User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Legal abortion is a matter of public health
On June 24, the U.S. Supreme Court overturned Roe v. Wade, a decision that was issued in 1973. From now on, each state will be able to choose the laws that it wants to put in place regarding abortion. Several states have already decided to ban abortion altogether. As a physician, but also as a woman, I am stunned to see this opposition to a right that, in my opinion, is also a matter of public health.
International data
In Belgium, voluntary termination of pregnancy (VTP) has been allowed since 1990. Except in the case of a serious medical problem, the abortion must take place before the end of the 12th week after conception. So, 14 weeks from the last menstrual period (LMP).
Beyond that time frame, a VTP can be performed only when the continuation of the pregnancy endangers the health of the woman or when it is certain that the unborn child will be affected by a condition of particular gravity and recognized as incurable at the time of diagnosis. This is referred to as termination for medical reasons (TFMR).
First observation
The annual number of VTPs did not climb following legalization. For the past 20 years in Belgium, that number has remained stable, hovering around 19,000. Abortion continues to be an action – neither trivialized nor minimized – that is difficult for any woman to take, no matter what her reason.
Second observation
Over 60% of women who had an abortion were using a form of contraception. So, while the burden of contraception still rests almost exclusively on the woman, it cannot be said that those who had a VTP did not use some method of birth control.
Even more important, legal abortions have very few complications, either physical or psychological. Studies show that pregnancy itself carries a higher risk for psychopathological manifestations than a VTP. These VTPs are safe, and women quickly recover from them. The most sensitive time seems to be the period before the abortion, and it’s at this stage that most of the psychological and psychopathological manifestations accumulate. The majority of women facing a VTP experience feelings of relief, and only a minority develop psychological problems, usually when there is already a history of mental disorder. The literature shows that the levels of anxiety and depression decrease in the month following the abortion. Being denied a VTP, on the other hand, significantly increases the woman’s risk of developing a mental disorder.
Should a VTP be denied, a woman, if she determines that she doesn’t have any other choice, may then end up turning to a back-alley abortion. The methods used for this are medieval, dangerous, and may not prove successful – things like using chemicals, piercing the amniotic sac with a needle or sharp object (the famous coat hanger), eating or drinking abortifacient herbs, taking large quantities of medication, punching the stomach, falling down stairs, and engaging in intense physical exercise.
From there, these risky methods inevitably lead to numerous complications: Incomplete abortions, infections, septicemia, breakthrough bleeding, subsequent sterility, laceration of the uterine wall, or death.
Around one-third of women who undergo risky abortions develop complications, while less than half receive care.
The World Health Organization estimates that back-alley abortions represent 49% of abortions worldwide. It puts the number of illegal abortions performed each year at 20 million.
Each year, around 60,000 women worldwide die as a result of an unsafe VTP. That’s one woman every 9 minutes. And odds are that these figures are underestimated.
Making the decision to resort to a VTP is always difficult. Ideally, you should be able to discuss it with your partner, when there is one, and with your close friends and family, to have someone go with you as support, to weigh the pros and cons, and to make a choice in line with your convictions and your conscience. But first and foremost, the law must guarantee the right to be able to ask oneself this question, because guaranteeing this right is also guaranteeing the health and safety of women, and that is why this remains a public health imperative.
A version of this article first appeared on Medscape.com. This article was translated from MediQuality.
On June 24, the U.S. Supreme Court overturned Roe v. Wade, a decision that was issued in 1973. From now on, each state will be able to choose the laws that it wants to put in place regarding abortion. Several states have already decided to ban abortion altogether. As a physician, but also as a woman, I am stunned to see this opposition to a right that, in my opinion, is also a matter of public health.
International data
In Belgium, voluntary termination of pregnancy (VTP) has been allowed since 1990. Except in the case of a serious medical problem, the abortion must take place before the end of the 12th week after conception. So, 14 weeks from the last menstrual period (LMP).
Beyond that time frame, a VTP can be performed only when the continuation of the pregnancy endangers the health of the woman or when it is certain that the unborn child will be affected by a condition of particular gravity and recognized as incurable at the time of diagnosis. This is referred to as termination for medical reasons (TFMR).
First observation
The annual number of VTPs did not climb following legalization. For the past 20 years in Belgium, that number has remained stable, hovering around 19,000. Abortion continues to be an action – neither trivialized nor minimized – that is difficult for any woman to take, no matter what her reason.
Second observation
Over 60% of women who had an abortion were using a form of contraception. So, while the burden of contraception still rests almost exclusively on the woman, it cannot be said that those who had a VTP did not use some method of birth control.
Even more important, legal abortions have very few complications, either physical or psychological. Studies show that pregnancy itself carries a higher risk for psychopathological manifestations than a VTP. These VTPs are safe, and women quickly recover from them. The most sensitive time seems to be the period before the abortion, and it’s at this stage that most of the psychological and psychopathological manifestations accumulate. The majority of women facing a VTP experience feelings of relief, and only a minority develop psychological problems, usually when there is already a history of mental disorder. The literature shows that the levels of anxiety and depression decrease in the month following the abortion. Being denied a VTP, on the other hand, significantly increases the woman’s risk of developing a mental disorder.
Should a VTP be denied, a woman, if she determines that she doesn’t have any other choice, may then end up turning to a back-alley abortion. The methods used for this are medieval, dangerous, and may not prove successful – things like using chemicals, piercing the amniotic sac with a needle or sharp object (the famous coat hanger), eating or drinking abortifacient herbs, taking large quantities of medication, punching the stomach, falling down stairs, and engaging in intense physical exercise.
From there, these risky methods inevitably lead to numerous complications: Incomplete abortions, infections, septicemia, breakthrough bleeding, subsequent sterility, laceration of the uterine wall, or death.
Around one-third of women who undergo risky abortions develop complications, while less than half receive care.
The World Health Organization estimates that back-alley abortions represent 49% of abortions worldwide. It puts the number of illegal abortions performed each year at 20 million.
Each year, around 60,000 women worldwide die as a result of an unsafe VTP. That’s one woman every 9 minutes. And odds are that these figures are underestimated.
Making the decision to resort to a VTP is always difficult. Ideally, you should be able to discuss it with your partner, when there is one, and with your close friends and family, to have someone go with you as support, to weigh the pros and cons, and to make a choice in line with your convictions and your conscience. But first and foremost, the law must guarantee the right to be able to ask oneself this question, because guaranteeing this right is also guaranteeing the health and safety of women, and that is why this remains a public health imperative.
A version of this article first appeared on Medscape.com. This article was translated from MediQuality.
On June 24, the U.S. Supreme Court overturned Roe v. Wade, a decision that was issued in 1973. From now on, each state will be able to choose the laws that it wants to put in place regarding abortion. Several states have already decided to ban abortion altogether. As a physician, but also as a woman, I am stunned to see this opposition to a right that, in my opinion, is also a matter of public health.
International data
In Belgium, voluntary termination of pregnancy (VTP) has been allowed since 1990. Except in the case of a serious medical problem, the abortion must take place before the end of the 12th week after conception. So, 14 weeks from the last menstrual period (LMP).
Beyond that time frame, a VTP can be performed only when the continuation of the pregnancy endangers the health of the woman or when it is certain that the unborn child will be affected by a condition of particular gravity and recognized as incurable at the time of diagnosis. This is referred to as termination for medical reasons (TFMR).
First observation
The annual number of VTPs did not climb following legalization. For the past 20 years in Belgium, that number has remained stable, hovering around 19,000. Abortion continues to be an action – neither trivialized nor minimized – that is difficult for any woman to take, no matter what her reason.
Second observation
Over 60% of women who had an abortion were using a form of contraception. So, while the burden of contraception still rests almost exclusively on the woman, it cannot be said that those who had a VTP did not use some method of birth control.
Even more important, legal abortions have very few complications, either physical or psychological. Studies show that pregnancy itself carries a higher risk for psychopathological manifestations than a VTP. These VTPs are safe, and women quickly recover from them. The most sensitive time seems to be the period before the abortion, and it’s at this stage that most of the psychological and psychopathological manifestations accumulate. The majority of women facing a VTP experience feelings of relief, and only a minority develop psychological problems, usually when there is already a history of mental disorder. The literature shows that the levels of anxiety and depression decrease in the month following the abortion. Being denied a VTP, on the other hand, significantly increases the woman’s risk of developing a mental disorder.
Should a VTP be denied, a woman, if she determines that she doesn’t have any other choice, may then end up turning to a back-alley abortion. The methods used for this are medieval, dangerous, and may not prove successful – things like using chemicals, piercing the amniotic sac with a needle or sharp object (the famous coat hanger), eating or drinking abortifacient herbs, taking large quantities of medication, punching the stomach, falling down stairs, and engaging in intense physical exercise.
From there, these risky methods inevitably lead to numerous complications: Incomplete abortions, infections, septicemia, breakthrough bleeding, subsequent sterility, laceration of the uterine wall, or death.
Around one-third of women who undergo risky abortions develop complications, while less than half receive care.
The World Health Organization estimates that back-alley abortions represent 49% of abortions worldwide. It puts the number of illegal abortions performed each year at 20 million.
Each year, around 60,000 women worldwide die as a result of an unsafe VTP. That’s one woman every 9 minutes. And odds are that these figures are underestimated.
Making the decision to resort to a VTP is always difficult. Ideally, you should be able to discuss it with your partner, when there is one, and with your close friends and family, to have someone go with you as support, to weigh the pros and cons, and to make a choice in line with your convictions and your conscience. But first and foremost, the law must guarantee the right to be able to ask oneself this question, because guaranteeing this right is also guaranteeing the health and safety of women, and that is why this remains a public health imperative.
A version of this article first appeared on Medscape.com. This article was translated from MediQuality.
Coming to a pill near you: The exercise molecule
Exercise in a pill? Sign us up
You just got home from a long shift and you know you should go to the gym, but the bed is calling and you just answered. We know sometimes we have to make sacrifices in the name of fitness, but there just aren’t enough hours in the day. Unless our prayers have been answered. There could be a pill that has the benefits of working out without having to work out.
In a study published in Nature, investigators reported that they have identified a molecule made during exercise and used it on mice, which took in less food after being given the pill, which may open doors to understanding how exercise affects hunger.

In the first part of the study, the researchers found the molecule, known as Lac-Phe – which is synthesized from lactate and phenylalanine – in the blood plasma of mice after they had run on a treadmill.
The investigators then gave a Lac-Phe supplement to mice on high-fat diets and found that their food intake was about 50% of what other mice were eating. The supplement also improved their glucose tolerance.
Because the research also found Lac-Phe in humans who exercised, they hope that this pill will be in our future. “Our next steps include finding more details about how Lac-Phe mediates its effects in the body, including the brain,” Yong Xu, MD, of Baylor College of Medicine, Houston, said in a written statement. “Our goal is to learn to modulate this exercise pathway for therapeutic interventions.”
As always, we are rooting for you, science!
Gonorrhea and grandparents: A match made in prehistoric heaven
*Editorial note: LOTME takes no responsibility for any unfortunate imagery the reader may have experienced from the above headline.
Old people are the greatest. Back pains, cognitive decline, aches in all the diodes down your left side, there’s nothing quite like your golden years. Notably, however, humans are one of the few animals who experience true old age, as most creatures are adapted to maximize reproductive potential. As such, living past menopause is rare in the animal kingdom.
This is where the “grandmother hypothesis” comes in: Back in Ye Olde Stone Age, women who lived into old age could provide child care for younger women, because human babies require a lot more time and attention than other animal offspring. But how did humans end up living so long? Enter a group of Californian researchers, who believe they have an answer. It was gonorrhea.
When compared with the chimpanzee genome (as well as with Neanderthals and Denisovans, our closest ancestors), humans have a unique mutated version of the CD33 gene that lacks a sugar-binding site; the standard version uses the sugar-binding site to protect against autoimmune response in the body, but that same site actually suppresses the brain’s ability to clear away damaged brain cells and amyloid, which eventually leads to diseases like dementia. The mutated version allows microglia (brain immune cells) to attack and clear out this unwanted material. People with higher levels of this mutated CD33 variant actually have higher protection against Alzheimer’s.
Interestingly, gonorrhea bacteria are coated in the same sugar that standard CD33 receptors bind to, thus allowing them to bypass the body’s immune system. According to the researchers, the mutated CD33 version likely emerged as a protection against gonorrhea, depriving the bacteria of their “molecular mimicry” abilities. In one of life’s happy accidents, it turned out this mutation also protects against age-related diseases, thus allowing humans with the mutation to live longer. Obviously, this was a good thing, and we ran with it until the modern day. Now we have senior citizens climbing Everest, and all our politicians keep on politicking into their 70s and 80s ... well, everything has its drawbacks.
Parents raise a glass to children’s food addiction
There can be something pretty addicting about processed foods. Have you ever eaten just one french fry? Or taken just one cookie? If so, your willpower is incredible. For many of us, it can be a struggle to stop.

A recent study from the University of Michigan, which considered the existence of an eating phenotype, suggests our parents’ habits could be to blame.
By administering a series of questionnaires that inquired about food addiction, alcohol use disorders, cannabis use disorder, nicotine/e-cigarette dependence, and their family tree, investigators found that participants with a “paternal history of problematic alcohol use” had higher risk of food addiction but not obesity.
Apparently about one in five people display a clinically significant addiction to highly processed foods. It was noted that foods like ice cream, pizza, and french fries have high amounts of refined carbs and fats, which could trigger an addictive response.
Lindzey Hoover, a graduate student at the university who was the study’s lead author, noted that living in an environment where these foods are cheap and accessible can be really challenging for those with a family history of addiction. The investigators suggested that public health approaches, like restriction of other substances and marketing to kids, should be put in place for highly processed foods.
Maybe french fries should come with a warning label.
A prescription for America’s traffic problems
Nostalgia is a funny thing. Do you ever feel nostalgic about things that really weren’t very pleasant in the first place? Take, for instance, the morning commute. Here in the Washington area, more than 2 years into the COVID era, the traffic is still not what it used to be … and we kind of miss it.

Nah, not really. That was just a way to get everyone thinking about driving, because AAA has something of an explanation for the situation out there on the highways and byways of America. It’s drugs. No, not those kinds of drugs. This time it’s prescription drugs that are the problem. Well, part of the problem, anyway.
AAA did a survey last summer and found that nearly 50% of drivers “used one or more potentially impairing medications in the past 30 days. … The proportion of those choosing to drive is higher among those taking multiple medications.” How much higher? More than 63% of those with two or more prescriptions were driving within 2 hours of taking at least one of those meds, as were 71% of those taking three or more.
The 2,657 respondents also were asked about the types of potentially impairing drugs they were taking: 61% of those using antidepressants had been on the road within 2 hours of use at least once in the past 30 days, as had 73% of those taking an amphetamine, AAA said.
So there you have it. That guy in the BMW who’s been tailgating you for the last 3 miles? He may be a jerk, but there’s a good chance he’s a jerk with a prescription … or two … or three.
Exercise in a pill? Sign us up
You just got home from a long shift and you know you should go to the gym, but the bed is calling and you just answered. We know sometimes we have to make sacrifices in the name of fitness, but there just aren’t enough hours in the day. Unless our prayers have been answered. There could be a pill that has the benefits of working out without having to work out.
In a study published in Nature, investigators reported that they have identified a molecule made during exercise and used it on mice, which took in less food after being given the pill, which may open doors to understanding how exercise affects hunger.
In the first part of the study, the researchers found the molecule, known as Lac-Phe – which is synthesized from lactate and phenylalanine – in the blood plasma of mice after they had run on a treadmill.
The investigators then gave a Lac-Phe supplement to mice on high-fat diets and found that their food intake was about 50% of what other mice were eating. The supplement also improved their glucose tolerance.
Because the research also found Lac-Phe in humans who exercised, they hope that this pill will be in our future. “Our next steps include finding more details about how Lac-Phe mediates its effects in the body, including the brain,” Yong Xu, MD, of Baylor College of Medicine, Houston, said in a written statement. “Our goal is to learn to modulate this exercise pathway for therapeutic interventions.”
As always, we are rooting for you, science!
Gonorrhea and grandparents: A match made in prehistoric heaven
*Editorial note: LOTME takes no responsibility for any unfortunate imagery the reader may have experienced from the above headline.
Old people are the greatest. Back pains, cognitive decline, aches in all the diodes down your left side, there’s nothing quite like your golden years. Notably, however, humans are one of the few animals who experience true old age, as most creatures are adapted to maximize reproductive potential. As such, living past menopause is rare in the animal kingdom.
This is where the “grandmother hypothesis” comes in: Back in Ye Olde Stone Age, women who lived into old age could provide child care for younger women, because human babies require a lot more time and attention than other animal offspring. But how did humans end up living so long? Enter a group of Californian researchers, who believe they have an answer. It was gonorrhea.
When compared with the chimpanzee genome (as well as with Neanderthals and Denisovans, our closest ancestors), humans have a unique mutated version of the CD33 gene that lacks a sugar-binding site; the standard version uses the sugar-binding site to protect against autoimmune response in the body, but that same site actually suppresses the brain’s ability to clear away damaged brain cells and amyloid, which eventually leads to diseases like dementia. The mutated version allows microglia (brain immune cells) to attack and clear out this unwanted material. People with higher levels of this mutated CD33 variant actually have higher protection against Alzheimer’s.
Interestingly, gonorrhea bacteria are coated in the same sugar that standard CD33 receptors bind to, thus allowing them to bypass the body’s immune system. According to the researchers, the mutated CD33 version likely emerged as a protection against gonorrhea, depriving the bacteria of their “molecular mimicry” abilities. In one of life’s happy accidents, it turned out this mutation also protects against age-related diseases, thus allowing humans with the mutation to live longer. Obviously, this was a good thing, and we ran with it until the modern day. Now we have senior citizens climbing Everest, and all our politicians keep on politicking into their 70s and 80s ... well, everything has its drawbacks.
Parents raise a glass to children’s food addiction
There can be something pretty addicting about processed foods. Have you ever eaten just one french fry? Or taken just one cookie? If so, your willpower is incredible. For many of us, it can be a struggle to stop.
A recent study from the University of Michigan, which considered the existence of an eating phenotype, suggests our parents’ habits could be to blame.
By administering a series of questionnaires that inquired about food addiction, alcohol use disorders, cannabis use disorder, nicotine/e-cigarette dependence, and their family tree, investigators found that participants with a “paternal history of problematic alcohol use” had higher risk of food addiction but not obesity.
Apparently about one in five people display a clinically significant addiction to highly processed foods. It was noted that foods like ice cream, pizza, and french fries have high amounts of refined carbs and fats, which could trigger an addictive response.
Lindzey Hoover, a graduate student at the university who was the study’s lead author, noted that living in an environment where these foods are cheap and accessible can be really challenging for those with a family history of addiction. The investigators suggested that public health approaches, like restriction of other substances and marketing to kids, should be put in place for highly processed foods.
Maybe french fries should come with a warning label.
A prescription for America’s traffic problems
Nostalgia is a funny thing. Do you ever feel nostalgic about things that really weren’t very pleasant in the first place? Take, for instance, the morning commute. Here in the Washington area, more than 2 years into the COVID era, the traffic is still not what it used to be … and we kind of miss it.
Nah, not really. That was just a way to get everyone thinking about driving, because AAA has something of an explanation for the situation out there on the highways and byways of America. It’s drugs. No, not those kinds of drugs. This time it’s prescription drugs that are the problem. Well, part of the problem, anyway.
AAA did a survey last summer and found that nearly 50% of drivers “used one or more potentially impairing medications in the past 30 days. … The proportion of those choosing to drive is higher among those taking multiple medications.” How much higher? More than 63% of those with two or more prescriptions were driving within 2 hours of taking at least one of those meds, as were 71% of those taking three or more.
The 2,657 respondents also were asked about the types of potentially impairing drugs they were taking: 61% of those using antidepressants had been on the road within 2 hours of use at least once in the past 30 days, as had 73% of those taking an amphetamine, AAA said.
So there you have it. That guy in the BMW who’s been tailgating you for the last 3 miles? He may be a jerk, but there’s a good chance he’s a jerk with a prescription … or two … or three.
Exercise in a pill? Sign us up
You just got home from a long shift and you know you should go to the gym, but the bed is calling and you just answered. We know sometimes we have to make sacrifices in the name of fitness, but there just aren’t enough hours in the day. Unless our prayers have been answered. There could be a pill that has the benefits of working out without having to work out.
In a study published in Nature, investigators reported that they have identified a molecule made during exercise and used it on mice, which took in less food after being given the pill, which may open doors to understanding how exercise affects hunger.
In the first part of the study, the researchers found the molecule, known as Lac-Phe – which is synthesized from lactate and phenylalanine – in the blood plasma of mice after they had run on a treadmill.
The investigators then gave a Lac-Phe supplement to mice on high-fat diets and found that their food intake was about 50% of what other mice were eating. The supplement also improved their glucose tolerance.
Because the research also found Lac-Phe in humans who exercised, they hope that this pill will be in our future. “Our next steps include finding more details about how Lac-Phe mediates its effects in the body, including the brain,” Yong Xu, MD, of Baylor College of Medicine, Houston, said in a written statement. “Our goal is to learn to modulate this exercise pathway for therapeutic interventions.”
As always, we are rooting for you, science!
Gonorrhea and grandparents: A match made in prehistoric heaven
*Editorial note: LOTME takes no responsibility for any unfortunate imagery the reader may have experienced from the above headline.
Old people are the greatest. Back pains, cognitive decline, aches in all the diodes down your left side, there’s nothing quite like your golden years. Notably, however, humans are one of the few animals who experience true old age, as most creatures are adapted to maximize reproductive potential. As such, living past menopause is rare in the animal kingdom.
This is where the “grandmother hypothesis” comes in: Back in Ye Olde Stone Age, women who lived into old age could provide child care for younger women, because human babies require a lot more time and attention than other animal offspring. But how did humans end up living so long? Enter a group of Californian researchers, who believe they have an answer. It was gonorrhea.
When compared with the chimpanzee genome (as well as with Neanderthals and Denisovans, our closest ancestors), humans have a unique mutated version of the CD33 gene that lacks a sugar-binding site; the standard version uses the sugar-binding site to protect against autoimmune response in the body, but that same site actually suppresses the brain’s ability to clear away damaged brain cells and amyloid, which eventually leads to diseases like dementia. The mutated version allows microglia (brain immune cells) to attack and clear out this unwanted material. People with higher levels of this mutated CD33 variant actually have higher protection against Alzheimer’s.
Interestingly, gonorrhea bacteria are coated in the same sugar that standard CD33 receptors bind to, thus allowing them to bypass the body’s immune system. According to the researchers, the mutated CD33 version likely emerged as a protection against gonorrhea, depriving the bacteria of their “molecular mimicry” abilities. In one of life’s happy accidents, it turned out this mutation also protects against age-related diseases, thus allowing humans with the mutation to live longer. Obviously, this was a good thing, and we ran with it until the modern day. Now we have senior citizens climbing Everest, and all our politicians keep on politicking into their 70s and 80s ... well, everything has its drawbacks.
Parents raise a glass to children’s food addiction
There can be something pretty addicting about processed foods. Have you ever eaten just one french fry? Or taken just one cookie? If so, your willpower is incredible. For many of us, it can be a struggle to stop.
A recent study from the University of Michigan, which considered the existence of an eating phenotype, suggests our parents’ habits could be to blame.
By administering a series of questionnaires that inquired about food addiction, alcohol use disorders, cannabis use disorder, nicotine/e-cigarette dependence, and their family tree, investigators found that participants with a “paternal history of problematic alcohol use” had higher risk of food addiction but not obesity.
Apparently about one in five people display a clinically significant addiction to highly processed foods. It was noted that foods like ice cream, pizza, and french fries have high amounts of refined carbs and fats, which could trigger an addictive response.
Lindzey Hoover, a graduate student at the university who was the study’s lead author, noted that living in an environment where these foods are cheap and accessible can be really challenging for those with a family history of addiction. The investigators suggested that public health approaches, like restriction of other substances and marketing to kids, should be put in place for highly processed foods.
Maybe french fries should come with a warning label.
A prescription for America’s traffic problems
Nostalgia is a funny thing. Do you ever feel nostalgic about things that really weren’t very pleasant in the first place? Take, for instance, the morning commute. Here in the Washington area, more than 2 years into the COVID era, the traffic is still not what it used to be … and we kind of miss it.
Nah, not really. That was just a way to get everyone thinking about driving, because AAA has something of an explanation for the situation out there on the highways and byways of America. It’s drugs. No, not those kinds of drugs. This time it’s prescription drugs that are the problem. Well, part of the problem, anyway.
AAA did a survey last summer and found that nearly 50% of drivers “used one or more potentially impairing medications in the past 30 days. … The proportion of those choosing to drive is higher among those taking multiple medications.” How much higher? More than 63% of those with two or more prescriptions were driving within 2 hours of taking at least one of those meds, as were 71% of those taking three or more.
The 2,657 respondents also were asked about the types of potentially impairing drugs they were taking: 61% of those using antidepressants had been on the road within 2 hours of use at least once in the past 30 days, as had 73% of those taking an amphetamine, AAA said.
So there you have it. That guy in the BMW who’s been tailgating you for the last 3 miles? He may be a jerk, but there’s a good chance he’s a jerk with a prescription … or two … or three.
Sugary drinks, rather than artificially sweetened beverages or juices, show link to IBD
Drinks sweetened with sugar – but not natural juices or drinks sweetened artificially – were linked to a higher risk of inflammatory bowel disease (IBD) in people who drank more than one a day in a study of more than 120,000 people.
IBD has previously been linked with high consumption of sugar, but population-based evidence has been inconclusive, and natural juices have not been studied, write lead author Tian Fu, with the department of gastroenterology, the Third Xiangya Hospital of Central South University in Changsha, China, and colleagues.
Their study compared the associations of sugar-sweetened drinks, artificially sweetened beverages, and natural juices (including pure fruit or vegetable juices) with IBD risk.
“As one of the major sources of free sugar, beverages have been related to inflammation-related health outcomes but received less attention in the field of IBD,” the authors wrote.
, especially Crohn’s disease (CD), but further studies are needed to confirm these findings and explore the underlying mechanism,” they write.
The study was published online in Alimentary Pharmacology and Therapeutics.
Link significant for Crohn’s disease but not ulcerative colitis
The researchers used data from 121,490 participants in the UK Biobank who did not have IBD at trial recruitment in 2006-2010. The average age of the participants was 56 years, and almost all (96.9%) were White. The researchers studied their intake of beverages with 24-hour diet recalls from 2009 to 2012.
Participants were sorted into three groups according to the consumption of each beverage: 0 unit (glasses, cans, or 250 mL/cartons) per day (reference group), 0-1 unit per day, and more than 1 unit per day.
While most (66.3%) did not drink any sugar-sweetened beverages, participants who reported drinking more than 1 unit per day were more likely to have a higher body mass index and consume higher amounts of total energy and sugar.
During an average follow-up of about 10 years, the investigators documented 510 incident IBD cases: 143 cases of CD and 367 cases of ulcerative colitis (UC).
Compared to people who did not drink sugar-sweetened beverages, those who drank at least 1 unit per day had a significantly higher IBD risk (hazard ratio, 1.51; 95% confidence interval, 1.11-2.05), but the trend was statistically nonsignificant.
The association was significant for CD (HR, 2.05; 95% CI, 1.22,3.46) but not for UC (HR, 1.31; 95% CI, 0.89-1.92). The positive association between sugar-sweetened drinks and risk of CD, but not UC, was in line with previous studies showing that dietary patterns were more associated with CD risk, the authors noted.
They also highlighted that there was no positive link between artificially sweetened beverages, natural juices, or total sugar intake and IBD risk. They noted that the inflammatory role of artificial sweeteners is still being debated.
Additionally, the effect of natural sugar in juices may be counteracted by fiber and bioactive compounds in the juices, the authors wrote.
A limitation of the study is that at baseline, all participants in the UK Biobank were older than 40 years, so the researchers could not examine any links with younger-onset IBD.
Additionally, the self-reported questionnaires are subject to recall bias, though the survey has been validated.
Study adds to previous evidence
Hasan Zaki, PhD, an assistant professor with the department of pathology at University of Texas Southwestern Medical Center, Dallas, said in an interview that the size of this population-based study adds evidence that simple sugar can increase the risk for IBD. Dr. Zaki studies the relationship of inflammatory disorders and diet and was not involved in the study.
“This study is very strong evidence of the association between high sugar and IBD,” he said. He noted that more studies are needed because there are few studies in this area and results have varied.
His lab conducted work on the subject previously in mice. In a 2020 study, they found that a high-sugar diet helped promote IBD development and gut microbiota dysfunction.
Dr. Zaki pointed out that, among people in the United Kingdom and those in the United States, diets, demographics, and IBD incidence are similar, a fact that may make the findings more generalizable.
However, studies comparing the categories of sweetened drinks should be conducted in a U.S. population to assess the results in a diverse group to see whether ethnicity plays a role, because almost all of the people in the UK group were White, he said.
Also important, Dr. Zaki said, will be follow-up studies of the link between sweet drinks and IBD in U.S. children, among whom consumption is particularly high and the IBD incidence is rising. One study showed the prevalence increased 133% from 2007 to 2016.
The results of this study should help gastroenterologists counsel patients on an ideal diet to avoid IBD or reduce IBD severity, he said.
The study was supported by the National Natural Science Foundation of China and Key Project of Research and Development Plan of Hunan Province. The study authors and Dr. Zaki report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Drinks sweetened with sugar – but not natural juices or drinks sweetened artificially – were linked to a higher risk of inflammatory bowel disease (IBD) in people who drank more than one a day in a study of more than 120,000 people.
IBD has previously been linked with high consumption of sugar, but population-based evidence has been inconclusive, and natural juices have not been studied, write lead author Tian Fu, with the department of gastroenterology, the Third Xiangya Hospital of Central South University in Changsha, China, and colleagues.
Their study compared the associations of sugar-sweetened drinks, artificially sweetened beverages, and natural juices (including pure fruit or vegetable juices) with IBD risk.
“As one of the major sources of free sugar, beverages have been related to inflammation-related health outcomes but received less attention in the field of IBD,” the authors wrote.
, especially Crohn’s disease (CD), but further studies are needed to confirm these findings and explore the underlying mechanism,” they write.
The study was published online in Alimentary Pharmacology and Therapeutics.
Link significant for Crohn’s disease but not ulcerative colitis
The researchers used data from 121,490 participants in the UK Biobank who did not have IBD at trial recruitment in 2006-2010. The average age of the participants was 56 years, and almost all (96.9%) were White. The researchers studied their intake of beverages with 24-hour diet recalls from 2009 to 2012.
Participants were sorted into three groups according to the consumption of each beverage: 0 unit (glasses, cans, or 250 mL/cartons) per day (reference group), 0-1 unit per day, and more than 1 unit per day.
While most (66.3%) did not drink any sugar-sweetened beverages, participants who reported drinking more than 1 unit per day were more likely to have a higher body mass index and consume higher amounts of total energy and sugar.
During an average follow-up of about 10 years, the investigators documented 510 incident IBD cases: 143 cases of CD and 367 cases of ulcerative colitis (UC).
Compared to people who did not drink sugar-sweetened beverages, those who drank at least 1 unit per day had a significantly higher IBD risk (hazard ratio, 1.51; 95% confidence interval, 1.11-2.05), but the trend was statistically nonsignificant.
The association was significant for CD (HR, 2.05; 95% CI, 1.22,3.46) but not for UC (HR, 1.31; 95% CI, 0.89-1.92). The positive association between sugar-sweetened drinks and risk of CD, but not UC, was in line with previous studies showing that dietary patterns were more associated with CD risk, the authors noted.
They also highlighted that there was no positive link between artificially sweetened beverages, natural juices, or total sugar intake and IBD risk. They noted that the inflammatory role of artificial sweeteners is still being debated.
Additionally, the effect of natural sugar in juices may be counteracted by fiber and bioactive compounds in the juices, the authors wrote.
A limitation of the study is that at baseline, all participants in the UK Biobank were older than 40 years, so the researchers could not examine any links with younger-onset IBD.
Additionally, the self-reported questionnaires are subject to recall bias, though the survey has been validated.
Study adds to previous evidence
Hasan Zaki, PhD, an assistant professor with the department of pathology at University of Texas Southwestern Medical Center, Dallas, said in an interview that the size of this population-based study adds evidence that simple sugar can increase the risk for IBD. Dr. Zaki studies the relationship of inflammatory disorders and diet and was not involved in the study.
“This study is very strong evidence of the association between high sugar and IBD,” he said. He noted that more studies are needed because there are few studies in this area and results have varied.
His lab conducted work on the subject previously in mice. In a 2020 study, they found that a high-sugar diet helped promote IBD development and gut microbiota dysfunction.
Dr. Zaki pointed out that, among people in the United Kingdom and those in the United States, diets, demographics, and IBD incidence are similar, a fact that may make the findings more generalizable.
However, studies comparing the categories of sweetened drinks should be conducted in a U.S. population to assess the results in a diverse group to see whether ethnicity plays a role, because almost all of the people in the UK group were White, he said.
Also important, Dr. Zaki said, will be follow-up studies of the link between sweet drinks and IBD in U.S. children, among whom consumption is particularly high and the IBD incidence is rising. One study showed the prevalence increased 133% from 2007 to 2016.
The results of this study should help gastroenterologists counsel patients on an ideal diet to avoid IBD or reduce IBD severity, he said.
The study was supported by the National Natural Science Foundation of China and Key Project of Research and Development Plan of Hunan Province. The study authors and Dr. Zaki report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Drinks sweetened with sugar – but not natural juices or drinks sweetened artificially – were linked to a higher risk of inflammatory bowel disease (IBD) in people who drank more than one a day in a study of more than 120,000 people.
IBD has previously been linked with high consumption of sugar, but population-based evidence has been inconclusive, and natural juices have not been studied, write lead author Tian Fu, with the department of gastroenterology, the Third Xiangya Hospital of Central South University in Changsha, China, and colleagues.
Their study compared the associations of sugar-sweetened drinks, artificially sweetened beverages, and natural juices (including pure fruit or vegetable juices) with IBD risk.
“As one of the major sources of free sugar, beverages have been related to inflammation-related health outcomes but received less attention in the field of IBD,” the authors wrote.
, especially Crohn’s disease (CD), but further studies are needed to confirm these findings and explore the underlying mechanism,” they write.
The study was published online in Alimentary Pharmacology and Therapeutics.
Link significant for Crohn’s disease but not ulcerative colitis
The researchers used data from 121,490 participants in the UK Biobank who did not have IBD at trial recruitment in 2006-2010. The average age of the participants was 56 years, and almost all (96.9%) were White. The researchers studied their intake of beverages with 24-hour diet recalls from 2009 to 2012.
Participants were sorted into three groups according to the consumption of each beverage: 0 unit (glasses, cans, or 250 mL/cartons) per day (reference group), 0-1 unit per day, and more than 1 unit per day.
While most (66.3%) did not drink any sugar-sweetened beverages, participants who reported drinking more than 1 unit per day were more likely to have a higher body mass index and consume higher amounts of total energy and sugar.
During an average follow-up of about 10 years, the investigators documented 510 incident IBD cases: 143 cases of CD and 367 cases of ulcerative colitis (UC).
Compared to people who did not drink sugar-sweetened beverages, those who drank at least 1 unit per day had a significantly higher IBD risk (hazard ratio, 1.51; 95% confidence interval, 1.11-2.05), but the trend was statistically nonsignificant.
The association was significant for CD (HR, 2.05; 95% CI, 1.22,3.46) but not for UC (HR, 1.31; 95% CI, 0.89-1.92). The positive association between sugar-sweetened drinks and risk of CD, but not UC, was in line with previous studies showing that dietary patterns were more associated with CD risk, the authors noted.
They also highlighted that there was no positive link between artificially sweetened beverages, natural juices, or total sugar intake and IBD risk. They noted that the inflammatory role of artificial sweeteners is still being debated.
Additionally, the effect of natural sugar in juices may be counteracted by fiber and bioactive compounds in the juices, the authors wrote.
A limitation of the study is that at baseline, all participants in the UK Biobank were older than 40 years, so the researchers could not examine any links with younger-onset IBD.
Additionally, the self-reported questionnaires are subject to recall bias, though the survey has been validated.
Study adds to previous evidence
Hasan Zaki, PhD, an assistant professor with the department of pathology at University of Texas Southwestern Medical Center, Dallas, said in an interview that the size of this population-based study adds evidence that simple sugar can increase the risk for IBD. Dr. Zaki studies the relationship of inflammatory disorders and diet and was not involved in the study.
“This study is very strong evidence of the association between high sugar and IBD,” he said. He noted that more studies are needed because there are few studies in this area and results have varied.
His lab conducted work on the subject previously in mice. In a 2020 study, they found that a high-sugar diet helped promote IBD development and gut microbiota dysfunction.
Dr. Zaki pointed out that, among people in the United Kingdom and those in the United States, diets, demographics, and IBD incidence are similar, a fact that may make the findings more generalizable.
However, studies comparing the categories of sweetened drinks should be conducted in a U.S. population to assess the results in a diverse group to see whether ethnicity plays a role, because almost all of the people in the UK group were White, he said.
Also important, Dr. Zaki said, will be follow-up studies of the link between sweet drinks and IBD in U.S. children, among whom consumption is particularly high and the IBD incidence is rising. One study showed the prevalence increased 133% from 2007 to 2016.
The results of this study should help gastroenterologists counsel patients on an ideal diet to avoid IBD or reduce IBD severity, he said.
The study was supported by the National Natural Science Foundation of China and Key Project of Research and Development Plan of Hunan Province. The study authors and Dr. Zaki report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ALIMENTARY PHARMACOLOGY AND THERAPEUTICS
Good news, bad news
“Children’s hospitals saw a more than 25% decline in injury-related emergency room visits during the first year of the pandemic.” There’s a headline that should soothe a nation starved for some good news. It was based on a study published in Pediatrics that reports on data collected in the Pediatric Health Information System between March 2020 and March 2021 using a 3-year period between 2017 and 2020 as a control. How could this not be good news? First, let’s not be too hasty in celebrating the good fortune of all those millions of children spared the pain and anxiety of an emergency department visit.
If you were an administrator of an emergency department attempting to match revenues with expenses, a 25% drop in visits may have hit your bottom line. Office-based pediatricians experienced a similar phenomenon when many parents quickly learned that they could ignore or self-manage minor illnesses and complaints.

A decrease in visits doesn’t necessarily mean that the conditions that drive the traffic flow in your facility have gone away. It may simply be that they are being managed somewhere else. However, it is equally likely that for some reason the pandemic created situations that made the usual illnesses and injuries that flood into emergency departments less likely to occur. And, here, other anecdotal evidence about weight gain and a decline in fitness point to the conclusion that when children are no longer in school, they settle into more sedentary and less injury-generating activities. Injuries from falling off the couch watching television or playing video games alone do occur but certainly with less frequency than the random collisions that are inevitable when scores of classmates are running around on the playground.
So while it may be tempting to view a decline in emergency department visits as a positive statistic, this pandemic should remind us to be careful about how we choose our metrics to measure the health of the community. A decline in injuries in the short term may be masking a more serious erosion in the health of the pediatric population over the long term. At times I worry that as a specialty we are so focused on injury prevention that we lose sight of the fact that being physically active comes with a risk. A risk that we may wish to minimize, but a risk we must accept if we want to encourage the physical activity that we know is so important in the bigger health picture. For example, emergency department visits caused by pedal cycles initially rose 60%, eventually settling into the 25%-30% range leading one to suspect there was a learning or relearning curve.
However, while visits for minor injuries declined 25%, those associated with firearms rose initially 22%, and then 42%, and finally over 35%. These numbers combined with significant increases in visits from suffocation, nonpedal transportation, and suicide intent make it clear that, for most children, being in school is significantly less dangerous than staying at home.
As the pandemic continues to tumble on and we are presented with future questions about whether to keep schools open or closed, I hope the results of this study and others will help school officials and their advisers step back and look beyond the simple metric of case numbers and appreciate that there are benefits to being in school that go far beyond what can be learned in class.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
“Children’s hospitals saw a more than 25% decline in injury-related emergency room visits during the first year of the pandemic.” There’s a headline that should soothe a nation starved for some good news. It was based on a study published in Pediatrics that reports on data collected in the Pediatric Health Information System between March 2020 and March 2021 using a 3-year period between 2017 and 2020 as a control. How could this not be good news? First, let’s not be too hasty in celebrating the good fortune of all those millions of children spared the pain and anxiety of an emergency department visit.
If you were an administrator of an emergency department attempting to match revenues with expenses, a 25% drop in visits may have hit your bottom line. Office-based pediatricians experienced a similar phenomenon when many parents quickly learned that they could ignore or self-manage minor illnesses and complaints.
A decrease in visits doesn’t necessarily mean that the conditions that drive the traffic flow in your facility have gone away. It may simply be that they are being managed somewhere else. However, it is equally likely that for some reason the pandemic created situations that made the usual illnesses and injuries that flood into emergency departments less likely to occur. And, here, other anecdotal evidence about weight gain and a decline in fitness point to the conclusion that when children are no longer in school, they settle into more sedentary and less injury-generating activities. Injuries from falling off the couch watching television or playing video games alone do occur but certainly with less frequency than the random collisions that are inevitable when scores of classmates are running around on the playground.
So while it may be tempting to view a decline in emergency department visits as a positive statistic, this pandemic should remind us to be careful about how we choose our metrics to measure the health of the community. A decline in injuries in the short term may be masking a more serious erosion in the health of the pediatric population over the long term. At times I worry that as a specialty we are so focused on injury prevention that we lose sight of the fact that being physically active comes with a risk. A risk that we may wish to minimize, but a risk we must accept if we want to encourage the physical activity that we know is so important in the bigger health picture. For example, emergency department visits caused by pedal cycles initially rose 60%, eventually settling into the 25%-30% range leading one to suspect there was a learning or relearning curve.
However, while visits for minor injuries declined 25%, those associated with firearms rose initially 22%, and then 42%, and finally over 35%. These numbers combined with significant increases in visits from suffocation, nonpedal transportation, and suicide intent make it clear that, for most children, being in school is significantly less dangerous than staying at home.
As the pandemic continues to tumble on and we are presented with future questions about whether to keep schools open or closed, I hope the results of this study and others will help school officials and their advisers step back and look beyond the simple metric of case numbers and appreciate that there are benefits to being in school that go far beyond what can be learned in class.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
“Children’s hospitals saw a more than 25% decline in injury-related emergency room visits during the first year of the pandemic.” There’s a headline that should soothe a nation starved for some good news. It was based on a study published in Pediatrics that reports on data collected in the Pediatric Health Information System between March 2020 and March 2021 using a 3-year period between 2017 and 2020 as a control. How could this not be good news? First, let’s not be too hasty in celebrating the good fortune of all those millions of children spared the pain and anxiety of an emergency department visit.
If you were an administrator of an emergency department attempting to match revenues with expenses, a 25% drop in visits may have hit your bottom line. Office-based pediatricians experienced a similar phenomenon when many parents quickly learned that they could ignore or self-manage minor illnesses and complaints.
A decrease in visits doesn’t necessarily mean that the conditions that drive the traffic flow in your facility have gone away. It may simply be that they are being managed somewhere else. However, it is equally likely that for some reason the pandemic created situations that made the usual illnesses and injuries that flood into emergency departments less likely to occur. And, here, other anecdotal evidence about weight gain and a decline in fitness point to the conclusion that when children are no longer in school, they settle into more sedentary and less injury-generating activities. Injuries from falling off the couch watching television or playing video games alone do occur but certainly with less frequency than the random collisions that are inevitable when scores of classmates are running around on the playground.
So while it may be tempting to view a decline in emergency department visits as a positive statistic, this pandemic should remind us to be careful about how we choose our metrics to measure the health of the community. A decline in injuries in the short term may be masking a more serious erosion in the health of the pediatric population over the long term. At times I worry that as a specialty we are so focused on injury prevention that we lose sight of the fact that being physically active comes with a risk. A risk that we may wish to minimize, but a risk we must accept if we want to encourage the physical activity that we know is so important in the bigger health picture. For example, emergency department visits caused by pedal cycles initially rose 60%, eventually settling into the 25%-30% range leading one to suspect there was a learning or relearning curve.
However, while visits for minor injuries declined 25%, those associated with firearms rose initially 22%, and then 42%, and finally over 35%. These numbers combined with significant increases in visits from suffocation, nonpedal transportation, and suicide intent make it clear that, for most children, being in school is significantly less dangerous than staying at home.
As the pandemic continues to tumble on and we are presented with future questions about whether to keep schools open or closed, I hope the results of this study and others will help school officials and their advisers step back and look beyond the simple metric of case numbers and appreciate that there are benefits to being in school that go far beyond what can be learned in class.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Potent cannabis linked to more worldwide addiction
Cannabis potency has increased worldwide in recent decades and is linked with more people becoming addicted to marijuana, according to a new study published in Lancet Psychiatry.
People who use higher concentrations of tetrahydrocannabinol, or THC, are more likely to have addiction and mental health problems, the study authors found.
For research, scientists have established a “standard THC unit” as 5 milligrams of THC, which produces a mild intoxication for nonregular users. Low-potency products are 5-10 milligrams per gram of THC, the researchers said.
“One of the highest-quality studies included in our publication found that Tom Freeman, PhD, the senior study author and director of the Addiction and Mental Health Group at the University of Bath (England), told CNN.
Dr. Freeman and colleagues reviewed studies that looked at the links between cannabis potency and mental health and addiction. They analyzed 20 studies that included reports on anxiety, depression, psychosis, and cannabis use disorder, or marijuana addiction.
Overall, the use of higher-potency cannabis was linked to a higher risk of cannabis use disorder, as compared with use of lower-potency cannabis.
The findings appear to line up with trends in cannabis addiction and treatment rates worldwide, “while cannabis potency continued to rise during the same time,” Dr. Freeman told CNN.
During the past decade, the European Monitoring Centre for Drugs and Drug Addiction found a 76% increase in people entering treatment for cannabis addiction. In the United States, about 3 in 10 people who use marijuana have cannabis use disorder, according to the Centers for Disease Control and Prevention.
What’s more, a report by the United Nations found that in the past 2 decades, the “proportion of people seeking treatment for cannabis addiction has risen in all world regions apart from Africa,” Dr. Freeman said.
In a gram of herbal cannabis, THC concentrations have increased by about 2.9 milligrams each year, according to another study by Dr. Freeman and colleagues. In the cannabis resin used to make extracts and concentrations, THC levels increased about 5.7 milligrams each year between 1975 to 2017.
Consumers may not know about the potency of their product or what the potency means, Dr. Freeman said. Those who buy from a store where marijuana is legally sold may be able to review a product label, but those who buy cannabis illegally “may not be able to access reliable information about the potency of the product they are using.”
Although people may try to adjust the amount that they consume by “adding less cannabis to their joint or inhaling less deeply,” Dr. Freeman said, it may not work as well as they intended. High-potency products still deliver a larger dose of THC than low-potency products.
In the review, Dr. Freeman and colleagues also found that more potent cannabis was linked to more cases of marijuana-associated psychosis. This could mean a “loss of contact with reality,” including delusions and hearing voices, he told CNN.
But the association with anxiety and depression was varied across the studies, “meaning that the impact is unclear for these other mental health outcomes,” Dr. Freeman said.
A version of this article first appeared on WebMD.com.
Cannabis potency has increased worldwide in recent decades and is linked with more people becoming addicted to marijuana, according to a new study published in Lancet Psychiatry.
People who use higher concentrations of tetrahydrocannabinol, or THC, are more likely to have addiction and mental health problems, the study authors found.
For research, scientists have established a “standard THC unit” as 5 milligrams of THC, which produces a mild intoxication for nonregular users. Low-potency products are 5-10 milligrams per gram of THC, the researchers said.
“One of the highest-quality studies included in our publication found that Tom Freeman, PhD, the senior study author and director of the Addiction and Mental Health Group at the University of Bath (England), told CNN.
Dr. Freeman and colleagues reviewed studies that looked at the links between cannabis potency and mental health and addiction. They analyzed 20 studies that included reports on anxiety, depression, psychosis, and cannabis use disorder, or marijuana addiction.
Overall, the use of higher-potency cannabis was linked to a higher risk of cannabis use disorder, as compared with use of lower-potency cannabis.
The findings appear to line up with trends in cannabis addiction and treatment rates worldwide, “while cannabis potency continued to rise during the same time,” Dr. Freeman told CNN.
During the past decade, the European Monitoring Centre for Drugs and Drug Addiction found a 76% increase in people entering treatment for cannabis addiction. In the United States, about 3 in 10 people who use marijuana have cannabis use disorder, according to the Centers for Disease Control and Prevention.
What’s more, a report by the United Nations found that in the past 2 decades, the “proportion of people seeking treatment for cannabis addiction has risen in all world regions apart from Africa,” Dr. Freeman said.
In a gram of herbal cannabis, THC concentrations have increased by about 2.9 milligrams each year, according to another study by Dr. Freeman and colleagues. In the cannabis resin used to make extracts and concentrations, THC levels increased about 5.7 milligrams each year between 1975 to 2017.
Consumers may not know about the potency of their product or what the potency means, Dr. Freeman said. Those who buy from a store where marijuana is legally sold may be able to review a product label, but those who buy cannabis illegally “may not be able to access reliable information about the potency of the product they are using.”
Although people may try to adjust the amount that they consume by “adding less cannabis to their joint or inhaling less deeply,” Dr. Freeman said, it may not work as well as they intended. High-potency products still deliver a larger dose of THC than low-potency products.
In the review, Dr. Freeman and colleagues also found that more potent cannabis was linked to more cases of marijuana-associated psychosis. This could mean a “loss of contact with reality,” including delusions and hearing voices, he told CNN.
But the association with anxiety and depression was varied across the studies, “meaning that the impact is unclear for these other mental health outcomes,” Dr. Freeman said.
A version of this article first appeared on WebMD.com.
Cannabis potency has increased worldwide in recent decades and is linked with more people becoming addicted to marijuana, according to a new study published in Lancet Psychiatry.
People who use higher concentrations of tetrahydrocannabinol, or THC, are more likely to have addiction and mental health problems, the study authors found.
For research, scientists have established a “standard THC unit” as 5 milligrams of THC, which produces a mild intoxication for nonregular users. Low-potency products are 5-10 milligrams per gram of THC, the researchers said.
“One of the highest-quality studies included in our publication found that Tom Freeman, PhD, the senior study author and director of the Addiction and Mental Health Group at the University of Bath (England), told CNN.
Dr. Freeman and colleagues reviewed studies that looked at the links between cannabis potency and mental health and addiction. They analyzed 20 studies that included reports on anxiety, depression, psychosis, and cannabis use disorder, or marijuana addiction.
Overall, the use of higher-potency cannabis was linked to a higher risk of cannabis use disorder, as compared with use of lower-potency cannabis.
The findings appear to line up with trends in cannabis addiction and treatment rates worldwide, “while cannabis potency continued to rise during the same time,” Dr. Freeman told CNN.
During the past decade, the European Monitoring Centre for Drugs and Drug Addiction found a 76% increase in people entering treatment for cannabis addiction. In the United States, about 3 in 10 people who use marijuana have cannabis use disorder, according to the Centers for Disease Control and Prevention.
What’s more, a report by the United Nations found that in the past 2 decades, the “proportion of people seeking treatment for cannabis addiction has risen in all world regions apart from Africa,” Dr. Freeman said.
In a gram of herbal cannabis, THC concentrations have increased by about 2.9 milligrams each year, according to another study by Dr. Freeman and colleagues. In the cannabis resin used to make extracts and concentrations, THC levels increased about 5.7 milligrams each year between 1975 to 2017.
Consumers may not know about the potency of their product or what the potency means, Dr. Freeman said. Those who buy from a store where marijuana is legally sold may be able to review a product label, but those who buy cannabis illegally “may not be able to access reliable information about the potency of the product they are using.”
Although people may try to adjust the amount that they consume by “adding less cannabis to their joint or inhaling less deeply,” Dr. Freeman said, it may not work as well as they intended. High-potency products still deliver a larger dose of THC than low-potency products.
In the review, Dr. Freeman and colleagues also found that more potent cannabis was linked to more cases of marijuana-associated psychosis. This could mean a “loss of contact with reality,” including delusions and hearing voices, he told CNN.
But the association with anxiety and depression was varied across the studies, “meaning that the impact is unclear for these other mental health outcomes,” Dr. Freeman said.
A version of this article first appeared on WebMD.com.
FROM THE LANCET PSYCHIATRY
Biologics for IBD may come with added risks in Hispanic patients
Biologic agents may not be as safe or effective in Hispanic patients with inflammatory bowel disease (IBD) as they are in non-Hispanic patients, suggest new data published online in Clinical Gastroenterology and Hepatology.
To compare risk for hospitalization, surgery, and serious infections, Nghia H. Nguyen, MD, and his team at the Inflammatory Bowel Disease Center at the University of California, San Diego, included a multicenter, electronic health record–based cohort of biologic-treated Hispanic and non-Hispanic patients with IBD and used 1:4 propensity score matching.
They compared 240 Hispanic patients (53% male; 45% with ulcerative colitis; 73% treated with tumor necrosis factor alpha [TNF-alpha] antagonist; 20% with prior biologic exposure) with 960 non-Hispanic patients (51% male; 44% with ulcerative colitis; 67% treated with TNF-alpha antagonist; 27% with prior biologic exposure). Patients were new users of biologics (TNF-alpha antagonist, ustekinumab, or vedolizumab).
Compared with non-Hispanic patients, Hispanic patients had a higher risk for all-cause hospitalization (31% vs. 23%) within 1 year of starting a biologic agent.
Hispanic patients also had almost twice the risk for IBD-related surgeries (7% vs. 4.6%, respectively) and trended toward a higher risk for serious infection (8.8% vs. 4.9%, respectively).
The findings are particularly important because incidence and prevalence of IBD in Hispanic adults are increasing rapidly, according to the authors.
“Currently, 1.2% of Hispanic adults in the United States report having IBD, and this number is expected to increase progressively over the next few years with global immigration patterns and changing demographics of the United States,” the authors write.
Potential drivers of disparities
Hispanic patients have been underrepresented in clinical trials of biologic agents in IBD, making up fewer than 5% of participants, the authors note. This has resulted in limited data and created challenges in discerning reasons for the disparity.
The authors note the potential role of genetics in the effectiveness of some biologic agents, although that has not been well studied in Hispanic patients.
Additionally, according to this study, Hispanic patients with IBD lived with more negative social determinants of health, particularly related to food insecurity (27%) and lack of adequate social support (83%), compared with non-Hispanic patients (unpublished data).
“In other studies on health care utilization, Hispanic patients were found to have limited access to appropriate specialist care and lack of insurance coverage,” the authors point out.
The authors acknowledge that limitations of their study include the inability to pinpoint the primary reason for hospitalization because data on primary versus secondary discharge diagnoses were not available. Also, they relied on prescription information in electronic health records and could not confirm that medications were dispensed or that patients took them.
They also acknowledged selection bias as a limitation, because the focus was only on patients treated with biologics and not on outcomes for those who may have warranted a biologic treatment but were unable to receive it.
“Future studies are needed to investigate the biological, social, and environmental drivers of these differences,” the authors write.
The authors’ complete financial disclosures are available with the full text of the paper.
A version of this article first appeared on Medscape.com.
Biologic agents may not be as safe or effective in Hispanic patients with inflammatory bowel disease (IBD) as they are in non-Hispanic patients, suggest new data published online in Clinical Gastroenterology and Hepatology.
To compare risk for hospitalization, surgery, and serious infections, Nghia H. Nguyen, MD, and his team at the Inflammatory Bowel Disease Center at the University of California, San Diego, included a multicenter, electronic health record–based cohort of biologic-treated Hispanic and non-Hispanic patients with IBD and used 1:4 propensity score matching.
They compared 240 Hispanic patients (53% male; 45% with ulcerative colitis; 73% treated with tumor necrosis factor alpha [TNF-alpha] antagonist; 20% with prior biologic exposure) with 960 non-Hispanic patients (51% male; 44% with ulcerative colitis; 67% treated with TNF-alpha antagonist; 27% with prior biologic exposure). Patients were new users of biologics (TNF-alpha antagonist, ustekinumab, or vedolizumab).
Compared with non-Hispanic patients, Hispanic patients had a higher risk for all-cause hospitalization (31% vs. 23%) within 1 year of starting a biologic agent.
Hispanic patients also had almost twice the risk for IBD-related surgeries (7% vs. 4.6%, respectively) and trended toward a higher risk for serious infection (8.8% vs. 4.9%, respectively).
The findings are particularly important because incidence and prevalence of IBD in Hispanic adults are increasing rapidly, according to the authors.
“Currently, 1.2% of Hispanic adults in the United States report having IBD, and this number is expected to increase progressively over the next few years with global immigration patterns and changing demographics of the United States,” the authors write.
Potential drivers of disparities
Hispanic patients have been underrepresented in clinical trials of biologic agents in IBD, making up fewer than 5% of participants, the authors note. This has resulted in limited data and created challenges in discerning reasons for the disparity.
The authors note the potential role of genetics in the effectiveness of some biologic agents, although that has not been well studied in Hispanic patients.
Additionally, according to this study, Hispanic patients with IBD lived with more negative social determinants of health, particularly related to food insecurity (27%) and lack of adequate social support (83%), compared with non-Hispanic patients (unpublished data).
“In other studies on health care utilization, Hispanic patients were found to have limited access to appropriate specialist care and lack of insurance coverage,” the authors point out.
The authors acknowledge that limitations of their study include the inability to pinpoint the primary reason for hospitalization because data on primary versus secondary discharge diagnoses were not available. Also, they relied on prescription information in electronic health records and could not confirm that medications were dispensed or that patients took them.
They also acknowledged selection bias as a limitation, because the focus was only on patients treated with biologics and not on outcomes for those who may have warranted a biologic treatment but were unable to receive it.
“Future studies are needed to investigate the biological, social, and environmental drivers of these differences,” the authors write.
The authors’ complete financial disclosures are available with the full text of the paper.
A version of this article first appeared on Medscape.com.
Biologic agents may not be as safe or effective in Hispanic patients with inflammatory bowel disease (IBD) as they are in non-Hispanic patients, suggest new data published online in Clinical Gastroenterology and Hepatology.
To compare risk for hospitalization, surgery, and serious infections, Nghia H. Nguyen, MD, and his team at the Inflammatory Bowel Disease Center at the University of California, San Diego, included a multicenter, electronic health record–based cohort of biologic-treated Hispanic and non-Hispanic patients with IBD and used 1:4 propensity score matching.
They compared 240 Hispanic patients (53% male; 45% with ulcerative colitis; 73% treated with tumor necrosis factor alpha [TNF-alpha] antagonist; 20% with prior biologic exposure) with 960 non-Hispanic patients (51% male; 44% with ulcerative colitis; 67% treated with TNF-alpha antagonist; 27% with prior biologic exposure). Patients were new users of biologics (TNF-alpha antagonist, ustekinumab, or vedolizumab).
Compared with non-Hispanic patients, Hispanic patients had a higher risk for all-cause hospitalization (31% vs. 23%) within 1 year of starting a biologic agent.
Hispanic patients also had almost twice the risk for IBD-related surgeries (7% vs. 4.6%, respectively) and trended toward a higher risk for serious infection (8.8% vs. 4.9%, respectively).
The findings are particularly important because incidence and prevalence of IBD in Hispanic adults are increasing rapidly, according to the authors.
“Currently, 1.2% of Hispanic adults in the United States report having IBD, and this number is expected to increase progressively over the next few years with global immigration patterns and changing demographics of the United States,” the authors write.
Potential drivers of disparities
Hispanic patients have been underrepresented in clinical trials of biologic agents in IBD, making up fewer than 5% of participants, the authors note. This has resulted in limited data and created challenges in discerning reasons for the disparity.
The authors note the potential role of genetics in the effectiveness of some biologic agents, although that has not been well studied in Hispanic patients.
Additionally, according to this study, Hispanic patients with IBD lived with more negative social determinants of health, particularly related to food insecurity (27%) and lack of adequate social support (83%), compared with non-Hispanic patients (unpublished data).
“In other studies on health care utilization, Hispanic patients were found to have limited access to appropriate specialist care and lack of insurance coverage,” the authors point out.
The authors acknowledge that limitations of their study include the inability to pinpoint the primary reason for hospitalization because data on primary versus secondary discharge diagnoses were not available. Also, they relied on prescription information in electronic health records and could not confirm that medications were dispensed or that patients took them.
They also acknowledged selection bias as a limitation, because the focus was only on patients treated with biologics and not on outcomes for those who may have warranted a biologic treatment but were unable to receive it.
“Future studies are needed to investigate the biological, social, and environmental drivers of these differences,” the authors write.
The authors’ complete financial disclosures are available with the full text of the paper.
A version of this article first appeared on Medscape.com.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Children and COVID: Many parents see vaccine as the greater risk
New COVID-19 cases rose for the second week in a row as cumulative cases among U.S. children passed the 14-million mark, but a recent survey shows that more than half of parents believe that the vaccine is a greater risk to children under age 5 years than the virus.
In a Kaiser Family Foundation survey conducted July 7-17, 53% of parents with children aged 6 months to 5 years said that the vaccine is “a bigger risk to their child’s health than getting infected with COVID-19, compared to 44% who say getting infected is the bigger risk,” KFF reported July 26.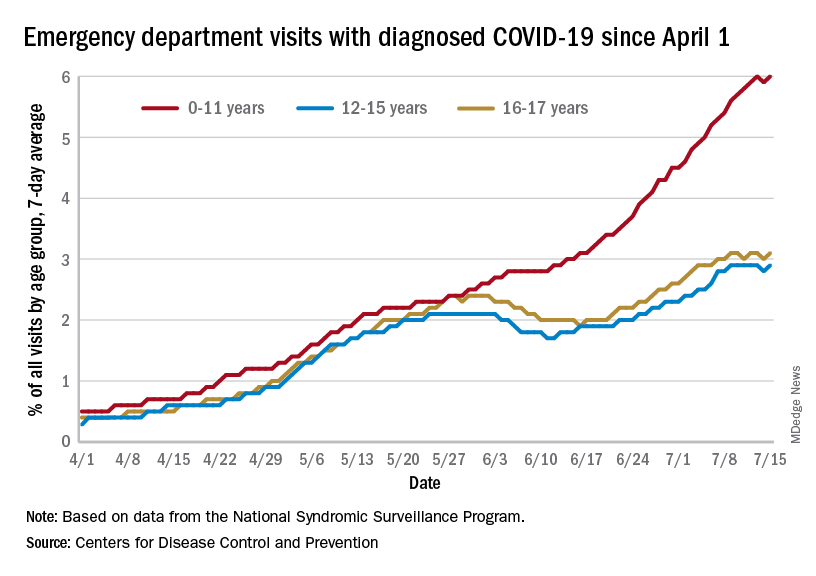
More than 4 out of 10 of respondents (43%) said that they will “definitely not” get their eligible children vaccinated, while only 7% said that their children had already received it and 10% said their children would get it as soon as possible, according to the KFF survey, which had an overall sample size of 1,847 adults, including an oversample of 471 parents of children under age 5.
Vaccine initiation has been slow in the first month since it was approved for the youngest children. Just 2.8% of all eligible children under age 5 had received an initial dose as of July 19, compared with first-month uptake figures of more than 18% for the 5- to 11-year-olds and 27% for those aged 12-15, based on data from the Centers for Disease Control and Prevention.
The current rates for vaccination in those aged 5 and older look like this: 70.2% of 12- to 17-year-olds have received at least one dose, versus 37.1% of those aged 5-11. Just over 60% of the older children were fully vaccinated as of July 19, as were 30.2% of the 5- to 11-year-olds, the CDC reported on its COVID Data Tracker.
Number of new cases hits 2-month high
Despite the vaccine, SARS-CoV-2 and its various mutations have continued with their summer travels. With 92,000 newly infected children added for the week of July 15-21, there have now been a total of 14,003,497 pediatric cases reported since the start of the pandemic, which works out to 18.6% of cases in all ages, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report.
The 92,000 new cases represent an increase of almost 22% over the previous week and mark the highest 1-week count since May, when the total passed 100,000 for 2 consecutive weeks. More recently the trend had seemed more stable as weekly cases dropped twice and rose twice as the total hovered around 70,000, based on the data collected by the AAP and CHA from state and territorial health departments.
A different scenario has played out for emergency department visits and hospital admissions, which have risen steadily since the beginning of April. The admission rate for children aged 0-17, which was just 0.13 new patients per 100,000 population on April 11, was up to 0.44 per 100,000 on July 21. By comparison, the highest rate reached last year during the Delta surge was 0.47 per 100,000, based on CDC data.
The 7-day average of emergency dept. visits among the youngest age group, 0-11 years, shows the same general increase as hospital admissions, but the older children have diverged form that path (see graph). For those aged 12-15 and 16-17, hospitalizations started dropping in late May and into mid-June before climbing again, although more slowly than for the youngest group, the CDC data show.
The ED visit rate with diagnosed COVID among those aged 0-11, measured at 6.1% of all visits on July 19, is, in fact, considerably higher than at any time during the Delta surge last year, when it never passed 4.0%, although much lower than peak Omicron (14.1%). That 6.1% was also higher than any other age group on that day, adults included, the CDC said.
New COVID-19 cases rose for the second week in a row as cumulative cases among U.S. children passed the 14-million mark, but a recent survey shows that more than half of parents believe that the vaccine is a greater risk to children under age 5 years than the virus.
In a Kaiser Family Foundation survey conducted July 7-17, 53% of parents with children aged 6 months to 5 years said that the vaccine is “a bigger risk to their child’s health than getting infected with COVID-19, compared to 44% who say getting infected is the bigger risk,” KFF reported July 26.
More than 4 out of 10 of respondents (43%) said that they will “definitely not” get their eligible children vaccinated, while only 7% said that their children had already received it and 10% said their children would get it as soon as possible, according to the KFF survey, which had an overall sample size of 1,847 adults, including an oversample of 471 parents of children under age 5.
Vaccine initiation has been slow in the first month since it was approved for the youngest children. Just 2.8% of all eligible children under age 5 had received an initial dose as of July 19, compared with first-month uptake figures of more than 18% for the 5- to 11-year-olds and 27% for those aged 12-15, based on data from the Centers for Disease Control and Prevention.
The current rates for vaccination in those aged 5 and older look like this: 70.2% of 12- to 17-year-olds have received at least one dose, versus 37.1% of those aged 5-11. Just over 60% of the older children were fully vaccinated as of July 19, as were 30.2% of the 5- to 11-year-olds, the CDC reported on its COVID Data Tracker.
Number of new cases hits 2-month high
Despite the vaccine, SARS-CoV-2 and its various mutations have continued with their summer travels. With 92,000 newly infected children added for the week of July 15-21, there have now been a total of 14,003,497 pediatric cases reported since the start of the pandemic, which works out to 18.6% of cases in all ages, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report.
The 92,000 new cases represent an increase of almost 22% over the previous week and mark the highest 1-week count since May, when the total passed 100,000 for 2 consecutive weeks. More recently the trend had seemed more stable as weekly cases dropped twice and rose twice as the total hovered around 70,000, based on the data collected by the AAP and CHA from state and territorial health departments.
A different scenario has played out for emergency department visits and hospital admissions, which have risen steadily since the beginning of April. The admission rate for children aged 0-17, which was just 0.13 new patients per 100,000 population on April 11, was up to 0.44 per 100,000 on July 21. By comparison, the highest rate reached last year during the Delta surge was 0.47 per 100,000, based on CDC data.
The 7-day average of emergency dept. visits among the youngest age group, 0-11 years, shows the same general increase as hospital admissions, but the older children have diverged form that path (see graph). For those aged 12-15 and 16-17, hospitalizations started dropping in late May and into mid-June before climbing again, although more slowly than for the youngest group, the CDC data show.
The ED visit rate with diagnosed COVID among those aged 0-11, measured at 6.1% of all visits on July 19, is, in fact, considerably higher than at any time during the Delta surge last year, when it never passed 4.0%, although much lower than peak Omicron (14.1%). That 6.1% was also higher than any other age group on that day, adults included, the CDC said.
New COVID-19 cases rose for the second week in a row as cumulative cases among U.S. children passed the 14-million mark, but a recent survey shows that more than half of parents believe that the vaccine is a greater risk to children under age 5 years than the virus.
In a Kaiser Family Foundation survey conducted July 7-17, 53% of parents with children aged 6 months to 5 years said that the vaccine is “a bigger risk to their child’s health than getting infected with COVID-19, compared to 44% who say getting infected is the bigger risk,” KFF reported July 26.
More than 4 out of 10 of respondents (43%) said that they will “definitely not” get their eligible children vaccinated, while only 7% said that their children had already received it and 10% said their children would get it as soon as possible, according to the KFF survey, which had an overall sample size of 1,847 adults, including an oversample of 471 parents of children under age 5.
Vaccine initiation has been slow in the first month since it was approved for the youngest children. Just 2.8% of all eligible children under age 5 had received an initial dose as of July 19, compared with first-month uptake figures of more than 18% for the 5- to 11-year-olds and 27% for those aged 12-15, based on data from the Centers for Disease Control and Prevention.
The current rates for vaccination in those aged 5 and older look like this: 70.2% of 12- to 17-year-olds have received at least one dose, versus 37.1% of those aged 5-11. Just over 60% of the older children were fully vaccinated as of July 19, as were 30.2% of the 5- to 11-year-olds, the CDC reported on its COVID Data Tracker.
Number of new cases hits 2-month high
Despite the vaccine, SARS-CoV-2 and its various mutations have continued with their summer travels. With 92,000 newly infected children added for the week of July 15-21, there have now been a total of 14,003,497 pediatric cases reported since the start of the pandemic, which works out to 18.6% of cases in all ages, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report.
The 92,000 new cases represent an increase of almost 22% over the previous week and mark the highest 1-week count since May, when the total passed 100,000 for 2 consecutive weeks. More recently the trend had seemed more stable as weekly cases dropped twice and rose twice as the total hovered around 70,000, based on the data collected by the AAP and CHA from state and territorial health departments.
A different scenario has played out for emergency department visits and hospital admissions, which have risen steadily since the beginning of April. The admission rate for children aged 0-17, which was just 0.13 new patients per 100,000 population on April 11, was up to 0.44 per 100,000 on July 21. By comparison, the highest rate reached last year during the Delta surge was 0.47 per 100,000, based on CDC data.
The 7-day average of emergency dept. visits among the youngest age group, 0-11 years, shows the same general increase as hospital admissions, but the older children have diverged form that path (see graph). For those aged 12-15 and 16-17, hospitalizations started dropping in late May and into mid-June before climbing again, although more slowly than for the youngest group, the CDC data show.
The ED visit rate with diagnosed COVID among those aged 0-11, measured at 6.1% of all visits on July 19, is, in fact, considerably higher than at any time during the Delta surge last year, when it never passed 4.0%, although much lower than peak Omicron (14.1%). That 6.1% was also higher than any other age group on that day, adults included, the CDC said.
U.S. News issues top hospitals list, now with expanded health equity measures
For the seventh consecutive year, the Mayo Clinic in Rochester, Minn., took the top spot in the annual honor roll of best hospitals, published July 26 by U.S. News & World Report.
The 2022 rankings, which marks the 33rd edition, showcase several methodology changes, including new ratings for ovarian, prostate, and uterine cancer surgeries that “provide patients ... with previously unavailable information to assist them in making a critical health care decision,” a news release from the publication explains.
said the release. Finally, a new metric called “home time” determines how successfully each hospital helps patients return home.
Mayo Clinic remains No. 1
For the 2022-2023 rankings and ratings, U.S. News compared more than 4,500 medical centers across the country in 15 specialties and 20 procedures and conditions. Of these, 493 were recognized as Best Regional Hospitals as a result of their overall strong performance.
The list was then narrowed to the top 20 hospitals, outlined in the honor roll below, that deliver “exceptional treatment across multiple areas of care.”
Following Mayo Clinic in the annual ranking’s top spot, Cedars-Sinai Medical Center in Los Angeles rises from No. 6 to No. 2, and New York University Langone Hospitals finish third, up from eighth in 2021.
Cleveland Clinic in Ohio holds the No. 4 spot, down two from 2021, while Johns Hopkins Hospital in Baltimore and UCLA Medical Center in Los Angeles tie for fifth place. Rounding out the top 10, in order, are: New York–Presbyterian Hospital–Columbia and Cornell, New York; Massachusetts General Hospital, Boston; Northwestern Memorial Hospital, Chicago; Stanford (Calif.) Health Care–Stanford Hospital.
The following hospitals complete the top 20 in the United States:
- 11. Barnes-Jewish Hospital, St. Louis
- 12. UCSF Medical Center, San Francisco
- 13. Hospitals of the University of Pennsylvania–Penn Presbyterian, Philadelphia
- 14. Brigham and Women’s Hospital, Boston
- 15. Houston Methodist Hospital
- 16. Mount Sinai Hospital, New York
- 17. University of Michigan Health–Michigan Medicine, Ann Arbor
- 18. Mayo Clinic–Phoenix
- 19. Vanderbilt University Medical Center, Nashville, Tenn.
- 20. Rush University Medical Center, Chicago
For the specialty rankings, the University of Texas MD Anderson Cancer Center, Houston, remains No. 1 in cancer care, the Cleveland Clinic is No. 1 in cardiology and heart surgery, and the Hospital for Special Surgery in New York is No. 1 in orthopedics.
Top five for cancer
- 1. University of Texas MD Anderson Cancer Center, Houston
- 2. Memorial Sloan Kettering Cancer Center, New York
- 3. Mayo Clinic, Rochester, Minn.
- 4. Dana-Farber/Brigham and Women’s Cancer Center, Boston
- 5. UCLA Medical Center, Los Angeles
Top five for cardiology and heart surgery
- 1. Cleveland Clinic
- 2. Mayo Clinic, Rochester, Minn.
- 3. Cedars-Sinai Medical Center, Los Angeles
- 4. New York–Presbyterian Hospital–Columbia and Cornell, New York
- 5. New York University Langone Hospitals
Top five for orthopedics
- 1. Hospital for Special Surgery, New York
- 2. Mayo Clinic, Rochester, Minn.
- 3. Cedars-Sinai Medical Center, Los Angeles
- 4. New York University Langone Hospitals
- 5. (tie) Rush University Medical Center, Chicago
- 5. (tie) UCLA Medical Center, Los Angeles
According to the news release, the procedures and conditions ratings are based entirely on objective patient care measures like survival rates, patient experience, home time, and level of nursing care. The Best Hospitals rankings consider a variety of data provided by the Centers for Medicare & Medicaid Services, American Hospital Association, professional organizations, and medical specialists.
The full report is available online.
A version of this article first appeared on Medscape.com.
For the seventh consecutive year, the Mayo Clinic in Rochester, Minn., took the top spot in the annual honor roll of best hospitals, published July 26 by U.S. News & World Report.
The 2022 rankings, which marks the 33rd edition, showcase several methodology changes, including new ratings for ovarian, prostate, and uterine cancer surgeries that “provide patients ... with previously unavailable information to assist them in making a critical health care decision,” a news release from the publication explains.
said the release. Finally, a new metric called “home time” determines how successfully each hospital helps patients return home.
Mayo Clinic remains No. 1
For the 2022-2023 rankings and ratings, U.S. News compared more than 4,500 medical centers across the country in 15 specialties and 20 procedures and conditions. Of these, 493 were recognized as Best Regional Hospitals as a result of their overall strong performance.
The list was then narrowed to the top 20 hospitals, outlined in the honor roll below, that deliver “exceptional treatment across multiple areas of care.”
Following Mayo Clinic in the annual ranking’s top spot, Cedars-Sinai Medical Center in Los Angeles rises from No. 6 to No. 2, and New York University Langone Hospitals finish third, up from eighth in 2021.
Cleveland Clinic in Ohio holds the No. 4 spot, down two from 2021, while Johns Hopkins Hospital in Baltimore and UCLA Medical Center in Los Angeles tie for fifth place. Rounding out the top 10, in order, are: New York–Presbyterian Hospital–Columbia and Cornell, New York; Massachusetts General Hospital, Boston; Northwestern Memorial Hospital, Chicago; Stanford (Calif.) Health Care–Stanford Hospital.
The following hospitals complete the top 20 in the United States:
- 11. Barnes-Jewish Hospital, St. Louis
- 12. UCSF Medical Center, San Francisco
- 13. Hospitals of the University of Pennsylvania–Penn Presbyterian, Philadelphia
- 14. Brigham and Women’s Hospital, Boston
- 15. Houston Methodist Hospital
- 16. Mount Sinai Hospital, New York
- 17. University of Michigan Health–Michigan Medicine, Ann Arbor
- 18. Mayo Clinic–Phoenix
- 19. Vanderbilt University Medical Center, Nashville, Tenn.
- 20. Rush University Medical Center, Chicago
For the specialty rankings, the University of Texas MD Anderson Cancer Center, Houston, remains No. 1 in cancer care, the Cleveland Clinic is No. 1 in cardiology and heart surgery, and the Hospital for Special Surgery in New York is No. 1 in orthopedics.
Top five for cancer
- 1. University of Texas MD Anderson Cancer Center, Houston
- 2. Memorial Sloan Kettering Cancer Center, New York
- 3. Mayo Clinic, Rochester, Minn.
- 4. Dana-Farber/Brigham and Women’s Cancer Center, Boston
- 5. UCLA Medical Center, Los Angeles
Top five for cardiology and heart surgery
- 1. Cleveland Clinic
- 2. Mayo Clinic, Rochester, Minn.
- 3. Cedars-Sinai Medical Center, Los Angeles
- 4. New York–Presbyterian Hospital–Columbia and Cornell, New York
- 5. New York University Langone Hospitals
Top five for orthopedics
- 1. Hospital for Special Surgery, New York
- 2. Mayo Clinic, Rochester, Minn.
- 3. Cedars-Sinai Medical Center, Los Angeles
- 4. New York University Langone Hospitals
- 5. (tie) Rush University Medical Center, Chicago
- 5. (tie) UCLA Medical Center, Los Angeles
According to the news release, the procedures and conditions ratings are based entirely on objective patient care measures like survival rates, patient experience, home time, and level of nursing care. The Best Hospitals rankings consider a variety of data provided by the Centers for Medicare & Medicaid Services, American Hospital Association, professional organizations, and medical specialists.
The full report is available online.
A version of this article first appeared on Medscape.com.
For the seventh consecutive year, the Mayo Clinic in Rochester, Minn., took the top spot in the annual honor roll of best hospitals, published July 26 by U.S. News & World Report.
The 2022 rankings, which marks the 33rd edition, showcase several methodology changes, including new ratings for ovarian, prostate, and uterine cancer surgeries that “provide patients ... with previously unavailable information to assist them in making a critical health care decision,” a news release from the publication explains.
said the release. Finally, a new metric called “home time” determines how successfully each hospital helps patients return home.
Mayo Clinic remains No. 1
For the 2022-2023 rankings and ratings, U.S. News compared more than 4,500 medical centers across the country in 15 specialties and 20 procedures and conditions. Of these, 493 were recognized as Best Regional Hospitals as a result of their overall strong performance.
The list was then narrowed to the top 20 hospitals, outlined in the honor roll below, that deliver “exceptional treatment across multiple areas of care.”
Following Mayo Clinic in the annual ranking’s top spot, Cedars-Sinai Medical Center in Los Angeles rises from No. 6 to No. 2, and New York University Langone Hospitals finish third, up from eighth in 2021.
Cleveland Clinic in Ohio holds the No. 4 spot, down two from 2021, while Johns Hopkins Hospital in Baltimore and UCLA Medical Center in Los Angeles tie for fifth place. Rounding out the top 10, in order, are: New York–Presbyterian Hospital–Columbia and Cornell, New York; Massachusetts General Hospital, Boston; Northwestern Memorial Hospital, Chicago; Stanford (Calif.) Health Care–Stanford Hospital.
The following hospitals complete the top 20 in the United States:
- 11. Barnes-Jewish Hospital, St. Louis
- 12. UCSF Medical Center, San Francisco
- 13. Hospitals of the University of Pennsylvania–Penn Presbyterian, Philadelphia
- 14. Brigham and Women’s Hospital, Boston
- 15. Houston Methodist Hospital
- 16. Mount Sinai Hospital, New York
- 17. University of Michigan Health–Michigan Medicine, Ann Arbor
- 18. Mayo Clinic–Phoenix
- 19. Vanderbilt University Medical Center, Nashville, Tenn.
- 20. Rush University Medical Center, Chicago
For the specialty rankings, the University of Texas MD Anderson Cancer Center, Houston, remains No. 1 in cancer care, the Cleveland Clinic is No. 1 in cardiology and heart surgery, and the Hospital for Special Surgery in New York is No. 1 in orthopedics.
Top five for cancer
- 1. University of Texas MD Anderson Cancer Center, Houston
- 2. Memorial Sloan Kettering Cancer Center, New York
- 3. Mayo Clinic, Rochester, Minn.
- 4. Dana-Farber/Brigham and Women’s Cancer Center, Boston
- 5. UCLA Medical Center, Los Angeles
Top five for cardiology and heart surgery
- 1. Cleveland Clinic
- 2. Mayo Clinic, Rochester, Minn.
- 3. Cedars-Sinai Medical Center, Los Angeles
- 4. New York–Presbyterian Hospital–Columbia and Cornell, New York
- 5. New York University Langone Hospitals
Top five for orthopedics
- 1. Hospital for Special Surgery, New York
- 2. Mayo Clinic, Rochester, Minn.
- 3. Cedars-Sinai Medical Center, Los Angeles
- 4. New York University Langone Hospitals
- 5. (tie) Rush University Medical Center, Chicago
- 5. (tie) UCLA Medical Center, Los Angeles
According to the news release, the procedures and conditions ratings are based entirely on objective patient care measures like survival rates, patient experience, home time, and level of nursing care. The Best Hospitals rankings consider a variety of data provided by the Centers for Medicare & Medicaid Services, American Hospital Association, professional organizations, and medical specialists.
The full report is available online.
A version of this article first appeared on Medscape.com.
Two distinct phenotypes of COVID-related myocarditis emerge
Researchers from France have identified two distinct phenotypes of fulminant COVID-19–related myocarditis in adults, with different clinical presentations, immunologic profiles, and outcomes.
Differentiation between the two bioclinical entities is important to understand for patient management and further pathophysiological studies, they said.
The first phenotype occurs early (within a few days) in acute SARS-CoV-2 infection, with active viral replication (polymerase chain reaction positive) in adults who meet criteria for multisystem inflammatory syndrome (MIS-A+).
In this early phenotype, there is “limited systemic inflammation without skin and mucosal involvement, but myocardial dysfunction is fulminant and frequently associated with large pericardial effusions. These cases more often require extracorporeal membrane oxygenation [ECMO],” Guy Gorochov, MD, PhD, Sorbonne University, Paris, said in an interview.
The second is a delayed, postinfectious, immune-driven phenotype that occurs in adults who fail to meet the criteria for MIS-A (MIS-A–).
This phenotype occurs weeks after SARS-CoV-2 infection, usually beyond detectable active viral replication (PCR–) in the context of specific immune response and severe systemic inflammation with skin and mucosal involvement. Myocardial dysfunction is more progressive and rarely associated with large pericardial effusions, Dr. Gorochov explained.
The study was published in the Journal of the American College of Cardiology.
Evolving understanding
The findings are based on a retrospective analysis of 38 patients without a history of COVID-19 vaccination who were admitted to the intensive care unit from March 2020 to June 2021 for suspected fulminant COVID-19 myocarditis.
Patients were confirmed to have SARS-CoV-2 infection by PCR and/or by serologic testing. As noted in other studies, the patients were predominantly young men (66%; median age, 27.5 years). Twenty-five (66%) patients were MIS-A+ and 13 (34%) were MIS-A–.
In general, the MIS-A– patients were sicker and had worse outcomes.
Specifically, compared with the MIS-A+ patients, MIS-A– patients had a shorter time between the onset of COVID-19 symptoms and the development of myocarditis, a shorter time to ICU admission, and more severe presentations assessed using lower left ventricular ejection fraction and sequential organ failure assessment scores.
MIS-A– patients also had higher lactate levels, were more likely to need venoarterial ECMO (92% vs 16%), had higher ICU mortality (31% vs. 4%), and a had lower probability of survival at 3 months (68% vs. 96%), compared with their MIS-A+ peers.
Immunologic differences
The immunologic profiles of these two distinct clinical phenotypes also differed.
In MIS-A– early-type COVID-19 myocarditis, RNA polymerase III autoantibodies are frequently positive and serum levels of antiviral interferon-alpha and granulocyte-attracting interleukin-8 are elevated.
In contrast, in MIS-A+ delayed-type COVID-19 myocarditis, RNA polymerase III autoantibodies are negative and serum levels of IL-17 and IL-22 are highly elevated.
“We suggest that IL-17 and IL-22 are novel criteria that should help to assess in adults the recently recognized MIS-A,” Dr. Gorochov told this news organization. “It should be tested whether IL-17 and IL-22 are also elevated in children with MIS-C.”
The researchers also observed “extremely” high serum IL-10 levels in both patient groups. This has been previously associated with severe myocardial injury and an increase in the risk for death in severe COVID-19 patients.
The researchers said the phenotypic clustering of patients with fulminant COVID-19–related myocarditis “seems relevant” for their management.
MIS-A– cases, owing to the high risk for evolution toward refractory cardiogenic shock, should be “urgently” referred to a center with venoarterial ECMO and closely monitored to prevent a “too-late” cannulation, especially under cardiopulmonary resuscitation, known to be associated with poor outcomes, they advised.
They noted that the five patients who died in their series had late venoarterial ECMO implantation, while undergoing multiple organ failures or resuscitation.
Conversely, the risk for evolution to refractory cardiogenic shock is lower in MIS-A+ cases. However, identifying MIS-A+ cases is “all the more important given that numerous data support the efficacy of corticosteroids and/or intravenous immunoglobulins in MIS-C,” Dr. Gorochov and colleagues wrote.
The authors of a linked editorial said the French team should be “commended on their work in furthering our understanding of fulminant myocarditis related to COVID-19 infection.”
Ajith Nair, MD, Baylor College of Medicine, and Anita Deswal, MD, MPH, University of Texas M.D. Anderson Cancer Center, both in Houston, noted that fulminant myocarditis is rare and can result from either of two mechanisms: viral tropism or an immune-mediated mechanism.
“It remains to be seen whether using antiviral therapy versus immunomodulatory therapy on the basis of clinical and cytokine profiles will yield benefits,” they wrote.
“Fulminant myocarditis invariably requires hemodynamic support and carries a high mortality risk if it is recognized late. However, the long-term prognosis in patients who survive the critical period is favorable, with recovery of myocardial function,” they added.
“This study highlights the ever-shifting understanding of the pathophysiology and therapeutic approaches to fulminant myocarditis,” Dr. Nair and Dr. Deswal concluded.
This research was supported in part by the Foundation of France, French National Research Agency, Sorbonne University, and Clinical Research Hospital. The researchers have filed a patent application based on these results. Dr. Nair and Dr. Deswal have no relevant disclosures.
A version of this article first appeared on Medscape.com.
Researchers from France have identified two distinct phenotypes of fulminant COVID-19–related myocarditis in adults, with different clinical presentations, immunologic profiles, and outcomes.
Differentiation between the two bioclinical entities is important to understand for patient management and further pathophysiological studies, they said.
The first phenotype occurs early (within a few days) in acute SARS-CoV-2 infection, with active viral replication (polymerase chain reaction positive) in adults who meet criteria for multisystem inflammatory syndrome (MIS-A+).
In this early phenotype, there is “limited systemic inflammation without skin and mucosal involvement, but myocardial dysfunction is fulminant and frequently associated with large pericardial effusions. These cases more often require extracorporeal membrane oxygenation [ECMO],” Guy Gorochov, MD, PhD, Sorbonne University, Paris, said in an interview.
The second is a delayed, postinfectious, immune-driven phenotype that occurs in adults who fail to meet the criteria for MIS-A (MIS-A–).
This phenotype occurs weeks after SARS-CoV-2 infection, usually beyond detectable active viral replication (PCR–) in the context of specific immune response and severe systemic inflammation with skin and mucosal involvement. Myocardial dysfunction is more progressive and rarely associated with large pericardial effusions, Dr. Gorochov explained.
The study was published in the Journal of the American College of Cardiology.
Evolving understanding
The findings are based on a retrospective analysis of 38 patients without a history of COVID-19 vaccination who were admitted to the intensive care unit from March 2020 to June 2021 for suspected fulminant COVID-19 myocarditis.
Patients were confirmed to have SARS-CoV-2 infection by PCR and/or by serologic testing. As noted in other studies, the patients were predominantly young men (66%; median age, 27.5 years). Twenty-five (66%) patients were MIS-A+ and 13 (34%) were MIS-A–.
In general, the MIS-A– patients were sicker and had worse outcomes.
Specifically, compared with the MIS-A+ patients, MIS-A– patients had a shorter time between the onset of COVID-19 symptoms and the development of myocarditis, a shorter time to ICU admission, and more severe presentations assessed using lower left ventricular ejection fraction and sequential organ failure assessment scores.
MIS-A– patients also had higher lactate levels, were more likely to need venoarterial ECMO (92% vs 16%), had higher ICU mortality (31% vs. 4%), and a had lower probability of survival at 3 months (68% vs. 96%), compared with their MIS-A+ peers.
Immunologic differences
The immunologic profiles of these two distinct clinical phenotypes also differed.
In MIS-A– early-type COVID-19 myocarditis, RNA polymerase III autoantibodies are frequently positive and serum levels of antiviral interferon-alpha and granulocyte-attracting interleukin-8 are elevated.
In contrast, in MIS-A+ delayed-type COVID-19 myocarditis, RNA polymerase III autoantibodies are negative and serum levels of IL-17 and IL-22 are highly elevated.
“We suggest that IL-17 and IL-22 are novel criteria that should help to assess in adults the recently recognized MIS-A,” Dr. Gorochov told this news organization. “It should be tested whether IL-17 and IL-22 are also elevated in children with MIS-C.”
The researchers also observed “extremely” high serum IL-10 levels in both patient groups. This has been previously associated with severe myocardial injury and an increase in the risk for death in severe COVID-19 patients.
The researchers said the phenotypic clustering of patients with fulminant COVID-19–related myocarditis “seems relevant” for their management.
MIS-A– cases, owing to the high risk for evolution toward refractory cardiogenic shock, should be “urgently” referred to a center with venoarterial ECMO and closely monitored to prevent a “too-late” cannulation, especially under cardiopulmonary resuscitation, known to be associated with poor outcomes, they advised.
They noted that the five patients who died in their series had late venoarterial ECMO implantation, while undergoing multiple organ failures or resuscitation.
Conversely, the risk for evolution to refractory cardiogenic shock is lower in MIS-A+ cases. However, identifying MIS-A+ cases is “all the more important given that numerous data support the efficacy of corticosteroids and/or intravenous immunoglobulins in MIS-C,” Dr. Gorochov and colleagues wrote.
The authors of a linked editorial said the French team should be “commended on their work in furthering our understanding of fulminant myocarditis related to COVID-19 infection.”
Ajith Nair, MD, Baylor College of Medicine, and Anita Deswal, MD, MPH, University of Texas M.D. Anderson Cancer Center, both in Houston, noted that fulminant myocarditis is rare and can result from either of two mechanisms: viral tropism or an immune-mediated mechanism.
“It remains to be seen whether using antiviral therapy versus immunomodulatory therapy on the basis of clinical and cytokine profiles will yield benefits,” they wrote.
“Fulminant myocarditis invariably requires hemodynamic support and carries a high mortality risk if it is recognized late. However, the long-term prognosis in patients who survive the critical period is favorable, with recovery of myocardial function,” they added.
“This study highlights the ever-shifting understanding of the pathophysiology and therapeutic approaches to fulminant myocarditis,” Dr. Nair and Dr. Deswal concluded.
This research was supported in part by the Foundation of France, French National Research Agency, Sorbonne University, and Clinical Research Hospital. The researchers have filed a patent application based on these results. Dr. Nair and Dr. Deswal have no relevant disclosures.
A version of this article first appeared on Medscape.com.
Researchers from France have identified two distinct phenotypes of fulminant COVID-19–related myocarditis in adults, with different clinical presentations, immunologic profiles, and outcomes.
Differentiation between the two bioclinical entities is important to understand for patient management and further pathophysiological studies, they said.
The first phenotype occurs early (within a few days) in acute SARS-CoV-2 infection, with active viral replication (polymerase chain reaction positive) in adults who meet criteria for multisystem inflammatory syndrome (MIS-A+).
In this early phenotype, there is “limited systemic inflammation without skin and mucosal involvement, but myocardial dysfunction is fulminant and frequently associated with large pericardial effusions. These cases more often require extracorporeal membrane oxygenation [ECMO],” Guy Gorochov, MD, PhD, Sorbonne University, Paris, said in an interview.
The second is a delayed, postinfectious, immune-driven phenotype that occurs in adults who fail to meet the criteria for MIS-A (MIS-A–).
This phenotype occurs weeks after SARS-CoV-2 infection, usually beyond detectable active viral replication (PCR–) in the context of specific immune response and severe systemic inflammation with skin and mucosal involvement. Myocardial dysfunction is more progressive and rarely associated with large pericardial effusions, Dr. Gorochov explained.
The study was published in the Journal of the American College of Cardiology.
Evolving understanding
The findings are based on a retrospective analysis of 38 patients without a history of COVID-19 vaccination who were admitted to the intensive care unit from March 2020 to June 2021 for suspected fulminant COVID-19 myocarditis.
Patients were confirmed to have SARS-CoV-2 infection by PCR and/or by serologic testing. As noted in other studies, the patients were predominantly young men (66%; median age, 27.5 years). Twenty-five (66%) patients were MIS-A+ and 13 (34%) were MIS-A–.
In general, the MIS-A– patients were sicker and had worse outcomes.
Specifically, compared with the MIS-A+ patients, MIS-A– patients had a shorter time between the onset of COVID-19 symptoms and the development of myocarditis, a shorter time to ICU admission, and more severe presentations assessed using lower left ventricular ejection fraction and sequential organ failure assessment scores.
MIS-A– patients also had higher lactate levels, were more likely to need venoarterial ECMO (92% vs 16%), had higher ICU mortality (31% vs. 4%), and a had lower probability of survival at 3 months (68% vs. 96%), compared with their MIS-A+ peers.
Immunologic differences
The immunologic profiles of these two distinct clinical phenotypes also differed.
In MIS-A– early-type COVID-19 myocarditis, RNA polymerase III autoantibodies are frequently positive and serum levels of antiviral interferon-alpha and granulocyte-attracting interleukin-8 are elevated.
In contrast, in MIS-A+ delayed-type COVID-19 myocarditis, RNA polymerase III autoantibodies are negative and serum levels of IL-17 and IL-22 are highly elevated.
“We suggest that IL-17 and IL-22 are novel criteria that should help to assess in adults the recently recognized MIS-A,” Dr. Gorochov told this news organization. “It should be tested whether IL-17 and IL-22 are also elevated in children with MIS-C.”
The researchers also observed “extremely” high serum IL-10 levels in both patient groups. This has been previously associated with severe myocardial injury and an increase in the risk for death in severe COVID-19 patients.
The researchers said the phenotypic clustering of patients with fulminant COVID-19–related myocarditis “seems relevant” for their management.
MIS-A– cases, owing to the high risk for evolution toward refractory cardiogenic shock, should be “urgently” referred to a center with venoarterial ECMO and closely monitored to prevent a “too-late” cannulation, especially under cardiopulmonary resuscitation, known to be associated with poor outcomes, they advised.
They noted that the five patients who died in their series had late venoarterial ECMO implantation, while undergoing multiple organ failures or resuscitation.
Conversely, the risk for evolution to refractory cardiogenic shock is lower in MIS-A+ cases. However, identifying MIS-A+ cases is “all the more important given that numerous data support the efficacy of corticosteroids and/or intravenous immunoglobulins in MIS-C,” Dr. Gorochov and colleagues wrote.
The authors of a linked editorial said the French team should be “commended on their work in furthering our understanding of fulminant myocarditis related to COVID-19 infection.”
Ajith Nair, MD, Baylor College of Medicine, and Anita Deswal, MD, MPH, University of Texas M.D. Anderson Cancer Center, both in Houston, noted that fulminant myocarditis is rare and can result from either of two mechanisms: viral tropism or an immune-mediated mechanism.
“It remains to be seen whether using antiviral therapy versus immunomodulatory therapy on the basis of clinical and cytokine profiles will yield benefits,” they wrote.
“Fulminant myocarditis invariably requires hemodynamic support and carries a high mortality risk if it is recognized late. However, the long-term prognosis in patients who survive the critical period is favorable, with recovery of myocardial function,” they added.
“This study highlights the ever-shifting understanding of the pathophysiology and therapeutic approaches to fulminant myocarditis,” Dr. Nair and Dr. Deswal concluded.
This research was supported in part by the Foundation of France, French National Research Agency, Sorbonne University, and Clinical Research Hospital. The researchers have filed a patent application based on these results. Dr. Nair and Dr. Deswal have no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Monkeypox: Large study highlights new symptoms
Single ulcers, anal lesions, and mouth sores are all unique symptoms of the current monkeypox outbreak, according to the largest international monkeypox case series to date. These findings underscore the need to broaden case definitions for the disease, researchers say.
“While we expected various skin problems and rashes, we also found that 1 in 10 people had only a single skin lesion in the genital area, and 15% had anal and/or rectal pain,” John Thornhill, MD, PhD, the lead author of the research, said in a press release. Dr. Thornhill is a consultant physician in sexual health and HIV and a clinical senior lecturer at Barts NHS Health Trust and Queen Mary University of London. “These different presentations highlight that monkeypox infections could be missed or easily confused with common sexually transmitted infections such as syphilis or herpes,” he said.
Since April 2022, more than 15,000 cases of monkeypox have been reported in 66 countries where the virus was previously not known to be present. The virus, a less severe cousin of smallpox, is endemic to areas of central and west Africa.
In a study published in the New England Journal of Medicine, researchers reported clinical details and outcomes of 528 monkeypox infections across 16 countries. All the cases were diagnosed between April 27 and June 24, 2022. Ninety-five percent of the cases were suspected to have been transmitted through sexual activity, 98% of patients identified as gay or bisexual men, and 75% of the patients were White. The median age of patients in this case series was 38 years, and 90% of infections occurred in Europe. Forty-one percent of patients were HIV-positive, and 96% of these individuals were receiving antiretroviral therapy. Among patients whose HIV status was negative or unknown, 57% reported using preexposure prophylaxis against HIV. About 3 in 10 (29%) individuals tested positive for concurrent sexually transmitted infections.
Nearly three out of four patients (73%) had anogenital lesions, and 41% had mucosal lesions. Fifty-four patients had one genital lesion, and 64% had fewer than 10 lesions in total. Fever (62%), swollen lymph nodes (56%), lethargy (41%), and myalgia (31%) were commonly reported symptoms prior to the development of the rash. Seventy patients (13%) required hospitalization, most commonly for severe anorectal pain and soft-tissue superinfection. Just 5% of patients received monkeypox-specific treatment: intravenous or topical cidofovir (2%), tecovirimat (2%), and vaccinia immune globulin (<1%).
The study “importantly reinforces our current understanding that the overwhelming majority of cases have been sexually associated, predominantly in men who have sex with men,” Jeffrey Klausner, MD, PhD, an infectious disease specialist at the University of Southern California, Los Angeles, said in an interview with this news organization. He was not involved with the research. “Anyone can get monkeypox, but it is most effectively spread through what we call dense networks – where there is a frequent, close personal contact,” he said. “It just happens that gay men and other men who have sex with men have some of those networks.”
The fact that most lesions are present in the genital and anal region – which is unique to this outbreak – points to transmission of the infection during intimate contact, he noted. Still, there is not enough evidence to suggest that monkeypox is spread through sexual transmission. While most semen samples in the study tested positive for monkeypox viral DNA, it is not known whether there is enough virus present to cause transmission, Dr. Thornhill said. He noted that more research is needed.
Dr. Klausner also emphasized the importance of developing new tests to diagnose monkeypox earlier to prevent spread. The lab test for monkeypox requires a swab from a lesion, but this study showed that most patients had notable symptoms prior to developing the standard rash or lesions, he said. Reliable tests using saliva or throat swabs could help detect infections faster, he noted. Patients are thought to be most contagious when they develop lesions, Dr. Klausner said, so diagnosing patients before this stage would allow them to be isolated sooner.
The California-based lab company Flow Health announced a saliva-based PCR test for monkeypox on July 9, although the Food and Drug Administration cautioned that test results from other sample types beside lesion swabs may be inaccurate. “The FDA is not aware of clinical data supporting the use of other sample types, such as blood or saliva, for monkeypox virus testing,” the agency said in a statement on July 15. “Testing samples not taken from a lesion may lead to false test results.”
Dr. Klausner reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Single ulcers, anal lesions, and mouth sores are all unique symptoms of the current monkeypox outbreak, according to the largest international monkeypox case series to date. These findings underscore the need to broaden case definitions for the disease, researchers say.
“While we expected various skin problems and rashes, we also found that 1 in 10 people had only a single skin lesion in the genital area, and 15% had anal and/or rectal pain,” John Thornhill, MD, PhD, the lead author of the research, said in a press release. Dr. Thornhill is a consultant physician in sexual health and HIV and a clinical senior lecturer at Barts NHS Health Trust and Queen Mary University of London. “These different presentations highlight that monkeypox infections could be missed or easily confused with common sexually transmitted infections such as syphilis or herpes,” he said.
Since April 2022, more than 15,000 cases of monkeypox have been reported in 66 countries where the virus was previously not known to be present. The virus, a less severe cousin of smallpox, is endemic to areas of central and west Africa.
In a study published in the New England Journal of Medicine, researchers reported clinical details and outcomes of 528 monkeypox infections across 16 countries. All the cases were diagnosed between April 27 and June 24, 2022. Ninety-five percent of the cases were suspected to have been transmitted through sexual activity, 98% of patients identified as gay or bisexual men, and 75% of the patients were White. The median age of patients in this case series was 38 years, and 90% of infections occurred in Europe. Forty-one percent of patients were HIV-positive, and 96% of these individuals were receiving antiretroviral therapy. Among patients whose HIV status was negative or unknown, 57% reported using preexposure prophylaxis against HIV. About 3 in 10 (29%) individuals tested positive for concurrent sexually transmitted infections.
Nearly three out of four patients (73%) had anogenital lesions, and 41% had mucosal lesions. Fifty-four patients had one genital lesion, and 64% had fewer than 10 lesions in total. Fever (62%), swollen lymph nodes (56%), lethargy (41%), and myalgia (31%) were commonly reported symptoms prior to the development of the rash. Seventy patients (13%) required hospitalization, most commonly for severe anorectal pain and soft-tissue superinfection. Just 5% of patients received monkeypox-specific treatment: intravenous or topical cidofovir (2%), tecovirimat (2%), and vaccinia immune globulin (<1%).
The study “importantly reinforces our current understanding that the overwhelming majority of cases have been sexually associated, predominantly in men who have sex with men,” Jeffrey Klausner, MD, PhD, an infectious disease specialist at the University of Southern California, Los Angeles, said in an interview with this news organization. He was not involved with the research. “Anyone can get monkeypox, but it is most effectively spread through what we call dense networks – where there is a frequent, close personal contact,” he said. “It just happens that gay men and other men who have sex with men have some of those networks.”
The fact that most lesions are present in the genital and anal region – which is unique to this outbreak – points to transmission of the infection during intimate contact, he noted. Still, there is not enough evidence to suggest that monkeypox is spread through sexual transmission. While most semen samples in the study tested positive for monkeypox viral DNA, it is not known whether there is enough virus present to cause transmission, Dr. Thornhill said. He noted that more research is needed.
Dr. Klausner also emphasized the importance of developing new tests to diagnose monkeypox earlier to prevent spread. The lab test for monkeypox requires a swab from a lesion, but this study showed that most patients had notable symptoms prior to developing the standard rash or lesions, he said. Reliable tests using saliva or throat swabs could help detect infections faster, he noted. Patients are thought to be most contagious when they develop lesions, Dr. Klausner said, so diagnosing patients before this stage would allow them to be isolated sooner.
The California-based lab company Flow Health announced a saliva-based PCR test for monkeypox on July 9, although the Food and Drug Administration cautioned that test results from other sample types beside lesion swabs may be inaccurate. “The FDA is not aware of clinical data supporting the use of other sample types, such as blood or saliva, for monkeypox virus testing,” the agency said in a statement on July 15. “Testing samples not taken from a lesion may lead to false test results.”
Dr. Klausner reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Single ulcers, anal lesions, and mouth sores are all unique symptoms of the current monkeypox outbreak, according to the largest international monkeypox case series to date. These findings underscore the need to broaden case definitions for the disease, researchers say.
“While we expected various skin problems and rashes, we also found that 1 in 10 people had only a single skin lesion in the genital area, and 15% had anal and/or rectal pain,” John Thornhill, MD, PhD, the lead author of the research, said in a press release. Dr. Thornhill is a consultant physician in sexual health and HIV and a clinical senior lecturer at Barts NHS Health Trust and Queen Mary University of London. “These different presentations highlight that monkeypox infections could be missed or easily confused with common sexually transmitted infections such as syphilis or herpes,” he said.
Since April 2022, more than 15,000 cases of monkeypox have been reported in 66 countries where the virus was previously not known to be present. The virus, a less severe cousin of smallpox, is endemic to areas of central and west Africa.
In a study published in the New England Journal of Medicine, researchers reported clinical details and outcomes of 528 monkeypox infections across 16 countries. All the cases were diagnosed between April 27 and June 24, 2022. Ninety-five percent of the cases were suspected to have been transmitted through sexual activity, 98% of patients identified as gay or bisexual men, and 75% of the patients were White. The median age of patients in this case series was 38 years, and 90% of infections occurred in Europe. Forty-one percent of patients were HIV-positive, and 96% of these individuals were receiving antiretroviral therapy. Among patients whose HIV status was negative or unknown, 57% reported using preexposure prophylaxis against HIV. About 3 in 10 (29%) individuals tested positive for concurrent sexually transmitted infections.
Nearly three out of four patients (73%) had anogenital lesions, and 41% had mucosal lesions. Fifty-four patients had one genital lesion, and 64% had fewer than 10 lesions in total. Fever (62%), swollen lymph nodes (56%), lethargy (41%), and myalgia (31%) were commonly reported symptoms prior to the development of the rash. Seventy patients (13%) required hospitalization, most commonly for severe anorectal pain and soft-tissue superinfection. Just 5% of patients received monkeypox-specific treatment: intravenous or topical cidofovir (2%), tecovirimat (2%), and vaccinia immune globulin (<1%).
The study “importantly reinforces our current understanding that the overwhelming majority of cases have been sexually associated, predominantly in men who have sex with men,” Jeffrey Klausner, MD, PhD, an infectious disease specialist at the University of Southern California, Los Angeles, said in an interview with this news organization. He was not involved with the research. “Anyone can get monkeypox, but it is most effectively spread through what we call dense networks – where there is a frequent, close personal contact,” he said. “It just happens that gay men and other men who have sex with men have some of those networks.”
The fact that most lesions are present in the genital and anal region – which is unique to this outbreak – points to transmission of the infection during intimate contact, he noted. Still, there is not enough evidence to suggest that monkeypox is spread through sexual transmission. While most semen samples in the study tested positive for monkeypox viral DNA, it is not known whether there is enough virus present to cause transmission, Dr. Thornhill said. He noted that more research is needed.
Dr. Klausner also emphasized the importance of developing new tests to diagnose monkeypox earlier to prevent spread. The lab test for monkeypox requires a swab from a lesion, but this study showed that most patients had notable symptoms prior to developing the standard rash or lesions, he said. Reliable tests using saliva or throat swabs could help detect infections faster, he noted. Patients are thought to be most contagious when they develop lesions, Dr. Klausner said, so diagnosing patients before this stage would allow them to be isolated sooner.
The California-based lab company Flow Health announced a saliva-based PCR test for monkeypox on July 9, although the Food and Drug Administration cautioned that test results from other sample types beside lesion swabs may be inaccurate. “The FDA is not aware of clinical data supporting the use of other sample types, such as blood or saliva, for monkeypox virus testing,” the agency said in a statement on July 15. “Testing samples not taken from a lesion may lead to false test results.”
Dr. Klausner reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.