User login
When does shyness become a disorder?
Social phobia was accorded official psychiatric diagnostic status in the United States less than 20 years ago, but has been described in the medical literature for centuries. Hippocrates described such a patient: “He dare not come in company for fear he should be misused, disgraced, overshoot himself in gestures or speeches or be sick; he thinks every man observes him.”1
This observation was made more than 2,000 years ago. Yet social anxiety disorder (SAD) was left largely unstudied until the mid-1980s.2 An estimated 20 million people in the U.S. suffer from this disorder.
What causes some people to break into a cold sweat at the thought of the most casual encounter with a checkout clerk, a coworker, or an acquaintance? Limited evidence points to underlying biological abnormalities in SAD, but there have been no conclusive findings.
Two main subtypes of SAD exist (Box 1). Roughly 25% of sufferers have discrete or nongeneralized SAD, that is, circumscribed social fears limited to one or two situations, such as speaking in public or performing before an audience. The remaining 75% suffer from generalized SAD, the more severe subtype in which all or nearly all interpersonal interactions are difficult.
Generalized SAD often begins early in life, with a mean onset at about age 15, but 35% of the time SAD occurs in individuals before age 10.3 This subtype appears to run in families, while the nongeneralized subtype does not, suggesting that a genetic inheritance is possible. From an etiological perspective, the possible effects of parenting styles of socially anxious parents, or acquisition of social anxiety conditioned by experiencing extreme embarrassment, may also contribute to the development of SAD in some people. Approximately twice as many females as males are affected, and almost all are affected before age 25.3,4 When social fears interfere with social, occupational, or family life, the affected individual is not suffering from normal "shyness," but rather a treatable anxiety disorder.
–Toastmasters slogan
Generalized
- Most social interactions
- Early onset
- Social skills deficit
- High comorbidity
- Lower achievement
- Remission rare
Nongeneralized
- Limited fears
- Later onset
- Social skills normal
- Less comorbidity
- Less Impairment
- Remits often
The National Comorbidity Survey (NCS) estimated lifetime prevalence of SAD at 13.3% and 12-month prevalence at 7.6%, making it the third most common psychiatric disorder, following only major depression and alcohol abuse/dependence.5 Despite this high rate, SAD remains woefully underdiagnosed.
Anyone who has had to speak in public, play a musical instrument at a recital, or perform in some way under the watchful expectation of an audience has experienced anxiety as he or she anticipates the "big moment” (Box 2). Once the performance is under way, the anxiety usually lessens to a more manageable level for most people. In fact, nearly one in three Americans will admit to moderate or great fear of speaking in public.

Mr. L, a 40-year-old eighth-grade teacher, consulted a psychiatrist because he was scheduled to be evaluated by a state education accreditation committee while teaching class. Though he had always passed these before, he had been worried sick for weeks and was experiencing panic attacks each time he thought about the accreditation visit.
He lived with his mother, had never dated, and had few friends. He was extremely inhibited outside the classroom, brought cash to stores to avoid being observed while writing a check or signing credit card slips, and avoided social gatherings outside of his church, which he attended with his mother and tolerated with distress.
Further history revealed that he had quit medical school during his third year because he had so much difficulty presenting cases to the attending on ward rounds that he chose to leave the profession in order to avoid feeling sick each morning and afternoon.
Enough people encounter the fear of public speaking to support the weekly Toastmasters meetings in most U.S. cities. Many people overcome their social anxiety about public speaking or performing with continued practice. However, those with nongeneralized SAD, who are among the most severely affected, may remain so fearful of speaking or performing under scrutiny that they avoid it at any cost—even if it means passing up a job or promotion or even choosing to change professions.
The majority (75%) of those with SAD—representing approximately 15 million individuals in the U.S.—suffer from generalized SAD, a much more severe, potentially disabling subtype. These unfortunate individuals fear and avoid most or all social interactions outside their home except those with family or close friends. When they encounter or even anticipate entering feared social situations, individuals with generalized SAD experience severe anxiety. Blushing, tremulousness, and sweating can be noticed by others, and thus are particularly distressing to those with SAD.
Recovery without treatment is rare. The typically early age at onset of generalized SAD3,4 imposes greater limitations on development of social competence than on those who develop more discrete fear of public speaking or performing later in life—after socialization skills have already developed.
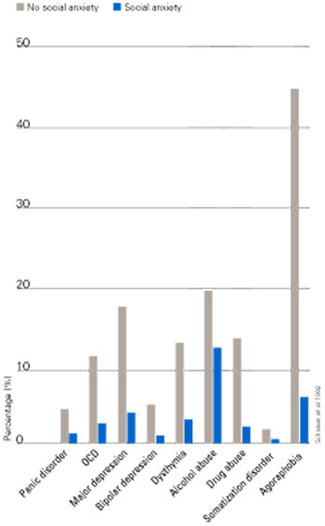
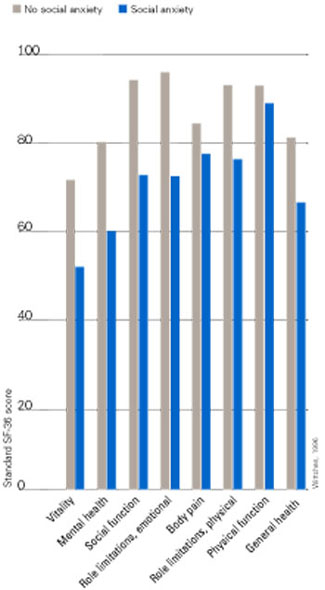
Individuals with SAD frequently suffer from comorbid psychiatric disorders, mostly depression and/or other anxiety disorders.6Figure 1 shows that individuals with SAD are at significantly increased risk for depression, other anxiety disorders, and alcohol and drug abuse. Since generalized SAD usually appears at an earlier age than other anxiety disorders, it represents a risk factor for subsequent depression. The level of functional impairment caused by SAD is similar to that caused by major depression7 (Figure 2).
As more comorbid psychiatric disorders accrue, impairment and increased risk for additional disorders may occur. Further, the risk of suicide is increased in those with comorbid SAD vs. those with SAD only. The findings suggest that if social anxiety were detected and treated effectively at an early age, it might be possible to prevent other psychiatric disorders—particularly depression—as well as the predictable morbidity and mortality that accompanies untreated SAD. Given the estimated $44 billion annual cost of anxiety disorders in the U.S.,8 research targeted at testing this hypothesis would appear to be a good investment.
Figure 1 HOW PREVALENT IS LIFETIME COMORBIDITY IN SAD?
- Inherent avoidance of scrutiny, (e.g., evaluation)
- Uncertain diagnostic threshold
- Acceptance of pathological shyness as ‘just my personality’
- Lack of understanding by professionals, family, friends
- Coping strategies that mask disability
- Comorbid psychiatric disorders that mask SAD
Figure 2 QUALITY OF LIFE IN PATIENTS WITH SOCIAL ANXIETY DISORDER
Seeing the unseen: making the diagnosis quickly
Although SAD is extremely common, a variety of factors may contribute to the low rate of recognition of the disorder (Box 3). Because of their intense discomfort toward scrutiny by authority figures such as their physician, individuals with SAD may not be willing to discuss their fears. Studies estimating the prevalence in primary care suggest that these individuals visit their referring physicians at about the same rate as the general population.6,9-11 Affected individuals are unlikely to seek psychiatric treatment unless they have a comorbid depression or anxiety.6,7
Table 1
DIFFERENTIAL DIAGNOSIS FOR SOCIAL ANXIETY DISORDER
| Condition | Diagnostic features |
|---|---|
| Posttraumatic stress disorder | Temporally follows traumatic event; cues related to trauma, not exclusively to social situations |
| Panic disorder | Unexpected panic attacks, not exclusively socially mediated anxiety |
| Agoraphobia | Fearful avoidance of situations in which panic attacks may occur, not limited to social situations |
| Major depression or atypical depression | Social withdrawal temporally related to mood disturbance, not to fear of humiliation or embarrassment; atypical depression with rejection sensitivity associated with other symptoms (e.g., hypersomnia, hyperphagia, anergy, mood reactivity) |
| Generalized anxiety disorder | Focus of worry not limited to social situations; social discomfort or avoidance not a key feature |
| Body dysmorphic disorder | Avoidance of social activity focused on concern over perceived ugliness |
| Avoidant personality disorder | Often present in generalized social anxiety disorder; may represent more severe end of social anxiety disorder spectrum; social activity desired but avoided |
| Schizotypal/schizoid personality disorders | Avoidance of social situations is preferred by individual and is not due to fear of embarrassment or humiliation |
| Normal shyness | Minimal or no interference with social, occupational, or family functioning |
| Adapted from Lydiard RB. Social anxiety disorder: comorbidity and its implications. J Clin Psychiatry.2001;62(suppl 1):17-23. | |
SAD can be difficult to tease apart from other coexisting conditions. Individuals who present for treatment of other anxiety disorders, depression, or substance abuse disorders should be considered at risk for current but undetected SAD. Many of the symptoms overlap (Table 1). The key diagnostic feature, which leads to the diagnosis of SAD, is that the fear and avoidance specifically are related to being in or anticipating a feared social situation (Box 4).
Social
- Attending parties, weddings etc.
- Conversing in a group
- Speaking on the telephone
- Interacting with authority figure (e.g., teacher or boss)
- Making eye contact
- Ordering in a restaurant
Performance
- Public speaking
- Eating in public
- Writing a check
- Using a public toilet
- Taking a test
- Trying on clothes in a store
- Speaking up at a meeting
Many clinicians mistake social anxiety for panic disorder, since panic attacks in people with SAD are often cued by social situations. There can be up to a 40% overlap of SAD with panic disorder.4 Without probing carefully into the focus on fear and avoidance, SAD can be easily overlooked. Individuals with panic disorder experience unexpected attacks and are terrified at the prospect of additional attacks, while those with SAD experience attacks linked to social situations and fear scrutiny and embarrassment more than the attacks themselves.
SAD and major depression frequently coexist,4,11,12 challenging clinicians to distinguish social reticence and withdrawal accompanying depression from the fearful avoidance that typifies SAD. SAD usually precedes depression. Asking if the patient experienced social anxiety prior to the onset of depression can help identify SAD with comorbid depression.
Alcohol-related disorders are twice as likely to occur in those affected by SAD as in those not affected. The risk for females increases more than it does for males.2-4 SAD most often precedes alcohol abuse. Studies show that about 30% of patients receiving treatment for alcohol abuse/dependence have SAD. If it remains undetected, the risk of rapid relapse is high. That’s because patients are highly unlikely to participate in psychosocial treatments that help sustain post-treatment abstinence, such as the Alcoholics Anonymous 12-step program. A recent study found that both social anxiety and alcohol abuse disorders improve when SAD in alcoholics is treated.13
A substantially higher percentage of adults with SAD, especially women, have histories of prior childhood sexual and/or physical abuse than the general population.14 Recent studies both in women following rape and in combat veterans with posttraumatic stress disorder (PTSD) suggest that those with perceived life-threatening events are at higher risk for developing secondary SAD than are individuals who experience less severe trauma.15,16 We do not yet know if secondary SAD in trauma victims is different in character or response to treatment.
Individuals with certain medical conditions can develop symptoms resembling SAD. These include stuttering, benign essential tremor,17 Parkinson’s disease, disfiguring burn injuries, and possibly irritable bowel syndrome. Such patients are technically excluded from being diagnosed with SAD, though they would meet criteria if the diagnostic rules were suspended. A limited body of literature and clinical experience suggests that symptoms secondary to physical conditions may respond to the same treatment as SAD in medically healthy persons. A treatment trial for selected patients with SAD symptoms associated with medical conditions may provide significant benefits. Clearly more research is needed in this area.
- “Being embarrassed or looking stupid are among my worst fears.”
- “Fear of embarrassment causes me to avoid doing things or speaking to people.”
- “I avoid activities in which I am the center of attention.”
Connor et al, Depress Anxiety 2001;14:137
A recently developed self-rating scale, the Social Phobia Inventory (SPIN), assesses the spectrum of cognitive, behavioral, and physiological symptoms associated with SAD.18 Three of the 17 SPIN items have been found to identify generalized SAD with a high degree of sensitivity (Box 5).
The 3 main goals of SAD treatment are
- Acute reduction and control of pathological anxiety and related phobic avoidance;
- Adequate treatment of depression or other comorbid conditions;
- Long-term management of the social phobia.
Significant advances in treatment have emerged over the past 2 decades. We now know that cognitive behavioral therapy (CBT), medication, and their combination are efficacious.
Social situations involving speaking or performance are usually predictable, and nongeneralized SAD is thus amenable to use of a beta-blocker or benzodiazepine (Box 6). Beta-blockers are often adequate for control of tremor and increased heart rate. Some patients may also benefit more from judicious use of a benzodiazepine prior to the event.
In contrast, generalized SAD is less predictable, and continual treatment is recommended. Ideally, a medication regimen would be easily tolerated long-term, and would have antidepressant effects and a broad spectrum of efficacy against commonly coexisting disorders. Because of the significant risk for depression in individuals with SAD, first-line antidepressant treatment is preferred when possible over other medications.
The selective serotonin reuptake inhibitors (SSRIs) are now considered the first-line pharmacological treatment for social phobia. Paroxetine was the first to receive FDA approval for generalized SAD.19 Large multicenter studies supporting the efficacy of two other SSRIs—sertraline and fluvoxamine—have been reported.12 The SSRIs also appear to work against the other psychiatric disorders with which SAD commonly co-occurs, such as panic disorder, major depression, generalized anxiety disorder, and PTSD.
The empirical database is very limited, but it appears that SSRI treatment for a significant percentage of patients with SAD may require higher doses (up to twice the amount) than are usually needed for depression.10 Approximately 50% to 65% of patients with generalized SAD respond to any given SSRI. In our experience, failure to respond to one SSRI does not preclude response to a second SSRI.
The irreversible monoamine oxidase (MAO) inhibitor phenelzine was the first antidepressant shown to be useful for SAD. Tranylcypromine is less well studied, but also appears to be effective. The significant side effects (weight gain, orthostatic hypotension, insomnia) and inconvenience of administration have reduced use of these agents.
Nongeneralized
- PRN treatment
- Beta-blockers
- Benzodiazepines
Generalized
- Continuous treatment
- Broad-spectrum antidepressants
- Benzodiazepines
- MAOIs
- Antiepileptic agents
The tricyclic antidepressants are probably not effective, with the exception of clomipramine (also a potent inhibitor of serotonin reuptake).12 Clomipramine, while an effective anxiolytic and antidepressant, causes prohibitive side effects in many patients (e.g., sexual dysfunction and weight gain).
Key elements for individual or group setting
- Cognitive “restructuring”
- Social skills enhancement
The newer antidepressants venlafaxine and nefazodone are less well studied than the SSRIs, but show promise as potential broad-spectrum agents. Bupropion, a novel antidepressant, and the azapirone anxiolytic buspirone do not appear to work against SAD.
The main role of the benzodiazepines in SAD treatment is adjunctive to antidepressants or in some patients intolerant of, or unresponsive to, other treatments. Clonazepam, alprazolam, and probably others are effective for SAD, but they may not effectively treat or prevent depression or other commonly associated disorders.
The anticonvulsant gabapentin has been shown in one controlled study to be effective in treating SAD.20 This agent may be particularly useful for complicated patients such as those with a history of alcohol-related disorders, bipolar-spectrum disorder, or intolerance to SSRIs.
In parallel with the development of effective psychopharmacological treatments, several types of behavioral and cognitive behavioral treatments have been investigated, including imaginal flooding, graduated exposure, social skills training, cognitive-behavior approaches, and combined cognitive restructuring and graduated exposure.21 These treatments involve similar elements targeted at the cognitive distortions and avoidance behaviors, which represent core features of SAD (Box 7).
Many clinicians believe that combined pharmacotherapy and CBT treatment are superior to either modality alone for treating SAD. The little empirical information available indicates that acute treatment differences between drug alone and drug in combination with CBT are not impressive. However, there appears to be a lower rate of relapse following CBT than after medication discontinuation.
Despite our ability to treat this disorder, only a small fraction of sufferers get treatment. If untreated, the risk of comorbidity is extremely high. Routine screening for SAD, especially in younger individuals, could provide for early detection and treatment. Psychiatrists can play an important role in early detection and treatment by educating consumers, teachers, school nurses, psychologists, and pediatricians.
Related resources
- Lydiard, R.B. Social anxiety disorder comorbidity and its implications J. Clin. Psychiatry. 2001;62(suppl):17-23.
- American Psychiatric Association, http://www.psych.org
- American Psychological Association, http://www.apa.org
- National Institute for Mental Health: Anxiety Disorders, http://www.nimh.nih.gov/anxiety/
- Anxiety Disorders Associations of America, http://www.adaa.org/
Drug brand names
- Alprazolam • Xanax
- Atenolol • Tenormin
- Bupropion • Wellbutrin
- Buspirone • Buspar
- Clomipramine • Anafranil
- Clonazepam • Klonopin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Lorazepam • Ativan
- Nefazodone • Serzone
- Paroxetine • Paxil
- Phenelzine • Nardil
- Propranolol • Inderal
- Sertraline • Zoloft
- Tranylcypromine • Parnate
- Venlafaxine • Effexor
Disclosure
The author reports that he has received grant/research support and has served as a consultant to and on the speaker's bureau of Bristol-Myers Squibb Co., GlaxoSmithKline, Pfizer Inc., Eli Lilly and Co., Parke-Davis, and Solvay Pharmaceuticals. He also has received grant/research support and served as a consultant for Forest Pharmaceuticals, Wyeth-Ayerst Pharmaceuticals, and Roche; received grant/research support from Sanofi-Synthelabo; and has served as consultant for Dupont Pharmaceuticals and AstraZeneca.
1. Burton R. The Anatomy of Melancholy, vol. 1, 11th ed. London, England. Thomas Tegg, Cheapside; 1845.
2. Liebowitz MR, Gorman JM, Fyer AJ, Klein DF. Social phobia: review of a neglected anxiety disorder. Arch Gen Psychiatry. 1985;42:729-736.
3. Magee WJ, Eaton WW, Wittchen HU, et al. Agoraphobia, simple phobia, and social phobia in the National Comorbidity Survey. Arch Gen Psychiatry. 1996;53:159-168.
4. Schneier FR, Johnson J, et al. Social phobia: comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry. 1992;49:282-288.
5. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51:8-19.
6. Goldenberg IM, et al. The infrequency of “pure culture” diagnosis among the anxiety disorders. J Clin Psychiatry. 1996;57:528-533.
7. Wittchen HU, Beloch E. The impact of social phobia on quality of life. Int Clin Psychopharmacol. 1996;11(suppl):15-23.
8. Greenberg PE, Sisitsky T, Kessler RC, et al. The economic burden of anxiety disorders in the 1990s. J Clin Psychiatry. 1999;60:427-435.
9. Weiller E, Bisserbe JC, Boyer P, et al. Social phobia in general health care. Br J Psychiatry. 1996;168:169-174.
10. Katzelnick DJ, Greist JH. Social anxiety disorder: an unrecognized problem in primary care. J Clin Psychiatry. 2001;62:11.-
11. Davidson J. Social anxiety disorder under scrutiny. Depress Anxiety. 2000;11:93-98.
12. Lydiard RB. Social anxiety disorder: treatment role of the SSRIs. In Montgomery SA, den Boer JA (eds). SSRIs in Depression and Anxiety Perspectives in Psychiatry ,vol 8. NY: Wiley, Chichester, 129-150, 2001.
13. Randall CL, et al. Paroxetine improves both social anxiety and alcohol use in dually-diagnosed patients at the American College of Neuropsychopharmacology. San Juan, Puerto Rico. Dec 10-15, 2000.
14. Stein MB, Walker JR, Anderson G, et al. Childhood physical and sexual abuse in patients with anxiety disorders and in a community sample. Am J Psychiatry. 1996;153:275-277.
15. Boudreaux E, Kilpatrick DG, Resnick HS, et al. Criminal victimization, posttraumatic stress disorder, and comorbid psychopathology among a community sample of women. J Trauma Stress. 1998;11:665-678.
16. Orsillo SM, Heimberg RG, Juster HR, Garrett J. Social phobia and PTSD in Vietnam veterans. J Trauma Stress. 1996;9:235-252.
17. George MS, Lydiard RB. Social phobia secondary to physical disability: a review of benign essential tremor (BET) and stuttering. Psychosomatics. 1994;35:520-523.
18. Connor KM, et al. Mini-SPIN: A brief screening assessment for generalized social anxiety disorder. Depress Anxiety. 2001;14:137-140.
19. Stein MB, Liebowitz MR, Lydiard RB, et al. Paroxetine treatment of generalized social phobia (social anxiety disorder): a randomized controlled trial. JAMA. 1998;280:708-713.
20. Pande AC, Davidson JR, Jefferson JW, et al. Treatment of social phobia with gabapentin: a placebo-controlled study. J Clin Psychopharmacol. 1999;19:341-348.
21. Heimberg RG. Specific issues in the cognitive behavioral treatment of social phobia. J Clin Psychiatry. 1993;54(suppl 12):36-45.
Social phobia was accorded official psychiatric diagnostic status in the United States less than 20 years ago, but has been described in the medical literature for centuries. Hippocrates described such a patient: “He dare not come in company for fear he should be misused, disgraced, overshoot himself in gestures or speeches or be sick; he thinks every man observes him.”1
This observation was made more than 2,000 years ago. Yet social anxiety disorder (SAD) was left largely unstudied until the mid-1980s.2 An estimated 20 million people in the U.S. suffer from this disorder.
What causes some people to break into a cold sweat at the thought of the most casual encounter with a checkout clerk, a coworker, or an acquaintance? Limited evidence points to underlying biological abnormalities in SAD, but there have been no conclusive findings.
Two main subtypes of SAD exist (Box 1). Roughly 25% of sufferers have discrete or nongeneralized SAD, that is, circumscribed social fears limited to one or two situations, such as speaking in public or performing before an audience. The remaining 75% suffer from generalized SAD, the more severe subtype in which all or nearly all interpersonal interactions are difficult.
Generalized SAD often begins early in life, with a mean onset at about age 15, but 35% of the time SAD occurs in individuals before age 10.3 This subtype appears to run in families, while the nongeneralized subtype does not, suggesting that a genetic inheritance is possible. From an etiological perspective, the possible effects of parenting styles of socially anxious parents, or acquisition of social anxiety conditioned by experiencing extreme embarrassment, may also contribute to the development of SAD in some people. Approximately twice as many females as males are affected, and almost all are affected before age 25.3,4 When social fears interfere with social, occupational, or family life, the affected individual is not suffering from normal "shyness," but rather a treatable anxiety disorder.
–Toastmasters slogan
Generalized
- Most social interactions
- Early onset
- Social skills deficit
- High comorbidity
- Lower achievement
- Remission rare
Nongeneralized
- Limited fears
- Later onset
- Social skills normal
- Less comorbidity
- Less Impairment
- Remits often
The National Comorbidity Survey (NCS) estimated lifetime prevalence of SAD at 13.3% and 12-month prevalence at 7.6%, making it the third most common psychiatric disorder, following only major depression and alcohol abuse/dependence.5 Despite this high rate, SAD remains woefully underdiagnosed.
Anyone who has had to speak in public, play a musical instrument at a recital, or perform in some way under the watchful expectation of an audience has experienced anxiety as he or she anticipates the "big moment” (Box 2). Once the performance is under way, the anxiety usually lessens to a more manageable level for most people. In fact, nearly one in three Americans will admit to moderate or great fear of speaking in public.
Mr. L, a 40-year-old eighth-grade teacher, consulted a psychiatrist because he was scheduled to be evaluated by a state education accreditation committee while teaching class. Though he had always passed these before, he had been worried sick for weeks and was experiencing panic attacks each time he thought about the accreditation visit.
He lived with his mother, had never dated, and had few friends. He was extremely inhibited outside the classroom, brought cash to stores to avoid being observed while writing a check or signing credit card slips, and avoided social gatherings outside of his church, which he attended with his mother and tolerated with distress.
Further history revealed that he had quit medical school during his third year because he had so much difficulty presenting cases to the attending on ward rounds that he chose to leave the profession in order to avoid feeling sick each morning and afternoon.
Enough people encounter the fear of public speaking to support the weekly Toastmasters meetings in most U.S. cities. Many people overcome their social anxiety about public speaking or performing with continued practice. However, those with nongeneralized SAD, who are among the most severely affected, may remain so fearful of speaking or performing under scrutiny that they avoid it at any cost—even if it means passing up a job or promotion or even choosing to change professions.
The majority (75%) of those with SAD—representing approximately 15 million individuals in the U.S.—suffer from generalized SAD, a much more severe, potentially disabling subtype. These unfortunate individuals fear and avoid most or all social interactions outside their home except those with family or close friends. When they encounter or even anticipate entering feared social situations, individuals with generalized SAD experience severe anxiety. Blushing, tremulousness, and sweating can be noticed by others, and thus are particularly distressing to those with SAD.
Recovery without treatment is rare. The typically early age at onset of generalized SAD3,4 imposes greater limitations on development of social competence than on those who develop more discrete fear of public speaking or performing later in life—after socialization skills have already developed.
Individuals with SAD frequently suffer from comorbid psychiatric disorders, mostly depression and/or other anxiety disorders.6Figure 1 shows that individuals with SAD are at significantly increased risk for depression, other anxiety disorders, and alcohol and drug abuse. Since generalized SAD usually appears at an earlier age than other anxiety disorders, it represents a risk factor for subsequent depression. The level of functional impairment caused by SAD is similar to that caused by major depression7 (Figure 2).
As more comorbid psychiatric disorders accrue, impairment and increased risk for additional disorders may occur. Further, the risk of suicide is increased in those with comorbid SAD vs. those with SAD only. The findings suggest that if social anxiety were detected and treated effectively at an early age, it might be possible to prevent other psychiatric disorders—particularly depression—as well as the predictable morbidity and mortality that accompanies untreated SAD. Given the estimated $44 billion annual cost of anxiety disorders in the U.S.,8 research targeted at testing this hypothesis would appear to be a good investment.
Figure 1 HOW PREVALENT IS LIFETIME COMORBIDITY IN SAD?
- Inherent avoidance of scrutiny, (e.g., evaluation)
- Uncertain diagnostic threshold
- Acceptance of pathological shyness as ‘just my personality’
- Lack of understanding by professionals, family, friends
- Coping strategies that mask disability
- Comorbid psychiatric disorders that mask SAD
Figure 2 QUALITY OF LIFE IN PATIENTS WITH SOCIAL ANXIETY DISORDER
Seeing the unseen: making the diagnosis quickly
Although SAD is extremely common, a variety of factors may contribute to the low rate of recognition of the disorder (Box 3). Because of their intense discomfort toward scrutiny by authority figures such as their physician, individuals with SAD may not be willing to discuss their fears. Studies estimating the prevalence in primary care suggest that these individuals visit their referring physicians at about the same rate as the general population.6,9-11 Affected individuals are unlikely to seek psychiatric treatment unless they have a comorbid depression or anxiety.6,7
Table 1
DIFFERENTIAL DIAGNOSIS FOR SOCIAL ANXIETY DISORDER
| Condition | Diagnostic features |
|---|---|
| Posttraumatic stress disorder | Temporally follows traumatic event; cues related to trauma, not exclusively to social situations |
| Panic disorder | Unexpected panic attacks, not exclusively socially mediated anxiety |
| Agoraphobia | Fearful avoidance of situations in which panic attacks may occur, not limited to social situations |
| Major depression or atypical depression | Social withdrawal temporally related to mood disturbance, not to fear of humiliation or embarrassment; atypical depression with rejection sensitivity associated with other symptoms (e.g., hypersomnia, hyperphagia, anergy, mood reactivity) |
| Generalized anxiety disorder | Focus of worry not limited to social situations; social discomfort or avoidance not a key feature |
| Body dysmorphic disorder | Avoidance of social activity focused on concern over perceived ugliness |
| Avoidant personality disorder | Often present in generalized social anxiety disorder; may represent more severe end of social anxiety disorder spectrum; social activity desired but avoided |
| Schizotypal/schizoid personality disorders | Avoidance of social situations is preferred by individual and is not due to fear of embarrassment or humiliation |
| Normal shyness | Minimal or no interference with social, occupational, or family functioning |
| Adapted from Lydiard RB. Social anxiety disorder: comorbidity and its implications. J Clin Psychiatry.2001;62(suppl 1):17-23. | |
SAD can be difficult to tease apart from other coexisting conditions. Individuals who present for treatment of other anxiety disorders, depression, or substance abuse disorders should be considered at risk for current but undetected SAD. Many of the symptoms overlap (Table 1). The key diagnostic feature, which leads to the diagnosis of SAD, is that the fear and avoidance specifically are related to being in or anticipating a feared social situation (Box 4).
Social
- Attending parties, weddings etc.
- Conversing in a group
- Speaking on the telephone
- Interacting with authority figure (e.g., teacher or boss)
- Making eye contact
- Ordering in a restaurant
Performance
- Public speaking
- Eating in public
- Writing a check
- Using a public toilet
- Taking a test
- Trying on clothes in a store
- Speaking up at a meeting
Many clinicians mistake social anxiety for panic disorder, since panic attacks in people with SAD are often cued by social situations. There can be up to a 40% overlap of SAD with panic disorder.4 Without probing carefully into the focus on fear and avoidance, SAD can be easily overlooked. Individuals with panic disorder experience unexpected attacks and are terrified at the prospect of additional attacks, while those with SAD experience attacks linked to social situations and fear scrutiny and embarrassment more than the attacks themselves.
SAD and major depression frequently coexist,4,11,12 challenging clinicians to distinguish social reticence and withdrawal accompanying depression from the fearful avoidance that typifies SAD. SAD usually precedes depression. Asking if the patient experienced social anxiety prior to the onset of depression can help identify SAD with comorbid depression.
Alcohol-related disorders are twice as likely to occur in those affected by SAD as in those not affected. The risk for females increases more than it does for males.2-4 SAD most often precedes alcohol abuse. Studies show that about 30% of patients receiving treatment for alcohol abuse/dependence have SAD. If it remains undetected, the risk of rapid relapse is high. That’s because patients are highly unlikely to participate in psychosocial treatments that help sustain post-treatment abstinence, such as the Alcoholics Anonymous 12-step program. A recent study found that both social anxiety and alcohol abuse disorders improve when SAD in alcoholics is treated.13
A substantially higher percentage of adults with SAD, especially women, have histories of prior childhood sexual and/or physical abuse than the general population.14 Recent studies both in women following rape and in combat veterans with posttraumatic stress disorder (PTSD) suggest that those with perceived life-threatening events are at higher risk for developing secondary SAD than are individuals who experience less severe trauma.15,16 We do not yet know if secondary SAD in trauma victims is different in character or response to treatment.
Individuals with certain medical conditions can develop symptoms resembling SAD. These include stuttering, benign essential tremor,17 Parkinson’s disease, disfiguring burn injuries, and possibly irritable bowel syndrome. Such patients are technically excluded from being diagnosed with SAD, though they would meet criteria if the diagnostic rules were suspended. A limited body of literature and clinical experience suggests that symptoms secondary to physical conditions may respond to the same treatment as SAD in medically healthy persons. A treatment trial for selected patients with SAD symptoms associated with medical conditions may provide significant benefits. Clearly more research is needed in this area.
- “Being embarrassed or looking stupid are among my worst fears.”
- “Fear of embarrassment causes me to avoid doing things or speaking to people.”
- “I avoid activities in which I am the center of attention.”
Connor et al, Depress Anxiety 2001;14:137
A recently developed self-rating scale, the Social Phobia Inventory (SPIN), assesses the spectrum of cognitive, behavioral, and physiological symptoms associated with SAD.18 Three of the 17 SPIN items have been found to identify generalized SAD with a high degree of sensitivity (Box 5).
The 3 main goals of SAD treatment are
- Acute reduction and control of pathological anxiety and related phobic avoidance;
- Adequate treatment of depression or other comorbid conditions;
- Long-term management of the social phobia.
Significant advances in treatment have emerged over the past 2 decades. We now know that cognitive behavioral therapy (CBT), medication, and their combination are efficacious.
Social situations involving speaking or performance are usually predictable, and nongeneralized SAD is thus amenable to use of a beta-blocker or benzodiazepine (Box 6). Beta-blockers are often adequate for control of tremor and increased heart rate. Some patients may also benefit more from judicious use of a benzodiazepine prior to the event.
In contrast, generalized SAD is less predictable, and continual treatment is recommended. Ideally, a medication regimen would be easily tolerated long-term, and would have antidepressant effects and a broad spectrum of efficacy against commonly coexisting disorders. Because of the significant risk for depression in individuals with SAD, first-line antidepressant treatment is preferred when possible over other medications.
The selective serotonin reuptake inhibitors (SSRIs) are now considered the first-line pharmacological treatment for social phobia. Paroxetine was the first to receive FDA approval for generalized SAD.19 Large multicenter studies supporting the efficacy of two other SSRIs—sertraline and fluvoxamine—have been reported.12 The SSRIs also appear to work against the other psychiatric disorders with which SAD commonly co-occurs, such as panic disorder, major depression, generalized anxiety disorder, and PTSD.
The empirical database is very limited, but it appears that SSRI treatment for a significant percentage of patients with SAD may require higher doses (up to twice the amount) than are usually needed for depression.10 Approximately 50% to 65% of patients with generalized SAD respond to any given SSRI. In our experience, failure to respond to one SSRI does not preclude response to a second SSRI.
The irreversible monoamine oxidase (MAO) inhibitor phenelzine was the first antidepressant shown to be useful for SAD. Tranylcypromine is less well studied, but also appears to be effective. The significant side effects (weight gain, orthostatic hypotension, insomnia) and inconvenience of administration have reduced use of these agents.
Nongeneralized
- PRN treatment
- Beta-blockers
- Benzodiazepines
Generalized
- Continuous treatment
- Broad-spectrum antidepressants
- Benzodiazepines
- MAOIs
- Antiepileptic agents
The tricyclic antidepressants are probably not effective, with the exception of clomipramine (also a potent inhibitor of serotonin reuptake).12 Clomipramine, while an effective anxiolytic and antidepressant, causes prohibitive side effects in many patients (e.g., sexual dysfunction and weight gain).
Key elements for individual or group setting
- Cognitive “restructuring”
- Social skills enhancement
The newer antidepressants venlafaxine and nefazodone are less well studied than the SSRIs, but show promise as potential broad-spectrum agents. Bupropion, a novel antidepressant, and the azapirone anxiolytic buspirone do not appear to work against SAD.
The main role of the benzodiazepines in SAD treatment is adjunctive to antidepressants or in some patients intolerant of, or unresponsive to, other treatments. Clonazepam, alprazolam, and probably others are effective for SAD, but they may not effectively treat or prevent depression or other commonly associated disorders.
The anticonvulsant gabapentin has been shown in one controlled study to be effective in treating SAD.20 This agent may be particularly useful for complicated patients such as those with a history of alcohol-related disorders, bipolar-spectrum disorder, or intolerance to SSRIs.
In parallel with the development of effective psychopharmacological treatments, several types of behavioral and cognitive behavioral treatments have been investigated, including imaginal flooding, graduated exposure, social skills training, cognitive-behavior approaches, and combined cognitive restructuring and graduated exposure.21 These treatments involve similar elements targeted at the cognitive distortions and avoidance behaviors, which represent core features of SAD (Box 7).
Many clinicians believe that combined pharmacotherapy and CBT treatment are superior to either modality alone for treating SAD. The little empirical information available indicates that acute treatment differences between drug alone and drug in combination with CBT are not impressive. However, there appears to be a lower rate of relapse following CBT than after medication discontinuation.
Despite our ability to treat this disorder, only a small fraction of sufferers get treatment. If untreated, the risk of comorbidity is extremely high. Routine screening for SAD, especially in younger individuals, could provide for early detection and treatment. Psychiatrists can play an important role in early detection and treatment by educating consumers, teachers, school nurses, psychologists, and pediatricians.
Related resources
- Lydiard, R.B. Social anxiety disorder comorbidity and its implications J. Clin. Psychiatry. 2001;62(suppl):17-23.
- American Psychiatric Association, http://www.psych.org
- American Psychological Association, http://www.apa.org
- National Institute for Mental Health: Anxiety Disorders, http://www.nimh.nih.gov/anxiety/
- Anxiety Disorders Associations of America, http://www.adaa.org/
Drug brand names
- Alprazolam • Xanax
- Atenolol • Tenormin
- Bupropion • Wellbutrin
- Buspirone • Buspar
- Clomipramine • Anafranil
- Clonazepam • Klonopin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Lorazepam • Ativan
- Nefazodone • Serzone
- Paroxetine • Paxil
- Phenelzine • Nardil
- Propranolol • Inderal
- Sertraline • Zoloft
- Tranylcypromine • Parnate
- Venlafaxine • Effexor
Disclosure
The author reports that he has received grant/research support and has served as a consultant to and on the speaker's bureau of Bristol-Myers Squibb Co., GlaxoSmithKline, Pfizer Inc., Eli Lilly and Co., Parke-Davis, and Solvay Pharmaceuticals. He also has received grant/research support and served as a consultant for Forest Pharmaceuticals, Wyeth-Ayerst Pharmaceuticals, and Roche; received grant/research support from Sanofi-Synthelabo; and has served as consultant for Dupont Pharmaceuticals and AstraZeneca.
Social phobia was accorded official psychiatric diagnostic status in the United States less than 20 years ago, but has been described in the medical literature for centuries. Hippocrates described such a patient: “He dare not come in company for fear he should be misused, disgraced, overshoot himself in gestures or speeches or be sick; he thinks every man observes him.”1
This observation was made more than 2,000 years ago. Yet social anxiety disorder (SAD) was left largely unstudied until the mid-1980s.2 An estimated 20 million people in the U.S. suffer from this disorder.
What causes some people to break into a cold sweat at the thought of the most casual encounter with a checkout clerk, a coworker, or an acquaintance? Limited evidence points to underlying biological abnormalities in SAD, but there have been no conclusive findings.
Two main subtypes of SAD exist (Box 1). Roughly 25% of sufferers have discrete or nongeneralized SAD, that is, circumscribed social fears limited to one or two situations, such as speaking in public or performing before an audience. The remaining 75% suffer from generalized SAD, the more severe subtype in which all or nearly all interpersonal interactions are difficult.
Generalized SAD often begins early in life, with a mean onset at about age 15, but 35% of the time SAD occurs in individuals before age 10.3 This subtype appears to run in families, while the nongeneralized subtype does not, suggesting that a genetic inheritance is possible. From an etiological perspective, the possible effects of parenting styles of socially anxious parents, or acquisition of social anxiety conditioned by experiencing extreme embarrassment, may also contribute to the development of SAD in some people. Approximately twice as many females as males are affected, and almost all are affected before age 25.3,4 When social fears interfere with social, occupational, or family life, the affected individual is not suffering from normal "shyness," but rather a treatable anxiety disorder.
–Toastmasters slogan
Generalized
- Most social interactions
- Early onset
- Social skills deficit
- High comorbidity
- Lower achievement
- Remission rare
Nongeneralized
- Limited fears
- Later onset
- Social skills normal
- Less comorbidity
- Less Impairment
- Remits often
The National Comorbidity Survey (NCS) estimated lifetime prevalence of SAD at 13.3% and 12-month prevalence at 7.6%, making it the third most common psychiatric disorder, following only major depression and alcohol abuse/dependence.5 Despite this high rate, SAD remains woefully underdiagnosed.
Anyone who has had to speak in public, play a musical instrument at a recital, or perform in some way under the watchful expectation of an audience has experienced anxiety as he or she anticipates the "big moment” (Box 2). Once the performance is under way, the anxiety usually lessens to a more manageable level for most people. In fact, nearly one in three Americans will admit to moderate or great fear of speaking in public.
Mr. L, a 40-year-old eighth-grade teacher, consulted a psychiatrist because he was scheduled to be evaluated by a state education accreditation committee while teaching class. Though he had always passed these before, he had been worried sick for weeks and was experiencing panic attacks each time he thought about the accreditation visit.
He lived with his mother, had never dated, and had few friends. He was extremely inhibited outside the classroom, brought cash to stores to avoid being observed while writing a check or signing credit card slips, and avoided social gatherings outside of his church, which he attended with his mother and tolerated with distress.
Further history revealed that he had quit medical school during his third year because he had so much difficulty presenting cases to the attending on ward rounds that he chose to leave the profession in order to avoid feeling sick each morning and afternoon.
Enough people encounter the fear of public speaking to support the weekly Toastmasters meetings in most U.S. cities. Many people overcome their social anxiety about public speaking or performing with continued practice. However, those with nongeneralized SAD, who are among the most severely affected, may remain so fearful of speaking or performing under scrutiny that they avoid it at any cost—even if it means passing up a job or promotion or even choosing to change professions.
The majority (75%) of those with SAD—representing approximately 15 million individuals in the U.S.—suffer from generalized SAD, a much more severe, potentially disabling subtype. These unfortunate individuals fear and avoid most or all social interactions outside their home except those with family or close friends. When they encounter or even anticipate entering feared social situations, individuals with generalized SAD experience severe anxiety. Blushing, tremulousness, and sweating can be noticed by others, and thus are particularly distressing to those with SAD.
Recovery without treatment is rare. The typically early age at onset of generalized SAD3,4 imposes greater limitations on development of social competence than on those who develop more discrete fear of public speaking or performing later in life—after socialization skills have already developed.
Individuals with SAD frequently suffer from comorbid psychiatric disorders, mostly depression and/or other anxiety disorders.6Figure 1 shows that individuals with SAD are at significantly increased risk for depression, other anxiety disorders, and alcohol and drug abuse. Since generalized SAD usually appears at an earlier age than other anxiety disorders, it represents a risk factor for subsequent depression. The level of functional impairment caused by SAD is similar to that caused by major depression7 (Figure 2).
As more comorbid psychiatric disorders accrue, impairment and increased risk for additional disorders may occur. Further, the risk of suicide is increased in those with comorbid SAD vs. those with SAD only. The findings suggest that if social anxiety were detected and treated effectively at an early age, it might be possible to prevent other psychiatric disorders—particularly depression—as well as the predictable morbidity and mortality that accompanies untreated SAD. Given the estimated $44 billion annual cost of anxiety disorders in the U.S.,8 research targeted at testing this hypothesis would appear to be a good investment.
Figure 1 HOW PREVALENT IS LIFETIME COMORBIDITY IN SAD?
- Inherent avoidance of scrutiny, (e.g., evaluation)
- Uncertain diagnostic threshold
- Acceptance of pathological shyness as ‘just my personality’
- Lack of understanding by professionals, family, friends
- Coping strategies that mask disability
- Comorbid psychiatric disorders that mask SAD
Figure 2 QUALITY OF LIFE IN PATIENTS WITH SOCIAL ANXIETY DISORDER
Seeing the unseen: making the diagnosis quickly
Although SAD is extremely common, a variety of factors may contribute to the low rate of recognition of the disorder (Box 3). Because of their intense discomfort toward scrutiny by authority figures such as their physician, individuals with SAD may not be willing to discuss their fears. Studies estimating the prevalence in primary care suggest that these individuals visit their referring physicians at about the same rate as the general population.6,9-11 Affected individuals are unlikely to seek psychiatric treatment unless they have a comorbid depression or anxiety.6,7
Table 1
DIFFERENTIAL DIAGNOSIS FOR SOCIAL ANXIETY DISORDER
| Condition | Diagnostic features |
|---|---|
| Posttraumatic stress disorder | Temporally follows traumatic event; cues related to trauma, not exclusively to social situations |
| Panic disorder | Unexpected panic attacks, not exclusively socially mediated anxiety |
| Agoraphobia | Fearful avoidance of situations in which panic attacks may occur, not limited to social situations |
| Major depression or atypical depression | Social withdrawal temporally related to mood disturbance, not to fear of humiliation or embarrassment; atypical depression with rejection sensitivity associated with other symptoms (e.g., hypersomnia, hyperphagia, anergy, mood reactivity) |
| Generalized anxiety disorder | Focus of worry not limited to social situations; social discomfort or avoidance not a key feature |
| Body dysmorphic disorder | Avoidance of social activity focused on concern over perceived ugliness |
| Avoidant personality disorder | Often present in generalized social anxiety disorder; may represent more severe end of social anxiety disorder spectrum; social activity desired but avoided |
| Schizotypal/schizoid personality disorders | Avoidance of social situations is preferred by individual and is not due to fear of embarrassment or humiliation |
| Normal shyness | Minimal or no interference with social, occupational, or family functioning |
| Adapted from Lydiard RB. Social anxiety disorder: comorbidity and its implications. J Clin Psychiatry.2001;62(suppl 1):17-23. | |
SAD can be difficult to tease apart from other coexisting conditions. Individuals who present for treatment of other anxiety disorders, depression, or substance abuse disorders should be considered at risk for current but undetected SAD. Many of the symptoms overlap (Table 1). The key diagnostic feature, which leads to the diagnosis of SAD, is that the fear and avoidance specifically are related to being in or anticipating a feared social situation (Box 4).
Social
- Attending parties, weddings etc.
- Conversing in a group
- Speaking on the telephone
- Interacting with authority figure (e.g., teacher or boss)
- Making eye contact
- Ordering in a restaurant
Performance
- Public speaking
- Eating in public
- Writing a check
- Using a public toilet
- Taking a test
- Trying on clothes in a store
- Speaking up at a meeting
Many clinicians mistake social anxiety for panic disorder, since panic attacks in people with SAD are often cued by social situations. There can be up to a 40% overlap of SAD with panic disorder.4 Without probing carefully into the focus on fear and avoidance, SAD can be easily overlooked. Individuals with panic disorder experience unexpected attacks and are terrified at the prospect of additional attacks, while those with SAD experience attacks linked to social situations and fear scrutiny and embarrassment more than the attacks themselves.
SAD and major depression frequently coexist,4,11,12 challenging clinicians to distinguish social reticence and withdrawal accompanying depression from the fearful avoidance that typifies SAD. SAD usually precedes depression. Asking if the patient experienced social anxiety prior to the onset of depression can help identify SAD with comorbid depression.
Alcohol-related disorders are twice as likely to occur in those affected by SAD as in those not affected. The risk for females increases more than it does for males.2-4 SAD most often precedes alcohol abuse. Studies show that about 30% of patients receiving treatment for alcohol abuse/dependence have SAD. If it remains undetected, the risk of rapid relapse is high. That’s because patients are highly unlikely to participate in psychosocial treatments that help sustain post-treatment abstinence, such as the Alcoholics Anonymous 12-step program. A recent study found that both social anxiety and alcohol abuse disorders improve when SAD in alcoholics is treated.13
A substantially higher percentage of adults with SAD, especially women, have histories of prior childhood sexual and/or physical abuse than the general population.14 Recent studies both in women following rape and in combat veterans with posttraumatic stress disorder (PTSD) suggest that those with perceived life-threatening events are at higher risk for developing secondary SAD than are individuals who experience less severe trauma.15,16 We do not yet know if secondary SAD in trauma victims is different in character or response to treatment.
Individuals with certain medical conditions can develop symptoms resembling SAD. These include stuttering, benign essential tremor,17 Parkinson’s disease, disfiguring burn injuries, and possibly irritable bowel syndrome. Such patients are technically excluded from being diagnosed with SAD, though they would meet criteria if the diagnostic rules were suspended. A limited body of literature and clinical experience suggests that symptoms secondary to physical conditions may respond to the same treatment as SAD in medically healthy persons. A treatment trial for selected patients with SAD symptoms associated with medical conditions may provide significant benefits. Clearly more research is needed in this area.
- “Being embarrassed or looking stupid are among my worst fears.”
- “Fear of embarrassment causes me to avoid doing things or speaking to people.”
- “I avoid activities in which I am the center of attention.”
Connor et al, Depress Anxiety 2001;14:137
A recently developed self-rating scale, the Social Phobia Inventory (SPIN), assesses the spectrum of cognitive, behavioral, and physiological symptoms associated with SAD.18 Three of the 17 SPIN items have been found to identify generalized SAD with a high degree of sensitivity (Box 5).
The 3 main goals of SAD treatment are
- Acute reduction and control of pathological anxiety and related phobic avoidance;
- Adequate treatment of depression or other comorbid conditions;
- Long-term management of the social phobia.
Significant advances in treatment have emerged over the past 2 decades. We now know that cognitive behavioral therapy (CBT), medication, and their combination are efficacious.
Social situations involving speaking or performance are usually predictable, and nongeneralized SAD is thus amenable to use of a beta-blocker or benzodiazepine (Box 6). Beta-blockers are often adequate for control of tremor and increased heart rate. Some patients may also benefit more from judicious use of a benzodiazepine prior to the event.
In contrast, generalized SAD is less predictable, and continual treatment is recommended. Ideally, a medication regimen would be easily tolerated long-term, and would have antidepressant effects and a broad spectrum of efficacy against commonly coexisting disorders. Because of the significant risk for depression in individuals with SAD, first-line antidepressant treatment is preferred when possible over other medications.
The selective serotonin reuptake inhibitors (SSRIs) are now considered the first-line pharmacological treatment for social phobia. Paroxetine was the first to receive FDA approval for generalized SAD.19 Large multicenter studies supporting the efficacy of two other SSRIs—sertraline and fluvoxamine—have been reported.12 The SSRIs also appear to work against the other psychiatric disorders with which SAD commonly co-occurs, such as panic disorder, major depression, generalized anxiety disorder, and PTSD.
The empirical database is very limited, but it appears that SSRI treatment for a significant percentage of patients with SAD may require higher doses (up to twice the amount) than are usually needed for depression.10 Approximately 50% to 65% of patients with generalized SAD respond to any given SSRI. In our experience, failure to respond to one SSRI does not preclude response to a second SSRI.
The irreversible monoamine oxidase (MAO) inhibitor phenelzine was the first antidepressant shown to be useful for SAD. Tranylcypromine is less well studied, but also appears to be effective. The significant side effects (weight gain, orthostatic hypotension, insomnia) and inconvenience of administration have reduced use of these agents.
Nongeneralized
- PRN treatment
- Beta-blockers
- Benzodiazepines
Generalized
- Continuous treatment
- Broad-spectrum antidepressants
- Benzodiazepines
- MAOIs
- Antiepileptic agents
The tricyclic antidepressants are probably not effective, with the exception of clomipramine (also a potent inhibitor of serotonin reuptake).12 Clomipramine, while an effective anxiolytic and antidepressant, causes prohibitive side effects in many patients (e.g., sexual dysfunction and weight gain).
Key elements for individual or group setting
- Cognitive “restructuring”
- Social skills enhancement
The newer antidepressants venlafaxine and nefazodone are less well studied than the SSRIs, but show promise as potential broad-spectrum agents. Bupropion, a novel antidepressant, and the azapirone anxiolytic buspirone do not appear to work against SAD.
The main role of the benzodiazepines in SAD treatment is adjunctive to antidepressants or in some patients intolerant of, or unresponsive to, other treatments. Clonazepam, alprazolam, and probably others are effective for SAD, but they may not effectively treat or prevent depression or other commonly associated disorders.
The anticonvulsant gabapentin has been shown in one controlled study to be effective in treating SAD.20 This agent may be particularly useful for complicated patients such as those with a history of alcohol-related disorders, bipolar-spectrum disorder, or intolerance to SSRIs.
In parallel with the development of effective psychopharmacological treatments, several types of behavioral and cognitive behavioral treatments have been investigated, including imaginal flooding, graduated exposure, social skills training, cognitive-behavior approaches, and combined cognitive restructuring and graduated exposure.21 These treatments involve similar elements targeted at the cognitive distortions and avoidance behaviors, which represent core features of SAD (Box 7).
Many clinicians believe that combined pharmacotherapy and CBT treatment are superior to either modality alone for treating SAD. The little empirical information available indicates that acute treatment differences between drug alone and drug in combination with CBT are not impressive. However, there appears to be a lower rate of relapse following CBT than after medication discontinuation.
Despite our ability to treat this disorder, only a small fraction of sufferers get treatment. If untreated, the risk of comorbidity is extremely high. Routine screening for SAD, especially in younger individuals, could provide for early detection and treatment. Psychiatrists can play an important role in early detection and treatment by educating consumers, teachers, school nurses, psychologists, and pediatricians.
Related resources
- Lydiard, R.B. Social anxiety disorder comorbidity and its implications J. Clin. Psychiatry. 2001;62(suppl):17-23.
- American Psychiatric Association, http://www.psych.org
- American Psychological Association, http://www.apa.org
- National Institute for Mental Health: Anxiety Disorders, http://www.nimh.nih.gov/anxiety/
- Anxiety Disorders Associations of America, http://www.adaa.org/
Drug brand names
- Alprazolam • Xanax
- Atenolol • Tenormin
- Bupropion • Wellbutrin
- Buspirone • Buspar
- Clomipramine • Anafranil
- Clonazepam • Klonopin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Lorazepam • Ativan
- Nefazodone • Serzone
- Paroxetine • Paxil
- Phenelzine • Nardil
- Propranolol • Inderal
- Sertraline • Zoloft
- Tranylcypromine • Parnate
- Venlafaxine • Effexor
Disclosure
The author reports that he has received grant/research support and has served as a consultant to and on the speaker's bureau of Bristol-Myers Squibb Co., GlaxoSmithKline, Pfizer Inc., Eli Lilly and Co., Parke-Davis, and Solvay Pharmaceuticals. He also has received grant/research support and served as a consultant for Forest Pharmaceuticals, Wyeth-Ayerst Pharmaceuticals, and Roche; received grant/research support from Sanofi-Synthelabo; and has served as consultant for Dupont Pharmaceuticals and AstraZeneca.
1. Burton R. The Anatomy of Melancholy, vol. 1, 11th ed. London, England. Thomas Tegg, Cheapside; 1845.
2. Liebowitz MR, Gorman JM, Fyer AJ, Klein DF. Social phobia: review of a neglected anxiety disorder. Arch Gen Psychiatry. 1985;42:729-736.
3. Magee WJ, Eaton WW, Wittchen HU, et al. Agoraphobia, simple phobia, and social phobia in the National Comorbidity Survey. Arch Gen Psychiatry. 1996;53:159-168.
4. Schneier FR, Johnson J, et al. Social phobia: comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry. 1992;49:282-288.
5. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51:8-19.
6. Goldenberg IM, et al. The infrequency of “pure culture” diagnosis among the anxiety disorders. J Clin Psychiatry. 1996;57:528-533.
7. Wittchen HU, Beloch E. The impact of social phobia on quality of life. Int Clin Psychopharmacol. 1996;11(suppl):15-23.
8. Greenberg PE, Sisitsky T, Kessler RC, et al. The economic burden of anxiety disorders in the 1990s. J Clin Psychiatry. 1999;60:427-435.
9. Weiller E, Bisserbe JC, Boyer P, et al. Social phobia in general health care. Br J Psychiatry. 1996;168:169-174.
10. Katzelnick DJ, Greist JH. Social anxiety disorder: an unrecognized problem in primary care. J Clin Psychiatry. 2001;62:11.-
11. Davidson J. Social anxiety disorder under scrutiny. Depress Anxiety. 2000;11:93-98.
12. Lydiard RB. Social anxiety disorder: treatment role of the SSRIs. In Montgomery SA, den Boer JA (eds). SSRIs in Depression and Anxiety Perspectives in Psychiatry ,vol 8. NY: Wiley, Chichester, 129-150, 2001.
13. Randall CL, et al. Paroxetine improves both social anxiety and alcohol use in dually-diagnosed patients at the American College of Neuropsychopharmacology. San Juan, Puerto Rico. Dec 10-15, 2000.
14. Stein MB, Walker JR, Anderson G, et al. Childhood physical and sexual abuse in patients with anxiety disorders and in a community sample. Am J Psychiatry. 1996;153:275-277.
15. Boudreaux E, Kilpatrick DG, Resnick HS, et al. Criminal victimization, posttraumatic stress disorder, and comorbid psychopathology among a community sample of women. J Trauma Stress. 1998;11:665-678.
16. Orsillo SM, Heimberg RG, Juster HR, Garrett J. Social phobia and PTSD in Vietnam veterans. J Trauma Stress. 1996;9:235-252.
17. George MS, Lydiard RB. Social phobia secondary to physical disability: a review of benign essential tremor (BET) and stuttering. Psychosomatics. 1994;35:520-523.
18. Connor KM, et al. Mini-SPIN: A brief screening assessment for generalized social anxiety disorder. Depress Anxiety. 2001;14:137-140.
19. Stein MB, Liebowitz MR, Lydiard RB, et al. Paroxetine treatment of generalized social phobia (social anxiety disorder): a randomized controlled trial. JAMA. 1998;280:708-713.
20. Pande AC, Davidson JR, Jefferson JW, et al. Treatment of social phobia with gabapentin: a placebo-controlled study. J Clin Psychopharmacol. 1999;19:341-348.
21. Heimberg RG. Specific issues in the cognitive behavioral treatment of social phobia. J Clin Psychiatry. 1993;54(suppl 12):36-45.
1. Burton R. The Anatomy of Melancholy, vol. 1, 11th ed. London, England. Thomas Tegg, Cheapside; 1845.
2. Liebowitz MR, Gorman JM, Fyer AJ, Klein DF. Social phobia: review of a neglected anxiety disorder. Arch Gen Psychiatry. 1985;42:729-736.
3. Magee WJ, Eaton WW, Wittchen HU, et al. Agoraphobia, simple phobia, and social phobia in the National Comorbidity Survey. Arch Gen Psychiatry. 1996;53:159-168.
4. Schneier FR, Johnson J, et al. Social phobia: comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry. 1992;49:282-288.
5. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51:8-19.
6. Goldenberg IM, et al. The infrequency of “pure culture” diagnosis among the anxiety disorders. J Clin Psychiatry. 1996;57:528-533.
7. Wittchen HU, Beloch E. The impact of social phobia on quality of life. Int Clin Psychopharmacol. 1996;11(suppl):15-23.
8. Greenberg PE, Sisitsky T, Kessler RC, et al. The economic burden of anxiety disorders in the 1990s. J Clin Psychiatry. 1999;60:427-435.
9. Weiller E, Bisserbe JC, Boyer P, et al. Social phobia in general health care. Br J Psychiatry. 1996;168:169-174.
10. Katzelnick DJ, Greist JH. Social anxiety disorder: an unrecognized problem in primary care. J Clin Psychiatry. 2001;62:11.-
11. Davidson J. Social anxiety disorder under scrutiny. Depress Anxiety. 2000;11:93-98.
12. Lydiard RB. Social anxiety disorder: treatment role of the SSRIs. In Montgomery SA, den Boer JA (eds). SSRIs in Depression and Anxiety Perspectives in Psychiatry ,vol 8. NY: Wiley, Chichester, 129-150, 2001.
13. Randall CL, et al. Paroxetine improves both social anxiety and alcohol use in dually-diagnosed patients at the American College of Neuropsychopharmacology. San Juan, Puerto Rico. Dec 10-15, 2000.
14. Stein MB, Walker JR, Anderson G, et al. Childhood physical and sexual abuse in patients with anxiety disorders and in a community sample. Am J Psychiatry. 1996;153:275-277.
15. Boudreaux E, Kilpatrick DG, Resnick HS, et al. Criminal victimization, posttraumatic stress disorder, and comorbid psychopathology among a community sample of women. J Trauma Stress. 1998;11:665-678.
16. Orsillo SM, Heimberg RG, Juster HR, Garrett J. Social phobia and PTSD in Vietnam veterans. J Trauma Stress. 1996;9:235-252.
17. George MS, Lydiard RB. Social phobia secondary to physical disability: a review of benign essential tremor (BET) and stuttering. Psychosomatics. 1994;35:520-523.
18. Connor KM, et al. Mini-SPIN: A brief screening assessment for generalized social anxiety disorder. Depress Anxiety. 2001;14:137-140.
19. Stein MB, Liebowitz MR, Lydiard RB, et al. Paroxetine treatment of generalized social phobia (social anxiety disorder): a randomized controlled trial. JAMA. 1998;280:708-713.
20. Pande AC, Davidson JR, Jefferson JW, et al. Treatment of social phobia with gabapentin: a placebo-controlled study. J Clin Psychopharmacol. 1999;19:341-348.
21. Heimberg RG. Specific issues in the cognitive behavioral treatment of social phobia. J Clin Psychiatry. 1993;54(suppl 12):36-45.
Cognitive enhancers for dementia: Do they work?
No psychiatrist likes to see the month-by-month deterioration in an Alzheimer’s patient—the losses in cognition, the declining ability to function, the behavioral aberrations that upset family and friends.
The problem will accelerate in the decades ahead as the proportion of elderly in the population increase. More than 4 million people in the United States are afflicted with this disorder. Prevalence rates as high as 10% have been estimated for individuals older than 65. Patients with the disease have estimated direct costs of $20,000 to $61,000 per year if the duration lasts 7 to 8 years.1
Although behavioral and functional deficits account for the high costs associated with Alzheimer’s disease (AD), the disorder is defined by cognitive criteria (Box 1). The majority of medication trials have been aimed at symptomatic treatment. More recently, studies have been designed to prevent or delay the onset of AD. Early on, initial therapies directed toward AD were aimed at reversing the cholinergic deficit (Box 2). Clinical trials utilizing lecithin (25-100 g/d) and choline (<16 g/d) as precursors of acetylcholine did not lead to significant benefit.6 Augmenting central cholinergic levels with acetylcholinesterase (AChE) inhibitors has consistently detected symptomatic improvement.
In recent years, the Food and Drug Administration has approved 4 AChE inhibitors—tacrine, donepezil, rivastigmine, and galantamine—for the treatment of AD. I will discuss only the latter 3, since tacrine, the first to Nshow benefit, has a high rate of adverse effects and is of limited use.7 The AChE inhibitors may improve cognition and behavioral symptoms and delay progression of the illness. They can also have beneficial effects on activities of daily living (ADL) and can reduce costs and improve caregiver burden.8
- The development of multiple cognitive deficits manifested by both:
- Memory impairment (impaired ability to learn new information or to recall previously learned information) and
- One (or more) of the following cognitive disturbances:
- Aphasia (language disturbance)
- Apraxia (impaired ability to carry out motor activities despite intact motor function)
- Agnosia (failure to recognize or identify objects despite intact sensory function)
- Disturbance in executive functioning (i.e., planning, organization, sequencing, abstracting)
- The cognitive deficits in Criteria A1 and A2 each cause significant impairment in social or occupational functioning and represent a significant decline from a previous level of functioning.
- The course is characterized by gradual onset and continuing cognitive decline.
Source: American Psychatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington DC: American Psychiatric Press., 1994.
The three AChE inhibitors have unique basic properties (Box 3). In order to maximize and prolong positive drug effects, it is important to start early and adjust dosage during the treatment9 (Table 1). Side effects are tolerable; the most common include nausea, vomiting, and diarrhea. Titrating the dosage slowly can reduce these. The cholinergic quality of these medications dictate that they be prescribed with caution in patients with bradycardic arrhythmias such as sick sinus syndrome, asthma, or chronic obstructive pulmonary disease.10
Effects on cognition and global assessments
Numerous efficacy studies examining cognition and global assessments in AD patients have been performed with the AChE inhibitors. Their major therapeutic effect is to maintain cognitive function at a constant level during a 6- to 12-month period of treatment, as compared to placebo. Comparison of clinical effects of all 3 agents demonstrates a similar magnitude of improvement. For some drugs, this may represent an upper limit, whereas for others it may still be possible to further increase the benefit.
The pathophysiologic processes implicated in Alzheimer’s disease (AD)include amyloid precursor protein metabolism, tau phosphorylation, apolipoprotein E, inflammation, oxidative stress, and apoptosis. Neuropathological features include amyloid plaques, neurofibrillary tangles, neuronal and synaptic loss, microgliosis, and astrocytosis. The resulting clinical syndrome of dementia is associated with neurotransmitter deficits and intracortical disconnection.
The central cholinergic neurotransmitter system is impaired in AD. This system is involved in learning and memory. The limbic system and neocortex receive projections from the cholinergic system in the septal nuclei and substantia innominata. This includes the medial septal nucleus, diagonal band, and nucleus basalis.2 Literature on animals has demonstrated that basal forebrain lesions impair learning and memory. Cholinergic agonists can improve this. Furthermore, cholinergic antagonists such as scopolamine and atropine can impair learning and memory in humans and animals.3 In AD, a 58% to 93% reduction in choline acetyltransferase levels (and other cholinergic markers) in the cortex and hippocampus can be observed and this correlates with dementia severity.4 Early AD is characterized by neuronal loss and tangles in the cholinergic nucleus basalis of Meynert.5
Results of 4 double-blind, placebo-controlled clinical trials of donepezil, involving more than 1,900 individuals with mild to moderate AD, have been published recently. In all, significant improvements in cognition were observed consistently for both therapeutic doses of donepezil (5 mg/d and 10 mg/d), relative to placebo. Similar benefits were reported for global functioning.
The long-term clinical efficacy and safety of donepezil versus placebo across 1 year in patients with mild to moderate AD was investigated.14 The Gottfries-Brane-Steen global assessment for rating dementia symptoms demonstrated the benefit of donepezil over placebo at weeks 24, 36, and 52, and at the study end point. Advantages of donepezil were also observed in cognition and ADL.
Donepezil also appears to work for patients with moderate to severe AD. In a recent 24-week study,15 patients receiving donepezil showed benefits on the Clinician’s Interview-Based Impression of Change with Caregiver Input (CIBIC+), compared with placebo, at all visits up to week 24 and at the study’s end point. All other secondary measures showed significant differences between the groups in favor of donepezil at the end of the study. These data suggest that donepezil’s benefits extend into more advanced stages of AD than those previously investigated, with good tolerability.
Clinical trials of rivastigmine (1.5-6 mg twice daily PO) have also demonstrated benefits on cognitive and global measures.16 The efficacy of rivastigmine tartrate (ENA 713) in patients with mild to moderately severe Alzheimer’s disease was evaluated in a 26-week open-label extension of a 26-week, double-blind, placebo-controlled study. By 52 weeks, patients originally treated with rivastigmine 6 to 12 mg/d had significantly better cognitive function than did patients originally treated with placebo.17- 19
Donepezil is a second-generation, piperidine-class, selective and reversible acetylcholinesterase (AChE) inhibitor. It is structurally dissimilar from other established AChE inhibitors.
Experimentally, donepezil inhibits AChE activity in human erythrocytes and increases extracellular acetylcholine levels in the cerebral cortex and the hippocampus of the rat. Pharmacologically, donepezil has a half-life of approximately 70h, lending itself to once-daily administration.11
Rivastigmine (ENA 713, or carbamoylatine) is an AChE inhibitor with brain-region selectivity and a long duration of action. Both preclinical studies and studies in human volunteers have shown that rivastigmine induces substantially greater inhibition of AChE in the central nervous system compartment than it does in the periphery (40% inhibition of central AChE compared with 10% inhibition of plasma butylcholinesterase in healthy volunteers). Rivastigmine also preferentially inhibits the G1 enzymatic form of AChE, which predominates in the brains of patients with Alzheimer’s disease (AD).
Evidence from animal studies also suggests that rivastigmine is a more potent inhibitor of AChE in the cortex and hippocampus, the brain regions most affected by AD. The principal metabolite of rivastigmine has at least 10-fold lower activity against AChE compared with the parent drug.
Rivastigmine is completely metabolized; the major route of elimination of the metabolites is renal. Rivastigmine is inactivated during the process of interacting with and inhibiting AChE, and, in contrast to other AChE inhibitors, the hepatic cytochrome P-450 (CYP-450) system is not involved in the metabolism of rivastigmine.12
Galantamine is an allosterically potentiating ligand that modulates nicotinic cholinergic receptors (nAChR) to increase acetylcholine release as well as acting as an AChE inhibitor. In preclinical experiments, the drug significantly improves learning, reduces AChE levels, and increases nicotinic receptor binding. Action of galantamine is on the most abundant nAChR in the human brain, the alpha4/beta2subtype.13
Clinical trials of galantamine (4-12 mg/bid PO) have demonstrated similar benefits.20 Following a 4-week placebo run-in, patients were randomized to 1 of 4 treatment arms: placebo or galantamine escalated to final maintenance dosages of 8, 16, or 24 mg/d for a 5-month treatment phase. At study’s end, the galantamine-place-bo differences on the cognitive subscale of the AD Assessment Scale were 3.3 points for the 16 mg/d group and 3.6 points for the 24 mg/d group. Treatment discontinuations due to adverse events were low in all galantamine groups (6% to 10%) and comparable with that in the placebo group (7%). The incidence of adverse events in the galantamine groups, notably gastrointestinal symptoms, was low and most adverse events were mild.
Other studies examining galantamine have demonstrated similar clinical benefits.8, 21
When using AChE inhibitors, the slope of cognitive decline is similar in treated and untreated patients after the initial improvement. These drugs essentially do not reverse the disorder’s course but shift upward the curve describing the time course of cognitive decline. This applies also to behavioral and functional benefits. Thus the benefit obtained is symptomatic and not neuroprotective, and is lost after discontinuing the medications.
Effects on functioning and behavior
In a 24-week multinational clinical trial, patients receiving donepezil (10 mg/d) were more able than placebo-treated patients to perform complex daily functioning tasks.22 Similar effects have been observed with rivastigmine and galantamine.16, 20
All 3 AChE inhibitors have demonstrated improvements in the behavioral changes associated with AD. Cummings et al23 tested the hypothesis that behavioral disturbances are reported at significantly lower rates by caregivers of AD patients receiving donepezil, compared with a group of patients not receiving a drug for treatment of dementia. Donepezil patients were described as significantly less likely to be threatening, destroy property, and talk loudly, and significantly fewer were treated with sedatives.
Table 1
COMPARING THEAChE INHIBITORS
| Donepezil | Rivastigmine | Galantamine | |
|---|---|---|---|
| Chemical class | Piperidine | Carbamate | Phenanthrene alkaloid |
| AChE inhibitor | Yes | Yes | Yes |
| BuChE inhibitor | Small | Yes | Small |
| Nicotinic modulation | No | No | Yes |
| Elimination half-life | 50-70 h | 0.6-2 h | 5-7 h |
| Administration | Once daily | Twice daily | Twice daily |
| Starting dosage | 5 mg/d | 1.5 mg bid | 4 mg bid |
| Total recommended dosage | 5-10 mg/d | 6-12 mg/d | 16-24 mg/d |
| Adapted from Conn DK. Cholinesterase inhibitors: Comparing the options for mild-to-moderate dementia. Geriatrics56: 56-57, 2001. | |||
An open-label study by Weiner et al24 examined the effects of donepezil on emotional and behavioral symptoms using the CERAD Behavior Rating Scale for Dementia and its subscales. In a group of 25 AD patients treated with donepezil, scores returned to baseline levels at 12 months. In contrast, the scores of the reference group worsened minimally.
Galantamine has also proved effective in treating behavioral symptoms associated with AD. In the Tariot et al20 study, galantamine at 16 mg/d and 24 mg/d had a significantly better outcome on CIBIC+, ADL, and behavioral symptoms versus placebo.
Rosler et al25 assessed the ability of rivastigmine to improve behavioral symptoms in AD. Using the behavioral component of the CIBIC+, results showed that long-term treatment with rivastigmine could slow the progression of symptoms. Symptoms showing stabilization included aggressiveness, activity disturbances, hallucinations, and paranoid features. The results also suggest that patients treated earlier with rivastigmine may attain a greater benefit than those whose treatment is delayed 6 months.
Rivastigmine also has significant effects on controlling behavioral symptoms in patients with Lewy body dementia.26 A placebo-controlled, double-blind, multicenter study was performed in 120 patients with Lewy body dementia. Individuals were given up to 12 mg/d rivastigmine or placebo for 20 weeks, followed by 3 weeks rest. Assessment by neuropsychiatric inventory was made at baseline, and again at weeks 12, 20, and 23.
Patients taking rivastigmine were significantly less apathetic and anxious than those on placebo, and had fewer delusions and hallucinations. Almost twice as many patients on rivastigmine as on placebo (37, 63% versus 18, 30%) showed at least a 30% improvement from baseline. In a computerized cognitive assessment system and neuropsychological tests, patients were significantly faster and better than those on placebo, particularly when performing tasks with a substantial attentional component.
Cost effectiveness
Numerous studies have demonstrated that AChE inhibitors are cost savers in AD treatment. Fillit et al27 examined the impact of donepezil in a multisite managed care organization for 2 years using claims data for 70 individuals with AD and related dementias. The median per diem medical costs were $1.22 lower post treatment than they were in the pretreatment phase. Moreover, posttreatment costs were reduced in 6 of 7 service settings, with median per diem savings of $0.77 in outpatient care and $0.65 in office visits.
Neumann et al28 utilized cost-effectiveness analysis to predict that for mild AD, donepezil would pay for itself in cost offsets if the drug’s effect exceeds 2 years. Donepezil costs were partially offset by a reduction in the costs of care due to enhanced cognitive functioning and the delay in placing the patient in more costly disease stages and settings.
One study used the disease-progression model to estimate potential per-patient savings resulting from the treatment of AD in Canada.29 Rivastigmine was estimated to delay the transition to more severe stages of AD by up to 188 days for patients with mild AD after 2 years of treatment. For patients with mild-to-moderate and moderate disease, this delay was estimated to be 106 and 44 days, respectively.
The Assessment of Health Economics in Alzheimer’s Disease model uses algorithms to predict the time until patients with AD require full-time care. A study, performed in Canada, compared treatment with galantamine to treatment without pharmacological interventions.30 Galantamine was predicted to reduce the duration of full-time care by almost 10%. Approximately 5.6 patients with mild-to-moderate disease must be placed on treatment to avoid 1 year of full-time care, resulting in savings averaging $528 per patient. For patients with moderate disease, 3.9 patients must be placed on treatment to avoid 1 year of full-time care, with savings predicted at $2,533 per patient.
Caregiving burden
Fillit et al addressed caregiver well-being in a self-administered, nationwide survey of AD caregivers. Caregivers of patients treated with donepezil (n = 274) were compared with caregivers of patients not treated with donepezil (n = 274).31 The Caregiver Burden Scale measured time demands and distress linked to commonly performed caregiving tasks. Donepezil caregivers reported significantly lower scores on difficulty of caregiving. Similar findings have been observed with galantamine.32
Related resources
- Bullock R. New drugs for Alzheimer’s disease and other dementias. Br J Psychiatry. 2002;180(2):135-139.
- Brodaty H, Ames D, et al. Pharmacological treatment of cognitive deficits in Alzheimer’s disease. Med J Aust. 2001;175(6):324-329.
- Ahmed MB. Alzheimer’s disease: recent advances in etiology, diagnosis, and management. Tex Med. 2001;97(12):50-58.
- Frisoni GB. Treatment of Alzheimer’s disease with acetyl-cholinesterase inhibitors: bridging the gap between evidence and practice. J Neurol. 2001;248(7):551-7.
Drug brand names
- Tacrine • Cognex
- Donepezil • Aricept
- Rivastigmine • Exelon
- Galantamine • Reminyl
Disclosure
The author reports that he receives grant/research support from, serves as a consultant to, and is on the speaker’s bureau of Janssen Pharmaceutica and Pfizer Inc., and serves as consultant to and is on the speaker’s bureau of Novartis Pharmaceuticals Corp.
1. Irizarry M, Hyman B. Alzheimer’s disease. In: Principles of neuroepidemiology. Batchelor T, Cudkowicz M, eds. Boston: Butterworth-Heinemann, 2001:69-98.
2. Mesulam MM, Mufson EJ, Levey AI, Warner BH. Cholinergic innervation of cortex by the basal forebrain: Cytochemistry and cortical connections of the septal area, diagonal band nuclei, nucleus basalis (substantia innominata), and hypothalamus in the rhesus monkey. J Comp Neurol. 1983a;214:170-197.
3. Drachman DA, Leavitt J. Human memory and the cholinergic system. A relationship to aging? Arch Neurol. 1974;30:113-121.
4. Davies P, Maloney AJ. Selective loss of central cholinergic neurons in Alzheimer’s disease. Lancet. 1976;2:1403.-
5. Whitehouse PJ, Price DL, Clark AW, Coyle JT, DeLong MR. Alzheimer disease: evidence for selective loss of cholinergic neurons in the nucleus basalis. Ann Neurol. 1981;10:122-126.
6. Higgins JPT, Flicker L. Lecithin and cognitive impairment. The Cochrane Database of Systematic Reviews. 2001.;
7. Knapp MJ, Knopman DS, Solomon PR, Pendlebury WW, Davis CS, Gracon SI. A 30-week randomized controlled trial of high-dose tacrine in patients with Alzheimer’s disease. The Tacrine Study Group. JAMA. 1994;271:985-991.
8. Raskind MA, Peskind ER, Wessel T, Yuan W. Galantamine in AD: A 6-month randomized, placebo-controlled trial with a 6-month extension. The Galantamine USA-1 Study Group. Neurology. 2000;54:2262-2268.
9. Giacobini E. Cholinesterase inhibitors stabilize Alzheimer’s disease. Methods Find Exp Clin Pharmacol. 2000;22:609-613.
10. Irizarry MC, Hyman BT. Alzhemier Disease Therapeutics. J Neuropathology Exp Neurology. 2001;60:923-928.
11. Wilkinson DG. The pharmacology of donepezil: a new treatment of Alzheimer’s disease. Expert Opin Pharmacother. 1999;1:121-135.
12. Polinsky RJ. Clinical pharmacology of rivastigmine: a new-generation acetyl-cholinesterase inhibitor for the treatment of Alzheimer’s disease. Clin Ther. 1998;20:634-647.
13. Samochocki M, Zerlin M, Jostock R, et al. Galantamine is an allosterically potentiating ligand of the human alpha4/beta2 nAChR. Acta Neurol Scand. 2000(Suppl);;176:68-73.
14. Winblad B, Engedal K, Soininen H, Verhey F, et al. A 1-year, randomized, placebo-controlled study of donepezil in patients with mild to moderate AD. Neurology. 2001;57:489-495.
15. Feldman H, Gauthier S, Hecker J, et al. Donepezil MSAD Study Investigators Group.A 24-week, randomized, double-blind study of donepezil in moderate to severe Alzheimer’s disease. Neurology. 2001;57:613-620.
16. Farlow M, Anand R, Messina J, Jr, Hartman R, Veach J. A 52-week study of the efficacy of rivastigmine in patients with mild to moderately severe Alzheimer’s disease. Eur Neurol. 2000;44:236-241.
17. Rogers S, Friedhoff L. Donepezil Study Group.The efficacy and safety of donepezil in patients with Alzhemier’s disease. Dementia. 1996;7:293-303.
18. Rogers S, Farlow M, Doody R, Morris R, Friedhoff L. A 24-week, double-blind, placebo-controlled trial of donepezil in patients with Alzheimer’s disease. Donepezil Study Group. Neurology. 1998;50:136-145.
19. Rosler M, Anand R, Cicin-Sain A, Gauthier S, Agid Y, DalBianco P, Stahelin HB, et al. Efficacy and safety of rivastigmine in patients with Alzheimer’s disease: International randomized controlled trial. BMJ. 1999;318:633-638.
20. Tariot PN, Solomon PR, Morris JC, Kershaw P, Lilienfeld S, Ding C. A 5-month, randomized, placebo-controlled trial of galantamine in AD. The Galantamine USA-10 Study Group. Neurology. 2000;54:2269-2276.
21. Wilcock GK, Lilienfeld S, Gaens E. Efficacy and safety of galantamine in patients with mild to moderate Alzheimer’s disease: Multicentre randomized controlled trial. Galantamine International - 1 Study Group. BMJ. 2000;321:1445-1449.
22. Knopman DS. Management of cognition and function: new results from the clinical trials programme of Aricept (R) (donepezil Hcl). Int J Neuropsychopharmacol. 2000;3:13-20.
23. Cummings JL, Donohue JA, Brooks RL. The relationship between donepezil and behavioral disturbances in patients with Alzheimer’s disease. Am J Geriatr Psychiatry. 2000;8:134-140.
24. Weiner MF, Martin-Cook K, Foster BM, Saine K, et al. Effects of donepezil on emotional/behavioral symptoms in Alzheimer’s disease patients. J Clin Psychiatry. 2000;487-492.
25. Rosler M, Retz W, Retz-Junginger P, Dennler HJ. Effects of two-year treatment with the cholinesterase inhibitor rivastigmine on behavioural symptoms in Alzheimer’s disease. Behav Neurol. 1998;11:211-216.
26. McKeith I, Del Ser T, Spano P, Emre M, et al. Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study. Lancet. 2000;356(9247):2031-2036.
27. Fillit H, Gutterman EM, Lewis B. Donepezil use in managed Medicare: effect on health care costs and utilization. Clin Ther. 1999;21:2173-2185.
28. Neumann PJ, Hermann RC, Kuntz KM, Araki SS, Duff SB, Leon J, Berenbaum PA, et al. Cost-effectiveness of donepezil in the treatment of mild or moderate Alzheimer’s disease. Neurology. 1999;52:1115-1116.
29. Hauber AB, Gnanasakthy A, Mauskopf JA. Savings in the cost of caring for patients with Alzheimer’s disease in Canada: an analysis of treatment with rivastigmine. Clin Ther. 2000;22:439-451.
30. Getsios D, Caro JJ, Caro G, Ishak K. The AHEAD Study Group. Assessment of health economics in Alzheimer’s disease (AHEAD): galantamine treatment in Canada. Neurology. 2001;57:972-978.
31. Fillit HM, Gutterman EM, Brooks RL. Impact of donepezil on caregiving burden for patients with Alzheimer’s disease. Int Psychogeriatr. 2000;12(3):389-401.
32. Blesa R. Galantamine: therapeutic effects beyond cognition. Dement Geriatr Cogn Disord. 2000;11(Suppl)1:28-34.
No psychiatrist likes to see the month-by-month deterioration in an Alzheimer’s patient—the losses in cognition, the declining ability to function, the behavioral aberrations that upset family and friends.
The problem will accelerate in the decades ahead as the proportion of elderly in the population increase. More than 4 million people in the United States are afflicted with this disorder. Prevalence rates as high as 10% have been estimated for individuals older than 65. Patients with the disease have estimated direct costs of $20,000 to $61,000 per year if the duration lasts 7 to 8 years.1
Although behavioral and functional deficits account for the high costs associated with Alzheimer’s disease (AD), the disorder is defined by cognitive criteria (Box 1). The majority of medication trials have been aimed at symptomatic treatment. More recently, studies have been designed to prevent or delay the onset of AD. Early on, initial therapies directed toward AD were aimed at reversing the cholinergic deficit (Box 2). Clinical trials utilizing lecithin (25-100 g/d) and choline (<16 g/d) as precursors of acetylcholine did not lead to significant benefit.6 Augmenting central cholinergic levels with acetylcholinesterase (AChE) inhibitors has consistently detected symptomatic improvement.
In recent years, the Food and Drug Administration has approved 4 AChE inhibitors—tacrine, donepezil, rivastigmine, and galantamine—for the treatment of AD. I will discuss only the latter 3, since tacrine, the first to Nshow benefit, has a high rate of adverse effects and is of limited use.7 The AChE inhibitors may improve cognition and behavioral symptoms and delay progression of the illness. They can also have beneficial effects on activities of daily living (ADL) and can reduce costs and improve caregiver burden.8
- The development of multiple cognitive deficits manifested by both:
- Memory impairment (impaired ability to learn new information or to recall previously learned information) and
- One (or more) of the following cognitive disturbances:
- Aphasia (language disturbance)
- Apraxia (impaired ability to carry out motor activities despite intact motor function)
- Agnosia (failure to recognize or identify objects despite intact sensory function)
- Disturbance in executive functioning (i.e., planning, organization, sequencing, abstracting)
- The cognitive deficits in Criteria A1 and A2 each cause significant impairment in social or occupational functioning and represent a significant decline from a previous level of functioning.
- The course is characterized by gradual onset and continuing cognitive decline.
Source: American Psychatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington DC: American Psychiatric Press., 1994.
The three AChE inhibitors have unique basic properties (Box 3). In order to maximize and prolong positive drug effects, it is important to start early and adjust dosage during the treatment9 (Table 1). Side effects are tolerable; the most common include nausea, vomiting, and diarrhea. Titrating the dosage slowly can reduce these. The cholinergic quality of these medications dictate that they be prescribed with caution in patients with bradycardic arrhythmias such as sick sinus syndrome, asthma, or chronic obstructive pulmonary disease.10
Effects on cognition and global assessments
Numerous efficacy studies examining cognition and global assessments in AD patients have been performed with the AChE inhibitors. Their major therapeutic effect is to maintain cognitive function at a constant level during a 6- to 12-month period of treatment, as compared to placebo. Comparison of clinical effects of all 3 agents demonstrates a similar magnitude of improvement. For some drugs, this may represent an upper limit, whereas for others it may still be possible to further increase the benefit.
The pathophysiologic processes implicated in Alzheimer’s disease (AD)include amyloid precursor protein metabolism, tau phosphorylation, apolipoprotein E, inflammation, oxidative stress, and apoptosis. Neuropathological features include amyloid plaques, neurofibrillary tangles, neuronal and synaptic loss, microgliosis, and astrocytosis. The resulting clinical syndrome of dementia is associated with neurotransmitter deficits and intracortical disconnection.
The central cholinergic neurotransmitter system is impaired in AD. This system is involved in learning and memory. The limbic system and neocortex receive projections from the cholinergic system in the septal nuclei and substantia innominata. This includes the medial septal nucleus, diagonal band, and nucleus basalis.2 Literature on animals has demonstrated that basal forebrain lesions impair learning and memory. Cholinergic agonists can improve this. Furthermore, cholinergic antagonists such as scopolamine and atropine can impair learning and memory in humans and animals.3 In AD, a 58% to 93% reduction in choline acetyltransferase levels (and other cholinergic markers) in the cortex and hippocampus can be observed and this correlates with dementia severity.4 Early AD is characterized by neuronal loss and tangles in the cholinergic nucleus basalis of Meynert.5
Results of 4 double-blind, placebo-controlled clinical trials of donepezil, involving more than 1,900 individuals with mild to moderate AD, have been published recently. In all, significant improvements in cognition were observed consistently for both therapeutic doses of donepezil (5 mg/d and 10 mg/d), relative to placebo. Similar benefits were reported for global functioning.
The long-term clinical efficacy and safety of donepezil versus placebo across 1 year in patients with mild to moderate AD was investigated.14 The Gottfries-Brane-Steen global assessment for rating dementia symptoms demonstrated the benefit of donepezil over placebo at weeks 24, 36, and 52, and at the study end point. Advantages of donepezil were also observed in cognition and ADL.
Donepezil also appears to work for patients with moderate to severe AD. In a recent 24-week study,15 patients receiving donepezil showed benefits on the Clinician’s Interview-Based Impression of Change with Caregiver Input (CIBIC+), compared with placebo, at all visits up to week 24 and at the study’s end point. All other secondary measures showed significant differences between the groups in favor of donepezil at the end of the study. These data suggest that donepezil’s benefits extend into more advanced stages of AD than those previously investigated, with good tolerability.
Clinical trials of rivastigmine (1.5-6 mg twice daily PO) have also demonstrated benefits on cognitive and global measures.16 The efficacy of rivastigmine tartrate (ENA 713) in patients with mild to moderately severe Alzheimer’s disease was evaluated in a 26-week open-label extension of a 26-week, double-blind, placebo-controlled study. By 52 weeks, patients originally treated with rivastigmine 6 to 12 mg/d had significantly better cognitive function than did patients originally treated with placebo.17- 19
Donepezil is a second-generation, piperidine-class, selective and reversible acetylcholinesterase (AChE) inhibitor. It is structurally dissimilar from other established AChE inhibitors.
Experimentally, donepezil inhibits AChE activity in human erythrocytes and increases extracellular acetylcholine levels in the cerebral cortex and the hippocampus of the rat. Pharmacologically, donepezil has a half-life of approximately 70h, lending itself to once-daily administration.11
Rivastigmine (ENA 713, or carbamoylatine) is an AChE inhibitor with brain-region selectivity and a long duration of action. Both preclinical studies and studies in human volunteers have shown that rivastigmine induces substantially greater inhibition of AChE in the central nervous system compartment than it does in the periphery (40% inhibition of central AChE compared with 10% inhibition of plasma butylcholinesterase in healthy volunteers). Rivastigmine also preferentially inhibits the G1 enzymatic form of AChE, which predominates in the brains of patients with Alzheimer’s disease (AD).
Evidence from animal studies also suggests that rivastigmine is a more potent inhibitor of AChE in the cortex and hippocampus, the brain regions most affected by AD. The principal metabolite of rivastigmine has at least 10-fold lower activity against AChE compared with the parent drug.
Rivastigmine is completely metabolized; the major route of elimination of the metabolites is renal. Rivastigmine is inactivated during the process of interacting with and inhibiting AChE, and, in contrast to other AChE inhibitors, the hepatic cytochrome P-450 (CYP-450) system is not involved in the metabolism of rivastigmine.12
Galantamine is an allosterically potentiating ligand that modulates nicotinic cholinergic receptors (nAChR) to increase acetylcholine release as well as acting as an AChE inhibitor. In preclinical experiments, the drug significantly improves learning, reduces AChE levels, and increases nicotinic receptor binding. Action of galantamine is on the most abundant nAChR in the human brain, the alpha4/beta2subtype.13
Clinical trials of galantamine (4-12 mg/bid PO) have demonstrated similar benefits.20 Following a 4-week placebo run-in, patients were randomized to 1 of 4 treatment arms: placebo or galantamine escalated to final maintenance dosages of 8, 16, or 24 mg/d for a 5-month treatment phase. At study’s end, the galantamine-place-bo differences on the cognitive subscale of the AD Assessment Scale were 3.3 points for the 16 mg/d group and 3.6 points for the 24 mg/d group. Treatment discontinuations due to adverse events were low in all galantamine groups (6% to 10%) and comparable with that in the placebo group (7%). The incidence of adverse events in the galantamine groups, notably gastrointestinal symptoms, was low and most adverse events were mild.
Other studies examining galantamine have demonstrated similar clinical benefits.8, 21
When using AChE inhibitors, the slope of cognitive decline is similar in treated and untreated patients after the initial improvement. These drugs essentially do not reverse the disorder’s course but shift upward the curve describing the time course of cognitive decline. This applies also to behavioral and functional benefits. Thus the benefit obtained is symptomatic and not neuroprotective, and is lost after discontinuing the medications.
Effects on functioning and behavior
In a 24-week multinational clinical trial, patients receiving donepezil (10 mg/d) were more able than placebo-treated patients to perform complex daily functioning tasks.22 Similar effects have been observed with rivastigmine and galantamine.16, 20
All 3 AChE inhibitors have demonstrated improvements in the behavioral changes associated with AD. Cummings et al23 tested the hypothesis that behavioral disturbances are reported at significantly lower rates by caregivers of AD patients receiving donepezil, compared with a group of patients not receiving a drug for treatment of dementia. Donepezil patients were described as significantly less likely to be threatening, destroy property, and talk loudly, and significantly fewer were treated with sedatives.
Table 1
COMPARING THEAChE INHIBITORS
| Donepezil | Rivastigmine | Galantamine | |
|---|---|---|---|
| Chemical class | Piperidine | Carbamate | Phenanthrene alkaloid |
| AChE inhibitor | Yes | Yes | Yes |
| BuChE inhibitor | Small | Yes | Small |
| Nicotinic modulation | No | No | Yes |
| Elimination half-life | 50-70 h | 0.6-2 h | 5-7 h |
| Administration | Once daily | Twice daily | Twice daily |
| Starting dosage | 5 mg/d | 1.5 mg bid | 4 mg bid |
| Total recommended dosage | 5-10 mg/d | 6-12 mg/d | 16-24 mg/d |
| Adapted from Conn DK. Cholinesterase inhibitors: Comparing the options for mild-to-moderate dementia. Geriatrics56: 56-57, 2001. | |||
An open-label study by Weiner et al24 examined the effects of donepezil on emotional and behavioral symptoms using the CERAD Behavior Rating Scale for Dementia and its subscales. In a group of 25 AD patients treated with donepezil, scores returned to baseline levels at 12 months. In contrast, the scores of the reference group worsened minimally.
Galantamine has also proved effective in treating behavioral symptoms associated with AD. In the Tariot et al20 study, galantamine at 16 mg/d and 24 mg/d had a significantly better outcome on CIBIC+, ADL, and behavioral symptoms versus placebo.
Rosler et al25 assessed the ability of rivastigmine to improve behavioral symptoms in AD. Using the behavioral component of the CIBIC+, results showed that long-term treatment with rivastigmine could slow the progression of symptoms. Symptoms showing stabilization included aggressiveness, activity disturbances, hallucinations, and paranoid features. The results also suggest that patients treated earlier with rivastigmine may attain a greater benefit than those whose treatment is delayed 6 months.
Rivastigmine also has significant effects on controlling behavioral symptoms in patients with Lewy body dementia.26 A placebo-controlled, double-blind, multicenter study was performed in 120 patients with Lewy body dementia. Individuals were given up to 12 mg/d rivastigmine or placebo for 20 weeks, followed by 3 weeks rest. Assessment by neuropsychiatric inventory was made at baseline, and again at weeks 12, 20, and 23.
Patients taking rivastigmine were significantly less apathetic and anxious than those on placebo, and had fewer delusions and hallucinations. Almost twice as many patients on rivastigmine as on placebo (37, 63% versus 18, 30%) showed at least a 30% improvement from baseline. In a computerized cognitive assessment system and neuropsychological tests, patients were significantly faster and better than those on placebo, particularly when performing tasks with a substantial attentional component.
Cost effectiveness
Numerous studies have demonstrated that AChE inhibitors are cost savers in AD treatment. Fillit et al27 examined the impact of donepezil in a multisite managed care organization for 2 years using claims data for 70 individuals with AD and related dementias. The median per diem medical costs were $1.22 lower post treatment than they were in the pretreatment phase. Moreover, posttreatment costs were reduced in 6 of 7 service settings, with median per diem savings of $0.77 in outpatient care and $0.65 in office visits.
Neumann et al28 utilized cost-effectiveness analysis to predict that for mild AD, donepezil would pay for itself in cost offsets if the drug’s effect exceeds 2 years. Donepezil costs were partially offset by a reduction in the costs of care due to enhanced cognitive functioning and the delay in placing the patient in more costly disease stages and settings.
One study used the disease-progression model to estimate potential per-patient savings resulting from the treatment of AD in Canada.29 Rivastigmine was estimated to delay the transition to more severe stages of AD by up to 188 days for patients with mild AD after 2 years of treatment. For patients with mild-to-moderate and moderate disease, this delay was estimated to be 106 and 44 days, respectively.
The Assessment of Health Economics in Alzheimer’s Disease model uses algorithms to predict the time until patients with AD require full-time care. A study, performed in Canada, compared treatment with galantamine to treatment without pharmacological interventions.30 Galantamine was predicted to reduce the duration of full-time care by almost 10%. Approximately 5.6 patients with mild-to-moderate disease must be placed on treatment to avoid 1 year of full-time care, resulting in savings averaging $528 per patient. For patients with moderate disease, 3.9 patients must be placed on treatment to avoid 1 year of full-time care, with savings predicted at $2,533 per patient.
Caregiving burden
Fillit et al addressed caregiver well-being in a self-administered, nationwide survey of AD caregivers. Caregivers of patients treated with donepezil (n = 274) were compared with caregivers of patients not treated with donepezil (n = 274).31 The Caregiver Burden Scale measured time demands and distress linked to commonly performed caregiving tasks. Donepezil caregivers reported significantly lower scores on difficulty of caregiving. Similar findings have been observed with galantamine.32
Related resources
- Bullock R. New drugs for Alzheimer’s disease and other dementias. Br J Psychiatry. 2002;180(2):135-139.
- Brodaty H, Ames D, et al. Pharmacological treatment of cognitive deficits in Alzheimer’s disease. Med J Aust. 2001;175(6):324-329.
- Ahmed MB. Alzheimer’s disease: recent advances in etiology, diagnosis, and management. Tex Med. 2001;97(12):50-58.
- Frisoni GB. Treatment of Alzheimer’s disease with acetyl-cholinesterase inhibitors: bridging the gap between evidence and practice. J Neurol. 2001;248(7):551-7.
Drug brand names
- Tacrine • Cognex
- Donepezil • Aricept
- Rivastigmine • Exelon
- Galantamine • Reminyl
Disclosure
The author reports that he receives grant/research support from, serves as a consultant to, and is on the speaker’s bureau of Janssen Pharmaceutica and Pfizer Inc., and serves as consultant to and is on the speaker’s bureau of Novartis Pharmaceuticals Corp.
No psychiatrist likes to see the month-by-month deterioration in an Alzheimer’s patient—the losses in cognition, the declining ability to function, the behavioral aberrations that upset family and friends.
The problem will accelerate in the decades ahead as the proportion of elderly in the population increase. More than 4 million people in the United States are afflicted with this disorder. Prevalence rates as high as 10% have been estimated for individuals older than 65. Patients with the disease have estimated direct costs of $20,000 to $61,000 per year if the duration lasts 7 to 8 years.1
Although behavioral and functional deficits account for the high costs associated with Alzheimer’s disease (AD), the disorder is defined by cognitive criteria (Box 1). The majority of medication trials have been aimed at symptomatic treatment. More recently, studies have been designed to prevent or delay the onset of AD. Early on, initial therapies directed toward AD were aimed at reversing the cholinergic deficit (Box 2). Clinical trials utilizing lecithin (25-100 g/d) and choline (<16 g/d) as precursors of acetylcholine did not lead to significant benefit.6 Augmenting central cholinergic levels with acetylcholinesterase (AChE) inhibitors has consistently detected symptomatic improvement.
In recent years, the Food and Drug Administration has approved 4 AChE inhibitors—tacrine, donepezil, rivastigmine, and galantamine—for the treatment of AD. I will discuss only the latter 3, since tacrine, the first to Nshow benefit, has a high rate of adverse effects and is of limited use.7 The AChE inhibitors may improve cognition and behavioral symptoms and delay progression of the illness. They can also have beneficial effects on activities of daily living (ADL) and can reduce costs and improve caregiver burden.8
- The development of multiple cognitive deficits manifested by both:
- Memory impairment (impaired ability to learn new information or to recall previously learned information) and
- One (or more) of the following cognitive disturbances:
- Aphasia (language disturbance)
- Apraxia (impaired ability to carry out motor activities despite intact motor function)
- Agnosia (failure to recognize or identify objects despite intact sensory function)
- Disturbance in executive functioning (i.e., planning, organization, sequencing, abstracting)
- The cognitive deficits in Criteria A1 and A2 each cause significant impairment in social or occupational functioning and represent a significant decline from a previous level of functioning.
- The course is characterized by gradual onset and continuing cognitive decline.
Source: American Psychatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington DC: American Psychiatric Press., 1994.
The three AChE inhibitors have unique basic properties (Box 3). In order to maximize and prolong positive drug effects, it is important to start early and adjust dosage during the treatment9 (Table 1). Side effects are tolerable; the most common include nausea, vomiting, and diarrhea. Titrating the dosage slowly can reduce these. The cholinergic quality of these medications dictate that they be prescribed with caution in patients with bradycardic arrhythmias such as sick sinus syndrome, asthma, or chronic obstructive pulmonary disease.10
Effects on cognition and global assessments
Numerous efficacy studies examining cognition and global assessments in AD patients have been performed with the AChE inhibitors. Their major therapeutic effect is to maintain cognitive function at a constant level during a 6- to 12-month period of treatment, as compared to placebo. Comparison of clinical effects of all 3 agents demonstrates a similar magnitude of improvement. For some drugs, this may represent an upper limit, whereas for others it may still be possible to further increase the benefit.
The pathophysiologic processes implicated in Alzheimer’s disease (AD)include amyloid precursor protein metabolism, tau phosphorylation, apolipoprotein E, inflammation, oxidative stress, and apoptosis. Neuropathological features include amyloid plaques, neurofibrillary tangles, neuronal and synaptic loss, microgliosis, and astrocytosis. The resulting clinical syndrome of dementia is associated with neurotransmitter deficits and intracortical disconnection.
The central cholinergic neurotransmitter system is impaired in AD. This system is involved in learning and memory. The limbic system and neocortex receive projections from the cholinergic system in the septal nuclei and substantia innominata. This includes the medial septal nucleus, diagonal band, and nucleus basalis.2 Literature on animals has demonstrated that basal forebrain lesions impair learning and memory. Cholinergic agonists can improve this. Furthermore, cholinergic antagonists such as scopolamine and atropine can impair learning and memory in humans and animals.3 In AD, a 58% to 93% reduction in choline acetyltransferase levels (and other cholinergic markers) in the cortex and hippocampus can be observed and this correlates with dementia severity.4 Early AD is characterized by neuronal loss and tangles in the cholinergic nucleus basalis of Meynert.5
Results of 4 double-blind, placebo-controlled clinical trials of donepezil, involving more than 1,900 individuals with mild to moderate AD, have been published recently. In all, significant improvements in cognition were observed consistently for both therapeutic doses of donepezil (5 mg/d and 10 mg/d), relative to placebo. Similar benefits were reported for global functioning.
The long-term clinical efficacy and safety of donepezil versus placebo across 1 year in patients with mild to moderate AD was investigated.14 The Gottfries-Brane-Steen global assessment for rating dementia symptoms demonstrated the benefit of donepezil over placebo at weeks 24, 36, and 52, and at the study end point. Advantages of donepezil were also observed in cognition and ADL.
Donepezil also appears to work for patients with moderate to severe AD. In a recent 24-week study,15 patients receiving donepezil showed benefits on the Clinician’s Interview-Based Impression of Change with Caregiver Input (CIBIC+), compared with placebo, at all visits up to week 24 and at the study’s end point. All other secondary measures showed significant differences between the groups in favor of donepezil at the end of the study. These data suggest that donepezil’s benefits extend into more advanced stages of AD than those previously investigated, with good tolerability.
Clinical trials of rivastigmine (1.5-6 mg twice daily PO) have also demonstrated benefits on cognitive and global measures.16 The efficacy of rivastigmine tartrate (ENA 713) in patients with mild to moderately severe Alzheimer’s disease was evaluated in a 26-week open-label extension of a 26-week, double-blind, placebo-controlled study. By 52 weeks, patients originally treated with rivastigmine 6 to 12 mg/d had significantly better cognitive function than did patients originally treated with placebo.17- 19
Donepezil is a second-generation, piperidine-class, selective and reversible acetylcholinesterase (AChE) inhibitor. It is structurally dissimilar from other established AChE inhibitors.
Experimentally, donepezil inhibits AChE activity in human erythrocytes and increases extracellular acetylcholine levels in the cerebral cortex and the hippocampus of the rat. Pharmacologically, donepezil has a half-life of approximately 70h, lending itself to once-daily administration.11
Rivastigmine (ENA 713, or carbamoylatine) is an AChE inhibitor with brain-region selectivity and a long duration of action. Both preclinical studies and studies in human volunteers have shown that rivastigmine induces substantially greater inhibition of AChE in the central nervous system compartment than it does in the periphery (40% inhibition of central AChE compared with 10% inhibition of plasma butylcholinesterase in healthy volunteers). Rivastigmine also preferentially inhibits the G1 enzymatic form of AChE, which predominates in the brains of patients with Alzheimer’s disease (AD).
Evidence from animal studies also suggests that rivastigmine is a more potent inhibitor of AChE in the cortex and hippocampus, the brain regions most affected by AD. The principal metabolite of rivastigmine has at least 10-fold lower activity against AChE compared with the parent drug.
Rivastigmine is completely metabolized; the major route of elimination of the metabolites is renal. Rivastigmine is inactivated during the process of interacting with and inhibiting AChE, and, in contrast to other AChE inhibitors, the hepatic cytochrome P-450 (CYP-450) system is not involved in the metabolism of rivastigmine.12
Galantamine is an allosterically potentiating ligand that modulates nicotinic cholinergic receptors (nAChR) to increase acetylcholine release as well as acting as an AChE inhibitor. In preclinical experiments, the drug significantly improves learning, reduces AChE levels, and increases nicotinic receptor binding. Action of galantamine is on the most abundant nAChR in the human brain, the alpha4/beta2subtype.13
Clinical trials of galantamine (4-12 mg/bid PO) have demonstrated similar benefits.20 Following a 4-week placebo run-in, patients were randomized to 1 of 4 treatment arms: placebo or galantamine escalated to final maintenance dosages of 8, 16, or 24 mg/d for a 5-month treatment phase. At study’s end, the galantamine-place-bo differences on the cognitive subscale of the AD Assessment Scale were 3.3 points for the 16 mg/d group and 3.6 points for the 24 mg/d group. Treatment discontinuations due to adverse events were low in all galantamine groups (6% to 10%) and comparable with that in the placebo group (7%). The incidence of adverse events in the galantamine groups, notably gastrointestinal symptoms, was low and most adverse events were mild.
Other studies examining galantamine have demonstrated similar clinical benefits.8, 21
When using AChE inhibitors, the slope of cognitive decline is similar in treated and untreated patients after the initial improvement. These drugs essentially do not reverse the disorder’s course but shift upward the curve describing the time course of cognitive decline. This applies also to behavioral and functional benefits. Thus the benefit obtained is symptomatic and not neuroprotective, and is lost after discontinuing the medications.
Effects on functioning and behavior
In a 24-week multinational clinical trial, patients receiving donepezil (10 mg/d) were more able than placebo-treated patients to perform complex daily functioning tasks.22 Similar effects have been observed with rivastigmine and galantamine.16, 20
All 3 AChE inhibitors have demonstrated improvements in the behavioral changes associated with AD. Cummings et al23 tested the hypothesis that behavioral disturbances are reported at significantly lower rates by caregivers of AD patients receiving donepezil, compared with a group of patients not receiving a drug for treatment of dementia. Donepezil patients were described as significantly less likely to be threatening, destroy property, and talk loudly, and significantly fewer were treated with sedatives.
Table 1
COMPARING THEAChE INHIBITORS
| Donepezil | Rivastigmine | Galantamine | |
|---|---|---|---|
| Chemical class | Piperidine | Carbamate | Phenanthrene alkaloid |
| AChE inhibitor | Yes | Yes | Yes |
| BuChE inhibitor | Small | Yes | Small |
| Nicotinic modulation | No | No | Yes |
| Elimination half-life | 50-70 h | 0.6-2 h | 5-7 h |
| Administration | Once daily | Twice daily | Twice daily |
| Starting dosage | 5 mg/d | 1.5 mg bid | 4 mg bid |
| Total recommended dosage | 5-10 mg/d | 6-12 mg/d | 16-24 mg/d |
| Adapted from Conn DK. Cholinesterase inhibitors: Comparing the options for mild-to-moderate dementia. Geriatrics56: 56-57, 2001. | |||
An open-label study by Weiner et al24 examined the effects of donepezil on emotional and behavioral symptoms using the CERAD Behavior Rating Scale for Dementia and its subscales. In a group of 25 AD patients treated with donepezil, scores returned to baseline levels at 12 months. In contrast, the scores of the reference group worsened minimally.
Galantamine has also proved effective in treating behavioral symptoms associated with AD. In the Tariot et al20 study, galantamine at 16 mg/d and 24 mg/d had a significantly better outcome on CIBIC+, ADL, and behavioral symptoms versus placebo.
Rosler et al25 assessed the ability of rivastigmine to improve behavioral symptoms in AD. Using the behavioral component of the CIBIC+, results showed that long-term treatment with rivastigmine could slow the progression of symptoms. Symptoms showing stabilization included aggressiveness, activity disturbances, hallucinations, and paranoid features. The results also suggest that patients treated earlier with rivastigmine may attain a greater benefit than those whose treatment is delayed 6 months.
Rivastigmine also has significant effects on controlling behavioral symptoms in patients with Lewy body dementia.26 A placebo-controlled, double-blind, multicenter study was performed in 120 patients with Lewy body dementia. Individuals were given up to 12 mg/d rivastigmine or placebo for 20 weeks, followed by 3 weeks rest. Assessment by neuropsychiatric inventory was made at baseline, and again at weeks 12, 20, and 23.
Patients taking rivastigmine were significantly less apathetic and anxious than those on placebo, and had fewer delusions and hallucinations. Almost twice as many patients on rivastigmine as on placebo (37, 63% versus 18, 30%) showed at least a 30% improvement from baseline. In a computerized cognitive assessment system and neuropsychological tests, patients were significantly faster and better than those on placebo, particularly when performing tasks with a substantial attentional component.
Cost effectiveness
Numerous studies have demonstrated that AChE inhibitors are cost savers in AD treatment. Fillit et al27 examined the impact of donepezil in a multisite managed care organization for 2 years using claims data for 70 individuals with AD and related dementias. The median per diem medical costs were $1.22 lower post treatment than they were in the pretreatment phase. Moreover, posttreatment costs were reduced in 6 of 7 service settings, with median per diem savings of $0.77 in outpatient care and $0.65 in office visits.
Neumann et al28 utilized cost-effectiveness analysis to predict that for mild AD, donepezil would pay for itself in cost offsets if the drug’s effect exceeds 2 years. Donepezil costs were partially offset by a reduction in the costs of care due to enhanced cognitive functioning and the delay in placing the patient in more costly disease stages and settings.
One study used the disease-progression model to estimate potential per-patient savings resulting from the treatment of AD in Canada.29 Rivastigmine was estimated to delay the transition to more severe stages of AD by up to 188 days for patients with mild AD after 2 years of treatment. For patients with mild-to-moderate and moderate disease, this delay was estimated to be 106 and 44 days, respectively.
The Assessment of Health Economics in Alzheimer’s Disease model uses algorithms to predict the time until patients with AD require full-time care. A study, performed in Canada, compared treatment with galantamine to treatment without pharmacological interventions.30 Galantamine was predicted to reduce the duration of full-time care by almost 10%. Approximately 5.6 patients with mild-to-moderate disease must be placed on treatment to avoid 1 year of full-time care, resulting in savings averaging $528 per patient. For patients with moderate disease, 3.9 patients must be placed on treatment to avoid 1 year of full-time care, with savings predicted at $2,533 per patient.
Caregiving burden
Fillit et al addressed caregiver well-being in a self-administered, nationwide survey of AD caregivers. Caregivers of patients treated with donepezil (n = 274) were compared with caregivers of patients not treated with donepezil (n = 274).31 The Caregiver Burden Scale measured time demands and distress linked to commonly performed caregiving tasks. Donepezil caregivers reported significantly lower scores on difficulty of caregiving. Similar findings have been observed with galantamine.32
Related resources
- Bullock R. New drugs for Alzheimer’s disease and other dementias. Br J Psychiatry. 2002;180(2):135-139.
- Brodaty H, Ames D, et al. Pharmacological treatment of cognitive deficits in Alzheimer’s disease. Med J Aust. 2001;175(6):324-329.
- Ahmed MB. Alzheimer’s disease: recent advances in etiology, diagnosis, and management. Tex Med. 2001;97(12):50-58.
- Frisoni GB. Treatment of Alzheimer’s disease with acetyl-cholinesterase inhibitors: bridging the gap between evidence and practice. J Neurol. 2001;248(7):551-7.
Drug brand names
- Tacrine • Cognex
- Donepezil • Aricept
- Rivastigmine • Exelon
- Galantamine • Reminyl
Disclosure
The author reports that he receives grant/research support from, serves as a consultant to, and is on the speaker’s bureau of Janssen Pharmaceutica and Pfizer Inc., and serves as consultant to and is on the speaker’s bureau of Novartis Pharmaceuticals Corp.
1. Irizarry M, Hyman B. Alzheimer’s disease. In: Principles of neuroepidemiology. Batchelor T, Cudkowicz M, eds. Boston: Butterworth-Heinemann, 2001:69-98.
2. Mesulam MM, Mufson EJ, Levey AI, Warner BH. Cholinergic innervation of cortex by the basal forebrain: Cytochemistry and cortical connections of the septal area, diagonal band nuclei, nucleus basalis (substantia innominata), and hypothalamus in the rhesus monkey. J Comp Neurol. 1983a;214:170-197.
3. Drachman DA, Leavitt J. Human memory and the cholinergic system. A relationship to aging? Arch Neurol. 1974;30:113-121.
4. Davies P, Maloney AJ. Selective loss of central cholinergic neurons in Alzheimer’s disease. Lancet. 1976;2:1403.-
5. Whitehouse PJ, Price DL, Clark AW, Coyle JT, DeLong MR. Alzheimer disease: evidence for selective loss of cholinergic neurons in the nucleus basalis. Ann Neurol. 1981;10:122-126.
6. Higgins JPT, Flicker L. Lecithin and cognitive impairment. The Cochrane Database of Systematic Reviews. 2001.;
7. Knapp MJ, Knopman DS, Solomon PR, Pendlebury WW, Davis CS, Gracon SI. A 30-week randomized controlled trial of high-dose tacrine in patients with Alzheimer’s disease. The Tacrine Study Group. JAMA. 1994;271:985-991.
8. Raskind MA, Peskind ER, Wessel T, Yuan W. Galantamine in AD: A 6-month randomized, placebo-controlled trial with a 6-month extension. The Galantamine USA-1 Study Group. Neurology. 2000;54:2262-2268.
9. Giacobini E. Cholinesterase inhibitors stabilize Alzheimer’s disease. Methods Find Exp Clin Pharmacol. 2000;22:609-613.
10. Irizarry MC, Hyman BT. Alzhemier Disease Therapeutics. J Neuropathology Exp Neurology. 2001;60:923-928.
11. Wilkinson DG. The pharmacology of donepezil: a new treatment of Alzheimer’s disease. Expert Opin Pharmacother. 1999;1:121-135.
12. Polinsky RJ. Clinical pharmacology of rivastigmine: a new-generation acetyl-cholinesterase inhibitor for the treatment of Alzheimer’s disease. Clin Ther. 1998;20:634-647.
13. Samochocki M, Zerlin M, Jostock R, et al. Galantamine is an allosterically potentiating ligand of the human alpha4/beta2 nAChR. Acta Neurol Scand. 2000(Suppl);;176:68-73.
14. Winblad B, Engedal K, Soininen H, Verhey F, et al. A 1-year, randomized, placebo-controlled study of donepezil in patients with mild to moderate AD. Neurology. 2001;57:489-495.
15. Feldman H, Gauthier S, Hecker J, et al. Donepezil MSAD Study Investigators Group.A 24-week, randomized, double-blind study of donepezil in moderate to severe Alzheimer’s disease. Neurology. 2001;57:613-620.
16. Farlow M, Anand R, Messina J, Jr, Hartman R, Veach J. A 52-week study of the efficacy of rivastigmine in patients with mild to moderately severe Alzheimer’s disease. Eur Neurol. 2000;44:236-241.
17. Rogers S, Friedhoff L. Donepezil Study Group.The efficacy and safety of donepezil in patients with Alzhemier’s disease. Dementia. 1996;7:293-303.
18. Rogers S, Farlow M, Doody R, Morris R, Friedhoff L. A 24-week, double-blind, placebo-controlled trial of donepezil in patients with Alzheimer’s disease. Donepezil Study Group. Neurology. 1998;50:136-145.
19. Rosler M, Anand R, Cicin-Sain A, Gauthier S, Agid Y, DalBianco P, Stahelin HB, et al. Efficacy and safety of rivastigmine in patients with Alzheimer’s disease: International randomized controlled trial. BMJ. 1999;318:633-638.
20. Tariot PN, Solomon PR, Morris JC, Kershaw P, Lilienfeld S, Ding C. A 5-month, randomized, placebo-controlled trial of galantamine in AD. The Galantamine USA-10 Study Group. Neurology. 2000;54:2269-2276.
21. Wilcock GK, Lilienfeld S, Gaens E. Efficacy and safety of galantamine in patients with mild to moderate Alzheimer’s disease: Multicentre randomized controlled trial. Galantamine International - 1 Study Group. BMJ. 2000;321:1445-1449.
22. Knopman DS. Management of cognition and function: new results from the clinical trials programme of Aricept (R) (donepezil Hcl). Int J Neuropsychopharmacol. 2000;3:13-20.
23. Cummings JL, Donohue JA, Brooks RL. The relationship between donepezil and behavioral disturbances in patients with Alzheimer’s disease. Am J Geriatr Psychiatry. 2000;8:134-140.
24. Weiner MF, Martin-Cook K, Foster BM, Saine K, et al. Effects of donepezil on emotional/behavioral symptoms in Alzheimer’s disease patients. J Clin Psychiatry. 2000;487-492.
25. Rosler M, Retz W, Retz-Junginger P, Dennler HJ. Effects of two-year treatment with the cholinesterase inhibitor rivastigmine on behavioural symptoms in Alzheimer’s disease. Behav Neurol. 1998;11:211-216.
26. McKeith I, Del Ser T, Spano P, Emre M, et al. Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study. Lancet. 2000;356(9247):2031-2036.
27. Fillit H, Gutterman EM, Lewis B. Donepezil use in managed Medicare: effect on health care costs and utilization. Clin Ther. 1999;21:2173-2185.
28. Neumann PJ, Hermann RC, Kuntz KM, Araki SS, Duff SB, Leon J, Berenbaum PA, et al. Cost-effectiveness of donepezil in the treatment of mild or moderate Alzheimer’s disease. Neurology. 1999;52:1115-1116.
29. Hauber AB, Gnanasakthy A, Mauskopf JA. Savings in the cost of caring for patients with Alzheimer’s disease in Canada: an analysis of treatment with rivastigmine. Clin Ther. 2000;22:439-451.
30. Getsios D, Caro JJ, Caro G, Ishak K. The AHEAD Study Group. Assessment of health economics in Alzheimer’s disease (AHEAD): galantamine treatment in Canada. Neurology. 2001;57:972-978.
31. Fillit HM, Gutterman EM, Brooks RL. Impact of donepezil on caregiving burden for patients with Alzheimer’s disease. Int Psychogeriatr. 2000;12(3):389-401.
32. Blesa R. Galantamine: therapeutic effects beyond cognition. Dement Geriatr Cogn Disord. 2000;11(Suppl)1:28-34.
1. Irizarry M, Hyman B. Alzheimer’s disease. In: Principles of neuroepidemiology. Batchelor T, Cudkowicz M, eds. Boston: Butterworth-Heinemann, 2001:69-98.
2. Mesulam MM, Mufson EJ, Levey AI, Warner BH. Cholinergic innervation of cortex by the basal forebrain: Cytochemistry and cortical connections of the septal area, diagonal band nuclei, nucleus basalis (substantia innominata), and hypothalamus in the rhesus monkey. J Comp Neurol. 1983a;214:170-197.
3. Drachman DA, Leavitt J. Human memory and the cholinergic system. A relationship to aging? Arch Neurol. 1974;30:113-121.
4. Davies P, Maloney AJ. Selective loss of central cholinergic neurons in Alzheimer’s disease. Lancet. 1976;2:1403.-
5. Whitehouse PJ, Price DL, Clark AW, Coyle JT, DeLong MR. Alzheimer disease: evidence for selective loss of cholinergic neurons in the nucleus basalis. Ann Neurol. 1981;10:122-126.
6. Higgins JPT, Flicker L. Lecithin and cognitive impairment. The Cochrane Database of Systematic Reviews. 2001.;
7. Knapp MJ, Knopman DS, Solomon PR, Pendlebury WW, Davis CS, Gracon SI. A 30-week randomized controlled trial of high-dose tacrine in patients with Alzheimer’s disease. The Tacrine Study Group. JAMA. 1994;271:985-991.
8. Raskind MA, Peskind ER, Wessel T, Yuan W. Galantamine in AD: A 6-month randomized, placebo-controlled trial with a 6-month extension. The Galantamine USA-1 Study Group. Neurology. 2000;54:2262-2268.
9. Giacobini E. Cholinesterase inhibitors stabilize Alzheimer’s disease. Methods Find Exp Clin Pharmacol. 2000;22:609-613.
10. Irizarry MC, Hyman BT. Alzhemier Disease Therapeutics. J Neuropathology Exp Neurology. 2001;60:923-928.
11. Wilkinson DG. The pharmacology of donepezil: a new treatment of Alzheimer’s disease. Expert Opin Pharmacother. 1999;1:121-135.
12. Polinsky RJ. Clinical pharmacology of rivastigmine: a new-generation acetyl-cholinesterase inhibitor for the treatment of Alzheimer’s disease. Clin Ther. 1998;20:634-647.
13. Samochocki M, Zerlin M, Jostock R, et al. Galantamine is an allosterically potentiating ligand of the human alpha4/beta2 nAChR. Acta Neurol Scand. 2000(Suppl);;176:68-73.
14. Winblad B, Engedal K, Soininen H, Verhey F, et al. A 1-year, randomized, placebo-controlled study of donepezil in patients with mild to moderate AD. Neurology. 2001;57:489-495.
15. Feldman H, Gauthier S, Hecker J, et al. Donepezil MSAD Study Investigators Group.A 24-week, randomized, double-blind study of donepezil in moderate to severe Alzheimer’s disease. Neurology. 2001;57:613-620.
16. Farlow M, Anand R, Messina J, Jr, Hartman R, Veach J. A 52-week study of the efficacy of rivastigmine in patients with mild to moderately severe Alzheimer’s disease. Eur Neurol. 2000;44:236-241.
17. Rogers S, Friedhoff L. Donepezil Study Group.The efficacy and safety of donepezil in patients with Alzhemier’s disease. Dementia. 1996;7:293-303.
18. Rogers S, Farlow M, Doody R, Morris R, Friedhoff L. A 24-week, double-blind, placebo-controlled trial of donepezil in patients with Alzheimer’s disease. Donepezil Study Group. Neurology. 1998;50:136-145.
19. Rosler M, Anand R, Cicin-Sain A, Gauthier S, Agid Y, DalBianco P, Stahelin HB, et al. Efficacy and safety of rivastigmine in patients with Alzheimer’s disease: International randomized controlled trial. BMJ. 1999;318:633-638.
20. Tariot PN, Solomon PR, Morris JC, Kershaw P, Lilienfeld S, Ding C. A 5-month, randomized, placebo-controlled trial of galantamine in AD. The Galantamine USA-10 Study Group. Neurology. 2000;54:2269-2276.
21. Wilcock GK, Lilienfeld S, Gaens E. Efficacy and safety of galantamine in patients with mild to moderate Alzheimer’s disease: Multicentre randomized controlled trial. Galantamine International - 1 Study Group. BMJ. 2000;321:1445-1449.
22. Knopman DS. Management of cognition and function: new results from the clinical trials programme of Aricept (R) (donepezil Hcl). Int J Neuropsychopharmacol. 2000;3:13-20.
23. Cummings JL, Donohue JA, Brooks RL. The relationship between donepezil and behavioral disturbances in patients with Alzheimer’s disease. Am J Geriatr Psychiatry. 2000;8:134-140.
24. Weiner MF, Martin-Cook K, Foster BM, Saine K, et al. Effects of donepezil on emotional/behavioral symptoms in Alzheimer’s disease patients. J Clin Psychiatry. 2000;487-492.
25. Rosler M, Retz W, Retz-Junginger P, Dennler HJ. Effects of two-year treatment with the cholinesterase inhibitor rivastigmine on behavioural symptoms in Alzheimer’s disease. Behav Neurol. 1998;11:211-216.
26. McKeith I, Del Ser T, Spano P, Emre M, et al. Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study. Lancet. 2000;356(9247):2031-2036.
27. Fillit H, Gutterman EM, Lewis B. Donepezil use in managed Medicare: effect on health care costs and utilization. Clin Ther. 1999;21:2173-2185.
28. Neumann PJ, Hermann RC, Kuntz KM, Araki SS, Duff SB, Leon J, Berenbaum PA, et al. Cost-effectiveness of donepezil in the treatment of mild or moderate Alzheimer’s disease. Neurology. 1999;52:1115-1116.
29. Hauber AB, Gnanasakthy A, Mauskopf JA. Savings in the cost of caring for patients with Alzheimer’s disease in Canada: an analysis of treatment with rivastigmine. Clin Ther. 2000;22:439-451.
30. Getsios D, Caro JJ, Caro G, Ishak K. The AHEAD Study Group. Assessment of health economics in Alzheimer’s disease (AHEAD): galantamine treatment in Canada. Neurology. 2001;57:972-978.
31. Fillit HM, Gutterman EM, Brooks RL. Impact of donepezil on caregiving burden for patients with Alzheimer’s disease. Int Psychogeriatr. 2000;12(3):389-401.
32. Blesa R. Galantamine: therapeutic effects beyond cognition. Dement Geriatr Cogn Disord. 2000;11(Suppl)1:28-34.
Chronic tension-type headache: Advice for the viselike-headache patient
Taking the tension out of tension-type headaches
Idiopathic retroperitoneal fibrosis: Prompt diagnosis preserves organ function
Advances in treatment of chronic hepatitis C: 'Pegylated' interferons
Diagnosis of lupus: A glass half full
Tired, aching, ANA-positive: Does your patient have lupus or fibromyalgia?
A 23-year-old man with a continuous heart murmur
Can high-dose supplementation with vitamins C and E, beta carotene, and zinc slow the progression of macular degeneration?
ABSTRACT
BACKGROUND: Age-related macular degeneration (ARMD) is the leading cause of blindness in the United States among people aged 65 years or older. Observational and experimental data suggest that antioxidant or zinc supplements may delay progression of ARMD and visual loss.
POPULATION STUDIED: Eleven retinal specialty clinics enrolled participants aged 55 to 80 years in 4 ARMD categories determined by the size and extent of drusen and retinal pigment epithelial abnormalities in each eye, the presence of advanced ARMD (each determined by evaluation of color photographs at a reading center), and visual acuity. Persons in category 1 had no ARMD; those in category 2 had mild or borderline ARMD; those in category 3 had moderate ARMD; and those in category 4 had advanced ARMD. At least 1 eye had a best corrected visual acuity of 20/32 or better (the study eye). Among participants, 56% were women, 96% were white, and the median age was 69 years. Potential participants were excluded for illness or disorders (history of cancer with a poor 7-year prognosis, major cardiovascular or cerebrovascular event within the previous year, or hemochromatosis) that would have made long-term follow-up or compliance with the study protocol unlikely or difficult.
STUDY DESIGN AND VALIDITY: This was a randomized, double-masked, placebo-controlled trial (concealed allocation assignment). Participants were assigned to 1 of 4 treatment groups: (1) antioxidants (500 mg vitamin C, 400 IU vitamin E, 15 mg beta carotene); (2) 80 mg zinc as zinc oxide and copper, 2 mg as cupric oxide; (3) antioxidants plus zinc; or (4) placebo. The groups did not differ in their baseline characteristics. Average follow-up was 6.3 years, with 2.4% lost to follow-up. Analysis was by intention to treat. The judicial assessors of outcomes were masked to treatment group assignment.
OUTCOMES MEASURED: Two primary outcomes were defined for study eyes in the ARMD trial: (1) progression to advanced ARMD and (2) at least a 15-letter decrease in visual acuity score.
RESULTS: Patients with no ARMD (category 1) and mild or borderline ARMD (category 2) did not benefit from antioxidant and/or zinc supplementation. However, participants in the moderate and advanced ARMD groups (categories 3 and 4) had a lower risk of progression to advanced ARMD and visual acuity loss in the good eye if they took both zinc and antioxidants compared with placebo for 7 years (35.7% vs 26.7%, respectively; P < .001; number needed to treat = 11).
Patients with moderate to advanced ARMD should consider taking an antioxidant/zinc supplement. Treatment of 11 such patients with high-dose supplementation of vitamin C, vitamin E, beta carotene, and zinc for 7 years will prevent progression of ARMD in one of them. Although some may argue that the results of this study justify routine screening for this condition, we need further evidence on both the number needed to screen for a benefit and the overall cost-to-benefit ratio of the intervention. In addition, we should remember that beta carotene has been linked to an increased risk of lung cancer in smokers.
ABSTRACT
BACKGROUND: Age-related macular degeneration (ARMD) is the leading cause of blindness in the United States among people aged 65 years or older. Observational and experimental data suggest that antioxidant or zinc supplements may delay progression of ARMD and visual loss.
POPULATION STUDIED: Eleven retinal specialty clinics enrolled participants aged 55 to 80 years in 4 ARMD categories determined by the size and extent of drusen and retinal pigment epithelial abnormalities in each eye, the presence of advanced ARMD (each determined by evaluation of color photographs at a reading center), and visual acuity. Persons in category 1 had no ARMD; those in category 2 had mild or borderline ARMD; those in category 3 had moderate ARMD; and those in category 4 had advanced ARMD. At least 1 eye had a best corrected visual acuity of 20/32 or better (the study eye). Among participants, 56% were women, 96% were white, and the median age was 69 years. Potential participants were excluded for illness or disorders (history of cancer with a poor 7-year prognosis, major cardiovascular or cerebrovascular event within the previous year, or hemochromatosis) that would have made long-term follow-up or compliance with the study protocol unlikely or difficult.
STUDY DESIGN AND VALIDITY: This was a randomized, double-masked, placebo-controlled trial (concealed allocation assignment). Participants were assigned to 1 of 4 treatment groups: (1) antioxidants (500 mg vitamin C, 400 IU vitamin E, 15 mg beta carotene); (2) 80 mg zinc as zinc oxide and copper, 2 mg as cupric oxide; (3) antioxidants plus zinc; or (4) placebo. The groups did not differ in their baseline characteristics. Average follow-up was 6.3 years, with 2.4% lost to follow-up. Analysis was by intention to treat. The judicial assessors of outcomes were masked to treatment group assignment.
OUTCOMES MEASURED: Two primary outcomes were defined for study eyes in the ARMD trial: (1) progression to advanced ARMD and (2) at least a 15-letter decrease in visual acuity score.
RESULTS: Patients with no ARMD (category 1) and mild or borderline ARMD (category 2) did not benefit from antioxidant and/or zinc supplementation. However, participants in the moderate and advanced ARMD groups (categories 3 and 4) had a lower risk of progression to advanced ARMD and visual acuity loss in the good eye if they took both zinc and antioxidants compared with placebo for 7 years (35.7% vs 26.7%, respectively; P < .001; number needed to treat = 11).
Patients with moderate to advanced ARMD should consider taking an antioxidant/zinc supplement. Treatment of 11 such patients with high-dose supplementation of vitamin C, vitamin E, beta carotene, and zinc for 7 years will prevent progression of ARMD in one of them. Although some may argue that the results of this study justify routine screening for this condition, we need further evidence on both the number needed to screen for a benefit and the overall cost-to-benefit ratio of the intervention. In addition, we should remember that beta carotene has been linked to an increased risk of lung cancer in smokers.
ABSTRACT
BACKGROUND: Age-related macular degeneration (ARMD) is the leading cause of blindness in the United States among people aged 65 years or older. Observational and experimental data suggest that antioxidant or zinc supplements may delay progression of ARMD and visual loss.
POPULATION STUDIED: Eleven retinal specialty clinics enrolled participants aged 55 to 80 years in 4 ARMD categories determined by the size and extent of drusen and retinal pigment epithelial abnormalities in each eye, the presence of advanced ARMD (each determined by evaluation of color photographs at a reading center), and visual acuity. Persons in category 1 had no ARMD; those in category 2 had mild or borderline ARMD; those in category 3 had moderate ARMD; and those in category 4 had advanced ARMD. At least 1 eye had a best corrected visual acuity of 20/32 or better (the study eye). Among participants, 56% were women, 96% were white, and the median age was 69 years. Potential participants were excluded for illness or disorders (history of cancer with a poor 7-year prognosis, major cardiovascular or cerebrovascular event within the previous year, or hemochromatosis) that would have made long-term follow-up or compliance with the study protocol unlikely or difficult.
STUDY DESIGN AND VALIDITY: This was a randomized, double-masked, placebo-controlled trial (concealed allocation assignment). Participants were assigned to 1 of 4 treatment groups: (1) antioxidants (500 mg vitamin C, 400 IU vitamin E, 15 mg beta carotene); (2) 80 mg zinc as zinc oxide and copper, 2 mg as cupric oxide; (3) antioxidants plus zinc; or (4) placebo. The groups did not differ in their baseline characteristics. Average follow-up was 6.3 years, with 2.4% lost to follow-up. Analysis was by intention to treat. The judicial assessors of outcomes were masked to treatment group assignment.
OUTCOMES MEASURED: Two primary outcomes were defined for study eyes in the ARMD trial: (1) progression to advanced ARMD and (2) at least a 15-letter decrease in visual acuity score.
RESULTS: Patients with no ARMD (category 1) and mild or borderline ARMD (category 2) did not benefit from antioxidant and/or zinc supplementation. However, participants in the moderate and advanced ARMD groups (categories 3 and 4) had a lower risk of progression to advanced ARMD and visual acuity loss in the good eye if they took both zinc and antioxidants compared with placebo for 7 years (35.7% vs 26.7%, respectively; P < .001; number needed to treat = 11).
Patients with moderate to advanced ARMD should consider taking an antioxidant/zinc supplement. Treatment of 11 such patients with high-dose supplementation of vitamin C, vitamin E, beta carotene, and zinc for 7 years will prevent progression of ARMD in one of them. Although some may argue that the results of this study justify routine screening for this condition, we need further evidence on both the number needed to screen for a benefit and the overall cost-to-benefit ratio of the intervention. In addition, we should remember that beta carotene has been linked to an increased risk of lung cancer in smokers.