User login
Study reveals mutation that causes aplastic anemia

of women in a family
By studying 3 generations of a family plagued by blood disorders, researchers discovered a genetic mutation that causes aplastic anemia.
The team performed whole-exome sequencing on DNA from the families and identified an inherited mutation on the ACD gene, which codes for the telomere-binding protein TPP1.
The mutation disrupts the interactions between telomeres and telomerase, which causes blood cells to die and results in aplastic anemia.
“Identifying this causal defect may help suggest future molecular-based treatments that bypass the gene defect and restore blood cell production,” said Hakon Hakonarson, MD, PhD, of The Children’s Hospital of Philadelphia in Pennsylvania.
Dr Hakonarson and his colleagues described this research in Blood.
The team studied an Australian family with aplastic anemia and other hematopoietic disorders, including leukemia. Whole-exome sequencing of the family’s DNA revealed an inherited mutation on the ACD gene.
The mutation is an amino acid deletion in the TEL patch of TPP1 (ΔK170). All of the family members with this mutation had short telomeres, and those with wild-type TPP1 did not.
The researchers introduced TPP1 with the ΔK170 mutation into 293T cells and found the protein could localize to telomeres but failed to recruit telomerase. The team said this indicates a causal relationship between the mutation and bone marrow disorders.
Without access to telomerase to help maintain telomeres, blood cells lose their structural integrity and die, resulting in bone marrow failure and aplastic anemia.
Nine other genes were previously found to play a role in bone marrow failure disorders. The current study adds ACD to the list and is the first time the gene has been shown to have a disease-causing role.
“This improved understanding of the underlying molecular mechanisms may suggest new approaches to treating disorders such as aplastic anemia,” Dr Hakonarson said. “For instance, investigators may identify other avenues for recruiting telomerase to telomeres to restore its protective function.” ![]()
of women in a family
By studying 3 generations of a family plagued by blood disorders, researchers discovered a genetic mutation that causes aplastic anemia.
The team performed whole-exome sequencing on DNA from the families and identified an inherited mutation on the ACD gene, which codes for the telomere-binding protein TPP1.
The mutation disrupts the interactions between telomeres and telomerase, which causes blood cells to die and results in aplastic anemia.
“Identifying this causal defect may help suggest future molecular-based treatments that bypass the gene defect and restore blood cell production,” said Hakon Hakonarson, MD, PhD, of The Children’s Hospital of Philadelphia in Pennsylvania.
Dr Hakonarson and his colleagues described this research in Blood.
The team studied an Australian family with aplastic anemia and other hematopoietic disorders, including leukemia. Whole-exome sequencing of the family’s DNA revealed an inherited mutation on the ACD gene.
The mutation is an amino acid deletion in the TEL patch of TPP1 (ΔK170). All of the family members with this mutation had short telomeres, and those with wild-type TPP1 did not.
The researchers introduced TPP1 with the ΔK170 mutation into 293T cells and found the protein could localize to telomeres but failed to recruit telomerase. The team said this indicates a causal relationship between the mutation and bone marrow disorders.
Without access to telomerase to help maintain telomeres, blood cells lose their structural integrity and die, resulting in bone marrow failure and aplastic anemia.
Nine other genes were previously found to play a role in bone marrow failure disorders. The current study adds ACD to the list and is the first time the gene has been shown to have a disease-causing role.
“This improved understanding of the underlying molecular mechanisms may suggest new approaches to treating disorders such as aplastic anemia,” Dr Hakonarson said. “For instance, investigators may identify other avenues for recruiting telomerase to telomeres to restore its protective function.” ![]()
of women in a family
By studying 3 generations of a family plagued by blood disorders, researchers discovered a genetic mutation that causes aplastic anemia.
The team performed whole-exome sequencing on DNA from the families and identified an inherited mutation on the ACD gene, which codes for the telomere-binding protein TPP1.
The mutation disrupts the interactions between telomeres and telomerase, which causes blood cells to die and results in aplastic anemia.
“Identifying this causal defect may help suggest future molecular-based treatments that bypass the gene defect and restore blood cell production,” said Hakon Hakonarson, MD, PhD, of The Children’s Hospital of Philadelphia in Pennsylvania.
Dr Hakonarson and his colleagues described this research in Blood.
The team studied an Australian family with aplastic anemia and other hematopoietic disorders, including leukemia. Whole-exome sequencing of the family’s DNA revealed an inherited mutation on the ACD gene.
The mutation is an amino acid deletion in the TEL patch of TPP1 (ΔK170). All of the family members with this mutation had short telomeres, and those with wild-type TPP1 did not.
The researchers introduced TPP1 with the ΔK170 mutation into 293T cells and found the protein could localize to telomeres but failed to recruit telomerase. The team said this indicates a causal relationship between the mutation and bone marrow disorders.
Without access to telomerase to help maintain telomeres, blood cells lose their structural integrity and die, resulting in bone marrow failure and aplastic anemia.
Nine other genes were previously found to play a role in bone marrow failure disorders. The current study adds ACD to the list and is the first time the gene has been shown to have a disease-causing role.
“This improved understanding of the underlying molecular mechanisms may suggest new approaches to treating disorders such as aplastic anemia,” Dr Hakonarson said. “For instance, investigators may identify other avenues for recruiting telomerase to telomeres to restore its protective function.” ![]()
FDA approves new treatment for PI

Credit: Baxter
The US Food and Drug Administration (FDA) has approved a subcutaneous immune globulin product for use in adults with primary immunodeficiency (PI).
The product, HyQvia, is an immune globulin with a recombinant human hyaluronidase. It requires a single infusion every 3 to 4 weeks and 1 injection site per infusion to deliver a full therapeutic dose of immune globulin.
Current therapies require weekly or bi-weekly treatment with multiple infusion sites per treatment.
Baxter International Inc. expects to launch HyQvia in the US in the coming weeks. The product has been FDA-approved with a black-box warning detailing the risk of thrombosis associated with immune globulin products.
The immune globulin component of HyQvia is a 10% solution prepared from large pools of human plasma consisting of at least 98% IgG. The recombinant human hyaluronidase increases the dispersion and absorption of the immune globulin.
In a phase 3 trial, HyQvia compared well with intravenous human immune globulin 10% (IVIG).
Researchers compared the treatments at different time periods in a cohort of PI patients with a median age of 35 (range, 4-78 years). All 87 patients studied received IVIG, and 83 of the patients received at least 1 dose of HyQvia.
Patients received HyQvia for a median of 366 days and IVIG for a median of 91 days. The median ratio (HyQvia:IVIG) for the IgG dosage administered was 1.088 (range, 0.986–1.382).
Trough IgG concentrations, the incidence of infection, and rates of adverse events were generally similar during the HyQvia treatment period and the IVIG treatment period.
For patients aged 12 years and older, the median IgG Ctrough values with HyQvia were approximately the same as with IVIG. The median trough ratio (HyQvia:IVIG) was 0.985.
For patients younger than 12 (n=11), the median IgG Ctrough values were 10.0 and 9.6 g/L after HyQvia and IVIG, respectively, with a median trough ratio of 1.038.
The overall infection rates were 2.97 per patient-year with HyQvia and 4.51 per patient-year with IVIG.
During the HyQvia treatment period, the rate of acute serious bacterial infection (SBI) was 0.025 per patient-year. The rate of acute SBIs occurring during IVIG treatment was not reported.
In patients age 18 and older (n=59), the rate of acute SBIs was 0.00 per patient-year, and the overall infection rate was 3.20 per patient-year.
For this same patient group, the local adverse reaction rate was 0.286 per infusion.
The rate of systemic adverse events temporally related to an infusion was 0.20 per infusion with HyQvia and 0.33 per infusion with IVIG. There were no serious adverse events reported in these patients with either treatment.
HyQvia was approved in Europe in 2013 for adults with PI syndromes and myeloma or chronic lymphocytic leukemia with severe secondary hypogammaglobulinemia and recurrent infections.
For more details on HyQvia, see the prescribing information. ![]()
Credit: Baxter
The US Food and Drug Administration (FDA) has approved a subcutaneous immune globulin product for use in adults with primary immunodeficiency (PI).
The product, HyQvia, is an immune globulin with a recombinant human hyaluronidase. It requires a single infusion every 3 to 4 weeks and 1 injection site per infusion to deliver a full therapeutic dose of immune globulin.
Current therapies require weekly or bi-weekly treatment with multiple infusion sites per treatment.
Baxter International Inc. expects to launch HyQvia in the US in the coming weeks. The product has been FDA-approved with a black-box warning detailing the risk of thrombosis associated with immune globulin products.
The immune globulin component of HyQvia is a 10% solution prepared from large pools of human plasma consisting of at least 98% IgG. The recombinant human hyaluronidase increases the dispersion and absorption of the immune globulin.
In a phase 3 trial, HyQvia compared well with intravenous human immune globulin 10% (IVIG).
Researchers compared the treatments at different time periods in a cohort of PI patients with a median age of 35 (range, 4-78 years). All 87 patients studied received IVIG, and 83 of the patients received at least 1 dose of HyQvia.
Patients received HyQvia for a median of 366 days and IVIG for a median of 91 days. The median ratio (HyQvia:IVIG) for the IgG dosage administered was 1.088 (range, 0.986–1.382).
Trough IgG concentrations, the incidence of infection, and rates of adverse events were generally similar during the HyQvia treatment period and the IVIG treatment period.
For patients aged 12 years and older, the median IgG Ctrough values with HyQvia were approximately the same as with IVIG. The median trough ratio (HyQvia:IVIG) was 0.985.
For patients younger than 12 (n=11), the median IgG Ctrough values were 10.0 and 9.6 g/L after HyQvia and IVIG, respectively, with a median trough ratio of 1.038.
The overall infection rates were 2.97 per patient-year with HyQvia and 4.51 per patient-year with IVIG.
During the HyQvia treatment period, the rate of acute serious bacterial infection (SBI) was 0.025 per patient-year. The rate of acute SBIs occurring during IVIG treatment was not reported.
In patients age 18 and older (n=59), the rate of acute SBIs was 0.00 per patient-year, and the overall infection rate was 3.20 per patient-year.
For this same patient group, the local adverse reaction rate was 0.286 per infusion.
The rate of systemic adverse events temporally related to an infusion was 0.20 per infusion with HyQvia and 0.33 per infusion with IVIG. There were no serious adverse events reported in these patients with either treatment.
HyQvia was approved in Europe in 2013 for adults with PI syndromes and myeloma or chronic lymphocytic leukemia with severe secondary hypogammaglobulinemia and recurrent infections.
For more details on HyQvia, see the prescribing information. ![]()
Credit: Baxter
The US Food and Drug Administration (FDA) has approved a subcutaneous immune globulin product for use in adults with primary immunodeficiency (PI).
The product, HyQvia, is an immune globulin with a recombinant human hyaluronidase. It requires a single infusion every 3 to 4 weeks and 1 injection site per infusion to deliver a full therapeutic dose of immune globulin.
Current therapies require weekly or bi-weekly treatment with multiple infusion sites per treatment.
Baxter International Inc. expects to launch HyQvia in the US in the coming weeks. The product has been FDA-approved with a black-box warning detailing the risk of thrombosis associated with immune globulin products.
The immune globulin component of HyQvia is a 10% solution prepared from large pools of human plasma consisting of at least 98% IgG. The recombinant human hyaluronidase increases the dispersion and absorption of the immune globulin.
In a phase 3 trial, HyQvia compared well with intravenous human immune globulin 10% (IVIG).
Researchers compared the treatments at different time periods in a cohort of PI patients with a median age of 35 (range, 4-78 years). All 87 patients studied received IVIG, and 83 of the patients received at least 1 dose of HyQvia.
Patients received HyQvia for a median of 366 days and IVIG for a median of 91 days. The median ratio (HyQvia:IVIG) for the IgG dosage administered was 1.088 (range, 0.986–1.382).
Trough IgG concentrations, the incidence of infection, and rates of adverse events were generally similar during the HyQvia treatment period and the IVIG treatment period.
For patients aged 12 years and older, the median IgG Ctrough values with HyQvia were approximately the same as with IVIG. The median trough ratio (HyQvia:IVIG) was 0.985.
For patients younger than 12 (n=11), the median IgG Ctrough values were 10.0 and 9.6 g/L after HyQvia and IVIG, respectively, with a median trough ratio of 1.038.
The overall infection rates were 2.97 per patient-year with HyQvia and 4.51 per patient-year with IVIG.
During the HyQvia treatment period, the rate of acute serious bacterial infection (SBI) was 0.025 per patient-year. The rate of acute SBIs occurring during IVIG treatment was not reported.
In patients age 18 and older (n=59), the rate of acute SBIs was 0.00 per patient-year, and the overall infection rate was 3.20 per patient-year.
For this same patient group, the local adverse reaction rate was 0.286 per infusion.
The rate of systemic adverse events temporally related to an infusion was 0.20 per infusion with HyQvia and 0.33 per infusion with IVIG. There were no serious adverse events reported in these patients with either treatment.
HyQvia was approved in Europe in 2013 for adults with PI syndromes and myeloma or chronic lymphocytic leukemia with severe secondary hypogammaglobulinemia and recurrent infections.
For more details on HyQvia, see the prescribing information. ![]()
Test allows for rapid diagnosis of anemia

Credit: Gary Meek
A simple device could provide more rapid diagnosis of anemia and allow for inexpensive at-home monitoring, according to a paper published in The Journal of Clinical Investigation.
The disposable device analyzes a single droplet of blood using a chemical reagent that produces visible color changes corresponding to different levels of anemia.
The test produces results in about 60 seconds, and a smartphone application can correlate the visual results to specific hemoglobin levels.
“Our goal is to get this device into patients’ hands so they can diagnose and monitor anemia themselves,” said Wilbur Lam, MD, PhD, of the Georgia Institute of Technology and Emory University in Atlanta.
“Patients could use this device in a way that’s very similar to how diabetics use glucose-monitoring devices, but this will be even simpler because this is a visual-based test that doesn’t require an additional electrical device to analyze the results.”
The device was developed through a collaboration between Emory University, Children’s Healthcare of Atlanta, and Georgia Tech. It grew out of a 2011 undergraduate senior design project in the Wallace H. Coulter Department of Biomedical Engineering at Georgia Tech and Emory University.
Using a 2-piece prototype device, the test works this way: A patient sticks a finger with a lance to produce a droplet of blood. The device’s cap, a small vial, is touched to the droplet, drawing in a precise amount of blood using capillary action.
The cap containing the blood sample is then placed onto the body of the clear plastic test kit, which contains the chemical reagent. After the cap is closed, the device is briefly shaken to mix the blood and reagent.
“When the capillary is filled, we have a very precise volume of blood, about 5 microliters, which is less than a droplet—much less than what is required by other anemia tests,” explained Erika Tyburski, the paper’s first author and leader of the team that developed the device.
Hemoglobin then serves as a catalyst for a reduction-oxidation reaction that takes place in the device. After about 45 seconds, the reaction is complete, and the user sees a color ranging from green-blue to red, indicating the degree of anemia.
A label on the device helps with interpretation of the color, or patients could use a smartphone app that automatically correlates the color to a specific hemoglobin level.
To evaluate sensitivity and specificity of the device, Tyburski studied blood taken from 238 pediatric and adult patients. Each blood sample was tested 4 times using the device, and the results were compared to reports provided by conventional hematology analyzers.
The results of the 1-minute test were consistent with those of the conventional analyses. The smartphone app produced the best results for measuring severe anemia.
“The test doesn’t require a skilled technician or a draw of venous blood, and you see the results immediately,” Dr Lam said. “We think this is an empowering system, both for the general public and for our patients.”
Tyburski and Dr Lam have teamed up with 2 other partners to launch a startup company called Sanguina to commercialize the test, which will be known as AnemoCheck™.
The test will require approval from the US Food and Drug Administration, but the researchers believe the device could be on pharmacy shelves sometime in 2016.
The team also plans to study how the test may be applied to sickle cell anemia and other diseases. ![]()
Credit: Gary Meek
A simple device could provide more rapid diagnosis of anemia and allow for inexpensive at-home monitoring, according to a paper published in The Journal of Clinical Investigation.
The disposable device analyzes a single droplet of blood using a chemical reagent that produces visible color changes corresponding to different levels of anemia.
The test produces results in about 60 seconds, and a smartphone application can correlate the visual results to specific hemoglobin levels.
“Our goal is to get this device into patients’ hands so they can diagnose and monitor anemia themselves,” said Wilbur Lam, MD, PhD, of the Georgia Institute of Technology and Emory University in Atlanta.
“Patients could use this device in a way that’s very similar to how diabetics use glucose-monitoring devices, but this will be even simpler because this is a visual-based test that doesn’t require an additional electrical device to analyze the results.”
The device was developed through a collaboration between Emory University, Children’s Healthcare of Atlanta, and Georgia Tech. It grew out of a 2011 undergraduate senior design project in the Wallace H. Coulter Department of Biomedical Engineering at Georgia Tech and Emory University.
Using a 2-piece prototype device, the test works this way: A patient sticks a finger with a lance to produce a droplet of blood. The device’s cap, a small vial, is touched to the droplet, drawing in a precise amount of blood using capillary action.
The cap containing the blood sample is then placed onto the body of the clear plastic test kit, which contains the chemical reagent. After the cap is closed, the device is briefly shaken to mix the blood and reagent.
“When the capillary is filled, we have a very precise volume of blood, about 5 microliters, which is less than a droplet—much less than what is required by other anemia tests,” explained Erika Tyburski, the paper’s first author and leader of the team that developed the device.
Hemoglobin then serves as a catalyst for a reduction-oxidation reaction that takes place in the device. After about 45 seconds, the reaction is complete, and the user sees a color ranging from green-blue to red, indicating the degree of anemia.
A label on the device helps with interpretation of the color, or patients could use a smartphone app that automatically correlates the color to a specific hemoglobin level.
To evaluate sensitivity and specificity of the device, Tyburski studied blood taken from 238 pediatric and adult patients. Each blood sample was tested 4 times using the device, and the results were compared to reports provided by conventional hematology analyzers.
The results of the 1-minute test were consistent with those of the conventional analyses. The smartphone app produced the best results for measuring severe anemia.
“The test doesn’t require a skilled technician or a draw of venous blood, and you see the results immediately,” Dr Lam said. “We think this is an empowering system, both for the general public and for our patients.”
Tyburski and Dr Lam have teamed up with 2 other partners to launch a startup company called Sanguina to commercialize the test, which will be known as AnemoCheck™.
The test will require approval from the US Food and Drug Administration, but the researchers believe the device could be on pharmacy shelves sometime in 2016.
The team also plans to study how the test may be applied to sickle cell anemia and other diseases. ![]()
Credit: Gary Meek
A simple device could provide more rapid diagnosis of anemia and allow for inexpensive at-home monitoring, according to a paper published in The Journal of Clinical Investigation.
The disposable device analyzes a single droplet of blood using a chemical reagent that produces visible color changes corresponding to different levels of anemia.
The test produces results in about 60 seconds, and a smartphone application can correlate the visual results to specific hemoglobin levels.
“Our goal is to get this device into patients’ hands so they can diagnose and monitor anemia themselves,” said Wilbur Lam, MD, PhD, of the Georgia Institute of Technology and Emory University in Atlanta.
“Patients could use this device in a way that’s very similar to how diabetics use glucose-monitoring devices, but this will be even simpler because this is a visual-based test that doesn’t require an additional electrical device to analyze the results.”
The device was developed through a collaboration between Emory University, Children’s Healthcare of Atlanta, and Georgia Tech. It grew out of a 2011 undergraduate senior design project in the Wallace H. Coulter Department of Biomedical Engineering at Georgia Tech and Emory University.
Using a 2-piece prototype device, the test works this way: A patient sticks a finger with a lance to produce a droplet of blood. The device’s cap, a small vial, is touched to the droplet, drawing in a precise amount of blood using capillary action.
The cap containing the blood sample is then placed onto the body of the clear plastic test kit, which contains the chemical reagent. After the cap is closed, the device is briefly shaken to mix the blood and reagent.
“When the capillary is filled, we have a very precise volume of blood, about 5 microliters, which is less than a droplet—much less than what is required by other anemia tests,” explained Erika Tyburski, the paper’s first author and leader of the team that developed the device.
Hemoglobin then serves as a catalyst for a reduction-oxidation reaction that takes place in the device. After about 45 seconds, the reaction is complete, and the user sees a color ranging from green-blue to red, indicating the degree of anemia.
A label on the device helps with interpretation of the color, or patients could use a smartphone app that automatically correlates the color to a specific hemoglobin level.
To evaluate sensitivity and specificity of the device, Tyburski studied blood taken from 238 pediatric and adult patients. Each blood sample was tested 4 times using the device, and the results were compared to reports provided by conventional hematology analyzers.
The results of the 1-minute test were consistent with those of the conventional analyses. The smartphone app produced the best results for measuring severe anemia.
“The test doesn’t require a skilled technician or a draw of venous blood, and you see the results immediately,” Dr Lam said. “We think this is an empowering system, both for the general public and for our patients.”
Tyburski and Dr Lam have teamed up with 2 other partners to launch a startup company called Sanguina to commercialize the test, which will be known as AnemoCheck™.
The test will require approval from the US Food and Drug Administration, but the researchers believe the device could be on pharmacy shelves sometime in 2016.
The team also plans to study how the test may be applied to sickle cell anemia and other diseases. ![]()
Antifungal shows promise in hematologic conditions
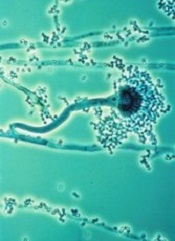
WASHINGTON, DC—A new antifungal agent is as effective as an existing drug against invasive mold infection in patients with hematologic disorders, results of a phase 3 trial suggest.
Overall response and all-cause mortality rates were comparable with the newer drug, isavuconazole (ISA), and the existing drug, voriconazole (VRC).
The overall rates of treatment-emergent adverse events were comparable as well, but ISA was associated with a significantly lower incidence of several events.
Kieren Marr, MD, of Johns Hopkins University in Baltimore, Maryland, and her colleagues presented these results in a subset of patients from the SECURE trial at the 54th Interscience Conference on Antimicrobial Agents and Chemotherapy (poster M-1757).
Patient characteristics and safety outcomes
Of the 433 patients with a hematologic disorder enrolled in the trial, 217 had proven or probable invasive mold infection. The researchers divided patients into 2 groups according to disease: those with acute myeloid leukemia (AML) and those with acute lymphoblastic leukemia (ALL) or other conditions.
In all, 102 patients had AML, and 115 had ALL (n=28) or other conditions, including non-Hodgkin lymphoma (n=19), chronic lymphocytic leukemia (n=15), refractory anemia with excess blasts (n=9), myelodysplastic syndrome (n=8), chronic myeloid leukemia (n=6), and “other” underlying conditions (n=30).
Patients were randomized to receive VRC (n=105) or ISA (N=112). Thirty patients in the ISA arm and 26 in the VRC arm had undergone allogeneic transplant prior to therapy.
The primary outcome was all-cause mortality at day 42. Overall response and safety were secondary endpoints.
The overall rates of treatment-emergent adverse events were similar between ISA and VRC arms. Ninety-seven percent of patients in the ISA arm and 98% of patients in the VRC arm reported at least 1 treatment-emergent adverse event.
However, patients in the ISA arm had significantly fewer (P<0.05) events for the cardiac disorders, eye, psychiatric disorders, renal and urinary, and vascular system organ classes.
Response and mortality
All-cause mortality rates were comparable between the ISA and VRC arms—22% and 24%, respectively—as were overall response rates—39% and 34%, respectively—and complete response rates—13% and 10%, respectively.
All-cause mortality rates among patients with AML were 18% in the ISA arm and 15% in the VRC arm. Overall response rates were 36% and 48%, respectively.
For patients with ALL or other hematologic conditions, all-cause mortality rates were 26% in the ISA arm and 32% in the VRC arm. Overall response rates were 42% and 21%, respectively.
In transplant patients, the all-cause mortality rate was 27% for both the ISA and VRC arms. The overall response rate was 27% for both arms as well.
“These results show the potential of isavuconazole as a potent antifungal in the fight against invasive mold disease,” Dr Marr said.
ISA is an investigational antifungal under development by Astellas and Basilea Pharmaceutica International Ltd. The SECURE trial was funded by Astellas.
The US Food and Drug Administration recently accepted a new drug application seeking approval for ISA for the treatment of invasive aspergillosis and invasive mucormycosis. ![]()
WASHINGTON, DC—A new antifungal agent is as effective as an existing drug against invasive mold infection in patients with hematologic disorders, results of a phase 3 trial suggest.
Overall response and all-cause mortality rates were comparable with the newer drug, isavuconazole (ISA), and the existing drug, voriconazole (VRC).
The overall rates of treatment-emergent adverse events were comparable as well, but ISA was associated with a significantly lower incidence of several events.
Kieren Marr, MD, of Johns Hopkins University in Baltimore, Maryland, and her colleagues presented these results in a subset of patients from the SECURE trial at the 54th Interscience Conference on Antimicrobial Agents and Chemotherapy (poster M-1757).
Patient characteristics and safety outcomes
Of the 433 patients with a hematologic disorder enrolled in the trial, 217 had proven or probable invasive mold infection. The researchers divided patients into 2 groups according to disease: those with acute myeloid leukemia (AML) and those with acute lymphoblastic leukemia (ALL) or other conditions.
In all, 102 patients had AML, and 115 had ALL (n=28) or other conditions, including non-Hodgkin lymphoma (n=19), chronic lymphocytic leukemia (n=15), refractory anemia with excess blasts (n=9), myelodysplastic syndrome (n=8), chronic myeloid leukemia (n=6), and “other” underlying conditions (n=30).
Patients were randomized to receive VRC (n=105) or ISA (N=112). Thirty patients in the ISA arm and 26 in the VRC arm had undergone allogeneic transplant prior to therapy.
The primary outcome was all-cause mortality at day 42. Overall response and safety were secondary endpoints.
The overall rates of treatment-emergent adverse events were similar between ISA and VRC arms. Ninety-seven percent of patients in the ISA arm and 98% of patients in the VRC arm reported at least 1 treatment-emergent adverse event.
However, patients in the ISA arm had significantly fewer (P<0.05) events for the cardiac disorders, eye, psychiatric disorders, renal and urinary, and vascular system organ classes.
Response and mortality
All-cause mortality rates were comparable between the ISA and VRC arms—22% and 24%, respectively—as were overall response rates—39% and 34%, respectively—and complete response rates—13% and 10%, respectively.
All-cause mortality rates among patients with AML were 18% in the ISA arm and 15% in the VRC arm. Overall response rates were 36% and 48%, respectively.
For patients with ALL or other hematologic conditions, all-cause mortality rates were 26% in the ISA arm and 32% in the VRC arm. Overall response rates were 42% and 21%, respectively.
In transplant patients, the all-cause mortality rate was 27% for both the ISA and VRC arms. The overall response rate was 27% for both arms as well.
“These results show the potential of isavuconazole as a potent antifungal in the fight against invasive mold disease,” Dr Marr said.
ISA is an investigational antifungal under development by Astellas and Basilea Pharmaceutica International Ltd. The SECURE trial was funded by Astellas.
The US Food and Drug Administration recently accepted a new drug application seeking approval for ISA for the treatment of invasive aspergillosis and invasive mucormycosis. ![]()
WASHINGTON, DC—A new antifungal agent is as effective as an existing drug against invasive mold infection in patients with hematologic disorders, results of a phase 3 trial suggest.
Overall response and all-cause mortality rates were comparable with the newer drug, isavuconazole (ISA), and the existing drug, voriconazole (VRC).
The overall rates of treatment-emergent adverse events were comparable as well, but ISA was associated with a significantly lower incidence of several events.
Kieren Marr, MD, of Johns Hopkins University in Baltimore, Maryland, and her colleagues presented these results in a subset of patients from the SECURE trial at the 54th Interscience Conference on Antimicrobial Agents and Chemotherapy (poster M-1757).
Patient characteristics and safety outcomes
Of the 433 patients with a hematologic disorder enrolled in the trial, 217 had proven or probable invasive mold infection. The researchers divided patients into 2 groups according to disease: those with acute myeloid leukemia (AML) and those with acute lymphoblastic leukemia (ALL) or other conditions.
In all, 102 patients had AML, and 115 had ALL (n=28) or other conditions, including non-Hodgkin lymphoma (n=19), chronic lymphocytic leukemia (n=15), refractory anemia with excess blasts (n=9), myelodysplastic syndrome (n=8), chronic myeloid leukemia (n=6), and “other” underlying conditions (n=30).
Patients were randomized to receive VRC (n=105) or ISA (N=112). Thirty patients in the ISA arm and 26 in the VRC arm had undergone allogeneic transplant prior to therapy.
The primary outcome was all-cause mortality at day 42. Overall response and safety were secondary endpoints.
The overall rates of treatment-emergent adverse events were similar between ISA and VRC arms. Ninety-seven percent of patients in the ISA arm and 98% of patients in the VRC arm reported at least 1 treatment-emergent adverse event.
However, patients in the ISA arm had significantly fewer (P<0.05) events for the cardiac disorders, eye, psychiatric disorders, renal and urinary, and vascular system organ classes.
Response and mortality
All-cause mortality rates were comparable between the ISA and VRC arms—22% and 24%, respectively—as were overall response rates—39% and 34%, respectively—and complete response rates—13% and 10%, respectively.
All-cause mortality rates among patients with AML were 18% in the ISA arm and 15% in the VRC arm. Overall response rates were 36% and 48%, respectively.
For patients with ALL or other hematologic conditions, all-cause mortality rates were 26% in the ISA arm and 32% in the VRC arm. Overall response rates were 42% and 21%, respectively.
In transplant patients, the all-cause mortality rate was 27% for both the ISA and VRC arms. The overall response rate was 27% for both arms as well.
“These results show the potential of isavuconazole as a potent antifungal in the fight against invasive mold disease,” Dr Marr said.
ISA is an investigational antifungal under development by Astellas and Basilea Pharmaceutica International Ltd. The SECURE trial was funded by Astellas.
The US Food and Drug Administration recently accepted a new drug application seeking approval for ISA for the treatment of invasive aspergillosis and invasive mucormycosis. ![]()
Discrimination may prompt non-adherence in SCD patients

attending physician looks on
Credit: NCI
Research has shown that many patients with sickle cell disease (SCD) do not consistently follow their doctor’s orders, and a new study suggests discrimination may be partly to blame.
Patients who felt they experienced discrimination because of their race or health status were 53% more likely than their peers to disregard physician recommendations.
However, reports of discrimination were also common among patients who said they followed doctors’ orders to the letter.
Carlton Haywood Jr, PhD, of the Johns Hopkins School of Medicine in Baltimore, Maryland, and his colleagues conducted this research and detailed the results in the Journal of General Internal Medicine.
Dr Haywood’s team monitored the experiences of 291 SCD patients (aged 15 and older) who were participating in the Improving Patient Outcomes with Respect and Trust (IMPORT) study.
Patients completed surveys to report perceived discrimination from healthcare providers and their adherence to physician recommendations.
More than a third of patients (36%) reported non-adherence to a doctor’s recommendations in the 2 years prior to completing the survey.
Fifty-eight percent of the non-adherent patients and 43% of the adherent group reported at least 1 incident of discrimination due to their race or health status.
Patients who had experienced discrimination were 53% more likely than their peers to follow physicians’ recommendations inconsistently.
Trust in medical professionals appeared to mediate the discrimination/non-adherence relationship. It accounted for 50% of the excess prevalence of non-adherence among patients who reported incidents of discrimination.
The researchers said these findings are consistent with previous studies among other chronically ill patient groups. They also show how discrimination affects a patient’s trust in the healthcare system, as well as the person’s subsequent willingness to follow prescribed treatment regimens.
Dr Haywood believes the perceptions and experiences of discrimination may increase the chances that SCD patients will not fully benefit from the care available to them.
“A good relationship between the patient and provider can facilitate adherence, while a problematic relationship can negatively impact patient adherence,” he said.
“Improving relationships between healthcare providers and such patients may improve their trust in medical professionals, which, in turn, may improve other outcomes among this underserved patient population.” ![]()
attending physician looks on
Credit: NCI
Research has shown that many patients with sickle cell disease (SCD) do not consistently follow their doctor’s orders, and a new study suggests discrimination may be partly to blame.
Patients who felt they experienced discrimination because of their race or health status were 53% more likely than their peers to disregard physician recommendations.
However, reports of discrimination were also common among patients who said they followed doctors’ orders to the letter.
Carlton Haywood Jr, PhD, of the Johns Hopkins School of Medicine in Baltimore, Maryland, and his colleagues conducted this research and detailed the results in the Journal of General Internal Medicine.
Dr Haywood’s team monitored the experiences of 291 SCD patients (aged 15 and older) who were participating in the Improving Patient Outcomes with Respect and Trust (IMPORT) study.
Patients completed surveys to report perceived discrimination from healthcare providers and their adherence to physician recommendations.
More than a third of patients (36%) reported non-adherence to a doctor’s recommendations in the 2 years prior to completing the survey.
Fifty-eight percent of the non-adherent patients and 43% of the adherent group reported at least 1 incident of discrimination due to their race or health status.
Patients who had experienced discrimination were 53% more likely than their peers to follow physicians’ recommendations inconsistently.
Trust in medical professionals appeared to mediate the discrimination/non-adherence relationship. It accounted for 50% of the excess prevalence of non-adherence among patients who reported incidents of discrimination.
The researchers said these findings are consistent with previous studies among other chronically ill patient groups. They also show how discrimination affects a patient’s trust in the healthcare system, as well as the person’s subsequent willingness to follow prescribed treatment regimens.
Dr Haywood believes the perceptions and experiences of discrimination may increase the chances that SCD patients will not fully benefit from the care available to them.
“A good relationship between the patient and provider can facilitate adherence, while a problematic relationship can negatively impact patient adherence,” he said.
“Improving relationships between healthcare providers and such patients may improve their trust in medical professionals, which, in turn, may improve other outcomes among this underserved patient population.” ![]()
attending physician looks on
Credit: NCI
Research has shown that many patients with sickle cell disease (SCD) do not consistently follow their doctor’s orders, and a new study suggests discrimination may be partly to blame.
Patients who felt they experienced discrimination because of their race or health status were 53% more likely than their peers to disregard physician recommendations.
However, reports of discrimination were also common among patients who said they followed doctors’ orders to the letter.
Carlton Haywood Jr, PhD, of the Johns Hopkins School of Medicine in Baltimore, Maryland, and his colleagues conducted this research and detailed the results in the Journal of General Internal Medicine.
Dr Haywood’s team monitored the experiences of 291 SCD patients (aged 15 and older) who were participating in the Improving Patient Outcomes with Respect and Trust (IMPORT) study.
Patients completed surveys to report perceived discrimination from healthcare providers and their adherence to physician recommendations.
More than a third of patients (36%) reported non-adherence to a doctor’s recommendations in the 2 years prior to completing the survey.
Fifty-eight percent of the non-adherent patients and 43% of the adherent group reported at least 1 incident of discrimination due to their race or health status.
Patients who had experienced discrimination were 53% more likely than their peers to follow physicians’ recommendations inconsistently.
Trust in medical professionals appeared to mediate the discrimination/non-adherence relationship. It accounted for 50% of the excess prevalence of non-adherence among patients who reported incidents of discrimination.
The researchers said these findings are consistent with previous studies among other chronically ill patient groups. They also show how discrimination affects a patient’s trust in the healthcare system, as well as the person’s subsequent willingness to follow prescribed treatment regimens.
Dr Haywood believes the perceptions and experiences of discrimination may increase the chances that SCD patients will not fully benefit from the care available to them.
“A good relationship between the patient and provider can facilitate adherence, while a problematic relationship can negatively impact patient adherence,” he said.
“Improving relationships between healthcare providers and such patients may improve their trust in medical professionals, which, in turn, may improve other outcomes among this underserved patient population.” ![]()
NICE recommends eculizumab for aHUS despite cost

Credit: Globovision
The UK’s National Institute for Health and Care Excellence (NICE) has issued a draft guidance recommending eculizumab (Soliris) to treat atypical hemolytic uremic syndrome (aHUS), despite the drug’s high cost.
NICE estimates that eculizumab will cost the National Health Service (NHS) up to £58 million in the first year, rising to £82 million after 5 years.
The drug is currently funded by NHS England through interim specialized commissioning arrangements.
Eculizumab is ‘breakthrough’ for aHUS
aHUS is an extremely rare but life-threatening disease that causes inflammation of blood vessels and the formation of blood clots throughout the body. Patients with aHUS are at constant risk of sudden and progressive damage to, and failure of, vital organs.
Roughly 10% to 15% of patients die in the initial, acute phase of aHUS. The majority of patients—up to 70%—develop end-stage kidney failure requiring dialysis. And 1 in 5 patients has aHUS affecting organs other than the kidneys, most commonly the brain or heart.
Eculizumab inhibits the disease by blocking pro-thrombotic and pro-inflammatory processes, which can lead to cellular damage in small blood vessels throughout the body, renal failure, and damage to other organs.
“Eculizumab radically improves the quality of life of the small number of people with aHUS,” said NICE Chief Executive Sir Andrew Dillon.
“From the available evidence and from the testimony of clinicians and patients, families, and carers, it is clear that eculizumab is a significant breakthrough in the management of aHUS. The drug offers people with the disease the possibility of avoiding end-stage renal failure, dialysis, and kidney transplantation, as well as other organ damage.”
Breakthrough comes with considerable cost
Eculizumab costs £3150 per 30 mL vial (excluding value-added tax). The net budget impact of eculizumab based on the developer’s predicted rate of uptake over a 5-year period is confidential.
However, to allow consultees and commentators to properly engage in the consultation process, NICE has prepared an illustration of the possible budget impact of eculizumab for aHUS, using information available in the public domain.
This is based on a treatment cost of £340,200 per adult patient in the first year (based on the acquisition cost of the drug and the recommended dosing for an adult), and assumes a patient cohort of 170, as estimated by NHS England in its interim commissioning policy.
If all of these adult patients with aHUS are treated with eculizumab, the budget impact for the first year would be £57.8 million.
If an additional 20 new patients are treated the following year (based on a worldwide incidence of 0.4 per million), the budget impact will rise to £62.5 million in year 2. That assumes all new patients are treated, and all existing patients continue to be treated at the maintenance cost of £327,600 per year.
Using the same assumptions, the budget impact will rise to £69 million in year 3 (190 existing and 20 new patients), £75 million in year 4 (210 existing and 20 new patients), and £82 million in year 5 (230 existing and 20 new patients).
Conditions of the recommendation
The expert committee advising NICE on eculizumab believes the budget impact of recommending the drug for aHUS in relation to the benefits it offers would be lower if the potential for dose adjustment and treatment discontinuation was taken into account, according to Sir Dillon.
“Therefore, the draft guidance recommends that eculizumab is funded only if important conditions are met,” he said. “These include coordinating the use of eculizumab through an expert center and putting in place systems for monitoring how many people are diagnosed with aHUS, how many receive the drug, at what dose, and for how long.”
“The program also needs to develop protocols for starting and stopping treatment with eculizumab for clinical reasons and introduce a research program to collect data to evaluate when stopping treatment or adjusting the dose of the drug might occur.”
Given that the budget impact of eculizumab for treating aHUS will be considerable, the draft guidance also recommends that NHS England and the drug’s developer, Alexion, should consider what opportunities might exist to reduce the overall cost of eculizumab to the NHS.
NICE has not yet issued final guidance to the NHS. These decisions may change after consultation. The public can comment on the preliminary recommendations, which will be available until midday on September 25.
Comments received during this consultation period will be considered by the advisory committee at its meeting in October and, following this meeting, the next draft guidance will be issued. ![]()
Credit: Globovision
The UK’s National Institute for Health and Care Excellence (NICE) has issued a draft guidance recommending eculizumab (Soliris) to treat atypical hemolytic uremic syndrome (aHUS), despite the drug’s high cost.
NICE estimates that eculizumab will cost the National Health Service (NHS) up to £58 million in the first year, rising to £82 million after 5 years.
The drug is currently funded by NHS England through interim specialized commissioning arrangements.
Eculizumab is ‘breakthrough’ for aHUS
aHUS is an extremely rare but life-threatening disease that causes inflammation of blood vessels and the formation of blood clots throughout the body. Patients with aHUS are at constant risk of sudden and progressive damage to, and failure of, vital organs.
Roughly 10% to 15% of patients die in the initial, acute phase of aHUS. The majority of patients—up to 70%—develop end-stage kidney failure requiring dialysis. And 1 in 5 patients has aHUS affecting organs other than the kidneys, most commonly the brain or heart.
Eculizumab inhibits the disease by blocking pro-thrombotic and pro-inflammatory processes, which can lead to cellular damage in small blood vessels throughout the body, renal failure, and damage to other organs.
“Eculizumab radically improves the quality of life of the small number of people with aHUS,” said NICE Chief Executive Sir Andrew Dillon.
“From the available evidence and from the testimony of clinicians and patients, families, and carers, it is clear that eculizumab is a significant breakthrough in the management of aHUS. The drug offers people with the disease the possibility of avoiding end-stage renal failure, dialysis, and kidney transplantation, as well as other organ damage.”
Breakthrough comes with considerable cost
Eculizumab costs £3150 per 30 mL vial (excluding value-added tax). The net budget impact of eculizumab based on the developer’s predicted rate of uptake over a 5-year period is confidential.
However, to allow consultees and commentators to properly engage in the consultation process, NICE has prepared an illustration of the possible budget impact of eculizumab for aHUS, using information available in the public domain.
This is based on a treatment cost of £340,200 per adult patient in the first year (based on the acquisition cost of the drug and the recommended dosing for an adult), and assumes a patient cohort of 170, as estimated by NHS England in its interim commissioning policy.
If all of these adult patients with aHUS are treated with eculizumab, the budget impact for the first year would be £57.8 million.
If an additional 20 new patients are treated the following year (based on a worldwide incidence of 0.4 per million), the budget impact will rise to £62.5 million in year 2. That assumes all new patients are treated, and all existing patients continue to be treated at the maintenance cost of £327,600 per year.
Using the same assumptions, the budget impact will rise to £69 million in year 3 (190 existing and 20 new patients), £75 million in year 4 (210 existing and 20 new patients), and £82 million in year 5 (230 existing and 20 new patients).
Conditions of the recommendation
The expert committee advising NICE on eculizumab believes the budget impact of recommending the drug for aHUS in relation to the benefits it offers would be lower if the potential for dose adjustment and treatment discontinuation was taken into account, according to Sir Dillon.
“Therefore, the draft guidance recommends that eculizumab is funded only if important conditions are met,” he said. “These include coordinating the use of eculizumab through an expert center and putting in place systems for monitoring how many people are diagnosed with aHUS, how many receive the drug, at what dose, and for how long.”
“The program also needs to develop protocols for starting and stopping treatment with eculizumab for clinical reasons and introduce a research program to collect data to evaluate when stopping treatment or adjusting the dose of the drug might occur.”
Given that the budget impact of eculizumab for treating aHUS will be considerable, the draft guidance also recommends that NHS England and the drug’s developer, Alexion, should consider what opportunities might exist to reduce the overall cost of eculizumab to the NHS.
NICE has not yet issued final guidance to the NHS. These decisions may change after consultation. The public can comment on the preliminary recommendations, which will be available until midday on September 25.
Comments received during this consultation period will be considered by the advisory committee at its meeting in October and, following this meeting, the next draft guidance will be issued. ![]()
Credit: Globovision
The UK’s National Institute for Health and Care Excellence (NICE) has issued a draft guidance recommending eculizumab (Soliris) to treat atypical hemolytic uremic syndrome (aHUS), despite the drug’s high cost.
NICE estimates that eculizumab will cost the National Health Service (NHS) up to £58 million in the first year, rising to £82 million after 5 years.
The drug is currently funded by NHS England through interim specialized commissioning arrangements.
Eculizumab is ‘breakthrough’ for aHUS
aHUS is an extremely rare but life-threatening disease that causes inflammation of blood vessels and the formation of blood clots throughout the body. Patients with aHUS are at constant risk of sudden and progressive damage to, and failure of, vital organs.
Roughly 10% to 15% of patients die in the initial, acute phase of aHUS. The majority of patients—up to 70%—develop end-stage kidney failure requiring dialysis. And 1 in 5 patients has aHUS affecting organs other than the kidneys, most commonly the brain or heart.
Eculizumab inhibits the disease by blocking pro-thrombotic and pro-inflammatory processes, which can lead to cellular damage in small blood vessels throughout the body, renal failure, and damage to other organs.
“Eculizumab radically improves the quality of life of the small number of people with aHUS,” said NICE Chief Executive Sir Andrew Dillon.
“From the available evidence and from the testimony of clinicians and patients, families, and carers, it is clear that eculizumab is a significant breakthrough in the management of aHUS. The drug offers people with the disease the possibility of avoiding end-stage renal failure, dialysis, and kidney transplantation, as well as other organ damage.”
Breakthrough comes with considerable cost
Eculizumab costs £3150 per 30 mL vial (excluding value-added tax). The net budget impact of eculizumab based on the developer’s predicted rate of uptake over a 5-year period is confidential.
However, to allow consultees and commentators to properly engage in the consultation process, NICE has prepared an illustration of the possible budget impact of eculizumab for aHUS, using information available in the public domain.
This is based on a treatment cost of £340,200 per adult patient in the first year (based on the acquisition cost of the drug and the recommended dosing for an adult), and assumes a patient cohort of 170, as estimated by NHS England in its interim commissioning policy.
If all of these adult patients with aHUS are treated with eculizumab, the budget impact for the first year would be £57.8 million.
If an additional 20 new patients are treated the following year (based on a worldwide incidence of 0.4 per million), the budget impact will rise to £62.5 million in year 2. That assumes all new patients are treated, and all existing patients continue to be treated at the maintenance cost of £327,600 per year.
Using the same assumptions, the budget impact will rise to £69 million in year 3 (190 existing and 20 new patients), £75 million in year 4 (210 existing and 20 new patients), and £82 million in year 5 (230 existing and 20 new patients).
Conditions of the recommendation
The expert committee advising NICE on eculizumab believes the budget impact of recommending the drug for aHUS in relation to the benefits it offers would be lower if the potential for dose adjustment and treatment discontinuation was taken into account, according to Sir Dillon.
“Therefore, the draft guidance recommends that eculizumab is funded only if important conditions are met,” he said. “These include coordinating the use of eculizumab through an expert center and putting in place systems for monitoring how many people are diagnosed with aHUS, how many receive the drug, at what dose, and for how long.”
“The program also needs to develop protocols for starting and stopping treatment with eculizumab for clinical reasons and introduce a research program to collect data to evaluate when stopping treatment or adjusting the dose of the drug might occur.”
Given that the budget impact of eculizumab for treating aHUS will be considerable, the draft guidance also recommends that NHS England and the drug’s developer, Alexion, should consider what opportunities might exist to reduce the overall cost of eculizumab to the NHS.
NICE has not yet issued final guidance to the NHS. These decisions may change after consultation. The public can comment on the preliminary recommendations, which will be available until midday on September 25.
Comments received during this consultation period will be considered by the advisory committee at its meeting in October and, following this meeting, the next draft guidance will be issued. ![]()
Recommendations for managing SCD lack supporting evidence

Credit: St Jude Children’s
Research Hospital
A new set of guidelines includes some strong recommendations for managing patients with sickle cell disease (SCD) that are not supported by high-quality evidence, according to researchers.
The group reviewed the medical literature to examine the quality of evidence supporting each of the guideline’s recommendations.
And they discovered a lack of randomized controlled trials in SCD patients that have left “extensive” gaps in our knowledge of the disease.
So while the guidelines do provide some helpful advice for managing patients with SCD, they also leave healthcare professionals with some uncertainties, according to the researchers.
The National Heart, Lung, and Blood Institute convened an expert panel to develop the guidelines, which are now available on the institute’s website.
Barbara P. Yawn, MD, of the Olmsted Medical Center in Rochester, Minnesota, and her colleagues examined the quality of evidence supporting the guidelines and reported their results in JAMA alongside a related editorial. Several examples of guideline recommendations and supporting evidence follow.
Health management recommendations
The guidelines strongly recommend oral penicillin prophylaxis twice daily until age 5 years in all children with HbSS to prevent invasive pneumococcal infection. And this recommendation is supported by moderate-quality evidence.
But the guidelines also strongly recommend referral to an ophthalmologist for dilated eye examination to screen for retinopathy beginning at age 10 years, and the quality of evidence supporting this recommendation is poor.
Acute SCD complications
The guidelines strongly recommend rapid initiation of parenteral opioids in adults and children with a vaso-occlusive crisis associated with severe pain, a suggestion supported by high-quality evidence.
However, the guidelines also strongly recommend treating SCD patients with acute chest syndrome with an intravenous cephalosporin, an oral macrolide antibiotic, and supplemental oxygen (to maintain oxygen saturation of >95%), as well as closely monitoring patients for bronchospasm, acute anemia, and hypoxemia. And this is supported by low-quality evidence.
Chronic complications
A strong recommendation supported by high-quality evidence is to treat avascular necrosis with analgesics and consult physical therapy and orthopedic departments for assessment and follow-up.
A strong recommendation supported by low-quality evidence is to evaluate all children and adults with SCD and intermittent or chronic hip pain for avascular necrosis by history, physical examination, radiography, and magnetic resonance imaging, as needed.
Use of hydroxyurea
Dr Yawn and her colleagues found that strong recommendations for hydroxyurea are all supported by moderate- or high-quality evidence.
A strong recommendation supported by high-quality evidence is to initiate hydroxyurea in adults who have at least 3 moderate-to-severe pain crises associated with SCD during a 12-month period.
A strong recommendation supported by moderate-quality evidence is to initiate hydroxyurea in adults who have sickle cell-associated pain that interferes with daily activities and quality of life.
Transfusion therapy
For this category, the only strong recommendation supported by high-quality evidence is to transfuse a child with a transcranial Doppler reading greater than 200 cm/s.
The guidelines strongly recommend transfusing red blood cells in adults and children with SCD to bring the hemoglobin level to 10 g/dL prior to undergoing a surgical procedure involving general anesthesia, but this is supported by moderate-quality evidence.
A strong recommendation supported by low-quality evidence is to perform an exchange transfusion in a patient with symptomatic, severe acute chest syndrome (defined by an oxygen saturation less than 90% despite supplemental oxygen).
Conclusions
Dr Yawn and her colleagues said this investigation confirms that developing guidelines for managing SCD is challenging because high-quality evidence is limited in virtually every area related to SCD management.
Therefore, the guidelines leave healthcare professionals with some uncertainties about managing SCD patients. But the researchers hope their analysis will prompt new research that might provide more definitive guidance. ![]()
Credit: St Jude Children’s
Research Hospital
A new set of guidelines includes some strong recommendations for managing patients with sickle cell disease (SCD) that are not supported by high-quality evidence, according to researchers.
The group reviewed the medical literature to examine the quality of evidence supporting each of the guideline’s recommendations.
And they discovered a lack of randomized controlled trials in SCD patients that have left “extensive” gaps in our knowledge of the disease.
So while the guidelines do provide some helpful advice for managing patients with SCD, they also leave healthcare professionals with some uncertainties, according to the researchers.
The National Heart, Lung, and Blood Institute convened an expert panel to develop the guidelines, which are now available on the institute’s website.
Barbara P. Yawn, MD, of the Olmsted Medical Center in Rochester, Minnesota, and her colleagues examined the quality of evidence supporting the guidelines and reported their results in JAMA alongside a related editorial. Several examples of guideline recommendations and supporting evidence follow.
Health management recommendations
The guidelines strongly recommend oral penicillin prophylaxis twice daily until age 5 years in all children with HbSS to prevent invasive pneumococcal infection. And this recommendation is supported by moderate-quality evidence.
But the guidelines also strongly recommend referral to an ophthalmologist for dilated eye examination to screen for retinopathy beginning at age 10 years, and the quality of evidence supporting this recommendation is poor.
Acute SCD complications
The guidelines strongly recommend rapid initiation of parenteral opioids in adults and children with a vaso-occlusive crisis associated with severe pain, a suggestion supported by high-quality evidence.
However, the guidelines also strongly recommend treating SCD patients with acute chest syndrome with an intravenous cephalosporin, an oral macrolide antibiotic, and supplemental oxygen (to maintain oxygen saturation of >95%), as well as closely monitoring patients for bronchospasm, acute anemia, and hypoxemia. And this is supported by low-quality evidence.
Chronic complications
A strong recommendation supported by high-quality evidence is to treat avascular necrosis with analgesics and consult physical therapy and orthopedic departments for assessment and follow-up.
A strong recommendation supported by low-quality evidence is to evaluate all children and adults with SCD and intermittent or chronic hip pain for avascular necrosis by history, physical examination, radiography, and magnetic resonance imaging, as needed.
Use of hydroxyurea
Dr Yawn and her colleagues found that strong recommendations for hydroxyurea are all supported by moderate- or high-quality evidence.
A strong recommendation supported by high-quality evidence is to initiate hydroxyurea in adults who have at least 3 moderate-to-severe pain crises associated with SCD during a 12-month period.
A strong recommendation supported by moderate-quality evidence is to initiate hydroxyurea in adults who have sickle cell-associated pain that interferes with daily activities and quality of life.
Transfusion therapy
For this category, the only strong recommendation supported by high-quality evidence is to transfuse a child with a transcranial Doppler reading greater than 200 cm/s.
The guidelines strongly recommend transfusing red blood cells in adults and children with SCD to bring the hemoglobin level to 10 g/dL prior to undergoing a surgical procedure involving general anesthesia, but this is supported by moderate-quality evidence.
A strong recommendation supported by low-quality evidence is to perform an exchange transfusion in a patient with symptomatic, severe acute chest syndrome (defined by an oxygen saturation less than 90% despite supplemental oxygen).
Conclusions
Dr Yawn and her colleagues said this investigation confirms that developing guidelines for managing SCD is challenging because high-quality evidence is limited in virtually every area related to SCD management.
Therefore, the guidelines leave healthcare professionals with some uncertainties about managing SCD patients. But the researchers hope their analysis will prompt new research that might provide more definitive guidance. ![]()
Credit: St Jude Children’s
Research Hospital
A new set of guidelines includes some strong recommendations for managing patients with sickle cell disease (SCD) that are not supported by high-quality evidence, according to researchers.
The group reviewed the medical literature to examine the quality of evidence supporting each of the guideline’s recommendations.
And they discovered a lack of randomized controlled trials in SCD patients that have left “extensive” gaps in our knowledge of the disease.
So while the guidelines do provide some helpful advice for managing patients with SCD, they also leave healthcare professionals with some uncertainties, according to the researchers.
The National Heart, Lung, and Blood Institute convened an expert panel to develop the guidelines, which are now available on the institute’s website.
Barbara P. Yawn, MD, of the Olmsted Medical Center in Rochester, Minnesota, and her colleagues examined the quality of evidence supporting the guidelines and reported their results in JAMA alongside a related editorial. Several examples of guideline recommendations and supporting evidence follow.
Health management recommendations
The guidelines strongly recommend oral penicillin prophylaxis twice daily until age 5 years in all children with HbSS to prevent invasive pneumococcal infection. And this recommendation is supported by moderate-quality evidence.
But the guidelines also strongly recommend referral to an ophthalmologist for dilated eye examination to screen for retinopathy beginning at age 10 years, and the quality of evidence supporting this recommendation is poor.
Acute SCD complications
The guidelines strongly recommend rapid initiation of parenteral opioids in adults and children with a vaso-occlusive crisis associated with severe pain, a suggestion supported by high-quality evidence.
However, the guidelines also strongly recommend treating SCD patients with acute chest syndrome with an intravenous cephalosporin, an oral macrolide antibiotic, and supplemental oxygen (to maintain oxygen saturation of >95%), as well as closely monitoring patients for bronchospasm, acute anemia, and hypoxemia. And this is supported by low-quality evidence.
Chronic complications
A strong recommendation supported by high-quality evidence is to treat avascular necrosis with analgesics and consult physical therapy and orthopedic departments for assessment and follow-up.
A strong recommendation supported by low-quality evidence is to evaluate all children and adults with SCD and intermittent or chronic hip pain for avascular necrosis by history, physical examination, radiography, and magnetic resonance imaging, as needed.
Use of hydroxyurea
Dr Yawn and her colleagues found that strong recommendations for hydroxyurea are all supported by moderate- or high-quality evidence.
A strong recommendation supported by high-quality evidence is to initiate hydroxyurea in adults who have at least 3 moderate-to-severe pain crises associated with SCD during a 12-month period.
A strong recommendation supported by moderate-quality evidence is to initiate hydroxyurea in adults who have sickle cell-associated pain that interferes with daily activities and quality of life.
Transfusion therapy
For this category, the only strong recommendation supported by high-quality evidence is to transfuse a child with a transcranial Doppler reading greater than 200 cm/s.
The guidelines strongly recommend transfusing red blood cells in adults and children with SCD to bring the hemoglobin level to 10 g/dL prior to undergoing a surgical procedure involving general anesthesia, but this is supported by moderate-quality evidence.
A strong recommendation supported by low-quality evidence is to perform an exchange transfusion in a patient with symptomatic, severe acute chest syndrome (defined by an oxygen saturation less than 90% despite supplemental oxygen).
Conclusions
Dr Yawn and her colleagues said this investigation confirms that developing guidelines for managing SCD is challenging because high-quality evidence is limited in virtually every area related to SCD management.
Therefore, the guidelines leave healthcare professionals with some uncertainties about managing SCD patients. But the researchers hope their analysis will prompt new research that might provide more definitive guidance.
NHLBI expert panel issues guideline on sickle cell disease
The "much anticipated" guideline to help primary care and emergency clinicians improve the management of sickle cell disease includes a consensus treatment protocol for implementing hydroxyurea therapy and more detailed guidance regarding long-term transfusion therapy, according to a summary report published online September 9 in Journal of the American Medical Association.
Sickle cell disease (SCD), a life-threatening genetically transmitted disorder affecting 70,000-100,000 Americans, is associated with a wide array of complex acute and chronic complications that require immediate medical attention. But high-quality data on which to base management decisions are sorely lacking, and clinicians get little in the way of guidance from existing recommendations. One result is that "the two most widely available disease-modifying therapies, hydroxyurea and long-term transfusions, are underused, and hematopoietic stem cell transplantation, the only curative approach, has been used in only a small proportion of affected individuals," said Dr. Barbara P. Yawn and her associates on the National Heart, Lung, and Blood Institute expert panel that issued the summary report.

Even this guideline is somewhat rudimentary due to the dearth of good data "in virtually every area related to SCD management," and cannot help but leave "many uncertainties for health professionals caring for individuals with SCD." But it is hoped that this guideline will furnish a critical foundation for future research and will now begin "to facilitate improved and more accessible care for all affected individuals," said Dr. Yawn, director of research at Olmsted Medical Center, Rochester, Minn., and her associates.
The guideline is based on an extensive literature review of more than 13,000 abstracts and articles, which was winnowed to 1,583 original studies regarding SCD. From this, a team of health care professionals in family medicine, internal medicine, pediatric and adult hematology, psychiatry and mental health, transfusion medicine, obstetrics and gynecology, maternal/fetal medicine, and emergency department nursing compiled the guideline as well as the summary, entitled Evidence-Based Management of Sickle Cell Disease: Expert Panel Report 2014 (JAMA 2014 September 9 [doi:10.1001/jama.2014.10517]).
In addition to establishing a protocol for implementing hydroxyurea therapy, the guideline addresses changes in pneumococcal vaccination recommendations for adults and children; annual transcranial Doppler screening coupled with long-term transfusion therapy when necessary to prevent stroke in children aged 2-16 years; rapid initiation of opioids for severe pain during vasoocclusive crises; analgesics and physical therapy for avascular necrosis; ACE inhibitor treatment for adults with microalbuminuria; referral to specialists for screening and treatment of proliferative retinopathy; echocardiography to assess signs of pulmonary hypertension; and monitoring for iron overload in patients receiving transfusion therapy.
Both the summary report and the full guideline are available at http://www.nhlbi.nih.gov/health-pro/guidelines/sickle-cell-disease-guidelines/.
Yawn et al. have made a monumental effort to produce practical, evidence-based guidelines, but they were hampered at every turn by a pervasive lack of good quality evidence on which to base their recommendations. Still missing from this guideline are suggestions for how often and when to screen for kidney disease, how to screen for and treat the common clinical problem of asthma-like symptoms (when standard therapies are contraindicated in SCD), how to advocate for patients with the common sequelae of silent cerebral infarcts, or when to consider hematopoietic stem-cell transplantation.
The expert panel also failed to include representatives from the people most affected by SCD: patients and their families. Failure to listen to the perspective of the families, understand which of these recommendations are important to them, and deal with the obstacles families face in implementing the recommendations is a critically important omission.
Dr. Michael R. DeBaun is in the department of pediatrics at the Vanderbilt-Meharry Center of Excellence in Sickle Cell Disease, Nashville. He made his remarks in an editorial accompanying Dr. Yawn’s report (JAMA 2014:312;1004-5). Dr. DeBaun reported no financial conflicts of interest.
Yawn et al. have made a monumental effort to produce practical, evidence-based guidelines, but they were hampered at every turn by a pervasive lack of good quality evidence on which to base their recommendations. Still missing from this guideline are suggestions for how often and when to screen for kidney disease, how to screen for and treat the common clinical problem of asthma-like symptoms (when standard therapies are contraindicated in SCD), how to advocate for patients with the common sequelae of silent cerebral infarcts, or when to consider hematopoietic stem-cell transplantation.
The expert panel also failed to include representatives from the people most affected by SCD: patients and their families. Failure to listen to the perspective of the families, understand which of these recommendations are important to them, and deal with the obstacles families face in implementing the recommendations is a critically important omission.
Dr. Michael R. DeBaun is in the department of pediatrics at the Vanderbilt-Meharry Center of Excellence in Sickle Cell Disease, Nashville. He made his remarks in an editorial accompanying Dr. Yawn’s report (JAMA 2014:312;1004-5). Dr. DeBaun reported no financial conflicts of interest.
Yawn et al. have made a monumental effort to produce practical, evidence-based guidelines, but they were hampered at every turn by a pervasive lack of good quality evidence on which to base their recommendations. Still missing from this guideline are suggestions for how often and when to screen for kidney disease, how to screen for and treat the common clinical problem of asthma-like symptoms (when standard therapies are contraindicated in SCD), how to advocate for patients with the common sequelae of silent cerebral infarcts, or when to consider hematopoietic stem-cell transplantation.
The expert panel also failed to include representatives from the people most affected by SCD: patients and their families. Failure to listen to the perspective of the families, understand which of these recommendations are important to them, and deal with the obstacles families face in implementing the recommendations is a critically important omission.
Dr. Michael R. DeBaun is in the department of pediatrics at the Vanderbilt-Meharry Center of Excellence in Sickle Cell Disease, Nashville. He made his remarks in an editorial accompanying Dr. Yawn’s report (JAMA 2014:312;1004-5). Dr. DeBaun reported no financial conflicts of interest.
The "much anticipated" guideline to help primary care and emergency clinicians improve the management of sickle cell disease includes a consensus treatment protocol for implementing hydroxyurea therapy and more detailed guidance regarding long-term transfusion therapy, according to a summary report published online September 9 in Journal of the American Medical Association.
Sickle cell disease (SCD), a life-threatening genetically transmitted disorder affecting 70,000-100,000 Americans, is associated with a wide array of complex acute and chronic complications that require immediate medical attention. But high-quality data on which to base management decisions are sorely lacking, and clinicians get little in the way of guidance from existing recommendations. One result is that "the two most widely available disease-modifying therapies, hydroxyurea and long-term transfusions, are underused, and hematopoietic stem cell transplantation, the only curative approach, has been used in only a small proportion of affected individuals," said Dr. Barbara P. Yawn and her associates on the National Heart, Lung, and Blood Institute expert panel that issued the summary report.
Even this guideline is somewhat rudimentary due to the dearth of good data "in virtually every area related to SCD management," and cannot help but leave "many uncertainties for health professionals caring for individuals with SCD." But it is hoped that this guideline will furnish a critical foundation for future research and will now begin "to facilitate improved and more accessible care for all affected individuals," said Dr. Yawn, director of research at Olmsted Medical Center, Rochester, Minn., and her associates.
The guideline is based on an extensive literature review of more than 13,000 abstracts and articles, which was winnowed to 1,583 original studies regarding SCD. From this, a team of health care professionals in family medicine, internal medicine, pediatric and adult hematology, psychiatry and mental health, transfusion medicine, obstetrics and gynecology, maternal/fetal medicine, and emergency department nursing compiled the guideline as well as the summary, entitled Evidence-Based Management of Sickle Cell Disease: Expert Panel Report 2014 (JAMA 2014 September 9 [doi:10.1001/jama.2014.10517]).
In addition to establishing a protocol for implementing hydroxyurea therapy, the guideline addresses changes in pneumococcal vaccination recommendations for adults and children; annual transcranial Doppler screening coupled with long-term transfusion therapy when necessary to prevent stroke in children aged 2-16 years; rapid initiation of opioids for severe pain during vasoocclusive crises; analgesics and physical therapy for avascular necrosis; ACE inhibitor treatment for adults with microalbuminuria; referral to specialists for screening and treatment of proliferative retinopathy; echocardiography to assess signs of pulmonary hypertension; and monitoring for iron overload in patients receiving transfusion therapy.
Both the summary report and the full guideline are available at http://www.nhlbi.nih.gov/health-pro/guidelines/sickle-cell-disease-guidelines/.
The "much anticipated" guideline to help primary care and emergency clinicians improve the management of sickle cell disease includes a consensus treatment protocol for implementing hydroxyurea therapy and more detailed guidance regarding long-term transfusion therapy, according to a summary report published online September 9 in Journal of the American Medical Association.
Sickle cell disease (SCD), a life-threatening genetically transmitted disorder affecting 70,000-100,000 Americans, is associated with a wide array of complex acute and chronic complications that require immediate medical attention. But high-quality data on which to base management decisions are sorely lacking, and clinicians get little in the way of guidance from existing recommendations. One result is that "the two most widely available disease-modifying therapies, hydroxyurea and long-term transfusions, are underused, and hematopoietic stem cell transplantation, the only curative approach, has been used in only a small proportion of affected individuals," said Dr. Barbara P. Yawn and her associates on the National Heart, Lung, and Blood Institute expert panel that issued the summary report.
Even this guideline is somewhat rudimentary due to the dearth of good data "in virtually every area related to SCD management," and cannot help but leave "many uncertainties for health professionals caring for individuals with SCD." But it is hoped that this guideline will furnish a critical foundation for future research and will now begin "to facilitate improved and more accessible care for all affected individuals," said Dr. Yawn, director of research at Olmsted Medical Center, Rochester, Minn., and her associates.
The guideline is based on an extensive literature review of more than 13,000 abstracts and articles, which was winnowed to 1,583 original studies regarding SCD. From this, a team of health care professionals in family medicine, internal medicine, pediatric and adult hematology, psychiatry and mental health, transfusion medicine, obstetrics and gynecology, maternal/fetal medicine, and emergency department nursing compiled the guideline as well as the summary, entitled Evidence-Based Management of Sickle Cell Disease: Expert Panel Report 2014 (JAMA 2014 September 9 [doi:10.1001/jama.2014.10517]).
In addition to establishing a protocol for implementing hydroxyurea therapy, the guideline addresses changes in pneumococcal vaccination recommendations for adults and children; annual transcranial Doppler screening coupled with long-term transfusion therapy when necessary to prevent stroke in children aged 2-16 years; rapid initiation of opioids for severe pain during vasoocclusive crises; analgesics and physical therapy for avascular necrosis; ACE inhibitor treatment for adults with microalbuminuria; referral to specialists for screening and treatment of proliferative retinopathy; echocardiography to assess signs of pulmonary hypertension; and monitoring for iron overload in patients receiving transfusion therapy.
Both the summary report and the full guideline are available at http://www.nhlbi.nih.gov/health-pro/guidelines/sickle-cell-disease-guidelines/.
FROM JAMA
Major finding: The two most widely available disease-modifying therapies for SCD, hydroxyurea and long-term transfusions, are underused, in large part because no evidence-based treatment protocols have been devised until now.
Data source: A review of the literature and compilation of management guidelines "to assist health care professionals in the management of common issues of sickle cell disease."
Disclosures: The National Heart, Lung, and Blood Institute sponsored the development of this guideline. All expert panel members served voluntarily. Many reported numerous ties to industry sources.

Drug shows early promise for hematologic malignancies
A drug that targets mitochondrial function is largely safe and can be active in heavily pretreated patients with hematologic malignancies, a phase 1 trial indicates.
The drug, CPI-613, prompted responses in only 4 of 21 evaluable patients. However, 2 of those responses lasted more than 2 years.
CPI-613 was generally well-tolerated and did not induce bone marrow suppression. Four patients experienced renal failure, but it was reversed in 3 of them.
These results appear in Clinical Cancer Research.
“This drug is selectively taken up by cancer cells and then shuts down the production of energy in the mitochondria,” said study author Timothy Pardee, MD, PhD, of the Comprehensive Cancer Center of Wake Forest University in Winston-Salem, North Carolina.
“This is the first drug to inhibit mitochondria in this way, and, if it proves effective in further clinical trials, it will open up a whole new approach to fighting cancer.”
Dr Pardee and his colleagues evaluated CPI-613 in 26 patients with relapsed or refractory hematologic malignancies—11 with acute myeloid leukemia, 6 with non-Hodgkin lymphoma, 4 with multiple myeloma, 4 with myelodysplastic syndrome (MDS), and 1 with Hodgkin lymphoma.
The median patient age was 65 years (range, 19-81), and the median number of prior therapies was 3 (range, 1-9).
Treatment dosing and toxicity
Patients received CPI-613 as a 2-hour infusion on days 1 and 4 for 3 weeks every 28 days.
When the infusion time was shortened to 1 hour, renal failure occurred in 2 patients. At 3780 mg/m2, there were 2 dose-limiting toxicities. There were no such toxicities at a dose of 2940 mg/m2 over 2 hours, so this was considered the maximum-tolerated dose.
The following grade 2 or higher toxicities were probably or definitely related to treatment: nausea (1 grade 2), vomiting (1 grade 3), diarrhea (3 grade 2), proteinuria (1 grade 2), renal failure (4 grade 3), hypotension (1 grade 2), hypocalcemia (1 grade 2), hypoalbuminemia (1 grade 2), and hyperkalemia (1 grade 3).
Renal failure was resolved in 3 of the 4 patients. The remaining patient chose hospice care.
Response data
Five patients discontinued treatment—1 refused therapy, 1 acquired an infection, and 3 developed acute kidney failure.
Of the 21 patients evaluable for response, 4 had an objective response following CPI-613 treatment, and 2 had prolonged stable disease.
One patient with MDS achieved a complete response that has been maintained for more than 3 years. A patient with acute myeloid leukemia achieved a morphologically leukemia-free state, went on to transplant, and is still alive and leukemia-free.
A patient with Burkitt lymphoma achieved a partial response after 3 cycles of therapy that was maintained for 17 cycles. She discontinued CPI-613 to have her residual disease resected, and has not received any treatment since. She is now disease-free more than 12 months later.
A patient with cutaneous T-cell lymphoma achieved a partial response that has been sustained for more than 2 years. At her request, she started to receive continuous therapy (no 1-week rest period), and she remains on treatment without significant toxicities and no evidence of marrow suppression.
The 2 patients with prolonged stable disease had MDS. Their disease was stable for 8 and 12 cycles, respectively. Two patients with multiple myeloma also initially had stable disease, but they progressed after 2 and 4 cycles, respectively.
Two patients died from disease progression while on study.
The researchers said these results suggest that agents targeting mitochondrial metabolism can be safe and active in hematologic malignancies. A phase 2 trial of CPI-613 is now underway.
Support for the phase 1 trial was provided by National Cancer Institute grants P30CA012197 and 1K08CA169809, the Doug Coley Foundation for Leukemia Research, the Frances P. Tutwiler Fund, The MacKay Foundation for Cancer Research, and Cornerstone Pharmaceuticals, which manufactured and provided CPI-613.
A drug that targets mitochondrial function is largely safe and can be active in heavily pretreated patients with hematologic malignancies, a phase 1 trial indicates.
The drug, CPI-613, prompted responses in only 4 of 21 evaluable patients. However, 2 of those responses lasted more than 2 years.
CPI-613 was generally well-tolerated and did not induce bone marrow suppression. Four patients experienced renal failure, but it was reversed in 3 of them.
These results appear in Clinical Cancer Research.
“This drug is selectively taken up by cancer cells and then shuts down the production of energy in the mitochondria,” said study author Timothy Pardee, MD, PhD, of the Comprehensive Cancer Center of Wake Forest University in Winston-Salem, North Carolina.
“This is the first drug to inhibit mitochondria in this way, and, if it proves effective in further clinical trials, it will open up a whole new approach to fighting cancer.”
Dr Pardee and his colleagues evaluated CPI-613 in 26 patients with relapsed or refractory hematologic malignancies—11 with acute myeloid leukemia, 6 with non-Hodgkin lymphoma, 4 with multiple myeloma, 4 with myelodysplastic syndrome (MDS), and 1 with Hodgkin lymphoma.
The median patient age was 65 years (range, 19-81), and the median number of prior therapies was 3 (range, 1-9).
Treatment dosing and toxicity
Patients received CPI-613 as a 2-hour infusion on days 1 and 4 for 3 weeks every 28 days.
When the infusion time was shortened to 1 hour, renal failure occurred in 2 patients. At 3780 mg/m2, there were 2 dose-limiting toxicities. There were no such toxicities at a dose of 2940 mg/m2 over 2 hours, so this was considered the maximum-tolerated dose.
The following grade 2 or higher toxicities were probably or definitely related to treatment: nausea (1 grade 2), vomiting (1 grade 3), diarrhea (3 grade 2), proteinuria (1 grade 2), renal failure (4 grade 3), hypotension (1 grade 2), hypocalcemia (1 grade 2), hypoalbuminemia (1 grade 2), and hyperkalemia (1 grade 3).
Renal failure was resolved in 3 of the 4 patients. The remaining patient chose hospice care.
Response data
Five patients discontinued treatment—1 refused therapy, 1 acquired an infection, and 3 developed acute kidney failure.
Of the 21 patients evaluable for response, 4 had an objective response following CPI-613 treatment, and 2 had prolonged stable disease.
One patient with MDS achieved a complete response that has been maintained for more than 3 years. A patient with acute myeloid leukemia achieved a morphologically leukemia-free state, went on to transplant, and is still alive and leukemia-free.
A patient with Burkitt lymphoma achieved a partial response after 3 cycles of therapy that was maintained for 17 cycles. She discontinued CPI-613 to have her residual disease resected, and has not received any treatment since. She is now disease-free more than 12 months later.
A patient with cutaneous T-cell lymphoma achieved a partial response that has been sustained for more than 2 years. At her request, she started to receive continuous therapy (no 1-week rest period), and she remains on treatment without significant toxicities and no evidence of marrow suppression.
The 2 patients with prolonged stable disease had MDS. Their disease was stable for 8 and 12 cycles, respectively. Two patients with multiple myeloma also initially had stable disease, but they progressed after 2 and 4 cycles, respectively.
Two patients died from disease progression while on study.
The researchers said these results suggest that agents targeting mitochondrial metabolism can be safe and active in hematologic malignancies. A phase 2 trial of CPI-613 is now underway.
Support for the phase 1 trial was provided by National Cancer Institute grants P30CA012197 and 1K08CA169809, the Doug Coley Foundation for Leukemia Research, the Frances P. Tutwiler Fund, The MacKay Foundation for Cancer Research, and Cornerstone Pharmaceuticals, which manufactured and provided CPI-613.
A drug that targets mitochondrial function is largely safe and can be active in heavily pretreated patients with hematologic malignancies, a phase 1 trial indicates.
The drug, CPI-613, prompted responses in only 4 of 21 evaluable patients. However, 2 of those responses lasted more than 2 years.
CPI-613 was generally well-tolerated and did not induce bone marrow suppression. Four patients experienced renal failure, but it was reversed in 3 of them.
These results appear in Clinical Cancer Research.
“This drug is selectively taken up by cancer cells and then shuts down the production of energy in the mitochondria,” said study author Timothy Pardee, MD, PhD, of the Comprehensive Cancer Center of Wake Forest University in Winston-Salem, North Carolina.
“This is the first drug to inhibit mitochondria in this way, and, if it proves effective in further clinical trials, it will open up a whole new approach to fighting cancer.”
Dr Pardee and his colleagues evaluated CPI-613 in 26 patients with relapsed or refractory hematologic malignancies—11 with acute myeloid leukemia, 6 with non-Hodgkin lymphoma, 4 with multiple myeloma, 4 with myelodysplastic syndrome (MDS), and 1 with Hodgkin lymphoma.
The median patient age was 65 years (range, 19-81), and the median number of prior therapies was 3 (range, 1-9).
Treatment dosing and toxicity
Patients received CPI-613 as a 2-hour infusion on days 1 and 4 for 3 weeks every 28 days.
When the infusion time was shortened to 1 hour, renal failure occurred in 2 patients. At 3780 mg/m2, there were 2 dose-limiting toxicities. There were no such toxicities at a dose of 2940 mg/m2 over 2 hours, so this was considered the maximum-tolerated dose.
The following grade 2 or higher toxicities were probably or definitely related to treatment: nausea (1 grade 2), vomiting (1 grade 3), diarrhea (3 grade 2), proteinuria (1 grade 2), renal failure (4 grade 3), hypotension (1 grade 2), hypocalcemia (1 grade 2), hypoalbuminemia (1 grade 2), and hyperkalemia (1 grade 3).
Renal failure was resolved in 3 of the 4 patients. The remaining patient chose hospice care.
Response data
Five patients discontinued treatment—1 refused therapy, 1 acquired an infection, and 3 developed acute kidney failure.
Of the 21 patients evaluable for response, 4 had an objective response following CPI-613 treatment, and 2 had prolonged stable disease.
One patient with MDS achieved a complete response that has been maintained for more than 3 years. A patient with acute myeloid leukemia achieved a morphologically leukemia-free state, went on to transplant, and is still alive and leukemia-free.
A patient with Burkitt lymphoma achieved a partial response after 3 cycles of therapy that was maintained for 17 cycles. She discontinued CPI-613 to have her residual disease resected, and has not received any treatment since. She is now disease-free more than 12 months later.
A patient with cutaneous T-cell lymphoma achieved a partial response that has been sustained for more than 2 years. At her request, she started to receive continuous therapy (no 1-week rest period), and she remains on treatment without significant toxicities and no evidence of marrow suppression.
The 2 patients with prolonged stable disease had MDS. Their disease was stable for 8 and 12 cycles, respectively. Two patients with multiple myeloma also initially had stable disease, but they progressed after 2 and 4 cycles, respectively.
Two patients died from disease progression while on study.
The researchers said these results suggest that agents targeting mitochondrial metabolism can be safe and active in hematologic malignancies. A phase 2 trial of CPI-613 is now underway.
Support for the phase 1 trial was provided by National Cancer Institute grants P30CA012197 and 1K08CA169809, the Doug Coley Foundation for Leukemia Research, the Frances P. Tutwiler Fund, The MacKay Foundation for Cancer Research, and Cornerstone Pharmaceuticals, which manufactured and provided CPI-613.
Overcoming an obstacle to RBC development

Researchers have discovered a natural barrier to hematopoiesis and a way to circumvent it, according to a paper published in Blood.
The group found that components of the exosome complex—exosc8 and exosc9—suppress red blood cell (RBC) maturation.
“From a fundamental perspective, this is very important because this mechanism counteracts the development of precursor cells into red blood cells, thereby establishing a balance between developed cells and the progenitor population,” said study author Emery Bresnick, PhD, of the UW School of Medicine and Public Health in Madison, Wisconsin.
“In the context of translation, if you want to maximize the output of end-stage red blood cells, which we’re not able to do at this time, our study provides a rational approach involving lowering the levels of these subunits.”
Specifically, the researchers found that GATA-1 and Foxo3 can repress the exosome components, thereby allowing for RBC maturation.
The barrier explained
Dr Bresnick and his colleagues noted that the primary obstacle in converting hematopoietic stem cells into RBCs involves late-stage maturation.
“The problem isn’t simply getting erythroid precursors produced by the bucket, but understanding how these cells systematically lose their nuclei and organelles to become a red blood cell, the final product,” Dr Bresnick said.
“This is the bottleneck, even in the stem cell world of embryonic and induced pluripotent stem cells. We know little about how the cell orchestrates the intricate processes that constitute late-stage maturation.”
At the end of RBC development, the erythroid precursor must eject its own genetic material via enucleation. Although it’s clear why enucleation is important (making the cell more flexible and allowing it to carry more oxygen), exactly how the cell does it has been unclear.
Besides ejecting the nucleus, the cell must be cleared of other organelles, such as the endoplasmic reticulum and mitochondria. This process (autophagy) is linked to a pair of transcription factors—GATA1 and Foxo3—that control gene expression important in RBC development.
Because they knew GATA1 and Foxo3 promote autophagy, Dr Bresnick and his colleagues wondered if the proteins these transcription factors repress play an important role in cell maturation.
This led them to identify exosc8 and exosc9, two units of the exosome that ultimately established the development barrier.
The researchers plan to continue studying the exosome because many RNAs in the cell are not degraded by the exosome. Determining exactly how the exosome decides what RNA to dispose of may provide an even better understanding of the newly discovered barrier.
“One goal we have is to establish the specific RNA targets the exosome is regulating that are responsible for the blockade,” Dr Bresnick said. “In doing so, we might even uncover targets that are easier to manipulate than the exosome itself.”
Researchers have discovered a natural barrier to hematopoiesis and a way to circumvent it, according to a paper published in Blood.
The group found that components of the exosome complex—exosc8 and exosc9—suppress red blood cell (RBC) maturation.
“From a fundamental perspective, this is very important because this mechanism counteracts the development of precursor cells into red blood cells, thereby establishing a balance between developed cells and the progenitor population,” said study author Emery Bresnick, PhD, of the UW School of Medicine and Public Health in Madison, Wisconsin.
“In the context of translation, if you want to maximize the output of end-stage red blood cells, which we’re not able to do at this time, our study provides a rational approach involving lowering the levels of these subunits.”
Specifically, the researchers found that GATA-1 and Foxo3 can repress the exosome components, thereby allowing for RBC maturation.
The barrier explained
Dr Bresnick and his colleagues noted that the primary obstacle in converting hematopoietic stem cells into RBCs involves late-stage maturation.
“The problem isn’t simply getting erythroid precursors produced by the bucket, but understanding how these cells systematically lose their nuclei and organelles to become a red blood cell, the final product,” Dr Bresnick said.
“This is the bottleneck, even in the stem cell world of embryonic and induced pluripotent stem cells. We know little about how the cell orchestrates the intricate processes that constitute late-stage maturation.”
At the end of RBC development, the erythroid precursor must eject its own genetic material via enucleation. Although it’s clear why enucleation is important (making the cell more flexible and allowing it to carry more oxygen), exactly how the cell does it has been unclear.
Besides ejecting the nucleus, the cell must be cleared of other organelles, such as the endoplasmic reticulum and mitochondria. This process (autophagy) is linked to a pair of transcription factors—GATA1 and Foxo3—that control gene expression important in RBC development.
Because they knew GATA1 and Foxo3 promote autophagy, Dr Bresnick and his colleagues wondered if the proteins these transcription factors repress play an important role in cell maturation.
This led them to identify exosc8 and exosc9, two units of the exosome that ultimately established the development barrier.
The researchers plan to continue studying the exosome because many RNAs in the cell are not degraded by the exosome. Determining exactly how the exosome decides what RNA to dispose of may provide an even better understanding of the newly discovered barrier.
“One goal we have is to establish the specific RNA targets the exosome is regulating that are responsible for the blockade,” Dr Bresnick said. “In doing so, we might even uncover targets that are easier to manipulate than the exosome itself.”
Researchers have discovered a natural barrier to hematopoiesis and a way to circumvent it, according to a paper published in Blood.
The group found that components of the exosome complex—exosc8 and exosc9—suppress red blood cell (RBC) maturation.
“From a fundamental perspective, this is very important because this mechanism counteracts the development of precursor cells into red blood cells, thereby establishing a balance between developed cells and the progenitor population,” said study author Emery Bresnick, PhD, of the UW School of Medicine and Public Health in Madison, Wisconsin.
“In the context of translation, if you want to maximize the output of end-stage red blood cells, which we’re not able to do at this time, our study provides a rational approach involving lowering the levels of these subunits.”
Specifically, the researchers found that GATA-1 and Foxo3 can repress the exosome components, thereby allowing for RBC maturation.
The barrier explained
Dr Bresnick and his colleagues noted that the primary obstacle in converting hematopoietic stem cells into RBCs involves late-stage maturation.
“The problem isn’t simply getting erythroid precursors produced by the bucket, but understanding how these cells systematically lose their nuclei and organelles to become a red blood cell, the final product,” Dr Bresnick said.
“This is the bottleneck, even in the stem cell world of embryonic and induced pluripotent stem cells. We know little about how the cell orchestrates the intricate processes that constitute late-stage maturation.”
At the end of RBC development, the erythroid precursor must eject its own genetic material via enucleation. Although it’s clear why enucleation is important (making the cell more flexible and allowing it to carry more oxygen), exactly how the cell does it has been unclear.
Besides ejecting the nucleus, the cell must be cleared of other organelles, such as the endoplasmic reticulum and mitochondria. This process (autophagy) is linked to a pair of transcription factors—GATA1 and Foxo3—that control gene expression important in RBC development.
Because they knew GATA1 and Foxo3 promote autophagy, Dr Bresnick and his colleagues wondered if the proteins these transcription factors repress play an important role in cell maturation.
This led them to identify exosc8 and exosc9, two units of the exosome that ultimately established the development barrier.
The researchers plan to continue studying the exosome because many RNAs in the cell are not degraded by the exosome. Determining exactly how the exosome decides what RNA to dispose of may provide an even better understanding of the newly discovered barrier.
“One goal we have is to establish the specific RNA targets the exosome is regulating that are responsible for the blockade,” Dr Bresnick said. “In doing so, we might even uncover targets that are easier to manipulate than the exosome itself.”