User login
Intrauterine vacuum device treatment of postpartum hemorrhage
Postpartum hemorrhage (PPH) is a common complication of birth. In 2019, 4.3% of births in the United States were complicated by at least one episode of PPH.1 Major causes of PPH include uterine atony, retained products of conception, reproductive tract trauma, and coagulopathy.2 Active management of the third stage of labor with the routine administration of postpartum uterotonics reduces the risk of PPH.3,4
PPH treatment requires a systematic approach using appropriate uterotonic medications, tranexamic acid, and procedures performed in a timely sequence to resolve the hemorrhage. Following vaginal birth, procedures that do not require a laparotomy to treat PPH include uterine massage, uterine evacuation to remove retained placental tissue, repair of lacerations, uterine balloon tamponade (UBT), uterine packing, a vacuum-induced hemorrhage control device (VHCD; JADA, Organon), and uterine artery embolization. Following cesarean birth, with an open laparotomy incision, interventions to treat PPH due to atony include vascular ligation, uterine compression sutures, UBT, VHCD, hysterectomy, and pelvic packing.2
Over the past 2 decades, UBT has been widely used for the treatment of PPH with a success rate in observational studies of approximately 86%.5 The uterine balloon creates pressure against the wall of the uterus permitting accumulation of platelets at bleeding sites, enhancing the activity of the clotting system. The uterine balloon provides direct pressure on the bleeding site(s). It is well known in trauma care that the first step to treat a bleeding wound is to apply direct pressure to the bleeding site. During the third stage of labor, a natural process is tetanic uterine contraction, which constricts myometrial vessels and the placenta bed. Placing a balloon in the uterus and inflating the balloon to 200 mL to 500 mL may delay the involution of the uterus that should occur following birth. An observation of great interest is the insight that inducing a vacuum in the uterine cavity may enhance tetanic uterine contraction and constriction of the myometrial vessels. Vacuum-induced hemorrhage control is discussed in detail in this editorial.
Vacuum-induced hemorrhage control device
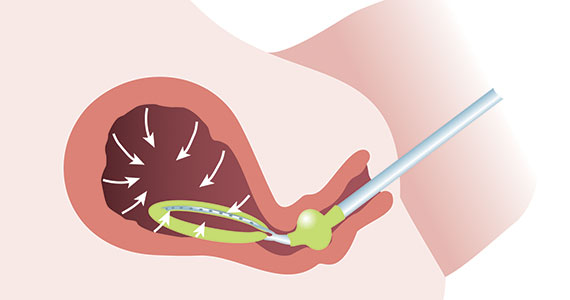
A new device for the treatment of PPH due to uterine atony is the JADA VHCD (FIGURE), which generates negative intrauterine pressure causing the uterus to contract, thereby constricting myometrial vessels and reducing uterine bleeding. The JADA VHCD system is indicated to provide control and treatment of abnormal postpartum uterine bleeding following vaginal or cesarean birth caused by uterine atony when conservative management is indicated.6
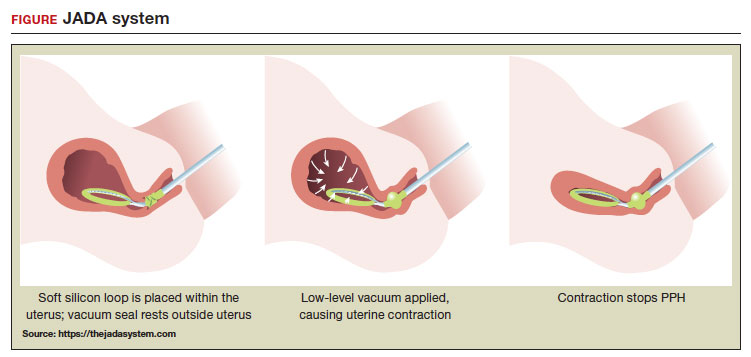 ILLUSTRATION: MARY ELLEN NIATAS FOR OBG MANAGEMENT
ILLUSTRATION: MARY ELLEN NIATAS FOR OBG MANAGEMENT
System components
The JADA VHCD consists of a leading portion intended to be inserted into the uterine cavity, which consists of a silicone elliptical loop with 20 vacuum pores. A soft shield covers the vacuum loop to reduce the risk of the vacuum pores being clogged with biological material, including blood and clots. The elliptical loop is attached to a catheter intended for connection to a vacuum source set to 80 mm Hg ±10 mm Hg (hospital wall suction or portable suction device) with an in-line cannister to collect blood. Approximately 16 cm from the tip of the elliptical loop is a balloon that should be positioned in the upper vagina, not inside the cervix, and inflated with fluid (60 mL to 120 mL) through a dedicated port to occlude the vagina, thereby preserving a stable intrauterine vacuum.
Continue to: Correct usage...
Correct usage
A simple mnemonic to facilitate use of the JADA VHCD is “120/80”—fill the vaginal balloon with 120 mL of sterile fluid and attach the tubing to a source that is set to provide 80 mm Hg of vacuum with an in-line collection cannister. The VHCD may not work correctly if there is a substantial amount of blood in the uterus. Clinical experts advise that an important step prior to placing the elliptical loop in the uterus is to perform a sweep of the uterine cavity with a hand or instrument to remove clots and ensure there is no retained placental tissue. It is preferable to assemble the suction tubing, syringe, sterile fluid, and other instruments (eg, forceps, speculum) needed to insert the device prior to attempting to place the VHCD. When the elliptical loop is compressed for insertion, it is about 2 cm in diameter, necessitating that the cervix be dilated sufficiently to accommodate the device.
Immediately after placing the VHCD, contractions can be monitored by physical examination and the amount of ongoing bleeding can be estimated by observing the amount of blood accumulating in the cannister. Rapid onset of a palpable increase in uterine tone is a prominent feature of successful treatment of PPH with the VHCD. The VHCD should be kept in the uterus with active suction for at least 1 hour. Taping the tubing to the inner thigh may help stabilize the device. Once bleeding is controlled, prior to removing the device, the vacuum should be discontinued, and bleeding activityshould be assessed for at least 30 minutes. If the patient is stable, the vaginal balloon can be deflated, followed by removal of the device. The VHCD should be removed within 24 hours of placement.6
The JADA VHCD system should not be used with ongoing intrauterine pregnancy, untreated uterine rupture, unresolved uterine inversion, current cervical cancer, or serious infection of the uterus.6 The VHCD has not been evaluated for effectiveness in the treatment of placenta accreta or coagulopathy. The VHCD has not been specifically evaluated for safety and effectiveness in patients < 34 weeks’ duration, but clinicians report successful use of the device in cases of PPH that have occurred in the second and early-third trimesters. If the device can be appropriately placed with the elliptical loop in the uterus and the balloon in the vagina, it is theoretically possible to use the device for cases of PPH occurring before 34 weeks’ gestation.
When using the JADA VHCD system, it is important to simultaneously provide cardiovascular support, appropriate transfusion of blood products and timely surgical intervention, if indicated. All obstetricians know that in complicated cases of PPH, where conservative measures have not worked, uterine artery embolization or hysterectomy may be the only interventions that will prevent serious patient morbidity.
Effectiveness data
The VHCD has not been evaluated against an alternative approach, such as UBT, in published randomized clinical trials. However, prospective cohort studies have reported that the JADA is often successful in the treatment of PPH.7-10
In a multicenter cohort study of 107 patients with PPH, including 91 vaginal and 16 cesarean births, 100 patients (93%) were successfully treated with the JADA VHCD.7 Median blood loss before application of the system was 870 mL with vaginal birth and 1,300 mL with cesarean birth. Definitive control of the hemorrhage was observed at a median of 3 minutes after initiation of the intrauterine vacuum. In this study, 32% of patients had reproductive tract lacerations that needed to be repaired, and 2 patients required a hysterectomy. Forty patients required a blood transfusion.
Two patients were treated with a Bakri UBT when the VHCD did not resolve the PPH. In this cohort, the vacuum was applied for a median duration of 144 minutes, and a median total device dwell time was 191 minutes. Compared with UBT, the JADA VHCD intrauterine dwell time was shorter, facilitating patient progression and early transfer to the postpartum unit. The physicians who participated in the study reported that the device was easy to use. The complications reported in this cohort were minor and included endometritis (5 cases), vaginal infection (2 cases), and disruption of a vaginal laceration repair (1 case).7
Novel approaches to generating an intrauterine vacuum to treat PPH
The JADA VHCD is the only vacuum device approved by the US Food and Drug Administration (FDA) for treatment of PPH. However, clinical innovators have reported alternative approaches to generating an intrauterine vacuum using equipment designed for other purposes. In one study, a Bakri balloon was used to generate intrauterine vacuum tamponade to treat PPH.11 In this study, a Bakri balloon was inserted into the uterus, and the balloon was inflated to 50 mL to 100 mL to seal the vacuum. The main Bakri port was attached to a suction aspiration device set to generate a vacuum of 450 mm Hg to 525 mm Hg, a much greater vacuum than used with the JADA VHCD. This study included 44 cases of PPH due to uterine atony and 22 cases due to placental pathology, with successful treatment of PPH in 86% and 73% of the cases, respectively.
Another approach to generate intrauterine vacuum tamponade involves using a Levin stomach tube (FG24 or FG36), which has an open end and 4 side ports near the open tip.12-14 The Levin stomach tube is low cost and has many favorable design features, including a rounded tip, wide-bore, and circumferentially placed side ports. The FG36 Levin stomach tube is 12 mm in diameter and has 10 mm side ports. A vacuum device set to deliver 100 mm Hg to 200 mm Hgwas used in some of the studies evaluating the Levin stomach tube for the treatment of PPH. In 3 cases of severe PPH unresponsive to standard interventions, creation of vacuum tamponade with flexible suction tubing with side ports was successful in controlling the hemorrhage.13
Dr. T.N. Vasudeva Panicker invented an intrauterine cannula 12 mm in diameter and 25 cm in length, with dozens of 4 mm side ports over the distal 12 cm of the cannula.15 The cannula, which is made of stainless steel or plastic, is inserted into the uterus and 700 mm Hgvacuum is applied, a level much greater than the 80 mm Hg vacuum recommended for use with the JADA VHCD. When successful, the high suction clears the uterus of blood and causes uterine contraction. In 4 cases of severe PPH, the device successfully controlled the hemorrhage. In 2 of the 4 cases the device that was initially placed became clogged with blood and needed to be replaced.
UBT vs VHCD
To date there are no published randomized controlled trials comparing Bakri UBT to the JADA VHCD. In one retrospective study, the frequency of massive transfusion of red blood cells (RBCs), defined as the transfusion of 4 units or greater of RBCs, was assessed among 78 patients treated with the Bakri UBT and 36 patients treated with the JADA VHCD.9 In this study, at baseline there was a non ̶ statistically significant trend for JADA VHCD to be used more frequently than the Bakri UBT in cases of PPH occurring during repeat cesarean delivery (33% vs 14%). The Bakri UBT was used more frequently than the JADA VHCD among patients having a PPH following a vaginal delivery (51% vs 31%). Both devices were used at similar rates for operative vaginal delivery (6%) and primary cesarean birth (31% VHCD and 28% UBT).
In this retrospective study, the percentage of patients treated with VHCD or UBT who received 4 or more units of RBCs was 3% and 21%, respectively (P < .01). Among patients treated with VHCD and UBT, the estimated median blood loss was 1,500 mL and 1,850 mL (P=.02), respectively. The median hemoglobin concentration at discharge was similar in the VHCD and UBT groups, 8.8 g/dL and 8.6 g/dL, respectively.9 A randomized controlled trial is necessary to refine our understanding of the comparative effectiveness of UBT and VHCD in controlling PPH following vaginal and cesarean birth.
A welcome addition to treatment options
Every obstetrician knows that, in the next 12 months of their practice, they will encounter multiple cases of PPH. One or two of these cases may require the physician to use every medication and procedure available for the treatment of PPH to save the life of the patient. To prepare to treat the next case of PPH rapidly and effectively, it is important for every obstetrician to develop a standardized cognitive plan for using all available treatmentmodalities in an appropriate and timely sequence, including both the Bakri balloon and the JADA VHCD. The insight that inducing an intrauterine vacuum causes uterine contraction, which may resolve PPH, is an important discovery. The JADA VHCD is a welcome addition to our armamentarium of treatments for PPH. ●
- Corbetta-Rastelli CM, Friedman AM, Sobhani NC, et al. Postpartum hemorrhage trends and outcomes in the United States, 2000-2019. Obstet Gynecol. 2023;141:152-161.
- Bienstock JL, Eke AC, Hueppchen NA. Postpartum hemorrhage. N Engl J Med. 2021;384:16351645.
- Salati JA, Leathersich SJ, Williams MJ, et al. Prophylactic oxytocin for the third stage of labour to prevent postpartum hemorrhage. Cochrane Database Syst Rev. 2019;CD001808.
- Begley CM, Gyte GMI, Devane D, et al. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2019;CD007412.
- Suarez S, Conde-Agudelo A, Borovac-Pinheiro A, et al. Uterine balloon tamponade for the treatment of postpartum hemorrhage: a systematic review and meta-analysis. Am J Obstet Gynecol. 2020;222:293.e1-e52.
- US Food and Drug Administration. JADA system approval. Accessed July 25, 2023. https://www .accessdata.fda.gov/cdrh_docs/pdf21/K212757 .pdf
- D’Alton ME, Rood KM, Smid MC, et al. Intrauterine vacuum-induced hemorrhage control device for rapid treatment of postpartum hemorrhage. Obstet Gynecol. 2020;136:882-891.
- D’Alton M, Rood K, Simhan H, et al. Profile of the JADA System: the vacuum-induced hemorrhage control device for treating abnormal postpartum uterine bleeding and postpartum hemorrhage. Expert Rev Med Devices. 2021; 18:849-853.
- Gulersen M, Gerber RP, Rochelson B, et al. Vacuum-induced hemorrhage control versus uterine balloon tamponade for postpartum hemorrhage. J Obstet Gynaecol Can. 2023;45:267-272.
- Purwosunnu Y, Sarkoen W, Arulkumaran S, et al. Control of postpartum hemorrhage using vacuum-induced uterine tamponade. Obstet Gynecol. 2016;128:33-36.
- Haslinger C, Weber K, Zimmerman R. Vacuuminduced tamponade for treatment of postpartum hemorrhage. Obstet Gynecol. 2021;138:361-365.
- Hofmeyr GJ, Middleton K, Singata-Madliki M. Randomized feasibility study of suction-tube uterine tamponade for postpartum hemorrhage. Int J Gynaecol Obstet. 2019;146:339-343.
- Hofmeyr GJ, Singata-Madliki M. Novel suction tube uterine tamponade for treating intractable postpartum hemorrhage: description of technique and report of three cases. BJOG. 2020;127:1280-1283.
- Cebekhulu SN, Abdul H, Batting J, et al. Suction tube uterine tamponade for treatment of refractory postpartum hemorrhage: internal feasibility and acceptability pilot of a randomized clinical trial. Int J Gynaecol Obstet. 2022;158: 79-85.
- Panicker TNV. Panicker’s vacuum suction haemostatic device for treating post-partum hemorrhage. J Obstet Gynaecol India. 2017;67:150-151.

Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair Emeritus, Department of Obstetrics and Gynecology
Brigham and Women’s Hospital
Kate Macy Ladd Distinguished Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Boston, Massachusetts
The author reports no conflict of interest related to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair Emeritus, Department of Obstetrics and Gynecology
Brigham and Women’s Hospital
Kate Macy Ladd Distinguished Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Boston, Massachusetts
The author reports no conflict of interest related to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair Emeritus, Department of Obstetrics and Gynecology
Brigham and Women’s Hospital
Kate Macy Ladd Distinguished Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Boston, Massachusetts
The author reports no conflict of interest related to this article.
Postpartum hemorrhage (PPH) is a common complication of birth. In 2019, 4.3% of births in the United States were complicated by at least one episode of PPH.1 Major causes of PPH include uterine atony, retained products of conception, reproductive tract trauma, and coagulopathy.2 Active management of the third stage of labor with the routine administration of postpartum uterotonics reduces the risk of PPH.3,4
PPH treatment requires a systematic approach using appropriate uterotonic medications, tranexamic acid, and procedures performed in a timely sequence to resolve the hemorrhage. Following vaginal birth, procedures that do not require a laparotomy to treat PPH include uterine massage, uterine evacuation to remove retained placental tissue, repair of lacerations, uterine balloon tamponade (UBT), uterine packing, a vacuum-induced hemorrhage control device (VHCD; JADA, Organon), and uterine artery embolization. Following cesarean birth, with an open laparotomy incision, interventions to treat PPH due to atony include vascular ligation, uterine compression sutures, UBT, VHCD, hysterectomy, and pelvic packing.2
Over the past 2 decades, UBT has been widely used for the treatment of PPH with a success rate in observational studies of approximately 86%.5 The uterine balloon creates pressure against the wall of the uterus permitting accumulation of platelets at bleeding sites, enhancing the activity of the clotting system. The uterine balloon provides direct pressure on the bleeding site(s). It is well known in trauma care that the first step to treat a bleeding wound is to apply direct pressure to the bleeding site. During the third stage of labor, a natural process is tetanic uterine contraction, which constricts myometrial vessels and the placenta bed. Placing a balloon in the uterus and inflating the balloon to 200 mL to 500 mL may delay the involution of the uterus that should occur following birth. An observation of great interest is the insight that inducing a vacuum in the uterine cavity may enhance tetanic uterine contraction and constriction of the myometrial vessels. Vacuum-induced hemorrhage control is discussed in detail in this editorial.
Vacuum-induced hemorrhage control device
A new device for the treatment of PPH due to uterine atony is the JADA VHCD (FIGURE), which generates negative intrauterine pressure causing the uterus to contract, thereby constricting myometrial vessels and reducing uterine bleeding. The JADA VHCD system is indicated to provide control and treatment of abnormal postpartum uterine bleeding following vaginal or cesarean birth caused by uterine atony when conservative management is indicated.6
ILLUSTRATION: MARY ELLEN NIATAS FOR OBG MANAGEMENT
System components
The JADA VHCD consists of a leading portion intended to be inserted into the uterine cavity, which consists of a silicone elliptical loop with 20 vacuum pores. A soft shield covers the vacuum loop to reduce the risk of the vacuum pores being clogged with biological material, including blood and clots. The elliptical loop is attached to a catheter intended for connection to a vacuum source set to 80 mm Hg ±10 mm Hg (hospital wall suction or portable suction device) with an in-line cannister to collect blood. Approximately 16 cm from the tip of the elliptical loop is a balloon that should be positioned in the upper vagina, not inside the cervix, and inflated with fluid (60 mL to 120 mL) through a dedicated port to occlude the vagina, thereby preserving a stable intrauterine vacuum.
Continue to: Correct usage...
Correct usage
A simple mnemonic to facilitate use of the JADA VHCD is “120/80”—fill the vaginal balloon with 120 mL of sterile fluid and attach the tubing to a source that is set to provide 80 mm Hg of vacuum with an in-line collection cannister. The VHCD may not work correctly if there is a substantial amount of blood in the uterus. Clinical experts advise that an important step prior to placing the elliptical loop in the uterus is to perform a sweep of the uterine cavity with a hand or instrument to remove clots and ensure there is no retained placental tissue. It is preferable to assemble the suction tubing, syringe, sterile fluid, and other instruments (eg, forceps, speculum) needed to insert the device prior to attempting to place the VHCD. When the elliptical loop is compressed for insertion, it is about 2 cm in diameter, necessitating that the cervix be dilated sufficiently to accommodate the device.
Immediately after placing the VHCD, contractions can be monitored by physical examination and the amount of ongoing bleeding can be estimated by observing the amount of blood accumulating in the cannister. Rapid onset of a palpable increase in uterine tone is a prominent feature of successful treatment of PPH with the VHCD. The VHCD should be kept in the uterus with active suction for at least 1 hour. Taping the tubing to the inner thigh may help stabilize the device. Once bleeding is controlled, prior to removing the device, the vacuum should be discontinued, and bleeding activityshould be assessed for at least 30 minutes. If the patient is stable, the vaginal balloon can be deflated, followed by removal of the device. The VHCD should be removed within 24 hours of placement.6
The JADA VHCD system should not be used with ongoing intrauterine pregnancy, untreated uterine rupture, unresolved uterine inversion, current cervical cancer, or serious infection of the uterus.6 The VHCD has not been evaluated for effectiveness in the treatment of placenta accreta or coagulopathy. The VHCD has not been specifically evaluated for safety and effectiveness in patients < 34 weeks’ duration, but clinicians report successful use of the device in cases of PPH that have occurred in the second and early-third trimesters. If the device can be appropriately placed with the elliptical loop in the uterus and the balloon in the vagina, it is theoretically possible to use the device for cases of PPH occurring before 34 weeks’ gestation.
When using the JADA VHCD system, it is important to simultaneously provide cardiovascular support, appropriate transfusion of blood products and timely surgical intervention, if indicated. All obstetricians know that in complicated cases of PPH, where conservative measures have not worked, uterine artery embolization or hysterectomy may be the only interventions that will prevent serious patient morbidity.
Effectiveness data
The VHCD has not been evaluated against an alternative approach, such as UBT, in published randomized clinical trials. However, prospective cohort studies have reported that the JADA is often successful in the treatment of PPH.7-10
In a multicenter cohort study of 107 patients with PPH, including 91 vaginal and 16 cesarean births, 100 patients (93%) were successfully treated with the JADA VHCD.7 Median blood loss before application of the system was 870 mL with vaginal birth and 1,300 mL with cesarean birth. Definitive control of the hemorrhage was observed at a median of 3 minutes after initiation of the intrauterine vacuum. In this study, 32% of patients had reproductive tract lacerations that needed to be repaired, and 2 patients required a hysterectomy. Forty patients required a blood transfusion.
Two patients were treated with a Bakri UBT when the VHCD did not resolve the PPH. In this cohort, the vacuum was applied for a median duration of 144 minutes, and a median total device dwell time was 191 minutes. Compared with UBT, the JADA VHCD intrauterine dwell time was shorter, facilitating patient progression and early transfer to the postpartum unit. The physicians who participated in the study reported that the device was easy to use. The complications reported in this cohort were minor and included endometritis (5 cases), vaginal infection (2 cases), and disruption of a vaginal laceration repair (1 case).7
Novel approaches to generating an intrauterine vacuum to treat PPH
The JADA VHCD is the only vacuum device approved by the US Food and Drug Administration (FDA) for treatment of PPH. However, clinical innovators have reported alternative approaches to generating an intrauterine vacuum using equipment designed for other purposes. In one study, a Bakri balloon was used to generate intrauterine vacuum tamponade to treat PPH.11 In this study, a Bakri balloon was inserted into the uterus, and the balloon was inflated to 50 mL to 100 mL to seal the vacuum. The main Bakri port was attached to a suction aspiration device set to generate a vacuum of 450 mm Hg to 525 mm Hg, a much greater vacuum than used with the JADA VHCD. This study included 44 cases of PPH due to uterine atony and 22 cases due to placental pathology, with successful treatment of PPH in 86% and 73% of the cases, respectively.
Another approach to generate intrauterine vacuum tamponade involves using a Levin stomach tube (FG24 or FG36), which has an open end and 4 side ports near the open tip.12-14 The Levin stomach tube is low cost and has many favorable design features, including a rounded tip, wide-bore, and circumferentially placed side ports. The FG36 Levin stomach tube is 12 mm in diameter and has 10 mm side ports. A vacuum device set to deliver 100 mm Hg to 200 mm Hgwas used in some of the studies evaluating the Levin stomach tube for the treatment of PPH. In 3 cases of severe PPH unresponsive to standard interventions, creation of vacuum tamponade with flexible suction tubing with side ports was successful in controlling the hemorrhage.13
Dr. T.N. Vasudeva Panicker invented an intrauterine cannula 12 mm in diameter and 25 cm in length, with dozens of 4 mm side ports over the distal 12 cm of the cannula.15 The cannula, which is made of stainless steel or plastic, is inserted into the uterus and 700 mm Hgvacuum is applied, a level much greater than the 80 mm Hg vacuum recommended for use with the JADA VHCD. When successful, the high suction clears the uterus of blood and causes uterine contraction. In 4 cases of severe PPH, the device successfully controlled the hemorrhage. In 2 of the 4 cases the device that was initially placed became clogged with blood and needed to be replaced.
UBT vs VHCD
To date there are no published randomized controlled trials comparing Bakri UBT to the JADA VHCD. In one retrospective study, the frequency of massive transfusion of red blood cells (RBCs), defined as the transfusion of 4 units or greater of RBCs, was assessed among 78 patients treated with the Bakri UBT and 36 patients treated with the JADA VHCD.9 In this study, at baseline there was a non ̶ statistically significant trend for JADA VHCD to be used more frequently than the Bakri UBT in cases of PPH occurring during repeat cesarean delivery (33% vs 14%). The Bakri UBT was used more frequently than the JADA VHCD among patients having a PPH following a vaginal delivery (51% vs 31%). Both devices were used at similar rates for operative vaginal delivery (6%) and primary cesarean birth (31% VHCD and 28% UBT).
In this retrospective study, the percentage of patients treated with VHCD or UBT who received 4 or more units of RBCs was 3% and 21%, respectively (P < .01). Among patients treated with VHCD and UBT, the estimated median blood loss was 1,500 mL and 1,850 mL (P=.02), respectively. The median hemoglobin concentration at discharge was similar in the VHCD and UBT groups, 8.8 g/dL and 8.6 g/dL, respectively.9 A randomized controlled trial is necessary to refine our understanding of the comparative effectiveness of UBT and VHCD in controlling PPH following vaginal and cesarean birth.
A welcome addition to treatment options
Every obstetrician knows that, in the next 12 months of their practice, they will encounter multiple cases of PPH. One or two of these cases may require the physician to use every medication and procedure available for the treatment of PPH to save the life of the patient. To prepare to treat the next case of PPH rapidly and effectively, it is important for every obstetrician to develop a standardized cognitive plan for using all available treatmentmodalities in an appropriate and timely sequence, including both the Bakri balloon and the JADA VHCD. The insight that inducing an intrauterine vacuum causes uterine contraction, which may resolve PPH, is an important discovery. The JADA VHCD is a welcome addition to our armamentarium of treatments for PPH. ●
Postpartum hemorrhage (PPH) is a common complication of birth. In 2019, 4.3% of births in the United States were complicated by at least one episode of PPH.1 Major causes of PPH include uterine atony, retained products of conception, reproductive tract trauma, and coagulopathy.2 Active management of the third stage of labor with the routine administration of postpartum uterotonics reduces the risk of PPH.3,4
PPH treatment requires a systematic approach using appropriate uterotonic medications, tranexamic acid, and procedures performed in a timely sequence to resolve the hemorrhage. Following vaginal birth, procedures that do not require a laparotomy to treat PPH include uterine massage, uterine evacuation to remove retained placental tissue, repair of lacerations, uterine balloon tamponade (UBT), uterine packing, a vacuum-induced hemorrhage control device (VHCD; JADA, Organon), and uterine artery embolization. Following cesarean birth, with an open laparotomy incision, interventions to treat PPH due to atony include vascular ligation, uterine compression sutures, UBT, VHCD, hysterectomy, and pelvic packing.2
Over the past 2 decades, UBT has been widely used for the treatment of PPH with a success rate in observational studies of approximately 86%.5 The uterine balloon creates pressure against the wall of the uterus permitting accumulation of platelets at bleeding sites, enhancing the activity of the clotting system. The uterine balloon provides direct pressure on the bleeding site(s). It is well known in trauma care that the first step to treat a bleeding wound is to apply direct pressure to the bleeding site. During the third stage of labor, a natural process is tetanic uterine contraction, which constricts myometrial vessels and the placenta bed. Placing a balloon in the uterus and inflating the balloon to 200 mL to 500 mL may delay the involution of the uterus that should occur following birth. An observation of great interest is the insight that inducing a vacuum in the uterine cavity may enhance tetanic uterine contraction and constriction of the myometrial vessels. Vacuum-induced hemorrhage control is discussed in detail in this editorial.
Vacuum-induced hemorrhage control device
A new device for the treatment of PPH due to uterine atony is the JADA VHCD (FIGURE), which generates negative intrauterine pressure causing the uterus to contract, thereby constricting myometrial vessels and reducing uterine bleeding. The JADA VHCD system is indicated to provide control and treatment of abnormal postpartum uterine bleeding following vaginal or cesarean birth caused by uterine atony when conservative management is indicated.6
ILLUSTRATION: MARY ELLEN NIATAS FOR OBG MANAGEMENT
System components
The JADA VHCD consists of a leading portion intended to be inserted into the uterine cavity, which consists of a silicone elliptical loop with 20 vacuum pores. A soft shield covers the vacuum loop to reduce the risk of the vacuum pores being clogged with biological material, including blood and clots. The elliptical loop is attached to a catheter intended for connection to a vacuum source set to 80 mm Hg ±10 mm Hg (hospital wall suction or portable suction device) with an in-line cannister to collect blood. Approximately 16 cm from the tip of the elliptical loop is a balloon that should be positioned in the upper vagina, not inside the cervix, and inflated with fluid (60 mL to 120 mL) through a dedicated port to occlude the vagina, thereby preserving a stable intrauterine vacuum.
Continue to: Correct usage...
Correct usage
A simple mnemonic to facilitate use of the JADA VHCD is “120/80”—fill the vaginal balloon with 120 mL of sterile fluid and attach the tubing to a source that is set to provide 80 mm Hg of vacuum with an in-line collection cannister. The VHCD may not work correctly if there is a substantial amount of blood in the uterus. Clinical experts advise that an important step prior to placing the elliptical loop in the uterus is to perform a sweep of the uterine cavity with a hand or instrument to remove clots and ensure there is no retained placental tissue. It is preferable to assemble the suction tubing, syringe, sterile fluid, and other instruments (eg, forceps, speculum) needed to insert the device prior to attempting to place the VHCD. When the elliptical loop is compressed for insertion, it is about 2 cm in diameter, necessitating that the cervix be dilated sufficiently to accommodate the device.
Immediately after placing the VHCD, contractions can be monitored by physical examination and the amount of ongoing bleeding can be estimated by observing the amount of blood accumulating in the cannister. Rapid onset of a palpable increase in uterine tone is a prominent feature of successful treatment of PPH with the VHCD. The VHCD should be kept in the uterus with active suction for at least 1 hour. Taping the tubing to the inner thigh may help stabilize the device. Once bleeding is controlled, prior to removing the device, the vacuum should be discontinued, and bleeding activityshould be assessed for at least 30 minutes. If the patient is stable, the vaginal balloon can be deflated, followed by removal of the device. The VHCD should be removed within 24 hours of placement.6
The JADA VHCD system should not be used with ongoing intrauterine pregnancy, untreated uterine rupture, unresolved uterine inversion, current cervical cancer, or serious infection of the uterus.6 The VHCD has not been evaluated for effectiveness in the treatment of placenta accreta or coagulopathy. The VHCD has not been specifically evaluated for safety and effectiveness in patients < 34 weeks’ duration, but clinicians report successful use of the device in cases of PPH that have occurred in the second and early-third trimesters. If the device can be appropriately placed with the elliptical loop in the uterus and the balloon in the vagina, it is theoretically possible to use the device for cases of PPH occurring before 34 weeks’ gestation.
When using the JADA VHCD system, it is important to simultaneously provide cardiovascular support, appropriate transfusion of blood products and timely surgical intervention, if indicated. All obstetricians know that in complicated cases of PPH, where conservative measures have not worked, uterine artery embolization or hysterectomy may be the only interventions that will prevent serious patient morbidity.
Effectiveness data
The VHCD has not been evaluated against an alternative approach, such as UBT, in published randomized clinical trials. However, prospective cohort studies have reported that the JADA is often successful in the treatment of PPH.7-10
In a multicenter cohort study of 107 patients with PPH, including 91 vaginal and 16 cesarean births, 100 patients (93%) were successfully treated with the JADA VHCD.7 Median blood loss before application of the system was 870 mL with vaginal birth and 1,300 mL with cesarean birth. Definitive control of the hemorrhage was observed at a median of 3 minutes after initiation of the intrauterine vacuum. In this study, 32% of patients had reproductive tract lacerations that needed to be repaired, and 2 patients required a hysterectomy. Forty patients required a blood transfusion.
Two patients were treated with a Bakri UBT when the VHCD did not resolve the PPH. In this cohort, the vacuum was applied for a median duration of 144 minutes, and a median total device dwell time was 191 minutes. Compared with UBT, the JADA VHCD intrauterine dwell time was shorter, facilitating patient progression and early transfer to the postpartum unit. The physicians who participated in the study reported that the device was easy to use. The complications reported in this cohort were minor and included endometritis (5 cases), vaginal infection (2 cases), and disruption of a vaginal laceration repair (1 case).7
Novel approaches to generating an intrauterine vacuum to treat PPH
The JADA VHCD is the only vacuum device approved by the US Food and Drug Administration (FDA) for treatment of PPH. However, clinical innovators have reported alternative approaches to generating an intrauterine vacuum using equipment designed for other purposes. In one study, a Bakri balloon was used to generate intrauterine vacuum tamponade to treat PPH.11 In this study, a Bakri balloon was inserted into the uterus, and the balloon was inflated to 50 mL to 100 mL to seal the vacuum. The main Bakri port was attached to a suction aspiration device set to generate a vacuum of 450 mm Hg to 525 mm Hg, a much greater vacuum than used with the JADA VHCD. This study included 44 cases of PPH due to uterine atony and 22 cases due to placental pathology, with successful treatment of PPH in 86% and 73% of the cases, respectively.
Another approach to generate intrauterine vacuum tamponade involves using a Levin stomach tube (FG24 or FG36), which has an open end and 4 side ports near the open tip.12-14 The Levin stomach tube is low cost and has many favorable design features, including a rounded tip, wide-bore, and circumferentially placed side ports. The FG36 Levin stomach tube is 12 mm in diameter and has 10 mm side ports. A vacuum device set to deliver 100 mm Hg to 200 mm Hgwas used in some of the studies evaluating the Levin stomach tube for the treatment of PPH. In 3 cases of severe PPH unresponsive to standard interventions, creation of vacuum tamponade with flexible suction tubing with side ports was successful in controlling the hemorrhage.13
Dr. T.N. Vasudeva Panicker invented an intrauterine cannula 12 mm in diameter and 25 cm in length, with dozens of 4 mm side ports over the distal 12 cm of the cannula.15 The cannula, which is made of stainless steel or plastic, is inserted into the uterus and 700 mm Hgvacuum is applied, a level much greater than the 80 mm Hg vacuum recommended for use with the JADA VHCD. When successful, the high suction clears the uterus of blood and causes uterine contraction. In 4 cases of severe PPH, the device successfully controlled the hemorrhage. In 2 of the 4 cases the device that was initially placed became clogged with blood and needed to be replaced.
UBT vs VHCD
To date there are no published randomized controlled trials comparing Bakri UBT to the JADA VHCD. In one retrospective study, the frequency of massive transfusion of red blood cells (RBCs), defined as the transfusion of 4 units or greater of RBCs, was assessed among 78 patients treated with the Bakri UBT and 36 patients treated with the JADA VHCD.9 In this study, at baseline there was a non ̶ statistically significant trend for JADA VHCD to be used more frequently than the Bakri UBT in cases of PPH occurring during repeat cesarean delivery (33% vs 14%). The Bakri UBT was used more frequently than the JADA VHCD among patients having a PPH following a vaginal delivery (51% vs 31%). Both devices were used at similar rates for operative vaginal delivery (6%) and primary cesarean birth (31% VHCD and 28% UBT).
In this retrospective study, the percentage of patients treated with VHCD or UBT who received 4 or more units of RBCs was 3% and 21%, respectively (P < .01). Among patients treated with VHCD and UBT, the estimated median blood loss was 1,500 mL and 1,850 mL (P=.02), respectively. The median hemoglobin concentration at discharge was similar in the VHCD and UBT groups, 8.8 g/dL and 8.6 g/dL, respectively.9 A randomized controlled trial is necessary to refine our understanding of the comparative effectiveness of UBT and VHCD in controlling PPH following vaginal and cesarean birth.
A welcome addition to treatment options
Every obstetrician knows that, in the next 12 months of their practice, they will encounter multiple cases of PPH. One or two of these cases may require the physician to use every medication and procedure available for the treatment of PPH to save the life of the patient. To prepare to treat the next case of PPH rapidly and effectively, it is important for every obstetrician to develop a standardized cognitive plan for using all available treatmentmodalities in an appropriate and timely sequence, including both the Bakri balloon and the JADA VHCD. The insight that inducing an intrauterine vacuum causes uterine contraction, which may resolve PPH, is an important discovery. The JADA VHCD is a welcome addition to our armamentarium of treatments for PPH. ●
- Corbetta-Rastelli CM, Friedman AM, Sobhani NC, et al. Postpartum hemorrhage trends and outcomes in the United States, 2000-2019. Obstet Gynecol. 2023;141:152-161.
- Bienstock JL, Eke AC, Hueppchen NA. Postpartum hemorrhage. N Engl J Med. 2021;384:16351645.
- Salati JA, Leathersich SJ, Williams MJ, et al. Prophylactic oxytocin for the third stage of labour to prevent postpartum hemorrhage. Cochrane Database Syst Rev. 2019;CD001808.
- Begley CM, Gyte GMI, Devane D, et al. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2019;CD007412.
- Suarez S, Conde-Agudelo A, Borovac-Pinheiro A, et al. Uterine balloon tamponade for the treatment of postpartum hemorrhage: a systematic review and meta-analysis. Am J Obstet Gynecol. 2020;222:293.e1-e52.
- US Food and Drug Administration. JADA system approval. Accessed July 25, 2023. https://www .accessdata.fda.gov/cdrh_docs/pdf21/K212757 .pdf
- D’Alton ME, Rood KM, Smid MC, et al. Intrauterine vacuum-induced hemorrhage control device for rapid treatment of postpartum hemorrhage. Obstet Gynecol. 2020;136:882-891.
- D’Alton M, Rood K, Simhan H, et al. Profile of the JADA System: the vacuum-induced hemorrhage control device for treating abnormal postpartum uterine bleeding and postpartum hemorrhage. Expert Rev Med Devices. 2021; 18:849-853.
- Gulersen M, Gerber RP, Rochelson B, et al. Vacuum-induced hemorrhage control versus uterine balloon tamponade for postpartum hemorrhage. J Obstet Gynaecol Can. 2023;45:267-272.
- Purwosunnu Y, Sarkoen W, Arulkumaran S, et al. Control of postpartum hemorrhage using vacuum-induced uterine tamponade. Obstet Gynecol. 2016;128:33-36.
- Haslinger C, Weber K, Zimmerman R. Vacuuminduced tamponade for treatment of postpartum hemorrhage. Obstet Gynecol. 2021;138:361-365.
- Hofmeyr GJ, Middleton K, Singata-Madliki M. Randomized feasibility study of suction-tube uterine tamponade for postpartum hemorrhage. Int J Gynaecol Obstet. 2019;146:339-343.
- Hofmeyr GJ, Singata-Madliki M. Novel suction tube uterine tamponade for treating intractable postpartum hemorrhage: description of technique and report of three cases. BJOG. 2020;127:1280-1283.
- Cebekhulu SN, Abdul H, Batting J, et al. Suction tube uterine tamponade for treatment of refractory postpartum hemorrhage: internal feasibility and acceptability pilot of a randomized clinical trial. Int J Gynaecol Obstet. 2022;158: 79-85.
- Panicker TNV. Panicker’s vacuum suction haemostatic device for treating post-partum hemorrhage. J Obstet Gynaecol India. 2017;67:150-151.
- Corbetta-Rastelli CM, Friedman AM, Sobhani NC, et al. Postpartum hemorrhage trends and outcomes in the United States, 2000-2019. Obstet Gynecol. 2023;141:152-161.
- Bienstock JL, Eke AC, Hueppchen NA. Postpartum hemorrhage. N Engl J Med. 2021;384:16351645.
- Salati JA, Leathersich SJ, Williams MJ, et al. Prophylactic oxytocin for the third stage of labour to prevent postpartum hemorrhage. Cochrane Database Syst Rev. 2019;CD001808.
- Begley CM, Gyte GMI, Devane D, et al. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst Rev. 2019;CD007412.
- Suarez S, Conde-Agudelo A, Borovac-Pinheiro A, et al. Uterine balloon tamponade for the treatment of postpartum hemorrhage: a systematic review and meta-analysis. Am J Obstet Gynecol. 2020;222:293.e1-e52.
- US Food and Drug Administration. JADA system approval. Accessed July 25, 2023. https://www .accessdata.fda.gov/cdrh_docs/pdf21/K212757 .pdf
- D’Alton ME, Rood KM, Smid MC, et al. Intrauterine vacuum-induced hemorrhage control device for rapid treatment of postpartum hemorrhage. Obstet Gynecol. 2020;136:882-891.
- D’Alton M, Rood K, Simhan H, et al. Profile of the JADA System: the vacuum-induced hemorrhage control device for treating abnormal postpartum uterine bleeding and postpartum hemorrhage. Expert Rev Med Devices. 2021; 18:849-853.
- Gulersen M, Gerber RP, Rochelson B, et al. Vacuum-induced hemorrhage control versus uterine balloon tamponade for postpartum hemorrhage. J Obstet Gynaecol Can. 2023;45:267-272.
- Purwosunnu Y, Sarkoen W, Arulkumaran S, et al. Control of postpartum hemorrhage using vacuum-induced uterine tamponade. Obstet Gynecol. 2016;128:33-36.
- Haslinger C, Weber K, Zimmerman R. Vacuuminduced tamponade for treatment of postpartum hemorrhage. Obstet Gynecol. 2021;138:361-365.
- Hofmeyr GJ, Middleton K, Singata-Madliki M. Randomized feasibility study of suction-tube uterine tamponade for postpartum hemorrhage. Int J Gynaecol Obstet. 2019;146:339-343.
- Hofmeyr GJ, Singata-Madliki M. Novel suction tube uterine tamponade for treating intractable postpartum hemorrhage: description of technique and report of three cases. BJOG. 2020;127:1280-1283.
- Cebekhulu SN, Abdul H, Batting J, et al. Suction tube uterine tamponade for treatment of refractory postpartum hemorrhage: internal feasibility and acceptability pilot of a randomized clinical trial. Int J Gynaecol Obstet. 2022;158: 79-85.
- Panicker TNV. Panicker’s vacuum suction haemostatic device for treating post-partum hemorrhage. J Obstet Gynaecol India. 2017;67:150-151.
Axial spondyloarthritis: Does visibility with x-rays make a difference in management?
Knowing whether a patient has radiographic or nonradiographic axial spondyloarthritis will not change management, experts say.
Out with the old, in with the new
Axial spondyloarthritis is characterized by chronic inflammation of the sacroiliac (SI) joints, and spine. It’s a modern term that includes ankylosing spondylitis (AS) and that refers to opposite ends of a disease spectrum.
Nonradiographic axial spondyloarthritis (nr-axSpA) is so termed because there are no definitive visible changes on plain x-rays, although inflammatory changes may be seen on MRI.
Radiographic axial spondyloarthritis (r-axSpA) is the same as AS to some extent and is associated with clear signs of joint damage (that is, of past inflammation) on x-rays.
“Axial spondyloarthritis is one disease, and whether it is radiographic or nonradiographic makes zero difference in the management of the patient,” says Atul Deodhar, MD, professor of medicine and medical director of rheumatology clinics at Oregon Health and Science University, Portland. The distinction came about in 2009 to facilitate scientific and clinical research, he explains, and to enable the use of tumor necrosis factor inhibitors, which were new at the time, for patients who could not be classified as having AS.
“We have known what ankylosing spondylitis is for a long time because we have been doing plain x-rays of the sacroiliac joints, and if we see classical changes of sacroiliitis, we have the diagnosis. However, MRI changed everything,” Dr. Deodhar says. Now it’s possible to see inflammatory changes in the SI joints and early joint damage, which was not possible to see on x-ray until many years later.
Reassuring for patients?
“Currently, we don’t really have different treatments,” Dr. Deodhar notes. Perhaps the only benefit is that it might be reassuring for patients to know that they have the nonradiographic form. Receiving a diagnosis of axial spondyloarthritis comes as quite a shock. It’s a diagnosis that is potentially going to affect them for the rest of their lives, and some patients worry that they’ll develop the classic “bamboo” spine of AS, he adds. So, being able to tell patients that they have nr-axSpA and that they are going to be treated early and aggressively may be somewhat comforting.
“It’s a continuum of a disease state, but a lot of people will stay at the nonradiographic stage,” points out Portland-based internist Beth Smith, DO, associate professor of medicine at OHSU.
“A good portion of individuals who may have an MRI that’s positive will either go into remission or just stay at that stage of the disease; they won’t necessarily progress to radiographic sacroiliitis,” she adds.
Spotting nr-axSpA in practice
Nr-axSpA can be tricky to spot in clinical practice, and its diagnosis in primary care largely relies on patients’ clinical presentation and identifying IBP. This is the key symptom. When someone younger than 45 years experiences back pain that is characterized by insidious and chronic onset and that improves with anti-inflammatory agents and activity but that worsens with rest and is worse at night, then imaging of the SI joints may be appropriate.
“You have to have that index of suspicion in order to even think about ordering the appropriate imaging test,” Dr. Smith says. IBP may be the big clue, but patients may also return on separate occasions with multiple associated complaints, such as plantar fasciitis, tennis elbow, or other conditions, such as psoriasis, she says.
Ordering HLA-B27 and C-reactive protein tests may be useful prior to conducting any imaging, Dr. Smith says, “and if imaging is ordered, make sure it is an x-ray of the sacroiliac joint, not the lumbar spine.”
Dr. Deodhar cautions: “A single anterior-posterior view of the pelvis is enough to look at the sacroiliac joint.” There is no need to order separate views of the right and left SI joints; doing so will provide no additional useful information and exposes the patient to unnecessary radiation.
Importantly, consider whether an x-ray of the lumbar spine is needed for a patient with chronic back pain, he says. “You should do an investigation that is going to make a difference to your management. If you take 100 patients with back pain, 95% of the time, it is going to be mechanical back pain. Why do an x-ray of the lumbar spine?” Dr. Deodhar asks rhetorically.
It should also be borne in mind that x-rays can be nonspecific, and several conditions may mimic sacroiliitis, such as osteitis condensans ilii in women who have given birth, osteoarthritis of the SI joints, and old infection of the SI joints.
MRIs need specialist interpretation
MRIs of the lumbar spine are overused to diagnose back pain, and while they might be sensitive to early inflammatory changes in SI joints, they require an expert eye for interpretation.
“MRI of the SI joints is to be used wisely in patients when there is enough clinical suspicion,” Dr. Deodhar advises. Even when an MRI is negative for sacroiliitis, patients could still have axial spondyloarthritis.
MRIs of the SI joints are needed, but not of the lumbar spine, he stresses. Views of the lumbar spine may show only signs of disk degeneration and perhaps osteoarthritis.
Moreover, Dr. Deodhar says, “MRI is so sensitive that we used to think that bone marrow edema is good enough for telling us there is sacroiliitis.” However, even people without IBP can have bone marrow edema; “exercise can show bone marrow edema,” he says.
So, “If there’s a suspicion of axial spondyloarthritis, the patient should be referred to a rheumatologist,” who will discuss the interpretation with highly specialized musculoskeletal radiologists.
Take-home messages
Whether it is nr-axSpA or r-axSpA, “the burden of disease for the patient is the same; treatment is the same,” says Dr. Deodhar. Patients should be referred to a rheumatologist as soon as possible if axial spondyloarthritis is suspected. A single x-ray of the pelvis should be performed to see the SI joints, but MRIs should be left to secondary care, he suggests.
Dr. Smith notes: “Having that index of suspicion of an inflammatory etiology for the back pain is essential.” It ensures that “patients can get early and appropriate treatment for a disease that’s very different from the mechanical back pain that we mostly see in primary care.”
Dr. Deodhar has received research grants or has acted as a consultant to multiple pharmaceutical companies, including AbbVie, Bristol-Myers Squibb, Celgene, Janssen, UCB, Novartis, Pfizer, and Eli Lilly. Dr. Smith reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Knowing whether a patient has radiographic or nonradiographic axial spondyloarthritis will not change management, experts say.
Out with the old, in with the new
Axial spondyloarthritis is characterized by chronic inflammation of the sacroiliac (SI) joints, and spine. It’s a modern term that includes ankylosing spondylitis (AS) and that refers to opposite ends of a disease spectrum.
Nonradiographic axial spondyloarthritis (nr-axSpA) is so termed because there are no definitive visible changes on plain x-rays, although inflammatory changes may be seen on MRI.
Radiographic axial spondyloarthritis (r-axSpA) is the same as AS to some extent and is associated with clear signs of joint damage (that is, of past inflammation) on x-rays.
“Axial spondyloarthritis is one disease, and whether it is radiographic or nonradiographic makes zero difference in the management of the patient,” says Atul Deodhar, MD, professor of medicine and medical director of rheumatology clinics at Oregon Health and Science University, Portland. The distinction came about in 2009 to facilitate scientific and clinical research, he explains, and to enable the use of tumor necrosis factor inhibitors, which were new at the time, for patients who could not be classified as having AS.
“We have known what ankylosing spondylitis is for a long time because we have been doing plain x-rays of the sacroiliac joints, and if we see classical changes of sacroiliitis, we have the diagnosis. However, MRI changed everything,” Dr. Deodhar says. Now it’s possible to see inflammatory changes in the SI joints and early joint damage, which was not possible to see on x-ray until many years later.
Reassuring for patients?
“Currently, we don’t really have different treatments,” Dr. Deodhar notes. Perhaps the only benefit is that it might be reassuring for patients to know that they have the nonradiographic form. Receiving a diagnosis of axial spondyloarthritis comes as quite a shock. It’s a diagnosis that is potentially going to affect them for the rest of their lives, and some patients worry that they’ll develop the classic “bamboo” spine of AS, he adds. So, being able to tell patients that they have nr-axSpA and that they are going to be treated early and aggressively may be somewhat comforting.
“It’s a continuum of a disease state, but a lot of people will stay at the nonradiographic stage,” points out Portland-based internist Beth Smith, DO, associate professor of medicine at OHSU.
“A good portion of individuals who may have an MRI that’s positive will either go into remission or just stay at that stage of the disease; they won’t necessarily progress to radiographic sacroiliitis,” she adds.
Spotting nr-axSpA in practice
Nr-axSpA can be tricky to spot in clinical practice, and its diagnosis in primary care largely relies on patients’ clinical presentation and identifying IBP. This is the key symptom. When someone younger than 45 years experiences back pain that is characterized by insidious and chronic onset and that improves with anti-inflammatory agents and activity but that worsens with rest and is worse at night, then imaging of the SI joints may be appropriate.
“You have to have that index of suspicion in order to even think about ordering the appropriate imaging test,” Dr. Smith says. IBP may be the big clue, but patients may also return on separate occasions with multiple associated complaints, such as plantar fasciitis, tennis elbow, or other conditions, such as psoriasis, she says.
Ordering HLA-B27 and C-reactive protein tests may be useful prior to conducting any imaging, Dr. Smith says, “and if imaging is ordered, make sure it is an x-ray of the sacroiliac joint, not the lumbar spine.”
Dr. Deodhar cautions: “A single anterior-posterior view of the pelvis is enough to look at the sacroiliac joint.” There is no need to order separate views of the right and left SI joints; doing so will provide no additional useful information and exposes the patient to unnecessary radiation.
Importantly, consider whether an x-ray of the lumbar spine is needed for a patient with chronic back pain, he says. “You should do an investigation that is going to make a difference to your management. If you take 100 patients with back pain, 95% of the time, it is going to be mechanical back pain. Why do an x-ray of the lumbar spine?” Dr. Deodhar asks rhetorically.
It should also be borne in mind that x-rays can be nonspecific, and several conditions may mimic sacroiliitis, such as osteitis condensans ilii in women who have given birth, osteoarthritis of the SI joints, and old infection of the SI joints.
MRIs need specialist interpretation
MRIs of the lumbar spine are overused to diagnose back pain, and while they might be sensitive to early inflammatory changes in SI joints, they require an expert eye for interpretation.
“MRI of the SI joints is to be used wisely in patients when there is enough clinical suspicion,” Dr. Deodhar advises. Even when an MRI is negative for sacroiliitis, patients could still have axial spondyloarthritis.
MRIs of the SI joints are needed, but not of the lumbar spine, he stresses. Views of the lumbar spine may show only signs of disk degeneration and perhaps osteoarthritis.
Moreover, Dr. Deodhar says, “MRI is so sensitive that we used to think that bone marrow edema is good enough for telling us there is sacroiliitis.” However, even people without IBP can have bone marrow edema; “exercise can show bone marrow edema,” he says.
So, “If there’s a suspicion of axial spondyloarthritis, the patient should be referred to a rheumatologist,” who will discuss the interpretation with highly specialized musculoskeletal radiologists.
Take-home messages
Whether it is nr-axSpA or r-axSpA, “the burden of disease for the patient is the same; treatment is the same,” says Dr. Deodhar. Patients should be referred to a rheumatologist as soon as possible if axial spondyloarthritis is suspected. A single x-ray of the pelvis should be performed to see the SI joints, but MRIs should be left to secondary care, he suggests.
Dr. Smith notes: “Having that index of suspicion of an inflammatory etiology for the back pain is essential.” It ensures that “patients can get early and appropriate treatment for a disease that’s very different from the mechanical back pain that we mostly see in primary care.”
Dr. Deodhar has received research grants or has acted as a consultant to multiple pharmaceutical companies, including AbbVie, Bristol-Myers Squibb, Celgene, Janssen, UCB, Novartis, Pfizer, and Eli Lilly. Dr. Smith reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Knowing whether a patient has radiographic or nonradiographic axial spondyloarthritis will not change management, experts say.
Out with the old, in with the new
Axial spondyloarthritis is characterized by chronic inflammation of the sacroiliac (SI) joints, and spine. It’s a modern term that includes ankylosing spondylitis (AS) and that refers to opposite ends of a disease spectrum.
Nonradiographic axial spondyloarthritis (nr-axSpA) is so termed because there are no definitive visible changes on plain x-rays, although inflammatory changes may be seen on MRI.
Radiographic axial spondyloarthritis (r-axSpA) is the same as AS to some extent and is associated with clear signs of joint damage (that is, of past inflammation) on x-rays.
“Axial spondyloarthritis is one disease, and whether it is radiographic or nonradiographic makes zero difference in the management of the patient,” says Atul Deodhar, MD, professor of medicine and medical director of rheumatology clinics at Oregon Health and Science University, Portland. The distinction came about in 2009 to facilitate scientific and clinical research, he explains, and to enable the use of tumor necrosis factor inhibitors, which were new at the time, for patients who could not be classified as having AS.
“We have known what ankylosing spondylitis is for a long time because we have been doing plain x-rays of the sacroiliac joints, and if we see classical changes of sacroiliitis, we have the diagnosis. However, MRI changed everything,” Dr. Deodhar says. Now it’s possible to see inflammatory changes in the SI joints and early joint damage, which was not possible to see on x-ray until many years later.
Reassuring for patients?
“Currently, we don’t really have different treatments,” Dr. Deodhar notes. Perhaps the only benefit is that it might be reassuring for patients to know that they have the nonradiographic form. Receiving a diagnosis of axial spondyloarthritis comes as quite a shock. It’s a diagnosis that is potentially going to affect them for the rest of their lives, and some patients worry that they’ll develop the classic “bamboo” spine of AS, he adds. So, being able to tell patients that they have nr-axSpA and that they are going to be treated early and aggressively may be somewhat comforting.
“It’s a continuum of a disease state, but a lot of people will stay at the nonradiographic stage,” points out Portland-based internist Beth Smith, DO, associate professor of medicine at OHSU.
“A good portion of individuals who may have an MRI that’s positive will either go into remission or just stay at that stage of the disease; they won’t necessarily progress to radiographic sacroiliitis,” she adds.
Spotting nr-axSpA in practice
Nr-axSpA can be tricky to spot in clinical practice, and its diagnosis in primary care largely relies on patients’ clinical presentation and identifying IBP. This is the key symptom. When someone younger than 45 years experiences back pain that is characterized by insidious and chronic onset and that improves with anti-inflammatory agents and activity but that worsens with rest and is worse at night, then imaging of the SI joints may be appropriate.
“You have to have that index of suspicion in order to even think about ordering the appropriate imaging test,” Dr. Smith says. IBP may be the big clue, but patients may also return on separate occasions with multiple associated complaints, such as plantar fasciitis, tennis elbow, or other conditions, such as psoriasis, she says.
Ordering HLA-B27 and C-reactive protein tests may be useful prior to conducting any imaging, Dr. Smith says, “and if imaging is ordered, make sure it is an x-ray of the sacroiliac joint, not the lumbar spine.”
Dr. Deodhar cautions: “A single anterior-posterior view of the pelvis is enough to look at the sacroiliac joint.” There is no need to order separate views of the right and left SI joints; doing so will provide no additional useful information and exposes the patient to unnecessary radiation.
Importantly, consider whether an x-ray of the lumbar spine is needed for a patient with chronic back pain, he says. “You should do an investigation that is going to make a difference to your management. If you take 100 patients with back pain, 95% of the time, it is going to be mechanical back pain. Why do an x-ray of the lumbar spine?” Dr. Deodhar asks rhetorically.
It should also be borne in mind that x-rays can be nonspecific, and several conditions may mimic sacroiliitis, such as osteitis condensans ilii in women who have given birth, osteoarthritis of the SI joints, and old infection of the SI joints.
MRIs need specialist interpretation
MRIs of the lumbar spine are overused to diagnose back pain, and while they might be sensitive to early inflammatory changes in SI joints, they require an expert eye for interpretation.
“MRI of the SI joints is to be used wisely in patients when there is enough clinical suspicion,” Dr. Deodhar advises. Even when an MRI is negative for sacroiliitis, patients could still have axial spondyloarthritis.
MRIs of the SI joints are needed, but not of the lumbar spine, he stresses. Views of the lumbar spine may show only signs of disk degeneration and perhaps osteoarthritis.
Moreover, Dr. Deodhar says, “MRI is so sensitive that we used to think that bone marrow edema is good enough for telling us there is sacroiliitis.” However, even people without IBP can have bone marrow edema; “exercise can show bone marrow edema,” he says.
So, “If there’s a suspicion of axial spondyloarthritis, the patient should be referred to a rheumatologist,” who will discuss the interpretation with highly specialized musculoskeletal radiologists.
Take-home messages
Whether it is nr-axSpA or r-axSpA, “the burden of disease for the patient is the same; treatment is the same,” says Dr. Deodhar. Patients should be referred to a rheumatologist as soon as possible if axial spondyloarthritis is suspected. A single x-ray of the pelvis should be performed to see the SI joints, but MRIs should be left to secondary care, he suggests.
Dr. Smith notes: “Having that index of suspicion of an inflammatory etiology for the back pain is essential.” It ensures that “patients can get early and appropriate treatment for a disease that’s very different from the mechanical back pain that we mostly see in primary care.”
Dr. Deodhar has received research grants or has acted as a consultant to multiple pharmaceutical companies, including AbbVie, Bristol-Myers Squibb, Celgene, Janssen, UCB, Novartis, Pfizer, and Eli Lilly. Dr. Smith reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
How much pain is in the mind? This doctor thinks the answer is, most
More than 3 decades ago, John E. Sarno, MD, published Healing Back Pain, a popular book that garnered something of a cult following. Looking at his own practice, Dr. Sarno, a rehabilitation medicine specialist in New York, saw that most of his patients with chronic pain did not have evidence of acute injury or degenerative disk disease. Their persistent pain appeared to be independent of any structural damage to the spine. Dr. Sarno attributed the pain to what he called tension myoneural syndrome (TMS), or the body’s reaction to suppressed stress and emotional turmoil. Resolving that psychological conflict, Dr. Sarno believed, would lead to an improvement in pain.
Dr. Sarno’s theory has met skepticism from the mainstream community, but glowing testimonies from patients who say they benefited from his strategies fill the Internet. Dr. Sarno wrote several books on his ideas before his death in 2017. But he published only one peer-reviewed study, a 2003 review in the Archives of Physical Medicine and Rehabilitation coauthored by Ira Rashbaum, MD.
The interview has been edited for length and clarity.
What is your theory of back pain?
Dr. Rashbaum: My null hypothesis is that back pain is not due to psychological issues, so as to not be a biased doctor, I try to accept the null hypothesis or reject the null hypothesis. In most cases chronic back pain is not due to structural etiology. My sense is it’s a mind-body issue – the avoidance of feeling strong emotions like anger, rage, sadness, fear, shame, and guilt. Patients can embrace psychoeducational programs and if they don’t get better, we work with a psychotherapist or a licensed mental health counselor to help work through the patient’s feelings. That’s my experience over a number of years.
How do you determine if a patient has back pain from a mind-body issue or another cause?
Dr. Rashbaum: I do a very careful medical history, including a physical examination and review of any diagnostic studies they’ve undergone. In most situations, there’s not really a medical cause of the back pain. For instance, a lot of asymptomatic individuals have all sorts of horrible findings on medical imaging like CTs and MRIs, and the reverse is also true – many people with negative findings on imaging tests experience significant pain. My job as a diagnostician is to see how much of this is really a mind-body problem or something that stems from structural pathology.
How well do your patients react to being told that their back pain is, in a way, “in their head?”
Dr. Rashbaum: I have a skewed population. I’m sort of like a guru in mind-body back pain, so the people who come to me are already thinking along those lines. I ask: “What’s going on in your life?” Maybe there are job issues, marital issues, health issues, and I’d say that it’s certainly possible that stress can be causing this back pain.
Sometimes when I see a patient referred from another physician, I’m a bit hesitant to ask about what’s going on in their life. Even earlier today, I’d seen a patient with back pain and I had a sense that they were not really going to be open to a mind-body approach. So I said, do physical therapy.
What do you recommend primary care clinicians do with patients with back pain?
Dr. Rashbaum: You have to do a proper neurologic examination and musculoskeletal examination. It’s a tough situation because doctors in primary care have limited time to take care of patients. It’s difficult to have a deeper dive just to kind of see what’s going on in their life. But you can recommend useful agents like acetaminophen and muscle relaxants, which are sometimes okay.
What sorts of things do you tell patients to say to themselves when they’re experiencing pain?
Dr. Rashbaum: If the pain is severe, I recommend they take medication – over-the-counter analgesics or a muscle relaxant, if they have them – and take a warm shower or bath. I prefer acetaminophen up to three times per day, if that’s okay with the patient’s primary care physician, over NSAIDs because most pain is noninflammatory in nature. Once the pain is more manageable, patients should journal about what’s going on in their lives and/or meditate, and try to feel any strong emotions, such as anger, sadness, or fear.
What do you say to clinicians who are dismissive of the notion that chronic pain may stem from emotional repression, and that addressing the latter can resolve the former – particularly those who point to a lack of peer-reviewed data for such a link?
Dr. Rashbaum: I would tell them they could be looking harder for that evidence. For example, in a patient page from JAMA from April 24, 2013, on low back pain, often the cause of back pain is unknown. There are data in spine surgical journals that patients with psychological issues do worse with spine surgery. And in 2016 JAMA published a study from Cherkin and colleagues, which found that, among adults with chronic low back pain, treatment with mindfulness-based stress reduction or cognitive behavioral therapy resulted in greater improvement in back pain and functional limitations at 26 weeks, compared with usual care.
My feeling is that these psychosocial interventions are easy to try, relatively inexpensive, noninvasive, and, in my experience, often can lead to marked improvements. I believe that, for the vast majority of people with chronic pain, it makes much more sense to start by addressing mind-body issues than turning to that approach as a last resort.
Dr. Rashbaum reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
More than 3 decades ago, John E. Sarno, MD, published Healing Back Pain, a popular book that garnered something of a cult following. Looking at his own practice, Dr. Sarno, a rehabilitation medicine specialist in New York, saw that most of his patients with chronic pain did not have evidence of acute injury or degenerative disk disease. Their persistent pain appeared to be independent of any structural damage to the spine. Dr. Sarno attributed the pain to what he called tension myoneural syndrome (TMS), or the body’s reaction to suppressed stress and emotional turmoil. Resolving that psychological conflict, Dr. Sarno believed, would lead to an improvement in pain.
Dr. Sarno’s theory has met skepticism from the mainstream community, but glowing testimonies from patients who say they benefited from his strategies fill the Internet. Dr. Sarno wrote several books on his ideas before his death in 2017. But he published only one peer-reviewed study, a 2003 review in the Archives of Physical Medicine and Rehabilitation coauthored by Ira Rashbaum, MD.
The interview has been edited for length and clarity.
What is your theory of back pain?
Dr. Rashbaum: My null hypothesis is that back pain is not due to psychological issues, so as to not be a biased doctor, I try to accept the null hypothesis or reject the null hypothesis. In most cases chronic back pain is not due to structural etiology. My sense is it’s a mind-body issue – the avoidance of feeling strong emotions like anger, rage, sadness, fear, shame, and guilt. Patients can embrace psychoeducational programs and if they don’t get better, we work with a psychotherapist or a licensed mental health counselor to help work through the patient’s feelings. That’s my experience over a number of years.
How do you determine if a patient has back pain from a mind-body issue or another cause?
Dr. Rashbaum: I do a very careful medical history, including a physical examination and review of any diagnostic studies they’ve undergone. In most situations, there’s not really a medical cause of the back pain. For instance, a lot of asymptomatic individuals have all sorts of horrible findings on medical imaging like CTs and MRIs, and the reverse is also true – many people with negative findings on imaging tests experience significant pain. My job as a diagnostician is to see how much of this is really a mind-body problem or something that stems from structural pathology.
How well do your patients react to being told that their back pain is, in a way, “in their head?”
Dr. Rashbaum: I have a skewed population. I’m sort of like a guru in mind-body back pain, so the people who come to me are already thinking along those lines. I ask: “What’s going on in your life?” Maybe there are job issues, marital issues, health issues, and I’d say that it’s certainly possible that stress can be causing this back pain.
Sometimes when I see a patient referred from another physician, I’m a bit hesitant to ask about what’s going on in their life. Even earlier today, I’d seen a patient with back pain and I had a sense that they were not really going to be open to a mind-body approach. So I said, do physical therapy.
What do you recommend primary care clinicians do with patients with back pain?
Dr. Rashbaum: You have to do a proper neurologic examination and musculoskeletal examination. It’s a tough situation because doctors in primary care have limited time to take care of patients. It’s difficult to have a deeper dive just to kind of see what’s going on in their life. But you can recommend useful agents like acetaminophen and muscle relaxants, which are sometimes okay.
What sorts of things do you tell patients to say to themselves when they’re experiencing pain?
Dr. Rashbaum: If the pain is severe, I recommend they take medication – over-the-counter analgesics or a muscle relaxant, if they have them – and take a warm shower or bath. I prefer acetaminophen up to three times per day, if that’s okay with the patient’s primary care physician, over NSAIDs because most pain is noninflammatory in nature. Once the pain is more manageable, patients should journal about what’s going on in their lives and/or meditate, and try to feel any strong emotions, such as anger, sadness, or fear.
What do you say to clinicians who are dismissive of the notion that chronic pain may stem from emotional repression, and that addressing the latter can resolve the former – particularly those who point to a lack of peer-reviewed data for such a link?
Dr. Rashbaum: I would tell them they could be looking harder for that evidence. For example, in a patient page from JAMA from April 24, 2013, on low back pain, often the cause of back pain is unknown. There are data in spine surgical journals that patients with psychological issues do worse with spine surgery. And in 2016 JAMA published a study from Cherkin and colleagues, which found that, among adults with chronic low back pain, treatment with mindfulness-based stress reduction or cognitive behavioral therapy resulted in greater improvement in back pain and functional limitations at 26 weeks, compared with usual care.
My feeling is that these psychosocial interventions are easy to try, relatively inexpensive, noninvasive, and, in my experience, often can lead to marked improvements. I believe that, for the vast majority of people with chronic pain, it makes much more sense to start by addressing mind-body issues than turning to that approach as a last resort.
Dr. Rashbaum reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
More than 3 decades ago, John E. Sarno, MD, published Healing Back Pain, a popular book that garnered something of a cult following. Looking at his own practice, Dr. Sarno, a rehabilitation medicine specialist in New York, saw that most of his patients with chronic pain did not have evidence of acute injury or degenerative disk disease. Their persistent pain appeared to be independent of any structural damage to the spine. Dr. Sarno attributed the pain to what he called tension myoneural syndrome (TMS), or the body’s reaction to suppressed stress and emotional turmoil. Resolving that psychological conflict, Dr. Sarno believed, would lead to an improvement in pain.
Dr. Sarno’s theory has met skepticism from the mainstream community, but glowing testimonies from patients who say they benefited from his strategies fill the Internet. Dr. Sarno wrote several books on his ideas before his death in 2017. But he published only one peer-reviewed study, a 2003 review in the Archives of Physical Medicine and Rehabilitation coauthored by Ira Rashbaum, MD.
The interview has been edited for length and clarity.
What is your theory of back pain?
Dr. Rashbaum: My null hypothesis is that back pain is not due to psychological issues, so as to not be a biased doctor, I try to accept the null hypothesis or reject the null hypothesis. In most cases chronic back pain is not due to structural etiology. My sense is it’s a mind-body issue – the avoidance of feeling strong emotions like anger, rage, sadness, fear, shame, and guilt. Patients can embrace psychoeducational programs and if they don’t get better, we work with a psychotherapist or a licensed mental health counselor to help work through the patient’s feelings. That’s my experience over a number of years.
How do you determine if a patient has back pain from a mind-body issue or another cause?
Dr. Rashbaum: I do a very careful medical history, including a physical examination and review of any diagnostic studies they’ve undergone. In most situations, there’s not really a medical cause of the back pain. For instance, a lot of asymptomatic individuals have all sorts of horrible findings on medical imaging like CTs and MRIs, and the reverse is also true – many people with negative findings on imaging tests experience significant pain. My job as a diagnostician is to see how much of this is really a mind-body problem or something that stems from structural pathology.
How well do your patients react to being told that their back pain is, in a way, “in their head?”
Dr. Rashbaum: I have a skewed population. I’m sort of like a guru in mind-body back pain, so the people who come to me are already thinking along those lines. I ask: “What’s going on in your life?” Maybe there are job issues, marital issues, health issues, and I’d say that it’s certainly possible that stress can be causing this back pain.
Sometimes when I see a patient referred from another physician, I’m a bit hesitant to ask about what’s going on in their life. Even earlier today, I’d seen a patient with back pain and I had a sense that they were not really going to be open to a mind-body approach. So I said, do physical therapy.
What do you recommend primary care clinicians do with patients with back pain?
Dr. Rashbaum: You have to do a proper neurologic examination and musculoskeletal examination. It’s a tough situation because doctors in primary care have limited time to take care of patients. It’s difficult to have a deeper dive just to kind of see what’s going on in their life. But you can recommend useful agents like acetaminophen and muscle relaxants, which are sometimes okay.
What sorts of things do you tell patients to say to themselves when they’re experiencing pain?
Dr. Rashbaum: If the pain is severe, I recommend they take medication – over-the-counter analgesics or a muscle relaxant, if they have them – and take a warm shower or bath. I prefer acetaminophen up to three times per day, if that’s okay with the patient’s primary care physician, over NSAIDs because most pain is noninflammatory in nature. Once the pain is more manageable, patients should journal about what’s going on in their lives and/or meditate, and try to feel any strong emotions, such as anger, sadness, or fear.
What do you say to clinicians who are dismissive of the notion that chronic pain may stem from emotional repression, and that addressing the latter can resolve the former – particularly those who point to a lack of peer-reviewed data for such a link?
Dr. Rashbaum: I would tell them they could be looking harder for that evidence. For example, in a patient page from JAMA from April 24, 2013, on low back pain, often the cause of back pain is unknown. There are data in spine surgical journals that patients with psychological issues do worse with spine surgery. And in 2016 JAMA published a study from Cherkin and colleagues, which found that, among adults with chronic low back pain, treatment with mindfulness-based stress reduction or cognitive behavioral therapy resulted in greater improvement in back pain and functional limitations at 26 weeks, compared with usual care.
My feeling is that these psychosocial interventions are easy to try, relatively inexpensive, noninvasive, and, in my experience, often can lead to marked improvements. I believe that, for the vast majority of people with chronic pain, it makes much more sense to start by addressing mind-body issues than turning to that approach as a last resort.
Dr. Rashbaum reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Nutritional psychiatry: Does it exist?
Matt was diagnosed with ADHD combined type when he was 6 years old. Given his age, the family was reluctant to try medications, but after a couple years of parenting classes and reward charts, the parents requested a stimulant. He had significant improvement in focus and impulsivity but also reduced appetite. Now at age 13, irritability and depressive symptoms have been increasing for 9 months. Skeptical of adding another medication, his parents ask whether nutrition might be an alternative tool to treat his symptoms?
What a healthy diet even consists of seems to be a moving target over decades and years. Trendy research, supplements, and dietary approaches proliferate alongside appealing theories of action. In the end, weighing which intervention is effective for which disorder and at what cost becomes murky.
Yet several fundamental principles seem clear and consistent over time and across studies.

Starting early
There is reliable evidence that in the perinatal environment, nutrition sets the stage for many aspects of healthy development. These effects are likely mediated variously through the hypothalamic-pituitary-adrenal axis, the trillions of gut bacteria that make up the microbiome, gene-environment interactions, and more. Maternal malnutrition and stress prenatally puts infants at risk for not only poor birth outcomes but also psychiatric challenges throughout childhood, such as ADHD, anxiety, depression, and autism.1
Intervening in the perinatal period has long-term benefits. A first step includes assessing food security, beginning with consistent access to nutritious food. It is important to inquire about the role of food and nutrition in the family’s history and culture, as well as identifying resources to support access to affordable nutrition. This can be paired with parenting interventions, such as family meals without screens. This may require scaffolding positive conversations in high-conflict family settings (see The Family Dinner Project).
Healthy diets promote mental health
If food security is achieved, what is next? Clinicians can inquire about the who, what, where, when, and why of nutrition to learn about a family’s eating habits.2 While randomized controlled data is very limited, both cross-sectional and longitudinal studies show that healthy diets in youth correlate with mental health – more healthy foods reducing internalizing and externalizing disorders, and more typical Western diets increasing the risk. On average, dietary interventions include higher levels of fruits and vegetables, fish, and nuts, and lower levels of processed foods.2 There is not evidence that restrictive diets or fasting is appropriate or safe for youth. Additionally, involving children in getting, growing, or preparing food with gradually increasing autonomy fosters self-confidence and skill development.
In those struggling with restrictive eating disorders, food is medicine – helping those with restrictive diets to develop more balanced and adequate intake for metabolic needs. Outside of diagnosable eating disorders, weight or body mass index is less of a goal or marker when it comes to mental health. Instead, look for participation in enjoyable activities, opportunities to move and rest, and a body image that supports self-care and self-confidence (see the National Institutes of Health’s We Can! Program). Creating dissonance with cultural ideals of appearance centered on thinness can prevent future eating disorders.3
Nutraceutical options
Outside of eating disorders, specific foods and plants with health or medicinal properties – variously called nutraceuticals, phytoceuticals, or micronutrients – have emerging evidence in mental health. A 2022 expert academic consensus panel reviewed the literature to create clinical guidelines in this area.4 For major depression, adding omega-3 fatty acids to standard antidepressant treatment or standalone St. John’s wort have adequate evidence to recommend, while adjunctive probiotics, zinc, saffron, and curcumin have sufficient though less robust evidence. S-adenosyl methionine, vitamin D, and methyfolate showed only weak evidence for depression, while vitamin C, magnesium, creatine, N-acetylcysteine, folate, and monotherapy omega-3s do not have sufficient evidence to be recommended. For ADHD there was weak support for vitamin D, but no clear evidence for omega-3s, zinc, gingko, or acetyl L-carnitine. For anxiety, there is moderate evidence for ashwagandha and lavender in adults. A child psychiatry review suggests also trying chamomile for generalized anxiety based on the evidence in young adults, and underscores some data for N-acetylcysteine for OCD in particular.5
Many of these nutraceuticals exhibit small or moderate effects in a limited number of trials, with generally much less data for youth, compared with adults. While the same could be said for many on- and off-label uses of psychiatric medications for kids, clinicians would be wise to consider these highly specific nutritional interventions as items on the menu of treatment options rather than stand-alone treatments.
Revisitng the case study
Reflecting on Matt’s care, his pediatrician first assessed his dietary patterns, noting late-night eating and caffeine use with minimal hydration or fiber across the day. Recommendations for keeping fruit and vegetable snacks easily accessible as well as carrying a water flask are well received. They also discuss adding omega-3 fatty acids and probiotics with his morning stimulant while he awaits a referral for cognitive-behavioral therapy in order to address his depressive symptoms and minimize medication needs.
Beyond addressing food security and balanced family meals, specific interventions may be appropriate as initial treatment adjuncts for mild and some moderate mental illness. For more intense moderate to severe illness, nutritional psychiatry may be considered in combination with treatments with stronger evidence. At a community level, clinicians can help advocate for universal school meal programs to address food security, and so-called salad bar interventions to increase fruit/vegetable uptake among school-age children.
Dr. Rosenfeld is associate professor of psychiatry and pediatrics at University of Vermont and the Vermont Center for Children, Youth, and Families, both in Burlington. He has no disclosures.
References
1 Vohr BR et al. Pediatrics. 2017;139:S38-49.
2. Hosker DK et al. Child Adol Psychiatr Clin N Am. 2019;28(2):171-93.
3. Stice E et al. Int J Eat Disord. 2013;46(5):478-85.
4. Sarris J et al. World J Biol Psychiatry. 2022;23(6):424-55.
5. Simkin DR et al. Child Adolesc Psychiatric Clin N Am. 2023;32:193-216.
Matt was diagnosed with ADHD combined type when he was 6 years old. Given his age, the family was reluctant to try medications, but after a couple years of parenting classes and reward charts, the parents requested a stimulant. He had significant improvement in focus and impulsivity but also reduced appetite. Now at age 13, irritability and depressive symptoms have been increasing for 9 months. Skeptical of adding another medication, his parents ask whether nutrition might be an alternative tool to treat his symptoms?
What a healthy diet even consists of seems to be a moving target over decades and years. Trendy research, supplements, and dietary approaches proliferate alongside appealing theories of action. In the end, weighing which intervention is effective for which disorder and at what cost becomes murky.
Yet several fundamental principles seem clear and consistent over time and across studies.
Starting early
There is reliable evidence that in the perinatal environment, nutrition sets the stage for many aspects of healthy development. These effects are likely mediated variously through the hypothalamic-pituitary-adrenal axis, the trillions of gut bacteria that make up the microbiome, gene-environment interactions, and more. Maternal malnutrition and stress prenatally puts infants at risk for not only poor birth outcomes but also psychiatric challenges throughout childhood, such as ADHD, anxiety, depression, and autism.1
Intervening in the perinatal period has long-term benefits. A first step includes assessing food security, beginning with consistent access to nutritious food. It is important to inquire about the role of food and nutrition in the family’s history and culture, as well as identifying resources to support access to affordable nutrition. This can be paired with parenting interventions, such as family meals without screens. This may require scaffolding positive conversations in high-conflict family settings (see The Family Dinner Project).
Healthy diets promote mental health
If food security is achieved, what is next? Clinicians can inquire about the who, what, where, when, and why of nutrition to learn about a family’s eating habits.2 While randomized controlled data is very limited, both cross-sectional and longitudinal studies show that healthy diets in youth correlate with mental health – more healthy foods reducing internalizing and externalizing disorders, and more typical Western diets increasing the risk. On average, dietary interventions include higher levels of fruits and vegetables, fish, and nuts, and lower levels of processed foods.2 There is not evidence that restrictive diets or fasting is appropriate or safe for youth. Additionally, involving children in getting, growing, or preparing food with gradually increasing autonomy fosters self-confidence and skill development.
In those struggling with restrictive eating disorders, food is medicine – helping those with restrictive diets to develop more balanced and adequate intake for metabolic needs. Outside of diagnosable eating disorders, weight or body mass index is less of a goal or marker when it comes to mental health. Instead, look for participation in enjoyable activities, opportunities to move and rest, and a body image that supports self-care and self-confidence (see the National Institutes of Health’s We Can! Program). Creating dissonance with cultural ideals of appearance centered on thinness can prevent future eating disorders.3
Nutraceutical options
Outside of eating disorders, specific foods and plants with health or medicinal properties – variously called nutraceuticals, phytoceuticals, or micronutrients – have emerging evidence in mental health. A 2022 expert academic consensus panel reviewed the literature to create clinical guidelines in this area.4 For major depression, adding omega-3 fatty acids to standard antidepressant treatment or standalone St. John’s wort have adequate evidence to recommend, while adjunctive probiotics, zinc, saffron, and curcumin have sufficient though less robust evidence. S-adenosyl methionine, vitamin D, and methyfolate showed only weak evidence for depression, while vitamin C, magnesium, creatine, N-acetylcysteine, folate, and monotherapy omega-3s do not have sufficient evidence to be recommended. For ADHD there was weak support for vitamin D, but no clear evidence for omega-3s, zinc, gingko, or acetyl L-carnitine. For anxiety, there is moderate evidence for ashwagandha and lavender in adults. A child psychiatry review suggests also trying chamomile for generalized anxiety based on the evidence in young adults, and underscores some data for N-acetylcysteine for OCD in particular.5
Many of these nutraceuticals exhibit small or moderate effects in a limited number of trials, with generally much less data for youth, compared with adults. While the same could be said for many on- and off-label uses of psychiatric medications for kids, clinicians would be wise to consider these highly specific nutritional interventions as items on the menu of treatment options rather than stand-alone treatments.
Revisitng the case study
Reflecting on Matt’s care, his pediatrician first assessed his dietary patterns, noting late-night eating and caffeine use with minimal hydration or fiber across the day. Recommendations for keeping fruit and vegetable snacks easily accessible as well as carrying a water flask are well received. They also discuss adding omega-3 fatty acids and probiotics with his morning stimulant while he awaits a referral for cognitive-behavioral therapy in order to address his depressive symptoms and minimize medication needs.
Beyond addressing food security and balanced family meals, specific interventions may be appropriate as initial treatment adjuncts for mild and some moderate mental illness. For more intense moderate to severe illness, nutritional psychiatry may be considered in combination with treatments with stronger evidence. At a community level, clinicians can help advocate for universal school meal programs to address food security, and so-called salad bar interventions to increase fruit/vegetable uptake among school-age children.
Dr. Rosenfeld is associate professor of psychiatry and pediatrics at University of Vermont and the Vermont Center for Children, Youth, and Families, both in Burlington. He has no disclosures.
References
1 Vohr BR et al. Pediatrics. 2017;139:S38-49.
2. Hosker DK et al. Child Adol Psychiatr Clin N Am. 2019;28(2):171-93.
3. Stice E et al. Int J Eat Disord. 2013;46(5):478-85.
4. Sarris J et al. World J Biol Psychiatry. 2022;23(6):424-55.
5. Simkin DR et al. Child Adolesc Psychiatric Clin N Am. 2023;32:193-216.
Matt was diagnosed with ADHD combined type when he was 6 years old. Given his age, the family was reluctant to try medications, but after a couple years of parenting classes and reward charts, the parents requested a stimulant. He had significant improvement in focus and impulsivity but also reduced appetite. Now at age 13, irritability and depressive symptoms have been increasing for 9 months. Skeptical of adding another medication, his parents ask whether nutrition might be an alternative tool to treat his symptoms?
What a healthy diet even consists of seems to be a moving target over decades and years. Trendy research, supplements, and dietary approaches proliferate alongside appealing theories of action. In the end, weighing which intervention is effective for which disorder and at what cost becomes murky.
Yet several fundamental principles seem clear and consistent over time and across studies.
Starting early
There is reliable evidence that in the perinatal environment, nutrition sets the stage for many aspects of healthy development. These effects are likely mediated variously through the hypothalamic-pituitary-adrenal axis, the trillions of gut bacteria that make up the microbiome, gene-environment interactions, and more. Maternal malnutrition and stress prenatally puts infants at risk for not only poor birth outcomes but also psychiatric challenges throughout childhood, such as ADHD, anxiety, depression, and autism.1
Intervening in the perinatal period has long-term benefits. A first step includes assessing food security, beginning with consistent access to nutritious food. It is important to inquire about the role of food and nutrition in the family’s history and culture, as well as identifying resources to support access to affordable nutrition. This can be paired with parenting interventions, such as family meals without screens. This may require scaffolding positive conversations in high-conflict family settings (see The Family Dinner Project).
Healthy diets promote mental health
If food security is achieved, what is next? Clinicians can inquire about the who, what, where, when, and why of nutrition to learn about a family’s eating habits.2 While randomized controlled data is very limited, both cross-sectional and longitudinal studies show that healthy diets in youth correlate with mental health – more healthy foods reducing internalizing and externalizing disorders, and more typical Western diets increasing the risk. On average, dietary interventions include higher levels of fruits and vegetables, fish, and nuts, and lower levels of processed foods.2 There is not evidence that restrictive diets or fasting is appropriate or safe for youth. Additionally, involving children in getting, growing, or preparing food with gradually increasing autonomy fosters self-confidence and skill development.
In those struggling with restrictive eating disorders, food is medicine – helping those with restrictive diets to develop more balanced and adequate intake for metabolic needs. Outside of diagnosable eating disorders, weight or body mass index is less of a goal or marker when it comes to mental health. Instead, look for participation in enjoyable activities, opportunities to move and rest, and a body image that supports self-care and self-confidence (see the National Institutes of Health’s We Can! Program). Creating dissonance with cultural ideals of appearance centered on thinness can prevent future eating disorders.3
Nutraceutical options
Outside of eating disorders, specific foods and plants with health or medicinal properties – variously called nutraceuticals, phytoceuticals, or micronutrients – have emerging evidence in mental health. A 2022 expert academic consensus panel reviewed the literature to create clinical guidelines in this area.4 For major depression, adding omega-3 fatty acids to standard antidepressant treatment or standalone St. John’s wort have adequate evidence to recommend, while adjunctive probiotics, zinc, saffron, and curcumin have sufficient though less robust evidence. S-adenosyl methionine, vitamin D, and methyfolate showed only weak evidence for depression, while vitamin C, magnesium, creatine, N-acetylcysteine, folate, and monotherapy omega-3s do not have sufficient evidence to be recommended. For ADHD there was weak support for vitamin D, but no clear evidence for omega-3s, zinc, gingko, or acetyl L-carnitine. For anxiety, there is moderate evidence for ashwagandha and lavender in adults. A child psychiatry review suggests also trying chamomile for generalized anxiety based on the evidence in young adults, and underscores some data for N-acetylcysteine for OCD in particular.5
Many of these nutraceuticals exhibit small or moderate effects in a limited number of trials, with generally much less data for youth, compared with adults. While the same could be said for many on- and off-label uses of psychiatric medications for kids, clinicians would be wise to consider these highly specific nutritional interventions as items on the menu of treatment options rather than stand-alone treatments.
Revisitng the case study
Reflecting on Matt’s care, his pediatrician first assessed his dietary patterns, noting late-night eating and caffeine use with minimal hydration or fiber across the day. Recommendations for keeping fruit and vegetable snacks easily accessible as well as carrying a water flask are well received. They also discuss adding omega-3 fatty acids and probiotics with his morning stimulant while he awaits a referral for cognitive-behavioral therapy in order to address his depressive symptoms and minimize medication needs.
Beyond addressing food security and balanced family meals, specific interventions may be appropriate as initial treatment adjuncts for mild and some moderate mental illness. For more intense moderate to severe illness, nutritional psychiatry may be considered in combination with treatments with stronger evidence. At a community level, clinicians can help advocate for universal school meal programs to address food security, and so-called salad bar interventions to increase fruit/vegetable uptake among school-age children.
Dr. Rosenfeld is associate professor of psychiatry and pediatrics at University of Vermont and the Vermont Center for Children, Youth, and Families, both in Burlington. He has no disclosures.
References
1 Vohr BR et al. Pediatrics. 2017;139:S38-49.
2. Hosker DK et al. Child Adol Psychiatr Clin N Am. 2019;28(2):171-93.
3. Stice E et al. Int J Eat Disord. 2013;46(5):478-85.
4. Sarris J et al. World J Biol Psychiatry. 2022;23(6):424-55.
5. Simkin DR et al. Child Adolesc Psychiatric Clin N Am. 2023;32:193-216.
West Nile infections rising in the U.S.
Several signs are pointing to an impending surge in the number of human cases of West Nile virus in several regions of the United States.
West Nile virus is spread by infected mosquitoes and currently there is no cure or virus-specific treatment. In rare cases, it can be deadly. It can infect humans, birds, horses, and other mammals.
West Nile Virus is the leading cause of mosquito-borne disease in the continental United States. As of Aug. 8, 126 human cases had been identified across 22 states, according to the Centers for Disease Control and Prevention.
“Particularly here in California, it’s peak risk right now,” said Vicki Kramer, PhD, chief of vector-borne diseases in the California Department of Public Health. She said scientists there are seeing higher mosquito and infected mosquito numbers.
“Peak risk right now”
Dead birds are tested for the virus and by Aug. 4, 181 of the 913 birds tested in California have been positive, three times the total testing positive by this time in 2022.
“Last year at this time, we had 60 positive dead birds out of 817 tested,” Dr. Kramer said.
Severe flooding and high heat can contribute to the rise in mosquito populations and many parts of the country have seen plenty of both.
One of the ways scientists track infected mosquito patterns in California is by using flocks of strategically placed sentinel chickens.
“Chickens are a mosquito magnet,” Dr. Kramer said.
Chickens don’t get sick with the virus, but they do build antibodies to it. Surveillance teams check their blood every other week to track the virus.
Daniel Pastula, MD, MHS, chief of neuroinfectious diseases and global neurology at the University of Colorado School of Medicine and the Colorado School of Public Health, said the state is watching troubling signs as well.
“The concern this year,” Dr. Pastula said, “particularly along the Front Range in Colorado, is we’ve found many more mosquitoes [that are] positive for West Nile earlier in the season compared with other years.
“We’re bracing for higher-than-baseline human cases,” he said.
Asked about this year’s first human case, reported in Toronto, a region with a long winter and low incidence of the virus, he said that provides a further example that people need to be prepared even in climates not known to be mosquito-dense.
He added, however, that climate is only one factor in the severity of the season. Others include birds’ immunity and migratory patterns.
Dr. Pastula said that fluctuations in temperature and rainfall are rising with climate change and are disrupting normal baseline levels of West Nile.
“That shows we need to be prepared for West Nile virus and other mosquito-borne diseases in any place in North America or really the world. We recently saw malaria cases in the southern United States. It just shows you how dangerous mosquitoes can be.”
Avoid mosquito bites
Dr. Pastula and Dr. Kramer list the precautions people can take to protect themselves from West Nile virus:
- Limit outdoor exposure particularly at dusk and dawn.
- Wear protective clothing.
- Use .
- Repair window screens so mosquitoes cannot fly through.
- Dump and drain standing water on your property and maintain swimming pools.
Dr. Pastula noted that summer is the time human cases start to mount – typically from July and August to the first hard freeze.
“We have been warning people here up and down the Front Range of Colorado to take prevention very seriously,” Dr. Pastula said.
He pointed out that 80% who are infected with West Nile will have no symptoms.
About 20% will have flu-like illness – high fever, body and joint aches, rash, diarrhea, or headaches. Symptoms may last for weeks. About 1% of the time, he said, people can get neuroinvasive West Nile.
Dr. Pastula explained that the virus can infect the covering of the brain and spinal cord causing meningitis with very high fever, severe headaches, stiff neck, and sensitivity to light.
So far this year, there have been 89 neuroinvasive cases reported nationally, according to the CDC.
With West Nile encephalitis, the virus “can infect the brain itself causing altered mental status, movement disorders, or weakness,” Dr. Pastula said.
Sometimes it can infect the gray matter of the spinal cord causing a West Nile virus poliomyelitis, which brings polio-like symptoms.
“The West Nile encephalitis and poliomyelitis can cause permanent deficits or even death,” he said. “It’s uncommon but it’s not trivial.”
Several vaccine candidates are in development, Dr. Pastula said, but none has reached clinical trials. Part of the reason for that, he said, is that scientists must be able to predict the timing of an outbreak.
“We’re not really great at predicting outbreaks,” he said.
Although the risk for neuroinvasive disease is small, it can be higher in certain groups, he said – those who are over age 60 years or are immunocompromised; those who have diabetes, cancer, or kidney disease; or those who have undergone organ transplants.
Those infected should see a health care professional and may be able to get relief with the usual medications for flu-like illness.
Some with severe infection may need to go to the hospital, Dr. Pastula said.
A version of this article first appeared on Medscape.com.
Several signs are pointing to an impending surge in the number of human cases of West Nile virus in several regions of the United States.
West Nile virus is spread by infected mosquitoes and currently there is no cure or virus-specific treatment. In rare cases, it can be deadly. It can infect humans, birds, horses, and other mammals.
West Nile Virus is the leading cause of mosquito-borne disease in the continental United States. As of Aug. 8, 126 human cases had been identified across 22 states, according to the Centers for Disease Control and Prevention.
“Particularly here in California, it’s peak risk right now,” said Vicki Kramer, PhD, chief of vector-borne diseases in the California Department of Public Health. She said scientists there are seeing higher mosquito and infected mosquito numbers.
“Peak risk right now”
Dead birds are tested for the virus and by Aug. 4, 181 of the 913 birds tested in California have been positive, three times the total testing positive by this time in 2022.
“Last year at this time, we had 60 positive dead birds out of 817 tested,” Dr. Kramer said.
Severe flooding and high heat can contribute to the rise in mosquito populations and many parts of the country have seen plenty of both.
One of the ways scientists track infected mosquito patterns in California is by using flocks of strategically placed sentinel chickens.
“Chickens are a mosquito magnet,” Dr. Kramer said.
Chickens don’t get sick with the virus, but they do build antibodies to it. Surveillance teams check their blood every other week to track the virus.
Daniel Pastula, MD, MHS, chief of neuroinfectious diseases and global neurology at the University of Colorado School of Medicine and the Colorado School of Public Health, said the state is watching troubling signs as well.
“The concern this year,” Dr. Pastula said, “particularly along the Front Range in Colorado, is we’ve found many more mosquitoes [that are] positive for West Nile earlier in the season compared with other years.
“We’re bracing for higher-than-baseline human cases,” he said.
Asked about this year’s first human case, reported in Toronto, a region with a long winter and low incidence of the virus, he said that provides a further example that people need to be prepared even in climates not known to be mosquito-dense.
He added, however, that climate is only one factor in the severity of the season. Others include birds’ immunity and migratory patterns.
Dr. Pastula said that fluctuations in temperature and rainfall are rising with climate change and are disrupting normal baseline levels of West Nile.
“That shows we need to be prepared for West Nile virus and other mosquito-borne diseases in any place in North America or really the world. We recently saw malaria cases in the southern United States. It just shows you how dangerous mosquitoes can be.”
Avoid mosquito bites
Dr. Pastula and Dr. Kramer list the precautions people can take to protect themselves from West Nile virus:
- Limit outdoor exposure particularly at dusk and dawn.
- Wear protective clothing.
- Use .
- Repair window screens so mosquitoes cannot fly through.
- Dump and drain standing water on your property and maintain swimming pools.
Dr. Pastula noted that summer is the time human cases start to mount – typically from July and August to the first hard freeze.
“We have been warning people here up and down the Front Range of Colorado to take prevention very seriously,” Dr. Pastula said.
He pointed out that 80% who are infected with West Nile will have no symptoms.
About 20% will have flu-like illness – high fever, body and joint aches, rash, diarrhea, or headaches. Symptoms may last for weeks. About 1% of the time, he said, people can get neuroinvasive West Nile.
Dr. Pastula explained that the virus can infect the covering of the brain and spinal cord causing meningitis with very high fever, severe headaches, stiff neck, and sensitivity to light.
So far this year, there have been 89 neuroinvasive cases reported nationally, according to the CDC.
With West Nile encephalitis, the virus “can infect the brain itself causing altered mental status, movement disorders, or weakness,” Dr. Pastula said.
Sometimes it can infect the gray matter of the spinal cord causing a West Nile virus poliomyelitis, which brings polio-like symptoms.
“The West Nile encephalitis and poliomyelitis can cause permanent deficits or even death,” he said. “It’s uncommon but it’s not trivial.”
Several vaccine candidates are in development, Dr. Pastula said, but none has reached clinical trials. Part of the reason for that, he said, is that scientists must be able to predict the timing of an outbreak.
“We’re not really great at predicting outbreaks,” he said.
Although the risk for neuroinvasive disease is small, it can be higher in certain groups, he said – those who are over age 60 years or are immunocompromised; those who have diabetes, cancer, or kidney disease; or those who have undergone organ transplants.
Those infected should see a health care professional and may be able to get relief with the usual medications for flu-like illness.
Some with severe infection may need to go to the hospital, Dr. Pastula said.
A version of this article first appeared on Medscape.com.
Several signs are pointing to an impending surge in the number of human cases of West Nile virus in several regions of the United States.
West Nile virus is spread by infected mosquitoes and currently there is no cure or virus-specific treatment. In rare cases, it can be deadly. It can infect humans, birds, horses, and other mammals.
West Nile Virus is the leading cause of mosquito-borne disease in the continental United States. As of Aug. 8, 126 human cases had been identified across 22 states, according to the Centers for Disease Control and Prevention.
“Particularly here in California, it’s peak risk right now,” said Vicki Kramer, PhD, chief of vector-borne diseases in the California Department of Public Health. She said scientists there are seeing higher mosquito and infected mosquito numbers.
“Peak risk right now”
Dead birds are tested for the virus and by Aug. 4, 181 of the 913 birds tested in California have been positive, three times the total testing positive by this time in 2022.
“Last year at this time, we had 60 positive dead birds out of 817 tested,” Dr. Kramer said.
Severe flooding and high heat can contribute to the rise in mosquito populations and many parts of the country have seen plenty of both.
One of the ways scientists track infected mosquito patterns in California is by using flocks of strategically placed sentinel chickens.
“Chickens are a mosquito magnet,” Dr. Kramer said.
Chickens don’t get sick with the virus, but they do build antibodies to it. Surveillance teams check their blood every other week to track the virus.
Daniel Pastula, MD, MHS, chief of neuroinfectious diseases and global neurology at the University of Colorado School of Medicine and the Colorado School of Public Health, said the state is watching troubling signs as well.
“The concern this year,” Dr. Pastula said, “particularly along the Front Range in Colorado, is we’ve found many more mosquitoes [that are] positive for West Nile earlier in the season compared with other years.
“We’re bracing for higher-than-baseline human cases,” he said.
Asked about this year’s first human case, reported in Toronto, a region with a long winter and low incidence of the virus, he said that provides a further example that people need to be prepared even in climates not known to be mosquito-dense.
He added, however, that climate is only one factor in the severity of the season. Others include birds’ immunity and migratory patterns.
Dr. Pastula said that fluctuations in temperature and rainfall are rising with climate change and are disrupting normal baseline levels of West Nile.
“That shows we need to be prepared for West Nile virus and other mosquito-borne diseases in any place in North America or really the world. We recently saw malaria cases in the southern United States. It just shows you how dangerous mosquitoes can be.”
Avoid mosquito bites
Dr. Pastula and Dr. Kramer list the precautions people can take to protect themselves from West Nile virus:
- Limit outdoor exposure particularly at dusk and dawn.
- Wear protective clothing.
- Use .
- Repair window screens so mosquitoes cannot fly through.
- Dump and drain standing water on your property and maintain swimming pools.
Dr. Pastula noted that summer is the time human cases start to mount – typically from July and August to the first hard freeze.
“We have been warning people here up and down the Front Range of Colorado to take prevention very seriously,” Dr. Pastula said.
He pointed out that 80% who are infected with West Nile will have no symptoms.
About 20% will have flu-like illness – high fever, body and joint aches, rash, diarrhea, or headaches. Symptoms may last for weeks. About 1% of the time, he said, people can get neuroinvasive West Nile.
Dr. Pastula explained that the virus can infect the covering of the brain and spinal cord causing meningitis with very high fever, severe headaches, stiff neck, and sensitivity to light.
So far this year, there have been 89 neuroinvasive cases reported nationally, according to the CDC.
With West Nile encephalitis, the virus “can infect the brain itself causing altered mental status, movement disorders, or weakness,” Dr. Pastula said.
Sometimes it can infect the gray matter of the spinal cord causing a West Nile virus poliomyelitis, which brings polio-like symptoms.
“The West Nile encephalitis and poliomyelitis can cause permanent deficits or even death,” he said. “It’s uncommon but it’s not trivial.”
Several vaccine candidates are in development, Dr. Pastula said, but none has reached clinical trials. Part of the reason for that, he said, is that scientists must be able to predict the timing of an outbreak.
“We’re not really great at predicting outbreaks,” he said.
Although the risk for neuroinvasive disease is small, it can be higher in certain groups, he said – those who are over age 60 years or are immunocompromised; those who have diabetes, cancer, or kidney disease; or those who have undergone organ transplants.
Those infected should see a health care professional and may be able to get relief with the usual medications for flu-like illness.
Some with severe infection may need to go to the hospital, Dr. Pastula said.
A version of this article first appeared on Medscape.com.
Zuranolone: A novel postpartum depression treatment, with lingering questions
Postpartum depression (PPD) remains the most common complication in modern obstetrics, and a leading cause of postpartum mortality in the first year of life. The last 15 years have brought considerable progress with respect to adoption of systematic screening for PPD across America. Screening for PPD, most often using the Edinburgh Postnatal Depression Scale (EPDS), has become part of routine obstetrical care, and is also widely used in pediatric settings.
That is the good news. But the flip side of the identification of those women whose scores on the EPDS suggest significant depressive symptoms is that the number of these patients who, following identification, receive referrals for adequate treatment that gets them well is unfortunately low. This “perinatal treatment cascade” refers to the majority of women who, on the other side of identification of PPD, fail to receive adequate treatment and continue to have persistent depression (Cox E. et al. J Clin Psychiatry. 2016 Sep;77[9]:1189-1200). This is perhaps the greatest challenge to the field and to clinicians – how do we, on the other side of screening, see that these women get access to care and get well with the available treatments at hand?

Recently, a widely read and circulated article was published in The Wall Street Journal about the challenges associated with navigating care resources for women suffering from PPD. In that article, it was made clear, based on clinical vignette after clinical vignette from postpartum women across America, that neither obstetricians, mental health professionals, nor pediatricians are the “clinical home” for women suffering from postpartum mood and anxiety disorders. The article painfully highlights the system-wide failure to coordinate mental health care for women suffering from postpartum psychiatric illness.
Within a day of the publication of The Wall Street Journal article, the Food and Drug Administration approved zuranolone (Zurzuvae; Sage Therapeutics; Cambridge, Mass.) for the treatment of PPD following the review of two studies demonstrating the superiority of the new medicine over placebo. Women who were enrolled met criteria for major depressive disorder based on Diagnostic and Statistical Manual of Mental Disorders criteria beginning in no earlier than the third trimester of pregnancy or later than 4 weeks of delivery. The two studies included a combined sample size of approximately 350 patients suffering from severe PPD. In the studies, women received either 50 mg or 40 mg of zuranolone, or placebo for 14 days. Treatment was associated with a significant change in the Hamilton Depression Rating Scale at day 15, and treatment response was maintained at day 42, which was 4 weeks after the last dose of study medication.
Zuranolone is a neuroactive steroid, which is taken orally, unlike brexanolone (Zulresso; Sage Therapeutics; Cambridge, Mass.), which requires intravenous administration. Zuranolone will be commercially available based on estimates around the fourth quarter of 2023. The most common side effects are drowsiness, dizziness, and sedation, and the FDA label will have a boxed warning about zuranolone’s potential to impact a person’s driving ability, and performance of potentially hazardous activities.
It is noteworthy that while this new medication received FDA approval for the PPD indication, it did not receive FDA approval for the treatment of major depressive disorder (MDD), and the agency issued a Complete Response Letter to the manufacturers noting their application did not provide substantial evidence of effectiveness in MDD. The FDA said in the Complete Response Letter that an additional study or studies will be needed; the manufacturers are currently evaluating next steps.
Where zuranolone fits into the treatment algorithm for severe PPD
Many clinicians who support women with PPD will wonder, upon hearing this news, where zuranolone fits into the treatment algorithm for severe postpartum major depression. Some relevant issues that may determine the answer are the following:
Cost. The cost of brexanolone was substantial, at $34,000 per year, and was viewed by some as a limiting factor in terms of its very limited uptake. As of this column’s publication, zuranolone’s manufacturer has not stated how much the medication will cost.
Breastfeeding. Unlike selective serotonin reuptake inhibitors, which have been demonstrated to be effective for the treatment of PPD and safe during pregnancy and lactation, we have sparse data on the safety of zuranolone for women who wish to breastfeed. It is also unclear whether women eligible for zuranolone would, based on the limited data on safety in lactation, choose deferral of breastfeeding for 14 days in exchange for treatment.
Duration of treatment. While zuranolone was studied in the context of 14 days of acute treatment, then out to day 42, we have no published data on what happens on the other side of this brief interval. As a simple example, in a patient with a history of recurrent major depression previously treated with antidepressants, but where antidepressants were perhaps deferred during pregnancy, is PPD to be treated with zuranolone for 14 days? Or, hypothetically, should it be followed by empiric antidepressant treatment at day 14? Alternatively, are patient and clinician supposed to wait until recurrence occurs before pursuing adjunctive antidepressant therapy whether it is pharmacologic, nonpharmacologic, or both?
Treatment in patients with bipolar disorder. It is also unclear whether treatment with zuranolone applies to other populations of postpartum women. Certainly, for women with bipolar depression, which is common in postpartum women given the vulnerability of bipolar women to new onset of depression or postpartum depressive relapse of underlying disorder, we simply have no data regarding where zuranolone might fit in with respect to this group of patients.
The answers to these questions may help to determine whether zuranolone, a new antidepressant with efficacy, quick time to onset, and a novel mechanism of action is a “game changer.” The article in The Wall Street Journal provided me with some optimism, as it gave PPD and the issues surrounding PPD the attention it deserves in a major periodical. As a new treatment, it may help alleviate suffering at a critical time for patients and their families. We are inching closer to mitigation of stigma associated with this common illness.
Thinking back across the last 3 decades of my treating women suffering from PPD, I have reflected on what has gotten these patients well. I concluded that , along with family and community-based support groups, as well as a culture that reduces stigma and by so doing lessens the toll of this important and too frequently incompletely-treated illness.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital (MGH) in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. The Center for Women’s Mental Health at MGH was a non-enrolling site for the pivotal phase 3 SKYLARK trial evaluating zuranolone. Full disclosure information for Dr. Cohen is available at womensmentalhealth.org. Email Dr. Cohen at [email protected].
Postpartum depression (PPD) remains the most common complication in modern obstetrics, and a leading cause of postpartum mortality in the first year of life. The last 15 years have brought considerable progress with respect to adoption of systematic screening for PPD across America. Screening for PPD, most often using the Edinburgh Postnatal Depression Scale (EPDS), has become part of routine obstetrical care, and is also widely used in pediatric settings.
That is the good news. But the flip side of the identification of those women whose scores on the EPDS suggest significant depressive symptoms is that the number of these patients who, following identification, receive referrals for adequate treatment that gets them well is unfortunately low. This “perinatal treatment cascade” refers to the majority of women who, on the other side of identification of PPD, fail to receive adequate treatment and continue to have persistent depression (Cox E. et al. J Clin Psychiatry. 2016 Sep;77[9]:1189-1200). This is perhaps the greatest challenge to the field and to clinicians – how do we, on the other side of screening, see that these women get access to care and get well with the available treatments at hand?
Recently, a widely read and circulated article was published in The Wall Street Journal about the challenges associated with navigating care resources for women suffering from PPD. In that article, it was made clear, based on clinical vignette after clinical vignette from postpartum women across America, that neither obstetricians, mental health professionals, nor pediatricians are the “clinical home” for women suffering from postpartum mood and anxiety disorders. The article painfully highlights the system-wide failure to coordinate mental health care for women suffering from postpartum psychiatric illness.
Within a day of the publication of The Wall Street Journal article, the Food and Drug Administration approved zuranolone (Zurzuvae; Sage Therapeutics; Cambridge, Mass.) for the treatment of PPD following the review of two studies demonstrating the superiority of the new medicine over placebo. Women who were enrolled met criteria for major depressive disorder based on Diagnostic and Statistical Manual of Mental Disorders criteria beginning in no earlier than the third trimester of pregnancy or later than 4 weeks of delivery. The two studies included a combined sample size of approximately 350 patients suffering from severe PPD. In the studies, women received either 50 mg or 40 mg of zuranolone, or placebo for 14 days. Treatment was associated with a significant change in the Hamilton Depression Rating Scale at day 15, and treatment response was maintained at day 42, which was 4 weeks after the last dose of study medication.
Zuranolone is a neuroactive steroid, which is taken orally, unlike brexanolone (Zulresso; Sage Therapeutics; Cambridge, Mass.), which requires intravenous administration. Zuranolone will be commercially available based on estimates around the fourth quarter of 2023. The most common side effects are drowsiness, dizziness, and sedation, and the FDA label will have a boxed warning about zuranolone’s potential to impact a person’s driving ability, and performance of potentially hazardous activities.
It is noteworthy that while this new medication received FDA approval for the PPD indication, it did not receive FDA approval for the treatment of major depressive disorder (MDD), and the agency issued a Complete Response Letter to the manufacturers noting their application did not provide substantial evidence of effectiveness in MDD. The FDA said in the Complete Response Letter that an additional study or studies will be needed; the manufacturers are currently evaluating next steps.
Where zuranolone fits into the treatment algorithm for severe PPD
Many clinicians who support women with PPD will wonder, upon hearing this news, where zuranolone fits into the treatment algorithm for severe postpartum major depression. Some relevant issues that may determine the answer are the following:
Cost. The cost of brexanolone was substantial, at $34,000 per year, and was viewed by some as a limiting factor in terms of its very limited uptake. As of this column’s publication, zuranolone’s manufacturer has not stated how much the medication will cost.
Breastfeeding. Unlike selective serotonin reuptake inhibitors, which have been demonstrated to be effective for the treatment of PPD and safe during pregnancy and lactation, we have sparse data on the safety of zuranolone for women who wish to breastfeed. It is also unclear whether women eligible for zuranolone would, based on the limited data on safety in lactation, choose deferral of breastfeeding for 14 days in exchange for treatment.
Duration of treatment. While zuranolone was studied in the context of 14 days of acute treatment, then out to day 42, we have no published data on what happens on the other side of this brief interval. As a simple example, in a patient with a history of recurrent major depression previously treated with antidepressants, but where antidepressants were perhaps deferred during pregnancy, is PPD to be treated with zuranolone for 14 days? Or, hypothetically, should it be followed by empiric antidepressant treatment at day 14? Alternatively, are patient and clinician supposed to wait until recurrence occurs before pursuing adjunctive antidepressant therapy whether it is pharmacologic, nonpharmacologic, or both?
Treatment in patients with bipolar disorder. It is also unclear whether treatment with zuranolone applies to other populations of postpartum women. Certainly, for women with bipolar depression, which is common in postpartum women given the vulnerability of bipolar women to new onset of depression or postpartum depressive relapse of underlying disorder, we simply have no data regarding where zuranolone might fit in with respect to this group of patients.
The answers to these questions may help to determine whether zuranolone, a new antidepressant with efficacy, quick time to onset, and a novel mechanism of action is a “game changer.” The article in The Wall Street Journal provided me with some optimism, as it gave PPD and the issues surrounding PPD the attention it deserves in a major periodical. As a new treatment, it may help alleviate suffering at a critical time for patients and their families. We are inching closer to mitigation of stigma associated with this common illness.
Thinking back across the last 3 decades of my treating women suffering from PPD, I have reflected on what has gotten these patients well. I concluded that , along with family and community-based support groups, as well as a culture that reduces stigma and by so doing lessens the toll of this important and too frequently incompletely-treated illness.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital (MGH) in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. The Center for Women’s Mental Health at MGH was a non-enrolling site for the pivotal phase 3 SKYLARK trial evaluating zuranolone. Full disclosure information for Dr. Cohen is available at womensmentalhealth.org. Email Dr. Cohen at [email protected].
Postpartum depression (PPD) remains the most common complication in modern obstetrics, and a leading cause of postpartum mortality in the first year of life. The last 15 years have brought considerable progress with respect to adoption of systematic screening for PPD across America. Screening for PPD, most often using the Edinburgh Postnatal Depression Scale (EPDS), has become part of routine obstetrical care, and is also widely used in pediatric settings.
That is the good news. But the flip side of the identification of those women whose scores on the EPDS suggest significant depressive symptoms is that the number of these patients who, following identification, receive referrals for adequate treatment that gets them well is unfortunately low. This “perinatal treatment cascade” refers to the majority of women who, on the other side of identification of PPD, fail to receive adequate treatment and continue to have persistent depression (Cox E. et al. J Clin Psychiatry. 2016 Sep;77[9]:1189-1200). This is perhaps the greatest challenge to the field and to clinicians – how do we, on the other side of screening, see that these women get access to care and get well with the available treatments at hand?
Recently, a widely read and circulated article was published in The Wall Street Journal about the challenges associated with navigating care resources for women suffering from PPD. In that article, it was made clear, based on clinical vignette after clinical vignette from postpartum women across America, that neither obstetricians, mental health professionals, nor pediatricians are the “clinical home” for women suffering from postpartum mood and anxiety disorders. The article painfully highlights the system-wide failure to coordinate mental health care for women suffering from postpartum psychiatric illness.
Within a day of the publication of The Wall Street Journal article, the Food and Drug Administration approved zuranolone (Zurzuvae; Sage Therapeutics; Cambridge, Mass.) for the treatment of PPD following the review of two studies demonstrating the superiority of the new medicine over placebo. Women who were enrolled met criteria for major depressive disorder based on Diagnostic and Statistical Manual of Mental Disorders criteria beginning in no earlier than the third trimester of pregnancy or later than 4 weeks of delivery. The two studies included a combined sample size of approximately 350 patients suffering from severe PPD. In the studies, women received either 50 mg or 40 mg of zuranolone, or placebo for 14 days. Treatment was associated with a significant change in the Hamilton Depression Rating Scale at day 15, and treatment response was maintained at day 42, which was 4 weeks after the last dose of study medication.
Zuranolone is a neuroactive steroid, which is taken orally, unlike brexanolone (Zulresso; Sage Therapeutics; Cambridge, Mass.), which requires intravenous administration. Zuranolone will be commercially available based on estimates around the fourth quarter of 2023. The most common side effects are drowsiness, dizziness, and sedation, and the FDA label will have a boxed warning about zuranolone’s potential to impact a person’s driving ability, and performance of potentially hazardous activities.
It is noteworthy that while this new medication received FDA approval for the PPD indication, it did not receive FDA approval for the treatment of major depressive disorder (MDD), and the agency issued a Complete Response Letter to the manufacturers noting their application did not provide substantial evidence of effectiveness in MDD. The FDA said in the Complete Response Letter that an additional study or studies will be needed; the manufacturers are currently evaluating next steps.
Where zuranolone fits into the treatment algorithm for severe PPD
Many clinicians who support women with PPD will wonder, upon hearing this news, where zuranolone fits into the treatment algorithm for severe postpartum major depression. Some relevant issues that may determine the answer are the following:
Cost. The cost of brexanolone was substantial, at $34,000 per year, and was viewed by some as a limiting factor in terms of its very limited uptake. As of this column’s publication, zuranolone’s manufacturer has not stated how much the medication will cost.
Breastfeeding. Unlike selective serotonin reuptake inhibitors, which have been demonstrated to be effective for the treatment of PPD and safe during pregnancy and lactation, we have sparse data on the safety of zuranolone for women who wish to breastfeed. It is also unclear whether women eligible for zuranolone would, based on the limited data on safety in lactation, choose deferral of breastfeeding for 14 days in exchange for treatment.
Duration of treatment. While zuranolone was studied in the context of 14 days of acute treatment, then out to day 42, we have no published data on what happens on the other side of this brief interval. As a simple example, in a patient with a history of recurrent major depression previously treated with antidepressants, but where antidepressants were perhaps deferred during pregnancy, is PPD to be treated with zuranolone for 14 days? Or, hypothetically, should it be followed by empiric antidepressant treatment at day 14? Alternatively, are patient and clinician supposed to wait until recurrence occurs before pursuing adjunctive antidepressant therapy whether it is pharmacologic, nonpharmacologic, or both?
Treatment in patients with bipolar disorder. It is also unclear whether treatment with zuranolone applies to other populations of postpartum women. Certainly, for women with bipolar depression, which is common in postpartum women given the vulnerability of bipolar women to new onset of depression or postpartum depressive relapse of underlying disorder, we simply have no data regarding where zuranolone might fit in with respect to this group of patients.
The answers to these questions may help to determine whether zuranolone, a new antidepressant with efficacy, quick time to onset, and a novel mechanism of action is a “game changer.” The article in The Wall Street Journal provided me with some optimism, as it gave PPD and the issues surrounding PPD the attention it deserves in a major periodical. As a new treatment, it may help alleviate suffering at a critical time for patients and their families. We are inching closer to mitigation of stigma associated with this common illness.
Thinking back across the last 3 decades of my treating women suffering from PPD, I have reflected on what has gotten these patients well. I concluded that , along with family and community-based support groups, as well as a culture that reduces stigma and by so doing lessens the toll of this important and too frequently incompletely-treated illness.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital (MGH) in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. The Center for Women’s Mental Health at MGH was a non-enrolling site for the pivotal phase 3 SKYLARK trial evaluating zuranolone. Full disclosure information for Dr. Cohen is available at womensmentalhealth.org. Email Dr. Cohen at [email protected].
Postpartum depression risk increased among sexual minority women
However, with sexual orientation highly underdocumented among women giving birth, understanding of the prevalence is lacking.
“To our knowledge, this cohort study was the first to examine perinatal depression screening and symptom endorsement among sexual minority women in a major medical center in the U.S.,” reported the authors of the study published in JAMA Psychiatry.
The results “highlight the need for investigations that include strategies for measuring sexual orientation because reliance on medical record review has substantial limitations with regard to the research questions and the validity of the data,” they noted.
Clinical guidelines recommend universal perinatal depression screening at obstetric and pediatric well-infant visits; however, there are significant gaps in data on the issue when it comes to sexual minority women.
To assess the prevalence of sexual minority people giving birth and compare perinatal depression screening rates and scores with those of heterosexual cisgender women, the authors conducted a review of medical records of 18,243 female patients who gave birth at a large, diverse, university-based medical center in Chicago between January and December of 2019.
Of the patients, 57.3% of whom were non-Hispanic White, 1.5% (280) had documentation of their sexual orientation, or sexual minority status.
The results show that those identified as being in sexual minorities, including lesbian, bisexual, queer, pansexual or asexual, were more likely than were heterosexual women to be more engaged in their care – they were more likely to have attended at least one prenatal visit (20.0% vs. 13.7%; P = .002) and at least one postpartum care visit (18.6% vs. 12.8%; P = .004), and more likely to be screened for depression during postpartum care (odds ratio, 1.77; P = .002).
Sexual minority women were also significantly more likely to screen positive for depression during the postpartum period than were heterosexual women (odds ratio, 2.38; P = .03); however, all other comparisons were not significantly different.
The finding regarding postpartum depression was consistent with recent literature, including a systematic review indicating that the stress of being in a sexual minority may be heightened during the postpartum period, the authors noted.
Reasons for the heightened stress may include “being perceived as inadequate parents, heteronormativity in perinatal care, such as intake forms asking for information about the child’s father, and lack of familial social support due to nonacceptance of the parents’ sexual orientation,” the researchers explained.
The rate of only 1.5% of people giving birth who identified as a sexual minority was significantly lower than expected, and much lower that the 17% reported in a recent nationally representative sample of women, first author Leiszle Lapping-Carr, PhD, director of the sexual and relationship health program, department of psychiatry and behavioral sciences, Northwestern University, Chicago, said in an interview.
“I did not expect a rate as low at 1.5%,” she said. “I anticipated it would not be as high as the 17%, but this was quite low. I think one primary reason is that women are not interested in disclosing their sexual orientation to their ob.gyns. if they don’t have to.”
Furthermore, Dr. Lapping-Carr said, “most medical systems do not have an easy way to document sexual orientation or gender identity, and even if it exists many physicians are unaware of the process.”
On a broader level, the lower rates may be indicative of a lack of acknowledgment of sexual minorities in the ob.gyn. setting, Dr. Lapping-Carr added.

“There is a heteronormative bias implicit in most obstetrics clinics, in which pregnant people are automatically gendered as women and assumed to be heterosexual, especially if they present with a male partner,” she said.
Because of those factors, even if a pregnant person discloses sexual identity, that person may request that it not be documented in the chart, she noted.
The higher rates of postpartum depression are consistent with higher rates of mental illness that are reported in general among sexual minority women, pregnant or not, including depression, anxiety, higher rates of substance abuse, stressful life events, and intimate partner violence, compared with heterosexual women, the authors noted.
Develop more supportive systems
To address postpartum depression among sexual minority women, Dr. Lapping-Carr suggested that clinicians generally start by avoiding language and behaviors that could suggest the potential bias that sexual minority patients can face.
“The main change [in treatment] that would likely be helpful for postpartum depression treatment is removing heteronormative language, e.g., not referring to partners as ‘fathers,’ ” she said.
Also, patients may benefit from “discussion of issues of relevance to people with sexual minority identities, such as the process of adoption for female non-birthing partners,” Dr. Lapping-Carr added.
“Starting to create spaces that are inclusive and welcoming for people of all identities will go a long way in increasing your patient’s trust in you,” she said.
While there is a lack of published data regarding increases in rates of sexual minority patients who are giving birth, societal trends suggest the rates may likely be on the rise, Dr. Lapping-Carr said.
“We do know that among adolescents, endorsement of sexual and gender minority identities is much higher than in previous generations, so it would follow that the proportion of birthing people with sexual and gender minority identities would also increase,” she said.
Commenting on the study, K. Ashley Brandt, DO, obstetrics section chief and medical director of Gender Affirming Surgery at Reading Hospital, in West Reading, Pa., noted that limitations include a lack of information about the bigger picture of patients’ risk factors.
“There is no documentation of other risks factors, including rates of depression in the antenatal period, which is higher in LGBTQ individuals and also a risk factor for postpartum depression,” Dr. Brandt told this news organization.
She agreed, however, that patients may be reluctant to report their sexual minority status on the record – but such issues are often addressed.

“I believe that obstetricians do ask this question far more than other providers, but it may not be easily captured in medical records, and patients may also hesitate to disclose sexual practices and sexual orientation due to fear of medical discrimination, which is still extremely prevalent,” Dr. Brandt said.
The study underscores, however, that “same-sex parents are a reality that providers will face,” she said. “They have unique social determinants for health that often go undocumented and unaddressed, which could contribute to higher rates of depression in the postpartum period.”
Factors that may be ignored or undocumented, such as sexual minorities’ religious beliefs or social and familial support, can play significant roles in health care outcomes, Dr. Brandt added.
“Providers need to find ways to better educate themselves about LGBTQ individuals and develop more supportive systems to ensure patients feel safe in disclosing their identities.”
The authors and Dr. Brandt had no disclosures to report.
However, with sexual orientation highly underdocumented among women giving birth, understanding of the prevalence is lacking.
“To our knowledge, this cohort study was the first to examine perinatal depression screening and symptom endorsement among sexual minority women in a major medical center in the U.S.,” reported the authors of the study published in JAMA Psychiatry.
The results “highlight the need for investigations that include strategies for measuring sexual orientation because reliance on medical record review has substantial limitations with regard to the research questions and the validity of the data,” they noted.
Clinical guidelines recommend universal perinatal depression screening at obstetric and pediatric well-infant visits; however, there are significant gaps in data on the issue when it comes to sexual minority women.
To assess the prevalence of sexual minority people giving birth and compare perinatal depression screening rates and scores with those of heterosexual cisgender women, the authors conducted a review of medical records of 18,243 female patients who gave birth at a large, diverse, university-based medical center in Chicago between January and December of 2019.
Of the patients, 57.3% of whom were non-Hispanic White, 1.5% (280) had documentation of their sexual orientation, or sexual minority status.
The results show that those identified as being in sexual minorities, including lesbian, bisexual, queer, pansexual or asexual, were more likely than were heterosexual women to be more engaged in their care – they were more likely to have attended at least one prenatal visit (20.0% vs. 13.7%; P = .002) and at least one postpartum care visit (18.6% vs. 12.8%; P = .004), and more likely to be screened for depression during postpartum care (odds ratio, 1.77; P = .002).
Sexual minority women were also significantly more likely to screen positive for depression during the postpartum period than were heterosexual women (odds ratio, 2.38; P = .03); however, all other comparisons were not significantly different.
The finding regarding postpartum depression was consistent with recent literature, including a systematic review indicating that the stress of being in a sexual minority may be heightened during the postpartum period, the authors noted.
Reasons for the heightened stress may include “being perceived as inadequate parents, heteronormativity in perinatal care, such as intake forms asking for information about the child’s father, and lack of familial social support due to nonacceptance of the parents’ sexual orientation,” the researchers explained.
The rate of only 1.5% of people giving birth who identified as a sexual minority was significantly lower than expected, and much lower that the 17% reported in a recent nationally representative sample of women, first author Leiszle Lapping-Carr, PhD, director of the sexual and relationship health program, department of psychiatry and behavioral sciences, Northwestern University, Chicago, said in an interview.
“I did not expect a rate as low at 1.5%,” she said. “I anticipated it would not be as high as the 17%, but this was quite low. I think one primary reason is that women are not interested in disclosing their sexual orientation to their ob.gyns. if they don’t have to.”
Furthermore, Dr. Lapping-Carr said, “most medical systems do not have an easy way to document sexual orientation or gender identity, and even if it exists many physicians are unaware of the process.”
On a broader level, the lower rates may be indicative of a lack of acknowledgment of sexual minorities in the ob.gyn. setting, Dr. Lapping-Carr added.
“There is a heteronormative bias implicit in most obstetrics clinics, in which pregnant people are automatically gendered as women and assumed to be heterosexual, especially if they present with a male partner,” she said.
Because of those factors, even if a pregnant person discloses sexual identity, that person may request that it not be documented in the chart, she noted.
The higher rates of postpartum depression are consistent with higher rates of mental illness that are reported in general among sexual minority women, pregnant or not, including depression, anxiety, higher rates of substance abuse, stressful life events, and intimate partner violence, compared with heterosexual women, the authors noted.
Develop more supportive systems
To address postpartum depression among sexual minority women, Dr. Lapping-Carr suggested that clinicians generally start by avoiding language and behaviors that could suggest the potential bias that sexual minority patients can face.
“The main change [in treatment] that would likely be helpful for postpartum depression treatment is removing heteronormative language, e.g., not referring to partners as ‘fathers,’ ” she said.
Also, patients may benefit from “discussion of issues of relevance to people with sexual minority identities, such as the process of adoption for female non-birthing partners,” Dr. Lapping-Carr added.
“Starting to create spaces that are inclusive and welcoming for people of all identities will go a long way in increasing your patient’s trust in you,” she said.
While there is a lack of published data regarding increases in rates of sexual minority patients who are giving birth, societal trends suggest the rates may likely be on the rise, Dr. Lapping-Carr said.
“We do know that among adolescents, endorsement of sexual and gender minority identities is much higher than in previous generations, so it would follow that the proportion of birthing people with sexual and gender minority identities would also increase,” she said.
Commenting on the study, K. Ashley Brandt, DO, obstetrics section chief and medical director of Gender Affirming Surgery at Reading Hospital, in West Reading, Pa., noted that limitations include a lack of information about the bigger picture of patients’ risk factors.
“There is no documentation of other risks factors, including rates of depression in the antenatal period, which is higher in LGBTQ individuals and also a risk factor for postpartum depression,” Dr. Brandt told this news organization.
She agreed, however, that patients may be reluctant to report their sexual minority status on the record – but such issues are often addressed.
“I believe that obstetricians do ask this question far more than other providers, but it may not be easily captured in medical records, and patients may also hesitate to disclose sexual practices and sexual orientation due to fear of medical discrimination, which is still extremely prevalent,” Dr. Brandt said.
The study underscores, however, that “same-sex parents are a reality that providers will face,” she said. “They have unique social determinants for health that often go undocumented and unaddressed, which could contribute to higher rates of depression in the postpartum period.”
Factors that may be ignored or undocumented, such as sexual minorities’ religious beliefs or social and familial support, can play significant roles in health care outcomes, Dr. Brandt added.
“Providers need to find ways to better educate themselves about LGBTQ individuals and develop more supportive systems to ensure patients feel safe in disclosing their identities.”
The authors and Dr. Brandt had no disclosures to report.
However, with sexual orientation highly underdocumented among women giving birth, understanding of the prevalence is lacking.
“To our knowledge, this cohort study was the first to examine perinatal depression screening and symptom endorsement among sexual minority women in a major medical center in the U.S.,” reported the authors of the study published in JAMA Psychiatry.
The results “highlight the need for investigations that include strategies for measuring sexual orientation because reliance on medical record review has substantial limitations with regard to the research questions and the validity of the data,” they noted.
Clinical guidelines recommend universal perinatal depression screening at obstetric and pediatric well-infant visits; however, there are significant gaps in data on the issue when it comes to sexual minority women.
To assess the prevalence of sexual minority people giving birth and compare perinatal depression screening rates and scores with those of heterosexual cisgender women, the authors conducted a review of medical records of 18,243 female patients who gave birth at a large, diverse, university-based medical center in Chicago between January and December of 2019.
Of the patients, 57.3% of whom were non-Hispanic White, 1.5% (280) had documentation of their sexual orientation, or sexual minority status.
The results show that those identified as being in sexual minorities, including lesbian, bisexual, queer, pansexual or asexual, were more likely than were heterosexual women to be more engaged in their care – they were more likely to have attended at least one prenatal visit (20.0% vs. 13.7%; P = .002) and at least one postpartum care visit (18.6% vs. 12.8%; P = .004), and more likely to be screened for depression during postpartum care (odds ratio, 1.77; P = .002).
Sexual minority women were also significantly more likely to screen positive for depression during the postpartum period than were heterosexual women (odds ratio, 2.38; P = .03); however, all other comparisons were not significantly different.
The finding regarding postpartum depression was consistent with recent literature, including a systematic review indicating that the stress of being in a sexual minority may be heightened during the postpartum period, the authors noted.
Reasons for the heightened stress may include “being perceived as inadequate parents, heteronormativity in perinatal care, such as intake forms asking for information about the child’s father, and lack of familial social support due to nonacceptance of the parents’ sexual orientation,” the researchers explained.
The rate of only 1.5% of people giving birth who identified as a sexual minority was significantly lower than expected, and much lower that the 17% reported in a recent nationally representative sample of women, first author Leiszle Lapping-Carr, PhD, director of the sexual and relationship health program, department of psychiatry and behavioral sciences, Northwestern University, Chicago, said in an interview.
“I did not expect a rate as low at 1.5%,” she said. “I anticipated it would not be as high as the 17%, but this was quite low. I think one primary reason is that women are not interested in disclosing their sexual orientation to their ob.gyns. if they don’t have to.”
Furthermore, Dr. Lapping-Carr said, “most medical systems do not have an easy way to document sexual orientation or gender identity, and even if it exists many physicians are unaware of the process.”
On a broader level, the lower rates may be indicative of a lack of acknowledgment of sexual minorities in the ob.gyn. setting, Dr. Lapping-Carr added.
“There is a heteronormative bias implicit in most obstetrics clinics, in which pregnant people are automatically gendered as women and assumed to be heterosexual, especially if they present with a male partner,” she said.
Because of those factors, even if a pregnant person discloses sexual identity, that person may request that it not be documented in the chart, she noted.
The higher rates of postpartum depression are consistent with higher rates of mental illness that are reported in general among sexual minority women, pregnant or not, including depression, anxiety, higher rates of substance abuse, stressful life events, and intimate partner violence, compared with heterosexual women, the authors noted.
Develop more supportive systems
To address postpartum depression among sexual minority women, Dr. Lapping-Carr suggested that clinicians generally start by avoiding language and behaviors that could suggest the potential bias that sexual minority patients can face.
“The main change [in treatment] that would likely be helpful for postpartum depression treatment is removing heteronormative language, e.g., not referring to partners as ‘fathers,’ ” she said.
Also, patients may benefit from “discussion of issues of relevance to people with sexual minority identities, such as the process of adoption for female non-birthing partners,” Dr. Lapping-Carr added.
“Starting to create spaces that are inclusive and welcoming for people of all identities will go a long way in increasing your patient’s trust in you,” she said.
While there is a lack of published data regarding increases in rates of sexual minority patients who are giving birth, societal trends suggest the rates may likely be on the rise, Dr. Lapping-Carr said.
“We do know that among adolescents, endorsement of sexual and gender minority identities is much higher than in previous generations, so it would follow that the proportion of birthing people with sexual and gender minority identities would also increase,” she said.
Commenting on the study, K. Ashley Brandt, DO, obstetrics section chief and medical director of Gender Affirming Surgery at Reading Hospital, in West Reading, Pa., noted that limitations include a lack of information about the bigger picture of patients’ risk factors.
“There is no documentation of other risks factors, including rates of depression in the antenatal period, which is higher in LGBTQ individuals and also a risk factor for postpartum depression,” Dr. Brandt told this news organization.
She agreed, however, that patients may be reluctant to report their sexual minority status on the record – but such issues are often addressed.
“I believe that obstetricians do ask this question far more than other providers, but it may not be easily captured in medical records, and patients may also hesitate to disclose sexual practices and sexual orientation due to fear of medical discrimination, which is still extremely prevalent,” Dr. Brandt said.
The study underscores, however, that “same-sex parents are a reality that providers will face,” she said. “They have unique social determinants for health that often go undocumented and unaddressed, which could contribute to higher rates of depression in the postpartum period.”
Factors that may be ignored or undocumented, such as sexual minorities’ religious beliefs or social and familial support, can play significant roles in health care outcomes, Dr. Brandt added.
“Providers need to find ways to better educate themselves about LGBTQ individuals and develop more supportive systems to ensure patients feel safe in disclosing their identities.”
The authors and Dr. Brandt had no disclosures to report.
FROM JAMA PSYCHIATRY
New weight loss drugs appeal to half of U.S. adults
A recent survey of more than 1,000 U.S. adults showed that 18% were “somewhat interested” in taking a “safe, effective” weight loss drug, 27% were “very interested,” and 4% said they were already using such an agent, together constituting 49% of the surveyed adults.
The newer, more potent and generally safe agents that work by stimulating receptors to nutrient-stimulated hormones, such as incretins like glucagonlike peptide–1, seem to drive this interest.
When asked: “How much have you heard, if anything, about a new class of drugs being used for weight loss, such as Ozempic [semaglutide formulated and approved for people with type 2 diabetes], Wegovy [semaglutide for weight loss], and Mounjaro [tirzepatide, currently approved for treating only people with type 2 diabetes]?” 43% said they had heard some, or a lot, about these agents.
This was particularly true among people at least 65 years old, who had a 55% prevalence of knowing some, or a lot, about these new weight-loss agents, while an additional 26% had heard at least “a little” about them, reported staff members of KFF (formerly the Kaiser Family Foundation) in a report posted online in early August.
Weight loss drugs garner ‘increasing’ attention
“A new class of prescription drugs, initially developed to treat type 2 diabetes, have been garnering an increasing amount of attention due to their ability to act as highly effective weight loss drugs for overweight or obese adults,” wrote the report’s authors.
However, surveyed interest fell markedly when respondents answered further questions that hinged on certain limitations of the newer weight loss formulations.
For example, the percent interested held nearly steady, at 44%, when told the weight loss agent in question was an oral pill, but when asked about formulations requiring weekly injections the prevalence of people who had some interest, or were very interested, dropped to 23%. And when presented with the premise that they would need to take the drug chronically to keep their weight off and that stopping the agent would mean weight regain, those with “higher levels of interest” in the agent fell to 14% of the study sample.
Other deal breakers for most survey respondents were lack of a weight-loss indication approved by the Food and Drug Administration, a hypothetical that left 16% still somewhat or very interested, and lack of insurance coverage, which also dropped the higher interest levels to 16% of respondents. On the flip side of that sentiment, 80% of survey respondents believe that health insurance should cover the cost for a prescription weight loss drug for people with overweight or obesity.
The survey was designed and analyzed by public-opinion researchers at KFF and run both online and by telephone in both English and Spanish during July 11-19, 2023. The margin of sampling error was plus or minus 3 percentage points for the full sample but may have been even higher for results based on subgroup analyses.
The survey report includes no funding or disclosure information. However, KFF describes itself as “independent” and “nonpartisan” and that it “does everything based on facts and data, and we do so objectively without taking policy positions and without affiliation to any political party or external interest.”
A version of this article first appeared on Medscape.com.
A recent survey of more than 1,000 U.S. adults showed that 18% were “somewhat interested” in taking a “safe, effective” weight loss drug, 27% were “very interested,” and 4% said they were already using such an agent, together constituting 49% of the surveyed adults.
The newer, more potent and generally safe agents that work by stimulating receptors to nutrient-stimulated hormones, such as incretins like glucagonlike peptide–1, seem to drive this interest.
When asked: “How much have you heard, if anything, about a new class of drugs being used for weight loss, such as Ozempic [semaglutide formulated and approved for people with type 2 diabetes], Wegovy [semaglutide for weight loss], and Mounjaro [tirzepatide, currently approved for treating only people with type 2 diabetes]?” 43% said they had heard some, or a lot, about these agents.
This was particularly true among people at least 65 years old, who had a 55% prevalence of knowing some, or a lot, about these new weight-loss agents, while an additional 26% had heard at least “a little” about them, reported staff members of KFF (formerly the Kaiser Family Foundation) in a report posted online in early August.
Weight loss drugs garner ‘increasing’ attention
“A new class of prescription drugs, initially developed to treat type 2 diabetes, have been garnering an increasing amount of attention due to their ability to act as highly effective weight loss drugs for overweight or obese adults,” wrote the report’s authors.
However, surveyed interest fell markedly when respondents answered further questions that hinged on certain limitations of the newer weight loss formulations.
For example, the percent interested held nearly steady, at 44%, when told the weight loss agent in question was an oral pill, but when asked about formulations requiring weekly injections the prevalence of people who had some interest, or were very interested, dropped to 23%. And when presented with the premise that they would need to take the drug chronically to keep their weight off and that stopping the agent would mean weight regain, those with “higher levels of interest” in the agent fell to 14% of the study sample.
Other deal breakers for most survey respondents were lack of a weight-loss indication approved by the Food and Drug Administration, a hypothetical that left 16% still somewhat or very interested, and lack of insurance coverage, which also dropped the higher interest levels to 16% of respondents. On the flip side of that sentiment, 80% of survey respondents believe that health insurance should cover the cost for a prescription weight loss drug for people with overweight or obesity.
The survey was designed and analyzed by public-opinion researchers at KFF and run both online and by telephone in both English and Spanish during July 11-19, 2023. The margin of sampling error was plus or minus 3 percentage points for the full sample but may have been even higher for results based on subgroup analyses.
The survey report includes no funding or disclosure information. However, KFF describes itself as “independent” and “nonpartisan” and that it “does everything based on facts and data, and we do so objectively without taking policy positions and without affiliation to any political party or external interest.”
A version of this article first appeared on Medscape.com.
A recent survey of more than 1,000 U.S. adults showed that 18% were “somewhat interested” in taking a “safe, effective” weight loss drug, 27% were “very interested,” and 4% said they were already using such an agent, together constituting 49% of the surveyed adults.
The newer, more potent and generally safe agents that work by stimulating receptors to nutrient-stimulated hormones, such as incretins like glucagonlike peptide–1, seem to drive this interest.
When asked: “How much have you heard, if anything, about a new class of drugs being used for weight loss, such as Ozempic [semaglutide formulated and approved for people with type 2 diabetes], Wegovy [semaglutide for weight loss], and Mounjaro [tirzepatide, currently approved for treating only people with type 2 diabetes]?” 43% said they had heard some, or a lot, about these agents.
This was particularly true among people at least 65 years old, who had a 55% prevalence of knowing some, or a lot, about these new weight-loss agents, while an additional 26% had heard at least “a little” about them, reported staff members of KFF (formerly the Kaiser Family Foundation) in a report posted online in early August.
Weight loss drugs garner ‘increasing’ attention
“A new class of prescription drugs, initially developed to treat type 2 diabetes, have been garnering an increasing amount of attention due to their ability to act as highly effective weight loss drugs for overweight or obese adults,” wrote the report’s authors.
However, surveyed interest fell markedly when respondents answered further questions that hinged on certain limitations of the newer weight loss formulations.
For example, the percent interested held nearly steady, at 44%, when told the weight loss agent in question was an oral pill, but when asked about formulations requiring weekly injections the prevalence of people who had some interest, or were very interested, dropped to 23%. And when presented with the premise that they would need to take the drug chronically to keep their weight off and that stopping the agent would mean weight regain, those with “higher levels of interest” in the agent fell to 14% of the study sample.
Other deal breakers for most survey respondents were lack of a weight-loss indication approved by the Food and Drug Administration, a hypothetical that left 16% still somewhat or very interested, and lack of insurance coverage, which also dropped the higher interest levels to 16% of respondents. On the flip side of that sentiment, 80% of survey respondents believe that health insurance should cover the cost for a prescription weight loss drug for people with overweight or obesity.
The survey was designed and analyzed by public-opinion researchers at KFF and run both online and by telephone in both English and Spanish during July 11-19, 2023. The margin of sampling error was plus or minus 3 percentage points for the full sample but may have been even higher for results based on subgroup analyses.
The survey report includes no funding or disclosure information. However, KFF describes itself as “independent” and “nonpartisan” and that it “does everything based on facts and data, and we do so objectively without taking policy positions and without affiliation to any political party or external interest.”
A version of this article first appeared on Medscape.com.
Too old for time out. Now what? Oppositional behavior in school-age children
But here is the family coming to see us, struggling to get cooperation, and often increasingly embarrassed and angry.
Sometimes the dynamics leading to this behavior seem obvious: the parent tells their child to put away the toys they have pulled out in your waiting room, is ignored, and cleans them up themselves without a word. The child smugly fiddles with their cell phone, reinforced by removal of the task. Even without a defined reward, this still constitutes positive reinforcement as it increases the likelihood of the same future behavior of ignoring a parental directive.

Preventing this “mild” oppositionality at a younger age may come from the parent jollying the child through the clean up, participating with them in a game-like way counting the toys or making it a race, or even using only one request before grasping the child’s hand and “assisting” them in picking up a toy while praising cooperation but these tactics become less appropriate with age.
Other factors that may have led to school-aged child refusal include yelling at them, shaming, comparing them with a more compliant sibling, threatening a punishment that is never carried out, or deferring a consequence to the other caregiver. Of course, no child would want to please a caregiver with this kind of interaction by obeying them. By school age, children have a greater need to exert autonomy and avoid humiliation and may do this by getting angry, talking back, insulting the parent, or leaving the scene. This is especially likely if peers or siblings are present and the child wants to show that they can’t be bossed around.
Practical advice
So what can we advise when habits of refusal have already been established? Keeping in mind the major school-age psychosocial tasks of developing autonomy and self-esteem, the parent may need to overdo opportunities for this child to have choices and experience respect. When the child has a generalized oppositional stance, the parent may feel that it is difficult to identify opportunities to do this. The key in that case is to set up for cooperation and focus on small positive or neutral bits of behavior to reinforce. For example, requesting that the child do something they want to do anyways, such as come for a snack or turn on the TV, can be met with a brief but sincere “thanks” or “thanks for hopping on that.”
Sarcasm is counterproductive at all times, as it is insulting. Asking the child’s opinion regularly then listening and reflecting, rephrasing what they said, and even checking to see if the parent “got it right” do not require that the parent agrees. Any disagreement that the parent feels is needed can be withheld for a few minutes to indicate respect for the child’s opinion. For a child to learn to make “good choices” of behavior comes also from noticing how “not so good choices” worked out, a reflection the parent can try to elicit nonjudgmentally. Rebuilding the relationship can be done over time with respectful communication and assuring daily times of showing interest in the child, fooling around together, or playing a game.
While giving more choices respects autonomy, the options must really be acceptable to the parent. They may allow the child to choose some aspects of family activities – a skate park, or a certain eatery, or parts of the outing could be optional. Sometimes the order of upcoming events can provide a choice even if attendance is required. Sometimes the dress code can be flexible (flip flops, okay sure!), or a friend (preferably a well-behaved one!) could be invited along.
Pitfalls to avoid
Avoiding humiliation may be obvious, such as not complementing a singing performance or insistence on the child self-reporting bad behavior. For some families the parents may need to avoid their own embarrassing habits of “bad jokes” or outlandish clothes as a reasonable accommodation. Other kinds of humiliation to avoid may be specific to the child’s weaknesses, such as insisting that a clumsy child play on a team or a shy child speak to strangers. While it may be valuable for the child to work on those weaknesses, this should be done in private, if possible, or even with a coach who is not the parent if the relationship is strained.
Sensitive or anxious children are more prone to embarrassment and may then react with oppositional responses. They often do better with notice or coaching for upcoming events that may be in a category that has upset them in the past; for example, a visit from an overly affectionate aunt. Children may gain respect for their parents by being given a task that serves as an early escape route for these situations (Oh, would you please run out to the car and get my sweater?) although progressively tolerating undesirable situations is also important practice. A kindly debrief later with praise for progress also builds skills.
Reinforcing behaviors and revisiting consequences
Gaining more privileges as the reward for cooperation and responsibility is the natural sequence with development but oppositional children may need a chart, ideally negotiated as a family, to be clear about this cause-effect plan and what is expected for them to earn more freedom. Another benefit of a chart is that it is an objective translator of rules that can literally be pointed to rather than a parent-child conversation that could become an argument. Parents need to make expectations clear and follow through on promised increased privileges or consequences to be seen as fair. Having regular routines for chores, not just for activities, reduces refusal as well. Such concrete steps are especially important for children with ADHD who are often easily distracted from parental requests even if they meant to follow them and have a weak sense of timing. I have seen some wise parents give their distracted or impulsive child “a minute to decide if that is their final choice” before levying a consequence.
“When-then” statements can be useful both for coaching appropriate behavior in advance, debriefs, and alerting to consequences when needed. For example: “When you ask your aunt a question right away when you meet her then her hugs will be shorter” is coaching. “When you come home an hour late then you will have an hour earlier curfew the next week” is a graded consequence.
The cell phone issue
I can’t omit mentioning the specific situation of a child on a cell phone or tablet ignoring or refusing requests. While having possession of such a device may be seen as a safety measure (How can he reach me?) and social coinage (All my friends have one!), they are distracting and addicting and now the most common reason I see for oppositional interactions. This has been discussed elsewhere, so let me just say that a device is a privilege and should not “belong” to a child. Delaying the age of “lending” the device, establishing rules for use to certain situations and durations, and removing it for defined periods if it is interfering with cooperation are basic principles, even though enforcing them may result in upsets. Parents may need to change their own device use to be able to address oppositional behavior in their child.
Strategies for building better behavior
How important is it for the parent to verbalize what they are doing to instruct or accommodate their school-aged child? In the presence of others, the fewer words highlighting that an intervention is underway the better. Sometimes having a secret signal to prompt or praise, even a wink, can be helpful without being humiliating. These should be decided on together in private and practiced at first in nonstressful situations. Comments of appreciation or praise are appropriate then and are often reinforcing but should be very specific; for example, “I’m glad you got ready right away when it was time to leave” rather than general or backwards praise “Ready on time today, huh?” For some, especially younger or special-needs children, marks, points, tickets, tokens, or little prizes may be beneficial reinforcers, especially when trying to establish new patterns of interaction. Praise should fairly quickly replace more concrete rewards, though, by weaning, first by intermittent delivery or spacing further apart.
When counseling about oppositional behavior in school-aged children eliciting specific examples is key to determining whether parents are overly rigid or lax, have realistic expectations for their individual child’s temperament, skills, and past experiences (for example, traumas). As Ross Greene, PhD, points out,1 assisting families in understanding the gaps in skills that bring out opposition and categorizing behaviors into the rare “must-do’s,” and the many “just drop it’s,” in order to focus on understanding and building strategies and cooperation for situations that are important but not critical (Plan B) may require regular counseling by a mental health professional to help a child develop adaptive behavior and facilitate family harmony.
Reference
1. Greene RW. The Explosive Child: A New Approach for Understanding and Parenting Easily Frustrated, Chronically Inflexible Children, Sixth Edition, (New York: Harper Paperbacks, 2021).
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. Email her at [email protected].
But here is the family coming to see us, struggling to get cooperation, and often increasingly embarrassed and angry.
Sometimes the dynamics leading to this behavior seem obvious: the parent tells their child to put away the toys they have pulled out in your waiting room, is ignored, and cleans them up themselves without a word. The child smugly fiddles with their cell phone, reinforced by removal of the task. Even without a defined reward, this still constitutes positive reinforcement as it increases the likelihood of the same future behavior of ignoring a parental directive.
Preventing this “mild” oppositionality at a younger age may come from the parent jollying the child through the clean up, participating with them in a game-like way counting the toys or making it a race, or even using only one request before grasping the child’s hand and “assisting” them in picking up a toy while praising cooperation but these tactics become less appropriate with age.
Other factors that may have led to school-aged child refusal include yelling at them, shaming, comparing them with a more compliant sibling, threatening a punishment that is never carried out, or deferring a consequence to the other caregiver. Of course, no child would want to please a caregiver with this kind of interaction by obeying them. By school age, children have a greater need to exert autonomy and avoid humiliation and may do this by getting angry, talking back, insulting the parent, or leaving the scene. This is especially likely if peers or siblings are present and the child wants to show that they can’t be bossed around.
Practical advice
So what can we advise when habits of refusal have already been established? Keeping in mind the major school-age psychosocial tasks of developing autonomy and self-esteem, the parent may need to overdo opportunities for this child to have choices and experience respect. When the child has a generalized oppositional stance, the parent may feel that it is difficult to identify opportunities to do this. The key in that case is to set up for cooperation and focus on small positive or neutral bits of behavior to reinforce. For example, requesting that the child do something they want to do anyways, such as come for a snack or turn on the TV, can be met with a brief but sincere “thanks” or “thanks for hopping on that.”
Sarcasm is counterproductive at all times, as it is insulting. Asking the child’s opinion regularly then listening and reflecting, rephrasing what they said, and even checking to see if the parent “got it right” do not require that the parent agrees. Any disagreement that the parent feels is needed can be withheld for a few minutes to indicate respect for the child’s opinion. For a child to learn to make “good choices” of behavior comes also from noticing how “not so good choices” worked out, a reflection the parent can try to elicit nonjudgmentally. Rebuilding the relationship can be done over time with respectful communication and assuring daily times of showing interest in the child, fooling around together, or playing a game.
While giving more choices respects autonomy, the options must really be acceptable to the parent. They may allow the child to choose some aspects of family activities – a skate park, or a certain eatery, or parts of the outing could be optional. Sometimes the order of upcoming events can provide a choice even if attendance is required. Sometimes the dress code can be flexible (flip flops, okay sure!), or a friend (preferably a well-behaved one!) could be invited along.
Pitfalls to avoid
Avoiding humiliation may be obvious, such as not complementing a singing performance or insistence on the child self-reporting bad behavior. For some families the parents may need to avoid their own embarrassing habits of “bad jokes” or outlandish clothes as a reasonable accommodation. Other kinds of humiliation to avoid may be specific to the child’s weaknesses, such as insisting that a clumsy child play on a team or a shy child speak to strangers. While it may be valuable for the child to work on those weaknesses, this should be done in private, if possible, or even with a coach who is not the parent if the relationship is strained.
Sensitive or anxious children are more prone to embarrassment and may then react with oppositional responses. They often do better with notice or coaching for upcoming events that may be in a category that has upset them in the past; for example, a visit from an overly affectionate aunt. Children may gain respect for their parents by being given a task that serves as an early escape route for these situations (Oh, would you please run out to the car and get my sweater?) although progressively tolerating undesirable situations is also important practice. A kindly debrief later with praise for progress also builds skills.
Reinforcing behaviors and revisiting consequences
Gaining more privileges as the reward for cooperation and responsibility is the natural sequence with development but oppositional children may need a chart, ideally negotiated as a family, to be clear about this cause-effect plan and what is expected for them to earn more freedom. Another benefit of a chart is that it is an objective translator of rules that can literally be pointed to rather than a parent-child conversation that could become an argument. Parents need to make expectations clear and follow through on promised increased privileges or consequences to be seen as fair. Having regular routines for chores, not just for activities, reduces refusal as well. Such concrete steps are especially important for children with ADHD who are often easily distracted from parental requests even if they meant to follow them and have a weak sense of timing. I have seen some wise parents give their distracted or impulsive child “a minute to decide if that is their final choice” before levying a consequence.
“When-then” statements can be useful both for coaching appropriate behavior in advance, debriefs, and alerting to consequences when needed. For example: “When you ask your aunt a question right away when you meet her then her hugs will be shorter” is coaching. “When you come home an hour late then you will have an hour earlier curfew the next week” is a graded consequence.
The cell phone issue
I can’t omit mentioning the specific situation of a child on a cell phone or tablet ignoring or refusing requests. While having possession of such a device may be seen as a safety measure (How can he reach me?) and social coinage (All my friends have one!), they are distracting and addicting and now the most common reason I see for oppositional interactions. This has been discussed elsewhere, so let me just say that a device is a privilege and should not “belong” to a child. Delaying the age of “lending” the device, establishing rules for use to certain situations and durations, and removing it for defined periods if it is interfering with cooperation are basic principles, even though enforcing them may result in upsets. Parents may need to change their own device use to be able to address oppositional behavior in their child.
Strategies for building better behavior
How important is it for the parent to verbalize what they are doing to instruct or accommodate their school-aged child? In the presence of others, the fewer words highlighting that an intervention is underway the better. Sometimes having a secret signal to prompt or praise, even a wink, can be helpful without being humiliating. These should be decided on together in private and practiced at first in nonstressful situations. Comments of appreciation or praise are appropriate then and are often reinforcing but should be very specific; for example, “I’m glad you got ready right away when it was time to leave” rather than general or backwards praise “Ready on time today, huh?” For some, especially younger or special-needs children, marks, points, tickets, tokens, or little prizes may be beneficial reinforcers, especially when trying to establish new patterns of interaction. Praise should fairly quickly replace more concrete rewards, though, by weaning, first by intermittent delivery or spacing further apart.
When counseling about oppositional behavior in school-aged children eliciting specific examples is key to determining whether parents are overly rigid or lax, have realistic expectations for their individual child’s temperament, skills, and past experiences (for example, traumas). As Ross Greene, PhD, points out,1 assisting families in understanding the gaps in skills that bring out opposition and categorizing behaviors into the rare “must-do’s,” and the many “just drop it’s,” in order to focus on understanding and building strategies and cooperation for situations that are important but not critical (Plan B) may require regular counseling by a mental health professional to help a child develop adaptive behavior and facilitate family harmony.
Reference
1. Greene RW. The Explosive Child: A New Approach for Understanding and Parenting Easily Frustrated, Chronically Inflexible Children, Sixth Edition, (New York: Harper Paperbacks, 2021).
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. Email her at [email protected].
But here is the family coming to see us, struggling to get cooperation, and often increasingly embarrassed and angry.
Sometimes the dynamics leading to this behavior seem obvious: the parent tells their child to put away the toys they have pulled out in your waiting room, is ignored, and cleans them up themselves without a word. The child smugly fiddles with their cell phone, reinforced by removal of the task. Even without a defined reward, this still constitutes positive reinforcement as it increases the likelihood of the same future behavior of ignoring a parental directive.
Preventing this “mild” oppositionality at a younger age may come from the parent jollying the child through the clean up, participating with them in a game-like way counting the toys or making it a race, or even using only one request before grasping the child’s hand and “assisting” them in picking up a toy while praising cooperation but these tactics become less appropriate with age.
Other factors that may have led to school-aged child refusal include yelling at them, shaming, comparing them with a more compliant sibling, threatening a punishment that is never carried out, or deferring a consequence to the other caregiver. Of course, no child would want to please a caregiver with this kind of interaction by obeying them. By school age, children have a greater need to exert autonomy and avoid humiliation and may do this by getting angry, talking back, insulting the parent, or leaving the scene. This is especially likely if peers or siblings are present and the child wants to show that they can’t be bossed around.
Practical advice
So what can we advise when habits of refusal have already been established? Keeping in mind the major school-age psychosocial tasks of developing autonomy and self-esteem, the parent may need to overdo opportunities for this child to have choices and experience respect. When the child has a generalized oppositional stance, the parent may feel that it is difficult to identify opportunities to do this. The key in that case is to set up for cooperation and focus on small positive or neutral bits of behavior to reinforce. For example, requesting that the child do something they want to do anyways, such as come for a snack or turn on the TV, can be met with a brief but sincere “thanks” or “thanks for hopping on that.”
Sarcasm is counterproductive at all times, as it is insulting. Asking the child’s opinion regularly then listening and reflecting, rephrasing what they said, and even checking to see if the parent “got it right” do not require that the parent agrees. Any disagreement that the parent feels is needed can be withheld for a few minutes to indicate respect for the child’s opinion. For a child to learn to make “good choices” of behavior comes also from noticing how “not so good choices” worked out, a reflection the parent can try to elicit nonjudgmentally. Rebuilding the relationship can be done over time with respectful communication and assuring daily times of showing interest in the child, fooling around together, or playing a game.
While giving more choices respects autonomy, the options must really be acceptable to the parent. They may allow the child to choose some aspects of family activities – a skate park, or a certain eatery, or parts of the outing could be optional. Sometimes the order of upcoming events can provide a choice even if attendance is required. Sometimes the dress code can be flexible (flip flops, okay sure!), or a friend (preferably a well-behaved one!) could be invited along.
Pitfalls to avoid
Avoiding humiliation may be obvious, such as not complementing a singing performance or insistence on the child self-reporting bad behavior. For some families the parents may need to avoid their own embarrassing habits of “bad jokes” or outlandish clothes as a reasonable accommodation. Other kinds of humiliation to avoid may be specific to the child’s weaknesses, such as insisting that a clumsy child play on a team or a shy child speak to strangers. While it may be valuable for the child to work on those weaknesses, this should be done in private, if possible, or even with a coach who is not the parent if the relationship is strained.
Sensitive or anxious children are more prone to embarrassment and may then react with oppositional responses. They often do better with notice or coaching for upcoming events that may be in a category that has upset them in the past; for example, a visit from an overly affectionate aunt. Children may gain respect for their parents by being given a task that serves as an early escape route for these situations (Oh, would you please run out to the car and get my sweater?) although progressively tolerating undesirable situations is also important practice. A kindly debrief later with praise for progress also builds skills.
Reinforcing behaviors and revisiting consequences
Gaining more privileges as the reward for cooperation and responsibility is the natural sequence with development but oppositional children may need a chart, ideally negotiated as a family, to be clear about this cause-effect plan and what is expected for them to earn more freedom. Another benefit of a chart is that it is an objective translator of rules that can literally be pointed to rather than a parent-child conversation that could become an argument. Parents need to make expectations clear and follow through on promised increased privileges or consequences to be seen as fair. Having regular routines for chores, not just for activities, reduces refusal as well. Such concrete steps are especially important for children with ADHD who are often easily distracted from parental requests even if they meant to follow them and have a weak sense of timing. I have seen some wise parents give their distracted or impulsive child “a minute to decide if that is their final choice” before levying a consequence.
“When-then” statements can be useful both for coaching appropriate behavior in advance, debriefs, and alerting to consequences when needed. For example: “When you ask your aunt a question right away when you meet her then her hugs will be shorter” is coaching. “When you come home an hour late then you will have an hour earlier curfew the next week” is a graded consequence.
The cell phone issue
I can’t omit mentioning the specific situation of a child on a cell phone or tablet ignoring or refusing requests. While having possession of such a device may be seen as a safety measure (How can he reach me?) and social coinage (All my friends have one!), they are distracting and addicting and now the most common reason I see for oppositional interactions. This has been discussed elsewhere, so let me just say that a device is a privilege and should not “belong” to a child. Delaying the age of “lending” the device, establishing rules for use to certain situations and durations, and removing it for defined periods if it is interfering with cooperation are basic principles, even though enforcing them may result in upsets. Parents may need to change their own device use to be able to address oppositional behavior in their child.
Strategies for building better behavior
How important is it for the parent to verbalize what they are doing to instruct or accommodate their school-aged child? In the presence of others, the fewer words highlighting that an intervention is underway the better. Sometimes having a secret signal to prompt or praise, even a wink, can be helpful without being humiliating. These should be decided on together in private and practiced at first in nonstressful situations. Comments of appreciation or praise are appropriate then and are often reinforcing but should be very specific; for example, “I’m glad you got ready right away when it was time to leave” rather than general or backwards praise “Ready on time today, huh?” For some, especially younger or special-needs children, marks, points, tickets, tokens, or little prizes may be beneficial reinforcers, especially when trying to establish new patterns of interaction. Praise should fairly quickly replace more concrete rewards, though, by weaning, first by intermittent delivery or spacing further apart.
When counseling about oppositional behavior in school-aged children eliciting specific examples is key to determining whether parents are overly rigid or lax, have realistic expectations for their individual child’s temperament, skills, and past experiences (for example, traumas). As Ross Greene, PhD, points out,1 assisting families in understanding the gaps in skills that bring out opposition and categorizing behaviors into the rare “must-do’s,” and the many “just drop it’s,” in order to focus on understanding and building strategies and cooperation for situations that are important but not critical (Plan B) may require regular counseling by a mental health professional to help a child develop adaptive behavior and facilitate family harmony.
Reference
1. Greene RW. The Explosive Child: A New Approach for Understanding and Parenting Easily Frustrated, Chronically Inflexible Children, Sixth Edition, (New York: Harper Paperbacks, 2021).
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. Email her at [email protected].
New COVID shots will be available in September
The updated vaccine still needs final sign-offs from the Food and Drug Administration and the CDC.
“We anticipate that they are going to be available for most folks by the third or fourth week of September,” Director Mandy Cohen, MD, MPH, said on a podcast hosted by former White House COVID adviser Andy Slavitt. “We are likely to see this as a recommendation as an annual COVID shot, just as we have an annual flu shot. I think that will give folks more clarity on whether they should get one or not.”
For people who are considering now whether they should get the currently available COVID vaccine or wait until the new one comes out, Dr. Cohen said that depends on a person’s individual risk. People who are 65 or older or who have multiple health conditions should go ahead and get the currently available shot if it’s been more than 6-8 months since their last dose. For all other people, it’s OK to wait for the new version.
Analysts expect low demand for the updated vaccine. About 240 million people in the United States got at least one dose when vaccines first became available in 2021, Reuters reported, but that number dropped to less than 50 million getting the most updated shot in the fall of 2022.
“Take a look at what happened last winter. It was 50 million in the U.S., and it seems likely to be lower than that, given that there’s less concern about COVID this year than last year,” Michael Yee, a health care industry analyst for the firm Jefferies, told Reuters.
Dr. Cohen noted during the podcast that the recent uptick in virus activity should be taken in context.
“What we’re seeing right now in August of 2023 are small increases of folks getting COVID. We are still at some of the lowest hospitalizations that we’ve been at in the past 3 years,” she said. “Even a 10% increase on a very, very small number is still very small. My level of concern continues to be low.”
A version of this article was first published on WebMD.com .
The updated vaccine still needs final sign-offs from the Food and Drug Administration and the CDC.
“We anticipate that they are going to be available for most folks by the third or fourth week of September,” Director Mandy Cohen, MD, MPH, said on a podcast hosted by former White House COVID adviser Andy Slavitt. “We are likely to see this as a recommendation as an annual COVID shot, just as we have an annual flu shot. I think that will give folks more clarity on whether they should get one or not.”
For people who are considering now whether they should get the currently available COVID vaccine or wait until the new one comes out, Dr. Cohen said that depends on a person’s individual risk. People who are 65 or older or who have multiple health conditions should go ahead and get the currently available shot if it’s been more than 6-8 months since their last dose. For all other people, it’s OK to wait for the new version.
Analysts expect low demand for the updated vaccine. About 240 million people in the United States got at least one dose when vaccines first became available in 2021, Reuters reported, but that number dropped to less than 50 million getting the most updated shot in the fall of 2022.
“Take a look at what happened last winter. It was 50 million in the U.S., and it seems likely to be lower than that, given that there’s less concern about COVID this year than last year,” Michael Yee, a health care industry analyst for the firm Jefferies, told Reuters.
Dr. Cohen noted during the podcast that the recent uptick in virus activity should be taken in context.
“What we’re seeing right now in August of 2023 are small increases of folks getting COVID. We are still at some of the lowest hospitalizations that we’ve been at in the past 3 years,” she said. “Even a 10% increase on a very, very small number is still very small. My level of concern continues to be low.”
A version of this article was first published on WebMD.com .
The updated vaccine still needs final sign-offs from the Food and Drug Administration and the CDC.
“We anticipate that they are going to be available for most folks by the third or fourth week of September,” Director Mandy Cohen, MD, MPH, said on a podcast hosted by former White House COVID adviser Andy Slavitt. “We are likely to see this as a recommendation as an annual COVID shot, just as we have an annual flu shot. I think that will give folks more clarity on whether they should get one or not.”
For people who are considering now whether they should get the currently available COVID vaccine or wait until the new one comes out, Dr. Cohen said that depends on a person’s individual risk. People who are 65 or older or who have multiple health conditions should go ahead and get the currently available shot if it’s been more than 6-8 months since their last dose. For all other people, it’s OK to wait for the new version.
Analysts expect low demand for the updated vaccine. About 240 million people in the United States got at least one dose when vaccines first became available in 2021, Reuters reported, but that number dropped to less than 50 million getting the most updated shot in the fall of 2022.
“Take a look at what happened last winter. It was 50 million in the U.S., and it seems likely to be lower than that, given that there’s less concern about COVID this year than last year,” Michael Yee, a health care industry analyst for the firm Jefferies, told Reuters.
Dr. Cohen noted during the podcast that the recent uptick in virus activity should be taken in context.
“What we’re seeing right now in August of 2023 are small increases of folks getting COVID. We are still at some of the lowest hospitalizations that we’ve been at in the past 3 years,” she said. “Even a 10% increase on a very, very small number is still very small. My level of concern continues to be low.”
A version of this article was first published on WebMD.com .