User login
Congrats to the Class of 2013
Clinical informatics, the principle of blending health information technology (HIT) with patient care, is going mainstream. The subspecialty, popular in hospitalist circles, is scheduled to offer board certification following its recent approval by the American Board of Medical Specialties. The first examination will be administered by the American Board of Preventative Medicine and could be held as early as fall 2012, with certificates awarded early in 2013.
AMIA, the informatics trade group, believes the recognition will help push more medical schools to integrate informatics into the curriculum, which will only further solidify the subspecialty place in modern medicine.
Clinical informatics, the principle of blending health information technology (HIT) with patient care, is going mainstream. The subspecialty, popular in hospitalist circles, is scheduled to offer board certification following its recent approval by the American Board of Medical Specialties. The first examination will be administered by the American Board of Preventative Medicine and could be held as early as fall 2012, with certificates awarded early in 2013.
AMIA, the informatics trade group, believes the recognition will help push more medical schools to integrate informatics into the curriculum, which will only further solidify the subspecialty place in modern medicine.
Clinical informatics, the principle of blending health information technology (HIT) with patient care, is going mainstream. The subspecialty, popular in hospitalist circles, is scheduled to offer board certification following its recent approval by the American Board of Medical Specialties. The first examination will be administered by the American Board of Preventative Medicine and could be held as early as fall 2012, with certificates awarded early in 2013.
AMIA, the informatics trade group, believes the recognition will help push more medical schools to integrate informatics into the curriculum, which will only further solidify the subspecialty place in modern medicine.
By the Numbers: 209,000
Projected total number of adult in-hospital cardiac arrests that are treated with a resuscitation response each year in U.S. hospitals.1 Raina Merchant, MD, and colleagues from the University of Pennsylvania Health System derived several estimates from the American Heart Association’s Get with the Guidelines-Resuscitation registry for 2003 to 2007, weighted for total U.S. hospital bed days. Survival rate for in-hospital cardiac arrests is 21%, compared with 10% for arrests in other settings. But the authors note that arrests might be rising, which is “important for understanding the burden of in-hospital cardiac arrest and developing strategies to improve care for hospitalized patients,” Dr. Merchant says.
Reference
Projected total number of adult in-hospital cardiac arrests that are treated with a resuscitation response each year in U.S. hospitals.1 Raina Merchant, MD, and colleagues from the University of Pennsylvania Health System derived several estimates from the American Heart Association’s Get with the Guidelines-Resuscitation registry for 2003 to 2007, weighted for total U.S. hospital bed days. Survival rate for in-hospital cardiac arrests is 21%, compared with 10% for arrests in other settings. But the authors note that arrests might be rising, which is “important for understanding the burden of in-hospital cardiac arrest and developing strategies to improve care for hospitalized patients,” Dr. Merchant says.
Reference
Projected total number of adult in-hospital cardiac arrests that are treated with a resuscitation response each year in U.S. hospitals.1 Raina Merchant, MD, and colleagues from the University of Pennsylvania Health System derived several estimates from the American Heart Association’s Get with the Guidelines-Resuscitation registry for 2003 to 2007, weighted for total U.S. hospital bed days. Survival rate for in-hospital cardiac arrests is 21%, compared with 10% for arrests in other settings. But the authors note that arrests might be rising, which is “important for understanding the burden of in-hospital cardiac arrest and developing strategies to improve care for hospitalized patients,” Dr. Merchant says.
Reference
Lost in Transition

It’s been nearly two decades since I graduated from medical school. I think back and I honestly do not remember any lectures about transitions of care.
During residency, I remember some attending physicians would insist that when I discharged patients from the hospital, the patients had to leave with post-discharge appointments in hand. Like any diligent intern, I did as I was told. I telephoned the administrative assistants in clinic and booked follow-up appointments for my patients. I always asked for the first available appointment. Why? Because that was what my senior resident told me to do. I suspect he learned that from his resident as well.
Sometimes the appointment was scheduled for the week following discharge; other times it was six months later. I honestly didn’t give it much thought. There was a blank on the discharge paperwork and I filled it in with a date and time. I was doing my job—or so I thought.
Can you imagine if someone just gave you a slip of paper today telling you when to show up to get your teeth cleaned without consulting your schedule? How about scheduling the oil change for your car at a garage 100 miles away? Seems pretty silly, doesn’t it? Nothing about it seems customer-centric or cost-efficient.
With such a system in place, why are we surprised when patients do not show up for their follow-up appointments? When the patient presents to the ED later and is readmitted to the hospital, we label them as “non-compliant” because they failed to show up for their follow-up appointment.
Inefficient, Ineffective, Inappropriate
There are multiple problems with the above situation. The first problem: Why are doctors calling to schedule follow-up appointments in the first place? Do we ask airline pilots to serve refreshments? I suppose they could, but I’d rather they concentrate on flying the plane. It also seems like an awful waste of money and resources when we could accomplish the same feat with less-expensive airline attendants who are better trained to interact with passengers.
At most teaching hospitals across the country, I suspect we still rely on trainees to book follow-up appointments for patients. At hospitals without trainees, I suspect some of this responsibility falls on nurses and unit coordinators. Again, I wonder how often these people are actually in a position to schedule an appointment that the patient is likely to keep—or whether they are filling in a box on a checklist like I used to do.
Common Problem?
How do other industries address this issue? Well, many utilize customer service representatives to help consumers book their appointments. Some industries have advanced software, which allows consumers to book their own appointment online. I have to tell you that I am chuckling as I write this. I’m chuckling not because this is funny—I am just amazed that something that is so common sense is not utilized consistently across the hospital industry. When was the last time you actually called a hotel to book a room? Most of us find it so much more convenient to book airline tickets or hotel rooms online.
If we were to create a system with the consumer’s satisfaction and cost in mind, would you rely on trainees, nurses, or unit coordinators to book follow-up appointments? I suppose Hypothetical System 2.0 would include consumer representatives speaking with patients to book appointments. Hypothetical System 3.0 would allow patients and/or a family member to book the appointment online.
I can tell you that folks at Beth Israel Deaconess Medical Center in Boston, where I work, have given this some thought. We are nowhere near a 3.0 version, but we do rely on professional appointment-makers to work with our hospitalized patients to book follow-up appointments. Inpatient providers put in the order online requesting follow-up appointments for their hospitalized patients. The online application asks the provider to specify the requests. Does the patient need follow-up with specialists, as well as their primary outpatient provider? The inpatient provider can specify the window of time in which they recommend follow-up for the patient. If I want my patient to follow up with their primary-care physician (PCP) within one week and with their cardiologist within two weeks, the appointment-maker will work with the patient and the respective doctors’ offices to make this happen. I am contacted only if any issues arise.
All of this information is provided to the patient with their other discharge paperwork. Some of you might be asking: How can the hospital afford to pay for this software and for the cadre of professional appointment-makers? I am wondering how hospitals can afford not to. It’s like worrying about the cost of a college degree until you realize how difficult it is trying to get a job without one.
Part of the PCP “access” problem we have in this country is due to the fact that not every patient shows up for scheduled appointments. Our appointment-makers minimize the “no show” rate because, by speaking with patients about their schedules, they are providing appointments to patients with knowledge that they are likely to make the appointment. One of the things we learned at Beth Israel was that our trainees were sometimes requesting appointments for patients within one week of discharge when I knew darn well that the patient was unlikely to make that appointment because the patient most likely would still be at rehab.
Prior to this system, we also had the occasional PCP who was upset because we booked their patient’s follow-up with a specialist who was outside that PCP’s “inner circle” of specialists. How in the world are any of us supposed to remember this information?
Well, our professional appointment-makers utilize this information as part of the algorithm they follow when booking appointments for patients. As our nation moves towards a value-based purchasing system for healthcare, we don’t need to recreate the wheel; we can adopt proven practices from other cost-effective industries—and we can improve customer satisfaction.
I am interested in hearing how appointments are arranged for your hospitalized patients. Send me your thoughts at [email protected].
Dr. Li is president of SHM.
It’s been nearly two decades since I graduated from medical school. I think back and I honestly do not remember any lectures about transitions of care.
During residency, I remember some attending physicians would insist that when I discharged patients from the hospital, the patients had to leave with post-discharge appointments in hand. Like any diligent intern, I did as I was told. I telephoned the administrative assistants in clinic and booked follow-up appointments for my patients. I always asked for the first available appointment. Why? Because that was what my senior resident told me to do. I suspect he learned that from his resident as well.
Sometimes the appointment was scheduled for the week following discharge; other times it was six months later. I honestly didn’t give it much thought. There was a blank on the discharge paperwork and I filled it in with a date and time. I was doing my job—or so I thought.
Can you imagine if someone just gave you a slip of paper today telling you when to show up to get your teeth cleaned without consulting your schedule? How about scheduling the oil change for your car at a garage 100 miles away? Seems pretty silly, doesn’t it? Nothing about it seems customer-centric or cost-efficient.
With such a system in place, why are we surprised when patients do not show up for their follow-up appointments? When the patient presents to the ED later and is readmitted to the hospital, we label them as “non-compliant” because they failed to show up for their follow-up appointment.
Inefficient, Ineffective, Inappropriate
There are multiple problems with the above situation. The first problem: Why are doctors calling to schedule follow-up appointments in the first place? Do we ask airline pilots to serve refreshments? I suppose they could, but I’d rather they concentrate on flying the plane. It also seems like an awful waste of money and resources when we could accomplish the same feat with less-expensive airline attendants who are better trained to interact with passengers.
At most teaching hospitals across the country, I suspect we still rely on trainees to book follow-up appointments for patients. At hospitals without trainees, I suspect some of this responsibility falls on nurses and unit coordinators. Again, I wonder how often these people are actually in a position to schedule an appointment that the patient is likely to keep—or whether they are filling in a box on a checklist like I used to do.
Common Problem?
How do other industries address this issue? Well, many utilize customer service representatives to help consumers book their appointments. Some industries have advanced software, which allows consumers to book their own appointment online. I have to tell you that I am chuckling as I write this. I’m chuckling not because this is funny—I am just amazed that something that is so common sense is not utilized consistently across the hospital industry. When was the last time you actually called a hotel to book a room? Most of us find it so much more convenient to book airline tickets or hotel rooms online.
If we were to create a system with the consumer’s satisfaction and cost in mind, would you rely on trainees, nurses, or unit coordinators to book follow-up appointments? I suppose Hypothetical System 2.0 would include consumer representatives speaking with patients to book appointments. Hypothetical System 3.0 would allow patients and/or a family member to book the appointment online.
I can tell you that folks at Beth Israel Deaconess Medical Center in Boston, where I work, have given this some thought. We are nowhere near a 3.0 version, but we do rely on professional appointment-makers to work with our hospitalized patients to book follow-up appointments. Inpatient providers put in the order online requesting follow-up appointments for their hospitalized patients. The online application asks the provider to specify the requests. Does the patient need follow-up with specialists, as well as their primary outpatient provider? The inpatient provider can specify the window of time in which they recommend follow-up for the patient. If I want my patient to follow up with their primary-care physician (PCP) within one week and with their cardiologist within two weeks, the appointment-maker will work with the patient and the respective doctors’ offices to make this happen. I am contacted only if any issues arise.
All of this information is provided to the patient with their other discharge paperwork. Some of you might be asking: How can the hospital afford to pay for this software and for the cadre of professional appointment-makers? I am wondering how hospitals can afford not to. It’s like worrying about the cost of a college degree until you realize how difficult it is trying to get a job without one.
Part of the PCP “access” problem we have in this country is due to the fact that not every patient shows up for scheduled appointments. Our appointment-makers minimize the “no show” rate because, by speaking with patients about their schedules, they are providing appointments to patients with knowledge that they are likely to make the appointment. One of the things we learned at Beth Israel was that our trainees were sometimes requesting appointments for patients within one week of discharge when I knew darn well that the patient was unlikely to make that appointment because the patient most likely would still be at rehab.
Prior to this system, we also had the occasional PCP who was upset because we booked their patient’s follow-up with a specialist who was outside that PCP’s “inner circle” of specialists. How in the world are any of us supposed to remember this information?
Well, our professional appointment-makers utilize this information as part of the algorithm they follow when booking appointments for patients. As our nation moves towards a value-based purchasing system for healthcare, we don’t need to recreate the wheel; we can adopt proven practices from other cost-effective industries—and we can improve customer satisfaction.
I am interested in hearing how appointments are arranged for your hospitalized patients. Send me your thoughts at [email protected].
Dr. Li is president of SHM.
It’s been nearly two decades since I graduated from medical school. I think back and I honestly do not remember any lectures about transitions of care.
During residency, I remember some attending physicians would insist that when I discharged patients from the hospital, the patients had to leave with post-discharge appointments in hand. Like any diligent intern, I did as I was told. I telephoned the administrative assistants in clinic and booked follow-up appointments for my patients. I always asked for the first available appointment. Why? Because that was what my senior resident told me to do. I suspect he learned that from his resident as well.
Sometimes the appointment was scheduled for the week following discharge; other times it was six months later. I honestly didn’t give it much thought. There was a blank on the discharge paperwork and I filled it in with a date and time. I was doing my job—or so I thought.
Can you imagine if someone just gave you a slip of paper today telling you when to show up to get your teeth cleaned without consulting your schedule? How about scheduling the oil change for your car at a garage 100 miles away? Seems pretty silly, doesn’t it? Nothing about it seems customer-centric or cost-efficient.
With such a system in place, why are we surprised when patients do not show up for their follow-up appointments? When the patient presents to the ED later and is readmitted to the hospital, we label them as “non-compliant” because they failed to show up for their follow-up appointment.
Inefficient, Ineffective, Inappropriate
There are multiple problems with the above situation. The first problem: Why are doctors calling to schedule follow-up appointments in the first place? Do we ask airline pilots to serve refreshments? I suppose they could, but I’d rather they concentrate on flying the plane. It also seems like an awful waste of money and resources when we could accomplish the same feat with less-expensive airline attendants who are better trained to interact with passengers.
At most teaching hospitals across the country, I suspect we still rely on trainees to book follow-up appointments for patients. At hospitals without trainees, I suspect some of this responsibility falls on nurses and unit coordinators. Again, I wonder how often these people are actually in a position to schedule an appointment that the patient is likely to keep—or whether they are filling in a box on a checklist like I used to do.
Common Problem?
How do other industries address this issue? Well, many utilize customer service representatives to help consumers book their appointments. Some industries have advanced software, which allows consumers to book their own appointment online. I have to tell you that I am chuckling as I write this. I’m chuckling not because this is funny—I am just amazed that something that is so common sense is not utilized consistently across the hospital industry. When was the last time you actually called a hotel to book a room? Most of us find it so much more convenient to book airline tickets or hotel rooms online.
If we were to create a system with the consumer’s satisfaction and cost in mind, would you rely on trainees, nurses, or unit coordinators to book follow-up appointments? I suppose Hypothetical System 2.0 would include consumer representatives speaking with patients to book appointments. Hypothetical System 3.0 would allow patients and/or a family member to book the appointment online.
I can tell you that folks at Beth Israel Deaconess Medical Center in Boston, where I work, have given this some thought. We are nowhere near a 3.0 version, but we do rely on professional appointment-makers to work with our hospitalized patients to book follow-up appointments. Inpatient providers put in the order online requesting follow-up appointments for their hospitalized patients. The online application asks the provider to specify the requests. Does the patient need follow-up with specialists, as well as their primary outpatient provider? The inpatient provider can specify the window of time in which they recommend follow-up for the patient. If I want my patient to follow up with their primary-care physician (PCP) within one week and with their cardiologist within two weeks, the appointment-maker will work with the patient and the respective doctors’ offices to make this happen. I am contacted only if any issues arise.
All of this information is provided to the patient with their other discharge paperwork. Some of you might be asking: How can the hospital afford to pay for this software and for the cadre of professional appointment-makers? I am wondering how hospitals can afford not to. It’s like worrying about the cost of a college degree until you realize how difficult it is trying to get a job without one.
Part of the PCP “access” problem we have in this country is due to the fact that not every patient shows up for scheduled appointments. Our appointment-makers minimize the “no show” rate because, by speaking with patients about their schedules, they are providing appointments to patients with knowledge that they are likely to make the appointment. One of the things we learned at Beth Israel was that our trainees were sometimes requesting appointments for patients within one week of discharge when I knew darn well that the patient was unlikely to make that appointment because the patient most likely would still be at rehab.
Prior to this system, we also had the occasional PCP who was upset because we booked their patient’s follow-up with a specialist who was outside that PCP’s “inner circle” of specialists. How in the world are any of us supposed to remember this information?
Well, our professional appointment-makers utilize this information as part of the algorithm they follow when booking appointments for patients. As our nation moves towards a value-based purchasing system for healthcare, we don’t need to recreate the wheel; we can adopt proven practices from other cost-effective industries—and we can improve customer satisfaction.
I am interested in hearing how appointments are arranged for your hospitalized patients. Send me your thoughts at [email protected].
Dr. Li is president of SHM.
Quality, Defined

Pornography. There can be few better hooks for readers than that. Just typing the word is a bit uncomfortable. As is, I imagine, reading it. But it’s effective, and likely why you’ve made it to word 37 of my column—34 words further than you usually get, I imagine.
“What about pornography?” you ask with bated breath. “What could pornography possibly have to do with hospital medicine?” your mind wonders. “Is this the column that (finally) gets Glasheen fired?” the ambulance chaser in you titillates.
By now, you’ve no doubt heard the famous Potter Stewart definition of pornography: “I know it when I see it.” That’s how the former U.S. Supreme Court justice described his threshold for recognizing pornography. It was made famous in a 1960s decision about whether a particular movie scene was protected by the 1st Amendment right to free speech or, indeed, a pornographic obscenity to be censured. Stewart, who clearly recognized the need to “define” pornography, also recognized the inherent challenges in doing so. The I-know-it-when-I-see-it benchmark is, of course, flawed, but I defy you to come up with a better definition.
Quality Is, of Course…
I was thinking about pornography (another discomforting phrase to type) recently—and Potter Stewart’s challenge in defining it, specifically—when I was asked about quality in healthcare. The query, which occurred during a several-hour, mind-numbing meeting (is there another type of several-hour meeting?), was “What is quality?” The question, laced with hostility and dripping with antagonism, was posed by a senior physician and directed pointedly at me. Indignantly, I cleared my throat, mentally stepping onto my pedestal to ceremoniously topple this academic egghead with my erudite response.
“Well, quality is, of course,” I confidently retorted, the “of course” added to demonstrate my moral superiority, “the ability to … uhhh, you see … ummmm, you know.” At which point I again cleared my throat not once, not twice, but a socially awkward three times before employing the timed-honored, full-body shock-twitch that signifies that you’ve just received an urgent vibrate page (faked, of course) and excused myself from the meeting, never to return.
The reality is that I struggle to define quality. Like Chief Justice Stewart, I think I know quality when I see it, but more precise definitions can be elusive.
And distracting.
It’s Not My Job
Just this morning, I read a news release from a respected physician group trumpeting the fact that their advocacy resulted in the federal government reducing the number of quality data-point requirements in their final rule for accountable-care organizations (ACOs) from 66 to 33. Trumpeting? Is this a good thing? Should we be supporting fewer quality measures? The article quoted a physician leader saying that the original reporting requirements were too burdensome. Too burdensome to whom? My guess is the recipients of our care, often referred to as our patients, wouldn’t categorize quality assurance as “too burdensome.”
I was at another meeting recently in which a respected colleague related her take on the physician role in improving quality. “I don’t think that’s a physician’s job. That’s what we have a quality department for,” she noted. “It’s just too expensive, time-consuming, and boring for physicians to do that kind of work.”
Too burdensome? Not a physician’s job to ensure the delivery of quality care? While I understand the sentiment (the need to have support staff collecting data, recognition of the huge infrastructure requirements, etc.), I can’t help but think that these types of responses are a large part of the struggle we are having with improving quality.
Then again, I would hazard that 0.0 percent of physicians would argue with the premise that we are obliged by the Hippocratic Oath, our moral compass, and our sense of professionalism to provide the best possible care to our patients. If we accept that we aren’t doing that—and we aren’t—then what is the disconnect? Why aren’t we seeking more quality data points? Why isn’t this “our job”?
Definitional Disconnect
Well, the truth is, it is our job. And we know it. The problem is that quality isn’t universally defined and the process of trying to define it often distracts us from the true task at hand—improving patient care.
Few of us would argue that a wrong-site surgery or anaphylaxis from administration of a medication known to have caused an allergy represents a suboptimal level of care. But more often than not, we see quality being measured and defined in less concrete, more obscure ways—ways that my eyes may not view as low-quality. These definitions are inherently flawed and breed contempt among providers who are told they aren’t passing muster in metrics they don’t see as “quality.”
So the real disconnect is definitional. Is quality defined by the Institute of Medicine characteristics of safe, effective, patient-centered, timely, efficient, and equitable care? Or is it the rates of underuse, overuse, and misuse of medical treatments and procedures? Or is it defined by individual quality metrics such as those captured by the Centers for Medicare & Medicaid Services (CMS)—you know, things like hospital fall rates, perioperative antibiotic usage, beta-blockers after MI, or whether a patient reported their bathroom as being clean?
Is 30% of the quality of care that we deliver referable to the patient experience (as measured by HCAHPS), as the new value-based purchasing program would have us believe? Is it hospital accreditation through the Joint Commission? Or physician certification through our parent boards? Is quality measured by a physician’s cognitive or technical skills, or where they went to school? Is it experience, medical knowledge, guideline usage?
We use such a mystifying array of metrics to define quality that it confuses the issue such that physicians who personally believe they are doing a good job can become disenfranchised. To a physician who provides clinically appropriate care around a surgical procedure or treatment of pneumonia, it can be demeaning and demoralizing to suggest that his or her patient did not receive “high quality” care because the bathroom wasn’t clean or the patient didn’t get a flu shot. Yet, this is the message we often send—a message that alienates many physicians, making them cynical about quality and disengaged in quality improvement. The result is that they seek fewer quality data points and defer the job of improving quality to someone else.
Make no mistake: Quality measures have an important role in our healthcare landscape. But to the degree that defining quality confuses, alienates, or disenfranchises providers, we should stop trying to define it. Quality is not a thing, a metric, or an outcome. It is not an elusive, unquantifiable creature that is achievable only by the elite. Quality is simply providing the best possible care. And quality improvement is simply closing the gap between the best possible care and actual care.
In this regard, we can learn a lot from Potter Stewart. We know quality when we see it. And we know what an absence of quality looks like.
Let’s close that gap by putting less energy into defining quality, and putting more energy into the tenacious pursuit of quality.
Dr. Glasheen is physician editor of The Hospitalist.
Pornography. There can be few better hooks for readers than that. Just typing the word is a bit uncomfortable. As is, I imagine, reading it. But it’s effective, and likely why you’ve made it to word 37 of my column—34 words further than you usually get, I imagine.
“What about pornography?” you ask with bated breath. “What could pornography possibly have to do with hospital medicine?” your mind wonders. “Is this the column that (finally) gets Glasheen fired?” the ambulance chaser in you titillates.
By now, you’ve no doubt heard the famous Potter Stewart definition of pornography: “I know it when I see it.” That’s how the former U.S. Supreme Court justice described his threshold for recognizing pornography. It was made famous in a 1960s decision about whether a particular movie scene was protected by the 1st Amendment right to free speech or, indeed, a pornographic obscenity to be censured. Stewart, who clearly recognized the need to “define” pornography, also recognized the inherent challenges in doing so. The I-know-it-when-I-see-it benchmark is, of course, flawed, but I defy you to come up with a better definition.
Quality Is, of Course…
I was thinking about pornography (another discomforting phrase to type) recently—and Potter Stewart’s challenge in defining it, specifically—when I was asked about quality in healthcare. The query, which occurred during a several-hour, mind-numbing meeting (is there another type of several-hour meeting?), was “What is quality?” The question, laced with hostility and dripping with antagonism, was posed by a senior physician and directed pointedly at me. Indignantly, I cleared my throat, mentally stepping onto my pedestal to ceremoniously topple this academic egghead with my erudite response.
“Well, quality is, of course,” I confidently retorted, the “of course” added to demonstrate my moral superiority, “the ability to … uhhh, you see … ummmm, you know.” At which point I again cleared my throat not once, not twice, but a socially awkward three times before employing the timed-honored, full-body shock-twitch that signifies that you’ve just received an urgent vibrate page (faked, of course) and excused myself from the meeting, never to return.
The reality is that I struggle to define quality. Like Chief Justice Stewart, I think I know quality when I see it, but more precise definitions can be elusive.
And distracting.
It’s Not My Job
Just this morning, I read a news release from a respected physician group trumpeting the fact that their advocacy resulted in the federal government reducing the number of quality data-point requirements in their final rule for accountable-care organizations (ACOs) from 66 to 33. Trumpeting? Is this a good thing? Should we be supporting fewer quality measures? The article quoted a physician leader saying that the original reporting requirements were too burdensome. Too burdensome to whom? My guess is the recipients of our care, often referred to as our patients, wouldn’t categorize quality assurance as “too burdensome.”
I was at another meeting recently in which a respected colleague related her take on the physician role in improving quality. “I don’t think that’s a physician’s job. That’s what we have a quality department for,” she noted. “It’s just too expensive, time-consuming, and boring for physicians to do that kind of work.”
Too burdensome? Not a physician’s job to ensure the delivery of quality care? While I understand the sentiment (the need to have support staff collecting data, recognition of the huge infrastructure requirements, etc.), I can’t help but think that these types of responses are a large part of the struggle we are having with improving quality.
Then again, I would hazard that 0.0 percent of physicians would argue with the premise that we are obliged by the Hippocratic Oath, our moral compass, and our sense of professionalism to provide the best possible care to our patients. If we accept that we aren’t doing that—and we aren’t—then what is the disconnect? Why aren’t we seeking more quality data points? Why isn’t this “our job”?
Definitional Disconnect
Well, the truth is, it is our job. And we know it. The problem is that quality isn’t universally defined and the process of trying to define it often distracts us from the true task at hand—improving patient care.
Few of us would argue that a wrong-site surgery or anaphylaxis from administration of a medication known to have caused an allergy represents a suboptimal level of care. But more often than not, we see quality being measured and defined in less concrete, more obscure ways—ways that my eyes may not view as low-quality. These definitions are inherently flawed and breed contempt among providers who are told they aren’t passing muster in metrics they don’t see as “quality.”
So the real disconnect is definitional. Is quality defined by the Institute of Medicine characteristics of safe, effective, patient-centered, timely, efficient, and equitable care? Or is it the rates of underuse, overuse, and misuse of medical treatments and procedures? Or is it defined by individual quality metrics such as those captured by the Centers for Medicare & Medicaid Services (CMS)—you know, things like hospital fall rates, perioperative antibiotic usage, beta-blockers after MI, or whether a patient reported their bathroom as being clean?
Is 30% of the quality of care that we deliver referable to the patient experience (as measured by HCAHPS), as the new value-based purchasing program would have us believe? Is it hospital accreditation through the Joint Commission? Or physician certification through our parent boards? Is quality measured by a physician’s cognitive or technical skills, or where they went to school? Is it experience, medical knowledge, guideline usage?
We use such a mystifying array of metrics to define quality that it confuses the issue such that physicians who personally believe they are doing a good job can become disenfranchised. To a physician who provides clinically appropriate care around a surgical procedure or treatment of pneumonia, it can be demeaning and demoralizing to suggest that his or her patient did not receive “high quality” care because the bathroom wasn’t clean or the patient didn’t get a flu shot. Yet, this is the message we often send—a message that alienates many physicians, making them cynical about quality and disengaged in quality improvement. The result is that they seek fewer quality data points and defer the job of improving quality to someone else.
Make no mistake: Quality measures have an important role in our healthcare landscape. But to the degree that defining quality confuses, alienates, or disenfranchises providers, we should stop trying to define it. Quality is not a thing, a metric, or an outcome. It is not an elusive, unquantifiable creature that is achievable only by the elite. Quality is simply providing the best possible care. And quality improvement is simply closing the gap between the best possible care and actual care.
In this regard, we can learn a lot from Potter Stewart. We know quality when we see it. And we know what an absence of quality looks like.
Let’s close that gap by putting less energy into defining quality, and putting more energy into the tenacious pursuit of quality.
Dr. Glasheen is physician editor of The Hospitalist.
Pornography. There can be few better hooks for readers than that. Just typing the word is a bit uncomfortable. As is, I imagine, reading it. But it’s effective, and likely why you’ve made it to word 37 of my column—34 words further than you usually get, I imagine.
“What about pornography?” you ask with bated breath. “What could pornography possibly have to do with hospital medicine?” your mind wonders. “Is this the column that (finally) gets Glasheen fired?” the ambulance chaser in you titillates.
By now, you’ve no doubt heard the famous Potter Stewart definition of pornography: “I know it when I see it.” That’s how the former U.S. Supreme Court justice described his threshold for recognizing pornography. It was made famous in a 1960s decision about whether a particular movie scene was protected by the 1st Amendment right to free speech or, indeed, a pornographic obscenity to be censured. Stewart, who clearly recognized the need to “define” pornography, also recognized the inherent challenges in doing so. The I-know-it-when-I-see-it benchmark is, of course, flawed, but I defy you to come up with a better definition.
Quality Is, of Course…
I was thinking about pornography (another discomforting phrase to type) recently—and Potter Stewart’s challenge in defining it, specifically—when I was asked about quality in healthcare. The query, which occurred during a several-hour, mind-numbing meeting (is there another type of several-hour meeting?), was “What is quality?” The question, laced with hostility and dripping with antagonism, was posed by a senior physician and directed pointedly at me. Indignantly, I cleared my throat, mentally stepping onto my pedestal to ceremoniously topple this academic egghead with my erudite response.
“Well, quality is, of course,” I confidently retorted, the “of course” added to demonstrate my moral superiority, “the ability to … uhhh, you see … ummmm, you know.” At which point I again cleared my throat not once, not twice, but a socially awkward three times before employing the timed-honored, full-body shock-twitch that signifies that you’ve just received an urgent vibrate page (faked, of course) and excused myself from the meeting, never to return.
The reality is that I struggle to define quality. Like Chief Justice Stewart, I think I know quality when I see it, but more precise definitions can be elusive.
And distracting.
It’s Not My Job
Just this morning, I read a news release from a respected physician group trumpeting the fact that their advocacy resulted in the federal government reducing the number of quality data-point requirements in their final rule for accountable-care organizations (ACOs) from 66 to 33. Trumpeting? Is this a good thing? Should we be supporting fewer quality measures? The article quoted a physician leader saying that the original reporting requirements were too burdensome. Too burdensome to whom? My guess is the recipients of our care, often referred to as our patients, wouldn’t categorize quality assurance as “too burdensome.”
I was at another meeting recently in which a respected colleague related her take on the physician role in improving quality. “I don’t think that’s a physician’s job. That’s what we have a quality department for,” she noted. “It’s just too expensive, time-consuming, and boring for physicians to do that kind of work.”
Too burdensome? Not a physician’s job to ensure the delivery of quality care? While I understand the sentiment (the need to have support staff collecting data, recognition of the huge infrastructure requirements, etc.), I can’t help but think that these types of responses are a large part of the struggle we are having with improving quality.
Then again, I would hazard that 0.0 percent of physicians would argue with the premise that we are obliged by the Hippocratic Oath, our moral compass, and our sense of professionalism to provide the best possible care to our patients. If we accept that we aren’t doing that—and we aren’t—then what is the disconnect? Why aren’t we seeking more quality data points? Why isn’t this “our job”?
Definitional Disconnect
Well, the truth is, it is our job. And we know it. The problem is that quality isn’t universally defined and the process of trying to define it often distracts us from the true task at hand—improving patient care.
Few of us would argue that a wrong-site surgery or anaphylaxis from administration of a medication known to have caused an allergy represents a suboptimal level of care. But more often than not, we see quality being measured and defined in less concrete, more obscure ways—ways that my eyes may not view as low-quality. These definitions are inherently flawed and breed contempt among providers who are told they aren’t passing muster in metrics they don’t see as “quality.”
So the real disconnect is definitional. Is quality defined by the Institute of Medicine characteristics of safe, effective, patient-centered, timely, efficient, and equitable care? Or is it the rates of underuse, overuse, and misuse of medical treatments and procedures? Or is it defined by individual quality metrics such as those captured by the Centers for Medicare & Medicaid Services (CMS)—you know, things like hospital fall rates, perioperative antibiotic usage, beta-blockers after MI, or whether a patient reported their bathroom as being clean?
Is 30% of the quality of care that we deliver referable to the patient experience (as measured by HCAHPS), as the new value-based purchasing program would have us believe? Is it hospital accreditation through the Joint Commission? Or physician certification through our parent boards? Is quality measured by a physician’s cognitive or technical skills, or where they went to school? Is it experience, medical knowledge, guideline usage?
We use such a mystifying array of metrics to define quality that it confuses the issue such that physicians who personally believe they are doing a good job can become disenfranchised. To a physician who provides clinically appropriate care around a surgical procedure or treatment of pneumonia, it can be demeaning and demoralizing to suggest that his or her patient did not receive “high quality” care because the bathroom wasn’t clean or the patient didn’t get a flu shot. Yet, this is the message we often send—a message that alienates many physicians, making them cynical about quality and disengaged in quality improvement. The result is that they seek fewer quality data points and defer the job of improving quality to someone else.
Make no mistake: Quality measures have an important role in our healthcare landscape. But to the degree that defining quality confuses, alienates, or disenfranchises providers, we should stop trying to define it. Quality is not a thing, a metric, or an outcome. It is not an elusive, unquantifiable creature that is achievable only by the elite. Quality is simply providing the best possible care. And quality improvement is simply closing the gap between the best possible care and actual care.
In this regard, we can learn a lot from Potter Stewart. We know quality when we see it. And we know what an absence of quality looks like.
Let’s close that gap by putting less energy into defining quality, and putting more energy into the tenacious pursuit of quality.
Dr. Glasheen is physician editor of The Hospitalist.
Holdout Hospitals

I think 70% to 80% of U.S. hospitals now have a hospitalist practice. (Some have more than one hospitalist group operating within their walls.) I arrived at this estimate by relying on both my anecdotal experience and on the annual American Hospital Association survey, which in 2009 showed 58% of hospitals have hospitalists, with an ongoing rapid rate of adoption.
No regular reader of The Hospitalist should be surprised that most U.S. hospitals now have hospitalists, but some might be surprised that 20% to 30% don’t. There are about 5,800 hospitals in the U.S. (a ballpark figure), so that means about 1,100 to 1,800 don’t have hospitalists. What is unique about them?
For some hospitals, the answer is easy. For example, the U.S. has something like 450 psychiatric hospitals. They vary a lot, but many simply don’t accept patients with active medical problems, so these facilities would have little need for medical hospitalists.
Variations in how the term “hospitalist” is used probably account for some facilities reporting no hospitalists. For example, long-term acute-care hospitals (LTACs) might have dedicated inpatient providers but simply don’t call them hospitalists.
Even accounting for these things, there are still a lot of “med-surg” hospitals that say they don’t have hospitalists.
The Holdouts
My experience suggests the two most important reasons some hospitals have not yet developed a hospitalist practice are an oversupply of primary-care physicians (PCPs) and an attractive payor mix in the unassigned patient population. In fact, it is hard for me to imagine a hospital that enjoys both of these attributes ever being able to support hospitalists.
Although it isn’t a common problem, an excess of PCPs (or dearth of patients) removes the most universal and powerful stimulus to develop a hospitalist practice: the desire of PCPs to be relieved of hospital work. And in most cases, those PCPs can offset the loss of hospital work and its associated revenue, with more work in the office. This can mean a better lifestyle (e.g. no trips to the hospital on nights and weekends) and the same or higher income. But if there are too many PCPs in the community, they may be unwilling to give up the hospital work, as there might be no way to replace it in the office. End result: no hospitalists.
For the rare hospital that has an attractive ED-unassigned payor mix, PCPs are more likely to want to continue taking ED call and not support a proposal to develop a hospitalist practice. And access to the ED call roster can be important to new PCPs building a community practice. I have seen situations in which a hospital has addressed the poor reimbursement of unattached ED admissions by paying PCPs to provide that care. Even though that same hospital might want a hospitalist practice, the ED call payment it is providing to PCPs may create a barrier that can’t be overcome. Such a hospital will face the very difficult decision of terminating the payments for ED call and redirecting that money to a hospitalist practice—something that is likely to lead to a lot of frustration on the part of PCPs who depend on the pay-for-call arrangement. A common outcome: no hospitalists.
An occasional reason hospitals are late to the hospitalist party is one or two (rarely more than that) of its private PCPs have simply chosen to work heroic amounts, and in addition to office and hospital care of their private patients, they accept referrals from other PCPs. I have met a number of doctors like this. Some are terrific doctors who actively participate in hospital initiatives; many appear chronically tired and harried, and hospital staff express frustration that they do things like make rounds at 3 a.m., take hours to respond to urgent calls, refuse to use protocols, etc. But because they’ve responded to the PCPs’ desire to be relieved of hospital work, other doctors may rally to their support and prevent the hospital from moving forward with a hospitalist program.
Will Every Hospital Have Hospitalists Eventually?
It is really interesting to think about whether every hospital, outside narrow specialty hospitals, will have hospitalists in the future. I wonder what informed people in the 1970s and early 1980s were predicting for emergency medicine’s future. At that point it probably wasn’t clear that, in the future, dedicated ED doctors essentially would staff every ED in the country, but I think that is exactly what has happened. (I once worked with an approximately 100-bed rural hospital that didn’t have ED physicians until 1999. I wonder if they were the last adopter.)
I think hospitalists are critically important for nearly all med-surg hospitals; however, maybe there will always be a small number that either have PCPs continue to practice in the traditional model, working both outpatient and inpatient, or some other effective configuration that makes hospitalists less necessary. We’ll have to wait and see. But I’m pretty confident
that almost no institutions that have hospitalists will ever return to the pre-hospitalist model of care. It seems there is no going back.
For those hospitals without hospitalists currently who will at some future time have hospitalists, the right time for this to happen is dependent on a combination of local factors. It could be something like the departure (i.e. relocation or retirement) of some of the current doctors, or simply the arrival of someone who has a vision and energy to successfully navigate the obstacles to build one. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.</p>
I think 70% to 80% of U.S. hospitals now have a hospitalist practice. (Some have more than one hospitalist group operating within their walls.) I arrived at this estimate by relying on both my anecdotal experience and on the annual American Hospital Association survey, which in 2009 showed 58% of hospitals have hospitalists, with an ongoing rapid rate of adoption.
No regular reader of The Hospitalist should be surprised that most U.S. hospitals now have hospitalists, but some might be surprised that 20% to 30% don’t. There are about 5,800 hospitals in the U.S. (a ballpark figure), so that means about 1,100 to 1,800 don’t have hospitalists. What is unique about them?
For some hospitals, the answer is easy. For example, the U.S. has something like 450 psychiatric hospitals. They vary a lot, but many simply don’t accept patients with active medical problems, so these facilities would have little need for medical hospitalists.
Variations in how the term “hospitalist” is used probably account for some facilities reporting no hospitalists. For example, long-term acute-care hospitals (LTACs) might have dedicated inpatient providers but simply don’t call them hospitalists.
Even accounting for these things, there are still a lot of “med-surg” hospitals that say they don’t have hospitalists.
The Holdouts
My experience suggests the two most important reasons some hospitals have not yet developed a hospitalist practice are an oversupply of primary-care physicians (PCPs) and an attractive payor mix in the unassigned patient population. In fact, it is hard for me to imagine a hospital that enjoys both of these attributes ever being able to support hospitalists.
Although it isn’t a common problem, an excess of PCPs (or dearth of patients) removes the most universal and powerful stimulus to develop a hospitalist practice: the desire of PCPs to be relieved of hospital work. And in most cases, those PCPs can offset the loss of hospital work and its associated revenue, with more work in the office. This can mean a better lifestyle (e.g. no trips to the hospital on nights and weekends) and the same or higher income. But if there are too many PCPs in the community, they may be unwilling to give up the hospital work, as there might be no way to replace it in the office. End result: no hospitalists.
For the rare hospital that has an attractive ED-unassigned payor mix, PCPs are more likely to want to continue taking ED call and not support a proposal to develop a hospitalist practice. And access to the ED call roster can be important to new PCPs building a community practice. I have seen situations in which a hospital has addressed the poor reimbursement of unattached ED admissions by paying PCPs to provide that care. Even though that same hospital might want a hospitalist practice, the ED call payment it is providing to PCPs may create a barrier that can’t be overcome. Such a hospital will face the very difficult decision of terminating the payments for ED call and redirecting that money to a hospitalist practice—something that is likely to lead to a lot of frustration on the part of PCPs who depend on the pay-for-call arrangement. A common outcome: no hospitalists.
An occasional reason hospitals are late to the hospitalist party is one or two (rarely more than that) of its private PCPs have simply chosen to work heroic amounts, and in addition to office and hospital care of their private patients, they accept referrals from other PCPs. I have met a number of doctors like this. Some are terrific doctors who actively participate in hospital initiatives; many appear chronically tired and harried, and hospital staff express frustration that they do things like make rounds at 3 a.m., take hours to respond to urgent calls, refuse to use protocols, etc. But because they’ve responded to the PCPs’ desire to be relieved of hospital work, other doctors may rally to their support and prevent the hospital from moving forward with a hospitalist program.
Will Every Hospital Have Hospitalists Eventually?
It is really interesting to think about whether every hospital, outside narrow specialty hospitals, will have hospitalists in the future. I wonder what informed people in the 1970s and early 1980s were predicting for emergency medicine’s future. At that point it probably wasn’t clear that, in the future, dedicated ED doctors essentially would staff every ED in the country, but I think that is exactly what has happened. (I once worked with an approximately 100-bed rural hospital that didn’t have ED physicians until 1999. I wonder if they were the last adopter.)
I think hospitalists are critically important for nearly all med-surg hospitals; however, maybe there will always be a small number that either have PCPs continue to practice in the traditional model, working both outpatient and inpatient, or some other effective configuration that makes hospitalists less necessary. We’ll have to wait and see. But I’m pretty confident
that almost no institutions that have hospitalists will ever return to the pre-hospitalist model of care. It seems there is no going back.
For those hospitals without hospitalists currently who will at some future time have hospitalists, the right time for this to happen is dependent on a combination of local factors. It could be something like the departure (i.e. relocation or retirement) of some of the current doctors, or simply the arrival of someone who has a vision and energy to successfully navigate the obstacles to build one. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.</p>
I think 70% to 80% of U.S. hospitals now have a hospitalist practice. (Some have more than one hospitalist group operating within their walls.) I arrived at this estimate by relying on both my anecdotal experience and on the annual American Hospital Association survey, which in 2009 showed 58% of hospitals have hospitalists, with an ongoing rapid rate of adoption.
No regular reader of The Hospitalist should be surprised that most U.S. hospitals now have hospitalists, but some might be surprised that 20% to 30% don’t. There are about 5,800 hospitals in the U.S. (a ballpark figure), so that means about 1,100 to 1,800 don’t have hospitalists. What is unique about them?
For some hospitals, the answer is easy. For example, the U.S. has something like 450 psychiatric hospitals. They vary a lot, but many simply don’t accept patients with active medical problems, so these facilities would have little need for medical hospitalists.
Variations in how the term “hospitalist” is used probably account for some facilities reporting no hospitalists. For example, long-term acute-care hospitals (LTACs) might have dedicated inpatient providers but simply don’t call them hospitalists.
Even accounting for these things, there are still a lot of “med-surg” hospitals that say they don’t have hospitalists.
The Holdouts
My experience suggests the two most important reasons some hospitals have not yet developed a hospitalist practice are an oversupply of primary-care physicians (PCPs) and an attractive payor mix in the unassigned patient population. In fact, it is hard for me to imagine a hospital that enjoys both of these attributes ever being able to support hospitalists.
Although it isn’t a common problem, an excess of PCPs (or dearth of patients) removes the most universal and powerful stimulus to develop a hospitalist practice: the desire of PCPs to be relieved of hospital work. And in most cases, those PCPs can offset the loss of hospital work and its associated revenue, with more work in the office. This can mean a better lifestyle (e.g. no trips to the hospital on nights and weekends) and the same or higher income. But if there are too many PCPs in the community, they may be unwilling to give up the hospital work, as there might be no way to replace it in the office. End result: no hospitalists.
For the rare hospital that has an attractive ED-unassigned payor mix, PCPs are more likely to want to continue taking ED call and not support a proposal to develop a hospitalist practice. And access to the ED call roster can be important to new PCPs building a community practice. I have seen situations in which a hospital has addressed the poor reimbursement of unattached ED admissions by paying PCPs to provide that care. Even though that same hospital might want a hospitalist practice, the ED call payment it is providing to PCPs may create a barrier that can’t be overcome. Such a hospital will face the very difficult decision of terminating the payments for ED call and redirecting that money to a hospitalist practice—something that is likely to lead to a lot of frustration on the part of PCPs who depend on the pay-for-call arrangement. A common outcome: no hospitalists.
An occasional reason hospitals are late to the hospitalist party is one or two (rarely more than that) of its private PCPs have simply chosen to work heroic amounts, and in addition to office and hospital care of their private patients, they accept referrals from other PCPs. I have met a number of doctors like this. Some are terrific doctors who actively participate in hospital initiatives; many appear chronically tired and harried, and hospital staff express frustration that they do things like make rounds at 3 a.m., take hours to respond to urgent calls, refuse to use protocols, etc. But because they’ve responded to the PCPs’ desire to be relieved of hospital work, other doctors may rally to their support and prevent the hospital from moving forward with a hospitalist program.
Will Every Hospital Have Hospitalists Eventually?
It is really interesting to think about whether every hospital, outside narrow specialty hospitals, will have hospitalists in the future. I wonder what informed people in the 1970s and early 1980s were predicting for emergency medicine’s future. At that point it probably wasn’t clear that, in the future, dedicated ED doctors essentially would staff every ED in the country, but I think that is exactly what has happened. (I once worked with an approximately 100-bed rural hospital that didn’t have ED physicians until 1999. I wonder if they were the last adopter.)
I think hospitalists are critically important for nearly all med-surg hospitals; however, maybe there will always be a small number that either have PCPs continue to practice in the traditional model, working both outpatient and inpatient, or some other effective configuration that makes hospitalists less necessary. We’ll have to wait and see. But I’m pretty confident
that almost no institutions that have hospitalists will ever return to the pre-hospitalist model of care. It seems there is no going back.
For those hospitals without hospitalists currently who will at some future time have hospitalists, the right time for this to happen is dependent on a combination of local factors. It could be something like the departure (i.e. relocation or retirement) of some of the current doctors, or simply the arrival of someone who has a vision and energy to successfully navigate the obstacles to build one. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.</p>
The Critical Question
Dr. Sali, the resident, asks his attending: Dr. Biba, are you saying that you can tell if a patient has marital problems in the first 5 minutes of an interview?
Dr. Biba: Yes. In fact, Jill Hooley says that you just need to ask one question of a patient: "How critical is your spouse of you?"
Dr. Sali: Okay, so I asked Jeanie "the Critical Question" at our first meeting. She said yes. Now what?
Dr. Biba: Now you bring in the husband and try to understand what is going on.
A week later:
Dr. Sali: So I met with Jeanie and her husband. He started right in with "So what’s wrong with my wife?" When I explained about depression, he said "What do you mean she’s depressed? She’s never said that before! Jeanie, why are you saying this stuff? Don’t you want to go to work?"
Dr. Biba: Wow, that sounds bad. What did you do then?
Dr. Sali: I explained some more about depression, all its symptoms and signs. I asked the husband to listen and said that we needed to work together to help Jeanie. Then he said, "That’s how her mother was!" He completely changed! He still was a bit agitated but he was okay and said, "So, let’s get this illness treated!" I am not sure I trust his quick change, but at least he has some idea of what needs to be done.
Dr. Biba: What did you tell him he needs to do?
Dr. Sali: I didn’t know what to tell him. I gave him a handout about depression and families that I found on the Internet. Can you meet with them and me next week?
High criticalness in families is often tied to a lack of understanding about illness. In the scenario described above, the patient’s husband thought he was being a good husband by standing tough with his wife. His intentions were good, but he did not understand the extent to which depression impairs energy and motivation.
High criticalness is a component of the concept of expressed emotion (EE), a robust research construct in family psychiatry. High levels of EE are found in patient-family interactions when patients relapse sooner and more frequently. EE was first described with schizophrenia, but high EE is associated with early relapse in many other psychiatric and medical illnesses (Arch. Gen. Psychiatry 1998;55:547-52).
EE consists of three components: criticalness, overt hostility, and emotional overinvolvement. It originally was measured with the 2-hour Camberwell Family Interview ("Expressed Emotion in Families." New York: Guilford Press, 1985). But shorter tools now exist, such as the critical question conceptualized by Jill Hooley, D.Phil., and the Five-Minute Speech Sample (FMSS). The FMSS consists of asking a family member to speak freely about the patient’s character and their relationships, without disturbance from the interviewer, for 5 minutes (Psychiatry Res. 1986;17:203-12).
Dr. Hooley measured marital distress and patients’ perceptions of criticism from spouses in hospitalized patients with major depression. EE and marital distress predicted the same relapse rates at 9 months. However, a patient’s response to the question, "How critical is your spouse of you?" accounted for more of the variance in relapse rates than did EE and marital distress combined (J. Abnorm. Psychol. 1989;98:229-35).
The good news is that EE is reduced with psychoeducational family interventions. In addition, many interventions that reduce EE are evidence based, and are effective across many illnesses and cultures. For example, a recent study of a family work intervention in Catalonia, Spain, found improvements in the clinical status as well as global and social functioning of patients with schizophrenia (Int. J. Soc. Psychiatry 2011 Aug. 1 [doi:10.1177/00207640114155]).
Dr. Julian Leff, one of the social psychiatrists who delineated EE, is still hard at work reducing EE, this time in the auditory hallucination of patients with schizophrenia in a new therapy called Avatar Therapy for people with persistent auditory hallucinations (Department of Psychiatry Grand Rounds, University of Colorado at Denver, Oct. 19, 2011).
Dr. Sali, the resident, asks his attending: Dr. Biba, are you saying that you can tell if a patient has marital problems in the first 5 minutes of an interview?
Dr. Biba: Yes. In fact, Jill Hooley says that you just need to ask one question of a patient: "How critical is your spouse of you?"
Dr. Sali: Okay, so I asked Jeanie "the Critical Question" at our first meeting. She said yes. Now what?
Dr. Biba: Now you bring in the husband and try to understand what is going on.
A week later:
Dr. Sali: So I met with Jeanie and her husband. He started right in with "So what’s wrong with my wife?" When I explained about depression, he said "What do you mean she’s depressed? She’s never said that before! Jeanie, why are you saying this stuff? Don’t you want to go to work?"
Dr. Biba: Wow, that sounds bad. What did you do then?
Dr. Sali: I explained some more about depression, all its symptoms and signs. I asked the husband to listen and said that we needed to work together to help Jeanie. Then he said, "That’s how her mother was!" He completely changed! He still was a bit agitated but he was okay and said, "So, let’s get this illness treated!" I am not sure I trust his quick change, but at least he has some idea of what needs to be done.
Dr. Biba: What did you tell him he needs to do?
Dr. Sali: I didn’t know what to tell him. I gave him a handout about depression and families that I found on the Internet. Can you meet with them and me next week?
High criticalness in families is often tied to a lack of understanding about illness. In the scenario described above, the patient’s husband thought he was being a good husband by standing tough with his wife. His intentions were good, but he did not understand the extent to which depression impairs energy and motivation.
High criticalness is a component of the concept of expressed emotion (EE), a robust research construct in family psychiatry. High levels of EE are found in patient-family interactions when patients relapse sooner and more frequently. EE was first described with schizophrenia, but high EE is associated with early relapse in many other psychiatric and medical illnesses (Arch. Gen. Psychiatry 1998;55:547-52).
EE consists of three components: criticalness, overt hostility, and emotional overinvolvement. It originally was measured with the 2-hour Camberwell Family Interview ("Expressed Emotion in Families." New York: Guilford Press, 1985). But shorter tools now exist, such as the critical question conceptualized by Jill Hooley, D.Phil., and the Five-Minute Speech Sample (FMSS). The FMSS consists of asking a family member to speak freely about the patient’s character and their relationships, without disturbance from the interviewer, for 5 minutes (Psychiatry Res. 1986;17:203-12).
Dr. Hooley measured marital distress and patients’ perceptions of criticism from spouses in hospitalized patients with major depression. EE and marital distress predicted the same relapse rates at 9 months. However, a patient’s response to the question, "How critical is your spouse of you?" accounted for more of the variance in relapse rates than did EE and marital distress combined (J. Abnorm. Psychol. 1989;98:229-35).
The good news is that EE is reduced with psychoeducational family interventions. In addition, many interventions that reduce EE are evidence based, and are effective across many illnesses and cultures. For example, a recent study of a family work intervention in Catalonia, Spain, found improvements in the clinical status as well as global and social functioning of patients with schizophrenia (Int. J. Soc. Psychiatry 2011 Aug. 1 [doi:10.1177/00207640114155]).
Dr. Julian Leff, one of the social psychiatrists who delineated EE, is still hard at work reducing EE, this time in the auditory hallucination of patients with schizophrenia in a new therapy called Avatar Therapy for people with persistent auditory hallucinations (Department of Psychiatry Grand Rounds, University of Colorado at Denver, Oct. 19, 2011).
Dr. Sali, the resident, asks his attending: Dr. Biba, are you saying that you can tell if a patient has marital problems in the first 5 minutes of an interview?
Dr. Biba: Yes. In fact, Jill Hooley says that you just need to ask one question of a patient: "How critical is your spouse of you?"
Dr. Sali: Okay, so I asked Jeanie "the Critical Question" at our first meeting. She said yes. Now what?
Dr. Biba: Now you bring in the husband and try to understand what is going on.
A week later:
Dr. Sali: So I met with Jeanie and her husband. He started right in with "So what’s wrong with my wife?" When I explained about depression, he said "What do you mean she’s depressed? She’s never said that before! Jeanie, why are you saying this stuff? Don’t you want to go to work?"
Dr. Biba: Wow, that sounds bad. What did you do then?
Dr. Sali: I explained some more about depression, all its symptoms and signs. I asked the husband to listen and said that we needed to work together to help Jeanie. Then he said, "That’s how her mother was!" He completely changed! He still was a bit agitated but he was okay and said, "So, let’s get this illness treated!" I am not sure I trust his quick change, but at least he has some idea of what needs to be done.
Dr. Biba: What did you tell him he needs to do?
Dr. Sali: I didn’t know what to tell him. I gave him a handout about depression and families that I found on the Internet. Can you meet with them and me next week?
High criticalness in families is often tied to a lack of understanding about illness. In the scenario described above, the patient’s husband thought he was being a good husband by standing tough with his wife. His intentions were good, but he did not understand the extent to which depression impairs energy and motivation.
High criticalness is a component of the concept of expressed emotion (EE), a robust research construct in family psychiatry. High levels of EE are found in patient-family interactions when patients relapse sooner and more frequently. EE was first described with schizophrenia, but high EE is associated with early relapse in many other psychiatric and medical illnesses (Arch. Gen. Psychiatry 1998;55:547-52).
EE consists of three components: criticalness, overt hostility, and emotional overinvolvement. It originally was measured with the 2-hour Camberwell Family Interview ("Expressed Emotion in Families." New York: Guilford Press, 1985). But shorter tools now exist, such as the critical question conceptualized by Jill Hooley, D.Phil., and the Five-Minute Speech Sample (FMSS). The FMSS consists of asking a family member to speak freely about the patient’s character and their relationships, without disturbance from the interviewer, for 5 minutes (Psychiatry Res. 1986;17:203-12).
Dr. Hooley measured marital distress and patients’ perceptions of criticism from spouses in hospitalized patients with major depression. EE and marital distress predicted the same relapse rates at 9 months. However, a patient’s response to the question, "How critical is your spouse of you?" accounted for more of the variance in relapse rates than did EE and marital distress combined (J. Abnorm. Psychol. 1989;98:229-35).
The good news is that EE is reduced with psychoeducational family interventions. In addition, many interventions that reduce EE are evidence based, and are effective across many illnesses and cultures. For example, a recent study of a family work intervention in Catalonia, Spain, found improvements in the clinical status as well as global and social functioning of patients with schizophrenia (Int. J. Soc. Psychiatry 2011 Aug. 1 [doi:10.1177/00207640114155]).
Dr. Julian Leff, one of the social psychiatrists who delineated EE, is still hard at work reducing EE, this time in the auditory hallucination of patients with schizophrenia in a new therapy called Avatar Therapy for people with persistent auditory hallucinations (Department of Psychiatry Grand Rounds, University of Colorado at Denver, Oct. 19, 2011).
Evaluation and Management of the Infant With Hypotonia
When you first observe or suspect an infant has hypotonia, you face a decision whether the condition is benign and likely to resolve over time vs. a more serious condition with an important neurologic basis.
You will be in a position to make that call in many cases in your practice. Related observations include spontaneous movement during a physical examination; basic laboratory testing; and any relevant family history of genetic-based disease. These can go a long way to guide your diagnosis. Any abnormality in growth, feeding patterns, or respiration also provides important clinical clues.

Pediatricians, depending on their experience, can determine when a "wait and watch" approach is appropriate. For example, benign hypotonia is more likely when there are no major delays in growth or motor milestones, no signs of abnormal respiration, and parents report normal feeding patterns.
Since we cannot test the strength of a 7- or 8-month-old infant by asking them to offer resistance with their arms and legs, it’s useful to observe the amount and quality of their spontaneous movements. Watch their head control when you pull the infant to sit from a supine position. Does the head lag behind at all? How vigorously does the infant kick or grasp? These signs can help examiners compare impressions of degree of weakness, if there is any, in hypotonic infants.
Parents may be unaware of any low muscle tone, so it’s important to include hypotonia on your physical examination checklist.
Ask parents about the strength of the infant during diaper or clothing changes. Often parents have a good sense of the amount of force their child displays, and it can be reassuring to make these observations in the examination room as well.
An infant with a benign form of congenital hypotonia will move her arms and legs frequently: batting, roving, and sometimes synchronous movements come and go depending on level of alertness. In contrast, an infant with hypotonia caused by a neurologic disease, such as spinal muscle atrophy, will move much less frequently and the initiation of the movement(s) is slower.
In some cases, the degree or cause of hypotonia may not be clear, and the question becomes what to do with that uncertainty. A creatine phosphokinase (CPK) assay, the most common initial laboratory test to assess low muscle tone, can be helpful, although a normal result doesn’t rule out muscle or nerve disease.
In addition, check the baby’s respiratory rate and listen for any stridor or other signs of obstruction in her breathing. Noisy breathing can suggest upper respiratory muscle involvement, in which case further work-up is warranted. How’s the head growth over time?
Testing deep tendon reflexes can be tricky. While the presence of reflexes is reassuring, absence suggests a peripheral nerve problem or anterior horn cell disease.
Ask parents about the baby’s typical feeding pattern. An infant that seems to take a long time to feed and/or has an interrupted pattern of feeding should raise your clinical suspicion about an important neurologic cause for their hypotonia.
Family history can be an independent risk factor for a more serious, inherited neurologic etiology. Many of the causes of hypotonia are genetic, and specialist input will be appropriate if you uncover relevant family history. Inquire about any first-degree relative or others with an inherited neurologic condition that could underlie the infant’s hypotonia. In some cases, a non-neurologic inherited disease such as Marfan syndrome can cause hypotonia as well.
Specialist input is indicated if you suspect a genetic basis for the hypotonia, even if the infant passes the other important elements of your evaluation (for example, normal milestones, eating, and breathing).
These patients are a pretty diverse group, and there are many infants with hypotonia who will ultimately do well. If you are unsure, it’s definitely worth tracking these patients a little closer using history and physical examination checklists. Check in with a specialist if you continue to be unsure as you move forward.
Dr. Bingham is a pediatric neurologist at Fletcher Allen Health Care and associate professor of neurology at the University of Vermont in Burlington. Dr. Bingham said he had no relevant financial disclosures.
When you first observe or suspect an infant has hypotonia, you face a decision whether the condition is benign and likely to resolve over time vs. a more serious condition with an important neurologic basis.
You will be in a position to make that call in many cases in your practice. Related observations include spontaneous movement during a physical examination; basic laboratory testing; and any relevant family history of genetic-based disease. These can go a long way to guide your diagnosis. Any abnormality in growth, feeding patterns, or respiration also provides important clinical clues.
Pediatricians, depending on their experience, can determine when a "wait and watch" approach is appropriate. For example, benign hypotonia is more likely when there are no major delays in growth or motor milestones, no signs of abnormal respiration, and parents report normal feeding patterns.
Since we cannot test the strength of a 7- or 8-month-old infant by asking them to offer resistance with their arms and legs, it’s useful to observe the amount and quality of their spontaneous movements. Watch their head control when you pull the infant to sit from a supine position. Does the head lag behind at all? How vigorously does the infant kick or grasp? These signs can help examiners compare impressions of degree of weakness, if there is any, in hypotonic infants.
Parents may be unaware of any low muscle tone, so it’s important to include hypotonia on your physical examination checklist.
Ask parents about the strength of the infant during diaper or clothing changes. Often parents have a good sense of the amount of force their child displays, and it can be reassuring to make these observations in the examination room as well.
An infant with a benign form of congenital hypotonia will move her arms and legs frequently: batting, roving, and sometimes synchronous movements come and go depending on level of alertness. In contrast, an infant with hypotonia caused by a neurologic disease, such as spinal muscle atrophy, will move much less frequently and the initiation of the movement(s) is slower.
In some cases, the degree or cause of hypotonia may not be clear, and the question becomes what to do with that uncertainty. A creatine phosphokinase (CPK) assay, the most common initial laboratory test to assess low muscle tone, can be helpful, although a normal result doesn’t rule out muscle or nerve disease.
In addition, check the baby’s respiratory rate and listen for any stridor or other signs of obstruction in her breathing. Noisy breathing can suggest upper respiratory muscle involvement, in which case further work-up is warranted. How’s the head growth over time?
Testing deep tendon reflexes can be tricky. While the presence of reflexes is reassuring, absence suggests a peripheral nerve problem or anterior horn cell disease.
Ask parents about the baby’s typical feeding pattern. An infant that seems to take a long time to feed and/or has an interrupted pattern of feeding should raise your clinical suspicion about an important neurologic cause for their hypotonia.
Family history can be an independent risk factor for a more serious, inherited neurologic etiology. Many of the causes of hypotonia are genetic, and specialist input will be appropriate if you uncover relevant family history. Inquire about any first-degree relative or others with an inherited neurologic condition that could underlie the infant’s hypotonia. In some cases, a non-neurologic inherited disease such as Marfan syndrome can cause hypotonia as well.
Specialist input is indicated if you suspect a genetic basis for the hypotonia, even if the infant passes the other important elements of your evaluation (for example, normal milestones, eating, and breathing).
These patients are a pretty diverse group, and there are many infants with hypotonia who will ultimately do well. If you are unsure, it’s definitely worth tracking these patients a little closer using history and physical examination checklists. Check in with a specialist if you continue to be unsure as you move forward.
Dr. Bingham is a pediatric neurologist at Fletcher Allen Health Care and associate professor of neurology at the University of Vermont in Burlington. Dr. Bingham said he had no relevant financial disclosures.
When you first observe or suspect an infant has hypotonia, you face a decision whether the condition is benign and likely to resolve over time vs. a more serious condition with an important neurologic basis.
You will be in a position to make that call in many cases in your practice. Related observations include spontaneous movement during a physical examination; basic laboratory testing; and any relevant family history of genetic-based disease. These can go a long way to guide your diagnosis. Any abnormality in growth, feeding patterns, or respiration also provides important clinical clues.
Pediatricians, depending on their experience, can determine when a "wait and watch" approach is appropriate. For example, benign hypotonia is more likely when there are no major delays in growth or motor milestones, no signs of abnormal respiration, and parents report normal feeding patterns.
Since we cannot test the strength of a 7- or 8-month-old infant by asking them to offer resistance with their arms and legs, it’s useful to observe the amount and quality of their spontaneous movements. Watch their head control when you pull the infant to sit from a supine position. Does the head lag behind at all? How vigorously does the infant kick or grasp? These signs can help examiners compare impressions of degree of weakness, if there is any, in hypotonic infants.
Parents may be unaware of any low muscle tone, so it’s important to include hypotonia on your physical examination checklist.
Ask parents about the strength of the infant during diaper or clothing changes. Often parents have a good sense of the amount of force their child displays, and it can be reassuring to make these observations in the examination room as well.
An infant with a benign form of congenital hypotonia will move her arms and legs frequently: batting, roving, and sometimes synchronous movements come and go depending on level of alertness. In contrast, an infant with hypotonia caused by a neurologic disease, such as spinal muscle atrophy, will move much less frequently and the initiation of the movement(s) is slower.
In some cases, the degree or cause of hypotonia may not be clear, and the question becomes what to do with that uncertainty. A creatine phosphokinase (CPK) assay, the most common initial laboratory test to assess low muscle tone, can be helpful, although a normal result doesn’t rule out muscle or nerve disease.
In addition, check the baby’s respiratory rate and listen for any stridor or other signs of obstruction in her breathing. Noisy breathing can suggest upper respiratory muscle involvement, in which case further work-up is warranted. How’s the head growth over time?
Testing deep tendon reflexes can be tricky. While the presence of reflexes is reassuring, absence suggests a peripheral nerve problem or anterior horn cell disease.
Ask parents about the baby’s typical feeding pattern. An infant that seems to take a long time to feed and/or has an interrupted pattern of feeding should raise your clinical suspicion about an important neurologic cause for their hypotonia.
Family history can be an independent risk factor for a more serious, inherited neurologic etiology. Many of the causes of hypotonia are genetic, and specialist input will be appropriate if you uncover relevant family history. Inquire about any first-degree relative or others with an inherited neurologic condition that could underlie the infant’s hypotonia. In some cases, a non-neurologic inherited disease such as Marfan syndrome can cause hypotonia as well.
Specialist input is indicated if you suspect a genetic basis for the hypotonia, even if the infant passes the other important elements of your evaluation (for example, normal milestones, eating, and breathing).
These patients are a pretty diverse group, and there are many infants with hypotonia who will ultimately do well. If you are unsure, it’s definitely worth tracking these patients a little closer using history and physical examination checklists. Check in with a specialist if you continue to be unsure as you move forward.
Dr. Bingham is a pediatric neurologist at Fletcher Allen Health Care and associate professor of neurology at the University of Vermont in Burlington. Dr. Bingham said he had no relevant financial disclosures.
Severe Comorbidity Doubles Death Risk in Multiple Myeloma
PARIS – Elderly patients with multiple myeloma and severe comorbid disease are more than twice as likely to die as were those with no comorbidities, data from a single-center, retrospective study show.
Mild or moderate comorbidities did not appear to influence overall survival significantly in the 179-patient study. The hazard ratio (HR) for death in patients with severe comorbidity vs. none was 2.36 (P = .01), which was associated with a median overall survival of 15.1 months.
Median overall survival was 43.1 months for those with no comorbidities and 31.5 and 35 months, respectively, in those with mild (HR, 1.38; P = .26) or moderate (HR, 1.5; P = .19) comorbidities.
"The severity of comorbidities is associated with poorer survival in older adults with multiple myeloma," said lead author Dr. Tanya M. Wildes of Washington University in St. Louis.
Nevertheless, comorbidities are not currently incorporated into any staging systems for the disease, Dr. Wildes observed in an interview at the annual meeting of the International Society of Geriatric Oncology.
The research is part of a wider project that is looking at the value of performing a geriatric assessment to help predict which elderly patients with hematological malignancies may be able to undergo standard cancer treatment, or require additional monitoring for adverse events, or more supportive care.
"The severity of comorbidities is associated with poorer survival in older adults with multiple myeloma."
In the current study, Dr. Wildes and her colleagues identified all patients who were diagnosed and treated for multiple myeloma at Barnes-Jewish Hospital, St. Louis, between January 2000 and March 2010. Demographic, clinical, and survival data were obtained, with concomitant conditions graded using the Adult Comorbidity Evaluation (ACE) 27 index as none, mild, moderate, or severe.
The primary end point of the study was overall survival, the duration of which was calculated from the date of diagnosis until the time of last follow-up.
The median age of patients at baseline was 69 years (range, 65-91 years). There was a similar percentage of men (48.4%) and women (51.4%), and 75% of the population was white. Most of the remainder were black (23.5%).
According to the ACE-27 index, 41.3% of patients had mild, 24.6% had moderate, and 15.6% had severe comorbidities. The remaining 18.5% had no comorbidities.
"The challenge with multiple myeloma is that some of the comorbidities may be disease related as opposed to patient’s underlying comorbidities," Dr. Wildes noted. That would require reviewing the patients’ medical records, which was not done in the current evaluation of this data set but is something that the researchers plan on looking at next.
"These are hypothesis-generating data at the moment," Dr. Wildes said. Further study, to evaluate the impact of comorbidities on survival in multiple myeloma and their influence on patients’ tolerance of therapy and treatment decisions, is needed.
"On average, three comorbidities can be expected in a patient [aged] 65 years and older," said Dr. Lazzaro Repetto of the Istituto Nazionale di Riposo e Cura per Anziani at the Istituto di Ricovero e Cura a Carattere Scientifico in Rome.
Speaking at separate session during the meeting, Dr. Repetto said common comorbidities in elderly cancer patients included cardiovascular disease, renal insufficiency, diabetes, dementia, depression, anemia, osteoporosis, arthritis and arthrosis, and chronic obstructive pulmonary disease. All of these may have an impact on survival.
Indeed, other research presented by a Danish team showed that colorectal and lung cancers in particular were associated with a high number of comorbidities when compared with the general elderly population. A high comorbidity burden was also linked to reduced overall survival, but only in those with lung cancer, reported Dr. Trine Lembrecht Jørgensen of Odense (Denmark) University Hospital and associates.
The presence of comorbidities can alter treatment decisions, influencing the type of treatment offered, said Dr. Repetto. However, although assessing comorbid disease is important, it should always be part of a wider geriatric assessment, he advised. This should include measures of cognition, emotional and physical functioning, medication use, socioeconomic and social support factors, and the patient’s wishes.
"Using the geriatric assessment we can personalize treatment, and optimize the balance between benefit and risk of our decisions," Dr. Repetto suggested.
Dr. Wildes’ research was supported by a grant from the U.S. National Cancer Institute. Dr. Wildes and Dr. Repetto had no conflicts of interest.
PARIS – Elderly patients with multiple myeloma and severe comorbid disease are more than twice as likely to die as were those with no comorbidities, data from a single-center, retrospective study show.
Mild or moderate comorbidities did not appear to influence overall survival significantly in the 179-patient study. The hazard ratio (HR) for death in patients with severe comorbidity vs. none was 2.36 (P = .01), which was associated with a median overall survival of 15.1 months.
Median overall survival was 43.1 months for those with no comorbidities and 31.5 and 35 months, respectively, in those with mild (HR, 1.38; P = .26) or moderate (HR, 1.5; P = .19) comorbidities.
"The severity of comorbidities is associated with poorer survival in older adults with multiple myeloma," said lead author Dr. Tanya M. Wildes of Washington University in St. Louis.
Nevertheless, comorbidities are not currently incorporated into any staging systems for the disease, Dr. Wildes observed in an interview at the annual meeting of the International Society of Geriatric Oncology.
The research is part of a wider project that is looking at the value of performing a geriatric assessment to help predict which elderly patients with hematological malignancies may be able to undergo standard cancer treatment, or require additional monitoring for adverse events, or more supportive care.
"The severity of comorbidities is associated with poorer survival in older adults with multiple myeloma."
In the current study, Dr. Wildes and her colleagues identified all patients who were diagnosed and treated for multiple myeloma at Barnes-Jewish Hospital, St. Louis, between January 2000 and March 2010. Demographic, clinical, and survival data were obtained, with concomitant conditions graded using the Adult Comorbidity Evaluation (ACE) 27 index as none, mild, moderate, or severe.
The primary end point of the study was overall survival, the duration of which was calculated from the date of diagnosis until the time of last follow-up.
The median age of patients at baseline was 69 years (range, 65-91 years). There was a similar percentage of men (48.4%) and women (51.4%), and 75% of the population was white. Most of the remainder were black (23.5%).
According to the ACE-27 index, 41.3% of patients had mild, 24.6% had moderate, and 15.6% had severe comorbidities. The remaining 18.5% had no comorbidities.
"The challenge with multiple myeloma is that some of the comorbidities may be disease related as opposed to patient’s underlying comorbidities," Dr. Wildes noted. That would require reviewing the patients’ medical records, which was not done in the current evaluation of this data set but is something that the researchers plan on looking at next.
"These are hypothesis-generating data at the moment," Dr. Wildes said. Further study, to evaluate the impact of comorbidities on survival in multiple myeloma and their influence on patients’ tolerance of therapy and treatment decisions, is needed.
"On average, three comorbidities can be expected in a patient [aged] 65 years and older," said Dr. Lazzaro Repetto of the Istituto Nazionale di Riposo e Cura per Anziani at the Istituto di Ricovero e Cura a Carattere Scientifico in Rome.
Speaking at separate session during the meeting, Dr. Repetto said common comorbidities in elderly cancer patients included cardiovascular disease, renal insufficiency, diabetes, dementia, depression, anemia, osteoporosis, arthritis and arthrosis, and chronic obstructive pulmonary disease. All of these may have an impact on survival.
Indeed, other research presented by a Danish team showed that colorectal and lung cancers in particular were associated with a high number of comorbidities when compared with the general elderly population. A high comorbidity burden was also linked to reduced overall survival, but only in those with lung cancer, reported Dr. Trine Lembrecht Jørgensen of Odense (Denmark) University Hospital and associates.
The presence of comorbidities can alter treatment decisions, influencing the type of treatment offered, said Dr. Repetto. However, although assessing comorbid disease is important, it should always be part of a wider geriatric assessment, he advised. This should include measures of cognition, emotional and physical functioning, medication use, socioeconomic and social support factors, and the patient’s wishes.
"Using the geriatric assessment we can personalize treatment, and optimize the balance between benefit and risk of our decisions," Dr. Repetto suggested.
Dr. Wildes’ research was supported by a grant from the U.S. National Cancer Institute. Dr. Wildes and Dr. Repetto had no conflicts of interest.
PARIS – Elderly patients with multiple myeloma and severe comorbid disease are more than twice as likely to die as were those with no comorbidities, data from a single-center, retrospective study show.
Mild or moderate comorbidities did not appear to influence overall survival significantly in the 179-patient study. The hazard ratio (HR) for death in patients with severe comorbidity vs. none was 2.36 (P = .01), which was associated with a median overall survival of 15.1 months.
Median overall survival was 43.1 months for those with no comorbidities and 31.5 and 35 months, respectively, in those with mild (HR, 1.38; P = .26) or moderate (HR, 1.5; P = .19) comorbidities.
"The severity of comorbidities is associated with poorer survival in older adults with multiple myeloma," said lead author Dr. Tanya M. Wildes of Washington University in St. Louis.
Nevertheless, comorbidities are not currently incorporated into any staging systems for the disease, Dr. Wildes observed in an interview at the annual meeting of the International Society of Geriatric Oncology.
The research is part of a wider project that is looking at the value of performing a geriatric assessment to help predict which elderly patients with hematological malignancies may be able to undergo standard cancer treatment, or require additional monitoring for adverse events, or more supportive care.
"The severity of comorbidities is associated with poorer survival in older adults with multiple myeloma."
In the current study, Dr. Wildes and her colleagues identified all patients who were diagnosed and treated for multiple myeloma at Barnes-Jewish Hospital, St. Louis, between January 2000 and March 2010. Demographic, clinical, and survival data were obtained, with concomitant conditions graded using the Adult Comorbidity Evaluation (ACE) 27 index as none, mild, moderate, or severe.
The primary end point of the study was overall survival, the duration of which was calculated from the date of diagnosis until the time of last follow-up.
The median age of patients at baseline was 69 years (range, 65-91 years). There was a similar percentage of men (48.4%) and women (51.4%), and 75% of the population was white. Most of the remainder were black (23.5%).
According to the ACE-27 index, 41.3% of patients had mild, 24.6% had moderate, and 15.6% had severe comorbidities. The remaining 18.5% had no comorbidities.
"The challenge with multiple myeloma is that some of the comorbidities may be disease related as opposed to patient’s underlying comorbidities," Dr. Wildes noted. That would require reviewing the patients’ medical records, which was not done in the current evaluation of this data set but is something that the researchers plan on looking at next.
"These are hypothesis-generating data at the moment," Dr. Wildes said. Further study, to evaluate the impact of comorbidities on survival in multiple myeloma and their influence on patients’ tolerance of therapy and treatment decisions, is needed.
"On average, three comorbidities can be expected in a patient [aged] 65 years and older," said Dr. Lazzaro Repetto of the Istituto Nazionale di Riposo e Cura per Anziani at the Istituto di Ricovero e Cura a Carattere Scientifico in Rome.
Speaking at separate session during the meeting, Dr. Repetto said common comorbidities in elderly cancer patients included cardiovascular disease, renal insufficiency, diabetes, dementia, depression, anemia, osteoporosis, arthritis and arthrosis, and chronic obstructive pulmonary disease. All of these may have an impact on survival.
Indeed, other research presented by a Danish team showed that colorectal and lung cancers in particular were associated with a high number of comorbidities when compared with the general elderly population. A high comorbidity burden was also linked to reduced overall survival, but only in those with lung cancer, reported Dr. Trine Lembrecht Jørgensen of Odense (Denmark) University Hospital and associates.
The presence of comorbidities can alter treatment decisions, influencing the type of treatment offered, said Dr. Repetto. However, although assessing comorbid disease is important, it should always be part of a wider geriatric assessment, he advised. This should include measures of cognition, emotional and physical functioning, medication use, socioeconomic and social support factors, and the patient’s wishes.
"Using the geriatric assessment we can personalize treatment, and optimize the balance between benefit and risk of our decisions," Dr. Repetto suggested.
Dr. Wildes’ research was supported by a grant from the U.S. National Cancer Institute. Dr. Wildes and Dr. Repetto had no conflicts of interest.
FROM THE ANNUAL MEETING OF THE INTERNATIONAL SOCIETY OF GERIATRIC ONCOLOGY
Major Finding: Median overall survival in patients with severe comorbidity was 15.1 months vs. 43.1 months in patients with no comorbidity (hazard ratio for death, 2.36; P less than .01).
Data Source: Retrospective, single center study of 179 patients with multiple myeloma aged 65 years or older.
Disclosures: Dr. Wildes’ research was supported by a grant from the US National Cancer Institute. Neither Dr. Wildes nor Dr. Repetto reported any conflicts of interest.
Online Exclusive: TK
Enter text here
Enter text here
Enter text here
Dabigatran Etexilate
Vitamin K antagonists (VKAs) such as warfarin have been the backbone of oral anticoagulation in clinical practice since the middle of the last century. Despite their efficacy, VKAs have well‐recognized limitations that have led to their underutilization in patients who would otherwise be candidates for oral anticoagulation.14 These limitations include a narrow therapeutic window and significant intra‐ and interindividual variability in dose requirements as well as numerous drugdrug and drugfood interactions.59 Therefore, VKAs require close laboratory monitoring to prevent excessive or under‐anticoagulation, and maintaining therapeutic anticoagulation with VKAs remains a challenging task in many patients.2 It has been shown that 30%50% of international normalized ratio (INR) results fall outside of the targeted therapeutic range.10, 11 Consequently, it is not surprising that warfarin is a common cause of medication‐related emergency room visits.12 Despite many fruitless years of searching for better alternatives, VKAs have remained the mainstay of oral anticoagulation for more than 60 years.8
An ideal anticoagulant would be orally administered, effective, safe, exhibit a predictable pharmacokinetic profile and a low potential for drug or dietary interactions, and therefore would not require routine laboratory monitoring.2, 5, 13 Other desirable characteristics would include a rapid onset of action to decrease or eliminate the need for bridging therapy, and rapid reversibility with or without an antidote.8, 13 To date, no oral anticoagulant has been developed that possesses all of these desired characteristics. Dabigatran etexilate (Pradaxa, Boehringer Ingelheim Pharmaceuticals, Inc.) has recently become the first oral anticoagulant to be available for wide clinical use since the 1950s.14 In the following sections, we provide an overview of dabigatran etexilate, with a special focus on issues that are pertinent to hospitalists and the hospitalized patient.
PHARMACOLOGY OF DABIGATRAN ETEXILATE
Pharmacokinetics and Pharmacodynamics of Dabigatran Etexilate
A comparison of the pharmacokinetic (PK) and pharmacodynamic (PD) properties of dabigatran etexilate (dabigatran) and warfarin are presented in Table 1. Dabigatran etexilate (referred to from this point as dabigatran) is a prodrug of dabigatran, which blocks the terminal coagulation cascade by binding to the active site of thrombin and selectively inhibiting this critical serine protease in a dose‐dependent and reversible fashion.15 Thrombin plays a central role in blood coagulation by converting fibrinogen to fibrin, amplifying its own generation by feedback activation of factors V, VIII, and XI, and by activating platelets (Figure 1).16 Dabigatran is a direct thrombin inhibitor that acts independently of anti‐thrombin to inhibit both free and clot‐bound thrombin.17, 18 The bioavailability of dabigatran after oral intake is low (6%7%).1923 After absorption, the prodrug is rapidly converted by plasma and hepatic esterases to the active drug dabigatran, but it is not metabolized by the CYP‐450 system, therefore reducing the potential for drugdrug interactions.8, 2328 The long half‐life of dabigatran allows for once or twice daily dosing.21, 24 The PK profile of dabigatran is predictable, with minimal inter‐ and intraindividual variation.21, 22
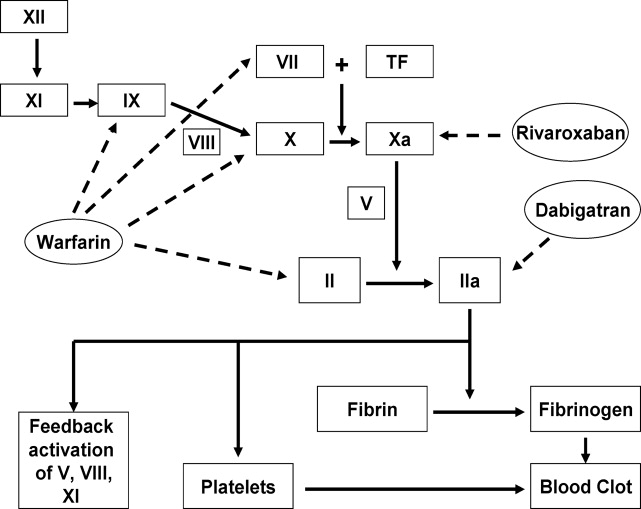
| Warfarin | Dabigatran | |
|---|---|---|
| Mechanism of action | Reduces functional levels of vitamin Kdependent factors II, VII, IX, and X by inhibiting vitamin K epoxide reductase | Binds to active site of thrombin (factor IIa) and reversibly inhibits free and clot‐bound thrombin |
| Prodrug | No | Yes |
| Bioavailability | >90%95% | 6%7% |
| Protein binding | 99% | 35% |
| Time to reach peak plasma levels | 7296 hr | 23 hr |
| Half‐life | 3644 hr | 1217 hr |
| Routine coagulation monitoring | Required, but frequency varies based on clinical situation | No requirement for routine monitoring |
| Schedule | INR‐adjusted, usually once daily | Fixed dose, once or twice daily |
| Metabolism | CYP‐450 hepatic microsomal enzymes, especially CYP2C9, CYP1A2, and CYP3A4 | Esterase‐catalyzed hydrolysis in plasma or liver after intestinal P‐gp transport |
| Clearance | Almost entirely hepatic | 80% unchanged renally (after an intravenous dose), 20% hepatic after conjugation |
| Drug interactions | Drugs that affect CYP‐450 hepatic microsomal enzymes and those that displace warfarin from plasma proteins | P‐gp inhibitors (CYP‐450 system not involved) |
| Antidote | Yes (vitamin K and plasma products) | No |
Dabigatran is packaged in capsules that are hygroscopic. Therefore, the capsules should be stored in the original container with the cap tightly closed. Exposure of dabigatran capsules to air for prolonged periods outside the original container can result in deterioration of the active compound and reduced efficacy.27, 28 Dabigatran capsules contain tartaric acid which is necessary to facilitate dissolution of the medication in the gastrointestinal tract for optimal absorption.2 Breaking the capsules or removing the drug from the capsule can result in increased exposure. Therefore, dabigatran capsules should be taken intact, and patients should be instructed that dabigatran capsules should not be broken, chewed, or opened before administration.28 Alternative anticoagulants should be used if patients cannot swallow the capsule intact for any reason (eg, intubated patients).
Dabigatran and Drug and Food Interactions
Dabigatran acts as a substrate of the transporter protein P‐glycoprotein (P‐gp), which is also involved in the transport of many other drugs.5, 16 P‐gp is an efflux pump that functions to prevent the absorption of drugs in the intestine or increase the renal excretion of drugs that are P‐gp substrates.25 Inhibitors of P‐gp increase the serum concentrations of P‐gp substrates, whereas P‐gp inducers reduce the concentrations of these medications.13 Examples of P‐gp inhibitors include clarithromycin, quinidine, and verapamil, whereas rifampin, pantoprazole, and St John's wort are known to induce P‐gp.5, 24, 26 As an illustration, the coadministration of dabigatran and amiodarone, a known P‐gp inhibitor, increases the area under the curve of drug plasmaconcentrationtime of dabigatran by 60% without significantly affecting levels of amiodarone.5, 27 Nevertheless, dagibatran's prescribing information in the United States advises that the P‐gp inhibitors ketoconazole, verapamil, amiodarone, quinidine, and clarithromycin do not require dose adjustments, although these results should not be extrapolated to other P‐gp inhibitors.28 In addition, the manufacturer recommends generally avoiding the concomitant use of the potent P‐gp inducer rifampin with dabigatran, whereas the European Medicines Agency advises caution in the coadministration of rifampin or St John's wort with dabigatran.27, 28
Not all P‐gp substrates result in clinically significant interactions with dabigatran (eg, digoxin, diclofenac, and atorvastatin).19, 29 The use of nonsteroidal anti‐inflammatory drugs and aspirin may increase the risk of bleeding in patients using dabigatran.5, 26, 27 It is not recommended to coadminister certain anti‐platelet agents (such as clopidogrel, prasugrel, or ticlopidine) with dabigatran.26, 30 Although the use of proton pump inhibitors such as pantoprazole leads to a 30% decrease in the area under the curve of dabigatran, coadministration of pantoprazole and other proton pump inhibitors with dabigatran in clinical trials did not affect bleeding risk or efficacy.27 Attention to potential drug interactions with dabigatran is important, because dabigatran is not usually monitored. Food interactions with dabigatran appear to be low, and therefore dabigatran can probably be taken with or without food, but caution is advised given the limited postmarketing experience with dabigatran.30 An excellent review of drug and dietary interactions of dabigatran has been published recently.5
Use of Dabigatran in Patients With Liver or Renal Impairment
Approximately 80% of dabigatran is excreted, largely unchanged, by the kidneys in healthy subjects.19 Patients with severe renal impairment (creatinine clearance [CrCL], 30 mL/min) were excluded from phase 3 trials that evaluated dabigatran.3135 A small study in patients with renal impairment showed a linear correlation between renal function and renal clearance of dabigatran, with proportional increases in the anticoagulant effects of dabigatran with decreasing renal function.36 For patients on hemodialysis, 62%68% of the dose was removed.36 The authors recommended avoidance of dabigatran in severe renal impairment, and a dose reduction was recommended for moderate renal impairment (CrCL, 3150 mL/min).13, 36 Despite exclusion of patients with CrCL of 30 mL/min from all phase 3 trials of dabigatran and the relative contraindication of the use of dabigatran in this patient population, the US Food and Drug Administration (FDA) approved a reduced dose of 75 mg twice daily for patients with CrCL of 1530 mL/min, but no dosing recommendations were made for patients with CrCL of 15 mL/min or for patients on dialysis.13, 28, 36 We believe that dabigatran should be used with great caution in patients with CrCl 1530 mL/min given the limited outcome data in these patients, and alternative anticoagulants should be strongly considered for these patients until more data are available.
Less than 20% of the dabigatran dose is conjugated in the liver and subsequently secreted in the biliary system.19, 23 Stangier et al. showed that moderate hepatic impairment does not affect the PK/PD or safety profile of dabigatran and concluded that dabigatran can be given to those patients without dose adjustment.37 On the other hand, severe hepatic impairment (Child‐Pugh class B or C cirrhosis) and an alanine aminotransferase level more than 2 to 3 times the upper limit of normal were used as exclusion criteria in most of the phase 3 trials that evaluated dabigatran.16, 24, 34, 35, 38 The hepatic toxicity noted with the first generation oral direct thrombin inhibitor, ximelagatran, has not been seen with dabigatran in clinical trials, although long‐term postmarketing data are lacking.32, 34, 35, 3840
The Effect of Dabigatran on Common Coagulation Laboratory Tests and Recommendations for Monitoring Dabigatran's Anticoagulant Effects
Despite the predictable PK profile of dabigatran, its effects on common coagulation assays remain incompletely defined.41 Most patients on dabigatran will have a prolonged activated partial thromboplastin time (aPTT) even at trough concentrations, but not in a linear predictable fashion.19, 20, 21, 36, 41 Dabigatran has few and unpredictable effects on prothrombin time (PT) and INR, and therapeutic concentrations of dabigatran usually result in only modest elevations of PT/INR.21, 42 Although thrombin time (TT) displays a good linear correlation with plasma concentrations of dabigatran, the reagents used to perform TT in most clinical laboratories are not standardized. Therefore, TT is better suited to detecting the presence of dabigatran rather than monitoring its anticoagulant effects.24, 42 Therefore, even a slightly prolonged aPTT or TT could reflect significant plasma dabigatran levels. The best assays for monitoring dabigatran are the ecarin clotting time (ECT), modified thrombelastographic evaluations of whole blood clot formation, and the Hemoclot Thrombin Inhibitor assay, but these tests are limited by lack of standardization and limited clinical availablity.24, 42, 43
EFFICACY OF DABIGATRAN
In this section, we provide a brief review of the major phase 3 trials that evaluated dabigatran for different indications (see references 13, 16, and 24 for recent detailed reviews of the clinical trials of dabigatran).
Dabigatran for Thromboprophylaxis in Patients with Atrial Fibrillation
The Randomized Evaluation of Long‐Term Anticoagulation Therapy (RE‐LY) trial was a prospective, noninferiority, phase 3 study of dabigatran that was the basis for its FDA approval in patients with nonvalvular AF.35, 44 In RE‐LY, 18,113 AF patients with another thromboembolic risk factor were randomized to receive fixed doses of dabigatran (110 mg or 150 mg twice daily) or adjusted‐dose warfarin.35 The median duration of follow‐up was 2 years and the primary outcome was stroke or systemic embolism. The primary outcome occurred in 1.69% per year in the warfarin group versus 1.53% per year in the group receiving 110 mg of dabigatran twice daily (relative risk with dabigatran, 0.91; 95% confidence interval [CI], 0.741.11; P 0.001 for noninferiority) and 1.11% per year in the group receiving 150 mg of dabigatran twice daily (relative risk, 0.66; 95% CI, 0.530.82; P 0.001 for superiority). The rate of major bleeding was 3.36% per year in the warfarin group versus 2.71% per year in the dabigatran 110 mg group (P = 0.003) and 3.11% per year in the dabigatran 150 mg group (P = 0.31). Intracranial bleeds were significantly less common in both dabigatran groups than with warfarin. Major gastrointestinal bleeding rate was significantly higher in the dabigatran group at the 150‐mg dose than in the warfarin group. The mortality rate was 4.13% per year in the warfarin group versus 3.75% per year with 110 mg of dabigatran (P = 0.13) and 3.64% per year with 150 mg of dabigatran (P = 0.051).35 The authors concluded that in patients with nonvalvular AF, dabigatran given at a dose of 110 mg twice daily was not inferior to warfarin, and was associated with lower rates of major hemorrhage than warfarin.35 Dabigatran given at a dose of 150 mg twice daily was associated with lower rates of stroke and systemic embolism than warfarin but had similar rates of major hemorrhage.35 These effects were maintained in patients with previous stroke or transient ischemic attack, and in these patients starting dabigatran with and without prior VKA treatment.45, 46
Dabigatran for Prevention of Venous Thromboembolism After Major Orthopedic Procedures
Without thromboprophylaxis, the incidence of venous thromboembolism (VTE) following major orthopedic surgery is 40%60%.47 Nevertheless, many patients do not receive appropriate thromboprophylaxis after orthopedic surgery, in part due to the limitations of VKAs and the inconvenience of low molecular weight heparin (LMWH) injections.48
RE‐NOVATE Trial
Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE‐NOVATE trail) was a prospective, noninferiority phase 3 trial in which 3494 patients undergoing total hip replacement (THR) were randomized in double‐blind fashion to 2835 days of dabigatran 220 mg or 150 mg once daily, starting with a half‐dose 14 hours after surgery, or subcutaneous (SC) enoxaparin 40 mg once daily, starting the evening before surgery.33 The primary efficacy outcome was the composite of total VTE (venographic or symptomatic) and death from all causes during treatment. The primary efficacy outcome occurred in 6.7% in the enoxaparin group versus 6.0% in the dabigatran 220 mg group (absolute difference [AD], 0.7%; 95% CI, 2.9% to 1.6%) and 8.6% in the 150 mg group (AD, 1.9%; 95% CI, 0.6% to 4.4%). There was no significant difference in major bleeding with either dose of dabigatran compared with enoxaparin (220 mg, P = 0.44; 150 mg, P = 0.60). It was concluded that oral dabigatran was not inferior to enoxaparin for prevention of VTE after THR surgery, with a similar safety profile.33
RE‐NOVATE II Trial
Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE‐NOVATE II trail) was a randomized, double‐blind, noninferiority phase 3 trial that compared dabigatran versus SC enoxaparin for extended thromboprophylaxis in patients undergoing THR.38 A total of 2055 patients were randomized to 2835 days of oral dabigatran, 220 mg once daily, starting with a half‐dose 14 hours after surgery, or SC enoxaparin 40 mg once daily, starting the evening before surgery. The primary efficacy outcome was the same as that in the RE‐NOVATE trial. The primary efficacy outcome occurred in 7.7% of the dabigatran group versus 8.8% of the enoxaparin group (risk difference, 1.1%; 95% CI, 3.8 to 1.6%; P 0.0001 for the prespecified noninferiority margin. Major VTE plus VTE‐related death occurred in 2.2% of the dabigatran group versus 4.2% of the enoxaparin group (risk difference, 1.9%; 95% CI, 3.6% to 0.2%; P = 0.03). Major bleeding occurred in 1.4% of the dabigatran group and 0.9% of the enoxaparin group (P = 0.40). It was concluded that extended prophylaxis with oral dabigatran 220 mg once daily was not inferior to SC enoxaparin 40 mg once daily for prevention of VTE after THR. The safety profiles were similar between the 2 arms.38
RE‐MODEL Trial
In the Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromblembloism after total knee replacement (RE‐MODEL trail) phase 3 trial, 2076 patients who underwent total knee replacement (TKR) were randomized to receive dabigatran 150 mg or 220 mg once daily starting with a half‐dose 14 hours after surgery, or SC enoxaparin 40 mg once daily starting the evening before surgery, for 610 days.32 Patients were followed‐up for 3 months. The primary efficacy outcome was a composite of total VTE (venographic or symptomatic) and mortality during treatment. The primary efficacy outcome occurred in 37.7% of the enoxaparin group versus 36.4% of the dabigatran 220 mg group (AD, 1.3%; 95% CI, 7.3 to 4.6) and 40.5% of the 150 mg group (AD, 2.8%; 95% CI, 3.1 to 8.7). The incidence of major bleeding did not differ between the groups (1.3% versus 1.5% and 1.3%, respectively). The conclusion was that dabigatran (220 mg or 150 mg) was not inferior to enoxaparin for prevention of VTE after TKR surgery and exhibited a similar safety profile.32
RE‐MOBILZE Trial
The oral thrombin inhibitor dabigatran etexilate vs the North American enoxaparin regimen for the prevention of venous thromboembolism after knee arthroplasty surgery (RE‐MOBILIZE trail) was a phase 3 trial that randomized 1896 patients after unilateral TKR to receive dabigatran 220 or 150 mg once daily versus enoxaparin 30 mg SC twice daily after surgery.40 Dosing stopped at contrast venography, 1215 days after surgery. Follow‐up was for 3 months. The primary outcome was a composite of total VTE events and all‐cause mortality during treatment. With respect to the primary outcome, dabigatran at 220 and 150 mg showed inferior efficacy to enoxaparin, with VTE rates of 31% (P = 0.02 vs enoxaparin), 34% (P 0.001 vs enoxaparin), and 25%, respectively. Major bleeding was similar. It was concluded that dabigatran was inferior to the twice‐daily North American enoxaparin regimen, probably because of the latter's more intense and prolonged dosing.40 It should be noted that the first dose of dabigatran in this study was given 612 hours after surgery, compared with 14 hours postoperatively in RE‐MODEL, which may have contributed to the inferior outcome.32, 40
Dabigatran for Treatment of Acute VTE
RE‐COVER was a large, randomized, noninferiority phase 3 trial that randomized 2564 patients with acute symptomatic proximal lower extremity deep vein thrombosis or pulmonary embolism to 6 months of dabigatran 150 mg twice daily or dose‐adjusted warfarin (INR 2/3).34 All patients initially received parenteral anticoagulation (LMWH or unfractionated heparin [UFH]) for a median of 9 days. Patients in the warfarin group spent 60% of the time in the therapeutic range. In the dabigatran arm, 2.4% had recurrent VTE versus 2.1% in the warfarin arm (P 0.001 for the prespecified noninferiority margin). Major bleeding occurred in 1.6% of patients in the dabigatran arm and 1.9% in the warfarin arm (hazards ratio, 0.82; 95% CI, 0.451.48). There was no difference in the other safety endpoints (acute coronary syndrome, abnormal liver function tests and deaths). Adverse events (especially gastrointestinal) leading to discontinuation of the study drug occurred in 9% of patients assigned to dabigatran and 6.8% of patients assigned to warfarin (P = 0.05). It was concluded that a fixed dose of dabigatran was not inferior to warfarin for treatment of VTE, with a similar safety profile.34 It is important to note that the first dose of dabigatran was given after a median of 9 days of parenteral anticoagulation therapy, so the findings of this study do not provide data regarding the use of dabigatran as initial monotherapy for acute VTE.34 The results of additional randomized trials evaluating the use of dabigatran for acute VTE treatment (RE‐COVER II) and secondary prevention of VTE (RE‐MEDY and RE‐SONATE) are expected soon.16
SAFETY OF DABIGATRAN
Aside from the bleeding risks discussed earlier, the most commonly reported side effect of dabigatran was dyspepsia. Dyspepsia occurred twice as frequently in patients taking dabigatran versus warfarin in the RE‐LY trial (11.5% vs 5.8%).35 One possible explanation for the higher incidence of dyspepsia is the tartaric acid component in dabigatran capsules.2 In the RE‐LY study, myocardial infarction occurred more commonly in the dabigatran arms (0.72% with 110 mg and 0.74% with 150 mg) than the warfarin arm (0.53%, P = 0.07 and 0.048, respectively).24, 35 It has been postulated that this observation could be related to a greater efficacy of warfarin for the prevention of myocardial infarction rather than an adverse effect of dabigatran.2 There was no increase in acute coronary syndrome rates noted with dabigatran in the other phase 3 trials.3234, 38, 40 No increased risk of elevated liver function test has been noted with dabigatran, but long‐term data are unavailable.32, 34, 35, 38
MANAGEMENT OF SPECIAL SITUATIONS THAT MAY ARISE IN THE USE OF DABIGATRAN
Switching From Warfarin to Dabigatran and Vice Versa
When converting patients from warfarin to dabigatran, it is recommended that dabigatran be started once the INR falls below the lower limit of the desired therapeutic range. Conversely, when switching from dabigatran to warfarin, the manufacturer recommends starting warfarin based on renal function (Table 2). It should be noted that because dabigatran can increase the INR, the INR will better reflect warfarin's effect after dabigatran has been stopped for at least 2 days.27, 28
| CrCL (mL/min) | Time of Warfarin Initiation |
|---|---|
| |
| 50 | 3 d before discontinuing dabigatran |
| 3150 | 2 d before discontinuing dabigatran |
| 1530 | 1 d before discontinuing dabigatran |
| 15 | No recommendations made |
Bridging from Dabigatran to Parenteral Anticoagulants and Vice Versa
For patients currently receiving a parenteral anticoagulant, the manufacturer recommends starting dabigatran 02 hours before the next administration time for parenteral anticoagulants (eg, LMWH) or at the time of discontinuation for continuously infused parenteral drugs (eg, intravenous UFH).28 For patients currently taking dabigatran who are transitioning to a parenteral anticoagulant, it is recommended to wait 12 hours (CrCl 30 mL/min) or 24 hours (CrCl 30 mL/min) after the last dose of dabigatran before initiating treatment with a parenteral anticoagulant.27, 28
Management of Dabigatran Before Elective and Urgent Invasive Procedures
Patients who undergo invasive procedures in the presence of therapeutic levels of dabigatran are at an increased risk of bleeding. The manufacturer recommends holding dabigatran for at least 24 hours before elective surgery depending on the degree of renal impairment and the risk of bleeding.28 Table 3 lists recommendations on the timing of discontinuation of dabigatran before a procedure. If emergent/urgent surgery is necessary for a patient who is on dabigatran, the risk of bleeding should be weighed against the urgency of the intervention.28, 42, 44 As mentioned earlier, the ECT or the Hemoclot Thrombin Inhibitor assay are the preferred tests for measurement of dabigatran effects, but they are not standardized or widely clinically available. Instead, prolongation of the TT (preferably) or the aPTT can be used to determine the presence of dabigatran.28, 42
| CrCL (mL/min) | Half‐Life (hr) | Suggested Timing of Discontinuation of Dabigatran Before Surgery | |
|---|---|---|---|
| Standard Risk of Bleeding | High Risk of Bleeding* | ||
| |||
| >80 | 13 (11‐22) | 24 hr | 24 d |
| 5180 | 15 (12‐34) | 24 hr | 24 d |
| 3150 | 18 (13‐23) | 48 hr | 4 d |
| 30 | 27 (22‐35) | 25 d | >5 d |
Overdose and Toxicity With Dabigatran
Accidental or intentional overdose, or accumulation of dabigatran due to renal impairment, may lead to hemorrhagic complications. Unlike warfarin and heparin, there is no antidote for dabigatran. There are no widely available, reliable laboratory tests to measure the anticoagulant activity of dabigatran, and evidence‐based guidelines to manage dabigatran toxicity do not exist. Therefore, in the event of dabigatran toxicity, treatment is largely supportive. Management of toxicity is dependent on whether the overdose/accumulation is accompanied by bleeding or not. For overdose, interventions include adequate diuresis and the use of activated charcoal to reduce the absorption of dabigatran (within 2 hours of ingestion).42 In the event of bleeding, proposed measures include application of mechanical pressure to the sites of bleeding and infusion of pro‐coagulant blood products such as activated prothrombin complex concentrates (eg, FEIBA VH, Baxter) or recombinant human activated factor VIIa (NovoSeven, Novo‐Nordisk) (reviewed in references 26 and 42). In life‐threatening situations, hemodialysis could be considered, because it can remove 60% of the drug within 23 hours.42 Hemoperfusion over a charcoal filter or large volume hemofiltration have also been suggested in extreme situations.27, 28, 36, 42 Acknowledging their limitations, the ECT, TT, or aPTT may be used to direct therapy.27, 42
Pregnancy and Dabigatran Therapy
Dabigatran is a class C drug during pregnancy, and there are no studies of dabigatran in pregnant women. Animal studies with dabigatran showed decreased fertility of pregnant rats; therefore, the risks and benefits of dabigatran therapy during pregnancy should be weighed carefully.27, 28, 44
CONCLUSIONS
Dabigatran is a novel, oral direct thrombin inhibitor that exhibits several advantages over warfarin. The predictable pharmacokinetic profile and minimal food and drug interactions of dabigatran allow for a fixed‐dosing regimen and obviate the need for routine laboratory monitoring. However, this apparent advantage is also a disadvantage. The lack of a reliable method to monitor dabigatran makes it more difficult to assess compliance, measure the impact of drug interactions, evaluate for toxicity, and determine bona fide therapeutic failure versus noncompliance in the event of breakthrough thromboembolism.28, 42 Other limitations of dabigatran include the lack of an antidote and the dependence on normal renal function for elimination, with the potential for drug accumulation and toxicity with renal impairment. The noninferiority design of the clinical trials that evaluated dabigatran, the absence of long‐term safety and efficacy data, and issues related to the cost effectiveness of dabigatran should be considered when prescribing this agent. More studies are needed to assess dabigatran in special patient populations (eg, the elderly, patients with renal and hepatic impairment, pediatric and pregnant patients) and to better understand dabigatrandrug interactions.
As more novel oral anticoagulant agents, such as factor Xa inhibitors, become available for clinical use, comparative studies will need to be performed to better define the role of each agent for specific indications. In the future, it might be possible to tailor the choice of the oral anticoagulant to the individual patient not only on the basis of the clinical indication but also the specific patient characteristics and possible drug interactions. For example, rivaroxaban (Xarelto) is an oral direct factor Xa that was recently approved in the United States for VTE thromboprophylaxis following orthopedic surgery and in patients with non‐valvular atrial fibrillation.2 Similar to dabigatran, rivaroxaban exhibits predictable PK and PD that allow fixed once or twice daily dosing and obviate the need for routine monitoring of its anticoagulant effects.2, 16 Unlike dabigatran, rivaroxaban is an active drug and not a prodrug, and has a significantly higher bioavailability than dabigatran (>80% vs 6%).16 In addition, the levels of rivaroxaban can be affected by drugs that interfere with both P‐gp and the hepatic CYP‐450 system, compared with dabigatran, which is affected only by drugs that affect P‐gp.8, 16
- ,,, et al.The use of antithrombotic therapies in the prevention and treatment of arterial and venous thrombosis: a survey of current knowledge and practice supporting the need for clinical education.Crit Pathw Cardiol.2010;9:41–48.
- .Warfarin versus new agents: interpreting the data.Hematology Am Soc Hematol Educ Program.2010;2010:221–228.
- ,,,,.Why do patients with atrial fibrillation not receive warfarin?Arch Intern Med.2000;160:41–46.
- ,,,,,.Warfarin use among ambulatory patients with nonvalvular atrial fibrillation: The anticoagulation and risk factors in atrial fibrillation (ATRIA) study.Ann Intern Med.1999;131:927–934.
- ,.Drug and dietary interactions of the new and emerging oral anticoagulants.Int J Clin Pract.2010;64:956–967.
- ,,, et al.The risk of bleeding complications in patients with cytochrome P450 CYP2C9*2 or CYP2C9*3 alleles on acenocoumarol or phenprocoumon.Thromb Haemost.2004;92:61–66.
- ,,, et al.Differentiating low‐molecular‐weight heparins based on chemical, biological, and pharmacologic properties: implications for the development of generic versions of low‐molecular‐weight heparins.Semin Thromb Hemost.2008;34:74–85.
- ,.Emerging anticoagulants.Expert Opin Emerg Drugs.2011;16:31–44.
- ,,, et al.Systematic overview of warfarin and its drug and food interactions.Arch Intern Med.2005;165:1095–1106.
- ,,,,,.Evaluation of the pattern of treatment, level of anticoagulation control, and outcome of treatment with warfarin in patients with non‐valvar atrial fibrillation: a record linkage study in a large british population.Heart.2005;91:472–477.
- ,,, et al.Comparison of outcomes among patients randomized to warfarin therapy according to anticoagulant control: results from SPORTIF III and V.Arch Intern Med.2007;167:239–245.
- ,,,.Medication use leading to emergency department visits for adverse drug events in older adults.Ann Intern Med.2007;147:755–765.
- .New oral anticoagulants: a practical guide for clinicians.J Thromb Thrombolysis.2010;29:182–191.
- ,,,.The quest for new anticoagulants: from clinical development to clinical practice [published ahead of print June 14, 2010].Cardiovasc Ther.2010. doi: 10.1111/j.1755–5922.2010.00160.x.
- ,,,,.In‐vitro profile and ex‐vivo anticoagulant activity of the direct thrombin inhibitor dabigatran and its orally active prodrug, dabigatran etexilate.Thromb Haemost.2007;98:155–162.
- ,,.Novel oral factor xa and thrombin inhibitors in the management of thromboembolism.Annu Rev Med.2011;62:41–57.
- ,,,,.Clot‐bound thrombin is protected from inhibition by heparin‐antithrombin III but is susceptible to inactivation by antithrombin III‐independent inhibitors.J Clin Invest.1990;86:385–391.
- ,,.Thrombin binds to soluble fibrin degradation products where it is protected from inhibition by heparin‐antithrombin but susceptible to inactivation by antithrombin‐independent inhibitors.Circulation.1998;97:544–552.
- .Clinical pharmacokinetics and pharmacodynamics of the oral direct thrombin inhibitor dabigatran etexilate.Clin Pharmacokinet.2008;47:285–295.
- ,.Pharmacology, pharmacokinetics, and pharmacodynamics of dabigatran etexilate, an oral direct thrombin inhibitor.Clin Appl Thromb Hemost.2009;15(suppl 1):9S–16S.
- ,,,,.The pharmacokinetics, pharmacodynamics and tolerability of dabigatran etexilate, a new oral direct thrombin inhibitor, in healthy male subjects.Br J Clin Pharmacol.2007;64:292–303.
- ,,,.Pharmacokinetics and pharmacodynamics of the direct oral thrombin inhibitor dabigatran in healthy elderly subjects.Clin Pharmacokinet.2008;47:47–59.
- ,,,,.The metabolism and disposition of the oral direct thrombin inhibitor, dabigatran, in humans.Drug Metab Dispos.2008;36:386–399.
- ,,.Dabigatran etexilate versus warfarin as the oral anticoagulant of choice? A review of clinical data.Pharmacol Ther.2011;129:185–194.
- .The role of P‐glycoprotein and organic anion‐transporting polypeptides in drug interactions.Drug Saf.2005;28:789–801.
- ,,.Novel oral anticoagulants: implications in the perioperative setting.Anesthesiology.2010;113:726–745.
- European Medicines Agency. Pradaxa (dabigatran etexilate) [product information]. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_‐_Product_Information/human/000829/WC 500041059.pdf. Accessed March 25,2011.
- Dabigatran medication guide. Available at: http://bidocs.boehringer‐ingelheim.com/BIWebAccess/ViewServlet.ser?docBase = renetnt9:59–68.
- ,,.Novel oral anticoagulants: the potential relegation of vitamin K antagonists in clinical practice.Int J Clin Pract.2010;64:835–838.
- .The RE‐LY study: Randomized Evaluation of Long‐term anticoagulant therapY: dabigatran vs. warfarin.Eur Heart J.2009;30:2554–2555.
- ,,, et al.Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: the RE‐MODEL randomized trial.J Thromb Haemost.2007;5:2178–2185.
- ,,, et al.Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: a randomised, double‐blind, non‐inferiority trial.Lancet.2007;370:949–956.
- ,,, et al.Dabigatran versus warfarin in the treatment of acute venous thromboembolism.N Engl J Med.2009;361:2342–2352.
- ,,, et al.Dabigatran versus warfarin in patients with atrial fibrillation.N Engl J Med.2009;361:1139–1151.
- ,,,.Influence of renal impairment on the pharmacokinetics and pharmacodynamics of oral dabigatran etexilate: an open‐label, parallel‐group, single‐centre study.Clin Pharmacokinet.2010;49:259–268.
- ,,,,.Pharmacokinetics and pharmacodynamics of dabigatran etexilate, an oral direct thrombin inhibitor, are not affected by moderate hepatic impairment.J Clin Pharmacol.2008;48:1411–1419.
- ,,, et al.Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE‐NOVATE II). A randomised, double‐blind, non‐inferiority trial.Thromb Haemost.2011;105:721–729.
- ,.Insights from the dabigatran versus warfarin trial in patients with venous thromboembolism (the RE‐COVER trial).Expert Opin Pharmacother.2010;11:1035–1037.
- RE‐MOBILIZE Writing Committee,,, et al.Oral thrombin inhibitor dabigatran etexilate vs north american enoxaparin regimen for prevention of venous thromboembolism after knee arthroplasty surgery.J Arthroplasty.2009;24:1–9.
- ,,, et al.Effects of the oral, direct thrombin inhibitor dabigatran on five common coagulation assays.Thromb Haemost.2011;105:371–378.
- ,,, et al.Dabigatran etexilate—a novel, reversible, oral direct thrombin inhibitor: interpretation of coagulation assays and reversal of anticoagulant activity.Thromb Haemost.2010;103:1116–1127.
- ,.A direct thrombin inhibitor studied by dynamic whole blood clot formation. haemostatic response to ex‐vivo addition of recombinant factor VIIa or activated prothrombin complex concentrate.Thromb Haemost.2006;96:446–453.
- US Food and Drug Administration. Dabigatran drug approval history. Available at: http://www.accessdata.fda.gov/drugsatfda_ docs/nda/2010/022512Orig1s000TOC.cfm. Accessed March 20,2011.
- ,,, et al.Dabigatran compared with warfarin in patients with atrial fibrillation and previous transient ischaemic attack or stroke: a subgroup analysis of the RE‐LY trial.Lancet Neurol.2010;9:1157–1163.
- ,,, et al.Dabigatran and warfarin in vitamin K antagonist‐naive and ‐experienced cohorts with atrial fibrillation.Circulation.2010;122:2246–2253.
- ,,, et al.Prevention of venous thromboembolism: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th edition).Chest.2008;133(6 suppl):381S–453S.
- ,,,.American Association of Orthopedic Surgeons and American College of Chest Physicians guidelines for venous thromboembolism prevention in hip and knee arthroplasty differ: what are the implications for clinicians and patients?Chest.2009;135:513–520.
Vitamin K antagonists (VKAs) such as warfarin have been the backbone of oral anticoagulation in clinical practice since the middle of the last century. Despite their efficacy, VKAs have well‐recognized limitations that have led to their underutilization in patients who would otherwise be candidates for oral anticoagulation.14 These limitations include a narrow therapeutic window and significant intra‐ and interindividual variability in dose requirements as well as numerous drugdrug and drugfood interactions.59 Therefore, VKAs require close laboratory monitoring to prevent excessive or under‐anticoagulation, and maintaining therapeutic anticoagulation with VKAs remains a challenging task in many patients.2 It has been shown that 30%50% of international normalized ratio (INR) results fall outside of the targeted therapeutic range.10, 11 Consequently, it is not surprising that warfarin is a common cause of medication‐related emergency room visits.12 Despite many fruitless years of searching for better alternatives, VKAs have remained the mainstay of oral anticoagulation for more than 60 years.8
An ideal anticoagulant would be orally administered, effective, safe, exhibit a predictable pharmacokinetic profile and a low potential for drug or dietary interactions, and therefore would not require routine laboratory monitoring.2, 5, 13 Other desirable characteristics would include a rapid onset of action to decrease or eliminate the need for bridging therapy, and rapid reversibility with or without an antidote.8, 13 To date, no oral anticoagulant has been developed that possesses all of these desired characteristics. Dabigatran etexilate (Pradaxa, Boehringer Ingelheim Pharmaceuticals, Inc.) has recently become the first oral anticoagulant to be available for wide clinical use since the 1950s.14 In the following sections, we provide an overview of dabigatran etexilate, with a special focus on issues that are pertinent to hospitalists and the hospitalized patient.
PHARMACOLOGY OF DABIGATRAN ETEXILATE
Pharmacokinetics and Pharmacodynamics of Dabigatran Etexilate
A comparison of the pharmacokinetic (PK) and pharmacodynamic (PD) properties of dabigatran etexilate (dabigatran) and warfarin are presented in Table 1. Dabigatran etexilate (referred to from this point as dabigatran) is a prodrug of dabigatran, which blocks the terminal coagulation cascade by binding to the active site of thrombin and selectively inhibiting this critical serine protease in a dose‐dependent and reversible fashion.15 Thrombin plays a central role in blood coagulation by converting fibrinogen to fibrin, amplifying its own generation by feedback activation of factors V, VIII, and XI, and by activating platelets (Figure 1).16 Dabigatran is a direct thrombin inhibitor that acts independently of anti‐thrombin to inhibit both free and clot‐bound thrombin.17, 18 The bioavailability of dabigatran after oral intake is low (6%7%).1923 After absorption, the prodrug is rapidly converted by plasma and hepatic esterases to the active drug dabigatran, but it is not metabolized by the CYP‐450 system, therefore reducing the potential for drugdrug interactions.8, 2328 The long half‐life of dabigatran allows for once or twice daily dosing.21, 24 The PK profile of dabigatran is predictable, with minimal inter‐ and intraindividual variation.21, 22
| Warfarin | Dabigatran | |
|---|---|---|
| Mechanism of action | Reduces functional levels of vitamin Kdependent factors II, VII, IX, and X by inhibiting vitamin K epoxide reductase | Binds to active site of thrombin (factor IIa) and reversibly inhibits free and clot‐bound thrombin |
| Prodrug | No | Yes |
| Bioavailability | >90%95% | 6%7% |
| Protein binding | 99% | 35% |
| Time to reach peak plasma levels | 7296 hr | 23 hr |
| Half‐life | 3644 hr | 1217 hr |
| Routine coagulation monitoring | Required, but frequency varies based on clinical situation | No requirement for routine monitoring |
| Schedule | INR‐adjusted, usually once daily | Fixed dose, once or twice daily |
| Metabolism | CYP‐450 hepatic microsomal enzymes, especially CYP2C9, CYP1A2, and CYP3A4 | Esterase‐catalyzed hydrolysis in plasma or liver after intestinal P‐gp transport |
| Clearance | Almost entirely hepatic | 80% unchanged renally (after an intravenous dose), 20% hepatic after conjugation |
| Drug interactions | Drugs that affect CYP‐450 hepatic microsomal enzymes and those that displace warfarin from plasma proteins | P‐gp inhibitors (CYP‐450 system not involved) |
| Antidote | Yes (vitamin K and plasma products) | No |
Dabigatran is packaged in capsules that are hygroscopic. Therefore, the capsules should be stored in the original container with the cap tightly closed. Exposure of dabigatran capsules to air for prolonged periods outside the original container can result in deterioration of the active compound and reduced efficacy.27, 28 Dabigatran capsules contain tartaric acid which is necessary to facilitate dissolution of the medication in the gastrointestinal tract for optimal absorption.2 Breaking the capsules or removing the drug from the capsule can result in increased exposure. Therefore, dabigatran capsules should be taken intact, and patients should be instructed that dabigatran capsules should not be broken, chewed, or opened before administration.28 Alternative anticoagulants should be used if patients cannot swallow the capsule intact for any reason (eg, intubated patients).
Dabigatran and Drug and Food Interactions
Dabigatran acts as a substrate of the transporter protein P‐glycoprotein (P‐gp), which is also involved in the transport of many other drugs.5, 16 P‐gp is an efflux pump that functions to prevent the absorption of drugs in the intestine or increase the renal excretion of drugs that are P‐gp substrates.25 Inhibitors of P‐gp increase the serum concentrations of P‐gp substrates, whereas P‐gp inducers reduce the concentrations of these medications.13 Examples of P‐gp inhibitors include clarithromycin, quinidine, and verapamil, whereas rifampin, pantoprazole, and St John's wort are known to induce P‐gp.5, 24, 26 As an illustration, the coadministration of dabigatran and amiodarone, a known P‐gp inhibitor, increases the area under the curve of drug plasmaconcentrationtime of dabigatran by 60% without significantly affecting levels of amiodarone.5, 27 Nevertheless, dagibatran's prescribing information in the United States advises that the P‐gp inhibitors ketoconazole, verapamil, amiodarone, quinidine, and clarithromycin do not require dose adjustments, although these results should not be extrapolated to other P‐gp inhibitors.28 In addition, the manufacturer recommends generally avoiding the concomitant use of the potent P‐gp inducer rifampin with dabigatran, whereas the European Medicines Agency advises caution in the coadministration of rifampin or St John's wort with dabigatran.27, 28
Not all P‐gp substrates result in clinically significant interactions with dabigatran (eg, digoxin, diclofenac, and atorvastatin).19, 29 The use of nonsteroidal anti‐inflammatory drugs and aspirin may increase the risk of bleeding in patients using dabigatran.5, 26, 27 It is not recommended to coadminister certain anti‐platelet agents (such as clopidogrel, prasugrel, or ticlopidine) with dabigatran.26, 30 Although the use of proton pump inhibitors such as pantoprazole leads to a 30% decrease in the area under the curve of dabigatran, coadministration of pantoprazole and other proton pump inhibitors with dabigatran in clinical trials did not affect bleeding risk or efficacy.27 Attention to potential drug interactions with dabigatran is important, because dabigatran is not usually monitored. Food interactions with dabigatran appear to be low, and therefore dabigatran can probably be taken with or without food, but caution is advised given the limited postmarketing experience with dabigatran.30 An excellent review of drug and dietary interactions of dabigatran has been published recently.5
Use of Dabigatran in Patients With Liver or Renal Impairment
Approximately 80% of dabigatran is excreted, largely unchanged, by the kidneys in healthy subjects.19 Patients with severe renal impairment (creatinine clearance [CrCL], 30 mL/min) were excluded from phase 3 trials that evaluated dabigatran.3135 A small study in patients with renal impairment showed a linear correlation between renal function and renal clearance of dabigatran, with proportional increases in the anticoagulant effects of dabigatran with decreasing renal function.36 For patients on hemodialysis, 62%68% of the dose was removed.36 The authors recommended avoidance of dabigatran in severe renal impairment, and a dose reduction was recommended for moderate renal impairment (CrCL, 3150 mL/min).13, 36 Despite exclusion of patients with CrCL of 30 mL/min from all phase 3 trials of dabigatran and the relative contraindication of the use of dabigatran in this patient population, the US Food and Drug Administration (FDA) approved a reduced dose of 75 mg twice daily for patients with CrCL of 1530 mL/min, but no dosing recommendations were made for patients with CrCL of 15 mL/min or for patients on dialysis.13, 28, 36 We believe that dabigatran should be used with great caution in patients with CrCl 1530 mL/min given the limited outcome data in these patients, and alternative anticoagulants should be strongly considered for these patients until more data are available.
Less than 20% of the dabigatran dose is conjugated in the liver and subsequently secreted in the biliary system.19, 23 Stangier et al. showed that moderate hepatic impairment does not affect the PK/PD or safety profile of dabigatran and concluded that dabigatran can be given to those patients without dose adjustment.37 On the other hand, severe hepatic impairment (Child‐Pugh class B or C cirrhosis) and an alanine aminotransferase level more than 2 to 3 times the upper limit of normal were used as exclusion criteria in most of the phase 3 trials that evaluated dabigatran.16, 24, 34, 35, 38 The hepatic toxicity noted with the first generation oral direct thrombin inhibitor, ximelagatran, has not been seen with dabigatran in clinical trials, although long‐term postmarketing data are lacking.32, 34, 35, 3840
The Effect of Dabigatran on Common Coagulation Laboratory Tests and Recommendations for Monitoring Dabigatran's Anticoagulant Effects
Despite the predictable PK profile of dabigatran, its effects on common coagulation assays remain incompletely defined.41 Most patients on dabigatran will have a prolonged activated partial thromboplastin time (aPTT) even at trough concentrations, but not in a linear predictable fashion.19, 20, 21, 36, 41 Dabigatran has few and unpredictable effects on prothrombin time (PT) and INR, and therapeutic concentrations of dabigatran usually result in only modest elevations of PT/INR.21, 42 Although thrombin time (TT) displays a good linear correlation with plasma concentrations of dabigatran, the reagents used to perform TT in most clinical laboratories are not standardized. Therefore, TT is better suited to detecting the presence of dabigatran rather than monitoring its anticoagulant effects.24, 42 Therefore, even a slightly prolonged aPTT or TT could reflect significant plasma dabigatran levels. The best assays for monitoring dabigatran are the ecarin clotting time (ECT), modified thrombelastographic evaluations of whole blood clot formation, and the Hemoclot Thrombin Inhibitor assay, but these tests are limited by lack of standardization and limited clinical availablity.24, 42, 43
EFFICACY OF DABIGATRAN
In this section, we provide a brief review of the major phase 3 trials that evaluated dabigatran for different indications (see references 13, 16, and 24 for recent detailed reviews of the clinical trials of dabigatran).
Dabigatran for Thromboprophylaxis in Patients with Atrial Fibrillation
The Randomized Evaluation of Long‐Term Anticoagulation Therapy (RE‐LY) trial was a prospective, noninferiority, phase 3 study of dabigatran that was the basis for its FDA approval in patients with nonvalvular AF.35, 44 In RE‐LY, 18,113 AF patients with another thromboembolic risk factor were randomized to receive fixed doses of dabigatran (110 mg or 150 mg twice daily) or adjusted‐dose warfarin.35 The median duration of follow‐up was 2 years and the primary outcome was stroke or systemic embolism. The primary outcome occurred in 1.69% per year in the warfarin group versus 1.53% per year in the group receiving 110 mg of dabigatran twice daily (relative risk with dabigatran, 0.91; 95% confidence interval [CI], 0.741.11; P 0.001 for noninferiority) and 1.11% per year in the group receiving 150 mg of dabigatran twice daily (relative risk, 0.66; 95% CI, 0.530.82; P 0.001 for superiority). The rate of major bleeding was 3.36% per year in the warfarin group versus 2.71% per year in the dabigatran 110 mg group (P = 0.003) and 3.11% per year in the dabigatran 150 mg group (P = 0.31). Intracranial bleeds were significantly less common in both dabigatran groups than with warfarin. Major gastrointestinal bleeding rate was significantly higher in the dabigatran group at the 150‐mg dose than in the warfarin group. The mortality rate was 4.13% per year in the warfarin group versus 3.75% per year with 110 mg of dabigatran (P = 0.13) and 3.64% per year with 150 mg of dabigatran (P = 0.051).35 The authors concluded that in patients with nonvalvular AF, dabigatran given at a dose of 110 mg twice daily was not inferior to warfarin, and was associated with lower rates of major hemorrhage than warfarin.35 Dabigatran given at a dose of 150 mg twice daily was associated with lower rates of stroke and systemic embolism than warfarin but had similar rates of major hemorrhage.35 These effects were maintained in patients with previous stroke or transient ischemic attack, and in these patients starting dabigatran with and without prior VKA treatment.45, 46
Dabigatran for Prevention of Venous Thromboembolism After Major Orthopedic Procedures
Without thromboprophylaxis, the incidence of venous thromboembolism (VTE) following major orthopedic surgery is 40%60%.47 Nevertheless, many patients do not receive appropriate thromboprophylaxis after orthopedic surgery, in part due to the limitations of VKAs and the inconvenience of low molecular weight heparin (LMWH) injections.48
RE‐NOVATE Trial
Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE‐NOVATE trail) was a prospective, noninferiority phase 3 trial in which 3494 patients undergoing total hip replacement (THR) were randomized in double‐blind fashion to 2835 days of dabigatran 220 mg or 150 mg once daily, starting with a half‐dose 14 hours after surgery, or subcutaneous (SC) enoxaparin 40 mg once daily, starting the evening before surgery.33 The primary efficacy outcome was the composite of total VTE (venographic or symptomatic) and death from all causes during treatment. The primary efficacy outcome occurred in 6.7% in the enoxaparin group versus 6.0% in the dabigatran 220 mg group (absolute difference [AD], 0.7%; 95% CI, 2.9% to 1.6%) and 8.6% in the 150 mg group (AD, 1.9%; 95% CI, 0.6% to 4.4%). There was no significant difference in major bleeding with either dose of dabigatran compared with enoxaparin (220 mg, P = 0.44; 150 mg, P = 0.60). It was concluded that oral dabigatran was not inferior to enoxaparin for prevention of VTE after THR surgery, with a similar safety profile.33
RE‐NOVATE II Trial
Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE‐NOVATE II trail) was a randomized, double‐blind, noninferiority phase 3 trial that compared dabigatran versus SC enoxaparin for extended thromboprophylaxis in patients undergoing THR.38 A total of 2055 patients were randomized to 2835 days of oral dabigatran, 220 mg once daily, starting with a half‐dose 14 hours after surgery, or SC enoxaparin 40 mg once daily, starting the evening before surgery. The primary efficacy outcome was the same as that in the RE‐NOVATE trial. The primary efficacy outcome occurred in 7.7% of the dabigatran group versus 8.8% of the enoxaparin group (risk difference, 1.1%; 95% CI, 3.8 to 1.6%; P 0.0001 for the prespecified noninferiority margin. Major VTE plus VTE‐related death occurred in 2.2% of the dabigatran group versus 4.2% of the enoxaparin group (risk difference, 1.9%; 95% CI, 3.6% to 0.2%; P = 0.03). Major bleeding occurred in 1.4% of the dabigatran group and 0.9% of the enoxaparin group (P = 0.40). It was concluded that extended prophylaxis with oral dabigatran 220 mg once daily was not inferior to SC enoxaparin 40 mg once daily for prevention of VTE after THR. The safety profiles were similar between the 2 arms.38
RE‐MODEL Trial
In the Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromblembloism after total knee replacement (RE‐MODEL trail) phase 3 trial, 2076 patients who underwent total knee replacement (TKR) were randomized to receive dabigatran 150 mg or 220 mg once daily starting with a half‐dose 14 hours after surgery, or SC enoxaparin 40 mg once daily starting the evening before surgery, for 610 days.32 Patients were followed‐up for 3 months. The primary efficacy outcome was a composite of total VTE (venographic or symptomatic) and mortality during treatment. The primary efficacy outcome occurred in 37.7% of the enoxaparin group versus 36.4% of the dabigatran 220 mg group (AD, 1.3%; 95% CI, 7.3 to 4.6) and 40.5% of the 150 mg group (AD, 2.8%; 95% CI, 3.1 to 8.7). The incidence of major bleeding did not differ between the groups (1.3% versus 1.5% and 1.3%, respectively). The conclusion was that dabigatran (220 mg or 150 mg) was not inferior to enoxaparin for prevention of VTE after TKR surgery and exhibited a similar safety profile.32
RE‐MOBILZE Trial
The oral thrombin inhibitor dabigatran etexilate vs the North American enoxaparin regimen for the prevention of venous thromboembolism after knee arthroplasty surgery (RE‐MOBILIZE trail) was a phase 3 trial that randomized 1896 patients after unilateral TKR to receive dabigatran 220 or 150 mg once daily versus enoxaparin 30 mg SC twice daily after surgery.40 Dosing stopped at contrast venography, 1215 days after surgery. Follow‐up was for 3 months. The primary outcome was a composite of total VTE events and all‐cause mortality during treatment. With respect to the primary outcome, dabigatran at 220 and 150 mg showed inferior efficacy to enoxaparin, with VTE rates of 31% (P = 0.02 vs enoxaparin), 34% (P 0.001 vs enoxaparin), and 25%, respectively. Major bleeding was similar. It was concluded that dabigatran was inferior to the twice‐daily North American enoxaparin regimen, probably because of the latter's more intense and prolonged dosing.40 It should be noted that the first dose of dabigatran in this study was given 612 hours after surgery, compared with 14 hours postoperatively in RE‐MODEL, which may have contributed to the inferior outcome.32, 40
Dabigatran for Treatment of Acute VTE
RE‐COVER was a large, randomized, noninferiority phase 3 trial that randomized 2564 patients with acute symptomatic proximal lower extremity deep vein thrombosis or pulmonary embolism to 6 months of dabigatran 150 mg twice daily or dose‐adjusted warfarin (INR 2/3).34 All patients initially received parenteral anticoagulation (LMWH or unfractionated heparin [UFH]) for a median of 9 days. Patients in the warfarin group spent 60% of the time in the therapeutic range. In the dabigatran arm, 2.4% had recurrent VTE versus 2.1% in the warfarin arm (P 0.001 for the prespecified noninferiority margin). Major bleeding occurred in 1.6% of patients in the dabigatran arm and 1.9% in the warfarin arm (hazards ratio, 0.82; 95% CI, 0.451.48). There was no difference in the other safety endpoints (acute coronary syndrome, abnormal liver function tests and deaths). Adverse events (especially gastrointestinal) leading to discontinuation of the study drug occurred in 9% of patients assigned to dabigatran and 6.8% of patients assigned to warfarin (P = 0.05). It was concluded that a fixed dose of dabigatran was not inferior to warfarin for treatment of VTE, with a similar safety profile.34 It is important to note that the first dose of dabigatran was given after a median of 9 days of parenteral anticoagulation therapy, so the findings of this study do not provide data regarding the use of dabigatran as initial monotherapy for acute VTE.34 The results of additional randomized trials evaluating the use of dabigatran for acute VTE treatment (RE‐COVER II) and secondary prevention of VTE (RE‐MEDY and RE‐SONATE) are expected soon.16
SAFETY OF DABIGATRAN
Aside from the bleeding risks discussed earlier, the most commonly reported side effect of dabigatran was dyspepsia. Dyspepsia occurred twice as frequently in patients taking dabigatran versus warfarin in the RE‐LY trial (11.5% vs 5.8%).35 One possible explanation for the higher incidence of dyspepsia is the tartaric acid component in dabigatran capsules.2 In the RE‐LY study, myocardial infarction occurred more commonly in the dabigatran arms (0.72% with 110 mg and 0.74% with 150 mg) than the warfarin arm (0.53%, P = 0.07 and 0.048, respectively).24, 35 It has been postulated that this observation could be related to a greater efficacy of warfarin for the prevention of myocardial infarction rather than an adverse effect of dabigatran.2 There was no increase in acute coronary syndrome rates noted with dabigatran in the other phase 3 trials.3234, 38, 40 No increased risk of elevated liver function test has been noted with dabigatran, but long‐term data are unavailable.32, 34, 35, 38
MANAGEMENT OF SPECIAL SITUATIONS THAT MAY ARISE IN THE USE OF DABIGATRAN
Switching From Warfarin to Dabigatran and Vice Versa
When converting patients from warfarin to dabigatran, it is recommended that dabigatran be started once the INR falls below the lower limit of the desired therapeutic range. Conversely, when switching from dabigatran to warfarin, the manufacturer recommends starting warfarin based on renal function (Table 2). It should be noted that because dabigatran can increase the INR, the INR will better reflect warfarin's effect after dabigatran has been stopped for at least 2 days.27, 28
| CrCL (mL/min) | Time of Warfarin Initiation |
|---|---|
| |
| 50 | 3 d before discontinuing dabigatran |
| 3150 | 2 d before discontinuing dabigatran |
| 1530 | 1 d before discontinuing dabigatran |
| 15 | No recommendations made |
Bridging from Dabigatran to Parenteral Anticoagulants and Vice Versa
For patients currently receiving a parenteral anticoagulant, the manufacturer recommends starting dabigatran 02 hours before the next administration time for parenteral anticoagulants (eg, LMWH) or at the time of discontinuation for continuously infused parenteral drugs (eg, intravenous UFH).28 For patients currently taking dabigatran who are transitioning to a parenteral anticoagulant, it is recommended to wait 12 hours (CrCl 30 mL/min) or 24 hours (CrCl 30 mL/min) after the last dose of dabigatran before initiating treatment with a parenteral anticoagulant.27, 28
Management of Dabigatran Before Elective and Urgent Invasive Procedures
Patients who undergo invasive procedures in the presence of therapeutic levels of dabigatran are at an increased risk of bleeding. The manufacturer recommends holding dabigatran for at least 24 hours before elective surgery depending on the degree of renal impairment and the risk of bleeding.28 Table 3 lists recommendations on the timing of discontinuation of dabigatran before a procedure. If emergent/urgent surgery is necessary for a patient who is on dabigatran, the risk of bleeding should be weighed against the urgency of the intervention.28, 42, 44 As mentioned earlier, the ECT or the Hemoclot Thrombin Inhibitor assay are the preferred tests for measurement of dabigatran effects, but they are not standardized or widely clinically available. Instead, prolongation of the TT (preferably) or the aPTT can be used to determine the presence of dabigatran.28, 42
| CrCL (mL/min) | Half‐Life (hr) | Suggested Timing of Discontinuation of Dabigatran Before Surgery | |
|---|---|---|---|
| Standard Risk of Bleeding | High Risk of Bleeding* | ||
| |||
| >80 | 13 (11‐22) | 24 hr | 24 d |
| 5180 | 15 (12‐34) | 24 hr | 24 d |
| 3150 | 18 (13‐23) | 48 hr | 4 d |
| 30 | 27 (22‐35) | 25 d | >5 d |
Overdose and Toxicity With Dabigatran
Accidental or intentional overdose, or accumulation of dabigatran due to renal impairment, may lead to hemorrhagic complications. Unlike warfarin and heparin, there is no antidote for dabigatran. There are no widely available, reliable laboratory tests to measure the anticoagulant activity of dabigatran, and evidence‐based guidelines to manage dabigatran toxicity do not exist. Therefore, in the event of dabigatran toxicity, treatment is largely supportive. Management of toxicity is dependent on whether the overdose/accumulation is accompanied by bleeding or not. For overdose, interventions include adequate diuresis and the use of activated charcoal to reduce the absorption of dabigatran (within 2 hours of ingestion).42 In the event of bleeding, proposed measures include application of mechanical pressure to the sites of bleeding and infusion of pro‐coagulant blood products such as activated prothrombin complex concentrates (eg, FEIBA VH, Baxter) or recombinant human activated factor VIIa (NovoSeven, Novo‐Nordisk) (reviewed in references 26 and 42). In life‐threatening situations, hemodialysis could be considered, because it can remove 60% of the drug within 23 hours.42 Hemoperfusion over a charcoal filter or large volume hemofiltration have also been suggested in extreme situations.27, 28, 36, 42 Acknowledging their limitations, the ECT, TT, or aPTT may be used to direct therapy.27, 42
Pregnancy and Dabigatran Therapy
Dabigatran is a class C drug during pregnancy, and there are no studies of dabigatran in pregnant women. Animal studies with dabigatran showed decreased fertility of pregnant rats; therefore, the risks and benefits of dabigatran therapy during pregnancy should be weighed carefully.27, 28, 44
CONCLUSIONS
Dabigatran is a novel, oral direct thrombin inhibitor that exhibits several advantages over warfarin. The predictable pharmacokinetic profile and minimal food and drug interactions of dabigatran allow for a fixed‐dosing regimen and obviate the need for routine laboratory monitoring. However, this apparent advantage is also a disadvantage. The lack of a reliable method to monitor dabigatran makes it more difficult to assess compliance, measure the impact of drug interactions, evaluate for toxicity, and determine bona fide therapeutic failure versus noncompliance in the event of breakthrough thromboembolism.28, 42 Other limitations of dabigatran include the lack of an antidote and the dependence on normal renal function for elimination, with the potential for drug accumulation and toxicity with renal impairment. The noninferiority design of the clinical trials that evaluated dabigatran, the absence of long‐term safety and efficacy data, and issues related to the cost effectiveness of dabigatran should be considered when prescribing this agent. More studies are needed to assess dabigatran in special patient populations (eg, the elderly, patients with renal and hepatic impairment, pediatric and pregnant patients) and to better understand dabigatrandrug interactions.
As more novel oral anticoagulant agents, such as factor Xa inhibitors, become available for clinical use, comparative studies will need to be performed to better define the role of each agent for specific indications. In the future, it might be possible to tailor the choice of the oral anticoagulant to the individual patient not only on the basis of the clinical indication but also the specific patient characteristics and possible drug interactions. For example, rivaroxaban (Xarelto) is an oral direct factor Xa that was recently approved in the United States for VTE thromboprophylaxis following orthopedic surgery and in patients with non‐valvular atrial fibrillation.2 Similar to dabigatran, rivaroxaban exhibits predictable PK and PD that allow fixed once or twice daily dosing and obviate the need for routine monitoring of its anticoagulant effects.2, 16 Unlike dabigatran, rivaroxaban is an active drug and not a prodrug, and has a significantly higher bioavailability than dabigatran (>80% vs 6%).16 In addition, the levels of rivaroxaban can be affected by drugs that interfere with both P‐gp and the hepatic CYP‐450 system, compared with dabigatran, which is affected only by drugs that affect P‐gp.8, 16
Vitamin K antagonists (VKAs) such as warfarin have been the backbone of oral anticoagulation in clinical practice since the middle of the last century. Despite their efficacy, VKAs have well‐recognized limitations that have led to their underutilization in patients who would otherwise be candidates for oral anticoagulation.14 These limitations include a narrow therapeutic window and significant intra‐ and interindividual variability in dose requirements as well as numerous drugdrug and drugfood interactions.59 Therefore, VKAs require close laboratory monitoring to prevent excessive or under‐anticoagulation, and maintaining therapeutic anticoagulation with VKAs remains a challenging task in many patients.2 It has been shown that 30%50% of international normalized ratio (INR) results fall outside of the targeted therapeutic range.10, 11 Consequently, it is not surprising that warfarin is a common cause of medication‐related emergency room visits.12 Despite many fruitless years of searching for better alternatives, VKAs have remained the mainstay of oral anticoagulation for more than 60 years.8
An ideal anticoagulant would be orally administered, effective, safe, exhibit a predictable pharmacokinetic profile and a low potential for drug or dietary interactions, and therefore would not require routine laboratory monitoring.2, 5, 13 Other desirable characteristics would include a rapid onset of action to decrease or eliminate the need for bridging therapy, and rapid reversibility with or without an antidote.8, 13 To date, no oral anticoagulant has been developed that possesses all of these desired characteristics. Dabigatran etexilate (Pradaxa, Boehringer Ingelheim Pharmaceuticals, Inc.) has recently become the first oral anticoagulant to be available for wide clinical use since the 1950s.14 In the following sections, we provide an overview of dabigatran etexilate, with a special focus on issues that are pertinent to hospitalists and the hospitalized patient.
PHARMACOLOGY OF DABIGATRAN ETEXILATE
Pharmacokinetics and Pharmacodynamics of Dabigatran Etexilate
A comparison of the pharmacokinetic (PK) and pharmacodynamic (PD) properties of dabigatran etexilate (dabigatran) and warfarin are presented in Table 1. Dabigatran etexilate (referred to from this point as dabigatran) is a prodrug of dabigatran, which blocks the terminal coagulation cascade by binding to the active site of thrombin and selectively inhibiting this critical serine protease in a dose‐dependent and reversible fashion.15 Thrombin plays a central role in blood coagulation by converting fibrinogen to fibrin, amplifying its own generation by feedback activation of factors V, VIII, and XI, and by activating platelets (Figure 1).16 Dabigatran is a direct thrombin inhibitor that acts independently of anti‐thrombin to inhibit both free and clot‐bound thrombin.17, 18 The bioavailability of dabigatran after oral intake is low (6%7%).1923 After absorption, the prodrug is rapidly converted by plasma and hepatic esterases to the active drug dabigatran, but it is not metabolized by the CYP‐450 system, therefore reducing the potential for drugdrug interactions.8, 2328 The long half‐life of dabigatran allows for once or twice daily dosing.21, 24 The PK profile of dabigatran is predictable, with minimal inter‐ and intraindividual variation.21, 22
| Warfarin | Dabigatran | |
|---|---|---|
| Mechanism of action | Reduces functional levels of vitamin Kdependent factors II, VII, IX, and X by inhibiting vitamin K epoxide reductase | Binds to active site of thrombin (factor IIa) and reversibly inhibits free and clot‐bound thrombin |
| Prodrug | No | Yes |
| Bioavailability | >90%95% | 6%7% |
| Protein binding | 99% | 35% |
| Time to reach peak plasma levels | 7296 hr | 23 hr |
| Half‐life | 3644 hr | 1217 hr |
| Routine coagulation monitoring | Required, but frequency varies based on clinical situation | No requirement for routine monitoring |
| Schedule | INR‐adjusted, usually once daily | Fixed dose, once or twice daily |
| Metabolism | CYP‐450 hepatic microsomal enzymes, especially CYP2C9, CYP1A2, and CYP3A4 | Esterase‐catalyzed hydrolysis in plasma or liver after intestinal P‐gp transport |
| Clearance | Almost entirely hepatic | 80% unchanged renally (after an intravenous dose), 20% hepatic after conjugation |
| Drug interactions | Drugs that affect CYP‐450 hepatic microsomal enzymes and those that displace warfarin from plasma proteins | P‐gp inhibitors (CYP‐450 system not involved) |
| Antidote | Yes (vitamin K and plasma products) | No |
Dabigatran is packaged in capsules that are hygroscopic. Therefore, the capsules should be stored in the original container with the cap tightly closed. Exposure of dabigatran capsules to air for prolonged periods outside the original container can result in deterioration of the active compound and reduced efficacy.27, 28 Dabigatran capsules contain tartaric acid which is necessary to facilitate dissolution of the medication in the gastrointestinal tract for optimal absorption.2 Breaking the capsules or removing the drug from the capsule can result in increased exposure. Therefore, dabigatran capsules should be taken intact, and patients should be instructed that dabigatran capsules should not be broken, chewed, or opened before administration.28 Alternative anticoagulants should be used if patients cannot swallow the capsule intact for any reason (eg, intubated patients).
Dabigatran and Drug and Food Interactions
Dabigatran acts as a substrate of the transporter protein P‐glycoprotein (P‐gp), which is also involved in the transport of many other drugs.5, 16 P‐gp is an efflux pump that functions to prevent the absorption of drugs in the intestine or increase the renal excretion of drugs that are P‐gp substrates.25 Inhibitors of P‐gp increase the serum concentrations of P‐gp substrates, whereas P‐gp inducers reduce the concentrations of these medications.13 Examples of P‐gp inhibitors include clarithromycin, quinidine, and verapamil, whereas rifampin, pantoprazole, and St John's wort are known to induce P‐gp.5, 24, 26 As an illustration, the coadministration of dabigatran and amiodarone, a known P‐gp inhibitor, increases the area under the curve of drug plasmaconcentrationtime of dabigatran by 60% without significantly affecting levels of amiodarone.5, 27 Nevertheless, dagibatran's prescribing information in the United States advises that the P‐gp inhibitors ketoconazole, verapamil, amiodarone, quinidine, and clarithromycin do not require dose adjustments, although these results should not be extrapolated to other P‐gp inhibitors.28 In addition, the manufacturer recommends generally avoiding the concomitant use of the potent P‐gp inducer rifampin with dabigatran, whereas the European Medicines Agency advises caution in the coadministration of rifampin or St John's wort with dabigatran.27, 28
Not all P‐gp substrates result in clinically significant interactions with dabigatran (eg, digoxin, diclofenac, and atorvastatin).19, 29 The use of nonsteroidal anti‐inflammatory drugs and aspirin may increase the risk of bleeding in patients using dabigatran.5, 26, 27 It is not recommended to coadminister certain anti‐platelet agents (such as clopidogrel, prasugrel, or ticlopidine) with dabigatran.26, 30 Although the use of proton pump inhibitors such as pantoprazole leads to a 30% decrease in the area under the curve of dabigatran, coadministration of pantoprazole and other proton pump inhibitors with dabigatran in clinical trials did not affect bleeding risk or efficacy.27 Attention to potential drug interactions with dabigatran is important, because dabigatran is not usually monitored. Food interactions with dabigatran appear to be low, and therefore dabigatran can probably be taken with or without food, but caution is advised given the limited postmarketing experience with dabigatran.30 An excellent review of drug and dietary interactions of dabigatran has been published recently.5
Use of Dabigatran in Patients With Liver or Renal Impairment
Approximately 80% of dabigatran is excreted, largely unchanged, by the kidneys in healthy subjects.19 Patients with severe renal impairment (creatinine clearance [CrCL], 30 mL/min) were excluded from phase 3 trials that evaluated dabigatran.3135 A small study in patients with renal impairment showed a linear correlation between renal function and renal clearance of dabigatran, with proportional increases in the anticoagulant effects of dabigatran with decreasing renal function.36 For patients on hemodialysis, 62%68% of the dose was removed.36 The authors recommended avoidance of dabigatran in severe renal impairment, and a dose reduction was recommended for moderate renal impairment (CrCL, 3150 mL/min).13, 36 Despite exclusion of patients with CrCL of 30 mL/min from all phase 3 trials of dabigatran and the relative contraindication of the use of dabigatran in this patient population, the US Food and Drug Administration (FDA) approved a reduced dose of 75 mg twice daily for patients with CrCL of 1530 mL/min, but no dosing recommendations were made for patients with CrCL of 15 mL/min or for patients on dialysis.13, 28, 36 We believe that dabigatran should be used with great caution in patients with CrCl 1530 mL/min given the limited outcome data in these patients, and alternative anticoagulants should be strongly considered for these patients until more data are available.
Less than 20% of the dabigatran dose is conjugated in the liver and subsequently secreted in the biliary system.19, 23 Stangier et al. showed that moderate hepatic impairment does not affect the PK/PD or safety profile of dabigatran and concluded that dabigatran can be given to those patients without dose adjustment.37 On the other hand, severe hepatic impairment (Child‐Pugh class B or C cirrhosis) and an alanine aminotransferase level more than 2 to 3 times the upper limit of normal were used as exclusion criteria in most of the phase 3 trials that evaluated dabigatran.16, 24, 34, 35, 38 The hepatic toxicity noted with the first generation oral direct thrombin inhibitor, ximelagatran, has not been seen with dabigatran in clinical trials, although long‐term postmarketing data are lacking.32, 34, 35, 3840
The Effect of Dabigatran on Common Coagulation Laboratory Tests and Recommendations for Monitoring Dabigatran's Anticoagulant Effects
Despite the predictable PK profile of dabigatran, its effects on common coagulation assays remain incompletely defined.41 Most patients on dabigatran will have a prolonged activated partial thromboplastin time (aPTT) even at trough concentrations, but not in a linear predictable fashion.19, 20, 21, 36, 41 Dabigatran has few and unpredictable effects on prothrombin time (PT) and INR, and therapeutic concentrations of dabigatran usually result in only modest elevations of PT/INR.21, 42 Although thrombin time (TT) displays a good linear correlation with plasma concentrations of dabigatran, the reagents used to perform TT in most clinical laboratories are not standardized. Therefore, TT is better suited to detecting the presence of dabigatran rather than monitoring its anticoagulant effects.24, 42 Therefore, even a slightly prolonged aPTT or TT could reflect significant plasma dabigatran levels. The best assays for monitoring dabigatran are the ecarin clotting time (ECT), modified thrombelastographic evaluations of whole blood clot formation, and the Hemoclot Thrombin Inhibitor assay, but these tests are limited by lack of standardization and limited clinical availablity.24, 42, 43
EFFICACY OF DABIGATRAN
In this section, we provide a brief review of the major phase 3 trials that evaluated dabigatran for different indications (see references 13, 16, and 24 for recent detailed reviews of the clinical trials of dabigatran).
Dabigatran for Thromboprophylaxis in Patients with Atrial Fibrillation
The Randomized Evaluation of Long‐Term Anticoagulation Therapy (RE‐LY) trial was a prospective, noninferiority, phase 3 study of dabigatran that was the basis for its FDA approval in patients with nonvalvular AF.35, 44 In RE‐LY, 18,113 AF patients with another thromboembolic risk factor were randomized to receive fixed doses of dabigatran (110 mg or 150 mg twice daily) or adjusted‐dose warfarin.35 The median duration of follow‐up was 2 years and the primary outcome was stroke or systemic embolism. The primary outcome occurred in 1.69% per year in the warfarin group versus 1.53% per year in the group receiving 110 mg of dabigatran twice daily (relative risk with dabigatran, 0.91; 95% confidence interval [CI], 0.741.11; P 0.001 for noninferiority) and 1.11% per year in the group receiving 150 mg of dabigatran twice daily (relative risk, 0.66; 95% CI, 0.530.82; P 0.001 for superiority). The rate of major bleeding was 3.36% per year in the warfarin group versus 2.71% per year in the dabigatran 110 mg group (P = 0.003) and 3.11% per year in the dabigatran 150 mg group (P = 0.31). Intracranial bleeds were significantly less common in both dabigatran groups than with warfarin. Major gastrointestinal bleeding rate was significantly higher in the dabigatran group at the 150‐mg dose than in the warfarin group. The mortality rate was 4.13% per year in the warfarin group versus 3.75% per year with 110 mg of dabigatran (P = 0.13) and 3.64% per year with 150 mg of dabigatran (P = 0.051).35 The authors concluded that in patients with nonvalvular AF, dabigatran given at a dose of 110 mg twice daily was not inferior to warfarin, and was associated with lower rates of major hemorrhage than warfarin.35 Dabigatran given at a dose of 150 mg twice daily was associated with lower rates of stroke and systemic embolism than warfarin but had similar rates of major hemorrhage.35 These effects were maintained in patients with previous stroke or transient ischemic attack, and in these patients starting dabigatran with and without prior VKA treatment.45, 46
Dabigatran for Prevention of Venous Thromboembolism After Major Orthopedic Procedures
Without thromboprophylaxis, the incidence of venous thromboembolism (VTE) following major orthopedic surgery is 40%60%.47 Nevertheless, many patients do not receive appropriate thromboprophylaxis after orthopedic surgery, in part due to the limitations of VKAs and the inconvenience of low molecular weight heparin (LMWH) injections.48
RE‐NOVATE Trial
Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE‐NOVATE trail) was a prospective, noninferiority phase 3 trial in which 3494 patients undergoing total hip replacement (THR) were randomized in double‐blind fashion to 2835 days of dabigatran 220 mg or 150 mg once daily, starting with a half‐dose 14 hours after surgery, or subcutaneous (SC) enoxaparin 40 mg once daily, starting the evening before surgery.33 The primary efficacy outcome was the composite of total VTE (venographic or symptomatic) and death from all causes during treatment. The primary efficacy outcome occurred in 6.7% in the enoxaparin group versus 6.0% in the dabigatran 220 mg group (absolute difference [AD], 0.7%; 95% CI, 2.9% to 1.6%) and 8.6% in the 150 mg group (AD, 1.9%; 95% CI, 0.6% to 4.4%). There was no significant difference in major bleeding with either dose of dabigatran compared with enoxaparin (220 mg, P = 0.44; 150 mg, P = 0.60). It was concluded that oral dabigatran was not inferior to enoxaparin for prevention of VTE after THR surgery, with a similar safety profile.33
RE‐NOVATE II Trial
Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE‐NOVATE II trail) was a randomized, double‐blind, noninferiority phase 3 trial that compared dabigatran versus SC enoxaparin for extended thromboprophylaxis in patients undergoing THR.38 A total of 2055 patients were randomized to 2835 days of oral dabigatran, 220 mg once daily, starting with a half‐dose 14 hours after surgery, or SC enoxaparin 40 mg once daily, starting the evening before surgery. The primary efficacy outcome was the same as that in the RE‐NOVATE trial. The primary efficacy outcome occurred in 7.7% of the dabigatran group versus 8.8% of the enoxaparin group (risk difference, 1.1%; 95% CI, 3.8 to 1.6%; P 0.0001 for the prespecified noninferiority margin. Major VTE plus VTE‐related death occurred in 2.2% of the dabigatran group versus 4.2% of the enoxaparin group (risk difference, 1.9%; 95% CI, 3.6% to 0.2%; P = 0.03). Major bleeding occurred in 1.4% of the dabigatran group and 0.9% of the enoxaparin group (P = 0.40). It was concluded that extended prophylaxis with oral dabigatran 220 mg once daily was not inferior to SC enoxaparin 40 mg once daily for prevention of VTE after THR. The safety profiles were similar between the 2 arms.38
RE‐MODEL Trial
In the Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromblembloism after total knee replacement (RE‐MODEL trail) phase 3 trial, 2076 patients who underwent total knee replacement (TKR) were randomized to receive dabigatran 150 mg or 220 mg once daily starting with a half‐dose 14 hours after surgery, or SC enoxaparin 40 mg once daily starting the evening before surgery, for 610 days.32 Patients were followed‐up for 3 months. The primary efficacy outcome was a composite of total VTE (venographic or symptomatic) and mortality during treatment. The primary efficacy outcome occurred in 37.7% of the enoxaparin group versus 36.4% of the dabigatran 220 mg group (AD, 1.3%; 95% CI, 7.3 to 4.6) and 40.5% of the 150 mg group (AD, 2.8%; 95% CI, 3.1 to 8.7). The incidence of major bleeding did not differ between the groups (1.3% versus 1.5% and 1.3%, respectively). The conclusion was that dabigatran (220 mg or 150 mg) was not inferior to enoxaparin for prevention of VTE after TKR surgery and exhibited a similar safety profile.32
RE‐MOBILZE Trial
The oral thrombin inhibitor dabigatran etexilate vs the North American enoxaparin regimen for the prevention of venous thromboembolism after knee arthroplasty surgery (RE‐MOBILIZE trail) was a phase 3 trial that randomized 1896 patients after unilateral TKR to receive dabigatran 220 or 150 mg once daily versus enoxaparin 30 mg SC twice daily after surgery.40 Dosing stopped at contrast venography, 1215 days after surgery. Follow‐up was for 3 months. The primary outcome was a composite of total VTE events and all‐cause mortality during treatment. With respect to the primary outcome, dabigatran at 220 and 150 mg showed inferior efficacy to enoxaparin, with VTE rates of 31% (P = 0.02 vs enoxaparin), 34% (P 0.001 vs enoxaparin), and 25%, respectively. Major bleeding was similar. It was concluded that dabigatran was inferior to the twice‐daily North American enoxaparin regimen, probably because of the latter's more intense and prolonged dosing.40 It should be noted that the first dose of dabigatran in this study was given 612 hours after surgery, compared with 14 hours postoperatively in RE‐MODEL, which may have contributed to the inferior outcome.32, 40
Dabigatran for Treatment of Acute VTE
RE‐COVER was a large, randomized, noninferiority phase 3 trial that randomized 2564 patients with acute symptomatic proximal lower extremity deep vein thrombosis or pulmonary embolism to 6 months of dabigatran 150 mg twice daily or dose‐adjusted warfarin (INR 2/3).34 All patients initially received parenteral anticoagulation (LMWH or unfractionated heparin [UFH]) for a median of 9 days. Patients in the warfarin group spent 60% of the time in the therapeutic range. In the dabigatran arm, 2.4% had recurrent VTE versus 2.1% in the warfarin arm (P 0.001 for the prespecified noninferiority margin). Major bleeding occurred in 1.6% of patients in the dabigatran arm and 1.9% in the warfarin arm (hazards ratio, 0.82; 95% CI, 0.451.48). There was no difference in the other safety endpoints (acute coronary syndrome, abnormal liver function tests and deaths). Adverse events (especially gastrointestinal) leading to discontinuation of the study drug occurred in 9% of patients assigned to dabigatran and 6.8% of patients assigned to warfarin (P = 0.05). It was concluded that a fixed dose of dabigatran was not inferior to warfarin for treatment of VTE, with a similar safety profile.34 It is important to note that the first dose of dabigatran was given after a median of 9 days of parenteral anticoagulation therapy, so the findings of this study do not provide data regarding the use of dabigatran as initial monotherapy for acute VTE.34 The results of additional randomized trials evaluating the use of dabigatran for acute VTE treatment (RE‐COVER II) and secondary prevention of VTE (RE‐MEDY and RE‐SONATE) are expected soon.16
SAFETY OF DABIGATRAN
Aside from the bleeding risks discussed earlier, the most commonly reported side effect of dabigatran was dyspepsia. Dyspepsia occurred twice as frequently in patients taking dabigatran versus warfarin in the RE‐LY trial (11.5% vs 5.8%).35 One possible explanation for the higher incidence of dyspepsia is the tartaric acid component in dabigatran capsules.2 In the RE‐LY study, myocardial infarction occurred more commonly in the dabigatran arms (0.72% with 110 mg and 0.74% with 150 mg) than the warfarin arm (0.53%, P = 0.07 and 0.048, respectively).24, 35 It has been postulated that this observation could be related to a greater efficacy of warfarin for the prevention of myocardial infarction rather than an adverse effect of dabigatran.2 There was no increase in acute coronary syndrome rates noted with dabigatran in the other phase 3 trials.3234, 38, 40 No increased risk of elevated liver function test has been noted with dabigatran, but long‐term data are unavailable.32, 34, 35, 38
MANAGEMENT OF SPECIAL SITUATIONS THAT MAY ARISE IN THE USE OF DABIGATRAN
Switching From Warfarin to Dabigatran and Vice Versa
When converting patients from warfarin to dabigatran, it is recommended that dabigatran be started once the INR falls below the lower limit of the desired therapeutic range. Conversely, when switching from dabigatran to warfarin, the manufacturer recommends starting warfarin based on renal function (Table 2). It should be noted that because dabigatran can increase the INR, the INR will better reflect warfarin's effect after dabigatran has been stopped for at least 2 days.27, 28
| CrCL (mL/min) | Time of Warfarin Initiation |
|---|---|
| |
| 50 | 3 d before discontinuing dabigatran |
| 3150 | 2 d before discontinuing dabigatran |
| 1530 | 1 d before discontinuing dabigatran |
| 15 | No recommendations made |
Bridging from Dabigatran to Parenteral Anticoagulants and Vice Versa
For patients currently receiving a parenteral anticoagulant, the manufacturer recommends starting dabigatran 02 hours before the next administration time for parenteral anticoagulants (eg, LMWH) or at the time of discontinuation for continuously infused parenteral drugs (eg, intravenous UFH).28 For patients currently taking dabigatran who are transitioning to a parenteral anticoagulant, it is recommended to wait 12 hours (CrCl 30 mL/min) or 24 hours (CrCl 30 mL/min) after the last dose of dabigatran before initiating treatment with a parenteral anticoagulant.27, 28
Management of Dabigatran Before Elective and Urgent Invasive Procedures
Patients who undergo invasive procedures in the presence of therapeutic levels of dabigatran are at an increased risk of bleeding. The manufacturer recommends holding dabigatran for at least 24 hours before elective surgery depending on the degree of renal impairment and the risk of bleeding.28 Table 3 lists recommendations on the timing of discontinuation of dabigatran before a procedure. If emergent/urgent surgery is necessary for a patient who is on dabigatran, the risk of bleeding should be weighed against the urgency of the intervention.28, 42, 44 As mentioned earlier, the ECT or the Hemoclot Thrombin Inhibitor assay are the preferred tests for measurement of dabigatran effects, but they are not standardized or widely clinically available. Instead, prolongation of the TT (preferably) or the aPTT can be used to determine the presence of dabigatran.28, 42
| CrCL (mL/min) | Half‐Life (hr) | Suggested Timing of Discontinuation of Dabigatran Before Surgery | |
|---|---|---|---|
| Standard Risk of Bleeding | High Risk of Bleeding* | ||
| |||
| >80 | 13 (11‐22) | 24 hr | 24 d |
| 5180 | 15 (12‐34) | 24 hr | 24 d |
| 3150 | 18 (13‐23) | 48 hr | 4 d |
| 30 | 27 (22‐35) | 25 d | >5 d |
Overdose and Toxicity With Dabigatran
Accidental or intentional overdose, or accumulation of dabigatran due to renal impairment, may lead to hemorrhagic complications. Unlike warfarin and heparin, there is no antidote for dabigatran. There are no widely available, reliable laboratory tests to measure the anticoagulant activity of dabigatran, and evidence‐based guidelines to manage dabigatran toxicity do not exist. Therefore, in the event of dabigatran toxicity, treatment is largely supportive. Management of toxicity is dependent on whether the overdose/accumulation is accompanied by bleeding or not. For overdose, interventions include adequate diuresis and the use of activated charcoal to reduce the absorption of dabigatran (within 2 hours of ingestion).42 In the event of bleeding, proposed measures include application of mechanical pressure to the sites of bleeding and infusion of pro‐coagulant blood products such as activated prothrombin complex concentrates (eg, FEIBA VH, Baxter) or recombinant human activated factor VIIa (NovoSeven, Novo‐Nordisk) (reviewed in references 26 and 42). In life‐threatening situations, hemodialysis could be considered, because it can remove 60% of the drug within 23 hours.42 Hemoperfusion over a charcoal filter or large volume hemofiltration have also been suggested in extreme situations.27, 28, 36, 42 Acknowledging their limitations, the ECT, TT, or aPTT may be used to direct therapy.27, 42
Pregnancy and Dabigatran Therapy
Dabigatran is a class C drug during pregnancy, and there are no studies of dabigatran in pregnant women. Animal studies with dabigatran showed decreased fertility of pregnant rats; therefore, the risks and benefits of dabigatran therapy during pregnancy should be weighed carefully.27, 28, 44
CONCLUSIONS
Dabigatran is a novel, oral direct thrombin inhibitor that exhibits several advantages over warfarin. The predictable pharmacokinetic profile and minimal food and drug interactions of dabigatran allow for a fixed‐dosing regimen and obviate the need for routine laboratory monitoring. However, this apparent advantage is also a disadvantage. The lack of a reliable method to monitor dabigatran makes it more difficult to assess compliance, measure the impact of drug interactions, evaluate for toxicity, and determine bona fide therapeutic failure versus noncompliance in the event of breakthrough thromboembolism.28, 42 Other limitations of dabigatran include the lack of an antidote and the dependence on normal renal function for elimination, with the potential for drug accumulation and toxicity with renal impairment. The noninferiority design of the clinical trials that evaluated dabigatran, the absence of long‐term safety and efficacy data, and issues related to the cost effectiveness of dabigatran should be considered when prescribing this agent. More studies are needed to assess dabigatran in special patient populations (eg, the elderly, patients with renal and hepatic impairment, pediatric and pregnant patients) and to better understand dabigatrandrug interactions.
As more novel oral anticoagulant agents, such as factor Xa inhibitors, become available for clinical use, comparative studies will need to be performed to better define the role of each agent for specific indications. In the future, it might be possible to tailor the choice of the oral anticoagulant to the individual patient not only on the basis of the clinical indication but also the specific patient characteristics and possible drug interactions. For example, rivaroxaban (Xarelto) is an oral direct factor Xa that was recently approved in the United States for VTE thromboprophylaxis following orthopedic surgery and in patients with non‐valvular atrial fibrillation.2 Similar to dabigatran, rivaroxaban exhibits predictable PK and PD that allow fixed once or twice daily dosing and obviate the need for routine monitoring of its anticoagulant effects.2, 16 Unlike dabigatran, rivaroxaban is an active drug and not a prodrug, and has a significantly higher bioavailability than dabigatran (>80% vs 6%).16 In addition, the levels of rivaroxaban can be affected by drugs that interfere with both P‐gp and the hepatic CYP‐450 system, compared with dabigatran, which is affected only by drugs that affect P‐gp.8, 16
- ,,, et al.The use of antithrombotic therapies in the prevention and treatment of arterial and venous thrombosis: a survey of current knowledge and practice supporting the need for clinical education.Crit Pathw Cardiol.2010;9:41–48.
- .Warfarin versus new agents: interpreting the data.Hematology Am Soc Hematol Educ Program.2010;2010:221–228.
- ,,,,.Why do patients with atrial fibrillation not receive warfarin?Arch Intern Med.2000;160:41–46.
- ,,,,,.Warfarin use among ambulatory patients with nonvalvular atrial fibrillation: The anticoagulation and risk factors in atrial fibrillation (ATRIA) study.Ann Intern Med.1999;131:927–934.
- ,.Drug and dietary interactions of the new and emerging oral anticoagulants.Int J Clin Pract.2010;64:956–967.
- ,,, et al.The risk of bleeding complications in patients with cytochrome P450 CYP2C9*2 or CYP2C9*3 alleles on acenocoumarol or phenprocoumon.Thromb Haemost.2004;92:61–66.
- ,,, et al.Differentiating low‐molecular‐weight heparins based on chemical, biological, and pharmacologic properties: implications for the development of generic versions of low‐molecular‐weight heparins.Semin Thromb Hemost.2008;34:74–85.
- ,.Emerging anticoagulants.Expert Opin Emerg Drugs.2011;16:31–44.
- ,,, et al.Systematic overview of warfarin and its drug and food interactions.Arch Intern Med.2005;165:1095–1106.
- ,,,,,.Evaluation of the pattern of treatment, level of anticoagulation control, and outcome of treatment with warfarin in patients with non‐valvar atrial fibrillation: a record linkage study in a large british population.Heart.2005;91:472–477.
- ,,, et al.Comparison of outcomes among patients randomized to warfarin therapy according to anticoagulant control: results from SPORTIF III and V.Arch Intern Med.2007;167:239–245.
- ,,,.Medication use leading to emergency department visits for adverse drug events in older adults.Ann Intern Med.2007;147:755–765.
- .New oral anticoagulants: a practical guide for clinicians.J Thromb Thrombolysis.2010;29:182–191.
- ,,,.The quest for new anticoagulants: from clinical development to clinical practice [published ahead of print June 14, 2010].Cardiovasc Ther.2010. doi: 10.1111/j.1755–5922.2010.00160.x.
- ,,,,.In‐vitro profile and ex‐vivo anticoagulant activity of the direct thrombin inhibitor dabigatran and its orally active prodrug, dabigatran etexilate.Thromb Haemost.2007;98:155–162.
- ,,.Novel oral factor xa and thrombin inhibitors in the management of thromboembolism.Annu Rev Med.2011;62:41–57.
- ,,,,.Clot‐bound thrombin is protected from inhibition by heparin‐antithrombin III but is susceptible to inactivation by antithrombin III‐independent inhibitors.J Clin Invest.1990;86:385–391.
- ,,.Thrombin binds to soluble fibrin degradation products where it is protected from inhibition by heparin‐antithrombin but susceptible to inactivation by antithrombin‐independent inhibitors.Circulation.1998;97:544–552.
- .Clinical pharmacokinetics and pharmacodynamics of the oral direct thrombin inhibitor dabigatran etexilate.Clin Pharmacokinet.2008;47:285–295.
- ,.Pharmacology, pharmacokinetics, and pharmacodynamics of dabigatran etexilate, an oral direct thrombin inhibitor.Clin Appl Thromb Hemost.2009;15(suppl 1):9S–16S.
- ,,,,.The pharmacokinetics, pharmacodynamics and tolerability of dabigatran etexilate, a new oral direct thrombin inhibitor, in healthy male subjects.Br J Clin Pharmacol.2007;64:292–303.
- ,,,.Pharmacokinetics and pharmacodynamics of the direct oral thrombin inhibitor dabigatran in healthy elderly subjects.Clin Pharmacokinet.2008;47:47–59.
- ,,,,.The metabolism and disposition of the oral direct thrombin inhibitor, dabigatran, in humans.Drug Metab Dispos.2008;36:386–399.
- ,,.Dabigatran etexilate versus warfarin as the oral anticoagulant of choice? A review of clinical data.Pharmacol Ther.2011;129:185–194.
- .The role of P‐glycoprotein and organic anion‐transporting polypeptides in drug interactions.Drug Saf.2005;28:789–801.
- ,,.Novel oral anticoagulants: implications in the perioperative setting.Anesthesiology.2010;113:726–745.
- European Medicines Agency. Pradaxa (dabigatran etexilate) [product information]. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_‐_Product_Information/human/000829/WC 500041059.pdf. Accessed March 25,2011.
- Dabigatran medication guide. Available at: http://bidocs.boehringer‐ingelheim.com/BIWebAccess/ViewServlet.ser?docBase = renetnt9:59–68.
- ,,.Novel oral anticoagulants: the potential relegation of vitamin K antagonists in clinical practice.Int J Clin Pract.2010;64:835–838.
- .The RE‐LY study: Randomized Evaluation of Long‐term anticoagulant therapY: dabigatran vs. warfarin.Eur Heart J.2009;30:2554–2555.
- ,,, et al.Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: the RE‐MODEL randomized trial.J Thromb Haemost.2007;5:2178–2185.
- ,,, et al.Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: a randomised, double‐blind, non‐inferiority trial.Lancet.2007;370:949–956.
- ,,, et al.Dabigatran versus warfarin in the treatment of acute venous thromboembolism.N Engl J Med.2009;361:2342–2352.
- ,,, et al.Dabigatran versus warfarin in patients with atrial fibrillation.N Engl J Med.2009;361:1139–1151.
- ,,,.Influence of renal impairment on the pharmacokinetics and pharmacodynamics of oral dabigatran etexilate: an open‐label, parallel‐group, single‐centre study.Clin Pharmacokinet.2010;49:259–268.
- ,,,,.Pharmacokinetics and pharmacodynamics of dabigatran etexilate, an oral direct thrombin inhibitor, are not affected by moderate hepatic impairment.J Clin Pharmacol.2008;48:1411–1419.
- ,,, et al.Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE‐NOVATE II). A randomised, double‐blind, non‐inferiority trial.Thromb Haemost.2011;105:721–729.
- ,.Insights from the dabigatran versus warfarin trial in patients with venous thromboembolism (the RE‐COVER trial).Expert Opin Pharmacother.2010;11:1035–1037.
- RE‐MOBILIZE Writing Committee,,, et al.Oral thrombin inhibitor dabigatran etexilate vs north american enoxaparin regimen for prevention of venous thromboembolism after knee arthroplasty surgery.J Arthroplasty.2009;24:1–9.
- ,,, et al.Effects of the oral, direct thrombin inhibitor dabigatran on five common coagulation assays.Thromb Haemost.2011;105:371–378.
- ,,, et al.Dabigatran etexilate—a novel, reversible, oral direct thrombin inhibitor: interpretation of coagulation assays and reversal of anticoagulant activity.Thromb Haemost.2010;103:1116–1127.
- ,.A direct thrombin inhibitor studied by dynamic whole blood clot formation. haemostatic response to ex‐vivo addition of recombinant factor VIIa or activated prothrombin complex concentrate.Thromb Haemost.2006;96:446–453.
- US Food and Drug Administration. Dabigatran drug approval history. Available at: http://www.accessdata.fda.gov/drugsatfda_ docs/nda/2010/022512Orig1s000TOC.cfm. Accessed March 20,2011.
- ,,, et al.Dabigatran compared with warfarin in patients with atrial fibrillation and previous transient ischaemic attack or stroke: a subgroup analysis of the RE‐LY trial.Lancet Neurol.2010;9:1157–1163.
- ,,, et al.Dabigatran and warfarin in vitamin K antagonist‐naive and ‐experienced cohorts with atrial fibrillation.Circulation.2010;122:2246–2253.
- ,,, et al.Prevention of venous thromboembolism: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th edition).Chest.2008;133(6 suppl):381S–453S.
- ,,,.American Association of Orthopedic Surgeons and American College of Chest Physicians guidelines for venous thromboembolism prevention in hip and knee arthroplasty differ: what are the implications for clinicians and patients?Chest.2009;135:513–520.
- ,,, et al.The use of antithrombotic therapies in the prevention and treatment of arterial and venous thrombosis: a survey of current knowledge and practice supporting the need for clinical education.Crit Pathw Cardiol.2010;9:41–48.
- .Warfarin versus new agents: interpreting the data.Hematology Am Soc Hematol Educ Program.2010;2010:221–228.
- ,,,,.Why do patients with atrial fibrillation not receive warfarin?Arch Intern Med.2000;160:41–46.
- ,,,,,.Warfarin use among ambulatory patients with nonvalvular atrial fibrillation: The anticoagulation and risk factors in atrial fibrillation (ATRIA) study.Ann Intern Med.1999;131:927–934.
- ,.Drug and dietary interactions of the new and emerging oral anticoagulants.Int J Clin Pract.2010;64:956–967.
- ,,, et al.The risk of bleeding complications in patients with cytochrome P450 CYP2C9*2 or CYP2C9*3 alleles on acenocoumarol or phenprocoumon.Thromb Haemost.2004;92:61–66.
- ,,, et al.Differentiating low‐molecular‐weight heparins based on chemical, biological, and pharmacologic properties: implications for the development of generic versions of low‐molecular‐weight heparins.Semin Thromb Hemost.2008;34:74–85.
- ,.Emerging anticoagulants.Expert Opin Emerg Drugs.2011;16:31–44.
- ,,, et al.Systematic overview of warfarin and its drug and food interactions.Arch Intern Med.2005;165:1095–1106.
- ,,,,,.Evaluation of the pattern of treatment, level of anticoagulation control, and outcome of treatment with warfarin in patients with non‐valvar atrial fibrillation: a record linkage study in a large british population.Heart.2005;91:472–477.
- ,,, et al.Comparison of outcomes among patients randomized to warfarin therapy according to anticoagulant control: results from SPORTIF III and V.Arch Intern Med.2007;167:239–245.
- ,,,.Medication use leading to emergency department visits for adverse drug events in older adults.Ann Intern Med.2007;147:755–765.
- .New oral anticoagulants: a practical guide for clinicians.J Thromb Thrombolysis.2010;29:182–191.
- ,,,.The quest for new anticoagulants: from clinical development to clinical practice [published ahead of print June 14, 2010].Cardiovasc Ther.2010. doi: 10.1111/j.1755–5922.2010.00160.x.
- ,,,,.In‐vitro profile and ex‐vivo anticoagulant activity of the direct thrombin inhibitor dabigatran and its orally active prodrug, dabigatran etexilate.Thromb Haemost.2007;98:155–162.
- ,,.Novel oral factor xa and thrombin inhibitors in the management of thromboembolism.Annu Rev Med.2011;62:41–57.
- ,,,,.Clot‐bound thrombin is protected from inhibition by heparin‐antithrombin III but is susceptible to inactivation by antithrombin III‐independent inhibitors.J Clin Invest.1990;86:385–391.
- ,,.Thrombin binds to soluble fibrin degradation products where it is protected from inhibition by heparin‐antithrombin but susceptible to inactivation by antithrombin‐independent inhibitors.Circulation.1998;97:544–552.
- .Clinical pharmacokinetics and pharmacodynamics of the oral direct thrombin inhibitor dabigatran etexilate.Clin Pharmacokinet.2008;47:285–295.
- ,.Pharmacology, pharmacokinetics, and pharmacodynamics of dabigatran etexilate, an oral direct thrombin inhibitor.Clin Appl Thromb Hemost.2009;15(suppl 1):9S–16S.
- ,,,,.The pharmacokinetics, pharmacodynamics and tolerability of dabigatran etexilate, a new oral direct thrombin inhibitor, in healthy male subjects.Br J Clin Pharmacol.2007;64:292–303.
- ,,,.Pharmacokinetics and pharmacodynamics of the direct oral thrombin inhibitor dabigatran in healthy elderly subjects.Clin Pharmacokinet.2008;47:47–59.
- ,,,,.The metabolism and disposition of the oral direct thrombin inhibitor, dabigatran, in humans.Drug Metab Dispos.2008;36:386–399.
- ,,.Dabigatran etexilate versus warfarin as the oral anticoagulant of choice? A review of clinical data.Pharmacol Ther.2011;129:185–194.
- .The role of P‐glycoprotein and organic anion‐transporting polypeptides in drug interactions.Drug Saf.2005;28:789–801.
- ,,.Novel oral anticoagulants: implications in the perioperative setting.Anesthesiology.2010;113:726–745.
- European Medicines Agency. Pradaxa (dabigatran etexilate) [product information]. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_‐_Product_Information/human/000829/WC 500041059.pdf. Accessed March 25,2011.
- Dabigatran medication guide. Available at: http://bidocs.boehringer‐ingelheim.com/BIWebAccess/ViewServlet.ser?docBase = renetnt9:59–68.
- ,,.Novel oral anticoagulants: the potential relegation of vitamin K antagonists in clinical practice.Int J Clin Pract.2010;64:835–838.
- .The RE‐LY study: Randomized Evaluation of Long‐term anticoagulant therapY: dabigatran vs. warfarin.Eur Heart J.2009;30:2554–2555.
- ,,, et al.Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: the RE‐MODEL randomized trial.J Thromb Haemost.2007;5:2178–2185.
- ,,, et al.Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: a randomised, double‐blind, non‐inferiority trial.Lancet.2007;370:949–956.
- ,,, et al.Dabigatran versus warfarin in the treatment of acute venous thromboembolism.N Engl J Med.2009;361:2342–2352.
- ,,, et al.Dabigatran versus warfarin in patients with atrial fibrillation.N Engl J Med.2009;361:1139–1151.
- ,,,.Influence of renal impairment on the pharmacokinetics and pharmacodynamics of oral dabigatran etexilate: an open‐label, parallel‐group, single‐centre study.Clin Pharmacokinet.2010;49:259–268.
- ,,,,.Pharmacokinetics and pharmacodynamics of dabigatran etexilate, an oral direct thrombin inhibitor, are not affected by moderate hepatic impairment.J Clin Pharmacol.2008;48:1411–1419.
- ,,, et al.Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE‐NOVATE II). A randomised, double‐blind, non‐inferiority trial.Thromb Haemost.2011;105:721–729.
- ,.Insights from the dabigatran versus warfarin trial in patients with venous thromboembolism (the RE‐COVER trial).Expert Opin Pharmacother.2010;11:1035–1037.
- RE‐MOBILIZE Writing Committee,,, et al.Oral thrombin inhibitor dabigatran etexilate vs north american enoxaparin regimen for prevention of venous thromboembolism after knee arthroplasty surgery.J Arthroplasty.2009;24:1–9.
- ,,, et al.Effects of the oral, direct thrombin inhibitor dabigatran on five common coagulation assays.Thromb Haemost.2011;105:371–378.
- ,,, et al.Dabigatran etexilate—a novel, reversible, oral direct thrombin inhibitor: interpretation of coagulation assays and reversal of anticoagulant activity.Thromb Haemost.2010;103:1116–1127.
- ,.A direct thrombin inhibitor studied by dynamic whole blood clot formation. haemostatic response to ex‐vivo addition of recombinant factor VIIa or activated prothrombin complex concentrate.Thromb Haemost.2006;96:446–453.
- US Food and Drug Administration. Dabigatran drug approval history. Available at: http://www.accessdata.fda.gov/drugsatfda_ docs/nda/2010/022512Orig1s000TOC.cfm. Accessed March 20,2011.
- ,,, et al.Dabigatran compared with warfarin in patients with atrial fibrillation and previous transient ischaemic attack or stroke: a subgroup analysis of the RE‐LY trial.Lancet Neurol.2010;9:1157–1163.
- ,,, et al.Dabigatran and warfarin in vitamin K antagonist‐naive and ‐experienced cohorts with atrial fibrillation.Circulation.2010;122:2246–2253.
- ,,, et al.Prevention of venous thromboembolism: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th edition).Chest.2008;133(6 suppl):381S–453S.
- ,,,.American Association of Orthopedic Surgeons and American College of Chest Physicians guidelines for venous thromboembolism prevention in hip and knee arthroplasty differ: what are the implications for clinicians and patients?Chest.2009;135:513–520.