User login
Cardiology News is an independent news source that provides cardiologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on cardiology and the cardiologist's practice. Cardiology News Digital Network is the online destination and multimedia properties of Cardiology News, the independent news publication for cardiologists. Cardiology news is the leading source of news and commentary about clinical developments in cardiology as well as health care policy and regulations that affect the cardiologist's practice. Cardiology News Digital Network is owned by Frontline Medical Communications.
New blood pressure thresholds: How do they affect the evaluation and treatment of hypertension?
In a major shift in the definition of hypertension, guidelines published in 2017 reclassified 130/80 mm Hg as high blood pressure, or stage 1 hypertension. Previous guidelines classified 130/80 mm Hg as elevated, and 140/90 mm Hg used to be the threshold for stage 1 hypertension.
“This shift in classification criteria may cause confusion among clinicians caring for patients with hypertension and has a significant impact on how we diagnose and manage hypertension in our practice,” said Shawna D. Nesbitt, MD, professor of internal medicine at the University of Texas Southwestern Medical Center and medical director at Parkland Hypertension Clinic in Dallas. Dr. Nesbitt is an expert in the diagnosis and treatment of hypertension, particularly complex and refractory cases.
Cardiovascular disease (CVD) is the leading cause of death in the United States, accounting for nearly one-quarter of all deaths in men and in women. Hypertension is a key factor contributing to CVD. The hypertension‐related CVD mortality is currently on the rise in many U.S. demographic groups, including younger individuals (35-64 years old), she said.
When asked about the potential causes of this trend, Dr. Nesbitt explained that the epidemics of obesity and overweight are critical contributors to the high prevalence of hypertension.
The new definition means a wider gap in the prevalence of hypertension between men and women, as well as between Black and White people in the United States. The U.S. rates of hypertension and hypertension‐related CVD mortality are much higher in Black than in White people in this country. Hypertension control rates are the lowest in Black, Hispanic, and Asian males, Dr. Nesbitt said.
Accurate measurement of blood pressure is crucial
The changes in classification criteria for hypertension have made accurate measurements of blood pressure important. A key challenge in the evaluation of hypertension in the clinic is the difference in the methods used to measure blood pressure between trials and real-world clinical practice.
“We can’t easily translate data collected in clinical trials into real-life scenarios, and this can have important implications in our expectations of treatment outcome,” Dr. Nesbitt cautioned.
Commenting on the best practices in blood pressure measurements in the office, Dr. Nesbitt said that patients need to be seated with their feet on the floor and their backs and arms supported. In addition, patients need to have at least 5 minutes of rest without talking.
“It is very important to help patients understand what triggers their blood pressure to be elevated and teach them how and when to measure their blood pressure at home using their own devices,” she added.
Another critical question is how to translate the new guidelines into changes in clinical care, she said.
Current treatment landscape of hypertension
Ensuring a healthy diet, weight, and sleep, participating in physical activity, avoiding nicotine, and managing blood pressure, cholesterol, and sugar levels are the new “Life’s Essential 8” strategies proposed by the American Heart Association (AHA) to reduce CVD risk.
“Sleep has recently been added to the AHA guidelines because it modulates many factors contributing to hypertension,” Dr. Nesbitt pointed out. She advised that clinicians should ask patients about their sleep and educate them on healthy sleeping habits.
Some of the evidence used to develop the new AHA guidelines is derived from the SPRINT trial, which showed that controlling blood pressure reduces the risk of major adverse cardiovascular events. “This is our ultimate goal for our patients with hypertension,” Dr. Nesbitt noted.
Regarding the best practice in hypertension management, Dr. Nesbitt explained that with the new blood pressure thresholds, more patients will be diagnosed with stage 1 hypertension and need the nonpharmacological therapy suggested by the AHA. But patients with stage 1 hypertension and with a high CVD risk (at least 10%) also should receive blood pressure-lowering medications, so an accurate assessment of the risk of clinical atherosclerotic cardiovascular disease (ASCVD) or the estimated 10-year CVD risk is crucial. “If we are not careful, we might miss some patients who need to be treated,” she said.
Calcium channel blockers, thiazide diuretics, and ACE inhibitors or angiotensin receptor blockers (ARBs) are the treatment of choice for patients with newly diagnosed hypertension. Although extensively used in the past, beta-blockers are no longer a first-line treatment for hypertension.
When asked why beta-blockers are no longer suitable for routine initial treatment of hypertension, Dr. Nesbitt said that they are effective in controlling palpitations but “other antihypertensive drugs have proven far better in controlling blood pressure.”
Hypertension is multifactorial and often occurs in combination with other conditions, including diabetes and chronic kidney disease. When developing a treatment plan for patients with hypertension, comorbidities need to be considered, because their management may also help control blood pressure, especially for conditions that may contribute to the development of hypertension.
Common conditions that contribute to and often coexist with hypertension include sleep apnea, obesity, anxiety, and depression. However, convincing people to seek mental health support can be very challenging, Dr. Nesbitt said.
She added that hypertension is a complex disease with a strong social component. Understanding its pathophysiology and social determinants is paramount for successfully managing hypertension at the individual level, as well as at the community level.
Identification and management of side effects is key
Dr. Nesbitt also discussed the importance of the identification and management of side effects associated with blood pressure-lowering drugs. She cautioned that, if not managed, side effects can lead to treatment nonadherence and pseudo‐resistance, both of which can jeopardize the successful management of hypertension.
When asked about her approach to managing side effects and convincing patients to continue taking their medications, Dr. Nesbitt noted that “setting realistic expectations and goals is key.”
In an interview after Dr. Nesbitt’s presentation, Jesica Naanous, MD, agreed that having an honest conversation with the patients is the best way to convince them to keep taking their medications. She also explains to patients that the complications of uncontrolled blood pressure are worse than the side effects of the drugs.
“As a last resort, I change a blood pressure-lowering agent to another,” added Dr. Naanous, an internist at the American British Cowdray (ABC) Medical Center in Mexico City. She explained that many antihypertensive drugs have different toxicity profiles, and simply changing to another agent can make treatment more tolerable for the patient.
Dr. Nesbitt reported no relationships with entities whose primary business is producing, marketing, selling, reselling, or distributing health care products used by or on patients.
In a major shift in the definition of hypertension, guidelines published in 2017 reclassified 130/80 mm Hg as high blood pressure, or stage 1 hypertension. Previous guidelines classified 130/80 mm Hg as elevated, and 140/90 mm Hg used to be the threshold for stage 1 hypertension.
“This shift in classification criteria may cause confusion among clinicians caring for patients with hypertension and has a significant impact on how we diagnose and manage hypertension in our practice,” said Shawna D. Nesbitt, MD, professor of internal medicine at the University of Texas Southwestern Medical Center and medical director at Parkland Hypertension Clinic in Dallas. Dr. Nesbitt is an expert in the diagnosis and treatment of hypertension, particularly complex and refractory cases.
Cardiovascular disease (CVD) is the leading cause of death in the United States, accounting for nearly one-quarter of all deaths in men and in women. Hypertension is a key factor contributing to CVD. The hypertension‐related CVD mortality is currently on the rise in many U.S. demographic groups, including younger individuals (35-64 years old), she said.
When asked about the potential causes of this trend, Dr. Nesbitt explained that the epidemics of obesity and overweight are critical contributors to the high prevalence of hypertension.
The new definition means a wider gap in the prevalence of hypertension between men and women, as well as between Black and White people in the United States. The U.S. rates of hypertension and hypertension‐related CVD mortality are much higher in Black than in White people in this country. Hypertension control rates are the lowest in Black, Hispanic, and Asian males, Dr. Nesbitt said.
Accurate measurement of blood pressure is crucial
The changes in classification criteria for hypertension have made accurate measurements of blood pressure important. A key challenge in the evaluation of hypertension in the clinic is the difference in the methods used to measure blood pressure between trials and real-world clinical practice.
“We can’t easily translate data collected in clinical trials into real-life scenarios, and this can have important implications in our expectations of treatment outcome,” Dr. Nesbitt cautioned.
Commenting on the best practices in blood pressure measurements in the office, Dr. Nesbitt said that patients need to be seated with their feet on the floor and their backs and arms supported. In addition, patients need to have at least 5 minutes of rest without talking.
“It is very important to help patients understand what triggers their blood pressure to be elevated and teach them how and when to measure their blood pressure at home using their own devices,” she added.
Another critical question is how to translate the new guidelines into changes in clinical care, she said.
Current treatment landscape of hypertension
Ensuring a healthy diet, weight, and sleep, participating in physical activity, avoiding nicotine, and managing blood pressure, cholesterol, and sugar levels are the new “Life’s Essential 8” strategies proposed by the American Heart Association (AHA) to reduce CVD risk.
“Sleep has recently been added to the AHA guidelines because it modulates many factors contributing to hypertension,” Dr. Nesbitt pointed out. She advised that clinicians should ask patients about their sleep and educate them on healthy sleeping habits.
Some of the evidence used to develop the new AHA guidelines is derived from the SPRINT trial, which showed that controlling blood pressure reduces the risk of major adverse cardiovascular events. “This is our ultimate goal for our patients with hypertension,” Dr. Nesbitt noted.
Regarding the best practice in hypertension management, Dr. Nesbitt explained that with the new blood pressure thresholds, more patients will be diagnosed with stage 1 hypertension and need the nonpharmacological therapy suggested by the AHA. But patients with stage 1 hypertension and with a high CVD risk (at least 10%) also should receive blood pressure-lowering medications, so an accurate assessment of the risk of clinical atherosclerotic cardiovascular disease (ASCVD) or the estimated 10-year CVD risk is crucial. “If we are not careful, we might miss some patients who need to be treated,” she said.
Calcium channel blockers, thiazide diuretics, and ACE inhibitors or angiotensin receptor blockers (ARBs) are the treatment of choice for patients with newly diagnosed hypertension. Although extensively used in the past, beta-blockers are no longer a first-line treatment for hypertension.
When asked why beta-blockers are no longer suitable for routine initial treatment of hypertension, Dr. Nesbitt said that they are effective in controlling palpitations but “other antihypertensive drugs have proven far better in controlling blood pressure.”
Hypertension is multifactorial and often occurs in combination with other conditions, including diabetes and chronic kidney disease. When developing a treatment plan for patients with hypertension, comorbidities need to be considered, because their management may also help control blood pressure, especially for conditions that may contribute to the development of hypertension.
Common conditions that contribute to and often coexist with hypertension include sleep apnea, obesity, anxiety, and depression. However, convincing people to seek mental health support can be very challenging, Dr. Nesbitt said.
She added that hypertension is a complex disease with a strong social component. Understanding its pathophysiology and social determinants is paramount for successfully managing hypertension at the individual level, as well as at the community level.
Identification and management of side effects is key
Dr. Nesbitt also discussed the importance of the identification and management of side effects associated with blood pressure-lowering drugs. She cautioned that, if not managed, side effects can lead to treatment nonadherence and pseudo‐resistance, both of which can jeopardize the successful management of hypertension.
When asked about her approach to managing side effects and convincing patients to continue taking their medications, Dr. Nesbitt noted that “setting realistic expectations and goals is key.”
In an interview after Dr. Nesbitt’s presentation, Jesica Naanous, MD, agreed that having an honest conversation with the patients is the best way to convince them to keep taking their medications. She also explains to patients that the complications of uncontrolled blood pressure are worse than the side effects of the drugs.
“As a last resort, I change a blood pressure-lowering agent to another,” added Dr. Naanous, an internist at the American British Cowdray (ABC) Medical Center in Mexico City. She explained that many antihypertensive drugs have different toxicity profiles, and simply changing to another agent can make treatment more tolerable for the patient.
Dr. Nesbitt reported no relationships with entities whose primary business is producing, marketing, selling, reselling, or distributing health care products used by or on patients.
In a major shift in the definition of hypertension, guidelines published in 2017 reclassified 130/80 mm Hg as high blood pressure, or stage 1 hypertension. Previous guidelines classified 130/80 mm Hg as elevated, and 140/90 mm Hg used to be the threshold for stage 1 hypertension.
“This shift in classification criteria may cause confusion among clinicians caring for patients with hypertension and has a significant impact on how we diagnose and manage hypertension in our practice,” said Shawna D. Nesbitt, MD, professor of internal medicine at the University of Texas Southwestern Medical Center and medical director at Parkland Hypertension Clinic in Dallas. Dr. Nesbitt is an expert in the diagnosis and treatment of hypertension, particularly complex and refractory cases.
Cardiovascular disease (CVD) is the leading cause of death in the United States, accounting for nearly one-quarter of all deaths in men and in women. Hypertension is a key factor contributing to CVD. The hypertension‐related CVD mortality is currently on the rise in many U.S. demographic groups, including younger individuals (35-64 years old), she said.
When asked about the potential causes of this trend, Dr. Nesbitt explained that the epidemics of obesity and overweight are critical contributors to the high prevalence of hypertension.
The new definition means a wider gap in the prevalence of hypertension between men and women, as well as between Black and White people in the United States. The U.S. rates of hypertension and hypertension‐related CVD mortality are much higher in Black than in White people in this country. Hypertension control rates are the lowest in Black, Hispanic, and Asian males, Dr. Nesbitt said.
Accurate measurement of blood pressure is crucial
The changes in classification criteria for hypertension have made accurate measurements of blood pressure important. A key challenge in the evaluation of hypertension in the clinic is the difference in the methods used to measure blood pressure between trials and real-world clinical practice.
“We can’t easily translate data collected in clinical trials into real-life scenarios, and this can have important implications in our expectations of treatment outcome,” Dr. Nesbitt cautioned.
Commenting on the best practices in blood pressure measurements in the office, Dr. Nesbitt said that patients need to be seated with their feet on the floor and their backs and arms supported. In addition, patients need to have at least 5 minutes of rest without talking.
“It is very important to help patients understand what triggers their blood pressure to be elevated and teach them how and when to measure their blood pressure at home using their own devices,” she added.
Another critical question is how to translate the new guidelines into changes in clinical care, she said.
Current treatment landscape of hypertension
Ensuring a healthy diet, weight, and sleep, participating in physical activity, avoiding nicotine, and managing blood pressure, cholesterol, and sugar levels are the new “Life’s Essential 8” strategies proposed by the American Heart Association (AHA) to reduce CVD risk.
“Sleep has recently been added to the AHA guidelines because it modulates many factors contributing to hypertension,” Dr. Nesbitt pointed out. She advised that clinicians should ask patients about their sleep and educate them on healthy sleeping habits.
Some of the evidence used to develop the new AHA guidelines is derived from the SPRINT trial, which showed that controlling blood pressure reduces the risk of major adverse cardiovascular events. “This is our ultimate goal for our patients with hypertension,” Dr. Nesbitt noted.
Regarding the best practice in hypertension management, Dr. Nesbitt explained that with the new blood pressure thresholds, more patients will be diagnosed with stage 1 hypertension and need the nonpharmacological therapy suggested by the AHA. But patients with stage 1 hypertension and with a high CVD risk (at least 10%) also should receive blood pressure-lowering medications, so an accurate assessment of the risk of clinical atherosclerotic cardiovascular disease (ASCVD) or the estimated 10-year CVD risk is crucial. “If we are not careful, we might miss some patients who need to be treated,” she said.
Calcium channel blockers, thiazide diuretics, and ACE inhibitors or angiotensin receptor blockers (ARBs) are the treatment of choice for patients with newly diagnosed hypertension. Although extensively used in the past, beta-blockers are no longer a first-line treatment for hypertension.
When asked why beta-blockers are no longer suitable for routine initial treatment of hypertension, Dr. Nesbitt said that they are effective in controlling palpitations but “other antihypertensive drugs have proven far better in controlling blood pressure.”
Hypertension is multifactorial and often occurs in combination with other conditions, including diabetes and chronic kidney disease. When developing a treatment plan for patients with hypertension, comorbidities need to be considered, because their management may also help control blood pressure, especially for conditions that may contribute to the development of hypertension.
Common conditions that contribute to and often coexist with hypertension include sleep apnea, obesity, anxiety, and depression. However, convincing people to seek mental health support can be very challenging, Dr. Nesbitt said.
She added that hypertension is a complex disease with a strong social component. Understanding its pathophysiology and social determinants is paramount for successfully managing hypertension at the individual level, as well as at the community level.
Identification and management of side effects is key
Dr. Nesbitt also discussed the importance of the identification and management of side effects associated with blood pressure-lowering drugs. She cautioned that, if not managed, side effects can lead to treatment nonadherence and pseudo‐resistance, both of which can jeopardize the successful management of hypertension.
When asked about her approach to managing side effects and convincing patients to continue taking their medications, Dr. Nesbitt noted that “setting realistic expectations and goals is key.”
In an interview after Dr. Nesbitt’s presentation, Jesica Naanous, MD, agreed that having an honest conversation with the patients is the best way to convince them to keep taking their medications. She also explains to patients that the complications of uncontrolled blood pressure are worse than the side effects of the drugs.
“As a last resort, I change a blood pressure-lowering agent to another,” added Dr. Naanous, an internist at the American British Cowdray (ABC) Medical Center in Mexico City. She explained that many antihypertensive drugs have different toxicity profiles, and simply changing to another agent can make treatment more tolerable for the patient.
Dr. Nesbitt reported no relationships with entities whose primary business is producing, marketing, selling, reselling, or distributing health care products used by or on patients.
AT INTERNAL MEDICINE 2023
Can an endoscopic procedure treat type 2 diabetes?
Called recellularization via electroporation therapy (ReCET), the technology, manufactured by Endogenex, uses a specialized catheter to deliver alternating electric pulses to the duodenum to induce cellular regeneration. This process is thought to improve insulin sensitivity, in part, by altering gut hormones and nutritional sensing, principal investigator Jacques Bergman, MD, PhD, said in a press briefing held in conjunction with the annual Digestive Disease Week® (DDW), where he will present the data on May 9.

In the first-in-human study of ReCET, 12 of 14 patients were able to come off insulin for up to a year following the procedure when combined with the use of the glucagonlike peptide–1 agonist semaglutide.
“This might be a game changer in the management of type 2 diabetes because a single outpatient endoscopic intervention was suggested to have a pretty long therapeutic effect, which is compliance-free, as opposed to drug therapy that relies on patients taking the drugs on a daily basis,” said Dr. Bergman, professor of gastrointestinal endoscopy at Amsterdam University Medical Center.
Moreover, he added, “this technique is disease-modifying, so it goes to the root cause of type 2 diabetes and tackles the insulin resistance, as opposed to drug therapy, which at best, is disease-controlling, and the effect is immediately gone if you stop the medication.”
ReCET is similar to another product, Fractyl’s Revita DMR, for which Dr. Bergman was involved in a randomized clinical trial. He said in an interview that the two technologies differ in that the Revita uses heat with submucosal lifting to avoid deeper heat penetration, whereas ReCET is nonthermal. He is also involved in a second randomized trial of the Revita.
Is semaglutide muddying the findings?
Asked to comment about the current study with ReCET, Ali Aminian, MD, professor of surgery and director of the Bariatric and Metabolic Institute at the Cleveland Clinic, said that the treatment effect is certainly plausible.

“The observation that hyperglycemia rapidly and substantially improves after bariatric surgery has prompted innovators to search for novel endoscopic procedures targeting the GI tract to improve diabetes and metabolic disease. Over the years, we learned that in addition to its role in digestion and absorption, the GI tract is actually a large endocrine organ which contributes to development of diabetes and metabolic disease.”
However, Dr. Aminian said that, “while these preliminary findings on a very small number of patients with a very short follow-up time are interesting,” he faulted the study design for including semaglutide. “When patients are treated with a combination of therapies, it will be hard to understand the true effect of each therapy,” and particularly, “when we add a strong diabetes medication like semaglutide.”
Dr. Bergman said semaglutide was used to “boost the insulin-resistant effect of the endoscopic treatment,” and that a planned double-blind, randomized trial will “show how much semaglutide actually contributed to the effect.” The ultimate goal, he noted, is to eliminate the need for all medications.
Moreover, when people with type 2 diabetes add semaglutide to insulin treatment, only about 20% typically are able to quit taking the insulin, in contrast to the 86% seen in this study, lead author Celine Busch, MBBS, a PhD candidate in gastroenterology at Amsterdam University, said in a DDW statement.
Dr. Aminian said, “I’m looking forward to better quality data ... from studies with a stronger design to prove safety, efficacy, and durability of this endoscopic intervention in patients with diabetes.”
But, he also cautioned, “in the past few years, other endoscopic procedures targeting the duodenum were introduced with exciting initial findings based on a small series [with a] short-term follow-up time. However, their safety, efficacy, and durability were not proven in subsequent studies.”
All patients stopped insulin, most for a year
The single-arm, single-center study involved 14 patients with type 2 diabetes taking basal but not premeal insulin. All underwent the 1-hour outpatient ReCET procedure, which involved placing a catheter into the first part of the small bowel and delivering electrical pulses to the duodenum.
Patients adhered to a calorie-controlled liquid diet for 2 weeks, after which they were initiated on semaglutide. All 14 patients were able to come off insulin for 3 months while maintaining glycemic control, and 12 were able to come off insulin for 12 months. They also experienced a 50% reduction in liver fat.
Dr. Bergman said a randomized, double-blind study using a sham procedure for controls is expected to start in about 2 months. “But for now, we are very encouraged by the potential for controlling type 2 diabetes with a single endoscopic treatment.”
Dr. Bergman has reported serving on the advisory board for Endogenex. Dr. Aminian has reported receiving research support and honorarium from Medtronic and Ethicon.
The meeting is sponsored by the American Gastroenterological Association, the American Association for the Study of Liver Diseases, the American Society for Gastrointestinal Endoscopy, and the Society for Surgery of the Alimentary Tract.
A version of this article first appeared on Medscape.com.
Called recellularization via electroporation therapy (ReCET), the technology, manufactured by Endogenex, uses a specialized catheter to deliver alternating electric pulses to the duodenum to induce cellular regeneration. This process is thought to improve insulin sensitivity, in part, by altering gut hormones and nutritional sensing, principal investigator Jacques Bergman, MD, PhD, said in a press briefing held in conjunction with the annual Digestive Disease Week® (DDW), where he will present the data on May 9.
In the first-in-human study of ReCET, 12 of 14 patients were able to come off insulin for up to a year following the procedure when combined with the use of the glucagonlike peptide–1 agonist semaglutide.
“This might be a game changer in the management of type 2 diabetes because a single outpatient endoscopic intervention was suggested to have a pretty long therapeutic effect, which is compliance-free, as opposed to drug therapy that relies on patients taking the drugs on a daily basis,” said Dr. Bergman, professor of gastrointestinal endoscopy at Amsterdam University Medical Center.
Moreover, he added, “this technique is disease-modifying, so it goes to the root cause of type 2 diabetes and tackles the insulin resistance, as opposed to drug therapy, which at best, is disease-controlling, and the effect is immediately gone if you stop the medication.”
ReCET is similar to another product, Fractyl’s Revita DMR, for which Dr. Bergman was involved in a randomized clinical trial. He said in an interview that the two technologies differ in that the Revita uses heat with submucosal lifting to avoid deeper heat penetration, whereas ReCET is nonthermal. He is also involved in a second randomized trial of the Revita.
Is semaglutide muddying the findings?
Asked to comment about the current study with ReCET, Ali Aminian, MD, professor of surgery and director of the Bariatric and Metabolic Institute at the Cleveland Clinic, said that the treatment effect is certainly plausible.
“The observation that hyperglycemia rapidly and substantially improves after bariatric surgery has prompted innovators to search for novel endoscopic procedures targeting the GI tract to improve diabetes and metabolic disease. Over the years, we learned that in addition to its role in digestion and absorption, the GI tract is actually a large endocrine organ which contributes to development of diabetes and metabolic disease.”
However, Dr. Aminian said that, “while these preliminary findings on a very small number of patients with a very short follow-up time are interesting,” he faulted the study design for including semaglutide. “When patients are treated with a combination of therapies, it will be hard to understand the true effect of each therapy,” and particularly, “when we add a strong diabetes medication like semaglutide.”
Dr. Bergman said semaglutide was used to “boost the insulin-resistant effect of the endoscopic treatment,” and that a planned double-blind, randomized trial will “show how much semaglutide actually contributed to the effect.” The ultimate goal, he noted, is to eliminate the need for all medications.
Moreover, when people with type 2 diabetes add semaglutide to insulin treatment, only about 20% typically are able to quit taking the insulin, in contrast to the 86% seen in this study, lead author Celine Busch, MBBS, a PhD candidate in gastroenterology at Amsterdam University, said in a DDW statement.
Dr. Aminian said, “I’m looking forward to better quality data ... from studies with a stronger design to prove safety, efficacy, and durability of this endoscopic intervention in patients with diabetes.”
But, he also cautioned, “in the past few years, other endoscopic procedures targeting the duodenum were introduced with exciting initial findings based on a small series [with a] short-term follow-up time. However, their safety, efficacy, and durability were not proven in subsequent studies.”
All patients stopped insulin, most for a year
The single-arm, single-center study involved 14 patients with type 2 diabetes taking basal but not premeal insulin. All underwent the 1-hour outpatient ReCET procedure, which involved placing a catheter into the first part of the small bowel and delivering electrical pulses to the duodenum.
Patients adhered to a calorie-controlled liquid diet for 2 weeks, after which they were initiated on semaglutide. All 14 patients were able to come off insulin for 3 months while maintaining glycemic control, and 12 were able to come off insulin for 12 months. They also experienced a 50% reduction in liver fat.
Dr. Bergman said a randomized, double-blind study using a sham procedure for controls is expected to start in about 2 months. “But for now, we are very encouraged by the potential for controlling type 2 diabetes with a single endoscopic treatment.”
Dr. Bergman has reported serving on the advisory board for Endogenex. Dr. Aminian has reported receiving research support and honorarium from Medtronic and Ethicon.
The meeting is sponsored by the American Gastroenterological Association, the American Association for the Study of Liver Diseases, the American Society for Gastrointestinal Endoscopy, and the Society for Surgery of the Alimentary Tract.
A version of this article first appeared on Medscape.com.
Called recellularization via electroporation therapy (ReCET), the technology, manufactured by Endogenex, uses a specialized catheter to deliver alternating electric pulses to the duodenum to induce cellular regeneration. This process is thought to improve insulin sensitivity, in part, by altering gut hormones and nutritional sensing, principal investigator Jacques Bergman, MD, PhD, said in a press briefing held in conjunction with the annual Digestive Disease Week® (DDW), where he will present the data on May 9.
In the first-in-human study of ReCET, 12 of 14 patients were able to come off insulin for up to a year following the procedure when combined with the use of the glucagonlike peptide–1 agonist semaglutide.
“This might be a game changer in the management of type 2 diabetes because a single outpatient endoscopic intervention was suggested to have a pretty long therapeutic effect, which is compliance-free, as opposed to drug therapy that relies on patients taking the drugs on a daily basis,” said Dr. Bergman, professor of gastrointestinal endoscopy at Amsterdam University Medical Center.
Moreover, he added, “this technique is disease-modifying, so it goes to the root cause of type 2 diabetes and tackles the insulin resistance, as opposed to drug therapy, which at best, is disease-controlling, and the effect is immediately gone if you stop the medication.”
ReCET is similar to another product, Fractyl’s Revita DMR, for which Dr. Bergman was involved in a randomized clinical trial. He said in an interview that the two technologies differ in that the Revita uses heat with submucosal lifting to avoid deeper heat penetration, whereas ReCET is nonthermal. He is also involved in a second randomized trial of the Revita.
Is semaglutide muddying the findings?
Asked to comment about the current study with ReCET, Ali Aminian, MD, professor of surgery and director of the Bariatric and Metabolic Institute at the Cleveland Clinic, said that the treatment effect is certainly plausible.
“The observation that hyperglycemia rapidly and substantially improves after bariatric surgery has prompted innovators to search for novel endoscopic procedures targeting the GI tract to improve diabetes and metabolic disease. Over the years, we learned that in addition to its role in digestion and absorption, the GI tract is actually a large endocrine organ which contributes to development of diabetes and metabolic disease.”
However, Dr. Aminian said that, “while these preliminary findings on a very small number of patients with a very short follow-up time are interesting,” he faulted the study design for including semaglutide. “When patients are treated with a combination of therapies, it will be hard to understand the true effect of each therapy,” and particularly, “when we add a strong diabetes medication like semaglutide.”
Dr. Bergman said semaglutide was used to “boost the insulin-resistant effect of the endoscopic treatment,” and that a planned double-blind, randomized trial will “show how much semaglutide actually contributed to the effect.” The ultimate goal, he noted, is to eliminate the need for all medications.
Moreover, when people with type 2 diabetes add semaglutide to insulin treatment, only about 20% typically are able to quit taking the insulin, in contrast to the 86% seen in this study, lead author Celine Busch, MBBS, a PhD candidate in gastroenterology at Amsterdam University, said in a DDW statement.
Dr. Aminian said, “I’m looking forward to better quality data ... from studies with a stronger design to prove safety, efficacy, and durability of this endoscopic intervention in patients with diabetes.”
But, he also cautioned, “in the past few years, other endoscopic procedures targeting the duodenum were introduced with exciting initial findings based on a small series [with a] short-term follow-up time. However, their safety, efficacy, and durability were not proven in subsequent studies.”
All patients stopped insulin, most for a year
The single-arm, single-center study involved 14 patients with type 2 diabetes taking basal but not premeal insulin. All underwent the 1-hour outpatient ReCET procedure, which involved placing a catheter into the first part of the small bowel and delivering electrical pulses to the duodenum.
Patients adhered to a calorie-controlled liquid diet for 2 weeks, after which they were initiated on semaglutide. All 14 patients were able to come off insulin for 3 months while maintaining glycemic control, and 12 were able to come off insulin for 12 months. They also experienced a 50% reduction in liver fat.
Dr. Bergman said a randomized, double-blind study using a sham procedure for controls is expected to start in about 2 months. “But for now, we are very encouraged by the potential for controlling type 2 diabetes with a single endoscopic treatment.”
Dr. Bergman has reported serving on the advisory board for Endogenex. Dr. Aminian has reported receiving research support and honorarium from Medtronic and Ethicon.
The meeting is sponsored by the American Gastroenterological Association, the American Association for the Study of Liver Diseases, the American Society for Gastrointestinal Endoscopy, and the Society for Surgery of the Alimentary Tract.
A version of this article first appeared on Medscape.com.
FROM DDW 2023
Novel strategy could improve heart transplant allocation
Prediction models that incorporate more than just treatment status could rank order heart transplant candidates by urgency more effectively than the current system, a modeling study suggests.
Since 2018, the U.S. heart transplant allocation system has ranked heart candidates according to six treatment-based “statuses” (up from three used previously), ignoring many objective patient characteristics, the authors write.
Their study showed no significant difference in survival between statuses four and six, and status five had lower survival than status four.
“We expected multivariable prediction models to outperform the six-status system when it comes to rank ordering patients by how likely they are to die on the wait list (medical urgency),” William F. Parker, MD, MS, PhD, of the University of Chicago, told this news organization.
“However, we were surprised to see that the statuses were out of order,” he said. “Status five patients are more urgent than status three or status four patients,” mainly because most are in renal failure and listed for multiorgan transplantation with a kidney.
Objective physiologic measurements, such as glomerular filtration rate (GFR), had high variable importance, offering a minimally invasive measurement with predictive power in assessing medical urgency. Therefore, including GFR and other variables such as extracorporeal membrane oxygenation (ECMO) could improve the accuracy of the allocation system in identifying the most medically urgent candidates, Dr. Parker and colleagues suggest.
The study was published online in JACC: Heart Failure.
‘Moderate ability’ to rank order
The investigators assessed the effectiveness of the standard six-status ranking system and several novel prediction models in identifying the most urgent heart transplant candidates. The primary outcome was death before receipt of a heart transplant.
The final data set contained 32,294 candidates (mean age, 53 years; 74%, men); 27,200 made up the prepolicy training set and 5,094 were included in the postpolicy test set.
The team evaluated the accuracy of the six-status system using Harrell’s C-index and log-rank tests of Kaplan-Meier estimated survival by status for candidates listed after the policy change (November 2018 to March 2020) in the Scientific Registry of Transplant Recipients data set.
They then developed Cox proportional hazards models and random survival forest models using prepolicy data (2010-2017). Predictor variables included age, diagnosis, laboratory measurements, hemodynamics, and supportive treatment at the time of listing.
They found that the six-status ranking at listing has had “moderate ability” to rank order candidates.
As Dr. Parker indicated, statuses four and six had no significant difference in survival, and status five had lower survival than status four.
The investigators’ multivariable prediction models derived with prepolicy data ranked candidates correctly more often than the six-status rankings. Objective physiologic measurements, such as GFR and ECMO, were identified as having significant importance with regard to ranking by urgency.
“The novel prediction models we developed … could be implemented by the Organ Procurement and Transplantation Network (OPTN) as allocation policy and would be better than the status quo,” Dr. Parker said. “However, I think we could do even better using the newer data collected after 2018.”
Modifications underway
The OPTN Heart Transplantation Committee is currently working on developing a new framework for allocating deceased donor hearts called Continuous Distribution.
“The six-tiered system works well, and it better stratifies the most medically urgent candidates than the previous allocation framework,” the leadership of the United Network for Organ Sharing Heart Transplantation Committee, including Chair Richard C. Daly, MD, Mayo Clinic; Vice-Chair Jondavid Menteer, MD, University of Southern California, Los Angeles; and former Chair Shelley Hall, MD, Baylor University Medical Center, told this news organization.
“That said, it is always appropriate to review and adjust variables that affect the medical urgency attribute for heart allocation.”
The new framework will change how patients are prioritized, they said. “Continuous distribution will consider all patient factors, including medical urgency, together to determine the order of an organ offer, and no single factor will decide an organ match.
“The goal is to increase fairness by moving to a points-based allocation framework that allows candidates to be compared using a single score composed of multiple factors.
“Furthermore,” they added, “continuous distribution provides a framework that will allow modifications of the criteria defining medical urgency (and other attributes of allocation) to a finer degree than the current policy. … Once continuous distribution is in place and the OPTN has policy monitoring data, the committee may consider and model different ways of defining medical urgency.”
Kiran K. Khush, MD, of Stanford (Calif.) University School of Medicine, coauthor of a related commentary, elaborated. “The composite allocation score (CAS) will consist of a ‘points-based system,’ in which candidates will be assigned points based on (1) medical urgency, (2) anticipated posttransplant survival, (3) candidate biology (eg., special characteristics that may result in higher prioritization, such as blood type O and allosensitization), (4) access (eg., prior living donor, pediatric patient), and (5) placement efficacy (travel, proximity).”
Candidates will be assigned points based on these categories, and will be rank ordered for each donor offer.
Dr. Khush and colleagues propose that a multivariable model – such as the ones described in the study – would be the best way to assign points for medical urgency.
“This system will be more equitable than the current system,” Dr. Khush said, “because it will better prioritize the sickest candidates while improving access for patients who are currently at a disadvantage [for example, blood O, highly sensitized patients], and will also remove artificial geographic boundaries [for example, the current 500-mile rule for heart allocation].”
Going further
Jesse D. Schold, PhD, of the University of Colorado at Denver, Aurora, raises concerns about other aspects of the heart allocation system in another related commentary.
“One big issue with our data in transplantation … is that, while it is very comprehensive for capturing transplant candidates and recipients, there is no data collection for patients and processes of care for patients prior to wait list placement,” he told this news organization. This phase of care is subject to wide variation in practice, he said, “and is likely as important as any to patients – the ability to be referred, evaluated, and placed on a waiting list.”
Report cards that measure quality of care after wait list placement ignore key phases prior to wait list placement, he said. “This may have the unintended consequences of limiting access to care and to the waiting list for patients perceived to be at higher risk, or the use of higher-risk donors, despite their potential survival advantage.
“In contrast,” he said, “quality report cards that incentivize treatment for all patients who may benefit would likely have a greater beneficial impact on patients with end-organ disease.”
There is also significant risk of underlying differences in patient populations between centers, despite the use of multivariable models, he added. This heterogeneity “may not be reflected accurately in the report cards [which] have significant impact for regulatory review, private payer contracting, and center reputation.”
Some of these concerns may be addressed in the new OPTN Modernization Initiative, according to David Bowman, a public affairs specialist at the Health Resources and Services Administration. One of the goals of the initiative “is to ensure that the OPTN Board of Directors is high functioning, has greater independence, and represents the diversity of communities served by the OPTN,” he told this news organization. “Strengthened governance will lead to effective policy development and implementation, and enhanced transparency and accountability of the process.”
Addressing another concern about the system, Savitri Fedson, MD, of the Michael E. DeBakey VA Medical Center and Baylor College of Medicine, Houston, wonders in a related editorial whether organ donors and recipients should know more about each other, and if so, could that reverse the ongoing downward trend in organ acceptance?
Although some organizations are in favor of sharing more information, Dr. Fedson notes that “less information may have the greater benefit.” She writes, “We might realize that the simplest approach is often the best: a fulsome thank you for the donor’s gift that is willingly given to a stranger without expectation of payment, and on the recipient side, the knowledge that an organ is of good quality.
“The transplant patient can be comforted with the understanding that the risk of disease transmission, while not zero, is low, and that their survival following acceptance of an organ is better than languishing on a waiting list.”
The study received no commercial funding. Dr. Parker, Dr. Khush, Dr. Schold, and Dr. Fedson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Prediction models that incorporate more than just treatment status could rank order heart transplant candidates by urgency more effectively than the current system, a modeling study suggests.
Since 2018, the U.S. heart transplant allocation system has ranked heart candidates according to six treatment-based “statuses” (up from three used previously), ignoring many objective patient characteristics, the authors write.
Their study showed no significant difference in survival between statuses four and six, and status five had lower survival than status four.
“We expected multivariable prediction models to outperform the six-status system when it comes to rank ordering patients by how likely they are to die on the wait list (medical urgency),” William F. Parker, MD, MS, PhD, of the University of Chicago, told this news organization.
“However, we were surprised to see that the statuses were out of order,” he said. “Status five patients are more urgent than status three or status four patients,” mainly because most are in renal failure and listed for multiorgan transplantation with a kidney.
Objective physiologic measurements, such as glomerular filtration rate (GFR), had high variable importance, offering a minimally invasive measurement with predictive power in assessing medical urgency. Therefore, including GFR and other variables such as extracorporeal membrane oxygenation (ECMO) could improve the accuracy of the allocation system in identifying the most medically urgent candidates, Dr. Parker and colleagues suggest.
The study was published online in JACC: Heart Failure.
‘Moderate ability’ to rank order
The investigators assessed the effectiveness of the standard six-status ranking system and several novel prediction models in identifying the most urgent heart transplant candidates. The primary outcome was death before receipt of a heart transplant.
The final data set contained 32,294 candidates (mean age, 53 years; 74%, men); 27,200 made up the prepolicy training set and 5,094 were included in the postpolicy test set.
The team evaluated the accuracy of the six-status system using Harrell’s C-index and log-rank tests of Kaplan-Meier estimated survival by status for candidates listed after the policy change (November 2018 to March 2020) in the Scientific Registry of Transplant Recipients data set.
They then developed Cox proportional hazards models and random survival forest models using prepolicy data (2010-2017). Predictor variables included age, diagnosis, laboratory measurements, hemodynamics, and supportive treatment at the time of listing.
They found that the six-status ranking at listing has had “moderate ability” to rank order candidates.
As Dr. Parker indicated, statuses four and six had no significant difference in survival, and status five had lower survival than status four.
The investigators’ multivariable prediction models derived with prepolicy data ranked candidates correctly more often than the six-status rankings. Objective physiologic measurements, such as GFR and ECMO, were identified as having significant importance with regard to ranking by urgency.
“The novel prediction models we developed … could be implemented by the Organ Procurement and Transplantation Network (OPTN) as allocation policy and would be better than the status quo,” Dr. Parker said. “However, I think we could do even better using the newer data collected after 2018.”
Modifications underway
The OPTN Heart Transplantation Committee is currently working on developing a new framework for allocating deceased donor hearts called Continuous Distribution.
“The six-tiered system works well, and it better stratifies the most medically urgent candidates than the previous allocation framework,” the leadership of the United Network for Organ Sharing Heart Transplantation Committee, including Chair Richard C. Daly, MD, Mayo Clinic; Vice-Chair Jondavid Menteer, MD, University of Southern California, Los Angeles; and former Chair Shelley Hall, MD, Baylor University Medical Center, told this news organization.
“That said, it is always appropriate to review and adjust variables that affect the medical urgency attribute for heart allocation.”
The new framework will change how patients are prioritized, they said. “Continuous distribution will consider all patient factors, including medical urgency, together to determine the order of an organ offer, and no single factor will decide an organ match.
“The goal is to increase fairness by moving to a points-based allocation framework that allows candidates to be compared using a single score composed of multiple factors.
“Furthermore,” they added, “continuous distribution provides a framework that will allow modifications of the criteria defining medical urgency (and other attributes of allocation) to a finer degree than the current policy. … Once continuous distribution is in place and the OPTN has policy monitoring data, the committee may consider and model different ways of defining medical urgency.”
Kiran K. Khush, MD, of Stanford (Calif.) University School of Medicine, coauthor of a related commentary, elaborated. “The composite allocation score (CAS) will consist of a ‘points-based system,’ in which candidates will be assigned points based on (1) medical urgency, (2) anticipated posttransplant survival, (3) candidate biology (eg., special characteristics that may result in higher prioritization, such as blood type O and allosensitization), (4) access (eg., prior living donor, pediatric patient), and (5) placement efficacy (travel, proximity).”
Candidates will be assigned points based on these categories, and will be rank ordered for each donor offer.
Dr. Khush and colleagues propose that a multivariable model – such as the ones described in the study – would be the best way to assign points for medical urgency.
“This system will be more equitable than the current system,” Dr. Khush said, “because it will better prioritize the sickest candidates while improving access for patients who are currently at a disadvantage [for example, blood O, highly sensitized patients], and will also remove artificial geographic boundaries [for example, the current 500-mile rule for heart allocation].”
Going further
Jesse D. Schold, PhD, of the University of Colorado at Denver, Aurora, raises concerns about other aspects of the heart allocation system in another related commentary.
“One big issue with our data in transplantation … is that, while it is very comprehensive for capturing transplant candidates and recipients, there is no data collection for patients and processes of care for patients prior to wait list placement,” he told this news organization. This phase of care is subject to wide variation in practice, he said, “and is likely as important as any to patients – the ability to be referred, evaluated, and placed on a waiting list.”
Report cards that measure quality of care after wait list placement ignore key phases prior to wait list placement, he said. “This may have the unintended consequences of limiting access to care and to the waiting list for patients perceived to be at higher risk, or the use of higher-risk donors, despite their potential survival advantage.
“In contrast,” he said, “quality report cards that incentivize treatment for all patients who may benefit would likely have a greater beneficial impact on patients with end-organ disease.”
There is also significant risk of underlying differences in patient populations between centers, despite the use of multivariable models, he added. This heterogeneity “may not be reflected accurately in the report cards [which] have significant impact for regulatory review, private payer contracting, and center reputation.”
Some of these concerns may be addressed in the new OPTN Modernization Initiative, according to David Bowman, a public affairs specialist at the Health Resources and Services Administration. One of the goals of the initiative “is to ensure that the OPTN Board of Directors is high functioning, has greater independence, and represents the diversity of communities served by the OPTN,” he told this news organization. “Strengthened governance will lead to effective policy development and implementation, and enhanced transparency and accountability of the process.”
Addressing another concern about the system, Savitri Fedson, MD, of the Michael E. DeBakey VA Medical Center and Baylor College of Medicine, Houston, wonders in a related editorial whether organ donors and recipients should know more about each other, and if so, could that reverse the ongoing downward trend in organ acceptance?
Although some organizations are in favor of sharing more information, Dr. Fedson notes that “less information may have the greater benefit.” She writes, “We might realize that the simplest approach is often the best: a fulsome thank you for the donor’s gift that is willingly given to a stranger without expectation of payment, and on the recipient side, the knowledge that an organ is of good quality.
“The transplant patient can be comforted with the understanding that the risk of disease transmission, while not zero, is low, and that their survival following acceptance of an organ is better than languishing on a waiting list.”
The study received no commercial funding. Dr. Parker, Dr. Khush, Dr. Schold, and Dr. Fedson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Prediction models that incorporate more than just treatment status could rank order heart transplant candidates by urgency more effectively than the current system, a modeling study suggests.
Since 2018, the U.S. heart transplant allocation system has ranked heart candidates according to six treatment-based “statuses” (up from three used previously), ignoring many objective patient characteristics, the authors write.
Their study showed no significant difference in survival between statuses four and six, and status five had lower survival than status four.
“We expected multivariable prediction models to outperform the six-status system when it comes to rank ordering patients by how likely they are to die on the wait list (medical urgency),” William F. Parker, MD, MS, PhD, of the University of Chicago, told this news organization.
“However, we were surprised to see that the statuses were out of order,” he said. “Status five patients are more urgent than status three or status four patients,” mainly because most are in renal failure and listed for multiorgan transplantation with a kidney.
Objective physiologic measurements, such as glomerular filtration rate (GFR), had high variable importance, offering a minimally invasive measurement with predictive power in assessing medical urgency. Therefore, including GFR and other variables such as extracorporeal membrane oxygenation (ECMO) could improve the accuracy of the allocation system in identifying the most medically urgent candidates, Dr. Parker and colleagues suggest.
The study was published online in JACC: Heart Failure.
‘Moderate ability’ to rank order
The investigators assessed the effectiveness of the standard six-status ranking system and several novel prediction models in identifying the most urgent heart transplant candidates. The primary outcome was death before receipt of a heart transplant.
The final data set contained 32,294 candidates (mean age, 53 years; 74%, men); 27,200 made up the prepolicy training set and 5,094 were included in the postpolicy test set.
The team evaluated the accuracy of the six-status system using Harrell’s C-index and log-rank tests of Kaplan-Meier estimated survival by status for candidates listed after the policy change (November 2018 to March 2020) in the Scientific Registry of Transplant Recipients data set.
They then developed Cox proportional hazards models and random survival forest models using prepolicy data (2010-2017). Predictor variables included age, diagnosis, laboratory measurements, hemodynamics, and supportive treatment at the time of listing.
They found that the six-status ranking at listing has had “moderate ability” to rank order candidates.
As Dr. Parker indicated, statuses four and six had no significant difference in survival, and status five had lower survival than status four.
The investigators’ multivariable prediction models derived with prepolicy data ranked candidates correctly more often than the six-status rankings. Objective physiologic measurements, such as GFR and ECMO, were identified as having significant importance with regard to ranking by urgency.
“The novel prediction models we developed … could be implemented by the Organ Procurement and Transplantation Network (OPTN) as allocation policy and would be better than the status quo,” Dr. Parker said. “However, I think we could do even better using the newer data collected after 2018.”
Modifications underway
The OPTN Heart Transplantation Committee is currently working on developing a new framework for allocating deceased donor hearts called Continuous Distribution.
“The six-tiered system works well, and it better stratifies the most medically urgent candidates than the previous allocation framework,” the leadership of the United Network for Organ Sharing Heart Transplantation Committee, including Chair Richard C. Daly, MD, Mayo Clinic; Vice-Chair Jondavid Menteer, MD, University of Southern California, Los Angeles; and former Chair Shelley Hall, MD, Baylor University Medical Center, told this news organization.
“That said, it is always appropriate to review and adjust variables that affect the medical urgency attribute for heart allocation.”
The new framework will change how patients are prioritized, they said. “Continuous distribution will consider all patient factors, including medical urgency, together to determine the order of an organ offer, and no single factor will decide an organ match.
“The goal is to increase fairness by moving to a points-based allocation framework that allows candidates to be compared using a single score composed of multiple factors.
“Furthermore,” they added, “continuous distribution provides a framework that will allow modifications of the criteria defining medical urgency (and other attributes of allocation) to a finer degree than the current policy. … Once continuous distribution is in place and the OPTN has policy monitoring data, the committee may consider and model different ways of defining medical urgency.”
Kiran K. Khush, MD, of Stanford (Calif.) University School of Medicine, coauthor of a related commentary, elaborated. “The composite allocation score (CAS) will consist of a ‘points-based system,’ in which candidates will be assigned points based on (1) medical urgency, (2) anticipated posttransplant survival, (3) candidate biology (eg., special characteristics that may result in higher prioritization, such as blood type O and allosensitization), (4) access (eg., prior living donor, pediatric patient), and (5) placement efficacy (travel, proximity).”
Candidates will be assigned points based on these categories, and will be rank ordered for each donor offer.
Dr. Khush and colleagues propose that a multivariable model – such as the ones described in the study – would be the best way to assign points for medical urgency.
“This system will be more equitable than the current system,” Dr. Khush said, “because it will better prioritize the sickest candidates while improving access for patients who are currently at a disadvantage [for example, blood O, highly sensitized patients], and will also remove artificial geographic boundaries [for example, the current 500-mile rule for heart allocation].”
Going further
Jesse D. Schold, PhD, of the University of Colorado at Denver, Aurora, raises concerns about other aspects of the heart allocation system in another related commentary.
“One big issue with our data in transplantation … is that, while it is very comprehensive for capturing transplant candidates and recipients, there is no data collection for patients and processes of care for patients prior to wait list placement,” he told this news organization. This phase of care is subject to wide variation in practice, he said, “and is likely as important as any to patients – the ability to be referred, evaluated, and placed on a waiting list.”
Report cards that measure quality of care after wait list placement ignore key phases prior to wait list placement, he said. “This may have the unintended consequences of limiting access to care and to the waiting list for patients perceived to be at higher risk, or the use of higher-risk donors, despite their potential survival advantage.
“In contrast,” he said, “quality report cards that incentivize treatment for all patients who may benefit would likely have a greater beneficial impact on patients with end-organ disease.”
There is also significant risk of underlying differences in patient populations between centers, despite the use of multivariable models, he added. This heterogeneity “may not be reflected accurately in the report cards [which] have significant impact for regulatory review, private payer contracting, and center reputation.”
Some of these concerns may be addressed in the new OPTN Modernization Initiative, according to David Bowman, a public affairs specialist at the Health Resources and Services Administration. One of the goals of the initiative “is to ensure that the OPTN Board of Directors is high functioning, has greater independence, and represents the diversity of communities served by the OPTN,” he told this news organization. “Strengthened governance will lead to effective policy development and implementation, and enhanced transparency and accountability of the process.”
Addressing another concern about the system, Savitri Fedson, MD, of the Michael E. DeBakey VA Medical Center and Baylor College of Medicine, Houston, wonders in a related editorial whether organ donors and recipients should know more about each other, and if so, could that reverse the ongoing downward trend in organ acceptance?
Although some organizations are in favor of sharing more information, Dr. Fedson notes that “less information may have the greater benefit.” She writes, “We might realize that the simplest approach is often the best: a fulsome thank you for the donor’s gift that is willingly given to a stranger without expectation of payment, and on the recipient side, the knowledge that an organ is of good quality.
“The transplant patient can be comforted with the understanding that the risk of disease transmission, while not zero, is low, and that their survival following acceptance of an organ is better than languishing on a waiting list.”
The study received no commercial funding. Dr. Parker, Dr. Khush, Dr. Schold, and Dr. Fedson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JACC: HEART FAILURE
Tirzepatide scores win in second obesity trial, SURMOUNT-2
The “twincretin” tirzepatide (Mounjaro) has proven successful in SURMOUNT-2, the second pivotal trial for the drug as an antiobesity agent, according to top-line results reported April 27 by tirzepatide’s manufacturer, Lilly, in a press release. The company reveals that tirzepatide achieved both of its primary endpoints in the trial, as well as all its key secondary endpoints.
The findings pave the way for tirzepatide to likely receive Food and Drug Administration approval as a treatment for obesity, perhaps before the end of 2023.
Tirzepatide received FDA approval in May 2022 for the treatment of type 2 diabetes in adults, under the brand name Mounjaro, and some people have already been using it off-label to treat obesity.
Tirzepatide is a dual glucagonlike peptide–1 (GLP-1) agonist and glucose-dependent insulinotropic polypeptide agonist. Several GLP-1 receptor agonists are already approved in the United States, including semaglutide, a once-weekly injection, which is approved as Wegovy for patients with obesity and as Ozempic for treatment of type 2 diabetes.
These agents have been incredibly popular among celebrity influencers, and with use of the #Ozempic hashtag and others on social media, this has led to unprecedented use of these products for weight loss, often among those who do not even have obesity or type 2 diabetes. Subsequently, patients with type 2 diabetes and obesity who need them have often struggled to obtain them, owing to shortages following this phenomenon.
SURMOUNT-2: Weight loss around 15%, less than seen in SURMOUNT-1
SURMOUNT-2 enrolled 938 adults with overweight or obesity and type 2 diabetes and had dual primary endpoints that both focused on weight loss, compared with placebo.
The first completed pivotal trial of tirzepatide for weight loss, SURMOUNT-1, enrolled people with overweight or obesity but no diabetes and had its main results reported in 2022. At the time, the weight loss achieved with tirzepatide, was described as “unprecedented,” with those given the highest dose in that trial (15 mg subcutaneously per week) losing an average of 20%-22% of body weight over 72 weeks, depending on the specific statistical analysis used.
For SURMOUNT-2’s first primary endpoint, 72 weeks of weekly subcutaneous injections with tirzepatide at dosages of 10 mg or 15 mg led to an average weight loss from baseline of 13.4% and 15.7%, respectively, compared with an average loss of 3.3% from baseline in the placebo-treated control arm.
For the second primary endpoint, 81.6% of people on the 10-mg dose and 86.4% on the 15-mg dose achieved at least 5% weight loss from baseline, compared with 30.5% of controls who had at least 5% weight loss from baseline.
In one key secondary endpoint, tirzepatide at dosages of 10 mg or 15 mg weekly produced at least a 15% cut in weight from baseline in 41.4% and 51.8% of participants, respectively, compared with a 2.6% rate of this endpoint in the placebo controls.
So the extent of weight loss seen in in SURMOUNT-2 was somewhat less than was reported in SURMOUNT-1, a finding consistent with many prior studies of incretin-based weight-loss agents, which seem to pack a more potent weight-loss punch in people without type 2 diabetes.
Lilly did not specifically report the treatment effect of tirzepatide on hemoglobin A1c in SURMOUNT-2, only saying that the effect was similar to what had been seen in the series of five SURPASS trials that led to the approval of tirzepatide for type 2 diabetes.
Lilly also reported that the safety profile of tirzepatide in SURMOUNT-2 generally matched what was seen in SURMOUNT-1 as well as in the SURPASS trials. The most common adverse events in SURMOUNT-2 involved gastrointestinal symptoms, such as nausea, diarrhea, and vomiting; these were generally mild to moderate in severity and clustered during the dose-escalation phase at the start of treatment. Treatment discontinuations caused by adverse effects were 3.8% on the 10-mg dosage, 7.4% on the 15-mg dosage, and 3.8% on placebo.
SURMOUNT-2 enrolled patients in the United States, Puerto Rico, and five other countries. All participants also received interventions designed to reduce their calorie intake and increase their physical activity.
More SURMOUNT-2 results at ADA in June
Lilly also announced that researchers would report more complete results from SURMOUNT-2 at the 2023 scientific sessions of the American Diabetes Association, being held in San Diego in late June, and publish the findings in a major medical journal.
Results from two additional phase 3 trials of tirzepatide in people with overweight or obesity, SURMOUNT-3 and SURMOUNT-4, are expected later in 2023.
Lilly started an application to the FDA for an indication for weight loss in October 2022 under a fast track designation by the agency, and the data collected in SURMOUNT-2 are expected to complete this application, which would then be subject to an FDA decision within about 6 months. Lilly said in its April 27 press release that it anticipates an FDA decision on this application may occur before the end of 2023.
SURMOUNT-2 and all of the other tirzepatide trials were sponsored by Lilly.
A version of this article first appeared on Medscape.com.
The “twincretin” tirzepatide (Mounjaro) has proven successful in SURMOUNT-2, the second pivotal trial for the drug as an antiobesity agent, according to top-line results reported April 27 by tirzepatide’s manufacturer, Lilly, in a press release. The company reveals that tirzepatide achieved both of its primary endpoints in the trial, as well as all its key secondary endpoints.
The findings pave the way for tirzepatide to likely receive Food and Drug Administration approval as a treatment for obesity, perhaps before the end of 2023.
Tirzepatide received FDA approval in May 2022 for the treatment of type 2 diabetes in adults, under the brand name Mounjaro, and some people have already been using it off-label to treat obesity.
Tirzepatide is a dual glucagonlike peptide–1 (GLP-1) agonist and glucose-dependent insulinotropic polypeptide agonist. Several GLP-1 receptor agonists are already approved in the United States, including semaglutide, a once-weekly injection, which is approved as Wegovy for patients with obesity and as Ozempic for treatment of type 2 diabetes.
These agents have been incredibly popular among celebrity influencers, and with use of the #Ozempic hashtag and others on social media, this has led to unprecedented use of these products for weight loss, often among those who do not even have obesity or type 2 diabetes. Subsequently, patients with type 2 diabetes and obesity who need them have often struggled to obtain them, owing to shortages following this phenomenon.
SURMOUNT-2: Weight loss around 15%, less than seen in SURMOUNT-1
SURMOUNT-2 enrolled 938 adults with overweight or obesity and type 2 diabetes and had dual primary endpoints that both focused on weight loss, compared with placebo.
The first completed pivotal trial of tirzepatide for weight loss, SURMOUNT-1, enrolled people with overweight or obesity but no diabetes and had its main results reported in 2022. At the time, the weight loss achieved with tirzepatide, was described as “unprecedented,” with those given the highest dose in that trial (15 mg subcutaneously per week) losing an average of 20%-22% of body weight over 72 weeks, depending on the specific statistical analysis used.
For SURMOUNT-2’s first primary endpoint, 72 weeks of weekly subcutaneous injections with tirzepatide at dosages of 10 mg or 15 mg led to an average weight loss from baseline of 13.4% and 15.7%, respectively, compared with an average loss of 3.3% from baseline in the placebo-treated control arm.
For the second primary endpoint, 81.6% of people on the 10-mg dose and 86.4% on the 15-mg dose achieved at least 5% weight loss from baseline, compared with 30.5% of controls who had at least 5% weight loss from baseline.
In one key secondary endpoint, tirzepatide at dosages of 10 mg or 15 mg weekly produced at least a 15% cut in weight from baseline in 41.4% and 51.8% of participants, respectively, compared with a 2.6% rate of this endpoint in the placebo controls.
So the extent of weight loss seen in in SURMOUNT-2 was somewhat less than was reported in SURMOUNT-1, a finding consistent with many prior studies of incretin-based weight-loss agents, which seem to pack a more potent weight-loss punch in people without type 2 diabetes.
Lilly did not specifically report the treatment effect of tirzepatide on hemoglobin A1c in SURMOUNT-2, only saying that the effect was similar to what had been seen in the series of five SURPASS trials that led to the approval of tirzepatide for type 2 diabetes.
Lilly also reported that the safety profile of tirzepatide in SURMOUNT-2 generally matched what was seen in SURMOUNT-1 as well as in the SURPASS trials. The most common adverse events in SURMOUNT-2 involved gastrointestinal symptoms, such as nausea, diarrhea, and vomiting; these were generally mild to moderate in severity and clustered during the dose-escalation phase at the start of treatment. Treatment discontinuations caused by adverse effects were 3.8% on the 10-mg dosage, 7.4% on the 15-mg dosage, and 3.8% on placebo.
SURMOUNT-2 enrolled patients in the United States, Puerto Rico, and five other countries. All participants also received interventions designed to reduce their calorie intake and increase their physical activity.
More SURMOUNT-2 results at ADA in June
Lilly also announced that researchers would report more complete results from SURMOUNT-2 at the 2023 scientific sessions of the American Diabetes Association, being held in San Diego in late June, and publish the findings in a major medical journal.
Results from two additional phase 3 trials of tirzepatide in people with overweight or obesity, SURMOUNT-3 and SURMOUNT-4, are expected later in 2023.
Lilly started an application to the FDA for an indication for weight loss in October 2022 under a fast track designation by the agency, and the data collected in SURMOUNT-2 are expected to complete this application, which would then be subject to an FDA decision within about 6 months. Lilly said in its April 27 press release that it anticipates an FDA decision on this application may occur before the end of 2023.
SURMOUNT-2 and all of the other tirzepatide trials were sponsored by Lilly.
A version of this article first appeared on Medscape.com.
The “twincretin” tirzepatide (Mounjaro) has proven successful in SURMOUNT-2, the second pivotal trial for the drug as an antiobesity agent, according to top-line results reported April 27 by tirzepatide’s manufacturer, Lilly, in a press release. The company reveals that tirzepatide achieved both of its primary endpoints in the trial, as well as all its key secondary endpoints.
The findings pave the way for tirzepatide to likely receive Food and Drug Administration approval as a treatment for obesity, perhaps before the end of 2023.
Tirzepatide received FDA approval in May 2022 for the treatment of type 2 diabetes in adults, under the brand name Mounjaro, and some people have already been using it off-label to treat obesity.
Tirzepatide is a dual glucagonlike peptide–1 (GLP-1) agonist and glucose-dependent insulinotropic polypeptide agonist. Several GLP-1 receptor agonists are already approved in the United States, including semaglutide, a once-weekly injection, which is approved as Wegovy for patients with obesity and as Ozempic for treatment of type 2 diabetes.
These agents have been incredibly popular among celebrity influencers, and with use of the #Ozempic hashtag and others on social media, this has led to unprecedented use of these products for weight loss, often among those who do not even have obesity or type 2 diabetes. Subsequently, patients with type 2 diabetes and obesity who need them have often struggled to obtain them, owing to shortages following this phenomenon.
SURMOUNT-2: Weight loss around 15%, less than seen in SURMOUNT-1
SURMOUNT-2 enrolled 938 adults with overweight or obesity and type 2 diabetes and had dual primary endpoints that both focused on weight loss, compared with placebo.
The first completed pivotal trial of tirzepatide for weight loss, SURMOUNT-1, enrolled people with overweight or obesity but no diabetes and had its main results reported in 2022. At the time, the weight loss achieved with tirzepatide, was described as “unprecedented,” with those given the highest dose in that trial (15 mg subcutaneously per week) losing an average of 20%-22% of body weight over 72 weeks, depending on the specific statistical analysis used.
For SURMOUNT-2’s first primary endpoint, 72 weeks of weekly subcutaneous injections with tirzepatide at dosages of 10 mg or 15 mg led to an average weight loss from baseline of 13.4% and 15.7%, respectively, compared with an average loss of 3.3% from baseline in the placebo-treated control arm.
For the second primary endpoint, 81.6% of people on the 10-mg dose and 86.4% on the 15-mg dose achieved at least 5% weight loss from baseline, compared with 30.5% of controls who had at least 5% weight loss from baseline.
In one key secondary endpoint, tirzepatide at dosages of 10 mg or 15 mg weekly produced at least a 15% cut in weight from baseline in 41.4% and 51.8% of participants, respectively, compared with a 2.6% rate of this endpoint in the placebo controls.
So the extent of weight loss seen in in SURMOUNT-2 was somewhat less than was reported in SURMOUNT-1, a finding consistent with many prior studies of incretin-based weight-loss agents, which seem to pack a more potent weight-loss punch in people without type 2 diabetes.
Lilly did not specifically report the treatment effect of tirzepatide on hemoglobin A1c in SURMOUNT-2, only saying that the effect was similar to what had been seen in the series of five SURPASS trials that led to the approval of tirzepatide for type 2 diabetes.
Lilly also reported that the safety profile of tirzepatide in SURMOUNT-2 generally matched what was seen in SURMOUNT-1 as well as in the SURPASS trials. The most common adverse events in SURMOUNT-2 involved gastrointestinal symptoms, such as nausea, diarrhea, and vomiting; these were generally mild to moderate in severity and clustered during the dose-escalation phase at the start of treatment. Treatment discontinuations caused by adverse effects were 3.8% on the 10-mg dosage, 7.4% on the 15-mg dosage, and 3.8% on placebo.
SURMOUNT-2 enrolled patients in the United States, Puerto Rico, and five other countries. All participants also received interventions designed to reduce their calorie intake and increase their physical activity.
More SURMOUNT-2 results at ADA in June
Lilly also announced that researchers would report more complete results from SURMOUNT-2 at the 2023 scientific sessions of the American Diabetes Association, being held in San Diego in late June, and publish the findings in a major medical journal.
Results from two additional phase 3 trials of tirzepatide in people with overweight or obesity, SURMOUNT-3 and SURMOUNT-4, are expected later in 2023.
Lilly started an application to the FDA for an indication for weight loss in October 2022 under a fast track designation by the agency, and the data collected in SURMOUNT-2 are expected to complete this application, which would then be subject to an FDA decision within about 6 months. Lilly said in its April 27 press release that it anticipates an FDA decision on this application may occur before the end of 2023.
SURMOUNT-2 and all of the other tirzepatide trials were sponsored by Lilly.
A version of this article first appeared on Medscape.com.
Drive, chip, and putt your way to osteoarthritis relief
Taking a swing against arthritis
Osteoarthritis is a tough disease to manage. Exercise helps ease the stiffness and pain of the joints, but at the same time, the disease makes it difficult to do that beneficial exercise. Even a relatively simple activity like jogging can hurt more than it helps. If only there were a low-impact exercise that was incredibly popular among the generally older population who are likely to have arthritis.
We love a good golf study here at LOTME, and a group of Australian and U.K. researchers have provided. Osteoarthritis affects 2 million people in the land down under, making it the most common source of disability there. In that population, only 64% reported their physical health to be good, very good, or excellent. Among the 459 golfers with OA that the study authors surveyed, however, the percentage reporting good health rose to more than 90%.
A similar story emerged when they looked at mental health. Nearly a quarter of nongolfers with OA reported high or very high levels of psychological distress, compared with just 8% of golfers. This pattern of improved physical and mental health remained when the researchers looked at the general, non-OA population.
This isn’t the first time golf’s been connected with improved health, and previous studies have shown golf to reduce the risks of cardiovascular disease, diabetes, and obesity, among other things. Just walking one 18-hole round significantly exceeds the CDC’s recommended 150 minutes of physical activity per week. Go out multiple times a week – leaving the cart and beer at home, American golfers – and you’ll be fit for a lifetime.
The golfers on our staff, however, are still waiting for those mental health benefits to kick in. Because when we’re adding up our scorecard after that string of four double bogeys to end the round, we’re most definitely thinking: “Yes, this sport is reducing my psychological distress. I am having fun right now.”
Battle of the sexes’ intestines
There are, we’re sure you’ve noticed, some differences between males and females. Females, for one thing, have longer small intestines than males. Everybody knows that, right? You didn’t know? Really? … Really?

Well, then, we’re guessing you haven’t read “Hidden diversity: Comparative functional morphology of humans and other species” by Erin A. McKenney, PhD, of North Carolina State University, Raleigh, and associates, which just appeared in PeerJ. We couldn’t put it down, even in the shower – a real page-turner/scroller. (It’s a great way to clean a phone, for those who also like to scroll, text, or talk on the toilet.)
The researchers got out their rulers, calipers, and string and took many measurements of the digestive systems of 45 human cadavers (21 female and 24 male), which were compared with data from 10 rats, 10 pigs, and 10 bullfrogs, which had been collected (the measurements, not the animals) by undergraduate students enrolled in a comparative anatomy laboratory course at the university.
There was little intestinal-length variation among the four-legged subjects, but when it comes to humans, females have “consistently and significantly longer small intestines than males,” the investigators noted.
The women’s small intestines, almost 14 feet long on average, were about a foot longer than the men’s, which suggests that women are better able to extract nutrients from food and “supports the canalization hypothesis, which posits that women are better able to survive during periods of stress,” coauthor Amanda Hale said in a written statement from the school. The way to a man’s heart may be through his stomach, but the way to a woman’s heart is through her duodenum, it seems.
Fascinating stuff, to be sure, but the thing that really caught our eye in the PeerJ article was the authors’ suggestion “that organs behave independently of one another, both within and across species.” Organs behaving independently? A somewhat ominous concept, no doubt, but it does explain a lot of the sounds we hear coming from our guts, which can get pretty frightening, especially on chili night.
Dog walking is dangerous business
Yes, you did read that right. A lot of strange things can send you to the emergency department. Go ahead and add dog walking onto that list.
Investigators from Johns Hopkins University estimate that over 422,000 adults presented to U.S. emergency departments with leash-dependent dog walking-related injuries between 2001 and 2020.
With almost 53% of U.S. households owning at least one dog in 2021-2022 in the wake of the COVID pet boom, this kind of occurrence is becoming more common than you think. The annual number of dog-walking injuries more than quadrupled from 7,300 to 32,000 over the course of the study, and the researchers link that spike to the promotion of dog walking for fitness, along with the boost of ownership itself.
The most common injuries listed in the National Electronic Injury Surveillance System database were finger fracture, traumatic brain injury, and shoulder sprain or strain. These mostly involved falls from being pulled, tripped, or tangled up in the leash while walking. For those aged 65 years and older, traumatic brain injury and hip fracture were the most common.
Women were 50% more likely to sustain a fracture than were men, and dog owners aged 65 and older were three times as likely to fall, twice as likely to get a fracture, and 60% more likely to have brain injury than were younger people. Now, that’s not to say younger people don’t also get hurt. After all, dogs aren’t ageists. The researchers have that data but it’s coming out later.
Meanwhile, the pitfalls involved with just trying to get our daily steps in while letting Muffin do her business have us on the lookout for random squirrels.
Taking a swing against arthritis
Osteoarthritis is a tough disease to manage. Exercise helps ease the stiffness and pain of the joints, but at the same time, the disease makes it difficult to do that beneficial exercise. Even a relatively simple activity like jogging can hurt more than it helps. If only there were a low-impact exercise that was incredibly popular among the generally older population who are likely to have arthritis.
We love a good golf study here at LOTME, and a group of Australian and U.K. researchers have provided. Osteoarthritis affects 2 million people in the land down under, making it the most common source of disability there. In that population, only 64% reported their physical health to be good, very good, or excellent. Among the 459 golfers with OA that the study authors surveyed, however, the percentage reporting good health rose to more than 90%.
A similar story emerged when they looked at mental health. Nearly a quarter of nongolfers with OA reported high or very high levels of psychological distress, compared with just 8% of golfers. This pattern of improved physical and mental health remained when the researchers looked at the general, non-OA population.
This isn’t the first time golf’s been connected with improved health, and previous studies have shown golf to reduce the risks of cardiovascular disease, diabetes, and obesity, among other things. Just walking one 18-hole round significantly exceeds the CDC’s recommended 150 minutes of physical activity per week. Go out multiple times a week – leaving the cart and beer at home, American golfers – and you’ll be fit for a lifetime.
The golfers on our staff, however, are still waiting for those mental health benefits to kick in. Because when we’re adding up our scorecard after that string of four double bogeys to end the round, we’re most definitely thinking: “Yes, this sport is reducing my psychological distress. I am having fun right now.”
Battle of the sexes’ intestines
There are, we’re sure you’ve noticed, some differences between males and females. Females, for one thing, have longer small intestines than males. Everybody knows that, right? You didn’t know? Really? … Really?
Well, then, we’re guessing you haven’t read “Hidden diversity: Comparative functional morphology of humans and other species” by Erin A. McKenney, PhD, of North Carolina State University, Raleigh, and associates, which just appeared in PeerJ. We couldn’t put it down, even in the shower – a real page-turner/scroller. (It’s a great way to clean a phone, for those who also like to scroll, text, or talk on the toilet.)
The researchers got out their rulers, calipers, and string and took many measurements of the digestive systems of 45 human cadavers (21 female and 24 male), which were compared with data from 10 rats, 10 pigs, and 10 bullfrogs, which had been collected (the measurements, not the animals) by undergraduate students enrolled in a comparative anatomy laboratory course at the university.
There was little intestinal-length variation among the four-legged subjects, but when it comes to humans, females have “consistently and significantly longer small intestines than males,” the investigators noted.
The women’s small intestines, almost 14 feet long on average, were about a foot longer than the men’s, which suggests that women are better able to extract nutrients from food and “supports the canalization hypothesis, which posits that women are better able to survive during periods of stress,” coauthor Amanda Hale said in a written statement from the school. The way to a man’s heart may be through his stomach, but the way to a woman’s heart is through her duodenum, it seems.
Fascinating stuff, to be sure, but the thing that really caught our eye in the PeerJ article was the authors’ suggestion “that organs behave independently of one another, both within and across species.” Organs behaving independently? A somewhat ominous concept, no doubt, but it does explain a lot of the sounds we hear coming from our guts, which can get pretty frightening, especially on chili night.
Dog walking is dangerous business
Yes, you did read that right. A lot of strange things can send you to the emergency department. Go ahead and add dog walking onto that list.
Investigators from Johns Hopkins University estimate that over 422,000 adults presented to U.S. emergency departments with leash-dependent dog walking-related injuries between 2001 and 2020.
With almost 53% of U.S. households owning at least one dog in 2021-2022 in the wake of the COVID pet boom, this kind of occurrence is becoming more common than you think. The annual number of dog-walking injuries more than quadrupled from 7,300 to 32,000 over the course of the study, and the researchers link that spike to the promotion of dog walking for fitness, along with the boost of ownership itself.
The most common injuries listed in the National Electronic Injury Surveillance System database were finger fracture, traumatic brain injury, and shoulder sprain or strain. These mostly involved falls from being pulled, tripped, or tangled up in the leash while walking. For those aged 65 years and older, traumatic brain injury and hip fracture were the most common.
Women were 50% more likely to sustain a fracture than were men, and dog owners aged 65 and older were three times as likely to fall, twice as likely to get a fracture, and 60% more likely to have brain injury than were younger people. Now, that’s not to say younger people don’t also get hurt. After all, dogs aren’t ageists. The researchers have that data but it’s coming out later.
Meanwhile, the pitfalls involved with just trying to get our daily steps in while letting Muffin do her business have us on the lookout for random squirrels.
Taking a swing against arthritis
Osteoarthritis is a tough disease to manage. Exercise helps ease the stiffness and pain of the joints, but at the same time, the disease makes it difficult to do that beneficial exercise. Even a relatively simple activity like jogging can hurt more than it helps. If only there were a low-impact exercise that was incredibly popular among the generally older population who are likely to have arthritis.
We love a good golf study here at LOTME, and a group of Australian and U.K. researchers have provided. Osteoarthritis affects 2 million people in the land down under, making it the most common source of disability there. In that population, only 64% reported their physical health to be good, very good, or excellent. Among the 459 golfers with OA that the study authors surveyed, however, the percentage reporting good health rose to more than 90%.
A similar story emerged when they looked at mental health. Nearly a quarter of nongolfers with OA reported high or very high levels of psychological distress, compared with just 8% of golfers. This pattern of improved physical and mental health remained when the researchers looked at the general, non-OA population.
This isn’t the first time golf’s been connected with improved health, and previous studies have shown golf to reduce the risks of cardiovascular disease, diabetes, and obesity, among other things. Just walking one 18-hole round significantly exceeds the CDC’s recommended 150 minutes of physical activity per week. Go out multiple times a week – leaving the cart and beer at home, American golfers – and you’ll be fit for a lifetime.
The golfers on our staff, however, are still waiting for those mental health benefits to kick in. Because when we’re adding up our scorecard after that string of four double bogeys to end the round, we’re most definitely thinking: “Yes, this sport is reducing my psychological distress. I am having fun right now.”
Battle of the sexes’ intestines
There are, we’re sure you’ve noticed, some differences between males and females. Females, for one thing, have longer small intestines than males. Everybody knows that, right? You didn’t know? Really? … Really?
Well, then, we’re guessing you haven’t read “Hidden diversity: Comparative functional morphology of humans and other species” by Erin A. McKenney, PhD, of North Carolina State University, Raleigh, and associates, which just appeared in PeerJ. We couldn’t put it down, even in the shower – a real page-turner/scroller. (It’s a great way to clean a phone, for those who also like to scroll, text, or talk on the toilet.)
The researchers got out their rulers, calipers, and string and took many measurements of the digestive systems of 45 human cadavers (21 female and 24 male), which were compared with data from 10 rats, 10 pigs, and 10 bullfrogs, which had been collected (the measurements, not the animals) by undergraduate students enrolled in a comparative anatomy laboratory course at the university.
There was little intestinal-length variation among the four-legged subjects, but when it comes to humans, females have “consistently and significantly longer small intestines than males,” the investigators noted.
The women’s small intestines, almost 14 feet long on average, were about a foot longer than the men’s, which suggests that women are better able to extract nutrients from food and “supports the canalization hypothesis, which posits that women are better able to survive during periods of stress,” coauthor Amanda Hale said in a written statement from the school. The way to a man’s heart may be through his stomach, but the way to a woman’s heart is through her duodenum, it seems.
Fascinating stuff, to be sure, but the thing that really caught our eye in the PeerJ article was the authors’ suggestion “that organs behave independently of one another, both within and across species.” Organs behaving independently? A somewhat ominous concept, no doubt, but it does explain a lot of the sounds we hear coming from our guts, which can get pretty frightening, especially on chili night.
Dog walking is dangerous business
Yes, you did read that right. A lot of strange things can send you to the emergency department. Go ahead and add dog walking onto that list.
Investigators from Johns Hopkins University estimate that over 422,000 adults presented to U.S. emergency departments with leash-dependent dog walking-related injuries between 2001 and 2020.
With almost 53% of U.S. households owning at least one dog in 2021-2022 in the wake of the COVID pet boom, this kind of occurrence is becoming more common than you think. The annual number of dog-walking injuries more than quadrupled from 7,300 to 32,000 over the course of the study, and the researchers link that spike to the promotion of dog walking for fitness, along with the boost of ownership itself.
The most common injuries listed in the National Electronic Injury Surveillance System database were finger fracture, traumatic brain injury, and shoulder sprain or strain. These mostly involved falls from being pulled, tripped, or tangled up in the leash while walking. For those aged 65 years and older, traumatic brain injury and hip fracture were the most common.
Women were 50% more likely to sustain a fracture than were men, and dog owners aged 65 and older were three times as likely to fall, twice as likely to get a fracture, and 60% more likely to have brain injury than were younger people. Now, that’s not to say younger people don’t also get hurt. After all, dogs aren’t ageists. The researchers have that data but it’s coming out later.
Meanwhile, the pitfalls involved with just trying to get our daily steps in while letting Muffin do her business have us on the lookout for random squirrels.

Hybrid ablation superior for persistent AFib: CEASE-AF
BARCELONA – Staged hybrid ablation provided superior freedom from atrial arrhythmias compared with endocardial catheter ablation alone, including the need for repeat ablations in patients with advanced atrial fibrillation (AF), new data show.
“We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase, so this is a huge difference,” concluded cardiac surgeon Nicholas Doll, MD, PhD, Schüchtermann Clinic, Bad Rothenfelde, Germany.
Dr. Doll presented the 12-month follow up results of the Combined Endoscopic Epicardial and Percutaneous Endocardial Ablation Versus Repeated Catheter Ablation in Persistent and Longstanding Persistent Atrial Fibrillation (CEASE-AF) trial at the European Heart Rhythm Association 2023 Congress, held recently in Barcelona and virtually.
He said CEASE-AF is the largest multicenter randomized clinical trial comparing these two approaches for control of atrial arrhythmias.
Safety outcomes were numerically higher in the hybrid ablation (HA) group of the trial but not statistically different from the catheter ablation (CA) group.
Unstable wavefront
As background, Dr. Doll explained that in advanced AF, there is a high degree of endocardial-epicardial dissociation with unstable wavefront propagation transitioning between the endocardial and epicardial surfaces. Endocardial mapping and ablation alone may be insufficient to address the mechanism of AF.
“So, the hypothesis of the CEASE-AF study was a minimally invasive hybrid ablation approach which combines endocardial and epicardial ablation to achieve superior effectiveness when compared to endocardial catheter ablation alone,” he said.
This prospective clinical trial randomized patients 2:1 at nine sites in five countries to HA (n = 102) or CA (n = 52). All had left atrial diameter of 4 cm to 6 cm and persistent AF for up to 1 year or longstanding persistent AF for greater than 1 year up to 10 years.
Any patient with a previous ablation procedure, BMI greater than 35 kg/m2, or left ventricular ejection fraction less than 30% was excluded.
For HA, stage 1 consisted of epicardial lesions for pulmonary vein isolation (PVI) plus the posterior wall box plus left atrial appendage exclusion using the AtriClip (AtriCure Inc.) left atrial appendage exclusion device. Stage 2 involved endocardial mapping and catheter ablation to address gaps.
For CA, the index procedure involved catheter-mediated PVI plus repeat endocardial ablation as clinically indicated. For both HA and CA, additional ablation techniques and lesions were allowed for nonparoxysmal AF.
The HA timeline was the first stage, index procedure at time 0 (n = 102), a 90-day blanking period, and then the second stage, endocardial procedure at 90 to 180 days from the index procedure (n = 93).
For the CA arm of the trial, endocardial catheter ablation was performed on a minimal endocardial lesion set at time 0. Then after a 90-day blanking period, repeat catheter ablation was performed if clinically indicated (6/52).
Repeat ablations and electrical or pharmaceutical cardioversions were allowed during the 12-month follow-up period from time 0.
The primary efficacy endpoint was freedom from AF, atrial flutter, or atrial tachycardia of greater than 30 seconds through 12 months in the absence of class I/III antiarrhythmic drugs except ones that previously had failed, at doses not exceeding those previously failed doses. The safety endpoint was a composite rate of major complications over the course of the study.
Even with relatively modest cohort sizes, the HA and CA arms of the trial were well matched at baseline for age (approximately 60 years), gender (75.5% and 73.1% male, respectively), BMI (29.7 and 29.8 kg/m2), and persistent AF (79.4% and 82.7%).
The groups had persistent AF for 2.94 ± 3.29 years and 3.34 ± 3.52 years, respectively. The mean left atrial size was 4.7 ± 0.5 cm for the HA group and 4.7 ± 0.4 cm for the CA group.
Outcomes favored hybrid ablation over catheter ablation, the researchers reported. “We never would have expected these huge differences,” Dr. Doll told the congress. “We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase.”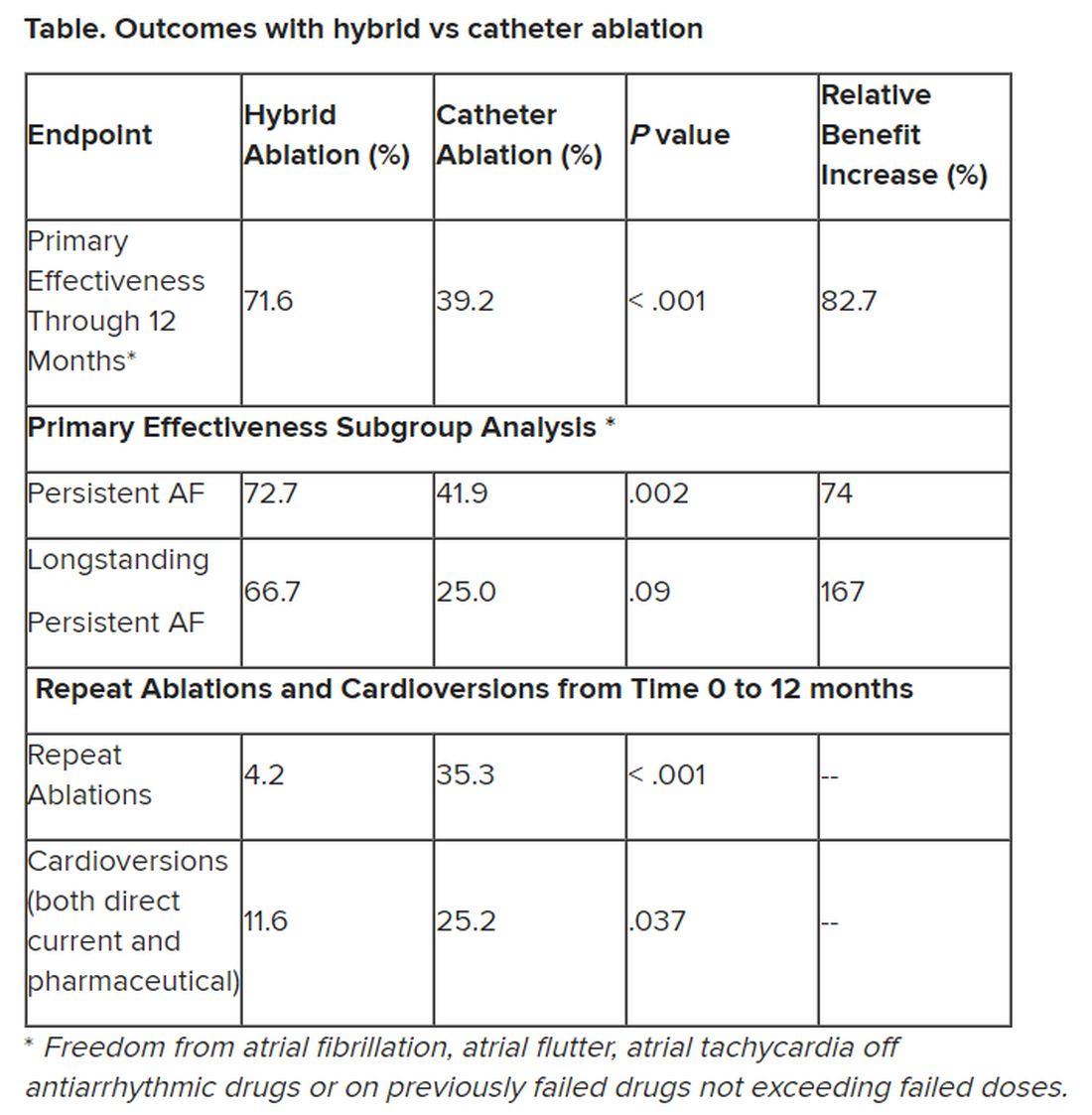
Subgroup analyses were consistent with the primary endpoint, but he said they would not be published because the trial was not powered for such comparisons.
Still, he noted that “there are only slightly reduced outcomes in the long-standing [persistent AF subgroup] in a really challenging patient arm, and we still have a success rate of 67%.” And the repeat ablations in about one-third of patients in the CA arm and need for cardioversions in about one quarter of them may have implications for reduced quality of life.
The total procedure duration was higher for the hybrid group at 336.4 ± 97 minutes, taking into account the index procedure plus the second stage procedure, vs. endocardial ablation at 251.9 ± 114 minutes, which includes the index procedure plus any repeat ablations (HA vs AF total duration, P < .001). Overall fluoroscopy time was approximately 8 minutes shorter for the HA arm.
Complications were assessed for 30 days post index procedure and 30 days post second stage procedure for the HA arm and for 30 days post index procedure and any repeat ablation for the CA arm.
The HA arm showed a complication rate of 7.8% vs. 5.8% for the CA arm (P = .751). Two patients in the former and three patients in the latter group had more than one major complication. There was one death in the HA group 93 days after the index procedure, and it was adjudicated as unrelated to the procedure.
“If you look back in the past, other studies showed a ... higher complication rate in the hybrid arm, so we feel very comfortable with these complication rates, which [are] very low and almost comparable,” Dr. Doll said.
Limitations of the study included symptom-driven electrocardiogram monitoring performed at unscheduled visits. Also, ablation beyond PVI in the CA arm and PVI/posterior box in the HA arm was not standardized and was performed according to standard practices in the participating countries.
“Success of epicardial-endocardial approach emphasizes the role of the collaborative heart team approach in the treatment of nonparoxysmal atrial fibrillation, and if I sum it up together, we can do it better” together, Dr. Doll advised.
‘Exceptional’ trial
After Dr. Doll’s presentation, appointed discussant Stylianos Tzeis, MD, PhD, head of the cardiology clinic and electrophysiology and pacing department at Mitera Hospital in Athens, congratulated the investigators and called CEASE-AF “an exceptional trial. It was really challenging to enroll patients in such a randomized controlled clinical trial.”
But Dr. Tzeis questioned whether pitting CA against HA was a fair comparison.
“Were the ablation targets similar between the two groups?” he asked. He noted that for the HA group, in the first stage the patients had PVI, posterior wall isolation, exclusion of the left atrial appendage, and additional lesions at the discretion of the operator. Ninety percent proceeded to the second stage, which was endocardial catheter ablation with verification of posterior wall isolation and PVI and additional lesions made if needed.
In the CA group, repeat catheter ablation could be performed after the 90-day blanking period if clinically indicated. “Please take note that only 10% were offered the second ablation. So at least in my perspective, this was a comparison of a two-stage approach versus a single-stage approach with a much more aggressive ablation protocol in the hybrid ablation group as compared to the endocardial group,” he said.
Seeing the higher success rate of the HA group in achieving the primary efficacy endpoint of freedom from all arrhythmias at 12 months, Dr. Tzeis asked, “Does this reflect the superiority of the epi-endo approach, or does it reflect the suboptimal performance of the catheter ablation approach?”
There was a 40% success rate in the CA patient population, a cohort that he deemed “not the most challenging persistent AF population in the world”: those with left atrial diameter of 47 millimeters and with 80% having an AF duration less than 12 months.
He also noted that “the average duration of the catheter ablation for the PVI in the vast majority of cases was 4 hours, which does not reflect what really happens in the everyday practice.”
All those critiques having been advanced, Dr. Tzeis said, “Definitely do not doubt my first comment that the authors should be congratulated, and I strongly believe that the main objective has been achieved to bring electrophysiologist and cardiac surgeons ... closer.”
The study sponsor was AtriCure Inc. with collaboration of Cardialysis BV. Doll has received consulting fees or royalties and/or has ownership or stockholder interest in AtriCure. Tzeis reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
BARCELONA – Staged hybrid ablation provided superior freedom from atrial arrhythmias compared with endocardial catheter ablation alone, including the need for repeat ablations in patients with advanced atrial fibrillation (AF), new data show.
“We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase, so this is a huge difference,” concluded cardiac surgeon Nicholas Doll, MD, PhD, Schüchtermann Clinic, Bad Rothenfelde, Germany.
Dr. Doll presented the 12-month follow up results of the Combined Endoscopic Epicardial and Percutaneous Endocardial Ablation Versus Repeated Catheter Ablation in Persistent and Longstanding Persistent Atrial Fibrillation (CEASE-AF) trial at the European Heart Rhythm Association 2023 Congress, held recently in Barcelona and virtually.
He said CEASE-AF is the largest multicenter randomized clinical trial comparing these two approaches for control of atrial arrhythmias.
Safety outcomes were numerically higher in the hybrid ablation (HA) group of the trial but not statistically different from the catheter ablation (CA) group.
Unstable wavefront
As background, Dr. Doll explained that in advanced AF, there is a high degree of endocardial-epicardial dissociation with unstable wavefront propagation transitioning between the endocardial and epicardial surfaces. Endocardial mapping and ablation alone may be insufficient to address the mechanism of AF.
“So, the hypothesis of the CEASE-AF study was a minimally invasive hybrid ablation approach which combines endocardial and epicardial ablation to achieve superior effectiveness when compared to endocardial catheter ablation alone,” he said.
This prospective clinical trial randomized patients 2:1 at nine sites in five countries to HA (n = 102) or CA (n = 52). All had left atrial diameter of 4 cm to 6 cm and persistent AF for up to 1 year or longstanding persistent AF for greater than 1 year up to 10 years.
Any patient with a previous ablation procedure, BMI greater than 35 kg/m2, or left ventricular ejection fraction less than 30% was excluded.
For HA, stage 1 consisted of epicardial lesions for pulmonary vein isolation (PVI) plus the posterior wall box plus left atrial appendage exclusion using the AtriClip (AtriCure Inc.) left atrial appendage exclusion device. Stage 2 involved endocardial mapping and catheter ablation to address gaps.
For CA, the index procedure involved catheter-mediated PVI plus repeat endocardial ablation as clinically indicated. For both HA and CA, additional ablation techniques and lesions were allowed for nonparoxysmal AF.
The HA timeline was the first stage, index procedure at time 0 (n = 102), a 90-day blanking period, and then the second stage, endocardial procedure at 90 to 180 days from the index procedure (n = 93).
For the CA arm of the trial, endocardial catheter ablation was performed on a minimal endocardial lesion set at time 0. Then after a 90-day blanking period, repeat catheter ablation was performed if clinically indicated (6/52).
Repeat ablations and electrical or pharmaceutical cardioversions were allowed during the 12-month follow-up period from time 0.
The primary efficacy endpoint was freedom from AF, atrial flutter, or atrial tachycardia of greater than 30 seconds through 12 months in the absence of class I/III antiarrhythmic drugs except ones that previously had failed, at doses not exceeding those previously failed doses. The safety endpoint was a composite rate of major complications over the course of the study.
Even with relatively modest cohort sizes, the HA and CA arms of the trial were well matched at baseline for age (approximately 60 years), gender (75.5% and 73.1% male, respectively), BMI (29.7 and 29.8 kg/m2), and persistent AF (79.4% and 82.7%).
The groups had persistent AF for 2.94 ± 3.29 years and 3.34 ± 3.52 years, respectively. The mean left atrial size was 4.7 ± 0.5 cm for the HA group and 4.7 ± 0.4 cm for the CA group.
Outcomes favored hybrid ablation over catheter ablation, the researchers reported. “We never would have expected these huge differences,” Dr. Doll told the congress. “We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase.”
Subgroup analyses were consistent with the primary endpoint, but he said they would not be published because the trial was not powered for such comparisons.
Still, he noted that “there are only slightly reduced outcomes in the long-standing [persistent AF subgroup] in a really challenging patient arm, and we still have a success rate of 67%.” And the repeat ablations in about one-third of patients in the CA arm and need for cardioversions in about one quarter of them may have implications for reduced quality of life.
The total procedure duration was higher for the hybrid group at 336.4 ± 97 minutes, taking into account the index procedure plus the second stage procedure, vs. endocardial ablation at 251.9 ± 114 minutes, which includes the index procedure plus any repeat ablations (HA vs AF total duration, P < .001). Overall fluoroscopy time was approximately 8 minutes shorter for the HA arm.
Complications were assessed for 30 days post index procedure and 30 days post second stage procedure for the HA arm and for 30 days post index procedure and any repeat ablation for the CA arm.
The HA arm showed a complication rate of 7.8% vs. 5.8% for the CA arm (P = .751). Two patients in the former and three patients in the latter group had more than one major complication. There was one death in the HA group 93 days after the index procedure, and it was adjudicated as unrelated to the procedure.
“If you look back in the past, other studies showed a ... higher complication rate in the hybrid arm, so we feel very comfortable with these complication rates, which [are] very low and almost comparable,” Dr. Doll said.
Limitations of the study included symptom-driven electrocardiogram monitoring performed at unscheduled visits. Also, ablation beyond PVI in the CA arm and PVI/posterior box in the HA arm was not standardized and was performed according to standard practices in the participating countries.
“Success of epicardial-endocardial approach emphasizes the role of the collaborative heart team approach in the treatment of nonparoxysmal atrial fibrillation, and if I sum it up together, we can do it better” together, Dr. Doll advised.
‘Exceptional’ trial
After Dr. Doll’s presentation, appointed discussant Stylianos Tzeis, MD, PhD, head of the cardiology clinic and electrophysiology and pacing department at Mitera Hospital in Athens, congratulated the investigators and called CEASE-AF “an exceptional trial. It was really challenging to enroll patients in such a randomized controlled clinical trial.”
But Dr. Tzeis questioned whether pitting CA against HA was a fair comparison.
“Were the ablation targets similar between the two groups?” he asked. He noted that for the HA group, in the first stage the patients had PVI, posterior wall isolation, exclusion of the left atrial appendage, and additional lesions at the discretion of the operator. Ninety percent proceeded to the second stage, which was endocardial catheter ablation with verification of posterior wall isolation and PVI and additional lesions made if needed.
In the CA group, repeat catheter ablation could be performed after the 90-day blanking period if clinically indicated. “Please take note that only 10% were offered the second ablation. So at least in my perspective, this was a comparison of a two-stage approach versus a single-stage approach with a much more aggressive ablation protocol in the hybrid ablation group as compared to the endocardial group,” he said.
Seeing the higher success rate of the HA group in achieving the primary efficacy endpoint of freedom from all arrhythmias at 12 months, Dr. Tzeis asked, “Does this reflect the superiority of the epi-endo approach, or does it reflect the suboptimal performance of the catheter ablation approach?”
There was a 40% success rate in the CA patient population, a cohort that he deemed “not the most challenging persistent AF population in the world”: those with left atrial diameter of 47 millimeters and with 80% having an AF duration less than 12 months.
He also noted that “the average duration of the catheter ablation for the PVI in the vast majority of cases was 4 hours, which does not reflect what really happens in the everyday practice.”
All those critiques having been advanced, Dr. Tzeis said, “Definitely do not doubt my first comment that the authors should be congratulated, and I strongly believe that the main objective has been achieved to bring electrophysiologist and cardiac surgeons ... closer.”
The study sponsor was AtriCure Inc. with collaboration of Cardialysis BV. Doll has received consulting fees or royalties and/or has ownership or stockholder interest in AtriCure. Tzeis reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
BARCELONA – Staged hybrid ablation provided superior freedom from atrial arrhythmias compared with endocardial catheter ablation alone, including the need for repeat ablations in patients with advanced atrial fibrillation (AF), new data show.
“We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase, so this is a huge difference,” concluded cardiac surgeon Nicholas Doll, MD, PhD, Schüchtermann Clinic, Bad Rothenfelde, Germany.
Dr. Doll presented the 12-month follow up results of the Combined Endoscopic Epicardial and Percutaneous Endocardial Ablation Versus Repeated Catheter Ablation in Persistent and Longstanding Persistent Atrial Fibrillation (CEASE-AF) trial at the European Heart Rhythm Association 2023 Congress, held recently in Barcelona and virtually.
He said CEASE-AF is the largest multicenter randomized clinical trial comparing these two approaches for control of atrial arrhythmias.
Safety outcomes were numerically higher in the hybrid ablation (HA) group of the trial but not statistically different from the catheter ablation (CA) group.
Unstable wavefront
As background, Dr. Doll explained that in advanced AF, there is a high degree of endocardial-epicardial dissociation with unstable wavefront propagation transitioning between the endocardial and epicardial surfaces. Endocardial mapping and ablation alone may be insufficient to address the mechanism of AF.
“So, the hypothesis of the CEASE-AF study was a minimally invasive hybrid ablation approach which combines endocardial and epicardial ablation to achieve superior effectiveness when compared to endocardial catheter ablation alone,” he said.
This prospective clinical trial randomized patients 2:1 at nine sites in five countries to HA (n = 102) or CA (n = 52). All had left atrial diameter of 4 cm to 6 cm and persistent AF for up to 1 year or longstanding persistent AF for greater than 1 year up to 10 years.
Any patient with a previous ablation procedure, BMI greater than 35 kg/m2, or left ventricular ejection fraction less than 30% was excluded.
For HA, stage 1 consisted of epicardial lesions for pulmonary vein isolation (PVI) plus the posterior wall box plus left atrial appendage exclusion using the AtriClip (AtriCure Inc.) left atrial appendage exclusion device. Stage 2 involved endocardial mapping and catheter ablation to address gaps.
For CA, the index procedure involved catheter-mediated PVI plus repeat endocardial ablation as clinically indicated. For both HA and CA, additional ablation techniques and lesions were allowed for nonparoxysmal AF.
The HA timeline was the first stage, index procedure at time 0 (n = 102), a 90-day blanking period, and then the second stage, endocardial procedure at 90 to 180 days from the index procedure (n = 93).
For the CA arm of the trial, endocardial catheter ablation was performed on a minimal endocardial lesion set at time 0. Then after a 90-day blanking period, repeat catheter ablation was performed if clinically indicated (6/52).
Repeat ablations and electrical or pharmaceutical cardioversions were allowed during the 12-month follow-up period from time 0.
The primary efficacy endpoint was freedom from AF, atrial flutter, or atrial tachycardia of greater than 30 seconds through 12 months in the absence of class I/III antiarrhythmic drugs except ones that previously had failed, at doses not exceeding those previously failed doses. The safety endpoint was a composite rate of major complications over the course of the study.
Even with relatively modest cohort sizes, the HA and CA arms of the trial were well matched at baseline for age (approximately 60 years), gender (75.5% and 73.1% male, respectively), BMI (29.7 and 29.8 kg/m2), and persistent AF (79.4% and 82.7%).
The groups had persistent AF for 2.94 ± 3.29 years and 3.34 ± 3.52 years, respectively. The mean left atrial size was 4.7 ± 0.5 cm for the HA group and 4.7 ± 0.4 cm for the CA group.
Outcomes favored hybrid ablation over catheter ablation, the researchers reported. “We never would have expected these huge differences,” Dr. Doll told the congress. “We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase.”
Subgroup analyses were consistent with the primary endpoint, but he said they would not be published because the trial was not powered for such comparisons.
Still, he noted that “there are only slightly reduced outcomes in the long-standing [persistent AF subgroup] in a really challenging patient arm, and we still have a success rate of 67%.” And the repeat ablations in about one-third of patients in the CA arm and need for cardioversions in about one quarter of them may have implications for reduced quality of life.
The total procedure duration was higher for the hybrid group at 336.4 ± 97 minutes, taking into account the index procedure plus the second stage procedure, vs. endocardial ablation at 251.9 ± 114 minutes, which includes the index procedure plus any repeat ablations (HA vs AF total duration, P < .001). Overall fluoroscopy time was approximately 8 minutes shorter for the HA arm.
Complications were assessed for 30 days post index procedure and 30 days post second stage procedure for the HA arm and for 30 days post index procedure and any repeat ablation for the CA arm.
The HA arm showed a complication rate of 7.8% vs. 5.8% for the CA arm (P = .751). Two patients in the former and three patients in the latter group had more than one major complication. There was one death in the HA group 93 days after the index procedure, and it was adjudicated as unrelated to the procedure.
“If you look back in the past, other studies showed a ... higher complication rate in the hybrid arm, so we feel very comfortable with these complication rates, which [are] very low and almost comparable,” Dr. Doll said.
Limitations of the study included symptom-driven electrocardiogram monitoring performed at unscheduled visits. Also, ablation beyond PVI in the CA arm and PVI/posterior box in the HA arm was not standardized and was performed according to standard practices in the participating countries.
“Success of epicardial-endocardial approach emphasizes the role of the collaborative heart team approach in the treatment of nonparoxysmal atrial fibrillation, and if I sum it up together, we can do it better” together, Dr. Doll advised.
‘Exceptional’ trial
After Dr. Doll’s presentation, appointed discussant Stylianos Tzeis, MD, PhD, head of the cardiology clinic and electrophysiology and pacing department at Mitera Hospital in Athens, congratulated the investigators and called CEASE-AF “an exceptional trial. It was really challenging to enroll patients in such a randomized controlled clinical trial.”
But Dr. Tzeis questioned whether pitting CA against HA was a fair comparison.
“Were the ablation targets similar between the two groups?” he asked. He noted that for the HA group, in the first stage the patients had PVI, posterior wall isolation, exclusion of the left atrial appendage, and additional lesions at the discretion of the operator. Ninety percent proceeded to the second stage, which was endocardial catheter ablation with verification of posterior wall isolation and PVI and additional lesions made if needed.
In the CA group, repeat catheter ablation could be performed after the 90-day blanking period if clinically indicated. “Please take note that only 10% were offered the second ablation. So at least in my perspective, this was a comparison of a two-stage approach versus a single-stage approach with a much more aggressive ablation protocol in the hybrid ablation group as compared to the endocardial group,” he said.
Seeing the higher success rate of the HA group in achieving the primary efficacy endpoint of freedom from all arrhythmias at 12 months, Dr. Tzeis asked, “Does this reflect the superiority of the epi-endo approach, or does it reflect the suboptimal performance of the catheter ablation approach?”
There was a 40% success rate in the CA patient population, a cohort that he deemed “not the most challenging persistent AF population in the world”: those with left atrial diameter of 47 millimeters and with 80% having an AF duration less than 12 months.
He also noted that “the average duration of the catheter ablation for the PVI in the vast majority of cases was 4 hours, which does not reflect what really happens in the everyday practice.”
All those critiques having been advanced, Dr. Tzeis said, “Definitely do not doubt my first comment that the authors should be congratulated, and I strongly believe that the main objective has been achieved to bring electrophysiologist and cardiac surgeons ... closer.”
The study sponsor was AtriCure Inc. with collaboration of Cardialysis BV. Doll has received consulting fees or royalties and/or has ownership or stockholder interest in AtriCure. Tzeis reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
AT EHRA 2023
Ablation for atrial fibrillation may protect the aging brain
BOSTON – , new research suggests.
Investigators found adults who had previously undergone catheter ablation were significantly less likely to be cognitively impaired during the 2-year study period, compared with those who receive medical management alone.
“Catheter ablation is intended to stop atrial fibrillation and restore the normal rhythm of the heart. By doing so, there is an improved cerebral hemodynamic profile,” said Bahadar S. Srichawla, DO, department of neurology, University of Massachusetts, Worcester.
“Thus, long-term cognitive outcomes may be improved due to improved blood flow to the brain by restoring the normal rhythm of the heart,” he added.
This research was presented at the 2023 annual meeting of the American Academy of Neurology.
Heart-brain connection
The study involved 887 older adults (mean age 75; 49% women) with atrial fibrillation participating in the SAGE-AF (Systematic Assessment of Geriatric Elements) study. A total of 193 (22%) participants underwent catheter ablation prior to enrollment. These individuals more frequently had an implantable cardiac device (46% vs. 28%, P < .001) and persistent atrial fibrillation (31% vs. 23%, P < .05).
Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA) tool at baseline and 1 and 2 years, with cognitive impairment defined as a MoCA score of 23 or below. Individuals who had catheter ablation had an average MoCA score of 25, compared with an average score of 23 in those who didn’t have catheter ablation.
After adjusting for potential confounding factors such as heart disease, renal disease, sleep apnea, and atrial fibrillation risk score, those who underwent catheter ablation were 36% less likely to develop cognitive impairment over 2 years than those who were treated only with medication (adjusted odds ratio, 0.64; 95% CI, 0.46-0.88).
During his presentation, Dr. Srichawla noted there is a hypothesis that individuals who are anticoagulated with warfarin may be prone to cerebral microbleeds and may be more cognitively impaired over time.
However, in a subgroup analysis, “cognitive function was similar at 2-year follow-up in those anticoagulated with warfarin, compared with all other anticoagulants. However, it should be noted that in this study, a direct head-to-head comparison was not done,” Dr. Srichawla told attendees.
“In patients with atrial fibrillation, catheter ablation should be discussed as a potential treatment strategy, particularly in patients who have or are at risk for cognitive decline and dementia,” Dr. Srichawla said.
Intriguing findings
Commenting on the research, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, said the study is “intriguing and adds to what we know from previous research connecting cardiovascular and cognitive health.”
“However, there are limitations to this study,” Dr. Griffin said, “including its predominantly White cohort and the use of only neuropsychiatric testing to diagnose dementia. More research is needed to fully understand the impact of atrial fibrillation on cognitive outcomes in all people.”
“It’s well known that the heart and the brain are intimately connected. Individuals experiencing any cardiovascular issues should speak to their doctor,” Dr. Griffin added.
Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, agreed. “If you ever get up too quickly and feel woozy, that is your brain not getting enough blood flow and you are getting all the warning signs to correct that – or else! Similarly, with atrial fibrillation, the heart is contracting, but not effectively pumping blood to the brain,” he said.
“This line of research shows that correcting the abnormal heart rhythm by zapping the faulty circuit with a catheter is actually better for your brain health than just taking medications alone,” added Dr. Lakhan, who was not involved with the study.
The study had no commercial funding. Dr. Srichawla, Dr. Griffin, and Dr. Lakhan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BOSTON – , new research suggests.
Investigators found adults who had previously undergone catheter ablation were significantly less likely to be cognitively impaired during the 2-year study period, compared with those who receive medical management alone.
“Catheter ablation is intended to stop atrial fibrillation and restore the normal rhythm of the heart. By doing so, there is an improved cerebral hemodynamic profile,” said Bahadar S. Srichawla, DO, department of neurology, University of Massachusetts, Worcester.
“Thus, long-term cognitive outcomes may be improved due to improved blood flow to the brain by restoring the normal rhythm of the heart,” he added.
This research was presented at the 2023 annual meeting of the American Academy of Neurology.
Heart-brain connection
The study involved 887 older adults (mean age 75; 49% women) with atrial fibrillation participating in the SAGE-AF (Systematic Assessment of Geriatric Elements) study. A total of 193 (22%) participants underwent catheter ablation prior to enrollment. These individuals more frequently had an implantable cardiac device (46% vs. 28%, P < .001) and persistent atrial fibrillation (31% vs. 23%, P < .05).
Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA) tool at baseline and 1 and 2 years, with cognitive impairment defined as a MoCA score of 23 or below. Individuals who had catheter ablation had an average MoCA score of 25, compared with an average score of 23 in those who didn’t have catheter ablation.
After adjusting for potential confounding factors such as heart disease, renal disease, sleep apnea, and atrial fibrillation risk score, those who underwent catheter ablation were 36% less likely to develop cognitive impairment over 2 years than those who were treated only with medication (adjusted odds ratio, 0.64; 95% CI, 0.46-0.88).
During his presentation, Dr. Srichawla noted there is a hypothesis that individuals who are anticoagulated with warfarin may be prone to cerebral microbleeds and may be more cognitively impaired over time.
However, in a subgroup analysis, “cognitive function was similar at 2-year follow-up in those anticoagulated with warfarin, compared with all other anticoagulants. However, it should be noted that in this study, a direct head-to-head comparison was not done,” Dr. Srichawla told attendees.
“In patients with atrial fibrillation, catheter ablation should be discussed as a potential treatment strategy, particularly in patients who have or are at risk for cognitive decline and dementia,” Dr. Srichawla said.
Intriguing findings
Commenting on the research, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, said the study is “intriguing and adds to what we know from previous research connecting cardiovascular and cognitive health.”
“However, there are limitations to this study,” Dr. Griffin said, “including its predominantly White cohort and the use of only neuropsychiatric testing to diagnose dementia. More research is needed to fully understand the impact of atrial fibrillation on cognitive outcomes in all people.”
“It’s well known that the heart and the brain are intimately connected. Individuals experiencing any cardiovascular issues should speak to their doctor,” Dr. Griffin added.
Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, agreed. “If you ever get up too quickly and feel woozy, that is your brain not getting enough blood flow and you are getting all the warning signs to correct that – or else! Similarly, with atrial fibrillation, the heart is contracting, but not effectively pumping blood to the brain,” he said.
“This line of research shows that correcting the abnormal heart rhythm by zapping the faulty circuit with a catheter is actually better for your brain health than just taking medications alone,” added Dr. Lakhan, who was not involved with the study.
The study had no commercial funding. Dr. Srichawla, Dr. Griffin, and Dr. Lakhan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BOSTON – , new research suggests.
Investigators found adults who had previously undergone catheter ablation were significantly less likely to be cognitively impaired during the 2-year study period, compared with those who receive medical management alone.
“Catheter ablation is intended to stop atrial fibrillation and restore the normal rhythm of the heart. By doing so, there is an improved cerebral hemodynamic profile,” said Bahadar S. Srichawla, DO, department of neurology, University of Massachusetts, Worcester.
“Thus, long-term cognitive outcomes may be improved due to improved blood flow to the brain by restoring the normal rhythm of the heart,” he added.
This research was presented at the 2023 annual meeting of the American Academy of Neurology.
Heart-brain connection
The study involved 887 older adults (mean age 75; 49% women) with atrial fibrillation participating in the SAGE-AF (Systematic Assessment of Geriatric Elements) study. A total of 193 (22%) participants underwent catheter ablation prior to enrollment. These individuals more frequently had an implantable cardiac device (46% vs. 28%, P < .001) and persistent atrial fibrillation (31% vs. 23%, P < .05).
Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA) tool at baseline and 1 and 2 years, with cognitive impairment defined as a MoCA score of 23 or below. Individuals who had catheter ablation had an average MoCA score of 25, compared with an average score of 23 in those who didn’t have catheter ablation.
After adjusting for potential confounding factors such as heart disease, renal disease, sleep apnea, and atrial fibrillation risk score, those who underwent catheter ablation were 36% less likely to develop cognitive impairment over 2 years than those who were treated only with medication (adjusted odds ratio, 0.64; 95% CI, 0.46-0.88).
During his presentation, Dr. Srichawla noted there is a hypothesis that individuals who are anticoagulated with warfarin may be prone to cerebral microbleeds and may be more cognitively impaired over time.
However, in a subgroup analysis, “cognitive function was similar at 2-year follow-up in those anticoagulated with warfarin, compared with all other anticoagulants. However, it should be noted that in this study, a direct head-to-head comparison was not done,” Dr. Srichawla told attendees.
“In patients with atrial fibrillation, catheter ablation should be discussed as a potential treatment strategy, particularly in patients who have or are at risk for cognitive decline and dementia,” Dr. Srichawla said.
Intriguing findings
Commenting on the research, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, said the study is “intriguing and adds to what we know from previous research connecting cardiovascular and cognitive health.”
“However, there are limitations to this study,” Dr. Griffin said, “including its predominantly White cohort and the use of only neuropsychiatric testing to diagnose dementia. More research is needed to fully understand the impact of atrial fibrillation on cognitive outcomes in all people.”
“It’s well known that the heart and the brain are intimately connected. Individuals experiencing any cardiovascular issues should speak to their doctor,” Dr. Griffin added.
Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, agreed. “If you ever get up too quickly and feel woozy, that is your brain not getting enough blood flow and you are getting all the warning signs to correct that – or else! Similarly, with atrial fibrillation, the heart is contracting, but not effectively pumping blood to the brain,” he said.
“This line of research shows that correcting the abnormal heart rhythm by zapping the faulty circuit with a catheter is actually better for your brain health than just taking medications alone,” added Dr. Lakhan, who was not involved with the study.
The study had no commercial funding. Dr. Srichawla, Dr. Griffin, and Dr. Lakhan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2023
What new cardiovascular disease risk factors have emerged?
Cardiovascular disease (CVD) is the main cause of premature death and disability in the general population, and according to the World Health Organization, the incidence of CVD is increasing throughout the world. Conventional risk factors that contribute to the occurrence and worsening of CVD have been identified and widely studied. They include high cholesterol levels, high blood pressure, diabetes, obesity, smoking, and lack of physical activity. Despite the introduction of measures to prevent and treat these risk factors with lipid-lowering drugs, antihypertensives, antiplatelet drugs, and anticoagulants, the mortality rate related to CVD remains high.
Despite the effectiveness of many currently available treatment options, there are still significant gaps in risk assessment and treatment of CVD.
They are detailed in an editorial published in The American Journal of Medicine that describes their role and their impact on our cardiovascular health.
Systemic inflammation
The new coronary risk factors include the following diseases characterized by systemic inflammation:
- Gout – Among patients who have experienced a recent flare of gout, the probability of experiencing an acute cardiovascular event such as a myocardial infarction or stroke is increased.
- Rheumatoid arthritis and systemic lupus erythematous – Patients with one or both of these conditions are at higher odds of experiencing concomitant premature and extremely premature coronary artery disease.
- Inflammatory bowel disease (Crohn’s disease or ulcerative colitis) – Patients with this disease have increased odds of developing coronary artery disease.
- Psoriasis – Patients with psoriasis are up to 50% more likely to develop CVD.
Maternal and childhood factors
The following maternal and childhood factors are associated with an increased risk of developing coronary artery disease: gestational diabetes; preeclampsia; delivering a child of low birth weight; preterm delivery; and premature or surgical menopause. The factor or factors that increase the risk of coronary artery disease associated with each of these conditions are not known but may be the result of increased cytokine and oxidative stress.
An unusual and yet unexplained association has been observed between migraine headaches with aura in women and incident CVD.
Also of interest is the association of early life trauma and the risk of adverse cardiovascular outcomes in young and middle-aged individuals who have a history of myocardial infarction.
Transgender patients who present for gender-affirming care are also at increased cardiovascular risk. Among these patients, the increase in coronary artery disease risk may be related to high rates of anxiety and depression.
Environmental factors
Low socioeconomic status has emerged as a risk factor. Increased psychosocial stressors, limited educational and economic opportunities, and lack of peer influence favoring healthier lifestyle choices may be causative elements leading to enhanced coronary artery disease among individuals with low socioeconomic living conditions.
Air pollution was estimated to have caused 9 million deaths worldwide in 2019, with 62% due to CVD and 31.7% to coronary artery disease. Severely polluted environmental aerosols contain several toxic metals, such as lead, mercury, arsenic, and cadmium. Transient exposure to various air pollutants may trigger the onset of an acute coronary syndrome.
Lifestyle factors
Long working hours by patients who have experienced a first myocardial infarction increase the risk for a recurrent event, possibly because of prolonged exposure to work stressors.
Skipping breakfast has been linked to increased cardiovascular and all-cause mortality.
Long-term consumption of drinks containing sugar and artificial sweeteners has also been associated with increased cardiovascular mortality.
Recognizing the presence of one or more of these new risk factors could help prompt and improve behaviors for reducing more conventional CV risk factors to a minimum.
This article was translated from Univadis Italy, which is part of the Medscape Professional Network.
A version of this article first appeared on Medscape.com.
Cardiovascular disease (CVD) is the main cause of premature death and disability in the general population, and according to the World Health Organization, the incidence of CVD is increasing throughout the world. Conventional risk factors that contribute to the occurrence and worsening of CVD have been identified and widely studied. They include high cholesterol levels, high blood pressure, diabetes, obesity, smoking, and lack of physical activity. Despite the introduction of measures to prevent and treat these risk factors with lipid-lowering drugs, antihypertensives, antiplatelet drugs, and anticoagulants, the mortality rate related to CVD remains high.
Despite the effectiveness of many currently available treatment options, there are still significant gaps in risk assessment and treatment of CVD.
They are detailed in an editorial published in The American Journal of Medicine that describes their role and their impact on our cardiovascular health.
Systemic inflammation
The new coronary risk factors include the following diseases characterized by systemic inflammation:
- Gout – Among patients who have experienced a recent flare of gout, the probability of experiencing an acute cardiovascular event such as a myocardial infarction or stroke is increased.
- Rheumatoid arthritis and systemic lupus erythematous – Patients with one or both of these conditions are at higher odds of experiencing concomitant premature and extremely premature coronary artery disease.
- Inflammatory bowel disease (Crohn’s disease or ulcerative colitis) – Patients with this disease have increased odds of developing coronary artery disease.
- Psoriasis – Patients with psoriasis are up to 50% more likely to develop CVD.
Maternal and childhood factors
The following maternal and childhood factors are associated with an increased risk of developing coronary artery disease: gestational diabetes; preeclampsia; delivering a child of low birth weight; preterm delivery; and premature or surgical menopause. The factor or factors that increase the risk of coronary artery disease associated with each of these conditions are not known but may be the result of increased cytokine and oxidative stress.
An unusual and yet unexplained association has been observed between migraine headaches with aura in women and incident CVD.
Also of interest is the association of early life trauma and the risk of adverse cardiovascular outcomes in young and middle-aged individuals who have a history of myocardial infarction.
Transgender patients who present for gender-affirming care are also at increased cardiovascular risk. Among these patients, the increase in coronary artery disease risk may be related to high rates of anxiety and depression.
Environmental factors
Low socioeconomic status has emerged as a risk factor. Increased psychosocial stressors, limited educational and economic opportunities, and lack of peer influence favoring healthier lifestyle choices may be causative elements leading to enhanced coronary artery disease among individuals with low socioeconomic living conditions.
Air pollution was estimated to have caused 9 million deaths worldwide in 2019, with 62% due to CVD and 31.7% to coronary artery disease. Severely polluted environmental aerosols contain several toxic metals, such as lead, mercury, arsenic, and cadmium. Transient exposure to various air pollutants may trigger the onset of an acute coronary syndrome.
Lifestyle factors
Long working hours by patients who have experienced a first myocardial infarction increase the risk for a recurrent event, possibly because of prolonged exposure to work stressors.
Skipping breakfast has been linked to increased cardiovascular and all-cause mortality.
Long-term consumption of drinks containing sugar and artificial sweeteners has also been associated with increased cardiovascular mortality.
Recognizing the presence of one or more of these new risk factors could help prompt and improve behaviors for reducing more conventional CV risk factors to a minimum.
This article was translated from Univadis Italy, which is part of the Medscape Professional Network.
A version of this article first appeared on Medscape.com.
Cardiovascular disease (CVD) is the main cause of premature death and disability in the general population, and according to the World Health Organization, the incidence of CVD is increasing throughout the world. Conventional risk factors that contribute to the occurrence and worsening of CVD have been identified and widely studied. They include high cholesterol levels, high blood pressure, diabetes, obesity, smoking, and lack of physical activity. Despite the introduction of measures to prevent and treat these risk factors with lipid-lowering drugs, antihypertensives, antiplatelet drugs, and anticoagulants, the mortality rate related to CVD remains high.
Despite the effectiveness of many currently available treatment options, there are still significant gaps in risk assessment and treatment of CVD.
They are detailed in an editorial published in The American Journal of Medicine that describes their role and their impact on our cardiovascular health.
Systemic inflammation
The new coronary risk factors include the following diseases characterized by systemic inflammation:
- Gout – Among patients who have experienced a recent flare of gout, the probability of experiencing an acute cardiovascular event such as a myocardial infarction or stroke is increased.
- Rheumatoid arthritis and systemic lupus erythematous – Patients with one or both of these conditions are at higher odds of experiencing concomitant premature and extremely premature coronary artery disease.
- Inflammatory bowel disease (Crohn’s disease or ulcerative colitis) – Patients with this disease have increased odds of developing coronary artery disease.
- Psoriasis – Patients with psoriasis are up to 50% more likely to develop CVD.
Maternal and childhood factors
The following maternal and childhood factors are associated with an increased risk of developing coronary artery disease: gestational diabetes; preeclampsia; delivering a child of low birth weight; preterm delivery; and premature or surgical menopause. The factor or factors that increase the risk of coronary artery disease associated with each of these conditions are not known but may be the result of increased cytokine and oxidative stress.
An unusual and yet unexplained association has been observed between migraine headaches with aura in women and incident CVD.
Also of interest is the association of early life trauma and the risk of adverse cardiovascular outcomes in young and middle-aged individuals who have a history of myocardial infarction.
Transgender patients who present for gender-affirming care are also at increased cardiovascular risk. Among these patients, the increase in coronary artery disease risk may be related to high rates of anxiety and depression.
Environmental factors
Low socioeconomic status has emerged as a risk factor. Increased psychosocial stressors, limited educational and economic opportunities, and lack of peer influence favoring healthier lifestyle choices may be causative elements leading to enhanced coronary artery disease among individuals with low socioeconomic living conditions.
Air pollution was estimated to have caused 9 million deaths worldwide in 2019, with 62% due to CVD and 31.7% to coronary artery disease. Severely polluted environmental aerosols contain several toxic metals, such as lead, mercury, arsenic, and cadmium. Transient exposure to various air pollutants may trigger the onset of an acute coronary syndrome.
Lifestyle factors
Long working hours by patients who have experienced a first myocardial infarction increase the risk for a recurrent event, possibly because of prolonged exposure to work stressors.
Skipping breakfast has been linked to increased cardiovascular and all-cause mortality.
Long-term consumption of drinks containing sugar and artificial sweeteners has also been associated with increased cardiovascular mortality.
Recognizing the presence of one or more of these new risk factors could help prompt and improve behaviors for reducing more conventional CV risk factors to a minimum.
This article was translated from Univadis Italy, which is part of the Medscape Professional Network.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF MEDICINE
FDA okays latest artificial pancreas, the MiniMed 780G
The Food and Drug Administration has approved Medtronic Minimed’s 780G automated insulin delivery system with the Guardian 4 sensor.
The latest so-called artificial pancreas system is approved for people aged 7 years and older who have type 1 diabetes. Medtronic will begin taking preorders for the 780G on May 15, 2023. Users of the current MiniMed 770G will be eligible for no-cost remote software upgrades.
The 780G is currently available in 105 countries. It has been available in Europe since 2020 and in the United Kingdom since 2021. It is the first automated insulin delivery system to automatically administer bolus correction insulin doses every 5 minutes to correct meal-related hyperglycemia.
This so-called meal detection technology doesn’t replace manual premeal boluses but does provide extra insulin if the premeal bolus is skipped or is insufficient.
As with other automated systems, the 780G automatically adjusts basal insulin doses up or down based on glucose levels and trends and shuts off insulin delivery to prevent hypoglycemia. The insulin pump’s infusion set can be worn for 7 days, rather than 3 days as with the older system, and the glucose target level can be set as low as 100 mg/dL.
And in contrast to the older MiniMed 670G system, which tended to frequently boot users out of automated mode, with the 780G, users spent an average of 95% of the time in the automated “SmartGuard” mode.
In the pivotal U.S. trial, overall, patients who used the 780G spent 75% of the time in ideal glucose range (70-180 mg/dL) and 1.8% of the time below that range. Overnight, the figures were 82% and 1.5%, respectively. With the glucose target set at 100 mg/dL and active insulin time set to 2 hours, patients spent 78.8% of time in range without increased hyperglycemia.
In the ADAPT study, with the 780G, there was a 26% increase in time in ideal glucose range and a 1.4% reduction in A1c compared with results for patients who received multiple daily insulin injections with intermittently scanned continuous glucose monitoring, without an increase in hypoglycemia. Overnight, time in range increased 30.2%. The results were sustained at 1 year.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved Medtronic Minimed’s 780G automated insulin delivery system with the Guardian 4 sensor.
The latest so-called artificial pancreas system is approved for people aged 7 years and older who have type 1 diabetes. Medtronic will begin taking preorders for the 780G on May 15, 2023. Users of the current MiniMed 770G will be eligible for no-cost remote software upgrades.
The 780G is currently available in 105 countries. It has been available in Europe since 2020 and in the United Kingdom since 2021. It is the first automated insulin delivery system to automatically administer bolus correction insulin doses every 5 minutes to correct meal-related hyperglycemia.
This so-called meal detection technology doesn’t replace manual premeal boluses but does provide extra insulin if the premeal bolus is skipped or is insufficient.
As with other automated systems, the 780G automatically adjusts basal insulin doses up or down based on glucose levels and trends and shuts off insulin delivery to prevent hypoglycemia. The insulin pump’s infusion set can be worn for 7 days, rather than 3 days as with the older system, and the glucose target level can be set as low as 100 mg/dL.
And in contrast to the older MiniMed 670G system, which tended to frequently boot users out of automated mode, with the 780G, users spent an average of 95% of the time in the automated “SmartGuard” mode.
In the pivotal U.S. trial, overall, patients who used the 780G spent 75% of the time in ideal glucose range (70-180 mg/dL) and 1.8% of the time below that range. Overnight, the figures were 82% and 1.5%, respectively. With the glucose target set at 100 mg/dL and active insulin time set to 2 hours, patients spent 78.8% of time in range without increased hyperglycemia.
In the ADAPT study, with the 780G, there was a 26% increase in time in ideal glucose range and a 1.4% reduction in A1c compared with results for patients who received multiple daily insulin injections with intermittently scanned continuous glucose monitoring, without an increase in hypoglycemia. Overnight, time in range increased 30.2%. The results were sustained at 1 year.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved Medtronic Minimed’s 780G automated insulin delivery system with the Guardian 4 sensor.
The latest so-called artificial pancreas system is approved for people aged 7 years and older who have type 1 diabetes. Medtronic will begin taking preorders for the 780G on May 15, 2023. Users of the current MiniMed 770G will be eligible for no-cost remote software upgrades.
The 780G is currently available in 105 countries. It has been available in Europe since 2020 and in the United Kingdom since 2021. It is the first automated insulin delivery system to automatically administer bolus correction insulin doses every 5 minutes to correct meal-related hyperglycemia.
This so-called meal detection technology doesn’t replace manual premeal boluses but does provide extra insulin if the premeal bolus is skipped or is insufficient.
As with other automated systems, the 780G automatically adjusts basal insulin doses up or down based on glucose levels and trends and shuts off insulin delivery to prevent hypoglycemia. The insulin pump’s infusion set can be worn for 7 days, rather than 3 days as with the older system, and the glucose target level can be set as low as 100 mg/dL.
And in contrast to the older MiniMed 670G system, which tended to frequently boot users out of automated mode, with the 780G, users spent an average of 95% of the time in the automated “SmartGuard” mode.
In the pivotal U.S. trial, overall, patients who used the 780G spent 75% of the time in ideal glucose range (70-180 mg/dL) and 1.8% of the time below that range. Overnight, the figures were 82% and 1.5%, respectively. With the glucose target set at 100 mg/dL and active insulin time set to 2 hours, patients spent 78.8% of time in range without increased hyperglycemia.
In the ADAPT study, with the 780G, there was a 26% increase in time in ideal glucose range and a 1.4% reduction in A1c compared with results for patients who received multiple daily insulin injections with intermittently scanned continuous glucose monitoring, without an increase in hypoglycemia. Overnight, time in range increased 30.2%. The results were sustained at 1 year.
A version of this article first appeared on Medscape.com.
New ACC guidance on heart failure with preserved ejection fraction
The American College of Cardiology has released an Expert Consensus Decision Pathway (ECDP) on the management of heart failure with preserved ejection fraction (HFpEF).
The 44-page document highlights the “critical need” to accurately diagnose HFpEF to permit timely implementation of evidence- and guideline-based therapies to improve patient outcomes.
Although the incidence of overall HF in the United States appears to be stable or declining, the incidence of HFpEF continues to rise in tandem with increasing age and burdens of obesity, sedentary lifestyle, and cardiometabolic disorders.
HFpEF now accounts for more than one half of HF cases but remains “underrecognized” in everyday clinical practice, said the writing group, led by Michelle Kittleson, MD, PhD, professor of medicine, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles.
HFpEF is a complex condition, often with multiple overlapping comorbidities, including hypertension, diabetes, obesity, and sleep apnea; optimal management requires a multidisciplinary approach, the writing group said.
The ECDP on HFpEF lays out a structure for diagnosis, clinical decision-making, management of comorbidities, implementation of the latest guideline-directed medical therapy (pharmacologic and nonpharmacologic), and equitable delivery of care.
The document was published online in the Journal of the American College of Cardiology.
It aligns with and builds on recommendations from the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
“HFpEF is one of the most pressing diagnostic and therapeutic challenges in clinical medicine today given its increasing prevalence, under diagnosis, poor prognosis, limited therapeutic options, and substantial burden on the health care system worldwide,” wrote the authors of a companion scientific statement on HFpEF.
Despite these challenges, the success of recent sodium-glucose cotransporter 2 inhibitor trials has shown that HFpEF is treatable, Barry Borlaug, MD, department of cardiovascular medicine, Mayo Clinic, Rochester, Minn., and coauthors pointed out.
They noted that “ongoing large-scale studies of HFpEF pathobiology, an increasing number of translational studies spanning the gap between the bedside and the bench, and numerous clinical trials of novel therapeutics in HFpEF offer a glimpse of hope toward a future of reduced prevalence, morbidity, and mortality associated with HFpEF, which would be a major advance for population health.”
A version of this article originally appeared on Medscape.com.
The American College of Cardiology has released an Expert Consensus Decision Pathway (ECDP) on the management of heart failure with preserved ejection fraction (HFpEF).
The 44-page document highlights the “critical need” to accurately diagnose HFpEF to permit timely implementation of evidence- and guideline-based therapies to improve patient outcomes.
Although the incidence of overall HF in the United States appears to be stable or declining, the incidence of HFpEF continues to rise in tandem with increasing age and burdens of obesity, sedentary lifestyle, and cardiometabolic disorders.
HFpEF now accounts for more than one half of HF cases but remains “underrecognized” in everyday clinical practice, said the writing group, led by Michelle Kittleson, MD, PhD, professor of medicine, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles.
HFpEF is a complex condition, often with multiple overlapping comorbidities, including hypertension, diabetes, obesity, and sleep apnea; optimal management requires a multidisciplinary approach, the writing group said.
The ECDP on HFpEF lays out a structure for diagnosis, clinical decision-making, management of comorbidities, implementation of the latest guideline-directed medical therapy (pharmacologic and nonpharmacologic), and equitable delivery of care.
The document was published online in the Journal of the American College of Cardiology.
It aligns with and builds on recommendations from the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
“HFpEF is one of the most pressing diagnostic and therapeutic challenges in clinical medicine today given its increasing prevalence, under diagnosis, poor prognosis, limited therapeutic options, and substantial burden on the health care system worldwide,” wrote the authors of a companion scientific statement on HFpEF.
Despite these challenges, the success of recent sodium-glucose cotransporter 2 inhibitor trials has shown that HFpEF is treatable, Barry Borlaug, MD, department of cardiovascular medicine, Mayo Clinic, Rochester, Minn., and coauthors pointed out.
They noted that “ongoing large-scale studies of HFpEF pathobiology, an increasing number of translational studies spanning the gap between the bedside and the bench, and numerous clinical trials of novel therapeutics in HFpEF offer a glimpse of hope toward a future of reduced prevalence, morbidity, and mortality associated with HFpEF, which would be a major advance for population health.”
A version of this article originally appeared on Medscape.com.
The American College of Cardiology has released an Expert Consensus Decision Pathway (ECDP) on the management of heart failure with preserved ejection fraction (HFpEF).
The 44-page document highlights the “critical need” to accurately diagnose HFpEF to permit timely implementation of evidence- and guideline-based therapies to improve patient outcomes.
Although the incidence of overall HF in the United States appears to be stable or declining, the incidence of HFpEF continues to rise in tandem with increasing age and burdens of obesity, sedentary lifestyle, and cardiometabolic disorders.
HFpEF now accounts for more than one half of HF cases but remains “underrecognized” in everyday clinical practice, said the writing group, led by Michelle Kittleson, MD, PhD, professor of medicine, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles.
HFpEF is a complex condition, often with multiple overlapping comorbidities, including hypertension, diabetes, obesity, and sleep apnea; optimal management requires a multidisciplinary approach, the writing group said.
The ECDP on HFpEF lays out a structure for diagnosis, clinical decision-making, management of comorbidities, implementation of the latest guideline-directed medical therapy (pharmacologic and nonpharmacologic), and equitable delivery of care.
The document was published online in the Journal of the American College of Cardiology.
It aligns with and builds on recommendations from the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
“HFpEF is one of the most pressing diagnostic and therapeutic challenges in clinical medicine today given its increasing prevalence, under diagnosis, poor prognosis, limited therapeutic options, and substantial burden on the health care system worldwide,” wrote the authors of a companion scientific statement on HFpEF.
Despite these challenges, the success of recent sodium-glucose cotransporter 2 inhibitor trials has shown that HFpEF is treatable, Barry Borlaug, MD, department of cardiovascular medicine, Mayo Clinic, Rochester, Minn., and coauthors pointed out.
They noted that “ongoing large-scale studies of HFpEF pathobiology, an increasing number of translational studies spanning the gap between the bedside and the bench, and numerous clinical trials of novel therapeutics in HFpEF offer a glimpse of hope toward a future of reduced prevalence, morbidity, and mortality associated with HFpEF, which would be a major advance for population health.”
A version of this article originally appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY