User login
AAN: Facial nerve stimulator relieves cluster headaches
WASHINGTON – An implantable device that stimulates the sphenopalatine ganglion nerve bundle either reduced or eliminated pain in 68% of more than 5,000 cluster headaches, a 3-year study has determined.
The device, which is approved in Europe, was more effective in attacks of moderate severity, with a 78% rate of pain reduction or elimination, Dr. Jose Miguel Lainez reported at the annual meeting of the American Academy of Neurology.
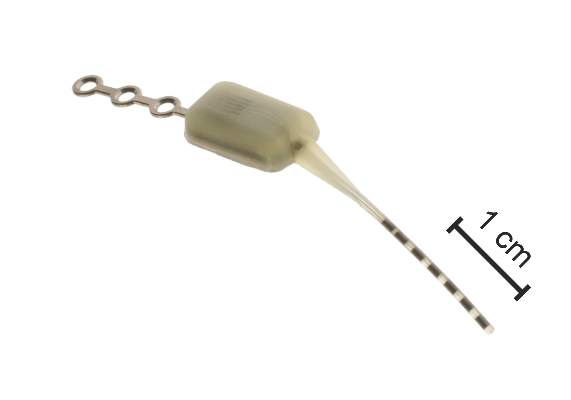
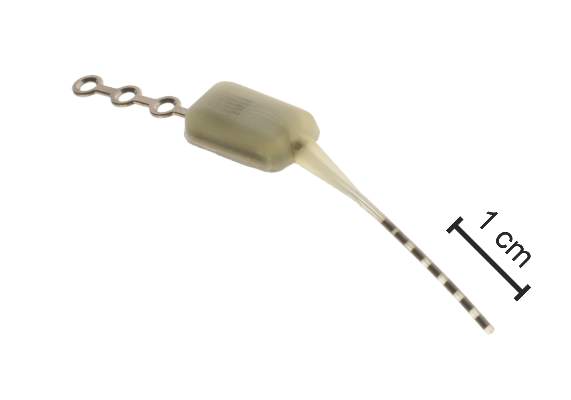
The Pulsante System, manufactured by Autonomic Technologiesof Redwood City, Calif., consists of a neurostimulator about the size of an almond, and a lead with six electrodes. It’s inserted under local anesthetic via a small incision in the upper gum on the side in which the patient experiences symptoms. The electrodes are positioned along the sphenopalatine ganglion (SPG) nerve and the neurostimulator is affixed to the zygomatic process.
A hand-held remote controller placed against the cheek activates the device and controls the intensity of stimulation, which is thought to work by blocking signals to the postganglionic parasympathetic fibers. Those fibers innervate facial structures and the cerebral and meningeal blood vessels and are implicated in the pain and accompanying autonomic symptoms of a cluster headache attack.
Dr. Lainez, professor of neurology at Catholic University of Valencia (Spain), presented 3-year follow-up data from Pathway CH-1, a randomized, sham-controlled trial of 43 patients with cluster headache. Of these, 33 completed the 3-year follow-up period. Of the remaining 10, 1 was lost from observation, 5 violated protocol, 1 had the device implanted incorrectly, and 3 had the device explanted because of incorrect placement or lead migration.
Most of the patients were male. Mean age was 41 years. They had a mean disease duration of 10 years and averaged 17 cluster headaches per week but ranged from 4 to 70 attacks per week. Over the 3 years, 5,130 attacks were treated; the mean stimulation duration for these was 14 minutes with a mean response time of 11 minutes. Therapy was considered effective in 65% (3,354) of these attacks based on a clinically meaningful reduction in pain or pain elimination.
Dr. Lainez did not parse these results. However, in the initial 28-week phase of the Pathway CH-1 study, pain was reduced in 68% of attacks treated with the device and 7% of those treated with the sham control. Pain freedom by 15 minutes was achieved in 34% of attacks with full stimulation, compared with 1.5% of those treated with sham.
In the follow-up study, the device seemed most effective in attacks of moderate severity (78% response rate of pain reduction or elimination). The response rate was 59% in mild attacks and 51% in severe attacks. Most attacks treated with the device (77%) did not involve the use of abortive therapy.
Dr. Lainez did not mention adverse events related to the device. However, in the 28-week study, there were 92, including parasthesias and numbness; facial and tooth pain; and swelling. Others were considered mild and included dry eye, nose bleed, and facial asymmetry.
The device is currently being investigated in a U.S. study. The open-label Pathway-CH2 study aims to recruit 120 patients. For information on Pathway CH-2, contact Anthony Caparso.
The trial was sponsored by Autonomic Technologies Inc. Dr. Lainez had no financial ties with the company.
On Twitter @alz_gal
WASHINGTON – An implantable device that stimulates the sphenopalatine ganglion nerve bundle either reduced or eliminated pain in 68% of more than 5,000 cluster headaches, a 3-year study has determined.
The device, which is approved in Europe, was more effective in attacks of moderate severity, with a 78% rate of pain reduction or elimination, Dr. Jose Miguel Lainez reported at the annual meeting of the American Academy of Neurology.
The Pulsante System, manufactured by Autonomic Technologiesof Redwood City, Calif., consists of a neurostimulator about the size of an almond, and a lead with six electrodes. It’s inserted under local anesthetic via a small incision in the upper gum on the side in which the patient experiences symptoms. The electrodes are positioned along the sphenopalatine ganglion (SPG) nerve and the neurostimulator is affixed to the zygomatic process.
A hand-held remote controller placed against the cheek activates the device and controls the intensity of stimulation, which is thought to work by blocking signals to the postganglionic parasympathetic fibers. Those fibers innervate facial structures and the cerebral and meningeal blood vessels and are implicated in the pain and accompanying autonomic symptoms of a cluster headache attack.
Dr. Lainez, professor of neurology at Catholic University of Valencia (Spain), presented 3-year follow-up data from Pathway CH-1, a randomized, sham-controlled trial of 43 patients with cluster headache. Of these, 33 completed the 3-year follow-up period. Of the remaining 10, 1 was lost from observation, 5 violated protocol, 1 had the device implanted incorrectly, and 3 had the device explanted because of incorrect placement or lead migration.
Most of the patients were male. Mean age was 41 years. They had a mean disease duration of 10 years and averaged 17 cluster headaches per week but ranged from 4 to 70 attacks per week. Over the 3 years, 5,130 attacks were treated; the mean stimulation duration for these was 14 minutes with a mean response time of 11 minutes. Therapy was considered effective in 65% (3,354) of these attacks based on a clinically meaningful reduction in pain or pain elimination.
Dr. Lainez did not parse these results. However, in the initial 28-week phase of the Pathway CH-1 study, pain was reduced in 68% of attacks treated with the device and 7% of those treated with the sham control. Pain freedom by 15 minutes was achieved in 34% of attacks with full stimulation, compared with 1.5% of those treated with sham.
In the follow-up study, the device seemed most effective in attacks of moderate severity (78% response rate of pain reduction or elimination). The response rate was 59% in mild attacks and 51% in severe attacks. Most attacks treated with the device (77%) did not involve the use of abortive therapy.
Dr. Lainez did not mention adverse events related to the device. However, in the 28-week study, there were 92, including parasthesias and numbness; facial and tooth pain; and swelling. Others were considered mild and included dry eye, nose bleed, and facial asymmetry.
The device is currently being investigated in a U.S. study. The open-label Pathway-CH2 study aims to recruit 120 patients. For information on Pathway CH-2, contact Anthony Caparso.
The trial was sponsored by Autonomic Technologies Inc. Dr. Lainez had no financial ties with the company.
On Twitter @alz_gal
WASHINGTON – An implantable device that stimulates the sphenopalatine ganglion nerve bundle either reduced or eliminated pain in 68% of more than 5,000 cluster headaches, a 3-year study has determined.
The device, which is approved in Europe, was more effective in attacks of moderate severity, with a 78% rate of pain reduction or elimination, Dr. Jose Miguel Lainez reported at the annual meeting of the American Academy of Neurology.
The Pulsante System, manufactured by Autonomic Technologiesof Redwood City, Calif., consists of a neurostimulator about the size of an almond, and a lead with six electrodes. It’s inserted under local anesthetic via a small incision in the upper gum on the side in which the patient experiences symptoms. The electrodes are positioned along the sphenopalatine ganglion (SPG) nerve and the neurostimulator is affixed to the zygomatic process.
A hand-held remote controller placed against the cheek activates the device and controls the intensity of stimulation, which is thought to work by blocking signals to the postganglionic parasympathetic fibers. Those fibers innervate facial structures and the cerebral and meningeal blood vessels and are implicated in the pain and accompanying autonomic symptoms of a cluster headache attack.
Dr. Lainez, professor of neurology at Catholic University of Valencia (Spain), presented 3-year follow-up data from Pathway CH-1, a randomized, sham-controlled trial of 43 patients with cluster headache. Of these, 33 completed the 3-year follow-up period. Of the remaining 10, 1 was lost from observation, 5 violated protocol, 1 had the device implanted incorrectly, and 3 had the device explanted because of incorrect placement or lead migration.
Most of the patients were male. Mean age was 41 years. They had a mean disease duration of 10 years and averaged 17 cluster headaches per week but ranged from 4 to 70 attacks per week. Over the 3 years, 5,130 attacks were treated; the mean stimulation duration for these was 14 minutes with a mean response time of 11 minutes. Therapy was considered effective in 65% (3,354) of these attacks based on a clinically meaningful reduction in pain or pain elimination.
Dr. Lainez did not parse these results. However, in the initial 28-week phase of the Pathway CH-1 study, pain was reduced in 68% of attacks treated with the device and 7% of those treated with the sham control. Pain freedom by 15 minutes was achieved in 34% of attacks with full stimulation, compared with 1.5% of those treated with sham.
In the follow-up study, the device seemed most effective in attacks of moderate severity (78% response rate of pain reduction or elimination). The response rate was 59% in mild attacks and 51% in severe attacks. Most attacks treated with the device (77%) did not involve the use of abortive therapy.
Dr. Lainez did not mention adverse events related to the device. However, in the 28-week study, there were 92, including parasthesias and numbness; facial and tooth pain; and swelling. Others were considered mild and included dry eye, nose bleed, and facial asymmetry.
The device is currently being investigated in a U.S. study. The open-label Pathway-CH2 study aims to recruit 120 patients. For information on Pathway CH-2, contact Anthony Caparso.
The trial was sponsored by Autonomic Technologies Inc. Dr. Lainez had no financial ties with the company.
On Twitter @alz_gal
AT THE AAN 2015 ANNUAL MEETING
Key clinical point: An implantable device that stimulates the sphenopalatine ganglion nerve provided pain relief in cluster headaches.
Major finding: The device reduced or eliminated pain in 68% of more than 5,000 cluster headaches.
Data source: A 3-year follow-up study that examined response in more than 5,000 cluster headaches.
Disclosures: The trial was sponsored by Autonomic Technologies Inc., which makes the Pulsante System. Dr. Lainez had no financial disclosures.
AAN: OnabotulinumtoxinA injections reduce migraine hospitalizations
WASHINGTON – OnabotulinumtoxinA injections significantly decreased both emergency department visits and hospitalizations for chronic migraine for up to 1 year among patients who had previously been admitted for the condition.
By 6 months after the first injection, ED visits were down 32% and hospitalizations were down 52%, Dr. Noah Rosen said at the annual meeting of the American Academy of Neurology.

Dr. Rosen of the Hofstra North Shore Headache Center in Great Neck, N.Y., based his findings on data from the MarketScan health resource utilization database, which captures about 66 million patient visits per year. The initial cohort included 3,840 patients who had a new diagnosis of chronic migraine with at least one subsequent onabotulinumtoxinA treatment within 6 months of diagnosis. These were followed for 1 year before the diagnosis and for 1 year after treatment began. The cohort comprised 1,831 patients at 6 months and 936 patients at 12 months.
Most (80%) of the population already had a diagnosis of migraine before the chronic migraine diagnosis; about half also had another headache disorder. They were a mean of 46 years old and were predominantly women. Depression was present in 20% and anxiety in about 11%. They also were taking one to three other headache medications, including triptans, opioids, nonsteroidal anti-inflammatory drugs, muscle relaxants, benzodiazepines, barbiturates, and ergots. The time from diagnosis to first injection was about a month, with subsequent injections 90 days apart.
The 6-month improvements in ED visits and hospitalizations remained steady, Dr. Rosen said. The reductions at 9 months in ED visits and hospitalizations were identical to those at 6 months. At 12 months, they had declined 25% and 47%, respectively, from baseline.
“This shows that the immediate benefits, which have been reported before, are maintained for at least a year,” he noted.
Dr. Rosen is on the speakers’ board and has been an advisor for Allergan and Zogenix. He also has received remuneration from Curelator.
On Twitter @alz_gal
WASHINGTON – OnabotulinumtoxinA injections significantly decreased both emergency department visits and hospitalizations for chronic migraine for up to 1 year among patients who had previously been admitted for the condition.
By 6 months after the first injection, ED visits were down 32% and hospitalizations were down 52%, Dr. Noah Rosen said at the annual meeting of the American Academy of Neurology.
Dr. Rosen of the Hofstra North Shore Headache Center in Great Neck, N.Y., based his findings on data from the MarketScan health resource utilization database, which captures about 66 million patient visits per year. The initial cohort included 3,840 patients who had a new diagnosis of chronic migraine with at least one subsequent onabotulinumtoxinA treatment within 6 months of diagnosis. These were followed for 1 year before the diagnosis and for 1 year after treatment began. The cohort comprised 1,831 patients at 6 months and 936 patients at 12 months.
Most (80%) of the population already had a diagnosis of migraine before the chronic migraine diagnosis; about half also had another headache disorder. They were a mean of 46 years old and were predominantly women. Depression was present in 20% and anxiety in about 11%. They also were taking one to three other headache medications, including triptans, opioids, nonsteroidal anti-inflammatory drugs, muscle relaxants, benzodiazepines, barbiturates, and ergots. The time from diagnosis to first injection was about a month, with subsequent injections 90 days apart.
The 6-month improvements in ED visits and hospitalizations remained steady, Dr. Rosen said. The reductions at 9 months in ED visits and hospitalizations were identical to those at 6 months. At 12 months, they had declined 25% and 47%, respectively, from baseline.
“This shows that the immediate benefits, which have been reported before, are maintained for at least a year,” he noted.
Dr. Rosen is on the speakers’ board and has been an advisor for Allergan and Zogenix. He also has received remuneration from Curelator.
On Twitter @alz_gal
WASHINGTON – OnabotulinumtoxinA injections significantly decreased both emergency department visits and hospitalizations for chronic migraine for up to 1 year among patients who had previously been admitted for the condition.
By 6 months after the first injection, ED visits were down 32% and hospitalizations were down 52%, Dr. Noah Rosen said at the annual meeting of the American Academy of Neurology.
Dr. Rosen of the Hofstra North Shore Headache Center in Great Neck, N.Y., based his findings on data from the MarketScan health resource utilization database, which captures about 66 million patient visits per year. The initial cohort included 3,840 patients who had a new diagnosis of chronic migraine with at least one subsequent onabotulinumtoxinA treatment within 6 months of diagnosis. These were followed for 1 year before the diagnosis and for 1 year after treatment began. The cohort comprised 1,831 patients at 6 months and 936 patients at 12 months.
Most (80%) of the population already had a diagnosis of migraine before the chronic migraine diagnosis; about half also had another headache disorder. They were a mean of 46 years old and were predominantly women. Depression was present in 20% and anxiety in about 11%. They also were taking one to three other headache medications, including triptans, opioids, nonsteroidal anti-inflammatory drugs, muscle relaxants, benzodiazepines, barbiturates, and ergots. The time from diagnosis to first injection was about a month, with subsequent injections 90 days apart.
The 6-month improvements in ED visits and hospitalizations remained steady, Dr. Rosen said. The reductions at 9 months in ED visits and hospitalizations were identical to those at 6 months. At 12 months, they had declined 25% and 47%, respectively, from baseline.
“This shows that the immediate benefits, which have been reported before, are maintained for at least a year,” he noted.
Dr. Rosen is on the speakers’ board and has been an advisor for Allergan and Zogenix. He also has received remuneration from Curelator.
On Twitter @alz_gal
AT THE AAN 2015 ANNUAL MEETING
Key clinical point: OnabotulinumtoxinA injections reduced hospital usage for chronic migraine for up to 1 year.
Major finding: By 6 months after the first injection, emergency dept. visits were down 32% and hospitalizations were down 52%. At 12 months, the reductions were 25% and 47% from baseline, respectively.
Data source: The retrospective database study comprised 3,840 patients.
Disclosures: Dr. Rosen is on the speakers’ board and has been an advisor for Allergan and Zogenix. He also has received remuneration from Curelator.

AAN: Intranasal sumatriptan powder works faster than tablet form
WASHINGTON – A low-dose intranasal sumatriptan powder worked faster than the 100-mg oral formulation on acute migraine, with a significantly lower rate of triptan-related chest tightening.
Additionally, the 22-mg powder formulation reduced or eliminated pain just as long as the 100-mg tablet did, with pain relief reported by 60% of each group and pain freedom by 50% at 48 hours, Dr. Stewart Tepper said at the annual meeting of the American Academy of Neurology.

“Oral was not superior to the powder in any of the efficacy outcomes” in the COMPASS trial, a phase III, placebo-controlled, crossover study, said Dr. Tepper of the Cleveland Clinic in Ohio.
Nor was the powder associated with the “foul” taste patients often complain of when they use a liquid sumatriptan nasal spray, he added.
The investigational drug, AVP-825 (Avanir Pharmaceuticals) is packaged in a unique intranasal delivery system. The breath-powered device holds a single-drug cartridge. Two cartridges equal one 22-mg dose; of this, about 16 mg are actually delivered.
Patients put the nasal piece into one nostril, seal their lips around a mouthpiece, and blow into it. “This elevates and closes the soft palate, so the powder doesn’t enter the oropharynx,” Dr. Tepper said. “The powder is delivered high into the nose. The top of the septum is open, so the breath comes out the other side.”
The trial enrolled 185 patients and assessed 1,531 migraines over 24 weeks. Patients were randomized to active powder or placebo tablet for 12 weeks or five migraines, and then crossed to placebo powder or active tablet. The primary endpoint was the change in SPID-30 (sum of pain intensity differences from baseline-30 minutes).
AVP-825 significantly outperformed oral sumatriptan on the SPID-30 measure, with a mean 11-point decrease on the pain scale, compared with a mean 7-point decrease.
Secondary endpoints were pain relief – from moderate or severe to none or mild – and pain freedom. These were measured every 15 minutes for the first hour and then again at 60, 90, and 120 minutes. Pain was also assessed 24 and 48 hours post dose.
AVP-825 showed its greatest advantage during the first 60 minutes, reducing pain in significantly more migraine attacks than did the oral form. By 30 minutes, response rates were 54% vs. 39%; by 1 hour, they were 72% vs. 63%. Thereafter, both forms were equally effective. There were no differences in 24- and 48-hour outcomes, with about 60% of each group reporting sustained pain relief.
The findings were similar for the outcome of pain freedom, although – as could be expected – response rates were much lower. Again, AVP-825 showed an early advantage, with 7% of migraines completely abating by 15 minutes. At 30 minutes, response rates were 18% vs. 11%. AVP-825 continued to show about a 10% advantage over oral through 90 minutes. By 2 hours, the response rate was about 60% for both treatments. At 24 and 48 hours about half of the migraines attacks were still completely abated.
The investigational drug was well tolerated. Although 54% of patients experienced some sort of treatment-related adverse event, most were mild (44%); a burning sensation in the nose was the most commonly reported.
Systemic adverse events occurred more frequently in those taking the oral medication. Triptan-related sensations – tightening in the chest and neck – occurred in 5% of those taking the tablet and 2% of those who used AVP-825.
Last fall, the Food and Drug Administration issued a Complete Response Letter to Avanir’s New Drug Application, requesting that the company address device use errors seen in some of the trials. The agency did not, however, find any clinical or nonclinical safety or efficacy issues or request that additional clinical trials be conducted prior to approval.
The study was cofunded by OptiNose U.S. and Avanir Pharmaceuticals. Dr. Tepper has received research funds from, serves as a consultant to, or sits the advisory board of Allergan, ATI, Impax, and a number of other pharmaceutical companies.
On Twitter @alz_gal
WASHINGTON – A low-dose intranasal sumatriptan powder worked faster than the 100-mg oral formulation on acute migraine, with a significantly lower rate of triptan-related chest tightening.
Additionally, the 22-mg powder formulation reduced or eliminated pain just as long as the 100-mg tablet did, with pain relief reported by 60% of each group and pain freedom by 50% at 48 hours, Dr. Stewart Tepper said at the annual meeting of the American Academy of Neurology.
“Oral was not superior to the powder in any of the efficacy outcomes” in the COMPASS trial, a phase III, placebo-controlled, crossover study, said Dr. Tepper of the Cleveland Clinic in Ohio.
Nor was the powder associated with the “foul” taste patients often complain of when they use a liquid sumatriptan nasal spray, he added.
The investigational drug, AVP-825 (Avanir Pharmaceuticals) is packaged in a unique intranasal delivery system. The breath-powered device holds a single-drug cartridge. Two cartridges equal one 22-mg dose; of this, about 16 mg are actually delivered.
Patients put the nasal piece into one nostril, seal their lips around a mouthpiece, and blow into it. “This elevates and closes the soft palate, so the powder doesn’t enter the oropharynx,” Dr. Tepper said. “The powder is delivered high into the nose. The top of the septum is open, so the breath comes out the other side.”
The trial enrolled 185 patients and assessed 1,531 migraines over 24 weeks. Patients were randomized to active powder or placebo tablet for 12 weeks or five migraines, and then crossed to placebo powder or active tablet. The primary endpoint was the change in SPID-30 (sum of pain intensity differences from baseline-30 minutes).
AVP-825 significantly outperformed oral sumatriptan on the SPID-30 measure, with a mean 11-point decrease on the pain scale, compared with a mean 7-point decrease.
Secondary endpoints were pain relief – from moderate or severe to none or mild – and pain freedom. These were measured every 15 minutes for the first hour and then again at 60, 90, and 120 minutes. Pain was also assessed 24 and 48 hours post dose.
AVP-825 showed its greatest advantage during the first 60 minutes, reducing pain in significantly more migraine attacks than did the oral form. By 30 minutes, response rates were 54% vs. 39%; by 1 hour, they were 72% vs. 63%. Thereafter, both forms were equally effective. There were no differences in 24- and 48-hour outcomes, with about 60% of each group reporting sustained pain relief.
The findings were similar for the outcome of pain freedom, although – as could be expected – response rates were much lower. Again, AVP-825 showed an early advantage, with 7% of migraines completely abating by 15 minutes. At 30 minutes, response rates were 18% vs. 11%. AVP-825 continued to show about a 10% advantage over oral through 90 minutes. By 2 hours, the response rate was about 60% for both treatments. At 24 and 48 hours about half of the migraines attacks were still completely abated.
The investigational drug was well tolerated. Although 54% of patients experienced some sort of treatment-related adverse event, most were mild (44%); a burning sensation in the nose was the most commonly reported.
Systemic adverse events occurred more frequently in those taking the oral medication. Triptan-related sensations – tightening in the chest and neck – occurred in 5% of those taking the tablet and 2% of those who used AVP-825.
Last fall, the Food and Drug Administration issued a Complete Response Letter to Avanir’s New Drug Application, requesting that the company address device use errors seen in some of the trials. The agency did not, however, find any clinical or nonclinical safety or efficacy issues or request that additional clinical trials be conducted prior to approval.
The study was cofunded by OptiNose U.S. and Avanir Pharmaceuticals. Dr. Tepper has received research funds from, serves as a consultant to, or sits the advisory board of Allergan, ATI, Impax, and a number of other pharmaceutical companies.
On Twitter @alz_gal
WASHINGTON – A low-dose intranasal sumatriptan powder worked faster than the 100-mg oral formulation on acute migraine, with a significantly lower rate of triptan-related chest tightening.
Additionally, the 22-mg powder formulation reduced or eliminated pain just as long as the 100-mg tablet did, with pain relief reported by 60% of each group and pain freedom by 50% at 48 hours, Dr. Stewart Tepper said at the annual meeting of the American Academy of Neurology.
“Oral was not superior to the powder in any of the efficacy outcomes” in the COMPASS trial, a phase III, placebo-controlled, crossover study, said Dr. Tepper of the Cleveland Clinic in Ohio.
Nor was the powder associated with the “foul” taste patients often complain of when they use a liquid sumatriptan nasal spray, he added.
The investigational drug, AVP-825 (Avanir Pharmaceuticals) is packaged in a unique intranasal delivery system. The breath-powered device holds a single-drug cartridge. Two cartridges equal one 22-mg dose; of this, about 16 mg are actually delivered.
Patients put the nasal piece into one nostril, seal their lips around a mouthpiece, and blow into it. “This elevates and closes the soft palate, so the powder doesn’t enter the oropharynx,” Dr. Tepper said. “The powder is delivered high into the nose. The top of the septum is open, so the breath comes out the other side.”
The trial enrolled 185 patients and assessed 1,531 migraines over 24 weeks. Patients were randomized to active powder or placebo tablet for 12 weeks or five migraines, and then crossed to placebo powder or active tablet. The primary endpoint was the change in SPID-30 (sum of pain intensity differences from baseline-30 minutes).
AVP-825 significantly outperformed oral sumatriptan on the SPID-30 measure, with a mean 11-point decrease on the pain scale, compared with a mean 7-point decrease.
Secondary endpoints were pain relief – from moderate or severe to none or mild – and pain freedom. These were measured every 15 minutes for the first hour and then again at 60, 90, and 120 minutes. Pain was also assessed 24 and 48 hours post dose.
AVP-825 showed its greatest advantage during the first 60 minutes, reducing pain in significantly more migraine attacks than did the oral form. By 30 minutes, response rates were 54% vs. 39%; by 1 hour, they were 72% vs. 63%. Thereafter, both forms were equally effective. There were no differences in 24- and 48-hour outcomes, with about 60% of each group reporting sustained pain relief.
The findings were similar for the outcome of pain freedom, although – as could be expected – response rates were much lower. Again, AVP-825 showed an early advantage, with 7% of migraines completely abating by 15 minutes. At 30 minutes, response rates were 18% vs. 11%. AVP-825 continued to show about a 10% advantage over oral through 90 minutes. By 2 hours, the response rate was about 60% for both treatments. At 24 and 48 hours about half of the migraines attacks were still completely abated.
The investigational drug was well tolerated. Although 54% of patients experienced some sort of treatment-related adverse event, most were mild (44%); a burning sensation in the nose was the most commonly reported.
Systemic adverse events occurred more frequently in those taking the oral medication. Triptan-related sensations – tightening in the chest and neck – occurred in 5% of those taking the tablet and 2% of those who used AVP-825.
Last fall, the Food and Drug Administration issued a Complete Response Letter to Avanir’s New Drug Application, requesting that the company address device use errors seen in some of the trials. The agency did not, however, find any clinical or nonclinical safety or efficacy issues or request that additional clinical trials be conducted prior to approval.
The study was cofunded by OptiNose U.S. and Avanir Pharmaceuticals. Dr. Tepper has received research funds from, serves as a consultant to, or sits the advisory board of Allergan, ATI, Impax, and a number of other pharmaceutical companies.
On Twitter @alz_gal
AT THE AAN 2015 ANNUAL MEETING
Key clinical point: An intranasal powdered sumatriptan worked fast and more effectively on acute migraine attacks than did the oral form of the drug.
Major finding: By 30 minutes, response rates were 54% for the inhaled powder vs. 39% for the tablet. By 1 hour, they were 72% vs. 63%. Thereafter, both forms were equally effective.
Data source: The placebo-controlled crossover trial involved 185 patients who experienced more than 1,500 migraines during 24 weeks.
Disclosures: The study was cofunded by OptiNose U.S. and Avanir Pharmaceuticals. Dr. Tepper has received research funds from, serves as a consultant to, or sits on the advisory board of Allergan, ATI, Impax, and a number of other pharmaceutical companies.

AAN: Migraine Knowledge Remains Suboptimal in Primary Care
WASHINGTON – Primary care providers are generally familiar with the prevalence and initial diagnosis of migraine but less so with the specifics of treating migraine or its psychiatric comorbidities.
Many primary care providers (PCPs) are uncomfortable with prescribing preventive medications, preferring to rely on abortives and other acute attack treatments, Dr. Mia Minen said at the annual meeting of the American Academy of Neurology. Her study on PCP knowledge of migraine also revealed a “concerning” lack of attention to depression and anxiety among migraine patients.
“Most of our participants did know that these are common comorbid conditions,” said Dr. Minen of New York University. “But only half of them were assessing patients for anxiety, and only 30% for depression. This is a significant problem, because we think there’s a bidirectional relationship here – treating the psychiatric problems may actually help the migraines as well.”
Migraine accounts for 5 million-9 million primary care visits each year, she said, and many migraine patients are managed by their PCPs. “Unfortunately, as many as 60% of these patients are unrecognized as having migraine,” and many go for as long as 4 years before being properly diagnosed. “Primary care physicians have limited time with patients, and a migraine intake and assessment is time-consuming – as is managing the patient. Studies show that treatment is often suboptimal, with simple analgesic prescribing. And few of those who do qualify for preventive treatment actually get it.”
Her study aimed to discover what PCPs know – and need to learn – about migraine.
The first portion was framed in three semi-structured 15-minute interviews, moderated by headache specialists. Eleven physicians from different backgrounds attended these. They were asked what they perceived as their knowledge gaps in migraine diagnosis and treatment, and what difficulties they had encountered in those areas.
“About half said they would order an MRI for a new type of headache,” Dr. Minen said. A quarter didn’t know that an MRI was indicated for a headache with neuralgic symptoms, and only a third knew to order one when a headache worsened or remained unresponsive to treatment.
“These four conditions are situations in which headache experts typically agree that imaging is necessary,” Dr. Minen said. “Our findings indicate that primary care physicians might not actually be ordering imaging studies in situations where it should be done.”
Participants were generally unaware of the AAN’s guidelines on preventive medications, or the “Choosing Wisely” campaign to limit opioids and imaging in migraine patients, except in particular cases.
While most had heard of medication overuse headache, they were uncertain about how to diagnose it and unaware of some of the medications implicated in it. Participants were comfortable with some abortive medications (sumatriptan and naratriptan) and only prescribed opioids as a last resort. Antiemetics were rarely offered without a specific patient request.
There was uncertainty and discomfort about prescribing preventive medications, particularly topiramate. Several physicians said that patients often don’t comply with a daily regimen, so they preferred to stick with abortives. None had used botulinum toxin.
The second part of the study was a more specific, online survey completed by about 80 PCPs.
Most (60%) weren’t familiar with the recommendation about limiting opioids. While 60% said they knew that nonsteroidal anti-inflammatories could spark medication overuse headache, only half know that butabital-containing drugs could. A third knew about the risks for it with acetaminophen and narcotics, and only 13% about the association of triptans with medication overuse headache.
Few patients were apparently referred to evidence-based nonpharmacologic treatments, like biofeedback and cognitive behavioral therapy (just 1% and 3% of physicians said that they did so).
“Doctors apparently just don’t know that these alternatives are supported by strong evidence,” Dr. Minen said.
She had no financial disclosures.
WASHINGTON – Primary care providers are generally familiar with the prevalence and initial diagnosis of migraine but less so with the specifics of treating migraine or its psychiatric comorbidities.
Many primary care providers (PCPs) are uncomfortable with prescribing preventive medications, preferring to rely on abortives and other acute attack treatments, Dr. Mia Minen said at the annual meeting of the American Academy of Neurology. Her study on PCP knowledge of migraine also revealed a “concerning” lack of attention to depression and anxiety among migraine patients.
“Most of our participants did know that these are common comorbid conditions,” said Dr. Minen of New York University. “But only half of them were assessing patients for anxiety, and only 30% for depression. This is a significant problem, because we think there’s a bidirectional relationship here – treating the psychiatric problems may actually help the migraines as well.”
Migraine accounts for 5 million-9 million primary care visits each year, she said, and many migraine patients are managed by their PCPs. “Unfortunately, as many as 60% of these patients are unrecognized as having migraine,” and many go for as long as 4 years before being properly diagnosed. “Primary care physicians have limited time with patients, and a migraine intake and assessment is time-consuming – as is managing the patient. Studies show that treatment is often suboptimal, with simple analgesic prescribing. And few of those who do qualify for preventive treatment actually get it.”
Her study aimed to discover what PCPs know – and need to learn – about migraine.
The first portion was framed in three semi-structured 15-minute interviews, moderated by headache specialists. Eleven physicians from different backgrounds attended these. They were asked what they perceived as their knowledge gaps in migraine diagnosis and treatment, and what difficulties they had encountered in those areas.
“About half said they would order an MRI for a new type of headache,” Dr. Minen said. A quarter didn’t know that an MRI was indicated for a headache with neuralgic symptoms, and only a third knew to order one when a headache worsened or remained unresponsive to treatment.
“These four conditions are situations in which headache experts typically agree that imaging is necessary,” Dr. Minen said. “Our findings indicate that primary care physicians might not actually be ordering imaging studies in situations where it should be done.”
Participants were generally unaware of the AAN’s guidelines on preventive medications, or the “Choosing Wisely” campaign to limit opioids and imaging in migraine patients, except in particular cases.
While most had heard of medication overuse headache, they were uncertain about how to diagnose it and unaware of some of the medications implicated in it. Participants were comfortable with some abortive medications (sumatriptan and naratriptan) and only prescribed opioids as a last resort. Antiemetics were rarely offered without a specific patient request.
There was uncertainty and discomfort about prescribing preventive medications, particularly topiramate. Several physicians said that patients often don’t comply with a daily regimen, so they preferred to stick with abortives. None had used botulinum toxin.
The second part of the study was a more specific, online survey completed by about 80 PCPs.
Most (60%) weren’t familiar with the recommendation about limiting opioids. While 60% said they knew that nonsteroidal anti-inflammatories could spark medication overuse headache, only half know that butabital-containing drugs could. A third knew about the risks for it with acetaminophen and narcotics, and only 13% about the association of triptans with medication overuse headache.
Few patients were apparently referred to evidence-based nonpharmacologic treatments, like biofeedback and cognitive behavioral therapy (just 1% and 3% of physicians said that they did so).
“Doctors apparently just don’t know that these alternatives are supported by strong evidence,” Dr. Minen said.
She had no financial disclosures.
WASHINGTON – Primary care providers are generally familiar with the prevalence and initial diagnosis of migraine but less so with the specifics of treating migraine or its psychiatric comorbidities.
Many primary care providers (PCPs) are uncomfortable with prescribing preventive medications, preferring to rely on abortives and other acute attack treatments, Dr. Mia Minen said at the annual meeting of the American Academy of Neurology. Her study on PCP knowledge of migraine also revealed a “concerning” lack of attention to depression and anxiety among migraine patients.
“Most of our participants did know that these are common comorbid conditions,” said Dr. Minen of New York University. “But only half of them were assessing patients for anxiety, and only 30% for depression. This is a significant problem, because we think there’s a bidirectional relationship here – treating the psychiatric problems may actually help the migraines as well.”
Migraine accounts for 5 million-9 million primary care visits each year, she said, and many migraine patients are managed by their PCPs. “Unfortunately, as many as 60% of these patients are unrecognized as having migraine,” and many go for as long as 4 years before being properly diagnosed. “Primary care physicians have limited time with patients, and a migraine intake and assessment is time-consuming – as is managing the patient. Studies show that treatment is often suboptimal, with simple analgesic prescribing. And few of those who do qualify for preventive treatment actually get it.”
Her study aimed to discover what PCPs know – and need to learn – about migraine.
The first portion was framed in three semi-structured 15-minute interviews, moderated by headache specialists. Eleven physicians from different backgrounds attended these. They were asked what they perceived as their knowledge gaps in migraine diagnosis and treatment, and what difficulties they had encountered in those areas.
“About half said they would order an MRI for a new type of headache,” Dr. Minen said. A quarter didn’t know that an MRI was indicated for a headache with neuralgic symptoms, and only a third knew to order one when a headache worsened or remained unresponsive to treatment.
“These four conditions are situations in which headache experts typically agree that imaging is necessary,” Dr. Minen said. “Our findings indicate that primary care physicians might not actually be ordering imaging studies in situations where it should be done.”
Participants were generally unaware of the AAN’s guidelines on preventive medications, or the “Choosing Wisely” campaign to limit opioids and imaging in migraine patients, except in particular cases.
While most had heard of medication overuse headache, they were uncertain about how to diagnose it and unaware of some of the medications implicated in it. Participants were comfortable with some abortive medications (sumatriptan and naratriptan) and only prescribed opioids as a last resort. Antiemetics were rarely offered without a specific patient request.
There was uncertainty and discomfort about prescribing preventive medications, particularly topiramate. Several physicians said that patients often don’t comply with a daily regimen, so they preferred to stick with abortives. None had used botulinum toxin.
The second part of the study was a more specific, online survey completed by about 80 PCPs.
Most (60%) weren’t familiar with the recommendation about limiting opioids. While 60% said they knew that nonsteroidal anti-inflammatories could spark medication overuse headache, only half know that butabital-containing drugs could. A third knew about the risks for it with acetaminophen and narcotics, and only 13% about the association of triptans with medication overuse headache.
Few patients were apparently referred to evidence-based nonpharmacologic treatments, like biofeedback and cognitive behavioral therapy (just 1% and 3% of physicians said that they did so).
“Doctors apparently just don’t know that these alternatives are supported by strong evidence,” Dr. Minen said.
She had no financial disclosures.
AT AAN 2015
AAN: Migraine knowledge remains suboptimal in primary care
WASHINGTON – Primary care providers are generally familiar with the prevalence and initial diagnosis of migraine but less so with the specifics of treating migraine or its psychiatric comorbidities.
Many primary care providers (PCPs) are uncomfortable with prescribing preventive medications, preferring to rely on abortives and other acute attack treatments, Dr. Mia Minen said at the annual meeting of the American Academy of Neurology. Her study on PCP knowledge of migraine also revealed a “concerning” lack of attention to depression and anxiety among migraine patients.
“Most of our participants did know that these are common comorbid conditions,” said Dr. Minen of New York University. “But only half of them were assessing patients for anxiety, and only 30% for depression. This is a significant problem, because we think there’s a bidirectional relationship here – treating the psychiatric problems may actually help the migraines as well.”
Migraine accounts for 5 million-9 million primary care visits each year, she said, and many migraine patients are managed by their PCPs. “Unfortunately, as many as 60% of these patients are unrecognized as having migraine,” and many go for as long as 4 years before being properly diagnosed. “Primary care physicians have limited time with patients, and a migraine intake and assessment is time-consuming – as is managing the patient. Studies show that treatment is often suboptimal, with simple analgesic prescribing. And few of those who do qualify for preventive treatment actually get it.”
Her study aimed to discover what PCPs know – and need to learn – about migraine.
The first portion was framed in three semi-structured 15-minute interviews, moderated by headache specialists. Eleven physicians from different backgrounds attended these. They were asked what they perceived as their knowledge gaps in migraine diagnosis and treatment, and what difficulties they had encountered in those areas.
“About half said they would order an MRI for a new type of headache,” Dr. Minen said. A quarter didn’t know that an MRI was indicated for a headache with neuralgic symptoms, and only a third knew to order one when a headache worsened or remained unresponsive to treatment.
“These four conditions are situations in which headache experts typically agree that imaging is necessary,” Dr. Minen said. “Our findings indicate that primary care physicians might not actually be ordering imaging studies in situations where it should be done.”
Participants were generally unaware of the AAN’s guidelines on preventive medications, or the “Choosing Wisely” campaign to limit opioids and imaging in migraine patients, except in particular cases.
While most had heard of medication overuse headache, they were uncertain about how to diagnose it and unaware of some of the medications implicated in it. Participants were comfortable with some abortive medications (sumatriptan and naratriptan) and only prescribed opioids as a last resort. Antiemetics were rarely offered without a specific patient request.
There was uncertainty and discomfort about prescribing preventive medications, particularly topiramate. Several physicians said that patients often don’t comply with a daily regimen, so they preferred to stick with abortives. None had used botulinum toxin.
The second part of the study was a more specific, online survey completed by about 80 PCPs.
Most (60%) weren’t familiar with the recommendation about limiting opioids. While 60% said they knew that nonsteroidal anti-inflammatories could spark medication overuse headache, only half know that butabital-containing drugs could. A third knew about the risks for it with acetaminophen and narcotics, and only 13% about the association of triptans with medication overuse headache.
Few patients were apparently referred to evidence-based nonpharmacologic treatments, like biofeedback and cognitive behavioral therapy (just 1% and 3% of physicians said that they did so).
“Doctors apparently just don’t know that these alternatives are supported by strong evidence,” Dr. Minen said.
She had no financial disclosures.
On Twitter @alz_gal
WASHINGTON – Primary care providers are generally familiar with the prevalence and initial diagnosis of migraine but less so with the specifics of treating migraine or its psychiatric comorbidities.
Many primary care providers (PCPs) are uncomfortable with prescribing preventive medications, preferring to rely on abortives and other acute attack treatments, Dr. Mia Minen said at the annual meeting of the American Academy of Neurology. Her study on PCP knowledge of migraine also revealed a “concerning” lack of attention to depression and anxiety among migraine patients.
“Most of our participants did know that these are common comorbid conditions,” said Dr. Minen of New York University. “But only half of them were assessing patients for anxiety, and only 30% for depression. This is a significant problem, because we think there’s a bidirectional relationship here – treating the psychiatric problems may actually help the migraines as well.”
Migraine accounts for 5 million-9 million primary care visits each year, she said, and many migraine patients are managed by their PCPs. “Unfortunately, as many as 60% of these patients are unrecognized as having migraine,” and many go for as long as 4 years before being properly diagnosed. “Primary care physicians have limited time with patients, and a migraine intake and assessment is time-consuming – as is managing the patient. Studies show that treatment is often suboptimal, with simple analgesic prescribing. And few of those who do qualify for preventive treatment actually get it.”
Her study aimed to discover what PCPs know – and need to learn – about migraine.
The first portion was framed in three semi-structured 15-minute interviews, moderated by headache specialists. Eleven physicians from different backgrounds attended these. They were asked what they perceived as their knowledge gaps in migraine diagnosis and treatment, and what difficulties they had encountered in those areas.
“About half said they would order an MRI for a new type of headache,” Dr. Minen said. A quarter didn’t know that an MRI was indicated for a headache with neuralgic symptoms, and only a third knew to order one when a headache worsened or remained unresponsive to treatment.
“These four conditions are situations in which headache experts typically agree that imaging is necessary,” Dr. Minen said. “Our findings indicate that primary care physicians might not actually be ordering imaging studies in situations where it should be done.”
Participants were generally unaware of the AAN’s guidelines on preventive medications, or the “Choosing Wisely” campaign to limit opioids and imaging in migraine patients, except in particular cases.
While most had heard of medication overuse headache, they were uncertain about how to diagnose it and unaware of some of the medications implicated in it. Participants were comfortable with some abortive medications (sumatriptan and naratriptan) and only prescribed opioids as a last resort. Antiemetics were rarely offered without a specific patient request.
There was uncertainty and discomfort about prescribing preventive medications, particularly topiramate. Several physicians said that patients often don’t comply with a daily regimen, so they preferred to stick with abortives. None had used botulinum toxin.
The second part of the study was a more specific, online survey completed by about 80 PCPs.
Most (60%) weren’t familiar with the recommendation about limiting opioids. While 60% said they knew that nonsteroidal anti-inflammatories could spark medication overuse headache, only half know that butabital-containing drugs could. A third knew about the risks for it with acetaminophen and narcotics, and only 13% about the association of triptans with medication overuse headache.
Few patients were apparently referred to evidence-based nonpharmacologic treatments, like biofeedback and cognitive behavioral therapy (just 1% and 3% of physicians said that they did so).
“Doctors apparently just don’t know that these alternatives are supported by strong evidence,” Dr. Minen said.
She had no financial disclosures.
On Twitter @alz_gal
WASHINGTON – Primary care providers are generally familiar with the prevalence and initial diagnosis of migraine but less so with the specifics of treating migraine or its psychiatric comorbidities.
Many primary care providers (PCPs) are uncomfortable with prescribing preventive medications, preferring to rely on abortives and other acute attack treatments, Dr. Mia Minen said at the annual meeting of the American Academy of Neurology. Her study on PCP knowledge of migraine also revealed a “concerning” lack of attention to depression and anxiety among migraine patients.
“Most of our participants did know that these are common comorbid conditions,” said Dr. Minen of New York University. “But only half of them were assessing patients for anxiety, and only 30% for depression. This is a significant problem, because we think there’s a bidirectional relationship here – treating the psychiatric problems may actually help the migraines as well.”
Migraine accounts for 5 million-9 million primary care visits each year, she said, and many migraine patients are managed by their PCPs. “Unfortunately, as many as 60% of these patients are unrecognized as having migraine,” and many go for as long as 4 years before being properly diagnosed. “Primary care physicians have limited time with patients, and a migraine intake and assessment is time-consuming – as is managing the patient. Studies show that treatment is often suboptimal, with simple analgesic prescribing. And few of those who do qualify for preventive treatment actually get it.”
Her study aimed to discover what PCPs know – and need to learn – about migraine.
The first portion was framed in three semi-structured 15-minute interviews, moderated by headache specialists. Eleven physicians from different backgrounds attended these. They were asked what they perceived as their knowledge gaps in migraine diagnosis and treatment, and what difficulties they had encountered in those areas.
“About half said they would order an MRI for a new type of headache,” Dr. Minen said. A quarter didn’t know that an MRI was indicated for a headache with neuralgic symptoms, and only a third knew to order one when a headache worsened or remained unresponsive to treatment.
“These four conditions are situations in which headache experts typically agree that imaging is necessary,” Dr. Minen said. “Our findings indicate that primary care physicians might not actually be ordering imaging studies in situations where it should be done.”
Participants were generally unaware of the AAN’s guidelines on preventive medications, or the “Choosing Wisely” campaign to limit opioids and imaging in migraine patients, except in particular cases.
While most had heard of medication overuse headache, they were uncertain about how to diagnose it and unaware of some of the medications implicated in it. Participants were comfortable with some abortive medications (sumatriptan and naratriptan) and only prescribed opioids as a last resort. Antiemetics were rarely offered without a specific patient request.
There was uncertainty and discomfort about prescribing preventive medications, particularly topiramate. Several physicians said that patients often don’t comply with a daily regimen, so they preferred to stick with abortives. None had used botulinum toxin.
The second part of the study was a more specific, online survey completed by about 80 PCPs.
Most (60%) weren’t familiar with the recommendation about limiting opioids. While 60% said they knew that nonsteroidal anti-inflammatories could spark medication overuse headache, only half know that butabital-containing drugs could. A third knew about the risks for it with acetaminophen and narcotics, and only 13% about the association of triptans with medication overuse headache.
Few patients were apparently referred to evidence-based nonpharmacologic treatments, like biofeedback and cognitive behavioral therapy (just 1% and 3% of physicians said that they did so).
“Doctors apparently just don’t know that these alternatives are supported by strong evidence,” Dr. Minen said.
She had no financial disclosures.
On Twitter @alz_gal
AT AAN 2015
Key clinical point: Primary care physicians say they need to know more about diagnosing and treating migraine.
Major finding: Imaging, preventive medications, and psychiatric comorbities were all areas physicians identified as needing improvement.
Data source: The interviews and survey comprised a total of about 100 primary care phyisicians.
Disclosures: Dr. Minen had no financial disclosures.
AAN: Maternal valproate linked to kids’ physical, cognitive problems
WASHINGTON – One-quarter of valproate-exposed children in an ongoing study had a major birth defect or reduced IQ, Dr. Kimford Meador reported at the annual meeting of the American Academy of Neurology.
The findings reconfirm just how dangerous the antiepileptic drug can be to a developing fetus, especially when viewed along with findings of increased risk associated with even low valproate doses, said Dr. Meador of Stanford (Calif.) University.

“I don’t think we have even yet captured all the risks that are there,” he said. In addition, he stressed that valproate is a poor choice in a woman who plans a pregnancy, and it should not be used, unless absolutely necessary, in any woman of childbearing age who maintains her fertility.
The drug also is commonly employed to treat depression and migraine, he added.
The Maternal Outcomes and Neurodevelopmental Effects of Antiepileptic Drugs (MONEAD) study assessed neurodevelopmental outcomes in 311 children whose mothers took valproate, phenytoin, carbamazepine, or lamotrigine for epilepsy during pregnancy. These drugs were chosen because they were the most commonly prescribed when the study began.
Analyses in the prior Neurodevelopmental Effects of Antiepileptic Drugs (NEAD) study have shown that valproate is linked to major congenital malformations and lower IQ in toddlers (N. Engl. J. Med. 2009;360:1597-605) and 6-year-olds (Lancet Neurol. 2013;12:244-52). In another study, the drug has also been linked to an increased risk of autism spectrum disorders and autism (hazard ratios of 3.0 and 5.2, respectively).
The new analysis examined the risk of either a negative physical or cognitive outcome, or a combination of both, among the entire NEAD group. The individual domain of verbal IQ also was examined because it was an area of particular concern in the previous analyses.
Because maternal IQ is the major predictor of child IQ in the general population, the analysis looked at how many children had an IQ less than one standard deviation lower than their mother’s IQ – about 15 points.
Of the children exposed to valproate, 7 of 69 children had some kind of a major congenital malformation, and 12 of 58 children had a decreased IQ, compared with the mother. A full 25% (17 of 69 children) had one or both of these problems.
All of the outcomes were significantly worse than those seen with carbamazepine (birth defect, 5%; low IQ, 11%; either or both, 10%); lamotrigine (birth defect, 1%; low IQ, 12%; either or both, 12%); and phenytoin (birth defect, 7%; low IQ, 6%; either or both, 13%).
The investigators also examined a variety of cognitive measures: verbal and nonverbal IQ, General Memory Index, Behavior Rating of Inventory of Executive Function, and Nepsy Executive Index.
“Whatever cognitive measure we employed, we saw a greater negative as the valproate dose increased,” Dr. Meador said. “At what level the dose confers no risk is unclear, though, because it’s hard to adjust for genetic risk factors and the individual drug absorption levels, among other things.”
However, a recent U.K. study showed an increased risk of both outcomes among children who were exposed to even a very low dose of the drug – below 800 mg daily (Neurology 2015;84:382-90).
It’s not clear how valproate might exert its deleterious effects, Dr. Meador noted.
“It may damage the developing brain by causing neuronal death, or causing dysfunction in the surviving cells. This risk of adverse drug-induced effects on the immature brain doesn't go away immediately when the baby comes out of the womb,” he observed. “It’s a complicated area to study, too, because we don’t normally expose neonates to antiepileptics unless they are already having seizures.”
There was also an “unexpected” finding in the analysis, Dr. Meador said. “We were collecting information on periconceptional folate as a confounding factor. There was a very robust positive effect of about a 6-point IQ gain in those children, compared to those whose mothers didn’t take folate at time of conception.
“This is consistent with the idea that periconceptual folate may not only be important for reducing fetal malformations, but may also have a positive effect on cognitive abilities,” Dr. Meador said. “So, I recommend that all women of childbearing age should be taking folate.”
Dr. Meador has received personal compensation for activities on behalf of the Epilepsy Study Consortium with Eisai, NeuroPace, Novartis, Supernus, UCB Pharma, Upsher-Smith Laboratories, and Vivus Pharmaceuticals as a consultant. He has received research support from Pfizer and UCB Pharma.
On Twitter @alz_gal
This article was updated May 5, 2015.
WASHINGTON – One-quarter of valproate-exposed children in an ongoing study had a major birth defect or reduced IQ, Dr. Kimford Meador reported at the annual meeting of the American Academy of Neurology.
The findings reconfirm just how dangerous the antiepileptic drug can be to a developing fetus, especially when viewed along with findings of increased risk associated with even low valproate doses, said Dr. Meador of Stanford (Calif.) University.
“I don’t think we have even yet captured all the risks that are there,” he said. In addition, he stressed that valproate is a poor choice in a woman who plans a pregnancy, and it should not be used, unless absolutely necessary, in any woman of childbearing age who maintains her fertility.
The drug also is commonly employed to treat depression and migraine, he added.
The Maternal Outcomes and Neurodevelopmental Effects of Antiepileptic Drugs (MONEAD) study assessed neurodevelopmental outcomes in 311 children whose mothers took valproate, phenytoin, carbamazepine, or lamotrigine for epilepsy during pregnancy. These drugs were chosen because they were the most commonly prescribed when the study began.
Analyses in the prior Neurodevelopmental Effects of Antiepileptic Drugs (NEAD) study have shown that valproate is linked to major congenital malformations and lower IQ in toddlers (N. Engl. J. Med. 2009;360:1597-605) and 6-year-olds (Lancet Neurol. 2013;12:244-52). In another study, the drug has also been linked to an increased risk of autism spectrum disorders and autism (hazard ratios of 3.0 and 5.2, respectively).
The new analysis examined the risk of either a negative physical or cognitive outcome, or a combination of both, among the entire NEAD group. The individual domain of verbal IQ also was examined because it was an area of particular concern in the previous analyses.
Because maternal IQ is the major predictor of child IQ in the general population, the analysis looked at how many children had an IQ less than one standard deviation lower than their mother’s IQ – about 15 points.
Of the children exposed to valproate, 7 of 69 children had some kind of a major congenital malformation, and 12 of 58 children had a decreased IQ, compared with the mother. A full 25% (17 of 69 children) had one or both of these problems.
All of the outcomes were significantly worse than those seen with carbamazepine (birth defect, 5%; low IQ, 11%; either or both, 10%); lamotrigine (birth defect, 1%; low IQ, 12%; either or both, 12%); and phenytoin (birth defect, 7%; low IQ, 6%; either or both, 13%).
The investigators also examined a variety of cognitive measures: verbal and nonverbal IQ, General Memory Index, Behavior Rating of Inventory of Executive Function, and Nepsy Executive Index.
“Whatever cognitive measure we employed, we saw a greater negative as the valproate dose increased,” Dr. Meador said. “At what level the dose confers no risk is unclear, though, because it’s hard to adjust for genetic risk factors and the individual drug absorption levels, among other things.”
However, a recent U.K. study showed an increased risk of both outcomes among children who were exposed to even a very low dose of the drug – below 800 mg daily (Neurology 2015;84:382-90).
It’s not clear how valproate might exert its deleterious effects, Dr. Meador noted.
“It may damage the developing brain by causing neuronal death, or causing dysfunction in the surviving cells. This risk of adverse drug-induced effects on the immature brain doesn't go away immediately when the baby comes out of the womb,” he observed. “It’s a complicated area to study, too, because we don’t normally expose neonates to antiepileptics unless they are already having seizures.”
There was also an “unexpected” finding in the analysis, Dr. Meador said. “We were collecting information on periconceptional folate as a confounding factor. There was a very robust positive effect of about a 6-point IQ gain in those children, compared to those whose mothers didn’t take folate at time of conception.
“This is consistent with the idea that periconceptual folate may not only be important for reducing fetal malformations, but may also have a positive effect on cognitive abilities,” Dr. Meador said. “So, I recommend that all women of childbearing age should be taking folate.”
Dr. Meador has received personal compensation for activities on behalf of the Epilepsy Study Consortium with Eisai, NeuroPace, Novartis, Supernus, UCB Pharma, Upsher-Smith Laboratories, and Vivus Pharmaceuticals as a consultant. He has received research support from Pfizer and UCB Pharma.
On Twitter @alz_gal
This article was updated May 5, 2015.
WASHINGTON – One-quarter of valproate-exposed children in an ongoing study had a major birth defect or reduced IQ, Dr. Kimford Meador reported at the annual meeting of the American Academy of Neurology.
The findings reconfirm just how dangerous the antiepileptic drug can be to a developing fetus, especially when viewed along with findings of increased risk associated with even low valproate doses, said Dr. Meador of Stanford (Calif.) University.
“I don’t think we have even yet captured all the risks that are there,” he said. In addition, he stressed that valproate is a poor choice in a woman who plans a pregnancy, and it should not be used, unless absolutely necessary, in any woman of childbearing age who maintains her fertility.
The drug also is commonly employed to treat depression and migraine, he added.
The Maternal Outcomes and Neurodevelopmental Effects of Antiepileptic Drugs (MONEAD) study assessed neurodevelopmental outcomes in 311 children whose mothers took valproate, phenytoin, carbamazepine, or lamotrigine for epilepsy during pregnancy. These drugs were chosen because they were the most commonly prescribed when the study began.
Analyses in the prior Neurodevelopmental Effects of Antiepileptic Drugs (NEAD) study have shown that valproate is linked to major congenital malformations and lower IQ in toddlers (N. Engl. J. Med. 2009;360:1597-605) and 6-year-olds (Lancet Neurol. 2013;12:244-52). In another study, the drug has also been linked to an increased risk of autism spectrum disorders and autism (hazard ratios of 3.0 and 5.2, respectively).
The new analysis examined the risk of either a negative physical or cognitive outcome, or a combination of both, among the entire NEAD group. The individual domain of verbal IQ also was examined because it was an area of particular concern in the previous analyses.
Because maternal IQ is the major predictor of child IQ in the general population, the analysis looked at how many children had an IQ less than one standard deviation lower than their mother’s IQ – about 15 points.
Of the children exposed to valproate, 7 of 69 children had some kind of a major congenital malformation, and 12 of 58 children had a decreased IQ, compared with the mother. A full 25% (17 of 69 children) had one or both of these problems.
All of the outcomes were significantly worse than those seen with carbamazepine (birth defect, 5%; low IQ, 11%; either or both, 10%); lamotrigine (birth defect, 1%; low IQ, 12%; either or both, 12%); and phenytoin (birth defect, 7%; low IQ, 6%; either or both, 13%).
The investigators also examined a variety of cognitive measures: verbal and nonverbal IQ, General Memory Index, Behavior Rating of Inventory of Executive Function, and Nepsy Executive Index.
“Whatever cognitive measure we employed, we saw a greater negative as the valproate dose increased,” Dr. Meador said. “At what level the dose confers no risk is unclear, though, because it’s hard to adjust for genetic risk factors and the individual drug absorption levels, among other things.”
However, a recent U.K. study showed an increased risk of both outcomes among children who were exposed to even a very low dose of the drug – below 800 mg daily (Neurology 2015;84:382-90).
It’s not clear how valproate might exert its deleterious effects, Dr. Meador noted.
“It may damage the developing brain by causing neuronal death, or causing dysfunction in the surviving cells. This risk of adverse drug-induced effects on the immature brain doesn't go away immediately when the baby comes out of the womb,” he observed. “It’s a complicated area to study, too, because we don’t normally expose neonates to antiepileptics unless they are already having seizures.”
There was also an “unexpected” finding in the analysis, Dr. Meador said. “We were collecting information on periconceptional folate as a confounding factor. There was a very robust positive effect of about a 6-point IQ gain in those children, compared to those whose mothers didn’t take folate at time of conception.
“This is consistent with the idea that periconceptual folate may not only be important for reducing fetal malformations, but may also have a positive effect on cognitive abilities,” Dr. Meador said. “So, I recommend that all women of childbearing age should be taking folate.”
Dr. Meador has received personal compensation for activities on behalf of the Epilepsy Study Consortium with Eisai, NeuroPace, Novartis, Supernus, UCB Pharma, Upsher-Smith Laboratories, and Vivus Pharmaceuticals as a consultant. He has received research support from Pfizer and UCB Pharma.
On Twitter @alz_gal
This article was updated May 5, 2015.
AT THE AAN 2015 ANNUAL MEETING
Key clinical point: Evidence continues to mount about the dangers of fetal exposure to maternal valproate.
Major finding: A quarter of children exposed prenatally to valproate had both a major congenital malformation and a relative decrease in IQ.
Data source: The MONEAD study continues to follow 311 children with in-utero exposure to valproate, carbamazepine, lamotrigine, or phenytoin.
Disclosures: Dr. Meador has received personal compensation for activities on behalf of the Epilepsy Study Consortium with Eisai, NeuroPace, Novartis, Supernus, UCB Pharma, Upsher-Smith Laboratories, and Vivus Pharmaceuticals as a consultant. He has received research support from Pfizer and UCB Pharma.

VIDEO: Don’t Forget Folate for Women on Antiepilepsy Drugs
WASHINGTON – Only 20% of women of childbearing age taking antiepileptic drugs also received a folate prescription, a small study revealed – but a brief intervention helped boost the rate above 60%.
Folic acid supplementation is de rigueur for women of childbearing age – and especially important in very early pregnancy. The need appears even greater in women who take antiepileptic drugs, many of which increase the risk of birth defects.
Despite current recommendations for folic acid supplementation in all women, prescription by neurologists seems low, according to Dr. Brian D. Moseley of the University of Cincinnati.
“We wanted to look at the rates of the prescription of folic acid to women on antiepileptic drugs who were seen in our general neurology clinic,” Dr. Moseley explained.
In an interview at the annual meeting of the American Academy of Neurology, Dr. Moseley discussed the study’s findings, how a brief intervention with the clinic’s physicians increased folic acid prescription rates, and which folic acid dosages may be optimal.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – Only 20% of women of childbearing age taking antiepileptic drugs also received a folate prescription, a small study revealed – but a brief intervention helped boost the rate above 60%.
Folic acid supplementation is de rigueur for women of childbearing age – and especially important in very early pregnancy. The need appears even greater in women who take antiepileptic drugs, many of which increase the risk of birth defects.
Despite current recommendations for folic acid supplementation in all women, prescription by neurologists seems low, according to Dr. Brian D. Moseley of the University of Cincinnati.
“We wanted to look at the rates of the prescription of folic acid to women on antiepileptic drugs who were seen in our general neurology clinic,” Dr. Moseley explained.
In an interview at the annual meeting of the American Academy of Neurology, Dr. Moseley discussed the study’s findings, how a brief intervention with the clinic’s physicians increased folic acid prescription rates, and which folic acid dosages may be optimal.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – Only 20% of women of childbearing age taking antiepileptic drugs also received a folate prescription, a small study revealed – but a brief intervention helped boost the rate above 60%.
Folic acid supplementation is de rigueur for women of childbearing age – and especially important in very early pregnancy. The need appears even greater in women who take antiepileptic drugs, many of which increase the risk of birth defects.
Despite current recommendations for folic acid supplementation in all women, prescription by neurologists seems low, according to Dr. Brian D. Moseley of the University of Cincinnati.
“We wanted to look at the rates of the prescription of folic acid to women on antiepileptic drugs who were seen in our general neurology clinic,” Dr. Moseley explained.
In an interview at the annual meeting of the American Academy of Neurology, Dr. Moseley discussed the study’s findings, how a brief intervention with the clinic’s physicians increased folic acid prescription rates, and which folic acid dosages may be optimal.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE AAN 2015 ANNUAL MEETING

VIDEO: Don’t forget folate for women on antiepilepsy drugs
WASHINGTON – Only 20% of women of childbearing age taking antiepileptic drugs also received a folate prescription, a small study revealed – but a brief intervention helped boost the rate above 60%.
Folic acid supplementation is de rigueur for women of childbearing age – and especially important in very early pregnancy. The need appears even greater in women who take antiepileptic drugs, many of which increase the risk of birth defects.
Despite current recommendations for folic acid supplementation in all women, prescription by neurologists seems low, according to Dr. Brian D. Moseley of the University of Cincinnati.
“We wanted to look at the rates of the prescription of folic acid to women on antiepileptic drugs who were seen in our general neurology clinic,” Dr. Moseley explained.
In an interview at the annual meeting of the American Academy of Neurology, Dr. Moseley discussed the study’s findings, how a brief intervention with the clinic’s physicians increased folic acid prescription rates, and which folic acid dosages may be optimal.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – Only 20% of women of childbearing age taking antiepileptic drugs also received a folate prescription, a small study revealed – but a brief intervention helped boost the rate above 60%.
Folic acid supplementation is de rigueur for women of childbearing age – and especially important in very early pregnancy. The need appears even greater in women who take antiepileptic drugs, many of which increase the risk of birth defects.
Despite current recommendations for folic acid supplementation in all women, prescription by neurologists seems low, according to Dr. Brian D. Moseley of the University of Cincinnati.
“We wanted to look at the rates of the prescription of folic acid to women on antiepileptic drugs who were seen in our general neurology clinic,” Dr. Moseley explained.
In an interview at the annual meeting of the American Academy of Neurology, Dr. Moseley discussed the study’s findings, how a brief intervention with the clinic’s physicians increased folic acid prescription rates, and which folic acid dosages may be optimal.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – Only 20% of women of childbearing age taking antiepileptic drugs also received a folate prescription, a small study revealed – but a brief intervention helped boost the rate above 60%.
Folic acid supplementation is de rigueur for women of childbearing age – and especially important in very early pregnancy. The need appears even greater in women who take antiepileptic drugs, many of which increase the risk of birth defects.
Despite current recommendations for folic acid supplementation in all women, prescription by neurologists seems low, according to Dr. Brian D. Moseley of the University of Cincinnati.
“We wanted to look at the rates of the prescription of folic acid to women on antiepileptic drugs who were seen in our general neurology clinic,” Dr. Moseley explained.
In an interview at the annual meeting of the American Academy of Neurology, Dr. Moseley discussed the study’s findings, how a brief intervention with the clinic’s physicians increased folic acid prescription rates, and which folic acid dosages may be optimal.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE AAN 2015 ANNUAL MEETING

VIDEO: Clinicians give perspectives on first unprovoked seizure guideline
WASHINGTON – Adult patients and their doctors should decide together whether to treat a first unprovoked seizure, according to a new recommendation issued by the American Academy of Neurology and the American Epilepsy Society. But although treatment reduces the risk of a recurrent seizure by 35%, it doesn’t appear to change the eventual prognosis – and balancing the risks of seizure and the risks of antiepileptic drugs is not easy.
In video interviews at the annual meeting of the American Academy of Neurology, Dr. Allan Krumholz of the University of Maryland, Baltimore, who headed the guideline writing committee, reviews the data, while Dr. Jacqueline French, professor of neurology at New York University puts it in clinical perspective.
But will the recommendations change practice? Dr. Derek Chong, a practicing neurologist at New York University’s Langone Comprehensive Epilepsy Center, shares his own thoughts in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
WASHINGTON – Adult patients and their doctors should decide together whether to treat a first unprovoked seizure, according to a new recommendation issued by the American Academy of Neurology and the American Epilepsy Society. But although treatment reduces the risk of a recurrent seizure by 35%, it doesn’t appear to change the eventual prognosis – and balancing the risks of seizure and the risks of antiepileptic drugs is not easy.
In video interviews at the annual meeting of the American Academy of Neurology, Dr. Allan Krumholz of the University of Maryland, Baltimore, who headed the guideline writing committee, reviews the data, while Dr. Jacqueline French, professor of neurology at New York University puts it in clinical perspective.
But will the recommendations change practice? Dr. Derek Chong, a practicing neurologist at New York University’s Langone Comprehensive Epilepsy Center, shares his own thoughts in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
WASHINGTON – Adult patients and their doctors should decide together whether to treat a first unprovoked seizure, according to a new recommendation issued by the American Academy of Neurology and the American Epilepsy Society. But although treatment reduces the risk of a recurrent seizure by 35%, it doesn’t appear to change the eventual prognosis – and balancing the risks of seizure and the risks of antiepileptic drugs is not easy.
In video interviews at the annual meeting of the American Academy of Neurology, Dr. Allan Krumholz of the University of Maryland, Baltimore, who headed the guideline writing committee, reviews the data, while Dr. Jacqueline French, professor of neurology at New York University puts it in clinical perspective.
But will the recommendations change practice? Dr. Derek Chong, a practicing neurologist at New York University’s Langone Comprehensive Epilepsy Center, shares his own thoughts in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
AT THE AAN 2015 ANNUAL MEETING

Guideline aids decision on whether to treat a first seizure in adults
WASHINGTON – A new set of recommendations issued by the American Academy of Neurology and the American Epilepsy Society should help clinicians to determine an individual approach for deciding whether to treat an adult patient with a first unprovoked seizure.
The new guideline notes that immediate treatment lowers the risk of a subsequent seizure by 35% over 5 years, but probably does not affect the eventual seizure outcome, first author Dr. Allan Krumholz said at the annual meeting of the American Academy of Neurology.
“Over the long term, immediate antiepileptic therapy won’t change the prognosis,” said Dr. Krumholz of the University of Maryland, Baltimore. “Over 5 years, it’s unlikely to improve the chance for sustained remission. However, I would add that, in general, the prognosis for these patients, whether they have immediate treatment or wait until after a second seizure, is generally good, with 75% of them becoming seizure-free on medication.”
Rather than providing a step-by-step treatment algorithm, the guideline stresses the importance of collaborative decision making between doctor and patient. It was cosponsored by the American Epilepsy Society and simultaneously published in Neurology (Neurology 2015;84:1705-13).
“This paper can’t give a simple, black-and-white recommendation about whether to immediately start antiepileptic medications,” Dr. Krumholz said at a press briefing. “What we can say – and what is most important – is that these decisions need to be made on an individual basis. Clinicians should weigh individual seizure recurrence risks against the risks and benefits of antiepileptic drugs [AEDs], and consider the preferences of patients.”
An AAN task force reviewed 47 studies on first-seizure treatment and trichotomized them based on their strength of evidence.
Ten studies (two class I and eight class II) addressed the risk of seizure recurrence. These found that the risk of a subsequent seizure is lowest shortly after the first, and increases over time, from 21% to 45% by 5 years. Seizure recurrence was lowest if the patient started an AED, although this finding was not based on randomized, controlled studies.
The risk of recurrence was doubled for patients who had a predisposing clinical factor: a prior brain lesion, abnormal structural imaging of the brain, an EEG with epileptiform waves, or a nocturnal seizure. Clinicians should take these findings into account when assessing patients for treatment, Dr. Krumholz noted.
Five studies (one class I and four class II) evaluated the risk of additional seizures over short- and long-term follow-up. These found that the majority will happen within the first year, and that immediate AED treatment reduces that risk by 35%.
Five studies identified the risk of adverse events associated with AED treatment (four class II and one class III). The incidence of side effects ranged from 7% to 31%. These studies included the medications phenytoin, phenobarbital, carbamazepine, valproic acid, and lamotrigine. However, the guideline noted, several of these are older medications that may not be as commonly used now as the newer-generation drugs. The document also noted that most side effects are dose-related and reversible on drug discontinuation.
The guideline is a good companion to AAN’s 2007 recommendations on evaluating an unprovoked first seizure in adults, Dr. Krumholz added.
Dr. Krumholz had no financial disclosures relevant to the guidelines.
On Twitter @alz_gal
WASHINGTON – A new set of recommendations issued by the American Academy of Neurology and the American Epilepsy Society should help clinicians to determine an individual approach for deciding whether to treat an adult patient with a first unprovoked seizure.
The new guideline notes that immediate treatment lowers the risk of a subsequent seizure by 35% over 5 years, but probably does not affect the eventual seizure outcome, first author Dr. Allan Krumholz said at the annual meeting of the American Academy of Neurology.
“Over the long term, immediate antiepileptic therapy won’t change the prognosis,” said Dr. Krumholz of the University of Maryland, Baltimore. “Over 5 years, it’s unlikely to improve the chance for sustained remission. However, I would add that, in general, the prognosis for these patients, whether they have immediate treatment or wait until after a second seizure, is generally good, with 75% of them becoming seizure-free on medication.”
Rather than providing a step-by-step treatment algorithm, the guideline stresses the importance of collaborative decision making between doctor and patient. It was cosponsored by the American Epilepsy Society and simultaneously published in Neurology (Neurology 2015;84:1705-13).
“This paper can’t give a simple, black-and-white recommendation about whether to immediately start antiepileptic medications,” Dr. Krumholz said at a press briefing. “What we can say – and what is most important – is that these decisions need to be made on an individual basis. Clinicians should weigh individual seizure recurrence risks against the risks and benefits of antiepileptic drugs [AEDs], and consider the preferences of patients.”
An AAN task force reviewed 47 studies on first-seizure treatment and trichotomized them based on their strength of evidence.
Ten studies (two class I and eight class II) addressed the risk of seizure recurrence. These found that the risk of a subsequent seizure is lowest shortly after the first, and increases over time, from 21% to 45% by 5 years. Seizure recurrence was lowest if the patient started an AED, although this finding was not based on randomized, controlled studies.
The risk of recurrence was doubled for patients who had a predisposing clinical factor: a prior brain lesion, abnormal structural imaging of the brain, an EEG with epileptiform waves, or a nocturnal seizure. Clinicians should take these findings into account when assessing patients for treatment, Dr. Krumholz noted.
Five studies (one class I and four class II) evaluated the risk of additional seizures over short- and long-term follow-up. These found that the majority will happen within the first year, and that immediate AED treatment reduces that risk by 35%.
Five studies identified the risk of adverse events associated with AED treatment (four class II and one class III). The incidence of side effects ranged from 7% to 31%. These studies included the medications phenytoin, phenobarbital, carbamazepine, valproic acid, and lamotrigine. However, the guideline noted, several of these are older medications that may not be as commonly used now as the newer-generation drugs. The document also noted that most side effects are dose-related and reversible on drug discontinuation.
The guideline is a good companion to AAN’s 2007 recommendations on evaluating an unprovoked first seizure in adults, Dr. Krumholz added.
Dr. Krumholz had no financial disclosures relevant to the guidelines.
On Twitter @alz_gal
WASHINGTON – A new set of recommendations issued by the American Academy of Neurology and the American Epilepsy Society should help clinicians to determine an individual approach for deciding whether to treat an adult patient with a first unprovoked seizure.
The new guideline notes that immediate treatment lowers the risk of a subsequent seizure by 35% over 5 years, but probably does not affect the eventual seizure outcome, first author Dr. Allan Krumholz said at the annual meeting of the American Academy of Neurology.
“Over the long term, immediate antiepileptic therapy won’t change the prognosis,” said Dr. Krumholz of the University of Maryland, Baltimore. “Over 5 years, it’s unlikely to improve the chance for sustained remission. However, I would add that, in general, the prognosis for these patients, whether they have immediate treatment or wait until after a second seizure, is generally good, with 75% of them becoming seizure-free on medication.”
Rather than providing a step-by-step treatment algorithm, the guideline stresses the importance of collaborative decision making between doctor and patient. It was cosponsored by the American Epilepsy Society and simultaneously published in Neurology (Neurology 2015;84:1705-13).
“This paper can’t give a simple, black-and-white recommendation about whether to immediately start antiepileptic medications,” Dr. Krumholz said at a press briefing. “What we can say – and what is most important – is that these decisions need to be made on an individual basis. Clinicians should weigh individual seizure recurrence risks against the risks and benefits of antiepileptic drugs [AEDs], and consider the preferences of patients.”
An AAN task force reviewed 47 studies on first-seizure treatment and trichotomized them based on their strength of evidence.
Ten studies (two class I and eight class II) addressed the risk of seizure recurrence. These found that the risk of a subsequent seizure is lowest shortly after the first, and increases over time, from 21% to 45% by 5 years. Seizure recurrence was lowest if the patient started an AED, although this finding was not based on randomized, controlled studies.
The risk of recurrence was doubled for patients who had a predisposing clinical factor: a prior brain lesion, abnormal structural imaging of the brain, an EEG with epileptiform waves, or a nocturnal seizure. Clinicians should take these findings into account when assessing patients for treatment, Dr. Krumholz noted.
Five studies (one class I and four class II) evaluated the risk of additional seizures over short- and long-term follow-up. These found that the majority will happen within the first year, and that immediate AED treatment reduces that risk by 35%.
Five studies identified the risk of adverse events associated with AED treatment (four class II and one class III). The incidence of side effects ranged from 7% to 31%. These studies included the medications phenytoin, phenobarbital, carbamazepine, valproic acid, and lamotrigine. However, the guideline noted, several of these are older medications that may not be as commonly used now as the newer-generation drugs. The document also noted that most side effects are dose-related and reversible on drug discontinuation.
The guideline is a good companion to AAN’s 2007 recommendations on evaluating an unprovoked first seizure in adults, Dr. Krumholz added.
Dr. Krumholz had no financial disclosures relevant to the guidelines.
On Twitter @alz_gal
AT THE AAN 2015 ANNUAL MEETING