User login
Evaluating Fontan failure risk after arrhythmia
People who have undergone the Fontan procedure have been known to be prone to developing arrhythmias, but few studies have evaluated their prognosis, so researchers from Australia and New Zealand analyzed results of more than 1,000 patients with Fontan circulation and found that two-thirds did not have any arrhythmia at 20 years, and that, among those who did have arrhythmias, almost three-quarters survived 10 years.
“After the first onset of an arrhythmia, close surveillance of ventricular function is required,” Thomas A. Carins, MD, and his colleagues reported (J Thorac Cardiovasc Surg. 2016;152:1355-63). They analyzed data from 1,034 patients who had Fontan procedures from 1975 to 2014 in the Australia and New Zealand Fontan Registry. “The development of an arrhythmia is associated with a heightened risk of subsequent failure of the Fontan circulation,” they wrote.
The study aimed to determine the type of arrhythmias Fontan patients had and what impact that had on long-term outcomes. The most common Fontan approach used in study patients was the extracardiac conduit (555), followed by the lateral tunnel approach (269) and atriopulmonary (210). Those who had the extracardiac Fontan were least likely to develop an arrhythmia, with a hazard ratio of 0.23 (P less than .001), which Dr. Carins and his coauthors noted was in line with previous reports of arrhythmias occurring in patients who had undergone the atriopulmonary connection (Circulation. 2004;109:2319-25; J Thorac Cardiovasc Surg. 1998;115:499-505).
Overall, 195 patients in the study developed arrhythmia, with 162 having tachyarrhythmia, 74 having bradyarrhythmia and 41 having both. “At 20 years, freedom from any arrhythmia, tachyarrhythmia, and bradyarrhythmia was 66%, 69%, and 85%, respectively,” the researchers said.
The following outcomes occurred after the first onset of arrhythmia – tachyarrhythmia in 153 patients and bradyarrhythmia in 42: Thirty-three died; 12 had heart transplants, 30 had a Fontan correction to an extracardiac conduit, three had a Fontan takedown, 12 developed enteropathy, and 25 developed New York Heart Association class III or IV symptoms. Eighty-four patients reached the composite endpoint of Fontan failure.
After they developed arrhythmias, most patients in all three Fontan procedure groups remained free from Fontan failure at 10 years: 67% in the extracardiac conduit group; 54% in the lateral tunnel group; and 51% in the atriopulmonary group.
Medical management of up to four medications was the preferred initial treatment for those with tachyarrhythmias (86%); 101 patients had a single episode of tachyarrhythmia at follow-up intervals of four to 13 years (7.6 year median). “Those who experienced a single versus multiple episodes of tachyarrhythmia showed comparable freedom from Fontan failure at 15 years,” noted Dr. Carins and his coauthors – with rates of 34% and 33%, respectively. Of the 74 patients with bradyarrhythmias, 66 received pacemakers.
“Survival after the onset of an arrhythmia was surprisingly good with 67% and 84% of patients alive at 10 years after the onset of a tachyarrhythmia and bradyarrhythmia, respectively,” the study authors said. “There was no association between occurrence of arrhythmia and survival.”
About 40% of the patients with a tachyarrhythmia or bradyarrhythmia in the study had reduced ventricular function at 10 years after onset, the researchers wrote. “Although the assessment of ventricular function in this study was clearly subjective, we nonetheless believe that these findings suggest that the onset of an arrhythmia is associated with a progressive deterioration in cardiac function,”they noted.
Coauthor Andrew Bullock, MBBS, disclosed receiving consulting fees from Actelion. Dr. Cairns and other coauthors had no financial relationships to disclose.
When interpreting the data that the Australian and New Zealand researchers analyzed, one must be cautious about viewing arrhythmia as an early indicator for Fontan revision, Mark E. Alexander, MD, of Boston Children’s Hospital and Harvard Medical School, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:1364-5).
The outcome of a Fontan revision after an arrhythmia “becomes self-fulfilling,” Dr. Alexander said. He questioned what the revision procedure would be when the initial operation was an extracardiac Fontan. “The complex risks of that procedure continue to keep decisions regarding Fontan revisions challenging,” he said. He also noted the study did not analyze the association of ventricular function and arrhythmias “in a substantive way.”
And Dr. Alexander did not interpret the study results as an endorsement of the extracardiac Fontan or a rejection of the lateral tunnel approach. The early adoption of the extracardiac Fontan by the groups the authors represented is itself a limitation of the study, he said. Challenges with follow-up of extracardiac techniques in this and other studies “limit our ability to declare a ‘victor’ in that debate,” he said. “It does remind the electrophysiologist that he or she needs to master the techniques of entering the pulmonary venous atrium in these patients.”
The precision of calculating risk after an operation grows weaker with time, he said, and at 15-20 years morbidity starts to increase and follow-up becomes “more diffuse,” Dr. Alexander said. “That reality means we look forward to this group continuing to enhance our understanding of how our changing management decisions can aid our patients.”
Dr. Alexander had no financial relationships to disclose.
When interpreting the data that the Australian and New Zealand researchers analyzed, one must be cautious about viewing arrhythmia as an early indicator for Fontan revision, Mark E. Alexander, MD, of Boston Children’s Hospital and Harvard Medical School, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:1364-5).
The outcome of a Fontan revision after an arrhythmia “becomes self-fulfilling,” Dr. Alexander said. He questioned what the revision procedure would be when the initial operation was an extracardiac Fontan. “The complex risks of that procedure continue to keep decisions regarding Fontan revisions challenging,” he said. He also noted the study did not analyze the association of ventricular function and arrhythmias “in a substantive way.”
And Dr. Alexander did not interpret the study results as an endorsement of the extracardiac Fontan or a rejection of the lateral tunnel approach. The early adoption of the extracardiac Fontan by the groups the authors represented is itself a limitation of the study, he said. Challenges with follow-up of extracardiac techniques in this and other studies “limit our ability to declare a ‘victor’ in that debate,” he said. “It does remind the electrophysiologist that he or she needs to master the techniques of entering the pulmonary venous atrium in these patients.”
The precision of calculating risk after an operation grows weaker with time, he said, and at 15-20 years morbidity starts to increase and follow-up becomes “more diffuse,” Dr. Alexander said. “That reality means we look forward to this group continuing to enhance our understanding of how our changing management decisions can aid our patients.”
Dr. Alexander had no financial relationships to disclose.
When interpreting the data that the Australian and New Zealand researchers analyzed, one must be cautious about viewing arrhythmia as an early indicator for Fontan revision, Mark E. Alexander, MD, of Boston Children’s Hospital and Harvard Medical School, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:1364-5).
The outcome of a Fontan revision after an arrhythmia “becomes self-fulfilling,” Dr. Alexander said. He questioned what the revision procedure would be when the initial operation was an extracardiac Fontan. “The complex risks of that procedure continue to keep decisions regarding Fontan revisions challenging,” he said. He also noted the study did not analyze the association of ventricular function and arrhythmias “in a substantive way.”
And Dr. Alexander did not interpret the study results as an endorsement of the extracardiac Fontan or a rejection of the lateral tunnel approach. The early adoption of the extracardiac Fontan by the groups the authors represented is itself a limitation of the study, he said. Challenges with follow-up of extracardiac techniques in this and other studies “limit our ability to declare a ‘victor’ in that debate,” he said. “It does remind the electrophysiologist that he or she needs to master the techniques of entering the pulmonary venous atrium in these patients.”
The precision of calculating risk after an operation grows weaker with time, he said, and at 15-20 years morbidity starts to increase and follow-up becomes “more diffuse,” Dr. Alexander said. “That reality means we look forward to this group continuing to enhance our understanding of how our changing management decisions can aid our patients.”
Dr. Alexander had no financial relationships to disclose.
People who have undergone the Fontan procedure have been known to be prone to developing arrhythmias, but few studies have evaluated their prognosis, so researchers from Australia and New Zealand analyzed results of more than 1,000 patients with Fontan circulation and found that two-thirds did not have any arrhythmia at 20 years, and that, among those who did have arrhythmias, almost three-quarters survived 10 years.
“After the first onset of an arrhythmia, close surveillance of ventricular function is required,” Thomas A. Carins, MD, and his colleagues reported (J Thorac Cardiovasc Surg. 2016;152:1355-63). They analyzed data from 1,034 patients who had Fontan procedures from 1975 to 2014 in the Australia and New Zealand Fontan Registry. “The development of an arrhythmia is associated with a heightened risk of subsequent failure of the Fontan circulation,” they wrote.
The study aimed to determine the type of arrhythmias Fontan patients had and what impact that had on long-term outcomes. The most common Fontan approach used in study patients was the extracardiac conduit (555), followed by the lateral tunnel approach (269) and atriopulmonary (210). Those who had the extracardiac Fontan were least likely to develop an arrhythmia, with a hazard ratio of 0.23 (P less than .001), which Dr. Carins and his coauthors noted was in line with previous reports of arrhythmias occurring in patients who had undergone the atriopulmonary connection (Circulation. 2004;109:2319-25; J Thorac Cardiovasc Surg. 1998;115:499-505).
Overall, 195 patients in the study developed arrhythmia, with 162 having tachyarrhythmia, 74 having bradyarrhythmia and 41 having both. “At 20 years, freedom from any arrhythmia, tachyarrhythmia, and bradyarrhythmia was 66%, 69%, and 85%, respectively,” the researchers said.
The following outcomes occurred after the first onset of arrhythmia – tachyarrhythmia in 153 patients and bradyarrhythmia in 42: Thirty-three died; 12 had heart transplants, 30 had a Fontan correction to an extracardiac conduit, three had a Fontan takedown, 12 developed enteropathy, and 25 developed New York Heart Association class III or IV symptoms. Eighty-four patients reached the composite endpoint of Fontan failure.
After they developed arrhythmias, most patients in all three Fontan procedure groups remained free from Fontan failure at 10 years: 67% in the extracardiac conduit group; 54% in the lateral tunnel group; and 51% in the atriopulmonary group.
Medical management of up to four medications was the preferred initial treatment for those with tachyarrhythmias (86%); 101 patients had a single episode of tachyarrhythmia at follow-up intervals of four to 13 years (7.6 year median). “Those who experienced a single versus multiple episodes of tachyarrhythmia showed comparable freedom from Fontan failure at 15 years,” noted Dr. Carins and his coauthors – with rates of 34% and 33%, respectively. Of the 74 patients with bradyarrhythmias, 66 received pacemakers.
“Survival after the onset of an arrhythmia was surprisingly good with 67% and 84% of patients alive at 10 years after the onset of a tachyarrhythmia and bradyarrhythmia, respectively,” the study authors said. “There was no association between occurrence of arrhythmia and survival.”
About 40% of the patients with a tachyarrhythmia or bradyarrhythmia in the study had reduced ventricular function at 10 years after onset, the researchers wrote. “Although the assessment of ventricular function in this study was clearly subjective, we nonetheless believe that these findings suggest that the onset of an arrhythmia is associated with a progressive deterioration in cardiac function,”they noted.
Coauthor Andrew Bullock, MBBS, disclosed receiving consulting fees from Actelion. Dr. Cairns and other coauthors had no financial relationships to disclose.
People who have undergone the Fontan procedure have been known to be prone to developing arrhythmias, but few studies have evaluated their prognosis, so researchers from Australia and New Zealand analyzed results of more than 1,000 patients with Fontan circulation and found that two-thirds did not have any arrhythmia at 20 years, and that, among those who did have arrhythmias, almost three-quarters survived 10 years.
“After the first onset of an arrhythmia, close surveillance of ventricular function is required,” Thomas A. Carins, MD, and his colleagues reported (J Thorac Cardiovasc Surg. 2016;152:1355-63). They analyzed data from 1,034 patients who had Fontan procedures from 1975 to 2014 in the Australia and New Zealand Fontan Registry. “The development of an arrhythmia is associated with a heightened risk of subsequent failure of the Fontan circulation,” they wrote.
The study aimed to determine the type of arrhythmias Fontan patients had and what impact that had on long-term outcomes. The most common Fontan approach used in study patients was the extracardiac conduit (555), followed by the lateral tunnel approach (269) and atriopulmonary (210). Those who had the extracardiac Fontan were least likely to develop an arrhythmia, with a hazard ratio of 0.23 (P less than .001), which Dr. Carins and his coauthors noted was in line with previous reports of arrhythmias occurring in patients who had undergone the atriopulmonary connection (Circulation. 2004;109:2319-25; J Thorac Cardiovasc Surg. 1998;115:499-505).
Overall, 195 patients in the study developed arrhythmia, with 162 having tachyarrhythmia, 74 having bradyarrhythmia and 41 having both. “At 20 years, freedom from any arrhythmia, tachyarrhythmia, and bradyarrhythmia was 66%, 69%, and 85%, respectively,” the researchers said.
The following outcomes occurred after the first onset of arrhythmia – tachyarrhythmia in 153 patients and bradyarrhythmia in 42: Thirty-three died; 12 had heart transplants, 30 had a Fontan correction to an extracardiac conduit, three had a Fontan takedown, 12 developed enteropathy, and 25 developed New York Heart Association class III or IV symptoms. Eighty-four patients reached the composite endpoint of Fontan failure.
After they developed arrhythmias, most patients in all three Fontan procedure groups remained free from Fontan failure at 10 years: 67% in the extracardiac conduit group; 54% in the lateral tunnel group; and 51% in the atriopulmonary group.
Medical management of up to four medications was the preferred initial treatment for those with tachyarrhythmias (86%); 101 patients had a single episode of tachyarrhythmia at follow-up intervals of four to 13 years (7.6 year median). “Those who experienced a single versus multiple episodes of tachyarrhythmia showed comparable freedom from Fontan failure at 15 years,” noted Dr. Carins and his coauthors – with rates of 34% and 33%, respectively. Of the 74 patients with bradyarrhythmias, 66 received pacemakers.
“Survival after the onset of an arrhythmia was surprisingly good with 67% and 84% of patients alive at 10 years after the onset of a tachyarrhythmia and bradyarrhythmia, respectively,” the study authors said. “There was no association between occurrence of arrhythmia and survival.”
About 40% of the patients with a tachyarrhythmia or bradyarrhythmia in the study had reduced ventricular function at 10 years after onset, the researchers wrote. “Although the assessment of ventricular function in this study was clearly subjective, we nonetheless believe that these findings suggest that the onset of an arrhythmia is associated with a progressive deterioration in cardiac function,”they noted.
Coauthor Andrew Bullock, MBBS, disclosed receiving consulting fees from Actelion. Dr. Cairns and other coauthors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: The development of arrhythmia is associated with a heightened risk of failure of Fontan circulation after a Fontan procedure.
Major finding: At 20 years, freedom from any arrhythmia was 66%, and after the onset of any arrhythmia freedom from Fontan failure was 55%.
Data source: 1,034 patients who had undergone a Fontan procedure from 1975 to 2014 as recorded in the Australian and New Zealand Fontan Registry.
Disclosures: Coauthor Andrew Bullock, MBBS, reported receiving consulting fees from Actelion. All other others have no financial relationships to disclose.
Revision technique treats graft dysfunction after esophageal reconstruction
Ingestion of caustic substances like alkali, acid, and bleaches that call for esophageal surgery is relatively rare, and the study of dealing with postsurgery complications even rarer, but a team of surgeons from a large public referral hospital in Paris has collected enough cases over the first years of this century to report that a form of revision surgery in these cases can yield good outcomes with acceptable morbidity, according to a study in the Journal of Thoracic and Cardiovascular Surgery (2016;152:1378-85).
Thibault Voron, MD, and coauthors at Hôpitaux Saint-Louis and the University of Paris performed revision cervicosternolaparotomy (CSLap) on 55 patients from 1999 to 2015. Two patients (4%) died and the severe morbidity rate was 27%, but the long-term functional success rate was 85%. “Of note, these figures compare favorably with results of primary esophageal reconstruction for caustic injuries in the literature,” Dr. Voron and colleagues said. Overall the study authors performed revision surgery on 100 patients, with the remaining 45 undergoing repair through a limited approach. There were no significant differences in characteristics between the two groups.
Primary esophageal reconstruction for caustic injuries can usually be done at referral centers with good results, but up to half of these patients can have late complications, consisting mostly of strictures and redundancy that can cause loss of function, Dr. Voron and coauthors said. Published series have reported revision surgery in 15%-38% of patients (Dis Esophagus. 2008;21:E1-5; Dis Esophagus. 1999;12:7-9), but revision surgery itself is difficult to accomplish.
CSLap involves a large operative field from the jaw to the pubis. It starts with a comprehensive neck exploration through the previous cervical incision or with a median laparotomy to rule out a limited-approach repair. CSLap was undertaken when the graft was too short for a tension-free anastomosis. After the upper part of the graft was dissected from the thoracic inlet, the abdomen was opened for dissection of the abdominal part of the transplant. All scar tissues and strictures were excised after the transplant release, and a new anastomosis was constructed in healthy tissues. In cases involving life-threatening complications, patient survival prevailed over graft preservation and reconstruction of digestive continuity. The operations took up to 10 hours, with 8 hours, 20 minutes the median.
Dr. Voron and coauthors identified two distinct indications for CSLap: graft strictures in 43 (78%) of patients to rescue the primary conduit and reconstruct the cervical anastomosis and a need to access the retrosternal space to treat graft-related complications. “Graft lengthening was definitely not the issue in this situation,” Dr. Voron and colleagues said of the latter indication.
Four patients had emergency revision CSLap for spontaneous graft perforation and complications related to caustic reingestion. None died and one patient had preservation of the primary conduit. “Retrosternal grafts can be quickly removed by blunt dissection in life-threatening circumstances; however, if reasonable chances to recover the transplant exist, CSLap exploration can be justified,” Dr. Voron and coauthors said.
CSLap offers a few advantages in these situations: Transplant release provides significant lengthening of the graft that enables preservation of the primary conduit and redo of the cervical anastomosis in most patients, and it allows direct access to the retrosternal space if needed, Dr. Voron and coauthors said.
Dr. Voron and coauthors had no financial relationships to disclose.
This series by Dr. Voron and coauthors was “truly remarkable,” given the rarity of esophageal caustic injuries and even rarer occasion of revision surgery, Victor A. Ferraris, MD, PhD, of the University of Kentucky, Lexington, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:1386-7). He attributed the series size to the authors’ clinical setting in a trauma entry point for Europe’s largest hospital system – the same hospital that received victims of the terrorist attack at the Bataclan concert hall in Paris in November 2015.
“Voron and coauthors clearly have the benefit of a large referral population and vast medical infrastructure in the Assistance Publique-Hôpitaux de Paris,” Dr. Ferraris said. That volume certainly factors into their ability to achieve “very good outcomes,” he said.
“This seems to be an argument in favor of localization of resources to a single center,” Dr. Ferraris said. “Dr. Voron and coauthors have translated their experience into knowledge that can help other surgeons deal with this difficult problem.”
Dr. Ferraris had no financial relationships to disclose.
This series by Dr. Voron and coauthors was “truly remarkable,” given the rarity of esophageal caustic injuries and even rarer occasion of revision surgery, Victor A. Ferraris, MD, PhD, of the University of Kentucky, Lexington, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:1386-7). He attributed the series size to the authors’ clinical setting in a trauma entry point for Europe’s largest hospital system – the same hospital that received victims of the terrorist attack at the Bataclan concert hall in Paris in November 2015.
“Voron and coauthors clearly have the benefit of a large referral population and vast medical infrastructure in the Assistance Publique-Hôpitaux de Paris,” Dr. Ferraris said. That volume certainly factors into their ability to achieve “very good outcomes,” he said.
“This seems to be an argument in favor of localization of resources to a single center,” Dr. Ferraris said. “Dr. Voron and coauthors have translated their experience into knowledge that can help other surgeons deal with this difficult problem.”
Dr. Ferraris had no financial relationships to disclose.
This series by Dr. Voron and coauthors was “truly remarkable,” given the rarity of esophageal caustic injuries and even rarer occasion of revision surgery, Victor A. Ferraris, MD, PhD, of the University of Kentucky, Lexington, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:1386-7). He attributed the series size to the authors’ clinical setting in a trauma entry point for Europe’s largest hospital system – the same hospital that received victims of the terrorist attack at the Bataclan concert hall in Paris in November 2015.
“Voron and coauthors clearly have the benefit of a large referral population and vast medical infrastructure in the Assistance Publique-Hôpitaux de Paris,” Dr. Ferraris said. That volume certainly factors into their ability to achieve “very good outcomes,” he said.
“This seems to be an argument in favor of localization of resources to a single center,” Dr. Ferraris said. “Dr. Voron and coauthors have translated their experience into knowledge that can help other surgeons deal with this difficult problem.”
Dr. Ferraris had no financial relationships to disclose.
Ingestion of caustic substances like alkali, acid, and bleaches that call for esophageal surgery is relatively rare, and the study of dealing with postsurgery complications even rarer, but a team of surgeons from a large public referral hospital in Paris has collected enough cases over the first years of this century to report that a form of revision surgery in these cases can yield good outcomes with acceptable morbidity, according to a study in the Journal of Thoracic and Cardiovascular Surgery (2016;152:1378-85).
Thibault Voron, MD, and coauthors at Hôpitaux Saint-Louis and the University of Paris performed revision cervicosternolaparotomy (CSLap) on 55 patients from 1999 to 2015. Two patients (4%) died and the severe morbidity rate was 27%, but the long-term functional success rate was 85%. “Of note, these figures compare favorably with results of primary esophageal reconstruction for caustic injuries in the literature,” Dr. Voron and colleagues said. Overall the study authors performed revision surgery on 100 patients, with the remaining 45 undergoing repair through a limited approach. There were no significant differences in characteristics between the two groups.
Primary esophageal reconstruction for caustic injuries can usually be done at referral centers with good results, but up to half of these patients can have late complications, consisting mostly of strictures and redundancy that can cause loss of function, Dr. Voron and coauthors said. Published series have reported revision surgery in 15%-38% of patients (Dis Esophagus. 2008;21:E1-5; Dis Esophagus. 1999;12:7-9), but revision surgery itself is difficult to accomplish.
CSLap involves a large operative field from the jaw to the pubis. It starts with a comprehensive neck exploration through the previous cervical incision or with a median laparotomy to rule out a limited-approach repair. CSLap was undertaken when the graft was too short for a tension-free anastomosis. After the upper part of the graft was dissected from the thoracic inlet, the abdomen was opened for dissection of the abdominal part of the transplant. All scar tissues and strictures were excised after the transplant release, and a new anastomosis was constructed in healthy tissues. In cases involving life-threatening complications, patient survival prevailed over graft preservation and reconstruction of digestive continuity. The operations took up to 10 hours, with 8 hours, 20 minutes the median.
Dr. Voron and coauthors identified two distinct indications for CSLap: graft strictures in 43 (78%) of patients to rescue the primary conduit and reconstruct the cervical anastomosis and a need to access the retrosternal space to treat graft-related complications. “Graft lengthening was definitely not the issue in this situation,” Dr. Voron and colleagues said of the latter indication.
Four patients had emergency revision CSLap for spontaneous graft perforation and complications related to caustic reingestion. None died and one patient had preservation of the primary conduit. “Retrosternal grafts can be quickly removed by blunt dissection in life-threatening circumstances; however, if reasonable chances to recover the transplant exist, CSLap exploration can be justified,” Dr. Voron and coauthors said.
CSLap offers a few advantages in these situations: Transplant release provides significant lengthening of the graft that enables preservation of the primary conduit and redo of the cervical anastomosis in most patients, and it allows direct access to the retrosternal space if needed, Dr. Voron and coauthors said.
Dr. Voron and coauthors had no financial relationships to disclose.
Ingestion of caustic substances like alkali, acid, and bleaches that call for esophageal surgery is relatively rare, and the study of dealing with postsurgery complications even rarer, but a team of surgeons from a large public referral hospital in Paris has collected enough cases over the first years of this century to report that a form of revision surgery in these cases can yield good outcomes with acceptable morbidity, according to a study in the Journal of Thoracic and Cardiovascular Surgery (2016;152:1378-85).
Thibault Voron, MD, and coauthors at Hôpitaux Saint-Louis and the University of Paris performed revision cervicosternolaparotomy (CSLap) on 55 patients from 1999 to 2015. Two patients (4%) died and the severe morbidity rate was 27%, but the long-term functional success rate was 85%. “Of note, these figures compare favorably with results of primary esophageal reconstruction for caustic injuries in the literature,” Dr. Voron and colleagues said. Overall the study authors performed revision surgery on 100 patients, with the remaining 45 undergoing repair through a limited approach. There were no significant differences in characteristics between the two groups.
Primary esophageal reconstruction for caustic injuries can usually be done at referral centers with good results, but up to half of these patients can have late complications, consisting mostly of strictures and redundancy that can cause loss of function, Dr. Voron and coauthors said. Published series have reported revision surgery in 15%-38% of patients (Dis Esophagus. 2008;21:E1-5; Dis Esophagus. 1999;12:7-9), but revision surgery itself is difficult to accomplish.
CSLap involves a large operative field from the jaw to the pubis. It starts with a comprehensive neck exploration through the previous cervical incision or with a median laparotomy to rule out a limited-approach repair. CSLap was undertaken when the graft was too short for a tension-free anastomosis. After the upper part of the graft was dissected from the thoracic inlet, the abdomen was opened for dissection of the abdominal part of the transplant. All scar tissues and strictures were excised after the transplant release, and a new anastomosis was constructed in healthy tissues. In cases involving life-threatening complications, patient survival prevailed over graft preservation and reconstruction of digestive continuity. The operations took up to 10 hours, with 8 hours, 20 minutes the median.
Dr. Voron and coauthors identified two distinct indications for CSLap: graft strictures in 43 (78%) of patients to rescue the primary conduit and reconstruct the cervical anastomosis and a need to access the retrosternal space to treat graft-related complications. “Graft lengthening was definitely not the issue in this situation,” Dr. Voron and colleagues said of the latter indication.
Four patients had emergency revision CSLap for spontaneous graft perforation and complications related to caustic reingestion. None died and one patient had preservation of the primary conduit. “Retrosternal grafts can be quickly removed by blunt dissection in life-threatening circumstances; however, if reasonable chances to recover the transplant exist, CSLap exploration can be justified,” Dr. Voron and coauthors said.
CSLap offers a few advantages in these situations: Transplant release provides significant lengthening of the graft that enables preservation of the primary conduit and redo of the cervical anastomosis in most patients, and it allows direct access to the retrosternal space if needed, Dr. Voron and coauthors said.
Dr. Voron and coauthors had no financial relationships to disclose.
Key clinical point: Cervicosternolaparotomy revision surgery for graft dysfunction after esophageal reconstruction for caustic injuries can achieve good results with acceptable morbidity.
Major finding: Functional success rate after revision CSLap was 85% after a mean follow-up of 4.4 years.
Data source: 55 patients who underwent CSLap revision surgery between 1999 and 2015 at a single center.
Disclosures: Dr. Voron and coauthors had no financial relationships to disclose.
SYNTAX analysis: Making the case for CABG over PCI
Whenever seminal clinical trials report results that challenge conventional thinking, physicians face the challenge of actually applying those findings in the clinic. A team of cardiac surgeons from Baylor University in Plano, Tex., has offered its take on the clinical implications of recent findings from the cause-of-death analysis of the SYNTAX trial that compared coronary artery bypass grafting with stenting: When counseling higher-risk patients with coronary artery disease about revascularization procedures, cardiologists and cardiac surgeons should clearly elucidate the dramatic advantage of coronary artery bypass grafting over stenting that SYNTAX had demonstrated.
Michael Mack, MD, and coauthors made their case in a featured expert opinion in the Journal of Thoracic and Cardiovascular Surgery (2016;152:1237-40).

“In fact, there was a significant survival advantage for CABG in the patients with intermediate and high SYNTAX scores, with the death rate of CABG versus PCI being 9.6% versus 16.3% (P less than .047) and 8.8% versus 17.8% (P less than .02), respectively,” they wrote.
The advantages of surgery “have been most striking for patients with intermediate or high SYNTAX scores, but seem to exist for patients with low scores as well, although requiring more follow-up,” Dr. Mack and colleagues said. But the situation is less clear in other subgroups, particularly in patients with less diffuse distal disease and lower SYNTAX scores, they added.
Complete revascularization after the procedure may explain the better outcomes with CABG, as 43.3% of those in the PCI arm had incomplete revascularization vs. 36.8% in the CABG arm. “Incomplete revascularization was associated with increased risk for major adverse cardiac or cerebrovascular events three years after PCI, but incomplete revascularization in the CABG group could not be identified as a predictor for worse outcomes,” Dr. Mack and colleagues noted.
The expert opinion authors debunk one of the recent criticisms of SYNTAX: that its reliance on first-generation drug-eluting stents is dated and not relevant today. They noted the more recent Bypass Surgery Vs. Everolimus-Eluting Stent Implantation for Multivessel Coronary Artery Disease trial found a similarly higher rate of death, heart attack, and target vessel revascularization occurred more frequently in the PCI group (15.3% vs. 10.6% in the CABG group) (N Engl J Med. 2015;372:1204-12).
Nonetheless, Dr. Mack and coauthors found room for improvement for CABG through increased use of atrial revascularization and appropriate measures to minimize stroke.
The latest SYNTAX findings can inform the approach surgeons take with high-risk patients, they said. This should include “a discussion of these data, particularly in regard to survival.” And physicians should base their therapeutic recommendations on these data. “At present, there are data seeming to indicate that the majority of patients with three-vessel disease receiving invasive treatment in the United States are being treated with PCI, an outcome that is not congruent with these outcome findings,” they said.
Taking into consideration other SYNTAX analyses that have shown that completeness of revascularization is a determining factor in post-PCI outcomes, Dr. Mack and coauthors said that physicians should calculate the degree of coronary artery disease (CAD) left untreated after intervention, “and those patients who are likely to have a high residual SYNTAX score should be strongly considered for CABG.” Doctors should also focus “intensive efforts” on adherence to optimal medical therapy after both CABG and PCI.
“Finally, although there is a strong patient preference for a less-invasive treatment of their CAD, patients with advanced disease should be made aware that the choice of PCI puts them at an increased risk of death relative to CABG, and a full and transparent discussion should occur regarding the implications of their decision,” Dr. Mack and coauthors concluded.
They had no relevant financial relationships to disclose.
In their invited editorial commentary, Saswata Deb, MD, and Stephen E. Fremes, MD, of the Schulich Heart Center at the University of Toronto, concurred with the conclusions of Dr. Mack and colleagues (J Thorac Cardiovasc Surg. 2016;152:1241-2). And Joseph F. Sabik III, MD, of the Cleveland Clinic arrived at a similar conclusion in an accompanying editorial (J. Thorac Cardiovasc Surg. 2016;152:1227-8).
Dr. Deb and Dr. Fremes found noteworthy the point Dr. Mack and coauthors raised about cardiologists and internists continuing to recommend PCI to patients with complex multivessel CAD despite evidence from SYNTAX and other trials. “This raises the importance of having a multidisciplinary heart team,” Dr. Deb and Dr. Fremes said.
But they also raised an important question about the difference in outcomes between CABG and PCI in complex multivessel disease. CABG should be the preferred intervention if the high rates of late fatal myocardial infarction after PCI are due to incomplete revascularization; however, if late stent thrombosis was the cause of this disparity in outcomes, then improvements in PCI could close that gap.
In his editorial, Dr. Sabik attributed the difference in outcomes between PCI and CABG to the ability of the former to both treat existing and prevent future stenosis. PCI can be “difficult, dangerous, and even impossible” when the target vessel is totally occluded or the stenosis is complex, hence leading to incomplete revascularization and residual ischemia. “Performing CABG to these vessels is no more difficult than for an isolated, noncomplex stenosis,” Dr. Sabik said.
Dr. Sabik disclosed he is the principal investigator for an Abbott Laboratories–sponsored trial of left main coronary disease, and is on the scientific advisory board of Medtronic.
Dr. Deb and Dr. Fremes had no relationships to disclose.
In their invited editorial commentary, Saswata Deb, MD, and Stephen E. Fremes, MD, of the Schulich Heart Center at the University of Toronto, concurred with the conclusions of Dr. Mack and colleagues (J Thorac Cardiovasc Surg. 2016;152:1241-2). And Joseph F. Sabik III, MD, of the Cleveland Clinic arrived at a similar conclusion in an accompanying editorial (J. Thorac Cardiovasc Surg. 2016;152:1227-8).
Dr. Deb and Dr. Fremes found noteworthy the point Dr. Mack and coauthors raised about cardiologists and internists continuing to recommend PCI to patients with complex multivessel CAD despite evidence from SYNTAX and other trials. “This raises the importance of having a multidisciplinary heart team,” Dr. Deb and Dr. Fremes said.
But they also raised an important question about the difference in outcomes between CABG and PCI in complex multivessel disease. CABG should be the preferred intervention if the high rates of late fatal myocardial infarction after PCI are due to incomplete revascularization; however, if late stent thrombosis was the cause of this disparity in outcomes, then improvements in PCI could close that gap.
In his editorial, Dr. Sabik attributed the difference in outcomes between PCI and CABG to the ability of the former to both treat existing and prevent future stenosis. PCI can be “difficult, dangerous, and even impossible” when the target vessel is totally occluded or the stenosis is complex, hence leading to incomplete revascularization and residual ischemia. “Performing CABG to these vessels is no more difficult than for an isolated, noncomplex stenosis,” Dr. Sabik said.
Dr. Sabik disclosed he is the principal investigator for an Abbott Laboratories–sponsored trial of left main coronary disease, and is on the scientific advisory board of Medtronic.
Dr. Deb and Dr. Fremes had no relationships to disclose.
In their invited editorial commentary, Saswata Deb, MD, and Stephen E. Fremes, MD, of the Schulich Heart Center at the University of Toronto, concurred with the conclusions of Dr. Mack and colleagues (J Thorac Cardiovasc Surg. 2016;152:1241-2). And Joseph F. Sabik III, MD, of the Cleveland Clinic arrived at a similar conclusion in an accompanying editorial (J. Thorac Cardiovasc Surg. 2016;152:1227-8).
Dr. Deb and Dr. Fremes found noteworthy the point Dr. Mack and coauthors raised about cardiologists and internists continuing to recommend PCI to patients with complex multivessel CAD despite evidence from SYNTAX and other trials. “This raises the importance of having a multidisciplinary heart team,” Dr. Deb and Dr. Fremes said.
But they also raised an important question about the difference in outcomes between CABG and PCI in complex multivessel disease. CABG should be the preferred intervention if the high rates of late fatal myocardial infarction after PCI are due to incomplete revascularization; however, if late stent thrombosis was the cause of this disparity in outcomes, then improvements in PCI could close that gap.
In his editorial, Dr. Sabik attributed the difference in outcomes between PCI and CABG to the ability of the former to both treat existing and prevent future stenosis. PCI can be “difficult, dangerous, and even impossible” when the target vessel is totally occluded or the stenosis is complex, hence leading to incomplete revascularization and residual ischemia. “Performing CABG to these vessels is no more difficult than for an isolated, noncomplex stenosis,” Dr. Sabik said.
Dr. Sabik disclosed he is the principal investigator for an Abbott Laboratories–sponsored trial of left main coronary disease, and is on the scientific advisory board of Medtronic.
Dr. Deb and Dr. Fremes had no relationships to disclose.
Whenever seminal clinical trials report results that challenge conventional thinking, physicians face the challenge of actually applying those findings in the clinic. A team of cardiac surgeons from Baylor University in Plano, Tex., has offered its take on the clinical implications of recent findings from the cause-of-death analysis of the SYNTAX trial that compared coronary artery bypass grafting with stenting: When counseling higher-risk patients with coronary artery disease about revascularization procedures, cardiologists and cardiac surgeons should clearly elucidate the dramatic advantage of coronary artery bypass grafting over stenting that SYNTAX had demonstrated.
Michael Mack, MD, and coauthors made their case in a featured expert opinion in the Journal of Thoracic and Cardiovascular Surgery (2016;152:1237-40).
“In fact, there was a significant survival advantage for CABG in the patients with intermediate and high SYNTAX scores, with the death rate of CABG versus PCI being 9.6% versus 16.3% (P less than .047) and 8.8% versus 17.8% (P less than .02), respectively,” they wrote.
The advantages of surgery “have been most striking for patients with intermediate or high SYNTAX scores, but seem to exist for patients with low scores as well, although requiring more follow-up,” Dr. Mack and colleagues said. But the situation is less clear in other subgroups, particularly in patients with less diffuse distal disease and lower SYNTAX scores, they added.
Complete revascularization after the procedure may explain the better outcomes with CABG, as 43.3% of those in the PCI arm had incomplete revascularization vs. 36.8% in the CABG arm. “Incomplete revascularization was associated with increased risk for major adverse cardiac or cerebrovascular events three years after PCI, but incomplete revascularization in the CABG group could not be identified as a predictor for worse outcomes,” Dr. Mack and colleagues noted.
The expert opinion authors debunk one of the recent criticisms of SYNTAX: that its reliance on first-generation drug-eluting stents is dated and not relevant today. They noted the more recent Bypass Surgery Vs. Everolimus-Eluting Stent Implantation for Multivessel Coronary Artery Disease trial found a similarly higher rate of death, heart attack, and target vessel revascularization occurred more frequently in the PCI group (15.3% vs. 10.6% in the CABG group) (N Engl J Med. 2015;372:1204-12).
Nonetheless, Dr. Mack and coauthors found room for improvement for CABG through increased use of atrial revascularization and appropriate measures to minimize stroke.
The latest SYNTAX findings can inform the approach surgeons take with high-risk patients, they said. This should include “a discussion of these data, particularly in regard to survival.” And physicians should base their therapeutic recommendations on these data. “At present, there are data seeming to indicate that the majority of patients with three-vessel disease receiving invasive treatment in the United States are being treated with PCI, an outcome that is not congruent with these outcome findings,” they said.
Taking into consideration other SYNTAX analyses that have shown that completeness of revascularization is a determining factor in post-PCI outcomes, Dr. Mack and coauthors said that physicians should calculate the degree of coronary artery disease (CAD) left untreated after intervention, “and those patients who are likely to have a high residual SYNTAX score should be strongly considered for CABG.” Doctors should also focus “intensive efforts” on adherence to optimal medical therapy after both CABG and PCI.
“Finally, although there is a strong patient preference for a less-invasive treatment of their CAD, patients with advanced disease should be made aware that the choice of PCI puts them at an increased risk of death relative to CABG, and a full and transparent discussion should occur regarding the implications of their decision,” Dr. Mack and coauthors concluded.
They had no relevant financial relationships to disclose.
Whenever seminal clinical trials report results that challenge conventional thinking, physicians face the challenge of actually applying those findings in the clinic. A team of cardiac surgeons from Baylor University in Plano, Tex., has offered its take on the clinical implications of recent findings from the cause-of-death analysis of the SYNTAX trial that compared coronary artery bypass grafting with stenting: When counseling higher-risk patients with coronary artery disease about revascularization procedures, cardiologists and cardiac surgeons should clearly elucidate the dramatic advantage of coronary artery bypass grafting over stenting that SYNTAX had demonstrated.
Michael Mack, MD, and coauthors made their case in a featured expert opinion in the Journal of Thoracic and Cardiovascular Surgery (2016;152:1237-40).
“In fact, there was a significant survival advantage for CABG in the patients with intermediate and high SYNTAX scores, with the death rate of CABG versus PCI being 9.6% versus 16.3% (P less than .047) and 8.8% versus 17.8% (P less than .02), respectively,” they wrote.
The advantages of surgery “have been most striking for patients with intermediate or high SYNTAX scores, but seem to exist for patients with low scores as well, although requiring more follow-up,” Dr. Mack and colleagues said. But the situation is less clear in other subgroups, particularly in patients with less diffuse distal disease and lower SYNTAX scores, they added.
Complete revascularization after the procedure may explain the better outcomes with CABG, as 43.3% of those in the PCI arm had incomplete revascularization vs. 36.8% in the CABG arm. “Incomplete revascularization was associated with increased risk for major adverse cardiac or cerebrovascular events three years after PCI, but incomplete revascularization in the CABG group could not be identified as a predictor for worse outcomes,” Dr. Mack and colleagues noted.
The expert opinion authors debunk one of the recent criticisms of SYNTAX: that its reliance on first-generation drug-eluting stents is dated and not relevant today. They noted the more recent Bypass Surgery Vs. Everolimus-Eluting Stent Implantation for Multivessel Coronary Artery Disease trial found a similarly higher rate of death, heart attack, and target vessel revascularization occurred more frequently in the PCI group (15.3% vs. 10.6% in the CABG group) (N Engl J Med. 2015;372:1204-12).
Nonetheless, Dr. Mack and coauthors found room for improvement for CABG through increased use of atrial revascularization and appropriate measures to minimize stroke.
The latest SYNTAX findings can inform the approach surgeons take with high-risk patients, they said. This should include “a discussion of these data, particularly in regard to survival.” And physicians should base their therapeutic recommendations on these data. “At present, there are data seeming to indicate that the majority of patients with three-vessel disease receiving invasive treatment in the United States are being treated with PCI, an outcome that is not congruent with these outcome findings,” they said.
Taking into consideration other SYNTAX analyses that have shown that completeness of revascularization is a determining factor in post-PCI outcomes, Dr. Mack and coauthors said that physicians should calculate the degree of coronary artery disease (CAD) left untreated after intervention, “and those patients who are likely to have a high residual SYNTAX score should be strongly considered for CABG.” Doctors should also focus “intensive efforts” on adherence to optimal medical therapy after both CABG and PCI.
“Finally, although there is a strong patient preference for a less-invasive treatment of their CAD, patients with advanced disease should be made aware that the choice of PCI puts them at an increased risk of death relative to CABG, and a full and transparent discussion should occur regarding the implications of their decision,” Dr. Mack and coauthors concluded.
They had no relevant financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Physicians should clearly communicate to patients with complex multivessel artery disease the key findings of the SYNTAX trial.
Major finding: The SYNTAX trials showed the risk of cardiac death from myocardial infarction after percutaneous coronary intervention (PCI) is 10 times greater than that after coronary artery bypass grafting in higher-risk patients.
Data source: A post hoc analysis of causes of death in all 3,075 trial and registry patients in the Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery (SYNTAX) trial.
Disclosures: Dr. Mack and coauthors reported having no financial disclosures.
Is regional anesthesia safer in CEA?
COLUMBUS, OHIO – General anesthesia during carotid endarterectomy carries almost twice the risk of complications and unplanned intubation as regional anesthesia, but the latter approach, which is not available in all hospitals, has its own issues, an analysis of procedures from a statewide database in Michigan found.
“This study is timely because of CMS [Center for Medicare & Medicaid Services] initiatives tying reimbursement to specific quality measures,” Ahmad S Hussain, MD, of Wayne State University in Detroit said in reporting the study results at the annual meeting of the Midwestern Vascular Surgery Society.

Regional anesthesia in CEA emerged in the 1990s, Dr. Hussain said, and allows for more reliable neurologic monitoring and more direct evaluation of the need for stenting during CEA than general anesthesia, which requires continuous monitoring of cerebral perfusion with carotid stump pressures, electroencephalogram, and transcranial doppler.
The researchers retrospectively analyzed 4,558 patients who had CEA at hospitals participating in the Michigan Surgical Quality Cooperative from 2012 to 2014 – 4,008 of whom had general anesthesia and 550 regional anesthesia.
“Advocates for carotid endarterectomy with regional anesthesia cite a reduction in hemodynamic instability and the ability for neurological monitoring, but many still prefer general anesthesia because the benefits of regional anesthesia have not been clearly demonstrated, allowing that regional anesthesia may not be available in all centers and allowing that a certain amount of patient movement during the procedure may not be uniformly tolerated,” Dr. Hussain said.
General anesthesia patients in the study had more than twice the rate of any morbidity at 30 days than those who had regional, 8.7% vs. 4.2%, and significantly higher rates of unplanned intervention, 2.1% vs. 0.6%. Dr. Hussain said. However, the study could not determine differences in 30-day mortality or other key outcomes, such as rates of pneumonia, sepsis, deep vein thrombosis, or pulmonary embolism, becauseof insufficient sample sizes, Dr. Hussain said
The study found less significant differences between general and regional anesthesia techniques, respectively, in rates of extended length of stay, 12.1% vs. 9.5%; readmissions, 9.2% vs. 6.1%; and reoperation, 4.5% vs. 3%.
The retrospective study used two models to analyze odds ratios: Model 1 adjusted for case mix; and model 2 adjusted for case mix as fixed effects and site as a random effect. While the retrospective nature of the study may be a limitation, the findings support the use of regional anesthesia for CEA when available, Dr. Hussain said.
Dr. Hussain had no relationships to disclose.
COLUMBUS, OHIO – General anesthesia during carotid endarterectomy carries almost twice the risk of complications and unplanned intubation as regional anesthesia, but the latter approach, which is not available in all hospitals, has its own issues, an analysis of procedures from a statewide database in Michigan found.
“This study is timely because of CMS [Center for Medicare & Medicaid Services] initiatives tying reimbursement to specific quality measures,” Ahmad S Hussain, MD, of Wayne State University in Detroit said in reporting the study results at the annual meeting of the Midwestern Vascular Surgery Society.
Regional anesthesia in CEA emerged in the 1990s, Dr. Hussain said, and allows for more reliable neurologic monitoring and more direct evaluation of the need for stenting during CEA than general anesthesia, which requires continuous monitoring of cerebral perfusion with carotid stump pressures, electroencephalogram, and transcranial doppler.
The researchers retrospectively analyzed 4,558 patients who had CEA at hospitals participating in the Michigan Surgical Quality Cooperative from 2012 to 2014 – 4,008 of whom had general anesthesia and 550 regional anesthesia.
“Advocates for carotid endarterectomy with regional anesthesia cite a reduction in hemodynamic instability and the ability for neurological monitoring, but many still prefer general anesthesia because the benefits of regional anesthesia have not been clearly demonstrated, allowing that regional anesthesia may not be available in all centers and allowing that a certain amount of patient movement during the procedure may not be uniformly tolerated,” Dr. Hussain said.
General anesthesia patients in the study had more than twice the rate of any morbidity at 30 days than those who had regional, 8.7% vs. 4.2%, and significantly higher rates of unplanned intervention, 2.1% vs. 0.6%. Dr. Hussain said. However, the study could not determine differences in 30-day mortality or other key outcomes, such as rates of pneumonia, sepsis, deep vein thrombosis, or pulmonary embolism, becauseof insufficient sample sizes, Dr. Hussain said
The study found less significant differences between general and regional anesthesia techniques, respectively, in rates of extended length of stay, 12.1% vs. 9.5%; readmissions, 9.2% vs. 6.1%; and reoperation, 4.5% vs. 3%.
The retrospective study used two models to analyze odds ratios: Model 1 adjusted for case mix; and model 2 adjusted for case mix as fixed effects and site as a random effect. While the retrospective nature of the study may be a limitation, the findings support the use of regional anesthesia for CEA when available, Dr. Hussain said.
Dr. Hussain had no relationships to disclose.
COLUMBUS, OHIO – General anesthesia during carotid endarterectomy carries almost twice the risk of complications and unplanned intubation as regional anesthesia, but the latter approach, which is not available in all hospitals, has its own issues, an analysis of procedures from a statewide database in Michigan found.
“This study is timely because of CMS [Center for Medicare & Medicaid Services] initiatives tying reimbursement to specific quality measures,” Ahmad S Hussain, MD, of Wayne State University in Detroit said in reporting the study results at the annual meeting of the Midwestern Vascular Surgery Society.
Regional anesthesia in CEA emerged in the 1990s, Dr. Hussain said, and allows for more reliable neurologic monitoring and more direct evaluation of the need for stenting during CEA than general anesthesia, which requires continuous monitoring of cerebral perfusion with carotid stump pressures, electroencephalogram, and transcranial doppler.
The researchers retrospectively analyzed 4,558 patients who had CEA at hospitals participating in the Michigan Surgical Quality Cooperative from 2012 to 2014 – 4,008 of whom had general anesthesia and 550 regional anesthesia.
“Advocates for carotid endarterectomy with regional anesthesia cite a reduction in hemodynamic instability and the ability for neurological monitoring, but many still prefer general anesthesia because the benefits of regional anesthesia have not been clearly demonstrated, allowing that regional anesthesia may not be available in all centers and allowing that a certain amount of patient movement during the procedure may not be uniformly tolerated,” Dr. Hussain said.
General anesthesia patients in the study had more than twice the rate of any morbidity at 30 days than those who had regional, 8.7% vs. 4.2%, and significantly higher rates of unplanned intervention, 2.1% vs. 0.6%. Dr. Hussain said. However, the study could not determine differences in 30-day mortality or other key outcomes, such as rates of pneumonia, sepsis, deep vein thrombosis, or pulmonary embolism, becauseof insufficient sample sizes, Dr. Hussain said
The study found less significant differences between general and regional anesthesia techniques, respectively, in rates of extended length of stay, 12.1% vs. 9.5%; readmissions, 9.2% vs. 6.1%; and reoperation, 4.5% vs. 3%.
The retrospective study used two models to analyze odds ratios: Model 1 adjusted for case mix; and model 2 adjusted for case mix as fixed effects and site as a random effect. While the retrospective nature of the study may be a limitation, the findings support the use of regional anesthesia for CEA when available, Dr. Hussain said.
Dr. Hussain had no relationships to disclose.
AT MIDWESTERN VASCULAR 2016
Key clinical point: General anesthesia for carotid endarterectomy carries a higher risk of complications and readmissions than regional anesthesia.
Major finding: Any morbidity after CEA with general anesthesia was 8.7% vs. 4.2% for regional anesthesia, and readmissions rates were 9.2% vs. 6.1%.
Data source: Retrospective analysis of 4,558 patients who had CEA between 2012 and 2014 at hospitals participating in the Michigan Surgical Quality Collaborative database.
Disclosures: Dr. Hussain reported having no financial disclosures.
CEA risk models fit for an app
COLUMBUS, OHIO – Carotid endarterectomy is an effective treatment for people with asymptomatic carotid artery disease when stroke rates are low and they survive long enough to benefit from the treatment. But determining who those patients are can be a challenge for vascular surgeons. A team of vascular specialists from around the country have developed risk prediction models to help surgeons better select asymptomatic patients for the procedure, Randall DeMartino, MD, said at the annual meeting of the Midwestern Vascular Surgical Society.
“These models will be used for mobile apps and web-based applications for point of care patient risk assessment,” said Dr. DeMartino of the Mayo Clinic in Rochester, Minn. He is the lead researcher for the study, which uses data from the Vascular Quality Initiative (VQI).

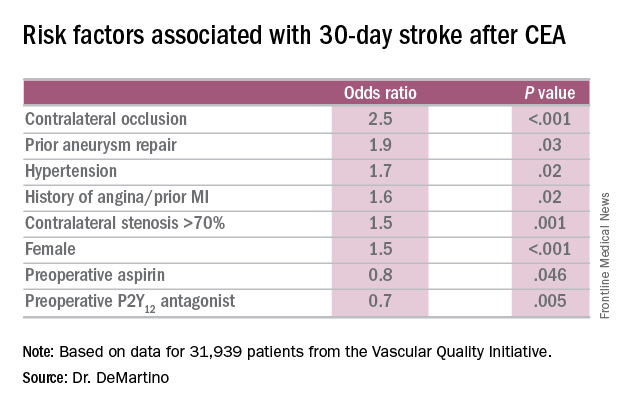
In developing the models, the researchers sampled asymptomatic patients in the VQI who had first-time elective CEA. There were 31,939 patients in the stroke analysis who had CEA from 2010-2015, and 24,086 patients in the mortality analysis who had procedures from 2010-2014. Dr. DeMartino and his colleagues evaluated all preoperative patient and surgeon characteristics, then used an algorithm to optimize the variables that were selected for the final logistic model.
The researchers also evaluated 30-day stroke rates and 1-year mortality at participating centers and found wide variability: an average of 0.9% for stroke, with a range of 0-8.3%; and 3.2% for mortality, with a range of 0-20%. “Actually, 22% of centers had a 1-year mortality rate that exceeded 5%,” Dr. DeMartino said.
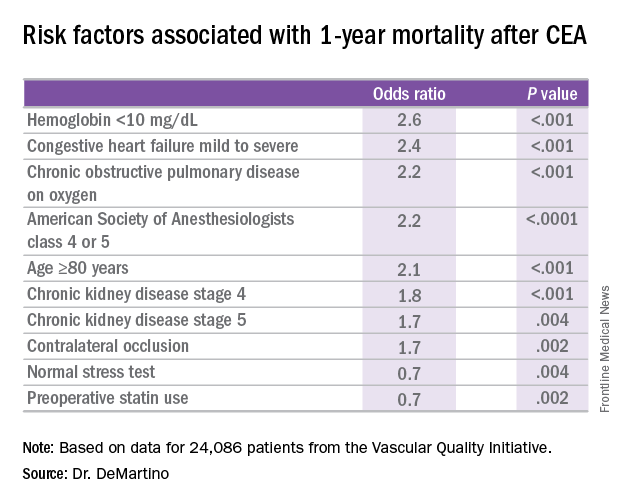
The model for 1-year mortality identified the following variables associated with the highest risk of death 1 year after CEA: age greater than or equal to 80 years; a preoperative hemoglobin less than 10 mg/dL; oxygen-dependent chronic obstructive pulmonary disease; mild to severe congestive heart failure; American Society of Anesthesiologists classification of IV or V; stage 4 or 5 chronic kidney disease; and a contralateral occlusion.
“Conversely, a normal stress test, when performed, and preoperative statin use were associated with reduced risk of death over a year,” Dr. DeMartino said.
“These data have been used to provide Center Opportunity for Improvement reports through VQI where centers can identify if they are selecting patients with risk factors for stroke or mortality more often compared to other centers,” Dr. DeMartino said. “This allows centers to see where opportunities for improvement exist.”
Also, physicians can see the proportion of patients they select with a predicted mortality risk over 5% at one year – “a group of patients who may gain little benefit from prophylactic CEA,” he said. “Physicians can compare their patient selection to those in their region or nationally.”
Dr. DeMartino had no relationships to disclose.
COLUMBUS, OHIO – Carotid endarterectomy is an effective treatment for people with asymptomatic carotid artery disease when stroke rates are low and they survive long enough to benefit from the treatment. But determining who those patients are can be a challenge for vascular surgeons. A team of vascular specialists from around the country have developed risk prediction models to help surgeons better select asymptomatic patients for the procedure, Randall DeMartino, MD, said at the annual meeting of the Midwestern Vascular Surgical Society.
“These models will be used for mobile apps and web-based applications for point of care patient risk assessment,” said Dr. DeMartino of the Mayo Clinic in Rochester, Minn. He is the lead researcher for the study, which uses data from the Vascular Quality Initiative (VQI).
In developing the models, the researchers sampled asymptomatic patients in the VQI who had first-time elective CEA. There were 31,939 patients in the stroke analysis who had CEA from 2010-2015, and 24,086 patients in the mortality analysis who had procedures from 2010-2014. Dr. DeMartino and his colleagues evaluated all preoperative patient and surgeon characteristics, then used an algorithm to optimize the variables that were selected for the final logistic model.
The researchers also evaluated 30-day stroke rates and 1-year mortality at participating centers and found wide variability: an average of 0.9% for stroke, with a range of 0-8.3%; and 3.2% for mortality, with a range of 0-20%. “Actually, 22% of centers had a 1-year mortality rate that exceeded 5%,” Dr. DeMartino said.
The model for 1-year mortality identified the following variables associated with the highest risk of death 1 year after CEA: age greater than or equal to 80 years; a preoperative hemoglobin less than 10 mg/dL; oxygen-dependent chronic obstructive pulmonary disease; mild to severe congestive heart failure; American Society of Anesthesiologists classification of IV or V; stage 4 or 5 chronic kidney disease; and a contralateral occlusion.
“Conversely, a normal stress test, when performed, and preoperative statin use were associated with reduced risk of death over a year,” Dr. DeMartino said.
“These data have been used to provide Center Opportunity for Improvement reports through VQI where centers can identify if they are selecting patients with risk factors for stroke or mortality more often compared to other centers,” Dr. DeMartino said. “This allows centers to see where opportunities for improvement exist.”
Also, physicians can see the proportion of patients they select with a predicted mortality risk over 5% at one year – “a group of patients who may gain little benefit from prophylactic CEA,” he said. “Physicians can compare their patient selection to those in their region or nationally.”
Dr. DeMartino had no relationships to disclose.
COLUMBUS, OHIO – Carotid endarterectomy is an effective treatment for people with asymptomatic carotid artery disease when stroke rates are low and they survive long enough to benefit from the treatment. But determining who those patients are can be a challenge for vascular surgeons. A team of vascular specialists from around the country have developed risk prediction models to help surgeons better select asymptomatic patients for the procedure, Randall DeMartino, MD, said at the annual meeting of the Midwestern Vascular Surgical Society.
“These models will be used for mobile apps and web-based applications for point of care patient risk assessment,” said Dr. DeMartino of the Mayo Clinic in Rochester, Minn. He is the lead researcher for the study, which uses data from the Vascular Quality Initiative (VQI).
In developing the models, the researchers sampled asymptomatic patients in the VQI who had first-time elective CEA. There were 31,939 patients in the stroke analysis who had CEA from 2010-2015, and 24,086 patients in the mortality analysis who had procedures from 2010-2014. Dr. DeMartino and his colleagues evaluated all preoperative patient and surgeon characteristics, then used an algorithm to optimize the variables that were selected for the final logistic model.
The researchers also evaluated 30-day stroke rates and 1-year mortality at participating centers and found wide variability: an average of 0.9% for stroke, with a range of 0-8.3%; and 3.2% for mortality, with a range of 0-20%. “Actually, 22% of centers had a 1-year mortality rate that exceeded 5%,” Dr. DeMartino said.
The model for 1-year mortality identified the following variables associated with the highest risk of death 1 year after CEA: age greater than or equal to 80 years; a preoperative hemoglobin less than 10 mg/dL; oxygen-dependent chronic obstructive pulmonary disease; mild to severe congestive heart failure; American Society of Anesthesiologists classification of IV or V; stage 4 or 5 chronic kidney disease; and a contralateral occlusion.
“Conversely, a normal stress test, when performed, and preoperative statin use were associated with reduced risk of death over a year,” Dr. DeMartino said.
“These data have been used to provide Center Opportunity for Improvement reports through VQI where centers can identify if they are selecting patients with risk factors for stroke or mortality more often compared to other centers,” Dr. DeMartino said. “This allows centers to see where opportunities for improvement exist.”
Also, physicians can see the proportion of patients they select with a predicted mortality risk over 5% at one year – “a group of patients who may gain little benefit from prophylactic CEA,” he said. “Physicians can compare their patient selection to those in their region or nationally.”
Dr. DeMartino had no relationships to disclose.
AT MIDWESTERN VASCULAR 2016
Key clinical point: Risk-prediction models may identify patients at greatest risk of stroke and 1-year death after carotid endarterectomy (CEA).
Major finding: Contralateral occlusion has odds ratios of 2.5 for 30-day stroke after CEA and 1.7 for death at 1 year.
Data source: Sampling of patients from the Vascular Quality Initiative who had first-time CEA: 31,939 in the stroke analysis and 24,086 in the mortality analysis.
Disclosures: Dr. DeMartino reported having no financial disclosures.
Infection, readmission linked after open lower-extremity procedures
COLUMBUS, OHIO – Infections account for more than one-third of readmissions after endovascular lower-extremity procedures, but an analysis of these procedures over a 6-year period has identified a handful of factors, including an extended hospital stay, that may help vascular surgeons identify patients at greatest risk and reduce infection-related readmissions.
“Of a little over 7,000 patients that we evaluated with peripheral artery disease who underwent an elective lower-extremity procedure, we found an overall readmission rate of 10.9%; about 9.5% for those who underwent an open procedure and just over 12% for those who underwent an endovascular procedure,” Joseph C. Melvin, MD, of the University of Missouri Hospitals & Clinics in Columbia said at the annual meeting of the Midwestern Vascular Surgery Society.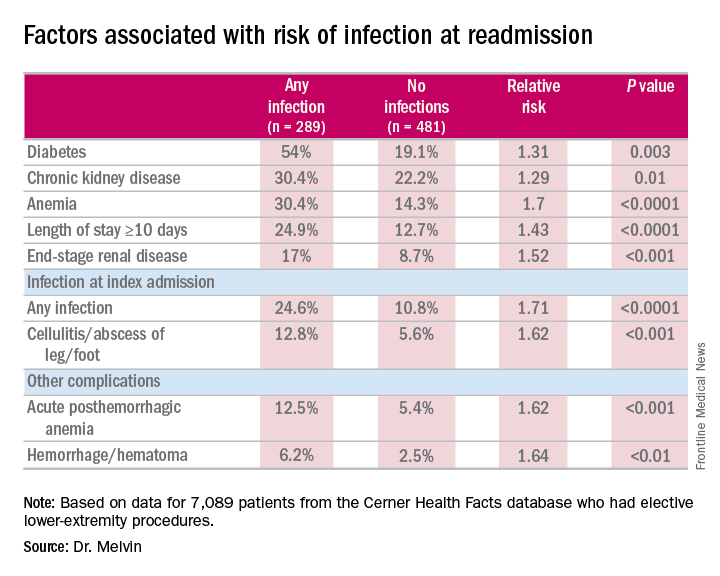
While the readmission rate for open operations was lower, the infection rate at readmission was higher for open procedures: 45.5% (157 of 345 readmissions) vs. 31.1% (132 of 425 readmissions), Dr. Melvin said.
“The risk factors for diagnosis of infection at readmission we found to be significant were anemia, chronic kidney disease, and end-stage renal disease, any infection at the time of the index admission, specifically cellulitis or abscess of the lower extremity given the patient’s peripheral artery disease status, diabetes, and then complications including posthemorrhagic anemia,” Dr. Melvin said. Laboratory testing values at the time of index admissions confirmed the risk factors.
The investigators also used multivariable logistic regression models in the analysis and found that factors most predictive of an infection-related readmission were length of stay, having the procedure at a teaching facility, anemia, and infection at the index admission, Dr. Melvin said.
The surgical site was the most common source of the infection, and Staphylococcus “not surprisingly” accounted for 25% of pathogens, Dr. Melvin said. “But what we did find to be interesting was that just over 40% of patients were found to have a gram-negative bacteria isolated, which would come into play with our decision with regards to antibiotic treatment,” he said.
The data suggest that further evaluation of ways to decrease postoperative infections and use of broad-spectrum antibiotics during readmissions may improve outcomes after open lower-extremity procedures, Dr. Melvin said.
Dr. Melvin had no financial relationships to disclose.
COLUMBUS, OHIO – Infections account for more than one-third of readmissions after endovascular lower-extremity procedures, but an analysis of these procedures over a 6-year period has identified a handful of factors, including an extended hospital stay, that may help vascular surgeons identify patients at greatest risk and reduce infection-related readmissions.
“Of a little over 7,000 patients that we evaluated with peripheral artery disease who underwent an elective lower-extremity procedure, we found an overall readmission rate of 10.9%; about 9.5% for those who underwent an open procedure and just over 12% for those who underwent an endovascular procedure,” Joseph C. Melvin, MD, of the University of Missouri Hospitals & Clinics in Columbia said at the annual meeting of the Midwestern Vascular Surgery Society.
While the readmission rate for open operations was lower, the infection rate at readmission was higher for open procedures: 45.5% (157 of 345 readmissions) vs. 31.1% (132 of 425 readmissions), Dr. Melvin said.
“The risk factors for diagnosis of infection at readmission we found to be significant were anemia, chronic kidney disease, and end-stage renal disease, any infection at the time of the index admission, specifically cellulitis or abscess of the lower extremity given the patient’s peripheral artery disease status, diabetes, and then complications including posthemorrhagic anemia,” Dr. Melvin said. Laboratory testing values at the time of index admissions confirmed the risk factors.
The investigators also used multivariable logistic regression models in the analysis and found that factors most predictive of an infection-related readmission were length of stay, having the procedure at a teaching facility, anemia, and infection at the index admission, Dr. Melvin said.
The surgical site was the most common source of the infection, and Staphylococcus “not surprisingly” accounted for 25% of pathogens, Dr. Melvin said. “But what we did find to be interesting was that just over 40% of patients were found to have a gram-negative bacteria isolated, which would come into play with our decision with regards to antibiotic treatment,” he said.
The data suggest that further evaluation of ways to decrease postoperative infections and use of broad-spectrum antibiotics during readmissions may improve outcomes after open lower-extremity procedures, Dr. Melvin said.
Dr. Melvin had no financial relationships to disclose.
COLUMBUS, OHIO – Infections account for more than one-third of readmissions after endovascular lower-extremity procedures, but an analysis of these procedures over a 6-year period has identified a handful of factors, including an extended hospital stay, that may help vascular surgeons identify patients at greatest risk and reduce infection-related readmissions.
“Of a little over 7,000 patients that we evaluated with peripheral artery disease who underwent an elective lower-extremity procedure, we found an overall readmission rate of 10.9%; about 9.5% for those who underwent an open procedure and just over 12% for those who underwent an endovascular procedure,” Joseph C. Melvin, MD, of the University of Missouri Hospitals & Clinics in Columbia said at the annual meeting of the Midwestern Vascular Surgery Society.
While the readmission rate for open operations was lower, the infection rate at readmission was higher for open procedures: 45.5% (157 of 345 readmissions) vs. 31.1% (132 of 425 readmissions), Dr. Melvin said.
“The risk factors for diagnosis of infection at readmission we found to be significant were anemia, chronic kidney disease, and end-stage renal disease, any infection at the time of the index admission, specifically cellulitis or abscess of the lower extremity given the patient’s peripheral artery disease status, diabetes, and then complications including posthemorrhagic anemia,” Dr. Melvin said. Laboratory testing values at the time of index admissions confirmed the risk factors.
The investigators also used multivariable logistic regression models in the analysis and found that factors most predictive of an infection-related readmission were length of stay, having the procedure at a teaching facility, anemia, and infection at the index admission, Dr. Melvin said.
The surgical site was the most common source of the infection, and Staphylococcus “not surprisingly” accounted for 25% of pathogens, Dr. Melvin said. “But what we did find to be interesting was that just over 40% of patients were found to have a gram-negative bacteria isolated, which would come into play with our decision with regards to antibiotic treatment,” he said.
The data suggest that further evaluation of ways to decrease postoperative infections and use of broad-spectrum antibiotics during readmissions may improve outcomes after open lower-extremity procedures, Dr. Melvin said.
Dr. Melvin had no financial relationships to disclose.
AT MIDWESTERN VASCULAR 2016
Key clinical point: Extended hospital stay and other factors can help identify patients at greatest risk for readmission due to infection.
Major finding: More than one-third of readmissions from lower-extremity procedures are the result of infections.
Data source: 7,089 elective lower extremity procedures selected from the Cerner Health Facts database.
Disclosures: Dr. Melvin reported having no financial disclosures.
Can carotid interventions affect cognitive function?
COLUMBUS, OHIO – The primary goal of carotid artery revascularization is to prevent stroke, heart attack or death, but carotid artery stenting and carotid endarterectomy may also cause changes in cognitive skills, according Raghu Motaganahalli, MD, of the Indiana University, Indianapolis.
“What about cognitive dysfunction as a result of carotid artery stenting (CAS) or carotid endarterectomy (CEA)?” Dr. Motaganahalli asked at the annual meeting of the Midwestern Vascular Surgical Society. “I think this is real, that there’s some truth to the matter. The question is how much and what domains of cognitive functions are affected?”

“Cerebrovascular hemodynamics status plays a role in cognitive function, but we need a better understanding of cerebrovascular hemodynamic failure and either improvement or decline of cognitive function after CAS or CEA,” he said.
A review of published trials shows that 10%-20% of patients who have either CAS or CEA have some degree of cognitive dysfunction as early as a day after the procedure. “It’s not a small number, compared to stoke, risk of myocardial infarction and death,” he said.
Some series have reported up to 40% of patients showed some cognitive dysfunction, and post–carotid endarterectomy cognitive dysfunction has been associated with early death, Dr. Motaganahalli said.
Cognitive dysfunction manifests in various forms, ranging from level of consciousness and memory to mood and ability to make calculations. Although the Mini-Mental State Examination Global Cognitive Assessment tool provides a method for evaluating cognitive function, “There is no uniformly accepted neurocognition test,” Dr. Motaganahalli said. That explains the wide variability of findings among published studies.
Vascular surgeons take a somewhat casual approach to their patients’ cognitive abilities after carotid revascularization, Dr. Motaganahalli said. “We don’t evaluate their memory and their cognitive functions on post-op day one; we just look to see whether they have neurologic dysfunction up front and that they’re capable of going home after that.”
But predicting in advance which patients are predisposed to cognitive decline after the procedures is difficult, he said. He cited a systematic review of 32 studies published between 1990-2007 that showed variable results (Stroke. 2008;39:3116-27): 11 studies during 1990-2005 suggested cognition actually improved after CEA; 9 studies during 1994-2006 suggested the opposite; 4 trials during 1992-2005 suggested no change in cognition after CEA; 5 studies during 2003-2007 showed improvement in cognition after CAS; and 3 trials comparing CAS and CEA and cognition found no differences in how the two procedures affect cognition.
Dr. Motaganahalli also cited a systematic review of 37 studies, 18 of which examined CEA, 12 CAS and seven compared CEA and CAS, found that either cognitive improvement or impairment for CEA and CAS separately were 10–15% of patients (Cerebrovasc Dis Extra. 2014;4:132-48).
“We have 69 papers that looked at cognitive function alone, but unfortunately, we don’t know whether cognitive function really improved based on this data set,” he said. “None of them are making the argument so clearly that there is cognitive improvement after revascularization.”
The variability in study findings can be due to differences in methodologies, the types of psychometric tests used, statistical analyses and the timing of cognitive assessments, Dr. Motaganahalli said.
Cognitive impairment after stroke caused by carotid disease is better understood than is cognitive impairment in the absence of a major stroke, Dr. Motaganahalli said.
“The mechanisms of how carotid disease can cause the cognitive impairment are threefold: It could be microembolism and hypoperfusion, which together can cause white matter disease and thereby some cognitive dysfunction in the long term,” he said (Neuroimaging Clin N Am. 2007 Aug;17:313-24).
Functional neurons may be a biomarker of cognitive outcome, he said. Hypoperfusion of functional neurons may lead to hypofunctional neurons, which can increase cerebral blood flow and cerebral metabolic rate for oxygen (CMRO2), and thus improve cognition. However, when additional variables are introduced to the hypofunctional neurons – such as microembolism, white matter disease, and prolonged hypoperfusion – that can lead to neuronal infarction that, while increasing cerebral blood flow, causes no change in CMRO2 and, thus, no cognitive improvement. The interval between hypofunctional neurons and neuronal infarction “is the time to do the revascularization, as long as you can demonstrate that there may be some truth to matter that it influences cognition,” Dr. Motaganahalli said.
While vascular surgeons may not be able to predict who will have cognitive decline after carotid interventions, “There are some pointers for possibly picking those patients who may benefit,” Dr. Motaganahalli said.
That choice of patients revolves around recognizing that chronic ischemia induces and increases the severity of cognitive dysfunction. Therefore, incorporating the pathophysiology of chronic ischemia into the algorithm for carotid artery disease may provide an opportunity to extend the goals of carotid artery revascularization to include preventing or reversing cognitive decline, he said.
Dr. Motaganahalli disclosed he is a consultant to Silk Road Medical.
COLUMBUS, OHIO – The primary goal of carotid artery revascularization is to prevent stroke, heart attack or death, but carotid artery stenting and carotid endarterectomy may also cause changes in cognitive skills, according Raghu Motaganahalli, MD, of the Indiana University, Indianapolis.
“What about cognitive dysfunction as a result of carotid artery stenting (CAS) or carotid endarterectomy (CEA)?” Dr. Motaganahalli asked at the annual meeting of the Midwestern Vascular Surgical Society. “I think this is real, that there’s some truth to the matter. The question is how much and what domains of cognitive functions are affected?”
“Cerebrovascular hemodynamics status plays a role in cognitive function, but we need a better understanding of cerebrovascular hemodynamic failure and either improvement or decline of cognitive function after CAS or CEA,” he said.
A review of published trials shows that 10%-20% of patients who have either CAS or CEA have some degree of cognitive dysfunction as early as a day after the procedure. “It’s not a small number, compared to stoke, risk of myocardial infarction and death,” he said.
Some series have reported up to 40% of patients showed some cognitive dysfunction, and post–carotid endarterectomy cognitive dysfunction has been associated with early death, Dr. Motaganahalli said.
Cognitive dysfunction manifests in various forms, ranging from level of consciousness and memory to mood and ability to make calculations. Although the Mini-Mental State Examination Global Cognitive Assessment tool provides a method for evaluating cognitive function, “There is no uniformly accepted neurocognition test,” Dr. Motaganahalli said. That explains the wide variability of findings among published studies.
Vascular surgeons take a somewhat casual approach to their patients’ cognitive abilities after carotid revascularization, Dr. Motaganahalli said. “We don’t evaluate their memory and their cognitive functions on post-op day one; we just look to see whether they have neurologic dysfunction up front and that they’re capable of going home after that.”
But predicting in advance which patients are predisposed to cognitive decline after the procedures is difficult, he said. He cited a systematic review of 32 studies published between 1990-2007 that showed variable results (Stroke. 2008;39:3116-27): 11 studies during 1990-2005 suggested cognition actually improved after CEA; 9 studies during 1994-2006 suggested the opposite; 4 trials during 1992-2005 suggested no change in cognition after CEA; 5 studies during 2003-2007 showed improvement in cognition after CAS; and 3 trials comparing CAS and CEA and cognition found no differences in how the two procedures affect cognition.
Dr. Motaganahalli also cited a systematic review of 37 studies, 18 of which examined CEA, 12 CAS and seven compared CEA and CAS, found that either cognitive improvement or impairment for CEA and CAS separately were 10–15% of patients (Cerebrovasc Dis Extra. 2014;4:132-48).
“We have 69 papers that looked at cognitive function alone, but unfortunately, we don’t know whether cognitive function really improved based on this data set,” he said. “None of them are making the argument so clearly that there is cognitive improvement after revascularization.”
The variability in study findings can be due to differences in methodologies, the types of psychometric tests used, statistical analyses and the timing of cognitive assessments, Dr. Motaganahalli said.
Cognitive impairment after stroke caused by carotid disease is better understood than is cognitive impairment in the absence of a major stroke, Dr. Motaganahalli said.
“The mechanisms of how carotid disease can cause the cognitive impairment are threefold: It could be microembolism and hypoperfusion, which together can cause white matter disease and thereby some cognitive dysfunction in the long term,” he said (Neuroimaging Clin N Am. 2007 Aug;17:313-24).
Functional neurons may be a biomarker of cognitive outcome, he said. Hypoperfusion of functional neurons may lead to hypofunctional neurons, which can increase cerebral blood flow and cerebral metabolic rate for oxygen (CMRO2), and thus improve cognition. However, when additional variables are introduced to the hypofunctional neurons – such as microembolism, white matter disease, and prolonged hypoperfusion – that can lead to neuronal infarction that, while increasing cerebral blood flow, causes no change in CMRO2 and, thus, no cognitive improvement. The interval between hypofunctional neurons and neuronal infarction “is the time to do the revascularization, as long as you can demonstrate that there may be some truth to matter that it influences cognition,” Dr. Motaganahalli said.
While vascular surgeons may not be able to predict who will have cognitive decline after carotid interventions, “There are some pointers for possibly picking those patients who may benefit,” Dr. Motaganahalli said.
That choice of patients revolves around recognizing that chronic ischemia induces and increases the severity of cognitive dysfunction. Therefore, incorporating the pathophysiology of chronic ischemia into the algorithm for carotid artery disease may provide an opportunity to extend the goals of carotid artery revascularization to include preventing or reversing cognitive decline, he said.
Dr. Motaganahalli disclosed he is a consultant to Silk Road Medical.
COLUMBUS, OHIO – The primary goal of carotid artery revascularization is to prevent stroke, heart attack or death, but carotid artery stenting and carotid endarterectomy may also cause changes in cognitive skills, according Raghu Motaganahalli, MD, of the Indiana University, Indianapolis.
“What about cognitive dysfunction as a result of carotid artery stenting (CAS) or carotid endarterectomy (CEA)?” Dr. Motaganahalli asked at the annual meeting of the Midwestern Vascular Surgical Society. “I think this is real, that there’s some truth to the matter. The question is how much and what domains of cognitive functions are affected?”
“Cerebrovascular hemodynamics status plays a role in cognitive function, but we need a better understanding of cerebrovascular hemodynamic failure and either improvement or decline of cognitive function after CAS or CEA,” he said.
A review of published trials shows that 10%-20% of patients who have either CAS or CEA have some degree of cognitive dysfunction as early as a day after the procedure. “It’s not a small number, compared to stoke, risk of myocardial infarction and death,” he said.
Some series have reported up to 40% of patients showed some cognitive dysfunction, and post–carotid endarterectomy cognitive dysfunction has been associated with early death, Dr. Motaganahalli said.
Cognitive dysfunction manifests in various forms, ranging from level of consciousness and memory to mood and ability to make calculations. Although the Mini-Mental State Examination Global Cognitive Assessment tool provides a method for evaluating cognitive function, “There is no uniformly accepted neurocognition test,” Dr. Motaganahalli said. That explains the wide variability of findings among published studies.
Vascular surgeons take a somewhat casual approach to their patients’ cognitive abilities after carotid revascularization, Dr. Motaganahalli said. “We don’t evaluate their memory and their cognitive functions on post-op day one; we just look to see whether they have neurologic dysfunction up front and that they’re capable of going home after that.”
But predicting in advance which patients are predisposed to cognitive decline after the procedures is difficult, he said. He cited a systematic review of 32 studies published between 1990-2007 that showed variable results (Stroke. 2008;39:3116-27): 11 studies during 1990-2005 suggested cognition actually improved after CEA; 9 studies during 1994-2006 suggested the opposite; 4 trials during 1992-2005 suggested no change in cognition after CEA; 5 studies during 2003-2007 showed improvement in cognition after CAS; and 3 trials comparing CAS and CEA and cognition found no differences in how the two procedures affect cognition.
Dr. Motaganahalli also cited a systematic review of 37 studies, 18 of which examined CEA, 12 CAS and seven compared CEA and CAS, found that either cognitive improvement or impairment for CEA and CAS separately were 10–15% of patients (Cerebrovasc Dis Extra. 2014;4:132-48).
“We have 69 papers that looked at cognitive function alone, but unfortunately, we don’t know whether cognitive function really improved based on this data set,” he said. “None of them are making the argument so clearly that there is cognitive improvement after revascularization.”
The variability in study findings can be due to differences in methodologies, the types of psychometric tests used, statistical analyses and the timing of cognitive assessments, Dr. Motaganahalli said.
Cognitive impairment after stroke caused by carotid disease is better understood than is cognitive impairment in the absence of a major stroke, Dr. Motaganahalli said.
“The mechanisms of how carotid disease can cause the cognitive impairment are threefold: It could be microembolism and hypoperfusion, which together can cause white matter disease and thereby some cognitive dysfunction in the long term,” he said (Neuroimaging Clin N Am. 2007 Aug;17:313-24).
Functional neurons may be a biomarker of cognitive outcome, he said. Hypoperfusion of functional neurons may lead to hypofunctional neurons, which can increase cerebral blood flow and cerebral metabolic rate for oxygen (CMRO2), and thus improve cognition. However, when additional variables are introduced to the hypofunctional neurons – such as microembolism, white matter disease, and prolonged hypoperfusion – that can lead to neuronal infarction that, while increasing cerebral blood flow, causes no change in CMRO2 and, thus, no cognitive improvement. The interval between hypofunctional neurons and neuronal infarction “is the time to do the revascularization, as long as you can demonstrate that there may be some truth to matter that it influences cognition,” Dr. Motaganahalli said.
While vascular surgeons may not be able to predict who will have cognitive decline after carotid interventions, “There are some pointers for possibly picking those patients who may benefit,” Dr. Motaganahalli said.
That choice of patients revolves around recognizing that chronic ischemia induces and increases the severity of cognitive dysfunction. Therefore, incorporating the pathophysiology of chronic ischemia into the algorithm for carotid artery disease may provide an opportunity to extend the goals of carotid artery revascularization to include preventing or reversing cognitive decline, he said.
Dr. Motaganahalli disclosed he is a consultant to Silk Road Medical.
AT THE ANNUAL MEETING OF THE MIDWESTERN VASCULAR SURGERY SOCIETY
Key clinical point: Incorporating the pathophysiology of chronic ischemia into the algorithm for carotid artery disease could expand the goals of revascularization to encompass cognitive decline.
Major finding: Cerebrovascular hemodynamic status plays a role in cognitive function after carotid artery interventions, but the mechanisms of either improvement or decline need better understanding.
Data source: Systematic review of 32 papers on neurocognition after carotid interventions published between 1990-2007 and analysis of 37 studies of CAS or CEA or both published since 2007.
Disclosures: Dr. Motaganahalli disclosed he is a consultant to Silk Road Medical Inc.
Study identifies SSI risk factors after open LEB
COLUMBUS, OHIO – A study of vascular procedures at 35 Michigan hospitals has identified three risk factors for surgical site infection after lower-extremity bypass that hospitals and vascular surgery teams may be able to modify.
“Patients who had iodine-only skin antiseptic preparation, a high-peak intraoperative glucose, or long operative times were more likely to have substantially increased risk for surgical site infection (SSI),” Frank Davis, MD, of the University of Michigan said in reporting the study results at the annual meeting of the Midwestern Vascular Surgical Society. Those risk factors are modifiable, Dr. Davis said.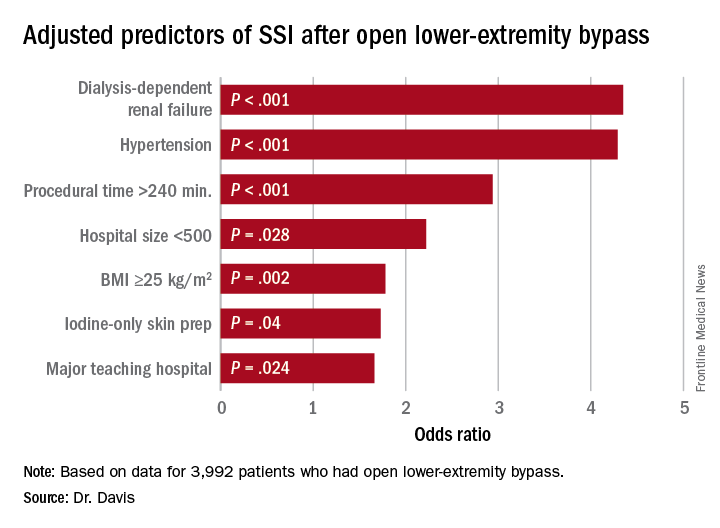
“Specific attention needs to be served moving forward in attempts to decrease the risk of SSI for lower-extremity bypass,” Dr. Davis said. “The incidence of SSI in our cohort across the state of Michigan was approximately 9.2%, and for those who did develop a SSI, there was a substantial increase in 30-day morbidity.”
Patients who had an SSI were more than three times more likely to have a major amputation (9% vs. 2.3%) than those without, and more than five times more likely to have a reoperation (3.9% vs. 0.7%), Dr. Davis said.
“With regard to preoperative symptomatology, those with lower peripheral artery questionnaire scores, resting pain, or acute ischemia were more likely to develop SSI postoperatively,” Dr. Davis said. “Patients who underwent an interim coronal bypass had a significant increase of SSI in comparison to all other bypass configurations.”
He also noted that major teaching hospitals or hospitals with 500 or fewer beds had higher rates of SSI.
“Targeted improvements in preoperative care may decrease complications and improve vascular patient outcomes,” Dr. Davis said.
Dr. Davis had no relationships to disclose.
COLUMBUS, OHIO – A study of vascular procedures at 35 Michigan hospitals has identified three risk factors for surgical site infection after lower-extremity bypass that hospitals and vascular surgery teams may be able to modify.
“Patients who had iodine-only skin antiseptic preparation, a high-peak intraoperative glucose, or long operative times were more likely to have substantially increased risk for surgical site infection (SSI),” Frank Davis, MD, of the University of Michigan said in reporting the study results at the annual meeting of the Midwestern Vascular Surgical Society. Those risk factors are modifiable, Dr. Davis said.
“Specific attention needs to be served moving forward in attempts to decrease the risk of SSI for lower-extremity bypass,” Dr. Davis said. “The incidence of SSI in our cohort across the state of Michigan was approximately 9.2%, and for those who did develop a SSI, there was a substantial increase in 30-day morbidity.”
Patients who had an SSI were more than three times more likely to have a major amputation (9% vs. 2.3%) than those without, and more than five times more likely to have a reoperation (3.9% vs. 0.7%), Dr. Davis said.
“With regard to preoperative symptomatology, those with lower peripheral artery questionnaire scores, resting pain, or acute ischemia were more likely to develop SSI postoperatively,” Dr. Davis said. “Patients who underwent an interim coronal bypass had a significant increase of SSI in comparison to all other bypass configurations.”
He also noted that major teaching hospitals or hospitals with 500 or fewer beds had higher rates of SSI.
“Targeted improvements in preoperative care may decrease complications and improve vascular patient outcomes,” Dr. Davis said.
Dr. Davis had no relationships to disclose.
COLUMBUS, OHIO – A study of vascular procedures at 35 Michigan hospitals has identified three risk factors for surgical site infection after lower-extremity bypass that hospitals and vascular surgery teams may be able to modify.
“Patients who had iodine-only skin antiseptic preparation, a high-peak intraoperative glucose, or long operative times were more likely to have substantially increased risk for surgical site infection (SSI),” Frank Davis, MD, of the University of Michigan said in reporting the study results at the annual meeting of the Midwestern Vascular Surgical Society. Those risk factors are modifiable, Dr. Davis said.
“Specific attention needs to be served moving forward in attempts to decrease the risk of SSI for lower-extremity bypass,” Dr. Davis said. “The incidence of SSI in our cohort across the state of Michigan was approximately 9.2%, and for those who did develop a SSI, there was a substantial increase in 30-day morbidity.”
Patients who had an SSI were more than three times more likely to have a major amputation (9% vs. 2.3%) than those without, and more than five times more likely to have a reoperation (3.9% vs. 0.7%), Dr. Davis said.
“With regard to preoperative symptomatology, those with lower peripheral artery questionnaire scores, resting pain, or acute ischemia were more likely to develop SSI postoperatively,” Dr. Davis said. “Patients who underwent an interim coronal bypass had a significant increase of SSI in comparison to all other bypass configurations.”
He also noted that major teaching hospitals or hospitals with 500 or fewer beds had higher rates of SSI.
“Targeted improvements in preoperative care may decrease complications and improve vascular patient outcomes,” Dr. Davis said.
Dr. Davis had no relationships to disclose.
AT MIDWESTERN VASCULAR 2016
Key clinical point: Study identified three key modifiable risk factors in surgical site infection (SSI) open after lower-extremity bypass (LEB).
Major finding: Incidence of SSI was 9.2% in the study cohort.
Data source: Blue Cross Blue Shield Michigan Vascular Intervention Collaborative database of 3,992 open LEB operations at 35 centers from January 2012 to June 2015.
Disclosures: Dr. Davis reported having no financial disclosures.
Using CHIMPS for type A dissection in a high-risk patient
Traditional open repair for type A aortic dissection in patients with Marfan syndrome and a previous cardiovascular surgery carries a high risk of morbidity and mortality, but a team of surgeons from China have reported on a hybrid technique that combines open and endovascular approaches to repair type A dissection in a patient with Marfan syndrome.
In the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:1191-3), Hong-wei Zhang, MD, and colleagues from West China Hospital of Sichuan University, explained their technique using chimney and sandwich grafts to repair a type A dissection in the patient late after Bentall surgery. “With great advancements in recent thoracic endovascular aortic repair technology, innovative hybrid operations combining open and endovascular techniques hold promising potential to expand treatment options,” Dr. Zhang and coauthors said.
They reported on a 33-year-old male with Marfan syndrome (MFS) who had elective aortic root and mechanical valve replacement 10 years earlier. Three days of persistent chest and back pain caused the patient to go to the emergency department, where computed tomography angiography (CTA) confirmed a type A aortic dissection from the distal ascending aorta to the iliac arteries and involving the proximal innominate artery and left common carotid artery (LCCA).
Because the patient refused another open surgery, Dr. Zhang and colleagues executed their hybrid approach, the first step of which was to create an LCCA-left axillar artery bypass with a 6-mm Gore-Tex graft (W.L. Gore & Associates). After they led the graft through the costoclavicular passage, they introduced the first (distal) thoracic stent (Valiant Captivia, Medtronic) from the right femoral artery and deployed it at the proximal descending aorta. They then inserted the second (proximal) thoracic stent graft into the previous ascending synthetic graft.
Next, they delivered the chimney grafts, two Fluency Plus covered stents (Bard Peripheral Vascular), from the right brachial and innominate artery into the ascending graft. Then they delivered two more Fluency grafts from the LCCA into the endolumen of the first (distal) thoracic stent graft.
After they deployed the second (proximal) thoracic stent graft, they deployed the precisely positioned stent grafts from the innominate artery and the LCCA, sandwiching the covered stents for the LCCA between the two thoracic stent grafts. They then occluded the left subclavian artery with a 10-mm double-disk vascular occlude.
Upon angiography at completion, Dr. Zhang and coauthors found an endoleak from the overlap zones between the two thoracic stent grafts.
However, the patient’s postoperative course was uneventful, and CTA 5 days after surgery showed complete sealing of the primary entry tear with patent chimney and sandwich grafts. The patient remained symptom-free at 30 days, when CTA again confirmed patency of the supra-arch grafts.
Dr. Zhang and coauthors acknowledge that carotid-to-carotid bypass could have been an alternative in order to use fewer stent grafts and to reduce the risk of endoleaks in this case, but they opted for this approach because of the dissection of the proximal innominate artery and LCCA and their concern of the long-term patency of a carotid-to-carotid bypass. “To our knowledge, this is the first reported case of a hybrid treatment for new-onset, type A aortic dissection in patients with MFS with a previous Bentall procedure,” Dr. Zhang and coauthors said. “Although further staged repairs are required in our case, this endovascular technique could be an effective and life-saving treatment option for the high-risk repeated surgical patients with MFS.”
Dr. Zhang and coauthors had no financial relationships to disclose.
In their invited commentary, Lars Svensson, MD, PhD, Matthew Eagleton, MD, and Eric Roselli, MD, of the Cleveland Clinic, said the approach Dr. Zhang and colleagues reported on is one of the “novel” endovascular CHIMPS methods for aortic arch repair – CHIMPS meaning chimneys, periscopes, snorkels, and sandwiches (J Thorac Cardiovasc Surg. 2016;152:958-9). But they noted that one of the ongoing challenges with these types of parallel grafts is the gutter leaks that occur between the sandwich grafts.
The commentators noted that CHIMPS procedures are easier alternatives to using spiral branch graft stents for the thoracoabdominal aorta or direct-connecting branch stems from an aortic stent in the arch, but they added, “An important caveat is that the blood supply maintenance and long-term durability may not be adequate.”
The patient Dr. Zhang and colleagues reported on “is young and will need a durable operation,” Dr. Svensson, Dr. Eagleton, and Dr. Roselli said. “Unfortunately, in our experience over time we have observed that these CHIMPS procedures tend to break down and leak into the arch, including the arch actually rupturing,” they said. These patients will need “intensive” monitoring. What’s more, patients with Marfan syndrome are prone to aneurysm formation “and are not good candidates for stenting,” the commentators said.
“Nevertheless, further engineering iterations of CHIMPS may address the problem with gutter leaks and become an alternative to the elephant trunk procedure for those patients who are at particularly high risk,” the commentators said.
Dr. Svensson disclosed he holds a patent with potential royalties for an aortic valve and aortic root stent graft with connecting branch grafts to the coronary ostia. Dr. Roselli is a consultant and investigator for Bolton, Gore, and Medtronic. Dr. Eagleton has no relationships to disclose.
In their invited commentary, Lars Svensson, MD, PhD, Matthew Eagleton, MD, and Eric Roselli, MD, of the Cleveland Clinic, said the approach Dr. Zhang and colleagues reported on is one of the “novel” endovascular CHIMPS methods for aortic arch repair – CHIMPS meaning chimneys, periscopes, snorkels, and sandwiches (J Thorac Cardiovasc Surg. 2016;152:958-9). But they noted that one of the ongoing challenges with these types of parallel grafts is the gutter leaks that occur between the sandwich grafts.
The commentators noted that CHIMPS procedures are easier alternatives to using spiral branch graft stents for the thoracoabdominal aorta or direct-connecting branch stems from an aortic stent in the arch, but they added, “An important caveat is that the blood supply maintenance and long-term durability may not be adequate.”
The patient Dr. Zhang and colleagues reported on “is young and will need a durable operation,” Dr. Svensson, Dr. Eagleton, and Dr. Roselli said. “Unfortunately, in our experience over time we have observed that these CHIMPS procedures tend to break down and leak into the arch, including the arch actually rupturing,” they said. These patients will need “intensive” monitoring. What’s more, patients with Marfan syndrome are prone to aneurysm formation “and are not good candidates for stenting,” the commentators said.
“Nevertheless, further engineering iterations of CHIMPS may address the problem with gutter leaks and become an alternative to the elephant trunk procedure for those patients who are at particularly high risk,” the commentators said.
Dr. Svensson disclosed he holds a patent with potential royalties for an aortic valve and aortic root stent graft with connecting branch grafts to the coronary ostia. Dr. Roselli is a consultant and investigator for Bolton, Gore, and Medtronic. Dr. Eagleton has no relationships to disclose.
In their invited commentary, Lars Svensson, MD, PhD, Matthew Eagleton, MD, and Eric Roselli, MD, of the Cleveland Clinic, said the approach Dr. Zhang and colleagues reported on is one of the “novel” endovascular CHIMPS methods for aortic arch repair – CHIMPS meaning chimneys, periscopes, snorkels, and sandwiches (J Thorac Cardiovasc Surg. 2016;152:958-9). But they noted that one of the ongoing challenges with these types of parallel grafts is the gutter leaks that occur between the sandwich grafts.
The commentators noted that CHIMPS procedures are easier alternatives to using spiral branch graft stents for the thoracoabdominal aorta or direct-connecting branch stems from an aortic stent in the arch, but they added, “An important caveat is that the blood supply maintenance and long-term durability may not be adequate.”
The patient Dr. Zhang and colleagues reported on “is young and will need a durable operation,” Dr. Svensson, Dr. Eagleton, and Dr. Roselli said. “Unfortunately, in our experience over time we have observed that these CHIMPS procedures tend to break down and leak into the arch, including the arch actually rupturing,” they said. These patients will need “intensive” monitoring. What’s more, patients with Marfan syndrome are prone to aneurysm formation “and are not good candidates for stenting,” the commentators said.
“Nevertheless, further engineering iterations of CHIMPS may address the problem with gutter leaks and become an alternative to the elephant trunk procedure for those patients who are at particularly high risk,” the commentators said.
Dr. Svensson disclosed he holds a patent with potential royalties for an aortic valve and aortic root stent graft with connecting branch grafts to the coronary ostia. Dr. Roselli is a consultant and investigator for Bolton, Gore, and Medtronic. Dr. Eagleton has no relationships to disclose.
Traditional open repair for type A aortic dissection in patients with Marfan syndrome and a previous cardiovascular surgery carries a high risk of morbidity and mortality, but a team of surgeons from China have reported on a hybrid technique that combines open and endovascular approaches to repair type A dissection in a patient with Marfan syndrome.
In the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:1191-3), Hong-wei Zhang, MD, and colleagues from West China Hospital of Sichuan University, explained their technique using chimney and sandwich grafts to repair a type A dissection in the patient late after Bentall surgery. “With great advancements in recent thoracic endovascular aortic repair technology, innovative hybrid operations combining open and endovascular techniques hold promising potential to expand treatment options,” Dr. Zhang and coauthors said.
They reported on a 33-year-old male with Marfan syndrome (MFS) who had elective aortic root and mechanical valve replacement 10 years earlier. Three days of persistent chest and back pain caused the patient to go to the emergency department, where computed tomography angiography (CTA) confirmed a type A aortic dissection from the distal ascending aorta to the iliac arteries and involving the proximal innominate artery and left common carotid artery (LCCA).
Because the patient refused another open surgery, Dr. Zhang and colleagues executed their hybrid approach, the first step of which was to create an LCCA-left axillar artery bypass with a 6-mm Gore-Tex graft (W.L. Gore & Associates). After they led the graft through the costoclavicular passage, they introduced the first (distal) thoracic stent (Valiant Captivia, Medtronic) from the right femoral artery and deployed it at the proximal descending aorta. They then inserted the second (proximal) thoracic stent graft into the previous ascending synthetic graft.
Next, they delivered the chimney grafts, two Fluency Plus covered stents (Bard Peripheral Vascular), from the right brachial and innominate artery into the ascending graft. Then they delivered two more Fluency grafts from the LCCA into the endolumen of the first (distal) thoracic stent graft.
After they deployed the second (proximal) thoracic stent graft, they deployed the precisely positioned stent grafts from the innominate artery and the LCCA, sandwiching the covered stents for the LCCA between the two thoracic stent grafts. They then occluded the left subclavian artery with a 10-mm double-disk vascular occlude.
Upon angiography at completion, Dr. Zhang and coauthors found an endoleak from the overlap zones between the two thoracic stent grafts.
However, the patient’s postoperative course was uneventful, and CTA 5 days after surgery showed complete sealing of the primary entry tear with patent chimney and sandwich grafts. The patient remained symptom-free at 30 days, when CTA again confirmed patency of the supra-arch grafts.
Dr. Zhang and coauthors acknowledge that carotid-to-carotid bypass could have been an alternative in order to use fewer stent grafts and to reduce the risk of endoleaks in this case, but they opted for this approach because of the dissection of the proximal innominate artery and LCCA and their concern of the long-term patency of a carotid-to-carotid bypass. “To our knowledge, this is the first reported case of a hybrid treatment for new-onset, type A aortic dissection in patients with MFS with a previous Bentall procedure,” Dr. Zhang and coauthors said. “Although further staged repairs are required in our case, this endovascular technique could be an effective and life-saving treatment option for the high-risk repeated surgical patients with MFS.”
Dr. Zhang and coauthors had no financial relationships to disclose.
Traditional open repair for type A aortic dissection in patients with Marfan syndrome and a previous cardiovascular surgery carries a high risk of morbidity and mortality, but a team of surgeons from China have reported on a hybrid technique that combines open and endovascular approaches to repair type A dissection in a patient with Marfan syndrome.
In the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:1191-3), Hong-wei Zhang, MD, and colleagues from West China Hospital of Sichuan University, explained their technique using chimney and sandwich grafts to repair a type A dissection in the patient late after Bentall surgery. “With great advancements in recent thoracic endovascular aortic repair technology, innovative hybrid operations combining open and endovascular techniques hold promising potential to expand treatment options,” Dr. Zhang and coauthors said.
They reported on a 33-year-old male with Marfan syndrome (MFS) who had elective aortic root and mechanical valve replacement 10 years earlier. Three days of persistent chest and back pain caused the patient to go to the emergency department, where computed tomography angiography (CTA) confirmed a type A aortic dissection from the distal ascending aorta to the iliac arteries and involving the proximal innominate artery and left common carotid artery (LCCA).
Because the patient refused another open surgery, Dr. Zhang and colleagues executed their hybrid approach, the first step of which was to create an LCCA-left axillar artery bypass with a 6-mm Gore-Tex graft (W.L. Gore & Associates). After they led the graft through the costoclavicular passage, they introduced the first (distal) thoracic stent (Valiant Captivia, Medtronic) from the right femoral artery and deployed it at the proximal descending aorta. They then inserted the second (proximal) thoracic stent graft into the previous ascending synthetic graft.
Next, they delivered the chimney grafts, two Fluency Plus covered stents (Bard Peripheral Vascular), from the right brachial and innominate artery into the ascending graft. Then they delivered two more Fluency grafts from the LCCA into the endolumen of the first (distal) thoracic stent graft.
After they deployed the second (proximal) thoracic stent graft, they deployed the precisely positioned stent grafts from the innominate artery and the LCCA, sandwiching the covered stents for the LCCA between the two thoracic stent grafts. They then occluded the left subclavian artery with a 10-mm double-disk vascular occlude.
Upon angiography at completion, Dr. Zhang and coauthors found an endoleak from the overlap zones between the two thoracic stent grafts.
However, the patient’s postoperative course was uneventful, and CTA 5 days after surgery showed complete sealing of the primary entry tear with patent chimney and sandwich grafts. The patient remained symptom-free at 30 days, when CTA again confirmed patency of the supra-arch grafts.
Dr. Zhang and coauthors acknowledge that carotid-to-carotid bypass could have been an alternative in order to use fewer stent grafts and to reduce the risk of endoleaks in this case, but they opted for this approach because of the dissection of the proximal innominate artery and LCCA and their concern of the long-term patency of a carotid-to-carotid bypass. “To our knowledge, this is the first reported case of a hybrid treatment for new-onset, type A aortic dissection in patients with MFS with a previous Bentall procedure,” Dr. Zhang and coauthors said. “Although further staged repairs are required in our case, this endovascular technique could be an effective and life-saving treatment option for the high-risk repeated surgical patients with MFS.”
Dr. Zhang and coauthors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Chimney and sandwich grafts facilitate hybrid repair of type A aortic dissection for a Marfan syndrome patient after Bentall surgery.
Major finding: A 33-year-old male with Marfan syndrome and a history of cardiac surgery was asymptomatic 30 days after hybrid repair for type A aortic dissection.
Data source: Case report of single patient at an academic medical center.
Disclosures: Dr. Zhang and coauthors reported having no financial disclosures.
Newborns with CHD have reduced cerebral oxygen delivery
Using a newer form of MRI to investigate oxygen levels in newborns with congenital heart disease, researchers in Canada reported that these patients may have impaired brain growth and development in the first weeks of life because of significantly lower cerebral oxygen delivery levels.
These findings suggest that oxygen delivery may impact brain growth, particularly in newborns with single-ventricle physiology, reported Jessie Mei Lim, BSc, of the University of Toronto, and her colleagues from McGill University, Montreal, and the Hospital for Sick Children, Toronto. The findings were published in the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:1095-103). Ms. Lim and her colleagues used cine phase-contrast (PC) MRI to measure cerebral blood flow in newborns with congenital heard disease (CHD). Previous studies used optical measures of tissue oxygenation and MRI arterial spin labeling to suggests that newborns with severe CHD have impaired CBF and cerebral oxygen delivery (CDO2) and CBF.
This single-center study involved 63 newborns from June 2013 to April 2015 at the Hospital for Sick Children. These subjects received an MRI of the head before surgery at an average of age 7.5 days. The scans were done without sedation or contrast while the infants were asleep. The study compared 31 age-matched controls with 32 subjects with various forms of CHD – 12 were managed surgically along a single-ventricle pathway (SVP), 4 had coarctation of the aorta, 13 had transposition of the great arteries (TGA), and 3 had other forms of CHD.
The researchers validated their method by reporting similarities between flows in the basilar and vertebral arteries in 14 controls, “suggesting good consistency and accuracy of our method for measuring CBF,” Ms. Lim and her coauthors noted. A comparison of CBF measured with an unpaired Student t test revealed no significant differences between the CHD group and controls. The average net CBF in CHD patients was 103.5 mL/min vs. 119.7 mL/min in controls.
However, when evaluating CDO2 using a Student t test, the researchers found significantly lower levels in the CHD group – an average of 1,1881 mLO2/min. vs. 2,712 mL O2/min in controls (P less than .0001). And when the researchers indexed CDO2 to brain volume yielding indexed oxygen delivery, the difference between the two groups was still significant: an average of 523.1 mL O2/min-1 .100 g-1 in the CHD group and 685.6 mL O2/min-1.100 g-1 in controls (P = .0006).
Among the CHD group, those with SVP and TGA had significantly lower CDO2 than that of controls. Brain volumes were also lower in those with CHD (mean of 338.5 mL vs. 377.7 mL in controls, P = .002).
The MRI findings were telling in the study population, Ms. Lim and her coauthors said. Five subjects in the CHD group had a combination of diffuse excessive high-signal intensity (DEHSI) and white-matter injury (WMI), 10 had an isolated finding of DEHSI, two had WMI alone and five others had other minor brain abnormalities. But the control group had no abnormal findings on conventional brain MRI.
The researchers acknowledged that, while the impact of reduced cerebral oxygen delivery is unknown, “theoretical reasons for thinking it might adversely impact ongoing brain growth and development during this period of rapid brain growth are considered.”
Cardiovascular surgeons should consider these findings when deciding on when to operate on newborns with CHD, the researchers said. “Further support for the concept that such a mechanism could lead to irreversible deficits in brain growth and development might result in attempts to expedite surgical repair of congenital cardiac lesions, which have conventionally not been addressed in the neonatal period,” they wrote.
Ms. Lim and her coauthors had no financial relationships to disclose.
Congenital heart disease (CHD) is heterogeneous and different types of lesions may cause different hemodynamics, Caitlin K. Rollins, MD, of Boston Children’s Hospital and Harvard Medical School said in her invited commentary (J Thorac Cardiovasc Surg. 2016;152-960-1).
Ms. Lim and her colleagues in this study confirmed that premise with their finding that newborns with CHD and controls had similar cerebral blood flow, but that those with CHD had reduced oxygen delivery. “These differences were most apparent in the neonates with single-ventricle physiology and transposition of the great arteries,” Dr. Rollins said. The study authors’ finding of an association between reduced oxygen delivery and impaired brain development, along with this group’s previous reports (Circulation 2015;131:1313-23) suggesting preserved cerebral blood flow in the late prenatal period, differ from other studies using traditional methods to show reduced cerebral blood flow in obstructive left-sided lesions, Dr. Rollins said. “Although technical differences may in part account for the discrepancy, the contrasting results also reflect that the relative contributions of abnormal cerebral blood flow and oxygenation differ among forms of CHD,” Dr. Rollins said.
Congenital heart disease (CHD) is heterogeneous and different types of lesions may cause different hemodynamics, Caitlin K. Rollins, MD, of Boston Children’s Hospital and Harvard Medical School said in her invited commentary (J Thorac Cardiovasc Surg. 2016;152-960-1).
Ms. Lim and her colleagues in this study confirmed that premise with their finding that newborns with CHD and controls had similar cerebral blood flow, but that those with CHD had reduced oxygen delivery. “These differences were most apparent in the neonates with single-ventricle physiology and transposition of the great arteries,” Dr. Rollins said. The study authors’ finding of an association between reduced oxygen delivery and impaired brain development, along with this group’s previous reports (Circulation 2015;131:1313-23) suggesting preserved cerebral blood flow in the late prenatal period, differ from other studies using traditional methods to show reduced cerebral blood flow in obstructive left-sided lesions, Dr. Rollins said. “Although technical differences may in part account for the discrepancy, the contrasting results also reflect that the relative contributions of abnormal cerebral blood flow and oxygenation differ among forms of CHD,” Dr. Rollins said.
Congenital heart disease (CHD) is heterogeneous and different types of lesions may cause different hemodynamics, Caitlin K. Rollins, MD, of Boston Children’s Hospital and Harvard Medical School said in her invited commentary (J Thorac Cardiovasc Surg. 2016;152-960-1).
Ms. Lim and her colleagues in this study confirmed that premise with their finding that newborns with CHD and controls had similar cerebral blood flow, but that those with CHD had reduced oxygen delivery. “These differences were most apparent in the neonates with single-ventricle physiology and transposition of the great arteries,” Dr. Rollins said. The study authors’ finding of an association between reduced oxygen delivery and impaired brain development, along with this group’s previous reports (Circulation 2015;131:1313-23) suggesting preserved cerebral blood flow in the late prenatal period, differ from other studies using traditional methods to show reduced cerebral blood flow in obstructive left-sided lesions, Dr. Rollins said. “Although technical differences may in part account for the discrepancy, the contrasting results also reflect that the relative contributions of abnormal cerebral blood flow and oxygenation differ among forms of CHD,” Dr. Rollins said.
Using a newer form of MRI to investigate oxygen levels in newborns with congenital heart disease, researchers in Canada reported that these patients may have impaired brain growth and development in the first weeks of life because of significantly lower cerebral oxygen delivery levels.
These findings suggest that oxygen delivery may impact brain growth, particularly in newborns with single-ventricle physiology, reported Jessie Mei Lim, BSc, of the University of Toronto, and her colleagues from McGill University, Montreal, and the Hospital for Sick Children, Toronto. The findings were published in the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:1095-103). Ms. Lim and her colleagues used cine phase-contrast (PC) MRI to measure cerebral blood flow in newborns with congenital heard disease (CHD). Previous studies used optical measures of tissue oxygenation and MRI arterial spin labeling to suggests that newborns with severe CHD have impaired CBF and cerebral oxygen delivery (CDO2) and CBF.
This single-center study involved 63 newborns from June 2013 to April 2015 at the Hospital for Sick Children. These subjects received an MRI of the head before surgery at an average of age 7.5 days. The scans were done without sedation or contrast while the infants were asleep. The study compared 31 age-matched controls with 32 subjects with various forms of CHD – 12 were managed surgically along a single-ventricle pathway (SVP), 4 had coarctation of the aorta, 13 had transposition of the great arteries (TGA), and 3 had other forms of CHD.
The researchers validated their method by reporting similarities between flows in the basilar and vertebral arteries in 14 controls, “suggesting good consistency and accuracy of our method for measuring CBF,” Ms. Lim and her coauthors noted. A comparison of CBF measured with an unpaired Student t test revealed no significant differences between the CHD group and controls. The average net CBF in CHD patients was 103.5 mL/min vs. 119.7 mL/min in controls.
However, when evaluating CDO2 using a Student t test, the researchers found significantly lower levels in the CHD group – an average of 1,1881 mLO2/min. vs. 2,712 mL O2/min in controls (P less than .0001). And when the researchers indexed CDO2 to brain volume yielding indexed oxygen delivery, the difference between the two groups was still significant: an average of 523.1 mL O2/min-1 .100 g-1 in the CHD group and 685.6 mL O2/min-1.100 g-1 in controls (P = .0006).
Among the CHD group, those with SVP and TGA had significantly lower CDO2 than that of controls. Brain volumes were also lower in those with CHD (mean of 338.5 mL vs. 377.7 mL in controls, P = .002).
The MRI findings were telling in the study population, Ms. Lim and her coauthors said. Five subjects in the CHD group had a combination of diffuse excessive high-signal intensity (DEHSI) and white-matter injury (WMI), 10 had an isolated finding of DEHSI, two had WMI alone and five others had other minor brain abnormalities. But the control group had no abnormal findings on conventional brain MRI.
The researchers acknowledged that, while the impact of reduced cerebral oxygen delivery is unknown, “theoretical reasons for thinking it might adversely impact ongoing brain growth and development during this period of rapid brain growth are considered.”
Cardiovascular surgeons should consider these findings when deciding on when to operate on newborns with CHD, the researchers said. “Further support for the concept that such a mechanism could lead to irreversible deficits in brain growth and development might result in attempts to expedite surgical repair of congenital cardiac lesions, which have conventionally not been addressed in the neonatal period,” they wrote.
Ms. Lim and her coauthors had no financial relationships to disclose.
Using a newer form of MRI to investigate oxygen levels in newborns with congenital heart disease, researchers in Canada reported that these patients may have impaired brain growth and development in the first weeks of life because of significantly lower cerebral oxygen delivery levels.
These findings suggest that oxygen delivery may impact brain growth, particularly in newborns with single-ventricle physiology, reported Jessie Mei Lim, BSc, of the University of Toronto, and her colleagues from McGill University, Montreal, and the Hospital for Sick Children, Toronto. The findings were published in the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:1095-103). Ms. Lim and her colleagues used cine phase-contrast (PC) MRI to measure cerebral blood flow in newborns with congenital heard disease (CHD). Previous studies used optical measures of tissue oxygenation and MRI arterial spin labeling to suggests that newborns with severe CHD have impaired CBF and cerebral oxygen delivery (CDO2) and CBF.
This single-center study involved 63 newborns from June 2013 to April 2015 at the Hospital for Sick Children. These subjects received an MRI of the head before surgery at an average of age 7.5 days. The scans were done without sedation or contrast while the infants were asleep. The study compared 31 age-matched controls with 32 subjects with various forms of CHD – 12 were managed surgically along a single-ventricle pathway (SVP), 4 had coarctation of the aorta, 13 had transposition of the great arteries (TGA), and 3 had other forms of CHD.
The researchers validated their method by reporting similarities between flows in the basilar and vertebral arteries in 14 controls, “suggesting good consistency and accuracy of our method for measuring CBF,” Ms. Lim and her coauthors noted. A comparison of CBF measured with an unpaired Student t test revealed no significant differences between the CHD group and controls. The average net CBF in CHD patients was 103.5 mL/min vs. 119.7 mL/min in controls.
However, when evaluating CDO2 using a Student t test, the researchers found significantly lower levels in the CHD group – an average of 1,1881 mLO2/min. vs. 2,712 mL O2/min in controls (P less than .0001). And when the researchers indexed CDO2 to brain volume yielding indexed oxygen delivery, the difference between the two groups was still significant: an average of 523.1 mL O2/min-1 .100 g-1 in the CHD group and 685.6 mL O2/min-1.100 g-1 in controls (P = .0006).
Among the CHD group, those with SVP and TGA had significantly lower CDO2 than that of controls. Brain volumes were also lower in those with CHD (mean of 338.5 mL vs. 377.7 mL in controls, P = .002).
The MRI findings were telling in the study population, Ms. Lim and her coauthors said. Five subjects in the CHD group had a combination of diffuse excessive high-signal intensity (DEHSI) and white-matter injury (WMI), 10 had an isolated finding of DEHSI, two had WMI alone and five others had other minor brain abnormalities. But the control group had no abnormal findings on conventional brain MRI.
The researchers acknowledged that, while the impact of reduced cerebral oxygen delivery is unknown, “theoretical reasons for thinking it might adversely impact ongoing brain growth and development during this period of rapid brain growth are considered.”
Cardiovascular surgeons should consider these findings when deciding on when to operate on newborns with CHD, the researchers said. “Further support for the concept that such a mechanism could lead to irreversible deficits in brain growth and development might result in attempts to expedite surgical repair of congenital cardiac lesions, which have conventionally not been addressed in the neonatal period,” they wrote.
Ms. Lim and her coauthors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Cerebral blood flow is maintained but cerebral oxygen delivery is decreased in preoperative newborns with cyanotic congenital heart disease (CHD).
Major finding: Average cerebral oxygen delivery measured 1,1881 mLO2/min in the CHD group when measured with Student t testing vs. 2,712 mLO2/min in controls (P less than .0001).
Data source: Single-center study of 32 neonates with various forms of CHD 31 age-matched controls.
Disclosures: Ms. Lim and coauthors have no financial relationships to disclose.