User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Complex surgery 10 times more likely with some ovarian tumors
according to a report at the Society of Gynecologic Oncology annual meeting.
Investigators found that women with those features, compared with those without them, are 10 times more likely to have a high-complexity surgery and almost 27 times more likely to have something other than a complete (RD0) resection.
The findings speak to a common dilemma in advanced ovarian cancer, whether women should have surgery or chemotherapy first. Part of the decision hinges on the likelihood of surgical success, explained lead investigator Diogo Torres, MD, a gynecologic oncologist at Ochsner Health in New Orleans.
He and his team concluded that “preoperative CT imaging combined with tumor molecular subtyping can identify a subset of women for whom successful primary surgery is unlikely. Preoperative tumor sampling may be useful in advanced [ovarian cancer] to better triage these cases to alternative approaches.”
For years “we’ve been trying to figure out” how best to make the call between primary debulking and neoadjuvant chemotherapy, said Pamela T. Soliman, MD, MPH,a gynecologic oncologist at the University of Texas MD Anderson Cancer Center, Houston, who discussed the abstract at the meeting.
Imaging alone or CA-125 are often used to make the decision, but they’re unreliable. Diagnostic laparoscopy is accurate, but it isn’t used much, she said.
What’s unique about Dr. Torres’s approach is that, by including tumor subtype, it incorporates tumor biology. It makes sense because his team previously found that women with mesenchymal (MES) tumors are more likely than those with other subtypes to have upper abdominal and miliary disease.
The approach needs validation in a larger study, but “I really commend” the team “for incorporating biology into the decision-making because it is clearly a step in the right direction,” Dr. Soliman said.
The study included 129 women who underwent primary debulking surgery for stage 3c or 4 high-grade serous ovarian cancer; 46x women (36%) had MES tumors according to RNA profiling of surgical specimens.
Preoperative CTs were reviewed to assess diaphragmatic disease; gastrohepatic/portahepatis lesions; root of superior mesenteric artery involvement; presence of moderate to severe ascites; intrahepatic lesions, and diffuse peritoneal thickening greater than 4 mm.
Fifty-nine women (46%) were classified as “CT high,” meaning that they had two or more of those findings. Women with no more than one were categorized as “CT low.”
Patients with MES tumors and CT-high disease had the lowest rates of complete resections, 8% versus 46% for the entire cohort and 72% for non-MES, CT-low women. MES, CT-high women were also the most likely to have high-complexity surgery (81% versus 35% in the non-MES, CT-low group).
Adjusting for age, stage, and American Society of Anesthesiologists score, the odds of high-complexity surgery were 9.53 times higher and the odds of something less than a complete resection were 26.73 times greater in MES, CT-high patients, compared with non-MES, CT-low women.
“Further studies are needed to evaluate and validate this model using preoperative biopsy specimens” instead of surgical specimens, the investigators said.
No funding was reported for the work. Dr. Torres didn’t have any disclosures. Dr. Soliman is an adviser for Eisai and Amgen, a consultant for Medscape, and receives research funding from Novartis and Incyte.
according to a report at the Society of Gynecologic Oncology annual meeting.
Investigators found that women with those features, compared with those without them, are 10 times more likely to have a high-complexity surgery and almost 27 times more likely to have something other than a complete (RD0) resection.
The findings speak to a common dilemma in advanced ovarian cancer, whether women should have surgery or chemotherapy first. Part of the decision hinges on the likelihood of surgical success, explained lead investigator Diogo Torres, MD, a gynecologic oncologist at Ochsner Health in New Orleans.
He and his team concluded that “preoperative CT imaging combined with tumor molecular subtyping can identify a subset of women for whom successful primary surgery is unlikely. Preoperative tumor sampling may be useful in advanced [ovarian cancer] to better triage these cases to alternative approaches.”
For years “we’ve been trying to figure out” how best to make the call between primary debulking and neoadjuvant chemotherapy, said Pamela T. Soliman, MD, MPH,a gynecologic oncologist at the University of Texas MD Anderson Cancer Center, Houston, who discussed the abstract at the meeting.
Imaging alone or CA-125 are often used to make the decision, but they’re unreliable. Diagnostic laparoscopy is accurate, but it isn’t used much, she said.
What’s unique about Dr. Torres’s approach is that, by including tumor subtype, it incorporates tumor biology. It makes sense because his team previously found that women with mesenchymal (MES) tumors are more likely than those with other subtypes to have upper abdominal and miliary disease.
The approach needs validation in a larger study, but “I really commend” the team “for incorporating biology into the decision-making because it is clearly a step in the right direction,” Dr. Soliman said.
The study included 129 women who underwent primary debulking surgery for stage 3c or 4 high-grade serous ovarian cancer; 46x women (36%) had MES tumors according to RNA profiling of surgical specimens.
Preoperative CTs were reviewed to assess diaphragmatic disease; gastrohepatic/portahepatis lesions; root of superior mesenteric artery involvement; presence of moderate to severe ascites; intrahepatic lesions, and diffuse peritoneal thickening greater than 4 mm.
Fifty-nine women (46%) were classified as “CT high,” meaning that they had two or more of those findings. Women with no more than one were categorized as “CT low.”
Patients with MES tumors and CT-high disease had the lowest rates of complete resections, 8% versus 46% for the entire cohort and 72% for non-MES, CT-low women. MES, CT-high women were also the most likely to have high-complexity surgery (81% versus 35% in the non-MES, CT-low group).
Adjusting for age, stage, and American Society of Anesthesiologists score, the odds of high-complexity surgery were 9.53 times higher and the odds of something less than a complete resection were 26.73 times greater in MES, CT-high patients, compared with non-MES, CT-low women.
“Further studies are needed to evaluate and validate this model using preoperative biopsy specimens” instead of surgical specimens, the investigators said.
No funding was reported for the work. Dr. Torres didn’t have any disclosures. Dr. Soliman is an adviser for Eisai and Amgen, a consultant for Medscape, and receives research funding from Novartis and Incyte.
according to a report at the Society of Gynecologic Oncology annual meeting.
Investigators found that women with those features, compared with those without them, are 10 times more likely to have a high-complexity surgery and almost 27 times more likely to have something other than a complete (RD0) resection.
The findings speak to a common dilemma in advanced ovarian cancer, whether women should have surgery or chemotherapy first. Part of the decision hinges on the likelihood of surgical success, explained lead investigator Diogo Torres, MD, a gynecologic oncologist at Ochsner Health in New Orleans.
He and his team concluded that “preoperative CT imaging combined with tumor molecular subtyping can identify a subset of women for whom successful primary surgery is unlikely. Preoperative tumor sampling may be useful in advanced [ovarian cancer] to better triage these cases to alternative approaches.”
For years “we’ve been trying to figure out” how best to make the call between primary debulking and neoadjuvant chemotherapy, said Pamela T. Soliman, MD, MPH,a gynecologic oncologist at the University of Texas MD Anderson Cancer Center, Houston, who discussed the abstract at the meeting.
Imaging alone or CA-125 are often used to make the decision, but they’re unreliable. Diagnostic laparoscopy is accurate, but it isn’t used much, she said.
What’s unique about Dr. Torres’s approach is that, by including tumor subtype, it incorporates tumor biology. It makes sense because his team previously found that women with mesenchymal (MES) tumors are more likely than those with other subtypes to have upper abdominal and miliary disease.
The approach needs validation in a larger study, but “I really commend” the team “for incorporating biology into the decision-making because it is clearly a step in the right direction,” Dr. Soliman said.
The study included 129 women who underwent primary debulking surgery for stage 3c or 4 high-grade serous ovarian cancer; 46x women (36%) had MES tumors according to RNA profiling of surgical specimens.
Preoperative CTs were reviewed to assess diaphragmatic disease; gastrohepatic/portahepatis lesions; root of superior mesenteric artery involvement; presence of moderate to severe ascites; intrahepatic lesions, and diffuse peritoneal thickening greater than 4 mm.
Fifty-nine women (46%) were classified as “CT high,” meaning that they had two or more of those findings. Women with no more than one were categorized as “CT low.”
Patients with MES tumors and CT-high disease had the lowest rates of complete resections, 8% versus 46% for the entire cohort and 72% for non-MES, CT-low women. MES, CT-high women were also the most likely to have high-complexity surgery (81% versus 35% in the non-MES, CT-low group).
Adjusting for age, stage, and American Society of Anesthesiologists score, the odds of high-complexity surgery were 9.53 times higher and the odds of something less than a complete resection were 26.73 times greater in MES, CT-high patients, compared with non-MES, CT-low women.
“Further studies are needed to evaluate and validate this model using preoperative biopsy specimens” instead of surgical specimens, the investigators said.
No funding was reported for the work. Dr. Torres didn’t have any disclosures. Dr. Soliman is an adviser for Eisai and Amgen, a consultant for Medscape, and receives research funding from Novartis and Incyte.
FROM SGO 2022
FDA approves new immunotherapy combo for metastatic melanoma
in adults and children 12 years or older, according to the drug’s manufacturer, Bristol-Myers Squibb.

Approval was based on the company’s RELATIVITY-047 trial, which found a median progression-free survival (PFS) of 10.1 months among 355 patients randomly assigned to the combination therapy compared with 4.6 months among 359 patients who received nivolumab alone (hazard ratio, 0.75; P = .0055).
In the combination therapy group, 18.9% of patients reported a grade 3/4 drug-related adverse event, compared with 9.7% in the nivolumab group; 14.6% of patients in the combination group had drug-related adverse events leading to discontinuation versus 6.7% of those receiving monotherapy, the company noted in a press release.
Relatlimab is the company’s third immune checkpoint inhibitor to reach the U.S. market, joining the PD-1 inhibitor nivolumab and the CTLA-4 blocker ipilimumab. Relatlimab targets LAG-3, a cell-surface receptor found on activated CD4+ T cells.
Nivolumab plus ipilimumab is currently the standard of care for previously untreated metastatic or inoperable melanoma. Both combinations produce similar PFS, but the incidence of grade 3/4 adverse events is higher with ipilimumab, according to a Jan. 6, 2022, editorial in the New England Journal of Medicine.
Musculoskeletal pain, fatigue, rash, pruritus, and diarrhea were the most common adverse reactions with combination nivolumab/relatlimab, occurring in 20% or more of RELATIVITY-047 trial participants.
Adrenal insufficiency, anemia, colitis, pneumonia, and myocardial infarction were the most frequent serious adverse reactions, but each occurred in less than 2% of patients. There were three fatal adverse events in the trial caused by hemophagocytic lymphohistiocytosis, acute lung edema, and pneumonitis.
The approved dosage is 480 mg nivolumab and 160 mg relatlimab administered intravenously every 4 weeks.
A version of this article first appeared on Medscape.com.
in adults and children 12 years or older, according to the drug’s manufacturer, Bristol-Myers Squibb.
Approval was based on the company’s RELATIVITY-047 trial, which found a median progression-free survival (PFS) of 10.1 months among 355 patients randomly assigned to the combination therapy compared with 4.6 months among 359 patients who received nivolumab alone (hazard ratio, 0.75; P = .0055).
In the combination therapy group, 18.9% of patients reported a grade 3/4 drug-related adverse event, compared with 9.7% in the nivolumab group; 14.6% of patients in the combination group had drug-related adverse events leading to discontinuation versus 6.7% of those receiving monotherapy, the company noted in a press release.
Relatlimab is the company’s third immune checkpoint inhibitor to reach the U.S. market, joining the PD-1 inhibitor nivolumab and the CTLA-4 blocker ipilimumab. Relatlimab targets LAG-3, a cell-surface receptor found on activated CD4+ T cells.
Nivolumab plus ipilimumab is currently the standard of care for previously untreated metastatic or inoperable melanoma. Both combinations produce similar PFS, but the incidence of grade 3/4 adverse events is higher with ipilimumab, according to a Jan. 6, 2022, editorial in the New England Journal of Medicine.
Musculoskeletal pain, fatigue, rash, pruritus, and diarrhea were the most common adverse reactions with combination nivolumab/relatlimab, occurring in 20% or more of RELATIVITY-047 trial participants.
Adrenal insufficiency, anemia, colitis, pneumonia, and myocardial infarction were the most frequent serious adverse reactions, but each occurred in less than 2% of patients. There were three fatal adverse events in the trial caused by hemophagocytic lymphohistiocytosis, acute lung edema, and pneumonitis.
The approved dosage is 480 mg nivolumab and 160 mg relatlimab administered intravenously every 4 weeks.
A version of this article first appeared on Medscape.com.
in adults and children 12 years or older, according to the drug’s manufacturer, Bristol-Myers Squibb.
Approval was based on the company’s RELATIVITY-047 trial, which found a median progression-free survival (PFS) of 10.1 months among 355 patients randomly assigned to the combination therapy compared with 4.6 months among 359 patients who received nivolumab alone (hazard ratio, 0.75; P = .0055).
In the combination therapy group, 18.9% of patients reported a grade 3/4 drug-related adverse event, compared with 9.7% in the nivolumab group; 14.6% of patients in the combination group had drug-related adverse events leading to discontinuation versus 6.7% of those receiving monotherapy, the company noted in a press release.
Relatlimab is the company’s third immune checkpoint inhibitor to reach the U.S. market, joining the PD-1 inhibitor nivolumab and the CTLA-4 blocker ipilimumab. Relatlimab targets LAG-3, a cell-surface receptor found on activated CD4+ T cells.
Nivolumab plus ipilimumab is currently the standard of care for previously untreated metastatic or inoperable melanoma. Both combinations produce similar PFS, but the incidence of grade 3/4 adverse events is higher with ipilimumab, according to a Jan. 6, 2022, editorial in the New England Journal of Medicine.
Musculoskeletal pain, fatigue, rash, pruritus, and diarrhea were the most common adverse reactions with combination nivolumab/relatlimab, occurring in 20% or more of RELATIVITY-047 trial participants.
Adrenal insufficiency, anemia, colitis, pneumonia, and myocardial infarction were the most frequent serious adverse reactions, but each occurred in less than 2% of patients. There were three fatal adverse events in the trial caused by hemophagocytic lymphohistiocytosis, acute lung edema, and pneumonitis.
The approved dosage is 480 mg nivolumab and 160 mg relatlimab administered intravenously every 4 weeks.
A version of this article first appeared on Medscape.com.
First-line CAR T-cell therapy could help cure some lymphomas
Results of the phase 2 ZUMA-12 trial suggest that axicabtagene ciloleucel (axi-cel), a chimeric antigen receptor (CAR) T-cell therapy approved to treat certain types of lymphoma, also shows promise as a treatment for another group of lymphoma patients – those with high-risk large B-cell lymphoma (LBCL) who failed two rounds of standard chemoimmunotherapy. In fact, a study author said, first-line treatment with this therapy could help usher some patients toward a cure.
The results appeared March 21, 2022, in Nature Medicine.
“The high efficacy with manageable safety profile suggest that further evaluation of axi-cel in first-line setting in patients with high-risk LBCL is warranted in a randomized, phase 3 trial comparing it to standard chemoimmunotherapy,” study lead author Sattva S. Neelapu, MD, of the University of Texas MD Anderson Cancer Center, Houston, said in an interview.
According to Dr. Neelapu, “patients with high-risk LBCL include those with high-intermediate or high International Prognostic Index score and those with certain molecular subtypes such as double- or triple-hit lymphoma. These patients have lower response rates and lower progression-free and overall survival with standard chemoimmunotherapy.”
Treatment of these patients can be especially challenging because they are underrepresented in clinical research, hematologist Michael Dickinson, MBBS, of the Peter MacCallum Cancer Center in Melbourne, said in an interview. “They often have disease that requires urgent treatment, so there is no time to recruit them into trials. A feature of ZUMA-12 is that it allowed patients to be recruited after short exposure to chemotherapy, which means that higher-risk patients could successfully be recruited into the trial.”
Axi-cel is already Food and Drug Administration approved for treatment of relapsed or refractory LBCL after 2 or more lines of systemic therapy plus relapsed or refractory follicular lymphoma, also after two or more lines of systemic therapy, Dr. Neelapu said.
For this study, researchers administered the treatment to 40 subjects with high-risk disease from 2019-2020 (median age, 61 years; 68% male; 95% at disease stage III or IV).
The researchers reported that 78% of 37 patients in the primary efficacy analysis reached complete response rate (95% confidence interval, 62-90); the median time to first complete response rate was 30 days (range, 27-207). About 89% of these subjects reached the secondary endpoint of objective response rate (95% CI, 75-97); the median time to first objective response was 29 days (range, 27-207).
At a median follow-up of 15.9 months, 73% were still in objective response.
“This is quite remarkable,” Dr. Neelapu said. “The durability of more than 70% is far higher than what would be expected with standard chemoimmunotherapy in these patients – under 40% durability with standard chemoimmunotherapy. Also, axi-cel induces durable responses in about 40% of patients in second- and third-line setting. However, when used as part of first-line therapy in this study, durable responses were observed in more than 70% of patients, suggesting that the efficacy of axi-cel may be much higher when used in first-line setting.”
Dr. Neelapu added: “Although the follow-up is short, it is highly likely that the majority of the patients with ongoing response beyond 1 year will likely be cured of their lymphoma.”
As for side effects, no treatment-related grade 5 events occurred, but 18 patients (45%) experienced serious adverse events. Grade 3 or higher cytokine release syndrome occurred in three patients (8%) and nine experienced neurologic events (23%).
“The majority of the higher-grade adverse events observed were due to cytopenias, which were expected due to the conditioning therapy,” Dr. Neelapu said. “Such cytopenias would also have been expected if these patients had received standard chemoimmunotherapy.”
Six patients (15%) died, 4 of progressive disease after going forward to other therapies.
As for cost, Dr. Neelapu said it should be similar to that of axi-cel as an FDA-approved third-line therapy. Axi-cel is highly expensive. Research has suggested that CAR T-cell therapy can boost costs beyond standard chemotherapy by $350,000-$490,000 with gains of 2-8 years of life (J Med Econ. Jan-Dec 2021;24[1]:458-68).
The study was funded by Kite. The authors reported various disclosures.
Results of the phase 2 ZUMA-12 trial suggest that axicabtagene ciloleucel (axi-cel), a chimeric antigen receptor (CAR) T-cell therapy approved to treat certain types of lymphoma, also shows promise as a treatment for another group of lymphoma patients – those with high-risk large B-cell lymphoma (LBCL) who failed two rounds of standard chemoimmunotherapy. In fact, a study author said, first-line treatment with this therapy could help usher some patients toward a cure.
The results appeared March 21, 2022, in Nature Medicine.
“The high efficacy with manageable safety profile suggest that further evaluation of axi-cel in first-line setting in patients with high-risk LBCL is warranted in a randomized, phase 3 trial comparing it to standard chemoimmunotherapy,” study lead author Sattva S. Neelapu, MD, of the University of Texas MD Anderson Cancer Center, Houston, said in an interview.
According to Dr. Neelapu, “patients with high-risk LBCL include those with high-intermediate or high International Prognostic Index score and those with certain molecular subtypes such as double- or triple-hit lymphoma. These patients have lower response rates and lower progression-free and overall survival with standard chemoimmunotherapy.”
Treatment of these patients can be especially challenging because they are underrepresented in clinical research, hematologist Michael Dickinson, MBBS, of the Peter MacCallum Cancer Center in Melbourne, said in an interview. “They often have disease that requires urgent treatment, so there is no time to recruit them into trials. A feature of ZUMA-12 is that it allowed patients to be recruited after short exposure to chemotherapy, which means that higher-risk patients could successfully be recruited into the trial.”
Axi-cel is already Food and Drug Administration approved for treatment of relapsed or refractory LBCL after 2 or more lines of systemic therapy plus relapsed or refractory follicular lymphoma, also after two or more lines of systemic therapy, Dr. Neelapu said.
For this study, researchers administered the treatment to 40 subjects with high-risk disease from 2019-2020 (median age, 61 years; 68% male; 95% at disease stage III or IV).
The researchers reported that 78% of 37 patients in the primary efficacy analysis reached complete response rate (95% confidence interval, 62-90); the median time to first complete response rate was 30 days (range, 27-207). About 89% of these subjects reached the secondary endpoint of objective response rate (95% CI, 75-97); the median time to first objective response was 29 days (range, 27-207).
At a median follow-up of 15.9 months, 73% were still in objective response.
“This is quite remarkable,” Dr. Neelapu said. “The durability of more than 70% is far higher than what would be expected with standard chemoimmunotherapy in these patients – under 40% durability with standard chemoimmunotherapy. Also, axi-cel induces durable responses in about 40% of patients in second- and third-line setting. However, when used as part of first-line therapy in this study, durable responses were observed in more than 70% of patients, suggesting that the efficacy of axi-cel may be much higher when used in first-line setting.”
Dr. Neelapu added: “Although the follow-up is short, it is highly likely that the majority of the patients with ongoing response beyond 1 year will likely be cured of their lymphoma.”
As for side effects, no treatment-related grade 5 events occurred, but 18 patients (45%) experienced serious adverse events. Grade 3 or higher cytokine release syndrome occurred in three patients (8%) and nine experienced neurologic events (23%).
“The majority of the higher-grade adverse events observed were due to cytopenias, which were expected due to the conditioning therapy,” Dr. Neelapu said. “Such cytopenias would also have been expected if these patients had received standard chemoimmunotherapy.”
Six patients (15%) died, 4 of progressive disease after going forward to other therapies.
As for cost, Dr. Neelapu said it should be similar to that of axi-cel as an FDA-approved third-line therapy. Axi-cel is highly expensive. Research has suggested that CAR T-cell therapy can boost costs beyond standard chemotherapy by $350,000-$490,000 with gains of 2-8 years of life (J Med Econ. Jan-Dec 2021;24[1]:458-68).
The study was funded by Kite. The authors reported various disclosures.
Results of the phase 2 ZUMA-12 trial suggest that axicabtagene ciloleucel (axi-cel), a chimeric antigen receptor (CAR) T-cell therapy approved to treat certain types of lymphoma, also shows promise as a treatment for another group of lymphoma patients – those with high-risk large B-cell lymphoma (LBCL) who failed two rounds of standard chemoimmunotherapy. In fact, a study author said, first-line treatment with this therapy could help usher some patients toward a cure.
The results appeared March 21, 2022, in Nature Medicine.
“The high efficacy with manageable safety profile suggest that further evaluation of axi-cel in first-line setting in patients with high-risk LBCL is warranted in a randomized, phase 3 trial comparing it to standard chemoimmunotherapy,” study lead author Sattva S. Neelapu, MD, of the University of Texas MD Anderson Cancer Center, Houston, said in an interview.
According to Dr. Neelapu, “patients with high-risk LBCL include those with high-intermediate or high International Prognostic Index score and those with certain molecular subtypes such as double- or triple-hit lymphoma. These patients have lower response rates and lower progression-free and overall survival with standard chemoimmunotherapy.”
Treatment of these patients can be especially challenging because they are underrepresented in clinical research, hematologist Michael Dickinson, MBBS, of the Peter MacCallum Cancer Center in Melbourne, said in an interview. “They often have disease that requires urgent treatment, so there is no time to recruit them into trials. A feature of ZUMA-12 is that it allowed patients to be recruited after short exposure to chemotherapy, which means that higher-risk patients could successfully be recruited into the trial.”
Axi-cel is already Food and Drug Administration approved for treatment of relapsed or refractory LBCL after 2 or more lines of systemic therapy plus relapsed or refractory follicular lymphoma, also after two or more lines of systemic therapy, Dr. Neelapu said.
For this study, researchers administered the treatment to 40 subjects with high-risk disease from 2019-2020 (median age, 61 years; 68% male; 95% at disease stage III or IV).
The researchers reported that 78% of 37 patients in the primary efficacy analysis reached complete response rate (95% confidence interval, 62-90); the median time to first complete response rate was 30 days (range, 27-207). About 89% of these subjects reached the secondary endpoint of objective response rate (95% CI, 75-97); the median time to first objective response was 29 days (range, 27-207).
At a median follow-up of 15.9 months, 73% were still in objective response.
“This is quite remarkable,” Dr. Neelapu said. “The durability of more than 70% is far higher than what would be expected with standard chemoimmunotherapy in these patients – under 40% durability with standard chemoimmunotherapy. Also, axi-cel induces durable responses in about 40% of patients in second- and third-line setting. However, when used as part of first-line therapy in this study, durable responses were observed in more than 70% of patients, suggesting that the efficacy of axi-cel may be much higher when used in first-line setting.”
Dr. Neelapu added: “Although the follow-up is short, it is highly likely that the majority of the patients with ongoing response beyond 1 year will likely be cured of their lymphoma.”
As for side effects, no treatment-related grade 5 events occurred, but 18 patients (45%) experienced serious adverse events. Grade 3 or higher cytokine release syndrome occurred in three patients (8%) and nine experienced neurologic events (23%).
“The majority of the higher-grade adverse events observed were due to cytopenias, which were expected due to the conditioning therapy,” Dr. Neelapu said. “Such cytopenias would also have been expected if these patients had received standard chemoimmunotherapy.”
Six patients (15%) died, 4 of progressive disease after going forward to other therapies.
As for cost, Dr. Neelapu said it should be similar to that of axi-cel as an FDA-approved third-line therapy. Axi-cel is highly expensive. Research has suggested that CAR T-cell therapy can boost costs beyond standard chemotherapy by $350,000-$490,000 with gains of 2-8 years of life (J Med Econ. Jan-Dec 2021;24[1]:458-68).
The study was funded by Kite. The authors reported various disclosures.
FROM NATURE MEDICINE
Eating olive oil may slow CLL disease progression
Olive oil is a major component of the Mediterranean diet, and olive phenols have been shown to convey antioxidant, anti-inflammatory, anticancer, neuroprotective, and antidiabetic effects by modulating various molecular pathways, Andrea Paola Rojas Gil, PhD, of the University of Peloponnese, Tripoli, Greece, and colleagues wrote.
In most patients, CLL is incurable, but those at the early stages do not need immediate therapy and may benefit from an intervention to prevent disease progression, the authors wrote. Previous research suggested that dietary intervention exerts a salutary effect on early CLL, and in vitro studies suggested that oleocanthal, a component of extra virgin olive oil, induced anticancer activity.
In a study published in Frontiers in Oncology, the researchers enrolled adults with early stage CLL who had not undergone chemotherapy or other treatment. All patients adhered to a Mediterranean-style diet.
After a washout period of 9-12 months, the researchers randomized 22 patients to extra virgin olive oil high in oleocanthal and oleacein (high OC/OL-EVOO). Patients in the intervention group consumed 40 mL/day of high OC/OL-EVOO before meals. Their average age was 71 years; 10 were women and 12 were men.
The primary outcomes included changes in hematological, biochemical, and apoptotic markers. After 6 months, patients in the intervention group showed a statistically significant reduction in white blood cells and lymphocyte count, compared with measurements taken 3 months before the intervention. The WBC decrease was greatest among patients with the highest WBC levels at baseline.
As for biochemical markers, the researchers observed a significant decrease in glucose levels during the intervention, but no significant effects on metabolic indexes or renal function.
After 3 months and also after 6 months of the olive oil intervention, patients showed a significant increase in the apoptotic markers ccK18 and Apo1-Fas (P ≤ .05 for both), as well as an increase in the cell cycle negative regulator p21. The dietary intervention also was associated with significant decreases in expression of the antiapoptotic protein survivin and in cyclin D, a positive cell cycle regulator protein.
Further, patients who had a high ccK18 level at baseline showed a significantly greater increase in ccK18 after the intervention, compared with those with lower ccK18 at baseline (P = .001).
Notably, “a negative correlation of the WBC at the end of the dietary intervention with the fluctuation of the protein expression of the apoptotic marker ccK18 (final – initial) was observed,” the researchers wrote in their discussion.
The study findings were limited by several factors including the small sample size, short intervention time, and pilot design, the researchers said. Other limitations include the possible effect of other unmeasured properties of olive oil.
However, the results reflect previous studies showing the benefits of a Mediterranean-type diet, and they represent the first clinical trial to indicate possible beneficial effects from oleocanthal and oleacein on the progression of CLL. Therefore, the authors concluded, the study is worthy of a large, multicenter trial.
Pilot data merit more research
In an interview, corresponding author Prokopios Magiatis, PhD, noted that CLL is “the most commonly diagnosed adult leukemia in Western countries and is responsible for about one in four cases of all leukemias.” CLL remains incurable in most patients, and ways to delay disease progression are needed.
“Oleocanthal is the active ingredient of early harvest olive oil with proven anticancer activities in vitro and in vivo,” Dr. Magiatis explained. “For this reason, it was a unique challenge to investigate the anticancer activity of this compound for the first time in humans through the dietary consumption of specifically selected olive oil.” He expressed surprise at the beneficial effects of high-oleocanthal olive oil, not only to the white blood cells, but also to glucose levels.
“It seems that oleocanthal can activate mechanisms related to the apoptosis of cancer cells, and also mechanisms related to blood glucose regulation without affecting any normal cells of the body,” he said. “All anticancer drugs usually have severe side effects, however the administration of 25 mg of oleocanthal through the dietary consumption of olive oil did not present any harmful effects for at least 6 months of everyday use.
“The addition of naturally produced high-oleocanthal olive oil in the diet of early-stage CLL patients at a dose of three tablespoons per day [40 mL] is a practice that may lower the cancerous white blood cells of the patients without any risk,” said Dr. Magiatis. “High-oleocanthal early-harvest olive oil has been consumed for centuries, and may be the key of longevity of several Mediterranean populations.
“In our study, the number of the white blood cells returned back to the number it was one year before the initiation of the study; this clearly shows that it could be a significant factor for the delay of the progress of the disease,” he said.
The current trial was a pilot study in one hospital with only 22 patients for 6 months, said Dr. Magiatis. “We are currently preparing the expansion of the study to other hospitals and other countries, and we aim to include at least 100 patients for at least 1 year, to validate the already-obtained beneficial results.”
The clinical trial is supported by the nonprofit organization World Olive Center for Health, he added.
The current study received no outside funding. The researchers had no financial conflicts to disclose.
Olive oil is a major component of the Mediterranean diet, and olive phenols have been shown to convey antioxidant, anti-inflammatory, anticancer, neuroprotective, and antidiabetic effects by modulating various molecular pathways, Andrea Paola Rojas Gil, PhD, of the University of Peloponnese, Tripoli, Greece, and colleagues wrote.
In most patients, CLL is incurable, but those at the early stages do not need immediate therapy and may benefit from an intervention to prevent disease progression, the authors wrote. Previous research suggested that dietary intervention exerts a salutary effect on early CLL, and in vitro studies suggested that oleocanthal, a component of extra virgin olive oil, induced anticancer activity.
In a study published in Frontiers in Oncology, the researchers enrolled adults with early stage CLL who had not undergone chemotherapy or other treatment. All patients adhered to a Mediterranean-style diet.
After a washout period of 9-12 months, the researchers randomized 22 patients to extra virgin olive oil high in oleocanthal and oleacein (high OC/OL-EVOO). Patients in the intervention group consumed 40 mL/day of high OC/OL-EVOO before meals. Their average age was 71 years; 10 were women and 12 were men.
The primary outcomes included changes in hematological, biochemical, and apoptotic markers. After 6 months, patients in the intervention group showed a statistically significant reduction in white blood cells and lymphocyte count, compared with measurements taken 3 months before the intervention. The WBC decrease was greatest among patients with the highest WBC levels at baseline.
As for biochemical markers, the researchers observed a significant decrease in glucose levels during the intervention, but no significant effects on metabolic indexes or renal function.
After 3 months and also after 6 months of the olive oil intervention, patients showed a significant increase in the apoptotic markers ccK18 and Apo1-Fas (P ≤ .05 for both), as well as an increase in the cell cycle negative regulator p21. The dietary intervention also was associated with significant decreases in expression of the antiapoptotic protein survivin and in cyclin D, a positive cell cycle regulator protein.
Further, patients who had a high ccK18 level at baseline showed a significantly greater increase in ccK18 after the intervention, compared with those with lower ccK18 at baseline (P = .001).
Notably, “a negative correlation of the WBC at the end of the dietary intervention with the fluctuation of the protein expression of the apoptotic marker ccK18 (final – initial) was observed,” the researchers wrote in their discussion.
The study findings were limited by several factors including the small sample size, short intervention time, and pilot design, the researchers said. Other limitations include the possible effect of other unmeasured properties of olive oil.
However, the results reflect previous studies showing the benefits of a Mediterranean-type diet, and they represent the first clinical trial to indicate possible beneficial effects from oleocanthal and oleacein on the progression of CLL. Therefore, the authors concluded, the study is worthy of a large, multicenter trial.
Pilot data merit more research
In an interview, corresponding author Prokopios Magiatis, PhD, noted that CLL is “the most commonly diagnosed adult leukemia in Western countries and is responsible for about one in four cases of all leukemias.” CLL remains incurable in most patients, and ways to delay disease progression are needed.
“Oleocanthal is the active ingredient of early harvest olive oil with proven anticancer activities in vitro and in vivo,” Dr. Magiatis explained. “For this reason, it was a unique challenge to investigate the anticancer activity of this compound for the first time in humans through the dietary consumption of specifically selected olive oil.” He expressed surprise at the beneficial effects of high-oleocanthal olive oil, not only to the white blood cells, but also to glucose levels.
“It seems that oleocanthal can activate mechanisms related to the apoptosis of cancer cells, and also mechanisms related to blood glucose regulation without affecting any normal cells of the body,” he said. “All anticancer drugs usually have severe side effects, however the administration of 25 mg of oleocanthal through the dietary consumption of olive oil did not present any harmful effects for at least 6 months of everyday use.
“The addition of naturally produced high-oleocanthal olive oil in the diet of early-stage CLL patients at a dose of three tablespoons per day [40 mL] is a practice that may lower the cancerous white blood cells of the patients without any risk,” said Dr. Magiatis. “High-oleocanthal early-harvest olive oil has been consumed for centuries, and may be the key of longevity of several Mediterranean populations.
“In our study, the number of the white blood cells returned back to the number it was one year before the initiation of the study; this clearly shows that it could be a significant factor for the delay of the progress of the disease,” he said.
The current trial was a pilot study in one hospital with only 22 patients for 6 months, said Dr. Magiatis. “We are currently preparing the expansion of the study to other hospitals and other countries, and we aim to include at least 100 patients for at least 1 year, to validate the already-obtained beneficial results.”
The clinical trial is supported by the nonprofit organization World Olive Center for Health, he added.
The current study received no outside funding. The researchers had no financial conflicts to disclose.
Olive oil is a major component of the Mediterranean diet, and olive phenols have been shown to convey antioxidant, anti-inflammatory, anticancer, neuroprotective, and antidiabetic effects by modulating various molecular pathways, Andrea Paola Rojas Gil, PhD, of the University of Peloponnese, Tripoli, Greece, and colleagues wrote.
In most patients, CLL is incurable, but those at the early stages do not need immediate therapy and may benefit from an intervention to prevent disease progression, the authors wrote. Previous research suggested that dietary intervention exerts a salutary effect on early CLL, and in vitro studies suggested that oleocanthal, a component of extra virgin olive oil, induced anticancer activity.
In a study published in Frontiers in Oncology, the researchers enrolled adults with early stage CLL who had not undergone chemotherapy or other treatment. All patients adhered to a Mediterranean-style diet.
After a washout period of 9-12 months, the researchers randomized 22 patients to extra virgin olive oil high in oleocanthal and oleacein (high OC/OL-EVOO). Patients in the intervention group consumed 40 mL/day of high OC/OL-EVOO before meals. Their average age was 71 years; 10 were women and 12 were men.
The primary outcomes included changes in hematological, biochemical, and apoptotic markers. After 6 months, patients in the intervention group showed a statistically significant reduction in white blood cells and lymphocyte count, compared with measurements taken 3 months before the intervention. The WBC decrease was greatest among patients with the highest WBC levels at baseline.
As for biochemical markers, the researchers observed a significant decrease in glucose levels during the intervention, but no significant effects on metabolic indexes or renal function.
After 3 months and also after 6 months of the olive oil intervention, patients showed a significant increase in the apoptotic markers ccK18 and Apo1-Fas (P ≤ .05 for both), as well as an increase in the cell cycle negative regulator p21. The dietary intervention also was associated with significant decreases in expression of the antiapoptotic protein survivin and in cyclin D, a positive cell cycle regulator protein.
Further, patients who had a high ccK18 level at baseline showed a significantly greater increase in ccK18 after the intervention, compared with those with lower ccK18 at baseline (P = .001).
Notably, “a negative correlation of the WBC at the end of the dietary intervention with the fluctuation of the protein expression of the apoptotic marker ccK18 (final – initial) was observed,” the researchers wrote in their discussion.
The study findings were limited by several factors including the small sample size, short intervention time, and pilot design, the researchers said. Other limitations include the possible effect of other unmeasured properties of olive oil.
However, the results reflect previous studies showing the benefits of a Mediterranean-type diet, and they represent the first clinical trial to indicate possible beneficial effects from oleocanthal and oleacein on the progression of CLL. Therefore, the authors concluded, the study is worthy of a large, multicenter trial.
Pilot data merit more research
In an interview, corresponding author Prokopios Magiatis, PhD, noted that CLL is “the most commonly diagnosed adult leukemia in Western countries and is responsible for about one in four cases of all leukemias.” CLL remains incurable in most patients, and ways to delay disease progression are needed.
“Oleocanthal is the active ingredient of early harvest olive oil with proven anticancer activities in vitro and in vivo,” Dr. Magiatis explained. “For this reason, it was a unique challenge to investigate the anticancer activity of this compound for the first time in humans through the dietary consumption of specifically selected olive oil.” He expressed surprise at the beneficial effects of high-oleocanthal olive oil, not only to the white blood cells, but also to glucose levels.
“It seems that oleocanthal can activate mechanisms related to the apoptosis of cancer cells, and also mechanisms related to blood glucose regulation without affecting any normal cells of the body,” he said. “All anticancer drugs usually have severe side effects, however the administration of 25 mg of oleocanthal through the dietary consumption of olive oil did not present any harmful effects for at least 6 months of everyday use.
“The addition of naturally produced high-oleocanthal olive oil in the diet of early-stage CLL patients at a dose of three tablespoons per day [40 mL] is a practice that may lower the cancerous white blood cells of the patients without any risk,” said Dr. Magiatis. “High-oleocanthal early-harvest olive oil has been consumed for centuries, and may be the key of longevity of several Mediterranean populations.
“In our study, the number of the white blood cells returned back to the number it was one year before the initiation of the study; this clearly shows that it could be a significant factor for the delay of the progress of the disease,” he said.
The current trial was a pilot study in one hospital with only 22 patients for 6 months, said Dr. Magiatis. “We are currently preparing the expansion of the study to other hospitals and other countries, and we aim to include at least 100 patients for at least 1 year, to validate the already-obtained beneficial results.”
The clinical trial is supported by the nonprofit organization World Olive Center for Health, he added.
The current study received no outside funding. The researchers had no financial conflicts to disclose.
FROM FRONTIERS IN ONCOLOGY
Adverse skin effects of cancer immunotherapy reviewed
Immune checkpoint inhibitors (ICIs) have unquestionably revolutionized the care of patients with malignant melanoma, non-small cell lung cancer, and other types of cancer.
, according to members of a European Academy of Dermatology and Venereology (EADV) task force.
“The desirable, immune-mediated oncologic response is often achieved at the cost of immune-related adverse events (irAEs) that may potentially affect any organ system,” they write in a position statement on the management of ICI-derived dermatologic adverse events.
Recommendations from the EADV “Dermatology for Cancer Patients” task force have been published in the Journal of the European Academy of Dermatology and Venereology.
Task force members developed the recommendations based on clinical experience from published data and came up with specific recommendations for treating cutaneous toxicities associated with dermatologic immune-related adverse events (dirAEs) that occur in patients receiving immunotherapy with an ICI.
ICIs include the cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4) inhibitor ipilimumab (Yervoy, Bristol Myers Squibb), and inhibitors of programmed death protein 1 (PD-1) and its ligand (PD-L1), including nivolumab (Opdivo, Bristol Myers Squibb), pembrolizumab (Keytruda, Merck), and other agents.
“The basic principle of management is that the interventions should be tailored to serve the equilibrium between patients’ relief from the symptoms and signs of skin toxicity and the preservation of an unimpeded oncologic treatment,” they write.
The recommendations are in line with those included in a 2021 update of the American Society of Clinical Oncology (ASCO) guidelines on the management of irAEs in patients treated with ICIs across the whole range of organ systems, said Milan J. Anadkat, MD, professor of dermatology and director of dermatology clinical trials at Washington University School of Medicine, St. Louis. Dr. Anadkat was a coauthor of the ASCO guideline update.
Although the European recommendations focus only on dermatologic side effects of ICIs in patients with cancer, “that doesn’t diminish their importance. They do a good job of summarizing how to approach and how to manage it depending on the severity of the toxicities and the various types of toxicities,” he told this news organization.
Having a paper focused exclusively on the dermatologic side effects of ICIs allows the inclusion of photographs that can help clinicians identify specific conditions that may require referral to a dermatologist, he said.
Both Dr. Anadkat and the authors of the European recommendations noted that dermatologic irAEs are more common with CTLA-4 inhibition than with PD-1/PD-L1 inhibition.
“It has to do with where the target is,” Dr. Anadkat said. “CTLA-4 inhibition works on a central aspect of the immune system, so it’s a much less specific site, whereas PD-1 affects an interaction at the site of the tumor cell itself, so it’s a little more specific.”
Pruritus
ICI-induced pruritus can occur without apparent skin changes, they write, noting that in a recent study of patients with dirAEs, about one-third had isolated pruritus.
The task force members cite a meta-analysis indicating a pruritus incidence of 13.2% for patients treated with nivolumab and 20.2% for patients treated with pembrolizumab but respective grade 3 pruritus rates of only 0.5% and 2.3%. The reported incidence of pruritus with ipilimumab was 47% in a different study.
Recommended treatments include topical moisturizers with or without medium-to-high potency corticosteroids for grade 1 reactions, non-sedating histamines and/or GABA agonists such as pregabalin, or gabapentin for grade 2 pruritus, and suspension of ICIs until pruritus improves in patients with grade 3 pruritus.
Maculopapular rash
Maculopapular or eczema-like rashes may occur in up to 68% of patients who receive a CTLA-4 inhibitor and up to 20% of those who receive a PD1/PD-L1 inhibitor, the authors note. Rashes commonly appear within 3-6 weeks of initiating therapy.
“The clinical presentation is nonspecific and consists of a rapid onset of multiple minimally scaly, erythematous macules and papules, congregating into plaques. Lesions are mostly located on trunk and extensor surfaces of the extremities and the face is generally spared,” they write.
Maculopapular rashes are typically accompanied by itching but could be asymptomatic, they noted.
Mild (grade 1) rashes may respond to moisturizers and topical potent or super-potent corticosteroids. Patients with grade 2 rash should also receive oral antihistamines. Systemic corticosteroids may be considered for patients with grade 3 rashes but only after other dirAEs that may require specific management, such as psoriasis, are ruled out.
Psoriasis-like rash
The most common form of psoriasis seen in patients treated with ICIs is psoriasis vulgaris with plaques, but other clinical variants are also seen, the authors note.
“Topical agents (corticosteroids, Vitamin D analogues) are prescribed in Grades 1/2 and supplementary” to systemic treatment for patients with grade 3 or recalcitrant lesions, they write. “If skin-directed therapies fail to provide symptomatic control,” systemic treatment and narrow band UVB phototherapy “should be considered,” they add.
Evidence regarding the use of systemic therapies to treat psoriasis-like rash associated with ICIs is sparse. Acitretin can be safely used in patients with cancer. Low-dose methotrexate is also safe to use except in patients with non-melanoma skin cancers. Cyclosporine, however, should be avoided because of the potential for tumor-promoting effects, they emphasized.
The recommendations also cover treatment of lichen planus-like and vitiligo-like rashes, as well as hair and nail changes, autoimmune bullous disorders, and oral mucosal dirAEs.
In addition, the recommendations cover severe cutaneous adverse reactions as well as serious, potentially life-threatening dirAEs, including Stevens-Johnson syndrome/TEN, acute generalized exanthematous pustulosis (AGEP), and drug reaction with eosinophilia and systemic symptoms/drug-induced hypersensitivity syndrome (DRESS/DIHS).
“The dose of corticosteroids may be adapted to the severity of DRESS. The therapeutic benefit of systemic corticosteroids in the management of SJS/TEN remains controversial, and some authors favor treatment with cyclosporine. However, the use of corticosteroids in this context of ICI treatment appears reasonable and should be proposed. Short courses of steroids seem also effective in AGEP,” the task force members write.
The recommendations did not have outside funding. Of the 19 authors, 6 disclosed relationships with various pharmaceutical companies, including AbbVie, Leo Pharma, Boehringer Ingelheim, Bristol Myers Squibb, and/or Janssen. Dr. Anadkat disclosed previous relationships with Merck, Bristol Myers Squibb, and current relationships with others.
A version of this article first appeared on Medscape.com.
Immune checkpoint inhibitors (ICIs) have unquestionably revolutionized the care of patients with malignant melanoma, non-small cell lung cancer, and other types of cancer.
, according to members of a European Academy of Dermatology and Venereology (EADV) task force.
“The desirable, immune-mediated oncologic response is often achieved at the cost of immune-related adverse events (irAEs) that may potentially affect any organ system,” they write in a position statement on the management of ICI-derived dermatologic adverse events.
Recommendations from the EADV “Dermatology for Cancer Patients” task force have been published in the Journal of the European Academy of Dermatology and Venereology.
Task force members developed the recommendations based on clinical experience from published data and came up with specific recommendations for treating cutaneous toxicities associated with dermatologic immune-related adverse events (dirAEs) that occur in patients receiving immunotherapy with an ICI.
ICIs include the cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4) inhibitor ipilimumab (Yervoy, Bristol Myers Squibb), and inhibitors of programmed death protein 1 (PD-1) and its ligand (PD-L1), including nivolumab (Opdivo, Bristol Myers Squibb), pembrolizumab (Keytruda, Merck), and other agents.
“The basic principle of management is that the interventions should be tailored to serve the equilibrium between patients’ relief from the symptoms and signs of skin toxicity and the preservation of an unimpeded oncologic treatment,” they write.
The recommendations are in line with those included in a 2021 update of the American Society of Clinical Oncology (ASCO) guidelines on the management of irAEs in patients treated with ICIs across the whole range of organ systems, said Milan J. Anadkat, MD, professor of dermatology and director of dermatology clinical trials at Washington University School of Medicine, St. Louis. Dr. Anadkat was a coauthor of the ASCO guideline update.
Although the European recommendations focus only on dermatologic side effects of ICIs in patients with cancer, “that doesn’t diminish their importance. They do a good job of summarizing how to approach and how to manage it depending on the severity of the toxicities and the various types of toxicities,” he told this news organization.
Having a paper focused exclusively on the dermatologic side effects of ICIs allows the inclusion of photographs that can help clinicians identify specific conditions that may require referral to a dermatologist, he said.
Both Dr. Anadkat and the authors of the European recommendations noted that dermatologic irAEs are more common with CTLA-4 inhibition than with PD-1/PD-L1 inhibition.
“It has to do with where the target is,” Dr. Anadkat said. “CTLA-4 inhibition works on a central aspect of the immune system, so it’s a much less specific site, whereas PD-1 affects an interaction at the site of the tumor cell itself, so it’s a little more specific.”
Pruritus
ICI-induced pruritus can occur without apparent skin changes, they write, noting that in a recent study of patients with dirAEs, about one-third had isolated pruritus.
The task force members cite a meta-analysis indicating a pruritus incidence of 13.2% for patients treated with nivolumab and 20.2% for patients treated with pembrolizumab but respective grade 3 pruritus rates of only 0.5% and 2.3%. The reported incidence of pruritus with ipilimumab was 47% in a different study.
Recommended treatments include topical moisturizers with or without medium-to-high potency corticosteroids for grade 1 reactions, non-sedating histamines and/or GABA agonists such as pregabalin, or gabapentin for grade 2 pruritus, and suspension of ICIs until pruritus improves in patients with grade 3 pruritus.
Maculopapular rash
Maculopapular or eczema-like rashes may occur in up to 68% of patients who receive a CTLA-4 inhibitor and up to 20% of those who receive a PD1/PD-L1 inhibitor, the authors note. Rashes commonly appear within 3-6 weeks of initiating therapy.
“The clinical presentation is nonspecific and consists of a rapid onset of multiple minimally scaly, erythematous macules and papules, congregating into plaques. Lesions are mostly located on trunk and extensor surfaces of the extremities and the face is generally spared,” they write.
Maculopapular rashes are typically accompanied by itching but could be asymptomatic, they noted.
Mild (grade 1) rashes may respond to moisturizers and topical potent or super-potent corticosteroids. Patients with grade 2 rash should also receive oral antihistamines. Systemic corticosteroids may be considered for patients with grade 3 rashes but only after other dirAEs that may require specific management, such as psoriasis, are ruled out.
Psoriasis-like rash
The most common form of psoriasis seen in patients treated with ICIs is psoriasis vulgaris with plaques, but other clinical variants are also seen, the authors note.
“Topical agents (corticosteroids, Vitamin D analogues) are prescribed in Grades 1/2 and supplementary” to systemic treatment for patients with grade 3 or recalcitrant lesions, they write. “If skin-directed therapies fail to provide symptomatic control,” systemic treatment and narrow band UVB phototherapy “should be considered,” they add.
Evidence regarding the use of systemic therapies to treat psoriasis-like rash associated with ICIs is sparse. Acitretin can be safely used in patients with cancer. Low-dose methotrexate is also safe to use except in patients with non-melanoma skin cancers. Cyclosporine, however, should be avoided because of the potential for tumor-promoting effects, they emphasized.
The recommendations also cover treatment of lichen planus-like and vitiligo-like rashes, as well as hair and nail changes, autoimmune bullous disorders, and oral mucosal dirAEs.
In addition, the recommendations cover severe cutaneous adverse reactions as well as serious, potentially life-threatening dirAEs, including Stevens-Johnson syndrome/TEN, acute generalized exanthematous pustulosis (AGEP), and drug reaction with eosinophilia and systemic symptoms/drug-induced hypersensitivity syndrome (DRESS/DIHS).
“The dose of corticosteroids may be adapted to the severity of DRESS. The therapeutic benefit of systemic corticosteroids in the management of SJS/TEN remains controversial, and some authors favor treatment with cyclosporine. However, the use of corticosteroids in this context of ICI treatment appears reasonable and should be proposed. Short courses of steroids seem also effective in AGEP,” the task force members write.
The recommendations did not have outside funding. Of the 19 authors, 6 disclosed relationships with various pharmaceutical companies, including AbbVie, Leo Pharma, Boehringer Ingelheim, Bristol Myers Squibb, and/or Janssen. Dr. Anadkat disclosed previous relationships with Merck, Bristol Myers Squibb, and current relationships with others.
A version of this article first appeared on Medscape.com.
Immune checkpoint inhibitors (ICIs) have unquestionably revolutionized the care of patients with malignant melanoma, non-small cell lung cancer, and other types of cancer.
, according to members of a European Academy of Dermatology and Venereology (EADV) task force.
“The desirable, immune-mediated oncologic response is often achieved at the cost of immune-related adverse events (irAEs) that may potentially affect any organ system,” they write in a position statement on the management of ICI-derived dermatologic adverse events.
Recommendations from the EADV “Dermatology for Cancer Patients” task force have been published in the Journal of the European Academy of Dermatology and Venereology.
Task force members developed the recommendations based on clinical experience from published data and came up with specific recommendations for treating cutaneous toxicities associated with dermatologic immune-related adverse events (dirAEs) that occur in patients receiving immunotherapy with an ICI.
ICIs include the cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4) inhibitor ipilimumab (Yervoy, Bristol Myers Squibb), and inhibitors of programmed death protein 1 (PD-1) and its ligand (PD-L1), including nivolumab (Opdivo, Bristol Myers Squibb), pembrolizumab (Keytruda, Merck), and other agents.
“The basic principle of management is that the interventions should be tailored to serve the equilibrium between patients’ relief from the symptoms and signs of skin toxicity and the preservation of an unimpeded oncologic treatment,” they write.
The recommendations are in line with those included in a 2021 update of the American Society of Clinical Oncology (ASCO) guidelines on the management of irAEs in patients treated with ICIs across the whole range of organ systems, said Milan J. Anadkat, MD, professor of dermatology and director of dermatology clinical trials at Washington University School of Medicine, St. Louis. Dr. Anadkat was a coauthor of the ASCO guideline update.
Although the European recommendations focus only on dermatologic side effects of ICIs in patients with cancer, “that doesn’t diminish their importance. They do a good job of summarizing how to approach and how to manage it depending on the severity of the toxicities and the various types of toxicities,” he told this news organization.
Having a paper focused exclusively on the dermatologic side effects of ICIs allows the inclusion of photographs that can help clinicians identify specific conditions that may require referral to a dermatologist, he said.
Both Dr. Anadkat and the authors of the European recommendations noted that dermatologic irAEs are more common with CTLA-4 inhibition than with PD-1/PD-L1 inhibition.
“It has to do with where the target is,” Dr. Anadkat said. “CTLA-4 inhibition works on a central aspect of the immune system, so it’s a much less specific site, whereas PD-1 affects an interaction at the site of the tumor cell itself, so it’s a little more specific.”
Pruritus
ICI-induced pruritus can occur without apparent skin changes, they write, noting that in a recent study of patients with dirAEs, about one-third had isolated pruritus.
The task force members cite a meta-analysis indicating a pruritus incidence of 13.2% for patients treated with nivolumab and 20.2% for patients treated with pembrolizumab but respective grade 3 pruritus rates of only 0.5% and 2.3%. The reported incidence of pruritus with ipilimumab was 47% in a different study.
Recommended treatments include topical moisturizers with or without medium-to-high potency corticosteroids for grade 1 reactions, non-sedating histamines and/or GABA agonists such as pregabalin, or gabapentin for grade 2 pruritus, and suspension of ICIs until pruritus improves in patients with grade 3 pruritus.
Maculopapular rash
Maculopapular or eczema-like rashes may occur in up to 68% of patients who receive a CTLA-4 inhibitor and up to 20% of those who receive a PD1/PD-L1 inhibitor, the authors note. Rashes commonly appear within 3-6 weeks of initiating therapy.
“The clinical presentation is nonspecific and consists of a rapid onset of multiple minimally scaly, erythematous macules and papules, congregating into plaques. Lesions are mostly located on trunk and extensor surfaces of the extremities and the face is generally spared,” they write.
Maculopapular rashes are typically accompanied by itching but could be asymptomatic, they noted.
Mild (grade 1) rashes may respond to moisturizers and topical potent or super-potent corticosteroids. Patients with grade 2 rash should also receive oral antihistamines. Systemic corticosteroids may be considered for patients with grade 3 rashes but only after other dirAEs that may require specific management, such as psoriasis, are ruled out.
Psoriasis-like rash
The most common form of psoriasis seen in patients treated with ICIs is psoriasis vulgaris with plaques, but other clinical variants are also seen, the authors note.
“Topical agents (corticosteroids, Vitamin D analogues) are prescribed in Grades 1/2 and supplementary” to systemic treatment for patients with grade 3 or recalcitrant lesions, they write. “If skin-directed therapies fail to provide symptomatic control,” systemic treatment and narrow band UVB phototherapy “should be considered,” they add.
Evidence regarding the use of systemic therapies to treat psoriasis-like rash associated with ICIs is sparse. Acitretin can be safely used in patients with cancer. Low-dose methotrexate is also safe to use except in patients with non-melanoma skin cancers. Cyclosporine, however, should be avoided because of the potential for tumor-promoting effects, they emphasized.
The recommendations also cover treatment of lichen planus-like and vitiligo-like rashes, as well as hair and nail changes, autoimmune bullous disorders, and oral mucosal dirAEs.
In addition, the recommendations cover severe cutaneous adverse reactions as well as serious, potentially life-threatening dirAEs, including Stevens-Johnson syndrome/TEN, acute generalized exanthematous pustulosis (AGEP), and drug reaction with eosinophilia and systemic symptoms/drug-induced hypersensitivity syndrome (DRESS/DIHS).
“The dose of corticosteroids may be adapted to the severity of DRESS. The therapeutic benefit of systemic corticosteroids in the management of SJS/TEN remains controversial, and some authors favor treatment with cyclosporine. However, the use of corticosteroids in this context of ICI treatment appears reasonable and should be proposed. Short courses of steroids seem also effective in AGEP,” the task force members write.
The recommendations did not have outside funding. Of the 19 authors, 6 disclosed relationships with various pharmaceutical companies, including AbbVie, Leo Pharma, Boehringer Ingelheim, Bristol Myers Squibb, and/or Janssen. Dr. Anadkat disclosed previous relationships with Merck, Bristol Myers Squibb, and current relationships with others.
A version of this article first appeared on Medscape.com.
Untargeted CT scans leads to overdiagnoses in lung cancer
Such overdiagnosis was illustrated in a recent study from JAMA Internal Medicine of women in Taiwan who were screened for lung cancer using low-dose CT (LDCT).
The study, and the accompanying editorial, pointed out the potential for large databases of routine clinical data to track long-term outcomes, and potentially identify patient subgroups that could benefit from early diagnosis using digital technologies.
The Taiwanese findings echo a similar trend identified in a 2018 post hoc analysis of the Danish Lung Cancer Screening Trial, which estimated that 67.2% of cancers found during that CT screening program for current or former smokers were overdiagnosed. The authors recommended that researchers report rates of overdiagnosis in future screening studies.
The authors of the Taiwan study noted that LDCT is low cost and is frequently offered to individuals who are not considered at high risk of lung cancer, and advertisements in Taiwan often target women, who rarely smoke. The researchers examined data from the Taiwan National Cancer Registry. They looked for evidence of an increased incidence of early-stage detection and reduced incidence of late-stage diagnosis. They found that, from 2004 to 2018, there was an increase of lung cancer incidence from 2.3 to 14.4 per 100,000 (difference, 12.1; 95% confidence interval, 11.3-12.8), but no significant difference in the incidence of late-stage disease (from 18.7 to 19.3 per 100,000; difference, 0.6; 95% CI, –0.5 to 1.7).
“This combination of findings, an additional 12.1 early-stage cancers per 100,000 population and no reduction in late-stage cancers, is strongly suggestive of overdiagnosis,” the authors wrote.
It can be difficult to convince people of the potential harms of overdiagnosis, especially when patients have a nodule removed and remain healthy years later. “It’s very counterintuitive, but it’s a reality, and I think this paper paints the reality very, very clearly,” said Daniel Capurro, MD, PhD, deputy director of the Centre for the Digital Transformation of Health at University of Melbourne, and an author of the editorial.
The issue is that some lung cancers progress so slowly that they may never cause a problem clinically, and their removal can lead to unnecessary cost and risk. And it’s not just cancer. “There are a bunch of other conditions that are defined by specific criteria, but we don’t add the prognosis to that definition. At the individual patient level, we don’t know the prognosis,” Dr. Capurro said.
Dr. Capurro discussed the increasing use of digital technologies like smartphone apps. Machine learning can potentially use such data to diagnose conditions like sleep or mood disorders before they become clinically significant, allowing earlier intervention, but they could also lead to overdiagnosis. Dr. Capurro proposed using longitudinal databases to track patient outcomes, which could be applied to digital screening technologies.
“You might be able to find unknown patterns that help discriminate between these pathological definitions. You should be able to train (digital screens) with the pathological definition plus the disease trajectory as a way to improve that label,” he said.
The study was funded by the Taiwan Ministry of Health and Welfare Clinical Trial Center.
Such overdiagnosis was illustrated in a recent study from JAMA Internal Medicine of women in Taiwan who were screened for lung cancer using low-dose CT (LDCT).
The study, and the accompanying editorial, pointed out the potential for large databases of routine clinical data to track long-term outcomes, and potentially identify patient subgroups that could benefit from early diagnosis using digital technologies.
The Taiwanese findings echo a similar trend identified in a 2018 post hoc analysis of the Danish Lung Cancer Screening Trial, which estimated that 67.2% of cancers found during that CT screening program for current or former smokers were overdiagnosed. The authors recommended that researchers report rates of overdiagnosis in future screening studies.
The authors of the Taiwan study noted that LDCT is low cost and is frequently offered to individuals who are not considered at high risk of lung cancer, and advertisements in Taiwan often target women, who rarely smoke. The researchers examined data from the Taiwan National Cancer Registry. They looked for evidence of an increased incidence of early-stage detection and reduced incidence of late-stage diagnosis. They found that, from 2004 to 2018, there was an increase of lung cancer incidence from 2.3 to 14.4 per 100,000 (difference, 12.1; 95% confidence interval, 11.3-12.8), but no significant difference in the incidence of late-stage disease (from 18.7 to 19.3 per 100,000; difference, 0.6; 95% CI, –0.5 to 1.7).
“This combination of findings, an additional 12.1 early-stage cancers per 100,000 population and no reduction in late-stage cancers, is strongly suggestive of overdiagnosis,” the authors wrote.
It can be difficult to convince people of the potential harms of overdiagnosis, especially when patients have a nodule removed and remain healthy years later. “It’s very counterintuitive, but it’s a reality, and I think this paper paints the reality very, very clearly,” said Daniel Capurro, MD, PhD, deputy director of the Centre for the Digital Transformation of Health at University of Melbourne, and an author of the editorial.
The issue is that some lung cancers progress so slowly that they may never cause a problem clinically, and their removal can lead to unnecessary cost and risk. And it’s not just cancer. “There are a bunch of other conditions that are defined by specific criteria, but we don’t add the prognosis to that definition. At the individual patient level, we don’t know the prognosis,” Dr. Capurro said.
Dr. Capurro discussed the increasing use of digital technologies like smartphone apps. Machine learning can potentially use such data to diagnose conditions like sleep or mood disorders before they become clinically significant, allowing earlier intervention, but they could also lead to overdiagnosis. Dr. Capurro proposed using longitudinal databases to track patient outcomes, which could be applied to digital screening technologies.
“You might be able to find unknown patterns that help discriminate between these pathological definitions. You should be able to train (digital screens) with the pathological definition plus the disease trajectory as a way to improve that label,” he said.
The study was funded by the Taiwan Ministry of Health and Welfare Clinical Trial Center.
Such overdiagnosis was illustrated in a recent study from JAMA Internal Medicine of women in Taiwan who were screened for lung cancer using low-dose CT (LDCT).
The study, and the accompanying editorial, pointed out the potential for large databases of routine clinical data to track long-term outcomes, and potentially identify patient subgroups that could benefit from early diagnosis using digital technologies.
The Taiwanese findings echo a similar trend identified in a 2018 post hoc analysis of the Danish Lung Cancer Screening Trial, which estimated that 67.2% of cancers found during that CT screening program for current or former smokers were overdiagnosed. The authors recommended that researchers report rates of overdiagnosis in future screening studies.
The authors of the Taiwan study noted that LDCT is low cost and is frequently offered to individuals who are not considered at high risk of lung cancer, and advertisements in Taiwan often target women, who rarely smoke. The researchers examined data from the Taiwan National Cancer Registry. They looked for evidence of an increased incidence of early-stage detection and reduced incidence of late-stage diagnosis. They found that, from 2004 to 2018, there was an increase of lung cancer incidence from 2.3 to 14.4 per 100,000 (difference, 12.1; 95% confidence interval, 11.3-12.8), but no significant difference in the incidence of late-stage disease (from 18.7 to 19.3 per 100,000; difference, 0.6; 95% CI, –0.5 to 1.7).
“This combination of findings, an additional 12.1 early-stage cancers per 100,000 population and no reduction in late-stage cancers, is strongly suggestive of overdiagnosis,” the authors wrote.
It can be difficult to convince people of the potential harms of overdiagnosis, especially when patients have a nodule removed and remain healthy years later. “It’s very counterintuitive, but it’s a reality, and I think this paper paints the reality very, very clearly,” said Daniel Capurro, MD, PhD, deputy director of the Centre for the Digital Transformation of Health at University of Melbourne, and an author of the editorial.
The issue is that some lung cancers progress so slowly that they may never cause a problem clinically, and their removal can lead to unnecessary cost and risk. And it’s not just cancer. “There are a bunch of other conditions that are defined by specific criteria, but we don’t add the prognosis to that definition. At the individual patient level, we don’t know the prognosis,” Dr. Capurro said.
Dr. Capurro discussed the increasing use of digital technologies like smartphone apps. Machine learning can potentially use such data to diagnose conditions like sleep or mood disorders before they become clinically significant, allowing earlier intervention, but they could also lead to overdiagnosis. Dr. Capurro proposed using longitudinal databases to track patient outcomes, which could be applied to digital screening technologies.
“You might be able to find unknown patterns that help discriminate between these pathological definitions. You should be able to train (digital screens) with the pathological definition plus the disease trajectory as a way to improve that label,” he said.
The study was funded by the Taiwan Ministry of Health and Welfare Clinical Trial Center.
FROM JAMA INTERNAL MEDICINE
What’s the future of microbiome therapies in C. diff, cancer?
WASHINGTON – Research on standardized microbiome-based therapies designed to prevent the recurrence of Clostridioides difficile infection (CDI) is moving “with a lot of momentum,” according to one expert, and modulation of the gut microbiome may even enhance responses to immunotherapy and/or abrogate toxicity, according to another.
Several products for prevention of CDI recurrence are poised for either phase 3 trials or upcoming Food and Drug Administration approval, Sahil Khanna, MBBS, MS, professor of medicine, gastroenterology, and hepatology at the Mayo Clinic in Rochester, Minn., reported at the annual Gut Microbiota for Health World Summit.
Jennifer A. Wargo, MD, MMSc, of the University of Texas MD Anderson Cancer Center, Houston, described her investigations of microbiome modulation’s role in cancer treatment. “I used to say yes [we can do this] somewhat enthusiastically without data, but now we have data to support this,” she said at the meeting, sponsored by the American Gastroenterological Association and the European Society for Neurogastroenterology and Motility. “The answer now is totally yes.”
New approaches for CDI
“Based on how the field is moving, we might be able to [offer our patients] earlier microbiome restoration” than is currently afforded with fecal microbiota transplantation (FMT), he said. “Right now the [Food and Drug Administration] and our clinical guidelines say we should do FMT after three or more episodes [of CDI] – that’s heartbreaking for patients.”
Several of the microbiome-based therapies under investigation – including two poised for phase 3 trials – have shown efficacy after a second episode of CDI, and one of these two has also had positive results after one episode of CDI in patients 65 at older, a group at particularly high risk of recurrence, said Dr. Khanna.
The value of standardized, mostly pill-form microbiome therapies has been heightened during the pandemic. “We’ve been doing conventional FMT for recurrent C. difficile for over a decade now, and it’s probably the most effective treatment we have,” said Colleen R. Kelly, MD, associate professor of medicine at Brown University, Providence, R.I., and moderator of the session on microbiota-based therapies.
Prepandemic “it got really hard, with issues of identifying donors, and quality control and safety ... And then when COVID hit the stool banks shut down,” she said in an interview after the meeting. With stool testing for SARS-CoV-2 now in place, some stool is again available, “but it made me realize how fragile our current system is,” Dr. Kelly said. “The fact that companies are putting these products through the FDA pipeline and investigating them in rigorous, scientific randomized controlled trials is really good for the field.”
The products vary in composition; some are live multi-strain biotherapeutics derived from donor stool, for instance, while others are defined live bacterial consortia not from stool. Most are oral formulations, given one or multiple times, that do not require any bowel preparation.
One of the products most advanced in the pipeline, RBX2660 (Rebiotix, Ferring Pharmaceuticals) is stool derived and rectally administered. In phase 3 research, 70.5% of patients who received one active enema after having had two or more CDI recurrences and standard-of-care antibiotic treatment had no additional recurrence at 8 weeks compared to 58.1% in the placebo group, Dr. Khanna said.
The other product with positive phase 3 results, SER-109 (Seres Therapeutics), is a donor stool-derived oral formulation of purified Firmicutes spores that is administered after bowel prep. In results published earlier this year, the percentage of patients with recurrence of CDI up to 8 weeks after standard antibiotic treatment was 12% in the SER-109 group and 40% in the placebo group.
Patients in this trial were required to have had three episodes of CDI, and interestingly, Dr. Khanna said, the diagnosis of CDI was made only by toxin enzyme immunoassay (EIA). Earlier phase 2 research, which allowed either toxin EIA or polymerase chain reaction testing for the diagnosis of CDI (as other trials have done), produced negative results, leading investigators to surmise that some of the included patients had been colonized with C. difficile rather than being actively infected, Dr. Khanna said.
Researchers of these trials are documenting not only resolution of CDI but what they believe are positive shifts in the gut microbiota after microbiome-based therapy, he said. For instance, a phase 1 trial he led of the product RBX7455 (Rebiotix, Ferring Pharmaceuticals) – an oral capsule of lyophilized stool-based bacteria that can be kept for several days at room temperature – showed increases in Bacteroidia and Clostridia.
And other trials’ analyses of microbiome engraftment have demonstrated that “you can restore [species] even when these bacteria aren’t [included in the therapy],” he noted. “As the milieu of the gut improves, species that were not detected start coming back up.”
Asked about rates of efficacy in the trials’ placebo arms, Dr. Khanna said that “we’ve become smarter with our antibiotic regimens ... the placebo response rate is the response to newer guideline-based therapies.”
In addition to CDI, microbiome-based therapies are being studied, mostly in phase 1 research, for indications such as Crohn’s disease, ulcerative colitis, autism spectrum disorder, hepatitis B, and hepatic encephalopathy, Dr. Khanna noted.
Dr. Kelly, whose own research has focused on FMT for CDI, said she anticipates an expansion of research into other indications once products to prevent CDI recurrence are on the market. “There have been a couple of promising ulcerative colitis trials that haven’t gone anywhere clinically yet,” she said in the interview. “But will we now identify patients with UC who may be more sensitive to microbial manipulation, for whom we can use these microbial therapies along with a biologic?”
Some of her patients with IBD and CDI who are treated with FMT have not only had their CDI eradicated but have subsequently seen improvements in their IBD, she noted.
The role of traditional FMT and of stool banks will likely change in the future with new standardized oral microbiome-based therapies that can be approved and regulated by the FDA, she said. However, “we think the stool banks will still have some value,” she said, certainly for clinical research and probably for some treatment purposes as well. Regarding new therapies, “I just really hope they’re affordable,” she said.
Gut microbiome manipulation for cancer
Dr. Wargo’s research at MD Anderson has focused on metastatic breast cancer and immunotherapeutic checkpoint blockade. By sequencing microbiota samples and performing immune profiling in hundreds of patients, her team found that responders to PD-1 blockage have a greater diversity of gut bacteria and that “favorable signatures in the gut microbiome” are associated with enhanced immune responses in the tumor microenvironment.
Studies published last year in Science from investigators in Israel (2021 Feb 5;371[6529]:602-9) and Pittsburgh (2021 Feb 5;371[6529]:595-602), demonstrated that FMT promotes response in immunotherapy-refractory melanoma patients. In one study, FMT provided clinical benefit in 6 of 15 patients whose cancer had progressed on prior anti-PD-1 therapy, “which is pretty remarkable,” Dr. Wargo said.
Both research groups, she noted, saw favorable changes in the gut microbiome and immune cell infiltrates both at the level of the colon and the tumor.
Current research on FMT and other microbiome modulation strategies for cancer is guided in part by knowledge that tumors have microbial signatures – these signatures are now being identified across all tumor types – and by findings of “cross talk” between the gut and tumor microbiomes, she explained.
“Researchers are working hard to identify optimal consortia to enhance immune responses in the cancer setting, with promising work in preclinical models,” she said, and clinical trials are in progress. The role of diet in modulating the microbiome and enhancing anti-tumor immunity, with a focus on high dietary fiber intake, is also being investigated, she said.
Dr. Wargo reported that she serves on the advisory boards and is a paid speaker of numerous pharmaceutical and biotechnology companies, and is the coinventor of a patent submitted by the Texas MD Anderson Cancer Center on modulating the microbiome to enhance response to checkpoint blockade, and another related patent. Dr. Khanna reported that he is involved in research with Ferring/Rebiotix, Finch, Seres, Pfizer and Vendata, and does consulting for Immuron and several other companies. Dr. Kelly said she serves as an unpaid adviser for OpenBiome, a nonprofit stool bank, and that her site has enrolled patients in two of the trials testing products for CDI.
WASHINGTON – Research on standardized microbiome-based therapies designed to prevent the recurrence of Clostridioides difficile infection (CDI) is moving “with a lot of momentum,” according to one expert, and modulation of the gut microbiome may even enhance responses to immunotherapy and/or abrogate toxicity, according to another.
Several products for prevention of CDI recurrence are poised for either phase 3 trials or upcoming Food and Drug Administration approval, Sahil Khanna, MBBS, MS, professor of medicine, gastroenterology, and hepatology at the Mayo Clinic in Rochester, Minn., reported at the annual Gut Microbiota for Health World Summit.
Jennifer A. Wargo, MD, MMSc, of the University of Texas MD Anderson Cancer Center, Houston, described her investigations of microbiome modulation’s role in cancer treatment. “I used to say yes [we can do this] somewhat enthusiastically without data, but now we have data to support this,” she said at the meeting, sponsored by the American Gastroenterological Association and the European Society for Neurogastroenterology and Motility. “The answer now is totally yes.”
New approaches for CDI
“Based on how the field is moving, we might be able to [offer our patients] earlier microbiome restoration” than is currently afforded with fecal microbiota transplantation (FMT), he said. “Right now the [Food and Drug Administration] and our clinical guidelines say we should do FMT after three or more episodes [of CDI] – that’s heartbreaking for patients.”
Several of the microbiome-based therapies under investigation – including two poised for phase 3 trials – have shown efficacy after a second episode of CDI, and one of these two has also had positive results after one episode of CDI in patients 65 at older, a group at particularly high risk of recurrence, said Dr. Khanna.
The value of standardized, mostly pill-form microbiome therapies has been heightened during the pandemic. “We’ve been doing conventional FMT for recurrent C. difficile for over a decade now, and it’s probably the most effective treatment we have,” said Colleen R. Kelly, MD, associate professor of medicine at Brown University, Providence, R.I., and moderator of the session on microbiota-based therapies.
Prepandemic “it got really hard, with issues of identifying donors, and quality control and safety ... And then when COVID hit the stool banks shut down,” she said in an interview after the meeting. With stool testing for SARS-CoV-2 now in place, some stool is again available, “but it made me realize how fragile our current system is,” Dr. Kelly said. “The fact that companies are putting these products through the FDA pipeline and investigating them in rigorous, scientific randomized controlled trials is really good for the field.”
The products vary in composition; some are live multi-strain biotherapeutics derived from donor stool, for instance, while others are defined live bacterial consortia not from stool. Most are oral formulations, given one or multiple times, that do not require any bowel preparation.
One of the products most advanced in the pipeline, RBX2660 (Rebiotix, Ferring Pharmaceuticals) is stool derived and rectally administered. In phase 3 research, 70.5% of patients who received one active enema after having had two or more CDI recurrences and standard-of-care antibiotic treatment had no additional recurrence at 8 weeks compared to 58.1% in the placebo group, Dr. Khanna said.
The other product with positive phase 3 results, SER-109 (Seres Therapeutics), is a donor stool-derived oral formulation of purified Firmicutes spores that is administered after bowel prep. In results published earlier this year, the percentage of patients with recurrence of CDI up to 8 weeks after standard antibiotic treatment was 12% in the SER-109 group and 40% in the placebo group.
Patients in this trial were required to have had three episodes of CDI, and interestingly, Dr. Khanna said, the diagnosis of CDI was made only by toxin enzyme immunoassay (EIA). Earlier phase 2 research, which allowed either toxin EIA or polymerase chain reaction testing for the diagnosis of CDI (as other trials have done), produced negative results, leading investigators to surmise that some of the included patients had been colonized with C. difficile rather than being actively infected, Dr. Khanna said.
Researchers of these trials are documenting not only resolution of CDI but what they believe are positive shifts in the gut microbiota after microbiome-based therapy, he said. For instance, a phase 1 trial he led of the product RBX7455 (Rebiotix, Ferring Pharmaceuticals) – an oral capsule of lyophilized stool-based bacteria that can be kept for several days at room temperature – showed increases in Bacteroidia and Clostridia.
And other trials’ analyses of microbiome engraftment have demonstrated that “you can restore [species] even when these bacteria aren’t [included in the therapy],” he noted. “As the milieu of the gut improves, species that were not detected start coming back up.”
Asked about rates of efficacy in the trials’ placebo arms, Dr. Khanna said that “we’ve become smarter with our antibiotic regimens ... the placebo response rate is the response to newer guideline-based therapies.”
In addition to CDI, microbiome-based therapies are being studied, mostly in phase 1 research, for indications such as Crohn’s disease, ulcerative colitis, autism spectrum disorder, hepatitis B, and hepatic encephalopathy, Dr. Khanna noted.
Dr. Kelly, whose own research has focused on FMT for CDI, said she anticipates an expansion of research into other indications once products to prevent CDI recurrence are on the market. “There have been a couple of promising ulcerative colitis trials that haven’t gone anywhere clinically yet,” she said in the interview. “But will we now identify patients with UC who may be more sensitive to microbial manipulation, for whom we can use these microbial therapies along with a biologic?”
Some of her patients with IBD and CDI who are treated with FMT have not only had their CDI eradicated but have subsequently seen improvements in their IBD, she noted.
The role of traditional FMT and of stool banks will likely change in the future with new standardized oral microbiome-based therapies that can be approved and regulated by the FDA, she said. However, “we think the stool banks will still have some value,” she said, certainly for clinical research and probably for some treatment purposes as well. Regarding new therapies, “I just really hope they’re affordable,” she said.
Gut microbiome manipulation for cancer
Dr. Wargo’s research at MD Anderson has focused on metastatic breast cancer and immunotherapeutic checkpoint blockade. By sequencing microbiota samples and performing immune profiling in hundreds of patients, her team found that responders to PD-1 blockage have a greater diversity of gut bacteria and that “favorable signatures in the gut microbiome” are associated with enhanced immune responses in the tumor microenvironment.
Studies published last year in Science from investigators in Israel (2021 Feb 5;371[6529]:602-9) and Pittsburgh (2021 Feb 5;371[6529]:595-602), demonstrated that FMT promotes response in immunotherapy-refractory melanoma patients. In one study, FMT provided clinical benefit in 6 of 15 patients whose cancer had progressed on prior anti-PD-1 therapy, “which is pretty remarkable,” Dr. Wargo said.
Both research groups, she noted, saw favorable changes in the gut microbiome and immune cell infiltrates both at the level of the colon and the tumor.
Current research on FMT and other microbiome modulation strategies for cancer is guided in part by knowledge that tumors have microbial signatures – these signatures are now being identified across all tumor types – and by findings of “cross talk” between the gut and tumor microbiomes, she explained.
“Researchers are working hard to identify optimal consortia to enhance immune responses in the cancer setting, with promising work in preclinical models,” she said, and clinical trials are in progress. The role of diet in modulating the microbiome and enhancing anti-tumor immunity, with a focus on high dietary fiber intake, is also being investigated, she said.
Dr. Wargo reported that she serves on the advisory boards and is a paid speaker of numerous pharmaceutical and biotechnology companies, and is the coinventor of a patent submitted by the Texas MD Anderson Cancer Center on modulating the microbiome to enhance response to checkpoint blockade, and another related patent. Dr. Khanna reported that he is involved in research with Ferring/Rebiotix, Finch, Seres, Pfizer and Vendata, and does consulting for Immuron and several other companies. Dr. Kelly said she serves as an unpaid adviser for OpenBiome, a nonprofit stool bank, and that her site has enrolled patients in two of the trials testing products for CDI.
WASHINGTON – Research on standardized microbiome-based therapies designed to prevent the recurrence of Clostridioides difficile infection (CDI) is moving “with a lot of momentum,” according to one expert, and modulation of the gut microbiome may even enhance responses to immunotherapy and/or abrogate toxicity, according to another.
Several products for prevention of CDI recurrence are poised for either phase 3 trials or upcoming Food and Drug Administration approval, Sahil Khanna, MBBS, MS, professor of medicine, gastroenterology, and hepatology at the Mayo Clinic in Rochester, Minn., reported at the annual Gut Microbiota for Health World Summit.
Jennifer A. Wargo, MD, MMSc, of the University of Texas MD Anderson Cancer Center, Houston, described her investigations of microbiome modulation’s role in cancer treatment. “I used to say yes [we can do this] somewhat enthusiastically without data, but now we have data to support this,” she said at the meeting, sponsored by the American Gastroenterological Association and the European Society for Neurogastroenterology and Motility. “The answer now is totally yes.”
New approaches for CDI
“Based on how the field is moving, we might be able to [offer our patients] earlier microbiome restoration” than is currently afforded with fecal microbiota transplantation (FMT), he said. “Right now the [Food and Drug Administration] and our clinical guidelines say we should do FMT after three or more episodes [of CDI] – that’s heartbreaking for patients.”
Several of the microbiome-based therapies under investigation – including two poised for phase 3 trials – have shown efficacy after a second episode of CDI, and one of these two has also had positive results after one episode of CDI in patients 65 at older, a group at particularly high risk of recurrence, said Dr. Khanna.
The value of standardized, mostly pill-form microbiome therapies has been heightened during the pandemic. “We’ve been doing conventional FMT for recurrent C. difficile for over a decade now, and it’s probably the most effective treatment we have,” said Colleen R. Kelly, MD, associate professor of medicine at Brown University, Providence, R.I., and moderator of the session on microbiota-based therapies.
Prepandemic “it got really hard, with issues of identifying donors, and quality control and safety ... And then when COVID hit the stool banks shut down,” she said in an interview after the meeting. With stool testing for SARS-CoV-2 now in place, some stool is again available, “but it made me realize how fragile our current system is,” Dr. Kelly said. “The fact that companies are putting these products through the FDA pipeline and investigating them in rigorous, scientific randomized controlled trials is really good for the field.”
The products vary in composition; some are live multi-strain biotherapeutics derived from donor stool, for instance, while others are defined live bacterial consortia not from stool. Most are oral formulations, given one or multiple times, that do not require any bowel preparation.
One of the products most advanced in the pipeline, RBX2660 (Rebiotix, Ferring Pharmaceuticals) is stool derived and rectally administered. In phase 3 research, 70.5% of patients who received one active enema after having had two or more CDI recurrences and standard-of-care antibiotic treatment had no additional recurrence at 8 weeks compared to 58.1% in the placebo group, Dr. Khanna said.
The other product with positive phase 3 results, SER-109 (Seres Therapeutics), is a donor stool-derived oral formulation of purified Firmicutes spores that is administered after bowel prep. In results published earlier this year, the percentage of patients with recurrence of CDI up to 8 weeks after standard antibiotic treatment was 12% in the SER-109 group and 40% in the placebo group.
Patients in this trial were required to have had three episodes of CDI, and interestingly, Dr. Khanna said, the diagnosis of CDI was made only by toxin enzyme immunoassay (EIA). Earlier phase 2 research, which allowed either toxin EIA or polymerase chain reaction testing for the diagnosis of CDI (as other trials have done), produced negative results, leading investigators to surmise that some of the included patients had been colonized with C. difficile rather than being actively infected, Dr. Khanna said.
Researchers of these trials are documenting not only resolution of CDI but what they believe are positive shifts in the gut microbiota after microbiome-based therapy, he said. For instance, a phase 1 trial he led of the product RBX7455 (Rebiotix, Ferring Pharmaceuticals) – an oral capsule of lyophilized stool-based bacteria that can be kept for several days at room temperature – showed increases in Bacteroidia and Clostridia.
And other trials’ analyses of microbiome engraftment have demonstrated that “you can restore [species] even when these bacteria aren’t [included in the therapy],” he noted. “As the milieu of the gut improves, species that were not detected start coming back up.”
Asked about rates of efficacy in the trials’ placebo arms, Dr. Khanna said that “we’ve become smarter with our antibiotic regimens ... the placebo response rate is the response to newer guideline-based therapies.”
In addition to CDI, microbiome-based therapies are being studied, mostly in phase 1 research, for indications such as Crohn’s disease, ulcerative colitis, autism spectrum disorder, hepatitis B, and hepatic encephalopathy, Dr. Khanna noted.
Dr. Kelly, whose own research has focused on FMT for CDI, said she anticipates an expansion of research into other indications once products to prevent CDI recurrence are on the market. “There have been a couple of promising ulcerative colitis trials that haven’t gone anywhere clinically yet,” she said in the interview. “But will we now identify patients with UC who may be more sensitive to microbial manipulation, for whom we can use these microbial therapies along with a biologic?”
Some of her patients with IBD and CDI who are treated with FMT have not only had their CDI eradicated but have subsequently seen improvements in their IBD, she noted.
The role of traditional FMT and of stool banks will likely change in the future with new standardized oral microbiome-based therapies that can be approved and regulated by the FDA, she said. However, “we think the stool banks will still have some value,” she said, certainly for clinical research and probably for some treatment purposes as well. Regarding new therapies, “I just really hope they’re affordable,” she said.
Gut microbiome manipulation for cancer
Dr. Wargo’s research at MD Anderson has focused on metastatic breast cancer and immunotherapeutic checkpoint blockade. By sequencing microbiota samples and performing immune profiling in hundreds of patients, her team found that responders to PD-1 blockage have a greater diversity of gut bacteria and that “favorable signatures in the gut microbiome” are associated with enhanced immune responses in the tumor microenvironment.
Studies published last year in Science from investigators in Israel (2021 Feb 5;371[6529]:602-9) and Pittsburgh (2021 Feb 5;371[6529]:595-602), demonstrated that FMT promotes response in immunotherapy-refractory melanoma patients. In one study, FMT provided clinical benefit in 6 of 15 patients whose cancer had progressed on prior anti-PD-1 therapy, “which is pretty remarkable,” Dr. Wargo said.
Both research groups, she noted, saw favorable changes in the gut microbiome and immune cell infiltrates both at the level of the colon and the tumor.
Current research on FMT and other microbiome modulation strategies for cancer is guided in part by knowledge that tumors have microbial signatures – these signatures are now being identified across all tumor types – and by findings of “cross talk” between the gut and tumor microbiomes, she explained.
“Researchers are working hard to identify optimal consortia to enhance immune responses in the cancer setting, with promising work in preclinical models,” she said, and clinical trials are in progress. The role of diet in modulating the microbiome and enhancing anti-tumor immunity, with a focus on high dietary fiber intake, is also being investigated, she said.
Dr. Wargo reported that she serves on the advisory boards and is a paid speaker of numerous pharmaceutical and biotechnology companies, and is the coinventor of a patent submitted by the Texas MD Anderson Cancer Center on modulating the microbiome to enhance response to checkpoint blockade, and another related patent. Dr. Khanna reported that he is involved in research with Ferring/Rebiotix, Finch, Seres, Pfizer and Vendata, and does consulting for Immuron and several other companies. Dr. Kelly said she serves as an unpaid adviser for OpenBiome, a nonprofit stool bank, and that her site has enrolled patients in two of the trials testing products for CDI.
REPORTING FROM GMFH 2022
Excess weight over lifetime hikes risk for colorectal cancer
Excess weight over a lifetime may play a greater role in a person’s risk for colorectal cancer (CRC) than previously thought, according to new research.
In their paper published online March 17 in JAMA Oncology, the authors liken the cumulative effects of a lifetime with overweight or obesity to the increased risk of cancer the more people smoke over time.
This population-based, case-control study was led by Xiangwei Li, MSc, of the division of clinical epidemiology and aging research at the German Cancer Research Center in Heidelberg.
It looked at height and self-reported weight documented in 10-year increments starting at age 20 years up to the current age for 5,635 people with CRC compared with 4,515 people in a control group.
Odds for colorectal cancer increased substantially over the decades when people carried the excess weight long term compared with participants who remained within the normal weight range during the period.

Coauthor Hermann Brenner, MD, MPH, a colleague in Li’s division at the German Cancer Research Center, said in an interview that a key message in the research is that “overweight and obesity are likely to increase the risk of colorectal cancer more strongly than suggested by previous studies that typically had considered body weight only at a single point of time.”
The researchers used a measure of weighted number of years lived with overweight or obesity (WYOs) determined by multiplying excess body mass index by number of years the person carried the excess weight.
They found a link between WYOs and CRC risk, with adjusted odds ratios (ORs) increasing from 1.25 (95% confidence interval [CI], 1.09-1.44) to 2.54 (95% CI, 2.24-2.89) from the first to the fourth quartile of WYOs, compared with people who stayed within normal weight parameters.
The odds went up substantially the longer the time carrying the excess weight.
“Each SD increment in WYOs was associated with an increase of CRC risk by 55% (adjusted OR, 1.55; 95% CI, 1.46-1.64),” the authors wrote. “This OR was higher than the OR per SD increase of excess body mass index at any single point of time, which ranged from 1.04 (95% CI, 0.93-1.16) to 1.27 (95% CI 1.16-1.39).”
Dr. Brenner said that although this study focused on colorectal cancer, “the same is likely to apply for other cancers and other chronic diseases.”
Prevention of overweight and obesity to reduce burden of cancer and other chronic diseases “should become a public health priority,” he said.
Preventing overweight in childhood is important
Overweight and obesity increasingly are starting in childhood, he noted, and may be a lifelong burden.
Therefore, “efforts to prevent their development in childhood, adolescence, and young adulthood are particularly important,” Dr. Brenner said.
The average age of the patients was 68 years in both the CRC and control groups. There were more men than women in both groups: 59.7% were men in the CRC group and 61.1% were men in the control group.
“Our proposed concept of WYOs is comparable to the concept of pack-years in that WYOs can be considered a weighted measure of years lived with the exposure, with weights reflecting the intensity of exposure,” the authors wrote.
Study helps confirm what is becoming more clear to researchers
Kimmie Ng, MD, MPH, a professor at Harvard Medical School and oncologist at Dana-Farber Cancer Institute, both in Boston, said in an interview that the study helps confirm what is becoming more clear to researchers.
“We do think that exposures over the life course are the ones that will be most strongly contributing to a risk of colorectal cancer as an adult,” she said. “With obesity, what we think is happening is that it’s setting up this milieu of chronic inflammation and insulin resistance and we know those two factors can lead to higher rates of colorectal cancer development and increased tumor growth.”
She said the ideal, but impractical, way to do the study would be to follow healthy people from childhood and document their weight over a lifetime. In this case-control study, people were asked to recall their weight at different time periods, which is a limitation and could lead to recall bias.
But the study is important, Dr. Ng said, and it adds convincing evidence that addressing the link between excess weight and CRC and chronic diseases should be a public health priority. “With the recent rise in young-onset colorectal cancer since the 1990s there has been a lot of interest in looking at whether obesity is a major contributor to that rising trend,” Dr. Ng noted. “If obesity is truly linked to colorectal cancer, these rising rates of obesity are very worrisome for potentially leading to more colorectal cancers in young adulthood and beyond.“
The study authors and Dr. Ng report no relevant financial relationships.
The new research was funded by the German Research Council, the Interdisciplinary Research Program of the National Center for Tumor Diseases, Germany, and the German Federal Ministry of Education and Research.
Excess weight over a lifetime may play a greater role in a person’s risk for colorectal cancer (CRC) than previously thought, according to new research.
In their paper published online March 17 in JAMA Oncology, the authors liken the cumulative effects of a lifetime with overweight or obesity to the increased risk of cancer the more people smoke over time.
This population-based, case-control study was led by Xiangwei Li, MSc, of the division of clinical epidemiology and aging research at the German Cancer Research Center in Heidelberg.
It looked at height and self-reported weight documented in 10-year increments starting at age 20 years up to the current age for 5,635 people with CRC compared with 4,515 people in a control group.
Odds for colorectal cancer increased substantially over the decades when people carried the excess weight long term compared with participants who remained within the normal weight range during the period.
Coauthor Hermann Brenner, MD, MPH, a colleague in Li’s division at the German Cancer Research Center, said in an interview that a key message in the research is that “overweight and obesity are likely to increase the risk of colorectal cancer more strongly than suggested by previous studies that typically had considered body weight only at a single point of time.”
The researchers used a measure of weighted number of years lived with overweight or obesity (WYOs) determined by multiplying excess body mass index by number of years the person carried the excess weight.
They found a link between WYOs and CRC risk, with adjusted odds ratios (ORs) increasing from 1.25 (95% confidence interval [CI], 1.09-1.44) to 2.54 (95% CI, 2.24-2.89) from the first to the fourth quartile of WYOs, compared with people who stayed within normal weight parameters.
The odds went up substantially the longer the time carrying the excess weight.
“Each SD increment in WYOs was associated with an increase of CRC risk by 55% (adjusted OR, 1.55; 95% CI, 1.46-1.64),” the authors wrote. “This OR was higher than the OR per SD increase of excess body mass index at any single point of time, which ranged from 1.04 (95% CI, 0.93-1.16) to 1.27 (95% CI 1.16-1.39).”
Dr. Brenner said that although this study focused on colorectal cancer, “the same is likely to apply for other cancers and other chronic diseases.”
Prevention of overweight and obesity to reduce burden of cancer and other chronic diseases “should become a public health priority,” he said.
Preventing overweight in childhood is important
Overweight and obesity increasingly are starting in childhood, he noted, and may be a lifelong burden.
Therefore, “efforts to prevent their development in childhood, adolescence, and young adulthood are particularly important,” Dr. Brenner said.
The average age of the patients was 68 years in both the CRC and control groups. There were more men than women in both groups: 59.7% were men in the CRC group and 61.1% were men in the control group.
“Our proposed concept of WYOs is comparable to the concept of pack-years in that WYOs can be considered a weighted measure of years lived with the exposure, with weights reflecting the intensity of exposure,” the authors wrote.
Study helps confirm what is becoming more clear to researchers
Kimmie Ng, MD, MPH, a professor at Harvard Medical School and oncologist at Dana-Farber Cancer Institute, both in Boston, said in an interview that the study helps confirm what is becoming more clear to researchers.
“We do think that exposures over the life course are the ones that will be most strongly contributing to a risk of colorectal cancer as an adult,” she said. “With obesity, what we think is happening is that it’s setting up this milieu of chronic inflammation and insulin resistance and we know those two factors can lead to higher rates of colorectal cancer development and increased tumor growth.”
She said the ideal, but impractical, way to do the study would be to follow healthy people from childhood and document their weight over a lifetime. In this case-control study, people were asked to recall their weight at different time periods, which is a limitation and could lead to recall bias.
But the study is important, Dr. Ng said, and it adds convincing evidence that addressing the link between excess weight and CRC and chronic diseases should be a public health priority. “With the recent rise in young-onset colorectal cancer since the 1990s there has been a lot of interest in looking at whether obesity is a major contributor to that rising trend,” Dr. Ng noted. “If obesity is truly linked to colorectal cancer, these rising rates of obesity are very worrisome for potentially leading to more colorectal cancers in young adulthood and beyond.“
The study authors and Dr. Ng report no relevant financial relationships.
The new research was funded by the German Research Council, the Interdisciplinary Research Program of the National Center for Tumor Diseases, Germany, and the German Federal Ministry of Education and Research.
Excess weight over a lifetime may play a greater role in a person’s risk for colorectal cancer (CRC) than previously thought, according to new research.
In their paper published online March 17 in JAMA Oncology, the authors liken the cumulative effects of a lifetime with overweight or obesity to the increased risk of cancer the more people smoke over time.
This population-based, case-control study was led by Xiangwei Li, MSc, of the division of clinical epidemiology and aging research at the German Cancer Research Center in Heidelberg.
It looked at height and self-reported weight documented in 10-year increments starting at age 20 years up to the current age for 5,635 people with CRC compared with 4,515 people in a control group.
Odds for colorectal cancer increased substantially over the decades when people carried the excess weight long term compared with participants who remained within the normal weight range during the period.
Coauthor Hermann Brenner, MD, MPH, a colleague in Li’s division at the German Cancer Research Center, said in an interview that a key message in the research is that “overweight and obesity are likely to increase the risk of colorectal cancer more strongly than suggested by previous studies that typically had considered body weight only at a single point of time.”
The researchers used a measure of weighted number of years lived with overweight or obesity (WYOs) determined by multiplying excess body mass index by number of years the person carried the excess weight.
They found a link between WYOs and CRC risk, with adjusted odds ratios (ORs) increasing from 1.25 (95% confidence interval [CI], 1.09-1.44) to 2.54 (95% CI, 2.24-2.89) from the first to the fourth quartile of WYOs, compared with people who stayed within normal weight parameters.
The odds went up substantially the longer the time carrying the excess weight.
“Each SD increment in WYOs was associated with an increase of CRC risk by 55% (adjusted OR, 1.55; 95% CI, 1.46-1.64),” the authors wrote. “This OR was higher than the OR per SD increase of excess body mass index at any single point of time, which ranged from 1.04 (95% CI, 0.93-1.16) to 1.27 (95% CI 1.16-1.39).”
Dr. Brenner said that although this study focused on colorectal cancer, “the same is likely to apply for other cancers and other chronic diseases.”
Prevention of overweight and obesity to reduce burden of cancer and other chronic diseases “should become a public health priority,” he said.
Preventing overweight in childhood is important
Overweight and obesity increasingly are starting in childhood, he noted, and may be a lifelong burden.
Therefore, “efforts to prevent their development in childhood, adolescence, and young adulthood are particularly important,” Dr. Brenner said.
The average age of the patients was 68 years in both the CRC and control groups. There were more men than women in both groups: 59.7% were men in the CRC group and 61.1% were men in the control group.
“Our proposed concept of WYOs is comparable to the concept of pack-years in that WYOs can be considered a weighted measure of years lived with the exposure, with weights reflecting the intensity of exposure,” the authors wrote.
Study helps confirm what is becoming more clear to researchers
Kimmie Ng, MD, MPH, a professor at Harvard Medical School and oncologist at Dana-Farber Cancer Institute, both in Boston, said in an interview that the study helps confirm what is becoming more clear to researchers.
“We do think that exposures over the life course are the ones that will be most strongly contributing to a risk of colorectal cancer as an adult,” she said. “With obesity, what we think is happening is that it’s setting up this milieu of chronic inflammation and insulin resistance and we know those two factors can lead to higher rates of colorectal cancer development and increased tumor growth.”
She said the ideal, but impractical, way to do the study would be to follow healthy people from childhood and document their weight over a lifetime. In this case-control study, people were asked to recall their weight at different time periods, which is a limitation and could lead to recall bias.
But the study is important, Dr. Ng said, and it adds convincing evidence that addressing the link between excess weight and CRC and chronic diseases should be a public health priority. “With the recent rise in young-onset colorectal cancer since the 1990s there has been a lot of interest in looking at whether obesity is a major contributor to that rising trend,” Dr. Ng noted. “If obesity is truly linked to colorectal cancer, these rising rates of obesity are very worrisome for potentially leading to more colorectal cancers in young adulthood and beyond.“
The study authors and Dr. Ng report no relevant financial relationships.
The new research was funded by the German Research Council, the Interdisciplinary Research Program of the National Center for Tumor Diseases, Germany, and the German Federal Ministry of Education and Research.
FROM JAMA ONCOLOGY
Ways to lessen toxic effects of chemo in older adults
Age-related changes that potentiate adverse drug reactions include alterations in absorption, distribution, metabolism, and excretion. As such, older patients often require adjustments in medications to optimize safety and use. Medication adjustment is especially important for older patients on complex medication regimens for multiple conditions, such as those undergoing cancer treatment. Three recent high-quality randomized trials evaluated the use of geriatric assessment (GA) in older adults with cancer.1-3
Interdisciplinary GA can identify aging-related conditions associated with poor outcomes in older patients with cancer (e.g., toxic effects of chemotherapy) and provide recommendations aimed at improving health outcomes. The results of these trials suggest that interdisciplinary GA can improve care outcomes and oncologists’ communication for older adults with cancer, and should be considered an emerging standard of care.
Geriatric assessment and chemotherapy-related toxic effects
A cluster randomized trial1 at City of Hope National Medical Center conducted between August 2015 and February 2019 enrolled 613 participants and randomly assigned them to receive a GA-guided intervention or usual standard of care in a 2-to-1 ratio. Participants were eligible for the study if they were aged ≥65 years; had a diagnosis of solid malignant neoplasm of any stage; were starting a new chemotherapy regimen; and were fluent in English, Spanish, or Chinese.
The intervention included a GA at baseline followed by assessments focused on six common areas: sleep problems, problems with eating and feeding, incontinence, confusion, evidence of falls, and skin breakdown. An interdisciplinary team (oncologist, nurse practitioner, pharmacist, physical therapist, occupational therapist, social worker, and nutritionist) performed the assessment and developed a plan of care. Interventions were multifactorial and could include referral to specialists; recommendations for medication changes; symptom management; nutritional intervention with diet recommendations and supplementation; and interventions targeting social, spiritual, and functional well-being. Follow-up by a nurse practitioner continued until completion of chemotherapy or 6 months after starting chemotherapy, whichever was earlier.
The primary outcome was grade 3 or higher chemotherapy-related toxic effects using National Cancer Institute criteria, and secondary outcomes were advance directive completion, emergency room visits and unplanned hospitalizations, and survival up to 12 months. Results showed a 10% absolute reduction in the incidence of grade 3 or higher toxic effects (P = .02), with a number needed to treat of 10. Advance directive completion also increased by 15%, but no differences were observed for other outcomes. This study offers high-quality evidence that a GA-based intervention can reduce toxic effects of chemotherapy regimens for older adults with cancer.
Geriatric assessment in community oncology practices
A recent study by Supriya G. Mohile, MD, and colleagues2 is the first nationwide multicenter clinical trial to demonstrate the effects of GA and GA-guided management. This study was conducted in 40 oncology practices from the University of Rochester National Cancer Institute Community Oncology Research Program network. Centers were randomly assigned to intervention or usual care (362 patients treated by 68 oncologists in the intervention group and 371 patients treated by 91 oncologists in the usual-care group). Eligibility criteria were age ≥70 years; impairment in at least one GA domain other than polypharmacy; incurable advanced solid tumor or lymphoma with a plan to start new cancer treatment with a high risk for toxic effects within 4 weeks; and English language fluency. Both study groups underwent a baseline GA that assessed patients’ physical performance, functional status, comorbidity, cognition, nutrition, social support, polypharmacy, and psychological status. For the intervention group, a summary and management recommendations were provided to the treating oncologists.
The primary outcome was grade 3 or higher toxic effects within 3 months of starting a new regimen; secondary outcomes included treatment intensity and survival and GA outcomes within 3 months. A smaller proportion of patients in the intervention group experienced toxicity (51% vs. 71%), with an absolute risk reduction of 20%. Patients in the intervention group also had fewer falls and a greater reduction in medications used; there were no other differences in secondary outcomes. This study offers very strong and generalizable evidence that incorporating GA in the care of older adults with cancer at risk for toxicity can reduce toxicity as well as improve other outcomes, such as falls and polypharmacy.
Geriatric assessment and oncologist-patient communication
A secondary analysis3 of data from Dr. Mohile and colleagues2 evaluated the effect of GA-guided recommendations on oncologist-patient communication regarding comorbidities. Patients (n = 541) included in this analysis were 76.6 years of age on average and had 3.2 (standard deviation, 1.9) comorbid conditions. All patients underwent GA, but only oncologists in the intervention arm received GA-based recommendations. Clinical encounters between oncologist and patient immediately following the GA were audio recorded and analyzed to examine communication between oncologists and participants as it relates to chronic comorbid conditions.
In the intervention arm, more discussions regarding comorbidities took place, and more participants’ concerns about comorbidities were acknowledged. More importantly, participants in the intervention group were 2.4 times more likely to have their concerns about comorbidities addressed through referral or education, compared with the usual-care group (P = .004). Moreover, 41% of oncologists in the intervention arm modified dosage or cancer treatment schedule because of concern about tolerability or comorbidities. This study demonstrates beneficial effects of GA in increasing communication and perhaps consideration of comorbidities of older adults when planning cancer treatment.
Dr. Hung is professor of geriatrics and palliative care at Mount Sinai Hospital, New York. He disclosed no relevant conflicts of interest.
References
1. Li D et al. JAMA Oncol. 2021;7:e214158.
2. Mohile SG et al. Lancet. 2021;398:1894-1904.
3. Kleckner AS et al. JCO Oncol Pract. 2022;18:e9-19.
A version of this article first appeared on Medscape.com.
Age-related changes that potentiate adverse drug reactions include alterations in absorption, distribution, metabolism, and excretion. As such, older patients often require adjustments in medications to optimize safety and use. Medication adjustment is especially important for older patients on complex medication regimens for multiple conditions, such as those undergoing cancer treatment. Three recent high-quality randomized trials evaluated the use of geriatric assessment (GA) in older adults with cancer.1-3
Interdisciplinary GA can identify aging-related conditions associated with poor outcomes in older patients with cancer (e.g., toxic effects of chemotherapy) and provide recommendations aimed at improving health outcomes. The results of these trials suggest that interdisciplinary GA can improve care outcomes and oncologists’ communication for older adults with cancer, and should be considered an emerging standard of care.
Geriatric assessment and chemotherapy-related toxic effects
A cluster randomized trial1 at City of Hope National Medical Center conducted between August 2015 and February 2019 enrolled 613 participants and randomly assigned them to receive a GA-guided intervention or usual standard of care in a 2-to-1 ratio. Participants were eligible for the study if they were aged ≥65 years; had a diagnosis of solid malignant neoplasm of any stage; were starting a new chemotherapy regimen; and were fluent in English, Spanish, or Chinese.
The intervention included a GA at baseline followed by assessments focused on six common areas: sleep problems, problems with eating and feeding, incontinence, confusion, evidence of falls, and skin breakdown. An interdisciplinary team (oncologist, nurse practitioner, pharmacist, physical therapist, occupational therapist, social worker, and nutritionist) performed the assessment and developed a plan of care. Interventions were multifactorial and could include referral to specialists; recommendations for medication changes; symptom management; nutritional intervention with diet recommendations and supplementation; and interventions targeting social, spiritual, and functional well-being. Follow-up by a nurse practitioner continued until completion of chemotherapy or 6 months after starting chemotherapy, whichever was earlier.
The primary outcome was grade 3 or higher chemotherapy-related toxic effects using National Cancer Institute criteria, and secondary outcomes were advance directive completion, emergency room visits and unplanned hospitalizations, and survival up to 12 months. Results showed a 10% absolute reduction in the incidence of grade 3 or higher toxic effects (P = .02), with a number needed to treat of 10. Advance directive completion also increased by 15%, but no differences were observed for other outcomes. This study offers high-quality evidence that a GA-based intervention can reduce toxic effects of chemotherapy regimens for older adults with cancer.
Geriatric assessment in community oncology practices
A recent study by Supriya G. Mohile, MD, and colleagues2 is the first nationwide multicenter clinical trial to demonstrate the effects of GA and GA-guided management. This study was conducted in 40 oncology practices from the University of Rochester National Cancer Institute Community Oncology Research Program network. Centers were randomly assigned to intervention or usual care (362 patients treated by 68 oncologists in the intervention group and 371 patients treated by 91 oncologists in the usual-care group). Eligibility criteria were age ≥70 years; impairment in at least one GA domain other than polypharmacy; incurable advanced solid tumor or lymphoma with a plan to start new cancer treatment with a high risk for toxic effects within 4 weeks; and English language fluency. Both study groups underwent a baseline GA that assessed patients’ physical performance, functional status, comorbidity, cognition, nutrition, social support, polypharmacy, and psychological status. For the intervention group, a summary and management recommendations were provided to the treating oncologists.
The primary outcome was grade 3 or higher toxic effects within 3 months of starting a new regimen; secondary outcomes included treatment intensity and survival and GA outcomes within 3 months. A smaller proportion of patients in the intervention group experienced toxicity (51% vs. 71%), with an absolute risk reduction of 20%. Patients in the intervention group also had fewer falls and a greater reduction in medications used; there were no other differences in secondary outcomes. This study offers very strong and generalizable evidence that incorporating GA in the care of older adults with cancer at risk for toxicity can reduce toxicity as well as improve other outcomes, such as falls and polypharmacy.
Geriatric assessment and oncologist-patient communication
A secondary analysis3 of data from Dr. Mohile and colleagues2 evaluated the effect of GA-guided recommendations on oncologist-patient communication regarding comorbidities. Patients (n = 541) included in this analysis were 76.6 years of age on average and had 3.2 (standard deviation, 1.9) comorbid conditions. All patients underwent GA, but only oncologists in the intervention arm received GA-based recommendations. Clinical encounters between oncologist and patient immediately following the GA were audio recorded and analyzed to examine communication between oncologists and participants as it relates to chronic comorbid conditions.
In the intervention arm, more discussions regarding comorbidities took place, and more participants’ concerns about comorbidities were acknowledged. More importantly, participants in the intervention group were 2.4 times more likely to have their concerns about comorbidities addressed through referral or education, compared with the usual-care group (P = .004). Moreover, 41% of oncologists in the intervention arm modified dosage or cancer treatment schedule because of concern about tolerability or comorbidities. This study demonstrates beneficial effects of GA in increasing communication and perhaps consideration of comorbidities of older adults when planning cancer treatment.
Dr. Hung is professor of geriatrics and palliative care at Mount Sinai Hospital, New York. He disclosed no relevant conflicts of interest.
References
1. Li D et al. JAMA Oncol. 2021;7:e214158.
2. Mohile SG et al. Lancet. 2021;398:1894-1904.
3. Kleckner AS et al. JCO Oncol Pract. 2022;18:e9-19.
A version of this article first appeared on Medscape.com.
Age-related changes that potentiate adverse drug reactions include alterations in absorption, distribution, metabolism, and excretion. As such, older patients often require adjustments in medications to optimize safety and use. Medication adjustment is especially important for older patients on complex medication regimens for multiple conditions, such as those undergoing cancer treatment. Three recent high-quality randomized trials evaluated the use of geriatric assessment (GA) in older adults with cancer.1-3
Interdisciplinary GA can identify aging-related conditions associated with poor outcomes in older patients with cancer (e.g., toxic effects of chemotherapy) and provide recommendations aimed at improving health outcomes. The results of these trials suggest that interdisciplinary GA can improve care outcomes and oncologists’ communication for older adults with cancer, and should be considered an emerging standard of care.
Geriatric assessment and chemotherapy-related toxic effects
A cluster randomized trial1 at City of Hope National Medical Center conducted between August 2015 and February 2019 enrolled 613 participants and randomly assigned them to receive a GA-guided intervention or usual standard of care in a 2-to-1 ratio. Participants were eligible for the study if they were aged ≥65 years; had a diagnosis of solid malignant neoplasm of any stage; were starting a new chemotherapy regimen; and were fluent in English, Spanish, or Chinese.
The intervention included a GA at baseline followed by assessments focused on six common areas: sleep problems, problems with eating and feeding, incontinence, confusion, evidence of falls, and skin breakdown. An interdisciplinary team (oncologist, nurse practitioner, pharmacist, physical therapist, occupational therapist, social worker, and nutritionist) performed the assessment and developed a plan of care. Interventions were multifactorial and could include referral to specialists; recommendations for medication changes; symptom management; nutritional intervention with diet recommendations and supplementation; and interventions targeting social, spiritual, and functional well-being. Follow-up by a nurse practitioner continued until completion of chemotherapy or 6 months after starting chemotherapy, whichever was earlier.
The primary outcome was grade 3 or higher chemotherapy-related toxic effects using National Cancer Institute criteria, and secondary outcomes were advance directive completion, emergency room visits and unplanned hospitalizations, and survival up to 12 months. Results showed a 10% absolute reduction in the incidence of grade 3 or higher toxic effects (P = .02), with a number needed to treat of 10. Advance directive completion also increased by 15%, but no differences were observed for other outcomes. This study offers high-quality evidence that a GA-based intervention can reduce toxic effects of chemotherapy regimens for older adults with cancer.
Geriatric assessment in community oncology practices
A recent study by Supriya G. Mohile, MD, and colleagues2 is the first nationwide multicenter clinical trial to demonstrate the effects of GA and GA-guided management. This study was conducted in 40 oncology practices from the University of Rochester National Cancer Institute Community Oncology Research Program network. Centers were randomly assigned to intervention or usual care (362 patients treated by 68 oncologists in the intervention group and 371 patients treated by 91 oncologists in the usual-care group). Eligibility criteria were age ≥70 years; impairment in at least one GA domain other than polypharmacy; incurable advanced solid tumor or lymphoma with a plan to start new cancer treatment with a high risk for toxic effects within 4 weeks; and English language fluency. Both study groups underwent a baseline GA that assessed patients’ physical performance, functional status, comorbidity, cognition, nutrition, social support, polypharmacy, and psychological status. For the intervention group, a summary and management recommendations were provided to the treating oncologists.
The primary outcome was grade 3 or higher toxic effects within 3 months of starting a new regimen; secondary outcomes included treatment intensity and survival and GA outcomes within 3 months. A smaller proportion of patients in the intervention group experienced toxicity (51% vs. 71%), with an absolute risk reduction of 20%. Patients in the intervention group also had fewer falls and a greater reduction in medications used; there were no other differences in secondary outcomes. This study offers very strong and generalizable evidence that incorporating GA in the care of older adults with cancer at risk for toxicity can reduce toxicity as well as improve other outcomes, such as falls and polypharmacy.
Geriatric assessment and oncologist-patient communication
A secondary analysis3 of data from Dr. Mohile and colleagues2 evaluated the effect of GA-guided recommendations on oncologist-patient communication regarding comorbidities. Patients (n = 541) included in this analysis were 76.6 years of age on average and had 3.2 (standard deviation, 1.9) comorbid conditions. All patients underwent GA, but only oncologists in the intervention arm received GA-based recommendations. Clinical encounters between oncologist and patient immediately following the GA were audio recorded and analyzed to examine communication between oncologists and participants as it relates to chronic comorbid conditions.
In the intervention arm, more discussions regarding comorbidities took place, and more participants’ concerns about comorbidities were acknowledged. More importantly, participants in the intervention group were 2.4 times more likely to have their concerns about comorbidities addressed through referral or education, compared with the usual-care group (P = .004). Moreover, 41% of oncologists in the intervention arm modified dosage or cancer treatment schedule because of concern about tolerability or comorbidities. This study demonstrates beneficial effects of GA in increasing communication and perhaps consideration of comorbidities of older adults when planning cancer treatment.
Dr. Hung is professor of geriatrics and palliative care at Mount Sinai Hospital, New York. He disclosed no relevant conflicts of interest.
References
1. Li D et al. JAMA Oncol. 2021;7:e214158.
2. Mohile SG et al. Lancet. 2021;398:1894-1904.
3. Kleckner AS et al. JCO Oncol Pract. 2022;18:e9-19.
A version of this article first appeared on Medscape.com.
Hematocrit, White Blood Cells, and Thrombotic Events in the Veteran Population With Polycythemia Vera
Polycythemia vera (PV) is a rare myeloproliferative neoplasm affecting 44 to 57 individuals per 100,000 in the United States.1,2 It is characterized by somatic mutations in the hematopoietic stem cell, resulting in hyperproliferation of mature myeloid lineage cells.2 Sustained erythrocytosis is a hallmark of PV, although many patients also have leukocytosis and thrombocytosis.2,3 These patients have increased inherent thrombotic risk with arterial events reported to occur at rates of 7 to 21/1000 person-years and venous thrombotic events at 5 to 20/1000 person-years.4-7 Thrombotic and cardiovascular events are leading causes of morbidity and mortality, resulting in a reduced overall survival of patients with PV compared with the general population.3,8-10
Blood Cell Counts and Thrombotic Events in PV
Treatment strategies for patients with PV mainly aim to prevent or manage thrombotic and bleeding complications through normalization of blood counts.11 Hematocrit (Hct) control has been reported to be associated with reduced thrombotic risk in patients with PV. This was shown and popularized by the prospective, randomized Cytoreductive Therapy in Polycythemia Vera (CYTO-PV) trial in which participants were randomized 1:1 to maintaining either a low (< 45%) or high (45%-50%) Hct for 5 years to examine the long-term effects of more- or less-intensive cytoreductive therapy.12 Patients in the low-Hct group were found to have a lower rate of death from cardiovascular events or major thrombosis (1.1/100 person-years in the low-Hct group vs 4.4 in the high-Hct group; hazard ratio [HR], 3.91; 95% confidence interval [CI], 1.45-10.53; P = .007). Likewise, cardiovascular events occurred at a lower rate in patients in the low-Hct group compared with the high-Hct group (4.4% vs 10.9% of patients, respectively; HR, 2.69; 95% CI, 1.19-6.12; P = .02).12
Leukocytosis has also been linked to elevated risk for vascular events as shown in several studies, including the real-world European Collaboration on Low-Dose Aspirin in PV (ECLAP) observational study and a post hoc subanalysis of the CYTO-PV study.13,14 In a multivariate, time-dependent analysis in ECLAP, patients with white blood cell (WBC) counts > 15 × 109/L had a significant increase in the risk of thrombosis compared with those who had lower WBC counts, with higher WBC count more strongly associated with arterial than venous thromboembolism.13 In CYTO-PV, a significant correlation between elevated WBC count (≥ 11 × 109/L vs reference level of < 7 × 109/L) and time-dependent risk of major thrombosis was shown (HR, 3.9; 95% CI, 1.24-12.3; P = .02).14 Likewise, WBC count ≥ 11 × 109/L was found to be a predictor of subsequent venous events in a separate single-center multivariate analysis of patients with PV.8
Although CYTO-PV remains one of the largest prospective landmark studies in PV demonstrating the impact of Hct control on thrombosis, it is worthwhile to note that the patients in the high-Hct group who received less frequent myelosuppressive therapy with hydroxyurea than the low-Hct group also had higher WBC counts.12,15 Work is needed to determine the relative effects of high Hct and high WBC counts on PV independent of each other.
The Veteran Population with PV
Two recently published retrospective analyses from Parasuraman and colleagues used data from the Veterans Health Administration (VHA), the largest integrated health care system in the US, with an aim to replicate findings from CYTO-PV in a real-world population.16,17 The 2 analyses focused independently on the effects of Hct control and WBC count on the risk of a thrombotic event in patients with PV.
In the first retrospective analysis, 213 patients with PV and no prior thrombosis were placed into groups based on whether Hct levels were consistently either < 45% or ≥ 45% throughout the study period.17 The mean follow-up time was 2.3 years, during which 44.1% of patients experienced a thrombotic event (Figure 1). Patients with Hct levels < 45% had a lower rate of thrombotic events compared to those with levels ≥ 45% (40.3% vs 54.2%, respectively; HR, 1.61; 95% CI, 1.03-2.51; P = .04). In a sensitivity analysis that included patients with pre-index thrombotic events (N = 342), similar results were noted (55.6% vs 76.9% between the < 45% and ≥ 45% groups, respectively; HR, 1.95; 95% CI, 1.46-2.61; P < .001).
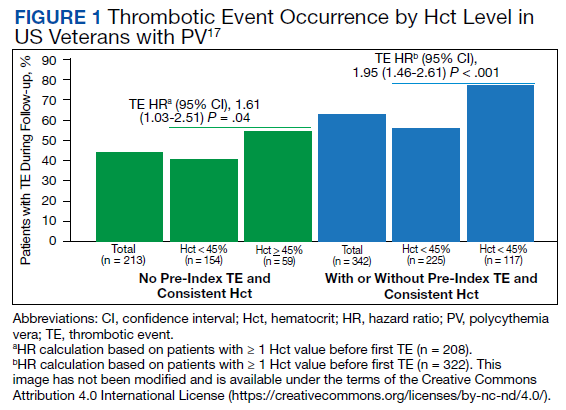
In the second analysis, the authors investigated the relationship between WBC counts and thrombotic events.16 Evaluable patients (N = 1565) were grouped into 1 of 4 cohorts based on the last WBC measurement taken during the study period before a thrombotic event or through the end of follow-up: (1) WBC < 7.0 × 109/L, (2) 7.0 to 8.4 × 109/L, (3) 8.5 to < 11.0 × 109/L, or (4) ≥ 11.0 × 109/L. Mean follow-up time ranged from 3.6 to 4.5 years among WBC count cohorts, during which 24.9% of patients experienced a thrombotic event. Compared with the reference cohort (WBC < 7.0 × 109/L), a significant positive association between WBC counts and thrombotic event occurrence was observed among patients with WBC counts of 8.5 to < 11.0 × 109/L (HR, 1.47; 95% CI, 1.10-1.96; P < .01) and ≥ 11 × 109/L (HR, 1.87; 95% CI, 1.44-2.43; P < .001) (Figure 2).16 When including all patients in a sensitivity analysis regardless of whether they experienced thrombotic events before the index date (N = 1876), similar results were obtained (7.0-8.4 × 109/L group: HR, 1.22; 95% CI, 0.97-1.55; P = .0959; 8.5 - 11.0 × 109/L group: HR, 1.41; 95% CI, 1.10-1.81; P = .0062; ≥ 11.0 × 109/L group: HR, 1.53; 95% CI, 1.23-1.91; P < .001; compared with < 7.0 × 109/L reference group). Rates of phlebotomy and cytoreductive treatments were similar across groups.16
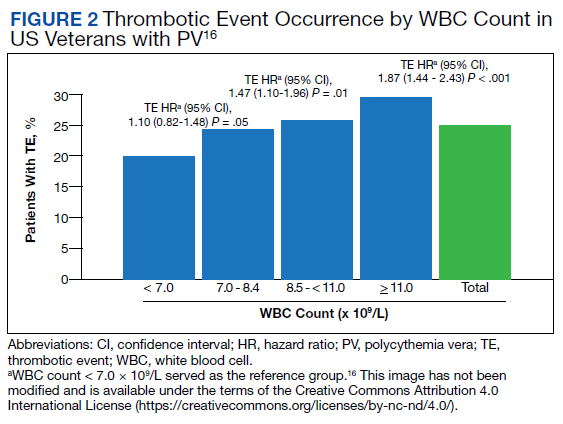
Some limitations to these studies are attributable to their retrospective design, reliance on health records, and the VHA population characteristics, which differ from the general population. For example, in this analysis, patients with PV in the VHA population had significantly increased risk of thrombotic events, even at a lower WBC count threshold (≥ 8.5 × 109/L) compared with those reported in CYTO-PV (≥ 11 × 109/L). Furthermore, approximately one-third of patients had elevated WBC levels, compared with 25.5% in the CYTO-PV study.14,16 This is most likely due to the unique nature of the VHA patient population, who are predominantly older adult men and generally have a higher comorbidity burden. A notable pre-index comorbidity burden was reported in the VHA population in the Hct analysis, even when compared to patients with PV in the general US population (Charlson Comorbidity Index score, 1.3 vs 0.8).6,17 Comorbid conditions such as hypertension, diabetes, and tobacco use, which are most common among the VHA population, are independently associated with higher risk of cardiovascular and thrombotic events.18,19 However, whether these higher levels of comorbidities affected the type of treatments they received was not elucidated, and the effectiveness of treatments to maintain target Hct levels was not addressed in the study.
Current PV Management and Future Implications
The National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology in myeloproliferative neoplasms recommend maintaining Hct levels < 45% in patients with PV.11 Patients with high-risk disease (age ≥ 60 years and/or history of thrombosis) are monitored for new thrombosis or bleeding and are managed for their cardiovascular risk factors. In addition, they receive low-dose aspirin (81-100 mg/day), undergo phlebotomy to maintain an Hct < 45%, and are managed with pharmacologic cytoreductive therapy. Cytoreductive therapy primarily consists of hydroxyurea or peginterferon alfa-2a for younger patients. Ruxolitinib, a Janus kinase (JAK1)/JAK2 inhibitor, is now approved by the US Food and Drug Administration as second-line treatment for those with PV that is intolerant or unresponsive to hydroxyurea or peginterferon alfa-2a treatments.11,20 However, the role of cytoreductive therapy is not clear for patients with low-risk disease (age < 60 years and no history of thrombosis). These patients are managed for their cardiovascular risk factors, undergo phlebotomy to maintain an Hct < 45%, are maintained on low-dose aspirin (81-100 mg/day), and are monitored for indications for cytoreductive therapy, which include any new thrombosis or disease-related major bleeding, frequent or persistent need for phlebotomy with poor tolerance for the procedure, splenomegaly, thrombocytosis, leukocytosis, and disease-related symptoms (eg, aquagenic pruritus, night sweats, fatigue).
Even though the current guidelines recommend maintaining a target Hct of < 45% in patients with high-risk PV, the role of Hct as the main determinant of thrombotic risk in patients with PV is still debated.21 In JAK2V617F-positive essential thrombocythemia, Hct levels are usually normal but risk of thrombosis is nevertheless still significant.22 The risk of thrombosis is significantly lower in primary familial and congenital polycythemia and much lower in secondary erythrocytosis such as cyanotic heart disease, long-term native dwellers of high altitude, and those with high-oxygen–affinity hemoglobins.21,23 In secondary erythrocytosis from hypoxia or upregulated hypoxic pathway such as hypoxia inducible factor-2α (HIF-2α) mutation and Chuvash erythrocytosis, the risk of thrombosis is more associated with the upregulated HIF pathway and its downstream consequences, rather than the elevated Hct level.24
However, most current literature supports the association of increased risk of thrombosis with higher Hct and high WBC count in patients with PV. In addition, the underlying mechanism of thrombogenesis still remains elusive; it is likely a complex process that involves interactions among multiple components, including elevated blood counts arising from clonal hematopoiesis, JAK2V617F allele burden, and platelet and WBC activation and their interaction with endothelial cells and inflammatory cytokines.25
Nevertheless, Hct control and aspirin use are current standard of care for patients with PV to mitigate thrombotic risk, and the results from the 2 analyses by Parasuraman and colleagues, using real-world data from the VHA, support the current practice guidelines to maintain Hct < 45% in these patients. They also provide additional support for considering WBC counts when determining patient risk and treatment plans. Although treatment response criteria from the European LeukemiaNet include achieving normal WBC levels to decrease the risk of thrombosis, current NCCN guidelines do not include WBC counts as a component for establishing patient risk or provide a target WBC count to guide patient management.11,26,27 Updates to these practice guidelines may be warranted. In addition, further study is needed to understand the mechanism of thrombogenesis in PV and other myeloproliferative disorders in order to develop novel therapeutic targets and improve patient outcomes.
Acknowledgments
Writing assistance was provided by Tania Iqbal, PhD, an employee of ICON (North Wales, PA), and was funded by Incyte Corporation (Wilmington, DE).
1. Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55(3):595-600. doi:10.3109/10428194.2013.813500
2. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. doi:10.1182/blood-2016-03-643544
3. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874-1881. doi:10.1038/leu.2013.163
4. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224-2232. doi:10.1200/JCO.2005.07.062
5. Vannucchi AM, Antonioli E, Guglielmelli P, et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110(3):840-846. doi:10.1182/blood-2006-12-064287
6. Goyal RK, Davis KL, Cote I, Mounedji N, Kaye JA. Increased incidence of thromboembolic event rates in patients diagnosed with polycythemia vera: results from an observational cohort study. Blood (ASH Annual Meeting Abstracts). 2014;124:4840. doi:10.1182/blood.V124.21.4840.4840
7. Barbui T, Carobbio A, Rumi E, et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood. 2014;124(19):3021-3023. doi:10.1182/blood-2014-07-591610 8. Cerquozzi S, Barraco D, Lasho T, et al. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017;7(12):662. doi:10.1038/s41408-017-0035-6
9. Stein BL, Moliterno AR, Tiu RV. Polycythemia vera disease burden: contributing factors, impact on quality of life, and emerging treatment options. Ann Hematol. 2014;93(12):1965-1976. doi:10.1007/s00277-014-2205-y
10. Hultcrantz M, Kristinsson SY, Andersson TM-L, et al. Patterns of survival among patients with myeloproliferative neoplasms diagnosed in Sweden from 1973 to 2008: a population-based study. J Clin Oncol. 2012;30(24):2995-3001. doi:10.1200/JCO.2012.42.1925
11. National Comprehensive Cancer Network. NCCN clinical practice guidelines in myeloproliferative neoplasms (Version 1.2020). Accessed March 3, 2022. https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
12. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22-33. doi:10.1056/NEJMoa1208500
13. Landolfi R, Di Gennaro L, Barbui T, et al. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood. 2007;109(6):2446-2452. doi:10.1182/blood-2006-08-042515
14. Barbui T, Masciulli A, Marfisi MR, et al. White blood cell counts and thrombosis in polycythemia vera: a subanalysis of the CYTO-PV study. Blood. 2015;126(4):560-561. doi:10.1182/blood-2015-04-638593
15. Prchal JT, Gordeuk VR. Treatment target in polycythemia vera. N Engl J Med. 2013;368(16):1555-1556. doi:10.1056/NEJMc1301262
16. Parasuraman S, Yu J, Paranagama D, et al. Elevated white blood cell levels and thrombotic events in patients with polycythemia vera: a real-world analysis of Veterans Health Administration data. Clin Lymphoma Myeloma Leuk. 2020;20(2):63-69. doi:10.1016/j.clml.2019.11.010
17. Parasuraman S, Yu J, Paranagama D, et al. Hematocrit levels and thrombotic events in patients with polycythemia vera: an analysis of Veterans Health Administration data. Ann Hematol. 2019;98(11):2533-2539. doi:10.1007/s00277-019-03793-w
18. WHO CVD Risk Chart Working Group. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7(10):e1332-e1345. doi:10.1016/S2214-109X(19)30318-3.
19. D’Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-753. doi:10.1161/CIRCULATIONAHA.107.699579
20. Jakafi. Package insert. Incyte Corporation; 2020.
21. Gordeuk VR, Key NS, Prchal JT. Re-evaluation of hematocrit as a determinant of thrombotic risk in erythrocytosis. Haematologica. 2019;104(4):653-658. doi:10.3324/haematol.2018.210732
22. Carobbio A, Thiele J, Passamonti F, et al. Risk factors for arterial and venous thrombosis in WHO-defined essential thrombocythemia: an international study of 891 patients. Blood. 2011;117(22):5857-5859. doi:10.1182/blood-2011-02-339002
23. Perloff JK, Marelli AJ, Miner PD. Risk of stroke in adults with cyanotic congenital heart disease. Circulation. 1993;87(6):1954-1959. doi:10.1161/01.cir.87.6.1954
24. Gordeuk VR, Miasnikova GY, Sergueeva AI, et al. Thrombotic risk in congenital erythrocytosis due to up-regulated hypoxia sensing is not associated with elevated hematocrit. Haematologica. 2020;105(3):e87-e90. doi:10.3324/haematol.2019.216267
25. Kroll MH, Michaelis LC, Verstovsek S. Mechanisms of thrombogenesis in polycythemia vera. Blood Rev. 2015;29(4):215-221. doi:10.1016/j.blre.2014.12.002
26. Barbui T, Tefferi A, Vannucchi AM, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018;32(5):1057-1069. doi:10.1038/s41375-018-0077-1
27. Barosi G, Mesa R, Finazzi G, et al. Revised response criteria for polycythemia vera and essential thrombocythemia: an ELN and IWG-MRT consensus project. Blood. 2013;121(23):4778-4781. doi:10.1182/blood-2013-01-478891
Polycythemia vera (PV) is a rare myeloproliferative neoplasm affecting 44 to 57 individuals per 100,000 in the United States.1,2 It is characterized by somatic mutations in the hematopoietic stem cell, resulting in hyperproliferation of mature myeloid lineage cells.2 Sustained erythrocytosis is a hallmark of PV, although many patients also have leukocytosis and thrombocytosis.2,3 These patients have increased inherent thrombotic risk with arterial events reported to occur at rates of 7 to 21/1000 person-years and venous thrombotic events at 5 to 20/1000 person-years.4-7 Thrombotic and cardiovascular events are leading causes of morbidity and mortality, resulting in a reduced overall survival of patients with PV compared with the general population.3,8-10
Blood Cell Counts and Thrombotic Events in PV
Treatment strategies for patients with PV mainly aim to prevent or manage thrombotic and bleeding complications through normalization of blood counts.11 Hematocrit (Hct) control has been reported to be associated with reduced thrombotic risk in patients with PV. This was shown and popularized by the prospective, randomized Cytoreductive Therapy in Polycythemia Vera (CYTO-PV) trial in which participants were randomized 1:1 to maintaining either a low (< 45%) or high (45%-50%) Hct for 5 years to examine the long-term effects of more- or less-intensive cytoreductive therapy.12 Patients in the low-Hct group were found to have a lower rate of death from cardiovascular events or major thrombosis (1.1/100 person-years in the low-Hct group vs 4.4 in the high-Hct group; hazard ratio [HR], 3.91; 95% confidence interval [CI], 1.45-10.53; P = .007). Likewise, cardiovascular events occurred at a lower rate in patients in the low-Hct group compared with the high-Hct group (4.4% vs 10.9% of patients, respectively; HR, 2.69; 95% CI, 1.19-6.12; P = .02).12
Leukocytosis has also been linked to elevated risk for vascular events as shown in several studies, including the real-world European Collaboration on Low-Dose Aspirin in PV (ECLAP) observational study and a post hoc subanalysis of the CYTO-PV study.13,14 In a multivariate, time-dependent analysis in ECLAP, patients with white blood cell (WBC) counts > 15 × 109/L had a significant increase in the risk of thrombosis compared with those who had lower WBC counts, with higher WBC count more strongly associated with arterial than venous thromboembolism.13 In CYTO-PV, a significant correlation between elevated WBC count (≥ 11 × 109/L vs reference level of < 7 × 109/L) and time-dependent risk of major thrombosis was shown (HR, 3.9; 95% CI, 1.24-12.3; P = .02).14 Likewise, WBC count ≥ 11 × 109/L was found to be a predictor of subsequent venous events in a separate single-center multivariate analysis of patients with PV.8
Although CYTO-PV remains one of the largest prospective landmark studies in PV demonstrating the impact of Hct control on thrombosis, it is worthwhile to note that the patients in the high-Hct group who received less frequent myelosuppressive therapy with hydroxyurea than the low-Hct group also had higher WBC counts.12,15 Work is needed to determine the relative effects of high Hct and high WBC counts on PV independent of each other.
The Veteran Population with PV
Two recently published retrospective analyses from Parasuraman and colleagues used data from the Veterans Health Administration (VHA), the largest integrated health care system in the US, with an aim to replicate findings from CYTO-PV in a real-world population.16,17 The 2 analyses focused independently on the effects of Hct control and WBC count on the risk of a thrombotic event in patients with PV.
In the first retrospective analysis, 213 patients with PV and no prior thrombosis were placed into groups based on whether Hct levels were consistently either < 45% or ≥ 45% throughout the study period.17 The mean follow-up time was 2.3 years, during which 44.1% of patients experienced a thrombotic event (Figure 1). Patients with Hct levels < 45% had a lower rate of thrombotic events compared to those with levels ≥ 45% (40.3% vs 54.2%, respectively; HR, 1.61; 95% CI, 1.03-2.51; P = .04). In a sensitivity analysis that included patients with pre-index thrombotic events (N = 342), similar results were noted (55.6% vs 76.9% between the < 45% and ≥ 45% groups, respectively; HR, 1.95; 95% CI, 1.46-2.61; P < .001).
In the second analysis, the authors investigated the relationship between WBC counts and thrombotic events.16 Evaluable patients (N = 1565) were grouped into 1 of 4 cohorts based on the last WBC measurement taken during the study period before a thrombotic event or through the end of follow-up: (1) WBC < 7.0 × 109/L, (2) 7.0 to 8.4 × 109/L, (3) 8.5 to < 11.0 × 109/L, or (4) ≥ 11.0 × 109/L. Mean follow-up time ranged from 3.6 to 4.5 years among WBC count cohorts, during which 24.9% of patients experienced a thrombotic event. Compared with the reference cohort (WBC < 7.0 × 109/L), a significant positive association between WBC counts and thrombotic event occurrence was observed among patients with WBC counts of 8.5 to < 11.0 × 109/L (HR, 1.47; 95% CI, 1.10-1.96; P < .01) and ≥ 11 × 109/L (HR, 1.87; 95% CI, 1.44-2.43; P < .001) (Figure 2).16 When including all patients in a sensitivity analysis regardless of whether they experienced thrombotic events before the index date (N = 1876), similar results were obtained (7.0-8.4 × 109/L group: HR, 1.22; 95% CI, 0.97-1.55; P = .0959; 8.5 - 11.0 × 109/L group: HR, 1.41; 95% CI, 1.10-1.81; P = .0062; ≥ 11.0 × 109/L group: HR, 1.53; 95% CI, 1.23-1.91; P < .001; compared with < 7.0 × 109/L reference group). Rates of phlebotomy and cytoreductive treatments were similar across groups.16
Some limitations to these studies are attributable to their retrospective design, reliance on health records, and the VHA population characteristics, which differ from the general population. For example, in this analysis, patients with PV in the VHA population had significantly increased risk of thrombotic events, even at a lower WBC count threshold (≥ 8.5 × 109/L) compared with those reported in CYTO-PV (≥ 11 × 109/L). Furthermore, approximately one-third of patients had elevated WBC levels, compared with 25.5% in the CYTO-PV study.14,16 This is most likely due to the unique nature of the VHA patient population, who are predominantly older adult men and generally have a higher comorbidity burden. A notable pre-index comorbidity burden was reported in the VHA population in the Hct analysis, even when compared to patients with PV in the general US population (Charlson Comorbidity Index score, 1.3 vs 0.8).6,17 Comorbid conditions such as hypertension, diabetes, and tobacco use, which are most common among the VHA population, are independently associated with higher risk of cardiovascular and thrombotic events.18,19 However, whether these higher levels of comorbidities affected the type of treatments they received was not elucidated, and the effectiveness of treatments to maintain target Hct levels was not addressed in the study.
Current PV Management and Future Implications
The National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology in myeloproliferative neoplasms recommend maintaining Hct levels < 45% in patients with PV.11 Patients with high-risk disease (age ≥ 60 years and/or history of thrombosis) are monitored for new thrombosis or bleeding and are managed for their cardiovascular risk factors. In addition, they receive low-dose aspirin (81-100 mg/day), undergo phlebotomy to maintain an Hct < 45%, and are managed with pharmacologic cytoreductive therapy. Cytoreductive therapy primarily consists of hydroxyurea or peginterferon alfa-2a for younger patients. Ruxolitinib, a Janus kinase (JAK1)/JAK2 inhibitor, is now approved by the US Food and Drug Administration as second-line treatment for those with PV that is intolerant or unresponsive to hydroxyurea or peginterferon alfa-2a treatments.11,20 However, the role of cytoreductive therapy is not clear for patients with low-risk disease (age < 60 years and no history of thrombosis). These patients are managed for their cardiovascular risk factors, undergo phlebotomy to maintain an Hct < 45%, are maintained on low-dose aspirin (81-100 mg/day), and are monitored for indications for cytoreductive therapy, which include any new thrombosis or disease-related major bleeding, frequent or persistent need for phlebotomy with poor tolerance for the procedure, splenomegaly, thrombocytosis, leukocytosis, and disease-related symptoms (eg, aquagenic pruritus, night sweats, fatigue).
Even though the current guidelines recommend maintaining a target Hct of < 45% in patients with high-risk PV, the role of Hct as the main determinant of thrombotic risk in patients with PV is still debated.21 In JAK2V617F-positive essential thrombocythemia, Hct levels are usually normal but risk of thrombosis is nevertheless still significant.22 The risk of thrombosis is significantly lower in primary familial and congenital polycythemia and much lower in secondary erythrocytosis such as cyanotic heart disease, long-term native dwellers of high altitude, and those with high-oxygen–affinity hemoglobins.21,23 In secondary erythrocytosis from hypoxia or upregulated hypoxic pathway such as hypoxia inducible factor-2α (HIF-2α) mutation and Chuvash erythrocytosis, the risk of thrombosis is more associated with the upregulated HIF pathway and its downstream consequences, rather than the elevated Hct level.24
However, most current literature supports the association of increased risk of thrombosis with higher Hct and high WBC count in patients with PV. In addition, the underlying mechanism of thrombogenesis still remains elusive; it is likely a complex process that involves interactions among multiple components, including elevated blood counts arising from clonal hematopoiesis, JAK2V617F allele burden, and platelet and WBC activation and their interaction with endothelial cells and inflammatory cytokines.25
Nevertheless, Hct control and aspirin use are current standard of care for patients with PV to mitigate thrombotic risk, and the results from the 2 analyses by Parasuraman and colleagues, using real-world data from the VHA, support the current practice guidelines to maintain Hct < 45% in these patients. They also provide additional support for considering WBC counts when determining patient risk and treatment plans. Although treatment response criteria from the European LeukemiaNet include achieving normal WBC levels to decrease the risk of thrombosis, current NCCN guidelines do not include WBC counts as a component for establishing patient risk or provide a target WBC count to guide patient management.11,26,27 Updates to these practice guidelines may be warranted. In addition, further study is needed to understand the mechanism of thrombogenesis in PV and other myeloproliferative disorders in order to develop novel therapeutic targets and improve patient outcomes.
Acknowledgments
Writing assistance was provided by Tania Iqbal, PhD, an employee of ICON (North Wales, PA), and was funded by Incyte Corporation (Wilmington, DE).
Polycythemia vera (PV) is a rare myeloproliferative neoplasm affecting 44 to 57 individuals per 100,000 in the United States.1,2 It is characterized by somatic mutations in the hematopoietic stem cell, resulting in hyperproliferation of mature myeloid lineage cells.2 Sustained erythrocytosis is a hallmark of PV, although many patients also have leukocytosis and thrombocytosis.2,3 These patients have increased inherent thrombotic risk with arterial events reported to occur at rates of 7 to 21/1000 person-years and venous thrombotic events at 5 to 20/1000 person-years.4-7 Thrombotic and cardiovascular events are leading causes of morbidity and mortality, resulting in a reduced overall survival of patients with PV compared with the general population.3,8-10
Blood Cell Counts and Thrombotic Events in PV
Treatment strategies for patients with PV mainly aim to prevent or manage thrombotic and bleeding complications through normalization of blood counts.11 Hematocrit (Hct) control has been reported to be associated with reduced thrombotic risk in patients with PV. This was shown and popularized by the prospective, randomized Cytoreductive Therapy in Polycythemia Vera (CYTO-PV) trial in which participants were randomized 1:1 to maintaining either a low (< 45%) or high (45%-50%) Hct for 5 years to examine the long-term effects of more- or less-intensive cytoreductive therapy.12 Patients in the low-Hct group were found to have a lower rate of death from cardiovascular events or major thrombosis (1.1/100 person-years in the low-Hct group vs 4.4 in the high-Hct group; hazard ratio [HR], 3.91; 95% confidence interval [CI], 1.45-10.53; P = .007). Likewise, cardiovascular events occurred at a lower rate in patients in the low-Hct group compared with the high-Hct group (4.4% vs 10.9% of patients, respectively; HR, 2.69; 95% CI, 1.19-6.12; P = .02).12
Leukocytosis has also been linked to elevated risk for vascular events as shown in several studies, including the real-world European Collaboration on Low-Dose Aspirin in PV (ECLAP) observational study and a post hoc subanalysis of the CYTO-PV study.13,14 In a multivariate, time-dependent analysis in ECLAP, patients with white blood cell (WBC) counts > 15 × 109/L had a significant increase in the risk of thrombosis compared with those who had lower WBC counts, with higher WBC count more strongly associated with arterial than venous thromboembolism.13 In CYTO-PV, a significant correlation between elevated WBC count (≥ 11 × 109/L vs reference level of < 7 × 109/L) and time-dependent risk of major thrombosis was shown (HR, 3.9; 95% CI, 1.24-12.3; P = .02).14 Likewise, WBC count ≥ 11 × 109/L was found to be a predictor of subsequent venous events in a separate single-center multivariate analysis of patients with PV.8
Although CYTO-PV remains one of the largest prospective landmark studies in PV demonstrating the impact of Hct control on thrombosis, it is worthwhile to note that the patients in the high-Hct group who received less frequent myelosuppressive therapy with hydroxyurea than the low-Hct group also had higher WBC counts.12,15 Work is needed to determine the relative effects of high Hct and high WBC counts on PV independent of each other.
The Veteran Population with PV
Two recently published retrospective analyses from Parasuraman and colleagues used data from the Veterans Health Administration (VHA), the largest integrated health care system in the US, with an aim to replicate findings from CYTO-PV in a real-world population.16,17 The 2 analyses focused independently on the effects of Hct control and WBC count on the risk of a thrombotic event in patients with PV.
In the first retrospective analysis, 213 patients with PV and no prior thrombosis were placed into groups based on whether Hct levels were consistently either < 45% or ≥ 45% throughout the study period.17 The mean follow-up time was 2.3 years, during which 44.1% of patients experienced a thrombotic event (Figure 1). Patients with Hct levels < 45% had a lower rate of thrombotic events compared to those with levels ≥ 45% (40.3% vs 54.2%, respectively; HR, 1.61; 95% CI, 1.03-2.51; P = .04). In a sensitivity analysis that included patients with pre-index thrombotic events (N = 342), similar results were noted (55.6% vs 76.9% between the < 45% and ≥ 45% groups, respectively; HR, 1.95; 95% CI, 1.46-2.61; P < .001).
In the second analysis, the authors investigated the relationship between WBC counts and thrombotic events.16 Evaluable patients (N = 1565) were grouped into 1 of 4 cohorts based on the last WBC measurement taken during the study period before a thrombotic event or through the end of follow-up: (1) WBC < 7.0 × 109/L, (2) 7.0 to 8.4 × 109/L, (3) 8.5 to < 11.0 × 109/L, or (4) ≥ 11.0 × 109/L. Mean follow-up time ranged from 3.6 to 4.5 years among WBC count cohorts, during which 24.9% of patients experienced a thrombotic event. Compared with the reference cohort (WBC < 7.0 × 109/L), a significant positive association between WBC counts and thrombotic event occurrence was observed among patients with WBC counts of 8.5 to < 11.0 × 109/L (HR, 1.47; 95% CI, 1.10-1.96; P < .01) and ≥ 11 × 109/L (HR, 1.87; 95% CI, 1.44-2.43; P < .001) (Figure 2).16 When including all patients in a sensitivity analysis regardless of whether they experienced thrombotic events before the index date (N = 1876), similar results were obtained (7.0-8.4 × 109/L group: HR, 1.22; 95% CI, 0.97-1.55; P = .0959; 8.5 - 11.0 × 109/L group: HR, 1.41; 95% CI, 1.10-1.81; P = .0062; ≥ 11.0 × 109/L group: HR, 1.53; 95% CI, 1.23-1.91; P < .001; compared with < 7.0 × 109/L reference group). Rates of phlebotomy and cytoreductive treatments were similar across groups.16
Some limitations to these studies are attributable to their retrospective design, reliance on health records, and the VHA population characteristics, which differ from the general population. For example, in this analysis, patients with PV in the VHA population had significantly increased risk of thrombotic events, even at a lower WBC count threshold (≥ 8.5 × 109/L) compared with those reported in CYTO-PV (≥ 11 × 109/L). Furthermore, approximately one-third of patients had elevated WBC levels, compared with 25.5% in the CYTO-PV study.14,16 This is most likely due to the unique nature of the VHA patient population, who are predominantly older adult men and generally have a higher comorbidity burden. A notable pre-index comorbidity burden was reported in the VHA population in the Hct analysis, even when compared to patients with PV in the general US population (Charlson Comorbidity Index score, 1.3 vs 0.8).6,17 Comorbid conditions such as hypertension, diabetes, and tobacco use, which are most common among the VHA population, are independently associated with higher risk of cardiovascular and thrombotic events.18,19 However, whether these higher levels of comorbidities affected the type of treatments they received was not elucidated, and the effectiveness of treatments to maintain target Hct levels was not addressed in the study.
Current PV Management and Future Implications
The National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology in myeloproliferative neoplasms recommend maintaining Hct levels < 45% in patients with PV.11 Patients with high-risk disease (age ≥ 60 years and/or history of thrombosis) are monitored for new thrombosis or bleeding and are managed for their cardiovascular risk factors. In addition, they receive low-dose aspirin (81-100 mg/day), undergo phlebotomy to maintain an Hct < 45%, and are managed with pharmacologic cytoreductive therapy. Cytoreductive therapy primarily consists of hydroxyurea or peginterferon alfa-2a for younger patients. Ruxolitinib, a Janus kinase (JAK1)/JAK2 inhibitor, is now approved by the US Food and Drug Administration as second-line treatment for those with PV that is intolerant or unresponsive to hydroxyurea or peginterferon alfa-2a treatments.11,20 However, the role of cytoreductive therapy is not clear for patients with low-risk disease (age < 60 years and no history of thrombosis). These patients are managed for their cardiovascular risk factors, undergo phlebotomy to maintain an Hct < 45%, are maintained on low-dose aspirin (81-100 mg/day), and are monitored for indications for cytoreductive therapy, which include any new thrombosis or disease-related major bleeding, frequent or persistent need for phlebotomy with poor tolerance for the procedure, splenomegaly, thrombocytosis, leukocytosis, and disease-related symptoms (eg, aquagenic pruritus, night sweats, fatigue).
Even though the current guidelines recommend maintaining a target Hct of < 45% in patients with high-risk PV, the role of Hct as the main determinant of thrombotic risk in patients with PV is still debated.21 In JAK2V617F-positive essential thrombocythemia, Hct levels are usually normal but risk of thrombosis is nevertheless still significant.22 The risk of thrombosis is significantly lower in primary familial and congenital polycythemia and much lower in secondary erythrocytosis such as cyanotic heart disease, long-term native dwellers of high altitude, and those with high-oxygen–affinity hemoglobins.21,23 In secondary erythrocytosis from hypoxia or upregulated hypoxic pathway such as hypoxia inducible factor-2α (HIF-2α) mutation and Chuvash erythrocytosis, the risk of thrombosis is more associated with the upregulated HIF pathway and its downstream consequences, rather than the elevated Hct level.24
However, most current literature supports the association of increased risk of thrombosis with higher Hct and high WBC count in patients with PV. In addition, the underlying mechanism of thrombogenesis still remains elusive; it is likely a complex process that involves interactions among multiple components, including elevated blood counts arising from clonal hematopoiesis, JAK2V617F allele burden, and platelet and WBC activation and their interaction with endothelial cells and inflammatory cytokines.25
Nevertheless, Hct control and aspirin use are current standard of care for patients with PV to mitigate thrombotic risk, and the results from the 2 analyses by Parasuraman and colleagues, using real-world data from the VHA, support the current practice guidelines to maintain Hct < 45% in these patients. They also provide additional support for considering WBC counts when determining patient risk and treatment plans. Although treatment response criteria from the European LeukemiaNet include achieving normal WBC levels to decrease the risk of thrombosis, current NCCN guidelines do not include WBC counts as a component for establishing patient risk or provide a target WBC count to guide patient management.11,26,27 Updates to these practice guidelines may be warranted. In addition, further study is needed to understand the mechanism of thrombogenesis in PV and other myeloproliferative disorders in order to develop novel therapeutic targets and improve patient outcomes.
Acknowledgments
Writing assistance was provided by Tania Iqbal, PhD, an employee of ICON (North Wales, PA), and was funded by Incyte Corporation (Wilmington, DE).
1. Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55(3):595-600. doi:10.3109/10428194.2013.813500
2. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. doi:10.1182/blood-2016-03-643544
3. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874-1881. doi:10.1038/leu.2013.163
4. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224-2232. doi:10.1200/JCO.2005.07.062
5. Vannucchi AM, Antonioli E, Guglielmelli P, et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110(3):840-846. doi:10.1182/blood-2006-12-064287
6. Goyal RK, Davis KL, Cote I, Mounedji N, Kaye JA. Increased incidence of thromboembolic event rates in patients diagnosed with polycythemia vera: results from an observational cohort study. Blood (ASH Annual Meeting Abstracts). 2014;124:4840. doi:10.1182/blood.V124.21.4840.4840
7. Barbui T, Carobbio A, Rumi E, et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood. 2014;124(19):3021-3023. doi:10.1182/blood-2014-07-591610 8. Cerquozzi S, Barraco D, Lasho T, et al. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017;7(12):662. doi:10.1038/s41408-017-0035-6
9. Stein BL, Moliterno AR, Tiu RV. Polycythemia vera disease burden: contributing factors, impact on quality of life, and emerging treatment options. Ann Hematol. 2014;93(12):1965-1976. doi:10.1007/s00277-014-2205-y
10. Hultcrantz M, Kristinsson SY, Andersson TM-L, et al. Patterns of survival among patients with myeloproliferative neoplasms diagnosed in Sweden from 1973 to 2008: a population-based study. J Clin Oncol. 2012;30(24):2995-3001. doi:10.1200/JCO.2012.42.1925
11. National Comprehensive Cancer Network. NCCN clinical practice guidelines in myeloproliferative neoplasms (Version 1.2020). Accessed March 3, 2022. https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
12. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22-33. doi:10.1056/NEJMoa1208500
13. Landolfi R, Di Gennaro L, Barbui T, et al. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood. 2007;109(6):2446-2452. doi:10.1182/blood-2006-08-042515
14. Barbui T, Masciulli A, Marfisi MR, et al. White blood cell counts and thrombosis in polycythemia vera: a subanalysis of the CYTO-PV study. Blood. 2015;126(4):560-561. doi:10.1182/blood-2015-04-638593
15. Prchal JT, Gordeuk VR. Treatment target in polycythemia vera. N Engl J Med. 2013;368(16):1555-1556. doi:10.1056/NEJMc1301262
16. Parasuraman S, Yu J, Paranagama D, et al. Elevated white blood cell levels and thrombotic events in patients with polycythemia vera: a real-world analysis of Veterans Health Administration data. Clin Lymphoma Myeloma Leuk. 2020;20(2):63-69. doi:10.1016/j.clml.2019.11.010
17. Parasuraman S, Yu J, Paranagama D, et al. Hematocrit levels and thrombotic events in patients with polycythemia vera: an analysis of Veterans Health Administration data. Ann Hematol. 2019;98(11):2533-2539. doi:10.1007/s00277-019-03793-w
18. WHO CVD Risk Chart Working Group. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7(10):e1332-e1345. doi:10.1016/S2214-109X(19)30318-3.
19. D’Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-753. doi:10.1161/CIRCULATIONAHA.107.699579
20. Jakafi. Package insert. Incyte Corporation; 2020.
21. Gordeuk VR, Key NS, Prchal JT. Re-evaluation of hematocrit as a determinant of thrombotic risk in erythrocytosis. Haematologica. 2019;104(4):653-658. doi:10.3324/haematol.2018.210732
22. Carobbio A, Thiele J, Passamonti F, et al. Risk factors for arterial and venous thrombosis in WHO-defined essential thrombocythemia: an international study of 891 patients. Blood. 2011;117(22):5857-5859. doi:10.1182/blood-2011-02-339002
23. Perloff JK, Marelli AJ, Miner PD. Risk of stroke in adults with cyanotic congenital heart disease. Circulation. 1993;87(6):1954-1959. doi:10.1161/01.cir.87.6.1954
24. Gordeuk VR, Miasnikova GY, Sergueeva AI, et al. Thrombotic risk in congenital erythrocytosis due to up-regulated hypoxia sensing is not associated with elevated hematocrit. Haematologica. 2020;105(3):e87-e90. doi:10.3324/haematol.2019.216267
25. Kroll MH, Michaelis LC, Verstovsek S. Mechanisms of thrombogenesis in polycythemia vera. Blood Rev. 2015;29(4):215-221. doi:10.1016/j.blre.2014.12.002
26. Barbui T, Tefferi A, Vannucchi AM, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018;32(5):1057-1069. doi:10.1038/s41375-018-0077-1
27. Barosi G, Mesa R, Finazzi G, et al. Revised response criteria for polycythemia vera and essential thrombocythemia: an ELN and IWG-MRT consensus project. Blood. 2013;121(23):4778-4781. doi:10.1182/blood-2013-01-478891
1. Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55(3):595-600. doi:10.3109/10428194.2013.813500
2. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. doi:10.1182/blood-2016-03-643544
3. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874-1881. doi:10.1038/leu.2013.163
4. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224-2232. doi:10.1200/JCO.2005.07.062
5. Vannucchi AM, Antonioli E, Guglielmelli P, et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110(3):840-846. doi:10.1182/blood-2006-12-064287
6. Goyal RK, Davis KL, Cote I, Mounedji N, Kaye JA. Increased incidence of thromboembolic event rates in patients diagnosed with polycythemia vera: results from an observational cohort study. Blood (ASH Annual Meeting Abstracts). 2014;124:4840. doi:10.1182/blood.V124.21.4840.4840
7. Barbui T, Carobbio A, Rumi E, et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood. 2014;124(19):3021-3023. doi:10.1182/blood-2014-07-591610 8. Cerquozzi S, Barraco D, Lasho T, et al. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017;7(12):662. doi:10.1038/s41408-017-0035-6
9. Stein BL, Moliterno AR, Tiu RV. Polycythemia vera disease burden: contributing factors, impact on quality of life, and emerging treatment options. Ann Hematol. 2014;93(12):1965-1976. doi:10.1007/s00277-014-2205-y
10. Hultcrantz M, Kristinsson SY, Andersson TM-L, et al. Patterns of survival among patients with myeloproliferative neoplasms diagnosed in Sweden from 1973 to 2008: a population-based study. J Clin Oncol. 2012;30(24):2995-3001. doi:10.1200/JCO.2012.42.1925
11. National Comprehensive Cancer Network. NCCN clinical practice guidelines in myeloproliferative neoplasms (Version 1.2020). Accessed March 3, 2022. https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
12. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22-33. doi:10.1056/NEJMoa1208500
13. Landolfi R, Di Gennaro L, Barbui T, et al. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood. 2007;109(6):2446-2452. doi:10.1182/blood-2006-08-042515
14. Barbui T, Masciulli A, Marfisi MR, et al. White blood cell counts and thrombosis in polycythemia vera: a subanalysis of the CYTO-PV study. Blood. 2015;126(4):560-561. doi:10.1182/blood-2015-04-638593
15. Prchal JT, Gordeuk VR. Treatment target in polycythemia vera. N Engl J Med. 2013;368(16):1555-1556. doi:10.1056/NEJMc1301262
16. Parasuraman S, Yu J, Paranagama D, et al. Elevated white blood cell levels and thrombotic events in patients with polycythemia vera: a real-world analysis of Veterans Health Administration data. Clin Lymphoma Myeloma Leuk. 2020;20(2):63-69. doi:10.1016/j.clml.2019.11.010
17. Parasuraman S, Yu J, Paranagama D, et al. Hematocrit levels and thrombotic events in patients with polycythemia vera: an analysis of Veterans Health Administration data. Ann Hematol. 2019;98(11):2533-2539. doi:10.1007/s00277-019-03793-w
18. WHO CVD Risk Chart Working Group. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7(10):e1332-e1345. doi:10.1016/S2214-109X(19)30318-3.
19. D’Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-753. doi:10.1161/CIRCULATIONAHA.107.699579
20. Jakafi. Package insert. Incyte Corporation; 2020.
21. Gordeuk VR, Key NS, Prchal JT. Re-evaluation of hematocrit as a determinant of thrombotic risk in erythrocytosis. Haematologica. 2019;104(4):653-658. doi:10.3324/haematol.2018.210732
22. Carobbio A, Thiele J, Passamonti F, et al. Risk factors for arterial and venous thrombosis in WHO-defined essential thrombocythemia: an international study of 891 patients. Blood. 2011;117(22):5857-5859. doi:10.1182/blood-2011-02-339002
23. Perloff JK, Marelli AJ, Miner PD. Risk of stroke in adults with cyanotic congenital heart disease. Circulation. 1993;87(6):1954-1959. doi:10.1161/01.cir.87.6.1954
24. Gordeuk VR, Miasnikova GY, Sergueeva AI, et al. Thrombotic risk in congenital erythrocytosis due to up-regulated hypoxia sensing is not associated with elevated hematocrit. Haematologica. 2020;105(3):e87-e90. doi:10.3324/haematol.2019.216267
25. Kroll MH, Michaelis LC, Verstovsek S. Mechanisms of thrombogenesis in polycythemia vera. Blood Rev. 2015;29(4):215-221. doi:10.1016/j.blre.2014.12.002
26. Barbui T, Tefferi A, Vannucchi AM, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018;32(5):1057-1069. doi:10.1038/s41375-018-0077-1
27. Barosi G, Mesa R, Finazzi G, et al. Revised response criteria for polycythemia vera and essential thrombocythemia: an ELN and IWG-MRT consensus project. Blood. 2013;121(23):4778-4781. doi:10.1182/blood-2013-01-478891