User login
› Assess the need for nonpharmacologic, behavioral interventions and for chemoprophylaxis based on a destination’s relative risk to travelers, planned and potential activities, and patient comorbidities. B
› Choose an antimalarial medication based on knowledge of area-specific drug effectiveness or resistance patterns, trip duration, drug cost, tolerance for adverse effects, and comorbidities. C
› Presume a diagnosis of malaria until proven otherwise in any traveler who is febrile after returning from a malaria-endemic region. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Although malaria was eradicated as an endemic disease in the United States in the early 1950s,1 it still returns yearly in approximately 1500 individuals who travel to foreign countries2—most of whom neglected to use prophylactic measures or use them properly.3 In more than 60 documented cases, these infected individuals have been the source of local transmission in their communities.2 To reduce the individual and public health risks associated with malaria, this article focuses on steps that international travelers can take to limit their risk of the disease.
What travelers need to know
In 2013, more than 61.5 million residents of the United States traveled abroad, approximately 30% of whom visited malaria-endemic regions: Mexico and equatorial nations in Central and South America; Africa; the Middle East; and South, East, and Southeast Asia.4 Counseling on appropriate preventive measures fits the Medical Home concept of comprehensive, preventive, patient-centered care, and pre-travel consultation—including a review of health data and itineraries, and patient education—can be a team-based effort.5
Begin your planning for malaria prophylaxis by assessing your patient’s individual risk. Key variables are a patient’s detailed itinerary, a credible and current source of information on location-specific malaria prevalence, personal risk factors, and risk tolerance. Shared decision-making is vital and enhances adherence to the prescribed regimen.
Endemicity varies regionally. Without chemoprophylaxis, risk of infection ranges from more than 20% in Papua New Guinea to 0.01% in Central America, with wide exposure risk variations likely, even within regions.6 Travel to areas of high endemicity requires more aggressive malaria prevention strategies than travel to low-endemicity regions.
Risk of exposure is lower with short visits,7 business-only travel, urban-only stays in some countries, day trips to endemic areas,7 and travel during seasons with lower mosquito burden. Likewise, travelers staying in a hotel with sealed windows will face lower nighttime Anopheles mosquito exposure. In these cases, nonpharmacologic measures alone may be appropriate.
Those at particularly high risk for complicated or lethal malarial infection are children, pregnant women, elderly individuals, and immunocompromised patients.7 In addition to counseling high-risk patients about prophylactic measures, consider advising against travel in certain circumstances. Among those at highest risk for acquiring malaria are immigrants and refugees traveling to their ancestral homelands to visit friends and relatives (VFR).2 Many VFR travelers fail to take appropriate prophylactic measures when “going home.”8 A significant number of cases of travel-acquired malaria occurs in VFR children.9
Individualizing prevention directives
The mainstays of malaria prevention include nonpharmacologic and behavioral interventions, as well as chemoprophylaxis. Most cases of malaria in travelers returning to the United States result from the improper implementation of prophylactic measures.3 Discussing individual risk with travelers is an easy way to bolster adherence to malaria prevention measures, and some evidence suggests it is effective10 (strength of recommendation [SOR]: C). Other limited studies have also shown that malaria education can improve knowledge about malaria transmission and increase the likelihood that preventive measures will be used.11,12
Recommend nonpharmacologic measures even for those using chemoprophylaxis
Nonpharmacologic interventions such as sleeping under permethrin-treated bednets, wearing long sleeves and full-length pants, treating clothes with permethrin, and applying DEET (N,N-diethyl-meta-toluamide) to exposed skin are effective and have the added benefit of preventing non-malarial arthropod-borne diseases4 (SOR: B). Studies have shown that, compared with sleeping without nets, the use of insecticide treated-nets can reduce child mortality by 17% and the incidence of uncomplicated malarial episodes by 50%.13 In areas with malaria transmission, 10% to 30% DEET—used alone or in combination with permethrin-treated clothing— can reduce bite load, although the American Academy of Pediatrics recommends against using DEET in children younger than 2 months of age.14,15
Using these measures in combination from dusk to dawn, when Anopheles mosquitoes are active, has been shown to be effective, although randomized, controlled studies are lacking.16 Remaining indoors during these peak biting periods is also advisable. In certain areas, and with the right itinerary, the traveler may only need to employ nonpharmacologic methods of preventing malarial infection. Recommend them to all patients traveling to malarial regions, even to individuals using pharmacologic prophylaxis.
Factors determining the need for, and selection of, chemoprophylaxis
When used properly, chemoprophylactic drugs are effective in preventing malaria (SOR: A). Atovaquone-proguanil achieves efficacy of 95% to 100%,17 while doxycycline, primaquine, and mefloquine are slightly less effective.18-20 Chloroquine is effective in 6 regions of the tropics and subtropics where Plasmodium falciparum resistance has not developed. Select a drug based on your assessment of an individual’s level of risk according to the personal itinerary, trip duration and accommodations, cost of medication, tolerance for adverse effects, and other factors (eg, comorbidities, concurrent drug usage, pregnancy).
Location matters. The risk of malaria transmission can vary considerably not only between countries, but also regionally within countries and even between a city and its immediate surroundings. Therefore, select a chemoprophylactic agent based on the specific itinerary, planned activities, the potential for unforeseen additional excursions, and local Plasmodium resistance patterns. For example, chloroquine is effective only in the Caribbean, Central America, and some countries in the Middle East.21 Mefloquine resistance has been reported in parts of Cambodia, Thailand, Vietnam, Burma, China, and Laos.21
On its Travelers’ Health Web site (www.cdc.gov/travel), the Centers for Disease Control and Prevention (CDC) reports for each country 1) the risk of malaria transmission, 2) areas within the country that pose a risk, 3) evidence of Plasmodium drug resistance, 4) which Plasmodium species are active, and 5) which chemoprophylactic medications are recommended.22 Additional Web sites, either free or subscription-based, allow users to view this same information on maps, advise on where insect precautions alone are sufficiently protective, and provide information about the traveler’s risk of contracting other diseases (TABLE 1).
TABLE 1
| Web resources on infectious diseases of concern to international travelers | |
| Resource | Notes |
Centers for Disease Control and Prevention | Free Site Go to Yellow Book » Contents » Chapter 3 » “Travel Vaccines & Malaria Information, by Country” for country-specific information about the risk of malaria transmission |
VHI Healthcare | Free Site Destination-specific information about travel alerts and vaccine recommendations Does not report malaria transmission data |
Gideon | Subscription only Online application that helps with diagnosing infectious diseases and keeping up to date with global health literature |
Travax | Subscription only Information about recommended vaccines and country-specific risk of malaria transmission |
Tropimed | Subscription only Information about recommended vaccines and country-specific risk of malaria transmission |
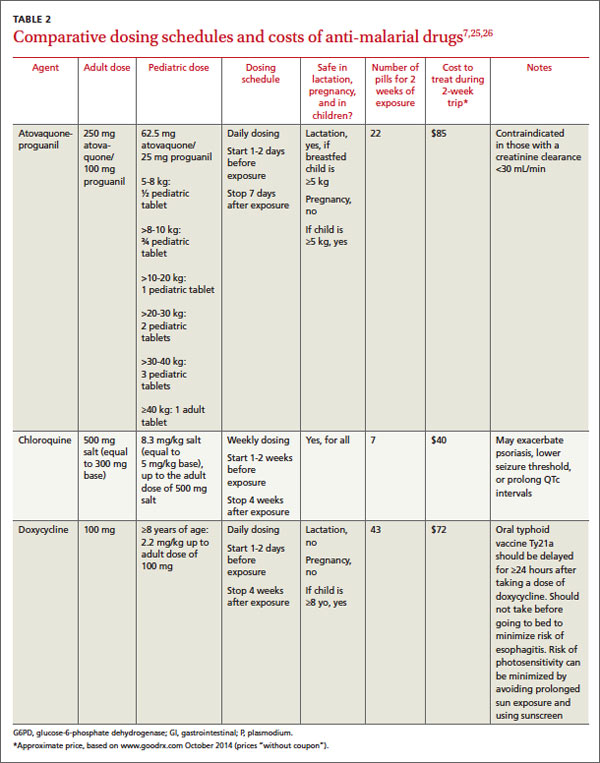
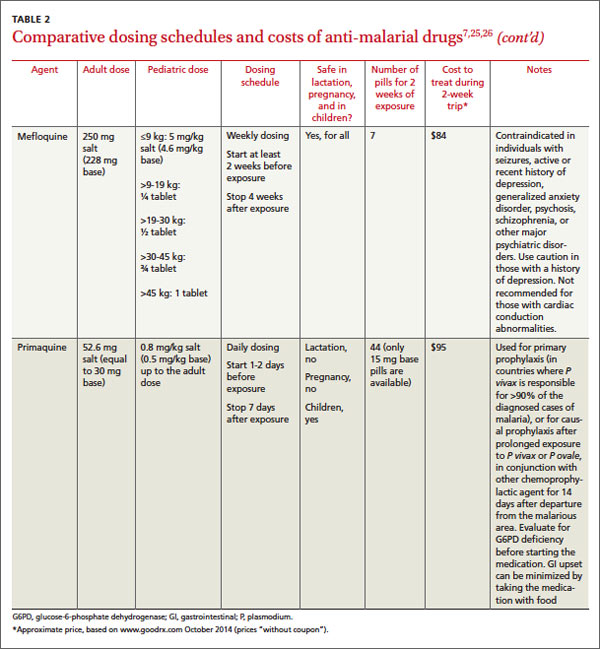
Comparative adverse effects of antimalarial agents. A Cochrane Review on the tolerability of chemoprophylactic agents concluded that atovaquone-proguanil and doxycycline were better tolerated than mefloquine (SOR: B). Compared with mefloquine, atovaquone-proguanil led to fewer reports of any adverse effects (relative risk [RR]=0.72), gastrointestinal adverse effects (RR=0.54), and neuropsychiatric adverse events (RR= 0.49-0.86, depending on the studies).23 Doxycycline users have reported fewer neuropsychiatric events (RR=0.84) than mefloquine users.23 These are relatively small differences, and the authors point out that these figures are based on low-quality evidence. Additional research is likely to have an impact on the confidence in the estimate of effect and to ultimately change the estimate.
Mefloquine is contraindicated in travelers with seizures, active or recent history of depression, generalized anxiety disorder, psychosis, schizophrenia, or other psychiatric disorders. Compared with mefloquine, atovaquone-proguanil and doxycycline cause fewer neuropsychiatric adverse effects (such as vivid dreams, dizziness, anxiety, depression, visual disturbance, or seizures).24 Caution is advised when prescribing chloroquine for patients with epilepsy because the medication has the potential to lower the seizure threshold.25
Use caution when prescribing mefloquine for patients with cardiac conduction disturbances. Electrocardiogram alterations such as sinus bradycardia, first-degree AV block, prolongation of QTc intervals, and abnormal T wave changes have been reported.26 Chloroquine can also prolong QTc intervals.26
Safety in pregnancy and breastfeeding. Malaria in pregnancy is associated with increased rates of anemia, low birth weight, prematurity, intrauterine growth restriction, and infant mortality.27 Chloroquine and mefloquine are considered safe during pregnancy and breastfeeding. Doxycycline has been associated with increased risk of harm to the fetus. Atovaquone-proguanil can be used in breastfeeding women if the child is ≥5 kg (≥11 lbs). Chemoprophylaxis taken by the mother while breastfeeding does not protect the infant from infection.
Dosing considerations. Mefloquine and chloroquine are dosed weekly; doxycycline and atovaquone-proguanil are taken daily. Travelers staying in a malaria-endemic region for longer periods (months rather than weeks) often prefer the weekly rather than daily medications; however, this may not be possible due to the adverse-effect profile of mefloquine or to traveling in an area with known chloroquine resistance. Some individuals prefer the routine of taking a medication daily, since remembering to take a single dose on the same day each week can be challenging. Others may not want to carry a large number of pills and therefore prefer weekly dosing. Have patients take medications before the trip, to assess tolerability and to ensure adequate blood concentrations before exposure.
Because mefloquine, doxycycline, and chloroquine target only the blood stages of Plasmodium, patients must continue these medications for 4 weeks following the exposure period to ensure adequate coverage as parasites are released from the liver. Because doxycycline is taken daily and has to be continued for 4 weeks following the exposure period, the total number of pills taken is higher for this regimen. Atovaquone-proguanil is active against hepatic and blood stages and can be discontinued a week following the exposure period.
With children, base dosing on body weight and do not exceed the recommended adult dose. When fractions of tablets are used (such as with mefloquine and atovaquone-proguanil dosing), pharmacists can crush tablets and place divided doses in capsules, to be sprinkled as needed into food such as applesauce or jelly. Mefloquine and chloroquine can be given to children of all ages and weights. Although atovaquone-proguanil is approved only for children ≥11 kg (24 lbs), dosing schedules have been calculated for children who weigh ≥5 kg.21 Doxycycline is recommended only for children who are at least 8 years of age.
Cost. For a 2-week exposure period, chloroquine is the least expensive medication (although regions in which it is recommended are limited due to resistance) (TABLE 27,25,26).
Ask about accommodations
Since Anopheles mosquitoes feed between dusk and dawn, inquiring about accommodations can further clarify a patient’s malaria risk. Staying in air-conditioned housing (implying that the interior can be sealed) or that has screened windows can reduce exposure to mosquitoes, although data are lacking regarding whether the latter practice reduces the incidence of malaria transmission28 (SOR: C).
Share decision making
After considering the key factors determining a patient’s level of risk, you may decide to recommend no specific interventions, to advise insect avoidance measures only, to combine insect avoidance with chemoprophylaxis, or to caution against traveling to a malaria-endemic region. The patient’s contribution to the final decision includes personal preferences, values, and risk tolerance—particularly when comorbidities are involved.
When preventive measures fail
Approximately 0.2% of travelers to malaria-endemic regions will become infected, despite proper pre-travel counseling and prophylaxis.29 In the United States, malaria is often misdiagnosed or improperly treated.30 The time from initial presentation to correct diagnosis of malaria has been reported as an astonishingly high 4 to 8.5 days, depending on the population.31,32
A high index of suspicion is needed and will ensure timely care when any febrile traveler returns from a malaria-endemic area.33 Be sure to advise patients to seek medical attention if they are feverish upon returning home.
Once suspected, the diagnosis of malaria can be readily confirmed through the use of antibody-, nucleic acid-, or microscopy-based techniques (the latter to directly visualize Plasmodium species in blood smears).
Although malaria chemoprophylaxis is relatively straightforward, malaria treatment—especially in cases of chemoprophylaxis failures—may not be, and the topic is beyond the scope of this article. For guidance on treating malaria, consult a knowledgeable physician or contact the CDC at www.cdc.gov/malaria/, or at (855) 856-4713 (weekdays, 9 am to 5 pm EST) or (770) 488-7100 (weekends or after normal business hours; ask for the Malaria Branch clinician on call).
CORRESPONDENCE
Mark K. Huntington, MD, PhD, Center for Family Medicine, 1115 East 20th Street, Sioux Falls, SD 57105; [email protected]
1. Mali S, Steele S, Slutsker L, et al; Centers for Disease Control and Prevention (CDC). Malaria surveillance - United States, 2008. MMWR Surveill Summ. 2010;59:1-15.
2. Centers for Disease Control and Prevention. Malaria facts. Centers for Disease Control and Prevention Web site. Available at: www.cdc.gov/malaria/about/facts.html. Accessed September 29, 2014.
3. Huntington MK. Healthy people, malaria and South Dakota. S D Med. 2012;65:297-300.
4. Office of Travel and Tourism Industries. U.S. citizen travel to international regions, 2013. Office of Travel and Tourism Industries Web site. Available at: http://travel.trade.gov/view/m-2013-O-001/index.html. Accessed September 29, 2014.
5. Bazemore AW, Huntington M. The pretravel consultation. Am Fam Physician. 2009;80:583-590.
6. Bradley DJ, Warhurst DC, Blaze M, et al. Malaria imported into the United Kingdom in 1996. Euro Surveill. 1998;3:40-42.
7. Arguin PM, Tan KR, et al; Centers for Disease Control and Prevention. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/malaria. Accessed October 15, 2014.
8. Pavli A, Maltezou HC. Malaria and travellers visiting friends and relatives. Travel Med Infect Dis. 2010;8:161-168.
9. Stäger K, Legros F, Krause G, et al. Imported malaria in children in industrialized countries, 1992-2002. Emerg Infect Dis. 2009;15:185-191.
10. Hartjes LB, Baumann LC, Henriques JB. Travel health risk perceptions and prevention behaviors of US study abroad students. J Travel Med. 2009;16:338-343.
11. Kishore J, Gupta VK, Singh SV, et al. Impact of health education intervention on knowledge and community action for malaria control in Delhi. J Commun Dis. 2008;40:183-192.
12. Chirdan OO, Zoakah AI, Ejembi CL. Impact of health education on home treatment and prevention of malaria in Jengre, North Central Nigeria. Ann Afr Med. 2008;7:112-119.
13. Lengeler C. Insecticide-treated bed nets and curtains for preventing malaria. Cochrane Database Syst Rev. 2004;(2): CD000363.
14. Centers for Disease Control and Prevention. Fight the bite for protection from malaria: Guidelines for DEET insect repellent use. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/malaria/toolkit/DEET.pdf. Accessed September 29, 2014.
15. American Academy of Pediatrics. Safety & prevention. Healthychildren.org Web site. Available at: http://www.healthychildren. org/English/safety-prevention/at-play/Pages/Insect-Repellents. aspx. Accessed September 29, 2014.
16. Croft AM, Baker D, von Bertele MJ. An evidence-based vector control strategy for military deployments: the British Army experience. Med Trop (Mars). 2001;61:91-98.
17. Boggild AK, Parise ME, Lewis LS, et al. Atovaquone-proguanil: report from the CDC expert meeting on malaria chemoprophylaxis (II). Am J Trop Med Hyg. 2007;76:208-223.
18. Tan KR, Magill AJ, Parise ME, et al; Centers for Disease Control and Prevention. Doxycycline for malaria chemoprophylaxis and treatment: report from the CDC expert meeting on malaria chemoprophylaxis. Am J Trop Med Hyg. 2011;84:517-531.
19. Hill DR, Baird JK, Parise ME, et al. Primaquine: report from CDC expert meeting on malaria chemoprophylaxis I. Am J Trop Med Hyg. 2006;75:402-415.
20. Steffen R, Fuchs E, Schildknecht J, et al. Mefloquine compared with other malaria chemoprophylactic regimens in tourists visiting east Africa. Lancet. 1993;341:1299-1303.
21. Centers for Disease Control and Prevention. CDC Health Information for International Travel 2014. New York, NY: Oxford University Press; 2014.
22. Gershman MD, Jentes ES, Johnson KJ, et al; Centers for Disease Control and Prevention. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-3- infectious-diseases-related-to-travel/yellow-fever-and-malaria- information-by-country.htm. Accessed September 29, 2014.
23. Jacquerioz FA, Croft AM. Drugs for preventing malaria in travellers. Cochrane Database Syst Rev. 2009;(4):CD006491.
24. Schlagenhauf P, Tschopp A, Johnson R, et al. Tolerability of malaria chemoprophylaxis in non-immune travellers to sub-Saharan Africa: multicentre, randomised, double blind, four arm study. BMJ. 2003;327:1078.
25. Chloroquine phosphate [package insert]. Eatontown, NJ: Westward Pharmaceutical Corp; 2010.
26. Lariam [package insert]. Roche Laboratories, Inc: Nutley, NJ; 2004.
27. Steketee RW, Nahlen BL, Parise ME, et al. The burden of malaria in pregnancy in malaria-endemic areas. Am J Trop Med Hyg. 2001;64(1-2 suppl):28-35.
28. Kirby MJ, Ameh D, Bottomley C, et al. Effect of two different house screening interventions on exposure to malaria vectors and on anaemia in children in The Gambia: a randomised controlled trial. Lancet. 2009;374:998-1009.
29. Steffen R, Amitirigala I, Mutsch M. Health risks among travelers--need for regular updates. J Travel Med. 2008;15:145-146.
30. Dorsey G, Gandhi M, Oyugi JH, et al. Difficulties in the prevention, diagnosis, and treatment of imported malaria. Arch Intern Med. 2000;160:2505-2510.
31. Newman RD, Parise ME, Barber AM, et al. Malaria-related deaths among U.S. travelers, 1963-2001. Ann Intern Med. 2004;141: 547-555.
32. Lesko CR, Arguin PM, Newman RD. Congenital malaria in the United States: a review of cases from 1966 to 2005. Arch Pediatr Adolesc Med. 2007;161:1062-1067.
33. Blair JE. Evaluation of fever in the international traveler. Unwanted ‘souvenir’ can have many causes. Postgrad Med. 2004;116: 13-20,29.
› Assess the need for nonpharmacologic, behavioral interventions and for chemoprophylaxis based on a destination’s relative risk to travelers, planned and potential activities, and patient comorbidities. B
› Choose an antimalarial medication based on knowledge of area-specific drug effectiveness or resistance patterns, trip duration, drug cost, tolerance for adverse effects, and comorbidities. C
› Presume a diagnosis of malaria until proven otherwise in any traveler who is febrile after returning from a malaria-endemic region. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Although malaria was eradicated as an endemic disease in the United States in the early 1950s,1 it still returns yearly in approximately 1500 individuals who travel to foreign countries2—most of whom neglected to use prophylactic measures or use them properly.3 In more than 60 documented cases, these infected individuals have been the source of local transmission in their communities.2 To reduce the individual and public health risks associated with malaria, this article focuses on steps that international travelers can take to limit their risk of the disease.
What travelers need to know
In 2013, more than 61.5 million residents of the United States traveled abroad, approximately 30% of whom visited malaria-endemic regions: Mexico and equatorial nations in Central and South America; Africa; the Middle East; and South, East, and Southeast Asia.4 Counseling on appropriate preventive measures fits the Medical Home concept of comprehensive, preventive, patient-centered care, and pre-travel consultation—including a review of health data and itineraries, and patient education—can be a team-based effort.5
Begin your planning for malaria prophylaxis by assessing your patient’s individual risk. Key variables are a patient’s detailed itinerary, a credible and current source of information on location-specific malaria prevalence, personal risk factors, and risk tolerance. Shared decision-making is vital and enhances adherence to the prescribed regimen.
Endemicity varies regionally. Without chemoprophylaxis, risk of infection ranges from more than 20% in Papua New Guinea to 0.01% in Central America, with wide exposure risk variations likely, even within regions.6 Travel to areas of high endemicity requires more aggressive malaria prevention strategies than travel to low-endemicity regions.
Risk of exposure is lower with short visits,7 business-only travel, urban-only stays in some countries, day trips to endemic areas,7 and travel during seasons with lower mosquito burden. Likewise, travelers staying in a hotel with sealed windows will face lower nighttime Anopheles mosquito exposure. In these cases, nonpharmacologic measures alone may be appropriate.
Those at particularly high risk for complicated or lethal malarial infection are children, pregnant women, elderly individuals, and immunocompromised patients.7 In addition to counseling high-risk patients about prophylactic measures, consider advising against travel in certain circumstances. Among those at highest risk for acquiring malaria are immigrants and refugees traveling to their ancestral homelands to visit friends and relatives (VFR).2 Many VFR travelers fail to take appropriate prophylactic measures when “going home.”8 A significant number of cases of travel-acquired malaria occurs in VFR children.9
Individualizing prevention directives
The mainstays of malaria prevention include nonpharmacologic and behavioral interventions, as well as chemoprophylaxis. Most cases of malaria in travelers returning to the United States result from the improper implementation of prophylactic measures.3 Discussing individual risk with travelers is an easy way to bolster adherence to malaria prevention measures, and some evidence suggests it is effective10 (strength of recommendation [SOR]: C). Other limited studies have also shown that malaria education can improve knowledge about malaria transmission and increase the likelihood that preventive measures will be used.11,12
Recommend nonpharmacologic measures even for those using chemoprophylaxis
Nonpharmacologic interventions such as sleeping under permethrin-treated bednets, wearing long sleeves and full-length pants, treating clothes with permethrin, and applying DEET (N,N-diethyl-meta-toluamide) to exposed skin are effective and have the added benefit of preventing non-malarial arthropod-borne diseases4 (SOR: B). Studies have shown that, compared with sleeping without nets, the use of insecticide treated-nets can reduce child mortality by 17% and the incidence of uncomplicated malarial episodes by 50%.13 In areas with malaria transmission, 10% to 30% DEET—used alone or in combination with permethrin-treated clothing— can reduce bite load, although the American Academy of Pediatrics recommends against using DEET in children younger than 2 months of age.14,15
Using these measures in combination from dusk to dawn, when Anopheles mosquitoes are active, has been shown to be effective, although randomized, controlled studies are lacking.16 Remaining indoors during these peak biting periods is also advisable. In certain areas, and with the right itinerary, the traveler may only need to employ nonpharmacologic methods of preventing malarial infection. Recommend them to all patients traveling to malarial regions, even to individuals using pharmacologic prophylaxis.
Factors determining the need for, and selection of, chemoprophylaxis
When used properly, chemoprophylactic drugs are effective in preventing malaria (SOR: A). Atovaquone-proguanil achieves efficacy of 95% to 100%,17 while doxycycline, primaquine, and mefloquine are slightly less effective.18-20 Chloroquine is effective in 6 regions of the tropics and subtropics where Plasmodium falciparum resistance has not developed. Select a drug based on your assessment of an individual’s level of risk according to the personal itinerary, trip duration and accommodations, cost of medication, tolerance for adverse effects, and other factors (eg, comorbidities, concurrent drug usage, pregnancy).
Location matters. The risk of malaria transmission can vary considerably not only between countries, but also regionally within countries and even between a city and its immediate surroundings. Therefore, select a chemoprophylactic agent based on the specific itinerary, planned activities, the potential for unforeseen additional excursions, and local Plasmodium resistance patterns. For example, chloroquine is effective only in the Caribbean, Central America, and some countries in the Middle East.21 Mefloquine resistance has been reported in parts of Cambodia, Thailand, Vietnam, Burma, China, and Laos.21
On its Travelers’ Health Web site (www.cdc.gov/travel), the Centers for Disease Control and Prevention (CDC) reports for each country 1) the risk of malaria transmission, 2) areas within the country that pose a risk, 3) evidence of Plasmodium drug resistance, 4) which Plasmodium species are active, and 5) which chemoprophylactic medications are recommended.22 Additional Web sites, either free or subscription-based, allow users to view this same information on maps, advise on where insect precautions alone are sufficiently protective, and provide information about the traveler’s risk of contracting other diseases (TABLE 1).
TABLE 1
| Web resources on infectious diseases of concern to international travelers | |
| Resource | Notes |
Centers for Disease Control and Prevention | Free Site Go to Yellow Book » Contents » Chapter 3 » “Travel Vaccines & Malaria Information, by Country” for country-specific information about the risk of malaria transmission |
VHI Healthcare | Free Site Destination-specific information about travel alerts and vaccine recommendations Does not report malaria transmission data |
Gideon | Subscription only Online application that helps with diagnosing infectious diseases and keeping up to date with global health literature |
Travax | Subscription only Information about recommended vaccines and country-specific risk of malaria transmission |
Tropimed | Subscription only Information about recommended vaccines and country-specific risk of malaria transmission |
Comparative adverse effects of antimalarial agents. A Cochrane Review on the tolerability of chemoprophylactic agents concluded that atovaquone-proguanil and doxycycline were better tolerated than mefloquine (SOR: B). Compared with mefloquine, atovaquone-proguanil led to fewer reports of any adverse effects (relative risk [RR]=0.72), gastrointestinal adverse effects (RR=0.54), and neuropsychiatric adverse events (RR= 0.49-0.86, depending on the studies).23 Doxycycline users have reported fewer neuropsychiatric events (RR=0.84) than mefloquine users.23 These are relatively small differences, and the authors point out that these figures are based on low-quality evidence. Additional research is likely to have an impact on the confidence in the estimate of effect and to ultimately change the estimate.
Mefloquine is contraindicated in travelers with seizures, active or recent history of depression, generalized anxiety disorder, psychosis, schizophrenia, or other psychiatric disorders. Compared with mefloquine, atovaquone-proguanil and doxycycline cause fewer neuropsychiatric adverse effects (such as vivid dreams, dizziness, anxiety, depression, visual disturbance, or seizures).24 Caution is advised when prescribing chloroquine for patients with epilepsy because the medication has the potential to lower the seizure threshold.25
Use caution when prescribing mefloquine for patients with cardiac conduction disturbances. Electrocardiogram alterations such as sinus bradycardia, first-degree AV block, prolongation of QTc intervals, and abnormal T wave changes have been reported.26 Chloroquine can also prolong QTc intervals.26
Safety in pregnancy and breastfeeding. Malaria in pregnancy is associated with increased rates of anemia, low birth weight, prematurity, intrauterine growth restriction, and infant mortality.27 Chloroquine and mefloquine are considered safe during pregnancy and breastfeeding. Doxycycline has been associated with increased risk of harm to the fetus. Atovaquone-proguanil can be used in breastfeeding women if the child is ≥5 kg (≥11 lbs). Chemoprophylaxis taken by the mother while breastfeeding does not protect the infant from infection.
Dosing considerations. Mefloquine and chloroquine are dosed weekly; doxycycline and atovaquone-proguanil are taken daily. Travelers staying in a malaria-endemic region for longer periods (months rather than weeks) often prefer the weekly rather than daily medications; however, this may not be possible due to the adverse-effect profile of mefloquine or to traveling in an area with known chloroquine resistance. Some individuals prefer the routine of taking a medication daily, since remembering to take a single dose on the same day each week can be challenging. Others may not want to carry a large number of pills and therefore prefer weekly dosing. Have patients take medications before the trip, to assess tolerability and to ensure adequate blood concentrations before exposure.
Because mefloquine, doxycycline, and chloroquine target only the blood stages of Plasmodium, patients must continue these medications for 4 weeks following the exposure period to ensure adequate coverage as parasites are released from the liver. Because doxycycline is taken daily and has to be continued for 4 weeks following the exposure period, the total number of pills taken is higher for this regimen. Atovaquone-proguanil is active against hepatic and blood stages and can be discontinued a week following the exposure period.
With children, base dosing on body weight and do not exceed the recommended adult dose. When fractions of tablets are used (such as with mefloquine and atovaquone-proguanil dosing), pharmacists can crush tablets and place divided doses in capsules, to be sprinkled as needed into food such as applesauce or jelly. Mefloquine and chloroquine can be given to children of all ages and weights. Although atovaquone-proguanil is approved only for children ≥11 kg (24 lbs), dosing schedules have been calculated for children who weigh ≥5 kg.21 Doxycycline is recommended only for children who are at least 8 years of age.
Cost. For a 2-week exposure period, chloroquine is the least expensive medication (although regions in which it is recommended are limited due to resistance) (TABLE 27,25,26).
Ask about accommodations
Since Anopheles mosquitoes feed between dusk and dawn, inquiring about accommodations can further clarify a patient’s malaria risk. Staying in air-conditioned housing (implying that the interior can be sealed) or that has screened windows can reduce exposure to mosquitoes, although data are lacking regarding whether the latter practice reduces the incidence of malaria transmission28 (SOR: C).
Share decision making
After considering the key factors determining a patient’s level of risk, you may decide to recommend no specific interventions, to advise insect avoidance measures only, to combine insect avoidance with chemoprophylaxis, or to caution against traveling to a malaria-endemic region. The patient’s contribution to the final decision includes personal preferences, values, and risk tolerance—particularly when comorbidities are involved.
When preventive measures fail
Approximately 0.2% of travelers to malaria-endemic regions will become infected, despite proper pre-travel counseling and prophylaxis.29 In the United States, malaria is often misdiagnosed or improperly treated.30 The time from initial presentation to correct diagnosis of malaria has been reported as an astonishingly high 4 to 8.5 days, depending on the population.31,32
A high index of suspicion is needed and will ensure timely care when any febrile traveler returns from a malaria-endemic area.33 Be sure to advise patients to seek medical attention if they are feverish upon returning home.
Once suspected, the diagnosis of malaria can be readily confirmed through the use of antibody-, nucleic acid-, or microscopy-based techniques (the latter to directly visualize Plasmodium species in blood smears).
Although malaria chemoprophylaxis is relatively straightforward, malaria treatment—especially in cases of chemoprophylaxis failures—may not be, and the topic is beyond the scope of this article. For guidance on treating malaria, consult a knowledgeable physician or contact the CDC at www.cdc.gov/malaria/, or at (855) 856-4713 (weekdays, 9 am to 5 pm EST) or (770) 488-7100 (weekends or after normal business hours; ask for the Malaria Branch clinician on call).
CORRESPONDENCE
Mark K. Huntington, MD, PhD, Center for Family Medicine, 1115 East 20th Street, Sioux Falls, SD 57105; [email protected]
› Assess the need for nonpharmacologic, behavioral interventions and for chemoprophylaxis based on a destination’s relative risk to travelers, planned and potential activities, and patient comorbidities. B
› Choose an antimalarial medication based on knowledge of area-specific drug effectiveness or resistance patterns, trip duration, drug cost, tolerance for adverse effects, and comorbidities. C
› Presume a diagnosis of malaria until proven otherwise in any traveler who is febrile after returning from a malaria-endemic region. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Although malaria was eradicated as an endemic disease in the United States in the early 1950s,1 it still returns yearly in approximately 1500 individuals who travel to foreign countries2—most of whom neglected to use prophylactic measures or use them properly.3 In more than 60 documented cases, these infected individuals have been the source of local transmission in their communities.2 To reduce the individual and public health risks associated with malaria, this article focuses on steps that international travelers can take to limit their risk of the disease.
What travelers need to know
In 2013, more than 61.5 million residents of the United States traveled abroad, approximately 30% of whom visited malaria-endemic regions: Mexico and equatorial nations in Central and South America; Africa; the Middle East; and South, East, and Southeast Asia.4 Counseling on appropriate preventive measures fits the Medical Home concept of comprehensive, preventive, patient-centered care, and pre-travel consultation—including a review of health data and itineraries, and patient education—can be a team-based effort.5
Begin your planning for malaria prophylaxis by assessing your patient’s individual risk. Key variables are a patient’s detailed itinerary, a credible and current source of information on location-specific malaria prevalence, personal risk factors, and risk tolerance. Shared decision-making is vital and enhances adherence to the prescribed regimen.
Endemicity varies regionally. Without chemoprophylaxis, risk of infection ranges from more than 20% in Papua New Guinea to 0.01% in Central America, with wide exposure risk variations likely, even within regions.6 Travel to areas of high endemicity requires more aggressive malaria prevention strategies than travel to low-endemicity regions.
Risk of exposure is lower with short visits,7 business-only travel, urban-only stays in some countries, day trips to endemic areas,7 and travel during seasons with lower mosquito burden. Likewise, travelers staying in a hotel with sealed windows will face lower nighttime Anopheles mosquito exposure. In these cases, nonpharmacologic measures alone may be appropriate.
Those at particularly high risk for complicated or lethal malarial infection are children, pregnant women, elderly individuals, and immunocompromised patients.7 In addition to counseling high-risk patients about prophylactic measures, consider advising against travel in certain circumstances. Among those at highest risk for acquiring malaria are immigrants and refugees traveling to their ancestral homelands to visit friends and relatives (VFR).2 Many VFR travelers fail to take appropriate prophylactic measures when “going home.”8 A significant number of cases of travel-acquired malaria occurs in VFR children.9
Individualizing prevention directives
The mainstays of malaria prevention include nonpharmacologic and behavioral interventions, as well as chemoprophylaxis. Most cases of malaria in travelers returning to the United States result from the improper implementation of prophylactic measures.3 Discussing individual risk with travelers is an easy way to bolster adherence to malaria prevention measures, and some evidence suggests it is effective10 (strength of recommendation [SOR]: C). Other limited studies have also shown that malaria education can improve knowledge about malaria transmission and increase the likelihood that preventive measures will be used.11,12
Recommend nonpharmacologic measures even for those using chemoprophylaxis
Nonpharmacologic interventions such as sleeping under permethrin-treated bednets, wearing long sleeves and full-length pants, treating clothes with permethrin, and applying DEET (N,N-diethyl-meta-toluamide) to exposed skin are effective and have the added benefit of preventing non-malarial arthropod-borne diseases4 (SOR: B). Studies have shown that, compared with sleeping without nets, the use of insecticide treated-nets can reduce child mortality by 17% and the incidence of uncomplicated malarial episodes by 50%.13 In areas with malaria transmission, 10% to 30% DEET—used alone or in combination with permethrin-treated clothing— can reduce bite load, although the American Academy of Pediatrics recommends against using DEET in children younger than 2 months of age.14,15
Using these measures in combination from dusk to dawn, when Anopheles mosquitoes are active, has been shown to be effective, although randomized, controlled studies are lacking.16 Remaining indoors during these peak biting periods is also advisable. In certain areas, and with the right itinerary, the traveler may only need to employ nonpharmacologic methods of preventing malarial infection. Recommend them to all patients traveling to malarial regions, even to individuals using pharmacologic prophylaxis.
Factors determining the need for, and selection of, chemoprophylaxis
When used properly, chemoprophylactic drugs are effective in preventing malaria (SOR: A). Atovaquone-proguanil achieves efficacy of 95% to 100%,17 while doxycycline, primaquine, and mefloquine are slightly less effective.18-20 Chloroquine is effective in 6 regions of the tropics and subtropics where Plasmodium falciparum resistance has not developed. Select a drug based on your assessment of an individual’s level of risk according to the personal itinerary, trip duration and accommodations, cost of medication, tolerance for adverse effects, and other factors (eg, comorbidities, concurrent drug usage, pregnancy).
Location matters. The risk of malaria transmission can vary considerably not only between countries, but also regionally within countries and even between a city and its immediate surroundings. Therefore, select a chemoprophylactic agent based on the specific itinerary, planned activities, the potential for unforeseen additional excursions, and local Plasmodium resistance patterns. For example, chloroquine is effective only in the Caribbean, Central America, and some countries in the Middle East.21 Mefloquine resistance has been reported in parts of Cambodia, Thailand, Vietnam, Burma, China, and Laos.21
On its Travelers’ Health Web site (www.cdc.gov/travel), the Centers for Disease Control and Prevention (CDC) reports for each country 1) the risk of malaria transmission, 2) areas within the country that pose a risk, 3) evidence of Plasmodium drug resistance, 4) which Plasmodium species are active, and 5) which chemoprophylactic medications are recommended.22 Additional Web sites, either free or subscription-based, allow users to view this same information on maps, advise on where insect precautions alone are sufficiently protective, and provide information about the traveler’s risk of contracting other diseases (TABLE 1).
TABLE 1
| Web resources on infectious diseases of concern to international travelers | |
| Resource | Notes |
Centers for Disease Control and Prevention | Free Site Go to Yellow Book » Contents » Chapter 3 » “Travel Vaccines & Malaria Information, by Country” for country-specific information about the risk of malaria transmission |
VHI Healthcare | Free Site Destination-specific information about travel alerts and vaccine recommendations Does not report malaria transmission data |
Gideon | Subscription only Online application that helps with diagnosing infectious diseases and keeping up to date with global health literature |
Travax | Subscription only Information about recommended vaccines and country-specific risk of malaria transmission |
Tropimed | Subscription only Information about recommended vaccines and country-specific risk of malaria transmission |
Comparative adverse effects of antimalarial agents. A Cochrane Review on the tolerability of chemoprophylactic agents concluded that atovaquone-proguanil and doxycycline were better tolerated than mefloquine (SOR: B). Compared with mefloquine, atovaquone-proguanil led to fewer reports of any adverse effects (relative risk [RR]=0.72), gastrointestinal adverse effects (RR=0.54), and neuropsychiatric adverse events (RR= 0.49-0.86, depending on the studies).23 Doxycycline users have reported fewer neuropsychiatric events (RR=0.84) than mefloquine users.23 These are relatively small differences, and the authors point out that these figures are based on low-quality evidence. Additional research is likely to have an impact on the confidence in the estimate of effect and to ultimately change the estimate.
Mefloquine is contraindicated in travelers with seizures, active or recent history of depression, generalized anxiety disorder, psychosis, schizophrenia, or other psychiatric disorders. Compared with mefloquine, atovaquone-proguanil and doxycycline cause fewer neuropsychiatric adverse effects (such as vivid dreams, dizziness, anxiety, depression, visual disturbance, or seizures).24 Caution is advised when prescribing chloroquine for patients with epilepsy because the medication has the potential to lower the seizure threshold.25
Use caution when prescribing mefloquine for patients with cardiac conduction disturbances. Electrocardiogram alterations such as sinus bradycardia, first-degree AV block, prolongation of QTc intervals, and abnormal T wave changes have been reported.26 Chloroquine can also prolong QTc intervals.26
Safety in pregnancy and breastfeeding. Malaria in pregnancy is associated with increased rates of anemia, low birth weight, prematurity, intrauterine growth restriction, and infant mortality.27 Chloroquine and mefloquine are considered safe during pregnancy and breastfeeding. Doxycycline has been associated with increased risk of harm to the fetus. Atovaquone-proguanil can be used in breastfeeding women if the child is ≥5 kg (≥11 lbs). Chemoprophylaxis taken by the mother while breastfeeding does not protect the infant from infection.
Dosing considerations. Mefloquine and chloroquine are dosed weekly; doxycycline and atovaquone-proguanil are taken daily. Travelers staying in a malaria-endemic region for longer periods (months rather than weeks) often prefer the weekly rather than daily medications; however, this may not be possible due to the adverse-effect profile of mefloquine or to traveling in an area with known chloroquine resistance. Some individuals prefer the routine of taking a medication daily, since remembering to take a single dose on the same day each week can be challenging. Others may not want to carry a large number of pills and therefore prefer weekly dosing. Have patients take medications before the trip, to assess tolerability and to ensure adequate blood concentrations before exposure.
Because mefloquine, doxycycline, and chloroquine target only the blood stages of Plasmodium, patients must continue these medications for 4 weeks following the exposure period to ensure adequate coverage as parasites are released from the liver. Because doxycycline is taken daily and has to be continued for 4 weeks following the exposure period, the total number of pills taken is higher for this regimen. Atovaquone-proguanil is active against hepatic and blood stages and can be discontinued a week following the exposure period.
With children, base dosing on body weight and do not exceed the recommended adult dose. When fractions of tablets are used (such as with mefloquine and atovaquone-proguanil dosing), pharmacists can crush tablets and place divided doses in capsules, to be sprinkled as needed into food such as applesauce or jelly. Mefloquine and chloroquine can be given to children of all ages and weights. Although atovaquone-proguanil is approved only for children ≥11 kg (24 lbs), dosing schedules have been calculated for children who weigh ≥5 kg.21 Doxycycline is recommended only for children who are at least 8 years of age.
Cost. For a 2-week exposure period, chloroquine is the least expensive medication (although regions in which it is recommended are limited due to resistance) (TABLE 27,25,26).
Ask about accommodations
Since Anopheles mosquitoes feed between dusk and dawn, inquiring about accommodations can further clarify a patient’s malaria risk. Staying in air-conditioned housing (implying that the interior can be sealed) or that has screened windows can reduce exposure to mosquitoes, although data are lacking regarding whether the latter practice reduces the incidence of malaria transmission28 (SOR: C).
Share decision making
After considering the key factors determining a patient’s level of risk, you may decide to recommend no specific interventions, to advise insect avoidance measures only, to combine insect avoidance with chemoprophylaxis, or to caution against traveling to a malaria-endemic region. The patient’s contribution to the final decision includes personal preferences, values, and risk tolerance—particularly when comorbidities are involved.
When preventive measures fail
Approximately 0.2% of travelers to malaria-endemic regions will become infected, despite proper pre-travel counseling and prophylaxis.29 In the United States, malaria is often misdiagnosed or improperly treated.30 The time from initial presentation to correct diagnosis of malaria has been reported as an astonishingly high 4 to 8.5 days, depending on the population.31,32
A high index of suspicion is needed and will ensure timely care when any febrile traveler returns from a malaria-endemic area.33 Be sure to advise patients to seek medical attention if they are feverish upon returning home.
Once suspected, the diagnosis of malaria can be readily confirmed through the use of antibody-, nucleic acid-, or microscopy-based techniques (the latter to directly visualize Plasmodium species in blood smears).
Although malaria chemoprophylaxis is relatively straightforward, malaria treatment—especially in cases of chemoprophylaxis failures—may not be, and the topic is beyond the scope of this article. For guidance on treating malaria, consult a knowledgeable physician or contact the CDC at www.cdc.gov/malaria/, or at (855) 856-4713 (weekdays, 9 am to 5 pm EST) or (770) 488-7100 (weekends or after normal business hours; ask for the Malaria Branch clinician on call).
CORRESPONDENCE
Mark K. Huntington, MD, PhD, Center for Family Medicine, 1115 East 20th Street, Sioux Falls, SD 57105; [email protected]
1. Mali S, Steele S, Slutsker L, et al; Centers for Disease Control and Prevention (CDC). Malaria surveillance - United States, 2008. MMWR Surveill Summ. 2010;59:1-15.
2. Centers for Disease Control and Prevention. Malaria facts. Centers for Disease Control and Prevention Web site. Available at: www.cdc.gov/malaria/about/facts.html. Accessed September 29, 2014.
3. Huntington MK. Healthy people, malaria and South Dakota. S D Med. 2012;65:297-300.
4. Office of Travel and Tourism Industries. U.S. citizen travel to international regions, 2013. Office of Travel and Tourism Industries Web site. Available at: http://travel.trade.gov/view/m-2013-O-001/index.html. Accessed September 29, 2014.
5. Bazemore AW, Huntington M. The pretravel consultation. Am Fam Physician. 2009;80:583-590.
6. Bradley DJ, Warhurst DC, Blaze M, et al. Malaria imported into the United Kingdom in 1996. Euro Surveill. 1998;3:40-42.
7. Arguin PM, Tan KR, et al; Centers for Disease Control and Prevention. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/malaria. Accessed October 15, 2014.
8. Pavli A, Maltezou HC. Malaria and travellers visiting friends and relatives. Travel Med Infect Dis. 2010;8:161-168.
9. Stäger K, Legros F, Krause G, et al. Imported malaria in children in industrialized countries, 1992-2002. Emerg Infect Dis. 2009;15:185-191.
10. Hartjes LB, Baumann LC, Henriques JB. Travel health risk perceptions and prevention behaviors of US study abroad students. J Travel Med. 2009;16:338-343.
11. Kishore J, Gupta VK, Singh SV, et al. Impact of health education intervention on knowledge and community action for malaria control in Delhi. J Commun Dis. 2008;40:183-192.
12. Chirdan OO, Zoakah AI, Ejembi CL. Impact of health education on home treatment and prevention of malaria in Jengre, North Central Nigeria. Ann Afr Med. 2008;7:112-119.
13. Lengeler C. Insecticide-treated bed nets and curtains for preventing malaria. Cochrane Database Syst Rev. 2004;(2): CD000363.
14. Centers for Disease Control and Prevention. Fight the bite for protection from malaria: Guidelines for DEET insect repellent use. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/malaria/toolkit/DEET.pdf. Accessed September 29, 2014.
15. American Academy of Pediatrics. Safety & prevention. Healthychildren.org Web site. Available at: http://www.healthychildren. org/English/safety-prevention/at-play/Pages/Insect-Repellents. aspx. Accessed September 29, 2014.
16. Croft AM, Baker D, von Bertele MJ. An evidence-based vector control strategy for military deployments: the British Army experience. Med Trop (Mars). 2001;61:91-98.
17. Boggild AK, Parise ME, Lewis LS, et al. Atovaquone-proguanil: report from the CDC expert meeting on malaria chemoprophylaxis (II). Am J Trop Med Hyg. 2007;76:208-223.
18. Tan KR, Magill AJ, Parise ME, et al; Centers for Disease Control and Prevention. Doxycycline for malaria chemoprophylaxis and treatment: report from the CDC expert meeting on malaria chemoprophylaxis. Am J Trop Med Hyg. 2011;84:517-531.
19. Hill DR, Baird JK, Parise ME, et al. Primaquine: report from CDC expert meeting on malaria chemoprophylaxis I. Am J Trop Med Hyg. 2006;75:402-415.
20. Steffen R, Fuchs E, Schildknecht J, et al. Mefloquine compared with other malaria chemoprophylactic regimens in tourists visiting east Africa. Lancet. 1993;341:1299-1303.
21. Centers for Disease Control and Prevention. CDC Health Information for International Travel 2014. New York, NY: Oxford University Press; 2014.
22. Gershman MD, Jentes ES, Johnson KJ, et al; Centers for Disease Control and Prevention. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-3- infectious-diseases-related-to-travel/yellow-fever-and-malaria- information-by-country.htm. Accessed September 29, 2014.
23. Jacquerioz FA, Croft AM. Drugs for preventing malaria in travellers. Cochrane Database Syst Rev. 2009;(4):CD006491.
24. Schlagenhauf P, Tschopp A, Johnson R, et al. Tolerability of malaria chemoprophylaxis in non-immune travellers to sub-Saharan Africa: multicentre, randomised, double blind, four arm study. BMJ. 2003;327:1078.
25. Chloroquine phosphate [package insert]. Eatontown, NJ: Westward Pharmaceutical Corp; 2010.
26. Lariam [package insert]. Roche Laboratories, Inc: Nutley, NJ; 2004.
27. Steketee RW, Nahlen BL, Parise ME, et al. The burden of malaria in pregnancy in malaria-endemic areas. Am J Trop Med Hyg. 2001;64(1-2 suppl):28-35.
28. Kirby MJ, Ameh D, Bottomley C, et al. Effect of two different house screening interventions on exposure to malaria vectors and on anaemia in children in The Gambia: a randomised controlled trial. Lancet. 2009;374:998-1009.
29. Steffen R, Amitirigala I, Mutsch M. Health risks among travelers--need for regular updates. J Travel Med. 2008;15:145-146.
30. Dorsey G, Gandhi M, Oyugi JH, et al. Difficulties in the prevention, diagnosis, and treatment of imported malaria. Arch Intern Med. 2000;160:2505-2510.
31. Newman RD, Parise ME, Barber AM, et al. Malaria-related deaths among U.S. travelers, 1963-2001. Ann Intern Med. 2004;141: 547-555.
32. Lesko CR, Arguin PM, Newman RD. Congenital malaria in the United States: a review of cases from 1966 to 2005. Arch Pediatr Adolesc Med. 2007;161:1062-1067.
33. Blair JE. Evaluation of fever in the international traveler. Unwanted ‘souvenir’ can have many causes. Postgrad Med. 2004;116: 13-20,29.
1. Mali S, Steele S, Slutsker L, et al; Centers for Disease Control and Prevention (CDC). Malaria surveillance - United States, 2008. MMWR Surveill Summ. 2010;59:1-15.
2. Centers for Disease Control and Prevention. Malaria facts. Centers for Disease Control and Prevention Web site. Available at: www.cdc.gov/malaria/about/facts.html. Accessed September 29, 2014.
3. Huntington MK. Healthy people, malaria and South Dakota. S D Med. 2012;65:297-300.
4. Office of Travel and Tourism Industries. U.S. citizen travel to international regions, 2013. Office of Travel and Tourism Industries Web site. Available at: http://travel.trade.gov/view/m-2013-O-001/index.html. Accessed September 29, 2014.
5. Bazemore AW, Huntington M. The pretravel consultation. Am Fam Physician. 2009;80:583-590.
6. Bradley DJ, Warhurst DC, Blaze M, et al. Malaria imported into the United Kingdom in 1996. Euro Surveill. 1998;3:40-42.
7. Arguin PM, Tan KR, et al; Centers for Disease Control and Prevention. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/malaria. Accessed October 15, 2014.
8. Pavli A, Maltezou HC. Malaria and travellers visiting friends and relatives. Travel Med Infect Dis. 2010;8:161-168.
9. Stäger K, Legros F, Krause G, et al. Imported malaria in children in industrialized countries, 1992-2002. Emerg Infect Dis. 2009;15:185-191.
10. Hartjes LB, Baumann LC, Henriques JB. Travel health risk perceptions and prevention behaviors of US study abroad students. J Travel Med. 2009;16:338-343.
11. Kishore J, Gupta VK, Singh SV, et al. Impact of health education intervention on knowledge and community action for malaria control in Delhi. J Commun Dis. 2008;40:183-192.
12. Chirdan OO, Zoakah AI, Ejembi CL. Impact of health education on home treatment and prevention of malaria in Jengre, North Central Nigeria. Ann Afr Med. 2008;7:112-119.
13. Lengeler C. Insecticide-treated bed nets and curtains for preventing malaria. Cochrane Database Syst Rev. 2004;(2): CD000363.
14. Centers for Disease Control and Prevention. Fight the bite for protection from malaria: Guidelines for DEET insect repellent use. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/malaria/toolkit/DEET.pdf. Accessed September 29, 2014.
15. American Academy of Pediatrics. Safety & prevention. Healthychildren.org Web site. Available at: http://www.healthychildren. org/English/safety-prevention/at-play/Pages/Insect-Repellents. aspx. Accessed September 29, 2014.
16. Croft AM, Baker D, von Bertele MJ. An evidence-based vector control strategy for military deployments: the British Army experience. Med Trop (Mars). 2001;61:91-98.
17. Boggild AK, Parise ME, Lewis LS, et al. Atovaquone-proguanil: report from the CDC expert meeting on malaria chemoprophylaxis (II). Am J Trop Med Hyg. 2007;76:208-223.
18. Tan KR, Magill AJ, Parise ME, et al; Centers for Disease Control and Prevention. Doxycycline for malaria chemoprophylaxis and treatment: report from the CDC expert meeting on malaria chemoprophylaxis. Am J Trop Med Hyg. 2011;84:517-531.
19. Hill DR, Baird JK, Parise ME, et al. Primaquine: report from CDC expert meeting on malaria chemoprophylaxis I. Am J Trop Med Hyg. 2006;75:402-415.
20. Steffen R, Fuchs E, Schildknecht J, et al. Mefloquine compared with other malaria chemoprophylactic regimens in tourists visiting east Africa. Lancet. 1993;341:1299-1303.
21. Centers for Disease Control and Prevention. CDC Health Information for International Travel 2014. New York, NY: Oxford University Press; 2014.
22. Gershman MD, Jentes ES, Johnson KJ, et al; Centers for Disease Control and Prevention. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-3- infectious-diseases-related-to-travel/yellow-fever-and-malaria- information-by-country.htm. Accessed September 29, 2014.
23. Jacquerioz FA, Croft AM. Drugs for preventing malaria in travellers. Cochrane Database Syst Rev. 2009;(4):CD006491.
24. Schlagenhauf P, Tschopp A, Johnson R, et al. Tolerability of malaria chemoprophylaxis in non-immune travellers to sub-Saharan Africa: multicentre, randomised, double blind, four arm study. BMJ. 2003;327:1078.
25. Chloroquine phosphate [package insert]. Eatontown, NJ: Westward Pharmaceutical Corp; 2010.
26. Lariam [package insert]. Roche Laboratories, Inc: Nutley, NJ; 2004.
27. Steketee RW, Nahlen BL, Parise ME, et al. The burden of malaria in pregnancy in malaria-endemic areas. Am J Trop Med Hyg. 2001;64(1-2 suppl):28-35.
28. Kirby MJ, Ameh D, Bottomley C, et al. Effect of two different house screening interventions on exposure to malaria vectors and on anaemia in children in The Gambia: a randomised controlled trial. Lancet. 2009;374:998-1009.
29. Steffen R, Amitirigala I, Mutsch M. Health risks among travelers--need for regular updates. J Travel Med. 2008;15:145-146.
30. Dorsey G, Gandhi M, Oyugi JH, et al. Difficulties in the prevention, diagnosis, and treatment of imported malaria. Arch Intern Med. 2000;160:2505-2510.
31. Newman RD, Parise ME, Barber AM, et al. Malaria-related deaths among U.S. travelers, 1963-2001. Ann Intern Med. 2004;141: 547-555.
32. Lesko CR, Arguin PM, Newman RD. Congenital malaria in the United States: a review of cases from 1966 to 2005. Arch Pediatr Adolesc Med. 2007;161:1062-1067.
33. Blair JE. Evaluation of fever in the international traveler. Unwanted ‘souvenir’ can have many causes. Postgrad Med. 2004;116: 13-20,29.