User login
Leukemia, lymphoma cause more distress in young adults

patient and her father
Photo by Rhoda Baer
Results of 2 new studies indicate that young adults (ages 18 to 39) who have survived leukemia or lymphoma are more likely to report high distress than older survivors (age 65 and older).
Specifically, 45% of younger survivors reported moderate-to-high distress, whereas only 18% of older survivors reported similarly elevated levels.
In both groups, this distress was not affected by the amount of time since a patient received treatment. Distress was just as likely to be high in survivors who had completed treatment 4 years prior as in survivors who were 3 months out of treatment.
Whitney Jones, PhD, of the University of Colorado Denver, and her colleagues reported these findings in the Journal of Psychosocial Oncology.
In the first study, Dr Jones and her colleagues surveyed 477 cancer survivors, using a widely used measure of distress after trauma and several items from a measure of quality of life in cancer survivors.
These measures allowed the researchers to ask which factors of a cancer survivor’s life after treatment are the best predictors of persistent distress after treatment completion.
And results showed that survivors younger than 40 had the highest prevalence of distress.
Dr Jones explained the effect of age on distress using a framework called the Lifespan Perspective. Because there is an expected social, cultural, and developmental course of a person’s life, an event that is highly disruptive in one lifespan stage may be less disruptive in another.
“For younger survivors, cancer is out of context,” Dr Jones said. “When you’re under 40, you’re finishing your education, entering the workforce, starting a family, and cancer may be interpreted as disruptive and unexpected in that phase.”
“On the other hand, some of our older survivors said things like, ‘Cancer isn’t the most difficult thing I’ve experienced in life.’ And they knew friends and family members who had dealt with similar cancer experiences.”
The study also showed that people who feared recurrence were most likely to report high overall distress levels. And high financial burden due to cancer treatment predicted distress.
In the second study, the researchers used interviews with 51 leukemia and lymphoma survivors to explore the human side of these numbers and better understand the sources of distress as articulated by survivors themselves.
“For example, this was before the Affordable Care Act, and we had one survivor who talked about having only the basic college student insurance when he was diagnosed,” Dr Jones said. “After treatment, he discovered he had substantial medical debt and was uninsurable.”
“It helped to hear survivors talk about their experiences in their own words. To hear them articulate it helped us understand the real struggles behind our data.”
The interviews also helped to explain why distress lingers even years after treatment ends.
“A patient told us that, after lymphoma treatment, her doctor said that it would take 2 years to recover physically and mentally, and that almost all the gains would be in these 2 years,” Dr Jones said.
“She said something like, ‘I was really patient for 2 years, then after those 2 years passed, I didn’t feel any better and realized this is what I was going to be living with.’”
Distress detection and treatment is increasingly being seen as part of the standard of care for cancer patients and post-treatment survivors, the researchers noted.
For example, organizations like the National Comprehensive Cancer Network and the American College of Surgeons Commission on Cancer mandate distress screening and treatment in order to earn accreditation from these institutions.
“Understanding which individuals are most likely to experience elevated distress can be useful in targeting interventions to potential participants,” Dr Jones said. ![]()
patient and her father
Photo by Rhoda Baer
Results of 2 new studies indicate that young adults (ages 18 to 39) who have survived leukemia or lymphoma are more likely to report high distress than older survivors (age 65 and older).
Specifically, 45% of younger survivors reported moderate-to-high distress, whereas only 18% of older survivors reported similarly elevated levels.
In both groups, this distress was not affected by the amount of time since a patient received treatment. Distress was just as likely to be high in survivors who had completed treatment 4 years prior as in survivors who were 3 months out of treatment.
Whitney Jones, PhD, of the University of Colorado Denver, and her colleagues reported these findings in the Journal of Psychosocial Oncology.
In the first study, Dr Jones and her colleagues surveyed 477 cancer survivors, using a widely used measure of distress after trauma and several items from a measure of quality of life in cancer survivors.
These measures allowed the researchers to ask which factors of a cancer survivor’s life after treatment are the best predictors of persistent distress after treatment completion.
And results showed that survivors younger than 40 had the highest prevalence of distress.
Dr Jones explained the effect of age on distress using a framework called the Lifespan Perspective. Because there is an expected social, cultural, and developmental course of a person’s life, an event that is highly disruptive in one lifespan stage may be less disruptive in another.
“For younger survivors, cancer is out of context,” Dr Jones said. “When you’re under 40, you’re finishing your education, entering the workforce, starting a family, and cancer may be interpreted as disruptive and unexpected in that phase.”
“On the other hand, some of our older survivors said things like, ‘Cancer isn’t the most difficult thing I’ve experienced in life.’ And they knew friends and family members who had dealt with similar cancer experiences.”
The study also showed that people who feared recurrence were most likely to report high overall distress levels. And high financial burden due to cancer treatment predicted distress.
In the second study, the researchers used interviews with 51 leukemia and lymphoma survivors to explore the human side of these numbers and better understand the sources of distress as articulated by survivors themselves.
“For example, this was before the Affordable Care Act, and we had one survivor who talked about having only the basic college student insurance when he was diagnosed,” Dr Jones said. “After treatment, he discovered he had substantial medical debt and was uninsurable.”
“It helped to hear survivors talk about their experiences in their own words. To hear them articulate it helped us understand the real struggles behind our data.”
The interviews also helped to explain why distress lingers even years after treatment ends.
“A patient told us that, after lymphoma treatment, her doctor said that it would take 2 years to recover physically and mentally, and that almost all the gains would be in these 2 years,” Dr Jones said.
“She said something like, ‘I was really patient for 2 years, then after those 2 years passed, I didn’t feel any better and realized this is what I was going to be living with.’”
Distress detection and treatment is increasingly being seen as part of the standard of care for cancer patients and post-treatment survivors, the researchers noted.
For example, organizations like the National Comprehensive Cancer Network and the American College of Surgeons Commission on Cancer mandate distress screening and treatment in order to earn accreditation from these institutions.
“Understanding which individuals are most likely to experience elevated distress can be useful in targeting interventions to potential participants,” Dr Jones said. ![]()
patient and her father
Photo by Rhoda Baer
Results of 2 new studies indicate that young adults (ages 18 to 39) who have survived leukemia or lymphoma are more likely to report high distress than older survivors (age 65 and older).
Specifically, 45% of younger survivors reported moderate-to-high distress, whereas only 18% of older survivors reported similarly elevated levels.
In both groups, this distress was not affected by the amount of time since a patient received treatment. Distress was just as likely to be high in survivors who had completed treatment 4 years prior as in survivors who were 3 months out of treatment.
Whitney Jones, PhD, of the University of Colorado Denver, and her colleagues reported these findings in the Journal of Psychosocial Oncology.
In the first study, Dr Jones and her colleagues surveyed 477 cancer survivors, using a widely used measure of distress after trauma and several items from a measure of quality of life in cancer survivors.
These measures allowed the researchers to ask which factors of a cancer survivor’s life after treatment are the best predictors of persistent distress after treatment completion.
And results showed that survivors younger than 40 had the highest prevalence of distress.
Dr Jones explained the effect of age on distress using a framework called the Lifespan Perspective. Because there is an expected social, cultural, and developmental course of a person’s life, an event that is highly disruptive in one lifespan stage may be less disruptive in another.
“For younger survivors, cancer is out of context,” Dr Jones said. “When you’re under 40, you’re finishing your education, entering the workforce, starting a family, and cancer may be interpreted as disruptive and unexpected in that phase.”
“On the other hand, some of our older survivors said things like, ‘Cancer isn’t the most difficult thing I’ve experienced in life.’ And they knew friends and family members who had dealt with similar cancer experiences.”
The study also showed that people who feared recurrence were most likely to report high overall distress levels. And high financial burden due to cancer treatment predicted distress.
In the second study, the researchers used interviews with 51 leukemia and lymphoma survivors to explore the human side of these numbers and better understand the sources of distress as articulated by survivors themselves.
“For example, this was before the Affordable Care Act, and we had one survivor who talked about having only the basic college student insurance when he was diagnosed,” Dr Jones said. “After treatment, he discovered he had substantial medical debt and was uninsurable.”
“It helped to hear survivors talk about their experiences in their own words. To hear them articulate it helped us understand the real struggles behind our data.”
The interviews also helped to explain why distress lingers even years after treatment ends.
“A patient told us that, after lymphoma treatment, her doctor said that it would take 2 years to recover physically and mentally, and that almost all the gains would be in these 2 years,” Dr Jones said.
“She said something like, ‘I was really patient for 2 years, then after those 2 years passed, I didn’t feel any better and realized this is what I was going to be living with.’”
Distress detection and treatment is increasingly being seen as part of the standard of care for cancer patients and post-treatment survivors, the researchers noted.
For example, organizations like the National Comprehensive Cancer Network and the American College of Surgeons Commission on Cancer mandate distress screening and treatment in order to earn accreditation from these institutions.
“Understanding which individuals are most likely to experience elevated distress can be useful in targeting interventions to potential participants,” Dr Jones said. ![]()
Survey results support shared decision-making

Photo by Rhoda Baer
A survey of cancer patients has shown that when physicians make treatment decisions alone, patients tend to rate the quality of care lower than when physicians include patients in the decision-making process.
Researchers found this to be the case even among patients who said they preferred it when physicians made treatment decisions alone.
Kenneth L. Kehl, MD, of MD Anderson Cancer Center in Houston, Texas, and his colleagues reported these findings in JAMA Oncology.
The researchers surveyed 5315 cancer patients who reported decision roles for 10,817 treatment decisions. The team assessed the association between patients’ roles in decisions with their reports on quality of care and physician communication.
Most of the patients (58%) said they preferred shared roles in decision-making, 36% preferred patient-controlled decisions, and 6% preferred physician-controlled decisions.
The patients reported that their actual decision-making process was patient-controlled in 39% of decisions, shared in 44%, and physician-controlled in 17%. Of the treatment decisions made by patients, 42% were regarding surgery, 36% were regarding chemotherapy, and 22% were regarding radiation.
The researchers found that patients’ preferred role in decision-making was not associated with how they rated the quality of care. But when they reported that treatment decisions were controlled by physicians, the patients were less likely to rate the quality of care as excellent, as compared to shared-decision making situations.
Patients said physician care was excellent in 67.8% of cases. And 55.8% of patients gave their physicians the highest possible rating of communication.
However, patients who preferred physician-controlled decisions to shared decision-making were less likely to give top ratings to their physicians, as were patients who reported actually experiencing physician-controlled vs shared decisions.
The researchers said these results highlight the benefits of promoting shared decision-making among all patients with cancer, even those who seem to prefer less active roles in the process.
In a related commentary, Sarah T. Hawley, PhD, and Reshma Jagsi, MD, DPhil, of the University of Michigan in Ann Arbor, said they were intrigued by the fact that the association between shared decision-making and patient appraisal of care quality remained even when controlling for a patient’s preferred role in the decision-making process.
“Kehl and colleagues conclude from this finding that it is important to promote [shared decision-making], even among patients who may seek less active roles,” Drs Hawley and Jagsi wrote.
“Yet . . . prior work . . . has suggested that it is the match between patients’ preferred and actual involvement that contributes to greater satisfaction with care. These conflicting results underscore the need for further work to better quantify and link measures of [shared decision-making] to patient appraisal of care.” ![]()
Photo by Rhoda Baer
A survey of cancer patients has shown that when physicians make treatment decisions alone, patients tend to rate the quality of care lower than when physicians include patients in the decision-making process.
Researchers found this to be the case even among patients who said they preferred it when physicians made treatment decisions alone.
Kenneth L. Kehl, MD, of MD Anderson Cancer Center in Houston, Texas, and his colleagues reported these findings in JAMA Oncology.
The researchers surveyed 5315 cancer patients who reported decision roles for 10,817 treatment decisions. The team assessed the association between patients’ roles in decisions with their reports on quality of care and physician communication.
Most of the patients (58%) said they preferred shared roles in decision-making, 36% preferred patient-controlled decisions, and 6% preferred physician-controlled decisions.
The patients reported that their actual decision-making process was patient-controlled in 39% of decisions, shared in 44%, and physician-controlled in 17%. Of the treatment decisions made by patients, 42% were regarding surgery, 36% were regarding chemotherapy, and 22% were regarding radiation.
The researchers found that patients’ preferred role in decision-making was not associated with how they rated the quality of care. But when they reported that treatment decisions were controlled by physicians, the patients were less likely to rate the quality of care as excellent, as compared to shared-decision making situations.
Patients said physician care was excellent in 67.8% of cases. And 55.8% of patients gave their physicians the highest possible rating of communication.
However, patients who preferred physician-controlled decisions to shared decision-making were less likely to give top ratings to their physicians, as were patients who reported actually experiencing physician-controlled vs shared decisions.
The researchers said these results highlight the benefits of promoting shared decision-making among all patients with cancer, even those who seem to prefer less active roles in the process.
In a related commentary, Sarah T. Hawley, PhD, and Reshma Jagsi, MD, DPhil, of the University of Michigan in Ann Arbor, said they were intrigued by the fact that the association between shared decision-making and patient appraisal of care quality remained even when controlling for a patient’s preferred role in the decision-making process.
“Kehl and colleagues conclude from this finding that it is important to promote [shared decision-making], even among patients who may seek less active roles,” Drs Hawley and Jagsi wrote.
“Yet . . . prior work . . . has suggested that it is the match between patients’ preferred and actual involvement that contributes to greater satisfaction with care. These conflicting results underscore the need for further work to better quantify and link measures of [shared decision-making] to patient appraisal of care.” ![]()
Photo by Rhoda Baer
A survey of cancer patients has shown that when physicians make treatment decisions alone, patients tend to rate the quality of care lower than when physicians include patients in the decision-making process.
Researchers found this to be the case even among patients who said they preferred it when physicians made treatment decisions alone.
Kenneth L. Kehl, MD, of MD Anderson Cancer Center in Houston, Texas, and his colleagues reported these findings in JAMA Oncology.
The researchers surveyed 5315 cancer patients who reported decision roles for 10,817 treatment decisions. The team assessed the association between patients’ roles in decisions with their reports on quality of care and physician communication.
Most of the patients (58%) said they preferred shared roles in decision-making, 36% preferred patient-controlled decisions, and 6% preferred physician-controlled decisions.
The patients reported that their actual decision-making process was patient-controlled in 39% of decisions, shared in 44%, and physician-controlled in 17%. Of the treatment decisions made by patients, 42% were regarding surgery, 36% were regarding chemotherapy, and 22% were regarding radiation.
The researchers found that patients’ preferred role in decision-making was not associated with how they rated the quality of care. But when they reported that treatment decisions were controlled by physicians, the patients were less likely to rate the quality of care as excellent, as compared to shared-decision making situations.
Patients said physician care was excellent in 67.8% of cases. And 55.8% of patients gave their physicians the highest possible rating of communication.
However, patients who preferred physician-controlled decisions to shared decision-making were less likely to give top ratings to their physicians, as were patients who reported actually experiencing physician-controlled vs shared decisions.
The researchers said these results highlight the benefits of promoting shared decision-making among all patients with cancer, even those who seem to prefer less active roles in the process.
In a related commentary, Sarah T. Hawley, PhD, and Reshma Jagsi, MD, DPhil, of the University of Michigan in Ann Arbor, said they were intrigued by the fact that the association between shared decision-making and patient appraisal of care quality remained even when controlling for a patient’s preferred role in the decision-making process.
“Kehl and colleagues conclude from this finding that it is important to promote [shared decision-making], even among patients who may seek less active roles,” Drs Hawley and Jagsi wrote.
“Yet . . . prior work . . . has suggested that it is the match between patients’ preferred and actual involvement that contributes to greater satisfaction with care. These conflicting results underscore the need for further work to better quantify and link measures of [shared decision-making] to patient appraisal of care.” ![]()
Cancer patients rarely make inappropriate requests, study shows

Photo courtesy of NIH
Although it makes sense that patient requests might drive physicians to practice defensive medicine, new research suggests that may not be the case with cancer patients.
The study, conducted at outpatient oncology centers, showed that patients rarely made clinically inappropriate requests.
Only 1% of more than 5000 patient-clinician encounters resulted in a clinically inappropriate request. And physicians rarely complied with these requests.
Keerthi Gogineni, MD, of the Hospital of the University of Pennsylvania in Philadelphia, and colleagues reported these findings in JAMA Oncology.
The researchers analyzed interviews with clinicians immediately after they visited with patients to assess whether a patient had made a request, the type of request made, and the clinical appropriateness of it.
The interviews were conducted at outpatient oncology facilities at 3 Philadelphia-area hospitals between October 2013 and June 2014.
The authors evaluated 5050 patient-clinician encounters involving 3624 patients and 60 clinicians. Most of the patients were women, and the most common cancer was hematologic.
Overall, 440 (8.7%) of the encounters included a patient demand or request, such as for imaging studies, treatments, or tests. And physicians complied with 365 (83%) of them.
Of all the patient-clinician encounters, 50 (1%) included a clinically inappropriate request. Clinicians complied with 7 of them. So, in 0.14% of encounters, clinicians ordered a test or treatment based on a clinically inappropriate request.
“At least in oncology, ‘demanding patients’ seem infrequent and may not account for a significant proportion of costs,” the researchers concluded.
In a related editorial, Anthony L. Back, MD, of the Seattle Cancer Care Alliance in Washington, wrote that inappropriate patient demands appear to be “more mythical than real.”
“[W]e have to stop blaming patients for being demanding,” he wrote. “In reality, it is hardly happening. The myth of the demanding patient is more about our own responses and how lackluster communication skills can contribute to difficult situations that stick in our throats and in our memories. And when we have calmed down enough to look up, we see that what is really happening between patients and physicians these days is something quite different.”
“It is possible that what the study by Gogineni et al documents is a point in the evolution of the patient-physician relationship when both sides recognize the complexity of cancer care belies a simple fix. Perhaps this ‘negative’ study is pointing to an important truth: that we need to redirect our attention from the myths that are distracting us.” ![]()
Photo courtesy of NIH
Although it makes sense that patient requests might drive physicians to practice defensive medicine, new research suggests that may not be the case with cancer patients.
The study, conducted at outpatient oncology centers, showed that patients rarely made clinically inappropriate requests.
Only 1% of more than 5000 patient-clinician encounters resulted in a clinically inappropriate request. And physicians rarely complied with these requests.
Keerthi Gogineni, MD, of the Hospital of the University of Pennsylvania in Philadelphia, and colleagues reported these findings in JAMA Oncology.
The researchers analyzed interviews with clinicians immediately after they visited with patients to assess whether a patient had made a request, the type of request made, and the clinical appropriateness of it.
The interviews were conducted at outpatient oncology facilities at 3 Philadelphia-area hospitals between October 2013 and June 2014.
The authors evaluated 5050 patient-clinician encounters involving 3624 patients and 60 clinicians. Most of the patients were women, and the most common cancer was hematologic.
Overall, 440 (8.7%) of the encounters included a patient demand or request, such as for imaging studies, treatments, or tests. And physicians complied with 365 (83%) of them.
Of all the patient-clinician encounters, 50 (1%) included a clinically inappropriate request. Clinicians complied with 7 of them. So, in 0.14% of encounters, clinicians ordered a test or treatment based on a clinically inappropriate request.
“At least in oncology, ‘demanding patients’ seem infrequent and may not account for a significant proportion of costs,” the researchers concluded.
In a related editorial, Anthony L. Back, MD, of the Seattle Cancer Care Alliance in Washington, wrote that inappropriate patient demands appear to be “more mythical than real.”
“[W]e have to stop blaming patients for being demanding,” he wrote. “In reality, it is hardly happening. The myth of the demanding patient is more about our own responses and how lackluster communication skills can contribute to difficult situations that stick in our throats and in our memories. And when we have calmed down enough to look up, we see that what is really happening between patients and physicians these days is something quite different.”
“It is possible that what the study by Gogineni et al documents is a point in the evolution of the patient-physician relationship when both sides recognize the complexity of cancer care belies a simple fix. Perhaps this ‘negative’ study is pointing to an important truth: that we need to redirect our attention from the myths that are distracting us.” ![]()
Photo courtesy of NIH
Although it makes sense that patient requests might drive physicians to practice defensive medicine, new research suggests that may not be the case with cancer patients.
The study, conducted at outpatient oncology centers, showed that patients rarely made clinically inappropriate requests.
Only 1% of more than 5000 patient-clinician encounters resulted in a clinically inappropriate request. And physicians rarely complied with these requests.
Keerthi Gogineni, MD, of the Hospital of the University of Pennsylvania in Philadelphia, and colleagues reported these findings in JAMA Oncology.
The researchers analyzed interviews with clinicians immediately after they visited with patients to assess whether a patient had made a request, the type of request made, and the clinical appropriateness of it.
The interviews were conducted at outpatient oncology facilities at 3 Philadelphia-area hospitals between October 2013 and June 2014.
The authors evaluated 5050 patient-clinician encounters involving 3624 patients and 60 clinicians. Most of the patients were women, and the most common cancer was hematologic.
Overall, 440 (8.7%) of the encounters included a patient demand or request, such as for imaging studies, treatments, or tests. And physicians complied with 365 (83%) of them.
Of all the patient-clinician encounters, 50 (1%) included a clinically inappropriate request. Clinicians complied with 7 of them. So, in 0.14% of encounters, clinicians ordered a test or treatment based on a clinically inappropriate request.
“At least in oncology, ‘demanding patients’ seem infrequent and may not account for a significant proportion of costs,” the researchers concluded.
In a related editorial, Anthony L. Back, MD, of the Seattle Cancer Care Alliance in Washington, wrote that inappropriate patient demands appear to be “more mythical than real.”
“[W]e have to stop blaming patients for being demanding,” he wrote. “In reality, it is hardly happening. The myth of the demanding patient is more about our own responses and how lackluster communication skills can contribute to difficult situations that stick in our throats and in our memories. And when we have calmed down enough to look up, we see that what is really happening between patients and physicians these days is something quite different.”
“It is possible that what the study by Gogineni et al documents is a point in the evolution of the patient-physician relationship when both sides recognize the complexity of cancer care belies a simple fix. Perhaps this ‘negative’ study is pointing to an important truth: that we need to redirect our attention from the myths that are distracting us.” ![]()
In-flight transfusions enable better outcomes in trauma patients

Photo by Elise Amendola
In-flight red blood cell (RBC) transfusions can improve outcomes in trauma patients, according to a study published in the Journal of the American College of Surgeons.
The research showed that air-lifted trauma victims who received blood transfusions in the helicopter had higher one-day survival rates and a lower risk of shock than air-lifted patients who did not receive transfusions until they arrived at the trauma unit.
Patients who received in-flight transfusions also required fewer RBCs once they arrived at the hospital.
Joshua Brown, MD, and his colleagues at the University of Pittsburgh Medical Center (UPMC) conducted this research, evaluating the air medical evacuation strategy at UPMC, which has a network of 18 helicopter bases in Pennsylvania, Ohio, and Maryland.
The STAT MedEvac helicopter teams have been carrying blood for transfusion on their flights for about 2 decades, but this is the first study that evaluated the use of transfused blood in civilian trauma victims air-evacuated directly from the injury scene and compared them with air-evacuated trauma victims who did not receive transfused blood.
It is also the largest study to date of a civilian in-flight trauma resuscitation protocol that has been used by the military in Iraq and Afghanistan.
The researchers evaluated 240 patients who received in-flight RBC transfusions and 480 patients who were not transfused until they reached the trauma center.
Receiving an in-flight transfusion was associated with better odds of 24-hour survival (adjusted odds ratio=4.92, P=0.01), decreased odds of shock (adjusted odds ratio=0.28, P=0.03), and lower 24-hour RBC requirement (coef -3.6 RBC units, P=0.04).
Based on these data, the UPMC may modify its protocol, Dr Brown said.
“It used to be the paramedics had to give the patient 2 liters of saline before giving them blood, and we dropped that down to only 1 liter of saline,” he noted. “Now, based on this study, we’re actually looking at giving patients blood without any saline who meet the criteria of low blood pressure and elevated heart rate and are clearly in shock.”
The UPMC protocol involves giving guidelines on when to administer transfusions to the paramedics and nurses onboard flights. All the STAT MedEvac flights at the institution carry 2 units of RBCs for transfusion.
Helicopter staff can communicate with the medical command doctor at the trauma center to get the go-ahead order to give blood to patients who may not meet the guidelines for transfusion but still may benefit from receiving it.
However, there are regulatory issues that may prevent such a protocol from being adopted universally, Dr Brown noted. In Pennsylvania, paramedics who have had additional training are allowed to start a blood transfusion without a physician present, but not all states allow this.
Dr Brown also explained the logistics and challenges of storing blood away from the blood bank.
“The blood needs to be refrigerated, the helicopter base must have a freezer, and the helicopters must have coolers when they’re actually out on a mission to keep the blood at an appropriate temperature,” he said.
Meeting these requirements involves close coordination with the blood bank and having a way to return unused blood after it expires in 30 days. The University of Pittsburgh has registered all of its helicopter bases as satellite blood banks to comply with the regulations. ![]()
Photo by Elise Amendola
In-flight red blood cell (RBC) transfusions can improve outcomes in trauma patients, according to a study published in the Journal of the American College of Surgeons.
The research showed that air-lifted trauma victims who received blood transfusions in the helicopter had higher one-day survival rates and a lower risk of shock than air-lifted patients who did not receive transfusions until they arrived at the trauma unit.
Patients who received in-flight transfusions also required fewer RBCs once they arrived at the hospital.
Joshua Brown, MD, and his colleagues at the University of Pittsburgh Medical Center (UPMC) conducted this research, evaluating the air medical evacuation strategy at UPMC, which has a network of 18 helicopter bases in Pennsylvania, Ohio, and Maryland.
The STAT MedEvac helicopter teams have been carrying blood for transfusion on their flights for about 2 decades, but this is the first study that evaluated the use of transfused blood in civilian trauma victims air-evacuated directly from the injury scene and compared them with air-evacuated trauma victims who did not receive transfused blood.
It is also the largest study to date of a civilian in-flight trauma resuscitation protocol that has been used by the military in Iraq and Afghanistan.
The researchers evaluated 240 patients who received in-flight RBC transfusions and 480 patients who were not transfused until they reached the trauma center.
Receiving an in-flight transfusion was associated with better odds of 24-hour survival (adjusted odds ratio=4.92, P=0.01), decreased odds of shock (adjusted odds ratio=0.28, P=0.03), and lower 24-hour RBC requirement (coef -3.6 RBC units, P=0.04).
Based on these data, the UPMC may modify its protocol, Dr Brown said.
“It used to be the paramedics had to give the patient 2 liters of saline before giving them blood, and we dropped that down to only 1 liter of saline,” he noted. “Now, based on this study, we’re actually looking at giving patients blood without any saline who meet the criteria of low blood pressure and elevated heart rate and are clearly in shock.”
The UPMC protocol involves giving guidelines on when to administer transfusions to the paramedics and nurses onboard flights. All the STAT MedEvac flights at the institution carry 2 units of RBCs for transfusion.
Helicopter staff can communicate with the medical command doctor at the trauma center to get the go-ahead order to give blood to patients who may not meet the guidelines for transfusion but still may benefit from receiving it.
However, there are regulatory issues that may prevent such a protocol from being adopted universally, Dr Brown noted. In Pennsylvania, paramedics who have had additional training are allowed to start a blood transfusion without a physician present, but not all states allow this.
Dr Brown also explained the logistics and challenges of storing blood away from the blood bank.
“The blood needs to be refrigerated, the helicopter base must have a freezer, and the helicopters must have coolers when they’re actually out on a mission to keep the blood at an appropriate temperature,” he said.
Meeting these requirements involves close coordination with the blood bank and having a way to return unused blood after it expires in 30 days. The University of Pittsburgh has registered all of its helicopter bases as satellite blood banks to comply with the regulations. ![]()
Photo by Elise Amendola
In-flight red blood cell (RBC) transfusions can improve outcomes in trauma patients, according to a study published in the Journal of the American College of Surgeons.
The research showed that air-lifted trauma victims who received blood transfusions in the helicopter had higher one-day survival rates and a lower risk of shock than air-lifted patients who did not receive transfusions until they arrived at the trauma unit.
Patients who received in-flight transfusions also required fewer RBCs once they arrived at the hospital.
Joshua Brown, MD, and his colleagues at the University of Pittsburgh Medical Center (UPMC) conducted this research, evaluating the air medical evacuation strategy at UPMC, which has a network of 18 helicopter bases in Pennsylvania, Ohio, and Maryland.
The STAT MedEvac helicopter teams have been carrying blood for transfusion on their flights for about 2 decades, but this is the first study that evaluated the use of transfused blood in civilian trauma victims air-evacuated directly from the injury scene and compared them with air-evacuated trauma victims who did not receive transfused blood.
It is also the largest study to date of a civilian in-flight trauma resuscitation protocol that has been used by the military in Iraq and Afghanistan.
The researchers evaluated 240 patients who received in-flight RBC transfusions and 480 patients who were not transfused until they reached the trauma center.
Receiving an in-flight transfusion was associated with better odds of 24-hour survival (adjusted odds ratio=4.92, P=0.01), decreased odds of shock (adjusted odds ratio=0.28, P=0.03), and lower 24-hour RBC requirement (coef -3.6 RBC units, P=0.04).
Based on these data, the UPMC may modify its protocol, Dr Brown said.
“It used to be the paramedics had to give the patient 2 liters of saline before giving them blood, and we dropped that down to only 1 liter of saline,” he noted. “Now, based on this study, we’re actually looking at giving patients blood without any saline who meet the criteria of low blood pressure and elevated heart rate and are clearly in shock.”
The UPMC protocol involves giving guidelines on when to administer transfusions to the paramedics and nurses onboard flights. All the STAT MedEvac flights at the institution carry 2 units of RBCs for transfusion.
Helicopter staff can communicate with the medical command doctor at the trauma center to get the go-ahead order to give blood to patients who may not meet the guidelines for transfusion but still may benefit from receiving it.
However, there are regulatory issues that may prevent such a protocol from being adopted universally, Dr Brown noted. In Pennsylvania, paramedics who have had additional training are allowed to start a blood transfusion without a physician present, but not all states allow this.
Dr Brown also explained the logistics and challenges of storing blood away from the blood bank.
“The blood needs to be refrigerated, the helicopter base must have a freezer, and the helicopters must have coolers when they’re actually out on a mission to keep the blood at an appropriate temperature,” he said.
Meeting these requirements involves close coordination with the blood bank and having a way to return unused blood after it expires in 30 days. The University of Pittsburgh has registered all of its helicopter bases as satellite blood banks to comply with the regulations. ![]()
Order of mutations impacts MPN behavior
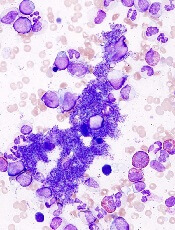
essential thrombocythemia
The order in which genetic mutations are acquired determines how myeloproliferative neoplasms (MPNs) behave, according to research published in NEJM.
Investigators found that mutation order impacts everything from the type of MPN a patient develops to how the disease responds to treatment.
“This surprising finding could help us offer more accurate prognoses to MPN patients based on their mutation order and tailor potential therapies towards them,” said study author David Kent, PhD, of the University of Cambridge in the UK.
“For example, our results predict that targeted JAK2 therapy would be more effective in patients with one mutation order but not the other.”
To uncover this finding, Dr Kent and his colleagues screened 246 MPN patients for mutations in JAK2 and TET2. By studying patients who carried both mutations, the team was able to determine which mutation came first and study the effect of mutation order on the behavior of hematopoietic stem cells.
The investigators found that patients who acquired mutations in JAK2 prior to those in TET2 displayed aberrant blood counts more than a decade earlier.
These patients were more likely to present with polycythemia vera than with essential thrombocythemia, and they were more likely to develop thromboses.
At the same time, JAK2-mutant progenitors from these patients exhibited increased sensitivity to the JAK1/2 inhibitor ruxolitinib in vitro.
“This is the first time that mutation order has been shown to affect any cancer, and it is likely that this phenomenon occurs in many types of malignancy,” said study author Tony Green, MD, PhD, of the University of Cambridge.
“These results show how the study of MPNs provides unparalleled access to the earliest stages of tumor development (inaccessible in other cancers, which usually cannot be detected until many mutations have accumulated). This should give us powerful insights into the origins of cancer.” ![]()
essential thrombocythemia
The order in which genetic mutations are acquired determines how myeloproliferative neoplasms (MPNs) behave, according to research published in NEJM.
Investigators found that mutation order impacts everything from the type of MPN a patient develops to how the disease responds to treatment.
“This surprising finding could help us offer more accurate prognoses to MPN patients based on their mutation order and tailor potential therapies towards them,” said study author David Kent, PhD, of the University of Cambridge in the UK.
“For example, our results predict that targeted JAK2 therapy would be more effective in patients with one mutation order but not the other.”
To uncover this finding, Dr Kent and his colleagues screened 246 MPN patients for mutations in JAK2 and TET2. By studying patients who carried both mutations, the team was able to determine which mutation came first and study the effect of mutation order on the behavior of hematopoietic stem cells.
The investigators found that patients who acquired mutations in JAK2 prior to those in TET2 displayed aberrant blood counts more than a decade earlier.
These patients were more likely to present with polycythemia vera than with essential thrombocythemia, and they were more likely to develop thromboses.
At the same time, JAK2-mutant progenitors from these patients exhibited increased sensitivity to the JAK1/2 inhibitor ruxolitinib in vitro.
“This is the first time that mutation order has been shown to affect any cancer, and it is likely that this phenomenon occurs in many types of malignancy,” said study author Tony Green, MD, PhD, of the University of Cambridge.
“These results show how the study of MPNs provides unparalleled access to the earliest stages of tumor development (inaccessible in other cancers, which usually cannot be detected until many mutations have accumulated). This should give us powerful insights into the origins of cancer.” ![]()
essential thrombocythemia
The order in which genetic mutations are acquired determines how myeloproliferative neoplasms (MPNs) behave, according to research published in NEJM.
Investigators found that mutation order impacts everything from the type of MPN a patient develops to how the disease responds to treatment.
“This surprising finding could help us offer more accurate prognoses to MPN patients based on their mutation order and tailor potential therapies towards them,” said study author David Kent, PhD, of the University of Cambridge in the UK.
“For example, our results predict that targeted JAK2 therapy would be more effective in patients with one mutation order but not the other.”
To uncover this finding, Dr Kent and his colleagues screened 246 MPN patients for mutations in JAK2 and TET2. By studying patients who carried both mutations, the team was able to determine which mutation came first and study the effect of mutation order on the behavior of hematopoietic stem cells.
The investigators found that patients who acquired mutations in JAK2 prior to those in TET2 displayed aberrant blood counts more than a decade earlier.
These patients were more likely to present with polycythemia vera than with essential thrombocythemia, and they were more likely to develop thromboses.
At the same time, JAK2-mutant progenitors from these patients exhibited increased sensitivity to the JAK1/2 inhibitor ruxolitinib in vitro.
“This is the first time that mutation order has been shown to affect any cancer, and it is likely that this phenomenon occurs in many types of malignancy,” said study author Tony Green, MD, PhD, of the University of Cambridge.
“These results show how the study of MPNs provides unparalleled access to the earliest stages of tumor development (inaccessible in other cancers, which usually cannot be detected until many mutations have accumulated). This should give us powerful insights into the origins of cancer.” ![]()
Robotic sock could prevent DVT, team says

the bio-inspired robotic sock
Photo courtesy of the National
University of Singapore
Researchers have invented a robotic sock that may be able to prevent deep vein thrombosis (DVT), although it has not yet been tested in clinical trials.
Equipped with soft actuators that mimic the tentacle movements of corals, the robotic sock emulates natural lower leg muscle contractions in the wearer’s leg, thereby promoting blood circulation throughout the body.
The device also allows the patient’s lower leg movements to be monitored to improve therapy outcomes.
The sock was created by Lim Jeong Hoon, MD, PhD, Raye Yeow Chen Hua, PhD, and Low Fanzhe (a PhD student), all from the National University of Singapore.
While exploring a way to prevent DVT, Dr Lim was inspired by the natural role of the human ankle muscles in facilitating venous blood flow back to the heart. He worked with Dr Yeow and Low to identify a way to perform this function for patients who are bedridden or unable to move their legs.
The team turned to nature for inspiration. They found similarities in the structural design of the coral tentacle, which can extend to grab food and contract to bring the food closer for consumption, and invented soft actuators that mimic this push-and-pull mechanism.
By integrating the actuators with a sock and the use of a programmable pneumatic pump-valve control system, the invention can create the desired robot-assisted ankle joint motions to facilitate blood flow in the leg.
“We chose to use only soft components and actuators to increase patient comfort during use, hence minimizing the risk of injury from excessive mechanical forces,” Low said. “Compression stockings are currently used in the hospital wards, so it makes sense to use a similar sock-based approach to provide comfort and minimize bulk on the ankle and foot.”
The researchers noted that the sock complements conventional ankle therapy exercises that therapists perform on patients, thereby optimizing therapy time and productivity.
In addition, the sock can be worn for prolonged periods to provide robot-assisted therapy, on top of the therapist-assisted sessions. The sock is also embedded with sensors to track the ankle joint angle, allowing the patient’s ankle motion to be monitored for better treatment.
“Given its compact size, modular design, and ease of use, the soft robotic sock can be adopted in hospital wards and rehabilitation centers for on-bed applications to prevent DVT among stroke patients or even at home for bedridden patients,” Dr Yeow said. “By reducing the risk of DVT using this device, we hope to improve survival rates of these patients.”
To investigate the effectiveness of the robotic sock, the researchers will be conducting pilot clinical trials with about 30 patients at the National University Hospital over 6 months, starting in March.
They hope the pilot trials will help them obtain patient and clinical feedback to further improve the design and capabilities of the device. The team intends to conduct trials across different local hospitals for better evaluation, and they also hope to commercialize the device in the future. ![]()
the bio-inspired robotic sock
Photo courtesy of the National
University of Singapore
Researchers have invented a robotic sock that may be able to prevent deep vein thrombosis (DVT), although it has not yet been tested in clinical trials.
Equipped with soft actuators that mimic the tentacle movements of corals, the robotic sock emulates natural lower leg muscle contractions in the wearer’s leg, thereby promoting blood circulation throughout the body.
The device also allows the patient’s lower leg movements to be monitored to improve therapy outcomes.
The sock was created by Lim Jeong Hoon, MD, PhD, Raye Yeow Chen Hua, PhD, and Low Fanzhe (a PhD student), all from the National University of Singapore.
While exploring a way to prevent DVT, Dr Lim was inspired by the natural role of the human ankle muscles in facilitating venous blood flow back to the heart. He worked with Dr Yeow and Low to identify a way to perform this function for patients who are bedridden or unable to move their legs.
The team turned to nature for inspiration. They found similarities in the structural design of the coral tentacle, which can extend to grab food and contract to bring the food closer for consumption, and invented soft actuators that mimic this push-and-pull mechanism.
By integrating the actuators with a sock and the use of a programmable pneumatic pump-valve control system, the invention can create the desired robot-assisted ankle joint motions to facilitate blood flow in the leg.
“We chose to use only soft components and actuators to increase patient comfort during use, hence minimizing the risk of injury from excessive mechanical forces,” Low said. “Compression stockings are currently used in the hospital wards, so it makes sense to use a similar sock-based approach to provide comfort and minimize bulk on the ankle and foot.”
The researchers noted that the sock complements conventional ankle therapy exercises that therapists perform on patients, thereby optimizing therapy time and productivity.
In addition, the sock can be worn for prolonged periods to provide robot-assisted therapy, on top of the therapist-assisted sessions. The sock is also embedded with sensors to track the ankle joint angle, allowing the patient’s ankle motion to be monitored for better treatment.
“Given its compact size, modular design, and ease of use, the soft robotic sock can be adopted in hospital wards and rehabilitation centers for on-bed applications to prevent DVT among stroke patients or even at home for bedridden patients,” Dr Yeow said. “By reducing the risk of DVT using this device, we hope to improve survival rates of these patients.”
To investigate the effectiveness of the robotic sock, the researchers will be conducting pilot clinical trials with about 30 patients at the National University Hospital over 6 months, starting in March.
They hope the pilot trials will help them obtain patient and clinical feedback to further improve the design and capabilities of the device. The team intends to conduct trials across different local hospitals for better evaluation, and they also hope to commercialize the device in the future. ![]()
the bio-inspired robotic sock
Photo courtesy of the National
University of Singapore
Researchers have invented a robotic sock that may be able to prevent deep vein thrombosis (DVT), although it has not yet been tested in clinical trials.
Equipped with soft actuators that mimic the tentacle movements of corals, the robotic sock emulates natural lower leg muscle contractions in the wearer’s leg, thereby promoting blood circulation throughout the body.
The device also allows the patient’s lower leg movements to be monitored to improve therapy outcomes.
The sock was created by Lim Jeong Hoon, MD, PhD, Raye Yeow Chen Hua, PhD, and Low Fanzhe (a PhD student), all from the National University of Singapore.
While exploring a way to prevent DVT, Dr Lim was inspired by the natural role of the human ankle muscles in facilitating venous blood flow back to the heart. He worked with Dr Yeow and Low to identify a way to perform this function for patients who are bedridden or unable to move their legs.
The team turned to nature for inspiration. They found similarities in the structural design of the coral tentacle, which can extend to grab food and contract to bring the food closer for consumption, and invented soft actuators that mimic this push-and-pull mechanism.
By integrating the actuators with a sock and the use of a programmable pneumatic pump-valve control system, the invention can create the desired robot-assisted ankle joint motions to facilitate blood flow in the leg.
“We chose to use only soft components and actuators to increase patient comfort during use, hence minimizing the risk of injury from excessive mechanical forces,” Low said. “Compression stockings are currently used in the hospital wards, so it makes sense to use a similar sock-based approach to provide comfort and minimize bulk on the ankle and foot.”
The researchers noted that the sock complements conventional ankle therapy exercises that therapists perform on patients, thereby optimizing therapy time and productivity.
In addition, the sock can be worn for prolonged periods to provide robot-assisted therapy, on top of the therapist-assisted sessions. The sock is also embedded with sensors to track the ankle joint angle, allowing the patient’s ankle motion to be monitored for better treatment.
“Given its compact size, modular design, and ease of use, the soft robotic sock can be adopted in hospital wards and rehabilitation centers for on-bed applications to prevent DVT among stroke patients or even at home for bedridden patients,” Dr Yeow said. “By reducing the risk of DVT using this device, we hope to improve survival rates of these patients.”
To investigate the effectiveness of the robotic sock, the researchers will be conducting pilot clinical trials with about 30 patients at the National University Hospital over 6 months, starting in March.
They hope the pilot trials will help them obtain patient and clinical feedback to further improve the design and capabilities of the device. The team intends to conduct trials across different local hospitals for better evaluation, and they also hope to commercialize the device in the future. ![]()
Gene variations tied to drug-related hearing loss

Photo by Peter Barta
New research has revealed inherited genetic variations associated with rapid hearing loss in young cancer patients who receive cisplatin.
The drug is used to treat a range of cancers and is known to pose a risk of severe hearing loss, but the risk factors involved are not completely understood.
Now, researchers have found that variations in the gene ACYP2 are associated with an increased risk of cisplatin-related hearing loss.
Jun J. Yang, PhD, of St Jude Children’s Research Hospital in Memphis, Tennessee, and his colleagues reported this discovery in Nature Genetics.
The researchers checked the DNA of 238 young patients with brain tumors for more than 1.7 million common genetic variations. The team found that variations in ACYP2 were associated with as much as a 4-fold greater risk of cisplatin-related hearing loss.
The screening is among the first to survey the genetic landscape for clues to help explain why the risk of cisplatin-related hearing loss varies so widely among patients.
“This is an important first step in being able to pinpoint patients who are at higher risk of developing cisplatin toxicity and to learn how to better manage that risk,” said study author Clinton Stewart, PharmD, also of St Jude.
The researchers confirmed the association between the high-risk ACYP2 variants and cisplatin-related hearing loss in a separate group of 68 brain tumor patients. The association was independent of other risk factors for cisplatin-related hearing loss, including patient age and receipt of radiation therapy.
Twenty-four of the 306 patients in this study had at least one copy of the high-risk ACYP2 variant. All 24 patients had measurable hearing loss that occurred as early as weeks after beginning cisplatin therapy.
Overall, however, the ACYP2 variant explained a relatively small proportion of hearing damage. Just 12.4% of the 194 patients in this study with cisplatin-related hearing loss carried the ACYP2 variant.
“This suggests that other genes also contribute to the risk of hearing loss and are yet to be identified,” Dr Yang said. “Further research is needed to understand how the ACYP2 variations modify the risk . . . of cisplatin toxicity.”
Such studies could potentially lead to new medications to protect high-risk patients from cisplatin-related toxicity or help identify candidates for intensive monitoring of their hearing, Dr Stewart said. Early intervention could then be offered if problems are identified.
This study included patients enrolled in 1 of 3 trials designed by St Jude investigators for newly diagnosed pediatric brain tumors. The protocols involved similar treatment, including surgery to remove as much of the tumor as possible, followed by radiation, which was modified based on patient age and other risk factors.
The patients were scheduled to receive 4 rounds of cisplatin therapy. Patients’ hearing was tested before treatment began, after radiation therapy, after each round of chemotherapy, and then at regular standardized intervals. Analysis of the resulting data led to identification of ACYP2 and other variants.
“Our primary goal is to cure children with brain tumors, but we also have a duty to help patients survive with a high quality of life,” said Giles Robinson, MD, also of St Jude.
“Hearing loss can have a significant impact on a child’s quality of life, language development, and academic performance. There is no easy fix, but the more we know about the risk factors, the better we will understand how to use cisplatin.” ![]()
Photo by Peter Barta
New research has revealed inherited genetic variations associated with rapid hearing loss in young cancer patients who receive cisplatin.
The drug is used to treat a range of cancers and is known to pose a risk of severe hearing loss, but the risk factors involved are not completely understood.
Now, researchers have found that variations in the gene ACYP2 are associated with an increased risk of cisplatin-related hearing loss.
Jun J. Yang, PhD, of St Jude Children’s Research Hospital in Memphis, Tennessee, and his colleagues reported this discovery in Nature Genetics.
The researchers checked the DNA of 238 young patients with brain tumors for more than 1.7 million common genetic variations. The team found that variations in ACYP2 were associated with as much as a 4-fold greater risk of cisplatin-related hearing loss.
The screening is among the first to survey the genetic landscape for clues to help explain why the risk of cisplatin-related hearing loss varies so widely among patients.
“This is an important first step in being able to pinpoint patients who are at higher risk of developing cisplatin toxicity and to learn how to better manage that risk,” said study author Clinton Stewart, PharmD, also of St Jude.
The researchers confirmed the association between the high-risk ACYP2 variants and cisplatin-related hearing loss in a separate group of 68 brain tumor patients. The association was independent of other risk factors for cisplatin-related hearing loss, including patient age and receipt of radiation therapy.
Twenty-four of the 306 patients in this study had at least one copy of the high-risk ACYP2 variant. All 24 patients had measurable hearing loss that occurred as early as weeks after beginning cisplatin therapy.
Overall, however, the ACYP2 variant explained a relatively small proportion of hearing damage. Just 12.4% of the 194 patients in this study with cisplatin-related hearing loss carried the ACYP2 variant.
“This suggests that other genes also contribute to the risk of hearing loss and are yet to be identified,” Dr Yang said. “Further research is needed to understand how the ACYP2 variations modify the risk . . . of cisplatin toxicity.”
Such studies could potentially lead to new medications to protect high-risk patients from cisplatin-related toxicity or help identify candidates for intensive monitoring of their hearing, Dr Stewart said. Early intervention could then be offered if problems are identified.
This study included patients enrolled in 1 of 3 trials designed by St Jude investigators for newly diagnosed pediatric brain tumors. The protocols involved similar treatment, including surgery to remove as much of the tumor as possible, followed by radiation, which was modified based on patient age and other risk factors.
The patients were scheduled to receive 4 rounds of cisplatin therapy. Patients’ hearing was tested before treatment began, after radiation therapy, after each round of chemotherapy, and then at regular standardized intervals. Analysis of the resulting data led to identification of ACYP2 and other variants.
“Our primary goal is to cure children with brain tumors, but we also have a duty to help patients survive with a high quality of life,” said Giles Robinson, MD, also of St Jude.
“Hearing loss can have a significant impact on a child’s quality of life, language development, and academic performance. There is no easy fix, but the more we know about the risk factors, the better we will understand how to use cisplatin.” ![]()
Photo by Peter Barta
New research has revealed inherited genetic variations associated with rapid hearing loss in young cancer patients who receive cisplatin.
The drug is used to treat a range of cancers and is known to pose a risk of severe hearing loss, but the risk factors involved are not completely understood.
Now, researchers have found that variations in the gene ACYP2 are associated with an increased risk of cisplatin-related hearing loss.
Jun J. Yang, PhD, of St Jude Children’s Research Hospital in Memphis, Tennessee, and his colleagues reported this discovery in Nature Genetics.
The researchers checked the DNA of 238 young patients with brain tumors for more than 1.7 million common genetic variations. The team found that variations in ACYP2 were associated with as much as a 4-fold greater risk of cisplatin-related hearing loss.
The screening is among the first to survey the genetic landscape for clues to help explain why the risk of cisplatin-related hearing loss varies so widely among patients.
“This is an important first step in being able to pinpoint patients who are at higher risk of developing cisplatin toxicity and to learn how to better manage that risk,” said study author Clinton Stewart, PharmD, also of St Jude.
The researchers confirmed the association between the high-risk ACYP2 variants and cisplatin-related hearing loss in a separate group of 68 brain tumor patients. The association was independent of other risk factors for cisplatin-related hearing loss, including patient age and receipt of radiation therapy.
Twenty-four of the 306 patients in this study had at least one copy of the high-risk ACYP2 variant. All 24 patients had measurable hearing loss that occurred as early as weeks after beginning cisplatin therapy.
Overall, however, the ACYP2 variant explained a relatively small proportion of hearing damage. Just 12.4% of the 194 patients in this study with cisplatin-related hearing loss carried the ACYP2 variant.
“This suggests that other genes also contribute to the risk of hearing loss and are yet to be identified,” Dr Yang said. “Further research is needed to understand how the ACYP2 variations modify the risk . . . of cisplatin toxicity.”
Such studies could potentially lead to new medications to protect high-risk patients from cisplatin-related toxicity or help identify candidates for intensive monitoring of their hearing, Dr Stewart said. Early intervention could then be offered if problems are identified.
This study included patients enrolled in 1 of 3 trials designed by St Jude investigators for newly diagnosed pediatric brain tumors. The protocols involved similar treatment, including surgery to remove as much of the tumor as possible, followed by radiation, which was modified based on patient age and other risk factors.
The patients were scheduled to receive 4 rounds of cisplatin therapy. Patients’ hearing was tested before treatment began, after radiation therapy, after each round of chemotherapy, and then at regular standardized intervals. Analysis of the resulting data led to identification of ACYP2 and other variants.
“Our primary goal is to cure children with brain tumors, but we also have a duty to help patients survive with a high quality of life,” said Giles Robinson, MD, also of St Jude.
“Hearing loss can have a significant impact on a child’s quality of life, language development, and academic performance. There is no easy fix, but the more we know about the risk factors, the better we will understand how to use cisplatin.”
Signs may predict death in cancer patients

Researchers have identified 8 highly specific physical and cognitive signs that seem to be associated with imminent death in cancer patients.
The findings, published in Cancer, could offer clinicians the ability to better communicate with patients and their families.
The research might also help guide the medical team and caregivers when it comes to complex decision making, such as discontinuing tests and therapy, plans for hospital discharge, and hospice referral.
Previous studies in end-of-life care have focused on physicians prognosticating better. However, research on how to tell if a patient has entered the final days of life has been minimal, according to David Hui, MD, of the University of Texas MD Anderson Cancer Center in Houston.
“In the past, studies trying to understand the signs associated with impending death were conducted in people who were recognized as dying, so there’s a potential bias built into this model,” Dr Hui said.
“With our study, we observed a list of signs in patients from the time they were admitted to the palliative care unit. They were observed systematically, twice a day, without knowing if the patient would die or be discharged.”
Dr Hui and his colleagues observed 357 cancer patients, 57% of whom ultimately died. The researchers observed 52 physical and cognitive signs—identified by Dr Hui and his colleagues in previous research—twice a day from the patient’s admission to discharge or death.
Of those 52 signs, the 8 most highly associated with impending death within 3 days were:
- Nonreactive pupils
- Decreased response to verbal stimuli
- Decreased response to visual stimuli
- Inability to close eyelids
- Drooping of the nasolabial fold
- Neck hyperextension
- Grunting of vocal cords
- Upper gastrointestinal bleeding.
“When cancer patients reach the last days of life, this is an extremely emotional time for families; their stress levels cannot be understated,” Dr Hui said.
“Knowing when death is imminent would provide more information so caregivers can plan appropriately. For clinicians, having this information could help reassure families that we are providing the best care possible.”
Dr Hui stressed that this research is not yet practice-changing, but is an important step in understanding these 8 signs and their relation to impending death. In addition, the findings are only representative of imminent cancer death and should not be generalized to other causes of death.
Follow-up studies in different settings are planned. Dr Hui and his colleagues plan to look at the reliability of the identified signs, as well as evaluate this research in other countries and in the hospice setting.
Researchers have identified 8 highly specific physical and cognitive signs that seem to be associated with imminent death in cancer patients.
The findings, published in Cancer, could offer clinicians the ability to better communicate with patients and their families.
The research might also help guide the medical team and caregivers when it comes to complex decision making, such as discontinuing tests and therapy, plans for hospital discharge, and hospice referral.
Previous studies in end-of-life care have focused on physicians prognosticating better. However, research on how to tell if a patient has entered the final days of life has been minimal, according to David Hui, MD, of the University of Texas MD Anderson Cancer Center in Houston.
“In the past, studies trying to understand the signs associated with impending death were conducted in people who were recognized as dying, so there’s a potential bias built into this model,” Dr Hui said.
“With our study, we observed a list of signs in patients from the time they were admitted to the palliative care unit. They were observed systematically, twice a day, without knowing if the patient would die or be discharged.”
Dr Hui and his colleagues observed 357 cancer patients, 57% of whom ultimately died. The researchers observed 52 physical and cognitive signs—identified by Dr Hui and his colleagues in previous research—twice a day from the patient’s admission to discharge or death.
Of those 52 signs, the 8 most highly associated with impending death within 3 days were:
- Nonreactive pupils
- Decreased response to verbal stimuli
- Decreased response to visual stimuli
- Inability to close eyelids
- Drooping of the nasolabial fold
- Neck hyperextension
- Grunting of vocal cords
- Upper gastrointestinal bleeding.
“When cancer patients reach the last days of life, this is an extremely emotional time for families; their stress levels cannot be understated,” Dr Hui said.
“Knowing when death is imminent would provide more information so caregivers can plan appropriately. For clinicians, having this information could help reassure families that we are providing the best care possible.”
Dr Hui stressed that this research is not yet practice-changing, but is an important step in understanding these 8 signs and their relation to impending death. In addition, the findings are only representative of imminent cancer death and should not be generalized to other causes of death.
Follow-up studies in different settings are planned. Dr Hui and his colleagues plan to look at the reliability of the identified signs, as well as evaluate this research in other countries and in the hospice setting.
Researchers have identified 8 highly specific physical and cognitive signs that seem to be associated with imminent death in cancer patients.
The findings, published in Cancer, could offer clinicians the ability to better communicate with patients and their families.
The research might also help guide the medical team and caregivers when it comes to complex decision making, such as discontinuing tests and therapy, plans for hospital discharge, and hospice referral.
Previous studies in end-of-life care have focused on physicians prognosticating better. However, research on how to tell if a patient has entered the final days of life has been minimal, according to David Hui, MD, of the University of Texas MD Anderson Cancer Center in Houston.
“In the past, studies trying to understand the signs associated with impending death were conducted in people who were recognized as dying, so there’s a potential bias built into this model,” Dr Hui said.
“With our study, we observed a list of signs in patients from the time they were admitted to the palliative care unit. They were observed systematically, twice a day, without knowing if the patient would die or be discharged.”
Dr Hui and his colleagues observed 357 cancer patients, 57% of whom ultimately died. The researchers observed 52 physical and cognitive signs—identified by Dr Hui and his colleagues in previous research—twice a day from the patient’s admission to discharge or death.
Of those 52 signs, the 8 most highly associated with impending death within 3 days were:
- Nonreactive pupils
- Decreased response to verbal stimuli
- Decreased response to visual stimuli
- Inability to close eyelids
- Drooping of the nasolabial fold
- Neck hyperextension
- Grunting of vocal cords
- Upper gastrointestinal bleeding.
“When cancer patients reach the last days of life, this is an extremely emotional time for families; their stress levels cannot be understated,” Dr Hui said.
“Knowing when death is imminent would provide more information so caregivers can plan appropriately. For clinicians, having this information could help reassure families that we are providing the best care possible.”
Dr Hui stressed that this research is not yet practice-changing, but is an important step in understanding these 8 signs and their relation to impending death. In addition, the findings are only representative of imminent cancer death and should not be generalized to other causes of death.
Follow-up studies in different settings are planned. Dr Hui and his colleagues plan to look at the reliability of the identified signs, as well as evaluate this research in other countries and in the hospice setting.
Donor telomere length linked to survival after HSCT
![]()
Photo by Chad McNeeley
Leukocyte telomere length is associated with survival in patients who undergo hematopoietic stem cell transplant (HSCT) to treat severe aplastic anemia, according to research published in JAMA.
But it’s the donor’s telomere length—not the recipient’s—that makes the difference, the study showed.
Patients who received an HSCT from an unrelated donor had better overall survival at 5 years if that donor’s leukocytes had longer telomeres.
Shahinaz M. Gadalla, MD, PhD, of the National Cancer Institute in Rockville, Maryland, and colleagues conducted this research.
The group compared recipient and donor leukocyte telomere length prior to transplant with outcomes after unrelated HSCT for 330 patients with severe aplastic anemia.
The patients and their donors had pre-HSCT blood samples and other clinical results available at the Center for International Blood and Marrow Transplant Research. Patients underwent HSCT between 1989 and 2007 in 84 centers and were followed until March 2013.
The researchers categorized leukocyte telomere length for both recipients and donors based on the leukocyte telomere length tertiles in the donors: long (third tertile) and short (first and second tertiles combined).
The team found that longer donor leukocyte telomere length was associated with a higher overall survival. The 5-year overall survival was 56% in the longer telomere group and 40% in the shorter telomere group (P=0.009).
After adjusting for donor age and clinical factors associated with survival following HSCT in severe aplastic anemia, the risk of post-HSCT all-cause mortality remained approximately 40% lower in patients receiving HSCT from donors with long vs short leukocyte telomeres (hazard ratio [HR]=0.61).
There was no association between donor leukocyte telomere length and engraftment at 28 days (HR=0.94). Likewise, there was no association between telomere length and acute (HR=0.77) or chronic graft-vs-host disease (HR=0.81).
And recipient telomere length was not associated with overall survival (HR=0.91).
The researchers said these results suggest that donor leukocyte telomere length may have a role in long-term post-transplant survival. Authors of a related editorial explored what this discovery could mean for transplant centers.
![]()
Photo by Chad McNeeley
Leukocyte telomere length is associated with survival in patients who undergo hematopoietic stem cell transplant (HSCT) to treat severe aplastic anemia, according to research published in JAMA.
But it’s the donor’s telomere length—not the recipient’s—that makes the difference, the study showed.
Patients who received an HSCT from an unrelated donor had better overall survival at 5 years if that donor’s leukocytes had longer telomeres.
Shahinaz M. Gadalla, MD, PhD, of the National Cancer Institute in Rockville, Maryland, and colleagues conducted this research.
The group compared recipient and donor leukocyte telomere length prior to transplant with outcomes after unrelated HSCT for 330 patients with severe aplastic anemia.
The patients and their donors had pre-HSCT blood samples and other clinical results available at the Center for International Blood and Marrow Transplant Research. Patients underwent HSCT between 1989 and 2007 in 84 centers and were followed until March 2013.
The researchers categorized leukocyte telomere length for both recipients and donors based on the leukocyte telomere length tertiles in the donors: long (third tertile) and short (first and second tertiles combined).
The team found that longer donor leukocyte telomere length was associated with a higher overall survival. The 5-year overall survival was 56% in the longer telomere group and 40% in the shorter telomere group (P=0.009).
After adjusting for donor age and clinical factors associated with survival following HSCT in severe aplastic anemia, the risk of post-HSCT all-cause mortality remained approximately 40% lower in patients receiving HSCT from donors with long vs short leukocyte telomeres (hazard ratio [HR]=0.61).
There was no association between donor leukocyte telomere length and engraftment at 28 days (HR=0.94). Likewise, there was no association between telomere length and acute (HR=0.77) or chronic graft-vs-host disease (HR=0.81).
And recipient telomere length was not associated with overall survival (HR=0.91).
The researchers said these results suggest that donor leukocyte telomere length may have a role in long-term post-transplant survival. Authors of a related editorial explored what this discovery could mean for transplant centers.
![]()
Photo by Chad McNeeley
Leukocyte telomere length is associated with survival in patients who undergo hematopoietic stem cell transplant (HSCT) to treat severe aplastic anemia, according to research published in JAMA.
But it’s the donor’s telomere length—not the recipient’s—that makes the difference, the study showed.
Patients who received an HSCT from an unrelated donor had better overall survival at 5 years if that donor’s leukocytes had longer telomeres.
Shahinaz M. Gadalla, MD, PhD, of the National Cancer Institute in Rockville, Maryland, and colleagues conducted this research.
The group compared recipient and donor leukocyte telomere length prior to transplant with outcomes after unrelated HSCT for 330 patients with severe aplastic anemia.
The patients and their donors had pre-HSCT blood samples and other clinical results available at the Center for International Blood and Marrow Transplant Research. Patients underwent HSCT between 1989 and 2007 in 84 centers and were followed until March 2013.
The researchers categorized leukocyte telomere length for both recipients and donors based on the leukocyte telomere length tertiles in the donors: long (third tertile) and short (first and second tertiles combined).
The team found that longer donor leukocyte telomere length was associated with a higher overall survival. The 5-year overall survival was 56% in the longer telomere group and 40% in the shorter telomere group (P=0.009).
After adjusting for donor age and clinical factors associated with survival following HSCT in severe aplastic anemia, the risk of post-HSCT all-cause mortality remained approximately 40% lower in patients receiving HSCT from donors with long vs short leukocyte telomeres (hazard ratio [HR]=0.61).
There was no association between donor leukocyte telomere length and engraftment at 28 days (HR=0.94). Likewise, there was no association between telomere length and acute (HR=0.77) or chronic graft-vs-host disease (HR=0.81).
And recipient telomere length was not associated with overall survival (HR=0.91).
The researchers said these results suggest that donor leukocyte telomere length may have a role in long-term post-transplant survival. Authors of a related editorial explored what this discovery could mean for transplant centers.
Approved TKI could treat drug-resistant CML, ALL

Photo courtesy of CDC
New research indicates that a tyrosine kinase inhibitor (TKI) approved to treat advanced renal cell carcinoma could prove useful in treating patients with drug-resistant chronic myeloid leukemia (CML) or acute lymphoblastic leukemia (ALL).
The study showed that the TKI, axitinib, can inhibit BCR-ABL1 (T315I), a mutation known to confer drug resistance in CML and ALL.
“Since axitinib is already used to treat cancer, its safety is known,” said Kimmo Porkka, MD, PhD, of the University of Helsinki in Finland.
“[A] formal exploration of its clinical utility in drug-resistant leukemia can now be done in a fast-track mode. Thus, the normally very long path from lab bench to bedside is now significantly shortened.”
Dr Porkka and his colleagues described the newfound activity of axitinib in Nature.
The researchers used a drug sensitivity and resistance testing method developed at the University of Helsinki’s Institute for Molecular Medicine Finland (FIMM) to examine how patient-derived leukemia cells responded to a large panel of drugs.
In this way, the group identified axitinib as a promising drug candidate for CML and ALL. Axitinib effectively eliminated drug-resistant leukemia cells.
The TKI inhibited BCR-ABL1 (T315I) at biochemical and cellular levels by binding to the active form of ABL1 (T315I) in a mutation-selective binding mode.
The researchers said this suggests the T315I mutation shifts the conformational equilibrium of the kinase in favor of an active (DFG-in) A-loop conformation, which has more optimal binding interactions with axitinib.
“If you think of the targeted protein as a lock into which the cancer drug fits in as a key, the resistant protein changes in such a way that we need a different key,” said study author Brion Murray, PhD, of Pfizer Worldwide Research & Development in San Diego, California.
“In the case of axitinib, it acts as two distinct keys—one for renal cell carcinoma and one for leukemia.”
The researchers also treated a CML patient with axitinib and observed a “rapid reduction” of T315I-positive cells in the patient’s bone marrow.
“Further research will determine whether these findings have the potential to significantly improve the standard of care for this select group of CML patients and patients with other related leukemias,” Dr Murray concluded.
Photo courtesy of CDC
New research indicates that a tyrosine kinase inhibitor (TKI) approved to treat advanced renal cell carcinoma could prove useful in treating patients with drug-resistant chronic myeloid leukemia (CML) or acute lymphoblastic leukemia (ALL).
The study showed that the TKI, axitinib, can inhibit BCR-ABL1 (T315I), a mutation known to confer drug resistance in CML and ALL.
“Since axitinib is already used to treat cancer, its safety is known,” said Kimmo Porkka, MD, PhD, of the University of Helsinki in Finland.
“[A] formal exploration of its clinical utility in drug-resistant leukemia can now be done in a fast-track mode. Thus, the normally very long path from lab bench to bedside is now significantly shortened.”
Dr Porkka and his colleagues described the newfound activity of axitinib in Nature.
The researchers used a drug sensitivity and resistance testing method developed at the University of Helsinki’s Institute for Molecular Medicine Finland (FIMM) to examine how patient-derived leukemia cells responded to a large panel of drugs.
In this way, the group identified axitinib as a promising drug candidate for CML and ALL. Axitinib effectively eliminated drug-resistant leukemia cells.
The TKI inhibited BCR-ABL1 (T315I) at biochemical and cellular levels by binding to the active form of ABL1 (T315I) in a mutation-selective binding mode.
The researchers said this suggests the T315I mutation shifts the conformational equilibrium of the kinase in favor of an active (DFG-in) A-loop conformation, which has more optimal binding interactions with axitinib.
“If you think of the targeted protein as a lock into which the cancer drug fits in as a key, the resistant protein changes in such a way that we need a different key,” said study author Brion Murray, PhD, of Pfizer Worldwide Research & Development in San Diego, California.
“In the case of axitinib, it acts as two distinct keys—one for renal cell carcinoma and one for leukemia.”
The researchers also treated a CML patient with axitinib and observed a “rapid reduction” of T315I-positive cells in the patient’s bone marrow.
“Further research will determine whether these findings have the potential to significantly improve the standard of care for this select group of CML patients and patients with other related leukemias,” Dr Murray concluded.
Photo courtesy of CDC
New research indicates that a tyrosine kinase inhibitor (TKI) approved to treat advanced renal cell carcinoma could prove useful in treating patients with drug-resistant chronic myeloid leukemia (CML) or acute lymphoblastic leukemia (ALL).
The study showed that the TKI, axitinib, can inhibit BCR-ABL1 (T315I), a mutation known to confer drug resistance in CML and ALL.
“Since axitinib is already used to treat cancer, its safety is known,” said Kimmo Porkka, MD, PhD, of the University of Helsinki in Finland.
“[A] formal exploration of its clinical utility in drug-resistant leukemia can now be done in a fast-track mode. Thus, the normally very long path from lab bench to bedside is now significantly shortened.”
Dr Porkka and his colleagues described the newfound activity of axitinib in Nature.
The researchers used a drug sensitivity and resistance testing method developed at the University of Helsinki’s Institute for Molecular Medicine Finland (FIMM) to examine how patient-derived leukemia cells responded to a large panel of drugs.
In this way, the group identified axitinib as a promising drug candidate for CML and ALL. Axitinib effectively eliminated drug-resistant leukemia cells.
The TKI inhibited BCR-ABL1 (T315I) at biochemical and cellular levels by binding to the active form of ABL1 (T315I) in a mutation-selective binding mode.
The researchers said this suggests the T315I mutation shifts the conformational equilibrium of the kinase in favor of an active (DFG-in) A-loop conformation, which has more optimal binding interactions with axitinib.
“If you think of the targeted protein as a lock into which the cancer drug fits in as a key, the resistant protein changes in such a way that we need a different key,” said study author Brion Murray, PhD, of Pfizer Worldwide Research & Development in San Diego, California.
“In the case of axitinib, it acts as two distinct keys—one for renal cell carcinoma and one for leukemia.”
The researchers also treated a CML patient with axitinib and observed a “rapid reduction” of T315I-positive cells in the patient’s bone marrow.
“Further research will determine whether these findings have the potential to significantly improve the standard of care for this select group of CML patients and patients with other related leukemias,” Dr Murray concluded.