User login
Clinical Psychiatry News is the online destination and multimedia properties of Clinica Psychiatry News, the independent news publication for psychiatrists. Since 1971, Clinical Psychiatry News has been the leading source of news and commentary about clinical developments in psychiatry as well as health care policy and regulations that affect the physician's practice.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
ketamine
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
suicide
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-cpn')]
div[contains(@class, 'pane-pub-home-cpn')]
div[contains(@class, 'pane-pub-topic-cpn')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Most children with ADHD are not receiving treatment
Just more than one-third (34.8%) had received either treatment.
Researchers, led by Mark Olfson, MD, MPH, Elizabeth K. Dollard Professor of Psychiatry, Medicine and Law and professor of epidemiology at New York State Psychiatric Institute and Columbia University Department of Psychiatry, New York, also found that girls were much less likely to get medications.

In this cross-sectional sample taken from 11, 723 children in the Adolescent Brain and Cognitive Development Study, 1,206 children aged 9 and 10 years had parent-reported ADHD, and of those children, 15.7% of boys and 7% of girls were currently receiving ADHD medications. The parents reported the children met ADHD criteria according to the Diagnostic and Statistical Manual of Mental Disorders.
Findings were published online in JAMA Network Open.
Diagnoses have doubled but treatment numbers lag
Report authors noted that the percentage of U.S. children whose parents report their child has been diagnosed with ADHD has nearly doubled over 2 decades from 5.5% in 1999 to 9.8% in 2018. That has led to misperceptions among professionals and the public that the disorder is overdiagnosed and overtreated, the authors wrote.
However, they wrote, “a focus on the increasing numbers of children treated for ADHD does not give a sense of what fraction of children in the population with ADHD receive treatment.”
Higher uptake at lower income and education levels
Researchers also found that, contrary to popular belief, children with ADHD from families with lower educational levels and lower income were more likely than those with higher educational levels and higher incomes to have received outpatient mental health care.
Among children with ADHD whose parents did not have a high school education, 32.2% of children were receiving medications while among children of parents with a bachelor’s degree 11.5% received medications.
Among children from families with incomes of less than $25 000, 36.5% were receiving outpatient mental health care, compared with 20.1% of those from families with incomes of $75,000 or more.
“These patterns suggest that attitudinal rather than socioeconomic factors often impede the flow of children with ADHD into treatment,” they wrote.
Black children less likely to receive medications
The researchers found that substantially more White children (14.8% [104 of 759]) than Black children (9.4% [22 of 206]), received medication, a finding consistent with previous research.
“Population-based racial and ethnic gradients exist in prescriptions for stimulants and other controlled substances, with the highest rates in majority-White areas,” the authors wrote. “As a result of structural racism, Black parents’ perspectives might further influence ADHD management decisions through mistrust in clinicians and concerns over safety and efficacy of stimulants.”
“Physician efforts to recognize and manage their own implicit biases, together with patient-centered clinical approaches that promote shared decision-making,” might help narrow the treatment gap, the authors wrote. That includes talking with Black parents about their knowledge and beliefs concerning managing ADHD, they added.
Confirming diagnosis critical
The authors noted that not all children with parent-reported ADHD need treatment or would benefit from it.
Lenard Adler, MD, director of the adult ADHD program and professor of Psychiatry and Child and Adolescent Psychiatry at New York University Langone Health, who was not part of the current study, said this research emphasizes the urgency of clinical diagnosis.
Dr. Adler was part of a team of researchers that found similar low numbers for treatment among adults with ADHD.
The current results highlight that “we want to get the diagnosis correct so that people who receive a diagnosis actually have it and, if they do, that they have access to care. Because the consequences for not having treatment for ADHD are significant,” Dr. Adler said.
He urged physicians who diagnose ADHD to make follow-up part of the care plan or these treatment gaps will persist.
The authors wrote that the results suggest a need to increase availability for mental health services and better communicate symptoms among parents, teachers, and primary care providers.
The authors declare no relevant financial relationships. Dr. Adler has consulted with Supernus Pharmaceuticals and Otsuka Pharmaceuticals, has done research with Takeda, and has received royalty payments from NYU for licensing of ADHD training materials.
Just more than one-third (34.8%) had received either treatment.
Researchers, led by Mark Olfson, MD, MPH, Elizabeth K. Dollard Professor of Psychiatry, Medicine and Law and professor of epidemiology at New York State Psychiatric Institute and Columbia University Department of Psychiatry, New York, also found that girls were much less likely to get medications.
In this cross-sectional sample taken from 11, 723 children in the Adolescent Brain and Cognitive Development Study, 1,206 children aged 9 and 10 years had parent-reported ADHD, and of those children, 15.7% of boys and 7% of girls were currently receiving ADHD medications. The parents reported the children met ADHD criteria according to the Diagnostic and Statistical Manual of Mental Disorders.
Findings were published online in JAMA Network Open.
Diagnoses have doubled but treatment numbers lag
Report authors noted that the percentage of U.S. children whose parents report their child has been diagnosed with ADHD has nearly doubled over 2 decades from 5.5% in 1999 to 9.8% in 2018. That has led to misperceptions among professionals and the public that the disorder is overdiagnosed and overtreated, the authors wrote.
However, they wrote, “a focus on the increasing numbers of children treated for ADHD does not give a sense of what fraction of children in the population with ADHD receive treatment.”
Higher uptake at lower income and education levels
Researchers also found that, contrary to popular belief, children with ADHD from families with lower educational levels and lower income were more likely than those with higher educational levels and higher incomes to have received outpatient mental health care.
Among children with ADHD whose parents did not have a high school education, 32.2% of children were receiving medications while among children of parents with a bachelor’s degree 11.5% received medications.
Among children from families with incomes of less than $25 000, 36.5% were receiving outpatient mental health care, compared with 20.1% of those from families with incomes of $75,000 or more.
“These patterns suggest that attitudinal rather than socioeconomic factors often impede the flow of children with ADHD into treatment,” they wrote.
Black children less likely to receive medications
The researchers found that substantially more White children (14.8% [104 of 759]) than Black children (9.4% [22 of 206]), received medication, a finding consistent with previous research.
“Population-based racial and ethnic gradients exist in prescriptions for stimulants and other controlled substances, with the highest rates in majority-White areas,” the authors wrote. “As a result of structural racism, Black parents’ perspectives might further influence ADHD management decisions through mistrust in clinicians and concerns over safety and efficacy of stimulants.”
“Physician efforts to recognize and manage their own implicit biases, together with patient-centered clinical approaches that promote shared decision-making,” might help narrow the treatment gap, the authors wrote. That includes talking with Black parents about their knowledge and beliefs concerning managing ADHD, they added.
Confirming diagnosis critical
The authors noted that not all children with parent-reported ADHD need treatment or would benefit from it.
Lenard Adler, MD, director of the adult ADHD program and professor of Psychiatry and Child and Adolescent Psychiatry at New York University Langone Health, who was not part of the current study, said this research emphasizes the urgency of clinical diagnosis.
Dr. Adler was part of a team of researchers that found similar low numbers for treatment among adults with ADHD.
The current results highlight that “we want to get the diagnosis correct so that people who receive a diagnosis actually have it and, if they do, that they have access to care. Because the consequences for not having treatment for ADHD are significant,” Dr. Adler said.
He urged physicians who diagnose ADHD to make follow-up part of the care plan or these treatment gaps will persist.
The authors wrote that the results suggest a need to increase availability for mental health services and better communicate symptoms among parents, teachers, and primary care providers.
The authors declare no relevant financial relationships. Dr. Adler has consulted with Supernus Pharmaceuticals and Otsuka Pharmaceuticals, has done research with Takeda, and has received royalty payments from NYU for licensing of ADHD training materials.
Just more than one-third (34.8%) had received either treatment.
Researchers, led by Mark Olfson, MD, MPH, Elizabeth K. Dollard Professor of Psychiatry, Medicine and Law and professor of epidemiology at New York State Psychiatric Institute and Columbia University Department of Psychiatry, New York, also found that girls were much less likely to get medications.
In this cross-sectional sample taken from 11, 723 children in the Adolescent Brain and Cognitive Development Study, 1,206 children aged 9 and 10 years had parent-reported ADHD, and of those children, 15.7% of boys and 7% of girls were currently receiving ADHD medications. The parents reported the children met ADHD criteria according to the Diagnostic and Statistical Manual of Mental Disorders.
Findings were published online in JAMA Network Open.
Diagnoses have doubled but treatment numbers lag
Report authors noted that the percentage of U.S. children whose parents report their child has been diagnosed with ADHD has nearly doubled over 2 decades from 5.5% in 1999 to 9.8% in 2018. That has led to misperceptions among professionals and the public that the disorder is overdiagnosed and overtreated, the authors wrote.
However, they wrote, “a focus on the increasing numbers of children treated for ADHD does not give a sense of what fraction of children in the population with ADHD receive treatment.”
Higher uptake at lower income and education levels
Researchers also found that, contrary to popular belief, children with ADHD from families with lower educational levels and lower income were more likely than those with higher educational levels and higher incomes to have received outpatient mental health care.
Among children with ADHD whose parents did not have a high school education, 32.2% of children were receiving medications while among children of parents with a bachelor’s degree 11.5% received medications.
Among children from families with incomes of less than $25 000, 36.5% were receiving outpatient mental health care, compared with 20.1% of those from families with incomes of $75,000 or more.
“These patterns suggest that attitudinal rather than socioeconomic factors often impede the flow of children with ADHD into treatment,” they wrote.
Black children less likely to receive medications
The researchers found that substantially more White children (14.8% [104 of 759]) than Black children (9.4% [22 of 206]), received medication, a finding consistent with previous research.
“Population-based racial and ethnic gradients exist in prescriptions for stimulants and other controlled substances, with the highest rates in majority-White areas,” the authors wrote. “As a result of structural racism, Black parents’ perspectives might further influence ADHD management decisions through mistrust in clinicians and concerns over safety and efficacy of stimulants.”
“Physician efforts to recognize and manage their own implicit biases, together with patient-centered clinical approaches that promote shared decision-making,” might help narrow the treatment gap, the authors wrote. That includes talking with Black parents about their knowledge and beliefs concerning managing ADHD, they added.
Confirming diagnosis critical
The authors noted that not all children with parent-reported ADHD need treatment or would benefit from it.
Lenard Adler, MD, director of the adult ADHD program and professor of Psychiatry and Child and Adolescent Psychiatry at New York University Langone Health, who was not part of the current study, said this research emphasizes the urgency of clinical diagnosis.
Dr. Adler was part of a team of researchers that found similar low numbers for treatment among adults with ADHD.
The current results highlight that “we want to get the diagnosis correct so that people who receive a diagnosis actually have it and, if they do, that they have access to care. Because the consequences for not having treatment for ADHD are significant,” Dr. Adler said.
He urged physicians who diagnose ADHD to make follow-up part of the care plan or these treatment gaps will persist.
The authors wrote that the results suggest a need to increase availability for mental health services and better communicate symptoms among parents, teachers, and primary care providers.
The authors declare no relevant financial relationships. Dr. Adler has consulted with Supernus Pharmaceuticals and Otsuka Pharmaceuticals, has done research with Takeda, and has received royalty payments from NYU for licensing of ADHD training materials.
FROM JAMA NETWORK OPEN
Long-term impact of childhood trauma explained
WASHINGTON –
“We already knew childhood trauma is associated with the later development of depressive and anxiety disorders, but it’s been unclear what makes sufferers of early trauma more likely to develop these psychiatric conditions,” study investigator Erika Kuzminskaite, PhD candidate, department of psychiatry, Amsterdam University Medical Center (UMC), the Netherlands, told this news organization.
“The evidence now points to unbalanced stress systems as a possible cause of this vulnerability, and now the most important question is, how we can develop preventive interventions,” she added.
The findings were presented as part of the Anxiety and Depression Association of America Anxiety & Depression conference.
Elevated cortisol, inflammation
The study included 2,779 adults from the Netherlands Study of Depression and Anxiety (NESDA). Two thirds of participants were female.
Participants retrospectively reported childhood trauma, defined as emotional, physical, or sexual abuse or emotional or physical neglect, before the age of 18 years. Severe trauma was defined as multiple types or increased frequency of abuse.
Of the total cohort, 48% reported experiencing some childhood trauma – 21% reported severe trauma, 27% reported mild trauma, and 42% reported no childhood trauma.
Among those with trauma, 89% had a current or remitted anxiety or depressive disorder, and 11% had no psychiatric sequelae. Among participants who reported no trauma, 68% had a current or remitted disorder, and 32% had no psychiatric disorders.
At baseline, researchers assessed markers of major bodily stress systems, including the hypothalamic-pituitary-adrenal (HPA) axis, the immune-inflammatory system, and the autonomic nervous system (ANS). They examined these markers separately and cumulatively.
In one model, investigators found that levels of cortisol and inflammation were significantly elevated in those with severe childhood trauma compared to those with no childhood trauma. The effects were largest for the cumulative markers for HPA-axis, inflammation, and all stress system markers (Cohen’s d = 0.23, 0.12, and 0.25, respectively). There was no association with ANS markers.
The results were partially explained by lifestyle, said Ms. Kuzminskaite, who noted that people with severe childhood trauma tend to have a higher body mass index, smoke more, and have other unhealthy habits that may represent a “coping” mechanism for trauma.
Those who experienced childhood trauma also have higher rates of other disorders, including asthma, diabetes, and cardiovascular disease. Ms. Kuzminskaite noted that people with childhood trauma have at least double the risk of cancer in later life.
When researchers adjusted for lifestyle factors and chronic conditions, the association for cortisol was reduced and that for inflammation disappeared. However, the cumulative inflammatory markers remained significant.
Another model examined lipopolysaccharide-stimulated (LPS) immune-inflammatory markers by childhood trauma severity. This provides a more “dynamic” measure of stress systems than looking only at static circulating levels in the blood, as was done in the first model, said Ms. Kuzminskaite.
“These levels should theoretically be more affected by experiences such as childhood trauma and they are also less sensitive to lifestyle.”
Here, researchers found significant positive associations with childhood trauma, especially severe trauma, after adjusting for lifestyle and health-related covariates (cumulative index d = 0.19).
“Almost all people with childhood trauma, especially severe trauma, had LPS-stimulated cytokines upregulated,” said Ms. Kuzminskaite. “So again, there is this dysregulation of immune system functioning in these subjects.”
And again, the strongest effect was for the cumulative index of all cytokines, she said.
Personalized interventions
Ms. Kuzminskaite noted the importance of learning the impact of early trauma on stress responses. “The goal is to eventually have personalized interventions for people with depression or anxiety related to childhood trauma, or even preventative interventions. If we know, for example, something is going wrong with a patient’s stress systems, we can suggest some therapeutic targets.”
Investigators in Amsterdam are examining the efficacy of mifepristone, which blocks progesterone and is used along with misoprostol for medication abortions and to treat high blood sugar. “The drug is supposed to reset the stress system functioning,” said Ms. Kuzminskaite.
It’s still important to target unhealthy lifestyle habits “that are really impacting the functioning of the stress systems,” she said. Lifestyle interventions could improve the efficacy of treatments for depression, for example, she added.
Luana Marques, PhD, associate professor, department of psychiatry, Harvard Medical School, Boston, said such research is important.
“It reveals the potentially extensive and long-lasting impact of childhood trauma on functioning. The findings underscore the importance of equipping at-risk and trauma-exposed youth with evidence-based skills for managing stress,” she said.
No conflicts of interest were reported.
A version of this article first appeared on Medscape.com.
WASHINGTON –
“We already knew childhood trauma is associated with the later development of depressive and anxiety disorders, but it’s been unclear what makes sufferers of early trauma more likely to develop these psychiatric conditions,” study investigator Erika Kuzminskaite, PhD candidate, department of psychiatry, Amsterdam University Medical Center (UMC), the Netherlands, told this news organization.
“The evidence now points to unbalanced stress systems as a possible cause of this vulnerability, and now the most important question is, how we can develop preventive interventions,” she added.
The findings were presented as part of the Anxiety and Depression Association of America Anxiety & Depression conference.
Elevated cortisol, inflammation
The study included 2,779 adults from the Netherlands Study of Depression and Anxiety (NESDA). Two thirds of participants were female.
Participants retrospectively reported childhood trauma, defined as emotional, physical, or sexual abuse or emotional or physical neglect, before the age of 18 years. Severe trauma was defined as multiple types or increased frequency of abuse.
Of the total cohort, 48% reported experiencing some childhood trauma – 21% reported severe trauma, 27% reported mild trauma, and 42% reported no childhood trauma.
Among those with trauma, 89% had a current or remitted anxiety or depressive disorder, and 11% had no psychiatric sequelae. Among participants who reported no trauma, 68% had a current or remitted disorder, and 32% had no psychiatric disorders.
At baseline, researchers assessed markers of major bodily stress systems, including the hypothalamic-pituitary-adrenal (HPA) axis, the immune-inflammatory system, and the autonomic nervous system (ANS). They examined these markers separately and cumulatively.
In one model, investigators found that levels of cortisol and inflammation were significantly elevated in those with severe childhood trauma compared to those with no childhood trauma. The effects were largest for the cumulative markers for HPA-axis, inflammation, and all stress system markers (Cohen’s d = 0.23, 0.12, and 0.25, respectively). There was no association with ANS markers.
The results were partially explained by lifestyle, said Ms. Kuzminskaite, who noted that people with severe childhood trauma tend to have a higher body mass index, smoke more, and have other unhealthy habits that may represent a “coping” mechanism for trauma.
Those who experienced childhood trauma also have higher rates of other disorders, including asthma, diabetes, and cardiovascular disease. Ms. Kuzminskaite noted that people with childhood trauma have at least double the risk of cancer in later life.
When researchers adjusted for lifestyle factors and chronic conditions, the association for cortisol was reduced and that for inflammation disappeared. However, the cumulative inflammatory markers remained significant.
Another model examined lipopolysaccharide-stimulated (LPS) immune-inflammatory markers by childhood trauma severity. This provides a more “dynamic” measure of stress systems than looking only at static circulating levels in the blood, as was done in the first model, said Ms. Kuzminskaite.
“These levels should theoretically be more affected by experiences such as childhood trauma and they are also less sensitive to lifestyle.”
Here, researchers found significant positive associations with childhood trauma, especially severe trauma, after adjusting for lifestyle and health-related covariates (cumulative index d = 0.19).
“Almost all people with childhood trauma, especially severe trauma, had LPS-stimulated cytokines upregulated,” said Ms. Kuzminskaite. “So again, there is this dysregulation of immune system functioning in these subjects.”
And again, the strongest effect was for the cumulative index of all cytokines, she said.
Personalized interventions
Ms. Kuzminskaite noted the importance of learning the impact of early trauma on stress responses. “The goal is to eventually have personalized interventions for people with depression or anxiety related to childhood trauma, or even preventative interventions. If we know, for example, something is going wrong with a patient’s stress systems, we can suggest some therapeutic targets.”
Investigators in Amsterdam are examining the efficacy of mifepristone, which blocks progesterone and is used along with misoprostol for medication abortions and to treat high blood sugar. “The drug is supposed to reset the stress system functioning,” said Ms. Kuzminskaite.
It’s still important to target unhealthy lifestyle habits “that are really impacting the functioning of the stress systems,” she said. Lifestyle interventions could improve the efficacy of treatments for depression, for example, she added.
Luana Marques, PhD, associate professor, department of psychiatry, Harvard Medical School, Boston, said such research is important.
“It reveals the potentially extensive and long-lasting impact of childhood trauma on functioning. The findings underscore the importance of equipping at-risk and trauma-exposed youth with evidence-based skills for managing stress,” she said.
No conflicts of interest were reported.
A version of this article first appeared on Medscape.com.
WASHINGTON –
“We already knew childhood trauma is associated with the later development of depressive and anxiety disorders, but it’s been unclear what makes sufferers of early trauma more likely to develop these psychiatric conditions,” study investigator Erika Kuzminskaite, PhD candidate, department of psychiatry, Amsterdam University Medical Center (UMC), the Netherlands, told this news organization.
“The evidence now points to unbalanced stress systems as a possible cause of this vulnerability, and now the most important question is, how we can develop preventive interventions,” she added.
The findings were presented as part of the Anxiety and Depression Association of America Anxiety & Depression conference.
Elevated cortisol, inflammation
The study included 2,779 adults from the Netherlands Study of Depression and Anxiety (NESDA). Two thirds of participants were female.
Participants retrospectively reported childhood trauma, defined as emotional, physical, or sexual abuse or emotional or physical neglect, before the age of 18 years. Severe trauma was defined as multiple types or increased frequency of abuse.
Of the total cohort, 48% reported experiencing some childhood trauma – 21% reported severe trauma, 27% reported mild trauma, and 42% reported no childhood trauma.
Among those with trauma, 89% had a current or remitted anxiety or depressive disorder, and 11% had no psychiatric sequelae. Among participants who reported no trauma, 68% had a current or remitted disorder, and 32% had no psychiatric disorders.
At baseline, researchers assessed markers of major bodily stress systems, including the hypothalamic-pituitary-adrenal (HPA) axis, the immune-inflammatory system, and the autonomic nervous system (ANS). They examined these markers separately and cumulatively.
In one model, investigators found that levels of cortisol and inflammation were significantly elevated in those with severe childhood trauma compared to those with no childhood trauma. The effects were largest for the cumulative markers for HPA-axis, inflammation, and all stress system markers (Cohen’s d = 0.23, 0.12, and 0.25, respectively). There was no association with ANS markers.
The results were partially explained by lifestyle, said Ms. Kuzminskaite, who noted that people with severe childhood trauma tend to have a higher body mass index, smoke more, and have other unhealthy habits that may represent a “coping” mechanism for trauma.
Those who experienced childhood trauma also have higher rates of other disorders, including asthma, diabetes, and cardiovascular disease. Ms. Kuzminskaite noted that people with childhood trauma have at least double the risk of cancer in later life.
When researchers adjusted for lifestyle factors and chronic conditions, the association for cortisol was reduced and that for inflammation disappeared. However, the cumulative inflammatory markers remained significant.
Another model examined lipopolysaccharide-stimulated (LPS) immune-inflammatory markers by childhood trauma severity. This provides a more “dynamic” measure of stress systems than looking only at static circulating levels in the blood, as was done in the first model, said Ms. Kuzminskaite.
“These levels should theoretically be more affected by experiences such as childhood trauma and they are also less sensitive to lifestyle.”
Here, researchers found significant positive associations with childhood trauma, especially severe trauma, after adjusting for lifestyle and health-related covariates (cumulative index d = 0.19).
“Almost all people with childhood trauma, especially severe trauma, had LPS-stimulated cytokines upregulated,” said Ms. Kuzminskaite. “So again, there is this dysregulation of immune system functioning in these subjects.”
And again, the strongest effect was for the cumulative index of all cytokines, she said.
Personalized interventions
Ms. Kuzminskaite noted the importance of learning the impact of early trauma on stress responses. “The goal is to eventually have personalized interventions for people with depression or anxiety related to childhood trauma, or even preventative interventions. If we know, for example, something is going wrong with a patient’s stress systems, we can suggest some therapeutic targets.”
Investigators in Amsterdam are examining the efficacy of mifepristone, which blocks progesterone and is used along with misoprostol for medication abortions and to treat high blood sugar. “The drug is supposed to reset the stress system functioning,” said Ms. Kuzminskaite.
It’s still important to target unhealthy lifestyle habits “that are really impacting the functioning of the stress systems,” she said. Lifestyle interventions could improve the efficacy of treatments for depression, for example, she added.
Luana Marques, PhD, associate professor, department of psychiatry, Harvard Medical School, Boston, said such research is important.
“It reveals the potentially extensive and long-lasting impact of childhood trauma on functioning. The findings underscore the importance of equipping at-risk and trauma-exposed youth with evidence-based skills for managing stress,” she said.
No conflicts of interest were reported.
A version of this article first appeared on Medscape.com.
AT ADAA 2023
ASCO updates treatment guidelines for anxiety and depression
Since the last guidelines, published in 2014, screening and assessment for depression and anxiety have improved, and a large new evidence base has emerged. To ensure the most up-to-date recommendations, a group of experts spanning psychology, psychiatry, medical and surgical oncology, internal medicine, and nursing convened to review the current literature on managing depression and anxiety. The review included 61 studies – 16 meta-analyses, 44 randomized controlled trials, and one systematic review – published between 2013 and 2021.
“The purpose of this guideline update is to gather and examine the evidence published since the 2014 guideline ... [with a] focus on management and treatment only.” The overall goal is to provide “the most effective and least resource-intensive intervention based on symptom severity” for patients with cancer, the experts write.
The new clinical practice guideline addresses the following question: What are the recommended treatment approaches in the management of anxiety and/or depression in survivors of adult cancer?
After an extensive literature search and analysis, the study was published online in the Journal of Clinical Oncology.
The expert panel’s recommendations fell into three broad categories – general management principles, treatment and care options for depressive symptoms, and treatment and care options for anxiety symptoms – with the guidelines for managing depression and anxiety largely mirroring each other.
The authors caution, however, that the guidelines “were developed in the context of mental health care being available and may not be applicable within other resource settings.”
General management principals
All patients with cancer, along with their caregivers, family members, or trusted confidants, should be offered information and resources on depression and anxiety. The panel gave this a “strong” recommendation but provided the caveat that the “information should be culturally informed and linguistically appropriate and can include a conversation between clinician and patient.”
Clinicians should select the most effective and least intensive intervention based on symptom severity when selecting treatment – what the panelists referred to as a stepped-care model. History of psychiatric diagnoses or substance use as well as prior responses to mental health treatment are some of the factors that may inform treatment choice.
For patients experiencing both depression and anxiety symptoms, treatment of depressive symptoms should be prioritized.
When referring a patient for further evaluation or care, clinicians “should make every effort to reduce barriers and facilitate patient follow-through,” the authors write. And health care professionals should regularly assess the treatment responses for patients receiving psychological or pharmacological interventions.
Overall, the treatments should be “supervised by a psychiatrist, and primary care or oncology providers work collaboratively with a nurse care manager to provide psychological interventions and monitor treatment compliance and outcomes,” the panelists write. “This type of collaborative care is found to be superior to usual care and is more cost-effective than face-to-face and pharmacologic treatment for depression.”
Treatment and care options for depressive and anxiety symptoms
For patients with moderate to severe depression symptoms, the panelists again stressed that clinicians should provide “culturally informed and linguistically appropriate information.” This information may include the frequency and symptoms of depression as well as signs these symptoms may be getting worse, with contact information for the medical team provided.
Among patients with moderate symptoms, clinicians can offer patients a range of individual or group therapy options, including cognitive-behavioral therapy (CBT), behavioral activation, mindfulness-based stress reduction, or structured physical activity and exercise. For patients with severe symptoms of depression, clinicians should offer individual therapy with one of these four treatment options: CBT, behavioral activation, mindfulness-based stress reduction, or interpersonal therapy.
The panelists offered almost identical recommendations for patients with anxiety, except mindfulness-based stress reduction was an option for patients with severe symptoms.
Clinicians can also provide pharmacologic options to treat depression or anxiety in certain patients, though the panelists provided the caveat that evidence for pharmacologic management is weak.
“These guidelines make no recommendations about any specific pharmacologic regimen being better than another,” the experts wrote. And “patients should be warned of potential harm or adverse effects.”
Overall, the panelists noted that, as highlighted in the 2014 ASCO guideline, the updated version continues to stress the importance of providing education on coping with stress, anxiety, and depression.
And “for individuals with elevated symptoms, validation and normalizing patients’ experiences is crucial,” the panelists write.
Although the timing of screening is not the focus of this updated review, the experts recognized that “how and when patients with cancer and survivors are screened are important determinants of timely management of anxiety and depression.”
And unlike the prior guideline, “pharmacotherapy is not recommended as a first-line treatment, neither alone nor in combination,” the authors say.
Overall, the panelists emphasize how widespread the mental health care crisis is and that problems accessing mental health care remain. “The choice of intervention to offer patients facing such obstacles should be based on shared decision-making, taking into account availability, accessibility, patient preference, likelihood of adverse events, adherence, and cost,” the experts conclude.
A version of this article first appeared on Medscape.com.
Since the last guidelines, published in 2014, screening and assessment for depression and anxiety have improved, and a large new evidence base has emerged. To ensure the most up-to-date recommendations, a group of experts spanning psychology, psychiatry, medical and surgical oncology, internal medicine, and nursing convened to review the current literature on managing depression and anxiety. The review included 61 studies – 16 meta-analyses, 44 randomized controlled trials, and one systematic review – published between 2013 and 2021.
“The purpose of this guideline update is to gather and examine the evidence published since the 2014 guideline ... [with a] focus on management and treatment only.” The overall goal is to provide “the most effective and least resource-intensive intervention based on symptom severity” for patients with cancer, the experts write.
The new clinical practice guideline addresses the following question: What are the recommended treatment approaches in the management of anxiety and/or depression in survivors of adult cancer?
After an extensive literature search and analysis, the study was published online in the Journal of Clinical Oncology.
The expert panel’s recommendations fell into three broad categories – general management principles, treatment and care options for depressive symptoms, and treatment and care options for anxiety symptoms – with the guidelines for managing depression and anxiety largely mirroring each other.
The authors caution, however, that the guidelines “were developed in the context of mental health care being available and may not be applicable within other resource settings.”
General management principals
All patients with cancer, along with their caregivers, family members, or trusted confidants, should be offered information and resources on depression and anxiety. The panel gave this a “strong” recommendation but provided the caveat that the “information should be culturally informed and linguistically appropriate and can include a conversation between clinician and patient.”
Clinicians should select the most effective and least intensive intervention based on symptom severity when selecting treatment – what the panelists referred to as a stepped-care model. History of psychiatric diagnoses or substance use as well as prior responses to mental health treatment are some of the factors that may inform treatment choice.
For patients experiencing both depression and anxiety symptoms, treatment of depressive symptoms should be prioritized.
When referring a patient for further evaluation or care, clinicians “should make every effort to reduce barriers and facilitate patient follow-through,” the authors write. And health care professionals should regularly assess the treatment responses for patients receiving psychological or pharmacological interventions.
Overall, the treatments should be “supervised by a psychiatrist, and primary care or oncology providers work collaboratively with a nurse care manager to provide psychological interventions and monitor treatment compliance and outcomes,” the panelists write. “This type of collaborative care is found to be superior to usual care and is more cost-effective than face-to-face and pharmacologic treatment for depression.”
Treatment and care options for depressive and anxiety symptoms
For patients with moderate to severe depression symptoms, the panelists again stressed that clinicians should provide “culturally informed and linguistically appropriate information.” This information may include the frequency and symptoms of depression as well as signs these symptoms may be getting worse, with contact information for the medical team provided.
Among patients with moderate symptoms, clinicians can offer patients a range of individual or group therapy options, including cognitive-behavioral therapy (CBT), behavioral activation, mindfulness-based stress reduction, or structured physical activity and exercise. For patients with severe symptoms of depression, clinicians should offer individual therapy with one of these four treatment options: CBT, behavioral activation, mindfulness-based stress reduction, or interpersonal therapy.
The panelists offered almost identical recommendations for patients with anxiety, except mindfulness-based stress reduction was an option for patients with severe symptoms.
Clinicians can also provide pharmacologic options to treat depression or anxiety in certain patients, though the panelists provided the caveat that evidence for pharmacologic management is weak.
“These guidelines make no recommendations about any specific pharmacologic regimen being better than another,” the experts wrote. And “patients should be warned of potential harm or adverse effects.”
Overall, the panelists noted that, as highlighted in the 2014 ASCO guideline, the updated version continues to stress the importance of providing education on coping with stress, anxiety, and depression.
And “for individuals with elevated symptoms, validation and normalizing patients’ experiences is crucial,” the panelists write.
Although the timing of screening is not the focus of this updated review, the experts recognized that “how and when patients with cancer and survivors are screened are important determinants of timely management of anxiety and depression.”
And unlike the prior guideline, “pharmacotherapy is not recommended as a first-line treatment, neither alone nor in combination,” the authors say.
Overall, the panelists emphasize how widespread the mental health care crisis is and that problems accessing mental health care remain. “The choice of intervention to offer patients facing such obstacles should be based on shared decision-making, taking into account availability, accessibility, patient preference, likelihood of adverse events, adherence, and cost,” the experts conclude.
A version of this article first appeared on Medscape.com.
Since the last guidelines, published in 2014, screening and assessment for depression and anxiety have improved, and a large new evidence base has emerged. To ensure the most up-to-date recommendations, a group of experts spanning psychology, psychiatry, medical and surgical oncology, internal medicine, and nursing convened to review the current literature on managing depression and anxiety. The review included 61 studies – 16 meta-analyses, 44 randomized controlled trials, and one systematic review – published between 2013 and 2021.
“The purpose of this guideline update is to gather and examine the evidence published since the 2014 guideline ... [with a] focus on management and treatment only.” The overall goal is to provide “the most effective and least resource-intensive intervention based on symptom severity” for patients with cancer, the experts write.
The new clinical practice guideline addresses the following question: What are the recommended treatment approaches in the management of anxiety and/or depression in survivors of adult cancer?
After an extensive literature search and analysis, the study was published online in the Journal of Clinical Oncology.
The expert panel’s recommendations fell into three broad categories – general management principles, treatment and care options for depressive symptoms, and treatment and care options for anxiety symptoms – with the guidelines for managing depression and anxiety largely mirroring each other.
The authors caution, however, that the guidelines “were developed in the context of mental health care being available and may not be applicable within other resource settings.”
General management principals
All patients with cancer, along with their caregivers, family members, or trusted confidants, should be offered information and resources on depression and anxiety. The panel gave this a “strong” recommendation but provided the caveat that the “information should be culturally informed and linguistically appropriate and can include a conversation between clinician and patient.”
Clinicians should select the most effective and least intensive intervention based on symptom severity when selecting treatment – what the panelists referred to as a stepped-care model. History of psychiatric diagnoses or substance use as well as prior responses to mental health treatment are some of the factors that may inform treatment choice.
For patients experiencing both depression and anxiety symptoms, treatment of depressive symptoms should be prioritized.
When referring a patient for further evaluation or care, clinicians “should make every effort to reduce barriers and facilitate patient follow-through,” the authors write. And health care professionals should regularly assess the treatment responses for patients receiving psychological or pharmacological interventions.
Overall, the treatments should be “supervised by a psychiatrist, and primary care or oncology providers work collaboratively with a nurse care manager to provide psychological interventions and monitor treatment compliance and outcomes,” the panelists write. “This type of collaborative care is found to be superior to usual care and is more cost-effective than face-to-face and pharmacologic treatment for depression.”
Treatment and care options for depressive and anxiety symptoms
For patients with moderate to severe depression symptoms, the panelists again stressed that clinicians should provide “culturally informed and linguistically appropriate information.” This information may include the frequency and symptoms of depression as well as signs these symptoms may be getting worse, with contact information for the medical team provided.
Among patients with moderate symptoms, clinicians can offer patients a range of individual or group therapy options, including cognitive-behavioral therapy (CBT), behavioral activation, mindfulness-based stress reduction, or structured physical activity and exercise. For patients with severe symptoms of depression, clinicians should offer individual therapy with one of these four treatment options: CBT, behavioral activation, mindfulness-based stress reduction, or interpersonal therapy.
The panelists offered almost identical recommendations for patients with anxiety, except mindfulness-based stress reduction was an option for patients with severe symptoms.
Clinicians can also provide pharmacologic options to treat depression or anxiety in certain patients, though the panelists provided the caveat that evidence for pharmacologic management is weak.
“These guidelines make no recommendations about any specific pharmacologic regimen being better than another,” the experts wrote. And “patients should be warned of potential harm or adverse effects.”
Overall, the panelists noted that, as highlighted in the 2014 ASCO guideline, the updated version continues to stress the importance of providing education on coping with stress, anxiety, and depression.
And “for individuals with elevated symptoms, validation and normalizing patients’ experiences is crucial,” the panelists write.
Although the timing of screening is not the focus of this updated review, the experts recognized that “how and when patients with cancer and survivors are screened are important determinants of timely management of anxiety and depression.”
And unlike the prior guideline, “pharmacotherapy is not recommended as a first-line treatment, neither alone nor in combination,” the authors say.
Overall, the panelists emphasize how widespread the mental health care crisis is and that problems accessing mental health care remain. “The choice of intervention to offer patients facing such obstacles should be based on shared decision-making, taking into account availability, accessibility, patient preference, likelihood of adverse events, adherence, and cost,” the experts conclude.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Transcranial magnetic stimulation during pregnancy: An alternative to antidepressant treatment?
A growing number of women ask about nonpharmacologic approaches for either the treatment of acute perinatal depression or for relapse prevention during pregnancy.
The last several decades have brought an increasing level of comfort with respect to antidepressant use during pregnancy, which derives from several factors.

First, it’s been well described that there’s an increased risk of relapse and morbidity associated with discontinuation of antidepressants proximate to pregnancy, particularly in women with histories of recurrent disease (JAMA Psychiatry. 2023;80[5]:441-50 and JAMA. 2006;295[5]:499-507).
Second, there’s an obvious increased confidence about using antidepressants during pregnancy given the robust reproductive safety data about antidepressants with respect to both teratogenesis and risk for organ malformation. Other studies also fail to demonstrate a relationship between fetal exposure to antidepressants and risk for subsequent development of attention-deficit/hyperactivity disorder (ADHD) and autism. These latter studies have been reviewed extensively in systematic reviews of meta-analyses addressing this question.
However, there are women who, as they approach the question of antidepressant use during pregnancy, would prefer a nonpharmacologic approach to managing depression in the setting of either a planned pregnancy, or sometimes in the setting of acute onset of depressive symptoms during pregnancy. Other women are more comfortable with the data in hand regarding the reproductive safety of antidepressants and continue antidepressants that have afforded emotional well-being, particularly if the road to well-being or euthymia has been a long one.
Still, we at Massachusetts General Hospital (MGH) Center for Women’s Mental Health along with multidisciplinary colleagues with whom we engage during our weekly Virtual Rounds community have observed a growing number of women asking about nonpharmacologic approaches for either the treatment of acute perinatal depression or for relapse prevention during pregnancy. They ask about these options for personal reasons, regardless of what we may know (and what we may not know) about existing pharmacologic interventions. In these scenarios, it is important to keep in mind that it is not about what we as clinicians necessarily know about these medicines per se that drives treatment, but rather about the private calculus that women and their partners apply about risk and benefit of pharmacologic treatment during pregnancy.
Nonpharmacologic treatment options
Mindfulness-based cognitive therapy (MBCT), cognitive behavioral therapy (CBT), and behavioral activation are therapies all of which have an evidence base with respect to their effectiveness for either the acute treatment of both depression (and perinatal depression specifically) or for mitigating risk for depressive relapse (MBCT). Several investigations are underway evaluating digital apps that utilize MBCT and CBT in these patient populations as well.
New treatments for which we have none or exceedingly sparse data to support use during pregnancy are neurosteroids. We are asked all the time about the use of neurosteroids such as brexanolone or zuranolone during pregnancy. Given the data on effectiveness of these agents for treatment of postpartum depression, the question about use during pregnancy is intuitive. But at this point in time, absent data, their use during pregnancy cannot be recommended.
With respect to newer nonpharmacologic approaches that have been looked at for treatment of major depressive disorder, the Food and Drug Administration has approved transcranial magnetic stimulation (TMS), a noninvasive form of neuromodulating therapy that use magnetic pulses to stimulate specific regions of the brain that have been implicated in psychiatric illness.
While there are no safety concerns that have been noted about use of TMS, the data regarding its use during pregnancy are still relatively limited, but it has been used to treat certain neurologic conditions during pregnancy. We now have a small randomized controlled study using TMS during pregnancy and multiple small case series suggesting a signal of efficacy in women with perinatal major depressive disorder. Side effects of TMS use during pregnancy have included hypotension, which has sometimes required repositioning of subjects, particularly later in pregnancy. Unlike electroconvulsive therapy, (ECT), often used when clinicians have exhausted other treatment options, TMS has no risk of seizure associated with its use.
TMS is now entering into the clinical arena in a more robust way. In certain settings, insurance companies are reimbursing for TMS treatment more often than was the case previously, making it a more viable option for a larger number of patients. There are also several exciting newer protocols, including theta burst stimulation, a new form of TMS treatment with less of a time commitment, and which may be more cost effective. However, data on this modality of treatment remain limited.
Where TMS fits in treating depression during pregnancy
The real question we are getting asked in clinic, both in person and during virtual rounds with multidisciplinary colleagues from across the world, is where TMS might fit into the algorithm for treating of depression during pregnancy. Where is it appropriate to be thinking about TMS in pregnancy, and where should it perhaps be deferred at this moment (and where is it not appropriate)?
It is probably of limited value (and possibly of potential harm) to switch to TMS in patients who have severe recurrent major depression and who are on maintenance antidepressant, and who believe that a switch to TMS will be effective for relapse prevention; there are simply no data currently suggesting that TMS can be used as a relapse prevention tool, unlike certain other nonpharmacologic interventions.
What about managing relapse of major depressive disorder during pregnancy in a patient who had responded to an antidepressant? We have seen patients with histories of severe recurrent disease who are managed well on antidepressants during pregnancy who then have breakthrough symptoms and inquire about using TMS as an augmentation strategy. Although we don’t have clear data supporting the use of TMS as an adjunct in that setting, in those patients, one could argue that a trial of TMS may be appropriate – as opposed to introducing multiple medicines to recapture euthymia during pregnancy where the benefit is unclear and where more exposure is implied by having to do potentially multiple trials.
Other patients with new onset of depression during pregnancy who, for personal reasons, will not take an antidepressant or pursue other nonpharmacologic interventions will frequently ask about TMS. and the increased availability of TMS in the community in various centers – as opposed to previously where it was more restricted to large academic medical centers.
I think it is a time of excitement in reproductive psychiatry where we have a growing number of tools to treat perinatal depression – from medications to digital tools. These tools – either alone or in combination with medicines that we’ve been using for years – are able to afford women a greater number of choices with respect to the treatment of perinatal depression than was available even 5 years ago. That takes us closer to an ability to use interventions that truly combine patient wishes and “precision perinatal psychiatry,” where we can match effective therapies with the individual clinical presentations and wishes with which patients come to us.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. Email Dr. Cohen at [email protected].
A growing number of women ask about nonpharmacologic approaches for either the treatment of acute perinatal depression or for relapse prevention during pregnancy.
The last several decades have brought an increasing level of comfort with respect to antidepressant use during pregnancy, which derives from several factors.
First, it’s been well described that there’s an increased risk of relapse and morbidity associated with discontinuation of antidepressants proximate to pregnancy, particularly in women with histories of recurrent disease (JAMA Psychiatry. 2023;80[5]:441-50 and JAMA. 2006;295[5]:499-507).
Second, there’s an obvious increased confidence about using antidepressants during pregnancy given the robust reproductive safety data about antidepressants with respect to both teratogenesis and risk for organ malformation. Other studies also fail to demonstrate a relationship between fetal exposure to antidepressants and risk for subsequent development of attention-deficit/hyperactivity disorder (ADHD) and autism. These latter studies have been reviewed extensively in systematic reviews of meta-analyses addressing this question.
However, there are women who, as they approach the question of antidepressant use during pregnancy, would prefer a nonpharmacologic approach to managing depression in the setting of either a planned pregnancy, or sometimes in the setting of acute onset of depressive symptoms during pregnancy. Other women are more comfortable with the data in hand regarding the reproductive safety of antidepressants and continue antidepressants that have afforded emotional well-being, particularly if the road to well-being or euthymia has been a long one.
Still, we at Massachusetts General Hospital (MGH) Center for Women’s Mental Health along with multidisciplinary colleagues with whom we engage during our weekly Virtual Rounds community have observed a growing number of women asking about nonpharmacologic approaches for either the treatment of acute perinatal depression or for relapse prevention during pregnancy. They ask about these options for personal reasons, regardless of what we may know (and what we may not know) about existing pharmacologic interventions. In these scenarios, it is important to keep in mind that it is not about what we as clinicians necessarily know about these medicines per se that drives treatment, but rather about the private calculus that women and their partners apply about risk and benefit of pharmacologic treatment during pregnancy.
Nonpharmacologic treatment options
Mindfulness-based cognitive therapy (MBCT), cognitive behavioral therapy (CBT), and behavioral activation are therapies all of which have an evidence base with respect to their effectiveness for either the acute treatment of both depression (and perinatal depression specifically) or for mitigating risk for depressive relapse (MBCT). Several investigations are underway evaluating digital apps that utilize MBCT and CBT in these patient populations as well.
New treatments for which we have none or exceedingly sparse data to support use during pregnancy are neurosteroids. We are asked all the time about the use of neurosteroids such as brexanolone or zuranolone during pregnancy. Given the data on effectiveness of these agents for treatment of postpartum depression, the question about use during pregnancy is intuitive. But at this point in time, absent data, their use during pregnancy cannot be recommended.
With respect to newer nonpharmacologic approaches that have been looked at for treatment of major depressive disorder, the Food and Drug Administration has approved transcranial magnetic stimulation (TMS), a noninvasive form of neuromodulating therapy that use magnetic pulses to stimulate specific regions of the brain that have been implicated in psychiatric illness.
While there are no safety concerns that have been noted about use of TMS, the data regarding its use during pregnancy are still relatively limited, but it has been used to treat certain neurologic conditions during pregnancy. We now have a small randomized controlled study using TMS during pregnancy and multiple small case series suggesting a signal of efficacy in women with perinatal major depressive disorder. Side effects of TMS use during pregnancy have included hypotension, which has sometimes required repositioning of subjects, particularly later in pregnancy. Unlike electroconvulsive therapy, (ECT), often used when clinicians have exhausted other treatment options, TMS has no risk of seizure associated with its use.
TMS is now entering into the clinical arena in a more robust way. In certain settings, insurance companies are reimbursing for TMS treatment more often than was the case previously, making it a more viable option for a larger number of patients. There are also several exciting newer protocols, including theta burst stimulation, a new form of TMS treatment with less of a time commitment, and which may be more cost effective. However, data on this modality of treatment remain limited.
Where TMS fits in treating depression during pregnancy
The real question we are getting asked in clinic, both in person and during virtual rounds with multidisciplinary colleagues from across the world, is where TMS might fit into the algorithm for treating of depression during pregnancy. Where is it appropriate to be thinking about TMS in pregnancy, and where should it perhaps be deferred at this moment (and where is it not appropriate)?
It is probably of limited value (and possibly of potential harm) to switch to TMS in patients who have severe recurrent major depression and who are on maintenance antidepressant, and who believe that a switch to TMS will be effective for relapse prevention; there are simply no data currently suggesting that TMS can be used as a relapse prevention tool, unlike certain other nonpharmacologic interventions.
What about managing relapse of major depressive disorder during pregnancy in a patient who had responded to an antidepressant? We have seen patients with histories of severe recurrent disease who are managed well on antidepressants during pregnancy who then have breakthrough symptoms and inquire about using TMS as an augmentation strategy. Although we don’t have clear data supporting the use of TMS as an adjunct in that setting, in those patients, one could argue that a trial of TMS may be appropriate – as opposed to introducing multiple medicines to recapture euthymia during pregnancy where the benefit is unclear and where more exposure is implied by having to do potentially multiple trials.
Other patients with new onset of depression during pregnancy who, for personal reasons, will not take an antidepressant or pursue other nonpharmacologic interventions will frequently ask about TMS. and the increased availability of TMS in the community in various centers – as opposed to previously where it was more restricted to large academic medical centers.
I think it is a time of excitement in reproductive psychiatry where we have a growing number of tools to treat perinatal depression – from medications to digital tools. These tools – either alone or in combination with medicines that we’ve been using for years – are able to afford women a greater number of choices with respect to the treatment of perinatal depression than was available even 5 years ago. That takes us closer to an ability to use interventions that truly combine patient wishes and “precision perinatal psychiatry,” where we can match effective therapies with the individual clinical presentations and wishes with which patients come to us.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. Email Dr. Cohen at [email protected].
A growing number of women ask about nonpharmacologic approaches for either the treatment of acute perinatal depression or for relapse prevention during pregnancy.
The last several decades have brought an increasing level of comfort with respect to antidepressant use during pregnancy, which derives from several factors.
First, it’s been well described that there’s an increased risk of relapse and morbidity associated with discontinuation of antidepressants proximate to pregnancy, particularly in women with histories of recurrent disease (JAMA Psychiatry. 2023;80[5]:441-50 and JAMA. 2006;295[5]:499-507).
Second, there’s an obvious increased confidence about using antidepressants during pregnancy given the robust reproductive safety data about antidepressants with respect to both teratogenesis and risk for organ malformation. Other studies also fail to demonstrate a relationship between fetal exposure to antidepressants and risk for subsequent development of attention-deficit/hyperactivity disorder (ADHD) and autism. These latter studies have been reviewed extensively in systematic reviews of meta-analyses addressing this question.
However, there are women who, as they approach the question of antidepressant use during pregnancy, would prefer a nonpharmacologic approach to managing depression in the setting of either a planned pregnancy, or sometimes in the setting of acute onset of depressive symptoms during pregnancy. Other women are more comfortable with the data in hand regarding the reproductive safety of antidepressants and continue antidepressants that have afforded emotional well-being, particularly if the road to well-being or euthymia has been a long one.
Still, we at Massachusetts General Hospital (MGH) Center for Women’s Mental Health along with multidisciplinary colleagues with whom we engage during our weekly Virtual Rounds community have observed a growing number of women asking about nonpharmacologic approaches for either the treatment of acute perinatal depression or for relapse prevention during pregnancy. They ask about these options for personal reasons, regardless of what we may know (and what we may not know) about existing pharmacologic interventions. In these scenarios, it is important to keep in mind that it is not about what we as clinicians necessarily know about these medicines per se that drives treatment, but rather about the private calculus that women and their partners apply about risk and benefit of pharmacologic treatment during pregnancy.
Nonpharmacologic treatment options
Mindfulness-based cognitive therapy (MBCT), cognitive behavioral therapy (CBT), and behavioral activation are therapies all of which have an evidence base with respect to their effectiveness for either the acute treatment of both depression (and perinatal depression specifically) or for mitigating risk for depressive relapse (MBCT). Several investigations are underway evaluating digital apps that utilize MBCT and CBT in these patient populations as well.
New treatments for which we have none or exceedingly sparse data to support use during pregnancy are neurosteroids. We are asked all the time about the use of neurosteroids such as brexanolone or zuranolone during pregnancy. Given the data on effectiveness of these agents for treatment of postpartum depression, the question about use during pregnancy is intuitive. But at this point in time, absent data, their use during pregnancy cannot be recommended.
With respect to newer nonpharmacologic approaches that have been looked at for treatment of major depressive disorder, the Food and Drug Administration has approved transcranial magnetic stimulation (TMS), a noninvasive form of neuromodulating therapy that use magnetic pulses to stimulate specific regions of the brain that have been implicated in psychiatric illness.
While there are no safety concerns that have been noted about use of TMS, the data regarding its use during pregnancy are still relatively limited, but it has been used to treat certain neurologic conditions during pregnancy. We now have a small randomized controlled study using TMS during pregnancy and multiple small case series suggesting a signal of efficacy in women with perinatal major depressive disorder. Side effects of TMS use during pregnancy have included hypotension, which has sometimes required repositioning of subjects, particularly later in pregnancy. Unlike electroconvulsive therapy, (ECT), often used when clinicians have exhausted other treatment options, TMS has no risk of seizure associated with its use.
TMS is now entering into the clinical arena in a more robust way. In certain settings, insurance companies are reimbursing for TMS treatment more often than was the case previously, making it a more viable option for a larger number of patients. There are also several exciting newer protocols, including theta burst stimulation, a new form of TMS treatment with less of a time commitment, and which may be more cost effective. However, data on this modality of treatment remain limited.
Where TMS fits in treating depression during pregnancy
The real question we are getting asked in clinic, both in person and during virtual rounds with multidisciplinary colleagues from across the world, is where TMS might fit into the algorithm for treating of depression during pregnancy. Where is it appropriate to be thinking about TMS in pregnancy, and where should it perhaps be deferred at this moment (and where is it not appropriate)?
It is probably of limited value (and possibly of potential harm) to switch to TMS in patients who have severe recurrent major depression and who are on maintenance antidepressant, and who believe that a switch to TMS will be effective for relapse prevention; there are simply no data currently suggesting that TMS can be used as a relapse prevention tool, unlike certain other nonpharmacologic interventions.
What about managing relapse of major depressive disorder during pregnancy in a patient who had responded to an antidepressant? We have seen patients with histories of severe recurrent disease who are managed well on antidepressants during pregnancy who then have breakthrough symptoms and inquire about using TMS as an augmentation strategy. Although we don’t have clear data supporting the use of TMS as an adjunct in that setting, in those patients, one could argue that a trial of TMS may be appropriate – as opposed to introducing multiple medicines to recapture euthymia during pregnancy where the benefit is unclear and where more exposure is implied by having to do potentially multiple trials.
Other patients with new onset of depression during pregnancy who, for personal reasons, will not take an antidepressant or pursue other nonpharmacologic interventions will frequently ask about TMS. and the increased availability of TMS in the community in various centers – as opposed to previously where it was more restricted to large academic medical centers.
I think it is a time of excitement in reproductive psychiatry where we have a growing number of tools to treat perinatal depression – from medications to digital tools. These tools – either alone or in combination with medicines that we’ve been using for years – are able to afford women a greater number of choices with respect to the treatment of perinatal depression than was available even 5 years ago. That takes us closer to an ability to use interventions that truly combine patient wishes and “precision perinatal psychiatry,” where we can match effective therapies with the individual clinical presentations and wishes with which patients come to us.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. Email Dr. Cohen at [email protected].
Survey reveals room for improvement in teen substance use screening
WASHINGTON – , Deepa Camenga, MD, said in a presentation at the 2023 Pediatric Academic Societies annual meeting.

The American Academy of Pediatrics recommends universal screening for substance use in adolescents during annual health visits, but current screening rates and practices among primary care pediatricians in the United States are unknown, said Dr. Camenga, an associate professor at Yale University, New Haven, Conn.
Uniformity in screening is lacking
Dr. Camenga presented data from the 2021 AAP Periodic Survey, which included 1,683 nonretired AAP members in the United States. Residents were excluded. The current analysis included 471 pediatricians who reported providing health supervision to adolescents. Overall, 284 of the 471 included respondents (60%) reported always screening adolescent patients for substance use during a health supervision visit. Of these, 42% reported using a standardized screening instrument, Dr. Camenga said.
The majority (70%) of pediatricians who used a standardized screening tool opted for the CRAFFT tool (Car, Relax, Alone, Forget, Friends, Trouble) designed for ages 12-21 years. Another 21% reported using an unspecified screening tool, 4% used RAAPS (Rapid Assessment for Adolescent Preventive Services), 3% used S2BI (Screening to Brief Intervention), and 1% used BSTAD (Brief Screener for Tobacco, Alcohol, and other Drugs).
A total of 77% of respondents reported screening their adolescent patients for substance use without a parent or guardian present. Approximately half (52%) used paper-based screening, 22% used electronic screening, 21% used verbal screening, and 6% reported other methods.
A total of 68% and 70% of respondents, respectively, agreed or strongly agreed that top barriers to screening were the lack of an onsite provider for counseling and the lack of readily available treatment options. Other reported barriers included lack of knowledge or information, patient reluctance to discuss substance use, too many other priorities during the visit, and inadequate payment. Only 6% of respondents strongly agreed that lack of time was a barrier, said Dr. Camenga.
Screening frequency and screening practices varied by geographic region, Dr. Camenga said. Pediatricians in the South and Midwest were only half as likely as those in the Northeast to report always screening adolescents for substance use (adjusted odds ratio, 0.43 and 0.53, respectively; P < .05). Similarly, compared with pediatricians in the Northeast, those in the South, Midwest, and West were significantly less likely to report using a standardized instrument for substance use screening (aOR, 0.53, 0.24, and 0.52, respectively; P < 0.001 for all).
The disparities in screening by geographic region show that there is room for improvement in this area, said Dr. Camenga. Systems-level interventions such as treatment financing and access to telehealth services could improve primary care access to substance use treatment professionals, she said.
At the practice level, embedding screening and referral tools into electronic health records could potentially improve screening rates. Many primary care pediatricians do not receive training in identifying and assessing substance use in their patients, or in first-line treatment, Dr. Camenga said.
“We have to invest in a ‘train the trainer’ type of model,” she emphasized.
Data highlight regional resource gaps
The current study is important because it highlights potential missed opportunities to screen adolescents for substance use, said Sarah Yale, MD, assistant professor of pediatrics at the Medical College of Wisconsin, Milwaukee, in an interview. Dr. Yale said that the disparities in screening by region are interesting and should serve as a focus for resource investment because the lack of specialists for referral and treatment options in these areas is likely a contributing factor.
However, lack of training also plays a role, said Dr. Yale, who was not involved in the study but served as a moderator of the presentation session at the meeting. Many pediatricians in practice have not been trained in substance use screening, and the fact that many of those who did try to screen were not using a standardized screening tool indicates a need for provider education, she said. The take-home message for clinicians is to find ways to include substance use screening in the care of their adolescent patients. Additionally, more research is needed to assess how best to integrate screening tools into visits, whether on paper, electronically, or verbally, and to include training on substance use screening during pediatric medical training.
The survey was conducted by the American Academy of Pediatrics Research Division. This year’s survey was supported by the Conrad N. Hilton Foundation. Dr. Camenga had no financial conflicts to disclose. Dr. Yale had no financial conflicts to disclose.
WASHINGTON – , Deepa Camenga, MD, said in a presentation at the 2023 Pediatric Academic Societies annual meeting.
The American Academy of Pediatrics recommends universal screening for substance use in adolescents during annual health visits, but current screening rates and practices among primary care pediatricians in the United States are unknown, said Dr. Camenga, an associate professor at Yale University, New Haven, Conn.
Uniformity in screening is lacking
Dr. Camenga presented data from the 2021 AAP Periodic Survey, which included 1,683 nonretired AAP members in the United States. Residents were excluded. The current analysis included 471 pediatricians who reported providing health supervision to adolescents. Overall, 284 of the 471 included respondents (60%) reported always screening adolescent patients for substance use during a health supervision visit. Of these, 42% reported using a standardized screening instrument, Dr. Camenga said.
The majority (70%) of pediatricians who used a standardized screening tool opted for the CRAFFT tool (Car, Relax, Alone, Forget, Friends, Trouble) designed for ages 12-21 years. Another 21% reported using an unspecified screening tool, 4% used RAAPS (Rapid Assessment for Adolescent Preventive Services), 3% used S2BI (Screening to Brief Intervention), and 1% used BSTAD (Brief Screener for Tobacco, Alcohol, and other Drugs).
A total of 77% of respondents reported screening their adolescent patients for substance use without a parent or guardian present. Approximately half (52%) used paper-based screening, 22% used electronic screening, 21% used verbal screening, and 6% reported other methods.
A total of 68% and 70% of respondents, respectively, agreed or strongly agreed that top barriers to screening were the lack of an onsite provider for counseling and the lack of readily available treatment options. Other reported barriers included lack of knowledge or information, patient reluctance to discuss substance use, too many other priorities during the visit, and inadequate payment. Only 6% of respondents strongly agreed that lack of time was a barrier, said Dr. Camenga.
Screening frequency and screening practices varied by geographic region, Dr. Camenga said. Pediatricians in the South and Midwest were only half as likely as those in the Northeast to report always screening adolescents for substance use (adjusted odds ratio, 0.43 and 0.53, respectively; P < .05). Similarly, compared with pediatricians in the Northeast, those in the South, Midwest, and West were significantly less likely to report using a standardized instrument for substance use screening (aOR, 0.53, 0.24, and 0.52, respectively; P < 0.001 for all).
The disparities in screening by geographic region show that there is room for improvement in this area, said Dr. Camenga. Systems-level interventions such as treatment financing and access to telehealth services could improve primary care access to substance use treatment professionals, she said.
At the practice level, embedding screening and referral tools into electronic health records could potentially improve screening rates. Many primary care pediatricians do not receive training in identifying and assessing substance use in their patients, or in first-line treatment, Dr. Camenga said.
“We have to invest in a ‘train the trainer’ type of model,” she emphasized.
Data highlight regional resource gaps
The current study is important because it highlights potential missed opportunities to screen adolescents for substance use, said Sarah Yale, MD, assistant professor of pediatrics at the Medical College of Wisconsin, Milwaukee, in an interview. Dr. Yale said that the disparities in screening by region are interesting and should serve as a focus for resource investment because the lack of specialists for referral and treatment options in these areas is likely a contributing factor.
However, lack of training also plays a role, said Dr. Yale, who was not involved in the study but served as a moderator of the presentation session at the meeting. Many pediatricians in practice have not been trained in substance use screening, and the fact that many of those who did try to screen were not using a standardized screening tool indicates a need for provider education, she said. The take-home message for clinicians is to find ways to include substance use screening in the care of their adolescent patients. Additionally, more research is needed to assess how best to integrate screening tools into visits, whether on paper, electronically, or verbally, and to include training on substance use screening during pediatric medical training.
The survey was conducted by the American Academy of Pediatrics Research Division. This year’s survey was supported by the Conrad N. Hilton Foundation. Dr. Camenga had no financial conflicts to disclose. Dr. Yale had no financial conflicts to disclose.
WASHINGTON – , Deepa Camenga, MD, said in a presentation at the 2023 Pediatric Academic Societies annual meeting.
The American Academy of Pediatrics recommends universal screening for substance use in adolescents during annual health visits, but current screening rates and practices among primary care pediatricians in the United States are unknown, said Dr. Camenga, an associate professor at Yale University, New Haven, Conn.
Uniformity in screening is lacking
Dr. Camenga presented data from the 2021 AAP Periodic Survey, which included 1,683 nonretired AAP members in the United States. Residents were excluded. The current analysis included 471 pediatricians who reported providing health supervision to adolescents. Overall, 284 of the 471 included respondents (60%) reported always screening adolescent patients for substance use during a health supervision visit. Of these, 42% reported using a standardized screening instrument, Dr. Camenga said.
The majority (70%) of pediatricians who used a standardized screening tool opted for the CRAFFT tool (Car, Relax, Alone, Forget, Friends, Trouble) designed for ages 12-21 years. Another 21% reported using an unspecified screening tool, 4% used RAAPS (Rapid Assessment for Adolescent Preventive Services), 3% used S2BI (Screening to Brief Intervention), and 1% used BSTAD (Brief Screener for Tobacco, Alcohol, and other Drugs).
A total of 77% of respondents reported screening their adolescent patients for substance use without a parent or guardian present. Approximately half (52%) used paper-based screening, 22% used electronic screening, 21% used verbal screening, and 6% reported other methods.
A total of 68% and 70% of respondents, respectively, agreed or strongly agreed that top barriers to screening were the lack of an onsite provider for counseling and the lack of readily available treatment options. Other reported barriers included lack of knowledge or information, patient reluctance to discuss substance use, too many other priorities during the visit, and inadequate payment. Only 6% of respondents strongly agreed that lack of time was a barrier, said Dr. Camenga.
Screening frequency and screening practices varied by geographic region, Dr. Camenga said. Pediatricians in the South and Midwest were only half as likely as those in the Northeast to report always screening adolescents for substance use (adjusted odds ratio, 0.43 and 0.53, respectively; P < .05). Similarly, compared with pediatricians in the Northeast, those in the South, Midwest, and West were significantly less likely to report using a standardized instrument for substance use screening (aOR, 0.53, 0.24, and 0.52, respectively; P < 0.001 for all).
The disparities in screening by geographic region show that there is room for improvement in this area, said Dr. Camenga. Systems-level interventions such as treatment financing and access to telehealth services could improve primary care access to substance use treatment professionals, she said.
At the practice level, embedding screening and referral tools into electronic health records could potentially improve screening rates. Many primary care pediatricians do not receive training in identifying and assessing substance use in their patients, or in first-line treatment, Dr. Camenga said.
“We have to invest in a ‘train the trainer’ type of model,” she emphasized.
Data highlight regional resource gaps
The current study is important because it highlights potential missed opportunities to screen adolescents for substance use, said Sarah Yale, MD, assistant professor of pediatrics at the Medical College of Wisconsin, Milwaukee, in an interview. Dr. Yale said that the disparities in screening by region are interesting and should serve as a focus for resource investment because the lack of specialists for referral and treatment options in these areas is likely a contributing factor.
However, lack of training also plays a role, said Dr. Yale, who was not involved in the study but served as a moderator of the presentation session at the meeting. Many pediatricians in practice have not been trained in substance use screening, and the fact that many of those who did try to screen were not using a standardized screening tool indicates a need for provider education, she said. The take-home message for clinicians is to find ways to include substance use screening in the care of their adolescent patients. Additionally, more research is needed to assess how best to integrate screening tools into visits, whether on paper, electronically, or verbally, and to include training on substance use screening during pediatric medical training.
The survey was conducted by the American Academy of Pediatrics Research Division. This year’s survey was supported by the Conrad N. Hilton Foundation. Dr. Camenga had no financial conflicts to disclose. Dr. Yale had no financial conflicts to disclose.
AT PAS 2023

Medical-level empathy? Yup, ChatGPT can fake that
Caution: Robotic uprisings in the rearview mirror are closer than they appear
ChatGPT. If you’ve been even in the proximity of the Internet lately, you may have heard of it. It’s quite an incredible piece of technology, an artificial intelligence that really could up-end a lot of industries. And lest doctors believe they’re safe from robotic replacement, consider this: ChatGPT took a test commonly used as a study resource by ophthalmologists and scored a 46%. Obviously, that’s not a passing grade. Job safe, right?
A month later, the researchers tried again. This time, ChatGPT got a 58%. Still not passing, and ChatGPT did especially poorly on ophthalmology specialty questions (it got 80% of general medicine questions right), but still, the jump in quality after just a month is ... concerning. It’s not like an AI will forget things. That score can only go up, and it’ll go up faster than you think.
“Sure, the robot is smart,” the doctors out there are thinking, “but how can an AI compete with human compassion, understanding, and bedside manner?”
And they’d be right. When it comes to bedside manner, there’s no competition between man and bot. ChatGPT is already winning.
In another study, researchers sampled nearly 200 questions from the subreddit r/AskDocs, which received verified physician responses. The researchers fed ChatGPT the questions – without the doctor’s answer – and a panel of health care professionals evaluated both the human doctor and ChatGPT in terms of quality and empathy.
Perhaps not surprisingly, the robot did better when it came to quality, providing a high-quality response 79% of the time, versus 22% for the human. But empathy? It was a bloodbath. ChatGPT provided an empathetic or very empathetic response 45% of the time, while humans could only do so 4.6% of the time. So much for bedside manner.
The researchers were suspiciously quick to note that ChatGPT isn’t a legitimate replacement for physicians, but could represent a tool to better provide care for patients. But let’s be honest, given ChatGPT’s quick advancement, how long before some intrepid stockholder says: “Hey, instead of paying doctors, why don’t we just use the free robot instead?” We give it a week. Or 11 minutes.
This week, on ‘As the sperm turns’
We’ve got a lot of spermy ground to cover, so let’s get right to it, starting with the small and working our way up.
We’re all pretty familiar with the basic structure of a sperm cell, yes? Bulbous head that contains all the important genetic information and a tail-like flagellum to propel it to its ultimate destination. Not much to work with there, you’d think, but what if Mother Nature, who clearly has a robust sense of humor, had something else in mind?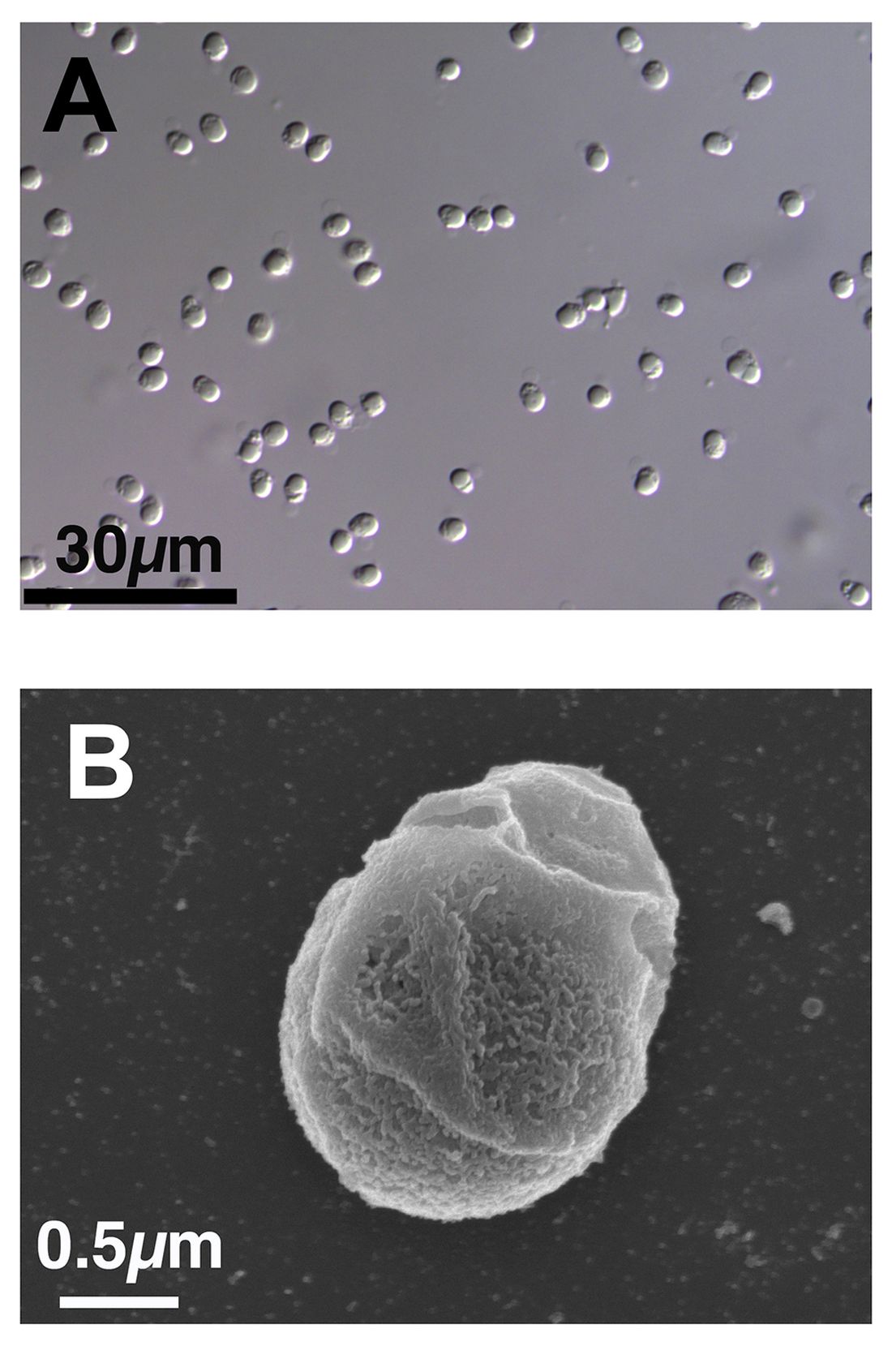
We present exhibit A, Paramormyorps kingsleyae, also known as the electric elephantfish, which happens to be the only known vertebrate species with tailless sperm. Sounds crazy to us, too, but Jason Gallant, PhD, of
Michigan State University, Lansing, has a theory: “A general notion in biology is that sperm are cheap, and eggs are expensive – but these fish may be telling us that sperm are more expensive than we might think. They could be saving energy by cutting back on sperm tails.”
He and his team think that finding the gene that turns off development of the flagellum in the elephant fish could benefit humans, specifically those with a genetic disorder called primary ciliary dyskinesia, whose lack of normally functioning cilia and flagella leads to chronic respiratory infection, abnormally positioned organs, fluid on the brain, and infertility.
And that – with “that” being infertility – brings us to exhibit B, a 41-year-old Dutch man named Jonathan Meijer who clearly has too much time on his hands.
A court in the Netherlands recently ordered him, and not for the first time, to stop donating sperm to fertility clinics after it was discovered that he had fathered between 500 and 600 children around the world. He had been banned from donating to Dutch clinics in 2017, at which point he had already fathered 100 children, but managed a workaround by donating internationally and online, sometimes using another name.
The judge ordered Mr. Meijer to contact all of the clinics abroad and ask them to destroy any of his sperm they still had in stock and threatened to fine him over $100,000 for each future violation.
Okay, so here’s the thing. We have been, um, let’s call it ... warned, about the evils of tastelessness in journalism, so we’re going to do what Mr. Meijer should have done and abstain. And we can last for longer than 11 minutes.
The realm of lost luggage and lost sleep
It may be convenient to live near an airport if you’re a frequent flyer, but it really doesn’t help your sleep numbers.
The first look at how such a common sound affects sleep duration showed that people exposed to even 45 decibels of airplane noise were less likely to get the 7-9 hours of sleep needed for healthy functioning, investigators said in Environmental Health Perspectives.
How loud is 45 dB exactly? A normal conversation is about 50 dB, while a whisper is 30 dB, to give you an idea. Airplane noise at 45 dB? You might not even notice it amongst the other noises in daily life.
The researchers looked at data from about 35,000 participants in the Nurses’ Health Study who live around 90 major U.S. airports. They examined plane noise every 5 years between 1995 and 2005, focusing on estimates of nighttime and daytime levels. Short sleep was most common among the nurses who lived on the West Coast, near major cargo airports or large bodies of water, and also among those who reported no hearing loss.
The investigators noted, however, that there was no consistent association between airplane noise and quality of sleep and stopped short of making any policy recommendations. Still, sleep is a very important, yet slept-on (pun intended) factor for our overall health, so it’s good to know if anything has the potential to cause disruption.
Caution: Robotic uprisings in the rearview mirror are closer than they appear
ChatGPT. If you’ve been even in the proximity of the Internet lately, you may have heard of it. It’s quite an incredible piece of technology, an artificial intelligence that really could up-end a lot of industries. And lest doctors believe they’re safe from robotic replacement, consider this: ChatGPT took a test commonly used as a study resource by ophthalmologists and scored a 46%. Obviously, that’s not a passing grade. Job safe, right?
A month later, the researchers tried again. This time, ChatGPT got a 58%. Still not passing, and ChatGPT did especially poorly on ophthalmology specialty questions (it got 80% of general medicine questions right), but still, the jump in quality after just a month is ... concerning. It’s not like an AI will forget things. That score can only go up, and it’ll go up faster than you think.
“Sure, the robot is smart,” the doctors out there are thinking, “but how can an AI compete with human compassion, understanding, and bedside manner?”
And they’d be right. When it comes to bedside manner, there’s no competition between man and bot. ChatGPT is already winning.
In another study, researchers sampled nearly 200 questions from the subreddit r/AskDocs, which received verified physician responses. The researchers fed ChatGPT the questions – without the doctor’s answer – and a panel of health care professionals evaluated both the human doctor and ChatGPT in terms of quality and empathy.
Perhaps not surprisingly, the robot did better when it came to quality, providing a high-quality response 79% of the time, versus 22% for the human. But empathy? It was a bloodbath. ChatGPT provided an empathetic or very empathetic response 45% of the time, while humans could only do so 4.6% of the time. So much for bedside manner.
The researchers were suspiciously quick to note that ChatGPT isn’t a legitimate replacement for physicians, but could represent a tool to better provide care for patients. But let’s be honest, given ChatGPT’s quick advancement, how long before some intrepid stockholder says: “Hey, instead of paying doctors, why don’t we just use the free robot instead?” We give it a week. Or 11 minutes.
This week, on ‘As the sperm turns’
We’ve got a lot of spermy ground to cover, so let’s get right to it, starting with the small and working our way up.
We’re all pretty familiar with the basic structure of a sperm cell, yes? Bulbous head that contains all the important genetic information and a tail-like flagellum to propel it to its ultimate destination. Not much to work with there, you’d think, but what if Mother Nature, who clearly has a robust sense of humor, had something else in mind?
We present exhibit A, Paramormyorps kingsleyae, also known as the electric elephantfish, which happens to be the only known vertebrate species with tailless sperm. Sounds crazy to us, too, but Jason Gallant, PhD, of
Michigan State University, Lansing, has a theory: “A general notion in biology is that sperm are cheap, and eggs are expensive – but these fish may be telling us that sperm are more expensive than we might think. They could be saving energy by cutting back on sperm tails.”
He and his team think that finding the gene that turns off development of the flagellum in the elephant fish could benefit humans, specifically those with a genetic disorder called primary ciliary dyskinesia, whose lack of normally functioning cilia and flagella leads to chronic respiratory infection, abnormally positioned organs, fluid on the brain, and infertility.
And that – with “that” being infertility – brings us to exhibit B, a 41-year-old Dutch man named Jonathan Meijer who clearly has too much time on his hands.
A court in the Netherlands recently ordered him, and not for the first time, to stop donating sperm to fertility clinics after it was discovered that he had fathered between 500 and 600 children around the world. He had been banned from donating to Dutch clinics in 2017, at which point he had already fathered 100 children, but managed a workaround by donating internationally and online, sometimes using another name.
The judge ordered Mr. Meijer to contact all of the clinics abroad and ask them to destroy any of his sperm they still had in stock and threatened to fine him over $100,000 for each future violation.
Okay, so here’s the thing. We have been, um, let’s call it ... warned, about the evils of tastelessness in journalism, so we’re going to do what Mr. Meijer should have done and abstain. And we can last for longer than 11 minutes.
The realm of lost luggage and lost sleep
It may be convenient to live near an airport if you’re a frequent flyer, but it really doesn’t help your sleep numbers.
The first look at how such a common sound affects sleep duration showed that people exposed to even 45 decibels of airplane noise were less likely to get the 7-9 hours of sleep needed for healthy functioning, investigators said in Environmental Health Perspectives.
How loud is 45 dB exactly? A normal conversation is about 50 dB, while a whisper is 30 dB, to give you an idea. Airplane noise at 45 dB? You might not even notice it amongst the other noises in daily life.
The researchers looked at data from about 35,000 participants in the Nurses’ Health Study who live around 90 major U.S. airports. They examined plane noise every 5 years between 1995 and 2005, focusing on estimates of nighttime and daytime levels. Short sleep was most common among the nurses who lived on the West Coast, near major cargo airports or large bodies of water, and also among those who reported no hearing loss.
The investigators noted, however, that there was no consistent association between airplane noise and quality of sleep and stopped short of making any policy recommendations. Still, sleep is a very important, yet slept-on (pun intended) factor for our overall health, so it’s good to know if anything has the potential to cause disruption.
Caution: Robotic uprisings in the rearview mirror are closer than they appear
ChatGPT. If you’ve been even in the proximity of the Internet lately, you may have heard of it. It’s quite an incredible piece of technology, an artificial intelligence that really could up-end a lot of industries. And lest doctors believe they’re safe from robotic replacement, consider this: ChatGPT took a test commonly used as a study resource by ophthalmologists and scored a 46%. Obviously, that’s not a passing grade. Job safe, right?
A month later, the researchers tried again. This time, ChatGPT got a 58%. Still not passing, and ChatGPT did especially poorly on ophthalmology specialty questions (it got 80% of general medicine questions right), but still, the jump in quality after just a month is ... concerning. It’s not like an AI will forget things. That score can only go up, and it’ll go up faster than you think.
“Sure, the robot is smart,” the doctors out there are thinking, “but how can an AI compete with human compassion, understanding, and bedside manner?”
And they’d be right. When it comes to bedside manner, there’s no competition between man and bot. ChatGPT is already winning.
In another study, researchers sampled nearly 200 questions from the subreddit r/AskDocs, which received verified physician responses. The researchers fed ChatGPT the questions – without the doctor’s answer – and a panel of health care professionals evaluated both the human doctor and ChatGPT in terms of quality and empathy.
Perhaps not surprisingly, the robot did better when it came to quality, providing a high-quality response 79% of the time, versus 22% for the human. But empathy? It was a bloodbath. ChatGPT provided an empathetic or very empathetic response 45% of the time, while humans could only do so 4.6% of the time. So much for bedside manner.
The researchers were suspiciously quick to note that ChatGPT isn’t a legitimate replacement for physicians, but could represent a tool to better provide care for patients. But let’s be honest, given ChatGPT’s quick advancement, how long before some intrepid stockholder says: “Hey, instead of paying doctors, why don’t we just use the free robot instead?” We give it a week. Or 11 minutes.
This week, on ‘As the sperm turns’
We’ve got a lot of spermy ground to cover, so let’s get right to it, starting with the small and working our way up.
We’re all pretty familiar with the basic structure of a sperm cell, yes? Bulbous head that contains all the important genetic information and a tail-like flagellum to propel it to its ultimate destination. Not much to work with there, you’d think, but what if Mother Nature, who clearly has a robust sense of humor, had something else in mind?
We present exhibit A, Paramormyorps kingsleyae, also known as the electric elephantfish, which happens to be the only known vertebrate species with tailless sperm. Sounds crazy to us, too, but Jason Gallant, PhD, of
Michigan State University, Lansing, has a theory: “A general notion in biology is that sperm are cheap, and eggs are expensive – but these fish may be telling us that sperm are more expensive than we might think. They could be saving energy by cutting back on sperm tails.”
He and his team think that finding the gene that turns off development of the flagellum in the elephant fish could benefit humans, specifically those with a genetic disorder called primary ciliary dyskinesia, whose lack of normally functioning cilia and flagella leads to chronic respiratory infection, abnormally positioned organs, fluid on the brain, and infertility.
And that – with “that” being infertility – brings us to exhibit B, a 41-year-old Dutch man named Jonathan Meijer who clearly has too much time on his hands.
A court in the Netherlands recently ordered him, and not for the first time, to stop donating sperm to fertility clinics after it was discovered that he had fathered between 500 and 600 children around the world. He had been banned from donating to Dutch clinics in 2017, at which point he had already fathered 100 children, but managed a workaround by donating internationally and online, sometimes using another name.
The judge ordered Mr. Meijer to contact all of the clinics abroad and ask them to destroy any of his sperm they still had in stock and threatened to fine him over $100,000 for each future violation.
Okay, so here’s the thing. We have been, um, let’s call it ... warned, about the evils of tastelessness in journalism, so we’re going to do what Mr. Meijer should have done and abstain. And we can last for longer than 11 minutes.
The realm of lost luggage and lost sleep
It may be convenient to live near an airport if you’re a frequent flyer, but it really doesn’t help your sleep numbers.
The first look at how such a common sound affects sleep duration showed that people exposed to even 45 decibels of airplane noise were less likely to get the 7-9 hours of sleep needed for healthy functioning, investigators said in Environmental Health Perspectives.
How loud is 45 dB exactly? A normal conversation is about 50 dB, while a whisper is 30 dB, to give you an idea. Airplane noise at 45 dB? You might not even notice it amongst the other noises in daily life.
The researchers looked at data from about 35,000 participants in the Nurses’ Health Study who live around 90 major U.S. airports. They examined plane noise every 5 years between 1995 and 2005, focusing on estimates of nighttime and daytime levels. Short sleep was most common among the nurses who lived on the West Coast, near major cargo airports or large bodies of water, and also among those who reported no hearing loss.
The investigators noted, however, that there was no consistent association between airplane noise and quality of sleep and stopped short of making any policy recommendations. Still, sleep is a very important, yet slept-on (pun intended) factor for our overall health, so it’s good to know if anything has the potential to cause disruption.
AHA backs screening for cognitive impairment after stroke
Screening for cognitive impairment should be part of multidisciplinary care for stroke survivors, the American Heart Association says in a new scientific statement.
“Cognitive impairment after stroke is very common, is associated with other post-stroke outcomes, and often has significant impact on the quality of life,” Nada El Husseini, MD, MHSc, chair of the scientific statement writing group, told this news organization.
“It is important to screen stroke survivors for cognitive impairment as well as for associated comorbidities such as mood and sleep disorders,” said Dr. El Husseini, associate professor of neurology at Duke University Medical Center in Durham, N.C.
The scientific statement was published online in Stroke. It’s the first to specifically focus on the cognitive impairment resulting from an overt stroke (ischemic or hemorrhagic).
‘Actionable’ considerations for care
The writing group performed a “scoping” review of the literature on the prevalence, diagnosis, and management of poststroke cognitive impairment (PSCI) to provide a framework for “actionable considerations” for clinical practice as well as to highlight gaps needing additional studies, Dr. El Husseini explained.
PSCI, ranging from mild to severe, occurs in up to 60% of stroke survivors in the first year after stroke; yet, it is often underreported and underdiagnosed, the writing group notes.
Up to 20% of stroke survivors who experience mild cognitive impairment fully recover cognitive function, and cognitive recovery is most likely within the first 6 months after a stroke.
However, improvement in cognitive impairment without return to prestroke levels is more frequent than is complete recovery. As many as one in three stroke survivors may develop dementia within 5 years of stroke.
The writing group also notes that PSCI is often associated with other conditions, including physical disability, sleep disorders, behavioral and personality changes, depression, and other neuropsychological changes – each of which may contribute to lower quality of life.
Currently, there is no “gold standard” for cognitive screening following stroke, but several brief cognitive screening tests, including the Mini–Mental State Examination and the Montreal Cognitive Assessment, are widely used to identify cognitive impairment after stroke.
The statement also highlights the importance of assessing cognitive changes over time after stroke. Stroke survivors who experience unexplained difficulties with cognitive-related activities of daily living, following care instructions, or providing a reliable health history may be candidates for additional cognitive screening.
Manage risk factors to prevent repeat stroke
“Anticipatory guidance regarding home and driving safety and, return to work (if applicable) along with interdisciplinary collaboration among different medical and ancillary specialists in the diagnosis and management of cognitive impairment is key for the holistic care of stroke survivors,” Dr. El Husseini told this news organization.
The multidisciplinary poststroke health care team could include neurologists, occupational therapists, speech therapists, nurses, neuropsychologists, gerontologists, and primary care providers.
“Because recurrent stroke is strongly associated with the development of cognitive impairment and dementia, prevention of recurrent strokes should be sought to decrease that risk,” Dr. El Husseini said. This includes addressing stroke risk factors, including high blood pressure, high cholesterol, type 2 diabetes, and atrial fibrillation.
The writing group says research is needed in the future to determine how cognitive impairment develops after stroke and the impact of nonbrain factors, including infection, frailty, and social factors.
Further research is also needed to determine best practices for cognitive screening after stroke, including the development and use of screening instruments that consider demographic, cultural, and linguistic factors in determining “normal” function.
“Perhaps the most pressing need, however, is the development of effective and culturally relevant treatments for poststroke cognitive impairment,” Dr. El Husseini said in a news release.
“We hope to see big enough clinical trials that assess various techniques, medications, and lifestyle changes in diverse groups of patients that may help improve cognitive function,” she added.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Stroke Council, the Council on Cardiovascular Radiology and Intervention, the Council on Hypertension, and the Council on Lifestyle and Cardiometabolic Health.
Screening for cognitive impairment should be part of multidisciplinary care for stroke survivors, the American Heart Association says in a new scientific statement.
“Cognitive impairment after stroke is very common, is associated with other post-stroke outcomes, and often has significant impact on the quality of life,” Nada El Husseini, MD, MHSc, chair of the scientific statement writing group, told this news organization.
“It is important to screen stroke survivors for cognitive impairment as well as for associated comorbidities such as mood and sleep disorders,” said Dr. El Husseini, associate professor of neurology at Duke University Medical Center in Durham, N.C.
The scientific statement was published online in Stroke. It’s the first to specifically focus on the cognitive impairment resulting from an overt stroke (ischemic or hemorrhagic).
‘Actionable’ considerations for care
The writing group performed a “scoping” review of the literature on the prevalence, diagnosis, and management of poststroke cognitive impairment (PSCI) to provide a framework for “actionable considerations” for clinical practice as well as to highlight gaps needing additional studies, Dr. El Husseini explained.
PSCI, ranging from mild to severe, occurs in up to 60% of stroke survivors in the first year after stroke; yet, it is often underreported and underdiagnosed, the writing group notes.
Up to 20% of stroke survivors who experience mild cognitive impairment fully recover cognitive function, and cognitive recovery is most likely within the first 6 months after a stroke.
However, improvement in cognitive impairment without return to prestroke levels is more frequent than is complete recovery. As many as one in three stroke survivors may develop dementia within 5 years of stroke.
The writing group also notes that PSCI is often associated with other conditions, including physical disability, sleep disorders, behavioral and personality changes, depression, and other neuropsychological changes – each of which may contribute to lower quality of life.
Currently, there is no “gold standard” for cognitive screening following stroke, but several brief cognitive screening tests, including the Mini–Mental State Examination and the Montreal Cognitive Assessment, are widely used to identify cognitive impairment after stroke.
The statement also highlights the importance of assessing cognitive changes over time after stroke. Stroke survivors who experience unexplained difficulties with cognitive-related activities of daily living, following care instructions, or providing a reliable health history may be candidates for additional cognitive screening.
Manage risk factors to prevent repeat stroke
“Anticipatory guidance regarding home and driving safety and, return to work (if applicable) along with interdisciplinary collaboration among different medical and ancillary specialists in the diagnosis and management of cognitive impairment is key for the holistic care of stroke survivors,” Dr. El Husseini told this news organization.
The multidisciplinary poststroke health care team could include neurologists, occupational therapists, speech therapists, nurses, neuropsychologists, gerontologists, and primary care providers.
“Because recurrent stroke is strongly associated with the development of cognitive impairment and dementia, prevention of recurrent strokes should be sought to decrease that risk,” Dr. El Husseini said. This includes addressing stroke risk factors, including high blood pressure, high cholesterol, type 2 diabetes, and atrial fibrillation.
The writing group says research is needed in the future to determine how cognitive impairment develops after stroke and the impact of nonbrain factors, including infection, frailty, and social factors.
Further research is also needed to determine best practices for cognitive screening after stroke, including the development and use of screening instruments that consider demographic, cultural, and linguistic factors in determining “normal” function.
“Perhaps the most pressing need, however, is the development of effective and culturally relevant treatments for poststroke cognitive impairment,” Dr. El Husseini said in a news release.
“We hope to see big enough clinical trials that assess various techniques, medications, and lifestyle changes in diverse groups of patients that may help improve cognitive function,” she added.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Stroke Council, the Council on Cardiovascular Radiology and Intervention, the Council on Hypertension, and the Council on Lifestyle and Cardiometabolic Health.
Screening for cognitive impairment should be part of multidisciplinary care for stroke survivors, the American Heart Association says in a new scientific statement.
“Cognitive impairment after stroke is very common, is associated with other post-stroke outcomes, and often has significant impact on the quality of life,” Nada El Husseini, MD, MHSc, chair of the scientific statement writing group, told this news organization.
“It is important to screen stroke survivors for cognitive impairment as well as for associated comorbidities such as mood and sleep disorders,” said Dr. El Husseini, associate professor of neurology at Duke University Medical Center in Durham, N.C.
The scientific statement was published online in Stroke. It’s the first to specifically focus on the cognitive impairment resulting from an overt stroke (ischemic or hemorrhagic).
‘Actionable’ considerations for care
The writing group performed a “scoping” review of the literature on the prevalence, diagnosis, and management of poststroke cognitive impairment (PSCI) to provide a framework for “actionable considerations” for clinical practice as well as to highlight gaps needing additional studies, Dr. El Husseini explained.
PSCI, ranging from mild to severe, occurs in up to 60% of stroke survivors in the first year after stroke; yet, it is often underreported and underdiagnosed, the writing group notes.
Up to 20% of stroke survivors who experience mild cognitive impairment fully recover cognitive function, and cognitive recovery is most likely within the first 6 months after a stroke.
However, improvement in cognitive impairment without return to prestroke levels is more frequent than is complete recovery. As many as one in three stroke survivors may develop dementia within 5 years of stroke.
The writing group also notes that PSCI is often associated with other conditions, including physical disability, sleep disorders, behavioral and personality changes, depression, and other neuropsychological changes – each of which may contribute to lower quality of life.
Currently, there is no “gold standard” for cognitive screening following stroke, but several brief cognitive screening tests, including the Mini–Mental State Examination and the Montreal Cognitive Assessment, are widely used to identify cognitive impairment after stroke.
The statement also highlights the importance of assessing cognitive changes over time after stroke. Stroke survivors who experience unexplained difficulties with cognitive-related activities of daily living, following care instructions, or providing a reliable health history may be candidates for additional cognitive screening.
Manage risk factors to prevent repeat stroke
“Anticipatory guidance regarding home and driving safety and, return to work (if applicable) along with interdisciplinary collaboration among different medical and ancillary specialists in the diagnosis and management of cognitive impairment is key for the holistic care of stroke survivors,” Dr. El Husseini told this news organization.
The multidisciplinary poststroke health care team could include neurologists, occupational therapists, speech therapists, nurses, neuropsychologists, gerontologists, and primary care providers.
“Because recurrent stroke is strongly associated with the development of cognitive impairment and dementia, prevention of recurrent strokes should be sought to decrease that risk,” Dr. El Husseini said. This includes addressing stroke risk factors, including high blood pressure, high cholesterol, type 2 diabetes, and atrial fibrillation.
The writing group says research is needed in the future to determine how cognitive impairment develops after stroke and the impact of nonbrain factors, including infection, frailty, and social factors.
Further research is also needed to determine best practices for cognitive screening after stroke, including the development and use of screening instruments that consider demographic, cultural, and linguistic factors in determining “normal” function.
“Perhaps the most pressing need, however, is the development of effective and culturally relevant treatments for poststroke cognitive impairment,” Dr. El Husseini said in a news release.
“We hope to see big enough clinical trials that assess various techniques, medications, and lifestyle changes in diverse groups of patients that may help improve cognitive function,” she added.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Stroke Council, the Council on Cardiovascular Radiology and Intervention, the Council on Hypertension, and the Council on Lifestyle and Cardiometabolic Health.
New tool accurately predicts suicide risk in serious mental illness
The 17-question Oxford Mental Illness and Suicide Tool (OxMIS) assessment is designed to predict 12-month suicide risk in people with schizophrenia spectrum disorders and bipolar disorder based on risk factors such as familial traits, antisocial traits, and information about self-harm.
“We have demonstrated the clinical utility of OxMIS in two separate studies and countries. As with any clinical risk prediction tool, it will not improve outcomes unless coupled with effective interventions,” lead investigator Amir Sariaslan, PhD, a senior research fellow in psychiatric epidemiology at the University of Oxford, England, told this news organization.
The findings were published online in Translational Psychiatry.
Twice validated
Dr. Sariaslan and his team originally developed and validated the OxMIS in a cohort of 75,000 people with SMI in Sweden. Recognizing the lack of externally validated prognostic models in the mental health field, the team wanted to validate the instrument in a new, population-based sample in Finland.
The investigators accessed information about patient diagnosis and treatment from the Finnish Care Register for Health Care, which contains de-identified information for all individuals between ages 15 and 65 years diagnosed with an SMI between Jan. 1, 1996, and Dec. 31, 2017.
They included 137,000 patients with somatic symptom disorder or bipolar disorder for a total of more than 5 million episodes of inpatient or outpatient treatment. Investigators linked the cohort to the Causes of Death Register to identify those who had died by suicide within 12 months of an index treatment episode, which investigators randomly selected for each person.
The investigators found that 1,475 individuals in the sample died by suicide within 1 year of their index episode (1.1%).
Each patient was assigned a clinical suicide risk score based on their clinical information, familial traits, prescription information, and comorbid conditions. Using OxMIS, the investigators found that the instrument accurately predicted suicide with an area under the curve of 0.70.
In other words, in 70% of the instances where the investigators randomly selected two people from the sample, one of whom died by suicide and the other of whom did not, the individual who died by suicide had a higher OxMIS risk score.
The investigators note the model overestimated the risk for patients who were at extremely high risk for suicide (those with a predicted suicide risk of > 5%). “In our complementary sensitivity analysis, we observed improved calibration in these patients when we assigned them a suicide risk prediction of no more than 5%,” they write.
Dr. Sariaslan said that the findings highlight the importance of safety planning interventions. “It is also essential to remember that OxMIS is not intended to replace clinical decision-making, but rather to support it,” he said.
As to whether the tool could be used in other populations, such as in the United States, Dr. Sariaslan said, “there is no good evidence that the contribution of risk factors to suicide in this population is different in the U.S. than in northern Europe, so there is no a priori reason to have to do multiple external validations before it can be used for research or clinical purposes.”
One size does not fit all
Commenting on the study, Ronald Kessler, PhD, McNeil Family Professor, department of health care policy at Harvard Medical School, Boston, said that he’d be “surprised” if OxMIS was adopted in the United States because there is already an existing tool that is “slightly more accurate,” which he helped develop.

“In addition, when we start thinking about uses for such scales, it becomes clear that different scales should be used for different segments of the population, depending on intervention options,” Dr. Kessler said.
“So, for example, a different scale would probably be optimal in deciding how to manage psychiatric inpatients in the transition back to the community after hospital discharge than [it would be], say, in deciding how to respond to suicidality among patients presenting at an emergency department. No one scale will fit for all the scenarios in which prediction is desired,” he added.
The study was funded by the Academy of Finland. Dr. Kessler receives funding from the National Institute of Mental Health, Department of Defense, and Veterans Administration to develop suicide prediction models. Dr. Sariaslan has no disclosures to report.
A version of this article first appeared on Medscape.com.
The 17-question Oxford Mental Illness and Suicide Tool (OxMIS) assessment is designed to predict 12-month suicide risk in people with schizophrenia spectrum disorders and bipolar disorder based on risk factors such as familial traits, antisocial traits, and information about self-harm.
“We have demonstrated the clinical utility of OxMIS in two separate studies and countries. As with any clinical risk prediction tool, it will not improve outcomes unless coupled with effective interventions,” lead investigator Amir Sariaslan, PhD, a senior research fellow in psychiatric epidemiology at the University of Oxford, England, told this news organization.
The findings were published online in Translational Psychiatry.
Twice validated
Dr. Sariaslan and his team originally developed and validated the OxMIS in a cohort of 75,000 people with SMI in Sweden. Recognizing the lack of externally validated prognostic models in the mental health field, the team wanted to validate the instrument in a new, population-based sample in Finland.
The investigators accessed information about patient diagnosis and treatment from the Finnish Care Register for Health Care, which contains de-identified information for all individuals between ages 15 and 65 years diagnosed with an SMI between Jan. 1, 1996, and Dec. 31, 2017.
They included 137,000 patients with somatic symptom disorder or bipolar disorder for a total of more than 5 million episodes of inpatient or outpatient treatment. Investigators linked the cohort to the Causes of Death Register to identify those who had died by suicide within 12 months of an index treatment episode, which investigators randomly selected for each person.
The investigators found that 1,475 individuals in the sample died by suicide within 1 year of their index episode (1.1%).
Each patient was assigned a clinical suicide risk score based on their clinical information, familial traits, prescription information, and comorbid conditions. Using OxMIS, the investigators found that the instrument accurately predicted suicide with an area under the curve of 0.70.
In other words, in 70% of the instances where the investigators randomly selected two people from the sample, one of whom died by suicide and the other of whom did not, the individual who died by suicide had a higher OxMIS risk score.
The investigators note the model overestimated the risk for patients who were at extremely high risk for suicide (those with a predicted suicide risk of > 5%). “In our complementary sensitivity analysis, we observed improved calibration in these patients when we assigned them a suicide risk prediction of no more than 5%,” they write.
Dr. Sariaslan said that the findings highlight the importance of safety planning interventions. “It is also essential to remember that OxMIS is not intended to replace clinical decision-making, but rather to support it,” he said.
As to whether the tool could be used in other populations, such as in the United States, Dr. Sariaslan said, “there is no good evidence that the contribution of risk factors to suicide in this population is different in the U.S. than in northern Europe, so there is no a priori reason to have to do multiple external validations before it can be used for research or clinical purposes.”
One size does not fit all
Commenting on the study, Ronald Kessler, PhD, McNeil Family Professor, department of health care policy at Harvard Medical School, Boston, said that he’d be “surprised” if OxMIS was adopted in the United States because there is already an existing tool that is “slightly more accurate,” which he helped develop.
“In addition, when we start thinking about uses for such scales, it becomes clear that different scales should be used for different segments of the population, depending on intervention options,” Dr. Kessler said.
“So, for example, a different scale would probably be optimal in deciding how to manage psychiatric inpatients in the transition back to the community after hospital discharge than [it would be], say, in deciding how to respond to suicidality among patients presenting at an emergency department. No one scale will fit for all the scenarios in which prediction is desired,” he added.
The study was funded by the Academy of Finland. Dr. Kessler receives funding from the National Institute of Mental Health, Department of Defense, and Veterans Administration to develop suicide prediction models. Dr. Sariaslan has no disclosures to report.
A version of this article first appeared on Medscape.com.
The 17-question Oxford Mental Illness and Suicide Tool (OxMIS) assessment is designed to predict 12-month suicide risk in people with schizophrenia spectrum disorders and bipolar disorder based on risk factors such as familial traits, antisocial traits, and information about self-harm.
“We have demonstrated the clinical utility of OxMIS in two separate studies and countries. As with any clinical risk prediction tool, it will not improve outcomes unless coupled with effective interventions,” lead investigator Amir Sariaslan, PhD, a senior research fellow in psychiatric epidemiology at the University of Oxford, England, told this news organization.
The findings were published online in Translational Psychiatry.
Twice validated
Dr. Sariaslan and his team originally developed and validated the OxMIS in a cohort of 75,000 people with SMI in Sweden. Recognizing the lack of externally validated prognostic models in the mental health field, the team wanted to validate the instrument in a new, population-based sample in Finland.
The investigators accessed information about patient diagnosis and treatment from the Finnish Care Register for Health Care, which contains de-identified information for all individuals between ages 15 and 65 years diagnosed with an SMI between Jan. 1, 1996, and Dec. 31, 2017.
They included 137,000 patients with somatic symptom disorder or bipolar disorder for a total of more than 5 million episodes of inpatient or outpatient treatment. Investigators linked the cohort to the Causes of Death Register to identify those who had died by suicide within 12 months of an index treatment episode, which investigators randomly selected for each person.
The investigators found that 1,475 individuals in the sample died by suicide within 1 year of their index episode (1.1%).
Each patient was assigned a clinical suicide risk score based on their clinical information, familial traits, prescription information, and comorbid conditions. Using OxMIS, the investigators found that the instrument accurately predicted suicide with an area under the curve of 0.70.
In other words, in 70% of the instances where the investigators randomly selected two people from the sample, one of whom died by suicide and the other of whom did not, the individual who died by suicide had a higher OxMIS risk score.
The investigators note the model overestimated the risk for patients who were at extremely high risk for suicide (those with a predicted suicide risk of > 5%). “In our complementary sensitivity analysis, we observed improved calibration in these patients when we assigned them a suicide risk prediction of no more than 5%,” they write.
Dr. Sariaslan said that the findings highlight the importance of safety planning interventions. “It is also essential to remember that OxMIS is not intended to replace clinical decision-making, but rather to support it,” he said.
As to whether the tool could be used in other populations, such as in the United States, Dr. Sariaslan said, “there is no good evidence that the contribution of risk factors to suicide in this population is different in the U.S. than in northern Europe, so there is no a priori reason to have to do multiple external validations before it can be used for research or clinical purposes.”
One size does not fit all
Commenting on the study, Ronald Kessler, PhD, McNeil Family Professor, department of health care policy at Harvard Medical School, Boston, said that he’d be “surprised” if OxMIS was adopted in the United States because there is already an existing tool that is “slightly more accurate,” which he helped develop.
“In addition, when we start thinking about uses for such scales, it becomes clear that different scales should be used for different segments of the population, depending on intervention options,” Dr. Kessler said.
“So, for example, a different scale would probably be optimal in deciding how to manage psychiatric inpatients in the transition back to the community after hospital discharge than [it would be], say, in deciding how to respond to suicidality among patients presenting at an emergency department. No one scale will fit for all the scenarios in which prediction is desired,” he added.
The study was funded by the Academy of Finland. Dr. Kessler receives funding from the National Institute of Mental Health, Department of Defense, and Veterans Administration to develop suicide prediction models. Dr. Sariaslan has no disclosures to report.
A version of this article first appeared on Medscape.com.
FROM TRANSLATIONAL PSYCHIATRY
Oral antiamyloid shows disease-modifying potential Phase 3 trial underway
BOSTON – , represented by positive changes in plasma and imaging biomarkers of Alzheimer’s disease pathology.
Use of the drug, ALZ-801 (Alzheon), led to a significant reduction of plasma phosphorylated–tau 181 (p-tau181) , a marker of amyloid-induced neuronal injury in Alzheimer’s disease, as well as slowing of hippocampal atrophy and stabilization of cognition.
“The 12-month results of our phase 2 trial support the finding that ALZ-801 blocks misfolding of amyloid monomers and subsequent formation of neurotoxic amyloid oligomers, the key initial step in the amyloid aggregation cascade, which leads to a rapid and sustained reduction of brain neurodegeneration as measured by plasma p-tau181,” John Hey, PhD, Alzheon’s chief scientific officer, said in a statement.
“The severalfold greater reduction on the p-tau181 biomarker in plasma compared to plaque-clearing antiamyloid antibodies, combined with preservation of brain hippocampal volume and their positive correlations with cognitive benefits, further validate the disease-modifying effects of ALZ-801 in Alzheimer’s patients,” Dr. Hey added.
The results were presented at the 2023 annual meeting of the American Academy of Neurology.
ALZ-801 is an optimized prodrug of tramiprosate that has been shown to inhibit amyloid-beta 42 aggregation into toxic oligomers.
The ongoing phase 2 study is evaluating the effects of oral ALZ-801 (265 mg twice daily) on biomarkers of Alzheimer’s disease pathology for 84 adults with early Alzheimer’s disease who have either the APOE4/4 or APOE3/4 genotype. These genotypes represent the majority of patients with Alzheimer’s disease.
The mean age of the cohort was 69 years, and 51% are women; 70% had mild cognitive impairment, and 30% had mild Alzheimer’s disease. The mean Mini-Mental State Examination score for the cohort was 26.0. Roughly half were taking a cholinesterase inhibitor.
Significant plasma p-tau181 reduction was observed at 13 weeks. Levels were reduced by 41% by 52 weeks (P = .016). There was also a significant 5% reduction in plasma amyloid-beta 42 and 40 at 52 weeks (P = .002 and P = .005, respectively), Dr. Hey reported.
After 12 months of treatment, hippocampal atrophy was reduced by about 23%, and expansion of ventricular volume was reduced by about 15%, both in comparison with matched controls from the Alzheimer’s Disease Neuroimaging Initiative.
Composite cognitive z-score improved significantly at 13 and 26 weeks and remained above baseline at 52 weeks in comparison with matched ADNI controls. “These are very promising data,” Dr. Hey told conference attendees.
He noted that the safety profile of ALZ-801 remains favorable and consistent with prior safety data. Common adverse events were mild nausea and SARS-CoV-2 infection. There were no drug-related serious events or amyloid-related imaging abnormalities–edema (ARIA-E).
The phase 3 APOLLOE4 study of ALZ-801 is underway. This double-blind, randomized study is comparing oral ALZ-801 with placebo over 78 weeks for roughly 300 adults with early Alzheimer’s disease who have the APOE4/4 genotype. APOLLOE4 is expected to be completed in mid 2024.
The APOLLOE4 study is supported by a $47 million grant from the National Institute on Aging. The U.S. Food and Drug Administration has granted ALZ-801 fast-track designation.
More accessible option?
Reached for comment, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, noted that the “biggest difference between this drug and others is that it is taken orally, rather than delivered through an infusion. This is important and valuable for reducing patient and caregiver burden and increasing ease of use and access.”
It’s also noteworthy that ALZ-801 was not associated with ARIA-E, “which has been reported in other antiamyloid trials and can occasionally be serious,” Dr. Griffin said.
Overall, he said the results are “encouraging, but more work is needed. If studies results continue to be positive, this treatment may provide a more accessible option for people who are at higher risk of ARIA,” Dr. Griffin said.
The study was funded by Alzheon. Dr. Hey is an employee of Alzheon and holds stock in the company. Dr. Griffin has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
BOSTON – , represented by positive changes in plasma and imaging biomarkers of Alzheimer’s disease pathology.
Use of the drug, ALZ-801 (Alzheon), led to a significant reduction of plasma phosphorylated–tau 181 (p-tau181) , a marker of amyloid-induced neuronal injury in Alzheimer’s disease, as well as slowing of hippocampal atrophy and stabilization of cognition.
“The 12-month results of our phase 2 trial support the finding that ALZ-801 blocks misfolding of amyloid monomers and subsequent formation of neurotoxic amyloid oligomers, the key initial step in the amyloid aggregation cascade, which leads to a rapid and sustained reduction of brain neurodegeneration as measured by plasma p-tau181,” John Hey, PhD, Alzheon’s chief scientific officer, said in a statement.
“The severalfold greater reduction on the p-tau181 biomarker in plasma compared to plaque-clearing antiamyloid antibodies, combined with preservation of brain hippocampal volume and their positive correlations with cognitive benefits, further validate the disease-modifying effects of ALZ-801 in Alzheimer’s patients,” Dr. Hey added.
The results were presented at the 2023 annual meeting of the American Academy of Neurology.
ALZ-801 is an optimized prodrug of tramiprosate that has been shown to inhibit amyloid-beta 42 aggregation into toxic oligomers.
The ongoing phase 2 study is evaluating the effects of oral ALZ-801 (265 mg twice daily) on biomarkers of Alzheimer’s disease pathology for 84 adults with early Alzheimer’s disease who have either the APOE4/4 or APOE3/4 genotype. These genotypes represent the majority of patients with Alzheimer’s disease.
The mean age of the cohort was 69 years, and 51% are women; 70% had mild cognitive impairment, and 30% had mild Alzheimer’s disease. The mean Mini-Mental State Examination score for the cohort was 26.0. Roughly half were taking a cholinesterase inhibitor.
Significant plasma p-tau181 reduction was observed at 13 weeks. Levels were reduced by 41% by 52 weeks (P = .016). There was also a significant 5% reduction in plasma amyloid-beta 42 and 40 at 52 weeks (P = .002 and P = .005, respectively), Dr. Hey reported.
After 12 months of treatment, hippocampal atrophy was reduced by about 23%, and expansion of ventricular volume was reduced by about 15%, both in comparison with matched controls from the Alzheimer’s Disease Neuroimaging Initiative.
Composite cognitive z-score improved significantly at 13 and 26 weeks and remained above baseline at 52 weeks in comparison with matched ADNI controls. “These are very promising data,” Dr. Hey told conference attendees.
He noted that the safety profile of ALZ-801 remains favorable and consistent with prior safety data. Common adverse events were mild nausea and SARS-CoV-2 infection. There were no drug-related serious events or amyloid-related imaging abnormalities–edema (ARIA-E).
The phase 3 APOLLOE4 study of ALZ-801 is underway. This double-blind, randomized study is comparing oral ALZ-801 with placebo over 78 weeks for roughly 300 adults with early Alzheimer’s disease who have the APOE4/4 genotype. APOLLOE4 is expected to be completed in mid 2024.
The APOLLOE4 study is supported by a $47 million grant from the National Institute on Aging. The U.S. Food and Drug Administration has granted ALZ-801 fast-track designation.
More accessible option?
Reached for comment, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, noted that the “biggest difference between this drug and others is that it is taken orally, rather than delivered through an infusion. This is important and valuable for reducing patient and caregiver burden and increasing ease of use and access.”
It’s also noteworthy that ALZ-801 was not associated with ARIA-E, “which has been reported in other antiamyloid trials and can occasionally be serious,” Dr. Griffin said.
Overall, he said the results are “encouraging, but more work is needed. If studies results continue to be positive, this treatment may provide a more accessible option for people who are at higher risk of ARIA,” Dr. Griffin said.
The study was funded by Alzheon. Dr. Hey is an employee of Alzheon and holds stock in the company. Dr. Griffin has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
BOSTON – , represented by positive changes in plasma and imaging biomarkers of Alzheimer’s disease pathology.
Use of the drug, ALZ-801 (Alzheon), led to a significant reduction of plasma phosphorylated–tau 181 (p-tau181) , a marker of amyloid-induced neuronal injury in Alzheimer’s disease, as well as slowing of hippocampal atrophy and stabilization of cognition.
“The 12-month results of our phase 2 trial support the finding that ALZ-801 blocks misfolding of amyloid monomers and subsequent formation of neurotoxic amyloid oligomers, the key initial step in the amyloid aggregation cascade, which leads to a rapid and sustained reduction of brain neurodegeneration as measured by plasma p-tau181,” John Hey, PhD, Alzheon’s chief scientific officer, said in a statement.
“The severalfold greater reduction on the p-tau181 biomarker in plasma compared to plaque-clearing antiamyloid antibodies, combined with preservation of brain hippocampal volume and their positive correlations with cognitive benefits, further validate the disease-modifying effects of ALZ-801 in Alzheimer’s patients,” Dr. Hey added.
The results were presented at the 2023 annual meeting of the American Academy of Neurology.
ALZ-801 is an optimized prodrug of tramiprosate that has been shown to inhibit amyloid-beta 42 aggregation into toxic oligomers.
The ongoing phase 2 study is evaluating the effects of oral ALZ-801 (265 mg twice daily) on biomarkers of Alzheimer’s disease pathology for 84 adults with early Alzheimer’s disease who have either the APOE4/4 or APOE3/4 genotype. These genotypes represent the majority of patients with Alzheimer’s disease.
The mean age of the cohort was 69 years, and 51% are women; 70% had mild cognitive impairment, and 30% had mild Alzheimer’s disease. The mean Mini-Mental State Examination score for the cohort was 26.0. Roughly half were taking a cholinesterase inhibitor.
Significant plasma p-tau181 reduction was observed at 13 weeks. Levels were reduced by 41% by 52 weeks (P = .016). There was also a significant 5% reduction in plasma amyloid-beta 42 and 40 at 52 weeks (P = .002 and P = .005, respectively), Dr. Hey reported.
After 12 months of treatment, hippocampal atrophy was reduced by about 23%, and expansion of ventricular volume was reduced by about 15%, both in comparison with matched controls from the Alzheimer’s Disease Neuroimaging Initiative.
Composite cognitive z-score improved significantly at 13 and 26 weeks and remained above baseline at 52 weeks in comparison with matched ADNI controls. “These are very promising data,” Dr. Hey told conference attendees.
He noted that the safety profile of ALZ-801 remains favorable and consistent with prior safety data. Common adverse events were mild nausea and SARS-CoV-2 infection. There were no drug-related serious events or amyloid-related imaging abnormalities–edema (ARIA-E).
The phase 3 APOLLOE4 study of ALZ-801 is underway. This double-blind, randomized study is comparing oral ALZ-801 with placebo over 78 weeks for roughly 300 adults with early Alzheimer’s disease who have the APOE4/4 genotype. APOLLOE4 is expected to be completed in mid 2024.
The APOLLOE4 study is supported by a $47 million grant from the National Institute on Aging. The U.S. Food and Drug Administration has granted ALZ-801 fast-track designation.
More accessible option?
Reached for comment, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, noted that the “biggest difference between this drug and others is that it is taken orally, rather than delivered through an infusion. This is important and valuable for reducing patient and caregiver burden and increasing ease of use and access.”
It’s also noteworthy that ALZ-801 was not associated with ARIA-E, “which has been reported in other antiamyloid trials and can occasionally be serious,” Dr. Griffin said.
Overall, he said the results are “encouraging, but more work is needed. If studies results continue to be positive, this treatment may provide a more accessible option for people who are at higher risk of ARIA,” Dr. Griffin said.
The study was funded by Alzheon. Dr. Hey is an employee of Alzheon and holds stock in the company. Dr. Griffin has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM AAN 2023
Why is buprenorphine use flatlining?
Opioid overdose deaths are at a record high in the United States, and many of these deaths can be prevented with medications such as buprenorphine, said lead author Kao-Ping Chua, MD, of the University of Michigan, Ann Arbor, in an interview. “However, buprenorphine cannot prevent opioid overdose deaths if patients are never started on the medication or only stay on the medication for a short time. For that reason, rates of buprenorphine initiation and retention are critical metrics for measuring how well the U.S. health care system is responding to the opioid epidemic,” he said.
“At the time we started our study, several other research groups had evaluated U.S. rates of buprenorphine initiation and retention using data through 2020. However, more recent national data were lacking,” Dr. Chua told this news organization. “We felt that this was an important knowledge gap given the many changes in society that have occurred since 2020,” he noted. “For example, it was possible that the relaxation of social distancing measures during 2021 and 2022 might have reduced barriers to health care visits, thereby increasing opportunities to initiate treatment for opioid addiction with buprenorphine,” he said.
Dr. Chua and colleagues used data from the IQVIA Longitudinal Prescription Database, which reports 92% of prescriptions dispensed from retail pharmacies in the United States. “Buprenorphine products included immediate-release and extended-release formulations approved for opioid use disorder but not formulations primarily used to treat pain,” they write.
Monthly buprenorphine initiation was defined as the number of patients initiating therapy per 100,000 individuals. For retention, the researchers used a National Quality Forum-endorsed quality measure that defined retention as continuous use of buprenorphine for at least 180 days.
A total of 3,006,629 patients began buprenorphine therapy during the study period; approximately 43% were female.
During the first years of the study period, from January 2016 through September 2018, the monthly buprenorphine initiation rate increased from 12.5 per 100,000 to 15.9 per 100,000, with a statistically significant monthly percentage change of 0.62% (P < .001).
However, from October 2018 through October 2022, the monthly percentage remained essentially the same (P = .62) with a monthly percentage change of −0.03%.
From March 2020 through December 2020, the median monthly buprenorphine initiation rate was 14.4 per 100,000, only slightly lower than the rates from January 2019 through February 2020 and from January 2021 through October 2022 (15.5 per 100,000 and 15.0 per 100,000, respectively).
Over the entire study period from January 2016 through October 2022, the median monthly retention rate for buprenorphine use was 22.2%. This rate increased minimally, with no significant changes in slope and a monthly percentage change of 0.08% (P = .04).
The study findings were limited by several factors, including a lack of data on race and ethnicity, in-clinic administration of buprenorphine, and buprenorphine dispensing through methadone outpatient programs, the researchers note. Also, data did not indicate whether some patients began buprenorphine to treat pain, they say. The timing of the flattening of buprenorphine use also suggests the influence of factors beyond the COVID-19 pandemic, they write.
However, the results were strengthened by the large sample size and suggest that efforts to date to increase buprenorphine use have been unsuccessful, the researchers write. “A comprehensive approach is needed to eliminate barriers to buprenorphine initiation and retention, such as stigma and uneven access to prescribers,” they conclude.
Study highlights underuse of buprenorphine option
“Our study shows that buprenorphine initiation rates have been flat since the end of 2018 and that rates of 180-day retention in buprenorphine therapy have remained low throughout 2016-2022,” Dr. Chua told this news organization. “Neither of these findings are particularly surprising, but they are disappointing,” he said. “There were a lot of policy and clinical efforts to maintain and expand access to buprenorphine during the COVID-19 pandemic, such as allowing buprenorphine to be prescribed via telehealth without an in-person visit and eliminating training requirements for the waiver that previously was required to prescribe buprenorphine.
“The fact that buprenorphine initiation and retention did not rise after these efforts were implemented suggests that they were insufficient to meet the rising need for this medication,” he said.
The current study “adds to a growing body of research suggesting that clinicians are not maximizing opportunities to initiate buprenorphine treatment among patients with opioid addiction,” Dr. Chua said. He cited another of his recent studies in which 1 in 12 patients were prescribed buprenorphine within 30 days of an emergency department visit for opioid overdose from August 2019 to April 2021, but half of patients with emergency department visits with anaphylaxis were prescribed anepinephrine auto-injector.
“My hope is that our new study will further underscore to clinicians how much the health care system is underusing a critical tool to prevent opioid overdose deaths,” he said.
The federal government’s recent elimination of the waiver needed to prescribe buprenorphine may move the needle, but to what degree remains to be seen, Dr. Chua added. “It is possible this intervention will be insufficient to overcome the many other barriers to buprenorphine initiation and retention, such as stigma about the drug among clinicians, patients, and pharmacists,” he said.
Lack of education remains a barrier to buprenorphine use
The current study is important to determine whether attempts to increase buprenorphine initiation and treatment retention are working, said Reuben J. Strayer, MD, director of addiction medicine in the emergency medicine department at Maimonides Medical Center, New York, in an interview.
Dr. Strayer was not involved in the current study, but said he was surprised that initiation of buprenorphine didn’t decrease more dramatically during the pandemic, given the significant barriers to accessing care during that time.
However, “efforts to increase buprenorphine initiation and retention have not been sufficiently effective,” Dr. Strayer said. “The rise of fentanyl as a primary street opioid, replacing heroin, has dissuaded both patients and providers from initiating buprenorphine for fear of precipitated withdrawal.”
The elimination of the DATA 2000 (X) waiver was the removal of a potential barrier to increased buprenorphine use, said Dr. Strayer. “Now that the DATA 2000 (X) waiver has been eliminated, the focus of buprenorphine access is educating primary care and inpatient providers on its use, so that patients with OUD [opioid use disorder] can be treated, regardless of the venue at which they seek care,” he said.
Looking ahead, “The priority in buprenorphine research is determining the most effective way to initiate buprenorphine without the risk of precipitated withdrawal,” Dr. Strayer added.
The study was supported in part by the Benter Foundation, the Michigan Department of Health and Human Services, and the Susan B. Meister Child Health Evaluation and Research Center in the department of pediatrics at the University of Michigan. Dr. Chua was supported by the National Institute on Drug Abuse. Dr. Strayer has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Opioid overdose deaths are at a record high in the United States, and many of these deaths can be prevented with medications such as buprenorphine, said lead author Kao-Ping Chua, MD, of the University of Michigan, Ann Arbor, in an interview. “However, buprenorphine cannot prevent opioid overdose deaths if patients are never started on the medication or only stay on the medication for a short time. For that reason, rates of buprenorphine initiation and retention are critical metrics for measuring how well the U.S. health care system is responding to the opioid epidemic,” he said.
“At the time we started our study, several other research groups had evaluated U.S. rates of buprenorphine initiation and retention using data through 2020. However, more recent national data were lacking,” Dr. Chua told this news organization. “We felt that this was an important knowledge gap given the many changes in society that have occurred since 2020,” he noted. “For example, it was possible that the relaxation of social distancing measures during 2021 and 2022 might have reduced barriers to health care visits, thereby increasing opportunities to initiate treatment for opioid addiction with buprenorphine,” he said.
Dr. Chua and colleagues used data from the IQVIA Longitudinal Prescription Database, which reports 92% of prescriptions dispensed from retail pharmacies in the United States. “Buprenorphine products included immediate-release and extended-release formulations approved for opioid use disorder but not formulations primarily used to treat pain,” they write.
Monthly buprenorphine initiation was defined as the number of patients initiating therapy per 100,000 individuals. For retention, the researchers used a National Quality Forum-endorsed quality measure that defined retention as continuous use of buprenorphine for at least 180 days.
A total of 3,006,629 patients began buprenorphine therapy during the study period; approximately 43% were female.
During the first years of the study period, from January 2016 through September 2018, the monthly buprenorphine initiation rate increased from 12.5 per 100,000 to 15.9 per 100,000, with a statistically significant monthly percentage change of 0.62% (P < .001).
However, from October 2018 through October 2022, the monthly percentage remained essentially the same (P = .62) with a monthly percentage change of −0.03%.
From March 2020 through December 2020, the median monthly buprenorphine initiation rate was 14.4 per 100,000, only slightly lower than the rates from January 2019 through February 2020 and from January 2021 through October 2022 (15.5 per 100,000 and 15.0 per 100,000, respectively).
Over the entire study period from January 2016 through October 2022, the median monthly retention rate for buprenorphine use was 22.2%. This rate increased minimally, with no significant changes in slope and a monthly percentage change of 0.08% (P = .04).
The study findings were limited by several factors, including a lack of data on race and ethnicity, in-clinic administration of buprenorphine, and buprenorphine dispensing through methadone outpatient programs, the researchers note. Also, data did not indicate whether some patients began buprenorphine to treat pain, they say. The timing of the flattening of buprenorphine use also suggests the influence of factors beyond the COVID-19 pandemic, they write.
However, the results were strengthened by the large sample size and suggest that efforts to date to increase buprenorphine use have been unsuccessful, the researchers write. “A comprehensive approach is needed to eliminate barriers to buprenorphine initiation and retention, such as stigma and uneven access to prescribers,” they conclude.
Study highlights underuse of buprenorphine option
“Our study shows that buprenorphine initiation rates have been flat since the end of 2018 and that rates of 180-day retention in buprenorphine therapy have remained low throughout 2016-2022,” Dr. Chua told this news organization. “Neither of these findings are particularly surprising, but they are disappointing,” he said. “There were a lot of policy and clinical efforts to maintain and expand access to buprenorphine during the COVID-19 pandemic, such as allowing buprenorphine to be prescribed via telehealth without an in-person visit and eliminating training requirements for the waiver that previously was required to prescribe buprenorphine.
“The fact that buprenorphine initiation and retention did not rise after these efforts were implemented suggests that they were insufficient to meet the rising need for this medication,” he said.
The current study “adds to a growing body of research suggesting that clinicians are not maximizing opportunities to initiate buprenorphine treatment among patients with opioid addiction,” Dr. Chua said. He cited another of his recent studies in which 1 in 12 patients were prescribed buprenorphine within 30 days of an emergency department visit for opioid overdose from August 2019 to April 2021, but half of patients with emergency department visits with anaphylaxis were prescribed anepinephrine auto-injector.
“My hope is that our new study will further underscore to clinicians how much the health care system is underusing a critical tool to prevent opioid overdose deaths,” he said.
The federal government’s recent elimination of the waiver needed to prescribe buprenorphine may move the needle, but to what degree remains to be seen, Dr. Chua added. “It is possible this intervention will be insufficient to overcome the many other barriers to buprenorphine initiation and retention, such as stigma about the drug among clinicians, patients, and pharmacists,” he said.
Lack of education remains a barrier to buprenorphine use
The current study is important to determine whether attempts to increase buprenorphine initiation and treatment retention are working, said Reuben J. Strayer, MD, director of addiction medicine in the emergency medicine department at Maimonides Medical Center, New York, in an interview.
Dr. Strayer was not involved in the current study, but said he was surprised that initiation of buprenorphine didn’t decrease more dramatically during the pandemic, given the significant barriers to accessing care during that time.
However, “efforts to increase buprenorphine initiation and retention have not been sufficiently effective,” Dr. Strayer said. “The rise of fentanyl as a primary street opioid, replacing heroin, has dissuaded both patients and providers from initiating buprenorphine for fear of precipitated withdrawal.”
The elimination of the DATA 2000 (X) waiver was the removal of a potential barrier to increased buprenorphine use, said Dr. Strayer. “Now that the DATA 2000 (X) waiver has been eliminated, the focus of buprenorphine access is educating primary care and inpatient providers on its use, so that patients with OUD [opioid use disorder] can be treated, regardless of the venue at which they seek care,” he said.
Looking ahead, “The priority in buprenorphine research is determining the most effective way to initiate buprenorphine without the risk of precipitated withdrawal,” Dr. Strayer added.
The study was supported in part by the Benter Foundation, the Michigan Department of Health and Human Services, and the Susan B. Meister Child Health Evaluation and Research Center in the department of pediatrics at the University of Michigan. Dr. Chua was supported by the National Institute on Drug Abuse. Dr. Strayer has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Opioid overdose deaths are at a record high in the United States, and many of these deaths can be prevented with medications such as buprenorphine, said lead author Kao-Ping Chua, MD, of the University of Michigan, Ann Arbor, in an interview. “However, buprenorphine cannot prevent opioid overdose deaths if patients are never started on the medication or only stay on the medication for a short time. For that reason, rates of buprenorphine initiation and retention are critical metrics for measuring how well the U.S. health care system is responding to the opioid epidemic,” he said.
“At the time we started our study, several other research groups had evaluated U.S. rates of buprenorphine initiation and retention using data through 2020. However, more recent national data were lacking,” Dr. Chua told this news organization. “We felt that this was an important knowledge gap given the many changes in society that have occurred since 2020,” he noted. “For example, it was possible that the relaxation of social distancing measures during 2021 and 2022 might have reduced barriers to health care visits, thereby increasing opportunities to initiate treatment for opioid addiction with buprenorphine,” he said.
Dr. Chua and colleagues used data from the IQVIA Longitudinal Prescription Database, which reports 92% of prescriptions dispensed from retail pharmacies in the United States. “Buprenorphine products included immediate-release and extended-release formulations approved for opioid use disorder but not formulations primarily used to treat pain,” they write.
Monthly buprenorphine initiation was defined as the number of patients initiating therapy per 100,000 individuals. For retention, the researchers used a National Quality Forum-endorsed quality measure that defined retention as continuous use of buprenorphine for at least 180 days.
A total of 3,006,629 patients began buprenorphine therapy during the study period; approximately 43% were female.
During the first years of the study period, from January 2016 through September 2018, the monthly buprenorphine initiation rate increased from 12.5 per 100,000 to 15.9 per 100,000, with a statistically significant monthly percentage change of 0.62% (P < .001).
However, from October 2018 through October 2022, the monthly percentage remained essentially the same (P = .62) with a monthly percentage change of −0.03%.
From March 2020 through December 2020, the median monthly buprenorphine initiation rate was 14.4 per 100,000, only slightly lower than the rates from January 2019 through February 2020 and from January 2021 through October 2022 (15.5 per 100,000 and 15.0 per 100,000, respectively).
Over the entire study period from January 2016 through October 2022, the median monthly retention rate for buprenorphine use was 22.2%. This rate increased minimally, with no significant changes in slope and a monthly percentage change of 0.08% (P = .04).
The study findings were limited by several factors, including a lack of data on race and ethnicity, in-clinic administration of buprenorphine, and buprenorphine dispensing through methadone outpatient programs, the researchers note. Also, data did not indicate whether some patients began buprenorphine to treat pain, they say. The timing of the flattening of buprenorphine use also suggests the influence of factors beyond the COVID-19 pandemic, they write.
However, the results were strengthened by the large sample size and suggest that efforts to date to increase buprenorphine use have been unsuccessful, the researchers write. “A comprehensive approach is needed to eliminate barriers to buprenorphine initiation and retention, such as stigma and uneven access to prescribers,” they conclude.
Study highlights underuse of buprenorphine option
“Our study shows that buprenorphine initiation rates have been flat since the end of 2018 and that rates of 180-day retention in buprenorphine therapy have remained low throughout 2016-2022,” Dr. Chua told this news organization. “Neither of these findings are particularly surprising, but they are disappointing,” he said. “There were a lot of policy and clinical efforts to maintain and expand access to buprenorphine during the COVID-19 pandemic, such as allowing buprenorphine to be prescribed via telehealth without an in-person visit and eliminating training requirements for the waiver that previously was required to prescribe buprenorphine.
“The fact that buprenorphine initiation and retention did not rise after these efforts were implemented suggests that they were insufficient to meet the rising need for this medication,” he said.
The current study “adds to a growing body of research suggesting that clinicians are not maximizing opportunities to initiate buprenorphine treatment among patients with opioid addiction,” Dr. Chua said. He cited another of his recent studies in which 1 in 12 patients were prescribed buprenorphine within 30 days of an emergency department visit for opioid overdose from August 2019 to April 2021, but half of patients with emergency department visits with anaphylaxis were prescribed anepinephrine auto-injector.
“My hope is that our new study will further underscore to clinicians how much the health care system is underusing a critical tool to prevent opioid overdose deaths,” he said.
The federal government’s recent elimination of the waiver needed to prescribe buprenorphine may move the needle, but to what degree remains to be seen, Dr. Chua added. “It is possible this intervention will be insufficient to overcome the many other barriers to buprenorphine initiation and retention, such as stigma about the drug among clinicians, patients, and pharmacists,” he said.
Lack of education remains a barrier to buprenorphine use
The current study is important to determine whether attempts to increase buprenorphine initiation and treatment retention are working, said Reuben J. Strayer, MD, director of addiction medicine in the emergency medicine department at Maimonides Medical Center, New York, in an interview.
Dr. Strayer was not involved in the current study, but said he was surprised that initiation of buprenorphine didn’t decrease more dramatically during the pandemic, given the significant barriers to accessing care during that time.
However, “efforts to increase buprenorphine initiation and retention have not been sufficiently effective,” Dr. Strayer said. “The rise of fentanyl as a primary street opioid, replacing heroin, has dissuaded both patients and providers from initiating buprenorphine for fear of precipitated withdrawal.”
The elimination of the DATA 2000 (X) waiver was the removal of a potential barrier to increased buprenorphine use, said Dr. Strayer. “Now that the DATA 2000 (X) waiver has been eliminated, the focus of buprenorphine access is educating primary care and inpatient providers on its use, so that patients with OUD [opioid use disorder] can be treated, regardless of the venue at which they seek care,” he said.
Looking ahead, “The priority in buprenorphine research is determining the most effective way to initiate buprenorphine without the risk of precipitated withdrawal,” Dr. Strayer added.
The study was supported in part by the Benter Foundation, the Michigan Department of Health and Human Services, and the Susan B. Meister Child Health Evaluation and Research Center in the department of pediatrics at the University of Michigan. Dr. Chua was supported by the National Institute on Drug Abuse. Dr. Strayer has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA