User login
Harnessing Doxycycline for STI Prevention: A Vital Role for Primary Care Physicians
Primary care physicians frequently offer postexposure prophylaxis for various infections, including influenza, pertussis, tetanus, hepatitis, and Lyme disease, among others. However, the scope of postexposure prophylaxis in primary care is expanding, presenting an opportunity to further integrate it into patient care. As primary care providers, we have the unique advantage of being involved in both preventive care and immediate response, particularly in urgent care or triage scenarios. This dual role is crucial, as timely administration of postexposure prophylaxis can prevent infections from taking hold, especially following high-risk exposures.
Recently, the use of doxycycline as a form of postexposure prophylaxis for sexually transmitted infections (STIs) has gained attention. Traditionally, doxycycline has been used as preexposure or postexposure prophylaxis for conditions like malaria and Lyme disease but has not been widely employed for STI prevention until now. Doxycycline is a relatively common medication, generally safe with side effects that typically resolve upon discontinuation. Several open-label studies have shown that taking 200 mg of doxycycline within 72 hours of condomless sex significantly reduces the incidence of chlamydia, gonorrhea, and syphilis among gay, bisexual, and other men who have sex with men, as well as transgender women who have previously had a bacterial STI. However, these benefits have not been consistently observed among cisgender women and heterosexual men.

Given these findings, the Centers for Disease Control and Prevention now recommends that clinicians discuss the risks and benefits of doxycycline PEP (Doxy PEP) with gay, bisexual, and other men who have sex with men, as well as transgender women who have had a bacterial STI in the past 12 months. This discussion should be part of a shared decision-making process, advising the use of 200 mg of doxycycline within 72 hours of oral, vaginal, or anal sex, with the recommendation not to exceed 200 mg every 24 hours and to reassess the need for continued use every 3-6 months. Doxy PEP can be safely prescribed with preexposure prophylaxis for HIV (PrEP). Patients who receive PrEP may often be eligible for Doxy PEP, though the groups are not always the same.
The shared decision-making process is essential when considering Doxy PEP. While cost-effective and proven to reduce the risk of gonorrhea, chlamydia, and syphilis, its benefits vary among different populations. Moreover, some patients may experience side effects such as photosensitivity and gastrointestinal discomfort. Since the effectiveness of prophylaxis is closely tied to the timing of exposure and the patient’s current risk factors, it is important to regularly evaluate whether Doxy PEP remains beneficial. As there is not yet clear benefit to heterosexual men and cisgender women, opportunities still need to be explored for them.
Integrating Doxy PEP into a primary care practice can be done efficiently. A standing order protocol could be established for telehealth visits or nurse triage, allowing timely administration when patients report an exposure within 72 hours. It could also be incorporated into electronic medical records as part of a smart set for easy access to orders and as standard educational material in after-visit instructions. As this option is new, it is also important to discuss it with patients before they may need it so that they are aware should the need arise. While concerns about antibiotic resistance are valid, studies have not yet shown significant resistance issues related to Doxy PEP use, though ongoing monitoring is necessary.
You might wonder why primary care should prioritize this intervention. As the first point of contact, primary care providers are well-positioned to identify the need for prophylaxis, particularly since its effectiveness diminishes over time. Furthermore, the established, trusting relationships that primary care physicians often have with their patients create a nonjudgmental environment that encourages disclosure of potential exposures. This trust, combined with easier access to care, can make a significant difference in the timely provision of postexposure prophylaxis. By offering comprehensive, holistic care, including prophylaxis, primary care physicians can prevent infections and address conditions before they lead to serious complications. Therefore, family medicine physicians should consider incorporating Doxy PEP into their practices as a standard of care.
Dr. Wheat is vice chair of Diversity, Equity, and Inclusion, Department of Family and Community Medicine, and associate professor, Family and Community Medicine, at Northwestern University’s Feinberg School of Medicine, Chicago. She has no relevant financial disclosures.
References
Bachmann LH et al. CDC Clinical Guidelines on the Use of Doxycycline Postexposure Prophylaxis for Bacterial Sexually Transmitted Infection Prevention, United States, 2024. MMWR Recomm Rep 2024;73(No. RR-2):1-8.
Traeger MW et al. Potential Impact of Doxycycline Postexposure Prophylaxis Prescribing Strategies on Incidence of Bacterial Sexually Transmitted Infections. (Clin Infect Dis. 2023 Aug 18. doi: 10.1093/cid/ciad488).
Primary care physicians frequently offer postexposure prophylaxis for various infections, including influenza, pertussis, tetanus, hepatitis, and Lyme disease, among others. However, the scope of postexposure prophylaxis in primary care is expanding, presenting an opportunity to further integrate it into patient care. As primary care providers, we have the unique advantage of being involved in both preventive care and immediate response, particularly in urgent care or triage scenarios. This dual role is crucial, as timely administration of postexposure prophylaxis can prevent infections from taking hold, especially following high-risk exposures.
Recently, the use of doxycycline as a form of postexposure prophylaxis for sexually transmitted infections (STIs) has gained attention. Traditionally, doxycycline has been used as preexposure or postexposure prophylaxis for conditions like malaria and Lyme disease but has not been widely employed for STI prevention until now. Doxycycline is a relatively common medication, generally safe with side effects that typically resolve upon discontinuation. Several open-label studies have shown that taking 200 mg of doxycycline within 72 hours of condomless sex significantly reduces the incidence of chlamydia, gonorrhea, and syphilis among gay, bisexual, and other men who have sex with men, as well as transgender women who have previously had a bacterial STI. However, these benefits have not been consistently observed among cisgender women and heterosexual men.
Given these findings, the Centers for Disease Control and Prevention now recommends that clinicians discuss the risks and benefits of doxycycline PEP (Doxy PEP) with gay, bisexual, and other men who have sex with men, as well as transgender women who have had a bacterial STI in the past 12 months. This discussion should be part of a shared decision-making process, advising the use of 200 mg of doxycycline within 72 hours of oral, vaginal, or anal sex, with the recommendation not to exceed 200 mg every 24 hours and to reassess the need for continued use every 3-6 months. Doxy PEP can be safely prescribed with preexposure prophylaxis for HIV (PrEP). Patients who receive PrEP may often be eligible for Doxy PEP, though the groups are not always the same.
The shared decision-making process is essential when considering Doxy PEP. While cost-effective and proven to reduce the risk of gonorrhea, chlamydia, and syphilis, its benefits vary among different populations. Moreover, some patients may experience side effects such as photosensitivity and gastrointestinal discomfort. Since the effectiveness of prophylaxis is closely tied to the timing of exposure and the patient’s current risk factors, it is important to regularly evaluate whether Doxy PEP remains beneficial. As there is not yet clear benefit to heterosexual men and cisgender women, opportunities still need to be explored for them.
Integrating Doxy PEP into a primary care practice can be done efficiently. A standing order protocol could be established for telehealth visits or nurse triage, allowing timely administration when patients report an exposure within 72 hours. It could also be incorporated into electronic medical records as part of a smart set for easy access to orders and as standard educational material in after-visit instructions. As this option is new, it is also important to discuss it with patients before they may need it so that they are aware should the need arise. While concerns about antibiotic resistance are valid, studies have not yet shown significant resistance issues related to Doxy PEP use, though ongoing monitoring is necessary.
You might wonder why primary care should prioritize this intervention. As the first point of contact, primary care providers are well-positioned to identify the need for prophylaxis, particularly since its effectiveness diminishes over time. Furthermore, the established, trusting relationships that primary care physicians often have with their patients create a nonjudgmental environment that encourages disclosure of potential exposures. This trust, combined with easier access to care, can make a significant difference in the timely provision of postexposure prophylaxis. By offering comprehensive, holistic care, including prophylaxis, primary care physicians can prevent infections and address conditions before they lead to serious complications. Therefore, family medicine physicians should consider incorporating Doxy PEP into their practices as a standard of care.
Dr. Wheat is vice chair of Diversity, Equity, and Inclusion, Department of Family and Community Medicine, and associate professor, Family and Community Medicine, at Northwestern University’s Feinberg School of Medicine, Chicago. She has no relevant financial disclosures.
References
Bachmann LH et al. CDC Clinical Guidelines on the Use of Doxycycline Postexposure Prophylaxis for Bacterial Sexually Transmitted Infection Prevention, United States, 2024. MMWR Recomm Rep 2024;73(No. RR-2):1-8.
Traeger MW et al. Potential Impact of Doxycycline Postexposure Prophylaxis Prescribing Strategies on Incidence of Bacterial Sexually Transmitted Infections. (Clin Infect Dis. 2023 Aug 18. doi: 10.1093/cid/ciad488).
Primary care physicians frequently offer postexposure prophylaxis for various infections, including influenza, pertussis, tetanus, hepatitis, and Lyme disease, among others. However, the scope of postexposure prophylaxis in primary care is expanding, presenting an opportunity to further integrate it into patient care. As primary care providers, we have the unique advantage of being involved in both preventive care and immediate response, particularly in urgent care or triage scenarios. This dual role is crucial, as timely administration of postexposure prophylaxis can prevent infections from taking hold, especially following high-risk exposures.
Recently, the use of doxycycline as a form of postexposure prophylaxis for sexually transmitted infections (STIs) has gained attention. Traditionally, doxycycline has been used as preexposure or postexposure prophylaxis for conditions like malaria and Lyme disease but has not been widely employed for STI prevention until now. Doxycycline is a relatively common medication, generally safe with side effects that typically resolve upon discontinuation. Several open-label studies have shown that taking 200 mg of doxycycline within 72 hours of condomless sex significantly reduces the incidence of chlamydia, gonorrhea, and syphilis among gay, bisexual, and other men who have sex with men, as well as transgender women who have previously had a bacterial STI. However, these benefits have not been consistently observed among cisgender women and heterosexual men.
Given these findings, the Centers for Disease Control and Prevention now recommends that clinicians discuss the risks and benefits of doxycycline PEP (Doxy PEP) with gay, bisexual, and other men who have sex with men, as well as transgender women who have had a bacterial STI in the past 12 months. This discussion should be part of a shared decision-making process, advising the use of 200 mg of doxycycline within 72 hours of oral, vaginal, or anal sex, with the recommendation not to exceed 200 mg every 24 hours and to reassess the need for continued use every 3-6 months. Doxy PEP can be safely prescribed with preexposure prophylaxis for HIV (PrEP). Patients who receive PrEP may often be eligible for Doxy PEP, though the groups are not always the same.
The shared decision-making process is essential when considering Doxy PEP. While cost-effective and proven to reduce the risk of gonorrhea, chlamydia, and syphilis, its benefits vary among different populations. Moreover, some patients may experience side effects such as photosensitivity and gastrointestinal discomfort. Since the effectiveness of prophylaxis is closely tied to the timing of exposure and the patient’s current risk factors, it is important to regularly evaluate whether Doxy PEP remains beneficial. As there is not yet clear benefit to heterosexual men and cisgender women, opportunities still need to be explored for them.
Integrating Doxy PEP into a primary care practice can be done efficiently. A standing order protocol could be established for telehealth visits or nurse triage, allowing timely administration when patients report an exposure within 72 hours. It could also be incorporated into electronic medical records as part of a smart set for easy access to orders and as standard educational material in after-visit instructions. As this option is new, it is also important to discuss it with patients before they may need it so that they are aware should the need arise. While concerns about antibiotic resistance are valid, studies have not yet shown significant resistance issues related to Doxy PEP use, though ongoing monitoring is necessary.
You might wonder why primary care should prioritize this intervention. As the first point of contact, primary care providers are well-positioned to identify the need for prophylaxis, particularly since its effectiveness diminishes over time. Furthermore, the established, trusting relationships that primary care physicians often have with their patients create a nonjudgmental environment that encourages disclosure of potential exposures. This trust, combined with easier access to care, can make a significant difference in the timely provision of postexposure prophylaxis. By offering comprehensive, holistic care, including prophylaxis, primary care physicians can prevent infections and address conditions before they lead to serious complications. Therefore, family medicine physicians should consider incorporating Doxy PEP into their practices as a standard of care.
Dr. Wheat is vice chair of Diversity, Equity, and Inclusion, Department of Family and Community Medicine, and associate professor, Family and Community Medicine, at Northwestern University’s Feinberg School of Medicine, Chicago. She has no relevant financial disclosures.
References
Bachmann LH et al. CDC Clinical Guidelines on the Use of Doxycycline Postexposure Prophylaxis for Bacterial Sexually Transmitted Infection Prevention, United States, 2024. MMWR Recomm Rep 2024;73(No. RR-2):1-8.
Traeger MW et al. Potential Impact of Doxycycline Postexposure Prophylaxis Prescribing Strategies on Incidence of Bacterial Sexually Transmitted Infections. (Clin Infect Dis. 2023 Aug 18. doi: 10.1093/cid/ciad488).
Imaging Tool Helps Identify Features of Nail Disorders
TOPLINE:
METHODOLOGY:
- The single-center, observational cross-sectional pilot study evaluated patients aged ≥ 7 years with newly diagnosed nail disorders between January 2022 and May 2023.
- A total of 128 patients (average age, 46.1 years; range, 8-84 years) with nail psoriasis, onychomycosis, idiopathic/traumatic onycholysis, brittle nail syndrome, nail lichen planus, retronychia, and other nail conditions and those with no nail findings (controls) were enrolled.
- Researchers performed nailfold capillaroscopy imaging and compared capillary features between patients with nail conditions and the controls.
TAKEAWAY:
- Patients with nail psoriasis had decreased capillary density and length (P < .001), more crossed and tortuous capillaries (P < .02), and increased abnormal capillary morphology (P = .03) compared with controls. Specific abnormalities, such as branching and meandering capillaries, were more common among those with nail psoriasis (both 26.5%).
- Patients with fingernail and toenail onychomycosis had a higher frequency of abnormal capillary morphology (P < .02), particularly meandering capillaries (75.0% for fingernails and 76.9% for toenails). However, other abnormalities were less frequently observed.
- Patients with nail lichen planus (P < .01), onychopapilloma (P = .01), and retronychia (P = .03) showed significantly shorter capillaries than controls. Retronychia was also associated with increased disorganized polymorphic capillaries (P = .02).
- Patients with brittle nail syndrome and eczema showed no significant differences compared with controls.
IN PRACTICE:
“Our findings highlight nailfold capillaroscopy as a potentially quick, cost-effective, and noninvasive imaging modality as an adjunct for diagnosis and treatment initiation for patients with onychodystrophies,” the authors wrote.
SOURCE:
This study was led by Jonathan K. Hwang, MD, Weill Cornell Medicine, New York City, and was published online in The Journal of the American Academy of Dermatology.
LIMITATIONS:
The study’s limitations included a small sample size for certain nail conditions and the single-center design, which limited generalizability. Additionally, the uneven surface, scaling, onycholysis, and thickening of toenails made some capillaroscopy images difficult to capture and interpret.
DISCLOSURES:
The study did not receive any funding. One author reported serving as a consultant for Eli Lilly, Ortho-Dermatologics, BelleTorus, and Moberg Pharma.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The single-center, observational cross-sectional pilot study evaluated patients aged ≥ 7 years with newly diagnosed nail disorders between January 2022 and May 2023.
- A total of 128 patients (average age, 46.1 years; range, 8-84 years) with nail psoriasis, onychomycosis, idiopathic/traumatic onycholysis, brittle nail syndrome, nail lichen planus, retronychia, and other nail conditions and those with no nail findings (controls) were enrolled.
- Researchers performed nailfold capillaroscopy imaging and compared capillary features between patients with nail conditions and the controls.
TAKEAWAY:
- Patients with nail psoriasis had decreased capillary density and length (P < .001), more crossed and tortuous capillaries (P < .02), and increased abnormal capillary morphology (P = .03) compared with controls. Specific abnormalities, such as branching and meandering capillaries, were more common among those with nail psoriasis (both 26.5%).
- Patients with fingernail and toenail onychomycosis had a higher frequency of abnormal capillary morphology (P < .02), particularly meandering capillaries (75.0% for fingernails and 76.9% for toenails). However, other abnormalities were less frequently observed.
- Patients with nail lichen planus (P < .01), onychopapilloma (P = .01), and retronychia (P = .03) showed significantly shorter capillaries than controls. Retronychia was also associated with increased disorganized polymorphic capillaries (P = .02).
- Patients with brittle nail syndrome and eczema showed no significant differences compared with controls.
IN PRACTICE:
“Our findings highlight nailfold capillaroscopy as a potentially quick, cost-effective, and noninvasive imaging modality as an adjunct for diagnosis and treatment initiation for patients with onychodystrophies,” the authors wrote.
SOURCE:
This study was led by Jonathan K. Hwang, MD, Weill Cornell Medicine, New York City, and was published online in The Journal of the American Academy of Dermatology.
LIMITATIONS:
The study’s limitations included a small sample size for certain nail conditions and the single-center design, which limited generalizability. Additionally, the uneven surface, scaling, onycholysis, and thickening of toenails made some capillaroscopy images difficult to capture and interpret.
DISCLOSURES:
The study did not receive any funding. One author reported serving as a consultant for Eli Lilly, Ortho-Dermatologics, BelleTorus, and Moberg Pharma.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The single-center, observational cross-sectional pilot study evaluated patients aged ≥ 7 years with newly diagnosed nail disorders between January 2022 and May 2023.
- A total of 128 patients (average age, 46.1 years; range, 8-84 years) with nail psoriasis, onychomycosis, idiopathic/traumatic onycholysis, brittle nail syndrome, nail lichen planus, retronychia, and other nail conditions and those with no nail findings (controls) were enrolled.
- Researchers performed nailfold capillaroscopy imaging and compared capillary features between patients with nail conditions and the controls.
TAKEAWAY:
- Patients with nail psoriasis had decreased capillary density and length (P < .001), more crossed and tortuous capillaries (P < .02), and increased abnormal capillary morphology (P = .03) compared with controls. Specific abnormalities, such as branching and meandering capillaries, were more common among those with nail psoriasis (both 26.5%).
- Patients with fingernail and toenail onychomycosis had a higher frequency of abnormal capillary morphology (P < .02), particularly meandering capillaries (75.0% for fingernails and 76.9% for toenails). However, other abnormalities were less frequently observed.
- Patients with nail lichen planus (P < .01), onychopapilloma (P = .01), and retronychia (P = .03) showed significantly shorter capillaries than controls. Retronychia was also associated with increased disorganized polymorphic capillaries (P = .02).
- Patients with brittle nail syndrome and eczema showed no significant differences compared with controls.
IN PRACTICE:
“Our findings highlight nailfold capillaroscopy as a potentially quick, cost-effective, and noninvasive imaging modality as an adjunct for diagnosis and treatment initiation for patients with onychodystrophies,” the authors wrote.
SOURCE:
This study was led by Jonathan K. Hwang, MD, Weill Cornell Medicine, New York City, and was published online in The Journal of the American Academy of Dermatology.
LIMITATIONS:
The study’s limitations included a small sample size for certain nail conditions and the single-center design, which limited generalizability. Additionally, the uneven surface, scaling, onycholysis, and thickening of toenails made some capillaroscopy images difficult to capture and interpret.
DISCLOSURES:
The study did not receive any funding. One author reported serving as a consultant for Eli Lilly, Ortho-Dermatologics, BelleTorus, and Moberg Pharma.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Locally Acquired Dengue Case Confirmed in California
A case of locally acquired dengue fever has been confirmed in a resident of Baldwin Park, California, according to a press release from the Los Angeles County Department of Public Health.
“Dengue is the most common insect-borne viral infection in the world, with a wide geographic spread; we know that we have mosquitoes capable of carrying and transmitting the virus in the United States already, and Los Angeles county is a major epicenter for international travel and trade,” James Lawler, MD, associate director for International Programs and Innovation at the Global Center for Health Security and professor in the Infectious Diseases Division at the University of Nebraska Medical Center, Omaha, Nebraska, said in an interview.
Although the patient had no known history of travel to a dengue-endemic area, the potential risk for widespread transmission of the virus in the Los Angeles County area remains low, and no additional suspected cases of locally acquired dengue have been identified, according to the release. However, the recent cases highlight the need for vigilance on the part of the public to reduce transmission of mosquito-borne infections, the public health department noted.
Most cases of dengue occur in people who have traveled to areas where the disease is more common, mainly tropical and subtropical areas, according to the press release. However, the types of mosquitoes that spread dengue exist in parts of the United States, so locally acquired infections can occur.
The Centers for Disease Control and Prevention (CDC) issued an official health advisory in June 2024 about an increased risk for dengue infections in the United States. According to the advisory, 745 cases of dengue were identified in US travelers to endemic areas between January 1, 2024, and June 24, 2024.
The CDC advises clinicians to maintain a high level of suspicion for dengue among individuals with fever and recent travel to areas with frequent dengue transmission, but also to consider locally acquired disease in areas of mosquito vectors.
In clinical practice, dengue may be difficult to differentiate from other febrile systemic infections, Dr. Lawler noted. “Joint pain, low back pain, and headache (often retro-orbital) are common and can be severe, and a rash often appears several days into illness,” he noted.
Do not delay treatment in suspected cases while waiting for test results, the CDC emphasized in the advisory. Food and Drug Administration–approved tests for dengue include RT-PCR and IgM antibody tests or NS1 and IgM antibody tests.
“Severe dengue can be life-threatening and progress to a hemorrhagic fever-like syndrome, and patients with severe dengue should be cared for on a high-acuity or intensive care setting, with close monitoring of labs and fluid status,” Dr. Lawler told this news organization.
The World Health Organization has published guidelines for the management of dengue, which Dr. Lawler strongly recommends to clinicians in the rare event that they are facing a severe case. The treatment for dengue is supportive care, according to the CDC; a vaccine that was deemed safe and effective is no longer being manufactured because of low demand.
Most symptoms last for 2-7 days, and most patients recover within a week, but approximately 1 in 20 may develop severe disease, according to the Los Angeles County Department of Public Health.
Approximately one quarter of dengue infections are symptomatic, and clinicians should know the signs of progression to severe disease, which include abdominal pain or tenderness, persistent vomiting, clinical fluid accumulation, mucosal bleeding, lethargy or restlessness, and liver enlargement, according to the CDC.
Local Dengue Not Unexpected
“Sadly, I am not surprised at another locally acquired case of dengue fever in the United States,” said Dr. Lawler. “We also have seen a trend of more historically tropical, insect-borne diseases popping up with locally acquired cases in the United States,” he noted.
Dr. Lawler suggested that “the erosion of state and local public health” is a major contributor to the increase in dengue cases. For more than 100 years, activities of state and local public health officials had significantly curtailed mosquito-borne diseases through aggressive control programs, “but we seem to be losing ground over the last several years,” he said.
“Locally acquired dengue cases are still rare in the United States,” he added. “However, people can protect themselves against dengue and more common arthropod-borne infections by taking precautions to cover up and wear insect repellent while outdoors.”
In addition, the Los Angeles County Department of Public Health emphasized in its press release that local residents reduce their risk for contact with mosquitoes by removing areas of standing water on their property and ensuring well-fitted screens on doors and windows.
Dr. Lawler had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
A case of locally acquired dengue fever has been confirmed in a resident of Baldwin Park, California, according to a press release from the Los Angeles County Department of Public Health.
“Dengue is the most common insect-borne viral infection in the world, with a wide geographic spread; we know that we have mosquitoes capable of carrying and transmitting the virus in the United States already, and Los Angeles county is a major epicenter for international travel and trade,” James Lawler, MD, associate director for International Programs and Innovation at the Global Center for Health Security and professor in the Infectious Diseases Division at the University of Nebraska Medical Center, Omaha, Nebraska, said in an interview.
Although the patient had no known history of travel to a dengue-endemic area, the potential risk for widespread transmission of the virus in the Los Angeles County area remains low, and no additional suspected cases of locally acquired dengue have been identified, according to the release. However, the recent cases highlight the need for vigilance on the part of the public to reduce transmission of mosquito-borne infections, the public health department noted.
Most cases of dengue occur in people who have traveled to areas where the disease is more common, mainly tropical and subtropical areas, according to the press release. However, the types of mosquitoes that spread dengue exist in parts of the United States, so locally acquired infections can occur.
The Centers for Disease Control and Prevention (CDC) issued an official health advisory in June 2024 about an increased risk for dengue infections in the United States. According to the advisory, 745 cases of dengue were identified in US travelers to endemic areas between January 1, 2024, and June 24, 2024.
The CDC advises clinicians to maintain a high level of suspicion for dengue among individuals with fever and recent travel to areas with frequent dengue transmission, but also to consider locally acquired disease in areas of mosquito vectors.
In clinical practice, dengue may be difficult to differentiate from other febrile systemic infections, Dr. Lawler noted. “Joint pain, low back pain, and headache (often retro-orbital) are common and can be severe, and a rash often appears several days into illness,” he noted.
Do not delay treatment in suspected cases while waiting for test results, the CDC emphasized in the advisory. Food and Drug Administration–approved tests for dengue include RT-PCR and IgM antibody tests or NS1 and IgM antibody tests.
“Severe dengue can be life-threatening and progress to a hemorrhagic fever-like syndrome, and patients with severe dengue should be cared for on a high-acuity or intensive care setting, with close monitoring of labs and fluid status,” Dr. Lawler told this news organization.
The World Health Organization has published guidelines for the management of dengue, which Dr. Lawler strongly recommends to clinicians in the rare event that they are facing a severe case. The treatment for dengue is supportive care, according to the CDC; a vaccine that was deemed safe and effective is no longer being manufactured because of low demand.
Most symptoms last for 2-7 days, and most patients recover within a week, but approximately 1 in 20 may develop severe disease, according to the Los Angeles County Department of Public Health.
Approximately one quarter of dengue infections are symptomatic, and clinicians should know the signs of progression to severe disease, which include abdominal pain or tenderness, persistent vomiting, clinical fluid accumulation, mucosal bleeding, lethargy or restlessness, and liver enlargement, according to the CDC.
Local Dengue Not Unexpected
“Sadly, I am not surprised at another locally acquired case of dengue fever in the United States,” said Dr. Lawler. “We also have seen a trend of more historically tropical, insect-borne diseases popping up with locally acquired cases in the United States,” he noted.
Dr. Lawler suggested that “the erosion of state and local public health” is a major contributor to the increase in dengue cases. For more than 100 years, activities of state and local public health officials had significantly curtailed mosquito-borne diseases through aggressive control programs, “but we seem to be losing ground over the last several years,” he said.
“Locally acquired dengue cases are still rare in the United States,” he added. “However, people can protect themselves against dengue and more common arthropod-borne infections by taking precautions to cover up and wear insect repellent while outdoors.”
In addition, the Los Angeles County Department of Public Health emphasized in its press release that local residents reduce their risk for contact with mosquitoes by removing areas of standing water on their property and ensuring well-fitted screens on doors and windows.
Dr. Lawler had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
A case of locally acquired dengue fever has been confirmed in a resident of Baldwin Park, California, according to a press release from the Los Angeles County Department of Public Health.
“Dengue is the most common insect-borne viral infection in the world, with a wide geographic spread; we know that we have mosquitoes capable of carrying and transmitting the virus in the United States already, and Los Angeles county is a major epicenter for international travel and trade,” James Lawler, MD, associate director for International Programs and Innovation at the Global Center for Health Security and professor in the Infectious Diseases Division at the University of Nebraska Medical Center, Omaha, Nebraska, said in an interview.
Although the patient had no known history of travel to a dengue-endemic area, the potential risk for widespread transmission of the virus in the Los Angeles County area remains low, and no additional suspected cases of locally acquired dengue have been identified, according to the release. However, the recent cases highlight the need for vigilance on the part of the public to reduce transmission of mosquito-borne infections, the public health department noted.
Most cases of dengue occur in people who have traveled to areas where the disease is more common, mainly tropical and subtropical areas, according to the press release. However, the types of mosquitoes that spread dengue exist in parts of the United States, so locally acquired infections can occur.
The Centers for Disease Control and Prevention (CDC) issued an official health advisory in June 2024 about an increased risk for dengue infections in the United States. According to the advisory, 745 cases of dengue were identified in US travelers to endemic areas between January 1, 2024, and June 24, 2024.
The CDC advises clinicians to maintain a high level of suspicion for dengue among individuals with fever and recent travel to areas with frequent dengue transmission, but also to consider locally acquired disease in areas of mosquito vectors.
In clinical practice, dengue may be difficult to differentiate from other febrile systemic infections, Dr. Lawler noted. “Joint pain, low back pain, and headache (often retro-orbital) are common and can be severe, and a rash often appears several days into illness,” he noted.
Do not delay treatment in suspected cases while waiting for test results, the CDC emphasized in the advisory. Food and Drug Administration–approved tests for dengue include RT-PCR and IgM antibody tests or NS1 and IgM antibody tests.
“Severe dengue can be life-threatening and progress to a hemorrhagic fever-like syndrome, and patients with severe dengue should be cared for on a high-acuity or intensive care setting, with close monitoring of labs and fluid status,” Dr. Lawler told this news organization.
The World Health Organization has published guidelines for the management of dengue, which Dr. Lawler strongly recommends to clinicians in the rare event that they are facing a severe case. The treatment for dengue is supportive care, according to the CDC; a vaccine that was deemed safe and effective is no longer being manufactured because of low demand.
Most symptoms last for 2-7 days, and most patients recover within a week, but approximately 1 in 20 may develop severe disease, according to the Los Angeles County Department of Public Health.
Approximately one quarter of dengue infections are symptomatic, and clinicians should know the signs of progression to severe disease, which include abdominal pain or tenderness, persistent vomiting, clinical fluid accumulation, mucosal bleeding, lethargy or restlessness, and liver enlargement, according to the CDC.
Local Dengue Not Unexpected
“Sadly, I am not surprised at another locally acquired case of dengue fever in the United States,” said Dr. Lawler. “We also have seen a trend of more historically tropical, insect-borne diseases popping up with locally acquired cases in the United States,” he noted.
Dr. Lawler suggested that “the erosion of state and local public health” is a major contributor to the increase in dengue cases. For more than 100 years, activities of state and local public health officials had significantly curtailed mosquito-borne diseases through aggressive control programs, “but we seem to be losing ground over the last several years,” he said.
“Locally acquired dengue cases are still rare in the United States,” he added. “However, people can protect themselves against dengue and more common arthropod-borne infections by taking precautions to cover up and wear insect repellent while outdoors.”
In addition, the Los Angeles County Department of Public Health emphasized in its press release that local residents reduce their risk for contact with mosquitoes by removing areas of standing water on their property and ensuring well-fitted screens on doors and windows.
Dr. Lawler had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Oropouche Virus
The pediatrician’s first patient of the day was a 15-year-old boy complaining of fever, chills, and profound arthralgias. His exam, including a careful assessment of his joints, yielded no clues, and the pediatrician was ready to diagnose this as a routine viral illness. An additional bit of history provided by the patient’s mother prompted the pediatrician to pause and reconsider.
“A week ago, we returned from a visit to Cuba,” the mother reported. “Could this be Oropouche virus infection?”

Oropouche virus disease is an arboviral disease caused by the Oropouche virus (OROV). It is transmitted to humans through midge or mosquito bites. Although largely unknown to most United States clinicians until recently, this vector-borne virus is not new. The first human Oropouche virus infection was identified in Trinidad and Tobago in 1955 and since then, there have been intermittent outbreaks in the Amazon region. In recent months, though, the epidemiology of Oropouche virus infections has changed. Infections are being identified in new geographic areas, including Cuba. According to the Pan American Health Organization, 506 cases of Oropouche virus infection have been identified in Cuba since May 27, 2024.
Two deaths from Oropouche virus infection have been reported in previously healthy people. Evolving data suggests adverse outcomes associated with vertical transmission during pregnancy. One fetal death and child with congenital anomalies have been reported in Brazil. Additional fetal deaths, miscarriages, and congenital anomalies are under investigation.
Travel-associated cases have been reported in the United States. As of September 10, 2024, 52 Oropouche virus disease cases had been reported from five states in the United States. The Centers for Disease Control and Prevention confirmed that the first 31 of these cases were travelers returning from Cuba. The CDC issued a health advisory on August 16, 2024: Increased Oropouche Virus Activity and Associated Risk to Travelers.
The pediatrician quickly reviewed the signs and symptoms of Oropouche virus infection. Disease typically presents as an abrupt onset of fever, severe headache, chills, myalgia, and arthralgia 3 to 10 days after the bite of infected mosquito. Some patients develop a maculopapular rash that starts on the trunk and spreads to the extremities. Meningitis and encephalitis develop in less than 1 in 20 people. The symptoms of Oropouche virus infection overlap with those of other arboviruses such as dengue, chikungunya, and Zika viruses. The disease can also mimic malaria or rickettsial infection. Approximately 60% of people with Oropouche virus infection experience a recurrence of symptoms within days to weeks of the initial resolution of symptoms.
Testing for Oropouche virus infection is available through the CDC’s Arbovirus Diagnostic Laboratory. In people who are acutely ill, reverse transcription-polymerase chain reaction testing can be used to identify the virus in serum and cerebrospinal fluid. Serologic testing is also available for people who have been symptomatic for at least 6 days.
The pediatrician contacted his local health department to discuss the possibility of Oropouche virus infection. After reviewing the case definition, public health authorities recommended laboratory testing for Oropouche virus, dengue, and Zika virus.
Back in the exam room, the pediatrician provided anticipatory guidance to the patient and his mother. There are no antiviral medications to treat Oropouche virus infection, so the pediatrician recommended supportive care, including acetaminophen for fever and pain. He also advised avoiding aspirin or other nonsteroidal anti-inflammatory drugs (NSAIDs) until dengue could be ruled out to reduce the risk of bleeding. After confirming that no one else in the home was sick with similar symptoms, he counseled about prevention strategies.
To date, transmission of Oropouche virus in the United States has not been documented, but vectors potentially capable of transmitting the virus are present in some areas of the United States. When people who are infected with Oropouche are bitten, they can spread the virus through their blood to biting midges or mosquitoes. The insects can then spread the virus to other people. To reduce to potential for local transmission, people who are sick with suspected Oropouche virus infection are advised to avoid biting-midge and mosquito bites for the first week of their illness. Any person who has recently traveled to an area where Oropouche virus transmission is occurring should also avoid insect bites for 3 weeks after returning home to account for the potential incubation period of the virus. This includes wearing an EPA-registered insect repellent.
A suspect case is a patient who has been in an area with documented or suspected OROV circulation* within 2 weeks of initial symptom onset (as patients may experience recurrent symptoms) and the following:
- Abrupt onset of reported fever, headache, and one or more of the following: myalgia, arthralgia, photophobia, retro-orbital/eye pain, or signs and symptoms of neuroinvasive disease (eg, stiff neck, altered mental status, seizures, limb weakness, or cerebrospinal fluid pleocytosis).
- Tested negative for other possible diseases, in particular dengue.†
- Absence of a more likely clinical explanation.
*If concern exists for local transmission in a nonendemic area, consider if the patient shared an exposure location with a person with confirmed OROV infection, lives in an area where travel-related cases have been identified, or has known vector exposure (eg, mosquitoes or biting midges).
†If strong suspicion of OROV disease exists based on the patient’s clinical features and history of travel to an area with virus circulation, do not wait on negative testing before sending specimens to CDC.
Adapted from: Centers for Disease Control and Prevention. Response to Oropouche Virus Disease Cases in U.S. States and Territories in the Americas. Available at: https.//www.cdc.gov/oropouche/media/pdfs/2024/09/response-to-oropouche-virus-disease.pdf
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She is a member of the AAP’s Committee on Infectious Diseases and one of the lead authors of the AAP’s Recommendations for Prevention and Control of Influenza in Children, 2022-2023. The opinions expressed in this article are her own. Dr. Bryant discloses that she has served as an investigator on clinical trials funded by Pfizer, Enanta and Gilead. Email her at [email protected]. (Also [email protected])
The pediatrician’s first patient of the day was a 15-year-old boy complaining of fever, chills, and profound arthralgias. His exam, including a careful assessment of his joints, yielded no clues, and the pediatrician was ready to diagnose this as a routine viral illness. An additional bit of history provided by the patient’s mother prompted the pediatrician to pause and reconsider.
“A week ago, we returned from a visit to Cuba,” the mother reported. “Could this be Oropouche virus infection?”
Oropouche virus disease is an arboviral disease caused by the Oropouche virus (OROV). It is transmitted to humans through midge or mosquito bites. Although largely unknown to most United States clinicians until recently, this vector-borne virus is not new. The first human Oropouche virus infection was identified in Trinidad and Tobago in 1955 and since then, there have been intermittent outbreaks in the Amazon region. In recent months, though, the epidemiology of Oropouche virus infections has changed. Infections are being identified in new geographic areas, including Cuba. According to the Pan American Health Organization, 506 cases of Oropouche virus infection have been identified in Cuba since May 27, 2024.
Two deaths from Oropouche virus infection have been reported in previously healthy people. Evolving data suggests adverse outcomes associated with vertical transmission during pregnancy. One fetal death and child with congenital anomalies have been reported in Brazil. Additional fetal deaths, miscarriages, and congenital anomalies are under investigation.
Travel-associated cases have been reported in the United States. As of September 10, 2024, 52 Oropouche virus disease cases had been reported from five states in the United States. The Centers for Disease Control and Prevention confirmed that the first 31 of these cases were travelers returning from Cuba. The CDC issued a health advisory on August 16, 2024: Increased Oropouche Virus Activity and Associated Risk to Travelers.
The pediatrician quickly reviewed the signs and symptoms of Oropouche virus infection. Disease typically presents as an abrupt onset of fever, severe headache, chills, myalgia, and arthralgia 3 to 10 days after the bite of infected mosquito. Some patients develop a maculopapular rash that starts on the trunk and spreads to the extremities. Meningitis and encephalitis develop in less than 1 in 20 people. The symptoms of Oropouche virus infection overlap with those of other arboviruses such as dengue, chikungunya, and Zika viruses. The disease can also mimic malaria or rickettsial infection. Approximately 60% of people with Oropouche virus infection experience a recurrence of symptoms within days to weeks of the initial resolution of symptoms.
Testing for Oropouche virus infection is available through the CDC’s Arbovirus Diagnostic Laboratory. In people who are acutely ill, reverse transcription-polymerase chain reaction testing can be used to identify the virus in serum and cerebrospinal fluid. Serologic testing is also available for people who have been symptomatic for at least 6 days.
The pediatrician contacted his local health department to discuss the possibility of Oropouche virus infection. After reviewing the case definition, public health authorities recommended laboratory testing for Oropouche virus, dengue, and Zika virus.
Back in the exam room, the pediatrician provided anticipatory guidance to the patient and his mother. There are no antiviral medications to treat Oropouche virus infection, so the pediatrician recommended supportive care, including acetaminophen for fever and pain. He also advised avoiding aspirin or other nonsteroidal anti-inflammatory drugs (NSAIDs) until dengue could be ruled out to reduce the risk of bleeding. After confirming that no one else in the home was sick with similar symptoms, he counseled about prevention strategies.
To date, transmission of Oropouche virus in the United States has not been documented, but vectors potentially capable of transmitting the virus are present in some areas of the United States. When people who are infected with Oropouche are bitten, they can spread the virus through their blood to biting midges or mosquitoes. The insects can then spread the virus to other people. To reduce to potential for local transmission, people who are sick with suspected Oropouche virus infection are advised to avoid biting-midge and mosquito bites for the first week of their illness. Any person who has recently traveled to an area where Oropouche virus transmission is occurring should also avoid insect bites for 3 weeks after returning home to account for the potential incubation period of the virus. This includes wearing an EPA-registered insect repellent.
A suspect case is a patient who has been in an area with documented or suspected OROV circulation* within 2 weeks of initial symptom onset (as patients may experience recurrent symptoms) and the following:
- Abrupt onset of reported fever, headache, and one or more of the following: myalgia, arthralgia, photophobia, retro-orbital/eye pain, or signs and symptoms of neuroinvasive disease (eg, stiff neck, altered mental status, seizures, limb weakness, or cerebrospinal fluid pleocytosis).
- Tested negative for other possible diseases, in particular dengue.†
- Absence of a more likely clinical explanation.
*If concern exists for local transmission in a nonendemic area, consider if the patient shared an exposure location with a person with confirmed OROV infection, lives in an area where travel-related cases have been identified, or has known vector exposure (eg, mosquitoes or biting midges).
†If strong suspicion of OROV disease exists based on the patient’s clinical features and history of travel to an area with virus circulation, do not wait on negative testing before sending specimens to CDC.
Adapted from: Centers for Disease Control and Prevention. Response to Oropouche Virus Disease Cases in U.S. States and Territories in the Americas. Available at: https.//www.cdc.gov/oropouche/media/pdfs/2024/09/response-to-oropouche-virus-disease.pdf
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She is a member of the AAP’s Committee on Infectious Diseases and one of the lead authors of the AAP’s Recommendations for Prevention and Control of Influenza in Children, 2022-2023. The opinions expressed in this article are her own. Dr. Bryant discloses that she has served as an investigator on clinical trials funded by Pfizer, Enanta and Gilead. Email her at [email protected]. (Also [email protected])
The pediatrician’s first patient of the day was a 15-year-old boy complaining of fever, chills, and profound arthralgias. His exam, including a careful assessment of his joints, yielded no clues, and the pediatrician was ready to diagnose this as a routine viral illness. An additional bit of history provided by the patient’s mother prompted the pediatrician to pause and reconsider.
“A week ago, we returned from a visit to Cuba,” the mother reported. “Could this be Oropouche virus infection?”
Oropouche virus disease is an arboviral disease caused by the Oropouche virus (OROV). It is transmitted to humans through midge or mosquito bites. Although largely unknown to most United States clinicians until recently, this vector-borne virus is not new. The first human Oropouche virus infection was identified in Trinidad and Tobago in 1955 and since then, there have been intermittent outbreaks in the Amazon region. In recent months, though, the epidemiology of Oropouche virus infections has changed. Infections are being identified in new geographic areas, including Cuba. According to the Pan American Health Organization, 506 cases of Oropouche virus infection have been identified in Cuba since May 27, 2024.
Two deaths from Oropouche virus infection have been reported in previously healthy people. Evolving data suggests adverse outcomes associated with vertical transmission during pregnancy. One fetal death and child with congenital anomalies have been reported in Brazil. Additional fetal deaths, miscarriages, and congenital anomalies are under investigation.
Travel-associated cases have been reported in the United States. As of September 10, 2024, 52 Oropouche virus disease cases had been reported from five states in the United States. The Centers for Disease Control and Prevention confirmed that the first 31 of these cases were travelers returning from Cuba. The CDC issued a health advisory on August 16, 2024: Increased Oropouche Virus Activity and Associated Risk to Travelers.
The pediatrician quickly reviewed the signs and symptoms of Oropouche virus infection. Disease typically presents as an abrupt onset of fever, severe headache, chills, myalgia, and arthralgia 3 to 10 days after the bite of infected mosquito. Some patients develop a maculopapular rash that starts on the trunk and spreads to the extremities. Meningitis and encephalitis develop in less than 1 in 20 people. The symptoms of Oropouche virus infection overlap with those of other arboviruses such as dengue, chikungunya, and Zika viruses. The disease can also mimic malaria or rickettsial infection. Approximately 60% of people with Oropouche virus infection experience a recurrence of symptoms within days to weeks of the initial resolution of symptoms.
Testing for Oropouche virus infection is available through the CDC’s Arbovirus Diagnostic Laboratory. In people who are acutely ill, reverse transcription-polymerase chain reaction testing can be used to identify the virus in serum and cerebrospinal fluid. Serologic testing is also available for people who have been symptomatic for at least 6 days.
The pediatrician contacted his local health department to discuss the possibility of Oropouche virus infection. After reviewing the case definition, public health authorities recommended laboratory testing for Oropouche virus, dengue, and Zika virus.
Back in the exam room, the pediatrician provided anticipatory guidance to the patient and his mother. There are no antiviral medications to treat Oropouche virus infection, so the pediatrician recommended supportive care, including acetaminophen for fever and pain. He also advised avoiding aspirin or other nonsteroidal anti-inflammatory drugs (NSAIDs) until dengue could be ruled out to reduce the risk of bleeding. After confirming that no one else in the home was sick with similar symptoms, he counseled about prevention strategies.
To date, transmission of Oropouche virus in the United States has not been documented, but vectors potentially capable of transmitting the virus are present in some areas of the United States. When people who are infected with Oropouche are bitten, they can spread the virus through their blood to biting midges or mosquitoes. The insects can then spread the virus to other people. To reduce to potential for local transmission, people who are sick with suspected Oropouche virus infection are advised to avoid biting-midge and mosquito bites for the first week of their illness. Any person who has recently traveled to an area where Oropouche virus transmission is occurring should also avoid insect bites for 3 weeks after returning home to account for the potential incubation period of the virus. This includes wearing an EPA-registered insect repellent.
A suspect case is a patient who has been in an area with documented or suspected OROV circulation* within 2 weeks of initial symptom onset (as patients may experience recurrent symptoms) and the following:
- Abrupt onset of reported fever, headache, and one or more of the following: myalgia, arthralgia, photophobia, retro-orbital/eye pain, or signs and symptoms of neuroinvasive disease (eg, stiff neck, altered mental status, seizures, limb weakness, or cerebrospinal fluid pleocytosis).
- Tested negative for other possible diseases, in particular dengue.†
- Absence of a more likely clinical explanation.
*If concern exists for local transmission in a nonendemic area, consider if the patient shared an exposure location with a person with confirmed OROV infection, lives in an area where travel-related cases have been identified, or has known vector exposure (eg, mosquitoes or biting midges).
†If strong suspicion of OROV disease exists based on the patient’s clinical features and history of travel to an area with virus circulation, do not wait on negative testing before sending specimens to CDC.
Adapted from: Centers for Disease Control and Prevention. Response to Oropouche Virus Disease Cases in U.S. States and Territories in the Americas. Available at: https.//www.cdc.gov/oropouche/media/pdfs/2024/09/response-to-oropouche-virus-disease.pdf
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She is a member of the AAP’s Committee on Infectious Diseases and one of the lead authors of the AAP’s Recommendations for Prevention and Control of Influenza in Children, 2022-2023. The opinions expressed in this article are her own. Dr. Bryant discloses that she has served as an investigator on clinical trials funded by Pfizer, Enanta and Gilead. Email her at [email protected]. (Also [email protected])
Could a Virus Reverse Antibiotic Resistance?
Peering through his microscope in 1910, Franco-Canadian microbiologist Félix d’Hérelle noticed some “clear spots” in his bacterial cultures, an anomaly that turned out to be viruses preying on the bacteria. Years later, Mr. d’Hérelle would come to use these viruses, which he called bacteriophages, to treat patients plagued with dysentery after World War I.
But now, with bacteria evolving resistance to more and more antibiotics, phage therapy is drawing a second look from researchers — sometimes with a novel twist. Instead of simply using the phages to kill bacteria directly, the new strategy aims to catch the bacteria in an evolutionary dilemma — one in which they cannot evade phages and antibiotics simultaneously.
This plan, which uses something called “phage steering,” has shown promising results in initial tests, but the scope of its usefulness remains to be proven.
There’s certainly need to find new ways to respond to bacterial infections. More than 70% of hospital-acquired bacterial infections in the United States are resistant to at least one type of antibiotic. And some pathogens, such as Acinetobacter, Pseudomonas, Escherichia coli, and Klebsiella — classified by the World Health Organization as some of the biggest threats to human health — are resistant to multiple antibiotics. In 2019, antibacterial resistance was linked to 4.95 million deaths globally, heightening the call for more effective treatment options.
One of the ways that bacteria can evolve resistance to antibiotics is by using structures in their membranes that are designed to move unwanted molecules out of the cell. By modifying these “efflux pumps” to recognize the antibiotic, bacteria can eliminate the drug before it poisons them.
As it turns out, some phages appear to use these same efflux pumps to invade the bacterial cell. The phage presumably attaches its tail to the outer portion of the pump protein, like a key slipping into a lock, and then injects its genetic material into the cell. This lucky coincidence led Paul Turner, PhD, an evolutionary biologist at Yale University, New Haven, Connecticut, to suggest that treating a patient with phages and antibiotics simultaneously could trap bacteria in a no-win situation: If they evolve to modify their efflux pumps so the phage can’t bind, the pumps will no longer expel antibiotics, and the bacteria will lose their resistance. But if they retain their antibiotic resistance, the phages will kill them, as Dr. Turner and colleagues explained in the 2023 Annual Review of Virology.
The result, in other words, is a two-pronged attack, said Michael Hochberg, PhD, an evolutionary biologist at the French National Centre for Scientific Research who studies how to prevent the evolution of bacterial resistance. “It’s kind of like a crisscross effect.” The same principle can target other bacterial molecules that play a dual role in resistance to viruses and antibiotics.
Turner tested this hypothesis on multidrug-resistant Pseudomonas aeruginosa, which causes dangerous infections, especially in healthcare settings. This bacterium has four efflux pumps involved in antibiotic resistance, and Dr. Turner predicted that if he could find a phage that used one of the pumps as a way into the cell, the bacterium would be forced to slam the door on the phage by mutating the receptor — thereby impeding its ability to pump out antibiotics.
Sampling from the environment, Dr. Turner’s team collected 42 phage strains that infect P aeruginosa. Out of all the phages, one, OMKO1, bound to an efflux pump, making it the perfect candidate for the experiment.
The researchers then cultured antibiotic-resistant P aeruginosa together with OMKO1, hoping this would force the bacterium to modify its efflux pump to resist the phage. They exposed these phage-resistant bacteria, as well as their normal, phage-sensitive counterparts, to four antibiotics the bacteria had been resistant to: tetracycline, erythromycin, ciprofloxacin, and ceftazidime.
As the theory predicted, the bacteria that had evolved resistance to the phage were more sensitive to the antibiotics than those that had not been exposed to the phage. This suggests that the bacteria had, indeed, been forced to lose their antibiotic resistance through their need to fight off the phage.
Other researchers have also shown that phage steering can resensitize bacteria to common antibiotics they’d become resistant to. One study, by an international research team, showed that a phage called Phab24 can be used to restore sensitivity to the antibiotic colistin in Acinetobacter baumannii, which causes life-threatening diseases.
In a second study, researchers at Monash University in Australia sampled infectious bacteria from patients. They found that several phages, including strains known as phi-FG02 and phi-CO01, were already present in some of the samples, and that A baumannii bacteria exposed to the phages had inactivated a gene that helps create the microbe’s important outer layer, or capsule. This layer serves as the entry point for the phages, but it also helps the bacterium to form biofilms that keep out antibiotics — so removing the layer rendered A baumannii susceptible to several antibiotics that it was previously resistant to.
In a third study, researchers from the University of Liverpool discovered that, when a P aeruginosa strain that was resistant to all antibiotics was exposed to phages, the bacterium became sensitive to two antibiotics that were otherwise considered ineffective against P aeruginosa.
Dr. Turner’s team has used phage steering in dozens of cases of personalized therapy in clinical settings, said Benjamin Chan, PhD, a microbiologist at Yale University who works with Dr. Turner. The results, many still unpublished, have been promising so far. Nonrespiratory infections are relatively easy to clear off, and lung infections, which the phage steering approach wouldn’t be expected to eradicate completely, often show some improvement.
“I would say that we have been quite successful in using phage steering to treat difficult-to-manage infections, reducing antimicrobial resistance in many cases,” he said. But he notes that it is sometimes difficult to determine whether phage steering really was responsible for the cures.
Devil in the details
Phage therapy may not work for all antibiotic-resistant bacteria, said molecular biologist Graham Hatfull, PhD, of the University of Pittsburgh in Pennsylvania. That’s because phages are very host specific, and for most phages, no one knows what target they bind to on the bacterial cell surface. For phage steering to work against antibiotic resistance, the phage has to bind to a molecule that’s involved in that resistance — and it’s not clear how often that fortuitous coincidence occurs.
Jason Gill, PhD, who studies bacteriophage biology at Texas A&M University, College Station, said that it is not easy to predict if a phage will induce antibiotic sensitivity. So you always have to hunt for the right virus each time.
Dr. Gill knows from experience how complicated the approach can get. He was part of a team of researchers and doctors who used phages to treat a patient with a multidrug-resistant A baumannii infection. Less than 4 days after the team administered phages intravenously and through the skin, the patient woke up from a coma and became responsive to the previously ineffective antibiotic minocycline — a striking success.
But when Dr. Gill tried a similar experiment in cell cultures, he got a different result. The A baumannii developed resistance to the phages, but they also maintained their resistance to minocycline. “There’s not a complete mechanistic understanding,” said Dr. Gill. “The linkage between phage resistance and antibiotic sensitivity probably varies by bacterial strain, phage and antibiotic.” That means phage steering may not always work.
Dr. Turner, for his part, pointed out another potential problem: That phages could work too well. If phage therapy kills large amounts of bacteria and deposits their remains in the bloodstream quickly, for example, this could trigger septic shock in patients. Scientists do not yet know how to address this problem.
Another concern is that doctors have less precise control over phages than antibiotics. “Phages can mutate, they can adapt, they have a genome,” said Dr. Hochberg. Safety concerns, he notes, are one factor inhibiting the routine use of phage therapy in countries like the United States, restricting it to case-by-case applications such as Dr. Turner and Dr. Chan’s.
Phage therapy may have been too high-tech for the 1940s, and even today, scientists grapple with how to use it. What we need now, said Dr. Turner, are rigorous experiments that will teach us how to make it work.
This article originally appeared in Knowable Magazine on September 09, 2024. Knowable Magazine is an independent journalistic endeavor from Annual Reviews, a nonprofit publisher dedicated to synthesizing and integrating knowledge for the progress of science and the benefit of society. Sign up for Knowable Magazine’s newsletter. A version of this article appeared on Medscape.com.
Peering through his microscope in 1910, Franco-Canadian microbiologist Félix d’Hérelle noticed some “clear spots” in his bacterial cultures, an anomaly that turned out to be viruses preying on the bacteria. Years later, Mr. d’Hérelle would come to use these viruses, which he called bacteriophages, to treat patients plagued with dysentery after World War I.
But now, with bacteria evolving resistance to more and more antibiotics, phage therapy is drawing a second look from researchers — sometimes with a novel twist. Instead of simply using the phages to kill bacteria directly, the new strategy aims to catch the bacteria in an evolutionary dilemma — one in which they cannot evade phages and antibiotics simultaneously.
This plan, which uses something called “phage steering,” has shown promising results in initial tests, but the scope of its usefulness remains to be proven.
There’s certainly need to find new ways to respond to bacterial infections. More than 70% of hospital-acquired bacterial infections in the United States are resistant to at least one type of antibiotic. And some pathogens, such as Acinetobacter, Pseudomonas, Escherichia coli, and Klebsiella — classified by the World Health Organization as some of the biggest threats to human health — are resistant to multiple antibiotics. In 2019, antibacterial resistance was linked to 4.95 million deaths globally, heightening the call for more effective treatment options.
One of the ways that bacteria can evolve resistance to antibiotics is by using structures in their membranes that are designed to move unwanted molecules out of the cell. By modifying these “efflux pumps” to recognize the antibiotic, bacteria can eliminate the drug before it poisons them.
As it turns out, some phages appear to use these same efflux pumps to invade the bacterial cell. The phage presumably attaches its tail to the outer portion of the pump protein, like a key slipping into a lock, and then injects its genetic material into the cell. This lucky coincidence led Paul Turner, PhD, an evolutionary biologist at Yale University, New Haven, Connecticut, to suggest that treating a patient with phages and antibiotics simultaneously could trap bacteria in a no-win situation: If they evolve to modify their efflux pumps so the phage can’t bind, the pumps will no longer expel antibiotics, and the bacteria will lose their resistance. But if they retain their antibiotic resistance, the phages will kill them, as Dr. Turner and colleagues explained in the 2023 Annual Review of Virology.
The result, in other words, is a two-pronged attack, said Michael Hochberg, PhD, an evolutionary biologist at the French National Centre for Scientific Research who studies how to prevent the evolution of bacterial resistance. “It’s kind of like a crisscross effect.” The same principle can target other bacterial molecules that play a dual role in resistance to viruses and antibiotics.
Turner tested this hypothesis on multidrug-resistant Pseudomonas aeruginosa, which causes dangerous infections, especially in healthcare settings. This bacterium has four efflux pumps involved in antibiotic resistance, and Dr. Turner predicted that if he could find a phage that used one of the pumps as a way into the cell, the bacterium would be forced to slam the door on the phage by mutating the receptor — thereby impeding its ability to pump out antibiotics.
Sampling from the environment, Dr. Turner’s team collected 42 phage strains that infect P aeruginosa. Out of all the phages, one, OMKO1, bound to an efflux pump, making it the perfect candidate for the experiment.
The researchers then cultured antibiotic-resistant P aeruginosa together with OMKO1, hoping this would force the bacterium to modify its efflux pump to resist the phage. They exposed these phage-resistant bacteria, as well as their normal, phage-sensitive counterparts, to four antibiotics the bacteria had been resistant to: tetracycline, erythromycin, ciprofloxacin, and ceftazidime.
As the theory predicted, the bacteria that had evolved resistance to the phage were more sensitive to the antibiotics than those that had not been exposed to the phage. This suggests that the bacteria had, indeed, been forced to lose their antibiotic resistance through their need to fight off the phage.
Other researchers have also shown that phage steering can resensitize bacteria to common antibiotics they’d become resistant to. One study, by an international research team, showed that a phage called Phab24 can be used to restore sensitivity to the antibiotic colistin in Acinetobacter baumannii, which causes life-threatening diseases.
In a second study, researchers at Monash University in Australia sampled infectious bacteria from patients. They found that several phages, including strains known as phi-FG02 and phi-CO01, were already present in some of the samples, and that A baumannii bacteria exposed to the phages had inactivated a gene that helps create the microbe’s important outer layer, or capsule. This layer serves as the entry point for the phages, but it also helps the bacterium to form biofilms that keep out antibiotics — so removing the layer rendered A baumannii susceptible to several antibiotics that it was previously resistant to.
In a third study, researchers from the University of Liverpool discovered that, when a P aeruginosa strain that was resistant to all antibiotics was exposed to phages, the bacterium became sensitive to two antibiotics that were otherwise considered ineffective against P aeruginosa.
Dr. Turner’s team has used phage steering in dozens of cases of personalized therapy in clinical settings, said Benjamin Chan, PhD, a microbiologist at Yale University who works with Dr. Turner. The results, many still unpublished, have been promising so far. Nonrespiratory infections are relatively easy to clear off, and lung infections, which the phage steering approach wouldn’t be expected to eradicate completely, often show some improvement.
“I would say that we have been quite successful in using phage steering to treat difficult-to-manage infections, reducing antimicrobial resistance in many cases,” he said. But he notes that it is sometimes difficult to determine whether phage steering really was responsible for the cures.
Devil in the details
Phage therapy may not work for all antibiotic-resistant bacteria, said molecular biologist Graham Hatfull, PhD, of the University of Pittsburgh in Pennsylvania. That’s because phages are very host specific, and for most phages, no one knows what target they bind to on the bacterial cell surface. For phage steering to work against antibiotic resistance, the phage has to bind to a molecule that’s involved in that resistance — and it’s not clear how often that fortuitous coincidence occurs.
Jason Gill, PhD, who studies bacteriophage biology at Texas A&M University, College Station, said that it is not easy to predict if a phage will induce antibiotic sensitivity. So you always have to hunt for the right virus each time.
Dr. Gill knows from experience how complicated the approach can get. He was part of a team of researchers and doctors who used phages to treat a patient with a multidrug-resistant A baumannii infection. Less than 4 days after the team administered phages intravenously and through the skin, the patient woke up from a coma and became responsive to the previously ineffective antibiotic minocycline — a striking success.
But when Dr. Gill tried a similar experiment in cell cultures, he got a different result. The A baumannii developed resistance to the phages, but they also maintained their resistance to minocycline. “There’s not a complete mechanistic understanding,” said Dr. Gill. “The linkage between phage resistance and antibiotic sensitivity probably varies by bacterial strain, phage and antibiotic.” That means phage steering may not always work.
Dr. Turner, for his part, pointed out another potential problem: That phages could work too well. If phage therapy kills large amounts of bacteria and deposits their remains in the bloodstream quickly, for example, this could trigger septic shock in patients. Scientists do not yet know how to address this problem.
Another concern is that doctors have less precise control over phages than antibiotics. “Phages can mutate, they can adapt, they have a genome,” said Dr. Hochberg. Safety concerns, he notes, are one factor inhibiting the routine use of phage therapy in countries like the United States, restricting it to case-by-case applications such as Dr. Turner and Dr. Chan’s.
Phage therapy may have been too high-tech for the 1940s, and even today, scientists grapple with how to use it. What we need now, said Dr. Turner, are rigorous experiments that will teach us how to make it work.
This article originally appeared in Knowable Magazine on September 09, 2024. Knowable Magazine is an independent journalistic endeavor from Annual Reviews, a nonprofit publisher dedicated to synthesizing and integrating knowledge for the progress of science and the benefit of society. Sign up for Knowable Magazine’s newsletter. A version of this article appeared on Medscape.com.
Peering through his microscope in 1910, Franco-Canadian microbiologist Félix d’Hérelle noticed some “clear spots” in his bacterial cultures, an anomaly that turned out to be viruses preying on the bacteria. Years later, Mr. d’Hérelle would come to use these viruses, which he called bacteriophages, to treat patients plagued with dysentery after World War I.
But now, with bacteria evolving resistance to more and more antibiotics, phage therapy is drawing a second look from researchers — sometimes with a novel twist. Instead of simply using the phages to kill bacteria directly, the new strategy aims to catch the bacteria in an evolutionary dilemma — one in which they cannot evade phages and antibiotics simultaneously.
This plan, which uses something called “phage steering,” has shown promising results in initial tests, but the scope of its usefulness remains to be proven.
There’s certainly need to find new ways to respond to bacterial infections. More than 70% of hospital-acquired bacterial infections in the United States are resistant to at least one type of antibiotic. And some pathogens, such as Acinetobacter, Pseudomonas, Escherichia coli, and Klebsiella — classified by the World Health Organization as some of the biggest threats to human health — are resistant to multiple antibiotics. In 2019, antibacterial resistance was linked to 4.95 million deaths globally, heightening the call for more effective treatment options.
One of the ways that bacteria can evolve resistance to antibiotics is by using structures in their membranes that are designed to move unwanted molecules out of the cell. By modifying these “efflux pumps” to recognize the antibiotic, bacteria can eliminate the drug before it poisons them.
As it turns out, some phages appear to use these same efflux pumps to invade the bacterial cell. The phage presumably attaches its tail to the outer portion of the pump protein, like a key slipping into a lock, and then injects its genetic material into the cell. This lucky coincidence led Paul Turner, PhD, an evolutionary biologist at Yale University, New Haven, Connecticut, to suggest that treating a patient with phages and antibiotics simultaneously could trap bacteria in a no-win situation: If they evolve to modify their efflux pumps so the phage can’t bind, the pumps will no longer expel antibiotics, and the bacteria will lose their resistance. But if they retain their antibiotic resistance, the phages will kill them, as Dr. Turner and colleagues explained in the 2023 Annual Review of Virology.
The result, in other words, is a two-pronged attack, said Michael Hochberg, PhD, an evolutionary biologist at the French National Centre for Scientific Research who studies how to prevent the evolution of bacterial resistance. “It’s kind of like a crisscross effect.” The same principle can target other bacterial molecules that play a dual role in resistance to viruses and antibiotics.
Turner tested this hypothesis on multidrug-resistant Pseudomonas aeruginosa, which causes dangerous infections, especially in healthcare settings. This bacterium has four efflux pumps involved in antibiotic resistance, and Dr. Turner predicted that if he could find a phage that used one of the pumps as a way into the cell, the bacterium would be forced to slam the door on the phage by mutating the receptor — thereby impeding its ability to pump out antibiotics.
Sampling from the environment, Dr. Turner’s team collected 42 phage strains that infect P aeruginosa. Out of all the phages, one, OMKO1, bound to an efflux pump, making it the perfect candidate for the experiment.
The researchers then cultured antibiotic-resistant P aeruginosa together with OMKO1, hoping this would force the bacterium to modify its efflux pump to resist the phage. They exposed these phage-resistant bacteria, as well as their normal, phage-sensitive counterparts, to four antibiotics the bacteria had been resistant to: tetracycline, erythromycin, ciprofloxacin, and ceftazidime.
As the theory predicted, the bacteria that had evolved resistance to the phage were more sensitive to the antibiotics than those that had not been exposed to the phage. This suggests that the bacteria had, indeed, been forced to lose their antibiotic resistance through their need to fight off the phage.
Other researchers have also shown that phage steering can resensitize bacteria to common antibiotics they’d become resistant to. One study, by an international research team, showed that a phage called Phab24 can be used to restore sensitivity to the antibiotic colistin in Acinetobacter baumannii, which causes life-threatening diseases.
In a second study, researchers at Monash University in Australia sampled infectious bacteria from patients. They found that several phages, including strains known as phi-FG02 and phi-CO01, were already present in some of the samples, and that A baumannii bacteria exposed to the phages had inactivated a gene that helps create the microbe’s important outer layer, or capsule. This layer serves as the entry point for the phages, but it also helps the bacterium to form biofilms that keep out antibiotics — so removing the layer rendered A baumannii susceptible to several antibiotics that it was previously resistant to.
In a third study, researchers from the University of Liverpool discovered that, when a P aeruginosa strain that was resistant to all antibiotics was exposed to phages, the bacterium became sensitive to two antibiotics that were otherwise considered ineffective against P aeruginosa.
Dr. Turner’s team has used phage steering in dozens of cases of personalized therapy in clinical settings, said Benjamin Chan, PhD, a microbiologist at Yale University who works with Dr. Turner. The results, many still unpublished, have been promising so far. Nonrespiratory infections are relatively easy to clear off, and lung infections, which the phage steering approach wouldn’t be expected to eradicate completely, often show some improvement.
“I would say that we have been quite successful in using phage steering to treat difficult-to-manage infections, reducing antimicrobial resistance in many cases,” he said. But he notes that it is sometimes difficult to determine whether phage steering really was responsible for the cures.
Devil in the details
Phage therapy may not work for all antibiotic-resistant bacteria, said molecular biologist Graham Hatfull, PhD, of the University of Pittsburgh in Pennsylvania. That’s because phages are very host specific, and for most phages, no one knows what target they bind to on the bacterial cell surface. For phage steering to work against antibiotic resistance, the phage has to bind to a molecule that’s involved in that resistance — and it’s not clear how often that fortuitous coincidence occurs.
Jason Gill, PhD, who studies bacteriophage biology at Texas A&M University, College Station, said that it is not easy to predict if a phage will induce antibiotic sensitivity. So you always have to hunt for the right virus each time.
Dr. Gill knows from experience how complicated the approach can get. He was part of a team of researchers and doctors who used phages to treat a patient with a multidrug-resistant A baumannii infection. Less than 4 days after the team administered phages intravenously and through the skin, the patient woke up from a coma and became responsive to the previously ineffective antibiotic minocycline — a striking success.
But when Dr. Gill tried a similar experiment in cell cultures, he got a different result. The A baumannii developed resistance to the phages, but they also maintained their resistance to minocycline. “There’s not a complete mechanistic understanding,” said Dr. Gill. “The linkage between phage resistance and antibiotic sensitivity probably varies by bacterial strain, phage and antibiotic.” That means phage steering may not always work.
Dr. Turner, for his part, pointed out another potential problem: That phages could work too well. If phage therapy kills large amounts of bacteria and deposits their remains in the bloodstream quickly, for example, this could trigger septic shock in patients. Scientists do not yet know how to address this problem.
Another concern is that doctors have less precise control over phages than antibiotics. “Phages can mutate, they can adapt, they have a genome,” said Dr. Hochberg. Safety concerns, he notes, are one factor inhibiting the routine use of phage therapy in countries like the United States, restricting it to case-by-case applications such as Dr. Turner and Dr. Chan’s.
Phage therapy may have been too high-tech for the 1940s, and even today, scientists grapple with how to use it. What we need now, said Dr. Turner, are rigorous experiments that will teach us how to make it work.
This article originally appeared in Knowable Magazine on September 09, 2024. Knowable Magazine is an independent journalistic endeavor from Annual Reviews, a nonprofit publisher dedicated to synthesizing and integrating knowledge for the progress of science and the benefit of society. Sign up for Knowable Magazine’s newsletter. A version of this article appeared on Medscape.com.
RSV Updates: Prophylaxis Approval and Hospitalization for Severe RSV
1. Pfizer announces positive top-line results from phase 3 study of ABRYSVO® in adults aged 18 to 59 at increased risk for RSV disease. Press release. Pfizer; April 9, 2024. Accessed May 22, 2024. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-positive-top-line-results-phase-3-study-1
2. Pfizer announces positive top-line data for full season two efficacy of ABRYSVO® for RSV in older adults. Press release. Pfizer; February 29, 2024. Accessed May 22, 2024. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-positive-top-line-data-full-season-two
3. CDC study shows effectiveness of RSV immunization for infants. Press release. US Centers for Disease Control and Prevention; March 7, 2024. Accessed May 22, 2024. https://www.cdc.gov/media/releases/2024/s0307-rsv-immunization.html
4. Moline HL, Tannis A, Toepfer AP, et al. Early estimate of nirsevimab effectiveness for prevention of respiratory syncytial virus–associated hospitalization among infants entering their first respiratory syncytial virus season — new vaccine surveillance network, October 2023–February 2024. MMWR Morb Mortal Wkly Rep. 2024;73(9):209-214. doi:10.15585/mmwr.mm7309a4
5. Havers FP, Whitaker M, Melgar M, et al; for the RSV-NET Surveillance Team. Characteristics and outcomes among adults aged ≥60 years hospitalized with laboratory-confirmed respiratory syncytial virus ─ RSV-NET, 12 states, July 2022–June 2023. MMWR Morb Mortal Wkly Rep. 2023;72(40):1075-1082. doi:10.15585/mmwr.mm7240a1
6. Walsh EE, Pérez Marc G, Zareba AM, et al; for the RENOIR Clinical Trial Group. Efficacy and safety of a bivalent RSV prefusion F vaccine in older adults. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
7. Fleming-Dutra KE, Jones JM, Roper LE, et al. Use of the Pfizer respiratory syncytial virus vaccine during pregnancy for the prevention of respiratory syncytial virus–associated lower respiratory tract disease in infants: recommendations of the Advisory Committee on Immunization Practices — United States, 2023. MMWR Morb Mortal Wkly Rep. 2023;72(41):1115-1122. doi:10.15585/mmwr.mm7241e1
8. Baker J, Aliabadi N, Munjal I, et al. Equivalent immunogenicity across three RSVpreF vaccine lots in healthy adults 18-49 years of age: results of a randomized phase 3 study. Vaccine. 2024;42(13):3172-3179. doi:10.1016/j.vaccine.2024.03.070
9. New data for AREXVY, GSK’s RSV vaccine, show potential to help protect adults aged 50 to 59 at increased risk for RSV disease. Press release. GSK; October 25, 2023. Accessed May 22, 2024. https://us.gsk.com/en-us/media/press-releases/new-data-for-arexvy/
1. Pfizer announces positive top-line results from phase 3 study of ABRYSVO® in adults aged 18 to 59 at increased risk for RSV disease. Press release. Pfizer; April 9, 2024. Accessed May 22, 2024. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-positive-top-line-results-phase-3-study-1
2. Pfizer announces positive top-line data for full season two efficacy of ABRYSVO® for RSV in older adults. Press release. Pfizer; February 29, 2024. Accessed May 22, 2024. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-positive-top-line-data-full-season-two
3. CDC study shows effectiveness of RSV immunization for infants. Press release. US Centers for Disease Control and Prevention; March 7, 2024. Accessed May 22, 2024. https://www.cdc.gov/media/releases/2024/s0307-rsv-immunization.html
4. Moline HL, Tannis A, Toepfer AP, et al. Early estimate of nirsevimab effectiveness for prevention of respiratory syncytial virus–associated hospitalization among infants entering their first respiratory syncytial virus season — new vaccine surveillance network, October 2023–February 2024. MMWR Morb Mortal Wkly Rep. 2024;73(9):209-214. doi:10.15585/mmwr.mm7309a4
5. Havers FP, Whitaker M, Melgar M, et al; for the RSV-NET Surveillance Team. Characteristics and outcomes among adults aged ≥60 years hospitalized with laboratory-confirmed respiratory syncytial virus ─ RSV-NET, 12 states, July 2022–June 2023. MMWR Morb Mortal Wkly Rep. 2023;72(40):1075-1082. doi:10.15585/mmwr.mm7240a1
6. Walsh EE, Pérez Marc G, Zareba AM, et al; for the RENOIR Clinical Trial Group. Efficacy and safety of a bivalent RSV prefusion F vaccine in older adults. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
7. Fleming-Dutra KE, Jones JM, Roper LE, et al. Use of the Pfizer respiratory syncytial virus vaccine during pregnancy for the prevention of respiratory syncytial virus–associated lower respiratory tract disease in infants: recommendations of the Advisory Committee on Immunization Practices — United States, 2023. MMWR Morb Mortal Wkly Rep. 2023;72(41):1115-1122. doi:10.15585/mmwr.mm7241e1
8. Baker J, Aliabadi N, Munjal I, et al. Equivalent immunogenicity across three RSVpreF vaccine lots in healthy adults 18-49 years of age: results of a randomized phase 3 study. Vaccine. 2024;42(13):3172-3179. doi:10.1016/j.vaccine.2024.03.070
9. New data for AREXVY, GSK’s RSV vaccine, show potential to help protect adults aged 50 to 59 at increased risk for RSV disease. Press release. GSK; October 25, 2023. Accessed May 22, 2024. https://us.gsk.com/en-us/media/press-releases/new-data-for-arexvy/
1. Pfizer announces positive top-line results from phase 3 study of ABRYSVO® in adults aged 18 to 59 at increased risk for RSV disease. Press release. Pfizer; April 9, 2024. Accessed May 22, 2024. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-positive-top-line-results-phase-3-study-1
2. Pfizer announces positive top-line data for full season two efficacy of ABRYSVO® for RSV in older adults. Press release. Pfizer; February 29, 2024. Accessed May 22, 2024. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-positive-top-line-data-full-season-two
3. CDC study shows effectiveness of RSV immunization for infants. Press release. US Centers for Disease Control and Prevention; March 7, 2024. Accessed May 22, 2024. https://www.cdc.gov/media/releases/2024/s0307-rsv-immunization.html
4. Moline HL, Tannis A, Toepfer AP, et al. Early estimate of nirsevimab effectiveness for prevention of respiratory syncytial virus–associated hospitalization among infants entering their first respiratory syncytial virus season — new vaccine surveillance network, October 2023–February 2024. MMWR Morb Mortal Wkly Rep. 2024;73(9):209-214. doi:10.15585/mmwr.mm7309a4
5. Havers FP, Whitaker M, Melgar M, et al; for the RSV-NET Surveillance Team. Characteristics and outcomes among adults aged ≥60 years hospitalized with laboratory-confirmed respiratory syncytial virus ─ RSV-NET, 12 states, July 2022–June 2023. MMWR Morb Mortal Wkly Rep. 2023;72(40):1075-1082. doi:10.15585/mmwr.mm7240a1
6. Walsh EE, Pérez Marc G, Zareba AM, et al; for the RENOIR Clinical Trial Group. Efficacy and safety of a bivalent RSV prefusion F vaccine in older adults. N Engl J Med. 2023;388(16):1465-1477. doi:10.1056/NEJMoa2213836
7. Fleming-Dutra KE, Jones JM, Roper LE, et al. Use of the Pfizer respiratory syncytial virus vaccine during pregnancy for the prevention of respiratory syncytial virus–associated lower respiratory tract disease in infants: recommendations of the Advisory Committee on Immunization Practices — United States, 2023. MMWR Morb Mortal Wkly Rep. 2023;72(41):1115-1122. doi:10.15585/mmwr.mm7241e1
8. Baker J, Aliabadi N, Munjal I, et al. Equivalent immunogenicity across three RSVpreF vaccine lots in healthy adults 18-49 years of age: results of a randomized phase 3 study. Vaccine. 2024;42(13):3172-3179. doi:10.1016/j.vaccine.2024.03.070
9. New data for AREXVY, GSK’s RSV vaccine, show potential to help protect adults aged 50 to 59 at increased risk for RSV disease. Press release. GSK; October 25, 2023. Accessed May 22, 2024. https://us.gsk.com/en-us/media/press-releases/new-data-for-arexvy/
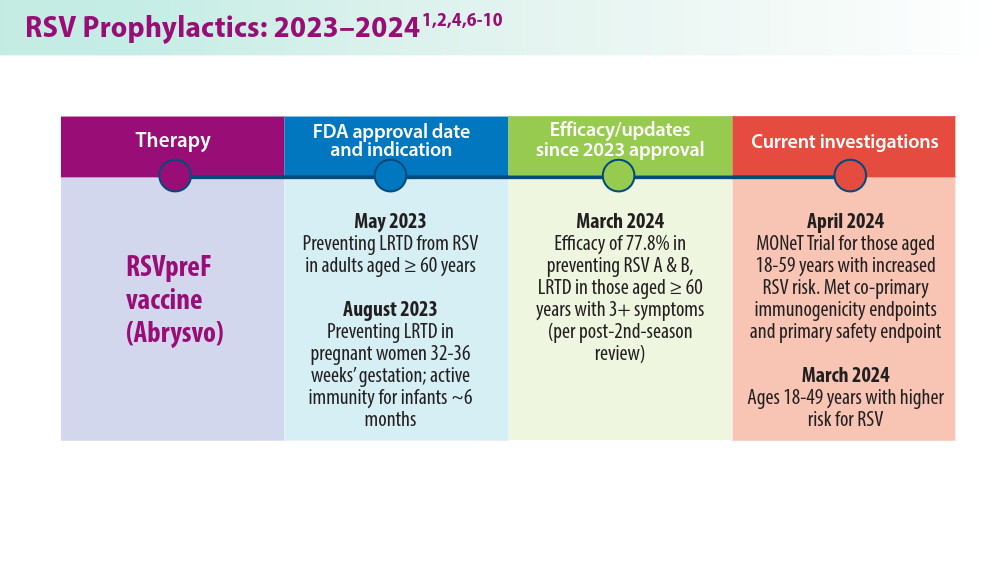
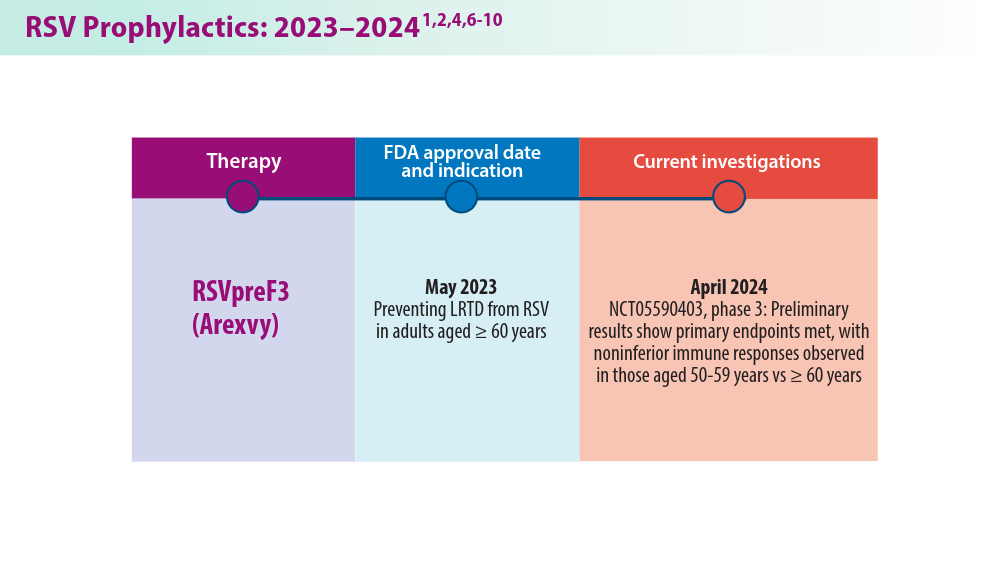
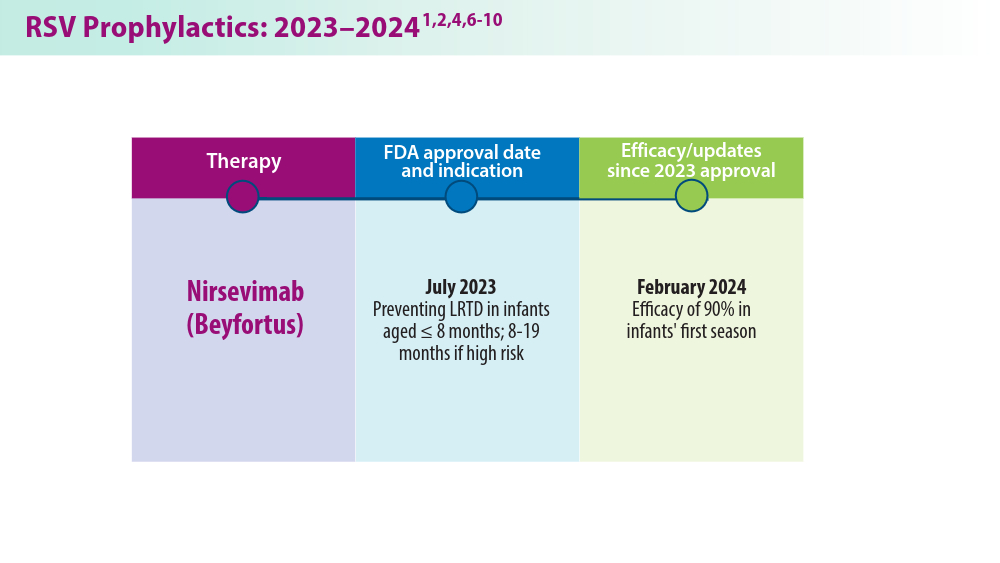
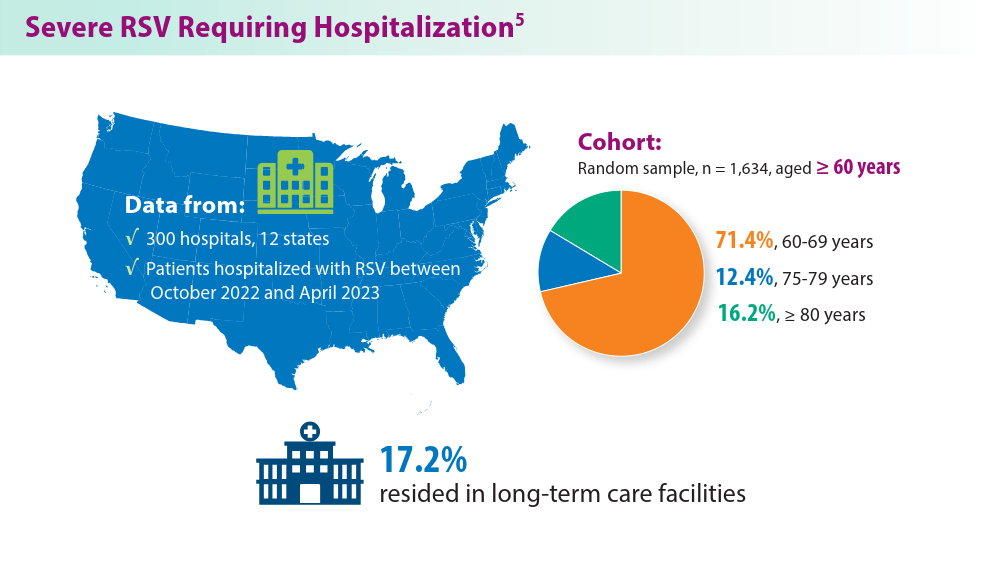
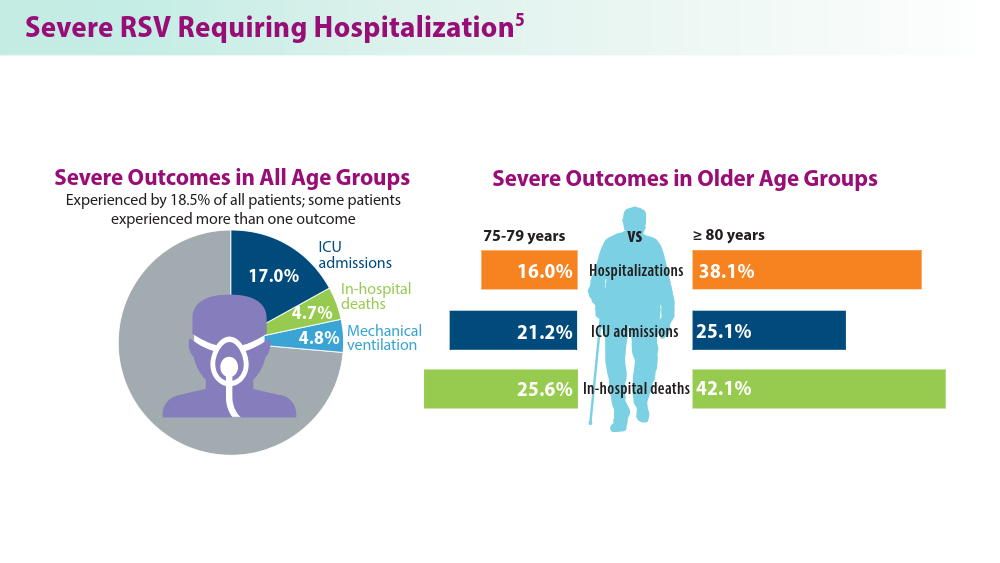
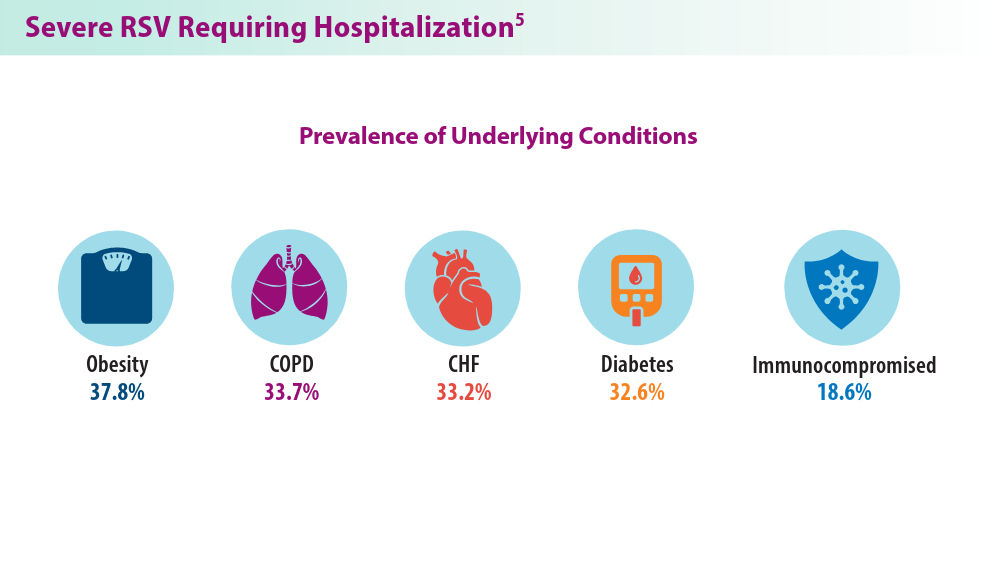
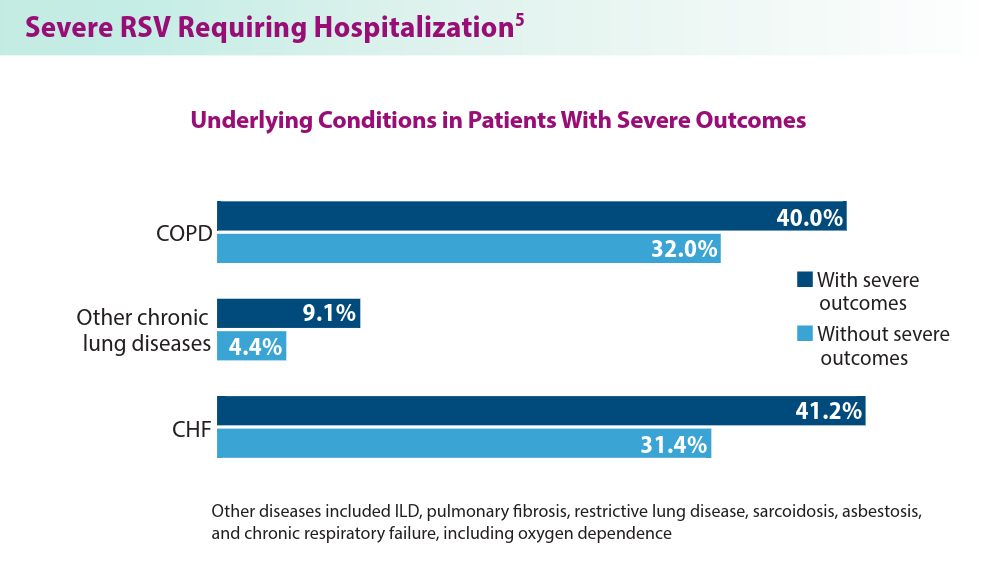
Pulmonology Data Trends 2024
Pulmonology Data Trends 2024 is a supplement to CHEST Physician highlighting the latest breakthroughs in pulmonology research and treatments through a series of infographics.
Read more:

Artificial Intelligence in Sleep Apnea
Ritwick Agrawal, MD, MS, FCCP
RSV Updates: Prophylaxis Approval and Hospitalization for Severe RSV
Riddhi Upadhyay, MD
Biologics in Asthma: Changing the Severe Asthma Paradigm
Shyam Subramanian, MD, FCCP
Updates in COPD Guidelines and Treatment
Dharani K. Narendra, MD, FCCP
Targeted Therapies and Surgical Resection for Lung Cancer: Evolving Treatment Options
Saadia A. Faiz, MD, FCCP
Closing the GAP in Idiopathic Pulmonary Fibrosis
Humayun Anjum, MD, FCCP
Severe Community-Acquired Pneumonia: Diagnostic Criteria, Treatment, and COVID-19
Sujith V. Cherian, MD, FCCP
Pulmonary Hypertension: Comorbidities and Novel Therapies
Mary Jo S. Farmer, MD, PhD, FCCP
The Genetic Side of Interstitial Lung Disease
Priya Balakrishnan, MD, MS, FCCP
Noninvasive Ventilation in Neuromuscular Disease
Sreelatha Naik, MD, FCCP, and Kelly Lobrutto, CRNP
Pulmonology Data Trends 2024 is a supplement to CHEST Physician highlighting the latest breakthroughs in pulmonology research and treatments through a series of infographics.
Read more:
Artificial Intelligence in Sleep Apnea
Ritwick Agrawal, MD, MS, FCCP
RSV Updates: Prophylaxis Approval and Hospitalization for Severe RSV
Riddhi Upadhyay, MD
Biologics in Asthma: Changing the Severe Asthma Paradigm
Shyam Subramanian, MD, FCCP
Updates in COPD Guidelines and Treatment
Dharani K. Narendra, MD, FCCP
Targeted Therapies and Surgical Resection for Lung Cancer: Evolving Treatment Options
Saadia A. Faiz, MD, FCCP
Closing the GAP in Idiopathic Pulmonary Fibrosis
Humayun Anjum, MD, FCCP
Severe Community-Acquired Pneumonia: Diagnostic Criteria, Treatment, and COVID-19
Sujith V. Cherian, MD, FCCP
Pulmonary Hypertension: Comorbidities and Novel Therapies
Mary Jo S. Farmer, MD, PhD, FCCP
The Genetic Side of Interstitial Lung Disease
Priya Balakrishnan, MD, MS, FCCP
Noninvasive Ventilation in Neuromuscular Disease
Sreelatha Naik, MD, FCCP, and Kelly Lobrutto, CRNP
Pulmonology Data Trends 2024 is a supplement to CHEST Physician highlighting the latest breakthroughs in pulmonology research and treatments through a series of infographics.
Read more:
Artificial Intelligence in Sleep Apnea
Ritwick Agrawal, MD, MS, FCCP
RSV Updates: Prophylaxis Approval and Hospitalization for Severe RSV
Riddhi Upadhyay, MD
Biologics in Asthma: Changing the Severe Asthma Paradigm
Shyam Subramanian, MD, FCCP
Updates in COPD Guidelines and Treatment
Dharani K. Narendra, MD, FCCP
Targeted Therapies and Surgical Resection for Lung Cancer: Evolving Treatment Options
Saadia A. Faiz, MD, FCCP
Closing the GAP in Idiopathic Pulmonary Fibrosis
Humayun Anjum, MD, FCCP
Severe Community-Acquired Pneumonia: Diagnostic Criteria, Treatment, and COVID-19
Sujith V. Cherian, MD, FCCP
Pulmonary Hypertension: Comorbidities and Novel Therapies
Mary Jo S. Farmer, MD, PhD, FCCP
The Genetic Side of Interstitial Lung Disease
Priya Balakrishnan, MD, MS, FCCP
Noninvasive Ventilation in Neuromuscular Disease
Sreelatha Naik, MD, FCCP, and Kelly Lobrutto, CRNP
Gram Stain Doesn’t Improve UTI Diagnosis in the ED
TOPLINE:
Compared with other urine analysis methods, urine Gram stain has a moderate predictive value for detecting gram-negative bacteria in urine culture but does not significantly improve urinary tract infection (UTI) diagnosis in the emergency department (ED).
METHODOLOGY:
- Researchers conducted an observational cohort study at the University Medical Center Groningen in the Netherlands, encompassing 1358 episodes across 1136 patients suspected of having a UTI.
- The study included the following predefined subgroups: patients using urinary catheters and patients with leukopenia (< 4.0×10⁹ leucocytes/L). Urine dipstick nitrite, automated urinalysis, Gram stain, and urine cultures were performed on urine samples collected from patients presenting at the ED.
- The sensitivity and specificity of Gram stain for “many” bacteria (quantified as > 15/high power field) were compared with those of urine dipstick nitrite and automated bacterial counting in urinalysis.
TAKEAWAY:
- The sensitivity and specificity of Gram stain for “many” bacteria were 51.3% and 91.0%, respectively, with an accuracy of 76.8%.
- Gram stain showed a positive predictive value (PPV) of 84.7% for gram-negative rods in urine culture; however, the PPV was only 38.4% for gram-positive cocci.
- In the catheter subgroup, the presence of monomorphic bacteria quantified as “many” had a higher PPV for diagnosing a UTI than the presence of polymorphic bacteria with the same quantification.
- The overall performance of Gram stain in diagnosing a UTI in the ED was comparable to that of automated bacterial counting in urinalysis but better than that of urine dipstick nitrite.
IN PRACTICE:
“With the exception of a moderate prediction of gram-negative bacteria in the UC [urine culture], urine GS [Gram stain] does not improve UTI diagnosis at the ED compared to other urine parameters,” the authors wrote.
SOURCE:
The study was led by Stephanie J.M. Middelkoop, University of Groningen, University Medical Center Groningen, the Netherlands. It was published online on August 16, 2024, in Infectious Diseases.
LIMITATIONS:
The study’s limitations included a small sample size within the leukopenia subgroup, which may have affected the generalizability of the findings. Additionally, the potential influence of refrigeration of urine samples on bacterial growth could have affected the results. In this study, indwelling catheters were not replaced before urine sample collection, which may have affected the accuracy of UTI diagnosis in patients using catheters.
DISCLOSURES:
No conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Compared with other urine analysis methods, urine Gram stain has a moderate predictive value for detecting gram-negative bacteria in urine culture but does not significantly improve urinary tract infection (UTI) diagnosis in the emergency department (ED).
METHODOLOGY:
- Researchers conducted an observational cohort study at the University Medical Center Groningen in the Netherlands, encompassing 1358 episodes across 1136 patients suspected of having a UTI.
- The study included the following predefined subgroups: patients using urinary catheters and patients with leukopenia (< 4.0×10⁹ leucocytes/L). Urine dipstick nitrite, automated urinalysis, Gram stain, and urine cultures were performed on urine samples collected from patients presenting at the ED.
- The sensitivity and specificity of Gram stain for “many” bacteria (quantified as > 15/high power field) were compared with those of urine dipstick nitrite and automated bacterial counting in urinalysis.
TAKEAWAY:
- The sensitivity and specificity of Gram stain for “many” bacteria were 51.3% and 91.0%, respectively, with an accuracy of 76.8%.
- Gram stain showed a positive predictive value (PPV) of 84.7% for gram-negative rods in urine culture; however, the PPV was only 38.4% for gram-positive cocci.
- In the catheter subgroup, the presence of monomorphic bacteria quantified as “many” had a higher PPV for diagnosing a UTI than the presence of polymorphic bacteria with the same quantification.
- The overall performance of Gram stain in diagnosing a UTI in the ED was comparable to that of automated bacterial counting in urinalysis but better than that of urine dipstick nitrite.
IN PRACTICE:
“With the exception of a moderate prediction of gram-negative bacteria in the UC [urine culture], urine GS [Gram stain] does not improve UTI diagnosis at the ED compared to other urine parameters,” the authors wrote.
SOURCE:
The study was led by Stephanie J.M. Middelkoop, University of Groningen, University Medical Center Groningen, the Netherlands. It was published online on August 16, 2024, in Infectious Diseases.
LIMITATIONS:
The study’s limitations included a small sample size within the leukopenia subgroup, which may have affected the generalizability of the findings. Additionally, the potential influence of refrigeration of urine samples on bacterial growth could have affected the results. In this study, indwelling catheters were not replaced before urine sample collection, which may have affected the accuracy of UTI diagnosis in patients using catheters.
DISCLOSURES:
No conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Compared with other urine analysis methods, urine Gram stain has a moderate predictive value for detecting gram-negative bacteria in urine culture but does not significantly improve urinary tract infection (UTI) diagnosis in the emergency department (ED).
METHODOLOGY:
- Researchers conducted an observational cohort study at the University Medical Center Groningen in the Netherlands, encompassing 1358 episodes across 1136 patients suspected of having a UTI.
- The study included the following predefined subgroups: patients using urinary catheters and patients with leukopenia (< 4.0×10⁹ leucocytes/L). Urine dipstick nitrite, automated urinalysis, Gram stain, and urine cultures were performed on urine samples collected from patients presenting at the ED.
- The sensitivity and specificity of Gram stain for “many” bacteria (quantified as > 15/high power field) were compared with those of urine dipstick nitrite and automated bacterial counting in urinalysis.
TAKEAWAY:
- The sensitivity and specificity of Gram stain for “many” bacteria were 51.3% and 91.0%, respectively, with an accuracy of 76.8%.
- Gram stain showed a positive predictive value (PPV) of 84.7% for gram-negative rods in urine culture; however, the PPV was only 38.4% for gram-positive cocci.
- In the catheter subgroup, the presence of monomorphic bacteria quantified as “many” had a higher PPV for diagnosing a UTI than the presence of polymorphic bacteria with the same quantification.
- The overall performance of Gram stain in diagnosing a UTI in the ED was comparable to that of automated bacterial counting in urinalysis but better than that of urine dipstick nitrite.
IN PRACTICE:
“With the exception of a moderate prediction of gram-negative bacteria in the UC [urine culture], urine GS [Gram stain] does not improve UTI diagnosis at the ED compared to other urine parameters,” the authors wrote.
SOURCE:
The study was led by Stephanie J.M. Middelkoop, University of Groningen, University Medical Center Groningen, the Netherlands. It was published online on August 16, 2024, in Infectious Diseases.
LIMITATIONS:
The study’s limitations included a small sample size within the leukopenia subgroup, which may have affected the generalizability of the findings. Additionally, the potential influence of refrigeration of urine samples on bacterial growth could have affected the results. In this study, indwelling catheters were not replaced before urine sample collection, which may have affected the accuracy of UTI diagnosis in patients using catheters.
DISCLOSURES:
No conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Listeriosis During Pregnancy Can Be Fatal for the Fetus
Listeriosis during pregnancy, when invasive, can be fatal for the fetus, with a rate of fetal loss or neonatal death of 29%, investigators reported in an article alerting clinicians to this condition.
The article was prompted when the Reproductive Infectious Diseases team at The University of British Columbia in Vancouver, British Columbia, Canada, “received many phone calls from concerned doctors and patients after the plant-based milk recall in early July,” Jeffrey Man Hay Wong, MD, told this news organization. “With such concerns, we updated our British Columbia guidelines for our patients but quickly realized that our recommendations would be useful across the country.”
The article was published online in the Canadian Medical Association Journal.
Five Key Points
Dr. Wong and colleagues provided the following five points and recommendations:
First, invasive listeriosis (bacteremia or meningitis) in pregnancy can have major fetal consequences, including fetal loss or neonatal death in 29% of cases. Affected patients can be asymptomatic or experience gastrointestinal symptoms, myalgias, fevers, acute respiratory distress syndrome, or sepsis.
Second, pregnant people should avoid foods at a high risk for Listeria monocytogenes contamination, including unpasteurized dairy products, luncheon meats, refrigerated meat spreads, and prepared salads. They also should stay aware of Health Canada recalls.
Third, it is not necessary to investigate or treat patients who may have ingested contaminated food but are asymptomatic. Listeriosis can present at 2-3 months after exposure because the incubation period can be as long as 70 days.
Fourth, for patients with mild gastroenteritis or flu-like symptoms who may have ingested contaminated food, obtaining blood cultures or starting a 2-week course of oral amoxicillin (500 mg, three times daily) could be considered.
Fifth, for patients with fever and possible exposure to L monocytogenes, blood cultures should be drawn immediately, and high-dose ampicillin should be initiated, along with electronic fetal heart rate monitoring.
“While choosing safer foods in pregnancy is recommended, it is most important to be aware of Health Canada food recalls and pay attention to symptoms if you’ve ingested these foods,” said Dr. Wong. “Working with the BC Centre for Disease Control, our teams are actively monitoring for cases of listeriosis in pregnancy here in British Columbia.
“Thankfully,” he said, “there haven’t been any confirmed cases in British Columbia related to the plant-based milk recall, though the bacteria’s incubation period can be up to 70 days in pregnancy.”
No Increase Suspected
Commenting on the article, Khady Diouf, MD, director of global obstetrics and gynecology at Brigham and Women’s Hospital in Boston, said, “It summarizes the main management, which is based mostly on expert opinion.”
US clinicians also should be reminded about listeriosis in pregnancy, she noted, pointing to “helpful guidance” from the American College of Obstetrics and Gynecology.
Although the United States similarly experienced a recent listeriosis outbreak resulting from contaminated deli meats, both Dr. Wong and Dr. Diouf said that these outbreaks do not seem to signal an increase in listeriosis cases overall.
“Food-borne listeriosis seems to come in waves,” said Dr. Wong. “At a public health level, we certainly have better surveillance programs for Listeria infections. In 2023, Health Canada updated its Policy on L monocytogenes in ready-to-eat foods, which emphasizes the good manufacturing practices recommended for food processing environments to identify outbreaks earlier.”
“I think we get these recalls yearly, and this has been the case for as long as I can remember,” Dr. Diouf agreed.
No funding was declared, and the authors declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Listeriosis during pregnancy, when invasive, can be fatal for the fetus, with a rate of fetal loss or neonatal death of 29%, investigators reported in an article alerting clinicians to this condition.
The article was prompted when the Reproductive Infectious Diseases team at The University of British Columbia in Vancouver, British Columbia, Canada, “received many phone calls from concerned doctors and patients after the plant-based milk recall in early July,” Jeffrey Man Hay Wong, MD, told this news organization. “With such concerns, we updated our British Columbia guidelines for our patients but quickly realized that our recommendations would be useful across the country.”
The article was published online in the Canadian Medical Association Journal.
Five Key Points
Dr. Wong and colleagues provided the following five points and recommendations:
First, invasive listeriosis (bacteremia or meningitis) in pregnancy can have major fetal consequences, including fetal loss or neonatal death in 29% of cases. Affected patients can be asymptomatic or experience gastrointestinal symptoms, myalgias, fevers, acute respiratory distress syndrome, or sepsis.
Second, pregnant people should avoid foods at a high risk for Listeria monocytogenes contamination, including unpasteurized dairy products, luncheon meats, refrigerated meat spreads, and prepared salads. They also should stay aware of Health Canada recalls.
Third, it is not necessary to investigate or treat patients who may have ingested contaminated food but are asymptomatic. Listeriosis can present at 2-3 months after exposure because the incubation period can be as long as 70 days.
Fourth, for patients with mild gastroenteritis or flu-like symptoms who may have ingested contaminated food, obtaining blood cultures or starting a 2-week course of oral amoxicillin (500 mg, three times daily) could be considered.
Fifth, for patients with fever and possible exposure to L monocytogenes, blood cultures should be drawn immediately, and high-dose ampicillin should be initiated, along with electronic fetal heart rate monitoring.
“While choosing safer foods in pregnancy is recommended, it is most important to be aware of Health Canada food recalls and pay attention to symptoms if you’ve ingested these foods,” said Dr. Wong. “Working with the BC Centre for Disease Control, our teams are actively monitoring for cases of listeriosis in pregnancy here in British Columbia.
“Thankfully,” he said, “there haven’t been any confirmed cases in British Columbia related to the plant-based milk recall, though the bacteria’s incubation period can be up to 70 days in pregnancy.”
No Increase Suspected
Commenting on the article, Khady Diouf, MD, director of global obstetrics and gynecology at Brigham and Women’s Hospital in Boston, said, “It summarizes the main management, which is based mostly on expert opinion.”
US clinicians also should be reminded about listeriosis in pregnancy, she noted, pointing to “helpful guidance” from the American College of Obstetrics and Gynecology.
Although the United States similarly experienced a recent listeriosis outbreak resulting from contaminated deli meats, both Dr. Wong and Dr. Diouf said that these outbreaks do not seem to signal an increase in listeriosis cases overall.
“Food-borne listeriosis seems to come in waves,” said Dr. Wong. “At a public health level, we certainly have better surveillance programs for Listeria infections. In 2023, Health Canada updated its Policy on L monocytogenes in ready-to-eat foods, which emphasizes the good manufacturing practices recommended for food processing environments to identify outbreaks earlier.”
“I think we get these recalls yearly, and this has been the case for as long as I can remember,” Dr. Diouf agreed.
No funding was declared, and the authors declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Listeriosis during pregnancy, when invasive, can be fatal for the fetus, with a rate of fetal loss or neonatal death of 29%, investigators reported in an article alerting clinicians to this condition.
The article was prompted when the Reproductive Infectious Diseases team at The University of British Columbia in Vancouver, British Columbia, Canada, “received many phone calls from concerned doctors and patients after the plant-based milk recall in early July,” Jeffrey Man Hay Wong, MD, told this news organization. “With such concerns, we updated our British Columbia guidelines for our patients but quickly realized that our recommendations would be useful across the country.”
The article was published online in the Canadian Medical Association Journal.
Five Key Points
Dr. Wong and colleagues provided the following five points and recommendations:
First, invasive listeriosis (bacteremia or meningitis) in pregnancy can have major fetal consequences, including fetal loss or neonatal death in 29% of cases. Affected patients can be asymptomatic or experience gastrointestinal symptoms, myalgias, fevers, acute respiratory distress syndrome, or sepsis.
Second, pregnant people should avoid foods at a high risk for Listeria monocytogenes contamination, including unpasteurized dairy products, luncheon meats, refrigerated meat spreads, and prepared salads. They also should stay aware of Health Canada recalls.
Third, it is not necessary to investigate or treat patients who may have ingested contaminated food but are asymptomatic. Listeriosis can present at 2-3 months after exposure because the incubation period can be as long as 70 days.
Fourth, for patients with mild gastroenteritis or flu-like symptoms who may have ingested contaminated food, obtaining blood cultures or starting a 2-week course of oral amoxicillin (500 mg, three times daily) could be considered.
Fifth, for patients with fever and possible exposure to L monocytogenes, blood cultures should be drawn immediately, and high-dose ampicillin should be initiated, along with electronic fetal heart rate monitoring.
“While choosing safer foods in pregnancy is recommended, it is most important to be aware of Health Canada food recalls and pay attention to symptoms if you’ve ingested these foods,” said Dr. Wong. “Working with the BC Centre for Disease Control, our teams are actively monitoring for cases of listeriosis in pregnancy here in British Columbia.
“Thankfully,” he said, “there haven’t been any confirmed cases in British Columbia related to the plant-based milk recall, though the bacteria’s incubation period can be up to 70 days in pregnancy.”
No Increase Suspected
Commenting on the article, Khady Diouf, MD, director of global obstetrics and gynecology at Brigham and Women’s Hospital in Boston, said, “It summarizes the main management, which is based mostly on expert opinion.”
US clinicians also should be reminded about listeriosis in pregnancy, she noted, pointing to “helpful guidance” from the American College of Obstetrics and Gynecology.
Although the United States similarly experienced a recent listeriosis outbreak resulting from contaminated deli meats, both Dr. Wong and Dr. Diouf said that these outbreaks do not seem to signal an increase in listeriosis cases overall.
“Food-borne listeriosis seems to come in waves,” said Dr. Wong. “At a public health level, we certainly have better surveillance programs for Listeria infections. In 2023, Health Canada updated its Policy on L monocytogenes in ready-to-eat foods, which emphasizes the good manufacturing practices recommended for food processing environments to identify outbreaks earlier.”
“I think we get these recalls yearly, and this has been the case for as long as I can remember,” Dr. Diouf agreed.
No funding was declared, and the authors declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE CANADIAN MEDICAL ASSOCIATION JOURNAL
Multiple Draining Sinus Tracts on the Thigh
The Diagnosis: Mycobacterial Infection
An injury sustained in a wet environment that results in chronic indolent abscesses, nodules, or draining sinus tracts suggests a mycobacterial infection. In our patient, a culture revealed MycobacteriuM fortuitum, which is classified in the rapid grower nontuberculous mycobacteria (NTM) group, along with Mycobacterium chelonae and Mycobacterium abscessus.1 The patient’s history of skin injury while cutting wet grass and the common presence of M fortuitum in the environment suggested that the organism entered the wound. The patient healed completely following surgical excision and a 2-month course of clarithromycin 1 g daily and rifampin 600 mg daily.
MycobacteriuM fortuitum was first isolated from an amphibian source in 1905 and later identified in a human with cutaneous infection in 1938. It commonly is found in soil and water.2 Skin and soft-tissue infections with M fortuitum usually are acquired from direct entry of the organism through a damaged skin barrier from trauma, medical injection, surgery, or tattoo placement.2,3
Skin lesions caused by NTM often are nonspecific and can mimic a variety of other dermatologic conditions, making clinical diagnosis challenging. As such, cutaneous manifestations of M fortuitum infection can include recurrent cutaneous abscesses, nodular lesions, chronic discharging sinuses, cellulitis, and surgical site infections.4 Although cutaneous infection with M fortuitum classically manifests with a single subcutaneous nodule at the site of trauma or surgery,5 it also can manifest as multiple draining sinus tracts, as seen in our patient. Hence, the diagnosis and treatment of cutaneous NTM infection is challenging, especially when M fortuitum skin manifestations can take up to 4 to 6 weeks to develop after inoculation. Diagnosis often requires a detailed patient history, tissue cultures, and histopathology.5
In recent years, rapid detection with polymerase chain reaction (PCR) techniques has been employed more widely. Notably, a molecular system based on multiplex real-time PCR with high-resolution melting was shown to have a sensitivity of up to 54% for distinguishing M fortuitum from other NTM.6 More recently, a 2-step real-time PCR method has demonstrated diagnostic sensitivity and specificity for differentiating NTM from Mycobacterium tuberculosis infections and identifying the causative NTM agent.7
Compared to immunocompetent individuals, those who are immunocompromised are more susceptible to less pathogenic strains of NTM, which can cause dissemination and lead to tenosynovitis, myositis, osteomyelitis, and septic arthritis.8-12 Nonetheless, cases of infections with NTM—including M fortuitum—are becoming harder to treat. Several single nucleotide polymorphisms and point mutations have been demonstrated in the ribosomal RNA methylase gene erm(39) related to clarithromycin resistance and in the rrl gene related to linezolid resistance.13 Due to increasing inducible resistance to common classes of antibiotics, such as macrolides and linezolid, treatment of M fortuitum requires multidrug regimens.13,14 Drug susceptibility testing also may be required, as M fortuitum has shown low resistance to tigecycline, tetracycline, cefmetazole, imipenem, and aminoglycosides (eg, amikacin, tobramycin, neomycin, gentamycin). Surgery is an important adjunctive tool in treating M fortuitum infections; patients with a single lesion are more likely to undergo surgical treatment alone or in combination with antibiotic therapy.15 More recently, antimicrobial photodynamic therapy has been explored as an alternative to eliminate NTM, including M fortuitum.16
The differential diagnosis for skin lesions manifesting with draining fistulae and sinus tracts includes conditions with infectious (cellulitis and chromomycosis) and inflammatory (pyoderma gangrenosum [PG] and hidradenitis suppurativa [HS]) causes.
Cellulitis is a common infection of the skin and subcutaneous tissue that predominantly is caused by gram-positive organisms such as β-hemolytic streptococci.17 Clinical manifestations include acute skin erythema, swelling, tenderness, and warmth. The legs are the most common sites of infection, but any area of the skin can be involved.17 Cellulitis comprises 10% of all infectious disease hospitalizations and up to 11% of all dermatologic admissions.18,19 It frequently is misdiagnosed, perhaps due to the lack of a reliable confirmatory laboratory test or imaging study, in addition to the plethora of diseases that mimic cellulitis, such as stasis dermatitis, lipodermatosclerosis, contact dermatitis, lymphedema, eosinophilic cellulitis, and papular urticaria.20,21 The consequences of misdiagnosis include but are not limited to unnecessary hospitalizations, inappropriate antibiotic use, and delayed management of the disease; thus, there is an urgent need for a reliable standard test to confirm the diagnosis, especially among nonspecialist physicians. 20 Most patients with uncomplicated cellulitis can be treated with empiric oral antibiotics that target β-hemolytic streptococci (ie, penicillin V potassium, amoxicillin).17 Methicillin-resistant Staphylococcus aureus coverage generally is unnecessary for nonpurulent cellulitis, but clinicians can consider adding amoxicillin-clavulanate, dicloxacillin, and cephalexin to the regimen. For purulent cellulitis, incision and drainage should be performed. In severe cases that manifest with sepsis, altered mental status, or hemodynamic instability, inpatient management is required.17
Chromomycosis (also known as chromoblastomycosis) is a chronic, indolent, granulomatous, suppurative mycosis of the skin and subcutaneous tissue22 that is caused by traumatic inoculation of various fungi of the order Chaetothyriales and family Herpotrichiellaceae, which are present in soil, plants, and decomposing wood. Chromomycosis is prevalent in tropical and subtropical regions.23,24 Clinically, it manifests as oligosymptomatic or asymptomatic lesions around an infection site that can manifest as papules with centrifugal growth evolving into nodular, verrucous, plaque, tumoral, or atrophic forms.22 Diagnosis is made with direct microscopy using potassium hydroxide, which reveals muriform bodies. Fungal culture in Sabouraud agar also can be used to isolate the causative pathogen.22 Unfortunately, chromomycosis is difficult to treat, with low cure rates and high relapse rates. Antifungal agents combined with surgery, cryotherapy, or thermotherapy often are used, with cure rates ranging from 15% to 80%.22,25
Pyoderma gangrenosum is a reactive noninfectious inflammatory dermatosis associated with inflammatory bowel disease and rheumatoid arthritis. The exact etiology is not clearly understood, but it generally is considered an autoinflammatory disorder.26 The most common form—classical PG—occurs in approximately 85% of cases and manifests as a painful erythematous lesion that progresses to a blistered or necrotic ulcer. It primarily affects the lower legs but can occur in other body sites.27 The diagnosis is based on clinical symptoms after excluding other similar conditions; histopathology of biopsied wound tissues often are required for confirmation. Treatment of PG starts with fast-acting immunosuppressive drugs (corticosteroids and/or cyclosporine) followed by slowacting immunosuppressive drugs (biologics).26
Hidradenitis suppurativa is a chronic recurrent disease of the hair follicle unit that develops after puberty.28 Clinically, HS manifests with painful nodules, abscesses, chronically draining fistulas, and scarring in areas of the body rich in apocrine glands.29,30 Treatment of HS is challenging due to its diverse clinical manifestations and unclear etiology. Topical therapy, systemic treatments, biologic agents, surgery, and light therapy have shown variable results.28,31
- Franco-Paredes C, Marcos LA, Henao-Martínez AF, et al. Cutaneous mycobacterial infections. Clin Microbiol Rev. 2018;32: E00069-18. doi:10.1128/CMR.00069-18
- Brown TH. The rapidly growing mycobacteria—MycobacteriuM fortuitum and Mycobacterium chelonae. Infect Control. 1985;6:283-238. doi:10.1017/s0195941700061762
- Hooper J; Beltrami EJ; Santoro F; et al. Remember the fite: a case of cutaneous MycobacteriuM fortuitum infection. Am J Dermatopathol. 2023;45:214-215. doi:10.1097/DAD.0000000000002336
- Franco-Paredes C, Chastain DB, Allen L, et al. Overview of cutaneous mycobacterial infections. Curr Trop Med Rep. 2018;5:228-232. doi:10.1007/s40475-018-0161-7
- Gonzalez-Santiago TM, Drage LA. Nontuberculous mycobacteria: skin and soft tissue infections. Dermatol Clin. 2015;33:563-77. doi:10.1016/j.det.2015.03.017
- Peixoto ADS, Montenegro LML, Lima AS, et al. Identification of nontuberculous mycobacteria species by multiplex real-time PCR with high-resolution melting. Rev Soc Bras Med Trop. 2020;53:E20200211. doi:10.1590/0037-8682-0211-2020
- Park J, Kwak N, Chae JC, et al. A two-step real-time PCR method to identify Mycobacterium tuberculosis infections and six dominant nontuberculous mycobacterial infections from clinical specimens. Microbiol Spectr. 2023:E0160623. doi:10.1128/spectrum.01606-23
- Fowler J, Mahlen SD. Localized cutaneous infections in immunocompetent individuals due to rapidly growing mycobacteria. Arch Pathol Lab Med. 2014;138:1106-1109. doi:10.5858/arpa.2012-0203-RS
- Gardini G, Gregori N, Matteelli A, et al. Mycobacterial skin infection. Curr Opin Infect Dis. 2022;35:79-87. doi:10.1097/QCO.0000000000000820
- Wang SH, Pancholi P. Mycobacterial skin and soft tissue infection. Curr Infect Dis Rep. 2014;16:438. doi:10.1007/s11908-014-0438-5
- Griffith DE, Aksamit T, Brown-Elliott BA, et al; ATS Mycobacterial Diseases Subcommittee; American Thoracic Society; Infectious Disease Society of America. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175:367-416. doi:10.1164/rccm.200604-571ST
- Mougari F, Guglielmetti L, Raskine L, et al. Infections caused by Mycobacterium abscessus: epidemiology, diagnostic tools and treatment. Expert Rev Anti Infect Ther. 2016;14:1139-1154. doi:10.1080/14787210.201 6.1238304
- Tu HZ, Lee HS, Chen YS, et al. High rates of antimicrobial resistance in rapidly growing mycobacterial infections in Taiwan. Pathogens. 2022;11:969. doi:10.3390/pathogens11090969
- Hashemzadeh M, Zadegan Dezfuli AA, Khosravi AD, et al. F requency of mutations in erm(39) related to clarithromycin resistance and in rrl related to linezolid resistance in clinical isolates of MycobacteriuM fortuitum in Iran. Acta Microbiol Immunol Hung. 2023;70:167-176. doi:10.1556/030.2023.02020
- Uslan DZ, Kowalski TJ, Wengenack NL, et al. Skin and soft tissue infections due to rapidly growing mycobacteria: comparison of clinical features, treatment, and susceptibility. Arch Dermatol. 2006;142:1287-1292. doi:10.1001/archderm.142.10.1287
- Miretti M, Juri L, Peralta A, et al. Photoinactivation of non-tuberculous mycobacteria using Zn-phthalocyanine loaded into liposomes. Tuberculosis (Edinb). 2022;136:102247. doi:10.1016/j.tube.2022.102247
- Bystritsky RJ. Cellulitis. Infect Dis Clin North Am. 2021;35:49-60. doi:10.1016/j.idc.2020.10.002
- Christensen K, Holman R, Steiner C, et al. Infectious disease hospitalizations in the United States. Clin Infect Dis. 2009;49:1025-1035. doi:10.1086/605562
- Yang JJ, Maloney NJ, Bach DQ, et al. Dermatology in the emergency department: prescriptions, rates of inpatient admission, and predictors of high utilization in the United States from 1996 to 2012. J Am Acad Dermatol. 2021;84:1480-1483. doi:10.1016/J.JAAD.2020.07.055
- Cutler TS, Jannat-Khah DP, Kam B, et al. Prevalence of misdiagnosis of cellulitis: a systematic review and meta-analysis. J Hosp Med. 2023;18:254-261. doi:10.1002/jhm.12977
- Keller EC, Tomecki KJ, Alraies MC. Distinguishing cellulitis from its mimics. Cleve Clin J Med. 2012;79:547-52. doi:10.3949/ccjm.79a.11121
- Brito AC, Bittencourt MJS. Chromoblastomycosis: an etiological, epidemiological, clinical, diagnostic, and treatment update. An Bras Dermatol. 2018;93:495-506. doi:10.1590/abd1806-4841.20187321
- McGinnis MR. Chromoblastomycosis and phaeohyphomycosis: new concepts, diagnosis, and mycology. J Am Acad Dermatol. 1983;8:1-16.
- Rubin HA, Bruce S, Rosen T, et al. Evidence for percutaneous inoculation as the mode of transmission for chromoblastomycosis. J Am Acad Dermatol. 1991;25:951-954.
- Bonifaz A, Paredes-Solís V, Saúl A. Treating chromoblastomycosis with systemic antifungals. Expert Opin Pharmacother. 2004;5:247-254.
- Maverakis E, Marzano AV, Le ST, et al. Pyoderma gangrenosum. Nat Rev Dis Primers. 2020;6:81. doi:10.1038/s41572-020-0213-x
- George C, Deroide F, Rustin M. Pyoderma gangrenosum—a guide to diagnosis and management. Clin Med (Lond). 2019;19:224-228. doi:10.7861/clinmedicine.19-3-224
- Narla S, Lyons AB, Hamzavi IH. The most recent advances in understanding and managing hidradenitis suppurativa. F1000Res. 2020;9:F1000 Faculty Rev-1049. doi:10.12688/f1000research.26083.1
- Garg A, Lavian J, Lin G, et al. Incidence of hidradenitis suppurativa in the United States: a sex- and age-adjusted population analysis. J Am Acad Dermatol. 2017;77:118-122. doi:10.1016/j.jaad.2017.02.005
- Daxhelet M, Suppa M, White J, et al. Proposed definitions of typical lesions in hidradenitis suppurativa. Dermatology. 2020;236:431-438. doi:10.1159/000507348
- Amat-Samaranch V, Agut-Busquet E, Vilarrasa E, et al. New perspectives on the treatment of hidradenitis suppurativa. Ther Adv Chronic Dis. 2021;12:20406223211055920. doi:10.1177/20406223211055920
The Diagnosis: Mycobacterial Infection
An injury sustained in a wet environment that results in chronic indolent abscesses, nodules, or draining sinus tracts suggests a mycobacterial infection. In our patient, a culture revealed MycobacteriuM fortuitum, which is classified in the rapid grower nontuberculous mycobacteria (NTM) group, along with Mycobacterium chelonae and Mycobacterium abscessus.1 The patient’s history of skin injury while cutting wet grass and the common presence of M fortuitum in the environment suggested that the organism entered the wound. The patient healed completely following surgical excision and a 2-month course of clarithromycin 1 g daily and rifampin 600 mg daily.
MycobacteriuM fortuitum was first isolated from an amphibian source in 1905 and later identified in a human with cutaneous infection in 1938. It commonly is found in soil and water.2 Skin and soft-tissue infections with M fortuitum usually are acquired from direct entry of the organism through a damaged skin barrier from trauma, medical injection, surgery, or tattoo placement.2,3
Skin lesions caused by NTM often are nonspecific and can mimic a variety of other dermatologic conditions, making clinical diagnosis challenging. As such, cutaneous manifestations of M fortuitum infection can include recurrent cutaneous abscesses, nodular lesions, chronic discharging sinuses, cellulitis, and surgical site infections.4 Although cutaneous infection with M fortuitum classically manifests with a single subcutaneous nodule at the site of trauma or surgery,5 it also can manifest as multiple draining sinus tracts, as seen in our patient. Hence, the diagnosis and treatment of cutaneous NTM infection is challenging, especially when M fortuitum skin manifestations can take up to 4 to 6 weeks to develop after inoculation. Diagnosis often requires a detailed patient history, tissue cultures, and histopathology.5
In recent years, rapid detection with polymerase chain reaction (PCR) techniques has been employed more widely. Notably, a molecular system based on multiplex real-time PCR with high-resolution melting was shown to have a sensitivity of up to 54% for distinguishing M fortuitum from other NTM.6 More recently, a 2-step real-time PCR method has demonstrated diagnostic sensitivity and specificity for differentiating NTM from Mycobacterium tuberculosis infections and identifying the causative NTM agent.7
Compared to immunocompetent individuals, those who are immunocompromised are more susceptible to less pathogenic strains of NTM, which can cause dissemination and lead to tenosynovitis, myositis, osteomyelitis, and septic arthritis.8-12 Nonetheless, cases of infections with NTM—including M fortuitum—are becoming harder to treat. Several single nucleotide polymorphisms and point mutations have been demonstrated in the ribosomal RNA methylase gene erm(39) related to clarithromycin resistance and in the rrl gene related to linezolid resistance.13 Due to increasing inducible resistance to common classes of antibiotics, such as macrolides and linezolid, treatment of M fortuitum requires multidrug regimens.13,14 Drug susceptibility testing also may be required, as M fortuitum has shown low resistance to tigecycline, tetracycline, cefmetazole, imipenem, and aminoglycosides (eg, amikacin, tobramycin, neomycin, gentamycin). Surgery is an important adjunctive tool in treating M fortuitum infections; patients with a single lesion are more likely to undergo surgical treatment alone or in combination with antibiotic therapy.15 More recently, antimicrobial photodynamic therapy has been explored as an alternative to eliminate NTM, including M fortuitum.16
The differential diagnosis for skin lesions manifesting with draining fistulae and sinus tracts includes conditions with infectious (cellulitis and chromomycosis) and inflammatory (pyoderma gangrenosum [PG] and hidradenitis suppurativa [HS]) causes.
Cellulitis is a common infection of the skin and subcutaneous tissue that predominantly is caused by gram-positive organisms such as β-hemolytic streptococci.17 Clinical manifestations include acute skin erythema, swelling, tenderness, and warmth. The legs are the most common sites of infection, but any area of the skin can be involved.17 Cellulitis comprises 10% of all infectious disease hospitalizations and up to 11% of all dermatologic admissions.18,19 It frequently is misdiagnosed, perhaps due to the lack of a reliable confirmatory laboratory test or imaging study, in addition to the plethora of diseases that mimic cellulitis, such as stasis dermatitis, lipodermatosclerosis, contact dermatitis, lymphedema, eosinophilic cellulitis, and papular urticaria.20,21 The consequences of misdiagnosis include but are not limited to unnecessary hospitalizations, inappropriate antibiotic use, and delayed management of the disease; thus, there is an urgent need for a reliable standard test to confirm the diagnosis, especially among nonspecialist physicians. 20 Most patients with uncomplicated cellulitis can be treated with empiric oral antibiotics that target β-hemolytic streptococci (ie, penicillin V potassium, amoxicillin).17 Methicillin-resistant Staphylococcus aureus coverage generally is unnecessary for nonpurulent cellulitis, but clinicians can consider adding amoxicillin-clavulanate, dicloxacillin, and cephalexin to the regimen. For purulent cellulitis, incision and drainage should be performed. In severe cases that manifest with sepsis, altered mental status, or hemodynamic instability, inpatient management is required.17
Chromomycosis (also known as chromoblastomycosis) is a chronic, indolent, granulomatous, suppurative mycosis of the skin and subcutaneous tissue22 that is caused by traumatic inoculation of various fungi of the order Chaetothyriales and family Herpotrichiellaceae, which are present in soil, plants, and decomposing wood. Chromomycosis is prevalent in tropical and subtropical regions.23,24 Clinically, it manifests as oligosymptomatic or asymptomatic lesions around an infection site that can manifest as papules with centrifugal growth evolving into nodular, verrucous, plaque, tumoral, or atrophic forms.22 Diagnosis is made with direct microscopy using potassium hydroxide, which reveals muriform bodies. Fungal culture in Sabouraud agar also can be used to isolate the causative pathogen.22 Unfortunately, chromomycosis is difficult to treat, with low cure rates and high relapse rates. Antifungal agents combined with surgery, cryotherapy, or thermotherapy often are used, with cure rates ranging from 15% to 80%.22,25
Pyoderma gangrenosum is a reactive noninfectious inflammatory dermatosis associated with inflammatory bowel disease and rheumatoid arthritis. The exact etiology is not clearly understood, but it generally is considered an autoinflammatory disorder.26 The most common form—classical PG—occurs in approximately 85% of cases and manifests as a painful erythematous lesion that progresses to a blistered or necrotic ulcer. It primarily affects the lower legs but can occur in other body sites.27 The diagnosis is based on clinical symptoms after excluding other similar conditions; histopathology of biopsied wound tissues often are required for confirmation. Treatment of PG starts with fast-acting immunosuppressive drugs (corticosteroids and/or cyclosporine) followed by slowacting immunosuppressive drugs (biologics).26
Hidradenitis suppurativa is a chronic recurrent disease of the hair follicle unit that develops after puberty.28 Clinically, HS manifests with painful nodules, abscesses, chronically draining fistulas, and scarring in areas of the body rich in apocrine glands.29,30 Treatment of HS is challenging due to its diverse clinical manifestations and unclear etiology. Topical therapy, systemic treatments, biologic agents, surgery, and light therapy have shown variable results.28,31
The Diagnosis: Mycobacterial Infection
An injury sustained in a wet environment that results in chronic indolent abscesses, nodules, or draining sinus tracts suggests a mycobacterial infection. In our patient, a culture revealed MycobacteriuM fortuitum, which is classified in the rapid grower nontuberculous mycobacteria (NTM) group, along with Mycobacterium chelonae and Mycobacterium abscessus.1 The patient’s history of skin injury while cutting wet grass and the common presence of M fortuitum in the environment suggested that the organism entered the wound. The patient healed completely following surgical excision and a 2-month course of clarithromycin 1 g daily and rifampin 600 mg daily.
MycobacteriuM fortuitum was first isolated from an amphibian source in 1905 and later identified in a human with cutaneous infection in 1938. It commonly is found in soil and water.2 Skin and soft-tissue infections with M fortuitum usually are acquired from direct entry of the organism through a damaged skin barrier from trauma, medical injection, surgery, or tattoo placement.2,3
Skin lesions caused by NTM often are nonspecific and can mimic a variety of other dermatologic conditions, making clinical diagnosis challenging. As such, cutaneous manifestations of M fortuitum infection can include recurrent cutaneous abscesses, nodular lesions, chronic discharging sinuses, cellulitis, and surgical site infections.4 Although cutaneous infection with M fortuitum classically manifests with a single subcutaneous nodule at the site of trauma or surgery,5 it also can manifest as multiple draining sinus tracts, as seen in our patient. Hence, the diagnosis and treatment of cutaneous NTM infection is challenging, especially when M fortuitum skin manifestations can take up to 4 to 6 weeks to develop after inoculation. Diagnosis often requires a detailed patient history, tissue cultures, and histopathology.5
In recent years, rapid detection with polymerase chain reaction (PCR) techniques has been employed more widely. Notably, a molecular system based on multiplex real-time PCR with high-resolution melting was shown to have a sensitivity of up to 54% for distinguishing M fortuitum from other NTM.6 More recently, a 2-step real-time PCR method has demonstrated diagnostic sensitivity and specificity for differentiating NTM from Mycobacterium tuberculosis infections and identifying the causative NTM agent.7
Compared to immunocompetent individuals, those who are immunocompromised are more susceptible to less pathogenic strains of NTM, which can cause dissemination and lead to tenosynovitis, myositis, osteomyelitis, and septic arthritis.8-12 Nonetheless, cases of infections with NTM—including M fortuitum—are becoming harder to treat. Several single nucleotide polymorphisms and point mutations have been demonstrated in the ribosomal RNA methylase gene erm(39) related to clarithromycin resistance and in the rrl gene related to linezolid resistance.13 Due to increasing inducible resistance to common classes of antibiotics, such as macrolides and linezolid, treatment of M fortuitum requires multidrug regimens.13,14 Drug susceptibility testing also may be required, as M fortuitum has shown low resistance to tigecycline, tetracycline, cefmetazole, imipenem, and aminoglycosides (eg, amikacin, tobramycin, neomycin, gentamycin). Surgery is an important adjunctive tool in treating M fortuitum infections; patients with a single lesion are more likely to undergo surgical treatment alone or in combination with antibiotic therapy.15 More recently, antimicrobial photodynamic therapy has been explored as an alternative to eliminate NTM, including M fortuitum.16
The differential diagnosis for skin lesions manifesting with draining fistulae and sinus tracts includes conditions with infectious (cellulitis and chromomycosis) and inflammatory (pyoderma gangrenosum [PG] and hidradenitis suppurativa [HS]) causes.
Cellulitis is a common infection of the skin and subcutaneous tissue that predominantly is caused by gram-positive organisms such as β-hemolytic streptococci.17 Clinical manifestations include acute skin erythema, swelling, tenderness, and warmth. The legs are the most common sites of infection, but any area of the skin can be involved.17 Cellulitis comprises 10% of all infectious disease hospitalizations and up to 11% of all dermatologic admissions.18,19 It frequently is misdiagnosed, perhaps due to the lack of a reliable confirmatory laboratory test or imaging study, in addition to the plethora of diseases that mimic cellulitis, such as stasis dermatitis, lipodermatosclerosis, contact dermatitis, lymphedema, eosinophilic cellulitis, and papular urticaria.20,21 The consequences of misdiagnosis include but are not limited to unnecessary hospitalizations, inappropriate antibiotic use, and delayed management of the disease; thus, there is an urgent need for a reliable standard test to confirm the diagnosis, especially among nonspecialist physicians. 20 Most patients with uncomplicated cellulitis can be treated with empiric oral antibiotics that target β-hemolytic streptococci (ie, penicillin V potassium, amoxicillin).17 Methicillin-resistant Staphylococcus aureus coverage generally is unnecessary for nonpurulent cellulitis, but clinicians can consider adding amoxicillin-clavulanate, dicloxacillin, and cephalexin to the regimen. For purulent cellulitis, incision and drainage should be performed. In severe cases that manifest with sepsis, altered mental status, or hemodynamic instability, inpatient management is required.17
Chromomycosis (also known as chromoblastomycosis) is a chronic, indolent, granulomatous, suppurative mycosis of the skin and subcutaneous tissue22 that is caused by traumatic inoculation of various fungi of the order Chaetothyriales and family Herpotrichiellaceae, which are present in soil, plants, and decomposing wood. Chromomycosis is prevalent in tropical and subtropical regions.23,24 Clinically, it manifests as oligosymptomatic or asymptomatic lesions around an infection site that can manifest as papules with centrifugal growth evolving into nodular, verrucous, plaque, tumoral, or atrophic forms.22 Diagnosis is made with direct microscopy using potassium hydroxide, which reveals muriform bodies. Fungal culture in Sabouraud agar also can be used to isolate the causative pathogen.22 Unfortunately, chromomycosis is difficult to treat, with low cure rates and high relapse rates. Antifungal agents combined with surgery, cryotherapy, or thermotherapy often are used, with cure rates ranging from 15% to 80%.22,25
Pyoderma gangrenosum is a reactive noninfectious inflammatory dermatosis associated with inflammatory bowel disease and rheumatoid arthritis. The exact etiology is not clearly understood, but it generally is considered an autoinflammatory disorder.26 The most common form—classical PG—occurs in approximately 85% of cases and manifests as a painful erythematous lesion that progresses to a blistered or necrotic ulcer. It primarily affects the lower legs but can occur in other body sites.27 The diagnosis is based on clinical symptoms after excluding other similar conditions; histopathology of biopsied wound tissues often are required for confirmation. Treatment of PG starts with fast-acting immunosuppressive drugs (corticosteroids and/or cyclosporine) followed by slowacting immunosuppressive drugs (biologics).26
Hidradenitis suppurativa is a chronic recurrent disease of the hair follicle unit that develops after puberty.28 Clinically, HS manifests with painful nodules, abscesses, chronically draining fistulas, and scarring in areas of the body rich in apocrine glands.29,30 Treatment of HS is challenging due to its diverse clinical manifestations and unclear etiology. Topical therapy, systemic treatments, biologic agents, surgery, and light therapy have shown variable results.28,31
- Franco-Paredes C, Marcos LA, Henao-Martínez AF, et al. Cutaneous mycobacterial infections. Clin Microbiol Rev. 2018;32: E00069-18. doi:10.1128/CMR.00069-18
- Brown TH. The rapidly growing mycobacteria—MycobacteriuM fortuitum and Mycobacterium chelonae. Infect Control. 1985;6:283-238. doi:10.1017/s0195941700061762
- Hooper J; Beltrami EJ; Santoro F; et al. Remember the fite: a case of cutaneous MycobacteriuM fortuitum infection. Am J Dermatopathol. 2023;45:214-215. doi:10.1097/DAD.0000000000002336
- Franco-Paredes C, Chastain DB, Allen L, et al. Overview of cutaneous mycobacterial infections. Curr Trop Med Rep. 2018;5:228-232. doi:10.1007/s40475-018-0161-7
- Gonzalez-Santiago TM, Drage LA. Nontuberculous mycobacteria: skin and soft tissue infections. Dermatol Clin. 2015;33:563-77. doi:10.1016/j.det.2015.03.017
- Peixoto ADS, Montenegro LML, Lima AS, et al. Identification of nontuberculous mycobacteria species by multiplex real-time PCR with high-resolution melting. Rev Soc Bras Med Trop. 2020;53:E20200211. doi:10.1590/0037-8682-0211-2020
- Park J, Kwak N, Chae JC, et al. A two-step real-time PCR method to identify Mycobacterium tuberculosis infections and six dominant nontuberculous mycobacterial infections from clinical specimens. Microbiol Spectr. 2023:E0160623. doi:10.1128/spectrum.01606-23
- Fowler J, Mahlen SD. Localized cutaneous infections in immunocompetent individuals due to rapidly growing mycobacteria. Arch Pathol Lab Med. 2014;138:1106-1109. doi:10.5858/arpa.2012-0203-RS
- Gardini G, Gregori N, Matteelli A, et al. Mycobacterial skin infection. Curr Opin Infect Dis. 2022;35:79-87. doi:10.1097/QCO.0000000000000820
- Wang SH, Pancholi P. Mycobacterial skin and soft tissue infection. Curr Infect Dis Rep. 2014;16:438. doi:10.1007/s11908-014-0438-5
- Griffith DE, Aksamit T, Brown-Elliott BA, et al; ATS Mycobacterial Diseases Subcommittee; American Thoracic Society; Infectious Disease Society of America. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175:367-416. doi:10.1164/rccm.200604-571ST
- Mougari F, Guglielmetti L, Raskine L, et al. Infections caused by Mycobacterium abscessus: epidemiology, diagnostic tools and treatment. Expert Rev Anti Infect Ther. 2016;14:1139-1154. doi:10.1080/14787210.201 6.1238304
- Tu HZ, Lee HS, Chen YS, et al. High rates of antimicrobial resistance in rapidly growing mycobacterial infections in Taiwan. Pathogens. 2022;11:969. doi:10.3390/pathogens11090969
- Hashemzadeh M, Zadegan Dezfuli AA, Khosravi AD, et al. F requency of mutations in erm(39) related to clarithromycin resistance and in rrl related to linezolid resistance in clinical isolates of MycobacteriuM fortuitum in Iran. Acta Microbiol Immunol Hung. 2023;70:167-176. doi:10.1556/030.2023.02020
- Uslan DZ, Kowalski TJ, Wengenack NL, et al. Skin and soft tissue infections due to rapidly growing mycobacteria: comparison of clinical features, treatment, and susceptibility. Arch Dermatol. 2006;142:1287-1292. doi:10.1001/archderm.142.10.1287
- Miretti M, Juri L, Peralta A, et al. Photoinactivation of non-tuberculous mycobacteria using Zn-phthalocyanine loaded into liposomes. Tuberculosis (Edinb). 2022;136:102247. doi:10.1016/j.tube.2022.102247
- Bystritsky RJ. Cellulitis. Infect Dis Clin North Am. 2021;35:49-60. doi:10.1016/j.idc.2020.10.002
- Christensen K, Holman R, Steiner C, et al. Infectious disease hospitalizations in the United States. Clin Infect Dis. 2009;49:1025-1035. doi:10.1086/605562
- Yang JJ, Maloney NJ, Bach DQ, et al. Dermatology in the emergency department: prescriptions, rates of inpatient admission, and predictors of high utilization in the United States from 1996 to 2012. J Am Acad Dermatol. 2021;84:1480-1483. doi:10.1016/J.JAAD.2020.07.055
- Cutler TS, Jannat-Khah DP, Kam B, et al. Prevalence of misdiagnosis of cellulitis: a systematic review and meta-analysis. J Hosp Med. 2023;18:254-261. doi:10.1002/jhm.12977
- Keller EC, Tomecki KJ, Alraies MC. Distinguishing cellulitis from its mimics. Cleve Clin J Med. 2012;79:547-52. doi:10.3949/ccjm.79a.11121
- Brito AC, Bittencourt MJS. Chromoblastomycosis: an etiological, epidemiological, clinical, diagnostic, and treatment update. An Bras Dermatol. 2018;93:495-506. doi:10.1590/abd1806-4841.20187321
- McGinnis MR. Chromoblastomycosis and phaeohyphomycosis: new concepts, diagnosis, and mycology. J Am Acad Dermatol. 1983;8:1-16.
- Rubin HA, Bruce S, Rosen T, et al. Evidence for percutaneous inoculation as the mode of transmission for chromoblastomycosis. J Am Acad Dermatol. 1991;25:951-954.
- Bonifaz A, Paredes-Solís V, Saúl A. Treating chromoblastomycosis with systemic antifungals. Expert Opin Pharmacother. 2004;5:247-254.
- Maverakis E, Marzano AV, Le ST, et al. Pyoderma gangrenosum. Nat Rev Dis Primers. 2020;6:81. doi:10.1038/s41572-020-0213-x
- George C, Deroide F, Rustin M. Pyoderma gangrenosum—a guide to diagnosis and management. Clin Med (Lond). 2019;19:224-228. doi:10.7861/clinmedicine.19-3-224
- Narla S, Lyons AB, Hamzavi IH. The most recent advances in understanding and managing hidradenitis suppurativa. F1000Res. 2020;9:F1000 Faculty Rev-1049. doi:10.12688/f1000research.26083.1
- Garg A, Lavian J, Lin G, et al. Incidence of hidradenitis suppurativa in the United States: a sex- and age-adjusted population analysis. J Am Acad Dermatol. 2017;77:118-122. doi:10.1016/j.jaad.2017.02.005
- Daxhelet M, Suppa M, White J, et al. Proposed definitions of typical lesions in hidradenitis suppurativa. Dermatology. 2020;236:431-438. doi:10.1159/000507348
- Amat-Samaranch V, Agut-Busquet E, Vilarrasa E, et al. New perspectives on the treatment of hidradenitis suppurativa. Ther Adv Chronic Dis. 2021;12:20406223211055920. doi:10.1177/20406223211055920
- Franco-Paredes C, Marcos LA, Henao-Martínez AF, et al. Cutaneous mycobacterial infections. Clin Microbiol Rev. 2018;32: E00069-18. doi:10.1128/CMR.00069-18
- Brown TH. The rapidly growing mycobacteria—MycobacteriuM fortuitum and Mycobacterium chelonae. Infect Control. 1985;6:283-238. doi:10.1017/s0195941700061762
- Hooper J; Beltrami EJ; Santoro F; et al. Remember the fite: a case of cutaneous MycobacteriuM fortuitum infection. Am J Dermatopathol. 2023;45:214-215. doi:10.1097/DAD.0000000000002336
- Franco-Paredes C, Chastain DB, Allen L, et al. Overview of cutaneous mycobacterial infections. Curr Trop Med Rep. 2018;5:228-232. doi:10.1007/s40475-018-0161-7
- Gonzalez-Santiago TM, Drage LA. Nontuberculous mycobacteria: skin and soft tissue infections. Dermatol Clin. 2015;33:563-77. doi:10.1016/j.det.2015.03.017
- Peixoto ADS, Montenegro LML, Lima AS, et al. Identification of nontuberculous mycobacteria species by multiplex real-time PCR with high-resolution melting. Rev Soc Bras Med Trop. 2020;53:E20200211. doi:10.1590/0037-8682-0211-2020
- Park J, Kwak N, Chae JC, et al. A two-step real-time PCR method to identify Mycobacterium tuberculosis infections and six dominant nontuberculous mycobacterial infections from clinical specimens. Microbiol Spectr. 2023:E0160623. doi:10.1128/spectrum.01606-23
- Fowler J, Mahlen SD. Localized cutaneous infections in immunocompetent individuals due to rapidly growing mycobacteria. Arch Pathol Lab Med. 2014;138:1106-1109. doi:10.5858/arpa.2012-0203-RS
- Gardini G, Gregori N, Matteelli A, et al. Mycobacterial skin infection. Curr Opin Infect Dis. 2022;35:79-87. doi:10.1097/QCO.0000000000000820
- Wang SH, Pancholi P. Mycobacterial skin and soft tissue infection. Curr Infect Dis Rep. 2014;16:438. doi:10.1007/s11908-014-0438-5
- Griffith DE, Aksamit T, Brown-Elliott BA, et al; ATS Mycobacterial Diseases Subcommittee; American Thoracic Society; Infectious Disease Society of America. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175:367-416. doi:10.1164/rccm.200604-571ST
- Mougari F, Guglielmetti L, Raskine L, et al. Infections caused by Mycobacterium abscessus: epidemiology, diagnostic tools and treatment. Expert Rev Anti Infect Ther. 2016;14:1139-1154. doi:10.1080/14787210.201 6.1238304
- Tu HZ, Lee HS, Chen YS, et al. High rates of antimicrobial resistance in rapidly growing mycobacterial infections in Taiwan. Pathogens. 2022;11:969. doi:10.3390/pathogens11090969
- Hashemzadeh M, Zadegan Dezfuli AA, Khosravi AD, et al. F requency of mutations in erm(39) related to clarithromycin resistance and in rrl related to linezolid resistance in clinical isolates of MycobacteriuM fortuitum in Iran. Acta Microbiol Immunol Hung. 2023;70:167-176. doi:10.1556/030.2023.02020
- Uslan DZ, Kowalski TJ, Wengenack NL, et al. Skin and soft tissue infections due to rapidly growing mycobacteria: comparison of clinical features, treatment, and susceptibility. Arch Dermatol. 2006;142:1287-1292. doi:10.1001/archderm.142.10.1287
- Miretti M, Juri L, Peralta A, et al. Photoinactivation of non-tuberculous mycobacteria using Zn-phthalocyanine loaded into liposomes. Tuberculosis (Edinb). 2022;136:102247. doi:10.1016/j.tube.2022.102247
- Bystritsky RJ. Cellulitis. Infect Dis Clin North Am. 2021;35:49-60. doi:10.1016/j.idc.2020.10.002
- Christensen K, Holman R, Steiner C, et al. Infectious disease hospitalizations in the United States. Clin Infect Dis. 2009;49:1025-1035. doi:10.1086/605562
- Yang JJ, Maloney NJ, Bach DQ, et al. Dermatology in the emergency department: prescriptions, rates of inpatient admission, and predictors of high utilization in the United States from 1996 to 2012. J Am Acad Dermatol. 2021;84:1480-1483. doi:10.1016/J.JAAD.2020.07.055
- Cutler TS, Jannat-Khah DP, Kam B, et al. Prevalence of misdiagnosis of cellulitis: a systematic review and meta-analysis. J Hosp Med. 2023;18:254-261. doi:10.1002/jhm.12977
- Keller EC, Tomecki KJ, Alraies MC. Distinguishing cellulitis from its mimics. Cleve Clin J Med. 2012;79:547-52. doi:10.3949/ccjm.79a.11121
- Brito AC, Bittencourt MJS. Chromoblastomycosis: an etiological, epidemiological, clinical, diagnostic, and treatment update. An Bras Dermatol. 2018;93:495-506. doi:10.1590/abd1806-4841.20187321
- McGinnis MR. Chromoblastomycosis and phaeohyphomycosis: new concepts, diagnosis, and mycology. J Am Acad Dermatol. 1983;8:1-16.
- Rubin HA, Bruce S, Rosen T, et al. Evidence for percutaneous inoculation as the mode of transmission for chromoblastomycosis. J Am Acad Dermatol. 1991;25:951-954.
- Bonifaz A, Paredes-Solís V, Saúl A. Treating chromoblastomycosis with systemic antifungals. Expert Opin Pharmacother. 2004;5:247-254.
- Maverakis E, Marzano AV, Le ST, et al. Pyoderma gangrenosum. Nat Rev Dis Primers. 2020;6:81. doi:10.1038/s41572-020-0213-x
- George C, Deroide F, Rustin M. Pyoderma gangrenosum—a guide to diagnosis and management. Clin Med (Lond). 2019;19:224-228. doi:10.7861/clinmedicine.19-3-224
- Narla S, Lyons AB, Hamzavi IH. The most recent advances in understanding and managing hidradenitis suppurativa. F1000Res. 2020;9:F1000 Faculty Rev-1049. doi:10.12688/f1000research.26083.1
- Garg A, Lavian J, Lin G, et al. Incidence of hidradenitis suppurativa in the United States: a sex- and age-adjusted population analysis. J Am Acad Dermatol. 2017;77:118-122. doi:10.1016/j.jaad.2017.02.005
- Daxhelet M, Suppa M, White J, et al. Proposed definitions of typical lesions in hidradenitis suppurativa. Dermatology. 2020;236:431-438. doi:10.1159/000507348
- Amat-Samaranch V, Agut-Busquet E, Vilarrasa E, et al. New perspectives on the treatment of hidradenitis suppurativa. Ther Adv Chronic Dis. 2021;12:20406223211055920. doi:10.1177/20406223211055920
A 40-year-old woman presented with multiple draining sinus tracts on the right thigh following an injury sustained weeks earlier while mowing wet grass.

