User login
For MD-IQ use only
When recommending photoprotection in dark skin, consider cosmesis
The according to a review of racial differences in the approach to photoprotection, presented at the virtual Skin of Color Update 2020.

“Using photoprotection is not second nature to people of color,” said Amy McMichael, MD, chair, department of dermatology, Wake Forest University, Winston-Salem, N.C. “It is important to understand the complexity of perception in photoprotection patients with skin of color,” she added.
One obstacle is appearance. For instance, some products appear chalky on dark skin.
“Consider cosmesis,” advised Dr. McMichael. As an alternative to oxybenzone and other organic sunscreen filters, she specifically recommended inorganic sunscreens with tint. Currently, zinc oxide and titanium dioxide are the only Food and Drug Administration–approved inorganic filters, she noted. The nanoparticle formulations are less than 100 nm in size. Tinted products blocking visible light of different shades have been developed for individuals of all Fitzpatrick skin types.
Many patients with dark skin will need convincing that sun protection offers benefits and does not impose significant risks. In one survey cited by Dr. McMichael, Blacks reported the lowest level of sunscreen use when compared with Whites, Asians, or Latinos. While the increased melanin content in the skin of people of color does provide natural photoprotection, it does not fully eliminate the many adverse consequences of excess sun exposure.
“Photoprotection is essential to minimize acute and chronic effects of exposure to UV light that includes erythema, pigment darkening, photoaging, and photocarcinogenesis,” Dr. McMichael noted.
Among Black people who do employ sun protection, a large proportion do so to reduce the risk or prevent exacerbation of dyschromias such as vitiligo, melasma, and postinflammatory hyperpigmentation, according to Dr. McMichael. However, there appears to be inadequate use of sunscreens even for these concerns.
According to a study she cited, dermatologists prescribed sunscreens to Black patients in only 1.8% of office visits. Yet, 5% of all dermatologist consultations by Black patients are made to address a dyschromia. After acne, generalized forms of dermatitis, seborrheic dermatitis, and atopic dermatitis, dyschromias are the fifth most common reason for Blacks to consult a dermatologist.
“We cannot know from the data what the provider was seeing, but we can see that sunscreens are not the first medication that providers are reaching for,” Dr. McMichael said.
There are some concerns about the use of sunscreen that can be dispelled. The risk of vitamin D deficiency is one. Dr. McMichael, citing National Health and Nutrition Examination Survey data, said there appears to be a low risk in Whites and essentially no risk in Blacks.
The potential for sunscreens to induce frontal fibrosing alopecia (FFA) is another concern, but Dr. McMichael sees several problems with the surveys that have associated sunscreens with FFA, including recall bias, temporal ambiguity regarding sunscreen exposure and FFA onset, and cases of FFA in areas of the world where sunscreen is not used.
For sunscreens and FFA, “there is no direct evidence of causation,” she said. For concerned patients, she does acknowledge that there are data supporting an association, but she explains that this “connection is very loose at best.”
When encouraging sun protection, Dr. McMichael discusses alternatives to sunscreens, including hats and clothing that are photoprotective, wrap-around sunglasses, and sun avoidance. For patients with dyschromias, it makes particular sense to employ multiple sun protection strategies, but Dr. McMichael suggested that everybody, including individuals with skin of color, should be considering how to reduce excess sun exposure. She indicated that messages should to be tailored for the Black population.
“It is important to understand the complexity of the perception in photoprotection in patients with skin of color,” she said. Success with increasing uptake of sunscreens in patients with darker skin might depend on allaying fears and directing patients to agents that are cosmetically acceptable.
Others have delivered the same or related messages in the past. Natasha Buchanan Lunsford, PhD, a researcher in the Division of Cancer Prevention and Control at the Centers for Disease Control and Prevention, led a study on perceptions about skin cancer among Blacks and Hispanics.
“Most participants perceived themselves to be at low skin cancer risk due to their darker skin tone,” reported Dr. Lundsford and her coinvestigators, a finding based on data collected from 18 focus groups with Black and Hispanic participants aged 18 through 44 years.
In this study, Hispanics reported sun protection behavior more often than Blacks, but the minority of both groups used sunscreen or other sun avoidance measures routinely. For those who did use sunscreens, skin darkening and photoaging, rather than prevention of skin cancer, was the most common motivation to do so.
One problem is that “while general skin cancer prevention messaging exists, tailored and culturally sensitive messaging is limited,” Dr. Lundsford and coauthors wrote.
Dr. McMichael has financial relationships with multiple pharmaceutical companies, including those that make skin care products.
The according to a review of racial differences in the approach to photoprotection, presented at the virtual Skin of Color Update 2020.
“Using photoprotection is not second nature to people of color,” said Amy McMichael, MD, chair, department of dermatology, Wake Forest University, Winston-Salem, N.C. “It is important to understand the complexity of perception in photoprotection patients with skin of color,” she added.
One obstacle is appearance. For instance, some products appear chalky on dark skin.
“Consider cosmesis,” advised Dr. McMichael. As an alternative to oxybenzone and other organic sunscreen filters, she specifically recommended inorganic sunscreens with tint. Currently, zinc oxide and titanium dioxide are the only Food and Drug Administration–approved inorganic filters, she noted. The nanoparticle formulations are less than 100 nm in size. Tinted products blocking visible light of different shades have been developed for individuals of all Fitzpatrick skin types.
Many patients with dark skin will need convincing that sun protection offers benefits and does not impose significant risks. In one survey cited by Dr. McMichael, Blacks reported the lowest level of sunscreen use when compared with Whites, Asians, or Latinos. While the increased melanin content in the skin of people of color does provide natural photoprotection, it does not fully eliminate the many adverse consequences of excess sun exposure.
“Photoprotection is essential to minimize acute and chronic effects of exposure to UV light that includes erythema, pigment darkening, photoaging, and photocarcinogenesis,” Dr. McMichael noted.
Among Black people who do employ sun protection, a large proportion do so to reduce the risk or prevent exacerbation of dyschromias such as vitiligo, melasma, and postinflammatory hyperpigmentation, according to Dr. McMichael. However, there appears to be inadequate use of sunscreens even for these concerns.
According to a study she cited, dermatologists prescribed sunscreens to Black patients in only 1.8% of office visits. Yet, 5% of all dermatologist consultations by Black patients are made to address a dyschromia. After acne, generalized forms of dermatitis, seborrheic dermatitis, and atopic dermatitis, dyschromias are the fifth most common reason for Blacks to consult a dermatologist.
“We cannot know from the data what the provider was seeing, but we can see that sunscreens are not the first medication that providers are reaching for,” Dr. McMichael said.
There are some concerns about the use of sunscreen that can be dispelled. The risk of vitamin D deficiency is one. Dr. McMichael, citing National Health and Nutrition Examination Survey data, said there appears to be a low risk in Whites and essentially no risk in Blacks.
The potential for sunscreens to induce frontal fibrosing alopecia (FFA) is another concern, but Dr. McMichael sees several problems with the surveys that have associated sunscreens with FFA, including recall bias, temporal ambiguity regarding sunscreen exposure and FFA onset, and cases of FFA in areas of the world where sunscreen is not used.
For sunscreens and FFA, “there is no direct evidence of causation,” she said. For concerned patients, she does acknowledge that there are data supporting an association, but she explains that this “connection is very loose at best.”
When encouraging sun protection, Dr. McMichael discusses alternatives to sunscreens, including hats and clothing that are photoprotective, wrap-around sunglasses, and sun avoidance. For patients with dyschromias, it makes particular sense to employ multiple sun protection strategies, but Dr. McMichael suggested that everybody, including individuals with skin of color, should be considering how to reduce excess sun exposure. She indicated that messages should to be tailored for the Black population.
“It is important to understand the complexity of the perception in photoprotection in patients with skin of color,” she said. Success with increasing uptake of sunscreens in patients with darker skin might depend on allaying fears and directing patients to agents that are cosmetically acceptable.
Others have delivered the same or related messages in the past. Natasha Buchanan Lunsford, PhD, a researcher in the Division of Cancer Prevention and Control at the Centers for Disease Control and Prevention, led a study on perceptions about skin cancer among Blacks and Hispanics.
“Most participants perceived themselves to be at low skin cancer risk due to their darker skin tone,” reported Dr. Lundsford and her coinvestigators, a finding based on data collected from 18 focus groups with Black and Hispanic participants aged 18 through 44 years.
In this study, Hispanics reported sun protection behavior more often than Blacks, but the minority of both groups used sunscreen or other sun avoidance measures routinely. For those who did use sunscreens, skin darkening and photoaging, rather than prevention of skin cancer, was the most common motivation to do so.
One problem is that “while general skin cancer prevention messaging exists, tailored and culturally sensitive messaging is limited,” Dr. Lundsford and coauthors wrote.
Dr. McMichael has financial relationships with multiple pharmaceutical companies, including those that make skin care products.
The according to a review of racial differences in the approach to photoprotection, presented at the virtual Skin of Color Update 2020.
“Using photoprotection is not second nature to people of color,” said Amy McMichael, MD, chair, department of dermatology, Wake Forest University, Winston-Salem, N.C. “It is important to understand the complexity of perception in photoprotection patients with skin of color,” she added.
One obstacle is appearance. For instance, some products appear chalky on dark skin.
“Consider cosmesis,” advised Dr. McMichael. As an alternative to oxybenzone and other organic sunscreen filters, she specifically recommended inorganic sunscreens with tint. Currently, zinc oxide and titanium dioxide are the only Food and Drug Administration–approved inorganic filters, she noted. The nanoparticle formulations are less than 100 nm in size. Tinted products blocking visible light of different shades have been developed for individuals of all Fitzpatrick skin types.
Many patients with dark skin will need convincing that sun protection offers benefits and does not impose significant risks. In one survey cited by Dr. McMichael, Blacks reported the lowest level of sunscreen use when compared with Whites, Asians, or Latinos. While the increased melanin content in the skin of people of color does provide natural photoprotection, it does not fully eliminate the many adverse consequences of excess sun exposure.
“Photoprotection is essential to minimize acute and chronic effects of exposure to UV light that includes erythema, pigment darkening, photoaging, and photocarcinogenesis,” Dr. McMichael noted.
Among Black people who do employ sun protection, a large proportion do so to reduce the risk or prevent exacerbation of dyschromias such as vitiligo, melasma, and postinflammatory hyperpigmentation, according to Dr. McMichael. However, there appears to be inadequate use of sunscreens even for these concerns.
According to a study she cited, dermatologists prescribed sunscreens to Black patients in only 1.8% of office visits. Yet, 5% of all dermatologist consultations by Black patients are made to address a dyschromia. After acne, generalized forms of dermatitis, seborrheic dermatitis, and atopic dermatitis, dyschromias are the fifth most common reason for Blacks to consult a dermatologist.
“We cannot know from the data what the provider was seeing, but we can see that sunscreens are not the first medication that providers are reaching for,” Dr. McMichael said.
There are some concerns about the use of sunscreen that can be dispelled. The risk of vitamin D deficiency is one. Dr. McMichael, citing National Health and Nutrition Examination Survey data, said there appears to be a low risk in Whites and essentially no risk in Blacks.
The potential for sunscreens to induce frontal fibrosing alopecia (FFA) is another concern, but Dr. McMichael sees several problems with the surveys that have associated sunscreens with FFA, including recall bias, temporal ambiguity regarding sunscreen exposure and FFA onset, and cases of FFA in areas of the world where sunscreen is not used.
For sunscreens and FFA, “there is no direct evidence of causation,” she said. For concerned patients, she does acknowledge that there are data supporting an association, but she explains that this “connection is very loose at best.”
When encouraging sun protection, Dr. McMichael discusses alternatives to sunscreens, including hats and clothing that are photoprotective, wrap-around sunglasses, and sun avoidance. For patients with dyschromias, it makes particular sense to employ multiple sun protection strategies, but Dr. McMichael suggested that everybody, including individuals with skin of color, should be considering how to reduce excess sun exposure. She indicated that messages should to be tailored for the Black population.
“It is important to understand the complexity of the perception in photoprotection in patients with skin of color,” she said. Success with increasing uptake of sunscreens in patients with darker skin might depend on allaying fears and directing patients to agents that are cosmetically acceptable.
Others have delivered the same or related messages in the past. Natasha Buchanan Lunsford, PhD, a researcher in the Division of Cancer Prevention and Control at the Centers for Disease Control and Prevention, led a study on perceptions about skin cancer among Blacks and Hispanics.
“Most participants perceived themselves to be at low skin cancer risk due to their darker skin tone,” reported Dr. Lundsford and her coinvestigators, a finding based on data collected from 18 focus groups with Black and Hispanic participants aged 18 through 44 years.
In this study, Hispanics reported sun protection behavior more often than Blacks, but the minority of both groups used sunscreen or other sun avoidance measures routinely. For those who did use sunscreens, skin darkening and photoaging, rather than prevention of skin cancer, was the most common motivation to do so.
One problem is that “while general skin cancer prevention messaging exists, tailored and culturally sensitive messaging is limited,” Dr. Lundsford and coauthors wrote.
Dr. McMichael has financial relationships with multiple pharmaceutical companies, including those that make skin care products.
FROM SOC 2020
September 2020 - Quick Quiz Question 2
Q2: Correct answer: D
Rationale
Episodic hepatic encephalopathy is usually precipitant induced in over 80% of cases and precipitants include dehydration, infections, over diuresis, gastrointestinal bleeding, constipation, and the use of narcotics and sedatives. The key is to identify and treat the precipitant. A diagnostic workup to rule out other disorders that can alter brain function and mimic hepatic encephalopathy should also be performed.
Reference
Viltstrup H et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology. 2014;60(2):715-35.
Q2: Correct answer: D
Rationale
Episodic hepatic encephalopathy is usually precipitant induced in over 80% of cases and precipitants include dehydration, infections, over diuresis, gastrointestinal bleeding, constipation, and the use of narcotics and sedatives. The key is to identify and treat the precipitant. A diagnostic workup to rule out other disorders that can alter brain function and mimic hepatic encephalopathy should also be performed.
Reference
Viltstrup H et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology. 2014;60(2):715-35.
Q2: Correct answer: D
Rationale
Episodic hepatic encephalopathy is usually precipitant induced in over 80% of cases and precipitants include dehydration, infections, over diuresis, gastrointestinal bleeding, constipation, and the use of narcotics and sedatives. The key is to identify and treat the precipitant. A diagnostic workup to rule out other disorders that can alter brain function and mimic hepatic encephalopathy should also be performed.
Reference
Viltstrup H et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology. 2014;60(2):715-35.
Q2. A 62-year-old man with hepatitis C cirrhosis is admitted with altered mental status. He had a recent dental procedure and was given pain medication and a short course of antibiotics. He is taking only spironolactone 50 mg for small ascites. The patient is alert but not oriented to place and time. He has evidence of asterixis. His mucous membranes are dry and he has no evidence of ascites on exam. His labs include WBC 4.7 x 103/mm3, AST 45 U/L, ALT 40 U/L, total bilirubin of 2.5 mg/dL, albumin of 3.7 g/dL, sodium 142 mEq/L, and a creatinine of 0.5 mg/dL.
September 2020 - Quick Quiz Question 1
Q1: Correct answer: B
Rationale
A serum ceruloplasmin less than 5 mg/L and a 24-hour urine copper excretion greater than 100 mcg/24 hours are both highly suggestive of Wilson's disease, a disorder of copper metabolism caused by a mutation in a P-type ATP-ase that mediates the excretion of copper into the bile. Treatment of Wilson's disease consists of copper chelation therapy. Commonly used therapies include D-penicillamine, trientine, and zinc. Patients on therapy should have 24-hour urine copper determination every 6-12 months. Patients on maintenance trientine or D-penicillamine should have urine copper excretion of 200-500 mcg/24 hours. Patients on zinc therapy should have much lower copper excretion, in the range of 75 mcg/24 hours.
References
1. European Association for the Study of the Liver. EASL clinical practice guidelines: Wilson's disease. J Hepatol. 2012;56:671-85.
2. Roberts EA, Schilsky ML. Diagnosis and treatment of Wilson disease: An update. Hepatology. 2008;47:2089-111.
Q1: Correct answer: B
Rationale
A serum ceruloplasmin less than 5 mg/L and a 24-hour urine copper excretion greater than 100 mcg/24 hours are both highly suggestive of Wilson's disease, a disorder of copper metabolism caused by a mutation in a P-type ATP-ase that mediates the excretion of copper into the bile. Treatment of Wilson's disease consists of copper chelation therapy. Commonly used therapies include D-penicillamine, trientine, and zinc. Patients on therapy should have 24-hour urine copper determination every 6-12 months. Patients on maintenance trientine or D-penicillamine should have urine copper excretion of 200-500 mcg/24 hours. Patients on zinc therapy should have much lower copper excretion, in the range of 75 mcg/24 hours.
References
1. European Association for the Study of the Liver. EASL clinical practice guidelines: Wilson's disease. J Hepatol. 2012;56:671-85.
2. Roberts EA, Schilsky ML. Diagnosis and treatment of Wilson disease: An update. Hepatology. 2008;47:2089-111.
Q1: Correct answer: B
Rationale
A serum ceruloplasmin less than 5 mg/L and a 24-hour urine copper excretion greater than 100 mcg/24 hours are both highly suggestive of Wilson's disease, a disorder of copper metabolism caused by a mutation in a P-type ATP-ase that mediates the excretion of copper into the bile. Treatment of Wilson's disease consists of copper chelation therapy. Commonly used therapies include D-penicillamine, trientine, and zinc. Patients on therapy should have 24-hour urine copper determination every 6-12 months. Patients on maintenance trientine or D-penicillamine should have urine copper excretion of 200-500 mcg/24 hours. Patients on zinc therapy should have much lower copper excretion, in the range of 75 mcg/24 hours.
References
1. European Association for the Study of the Liver. EASL clinical practice guidelines: Wilson's disease. J Hepatol. 2012;56:671-85.
2. Roberts EA, Schilsky ML. Diagnosis and treatment of Wilson disease: An update. Hepatology. 2008;47:2089-111.
Q1. A 19-year-old male with elevated liver enzymes is found to have a serum ceruloplasmin of 3 mg/L, and a urine copper excretion of 210 mcg/24 hours. He is started on trientine to treat his illness.
Dr. Anique K. Forrester joins editorial advisory board of Clinical Psychiatry News
Clinical Psychiatry News is pleased to announce that Anique K. Forrester, MD, has joined its editorial advisory board.

Dr. Forrester, who is board certified in the subspecialty of psychosomatic medicine (consultation-liaison psychiatry), holds numerous leadership positions at the University of Maryland, Baltimore. She is director of the consultation-liaison psychiatry fellowship at the university and serves as director of education for the C-L psychiatry PGY-2 rotation. Dr. Forrester, an assistant professor, also serves as chair of the department of psychiatry’s diversity committee and is the coordinator of the cultural psychiatry resident course.
Dr. Forrester completed her psychiatry residency training as well as psychosomatic medicine fellowship training at Sidney Kimmel Medical College, Philadelphia. She is a diplomate of the American Board of Psychiatry and Neurology. In addition, Dr. Forrester is a member of the Academy of Consultation-Liaison Psychiatry. She is a graduate of Howard University, Washington.
Her research interests include perinatal psychiatry, psycho-oncology, and cultural competence in medicine.
Welcome aboard, Dr. Forrester!
Clinical Psychiatry News is pleased to announce that Anique K. Forrester, MD, has joined its editorial advisory board.
Dr. Forrester, who is board certified in the subspecialty of psychosomatic medicine (consultation-liaison psychiatry), holds numerous leadership positions at the University of Maryland, Baltimore. She is director of the consultation-liaison psychiatry fellowship at the university and serves as director of education for the C-L psychiatry PGY-2 rotation. Dr. Forrester, an assistant professor, also serves as chair of the department of psychiatry’s diversity committee and is the coordinator of the cultural psychiatry resident course.
Dr. Forrester completed her psychiatry residency training as well as psychosomatic medicine fellowship training at Sidney Kimmel Medical College, Philadelphia. She is a diplomate of the American Board of Psychiatry and Neurology. In addition, Dr. Forrester is a member of the Academy of Consultation-Liaison Psychiatry. She is a graduate of Howard University, Washington.
Her research interests include perinatal psychiatry, psycho-oncology, and cultural competence in medicine.
Welcome aboard, Dr. Forrester!
Clinical Psychiatry News is pleased to announce that Anique K. Forrester, MD, has joined its editorial advisory board.
Dr. Forrester, who is board certified in the subspecialty of psychosomatic medicine (consultation-liaison psychiatry), holds numerous leadership positions at the University of Maryland, Baltimore. She is director of the consultation-liaison psychiatry fellowship at the university and serves as director of education for the C-L psychiatry PGY-2 rotation. Dr. Forrester, an assistant professor, also serves as chair of the department of psychiatry’s diversity committee and is the coordinator of the cultural psychiatry resident course.
Dr. Forrester completed her psychiatry residency training as well as psychosomatic medicine fellowship training at Sidney Kimmel Medical College, Philadelphia. She is a diplomate of the American Board of Psychiatry and Neurology. In addition, Dr. Forrester is a member of the Academy of Consultation-Liaison Psychiatry. She is a graduate of Howard University, Washington.
Her research interests include perinatal psychiatry, psycho-oncology, and cultural competence in medicine.
Welcome aboard, Dr. Forrester!
Red hair in women linked to elevated CRP levels in Nurses’ Health Study
Red-haired women were significantly more likely than were women with nonred hair to have elevated levels of C-reactive protein that may increase risk for cardiovascular conditions, according to data from nearly 9,000 women participating in the Nurses’ Health Study.
“Positive associations between red hair and cardiovascular disease and cancer in women, but not men, have been reported,” wrote Rebecca I. Hartman, MD, of Brigham and Women’s Hospital, Harvard Medical School, Boston, and colleagues.
In a study published in the Journal of Investigative Dermatology, they reviewed data from the Nurses’ Health Study, a 1976 cohort study of 121,700 women registered nurses in the United States. They analyzed blood specimens from 8,994 women that were collected between 1989 and 1990. Participants’ natural hair color was determined by asking them their natural hair color at age 21 years, with choices of red, blonde, light brown, dark brown, or black. Overall, dark brown/black hair was the most common color (45%) and 390 of the women (4.3%) had red hair.
The average CRP levels were significantly higher for women with red hair (3.7 mg/L), compared with those with blonde (3.3 mg/L), light brown (3.0 mg/mL), or dark brown/black (3.2 mg/L).
Using the CRP levels for red-haired women as a reference, women with blond, light brown, and dark brown/black hair averaged significantly lower CRP levels than those of red-haired women in an age-adjusted model (–15.2%, –18/1%, and –14.2%, respectively) and in a multivariate analysis (–12.7%, –14.1%, and –10.9%, respectively).
Non-red-haired women had significantly lower odds of high CRP levels compared with red-haired women, with odds ratios of 0.62, 0.60, and 0.67 for women with blonde, light brown, and dark brown/black hair, respectively, in multivariate analysis, the researchers found.
The study was limited by several factors including the use of self-reports for hair color and the relative homogeneity of the Nurses’ Health Study, which has a population of mostly white, female health professionals, the researchers noted.
However, the findings of significantly increased CRP levels “could potentially explain a prior report of increased risks of cardiovascular disease and cancer in red-haired women,” they said. “Although, we observed similar associations in the NHS between red hair and cardiovascular disease and cancer, they were not statistically significant,” they added.
Additional studies are needed to validate and examine the clinical significance of the results, they concluded.
“Elevated CRP levels, a marker of inflammation, have been associated with increased risk for several diseases, including colon cancer and heart disease,” lead author Dr. Hartman said in an interview. “Another study suggested red-haired women have elevated risks of cardiovascular disease and cancer. We wanted to see if different levels of inflammation in red-haired women could possibly explain these findings.”
She said she was not surprised by the findings, “as they were in line with our hypothesis.” In addition, “animal studies suggest that the gene most responsible for red hair, MC1R, may be linked to inflammation,” she said.
While red-haired women were found to have higher CRP levels in the study, “the underlying mechanism and clinical significance remain unknown,” and more research is needed, Dr. Hartman emphasized. “First, our findings need to be validated in women and also examined in men. If our findings are validated, future studies should examine the mechanism of CRP elevation in red-haired women, and whether these women have elevated risks of colon cancer and heart disease,” she said.
“If red-haired women do have increased levels of inflammation, and as a result have elevated risks of colon cancer and heart disease, then future interventions can focus on enhanced screening and possibly chemoprevention in this population,” she added.
The study was supported by the National Institutes of Health. Lead author Dr. Hartman was supported by an American Skin Association Research Grant.
SOURCE: Hartman RI et al. J Invest Dermatol. 2020 Oct 12. doi: 10.1016/j.jid.2020.09.015.
Red-haired women were significantly more likely than were women with nonred hair to have elevated levels of C-reactive protein that may increase risk for cardiovascular conditions, according to data from nearly 9,000 women participating in the Nurses’ Health Study.
“Positive associations between red hair and cardiovascular disease and cancer in women, but not men, have been reported,” wrote Rebecca I. Hartman, MD, of Brigham and Women’s Hospital, Harvard Medical School, Boston, and colleagues.
In a study published in the Journal of Investigative Dermatology, they reviewed data from the Nurses’ Health Study, a 1976 cohort study of 121,700 women registered nurses in the United States. They analyzed blood specimens from 8,994 women that were collected between 1989 and 1990. Participants’ natural hair color was determined by asking them their natural hair color at age 21 years, with choices of red, blonde, light brown, dark brown, or black. Overall, dark brown/black hair was the most common color (45%) and 390 of the women (4.3%) had red hair.
The average CRP levels were significantly higher for women with red hair (3.7 mg/L), compared with those with blonde (3.3 mg/L), light brown (3.0 mg/mL), or dark brown/black (3.2 mg/L).
Using the CRP levels for red-haired women as a reference, women with blond, light brown, and dark brown/black hair averaged significantly lower CRP levels than those of red-haired women in an age-adjusted model (–15.2%, –18/1%, and –14.2%, respectively) and in a multivariate analysis (–12.7%, –14.1%, and –10.9%, respectively).
Non-red-haired women had significantly lower odds of high CRP levels compared with red-haired women, with odds ratios of 0.62, 0.60, and 0.67 for women with blonde, light brown, and dark brown/black hair, respectively, in multivariate analysis, the researchers found.
The study was limited by several factors including the use of self-reports for hair color and the relative homogeneity of the Nurses’ Health Study, which has a population of mostly white, female health professionals, the researchers noted.
However, the findings of significantly increased CRP levels “could potentially explain a prior report of increased risks of cardiovascular disease and cancer in red-haired women,” they said. “Although, we observed similar associations in the NHS between red hair and cardiovascular disease and cancer, they were not statistically significant,” they added.
Additional studies are needed to validate and examine the clinical significance of the results, they concluded.
“Elevated CRP levels, a marker of inflammation, have been associated with increased risk for several diseases, including colon cancer and heart disease,” lead author Dr. Hartman said in an interview. “Another study suggested red-haired women have elevated risks of cardiovascular disease and cancer. We wanted to see if different levels of inflammation in red-haired women could possibly explain these findings.”
She said she was not surprised by the findings, “as they were in line with our hypothesis.” In addition, “animal studies suggest that the gene most responsible for red hair, MC1R, may be linked to inflammation,” she said.
While red-haired women were found to have higher CRP levels in the study, “the underlying mechanism and clinical significance remain unknown,” and more research is needed, Dr. Hartman emphasized. “First, our findings need to be validated in women and also examined in men. If our findings are validated, future studies should examine the mechanism of CRP elevation in red-haired women, and whether these women have elevated risks of colon cancer and heart disease,” she said.
“If red-haired women do have increased levels of inflammation, and as a result have elevated risks of colon cancer and heart disease, then future interventions can focus on enhanced screening and possibly chemoprevention in this population,” she added.
The study was supported by the National Institutes of Health. Lead author Dr. Hartman was supported by an American Skin Association Research Grant.
SOURCE: Hartman RI et al. J Invest Dermatol. 2020 Oct 12. doi: 10.1016/j.jid.2020.09.015.
Red-haired women were significantly more likely than were women with nonred hair to have elevated levels of C-reactive protein that may increase risk for cardiovascular conditions, according to data from nearly 9,000 women participating in the Nurses’ Health Study.
“Positive associations between red hair and cardiovascular disease and cancer in women, but not men, have been reported,” wrote Rebecca I. Hartman, MD, of Brigham and Women’s Hospital, Harvard Medical School, Boston, and colleagues.
In a study published in the Journal of Investigative Dermatology, they reviewed data from the Nurses’ Health Study, a 1976 cohort study of 121,700 women registered nurses in the United States. They analyzed blood specimens from 8,994 women that were collected between 1989 and 1990. Participants’ natural hair color was determined by asking them their natural hair color at age 21 years, with choices of red, blonde, light brown, dark brown, or black. Overall, dark brown/black hair was the most common color (45%) and 390 of the women (4.3%) had red hair.
The average CRP levels were significantly higher for women with red hair (3.7 mg/L), compared with those with blonde (3.3 mg/L), light brown (3.0 mg/mL), or dark brown/black (3.2 mg/L).
Using the CRP levels for red-haired women as a reference, women with blond, light brown, and dark brown/black hair averaged significantly lower CRP levels than those of red-haired women in an age-adjusted model (–15.2%, –18/1%, and –14.2%, respectively) and in a multivariate analysis (–12.7%, –14.1%, and –10.9%, respectively).
Non-red-haired women had significantly lower odds of high CRP levels compared with red-haired women, with odds ratios of 0.62, 0.60, and 0.67 for women with blonde, light brown, and dark brown/black hair, respectively, in multivariate analysis, the researchers found.
The study was limited by several factors including the use of self-reports for hair color and the relative homogeneity of the Nurses’ Health Study, which has a population of mostly white, female health professionals, the researchers noted.
However, the findings of significantly increased CRP levels “could potentially explain a prior report of increased risks of cardiovascular disease and cancer in red-haired women,” they said. “Although, we observed similar associations in the NHS between red hair and cardiovascular disease and cancer, they were not statistically significant,” they added.
Additional studies are needed to validate and examine the clinical significance of the results, they concluded.
“Elevated CRP levels, a marker of inflammation, have been associated with increased risk for several diseases, including colon cancer and heart disease,” lead author Dr. Hartman said in an interview. “Another study suggested red-haired women have elevated risks of cardiovascular disease and cancer. We wanted to see if different levels of inflammation in red-haired women could possibly explain these findings.”
She said she was not surprised by the findings, “as they were in line with our hypothesis.” In addition, “animal studies suggest that the gene most responsible for red hair, MC1R, may be linked to inflammation,” she said.
While red-haired women were found to have higher CRP levels in the study, “the underlying mechanism and clinical significance remain unknown,” and more research is needed, Dr. Hartman emphasized. “First, our findings need to be validated in women and also examined in men. If our findings are validated, future studies should examine the mechanism of CRP elevation in red-haired women, and whether these women have elevated risks of colon cancer and heart disease,” she said.
“If red-haired women do have increased levels of inflammation, and as a result have elevated risks of colon cancer and heart disease, then future interventions can focus on enhanced screening and possibly chemoprevention in this population,” she added.
The study was supported by the National Institutes of Health. Lead author Dr. Hartman was supported by an American Skin Association Research Grant.
SOURCE: Hartman RI et al. J Invest Dermatol. 2020 Oct 12. doi: 10.1016/j.jid.2020.09.015.
FROM THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
Popularity of virtual conferences may mean a permanent shift
Fifteen days. That’s how much time the American College of Cardiology (ACC) had to convert its annual conference, scheduled for the end of March this year in Chicago, into a virtual meeting for the estimated 17,000 people who had planned to attend.
Because of the coronavirus pandemic, Illinois announced restrictions on the size of gatherings on March 13, causing the ACC to pivot to an online-only model.
“One big advantage was that we already had all of our content planned,” Janice Sibley, the ACC’s executive vice president of education, told Medscape Medical News. “We knew who the faculty would be for different sessions, and many of them had already planned their slides.”
But determining how to present those hundreds of presentations at an online conference, not to mention addressing the logistics related to registrations, tech platforms, exhibit hall sponsors, and other aspects of an annual meeting, would be no small task.
But according to a Medscape poll, many physicians think that, while the virtual experience is worthwhile and getting better, it’s never going to be the same as spending several days on site, immersed in the experience of an annual meeting.
As one respondent commented, “I miss the intellectual excitement, the electricity in the room, when there is a live presentation that announces a major breakthrough.”
Large medical societies have an advantage
As ACC rapidly prepared for its virtual conference, the society first refunded all registration and expo fees and worked with the vendor partners to resolve the cancellation of rental space, food and beverage services, and decorating. Then they organized a team of 15 people split into three groups. One group focused on the intellectual, scientific, and educational elements of the virtual conference. They chose 24 sessions to livestream and decided to prerecord the rest for on-demand access, limiting the number of presenters they needed to train for online presentation.
A second team focused on business and worked with industry partners on how to translate a large expo into digital offerings. They developed virtual pages, advertisements, promotions, and industry-sponsored education.
The third team’s focus, Ms. Sibley said, was most critical, and the hardest: addressing socio-emotional needs.
“That group was responsible for trying to create the buzz and excitement we would have had at the event,” she said, “pivoting that experience we would have had in a live event to a virtual environment. What we were worried about was, would anyone even come?”
But ACC built it, and they did indeed come. Within a half hour of the opening session, nearly 13,000 people logged on from around the world. “It worked beautifully,” Ms. Sibley said.
By the end of the 3-day event, approximately 34,000 unique visitors had logged in for live or prerecorded sessions. Although ACC worried at first about technical glitches and bandwidth needs, everything ran smoothly. By 90 days after the meeting, 63,000 unique users had logged in to access the conference content.
ACC was among the first organizations forced to switch from an in-person to all-online meeting, but dozens of other organizations have now done the same, discovering the benefits and drawbacks of a virtual environment while experimenting with different formats and offerings. Talks with a few large medical societies about the experience revealed several common themes, including the following:
- Finding new ways to attract and measure attendance.
- Ensuring the actual scientific content was as robust online as in person.
- Realizing the value of social media in enhancing the socio-emotional experience.
- Believing that virtual meetings will become a permanent fixture in a future of “hybrid” conferences.
New ways of attracting and measuring attendance
Previous ways to measure meeting attendance were straightforward: number of registrations and number of people physically walking into sessions. An online conference, however, offers dozens of ways to measure attendance. While the number of registrations remained one tool – and all the organizations interviewed reported record numbers of registrations – organizations also used other metrics to measure success, such as “participation,” “engagement,” and “viewing time.”
ACC defined “participation” as a unique user logging in, and it defined “engagement” as sticking around for a while, possibly using chat functions or discussing the content on social media. The American Society of Clinical Oncology (ASCO) annual conference in May, which attracted more than 44,000 registered attendees, also measured total content views – more than 2.5 million during the meeting – and monitored social media. More than 8,800 Twitter users posted more than 45,000 tweets with the #ASCO20 hashtag during the meeting, generating 750 million likes, shares, and comments. The European League Against Rheumatism (EULAR) annual congress registered a record 18,700 delegates – up from 14,500 in 2019 – but it also measured attendance by average viewing time and visits by congress day and by category.
Organizations shifted fee structures as well. While ACC refunded fees for its first online meeting, it has since developed tiers to match fees to anticipated value, such as charging more for livestreamed sessions that allow interactivity than for viewing recordings. ASCO offered a one-time fee waiver for members plus free registration to cancer survivors and caregivers, discounted registration for patient advocates, and reduced fees for other categories. But adjusting how to measure attendance and charge for events were the easy parts of transitioning to online.
Priority for having robust content
The biggest difficulty for most organizations was the short time they had to move online, with a host of challenges accompanying the switch, said the executive director of EULAR, Julia Rautenstrauch, DrMed. These included technical requirements, communication, training, finances, legal issues, compliance rules, and other logistics.
“The year 2020 will be remembered for being the year of unexpected transformation,” said a spokesperson from European Society for Medical Oncology (ESMO), who declined to be named. “The number of fundamental questions we had to ask ourselves is pages long. The solutions we have implemented so far have been successful, but we won’t rest on our laurels.”
ASCO had an advantage in the pivot, despite only 6 weeks to make the switch, because they already had a robust online platform to build on. “We weren’t starting from scratch, but we were sure changing the way we prepared,” ASCO CEO Clifford Hudis, MD, said.
All of the organizations made the breadth and quality of scientific and educational content a top priority, and those who have already hosted meetings this year report positive feedback.
“The rating of the scientific content was excellent, and the event did indeed fulfill the educational goals and expected learning outcomes for the vast majority of delegates,” EULAR’s Dr. Rautenstrauch said.
“Our goal, when we went into this, was that, in the future when somebody looks back at ASCO20, they should not be able to tell that it was a different year from any other in terms of the science,” Dr. Hudis said.
Missing out on networking and social interaction
Even when logistics run smoothly, virtual conferences must overcome two other challenges: the loss of in-person interactions and the potential for “Zoom burnout.”
“You do miss that human contact, the unsaid reactions in the room when you’re speaking or providing a controversial statement, even the facial expression or seeing people lean in or being distracted,” Ms. Sibley said.
Taher Modarressi, MD, an endocrinologist with Diabetes and Endocrine Associates of Hunterdon in Flemington, N.J., said all the digital conferences he has attended were missing those key social elements: “seeing old friends, sideline discussions that generate new ideas, and meeting new colleagues. However, this has been partly alleviated with the robust rise of social media and ‘MedTwitter,’ in particular, where these discussions and interactions continue.”
To attempt to meet that need for social interaction, societies came up with a variety of options. EULAR offered chatrooms, “Meet the Expert” sessions, and other virtual opportunities for live interaction. ASCO hosted discussion groups with subsets of participants, such as virtual meetings with oncology fellows, and it plans to offer networking sessions and “poster walks” during future meetings.
“The value of an in-person meeting is connecting with people, exchanging ideas over coffee, and making new contacts,” ASCO’s Dr. Hudis said. While virtual meetings lose many of those personal interactions, knowledge can also be shared with more people, he said.
The key to combating digital fatigue is focusing on opportunities for interactivity, ACC’s Ms. Sibley said. “When you are creating a virtual environment, it’s important that you offer choices.” Online learners tend to have shorter attention spans than in-person learners, so people need opportunities to flip between sessions, like flipping between TV channels. Different engagement options are also essential, such as chat functions on the video platforms, asking questions of presenters orally or in writing, and using the familiar hashtags for social media discussion.
“We set up all those different ways to interact, and you allow the user to choose,” Ms. Sibley said.
Some conferences, however, had less time or fewer resources to adjust to a virtual format and couldn’t make up for the lost social interaction. Andy Bowman, MD, a neonatologist in Lubbock, Tex., was supposed to attend the Neonatal & Pediatric Airborne Transport Conference sponsored by International Biomed in the spring, but it was canceled at the last minute. Several weeks later, the organizers released videos of scheduled speakers giving their talks, but it was less engaging and too easy to get distracted, Dr. Bowman said.
“There is a noticeable decrease in energy – you can’t look around to feed off other’s reactions when a speaker says something off the wall, or new, or contrary to expectations,” he said. He also especially missed the social interactions, such as “missing out on the chance encounters in the hallway or seeing the same face in back-to-back sessions and figuring out you have shared interest.” He was also sorry to miss the expo because neonatal transport requires a lot of specialty equipment, and he appreciates the chance to actually touch and see it in person.
Advantages of an online meeting
Despite the challenges, online meetings can overcome obstacles of in-person meetings, particularly for those in low- and middle-income countries, such as travel and registration costs, the hardships of being away from practice, and visa restrictions.
“You really have the potential to broaden your reach,” Ms. Sibley said, noting that people in 157 countries participated in ACC.20.
Another advantage is keeping the experience available to people after the livestreamed event.
“Virtual events have demonstrated the potential for a more democratic conference world, expanding the dissemination of information to a much wider community of stakeholders,” ESMO’s spokesperson said.
Not traveling can actually mean getting more out of the conference, said Atisha Patel Manhas, MD, a hematologist/oncologist in Dallas, who attended ASCO. “I have really enjoyed the access aspect – on the virtual platform there is so much more content available to you, and travel time doesn’t cut into conference time,” she said, though she also missed the interaction with colleagues.
Others found that virtual conferences provided more engagement than in-person conferences. Marwah Abdalla, MD, MPH, an assistant professor of medicine and director of education for the Cardiac Intensive Care Unit at Columbia University Medical Center, New York, felt that moderated Q&A sessions offered more interaction among participants. She attended and spoke on a panel during virtual SLEEP 2020, a joint meeting of the American Academy of Sleep Medicine (AASM) and the Sleep Research Society (SRS).
“Usually during in-person sessions, only a few questions are possible, and participants rarely have an opportunity to discuss the presentations within the session due to time limits,” Dr. Abdalla said. “Because the conference presentations can also be viewed asynchronously, participants have been able to comment on lectures and continue the discussion offline, either via social media or via email.” She acknowledged drawbacks of the virtual experience, such as an inability to socialize in person and participate in activities but appreciated the new opportunities to network and learn from international colleagues who would not have been able to attend in person.
Ritu Thamman, MD, assistant professor of medicine at the University of Pittsburgh School of Medicine, pointed out that many institutions have cut their travel budgets, and physicians would be unable to attend in-person conferences for financial or other reasons. She especially appreciated that the European Society of Cardiology had no registration fee for ESC 2020 and made their content free for all of September, which led to more than 100,000 participants.
“That meant anyone anywhere could learn,” she said. “It makes it much more diverse and more egalitarian. That feels like a good step in the right direction for all of us.”
Dr. Modarressi, who found ESC “exhilarating,” similarly noted the benefit of such an equitably accessible conference. “Decreasing barriers and improving access to top-line results and up-to-date information has always been a challenge to the global health community,” he said, noting that the map of attendance for the virtual meeting was “astonishing.”
Given these benefits, organizers said they expect a future of hybrid conferences: physical meetings for those able to attend in person and virtual ones for those who cannot.
“We also expect that the hybrid congress will cater to the needs of people on-site by allowing them additional access to more scientific content than by physical attendance alone,” Dr. Rautenstrauch said.
Everyone has been in reactive mode this year, Ms. Sibley said, but the future looks bright as they seek ways to overcome challenges such as socio-emotional needs and virtual expo spaces.
“We’ve been thrust into the virtual world much faster than we expected, but we’re finding it’s opening more opportunities than we had live,” Ms. Sibley said. “This has catapulted us, for better or worse, into a new way to deliver education and other types of information.
“I think, if we’re smart, we’ll continue to think of ways this can augment our live environment and not replace it.”
A version of this article originally appeared on Medscape.com.
Fifteen days. That’s how much time the American College of Cardiology (ACC) had to convert its annual conference, scheduled for the end of March this year in Chicago, into a virtual meeting for the estimated 17,000 people who had planned to attend.
Because of the coronavirus pandemic, Illinois announced restrictions on the size of gatherings on March 13, causing the ACC to pivot to an online-only model.
“One big advantage was that we already had all of our content planned,” Janice Sibley, the ACC’s executive vice president of education, told Medscape Medical News. “We knew who the faculty would be for different sessions, and many of them had already planned their slides.”
But determining how to present those hundreds of presentations at an online conference, not to mention addressing the logistics related to registrations, tech platforms, exhibit hall sponsors, and other aspects of an annual meeting, would be no small task.
But according to a Medscape poll, many physicians think that, while the virtual experience is worthwhile and getting better, it’s never going to be the same as spending several days on site, immersed in the experience of an annual meeting.
As one respondent commented, “I miss the intellectual excitement, the electricity in the room, when there is a live presentation that announces a major breakthrough.”
Large medical societies have an advantage
As ACC rapidly prepared for its virtual conference, the society first refunded all registration and expo fees and worked with the vendor partners to resolve the cancellation of rental space, food and beverage services, and decorating. Then they organized a team of 15 people split into three groups. One group focused on the intellectual, scientific, and educational elements of the virtual conference. They chose 24 sessions to livestream and decided to prerecord the rest for on-demand access, limiting the number of presenters they needed to train for online presentation.
A second team focused on business and worked with industry partners on how to translate a large expo into digital offerings. They developed virtual pages, advertisements, promotions, and industry-sponsored education.
The third team’s focus, Ms. Sibley said, was most critical, and the hardest: addressing socio-emotional needs.
“That group was responsible for trying to create the buzz and excitement we would have had at the event,” she said, “pivoting that experience we would have had in a live event to a virtual environment. What we were worried about was, would anyone even come?”
But ACC built it, and they did indeed come. Within a half hour of the opening session, nearly 13,000 people logged on from around the world. “It worked beautifully,” Ms. Sibley said.
By the end of the 3-day event, approximately 34,000 unique visitors had logged in for live or prerecorded sessions. Although ACC worried at first about technical glitches and bandwidth needs, everything ran smoothly. By 90 days after the meeting, 63,000 unique users had logged in to access the conference content.
ACC was among the first organizations forced to switch from an in-person to all-online meeting, but dozens of other organizations have now done the same, discovering the benefits and drawbacks of a virtual environment while experimenting with different formats and offerings. Talks with a few large medical societies about the experience revealed several common themes, including the following:
- Finding new ways to attract and measure attendance.
- Ensuring the actual scientific content was as robust online as in person.
- Realizing the value of social media in enhancing the socio-emotional experience.
- Believing that virtual meetings will become a permanent fixture in a future of “hybrid” conferences.
New ways of attracting and measuring attendance
Previous ways to measure meeting attendance were straightforward: number of registrations and number of people physically walking into sessions. An online conference, however, offers dozens of ways to measure attendance. While the number of registrations remained one tool – and all the organizations interviewed reported record numbers of registrations – organizations also used other metrics to measure success, such as “participation,” “engagement,” and “viewing time.”
ACC defined “participation” as a unique user logging in, and it defined “engagement” as sticking around for a while, possibly using chat functions or discussing the content on social media. The American Society of Clinical Oncology (ASCO) annual conference in May, which attracted more than 44,000 registered attendees, also measured total content views – more than 2.5 million during the meeting – and monitored social media. More than 8,800 Twitter users posted more than 45,000 tweets with the #ASCO20 hashtag during the meeting, generating 750 million likes, shares, and comments. The European League Against Rheumatism (EULAR) annual congress registered a record 18,700 delegates – up from 14,500 in 2019 – but it also measured attendance by average viewing time and visits by congress day and by category.
Organizations shifted fee structures as well. While ACC refunded fees for its first online meeting, it has since developed tiers to match fees to anticipated value, such as charging more for livestreamed sessions that allow interactivity than for viewing recordings. ASCO offered a one-time fee waiver for members plus free registration to cancer survivors and caregivers, discounted registration for patient advocates, and reduced fees for other categories. But adjusting how to measure attendance and charge for events were the easy parts of transitioning to online.
Priority for having robust content
The biggest difficulty for most organizations was the short time they had to move online, with a host of challenges accompanying the switch, said the executive director of EULAR, Julia Rautenstrauch, DrMed. These included technical requirements, communication, training, finances, legal issues, compliance rules, and other logistics.
“The year 2020 will be remembered for being the year of unexpected transformation,” said a spokesperson from European Society for Medical Oncology (ESMO), who declined to be named. “The number of fundamental questions we had to ask ourselves is pages long. The solutions we have implemented so far have been successful, but we won’t rest on our laurels.”
ASCO had an advantage in the pivot, despite only 6 weeks to make the switch, because they already had a robust online platform to build on. “We weren’t starting from scratch, but we were sure changing the way we prepared,” ASCO CEO Clifford Hudis, MD, said.
All of the organizations made the breadth and quality of scientific and educational content a top priority, and those who have already hosted meetings this year report positive feedback.
“The rating of the scientific content was excellent, and the event did indeed fulfill the educational goals and expected learning outcomes for the vast majority of delegates,” EULAR’s Dr. Rautenstrauch said.
“Our goal, when we went into this, was that, in the future when somebody looks back at ASCO20, they should not be able to tell that it was a different year from any other in terms of the science,” Dr. Hudis said.
Missing out on networking and social interaction
Even when logistics run smoothly, virtual conferences must overcome two other challenges: the loss of in-person interactions and the potential for “Zoom burnout.”
“You do miss that human contact, the unsaid reactions in the room when you’re speaking or providing a controversial statement, even the facial expression or seeing people lean in or being distracted,” Ms. Sibley said.
Taher Modarressi, MD, an endocrinologist with Diabetes and Endocrine Associates of Hunterdon in Flemington, N.J., said all the digital conferences he has attended were missing those key social elements: “seeing old friends, sideline discussions that generate new ideas, and meeting new colleagues. However, this has been partly alleviated with the robust rise of social media and ‘MedTwitter,’ in particular, where these discussions and interactions continue.”
To attempt to meet that need for social interaction, societies came up with a variety of options. EULAR offered chatrooms, “Meet the Expert” sessions, and other virtual opportunities for live interaction. ASCO hosted discussion groups with subsets of participants, such as virtual meetings with oncology fellows, and it plans to offer networking sessions and “poster walks” during future meetings.
“The value of an in-person meeting is connecting with people, exchanging ideas over coffee, and making new contacts,” ASCO’s Dr. Hudis said. While virtual meetings lose many of those personal interactions, knowledge can also be shared with more people, he said.
The key to combating digital fatigue is focusing on opportunities for interactivity, ACC’s Ms. Sibley said. “When you are creating a virtual environment, it’s important that you offer choices.” Online learners tend to have shorter attention spans than in-person learners, so people need opportunities to flip between sessions, like flipping between TV channels. Different engagement options are also essential, such as chat functions on the video platforms, asking questions of presenters orally or in writing, and using the familiar hashtags for social media discussion.
“We set up all those different ways to interact, and you allow the user to choose,” Ms. Sibley said.
Some conferences, however, had less time or fewer resources to adjust to a virtual format and couldn’t make up for the lost social interaction. Andy Bowman, MD, a neonatologist in Lubbock, Tex., was supposed to attend the Neonatal & Pediatric Airborne Transport Conference sponsored by International Biomed in the spring, but it was canceled at the last minute. Several weeks later, the organizers released videos of scheduled speakers giving their talks, but it was less engaging and too easy to get distracted, Dr. Bowman said.
“There is a noticeable decrease in energy – you can’t look around to feed off other’s reactions when a speaker says something off the wall, or new, or contrary to expectations,” he said. He also especially missed the social interactions, such as “missing out on the chance encounters in the hallway or seeing the same face in back-to-back sessions and figuring out you have shared interest.” He was also sorry to miss the expo because neonatal transport requires a lot of specialty equipment, and he appreciates the chance to actually touch and see it in person.
Advantages of an online meeting
Despite the challenges, online meetings can overcome obstacles of in-person meetings, particularly for those in low- and middle-income countries, such as travel and registration costs, the hardships of being away from practice, and visa restrictions.
“You really have the potential to broaden your reach,” Ms. Sibley said, noting that people in 157 countries participated in ACC.20.
Another advantage is keeping the experience available to people after the livestreamed event.
“Virtual events have demonstrated the potential for a more democratic conference world, expanding the dissemination of information to a much wider community of stakeholders,” ESMO’s spokesperson said.
Not traveling can actually mean getting more out of the conference, said Atisha Patel Manhas, MD, a hematologist/oncologist in Dallas, who attended ASCO. “I have really enjoyed the access aspect – on the virtual platform there is so much more content available to you, and travel time doesn’t cut into conference time,” she said, though she also missed the interaction with colleagues.
Others found that virtual conferences provided more engagement than in-person conferences. Marwah Abdalla, MD, MPH, an assistant professor of medicine and director of education for the Cardiac Intensive Care Unit at Columbia University Medical Center, New York, felt that moderated Q&A sessions offered more interaction among participants. She attended and spoke on a panel during virtual SLEEP 2020, a joint meeting of the American Academy of Sleep Medicine (AASM) and the Sleep Research Society (SRS).
“Usually during in-person sessions, only a few questions are possible, and participants rarely have an opportunity to discuss the presentations within the session due to time limits,” Dr. Abdalla said. “Because the conference presentations can also be viewed asynchronously, participants have been able to comment on lectures and continue the discussion offline, either via social media or via email.” She acknowledged drawbacks of the virtual experience, such as an inability to socialize in person and participate in activities but appreciated the new opportunities to network and learn from international colleagues who would not have been able to attend in person.
Ritu Thamman, MD, assistant professor of medicine at the University of Pittsburgh School of Medicine, pointed out that many institutions have cut their travel budgets, and physicians would be unable to attend in-person conferences for financial or other reasons. She especially appreciated that the European Society of Cardiology had no registration fee for ESC 2020 and made their content free for all of September, which led to more than 100,000 participants.
“That meant anyone anywhere could learn,” she said. “It makes it much more diverse and more egalitarian. That feels like a good step in the right direction for all of us.”
Dr. Modarressi, who found ESC “exhilarating,” similarly noted the benefit of such an equitably accessible conference. “Decreasing barriers and improving access to top-line results and up-to-date information has always been a challenge to the global health community,” he said, noting that the map of attendance for the virtual meeting was “astonishing.”
Given these benefits, organizers said they expect a future of hybrid conferences: physical meetings for those able to attend in person and virtual ones for those who cannot.
“We also expect that the hybrid congress will cater to the needs of people on-site by allowing them additional access to more scientific content than by physical attendance alone,” Dr. Rautenstrauch said.
Everyone has been in reactive mode this year, Ms. Sibley said, but the future looks bright as they seek ways to overcome challenges such as socio-emotional needs and virtual expo spaces.
“We’ve been thrust into the virtual world much faster than we expected, but we’re finding it’s opening more opportunities than we had live,” Ms. Sibley said. “This has catapulted us, for better or worse, into a new way to deliver education and other types of information.
“I think, if we’re smart, we’ll continue to think of ways this can augment our live environment and not replace it.”
A version of this article originally appeared on Medscape.com.
Fifteen days. That’s how much time the American College of Cardiology (ACC) had to convert its annual conference, scheduled for the end of March this year in Chicago, into a virtual meeting for the estimated 17,000 people who had planned to attend.
Because of the coronavirus pandemic, Illinois announced restrictions on the size of gatherings on March 13, causing the ACC to pivot to an online-only model.
“One big advantage was that we already had all of our content planned,” Janice Sibley, the ACC’s executive vice president of education, told Medscape Medical News. “We knew who the faculty would be for different sessions, and many of them had already planned their slides.”
But determining how to present those hundreds of presentations at an online conference, not to mention addressing the logistics related to registrations, tech platforms, exhibit hall sponsors, and other aspects of an annual meeting, would be no small task.
But according to a Medscape poll, many physicians think that, while the virtual experience is worthwhile and getting better, it’s never going to be the same as spending several days on site, immersed in the experience of an annual meeting.
As one respondent commented, “I miss the intellectual excitement, the electricity in the room, when there is a live presentation that announces a major breakthrough.”
Large medical societies have an advantage
As ACC rapidly prepared for its virtual conference, the society first refunded all registration and expo fees and worked with the vendor partners to resolve the cancellation of rental space, food and beverage services, and decorating. Then they organized a team of 15 people split into three groups. One group focused on the intellectual, scientific, and educational elements of the virtual conference. They chose 24 sessions to livestream and decided to prerecord the rest for on-demand access, limiting the number of presenters they needed to train for online presentation.
A second team focused on business and worked with industry partners on how to translate a large expo into digital offerings. They developed virtual pages, advertisements, promotions, and industry-sponsored education.
The third team’s focus, Ms. Sibley said, was most critical, and the hardest: addressing socio-emotional needs.
“That group was responsible for trying to create the buzz and excitement we would have had at the event,” she said, “pivoting that experience we would have had in a live event to a virtual environment. What we were worried about was, would anyone even come?”
But ACC built it, and they did indeed come. Within a half hour of the opening session, nearly 13,000 people logged on from around the world. “It worked beautifully,” Ms. Sibley said.
By the end of the 3-day event, approximately 34,000 unique visitors had logged in for live or prerecorded sessions. Although ACC worried at first about technical glitches and bandwidth needs, everything ran smoothly. By 90 days after the meeting, 63,000 unique users had logged in to access the conference content.
ACC was among the first organizations forced to switch from an in-person to all-online meeting, but dozens of other organizations have now done the same, discovering the benefits and drawbacks of a virtual environment while experimenting with different formats and offerings. Talks with a few large medical societies about the experience revealed several common themes, including the following:
- Finding new ways to attract and measure attendance.
- Ensuring the actual scientific content was as robust online as in person.
- Realizing the value of social media in enhancing the socio-emotional experience.
- Believing that virtual meetings will become a permanent fixture in a future of “hybrid” conferences.
New ways of attracting and measuring attendance
Previous ways to measure meeting attendance were straightforward: number of registrations and number of people physically walking into sessions. An online conference, however, offers dozens of ways to measure attendance. While the number of registrations remained one tool – and all the organizations interviewed reported record numbers of registrations – organizations also used other metrics to measure success, such as “participation,” “engagement,” and “viewing time.”
ACC defined “participation” as a unique user logging in, and it defined “engagement” as sticking around for a while, possibly using chat functions or discussing the content on social media. The American Society of Clinical Oncology (ASCO) annual conference in May, which attracted more than 44,000 registered attendees, also measured total content views – more than 2.5 million during the meeting – and monitored social media. More than 8,800 Twitter users posted more than 45,000 tweets with the #ASCO20 hashtag during the meeting, generating 750 million likes, shares, and comments. The European League Against Rheumatism (EULAR) annual congress registered a record 18,700 delegates – up from 14,500 in 2019 – but it also measured attendance by average viewing time and visits by congress day and by category.
Organizations shifted fee structures as well. While ACC refunded fees for its first online meeting, it has since developed tiers to match fees to anticipated value, such as charging more for livestreamed sessions that allow interactivity than for viewing recordings. ASCO offered a one-time fee waiver for members plus free registration to cancer survivors and caregivers, discounted registration for patient advocates, and reduced fees for other categories. But adjusting how to measure attendance and charge for events were the easy parts of transitioning to online.
Priority for having robust content
The biggest difficulty for most organizations was the short time they had to move online, with a host of challenges accompanying the switch, said the executive director of EULAR, Julia Rautenstrauch, DrMed. These included technical requirements, communication, training, finances, legal issues, compliance rules, and other logistics.
“The year 2020 will be remembered for being the year of unexpected transformation,” said a spokesperson from European Society for Medical Oncology (ESMO), who declined to be named. “The number of fundamental questions we had to ask ourselves is pages long. The solutions we have implemented so far have been successful, but we won’t rest on our laurels.”
ASCO had an advantage in the pivot, despite only 6 weeks to make the switch, because they already had a robust online platform to build on. “We weren’t starting from scratch, but we were sure changing the way we prepared,” ASCO CEO Clifford Hudis, MD, said.
All of the organizations made the breadth and quality of scientific and educational content a top priority, and those who have already hosted meetings this year report positive feedback.
“The rating of the scientific content was excellent, and the event did indeed fulfill the educational goals and expected learning outcomes for the vast majority of delegates,” EULAR’s Dr. Rautenstrauch said.
“Our goal, when we went into this, was that, in the future when somebody looks back at ASCO20, they should not be able to tell that it was a different year from any other in terms of the science,” Dr. Hudis said.
Missing out on networking and social interaction
Even when logistics run smoothly, virtual conferences must overcome two other challenges: the loss of in-person interactions and the potential for “Zoom burnout.”
“You do miss that human contact, the unsaid reactions in the room when you’re speaking or providing a controversial statement, even the facial expression or seeing people lean in or being distracted,” Ms. Sibley said.
Taher Modarressi, MD, an endocrinologist with Diabetes and Endocrine Associates of Hunterdon in Flemington, N.J., said all the digital conferences he has attended were missing those key social elements: “seeing old friends, sideline discussions that generate new ideas, and meeting new colleagues. However, this has been partly alleviated with the robust rise of social media and ‘MedTwitter,’ in particular, where these discussions and interactions continue.”
To attempt to meet that need for social interaction, societies came up with a variety of options. EULAR offered chatrooms, “Meet the Expert” sessions, and other virtual opportunities for live interaction. ASCO hosted discussion groups with subsets of participants, such as virtual meetings with oncology fellows, and it plans to offer networking sessions and “poster walks” during future meetings.
“The value of an in-person meeting is connecting with people, exchanging ideas over coffee, and making new contacts,” ASCO’s Dr. Hudis said. While virtual meetings lose many of those personal interactions, knowledge can also be shared with more people, he said.
The key to combating digital fatigue is focusing on opportunities for interactivity, ACC’s Ms. Sibley said. “When you are creating a virtual environment, it’s important that you offer choices.” Online learners tend to have shorter attention spans than in-person learners, so people need opportunities to flip between sessions, like flipping between TV channels. Different engagement options are also essential, such as chat functions on the video platforms, asking questions of presenters orally or in writing, and using the familiar hashtags for social media discussion.
“We set up all those different ways to interact, and you allow the user to choose,” Ms. Sibley said.
Some conferences, however, had less time or fewer resources to adjust to a virtual format and couldn’t make up for the lost social interaction. Andy Bowman, MD, a neonatologist in Lubbock, Tex., was supposed to attend the Neonatal & Pediatric Airborne Transport Conference sponsored by International Biomed in the spring, but it was canceled at the last minute. Several weeks later, the organizers released videos of scheduled speakers giving their talks, but it was less engaging and too easy to get distracted, Dr. Bowman said.
“There is a noticeable decrease in energy – you can’t look around to feed off other’s reactions when a speaker says something off the wall, or new, or contrary to expectations,” he said. He also especially missed the social interactions, such as “missing out on the chance encounters in the hallway or seeing the same face in back-to-back sessions and figuring out you have shared interest.” He was also sorry to miss the expo because neonatal transport requires a lot of specialty equipment, and he appreciates the chance to actually touch and see it in person.
Advantages of an online meeting
Despite the challenges, online meetings can overcome obstacles of in-person meetings, particularly for those in low- and middle-income countries, such as travel and registration costs, the hardships of being away from practice, and visa restrictions.
“You really have the potential to broaden your reach,” Ms. Sibley said, noting that people in 157 countries participated in ACC.20.
Another advantage is keeping the experience available to people after the livestreamed event.
“Virtual events have demonstrated the potential for a more democratic conference world, expanding the dissemination of information to a much wider community of stakeholders,” ESMO’s spokesperson said.
Not traveling can actually mean getting more out of the conference, said Atisha Patel Manhas, MD, a hematologist/oncologist in Dallas, who attended ASCO. “I have really enjoyed the access aspect – on the virtual platform there is so much more content available to you, and travel time doesn’t cut into conference time,” she said, though she also missed the interaction with colleagues.
Others found that virtual conferences provided more engagement than in-person conferences. Marwah Abdalla, MD, MPH, an assistant professor of medicine and director of education for the Cardiac Intensive Care Unit at Columbia University Medical Center, New York, felt that moderated Q&A sessions offered more interaction among participants. She attended and spoke on a panel during virtual SLEEP 2020, a joint meeting of the American Academy of Sleep Medicine (AASM) and the Sleep Research Society (SRS).
“Usually during in-person sessions, only a few questions are possible, and participants rarely have an opportunity to discuss the presentations within the session due to time limits,” Dr. Abdalla said. “Because the conference presentations can also be viewed asynchronously, participants have been able to comment on lectures and continue the discussion offline, either via social media or via email.” She acknowledged drawbacks of the virtual experience, such as an inability to socialize in person and participate in activities but appreciated the new opportunities to network and learn from international colleagues who would not have been able to attend in person.
Ritu Thamman, MD, assistant professor of medicine at the University of Pittsburgh School of Medicine, pointed out that many institutions have cut their travel budgets, and physicians would be unable to attend in-person conferences for financial or other reasons. She especially appreciated that the European Society of Cardiology had no registration fee for ESC 2020 and made their content free for all of September, which led to more than 100,000 participants.
“That meant anyone anywhere could learn,” she said. “It makes it much more diverse and more egalitarian. That feels like a good step in the right direction for all of us.”
Dr. Modarressi, who found ESC “exhilarating,” similarly noted the benefit of such an equitably accessible conference. “Decreasing barriers and improving access to top-line results and up-to-date information has always been a challenge to the global health community,” he said, noting that the map of attendance for the virtual meeting was “astonishing.”
Given these benefits, organizers said they expect a future of hybrid conferences: physical meetings for those able to attend in person and virtual ones for those who cannot.
“We also expect that the hybrid congress will cater to the needs of people on-site by allowing them additional access to more scientific content than by physical attendance alone,” Dr. Rautenstrauch said.
Everyone has been in reactive mode this year, Ms. Sibley said, but the future looks bright as they seek ways to overcome challenges such as socio-emotional needs and virtual expo spaces.
“We’ve been thrust into the virtual world much faster than we expected, but we’re finding it’s opening more opportunities than we had live,” Ms. Sibley said. “This has catapulted us, for better or worse, into a new way to deliver education and other types of information.
“I think, if we’re smart, we’ll continue to think of ways this can augment our live environment and not replace it.”
A version of this article originally appeared on Medscape.com.
EMA panel backs peanut allergy desensitizing powder Palforzia
The product is intended for desensitizing children and adolescents to peanut allergy.
Palforzia will be available as an oral powder in capsules (0.5, 1, 10, 20, and 100 mg) and as oral powder in sachet (300 mg). The active substance is defatted powder of Arachis hypogaea.
Through use of the product, children with a peanut allergy receive controlled exposure to precise, increasing amounts of peanut protein, mixed with soft food, every day. Over time, this may help to decrease their sensitivity to small amounts of peanuts.
According to the press release from the EMA, Palforzia can mitigate accidental exposure to small amounts of peanut protein. “[A] single dose of a least 1 gram of peanut protein would cause no more than mild allergy symptoms,” the EMA said.
The treatment is indicated for patients aged 4 to 17 years who have received a confirmed diagnosis of peanut allergy. Treatment may be continued for patients aged 18 years or older, according to the press release.
It should be administered under the supervision of a healthcare provider qualified in the diagnosis and treatment of allergic diseases and should be used in conjunction with a peanut-avoidant diet, the EMA notes.
The most common side effects that have been reported are abdominal pain, throat irritation, itch, nausea, vomiting, urticaria, and upper abdominal discomfort.
The next step in the approval process is to obtain market authorization from the European Commission. Detailed recommendations for use will be described in the summary of product characteristics, which will be published in the European public assessment report and will be made available throughout Europe.
“We are encouraged by the CHMP opinion, which recommends Palforzia as the first and only treatment option in the European Union for patients with peanut allergy and their families,” Andrew Oxtoby, president and chief executive officer of Aimmune Therapeutics, said in a statement. “Today’s decision underscores the strong and compelling data from our Palforzia clinical trials and follows the US FDA approval of Palforzia earlier this year. We look forward to the European Commission’s final decision for the marketing approval of Palforzia, which we expect later this year.”
The FDA said in granting its approval that patients, parents, or caregivers must be counseled on the need for always-available injectable epinephrine, the need for continued peanut avoidance, and on how to recognize signs of anaphylaxis.
This article originally appeared on Medscape.com.
The product is intended for desensitizing children and adolescents to peanut allergy.
Palforzia will be available as an oral powder in capsules (0.5, 1, 10, 20, and 100 mg) and as oral powder in sachet (300 mg). The active substance is defatted powder of Arachis hypogaea.
Through use of the product, children with a peanut allergy receive controlled exposure to precise, increasing amounts of peanut protein, mixed with soft food, every day. Over time, this may help to decrease their sensitivity to small amounts of peanuts.
According to the press release from the EMA, Palforzia can mitigate accidental exposure to small amounts of peanut protein. “[A] single dose of a least 1 gram of peanut protein would cause no more than mild allergy symptoms,” the EMA said.
The treatment is indicated for patients aged 4 to 17 years who have received a confirmed diagnosis of peanut allergy. Treatment may be continued for patients aged 18 years or older, according to the press release.
It should be administered under the supervision of a healthcare provider qualified in the diagnosis and treatment of allergic diseases and should be used in conjunction with a peanut-avoidant diet, the EMA notes.
The most common side effects that have been reported are abdominal pain, throat irritation, itch, nausea, vomiting, urticaria, and upper abdominal discomfort.
The next step in the approval process is to obtain market authorization from the European Commission. Detailed recommendations for use will be described in the summary of product characteristics, which will be published in the European public assessment report and will be made available throughout Europe.
“We are encouraged by the CHMP opinion, which recommends Palforzia as the first and only treatment option in the European Union for patients with peanut allergy and their families,” Andrew Oxtoby, president and chief executive officer of Aimmune Therapeutics, said in a statement. “Today’s decision underscores the strong and compelling data from our Palforzia clinical trials and follows the US FDA approval of Palforzia earlier this year. We look forward to the European Commission’s final decision for the marketing approval of Palforzia, which we expect later this year.”
The FDA said in granting its approval that patients, parents, or caregivers must be counseled on the need for always-available injectable epinephrine, the need for continued peanut avoidance, and on how to recognize signs of anaphylaxis.
This article originally appeared on Medscape.com.
The product is intended for desensitizing children and adolescents to peanut allergy.
Palforzia will be available as an oral powder in capsules (0.5, 1, 10, 20, and 100 mg) and as oral powder in sachet (300 mg). The active substance is defatted powder of Arachis hypogaea.
Through use of the product, children with a peanut allergy receive controlled exposure to precise, increasing amounts of peanut protein, mixed with soft food, every day. Over time, this may help to decrease their sensitivity to small amounts of peanuts.
According to the press release from the EMA, Palforzia can mitigate accidental exposure to small amounts of peanut protein. “[A] single dose of a least 1 gram of peanut protein would cause no more than mild allergy symptoms,” the EMA said.
The treatment is indicated for patients aged 4 to 17 years who have received a confirmed diagnosis of peanut allergy. Treatment may be continued for patients aged 18 years or older, according to the press release.
It should be administered under the supervision of a healthcare provider qualified in the diagnosis and treatment of allergic diseases and should be used in conjunction with a peanut-avoidant diet, the EMA notes.
The most common side effects that have been reported are abdominal pain, throat irritation, itch, nausea, vomiting, urticaria, and upper abdominal discomfort.
The next step in the approval process is to obtain market authorization from the European Commission. Detailed recommendations for use will be described in the summary of product characteristics, which will be published in the European public assessment report and will be made available throughout Europe.
“We are encouraged by the CHMP opinion, which recommends Palforzia as the first and only treatment option in the European Union for patients with peanut allergy and their families,” Andrew Oxtoby, president and chief executive officer of Aimmune Therapeutics, said in a statement. “Today’s decision underscores the strong and compelling data from our Palforzia clinical trials and follows the US FDA approval of Palforzia earlier this year. We look forward to the European Commission’s final decision for the marketing approval of Palforzia, which we expect later this year.”
The FDA said in granting its approval that patients, parents, or caregivers must be counseled on the need for always-available injectable epinephrine, the need for continued peanut avoidance, and on how to recognize signs of anaphylaxis.
This article originally appeared on Medscape.com.
SHM announces 2021 virtual annual conference: SHM Converge
The Society of Hospital Medicine has announced its virtual annual conference for 2021: SHM Converge. Formerly known as Hospital Medicine 2021, SHM Converge will take place virtually from May 3-7, 2021, and will offer a fully digital experience with the same education, professional development, and networking hospitalists have come to expect from SHM’s annual conference.

“This year, COVID-19 has challenged us to embrace change and to innovate to better serve our hospital medicine community,” said Danielle Scheurer, MD, MSCR, SFHM, president of SHM’s board of directors. “In that spirit, not only are we introducing an exciting new brand for the SHM annual conference, we are unveiling a reimagined experience for attendees, complete with sessions highlighting the latest research, best practices and innovations in the field.”
The SHM Converge schedule features 20 educational tracks, including the addition of four new tracks to support hospital medicine professionals in some of the most relevant topics affecting health care: diagnostic safety; diversity, equity, and inclusion; leadership; and wellness and resilience
Attendees will also have the option to follow many of the most popular tracks from previous SHM annual conferences, including Rapid Fire, Clinical Updates, and High-Value Care, among others. In many sessions, speakers will present the latest data and information available about COVID-19’s impact on the practice of hospital medicine. Precourses will be held on May 3.
SHM Converge will also offer additional professional development opportunities, including the Research, Innovations, and Clinical Vignettes scientific abstract competition and a speed mentoring session. Networking will be an integral component of SHM Converge. Attendees will be able to choose from more than 20 Special Interest forums, live Q&A sessions and networking events through the interactive conference platform.
“While SHM Converge may look a bit different than the SHM annual conference we are accustomed to, I am confident the content will be among the best we have ever offered, spanning a broad range of clinical topics and issues affecting hospitalists and their patients,” said Daniel Steinberg, MD, SFHM, course director for SHM Converge. “This virtual experience will unite hospitalists from around the globe and connect them with renowned faculty members and thought leaders in hospital medicine – as well as with their hospitalist colleagues they look forward to reconnecting with each year.”
Keynote speaker announcements are forthcoming.
Registration for SHM Converge opens in November 2020. Learn more at shmconverge.org.
Members of the media can obtain press passes beginning in November 2020 by contacting [email protected].
The Society of Hospital Medicine has announced its virtual annual conference for 2021: SHM Converge. Formerly known as Hospital Medicine 2021, SHM Converge will take place virtually from May 3-7, 2021, and will offer a fully digital experience with the same education, professional development, and networking hospitalists have come to expect from SHM’s annual conference.
“This year, COVID-19 has challenged us to embrace change and to innovate to better serve our hospital medicine community,” said Danielle Scheurer, MD, MSCR, SFHM, president of SHM’s board of directors. “In that spirit, not only are we introducing an exciting new brand for the SHM annual conference, we are unveiling a reimagined experience for attendees, complete with sessions highlighting the latest research, best practices and innovations in the field.”
The SHM Converge schedule features 20 educational tracks, including the addition of four new tracks to support hospital medicine professionals in some of the most relevant topics affecting health care: diagnostic safety; diversity, equity, and inclusion; leadership; and wellness and resilience
Attendees will also have the option to follow many of the most popular tracks from previous SHM annual conferences, including Rapid Fire, Clinical Updates, and High-Value Care, among others. In many sessions, speakers will present the latest data and information available about COVID-19’s impact on the practice of hospital medicine. Precourses will be held on May 3.
SHM Converge will also offer additional professional development opportunities, including the Research, Innovations, and Clinical Vignettes scientific abstract competition and a speed mentoring session. Networking will be an integral component of SHM Converge. Attendees will be able to choose from more than 20 Special Interest forums, live Q&A sessions and networking events through the interactive conference platform.
“While SHM Converge may look a bit different than the SHM annual conference we are accustomed to, I am confident the content will be among the best we have ever offered, spanning a broad range of clinical topics and issues affecting hospitalists and their patients,” said Daniel Steinberg, MD, SFHM, course director for SHM Converge. “This virtual experience will unite hospitalists from around the globe and connect them with renowned faculty members and thought leaders in hospital medicine – as well as with their hospitalist colleagues they look forward to reconnecting with each year.”
Keynote speaker announcements are forthcoming.
Registration for SHM Converge opens in November 2020. Learn more at shmconverge.org.
Members of the media can obtain press passes beginning in November 2020 by contacting [email protected].
The Society of Hospital Medicine has announced its virtual annual conference for 2021: SHM Converge. Formerly known as Hospital Medicine 2021, SHM Converge will take place virtually from May 3-7, 2021, and will offer a fully digital experience with the same education, professional development, and networking hospitalists have come to expect from SHM’s annual conference.
“This year, COVID-19 has challenged us to embrace change and to innovate to better serve our hospital medicine community,” said Danielle Scheurer, MD, MSCR, SFHM, president of SHM’s board of directors. “In that spirit, not only are we introducing an exciting new brand for the SHM annual conference, we are unveiling a reimagined experience for attendees, complete with sessions highlighting the latest research, best practices and innovations in the field.”
The SHM Converge schedule features 20 educational tracks, including the addition of four new tracks to support hospital medicine professionals in some of the most relevant topics affecting health care: diagnostic safety; diversity, equity, and inclusion; leadership; and wellness and resilience
Attendees will also have the option to follow many of the most popular tracks from previous SHM annual conferences, including Rapid Fire, Clinical Updates, and High-Value Care, among others. In many sessions, speakers will present the latest data and information available about COVID-19’s impact on the practice of hospital medicine. Precourses will be held on May 3.
SHM Converge will also offer additional professional development opportunities, including the Research, Innovations, and Clinical Vignettes scientific abstract competition and a speed mentoring session. Networking will be an integral component of SHM Converge. Attendees will be able to choose from more than 20 Special Interest forums, live Q&A sessions and networking events through the interactive conference platform.
“While SHM Converge may look a bit different than the SHM annual conference we are accustomed to, I am confident the content will be among the best we have ever offered, spanning a broad range of clinical topics and issues affecting hospitalists and their patients,” said Daniel Steinberg, MD, SFHM, course director for SHM Converge. “This virtual experience will unite hospitalists from around the globe and connect them with renowned faculty members and thought leaders in hospital medicine – as well as with their hospitalist colleagues they look forward to reconnecting with each year.”
Keynote speaker announcements are forthcoming.
Registration for SHM Converge opens in November 2020. Learn more at shmconverge.org.
Members of the media can obtain press passes beginning in November 2020 by contacting [email protected].
Increasing racial diversity in hospital medicine’s leadership ranks
Have you ever done something where you’re not quite sure why you did it at the time, but later on you realize it was part of some larger cosmic purpose, and you go, “Ahhh, now I understand…that’s why!”? Call it a fortuitous coincidence. Or a subconscious act of anticipation. Maybe a little push from God.

Last summer, as SHM’s Practice Analysis Committee was planning the State of Hospital Medicine survey for 2020, we received a request from SHM’s Diversity, Equity & Inclusion (DEI) Special Interest Group (SIG) to include a series of questions related to hospitalist gender, race and ethnic distribution in the new survey. We’ve generally resisted doing things like this because the SoHM is designed to capture data at the group level, not the individual level – and honestly, it’s as much as a lot of groups can do to tell us reliably how many FTEs they have, much less provide details about individual providers. In addition, the survey is already really long, and we are always looking for ways to make it shorter and easier for participants while still collecting the information report users care most about.
But we wanted to take the asks from the DEI SIG seriously, and as we considered their request, we realized that though it wasn’t practical to collect this information for individual hospital medicine group (HMG) members, we could collect it for group leaders. Little did we know last summer that issues of gender and racial diversity and equity would be so front-and-center right now, as we prepare to release the 2020 SoHM Report in early September. Ahhh, now I understand…that’s why – with the prompting of the DEI SIG – we so fortuitously chose to include those questions this year!
Here’s a sneak preview of what we learned. Among SoHM respondents, 57.1% reported that the highest-ranking leader in their HMG is White, and 23.5% of highest-ranking leaders are Asian. Only 5.5% of HMG leaders were Black/African American. Ethnicity was a separate question, and only 2.2% of HMG leaders were reported as Hispanic/Latino.
I have been profoundly moved by the wretched deaths of George Floyd and other people of color at the hands of police in recent months, and by the subsequent protests and our growing national reckoning over issues of racial equity and justice. In my efforts to understand more about race in America, I have been challenged by my friend Ryan Brown, MD, specialty medical director for hospital medicine with Atrium Health in Charlotte, N.C., and others to go beyond just learning about these issues. I want to use my voice to advocate for change, and my actions to participate in effecting change, within the context of my sphere of influence.
So, what does that have to do with the SoHM data on HMG leader demographics? Well, it’s clear that Black and brown people are woefully underrepresented in the ranks of hospital medicine leadership.
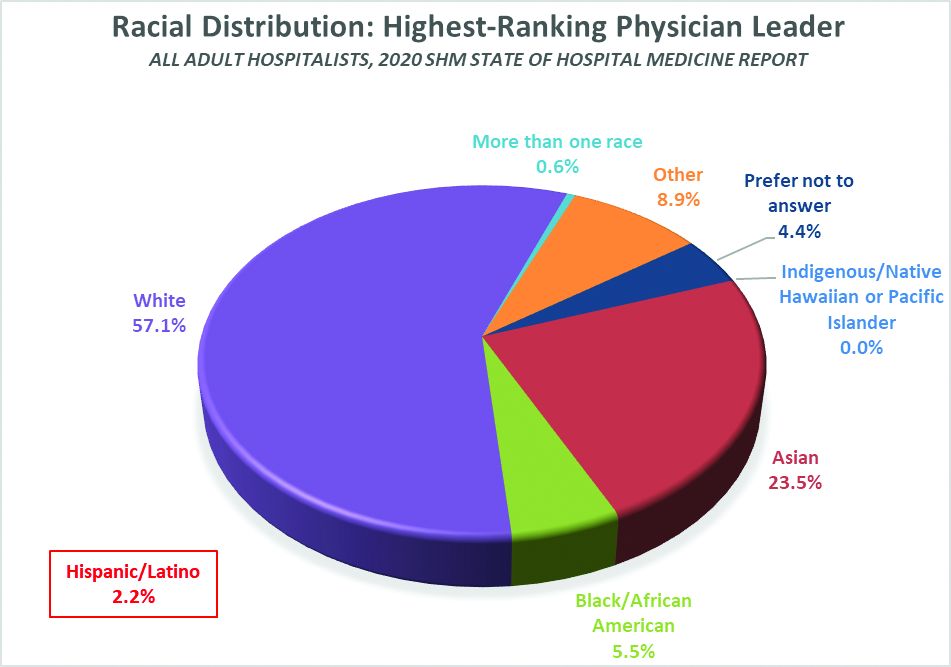
Unfortunately, we don’t have good information on racial diversity for hospitalists as a specialty, though I understand that SHM is working on plans to update membership profiles to begin collecting this information. In searching the Internet, I found a 2018 paper from the Journal of Health Care for the Poor and Underserved that studied racial and ethnic distribution of U.S. primary care physicians (doi: 10.1353/hpu.2018.0036). It reported that, in 2012, 7.8% of general internists were Black, along with 5.8% of family medicine/general practice physicians and 6.8% of pediatricians. A separate data set issued by the Association of American Medical Colleges reported that, in 2019, 6.4% of all actively practicing general internal medicine doctors were Black (5.5% of male IM physicians and 7.9% of female IM physicians). While this doesn’t mean hospitalists have the same racial and ethnic distribution, this is probably the best proxy we can come up with.
At first glance, having 5.5% of HMG leaders who are Black doesn’t seem terribly out of line with the reported range of 6.4 to 7.8% in the general population of internal medicine physicians (apologies to the family medicine and pediatric hospitalists reading this, but I’ll confine my discussion to internists for ease and brevity, since they represent the vast majority of the nation’s hospitalists). But do the math. It means Black hospitalists are likely underrepresented in HMG leadership ranks by something like 14% to 29% compared to their likely presence among hospitalists in general.
The real problem, of course, is that according the U.S. Census Bureau, 13.4% of the U.S. population is Black. So even if the racial distribution of HMG leaders catches up to the general hospitalist population, hospital medicine is still woefully underrepresenting the racial and ethnic distribution of our patient population.
The disconnect between the ethnic distribution of HMG leaders vs. hospitalists (based on general internal medicine distribution) is even more pronounced for Latinos. The JHCPU paper reported that, in 2012, 5.6% of general internists were Hispanic. The AAMC data set reported 5.8% of IM doctors were Hispanic/Latino. But only 2.2% of SoHM respondent HMGs reported a Hispanic/Latino leader, which means Latinos are underrepresented by somewhere around 61% or so relative to the likely hospitalist population, and by a whole lot more considering the fact that Latinos make up about 18.5% of the U.S. population.
I’m not saying that a White or Asian doctor can’t provide skilled, compassionate care to a Black or Latino patient, or vice-versa. It happens every day. I guess what I am saying is that we as a country and in the medical profession need to do a better job of creating pathways and promoting careers in medicine for people of color. A JAMA paper from 2019 reported that while the numbers and proportions of minority medical school matriculants has slowly been increasing from 2002 to 2017, the rate of increase was “slower than their age-matched counterparts in the U.S. population, resulting in increased underrepresentation” (doi:10.1001/jamanetworkopen.2019.10490). This means we’re falling behind, not catching up.
We need to make sure that people like Dr. Ryan Brown aren’t discouraged from pursuing medicine by teachers or school counselors because of their skin color or accent, or their gender or sexual orientation. And among those who become doctors, we need to promote hospital medicine as a desirable specialty for people of color and actively invite them in.
In my view, much of this starts with creating more and better paths to leadership within hospital medicine for people of color. Hospital medicine group leaders wield enormous – and increasing – influence, not only within their HMGs and within SHM, but within their institutions and health care systems. We need their voices and their influence to promote diversity within their groups, their institutions, within hospital medicine, and within medicine and the U.S. health care system more broadly.
The Society of Hospital Medicine is already taking steps to promote diversity, equity and inclusion. These include issuing a formal Diversity and Inclusion Statement, creating the DEI SIG, and the recent formation of a Board-designated DEI task force charged with making recommendations to promote DEI within SHM and in hospital medicine more broadly. But I want to challenge SHM to do more, particularly with regard to promoting diversity in leadership. Here are a few ideas to consider:
- Create and sponsor a mentoring program in which hospitalists volunteer to mentor minority junior high and high school students and help them prepare to pursue a career in medicine.
- Develop a formal, structured advocacy or collaboration effort with organizations like AAMC and the Accreditation Council for Graduate Medical Education designed to promote meaningful increases in the proportion of medical school students and residents who are people of color, and in the proportion who choose primary care – and ultimately, hospital medicine.
- Work hard to collect reliable racial, ethnic and gender information about SHM members and consider collaborating with MGMA to incorporate demographic questions into its survey tool for individual hospitalist compensation and productivity data. Challenge us on the Practice Analysis Committee who are responsible for the SoHM survey to continue surveying leadership demographics, and to consider how we can expand our collection of DEI information in 2022.
- Undertake a public relations campaign to highlight to health systems and other employers the under-representation of Black and Latino hospitalists in leadership positions, and to promote conscious efforts to increase those ranks.
- Create scholarships for hospitalists from underrepresented racial and ethnic groups to attend SHM-sponsored leadership development programs such as Leadership Academy, Academic Hospitalist Academy, and Quality and Safety Educators Academy, with the goal of increasing their ranks in positions of influence throughout healthcare. A scholarship program might even include raising funds to help minority hospitalists pursue Master’s-level programs such as an MBA, MHA, or MMM.
- Develop an educational track, mentoring program, or other support initiative for early-career hospitalist leaders and those interested in developing leadership skills, and ensure it gives specific attention to strategies for increasing the proportion of hospitalists of color in leadership positions.
- Review and revise existing SHM documents such as The Key Principles and Characteristics of an Effective Hospital Medicine Group, the Core Competencies in Hospital Medicine, and various white papers and position statements to ensure they address diversity, equity and inclusion – both with regard to the hospital medicine workforce and leadership, and with regard to patient care and eliminating health disparities.
I’m sure there are plenty of other similar actions we can take that I haven’t thought of. But we need to start the conversation about concrete steps our Society, and the medical specialty we represent, can take to foster real change. And then, we need to follow our words up with actions.
Ms. Flores is a partner at Nelson Flores Hospital Medicine Consultants in La Quinta, Calif. She serves on SHM’s Practice Analysis and Annual Conference Committees and helps to coordinate SHM’s biannual State of Hospital Medicine survey.
Have you ever done something where you’re not quite sure why you did it at the time, but later on you realize it was part of some larger cosmic purpose, and you go, “Ahhh, now I understand…that’s why!”? Call it a fortuitous coincidence. Or a subconscious act of anticipation. Maybe a little push from God.
Last summer, as SHM’s Practice Analysis Committee was planning the State of Hospital Medicine survey for 2020, we received a request from SHM’s Diversity, Equity & Inclusion (DEI) Special Interest Group (SIG) to include a series of questions related to hospitalist gender, race and ethnic distribution in the new survey. We’ve generally resisted doing things like this because the SoHM is designed to capture data at the group level, not the individual level – and honestly, it’s as much as a lot of groups can do to tell us reliably how many FTEs they have, much less provide details about individual providers. In addition, the survey is already really long, and we are always looking for ways to make it shorter and easier for participants while still collecting the information report users care most about.
But we wanted to take the asks from the DEI SIG seriously, and as we considered their request, we realized that though it wasn’t practical to collect this information for individual hospital medicine group (HMG) members, we could collect it for group leaders. Little did we know last summer that issues of gender and racial diversity and equity would be so front-and-center right now, as we prepare to release the 2020 SoHM Report in early September. Ahhh, now I understand…that’s why – with the prompting of the DEI SIG – we so fortuitously chose to include those questions this year!
Here’s a sneak preview of what we learned. Among SoHM respondents, 57.1% reported that the highest-ranking leader in their HMG is White, and 23.5% of highest-ranking leaders are Asian. Only 5.5% of HMG leaders were Black/African American. Ethnicity was a separate question, and only 2.2% of HMG leaders were reported as Hispanic/Latino.
I have been profoundly moved by the wretched deaths of George Floyd and other people of color at the hands of police in recent months, and by the subsequent protests and our growing national reckoning over issues of racial equity and justice. In my efforts to understand more about race in America, I have been challenged by my friend Ryan Brown, MD, specialty medical director for hospital medicine with Atrium Health in Charlotte, N.C., and others to go beyond just learning about these issues. I want to use my voice to advocate for change, and my actions to participate in effecting change, within the context of my sphere of influence.
So, what does that have to do with the SoHM data on HMG leader demographics? Well, it’s clear that Black and brown people are woefully underrepresented in the ranks of hospital medicine leadership.
Unfortunately, we don’t have good information on racial diversity for hospitalists as a specialty, though I understand that SHM is working on plans to update membership profiles to begin collecting this information. In searching the Internet, I found a 2018 paper from the Journal of Health Care for the Poor and Underserved that studied racial and ethnic distribution of U.S. primary care physicians (doi: 10.1353/hpu.2018.0036). It reported that, in 2012, 7.8% of general internists were Black, along with 5.8% of family medicine/general practice physicians and 6.8% of pediatricians. A separate data set issued by the Association of American Medical Colleges reported that, in 2019, 6.4% of all actively practicing general internal medicine doctors were Black (5.5% of male IM physicians and 7.9% of female IM physicians). While this doesn’t mean hospitalists have the same racial and ethnic distribution, this is probably the best proxy we can come up with.
At first glance, having 5.5% of HMG leaders who are Black doesn’t seem terribly out of line with the reported range of 6.4 to 7.8% in the general population of internal medicine physicians (apologies to the family medicine and pediatric hospitalists reading this, but I’ll confine my discussion to internists for ease and brevity, since they represent the vast majority of the nation’s hospitalists). But do the math. It means Black hospitalists are likely underrepresented in HMG leadership ranks by something like 14% to 29% compared to their likely presence among hospitalists in general.
The real problem, of course, is that according the U.S. Census Bureau, 13.4% of the U.S. population is Black. So even if the racial distribution of HMG leaders catches up to the general hospitalist population, hospital medicine is still woefully underrepresenting the racial and ethnic distribution of our patient population.
The disconnect between the ethnic distribution of HMG leaders vs. hospitalists (based on general internal medicine distribution) is even more pronounced for Latinos. The JHCPU paper reported that, in 2012, 5.6% of general internists were Hispanic. The AAMC data set reported 5.8% of IM doctors were Hispanic/Latino. But only 2.2% of SoHM respondent HMGs reported a Hispanic/Latino leader, which means Latinos are underrepresented by somewhere around 61% or so relative to the likely hospitalist population, and by a whole lot more considering the fact that Latinos make up about 18.5% of the U.S. population.
I’m not saying that a White or Asian doctor can’t provide skilled, compassionate care to a Black or Latino patient, or vice-versa. It happens every day. I guess what I am saying is that we as a country and in the medical profession need to do a better job of creating pathways and promoting careers in medicine for people of color. A JAMA paper from 2019 reported that while the numbers and proportions of minority medical school matriculants has slowly been increasing from 2002 to 2017, the rate of increase was “slower than their age-matched counterparts in the U.S. population, resulting in increased underrepresentation” (doi:10.1001/jamanetworkopen.2019.10490). This means we’re falling behind, not catching up.
We need to make sure that people like Dr. Ryan Brown aren’t discouraged from pursuing medicine by teachers or school counselors because of their skin color or accent, or their gender or sexual orientation. And among those who become doctors, we need to promote hospital medicine as a desirable specialty for people of color and actively invite them in.
In my view, much of this starts with creating more and better paths to leadership within hospital medicine for people of color. Hospital medicine group leaders wield enormous – and increasing – influence, not only within their HMGs and within SHM, but within their institutions and health care systems. We need their voices and their influence to promote diversity within their groups, their institutions, within hospital medicine, and within medicine and the U.S. health care system more broadly.
The Society of Hospital Medicine is already taking steps to promote diversity, equity and inclusion. These include issuing a formal Diversity and Inclusion Statement, creating the DEI SIG, and the recent formation of a Board-designated DEI task force charged with making recommendations to promote DEI within SHM and in hospital medicine more broadly. But I want to challenge SHM to do more, particularly with regard to promoting diversity in leadership. Here are a few ideas to consider:
- Create and sponsor a mentoring program in which hospitalists volunteer to mentor minority junior high and high school students and help them prepare to pursue a career in medicine.
- Develop a formal, structured advocacy or collaboration effort with organizations like AAMC and the Accreditation Council for Graduate Medical Education designed to promote meaningful increases in the proportion of medical school students and residents who are people of color, and in the proportion who choose primary care – and ultimately, hospital medicine.
- Work hard to collect reliable racial, ethnic and gender information about SHM members and consider collaborating with MGMA to incorporate demographic questions into its survey tool for individual hospitalist compensation and productivity data. Challenge us on the Practice Analysis Committee who are responsible for the SoHM survey to continue surveying leadership demographics, and to consider how we can expand our collection of DEI information in 2022.
- Undertake a public relations campaign to highlight to health systems and other employers the under-representation of Black and Latino hospitalists in leadership positions, and to promote conscious efforts to increase those ranks.
- Create scholarships for hospitalists from underrepresented racial and ethnic groups to attend SHM-sponsored leadership development programs such as Leadership Academy, Academic Hospitalist Academy, and Quality and Safety Educators Academy, with the goal of increasing their ranks in positions of influence throughout healthcare. A scholarship program might even include raising funds to help minority hospitalists pursue Master’s-level programs such as an MBA, MHA, or MMM.
- Develop an educational track, mentoring program, or other support initiative for early-career hospitalist leaders and those interested in developing leadership skills, and ensure it gives specific attention to strategies for increasing the proportion of hospitalists of color in leadership positions.
- Review and revise existing SHM documents such as The Key Principles and Characteristics of an Effective Hospital Medicine Group, the Core Competencies in Hospital Medicine, and various white papers and position statements to ensure they address diversity, equity and inclusion – both with regard to the hospital medicine workforce and leadership, and with regard to patient care and eliminating health disparities.
I’m sure there are plenty of other similar actions we can take that I haven’t thought of. But we need to start the conversation about concrete steps our Society, and the medical specialty we represent, can take to foster real change. And then, we need to follow our words up with actions.
Ms. Flores is a partner at Nelson Flores Hospital Medicine Consultants in La Quinta, Calif. She serves on SHM’s Practice Analysis and Annual Conference Committees and helps to coordinate SHM’s biannual State of Hospital Medicine survey.
Have you ever done something where you’re not quite sure why you did it at the time, but later on you realize it was part of some larger cosmic purpose, and you go, “Ahhh, now I understand…that’s why!”? Call it a fortuitous coincidence. Or a subconscious act of anticipation. Maybe a little push from God.
Last summer, as SHM’s Practice Analysis Committee was planning the State of Hospital Medicine survey for 2020, we received a request from SHM’s Diversity, Equity & Inclusion (DEI) Special Interest Group (SIG) to include a series of questions related to hospitalist gender, race and ethnic distribution in the new survey. We’ve generally resisted doing things like this because the SoHM is designed to capture data at the group level, not the individual level – and honestly, it’s as much as a lot of groups can do to tell us reliably how many FTEs they have, much less provide details about individual providers. In addition, the survey is already really long, and we are always looking for ways to make it shorter and easier for participants while still collecting the information report users care most about.
But we wanted to take the asks from the DEI SIG seriously, and as we considered their request, we realized that though it wasn’t practical to collect this information for individual hospital medicine group (HMG) members, we could collect it for group leaders. Little did we know last summer that issues of gender and racial diversity and equity would be so front-and-center right now, as we prepare to release the 2020 SoHM Report in early September. Ahhh, now I understand…that’s why – with the prompting of the DEI SIG – we so fortuitously chose to include those questions this year!
Here’s a sneak preview of what we learned. Among SoHM respondents, 57.1% reported that the highest-ranking leader in their HMG is White, and 23.5% of highest-ranking leaders are Asian. Only 5.5% of HMG leaders were Black/African American. Ethnicity was a separate question, and only 2.2% of HMG leaders were reported as Hispanic/Latino.
I have been profoundly moved by the wretched deaths of George Floyd and other people of color at the hands of police in recent months, and by the subsequent protests and our growing national reckoning over issues of racial equity and justice. In my efforts to understand more about race in America, I have been challenged by my friend Ryan Brown, MD, specialty medical director for hospital medicine with Atrium Health in Charlotte, N.C., and others to go beyond just learning about these issues. I want to use my voice to advocate for change, and my actions to participate in effecting change, within the context of my sphere of influence.
So, what does that have to do with the SoHM data on HMG leader demographics? Well, it’s clear that Black and brown people are woefully underrepresented in the ranks of hospital medicine leadership.
Unfortunately, we don’t have good information on racial diversity for hospitalists as a specialty, though I understand that SHM is working on plans to update membership profiles to begin collecting this information. In searching the Internet, I found a 2018 paper from the Journal of Health Care for the Poor and Underserved that studied racial and ethnic distribution of U.S. primary care physicians (doi: 10.1353/hpu.2018.0036). It reported that, in 2012, 7.8% of general internists were Black, along with 5.8% of family medicine/general practice physicians and 6.8% of pediatricians. A separate data set issued by the Association of American Medical Colleges reported that, in 2019, 6.4% of all actively practicing general internal medicine doctors were Black (5.5% of male IM physicians and 7.9% of female IM physicians). While this doesn’t mean hospitalists have the same racial and ethnic distribution, this is probably the best proxy we can come up with.
At first glance, having 5.5% of HMG leaders who are Black doesn’t seem terribly out of line with the reported range of 6.4 to 7.8% in the general population of internal medicine physicians (apologies to the family medicine and pediatric hospitalists reading this, but I’ll confine my discussion to internists for ease and brevity, since they represent the vast majority of the nation’s hospitalists). But do the math. It means Black hospitalists are likely underrepresented in HMG leadership ranks by something like 14% to 29% compared to their likely presence among hospitalists in general.
The real problem, of course, is that according the U.S. Census Bureau, 13.4% of the U.S. population is Black. So even if the racial distribution of HMG leaders catches up to the general hospitalist population, hospital medicine is still woefully underrepresenting the racial and ethnic distribution of our patient population.
The disconnect between the ethnic distribution of HMG leaders vs. hospitalists (based on general internal medicine distribution) is even more pronounced for Latinos. The JHCPU paper reported that, in 2012, 5.6% of general internists were Hispanic. The AAMC data set reported 5.8% of IM doctors were Hispanic/Latino. But only 2.2% of SoHM respondent HMGs reported a Hispanic/Latino leader, which means Latinos are underrepresented by somewhere around 61% or so relative to the likely hospitalist population, and by a whole lot more considering the fact that Latinos make up about 18.5% of the U.S. population.
I’m not saying that a White or Asian doctor can’t provide skilled, compassionate care to a Black or Latino patient, or vice-versa. It happens every day. I guess what I am saying is that we as a country and in the medical profession need to do a better job of creating pathways and promoting careers in medicine for people of color. A JAMA paper from 2019 reported that while the numbers and proportions of minority medical school matriculants has slowly been increasing from 2002 to 2017, the rate of increase was “slower than their age-matched counterparts in the U.S. population, resulting in increased underrepresentation” (doi:10.1001/jamanetworkopen.2019.10490). This means we’re falling behind, not catching up.
We need to make sure that people like Dr. Ryan Brown aren’t discouraged from pursuing medicine by teachers or school counselors because of their skin color or accent, or their gender or sexual orientation. And among those who become doctors, we need to promote hospital medicine as a desirable specialty for people of color and actively invite them in.
In my view, much of this starts with creating more and better paths to leadership within hospital medicine for people of color. Hospital medicine group leaders wield enormous – and increasing – influence, not only within their HMGs and within SHM, but within their institutions and health care systems. We need their voices and their influence to promote diversity within their groups, their institutions, within hospital medicine, and within medicine and the U.S. health care system more broadly.
The Society of Hospital Medicine is already taking steps to promote diversity, equity and inclusion. These include issuing a formal Diversity and Inclusion Statement, creating the DEI SIG, and the recent formation of a Board-designated DEI task force charged with making recommendations to promote DEI within SHM and in hospital medicine more broadly. But I want to challenge SHM to do more, particularly with regard to promoting diversity in leadership. Here are a few ideas to consider:
- Create and sponsor a mentoring program in which hospitalists volunteer to mentor minority junior high and high school students and help them prepare to pursue a career in medicine.
- Develop a formal, structured advocacy or collaboration effort with organizations like AAMC and the Accreditation Council for Graduate Medical Education designed to promote meaningful increases in the proportion of medical school students and residents who are people of color, and in the proportion who choose primary care – and ultimately, hospital medicine.
- Work hard to collect reliable racial, ethnic and gender information about SHM members and consider collaborating with MGMA to incorporate demographic questions into its survey tool for individual hospitalist compensation and productivity data. Challenge us on the Practice Analysis Committee who are responsible for the SoHM survey to continue surveying leadership demographics, and to consider how we can expand our collection of DEI information in 2022.
- Undertake a public relations campaign to highlight to health systems and other employers the under-representation of Black and Latino hospitalists in leadership positions, and to promote conscious efforts to increase those ranks.
- Create scholarships for hospitalists from underrepresented racial and ethnic groups to attend SHM-sponsored leadership development programs such as Leadership Academy, Academic Hospitalist Academy, and Quality and Safety Educators Academy, with the goal of increasing their ranks in positions of influence throughout healthcare. A scholarship program might even include raising funds to help minority hospitalists pursue Master’s-level programs such as an MBA, MHA, or MMM.
- Develop an educational track, mentoring program, or other support initiative for early-career hospitalist leaders and those interested in developing leadership skills, and ensure it gives specific attention to strategies for increasing the proportion of hospitalists of color in leadership positions.
- Review and revise existing SHM documents such as The Key Principles and Characteristics of an Effective Hospital Medicine Group, the Core Competencies in Hospital Medicine, and various white papers and position statements to ensure they address diversity, equity and inclusion – both with regard to the hospital medicine workforce and leadership, and with regard to patient care and eliminating health disparities.
I’m sure there are plenty of other similar actions we can take that I haven’t thought of. But we need to start the conversation about concrete steps our Society, and the medical specialty we represent, can take to foster real change. And then, we need to follow our words up with actions.
Ms. Flores is a partner at Nelson Flores Hospital Medicine Consultants in La Quinta, Calif. She serves on SHM’s Practice Analysis and Annual Conference Committees and helps to coordinate SHM’s biannual State of Hospital Medicine survey.
Calendar
For more information about upcoming events and award deadlines, please visit http://agau.gastro.org and http://www.gastro.org/research-funding.
UPCOMING EVENTS
Jan. 15-17, 2021
Gastrointestinal Cancers Symposium
Through an engaging lineup of novel science, education, and exhibits, the virtual 2021 Gastrointestinal (GI) Cancers Symposium offers new, innovative findings in GI cancer treatment, research, and care.
Early-bird deadline: Dec. 16, 2020.

Jan. 21-24, 2021
Crohn’s & Colitis Congress®Join health care professionals and researchers virtually at the Crohn’s & Colitis Congress® for the premier conference on IBD. Discover different perspectives, practical information you can immediately implement, and potential treatments on the horizon.
Early-bird deadline: Friday, Nov. 6, 2020.
May 21-23, 2021
Digestive Disease Week® (DDW)
Save the date for the world’s leading event in digestive disease. DDW® brings professionals in gastroenterology, hepatology, endoscopy, and GI surgery together. Experience growth when you share your research, converge with trailblazers, and improve the lives of patients suffering from GI and liver diseases.
Abstract submission window Oct. 15 to Dec. 3, 2020.
AWARD DEADLINES
American Gastroenterological Association (AGA) Student Abstract Award
This $500 travel award supports recipients who are graduate students, medical students,or medical residents (residents up to postgraduate year 3) giving abstract-based oral or poster presentations at Digestive Disease Week® (DDW). The top-scoring abstract will be designated the Student Abstract of the Year and receive a $1,000 award.
Application deadline: Feb. 24, 2021
AGA–Moti L. & Kamla Rustgi International Travel Awards
This $750 travel award provides support to early-career (that is, 35 years of age or younger at the time of DDW) basic, translational or clinical investigators residing outside North America to offset travel and related expenses to attend DDW.
Application deadline: Feb. 24, 2021
AGA Fellow Abstract Award
This $500 travel award supports recipients who are MD, PhD, or equivalent fellows giving abstract-based oral or poster presentations DDW. The top-scoring abstract will be designated the Fellow Abstract of the Year and receive a $1,000 award.
Application deadline: Feb. 24, 2021
For more information about upcoming events and award deadlines, please visit http://agau.gastro.org and http://www.gastro.org/research-funding.
UPCOMING EVENTS
Jan. 15-17, 2021
Gastrointestinal Cancers Symposium
Through an engaging lineup of novel science, education, and exhibits, the virtual 2021 Gastrointestinal (GI) Cancers Symposium offers new, innovative findings in GI cancer treatment, research, and care.
Early-bird deadline: Dec. 16, 2020.
Jan. 21-24, 2021
Crohn’s & Colitis Congress®Join health care professionals and researchers virtually at the Crohn’s & Colitis Congress® for the premier conference on IBD. Discover different perspectives, practical information you can immediately implement, and potential treatments on the horizon.
Early-bird deadline: Friday, Nov. 6, 2020.
May 21-23, 2021
Digestive Disease Week® (DDW)
Save the date for the world’s leading event in digestive disease. DDW® brings professionals in gastroenterology, hepatology, endoscopy, and GI surgery together. Experience growth when you share your research, converge with trailblazers, and improve the lives of patients suffering from GI and liver diseases.
Abstract submission window Oct. 15 to Dec. 3, 2020.
AWARD DEADLINES
American Gastroenterological Association (AGA) Student Abstract Award
This $500 travel award supports recipients who are graduate students, medical students,or medical residents (residents up to postgraduate year 3) giving abstract-based oral or poster presentations at Digestive Disease Week® (DDW). The top-scoring abstract will be designated the Student Abstract of the Year and receive a $1,000 award.
Application deadline: Feb. 24, 2021
AGA–Moti L. & Kamla Rustgi International Travel Awards
This $750 travel award provides support to early-career (that is, 35 years of age or younger at the time of DDW) basic, translational or clinical investigators residing outside North America to offset travel and related expenses to attend DDW.
Application deadline: Feb. 24, 2021
AGA Fellow Abstract Award
This $500 travel award supports recipients who are MD, PhD, or equivalent fellows giving abstract-based oral or poster presentations DDW. The top-scoring abstract will be designated the Fellow Abstract of the Year and receive a $1,000 award.
Application deadline: Feb. 24, 2021
For more information about upcoming events and award deadlines, please visit http://agau.gastro.org and http://www.gastro.org/research-funding.
UPCOMING EVENTS
Jan. 15-17, 2021
Gastrointestinal Cancers Symposium
Through an engaging lineup of novel science, education, and exhibits, the virtual 2021 Gastrointestinal (GI) Cancers Symposium offers new, innovative findings in GI cancer treatment, research, and care.
Early-bird deadline: Dec. 16, 2020.
Jan. 21-24, 2021
Crohn’s & Colitis Congress®Join health care professionals and researchers virtually at the Crohn’s & Colitis Congress® for the premier conference on IBD. Discover different perspectives, practical information you can immediately implement, and potential treatments on the horizon.
Early-bird deadline: Friday, Nov. 6, 2020.
May 21-23, 2021
Digestive Disease Week® (DDW)
Save the date for the world’s leading event in digestive disease. DDW® brings professionals in gastroenterology, hepatology, endoscopy, and GI surgery together. Experience growth when you share your research, converge with trailblazers, and improve the lives of patients suffering from GI and liver diseases.
Abstract submission window Oct. 15 to Dec. 3, 2020.
AWARD DEADLINES
American Gastroenterological Association (AGA) Student Abstract Award
This $500 travel award supports recipients who are graduate students, medical students,or medical residents (residents up to postgraduate year 3) giving abstract-based oral or poster presentations at Digestive Disease Week® (DDW). The top-scoring abstract will be designated the Student Abstract of the Year and receive a $1,000 award.
Application deadline: Feb. 24, 2021
AGA–Moti L. & Kamla Rustgi International Travel Awards
This $750 travel award provides support to early-career (that is, 35 years of age or younger at the time of DDW) basic, translational or clinical investigators residing outside North America to offset travel and related expenses to attend DDW.
Application deadline: Feb. 24, 2021
AGA Fellow Abstract Award
This $500 travel award supports recipients who are MD, PhD, or equivalent fellows giving abstract-based oral or poster presentations DDW. The top-scoring abstract will be designated the Fellow Abstract of the Year and receive a $1,000 award.
Application deadline: Feb. 24, 2021
