User login
Trump nominates Neil Gorsuch as 9th Supreme Court justice
President Donald Trump has chosen Neil Gorsuch, a conservative judge who presides over Denver’s 10th Circuit as his nominee for U.S. Supreme Court justice. A federal judge for 10 years, Judge Gorsuch is a long-time comrade of deceased Supreme Court Justice Antonin Scalia with a strong record of supporting religious freedom and less government control.
At a White House East Room ceremony on Jan. 31, Judge Gorsuch said he was honored and humbled by President’s Trump’s nomination and that he looked forward to answering questions during his Senate nomination hearing.
President Trump hailed Judge Gorsuch’s credentials as the “best he has ever seen,” and called him more than qualified to take the reins as the next Supreme Court justice.
“He has an extraordinary resume, as good as it gets,” President Trump said. “The qualifications of Judge Gorsuch are beyond dispute. He is a man of our country and a man who our country needs – and needs badly – to uphold the rule of law and the rule of justice.”
Judge Gorsuch, 49,was appointed to the 10th U.S. Circuit Court of Appeals in Denver, by President George W. Bush. His nomination was confirmed unanimously in the Senate. He holds a doctoral degree from Oxford University, (England), a law degree from Harvard Law School, Cambridge, Mass., and an undergraduate degree from Columbia University, New York. Judge Gorsuch began his legal career as a law clerk to Supreme Court justices Byron R. White and Anthony M. Kennedy, as well as to Judge David B. Sentelle of the U.S. Court of Appeals for the D.C. Circuit. Prior to his judicial appointment, Judge Gorsuch served as principal deputy associate attorney general at the Justice Department under George W. Bush.

A Senate confirmation hearing had not been announced at press time. Judge Gorsuch has pledged to work with both parties during the hearing to answer questions and alleviate any concerns.
“I look forward to speaking with members from both sides of the aisle,” he said. “I consider the United States Senate the greatest deliberative body in the world, and I respect the important role the Constitution affords it in the confirmation of our judges.”
Justice Antonin Scalia died suddenly on Feb. 13, 2016, leaving the high court with only eight members. Then-President Barack Obama nominated Judge Merrick Garland of the U.S. Court of Appeals for the District of Columbia Circuit to fill Scalia’s seat. However, the Republican-controlled Senate blocked Judge Garland from ever having a hearing and his nomination was never fully considered.
[email protected]
On Twitter @legal_med
President Donald Trump has chosen Neil Gorsuch, a conservative judge who presides over Denver’s 10th Circuit as his nominee for U.S. Supreme Court justice. A federal judge for 10 years, Judge Gorsuch is a long-time comrade of deceased Supreme Court Justice Antonin Scalia with a strong record of supporting religious freedom and less government control.
At a White House East Room ceremony on Jan. 31, Judge Gorsuch said he was honored and humbled by President’s Trump’s nomination and that he looked forward to answering questions during his Senate nomination hearing.
President Trump hailed Judge Gorsuch’s credentials as the “best he has ever seen,” and called him more than qualified to take the reins as the next Supreme Court justice.
“He has an extraordinary resume, as good as it gets,” President Trump said. “The qualifications of Judge Gorsuch are beyond dispute. He is a man of our country and a man who our country needs – and needs badly – to uphold the rule of law and the rule of justice.”
Judge Gorsuch, 49,was appointed to the 10th U.S. Circuit Court of Appeals in Denver, by President George W. Bush. His nomination was confirmed unanimously in the Senate. He holds a doctoral degree from Oxford University, (England), a law degree from Harvard Law School, Cambridge, Mass., and an undergraduate degree from Columbia University, New York. Judge Gorsuch began his legal career as a law clerk to Supreme Court justices Byron R. White and Anthony M. Kennedy, as well as to Judge David B. Sentelle of the U.S. Court of Appeals for the D.C. Circuit. Prior to his judicial appointment, Judge Gorsuch served as principal deputy associate attorney general at the Justice Department under George W. Bush.
A Senate confirmation hearing had not been announced at press time. Judge Gorsuch has pledged to work with both parties during the hearing to answer questions and alleviate any concerns.
“I look forward to speaking with members from both sides of the aisle,” he said. “I consider the United States Senate the greatest deliberative body in the world, and I respect the important role the Constitution affords it in the confirmation of our judges.”
Justice Antonin Scalia died suddenly on Feb. 13, 2016, leaving the high court with only eight members. Then-President Barack Obama nominated Judge Merrick Garland of the U.S. Court of Appeals for the District of Columbia Circuit to fill Scalia’s seat. However, the Republican-controlled Senate blocked Judge Garland from ever having a hearing and his nomination was never fully considered.
[email protected]
On Twitter @legal_med
President Donald Trump has chosen Neil Gorsuch, a conservative judge who presides over Denver’s 10th Circuit as his nominee for U.S. Supreme Court justice. A federal judge for 10 years, Judge Gorsuch is a long-time comrade of deceased Supreme Court Justice Antonin Scalia with a strong record of supporting religious freedom and less government control.
At a White House East Room ceremony on Jan. 31, Judge Gorsuch said he was honored and humbled by President’s Trump’s nomination and that he looked forward to answering questions during his Senate nomination hearing.
President Trump hailed Judge Gorsuch’s credentials as the “best he has ever seen,” and called him more than qualified to take the reins as the next Supreme Court justice.
“He has an extraordinary resume, as good as it gets,” President Trump said. “The qualifications of Judge Gorsuch are beyond dispute. He is a man of our country and a man who our country needs – and needs badly – to uphold the rule of law and the rule of justice.”
Judge Gorsuch, 49,was appointed to the 10th U.S. Circuit Court of Appeals in Denver, by President George W. Bush. His nomination was confirmed unanimously in the Senate. He holds a doctoral degree from Oxford University, (England), a law degree from Harvard Law School, Cambridge, Mass., and an undergraduate degree from Columbia University, New York. Judge Gorsuch began his legal career as a law clerk to Supreme Court justices Byron R. White and Anthony M. Kennedy, as well as to Judge David B. Sentelle of the U.S. Court of Appeals for the D.C. Circuit. Prior to his judicial appointment, Judge Gorsuch served as principal deputy associate attorney general at the Justice Department under George W. Bush.
A Senate confirmation hearing had not been announced at press time. Judge Gorsuch has pledged to work with both parties during the hearing to answer questions and alleviate any concerns.
“I look forward to speaking with members from both sides of the aisle,” he said. “I consider the United States Senate the greatest deliberative body in the world, and I respect the important role the Constitution affords it in the confirmation of our judges.”
Justice Antonin Scalia died suddenly on Feb. 13, 2016, leaving the high court with only eight members. Then-President Barack Obama nominated Judge Merrick Garland of the U.S. Court of Appeals for the District of Columbia Circuit to fill Scalia’s seat. However, the Republican-controlled Senate blocked Judge Garland from ever having a hearing and his nomination was never fully considered.
[email protected]
On Twitter @legal_med
Judge blocks Aetna-Humana merger
A federal judge has blocked a megamerger between health insurance giants Aetna and Humana, ruling that the consolidation would violate antitrust laws and reduce competition.
In a Jan. 23 decision, Judge John D. Bates of the U.S. District Court for the District of Columbia denied Aetna’s $37 billion plan to purchase Humana, following a month-long trial that began in early December. The court was unpersuaded that the efficiencies generated by the merger would be “sufficient to mitigate the anticompetitive effects for consumers in the challenged markets,” Judge Bates said in his opinion.
The U.S. Department of Justice, which challenged the merger, called the ruling a victory for patients, particularly seniors and working families.
“Competition spurs health insurers to offer higher quality and more affordable health insurance to seniors who choose Medicare Advantage plans and to low-income families and individuals who purchase insurance from public exchanges,” Brent Snyder, deputy assistant attorney general, said in a statement. “Aetna attempted to buy a formidable rival, Humana, instead of competing independently to win customers. Millions of consumers have benefited from competition between Aetna and Humana, and will continue to benefit because of today’s decision to block this merger.”
The Department of Justice, eight states, and the District of Columbia sued Aetna and Humana after an investigation into their proposed July 2015 merger. The government argued that the companies compete head-to-head in the Medicare Advantage and public exchange markets, and that such competition would be lost following the merger to the significant detriment of patients. Aetna and Humana argued their proposed merger would not substantially lessen competition because of the government’s regulatory authority over Medicare Advantage, the threat of entry by new competitors, and the defendants’ proposed divestiture of a portion of their Medicare Advantage business to insurer Molina Healthcare. The insurers also asserted that no current competition between the two companies exists in the 17 complaint counties because Aetna has decided not to compete in those counties in 2017. Judge Bates disagreed.
“The merger would likely substantially lessen competition in the market for individual Medicare Advantage in all 364 complaint counties,” Judge Bates said in his opinion. “This conclusion is based on identification of the proper product market, the overwhelming market concentration figures generated by the merger, and the considerable evidence of valuable head-to-head competition between Aetna and Humana, which the merger would eliminate. The companies’ rebuttal arguments are unpersuasive.”
The American Medical Association praised the ruling.
“Elderly patients were the big winners today as a federal court imposed an injunction on Aetna’s $37 billion acquisition of Humana,” AMA president Andrew W. Gurman, MD, said in a statement. “Aetna’s strategy to eliminate head-to-head competition with rival Humana posed a clear and present threat to the quality, accessibility, and affordability of health care for millions of seniors. The AMA applauds the extraordinarily well-documented, comprehensive, fact-based ruling of U.S. District Judge John D. Bates, which acknowledged that meaningful action was needed to preserve competition and protect high-quality medical care from unprecedented market power that Aetna would acquire from the merger deal.”
Another ruling is expected soon in the $48 billion planned merger between Anthem and Cigna, which is also being challenged by the Justice department. A trial in that case wrapped up in late December in front of U.S. District Court for the District of Columbia Judge Amy Berman.
[email protected]
On Twitter @legal_med
A federal judge has blocked a megamerger between health insurance giants Aetna and Humana, ruling that the consolidation would violate antitrust laws and reduce competition.
In a Jan. 23 decision, Judge John D. Bates of the U.S. District Court for the District of Columbia denied Aetna’s $37 billion plan to purchase Humana, following a month-long trial that began in early December. The court was unpersuaded that the efficiencies generated by the merger would be “sufficient to mitigate the anticompetitive effects for consumers in the challenged markets,” Judge Bates said in his opinion.
The U.S. Department of Justice, which challenged the merger, called the ruling a victory for patients, particularly seniors and working families.
“Competition spurs health insurers to offer higher quality and more affordable health insurance to seniors who choose Medicare Advantage plans and to low-income families and individuals who purchase insurance from public exchanges,” Brent Snyder, deputy assistant attorney general, said in a statement. “Aetna attempted to buy a formidable rival, Humana, instead of competing independently to win customers. Millions of consumers have benefited from competition between Aetna and Humana, and will continue to benefit because of today’s decision to block this merger.”
The Department of Justice, eight states, and the District of Columbia sued Aetna and Humana after an investigation into their proposed July 2015 merger. The government argued that the companies compete head-to-head in the Medicare Advantage and public exchange markets, and that such competition would be lost following the merger to the significant detriment of patients. Aetna and Humana argued their proposed merger would not substantially lessen competition because of the government’s regulatory authority over Medicare Advantage, the threat of entry by new competitors, and the defendants’ proposed divestiture of a portion of their Medicare Advantage business to insurer Molina Healthcare. The insurers also asserted that no current competition between the two companies exists in the 17 complaint counties because Aetna has decided not to compete in those counties in 2017. Judge Bates disagreed.
“The merger would likely substantially lessen competition in the market for individual Medicare Advantage in all 364 complaint counties,” Judge Bates said in his opinion. “This conclusion is based on identification of the proper product market, the overwhelming market concentration figures generated by the merger, and the considerable evidence of valuable head-to-head competition between Aetna and Humana, which the merger would eliminate. The companies’ rebuttal arguments are unpersuasive.”
The American Medical Association praised the ruling.
“Elderly patients were the big winners today as a federal court imposed an injunction on Aetna’s $37 billion acquisition of Humana,” AMA president Andrew W. Gurman, MD, said in a statement. “Aetna’s strategy to eliminate head-to-head competition with rival Humana posed a clear and present threat to the quality, accessibility, and affordability of health care for millions of seniors. The AMA applauds the extraordinarily well-documented, comprehensive, fact-based ruling of U.S. District Judge John D. Bates, which acknowledged that meaningful action was needed to preserve competition and protect high-quality medical care from unprecedented market power that Aetna would acquire from the merger deal.”
Another ruling is expected soon in the $48 billion planned merger between Anthem and Cigna, which is also being challenged by the Justice department. A trial in that case wrapped up in late December in front of U.S. District Court for the District of Columbia Judge Amy Berman.
[email protected]
On Twitter @legal_med
A federal judge has blocked a megamerger between health insurance giants Aetna and Humana, ruling that the consolidation would violate antitrust laws and reduce competition.
In a Jan. 23 decision, Judge John D. Bates of the U.S. District Court for the District of Columbia denied Aetna’s $37 billion plan to purchase Humana, following a month-long trial that began in early December. The court was unpersuaded that the efficiencies generated by the merger would be “sufficient to mitigate the anticompetitive effects for consumers in the challenged markets,” Judge Bates said in his opinion.
The U.S. Department of Justice, which challenged the merger, called the ruling a victory for patients, particularly seniors and working families.
“Competition spurs health insurers to offer higher quality and more affordable health insurance to seniors who choose Medicare Advantage plans and to low-income families and individuals who purchase insurance from public exchanges,” Brent Snyder, deputy assistant attorney general, said in a statement. “Aetna attempted to buy a formidable rival, Humana, instead of competing independently to win customers. Millions of consumers have benefited from competition between Aetna and Humana, and will continue to benefit because of today’s decision to block this merger.”
The Department of Justice, eight states, and the District of Columbia sued Aetna and Humana after an investigation into their proposed July 2015 merger. The government argued that the companies compete head-to-head in the Medicare Advantage and public exchange markets, and that such competition would be lost following the merger to the significant detriment of patients. Aetna and Humana argued their proposed merger would not substantially lessen competition because of the government’s regulatory authority over Medicare Advantage, the threat of entry by new competitors, and the defendants’ proposed divestiture of a portion of their Medicare Advantage business to insurer Molina Healthcare. The insurers also asserted that no current competition between the two companies exists in the 17 complaint counties because Aetna has decided not to compete in those counties in 2017. Judge Bates disagreed.
“The merger would likely substantially lessen competition in the market for individual Medicare Advantage in all 364 complaint counties,” Judge Bates said in his opinion. “This conclusion is based on identification of the proper product market, the overwhelming market concentration figures generated by the merger, and the considerable evidence of valuable head-to-head competition between Aetna and Humana, which the merger would eliminate. The companies’ rebuttal arguments are unpersuasive.”
The American Medical Association praised the ruling.
“Elderly patients were the big winners today as a federal court imposed an injunction on Aetna’s $37 billion acquisition of Humana,” AMA president Andrew W. Gurman, MD, said in a statement. “Aetna’s strategy to eliminate head-to-head competition with rival Humana posed a clear and present threat to the quality, accessibility, and affordability of health care for millions of seniors. The AMA applauds the extraordinarily well-documented, comprehensive, fact-based ruling of U.S. District Judge John D. Bates, which acknowledged that meaningful action was needed to preserve competition and protect high-quality medical care from unprecedented market power that Aetna would acquire from the merger deal.”
Another ruling is expected soon in the $48 billion planned merger between Anthem and Cigna, which is also being challenged by the Justice department. A trial in that case wrapped up in late December in front of U.S. District Court for the District of Columbia Judge Amy Berman.
[email protected]
On Twitter @legal_med

VIDEO: Health law changes under new administration
WASHINGTON – A new president is taking office along with new staffers to lead the country’s top health care agencies.
In this video, Joyce Hall, chair of the American Bar Association Health Law Section, discusses what changes she foresees in health law issues under the new administration and what to expect from the leadership transition. Ms. Hall also speaks on potential alterations to the Medicare Access and CHIP Reauthorization Act of 2015 and whether the potential appointment of Rep. Tom Price (R-Ga.) as U.S. Department of Health and Human Services Secretary will be positive or negative for health care providers.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @legal_med
WASHINGTON – A new president is taking office along with new staffers to lead the country’s top health care agencies.
In this video, Joyce Hall, chair of the American Bar Association Health Law Section, discusses what changes she foresees in health law issues under the new administration and what to expect from the leadership transition. Ms. Hall also speaks on potential alterations to the Medicare Access and CHIP Reauthorization Act of 2015 and whether the potential appointment of Rep. Tom Price (R-Ga.) as U.S. Department of Health and Human Services Secretary will be positive or negative for health care providers.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @legal_med
WASHINGTON – A new president is taking office along with new staffers to lead the country’s top health care agencies.
In this video, Joyce Hall, chair of the American Bar Association Health Law Section, discusses what changes she foresees in health law issues under the new administration and what to expect from the leadership transition. Ms. Hall also speaks on potential alterations to the Medicare Access and CHIP Reauthorization Act of 2015 and whether the potential appointment of Rep. Tom Price (R-Ga.) as U.S. Department of Health and Human Services Secretary will be positive or negative for health care providers.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @legal_med
AT THE WASHINGTON HEALTH LAW SUMMIT

FDA, EPA clarify which fish pregnant women and young children should eat
The Food and Drug Administration and the Environmental Protection Agency have issued updated guidance about fish consumption for pregnant women and young children, clarifying which types of fish are recommended and what types of fish to avoid.
In guidance issued Jan. 18, the agencies sort 62 types of fish into three categories based on mercury level: best choices, good choices, and fish to avoid. They recommend that women who are pregnant, women who may become pregnant, breastfeeding mothers, and young children eat two to three servings of fish in the “best choices” category per week. Women and young children are advised to eat one serving per week of fish in the “good choices” category, according to the announcement. Fish in the “best choices” category make up nearly 90% of fish eaten in the United States, according to the FDA.
“Fish are an important source of protein and other nutrients for young children and women who are or may become pregnant or are breastfeeding,” Stephen Ostroff, MD, FDA’s deputy commissioner for Foods and Veterinary Medicine, said in a statement. “This advice clearly shows the great diversity of fish in the U.S. market that they can consume safely. This new, clear and concrete advice is an excellent tool for making safe and healthy choices when buying fish.”
The updated advice cautions pregnant women and others to avoid seven types of fish that generally have higher mercury levels. This includes tilefish from the Gulf of Mexico, shark; swordfish; orange roughy, bigeye tuna; marlin, and king mackerel. Meanwhile, recommended choices lower in mercury include such fish as shrimp, pollock, salmon, canned light tuna, tilapia, catfish, and cod.
Consumers are urged to check local advisories for fish caught recreationally and gauge their fish consumption based on any local and state advisories for those waters. If no information on fishing advisories is available, the FDA recommends eating just one fish meal a week from local waters and to avoid other fish that week.
[email protected]
On Twitter @legal_med
The Food and Drug Administration and the Environmental Protection Agency have issued updated guidance about fish consumption for pregnant women and young children, clarifying which types of fish are recommended and what types of fish to avoid.
In guidance issued Jan. 18, the agencies sort 62 types of fish into three categories based on mercury level: best choices, good choices, and fish to avoid. They recommend that women who are pregnant, women who may become pregnant, breastfeeding mothers, and young children eat two to three servings of fish in the “best choices” category per week. Women and young children are advised to eat one serving per week of fish in the “good choices” category, according to the announcement. Fish in the “best choices” category make up nearly 90% of fish eaten in the United States, according to the FDA.
“Fish are an important source of protein and other nutrients for young children and women who are or may become pregnant or are breastfeeding,” Stephen Ostroff, MD, FDA’s deputy commissioner for Foods and Veterinary Medicine, said in a statement. “This advice clearly shows the great diversity of fish in the U.S. market that they can consume safely. This new, clear and concrete advice is an excellent tool for making safe and healthy choices when buying fish.”
The updated advice cautions pregnant women and others to avoid seven types of fish that generally have higher mercury levels. This includes tilefish from the Gulf of Mexico, shark; swordfish; orange roughy, bigeye tuna; marlin, and king mackerel. Meanwhile, recommended choices lower in mercury include such fish as shrimp, pollock, salmon, canned light tuna, tilapia, catfish, and cod.
Consumers are urged to check local advisories for fish caught recreationally and gauge their fish consumption based on any local and state advisories for those waters. If no information on fishing advisories is available, the FDA recommends eating just one fish meal a week from local waters and to avoid other fish that week.
[email protected]
On Twitter @legal_med
The Food and Drug Administration and the Environmental Protection Agency have issued updated guidance about fish consumption for pregnant women and young children, clarifying which types of fish are recommended and what types of fish to avoid.
In guidance issued Jan. 18, the agencies sort 62 types of fish into three categories based on mercury level: best choices, good choices, and fish to avoid. They recommend that women who are pregnant, women who may become pregnant, breastfeeding mothers, and young children eat two to three servings of fish in the “best choices” category per week. Women and young children are advised to eat one serving per week of fish in the “good choices” category, according to the announcement. Fish in the “best choices” category make up nearly 90% of fish eaten in the United States, according to the FDA.
“Fish are an important source of protein and other nutrients for young children and women who are or may become pregnant or are breastfeeding,” Stephen Ostroff, MD, FDA’s deputy commissioner for Foods and Veterinary Medicine, said in a statement. “This advice clearly shows the great diversity of fish in the U.S. market that they can consume safely. This new, clear and concrete advice is an excellent tool for making safe and healthy choices when buying fish.”
The updated advice cautions pregnant women and others to avoid seven types of fish that generally have higher mercury levels. This includes tilefish from the Gulf of Mexico, shark; swordfish; orange roughy, bigeye tuna; marlin, and king mackerel. Meanwhile, recommended choices lower in mercury include such fish as shrimp, pollock, salmon, canned light tuna, tilapia, catfish, and cod.
Consumers are urged to check local advisories for fish caught recreationally and gauge their fish consumption based on any local and state advisories for those waters. If no information on fishing advisories is available, the FDA recommends eating just one fish meal a week from local waters and to avoid other fish that week.
[email protected]
On Twitter @legal_med
What’s in store for CMS under Seema Verma?
WASHINGTON – Big changes could be in store for the Medicaid program under the potential leadership of Seema Verma as administrator of the Centers for Medicare & Medicaid Services.
In nominating Ms. Verma, President Trump called her a leading expert on Medicaid and Medicare who will help “transform our health care system for the benefit of all Americans.”
A relative unknown, Ms. Verma is a health policy consultant who has spent 20 years quietly designing policy projects involving Medicaid, including the crafting of Indiana’s Medicaid expansion under the Affordable Care Act in which she worked closely with Vice President Pence.
How the savvy consultant could alter the Medicaid program during her potential CMS tenure has been the source of much speculation. President Trump and Rep. Tom Price (R-Ga.), Health & Human Services secretary–designee, have called for the restructuring of Medicaid, including the possibility of block grants that would set limits on total annual spending regardless of enrollment or caps that would limit average spending per enrollee.
Ms. Verma’s role in the revamp will largely depend on what Congress allows, said Mark Polston, a Washington, D.C.–based health law attorney and former associate general counsel for litigation in the HHS Office of General Counsel, CMS division, under President George W. Bush.
“We don’t know what cards she has in her hands – let alone what’s in the deck for her to deal from,” Mr. Polston said at a meeting sponsored by the American Bar Association. “That’s really going to be set by Congress.”

“From a CMS perspective, the Medicaid program is in large part run by the states,” Mr. Blum said at the ABA meeting. “What the new nominee says to me is that there is going to be a very high priority placed upon working with states, working with governors to modify Medicaid programs and to shape them to meet different state priorities.”
Look no further than the Healthy Indiana Plan 2.0 to get an idea of what such plans could look like, said Leslie V. Norwalk, a Washington, D.C.–based health law attorney and a former acting CMS administrator under President George W. Bush. The Indiana plan requires patients to pay a small amount to receive health coverage and includes a lockout period if payments are missed. Ms. Verma could work with governors to develop similar model waivers, Ms. Norwalk said.

Mr. Blum said he believes a top priority for Ms. Verma will be limiting the disruption that could come if the ACA is repealed and finding ways to cover those who lose coverage.
“What the next team really needs to really realize [is] that those who sign up for coverage – with the exchanges or through the new state expansions – are sicker on average, have lower income on average, and they’re going to have to think very carefully about the transitions going on,” Mr. Blum said at the meeting. “How you think about the transitions, how you think about continuity of care, how you think about disruptions – those will be very real and very tangible for the next team.”

“If she’s smart, she’ll find a deputy who’s very strong on Medicare. She’ll probably also try to find a former Hill staffer who can help her on the Hill,” Mr. Scully said. “The best news for her is that they picked her really early, so she’s got a head start.”
Hiring a deputy with a strong insurance background will also be key, Ms. Norwalk said in an interview. Even if the exchanges are repealed, other CMS programs, such as Medicare Part D and Medicare Advantage rely heavily on insurers, she said.
Ms. Norwalk noted that Ms. Verma may be surprised to find that much of the CMS agenda is controlled by the requirements of Medicare’s regulatory cycle. “[It] will take up a lot of her time, perhaps more than she might anticipate,” she said. “But in addition, you’ll have governors coming in wanting to do waivers. ... The third component will be how much time she spends on Capitol Hill working on whether repeal is done or not, and certainly the replace function and how that works will be a critical component of what she does. [If she’s confirmed,] she’ll be a very busy lady.”
[email protected]
On Twitter @legal_med
WASHINGTON – Big changes could be in store for the Medicaid program under the potential leadership of Seema Verma as administrator of the Centers for Medicare & Medicaid Services.
In nominating Ms. Verma, President Trump called her a leading expert on Medicaid and Medicare who will help “transform our health care system for the benefit of all Americans.”
A relative unknown, Ms. Verma is a health policy consultant who has spent 20 years quietly designing policy projects involving Medicaid, including the crafting of Indiana’s Medicaid expansion under the Affordable Care Act in which she worked closely with Vice President Pence.
How the savvy consultant could alter the Medicaid program during her potential CMS tenure has been the source of much speculation. President Trump and Rep. Tom Price (R-Ga.), Health & Human Services secretary–designee, have called for the restructuring of Medicaid, including the possibility of block grants that would set limits on total annual spending regardless of enrollment or caps that would limit average spending per enrollee.
Ms. Verma’s role in the revamp will largely depend on what Congress allows, said Mark Polston, a Washington, D.C.–based health law attorney and former associate general counsel for litigation in the HHS Office of General Counsel, CMS division, under President George W. Bush.
“We don’t know what cards she has in her hands – let alone what’s in the deck for her to deal from,” Mr. Polston said at a meeting sponsored by the American Bar Association. “That’s really going to be set by Congress.”
“From a CMS perspective, the Medicaid program is in large part run by the states,” Mr. Blum said at the ABA meeting. “What the new nominee says to me is that there is going to be a very high priority placed upon working with states, working with governors to modify Medicaid programs and to shape them to meet different state priorities.”
Look no further than the Healthy Indiana Plan 2.0 to get an idea of what such plans could look like, said Leslie V. Norwalk, a Washington, D.C.–based health law attorney and a former acting CMS administrator under President George W. Bush. The Indiana plan requires patients to pay a small amount to receive health coverage and includes a lockout period if payments are missed. Ms. Verma could work with governors to develop similar model waivers, Ms. Norwalk said.
Mr. Blum said he believes a top priority for Ms. Verma will be limiting the disruption that could come if the ACA is repealed and finding ways to cover those who lose coverage.
“What the next team really needs to really realize [is] that those who sign up for coverage – with the exchanges or through the new state expansions – are sicker on average, have lower income on average, and they’re going to have to think very carefully about the transitions going on,” Mr. Blum said at the meeting. “How you think about the transitions, how you think about continuity of care, how you think about disruptions – those will be very real and very tangible for the next team.”
“If she’s smart, she’ll find a deputy who’s very strong on Medicare. She’ll probably also try to find a former Hill staffer who can help her on the Hill,” Mr. Scully said. “The best news for her is that they picked her really early, so she’s got a head start.”
Hiring a deputy with a strong insurance background will also be key, Ms. Norwalk said in an interview. Even if the exchanges are repealed, other CMS programs, such as Medicare Part D and Medicare Advantage rely heavily on insurers, she said.
Ms. Norwalk noted that Ms. Verma may be surprised to find that much of the CMS agenda is controlled by the requirements of Medicare’s regulatory cycle. “[It] will take up a lot of her time, perhaps more than she might anticipate,” she said. “But in addition, you’ll have governors coming in wanting to do waivers. ... The third component will be how much time she spends on Capitol Hill working on whether repeal is done or not, and certainly the replace function and how that works will be a critical component of what she does. [If she’s confirmed,] she’ll be a very busy lady.”
[email protected]
On Twitter @legal_med
WASHINGTON – Big changes could be in store for the Medicaid program under the potential leadership of Seema Verma as administrator of the Centers for Medicare & Medicaid Services.
In nominating Ms. Verma, President Trump called her a leading expert on Medicaid and Medicare who will help “transform our health care system for the benefit of all Americans.”
A relative unknown, Ms. Verma is a health policy consultant who has spent 20 years quietly designing policy projects involving Medicaid, including the crafting of Indiana’s Medicaid expansion under the Affordable Care Act in which she worked closely with Vice President Pence.
How the savvy consultant could alter the Medicaid program during her potential CMS tenure has been the source of much speculation. President Trump and Rep. Tom Price (R-Ga.), Health & Human Services secretary–designee, have called for the restructuring of Medicaid, including the possibility of block grants that would set limits on total annual spending regardless of enrollment or caps that would limit average spending per enrollee.
Ms. Verma’s role in the revamp will largely depend on what Congress allows, said Mark Polston, a Washington, D.C.–based health law attorney and former associate general counsel for litigation in the HHS Office of General Counsel, CMS division, under President George W. Bush.
“We don’t know what cards she has in her hands – let alone what’s in the deck for her to deal from,” Mr. Polston said at a meeting sponsored by the American Bar Association. “That’s really going to be set by Congress.”
“From a CMS perspective, the Medicaid program is in large part run by the states,” Mr. Blum said at the ABA meeting. “What the new nominee says to me is that there is going to be a very high priority placed upon working with states, working with governors to modify Medicaid programs and to shape them to meet different state priorities.”
Look no further than the Healthy Indiana Plan 2.0 to get an idea of what such plans could look like, said Leslie V. Norwalk, a Washington, D.C.–based health law attorney and a former acting CMS administrator under President George W. Bush. The Indiana plan requires patients to pay a small amount to receive health coverage and includes a lockout period if payments are missed. Ms. Verma could work with governors to develop similar model waivers, Ms. Norwalk said.
Mr. Blum said he believes a top priority for Ms. Verma will be limiting the disruption that could come if the ACA is repealed and finding ways to cover those who lose coverage.
“What the next team really needs to really realize [is] that those who sign up for coverage – with the exchanges or through the new state expansions – are sicker on average, have lower income on average, and they’re going to have to think very carefully about the transitions going on,” Mr. Blum said at the meeting. “How you think about the transitions, how you think about continuity of care, how you think about disruptions – those will be very real and very tangible for the next team.”
“If she’s smart, she’ll find a deputy who’s very strong on Medicare. She’ll probably also try to find a former Hill staffer who can help her on the Hill,” Mr. Scully said. “The best news for her is that they picked her really early, so she’s got a head start.”
Hiring a deputy with a strong insurance background will also be key, Ms. Norwalk said in an interview. Even if the exchanges are repealed, other CMS programs, such as Medicare Part D and Medicare Advantage rely heavily on insurers, she said.
Ms. Norwalk noted that Ms. Verma may be surprised to find that much of the CMS agenda is controlled by the requirements of Medicare’s regulatory cycle. “[It] will take up a lot of her time, perhaps more than she might anticipate,” she said. “But in addition, you’ll have governors coming in wanting to do waivers. ... The third component will be how much time she spends on Capitol Hill working on whether repeal is done or not, and certainly the replace function and how that works will be a critical component of what she does. [If she’s confirmed,] she’ll be a very busy lady.”
[email protected]
On Twitter @legal_med
AT THE AMERICAN BAR ASSOCIATION HEALTH LAW SUMMIT

Ohio governor vetoes 6-week abortion ban in favor of 20 weeks
Ohio Gov. John Kasich (R) has rejected a controversial bill that would have barred women in the state from having abortions as early as 6 weeks, but he signed another measure banning the procedure at 20 weeks.
The legislation, known as “the heartbeat bill,” would have prohibited abortions if a fetal heartbeat could be detected – usually around 6 weeks – and jailed physicians who performed the procedure without checking for a heartbeat or who provided an abortion after a heartbeat was found. The Ohio House approved the measure on Dec. 6 after earlier passage by the state senate. In his veto of the 6-week ban, Gov. Kasich noted that federal courts have struck down similar legislation in Arkansas and North Dakota, and that he did not want Ohio taxpayers to fund a losing legal challenge.
“Because the federal courts are bound to follow the Supreme Court’s rulings on abortion, the amendment ... will be struck down,” Gov. Kasich said in a statement. “The state of Ohio will be the losing party in that lawsuit and ... be forced to pay hundreds of thousands of taxpayer dollars to cover the legal fees of the pro-choice activists’ lawyers. Furthermore, such a defeat invites additional challenges to Ohio’s strong legal protections for unborn life. Therefore, this veto is in the public interest.”
Abortion rights advocates were quick to criticize the 20-week ban (SB 127), saying that Ohio lawmakers still intend to effectively end abortion in the state.
“The 20-week ban will force women to travel long distances and cross state lines in order to access safe, legal abortion – a barrier that many women simply cannot afford,” Dawn Laguens, Planned Parenthood Action Fund executive vice president said in a statement.
The American Congress of Obstetricians and Gynecologists Ohio Section also opposes the 20-week ban. In a Dec. 9 letter to Gov. Kasich, Wayne Trout, MD, chair of ACOG’s Ohio Section, said these types of laws come between physicians and patients and create unnecessary medical risks.
“A great number of pregnancy terminations beyond 20 weeks are due to identification of serious and fatal birth defects in otherwise highly desired pregnancies,” Dr. Trout wrote. “Continuation of these pregnancies would result in certain death of the baby and expose the newborn to needless pain. Meanwhile the mother is forced to carry the fetus to term and may be exposed to a myriad of medical and reproductive risks.”
The Ohio law also places doctors in a “precarious situation,” he noted, by criminalizing a medical procedure that is recognized by ACOG as a standard of care when women have a medical indication for termination of pregnancy.
Abortion opponents meanwhile, praised the 20-week ban, calling it a vehicle to end abortion. “It challenges the current national abortion standard and properly moves the legal needle from viability to the baby’s ability to feel pain,” Mike Gonidakis, President of Ohio Right to Life said in a statement.
[email protected]
On Twitter @legal_med
Ohio Gov. John Kasich (R) has rejected a controversial bill that would have barred women in the state from having abortions as early as 6 weeks, but he signed another measure banning the procedure at 20 weeks.
The legislation, known as “the heartbeat bill,” would have prohibited abortions if a fetal heartbeat could be detected – usually around 6 weeks – and jailed physicians who performed the procedure without checking for a heartbeat or who provided an abortion after a heartbeat was found. The Ohio House approved the measure on Dec. 6 after earlier passage by the state senate. In his veto of the 6-week ban, Gov. Kasich noted that federal courts have struck down similar legislation in Arkansas and North Dakota, and that he did not want Ohio taxpayers to fund a losing legal challenge.
“Because the federal courts are bound to follow the Supreme Court’s rulings on abortion, the amendment ... will be struck down,” Gov. Kasich said in a statement. “The state of Ohio will be the losing party in that lawsuit and ... be forced to pay hundreds of thousands of taxpayer dollars to cover the legal fees of the pro-choice activists’ lawyers. Furthermore, such a defeat invites additional challenges to Ohio’s strong legal protections for unborn life. Therefore, this veto is in the public interest.”
Abortion rights advocates were quick to criticize the 20-week ban (SB 127), saying that Ohio lawmakers still intend to effectively end abortion in the state.
“The 20-week ban will force women to travel long distances and cross state lines in order to access safe, legal abortion – a barrier that many women simply cannot afford,” Dawn Laguens, Planned Parenthood Action Fund executive vice president said in a statement.
The American Congress of Obstetricians and Gynecologists Ohio Section also opposes the 20-week ban. In a Dec. 9 letter to Gov. Kasich, Wayne Trout, MD, chair of ACOG’s Ohio Section, said these types of laws come between physicians and patients and create unnecessary medical risks.
“A great number of pregnancy terminations beyond 20 weeks are due to identification of serious and fatal birth defects in otherwise highly desired pregnancies,” Dr. Trout wrote. “Continuation of these pregnancies would result in certain death of the baby and expose the newborn to needless pain. Meanwhile the mother is forced to carry the fetus to term and may be exposed to a myriad of medical and reproductive risks.”
The Ohio law also places doctors in a “precarious situation,” he noted, by criminalizing a medical procedure that is recognized by ACOG as a standard of care when women have a medical indication for termination of pregnancy.
Abortion opponents meanwhile, praised the 20-week ban, calling it a vehicle to end abortion. “It challenges the current national abortion standard and properly moves the legal needle from viability to the baby’s ability to feel pain,” Mike Gonidakis, President of Ohio Right to Life said in a statement.
[email protected]
On Twitter @legal_med
Ohio Gov. John Kasich (R) has rejected a controversial bill that would have barred women in the state from having abortions as early as 6 weeks, but he signed another measure banning the procedure at 20 weeks.
The legislation, known as “the heartbeat bill,” would have prohibited abortions if a fetal heartbeat could be detected – usually around 6 weeks – and jailed physicians who performed the procedure without checking for a heartbeat or who provided an abortion after a heartbeat was found. The Ohio House approved the measure on Dec. 6 after earlier passage by the state senate. In his veto of the 6-week ban, Gov. Kasich noted that federal courts have struck down similar legislation in Arkansas and North Dakota, and that he did not want Ohio taxpayers to fund a losing legal challenge.
“Because the federal courts are bound to follow the Supreme Court’s rulings on abortion, the amendment ... will be struck down,” Gov. Kasich said in a statement. “The state of Ohio will be the losing party in that lawsuit and ... be forced to pay hundreds of thousands of taxpayer dollars to cover the legal fees of the pro-choice activists’ lawyers. Furthermore, such a defeat invites additional challenges to Ohio’s strong legal protections for unborn life. Therefore, this veto is in the public interest.”
Abortion rights advocates were quick to criticize the 20-week ban (SB 127), saying that Ohio lawmakers still intend to effectively end abortion in the state.
“The 20-week ban will force women to travel long distances and cross state lines in order to access safe, legal abortion – a barrier that many women simply cannot afford,” Dawn Laguens, Planned Parenthood Action Fund executive vice president said in a statement.
The American Congress of Obstetricians and Gynecologists Ohio Section also opposes the 20-week ban. In a Dec. 9 letter to Gov. Kasich, Wayne Trout, MD, chair of ACOG’s Ohio Section, said these types of laws come between physicians and patients and create unnecessary medical risks.
“A great number of pregnancy terminations beyond 20 weeks are due to identification of serious and fatal birth defects in otherwise highly desired pregnancies,” Dr. Trout wrote. “Continuation of these pregnancies would result in certain death of the baby and expose the newborn to needless pain. Meanwhile the mother is forced to carry the fetus to term and may be exposed to a myriad of medical and reproductive risks.”
The Ohio law also places doctors in a “precarious situation,” he noted, by criminalizing a medical procedure that is recognized by ACOG as a standard of care when women have a medical indication for termination of pregnancy.
Abortion opponents meanwhile, praised the 20-week ban, calling it a vehicle to end abortion. “It challenges the current national abortion standard and properly moves the legal needle from viability to the baby’s ability to feel pain,” Mike Gonidakis, President of Ohio Right to Life said in a statement.
[email protected]
On Twitter @legal_med
Trump administration to focus on ACA reform, tort reform
Look for three things from the Trump administration: significant changes to the Affordable Care Act, few changes to MACRA’s Quality Payment Program, and a conservative swing in the courts.
Republicans have had their sights on the Affordable Care Act since its passage in 2010; with majorities in both the House and the Senate, the question is not if, but when President Obama’s signature piece of legislation will be dismantled.
President-elect Donald Trump ran on the promise of ACA repeal. Health policy priorities on his transition website focus on greater use of health savings accounts, the ability to purchase insurance across state lines, and the reestablishment of high-risk pools.
Health policy experts differ in how they see ACA reform coming about, with some predicting a quick repeal coupled with an immediate legislative replacement, while others envision repeal with more time to craft replacement legislation. Reform also could come as a series of smaller bills rather than one comprehensive package.
Using budget reconciliation would not allow for full ACA repeal since only provisions that involve revenue generation or spending could be altered. However, since budget reconciliation bills cannot be filibustered, only a simple majority is needed for Senate passage. With their razor-thin majority – 51 seats – Republicans will need some support from outside of their own party.
“Twenty-some Democrats, many in very-deep ‘red states’ including North Dakota, are up for reelection in 2018,” Ms. Turner said. “They saw what happened to the candidates who supported Obamacare in 2016 – many of them went down. It happened with Evan Bayh in Indiana, who was running again to reclaim the Senate seat he left in 2010. And the Republican candidate [Todd Young] reminded the voters over and over that Evan Bayh voted for Obamacare. Same thing happened in Wisconsin with [Republican] Sen. Ron Johnson being challenged by Russ Feingold, who also was in the Senate when Obamacare passed. Feingold went down to defeat again. I think the lot of Democratic senators are going to be looking at what happened to those people and think ‘Maybe I better participate in coming up with a more sensible solution.’ ”
More importantly, the GOP may be looking for bipartisan support, especially since the ACA passed on a strict party-line vote. To that end, it could make more sense to delay reform efforts until a broader coalition can be formed and simultaneous repeal/replace package could be brought to both the House and the Senate floors.

In the new Congress, Senate Republicans might face some of the same obstructionist tactics they used during the Obama administration, which could complicate efforts to get bipartisan support.
“When you have people like Sen. [Bernie] Sanders (I-Vt.) and Sen. [Elizabeth] Warren (D-Mass.) saying they are going to adapt a scorched earth approach going forward, they and their followers don’t have any intention of doing anything that would in any way appear to cooperate with the Republicans,” Dr. Wilensky said. “Of course, there are other Democrats, especially some of the ones who will be up in 2018, who might not be quite so adamant.”

“Repeal without a clear idea of what the replacement would be would really throw that market into chaos, where right now we are at a place where the markets are relatively stable,” Dr. Collins said in an interview.“The best way to think about the ACA, and particularly on the marketplaces and what repeal means, is this image of the three-legged stool. The individual market is the seat and the legs include consumer protections, particularly guaranteed issue; the individual requirement to have insurance; and the subsidies to make that coverage affordable – Medicaid expansion is part of that as well. If you start to remove any one of those legs, the market becomes extremely unstable.”
Repealing the individual mandate is problematic as it goes hand in hand with the ban on coverage denial because of preexisting conditions, something President-elect Trump has signaled he is looking to maintain, Ms. Turner said, adding that free market solutions with appropriate incentives could be a different way to encourage healthy people to get coverage to help generate premium revenue to cover patients with preexisting conditions.
While the ACA will be in the crosshairs, experts expect MACRA to remain more or less intact, maybe with some minor tweaks, at least early on.
While the Medicare Access and CHIP Reauthorization Act of 2015 passed with overwhelming support from both parties, “the [implementing regulations] are just a nightmare and I think the Trump administration is going to have to take a look at them,” Ms. Turner said. She added that physicians are weary of the ever-growing federal administrative hassles. “You do not want doctors to leave private practice in droves, and they are looking at this cost of compliance.”
“I think that [MACRA] is just way too much of an in-the-weeds policy thing for the Trump administration to have addressed yet,” Ms. Turner continued. “But this certainly is going to have to be on the agenda because they are going to hear from a lot of doctors that this is not acceptable.”

Mr. Trump also has called for Medicaid reform, with block grants to the states.
“Everyone keeps talking about a block grant, but that is a clumsy way of doing it,” Ms. Turner said, suggesting the program be even more refined to cover people in different baskets, including dual-eligibles, healthy adults that were part of the ACA Medicaid expansion, mothers and infants, and disabled individuals. “A capitated allotment [allows the government to provide more support to] the people who need it.”
Dr. Wilensky suggested that the Trump administration could revisit the 1332 waiver process, another provision of the ACA.
“The current administration has taken a very-rigid view on that you have to keep savings from Medicaid and the ACA separate and any changes have to be budget neutral to each, which is an extremely rigid set of requirements,” she said. Instead “Medicaid and ACA savings could count together and it just needs to be budget neutral over a 3- or 5-year period. That would then allow states to come in and request a lot of flexibility that the current administration hasn’t been inclined to give them.”
Likewise, the Children’s Health Insurance Plan (CHIP) is up for reauthorization. While the program remains relatively popular, it could be due for some reforms as well. Dr. Wilensky said it might be time for the program to go away, though doing that would face resistance from congressional Democrats.
Likewise, Ms. Turner suggested it could be time to fold CHIP into another program like Medicaid.
“Does it really make sense for a mother who is overwhelmed, maybe even with two jobs, to have her kids on a different health insurance program than she’s on?” Ms. Turner said. “It just adds to the burden and the paperwork. Would it make more sense to blend some of these programs together, making sure the people get the health coverage they need, but without all these artificial silos that really make it much more difficult for the user at the other end. I think they are going to take a look at that.”
Whether the ACA is amended or repealed may affect some – but not all – of the ACA-related cases lingering in the courts.
Zubik v. Burwell for instance, may become irrelevant if President-elect Trump eliminates the ACA’s birth control mandate or its accommodation clause. Zubik centers on an exception to the birth control mandate for organizations that oppose coverage for contraceptives but are not exempted entities, such as churches. The plaintiffs argue that the government’s opt-out process makes them complicit in offering contraception coverage indirectly.

The Trump administration could choose to broaden the mandate’s exemption to include the religious organizations, thus satisfying the plaintiffs, said Timothy S. Jost, a health law professor at Washington and Lee University in Lexington, Va., who added that the case would become moot if the ACA is repealed wholesale.
“Millions of women [currently] get access to birth control without cost sharing through the Affordable Care Act,” he said in an interview. “That’s an issue [the new administration] is going to have to confront.”
In March, U.S. Supreme Court justices requested that both sides provide new briefs that outlined how contraception could be provided without requiring notice on the part of the suing employers. Then, in light of the briefs, the high court vacated the lower court rulings related to Zubik and remanded the case to the four appeals courts that had originally ruled on the issue.
If the case makes its way back to the Supreme Court, the ultimate ruling will largely depend on the makeup of the court at the time, said Eric D. Fader, a New York–based health law attorney.
“As long as we have a 4-4 Supreme Court, everything is up in the air,” Mr. Fader said in an interview. “As soon as that ninth slot is filled, I think we’re going to see some decisions that are going to be in line with traditional Republican conservative positions.”
However, a set of ACA-related cases that involve payments to insurers will continue litigating, regardless of actions by the new administration, analysts said. A half-dozen health insurers have sued the Health & Human Services department over alleged underpayments under the ACA’s risk corridor program.
“Even if you do away with the ACA, these cases all pertain to conduct that has already occurred, so they’re not going to be automatically moot,” Mr. Fader said in an interview. “They may struggle along for a while.”
The cases stem from the ACA’s risk corridor program, which requires HHS to collect funds from excessively profitable insurers that offer qualified health plans under the exchanges, while paying out funds to QHP insurers that have excessive losses. Collections from profitable insurers under the program fell short in 2014 and again in 2015, resulting in HHS paying about 12 cents on the dollar in payments to insurers.
The plaintiffs allege they’ve been shortchanged and that the government must reimburse them full payments for 2014. The Department of Justice (DOJ) argues the cases are premature because the full amount owed under the program is not due until 2016, after the program runs its course.
The Trump administration may surrender another ACA-linked challenge that questions billions in payments made to insurers, Mr. Jost said in an interview. In House v. Burwell, the House of Representatives accuses HHS of wrongly spending billions to repay insurers for health insurance provided to certain low-income patients under the ACA. The House claims HHS is illegally spending monies that Congress never appropriated. HHS argues that other statutory provisions of the ACA authorize expenditures for cost-sharing reimbursements. In May, the U.S. District Court for the District of Columbia decided in favor of the House, ruling that Congress never appropriated money for the payments and that no public money can be spent without an appropriation.
There is speculation that the Trump administration may not pursue an appeal, Mr. Jost said. “I think they better think long and hard about that because I don’t know why any president would want court precedent saying one house of Congress can sue the president whenever it disagrees,” he said. “If the Trump administration would give in on the lawsuit or the House would win … there would be some very large losses and some very large premium increases next year. There could be some very significant disruption of insurance markets.”
Again, if the ACA is repealed, the case may become irrelevant, Mr. Fader said. “If you get rid of the ACA and eliminate the cost sharing structure, than House v. Burwell is going to just be moot.”

“We have seen a substantial uptick in antitrust enforcement activity in health care over the last several years,” he said in an interview. “The Trump administration has said that one of its themes is reducing the regulatory burden on businesses. People will be watching to see if that means an attempt to back off of some of the more-aggressive antitrust enforcement activities in health care and other industries.”
The Obama administration is currently fighting to block two mega-mergers among four of the largest health insurers in the nation. The DOJ filed legal challenges earlier this year seeking to ban Anthem’s proposed acquisition of Cigna and Aetna’s proposed acquisition of Humana. The lawsuits allege the mergers – valued at $54 billion and $37 billion respectively – would negatively affect doctors, patients, and employers by limiting price competition, reducing benefits, and lowering quality of care. A majority of physician associations and patient groups oppose the mergers. But experts said the new administration could drop the challenges.
Similarly, the Trump administration could be more lax in its enforcement of the Stark Law. “You could certainly say if the administration is committed to reducing regulatory burden, one thing the administration might push forward is reducing some of the enforcement with respect to technical violations of Stark,” Mr. Horton said, noting that the Senate recently questioned if the government is going too far in regulating physician relationships under Stark. “If your theme is ‘Let’s cut back on regulation,’ that would be an area that you would think the administration would look at.”

Meanwhile, stronger medical malpractice reforms could be on the horizon in light of a Republican-controlled Congress. Tort reform advocates have a good chance at passing federal medical liability reforms that were left out of the ACA’s passage in 2010, said Dennis A. Cardoza, public affairs director and cochair of the federal public affairs practice at a national health law firm.
Earlier versions of the ACA included amendments that mandated lawsuits go through a state or federal alternative dispute resolution system prior to being filed in court. Another provision that failed would have provided federal grants to states that created special health courts for medical malpractice claims. The amendment would have allowed states to create expert panels, administrative health care tribunals, or a combination of the two.
“There’s much stronger support for tort reform among the Republicans in Congress,” Mr. Cardoza said in an interview. “There’s a shot [now]. If the reforms don’t go too far where they would penalize injured patients, I think they could get additional support and be well received by the Congress.”
Tougher abortion restrictions are likely under the Trump administration, experts said. President-elect Trump has said he is committed to nominating a ninth Supreme Court justice who opposes Roe v. Wade.

Vice President-elect Mike Pence, who is considered a strong voice for the religious right, will likely influence who Mr. Trump nominates for the high court, said Rep-elect Raskin, who added that if ever there was time that abortion rights are in jeopardy, it’s now.
“This really puts the Republicans to the test,” he said in an interview. “For decades now, they have been calling for the overruling of Roe v. Wade. The religious right will never forgive them if it doesn’t happen now. [Republicans] control the House, the Senate, and the White House. They have it within their reach to create a five-justice majority on the court.”
[email protected]
[email protected]
On Twitter @legal_med
Look for three things from the Trump administration: significant changes to the Affordable Care Act, few changes to MACRA’s Quality Payment Program, and a conservative swing in the courts.
Republicans have had their sights on the Affordable Care Act since its passage in 2010; with majorities in both the House and the Senate, the question is not if, but when President Obama’s signature piece of legislation will be dismantled.
President-elect Donald Trump ran on the promise of ACA repeal. Health policy priorities on his transition website focus on greater use of health savings accounts, the ability to purchase insurance across state lines, and the reestablishment of high-risk pools.
Health policy experts differ in how they see ACA reform coming about, with some predicting a quick repeal coupled with an immediate legislative replacement, while others envision repeal with more time to craft replacement legislation. Reform also could come as a series of smaller bills rather than one comprehensive package.
Using budget reconciliation would not allow for full ACA repeal since only provisions that involve revenue generation or spending could be altered. However, since budget reconciliation bills cannot be filibustered, only a simple majority is needed for Senate passage. With their razor-thin majority – 51 seats – Republicans will need some support from outside of their own party.
“Twenty-some Democrats, many in very-deep ‘red states’ including North Dakota, are up for reelection in 2018,” Ms. Turner said. “They saw what happened to the candidates who supported Obamacare in 2016 – many of them went down. It happened with Evan Bayh in Indiana, who was running again to reclaim the Senate seat he left in 2010. And the Republican candidate [Todd Young] reminded the voters over and over that Evan Bayh voted for Obamacare. Same thing happened in Wisconsin with [Republican] Sen. Ron Johnson being challenged by Russ Feingold, who also was in the Senate when Obamacare passed. Feingold went down to defeat again. I think the lot of Democratic senators are going to be looking at what happened to those people and think ‘Maybe I better participate in coming up with a more sensible solution.’ ”
More importantly, the GOP may be looking for bipartisan support, especially since the ACA passed on a strict party-line vote. To that end, it could make more sense to delay reform efforts until a broader coalition can be formed and simultaneous repeal/replace package could be brought to both the House and the Senate floors.
In the new Congress, Senate Republicans might face some of the same obstructionist tactics they used during the Obama administration, which could complicate efforts to get bipartisan support.
“When you have people like Sen. [Bernie] Sanders (I-Vt.) and Sen. [Elizabeth] Warren (D-Mass.) saying they are going to adapt a scorched earth approach going forward, they and their followers don’t have any intention of doing anything that would in any way appear to cooperate with the Republicans,” Dr. Wilensky said. “Of course, there are other Democrats, especially some of the ones who will be up in 2018, who might not be quite so adamant.”
“Repeal without a clear idea of what the replacement would be would really throw that market into chaos, where right now we are at a place where the markets are relatively stable,” Dr. Collins said in an interview.“The best way to think about the ACA, and particularly on the marketplaces and what repeal means, is this image of the three-legged stool. The individual market is the seat and the legs include consumer protections, particularly guaranteed issue; the individual requirement to have insurance; and the subsidies to make that coverage affordable – Medicaid expansion is part of that as well. If you start to remove any one of those legs, the market becomes extremely unstable.”
Repealing the individual mandate is problematic as it goes hand in hand with the ban on coverage denial because of preexisting conditions, something President-elect Trump has signaled he is looking to maintain, Ms. Turner said, adding that free market solutions with appropriate incentives could be a different way to encourage healthy people to get coverage to help generate premium revenue to cover patients with preexisting conditions.
While the ACA will be in the crosshairs, experts expect MACRA to remain more or less intact, maybe with some minor tweaks, at least early on.
While the Medicare Access and CHIP Reauthorization Act of 2015 passed with overwhelming support from both parties, “the [implementing regulations] are just a nightmare and I think the Trump administration is going to have to take a look at them,” Ms. Turner said. She added that physicians are weary of the ever-growing federal administrative hassles. “You do not want doctors to leave private practice in droves, and they are looking at this cost of compliance.”
“I think that [MACRA] is just way too much of an in-the-weeds policy thing for the Trump administration to have addressed yet,” Ms. Turner continued. “But this certainly is going to have to be on the agenda because they are going to hear from a lot of doctors that this is not acceptable.”
Mr. Trump also has called for Medicaid reform, with block grants to the states.
“Everyone keeps talking about a block grant, but that is a clumsy way of doing it,” Ms. Turner said, suggesting the program be even more refined to cover people in different baskets, including dual-eligibles, healthy adults that were part of the ACA Medicaid expansion, mothers and infants, and disabled individuals. “A capitated allotment [allows the government to provide more support to] the people who need it.”
Dr. Wilensky suggested that the Trump administration could revisit the 1332 waiver process, another provision of the ACA.
“The current administration has taken a very-rigid view on that you have to keep savings from Medicaid and the ACA separate and any changes have to be budget neutral to each, which is an extremely rigid set of requirements,” she said. Instead “Medicaid and ACA savings could count together and it just needs to be budget neutral over a 3- or 5-year period. That would then allow states to come in and request a lot of flexibility that the current administration hasn’t been inclined to give them.”
Likewise, the Children’s Health Insurance Plan (CHIP) is up for reauthorization. While the program remains relatively popular, it could be due for some reforms as well. Dr. Wilensky said it might be time for the program to go away, though doing that would face resistance from congressional Democrats.
Likewise, Ms. Turner suggested it could be time to fold CHIP into another program like Medicaid.
“Does it really make sense for a mother who is overwhelmed, maybe even with two jobs, to have her kids on a different health insurance program than she’s on?” Ms. Turner said. “It just adds to the burden and the paperwork. Would it make more sense to blend some of these programs together, making sure the people get the health coverage they need, but without all these artificial silos that really make it much more difficult for the user at the other end. I think they are going to take a look at that.”
Whether the ACA is amended or repealed may affect some – but not all – of the ACA-related cases lingering in the courts.
Zubik v. Burwell for instance, may become irrelevant if President-elect Trump eliminates the ACA’s birth control mandate or its accommodation clause. Zubik centers on an exception to the birth control mandate for organizations that oppose coverage for contraceptives but are not exempted entities, such as churches. The plaintiffs argue that the government’s opt-out process makes them complicit in offering contraception coverage indirectly.
The Trump administration could choose to broaden the mandate’s exemption to include the religious organizations, thus satisfying the plaintiffs, said Timothy S. Jost, a health law professor at Washington and Lee University in Lexington, Va., who added that the case would become moot if the ACA is repealed wholesale.
“Millions of women [currently] get access to birth control without cost sharing through the Affordable Care Act,” he said in an interview. “That’s an issue [the new administration] is going to have to confront.”
In March, U.S. Supreme Court justices requested that both sides provide new briefs that outlined how contraception could be provided without requiring notice on the part of the suing employers. Then, in light of the briefs, the high court vacated the lower court rulings related to Zubik and remanded the case to the four appeals courts that had originally ruled on the issue.
If the case makes its way back to the Supreme Court, the ultimate ruling will largely depend on the makeup of the court at the time, said Eric D. Fader, a New York–based health law attorney.
“As long as we have a 4-4 Supreme Court, everything is up in the air,” Mr. Fader said in an interview. “As soon as that ninth slot is filled, I think we’re going to see some decisions that are going to be in line with traditional Republican conservative positions.”
However, a set of ACA-related cases that involve payments to insurers will continue litigating, regardless of actions by the new administration, analysts said. A half-dozen health insurers have sued the Health & Human Services department over alleged underpayments under the ACA’s risk corridor program.
“Even if you do away with the ACA, these cases all pertain to conduct that has already occurred, so they’re not going to be automatically moot,” Mr. Fader said in an interview. “They may struggle along for a while.”
The cases stem from the ACA’s risk corridor program, which requires HHS to collect funds from excessively profitable insurers that offer qualified health plans under the exchanges, while paying out funds to QHP insurers that have excessive losses. Collections from profitable insurers under the program fell short in 2014 and again in 2015, resulting in HHS paying about 12 cents on the dollar in payments to insurers.
The plaintiffs allege they’ve been shortchanged and that the government must reimburse them full payments for 2014. The Department of Justice (DOJ) argues the cases are premature because the full amount owed under the program is not due until 2016, after the program runs its course.
The Trump administration may surrender another ACA-linked challenge that questions billions in payments made to insurers, Mr. Jost said in an interview. In House v. Burwell, the House of Representatives accuses HHS of wrongly spending billions to repay insurers for health insurance provided to certain low-income patients under the ACA. The House claims HHS is illegally spending monies that Congress never appropriated. HHS argues that other statutory provisions of the ACA authorize expenditures for cost-sharing reimbursements. In May, the U.S. District Court for the District of Columbia decided in favor of the House, ruling that Congress never appropriated money for the payments and that no public money can be spent without an appropriation.
There is speculation that the Trump administration may not pursue an appeal, Mr. Jost said. “I think they better think long and hard about that because I don’t know why any president would want court precedent saying one house of Congress can sue the president whenever it disagrees,” he said. “If the Trump administration would give in on the lawsuit or the House would win … there would be some very large losses and some very large premium increases next year. There could be some very significant disruption of insurance markets.”
Again, if the ACA is repealed, the case may become irrelevant, Mr. Fader said. “If you get rid of the ACA and eliminate the cost sharing structure, than House v. Burwell is going to just be moot.”
“We have seen a substantial uptick in antitrust enforcement activity in health care over the last several years,” he said in an interview. “The Trump administration has said that one of its themes is reducing the regulatory burden on businesses. People will be watching to see if that means an attempt to back off of some of the more-aggressive antitrust enforcement activities in health care and other industries.”
The Obama administration is currently fighting to block two mega-mergers among four of the largest health insurers in the nation. The DOJ filed legal challenges earlier this year seeking to ban Anthem’s proposed acquisition of Cigna and Aetna’s proposed acquisition of Humana. The lawsuits allege the mergers – valued at $54 billion and $37 billion respectively – would negatively affect doctors, patients, and employers by limiting price competition, reducing benefits, and lowering quality of care. A majority of physician associations and patient groups oppose the mergers. But experts said the new administration could drop the challenges.
Similarly, the Trump administration could be more lax in its enforcement of the Stark Law. “You could certainly say if the administration is committed to reducing regulatory burden, one thing the administration might push forward is reducing some of the enforcement with respect to technical violations of Stark,” Mr. Horton said, noting that the Senate recently questioned if the government is going too far in regulating physician relationships under Stark. “If your theme is ‘Let’s cut back on regulation,’ that would be an area that you would think the administration would look at.”
Meanwhile, stronger medical malpractice reforms could be on the horizon in light of a Republican-controlled Congress. Tort reform advocates have a good chance at passing federal medical liability reforms that were left out of the ACA’s passage in 2010, said Dennis A. Cardoza, public affairs director and cochair of the federal public affairs practice at a national health law firm.
Earlier versions of the ACA included amendments that mandated lawsuits go through a state or federal alternative dispute resolution system prior to being filed in court. Another provision that failed would have provided federal grants to states that created special health courts for medical malpractice claims. The amendment would have allowed states to create expert panels, administrative health care tribunals, or a combination of the two.
“There’s much stronger support for tort reform among the Republicans in Congress,” Mr. Cardoza said in an interview. “There’s a shot [now]. If the reforms don’t go too far where they would penalize injured patients, I think they could get additional support and be well received by the Congress.”
Tougher abortion restrictions are likely under the Trump administration, experts said. President-elect Trump has said he is committed to nominating a ninth Supreme Court justice who opposes Roe v. Wade.
Vice President-elect Mike Pence, who is considered a strong voice for the religious right, will likely influence who Mr. Trump nominates for the high court, said Rep-elect Raskin, who added that if ever there was time that abortion rights are in jeopardy, it’s now.
“This really puts the Republicans to the test,” he said in an interview. “For decades now, they have been calling for the overruling of Roe v. Wade. The religious right will never forgive them if it doesn’t happen now. [Republicans] control the House, the Senate, and the White House. They have it within their reach to create a five-justice majority on the court.”
[email protected]
[email protected]
On Twitter @legal_med
Look for three things from the Trump administration: significant changes to the Affordable Care Act, few changes to MACRA’s Quality Payment Program, and a conservative swing in the courts.
Republicans have had their sights on the Affordable Care Act since its passage in 2010; with majorities in both the House and the Senate, the question is not if, but when President Obama’s signature piece of legislation will be dismantled.
President-elect Donald Trump ran on the promise of ACA repeal. Health policy priorities on his transition website focus on greater use of health savings accounts, the ability to purchase insurance across state lines, and the reestablishment of high-risk pools.
Health policy experts differ in how they see ACA reform coming about, with some predicting a quick repeal coupled with an immediate legislative replacement, while others envision repeal with more time to craft replacement legislation. Reform also could come as a series of smaller bills rather than one comprehensive package.
Using budget reconciliation would not allow for full ACA repeal since only provisions that involve revenue generation or spending could be altered. However, since budget reconciliation bills cannot be filibustered, only a simple majority is needed for Senate passage. With their razor-thin majority – 51 seats – Republicans will need some support from outside of their own party.
“Twenty-some Democrats, many in very-deep ‘red states’ including North Dakota, are up for reelection in 2018,” Ms. Turner said. “They saw what happened to the candidates who supported Obamacare in 2016 – many of them went down. It happened with Evan Bayh in Indiana, who was running again to reclaim the Senate seat he left in 2010. And the Republican candidate [Todd Young] reminded the voters over and over that Evan Bayh voted for Obamacare. Same thing happened in Wisconsin with [Republican] Sen. Ron Johnson being challenged by Russ Feingold, who also was in the Senate when Obamacare passed. Feingold went down to defeat again. I think the lot of Democratic senators are going to be looking at what happened to those people and think ‘Maybe I better participate in coming up with a more sensible solution.’ ”
More importantly, the GOP may be looking for bipartisan support, especially since the ACA passed on a strict party-line vote. To that end, it could make more sense to delay reform efforts until a broader coalition can be formed and simultaneous repeal/replace package could be brought to both the House and the Senate floors.
In the new Congress, Senate Republicans might face some of the same obstructionist tactics they used during the Obama administration, which could complicate efforts to get bipartisan support.
“When you have people like Sen. [Bernie] Sanders (I-Vt.) and Sen. [Elizabeth] Warren (D-Mass.) saying they are going to adapt a scorched earth approach going forward, they and their followers don’t have any intention of doing anything that would in any way appear to cooperate with the Republicans,” Dr. Wilensky said. “Of course, there are other Democrats, especially some of the ones who will be up in 2018, who might not be quite so adamant.”
“Repeal without a clear idea of what the replacement would be would really throw that market into chaos, where right now we are at a place where the markets are relatively stable,” Dr. Collins said in an interview.“The best way to think about the ACA, and particularly on the marketplaces and what repeal means, is this image of the three-legged stool. The individual market is the seat and the legs include consumer protections, particularly guaranteed issue; the individual requirement to have insurance; and the subsidies to make that coverage affordable – Medicaid expansion is part of that as well. If you start to remove any one of those legs, the market becomes extremely unstable.”
Repealing the individual mandate is problematic as it goes hand in hand with the ban on coverage denial because of preexisting conditions, something President-elect Trump has signaled he is looking to maintain, Ms. Turner said, adding that free market solutions with appropriate incentives could be a different way to encourage healthy people to get coverage to help generate premium revenue to cover patients with preexisting conditions.
While the ACA will be in the crosshairs, experts expect MACRA to remain more or less intact, maybe with some minor tweaks, at least early on.
While the Medicare Access and CHIP Reauthorization Act of 2015 passed with overwhelming support from both parties, “the [implementing regulations] are just a nightmare and I think the Trump administration is going to have to take a look at them,” Ms. Turner said. She added that physicians are weary of the ever-growing federal administrative hassles. “You do not want doctors to leave private practice in droves, and they are looking at this cost of compliance.”
“I think that [MACRA] is just way too much of an in-the-weeds policy thing for the Trump administration to have addressed yet,” Ms. Turner continued. “But this certainly is going to have to be on the agenda because they are going to hear from a lot of doctors that this is not acceptable.”
Mr. Trump also has called for Medicaid reform, with block grants to the states.
“Everyone keeps talking about a block grant, but that is a clumsy way of doing it,” Ms. Turner said, suggesting the program be even more refined to cover people in different baskets, including dual-eligibles, healthy adults that were part of the ACA Medicaid expansion, mothers and infants, and disabled individuals. “A capitated allotment [allows the government to provide more support to] the people who need it.”
Dr. Wilensky suggested that the Trump administration could revisit the 1332 waiver process, another provision of the ACA.
“The current administration has taken a very-rigid view on that you have to keep savings from Medicaid and the ACA separate and any changes have to be budget neutral to each, which is an extremely rigid set of requirements,” she said. Instead “Medicaid and ACA savings could count together and it just needs to be budget neutral over a 3- or 5-year period. That would then allow states to come in and request a lot of flexibility that the current administration hasn’t been inclined to give them.”
Likewise, the Children’s Health Insurance Plan (CHIP) is up for reauthorization. While the program remains relatively popular, it could be due for some reforms as well. Dr. Wilensky said it might be time for the program to go away, though doing that would face resistance from congressional Democrats.
Likewise, Ms. Turner suggested it could be time to fold CHIP into another program like Medicaid.
“Does it really make sense for a mother who is overwhelmed, maybe even with two jobs, to have her kids on a different health insurance program than she’s on?” Ms. Turner said. “It just adds to the burden and the paperwork. Would it make more sense to blend some of these programs together, making sure the people get the health coverage they need, but without all these artificial silos that really make it much more difficult for the user at the other end. I think they are going to take a look at that.”
Whether the ACA is amended or repealed may affect some – but not all – of the ACA-related cases lingering in the courts.
Zubik v. Burwell for instance, may become irrelevant if President-elect Trump eliminates the ACA’s birth control mandate or its accommodation clause. Zubik centers on an exception to the birth control mandate for organizations that oppose coverage for contraceptives but are not exempted entities, such as churches. The plaintiffs argue that the government’s opt-out process makes them complicit in offering contraception coverage indirectly.
The Trump administration could choose to broaden the mandate’s exemption to include the religious organizations, thus satisfying the plaintiffs, said Timothy S. Jost, a health law professor at Washington and Lee University in Lexington, Va., who added that the case would become moot if the ACA is repealed wholesale.
“Millions of women [currently] get access to birth control without cost sharing through the Affordable Care Act,” he said in an interview. “That’s an issue [the new administration] is going to have to confront.”
In March, U.S. Supreme Court justices requested that both sides provide new briefs that outlined how contraception could be provided without requiring notice on the part of the suing employers. Then, in light of the briefs, the high court vacated the lower court rulings related to Zubik and remanded the case to the four appeals courts that had originally ruled on the issue.
If the case makes its way back to the Supreme Court, the ultimate ruling will largely depend on the makeup of the court at the time, said Eric D. Fader, a New York–based health law attorney.
“As long as we have a 4-4 Supreme Court, everything is up in the air,” Mr. Fader said in an interview. “As soon as that ninth slot is filled, I think we’re going to see some decisions that are going to be in line with traditional Republican conservative positions.”
However, a set of ACA-related cases that involve payments to insurers will continue litigating, regardless of actions by the new administration, analysts said. A half-dozen health insurers have sued the Health & Human Services department over alleged underpayments under the ACA’s risk corridor program.
“Even if you do away with the ACA, these cases all pertain to conduct that has already occurred, so they’re not going to be automatically moot,” Mr. Fader said in an interview. “They may struggle along for a while.”
The cases stem from the ACA’s risk corridor program, which requires HHS to collect funds from excessively profitable insurers that offer qualified health plans under the exchanges, while paying out funds to QHP insurers that have excessive losses. Collections from profitable insurers under the program fell short in 2014 and again in 2015, resulting in HHS paying about 12 cents on the dollar in payments to insurers.
The plaintiffs allege they’ve been shortchanged and that the government must reimburse them full payments for 2014. The Department of Justice (DOJ) argues the cases are premature because the full amount owed under the program is not due until 2016, after the program runs its course.
The Trump administration may surrender another ACA-linked challenge that questions billions in payments made to insurers, Mr. Jost said in an interview. In House v. Burwell, the House of Representatives accuses HHS of wrongly spending billions to repay insurers for health insurance provided to certain low-income patients under the ACA. The House claims HHS is illegally spending monies that Congress never appropriated. HHS argues that other statutory provisions of the ACA authorize expenditures for cost-sharing reimbursements. In May, the U.S. District Court for the District of Columbia decided in favor of the House, ruling that Congress never appropriated money for the payments and that no public money can be spent without an appropriation.
There is speculation that the Trump administration may not pursue an appeal, Mr. Jost said. “I think they better think long and hard about that because I don’t know why any president would want court precedent saying one house of Congress can sue the president whenever it disagrees,” he said. “If the Trump administration would give in on the lawsuit or the House would win … there would be some very large losses and some very large premium increases next year. There could be some very significant disruption of insurance markets.”
Again, if the ACA is repealed, the case may become irrelevant, Mr. Fader said. “If you get rid of the ACA and eliminate the cost sharing structure, than House v. Burwell is going to just be moot.”
“We have seen a substantial uptick in antitrust enforcement activity in health care over the last several years,” he said in an interview. “The Trump administration has said that one of its themes is reducing the regulatory burden on businesses. People will be watching to see if that means an attempt to back off of some of the more-aggressive antitrust enforcement activities in health care and other industries.”
The Obama administration is currently fighting to block two mega-mergers among four of the largest health insurers in the nation. The DOJ filed legal challenges earlier this year seeking to ban Anthem’s proposed acquisition of Cigna and Aetna’s proposed acquisition of Humana. The lawsuits allege the mergers – valued at $54 billion and $37 billion respectively – would negatively affect doctors, patients, and employers by limiting price competition, reducing benefits, and lowering quality of care. A majority of physician associations and patient groups oppose the mergers. But experts said the new administration could drop the challenges.
Similarly, the Trump administration could be more lax in its enforcement of the Stark Law. “You could certainly say if the administration is committed to reducing regulatory burden, one thing the administration might push forward is reducing some of the enforcement with respect to technical violations of Stark,” Mr. Horton said, noting that the Senate recently questioned if the government is going too far in regulating physician relationships under Stark. “If your theme is ‘Let’s cut back on regulation,’ that would be an area that you would think the administration would look at.”
Meanwhile, stronger medical malpractice reforms could be on the horizon in light of a Republican-controlled Congress. Tort reform advocates have a good chance at passing federal medical liability reforms that were left out of the ACA’s passage in 2010, said Dennis A. Cardoza, public affairs director and cochair of the federal public affairs practice at a national health law firm.
Earlier versions of the ACA included amendments that mandated lawsuits go through a state or federal alternative dispute resolution system prior to being filed in court. Another provision that failed would have provided federal grants to states that created special health courts for medical malpractice claims. The amendment would have allowed states to create expert panels, administrative health care tribunals, or a combination of the two.
“There’s much stronger support for tort reform among the Republicans in Congress,” Mr. Cardoza said in an interview. “There’s a shot [now]. If the reforms don’t go too far where they would penalize injured patients, I think they could get additional support and be well received by the Congress.”
Tougher abortion restrictions are likely under the Trump administration, experts said. President-elect Trump has said he is committed to nominating a ninth Supreme Court justice who opposes Roe v. Wade.
Vice President-elect Mike Pence, who is considered a strong voice for the religious right, will likely influence who Mr. Trump nominates for the high court, said Rep-elect Raskin, who added that if ever there was time that abortion rights are in jeopardy, it’s now.
“This really puts the Republicans to the test,” he said in an interview. “For decades now, they have been calling for the overruling of Roe v. Wade. The religious right will never forgive them if it doesn’t happen now. [Republicans] control the House, the Senate, and the White House. They have it within their reach to create a five-justice majority on the court.”
[email protected]
[email protected]
On Twitter @legal_med
Trump HHS nominee could curb regulations, reshape health insurance
Opinions are mixed on what the nominations of Rep. Tom Price (R-Ga.) as Secretary of Health & Human Services will mean for medicine and health care.
An orthopedic surgeon and six-term congressman, Dr. Price is an outspoken critic of the Affordable Care Act and has sponsored or cosponsored numerous bills to replace it. President-elect Trump called Rep. Price “a renowned physician” who has “earned a reputation for being a tireless problem solver and the go-to expert on health care policy,” according to a statement.
Not everyone agrees.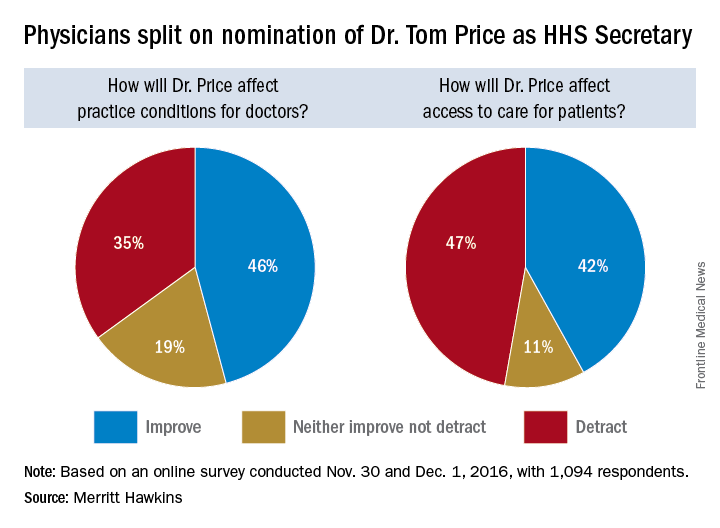
But Adam Gaffney, MD, a pulmonologist at the Cambridge (Mass.) Health Alliance, said physicians’ ability to care for their patients would be compromised if Rep. Price succeeds with many of his proposals, such as the privatization of Medicare and block grants for Medicaid.
“If these reforms go through, we’re going to see the insurance protections of our patients get worse,” said Dr. Gaffney, a board member for Physicians for a National Health Program, which advocates for a single-payer health care system. “If [his] agenda is successful, I think it’s going to have a detrimental impact on our ability to provide the care that our patients need.”
ACA repeal, malpractice reform
In the House, Rep. Price has introduced the Empowering Patients First Act, legislation, which would allow doctors to opt out of Medicare and enter into private contracts with Medicare patients. The bill is seen by many as a potential blueprint for Trump administration health reform. Rep. Price is also a proponent of malpractice reform that would make it tougher for patients to sue doctors and would lower liability insurance premiums.
The Empowering Patients First Act would repeal the ACA and offer tax credits for the purchase of individual and family health insurance policies. It would also create incentives for patients to contribute to health savings accounts, offer state grants to subsidize coverage for high-risk patients, and authorize businesses to cover members through association health plans.
The American Medical Association praised Rep. Price’s nomination, expressing support for ability to lead HHS.
“Dr. Price has been a leader in the development of health policies to advance patient choice and market-based solutions as well as reduce excessive regulatory burdens that diminish time devoted to patient care and increase costs,” AMA Board of Trustees Chair Patrice A. Harris, MD, said in a statement.
The American College of Surgeons' Executive Director, David B. Hoyt, MD, FACS, issued a supportive statement about the nomination of Dr. Price. "“Dr. Price is a stalwart champion for patients and their surgeons, and the ACS looks forward to working with him on key issues, such as the implementation of the Medicare Access and CHIP Reauthorization Act,” said Dr. Hoyt in a statement. “The ACS encourages the Senate to swiftly confirm Dr. Price’s nomination as Secretary of HHS."
But thousands of physicians disagree. Rep. Price’s proposals on Medicaid and Medicare threaten to harm vulnerable patients and limit access to healthcare, according to an open letter to the AMA published on Medium and credited to Clinician Action Network, a nonpartisan group that supports evidence-based policies. The group was started in opposition to the nomination of Rep. Price.
“We cannot support the dismantling of Medicaid, which has helped 15 million Americans gain health coverage since 2014,” the letter states. “We oppose Dr. Price’s proposals to reduce funding for the Children’s Health Insurance Program, a critical mechanism by which poor children access preventative care.”
Value-based payment or fee for service?
Rep. Price’s experience as a physician fuels his efforts to reduce burdensome regulations for doctors and enhance care efficiency, according to one of his predecessors, Louis W. Sullivan, MD. If confirmed, Rep. Price will become the third physician to be HHS secretary; Dr. Sullivan served in the George H.W. Bush administration and Otis R. Bowen, MD, served in the Reagan administration.
“He is very much aware of the challenges that physicians face in trying to delivery care,” said Dr. Sullivan. “I know that he’ll be working to reduce regulation when feasible so that the cost and delays that some regulatory issues present will hopefully be relieved,”
Some of those regulatory modifications could affect value-based care programs, Dr. Rodriguez said. Rep. Price has been critical of the move from fee for service to quality-based care and has opposed some corresponding programs, such as bundled payment initiatives. Rep. Price and members of the GOP Doctors Caucus wrote to Centers for Medicare & Medicaid Services in October to protest the regulations to implement the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) as too burdensome for smaller practices and calling for flexibility in quality reporting.
Rep. Price voted for passage of MACRA.
“He has been cautious about some of the changes that are being promoted in health care,” Dr. Rodriguez said. “He could slow that down – the processes being put in place. That might delay the impact those systems have in bringing about the improved quality that we want. [This would be] enormous, given the amount of work that we’ve been doing.”
A fair medical liability system also is a priority for Rep. Price, Dr. Sullivan said. His Empowering Patients First bill would require collaboration between HHS and physician associations to develop best practice guidelines that would provide a litigation safe harbor to physicians who practiced in accordance with the standards.
“I know that he will be working to develop strategies to reduce litigation in the health space,” Dr. Sullivan said in an interview. “That is one of the challenges that adds to health care costs, adds tension, and enhances an adversarial relationship between physicians and patients.”
But Dr. Gaffney said that he believes Rep. Price’s views on reproductive rights and gay marriage are regressive and that his agenda regarding health policy issues is bad for medicine.
“The overall [theme] of that agenda can be summed up as ‘take from the poor and sick and give to the rich,’ ” Dr. Gaffney said in an interview. “I think the financing of this [new health reform] system will be much more aggressive, and the result will be greater health care inequity.”
Rep. Price also has supported a ban on federal funding for Planned Parenthood, calling some of their practices barbaric. He has also voted to prohibit the importation of prescription drugs by nonsanctioned importers and has voted to repeal the medical device excise tax.
[email protected]
On Twitter @legal_med
Opinions are mixed on what the nominations of Rep. Tom Price (R-Ga.) as Secretary of Health & Human Services will mean for medicine and health care.
An orthopedic surgeon and six-term congressman, Dr. Price is an outspoken critic of the Affordable Care Act and has sponsored or cosponsored numerous bills to replace it. President-elect Trump called Rep. Price “a renowned physician” who has “earned a reputation for being a tireless problem solver and the go-to expert on health care policy,” according to a statement.
Not everyone agrees.
But Adam Gaffney, MD, a pulmonologist at the Cambridge (Mass.) Health Alliance, said physicians’ ability to care for their patients would be compromised if Rep. Price succeeds with many of his proposals, such as the privatization of Medicare and block grants for Medicaid.
“If these reforms go through, we’re going to see the insurance protections of our patients get worse,” said Dr. Gaffney, a board member for Physicians for a National Health Program, which advocates for a single-payer health care system. “If [his] agenda is successful, I think it’s going to have a detrimental impact on our ability to provide the care that our patients need.”
ACA repeal, malpractice reform
In the House, Rep. Price has introduced the Empowering Patients First Act, legislation, which would allow doctors to opt out of Medicare and enter into private contracts with Medicare patients. The bill is seen by many as a potential blueprint for Trump administration health reform. Rep. Price is also a proponent of malpractice reform that would make it tougher for patients to sue doctors and would lower liability insurance premiums.
The Empowering Patients First Act would repeal the ACA and offer tax credits for the purchase of individual and family health insurance policies. It would also create incentives for patients to contribute to health savings accounts, offer state grants to subsidize coverage for high-risk patients, and authorize businesses to cover members through association health plans.
The American Medical Association praised Rep. Price’s nomination, expressing support for ability to lead HHS.
“Dr. Price has been a leader in the development of health policies to advance patient choice and market-based solutions as well as reduce excessive regulatory burdens that diminish time devoted to patient care and increase costs,” AMA Board of Trustees Chair Patrice A. Harris, MD, said in a statement.
The American College of Surgeons' Executive Director, David B. Hoyt, MD, FACS, issued a supportive statement about the nomination of Dr. Price. "“Dr. Price is a stalwart champion for patients and their surgeons, and the ACS looks forward to working with him on key issues, such as the implementation of the Medicare Access and CHIP Reauthorization Act,” said Dr. Hoyt in a statement. “The ACS encourages the Senate to swiftly confirm Dr. Price’s nomination as Secretary of HHS."
But thousands of physicians disagree. Rep. Price’s proposals on Medicaid and Medicare threaten to harm vulnerable patients and limit access to healthcare, according to an open letter to the AMA published on Medium and credited to Clinician Action Network, a nonpartisan group that supports evidence-based policies. The group was started in opposition to the nomination of Rep. Price.
“We cannot support the dismantling of Medicaid, which has helped 15 million Americans gain health coverage since 2014,” the letter states. “We oppose Dr. Price’s proposals to reduce funding for the Children’s Health Insurance Program, a critical mechanism by which poor children access preventative care.”
Value-based payment or fee for service?
Rep. Price’s experience as a physician fuels his efforts to reduce burdensome regulations for doctors and enhance care efficiency, according to one of his predecessors, Louis W. Sullivan, MD. If confirmed, Rep. Price will become the third physician to be HHS secretary; Dr. Sullivan served in the George H.W. Bush administration and Otis R. Bowen, MD, served in the Reagan administration.
“He is very much aware of the challenges that physicians face in trying to delivery care,” said Dr. Sullivan. “I know that he’ll be working to reduce regulation when feasible so that the cost and delays that some regulatory issues present will hopefully be relieved,”
Some of those regulatory modifications could affect value-based care programs, Dr. Rodriguez said. Rep. Price has been critical of the move from fee for service to quality-based care and has opposed some corresponding programs, such as bundled payment initiatives. Rep. Price and members of the GOP Doctors Caucus wrote to Centers for Medicare & Medicaid Services in October to protest the regulations to implement the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) as too burdensome for smaller practices and calling for flexibility in quality reporting.
Rep. Price voted for passage of MACRA.
“He has been cautious about some of the changes that are being promoted in health care,” Dr. Rodriguez said. “He could slow that down – the processes being put in place. That might delay the impact those systems have in bringing about the improved quality that we want. [This would be] enormous, given the amount of work that we’ve been doing.”
A fair medical liability system also is a priority for Rep. Price, Dr. Sullivan said. His Empowering Patients First bill would require collaboration between HHS and physician associations to develop best practice guidelines that would provide a litigation safe harbor to physicians who practiced in accordance with the standards.
“I know that he will be working to develop strategies to reduce litigation in the health space,” Dr. Sullivan said in an interview. “That is one of the challenges that adds to health care costs, adds tension, and enhances an adversarial relationship between physicians and patients.”
But Dr. Gaffney said that he believes Rep. Price’s views on reproductive rights and gay marriage are regressive and that his agenda regarding health policy issues is bad for medicine.
“The overall [theme] of that agenda can be summed up as ‘take from the poor and sick and give to the rich,’ ” Dr. Gaffney said in an interview. “I think the financing of this [new health reform] system will be much more aggressive, and the result will be greater health care inequity.”
Rep. Price also has supported a ban on federal funding for Planned Parenthood, calling some of their practices barbaric. He has also voted to prohibit the importation of prescription drugs by nonsanctioned importers and has voted to repeal the medical device excise tax.
[email protected]
On Twitter @legal_med
Opinions are mixed on what the nominations of Rep. Tom Price (R-Ga.) as Secretary of Health & Human Services will mean for medicine and health care.
An orthopedic surgeon and six-term congressman, Dr. Price is an outspoken critic of the Affordable Care Act and has sponsored or cosponsored numerous bills to replace it. President-elect Trump called Rep. Price “a renowned physician” who has “earned a reputation for being a tireless problem solver and the go-to expert on health care policy,” according to a statement.
Not everyone agrees.
But Adam Gaffney, MD, a pulmonologist at the Cambridge (Mass.) Health Alliance, said physicians’ ability to care for their patients would be compromised if Rep. Price succeeds with many of his proposals, such as the privatization of Medicare and block grants for Medicaid.
“If these reforms go through, we’re going to see the insurance protections of our patients get worse,” said Dr. Gaffney, a board member for Physicians for a National Health Program, which advocates for a single-payer health care system. “If [his] agenda is successful, I think it’s going to have a detrimental impact on our ability to provide the care that our patients need.”
ACA repeal, malpractice reform
In the House, Rep. Price has introduced the Empowering Patients First Act, legislation, which would allow doctors to opt out of Medicare and enter into private contracts with Medicare patients. The bill is seen by many as a potential blueprint for Trump administration health reform. Rep. Price is also a proponent of malpractice reform that would make it tougher for patients to sue doctors and would lower liability insurance premiums.
The Empowering Patients First Act would repeal the ACA and offer tax credits for the purchase of individual and family health insurance policies. It would also create incentives for patients to contribute to health savings accounts, offer state grants to subsidize coverage for high-risk patients, and authorize businesses to cover members through association health plans.
The American Medical Association praised Rep. Price’s nomination, expressing support for ability to lead HHS.
“Dr. Price has been a leader in the development of health policies to advance patient choice and market-based solutions as well as reduce excessive regulatory burdens that diminish time devoted to patient care and increase costs,” AMA Board of Trustees Chair Patrice A. Harris, MD, said in a statement.
The American College of Surgeons' Executive Director, David B. Hoyt, MD, FACS, issued a supportive statement about the nomination of Dr. Price. "“Dr. Price is a stalwart champion for patients and their surgeons, and the ACS looks forward to working with him on key issues, such as the implementation of the Medicare Access and CHIP Reauthorization Act,” said Dr. Hoyt in a statement. “The ACS encourages the Senate to swiftly confirm Dr. Price’s nomination as Secretary of HHS."
But thousands of physicians disagree. Rep. Price’s proposals on Medicaid and Medicare threaten to harm vulnerable patients and limit access to healthcare, according to an open letter to the AMA published on Medium and credited to Clinician Action Network, a nonpartisan group that supports evidence-based policies. The group was started in opposition to the nomination of Rep. Price.
“We cannot support the dismantling of Medicaid, which has helped 15 million Americans gain health coverage since 2014,” the letter states. “We oppose Dr. Price’s proposals to reduce funding for the Children’s Health Insurance Program, a critical mechanism by which poor children access preventative care.”
Value-based payment or fee for service?
Rep. Price’s experience as a physician fuels his efforts to reduce burdensome regulations for doctors and enhance care efficiency, according to one of his predecessors, Louis W. Sullivan, MD. If confirmed, Rep. Price will become the third physician to be HHS secretary; Dr. Sullivan served in the George H.W. Bush administration and Otis R. Bowen, MD, served in the Reagan administration.
“He is very much aware of the challenges that physicians face in trying to delivery care,” said Dr. Sullivan. “I know that he’ll be working to reduce regulation when feasible so that the cost and delays that some regulatory issues present will hopefully be relieved,”
Some of those regulatory modifications could affect value-based care programs, Dr. Rodriguez said. Rep. Price has been critical of the move from fee for service to quality-based care and has opposed some corresponding programs, such as bundled payment initiatives. Rep. Price and members of the GOP Doctors Caucus wrote to Centers for Medicare & Medicaid Services in October to protest the regulations to implement the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) as too burdensome for smaller practices and calling for flexibility in quality reporting.
Rep. Price voted for passage of MACRA.
“He has been cautious about some of the changes that are being promoted in health care,” Dr. Rodriguez said. “He could slow that down – the processes being put in place. That might delay the impact those systems have in bringing about the improved quality that we want. [This would be] enormous, given the amount of work that we’ve been doing.”
A fair medical liability system also is a priority for Rep. Price, Dr. Sullivan said. His Empowering Patients First bill would require collaboration between HHS and physician associations to develop best practice guidelines that would provide a litigation safe harbor to physicians who practiced in accordance with the standards.
“I know that he will be working to develop strategies to reduce litigation in the health space,” Dr. Sullivan said in an interview. “That is one of the challenges that adds to health care costs, adds tension, and enhances an adversarial relationship between physicians and patients.”
But Dr. Gaffney said that he believes Rep. Price’s views on reproductive rights and gay marriage are regressive and that his agenda regarding health policy issues is bad for medicine.
“The overall [theme] of that agenda can be summed up as ‘take from the poor and sick and give to the rich,’ ” Dr. Gaffney said in an interview. “I think the financing of this [new health reform] system will be much more aggressive, and the result will be greater health care inequity.”
Rep. Price also has supported a ban on federal funding for Planned Parenthood, calling some of their practices barbaric. He has also voted to prohibit the importation of prescription drugs by nonsanctioned importers and has voted to repeal the medical device excise tax.
[email protected]
On Twitter @legal_med
50 years of ob.gyn.: Has practice changed for the better?
As a practicing obstetrician-gynecologist for nearly 40 years, Leonard Brabson, MD, has watched his specialty transform in ways both large and small.
For starters, his regular work attire in 1977 – a shirt and tie – is now scrubs. The paper charts that once filled his office shelves have been replaced with electronic records. And the cumbersome machines that once took blurry, still pictures of a fetus have advanced by leaps and bounds and become a staple of prenatal care.

“Back then, we were expected to be generalists. If [a patient] had a cancer, you took care of it. If [she] had a fertility problem or problem with endocrinology, you took care of it. Of course, now if I have a female cancer, we refer them to the gyn-oncologist. But when you go back 40 years and beyond, we did mostly everything.”
The ob.gyns. of today are practicing in a vastly different environment than their predecessors, and while many of the differences have improved patient care and enhanced efficiency, physicians also note that some changes have harmed the doctor-patient relationship and created career dissatisfaction.
“Certainly, the advances of modern medicine have enabled the current physician to provide the patient a level of care unparalleled in history,” said Charles E. Miller, MD, a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.

More volume, less time
Most long-time physicians agree that higher patient volumes and increasing administrative burdens have diminished the time they are able to spend with patients.

Rising clinical documentation and coding are the top administrative tasks taking away from one-on-one patient care, said Kristen Zeligs, MD, chair of the American Congress of Obstetricians and Gynecologists’ Junior Fellow Congress Advisory Council and a gynecologic oncology fellow at Walter Reed National Military Medical Center in Bethesda, Md.

But there are other factors straining the doctor-patient relationship. Decades ago, first-time mothers often stayed with one doctor for a lifetime, Dr. Brabson recalled, having all of her babies delivered by a single ob.gyn. The same can’t be said for today, where insurance changes, job relocations, and a lack of connections often lead patients to switch physicians frequently.
“Now a lot of patients [move on] from one year to the next,” Dr. Brabson said. “There’s not that same loyalty.”
Doctors, too, traditionally stuck with patients over the long haul, he added. In the past, if an ob.gyn treated a patient during pregnancy, that same physician was present during the delivery, even if it meant leaving a vacation early or coming in on a night off.
“Now the younger docs, especially those that have families with small children, when it’s not their night on call and it’s 5 o’clock, they’re checking out,” Dr. Brabson said. “One of my partners right now, she started inducing someone yesterday. Well today’s her day off, so I’m going to do the delivery. That’s been a big change.”
Highs and lows of liability premiums
Another pressure on the specialty over the last couple of decades has been the high cost of liability insurance.

“2003 was really the peak of the liability crisis,” Dr. Montgomery said. “Hospitals were closing. Doctors were giving up practice. It’s a little better now than it was.”
While ob.gyns. still pay higher premiums than many other specialties, the legal climate has improved in recent years, said Paul Greve Jr., executive vice president and senior consultant for the Willis Healthcare Practice, and author of the 2016 Medical Liability Monitor, an annual report that surveys medical liability premiums.
“The best way to characterize the overall environment for medical professional liability is stable,” he said. “In the area of obstetrics, for the first time ever in recent years, we are seeing lower frequency and lower severity [of lawsuits].”
The lower number of filings are largely due to patient safety initiatives among ob.gyn. programs and tort reforms – many of which have been upheld by courts in the last decade, Mr. Greve said.
Of course, the rate of premiums greatly differs depending on location, with ob.gyns. in Eastern New York paying a high of $214,999 and ob.gyns. in Minnesota paying a low of $16,449 in 2016, according to the Medical Liability Monitor.
“The environment is specific to the region,” Mr. Greve said. “New York City is still very problematic. Chicago is still very problematic. There are some pockets around the country where there’s no damage caps, and it’s really tough to defend claims.”
Technology ups and downs
Another fairly new pressure on ob.gyns. is the integration of the electronic health record and the federal reporting requirements that go along with it.
“Most practicing ob.gyns. are really fed up with the computerization of medicine and the tasking and the charting,” Dr. Montgomery said. “For every hour you spend seeing patients, you spend 1 or 2 hours doing computer chart work and paperwork. Most doctors don’t go into medicine so they can type; they go into medicine to take care of patients.”
The Internet age also poses challenges when it comes to patients conducting their own “research,” said Megan Evans, MD, an ob.gyn. at Tufts Medical Center, Boston.

Protecting the security of patients’ medical records in the digital age is another worry, she said.
But for Dr. Evans, who completed her residency training in 2015, having dozens of digital tools at her disposal as she treats patients is definitely an upside to today’s practice environment.
“I can review a practice bulletin, look up the latest treatment regimens, and contact my colleagues with a quick question – all on my iPhone,” she said. “I also believe there is so much potential for electronic medical records and how they communicate with each other.”
Advancements in ultrasound, fetal monitoring, and other medical technologies have also allowed ob.gyns. to intervene earlier and save lives.
Dr. Brabson recalled the helplessness he and other physicians felt in the 1970s when it came to delivering extremely premature babies.
“We didn’t really feel like you could save a baby under 2 pounds,” he said. “When I was a medical student, if you had a baby under 2 pounds, very commonly what they would do is lay the baby up on the table and watch and see how vigorous it was going to be, and if it really did breathe and carry on for awhile, then you might take it to the nursery. The equipment that we have to save babies with today, compared to 40 years ago, that’s a dramatic change.”
A changing focus for the future
If current trends continue, Dr. Brabson’s early experience of being a generalist ob.gyn. won’t be the norm. Instead, more ob.gyns. will choose to subspecialize. Whether this change is positive or negative for the specialty depends on who you ask.
“You could argue the pros and cons for both sides,” Dr. Zeligs said. “For me, it takes away from what drew me to the specialty – the breadth that ob.gyn. offers, both as a primary care specialty and as a surgical subspecialty.”
However, choosing one focus may offer some doctors a way to capture that elusive professional and personal balance, she added.
Despite the changing landscape of clinical duties and business operations, some parts of ob.gyn. practice have remained intact, according to Dr. Brabson. “The most rewarding and enjoyable part of the job is developing a relationship of mutual trust and respect,” he said. “As a result of developing such a relationship, both the patient and the doctor come away with positive feelings. This has not changed.”
[email protected]
On Twitter @legal_med
As a practicing obstetrician-gynecologist for nearly 40 years, Leonard Brabson, MD, has watched his specialty transform in ways both large and small.
For starters, his regular work attire in 1977 – a shirt and tie – is now scrubs. The paper charts that once filled his office shelves have been replaced with electronic records. And the cumbersome machines that once took blurry, still pictures of a fetus have advanced by leaps and bounds and become a staple of prenatal care.
“Back then, we were expected to be generalists. If [a patient] had a cancer, you took care of it. If [she] had a fertility problem or problem with endocrinology, you took care of it. Of course, now if I have a female cancer, we refer them to the gyn-oncologist. But when you go back 40 years and beyond, we did mostly everything.”
The ob.gyns. of today are practicing in a vastly different environment than their predecessors, and while many of the differences have improved patient care and enhanced efficiency, physicians also note that some changes have harmed the doctor-patient relationship and created career dissatisfaction.
“Certainly, the advances of modern medicine have enabled the current physician to provide the patient a level of care unparalleled in history,” said Charles E. Miller, MD, a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.
More volume, less time
Most long-time physicians agree that higher patient volumes and increasing administrative burdens have diminished the time they are able to spend with patients.
Rising clinical documentation and coding are the top administrative tasks taking away from one-on-one patient care, said Kristen Zeligs, MD, chair of the American Congress of Obstetricians and Gynecologists’ Junior Fellow Congress Advisory Council and a gynecologic oncology fellow at Walter Reed National Military Medical Center in Bethesda, Md.
But there are other factors straining the doctor-patient relationship. Decades ago, first-time mothers often stayed with one doctor for a lifetime, Dr. Brabson recalled, having all of her babies delivered by a single ob.gyn. The same can’t be said for today, where insurance changes, job relocations, and a lack of connections often lead patients to switch physicians frequently.
“Now a lot of patients [move on] from one year to the next,” Dr. Brabson said. “There’s not that same loyalty.”
Doctors, too, traditionally stuck with patients over the long haul, he added. In the past, if an ob.gyn treated a patient during pregnancy, that same physician was present during the delivery, even if it meant leaving a vacation early or coming in on a night off.
“Now the younger docs, especially those that have families with small children, when it’s not their night on call and it’s 5 o’clock, they’re checking out,” Dr. Brabson said. “One of my partners right now, she started inducing someone yesterday. Well today’s her day off, so I’m going to do the delivery. That’s been a big change.”
Highs and lows of liability premiums
Another pressure on the specialty over the last couple of decades has been the high cost of liability insurance.
“2003 was really the peak of the liability crisis,” Dr. Montgomery said. “Hospitals were closing. Doctors were giving up practice. It’s a little better now than it was.”
While ob.gyns. still pay higher premiums than many other specialties, the legal climate has improved in recent years, said Paul Greve Jr., executive vice president and senior consultant for the Willis Healthcare Practice, and author of the 2016 Medical Liability Monitor, an annual report that surveys medical liability premiums.
“The best way to characterize the overall environment for medical professional liability is stable,” he said. “In the area of obstetrics, for the first time ever in recent years, we are seeing lower frequency and lower severity [of lawsuits].”
The lower number of filings are largely due to patient safety initiatives among ob.gyn. programs and tort reforms – many of which have been upheld by courts in the last decade, Mr. Greve said.
Of course, the rate of premiums greatly differs depending on location, with ob.gyns. in Eastern New York paying a high of $214,999 and ob.gyns. in Minnesota paying a low of $16,449 in 2016, according to the Medical Liability Monitor.
“The environment is specific to the region,” Mr. Greve said. “New York City is still very problematic. Chicago is still very problematic. There are some pockets around the country where there’s no damage caps, and it’s really tough to defend claims.”
Technology ups and downs
Another fairly new pressure on ob.gyns. is the integration of the electronic health record and the federal reporting requirements that go along with it.
“Most practicing ob.gyns. are really fed up with the computerization of medicine and the tasking and the charting,” Dr. Montgomery said. “For every hour you spend seeing patients, you spend 1 or 2 hours doing computer chart work and paperwork. Most doctors don’t go into medicine so they can type; they go into medicine to take care of patients.”
The Internet age also poses challenges when it comes to patients conducting their own “research,” said Megan Evans, MD, an ob.gyn. at Tufts Medical Center, Boston.
Protecting the security of patients’ medical records in the digital age is another worry, she said.
But for Dr. Evans, who completed her residency training in 2015, having dozens of digital tools at her disposal as she treats patients is definitely an upside to today’s practice environment.
“I can review a practice bulletin, look up the latest treatment regimens, and contact my colleagues with a quick question – all on my iPhone,” she said. “I also believe there is so much potential for electronic medical records and how they communicate with each other.”
Advancements in ultrasound, fetal monitoring, and other medical technologies have also allowed ob.gyns. to intervene earlier and save lives.
Dr. Brabson recalled the helplessness he and other physicians felt in the 1970s when it came to delivering extremely premature babies.
“We didn’t really feel like you could save a baby under 2 pounds,” he said. “When I was a medical student, if you had a baby under 2 pounds, very commonly what they would do is lay the baby up on the table and watch and see how vigorous it was going to be, and if it really did breathe and carry on for awhile, then you might take it to the nursery. The equipment that we have to save babies with today, compared to 40 years ago, that’s a dramatic change.”
A changing focus for the future
If current trends continue, Dr. Brabson’s early experience of being a generalist ob.gyn. won’t be the norm. Instead, more ob.gyns. will choose to subspecialize. Whether this change is positive or negative for the specialty depends on who you ask.
“You could argue the pros and cons for both sides,” Dr. Zeligs said. “For me, it takes away from what drew me to the specialty – the breadth that ob.gyn. offers, both as a primary care specialty and as a surgical subspecialty.”
However, choosing one focus may offer some doctors a way to capture that elusive professional and personal balance, she added.
Despite the changing landscape of clinical duties and business operations, some parts of ob.gyn. practice have remained intact, according to Dr. Brabson. “The most rewarding and enjoyable part of the job is developing a relationship of mutual trust and respect,” he said. “As a result of developing such a relationship, both the patient and the doctor come away with positive feelings. This has not changed.”
[email protected]
On Twitter @legal_med
As a practicing obstetrician-gynecologist for nearly 40 years, Leonard Brabson, MD, has watched his specialty transform in ways both large and small.
For starters, his regular work attire in 1977 – a shirt and tie – is now scrubs. The paper charts that once filled his office shelves have been replaced with electronic records. And the cumbersome machines that once took blurry, still pictures of a fetus have advanced by leaps and bounds and become a staple of prenatal care.
“Back then, we were expected to be generalists. If [a patient] had a cancer, you took care of it. If [she] had a fertility problem or problem with endocrinology, you took care of it. Of course, now if I have a female cancer, we refer them to the gyn-oncologist. But when you go back 40 years and beyond, we did mostly everything.”
The ob.gyns. of today are practicing in a vastly different environment than their predecessors, and while many of the differences have improved patient care and enhanced efficiency, physicians also note that some changes have harmed the doctor-patient relationship and created career dissatisfaction.
“Certainly, the advances of modern medicine have enabled the current physician to provide the patient a level of care unparalleled in history,” said Charles E. Miller, MD, a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill.
More volume, less time
Most long-time physicians agree that higher patient volumes and increasing administrative burdens have diminished the time they are able to spend with patients.
Rising clinical documentation and coding are the top administrative tasks taking away from one-on-one patient care, said Kristen Zeligs, MD, chair of the American Congress of Obstetricians and Gynecologists’ Junior Fellow Congress Advisory Council and a gynecologic oncology fellow at Walter Reed National Military Medical Center in Bethesda, Md.
But there are other factors straining the doctor-patient relationship. Decades ago, first-time mothers often stayed with one doctor for a lifetime, Dr. Brabson recalled, having all of her babies delivered by a single ob.gyn. The same can’t be said for today, where insurance changes, job relocations, and a lack of connections often lead patients to switch physicians frequently.
“Now a lot of patients [move on] from one year to the next,” Dr. Brabson said. “There’s not that same loyalty.”
Doctors, too, traditionally stuck with patients over the long haul, he added. In the past, if an ob.gyn treated a patient during pregnancy, that same physician was present during the delivery, even if it meant leaving a vacation early or coming in on a night off.
“Now the younger docs, especially those that have families with small children, when it’s not their night on call and it’s 5 o’clock, they’re checking out,” Dr. Brabson said. “One of my partners right now, she started inducing someone yesterday. Well today’s her day off, so I’m going to do the delivery. That’s been a big change.”
Highs and lows of liability premiums
Another pressure on the specialty over the last couple of decades has been the high cost of liability insurance.
“2003 was really the peak of the liability crisis,” Dr. Montgomery said. “Hospitals were closing. Doctors were giving up practice. It’s a little better now than it was.”
While ob.gyns. still pay higher premiums than many other specialties, the legal climate has improved in recent years, said Paul Greve Jr., executive vice president and senior consultant for the Willis Healthcare Practice, and author of the 2016 Medical Liability Monitor, an annual report that surveys medical liability premiums.
“The best way to characterize the overall environment for medical professional liability is stable,” he said. “In the area of obstetrics, for the first time ever in recent years, we are seeing lower frequency and lower severity [of lawsuits].”
The lower number of filings are largely due to patient safety initiatives among ob.gyn. programs and tort reforms – many of which have been upheld by courts in the last decade, Mr. Greve said.
Of course, the rate of premiums greatly differs depending on location, with ob.gyns. in Eastern New York paying a high of $214,999 and ob.gyns. in Minnesota paying a low of $16,449 in 2016, according to the Medical Liability Monitor.
“The environment is specific to the region,” Mr. Greve said. “New York City is still very problematic. Chicago is still very problematic. There are some pockets around the country where there’s no damage caps, and it’s really tough to defend claims.”
Technology ups and downs
Another fairly new pressure on ob.gyns. is the integration of the electronic health record and the federal reporting requirements that go along with it.
“Most practicing ob.gyns. are really fed up with the computerization of medicine and the tasking and the charting,” Dr. Montgomery said. “For every hour you spend seeing patients, you spend 1 or 2 hours doing computer chart work and paperwork. Most doctors don’t go into medicine so they can type; they go into medicine to take care of patients.”
The Internet age also poses challenges when it comes to patients conducting their own “research,” said Megan Evans, MD, an ob.gyn. at Tufts Medical Center, Boston.
Protecting the security of patients’ medical records in the digital age is another worry, she said.
But for Dr. Evans, who completed her residency training in 2015, having dozens of digital tools at her disposal as she treats patients is definitely an upside to today’s practice environment.
“I can review a practice bulletin, look up the latest treatment regimens, and contact my colleagues with a quick question – all on my iPhone,” she said. “I also believe there is so much potential for electronic medical records and how they communicate with each other.”
Advancements in ultrasound, fetal monitoring, and other medical technologies have also allowed ob.gyns. to intervene earlier and save lives.
Dr. Brabson recalled the helplessness he and other physicians felt in the 1970s when it came to delivering extremely premature babies.
“We didn’t really feel like you could save a baby under 2 pounds,” he said. “When I was a medical student, if you had a baby under 2 pounds, very commonly what they would do is lay the baby up on the table and watch and see how vigorous it was going to be, and if it really did breathe and carry on for awhile, then you might take it to the nursery. The equipment that we have to save babies with today, compared to 40 years ago, that’s a dramatic change.”
A changing focus for the future
If current trends continue, Dr. Brabson’s early experience of being a generalist ob.gyn. won’t be the norm. Instead, more ob.gyns. will choose to subspecialize. Whether this change is positive or negative for the specialty depends on who you ask.
“You could argue the pros and cons for both sides,” Dr. Zeligs said. “For me, it takes away from what drew me to the specialty – the breadth that ob.gyn. offers, both as a primary care specialty and as a surgical subspecialty.”
However, choosing one focus may offer some doctors a way to capture that elusive professional and personal balance, she added.
Despite the changing landscape of clinical duties and business operations, some parts of ob.gyn. practice have remained intact, according to Dr. Brabson. “The most rewarding and enjoyable part of the job is developing a relationship of mutual trust and respect,” he said. “As a result of developing such a relationship, both the patient and the doctor come away with positive feelings. This has not changed.”
[email protected]
On Twitter @legal_med

STUDY: More children have access to care, insurance
Children’s access to pediatricians has improved since 2000 with markedly more patients carrying health insurance, according to a new study.
An analysis showed the rate of uninsured children dropped from 12% in 2000 to 5% in 2014, while children’s access rose for physician visits and regular care.
Kandyce Larson, PhD, of the American Academy of Pediatrics and her colleagues reviewed trends for 178,038 children in the Centers for Disease Control & Prevention’ National Health Interview Survey from 2000 to 2014. Researchers examined statistics for health insurance and trends across five access indicators: well-child visits, doctor office visits, dental visits, usual source of care, and unmet health needs. Results showed the uninsured rate declined by more than 50% from 12% of children in 2000 to 5% in 2014. Findings showed an accompanying increase in public health insurance coverage (19% to 39%), while private coverage decreased (69% to 56%) during the same time period (Pediatrics. 2016 Nov 15. doi: 10.1542/peds.2016-2176).
Uninsured rates for minority and poor children showed the largest decreases, the study found. The uninsured rate for Hispanic children decreased from 26% in 2000 to 9% in 2014, while uninsured black children dropped from 12% to 3%, according to the study. Significant declines in the uninsured rate also were seen for children in poor families (22% to 6%) and near-poor families (21% to 9%).
Health care access improved across all five indicators. Rates for no well-child visit declined from 29% in 2000 to 16% in 2014, while no doctor office visit went from 13% to 9%, and no dental visit decreased from 30% to 21%. No usual source of care dropped from 7% to 4%, and unmet health care needs decreased from 8% to 6%. The results amounted to an additional 9 million children receiving a well-child visit in 2014, compared with 2000. Improvements in access were generally greater for black and Hispanic children and those in poor and near-poor families, according to the study.

“It’s critical for our nation’s future health that we provide children at all income levels access to quality health care,” he said in a statement.
The rise in children who have a usual source of care and are undergoing regular well-child visits is especially heartening, added pediatrician Andrew D. Racine, MD, PhD, coauthor of the study and a member of the AAP Committee on Child Health Financing.
“When children see providers who know their medical history and can monitor their physical and socio-emotional development, they are more likely to have better overall health, be up to date on immunizations, perform better in school, and receive care in the most cost-effective way,” he said in a statement. Dr. Racine is a professor of clinical pediatrics at Albert Einstein College of Medicine, Bronx, N.Y.
[email protected]
On Twitter @legal_med
The findings of the current study have important implications for future child health care policy decisions.
First, children should have coverage, and strong efforts must be made to reach the 5.3% of children who remain uninsured. Second, the reauthorization and continued funding of the Children’s Health Insurance Plan, due to terminate in 2019, is essential and should be addressed sooner rather than later.
In addition, while this study focuses attention on health care access measures, advocates and policy makers need to address having meaningful health outcomes. Because health care only contributes 10% to 20% to maximizing population health, a new child health policy should focus on addressing the social determinants of health and the reduction of behaviors that compromise health, such as smoking, excessive alcohol intake, substance abuse, and poor nutrition.
Stephen Berman, MD, is a professor of pediatrics at the University of Colorado at Denver, holds an endowed chair in academic general pediatrics at the Children’s Hospital Colorado, and is the director of the Center for Global Health in the Colorado School of Public Health, all in Aurora. These remarks are excerpted from an accompanying editorial (Pediatrics. 2016 Nov 15. doi: 10.1542/peds.2016-2823). He reported having no relevant financial disclosures.
The findings of the current study have important implications for future child health care policy decisions.
First, children should have coverage, and strong efforts must be made to reach the 5.3% of children who remain uninsured. Second, the reauthorization and continued funding of the Children’s Health Insurance Plan, due to terminate in 2019, is essential and should be addressed sooner rather than later.
In addition, while this study focuses attention on health care access measures, advocates and policy makers need to address having meaningful health outcomes. Because health care only contributes 10% to 20% to maximizing population health, a new child health policy should focus on addressing the social determinants of health and the reduction of behaviors that compromise health, such as smoking, excessive alcohol intake, substance abuse, and poor nutrition.
Stephen Berman, MD, is a professor of pediatrics at the University of Colorado at Denver, holds an endowed chair in academic general pediatrics at the Children’s Hospital Colorado, and is the director of the Center for Global Health in the Colorado School of Public Health, all in Aurora. These remarks are excerpted from an accompanying editorial (Pediatrics. 2016 Nov 15. doi: 10.1542/peds.2016-2823). He reported having no relevant financial disclosures.
The findings of the current study have important implications for future child health care policy decisions.
First, children should have coverage, and strong efforts must be made to reach the 5.3% of children who remain uninsured. Second, the reauthorization and continued funding of the Children’s Health Insurance Plan, due to terminate in 2019, is essential and should be addressed sooner rather than later.
In addition, while this study focuses attention on health care access measures, advocates and policy makers need to address having meaningful health outcomes. Because health care only contributes 10% to 20% to maximizing population health, a new child health policy should focus on addressing the social determinants of health and the reduction of behaviors that compromise health, such as smoking, excessive alcohol intake, substance abuse, and poor nutrition.
Stephen Berman, MD, is a professor of pediatrics at the University of Colorado at Denver, holds an endowed chair in academic general pediatrics at the Children’s Hospital Colorado, and is the director of the Center for Global Health in the Colorado School of Public Health, all in Aurora. These remarks are excerpted from an accompanying editorial (Pediatrics. 2016 Nov 15. doi: 10.1542/peds.2016-2823). He reported having no relevant financial disclosures.
Children’s access to pediatricians has improved since 2000 with markedly more patients carrying health insurance, according to a new study.
An analysis showed the rate of uninsured children dropped from 12% in 2000 to 5% in 2014, while children’s access rose for physician visits and regular care.
Kandyce Larson, PhD, of the American Academy of Pediatrics and her colleagues reviewed trends for 178,038 children in the Centers for Disease Control & Prevention’ National Health Interview Survey from 2000 to 2014. Researchers examined statistics for health insurance and trends across five access indicators: well-child visits, doctor office visits, dental visits, usual source of care, and unmet health needs. Results showed the uninsured rate declined by more than 50% from 12% of children in 2000 to 5% in 2014. Findings showed an accompanying increase in public health insurance coverage (19% to 39%), while private coverage decreased (69% to 56%) during the same time period (Pediatrics. 2016 Nov 15. doi: 10.1542/peds.2016-2176).
Uninsured rates for minority and poor children showed the largest decreases, the study found. The uninsured rate for Hispanic children decreased from 26% in 2000 to 9% in 2014, while uninsured black children dropped from 12% to 3%, according to the study. Significant declines in the uninsured rate also were seen for children in poor families (22% to 6%) and near-poor families (21% to 9%).
Health care access improved across all five indicators. Rates for no well-child visit declined from 29% in 2000 to 16% in 2014, while no doctor office visit went from 13% to 9%, and no dental visit decreased from 30% to 21%. No usual source of care dropped from 7% to 4%, and unmet health care needs decreased from 8% to 6%. The results amounted to an additional 9 million children receiving a well-child visit in 2014, compared with 2000. Improvements in access were generally greater for black and Hispanic children and those in poor and near-poor families, according to the study.
“It’s critical for our nation’s future health that we provide children at all income levels access to quality health care,” he said in a statement.
The rise in children who have a usual source of care and are undergoing regular well-child visits is especially heartening, added pediatrician Andrew D. Racine, MD, PhD, coauthor of the study and a member of the AAP Committee on Child Health Financing.
“When children see providers who know their medical history and can monitor their physical and socio-emotional development, they are more likely to have better overall health, be up to date on immunizations, perform better in school, and receive care in the most cost-effective way,” he said in a statement. Dr. Racine is a professor of clinical pediatrics at Albert Einstein College of Medicine, Bronx, N.Y.
[email protected]
On Twitter @legal_med
Children’s access to pediatricians has improved since 2000 with markedly more patients carrying health insurance, according to a new study.
An analysis showed the rate of uninsured children dropped from 12% in 2000 to 5% in 2014, while children’s access rose for physician visits and regular care.
Kandyce Larson, PhD, of the American Academy of Pediatrics and her colleagues reviewed trends for 178,038 children in the Centers for Disease Control & Prevention’ National Health Interview Survey from 2000 to 2014. Researchers examined statistics for health insurance and trends across five access indicators: well-child visits, doctor office visits, dental visits, usual source of care, and unmet health needs. Results showed the uninsured rate declined by more than 50% from 12% of children in 2000 to 5% in 2014. Findings showed an accompanying increase in public health insurance coverage (19% to 39%), while private coverage decreased (69% to 56%) during the same time period (Pediatrics. 2016 Nov 15. doi: 10.1542/peds.2016-2176).
Uninsured rates for minority and poor children showed the largest decreases, the study found. The uninsured rate for Hispanic children decreased from 26% in 2000 to 9% in 2014, while uninsured black children dropped from 12% to 3%, according to the study. Significant declines in the uninsured rate also were seen for children in poor families (22% to 6%) and near-poor families (21% to 9%).
Health care access improved across all five indicators. Rates for no well-child visit declined from 29% in 2000 to 16% in 2014, while no doctor office visit went from 13% to 9%, and no dental visit decreased from 30% to 21%. No usual source of care dropped from 7% to 4%, and unmet health care needs decreased from 8% to 6%. The results amounted to an additional 9 million children receiving a well-child visit in 2014, compared with 2000. Improvements in access were generally greater for black and Hispanic children and those in poor and near-poor families, according to the study.
“It’s critical for our nation’s future health that we provide children at all income levels access to quality health care,” he said in a statement.
The rise in children who have a usual source of care and are undergoing regular well-child visits is especially heartening, added pediatrician Andrew D. Racine, MD, PhD, coauthor of the study and a member of the AAP Committee on Child Health Financing.
“When children see providers who know their medical history and can monitor their physical and socio-emotional development, they are more likely to have better overall health, be up to date on immunizations, perform better in school, and receive care in the most cost-effective way,” he said in a statement. Dr. Racine is a professor of clinical pediatrics at Albert Einstein College of Medicine, Bronx, N.Y.
[email protected]
On Twitter @legal_med
Key clinical point:
Major finding: The rate of uninsured children dropped from 12% in 2000 to 5% in 2014.
Data source: Study of survey data of 178,038 children.
Disclosures: The authors have indicated they have no relevant financial disclosures.