User login
Doug Brunk is a San Diego-based award-winning reporter who began covering health care in 1991. Before joining the company, he wrote for the health sciences division of Columbia University and was an associate editor at Contemporary Long Term Care magazine when it won a Jesse H. Neal Award. His work has been syndicated by the Los Angeles Times and he is the author of two books related to the University of Kentucky Wildcats men's basketball program. Doug has a master’s degree in magazine journalism from the S.I. Newhouse School of Public Communications at Syracuse University. Follow him on Twitter @dougbrunk.
Readmission to non-index hospital following acute stroke linked to worse outcomes
ATLANTA – Following an acute stroke, optimizing stroke secondary prevention measures, medical complications, and transitions of care is essential to reducing 30-day readmissions and improving patient outcomes, a large analysis of national data showed.
“Care that is fragmented with readmissions to other hospitals results not only in more expensive care and longer length of stay but also increased mortality for our acute stroke patients,” lead study author Laura K. Stein, MD, said in an interview in advance of the annual meeting of the American Neurological Association.
In 2017, a study of the Nationwide Readmissions Database demonstrated that 12.1% of patients with acute ischemic stroke were readmitted within 30 days (Stroke 2017;48:1386-8). It cited that 89.6% were unplanned and 12.9% were preventable. “However, this study did not examine whether patients were admitted to the discharging hospital or a different hospital,” said Dr. Stein, a neurologist at the Icahn School of Medicine at Mount Sinai, New York. “Furthermore, it did not include metrics such as cost, length of stay, and mortality with 30-day readmissions. Hospitals are increasingly held accountable and penalized for metrics such as length of stay and 30-day readmissions.”
In 2010, the Centers for Medicare & Medicaid Services introduced the Hospital Readmissions Reduction Program in an attempt to decrease readmissions following hospitalizations for acute myocardial infarction, heart failure, and pneumonia. “In 2012, CMS started reducing Medicare payments for hospitals with excess readmissions,” said Dr. Stein, who is a fellowship-trained stroke specialist. “While readmission to the same hospital has great implications for hospital systems, any readmission has great implications for patients.”
In what is believed to be the first study of its kind, Dr. Stein and her colleagues drew from the 2013 Nationwide Readmissions Database to examine in-hospital outcomes associated with 30-day readmission to a different hospital for acute ischemic stroke. They used ICD-9 codes to identify index stroke admissions and all-cause readmissions. Outcomes of interest were length of stay, total charges, and in-hospital mortality during the 30-day readmission. The main predictor was readmission to another hospital, compared with readmission to the same hospital as the index acute stroke admission. The researchers used linear regression for the outcomes of length of stay and charges, and logistic regression for in-hospital mortality. They adjusted for several variables during the index admission, including age, sex, vascular risk factors, hospital bed size, teaching hospital status, insurance status, discharge destination, National Center for Health Statistics urban-rural location classification, length of stay, and total charges.
Of 24,545 acute stroke patients readmitted within 30 days, 7,274 (30%) were readmitted to a different hospital. The top three reasons for readmission were acute cerebrovascular disease, septicemia, and renal failure. In fully adjusted models, readmission to a different hospital was associated with an increased length of stay of 0.97 days (P less than .0001) and a mean of $7,677.28 greater total charges, compared with readmission to the same hospital (P less than .0001). The fully adjusted odds ratio for in-hospital mortality during readmission was 1.17 for readmission to another hospital vs. readmission to the same hospital (P = .0079).
“While it is conceivable that cost and length of stay could be higher with readmission to a different hospital because of a need for additional testing with a lack of familiarity with the patient, it is concerning that mortality is higher,” Dr. Stein said. “These findings emphasize the importance of optimizing secondary stroke prevention and medical complications following acute stroke before discharge. Additionally, they emphasize the importance of good transitions of care from the inpatient to outpatient setting (whether that’s to a rehabilitation facility, skilled nursing facility, or home) and accessibility of the discharging stroke team after discharge.”
She acknowledged certain limitations of the analysis, including its reliance of administrative data, which could include misclassification of diagnoses and comorbidities based on ICD-9 codes. “However, we have chosen ICD-9 codes for stroke that have been previously validated in the literature,” Dr. Stein said. “For instance, the validated codes for stroke as the primary discharge diagnosis have a sensitivity of 74%, specificity of 95%, and positive predictive value of 88%. Second, we do not know stroke subtype or severity of stroke. Third, we do not know what the transitions of care plan were when the patients left the hospital following index acute ischemic stroke admission and why these patients ended up being readmitted to a different hospital rather than the one that treated them for their acute stroke.”
The researchers reported having no financial disclosures.
SOURCE: Stein L et al. Ann Neurol. 2018;84[S22]:S149. Abstract M127.
ATLANTA – Following an acute stroke, optimizing stroke secondary prevention measures, medical complications, and transitions of care is essential to reducing 30-day readmissions and improving patient outcomes, a large analysis of national data showed.
“Care that is fragmented with readmissions to other hospitals results not only in more expensive care and longer length of stay but also increased mortality for our acute stroke patients,” lead study author Laura K. Stein, MD, said in an interview in advance of the annual meeting of the American Neurological Association.
In 2017, a study of the Nationwide Readmissions Database demonstrated that 12.1% of patients with acute ischemic stroke were readmitted within 30 days (Stroke 2017;48:1386-8). It cited that 89.6% were unplanned and 12.9% were preventable. “However, this study did not examine whether patients were admitted to the discharging hospital or a different hospital,” said Dr. Stein, a neurologist at the Icahn School of Medicine at Mount Sinai, New York. “Furthermore, it did not include metrics such as cost, length of stay, and mortality with 30-day readmissions. Hospitals are increasingly held accountable and penalized for metrics such as length of stay and 30-day readmissions.”
In 2010, the Centers for Medicare & Medicaid Services introduced the Hospital Readmissions Reduction Program in an attempt to decrease readmissions following hospitalizations for acute myocardial infarction, heart failure, and pneumonia. “In 2012, CMS started reducing Medicare payments for hospitals with excess readmissions,” said Dr. Stein, who is a fellowship-trained stroke specialist. “While readmission to the same hospital has great implications for hospital systems, any readmission has great implications for patients.”
In what is believed to be the first study of its kind, Dr. Stein and her colleagues drew from the 2013 Nationwide Readmissions Database to examine in-hospital outcomes associated with 30-day readmission to a different hospital for acute ischemic stroke. They used ICD-9 codes to identify index stroke admissions and all-cause readmissions. Outcomes of interest were length of stay, total charges, and in-hospital mortality during the 30-day readmission. The main predictor was readmission to another hospital, compared with readmission to the same hospital as the index acute stroke admission. The researchers used linear regression for the outcomes of length of stay and charges, and logistic regression for in-hospital mortality. They adjusted for several variables during the index admission, including age, sex, vascular risk factors, hospital bed size, teaching hospital status, insurance status, discharge destination, National Center for Health Statistics urban-rural location classification, length of stay, and total charges.
Of 24,545 acute stroke patients readmitted within 30 days, 7,274 (30%) were readmitted to a different hospital. The top three reasons for readmission were acute cerebrovascular disease, septicemia, and renal failure. In fully adjusted models, readmission to a different hospital was associated with an increased length of stay of 0.97 days (P less than .0001) and a mean of $7,677.28 greater total charges, compared with readmission to the same hospital (P less than .0001). The fully adjusted odds ratio for in-hospital mortality during readmission was 1.17 for readmission to another hospital vs. readmission to the same hospital (P = .0079).
“While it is conceivable that cost and length of stay could be higher with readmission to a different hospital because of a need for additional testing with a lack of familiarity with the patient, it is concerning that mortality is higher,” Dr. Stein said. “These findings emphasize the importance of optimizing secondary stroke prevention and medical complications following acute stroke before discharge. Additionally, they emphasize the importance of good transitions of care from the inpatient to outpatient setting (whether that’s to a rehabilitation facility, skilled nursing facility, or home) and accessibility of the discharging stroke team after discharge.”
She acknowledged certain limitations of the analysis, including its reliance of administrative data, which could include misclassification of diagnoses and comorbidities based on ICD-9 codes. “However, we have chosen ICD-9 codes for stroke that have been previously validated in the literature,” Dr. Stein said. “For instance, the validated codes for stroke as the primary discharge diagnosis have a sensitivity of 74%, specificity of 95%, and positive predictive value of 88%. Second, we do not know stroke subtype or severity of stroke. Third, we do not know what the transitions of care plan were when the patients left the hospital following index acute ischemic stroke admission and why these patients ended up being readmitted to a different hospital rather than the one that treated them for their acute stroke.”
The researchers reported having no financial disclosures.
SOURCE: Stein L et al. Ann Neurol. 2018;84[S22]:S149. Abstract M127.
ATLANTA – Following an acute stroke, optimizing stroke secondary prevention measures, medical complications, and transitions of care is essential to reducing 30-day readmissions and improving patient outcomes, a large analysis of national data showed.
“Care that is fragmented with readmissions to other hospitals results not only in more expensive care and longer length of stay but also increased mortality for our acute stroke patients,” lead study author Laura K. Stein, MD, said in an interview in advance of the annual meeting of the American Neurological Association.
In 2017, a study of the Nationwide Readmissions Database demonstrated that 12.1% of patients with acute ischemic stroke were readmitted within 30 days (Stroke 2017;48:1386-8). It cited that 89.6% were unplanned and 12.9% were preventable. “However, this study did not examine whether patients were admitted to the discharging hospital or a different hospital,” said Dr. Stein, a neurologist at the Icahn School of Medicine at Mount Sinai, New York. “Furthermore, it did not include metrics such as cost, length of stay, and mortality with 30-day readmissions. Hospitals are increasingly held accountable and penalized for metrics such as length of stay and 30-day readmissions.”
In 2010, the Centers for Medicare & Medicaid Services introduced the Hospital Readmissions Reduction Program in an attempt to decrease readmissions following hospitalizations for acute myocardial infarction, heart failure, and pneumonia. “In 2012, CMS started reducing Medicare payments for hospitals with excess readmissions,” said Dr. Stein, who is a fellowship-trained stroke specialist. “While readmission to the same hospital has great implications for hospital systems, any readmission has great implications for patients.”
In what is believed to be the first study of its kind, Dr. Stein and her colleagues drew from the 2013 Nationwide Readmissions Database to examine in-hospital outcomes associated with 30-day readmission to a different hospital for acute ischemic stroke. They used ICD-9 codes to identify index stroke admissions and all-cause readmissions. Outcomes of interest were length of stay, total charges, and in-hospital mortality during the 30-day readmission. The main predictor was readmission to another hospital, compared with readmission to the same hospital as the index acute stroke admission. The researchers used linear regression for the outcomes of length of stay and charges, and logistic regression for in-hospital mortality. They adjusted for several variables during the index admission, including age, sex, vascular risk factors, hospital bed size, teaching hospital status, insurance status, discharge destination, National Center for Health Statistics urban-rural location classification, length of stay, and total charges.
Of 24,545 acute stroke patients readmitted within 30 days, 7,274 (30%) were readmitted to a different hospital. The top three reasons for readmission were acute cerebrovascular disease, septicemia, and renal failure. In fully adjusted models, readmission to a different hospital was associated with an increased length of stay of 0.97 days (P less than .0001) and a mean of $7,677.28 greater total charges, compared with readmission to the same hospital (P less than .0001). The fully adjusted odds ratio for in-hospital mortality during readmission was 1.17 for readmission to another hospital vs. readmission to the same hospital (P = .0079).
“While it is conceivable that cost and length of stay could be higher with readmission to a different hospital because of a need for additional testing with a lack of familiarity with the patient, it is concerning that mortality is higher,” Dr. Stein said. “These findings emphasize the importance of optimizing secondary stroke prevention and medical complications following acute stroke before discharge. Additionally, they emphasize the importance of good transitions of care from the inpatient to outpatient setting (whether that’s to a rehabilitation facility, skilled nursing facility, or home) and accessibility of the discharging stroke team after discharge.”
She acknowledged certain limitations of the analysis, including its reliance of administrative data, which could include misclassification of diagnoses and comorbidities based on ICD-9 codes. “However, we have chosen ICD-9 codes for stroke that have been previously validated in the literature,” Dr. Stein said. “For instance, the validated codes for stroke as the primary discharge diagnosis have a sensitivity of 74%, specificity of 95%, and positive predictive value of 88%. Second, we do not know stroke subtype or severity of stroke. Third, we do not know what the transitions of care plan were when the patients left the hospital following index acute ischemic stroke admission and why these patients ended up being readmitted to a different hospital rather than the one that treated them for their acute stroke.”
The researchers reported having no financial disclosures.
SOURCE: Stein L et al. Ann Neurol. 2018;84[S22]:S149. Abstract M127.
REPORTING FROM ANA 2018
Key clinical point:
Major finding: The adjusted odds ratio for in-hospital mortality during readmission was 1.17 for readmission to another hospital vs. readmission to the same hospital (P = .0079).
Study details: A review of 24,545 acute stroke patients 2013 from the Nationwide Readmissions Database.
Disclosures: The researchers reported having no financial disclosures.
Source: Stein L et al. Ann Neurol. 2018;84[S22]:S149. Abstract M127.
High systemic inflammation at midlife portends cognitive changes in later life
ATLANTA – results from a long-term analysis showed.

“There is considerable evidence suggesting that abnormal immune functioning and inflammation may influence cognitive functioning and promote dementia,” lead study author Keenan Walker, PhD, said in an interview in advance of the annual meeting of the American Neurological Association. “For example, several studies have found higher levels of inflammatory markers in the blood and cerebral spinal fluid of patients with dementia, compared to nondemented individuals of a comparable age. What is less clear, however, is whether inflammation actually promotes cognitive decline or occurs simply as a result of the brain changes underlying dementia.”
To help answer this question, Dr. Walker, of Johns Hopkins University, Baltimore, and his colleagues evaluated blood biomarkers of inflammation in 12,727 middle-aged participants during visits one and two of the Atherosclerosis Risk in Communities (ARIC) study, a prospective epidemiologic analysis conducted in four U.S. communities and funded by the National Heart, Lung, and Blood Institute. Visit one occurred between 1987 and 1989, while visit two took place between 1990 and 1992. The researchers related these markers to cognitive change over the subsequent decades. Specifically, they used four biomarkers (fibrinogen, white blood cell count, von Willebrand factor, and Factor VIII) to create an inflammation composite score at visit one, and measured C-reactive protein (CRP) at visit two. Next, they used measures of memory, executive function, and language assess cognition over three visits spanning 20 years.
The average age of study participants at first cognitive assessment was 57 years, 56% were women, and 21% were black. After controlling for differences in demographic variables, vascular risk factors and comorbidities, the researchers observed that each standard deviation (SD) increase in the midlife inflammation composite score was associated with an additional 20-year global cognitive decline of –0.035 SD (P less than .01). They found a similar association between each SD higher midlife CRP level and additional 20-year decline in global cognition (–0.038 SD; P less than .01). In addition, study participants with a midlife inflammation composite score in the top quartile had a 7.6% steeper decline in global cognition, compared with participants in the lowest quartile; a similar association was observed for CRP.
“We were surprised at what we found when we looked at inflammation’s effect on individual cognitive domains,” Dr. Walker said. “Specifically, we found that inflammation was associated with declines in memory, but not declines in other domains, such as executive function or language. One possible interpretation for these findings is that inflammation may selectively influence brain regions such as the hippocampus, which are necessary for memory consolidation and are also most vulnerable to Alzheimer’s disease.” He added that the current findings “provide support for the idea that systemic inflammation may have an early pathogenic role in the cognitive decline that occurs in the decades leading up to older adulthood.”
Dr. Walker acknowledged certain limitations of the study, including the attrition of participants because of deaths and dropouts over the 20-year follow-up period. “Because high levels of inflammation and comorbid disease are related to death and risk of study dropout, the sample of participants who completed the entirety of the study may represent a group that is healthier overall than the general population,” he said. “However, we took several steps to reduce any potential attrition bias using advanced statistical techniques.”
Dr. Walker disclosed that he receives funding support from the National Institutes of Health.
Source: Walker et al. ANA 2018, Abstract 305.
ATLANTA – results from a long-term analysis showed.
“There is considerable evidence suggesting that abnormal immune functioning and inflammation may influence cognitive functioning and promote dementia,” lead study author Keenan Walker, PhD, said in an interview in advance of the annual meeting of the American Neurological Association. “For example, several studies have found higher levels of inflammatory markers in the blood and cerebral spinal fluid of patients with dementia, compared to nondemented individuals of a comparable age. What is less clear, however, is whether inflammation actually promotes cognitive decline or occurs simply as a result of the brain changes underlying dementia.”
To help answer this question, Dr. Walker, of Johns Hopkins University, Baltimore, and his colleagues evaluated blood biomarkers of inflammation in 12,727 middle-aged participants during visits one and two of the Atherosclerosis Risk in Communities (ARIC) study, a prospective epidemiologic analysis conducted in four U.S. communities and funded by the National Heart, Lung, and Blood Institute. Visit one occurred between 1987 and 1989, while visit two took place between 1990 and 1992. The researchers related these markers to cognitive change over the subsequent decades. Specifically, they used four biomarkers (fibrinogen, white blood cell count, von Willebrand factor, and Factor VIII) to create an inflammation composite score at visit one, and measured C-reactive protein (CRP) at visit two. Next, they used measures of memory, executive function, and language assess cognition over three visits spanning 20 years.
The average age of study participants at first cognitive assessment was 57 years, 56% were women, and 21% were black. After controlling for differences in demographic variables, vascular risk factors and comorbidities, the researchers observed that each standard deviation (SD) increase in the midlife inflammation composite score was associated with an additional 20-year global cognitive decline of –0.035 SD (P less than .01). They found a similar association between each SD higher midlife CRP level and additional 20-year decline in global cognition (–0.038 SD; P less than .01). In addition, study participants with a midlife inflammation composite score in the top quartile had a 7.6% steeper decline in global cognition, compared with participants in the lowest quartile; a similar association was observed for CRP.
“We were surprised at what we found when we looked at inflammation’s effect on individual cognitive domains,” Dr. Walker said. “Specifically, we found that inflammation was associated with declines in memory, but not declines in other domains, such as executive function or language. One possible interpretation for these findings is that inflammation may selectively influence brain regions such as the hippocampus, which are necessary for memory consolidation and are also most vulnerable to Alzheimer’s disease.” He added that the current findings “provide support for the idea that systemic inflammation may have an early pathogenic role in the cognitive decline that occurs in the decades leading up to older adulthood.”
Dr. Walker acknowledged certain limitations of the study, including the attrition of participants because of deaths and dropouts over the 20-year follow-up period. “Because high levels of inflammation and comorbid disease are related to death and risk of study dropout, the sample of participants who completed the entirety of the study may represent a group that is healthier overall than the general population,” he said. “However, we took several steps to reduce any potential attrition bias using advanced statistical techniques.”
Dr. Walker disclosed that he receives funding support from the National Institutes of Health.
Source: Walker et al. ANA 2018, Abstract 305.
ATLANTA – results from a long-term analysis showed.
“There is considerable evidence suggesting that abnormal immune functioning and inflammation may influence cognitive functioning and promote dementia,” lead study author Keenan Walker, PhD, said in an interview in advance of the annual meeting of the American Neurological Association. “For example, several studies have found higher levels of inflammatory markers in the blood and cerebral spinal fluid of patients with dementia, compared to nondemented individuals of a comparable age. What is less clear, however, is whether inflammation actually promotes cognitive decline or occurs simply as a result of the brain changes underlying dementia.”
To help answer this question, Dr. Walker, of Johns Hopkins University, Baltimore, and his colleagues evaluated blood biomarkers of inflammation in 12,727 middle-aged participants during visits one and two of the Atherosclerosis Risk in Communities (ARIC) study, a prospective epidemiologic analysis conducted in four U.S. communities and funded by the National Heart, Lung, and Blood Institute. Visit one occurred between 1987 and 1989, while visit two took place between 1990 and 1992. The researchers related these markers to cognitive change over the subsequent decades. Specifically, they used four biomarkers (fibrinogen, white blood cell count, von Willebrand factor, and Factor VIII) to create an inflammation composite score at visit one, and measured C-reactive protein (CRP) at visit two. Next, they used measures of memory, executive function, and language assess cognition over three visits spanning 20 years.
The average age of study participants at first cognitive assessment was 57 years, 56% were women, and 21% were black. After controlling for differences in demographic variables, vascular risk factors and comorbidities, the researchers observed that each standard deviation (SD) increase in the midlife inflammation composite score was associated with an additional 20-year global cognitive decline of –0.035 SD (P less than .01). They found a similar association between each SD higher midlife CRP level and additional 20-year decline in global cognition (–0.038 SD; P less than .01). In addition, study participants with a midlife inflammation composite score in the top quartile had a 7.6% steeper decline in global cognition, compared with participants in the lowest quartile; a similar association was observed for CRP.
“We were surprised at what we found when we looked at inflammation’s effect on individual cognitive domains,” Dr. Walker said. “Specifically, we found that inflammation was associated with declines in memory, but not declines in other domains, such as executive function or language. One possible interpretation for these findings is that inflammation may selectively influence brain regions such as the hippocampus, which are necessary for memory consolidation and are also most vulnerable to Alzheimer’s disease.” He added that the current findings “provide support for the idea that systemic inflammation may have an early pathogenic role in the cognitive decline that occurs in the decades leading up to older adulthood.”
Dr. Walker acknowledged certain limitations of the study, including the attrition of participants because of deaths and dropouts over the 20-year follow-up period. “Because high levels of inflammation and comorbid disease are related to death and risk of study dropout, the sample of participants who completed the entirety of the study may represent a group that is healthier overall than the general population,” he said. “However, we took several steps to reduce any potential attrition bias using advanced statistical techniques.”
Dr. Walker disclosed that he receives funding support from the National Institutes of Health.
Source: Walker et al. ANA 2018, Abstract 305.
REPORTING FROM ANA 2018
Key clinical point: Inflammation was associated with declines in memory, but not declines in other domains, such as executive function or language.
Major finding: Each standard deviation (SD) increase in the midlife inflammation composite score was associated with an additional 20-year global cognitive decline of –0.035 SD (P less than .01).
Study details: An evaluation of blood biomarkers of inflammation in 12,727 middle-aged participants in the Atherosclerosis Risk in Communities Study.
Disclosures: Dr. Walker disclosed that he receives funding support from the National Institutes of Health.
Source: Walker et al. ANA 2018, Abstract 305.
Study explores link between GERD and poor sleep quality
ATLANTA – results from an ongoing longitudinal analysis demonstrated.
“We have little longitudinal information on GERD in the general population; the last published article on GERD incidence was 20 years ago,” lead study author Maurice M. Ohayon, MD, DSc, PhD, said in an interview in advance of the annual meeting of the American Neurological Association. “As a sleep specialist, I am always interested to see how a specific medical condition may affect the sleep quality of the individuals with that condition. How we live our day has an impact on our night; it works together.”
In an effort to examine the long-term effects of GERD on sleep disturbances, Dr. Ohayon, director of the Stanford (Calif.) Sleep Epidemiology Research Center, and his colleagues used U.S. Census data to identify a random sample of adults in Arizona, California, Colorado, Idaho, New York, Oregon, Pennsylvania, and Texas. The researchers conducted two waves of phone interviews with the subjects 3 years apart, beginning in 2004. They limited their analysis to 10,930 subjects with a mean age of 43 years who participated in both interviews.
Between wave 1 and wave 2 of phone interviews, the proportion of adults who reported having GERD rose from 10.6% to 12.4% and the prevalence of new GERD cases was 8.5% per year, while the incidence was 3.2% per year. Chronic GERD, defined as that present during both interview periods, was observed in 3.9% of the sample.
The researchers found that 77.3% of GERD subjects were taking a treatment to alleviate their symptoms, mostly proton-pump inhibitors. Those with chronic GERD were more likely to report being dissatisfied with their sleep during wave 2 of the study, compared with wave 1 (24.2% vs. 13.5%; P less than .001). In addition, compared with their non-GERD counterparts, those with chronic GERD were more likely to wake up at night (33.9% vs. 28.3%; P less than .001) and to have nonrestorative sleep (15.6% vs. 10.5%; P less than .001).
“Discomfort related to GERD may happen while you are sleeping,” said Dr. Ohayon, who is also a professor of psychiatry and behavioral sciences at Stanford University. “It may wake you up and, if not, it may make you feel unrested when you wake up. We observed both of these symptoms in our GERD participants. Insomnia disorders were also rampant in the chronic GERD group (24.5%, compared with 14.4% in non-GERD participants). An insomnia disorder is more than just having difficulty falling asleep or waking up at night, it means that your daytime functioning is affected by the poor quality of your night.”
Dr. Ohayon said other findings from the study were “rather alarming.” For example, individuals with GERD, especially those with the chronic form, weighed much more than those with no GERD did. “Over a 3-year period, the chronic GERD individuals gained one point in the body mass index, which for a 6-foot tall man translates into a weight gain of 30 pounds,” he said. “Of course, with that follows high blood pressure, high cholesterol, diabetes, chronic pain, and heart disease.”
He concluded that GERD has its main manifestations when affected individuals are sleeping on their backs. “The impact of GERD on the quality of sleep is major,” he said. “Sleepiness and fatigue during the day are the consequences impacting work, family, and quality of life.”
Dr. Ohayon acknowledged certain limitations of the study, including the fact that GERD was based on self-report. The study was supported by an unrestricted grant from Takeda.
Source: Oyahon et al. ANA 2018, Abstract 625.
ATLANTA – results from an ongoing longitudinal analysis demonstrated.
“We have little longitudinal information on GERD in the general population; the last published article on GERD incidence was 20 years ago,” lead study author Maurice M. Ohayon, MD, DSc, PhD, said in an interview in advance of the annual meeting of the American Neurological Association. “As a sleep specialist, I am always interested to see how a specific medical condition may affect the sleep quality of the individuals with that condition. How we live our day has an impact on our night; it works together.”
In an effort to examine the long-term effects of GERD on sleep disturbances, Dr. Ohayon, director of the Stanford (Calif.) Sleep Epidemiology Research Center, and his colleagues used U.S. Census data to identify a random sample of adults in Arizona, California, Colorado, Idaho, New York, Oregon, Pennsylvania, and Texas. The researchers conducted two waves of phone interviews with the subjects 3 years apart, beginning in 2004. They limited their analysis to 10,930 subjects with a mean age of 43 years who participated in both interviews.
Between wave 1 and wave 2 of phone interviews, the proportion of adults who reported having GERD rose from 10.6% to 12.4% and the prevalence of new GERD cases was 8.5% per year, while the incidence was 3.2% per year. Chronic GERD, defined as that present during both interview periods, was observed in 3.9% of the sample.
The researchers found that 77.3% of GERD subjects were taking a treatment to alleviate their symptoms, mostly proton-pump inhibitors. Those with chronic GERD were more likely to report being dissatisfied with their sleep during wave 2 of the study, compared with wave 1 (24.2% vs. 13.5%; P less than .001). In addition, compared with their non-GERD counterparts, those with chronic GERD were more likely to wake up at night (33.9% vs. 28.3%; P less than .001) and to have nonrestorative sleep (15.6% vs. 10.5%; P less than .001).
“Discomfort related to GERD may happen while you are sleeping,” said Dr. Ohayon, who is also a professor of psychiatry and behavioral sciences at Stanford University. “It may wake you up and, if not, it may make you feel unrested when you wake up. We observed both of these symptoms in our GERD participants. Insomnia disorders were also rampant in the chronic GERD group (24.5%, compared with 14.4% in non-GERD participants). An insomnia disorder is more than just having difficulty falling asleep or waking up at night, it means that your daytime functioning is affected by the poor quality of your night.”
Dr. Ohayon said other findings from the study were “rather alarming.” For example, individuals with GERD, especially those with the chronic form, weighed much more than those with no GERD did. “Over a 3-year period, the chronic GERD individuals gained one point in the body mass index, which for a 6-foot tall man translates into a weight gain of 30 pounds,” he said. “Of course, with that follows high blood pressure, high cholesterol, diabetes, chronic pain, and heart disease.”
He concluded that GERD has its main manifestations when affected individuals are sleeping on their backs. “The impact of GERD on the quality of sleep is major,” he said. “Sleepiness and fatigue during the day are the consequences impacting work, family, and quality of life.”
Dr. Ohayon acknowledged certain limitations of the study, including the fact that GERD was based on self-report. The study was supported by an unrestricted grant from Takeda.
Source: Oyahon et al. ANA 2018, Abstract 625.
ATLANTA – results from an ongoing longitudinal analysis demonstrated.
“We have little longitudinal information on GERD in the general population; the last published article on GERD incidence was 20 years ago,” lead study author Maurice M. Ohayon, MD, DSc, PhD, said in an interview in advance of the annual meeting of the American Neurological Association. “As a sleep specialist, I am always interested to see how a specific medical condition may affect the sleep quality of the individuals with that condition. How we live our day has an impact on our night; it works together.”
In an effort to examine the long-term effects of GERD on sleep disturbances, Dr. Ohayon, director of the Stanford (Calif.) Sleep Epidemiology Research Center, and his colleagues used U.S. Census data to identify a random sample of adults in Arizona, California, Colorado, Idaho, New York, Oregon, Pennsylvania, and Texas. The researchers conducted two waves of phone interviews with the subjects 3 years apart, beginning in 2004. They limited their analysis to 10,930 subjects with a mean age of 43 years who participated in both interviews.
Between wave 1 and wave 2 of phone interviews, the proportion of adults who reported having GERD rose from 10.6% to 12.4% and the prevalence of new GERD cases was 8.5% per year, while the incidence was 3.2% per year. Chronic GERD, defined as that present during both interview periods, was observed in 3.9% of the sample.
The researchers found that 77.3% of GERD subjects were taking a treatment to alleviate their symptoms, mostly proton-pump inhibitors. Those with chronic GERD were more likely to report being dissatisfied with their sleep during wave 2 of the study, compared with wave 1 (24.2% vs. 13.5%; P less than .001). In addition, compared with their non-GERD counterparts, those with chronic GERD were more likely to wake up at night (33.9% vs. 28.3%; P less than .001) and to have nonrestorative sleep (15.6% vs. 10.5%; P less than .001).
“Discomfort related to GERD may happen while you are sleeping,” said Dr. Ohayon, who is also a professor of psychiatry and behavioral sciences at Stanford University. “It may wake you up and, if not, it may make you feel unrested when you wake up. We observed both of these symptoms in our GERD participants. Insomnia disorders were also rampant in the chronic GERD group (24.5%, compared with 14.4% in non-GERD participants). An insomnia disorder is more than just having difficulty falling asleep or waking up at night, it means that your daytime functioning is affected by the poor quality of your night.”
Dr. Ohayon said other findings from the study were “rather alarming.” For example, individuals with GERD, especially those with the chronic form, weighed much more than those with no GERD did. “Over a 3-year period, the chronic GERD individuals gained one point in the body mass index, which for a 6-foot tall man translates into a weight gain of 30 pounds,” he said. “Of course, with that follows high blood pressure, high cholesterol, diabetes, chronic pain, and heart disease.”
He concluded that GERD has its main manifestations when affected individuals are sleeping on their backs. “The impact of GERD on the quality of sleep is major,” he said. “Sleepiness and fatigue during the day are the consequences impacting work, family, and quality of life.”
Dr. Ohayon acknowledged certain limitations of the study, including the fact that GERD was based on self-report. The study was supported by an unrestricted grant from Takeda.
Source: Oyahon et al. ANA 2018, Abstract 625.
REPORTING FROM ANA 2018
Key clinical point: GERD has a major impact on quality of sleep.
Major finding: Study participants with chronic GERD were more likely to report being dissatisfied with their sleep during wave 2 of the study, compared with wave 1 (24.2% vs. 13.5%; P less than .001).
Study details: A telephone-based survey of 10,930 U.S. adults who were interviewed during two waves 3 years apart.
Disclosures: The study was supported by an unrestricted grant from Takeda.
Source: Oyahon et al. ANA 2018, Abstract 625.
Survey sheds light on fellows’ perceptions of health care disparities
SAN DIEGO – About 25% of Fellows of the American College of Emergency Physicians acknowledged that health care disparities exist in their practices, according to a survey completed by 945 ACEP fellows in 36 states.

In conjunction with the American College of Emergency Physicians, Cheryl K. Zogg, MSPH, MHS, and her colleagues surveyed a nationally representative subset of ACEP fellows between September and December of 2017 to determine the extent to which emergency medicine physicians perceive that various forms of disparities exist and that there is “strong evidence” to support the existence of disparities.
The results were reported in an abstract presented during the annual meeting of the American College of Emergency Physicians.
“The existence of disparities in medicine has been widely acknowledged,” she said. “A lot of the modern conversation began in 2002, when the Institute of Medicine published its now-famous report, ‘Unequal Treatment.’ Since that time, a growing body of literature has discussed the existence of disparities in various medical fields and related to a number of factors including but not limited to race and ethnicity.”
The survey contained questions about perceptions of disparities related to insurance status, type of insurance, ability to speak English, educational attainment, race/ethnicity, sexual identity, and sexual orientation as well as the perceived strength of the evidence to support the existence of disparities in medicine in general and in emergency medicine specifically.
Ms. Zogg, an MD-PhD candidate at Yale University, New Haven, Conn., found that disparities of insurance status (85.6%) and type of insurance (81.3%) were the most widely acknowledged, followed by variations in care as a result of patients’ ability to speak English (73.7%) and level of educational attainment (61.5%).
Slightly more than half of respondents (51.9%) acknowledged the existence of disparities based on race/ethnicity in United States, but only 20.9% believe that such disparities exist in their hospitals and even fewer (3.9%) believe that they exist in their own personal practices. At the same time, more than one-third of respondents (40.6%) acknowledged the existence of disparities based on gender identity in the United States, but 22.4% believe that such disparities exist in their hospitals and even fewer (5.7%) believe that they exist in their own practices. Similar percentages were observed when respondents were asked about issues of sexual orientation (33.7%, 10.6%, and 2.3%, respectively).
Perceived strength of the evidence supporting the existence of disparities followed a similar trend. Between 74.7% and 82.2% of respondents believe there is strong evidence in medicine to support the existence of racial disparities in insurance status and insurance type, respectively. However, between 47% and 49.4% of respondents rated such evidence as strong in emergency medicine, and between 25.9% and 26.5% rated such evidence as strong in their own personal practices.
“While acknowledgment of disparities in the U.S. was strongly associated with perceived strength of the evidence in medicine in general (P less than .001), acknowledgment of disparities in one’s own practice was not associated with perceived strength of evidence in emergency medicine or with medicine in general,” Ms. Zogg said. “As evidence documenting disparities continues to increase, action is needed to address disparities in emergency care. This is important because as frontline providers of care, emergency physicians often act as the first point of contact for these patients within the U.S. health system. Ultimately, despite recognition of health care providers as a contributing factor to the existence of disparities and evidence to suggest the presence of disparities in emergency medicine, only one-fourth of FACEP openly acknowledge the potential for disparities in their personal practice.”
Ms. Zogg is supported by a National Institutes of Health Medical Scientist Training Program grant. The study was supported in part by a grant from the Emergency Medicine Foundation and the Society for Academic Emergency Medicine.
SOURCE: Zogg C et al. Ann Emerg Med. 2018 Oct;72(4):S118-9. doi: 10.1016/j.annemergmed.2018.08.306.
SAN DIEGO – About 25% of Fellows of the American College of Emergency Physicians acknowledged that health care disparities exist in their practices, according to a survey completed by 945 ACEP fellows in 36 states.
In conjunction with the American College of Emergency Physicians, Cheryl K. Zogg, MSPH, MHS, and her colleagues surveyed a nationally representative subset of ACEP fellows between September and December of 2017 to determine the extent to which emergency medicine physicians perceive that various forms of disparities exist and that there is “strong evidence” to support the existence of disparities.
The results were reported in an abstract presented during the annual meeting of the American College of Emergency Physicians.
“The existence of disparities in medicine has been widely acknowledged,” she said. “A lot of the modern conversation began in 2002, when the Institute of Medicine published its now-famous report, ‘Unequal Treatment.’ Since that time, a growing body of literature has discussed the existence of disparities in various medical fields and related to a number of factors including but not limited to race and ethnicity.”
The survey contained questions about perceptions of disparities related to insurance status, type of insurance, ability to speak English, educational attainment, race/ethnicity, sexual identity, and sexual orientation as well as the perceived strength of the evidence to support the existence of disparities in medicine in general and in emergency medicine specifically.
Ms. Zogg, an MD-PhD candidate at Yale University, New Haven, Conn., found that disparities of insurance status (85.6%) and type of insurance (81.3%) were the most widely acknowledged, followed by variations in care as a result of patients’ ability to speak English (73.7%) and level of educational attainment (61.5%).
Slightly more than half of respondents (51.9%) acknowledged the existence of disparities based on race/ethnicity in United States, but only 20.9% believe that such disparities exist in their hospitals and even fewer (3.9%) believe that they exist in their own personal practices. At the same time, more than one-third of respondents (40.6%) acknowledged the existence of disparities based on gender identity in the United States, but 22.4% believe that such disparities exist in their hospitals and even fewer (5.7%) believe that they exist in their own practices. Similar percentages were observed when respondents were asked about issues of sexual orientation (33.7%, 10.6%, and 2.3%, respectively).
Perceived strength of the evidence supporting the existence of disparities followed a similar trend. Between 74.7% and 82.2% of respondents believe there is strong evidence in medicine to support the existence of racial disparities in insurance status and insurance type, respectively. However, between 47% and 49.4% of respondents rated such evidence as strong in emergency medicine, and between 25.9% and 26.5% rated such evidence as strong in their own personal practices.
“While acknowledgment of disparities in the U.S. was strongly associated with perceived strength of the evidence in medicine in general (P less than .001), acknowledgment of disparities in one’s own practice was not associated with perceived strength of evidence in emergency medicine or with medicine in general,” Ms. Zogg said. “As evidence documenting disparities continues to increase, action is needed to address disparities in emergency care. This is important because as frontline providers of care, emergency physicians often act as the first point of contact for these patients within the U.S. health system. Ultimately, despite recognition of health care providers as a contributing factor to the existence of disparities and evidence to suggest the presence of disparities in emergency medicine, only one-fourth of FACEP openly acknowledge the potential for disparities in their personal practice.”
Ms. Zogg is supported by a National Institutes of Health Medical Scientist Training Program grant. The study was supported in part by a grant from the Emergency Medicine Foundation and the Society for Academic Emergency Medicine.
SOURCE: Zogg C et al. Ann Emerg Med. 2018 Oct;72(4):S118-9. doi: 10.1016/j.annemergmed.2018.08.306.
SAN DIEGO – About 25% of Fellows of the American College of Emergency Physicians acknowledged that health care disparities exist in their practices, according to a survey completed by 945 ACEP fellows in 36 states.
In conjunction with the American College of Emergency Physicians, Cheryl K. Zogg, MSPH, MHS, and her colleagues surveyed a nationally representative subset of ACEP fellows between September and December of 2017 to determine the extent to which emergency medicine physicians perceive that various forms of disparities exist and that there is “strong evidence” to support the existence of disparities.
The results were reported in an abstract presented during the annual meeting of the American College of Emergency Physicians.
“The existence of disparities in medicine has been widely acknowledged,” she said. “A lot of the modern conversation began in 2002, when the Institute of Medicine published its now-famous report, ‘Unequal Treatment.’ Since that time, a growing body of literature has discussed the existence of disparities in various medical fields and related to a number of factors including but not limited to race and ethnicity.”
The survey contained questions about perceptions of disparities related to insurance status, type of insurance, ability to speak English, educational attainment, race/ethnicity, sexual identity, and sexual orientation as well as the perceived strength of the evidence to support the existence of disparities in medicine in general and in emergency medicine specifically.
Ms. Zogg, an MD-PhD candidate at Yale University, New Haven, Conn., found that disparities of insurance status (85.6%) and type of insurance (81.3%) were the most widely acknowledged, followed by variations in care as a result of patients’ ability to speak English (73.7%) and level of educational attainment (61.5%).
Slightly more than half of respondents (51.9%) acknowledged the existence of disparities based on race/ethnicity in United States, but only 20.9% believe that such disparities exist in their hospitals and even fewer (3.9%) believe that they exist in their own personal practices. At the same time, more than one-third of respondents (40.6%) acknowledged the existence of disparities based on gender identity in the United States, but 22.4% believe that such disparities exist in their hospitals and even fewer (5.7%) believe that they exist in their own practices. Similar percentages were observed when respondents were asked about issues of sexual orientation (33.7%, 10.6%, and 2.3%, respectively).
Perceived strength of the evidence supporting the existence of disparities followed a similar trend. Between 74.7% and 82.2% of respondents believe there is strong evidence in medicine to support the existence of racial disparities in insurance status and insurance type, respectively. However, between 47% and 49.4% of respondents rated such evidence as strong in emergency medicine, and between 25.9% and 26.5% rated such evidence as strong in their own personal practices.
“While acknowledgment of disparities in the U.S. was strongly associated with perceived strength of the evidence in medicine in general (P less than .001), acknowledgment of disparities in one’s own practice was not associated with perceived strength of evidence in emergency medicine or with medicine in general,” Ms. Zogg said. “As evidence documenting disparities continues to increase, action is needed to address disparities in emergency care. This is important because as frontline providers of care, emergency physicians often act as the first point of contact for these patients within the U.S. health system. Ultimately, despite recognition of health care providers as a contributing factor to the existence of disparities and evidence to suggest the presence of disparities in emergency medicine, only one-fourth of FACEP openly acknowledge the potential for disparities in their personal practice.”
Ms. Zogg is supported by a National Institutes of Health Medical Scientist Training Program grant. The study was supported in part by a grant from the Emergency Medicine Foundation and the Society for Academic Emergency Medicine.
SOURCE: Zogg C et al. Ann Emerg Med. 2018 Oct;72(4):S118-9. doi: 10.1016/j.annemergmed.2018.08.306.
AT ACEP18
Key clinical point: As evidence documenting disparities continues to increase, action is needed to address disparities in EM care.
Major finding: Only one-fourth of ACEP fellows openly acknowledge the potential for disparities in their practices.
Study details: A survey of 945 ACEP fellows in 36 states.
Disclosures: Ms. Zogg is supported by a National Institutes of Health Medical Scientist Training Program grant. The study was supported in part by a grant from the Emergency Medicine Foundation and the Society for Academic Emergency Medicine.
Source: Zogg C et al. Ann Emerg Med. 2018 Oct;72(4):S118-9. doi: 10.1016/j.annemergmed.2018.08.306.
Pharmacist-led clinic boosted hypertension control after discharge
SAN DIEGO – Pharmacist-physician collaboration on hypertension management was effective for controlling blood pressure in patients discharged from an urban ED, results from a pilot study showed.

“Hypertension is the leading risk factor for cardiovascular events and stroke in this country,” Brittany Stewart, RD, PharmD, said at the annual meeting of the American College of Emergency Physicians. “The good news is that we’re not trying to figure out how to treat this disease, but the bad news is that we have 50% of people with uncontrolled high blood pressure.”
“Pharmacists are highly accessible in the community in outpatient settings,” Dr. Stewart of the department of pharmacy practice at Wayne State University, Detroit, said. “This is where ED providers can really integrate and work on a team to refer patients for their chronic diseases on an outpatient basis.”
In a prospective pilot trial, Dr. Stewart and her colleagues recruited 89 patients with uncontrolled hypertension who presented to the ED at Wayne State during May 24, 2017–May 18, 2018. Their average age was 43 years, 51% were male, 94% were black, 51% were current smokers, the mean body mass index was 34.5 kg/m2, and 18% had no health insurance.
“In Detroit, we have significant health disparities with our patient population,” she said. “They are high utilizers of the emergency department, not only for their acute illness but for chronic illness as well. There are several studies showing that team-based care has improved hypertension and blood pressure control. However, the adoption and sustainability of these models haven’t really taken off in our health care landscape yet.”
Over a period of 1.5 years, Dr. Stewart and two physicians developed a transitional care clinic, based on a collaborative practice agreement with emergency physicians. Per protocol, five follow-up visits were planned in an outpatient pharmacy clinic, where Dr. Stewart initiated and titrated antihypertensive medications and handled refills.
“The physician does not have to physically be at the clinic,” she said. “We work closely over the phone to make the best decisions, but it’s not typical ambulatory care where the physician has to be sitting right next to the pharmacist to make the best decisions for the patients.” The primary outcome was the transitional care clinic’s impact on blood pressure.
Dr. Stewart reported results from 47 medication interventions that were provided over 97 follow-up visits. The researchers found that the median blood pressure dropped from an initial reading of 160/102 mm Hg to 130/93 mm Hg by the fifth transitional care clinic visit. Across all patients, systolic blood pressure decreased by an average of 48 mm Hg. “I don’t think we were surprised by these results; we are getting people very much in need down to their blood pressure goals,” she said. “By the end of the study, patients were on an average of three antihypertensive medications.”
She and her colleagues plan to conduct a larger randomized, clinical trial of this care model. The research was supported by a faculty award from the Eugene Applebaum College of Pharmacy and Health Sciences at Wayne State University and by the National Association of Chain Drug Stores Foundation.
Source: Brody A et al. Ann Emerg Med. 2018 Oct;72;4:S36-7. doi. 10.1016/j.annemergmed.2018.08.088.
SAN DIEGO – Pharmacist-physician collaboration on hypertension management was effective for controlling blood pressure in patients discharged from an urban ED, results from a pilot study showed.
“Hypertension is the leading risk factor for cardiovascular events and stroke in this country,” Brittany Stewart, RD, PharmD, said at the annual meeting of the American College of Emergency Physicians. “The good news is that we’re not trying to figure out how to treat this disease, but the bad news is that we have 50% of people with uncontrolled high blood pressure.”
“Pharmacists are highly accessible in the community in outpatient settings,” Dr. Stewart of the department of pharmacy practice at Wayne State University, Detroit, said. “This is where ED providers can really integrate and work on a team to refer patients for their chronic diseases on an outpatient basis.”
In a prospective pilot trial, Dr. Stewart and her colleagues recruited 89 patients with uncontrolled hypertension who presented to the ED at Wayne State during May 24, 2017–May 18, 2018. Their average age was 43 years, 51% were male, 94% were black, 51% were current smokers, the mean body mass index was 34.5 kg/m2, and 18% had no health insurance.
“In Detroit, we have significant health disparities with our patient population,” she said. “They are high utilizers of the emergency department, not only for their acute illness but for chronic illness as well. There are several studies showing that team-based care has improved hypertension and blood pressure control. However, the adoption and sustainability of these models haven’t really taken off in our health care landscape yet.”
Over a period of 1.5 years, Dr. Stewart and two physicians developed a transitional care clinic, based on a collaborative practice agreement with emergency physicians. Per protocol, five follow-up visits were planned in an outpatient pharmacy clinic, where Dr. Stewart initiated and titrated antihypertensive medications and handled refills.
“The physician does not have to physically be at the clinic,” she said. “We work closely over the phone to make the best decisions, but it’s not typical ambulatory care where the physician has to be sitting right next to the pharmacist to make the best decisions for the patients.” The primary outcome was the transitional care clinic’s impact on blood pressure.
Dr. Stewart reported results from 47 medication interventions that were provided over 97 follow-up visits. The researchers found that the median blood pressure dropped from an initial reading of 160/102 mm Hg to 130/93 mm Hg by the fifth transitional care clinic visit. Across all patients, systolic blood pressure decreased by an average of 48 mm Hg. “I don’t think we were surprised by these results; we are getting people very much in need down to their blood pressure goals,” she said. “By the end of the study, patients were on an average of three antihypertensive medications.”
She and her colleagues plan to conduct a larger randomized, clinical trial of this care model. The research was supported by a faculty award from the Eugene Applebaum College of Pharmacy and Health Sciences at Wayne State University and by the National Association of Chain Drug Stores Foundation.
Source: Brody A et al. Ann Emerg Med. 2018 Oct;72;4:S36-7. doi. 10.1016/j.annemergmed.2018.08.088.
SAN DIEGO – Pharmacist-physician collaboration on hypertension management was effective for controlling blood pressure in patients discharged from an urban ED, results from a pilot study showed.
“Hypertension is the leading risk factor for cardiovascular events and stroke in this country,” Brittany Stewart, RD, PharmD, said at the annual meeting of the American College of Emergency Physicians. “The good news is that we’re not trying to figure out how to treat this disease, but the bad news is that we have 50% of people with uncontrolled high blood pressure.”
“Pharmacists are highly accessible in the community in outpatient settings,” Dr. Stewart of the department of pharmacy practice at Wayne State University, Detroit, said. “This is where ED providers can really integrate and work on a team to refer patients for their chronic diseases on an outpatient basis.”
In a prospective pilot trial, Dr. Stewart and her colleagues recruited 89 patients with uncontrolled hypertension who presented to the ED at Wayne State during May 24, 2017–May 18, 2018. Their average age was 43 years, 51% were male, 94% were black, 51% were current smokers, the mean body mass index was 34.5 kg/m2, and 18% had no health insurance.
“In Detroit, we have significant health disparities with our patient population,” she said. “They are high utilizers of the emergency department, not only for their acute illness but for chronic illness as well. There are several studies showing that team-based care has improved hypertension and blood pressure control. However, the adoption and sustainability of these models haven’t really taken off in our health care landscape yet.”
Over a period of 1.5 years, Dr. Stewart and two physicians developed a transitional care clinic, based on a collaborative practice agreement with emergency physicians. Per protocol, five follow-up visits were planned in an outpatient pharmacy clinic, where Dr. Stewart initiated and titrated antihypertensive medications and handled refills.
“The physician does not have to physically be at the clinic,” she said. “We work closely over the phone to make the best decisions, but it’s not typical ambulatory care where the physician has to be sitting right next to the pharmacist to make the best decisions for the patients.” The primary outcome was the transitional care clinic’s impact on blood pressure.
Dr. Stewart reported results from 47 medication interventions that were provided over 97 follow-up visits. The researchers found that the median blood pressure dropped from an initial reading of 160/102 mm Hg to 130/93 mm Hg by the fifth transitional care clinic visit. Across all patients, systolic blood pressure decreased by an average of 48 mm Hg. “I don’t think we were surprised by these results; we are getting people very much in need down to their blood pressure goals,” she said. “By the end of the study, patients were on an average of three antihypertensive medications.”
She and her colleagues plan to conduct a larger randomized, clinical trial of this care model. The research was supported by a faculty award from the Eugene Applebaum College of Pharmacy and Health Sciences at Wayne State University and by the National Association of Chain Drug Stores Foundation.
Source: Brody A et al. Ann Emerg Med. 2018 Oct;72;4:S36-7. doi. 10.1016/j.annemergmed.2018.08.088.
REPORTING FROM ACEP18
Key clinical point: Hypertensive patients discharged from an urban ED benefited from a pharmacist-led clinic.
Major finding: By the last follow-up visit, patients’ mean systolic blood pressure had decreased by 48 mm Hg.
Study details: A pilot study of 89 patients with uncontrolled blood pressure.
Disclosures: The research was supported by a faculty award from the Eugene Applebaum College of Pharmacy and Health Sciences at Wayne State University and by the National Association of Chain Drug Stores Foundation.
Source: Brody A et al. Ann Emerg Med. 2018 Oct;72;4:S36-7. doi. 10.1016/j.annemergmed.2018.08.088.
How to manage difficult dislocations
SAN DIEGO – Being prepared to manage difficult dislocations is key to maintaining the flow of patient care in any emergency department.
In a video interview at the annual meeting of the American College of Emergency Physicians, Danielle D. Campagne, MD, FACEP, shared her clinical pearls for managing dislocations of the jaw, hip, ankle, and shoulder.
Dr. Campagne is an emergency medicine physician who practices at Community Regional Medical Center in Fresno, Calif. She is also vice chief of emergency medicine at University of California, San Francisco, Fresno. She reported having no financial disclosures.
SAN DIEGO – Being prepared to manage difficult dislocations is key to maintaining the flow of patient care in any emergency department.
In a video interview at the annual meeting of the American College of Emergency Physicians, Danielle D. Campagne, MD, FACEP, shared her clinical pearls for managing dislocations of the jaw, hip, ankle, and shoulder.
Dr. Campagne is an emergency medicine physician who practices at Community Regional Medical Center in Fresno, Calif. She is also vice chief of emergency medicine at University of California, San Francisco, Fresno. She reported having no financial disclosures.
SAN DIEGO – Being prepared to manage difficult dislocations is key to maintaining the flow of patient care in any emergency department.
In a video interview at the annual meeting of the American College of Emergency Physicians, Danielle D. Campagne, MD, FACEP, shared her clinical pearls for managing dislocations of the jaw, hip, ankle, and shoulder.
Dr. Campagne is an emergency medicine physician who practices at Community Regional Medical Center in Fresno, Calif. She is also vice chief of emergency medicine at University of California, San Francisco, Fresno. She reported having no financial disclosures.
REPORTING FROM ACEP18

Five “can’t miss” oncologic emergencies
SAN DIEGO – Acute promyelocytic leukemia is one of five “can’t miss” oncologic emergencies, Megan Boysen Osborn, MD, MHPE, told a standing-room-only crowd at the annual meeting of the American College of Emergency Physicians.
In our exclusive video interview, Dr. Osborn, vice chair of education and the residency program director in the department of emergency medicine at the University of California, Irvine, offered tips on how to recognize acute promyelocytic leukemia, leukostasis, neutropenic fever, tumor lysis syndrome, and disseminated intravascular coagulation.
“All patients with suspected leukemias should be admitted,” she said. “Time is of the essence.”
Dr. Osborn reported having no financial disclosures related to her presentation.
SAN DIEGO – Acute promyelocytic leukemia is one of five “can’t miss” oncologic emergencies, Megan Boysen Osborn, MD, MHPE, told a standing-room-only crowd at the annual meeting of the American College of Emergency Physicians.
In our exclusive video interview, Dr. Osborn, vice chair of education and the residency program director in the department of emergency medicine at the University of California, Irvine, offered tips on how to recognize acute promyelocytic leukemia, leukostasis, neutropenic fever, tumor lysis syndrome, and disseminated intravascular coagulation.
“All patients with suspected leukemias should be admitted,” she said. “Time is of the essence.”
Dr. Osborn reported having no financial disclosures related to her presentation.
SAN DIEGO – Acute promyelocytic leukemia is one of five “can’t miss” oncologic emergencies, Megan Boysen Osborn, MD, MHPE, told a standing-room-only crowd at the annual meeting of the American College of Emergency Physicians.
In our exclusive video interview, Dr. Osborn, vice chair of education and the residency program director in the department of emergency medicine at the University of California, Irvine, offered tips on how to recognize acute promyelocytic leukemia, leukostasis, neutropenic fever, tumor lysis syndrome, and disseminated intravascular coagulation.
“All patients with suspected leukemias should be admitted,” she said. “Time is of the essence.”
Dr. Osborn reported having no financial disclosures related to her presentation.
REPORTING FROM ACEP18

Physical assaults in the emergency department on the rise, survey finds

Those are key findings from an email-based survey administered to ACEP members in August of 2018.
“The results are quite troubling,” Vidor E. Friedman, MD, FACEP, president of ACEP, said during a press briefing at the group’s annual meeting. “Emergency physicians are reporting that violence in emergency departments is increasing and that it’s harming not only physicians and nurses, but also patients and the care that’s being provided to them.”
Dr. Friedman, who practices emergency medicine in Maitland, Fla., recalled one afternoon shift when police brought in a drunk man they had cited for vagrancy after finding him in a ditch by the roadside. It was the man’s first day out of jail in 10 years. “He was a pretty intimidating looking guy,” Dr. Friedman said. “He threatened me and he threatened the staff, so we appropriately restrained him, which only increased his agitation. The fourth time he said he was going to kill me, he told me he was going to put an ice pick in my heart. When his buddies came to pick him up, I had the police escort him to the city limits, and I didn’t sleep at home for a week. This is the kind of thing that health care workers are exposed to on a fairly regular basis.”
The ACEP survey found that emergency physicians across all demographics experience various forms of violence and are increasingly concerned about violence in the ED. “We know that there is gross underreporting of [violence in the ED],” said Terry Kowalenko, MD, FACEP, chair of emergency medicine at Oakland University William Beaumont School of Medicine, Rochester, Mich., and coauthor of a new study that assessed violence against emergency physicians in that state. “Some studies have shown it to be under 50%. The other thing is, it’s very difficult to predict who the perpetrator will be, or who the victim will be. We did find that the time you spend with the patient certainly increases your chances of violence perpetrated against you. Clearly, there are consequences to the victim, the perpetrator, the institution, and potentially, other patients.”

According to Dr. Kowalenko’s own research, 72% of emergency medicine physicians in Michigan reported experiencing violence in the past year. In 2018, an increasing proportion of that state’s emergency physicians reported feeling “constantly fearful” of becoming a victim of violence (8.1% vs. 1.2% in 2005), with 22% reporting feeling frequently fearful (up from 9.4% in 2005).
For the ACEP-sponsored survey, on Aug. 21, 2018, Alexandria, Va.–based Marketing General sent an email to 31,389 ACEP members, inviting them to answer 22 questions in an effort to understand emergency physicians’ views on the level, type, frequency, and impact of violence experienced in the ED. By the time polling closed 6 days later, 3,539 surveys were completed, for a response rate of about 11%. Clinicians in California led the way with 8% of total responses, followed by those in Texas (7%), New York (7%), Florida (5%), Pennsylvania (5%), and Ohio (5%). Nearly two-thirds of respondents (71%) were male, and 25% work for emergency departments with annual patient volumes between 50,001 and 75,000, while another 39% work for departments with even higher volumes.
Nearly half of respondents (47%) reported being physically assaulted while at work in the ED, while 71% have witnessed an assault. Only 10% have experienced neither. The majority of assaults were committed by patients (97%), but 28% involved a patient’s family member or friend. The most common form of assault was a hit or a slap (44%), while other frequent forms of violence included being spit on (30%), punched (28%), or kicked (27%).
Among those who have been physically assaulted, 48% reported that at least half of all assaults were committed by people believed to be seeking drugs or who were under the influence of drugs or alcohol, while 41% said that more than half of assaults were committed by psychiatric patients.
“Our emergency departments are kind of a microcosm of all the challenges that we face today in society: gang violence, gun violence, domestic violence, and psychiatric illnesses [for which] we have a shortage of beds,” said Leigh Vinocur, MD, FACEP, former chair of ACEP’s Emergency Department Violence Committee. “Then there is the opioid crisis.” She added that being in an emergency department can be “an emotionally volatile experience for people from all walks of life. People come in hurt. They’re at their worst; they’re frightened, they’re vulnerable and stressed.”
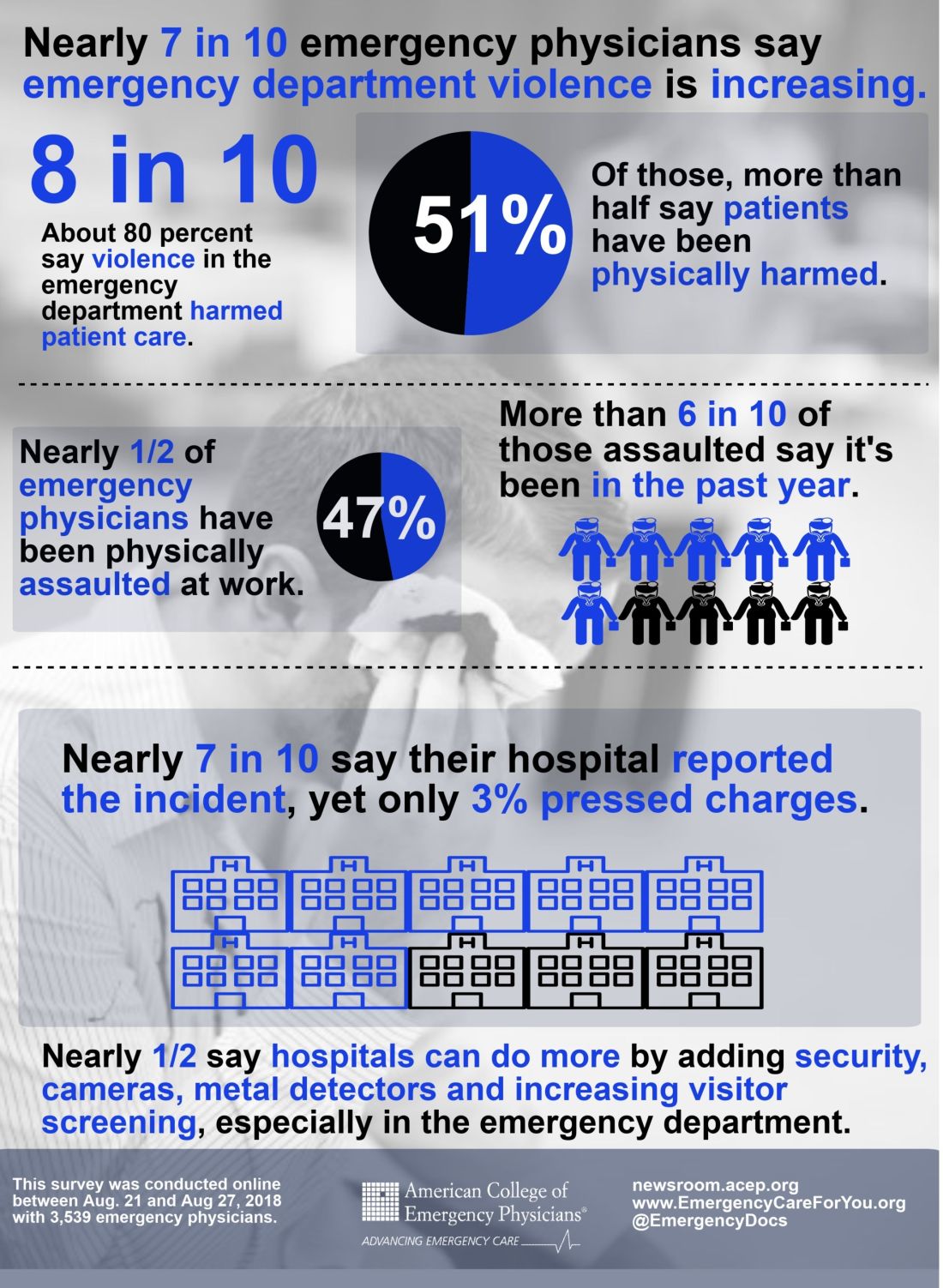
More than three-quarters of ACEP survey respondents (77%) believe that violence in the ED has harmed patient care, primarily by loss of productivity (81%), emotional trauma (81%), increased wait times (80%), and less focus from emergency staff or physicians (76%). In addition, 49% ranked “increase security” as the most important step hospitals can take to increase ED safety, while the top three contributing factors to violence in the ED were no adequate punitive consequence or response toward the attacker (34%), behavioral health patients (32%), and absence of adequate protective mechanisms for physicians/staff (15%).
When asked how the hospital administration or hospital security responded to the assault, 28% said that the hospital or nursing staff put a behavioral flag in the patient’s medical chart, while 21% said that hospital security arrested the patient for the assault or enlisted law enforcement to arrest the patient.
Finally, nearly half of respondents indicated that hospitals could do more by adding security cameras, metal detectors, and increasing visitor screening. “Obviously this is site-specific,” Dr. Friedman said. “We’re not saying that every emergency department in America needs to have a metal detector out front, but this needs to be something that institutions take seriously, to protect both patients and the providers that work there.”
[email protected]
Those are key findings from an email-based survey administered to ACEP members in August of 2018.
“The results are quite troubling,” Vidor E. Friedman, MD, FACEP, president of ACEP, said during a press briefing at the group’s annual meeting. “Emergency physicians are reporting that violence in emergency departments is increasing and that it’s harming not only physicians and nurses, but also patients and the care that’s being provided to them.”
Dr. Friedman, who practices emergency medicine in Maitland, Fla., recalled one afternoon shift when police brought in a drunk man they had cited for vagrancy after finding him in a ditch by the roadside. It was the man’s first day out of jail in 10 years. “He was a pretty intimidating looking guy,” Dr. Friedman said. “He threatened me and he threatened the staff, so we appropriately restrained him, which only increased his agitation. The fourth time he said he was going to kill me, he told me he was going to put an ice pick in my heart. When his buddies came to pick him up, I had the police escort him to the city limits, and I didn’t sleep at home for a week. This is the kind of thing that health care workers are exposed to on a fairly regular basis.”
The ACEP survey found that emergency physicians across all demographics experience various forms of violence and are increasingly concerned about violence in the ED. “We know that there is gross underreporting of [violence in the ED],” said Terry Kowalenko, MD, FACEP, chair of emergency medicine at Oakland University William Beaumont School of Medicine, Rochester, Mich., and coauthor of a new study that assessed violence against emergency physicians in that state. “Some studies have shown it to be under 50%. The other thing is, it’s very difficult to predict who the perpetrator will be, or who the victim will be. We did find that the time you spend with the patient certainly increases your chances of violence perpetrated against you. Clearly, there are consequences to the victim, the perpetrator, the institution, and potentially, other patients.”
According to Dr. Kowalenko’s own research, 72% of emergency medicine physicians in Michigan reported experiencing violence in the past year. In 2018, an increasing proportion of that state’s emergency physicians reported feeling “constantly fearful” of becoming a victim of violence (8.1% vs. 1.2% in 2005), with 22% reporting feeling frequently fearful (up from 9.4% in 2005).
For the ACEP-sponsored survey, on Aug. 21, 2018, Alexandria, Va.–based Marketing General sent an email to 31,389 ACEP members, inviting them to answer 22 questions in an effort to understand emergency physicians’ views on the level, type, frequency, and impact of violence experienced in the ED. By the time polling closed 6 days later, 3,539 surveys were completed, for a response rate of about 11%. Clinicians in California led the way with 8% of total responses, followed by those in Texas (7%), New York (7%), Florida (5%), Pennsylvania (5%), and Ohio (5%). Nearly two-thirds of respondents (71%) were male, and 25% work for emergency departments with annual patient volumes between 50,001 and 75,000, while another 39% work for departments with even higher volumes.
Nearly half of respondents (47%) reported being physically assaulted while at work in the ED, while 71% have witnessed an assault. Only 10% have experienced neither. The majority of assaults were committed by patients (97%), but 28% involved a patient’s family member or friend. The most common form of assault was a hit or a slap (44%), while other frequent forms of violence included being spit on (30%), punched (28%), or kicked (27%).
Among those who have been physically assaulted, 48% reported that at least half of all assaults were committed by people believed to be seeking drugs or who were under the influence of drugs or alcohol, while 41% said that more than half of assaults were committed by psychiatric patients.
“Our emergency departments are kind of a microcosm of all the challenges that we face today in society: gang violence, gun violence, domestic violence, and psychiatric illnesses [for which] we have a shortage of beds,” said Leigh Vinocur, MD, FACEP, former chair of ACEP’s Emergency Department Violence Committee. “Then there is the opioid crisis.” She added that being in an emergency department can be “an emotionally volatile experience for people from all walks of life. People come in hurt. They’re at their worst; they’re frightened, they’re vulnerable and stressed.”
More than three-quarters of ACEP survey respondents (77%) believe that violence in the ED has harmed patient care, primarily by loss of productivity (81%), emotional trauma (81%), increased wait times (80%), and less focus from emergency staff or physicians (76%). In addition, 49% ranked “increase security” as the most important step hospitals can take to increase ED safety, while the top three contributing factors to violence in the ED were no adequate punitive consequence or response toward the attacker (34%), behavioral health patients (32%), and absence of adequate protective mechanisms for physicians/staff (15%).
When asked how the hospital administration or hospital security responded to the assault, 28% said that the hospital or nursing staff put a behavioral flag in the patient’s medical chart, while 21% said that hospital security arrested the patient for the assault or enlisted law enforcement to arrest the patient.
Finally, nearly half of respondents indicated that hospitals could do more by adding security cameras, metal detectors, and increasing visitor screening. “Obviously this is site-specific,” Dr. Friedman said. “We’re not saying that every emergency department in America needs to have a metal detector out front, but this needs to be something that institutions take seriously, to protect both patients and the providers that work there.”
[email protected]
Those are key findings from an email-based survey administered to ACEP members in August of 2018.
“The results are quite troubling,” Vidor E. Friedman, MD, FACEP, president of ACEP, said during a press briefing at the group’s annual meeting. “Emergency physicians are reporting that violence in emergency departments is increasing and that it’s harming not only physicians and nurses, but also patients and the care that’s being provided to them.”
Dr. Friedman, who practices emergency medicine in Maitland, Fla., recalled one afternoon shift when police brought in a drunk man they had cited for vagrancy after finding him in a ditch by the roadside. It was the man’s first day out of jail in 10 years. “He was a pretty intimidating looking guy,” Dr. Friedman said. “He threatened me and he threatened the staff, so we appropriately restrained him, which only increased his agitation. The fourth time he said he was going to kill me, he told me he was going to put an ice pick in my heart. When his buddies came to pick him up, I had the police escort him to the city limits, and I didn’t sleep at home for a week. This is the kind of thing that health care workers are exposed to on a fairly regular basis.”
The ACEP survey found that emergency physicians across all demographics experience various forms of violence and are increasingly concerned about violence in the ED. “We know that there is gross underreporting of [violence in the ED],” said Terry Kowalenko, MD, FACEP, chair of emergency medicine at Oakland University William Beaumont School of Medicine, Rochester, Mich., and coauthor of a new study that assessed violence against emergency physicians in that state. “Some studies have shown it to be under 50%. The other thing is, it’s very difficult to predict who the perpetrator will be, or who the victim will be. We did find that the time you spend with the patient certainly increases your chances of violence perpetrated against you. Clearly, there are consequences to the victim, the perpetrator, the institution, and potentially, other patients.”
According to Dr. Kowalenko’s own research, 72% of emergency medicine physicians in Michigan reported experiencing violence in the past year. In 2018, an increasing proportion of that state’s emergency physicians reported feeling “constantly fearful” of becoming a victim of violence (8.1% vs. 1.2% in 2005), with 22% reporting feeling frequently fearful (up from 9.4% in 2005).
For the ACEP-sponsored survey, on Aug. 21, 2018, Alexandria, Va.–based Marketing General sent an email to 31,389 ACEP members, inviting them to answer 22 questions in an effort to understand emergency physicians’ views on the level, type, frequency, and impact of violence experienced in the ED. By the time polling closed 6 days later, 3,539 surveys were completed, for a response rate of about 11%. Clinicians in California led the way with 8% of total responses, followed by those in Texas (7%), New York (7%), Florida (5%), Pennsylvania (5%), and Ohio (5%). Nearly two-thirds of respondents (71%) were male, and 25% work for emergency departments with annual patient volumes between 50,001 and 75,000, while another 39% work for departments with even higher volumes.
Nearly half of respondents (47%) reported being physically assaulted while at work in the ED, while 71% have witnessed an assault. Only 10% have experienced neither. The majority of assaults were committed by patients (97%), but 28% involved a patient’s family member or friend. The most common form of assault was a hit or a slap (44%), while other frequent forms of violence included being spit on (30%), punched (28%), or kicked (27%).
Among those who have been physically assaulted, 48% reported that at least half of all assaults were committed by people believed to be seeking drugs or who were under the influence of drugs or alcohol, while 41% said that more than half of assaults were committed by psychiatric patients.
“Our emergency departments are kind of a microcosm of all the challenges that we face today in society: gang violence, gun violence, domestic violence, and psychiatric illnesses [for which] we have a shortage of beds,” said Leigh Vinocur, MD, FACEP, former chair of ACEP’s Emergency Department Violence Committee. “Then there is the opioid crisis.” She added that being in an emergency department can be “an emotionally volatile experience for people from all walks of life. People come in hurt. They’re at their worst; they’re frightened, they’re vulnerable and stressed.”
More than three-quarters of ACEP survey respondents (77%) believe that violence in the ED has harmed patient care, primarily by loss of productivity (81%), emotional trauma (81%), increased wait times (80%), and less focus from emergency staff or physicians (76%). In addition, 49% ranked “increase security” as the most important step hospitals can take to increase ED safety, while the top three contributing factors to violence in the ED were no adequate punitive consequence or response toward the attacker (34%), behavioral health patients (32%), and absence of adequate protective mechanisms for physicians/staff (15%).
When asked how the hospital administration or hospital security responded to the assault, 28% said that the hospital or nursing staff put a behavioral flag in the patient’s medical chart, while 21% said that hospital security arrested the patient for the assault or enlisted law enforcement to arrest the patient.
Finally, nearly half of respondents indicated that hospitals could do more by adding security cameras, metal detectors, and increasing visitor screening. “Obviously this is site-specific,” Dr. Friedman said. “We’re not saying that every emergency department in America needs to have a metal detector out front, but this needs to be something that institutions take seriously, to protect both patients and the providers that work there.”
[email protected]
AT ACEP18
Previous psychiatric admissions predict suicide attempts
SAN DIEGO – Among patients presenting to the emergency department with suicidal ideation, the number of previous psychiatric admissions is the most important predictor of a subsequent suicide attempt, results from a 2-year-long study showed.

Momentary measures – significant current difficulties with sleep, energy, or appetite, and anhedonia – “are important considerations during suicide risk assessment, regardless of whether the patient meets the threshold for major depressive disorder, lead study author Anne C. Knorr said in an interview in advance of the annual meeting of the American College of Emergency Physicians.
“Many traditionally studied psychiatric risk factors do not significantly differ between individuals who think about suicide and those who act on their suicidal thoughts, an important distinction as only one-third of those who think about suicide carry out a suicide attempt. While there is support for some psychiatric factors – for example, anxiety, substance use disorders, sleep disturbance – being useful in differentiating these groups, the current study is unique in its use of a longitudinal design to identify influential risk factors that predict future suicide attempt among those with suicidal ideation,” she said.
Ms. Knorr, a research project manager at Geisinger Medical Center, Danville, Pa., and her colleagues collected electronic medical record data from 908 patients who had received a psychiatric evaluation at an index emergency department visit for suicidal ideation over a 2-year period. The mean age of patients was 39 years. The target sample was 30 patients who had returned to the ED following a suicide attempt within 6 months of their index ED visit.
The researchers analyzed 32 predictor variables from patient charts, including demographics, psychiatric history, and current psychiatric presentation. The evaluation was done with “a machine learning statistical approach which is more capable than traditional statistical approaches in handling a large number of predictor variables,” Ms. Knorr said.
The number of previous psychiatric admissions was the most important predictor of a subsequent suicide attempt. The next nine most important variables were sleep disturbance, history of family suicide, low energy, patient age, psychiatrist determination of severe suicide risk, psychiatrist determination of moderate suicide risk, appetite issues, presence of a support system, and loss of interest/pleasure.
These symptoms may not typically be weighed heavily in risk assessments, Ms. Knorr said. “Additionally, given that research suggests that the clinical determination of suicide risk is historically poor, it was interesting that psychiatrist determination of moderate or high risk was influential in predicting a return visit for suicide attempt. Finally, we were surprised that a past history of suicide attempt, often viewed as the strongest predictor of a future suicide attempt, did not emerge as one of the top 10 influential predictors.
“Limitations of this study include the use of a return visit to a Geisinger emergency department as the only measure of a future suicide attempt and the utilization of data from only one health system,” she noted.
The study was funded by the Geisinger Clinic Research Fund. One of the coauthors, Andrei Nemoianu, MD, reported receipt of a research grant from Takeda Pharmaceuticals for a separate study.
SOURCE: Knorr A et al. Ann Emerg Med. 2018 Oct;72;4:S23. doi. 10.1016/j.annemergmed.2018.08.055.
SAN DIEGO – Among patients presenting to the emergency department with suicidal ideation, the number of previous psychiatric admissions is the most important predictor of a subsequent suicide attempt, results from a 2-year-long study showed.
Momentary measures – significant current difficulties with sleep, energy, or appetite, and anhedonia – “are important considerations during suicide risk assessment, regardless of whether the patient meets the threshold for major depressive disorder, lead study author Anne C. Knorr said in an interview in advance of the annual meeting of the American College of Emergency Physicians.
“Many traditionally studied psychiatric risk factors do not significantly differ between individuals who think about suicide and those who act on their suicidal thoughts, an important distinction as only one-third of those who think about suicide carry out a suicide attempt. While there is support for some psychiatric factors – for example, anxiety, substance use disorders, sleep disturbance – being useful in differentiating these groups, the current study is unique in its use of a longitudinal design to identify influential risk factors that predict future suicide attempt among those with suicidal ideation,” she said.
Ms. Knorr, a research project manager at Geisinger Medical Center, Danville, Pa., and her colleagues collected electronic medical record data from 908 patients who had received a psychiatric evaluation at an index emergency department visit for suicidal ideation over a 2-year period. The mean age of patients was 39 years. The target sample was 30 patients who had returned to the ED following a suicide attempt within 6 months of their index ED visit.
The researchers analyzed 32 predictor variables from patient charts, including demographics, psychiatric history, and current psychiatric presentation. The evaluation was done with “a machine learning statistical approach which is more capable than traditional statistical approaches in handling a large number of predictor variables,” Ms. Knorr said.
The number of previous psychiatric admissions was the most important predictor of a subsequent suicide attempt. The next nine most important variables were sleep disturbance, history of family suicide, low energy, patient age, psychiatrist determination of severe suicide risk, psychiatrist determination of moderate suicide risk, appetite issues, presence of a support system, and loss of interest/pleasure.
These symptoms may not typically be weighed heavily in risk assessments, Ms. Knorr said. “Additionally, given that research suggests that the clinical determination of suicide risk is historically poor, it was interesting that psychiatrist determination of moderate or high risk was influential in predicting a return visit for suicide attempt. Finally, we were surprised that a past history of suicide attempt, often viewed as the strongest predictor of a future suicide attempt, did not emerge as one of the top 10 influential predictors.
“Limitations of this study include the use of a return visit to a Geisinger emergency department as the only measure of a future suicide attempt and the utilization of data from only one health system,” she noted.
The study was funded by the Geisinger Clinic Research Fund. One of the coauthors, Andrei Nemoianu, MD, reported receipt of a research grant from Takeda Pharmaceuticals for a separate study.
SOURCE: Knorr A et al. Ann Emerg Med. 2018 Oct;72;4:S23. doi. 10.1016/j.annemergmed.2018.08.055.
SAN DIEGO – Among patients presenting to the emergency department with suicidal ideation, the number of previous psychiatric admissions is the most important predictor of a subsequent suicide attempt, results from a 2-year-long study showed.
Momentary measures – significant current difficulties with sleep, energy, or appetite, and anhedonia – “are important considerations during suicide risk assessment, regardless of whether the patient meets the threshold for major depressive disorder, lead study author Anne C. Knorr said in an interview in advance of the annual meeting of the American College of Emergency Physicians.
“Many traditionally studied psychiatric risk factors do not significantly differ between individuals who think about suicide and those who act on their suicidal thoughts, an important distinction as only one-third of those who think about suicide carry out a suicide attempt. While there is support for some psychiatric factors – for example, anxiety, substance use disorders, sleep disturbance – being useful in differentiating these groups, the current study is unique in its use of a longitudinal design to identify influential risk factors that predict future suicide attempt among those with suicidal ideation,” she said.
Ms. Knorr, a research project manager at Geisinger Medical Center, Danville, Pa., and her colleagues collected electronic medical record data from 908 patients who had received a psychiatric evaluation at an index emergency department visit for suicidal ideation over a 2-year period. The mean age of patients was 39 years. The target sample was 30 patients who had returned to the ED following a suicide attempt within 6 months of their index ED visit.
The researchers analyzed 32 predictor variables from patient charts, including demographics, psychiatric history, and current psychiatric presentation. The evaluation was done with “a machine learning statistical approach which is more capable than traditional statistical approaches in handling a large number of predictor variables,” Ms. Knorr said.
The number of previous psychiatric admissions was the most important predictor of a subsequent suicide attempt. The next nine most important variables were sleep disturbance, history of family suicide, low energy, patient age, psychiatrist determination of severe suicide risk, psychiatrist determination of moderate suicide risk, appetite issues, presence of a support system, and loss of interest/pleasure.
These symptoms may not typically be weighed heavily in risk assessments, Ms. Knorr said. “Additionally, given that research suggests that the clinical determination of suicide risk is historically poor, it was interesting that psychiatrist determination of moderate or high risk was influential in predicting a return visit for suicide attempt. Finally, we were surprised that a past history of suicide attempt, often viewed as the strongest predictor of a future suicide attempt, did not emerge as one of the top 10 influential predictors.
“Limitations of this study include the use of a return visit to a Geisinger emergency department as the only measure of a future suicide attempt and the utilization of data from only one health system,” she noted.
The study was funded by the Geisinger Clinic Research Fund. One of the coauthors, Andrei Nemoianu, MD, reported receipt of a research grant from Takeda Pharmaceuticals for a separate study.
SOURCE: Knorr A et al. Ann Emerg Med. 2018 Oct;72;4:S23. doi. 10.1016/j.annemergmed.2018.08.055.
AT ACEP18
Key clinical point: A number of factors representing momentary experiences such as low energy emerged as predictors of suicide attempts among suicidal ideators following an ED visit.
Major finding: The number of past psychiatric admissions was the most influential predictor of a subsequent suicide attempt.
Study details: A study of 30 patients who had returned to the ED following a suicide attempt within 6 months of their index ED visit.
Disclosures: The Geisinger Clinic Research Fund supported the study. A coauthor, Andrei Nemoianu, MD, reported receipt of a research grant from Takeda Pharmaceuticals for a separate study.
Source: Knorr A et al. Ann Emerg Med. 2018 Oct;72;4:S23.
ED visits related to psychiatric complaints are up 20% among elderly
SAN DIEGO – Between 2011 and 2015, the proportion of elderly patients presenting to the emergency department with psychiatric complaints increased by 20%, according to a retrospective analysis of national hospital data.
In addition, 10-year increases in age, male sex, nursing home status, and Medicare insurance were associated with an increased likelihood of hospital admission.
“The growing geriatric patient population is a well-known phenomenon across every developed country,” lead researcher Derrick Huang said in an interview in advance of the annual meeting of the American College of Emergency Physicians. “A potent mix of increasing life expectancy, greater disease severity and comorbidities in the elderly, and large-scale demographic shifts has placed a significant strain on both our financial and health care resources. This study corroborates these trends in the emergency department and is a preliminary exploration of potential, newly evolving clinical challenges that the ED team will increasingly face into the future.”
For the study, Mr. Huang, a fourth-year medical student at Oakland University William Beaumont School of Medicine in Rochester, Mich., and his colleagues examined National Ambulatory Medical Care Survey (NAMCS) data between 2011 and 2015. They limited the analysis to emergency department visits with patients in the age groups of 65-74, 75-84, and 85 or older. For the primary outcome of interest, the researchers evaluated demographic variables of age group, sex, residential status, race and ethnicity, and insurance for association with hospital admission. For the secondary outcome of interest, they evaluated presenting ED complaints related to the clinical domains of cardiopulmonary disease, psychiatric disease, and fractures and dislocations for potential trends in the ED geriatric age group between 2011 and 2015.
Mr. Huang and his associates found that, as a percentage of total ED visits, those among patients aged 65 or older rose from 14.9% in 2011 to 15.6% in 2015, an increase of 4.7%. By age group, the proportion of visits during the study period was highest for those aged 65-74 years (43.8%), followed by those aged 75-84 years (34.7%) and those aged 85 and older (21.5%). On multivariate analysis, the 75-84 and age-85-and-older groups were 1.30 and 1.71 times more likely to be admitted to the hospital, compared with the 65-74 group, respectively (P less than .000 for both).
Men were 1.19 times more likely than were women to be admitted (P less than .000). In addition, elderly patients who reside in nursing homes were 1.70 times more likely to be admitted to the hospital, compared with those who lived in private homes (P less than .000), while those with Medicare insurance were 1.57 more likely to be admitted, compared with those who did not have insurance (P = .004).
On trend analysis, ED psychiatric complaints rose incrementally during the study period, from 3.9% in 2011 to 4.7% in 2015, a relative increase of 20.5%. The researchers identified no consistent trend with visit complaints related to cardiopulmonary disease, and fractures and dislocations.
“This was not too surprising, because these difficulties with older patients are not new and many investigators have sought out solutions,” Mr. Huang said. “For example, there have been many interventions both in the ED as well as in the primary care setting designed to identify risk factors and facilitate postdischarge care to prevent falls. These approaches are constantly evolving and will be of increasing importance.”
“For example, we may be seeing a larger of proportion of patients with acute mental health complaints,” Mr. Huang said. “We will need to continue developing our multidisciplinary approach to care by improving coordination with different specialties – and especially outpatient and community health care providers.”
The study’s senior author was Jason Wasserman, PhD of Oakland University William Beaumont School of Medicine. The researchers reported having no financial disclosures.
SOURCE: Huang D et al. Ann Emerg Med. 2018 Oct. doi: 10.1016/j.annemergmed.2018.08.212.
SAN DIEGO – Between 2011 and 2015, the proportion of elderly patients presenting to the emergency department with psychiatric complaints increased by 20%, according to a retrospective analysis of national hospital data.
In addition, 10-year increases in age, male sex, nursing home status, and Medicare insurance were associated with an increased likelihood of hospital admission.
“The growing geriatric patient population is a well-known phenomenon across every developed country,” lead researcher Derrick Huang said in an interview in advance of the annual meeting of the American College of Emergency Physicians. “A potent mix of increasing life expectancy, greater disease severity and comorbidities in the elderly, and large-scale demographic shifts has placed a significant strain on both our financial and health care resources. This study corroborates these trends in the emergency department and is a preliminary exploration of potential, newly evolving clinical challenges that the ED team will increasingly face into the future.”
For the study, Mr. Huang, a fourth-year medical student at Oakland University William Beaumont School of Medicine in Rochester, Mich., and his colleagues examined National Ambulatory Medical Care Survey (NAMCS) data between 2011 and 2015. They limited the analysis to emergency department visits with patients in the age groups of 65-74, 75-84, and 85 or older. For the primary outcome of interest, the researchers evaluated demographic variables of age group, sex, residential status, race and ethnicity, and insurance for association with hospital admission. For the secondary outcome of interest, they evaluated presenting ED complaints related to the clinical domains of cardiopulmonary disease, psychiatric disease, and fractures and dislocations for potential trends in the ED geriatric age group between 2011 and 2015.
Mr. Huang and his associates found that, as a percentage of total ED visits, those among patients aged 65 or older rose from 14.9% in 2011 to 15.6% in 2015, an increase of 4.7%. By age group, the proportion of visits during the study period was highest for those aged 65-74 years (43.8%), followed by those aged 75-84 years (34.7%) and those aged 85 and older (21.5%). On multivariate analysis, the 75-84 and age-85-and-older groups were 1.30 and 1.71 times more likely to be admitted to the hospital, compared with the 65-74 group, respectively (P less than .000 for both).
Men were 1.19 times more likely than were women to be admitted (P less than .000). In addition, elderly patients who reside in nursing homes were 1.70 times more likely to be admitted to the hospital, compared with those who lived in private homes (P less than .000), while those with Medicare insurance were 1.57 more likely to be admitted, compared with those who did not have insurance (P = .004).
On trend analysis, ED psychiatric complaints rose incrementally during the study period, from 3.9% in 2011 to 4.7% in 2015, a relative increase of 20.5%. The researchers identified no consistent trend with visit complaints related to cardiopulmonary disease, and fractures and dislocations.
“This was not too surprising, because these difficulties with older patients are not new and many investigators have sought out solutions,” Mr. Huang said. “For example, there have been many interventions both in the ED as well as in the primary care setting designed to identify risk factors and facilitate postdischarge care to prevent falls. These approaches are constantly evolving and will be of increasing importance.”
“For example, we may be seeing a larger of proportion of patients with acute mental health complaints,” Mr. Huang said. “We will need to continue developing our multidisciplinary approach to care by improving coordination with different specialties – and especially outpatient and community health care providers.”
The study’s senior author was Jason Wasserman, PhD of Oakland University William Beaumont School of Medicine. The researchers reported having no financial disclosures.
SOURCE: Huang D et al. Ann Emerg Med. 2018 Oct. doi: 10.1016/j.annemergmed.2018.08.212.
SAN DIEGO – Between 2011 and 2015, the proportion of elderly patients presenting to the emergency department with psychiatric complaints increased by 20%, according to a retrospective analysis of national hospital data.
In addition, 10-year increases in age, male sex, nursing home status, and Medicare insurance were associated with an increased likelihood of hospital admission.
“The growing geriatric patient population is a well-known phenomenon across every developed country,” lead researcher Derrick Huang said in an interview in advance of the annual meeting of the American College of Emergency Physicians. “A potent mix of increasing life expectancy, greater disease severity and comorbidities in the elderly, and large-scale demographic shifts has placed a significant strain on both our financial and health care resources. This study corroborates these trends in the emergency department and is a preliminary exploration of potential, newly evolving clinical challenges that the ED team will increasingly face into the future.”
For the study, Mr. Huang, a fourth-year medical student at Oakland University William Beaumont School of Medicine in Rochester, Mich., and his colleagues examined National Ambulatory Medical Care Survey (NAMCS) data between 2011 and 2015. They limited the analysis to emergency department visits with patients in the age groups of 65-74, 75-84, and 85 or older. For the primary outcome of interest, the researchers evaluated demographic variables of age group, sex, residential status, race and ethnicity, and insurance for association with hospital admission. For the secondary outcome of interest, they evaluated presenting ED complaints related to the clinical domains of cardiopulmonary disease, psychiatric disease, and fractures and dislocations for potential trends in the ED geriatric age group between 2011 and 2015.
Mr. Huang and his associates found that, as a percentage of total ED visits, those among patients aged 65 or older rose from 14.9% in 2011 to 15.6% in 2015, an increase of 4.7%. By age group, the proportion of visits during the study period was highest for those aged 65-74 years (43.8%), followed by those aged 75-84 years (34.7%) and those aged 85 and older (21.5%). On multivariate analysis, the 75-84 and age-85-and-older groups were 1.30 and 1.71 times more likely to be admitted to the hospital, compared with the 65-74 group, respectively (P less than .000 for both).
Men were 1.19 times more likely than were women to be admitted (P less than .000). In addition, elderly patients who reside in nursing homes were 1.70 times more likely to be admitted to the hospital, compared with those who lived in private homes (P less than .000), while those with Medicare insurance were 1.57 more likely to be admitted, compared with those who did not have insurance (P = .004).
On trend analysis, ED psychiatric complaints rose incrementally during the study period, from 3.9% in 2011 to 4.7% in 2015, a relative increase of 20.5%. The researchers identified no consistent trend with visit complaints related to cardiopulmonary disease, and fractures and dislocations.
“This was not too surprising, because these difficulties with older patients are not new and many investigators have sought out solutions,” Mr. Huang said. “For example, there have been many interventions both in the ED as well as in the primary care setting designed to identify risk factors and facilitate postdischarge care to prevent falls. These approaches are constantly evolving and will be of increasing importance.”
“For example, we may be seeing a larger of proportion of patients with acute mental health complaints,” Mr. Huang said. “We will need to continue developing our multidisciplinary approach to care by improving coordination with different specialties – and especially outpatient and community health care providers.”
The study’s senior author was Jason Wasserman, PhD of Oakland University William Beaumont School of Medicine. The researchers reported having no financial disclosures.
SOURCE: Huang D et al. Ann Emerg Med. 2018 Oct. doi: 10.1016/j.annemergmed.2018.08.212.
REPORTING FROM ACEP18
Key clinical point: An increasing proportion of elderly patients are presenting to the emergency department with mental health complaints.
Major finding: Emergency department psychiatric complaints among elderly patients rose from 3.9% in 2011, to 4.7% in 2015, a relative increase of 20.5%.
Study details: A retrospective analysis of National Ambulatory Medical Care Survey data between 2011 and 2015.
Disclosures: The researchers reported having no financial disclosures.
Source: Huang D et al. Ann Emerg Med. 2018 Oct. doi: 10.1016/j.annemergmed.2018.08.212.