User login
Predictors of minimal disease activity achievement in upadacitinib-treated PsA
Key clinical point: This real-world study validated the efficacy of upadacitinib and elucidated the variables influencing the attainment of minimal disease activity (MDA) in response to upadacitinib therapy in patients with psoriatic arthritis (PsA).
Major finding: At week 24, nearly half (47%) of the patients treated with upadacitinib achieved MDA, with males (odds ratio [OR] 2.54; P = .043), patients naive to biologic disease-modifying antirheumatic drugs (OR 4.13; P = .013), and patients with high baseline C-reactive protein levels (OR 2.49; P = .046) having higher odds of achieving MDA.
Study details: Findings are from the preliminary results of the ongoing UPREAL-PsA study including 126 patients with peripheral or axial PsA who received 15 mg upadacitinib once daily.
Disclosures: This study did not receive any specific funding. The authors declared no conflicts of interest.
Source: Luchetti Gentiloni MM et al. Upadacitinib effectiveness and factors associated with minimal disease activity achievement in patients with psoriatic arthritis: Preliminary data of a real-life multicenter study. Arthritis Res Ther. 2023;25:196. (Oct 11). doi: 10.1186/s13075-023-03182-9
Key clinical point: This real-world study validated the efficacy of upadacitinib and elucidated the variables influencing the attainment of minimal disease activity (MDA) in response to upadacitinib therapy in patients with psoriatic arthritis (PsA).
Major finding: At week 24, nearly half (47%) of the patients treated with upadacitinib achieved MDA, with males (odds ratio [OR] 2.54; P = .043), patients naive to biologic disease-modifying antirheumatic drugs (OR 4.13; P = .013), and patients with high baseline C-reactive protein levels (OR 2.49; P = .046) having higher odds of achieving MDA.
Study details: Findings are from the preliminary results of the ongoing UPREAL-PsA study including 126 patients with peripheral or axial PsA who received 15 mg upadacitinib once daily.
Disclosures: This study did not receive any specific funding. The authors declared no conflicts of interest.
Source: Luchetti Gentiloni MM et al. Upadacitinib effectiveness and factors associated with minimal disease activity achievement in patients with psoriatic arthritis: Preliminary data of a real-life multicenter study. Arthritis Res Ther. 2023;25:196. (Oct 11). doi: 10.1186/s13075-023-03182-9
Key clinical point: This real-world study validated the efficacy of upadacitinib and elucidated the variables influencing the attainment of minimal disease activity (MDA) in response to upadacitinib therapy in patients with psoriatic arthritis (PsA).
Major finding: At week 24, nearly half (47%) of the patients treated with upadacitinib achieved MDA, with males (odds ratio [OR] 2.54; P = .043), patients naive to biologic disease-modifying antirheumatic drugs (OR 4.13; P = .013), and patients with high baseline C-reactive protein levels (OR 2.49; P = .046) having higher odds of achieving MDA.
Study details: Findings are from the preliminary results of the ongoing UPREAL-PsA study including 126 patients with peripheral or axial PsA who received 15 mg upadacitinib once daily.
Disclosures: This study did not receive any specific funding. The authors declared no conflicts of interest.
Source: Luchetti Gentiloni MM et al. Upadacitinib effectiveness and factors associated with minimal disease activity achievement in patients with psoriatic arthritis: Preliminary data of a real-life multicenter study. Arthritis Res Ther. 2023;25:196. (Oct 11). doi: 10.1186/s13075-023-03182-9
Study eases fears: Knee surgery surge not linked to premature intervention
“Both the total number [of surgeons performing primary TKA] and the number of surgeons per capita have been generally increasing,” wrote Peter Dust, MD, of McGill University, Montreal, and coauthors. “Reassuringly, however, our results suggest that despite the increasing number of surgeons, the indications for surgery are not being eroded by operating on healthier patients to fill operating room time.”
The study was published in the Canadian Journal of Surgery.
Rising demand
In the paper, Dr. Dust and colleagues noted that there was a 162% increase in volume of total knee arthroplasties among people enrolled in the Medicare program between 1991 and 2010.
Unrelated to the study, the Canadian Institute for Health Information (CIHI) has reported similar trends. In 2018-2019, about 75,000 knee replacements were performed in Canada; an increase of 22.5% over the previous 5 years. The numbers dropped in 2020-2021 during the pandemic because of limited access to medical facilities during that time, but then rebounded between April and September 2022 to close to prepandemic numbers. However, about 50% of patients were waiting longer during that time than the recommended 6 months (182 days) for their surgery.
So, what’s happening?
The trends for rising numbers of knee surgeries cannot be fully explained by population growth and increasing rates of obesity, Dr. Dust and colleagues wrote. That led them to ask whether some patients were undergoing surgery with a higher level of preoperative function compared with the past.
They conducted a systematic review and meta-analysis of the MEDLINE, Embase, and Cochrane databases with the aim of determining the effect of time, age, and sex on preoperative functional status. A total of 149 studies were ultimately included in the study, with data from 257 independent groups and 57,844 patients recruited from 1991 to 2015.
The analysis revealed that patients are undergoing TKA with a level of preoperative function similar to that in the past. Also, patient age, sex, and location did not influence the functional status at which patients were considered for surgery.
Jasvinder Singh, MD, professor of medicine and epidemiology at University of Alabama at Birmingham, who was not involved with the research, offered another suggestion to explain the trend: People today are more familiar with knee replacement surgery and thus find it a less daunting option.
“Everybody knows somebody who has had a knee done or a hip done,” Singh said in an interview.”People are a lot more familiar with these things than they were 30 years ago.”
Subjective criteria persists
In the paper, Dr. Dust said that he and his colleagues had hoped this study might reveal a target physical component summary (PCS) score, used to assess functional status, based on which patients could be considered for surgery. Their findings, however, did not enable such a recommendation to be made.
In an interview, Claudette M. Lajam, MD, a spokesperson for the American Academy of Orthopedic Surgeons (AAOS), agreed that there does not appear to be a trend toward earlier intervention. Also, a precise number or score that can be used to determine when patients should undergo TKA still does not exist. Dr. Lajam is professor of orthopedic surgery and system chief for orthopedic quality and risk at NYU Langone Health, New York.
The “sweet spot time” for TKA is still not clear based on available metrics, Dr. Lajam said. Physicians need to consider not only patient level of function before surgery, but also when to intervene so they will get the most benefit from these procedures.
The knee has to be “bad enough to justify major surgery,” she said, while waiting too long might lead to inferior outcomes.
In time, she thinks artificial intelligence (AI) could help in identifying when primary care clinicians should advise patients to seek specialist care for ailing knees.
AI could allow physicians and researchers to search for clues about the best timing for surgery by combing through millions of x-rays, a variety of functional scores used in assessing patients, and other sources of information, she explained. At this time, the PCS used by Dr. Dust and colleagues is just one of many measures used to assess patient level of function. AI might be able to bring these data together for scientists to review.
“AI can see patterns that I can’t see right now,” Dr. Lajam said.
But she emphasized that any AI application would be an aid to physicians in counseling patients. Evaluation by an experienced surgeon, together with guidance from any AI tool, could provide a greater understanding of how TKA could help patients with arthritis of the knee.
“The physician sees intangibles that AI would not see because we actually talk to the patient,” she explained.
Dr. Dust said there was no outside funding for the study and the authors and Dr. Lajam reported no relevant financial relationships. Dr. Singh said he has received consulting fees from AstraZeneca and institutional research support from Zimmer Biomet Holdings. He has received food and beverage payments from Intuitive Surgical Inc./Philips Electronics North America, and owns stock options in Atai Life Sciences. He is a member of the executive committee of Outcome Measures in Rheumatology (OMERACT), an organization that receives arms-length funding from eight companies.
A version of this article appeared on Medscape.com.
“Both the total number [of surgeons performing primary TKA] and the number of surgeons per capita have been generally increasing,” wrote Peter Dust, MD, of McGill University, Montreal, and coauthors. “Reassuringly, however, our results suggest that despite the increasing number of surgeons, the indications for surgery are not being eroded by operating on healthier patients to fill operating room time.”
The study was published in the Canadian Journal of Surgery.
Rising demand
In the paper, Dr. Dust and colleagues noted that there was a 162% increase in volume of total knee arthroplasties among people enrolled in the Medicare program between 1991 and 2010.
Unrelated to the study, the Canadian Institute for Health Information (CIHI) has reported similar trends. In 2018-2019, about 75,000 knee replacements were performed in Canada; an increase of 22.5% over the previous 5 years. The numbers dropped in 2020-2021 during the pandemic because of limited access to medical facilities during that time, but then rebounded between April and September 2022 to close to prepandemic numbers. However, about 50% of patients were waiting longer during that time than the recommended 6 months (182 days) for their surgery.
So, what’s happening?
The trends for rising numbers of knee surgeries cannot be fully explained by population growth and increasing rates of obesity, Dr. Dust and colleagues wrote. That led them to ask whether some patients were undergoing surgery with a higher level of preoperative function compared with the past.
They conducted a systematic review and meta-analysis of the MEDLINE, Embase, and Cochrane databases with the aim of determining the effect of time, age, and sex on preoperative functional status. A total of 149 studies were ultimately included in the study, with data from 257 independent groups and 57,844 patients recruited from 1991 to 2015.
The analysis revealed that patients are undergoing TKA with a level of preoperative function similar to that in the past. Also, patient age, sex, and location did not influence the functional status at which patients were considered for surgery.
Jasvinder Singh, MD, professor of medicine and epidemiology at University of Alabama at Birmingham, who was not involved with the research, offered another suggestion to explain the trend: People today are more familiar with knee replacement surgery and thus find it a less daunting option.
“Everybody knows somebody who has had a knee done or a hip done,” Singh said in an interview.”People are a lot more familiar with these things than they were 30 years ago.”
Subjective criteria persists
In the paper, Dr. Dust said that he and his colleagues had hoped this study might reveal a target physical component summary (PCS) score, used to assess functional status, based on which patients could be considered for surgery. Their findings, however, did not enable such a recommendation to be made.
In an interview, Claudette M. Lajam, MD, a spokesperson for the American Academy of Orthopedic Surgeons (AAOS), agreed that there does not appear to be a trend toward earlier intervention. Also, a precise number or score that can be used to determine when patients should undergo TKA still does not exist. Dr. Lajam is professor of orthopedic surgery and system chief for orthopedic quality and risk at NYU Langone Health, New York.
The “sweet spot time” for TKA is still not clear based on available metrics, Dr. Lajam said. Physicians need to consider not only patient level of function before surgery, but also when to intervene so they will get the most benefit from these procedures.
The knee has to be “bad enough to justify major surgery,” she said, while waiting too long might lead to inferior outcomes.
In time, she thinks artificial intelligence (AI) could help in identifying when primary care clinicians should advise patients to seek specialist care for ailing knees.
AI could allow physicians and researchers to search for clues about the best timing for surgery by combing through millions of x-rays, a variety of functional scores used in assessing patients, and other sources of information, she explained. At this time, the PCS used by Dr. Dust and colleagues is just one of many measures used to assess patient level of function. AI might be able to bring these data together for scientists to review.
“AI can see patterns that I can’t see right now,” Dr. Lajam said.
But she emphasized that any AI application would be an aid to physicians in counseling patients. Evaluation by an experienced surgeon, together with guidance from any AI tool, could provide a greater understanding of how TKA could help patients with arthritis of the knee.
“The physician sees intangibles that AI would not see because we actually talk to the patient,” she explained.
Dr. Dust said there was no outside funding for the study and the authors and Dr. Lajam reported no relevant financial relationships. Dr. Singh said he has received consulting fees from AstraZeneca and institutional research support from Zimmer Biomet Holdings. He has received food and beverage payments from Intuitive Surgical Inc./Philips Electronics North America, and owns stock options in Atai Life Sciences. He is a member of the executive committee of Outcome Measures in Rheumatology (OMERACT), an organization that receives arms-length funding from eight companies.
A version of this article appeared on Medscape.com.
“Both the total number [of surgeons performing primary TKA] and the number of surgeons per capita have been generally increasing,” wrote Peter Dust, MD, of McGill University, Montreal, and coauthors. “Reassuringly, however, our results suggest that despite the increasing number of surgeons, the indications for surgery are not being eroded by operating on healthier patients to fill operating room time.”
The study was published in the Canadian Journal of Surgery.
Rising demand
In the paper, Dr. Dust and colleagues noted that there was a 162% increase in volume of total knee arthroplasties among people enrolled in the Medicare program between 1991 and 2010.
Unrelated to the study, the Canadian Institute for Health Information (CIHI) has reported similar trends. In 2018-2019, about 75,000 knee replacements were performed in Canada; an increase of 22.5% over the previous 5 years. The numbers dropped in 2020-2021 during the pandemic because of limited access to medical facilities during that time, but then rebounded between April and September 2022 to close to prepandemic numbers. However, about 50% of patients were waiting longer during that time than the recommended 6 months (182 days) for their surgery.
So, what’s happening?
The trends for rising numbers of knee surgeries cannot be fully explained by population growth and increasing rates of obesity, Dr. Dust and colleagues wrote. That led them to ask whether some patients were undergoing surgery with a higher level of preoperative function compared with the past.
They conducted a systematic review and meta-analysis of the MEDLINE, Embase, and Cochrane databases with the aim of determining the effect of time, age, and sex on preoperative functional status. A total of 149 studies were ultimately included in the study, with data from 257 independent groups and 57,844 patients recruited from 1991 to 2015.
The analysis revealed that patients are undergoing TKA with a level of preoperative function similar to that in the past. Also, patient age, sex, and location did not influence the functional status at which patients were considered for surgery.
Jasvinder Singh, MD, professor of medicine and epidemiology at University of Alabama at Birmingham, who was not involved with the research, offered another suggestion to explain the trend: People today are more familiar with knee replacement surgery and thus find it a less daunting option.
“Everybody knows somebody who has had a knee done or a hip done,” Singh said in an interview.”People are a lot more familiar with these things than they were 30 years ago.”
Subjective criteria persists
In the paper, Dr. Dust said that he and his colleagues had hoped this study might reveal a target physical component summary (PCS) score, used to assess functional status, based on which patients could be considered for surgery. Their findings, however, did not enable such a recommendation to be made.
In an interview, Claudette M. Lajam, MD, a spokesperson for the American Academy of Orthopedic Surgeons (AAOS), agreed that there does not appear to be a trend toward earlier intervention. Also, a precise number or score that can be used to determine when patients should undergo TKA still does not exist. Dr. Lajam is professor of orthopedic surgery and system chief for orthopedic quality and risk at NYU Langone Health, New York.
The “sweet spot time” for TKA is still not clear based on available metrics, Dr. Lajam said. Physicians need to consider not only patient level of function before surgery, but also when to intervene so they will get the most benefit from these procedures.
The knee has to be “bad enough to justify major surgery,” she said, while waiting too long might lead to inferior outcomes.
In time, she thinks artificial intelligence (AI) could help in identifying when primary care clinicians should advise patients to seek specialist care for ailing knees.
AI could allow physicians and researchers to search for clues about the best timing for surgery by combing through millions of x-rays, a variety of functional scores used in assessing patients, and other sources of information, she explained. At this time, the PCS used by Dr. Dust and colleagues is just one of many measures used to assess patient level of function. AI might be able to bring these data together for scientists to review.
“AI can see patterns that I can’t see right now,” Dr. Lajam said.
But she emphasized that any AI application would be an aid to physicians in counseling patients. Evaluation by an experienced surgeon, together with guidance from any AI tool, could provide a greater understanding of how TKA could help patients with arthritis of the knee.
“The physician sees intangibles that AI would not see because we actually talk to the patient,” she explained.
Dr. Dust said there was no outside funding for the study and the authors and Dr. Lajam reported no relevant financial relationships. Dr. Singh said he has received consulting fees from AstraZeneca and institutional research support from Zimmer Biomet Holdings. He has received food and beverage payments from Intuitive Surgical Inc./Philips Electronics North America, and owns stock options in Atai Life Sciences. He is a member of the executive committee of Outcome Measures in Rheumatology (OMERACT), an organization that receives arms-length funding from eight companies.
A version of this article appeared on Medscape.com.
Children and preteen use of melatonin as sleep aid increased
More children and preteens are taking melatonin to help them sleep, a new study found, while experts cautioned parents may be unaware of some risks, particularly with long-term use.
The investigators noted not all melatonin supplements contain what they say they do – some tested in a separate study contained two to three times the amount of melatonin on the label, and one supplement contained none at all.
A matter of timing?
While not completely advising against the sleep supplement, the study researchers pointed out that short-term use is likely safer.
“We are not saying that melatonin is necessarily harmful to children. But much more research needs to be done before we can state with confidence that it is safe for kids to be taking long term,” lead study author Lauren Hartstein, PhD, a postdoctoral fellow in the Sleep and Development Lab at the University of Colorado in Boulder, said in a news release.
“If, after weighing potential risks and benefits, melatonin is recommended as the appropriate treatment, [a sleep medicine specialist] can recommend a dose and timing to treat the sleep issue,” said Raj Bhui, MD, a sleep medicine specialist and American Academy of Sleep Medicine spokesperson, who was not involved in the study.
An increasing trend
From 2017 to 2018, only about 1.3% of parents reported their children used melatonin in national data looking at supplement use in children and teenagers. In fact, usage more than doubled in this younger population from 2017 to 2020, another study revealed. “All of a sudden, in 2022, we started noticing a lot of parents telling us that their healthy child was regularly taking melatonin,” Dr. Hartstein said.
She and colleagues surveyed the parents of 993 children, aged 1 to less than 14, from January to April 2023. They found about 20% of these school-aged children and preteens took melatonin as a sleep aid. The findings, published in the journal JAMA Pediatrics, also suggest that some parents routinely give their preschool children melatonin.
They found nearly 6% of preschoolers aged 1-4, 18.5% of children aged 5-9, and 19.4% of kids aged 10-13 had taken melatonin in the previous month.
The researchers also discovered that many took melatonin for longer than a few nights. Preschool children took the supplement for a median of 1 year, grade school children for a median 18 months, and preteens for 21 months.
What’s in your supplement?
In a different study published April 25 (JAMA. 2023. doi: 10.1001/jama.2023.2296), researchers looked at 25 melatonin gummy products and found that 22 of them contained different amounts of melatonin than listed on the label. In fact, one called Sleep Plus Immune contained more than three times the amount, and with a supplement called Sleep Support, researchers could not detect any melatonin.
There is a general misconception that supplements are natural and therefore safe, Dr. Bhui said. “Multiple investigations of commercially available supplements have shown we cannot assume that what is on the label is in the pill or that what is in the pill is disclosed on the label. Formal laboratory testing has revealed some supplements to be adulterated with unapproved pharmaceutical ingredients, contaminated with microbes, or even tainted with toxins like arsenic, lead, and mercury.”
Choosing a product with the “USP Verified Mark” may give parents some comfort regarding melatonin content and consistency with labeling, Dr. Bhui said. Taking steps to safeguard the supply at home is also important in making sure children don’t take the supplements by accident. “With the increased use of melatonin, this has been a growing problem.”
A version of this article first appeared on WebMD.com.
More children and preteens are taking melatonin to help them sleep, a new study found, while experts cautioned parents may be unaware of some risks, particularly with long-term use.
The investigators noted not all melatonin supplements contain what they say they do – some tested in a separate study contained two to three times the amount of melatonin on the label, and one supplement contained none at all.
A matter of timing?
While not completely advising against the sleep supplement, the study researchers pointed out that short-term use is likely safer.
“We are not saying that melatonin is necessarily harmful to children. But much more research needs to be done before we can state with confidence that it is safe for kids to be taking long term,” lead study author Lauren Hartstein, PhD, a postdoctoral fellow in the Sleep and Development Lab at the University of Colorado in Boulder, said in a news release.
“If, after weighing potential risks and benefits, melatonin is recommended as the appropriate treatment, [a sleep medicine specialist] can recommend a dose and timing to treat the sleep issue,” said Raj Bhui, MD, a sleep medicine specialist and American Academy of Sleep Medicine spokesperson, who was not involved in the study.
An increasing trend
From 2017 to 2018, only about 1.3% of parents reported their children used melatonin in national data looking at supplement use in children and teenagers. In fact, usage more than doubled in this younger population from 2017 to 2020, another study revealed. “All of a sudden, in 2022, we started noticing a lot of parents telling us that their healthy child was regularly taking melatonin,” Dr. Hartstein said.
She and colleagues surveyed the parents of 993 children, aged 1 to less than 14, from January to April 2023. They found about 20% of these school-aged children and preteens took melatonin as a sleep aid. The findings, published in the journal JAMA Pediatrics, also suggest that some parents routinely give their preschool children melatonin.
They found nearly 6% of preschoolers aged 1-4, 18.5% of children aged 5-9, and 19.4% of kids aged 10-13 had taken melatonin in the previous month.
The researchers also discovered that many took melatonin for longer than a few nights. Preschool children took the supplement for a median of 1 year, grade school children for a median 18 months, and preteens for 21 months.
What’s in your supplement?
In a different study published April 25 (JAMA. 2023. doi: 10.1001/jama.2023.2296), researchers looked at 25 melatonin gummy products and found that 22 of them contained different amounts of melatonin than listed on the label. In fact, one called Sleep Plus Immune contained more than three times the amount, and with a supplement called Sleep Support, researchers could not detect any melatonin.
There is a general misconception that supplements are natural and therefore safe, Dr. Bhui said. “Multiple investigations of commercially available supplements have shown we cannot assume that what is on the label is in the pill or that what is in the pill is disclosed on the label. Formal laboratory testing has revealed some supplements to be adulterated with unapproved pharmaceutical ingredients, contaminated with microbes, or even tainted with toxins like arsenic, lead, and mercury.”
Choosing a product with the “USP Verified Mark” may give parents some comfort regarding melatonin content and consistency with labeling, Dr. Bhui said. Taking steps to safeguard the supply at home is also important in making sure children don’t take the supplements by accident. “With the increased use of melatonin, this has been a growing problem.”
A version of this article first appeared on WebMD.com.
More children and preteens are taking melatonin to help them sleep, a new study found, while experts cautioned parents may be unaware of some risks, particularly with long-term use.
The investigators noted not all melatonin supplements contain what they say they do – some tested in a separate study contained two to three times the amount of melatonin on the label, and one supplement contained none at all.
A matter of timing?
While not completely advising against the sleep supplement, the study researchers pointed out that short-term use is likely safer.
“We are not saying that melatonin is necessarily harmful to children. But much more research needs to be done before we can state with confidence that it is safe for kids to be taking long term,” lead study author Lauren Hartstein, PhD, a postdoctoral fellow in the Sleep and Development Lab at the University of Colorado in Boulder, said in a news release.
“If, after weighing potential risks and benefits, melatonin is recommended as the appropriate treatment, [a sleep medicine specialist] can recommend a dose and timing to treat the sleep issue,” said Raj Bhui, MD, a sleep medicine specialist and American Academy of Sleep Medicine spokesperson, who was not involved in the study.
An increasing trend
From 2017 to 2018, only about 1.3% of parents reported their children used melatonin in national data looking at supplement use in children and teenagers. In fact, usage more than doubled in this younger population from 2017 to 2020, another study revealed. “All of a sudden, in 2022, we started noticing a lot of parents telling us that their healthy child was regularly taking melatonin,” Dr. Hartstein said.
She and colleagues surveyed the parents of 993 children, aged 1 to less than 14, from January to April 2023. They found about 20% of these school-aged children and preteens took melatonin as a sleep aid. The findings, published in the journal JAMA Pediatrics, also suggest that some parents routinely give their preschool children melatonin.
They found nearly 6% of preschoolers aged 1-4, 18.5% of children aged 5-9, and 19.4% of kids aged 10-13 had taken melatonin in the previous month.
The researchers also discovered that many took melatonin for longer than a few nights. Preschool children took the supplement for a median of 1 year, grade school children for a median 18 months, and preteens for 21 months.
What’s in your supplement?
In a different study published April 25 (JAMA. 2023. doi: 10.1001/jama.2023.2296), researchers looked at 25 melatonin gummy products and found that 22 of them contained different amounts of melatonin than listed on the label. In fact, one called Sleep Plus Immune contained more than three times the amount, and with a supplement called Sleep Support, researchers could not detect any melatonin.
There is a general misconception that supplements are natural and therefore safe, Dr. Bhui said. “Multiple investigations of commercially available supplements have shown we cannot assume that what is on the label is in the pill or that what is in the pill is disclosed on the label. Formal laboratory testing has revealed some supplements to be adulterated with unapproved pharmaceutical ingredients, contaminated with microbes, or even tainted with toxins like arsenic, lead, and mercury.”
Choosing a product with the “USP Verified Mark” may give parents some comfort regarding melatonin content and consistency with labeling, Dr. Bhui said. Taking steps to safeguard the supply at home is also important in making sure children don’t take the supplements by accident. “With the increased use of melatonin, this has been a growing problem.”
A version of this article first appeared on WebMD.com.
FROM JAMA PEDIATRICS
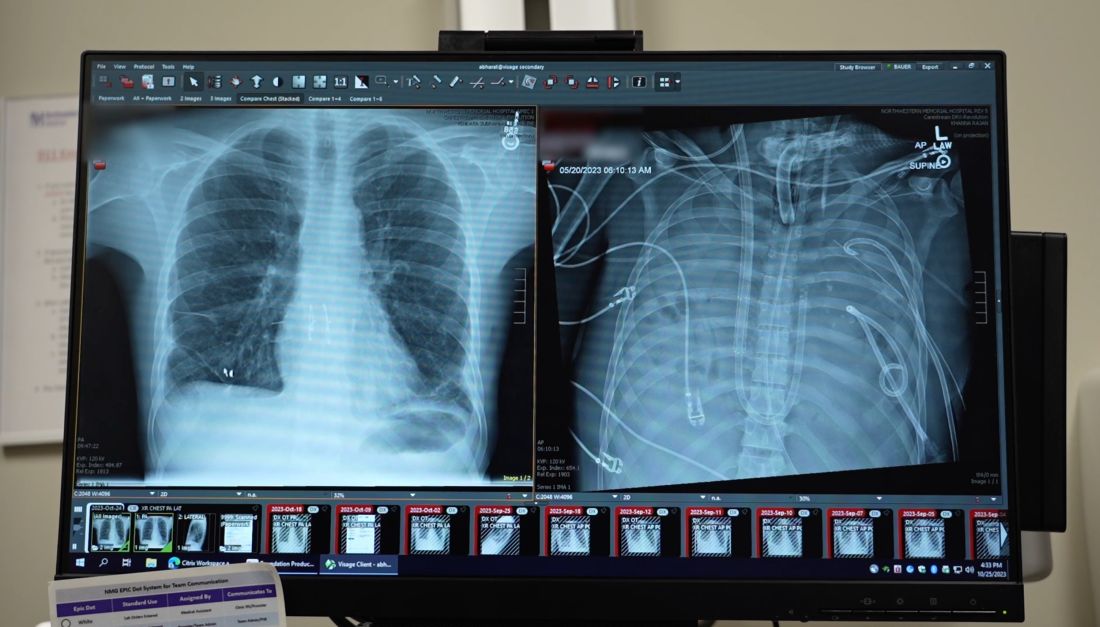
Breast implants used in double lung transplant post infection
An innovative surgical procedure combining breast implants and an artificial lung may help more patients with severe lung disease survive to receive transplants. The case was described in a press conference sponsored by Northwestern University, Evanston, Ill.
In May 2023, a surgical team at Northwestern removed both infected lungs from David “Davey” Bauer, aged 34 years, and temporarily used breast implants to hold his heart in place until new lungs were available.
In April 2023, Mr. Bauer, a longtime smoker and vaper, experienced shortness of breath. His girlfriend, Susan Gore, took him to an urgent care center, and he returned home, but “the next morning he couldn’t walk,” Ms. Gore said in the press conference. A trip to the ED yielded a diagnosis of influenza A, followed rapidly by a bacterial lung infection that proved resistant to antibiotics. Mr. Bauer had no prior medical history of serious illness, but he was soon in an intensive care unit. His condition continued to decline, and a double lung transplant was his only option.
The Northwestern Medicine Canning Thoracic Institute specializes in challenging cases, and Mr. Bauer was transferred there.
Back from the brink
Mr. Bauer made the transfer to Chicago despite being critically ill. He was in dire need of a lung transplant, and the only way to resolve his infection was to remove the lungs, said Ankit Bharat, MD, chief of thoracic surgery and director of Northwestern Medicine Canning Thoracic Institute, in the press conference.

“Something needed to be done right away,” Dr. Bharat said. Mr. Bauer’s lungs were removed and the chest cavity was extensively debrided to remove the infection.
Then it was time for outside-the-box thinking. “With the lungs taken out, we needed something to support the heart,” he said. Breast implants came to mind, and double Ds were the largest available.
In addition, the surgeons created an artificial lung system of conduits to keep Mr. Bauer’s blood pumping. “We wanted to maintain the natural blood flow in the body that would be present if the lungs were there,” Dr. Bharat explained.
Plastic surgeons at Northwestern gave Mr. Bauer’s surgical team “a crash course” in managing the breast implants, Dr. Bharat said. The team anticipated that their novel surgical solution would need to last for weeks, but Mr. Bauer’s condition improved immediately once the infected lungs were removed. He was placed on a double-lung transplant list, and the team received an offer of new lungs within 24 hours.
The breast implants were removed, the new lungs were implanted, and Bauer spent several months in the ICU before his discharge to rehabilitation therapy at the end of September, according to a Northwestern press release.
This type of procedure could help patients with infections who need transplants but are too sick to undergo them, Dr. Bharat said in the press conference. In Mr. Bauer’s case, “a lot of stars aligned,” including Bauer’s rapid improvement and the quick availability of a perfect lung match, Dr. Bharat said. Many patients don’t survive to the point of transplant.
“We were surprised how quickly he recovered once we removed the infected lungs,” Dr. Bharat noted. The quick recovery may be in part because of Bauer’s youth and relative good health, but “this was uncharted territory.”
Mr. Bauer’s case is the first use of this particular surgical technique, although the team drew on lessons learned in other surgical settings, such as removal of both lungs to prevent cross-contamination in patients with cancer, he added.
Causes and effects
As for the factors that contributed to Mr. Bauer’s initial infection, “there is a lot we don’t know, but we can try to put things together,” said Dr. Bharat. Just as many factors lined up to promote Mr. Bauer’s recovery, many factors lined up to cause the problem, including long-standing smoking and vaping. Although some still view vaping as a safer alternative to smoking, patient data and experiences do not support this claim. “We know for a fact that both of them cause harm,” he added.
Mr. Bauer started smoking cigarettes at age 21 and typically smoked a pack of cigarettes each day before switching to vaping in 2014. In addition, Mr. Bauer had not been vaccinated against the flu, and his flu infection was followed by a bacterial infection.
Bacterial infections followed by hospitalizations are not new as an effect of vaping; a series of articles described the ongoing epidemic of e-cigarette or vaping product use–associated lung injury (EVALI). Patients with EVALI often present at urgent care centers, as Bauer did, with symptoms of flu or pneumonia, and they are often given medication and sent home.
Looking ahead: “We expect that Davey will fully recover and live a normal life,” although he will remain in Chicago for another year for monitoring, said Rade Tomic, MD, pulmonologist and medical director of the Northwestern Medicine Canning Thoracic Institute lung transplant program, in the press conference.
Mr. Bauer expressed his thanks to the surgical team, who also presented him with another gift: a T-shirt with his newly chosen nickname, “DD Davey.” “I feel so blessed, I got a second chance at life,” Mr. Bauer said in the press conference. “You should not inhale anything into your lungs except oxygen.”
A version of this article first appeared on Medscape.com.
An innovative surgical procedure combining breast implants and an artificial lung may help more patients with severe lung disease survive to receive transplants. The case was described in a press conference sponsored by Northwestern University, Evanston, Ill.
In May 2023, a surgical team at Northwestern removed both infected lungs from David “Davey” Bauer, aged 34 years, and temporarily used breast implants to hold his heart in place until new lungs were available.
In April 2023, Mr. Bauer, a longtime smoker and vaper, experienced shortness of breath. His girlfriend, Susan Gore, took him to an urgent care center, and he returned home, but “the next morning he couldn’t walk,” Ms. Gore said in the press conference. A trip to the ED yielded a diagnosis of influenza A, followed rapidly by a bacterial lung infection that proved resistant to antibiotics. Mr. Bauer had no prior medical history of serious illness, but he was soon in an intensive care unit. His condition continued to decline, and a double lung transplant was his only option.
The Northwestern Medicine Canning Thoracic Institute specializes in challenging cases, and Mr. Bauer was transferred there.
Back from the brink
Mr. Bauer made the transfer to Chicago despite being critically ill. He was in dire need of a lung transplant, and the only way to resolve his infection was to remove the lungs, said Ankit Bharat, MD, chief of thoracic surgery and director of Northwestern Medicine Canning Thoracic Institute, in the press conference.
“Something needed to be done right away,” Dr. Bharat said. Mr. Bauer’s lungs were removed and the chest cavity was extensively debrided to remove the infection.
Then it was time for outside-the-box thinking. “With the lungs taken out, we needed something to support the heart,” he said. Breast implants came to mind, and double Ds were the largest available.
In addition, the surgeons created an artificial lung system of conduits to keep Mr. Bauer’s blood pumping. “We wanted to maintain the natural blood flow in the body that would be present if the lungs were there,” Dr. Bharat explained.
Plastic surgeons at Northwestern gave Mr. Bauer’s surgical team “a crash course” in managing the breast implants, Dr. Bharat said. The team anticipated that their novel surgical solution would need to last for weeks, but Mr. Bauer’s condition improved immediately once the infected lungs were removed. He was placed on a double-lung transplant list, and the team received an offer of new lungs within 24 hours.
The breast implants were removed, the new lungs were implanted, and Bauer spent several months in the ICU before his discharge to rehabilitation therapy at the end of September, according to a Northwestern press release.
This type of procedure could help patients with infections who need transplants but are too sick to undergo them, Dr. Bharat said in the press conference. In Mr. Bauer’s case, “a lot of stars aligned,” including Bauer’s rapid improvement and the quick availability of a perfect lung match, Dr. Bharat said. Many patients don’t survive to the point of transplant.
“We were surprised how quickly he recovered once we removed the infected lungs,” Dr. Bharat noted. The quick recovery may be in part because of Bauer’s youth and relative good health, but “this was uncharted territory.”
Mr. Bauer’s case is the first use of this particular surgical technique, although the team drew on lessons learned in other surgical settings, such as removal of both lungs to prevent cross-contamination in patients with cancer, he added.
Causes and effects
As for the factors that contributed to Mr. Bauer’s initial infection, “there is a lot we don’t know, but we can try to put things together,” said Dr. Bharat. Just as many factors lined up to promote Mr. Bauer’s recovery, many factors lined up to cause the problem, including long-standing smoking and vaping. Although some still view vaping as a safer alternative to smoking, patient data and experiences do not support this claim. “We know for a fact that both of them cause harm,” he added.
Mr. Bauer started smoking cigarettes at age 21 and typically smoked a pack of cigarettes each day before switching to vaping in 2014. In addition, Mr. Bauer had not been vaccinated against the flu, and his flu infection was followed by a bacterial infection.
Bacterial infections followed by hospitalizations are not new as an effect of vaping; a series of articles described the ongoing epidemic of e-cigarette or vaping product use–associated lung injury (EVALI). Patients with EVALI often present at urgent care centers, as Bauer did, with symptoms of flu or pneumonia, and they are often given medication and sent home.
Looking ahead: “We expect that Davey will fully recover and live a normal life,” although he will remain in Chicago for another year for monitoring, said Rade Tomic, MD, pulmonologist and medical director of the Northwestern Medicine Canning Thoracic Institute lung transplant program, in the press conference.
Mr. Bauer expressed his thanks to the surgical team, who also presented him with another gift: a T-shirt with his newly chosen nickname, “DD Davey.” “I feel so blessed, I got a second chance at life,” Mr. Bauer said in the press conference. “You should not inhale anything into your lungs except oxygen.”
A version of this article first appeared on Medscape.com.
An innovative surgical procedure combining breast implants and an artificial lung may help more patients with severe lung disease survive to receive transplants. The case was described in a press conference sponsored by Northwestern University, Evanston, Ill.
In May 2023, a surgical team at Northwestern removed both infected lungs from David “Davey” Bauer, aged 34 years, and temporarily used breast implants to hold his heart in place until new lungs were available.
In April 2023, Mr. Bauer, a longtime smoker and vaper, experienced shortness of breath. His girlfriend, Susan Gore, took him to an urgent care center, and he returned home, but “the next morning he couldn’t walk,” Ms. Gore said in the press conference. A trip to the ED yielded a diagnosis of influenza A, followed rapidly by a bacterial lung infection that proved resistant to antibiotics. Mr. Bauer had no prior medical history of serious illness, but he was soon in an intensive care unit. His condition continued to decline, and a double lung transplant was his only option.
The Northwestern Medicine Canning Thoracic Institute specializes in challenging cases, and Mr. Bauer was transferred there.
Back from the brink
Mr. Bauer made the transfer to Chicago despite being critically ill. He was in dire need of a lung transplant, and the only way to resolve his infection was to remove the lungs, said Ankit Bharat, MD, chief of thoracic surgery and director of Northwestern Medicine Canning Thoracic Institute, in the press conference.
“Something needed to be done right away,” Dr. Bharat said. Mr. Bauer’s lungs were removed and the chest cavity was extensively debrided to remove the infection.
Then it was time for outside-the-box thinking. “With the lungs taken out, we needed something to support the heart,” he said. Breast implants came to mind, and double Ds were the largest available.
In addition, the surgeons created an artificial lung system of conduits to keep Mr. Bauer’s blood pumping. “We wanted to maintain the natural blood flow in the body that would be present if the lungs were there,” Dr. Bharat explained.
Plastic surgeons at Northwestern gave Mr. Bauer’s surgical team “a crash course” in managing the breast implants, Dr. Bharat said. The team anticipated that their novel surgical solution would need to last for weeks, but Mr. Bauer’s condition improved immediately once the infected lungs were removed. He was placed on a double-lung transplant list, and the team received an offer of new lungs within 24 hours.
The breast implants were removed, the new lungs were implanted, and Bauer spent several months in the ICU before his discharge to rehabilitation therapy at the end of September, according to a Northwestern press release.
This type of procedure could help patients with infections who need transplants but are too sick to undergo them, Dr. Bharat said in the press conference. In Mr. Bauer’s case, “a lot of stars aligned,” including Bauer’s rapid improvement and the quick availability of a perfect lung match, Dr. Bharat said. Many patients don’t survive to the point of transplant.
“We were surprised how quickly he recovered once we removed the infected lungs,” Dr. Bharat noted. The quick recovery may be in part because of Bauer’s youth and relative good health, but “this was uncharted territory.”
Mr. Bauer’s case is the first use of this particular surgical technique, although the team drew on lessons learned in other surgical settings, such as removal of both lungs to prevent cross-contamination in patients with cancer, he added.
Causes and effects
As for the factors that contributed to Mr. Bauer’s initial infection, “there is a lot we don’t know, but we can try to put things together,” said Dr. Bharat. Just as many factors lined up to promote Mr. Bauer’s recovery, many factors lined up to cause the problem, including long-standing smoking and vaping. Although some still view vaping as a safer alternative to smoking, patient data and experiences do not support this claim. “We know for a fact that both of them cause harm,” he added.
Mr. Bauer started smoking cigarettes at age 21 and typically smoked a pack of cigarettes each day before switching to vaping in 2014. In addition, Mr. Bauer had not been vaccinated against the flu, and his flu infection was followed by a bacterial infection.
Bacterial infections followed by hospitalizations are not new as an effect of vaping; a series of articles described the ongoing epidemic of e-cigarette or vaping product use–associated lung injury (EVALI). Patients with EVALI often present at urgent care centers, as Bauer did, with symptoms of flu or pneumonia, and they are often given medication and sent home.
Looking ahead: “We expect that Davey will fully recover and live a normal life,” although he will remain in Chicago for another year for monitoring, said Rade Tomic, MD, pulmonologist and medical director of the Northwestern Medicine Canning Thoracic Institute lung transplant program, in the press conference.
Mr. Bauer expressed his thanks to the surgical team, who also presented him with another gift: a T-shirt with his newly chosen nickname, “DD Davey.” “I feel so blessed, I got a second chance at life,” Mr. Bauer said in the press conference. “You should not inhale anything into your lungs except oxygen.”
A version of this article first appeared on Medscape.com.
Physician’s dispute with Mayo Clinic raises free speech, academic freedom concerns
Michael J. Joyner, MD, claims that the Mayo Clinic violated its own policies by muzzling him, slapping him with an unpaid 1-week suspension, and labeling his comments to the media “unprofessional.”
In his Nov. 13 lawsuit, filed in Minnesota state court, Dr. Joyner asks that a judge order Mayo Clinic to stop its “retaliation and interference” with his “communications about his research.” He that claims the retaliation stems from his 2020 report about a Mayo Clinic business partner’s “attempt to unlawfully access and use protected patient data.”
Medical institutions often refuse to comment on pending litigation. But in a pair of unusual statements, the Mayo Clinic forcefully rebutted Joyner’s claims in some detail: “Dr. Joyner’s lawsuit is yet another manifestation of his refusal to recognize or accept responsibility for his inappropriate behaviors,” it told Becker’s Hospital Review.
In a June letter to colleagues, the institution’s communications head said Dr. Joyner was not punished over his transgender athlete comments but instead because he mistreated coworkers and made “unprofessional” comments to The New York Times.
Dr. Joyner, a prominent physiologist and anesthesiologist who has worked for Mayo Clinic for 36 years, has become a cause célèbre in academic and free-speech circles over the past several months.
Two conversations with journalists appear to be at the heart of the Mayo Clinic’s complaints.
First, a 2022 New York Times article about transgender athletes quoted him about how testosterone dramatically affects performance in males: “There are social aspects to sport, but physiology and biology underpin it. Testosterone is the 800-pound gorilla.”
“The language was at best, insensitive. At worst, transphobic,” an LGBTQ advocate told a TV news station in Rochester, Minn., where the Mayo Clinic is based. The article didn’t elaborate on why the advocate believed the language could be transphobic.
Then, a CNN story in 2023 noted that Dr. Joyner has studied convalescent plasma as a treatment for COVID-19 and quoted him about how the National Institutes of Health declined to take a stand on the use of the therapy: “Joyner said he’s ‘frustrated’ with the NIH’s ‘bureaucratic rope-a-dope,’ calling the agency’s guidelines ‘a wet blanket.’ ”
It is not unusual for medical researchers to comment bluntly to the media about federal agencies.
For example, a 2020 New York Times story that unraveled the Trump Administration’s apparent mischaracterization of Dr. Joyner’s research into convalescent plasma quoted a University of Pittsburgh physician as saying, “For the first time ever, I feel like official people in communications and people at the FDA grossly misrepresented data about a therapy.”
In a March 5 letter, a Mayo Clinic administrator wrote to Dr. Joyner to complain that his comments regarding the NIH were an example of his “problematic” use of “idiomatic language” that “reflects poorly on Mayo Clinic’s brand and reputation.” A paragraph in the letter is redacted in the version posted by the Foundation for Individual Rights and Expression, which supports Dr. Joyner.
The letter adds that Dr. Joyner’s comments to The New York Times “were problematic in the media and the LGBTQI+ community at Mayo Clinic.” The letter, which didn’t elaborate about the blowback, also says that “concerns remain with disrespectful communications with colleagues who describe your tone as unpleasant and having a ‘bullying’ quality to it.”
Kellie Miller, one of Dr. Joyner’s attorneys, noted in a statement that “Dr. Joyner’s personnel file is free of any documentation of Mayo’s ongoing and vague allegations of bullying and unprofessionalism with colleagues.”
The letter also ordered Dr. Joyner to not be rude or criticize the work of others and repair his relationship with Mayo Clinic’s public affairs staff: “This will take individual effort on your part.” It also ordered him to “discuss approved topics only” with reporters, “stick to prescribed messaging,” and not resist if the public affairs department doesn’t let him be interviewed: “Accept ‘no’ for an answer and move forward.”
Medical institutions often monitor how their employees interact with the media in order to control “messaging.” But firm rules at academic medical institutions like the Mayo Clinic may run the risk of running afoul of the tenets of academic freedom.
The institution and its CEO then retaliated by calling his claims “unprofessional,” according to the lawsuit, which provided no further details about the situation.
In a statement, the Mayo Clinic said it “hired an outside attorney to investigate these concerns. The attorney, who is now a federal judge, found there was no retaliation and that Dr. Joyner had engaged in a pattern of asserting inflammatory allegations grounded almost entirely in speculation.”
A petition signed by dozens of professors demands that Mayo Clinic “revoke the penalties and constraints it has imposed on him.”
“Dr. Joyner, a faculty member at a medical school that avows a commitment to academic freedom and to free expression, did not exceed the limits of his expertise in any of his statements to the press that led to these sanctions,” they wrote. “At no time did he claim to be speaking for the Mayo Clinic, and his remarks were well within the mainstream of the range of scientific opinion on topics in which he is expert.”
A version of this article first appeared on Medscape.com.
Michael J. Joyner, MD, claims that the Mayo Clinic violated its own policies by muzzling him, slapping him with an unpaid 1-week suspension, and labeling his comments to the media “unprofessional.”
In his Nov. 13 lawsuit, filed in Minnesota state court, Dr. Joyner asks that a judge order Mayo Clinic to stop its “retaliation and interference” with his “communications about his research.” He that claims the retaliation stems from his 2020 report about a Mayo Clinic business partner’s “attempt to unlawfully access and use protected patient data.”
Medical institutions often refuse to comment on pending litigation. But in a pair of unusual statements, the Mayo Clinic forcefully rebutted Joyner’s claims in some detail: “Dr. Joyner’s lawsuit is yet another manifestation of his refusal to recognize or accept responsibility for his inappropriate behaviors,” it told Becker’s Hospital Review.
In a June letter to colleagues, the institution’s communications head said Dr. Joyner was not punished over his transgender athlete comments but instead because he mistreated coworkers and made “unprofessional” comments to The New York Times.
Dr. Joyner, a prominent physiologist and anesthesiologist who has worked for Mayo Clinic for 36 years, has become a cause célèbre in academic and free-speech circles over the past several months.
Two conversations with journalists appear to be at the heart of the Mayo Clinic’s complaints.
First, a 2022 New York Times article about transgender athletes quoted him about how testosterone dramatically affects performance in males: “There are social aspects to sport, but physiology and biology underpin it. Testosterone is the 800-pound gorilla.”
“The language was at best, insensitive. At worst, transphobic,” an LGBTQ advocate told a TV news station in Rochester, Minn., where the Mayo Clinic is based. The article didn’t elaborate on why the advocate believed the language could be transphobic.
Then, a CNN story in 2023 noted that Dr. Joyner has studied convalescent plasma as a treatment for COVID-19 and quoted him about how the National Institutes of Health declined to take a stand on the use of the therapy: “Joyner said he’s ‘frustrated’ with the NIH’s ‘bureaucratic rope-a-dope,’ calling the agency’s guidelines ‘a wet blanket.’ ”
It is not unusual for medical researchers to comment bluntly to the media about federal agencies.
For example, a 2020 New York Times story that unraveled the Trump Administration’s apparent mischaracterization of Dr. Joyner’s research into convalescent plasma quoted a University of Pittsburgh physician as saying, “For the first time ever, I feel like official people in communications and people at the FDA grossly misrepresented data about a therapy.”
In a March 5 letter, a Mayo Clinic administrator wrote to Dr. Joyner to complain that his comments regarding the NIH were an example of his “problematic” use of “idiomatic language” that “reflects poorly on Mayo Clinic’s brand and reputation.” A paragraph in the letter is redacted in the version posted by the Foundation for Individual Rights and Expression, which supports Dr. Joyner.
The letter adds that Dr. Joyner’s comments to The New York Times “were problematic in the media and the LGBTQI+ community at Mayo Clinic.” The letter, which didn’t elaborate about the blowback, also says that “concerns remain with disrespectful communications with colleagues who describe your tone as unpleasant and having a ‘bullying’ quality to it.”
Kellie Miller, one of Dr. Joyner’s attorneys, noted in a statement that “Dr. Joyner’s personnel file is free of any documentation of Mayo’s ongoing and vague allegations of bullying and unprofessionalism with colleagues.”
The letter also ordered Dr. Joyner to not be rude or criticize the work of others and repair his relationship with Mayo Clinic’s public affairs staff: “This will take individual effort on your part.” It also ordered him to “discuss approved topics only” with reporters, “stick to prescribed messaging,” and not resist if the public affairs department doesn’t let him be interviewed: “Accept ‘no’ for an answer and move forward.”
Medical institutions often monitor how their employees interact with the media in order to control “messaging.” But firm rules at academic medical institutions like the Mayo Clinic may run the risk of running afoul of the tenets of academic freedom.
The institution and its CEO then retaliated by calling his claims “unprofessional,” according to the lawsuit, which provided no further details about the situation.
In a statement, the Mayo Clinic said it “hired an outside attorney to investigate these concerns. The attorney, who is now a federal judge, found there was no retaliation and that Dr. Joyner had engaged in a pattern of asserting inflammatory allegations grounded almost entirely in speculation.”
A petition signed by dozens of professors demands that Mayo Clinic “revoke the penalties and constraints it has imposed on him.”
“Dr. Joyner, a faculty member at a medical school that avows a commitment to academic freedom and to free expression, did not exceed the limits of his expertise in any of his statements to the press that led to these sanctions,” they wrote. “At no time did he claim to be speaking for the Mayo Clinic, and his remarks were well within the mainstream of the range of scientific opinion on topics in which he is expert.”
A version of this article first appeared on Medscape.com.
Michael J. Joyner, MD, claims that the Mayo Clinic violated its own policies by muzzling him, slapping him with an unpaid 1-week suspension, and labeling his comments to the media “unprofessional.”
In his Nov. 13 lawsuit, filed in Minnesota state court, Dr. Joyner asks that a judge order Mayo Clinic to stop its “retaliation and interference” with his “communications about his research.” He that claims the retaliation stems from his 2020 report about a Mayo Clinic business partner’s “attempt to unlawfully access and use protected patient data.”
Medical institutions often refuse to comment on pending litigation. But in a pair of unusual statements, the Mayo Clinic forcefully rebutted Joyner’s claims in some detail: “Dr. Joyner’s lawsuit is yet another manifestation of his refusal to recognize or accept responsibility for his inappropriate behaviors,” it told Becker’s Hospital Review.
In a June letter to colleagues, the institution’s communications head said Dr. Joyner was not punished over his transgender athlete comments but instead because he mistreated coworkers and made “unprofessional” comments to The New York Times.
Dr. Joyner, a prominent physiologist and anesthesiologist who has worked for Mayo Clinic for 36 years, has become a cause célèbre in academic and free-speech circles over the past several months.
Two conversations with journalists appear to be at the heart of the Mayo Clinic’s complaints.
First, a 2022 New York Times article about transgender athletes quoted him about how testosterone dramatically affects performance in males: “There are social aspects to sport, but physiology and biology underpin it. Testosterone is the 800-pound gorilla.”
“The language was at best, insensitive. At worst, transphobic,” an LGBTQ advocate told a TV news station in Rochester, Minn., where the Mayo Clinic is based. The article didn’t elaborate on why the advocate believed the language could be transphobic.
Then, a CNN story in 2023 noted that Dr. Joyner has studied convalescent plasma as a treatment for COVID-19 and quoted him about how the National Institutes of Health declined to take a stand on the use of the therapy: “Joyner said he’s ‘frustrated’ with the NIH’s ‘bureaucratic rope-a-dope,’ calling the agency’s guidelines ‘a wet blanket.’ ”
It is not unusual for medical researchers to comment bluntly to the media about federal agencies.
For example, a 2020 New York Times story that unraveled the Trump Administration’s apparent mischaracterization of Dr. Joyner’s research into convalescent plasma quoted a University of Pittsburgh physician as saying, “For the first time ever, I feel like official people in communications and people at the FDA grossly misrepresented data about a therapy.”
In a March 5 letter, a Mayo Clinic administrator wrote to Dr. Joyner to complain that his comments regarding the NIH were an example of his “problematic” use of “idiomatic language” that “reflects poorly on Mayo Clinic’s brand and reputation.” A paragraph in the letter is redacted in the version posted by the Foundation for Individual Rights and Expression, which supports Dr. Joyner.
The letter adds that Dr. Joyner’s comments to The New York Times “were problematic in the media and the LGBTQI+ community at Mayo Clinic.” The letter, which didn’t elaborate about the blowback, also says that “concerns remain with disrespectful communications with colleagues who describe your tone as unpleasant and having a ‘bullying’ quality to it.”
Kellie Miller, one of Dr. Joyner’s attorneys, noted in a statement that “Dr. Joyner’s personnel file is free of any documentation of Mayo’s ongoing and vague allegations of bullying and unprofessionalism with colleagues.”
The letter also ordered Dr. Joyner to not be rude or criticize the work of others and repair his relationship with Mayo Clinic’s public affairs staff: “This will take individual effort on your part.” It also ordered him to “discuss approved topics only” with reporters, “stick to prescribed messaging,” and not resist if the public affairs department doesn’t let him be interviewed: “Accept ‘no’ for an answer and move forward.”
Medical institutions often monitor how their employees interact with the media in order to control “messaging.” But firm rules at academic medical institutions like the Mayo Clinic may run the risk of running afoul of the tenets of academic freedom.
The institution and its CEO then retaliated by calling his claims “unprofessional,” according to the lawsuit, which provided no further details about the situation.
In a statement, the Mayo Clinic said it “hired an outside attorney to investigate these concerns. The attorney, who is now a federal judge, found there was no retaliation and that Dr. Joyner had engaged in a pattern of asserting inflammatory allegations grounded almost entirely in speculation.”
A petition signed by dozens of professors demands that Mayo Clinic “revoke the penalties and constraints it has imposed on him.”
“Dr. Joyner, a faculty member at a medical school that avows a commitment to academic freedom and to free expression, did not exceed the limits of his expertise in any of his statements to the press that led to these sanctions,” they wrote. “At no time did he claim to be speaking for the Mayo Clinic, and his remarks were well within the mainstream of the range of scientific opinion on topics in which he is expert.”
A version of this article first appeared on Medscape.com.
AI-ECG gets STEMI patients to cath lab sooner
PHILADELPHIA – An artificial intelligence platform that sends alerts based on electrocardiography results enabled cardiologists and emergency department physicians at a major hospital in Taiwan to move patients with ST-elevation myocardial infarction (STEMI) into the catheterization laboratory 9 minutes sooner than the conventional protocol that did not use AI.
“This is the first randomized clinical trial to demonstrate the reduction of electrocardiography to coronary cath lab activation time" from 52.3 to 43.3 minutes (P = .003), Chin Sheng Lin, MD, PhD, director of cardiology at the National Defense Medical Center Tri-Service General Hospital in Taipei City, said in presenting the results at the American Heart Association scientific sessions.

Dr. Lin reported results from the Artificial Intelligence Enabled Rapid Identify of ST-Elevation Myocardial Infarction Using Electrocardiogram (ARISE) trial. The trial included 43,994 patients who came to the hospital’s emergency and inpatient departments with at least one ECG but no history of coronary angiography (CAG) in the previous 3 days between May 2022 and April 2023.
They were randomly assigned by date to either AI-ECG for rapid identification and triage of STEMI or standard care. Overall, 145 patients were finally diagnosed with STEMI based on CAG, 77 in the intervention group and 68 in the control group. All patients were seen by one of 20 cardiologists who participated in the study.
Dr. Lin and his group developed an AI algorithm that captures the ECG readout in the emergency department, analyzes the data and then sends a high-risk alarm to the front-line physician and on-duty cardiologist to activate the primary percutaneous coronary intervention (PCI).
Trial results
The differentiation between groups was even more pronounced in ED patients during regular working hours, Dr. Lin said, at 61.6 minutes for the intervention group vs. 33.1 minutes for controls (P = .001).*
He noted that the AI group showed a trend towards fewer cases of clinically suspected STEMI but not getting CAG, 6.5% vs. 15.8%, for an odds ratio of 0.37 (95% confidence interval, 0.14-0.94).
The AI-ECG model also demonstrated a high diagnostic accuracy. “With this AI-ECG system, because it has a very high accuracy and a high positive predictive variable that reach 88%, we can send a message to the on-duty cardiologists and also the emergency room physician and they can send the patients to receive the operation or the PCI as soon as possible,” Dr. Lin said in an interview.
The time differential is critical, Dr. Lin said. “For the patient with acute myocardial infarction, 1 minute is critical, because the patients can die within minutes,” he said. “If we can save 9 minutes I think we can save more lives, but it needs a larger study to evaluate that.”
Dr. Lin acknowledged a few limitations with the trial, among them its single-center nature, relatively small sample size of STEMI patients and the short-term of follow-up. Future study should involve multiple centers along with a prehospital, emergency medical services AI-ECG model.
‘Novel’ for an AI trial
“This is an incredible application of an AI technology in a real-world problem,” said Brahmajee K. Nallamothu, MD, MPH, an interventional cardiologist at the University of Michigan, Ann Arbor, who did not participate in the study. “What I really love about this study is it’s actually a clinical problem that has large implications, particularly for under-resourced areas.”

Using a randomized clinical trial to evaluate the AI platform is “very, very novel,” he said, and called the time improvement “enormous.” Referencing Dr. Lin’s next steps for studying the AI-ECG platform, Dr. Nallamothu said, “if we could push this up even earlier to paramedics and EMTs and prehospital systems, there would be a lot of excitement there.”
He noted the sensitivity analysis resulted in a rate of 88.8% along with the positive predictive value of 88%. “Missing 1 out of 10 ST-elevation MIs in my eyes can still be considered a big deal, so we need to know if this is happening in particular types of patients, for example women versus men, or other groups.”
However, some investigations reported false activation rates as high as 33%, he said. “So, to say that, the positive predictive value is at 88% is really exciting and I think it can make a real inroads,” Dr. Nallamothu said.
Dr. Lin and Dr. Nallamothu have no relevant disclosures.
*Correction, 11/20/23: An earlier version of this article misstated in both trial arms the time to coronary catheterization lab activation.
PHILADELPHIA – An artificial intelligence platform that sends alerts based on electrocardiography results enabled cardiologists and emergency department physicians at a major hospital in Taiwan to move patients with ST-elevation myocardial infarction (STEMI) into the catheterization laboratory 9 minutes sooner than the conventional protocol that did not use AI.
“This is the first randomized clinical trial to demonstrate the reduction of electrocardiography to coronary cath lab activation time" from 52.3 to 43.3 minutes (P = .003), Chin Sheng Lin, MD, PhD, director of cardiology at the National Defense Medical Center Tri-Service General Hospital in Taipei City, said in presenting the results at the American Heart Association scientific sessions.
Dr. Lin reported results from the Artificial Intelligence Enabled Rapid Identify of ST-Elevation Myocardial Infarction Using Electrocardiogram (ARISE) trial. The trial included 43,994 patients who came to the hospital’s emergency and inpatient departments with at least one ECG but no history of coronary angiography (CAG) in the previous 3 days between May 2022 and April 2023.
They were randomly assigned by date to either AI-ECG for rapid identification and triage of STEMI or standard care. Overall, 145 patients were finally diagnosed with STEMI based on CAG, 77 in the intervention group and 68 in the control group. All patients were seen by one of 20 cardiologists who participated in the study.
Dr. Lin and his group developed an AI algorithm that captures the ECG readout in the emergency department, analyzes the data and then sends a high-risk alarm to the front-line physician and on-duty cardiologist to activate the primary percutaneous coronary intervention (PCI).
Trial results
The differentiation between groups was even more pronounced in ED patients during regular working hours, Dr. Lin said, at 61.6 minutes for the intervention group vs. 33.1 minutes for controls (P = .001).*
He noted that the AI group showed a trend towards fewer cases of clinically suspected STEMI but not getting CAG, 6.5% vs. 15.8%, for an odds ratio of 0.37 (95% confidence interval, 0.14-0.94).
The AI-ECG model also demonstrated a high diagnostic accuracy. “With this AI-ECG system, because it has a very high accuracy and a high positive predictive variable that reach 88%, we can send a message to the on-duty cardiologists and also the emergency room physician and they can send the patients to receive the operation or the PCI as soon as possible,” Dr. Lin said in an interview.
The time differential is critical, Dr. Lin said. “For the patient with acute myocardial infarction, 1 minute is critical, because the patients can die within minutes,” he said. “If we can save 9 minutes I think we can save more lives, but it needs a larger study to evaluate that.”
Dr. Lin acknowledged a few limitations with the trial, among them its single-center nature, relatively small sample size of STEMI patients and the short-term of follow-up. Future study should involve multiple centers along with a prehospital, emergency medical services AI-ECG model.
‘Novel’ for an AI trial
“This is an incredible application of an AI technology in a real-world problem,” said Brahmajee K. Nallamothu, MD, MPH, an interventional cardiologist at the University of Michigan, Ann Arbor, who did not participate in the study. “What I really love about this study is it’s actually a clinical problem that has large implications, particularly for under-resourced areas.”
Using a randomized clinical trial to evaluate the AI platform is “very, very novel,” he said, and called the time improvement “enormous.” Referencing Dr. Lin’s next steps for studying the AI-ECG platform, Dr. Nallamothu said, “if we could push this up even earlier to paramedics and EMTs and prehospital systems, there would be a lot of excitement there.”
He noted the sensitivity analysis resulted in a rate of 88.8% along with the positive predictive value of 88%. “Missing 1 out of 10 ST-elevation MIs in my eyes can still be considered a big deal, so we need to know if this is happening in particular types of patients, for example women versus men, or other groups.”
However, some investigations reported false activation rates as high as 33%, he said. “So, to say that, the positive predictive value is at 88% is really exciting and I think it can make a real inroads,” Dr. Nallamothu said.
Dr. Lin and Dr. Nallamothu have no relevant disclosures.
*Correction, 11/20/23: An earlier version of this article misstated in both trial arms the time to coronary catheterization lab activation.
PHILADELPHIA – An artificial intelligence platform that sends alerts based on electrocardiography results enabled cardiologists and emergency department physicians at a major hospital in Taiwan to move patients with ST-elevation myocardial infarction (STEMI) into the catheterization laboratory 9 minutes sooner than the conventional protocol that did not use AI.
“This is the first randomized clinical trial to demonstrate the reduction of electrocardiography to coronary cath lab activation time" from 52.3 to 43.3 minutes (P = .003), Chin Sheng Lin, MD, PhD, director of cardiology at the National Defense Medical Center Tri-Service General Hospital in Taipei City, said in presenting the results at the American Heart Association scientific sessions.
Dr. Lin reported results from the Artificial Intelligence Enabled Rapid Identify of ST-Elevation Myocardial Infarction Using Electrocardiogram (ARISE) trial. The trial included 43,994 patients who came to the hospital’s emergency and inpatient departments with at least one ECG but no history of coronary angiography (CAG) in the previous 3 days between May 2022 and April 2023.
They were randomly assigned by date to either AI-ECG for rapid identification and triage of STEMI or standard care. Overall, 145 patients were finally diagnosed with STEMI based on CAG, 77 in the intervention group and 68 in the control group. All patients were seen by one of 20 cardiologists who participated in the study.
Dr. Lin and his group developed an AI algorithm that captures the ECG readout in the emergency department, analyzes the data and then sends a high-risk alarm to the front-line physician and on-duty cardiologist to activate the primary percutaneous coronary intervention (PCI).
Trial results
The differentiation between groups was even more pronounced in ED patients during regular working hours, Dr. Lin said, at 61.6 minutes for the intervention group vs. 33.1 minutes for controls (P = .001).*
He noted that the AI group showed a trend towards fewer cases of clinically suspected STEMI but not getting CAG, 6.5% vs. 15.8%, for an odds ratio of 0.37 (95% confidence interval, 0.14-0.94).
The AI-ECG model also demonstrated a high diagnostic accuracy. “With this AI-ECG system, because it has a very high accuracy and a high positive predictive variable that reach 88%, we can send a message to the on-duty cardiologists and also the emergency room physician and they can send the patients to receive the operation or the PCI as soon as possible,” Dr. Lin said in an interview.
The time differential is critical, Dr. Lin said. “For the patient with acute myocardial infarction, 1 minute is critical, because the patients can die within minutes,” he said. “If we can save 9 minutes I think we can save more lives, but it needs a larger study to evaluate that.”
Dr. Lin acknowledged a few limitations with the trial, among them its single-center nature, relatively small sample size of STEMI patients and the short-term of follow-up. Future study should involve multiple centers along with a prehospital, emergency medical services AI-ECG model.
‘Novel’ for an AI trial
“This is an incredible application of an AI technology in a real-world problem,” said Brahmajee K. Nallamothu, MD, MPH, an interventional cardiologist at the University of Michigan, Ann Arbor, who did not participate in the study. “What I really love about this study is it’s actually a clinical problem that has large implications, particularly for under-resourced areas.”
Using a randomized clinical trial to evaluate the AI platform is “very, very novel,” he said, and called the time improvement “enormous.” Referencing Dr. Lin’s next steps for studying the AI-ECG platform, Dr. Nallamothu said, “if we could push this up even earlier to paramedics and EMTs and prehospital systems, there would be a lot of excitement there.”
He noted the sensitivity analysis resulted in a rate of 88.8% along with the positive predictive value of 88%. “Missing 1 out of 10 ST-elevation MIs in my eyes can still be considered a big deal, so we need to know if this is happening in particular types of patients, for example women versus men, or other groups.”
However, some investigations reported false activation rates as high as 33%, he said. “So, to say that, the positive predictive value is at 88% is really exciting and I think it can make a real inroads,” Dr. Nallamothu said.
Dr. Lin and Dr. Nallamothu have no relevant disclosures.
*Correction, 11/20/23: An earlier version of this article misstated in both trial arms the time to coronary catheterization lab activation.
AT AHA 2023
Sleeping beats sitting? What a new study means for your patients
Sit less, move more. Or stand more. Or sleep more.
Replacing 30 minutes of sitting a day with equal time standing or even sleeping could improve obesity markers like body weight and waist circumference, according to a new cross-sectional study investigating the impact of movement behavior on cardiometabolic health.
The findings suggest that, while higher-intensity activity may confer benefits sooner, adding more light activity or more standing, or even going to bed earlier, could improve heart health measures over time.
“Our study highlights that replacing sedentary behavior with any other behavior can be beneficial,” said study author Joanna M. Blodgett, PhD, a researcher at University College London’s Institute of Sport, Exercise and Health, and department of targeted intervention.
The study builds on a large and growing body of evidence that movement behaviors impact cardiometabolic health. Increasing physical activity to 150 minutes a week has been shown to reduce the risk for cardiovascular disease by 17% and type 2 diabetes by 26%. Other studies suggest that even modest increases in physical activity can be beneficial. A prospective study published in October found that even short activity bouts of a few minutes a day may lower risks for heart attack, stroke, and early death.
In the new study, researchers analyzed data from six studies and more than 15,000 participants, ranking behaviors according to their association with heart health. Moderate-to-vigorous activity was linked to the greatest benefit, followed by light activity, standing, sleeping, and finally – dead last on the list – sitting.
A thigh-worn device tracked participants’ activity throughout the day, and six measures gauged heart health: body mass index (BMI), waist circumference, HDL cholesterol, total-cholesterol-to-HDL ratio, triglycerides, and glycated hemoglobin.
Researchers modeled what would happen if people swapped various amounts of one activity for another every day for a week. Replacing just 4-13 minutes of sitting with moderate to vigorous activity improved heart health markers.
The cardiovascular demands of regular intense activity like running, cycling, dancing, or playing sports – even in small bouts – strengthen the heart and improve blood flow throughout the body, Dr. Blodgett said. “This can lower cholesterol, blood pressure, and resting heart rate.”
Even if adding moderate to vigorous activity is not an option, the findings suggest that people can still see benefits by replacing sitting with virtually any other activity – walking, standing, even sleeping.
Limitations
Because the study was observational, results can’t be used to infer causality.
“We cannot directly lean on the study results to guide prescriptions for particular exercise or lifestyle changes,” said Matthew Tomey, MD, a cardiologist with the Mount Sinai Health System, New York, who was not involved with the study. An interventional trial would be needed to confirm the findings.
The finding that sleep was better for participants than sitting is a good example. The benefits of replacing sitting with sleep were “clear” for adiposity measures like BMI and waist circumference, but negligible for blood markers such as cholesterol, triglycerides, and blood glucose, Dr. Blodgett said.
One explanation: “The negative impact of sitting on these obesity measures is likely due to related unhealthy behaviors like snacking rather than the physiological benefits of sleep itself,” Dr. Blodgett said.
What’s more, study participants were relatively young, healthy, and active. The average age was 54, and they averaged nearly 8 hours of sleep, 10 hours of sitting, 3 hours of standing, 1.5 hours of light activity, and more than an hour of moderate to vigorous activity per day. So it’s difficult to draw conclusions about patients who don’t fit those metrics.
Impact on patient care
That said, the results could help tailor recommendations for patients, Dr. Blodgett said.
If a patient is struggling to exercise or is unable to exercise because of health or ability restrictions, you could help them find ways to add a lighter activity to their day, such as taking the stairs or walking briskly to catch the bus. Even swapping a regular desk for a standing one, or going to bed 30 minutes earlier, could be a more practical and effective suggestion.
More than that: The research could be used to educate patients on the power of small changes. It shows that shifting daily habits even in small ways can make a difference, and people who are the least active stand to benefit the most.
You can also remind patients that moderate or vigorous activity doesn’t need to happen at the gym. It could be lawn work, taking a walk, or moving heavy boxes. In fact, many activities can be “moderate” or even “vigorous” depending on the effort put into them.
Share this rule of thumb: “An activity is classified as moderate intensity if you can talk but not sing while doing it, and an activity is generally considered vigorous intensity if you can’t say more than a few words without stopping to breathe,” Dr. Blodgett said.
The study also has implications for the potential of wearable activity trackers to monitor progress. Combining objective activity data with results from studies like this, and longer prospective studies, could help inform more helpful advice.
“Ultimately, this research helps move us closer to more personalized guidance of how changing behaviors can improve your health,” Dr. Blodgett said.
A version of this article first appeared on Medscape.com.
Sit less, move more. Or stand more. Or sleep more.
Replacing 30 minutes of sitting a day with equal time standing or even sleeping could improve obesity markers like body weight and waist circumference, according to a new cross-sectional study investigating the impact of movement behavior on cardiometabolic health.
The findings suggest that, while higher-intensity activity may confer benefits sooner, adding more light activity or more standing, or even going to bed earlier, could improve heart health measures over time.
“Our study highlights that replacing sedentary behavior with any other behavior can be beneficial,” said study author Joanna M. Blodgett, PhD, a researcher at University College London’s Institute of Sport, Exercise and Health, and department of targeted intervention.
The study builds on a large and growing body of evidence that movement behaviors impact cardiometabolic health. Increasing physical activity to 150 minutes a week has been shown to reduce the risk for cardiovascular disease by 17% and type 2 diabetes by 26%. Other studies suggest that even modest increases in physical activity can be beneficial. A prospective study published in October found that even short activity bouts of a few minutes a day may lower risks for heart attack, stroke, and early death.
In the new study, researchers analyzed data from six studies and more than 15,000 participants, ranking behaviors according to their association with heart health. Moderate-to-vigorous activity was linked to the greatest benefit, followed by light activity, standing, sleeping, and finally – dead last on the list – sitting.
A thigh-worn device tracked participants’ activity throughout the day, and six measures gauged heart health: body mass index (BMI), waist circumference, HDL cholesterol, total-cholesterol-to-HDL ratio, triglycerides, and glycated hemoglobin.
Researchers modeled what would happen if people swapped various amounts of one activity for another every day for a week. Replacing just 4-13 minutes of sitting with moderate to vigorous activity improved heart health markers.
The cardiovascular demands of regular intense activity like running, cycling, dancing, or playing sports – even in small bouts – strengthen the heart and improve blood flow throughout the body, Dr. Blodgett said. “This can lower cholesterol, blood pressure, and resting heart rate.”
Even if adding moderate to vigorous activity is not an option, the findings suggest that people can still see benefits by replacing sitting with virtually any other activity – walking, standing, even sleeping.
Limitations
Because the study was observational, results can’t be used to infer causality.
“We cannot directly lean on the study results to guide prescriptions for particular exercise or lifestyle changes,” said Matthew Tomey, MD, a cardiologist with the Mount Sinai Health System, New York, who was not involved with the study. An interventional trial would be needed to confirm the findings.
The finding that sleep was better for participants than sitting is a good example. The benefits of replacing sitting with sleep were “clear” for adiposity measures like BMI and waist circumference, but negligible for blood markers such as cholesterol, triglycerides, and blood glucose, Dr. Blodgett said.
One explanation: “The negative impact of sitting on these obesity measures is likely due to related unhealthy behaviors like snacking rather than the physiological benefits of sleep itself,” Dr. Blodgett said.
What’s more, study participants were relatively young, healthy, and active. The average age was 54, and they averaged nearly 8 hours of sleep, 10 hours of sitting, 3 hours of standing, 1.5 hours of light activity, and more than an hour of moderate to vigorous activity per day. So it’s difficult to draw conclusions about patients who don’t fit those metrics.
Impact on patient care
That said, the results could help tailor recommendations for patients, Dr. Blodgett said.
If a patient is struggling to exercise or is unable to exercise because of health or ability restrictions, you could help them find ways to add a lighter activity to their day, such as taking the stairs or walking briskly to catch the bus. Even swapping a regular desk for a standing one, or going to bed 30 minutes earlier, could be a more practical and effective suggestion.
More than that: The research could be used to educate patients on the power of small changes. It shows that shifting daily habits even in small ways can make a difference, and people who are the least active stand to benefit the most.
You can also remind patients that moderate or vigorous activity doesn’t need to happen at the gym. It could be lawn work, taking a walk, or moving heavy boxes. In fact, many activities can be “moderate” or even “vigorous” depending on the effort put into them.
Share this rule of thumb: “An activity is classified as moderate intensity if you can talk but not sing while doing it, and an activity is generally considered vigorous intensity if you can’t say more than a few words without stopping to breathe,” Dr. Blodgett said.
The study also has implications for the potential of wearable activity trackers to monitor progress. Combining objective activity data with results from studies like this, and longer prospective studies, could help inform more helpful advice.
“Ultimately, this research helps move us closer to more personalized guidance of how changing behaviors can improve your health,” Dr. Blodgett said.
A version of this article first appeared on Medscape.com.
Sit less, move more. Or stand more. Or sleep more.
Replacing 30 minutes of sitting a day with equal time standing or even sleeping could improve obesity markers like body weight and waist circumference, according to a new cross-sectional study investigating the impact of movement behavior on cardiometabolic health.
The findings suggest that, while higher-intensity activity may confer benefits sooner, adding more light activity or more standing, or even going to bed earlier, could improve heart health measures over time.
“Our study highlights that replacing sedentary behavior with any other behavior can be beneficial,” said study author Joanna M. Blodgett, PhD, a researcher at University College London’s Institute of Sport, Exercise and Health, and department of targeted intervention.
The study builds on a large and growing body of evidence that movement behaviors impact cardiometabolic health. Increasing physical activity to 150 minutes a week has been shown to reduce the risk for cardiovascular disease by 17% and type 2 diabetes by 26%. Other studies suggest that even modest increases in physical activity can be beneficial. A prospective study published in October found that even short activity bouts of a few minutes a day may lower risks for heart attack, stroke, and early death.
In the new study, researchers analyzed data from six studies and more than 15,000 participants, ranking behaviors according to their association with heart health. Moderate-to-vigorous activity was linked to the greatest benefit, followed by light activity, standing, sleeping, and finally – dead last on the list – sitting.
A thigh-worn device tracked participants’ activity throughout the day, and six measures gauged heart health: body mass index (BMI), waist circumference, HDL cholesterol, total-cholesterol-to-HDL ratio, triglycerides, and glycated hemoglobin.
Researchers modeled what would happen if people swapped various amounts of one activity for another every day for a week. Replacing just 4-13 minutes of sitting with moderate to vigorous activity improved heart health markers.
The cardiovascular demands of regular intense activity like running, cycling, dancing, or playing sports – even in small bouts – strengthen the heart and improve blood flow throughout the body, Dr. Blodgett said. “This can lower cholesterol, blood pressure, and resting heart rate.”
Even if adding moderate to vigorous activity is not an option, the findings suggest that people can still see benefits by replacing sitting with virtually any other activity – walking, standing, even sleeping.
Limitations
Because the study was observational, results can’t be used to infer causality.
“We cannot directly lean on the study results to guide prescriptions for particular exercise or lifestyle changes,” said Matthew Tomey, MD, a cardiologist with the Mount Sinai Health System, New York, who was not involved with the study. An interventional trial would be needed to confirm the findings.
The finding that sleep was better for participants than sitting is a good example. The benefits of replacing sitting with sleep were “clear” for adiposity measures like BMI and waist circumference, but negligible for blood markers such as cholesterol, triglycerides, and blood glucose, Dr. Blodgett said.
One explanation: “The negative impact of sitting on these obesity measures is likely due to related unhealthy behaviors like snacking rather than the physiological benefits of sleep itself,” Dr. Blodgett said.
What’s more, study participants were relatively young, healthy, and active. The average age was 54, and they averaged nearly 8 hours of sleep, 10 hours of sitting, 3 hours of standing, 1.5 hours of light activity, and more than an hour of moderate to vigorous activity per day. So it’s difficult to draw conclusions about patients who don’t fit those metrics.
Impact on patient care
That said, the results could help tailor recommendations for patients, Dr. Blodgett said.
If a patient is struggling to exercise or is unable to exercise because of health or ability restrictions, you could help them find ways to add a lighter activity to their day, such as taking the stairs or walking briskly to catch the bus. Even swapping a regular desk for a standing one, or going to bed 30 minutes earlier, could be a more practical and effective suggestion.
More than that: The research could be used to educate patients on the power of small changes. It shows that shifting daily habits even in small ways can make a difference, and people who are the least active stand to benefit the most.
You can also remind patients that moderate or vigorous activity doesn’t need to happen at the gym. It could be lawn work, taking a walk, or moving heavy boxes. In fact, many activities can be “moderate” or even “vigorous” depending on the effort put into them.
Share this rule of thumb: “An activity is classified as moderate intensity if you can talk but not sing while doing it, and an activity is generally considered vigorous intensity if you can’t say more than a few words without stopping to breathe,” Dr. Blodgett said.
The study also has implications for the potential of wearable activity trackers to monitor progress. Combining objective activity data with results from studies like this, and longer prospective studies, could help inform more helpful advice.
“Ultimately, this research helps move us closer to more personalized guidance of how changing behaviors can improve your health,” Dr. Blodgett said.
A version of this article first appeared on Medscape.com.
FROM THE EUROPEAN HEART JOURNAL
‘Love more’: Why doctors should promote social connection
Those who embrace lifestyle medicine are familiar with the slogan Dean Ornish, MD, likes to use: Eat well, move more, stress less, love more.
That last one, love, was the renowned physician and author’s focus at the recent American College of Lifestyle Medicine Conference in Denver. That’s because love – essentially the support, connectedness, and caring that patients feel when they join a lifestyle-change program – is “where healing occurs at the deepest level.”
Indeed, social connectedness is emerging as a vital pillar in the burgeoning field of lifestyle medicine, a specialty that uses lifestyle interventions to treat chronic conditions. About 300 lifestyle medicine programs are now integrated into residencies in medical schools across the country, up from a handful just 5 years ago, said Meagan Grega, MD, the conference chair.
“The energy and growth in American lifestyle medicine is unparalleled by anything else I see in the health care world right now,” said Dr. Grega, a family physician for 25 years in eastern Pennsylvania.
The field applies volumes of research, from the 1990s to today, demonstrating the healing effects of lifestyle changes. Dr. Ornish’s Preventive Medicine Research Institute has published research on small changes (like pomegranate juice helping blood flow in the heart) and huge ones: Coronary heart patients reversed the narrowing of arteries without lipid-lowering drugs after 1 year of lifestyle changes, including a vegetarian diet, aerobic exercise, stress management, and group support.
Ranking alongside bedrocks such as healthy diet, sleep, exercise, and stress management is positive social connection. That part, the “love more” part, often draws skepticism but is vital, said Dr. Ornish, who is sometimes referred to as the father of lifestyle medicine.
It’s “invariably the part that’s the most meaningful – that sense of connection to community that can come when you bring total strangers together,” Dr. Ornish said. “The ‘love more’ part, in many ways, is not only as important, but in some ways even more because everything really flows from that.”
Patients in a support group, who can “let down their emotional defenses and talk openly and authentically,” are much more likely to make and maintain healthy changes, Dr. Ornish said.
Love as medicine
Mounting evidence links loneliness and isolation with a range of health issues, from mood disorders such as depression to chronic conditions such as cardiovascular disease. What’s more, data suggest that loneliness and social isolation in the United States are on the rise, and the COVID pandemic made that more clear. In May 2023, Surgeon General Vivek Murthy, MD, called loneliness, isolation, and lack of connection in the United States a “public health crisis.”
“Good relationships keep us happier and healthier,” said Robert Waldinger, MD, a psychiatrist at Massachusetts General Hospital, Boston.
Dr. Waldinger, who was not affiliated with the conference, is head of the Harvard Study of Adult Development, one of the longest studies of adult life. Beginning in 1938, the study has tracked 724 people plus more than 1,300 of their descendants and found that embracing community and close relationships helps us live longer and be happier.
In the study, the people who were most satisfied with their relationships at age 50 years were the healthiest at age 80 years. Knowing you have someone to rely on protects the brain: “Those people’s memories stay sharper longer,” Dr. Waldinger said.
He draws a distinction between connection and love. “Love is, I think, more of a feeling,” Dr. Waldinger noted. “Connection is a feeling, but it’s also an activity.”
One in five Americans say they’re lonely, he said, “and loneliness is a stressor.” People who are isolated don’t sleep as well, he added. Their health declines earlier in midlife, brain function slips sooner, and their lives are shorter.
“You don’t have anyone to complain to,” he said. If you do, “you can feel your body start to calm down.” Those without social connections may stay in a low-level “fight-or-flight mode.”
“What we think happens is that you have low levels of inflammation chronically, and those can gradually break down body systems.” Moreover, higher rates of cardiac reactivity, for instance, a racing heartbeat when upset, can lead to high blood pressure and lower immune function.
In his talk, Dr. Ornish said, “Anger is that one emotion that has consistently been shown to make heart disease worse.”
Helping people in those straits is gratifying, Dr. Ornish said. “If we can work with people as lifestyle medicine practitioners when they’re suffering, there’s an opportunity for transformation.”
Future
Of course, that can be easier said than done. Dr. Ornish relayed a patient’s typical reaction to a lifestyle program: “This is kind of weird stuff. Like, I get diet. But a plant-based diet, really? Meditation? Loving more? Really?”
He told the conference, “Part of our job as lifestyle medicine practitioners is to spend a little extra time with them. It doesn’t even take that much time. And to really help them understand what brings them a sense of hope and meaning and purpose.”
The results can be motivating. “Most people feel so much better so quickly,” Dr. Ornish said. “It reframes the reason for change from fear of dying to joy of living.”
Dr. Grega, for one, is optimistic for the future, citing survey results showing that 95% of medical students think that they›d be better counselors with lifestyle training. ‘They passionately want this type of thing,” she said.
A version of this article first appeared on Medscape.com.
Those who embrace lifestyle medicine are familiar with the slogan Dean Ornish, MD, likes to use: Eat well, move more, stress less, love more.
That last one, love, was the renowned physician and author’s focus at the recent American College of Lifestyle Medicine Conference in Denver. That’s because love – essentially the support, connectedness, and caring that patients feel when they join a lifestyle-change program – is “where healing occurs at the deepest level.”
Indeed, social connectedness is emerging as a vital pillar in the burgeoning field of lifestyle medicine, a specialty that uses lifestyle interventions to treat chronic conditions. About 300 lifestyle medicine programs are now integrated into residencies in medical schools across the country, up from a handful just 5 years ago, said Meagan Grega, MD, the conference chair.
“The energy and growth in American lifestyle medicine is unparalleled by anything else I see in the health care world right now,” said Dr. Grega, a family physician for 25 years in eastern Pennsylvania.
The field applies volumes of research, from the 1990s to today, demonstrating the healing effects of lifestyle changes. Dr. Ornish’s Preventive Medicine Research Institute has published research on small changes (like pomegranate juice helping blood flow in the heart) and huge ones: Coronary heart patients reversed the narrowing of arteries without lipid-lowering drugs after 1 year of lifestyle changes, including a vegetarian diet, aerobic exercise, stress management, and group support.
Ranking alongside bedrocks such as healthy diet, sleep, exercise, and stress management is positive social connection. That part, the “love more” part, often draws skepticism but is vital, said Dr. Ornish, who is sometimes referred to as the father of lifestyle medicine.
It’s “invariably the part that’s the most meaningful – that sense of connection to community that can come when you bring total strangers together,” Dr. Ornish said. “The ‘love more’ part, in many ways, is not only as important, but in some ways even more because everything really flows from that.”
Patients in a support group, who can “let down their emotional defenses and talk openly and authentically,” are much more likely to make and maintain healthy changes, Dr. Ornish said.
Love as medicine
Mounting evidence links loneliness and isolation with a range of health issues, from mood disorders such as depression to chronic conditions such as cardiovascular disease. What’s more, data suggest that loneliness and social isolation in the United States are on the rise, and the COVID pandemic made that more clear. In May 2023, Surgeon General Vivek Murthy, MD, called loneliness, isolation, and lack of connection in the United States a “public health crisis.”
“Good relationships keep us happier and healthier,” said Robert Waldinger, MD, a psychiatrist at Massachusetts General Hospital, Boston.
Dr. Waldinger, who was not affiliated with the conference, is head of the Harvard Study of Adult Development, one of the longest studies of adult life. Beginning in 1938, the study has tracked 724 people plus more than 1,300 of their descendants and found that embracing community and close relationships helps us live longer and be happier.
In the study, the people who were most satisfied with their relationships at age 50 years were the healthiest at age 80 years. Knowing you have someone to rely on protects the brain: “Those people’s memories stay sharper longer,” Dr. Waldinger said.
He draws a distinction between connection and love. “Love is, I think, more of a feeling,” Dr. Waldinger noted. “Connection is a feeling, but it’s also an activity.”
One in five Americans say they’re lonely, he said, “and loneliness is a stressor.” People who are isolated don’t sleep as well, he added. Their health declines earlier in midlife, brain function slips sooner, and their lives are shorter.
“You don’t have anyone to complain to,” he said. If you do, “you can feel your body start to calm down.” Those without social connections may stay in a low-level “fight-or-flight mode.”
“What we think happens is that you have low levels of inflammation chronically, and those can gradually break down body systems.” Moreover, higher rates of cardiac reactivity, for instance, a racing heartbeat when upset, can lead to high blood pressure and lower immune function.
In his talk, Dr. Ornish said, “Anger is that one emotion that has consistently been shown to make heart disease worse.”
Helping people in those straits is gratifying, Dr. Ornish said. “If we can work with people as lifestyle medicine practitioners when they’re suffering, there’s an opportunity for transformation.”
Future
Of course, that can be easier said than done. Dr. Ornish relayed a patient’s typical reaction to a lifestyle program: “This is kind of weird stuff. Like, I get diet. But a plant-based diet, really? Meditation? Loving more? Really?”
He told the conference, “Part of our job as lifestyle medicine practitioners is to spend a little extra time with them. It doesn’t even take that much time. And to really help them understand what brings them a sense of hope and meaning and purpose.”
The results can be motivating. “Most people feel so much better so quickly,” Dr. Ornish said. “It reframes the reason for change from fear of dying to joy of living.”
Dr. Grega, for one, is optimistic for the future, citing survey results showing that 95% of medical students think that they›d be better counselors with lifestyle training. ‘They passionately want this type of thing,” she said.
A version of this article first appeared on Medscape.com.
Those who embrace lifestyle medicine are familiar with the slogan Dean Ornish, MD, likes to use: Eat well, move more, stress less, love more.
That last one, love, was the renowned physician and author’s focus at the recent American College of Lifestyle Medicine Conference in Denver. That’s because love – essentially the support, connectedness, and caring that patients feel when they join a lifestyle-change program – is “where healing occurs at the deepest level.”
Indeed, social connectedness is emerging as a vital pillar in the burgeoning field of lifestyle medicine, a specialty that uses lifestyle interventions to treat chronic conditions. About 300 lifestyle medicine programs are now integrated into residencies in medical schools across the country, up from a handful just 5 years ago, said Meagan Grega, MD, the conference chair.
“The energy and growth in American lifestyle medicine is unparalleled by anything else I see in the health care world right now,” said Dr. Grega, a family physician for 25 years in eastern Pennsylvania.
The field applies volumes of research, from the 1990s to today, demonstrating the healing effects of lifestyle changes. Dr. Ornish’s Preventive Medicine Research Institute has published research on small changes (like pomegranate juice helping blood flow in the heart) and huge ones: Coronary heart patients reversed the narrowing of arteries without lipid-lowering drugs after 1 year of lifestyle changes, including a vegetarian diet, aerobic exercise, stress management, and group support.
Ranking alongside bedrocks such as healthy diet, sleep, exercise, and stress management is positive social connection. That part, the “love more” part, often draws skepticism but is vital, said Dr. Ornish, who is sometimes referred to as the father of lifestyle medicine.
It’s “invariably the part that’s the most meaningful – that sense of connection to community that can come when you bring total strangers together,” Dr. Ornish said. “The ‘love more’ part, in many ways, is not only as important, but in some ways even more because everything really flows from that.”
Patients in a support group, who can “let down their emotional defenses and talk openly and authentically,” are much more likely to make and maintain healthy changes, Dr. Ornish said.
Love as medicine
Mounting evidence links loneliness and isolation with a range of health issues, from mood disorders such as depression to chronic conditions such as cardiovascular disease. What’s more, data suggest that loneliness and social isolation in the United States are on the rise, and the COVID pandemic made that more clear. In May 2023, Surgeon General Vivek Murthy, MD, called loneliness, isolation, and lack of connection in the United States a “public health crisis.”
“Good relationships keep us happier and healthier,” said Robert Waldinger, MD, a psychiatrist at Massachusetts General Hospital, Boston.
Dr. Waldinger, who was not affiliated with the conference, is head of the Harvard Study of Adult Development, one of the longest studies of adult life. Beginning in 1938, the study has tracked 724 people plus more than 1,300 of their descendants and found that embracing community and close relationships helps us live longer and be happier.
In the study, the people who were most satisfied with their relationships at age 50 years were the healthiest at age 80 years. Knowing you have someone to rely on protects the brain: “Those people’s memories stay sharper longer,” Dr. Waldinger said.
He draws a distinction between connection and love. “Love is, I think, more of a feeling,” Dr. Waldinger noted. “Connection is a feeling, but it’s also an activity.”
One in five Americans say they’re lonely, he said, “and loneliness is a stressor.” People who are isolated don’t sleep as well, he added. Their health declines earlier in midlife, brain function slips sooner, and their lives are shorter.
“You don’t have anyone to complain to,” he said. If you do, “you can feel your body start to calm down.” Those without social connections may stay in a low-level “fight-or-flight mode.”
“What we think happens is that you have low levels of inflammation chronically, and those can gradually break down body systems.” Moreover, higher rates of cardiac reactivity, for instance, a racing heartbeat when upset, can lead to high blood pressure and lower immune function.
In his talk, Dr. Ornish said, “Anger is that one emotion that has consistently been shown to make heart disease worse.”
Helping people in those straits is gratifying, Dr. Ornish said. “If we can work with people as lifestyle medicine practitioners when they’re suffering, there’s an opportunity for transformation.”
Future
Of course, that can be easier said than done. Dr. Ornish relayed a patient’s typical reaction to a lifestyle program: “This is kind of weird stuff. Like, I get diet. But a plant-based diet, really? Meditation? Loving more? Really?”
He told the conference, “Part of our job as lifestyle medicine practitioners is to spend a little extra time with them. It doesn’t even take that much time. And to really help them understand what brings them a sense of hope and meaning and purpose.”
The results can be motivating. “Most people feel so much better so quickly,” Dr. Ornish said. “It reframes the reason for change from fear of dying to joy of living.”
Dr. Grega, for one, is optimistic for the future, citing survey results showing that 95% of medical students think that they›d be better counselors with lifestyle training. ‘They passionately want this type of thing,” she said.
A version of this article first appeared on Medscape.com.
Dupilumab for Dyshidrotic Eczema With Secondary Improvement in Eosinophilic Interstitial Lung Disease
To the Editor:
Biologic medications are increasingly utilized in adults with moderate to severe atopic dermatitis (AD) that is inadequately controlled with topical medication. By targeting the IL-4 receptor alpha subunit, dupilumab inhibits the biologic effects of IL-4 and IL-13, resulting in remarkable improvement in disease and quality of life for many patients with refractory AD.1
In 2017, the US Food and Drug Administration approved dupilumab for use in AD, asthma, and chronic rhinosinusitis. However, there is evidence of the drug’s off-label efficacy in conditions such as eosinophilic annular erythema.2 We present a patient with dyshidrotic eczema treated with dupilumab who experienced contemporaneous secondary improvement in chronic eosinophilic pneumonia (CEP) and interstitial lung disease (ILD).
A 45-year-old man was referred to our dermatology clinic for chronic hand dermatitis refractory to increasing strengths of topical corticosteroids. He had a history of progressive shortness of breath of unknown cause, which began 2 years prior, and he was being followed at our institution’s ILD clinic. Earlier pulmonary function testing revealed a restrictive pattern with interstitial infiltrates seen on chest computed tomography. A lung biopsy demonstrated features of fibrotic nonspecific interstitial pneumonitis with superimposed eosinophilic pneumonia. His pulmonary symptoms had progressively worsened; over a period of several months, the supplemental oxygen requirement had increased to 6 L at rest and 12 L upon exertion. Prednisone therapy was initiated, which alleviated respiratory symptoms; however, the patient was unable to tolerate a gradual wean of the medication, which rendered him steroid dependent at 30 mg/d.
Along with respiratory symptoms, the patient reported symptoms consistent with an autoimmune process, including dry eyes. Muscle weakness and tenderness also were noted. Ultimately, a diagnosis of anti–PL-7 (anti-threonyl-transfer RNA synthetase) antisynthetase syndrome was rendered by identification of anti–PL-7 antibodies and an elevated level of creatinine kinase.
Physical examination at our clinic revealed subtle palmar scaling on the hands and multiple small clear vesicles on the lateral aspects of the digits (Figure, A), consistent with dyshidrotic eczema. He initially was treated with clobetasol propionate ointment 0.05%. Despite adherence to this high-potency topical corticosteroid, he experienced only minimal improvement over a period of 3 months. Dupilumab was started at standard dosing—600 mg at initiation, followed by 300 mg every 2 weeks. The patient reported rapid improvement in dyshidrotic eczema over several months with near-complete resolution (Figure, B).

Concurrent with initiation and continued use of dupilumab, without other changes in his medication regimen, the patient noted gradual improvement in respiratory symptoms. At 6-month follow-up he reported notable improvement in respiratory function and quality of life. He then tolerated a gradual wean of prednisone to 10 mg/d, with a similar reduction in supplemental oxygen.
Off-label use of dupilumab for various eosinophilic conditions has shown promising efficacy. Our patient experienced improvement in CEP shortly after initiation of dupilumab, enabling weaning of prednisone, which has a well established adverse effect profile associated with long term use.3,4 In comparison, dupilumab generally is well tolerated, with rare ophthalmologic complications and injection-site reactions.5
One case report suggested that CEP may represent a potential rare adverse effect of dupilumab initiation.6 However, prior to initiation of dupilumab, that patient had poorly controlled asthma requiring frequent oral corticosteroid therapy. It is possible that CEP was subclinical prior to initiation of dupilumab and became more noticeable once the patient was weaned from corticosteroids, which had served as an indirect treatment.6 Nonetheless, more research is needed to definitively establish the efficacy of dupilumab in CEP prior to more widespread use.
Irrespective of the potential efficacy of dupilumab for the treatment of CEP, our case highlights the growing body of evidence that dupilumab should be considered in the treatment of dyshidrotic eczema, particularly in cases refractory to topical treatment.7 When a systemic medication is preferred, dupilumab likely represents an option with a relatively well-tolerated adverse effect profile compared to traditional systemic treatments for dyshidrotic eczema.
1. Barbarot S, Wollenberg A, Silverberg JI, et al. Dupilumab provides rapid and sustained improvement in SCORAD outcomes in adults with moderate-to-severe atopic dermatitis: combined results ofour randomized phase 3 trials. J Dermatolog Treat. 2022;33:266-277. doi:10.1080/09546634.2020.1750550
2. Gordon SC, Robinson SN, Abudu M, et al. Eosinophilic annular erythema treated with dupilumab. Pediatr Dermatol. 2018;35:E255-E256. doi:10.1111/pde.13533
3. Callaghan DJ 3rd. Use of Google Trends to examine interest in Mohs micrographic surgery: 2004 to 2016. Dermatol Surg. 2018;44:186-192. doi:10.1097/DSS.0000000000001270
4. Fowler C, Hoover W. Dupilumab for chronic eosinophilic pneumonia. Pediatr Pulmonol. 2020;55:3229-3230. doi:10.1002/ppul.25096
5. Simpson EL, Akinlade B, Ardeleanu M. Two phase 3 trials of dupilumab versus placebo in atopic dermatitis. N Engl J Med. 2017;376:1090-1091. doi:10.1056/NEJMc1700366
6. Menzella F, Montanari G, Patricelli G, et al. A case of chronic eosinophilic pneumonia in a patient treated with dupilumab. Ther Clin Risk Manag. 2019;15:869-875. doi:10.2147/TCRM.S207402
7. Waldman RA, DeWane ME, Sloan B, et al. Dupilumab for the treatment of dyshidrotic eczema in 15 consecutive patients. J Am Acad Dermatol. 2020;82:1251-1252. doi:10.1016/j.jaad.2019.12.053
To the Editor:
Biologic medications are increasingly utilized in adults with moderate to severe atopic dermatitis (AD) that is inadequately controlled with topical medication. By targeting the IL-4 receptor alpha subunit, dupilumab inhibits the biologic effects of IL-4 and IL-13, resulting in remarkable improvement in disease and quality of life for many patients with refractory AD.1
In 2017, the US Food and Drug Administration approved dupilumab for use in AD, asthma, and chronic rhinosinusitis. However, there is evidence of the drug’s off-label efficacy in conditions such as eosinophilic annular erythema.2 We present a patient with dyshidrotic eczema treated with dupilumab who experienced contemporaneous secondary improvement in chronic eosinophilic pneumonia (CEP) and interstitial lung disease (ILD).
A 45-year-old man was referred to our dermatology clinic for chronic hand dermatitis refractory to increasing strengths of topical corticosteroids. He had a history of progressive shortness of breath of unknown cause, which began 2 years prior, and he was being followed at our institution’s ILD clinic. Earlier pulmonary function testing revealed a restrictive pattern with interstitial infiltrates seen on chest computed tomography. A lung biopsy demonstrated features of fibrotic nonspecific interstitial pneumonitis with superimposed eosinophilic pneumonia. His pulmonary symptoms had progressively worsened; over a period of several months, the supplemental oxygen requirement had increased to 6 L at rest and 12 L upon exertion. Prednisone therapy was initiated, which alleviated respiratory symptoms; however, the patient was unable to tolerate a gradual wean of the medication, which rendered him steroid dependent at 30 mg/d.
Along with respiratory symptoms, the patient reported symptoms consistent with an autoimmune process, including dry eyes. Muscle weakness and tenderness also were noted. Ultimately, a diagnosis of anti–PL-7 (anti-threonyl-transfer RNA synthetase) antisynthetase syndrome was rendered by identification of anti–PL-7 antibodies and an elevated level of creatinine kinase.
Physical examination at our clinic revealed subtle palmar scaling on the hands and multiple small clear vesicles on the lateral aspects of the digits (Figure, A), consistent with dyshidrotic eczema. He initially was treated with clobetasol propionate ointment 0.05%. Despite adherence to this high-potency topical corticosteroid, he experienced only minimal improvement over a period of 3 months. Dupilumab was started at standard dosing—600 mg at initiation, followed by 300 mg every 2 weeks. The patient reported rapid improvement in dyshidrotic eczema over several months with near-complete resolution (Figure, B).
Concurrent with initiation and continued use of dupilumab, without other changes in his medication regimen, the patient noted gradual improvement in respiratory symptoms. At 6-month follow-up he reported notable improvement in respiratory function and quality of life. He then tolerated a gradual wean of prednisone to 10 mg/d, with a similar reduction in supplemental oxygen.
Off-label use of dupilumab for various eosinophilic conditions has shown promising efficacy. Our patient experienced improvement in CEP shortly after initiation of dupilumab, enabling weaning of prednisone, which has a well established adverse effect profile associated with long term use.3,4 In comparison, dupilumab generally is well tolerated, with rare ophthalmologic complications and injection-site reactions.5
One case report suggested that CEP may represent a potential rare adverse effect of dupilumab initiation.6 However, prior to initiation of dupilumab, that patient had poorly controlled asthma requiring frequent oral corticosteroid therapy. It is possible that CEP was subclinical prior to initiation of dupilumab and became more noticeable once the patient was weaned from corticosteroids, which had served as an indirect treatment.6 Nonetheless, more research is needed to definitively establish the efficacy of dupilumab in CEP prior to more widespread use.
Irrespective of the potential efficacy of dupilumab for the treatment of CEP, our case highlights the growing body of evidence that dupilumab should be considered in the treatment of dyshidrotic eczema, particularly in cases refractory to topical treatment.7 When a systemic medication is preferred, dupilumab likely represents an option with a relatively well-tolerated adverse effect profile compared to traditional systemic treatments for dyshidrotic eczema.
To the Editor:
Biologic medications are increasingly utilized in adults with moderate to severe atopic dermatitis (AD) that is inadequately controlled with topical medication. By targeting the IL-4 receptor alpha subunit, dupilumab inhibits the biologic effects of IL-4 and IL-13, resulting in remarkable improvement in disease and quality of life for many patients with refractory AD.1
In 2017, the US Food and Drug Administration approved dupilumab for use in AD, asthma, and chronic rhinosinusitis. However, there is evidence of the drug’s off-label efficacy in conditions such as eosinophilic annular erythema.2 We present a patient with dyshidrotic eczema treated with dupilumab who experienced contemporaneous secondary improvement in chronic eosinophilic pneumonia (CEP) and interstitial lung disease (ILD).
A 45-year-old man was referred to our dermatology clinic for chronic hand dermatitis refractory to increasing strengths of topical corticosteroids. He had a history of progressive shortness of breath of unknown cause, which began 2 years prior, and he was being followed at our institution’s ILD clinic. Earlier pulmonary function testing revealed a restrictive pattern with interstitial infiltrates seen on chest computed tomography. A lung biopsy demonstrated features of fibrotic nonspecific interstitial pneumonitis with superimposed eosinophilic pneumonia. His pulmonary symptoms had progressively worsened; over a period of several months, the supplemental oxygen requirement had increased to 6 L at rest and 12 L upon exertion. Prednisone therapy was initiated, which alleviated respiratory symptoms; however, the patient was unable to tolerate a gradual wean of the medication, which rendered him steroid dependent at 30 mg/d.
Along with respiratory symptoms, the patient reported symptoms consistent with an autoimmune process, including dry eyes. Muscle weakness and tenderness also were noted. Ultimately, a diagnosis of anti–PL-7 (anti-threonyl-transfer RNA synthetase) antisynthetase syndrome was rendered by identification of anti–PL-7 antibodies and an elevated level of creatinine kinase.
Physical examination at our clinic revealed subtle palmar scaling on the hands and multiple small clear vesicles on the lateral aspects of the digits (Figure, A), consistent with dyshidrotic eczema. He initially was treated with clobetasol propionate ointment 0.05%. Despite adherence to this high-potency topical corticosteroid, he experienced only minimal improvement over a period of 3 months. Dupilumab was started at standard dosing—600 mg at initiation, followed by 300 mg every 2 weeks. The patient reported rapid improvement in dyshidrotic eczema over several months with near-complete resolution (Figure, B).
Concurrent with initiation and continued use of dupilumab, without other changes in his medication regimen, the patient noted gradual improvement in respiratory symptoms. At 6-month follow-up he reported notable improvement in respiratory function and quality of life. He then tolerated a gradual wean of prednisone to 10 mg/d, with a similar reduction in supplemental oxygen.
Off-label use of dupilumab for various eosinophilic conditions has shown promising efficacy. Our patient experienced improvement in CEP shortly after initiation of dupilumab, enabling weaning of prednisone, which has a well established adverse effect profile associated with long term use.3,4 In comparison, dupilumab generally is well tolerated, with rare ophthalmologic complications and injection-site reactions.5
One case report suggested that CEP may represent a potential rare adverse effect of dupilumab initiation.6 However, prior to initiation of dupilumab, that patient had poorly controlled asthma requiring frequent oral corticosteroid therapy. It is possible that CEP was subclinical prior to initiation of dupilumab and became more noticeable once the patient was weaned from corticosteroids, which had served as an indirect treatment.6 Nonetheless, more research is needed to definitively establish the efficacy of dupilumab in CEP prior to more widespread use.
Irrespective of the potential efficacy of dupilumab for the treatment of CEP, our case highlights the growing body of evidence that dupilumab should be considered in the treatment of dyshidrotic eczema, particularly in cases refractory to topical treatment.7 When a systemic medication is preferred, dupilumab likely represents an option with a relatively well-tolerated adverse effect profile compared to traditional systemic treatments for dyshidrotic eczema.
1. Barbarot S, Wollenberg A, Silverberg JI, et al. Dupilumab provides rapid and sustained improvement in SCORAD outcomes in adults with moderate-to-severe atopic dermatitis: combined results ofour randomized phase 3 trials. J Dermatolog Treat. 2022;33:266-277. doi:10.1080/09546634.2020.1750550
2. Gordon SC, Robinson SN, Abudu M, et al. Eosinophilic annular erythema treated with dupilumab. Pediatr Dermatol. 2018;35:E255-E256. doi:10.1111/pde.13533
3. Callaghan DJ 3rd. Use of Google Trends to examine interest in Mohs micrographic surgery: 2004 to 2016. Dermatol Surg. 2018;44:186-192. doi:10.1097/DSS.0000000000001270
4. Fowler C, Hoover W. Dupilumab for chronic eosinophilic pneumonia. Pediatr Pulmonol. 2020;55:3229-3230. doi:10.1002/ppul.25096
5. Simpson EL, Akinlade B, Ardeleanu M. Two phase 3 trials of dupilumab versus placebo in atopic dermatitis. N Engl J Med. 2017;376:1090-1091. doi:10.1056/NEJMc1700366
6. Menzella F, Montanari G, Patricelli G, et al. A case of chronic eosinophilic pneumonia in a patient treated with dupilumab. Ther Clin Risk Manag. 2019;15:869-875. doi:10.2147/TCRM.S207402
7. Waldman RA, DeWane ME, Sloan B, et al. Dupilumab for the treatment of dyshidrotic eczema in 15 consecutive patients. J Am Acad Dermatol. 2020;82:1251-1252. doi:10.1016/j.jaad.2019.12.053
1. Barbarot S, Wollenberg A, Silverberg JI, et al. Dupilumab provides rapid and sustained improvement in SCORAD outcomes in adults with moderate-to-severe atopic dermatitis: combined results ofour randomized phase 3 trials. J Dermatolog Treat. 2022;33:266-277. doi:10.1080/09546634.2020.1750550
2. Gordon SC, Robinson SN, Abudu M, et al. Eosinophilic annular erythema treated with dupilumab. Pediatr Dermatol. 2018;35:E255-E256. doi:10.1111/pde.13533
3. Callaghan DJ 3rd. Use of Google Trends to examine interest in Mohs micrographic surgery: 2004 to 2016. Dermatol Surg. 2018;44:186-192. doi:10.1097/DSS.0000000000001270
4. Fowler C, Hoover W. Dupilumab for chronic eosinophilic pneumonia. Pediatr Pulmonol. 2020;55:3229-3230. doi:10.1002/ppul.25096
5. Simpson EL, Akinlade B, Ardeleanu M. Two phase 3 trials of dupilumab versus placebo in atopic dermatitis. N Engl J Med. 2017;376:1090-1091. doi:10.1056/NEJMc1700366
6. Menzella F, Montanari G, Patricelli G, et al. A case of chronic eosinophilic pneumonia in a patient treated with dupilumab. Ther Clin Risk Manag. 2019;15:869-875. doi:10.2147/TCRM.S207402
7. Waldman RA, DeWane ME, Sloan B, et al. Dupilumab for the treatment of dyshidrotic eczema in 15 consecutive patients. J Am Acad Dermatol. 2020;82:1251-1252. doi:10.1016/j.jaad.2019.12.053
Practice Points
- Dupilumab can be considered for treatment of refractory dyshidrotic eczema.
- Dupilumab may provide secondary efficacy in patients with dyshidrotic eczema who also have an eosinophilic condition such as eosinophilic pneumonia.

Paradoxical Reaction to TNF-α Inhibitor Therapy in a Patient With Hidradenitis Suppurativa
To the Editor:
Hidradenitis suppurativa (HS) is a chronic inflammatory condition of the pilosebaceous unit that occurs in concert with elevations of various cytokines, including tumor necrosis factor α (TNF-α), IL-1β, IL-10, and IL-17.1,2 Adalimumab is a TNF-α inhibitor approved by the US Food and Drug Administration for the treatment of HS. Although TNF-α inhibitors are effective for many immune-mediated inflammatory disorders, paradoxical drug reactions have been reported following treatment with these agents.3-6 True paradoxical drug reactions likely are immune mediated and directly lead to new onset of a pathologic condition that would otherwise respond to that drug. For example, there are reports of rheumatoid arthritis patients who were treated with a TNF-α inhibitor and developed psoriatic skin lesions.3,6 Paradoxical drug reactions also have been reported with acute-onset inflammatory bowel disease and HS or less commonly pyoderma gangrenosum (PG), uveitis, granulomatous reactions, and vasculitis.4,5 We present the case of a patient with HS who was treated with a TNF-α inhibitor and developed 2 distinct paradoxical drug reactions. We also provide an overview of paradoxical drug reactions associated with TNF-α inhibitors.
A 38-year-old woman developed a painful “boil” on the right leg that was previously treated in the emergency department with incision and drainage as well as oral clindamycin for 7 days, but the lesion spread and continued to worsen. She had a history of HS in the axillae and groin region that had been present since 12 years of age. The condition was poorly controlled despite multiple courses of oral antibiotics and surgical resections. An oral contraceptive also was attempted, but the patient discontinued treatment when liver enzyme levels became elevated. The patient had no other notable medical history, including skin disease. There was a family history of HS in her father and a sibling. Seeking more effective treatment, the patient was offered adalimumab approximately 4 months prior to clinical presentation and agreed to start a course of the drug. She received a loading dose of 160 mg on day 1 and 80 mg on day 15 followed by a maintenance dosage of 40 mg weekly. She experienced improvement in HS symptoms after 3 months on adalimumab; however, she developed scaly pruritic patches on the scalp, arms, and legs that were consistent with psoriasis. Because of the absence of a personal or family history of psoriasis, the patient was informed of the probability of paradoxical psoriasis resulting from adalimumab. She elected to continue adalimumab because of the improvement in HS symptoms, and the psoriatic lesions were mild and adequately controlled with a topical steroid.
At the current presentation 1 month later, physical examination revealed a large indurated and ulcerated area with jagged edges at the incision and drainage site (Figure 1). Pyoderma gangrenosum was clinically suspected; a biopsy was performed, and the patient was started on oral prednisone. At 2-week follow-up, the ulcer was found to be rapidly resolving with prednisone and healing with cribriform scarring (Figure 2). Histopathology revealed an undermining neutrophilic inflammatory process that was consistent with PG. A diagnosis of PG was made based on previously published criteria7 and the following major/minor criteria in the patient: pathology; absence of infection on histologic analysis; history of pathergy related to worsening ulceration at the site of incision and drainage of the initial boil; clinical findings of an ulcer with peripheral violaceous erythema; undermined borders and tenderness at the site; and rapid resolution of the ulcer with prednisone.

Cessation of adalimumab gradually led to clearance of both psoriasiform lesions and PG; however, HS lesions persisted.

Although the precise pathogenesis of HS is unclear, both genetic abnormalities of the pilosebaceous unit and a dysregulated immune reaction appear to lead to the clinical characteristics of chronic inflammation and scarring seen in HS. A key effector appears to be helper T-cell (TH17) lymphocyte activation, with increased secretion of TNF-α, IL-1β, and IL-17.1,2 In turn, IL-17 induces higher expression of TNF-α, leading to a persistent cycle of inflammation. Peripheral recruitment of IL-17–producing neutrophils also may contribute to chronic inflammation.8
Adalimumab is the only US Food and Drug Administration–approved biologic indicated for the treatment of HS. Our patient initially responded to adalimumab with improvement of HS; however, treatment had to be discontinued because of the unusual occurrence of 2 distinct paradoxical reactions in a short span of time. Psoriasis and PG are both considered true paradoxical reactions because primary occurrences of both diseases usually are responsive to treatment with adalimumab.
Tumor necrosis factor α inhibitor–induced psoriasis arises de novo and is estimated to occur in approximately 5% of patients with rheumatoid arthritis.3,6 Palmoplantar pustular psoriasiform reactions are the most common form of paradoxical psoriasis. Topical medications can be used to treat skin lesions, but systemic treatment is required in many cases. Switching to an alternate class of a biologic, such as an IL-17, IL-12/23, or IL-23 inhibitor, can improve the skin reaction; however, such treatment is inconsistently successful, and paradoxical drug reactions also have been seen with these other classes of biologics.4,9
Recent studies support distinct immune causes for classical and paradoxical psoriasis. In classical psoriasis, plasmacytoid dendritic cells (pDCs) produce IFN-α, which stimulates conventional dendritic cells to produce TNF-α. However, TNF-α matures both pDCs and conventional dendritic cells; upon maturation, both types of dendritic cells lose the ability to produce IFN-α, thus allowing TNF-α to become dominant.10 The blockade of TNF-α prevents pDC maturation, leading to uninhibited IFN-α, which appears to drive inflammation in paradoxical psoriasis. In classical psoriasis, oligoclonal dermal CD4+ T cells and epidermal CD8+ T cells remain, even in resolved skin lesions, and can cause disease recurrence through reactivation of skin-resident memory T cells.11 No relapse of paradoxical psoriasis occurs with discontinuation of anti-TNF-α therapy, which supports the notion of an absence of memory T cells.
The incidence of paradoxical psoriasis in patients receiving a TNF-α inhibitor for HS is unclear.12 There are case series in which patients who had concurrent psoriasis and HS were successfully treated with a TNF-α inhibitor.13 A recently recognized condition—PASH syndrome—encompasses the clinical triad of PG, acne, and HS.10
Our patient had no history of acne or PG, only a long-standing history of HS. New-onset PG occurred only after a TNF-α inhibitor was initiated. Notably, PASH syndrome has been successfully treated with TNF-α inhibitors, highlighting the shared inflammatory etiology of HS and PG.14 In patients with concurrent PG and HS, TNF-α inhibitors were more effective for treating PG than for HS.
Pyoderma gangrenosum is an inflammatory disorder that often occurs concomitantly with other conditions, such as inflammatory bowel disease. The exact underlying cause of PG is unclear, but there appears to be both neutrophil and T-cell dysfunction in PG, with excess inflammatory cytokine production (eg, IL-1β, TNF-α, IL-17).15
The mainstay of treatment of PG is systemic corticosteroids and immunosuppressives, such as cyclosporine. Tumor necrosis factor α inhibitors as well as other interleukin inhibitors are increasingly utilized as potential therapeutic alternatives for PG.16,17
Unlike paradoxical psoriasis, the underlying cause of paradoxical PG is unclear.18,19 A similar mechanism may be postulated whereby inhibition of TNF-α leads to excessive activation of alternative inflammatory pathways that result in paradoxical PG. In one study, the prevalence of PG among 68,232 patients with HS was 0.18% compared with 0.01% among those without HS; therefore, patients with HS appear to be more predisposed to PG.20
This case illustrates the complex, often conflicting effects of cytokine inhibition in the paradoxical elicitation of alternative inflammatory disorders as an unintended consequence of the initial cytokine blockade. It is likely that genetic predisposition allows for paradoxical reactions in some patients when there is predominant inhibition of one cytokine in the inflammatory pathway. In rare cases, multiple paradoxical reactions are possible.
1. Vossen ARJV, van der Zee HH, Prens EP. Hidradenitis suppurativa: a systematic review integrating inflammatory pathways into a cohesive pathogenic model. Front Immunol. 2018;9:2965. doi:10.3389/fimmu.2018.02965
2. Goldburg SR, Strober BE, Payette MJ. Hidradenitis suppurativa: epidemiology, clinical presentation and pathogenesis. J Am Acad Dermatol. 2020; 82:1045-1058. doi:10.1016/j.jaad.2019.08.090
3. Brown G, Wang E, Leon A, et al. Tumor necrosis factor-α inhibitor-induced psoriasis: systematic review of clinical features, histopathological findings, and management experience. J Am Acad Dermatol. 2017;76:334-341. doi:10.1016/j.jaad.2016.08.012
4. Puig L. Paradoxical reactions: anti-tumor necrosis factor alpha agents, ustekinumab, secukinumab, ixekizumab and others. Curr Prob Dermatol. 2018;53:49-63. doi:10.1159/000479475
5. Faivre C, Villani AP, Aubin F, et al; . Hidradenitis suppurativa (HS): an unrecognized paradoxical effect of biologic agents (BA) used in chronic inflammatory diseases. J Am Acad Dermatol. 2016;74:1153-1159. doi:10.1016/j.jaad.2016.01.018
6. Ko JM, Gottlieb AB, Kerbleski JF. Induction and exacerbation of psoriasis with TNF-blockade therapy: a review and analysis of 127 cases. J Dermatolog Treat. 2009;20:100-108. doi:10.1080/09546630802441234
7. Maverakis E, Ma C, Shinkai K, et al. Diagnostic criteria of ulcerative pyoderma gangrenosum: a delphi consensus of international experts. JAMA Dermatol. 2018;154:461-466. doi:10.1001/jamadermatol.2017.5980
8. Lima AL, Karl I, Giner T, et al. Keratinocytes and neutrophils are important sources of proinflammatory molecules in hidradenitis suppurativa. Br J Dermatol. 2016;174:514-521. doi:10.1111/bjd.14214
9. Li SJ, Perez-Chada LM, Merola JF. TNF inhibitor-induced psoriasis: proposed algorithm for treatment and management. J Psoriasis Psoriatic Arthritis. 2019;4:70-80. doi:10.1177/2475530318810851
10. Conrad C, Di Domizio J, Mylonas A, et al. TNF blockade induces a dysregulated type I interferon response without autoimmunity in paradoxical psoriasis. Nat Commun. 2018;9:25. doi:10.1038/s41467-017-02466-4
11. Matos TR, O’Malley JT, Lowry EL, et al. Clinically resolved psoriatic lesions contain psoriasis-specific IL-17-producing αβ T cell clones. J Clin Invest. 2017;127:4031-4041. doi:10.1172/JCI93396
12. Faivre C, Villani AP, Aubin F, et al. Hidradenitis suppurativa (HS): an unrecognized paradoxical effect of biologic agents (BA) used in chronic inflammatory diseases. J Am Acad Dermatol. 2016;74:1153-1159. doi:10.1016/j.jaad.2016.01.018
13. Marzano AV, Damiani G, Ceccherini I, et al. Autoinflammation in pyoderma gangrenosum and its syndromic form (pyoderma gangrenosum, acne and suppurative hidradenitis). Br J Dermatol. 2017;176:1588-1598. doi:10.1111/bjd.15226
14. Cugno M, Borghi A, Marzano AV. PAPA, PASH, PAPASH syndromes: pathophysiology, presentation and treatment. Am J Clin Dermatol. 2017;18:555-562. doi:10.1007/s40257-017-0265-1
15. Wang EA, Steel A, Luxardi G, et al. Classic ulcerative pyoderma gangrenosum is a T cell-mediated disease targeting follicular adnexal structures: a hypothesis based on molecular and clinicopathologic studies. Front Immunol. 2018;8:1980. doi:10.3389/fimmu.2017.01980
16. Patel F, Fitzmaurice S, Duong C, et al. Effective strategies for the management of pyoderma gangrenosum: a comprehensive review. Acta Derm Venereol. 2015;95:525-531. doi:10.2340/00015555-2008
17. Partridge ACR, Bai JW, Rosen CF, et al. Effectiveness of systemic treatments for pyoderma gangrenosum: a systematic review of observational studies and clinical trials. Br J Dermatol. 2018;179:290-295. doi:10.1111/bjd.16485
18. Benzaquen M, Monnier J, Beaussault Y, et al. Pyoderma gangrenosum arising during treatment of psoriasis with adalimumab: effectiveness of ustekinumab. Australas J Dermatol. 2017;58:e270-e271. doi:10.1111/ajd.12545
19. Fujimoto N, Yamasaki Y, Watanabe RJ. Paradoxical uveitis and pyoderma gangrenosum in a patient with psoriatic arthritis under infliximab treatment. J Dtsch Dermatol Ges. 2018;16:1139-1140. doi:10.1111/ddg.13632
20. Tannenbaum R, Strunk A, Garg A. Overall and subgroup prevalence of pyoderma gangrenosum among patients with hidradenitis suppurativa: a population-based analysis in the United States. J Am Acad Dermatol. 2019;80:1533-1537. doi:10.1016/j.jaad.2019.02.004
To the Editor:
Hidradenitis suppurativa (HS) is a chronic inflammatory condition of the pilosebaceous unit that occurs in concert with elevations of various cytokines, including tumor necrosis factor α (TNF-α), IL-1β, IL-10, and IL-17.1,2 Adalimumab is a TNF-α inhibitor approved by the US Food and Drug Administration for the treatment of HS. Although TNF-α inhibitors are effective for many immune-mediated inflammatory disorders, paradoxical drug reactions have been reported following treatment with these agents.3-6 True paradoxical drug reactions likely are immune mediated and directly lead to new onset of a pathologic condition that would otherwise respond to that drug. For example, there are reports of rheumatoid arthritis patients who were treated with a TNF-α inhibitor and developed psoriatic skin lesions.3,6 Paradoxical drug reactions also have been reported with acute-onset inflammatory bowel disease and HS or less commonly pyoderma gangrenosum (PG), uveitis, granulomatous reactions, and vasculitis.4,5 We present the case of a patient with HS who was treated with a TNF-α inhibitor and developed 2 distinct paradoxical drug reactions. We also provide an overview of paradoxical drug reactions associated with TNF-α inhibitors.
A 38-year-old woman developed a painful “boil” on the right leg that was previously treated in the emergency department with incision and drainage as well as oral clindamycin for 7 days, but the lesion spread and continued to worsen. She had a history of HS in the axillae and groin region that had been present since 12 years of age. The condition was poorly controlled despite multiple courses of oral antibiotics and surgical resections. An oral contraceptive also was attempted, but the patient discontinued treatment when liver enzyme levels became elevated. The patient had no other notable medical history, including skin disease. There was a family history of HS in her father and a sibling. Seeking more effective treatment, the patient was offered adalimumab approximately 4 months prior to clinical presentation and agreed to start a course of the drug. She received a loading dose of 160 mg on day 1 and 80 mg on day 15 followed by a maintenance dosage of 40 mg weekly. She experienced improvement in HS symptoms after 3 months on adalimumab; however, she developed scaly pruritic patches on the scalp, arms, and legs that were consistent with psoriasis. Because of the absence of a personal or family history of psoriasis, the patient was informed of the probability of paradoxical psoriasis resulting from adalimumab. She elected to continue adalimumab because of the improvement in HS symptoms, and the psoriatic lesions were mild and adequately controlled with a topical steroid.
At the current presentation 1 month later, physical examination revealed a large indurated and ulcerated area with jagged edges at the incision and drainage site (Figure 1). Pyoderma gangrenosum was clinically suspected; a biopsy was performed, and the patient was started on oral prednisone. At 2-week follow-up, the ulcer was found to be rapidly resolving with prednisone and healing with cribriform scarring (Figure 2). Histopathology revealed an undermining neutrophilic inflammatory process that was consistent with PG. A diagnosis of PG was made based on previously published criteria7 and the following major/minor criteria in the patient: pathology; absence of infection on histologic analysis; history of pathergy related to worsening ulceration at the site of incision and drainage of the initial boil; clinical findings of an ulcer with peripheral violaceous erythema; undermined borders and tenderness at the site; and rapid resolution of the ulcer with prednisone.
Cessation of adalimumab gradually led to clearance of both psoriasiform lesions and PG; however, HS lesions persisted.
Although the precise pathogenesis of HS is unclear, both genetic abnormalities of the pilosebaceous unit and a dysregulated immune reaction appear to lead to the clinical characteristics of chronic inflammation and scarring seen in HS. A key effector appears to be helper T-cell (TH17) lymphocyte activation, with increased secretion of TNF-α, IL-1β, and IL-17.1,2 In turn, IL-17 induces higher expression of TNF-α, leading to a persistent cycle of inflammation. Peripheral recruitment of IL-17–producing neutrophils also may contribute to chronic inflammation.8
Adalimumab is the only US Food and Drug Administration–approved biologic indicated for the treatment of HS. Our patient initially responded to adalimumab with improvement of HS; however, treatment had to be discontinued because of the unusual occurrence of 2 distinct paradoxical reactions in a short span of time. Psoriasis and PG are both considered true paradoxical reactions because primary occurrences of both diseases usually are responsive to treatment with adalimumab.
Tumor necrosis factor α inhibitor–induced psoriasis arises de novo and is estimated to occur in approximately 5% of patients with rheumatoid arthritis.3,6 Palmoplantar pustular psoriasiform reactions are the most common form of paradoxical psoriasis. Topical medications can be used to treat skin lesions, but systemic treatment is required in many cases. Switching to an alternate class of a biologic, such as an IL-17, IL-12/23, or IL-23 inhibitor, can improve the skin reaction; however, such treatment is inconsistently successful, and paradoxical drug reactions also have been seen with these other classes of biologics.4,9
Recent studies support distinct immune causes for classical and paradoxical psoriasis. In classical psoriasis, plasmacytoid dendritic cells (pDCs) produce IFN-α, which stimulates conventional dendritic cells to produce TNF-α. However, TNF-α matures both pDCs and conventional dendritic cells; upon maturation, both types of dendritic cells lose the ability to produce IFN-α, thus allowing TNF-α to become dominant.10 The blockade of TNF-α prevents pDC maturation, leading to uninhibited IFN-α, which appears to drive inflammation in paradoxical psoriasis. In classical psoriasis, oligoclonal dermal CD4+ T cells and epidermal CD8+ T cells remain, even in resolved skin lesions, and can cause disease recurrence through reactivation of skin-resident memory T cells.11 No relapse of paradoxical psoriasis occurs with discontinuation of anti-TNF-α therapy, which supports the notion of an absence of memory T cells.
The incidence of paradoxical psoriasis in patients receiving a TNF-α inhibitor for HS is unclear.12 There are case series in which patients who had concurrent psoriasis and HS were successfully treated with a TNF-α inhibitor.13 A recently recognized condition—PASH syndrome—encompasses the clinical triad of PG, acne, and HS.10
Our patient had no history of acne or PG, only a long-standing history of HS. New-onset PG occurred only after a TNF-α inhibitor was initiated. Notably, PASH syndrome has been successfully treated with TNF-α inhibitors, highlighting the shared inflammatory etiology of HS and PG.14 In patients with concurrent PG and HS, TNF-α inhibitors were more effective for treating PG than for HS.
Pyoderma gangrenosum is an inflammatory disorder that often occurs concomitantly with other conditions, such as inflammatory bowel disease. The exact underlying cause of PG is unclear, but there appears to be both neutrophil and T-cell dysfunction in PG, with excess inflammatory cytokine production (eg, IL-1β, TNF-α, IL-17).15
The mainstay of treatment of PG is systemic corticosteroids and immunosuppressives, such as cyclosporine. Tumor necrosis factor α inhibitors as well as other interleukin inhibitors are increasingly utilized as potential therapeutic alternatives for PG.16,17
Unlike paradoxical psoriasis, the underlying cause of paradoxical PG is unclear.18,19 A similar mechanism may be postulated whereby inhibition of TNF-α leads to excessive activation of alternative inflammatory pathways that result in paradoxical PG. In one study, the prevalence of PG among 68,232 patients with HS was 0.18% compared with 0.01% among those without HS; therefore, patients with HS appear to be more predisposed to PG.20
This case illustrates the complex, often conflicting effects of cytokine inhibition in the paradoxical elicitation of alternative inflammatory disorders as an unintended consequence of the initial cytokine blockade. It is likely that genetic predisposition allows for paradoxical reactions in some patients when there is predominant inhibition of one cytokine in the inflammatory pathway. In rare cases, multiple paradoxical reactions are possible.
To the Editor:
Hidradenitis suppurativa (HS) is a chronic inflammatory condition of the pilosebaceous unit that occurs in concert with elevations of various cytokines, including tumor necrosis factor α (TNF-α), IL-1β, IL-10, and IL-17.1,2 Adalimumab is a TNF-α inhibitor approved by the US Food and Drug Administration for the treatment of HS. Although TNF-α inhibitors are effective for many immune-mediated inflammatory disorders, paradoxical drug reactions have been reported following treatment with these agents.3-6 True paradoxical drug reactions likely are immune mediated and directly lead to new onset of a pathologic condition that would otherwise respond to that drug. For example, there are reports of rheumatoid arthritis patients who were treated with a TNF-α inhibitor and developed psoriatic skin lesions.3,6 Paradoxical drug reactions also have been reported with acute-onset inflammatory bowel disease and HS or less commonly pyoderma gangrenosum (PG), uveitis, granulomatous reactions, and vasculitis.4,5 We present the case of a patient with HS who was treated with a TNF-α inhibitor and developed 2 distinct paradoxical drug reactions. We also provide an overview of paradoxical drug reactions associated with TNF-α inhibitors.
A 38-year-old woman developed a painful “boil” on the right leg that was previously treated in the emergency department with incision and drainage as well as oral clindamycin for 7 days, but the lesion spread and continued to worsen. She had a history of HS in the axillae and groin region that had been present since 12 years of age. The condition was poorly controlled despite multiple courses of oral antibiotics and surgical resections. An oral contraceptive also was attempted, but the patient discontinued treatment when liver enzyme levels became elevated. The patient had no other notable medical history, including skin disease. There was a family history of HS in her father and a sibling. Seeking more effective treatment, the patient was offered adalimumab approximately 4 months prior to clinical presentation and agreed to start a course of the drug. She received a loading dose of 160 mg on day 1 and 80 mg on day 15 followed by a maintenance dosage of 40 mg weekly. She experienced improvement in HS symptoms after 3 months on adalimumab; however, she developed scaly pruritic patches on the scalp, arms, and legs that were consistent with psoriasis. Because of the absence of a personal or family history of psoriasis, the patient was informed of the probability of paradoxical psoriasis resulting from adalimumab. She elected to continue adalimumab because of the improvement in HS symptoms, and the psoriatic lesions were mild and adequately controlled with a topical steroid.
At the current presentation 1 month later, physical examination revealed a large indurated and ulcerated area with jagged edges at the incision and drainage site (Figure 1). Pyoderma gangrenosum was clinically suspected; a biopsy was performed, and the patient was started on oral prednisone. At 2-week follow-up, the ulcer was found to be rapidly resolving with prednisone and healing with cribriform scarring (Figure 2). Histopathology revealed an undermining neutrophilic inflammatory process that was consistent with PG. A diagnosis of PG was made based on previously published criteria7 and the following major/minor criteria in the patient: pathology; absence of infection on histologic analysis; history of pathergy related to worsening ulceration at the site of incision and drainage of the initial boil; clinical findings of an ulcer with peripheral violaceous erythema; undermined borders and tenderness at the site; and rapid resolution of the ulcer with prednisone.
Cessation of adalimumab gradually led to clearance of both psoriasiform lesions and PG; however, HS lesions persisted.
Although the precise pathogenesis of HS is unclear, both genetic abnormalities of the pilosebaceous unit and a dysregulated immune reaction appear to lead to the clinical characteristics of chronic inflammation and scarring seen in HS. A key effector appears to be helper T-cell (TH17) lymphocyte activation, with increased secretion of TNF-α, IL-1β, and IL-17.1,2 In turn, IL-17 induces higher expression of TNF-α, leading to a persistent cycle of inflammation. Peripheral recruitment of IL-17–producing neutrophils also may contribute to chronic inflammation.8
Adalimumab is the only US Food and Drug Administration–approved biologic indicated for the treatment of HS. Our patient initially responded to adalimumab with improvement of HS; however, treatment had to be discontinued because of the unusual occurrence of 2 distinct paradoxical reactions in a short span of time. Psoriasis and PG are both considered true paradoxical reactions because primary occurrences of both diseases usually are responsive to treatment with adalimumab.
Tumor necrosis factor α inhibitor–induced psoriasis arises de novo and is estimated to occur in approximately 5% of patients with rheumatoid arthritis.3,6 Palmoplantar pustular psoriasiform reactions are the most common form of paradoxical psoriasis. Topical medications can be used to treat skin lesions, but systemic treatment is required in many cases. Switching to an alternate class of a biologic, such as an IL-17, IL-12/23, or IL-23 inhibitor, can improve the skin reaction; however, such treatment is inconsistently successful, and paradoxical drug reactions also have been seen with these other classes of biologics.4,9
Recent studies support distinct immune causes for classical and paradoxical psoriasis. In classical psoriasis, plasmacytoid dendritic cells (pDCs) produce IFN-α, which stimulates conventional dendritic cells to produce TNF-α. However, TNF-α matures both pDCs and conventional dendritic cells; upon maturation, both types of dendritic cells lose the ability to produce IFN-α, thus allowing TNF-α to become dominant.10 The blockade of TNF-α prevents pDC maturation, leading to uninhibited IFN-α, which appears to drive inflammation in paradoxical psoriasis. In classical psoriasis, oligoclonal dermal CD4+ T cells and epidermal CD8+ T cells remain, even in resolved skin lesions, and can cause disease recurrence through reactivation of skin-resident memory T cells.11 No relapse of paradoxical psoriasis occurs with discontinuation of anti-TNF-α therapy, which supports the notion of an absence of memory T cells.
The incidence of paradoxical psoriasis in patients receiving a TNF-α inhibitor for HS is unclear.12 There are case series in which patients who had concurrent psoriasis and HS were successfully treated with a TNF-α inhibitor.13 A recently recognized condition—PASH syndrome—encompasses the clinical triad of PG, acne, and HS.10
Our patient had no history of acne or PG, only a long-standing history of HS. New-onset PG occurred only after a TNF-α inhibitor was initiated. Notably, PASH syndrome has been successfully treated with TNF-α inhibitors, highlighting the shared inflammatory etiology of HS and PG.14 In patients with concurrent PG and HS, TNF-α inhibitors were more effective for treating PG than for HS.
Pyoderma gangrenosum is an inflammatory disorder that often occurs concomitantly with other conditions, such as inflammatory bowel disease. The exact underlying cause of PG is unclear, but there appears to be both neutrophil and T-cell dysfunction in PG, with excess inflammatory cytokine production (eg, IL-1β, TNF-α, IL-17).15
The mainstay of treatment of PG is systemic corticosteroids and immunosuppressives, such as cyclosporine. Tumor necrosis factor α inhibitors as well as other interleukin inhibitors are increasingly utilized as potential therapeutic alternatives for PG.16,17
Unlike paradoxical psoriasis, the underlying cause of paradoxical PG is unclear.18,19 A similar mechanism may be postulated whereby inhibition of TNF-α leads to excessive activation of alternative inflammatory pathways that result in paradoxical PG. In one study, the prevalence of PG among 68,232 patients with HS was 0.18% compared with 0.01% among those without HS; therefore, patients with HS appear to be more predisposed to PG.20
This case illustrates the complex, often conflicting effects of cytokine inhibition in the paradoxical elicitation of alternative inflammatory disorders as an unintended consequence of the initial cytokine blockade. It is likely that genetic predisposition allows for paradoxical reactions in some patients when there is predominant inhibition of one cytokine in the inflammatory pathway. In rare cases, multiple paradoxical reactions are possible.
1. Vossen ARJV, van der Zee HH, Prens EP. Hidradenitis suppurativa: a systematic review integrating inflammatory pathways into a cohesive pathogenic model. Front Immunol. 2018;9:2965. doi:10.3389/fimmu.2018.02965
2. Goldburg SR, Strober BE, Payette MJ. Hidradenitis suppurativa: epidemiology, clinical presentation and pathogenesis. J Am Acad Dermatol. 2020; 82:1045-1058. doi:10.1016/j.jaad.2019.08.090
3. Brown G, Wang E, Leon A, et al. Tumor necrosis factor-α inhibitor-induced psoriasis: systematic review of clinical features, histopathological findings, and management experience. J Am Acad Dermatol. 2017;76:334-341. doi:10.1016/j.jaad.2016.08.012
4. Puig L. Paradoxical reactions: anti-tumor necrosis factor alpha agents, ustekinumab, secukinumab, ixekizumab and others. Curr Prob Dermatol. 2018;53:49-63. doi:10.1159/000479475
5. Faivre C, Villani AP, Aubin F, et al; . Hidradenitis suppurativa (HS): an unrecognized paradoxical effect of biologic agents (BA) used in chronic inflammatory diseases. J Am Acad Dermatol. 2016;74:1153-1159. doi:10.1016/j.jaad.2016.01.018
6. Ko JM, Gottlieb AB, Kerbleski JF. Induction and exacerbation of psoriasis with TNF-blockade therapy: a review and analysis of 127 cases. J Dermatolog Treat. 2009;20:100-108. doi:10.1080/09546630802441234
7. Maverakis E, Ma C, Shinkai K, et al. Diagnostic criteria of ulcerative pyoderma gangrenosum: a delphi consensus of international experts. JAMA Dermatol. 2018;154:461-466. doi:10.1001/jamadermatol.2017.5980
8. Lima AL, Karl I, Giner T, et al. Keratinocytes and neutrophils are important sources of proinflammatory molecules in hidradenitis suppurativa. Br J Dermatol. 2016;174:514-521. doi:10.1111/bjd.14214
9. Li SJ, Perez-Chada LM, Merola JF. TNF inhibitor-induced psoriasis: proposed algorithm for treatment and management. J Psoriasis Psoriatic Arthritis. 2019;4:70-80. doi:10.1177/2475530318810851
10. Conrad C, Di Domizio J, Mylonas A, et al. TNF blockade induces a dysregulated type I interferon response without autoimmunity in paradoxical psoriasis. Nat Commun. 2018;9:25. doi:10.1038/s41467-017-02466-4
11. Matos TR, O’Malley JT, Lowry EL, et al. Clinically resolved psoriatic lesions contain psoriasis-specific IL-17-producing αβ T cell clones. J Clin Invest. 2017;127:4031-4041. doi:10.1172/JCI93396
12. Faivre C, Villani AP, Aubin F, et al. Hidradenitis suppurativa (HS): an unrecognized paradoxical effect of biologic agents (BA) used in chronic inflammatory diseases. J Am Acad Dermatol. 2016;74:1153-1159. doi:10.1016/j.jaad.2016.01.018
13. Marzano AV, Damiani G, Ceccherini I, et al. Autoinflammation in pyoderma gangrenosum and its syndromic form (pyoderma gangrenosum, acne and suppurative hidradenitis). Br J Dermatol. 2017;176:1588-1598. doi:10.1111/bjd.15226
14. Cugno M, Borghi A, Marzano AV. PAPA, PASH, PAPASH syndromes: pathophysiology, presentation and treatment. Am J Clin Dermatol. 2017;18:555-562. doi:10.1007/s40257-017-0265-1
15. Wang EA, Steel A, Luxardi G, et al. Classic ulcerative pyoderma gangrenosum is a T cell-mediated disease targeting follicular adnexal structures: a hypothesis based on molecular and clinicopathologic studies. Front Immunol. 2018;8:1980. doi:10.3389/fimmu.2017.01980
16. Patel F, Fitzmaurice S, Duong C, et al. Effective strategies for the management of pyoderma gangrenosum: a comprehensive review. Acta Derm Venereol. 2015;95:525-531. doi:10.2340/00015555-2008
17. Partridge ACR, Bai JW, Rosen CF, et al. Effectiveness of systemic treatments for pyoderma gangrenosum: a systematic review of observational studies and clinical trials. Br J Dermatol. 2018;179:290-295. doi:10.1111/bjd.16485
18. Benzaquen M, Monnier J, Beaussault Y, et al. Pyoderma gangrenosum arising during treatment of psoriasis with adalimumab: effectiveness of ustekinumab. Australas J Dermatol. 2017;58:e270-e271. doi:10.1111/ajd.12545
19. Fujimoto N, Yamasaki Y, Watanabe RJ. Paradoxical uveitis and pyoderma gangrenosum in a patient with psoriatic arthritis under infliximab treatment. J Dtsch Dermatol Ges. 2018;16:1139-1140. doi:10.1111/ddg.13632
20. Tannenbaum R, Strunk A, Garg A. Overall and subgroup prevalence of pyoderma gangrenosum among patients with hidradenitis suppurativa: a population-based analysis in the United States. J Am Acad Dermatol. 2019;80:1533-1537. doi:10.1016/j.jaad.2019.02.004
1. Vossen ARJV, van der Zee HH, Prens EP. Hidradenitis suppurativa: a systematic review integrating inflammatory pathways into a cohesive pathogenic model. Front Immunol. 2018;9:2965. doi:10.3389/fimmu.2018.02965
2. Goldburg SR, Strober BE, Payette MJ. Hidradenitis suppurativa: epidemiology, clinical presentation and pathogenesis. J Am Acad Dermatol. 2020; 82:1045-1058. doi:10.1016/j.jaad.2019.08.090
3. Brown G, Wang E, Leon A, et al. Tumor necrosis factor-α inhibitor-induced psoriasis: systematic review of clinical features, histopathological findings, and management experience. J Am Acad Dermatol. 2017;76:334-341. doi:10.1016/j.jaad.2016.08.012
4. Puig L. Paradoxical reactions: anti-tumor necrosis factor alpha agents, ustekinumab, secukinumab, ixekizumab and others. Curr Prob Dermatol. 2018;53:49-63. doi:10.1159/000479475
5. Faivre C, Villani AP, Aubin F, et al; . Hidradenitis suppurativa (HS): an unrecognized paradoxical effect of biologic agents (BA) used in chronic inflammatory diseases. J Am Acad Dermatol. 2016;74:1153-1159. doi:10.1016/j.jaad.2016.01.018
6. Ko JM, Gottlieb AB, Kerbleski JF. Induction and exacerbation of psoriasis with TNF-blockade therapy: a review and analysis of 127 cases. J Dermatolog Treat. 2009;20:100-108. doi:10.1080/09546630802441234
7. Maverakis E, Ma C, Shinkai K, et al. Diagnostic criteria of ulcerative pyoderma gangrenosum: a delphi consensus of international experts. JAMA Dermatol. 2018;154:461-466. doi:10.1001/jamadermatol.2017.5980
8. Lima AL, Karl I, Giner T, et al. Keratinocytes and neutrophils are important sources of proinflammatory molecules in hidradenitis suppurativa. Br J Dermatol. 2016;174:514-521. doi:10.1111/bjd.14214
9. Li SJ, Perez-Chada LM, Merola JF. TNF inhibitor-induced psoriasis: proposed algorithm for treatment and management. J Psoriasis Psoriatic Arthritis. 2019;4:70-80. doi:10.1177/2475530318810851
10. Conrad C, Di Domizio J, Mylonas A, et al. TNF blockade induces a dysregulated type I interferon response without autoimmunity in paradoxical psoriasis. Nat Commun. 2018;9:25. doi:10.1038/s41467-017-02466-4
11. Matos TR, O’Malley JT, Lowry EL, et al. Clinically resolved psoriatic lesions contain psoriasis-specific IL-17-producing αβ T cell clones. J Clin Invest. 2017;127:4031-4041. doi:10.1172/JCI93396
12. Faivre C, Villani AP, Aubin F, et al. Hidradenitis suppurativa (HS): an unrecognized paradoxical effect of biologic agents (BA) used in chronic inflammatory diseases. J Am Acad Dermatol. 2016;74:1153-1159. doi:10.1016/j.jaad.2016.01.018
13. Marzano AV, Damiani G, Ceccherini I, et al. Autoinflammation in pyoderma gangrenosum and its syndromic form (pyoderma gangrenosum, acne and suppurative hidradenitis). Br J Dermatol. 2017;176:1588-1598. doi:10.1111/bjd.15226
14. Cugno M, Borghi A, Marzano AV. PAPA, PASH, PAPASH syndromes: pathophysiology, presentation and treatment. Am J Clin Dermatol. 2017;18:555-562. doi:10.1007/s40257-017-0265-1
15. Wang EA, Steel A, Luxardi G, et al. Classic ulcerative pyoderma gangrenosum is a T cell-mediated disease targeting follicular adnexal structures: a hypothesis based on molecular and clinicopathologic studies. Front Immunol. 2018;8:1980. doi:10.3389/fimmu.2017.01980
16. Patel F, Fitzmaurice S, Duong C, et al. Effective strategies for the management of pyoderma gangrenosum: a comprehensive review. Acta Derm Venereol. 2015;95:525-531. doi:10.2340/00015555-2008
17. Partridge ACR, Bai JW, Rosen CF, et al. Effectiveness of systemic treatments for pyoderma gangrenosum: a systematic review of observational studies and clinical trials. Br J Dermatol. 2018;179:290-295. doi:10.1111/bjd.16485
18. Benzaquen M, Monnier J, Beaussault Y, et al. Pyoderma gangrenosum arising during treatment of psoriasis with adalimumab: effectiveness of ustekinumab. Australas J Dermatol. 2017;58:e270-e271. doi:10.1111/ajd.12545
19. Fujimoto N, Yamasaki Y, Watanabe RJ. Paradoxical uveitis and pyoderma gangrenosum in a patient with psoriatic arthritis under infliximab treatment. J Dtsch Dermatol Ges. 2018;16:1139-1140. doi:10.1111/ddg.13632
20. Tannenbaum R, Strunk A, Garg A. Overall and subgroup prevalence of pyoderma gangrenosum among patients with hidradenitis suppurativa: a population-based analysis in the United States. J Am Acad Dermatol. 2019;80:1533-1537. doi:10.1016/j.jaad.2019.02.004
Practice Points
- Clinicians need to be aware of the potential risk for a paradoxical reaction in patients receiving a tumor necrosis factor α (TNF-α) inhibitor for hidradenitis suppurativa.
- Although uncommon, developing more than 1 type of paradoxical skin reaction is possible with a TNF-α inhibitor.
- Early recognition and appropriate management of these paradoxical reactions are critical.
