User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Can lung cancer ID be as easy as breathing into an analyzer?
A study published in May in The Lancet journal eClinicalMedicine reports that
The tool was successfully used to identify, in 84 patients, 16 lung cancer–related carcinogenic volatile compounds (VOCs), such as aldehydes, hydrocarbons, ketones, carboxylic acids, and furan – some of which are compounds used in the production of common household goods, such as furniture, carpeting, and wood floors.
“The test is anticipated to be highlighted for primary screening of lung cancer but not the final diagnosis,” according to study authors who were led by Peiyu Wang, MD, PhD, chair of social medicine and health at Peking (China) University.
While early diagnosis and treatment are critical for improving lung cancer survival, early detection of lung cancer is challenging because of the lack of clinical manifestations and specific biomarkers. Annual CT scans are costly and include radiation exposure, Dr. Wang and his associates wrote.
Breathomics testing is considered a promising method for detection and screening for lung cancer. It has been under study for years and in 2014, researchers from Belgium published a review in Cancer Epidemiology Biomarkers and Prevention documenting the use of VOCs as early diagnostic or prognostic biomarkers for mesothelioma.
Lung cancer breath biomarkers identified in various studies have been highly heterogeneous because of differing sample collection methods, varying patient conditions, testing environments, and analysis methods. As a result, there currently is no breathomics test for lung cancer screening, Dr. Wang said in an interview.
In terms of its potential as a lung cancer screening tool, “Clinicians may introduce this test for people with high risk for lung cancer, such as elderly smokers, or people with suspected symptoms. It may also be introduced for young populations with subjective or objective needs to screen for lung cancer. As the proportion of lung adenocarcinoma in nonsmoking young women is increasing, the test may be a good method for lung cancer screening in this population,” Dr. Wang said.
After adjusting for age, sex, smoking, and comorbidities, researchers found elevated levels for 16 VOCs in patients with lung cancer. A diagnostic model including the 16 VOCs achieved an area under the curve of 0.952, sensitivity of 89.2%, specificity of 89.1%, and accuracy of 89.1% in lung cancer diagnosis. A model including the top eight VOCs achieved an area under the curve of 0.931, sensitivity of 86.0%, specificity of 87.2%, and accuracy of 86.9%.
After selecting 28 VOCs as candidates through a literature review, Dr. Wang and associates conducted a prospective discovery study from Sept. 1 to Dec. 31, 2020, using high-pressure photon ionization time-of-flight mass spectrometry to evaluate their performance for lung cancer diagnosis. The validation study included 157 lung cancer patients (mean age 57.0 years; 54.1 percent female) and 368 volunteers (mean age 44.5 years; 31.3% female).
“The external validation confirmed good performance of these biomarkers in lung cancer detection,” the researchers stated. It helped, they added, to solve the heterogeneity among published studies, establishing both 16 VOCs and 8 VOCS for lung cancer screening.
The authors stated that a large gap exists between breathomics research and clinical practices in lung cancer detection and screening. While the validated 16 VOCs, mainly aldehydes and hydrocarbon, showed potential for promoting this lung cancer screening strategy, more scientific studies are warranted to investigate the underlying mechanisms of identified lung cancer VOCs.
Dr. Wang declared no competing interests.
A study published in May in The Lancet journal eClinicalMedicine reports that
The tool was successfully used to identify, in 84 patients, 16 lung cancer–related carcinogenic volatile compounds (VOCs), such as aldehydes, hydrocarbons, ketones, carboxylic acids, and furan – some of which are compounds used in the production of common household goods, such as furniture, carpeting, and wood floors.
“The test is anticipated to be highlighted for primary screening of lung cancer but not the final diagnosis,” according to study authors who were led by Peiyu Wang, MD, PhD, chair of social medicine and health at Peking (China) University.
While early diagnosis and treatment are critical for improving lung cancer survival, early detection of lung cancer is challenging because of the lack of clinical manifestations and specific biomarkers. Annual CT scans are costly and include radiation exposure, Dr. Wang and his associates wrote.
Breathomics testing is considered a promising method for detection and screening for lung cancer. It has been under study for years and in 2014, researchers from Belgium published a review in Cancer Epidemiology Biomarkers and Prevention documenting the use of VOCs as early diagnostic or prognostic biomarkers for mesothelioma.
Lung cancer breath biomarkers identified in various studies have been highly heterogeneous because of differing sample collection methods, varying patient conditions, testing environments, and analysis methods. As a result, there currently is no breathomics test for lung cancer screening, Dr. Wang said in an interview.
In terms of its potential as a lung cancer screening tool, “Clinicians may introduce this test for people with high risk for lung cancer, such as elderly smokers, or people with suspected symptoms. It may also be introduced for young populations with subjective or objective needs to screen for lung cancer. As the proportion of lung adenocarcinoma in nonsmoking young women is increasing, the test may be a good method for lung cancer screening in this population,” Dr. Wang said.
After adjusting for age, sex, smoking, and comorbidities, researchers found elevated levels for 16 VOCs in patients with lung cancer. A diagnostic model including the 16 VOCs achieved an area under the curve of 0.952, sensitivity of 89.2%, specificity of 89.1%, and accuracy of 89.1% in lung cancer diagnosis. A model including the top eight VOCs achieved an area under the curve of 0.931, sensitivity of 86.0%, specificity of 87.2%, and accuracy of 86.9%.
After selecting 28 VOCs as candidates through a literature review, Dr. Wang and associates conducted a prospective discovery study from Sept. 1 to Dec. 31, 2020, using high-pressure photon ionization time-of-flight mass spectrometry to evaluate their performance for lung cancer diagnosis. The validation study included 157 lung cancer patients (mean age 57.0 years; 54.1 percent female) and 368 volunteers (mean age 44.5 years; 31.3% female).
“The external validation confirmed good performance of these biomarkers in lung cancer detection,” the researchers stated. It helped, they added, to solve the heterogeneity among published studies, establishing both 16 VOCs and 8 VOCS for lung cancer screening.
The authors stated that a large gap exists between breathomics research and clinical practices in lung cancer detection and screening. While the validated 16 VOCs, mainly aldehydes and hydrocarbon, showed potential for promoting this lung cancer screening strategy, more scientific studies are warranted to investigate the underlying mechanisms of identified lung cancer VOCs.
Dr. Wang declared no competing interests.
A study published in May in The Lancet journal eClinicalMedicine reports that
The tool was successfully used to identify, in 84 patients, 16 lung cancer–related carcinogenic volatile compounds (VOCs), such as aldehydes, hydrocarbons, ketones, carboxylic acids, and furan – some of which are compounds used in the production of common household goods, such as furniture, carpeting, and wood floors.
“The test is anticipated to be highlighted for primary screening of lung cancer but not the final diagnosis,” according to study authors who were led by Peiyu Wang, MD, PhD, chair of social medicine and health at Peking (China) University.
While early diagnosis and treatment are critical for improving lung cancer survival, early detection of lung cancer is challenging because of the lack of clinical manifestations and specific biomarkers. Annual CT scans are costly and include radiation exposure, Dr. Wang and his associates wrote.
Breathomics testing is considered a promising method for detection and screening for lung cancer. It has been under study for years and in 2014, researchers from Belgium published a review in Cancer Epidemiology Biomarkers and Prevention documenting the use of VOCs as early diagnostic or prognostic biomarkers for mesothelioma.
Lung cancer breath biomarkers identified in various studies have been highly heterogeneous because of differing sample collection methods, varying patient conditions, testing environments, and analysis methods. As a result, there currently is no breathomics test for lung cancer screening, Dr. Wang said in an interview.
In terms of its potential as a lung cancer screening tool, “Clinicians may introduce this test for people with high risk for lung cancer, such as elderly smokers, or people with suspected symptoms. It may also be introduced for young populations with subjective or objective needs to screen for lung cancer. As the proportion of lung adenocarcinoma in nonsmoking young women is increasing, the test may be a good method for lung cancer screening in this population,” Dr. Wang said.
After adjusting for age, sex, smoking, and comorbidities, researchers found elevated levels for 16 VOCs in patients with lung cancer. A diagnostic model including the 16 VOCs achieved an area under the curve of 0.952, sensitivity of 89.2%, specificity of 89.1%, and accuracy of 89.1% in lung cancer diagnosis. A model including the top eight VOCs achieved an area under the curve of 0.931, sensitivity of 86.0%, specificity of 87.2%, and accuracy of 86.9%.
After selecting 28 VOCs as candidates through a literature review, Dr. Wang and associates conducted a prospective discovery study from Sept. 1 to Dec. 31, 2020, using high-pressure photon ionization time-of-flight mass spectrometry to evaluate their performance for lung cancer diagnosis. The validation study included 157 lung cancer patients (mean age 57.0 years; 54.1 percent female) and 368 volunteers (mean age 44.5 years; 31.3% female).
“The external validation confirmed good performance of these biomarkers in lung cancer detection,” the researchers stated. It helped, they added, to solve the heterogeneity among published studies, establishing both 16 VOCs and 8 VOCS for lung cancer screening.
The authors stated that a large gap exists between breathomics research and clinical practices in lung cancer detection and screening. While the validated 16 VOCs, mainly aldehydes and hydrocarbon, showed potential for promoting this lung cancer screening strategy, more scientific studies are warranted to investigate the underlying mechanisms of identified lung cancer VOCs.
Dr. Wang declared no competing interests.
FROM ECLINICAL MEDICINE
Parents fall short on infant sleep safety
Less than 10% of parents followed recommended safe sleep practices for their infants aged 12 months and younger at both sleep onset and after nighttime waking, based on data from a survey of 1,500 parents published in Pediatrics.
Sleep-related death remains a major cause of infant mortality in the United States despite the early success of public health campaigns for safe sleep practices, such as “Back to Sleep,” and many parents persist in unsafe practices such as prone positioning and bed-sharing, Mersine A. Bryan, MD, of the University of Washington, Seattle, and colleagues wrote. “Though nighttime waking is common for infants, less attention has been paid to the safety of second-sleep practices.”
To examine the prevalence and safety of infant second-sleep practices, the researchers used a cross-sectional online survey to collect information on sleep practices from parents of infants aged 12 months and younger; 74% of the respondents were female, 65% were White, 12% were Black, and 17% were Hispanic. The mean age of the infants was 6.6 months, and 24% were aged 3 months and younger.
The survey included parent reports of three safe sleep practices based on the American Academy of Pediatrics 2016 Safe Infant Sleep Guidelines: supine infant sleep position, use of a separate sleep space (vs. bed sharing), and use of an approved surface/safe location (such as a bassinet, crib, cradle, or play yard vs. an adult bed).
Parents were asked to report sleep practices at sleep onset and at nighttime waking, and the researchers used a composite score to determine safe practices were met at each of these two time points.
Of the 1,500 participants, 581 (39%), reported any second-sleep practice. Of the 482 who reported on all three sleep practices at both time points, 29% met all three safe sleep criteria at sleep onset and 9% met all three safe sleep criteria at sleep onset and nighttime waking.
Of the parents who reported second sleep practices, 39% reported changes in practice after nighttime waking from sleep onset. Significantly more parents who switched practices between sleep onset and nighttime waking shifted from a safer to a less safe practice, the researchers noted.
For positioning, 67% of respondents overall reported placing infants on their backs at sleep onset. Among the 564 who reported a second sleep position, 42% placed infants on their backs again; 13% switched from supine to nonsupine positions and 7% changed from nonsupine to supine.
For sleep spaces, 72% of participants overall reported a separate sleep space for infants at sleep onset. Of the 508 who reported on second-sleep spaces, 54% kept infants in a separate space after nighttime waking, 18% shifted to a shared space after nighttime waking. Of those in shared spaces at sleep onset, 8% shifted to separate spaces after nighttime waking.
For sleep location, 71% of respondents overall used an approved sleep surface at sleep onset. Of the 560 who reported sleep location at both time points, 42% remained in a safe location after nighttime waking, while 30% were moved from a safe to an unsafe location, and 10% of those in an unsafe location were moved from an unsafe to a safe location.
In a multivariate analysis, the researchers examined the demographics associated with changes in sleep practice after nighttime waking. Parents younger than 25 years, first-time parents, those who identified as Black non-Hispanic or Hispanic, smokers, and those with preterm infants (less than 37 weeks’ gestation) were more likely to change sleep practices after nighttime waking. However, parents who reported a safe sleep practice at sleep onset were more likely to do so after nighttime waking.
“We hypothesize that expansion of existing strategies to promote infant safe sleep practices to include sleep practices after nighttime waking can have a positive impact on infant safe sleep,” the researchers wrote.
The study findings were limited by several factors including the use of an online survey, which limited the study population to those with internet and computer access, and the reliance on self-reports and only two time points, the researchers noted. Other limitations included the inclusion of only three of the AAP sleep recommendations, and the inclusion of only English speakers.
However, the results were strengthened by the large, diverse, and geographically representative sample of parents.
“When advising families about infant sleep, pediatricians should discuss nighttime wakings with parents because they are common and reinforce the need for safe sleep practices every time,” the researchers noted.
Increase opportunities for education
The current study is important because infants continue to die or experience life-long catastrophic health outcomes as a result of not following safe sleep practices, Cathy Haut, DNP, CPNP-AC, CPNP-PC, a pediatric nurse practitioner in Rehoboth Beach, Del., said in an interview.

“I am not surprised by the study findings,” said Dr. Haut, who was not involved in the study. “As a pediatric nurse practitioner for over 35 years, I see infant sleep as a continuing challenge for families. In today’s fast-paced world, multiple priorities leave parents few resources for managing their own well-being, with adequate sleep being one health requirement that is often not met for them.”
To improve safe sleep practices, “it is imperative for health care providers in any setting to address safe sleep practices for infants and children,” said Dr. Haut. “In addition to safety, opportunity for adequate hours of sleep is also important.” She acknowledged that, “in the office setting, time is a huge barrier to completing comprehensive anticipatory guidance. When parents ask questions about sleep, they are often doing everything they can to physically make it through the night with a crying infant. Enforcing safe practices at this point is extremely difficult.”
However, some opportunities for safe sleep education include the prenatal period when parents can take time to listen and plan, not just for feeding preferences but for safe infant sleep practices, Dr. Haut noted.
“When sleep is a problem, families can be invited back to the office for additional counseling and education, which allows more time than within a scheduled health visit,” Dr. Haut emphasized. “Finally, enhanced public awareness is an aspect of learning. In my career I have seen the devastating results of suffocation while cosleeping as well as injuries from falling from a bed or inappropriate sleeping space, and other poor outcomes from inadequate support for safe sleep habits.”
As for additional research, studies are needed to include larger populations and “to further quantify positive outcomes of following safe sleeping practices,” said Dr. Haut. The results of these studies should be made available to the general public, not only to health care professionals.
The study was supported by Seattle Children’s Research Institute. The researchers had no financial conflicts to disclose. Dr. Haut had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
Less than 10% of parents followed recommended safe sleep practices for their infants aged 12 months and younger at both sleep onset and after nighttime waking, based on data from a survey of 1,500 parents published in Pediatrics.
Sleep-related death remains a major cause of infant mortality in the United States despite the early success of public health campaigns for safe sleep practices, such as “Back to Sleep,” and many parents persist in unsafe practices such as prone positioning and bed-sharing, Mersine A. Bryan, MD, of the University of Washington, Seattle, and colleagues wrote. “Though nighttime waking is common for infants, less attention has been paid to the safety of second-sleep practices.”
To examine the prevalence and safety of infant second-sleep practices, the researchers used a cross-sectional online survey to collect information on sleep practices from parents of infants aged 12 months and younger; 74% of the respondents were female, 65% were White, 12% were Black, and 17% were Hispanic. The mean age of the infants was 6.6 months, and 24% were aged 3 months and younger.
The survey included parent reports of three safe sleep practices based on the American Academy of Pediatrics 2016 Safe Infant Sleep Guidelines: supine infant sleep position, use of a separate sleep space (vs. bed sharing), and use of an approved surface/safe location (such as a bassinet, crib, cradle, or play yard vs. an adult bed).
Parents were asked to report sleep practices at sleep onset and at nighttime waking, and the researchers used a composite score to determine safe practices were met at each of these two time points.
Of the 1,500 participants, 581 (39%), reported any second-sleep practice. Of the 482 who reported on all three sleep practices at both time points, 29% met all three safe sleep criteria at sleep onset and 9% met all three safe sleep criteria at sleep onset and nighttime waking.
Of the parents who reported second sleep practices, 39% reported changes in practice after nighttime waking from sleep onset. Significantly more parents who switched practices between sleep onset and nighttime waking shifted from a safer to a less safe practice, the researchers noted.
For positioning, 67% of respondents overall reported placing infants on their backs at sleep onset. Among the 564 who reported a second sleep position, 42% placed infants on their backs again; 13% switched from supine to nonsupine positions and 7% changed from nonsupine to supine.
For sleep spaces, 72% of participants overall reported a separate sleep space for infants at sleep onset. Of the 508 who reported on second-sleep spaces, 54% kept infants in a separate space after nighttime waking, 18% shifted to a shared space after nighttime waking. Of those in shared spaces at sleep onset, 8% shifted to separate spaces after nighttime waking.
For sleep location, 71% of respondents overall used an approved sleep surface at sleep onset. Of the 560 who reported sleep location at both time points, 42% remained in a safe location after nighttime waking, while 30% were moved from a safe to an unsafe location, and 10% of those in an unsafe location were moved from an unsafe to a safe location.
In a multivariate analysis, the researchers examined the demographics associated with changes in sleep practice after nighttime waking. Parents younger than 25 years, first-time parents, those who identified as Black non-Hispanic or Hispanic, smokers, and those with preterm infants (less than 37 weeks’ gestation) were more likely to change sleep practices after nighttime waking. However, parents who reported a safe sleep practice at sleep onset were more likely to do so after nighttime waking.
“We hypothesize that expansion of existing strategies to promote infant safe sleep practices to include sleep practices after nighttime waking can have a positive impact on infant safe sleep,” the researchers wrote.
The study findings were limited by several factors including the use of an online survey, which limited the study population to those with internet and computer access, and the reliance on self-reports and only two time points, the researchers noted. Other limitations included the inclusion of only three of the AAP sleep recommendations, and the inclusion of only English speakers.
However, the results were strengthened by the large, diverse, and geographically representative sample of parents.
“When advising families about infant sleep, pediatricians should discuss nighttime wakings with parents because they are common and reinforce the need for safe sleep practices every time,” the researchers noted.
Increase opportunities for education
The current study is important because infants continue to die or experience life-long catastrophic health outcomes as a result of not following safe sleep practices, Cathy Haut, DNP, CPNP-AC, CPNP-PC, a pediatric nurse practitioner in Rehoboth Beach, Del., said in an interview.
“I am not surprised by the study findings,” said Dr. Haut, who was not involved in the study. “As a pediatric nurse practitioner for over 35 years, I see infant sleep as a continuing challenge for families. In today’s fast-paced world, multiple priorities leave parents few resources for managing their own well-being, with adequate sleep being one health requirement that is often not met for them.”
To improve safe sleep practices, “it is imperative for health care providers in any setting to address safe sleep practices for infants and children,” said Dr. Haut. “In addition to safety, opportunity for adequate hours of sleep is also important.” She acknowledged that, “in the office setting, time is a huge barrier to completing comprehensive anticipatory guidance. When parents ask questions about sleep, they are often doing everything they can to physically make it through the night with a crying infant. Enforcing safe practices at this point is extremely difficult.”
However, some opportunities for safe sleep education include the prenatal period when parents can take time to listen and plan, not just for feeding preferences but for safe infant sleep practices, Dr. Haut noted.
“When sleep is a problem, families can be invited back to the office for additional counseling and education, which allows more time than within a scheduled health visit,” Dr. Haut emphasized. “Finally, enhanced public awareness is an aspect of learning. In my career I have seen the devastating results of suffocation while cosleeping as well as injuries from falling from a bed or inappropriate sleeping space, and other poor outcomes from inadequate support for safe sleep habits.”
As for additional research, studies are needed to include larger populations and “to further quantify positive outcomes of following safe sleeping practices,” said Dr. Haut. The results of these studies should be made available to the general public, not only to health care professionals.
The study was supported by Seattle Children’s Research Institute. The researchers had no financial conflicts to disclose. Dr. Haut had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
Less than 10% of parents followed recommended safe sleep practices for their infants aged 12 months and younger at both sleep onset and after nighttime waking, based on data from a survey of 1,500 parents published in Pediatrics.
Sleep-related death remains a major cause of infant mortality in the United States despite the early success of public health campaigns for safe sleep practices, such as “Back to Sleep,” and many parents persist in unsafe practices such as prone positioning and bed-sharing, Mersine A. Bryan, MD, of the University of Washington, Seattle, and colleagues wrote. “Though nighttime waking is common for infants, less attention has been paid to the safety of second-sleep practices.”
To examine the prevalence and safety of infant second-sleep practices, the researchers used a cross-sectional online survey to collect information on sleep practices from parents of infants aged 12 months and younger; 74% of the respondents were female, 65% were White, 12% were Black, and 17% were Hispanic. The mean age of the infants was 6.6 months, and 24% were aged 3 months and younger.
The survey included parent reports of three safe sleep practices based on the American Academy of Pediatrics 2016 Safe Infant Sleep Guidelines: supine infant sleep position, use of a separate sleep space (vs. bed sharing), and use of an approved surface/safe location (such as a bassinet, crib, cradle, or play yard vs. an adult bed).
Parents were asked to report sleep practices at sleep onset and at nighttime waking, and the researchers used a composite score to determine safe practices were met at each of these two time points.
Of the 1,500 participants, 581 (39%), reported any second-sleep practice. Of the 482 who reported on all three sleep practices at both time points, 29% met all three safe sleep criteria at sleep onset and 9% met all three safe sleep criteria at sleep onset and nighttime waking.
Of the parents who reported second sleep practices, 39% reported changes in practice after nighttime waking from sleep onset. Significantly more parents who switched practices between sleep onset and nighttime waking shifted from a safer to a less safe practice, the researchers noted.
For positioning, 67% of respondents overall reported placing infants on their backs at sleep onset. Among the 564 who reported a second sleep position, 42% placed infants on their backs again; 13% switched from supine to nonsupine positions and 7% changed from nonsupine to supine.
For sleep spaces, 72% of participants overall reported a separate sleep space for infants at sleep onset. Of the 508 who reported on second-sleep spaces, 54% kept infants in a separate space after nighttime waking, 18% shifted to a shared space after nighttime waking. Of those in shared spaces at sleep onset, 8% shifted to separate spaces after nighttime waking.
For sleep location, 71% of respondents overall used an approved sleep surface at sleep onset. Of the 560 who reported sleep location at both time points, 42% remained in a safe location after nighttime waking, while 30% were moved from a safe to an unsafe location, and 10% of those in an unsafe location were moved from an unsafe to a safe location.
In a multivariate analysis, the researchers examined the demographics associated with changes in sleep practice after nighttime waking. Parents younger than 25 years, first-time parents, those who identified as Black non-Hispanic or Hispanic, smokers, and those with preterm infants (less than 37 weeks’ gestation) were more likely to change sleep practices after nighttime waking. However, parents who reported a safe sleep practice at sleep onset were more likely to do so after nighttime waking.
“We hypothesize that expansion of existing strategies to promote infant safe sleep practices to include sleep practices after nighttime waking can have a positive impact on infant safe sleep,” the researchers wrote.
The study findings were limited by several factors including the use of an online survey, which limited the study population to those with internet and computer access, and the reliance on self-reports and only two time points, the researchers noted. Other limitations included the inclusion of only three of the AAP sleep recommendations, and the inclusion of only English speakers.
However, the results were strengthened by the large, diverse, and geographically representative sample of parents.
“When advising families about infant sleep, pediatricians should discuss nighttime wakings with parents because they are common and reinforce the need for safe sleep practices every time,” the researchers noted.
Increase opportunities for education
The current study is important because infants continue to die or experience life-long catastrophic health outcomes as a result of not following safe sleep practices, Cathy Haut, DNP, CPNP-AC, CPNP-PC, a pediatric nurse practitioner in Rehoboth Beach, Del., said in an interview.
“I am not surprised by the study findings,” said Dr. Haut, who was not involved in the study. “As a pediatric nurse practitioner for over 35 years, I see infant sleep as a continuing challenge for families. In today’s fast-paced world, multiple priorities leave parents few resources for managing their own well-being, with adequate sleep being one health requirement that is often not met for them.”
To improve safe sleep practices, “it is imperative for health care providers in any setting to address safe sleep practices for infants and children,” said Dr. Haut. “In addition to safety, opportunity for adequate hours of sleep is also important.” She acknowledged that, “in the office setting, time is a huge barrier to completing comprehensive anticipatory guidance. When parents ask questions about sleep, they are often doing everything they can to physically make it through the night with a crying infant. Enforcing safe practices at this point is extremely difficult.”
However, some opportunities for safe sleep education include the prenatal period when parents can take time to listen and plan, not just for feeding preferences but for safe infant sleep practices, Dr. Haut noted.
“When sleep is a problem, families can be invited back to the office for additional counseling and education, which allows more time than within a scheduled health visit,” Dr. Haut emphasized. “Finally, enhanced public awareness is an aspect of learning. In my career I have seen the devastating results of suffocation while cosleeping as well as injuries from falling from a bed or inappropriate sleeping space, and other poor outcomes from inadequate support for safe sleep habits.”
As for additional research, studies are needed to include larger populations and “to further quantify positive outcomes of following safe sleeping practices,” said Dr. Haut. The results of these studies should be made available to the general public, not only to health care professionals.
The study was supported by Seattle Children’s Research Institute. The researchers had no financial conflicts to disclose. Dr. Haut had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
FROM PEDIATRICS
Coffee drinkers – even those with a sweet tooth – live longer
Among more than 170,000 people in the United Kingdom, those who drank about two to four cups of coffee a day, with or without sugar, had a lower rate of death than those who didn’t drink coffee, reported lead author Dan Liu, MD, of the department of epidemiology at Southern Medical University, Guangzhou, China.
“Previous observational studies have suggested an association between coffee intake and reduced risk for death, but they did not distinguish between coffee consumed with sugar or artificial sweeteners and coffee consumed without,” Dr. Liu, who is also of the department of public health and preventive medicine, Jinan University, Guangzhou, China, and colleagues wrote in Annals of Internal Medicine.
To learn more, the investigators turned to the UK Biobank, which recruited approximately half a million participants in the United Kingdom between 2006 and 2010 to undergo a variety of questionnaires, interviews, physical measurements, and medical tests. Out of this group, 171,616 participants completed at least one dietary questionnaire and met the criteria for the present study, including lack of cancer or cardiovascular disease upon enrollment.
Results from these questionnaires showed that 55.4% of participants drank coffee without any sweetener, 14.3% drank coffee with sugar, 6.1% drank coffee with artificial sweetener, and 24.2% did not drink coffee at all. Coffee drinkers were further sorted into groups based on how many cups of coffee they drank per day.
Coffee drinkers were significantly less likely to die from any cause
Over the course of about 7 years, 3,177 of the participants died, including 1,725 who died from cancer and 628 who died from cardiovascular disease.
After accounting for other factors that might impact risk of death, like lifestyle choices, the investigators found that coffee drinkers were significantly less likely to die from any cause, cardiovascular disease, or cancer, than those who didn’t drink coffee at all. This benefit was observed across types of coffee, including ground, instant, and decaffeinated varieties. The protective effects of coffee were most apparent in people who drank about two to four cups a day, among whom death was about 30% less likely, regardless of whether they added sugar to their coffee or not. Individuals who drank coffee with artificial sweetener did not live significantly longer than those who drank no coffee at all; however, the investigators suggested that this result may have been skewed by higher rates of negative health factors, such as obesity and hypertension, in the artificial sweetener group.
Dr. Liu and colleagues noted that their findings align with previous studies linking coffee consumption with survival. Like those other studies, the present data revealed a “U-shaped” benefit curve, in which moderate coffee consumption was associated with longer life, whereas low or no consumption and high consumption were not.
Experts caution against drinking sweetened beverages despite new findings
Although the present findings suggested that adding sugar did not eliminate the health benefits of coffee, Dr. Liu and colleagues still cautioned against sweetened beverages, citing widely known associations between sugar consumption and poor health.
In an accompanying editorial, Christina C. Wee, MD, MPH, deputy editor of Annals of Internal Medicine, pointed out a key detail from the data: the amount of sugar added to coffee in the U.K. study may be dwarfed by the amount consumed by some coffee drinkers across the pond.
“The average dose of added sugar per cup of sweetened coffee [in the study] was only a little over a teaspoon, or about 4 grams,” Dr. Wee wrote. “This is a far cry from the 15 grams of sugar in an 8-ounce cup of caramel macchiato at a popular U.S. coffee chain.”
Still, Dr. Wee, an associate professor of medicine at Harvard Medical School, Boston, and director of the obesity research program in the division of general medicine at Beth Israel Deaconess Medical Center, Boston, suggested that your typical coffee drinker can feel safe in their daily habit.
“The evidence does not suggest a need for most coffee drinkers – particularly those who drink it with no or modest amounts of sugar – to eliminate coffee,” she wrote. “So drink up – but it would be prudent to avoid too many caramel macchiatos while more evidence brews.”
Estefanía Toledo, MD, MPH, PhD, of the department of preventive medicine and public health at the University of Navarra, Pamplona, Spain, offered a similar takeaway.

“For those who enjoy drinking coffee, are not pregnant or lactating, and do not have special health conditions, coffee consumption could be considered part of a healthy lifestyle,” Dr. Toledo said in a written comment. “I would recommend adding as little sugar as possible to coffee until more evidence has been accrued.”
Dr. Toledo, who previously published a study showing a link between coffee and extended survival, noted that moderate coffee consumption has “repeatedly” been associated with lower rates of “several chronic diseases” and death, but there still isn’t enough evidence to recommend coffee for those who don’t already drink it.
More long-term research is needed, Dr. Toledo said, ideally with studies comparing changes in coffee consumption and health outcomes over time. These may not be forthcoming, however, as such trials are “not easy and feasible to conduct.”
David Kao, MD, assistant professor of medicine-cardiology and medical director of the school of medicine at the University of Colorado at Denver, Aurora, said that the study conducted by Dr. Liu and colleagues is a “very well-executed analysis” that strengthens our confidence in the safety of long-term coffee consumption, even for patients with heart disease.
Dr. Kao, who recently published an analysis showing that higher coffee intake is associated with a lower risk of heart failure, refrained from advising anyone to up their coffee quota.
“I remain cautious about stating too strongly that people should increase coffee intake purely to improve survival,” Dr. Kao said in a written comment. “That said, it does not appear harmful to increase it some, until you drink consistently more than six to seven cups per day.”
The study was supported by the National Natural Science Foundation of China, the Young Elite Scientist Sponsorship Program by CAST, the Guangdong Basic and Applied Basic Research Foundation, and others. Dr. Toledo and Dr. Kao disclosed no relevant conflicts of interest.
Among more than 170,000 people in the United Kingdom, those who drank about two to four cups of coffee a day, with or without sugar, had a lower rate of death than those who didn’t drink coffee, reported lead author Dan Liu, MD, of the department of epidemiology at Southern Medical University, Guangzhou, China.
“Previous observational studies have suggested an association between coffee intake and reduced risk for death, but they did not distinguish between coffee consumed with sugar or artificial sweeteners and coffee consumed without,” Dr. Liu, who is also of the department of public health and preventive medicine, Jinan University, Guangzhou, China, and colleagues wrote in Annals of Internal Medicine.
To learn more, the investigators turned to the UK Biobank, which recruited approximately half a million participants in the United Kingdom between 2006 and 2010 to undergo a variety of questionnaires, interviews, physical measurements, and medical tests. Out of this group, 171,616 participants completed at least one dietary questionnaire and met the criteria for the present study, including lack of cancer or cardiovascular disease upon enrollment.
Results from these questionnaires showed that 55.4% of participants drank coffee without any sweetener, 14.3% drank coffee with sugar, 6.1% drank coffee with artificial sweetener, and 24.2% did not drink coffee at all. Coffee drinkers were further sorted into groups based on how many cups of coffee they drank per day.
Coffee drinkers were significantly less likely to die from any cause
Over the course of about 7 years, 3,177 of the participants died, including 1,725 who died from cancer and 628 who died from cardiovascular disease.
After accounting for other factors that might impact risk of death, like lifestyle choices, the investigators found that coffee drinkers were significantly less likely to die from any cause, cardiovascular disease, or cancer, than those who didn’t drink coffee at all. This benefit was observed across types of coffee, including ground, instant, and decaffeinated varieties. The protective effects of coffee were most apparent in people who drank about two to four cups a day, among whom death was about 30% less likely, regardless of whether they added sugar to their coffee or not. Individuals who drank coffee with artificial sweetener did not live significantly longer than those who drank no coffee at all; however, the investigators suggested that this result may have been skewed by higher rates of negative health factors, such as obesity and hypertension, in the artificial sweetener group.
Dr. Liu and colleagues noted that their findings align with previous studies linking coffee consumption with survival. Like those other studies, the present data revealed a “U-shaped” benefit curve, in which moderate coffee consumption was associated with longer life, whereas low or no consumption and high consumption were not.
Experts caution against drinking sweetened beverages despite new findings
Although the present findings suggested that adding sugar did not eliminate the health benefits of coffee, Dr. Liu and colleagues still cautioned against sweetened beverages, citing widely known associations between sugar consumption and poor health.
In an accompanying editorial, Christina C. Wee, MD, MPH, deputy editor of Annals of Internal Medicine, pointed out a key detail from the data: the amount of sugar added to coffee in the U.K. study may be dwarfed by the amount consumed by some coffee drinkers across the pond.
“The average dose of added sugar per cup of sweetened coffee [in the study] was only a little over a teaspoon, or about 4 grams,” Dr. Wee wrote. “This is a far cry from the 15 grams of sugar in an 8-ounce cup of caramel macchiato at a popular U.S. coffee chain.”
Still, Dr. Wee, an associate professor of medicine at Harvard Medical School, Boston, and director of the obesity research program in the division of general medicine at Beth Israel Deaconess Medical Center, Boston, suggested that your typical coffee drinker can feel safe in their daily habit.
“The evidence does not suggest a need for most coffee drinkers – particularly those who drink it with no or modest amounts of sugar – to eliminate coffee,” she wrote. “So drink up – but it would be prudent to avoid too many caramel macchiatos while more evidence brews.”
Estefanía Toledo, MD, MPH, PhD, of the department of preventive medicine and public health at the University of Navarra, Pamplona, Spain, offered a similar takeaway.
“For those who enjoy drinking coffee, are not pregnant or lactating, and do not have special health conditions, coffee consumption could be considered part of a healthy lifestyle,” Dr. Toledo said in a written comment. “I would recommend adding as little sugar as possible to coffee until more evidence has been accrued.”
Dr. Toledo, who previously published a study showing a link between coffee and extended survival, noted that moderate coffee consumption has “repeatedly” been associated with lower rates of “several chronic diseases” and death, but there still isn’t enough evidence to recommend coffee for those who don’t already drink it.
More long-term research is needed, Dr. Toledo said, ideally with studies comparing changes in coffee consumption and health outcomes over time. These may not be forthcoming, however, as such trials are “not easy and feasible to conduct.”
David Kao, MD, assistant professor of medicine-cardiology and medical director of the school of medicine at the University of Colorado at Denver, Aurora, said that the study conducted by Dr. Liu and colleagues is a “very well-executed analysis” that strengthens our confidence in the safety of long-term coffee consumption, even for patients with heart disease.
Dr. Kao, who recently published an analysis showing that higher coffee intake is associated with a lower risk of heart failure, refrained from advising anyone to up their coffee quota.
“I remain cautious about stating too strongly that people should increase coffee intake purely to improve survival,” Dr. Kao said in a written comment. “That said, it does not appear harmful to increase it some, until you drink consistently more than six to seven cups per day.”
The study was supported by the National Natural Science Foundation of China, the Young Elite Scientist Sponsorship Program by CAST, the Guangdong Basic and Applied Basic Research Foundation, and others. Dr. Toledo and Dr. Kao disclosed no relevant conflicts of interest.
Among more than 170,000 people in the United Kingdom, those who drank about two to four cups of coffee a day, with or without sugar, had a lower rate of death than those who didn’t drink coffee, reported lead author Dan Liu, MD, of the department of epidemiology at Southern Medical University, Guangzhou, China.
“Previous observational studies have suggested an association between coffee intake and reduced risk for death, but they did not distinguish between coffee consumed with sugar or artificial sweeteners and coffee consumed without,” Dr. Liu, who is also of the department of public health and preventive medicine, Jinan University, Guangzhou, China, and colleagues wrote in Annals of Internal Medicine.
To learn more, the investigators turned to the UK Biobank, which recruited approximately half a million participants in the United Kingdom between 2006 and 2010 to undergo a variety of questionnaires, interviews, physical measurements, and medical tests. Out of this group, 171,616 participants completed at least one dietary questionnaire and met the criteria for the present study, including lack of cancer or cardiovascular disease upon enrollment.
Results from these questionnaires showed that 55.4% of participants drank coffee without any sweetener, 14.3% drank coffee with sugar, 6.1% drank coffee with artificial sweetener, and 24.2% did not drink coffee at all. Coffee drinkers were further sorted into groups based on how many cups of coffee they drank per day.
Coffee drinkers were significantly less likely to die from any cause
Over the course of about 7 years, 3,177 of the participants died, including 1,725 who died from cancer and 628 who died from cardiovascular disease.
After accounting for other factors that might impact risk of death, like lifestyle choices, the investigators found that coffee drinkers were significantly less likely to die from any cause, cardiovascular disease, or cancer, than those who didn’t drink coffee at all. This benefit was observed across types of coffee, including ground, instant, and decaffeinated varieties. The protective effects of coffee were most apparent in people who drank about two to four cups a day, among whom death was about 30% less likely, regardless of whether they added sugar to their coffee or not. Individuals who drank coffee with artificial sweetener did not live significantly longer than those who drank no coffee at all; however, the investigators suggested that this result may have been skewed by higher rates of negative health factors, such as obesity and hypertension, in the artificial sweetener group.
Dr. Liu and colleagues noted that their findings align with previous studies linking coffee consumption with survival. Like those other studies, the present data revealed a “U-shaped” benefit curve, in which moderate coffee consumption was associated with longer life, whereas low or no consumption and high consumption were not.
Experts caution against drinking sweetened beverages despite new findings
Although the present findings suggested that adding sugar did not eliminate the health benefits of coffee, Dr. Liu and colleagues still cautioned against sweetened beverages, citing widely known associations between sugar consumption and poor health.
In an accompanying editorial, Christina C. Wee, MD, MPH, deputy editor of Annals of Internal Medicine, pointed out a key detail from the data: the amount of sugar added to coffee in the U.K. study may be dwarfed by the amount consumed by some coffee drinkers across the pond.
“The average dose of added sugar per cup of sweetened coffee [in the study] was only a little over a teaspoon, or about 4 grams,” Dr. Wee wrote. “This is a far cry from the 15 grams of sugar in an 8-ounce cup of caramel macchiato at a popular U.S. coffee chain.”
Still, Dr. Wee, an associate professor of medicine at Harvard Medical School, Boston, and director of the obesity research program in the division of general medicine at Beth Israel Deaconess Medical Center, Boston, suggested that your typical coffee drinker can feel safe in their daily habit.
“The evidence does not suggest a need for most coffee drinkers – particularly those who drink it with no or modest amounts of sugar – to eliminate coffee,” she wrote. “So drink up – but it would be prudent to avoid too many caramel macchiatos while more evidence brews.”
Estefanía Toledo, MD, MPH, PhD, of the department of preventive medicine and public health at the University of Navarra, Pamplona, Spain, offered a similar takeaway.
“For those who enjoy drinking coffee, are not pregnant or lactating, and do not have special health conditions, coffee consumption could be considered part of a healthy lifestyle,” Dr. Toledo said in a written comment. “I would recommend adding as little sugar as possible to coffee until more evidence has been accrued.”
Dr. Toledo, who previously published a study showing a link between coffee and extended survival, noted that moderate coffee consumption has “repeatedly” been associated with lower rates of “several chronic diseases” and death, but there still isn’t enough evidence to recommend coffee for those who don’t already drink it.
More long-term research is needed, Dr. Toledo said, ideally with studies comparing changes in coffee consumption and health outcomes over time. These may not be forthcoming, however, as such trials are “not easy and feasible to conduct.”
David Kao, MD, assistant professor of medicine-cardiology and medical director of the school of medicine at the University of Colorado at Denver, Aurora, said that the study conducted by Dr. Liu and colleagues is a “very well-executed analysis” that strengthens our confidence in the safety of long-term coffee consumption, even for patients with heart disease.
Dr. Kao, who recently published an analysis showing that higher coffee intake is associated with a lower risk of heart failure, refrained from advising anyone to up their coffee quota.
“I remain cautious about stating too strongly that people should increase coffee intake purely to improve survival,” Dr. Kao said in a written comment. “That said, it does not appear harmful to increase it some, until you drink consistently more than six to seven cups per day.”
The study was supported by the National Natural Science Foundation of China, the Young Elite Scientist Sponsorship Program by CAST, the Guangdong Basic and Applied Basic Research Foundation, and others. Dr. Toledo and Dr. Kao disclosed no relevant conflicts of interest.
FROM ANNALS OF INTERNAL MEDICINE
Abortion debate may affect Rx decisions for pregnant women
Obstetrician Beverly Gray, MD, is already seeing the effects of the Roe v. Wade abortion debate in her North Carolina practice.

The state allows abortion but requires that women get counseling with a qualified health professional 72 hours before the procedure. “Aside from that, we still have patients asking for more efficacious contraceptive methods just in case,” said Dr. Gray, residency director and division director for women’s community and population health and associate professor for obstetrics and gynecology at Duke University, Durham, N.C.
Patients and staff in her clinic have also been approaching her about tubal ligation. “They’re asking about additional birth control methods because they’re concerned about what’s going to happen” with the challenge to the historic Roe v. Wade decision in the Supreme Court and subsequent actions in the states to restrict or ban abortion, she said.
This has implications not just for abortion but for medications known to affect pregnancy. “What I’m really worried about is physicians will be withholding medicine because they’re concerned about teratogenic effects,” said Dr. Gray.
With more states issuing restrictions on abortion, doctors are worried that patients needing certain drugs to maintain their lupus flares, cancer, or other diseases may decide not to take them in the event they accidentally become pregnant. If the drug is known to affect the fetus, the fear is a patient who lives in a state with abortion restrictions will no longer have the option to terminate a pregnancy.

Instead, a scenario may arise in which the patient – and their physician – may opt not to treat at all with an otherwise lifesaving medication, experts told this news organization.
The U.S. landscape on abortion restrictions
A leaked draft of a U.S. Supreme Court opinion on Mississippi’s 15-week abortion ban has sent the medical community into a tailspin. The case, Dobbs v. Jackson Women’s Health Organization, challenges the 1973 Roe v. Wade decision that affirms the constitutional right to abortion. It’s anticipated the high court will decide on the case in June.
Although the upcoming decision is subject to change, the draft indicated the high court would uphold the Mississippi ban. This would essentially overturn the 1973 ruling. An earlier Supreme Court decision allowing a Texas law banning abortion at 6 weeks suggests the court may already be heading in this direction. At the state level, legislatures have been moving on divergent paths – some taking steps to preserve abortion rights, others initiating restrictions.
More than 100 abortion restrictions in 19 states took effect in 2021, according to the Guttmacher Institute, which tracks such metrics. In 2022, “two key themes are anti-abortion policymakers’ continued pursuit of various types of abortion bans and restrictions on medication abortion,” the institute reported.
Forty-six states and the District of Columbia have introduced 2,025 restrictions or proactive measures on sexual and reproductive health and rights so far this year. The latest tally from Guttmacher, updated in late May, revealed that 11 states so far have enacted 42 abortion restrictions. A total of 6 states (Arizona, Florida, Idaho, Kentucky, Oklahoma, and Wyoming) have issued nine bans on abortion.
Comparatively, 11 states have enacted 19 protective abortion measures.
Twenty-two states have introduced 117 restrictions on medication abortions, which account for 54% of U.S. abortions. This includes seven measures that would ban medication abortion outright, according to Guttmacher. Kentucky and South Dakota collectively have enacted 14 restrictions on medication abortion, as well as provisions that ban mailing of abortion pills.
Chilling effect on prescribing
Some physicians anticipate that drugs such as the “morning-after” pill (levonorgestrel) will become less available as restrictions go into effect, since these are medications designed to prevent pregnancy.*
However, the ongoing effort to put a lid on abortion measures has prompted concerns about a trickle-down effect on other medications that are otherwise life-changing or lifesaving to patients but pose a risk to the fetus.
Several drugs are well documented to affect fetal growth and development of the fetus, ranging from mild, transitory effects to severe, permanent birth defects, said Ronald G. Grifka, MD, chief medical officer of University of Michigan Health-West and clinical professor of pediatrics at the University of Michigan Medical School, Ann Arbor. “As new medications are developed, we will need heightened attention to make sure they are safe for the fetus,” he added.

Certain teratogenic medications are associated with a high risk of abortion even though this isn’t their primary use, noted Christina Chambers, PhD, MPH, co-director of the Center for Better Beginnings and associate director with the Altman Clinical & Translational Research Institute at the University of California, San Diego.

“I don’t think anyone would intentionally take these drugs to induce spontaneous abortion. But if the drugs pose a risk for it, I can see how the laws might be stretched” to include them, said Dr. Chambers.
Methotrexate, a medication for autoimmune disorders, has a high risk of spontaneous abortion. So do acne medications such as isotretinoin.
Patients are usually told they’re not supposed to get pregnant on these drugs because there’s a high risk of pregnancy loss and risk of malformations and potential learning problems in the fetus. But many pregnancies aren’t planned, said Dr. Chambers. “Patients may forget about the side effects or think their birth control will protect them. And the next time they refill the medication, they may not hear about the warnings again.”
With a restrictive abortion law or ban in effect, a woman might think: “I won’t take this drug because if there’s any potential that I might get pregnant, I won’t have the option to abort an at-risk pregnancy.” Women and their doctors, for that matter, don’t want to put themselves in this position, said Dr. Chambers.
Rheumatologist Megan Clowse, MD, who prescribes several medications that potentially cause major birth defects and pregnancy loss, worries about the ramifications of these accumulating bans.

“Methotrexate has been a leading drug for us for decades for rheumatoid arthritis. Mycophenolate is a vital drug for lupus,” said Dr. Clowse, associate professor of medicine at Duke University’s division of rheumatology and immunology.
Both methotrexate and mycophenolate pose about a 40% risk of pregnancy loss and significantly increase the risk for birth defects. “I’m definitely concerned that there might be doctors or women who elect not to use those medications in women of reproductive age because of the potential risk for pregnancy and absence of abortion rights,” said Dr. Clowse.
These situations might force women to use contraceptives they don’t want to use, such as hormonal implants or intrauterine devices, she added. Another side effect is that women and their partners may decide to abstain from sex.
The iPLEDGE factor
Some rheumatology drugs like lenalidomide (Revlimid) require a valid negative pregnancy test in a lab every month. Similarly, the iPLEDGE Risk Evaluation and Mitigation Strategy seeks to reduce the teratogenicity of isotretinoin by requiring two types of birth control and regular pregnancy tests by users.
For isotretinoin specifically, abortion restrictions “could lead to increased adherence to pregnancy prevention measures which are already stringent in iPLEDGE. But on the other hand, it could lead to reduced willingness of physicians to prescribe or patients to take the medication,” said Dr. Chambers.
With programs like iPLEDGE in effect, the rate of pregnancies and abortions that occur in dermatology are relatively low, said Jenny Murase, MD, associate clinical professor of dermatology at the University of California, San Francisco.

Nevertheless, as a physician who regularly prescribes medications like isotretinoin in women of childbearing age, “it’s terrifying to me that a woman wouldn’t have the option to terminate the pregnancy if a teratogenic effect from the medication caused a severe birth defect,” said Dr. Murase.
Dermatologists use other teratogenic medications such as thalidomide, mycophenolate mofetil, and methotrexate for chronic dermatologic disease like psoriasis and atopic dermatitis.
The situation is especially tricky for dermatologists since most patients – about 80% – never discuss their pregnancy with their specialist prior to pregnancy initiation. Dr. Murase recalls when a patient with chronic plaque psoriasis on methotrexate in her late 40s became pregnant and had an abortion even before Dr. Murase became aware of the pregnancy.
Because dermatologists routinely prescribe long-term medications for chronic diseases like acne, psoriasis, and atopic dermatitis, it is important to have a conversation regarding the risks and benefits of long-term medication should a pregnancy occur in any woman of childbearing age, she said.
Fewer women in clinical trials?
Abortion restrictions could possibly discourage women of reproductive age to participate in a clinical trial for a new medication, said Dr. Chambers.
A female patient with a chronic disease who’s randomized to receive a new medication may be required to use certain types of birth control because of unknown potential adverse effects the drug may have on the fetus. But in some cases, accidental pregnancies happen.
The participant in the trial may say, “I don’t know enough about the safety of this drug in pregnancy, and I’ve already taken it. I want to terminate the pregnancy,” said Dr. Chambers. Thinking ahead, a woman may decide not to do the trial to avoid the risk of getting pregnant and not having the option to terminate the pregnancy.
This could apply to new drugs such as antiviral treatments, or medications for severe chronic disease that typically have no clinical trial data in pregnancy prior to initial release into the market.
Women may start taking the drug without thinking about getting pregnant, then realize there are no safety data and become concerned about its effects on a future pregnancy.
The question is: Will abortion restrictions have a chilling effect on these new drugs as well? Patients and their doctors may decide not to try it until more data are available. “I can see where abortion restrictions would change the risk or benefit calculation in thinking about what you do or don’t prescribe or take during reproductive age,” said Dr. Chambers.
The upside of restrictions?
If there’s a positive side to these developments with abortion bans, it may encourage women taking new medications or joining clinical trials to think even more carefully about adherence to effective contraception, said Dr. Chambers.
Some methods are more effective than others, she emphasized. “When you have an unplanned pregnancy, it could mean that the method you used wasn’t optimal or you weren’t using it as recommended.” A goal moving forward is to encourage more thoughtful use of highly effective contraceptives, thus reducing the number of unplanned pregnancies, she added.
If patients are taking methotrexate, “the time to think about pregnancy is before getting pregnant so you can switch to a drug that’s compatible with pregnancy,” she said.
This whole thought process regarding pregnancy planning could work toward useful health goals, said Dr. Chambers. “Nobody thinks termination is the preferred method, but planning ahead should involve a discussion of what works best for the patient.”
Patients do have other choices, said Dr. Grifka. “Fortunately, there are many commonly prescribed medications which cross the placenta and have no ill effects on the fetus.”
Talking to patients about choices
Dr. Clowse, who spends a lot of time training rheumatologists, encourages them to have conversations with patients about pregnancy planning. It’s a lot to manage, getting the right drug to a female patient with chronic illness, especially in this current climate of abortion upheaval, she noted.
Her approach is to have an open and honest conversation with patients about their concerns and fears, what the realities are, and what the potential future options are for certain rheumatology drugs in the United States.
Some women who see what’s happening across the country may become so risk averse that they may choose to die rather than take a lifesaving drug that poses certain risks under new restrictions.
“I think that’s tragic,” said Dr. Clowse.
To help their patients, Dr. Gray believes physicians across specialties should better educate themselves about physiology in pregnancy and how to counsel patients on the impact of not taking medications in pregnancy.
In her view, it’s almost coercive to say to a patient, “You really need to have effective contraception if I’m going to give you this lifesaving or quality-of-life-improving medication.”
When confronting such scenarios, Dr. Gray doesn’t think physicians need to change how they counsel patients about contraception. “I don’t think we should be putting pressure on patients to consider other permanent methods just because there’s a lack of abortion options.”
Patients will eventually make those decisions for themselves, she said. “They’re going to want a more efficacious method because they’re worried about not having access to abortion if they get pregnant.”
Dr. Gray reports being a site principal investigator for a phase 3 trial for VeraCept IUD, funded by Sebela Pharmaceuticals. Dr. Clowse reports receiving research funding and doing consulting for GlaxoSmithKline.
*Correction, 6/2/2022: A previous version of this article misstated the intended use of drugs such as the “morning-after” pill (levonorgestrel). They are taken to prevent unintended pregnancy.
A version of this article first appeared on Medscape.com .
Obstetrician Beverly Gray, MD, is already seeing the effects of the Roe v. Wade abortion debate in her North Carolina practice.
The state allows abortion but requires that women get counseling with a qualified health professional 72 hours before the procedure. “Aside from that, we still have patients asking for more efficacious contraceptive methods just in case,” said Dr. Gray, residency director and division director for women’s community and population health and associate professor for obstetrics and gynecology at Duke University, Durham, N.C.
Patients and staff in her clinic have also been approaching her about tubal ligation. “They’re asking about additional birth control methods because they’re concerned about what’s going to happen” with the challenge to the historic Roe v. Wade decision in the Supreme Court and subsequent actions in the states to restrict or ban abortion, she said.
This has implications not just for abortion but for medications known to affect pregnancy. “What I’m really worried about is physicians will be withholding medicine because they’re concerned about teratogenic effects,” said Dr. Gray.
With more states issuing restrictions on abortion, doctors are worried that patients needing certain drugs to maintain their lupus flares, cancer, or other diseases may decide not to take them in the event they accidentally become pregnant. If the drug is known to affect the fetus, the fear is a patient who lives in a state with abortion restrictions will no longer have the option to terminate a pregnancy.
Instead, a scenario may arise in which the patient – and their physician – may opt not to treat at all with an otherwise lifesaving medication, experts told this news organization.
The U.S. landscape on abortion restrictions
A leaked draft of a U.S. Supreme Court opinion on Mississippi’s 15-week abortion ban has sent the medical community into a tailspin. The case, Dobbs v. Jackson Women’s Health Organization, challenges the 1973 Roe v. Wade decision that affirms the constitutional right to abortion. It’s anticipated the high court will decide on the case in June.
Although the upcoming decision is subject to change, the draft indicated the high court would uphold the Mississippi ban. This would essentially overturn the 1973 ruling. An earlier Supreme Court decision allowing a Texas law banning abortion at 6 weeks suggests the court may already be heading in this direction. At the state level, legislatures have been moving on divergent paths – some taking steps to preserve abortion rights, others initiating restrictions.
More than 100 abortion restrictions in 19 states took effect in 2021, according to the Guttmacher Institute, which tracks such metrics. In 2022, “two key themes are anti-abortion policymakers’ continued pursuit of various types of abortion bans and restrictions on medication abortion,” the institute reported.
Forty-six states and the District of Columbia have introduced 2,025 restrictions or proactive measures on sexual and reproductive health and rights so far this year. The latest tally from Guttmacher, updated in late May, revealed that 11 states so far have enacted 42 abortion restrictions. A total of 6 states (Arizona, Florida, Idaho, Kentucky, Oklahoma, and Wyoming) have issued nine bans on abortion.
Comparatively, 11 states have enacted 19 protective abortion measures.
Twenty-two states have introduced 117 restrictions on medication abortions, which account for 54% of U.S. abortions. This includes seven measures that would ban medication abortion outright, according to Guttmacher. Kentucky and South Dakota collectively have enacted 14 restrictions on medication abortion, as well as provisions that ban mailing of abortion pills.
Chilling effect on prescribing
Some physicians anticipate that drugs such as the “morning-after” pill (levonorgestrel) will become less available as restrictions go into effect, since these are medications designed to prevent pregnancy.*
However, the ongoing effort to put a lid on abortion measures has prompted concerns about a trickle-down effect on other medications that are otherwise life-changing or lifesaving to patients but pose a risk to the fetus.
Several drugs are well documented to affect fetal growth and development of the fetus, ranging from mild, transitory effects to severe, permanent birth defects, said Ronald G. Grifka, MD, chief medical officer of University of Michigan Health-West and clinical professor of pediatrics at the University of Michigan Medical School, Ann Arbor. “As new medications are developed, we will need heightened attention to make sure they are safe for the fetus,” he added.
Certain teratogenic medications are associated with a high risk of abortion even though this isn’t their primary use, noted Christina Chambers, PhD, MPH, co-director of the Center for Better Beginnings and associate director with the Altman Clinical & Translational Research Institute at the University of California, San Diego.
“I don’t think anyone would intentionally take these drugs to induce spontaneous abortion. But if the drugs pose a risk for it, I can see how the laws might be stretched” to include them, said Dr. Chambers.
Methotrexate, a medication for autoimmune disorders, has a high risk of spontaneous abortion. So do acne medications such as isotretinoin.
Patients are usually told they’re not supposed to get pregnant on these drugs because there’s a high risk of pregnancy loss and risk of malformations and potential learning problems in the fetus. But many pregnancies aren’t planned, said Dr. Chambers. “Patients may forget about the side effects or think their birth control will protect them. And the next time they refill the medication, they may not hear about the warnings again.”
With a restrictive abortion law or ban in effect, a woman might think: “I won’t take this drug because if there’s any potential that I might get pregnant, I won’t have the option to abort an at-risk pregnancy.” Women and their doctors, for that matter, don’t want to put themselves in this position, said Dr. Chambers.
Rheumatologist Megan Clowse, MD, who prescribes several medications that potentially cause major birth defects and pregnancy loss, worries about the ramifications of these accumulating bans.
“Methotrexate has been a leading drug for us for decades for rheumatoid arthritis. Mycophenolate is a vital drug for lupus,” said Dr. Clowse, associate professor of medicine at Duke University’s division of rheumatology and immunology.
Both methotrexate and mycophenolate pose about a 40% risk of pregnancy loss and significantly increase the risk for birth defects. “I’m definitely concerned that there might be doctors or women who elect not to use those medications in women of reproductive age because of the potential risk for pregnancy and absence of abortion rights,” said Dr. Clowse.
These situations might force women to use contraceptives they don’t want to use, such as hormonal implants or intrauterine devices, she added. Another side effect is that women and their partners may decide to abstain from sex.
The iPLEDGE factor
Some rheumatology drugs like lenalidomide (Revlimid) require a valid negative pregnancy test in a lab every month. Similarly, the iPLEDGE Risk Evaluation and Mitigation Strategy seeks to reduce the teratogenicity of isotretinoin by requiring two types of birth control and regular pregnancy tests by users.
For isotretinoin specifically, abortion restrictions “could lead to increased adherence to pregnancy prevention measures which are already stringent in iPLEDGE. But on the other hand, it could lead to reduced willingness of physicians to prescribe or patients to take the medication,” said Dr. Chambers.
With programs like iPLEDGE in effect, the rate of pregnancies and abortions that occur in dermatology are relatively low, said Jenny Murase, MD, associate clinical professor of dermatology at the University of California, San Francisco.
Nevertheless, as a physician who regularly prescribes medications like isotretinoin in women of childbearing age, “it’s terrifying to me that a woman wouldn’t have the option to terminate the pregnancy if a teratogenic effect from the medication caused a severe birth defect,” said Dr. Murase.
Dermatologists use other teratogenic medications such as thalidomide, mycophenolate mofetil, and methotrexate for chronic dermatologic disease like psoriasis and atopic dermatitis.
The situation is especially tricky for dermatologists since most patients – about 80% – never discuss their pregnancy with their specialist prior to pregnancy initiation. Dr. Murase recalls when a patient with chronic plaque psoriasis on methotrexate in her late 40s became pregnant and had an abortion even before Dr. Murase became aware of the pregnancy.
Because dermatologists routinely prescribe long-term medications for chronic diseases like acne, psoriasis, and atopic dermatitis, it is important to have a conversation regarding the risks and benefits of long-term medication should a pregnancy occur in any woman of childbearing age, she said.
Fewer women in clinical trials?
Abortion restrictions could possibly discourage women of reproductive age to participate in a clinical trial for a new medication, said Dr. Chambers.
A female patient with a chronic disease who’s randomized to receive a new medication may be required to use certain types of birth control because of unknown potential adverse effects the drug may have on the fetus. But in some cases, accidental pregnancies happen.
The participant in the trial may say, “I don’t know enough about the safety of this drug in pregnancy, and I’ve already taken it. I want to terminate the pregnancy,” said Dr. Chambers. Thinking ahead, a woman may decide not to do the trial to avoid the risk of getting pregnant and not having the option to terminate the pregnancy.
This could apply to new drugs such as antiviral treatments, or medications for severe chronic disease that typically have no clinical trial data in pregnancy prior to initial release into the market.
Women may start taking the drug without thinking about getting pregnant, then realize there are no safety data and become concerned about its effects on a future pregnancy.
The question is: Will abortion restrictions have a chilling effect on these new drugs as well? Patients and their doctors may decide not to try it until more data are available. “I can see where abortion restrictions would change the risk or benefit calculation in thinking about what you do or don’t prescribe or take during reproductive age,” said Dr. Chambers.
The upside of restrictions?
If there’s a positive side to these developments with abortion bans, it may encourage women taking new medications or joining clinical trials to think even more carefully about adherence to effective contraception, said Dr. Chambers.
Some methods are more effective than others, she emphasized. “When you have an unplanned pregnancy, it could mean that the method you used wasn’t optimal or you weren’t using it as recommended.” A goal moving forward is to encourage more thoughtful use of highly effective contraceptives, thus reducing the number of unplanned pregnancies, she added.
If patients are taking methotrexate, “the time to think about pregnancy is before getting pregnant so you can switch to a drug that’s compatible with pregnancy,” she said.
This whole thought process regarding pregnancy planning could work toward useful health goals, said Dr. Chambers. “Nobody thinks termination is the preferred method, but planning ahead should involve a discussion of what works best for the patient.”
Patients do have other choices, said Dr. Grifka. “Fortunately, there are many commonly prescribed medications which cross the placenta and have no ill effects on the fetus.”
Talking to patients about choices
Dr. Clowse, who spends a lot of time training rheumatologists, encourages them to have conversations with patients about pregnancy planning. It’s a lot to manage, getting the right drug to a female patient with chronic illness, especially in this current climate of abortion upheaval, she noted.
Her approach is to have an open and honest conversation with patients about their concerns and fears, what the realities are, and what the potential future options are for certain rheumatology drugs in the United States.
Some women who see what’s happening across the country may become so risk averse that they may choose to die rather than take a lifesaving drug that poses certain risks under new restrictions.
“I think that’s tragic,” said Dr. Clowse.
To help their patients, Dr. Gray believes physicians across specialties should better educate themselves about physiology in pregnancy and how to counsel patients on the impact of not taking medications in pregnancy.
In her view, it’s almost coercive to say to a patient, “You really need to have effective contraception if I’m going to give you this lifesaving or quality-of-life-improving medication.”
When confronting such scenarios, Dr. Gray doesn’t think physicians need to change how they counsel patients about contraception. “I don’t think we should be putting pressure on patients to consider other permanent methods just because there’s a lack of abortion options.”
Patients will eventually make those decisions for themselves, she said. “They’re going to want a more efficacious method because they’re worried about not having access to abortion if they get pregnant.”
Dr. Gray reports being a site principal investigator for a phase 3 trial for VeraCept IUD, funded by Sebela Pharmaceuticals. Dr. Clowse reports receiving research funding and doing consulting for GlaxoSmithKline.
*Correction, 6/2/2022: A previous version of this article misstated the intended use of drugs such as the “morning-after” pill (levonorgestrel). They are taken to prevent unintended pregnancy.
A version of this article first appeared on Medscape.com .
Obstetrician Beverly Gray, MD, is already seeing the effects of the Roe v. Wade abortion debate in her North Carolina practice.
The state allows abortion but requires that women get counseling with a qualified health professional 72 hours before the procedure. “Aside from that, we still have patients asking for more efficacious contraceptive methods just in case,” said Dr. Gray, residency director and division director for women’s community and population health and associate professor for obstetrics and gynecology at Duke University, Durham, N.C.
Patients and staff in her clinic have also been approaching her about tubal ligation. “They’re asking about additional birth control methods because they’re concerned about what’s going to happen” with the challenge to the historic Roe v. Wade decision in the Supreme Court and subsequent actions in the states to restrict or ban abortion, she said.
This has implications not just for abortion but for medications known to affect pregnancy. “What I’m really worried about is physicians will be withholding medicine because they’re concerned about teratogenic effects,” said Dr. Gray.
With more states issuing restrictions on abortion, doctors are worried that patients needing certain drugs to maintain their lupus flares, cancer, or other diseases may decide not to take them in the event they accidentally become pregnant. If the drug is known to affect the fetus, the fear is a patient who lives in a state with abortion restrictions will no longer have the option to terminate a pregnancy.
Instead, a scenario may arise in which the patient – and their physician – may opt not to treat at all with an otherwise lifesaving medication, experts told this news organization.
The U.S. landscape on abortion restrictions
A leaked draft of a U.S. Supreme Court opinion on Mississippi’s 15-week abortion ban has sent the medical community into a tailspin. The case, Dobbs v. Jackson Women’s Health Organization, challenges the 1973 Roe v. Wade decision that affirms the constitutional right to abortion. It’s anticipated the high court will decide on the case in June.
Although the upcoming decision is subject to change, the draft indicated the high court would uphold the Mississippi ban. This would essentially overturn the 1973 ruling. An earlier Supreme Court decision allowing a Texas law banning abortion at 6 weeks suggests the court may already be heading in this direction. At the state level, legislatures have been moving on divergent paths – some taking steps to preserve abortion rights, others initiating restrictions.
More than 100 abortion restrictions in 19 states took effect in 2021, according to the Guttmacher Institute, which tracks such metrics. In 2022, “two key themes are anti-abortion policymakers’ continued pursuit of various types of abortion bans and restrictions on medication abortion,” the institute reported.
Forty-six states and the District of Columbia have introduced 2,025 restrictions or proactive measures on sexual and reproductive health and rights so far this year. The latest tally from Guttmacher, updated in late May, revealed that 11 states so far have enacted 42 abortion restrictions. A total of 6 states (Arizona, Florida, Idaho, Kentucky, Oklahoma, and Wyoming) have issued nine bans on abortion.
Comparatively, 11 states have enacted 19 protective abortion measures.
Twenty-two states have introduced 117 restrictions on medication abortions, which account for 54% of U.S. abortions. This includes seven measures that would ban medication abortion outright, according to Guttmacher. Kentucky and South Dakota collectively have enacted 14 restrictions on medication abortion, as well as provisions that ban mailing of abortion pills.
Chilling effect on prescribing
Some physicians anticipate that drugs such as the “morning-after” pill (levonorgestrel) will become less available as restrictions go into effect, since these are medications designed to prevent pregnancy.*
However, the ongoing effort to put a lid on abortion measures has prompted concerns about a trickle-down effect on other medications that are otherwise life-changing or lifesaving to patients but pose a risk to the fetus.
Several drugs are well documented to affect fetal growth and development of the fetus, ranging from mild, transitory effects to severe, permanent birth defects, said Ronald G. Grifka, MD, chief medical officer of University of Michigan Health-West and clinical professor of pediatrics at the University of Michigan Medical School, Ann Arbor. “As new medications are developed, we will need heightened attention to make sure they are safe for the fetus,” he added.
Certain teratogenic medications are associated with a high risk of abortion even though this isn’t their primary use, noted Christina Chambers, PhD, MPH, co-director of the Center for Better Beginnings and associate director with the Altman Clinical & Translational Research Institute at the University of California, San Diego.
“I don’t think anyone would intentionally take these drugs to induce spontaneous abortion. But if the drugs pose a risk for it, I can see how the laws might be stretched” to include them, said Dr. Chambers.
Methotrexate, a medication for autoimmune disorders, has a high risk of spontaneous abortion. So do acne medications such as isotretinoin.
Patients are usually told they’re not supposed to get pregnant on these drugs because there’s a high risk of pregnancy loss and risk of malformations and potential learning problems in the fetus. But many pregnancies aren’t planned, said Dr. Chambers. “Patients may forget about the side effects or think their birth control will protect them. And the next time they refill the medication, they may not hear about the warnings again.”
With a restrictive abortion law or ban in effect, a woman might think: “I won’t take this drug because if there’s any potential that I might get pregnant, I won’t have the option to abort an at-risk pregnancy.” Women and their doctors, for that matter, don’t want to put themselves in this position, said Dr. Chambers.
Rheumatologist Megan Clowse, MD, who prescribes several medications that potentially cause major birth defects and pregnancy loss, worries about the ramifications of these accumulating bans.
“Methotrexate has been a leading drug for us for decades for rheumatoid arthritis. Mycophenolate is a vital drug for lupus,” said Dr. Clowse, associate professor of medicine at Duke University’s division of rheumatology and immunology.
Both methotrexate and mycophenolate pose about a 40% risk of pregnancy loss and significantly increase the risk for birth defects. “I’m definitely concerned that there might be doctors or women who elect not to use those medications in women of reproductive age because of the potential risk for pregnancy and absence of abortion rights,” said Dr. Clowse.
These situations might force women to use contraceptives they don’t want to use, such as hormonal implants or intrauterine devices, she added. Another side effect is that women and their partners may decide to abstain from sex.
The iPLEDGE factor
Some rheumatology drugs like lenalidomide (Revlimid) require a valid negative pregnancy test in a lab every month. Similarly, the iPLEDGE Risk Evaluation and Mitigation Strategy seeks to reduce the teratogenicity of isotretinoin by requiring two types of birth control and regular pregnancy tests by users.
For isotretinoin specifically, abortion restrictions “could lead to increased adherence to pregnancy prevention measures which are already stringent in iPLEDGE. But on the other hand, it could lead to reduced willingness of physicians to prescribe or patients to take the medication,” said Dr. Chambers.
With programs like iPLEDGE in effect, the rate of pregnancies and abortions that occur in dermatology are relatively low, said Jenny Murase, MD, associate clinical professor of dermatology at the University of California, San Francisco.
Nevertheless, as a physician who regularly prescribes medications like isotretinoin in women of childbearing age, “it’s terrifying to me that a woman wouldn’t have the option to terminate the pregnancy if a teratogenic effect from the medication caused a severe birth defect,” said Dr. Murase.
Dermatologists use other teratogenic medications such as thalidomide, mycophenolate mofetil, and methotrexate for chronic dermatologic disease like psoriasis and atopic dermatitis.
The situation is especially tricky for dermatologists since most patients – about 80% – never discuss their pregnancy with their specialist prior to pregnancy initiation. Dr. Murase recalls when a patient with chronic plaque psoriasis on methotrexate in her late 40s became pregnant and had an abortion even before Dr. Murase became aware of the pregnancy.
Because dermatologists routinely prescribe long-term medications for chronic diseases like acne, psoriasis, and atopic dermatitis, it is important to have a conversation regarding the risks and benefits of long-term medication should a pregnancy occur in any woman of childbearing age, she said.
Fewer women in clinical trials?
Abortion restrictions could possibly discourage women of reproductive age to participate in a clinical trial for a new medication, said Dr. Chambers.
A female patient with a chronic disease who’s randomized to receive a new medication may be required to use certain types of birth control because of unknown potential adverse effects the drug may have on the fetus. But in some cases, accidental pregnancies happen.
The participant in the trial may say, “I don’t know enough about the safety of this drug in pregnancy, and I’ve already taken it. I want to terminate the pregnancy,” said Dr. Chambers. Thinking ahead, a woman may decide not to do the trial to avoid the risk of getting pregnant and not having the option to terminate the pregnancy.
This could apply to new drugs such as antiviral treatments, or medications for severe chronic disease that typically have no clinical trial data in pregnancy prior to initial release into the market.
Women may start taking the drug without thinking about getting pregnant, then realize there are no safety data and become concerned about its effects on a future pregnancy.
The question is: Will abortion restrictions have a chilling effect on these new drugs as well? Patients and their doctors may decide not to try it until more data are available. “I can see where abortion restrictions would change the risk or benefit calculation in thinking about what you do or don’t prescribe or take during reproductive age,” said Dr. Chambers.
The upside of restrictions?
If there’s a positive side to these developments with abortion bans, it may encourage women taking new medications or joining clinical trials to think even more carefully about adherence to effective contraception, said Dr. Chambers.
Some methods are more effective than others, she emphasized. “When you have an unplanned pregnancy, it could mean that the method you used wasn’t optimal or you weren’t using it as recommended.” A goal moving forward is to encourage more thoughtful use of highly effective contraceptives, thus reducing the number of unplanned pregnancies, she added.
If patients are taking methotrexate, “the time to think about pregnancy is before getting pregnant so you can switch to a drug that’s compatible with pregnancy,” she said.
This whole thought process regarding pregnancy planning could work toward useful health goals, said Dr. Chambers. “Nobody thinks termination is the preferred method, but planning ahead should involve a discussion of what works best for the patient.”
Patients do have other choices, said Dr. Grifka. “Fortunately, there are many commonly prescribed medications which cross the placenta and have no ill effects on the fetus.”
Talking to patients about choices
Dr. Clowse, who spends a lot of time training rheumatologists, encourages them to have conversations with patients about pregnancy planning. It’s a lot to manage, getting the right drug to a female patient with chronic illness, especially in this current climate of abortion upheaval, she noted.
Her approach is to have an open and honest conversation with patients about their concerns and fears, what the realities are, and what the potential future options are for certain rheumatology drugs in the United States.
Some women who see what’s happening across the country may become so risk averse that they may choose to die rather than take a lifesaving drug that poses certain risks under new restrictions.
“I think that’s tragic,” said Dr. Clowse.
To help their patients, Dr. Gray believes physicians across specialties should better educate themselves about physiology in pregnancy and how to counsel patients on the impact of not taking medications in pregnancy.
In her view, it’s almost coercive to say to a patient, “You really need to have effective contraception if I’m going to give you this lifesaving or quality-of-life-improving medication.”
When confronting such scenarios, Dr. Gray doesn’t think physicians need to change how they counsel patients about contraception. “I don’t think we should be putting pressure on patients to consider other permanent methods just because there’s a lack of abortion options.”
Patients will eventually make those decisions for themselves, she said. “They’re going to want a more efficacious method because they’re worried about not having access to abortion if they get pregnant.”
Dr. Gray reports being a site principal investigator for a phase 3 trial for VeraCept IUD, funded by Sebela Pharmaceuticals. Dr. Clowse reports receiving research funding and doing consulting for GlaxoSmithKline.
*Correction, 6/2/2022: A previous version of this article misstated the intended use of drugs such as the “morning-after” pill (levonorgestrel). They are taken to prevent unintended pregnancy.
A version of this article first appeared on Medscape.com .
Are docs getting fed up with hearing about burnout?
There is a feeling of exhaustion, being unable to shake a lingering cold, suffering from frequent headaches and gastrointestinal disturbances, sleeplessness and shortness of breath ...
That was how burnout was described by clinical psychologist Herbert Freudenberger, PhD, who first used the phrase in a paper back in 1974, after observing the emotional depletion and accompanying psychosomatic symptoms among volunteer staff of a free clinic in New York City. He called it “burnout,” a term borrowed from the slang of substance abusers.
It has now been established beyond a shadow of a doubt that burnout is a serious issue facing physicians across specialties, albeit some more intensely than others. But with the constant barrage of stories published on an almost daily basis, along with studies and surveys, it begs the question:
Some have suggested that the focus should be more on tackling burnout and instituting viable solutions rather than rehashing the problem.
There haven’t been studies or surveys on this question, but several experts have offered their opinion.
Jonathan Fisher, MD, a cardiologist and organizational well-being and resiliency leader at Novant Health, Charlotte, N.C., cautioned that he hesitates to speak about what physicians in general believe. “We are a diverse group of nearly 1 million in the United States alone,” he said.
But he noted that there is a specific phenomenon among burned-out health care providers who are “burned out on burnout.”
“Essentially, the underlying thought is ‘talk is cheap and we want action,’” said Dr. Fisher, who is chair and co-founder of the Ending Physician Burnout Global Summit that was held in 2021. “This reaction is often a reflection of disheartened physicians’ sense of hopelessness and cynicism that systemic change to improve working conditions will happen in our lifetime.”
Dr. Fisher explained that “typically, anyone suffering – physicians or nonphysicians – cares more about ending the suffering as soon as possible than learning its causes, but to alleviate suffering at its core – including the emotional suffering of burnout – we must understand the many causes.”
“To address both the organizational and individual drivers of burnout requires a keen awareness of the thoughts, fears, and dreams of physicians, health care executives, and all other stakeholders in health care,” he added.
Burnout, of course, is a very real problem. The 2022 Medscape Physician Burnout & Depression Report found that nearly half of all respondents (47%) said they are burned out, which was higher than the prior year. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, jumping from 43% in 2021 to 60% this year. More than half of critical care physicians (56%) also reported that they were burned out.
The World Health Organization’s International Classification of Diseases (ICD-11) – the official compendium of diseases – has categorized burnout as a “syndrome” that results from “chronic workplace stress that has not been successfully managed.” It is considered to be an occupational phenomenon and is not classified as a medical condition.
But whether or not physicians are burned out on hearing about burnout remains unclear. “I am not sure if physicians are tired of hearing about ‘burnout,’ but I do think that they want to hear about solutions that go beyond just telling them to take better care of themselves,” said Anne Thorndike, MD, MPH, an internal medicine physician at Massachusetts General Hospital and associate professor of medicine at Harvard Medical School, Boston. “There are major systematic factors that contribute to physicians burning out.”
Why talk about negative outcomes?
Jonathan Ripp, MD, MPH, however, is familiar with this sentiment. “‘Why do we keep identifying a problem without solutions’ is certainly a sentiment that is being expressed,” he said. “It’s a negative outcome, so why do we keep talking about negative outcomes?”
Dr. Ripp, who is a professor of medicine, medical education, and geriatrics and palliative medicine; the senior associate dean for well-being and resilience; and chief wellness officer at Icahn School of Medicine at Mount Sinai, New York, is also a well-known expert and researcher in burnout and physician well-being.
He noted that burnout was one of the first “tools” used as a metric to measure well-being, but it is a negative measurement. “It’s been around a long time, so it has a lot of evidence,” said Dr. Ripp. “But that said, there are other ways of measuring well-being without a negative association, and ways of measuring meaning in work – fulfillment and satisfaction, and so on. It should be balanced.”
But for the average physician not familiar with the long legacy of research, they may be frustrated by this situation. “Then they ask, ‘Why are you just showing me more of this instead of doing something about it?’ but we are actually doing something about it,” said Dr. Ripp.
There are many efforts underway, he explained, but it’s a challenging and complex issue. “There are numerous drivers impacting the well-being of any given segment within the health care workforce,” he said. “It will also vary by discipline and location, and there are also a host of individual factors that may have very little to do with the work environment. There are some very well-established efforts for an organizational approach, but it remains to be seen which is the most effective.”
But in broad strokes, he continued, it’s about tackling the system and not about making an individual more resilient. “Individuals that do engage in activities that improve resilience do better, but that’s not what this is about – it’s not going to solve the problem,” said Dr. Ripp. “Those of us like myself, who are working in this space, are trying to promote a culture of well-being – at the system level.”
The question is how to enable the workforce to do their best work in an efficient way so that the balance of their activities are not the meaningless aspects. “And instead, shoot that balance to the meaningful aspects of work,” he added. “There are enormous challenges, but even though we are working on solutions, I can see how the individual may not see that – they may say, ‘Stop telling me to be resilient, stop telling me there’s a problem,’ but we’re working on it.”
Moving medicine forward
James Jerzak, MD, a family physician in Green Bay, Wisc., and physician lead at Bellin Health, noted that “it seems to me that doctors aren’t burned out talking about burnout, but they are burned out hearing that the solution to burnout is simply for them to become more resilient,” he said. “In actuality, the path to dealing with this huge problem is to make meaningful systemic changes in how medicine is practiced.”
He reiterated that medical care has become increasingly complex, with the aging of the population; the increasing incidence of chronic diseases, such as diabetes; the challenges with the increasing cost of care, higher copays, and lack of health insurance for a large portion of the country; and general incivility toward health care workers that was exacerbated by the pandemic.
“This has all led to significantly increased stress levels for medical workers,” he said. “Couple all of that with the increased work involved in meeting the demands of the electronic health record, and it is clear that the current situation is unsustainable.”
In his own health care system, moving medicine forward has meant advancing team-based care, which translates to expanding teams to include adequate support for physicians. This strategy addressed problems in health care delivery, part of which is burnout.
“In many systems practicing advanced team-based care, the ancillary staff – medical assistants, LPNs, and RNs – play an enhanced role in the patient visit and perform functions such as quality care gap closure, medication review and refill pending, pending orders, and helping with documentation,” he said. “Although the current health care workforce shortages has created challenges, there are a lot of innovative approaches being tried [that are] aimed at providing solutions.”
The second key factor is for systems is to develop robust support for their providers with a broad range of team members, such as case managers, clinical pharmacists, diabetic educators, care coordinators, and others. “The day has passed where individual physicians can effectivity manage all of the complexities of care, especially since there are so many nonclinical factors affecting care,” said Dr. Jerzak.
“The recent focus on the social determinants of health and health equity underlies the fact that it truly takes a team of health care professionals working together to provide optimal care for patients,” he said.
Dr. Thorndike, who mentors premedical and medical trainees, has pointed out that burnout begins way before an individual enters the workplace as a doctor. Burnout begins in the earliest stages of medical practice, with the application process to medical school. The admissions process extends over a 12-month period, causing a great deal of “toxic stress.”
One study found that, compared with non-premedical students, premedical students had greater depression severity and emotional exhaustion.
“The current system of medical school admissions ignores the toll that the lengthy and emotionally exhausting process takes on aspiring physicians,” she said. “This is just one example of many in training and health care that requires physicians to set aside their own lives to achieve their goals and to provide the best possible care to others.”
A version of this article first appeared on Medscape.com.
There is a feeling of exhaustion, being unable to shake a lingering cold, suffering from frequent headaches and gastrointestinal disturbances, sleeplessness and shortness of breath ...
That was how burnout was described by clinical psychologist Herbert Freudenberger, PhD, who first used the phrase in a paper back in 1974, after observing the emotional depletion and accompanying psychosomatic symptoms among volunteer staff of a free clinic in New York City. He called it “burnout,” a term borrowed from the slang of substance abusers.
It has now been established beyond a shadow of a doubt that burnout is a serious issue facing physicians across specialties, albeit some more intensely than others. But with the constant barrage of stories published on an almost daily basis, along with studies and surveys, it begs the question:
Some have suggested that the focus should be more on tackling burnout and instituting viable solutions rather than rehashing the problem.
There haven’t been studies or surveys on this question, but several experts have offered their opinion.
Jonathan Fisher, MD, a cardiologist and organizational well-being and resiliency leader at Novant Health, Charlotte, N.C., cautioned that he hesitates to speak about what physicians in general believe. “We are a diverse group of nearly 1 million in the United States alone,” he said.
But he noted that there is a specific phenomenon among burned-out health care providers who are “burned out on burnout.”
“Essentially, the underlying thought is ‘talk is cheap and we want action,’” said Dr. Fisher, who is chair and co-founder of the Ending Physician Burnout Global Summit that was held in 2021. “This reaction is often a reflection of disheartened physicians’ sense of hopelessness and cynicism that systemic change to improve working conditions will happen in our lifetime.”
Dr. Fisher explained that “typically, anyone suffering – physicians or nonphysicians – cares more about ending the suffering as soon as possible than learning its causes, but to alleviate suffering at its core – including the emotional suffering of burnout – we must understand the many causes.”
“To address both the organizational and individual drivers of burnout requires a keen awareness of the thoughts, fears, and dreams of physicians, health care executives, and all other stakeholders in health care,” he added.
Burnout, of course, is a very real problem. The 2022 Medscape Physician Burnout & Depression Report found that nearly half of all respondents (47%) said they are burned out, which was higher than the prior year. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, jumping from 43% in 2021 to 60% this year. More than half of critical care physicians (56%) also reported that they were burned out.
The World Health Organization’s International Classification of Diseases (ICD-11) – the official compendium of diseases – has categorized burnout as a “syndrome” that results from “chronic workplace stress that has not been successfully managed.” It is considered to be an occupational phenomenon and is not classified as a medical condition.
But whether or not physicians are burned out on hearing about burnout remains unclear. “I am not sure if physicians are tired of hearing about ‘burnout,’ but I do think that they want to hear about solutions that go beyond just telling them to take better care of themselves,” said Anne Thorndike, MD, MPH, an internal medicine physician at Massachusetts General Hospital and associate professor of medicine at Harvard Medical School, Boston. “There are major systematic factors that contribute to physicians burning out.”
Why talk about negative outcomes?
Jonathan Ripp, MD, MPH, however, is familiar with this sentiment. “‘Why do we keep identifying a problem without solutions’ is certainly a sentiment that is being expressed,” he said. “It’s a negative outcome, so why do we keep talking about negative outcomes?”
Dr. Ripp, who is a professor of medicine, medical education, and geriatrics and palliative medicine; the senior associate dean for well-being and resilience; and chief wellness officer at Icahn School of Medicine at Mount Sinai, New York, is also a well-known expert and researcher in burnout and physician well-being.
He noted that burnout was one of the first “tools” used as a metric to measure well-being, but it is a negative measurement. “It’s been around a long time, so it has a lot of evidence,” said Dr. Ripp. “But that said, there are other ways of measuring well-being without a negative association, and ways of measuring meaning in work – fulfillment and satisfaction, and so on. It should be balanced.”
But for the average physician not familiar with the long legacy of research, they may be frustrated by this situation. “Then they ask, ‘Why are you just showing me more of this instead of doing something about it?’ but we are actually doing something about it,” said Dr. Ripp.
There are many efforts underway, he explained, but it’s a challenging and complex issue. “There are numerous drivers impacting the well-being of any given segment within the health care workforce,” he said. “It will also vary by discipline and location, and there are also a host of individual factors that may have very little to do with the work environment. There are some very well-established efforts for an organizational approach, but it remains to be seen which is the most effective.”
But in broad strokes, he continued, it’s about tackling the system and not about making an individual more resilient. “Individuals that do engage in activities that improve resilience do better, but that’s not what this is about – it’s not going to solve the problem,” said Dr. Ripp. “Those of us like myself, who are working in this space, are trying to promote a culture of well-being – at the system level.”
The question is how to enable the workforce to do their best work in an efficient way so that the balance of their activities are not the meaningless aspects. “And instead, shoot that balance to the meaningful aspects of work,” he added. “There are enormous challenges, but even though we are working on solutions, I can see how the individual may not see that – they may say, ‘Stop telling me to be resilient, stop telling me there’s a problem,’ but we’re working on it.”
Moving medicine forward
James Jerzak, MD, a family physician in Green Bay, Wisc., and physician lead at Bellin Health, noted that “it seems to me that doctors aren’t burned out talking about burnout, but they are burned out hearing that the solution to burnout is simply for them to become more resilient,” he said. “In actuality, the path to dealing with this huge problem is to make meaningful systemic changes in how medicine is practiced.”
He reiterated that medical care has become increasingly complex, with the aging of the population; the increasing incidence of chronic diseases, such as diabetes; the challenges with the increasing cost of care, higher copays, and lack of health insurance for a large portion of the country; and general incivility toward health care workers that was exacerbated by the pandemic.
“This has all led to significantly increased stress levels for medical workers,” he said. “Couple all of that with the increased work involved in meeting the demands of the electronic health record, and it is clear that the current situation is unsustainable.”
In his own health care system, moving medicine forward has meant advancing team-based care, which translates to expanding teams to include adequate support for physicians. This strategy addressed problems in health care delivery, part of which is burnout.
“In many systems practicing advanced team-based care, the ancillary staff – medical assistants, LPNs, and RNs – play an enhanced role in the patient visit and perform functions such as quality care gap closure, medication review and refill pending, pending orders, and helping with documentation,” he said. “Although the current health care workforce shortages has created challenges, there are a lot of innovative approaches being tried [that are] aimed at providing solutions.”
The second key factor is for systems is to develop robust support for their providers with a broad range of team members, such as case managers, clinical pharmacists, diabetic educators, care coordinators, and others. “The day has passed where individual physicians can effectivity manage all of the complexities of care, especially since there are so many nonclinical factors affecting care,” said Dr. Jerzak.
“The recent focus on the social determinants of health and health equity underlies the fact that it truly takes a team of health care professionals working together to provide optimal care for patients,” he said.
Dr. Thorndike, who mentors premedical and medical trainees, has pointed out that burnout begins way before an individual enters the workplace as a doctor. Burnout begins in the earliest stages of medical practice, with the application process to medical school. The admissions process extends over a 12-month period, causing a great deal of “toxic stress.”
One study found that, compared with non-premedical students, premedical students had greater depression severity and emotional exhaustion.
“The current system of medical school admissions ignores the toll that the lengthy and emotionally exhausting process takes on aspiring physicians,” she said. “This is just one example of many in training and health care that requires physicians to set aside their own lives to achieve their goals and to provide the best possible care to others.”
A version of this article first appeared on Medscape.com.
There is a feeling of exhaustion, being unable to shake a lingering cold, suffering from frequent headaches and gastrointestinal disturbances, sleeplessness and shortness of breath ...
That was how burnout was described by clinical psychologist Herbert Freudenberger, PhD, who first used the phrase in a paper back in 1974, after observing the emotional depletion and accompanying psychosomatic symptoms among volunteer staff of a free clinic in New York City. He called it “burnout,” a term borrowed from the slang of substance abusers.
It has now been established beyond a shadow of a doubt that burnout is a serious issue facing physicians across specialties, albeit some more intensely than others. But with the constant barrage of stories published on an almost daily basis, along with studies and surveys, it begs the question:
Some have suggested that the focus should be more on tackling burnout and instituting viable solutions rather than rehashing the problem.
There haven’t been studies or surveys on this question, but several experts have offered their opinion.
Jonathan Fisher, MD, a cardiologist and organizational well-being and resiliency leader at Novant Health, Charlotte, N.C., cautioned that he hesitates to speak about what physicians in general believe. “We are a diverse group of nearly 1 million in the United States alone,” he said.
But he noted that there is a specific phenomenon among burned-out health care providers who are “burned out on burnout.”
“Essentially, the underlying thought is ‘talk is cheap and we want action,’” said Dr. Fisher, who is chair and co-founder of the Ending Physician Burnout Global Summit that was held in 2021. “This reaction is often a reflection of disheartened physicians’ sense of hopelessness and cynicism that systemic change to improve working conditions will happen in our lifetime.”
Dr. Fisher explained that “typically, anyone suffering – physicians or nonphysicians – cares more about ending the suffering as soon as possible than learning its causes, but to alleviate suffering at its core – including the emotional suffering of burnout – we must understand the many causes.”
“To address both the organizational and individual drivers of burnout requires a keen awareness of the thoughts, fears, and dreams of physicians, health care executives, and all other stakeholders in health care,” he added.
Burnout, of course, is a very real problem. The 2022 Medscape Physician Burnout & Depression Report found that nearly half of all respondents (47%) said they are burned out, which was higher than the prior year. Perhaps not surprisingly, burnout among emergency physicians took the biggest leap, jumping from 43% in 2021 to 60% this year. More than half of critical care physicians (56%) also reported that they were burned out.
The World Health Organization’s International Classification of Diseases (ICD-11) – the official compendium of diseases – has categorized burnout as a “syndrome” that results from “chronic workplace stress that has not been successfully managed.” It is considered to be an occupational phenomenon and is not classified as a medical condition.
But whether or not physicians are burned out on hearing about burnout remains unclear. “I am not sure if physicians are tired of hearing about ‘burnout,’ but I do think that they want to hear about solutions that go beyond just telling them to take better care of themselves,” said Anne Thorndike, MD, MPH, an internal medicine physician at Massachusetts General Hospital and associate professor of medicine at Harvard Medical School, Boston. “There are major systematic factors that contribute to physicians burning out.”
Why talk about negative outcomes?
Jonathan Ripp, MD, MPH, however, is familiar with this sentiment. “‘Why do we keep identifying a problem without solutions’ is certainly a sentiment that is being expressed,” he said. “It’s a negative outcome, so why do we keep talking about negative outcomes?”
Dr. Ripp, who is a professor of medicine, medical education, and geriatrics and palliative medicine; the senior associate dean for well-being and resilience; and chief wellness officer at Icahn School of Medicine at Mount Sinai, New York, is also a well-known expert and researcher in burnout and physician well-being.
He noted that burnout was one of the first “tools” used as a metric to measure well-being, but it is a negative measurement. “It’s been around a long time, so it has a lot of evidence,” said Dr. Ripp. “But that said, there are other ways of measuring well-being without a negative association, and ways of measuring meaning in work – fulfillment and satisfaction, and so on. It should be balanced.”
But for the average physician not familiar with the long legacy of research, they may be frustrated by this situation. “Then they ask, ‘Why are you just showing me more of this instead of doing something about it?’ but we are actually doing something about it,” said Dr. Ripp.
There are many efforts underway, he explained, but it’s a challenging and complex issue. “There are numerous drivers impacting the well-being of any given segment within the health care workforce,” he said. “It will also vary by discipline and location, and there are also a host of individual factors that may have very little to do with the work environment. There are some very well-established efforts for an organizational approach, but it remains to be seen which is the most effective.”
But in broad strokes, he continued, it’s about tackling the system and not about making an individual more resilient. “Individuals that do engage in activities that improve resilience do better, but that’s not what this is about – it’s not going to solve the problem,” said Dr. Ripp. “Those of us like myself, who are working in this space, are trying to promote a culture of well-being – at the system level.”
The question is how to enable the workforce to do their best work in an efficient way so that the balance of their activities are not the meaningless aspects. “And instead, shoot that balance to the meaningful aspects of work,” he added. “There are enormous challenges, but even though we are working on solutions, I can see how the individual may not see that – they may say, ‘Stop telling me to be resilient, stop telling me there’s a problem,’ but we’re working on it.”
Moving medicine forward
James Jerzak, MD, a family physician in Green Bay, Wisc., and physician lead at Bellin Health, noted that “it seems to me that doctors aren’t burned out talking about burnout, but they are burned out hearing that the solution to burnout is simply for them to become more resilient,” he said. “In actuality, the path to dealing with this huge problem is to make meaningful systemic changes in how medicine is practiced.”
He reiterated that medical care has become increasingly complex, with the aging of the population; the increasing incidence of chronic diseases, such as diabetes; the challenges with the increasing cost of care, higher copays, and lack of health insurance for a large portion of the country; and general incivility toward health care workers that was exacerbated by the pandemic.
“This has all led to significantly increased stress levels for medical workers,” he said. “Couple all of that with the increased work involved in meeting the demands of the electronic health record, and it is clear that the current situation is unsustainable.”
In his own health care system, moving medicine forward has meant advancing team-based care, which translates to expanding teams to include adequate support for physicians. This strategy addressed problems in health care delivery, part of which is burnout.
“In many systems practicing advanced team-based care, the ancillary staff – medical assistants, LPNs, and RNs – play an enhanced role in the patient visit and perform functions such as quality care gap closure, medication review and refill pending, pending orders, and helping with documentation,” he said. “Although the current health care workforce shortages has created challenges, there are a lot of innovative approaches being tried [that are] aimed at providing solutions.”
The second key factor is for systems is to develop robust support for their providers with a broad range of team members, such as case managers, clinical pharmacists, diabetic educators, care coordinators, and others. “The day has passed where individual physicians can effectivity manage all of the complexities of care, especially since there are so many nonclinical factors affecting care,” said Dr. Jerzak.
“The recent focus on the social determinants of health and health equity underlies the fact that it truly takes a team of health care professionals working together to provide optimal care for patients,” he said.
Dr. Thorndike, who mentors premedical and medical trainees, has pointed out that burnout begins way before an individual enters the workplace as a doctor. Burnout begins in the earliest stages of medical practice, with the application process to medical school. The admissions process extends over a 12-month period, causing a great deal of “toxic stress.”
One study found that, compared with non-premedical students, premedical students had greater depression severity and emotional exhaustion.
“The current system of medical school admissions ignores the toll that the lengthy and emotionally exhausting process takes on aspiring physicians,” she said. “This is just one example of many in training and health care that requires physicians to set aside their own lives to achieve their goals and to provide the best possible care to others.”
A version of this article first appeared on Medscape.com.
Very high HDL-C: Too much of a good thing?
A new study suggests that .
Investigators studied close to 10,000 patients with CAD in two separate cohorts. After adjusting for an array of covariates, they found that individuals with HDL-C levels greater than 80 mg/dL had a 96% higher risk for all-cause mortality and a 71% higher risk for cardiovascular mortality than those with HDL-C levels between 40 and 60 mg/dL.
A U-shaped association was found, with higher risk for all-cause and cardiovascular mortality in patients with both very low and very high, compared with midrange, HDL-C values.
“Very high HDL levels are associated with increased risk of adverse outcomes, not lower risk, as previously thought. This is true not only in the general population, but also in people with known coronary artery disease,” senior author Arshed A. Quyyumi, MD, professor of medicine, division of cardiology, Emory University, Atlanta, told this news organization.
“Physicians have to be cognizant of the fact that, at levels of HDL-C above 80 mg/dL, they [should be] more aggressive with risk reduction and not believe that the patient is at ‘low risk’ because of high levels of ‘good’ cholesterol,” said Dr. Quyyumi, director of the Emory Clinical Cardiovascular Research Institute.
The study was published online in JAMA Cardiology.
Inverse association?
HDL-C levels have “historically been inversely associated with increased cardiovascular disease (CVD) risk; however, recent studies have questioned the efficacy of therapies designed to increase HDL-C levels,” the authors wrote. Moreover, genetic variants associated with HDL-C have not been found to be linked to CVD risk.
Whether “very high HDL-C levels in patients with coronary artery disease (CAD) are associated with mortality risk remains unknown,” they wrote. In this study, the researchers investigated not only the potential risk of elevated HDL-C levels in these patients, but also the association of known HDL-C genetic variants with this risk.
To do so, they analyzed data from a subset of patients with CAD in two independent study groups: the UK Biobank (UKB; n = 14,478; mean [standard deviation] age, 61.2 [5.8] years; 76.2% male; 93.8% White) and the Emory Cardiovascular Biobank (EmCAB; n = 5,467; mean age, 63.8 [12.3] years; 66.4% male; 73.2% White). Participants were followed prospectively for a median of 8.9 (interquartile range, 8.0-9.7) years and 6.7 (IQR, 4.0-10.8) years, respectively.
Additional data collected included medical and medication history and demographic characteristics, which were used as covariates, as well as genomic information.
Of the UKB cohort, 12.4% and 7.9% sustained all-cause or cardiovascular death, respectively, during the follow-up period, and 1.8% of participants had an HDL-C level above 80 mg/dL.
Among these participants with very high HDL-C levels, 16.9% and 8.6% had all-cause or cardiovascular death, respectively. Compared with the reference category (HDL-C level of 40-60 mg/dL), those with low HDL-C levels (≤ 30 mg/dL) had an expected higher risk for both all-cause and cardiovascular mortality, even after adjustment for covariates (hazard ratio, 1.33; 95% confidence interval, 1.07-1.64 and HR, 1.42; 95% CI, 1.09-1.85, respectively; P = .009).
“Importantly,” the authors stated, “compared with the reference category, individuals with very high HDL-C levels (>80 mg/dL) also had a higher risk of all-cause death (HR, 1.58 [1.16-2.14], P = .004).”
Although cardiovascular death rates were not significantly greater in unadjusted analyses, after adjustment, the highest HDL-C group had an increased risk for all-cause and cardiovascular death (HR, 1.96; 95% CI, 1.42-2.71; P < .001 and HR, 1.71; 95% CI, 1.09-2.68, respectively; P = .02).
Compared with females, males with HDL-C levels above 80 mg/dL had a higher risk for all-cause and cardiovascular death.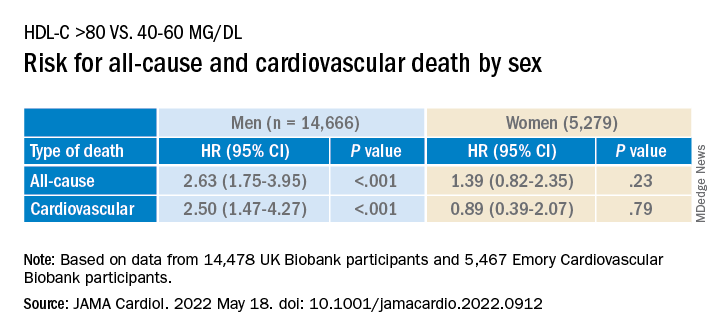
Similar findings were obtained in the EmCAB patients, 1.6% of whom had HDL-C levels above 80 mg/dL. During the follow-up period, 26.9% and 13.8% of participants sustained all-cause and cardiovascular death, respectively. Of those with HDL-C levels above 80 mg/dL, 30.0% and 16.7% experienced all-cause and cardiovascular death, respectively.
Compared with those with HDL-C levels of 40-60 mg/dL, those in the lowest (≤30 mg/dL) and highest (>80 mg/dL) groups had a “significant or near-significant greater risk for all-cause death in both unadjusted and fully adjusted models.
“Using adjusted HR curves, a U-shaped association between HDL-C and adverse events was evident with higher mortality at both very high and low HDL-C levels,” the authors noted.
Compared with patients without diabetes, those with diabetes and an HDL-C level above 80 mg/dL had a higher risk for all-cause and cardiovascular death, and patients younger than 65 years had a higher risk for cardiovascular death than patients 65 years and older.
The researchers found a “positive linear association” between the HDL-C genetic risk score (GRS) and HDL levels, wherein a 1-SD higher HDL-C GRS was associated with a 3.03 mg/dL higher HDL-C level (2.83-3.22; P < .001; R 2 = 0.06).
The HDL-C GRS was not associated with the risk for all-cause or cardiovascular death in unadjusted models, and after the HDL-C GRS was added to the fully adjusted models, the association with HDL-C level above 80 mg/dL was not attenuated, “indicating that HDL-C genetic variations in the GRS do not contribute substantially to the risk.”
“Potential mechanisms through which very high HDL-C might cause adverse cardiovascular outcomes in patients with CAD need to be studied,” Dr. Quyyumi said. “Whether the functional capacity of the HDL particle is altered when the level is very high remains unknown. Whether it is more able to oxidize and thus shift from being protective to harmful also needs to be investigated.”
Red flag
Commenting for this news organization, Sadiya Sana Khan, MD, MSc, assistant professor of medicine (cardiology) and preventive medicine (epidemiology), Northwestern University, Chicago, said: “I think the most important point [of the study] is to identify people with very high HDL-C. This can serve as a reminder to discuss heart-healthy lifestyles and discussion of statin therapy if needed, based on LDL-C.”
In an accompanying editorial coauthored with Gregg Fonarow, MD, Ahmanson-UCLA Cardiomyopathy Center, University of California, Los Angeles, the pair wrote: “Although the present findings may be related to residual confounding, high HDL-C levels should not automatically be assumed to be protective.”
They advised clinicians to “use HDL-C levels as a surrogate marker, with very low and very high levels as a red flag to target for more intensive primary and secondary prevention, as the maxim for HDL-C as ‘good’ cholesterol only holds for HDL-C levels of 80 mg/dL or less.”
This study was supported in part by grants from the National Institutes of Health, the American Heart Association, and the Abraham J. & Phyllis Katz Foundation. Dr. Quyyumi and coauthors report no relevant financial relationships. Dr. Khan reports receiving grants from the American Heart Association and the National Institutes of Health outside the submitted work. Dr. Fonarow reports receiving personal fees from Abbott, Amgen, AstraZeneca, Bayer, Cytokinetics, Edwards, Janssen, Medtronic, Merck, and Novartis outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
A new study suggests that .
Investigators studied close to 10,000 patients with CAD in two separate cohorts. After adjusting for an array of covariates, they found that individuals with HDL-C levels greater than 80 mg/dL had a 96% higher risk for all-cause mortality and a 71% higher risk for cardiovascular mortality than those with HDL-C levels between 40 and 60 mg/dL.
A U-shaped association was found, with higher risk for all-cause and cardiovascular mortality in patients with both very low and very high, compared with midrange, HDL-C values.
“Very high HDL levels are associated with increased risk of adverse outcomes, not lower risk, as previously thought. This is true not only in the general population, but also in people with known coronary artery disease,” senior author Arshed A. Quyyumi, MD, professor of medicine, division of cardiology, Emory University, Atlanta, told this news organization.
“Physicians have to be cognizant of the fact that, at levels of HDL-C above 80 mg/dL, they [should be] more aggressive with risk reduction and not believe that the patient is at ‘low risk’ because of high levels of ‘good’ cholesterol,” said Dr. Quyyumi, director of the Emory Clinical Cardiovascular Research Institute.
The study was published online in JAMA Cardiology.
Inverse association?
HDL-C levels have “historically been inversely associated with increased cardiovascular disease (CVD) risk; however, recent studies have questioned the efficacy of therapies designed to increase HDL-C levels,” the authors wrote. Moreover, genetic variants associated with HDL-C have not been found to be linked to CVD risk.
Whether “very high HDL-C levels in patients with coronary artery disease (CAD) are associated with mortality risk remains unknown,” they wrote. In this study, the researchers investigated not only the potential risk of elevated HDL-C levels in these patients, but also the association of known HDL-C genetic variants with this risk.
To do so, they analyzed data from a subset of patients with CAD in two independent study groups: the UK Biobank (UKB; n = 14,478; mean [standard deviation] age, 61.2 [5.8] years; 76.2% male; 93.8% White) and the Emory Cardiovascular Biobank (EmCAB; n = 5,467; mean age, 63.8 [12.3] years; 66.4% male; 73.2% White). Participants were followed prospectively for a median of 8.9 (interquartile range, 8.0-9.7) years and 6.7 (IQR, 4.0-10.8) years, respectively.
Additional data collected included medical and medication history and demographic characteristics, which were used as covariates, as well as genomic information.
Of the UKB cohort, 12.4% and 7.9% sustained all-cause or cardiovascular death, respectively, during the follow-up period, and 1.8% of participants had an HDL-C level above 80 mg/dL.
Among these participants with very high HDL-C levels, 16.9% and 8.6% had all-cause or cardiovascular death, respectively. Compared with the reference category (HDL-C level of 40-60 mg/dL), those with low HDL-C levels (≤ 30 mg/dL) had an expected higher risk for both all-cause and cardiovascular mortality, even after adjustment for covariates (hazard ratio, 1.33; 95% confidence interval, 1.07-1.64 and HR, 1.42; 95% CI, 1.09-1.85, respectively; P = .009).
“Importantly,” the authors stated, “compared with the reference category, individuals with very high HDL-C levels (>80 mg/dL) also had a higher risk of all-cause death (HR, 1.58 [1.16-2.14], P = .004).”
Although cardiovascular death rates were not significantly greater in unadjusted analyses, after adjustment, the highest HDL-C group had an increased risk for all-cause and cardiovascular death (HR, 1.96; 95% CI, 1.42-2.71; P < .001 and HR, 1.71; 95% CI, 1.09-2.68, respectively; P = .02).
Compared with females, males with HDL-C levels above 80 mg/dL had a higher risk for all-cause and cardiovascular death.
Similar findings were obtained in the EmCAB patients, 1.6% of whom had HDL-C levels above 80 mg/dL. During the follow-up period, 26.9% and 13.8% of participants sustained all-cause and cardiovascular death, respectively. Of those with HDL-C levels above 80 mg/dL, 30.0% and 16.7% experienced all-cause and cardiovascular death, respectively.
Compared with those with HDL-C levels of 40-60 mg/dL, those in the lowest (≤30 mg/dL) and highest (>80 mg/dL) groups had a “significant or near-significant greater risk for all-cause death in both unadjusted and fully adjusted models.
“Using adjusted HR curves, a U-shaped association between HDL-C and adverse events was evident with higher mortality at both very high and low HDL-C levels,” the authors noted.
Compared with patients without diabetes, those with diabetes and an HDL-C level above 80 mg/dL had a higher risk for all-cause and cardiovascular death, and patients younger than 65 years had a higher risk for cardiovascular death than patients 65 years and older.
The researchers found a “positive linear association” between the HDL-C genetic risk score (GRS) and HDL levels, wherein a 1-SD higher HDL-C GRS was associated with a 3.03 mg/dL higher HDL-C level (2.83-3.22; P < .001; R 2 = 0.06).
The HDL-C GRS was not associated with the risk for all-cause or cardiovascular death in unadjusted models, and after the HDL-C GRS was added to the fully adjusted models, the association with HDL-C level above 80 mg/dL was not attenuated, “indicating that HDL-C genetic variations in the GRS do not contribute substantially to the risk.”
“Potential mechanisms through which very high HDL-C might cause adverse cardiovascular outcomes in patients with CAD need to be studied,” Dr. Quyyumi said. “Whether the functional capacity of the HDL particle is altered when the level is very high remains unknown. Whether it is more able to oxidize and thus shift from being protective to harmful also needs to be investigated.”
Red flag
Commenting for this news organization, Sadiya Sana Khan, MD, MSc, assistant professor of medicine (cardiology) and preventive medicine (epidemiology), Northwestern University, Chicago, said: “I think the most important point [of the study] is to identify people with very high HDL-C. This can serve as a reminder to discuss heart-healthy lifestyles and discussion of statin therapy if needed, based on LDL-C.”
In an accompanying editorial coauthored with Gregg Fonarow, MD, Ahmanson-UCLA Cardiomyopathy Center, University of California, Los Angeles, the pair wrote: “Although the present findings may be related to residual confounding, high HDL-C levels should not automatically be assumed to be protective.”
They advised clinicians to “use HDL-C levels as a surrogate marker, with very low and very high levels as a red flag to target for more intensive primary and secondary prevention, as the maxim for HDL-C as ‘good’ cholesterol only holds for HDL-C levels of 80 mg/dL or less.”
This study was supported in part by grants from the National Institutes of Health, the American Heart Association, and the Abraham J. & Phyllis Katz Foundation. Dr. Quyyumi and coauthors report no relevant financial relationships. Dr. Khan reports receiving grants from the American Heart Association and the National Institutes of Health outside the submitted work. Dr. Fonarow reports receiving personal fees from Abbott, Amgen, AstraZeneca, Bayer, Cytokinetics, Edwards, Janssen, Medtronic, Merck, and Novartis outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
A new study suggests that .
Investigators studied close to 10,000 patients with CAD in two separate cohorts. After adjusting for an array of covariates, they found that individuals with HDL-C levels greater than 80 mg/dL had a 96% higher risk for all-cause mortality and a 71% higher risk for cardiovascular mortality than those with HDL-C levels between 40 and 60 mg/dL.
A U-shaped association was found, with higher risk for all-cause and cardiovascular mortality in patients with both very low and very high, compared with midrange, HDL-C values.
“Very high HDL levels are associated with increased risk of adverse outcomes, not lower risk, as previously thought. This is true not only in the general population, but also in people with known coronary artery disease,” senior author Arshed A. Quyyumi, MD, professor of medicine, division of cardiology, Emory University, Atlanta, told this news organization.
“Physicians have to be cognizant of the fact that, at levels of HDL-C above 80 mg/dL, they [should be] more aggressive with risk reduction and not believe that the patient is at ‘low risk’ because of high levels of ‘good’ cholesterol,” said Dr. Quyyumi, director of the Emory Clinical Cardiovascular Research Institute.
The study was published online in JAMA Cardiology.
Inverse association?
HDL-C levels have “historically been inversely associated with increased cardiovascular disease (CVD) risk; however, recent studies have questioned the efficacy of therapies designed to increase HDL-C levels,” the authors wrote. Moreover, genetic variants associated with HDL-C have not been found to be linked to CVD risk.
Whether “very high HDL-C levels in patients with coronary artery disease (CAD) are associated with mortality risk remains unknown,” they wrote. In this study, the researchers investigated not only the potential risk of elevated HDL-C levels in these patients, but also the association of known HDL-C genetic variants with this risk.
To do so, they analyzed data from a subset of patients with CAD in two independent study groups: the UK Biobank (UKB; n = 14,478; mean [standard deviation] age, 61.2 [5.8] years; 76.2% male; 93.8% White) and the Emory Cardiovascular Biobank (EmCAB; n = 5,467; mean age, 63.8 [12.3] years; 66.4% male; 73.2% White). Participants were followed prospectively for a median of 8.9 (interquartile range, 8.0-9.7) years and 6.7 (IQR, 4.0-10.8) years, respectively.
Additional data collected included medical and medication history and demographic characteristics, which were used as covariates, as well as genomic information.
Of the UKB cohort, 12.4% and 7.9% sustained all-cause or cardiovascular death, respectively, during the follow-up period, and 1.8% of participants had an HDL-C level above 80 mg/dL.
Among these participants with very high HDL-C levels, 16.9% and 8.6% had all-cause or cardiovascular death, respectively. Compared with the reference category (HDL-C level of 40-60 mg/dL), those with low HDL-C levels (≤ 30 mg/dL) had an expected higher risk for both all-cause and cardiovascular mortality, even after adjustment for covariates (hazard ratio, 1.33; 95% confidence interval, 1.07-1.64 and HR, 1.42; 95% CI, 1.09-1.85, respectively; P = .009).
“Importantly,” the authors stated, “compared with the reference category, individuals with very high HDL-C levels (>80 mg/dL) also had a higher risk of all-cause death (HR, 1.58 [1.16-2.14], P = .004).”
Although cardiovascular death rates were not significantly greater in unadjusted analyses, after adjustment, the highest HDL-C group had an increased risk for all-cause and cardiovascular death (HR, 1.96; 95% CI, 1.42-2.71; P < .001 and HR, 1.71; 95% CI, 1.09-2.68, respectively; P = .02).
Compared with females, males with HDL-C levels above 80 mg/dL had a higher risk for all-cause and cardiovascular death.
Similar findings were obtained in the EmCAB patients, 1.6% of whom had HDL-C levels above 80 mg/dL. During the follow-up period, 26.9% and 13.8% of participants sustained all-cause and cardiovascular death, respectively. Of those with HDL-C levels above 80 mg/dL, 30.0% and 16.7% experienced all-cause and cardiovascular death, respectively.
Compared with those with HDL-C levels of 40-60 mg/dL, those in the lowest (≤30 mg/dL) and highest (>80 mg/dL) groups had a “significant or near-significant greater risk for all-cause death in both unadjusted and fully adjusted models.
“Using adjusted HR curves, a U-shaped association between HDL-C and adverse events was evident with higher mortality at both very high and low HDL-C levels,” the authors noted.
Compared with patients without diabetes, those with diabetes and an HDL-C level above 80 mg/dL had a higher risk for all-cause and cardiovascular death, and patients younger than 65 years had a higher risk for cardiovascular death than patients 65 years and older.
The researchers found a “positive linear association” between the HDL-C genetic risk score (GRS) and HDL levels, wherein a 1-SD higher HDL-C GRS was associated with a 3.03 mg/dL higher HDL-C level (2.83-3.22; P < .001; R 2 = 0.06).
The HDL-C GRS was not associated with the risk for all-cause or cardiovascular death in unadjusted models, and after the HDL-C GRS was added to the fully adjusted models, the association with HDL-C level above 80 mg/dL was not attenuated, “indicating that HDL-C genetic variations in the GRS do not contribute substantially to the risk.”
“Potential mechanisms through which very high HDL-C might cause adverse cardiovascular outcomes in patients with CAD need to be studied,” Dr. Quyyumi said. “Whether the functional capacity of the HDL particle is altered when the level is very high remains unknown. Whether it is more able to oxidize and thus shift from being protective to harmful also needs to be investigated.”
Red flag
Commenting for this news organization, Sadiya Sana Khan, MD, MSc, assistant professor of medicine (cardiology) and preventive medicine (epidemiology), Northwestern University, Chicago, said: “I think the most important point [of the study] is to identify people with very high HDL-C. This can serve as a reminder to discuss heart-healthy lifestyles and discussion of statin therapy if needed, based on LDL-C.”
In an accompanying editorial coauthored with Gregg Fonarow, MD, Ahmanson-UCLA Cardiomyopathy Center, University of California, Los Angeles, the pair wrote: “Although the present findings may be related to residual confounding, high HDL-C levels should not automatically be assumed to be protective.”
They advised clinicians to “use HDL-C levels as a surrogate marker, with very low and very high levels as a red flag to target for more intensive primary and secondary prevention, as the maxim for HDL-C as ‘good’ cholesterol only holds for HDL-C levels of 80 mg/dL or less.”
This study was supported in part by grants from the National Institutes of Health, the American Heart Association, and the Abraham J. & Phyllis Katz Foundation. Dr. Quyyumi and coauthors report no relevant financial relationships. Dr. Khan reports receiving grants from the American Heart Association and the National Institutes of Health outside the submitted work. Dr. Fonarow reports receiving personal fees from Abbott, Amgen, AstraZeneca, Bayer, Cytokinetics, Edwards, Janssen, Medtronic, Merck, and Novartis outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
FROM JAMA CARDIOLOGY
Exercise response divides COPD patients into four groups
Not all patients with chronic obstructive pulmonary disease (COPD) respond equally well to pulmonary rehabilitation (PR).
Now, physicians can better categorize which patients will do well with PR and which ones less well or not well at all based on a new system of clustering of COPD patients according to their response to exercise therapy.
“We identified four clusters of COPD patients and their response to PR in the aim to better understand PR outcome and [adapt] it to patients’ profiles and needs,” lead author Yara Al Chikhanie, MD, of the cardiopulmonary rehabilitation center Dieulefit Sante (France), and colleagues observed.
“Identification of patients likely to show smaller responses to PR may help to target patients benefiting the most and to adapt PR settings for nonresponders to standard PR,” they suggested.
The study was published online in Respiratory Medicine.
Single-center cohort
The cohort consisted of 835 patients from a single center who had been admitted to a cardiopulmonary rehabilitation center over a 6-year period from 2021 to 2017. “The PR program used in the center was the same over the 6-year period,” the authors note – consisting of a 3- to 4-week, inpatient program with activities 5 days a week.
Each day, patients attended a 25-minute aerobic training session on a cycling ergometer or a treadmill; a 30-minute low-intensity gym session; a 30-minute group walk outdoors, and 30 minutes of strength training. “We aimed to cluster patients with COPD admitted to PR based on patients’ clinical characteristics and 6-meter walk test results (6MWT), pulse oxygen saturation (SPO2), heart rate (HR), and dyspnea,” the authors explained.
They then evaluated patient response to PR in each of these clusters based on the amount of improvement in the 6-meter walk distance (6MWD), lung function, and quality of life observed, they added.
The population consisted of seniors, equally men and women, mostly GOLD II and III patients (a measure of lung function) with a limited walking capacity, some 84% of the cohort having a 6MWD <80% predicted. The characteristics of the four identified clusters were as follows:
- Cluster 1: Consisted of younger men, GOLD I to II, average walkers, obese. The average 6MWD was 430 meters and patients had a large exercise HR response to PR. This cluster had a 76 meter improvement in their 6MWD, although 16% of the same cluster still did not respond to PR.
- Cluster 2: Consisted of older women, GOLD II-III, who were slow walkers. This cluster had a reduced 6MWD of 362 meters, but they also had a significant 97-meter improvement in their 6MWD following PR. Some 18% were still nonresponders to PR.
- Cluster 3: Consisted of older men, GOLD II to III, dyspneic, slow walkers, some 32% of whom responded to PR. This cluster also had a reduced 6MWD at 388 meters, but again, they also had a significant improvement of 79 meters in their 6MWD following the introduction of PR. Some 11% were nonresponders to PR.
- Cluster 4: Consisted of older men, GOLD III to IV, very slow walkers, oxygen-dependent, very dyspneic. This cluster had a severely reduced 6MWD of only 290 meters with severe exercise desaturation and dyspnea, and almost all of them were on long-term oxygen therapy. Nevertheless, this cluster also had a significant, 66-meter improvement in their 6MWD. Twenty-eight percent of them were nonresponders to PR.
Clinical practice
“The highly heterogeneous nature of the enrolled patient population reflects clinical practice,” the authors point out. For example, cluster 1 included patients with the best lung function, compared with those in clusters 2, 3, and 4 – which may be due, at least in part, to the aggravation in disease severity with age given that patients in cluster 1 were the youngest overall.
The fact that those in cluster 4 had the worst performance may also have been because of age and disease severity, the authors note, as those in cluster 4 had the highest proportion of patients on long-term oxygen therapy, again suggestive of disease severity. “Of note, these patients show the most impaired 6MWT responses despite the use of oxygen supplementation during walking,” the researchers added.
The authors also suggest that patients such as those in cluster 4 may require specific PR modalities in order to optimize their functional benefits. In contrast, those in cluster 1 had a significantly higher body mass index, compared with those in the other 3 clusters, which, interestingly enough, was not associated with more severe functional exercise impairment. The fact that older age participants, such as those in cluster 3 as well as those with high BMI in cluster 1, were both able to improve their 6MWD post-PR to the same extent as younger patients without obesity suggests that most older or overweight/obese patients can still show clinically significant improvement in 6MWD post PR, as the authors suggest.
Notably, the 6MWT was the only test available both pre-and post PR, making this an important limitation of the study, because only one aspect of the effect of PR was evaluated, omitting other physical and psychosocial benefits of PR, investigators suggest.
Adds to the literature
Asked to comment on the findings, Sachin Gupta, MD, attending physician, pulmonary & critical care medicine, Alameda Health System, Highland Hospital, Oakland, Calif., felt that these data add to the literature in defining COPD patient profiles, helping to categorize those in whom to expect greater walk distance improvements with PR versus those who will respond less well.
“Because 6MWD is a surrogate marker for quality of life (QOL) and mortality, further analysis in the form of a randomized controlled trial to determine long-term outcomes among the four clusters with adjustment for baseline characteristics would help determine the extent to which certain patient clusters may respond to PR,” Dr. Gupta told this news organization in an email.
At the same time, he suggested that while patients may not experience much net benefit in their 6MWD, their QOL or mortality risk may still improve with PR. “I cannot recall a patient ever describing their experience with PR as anything other than positive,” Dr. Gupta stressed.
“And as the authors [themselves] note, because PR serves to benefit patients beyond the 6MWD, I would not recommend limiting PR referrals based on the patient clusters identified,” he said.
The authors had no conflicts of interest to declare. Dr. Gupta declared that he is an employee and shareholder at Genentech.
Not all patients with chronic obstructive pulmonary disease (COPD) respond equally well to pulmonary rehabilitation (PR).
Now, physicians can better categorize which patients will do well with PR and which ones less well or not well at all based on a new system of clustering of COPD patients according to their response to exercise therapy.
“We identified four clusters of COPD patients and their response to PR in the aim to better understand PR outcome and [adapt] it to patients’ profiles and needs,” lead author Yara Al Chikhanie, MD, of the cardiopulmonary rehabilitation center Dieulefit Sante (France), and colleagues observed.
“Identification of patients likely to show smaller responses to PR may help to target patients benefiting the most and to adapt PR settings for nonresponders to standard PR,” they suggested.
The study was published online in Respiratory Medicine.
Single-center cohort
The cohort consisted of 835 patients from a single center who had been admitted to a cardiopulmonary rehabilitation center over a 6-year period from 2021 to 2017. “The PR program used in the center was the same over the 6-year period,” the authors note – consisting of a 3- to 4-week, inpatient program with activities 5 days a week.
Each day, patients attended a 25-minute aerobic training session on a cycling ergometer or a treadmill; a 30-minute low-intensity gym session; a 30-minute group walk outdoors, and 30 minutes of strength training. “We aimed to cluster patients with COPD admitted to PR based on patients’ clinical characteristics and 6-meter walk test results (6MWT), pulse oxygen saturation (SPO2), heart rate (HR), and dyspnea,” the authors explained.
They then evaluated patient response to PR in each of these clusters based on the amount of improvement in the 6-meter walk distance (6MWD), lung function, and quality of life observed, they added.
The population consisted of seniors, equally men and women, mostly GOLD II and III patients (a measure of lung function) with a limited walking capacity, some 84% of the cohort having a 6MWD <80% predicted. The characteristics of the four identified clusters were as follows:
- Cluster 1: Consisted of younger men, GOLD I to II, average walkers, obese. The average 6MWD was 430 meters and patients had a large exercise HR response to PR. This cluster had a 76 meter improvement in their 6MWD, although 16% of the same cluster still did not respond to PR.
- Cluster 2: Consisted of older women, GOLD II-III, who were slow walkers. This cluster had a reduced 6MWD of 362 meters, but they also had a significant 97-meter improvement in their 6MWD following PR. Some 18% were still nonresponders to PR.
- Cluster 3: Consisted of older men, GOLD II to III, dyspneic, slow walkers, some 32% of whom responded to PR. This cluster also had a reduced 6MWD at 388 meters, but again, they also had a significant improvement of 79 meters in their 6MWD following the introduction of PR. Some 11% were nonresponders to PR.
- Cluster 4: Consisted of older men, GOLD III to IV, very slow walkers, oxygen-dependent, very dyspneic. This cluster had a severely reduced 6MWD of only 290 meters with severe exercise desaturation and dyspnea, and almost all of them were on long-term oxygen therapy. Nevertheless, this cluster also had a significant, 66-meter improvement in their 6MWD. Twenty-eight percent of them were nonresponders to PR.
Clinical practice
“The highly heterogeneous nature of the enrolled patient population reflects clinical practice,” the authors point out. For example, cluster 1 included patients with the best lung function, compared with those in clusters 2, 3, and 4 – which may be due, at least in part, to the aggravation in disease severity with age given that patients in cluster 1 were the youngest overall.
The fact that those in cluster 4 had the worst performance may also have been because of age and disease severity, the authors note, as those in cluster 4 had the highest proportion of patients on long-term oxygen therapy, again suggestive of disease severity. “Of note, these patients show the most impaired 6MWT responses despite the use of oxygen supplementation during walking,” the researchers added.
The authors also suggest that patients such as those in cluster 4 may require specific PR modalities in order to optimize their functional benefits. In contrast, those in cluster 1 had a significantly higher body mass index, compared with those in the other 3 clusters, which, interestingly enough, was not associated with more severe functional exercise impairment. The fact that older age participants, such as those in cluster 3 as well as those with high BMI in cluster 1, were both able to improve their 6MWD post-PR to the same extent as younger patients without obesity suggests that most older or overweight/obese patients can still show clinically significant improvement in 6MWD post PR, as the authors suggest.
Notably, the 6MWT was the only test available both pre-and post PR, making this an important limitation of the study, because only one aspect of the effect of PR was evaluated, omitting other physical and psychosocial benefits of PR, investigators suggest.
Adds to the literature
Asked to comment on the findings, Sachin Gupta, MD, attending physician, pulmonary & critical care medicine, Alameda Health System, Highland Hospital, Oakland, Calif., felt that these data add to the literature in defining COPD patient profiles, helping to categorize those in whom to expect greater walk distance improvements with PR versus those who will respond less well.
“Because 6MWD is a surrogate marker for quality of life (QOL) and mortality, further analysis in the form of a randomized controlled trial to determine long-term outcomes among the four clusters with adjustment for baseline characteristics would help determine the extent to which certain patient clusters may respond to PR,” Dr. Gupta told this news organization in an email.
At the same time, he suggested that while patients may not experience much net benefit in their 6MWD, their QOL or mortality risk may still improve with PR. “I cannot recall a patient ever describing their experience with PR as anything other than positive,” Dr. Gupta stressed.
“And as the authors [themselves] note, because PR serves to benefit patients beyond the 6MWD, I would not recommend limiting PR referrals based on the patient clusters identified,” he said.
The authors had no conflicts of interest to declare. Dr. Gupta declared that he is an employee and shareholder at Genentech.
Not all patients with chronic obstructive pulmonary disease (COPD) respond equally well to pulmonary rehabilitation (PR).
Now, physicians can better categorize which patients will do well with PR and which ones less well or not well at all based on a new system of clustering of COPD patients according to their response to exercise therapy.
“We identified four clusters of COPD patients and their response to PR in the aim to better understand PR outcome and [adapt] it to patients’ profiles and needs,” lead author Yara Al Chikhanie, MD, of the cardiopulmonary rehabilitation center Dieulefit Sante (France), and colleagues observed.
“Identification of patients likely to show smaller responses to PR may help to target patients benefiting the most and to adapt PR settings for nonresponders to standard PR,” they suggested.
The study was published online in Respiratory Medicine.
Single-center cohort
The cohort consisted of 835 patients from a single center who had been admitted to a cardiopulmonary rehabilitation center over a 6-year period from 2021 to 2017. “The PR program used in the center was the same over the 6-year period,” the authors note – consisting of a 3- to 4-week, inpatient program with activities 5 days a week.
Each day, patients attended a 25-minute aerobic training session on a cycling ergometer or a treadmill; a 30-minute low-intensity gym session; a 30-minute group walk outdoors, and 30 minutes of strength training. “We aimed to cluster patients with COPD admitted to PR based on patients’ clinical characteristics and 6-meter walk test results (6MWT), pulse oxygen saturation (SPO2), heart rate (HR), and dyspnea,” the authors explained.
They then evaluated patient response to PR in each of these clusters based on the amount of improvement in the 6-meter walk distance (6MWD), lung function, and quality of life observed, they added.
The population consisted of seniors, equally men and women, mostly GOLD II and III patients (a measure of lung function) with a limited walking capacity, some 84% of the cohort having a 6MWD <80% predicted. The characteristics of the four identified clusters were as follows:
- Cluster 1: Consisted of younger men, GOLD I to II, average walkers, obese. The average 6MWD was 430 meters and patients had a large exercise HR response to PR. This cluster had a 76 meter improvement in their 6MWD, although 16% of the same cluster still did not respond to PR.
- Cluster 2: Consisted of older women, GOLD II-III, who were slow walkers. This cluster had a reduced 6MWD of 362 meters, but they also had a significant 97-meter improvement in their 6MWD following PR. Some 18% were still nonresponders to PR.
- Cluster 3: Consisted of older men, GOLD II to III, dyspneic, slow walkers, some 32% of whom responded to PR. This cluster also had a reduced 6MWD at 388 meters, but again, they also had a significant improvement of 79 meters in their 6MWD following the introduction of PR. Some 11% were nonresponders to PR.
- Cluster 4: Consisted of older men, GOLD III to IV, very slow walkers, oxygen-dependent, very dyspneic. This cluster had a severely reduced 6MWD of only 290 meters with severe exercise desaturation and dyspnea, and almost all of them were on long-term oxygen therapy. Nevertheless, this cluster also had a significant, 66-meter improvement in their 6MWD. Twenty-eight percent of them were nonresponders to PR.
Clinical practice
“The highly heterogeneous nature of the enrolled patient population reflects clinical practice,” the authors point out. For example, cluster 1 included patients with the best lung function, compared with those in clusters 2, 3, and 4 – which may be due, at least in part, to the aggravation in disease severity with age given that patients in cluster 1 were the youngest overall.
The fact that those in cluster 4 had the worst performance may also have been because of age and disease severity, the authors note, as those in cluster 4 had the highest proportion of patients on long-term oxygen therapy, again suggestive of disease severity. “Of note, these patients show the most impaired 6MWT responses despite the use of oxygen supplementation during walking,” the researchers added.
The authors also suggest that patients such as those in cluster 4 may require specific PR modalities in order to optimize their functional benefits. In contrast, those in cluster 1 had a significantly higher body mass index, compared with those in the other 3 clusters, which, interestingly enough, was not associated with more severe functional exercise impairment. The fact that older age participants, such as those in cluster 3 as well as those with high BMI in cluster 1, were both able to improve their 6MWD post-PR to the same extent as younger patients without obesity suggests that most older or overweight/obese patients can still show clinically significant improvement in 6MWD post PR, as the authors suggest.
Notably, the 6MWT was the only test available both pre-and post PR, making this an important limitation of the study, because only one aspect of the effect of PR was evaluated, omitting other physical and psychosocial benefits of PR, investigators suggest.
Adds to the literature
Asked to comment on the findings, Sachin Gupta, MD, attending physician, pulmonary & critical care medicine, Alameda Health System, Highland Hospital, Oakland, Calif., felt that these data add to the literature in defining COPD patient profiles, helping to categorize those in whom to expect greater walk distance improvements with PR versus those who will respond less well.
“Because 6MWD is a surrogate marker for quality of life (QOL) and mortality, further analysis in the form of a randomized controlled trial to determine long-term outcomes among the four clusters with adjustment for baseline characteristics would help determine the extent to which certain patient clusters may respond to PR,” Dr. Gupta told this news organization in an email.
At the same time, he suggested that while patients may not experience much net benefit in their 6MWD, their QOL or mortality risk may still improve with PR. “I cannot recall a patient ever describing their experience with PR as anything other than positive,” Dr. Gupta stressed.
“And as the authors [themselves] note, because PR serves to benefit patients beyond the 6MWD, I would not recommend limiting PR referrals based on the patient clusters identified,” he said.
The authors had no conflicts of interest to declare. Dr. Gupta declared that he is an employee and shareholder at Genentech.
FROM RESPIRATORY MEDICINE
Paradigm-challenging heart failure treatment strategy hopeful in early trial
A small group of patients with heart failure (HF) who underwent a novel transcatheter nerve-ablation procedure seemed to benefit with improved hemodynamics, symptoms, and quality of life in an admittedly limited observational series.
All had HF with preserved ejection fraction (HFpEF) and remained on guideline-directed medical therapy during the study.
The open-label experience has launched a randomized trial, featuring a sham control group, that could ultimately challenge dogma about volume overload in patients with chronic and acute HF and the perceived essential role of diuretics.
Researchers see transvenous ablation of the right greater splanchnic nerve (GSN) as potentially appropriate for patients with HF, regardless of ventricular function or acuity. But the ongoing REBALANCE-HF trial aims to enroll up to 80 patients with chronic HFpEF.
Meanwhile, the current 18 patients with elevated resting or exertional pulmonary capillary wedge pressure (PCWP), given the procedure as part of the main trial’s “roll-in” phase, showed declines in exercise PCWP after 1 month (P = .007) and improved quality-of-life scores at both 1 and 3 months (P < .01). Also at 1 month, a third of the patients improved by at least one step in NYHA functional class.
The procedure, called splanchnic ablation for volume management (SAVM), could potentially be used “across the spectrum of acute and chronic heart failure, maybe even with reduced ejection fraction (HFrEF) and preserved ejection fraction,” Marat Fudim, MD, MHS, Duke University Medical Center, Durham, N.C., told this news organization.
However, “for outcomes, we’ve really only looked in the ambulatory setting,” and only at symptomatic and functional responses. To that extent, based on the current experience and a few small previous studies, Dr. Fudim said, SAVM seems to benefit patients with HF in general who have dyspnea at exercise. Beyond that, the kind of patient who may be most suitable for it “is something I hope we will be able answer once the randomized dataset is in.”
Dr. Fudim reported the REBALANCE-HF roll-in results at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2022 sessions, held virtually and live in Madrid. He is also lead author on the same-day publication in the European Journal of Heart Failure.
A different treatment paradigm
Splanchnic-nerve blockade as a possible HF treatment is based on growing evidence that volume overload in patients with HF is not always the cause, at least not a main cause, of congestion and dyspnea. Rather, those classic HF signs and symptoms may often be triggered by adverse redistribution of stable fluid volume from primarily the splanchnic vascular compartment to the intrathoracic space.
In other words, what might seem like classic volume overload calling for diuresis often might actually be euvolemic redistribution of fluid from the abdomen to the chest, raising intracardiac pressures and causing dyspnea.
In that scenario, loop diuretics might only dehydrate the patient and potentially put the kidneys at risk, Dr. Fudim proposed. His recent experience with HF patients implanted with a pulmonary-artery pressure monitor, he said, suggests many who received standard volume-overload therapy had actually been normo- or hypovolemic.
More then half the patients “did not have high volume, they just had high pressures,” he said. “So there is a significant portion of the population that has pathological processes leading to high pressures, but it’s not volume overload. Diuresing those patients would probably not be the right decision.”
The unilateral SAVM procedure appears to attenuate sympathetically mediated splanchnic volume redistribution to the heart and lungs, but as it doesn’t affect the left GSN, preserves some normal sympathetic response.
Sometimes in studies of surgical or catheter-based SAVM, Dr. Fudim said, “we have observationally seen that people discontinued diuretics or decreased doses in the treatment arm.”
‘Beyond our classical thinking’
It’s “impressive” that such right-GSN ablation seemed to reduce exercise-filling pressures, but one should be circumspect because “it’s way beyond our classical thinking,” Wilfried Mullens, MD, PhD, Hospital Oost-Limburg, Genk, Belgium, said as a panelist after Dr. Fudim’s presentation.
“These are invasive procedures,” he noted, “and our physiological understanding does not always match up with what we’re doing in real life, if you look at other interventional procedures, like renal denervation, which showed neutral effects, or if you look at even interatrial shunt devices, which might even be dangerous.”
The field should be “very prudent” before using SAVM in practice, which shouldn’t be “before we have sufficient data to support the efficacy and safety,” Dr. Mullens said. “It remains to be seen how treatment success will be defined. Is it during exercise? How long does the treatment last? What is the effect of the treatment over time; is it not harmful? These are things that we don’t know yet.”
The procedure was considered successful in all 18 patients, 14 of whom were women and 16 of whom were in NYHA class 3. Their average age was 75, and their mean left ventricular ejection fraction (LVEF) at baseline was 61%. The primary efficacy endpoints were a reduction in PCWP at rest, with legs raised, and at 20W exercise at 1 month. Their baseline invasively measured peak exercise PCWP was at least 25 mm Hg.
At 1 month, mean PCWP at 20W exercise fell from 36.4 mm Hg to 28.9 mm Hg (P = .007) and peak PCWP declined from 39.5 mm Hg to 31.9 mm Hg (P = .013); resting PCWP wasn’t significantly affected. Twelve patients improved by at least one NYHA functional class (P = .02).
Scores on the Kansas City Cardiomyopathy Questionnaire (KCCQ), which assesses quality of life, improved by 22 points at 1 month and 18.3 points at 3 months (P < .01 for both differences).
No significant effects on 6-minute walk distance or natriuretic peptide levels were observed, nor were any observed on LVEF or echocardiographic measures of diastolic function, left ventricular (LV) atrial volume, or LV mass at 3 months.
Three “nonserious” device-related adverse events were observed, including one case of acute decompensation early in the experience, ostensibly due to excessive saline administration, Dr. Fudim reported. There was also one case of transient periprocedural hypertension and one instance of postprocedure back pain.
The SAVM procedure is performed transvenously and in general is technically “really not that challenging,” Dr. Fudim said. In most cases, the necessary skills would be accessible not only to interventional cardiologists but also heart failure specialists. “I have performed this procedure myself, and I’m a heart failure guy.”
The REBALANCE-HF roll-in phase and main trial are supported by Axon Therapies. Dr. Fudim discloses receiving support from Bayer, Bodyport, and BTG Specialty Pharmaceuticals; and consulting fees from Abbott, Audicor, Axon Therapies, Bodyguide, Bodyport, Boston Scientific, CVRx, Daxor, Edwards LifeSciences, Feldschuh Foundation, Fire1, Gradient, Intershunt, NXT Biomedical, Pharmacosmos, PreHealth, Splendo, Vironix, Viscardia, and Zoll. Dr. Mullens discloses receiving fees for speaking from Medtronic, Abbott, Novartis, Boston Scientific, AstraZeneca, and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
A small group of patients with heart failure (HF) who underwent a novel transcatheter nerve-ablation procedure seemed to benefit with improved hemodynamics, symptoms, and quality of life in an admittedly limited observational series.
All had HF with preserved ejection fraction (HFpEF) and remained on guideline-directed medical therapy during the study.
The open-label experience has launched a randomized trial, featuring a sham control group, that could ultimately challenge dogma about volume overload in patients with chronic and acute HF and the perceived essential role of diuretics.
Researchers see transvenous ablation of the right greater splanchnic nerve (GSN) as potentially appropriate for patients with HF, regardless of ventricular function or acuity. But the ongoing REBALANCE-HF trial aims to enroll up to 80 patients with chronic HFpEF.
Meanwhile, the current 18 patients with elevated resting or exertional pulmonary capillary wedge pressure (PCWP), given the procedure as part of the main trial’s “roll-in” phase, showed declines in exercise PCWP after 1 month (P = .007) and improved quality-of-life scores at both 1 and 3 months (P < .01). Also at 1 month, a third of the patients improved by at least one step in NYHA functional class.
The procedure, called splanchnic ablation for volume management (SAVM), could potentially be used “across the spectrum of acute and chronic heart failure, maybe even with reduced ejection fraction (HFrEF) and preserved ejection fraction,” Marat Fudim, MD, MHS, Duke University Medical Center, Durham, N.C., told this news organization.
However, “for outcomes, we’ve really only looked in the ambulatory setting,” and only at symptomatic and functional responses. To that extent, based on the current experience and a few small previous studies, Dr. Fudim said, SAVM seems to benefit patients with HF in general who have dyspnea at exercise. Beyond that, the kind of patient who may be most suitable for it “is something I hope we will be able answer once the randomized dataset is in.”
Dr. Fudim reported the REBALANCE-HF roll-in results at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2022 sessions, held virtually and live in Madrid. He is also lead author on the same-day publication in the European Journal of Heart Failure.
A different treatment paradigm
Splanchnic-nerve blockade as a possible HF treatment is based on growing evidence that volume overload in patients with HF is not always the cause, at least not a main cause, of congestion and dyspnea. Rather, those classic HF signs and symptoms may often be triggered by adverse redistribution of stable fluid volume from primarily the splanchnic vascular compartment to the intrathoracic space.
In other words, what might seem like classic volume overload calling for diuresis often might actually be euvolemic redistribution of fluid from the abdomen to the chest, raising intracardiac pressures and causing dyspnea.
In that scenario, loop diuretics might only dehydrate the patient and potentially put the kidneys at risk, Dr. Fudim proposed. His recent experience with HF patients implanted with a pulmonary-artery pressure monitor, he said, suggests many who received standard volume-overload therapy had actually been normo- or hypovolemic.
More then half the patients “did not have high volume, they just had high pressures,” he said. “So there is a significant portion of the population that has pathological processes leading to high pressures, but it’s not volume overload. Diuresing those patients would probably not be the right decision.”
The unilateral SAVM procedure appears to attenuate sympathetically mediated splanchnic volume redistribution to the heart and lungs, but as it doesn’t affect the left GSN, preserves some normal sympathetic response.
Sometimes in studies of surgical or catheter-based SAVM, Dr. Fudim said, “we have observationally seen that people discontinued diuretics or decreased doses in the treatment arm.”
‘Beyond our classical thinking’
It’s “impressive” that such right-GSN ablation seemed to reduce exercise-filling pressures, but one should be circumspect because “it’s way beyond our classical thinking,” Wilfried Mullens, MD, PhD, Hospital Oost-Limburg, Genk, Belgium, said as a panelist after Dr. Fudim’s presentation.
“These are invasive procedures,” he noted, “and our physiological understanding does not always match up with what we’re doing in real life, if you look at other interventional procedures, like renal denervation, which showed neutral effects, or if you look at even interatrial shunt devices, which might even be dangerous.”
The field should be “very prudent” before using SAVM in practice, which shouldn’t be “before we have sufficient data to support the efficacy and safety,” Dr. Mullens said. “It remains to be seen how treatment success will be defined. Is it during exercise? How long does the treatment last? What is the effect of the treatment over time; is it not harmful? These are things that we don’t know yet.”
The procedure was considered successful in all 18 patients, 14 of whom were women and 16 of whom were in NYHA class 3. Their average age was 75, and their mean left ventricular ejection fraction (LVEF) at baseline was 61%. The primary efficacy endpoints were a reduction in PCWP at rest, with legs raised, and at 20W exercise at 1 month. Their baseline invasively measured peak exercise PCWP was at least 25 mm Hg.
At 1 month, mean PCWP at 20W exercise fell from 36.4 mm Hg to 28.9 mm Hg (P = .007) and peak PCWP declined from 39.5 mm Hg to 31.9 mm Hg (P = .013); resting PCWP wasn’t significantly affected. Twelve patients improved by at least one NYHA functional class (P = .02).
Scores on the Kansas City Cardiomyopathy Questionnaire (KCCQ), which assesses quality of life, improved by 22 points at 1 month and 18.3 points at 3 months (P < .01 for both differences).
No significant effects on 6-minute walk distance or natriuretic peptide levels were observed, nor were any observed on LVEF or echocardiographic measures of diastolic function, left ventricular (LV) atrial volume, or LV mass at 3 months.
Three “nonserious” device-related adverse events were observed, including one case of acute decompensation early in the experience, ostensibly due to excessive saline administration, Dr. Fudim reported. There was also one case of transient periprocedural hypertension and one instance of postprocedure back pain.
The SAVM procedure is performed transvenously and in general is technically “really not that challenging,” Dr. Fudim said. In most cases, the necessary skills would be accessible not only to interventional cardiologists but also heart failure specialists. “I have performed this procedure myself, and I’m a heart failure guy.”
The REBALANCE-HF roll-in phase and main trial are supported by Axon Therapies. Dr. Fudim discloses receiving support from Bayer, Bodyport, and BTG Specialty Pharmaceuticals; and consulting fees from Abbott, Audicor, Axon Therapies, Bodyguide, Bodyport, Boston Scientific, CVRx, Daxor, Edwards LifeSciences, Feldschuh Foundation, Fire1, Gradient, Intershunt, NXT Biomedical, Pharmacosmos, PreHealth, Splendo, Vironix, Viscardia, and Zoll. Dr. Mullens discloses receiving fees for speaking from Medtronic, Abbott, Novartis, Boston Scientific, AstraZeneca, and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
A small group of patients with heart failure (HF) who underwent a novel transcatheter nerve-ablation procedure seemed to benefit with improved hemodynamics, symptoms, and quality of life in an admittedly limited observational series.
All had HF with preserved ejection fraction (HFpEF) and remained on guideline-directed medical therapy during the study.
The open-label experience has launched a randomized trial, featuring a sham control group, that could ultimately challenge dogma about volume overload in patients with chronic and acute HF and the perceived essential role of diuretics.
Researchers see transvenous ablation of the right greater splanchnic nerve (GSN) as potentially appropriate for patients with HF, regardless of ventricular function or acuity. But the ongoing REBALANCE-HF trial aims to enroll up to 80 patients with chronic HFpEF.
Meanwhile, the current 18 patients with elevated resting or exertional pulmonary capillary wedge pressure (PCWP), given the procedure as part of the main trial’s “roll-in” phase, showed declines in exercise PCWP after 1 month (P = .007) and improved quality-of-life scores at both 1 and 3 months (P < .01). Also at 1 month, a third of the patients improved by at least one step in NYHA functional class.
The procedure, called splanchnic ablation for volume management (SAVM), could potentially be used “across the spectrum of acute and chronic heart failure, maybe even with reduced ejection fraction (HFrEF) and preserved ejection fraction,” Marat Fudim, MD, MHS, Duke University Medical Center, Durham, N.C., told this news organization.
However, “for outcomes, we’ve really only looked in the ambulatory setting,” and only at symptomatic and functional responses. To that extent, based on the current experience and a few small previous studies, Dr. Fudim said, SAVM seems to benefit patients with HF in general who have dyspnea at exercise. Beyond that, the kind of patient who may be most suitable for it “is something I hope we will be able answer once the randomized dataset is in.”
Dr. Fudim reported the REBALANCE-HF roll-in results at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2022 sessions, held virtually and live in Madrid. He is also lead author on the same-day publication in the European Journal of Heart Failure.
A different treatment paradigm
Splanchnic-nerve blockade as a possible HF treatment is based on growing evidence that volume overload in patients with HF is not always the cause, at least not a main cause, of congestion and dyspnea. Rather, those classic HF signs and symptoms may often be triggered by adverse redistribution of stable fluid volume from primarily the splanchnic vascular compartment to the intrathoracic space.
In other words, what might seem like classic volume overload calling for diuresis often might actually be euvolemic redistribution of fluid from the abdomen to the chest, raising intracardiac pressures and causing dyspnea.
In that scenario, loop diuretics might only dehydrate the patient and potentially put the kidneys at risk, Dr. Fudim proposed. His recent experience with HF patients implanted with a pulmonary-artery pressure monitor, he said, suggests many who received standard volume-overload therapy had actually been normo- or hypovolemic.
More then half the patients “did not have high volume, they just had high pressures,” he said. “So there is a significant portion of the population that has pathological processes leading to high pressures, but it’s not volume overload. Diuresing those patients would probably not be the right decision.”
The unilateral SAVM procedure appears to attenuate sympathetically mediated splanchnic volume redistribution to the heart and lungs, but as it doesn’t affect the left GSN, preserves some normal sympathetic response.
Sometimes in studies of surgical or catheter-based SAVM, Dr. Fudim said, “we have observationally seen that people discontinued diuretics or decreased doses in the treatment arm.”
‘Beyond our classical thinking’
It’s “impressive” that such right-GSN ablation seemed to reduce exercise-filling pressures, but one should be circumspect because “it’s way beyond our classical thinking,” Wilfried Mullens, MD, PhD, Hospital Oost-Limburg, Genk, Belgium, said as a panelist after Dr. Fudim’s presentation.
“These are invasive procedures,” he noted, “and our physiological understanding does not always match up with what we’re doing in real life, if you look at other interventional procedures, like renal denervation, which showed neutral effects, or if you look at even interatrial shunt devices, which might even be dangerous.”
The field should be “very prudent” before using SAVM in practice, which shouldn’t be “before we have sufficient data to support the efficacy and safety,” Dr. Mullens said. “It remains to be seen how treatment success will be defined. Is it during exercise? How long does the treatment last? What is the effect of the treatment over time; is it not harmful? These are things that we don’t know yet.”
The procedure was considered successful in all 18 patients, 14 of whom were women and 16 of whom were in NYHA class 3. Their average age was 75, and their mean left ventricular ejection fraction (LVEF) at baseline was 61%. The primary efficacy endpoints were a reduction in PCWP at rest, with legs raised, and at 20W exercise at 1 month. Their baseline invasively measured peak exercise PCWP was at least 25 mm Hg.
At 1 month, mean PCWP at 20W exercise fell from 36.4 mm Hg to 28.9 mm Hg (P = .007) and peak PCWP declined from 39.5 mm Hg to 31.9 mm Hg (P = .013); resting PCWP wasn’t significantly affected. Twelve patients improved by at least one NYHA functional class (P = .02).
Scores on the Kansas City Cardiomyopathy Questionnaire (KCCQ), which assesses quality of life, improved by 22 points at 1 month and 18.3 points at 3 months (P < .01 for both differences).
No significant effects on 6-minute walk distance or natriuretic peptide levels were observed, nor were any observed on LVEF or echocardiographic measures of diastolic function, left ventricular (LV) atrial volume, or LV mass at 3 months.
Three “nonserious” device-related adverse events were observed, including one case of acute decompensation early in the experience, ostensibly due to excessive saline administration, Dr. Fudim reported. There was also one case of transient periprocedural hypertension and one instance of postprocedure back pain.
The SAVM procedure is performed transvenously and in general is technically “really not that challenging,” Dr. Fudim said. In most cases, the necessary skills would be accessible not only to interventional cardiologists but also heart failure specialists. “I have performed this procedure myself, and I’m a heart failure guy.”
The REBALANCE-HF roll-in phase and main trial are supported by Axon Therapies. Dr. Fudim discloses receiving support from Bayer, Bodyport, and BTG Specialty Pharmaceuticals; and consulting fees from Abbott, Audicor, Axon Therapies, Bodyguide, Bodyport, Boston Scientific, CVRx, Daxor, Edwards LifeSciences, Feldschuh Foundation, Fire1, Gradient, Intershunt, NXT Biomedical, Pharmacosmos, PreHealth, Splendo, Vironix, Viscardia, and Zoll. Dr. Mullens discloses receiving fees for speaking from Medtronic, Abbott, Novartis, Boston Scientific, AstraZeneca, and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
FROM ESC HEART FAILURE 2022
Airway injuries ‘devastating’ after battery ingestions: Review
Severe airway injuries are a “not infrequent” consequence after children swallow button batteries, which are commonly found in many household electronics, according to a systematic review published online in JAMA Otolaryngology–Head & Neck Surgery.
Most literature has focused on esophageal injury, but “the direct apposition of the esophagus to the trachea and recurrent laryngeal nerves also places these children at risk of airway injury, such as tracheoesophageal fistula (TEF) (a life-threatening complication), vocal cord paresis and paralysis, tracheal stenosis, and tracheomalacia,” the researchers wrote.
Led by Justine Philteos, MD, of the department of otolaryngology–head and neck surgery at the University of Toronto, the researchers found that tracheoesophageal fistula and vocal cord paralyses were the two most common airway injuries and often required tracheostomy.
The review included 195 children pulled from the National Capital Poison Center (NCPC) database – more often young children – who had ingested the batteries. The average age at ingestion was 17.8 months and the average time between ingestion and removal was 5.8 days.
Of the 195 children, 29 (15%) underwent tracheostomy, and 11 of the 29 children (38%) ultimately had decannulation. There were 14 deaths from swallowing the batteries. All 14 patients had a TEF. The cause of death was identified for 12 of the patients: Four died of pneumonia or respiratory failure; three of massive hematemesis; three of sepsis; one of multiorgan failure, and one of anoxic encephalopathy.
Vocal cord injury occurred after a shorter button battery exposure than other airway injuries.
The authors concluded that prioritizing quick button battery removal is essential “to decrease the devastating consequences of these injuries.”
In an invited commentary, Hannah Gibbs, and Kris R. Jatana, MD, of The Ohio State University in Columbus, described what’s being done to prevent and treat these injuries and what’s next.
They noted that ingestion is often unseen so diagnosis is difficult. Therefore, they wrote, a novel coin-battery metal detector could be a radiation-free, quick screening tool. They noted a patent-pending technology has been developed at Ohio State and Nationwide Children’s Hospital.
Honey can help slow injury
Some measures can be taken at home or in the hospital if battery swallowing is discovered, the editorialists noted.
In the home or in transport to the hospital, caregivers can give 10 mL of honey every 10 minutes until arrival if the child is older than 12 months.
At the hospital, 10 mL of either honey or sucralfate may be given every 10 minutes to slow the rate of injury until the battery can be surgically removed.
“The current NCPC guidelines suggest up to six doses may be given in the prehospital setting, with three additional doses administered in the hospital,” they wrote.
“These strategies should be considered earlier than 12 hours from ingestion, when there is no clinical concern for mediastinitis or sepsis. A child with an esophageal button battery should proceed to the operating room immediately regardless of whether he or she has recently eaten,” Ms. Gibbs and Dr. Jatana wrote.
App adds convenience to boost physician reporting
Foreign body ingestions are also severely underreported, they noted. They cited a survey of more than 400 physicians who directly manage foreign body ingestions that found only 11% of button battery injuries and 4% of all foreign body ingestion or aspiration events were reported. The great majority (92%) of respondents said they would report the events if that were more convenient.
To that end, the Global Injury Research Collaborative (GIRC) has created and released a free smartphone application, the GIRC App. It is available free on the iOS system (through App Store) and soon will be available on the Android system (through Google Play), they wrote.
Ms. Gibbs and Dr. Jatana urge other measures, including safer battery compartments and battery design, to reduce the likelihood of ingestion.
They pointed out that a bill was introduced in Congress that would require the Consumer Product Safety Commission to mandate a new standard for child-resistant compartments on products containing button batteries. The act, called Reese’s Law, has been referred to the Committee on Energy and Commerce and is under review.
Dr. Jatana reported having a patent pending for a coin or battery metal detector device under development; being a shareholder in Zotarix, Landsdowne Labs, and Tivic Health Systems; serving in a leadership position on the National Button Battery Task Force; and being a board member of the Global Injury Research Collaborative, which is a U.S. Internal Revenue Service–designated, 501(c)(3) nonprofit research organization. No other relevant disclosures were reported.
Severe airway injuries are a “not infrequent” consequence after children swallow button batteries, which are commonly found in many household electronics, according to a systematic review published online in JAMA Otolaryngology–Head & Neck Surgery.
Most literature has focused on esophageal injury, but “the direct apposition of the esophagus to the trachea and recurrent laryngeal nerves also places these children at risk of airway injury, such as tracheoesophageal fistula (TEF) (a life-threatening complication), vocal cord paresis and paralysis, tracheal stenosis, and tracheomalacia,” the researchers wrote.
Led by Justine Philteos, MD, of the department of otolaryngology–head and neck surgery at the University of Toronto, the researchers found that tracheoesophageal fistula and vocal cord paralyses were the two most common airway injuries and often required tracheostomy.
The review included 195 children pulled from the National Capital Poison Center (NCPC) database – more often young children – who had ingested the batteries. The average age at ingestion was 17.8 months and the average time between ingestion and removal was 5.8 days.
Of the 195 children, 29 (15%) underwent tracheostomy, and 11 of the 29 children (38%) ultimately had decannulation. There were 14 deaths from swallowing the batteries. All 14 patients had a TEF. The cause of death was identified for 12 of the patients: Four died of pneumonia or respiratory failure; three of massive hematemesis; three of sepsis; one of multiorgan failure, and one of anoxic encephalopathy.
Vocal cord injury occurred after a shorter button battery exposure than other airway injuries.
The authors concluded that prioritizing quick button battery removal is essential “to decrease the devastating consequences of these injuries.”
In an invited commentary, Hannah Gibbs, and Kris R. Jatana, MD, of The Ohio State University in Columbus, described what’s being done to prevent and treat these injuries and what’s next.
They noted that ingestion is often unseen so diagnosis is difficult. Therefore, they wrote, a novel coin-battery metal detector could be a radiation-free, quick screening tool. They noted a patent-pending technology has been developed at Ohio State and Nationwide Children’s Hospital.
Honey can help slow injury
Some measures can be taken at home or in the hospital if battery swallowing is discovered, the editorialists noted.
In the home or in transport to the hospital, caregivers can give 10 mL of honey every 10 minutes until arrival if the child is older than 12 months.
At the hospital, 10 mL of either honey or sucralfate may be given every 10 minutes to slow the rate of injury until the battery can be surgically removed.
“The current NCPC guidelines suggest up to six doses may be given in the prehospital setting, with three additional doses administered in the hospital,” they wrote.
“These strategies should be considered earlier than 12 hours from ingestion, when there is no clinical concern for mediastinitis or sepsis. A child with an esophageal button battery should proceed to the operating room immediately regardless of whether he or she has recently eaten,” Ms. Gibbs and Dr. Jatana wrote.
App adds convenience to boost physician reporting
Foreign body ingestions are also severely underreported, they noted. They cited a survey of more than 400 physicians who directly manage foreign body ingestions that found only 11% of button battery injuries and 4% of all foreign body ingestion or aspiration events were reported. The great majority (92%) of respondents said they would report the events if that were more convenient.
To that end, the Global Injury Research Collaborative (GIRC) has created and released a free smartphone application, the GIRC App. It is available free on the iOS system (through App Store) and soon will be available on the Android system (through Google Play), they wrote.
Ms. Gibbs and Dr. Jatana urge other measures, including safer battery compartments and battery design, to reduce the likelihood of ingestion.
They pointed out that a bill was introduced in Congress that would require the Consumer Product Safety Commission to mandate a new standard for child-resistant compartments on products containing button batteries. The act, called Reese’s Law, has been referred to the Committee on Energy and Commerce and is under review.
Dr. Jatana reported having a patent pending for a coin or battery metal detector device under development; being a shareholder in Zotarix, Landsdowne Labs, and Tivic Health Systems; serving in a leadership position on the National Button Battery Task Force; and being a board member of the Global Injury Research Collaborative, which is a U.S. Internal Revenue Service–designated, 501(c)(3) nonprofit research organization. No other relevant disclosures were reported.
Severe airway injuries are a “not infrequent” consequence after children swallow button batteries, which are commonly found in many household electronics, according to a systematic review published online in JAMA Otolaryngology–Head & Neck Surgery.
Most literature has focused on esophageal injury, but “the direct apposition of the esophagus to the trachea and recurrent laryngeal nerves also places these children at risk of airway injury, such as tracheoesophageal fistula (TEF) (a life-threatening complication), vocal cord paresis and paralysis, tracheal stenosis, and tracheomalacia,” the researchers wrote.
Led by Justine Philteos, MD, of the department of otolaryngology–head and neck surgery at the University of Toronto, the researchers found that tracheoesophageal fistula and vocal cord paralyses were the two most common airway injuries and often required tracheostomy.
The review included 195 children pulled from the National Capital Poison Center (NCPC) database – more often young children – who had ingested the batteries. The average age at ingestion was 17.8 months and the average time between ingestion and removal was 5.8 days.
Of the 195 children, 29 (15%) underwent tracheostomy, and 11 of the 29 children (38%) ultimately had decannulation. There were 14 deaths from swallowing the batteries. All 14 patients had a TEF. The cause of death was identified for 12 of the patients: Four died of pneumonia or respiratory failure; three of massive hematemesis; three of sepsis; one of multiorgan failure, and one of anoxic encephalopathy.
Vocal cord injury occurred after a shorter button battery exposure than other airway injuries.
The authors concluded that prioritizing quick button battery removal is essential “to decrease the devastating consequences of these injuries.”
In an invited commentary, Hannah Gibbs, and Kris R. Jatana, MD, of The Ohio State University in Columbus, described what’s being done to prevent and treat these injuries and what’s next.
They noted that ingestion is often unseen so diagnosis is difficult. Therefore, they wrote, a novel coin-battery metal detector could be a radiation-free, quick screening tool. They noted a patent-pending technology has been developed at Ohio State and Nationwide Children’s Hospital.
Honey can help slow injury
Some measures can be taken at home or in the hospital if battery swallowing is discovered, the editorialists noted.
In the home or in transport to the hospital, caregivers can give 10 mL of honey every 10 minutes until arrival if the child is older than 12 months.
At the hospital, 10 mL of either honey or sucralfate may be given every 10 minutes to slow the rate of injury until the battery can be surgically removed.
“The current NCPC guidelines suggest up to six doses may be given in the prehospital setting, with three additional doses administered in the hospital,” they wrote.
“These strategies should be considered earlier than 12 hours from ingestion, when there is no clinical concern for mediastinitis or sepsis. A child with an esophageal button battery should proceed to the operating room immediately regardless of whether he or she has recently eaten,” Ms. Gibbs and Dr. Jatana wrote.
App adds convenience to boost physician reporting
Foreign body ingestions are also severely underreported, they noted. They cited a survey of more than 400 physicians who directly manage foreign body ingestions that found only 11% of button battery injuries and 4% of all foreign body ingestion or aspiration events were reported. The great majority (92%) of respondents said they would report the events if that were more convenient.
To that end, the Global Injury Research Collaborative (GIRC) has created and released a free smartphone application, the GIRC App. It is available free on the iOS system (through App Store) and soon will be available on the Android system (through Google Play), they wrote.
Ms. Gibbs and Dr. Jatana urge other measures, including safer battery compartments and battery design, to reduce the likelihood of ingestion.
They pointed out that a bill was introduced in Congress that would require the Consumer Product Safety Commission to mandate a new standard for child-resistant compartments on products containing button batteries. The act, called Reese’s Law, has been referred to the Committee on Energy and Commerce and is under review.
Dr. Jatana reported having a patent pending for a coin or battery metal detector device under development; being a shareholder in Zotarix, Landsdowne Labs, and Tivic Health Systems; serving in a leadership position on the National Button Battery Task Force; and being a board member of the Global Injury Research Collaborative, which is a U.S. Internal Revenue Service–designated, 501(c)(3) nonprofit research organization. No other relevant disclosures were reported.
FROM JAMA OTOLARYNGOLOGY–HEAD & NECK SURGERY
Most COVID long-haulers suffer long-term debilitating neurologic symptoms
Most COVID-19 long-haulers continue to have brain fog, fatigue, and compromised quality of life more than a year after the initial infection, results from the most extensive follow-up to date of a group of long COVID patients show.
Most patients continue to experience debilitating neurologic symptoms an average of 15 months from symptom onset, Igor Koralnik, MD, who oversees the Neuro COVID-19 Clinic at Northwestern Medicine in Chicago, said during a press briefing.
Surprisingly, in some cases, new symptoms appear that didn’t exist before, including variation of heart rate and blood pressure, and gastrointestinal symptoms, indicating there may be a late appearance in dysfunction of the autonomic nervous system in those patients, Dr. Koralnik said.
The study was published online in Annals of Clinical and Translational Neurology.
Evolving symptoms
The investigators evaluated the evolution of neurologic symptoms in 52 adults who had mild COVID-19 symptoms and were not admitted to the hospital.
Their mean age was 43 years, 73% were women and 77% had received a COVID-19 vaccine. These patients have now been followed for between 11 and 18 months since their initial infection.
Overall, between first and follow-up evaluations, there was no significant change in the frequency of most neurologic symptoms, including brain fog (81% vs. 71%), numbness/tingling (69% vs. 65%), headache (67% vs. 54%), dizziness (50% vs. 54%), blurred vision (34% vs. 44%), tinnitus (33% vs. 42%), and fatigue (87% vs. 81%).
The only neurologic symptoms that decreased over time were loss of taste (63% vs. 27%) and smell (58% vs. 21%).
Conversely, heart rate and blood pressure variation (35% vs. 56%) and gastrointestinal symptoms (27% vs. 48%; P = .04) increased at follow-up evaluations.
Patients reported subjective improvements in their recovery, cognitive function and fatigue, but quality of life measures remained lower than the average population of the United States.
There was a neutral effect of COVID vaccination on long COVID symptoms – it didn’t cure long COVID or make long COVID worse, which is a reason given by some long-haulers for not getting vaccinated, Dr. Koralnik told the briefing.
Therefore, “we continue to encourage our patients to get vaccinated and boosted according to the Centers for Disease Control and Prevention recommendation,” he said.
Escape from the ‘pit of despair’
To date, the Northwestern Medicine Neuro COVID-19 Clinic has treated nearly 1,400 COVID long-haulers from across the United States.
Emily Caffee, a physical therapist from Wheaton, Ill., is one of them.
Speaking at the briefing, the 36-year-old described her saga and roller coaster of recovering from long COVID in three acts: her initial infection, followed by a descent into a pit of physical and emotional despair, followed by her eventual escape from that pit more than two years later.
Following a fairly mild case of COVID, Ms. Caffee said worsening neurologic symptoms forced her to take medical leave from her very physical and cognitively demanding job.
Ms. Caffee said she experienced crushing fatigue and brain fog, as well as rapid heart rate and blood pressure changes going from sitting to standing position.
She went from being a competitive athlete to someone who could barely get off the couch or empty the dishwasher.
With the ongoing help of her medical team, she slowly returned to daily activities and eventually to work on a limited basis.
Today, Ms. Caffee says she’s 90%-95% better but still she has some lingering symptoms and does not yet feel like her pre-COVID self.
It’s been a very slow climb out of the pit, Ms. Caffee said.
This study has no specific funding. The authors disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Most COVID-19 long-haulers continue to have brain fog, fatigue, and compromised quality of life more than a year after the initial infection, results from the most extensive follow-up to date of a group of long COVID patients show.
Most patients continue to experience debilitating neurologic symptoms an average of 15 months from symptom onset, Igor Koralnik, MD, who oversees the Neuro COVID-19 Clinic at Northwestern Medicine in Chicago, said during a press briefing.
Surprisingly, in some cases, new symptoms appear that didn’t exist before, including variation of heart rate and blood pressure, and gastrointestinal symptoms, indicating there may be a late appearance in dysfunction of the autonomic nervous system in those patients, Dr. Koralnik said.
The study was published online in Annals of Clinical and Translational Neurology.
Evolving symptoms
The investigators evaluated the evolution of neurologic symptoms in 52 adults who had mild COVID-19 symptoms and were not admitted to the hospital.
Their mean age was 43 years, 73% were women and 77% had received a COVID-19 vaccine. These patients have now been followed for between 11 and 18 months since their initial infection.
Overall, between first and follow-up evaluations, there was no significant change in the frequency of most neurologic symptoms, including brain fog (81% vs. 71%), numbness/tingling (69% vs. 65%), headache (67% vs. 54%), dizziness (50% vs. 54%), blurred vision (34% vs. 44%), tinnitus (33% vs. 42%), and fatigue (87% vs. 81%).
The only neurologic symptoms that decreased over time were loss of taste (63% vs. 27%) and smell (58% vs. 21%).
Conversely, heart rate and blood pressure variation (35% vs. 56%) and gastrointestinal symptoms (27% vs. 48%; P = .04) increased at follow-up evaluations.
Patients reported subjective improvements in their recovery, cognitive function and fatigue, but quality of life measures remained lower than the average population of the United States.
There was a neutral effect of COVID vaccination on long COVID symptoms – it didn’t cure long COVID or make long COVID worse, which is a reason given by some long-haulers for not getting vaccinated, Dr. Koralnik told the briefing.
Therefore, “we continue to encourage our patients to get vaccinated and boosted according to the Centers for Disease Control and Prevention recommendation,” he said.
Escape from the ‘pit of despair’
To date, the Northwestern Medicine Neuro COVID-19 Clinic has treated nearly 1,400 COVID long-haulers from across the United States.
Emily Caffee, a physical therapist from Wheaton, Ill., is one of them.
Speaking at the briefing, the 36-year-old described her saga and roller coaster of recovering from long COVID in three acts: her initial infection, followed by a descent into a pit of physical and emotional despair, followed by her eventual escape from that pit more than two years later.
Following a fairly mild case of COVID, Ms. Caffee said worsening neurologic symptoms forced her to take medical leave from her very physical and cognitively demanding job.
Ms. Caffee said she experienced crushing fatigue and brain fog, as well as rapid heart rate and blood pressure changes going from sitting to standing position.
She went from being a competitive athlete to someone who could barely get off the couch or empty the dishwasher.
With the ongoing help of her medical team, she slowly returned to daily activities and eventually to work on a limited basis.
Today, Ms. Caffee says she’s 90%-95% better but still she has some lingering symptoms and does not yet feel like her pre-COVID self.
It’s been a very slow climb out of the pit, Ms. Caffee said.
This study has no specific funding. The authors disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Most COVID-19 long-haulers continue to have brain fog, fatigue, and compromised quality of life more than a year after the initial infection, results from the most extensive follow-up to date of a group of long COVID patients show.
Most patients continue to experience debilitating neurologic symptoms an average of 15 months from symptom onset, Igor Koralnik, MD, who oversees the Neuro COVID-19 Clinic at Northwestern Medicine in Chicago, said during a press briefing.
Surprisingly, in some cases, new symptoms appear that didn’t exist before, including variation of heart rate and blood pressure, and gastrointestinal symptoms, indicating there may be a late appearance in dysfunction of the autonomic nervous system in those patients, Dr. Koralnik said.
The study was published online in Annals of Clinical and Translational Neurology.
Evolving symptoms
The investigators evaluated the evolution of neurologic symptoms in 52 adults who had mild COVID-19 symptoms and were not admitted to the hospital.
Their mean age was 43 years, 73% were women and 77% had received a COVID-19 vaccine. These patients have now been followed for between 11 and 18 months since their initial infection.
Overall, between first and follow-up evaluations, there was no significant change in the frequency of most neurologic symptoms, including brain fog (81% vs. 71%), numbness/tingling (69% vs. 65%), headache (67% vs. 54%), dizziness (50% vs. 54%), blurred vision (34% vs. 44%), tinnitus (33% vs. 42%), and fatigue (87% vs. 81%).
The only neurologic symptoms that decreased over time were loss of taste (63% vs. 27%) and smell (58% vs. 21%).
Conversely, heart rate and blood pressure variation (35% vs. 56%) and gastrointestinal symptoms (27% vs. 48%; P = .04) increased at follow-up evaluations.
Patients reported subjective improvements in their recovery, cognitive function and fatigue, but quality of life measures remained lower than the average population of the United States.
There was a neutral effect of COVID vaccination on long COVID symptoms – it didn’t cure long COVID or make long COVID worse, which is a reason given by some long-haulers for not getting vaccinated, Dr. Koralnik told the briefing.
Therefore, “we continue to encourage our patients to get vaccinated and boosted according to the Centers for Disease Control and Prevention recommendation,” he said.
Escape from the ‘pit of despair’
To date, the Northwestern Medicine Neuro COVID-19 Clinic has treated nearly 1,400 COVID long-haulers from across the United States.
Emily Caffee, a physical therapist from Wheaton, Ill., is one of them.
Speaking at the briefing, the 36-year-old described her saga and roller coaster of recovering from long COVID in three acts: her initial infection, followed by a descent into a pit of physical and emotional despair, followed by her eventual escape from that pit more than two years later.
Following a fairly mild case of COVID, Ms. Caffee said worsening neurologic symptoms forced her to take medical leave from her very physical and cognitively demanding job.
Ms. Caffee said she experienced crushing fatigue and brain fog, as well as rapid heart rate and blood pressure changes going from sitting to standing position.
She went from being a competitive athlete to someone who could barely get off the couch or empty the dishwasher.
With the ongoing help of her medical team, she slowly returned to daily activities and eventually to work on a limited basis.
Today, Ms. Caffee says she’s 90%-95% better but still she has some lingering symptoms and does not yet feel like her pre-COVID self.
It’s been a very slow climb out of the pit, Ms. Caffee said.
This study has no specific funding. The authors disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF CLINICAL AND TRANSLATIONAL NEUROLOGY