User login
BE: Surveillance endoscopy frequency improving but still overdone
A new analysis of a U.S. national database suggests that surveillance endoscopies are being initiated unnecessarily in patients without a diagnosis of Barrett’s esophagus, and sooner than the recommended interval in patients with nondysplastic Barrett’s esophagus. The study, published in the American Journal of Gastroenterology, found some improvements, suggesting that 2016 recommendations from the American College of Gastroenterology and the American Board of Internal Medicine have had some impact in reducing unnecessary surveillance, but more work may need to be done. The guidelines recommend surveillance of nondysplastic Barrett’s esophagus every 3-5 years, and no biopsy for normal or irregular Z-line (<1 cm of variability).
“There was a notable change in practice after the 2016 ACG guidelines,” said Ziad Gellad, MD, an associate professor of medicine at Duke University, Durham, N.C., in an interview. He noted that fewer providers were recommending 1-2-year surveillance intervals for nondysplastic Barrett’s esophagus and an increase in those who recommended a 3-year interval.
But the study also found frequent biopsies of irregular Z-line. Whether that’s a clear signal of overuse of biopsy is unclear, since the researchers couldn’t determine if other macroscopic or endoscopically visible abnormalities may have been present and driven a decision. “We can’t assume that there wasn’t any other abnormality in the esophagus that deserved to be biopsied,” said Dr. Gellad, who was not involved in the study.
The authors, led by Sachin Wani, MD, of the University of Colorado at Denver, Aurora, and Nicholas J. Shaheen, MD, MPH, of the University of North Carolina at Chapel Hill, analyzed data from the GI Quality Improvement Consortium Registry on 135,704 endoscopies in 114,894 patients, performed between January 2013 and December 2019. Analyzed data included procedure indication, demographics, endoscopy and histology findings, and recommendations for further endoscopy.
Just over 61% of subjects were men, and 91.0% were White. The mean age at time of endoscopy was 61.7 years. 50.2% of procedures produced a pathology-confirmed diagnosis of intestinal metaplasia (IM). Of these, 5.9% were indefinite for dysplasia or low-grade dysplasia (LGD), and 1.5% were high-grade dysplasia (HGD).
In 81.4% of cases with IM and a normal Z-line, the endoscopist recommended surveillance endoscopy. In 44.2%, the repeat was recommended in 3 years. 26.1% were recommended for surveillance in 1-2 years. Surveillance was recommended in 80.7% of cases with IM and an irregular Z-line; 51.5% in 3 years and 19.5% in 1-2 years. Almost 20% of subjects with normal Z-line and no IM were recommended for surveillance endoscopy, most often in 3 years (8.6%). 24% of those with irregular Z-line and no IM were recommended for surveillance endoscopy (15.8% in 3 years). Overall, between 2016 and 2019, compared with 2013-2015, the researchers found an increase in the frequency of recommendation of 3-year intervals, and a decrease in recommendation of 1-2-year intervals.
Among patients with columnar-lined esophagus and confirmed Barrett’s esophagus, 53.4% of the 1- to 3-cm group and 41.8% of the >3-cm group were recommended surveillance endoscopy at 3 years. 21.9% of the 1- to 3-cm group and 30.3% of the >3-cm group were recommended for surveillance endoscopy sooner than 3 years.
“It confirms overuse of upper endoscopy in the management of Barrett’s. However, there is also a nagging question in my mind about what to do about an irregular Z-line,” said Dr. Gellad. He noted that 33.8% of individuals with irregular Z-line had IM, while 3.8% had LGD and 0.7% had HGD. Those patients would have been missed if biopsies had not been taken, which would have been consistent with the new guidelines. However, he noted that pathology findings were not reviewed by an expert pathologist. “Does this data suggest because you find HGD in irregular Z-line, should we now in fact biopsy irregular Z-line? That’s one of the interesting pieces of this,” said Dr. Gellad.
He also believes that there is much more to be learned about what drives the decisions and timing surrounding surveillance endoscopy. “I think that’s an area that’s ripe for research,” said Dr. Gellad.
The study was funded by the University of Colorado department of medicine. The article authors have consulted for various companies. Dr. Gellad has no relevant financial disclosures.
SOURCE: Wani S et al. Am J Gastroenterol. 2020 Oct 11. doi: 10.14309/ajg.0000000000000960.
A new analysis of a U.S. national database suggests that surveillance endoscopies are being initiated unnecessarily in patients without a diagnosis of Barrett’s esophagus, and sooner than the recommended interval in patients with nondysplastic Barrett’s esophagus. The study, published in the American Journal of Gastroenterology, found some improvements, suggesting that 2016 recommendations from the American College of Gastroenterology and the American Board of Internal Medicine have had some impact in reducing unnecessary surveillance, but more work may need to be done. The guidelines recommend surveillance of nondysplastic Barrett’s esophagus every 3-5 years, and no biopsy for normal or irregular Z-line (<1 cm of variability).
“There was a notable change in practice after the 2016 ACG guidelines,” said Ziad Gellad, MD, an associate professor of medicine at Duke University, Durham, N.C., in an interview. He noted that fewer providers were recommending 1-2-year surveillance intervals for nondysplastic Barrett’s esophagus and an increase in those who recommended a 3-year interval.
But the study also found frequent biopsies of irregular Z-line. Whether that’s a clear signal of overuse of biopsy is unclear, since the researchers couldn’t determine if other macroscopic or endoscopically visible abnormalities may have been present and driven a decision. “We can’t assume that there wasn’t any other abnormality in the esophagus that deserved to be biopsied,” said Dr. Gellad, who was not involved in the study.
The authors, led by Sachin Wani, MD, of the University of Colorado at Denver, Aurora, and Nicholas J. Shaheen, MD, MPH, of the University of North Carolina at Chapel Hill, analyzed data from the GI Quality Improvement Consortium Registry on 135,704 endoscopies in 114,894 patients, performed between January 2013 and December 2019. Analyzed data included procedure indication, demographics, endoscopy and histology findings, and recommendations for further endoscopy.
Just over 61% of subjects were men, and 91.0% were White. The mean age at time of endoscopy was 61.7 years. 50.2% of procedures produced a pathology-confirmed diagnosis of intestinal metaplasia (IM). Of these, 5.9% were indefinite for dysplasia or low-grade dysplasia (LGD), and 1.5% were high-grade dysplasia (HGD).
In 81.4% of cases with IM and a normal Z-line, the endoscopist recommended surveillance endoscopy. In 44.2%, the repeat was recommended in 3 years. 26.1% were recommended for surveillance in 1-2 years. Surveillance was recommended in 80.7% of cases with IM and an irregular Z-line; 51.5% in 3 years and 19.5% in 1-2 years. Almost 20% of subjects with normal Z-line and no IM were recommended for surveillance endoscopy, most often in 3 years (8.6%). 24% of those with irregular Z-line and no IM were recommended for surveillance endoscopy (15.8% in 3 years). Overall, between 2016 and 2019, compared with 2013-2015, the researchers found an increase in the frequency of recommendation of 3-year intervals, and a decrease in recommendation of 1-2-year intervals.
Among patients with columnar-lined esophagus and confirmed Barrett’s esophagus, 53.4% of the 1- to 3-cm group and 41.8% of the >3-cm group were recommended surveillance endoscopy at 3 years. 21.9% of the 1- to 3-cm group and 30.3% of the >3-cm group were recommended for surveillance endoscopy sooner than 3 years.
“It confirms overuse of upper endoscopy in the management of Barrett’s. However, there is also a nagging question in my mind about what to do about an irregular Z-line,” said Dr. Gellad. He noted that 33.8% of individuals with irregular Z-line had IM, while 3.8% had LGD and 0.7% had HGD. Those patients would have been missed if biopsies had not been taken, which would have been consistent with the new guidelines. However, he noted that pathology findings were not reviewed by an expert pathologist. “Does this data suggest because you find HGD in irregular Z-line, should we now in fact biopsy irregular Z-line? That’s one of the interesting pieces of this,” said Dr. Gellad.
He also believes that there is much more to be learned about what drives the decisions and timing surrounding surveillance endoscopy. “I think that’s an area that’s ripe for research,” said Dr. Gellad.
The study was funded by the University of Colorado department of medicine. The article authors have consulted for various companies. Dr. Gellad has no relevant financial disclosures.
SOURCE: Wani S et al. Am J Gastroenterol. 2020 Oct 11. doi: 10.14309/ajg.0000000000000960.
A new analysis of a U.S. national database suggests that surveillance endoscopies are being initiated unnecessarily in patients without a diagnosis of Barrett’s esophagus, and sooner than the recommended interval in patients with nondysplastic Barrett’s esophagus. The study, published in the American Journal of Gastroenterology, found some improvements, suggesting that 2016 recommendations from the American College of Gastroenterology and the American Board of Internal Medicine have had some impact in reducing unnecessary surveillance, but more work may need to be done. The guidelines recommend surveillance of nondysplastic Barrett’s esophagus every 3-5 years, and no biopsy for normal or irregular Z-line (<1 cm of variability).
“There was a notable change in practice after the 2016 ACG guidelines,” said Ziad Gellad, MD, an associate professor of medicine at Duke University, Durham, N.C., in an interview. He noted that fewer providers were recommending 1-2-year surveillance intervals for nondysplastic Barrett’s esophagus and an increase in those who recommended a 3-year interval.
But the study also found frequent biopsies of irregular Z-line. Whether that’s a clear signal of overuse of biopsy is unclear, since the researchers couldn’t determine if other macroscopic or endoscopically visible abnormalities may have been present and driven a decision. “We can’t assume that there wasn’t any other abnormality in the esophagus that deserved to be biopsied,” said Dr. Gellad, who was not involved in the study.
The authors, led by Sachin Wani, MD, of the University of Colorado at Denver, Aurora, and Nicholas J. Shaheen, MD, MPH, of the University of North Carolina at Chapel Hill, analyzed data from the GI Quality Improvement Consortium Registry on 135,704 endoscopies in 114,894 patients, performed between January 2013 and December 2019. Analyzed data included procedure indication, demographics, endoscopy and histology findings, and recommendations for further endoscopy.
Just over 61% of subjects were men, and 91.0% were White. The mean age at time of endoscopy was 61.7 years. 50.2% of procedures produced a pathology-confirmed diagnosis of intestinal metaplasia (IM). Of these, 5.9% were indefinite for dysplasia or low-grade dysplasia (LGD), and 1.5% were high-grade dysplasia (HGD).
In 81.4% of cases with IM and a normal Z-line, the endoscopist recommended surveillance endoscopy. In 44.2%, the repeat was recommended in 3 years. 26.1% were recommended for surveillance in 1-2 years. Surveillance was recommended in 80.7% of cases with IM and an irregular Z-line; 51.5% in 3 years and 19.5% in 1-2 years. Almost 20% of subjects with normal Z-line and no IM were recommended for surveillance endoscopy, most often in 3 years (8.6%). 24% of those with irregular Z-line and no IM were recommended for surveillance endoscopy (15.8% in 3 years). Overall, between 2016 and 2019, compared with 2013-2015, the researchers found an increase in the frequency of recommendation of 3-year intervals, and a decrease in recommendation of 1-2-year intervals.
Among patients with columnar-lined esophagus and confirmed Barrett’s esophagus, 53.4% of the 1- to 3-cm group and 41.8% of the >3-cm group were recommended surveillance endoscopy at 3 years. 21.9% of the 1- to 3-cm group and 30.3% of the >3-cm group were recommended for surveillance endoscopy sooner than 3 years.
“It confirms overuse of upper endoscopy in the management of Barrett’s. However, there is also a nagging question in my mind about what to do about an irregular Z-line,” said Dr. Gellad. He noted that 33.8% of individuals with irregular Z-line had IM, while 3.8% had LGD and 0.7% had HGD. Those patients would have been missed if biopsies had not been taken, which would have been consistent with the new guidelines. However, he noted that pathology findings were not reviewed by an expert pathologist. “Does this data suggest because you find HGD in irregular Z-line, should we now in fact biopsy irregular Z-line? That’s one of the interesting pieces of this,” said Dr. Gellad.
He also believes that there is much more to be learned about what drives the decisions and timing surrounding surveillance endoscopy. “I think that’s an area that’s ripe for research,” said Dr. Gellad.
The study was funded by the University of Colorado department of medicine. The article authors have consulted for various companies. Dr. Gellad has no relevant financial disclosures.
SOURCE: Wani S et al. Am J Gastroenterol. 2020 Oct 11. doi: 10.14309/ajg.0000000000000960.
FROM THE AMERICAN JOURNAL OF GASTROENTEROLOGY
Chronic daily migraine from medication overuse: How worried should you be?
. Physicians worry about episodic migraine converting to chronic daily headache, but this worry can also lead to under-treatment and even stigmatization of patients who aggressively treat their symptoms.
These concerns and others were a topic of a debate at the Headache Cooperative of New England’s 20th Annual HCNE Boston Fall Headache Symposium, which was conducted virtually.
The International Classification of Headache-3 (ICHD-3) defines medication overuse headache as a headache that occurs on 15 or more days per month in a patient with pre-existing primary headache, and that develops because of regular overuse of acute or symptomatic headache medication. The ICHD-3 also says that headache usually resolves when overuse is stopped, though not always.
Paul Rizzoli, MD, took issue with that definition. “If you have a lot of headaches and you take medication for them, then you likely have medication overuse headache. They say the most common cause of symptoms suggestive of chronic migraine is medication overuse. That’s like saying, if you have a rash on your arm, then it is an allergic sun exposure rash. No need to characterize the rash,” said Dr. Rizzoli, who is clinical director of the John R. Graham Headache Center at Brigham and Women’s Faulkner Hospital in Boston, during the session.
Is medication overuse really the culprit?

Dr. Rizzoli began by emphasizing that taking a lot of medication is always a concern. “Significant hepatic and renal and GI toxicities can result from taking and overusing medication of all sorts. What (I am) questioning is whether or not this rather strange, arbitrary, fluidly-defined concept of abortive migraine medicine overuse is truly responsible for causing all of the ills of which it is accused – and just as importantly, if the proposed solution for it, which is to just stop the overused medication and all will be better – if that solution is the right or wrong advice to give to a patient,” he said.
Much of Dr. Rizzoli’s criticism rested on the definition of medication overuse syndrome. He believes that many concerns about medication overuse can be traced to the use of opiates or barbiturate-containing medications, which have known propensities to lead to headaches. Other cases are less well defined, and “it’s not quite clear what the pathophysiology of the condition is – whether or not it’s the same as rebound or withdrawal headache, or if it is the same as a pronociceptive effect of analgesics, also called medicine-induced headache. Both are well documented and accepted, and the idea of opioid-induced analgesia tolerance is well documented and has several plausible mechanisms attributed to it,” said Dr. Rizzoli.
He said that changes in structural imaging in the brain suggest there at least two subgroups of patients that are both labeled as having medication overuse headache, one from medication overuse and one from progression of migraine disease. “Based on physiology, medication overuse headache cannot be clearly seen as a unitary condition,” he said.
Dr. Rizzoli cited other research on triptans, opioids, and barbiturates that showed an overall conversion from episodic migraine to chronic migraine, with the lowest frequency occurring in patients taking acetaminophen, aspirin, and caffeine (2%), followed by NSAIDs (4%), triptans (4%), opioids (5%), and barbiturates (6%). A total of 52 patients who became chronic were taking triptans, on average 7 days per month. The 1,370 triptan-using patients who remained episodic took triptans on average 5 days per month. “Does this seem like a huge difference between these two groups? The transformation rate in just this triptan subgroup was about 3%-4%, suggesting that, compared with the overall transformation rate of 3%, use of triptans did not exert much force overall on the baseline rate,” he said. Similar patterns were visible with use of other classes of drugs.
Meanwhile, the higher rates of conversion seen with opioids and barbiturates suggests an effect from these drugs. “Perhaps this data suggests the previously known effect is at play here and argues against the need for a separate diagnosis of medication overuse headache,” Dr. Rizzoli said.
“The evidence that simple analgesics can cause medication overuse headache is especially weak, and the evidence that NSAIDs do is conflicting, with some evidence suggesting they’re protective at some doses.” Other population studies suggested most patients with daily headache do not overuse medications, and studies in India, where analgesics are rarely used, still showed a similar rate of conversion to daily headache. Other studies failed to show evidence that withdrawal of overused medication leads to improvement. “Studies of populations after aggressive management of medicine overuse headache indicate that, for the majority of the headaches, for the most part did not clear after treatment, except maybe for a short time,” said Dr. Rizzoli.
A systematic review of 18 population studies showed the prevalence of medical overuse headache ranged from 11% to 68%. “That indicates substantial uncertainty about the magnitude of the problem,” said Dr. Rizzoli.
He also noted potential harms to patients. Many patients come in experience between 10 and 20 headaches per month. “To see them out of medical overuse would have us advising not to treat half of their headaches monthly in order to avoid this evil. Many patients who have read or heard about this condition are themselves restricting treatment so as to avoid medication overuse headache. The harms of such undertreatment have not been fully investigated.”
To get at the issue, he recommended adapting the traditional number-needed-to-treat calculation. “You could calculate a number needed to overtreat. If medication use is assumed to be the sole cause of headache chronification, the calculations could suggest you would need to restrict therapy for about 4 people for each person you protect from going chronic. That’s a lot of undertreatment,” said Dr. Rizzoli.
He summed up by saying that some patients may have a progressive disorder with structure and physiological changes in the brain that result in chronic pain, and such patients should be identified and studied. In others with frequent headache, high medication use may simply be associated with the condition becoming chronic, but not causative. “These diagnostic groups may be mixed and may be difficult to untangle,” said Dr. Rizzoli.
Medication overuse is to blame

Dr. Rizzoli’s debate lecture was followed by Barbara Nye, MD, who argued that concerns over medication overuse headache are valid. She noted a more unifying definition in ICHD-3, which requires regular medication overuse for at least 3 months, along with primary headache disorder.
Dr. Nye, who is codirector of the Headache Clinic at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., related her experience that medication overuse headache often occurs more quickly than the 3-month time frame contained in ICHD-3, especially in patients who were given pain medications after undergoing surgery. She echoed Dr. Rizzoli’s concerns about opiates and barbiturates. “Medicine overuse headache should be something we focus on, and we should be warning providers both in neurology and primary care about the frequent use of opiate and butalbital-containing medications, and frequent over-the-counter medicine use in high-frequency headache disorders,” Dr. Nye said during her talk.
She cited research showing risk factors for conversion from episodic to chronic daily headache. As well as medication overuse, these include White race, lower education status, previous marriage, obesity, diabetes, arthritis, top-quartile caffeine use, stressful life events, and higher headache frequency.
Risks vary by medication class. Opiates and narcotics used more than 2 or 3 times per week are of particular concern, as are short-acting over-the-counter medicines used more than three times per week or 10-15 days per month. She agreed that NSAIDs may have a protective effect, but only at much lower doses and when used about five (or fewer) times per month. One study showed a possible protection effect of NSAIDs, though when used more than 10 days/month, they were associated with medication overuse headache.
Fioricet and Fiorinal, used more than 1 day/week, have an early and robust medicine overuse effect. “Limiting that use is very important,” said Dr. Nye. Other medicines and doses of concern include Tramadol/Ultram used at a higher than 50 mg/day dose, which has a metabolite that causes headache, and triptans used more than 10 days/month.
These concerns came about after analysis of large trials in patients with other conditions who also suffer from episodic migraines. A study of patients with irritable bowel syndrome and migraine showed a risk of conversion with opioid treatment. Another study of patients with arthritis and episodic migraine showed an association between conversion and NSAIDs alone, NSAIDs combined with Tylenol, and NSAIDs combined with opioids.
Risks of medication overuse also included collateral damage to the gastrointestinal and kidney systems, development of dependence, exacerbation of depression, and opioid-induced hyperalgesia, according to Dr. Nye. The overused medication may also interfere with the use of preventive medication. Those concerns drive the conventional wisdom of weaning patients off the overused medication, Dr. Nye said.
Dr. Nye discussed some of the observations of structural changes in the brain found in episodic migraine and chronic migraine associated with medication overuse. Functional MRI showed changes in grey matter, both as a result of medication overuse headache and further changes after medication withdrawal. “A lot of neuroplasticity and neuroadaptation occurs, and these effects seem to be sustained anywhere from 4-6 months after (medicine) discontinuation,” said Dr. Nye.
Common ground
Dr. Nye emphasized the need to be aware of the dangers of medication overuse headache, but noted that clinicians should address the problem to ensure that patients are empowered, potentially providing preventive medications and encouraging more effective use of daily abortive medications.
In response, Dr. Rizzoli suggested that the two agreed on many issues. For her part, Dr. Nye agreed that medication overuse headache is a muddy concept that needs more research to understand the relationship between opiate use and chronic migraine, “but I do think there have been some good studies of fMRI evaluating the difference between those with medication overuse headache and seeing how they convert back to a different underlying network (following medication withdrawal). I do agree that there is probably a subpopulation that is not affected by medication overuse headache,” Dr. Nye said.
In the end, both expressed concerns for the patient. “I share Barbara’s concern that we need to be mindful and protect our patients from medication use, but on the other hand I think we also need to protect our patients from the complications of having a diagnosis of medical overuse and the stigmatization that goes with that. That particular issue goes both ways,” said Dr. Rizzoli.
“I absolutely agree with that,” responded Dr. Nye.
Dr. Nye is on the advisory boards for Biohaven, Upsher Smith, and Impel. She is a trial site principal investigator for Allergan, Amgen, and Satsuma. Dr. Rizzoli has been a consultant for Nestle and served on the scientific advisory or data safety monitoring board for Biohaven and Xoc Pharma. He has also received research support from Allergan.
. Physicians worry about episodic migraine converting to chronic daily headache, but this worry can also lead to under-treatment and even stigmatization of patients who aggressively treat their symptoms.
These concerns and others were a topic of a debate at the Headache Cooperative of New England’s 20th Annual HCNE Boston Fall Headache Symposium, which was conducted virtually.
The International Classification of Headache-3 (ICHD-3) defines medication overuse headache as a headache that occurs on 15 or more days per month in a patient with pre-existing primary headache, and that develops because of regular overuse of acute or symptomatic headache medication. The ICHD-3 also says that headache usually resolves when overuse is stopped, though not always.
Paul Rizzoli, MD, took issue with that definition. “If you have a lot of headaches and you take medication for them, then you likely have medication overuse headache. They say the most common cause of symptoms suggestive of chronic migraine is medication overuse. That’s like saying, if you have a rash on your arm, then it is an allergic sun exposure rash. No need to characterize the rash,” said Dr. Rizzoli, who is clinical director of the John R. Graham Headache Center at Brigham and Women’s Faulkner Hospital in Boston, during the session.
Is medication overuse really the culprit?
Dr. Rizzoli began by emphasizing that taking a lot of medication is always a concern. “Significant hepatic and renal and GI toxicities can result from taking and overusing medication of all sorts. What (I am) questioning is whether or not this rather strange, arbitrary, fluidly-defined concept of abortive migraine medicine overuse is truly responsible for causing all of the ills of which it is accused – and just as importantly, if the proposed solution for it, which is to just stop the overused medication and all will be better – if that solution is the right or wrong advice to give to a patient,” he said.
Much of Dr. Rizzoli’s criticism rested on the definition of medication overuse syndrome. He believes that many concerns about medication overuse can be traced to the use of opiates or barbiturate-containing medications, which have known propensities to lead to headaches. Other cases are less well defined, and “it’s not quite clear what the pathophysiology of the condition is – whether or not it’s the same as rebound or withdrawal headache, or if it is the same as a pronociceptive effect of analgesics, also called medicine-induced headache. Both are well documented and accepted, and the idea of opioid-induced analgesia tolerance is well documented and has several plausible mechanisms attributed to it,” said Dr. Rizzoli.
He said that changes in structural imaging in the brain suggest there at least two subgroups of patients that are both labeled as having medication overuse headache, one from medication overuse and one from progression of migraine disease. “Based on physiology, medication overuse headache cannot be clearly seen as a unitary condition,” he said.
Dr. Rizzoli cited other research on triptans, opioids, and barbiturates that showed an overall conversion from episodic migraine to chronic migraine, with the lowest frequency occurring in patients taking acetaminophen, aspirin, and caffeine (2%), followed by NSAIDs (4%), triptans (4%), opioids (5%), and barbiturates (6%). A total of 52 patients who became chronic were taking triptans, on average 7 days per month. The 1,370 triptan-using patients who remained episodic took triptans on average 5 days per month. “Does this seem like a huge difference between these two groups? The transformation rate in just this triptan subgroup was about 3%-4%, suggesting that, compared with the overall transformation rate of 3%, use of triptans did not exert much force overall on the baseline rate,” he said. Similar patterns were visible with use of other classes of drugs.
Meanwhile, the higher rates of conversion seen with opioids and barbiturates suggests an effect from these drugs. “Perhaps this data suggests the previously known effect is at play here and argues against the need for a separate diagnosis of medication overuse headache,” Dr. Rizzoli said.
“The evidence that simple analgesics can cause medication overuse headache is especially weak, and the evidence that NSAIDs do is conflicting, with some evidence suggesting they’re protective at some doses.” Other population studies suggested most patients with daily headache do not overuse medications, and studies in India, where analgesics are rarely used, still showed a similar rate of conversion to daily headache. Other studies failed to show evidence that withdrawal of overused medication leads to improvement. “Studies of populations after aggressive management of medicine overuse headache indicate that, for the majority of the headaches, for the most part did not clear after treatment, except maybe for a short time,” said Dr. Rizzoli.
A systematic review of 18 population studies showed the prevalence of medical overuse headache ranged from 11% to 68%. “That indicates substantial uncertainty about the magnitude of the problem,” said Dr. Rizzoli.
He also noted potential harms to patients. Many patients come in experience between 10 and 20 headaches per month. “To see them out of medical overuse would have us advising not to treat half of their headaches monthly in order to avoid this evil. Many patients who have read or heard about this condition are themselves restricting treatment so as to avoid medication overuse headache. The harms of such undertreatment have not been fully investigated.”
To get at the issue, he recommended adapting the traditional number-needed-to-treat calculation. “You could calculate a number needed to overtreat. If medication use is assumed to be the sole cause of headache chronification, the calculations could suggest you would need to restrict therapy for about 4 people for each person you protect from going chronic. That’s a lot of undertreatment,” said Dr. Rizzoli.
He summed up by saying that some patients may have a progressive disorder with structure and physiological changes in the brain that result in chronic pain, and such patients should be identified and studied. In others with frequent headache, high medication use may simply be associated with the condition becoming chronic, but not causative. “These diagnostic groups may be mixed and may be difficult to untangle,” said Dr. Rizzoli.
Medication overuse is to blame
Dr. Rizzoli’s debate lecture was followed by Barbara Nye, MD, who argued that concerns over medication overuse headache are valid. She noted a more unifying definition in ICHD-3, which requires regular medication overuse for at least 3 months, along with primary headache disorder.
Dr. Nye, who is codirector of the Headache Clinic at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., related her experience that medication overuse headache often occurs more quickly than the 3-month time frame contained in ICHD-3, especially in patients who were given pain medications after undergoing surgery. She echoed Dr. Rizzoli’s concerns about opiates and barbiturates. “Medicine overuse headache should be something we focus on, and we should be warning providers both in neurology and primary care about the frequent use of opiate and butalbital-containing medications, and frequent over-the-counter medicine use in high-frequency headache disorders,” Dr. Nye said during her talk.
She cited research showing risk factors for conversion from episodic to chronic daily headache. As well as medication overuse, these include White race, lower education status, previous marriage, obesity, diabetes, arthritis, top-quartile caffeine use, stressful life events, and higher headache frequency.
Risks vary by medication class. Opiates and narcotics used more than 2 or 3 times per week are of particular concern, as are short-acting over-the-counter medicines used more than three times per week or 10-15 days per month. She agreed that NSAIDs may have a protective effect, but only at much lower doses and when used about five (or fewer) times per month. One study showed a possible protection effect of NSAIDs, though when used more than 10 days/month, they were associated with medication overuse headache.
Fioricet and Fiorinal, used more than 1 day/week, have an early and robust medicine overuse effect. “Limiting that use is very important,” said Dr. Nye. Other medicines and doses of concern include Tramadol/Ultram used at a higher than 50 mg/day dose, which has a metabolite that causes headache, and triptans used more than 10 days/month.
These concerns came about after analysis of large trials in patients with other conditions who also suffer from episodic migraines. A study of patients with irritable bowel syndrome and migraine showed a risk of conversion with opioid treatment. Another study of patients with arthritis and episodic migraine showed an association between conversion and NSAIDs alone, NSAIDs combined with Tylenol, and NSAIDs combined with opioids.
Risks of medication overuse also included collateral damage to the gastrointestinal and kidney systems, development of dependence, exacerbation of depression, and opioid-induced hyperalgesia, according to Dr. Nye. The overused medication may also interfere with the use of preventive medication. Those concerns drive the conventional wisdom of weaning patients off the overused medication, Dr. Nye said.
Dr. Nye discussed some of the observations of structural changes in the brain found in episodic migraine and chronic migraine associated with medication overuse. Functional MRI showed changes in grey matter, both as a result of medication overuse headache and further changes after medication withdrawal. “A lot of neuroplasticity and neuroadaptation occurs, and these effects seem to be sustained anywhere from 4-6 months after (medicine) discontinuation,” said Dr. Nye.
Common ground
Dr. Nye emphasized the need to be aware of the dangers of medication overuse headache, but noted that clinicians should address the problem to ensure that patients are empowered, potentially providing preventive medications and encouraging more effective use of daily abortive medications.
In response, Dr. Rizzoli suggested that the two agreed on many issues. For her part, Dr. Nye agreed that medication overuse headache is a muddy concept that needs more research to understand the relationship between opiate use and chronic migraine, “but I do think there have been some good studies of fMRI evaluating the difference between those with medication overuse headache and seeing how they convert back to a different underlying network (following medication withdrawal). I do agree that there is probably a subpopulation that is not affected by medication overuse headache,” Dr. Nye said.
In the end, both expressed concerns for the patient. “I share Barbara’s concern that we need to be mindful and protect our patients from medication use, but on the other hand I think we also need to protect our patients from the complications of having a diagnosis of medical overuse and the stigmatization that goes with that. That particular issue goes both ways,” said Dr. Rizzoli.
“I absolutely agree with that,” responded Dr. Nye.
Dr. Nye is on the advisory boards for Biohaven, Upsher Smith, and Impel. She is a trial site principal investigator for Allergan, Amgen, and Satsuma. Dr. Rizzoli has been a consultant for Nestle and served on the scientific advisory or data safety monitoring board for Biohaven and Xoc Pharma. He has also received research support from Allergan.
. Physicians worry about episodic migraine converting to chronic daily headache, but this worry can also lead to under-treatment and even stigmatization of patients who aggressively treat their symptoms.
These concerns and others were a topic of a debate at the Headache Cooperative of New England’s 20th Annual HCNE Boston Fall Headache Symposium, which was conducted virtually.
The International Classification of Headache-3 (ICHD-3) defines medication overuse headache as a headache that occurs on 15 or more days per month in a patient with pre-existing primary headache, and that develops because of regular overuse of acute or symptomatic headache medication. The ICHD-3 also says that headache usually resolves when overuse is stopped, though not always.
Paul Rizzoli, MD, took issue with that definition. “If you have a lot of headaches and you take medication for them, then you likely have medication overuse headache. They say the most common cause of symptoms suggestive of chronic migraine is medication overuse. That’s like saying, if you have a rash on your arm, then it is an allergic sun exposure rash. No need to characterize the rash,” said Dr. Rizzoli, who is clinical director of the John R. Graham Headache Center at Brigham and Women’s Faulkner Hospital in Boston, during the session.
Is medication overuse really the culprit?
Dr. Rizzoli began by emphasizing that taking a lot of medication is always a concern. “Significant hepatic and renal and GI toxicities can result from taking and overusing medication of all sorts. What (I am) questioning is whether or not this rather strange, arbitrary, fluidly-defined concept of abortive migraine medicine overuse is truly responsible for causing all of the ills of which it is accused – and just as importantly, if the proposed solution for it, which is to just stop the overused medication and all will be better – if that solution is the right or wrong advice to give to a patient,” he said.
Much of Dr. Rizzoli’s criticism rested on the definition of medication overuse syndrome. He believes that many concerns about medication overuse can be traced to the use of opiates or barbiturate-containing medications, which have known propensities to lead to headaches. Other cases are less well defined, and “it’s not quite clear what the pathophysiology of the condition is – whether or not it’s the same as rebound or withdrawal headache, or if it is the same as a pronociceptive effect of analgesics, also called medicine-induced headache. Both are well documented and accepted, and the idea of opioid-induced analgesia tolerance is well documented and has several plausible mechanisms attributed to it,” said Dr. Rizzoli.
He said that changes in structural imaging in the brain suggest there at least two subgroups of patients that are both labeled as having medication overuse headache, one from medication overuse and one from progression of migraine disease. “Based on physiology, medication overuse headache cannot be clearly seen as a unitary condition,” he said.
Dr. Rizzoli cited other research on triptans, opioids, and barbiturates that showed an overall conversion from episodic migraine to chronic migraine, with the lowest frequency occurring in patients taking acetaminophen, aspirin, and caffeine (2%), followed by NSAIDs (4%), triptans (4%), opioids (5%), and barbiturates (6%). A total of 52 patients who became chronic were taking triptans, on average 7 days per month. The 1,370 triptan-using patients who remained episodic took triptans on average 5 days per month. “Does this seem like a huge difference between these two groups? The transformation rate in just this triptan subgroup was about 3%-4%, suggesting that, compared with the overall transformation rate of 3%, use of triptans did not exert much force overall on the baseline rate,” he said. Similar patterns were visible with use of other classes of drugs.
Meanwhile, the higher rates of conversion seen with opioids and barbiturates suggests an effect from these drugs. “Perhaps this data suggests the previously known effect is at play here and argues against the need for a separate diagnosis of medication overuse headache,” Dr. Rizzoli said.
“The evidence that simple analgesics can cause medication overuse headache is especially weak, and the evidence that NSAIDs do is conflicting, with some evidence suggesting they’re protective at some doses.” Other population studies suggested most patients with daily headache do not overuse medications, and studies in India, where analgesics are rarely used, still showed a similar rate of conversion to daily headache. Other studies failed to show evidence that withdrawal of overused medication leads to improvement. “Studies of populations after aggressive management of medicine overuse headache indicate that, for the majority of the headaches, for the most part did not clear after treatment, except maybe for a short time,” said Dr. Rizzoli.
A systematic review of 18 population studies showed the prevalence of medical overuse headache ranged from 11% to 68%. “That indicates substantial uncertainty about the magnitude of the problem,” said Dr. Rizzoli.
He also noted potential harms to patients. Many patients come in experience between 10 and 20 headaches per month. “To see them out of medical overuse would have us advising not to treat half of their headaches monthly in order to avoid this evil. Many patients who have read or heard about this condition are themselves restricting treatment so as to avoid medication overuse headache. The harms of such undertreatment have not been fully investigated.”
To get at the issue, he recommended adapting the traditional number-needed-to-treat calculation. “You could calculate a number needed to overtreat. If medication use is assumed to be the sole cause of headache chronification, the calculations could suggest you would need to restrict therapy for about 4 people for each person you protect from going chronic. That’s a lot of undertreatment,” said Dr. Rizzoli.
He summed up by saying that some patients may have a progressive disorder with structure and physiological changes in the brain that result in chronic pain, and such patients should be identified and studied. In others with frequent headache, high medication use may simply be associated with the condition becoming chronic, but not causative. “These diagnostic groups may be mixed and may be difficult to untangle,” said Dr. Rizzoli.
Medication overuse is to blame
Dr. Rizzoli’s debate lecture was followed by Barbara Nye, MD, who argued that concerns over medication overuse headache are valid. She noted a more unifying definition in ICHD-3, which requires regular medication overuse for at least 3 months, along with primary headache disorder.
Dr. Nye, who is codirector of the Headache Clinic at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., related her experience that medication overuse headache often occurs more quickly than the 3-month time frame contained in ICHD-3, especially in patients who were given pain medications after undergoing surgery. She echoed Dr. Rizzoli’s concerns about opiates and barbiturates. “Medicine overuse headache should be something we focus on, and we should be warning providers both in neurology and primary care about the frequent use of opiate and butalbital-containing medications, and frequent over-the-counter medicine use in high-frequency headache disorders,” Dr. Nye said during her talk.
She cited research showing risk factors for conversion from episodic to chronic daily headache. As well as medication overuse, these include White race, lower education status, previous marriage, obesity, diabetes, arthritis, top-quartile caffeine use, stressful life events, and higher headache frequency.
Risks vary by medication class. Opiates and narcotics used more than 2 or 3 times per week are of particular concern, as are short-acting over-the-counter medicines used more than three times per week or 10-15 days per month. She agreed that NSAIDs may have a protective effect, but only at much lower doses and when used about five (or fewer) times per month. One study showed a possible protection effect of NSAIDs, though when used more than 10 days/month, they were associated with medication overuse headache.
Fioricet and Fiorinal, used more than 1 day/week, have an early and robust medicine overuse effect. “Limiting that use is very important,” said Dr. Nye. Other medicines and doses of concern include Tramadol/Ultram used at a higher than 50 mg/day dose, which has a metabolite that causes headache, and triptans used more than 10 days/month.
These concerns came about after analysis of large trials in patients with other conditions who also suffer from episodic migraines. A study of patients with irritable bowel syndrome and migraine showed a risk of conversion with opioid treatment. Another study of patients with arthritis and episodic migraine showed an association between conversion and NSAIDs alone, NSAIDs combined with Tylenol, and NSAIDs combined with opioids.
Risks of medication overuse also included collateral damage to the gastrointestinal and kidney systems, development of dependence, exacerbation of depression, and opioid-induced hyperalgesia, according to Dr. Nye. The overused medication may also interfere with the use of preventive medication. Those concerns drive the conventional wisdom of weaning patients off the overused medication, Dr. Nye said.
Dr. Nye discussed some of the observations of structural changes in the brain found in episodic migraine and chronic migraine associated with medication overuse. Functional MRI showed changes in grey matter, both as a result of medication overuse headache and further changes after medication withdrawal. “A lot of neuroplasticity and neuroadaptation occurs, and these effects seem to be sustained anywhere from 4-6 months after (medicine) discontinuation,” said Dr. Nye.
Common ground
Dr. Nye emphasized the need to be aware of the dangers of medication overuse headache, but noted that clinicians should address the problem to ensure that patients are empowered, potentially providing preventive medications and encouraging more effective use of daily abortive medications.
In response, Dr. Rizzoli suggested that the two agreed on many issues. For her part, Dr. Nye agreed that medication overuse headache is a muddy concept that needs more research to understand the relationship between opiate use and chronic migraine, “but I do think there have been some good studies of fMRI evaluating the difference between those with medication overuse headache and seeing how they convert back to a different underlying network (following medication withdrawal). I do agree that there is probably a subpopulation that is not affected by medication overuse headache,” Dr. Nye said.
In the end, both expressed concerns for the patient. “I share Barbara’s concern that we need to be mindful and protect our patients from medication use, but on the other hand I think we also need to protect our patients from the complications of having a diagnosis of medical overuse and the stigmatization that goes with that. That particular issue goes both ways,” said Dr. Rizzoli.
“I absolutely agree with that,” responded Dr. Nye.
Dr. Nye is on the advisory boards for Biohaven, Upsher Smith, and Impel. She is a trial site principal investigator for Allergan, Amgen, and Satsuma. Dr. Rizzoli has been a consultant for Nestle and served on the scientific advisory or data safety monitoring board for Biohaven and Xoc Pharma. He has also received research support from Allergan.
FROM HCNE’S 20TH ANNUAL BOSTON FALL HEADACHE SYMPOSIUM
A closer look at migraine aura
Migraine aura sometimes accompanies or precedes migraine pain, but the phenomenon is difficult to treat and poorly understood. However, some evidence points to potential neurological mechanisms, and migraine aura is associated with cardiovascular disease risk.

Andrea Harriott, MD, PhD, said at the Stowe Headache Symposium sponsored by the Headache Cooperative of New England, which was conducted virtually. Dr. Harriott is assistant professor of neurology at Massachusetts General Hospital in Boston.
Somewhere between 20% and 40% of patients with migraine experience aura. It is most often visual, though it can also include sensory, aphasic, and motor symptoms. Visual aura usually begins as a flickering zigzag pattern in the central visual field that moves slowly toward the periphery and often leaves a scotoma. Typical duration is 15-30 minutes. Aura symptoms are more common in females.
Research in the 1940s conducted by the Brazilian researcher Aristides de Azevedo Pacheco Leão, PhD, then at Harvard Medical School, Boston, showed evidence of CSD in rabbits after electrical or mechanical stimulation. He observed a wave of vasodilation and increased blood flow over the cortex that spread over nearly the entire dorsolateral cortex within 3-6 minutes.
In the 1940s and 1950s, researchers sketched on paper the visual disturbance over 10 minutes, tracking the expanding spectrum across the visual field, from the center toward the periphery. The resulting scotoma advanced across the visual cortex at a rate very similar to that of the cortical spreading observed by Dr. Leão, “potentially linking this electrical event that was described with the aura event of migraine,” said Dr. Harriott. Those researchers hypothesized that the aura was produced by a strong excitation phase, followed by a wave of total inhibition.
More recent functional magnetic resonance imaging studies have also shown that CSD-like disturbances occur when patients experience migraine aura. In one study, researchers observed an initial increase and then a decrease in the blood oxygenation level dependent (BOLD) signal, which spread slowly across the visual cortex and correlated with the aura event. “This study was really important in confirming that a CSD-like phenomenon was likely the underlying perturbation that produced the visual aura of migraine,” said Dr. Harriott.
Despite the evidence that CSD causes migraine aura, its connection to migraine pain hasn’t been firmly established. But Dr. Harriott presented some evidence linking the two. Migraine aura is usually followed by pain, and aura precedes migraine attacks 78%-93% of the time. Cephalic allodynia occurs in migraine about 70% to 80% of the time, and migraine with aura is more often associated with severe cutaneous allodynia than is migraine without aura. Finally, migraine patients with comorbidities have more severe disability, and more frequent cutaneous allodynia and aura than does the general migraine population (40% vs. 29%).
All of that suggests that activation of trigeminal nociceptors is involved with migraine aura, according to Dr. Harriott. Preclinical studies have also suggested links between CSD and activation of trigeminal nociceptors, with both immunohistochemical and electrophysiological lines of evidence. “These data suggest that spreading depression actually activates trigeminal nociceptors that we know are involved in signal pain in the head and neck, and that we know are involved in cephalic allodynia as well,” Dr. Harriott said.
The evidence impressed Allan Purdy, MD, professor of medicine at Dalhousie University, Halifax, N.S., who was the discussant for the presentation. “It’s an excellent case that CSD is a remarkably good correlate for aura,” he said during the session.
Along with potential impacts on migraine pain, aura is also associated with cardiovascular risk. “This is really important to know about in our clinical population,” said Dr. Harriott.
Meta-analyses of case control and cohort studies have shown associations between migraine aura and vascular disorders such as ischemic stroke. One meta-analysis showed about a twofold increased risk associated with migraine compared with the nonmigraine population. This difference was driven by migraine with aura (relative risk [RR], 2.25; 95% confidence interval [CI], 1.53-3.33) rather than migraine without aura (RR, 1.24; 95% CI, 0.86-1.79). Migraine generally is associated with greater risk of myocardial infarction (adjusted hazard ratio, 1.33; 95% CI, 1.08-1.64), and that association may be stronger in the aura phenotype.
There doesn’t appear to be evidence that traditional risk factors for heart disease – such as hypertension, diabetes, or high cholesterol – play a role in the association between aura and heart disease. One possibility is that variables like platelet activation, hypercoagulable state, or genetic susceptibility could be responsible.
The risks associated with migraine aura should be noted, but with a caveat, according to Dr. Purdy. “Even though the relative risk is high, the absolute risk is still relatively low, and patients with migraine with aura, who smoke or are female and over 45, those are the cases where the worry comes in.”
Dr. Harriott and Dr. Purdy have nothing to disclose.
Migraine aura sometimes accompanies or precedes migraine pain, but the phenomenon is difficult to treat and poorly understood. However, some evidence points to potential neurological mechanisms, and migraine aura is associated with cardiovascular disease risk.
Andrea Harriott, MD, PhD, said at the Stowe Headache Symposium sponsored by the Headache Cooperative of New England, which was conducted virtually. Dr. Harriott is assistant professor of neurology at Massachusetts General Hospital in Boston.
Somewhere between 20% and 40% of patients with migraine experience aura. It is most often visual, though it can also include sensory, aphasic, and motor symptoms. Visual aura usually begins as a flickering zigzag pattern in the central visual field that moves slowly toward the periphery and often leaves a scotoma. Typical duration is 15-30 minutes. Aura symptoms are more common in females.
Research in the 1940s conducted by the Brazilian researcher Aristides de Azevedo Pacheco Leão, PhD, then at Harvard Medical School, Boston, showed evidence of CSD in rabbits after electrical or mechanical stimulation. He observed a wave of vasodilation and increased blood flow over the cortex that spread over nearly the entire dorsolateral cortex within 3-6 minutes.
In the 1940s and 1950s, researchers sketched on paper the visual disturbance over 10 minutes, tracking the expanding spectrum across the visual field, from the center toward the periphery. The resulting scotoma advanced across the visual cortex at a rate very similar to that of the cortical spreading observed by Dr. Leão, “potentially linking this electrical event that was described with the aura event of migraine,” said Dr. Harriott. Those researchers hypothesized that the aura was produced by a strong excitation phase, followed by a wave of total inhibition.
More recent functional magnetic resonance imaging studies have also shown that CSD-like disturbances occur when patients experience migraine aura. In one study, researchers observed an initial increase and then a decrease in the blood oxygenation level dependent (BOLD) signal, which spread slowly across the visual cortex and correlated with the aura event. “This study was really important in confirming that a CSD-like phenomenon was likely the underlying perturbation that produced the visual aura of migraine,” said Dr. Harriott.
Despite the evidence that CSD causes migraine aura, its connection to migraine pain hasn’t been firmly established. But Dr. Harriott presented some evidence linking the two. Migraine aura is usually followed by pain, and aura precedes migraine attacks 78%-93% of the time. Cephalic allodynia occurs in migraine about 70% to 80% of the time, and migraine with aura is more often associated with severe cutaneous allodynia than is migraine without aura. Finally, migraine patients with comorbidities have more severe disability, and more frequent cutaneous allodynia and aura than does the general migraine population (40% vs. 29%).
All of that suggests that activation of trigeminal nociceptors is involved with migraine aura, according to Dr. Harriott. Preclinical studies have also suggested links between CSD and activation of trigeminal nociceptors, with both immunohistochemical and electrophysiological lines of evidence. “These data suggest that spreading depression actually activates trigeminal nociceptors that we know are involved in signal pain in the head and neck, and that we know are involved in cephalic allodynia as well,” Dr. Harriott said.
The evidence impressed Allan Purdy, MD, professor of medicine at Dalhousie University, Halifax, N.S., who was the discussant for the presentation. “It’s an excellent case that CSD is a remarkably good correlate for aura,” he said during the session.
Along with potential impacts on migraine pain, aura is also associated with cardiovascular risk. “This is really important to know about in our clinical population,” said Dr. Harriott.
Meta-analyses of case control and cohort studies have shown associations between migraine aura and vascular disorders such as ischemic stroke. One meta-analysis showed about a twofold increased risk associated with migraine compared with the nonmigraine population. This difference was driven by migraine with aura (relative risk [RR], 2.25; 95% confidence interval [CI], 1.53-3.33) rather than migraine without aura (RR, 1.24; 95% CI, 0.86-1.79). Migraine generally is associated with greater risk of myocardial infarction (adjusted hazard ratio, 1.33; 95% CI, 1.08-1.64), and that association may be stronger in the aura phenotype.
There doesn’t appear to be evidence that traditional risk factors for heart disease – such as hypertension, diabetes, or high cholesterol – play a role in the association between aura and heart disease. One possibility is that variables like platelet activation, hypercoagulable state, or genetic susceptibility could be responsible.
The risks associated with migraine aura should be noted, but with a caveat, according to Dr. Purdy. “Even though the relative risk is high, the absolute risk is still relatively low, and patients with migraine with aura, who smoke or are female and over 45, those are the cases where the worry comes in.”
Dr. Harriott and Dr. Purdy have nothing to disclose.
Migraine aura sometimes accompanies or precedes migraine pain, but the phenomenon is difficult to treat and poorly understood. However, some evidence points to potential neurological mechanisms, and migraine aura is associated with cardiovascular disease risk.
Andrea Harriott, MD, PhD, said at the Stowe Headache Symposium sponsored by the Headache Cooperative of New England, which was conducted virtually. Dr. Harriott is assistant professor of neurology at Massachusetts General Hospital in Boston.
Somewhere between 20% and 40% of patients with migraine experience aura. It is most often visual, though it can also include sensory, aphasic, and motor symptoms. Visual aura usually begins as a flickering zigzag pattern in the central visual field that moves slowly toward the periphery and often leaves a scotoma. Typical duration is 15-30 minutes. Aura symptoms are more common in females.
Research in the 1940s conducted by the Brazilian researcher Aristides de Azevedo Pacheco Leão, PhD, then at Harvard Medical School, Boston, showed evidence of CSD in rabbits after electrical or mechanical stimulation. He observed a wave of vasodilation and increased blood flow over the cortex that spread over nearly the entire dorsolateral cortex within 3-6 minutes.
In the 1940s and 1950s, researchers sketched on paper the visual disturbance over 10 minutes, tracking the expanding spectrum across the visual field, from the center toward the periphery. The resulting scotoma advanced across the visual cortex at a rate very similar to that of the cortical spreading observed by Dr. Leão, “potentially linking this electrical event that was described with the aura event of migraine,” said Dr. Harriott. Those researchers hypothesized that the aura was produced by a strong excitation phase, followed by a wave of total inhibition.
More recent functional magnetic resonance imaging studies have also shown that CSD-like disturbances occur when patients experience migraine aura. In one study, researchers observed an initial increase and then a decrease in the blood oxygenation level dependent (BOLD) signal, which spread slowly across the visual cortex and correlated with the aura event. “This study was really important in confirming that a CSD-like phenomenon was likely the underlying perturbation that produced the visual aura of migraine,” said Dr. Harriott.
Despite the evidence that CSD causes migraine aura, its connection to migraine pain hasn’t been firmly established. But Dr. Harriott presented some evidence linking the two. Migraine aura is usually followed by pain, and aura precedes migraine attacks 78%-93% of the time. Cephalic allodynia occurs in migraine about 70% to 80% of the time, and migraine with aura is more often associated with severe cutaneous allodynia than is migraine without aura. Finally, migraine patients with comorbidities have more severe disability, and more frequent cutaneous allodynia and aura than does the general migraine population (40% vs. 29%).
All of that suggests that activation of trigeminal nociceptors is involved with migraine aura, according to Dr. Harriott. Preclinical studies have also suggested links between CSD and activation of trigeminal nociceptors, with both immunohistochemical and electrophysiological lines of evidence. “These data suggest that spreading depression actually activates trigeminal nociceptors that we know are involved in signal pain in the head and neck, and that we know are involved in cephalic allodynia as well,” Dr. Harriott said.
The evidence impressed Allan Purdy, MD, professor of medicine at Dalhousie University, Halifax, N.S., who was the discussant for the presentation. “It’s an excellent case that CSD is a remarkably good correlate for aura,” he said during the session.
Along with potential impacts on migraine pain, aura is also associated with cardiovascular risk. “This is really important to know about in our clinical population,” said Dr. Harriott.
Meta-analyses of case control and cohort studies have shown associations between migraine aura and vascular disorders such as ischemic stroke. One meta-analysis showed about a twofold increased risk associated with migraine compared with the nonmigraine population. This difference was driven by migraine with aura (relative risk [RR], 2.25; 95% confidence interval [CI], 1.53-3.33) rather than migraine without aura (RR, 1.24; 95% CI, 0.86-1.79). Migraine generally is associated with greater risk of myocardial infarction (adjusted hazard ratio, 1.33; 95% CI, 1.08-1.64), and that association may be stronger in the aura phenotype.
There doesn’t appear to be evidence that traditional risk factors for heart disease – such as hypertension, diabetes, or high cholesterol – play a role in the association between aura and heart disease. One possibility is that variables like platelet activation, hypercoagulable state, or genetic susceptibility could be responsible.
The risks associated with migraine aura should be noted, but with a caveat, according to Dr. Purdy. “Even though the relative risk is high, the absolute risk is still relatively low, and patients with migraine with aura, who smoke or are female and over 45, those are the cases where the worry comes in.”
Dr. Harriott and Dr. Purdy have nothing to disclose.
FROM HCNE STOWE 2020
Stopping methotrexate, staying on etanercept provides best RA outcomes after remission
In patients with RA whose disease is well controlled by methotrexate combined with etanercept, withdrawal of methotrexate led to long-term outcomes that were nearly as good as continuation of combination therapy. The finding comes from the randomized, controlled SEAM-RA trial that sought to address weaknesses of previous studies. It included a long lead-in time with stringent criteria to ensure that participants had very good disease control.

Both the American College of Rheumatology and the European League Against Rheumatism recommend tapering medication in RA patients who are in long-term remission, but there is no established optimal strategy.
“There have been some prior RA trials that have looked at therapy reduction or withdrawal, but most did not use a very stringent definition of how well people were when they began. Were they in remission, or only in low disease activity?” said Jeffrey R. Curtis, MD, during a presentation of the results at the virtual annual meeting of the ACR. The study was also published online Nov. 18 in Arthritis & Rheumatology.
Stringent remission criteria
The key feature of the trial was the 6-month run-in period, when subjects were taking 50 mg etanercept once per week and 10-25 mg of oral methotrexate once per week, and had to complete at least three visits. They were excluded from the ensuing randomization if they had a Simplified Disease Activity Index (SDAI) score >3.3 and ≤11 at two or more visits, had an SDAI >11 at any time during the run-in period, or had an SDAI >3.3 at the third run-in visit.
“We [wanted them] to be doing quite well for a long period of time. That was empirically confirmed under observation as part of the lead-in period, and even before that, the clinical investigator had to affirm that they believed the patient was doing well for 6 or more months even before they were screened to enter the trial,” said Dr. Curtis, professor of medicine in the division of clinical immunology and rheumatology at the University of Alabama at Birmingham.
Once enrolled in the trial, patients were randomized 2:2:1 to continuing etanercept only (n = 101), continuing methotrexate only (n = 101), or continuing both medications (n = 51). Patients were eligible for rescue after randomization if they had an SDAI score >11 at any time, SDAI between 3.3 and 11 on three separate visits, or between 3.3 and 11 at two consecutive visits at least 2 weeks apart. About three-quarters of patients in each treatment arm were female, with a mean age of about 55 years, and 82%-91% were White.
Good remission recovery with rescue therapy
At week 48, 28.7% of the methotrexate-only group were in remission (SDAI ≤3.3), compared with 49.5% of the etanercept-only group (P = .004) and 52.9% of the combination group (P = .006). Time to disease worsening was shorter in the methotrexate-only group (median, 198 days) than in the etanercept-only group (median, not estimable; P < .001) and the combined therapy group (median, not estimable; P < .001).
The researchers also found that most patients who underwent rescue therapy once again achieved remission, including 71% of the methotrexate-only group, 75% of the etanercept-only group, and 80% of the combination therapy group. There was no between-group differences in the time required to reattain remission.
The high rate of remission recovery was a good sign, Dr. Curtis said. “To me as a clinician, the risk to try [withdrawing a medication] is quite low because the likelihood you can regain where you were before is quite good. It’s obviously more successful if you stop methotrexate and continue etanercept than if you do the reverse, but to me, this is quite a practical trial, and in fact the rigor of the inclusion criteria are much more like the patients I’m talking to about stopping therapy than some of the past studies in this regard. I think it’s quite useful in terms of generalizability. We want people that are doing this well or close to it before we take away medication.”
Positive reactions from rheumatologists
The reaction from the viewing audience was also positive. “I think this study fills a big data gap for what we do in clinical practice,” wrote Janet Pope, MD, in comments during the session.

Dr. Pope, who is a professor of medicine at the University of Western Ontario and head of rheumatology at St. Joseph’s Health Centre, both in London, said that the results build on previous work, including the CAMEO study, which showed that discontinuation of methotrexate in patients taking methotrexate and etanercept failed to achieve noninferiority to continuation of both medications, and the PRIZE study, which showed that continuing combination therapy at a reduced dose led to better outcomes than did switching to methotrexate alone or placebo. “This may be for some patients what they prefer if they don’t tolerate methotrexate,” she added.
“It’s wonderful to have these data to counsel patients. This is something we face every day,” wrote Elizabeth Wahl, MD, who is an acting assistant professor at the University of Washington, Seattle, and acting chief of rheumatology at the VA Puget Sound Healthcare System.
The study was funded by Amgen. Dr. Curtis has received grants or research support from AbbVie, Amgen, Bristol-Myers Squibb, Corrona, Janssen, Lilly, Myriad, Pfizer, Regeneron, Roche, and UCB. Dr. Pope consults for a variety of pharmaceutical companies. Dr. Wahl has no relevant financial disclosures.
SOURCE: Curtis JR et al. Arthritis Rheumatol. 2020;72(suppl 10), Abstract 0939.
In patients with RA whose disease is well controlled by methotrexate combined with etanercept, withdrawal of methotrexate led to long-term outcomes that were nearly as good as continuation of combination therapy. The finding comes from the randomized, controlled SEAM-RA trial that sought to address weaknesses of previous studies. It included a long lead-in time with stringent criteria to ensure that participants had very good disease control.
Both the American College of Rheumatology and the European League Against Rheumatism recommend tapering medication in RA patients who are in long-term remission, but there is no established optimal strategy.
“There have been some prior RA trials that have looked at therapy reduction or withdrawal, but most did not use a very stringent definition of how well people were when they began. Were they in remission, or only in low disease activity?” said Jeffrey R. Curtis, MD, during a presentation of the results at the virtual annual meeting of the ACR. The study was also published online Nov. 18 in Arthritis & Rheumatology.
Stringent remission criteria
The key feature of the trial was the 6-month run-in period, when subjects were taking 50 mg etanercept once per week and 10-25 mg of oral methotrexate once per week, and had to complete at least three visits. They were excluded from the ensuing randomization if they had a Simplified Disease Activity Index (SDAI) score >3.3 and ≤11 at two or more visits, had an SDAI >11 at any time during the run-in period, or had an SDAI >3.3 at the third run-in visit.
“We [wanted them] to be doing quite well for a long period of time. That was empirically confirmed under observation as part of the lead-in period, and even before that, the clinical investigator had to affirm that they believed the patient was doing well for 6 or more months even before they were screened to enter the trial,” said Dr. Curtis, professor of medicine in the division of clinical immunology and rheumatology at the University of Alabama at Birmingham.
Once enrolled in the trial, patients were randomized 2:2:1 to continuing etanercept only (n = 101), continuing methotrexate only (n = 101), or continuing both medications (n = 51). Patients were eligible for rescue after randomization if they had an SDAI score >11 at any time, SDAI between 3.3 and 11 on three separate visits, or between 3.3 and 11 at two consecutive visits at least 2 weeks apart. About three-quarters of patients in each treatment arm were female, with a mean age of about 55 years, and 82%-91% were White.
Good remission recovery with rescue therapy
At week 48, 28.7% of the methotrexate-only group were in remission (SDAI ≤3.3), compared with 49.5% of the etanercept-only group (P = .004) and 52.9% of the combination group (P = .006). Time to disease worsening was shorter in the methotrexate-only group (median, 198 days) than in the etanercept-only group (median, not estimable; P < .001) and the combined therapy group (median, not estimable; P < .001).
The researchers also found that most patients who underwent rescue therapy once again achieved remission, including 71% of the methotrexate-only group, 75% of the etanercept-only group, and 80% of the combination therapy group. There was no between-group differences in the time required to reattain remission.
The high rate of remission recovery was a good sign, Dr. Curtis said. “To me as a clinician, the risk to try [withdrawing a medication] is quite low because the likelihood you can regain where you were before is quite good. It’s obviously more successful if you stop methotrexate and continue etanercept than if you do the reverse, but to me, this is quite a practical trial, and in fact the rigor of the inclusion criteria are much more like the patients I’m talking to about stopping therapy than some of the past studies in this regard. I think it’s quite useful in terms of generalizability. We want people that are doing this well or close to it before we take away medication.”
Positive reactions from rheumatologists
The reaction from the viewing audience was also positive. “I think this study fills a big data gap for what we do in clinical practice,” wrote Janet Pope, MD, in comments during the session.
Dr. Pope, who is a professor of medicine at the University of Western Ontario and head of rheumatology at St. Joseph’s Health Centre, both in London, said that the results build on previous work, including the CAMEO study, which showed that discontinuation of methotrexate in patients taking methotrexate and etanercept failed to achieve noninferiority to continuation of both medications, and the PRIZE study, which showed that continuing combination therapy at a reduced dose led to better outcomes than did switching to methotrexate alone or placebo. “This may be for some patients what they prefer if they don’t tolerate methotrexate,” she added.
“It’s wonderful to have these data to counsel patients. This is something we face every day,” wrote Elizabeth Wahl, MD, who is an acting assistant professor at the University of Washington, Seattle, and acting chief of rheumatology at the VA Puget Sound Healthcare System.
The study was funded by Amgen. Dr. Curtis has received grants or research support from AbbVie, Amgen, Bristol-Myers Squibb, Corrona, Janssen, Lilly, Myriad, Pfizer, Regeneron, Roche, and UCB. Dr. Pope consults for a variety of pharmaceutical companies. Dr. Wahl has no relevant financial disclosures.
SOURCE: Curtis JR et al. Arthritis Rheumatol. 2020;72(suppl 10), Abstract 0939.
In patients with RA whose disease is well controlled by methotrexate combined with etanercept, withdrawal of methotrexate led to long-term outcomes that were nearly as good as continuation of combination therapy. The finding comes from the randomized, controlled SEAM-RA trial that sought to address weaknesses of previous studies. It included a long lead-in time with stringent criteria to ensure that participants had very good disease control.
Both the American College of Rheumatology and the European League Against Rheumatism recommend tapering medication in RA patients who are in long-term remission, but there is no established optimal strategy.
“There have been some prior RA trials that have looked at therapy reduction or withdrawal, but most did not use a very stringent definition of how well people were when they began. Were they in remission, or only in low disease activity?” said Jeffrey R. Curtis, MD, during a presentation of the results at the virtual annual meeting of the ACR. The study was also published online Nov. 18 in Arthritis & Rheumatology.
Stringent remission criteria
The key feature of the trial was the 6-month run-in period, when subjects were taking 50 mg etanercept once per week and 10-25 mg of oral methotrexate once per week, and had to complete at least three visits. They were excluded from the ensuing randomization if they had a Simplified Disease Activity Index (SDAI) score >3.3 and ≤11 at two or more visits, had an SDAI >11 at any time during the run-in period, or had an SDAI >3.3 at the third run-in visit.
“We [wanted them] to be doing quite well for a long period of time. That was empirically confirmed under observation as part of the lead-in period, and even before that, the clinical investigator had to affirm that they believed the patient was doing well for 6 or more months even before they were screened to enter the trial,” said Dr. Curtis, professor of medicine in the division of clinical immunology and rheumatology at the University of Alabama at Birmingham.
Once enrolled in the trial, patients were randomized 2:2:1 to continuing etanercept only (n = 101), continuing methotrexate only (n = 101), or continuing both medications (n = 51). Patients were eligible for rescue after randomization if they had an SDAI score >11 at any time, SDAI between 3.3 and 11 on three separate visits, or between 3.3 and 11 at two consecutive visits at least 2 weeks apart. About three-quarters of patients in each treatment arm were female, with a mean age of about 55 years, and 82%-91% were White.
Good remission recovery with rescue therapy
At week 48, 28.7% of the methotrexate-only group were in remission (SDAI ≤3.3), compared with 49.5% of the etanercept-only group (P = .004) and 52.9% of the combination group (P = .006). Time to disease worsening was shorter in the methotrexate-only group (median, 198 days) than in the etanercept-only group (median, not estimable; P < .001) and the combined therapy group (median, not estimable; P < .001).
The researchers also found that most patients who underwent rescue therapy once again achieved remission, including 71% of the methotrexate-only group, 75% of the etanercept-only group, and 80% of the combination therapy group. There was no between-group differences in the time required to reattain remission.
The high rate of remission recovery was a good sign, Dr. Curtis said. “To me as a clinician, the risk to try [withdrawing a medication] is quite low because the likelihood you can regain where you were before is quite good. It’s obviously more successful if you stop methotrexate and continue etanercept than if you do the reverse, but to me, this is quite a practical trial, and in fact the rigor of the inclusion criteria are much more like the patients I’m talking to about stopping therapy than some of the past studies in this regard. I think it’s quite useful in terms of generalizability. We want people that are doing this well or close to it before we take away medication.”
Positive reactions from rheumatologists
The reaction from the viewing audience was also positive. “I think this study fills a big data gap for what we do in clinical practice,” wrote Janet Pope, MD, in comments during the session.
Dr. Pope, who is a professor of medicine at the University of Western Ontario and head of rheumatology at St. Joseph’s Health Centre, both in London, said that the results build on previous work, including the CAMEO study, which showed that discontinuation of methotrexate in patients taking methotrexate and etanercept failed to achieve noninferiority to continuation of both medications, and the PRIZE study, which showed that continuing combination therapy at a reduced dose led to better outcomes than did switching to methotrexate alone or placebo. “This may be for some patients what they prefer if they don’t tolerate methotrexate,” she added.
“It’s wonderful to have these data to counsel patients. This is something we face every day,” wrote Elizabeth Wahl, MD, who is an acting assistant professor at the University of Washington, Seattle, and acting chief of rheumatology at the VA Puget Sound Healthcare System.
The study was funded by Amgen. Dr. Curtis has received grants or research support from AbbVie, Amgen, Bristol-Myers Squibb, Corrona, Janssen, Lilly, Myriad, Pfizer, Regeneron, Roche, and UCB. Dr. Pope consults for a variety of pharmaceutical companies. Dr. Wahl has no relevant financial disclosures.
SOURCE: Curtis JR et al. Arthritis Rheumatol. 2020;72(suppl 10), Abstract 0939.
FROM ACR 2020

Telehealth finds acceptance among patients with CF, clinicians
(CF) and the physicians who treat them, according to three new studies. The surveys examined attitudes during the COVID-19 pandemic, which complicates interpretation of the survey, but the results nevertheless bode well for telehealth’s future in the management of CF.

“Patients could be responding positively just because they could have a visit during the pandemic,” said Andrew NeSmith, during a presentation of a survey of adults with CF at the virtual North American Cystic Fibrosis Conference. Mr. NeSmith is the clinical data coordinator at the University of Alabama at Birmingham Cystic Fibrosis Center.
Other posters at the conference examined attitudes among pediatric populations and treating physicians, with generally positive results, which has generated optimism that telehealth could become an important element of care after the pandemic fades. “This data suggests that telehealth could be integrated into routine follow-up care in the CF chronic care model,” said Mr. NeSmith.
His team collected responses from 119 individuals at the University of Alabama at Birmingham; Boston Children’s Hospital; Brigham and Women’s Hospital, Boston; Virginia Commonwealth University, Richmond; and West Virginia University, Morgantown. A total of 28% had conducted a prior telehealth visit before the study; 92% of visits were conducted with a medical doctor. Only 13% reported experiencing difficulties with their first telehealth visit. Eighty-five percent rated convenience, and 77% rated their satisfaction with telehealth as “high.” Most (92%) said they were able to see their desired disciplines, 95% felt all of their issues had been addressed, and 83% strongly agreed that telehealth visits were of adequate length.
Not everything was rosy. A total of 48% of participants expressed at least moderate concern over a lack of pulmonary function test or throat/sputum culture. There were much fewer concerns over missing vital signs or weight measurements.
The overall results weren’t surprising to Robert Giusti, MD, clinical professor of pediatrics at New York University and director of the Pediatric Cystic Fibrosis Center, New York, who was not involved in the study. “I was expecting that patients were going to like it. It makes their life easier,” he said in an interview.
A survey of families of pediatric individuals with CF at seven centers found similar levels of satisfaction. A total of 23% had used telehealth previously; 96% rated convenience, and 93% rated satisfaction as “high.” Almost all (99%) felt that all concerns were met, 98% said that sessions were adequately long, and 87% had no trouble connecting to the visit.
Some participants in this survey had concerns about what might be missing with a televisit. Half (52%) had at least a moderate concern over lack of pulmonary function tests, 45% over lack of vital signs, 29% about lack of weight measurements, and 64% about the need for throat/sputum culture. Despite those issues, 69% preferred that “some” and 22% preferred that “most” future visits be conducted by telehealth.
A survey of physicians who used telehealth with CF patients also found broad support. They reported some challenges, with 70% saying they experienced technical difficulty, and 77% saying it “took time” to resolve a visit with only 18% reporting that visits were “quickly resolved.” Most (86%) said they were satisfied with telehealth for care delivery, and 78% said it was appropriate for most patients. Most said telehealth improved the patient-physician relationship, and they believed visits were more efficient when conducted via telehealth than in person. A majority (81%) endorsed using telehealth for some visits, and 12% for most visits.
A key question will be how telehealth affects patient outcomes, according to Ryan Perkins, MD, who was a coauthor of the survey of physicians. “If they’re not doing as well from an outcomes perspective, that would be a huge limitation to our patients,” said Dr. Perkins, who is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital.
Although the study examined only models of care that were entirely virtual, Dr. Perkins noted that hybrid in-person/virtual care models are also possible. “Do we have better outcomes doing it that way? Is there higher patient satisfaction? I’m sure that will be a hot topic moving forward.”
Dr. Perkins noted that patients expressed concern about not being able to get sputum cultures and spirometry recordings during telehealth sessions. “That’s not really surprising to me, but I think it raises the question as we’re imagining care models for the future – how can we implement those components into future care delivery?”
Another hurdle will be insurance coverage. “My fear is that insurance companies are going to cut down the amount of reimbursement for telehealth visits in the future and just going to make it more complicated,” said Dr. Giusti. “Certainly, though, I think telehealth is an important outreach that we’d like to continue with our patients.”
Mr. NeSmith, Dr. Giusti, and Dr. Perkins reported no relevant financial disclosures.
SOURCE: NeSmith A et al. NACFC 2020, Abstracts 797, 799, 810.
(CF) and the physicians who treat them, according to three new studies. The surveys examined attitudes during the COVID-19 pandemic, which complicates interpretation of the survey, but the results nevertheless bode well for telehealth’s future in the management of CF.
“Patients could be responding positively just because they could have a visit during the pandemic,” said Andrew NeSmith, during a presentation of a survey of adults with CF at the virtual North American Cystic Fibrosis Conference. Mr. NeSmith is the clinical data coordinator at the University of Alabama at Birmingham Cystic Fibrosis Center.
Other posters at the conference examined attitudes among pediatric populations and treating physicians, with generally positive results, which has generated optimism that telehealth could become an important element of care after the pandemic fades. “This data suggests that telehealth could be integrated into routine follow-up care in the CF chronic care model,” said Mr. NeSmith.
His team collected responses from 119 individuals at the University of Alabama at Birmingham; Boston Children’s Hospital; Brigham and Women’s Hospital, Boston; Virginia Commonwealth University, Richmond; and West Virginia University, Morgantown. A total of 28% had conducted a prior telehealth visit before the study; 92% of visits were conducted with a medical doctor. Only 13% reported experiencing difficulties with their first telehealth visit. Eighty-five percent rated convenience, and 77% rated their satisfaction with telehealth as “high.” Most (92%) said they were able to see their desired disciplines, 95% felt all of their issues had been addressed, and 83% strongly agreed that telehealth visits were of adequate length.
Not everything was rosy. A total of 48% of participants expressed at least moderate concern over a lack of pulmonary function test or throat/sputum culture. There were much fewer concerns over missing vital signs or weight measurements.
The overall results weren’t surprising to Robert Giusti, MD, clinical professor of pediatrics at New York University and director of the Pediatric Cystic Fibrosis Center, New York, who was not involved in the study. “I was expecting that patients were going to like it. It makes their life easier,” he said in an interview.
A survey of families of pediatric individuals with CF at seven centers found similar levels of satisfaction. A total of 23% had used telehealth previously; 96% rated convenience, and 93% rated satisfaction as “high.” Almost all (99%) felt that all concerns were met, 98% said that sessions were adequately long, and 87% had no trouble connecting to the visit.
Some participants in this survey had concerns about what might be missing with a televisit. Half (52%) had at least a moderate concern over lack of pulmonary function tests, 45% over lack of vital signs, 29% about lack of weight measurements, and 64% about the need for throat/sputum culture. Despite those issues, 69% preferred that “some” and 22% preferred that “most” future visits be conducted by telehealth.
A survey of physicians who used telehealth with CF patients also found broad support. They reported some challenges, with 70% saying they experienced technical difficulty, and 77% saying it “took time” to resolve a visit with only 18% reporting that visits were “quickly resolved.” Most (86%) said they were satisfied with telehealth for care delivery, and 78% said it was appropriate for most patients. Most said telehealth improved the patient-physician relationship, and they believed visits were more efficient when conducted via telehealth than in person. A majority (81%) endorsed using telehealth for some visits, and 12% for most visits.
A key question will be how telehealth affects patient outcomes, according to Ryan Perkins, MD, who was a coauthor of the survey of physicians. “If they’re not doing as well from an outcomes perspective, that would be a huge limitation to our patients,” said Dr. Perkins, who is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital.
Although the study examined only models of care that were entirely virtual, Dr. Perkins noted that hybrid in-person/virtual care models are also possible. “Do we have better outcomes doing it that way? Is there higher patient satisfaction? I’m sure that will be a hot topic moving forward.”
Dr. Perkins noted that patients expressed concern about not being able to get sputum cultures and spirometry recordings during telehealth sessions. “That’s not really surprising to me, but I think it raises the question as we’re imagining care models for the future – how can we implement those components into future care delivery?”
Another hurdle will be insurance coverage. “My fear is that insurance companies are going to cut down the amount of reimbursement for telehealth visits in the future and just going to make it more complicated,” said Dr. Giusti. “Certainly, though, I think telehealth is an important outreach that we’d like to continue with our patients.”
Mr. NeSmith, Dr. Giusti, and Dr. Perkins reported no relevant financial disclosures.
SOURCE: NeSmith A et al. NACFC 2020, Abstracts 797, 799, 810.
(CF) and the physicians who treat them, according to three new studies. The surveys examined attitudes during the COVID-19 pandemic, which complicates interpretation of the survey, but the results nevertheless bode well for telehealth’s future in the management of CF.
“Patients could be responding positively just because they could have a visit during the pandemic,” said Andrew NeSmith, during a presentation of a survey of adults with CF at the virtual North American Cystic Fibrosis Conference. Mr. NeSmith is the clinical data coordinator at the University of Alabama at Birmingham Cystic Fibrosis Center.
Other posters at the conference examined attitudes among pediatric populations and treating physicians, with generally positive results, which has generated optimism that telehealth could become an important element of care after the pandemic fades. “This data suggests that telehealth could be integrated into routine follow-up care in the CF chronic care model,” said Mr. NeSmith.
His team collected responses from 119 individuals at the University of Alabama at Birmingham; Boston Children’s Hospital; Brigham and Women’s Hospital, Boston; Virginia Commonwealth University, Richmond; and West Virginia University, Morgantown. A total of 28% had conducted a prior telehealth visit before the study; 92% of visits were conducted with a medical doctor. Only 13% reported experiencing difficulties with their first telehealth visit. Eighty-five percent rated convenience, and 77% rated their satisfaction with telehealth as “high.” Most (92%) said they were able to see their desired disciplines, 95% felt all of their issues had been addressed, and 83% strongly agreed that telehealth visits were of adequate length.
Not everything was rosy. A total of 48% of participants expressed at least moderate concern over a lack of pulmonary function test or throat/sputum culture. There were much fewer concerns over missing vital signs or weight measurements.
The overall results weren’t surprising to Robert Giusti, MD, clinical professor of pediatrics at New York University and director of the Pediatric Cystic Fibrosis Center, New York, who was not involved in the study. “I was expecting that patients were going to like it. It makes their life easier,” he said in an interview.
A survey of families of pediatric individuals with CF at seven centers found similar levels of satisfaction. A total of 23% had used telehealth previously; 96% rated convenience, and 93% rated satisfaction as “high.” Almost all (99%) felt that all concerns were met, 98% said that sessions were adequately long, and 87% had no trouble connecting to the visit.
Some participants in this survey had concerns about what might be missing with a televisit. Half (52%) had at least a moderate concern over lack of pulmonary function tests, 45% over lack of vital signs, 29% about lack of weight measurements, and 64% about the need for throat/sputum culture. Despite those issues, 69% preferred that “some” and 22% preferred that “most” future visits be conducted by telehealth.
A survey of physicians who used telehealth with CF patients also found broad support. They reported some challenges, with 70% saying they experienced technical difficulty, and 77% saying it “took time” to resolve a visit with only 18% reporting that visits were “quickly resolved.” Most (86%) said they were satisfied with telehealth for care delivery, and 78% said it was appropriate for most patients. Most said telehealth improved the patient-physician relationship, and they believed visits were more efficient when conducted via telehealth than in person. A majority (81%) endorsed using telehealth for some visits, and 12% for most visits.
A key question will be how telehealth affects patient outcomes, according to Ryan Perkins, MD, who was a coauthor of the survey of physicians. “If they’re not doing as well from an outcomes perspective, that would be a huge limitation to our patients,” said Dr. Perkins, who is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital.
Although the study examined only models of care that were entirely virtual, Dr. Perkins noted that hybrid in-person/virtual care models are also possible. “Do we have better outcomes doing it that way? Is there higher patient satisfaction? I’m sure that will be a hot topic moving forward.”
Dr. Perkins noted that patients expressed concern about not being able to get sputum cultures and spirometry recordings during telehealth sessions. “That’s not really surprising to me, but I think it raises the question as we’re imagining care models for the future – how can we implement those components into future care delivery?”
Another hurdle will be insurance coverage. “My fear is that insurance companies are going to cut down the amount of reimbursement for telehealth visits in the future and just going to make it more complicated,” said Dr. Giusti. “Certainly, though, I think telehealth is an important outreach that we’d like to continue with our patients.”
Mr. NeSmith, Dr. Giusti, and Dr. Perkins reported no relevant financial disclosures.
SOURCE: NeSmith A et al. NACFC 2020, Abstracts 797, 799, 810.
FROM NACFC 2020
Poverty raises depression risk in patients with cystic fibrosis
Poor people with chronic illness have greater difficulty managing their disease than do their better-off counterparts, and a new study confirms this reality for patients with cystic fibrosis.
and anxiety symptoms, according to a new cross-sectional study. The data were drawn from the Cystic Fibrosis Foundation’s Success with Therapies Research Consortium.
“Assessing the special challenges that individuals with lower SES face, including financial barriers, is essential to understand how we can address the unique combinations of adherence barriers. In other chronic disorders, financial barriers or lower socioeconomic status is associated with nonadherence, but this relationship has not been well established in cystic fibrosis,” said Kimberly Dickinson, MD, MPH, of Johns Hopkins University, Baltimore, during her presentation of the results at the virtual North American Cystic Fibrosis Conference.

“I’ve always thought that my patients in the poorer population were doing worse, and I think this demonstrates that that’s true,” said Robert Giusti, MD, in an interview. Dr. Giusti is a clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center in New York. He was not involved in the study.
“These are very pertinent issues, especially if you think about the pandemic, and some of the issues related to mental health. It just highlights the importance of socioeconomic status and screening for some of the known risk factors so that we can develop interventions or programs to provide equitable care to all of our cystic fibrosis patients,” said Ryan Perkins, MD, who moderated the session where the study was presented. He is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, also in Boston.
The researchers looked retrospectively at 1 year’s worth of pharmacy refill receipts and number of times prescriptions were refilled versus the number of times prescribed, then calculated medicinal possession ratios. This was cross-referenced with annual household income and insurance status of patients with CF at 12 pediatric and 9 adult CF care centers, for a total of 376 patients (128 pediatric and 248 adult).
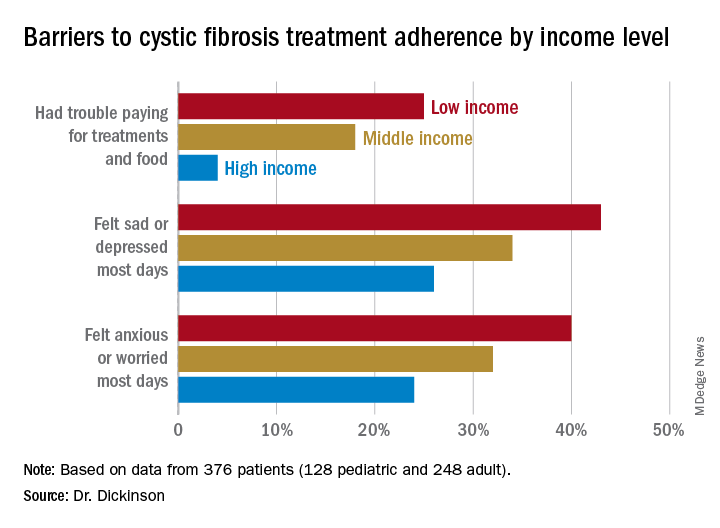
In this population, 32% of participants had public or no insurance, 68% had private or military insurance. The public/no insurance group was more likely than the private/military insurance group to report having trouble paying for treatments, food, or critical expenses related to CF care (23.3% vs. 12.1%, respectively); feeling symptoms on most days of depression (42.5% vs. 31.3%) or anxiety (40.0% vs. 28.5%); and experiencing conflict or stress with loved ones over treatments (30.0% vs. 20.3%) (P < .05 for all).
In all, 35% had a household income less than $40,000 per year, 33% between $44,000 and $100,000, and 32% higher than $100,000. The low-income group had a lower composite medication possession ratio (0.41) than the middle- (0.44) or high-income (0.52) groups, were more likely to have trouble paying for treatments, food, or treatment-related expenses (25%, 18%, 4%, respectively); were more likely most days to report symptoms of depression (43%, 34%, 26%) or anxiety (40%, 32%, 24%), and to have concerns about whether treatments were effective (42%, 27%, 29%). They were more likely to not be able to maintain a daily schedule or routine for treatments (28%, 22%, 14%).
The study showed that adherence barriers and suboptimal adherence are issues that cross all socioeconomic categories, though they were more problematic in the lowest bracket. Greater anxiety and depression among lower income individuals and those with private or no insurance was a key finding, according to Dr. Dickinson. “It highlights the importance of screening for mental health comorbidities that may impact non-adherence,” she said.
The study received funding from the Cystic Fibrosis Foundation. Dr. Dickinson, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
Poor people with chronic illness have greater difficulty managing their disease than do their better-off counterparts, and a new study confirms this reality for patients with cystic fibrosis.
and anxiety symptoms, according to a new cross-sectional study. The data were drawn from the Cystic Fibrosis Foundation’s Success with Therapies Research Consortium.
“Assessing the special challenges that individuals with lower SES face, including financial barriers, is essential to understand how we can address the unique combinations of adherence barriers. In other chronic disorders, financial barriers or lower socioeconomic status is associated with nonadherence, but this relationship has not been well established in cystic fibrosis,” said Kimberly Dickinson, MD, MPH, of Johns Hopkins University, Baltimore, during her presentation of the results at the virtual North American Cystic Fibrosis Conference.
“I’ve always thought that my patients in the poorer population were doing worse, and I think this demonstrates that that’s true,” said Robert Giusti, MD, in an interview. Dr. Giusti is a clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center in New York. He was not involved in the study.
“These are very pertinent issues, especially if you think about the pandemic, and some of the issues related to mental health. It just highlights the importance of socioeconomic status and screening for some of the known risk factors so that we can develop interventions or programs to provide equitable care to all of our cystic fibrosis patients,” said Ryan Perkins, MD, who moderated the session where the study was presented. He is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, also in Boston.
The researchers looked retrospectively at 1 year’s worth of pharmacy refill receipts and number of times prescriptions were refilled versus the number of times prescribed, then calculated medicinal possession ratios. This was cross-referenced with annual household income and insurance status of patients with CF at 12 pediatric and 9 adult CF care centers, for a total of 376 patients (128 pediatric and 248 adult).
In this population, 32% of participants had public or no insurance, 68% had private or military insurance. The public/no insurance group was more likely than the private/military insurance group to report having trouble paying for treatments, food, or critical expenses related to CF care (23.3% vs. 12.1%, respectively); feeling symptoms on most days of depression (42.5% vs. 31.3%) or anxiety (40.0% vs. 28.5%); and experiencing conflict or stress with loved ones over treatments (30.0% vs. 20.3%) (P < .05 for all).
In all, 35% had a household income less than $40,000 per year, 33% between $44,000 and $100,000, and 32% higher than $100,000. The low-income group had a lower composite medication possession ratio (0.41) than the middle- (0.44) or high-income (0.52) groups, were more likely to have trouble paying for treatments, food, or treatment-related expenses (25%, 18%, 4%, respectively); were more likely most days to report symptoms of depression (43%, 34%, 26%) or anxiety (40%, 32%, 24%), and to have concerns about whether treatments were effective (42%, 27%, 29%). They were more likely to not be able to maintain a daily schedule or routine for treatments (28%, 22%, 14%).
The study showed that adherence barriers and suboptimal adherence are issues that cross all socioeconomic categories, though they were more problematic in the lowest bracket. Greater anxiety and depression among lower income individuals and those with private or no insurance was a key finding, according to Dr. Dickinson. “It highlights the importance of screening for mental health comorbidities that may impact non-adherence,” she said.
The study received funding from the Cystic Fibrosis Foundation. Dr. Dickinson, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
Poor people with chronic illness have greater difficulty managing their disease than do their better-off counterparts, and a new study confirms this reality for patients with cystic fibrosis.
and anxiety symptoms, according to a new cross-sectional study. The data were drawn from the Cystic Fibrosis Foundation’s Success with Therapies Research Consortium.
“Assessing the special challenges that individuals with lower SES face, including financial barriers, is essential to understand how we can address the unique combinations of adherence barriers. In other chronic disorders, financial barriers or lower socioeconomic status is associated with nonadherence, but this relationship has not been well established in cystic fibrosis,” said Kimberly Dickinson, MD, MPH, of Johns Hopkins University, Baltimore, during her presentation of the results at the virtual North American Cystic Fibrosis Conference.
“I’ve always thought that my patients in the poorer population were doing worse, and I think this demonstrates that that’s true,” said Robert Giusti, MD, in an interview. Dr. Giusti is a clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center in New York. He was not involved in the study.
“These are very pertinent issues, especially if you think about the pandemic, and some of the issues related to mental health. It just highlights the importance of socioeconomic status and screening for some of the known risk factors so that we can develop interventions or programs to provide equitable care to all of our cystic fibrosis patients,” said Ryan Perkins, MD, who moderated the session where the study was presented. He is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, also in Boston.
The researchers looked retrospectively at 1 year’s worth of pharmacy refill receipts and number of times prescriptions were refilled versus the number of times prescribed, then calculated medicinal possession ratios. This was cross-referenced with annual household income and insurance status of patients with CF at 12 pediatric and 9 adult CF care centers, for a total of 376 patients (128 pediatric and 248 adult).
In this population, 32% of participants had public or no insurance, 68% had private or military insurance. The public/no insurance group was more likely than the private/military insurance group to report having trouble paying for treatments, food, or critical expenses related to CF care (23.3% vs. 12.1%, respectively); feeling symptoms on most days of depression (42.5% vs. 31.3%) or anxiety (40.0% vs. 28.5%); and experiencing conflict or stress with loved ones over treatments (30.0% vs. 20.3%) (P < .05 for all).
In all, 35% had a household income less than $40,000 per year, 33% between $44,000 and $100,000, and 32% higher than $100,000. The low-income group had a lower composite medication possession ratio (0.41) than the middle- (0.44) or high-income (0.52) groups, were more likely to have trouble paying for treatments, food, or treatment-related expenses (25%, 18%, 4%, respectively); were more likely most days to report symptoms of depression (43%, 34%, 26%) or anxiety (40%, 32%, 24%), and to have concerns about whether treatments were effective (42%, 27%, 29%). They were more likely to not be able to maintain a daily schedule or routine for treatments (28%, 22%, 14%).
The study showed that adherence barriers and suboptimal adherence are issues that cross all socioeconomic categories, though they were more problematic in the lowest bracket. Greater anxiety and depression among lower income individuals and those with private or no insurance was a key finding, according to Dr. Dickinson. “It highlights the importance of screening for mental health comorbidities that may impact non-adherence,” she said.
The study received funding from the Cystic Fibrosis Foundation. Dr. Dickinson, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
FROM NACFC 2020
.
Triple combination therapy for cystic fibrosis linked to plunging hospitalizations
.
The triple combination therapy elexacaftor/tezacaftor/ivacaftor was associated with a near elimination of hospital stays in one hospital in Oregon, according to a new report. The hospital savings still weren’t nearly enough to pay for the cost of therapy, but the study underscores what many institutions have observed and adds a new layer to the view of quality of life improvements that the new therapy brings.
“After we started prescribing it, we noticed pretty quickly that hospitalizations appeared to be declining after patients started triple combination therapy, and we were hearing [similar reports] from other centers as well. We wanted to quantify this,” Eric C. Walter, MD, a pulmonologist at the Kaiser Permanente Cystic Fibrosis Clinic in Portland, Ore., said during a presentation of the results at the virtual North American Cystic Fibrosis Conference.
“We’re seeing that across the board in real practice, the number of cystic fibrosis patients that have to be hospitalized since starting this triple combination has gone down,” Robert Giusti, MD, said in an interview. “When they’ve had pulmonary exacerbations in the past, it was frequently because they failed outpatient antibiotics, but I think with triple combination therapy, if they do get sick, the likelihood is they will respond to oral antibiotics, so they may not need that prolonged IV course in the hospital.” Dr. Giusti is clinical professor of pediatrics at New York University and director of the Pediatric Cystic Fibrosis Center. He was not involved in the study.
The therapy gained Food and Drug Administration approval in 2019 for the treatment of individuals with CF who are aged 12 years and older, and who have at least one copy of the F508del mutation. Its cost is about $317,000 per year within the Kaiser Permanente system, according to Dr. Walter. His group compared hospitalization days for CF-related diagnoses from Jan. 1 through Aug. 31, 2020, before and after initiation of triple combination therapy.
Of 47 eligible patients, 32 initiated therapy during the study period; 38% had severe lung disease, defined by forced expiratory volume in 1 second (FEV1) value less than 40%. In 2020, before initiation of therapy, there were an average of 27 hospital days per month, all among patients with severe lung disease.
Among the therapy group, there were no hospitalizations after initiation of therapy through Aug. 31. Dr. Walter noted that the first hospitalization of a patient on triple combination therapy didn’t occur until early October.
At an average daily cost of $6,700, the researchers calculated that triple combination therapy saved about $189,000 per month in this group of patients. Comparing numbers to previous years, in which some patients with FEV1 greater than 40% were hospitalized, the researchers calculated that the therapy saved about $151,000 per month among individuals with severe lung disease: Patients with severe lung disease contributed about 80% to total hospital costs.
The drug itself for the whole group cost $845,000, dwarfing the $189,000 savings overall. But among patients with severe disease, hospitalization savings were about $151,000 per month, while the drug cost in this group was $316,800 per month.
Cost savings are important, but the improvement in quality of life for a patient – avoiding hospitalization, fewer impacts on work and education – should not be overlooked, according to Ryan Perkins, MD, a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, who moderated the session. “Some of these aren’t things people typically quantify and assign a price tag to,” Dr. Perkins said in an interview.
A big limitation of the work is that it was conducted during the COVID-19 pandemic, which may have reduced hospitalizations. “We did have patients that called in, told us they were sick, that they needed to be treated for an exacerbation but didn’t want to go to the hospital,” said Dr. Walter. To help adjust for this, Dr. Walter’s team plans to compare intravenous antibiotic exposure before and after triple combination therapy, reasoning that it could help clarify the pandemic’s impact on hospitalizations.
Dr. Walter, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
SOURCE: Walter E et al. NACFC 2020. Abstract 795.
.
The triple combination therapy elexacaftor/tezacaftor/ivacaftor was associated with a near elimination of hospital stays in one hospital in Oregon, according to a new report. The hospital savings still weren’t nearly enough to pay for the cost of therapy, but the study underscores what many institutions have observed and adds a new layer to the view of quality of life improvements that the new therapy brings.
“After we started prescribing it, we noticed pretty quickly that hospitalizations appeared to be declining after patients started triple combination therapy, and we were hearing [similar reports] from other centers as well. We wanted to quantify this,” Eric C. Walter, MD, a pulmonologist at the Kaiser Permanente Cystic Fibrosis Clinic in Portland, Ore., said during a presentation of the results at the virtual North American Cystic Fibrosis Conference.
“We’re seeing that across the board in real practice, the number of cystic fibrosis patients that have to be hospitalized since starting this triple combination has gone down,” Robert Giusti, MD, said in an interview. “When they’ve had pulmonary exacerbations in the past, it was frequently because they failed outpatient antibiotics, but I think with triple combination therapy, if they do get sick, the likelihood is they will respond to oral antibiotics, so they may not need that prolonged IV course in the hospital.” Dr. Giusti is clinical professor of pediatrics at New York University and director of the Pediatric Cystic Fibrosis Center. He was not involved in the study.
The therapy gained Food and Drug Administration approval in 2019 for the treatment of individuals with CF who are aged 12 years and older, and who have at least one copy of the F508del mutation. Its cost is about $317,000 per year within the Kaiser Permanente system, according to Dr. Walter. His group compared hospitalization days for CF-related diagnoses from Jan. 1 through Aug. 31, 2020, before and after initiation of triple combination therapy.
Of 47 eligible patients, 32 initiated therapy during the study period; 38% had severe lung disease, defined by forced expiratory volume in 1 second (FEV1) value less than 40%. In 2020, before initiation of therapy, there were an average of 27 hospital days per month, all among patients with severe lung disease.
Among the therapy group, there were no hospitalizations after initiation of therapy through Aug. 31. Dr. Walter noted that the first hospitalization of a patient on triple combination therapy didn’t occur until early October.
At an average daily cost of $6,700, the researchers calculated that triple combination therapy saved about $189,000 per month in this group of patients. Comparing numbers to previous years, in which some patients with FEV1 greater than 40% were hospitalized, the researchers calculated that the therapy saved about $151,000 per month among individuals with severe lung disease: Patients with severe lung disease contributed about 80% to total hospital costs.
The drug itself for the whole group cost $845,000, dwarfing the $189,000 savings overall. But among patients with severe disease, hospitalization savings were about $151,000 per month, while the drug cost in this group was $316,800 per month.
Cost savings are important, but the improvement in quality of life for a patient – avoiding hospitalization, fewer impacts on work and education – should not be overlooked, according to Ryan Perkins, MD, a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, who moderated the session. “Some of these aren’t things people typically quantify and assign a price tag to,” Dr. Perkins said in an interview.
A big limitation of the work is that it was conducted during the COVID-19 pandemic, which may have reduced hospitalizations. “We did have patients that called in, told us they were sick, that they needed to be treated for an exacerbation but didn’t want to go to the hospital,” said Dr. Walter. To help adjust for this, Dr. Walter’s team plans to compare intravenous antibiotic exposure before and after triple combination therapy, reasoning that it could help clarify the pandemic’s impact on hospitalizations.
Dr. Walter, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
SOURCE: Walter E et al. NACFC 2020. Abstract 795.
.
The triple combination therapy elexacaftor/tezacaftor/ivacaftor was associated with a near elimination of hospital stays in one hospital in Oregon, according to a new report. The hospital savings still weren’t nearly enough to pay for the cost of therapy, but the study underscores what many institutions have observed and adds a new layer to the view of quality of life improvements that the new therapy brings.
“After we started prescribing it, we noticed pretty quickly that hospitalizations appeared to be declining after patients started triple combination therapy, and we were hearing [similar reports] from other centers as well. We wanted to quantify this,” Eric C. Walter, MD, a pulmonologist at the Kaiser Permanente Cystic Fibrosis Clinic in Portland, Ore., said during a presentation of the results at the virtual North American Cystic Fibrosis Conference.
“We’re seeing that across the board in real practice, the number of cystic fibrosis patients that have to be hospitalized since starting this triple combination has gone down,” Robert Giusti, MD, said in an interview. “When they’ve had pulmonary exacerbations in the past, it was frequently because they failed outpatient antibiotics, but I think with triple combination therapy, if they do get sick, the likelihood is they will respond to oral antibiotics, so they may not need that prolonged IV course in the hospital.” Dr. Giusti is clinical professor of pediatrics at New York University and director of the Pediatric Cystic Fibrosis Center. He was not involved in the study.
The therapy gained Food and Drug Administration approval in 2019 for the treatment of individuals with CF who are aged 12 years and older, and who have at least one copy of the F508del mutation. Its cost is about $317,000 per year within the Kaiser Permanente system, according to Dr. Walter. His group compared hospitalization days for CF-related diagnoses from Jan. 1 through Aug. 31, 2020, before and after initiation of triple combination therapy.
Of 47 eligible patients, 32 initiated therapy during the study period; 38% had severe lung disease, defined by forced expiratory volume in 1 second (FEV1) value less than 40%. In 2020, before initiation of therapy, there were an average of 27 hospital days per month, all among patients with severe lung disease.
Among the therapy group, there were no hospitalizations after initiation of therapy through Aug. 31. Dr. Walter noted that the first hospitalization of a patient on triple combination therapy didn’t occur until early October.
At an average daily cost of $6,700, the researchers calculated that triple combination therapy saved about $189,000 per month in this group of patients. Comparing numbers to previous years, in which some patients with FEV1 greater than 40% were hospitalized, the researchers calculated that the therapy saved about $151,000 per month among individuals with severe lung disease: Patients with severe lung disease contributed about 80% to total hospital costs.
The drug itself for the whole group cost $845,000, dwarfing the $189,000 savings overall. But among patients with severe disease, hospitalization savings were about $151,000 per month, while the drug cost in this group was $316,800 per month.
Cost savings are important, but the improvement in quality of life for a patient – avoiding hospitalization, fewer impacts on work and education – should not be overlooked, according to Ryan Perkins, MD, a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, who moderated the session. “Some of these aren’t things people typically quantify and assign a price tag to,” Dr. Perkins said in an interview.
A big limitation of the work is that it was conducted during the COVID-19 pandemic, which may have reduced hospitalizations. “We did have patients that called in, told us they were sick, that they needed to be treated for an exacerbation but didn’t want to go to the hospital,” said Dr. Walter. To help adjust for this, Dr. Walter’s team plans to compare intravenous antibiotic exposure before and after triple combination therapy, reasoning that it could help clarify the pandemic’s impact on hospitalizations.
Dr. Walter, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
SOURCE: Walter E et al. NACFC 2020. Abstract 795.
FROM NACFC 2020
Cystic fibrosis patients’ vulnerability to COVID-19 infection: Preliminary data ease fears
But early results suggest that social distance measures and perhaps the younger average age of individuals with CF have prevented a severe impact on this patient population.
Not all of the news is good. Some research suggests that posttransplant individuals may be at greater risk of severe outcomes. However, researchers warned that the data are too sparse to draw firm conclusions, and ongoing analyses of patient registries and other sources should lend greater insight into the burden of COVID-19 among individuals with CF. Those were some of the conclusions presented at a session of the virtual North American Cystic Fibrosis Conference.
D.B. Sanders, MD, who is a pediatric pulmonologist at Riley Hospital for Children and the Indiana University, both in Indianapolis, presented data from the Cystic Fibrosis Foundation’s Patient Registry, which includes patients in the United States. As in other populations, he showed that health care use has gone down among individuals with CF. From April to September 2019, 81% of clinical encounters were in the clinic and 12% in the hospital. Over the same period in 2020, those numbers dropped to 35% and 4%, respectively, with 30% by phone or computer. In-person health care use rebounded somewhat between July 1 and Sept. 16, with 53% of encounters at the clinic, 5% at the hospital, and 28% conducted virtually. There were also dips in forced expiratory volume in one second (FEV1) and microbiology testing, from about 90% occurring during health encounters at the end of 2019 to fewer than 10% of encounters by April.
As of Aug. 17, Dr. Sanders reported that 3,048 individuals with CF had been tested for COVID-19, with 174 positive results.
Racial and ethnic disparities in positive test results seen in other populations were also observable among individuals with CF. Several groups made up a higher proportion of COVID-19–positive CF patients than the general CF population, including Hispanics (18% vs. 9%), Blacks (7% vs. 5%), and individuals with FEV1 value less than 40% predicted (14% vs. 8%).
As of Sept. 17, there had been 51 hospitalizations and two deaths in the United States among 212 individuals with CF who tested positive for COVID-19, with increasing numbers that mirror trends in the U.S. population. One death occurred in a patient with advanced lung disease, the other in a post–lung transplant patient. “Thankfully [the numbers are] not higher, but this is being followed very closely,” said Dr. Sanders during his presentation.
One encouraging bit of news was that hospitalizations among individuals with CF have dropped since the start of the pandemic. “I think this shows how good our families are at socially distancing, wearing masks, and now that they not being exposed to viruses, I think we’re seeing the fruits of this with fewer hospitalizations,” said Dr. Sanders. He noted that it’s possible some of the decline could have been to reluctance to go to the hospital, and the introduction of triple combination cystic fibrosis transmembrane conductance regulator modulator therapy has also likely contributed. “We were already seeing fewer hospitalizations even before the pandemic hit,” he said.
At the session, Rebecca Cosgriff, director of data and quality improvement at the Cystic Fibrosis Trust in the United Kingdom, presented an international perspective on COVID-19 cases among individuals with CF. At the beginning of the pandemic, the Cystic Fibrosis Global Registry Harmonization Group recruited country coordinators to collect anonymized data on infections, hospitalizations, and other outcomes. In April, the group published its initial findings from 40 cases in eight countries, which concluded that these cases generally resembled the broader population in clinical course, which assuaged initial fears.
Ms. Cosgriff reported on results from a second round of data collection with a cutoff date of June 19, which expanded to 19 countries and included many from South America and more in Europe. The network encompassed about 85,000 individuals with CF, and tallied 181 cases of COVID-19. A total of 149 cases were nontransplant, and 32 were posttransplant (28 lung only). Fully 15% of the nontransplant group were over age 40 years, compared with 41% in the transplant group. Homozygous F508del mutations were more common in the posttransplant group (59% vs. 36%). However, lung function, as estimated by the best FEV1 measured in the previous year prior to infection, differed between the nontransplant (73%) and posttransplant (80%) COVID-19 patients.
Across all age groups, hospitalizations were more common in patients with best FEV1 percentage predicted values less than 70% (P = .001). Ms. Cosgriff also expressed concern about the posttransplant group. “Across all outcomes that might be indicative of infection severity – hospitalization, ICU admission, new supplementary oxygen, and non-invasive ventilation – the proportion of the posttransplant group was higher across the board,” she said during her presentation.
There were seven deaths. Ms. Cosgriff noted that there were too few deaths to analyze trends, but she presented a slide showing characteristics of deceased patients. “Factors like being post–lung transplant, being male, having less FEV1 than predicted, being over 40, or having CF-related diabetes, all appear pretty frequently amongst the cohort of people who died,” she said.
Overall, the results of these surveys are encouraging, suggesting that early fears that COVID-19 cases could be more severe among individuals with CF may not have been borne out so far. Dr. Sanders noted in his talk that there aren’t enough cases in the U.S. cohort to show links to risk factors with statistical significance. “But thankfully we’re not seeing a host of negative outcomes,” he said.
Dr. Sanders and Ms Cosgriff have no relevant financial disclosures.
But early results suggest that social distance measures and perhaps the younger average age of individuals with CF have prevented a severe impact on this patient population.
Not all of the news is good. Some research suggests that posttransplant individuals may be at greater risk of severe outcomes. However, researchers warned that the data are too sparse to draw firm conclusions, and ongoing analyses of patient registries and other sources should lend greater insight into the burden of COVID-19 among individuals with CF. Those were some of the conclusions presented at a session of the virtual North American Cystic Fibrosis Conference.
D.B. Sanders, MD, who is a pediatric pulmonologist at Riley Hospital for Children and the Indiana University, both in Indianapolis, presented data from the Cystic Fibrosis Foundation’s Patient Registry, which includes patients in the United States. As in other populations, he showed that health care use has gone down among individuals with CF. From April to September 2019, 81% of clinical encounters were in the clinic and 12% in the hospital. Over the same period in 2020, those numbers dropped to 35% and 4%, respectively, with 30% by phone or computer. In-person health care use rebounded somewhat between July 1 and Sept. 16, with 53% of encounters at the clinic, 5% at the hospital, and 28% conducted virtually. There were also dips in forced expiratory volume in one second (FEV1) and microbiology testing, from about 90% occurring during health encounters at the end of 2019 to fewer than 10% of encounters by April.
As of Aug. 17, Dr. Sanders reported that 3,048 individuals with CF had been tested for COVID-19, with 174 positive results.
Racial and ethnic disparities in positive test results seen in other populations were also observable among individuals with CF. Several groups made up a higher proportion of COVID-19–positive CF patients than the general CF population, including Hispanics (18% vs. 9%), Blacks (7% vs. 5%), and individuals with FEV1 value less than 40% predicted (14% vs. 8%).
As of Sept. 17, there had been 51 hospitalizations and two deaths in the United States among 212 individuals with CF who tested positive for COVID-19, with increasing numbers that mirror trends in the U.S. population. One death occurred in a patient with advanced lung disease, the other in a post–lung transplant patient. “Thankfully [the numbers are] not higher, but this is being followed very closely,” said Dr. Sanders during his presentation.
One encouraging bit of news was that hospitalizations among individuals with CF have dropped since the start of the pandemic. “I think this shows how good our families are at socially distancing, wearing masks, and now that they not being exposed to viruses, I think we’re seeing the fruits of this with fewer hospitalizations,” said Dr. Sanders. He noted that it’s possible some of the decline could have been to reluctance to go to the hospital, and the introduction of triple combination cystic fibrosis transmembrane conductance regulator modulator therapy has also likely contributed. “We were already seeing fewer hospitalizations even before the pandemic hit,” he said.
At the session, Rebecca Cosgriff, director of data and quality improvement at the Cystic Fibrosis Trust in the United Kingdom, presented an international perspective on COVID-19 cases among individuals with CF. At the beginning of the pandemic, the Cystic Fibrosis Global Registry Harmonization Group recruited country coordinators to collect anonymized data on infections, hospitalizations, and other outcomes. In April, the group published its initial findings from 40 cases in eight countries, which concluded that these cases generally resembled the broader population in clinical course, which assuaged initial fears.
Ms. Cosgriff reported on results from a second round of data collection with a cutoff date of June 19, which expanded to 19 countries and included many from South America and more in Europe. The network encompassed about 85,000 individuals with CF, and tallied 181 cases of COVID-19. A total of 149 cases were nontransplant, and 32 were posttransplant (28 lung only). Fully 15% of the nontransplant group were over age 40 years, compared with 41% in the transplant group. Homozygous F508del mutations were more common in the posttransplant group (59% vs. 36%). However, lung function, as estimated by the best FEV1 measured in the previous year prior to infection, differed between the nontransplant (73%) and posttransplant (80%) COVID-19 patients.
Across all age groups, hospitalizations were more common in patients with best FEV1 percentage predicted values less than 70% (P = .001). Ms. Cosgriff also expressed concern about the posttransplant group. “Across all outcomes that might be indicative of infection severity – hospitalization, ICU admission, new supplementary oxygen, and non-invasive ventilation – the proportion of the posttransplant group was higher across the board,” she said during her presentation.
There were seven deaths. Ms. Cosgriff noted that there were too few deaths to analyze trends, but she presented a slide showing characteristics of deceased patients. “Factors like being post–lung transplant, being male, having less FEV1 than predicted, being over 40, or having CF-related diabetes, all appear pretty frequently amongst the cohort of people who died,” she said.
Overall, the results of these surveys are encouraging, suggesting that early fears that COVID-19 cases could be more severe among individuals with CF may not have been borne out so far. Dr. Sanders noted in his talk that there aren’t enough cases in the U.S. cohort to show links to risk factors with statistical significance. “But thankfully we’re not seeing a host of negative outcomes,” he said.
Dr. Sanders and Ms Cosgriff have no relevant financial disclosures.
But early results suggest that social distance measures and perhaps the younger average age of individuals with CF have prevented a severe impact on this patient population.
Not all of the news is good. Some research suggests that posttransplant individuals may be at greater risk of severe outcomes. However, researchers warned that the data are too sparse to draw firm conclusions, and ongoing analyses of patient registries and other sources should lend greater insight into the burden of COVID-19 among individuals with CF. Those were some of the conclusions presented at a session of the virtual North American Cystic Fibrosis Conference.
D.B. Sanders, MD, who is a pediatric pulmonologist at Riley Hospital for Children and the Indiana University, both in Indianapolis, presented data from the Cystic Fibrosis Foundation’s Patient Registry, which includes patients in the United States. As in other populations, he showed that health care use has gone down among individuals with CF. From April to September 2019, 81% of clinical encounters were in the clinic and 12% in the hospital. Over the same period in 2020, those numbers dropped to 35% and 4%, respectively, with 30% by phone or computer. In-person health care use rebounded somewhat between July 1 and Sept. 16, with 53% of encounters at the clinic, 5% at the hospital, and 28% conducted virtually. There were also dips in forced expiratory volume in one second (FEV1) and microbiology testing, from about 90% occurring during health encounters at the end of 2019 to fewer than 10% of encounters by April.
As of Aug. 17, Dr. Sanders reported that 3,048 individuals with CF had been tested for COVID-19, with 174 positive results.
Racial and ethnic disparities in positive test results seen in other populations were also observable among individuals with CF. Several groups made up a higher proportion of COVID-19–positive CF patients than the general CF population, including Hispanics (18% vs. 9%), Blacks (7% vs. 5%), and individuals with FEV1 value less than 40% predicted (14% vs. 8%).
As of Sept. 17, there had been 51 hospitalizations and two deaths in the United States among 212 individuals with CF who tested positive for COVID-19, with increasing numbers that mirror trends in the U.S. population. One death occurred in a patient with advanced lung disease, the other in a post–lung transplant patient. “Thankfully [the numbers are] not higher, but this is being followed very closely,” said Dr. Sanders during his presentation.
One encouraging bit of news was that hospitalizations among individuals with CF have dropped since the start of the pandemic. “I think this shows how good our families are at socially distancing, wearing masks, and now that they not being exposed to viruses, I think we’re seeing the fruits of this with fewer hospitalizations,” said Dr. Sanders. He noted that it’s possible some of the decline could have been to reluctance to go to the hospital, and the introduction of triple combination cystic fibrosis transmembrane conductance regulator modulator therapy has also likely contributed. “We were already seeing fewer hospitalizations even before the pandemic hit,” he said.
At the session, Rebecca Cosgriff, director of data and quality improvement at the Cystic Fibrosis Trust in the United Kingdom, presented an international perspective on COVID-19 cases among individuals with CF. At the beginning of the pandemic, the Cystic Fibrosis Global Registry Harmonization Group recruited country coordinators to collect anonymized data on infections, hospitalizations, and other outcomes. In April, the group published its initial findings from 40 cases in eight countries, which concluded that these cases generally resembled the broader population in clinical course, which assuaged initial fears.
Ms. Cosgriff reported on results from a second round of data collection with a cutoff date of June 19, which expanded to 19 countries and included many from South America and more in Europe. The network encompassed about 85,000 individuals with CF, and tallied 181 cases of COVID-19. A total of 149 cases were nontransplant, and 32 were posttransplant (28 lung only). Fully 15% of the nontransplant group were over age 40 years, compared with 41% in the transplant group. Homozygous F508del mutations were more common in the posttransplant group (59% vs. 36%). However, lung function, as estimated by the best FEV1 measured in the previous year prior to infection, differed between the nontransplant (73%) and posttransplant (80%) COVID-19 patients.
Across all age groups, hospitalizations were more common in patients with best FEV1 percentage predicted values less than 70% (P = .001). Ms. Cosgriff also expressed concern about the posttransplant group. “Across all outcomes that might be indicative of infection severity – hospitalization, ICU admission, new supplementary oxygen, and non-invasive ventilation – the proportion of the posttransplant group was higher across the board,” she said during her presentation.
There were seven deaths. Ms. Cosgriff noted that there were too few deaths to analyze trends, but she presented a slide showing characteristics of deceased patients. “Factors like being post–lung transplant, being male, having less FEV1 than predicted, being over 40, or having CF-related diabetes, all appear pretty frequently amongst the cohort of people who died,” she said.
Overall, the results of these surveys are encouraging, suggesting that early fears that COVID-19 cases could be more severe among individuals with CF may not have been borne out so far. Dr. Sanders noted in his talk that there aren’t enough cases in the U.S. cohort to show links to risk factors with statistical significance. “But thankfully we’re not seeing a host of negative outcomes,” he said.
Dr. Sanders and Ms Cosgriff have no relevant financial disclosures.
FROM NACFC 2020
Home spirometry improved monitoring of cystic fibrosis patients during COVID-19 pandemic
Home spirometry has become increasingly used among cystic fibrosis patients during the COVID-19 pandemic, and new research suggests that home devices perform reasonably well. Forced expiratory volume in 1 second (FEV1) values were a bit lower than values seen in clinical spirometry performed in the same patient at a nearby time point, but the procedure reliably picked up decreases in FEV1, potentially helping patients and clinicians spot exacerbations early.
“Home spirometry was sort of a curiosity that was slowly working its way into cystic fibrosis research in 2019, and then all of a sudden in 2020 it became front and center as the only way to continue with clinical monitoring and research in many cases,” Alexander Paynter, MS, a biostatistician at the Cystic Fibrosis Foundation’s Therapeutic Development Network Coordinating Center, said during a talk at the virtual North American Cystic Fibrosis Conference.
To better determine how closely home spirometry matches clinical spirometry, Mr. Paynter and his colleagues analyzed data from the eICE study, which included 267 cystic fibrosis patients aged 14 and over at 14 cystic fibrosis centers. They were randomized to use home spirometry as an early intervention to detect exacerbations, or to continue usual clinic care with visits to the clinic every 3 months. The dataset includes twice-weekly home spirometry values, with a full-year of follow-up data. The researchers compared the home spirometry data to the clinical data closest in time to it. Clinic spirometry data with no corresponding home data within 7 days were discarded.
There was an estimated difference of –2.01 mL between home and clinic tests, with home spirometry producing lower values (95% confidence interval, –3.56 to –0.45). “There is actually a bias in home spirometry as compared to clinic spirometry,” concluded Mr. Paynter.
One explanation for lower values in home spirometry is that users are inexperienced with the device. If that’s true, then agreement should improve over time, but the researchers didn’t see strong evidence of that. Among 44 patients who completed five clinical visits, there was a difference of –2.97 (standard deviation [SD], 10.51) at baseline, –1.66 at 3 months (SD, 13.49), –3.7 at 6 months (SD, 12.44), –0.86 at 9 months (SD, 13.73), and –0.53 at 12 months (SD, 13.35). Though there was improvement over time, “we don’t find a lot of evidence that this bias completely resolves,” said Mr. Paynter.
In fact, a more likely explanation is the presence of coaching by a technician during clinical spirometry, according to Robert J. Giusti, MD, clinical professor of pediatrics and director of the Pediatric Cystic Fibrosis Center at New York University. “When they’re doing it at home, they don’t do it with the same effort, so I think that coaching through telemedicine during the home spirometry would make that difference disappear,” he said when asked to comment on the study.
The researchers found that change-based endpoints were similar between clinic and at-home spirometry. Compared to baseline, the two showed similar declines over time. “The clinic and home observations tend to track each other pretty well. At 6 months, for instance, it’s about a change of three points decrease (in both). But the bad news is that the variability is much greater in home devices,” said Mr. Paynter, noting larger confidence intervals and standard deviation values associated with home spirometry. That could influence future clinical designs that may rely on home spirometry, since a larger confidence interval means reduced power, which could double or even quadruple the number of participants needed to achieve the required power, he said.
But from a clinical standpoint, the ability of home spirometry to consistently detect a change from baseline could be quite valuable to future patient management, according to Dr. Giusti. “It looks like home spirometry will show that kind of a decrease, so that it’s still sensitive to pick up the concern that a patient is getting worse at home,” he said.
That could be useful even after the COVID-19 pandemic passes, as patients continue to embrace home monitoring. Physicians could keep track of patients and keep them focused on their care and treatment through frequent telemedicine visits combined with home spirometry. “I really think home spirometry will keep us more focused on how the patients are doing and make for better outcomes,” said Dr. Giusti.
Mr. Paynter and Dr. Giusti have no relevant financial disclosures.
SOURCE: Alex Paynter et al. NACFC 2020. Poster 643.
Home spirometry has become increasingly used among cystic fibrosis patients during the COVID-19 pandemic, and new research suggests that home devices perform reasonably well. Forced expiratory volume in 1 second (FEV1) values were a bit lower than values seen in clinical spirometry performed in the same patient at a nearby time point, but the procedure reliably picked up decreases in FEV1, potentially helping patients and clinicians spot exacerbations early.
“Home spirometry was sort of a curiosity that was slowly working its way into cystic fibrosis research in 2019, and then all of a sudden in 2020 it became front and center as the only way to continue with clinical monitoring and research in many cases,” Alexander Paynter, MS, a biostatistician at the Cystic Fibrosis Foundation’s Therapeutic Development Network Coordinating Center, said during a talk at the virtual North American Cystic Fibrosis Conference.
To better determine how closely home spirometry matches clinical spirometry, Mr. Paynter and his colleagues analyzed data from the eICE study, which included 267 cystic fibrosis patients aged 14 and over at 14 cystic fibrosis centers. They were randomized to use home spirometry as an early intervention to detect exacerbations, or to continue usual clinic care with visits to the clinic every 3 months. The dataset includes twice-weekly home spirometry values, with a full-year of follow-up data. The researchers compared the home spirometry data to the clinical data closest in time to it. Clinic spirometry data with no corresponding home data within 7 days were discarded.
There was an estimated difference of –2.01 mL between home and clinic tests, with home spirometry producing lower values (95% confidence interval, –3.56 to –0.45). “There is actually a bias in home spirometry as compared to clinic spirometry,” concluded Mr. Paynter.
One explanation for lower values in home spirometry is that users are inexperienced with the device. If that’s true, then agreement should improve over time, but the researchers didn’t see strong evidence of that. Among 44 patients who completed five clinical visits, there was a difference of –2.97 (standard deviation [SD], 10.51) at baseline, –1.66 at 3 months (SD, 13.49), –3.7 at 6 months (SD, 12.44), –0.86 at 9 months (SD, 13.73), and –0.53 at 12 months (SD, 13.35). Though there was improvement over time, “we don’t find a lot of evidence that this bias completely resolves,” said Mr. Paynter.
In fact, a more likely explanation is the presence of coaching by a technician during clinical spirometry, according to Robert J. Giusti, MD, clinical professor of pediatrics and director of the Pediatric Cystic Fibrosis Center at New York University. “When they’re doing it at home, they don’t do it with the same effort, so I think that coaching through telemedicine during the home spirometry would make that difference disappear,” he said when asked to comment on the study.
The researchers found that change-based endpoints were similar between clinic and at-home spirometry. Compared to baseline, the two showed similar declines over time. “The clinic and home observations tend to track each other pretty well. At 6 months, for instance, it’s about a change of three points decrease (in both). But the bad news is that the variability is much greater in home devices,” said Mr. Paynter, noting larger confidence intervals and standard deviation values associated with home spirometry. That could influence future clinical designs that may rely on home spirometry, since a larger confidence interval means reduced power, which could double or even quadruple the number of participants needed to achieve the required power, he said.
But from a clinical standpoint, the ability of home spirometry to consistently detect a change from baseline could be quite valuable to future patient management, according to Dr. Giusti. “It looks like home spirometry will show that kind of a decrease, so that it’s still sensitive to pick up the concern that a patient is getting worse at home,” he said.
That could be useful even after the COVID-19 pandemic passes, as patients continue to embrace home monitoring. Physicians could keep track of patients and keep them focused on their care and treatment through frequent telemedicine visits combined with home spirometry. “I really think home spirometry will keep us more focused on how the patients are doing and make for better outcomes,” said Dr. Giusti.
Mr. Paynter and Dr. Giusti have no relevant financial disclosures.
SOURCE: Alex Paynter et al. NACFC 2020. Poster 643.
Home spirometry has become increasingly used among cystic fibrosis patients during the COVID-19 pandemic, and new research suggests that home devices perform reasonably well. Forced expiratory volume in 1 second (FEV1) values were a bit lower than values seen in clinical spirometry performed in the same patient at a nearby time point, but the procedure reliably picked up decreases in FEV1, potentially helping patients and clinicians spot exacerbations early.
“Home spirometry was sort of a curiosity that was slowly working its way into cystic fibrosis research in 2019, and then all of a sudden in 2020 it became front and center as the only way to continue with clinical monitoring and research in many cases,” Alexander Paynter, MS, a biostatistician at the Cystic Fibrosis Foundation’s Therapeutic Development Network Coordinating Center, said during a talk at the virtual North American Cystic Fibrosis Conference.
To better determine how closely home spirometry matches clinical spirometry, Mr. Paynter and his colleagues analyzed data from the eICE study, which included 267 cystic fibrosis patients aged 14 and over at 14 cystic fibrosis centers. They were randomized to use home spirometry as an early intervention to detect exacerbations, or to continue usual clinic care with visits to the clinic every 3 months. The dataset includes twice-weekly home spirometry values, with a full-year of follow-up data. The researchers compared the home spirometry data to the clinical data closest in time to it. Clinic spirometry data with no corresponding home data within 7 days were discarded.
There was an estimated difference of –2.01 mL between home and clinic tests, with home spirometry producing lower values (95% confidence interval, –3.56 to –0.45). “There is actually a bias in home spirometry as compared to clinic spirometry,” concluded Mr. Paynter.
One explanation for lower values in home spirometry is that users are inexperienced with the device. If that’s true, then agreement should improve over time, but the researchers didn’t see strong evidence of that. Among 44 patients who completed five clinical visits, there was a difference of –2.97 (standard deviation [SD], 10.51) at baseline, –1.66 at 3 months (SD, 13.49), –3.7 at 6 months (SD, 12.44), –0.86 at 9 months (SD, 13.73), and –0.53 at 12 months (SD, 13.35). Though there was improvement over time, “we don’t find a lot of evidence that this bias completely resolves,” said Mr. Paynter.
In fact, a more likely explanation is the presence of coaching by a technician during clinical spirometry, according to Robert J. Giusti, MD, clinical professor of pediatrics and director of the Pediatric Cystic Fibrosis Center at New York University. “When they’re doing it at home, they don’t do it with the same effort, so I think that coaching through telemedicine during the home spirometry would make that difference disappear,” he said when asked to comment on the study.
The researchers found that change-based endpoints were similar between clinic and at-home spirometry. Compared to baseline, the two showed similar declines over time. “The clinic and home observations tend to track each other pretty well. At 6 months, for instance, it’s about a change of three points decrease (in both). But the bad news is that the variability is much greater in home devices,” said Mr. Paynter, noting larger confidence intervals and standard deviation values associated with home spirometry. That could influence future clinical designs that may rely on home spirometry, since a larger confidence interval means reduced power, which could double or even quadruple the number of participants needed to achieve the required power, he said.
But from a clinical standpoint, the ability of home spirometry to consistently detect a change from baseline could be quite valuable to future patient management, according to Dr. Giusti. “It looks like home spirometry will show that kind of a decrease, so that it’s still sensitive to pick up the concern that a patient is getting worse at home,” he said.
That could be useful even after the COVID-19 pandemic passes, as patients continue to embrace home monitoring. Physicians could keep track of patients and keep them focused on their care and treatment through frequent telemedicine visits combined with home spirometry. “I really think home spirometry will keep us more focused on how the patients are doing and make for better outcomes,” said Dr. Giusti.
Mr. Paynter and Dr. Giusti have no relevant financial disclosures.
SOURCE: Alex Paynter et al. NACFC 2020. Poster 643.
FROM NACFC 2020
Cystic fibrosis treatment: Triple combination benefits patients with advanced disease
New CFTR [cystic fibrosis transmembrane conductance regulator] modulator therapies can offer life-altering benefits to some patients with cystic fibrosis, even those with advanced disease.
, according to a multicenter analysis of patients taking elexacaftor, tezacaftor, and ivacaftor.
The study participants had a percent predicted forced expiratory volume in 1 second (ppFEV1) of 40% or below, or other high-risk factors. Researchers compared them to control patients who were genetically ineligible for triple combination therapy.
Previous studies of such patients on individual drugs or previous combinations showed increases in lung function in patients with advanced disease, though the magnitude of improvement varied across regimens. “With this improvement, it’s unclear how CFTR modulators should affect lung transplant referral timing,” Brent Bermingham, MD, said during a presentation of the study at the virtual North American Cystic Fibrosis Conference.
“The rationale for our study was that despite patients with advanced lung disease being excluded from phase III trials (of elexacaftor, tezacaftor, and ivacaftor), they are receiving a therapy with an unknown clinical efficacy and safety profile,” said Dr. Bermingham, a pulmonary and critical care fellow at the Medical University of South Carolina, Charleston.
Lung transplant referral guidelines recommend that physicians initiate discussions about the potential benefit of lung transplant when FEV1 drops below 50% of the predicted value. Patients should be referred for a transplant when the value is below 50% and rapidly declining (>20% decline in the past 12 months), when it drops below 40% with accompanying predictors of shortened survival, or when it drops below 30%. The guidelines were published before approval of triple combination therapy.
The researchers conducted an open-label retrospective analysis of 60 patients started on triple combination therapy between September 2019 and February 2020 at three centers in the Southeast. They compared percent predicted ppFEV1 values prior to initiation of therapy to ppFEV1 values obtained 2-12 weeks after the start of therapy. Patients on therapy were compared with 10 genetically ineligible controls. The two groups were generally similar aside from genetic status, though 100% of the therapy group had pancreatic insufficiency, compared with 90% of controls (P = .013).
The therapeutic group experienced a 7.8% increase in ppFEV1 after starting therapy (P < .001), compared with a 0.5% decrease in controls (P = .65). Before initiation of therapy, 33% of the therapy group met the criteria for initiating a transplant discussion, while 67% had been recommended for transplant. After therapy, 55% met the criteria for discussion, 33% were recommended for transplant, and 12% no longer met the criteria for discussion of transplantation. Fifty percent of controls were in discussion, and this dropped to 40%, while 50% were referred for transplantation, and this increased to 60%. On therapy, transplant referral candidates had an increase of forced vital capacity from 48.9 to 59.16 (P < .001).
Adverse events were rare, with only one discontinuation that occurred following a lung transplant and was not believed to be treatment related.
“Our study had a large number of patients taken from multiple centers, which suggests generalizabilty and real-world experience,” said Dr. Bermingham.
The results are encouraging, said Robert J. Giusti, MD, clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center.
“We’re all remarking how wonderful patients feel these days. It’s really a disease-altering treatment. But for the high-risk group, whose FEV1 is less than 40%, those are the patients we’re more concerned about because we thought maybe they had too much lung disease, and that they wouldn’t benefit from triple combination. But they seem to be improving, so that’s very reassuring,” said Dr. Giusti, who was not involved in the study.
The study received funding from the Cystic Fibrosis Foundation and Dartmouth College. Dr. Bermingham and Dr. Giusti have no relevant financial disclosures.
SOURCE: Bermingham B et al. NACFC 2020, Abstract 645.
New CFTR [cystic fibrosis transmembrane conductance regulator] modulator therapies can offer life-altering benefits to some patients with cystic fibrosis, even those with advanced disease.
, according to a multicenter analysis of patients taking elexacaftor, tezacaftor, and ivacaftor.
The study participants had a percent predicted forced expiratory volume in 1 second (ppFEV1) of 40% or below, or other high-risk factors. Researchers compared them to control patients who were genetically ineligible for triple combination therapy.
Previous studies of such patients on individual drugs or previous combinations showed increases in lung function in patients with advanced disease, though the magnitude of improvement varied across regimens. “With this improvement, it’s unclear how CFTR modulators should affect lung transplant referral timing,” Brent Bermingham, MD, said during a presentation of the study at the virtual North American Cystic Fibrosis Conference.
“The rationale for our study was that despite patients with advanced lung disease being excluded from phase III trials (of elexacaftor, tezacaftor, and ivacaftor), they are receiving a therapy with an unknown clinical efficacy and safety profile,” said Dr. Bermingham, a pulmonary and critical care fellow at the Medical University of South Carolina, Charleston.
Lung transplant referral guidelines recommend that physicians initiate discussions about the potential benefit of lung transplant when FEV1 drops below 50% of the predicted value. Patients should be referred for a transplant when the value is below 50% and rapidly declining (>20% decline in the past 12 months), when it drops below 40% with accompanying predictors of shortened survival, or when it drops below 30%. The guidelines were published before approval of triple combination therapy.
The researchers conducted an open-label retrospective analysis of 60 patients started on triple combination therapy between September 2019 and February 2020 at three centers in the Southeast. They compared percent predicted ppFEV1 values prior to initiation of therapy to ppFEV1 values obtained 2-12 weeks after the start of therapy. Patients on therapy were compared with 10 genetically ineligible controls. The two groups were generally similar aside from genetic status, though 100% of the therapy group had pancreatic insufficiency, compared with 90% of controls (P = .013).
The therapeutic group experienced a 7.8% increase in ppFEV1 after starting therapy (P < .001), compared with a 0.5% decrease in controls (P = .65). Before initiation of therapy, 33% of the therapy group met the criteria for initiating a transplant discussion, while 67% had been recommended for transplant. After therapy, 55% met the criteria for discussion, 33% were recommended for transplant, and 12% no longer met the criteria for discussion of transplantation. Fifty percent of controls were in discussion, and this dropped to 40%, while 50% were referred for transplantation, and this increased to 60%. On therapy, transplant referral candidates had an increase of forced vital capacity from 48.9 to 59.16 (P < .001).
Adverse events were rare, with only one discontinuation that occurred following a lung transplant and was not believed to be treatment related.
“Our study had a large number of patients taken from multiple centers, which suggests generalizabilty and real-world experience,” said Dr. Bermingham.
The results are encouraging, said Robert J. Giusti, MD, clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center.
“We’re all remarking how wonderful patients feel these days. It’s really a disease-altering treatment. But for the high-risk group, whose FEV1 is less than 40%, those are the patients we’re more concerned about because we thought maybe they had too much lung disease, and that they wouldn’t benefit from triple combination. But they seem to be improving, so that’s very reassuring,” said Dr. Giusti, who was not involved in the study.
The study received funding from the Cystic Fibrosis Foundation and Dartmouth College. Dr. Bermingham and Dr. Giusti have no relevant financial disclosures.
SOURCE: Bermingham B et al. NACFC 2020, Abstract 645.
New CFTR [cystic fibrosis transmembrane conductance regulator] modulator therapies can offer life-altering benefits to some patients with cystic fibrosis, even those with advanced disease.
, according to a multicenter analysis of patients taking elexacaftor, tezacaftor, and ivacaftor.
The study participants had a percent predicted forced expiratory volume in 1 second (ppFEV1) of 40% or below, or other high-risk factors. Researchers compared them to control patients who were genetically ineligible for triple combination therapy.
Previous studies of such patients on individual drugs or previous combinations showed increases in lung function in patients with advanced disease, though the magnitude of improvement varied across regimens. “With this improvement, it’s unclear how CFTR modulators should affect lung transplant referral timing,” Brent Bermingham, MD, said during a presentation of the study at the virtual North American Cystic Fibrosis Conference.
“The rationale for our study was that despite patients with advanced lung disease being excluded from phase III trials (of elexacaftor, tezacaftor, and ivacaftor), they are receiving a therapy with an unknown clinical efficacy and safety profile,” said Dr. Bermingham, a pulmonary and critical care fellow at the Medical University of South Carolina, Charleston.
Lung transplant referral guidelines recommend that physicians initiate discussions about the potential benefit of lung transplant when FEV1 drops below 50% of the predicted value. Patients should be referred for a transplant when the value is below 50% and rapidly declining (>20% decline in the past 12 months), when it drops below 40% with accompanying predictors of shortened survival, or when it drops below 30%. The guidelines were published before approval of triple combination therapy.
The researchers conducted an open-label retrospective analysis of 60 patients started on triple combination therapy between September 2019 and February 2020 at three centers in the Southeast. They compared percent predicted ppFEV1 values prior to initiation of therapy to ppFEV1 values obtained 2-12 weeks after the start of therapy. Patients on therapy were compared with 10 genetically ineligible controls. The two groups were generally similar aside from genetic status, though 100% of the therapy group had pancreatic insufficiency, compared with 90% of controls (P = .013).
The therapeutic group experienced a 7.8% increase in ppFEV1 after starting therapy (P < .001), compared with a 0.5% decrease in controls (P = .65). Before initiation of therapy, 33% of the therapy group met the criteria for initiating a transplant discussion, while 67% had been recommended for transplant. After therapy, 55% met the criteria for discussion, 33% were recommended for transplant, and 12% no longer met the criteria for discussion of transplantation. Fifty percent of controls were in discussion, and this dropped to 40%, while 50% were referred for transplantation, and this increased to 60%. On therapy, transplant referral candidates had an increase of forced vital capacity from 48.9 to 59.16 (P < .001).
Adverse events were rare, with only one discontinuation that occurred following a lung transplant and was not believed to be treatment related.
“Our study had a large number of patients taken from multiple centers, which suggests generalizabilty and real-world experience,” said Dr. Bermingham.
The results are encouraging, said Robert J. Giusti, MD, clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center.
“We’re all remarking how wonderful patients feel these days. It’s really a disease-altering treatment. But for the high-risk group, whose FEV1 is less than 40%, those are the patients we’re more concerned about because we thought maybe they had too much lung disease, and that they wouldn’t benefit from triple combination. But they seem to be improving, so that’s very reassuring,” said Dr. Giusti, who was not involved in the study.
The study received funding from the Cystic Fibrosis Foundation and Dartmouth College. Dr. Bermingham and Dr. Giusti have no relevant financial disclosures.
SOURCE: Bermingham B et al. NACFC 2020, Abstract 645.
FROM NACFC 2020