User login
Doug Brunk is a San Diego-based award-winning reporter who began covering health care in 1991. Before joining the company, he wrote for the health sciences division of Columbia University and was an associate editor at Contemporary Long Term Care magazine when it won a Jesse H. Neal Award. His work has been syndicated by the Los Angeles Times and he is the author of two books related to the University of Kentucky Wildcats men's basketball program. Doug has a master’s degree in magazine journalism from the S.I. Newhouse School of Public Communications at Syracuse University. Follow him on Twitter @dougbrunk.
Children with single ventricle CHD at risk for behavioral, emotional problems
NEW ORLEANS – Single ventricle congenital heart disease (CHD) and worse social determinants of health are associated with more behavior problems and less total competency in children, and this relationship is mediated by disease-related chronic stress, self-perception, and family environment.

Those are key findings from a large analysis of existing cross-sectional data presented at the annual meeting of the American Academy of Pediatrics. The study set out to assess what factors mediate the relationship between CHD severity, social determinants of health, and behavioral and emotional outcomes.
“We know that worse CHD severity is associated with worse parent-reported and self-reported behavioral and emotional functioning in children and adolescents survivors,” lead author Asad Qadir, MD, said in an interview. “ by taking measures that would decrease their and their caregivers’ disease-related chronic stress, improve family functioning, and improve the self-perception of the child. While social determinants of health are not modifiable, they are important for predicting which children may be at risk for behavior problems.”
Dr. Qadir, a cardiology fellow in the department of pediatrics at Northwestern University, Chicago, and colleagues performed a corollary analysis of the Pediatric Cardiac Quality of Life Inventory Testing study, an international, multicenter, cross-sectional study in which parents and patients with CHD completed questionnaires measuring behavioral and emotional functioning, self-perception, family environment, family coping, posttraumatic stress, and illness-related parenting stress (see Qual Life Res. 2008;17:613-26, Pediatrics. 2010;126[3]:498-508, and Cardiol Young. 2014;[2]:220-8). They assessed the relationships between CHD severity and social determinants of health (predictors), disease-related stress and psychosocial adaptation (mediators), and behavioral and emotional outcomes. They used structural equation modeling to determine the effects of predictors and mediators on outcomes, and created multivariable models for each patient- and parent-reported outcome.
The analysis included 981 patient-parent dyads. Of these, 210 patients had mild biventricular CHD, 620 had moderate biventricular CHD, and 151 had single ventricle CHD. The mean age of patients was 13 years and 55% were male. The researchers found that single ventricle CHD and worse social determinants of health were significant predictors of greater disease-related chronic stress for patients and caregivers and worse psychosocial adaptation in CHD survivors, including self-perception and family functioning constructs of cohesion and expressiveness (P less than .001 for all associations). In addition, single ventricle CHD and worse social determinants of health were associated with worse behavioral and emotional outcomes as reported by patients and parents, including internalizing behaviors, externalizing behaviors, and total competency (P less than .001 for all associations).
In multivariable models for all parent-reported outcomes, significant associations were observed between single ventricle CHD, social determinants of health, disease-related stress, child receiving mental health services, and cohesion/conflict in the family environment (P less than .001). In multivariable models for all patient-reported outcomes, significant associations were seen between single ventricle CHD, self-perception, and cohesion/conflict in the family environment (P less than 0.001).
Patient disease-related stress had the strongest association with externalizing problems, and worse social determinants of health significantly lowered patient-reported total competency.
“Many of the relationships found in the study make intuitive sense,” Dr. Qadir said. “For example, less favorable social determinants of health were associated with more parent disease-related chronic stress, which in turn was associated with parent-reported behavior problems in children. What was surprising was that worse behavioral outcomes were specifically associated with single ventricle disease only. Complex biventricular congenital heart disease patients (CHD that required a surgical- or catheter-based intervention) often have worse behavioral and emotional outcomes, similar to single ventricle patients. However, our model would argue that biventricular congenital heart disease complexity patients have more behavioral and emotional issues not because of their disease complexity, but due to their social determinants of health and the amount of disease-related chronic stress in the child and the parent and the amount of psychosocial adaptation found in the child and parent.”
Parent and patient disease-related chronic stress was not only an important mediator of the effect of CHD severity and social determinants of health on behavioral and emotional outcomes, he added, but it also had indirect effects that were mediated by family cohesion/conflict and patient self-perception.
“These data suggest that for those children with worse social determinants of health and single ventricle congenital heart disease, interventions that mitigate disease-related chronic stress, promote family functioning, and promote self-perception in the child may improve or optimize behavioral and emotional functioning during childhood and adolescence in CHD surgical survivors,” Dr. Qadir concluded.
He acknowledged certain limitations of the analysis, including the fact that it was a corollary cross-sectional analysis of an existing data set. “The results do not reflect possible changes over time,” he added. “There was also selection bias as non-English speakers were excluded, and the study population had a greater percentage of Caucasian and highly educated parents with higher income than the general population, which may affect the generalizability of our results.”
The researchers reported having no relevant financial disclosures.
NEW ORLEANS – Single ventricle congenital heart disease (CHD) and worse social determinants of health are associated with more behavior problems and less total competency in children, and this relationship is mediated by disease-related chronic stress, self-perception, and family environment.
Those are key findings from a large analysis of existing cross-sectional data presented at the annual meeting of the American Academy of Pediatrics. The study set out to assess what factors mediate the relationship between CHD severity, social determinants of health, and behavioral and emotional outcomes.
“We know that worse CHD severity is associated with worse parent-reported and self-reported behavioral and emotional functioning in children and adolescents survivors,” lead author Asad Qadir, MD, said in an interview. “ by taking measures that would decrease their and their caregivers’ disease-related chronic stress, improve family functioning, and improve the self-perception of the child. While social determinants of health are not modifiable, they are important for predicting which children may be at risk for behavior problems.”
Dr. Qadir, a cardiology fellow in the department of pediatrics at Northwestern University, Chicago, and colleagues performed a corollary analysis of the Pediatric Cardiac Quality of Life Inventory Testing study, an international, multicenter, cross-sectional study in which parents and patients with CHD completed questionnaires measuring behavioral and emotional functioning, self-perception, family environment, family coping, posttraumatic stress, and illness-related parenting stress (see Qual Life Res. 2008;17:613-26, Pediatrics. 2010;126[3]:498-508, and Cardiol Young. 2014;[2]:220-8). They assessed the relationships between CHD severity and social determinants of health (predictors), disease-related stress and psychosocial adaptation (mediators), and behavioral and emotional outcomes. They used structural equation modeling to determine the effects of predictors and mediators on outcomes, and created multivariable models for each patient- and parent-reported outcome.
The analysis included 981 patient-parent dyads. Of these, 210 patients had mild biventricular CHD, 620 had moderate biventricular CHD, and 151 had single ventricle CHD. The mean age of patients was 13 years and 55% were male. The researchers found that single ventricle CHD and worse social determinants of health were significant predictors of greater disease-related chronic stress for patients and caregivers and worse psychosocial adaptation in CHD survivors, including self-perception and family functioning constructs of cohesion and expressiveness (P less than .001 for all associations). In addition, single ventricle CHD and worse social determinants of health were associated with worse behavioral and emotional outcomes as reported by patients and parents, including internalizing behaviors, externalizing behaviors, and total competency (P less than .001 for all associations).
In multivariable models for all parent-reported outcomes, significant associations were observed between single ventricle CHD, social determinants of health, disease-related stress, child receiving mental health services, and cohesion/conflict in the family environment (P less than .001). In multivariable models for all patient-reported outcomes, significant associations were seen between single ventricle CHD, self-perception, and cohesion/conflict in the family environment (P less than 0.001).
Patient disease-related stress had the strongest association with externalizing problems, and worse social determinants of health significantly lowered patient-reported total competency.
“Many of the relationships found in the study make intuitive sense,” Dr. Qadir said. “For example, less favorable social determinants of health were associated with more parent disease-related chronic stress, which in turn was associated with parent-reported behavior problems in children. What was surprising was that worse behavioral outcomes were specifically associated with single ventricle disease only. Complex biventricular congenital heart disease patients (CHD that required a surgical- or catheter-based intervention) often have worse behavioral and emotional outcomes, similar to single ventricle patients. However, our model would argue that biventricular congenital heart disease complexity patients have more behavioral and emotional issues not because of their disease complexity, but due to their social determinants of health and the amount of disease-related chronic stress in the child and the parent and the amount of psychosocial adaptation found in the child and parent.”
Parent and patient disease-related chronic stress was not only an important mediator of the effect of CHD severity and social determinants of health on behavioral and emotional outcomes, he added, but it also had indirect effects that were mediated by family cohesion/conflict and patient self-perception.
“These data suggest that for those children with worse social determinants of health and single ventricle congenital heart disease, interventions that mitigate disease-related chronic stress, promote family functioning, and promote self-perception in the child may improve or optimize behavioral and emotional functioning during childhood and adolescence in CHD surgical survivors,” Dr. Qadir concluded.
He acknowledged certain limitations of the analysis, including the fact that it was a corollary cross-sectional analysis of an existing data set. “The results do not reflect possible changes over time,” he added. “There was also selection bias as non-English speakers were excluded, and the study population had a greater percentage of Caucasian and highly educated parents with higher income than the general population, which may affect the generalizability of our results.”
The researchers reported having no relevant financial disclosures.
NEW ORLEANS – Single ventricle congenital heart disease (CHD) and worse social determinants of health are associated with more behavior problems and less total competency in children, and this relationship is mediated by disease-related chronic stress, self-perception, and family environment.
Those are key findings from a large analysis of existing cross-sectional data presented at the annual meeting of the American Academy of Pediatrics. The study set out to assess what factors mediate the relationship between CHD severity, social determinants of health, and behavioral and emotional outcomes.
“We know that worse CHD severity is associated with worse parent-reported and self-reported behavioral and emotional functioning in children and adolescents survivors,” lead author Asad Qadir, MD, said in an interview. “ by taking measures that would decrease their and their caregivers’ disease-related chronic stress, improve family functioning, and improve the self-perception of the child. While social determinants of health are not modifiable, they are important for predicting which children may be at risk for behavior problems.”
Dr. Qadir, a cardiology fellow in the department of pediatrics at Northwestern University, Chicago, and colleagues performed a corollary analysis of the Pediatric Cardiac Quality of Life Inventory Testing study, an international, multicenter, cross-sectional study in which parents and patients with CHD completed questionnaires measuring behavioral and emotional functioning, self-perception, family environment, family coping, posttraumatic stress, and illness-related parenting stress (see Qual Life Res. 2008;17:613-26, Pediatrics. 2010;126[3]:498-508, and Cardiol Young. 2014;[2]:220-8). They assessed the relationships between CHD severity and social determinants of health (predictors), disease-related stress and psychosocial adaptation (mediators), and behavioral and emotional outcomes. They used structural equation modeling to determine the effects of predictors and mediators on outcomes, and created multivariable models for each patient- and parent-reported outcome.
The analysis included 981 patient-parent dyads. Of these, 210 patients had mild biventricular CHD, 620 had moderate biventricular CHD, and 151 had single ventricle CHD. The mean age of patients was 13 years and 55% were male. The researchers found that single ventricle CHD and worse social determinants of health were significant predictors of greater disease-related chronic stress for patients and caregivers and worse psychosocial adaptation in CHD survivors, including self-perception and family functioning constructs of cohesion and expressiveness (P less than .001 for all associations). In addition, single ventricle CHD and worse social determinants of health were associated with worse behavioral and emotional outcomes as reported by patients and parents, including internalizing behaviors, externalizing behaviors, and total competency (P less than .001 for all associations).
In multivariable models for all parent-reported outcomes, significant associations were observed between single ventricle CHD, social determinants of health, disease-related stress, child receiving mental health services, and cohesion/conflict in the family environment (P less than .001). In multivariable models for all patient-reported outcomes, significant associations were seen between single ventricle CHD, self-perception, and cohesion/conflict in the family environment (P less than 0.001).
Patient disease-related stress had the strongest association with externalizing problems, and worse social determinants of health significantly lowered patient-reported total competency.
“Many of the relationships found in the study make intuitive sense,” Dr. Qadir said. “For example, less favorable social determinants of health were associated with more parent disease-related chronic stress, which in turn was associated with parent-reported behavior problems in children. What was surprising was that worse behavioral outcomes were specifically associated with single ventricle disease only. Complex biventricular congenital heart disease patients (CHD that required a surgical- or catheter-based intervention) often have worse behavioral and emotional outcomes, similar to single ventricle patients. However, our model would argue that biventricular congenital heart disease complexity patients have more behavioral and emotional issues not because of their disease complexity, but due to their social determinants of health and the amount of disease-related chronic stress in the child and the parent and the amount of psychosocial adaptation found in the child and parent.”
Parent and patient disease-related chronic stress was not only an important mediator of the effect of CHD severity and social determinants of health on behavioral and emotional outcomes, he added, but it also had indirect effects that were mediated by family cohesion/conflict and patient self-perception.
“These data suggest that for those children with worse social determinants of health and single ventricle congenital heart disease, interventions that mitigate disease-related chronic stress, promote family functioning, and promote self-perception in the child may improve or optimize behavioral and emotional functioning during childhood and adolescence in CHD surgical survivors,” Dr. Qadir concluded.
He acknowledged certain limitations of the analysis, including the fact that it was a corollary cross-sectional analysis of an existing data set. “The results do not reflect possible changes over time,” he added. “There was also selection bias as non-English speakers were excluded, and the study population had a greater percentage of Caucasian and highly educated parents with higher income than the general population, which may affect the generalizability of our results.”
The researchers reported having no relevant financial disclosures.
AT AAP 2019
Recurrent intussusception rare in young children
NEW ORLEANS – Recurrent intussusception after discharge may be far less common in young children than previously reported, and significant morbidity associated with the condition is rare, results from an analysis of national data show.
“Recurrent intussusception following successful nonoperative reduction has previously been reported with a frequency of 8-12% based on data from individual institutions,” researchers led by Anthony R. Ferrantella, MD, wrote in an abstract presented at the annual meeting of the American Academy of Pediatrics. “Timing of discharge following successful non-operative reduction continues to be debated, but recent studies suggest it is safe to discharge home from the emergency department. However, the practice of hospital admission for an observation period of 24-48 hours following successful nonoperative reduction persists today among many pediatric surgeons.”
In an effort to evaluate readmissions for recurrent intussusception in young children on a large scale, Dr. Ferrantella, a surgery resident at the University of Miami, and his colleagues queried the Nationwide Readmissions Database during 2010-2014 to identify children younger than 5 years of age diagnosed with ileocolic intussusception. They compared the management during index admission and frequency of readmissions for recurrent intussusception up to one year after discharge. They excluded patients lacking procedure data, weighted the results for national estimates, and used chi-square analysis to compare cohorts.
The search yielded 8,289 young children who were diagnosed with ileocolic intussusception during an index admission. Of these, 43% received definitive treatment with nonoperative reduction alone, 42% underwent surgical reduction without bowel resection, and 15% underwent surgery with bowel resection. Among the hospitals where patients were treated, 75% were large, 80% were not-for-profit, and 94% were metropolitan teaching hospitals.
The researchers found that readmission for recurrent intussusception was required for only 4% of patients managed with nonoperative reduction alone, 2% of patients who underwent surgical reduction, and 0% of those who underwent bowel resection. The median time to readmission was 4 days for those managed with nonoperative reduction only and 64 days for those managed with surgery.
Among patients managed with nonoperative reduction alone during index admission, 71% were again managed successfully with nonoperative reduction alone, 24 underwent surgical reduction, and only 5% required bowel resection. No deaths occurred during any readmissions.
The findings “suggest and support the idea that if you can successfully perform a nonoperative reduction on a child that comes in with an intussusception, you can safely discharge them,” Dr. Ferrantella said in an interview. “If you were to keep them in the hospital, the [rate] of recurrences are very low. Even when they do recur, only 30%-40% will happen within the first 24-48 hours, so the majority will not benefit from a hospital admission.”
He acknowledged certain limitations of the analysis, including that the data came from a retrospectively collected database and that he and his colleagues were unable to track readmissions across state lines.
Dr. Ferrantella reported having no financial disclosures.
SOURCE: Ferrantella A. AAP 2019, Section on Surgery session.
NEW ORLEANS – Recurrent intussusception after discharge may be far less common in young children than previously reported, and significant morbidity associated with the condition is rare, results from an analysis of national data show.
“Recurrent intussusception following successful nonoperative reduction has previously been reported with a frequency of 8-12% based on data from individual institutions,” researchers led by Anthony R. Ferrantella, MD, wrote in an abstract presented at the annual meeting of the American Academy of Pediatrics. “Timing of discharge following successful non-operative reduction continues to be debated, but recent studies suggest it is safe to discharge home from the emergency department. However, the practice of hospital admission for an observation period of 24-48 hours following successful nonoperative reduction persists today among many pediatric surgeons.”
In an effort to evaluate readmissions for recurrent intussusception in young children on a large scale, Dr. Ferrantella, a surgery resident at the University of Miami, and his colleagues queried the Nationwide Readmissions Database during 2010-2014 to identify children younger than 5 years of age diagnosed with ileocolic intussusception. They compared the management during index admission and frequency of readmissions for recurrent intussusception up to one year after discharge. They excluded patients lacking procedure data, weighted the results for national estimates, and used chi-square analysis to compare cohorts.
The search yielded 8,289 young children who were diagnosed with ileocolic intussusception during an index admission. Of these, 43% received definitive treatment with nonoperative reduction alone, 42% underwent surgical reduction without bowel resection, and 15% underwent surgery with bowel resection. Among the hospitals where patients were treated, 75% were large, 80% were not-for-profit, and 94% were metropolitan teaching hospitals.
The researchers found that readmission for recurrent intussusception was required for only 4% of patients managed with nonoperative reduction alone, 2% of patients who underwent surgical reduction, and 0% of those who underwent bowel resection. The median time to readmission was 4 days for those managed with nonoperative reduction only and 64 days for those managed with surgery.
Among patients managed with nonoperative reduction alone during index admission, 71% were again managed successfully with nonoperative reduction alone, 24 underwent surgical reduction, and only 5% required bowel resection. No deaths occurred during any readmissions.
The findings “suggest and support the idea that if you can successfully perform a nonoperative reduction on a child that comes in with an intussusception, you can safely discharge them,” Dr. Ferrantella said in an interview. “If you were to keep them in the hospital, the [rate] of recurrences are very low. Even when they do recur, only 30%-40% will happen within the first 24-48 hours, so the majority will not benefit from a hospital admission.”
He acknowledged certain limitations of the analysis, including that the data came from a retrospectively collected database and that he and his colleagues were unable to track readmissions across state lines.
Dr. Ferrantella reported having no financial disclosures.
SOURCE: Ferrantella A. AAP 2019, Section on Surgery session.
NEW ORLEANS – Recurrent intussusception after discharge may be far less common in young children than previously reported, and significant morbidity associated with the condition is rare, results from an analysis of national data show.
“Recurrent intussusception following successful nonoperative reduction has previously been reported with a frequency of 8-12% based on data from individual institutions,” researchers led by Anthony R. Ferrantella, MD, wrote in an abstract presented at the annual meeting of the American Academy of Pediatrics. “Timing of discharge following successful non-operative reduction continues to be debated, but recent studies suggest it is safe to discharge home from the emergency department. However, the practice of hospital admission for an observation period of 24-48 hours following successful nonoperative reduction persists today among many pediatric surgeons.”
In an effort to evaluate readmissions for recurrent intussusception in young children on a large scale, Dr. Ferrantella, a surgery resident at the University of Miami, and his colleagues queried the Nationwide Readmissions Database during 2010-2014 to identify children younger than 5 years of age diagnosed with ileocolic intussusception. They compared the management during index admission and frequency of readmissions for recurrent intussusception up to one year after discharge. They excluded patients lacking procedure data, weighted the results for national estimates, and used chi-square analysis to compare cohorts.
The search yielded 8,289 young children who were diagnosed with ileocolic intussusception during an index admission. Of these, 43% received definitive treatment with nonoperative reduction alone, 42% underwent surgical reduction without bowel resection, and 15% underwent surgery with bowel resection. Among the hospitals where patients were treated, 75% were large, 80% were not-for-profit, and 94% were metropolitan teaching hospitals.
The researchers found that readmission for recurrent intussusception was required for only 4% of patients managed with nonoperative reduction alone, 2% of patients who underwent surgical reduction, and 0% of those who underwent bowel resection. The median time to readmission was 4 days for those managed with nonoperative reduction only and 64 days for those managed with surgery.
Among patients managed with nonoperative reduction alone during index admission, 71% were again managed successfully with nonoperative reduction alone, 24 underwent surgical reduction, and only 5% required bowel resection. No deaths occurred during any readmissions.
The findings “suggest and support the idea that if you can successfully perform a nonoperative reduction on a child that comes in with an intussusception, you can safely discharge them,” Dr. Ferrantella said in an interview. “If you were to keep them in the hospital, the [rate] of recurrences are very low. Even when they do recur, only 30%-40% will happen within the first 24-48 hours, so the majority will not benefit from a hospital admission.”
He acknowledged certain limitations of the analysis, including that the data came from a retrospectively collected database and that he and his colleagues were unable to track readmissions across state lines.
Dr. Ferrantella reported having no financial disclosures.
SOURCE: Ferrantella A. AAP 2019, Section on Surgery session.
AT AAP 2016
Urban or rural, children’s gun-related injuries equally deadly
NEW ORLEANS – Accidental firearm-related injuries among children occur more frequently in rural than in urban locations, and nearly 60% of such cases are potentially preventable, results from a single-center study suggest.
Furthermore, these gun injuries carry the same mortality and disability risk.
“Firearm-related injury is an understudied topic,” lead study author Amelia Lucisano, MD, said in an interview in advance of the annual meeting of the American Academy of Pediatrics. “In particular there is a lack of granular level research on firearm-related injury in the population.”
At the meeting, she presented findings from an analysis which set out to investigate the location, preventability, and temporal trends of pediatric firearm-related injury in 184 patients age 18 and younger who were treated in the pediatric trauma program at University of Pittsburgh Medical Center during 2008-2017. Dr. Lucisano, a surgical resident at the university, and her colleagues focused their work on efforts to illustrate the differences and similarities in the demographics, injury-related characteristics, and outcomes between the rural and urban populations of children who are injured by firearms in Southwestern Pennsylvania. They classified the location as rural if the injury occurred outside the region’s central metropolitan county, and classified the injury as potentially preventable if the firearm was not stored securely and was used without permission. Statistical analyses included Wilcoxon rank-sum and chi-square analyses.
Of the 184 children who sustained a firearm-related injury during the study period, 43% occurred in a rural location. Compared with children who were injured in an urban setting, those who were injured in a rural setting were younger (a mean of 13 vs. 14 years; P = 0.0003), were more frequently white (81% vs. 14%; P less than 0.0001), and were more frequently injured by accident (70% vs. 15%; P less than 0.0001). They were also more likely to be injured by rifle or shotgun (24.1% vs. 6.67%; P = 0.001).
The rates of death or disability and lengths of stay did not differ significantly based on location of injury, occurring in 16.5% of rural and 13.3% of urban patients.
Nearly three-quarters of accidental injuries (72%) occurred on the gun-owner’s property and 58% were considered by the researchers to be potentially preventable.
“As expected, rural injuries are more frequently unintentional while urban injuries are more frequently assaults,” Dr. Lucisano said. “However, markers of injury severity and outcomes are equivalent between the groups, meaning that morbidity and mortality of injuries in the rural setting are similar to those in the urban setting.”
She emphasized that while clinician bias may be to consider rural firearm-based injuries as less severe, “our study shows that they carry the same burden of morbidity and mortality as urban injuries and thus should be cared for with the same intensity and anticipation of a possible poor outcome. Furthermore, the large number of potentially preventable injuries among those that were unintentional represents a significant burden of morbidity and mortality that could have been avoided through safer firearm storage. Programs to promote safe firearm storage should be targeted to populations that have high rates of potentially preventable injuries.”
Dr. Lucisano and her colleagues observed that the rates of all forms of firearm-related injury appear to be on the rise in both rural and urban areas: accidental, self-inflicted, and assault, in particular. She acknowledged certain limitations of the study, including its retrospective, single-center design. “We did not capture children who died in the field or who were treated at other hospitals, though as our center is the only pediatric Level 1 trauma center, we capture a large majority of pediatric trauma patients in the region,” she said.
The researchers reported having no disclosures.
SOURCE: Lucisano A. AAP 2019, Section on Surgery program.
NEW ORLEANS – Accidental firearm-related injuries among children occur more frequently in rural than in urban locations, and nearly 60% of such cases are potentially preventable, results from a single-center study suggest.
Furthermore, these gun injuries carry the same mortality and disability risk.
“Firearm-related injury is an understudied topic,” lead study author Amelia Lucisano, MD, said in an interview in advance of the annual meeting of the American Academy of Pediatrics. “In particular there is a lack of granular level research on firearm-related injury in the population.”
At the meeting, she presented findings from an analysis which set out to investigate the location, preventability, and temporal trends of pediatric firearm-related injury in 184 patients age 18 and younger who were treated in the pediatric trauma program at University of Pittsburgh Medical Center during 2008-2017. Dr. Lucisano, a surgical resident at the university, and her colleagues focused their work on efforts to illustrate the differences and similarities in the demographics, injury-related characteristics, and outcomes between the rural and urban populations of children who are injured by firearms in Southwestern Pennsylvania. They classified the location as rural if the injury occurred outside the region’s central metropolitan county, and classified the injury as potentially preventable if the firearm was not stored securely and was used without permission. Statistical analyses included Wilcoxon rank-sum and chi-square analyses.
Of the 184 children who sustained a firearm-related injury during the study period, 43% occurred in a rural location. Compared with children who were injured in an urban setting, those who were injured in a rural setting were younger (a mean of 13 vs. 14 years; P = 0.0003), were more frequently white (81% vs. 14%; P less than 0.0001), and were more frequently injured by accident (70% vs. 15%; P less than 0.0001). They were also more likely to be injured by rifle or shotgun (24.1% vs. 6.67%; P = 0.001).
The rates of death or disability and lengths of stay did not differ significantly based on location of injury, occurring in 16.5% of rural and 13.3% of urban patients.
Nearly three-quarters of accidental injuries (72%) occurred on the gun-owner’s property and 58% were considered by the researchers to be potentially preventable.
“As expected, rural injuries are more frequently unintentional while urban injuries are more frequently assaults,” Dr. Lucisano said. “However, markers of injury severity and outcomes are equivalent between the groups, meaning that morbidity and mortality of injuries in the rural setting are similar to those in the urban setting.”
She emphasized that while clinician bias may be to consider rural firearm-based injuries as less severe, “our study shows that they carry the same burden of morbidity and mortality as urban injuries and thus should be cared for with the same intensity and anticipation of a possible poor outcome. Furthermore, the large number of potentially preventable injuries among those that were unintentional represents a significant burden of morbidity and mortality that could have been avoided through safer firearm storage. Programs to promote safe firearm storage should be targeted to populations that have high rates of potentially preventable injuries.”
Dr. Lucisano and her colleagues observed that the rates of all forms of firearm-related injury appear to be on the rise in both rural and urban areas: accidental, self-inflicted, and assault, in particular. She acknowledged certain limitations of the study, including its retrospective, single-center design. “We did not capture children who died in the field or who were treated at other hospitals, though as our center is the only pediatric Level 1 trauma center, we capture a large majority of pediatric trauma patients in the region,” she said.
The researchers reported having no disclosures.
SOURCE: Lucisano A. AAP 2019, Section on Surgery program.
NEW ORLEANS – Accidental firearm-related injuries among children occur more frequently in rural than in urban locations, and nearly 60% of such cases are potentially preventable, results from a single-center study suggest.
Furthermore, these gun injuries carry the same mortality and disability risk.
“Firearm-related injury is an understudied topic,” lead study author Amelia Lucisano, MD, said in an interview in advance of the annual meeting of the American Academy of Pediatrics. “In particular there is a lack of granular level research on firearm-related injury in the population.”
At the meeting, she presented findings from an analysis which set out to investigate the location, preventability, and temporal trends of pediatric firearm-related injury in 184 patients age 18 and younger who were treated in the pediatric trauma program at University of Pittsburgh Medical Center during 2008-2017. Dr. Lucisano, a surgical resident at the university, and her colleagues focused their work on efforts to illustrate the differences and similarities in the demographics, injury-related characteristics, and outcomes between the rural and urban populations of children who are injured by firearms in Southwestern Pennsylvania. They classified the location as rural if the injury occurred outside the region’s central metropolitan county, and classified the injury as potentially preventable if the firearm was not stored securely and was used without permission. Statistical analyses included Wilcoxon rank-sum and chi-square analyses.
Of the 184 children who sustained a firearm-related injury during the study period, 43% occurred in a rural location. Compared with children who were injured in an urban setting, those who were injured in a rural setting were younger (a mean of 13 vs. 14 years; P = 0.0003), were more frequently white (81% vs. 14%; P less than 0.0001), and were more frequently injured by accident (70% vs. 15%; P less than 0.0001). They were also more likely to be injured by rifle or shotgun (24.1% vs. 6.67%; P = 0.001).
The rates of death or disability and lengths of stay did not differ significantly based on location of injury, occurring in 16.5% of rural and 13.3% of urban patients.
Nearly three-quarters of accidental injuries (72%) occurred on the gun-owner’s property and 58% were considered by the researchers to be potentially preventable.
“As expected, rural injuries are more frequently unintentional while urban injuries are more frequently assaults,” Dr. Lucisano said. “However, markers of injury severity and outcomes are equivalent between the groups, meaning that morbidity and mortality of injuries in the rural setting are similar to those in the urban setting.”
She emphasized that while clinician bias may be to consider rural firearm-based injuries as less severe, “our study shows that they carry the same burden of morbidity and mortality as urban injuries and thus should be cared for with the same intensity and anticipation of a possible poor outcome. Furthermore, the large number of potentially preventable injuries among those that were unintentional represents a significant burden of morbidity and mortality that could have been avoided through safer firearm storage. Programs to promote safe firearm storage should be targeted to populations that have high rates of potentially preventable injuries.”
Dr. Lucisano and her colleagues observed that the rates of all forms of firearm-related injury appear to be on the rise in both rural and urban areas: accidental, self-inflicted, and assault, in particular. She acknowledged certain limitations of the study, including its retrospective, single-center design. “We did not capture children who died in the field or who were treated at other hospitals, though as our center is the only pediatric Level 1 trauma center, we capture a large majority of pediatric trauma patients in the region,” she said.
The researchers reported having no disclosures.
SOURCE: Lucisano A. AAP 2019, Section on Surgery program.
AT AAP 2019
Long catheters best standard-sized ones in trial of pediatric surgery patients
NEW ORLEANS – Children who require more than 48 hours of intravenous therapy should receive long peripheral catheters initially rather than standard peripheral intravenous catheters, results from a randomized, controlled trial suggest.

Long peripheral catheters (LPCs) are relatively new, 8- to 15-cm long peripheral vascular devices that have been investigated extensively in adults. “It has been shown that these devices are safe and reliable peripheral vascular access devices for use in this population,” lead study author Maurizio Pacilli, MD, said in an interview in advance of the annual meeting of the American Academy of Pediatrics.
“In addition, LPCs may represent an improvement to the quality of care in adults, as demonstrated by multiple randomized controlled trials, where they outperformed peripheral intravenous catheters (PIVCs). There remains, however, a lack of controlled studies to determine if this effect is replicable in children.”
In what he said is the first study of its kind, Dr. Pacilli, a senior research fellow at Monash Children’s Hospital and Monash University, Melbourne, and colleagues performed an open-label randomized trial of 72 pediatric surgical patients aged 1 year and older who required more than 48 hours of IV therapy. They assigned 36 to receive a PIVCs while the remaining 36 children received an 8-cm 22-gauge LPC.
The mean age of patients was 9 years and 71% were boys. Dr. Pacilli reported that the IV therapy duration was a mean of 5 days, and that gender, age, weight, emergency status, and IV therapy duration were similar between the two groups. However, the mean lifespan of catheters was 3 days in PIVC group, compared with 5 days in the LPC group, a difference that reached statistical significance (P = .003). Patients in the PIVC group received a median of two catheters, compared with one in the LPC group (P = .0002). The researchers found that patients in the PIVC group were less likely than were those in the LPC group to complete treatment with a single catheter (39% vs. 81%, relative risk [RR] 2.1, P = .0006), while the rate of catheter failure was higher for PIVCs than for LPCs (67% vs. 19%, RR 3.4, P = .0001; 187 vs. 43 failures per 1,000 catheter days). Infiltration was the most common complication, and occurred in 33% of patients in the PIVC group vs. 3% in LPC group (RR 12, P = .001).
“Our results showed for the first time, without doubt, that children requiring more than 48 hours of intravenous therapy benefit from receiving LPCs, compared with traditional PIVCs,” Dr. Pacilli said. “Of failed catheters, PIVCs are most likely to infiltrate, while LPCs are most likely to occlude. This indicates an additional benefit of LPCs as occlusion is a relatively benign complication. In addition, in all domains of satisfaction, parents favor LPCs. According to the parents, there is a significant improvement in ‘pain and discomfort’ and ‘overall satisfaction’ with the use of LPCs in children.”
He acknowledged certain limitations of the study, including the fact that children younger than 1 year of age were not included in the analysis. “New devices, suitable for very young children, need to be developed, and further studies are needed to confirm the findings from our trial in children younger than 1 year,” he said.
Dr. Pacilli reported having no financial disclosures.
NEW ORLEANS – Children who require more than 48 hours of intravenous therapy should receive long peripheral catheters initially rather than standard peripheral intravenous catheters, results from a randomized, controlled trial suggest.
Long peripheral catheters (LPCs) are relatively new, 8- to 15-cm long peripheral vascular devices that have been investigated extensively in adults. “It has been shown that these devices are safe and reliable peripheral vascular access devices for use in this population,” lead study author Maurizio Pacilli, MD, said in an interview in advance of the annual meeting of the American Academy of Pediatrics.
“In addition, LPCs may represent an improvement to the quality of care in adults, as demonstrated by multiple randomized controlled trials, where they outperformed peripheral intravenous catheters (PIVCs). There remains, however, a lack of controlled studies to determine if this effect is replicable in children.”
In what he said is the first study of its kind, Dr. Pacilli, a senior research fellow at Monash Children’s Hospital and Monash University, Melbourne, and colleagues performed an open-label randomized trial of 72 pediatric surgical patients aged 1 year and older who required more than 48 hours of IV therapy. They assigned 36 to receive a PIVCs while the remaining 36 children received an 8-cm 22-gauge LPC.
The mean age of patients was 9 years and 71% were boys. Dr. Pacilli reported that the IV therapy duration was a mean of 5 days, and that gender, age, weight, emergency status, and IV therapy duration were similar between the two groups. However, the mean lifespan of catheters was 3 days in PIVC group, compared with 5 days in the LPC group, a difference that reached statistical significance (P = .003). Patients in the PIVC group received a median of two catheters, compared with one in the LPC group (P = .0002). The researchers found that patients in the PIVC group were less likely than were those in the LPC group to complete treatment with a single catheter (39% vs. 81%, relative risk [RR] 2.1, P = .0006), while the rate of catheter failure was higher for PIVCs than for LPCs (67% vs. 19%, RR 3.4, P = .0001; 187 vs. 43 failures per 1,000 catheter days). Infiltration was the most common complication, and occurred in 33% of patients in the PIVC group vs. 3% in LPC group (RR 12, P = .001).
“Our results showed for the first time, without doubt, that children requiring more than 48 hours of intravenous therapy benefit from receiving LPCs, compared with traditional PIVCs,” Dr. Pacilli said. “Of failed catheters, PIVCs are most likely to infiltrate, while LPCs are most likely to occlude. This indicates an additional benefit of LPCs as occlusion is a relatively benign complication. In addition, in all domains of satisfaction, parents favor LPCs. According to the parents, there is a significant improvement in ‘pain and discomfort’ and ‘overall satisfaction’ with the use of LPCs in children.”
He acknowledged certain limitations of the study, including the fact that children younger than 1 year of age were not included in the analysis. “New devices, suitable for very young children, need to be developed, and further studies are needed to confirm the findings from our trial in children younger than 1 year,” he said.
Dr. Pacilli reported having no financial disclosures.
NEW ORLEANS – Children who require more than 48 hours of intravenous therapy should receive long peripheral catheters initially rather than standard peripheral intravenous catheters, results from a randomized, controlled trial suggest.
Long peripheral catheters (LPCs) are relatively new, 8- to 15-cm long peripheral vascular devices that have been investigated extensively in adults. “It has been shown that these devices are safe and reliable peripheral vascular access devices for use in this population,” lead study author Maurizio Pacilli, MD, said in an interview in advance of the annual meeting of the American Academy of Pediatrics.
“In addition, LPCs may represent an improvement to the quality of care in adults, as demonstrated by multiple randomized controlled trials, where they outperformed peripheral intravenous catheters (PIVCs). There remains, however, a lack of controlled studies to determine if this effect is replicable in children.”
In what he said is the first study of its kind, Dr. Pacilli, a senior research fellow at Monash Children’s Hospital and Monash University, Melbourne, and colleagues performed an open-label randomized trial of 72 pediatric surgical patients aged 1 year and older who required more than 48 hours of IV therapy. They assigned 36 to receive a PIVCs while the remaining 36 children received an 8-cm 22-gauge LPC.
The mean age of patients was 9 years and 71% were boys. Dr. Pacilli reported that the IV therapy duration was a mean of 5 days, and that gender, age, weight, emergency status, and IV therapy duration were similar between the two groups. However, the mean lifespan of catheters was 3 days in PIVC group, compared with 5 days in the LPC group, a difference that reached statistical significance (P = .003). Patients in the PIVC group received a median of two catheters, compared with one in the LPC group (P = .0002). The researchers found that patients in the PIVC group were less likely than were those in the LPC group to complete treatment with a single catheter (39% vs. 81%, relative risk [RR] 2.1, P = .0006), while the rate of catheter failure was higher for PIVCs than for LPCs (67% vs. 19%, RR 3.4, P = .0001; 187 vs. 43 failures per 1,000 catheter days). Infiltration was the most common complication, and occurred in 33% of patients in the PIVC group vs. 3% in LPC group (RR 12, P = .001).
“Our results showed for the first time, without doubt, that children requiring more than 48 hours of intravenous therapy benefit from receiving LPCs, compared with traditional PIVCs,” Dr. Pacilli said. “Of failed catheters, PIVCs are most likely to infiltrate, while LPCs are most likely to occlude. This indicates an additional benefit of LPCs as occlusion is a relatively benign complication. In addition, in all domains of satisfaction, parents favor LPCs. According to the parents, there is a significant improvement in ‘pain and discomfort’ and ‘overall satisfaction’ with the use of LPCs in children.”
He acknowledged certain limitations of the study, including the fact that children younger than 1 year of age were not included in the analysis. “New devices, suitable for very young children, need to be developed, and further studies are needed to confirm the findings from our trial in children younger than 1 year,” he said.
Dr. Pacilli reported having no financial disclosures.
REPORTING FROM AAP 2019
Key clinical point:
Major finding: The mean lifespan of catheters was 3 days in the peripheral intravenous catheters group, compared with 5 days in the long peripheral catheters group, a difference that reached statistical significance (P = .003).
Study details: An open-label, randomized trial of 72 pediatric surgical patients.
Disclosures: Dr. Pacilli reported having no financial disclosures.
Source: Pacilli M et al. AAP 2019, Section on Surgery program.
Strong showing for TAVR after 5 years in PARTNER 2A
SAN FRANCISCO – At 5 years, the rates of disabling stroke or death were similar among patients with severe aortic stenosis and intermediate surgical risk who underwent transcatheter aortic valve replacement or surgical aortic valve replacement.

At the same time, patients who underwent TAVR using a transthoracic approach had poorer outcomes, compared with their counterparts who underwent SAVR, Vinod H. Thourani, MD, reported at the Transcatheter Cardiovascular Therapeutics annual meeting. The findings come from an analysis of the PARTNER 2A trial, the largest randomized study ever conducted in the field of TAVR and SAVR.
In an effort to compare the key clinical outcomes, bioprosthetic valve function, and quality-of-life measures at 5 years for TAVR versus surgery, Dr. Thourani and his colleagues used data from 2,032 intermediate-risk patients with severe AS assigned to either TAVR or SAVR at 57 centers in the PARTNER 2A trial. Their mean age was 82 years, and their average Society of Thoracic Surgery risk score was 5.8%. The 2-year primary endpoint was all-cause death or disabling stroke in the intention-to-treat (ITT) population. At 5 years, the researchers analyzed all primary and secondary clinical and echo endpoints in both ITT and prespecified as-treated populations.
At 5 years, the primary endpoint of death and disabling stroke at 5 years was 47.9% in the TAVR group and 43.4% in the surgery group, a difference that did not reach statistical significance (hazard ratio, 1.09; P = .21). In the transfemoral cohort, rates of the primary endpoint were also similar between TAVR and SAVR (44.5% vs. 42%, respectively; HR, 1.02; P = .80). In the transthoracic cohort, however, the researchers observed a divergence in the primary outcome starting at year 1, such that it was higher with TAVR at 5 years, compared with SAVR (59.3% vs. 48.3%; P = .03), reported Dr. Thourani, chair of cardiac surgery at Medstar Heart and Vascular Institute, Washington.
When he and his colleagues examined freedom from aortic valve reintervention at 5 years, the hazard ratios showed some difference between TAVR and SAVR (HR, 3.93; P = .003), yet clinically the freedom from reintervention rate was very high (96.8% vs. 99.4%, respectively). “The other issue we’ve been interested in is the difference between mean aortic valve gradients between the groups,” Dr. Thourani said at the meeting. “There was no difference in mean aortic valve gradients between TAVR and SAVR at 5 years (a mean of 11.4 mm Hg vs. 10.8 mm Hg, respectively; P = .23).”
Paravalvular regurgitation (PVR) was more common in the TAVR vs. SAVR group at all follow-up times (P less than .001 in all categories). By year 5, the proportion of patients with moderate to severe PVR was 6.5% in the TAVR group vs. 0.4% in the SAVR group, respectively, while the proportion of those with mild PVR was 26.8%, compared with 5.9%.
In other findings, no difference in mortality was seen in the TAVR cohort between those with mild PVR and no or trace PVR (48.7% vs. 41.1%; P = .07). However, those with moderate to severe PVR at the end of the procedure had an increased mortality at the end of 5 years (64.8%; P = .007). “If you had none or trace PVR at baseline, there was no major difference in mortality between the two groups at 2 years,” Dr. Thourani said. “That difference was maintained at 5 years.”
The overall findings, he continued, support the notion that TAVR should be considered as an alternative to surgery in intermediate-risk patients with severe aortic stenosis. “However, in patients without acceptable transfemoral access, surgery may be the preferred alternative,” he said.
Roxana Mehran, MD,, director of interventional cardiovascular research and clinical trials at Mount Sinai School of Medicine, New York, commented that the reassurance of the same outcomes at 5 years between the two approaches “makes TAVR superior. It’s a less invasive and durable result. One of the things we have yet to figure out is the need for anticoagulation to prevent stroke in these patients. We have very little data and understanding about that.”
The PARTNER 2A study was funded by Edwards Lifesciences. Dr. Thourani has received grant or research support from and participation in steering committees for Edwards Lifesciences, Abbott Vascular, Boston Scientific, Gore Vascular, JenaValve, and Cryolife.
SAN FRANCISCO – At 5 years, the rates of disabling stroke or death were similar among patients with severe aortic stenosis and intermediate surgical risk who underwent transcatheter aortic valve replacement or surgical aortic valve replacement.
At the same time, patients who underwent TAVR using a transthoracic approach had poorer outcomes, compared with their counterparts who underwent SAVR, Vinod H. Thourani, MD, reported at the Transcatheter Cardiovascular Therapeutics annual meeting. The findings come from an analysis of the PARTNER 2A trial, the largest randomized study ever conducted in the field of TAVR and SAVR.
In an effort to compare the key clinical outcomes, bioprosthetic valve function, and quality-of-life measures at 5 years for TAVR versus surgery, Dr. Thourani and his colleagues used data from 2,032 intermediate-risk patients with severe AS assigned to either TAVR or SAVR at 57 centers in the PARTNER 2A trial. Their mean age was 82 years, and their average Society of Thoracic Surgery risk score was 5.8%. The 2-year primary endpoint was all-cause death or disabling stroke in the intention-to-treat (ITT) population. At 5 years, the researchers analyzed all primary and secondary clinical and echo endpoints in both ITT and prespecified as-treated populations.
At 5 years, the primary endpoint of death and disabling stroke at 5 years was 47.9% in the TAVR group and 43.4% in the surgery group, a difference that did not reach statistical significance (hazard ratio, 1.09; P = .21). In the transfemoral cohort, rates of the primary endpoint were also similar between TAVR and SAVR (44.5% vs. 42%, respectively; HR, 1.02; P = .80). In the transthoracic cohort, however, the researchers observed a divergence in the primary outcome starting at year 1, such that it was higher with TAVR at 5 years, compared with SAVR (59.3% vs. 48.3%; P = .03), reported Dr. Thourani, chair of cardiac surgery at Medstar Heart and Vascular Institute, Washington.
When he and his colleagues examined freedom from aortic valve reintervention at 5 years, the hazard ratios showed some difference between TAVR and SAVR (HR, 3.93; P = .003), yet clinically the freedom from reintervention rate was very high (96.8% vs. 99.4%, respectively). “The other issue we’ve been interested in is the difference between mean aortic valve gradients between the groups,” Dr. Thourani said at the meeting. “There was no difference in mean aortic valve gradients between TAVR and SAVR at 5 years (a mean of 11.4 mm Hg vs. 10.8 mm Hg, respectively; P = .23).”
Paravalvular regurgitation (PVR) was more common in the TAVR vs. SAVR group at all follow-up times (P less than .001 in all categories). By year 5, the proportion of patients with moderate to severe PVR was 6.5% in the TAVR group vs. 0.4% in the SAVR group, respectively, while the proportion of those with mild PVR was 26.8%, compared with 5.9%.
In other findings, no difference in mortality was seen in the TAVR cohort between those with mild PVR and no or trace PVR (48.7% vs. 41.1%; P = .07). However, those with moderate to severe PVR at the end of the procedure had an increased mortality at the end of 5 years (64.8%; P = .007). “If you had none or trace PVR at baseline, there was no major difference in mortality between the two groups at 2 years,” Dr. Thourani said. “That difference was maintained at 5 years.”
The overall findings, he continued, support the notion that TAVR should be considered as an alternative to surgery in intermediate-risk patients with severe aortic stenosis. “However, in patients without acceptable transfemoral access, surgery may be the preferred alternative,” he said.
Roxana Mehran, MD,, director of interventional cardiovascular research and clinical trials at Mount Sinai School of Medicine, New York, commented that the reassurance of the same outcomes at 5 years between the two approaches “makes TAVR superior. It’s a less invasive and durable result. One of the things we have yet to figure out is the need for anticoagulation to prevent stroke in these patients. We have very little data and understanding about that.”
The PARTNER 2A study was funded by Edwards Lifesciences. Dr. Thourani has received grant or research support from and participation in steering committees for Edwards Lifesciences, Abbott Vascular, Boston Scientific, Gore Vascular, JenaValve, and Cryolife.
SAN FRANCISCO – At 5 years, the rates of disabling stroke or death were similar among patients with severe aortic stenosis and intermediate surgical risk who underwent transcatheter aortic valve replacement or surgical aortic valve replacement.
At the same time, patients who underwent TAVR using a transthoracic approach had poorer outcomes, compared with their counterparts who underwent SAVR, Vinod H. Thourani, MD, reported at the Transcatheter Cardiovascular Therapeutics annual meeting. The findings come from an analysis of the PARTNER 2A trial, the largest randomized study ever conducted in the field of TAVR and SAVR.
In an effort to compare the key clinical outcomes, bioprosthetic valve function, and quality-of-life measures at 5 years for TAVR versus surgery, Dr. Thourani and his colleagues used data from 2,032 intermediate-risk patients with severe AS assigned to either TAVR or SAVR at 57 centers in the PARTNER 2A trial. Their mean age was 82 years, and their average Society of Thoracic Surgery risk score was 5.8%. The 2-year primary endpoint was all-cause death or disabling stroke in the intention-to-treat (ITT) population. At 5 years, the researchers analyzed all primary and secondary clinical and echo endpoints in both ITT and prespecified as-treated populations.
At 5 years, the primary endpoint of death and disabling stroke at 5 years was 47.9% in the TAVR group and 43.4% in the surgery group, a difference that did not reach statistical significance (hazard ratio, 1.09; P = .21). In the transfemoral cohort, rates of the primary endpoint were also similar between TAVR and SAVR (44.5% vs. 42%, respectively; HR, 1.02; P = .80). In the transthoracic cohort, however, the researchers observed a divergence in the primary outcome starting at year 1, such that it was higher with TAVR at 5 years, compared with SAVR (59.3% vs. 48.3%; P = .03), reported Dr. Thourani, chair of cardiac surgery at Medstar Heart and Vascular Institute, Washington.
When he and his colleagues examined freedom from aortic valve reintervention at 5 years, the hazard ratios showed some difference between TAVR and SAVR (HR, 3.93; P = .003), yet clinically the freedom from reintervention rate was very high (96.8% vs. 99.4%, respectively). “The other issue we’ve been interested in is the difference between mean aortic valve gradients between the groups,” Dr. Thourani said at the meeting. “There was no difference in mean aortic valve gradients between TAVR and SAVR at 5 years (a mean of 11.4 mm Hg vs. 10.8 mm Hg, respectively; P = .23).”
Paravalvular regurgitation (PVR) was more common in the TAVR vs. SAVR group at all follow-up times (P less than .001 in all categories). By year 5, the proportion of patients with moderate to severe PVR was 6.5% in the TAVR group vs. 0.4% in the SAVR group, respectively, while the proportion of those with mild PVR was 26.8%, compared with 5.9%.
In other findings, no difference in mortality was seen in the TAVR cohort between those with mild PVR and no or trace PVR (48.7% vs. 41.1%; P = .07). However, those with moderate to severe PVR at the end of the procedure had an increased mortality at the end of 5 years (64.8%; P = .007). “If you had none or trace PVR at baseline, there was no major difference in mortality between the two groups at 2 years,” Dr. Thourani said. “That difference was maintained at 5 years.”
The overall findings, he continued, support the notion that TAVR should be considered as an alternative to surgery in intermediate-risk patients with severe aortic stenosis. “However, in patients without acceptable transfemoral access, surgery may be the preferred alternative,” he said.
Roxana Mehran, MD,, director of interventional cardiovascular research and clinical trials at Mount Sinai School of Medicine, New York, commented that the reassurance of the same outcomes at 5 years between the two approaches “makes TAVR superior. It’s a less invasive and durable result. One of the things we have yet to figure out is the need for anticoagulation to prevent stroke in these patients. We have very little data and understanding about that.”
The PARTNER 2A study was funded by Edwards Lifesciences. Dr. Thourani has received grant or research support from and participation in steering committees for Edwards Lifesciences, Abbott Vascular, Boston Scientific, Gore Vascular, JenaValve, and Cryolife.
AT TCT 2019
Investigative device cut risk of contrast-induced AKI
SAN FRANCISCO – A urine flow rate (UFR)–guided approach was superior to the left ventricular end-diastolic pressure (LVEDP)-guided hydration regimen in preventing contrast-induced acute kidney injury and acute pulmonary edema in high-risk patients.

The results come from a randomized, multicenter, investigator-initiated trial designed to compare two hydration strategies for reducing the risk of acute kidney injury that Carlo Briguori, MD, PhD, presented at the Transcatheter Cardiovascular Therapeutics annual meeting.
Between July 15, 2015 and June 6, 2019, Dr. Briguori, chief of the laboratory of interventional cardiology at the Mediterranea Cardiocentro in Naples, Italy, and his colleagues enrolled 708 patients with an estimated glomerular filtration rate of 45 mL/min per 1.73 m2 or less and/or with a Mehran’s score greater of at least 11 and/or a Gurm’s score greater than 7. Of these, 355 were assigned to LVEDP-guided hydration with normal saline, while 353 were assigned to UFR-guided hydration controlled by the RenalGuard system. Iobitridol, a low-osmolar, nonionic contrast agent, was administered in all cases.
The primary endpoint for the trial, known as Renal Insufficiency Following Contrast Media Administration Trial III (REMEDIAL III), was the composite of contrast-induced acute kidney injury (defined as a serum creatinine increase of at least 25% and/or at least 0.5 mg/dL from baseline to 48 hours) and/or acute pulmonary edema. That endpoint occurred in 5.7% of patients in the UFR-guided group and in 10.3% of patients in the LVEDP-guided group (relative risk, 0.56; P = .036). As for side effects, three patients in the UFR-guided group (0.8%) experienced complications related to Foley insertion, including one case of hematuria and two cases of pain on micturition. No patients developed a urinary tract infection, Dr. Briguori reported at the meeting, which was sponsored by the Cardiovascular Research Foundation.
Hypokalemia occurred in 6.2% of patients in the UFR-guided group and 2.3% of patients in the LVEDP-guided group (RR, 2.70; P = .013), while potassium replacement was required in 5.1% of patients in the UFR-guided group, compared with 1.4% of LVEDP-guided patients (RR, 3.74; P = .009). Meanwhile, hypernatremia was observed in 1.2% of patients in both groups (P = 1.00).
“For the longest time, the interventional field has been trying to find ways to minimize acute kidney injury related to interventional procedures,” Juan F. Granada, MD, president and CEO of the Cardiovascular Research Foundation said in a media briefing. “We have a lot of data with multiple approaches with different results – mostly negative. This is important because, as procedures get more complex, longer, and contrast media is used, there is continuous interest in minimizing the potential kidney injury.”
A discussant at the briefing, Gary S. Mintz, MD, a senior medical adviser for the CRF, suggested a different approach to preventing contrast-induced nephropathy. “If you do imaging-guided zero-contrast percutaneous coronary intervention, you do not get contrast-induced nephropathy, period,” he said. “If you get rid of contrast, you get rid of contrast nephropathy. Anybody who has worked with patients who transition to dialysis understands that once you go on dialysis, your life changes for the worse no matter what you do. There has been no improvement in dialysis therapy in decades. But to me, the solution is to get rid of contrast, which can be done if you think differently and plan differently.”
For his part, Dr. Briguori said that he and his colleagues in REMEDIAL III “tried to use the least amount of contrast possible. The mean volume of contrast media in this trial was 70 mL, which is very low.”
The RenalGuard device (RenalGuard Solutions) is CE-marked for sale in Europe and is under investigation in the United States. The REMEDIAL III study was supported by an unrestricted grant from Guerbet (Villepinte, France) provided to the Mediterranea Cardiocentro. Dr. Briguori reported having no relevant disclosures.
SOURCE: Briguori C. TCT 2019, Late Breaking Trials 4 Session.
SAN FRANCISCO – A urine flow rate (UFR)–guided approach was superior to the left ventricular end-diastolic pressure (LVEDP)-guided hydration regimen in preventing contrast-induced acute kidney injury and acute pulmonary edema in high-risk patients.
The results come from a randomized, multicenter, investigator-initiated trial designed to compare two hydration strategies for reducing the risk of acute kidney injury that Carlo Briguori, MD, PhD, presented at the Transcatheter Cardiovascular Therapeutics annual meeting.
Between July 15, 2015 and June 6, 2019, Dr. Briguori, chief of the laboratory of interventional cardiology at the Mediterranea Cardiocentro in Naples, Italy, and his colleagues enrolled 708 patients with an estimated glomerular filtration rate of 45 mL/min per 1.73 m2 or less and/or with a Mehran’s score greater of at least 11 and/or a Gurm’s score greater than 7. Of these, 355 were assigned to LVEDP-guided hydration with normal saline, while 353 were assigned to UFR-guided hydration controlled by the RenalGuard system. Iobitridol, a low-osmolar, nonionic contrast agent, was administered in all cases.
The primary endpoint for the trial, known as Renal Insufficiency Following Contrast Media Administration Trial III (REMEDIAL III), was the composite of contrast-induced acute kidney injury (defined as a serum creatinine increase of at least 25% and/or at least 0.5 mg/dL from baseline to 48 hours) and/or acute pulmonary edema. That endpoint occurred in 5.7% of patients in the UFR-guided group and in 10.3% of patients in the LVEDP-guided group (relative risk, 0.56; P = .036). As for side effects, three patients in the UFR-guided group (0.8%) experienced complications related to Foley insertion, including one case of hematuria and two cases of pain on micturition. No patients developed a urinary tract infection, Dr. Briguori reported at the meeting, which was sponsored by the Cardiovascular Research Foundation.
Hypokalemia occurred in 6.2% of patients in the UFR-guided group and 2.3% of patients in the LVEDP-guided group (RR, 2.70; P = .013), while potassium replacement was required in 5.1% of patients in the UFR-guided group, compared with 1.4% of LVEDP-guided patients (RR, 3.74; P = .009). Meanwhile, hypernatremia was observed in 1.2% of patients in both groups (P = 1.00).
“For the longest time, the interventional field has been trying to find ways to minimize acute kidney injury related to interventional procedures,” Juan F. Granada, MD, president and CEO of the Cardiovascular Research Foundation said in a media briefing. “We have a lot of data with multiple approaches with different results – mostly negative. This is important because, as procedures get more complex, longer, and contrast media is used, there is continuous interest in minimizing the potential kidney injury.”
A discussant at the briefing, Gary S. Mintz, MD, a senior medical adviser for the CRF, suggested a different approach to preventing contrast-induced nephropathy. “If you do imaging-guided zero-contrast percutaneous coronary intervention, you do not get contrast-induced nephropathy, period,” he said. “If you get rid of contrast, you get rid of contrast nephropathy. Anybody who has worked with patients who transition to dialysis understands that once you go on dialysis, your life changes for the worse no matter what you do. There has been no improvement in dialysis therapy in decades. But to me, the solution is to get rid of contrast, which can be done if you think differently and plan differently.”
For his part, Dr. Briguori said that he and his colleagues in REMEDIAL III “tried to use the least amount of contrast possible. The mean volume of contrast media in this trial was 70 mL, which is very low.”
The RenalGuard device (RenalGuard Solutions) is CE-marked for sale in Europe and is under investigation in the United States. The REMEDIAL III study was supported by an unrestricted grant from Guerbet (Villepinte, France) provided to the Mediterranea Cardiocentro. Dr. Briguori reported having no relevant disclosures.
SOURCE: Briguori C. TCT 2019, Late Breaking Trials 4 Session.
SAN FRANCISCO – A urine flow rate (UFR)–guided approach was superior to the left ventricular end-diastolic pressure (LVEDP)-guided hydration regimen in preventing contrast-induced acute kidney injury and acute pulmonary edema in high-risk patients.
The results come from a randomized, multicenter, investigator-initiated trial designed to compare two hydration strategies for reducing the risk of acute kidney injury that Carlo Briguori, MD, PhD, presented at the Transcatheter Cardiovascular Therapeutics annual meeting.
Between July 15, 2015 and June 6, 2019, Dr. Briguori, chief of the laboratory of interventional cardiology at the Mediterranea Cardiocentro in Naples, Italy, and his colleagues enrolled 708 patients with an estimated glomerular filtration rate of 45 mL/min per 1.73 m2 or less and/or with a Mehran’s score greater of at least 11 and/or a Gurm’s score greater than 7. Of these, 355 were assigned to LVEDP-guided hydration with normal saline, while 353 were assigned to UFR-guided hydration controlled by the RenalGuard system. Iobitridol, a low-osmolar, nonionic contrast agent, was administered in all cases.
The primary endpoint for the trial, known as Renal Insufficiency Following Contrast Media Administration Trial III (REMEDIAL III), was the composite of contrast-induced acute kidney injury (defined as a serum creatinine increase of at least 25% and/or at least 0.5 mg/dL from baseline to 48 hours) and/or acute pulmonary edema. That endpoint occurred in 5.7% of patients in the UFR-guided group and in 10.3% of patients in the LVEDP-guided group (relative risk, 0.56; P = .036). As for side effects, three patients in the UFR-guided group (0.8%) experienced complications related to Foley insertion, including one case of hematuria and two cases of pain on micturition. No patients developed a urinary tract infection, Dr. Briguori reported at the meeting, which was sponsored by the Cardiovascular Research Foundation.
Hypokalemia occurred in 6.2% of patients in the UFR-guided group and 2.3% of patients in the LVEDP-guided group (RR, 2.70; P = .013), while potassium replacement was required in 5.1% of patients in the UFR-guided group, compared with 1.4% of LVEDP-guided patients (RR, 3.74; P = .009). Meanwhile, hypernatremia was observed in 1.2% of patients in both groups (P = 1.00).
“For the longest time, the interventional field has been trying to find ways to minimize acute kidney injury related to interventional procedures,” Juan F. Granada, MD, president and CEO of the Cardiovascular Research Foundation said in a media briefing. “We have a lot of data with multiple approaches with different results – mostly negative. This is important because, as procedures get more complex, longer, and contrast media is used, there is continuous interest in minimizing the potential kidney injury.”
A discussant at the briefing, Gary S. Mintz, MD, a senior medical adviser for the CRF, suggested a different approach to preventing contrast-induced nephropathy. “If you do imaging-guided zero-contrast percutaneous coronary intervention, you do not get contrast-induced nephropathy, period,” he said. “If you get rid of contrast, you get rid of contrast nephropathy. Anybody who has worked with patients who transition to dialysis understands that once you go on dialysis, your life changes for the worse no matter what you do. There has been no improvement in dialysis therapy in decades. But to me, the solution is to get rid of contrast, which can be done if you think differently and plan differently.”
For his part, Dr. Briguori said that he and his colleagues in REMEDIAL III “tried to use the least amount of contrast possible. The mean volume of contrast media in this trial was 70 mL, which is very low.”
The RenalGuard device (RenalGuard Solutions) is CE-marked for sale in Europe and is under investigation in the United States. The REMEDIAL III study was supported by an unrestricted grant from Guerbet (Villepinte, France) provided to the Mediterranea Cardiocentro. Dr. Briguori reported having no relevant disclosures.
SOURCE: Briguori C. TCT 2019, Late Breaking Trials 4 Session.
REPORTING FROM TCT 2019
Portico system safe, effective for high-risk TAVR patients
SAN FRANCISCO – An investigational device exemption trial of the Portico valve with FlexNav delivery system showed 1-year clinical results on par with commercially available valves, Gregory P. Fontana, MD, reported at the Transcatheter Cardiovascular Therapeutics annual meeting.

In a prospective, open-label study conducted at 52 sites known as PORTICO, Dr. Fontana and colleagues conducted a noninferiority intention-to-treat evaluation of the safety and effectiveness of the self-expanding Portico transcatheter aortic valve replacement system, compared with Food and Drug Administration–approved and commercially available TAVR systems for patients with severe aortic stenosis at high or extreme risk for surgery. Between May 2014 and June 2019, 750 patients from 69 sites were randomized 1:1 to each group. The prespecified primary safety composite endpoint was all-cause mortality, disabling stroke, life-threatening bleeding requiring blood transfusion, acute kidney injury requiring dialysis, or major vascular complications at 30 days, while the primary effectiveness composite endpoint was all-cause mortality or disabling stroke at 1 year.
The mean baseline age of patients was 83 years, 53% were female, and their mean Society of Thoracic Surgeons score was 6.5%. Dr. Fontana, director and chairman of cardiothoracic surgery at the CardioVascular Institute of Los Robles Regional Medical Center, Thousand Oaks, Calif., reported at the meeting sponsored by the Cardiovascular Research Foundation that procedural success was comparable between groups (96.5% for Portico vs, 98.3% for commercially available TAVR, respectively). In addition, patients in both groups met the prespecified primary safety composite endpoint (13.8% vs. 9.6%; P for noninferiority = .03) and the primary effectiveness composite endpoint (14.9% vs. 13.4%, P for noninferiority = .006).
However, the rate of moderate to severe paravalvular leak at 30 days was 6.3% among patients in the Portico valve group, compared with 2.1% of their counterparts in the commercially available TAVR group, a difference that did not reach noninferiority. Dr. Fontana said that a next-generation valve with design modifications to reduce paravalvular leak is being tested in clinical trials.
PORTICO included a separate cohort of 100 patients who underwent Portico valve implantation using the FlexNav Delivery System, which became available after the trial had launched. The primary safety endpoint for the FlexNav cohort was major vascular complication rate at 30 days. This cohort demonstrated no deaths or strokes, low rates of major vascular complications (7.0%) and new permanent pacemaker implants (14.6%), as well as a safety profile comparable with the commercially available valve group in the randomized study (8.0% vs. 9.6%).
“My sense of this device is that presumably it will be another valve we have available to us in the United States,” Pinak B. Shah, MD, a cardiologist at Brigham and Women’s Hospital, Boston, said during a media briefing. “The challenge to all of us is to figure out where it fits in our armamentarium. Is it going to be worth individuals to learn a whole new device when at this point it’s hard to say if there’s a major difference compared to the other self-expanding devices we have now?”
With the new FlexNav delivery system, the Portico valve is characterized by “a very calm, slow delivery,” said Dr. Fontana, who was the study’s coprincipal investigator, along with Raj R. Makkar, MD, director of interventional cardiology at Cedars-Sinai Medical Center, Los Angeles. “The operator can land the valve exactly where they want it. If they’re not happy, they can make some adjustments. I haven’t yet a system in my hands that is as stable as this. The option of having excellent hemodynamics and large cells to engage the coronary system is a unique combination for us in the United States.”
The Portico valve is not currently FDA approved. The PORTICO study was funded by Abbott. Dr. Fontana disclosed grant/research support from Abbott and Medtronic and consulting fees/honoraria from Abbott, Medtronic, and LivaNova.
SAN FRANCISCO – An investigational device exemption trial of the Portico valve with FlexNav delivery system showed 1-year clinical results on par with commercially available valves, Gregory P. Fontana, MD, reported at the Transcatheter Cardiovascular Therapeutics annual meeting.
In a prospective, open-label study conducted at 52 sites known as PORTICO, Dr. Fontana and colleagues conducted a noninferiority intention-to-treat evaluation of the safety and effectiveness of the self-expanding Portico transcatheter aortic valve replacement system, compared with Food and Drug Administration–approved and commercially available TAVR systems for patients with severe aortic stenosis at high or extreme risk for surgery. Between May 2014 and June 2019, 750 patients from 69 sites were randomized 1:1 to each group. The prespecified primary safety composite endpoint was all-cause mortality, disabling stroke, life-threatening bleeding requiring blood transfusion, acute kidney injury requiring dialysis, or major vascular complications at 30 days, while the primary effectiveness composite endpoint was all-cause mortality or disabling stroke at 1 year.
The mean baseline age of patients was 83 years, 53% were female, and their mean Society of Thoracic Surgeons score was 6.5%. Dr. Fontana, director and chairman of cardiothoracic surgery at the CardioVascular Institute of Los Robles Regional Medical Center, Thousand Oaks, Calif., reported at the meeting sponsored by the Cardiovascular Research Foundation that procedural success was comparable between groups (96.5% for Portico vs, 98.3% for commercially available TAVR, respectively). In addition, patients in both groups met the prespecified primary safety composite endpoint (13.8% vs. 9.6%; P for noninferiority = .03) and the primary effectiveness composite endpoint (14.9% vs. 13.4%, P for noninferiority = .006).
However, the rate of moderate to severe paravalvular leak at 30 days was 6.3% among patients in the Portico valve group, compared with 2.1% of their counterparts in the commercially available TAVR group, a difference that did not reach noninferiority. Dr. Fontana said that a next-generation valve with design modifications to reduce paravalvular leak is being tested in clinical trials.
PORTICO included a separate cohort of 100 patients who underwent Portico valve implantation using the FlexNav Delivery System, which became available after the trial had launched. The primary safety endpoint for the FlexNav cohort was major vascular complication rate at 30 days. This cohort demonstrated no deaths or strokes, low rates of major vascular complications (7.0%) and new permanent pacemaker implants (14.6%), as well as a safety profile comparable with the commercially available valve group in the randomized study (8.0% vs. 9.6%).
“My sense of this device is that presumably it will be another valve we have available to us in the United States,” Pinak B. Shah, MD, a cardiologist at Brigham and Women’s Hospital, Boston, said during a media briefing. “The challenge to all of us is to figure out where it fits in our armamentarium. Is it going to be worth individuals to learn a whole new device when at this point it’s hard to say if there’s a major difference compared to the other self-expanding devices we have now?”
With the new FlexNav delivery system, the Portico valve is characterized by “a very calm, slow delivery,” said Dr. Fontana, who was the study’s coprincipal investigator, along with Raj R. Makkar, MD, director of interventional cardiology at Cedars-Sinai Medical Center, Los Angeles. “The operator can land the valve exactly where they want it. If they’re not happy, they can make some adjustments. I haven’t yet a system in my hands that is as stable as this. The option of having excellent hemodynamics and large cells to engage the coronary system is a unique combination for us in the United States.”
The Portico valve is not currently FDA approved. The PORTICO study was funded by Abbott. Dr. Fontana disclosed grant/research support from Abbott and Medtronic and consulting fees/honoraria from Abbott, Medtronic, and LivaNova.
SAN FRANCISCO – An investigational device exemption trial of the Portico valve with FlexNav delivery system showed 1-year clinical results on par with commercially available valves, Gregory P. Fontana, MD, reported at the Transcatheter Cardiovascular Therapeutics annual meeting.
In a prospective, open-label study conducted at 52 sites known as PORTICO, Dr. Fontana and colleagues conducted a noninferiority intention-to-treat evaluation of the safety and effectiveness of the self-expanding Portico transcatheter aortic valve replacement system, compared with Food and Drug Administration–approved and commercially available TAVR systems for patients with severe aortic stenosis at high or extreme risk for surgery. Between May 2014 and June 2019, 750 patients from 69 sites were randomized 1:1 to each group. The prespecified primary safety composite endpoint was all-cause mortality, disabling stroke, life-threatening bleeding requiring blood transfusion, acute kidney injury requiring dialysis, or major vascular complications at 30 days, while the primary effectiveness composite endpoint was all-cause mortality or disabling stroke at 1 year.
The mean baseline age of patients was 83 years, 53% were female, and their mean Society of Thoracic Surgeons score was 6.5%. Dr. Fontana, director and chairman of cardiothoracic surgery at the CardioVascular Institute of Los Robles Regional Medical Center, Thousand Oaks, Calif., reported at the meeting sponsored by the Cardiovascular Research Foundation that procedural success was comparable between groups (96.5% for Portico vs, 98.3% for commercially available TAVR, respectively). In addition, patients in both groups met the prespecified primary safety composite endpoint (13.8% vs. 9.6%; P for noninferiority = .03) and the primary effectiveness composite endpoint (14.9% vs. 13.4%, P for noninferiority = .006).
However, the rate of moderate to severe paravalvular leak at 30 days was 6.3% among patients in the Portico valve group, compared with 2.1% of their counterparts in the commercially available TAVR group, a difference that did not reach noninferiority. Dr. Fontana said that a next-generation valve with design modifications to reduce paravalvular leak is being tested in clinical trials.
PORTICO included a separate cohort of 100 patients who underwent Portico valve implantation using the FlexNav Delivery System, which became available after the trial had launched. The primary safety endpoint for the FlexNav cohort was major vascular complication rate at 30 days. This cohort demonstrated no deaths or strokes, low rates of major vascular complications (7.0%) and new permanent pacemaker implants (14.6%), as well as a safety profile comparable with the commercially available valve group in the randomized study (8.0% vs. 9.6%).
“My sense of this device is that presumably it will be another valve we have available to us in the United States,” Pinak B. Shah, MD, a cardiologist at Brigham and Women’s Hospital, Boston, said during a media briefing. “The challenge to all of us is to figure out where it fits in our armamentarium. Is it going to be worth individuals to learn a whole new device when at this point it’s hard to say if there’s a major difference compared to the other self-expanding devices we have now?”
With the new FlexNav delivery system, the Portico valve is characterized by “a very calm, slow delivery,” said Dr. Fontana, who was the study’s coprincipal investigator, along with Raj R. Makkar, MD, director of interventional cardiology at Cedars-Sinai Medical Center, Los Angeles. “The operator can land the valve exactly where they want it. If they’re not happy, they can make some adjustments. I haven’t yet a system in my hands that is as stable as this. The option of having excellent hemodynamics and large cells to engage the coronary system is a unique combination for us in the United States.”
The Portico valve is not currently FDA approved. The PORTICO study was funded by Abbott. Dr. Fontana disclosed grant/research support from Abbott and Medtronic and consulting fees/honoraria from Abbott, Medtronic, and LivaNova.
REPORTING FROM TCT 2019
5-year outcomes similar between PCI and CABG for left main CAD
SAN FRANCISCO – Among patients with left main coronary artery disease and low or intermediate coronary disease complexity, no significant differences were observed between percutaneous coronary intervention and coronary artery bypass graft surgery with respect to the composite rate of death, stroke, or myocardial infarction at 5 years.

The findings come from an analysis of data from the EXCEL trial, which lead investigator Gregg W. Stone, MD, presented at the Transcatheter Cardiovascular Therapeutics annual meeting.
“PCI may be considered an acceptable revascularization modality for selected patients with left main coronary artery disease, a decision which should be made after heart team discussion, taking into account each patient’s individual risk factors and preferences,” said Dr. Stone, professor of medicine and professor of population health sciences and policy at the Icahn School of Medicine at Mount Sinai, New York.
Between September 2010 and March 2014, Dr. Stone and his colleagues at 126 sites in 17 countries enrolled 1,905 patients with left main CAD and site-assessed low or intermediate CAD complexity (SYNTAX score of up to 32) for randomization into one of two arms: 948 to revascularization with the Xience everolimus-eluting stent and 957 to coronary artery bypass graft surgery (CABG). The primary outcome was the composite of death, stroke, or myocardial infarction at 5 years. Long-term additional secondary outcomes included their components at 5 years, as well as therapy failure (definite stent thrombosis or symptomatic graft stenosis or occlusion), all revascularizations, and all cerebrovascular events (stroke or transient ischemic attack).
Dr. Stone reported that at 5 years, the primary composite of death, stroke, or MI occurred in 22.0% of patients in the PCI group and 19.2% of patients in the CABG group, a nonsignificant difference at P = 0.13).
However, when the researchers broke the results into three distinct risk periods within the 5-year time frame, they found that, with longer follow-up, came more of an advantage for CABG. The relative risk of PCI vs. CABG for the primary outcome favored PCI over CABG in the first 30 days (4.9% vs. 8%; hazard ratio, 0.61; P = .008), was neutral at 30 days to 1 year (4.1 vs. 3.8%; HR, 1.07; P = .76), and reversed at 1-5 years (15.1% vs. 9.7%; HR, 1.61; P less than .001). Using restricted mean survival time analysis, Dr. Stone and his colleagues found that, at the end of the 5-year follow-up period, event-free survival time was 5.2 days longer after PCI, compared with CABG. This translates into “a very similar event-free survival of a burden of disease from these two therapies at the end of 5 years,” he said.
In their analysis of secondary endpoints, some differences were noted, including an elevated risk of all-cause mortality in the PCI group, compared with the CABG group (13% vs. 9.9%, respectively; odds ratio, 1.38), yet no differences in definite cardiovascular mortality (5% vs. 4.5%; OR, 1.13) or in MI (10.6% vs. 9.1%; OR 1.14). In addition, there were fewer cerebrovascular events in the PCI vs. CABG groups (3.3% vs. 5.2%; OR, 0.61). “Overall, all of these differences were relatively small given the 5-year perspective,” Dr. Stone said at the meeting sponsored by the Cardiovascular Research Foundation. He concluded that the early benefits of PCI attributable to reduced periprocedural risk “were attenuated by the greater number of events occurring during follow-up with CABG, such that at 5 years the cumulative mean time free from adverse events was similar with both treatments.” He noted that a 10-year or longer follow-up is required to characterize the very late safety profile of PCI and CABG as both stents and bypass grafts progressively fail over time.
Discussant Dharam Kumbhani, MD, an interventional cardiologist at UT Southwestern Medical Center, Dallas, said that the findings from EXCEL “help us move the field forward and help us understand this concept of risk with PCI versus CABG. It really does help inform shared decision-making with patients.”
Results of the study were published online at the time of presentation (N Engl J Med. 2019 Sep 28. doi: 10.1056/NEJMoa1909406). The EXCEL trial was funded by Abbott Vascular. Dr. Stone disclosed having relationships with numerous device and pharmaceutical companies but had no relevant disclosures for this study.
SOURCE: Stone G et al. TCT 2019. N Engl J Med. 2019 Sep 28. doi: 10.1056/NEJMoa1909406.
SAN FRANCISCO – Among patients with left main coronary artery disease and low or intermediate coronary disease complexity, no significant differences were observed between percutaneous coronary intervention and coronary artery bypass graft surgery with respect to the composite rate of death, stroke, or myocardial infarction at 5 years.
The findings come from an analysis of data from the EXCEL trial, which lead investigator Gregg W. Stone, MD, presented at the Transcatheter Cardiovascular Therapeutics annual meeting.
“PCI may be considered an acceptable revascularization modality for selected patients with left main coronary artery disease, a decision which should be made after heart team discussion, taking into account each patient’s individual risk factors and preferences,” said Dr. Stone, professor of medicine and professor of population health sciences and policy at the Icahn School of Medicine at Mount Sinai, New York.
Between September 2010 and March 2014, Dr. Stone and his colleagues at 126 sites in 17 countries enrolled 1,905 patients with left main CAD and site-assessed low or intermediate CAD complexity (SYNTAX score of up to 32) for randomization into one of two arms: 948 to revascularization with the Xience everolimus-eluting stent and 957 to coronary artery bypass graft surgery (CABG). The primary outcome was the composite of death, stroke, or myocardial infarction at 5 years. Long-term additional secondary outcomes included their components at 5 years, as well as therapy failure (definite stent thrombosis or symptomatic graft stenosis or occlusion), all revascularizations, and all cerebrovascular events (stroke or transient ischemic attack).
Dr. Stone reported that at 5 years, the primary composite of death, stroke, or MI occurred in 22.0% of patients in the PCI group and 19.2% of patients in the CABG group, a nonsignificant difference at P = 0.13).
However, when the researchers broke the results into three distinct risk periods within the 5-year time frame, they found that, with longer follow-up, came more of an advantage for CABG. The relative risk of PCI vs. CABG for the primary outcome favored PCI over CABG in the first 30 days (4.9% vs. 8%; hazard ratio, 0.61; P = .008), was neutral at 30 days to 1 year (4.1 vs. 3.8%; HR, 1.07; P = .76), and reversed at 1-5 years (15.1% vs. 9.7%; HR, 1.61; P less than .001). Using restricted mean survival time analysis, Dr. Stone and his colleagues found that, at the end of the 5-year follow-up period, event-free survival time was 5.2 days longer after PCI, compared with CABG. This translates into “a very similar event-free survival of a burden of disease from these two therapies at the end of 5 years,” he said.
In their analysis of secondary endpoints, some differences were noted, including an elevated risk of all-cause mortality in the PCI group, compared with the CABG group (13% vs. 9.9%, respectively; odds ratio, 1.38), yet no differences in definite cardiovascular mortality (5% vs. 4.5%; OR, 1.13) or in MI (10.6% vs. 9.1%; OR 1.14). In addition, there were fewer cerebrovascular events in the PCI vs. CABG groups (3.3% vs. 5.2%; OR, 0.61). “Overall, all of these differences were relatively small given the 5-year perspective,” Dr. Stone said at the meeting sponsored by the Cardiovascular Research Foundation. He concluded that the early benefits of PCI attributable to reduced periprocedural risk “were attenuated by the greater number of events occurring during follow-up with CABG, such that at 5 years the cumulative mean time free from adverse events was similar with both treatments.” He noted that a 10-year or longer follow-up is required to characterize the very late safety profile of PCI and CABG as both stents and bypass grafts progressively fail over time.
Discussant Dharam Kumbhani, MD, an interventional cardiologist at UT Southwestern Medical Center, Dallas, said that the findings from EXCEL “help us move the field forward and help us understand this concept of risk with PCI versus CABG. It really does help inform shared decision-making with patients.”
Results of the study were published online at the time of presentation (N Engl J Med. 2019 Sep 28. doi: 10.1056/NEJMoa1909406). The EXCEL trial was funded by Abbott Vascular. Dr. Stone disclosed having relationships with numerous device and pharmaceutical companies but had no relevant disclosures for this study.
SOURCE: Stone G et al. TCT 2019. N Engl J Med. 2019 Sep 28. doi: 10.1056/NEJMoa1909406.
SAN FRANCISCO – Among patients with left main coronary artery disease and low or intermediate coronary disease complexity, no significant differences were observed between percutaneous coronary intervention and coronary artery bypass graft surgery with respect to the composite rate of death, stroke, or myocardial infarction at 5 years.
The findings come from an analysis of data from the EXCEL trial, which lead investigator Gregg W. Stone, MD, presented at the Transcatheter Cardiovascular Therapeutics annual meeting.
“PCI may be considered an acceptable revascularization modality for selected patients with left main coronary artery disease, a decision which should be made after heart team discussion, taking into account each patient’s individual risk factors and preferences,” said Dr. Stone, professor of medicine and professor of population health sciences and policy at the Icahn School of Medicine at Mount Sinai, New York.
Between September 2010 and March 2014, Dr. Stone and his colleagues at 126 sites in 17 countries enrolled 1,905 patients with left main CAD and site-assessed low or intermediate CAD complexity (SYNTAX score of up to 32) for randomization into one of two arms: 948 to revascularization with the Xience everolimus-eluting stent and 957 to coronary artery bypass graft surgery (CABG). The primary outcome was the composite of death, stroke, or myocardial infarction at 5 years. Long-term additional secondary outcomes included their components at 5 years, as well as therapy failure (definite stent thrombosis or symptomatic graft stenosis or occlusion), all revascularizations, and all cerebrovascular events (stroke or transient ischemic attack).
Dr. Stone reported that at 5 years, the primary composite of death, stroke, or MI occurred in 22.0% of patients in the PCI group and 19.2% of patients in the CABG group, a nonsignificant difference at P = 0.13).
However, when the researchers broke the results into three distinct risk periods within the 5-year time frame, they found that, with longer follow-up, came more of an advantage for CABG. The relative risk of PCI vs. CABG for the primary outcome favored PCI over CABG in the first 30 days (4.9% vs. 8%; hazard ratio, 0.61; P = .008), was neutral at 30 days to 1 year (4.1 vs. 3.8%; HR, 1.07; P = .76), and reversed at 1-5 years (15.1% vs. 9.7%; HR, 1.61; P less than .001). Using restricted mean survival time analysis, Dr. Stone and his colleagues found that, at the end of the 5-year follow-up period, event-free survival time was 5.2 days longer after PCI, compared with CABG. This translates into “a very similar event-free survival of a burden of disease from these two therapies at the end of 5 years,” he said.
In their analysis of secondary endpoints, some differences were noted, including an elevated risk of all-cause mortality in the PCI group, compared with the CABG group (13% vs. 9.9%, respectively; odds ratio, 1.38), yet no differences in definite cardiovascular mortality (5% vs. 4.5%; OR, 1.13) or in MI (10.6% vs. 9.1%; OR 1.14). In addition, there were fewer cerebrovascular events in the PCI vs. CABG groups (3.3% vs. 5.2%; OR, 0.61). “Overall, all of these differences were relatively small given the 5-year perspective,” Dr. Stone said at the meeting sponsored by the Cardiovascular Research Foundation. He concluded that the early benefits of PCI attributable to reduced periprocedural risk “were attenuated by the greater number of events occurring during follow-up with CABG, such that at 5 years the cumulative mean time free from adverse events was similar with both treatments.” He noted that a 10-year or longer follow-up is required to characterize the very late safety profile of PCI and CABG as both stents and bypass grafts progressively fail over time.
Discussant Dharam Kumbhani, MD, an interventional cardiologist at UT Southwestern Medical Center, Dallas, said that the findings from EXCEL “help us move the field forward and help us understand this concept of risk with PCI versus CABG. It really does help inform shared decision-making with patients.”
Results of the study were published online at the time of presentation (N Engl J Med. 2019 Sep 28. doi: 10.1056/NEJMoa1909406). The EXCEL trial was funded by Abbott Vascular. Dr. Stone disclosed having relationships with numerous device and pharmaceutical companies but had no relevant disclosures for this study.
SOURCE: Stone G et al. TCT 2019. N Engl J Med. 2019 Sep 28. doi: 10.1056/NEJMoa1909406.
AT TCT 2019
Wildfire smoke impact, part 2: Resources, advice for patients
Wildfires are on the move in California and communities from the Bay Area to Los Angeles County are once again coping with evacuation, possible destruction of homes, and health concerns related to poor air quality and smoke.

What can doctors tell their patients with cardiovascular and pulmonary conditions about the risks of smoke from wildfires?
EPA resources online
AirNow, a website managed by the Environmental Protection Agency, provides a variety of resources for the public and for health providers, including links to online tutorials, printable health fact sheets, and the newly updated document “Wildfire Smoke: Guide for Public Health Officials 2019.” When wildfire smoke generates an Air Quality Index (AQI) from 101-150, at-risk subgroups like people with asthma, chronic obstructive pulmonary disease (COPD), or heart disease should take precautions.
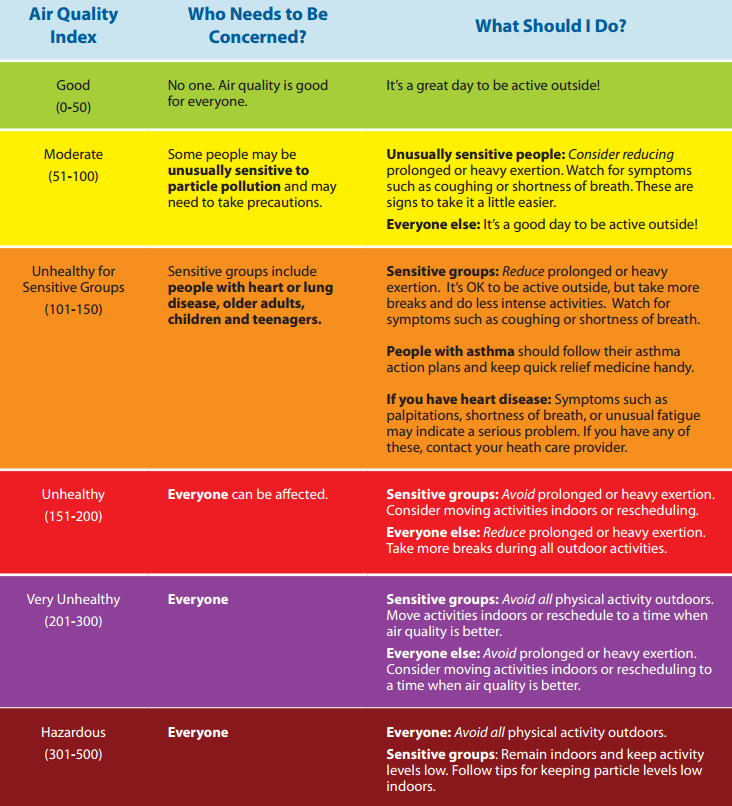
“An AQI of 151-200 is unhealthy for everyone, and an AQI above 200 is very unhealthy,” John R. Balmes, MD, a pulmonologist at the University of California, San Francisco, and an expert on the respiratory and cardiovascular effects of air pollutants, said in an interview. “That does not mean that everybody is going to die, though. You’re going to have some symptoms of scratchy throat, and you may cough once or twice an hour [from exposure to wildfire smoke], but people who don’t have any preexisting health problems are probably going to be fine and don’t necessarily have to wear an N95 mask. People should wear one if they need to feel comfortable.”
Masks – How much protection?

Wayne Cascio, MD, who directs the EPA’s National Health and Environmental Effects Research Laboratory, notes that some public health officials don’t recommend wearing N95 masks during wildfire smoke events. “There’s a lot of concern that people won’t use them correctly and will therefore feel like they’re protected and will spend more time outdoors than they should and still not get the benefit,” he said. “The masks also pose a challenge for children and for people with severe asthma and COPD.”
Masks also have to fit properly, which can be problematic for kids, added Dr. Balmes, one of the authors of “Wildfires Disaster Guidance: Tips for Staying Healthy During Wildfires” (Am J Respir Crit Care Med. 2019;199[2]:3-4).
“Even the small versions don’t necessarily fit kids well, so they’re not recommended for kids,” he said. “It doesn’t mean a kid couldn’t wear them, but it’s not officially recommended. The actual physiologic work of breathing isn’t much increased by using the N95 mask, but if you’re already struggling to get your breath, or experience dyspnea, then it might be hard to wear one. People with milder COPD can wear an N95 mask just like people with mild asthma if they have to go out.”
The EPA published a tip sheet about where and when to use an N95 or P100 mask, with warnings about the limited protection these devices offer, especially if not used correctly. Most masks do not protect the wearer from harmful gases that can be in wildfire smoke.
Ventilation systems
The EPA also recommends that people with more severe disease should stay indoors and avoid using air conditioning units that only draw in air from the outside or do not have a recirculating option. “If you have to bring in outside air because that’s how your system works, you should have a MERV 13 or better filter to filter out the fine particles,” Dr. Balmes said. “Not every ventilation system can handle it, but most can. That will help the house.”
Dr. Cascio pointed out that the instruction to close all windows and doors is a difficult proposition for people who live in states with moderate weather climates such as Montana and Colorado, where few homes have central air conditioning. “The treatment may be worse than the disease in this case, because it may exacerbate heat stress,” he said. “Try to find a place that has cleaner air. That might be a public building, a school, a fitness center, or a library. Yet we don’t know a lot about whether those areas are cleaner or not. That is currently the subject of some research on our part.”
Traveling away from an area affected by wildfire smoke to ride out the conditions is one option, but that can backfire. One weekend when smoke from the 2008 North Carolina peat fire was particularly troublesome, Dr. Cascio and his family drove about 60 miles west of Greenville to the town of Zebulon, where a minor league baseball game was being played and the air quality was good.
“My thought was to get the family to a better environment for at least a few hours,” Dr. Cascio recalled. “When we arrived in Zebulon the air quality was good as advertised. However, the direction of the wind shifted and the smoke started to move due west and within a short time you could barely see the players on the field. This experience also pointed out one of the lessons of wildfire smoke. That is, in the short term, it is sometimes difficult to predict where it will be present because of the nature of changes in weather and wind.”
Consumer tools to monitor air quality

Colleen E. Reid, PhD, of the department of geography at the University of Colorado, Boulder, an expert on the impact of wildfire smoke on human health, has observed in increase in consumer action to counter smoke inhalation during wildfire events. She said that consumers are buying personal laser particle counters, like the ones made by PurpleAir, to provide a real-time assessment of air quality.
“There is a lot of error with these smaller, cheaper monitors, but I think they give you a sense of trends over time,” Dr. Reid said. “People are trying to figure out how we can work with this sort of real-time data along with the high-quality EPA monitors. If everybody has their own monitor, or ways to better calibrate them to the high-quality data, that would be amazing. Researchers are trying to see how they can use that data to inform our understanding of the spatial and temporal patterning of air pollution.”

The EPA’s Smoke Sense app also holds promise. Characterized on its website as “a citizen science project,” the study uses a free mobile app to engage people living in affected communities to monitor their air quality and their cardiorespiratory symptoms. “Through engagement over time, you learn what the effects on your body are and what the expected effects are, so you can recognize the hazards and change the behavior when you’re experiencing it,” said Ana G. Rappold, PhD, who is the app’s principal investigator at the National Health and Environmental Effects Research Laboratory. One component of the app is time of last measurement of fine particulate matter and ozone based on the user’s location. Another is a module called Be Smoke Smart, which tests the user’s knowledge of wildfire smoke exposure. For example, one question is: “How likely are you to reduce your exposure on an Orange AQI alert day?” (which indicates that sensitive populations may experience health effects).
“Through gamification, they’re engaging with the issue,” Dr. Rappold said. “Then they learn about what others are reporting. In that part we also study how different messages change individuals’ perspective on how likely they are to make a change the next time they’re impacted by smoke.”
Wildfires are on the move in California and communities from the Bay Area to Los Angeles County are once again coping with evacuation, possible destruction of homes, and health concerns related to poor air quality and smoke.
What can doctors tell their patients with cardiovascular and pulmonary conditions about the risks of smoke from wildfires?
EPA resources online
AirNow, a website managed by the Environmental Protection Agency, provides a variety of resources for the public and for health providers, including links to online tutorials, printable health fact sheets, and the newly updated document “Wildfire Smoke: Guide for Public Health Officials 2019.” When wildfire smoke generates an Air Quality Index (AQI) from 101-150, at-risk subgroups like people with asthma, chronic obstructive pulmonary disease (COPD), or heart disease should take precautions.
“An AQI of 151-200 is unhealthy for everyone, and an AQI above 200 is very unhealthy,” John R. Balmes, MD, a pulmonologist at the University of California, San Francisco, and an expert on the respiratory and cardiovascular effects of air pollutants, said in an interview. “That does not mean that everybody is going to die, though. You’re going to have some symptoms of scratchy throat, and you may cough once or twice an hour [from exposure to wildfire smoke], but people who don’t have any preexisting health problems are probably going to be fine and don’t necessarily have to wear an N95 mask. People should wear one if they need to feel comfortable.”
Masks – How much protection?
Wayne Cascio, MD, who directs the EPA’s National Health and Environmental Effects Research Laboratory, notes that some public health officials don’t recommend wearing N95 masks during wildfire smoke events. “There’s a lot of concern that people won’t use them correctly and will therefore feel like they’re protected and will spend more time outdoors than they should and still not get the benefit,” he said. “The masks also pose a challenge for children and for people with severe asthma and COPD.”
Masks also have to fit properly, which can be problematic for kids, added Dr. Balmes, one of the authors of “Wildfires Disaster Guidance: Tips for Staying Healthy During Wildfires” (Am J Respir Crit Care Med. 2019;199[2]:3-4).
“Even the small versions don’t necessarily fit kids well, so they’re not recommended for kids,” he said. “It doesn’t mean a kid couldn’t wear them, but it’s not officially recommended. The actual physiologic work of breathing isn’t much increased by using the N95 mask, but if you’re already struggling to get your breath, or experience dyspnea, then it might be hard to wear one. People with milder COPD can wear an N95 mask just like people with mild asthma if they have to go out.”
The EPA published a tip sheet about where and when to use an N95 or P100 mask, with warnings about the limited protection these devices offer, especially if not used correctly. Most masks do not protect the wearer from harmful gases that can be in wildfire smoke.
Ventilation systems
The EPA also recommends that people with more severe disease should stay indoors and avoid using air conditioning units that only draw in air from the outside or do not have a recirculating option. “If you have to bring in outside air because that’s how your system works, you should have a MERV 13 or better filter to filter out the fine particles,” Dr. Balmes said. “Not every ventilation system can handle it, but most can. That will help the house.”
Dr. Cascio pointed out that the instruction to close all windows and doors is a difficult proposition for people who live in states with moderate weather climates such as Montana and Colorado, where few homes have central air conditioning. “The treatment may be worse than the disease in this case, because it may exacerbate heat stress,” he said. “Try to find a place that has cleaner air. That might be a public building, a school, a fitness center, or a library. Yet we don’t know a lot about whether those areas are cleaner or not. That is currently the subject of some research on our part.”
Traveling away from an area affected by wildfire smoke to ride out the conditions is one option, but that can backfire. One weekend when smoke from the 2008 North Carolina peat fire was particularly troublesome, Dr. Cascio and his family drove about 60 miles west of Greenville to the town of Zebulon, where a minor league baseball game was being played and the air quality was good.
“My thought was to get the family to a better environment for at least a few hours,” Dr. Cascio recalled. “When we arrived in Zebulon the air quality was good as advertised. However, the direction of the wind shifted and the smoke started to move due west and within a short time you could barely see the players on the field. This experience also pointed out one of the lessons of wildfire smoke. That is, in the short term, it is sometimes difficult to predict where it will be present because of the nature of changes in weather and wind.”
Consumer tools to monitor air quality
Colleen E. Reid, PhD, of the department of geography at the University of Colorado, Boulder, an expert on the impact of wildfire smoke on human health, has observed in increase in consumer action to counter smoke inhalation during wildfire events. She said that consumers are buying personal laser particle counters, like the ones made by PurpleAir, to provide a real-time assessment of air quality.
“There is a lot of error with these smaller, cheaper monitors, but I think they give you a sense of trends over time,” Dr. Reid said. “People are trying to figure out how we can work with this sort of real-time data along with the high-quality EPA monitors. If everybody has their own monitor, or ways to better calibrate them to the high-quality data, that would be amazing. Researchers are trying to see how they can use that data to inform our understanding of the spatial and temporal patterning of air pollution.”
The EPA’s Smoke Sense app also holds promise. Characterized on its website as “a citizen science project,” the study uses a free mobile app to engage people living in affected communities to monitor their air quality and their cardiorespiratory symptoms. “Through engagement over time, you learn what the effects on your body are and what the expected effects are, so you can recognize the hazards and change the behavior when you’re experiencing it,” said Ana G. Rappold, PhD, who is the app’s principal investigator at the National Health and Environmental Effects Research Laboratory. One component of the app is time of last measurement of fine particulate matter and ozone based on the user’s location. Another is a module called Be Smoke Smart, which tests the user’s knowledge of wildfire smoke exposure. For example, one question is: “How likely are you to reduce your exposure on an Orange AQI alert day?” (which indicates that sensitive populations may experience health effects).
“Through gamification, they’re engaging with the issue,” Dr. Rappold said. “Then they learn about what others are reporting. In that part we also study how different messages change individuals’ perspective on how likely they are to make a change the next time they’re impacted by smoke.”
Wildfires are on the move in California and communities from the Bay Area to Los Angeles County are once again coping with evacuation, possible destruction of homes, and health concerns related to poor air quality and smoke.
What can doctors tell their patients with cardiovascular and pulmonary conditions about the risks of smoke from wildfires?
EPA resources online
AirNow, a website managed by the Environmental Protection Agency, provides a variety of resources for the public and for health providers, including links to online tutorials, printable health fact sheets, and the newly updated document “Wildfire Smoke: Guide for Public Health Officials 2019.” When wildfire smoke generates an Air Quality Index (AQI) from 101-150, at-risk subgroups like people with asthma, chronic obstructive pulmonary disease (COPD), or heart disease should take precautions.
“An AQI of 151-200 is unhealthy for everyone, and an AQI above 200 is very unhealthy,” John R. Balmes, MD, a pulmonologist at the University of California, San Francisco, and an expert on the respiratory and cardiovascular effects of air pollutants, said in an interview. “That does not mean that everybody is going to die, though. You’re going to have some symptoms of scratchy throat, and you may cough once or twice an hour [from exposure to wildfire smoke], but people who don’t have any preexisting health problems are probably going to be fine and don’t necessarily have to wear an N95 mask. People should wear one if they need to feel comfortable.”
Masks – How much protection?
Wayne Cascio, MD, who directs the EPA’s National Health and Environmental Effects Research Laboratory, notes that some public health officials don’t recommend wearing N95 masks during wildfire smoke events. “There’s a lot of concern that people won’t use them correctly and will therefore feel like they’re protected and will spend more time outdoors than they should and still not get the benefit,” he said. “The masks also pose a challenge for children and for people with severe asthma and COPD.”
Masks also have to fit properly, which can be problematic for kids, added Dr. Balmes, one of the authors of “Wildfires Disaster Guidance: Tips for Staying Healthy During Wildfires” (Am J Respir Crit Care Med. 2019;199[2]:3-4).
“Even the small versions don’t necessarily fit kids well, so they’re not recommended for kids,” he said. “It doesn’t mean a kid couldn’t wear them, but it’s not officially recommended. The actual physiologic work of breathing isn’t much increased by using the N95 mask, but if you’re already struggling to get your breath, or experience dyspnea, then it might be hard to wear one. People with milder COPD can wear an N95 mask just like people with mild asthma if they have to go out.”
The EPA published a tip sheet about where and when to use an N95 or P100 mask, with warnings about the limited protection these devices offer, especially if not used correctly. Most masks do not protect the wearer from harmful gases that can be in wildfire smoke.
Ventilation systems
The EPA also recommends that people with more severe disease should stay indoors and avoid using air conditioning units that only draw in air from the outside or do not have a recirculating option. “If you have to bring in outside air because that’s how your system works, you should have a MERV 13 or better filter to filter out the fine particles,” Dr. Balmes said. “Not every ventilation system can handle it, but most can. That will help the house.”
Dr. Cascio pointed out that the instruction to close all windows and doors is a difficult proposition for people who live in states with moderate weather climates such as Montana and Colorado, where few homes have central air conditioning. “The treatment may be worse than the disease in this case, because it may exacerbate heat stress,” he said. “Try to find a place that has cleaner air. That might be a public building, a school, a fitness center, or a library. Yet we don’t know a lot about whether those areas are cleaner or not. That is currently the subject of some research on our part.”
Traveling away from an area affected by wildfire smoke to ride out the conditions is one option, but that can backfire. One weekend when smoke from the 2008 North Carolina peat fire was particularly troublesome, Dr. Cascio and his family drove about 60 miles west of Greenville to the town of Zebulon, where a minor league baseball game was being played and the air quality was good.
“My thought was to get the family to a better environment for at least a few hours,” Dr. Cascio recalled. “When we arrived in Zebulon the air quality was good as advertised. However, the direction of the wind shifted and the smoke started to move due west and within a short time you could barely see the players on the field. This experience also pointed out one of the lessons of wildfire smoke. That is, in the short term, it is sometimes difficult to predict where it will be present because of the nature of changes in weather and wind.”
Consumer tools to monitor air quality
Colleen E. Reid, PhD, of the department of geography at the University of Colorado, Boulder, an expert on the impact of wildfire smoke on human health, has observed in increase in consumer action to counter smoke inhalation during wildfire events. She said that consumers are buying personal laser particle counters, like the ones made by PurpleAir, to provide a real-time assessment of air quality.
“There is a lot of error with these smaller, cheaper monitors, but I think they give you a sense of trends over time,” Dr. Reid said. “People are trying to figure out how we can work with this sort of real-time data along with the high-quality EPA monitors. If everybody has their own monitor, or ways to better calibrate them to the high-quality data, that would be amazing. Researchers are trying to see how they can use that data to inform our understanding of the spatial and temporal patterning of air pollution.”
The EPA’s Smoke Sense app also holds promise. Characterized on its website as “a citizen science project,” the study uses a free mobile app to engage people living in affected communities to monitor their air quality and their cardiorespiratory symptoms. “Through engagement over time, you learn what the effects on your body are and what the expected effects are, so you can recognize the hazards and change the behavior when you’re experiencing it,” said Ana G. Rappold, PhD, who is the app’s principal investigator at the National Health and Environmental Effects Research Laboratory. One component of the app is time of last measurement of fine particulate matter and ozone based on the user’s location. Another is a module called Be Smoke Smart, which tests the user’s knowledge of wildfire smoke exposure. For example, one question is: “How likely are you to reduce your exposure on an Orange AQI alert day?” (which indicates that sensitive populations may experience health effects).
“Through gamification, they’re engaging with the issue,” Dr. Rappold said. “Then they learn about what others are reporting. In that part we also study how different messages change individuals’ perspective on how likely they are to make a change the next time they’re impacted by smoke.”
Short DAPT found noninferior to longer DAPT post stent implantation

In addition, P2Y12 inhibitor monotherapy was almost equivalent to aspirin monotherapy after 3 months in terms of both bleeding and thrombotic events.
“Recent guidelines recommend short DAPT up to 3 months, only in high bleeding risk patients,” lead investigator Ken Kozuma, MD, said during a media briefing at the Transcatheter Cardiovascular Therapeutics annual meeting. “However, short-term DAPT may be beneficial for any patients. Aspirin may be more associated with bleeding complication than P2Y12 receptor inhibitors.”
In a single-arm registry trial known as MODEL U-SES, Dr. Kozuma, of Teikyo University Hospital in Tokyo, and colleagues at 65 sites in Japan prospectively evaluated the safety of 3-month DAPT after implantation of the Ultimaster bioresorbable polymer sirolimus-eluting stent (BP-SES). The secondary objective was to investigate the appropriateness of P2Y12 receptor inhibitor monotherapy compared with aspirin monotherapy after 3 months. The researchers enrolled 1,695 patients with a mean age of 70 years who were treated with U-SES and considered appropriate for 3-month DAPT after implantation.
The primary endpoint was a composite endpoint of all-cause death, myocardial infarction, stroke (ischemic and hemorrhagic), Academic Research Consortium (ARC) definite/probable stent thrombosis, and serious bleeding (Bleeding Academic Research Consortium [BARC] 3 or 5) during the 12 months after stent implantation. Major secondary endpoints included a comparison of the incidence of each event for each continued antiplatelet drug.
Of the 1,695 patients enrolled, 1,686 completed 3-month clinical follow-up while 1,616 completed 1-year clinical follow-up. Patient-level adjusted historical data from 542 subjects in the CENTURY II cohort was used as the control group. Patients in that trial received the same stent but took DAPT for 1 year.
Dr. Kozuma reported that the primary endpoint occurred in 4.3% of patients in the MODEL U-SES group, compared with 5.7% of patients in the CENTURY II BP-SES group, a difference of –3.17%, which demonstrated noninferiority of the trial (P less than .001). At 3 months, P2Y12 inhibitor monotherapy was equivalent to aspirin monotherapy in terms of both bleeding and thrombotic events (2.5% in each modality; hazard ratio, 1.14; P = 0.71).
Dr. Kozuma acknowledged certain limitations of the trial, including the fact that propensity score adjusted analysis “may not compensate the selection bias of this study sufficiently, since considerable baseline difference was observed. Also, comparison between aspirin and P2Y12 receptor inhibitors was not randomized so that the safety and efficacy of each antiplatelet monotherapy cannot be conclusive.”
Despite these limitations, he concluded that the trial “demonstrated that 3-month DAPT was noninferior to an adjusted cohort of longer DAPT after BP-SES implantation in net adverse clinical events. Direct comparison between P2Y12 inhibitor and aspirin would be necessary to confirm the efficacy and safety of P2Y12 inhibitor monotherapy in a randomized fashion.”
The meeting was sponsored by the Cardiovascular Research Foundation.
Terumo sponsored the trial. Dr. Kozuma disclosed that he serves on the scientific advisory boards for and has received honoraria from Terumo, Abbott Vascular Japan, Boston Scientific Japan, Daiichi-Sankyo, Sanofi, Bayer, Boehringer Ingelheim and Bristol-Meyers Squibb.
SOURCE: Kozuma K et al. TCT 2019, late-breaking presentation.
In addition, P2Y12 inhibitor monotherapy was almost equivalent to aspirin monotherapy after 3 months in terms of both bleeding and thrombotic events.
“Recent guidelines recommend short DAPT up to 3 months, only in high bleeding risk patients,” lead investigator Ken Kozuma, MD, said during a media briefing at the Transcatheter Cardiovascular Therapeutics annual meeting. “However, short-term DAPT may be beneficial for any patients. Aspirin may be more associated with bleeding complication than P2Y12 receptor inhibitors.”
In a single-arm registry trial known as MODEL U-SES, Dr. Kozuma, of Teikyo University Hospital in Tokyo, and colleagues at 65 sites in Japan prospectively evaluated the safety of 3-month DAPT after implantation of the Ultimaster bioresorbable polymer sirolimus-eluting stent (BP-SES). The secondary objective was to investigate the appropriateness of P2Y12 receptor inhibitor monotherapy compared with aspirin monotherapy after 3 months. The researchers enrolled 1,695 patients with a mean age of 70 years who were treated with U-SES and considered appropriate for 3-month DAPT after implantation.
The primary endpoint was a composite endpoint of all-cause death, myocardial infarction, stroke (ischemic and hemorrhagic), Academic Research Consortium (ARC) definite/probable stent thrombosis, and serious bleeding (Bleeding Academic Research Consortium [BARC] 3 or 5) during the 12 months after stent implantation. Major secondary endpoints included a comparison of the incidence of each event for each continued antiplatelet drug.
Of the 1,695 patients enrolled, 1,686 completed 3-month clinical follow-up while 1,616 completed 1-year clinical follow-up. Patient-level adjusted historical data from 542 subjects in the CENTURY II cohort was used as the control group. Patients in that trial received the same stent but took DAPT for 1 year.
Dr. Kozuma reported that the primary endpoint occurred in 4.3% of patients in the MODEL U-SES group, compared with 5.7% of patients in the CENTURY II BP-SES group, a difference of –3.17%, which demonstrated noninferiority of the trial (P less than .001). At 3 months, P2Y12 inhibitor monotherapy was equivalent to aspirin monotherapy in terms of both bleeding and thrombotic events (2.5% in each modality; hazard ratio, 1.14; P = 0.71).
Dr. Kozuma acknowledged certain limitations of the trial, including the fact that propensity score adjusted analysis “may not compensate the selection bias of this study sufficiently, since considerable baseline difference was observed. Also, comparison between aspirin and P2Y12 receptor inhibitors was not randomized so that the safety and efficacy of each antiplatelet monotherapy cannot be conclusive.”
Despite these limitations, he concluded that the trial “demonstrated that 3-month DAPT was noninferior to an adjusted cohort of longer DAPT after BP-SES implantation in net adverse clinical events. Direct comparison between P2Y12 inhibitor and aspirin would be necessary to confirm the efficacy and safety of P2Y12 inhibitor monotherapy in a randomized fashion.”
The meeting was sponsored by the Cardiovascular Research Foundation.
Terumo sponsored the trial. Dr. Kozuma disclosed that he serves on the scientific advisory boards for and has received honoraria from Terumo, Abbott Vascular Japan, Boston Scientific Japan, Daiichi-Sankyo, Sanofi, Bayer, Boehringer Ingelheim and Bristol-Meyers Squibb.
SOURCE: Kozuma K et al. TCT 2019, late-breaking presentation.
In addition, P2Y12 inhibitor monotherapy was almost equivalent to aspirin monotherapy after 3 months in terms of both bleeding and thrombotic events.
“Recent guidelines recommend short DAPT up to 3 months, only in high bleeding risk patients,” lead investigator Ken Kozuma, MD, said during a media briefing at the Transcatheter Cardiovascular Therapeutics annual meeting. “However, short-term DAPT may be beneficial for any patients. Aspirin may be more associated with bleeding complication than P2Y12 receptor inhibitors.”
In a single-arm registry trial known as MODEL U-SES, Dr. Kozuma, of Teikyo University Hospital in Tokyo, and colleagues at 65 sites in Japan prospectively evaluated the safety of 3-month DAPT after implantation of the Ultimaster bioresorbable polymer sirolimus-eluting stent (BP-SES). The secondary objective was to investigate the appropriateness of P2Y12 receptor inhibitor monotherapy compared with aspirin monotherapy after 3 months. The researchers enrolled 1,695 patients with a mean age of 70 years who were treated with U-SES and considered appropriate for 3-month DAPT after implantation.
The primary endpoint was a composite endpoint of all-cause death, myocardial infarction, stroke (ischemic and hemorrhagic), Academic Research Consortium (ARC) definite/probable stent thrombosis, and serious bleeding (Bleeding Academic Research Consortium [BARC] 3 or 5) during the 12 months after stent implantation. Major secondary endpoints included a comparison of the incidence of each event for each continued antiplatelet drug.
Of the 1,695 patients enrolled, 1,686 completed 3-month clinical follow-up while 1,616 completed 1-year clinical follow-up. Patient-level adjusted historical data from 542 subjects in the CENTURY II cohort was used as the control group. Patients in that trial received the same stent but took DAPT for 1 year.
Dr. Kozuma reported that the primary endpoint occurred in 4.3% of patients in the MODEL U-SES group, compared with 5.7% of patients in the CENTURY II BP-SES group, a difference of –3.17%, which demonstrated noninferiority of the trial (P less than .001). At 3 months, P2Y12 inhibitor monotherapy was equivalent to aspirin monotherapy in terms of both bleeding and thrombotic events (2.5% in each modality; hazard ratio, 1.14; P = 0.71).
Dr. Kozuma acknowledged certain limitations of the trial, including the fact that propensity score adjusted analysis “may not compensate the selection bias of this study sufficiently, since considerable baseline difference was observed. Also, comparison between aspirin and P2Y12 receptor inhibitors was not randomized so that the safety and efficacy of each antiplatelet monotherapy cannot be conclusive.”
Despite these limitations, he concluded that the trial “demonstrated that 3-month DAPT was noninferior to an adjusted cohort of longer DAPT after BP-SES implantation in net adverse clinical events. Direct comparison between P2Y12 inhibitor and aspirin would be necessary to confirm the efficacy and safety of P2Y12 inhibitor monotherapy in a randomized fashion.”
The meeting was sponsored by the Cardiovascular Research Foundation.
Terumo sponsored the trial. Dr. Kozuma disclosed that he serves on the scientific advisory boards for and has received honoraria from Terumo, Abbott Vascular Japan, Boston Scientific Japan, Daiichi-Sankyo, Sanofi, Bayer, Boehringer Ingelheim and Bristol-Meyers Squibb.
SOURCE: Kozuma K et al. TCT 2019, late-breaking presentation.
AT TCT 2019