User login
Official Newspaper of the American College of Surgeons
Should you communicate with patients online?
A lot of mythology regarding the new Health Insurance Portability and Accountability Act rules (which I discussed in detail a few months ago) continues to circulate. One of the biggest myths is that e-mail communication with patients is now forbidden, so let’s debunk that one right now.
Here is a statement lifted verbatim from the official HIPAA web site (FAQ section):
"Patients may initiate communications with a provider using e-mail. If this situation occurs, the health care provider can assume (unless the patient has explicitly stated otherwise) that e-mail communications are acceptable to the individual.
"If the provider feels the patient may not be aware of the possible risks of using unencrypted e-mail, or has concerns about potential liability, the provider can alert the patient of those risks, and let the patient decide whether to continue e-mail communications."
Okay, so it’s permissible – but is it a good idea? Aside from the obvious privacy issues, many physicians balk at taking on one more unreimbursed demand on their time. While no one denies that these concerns are real, there also are real benefits to be gained from properly managed online communication – among them increased practice efficiency, and increased quality of care and satisfaction for patients.
I started giving one of my e-mail addresses to selected patients several years ago as an experiment, hoping to take some pressure off of our overloaded telephone system. The patients were grateful for simplified and more direct access, and I appreciated the decrease in phone messages and interruptions while I was seeing patients. I also noticed a decrease in those frustrating, unnecessary office visits – you know, "The rash is completely gone, but you told me to come back ..."
In general, I have found that the advantages for everyone involved (not least my nurses and receptionists) far outweigh the problems. And now, newer technologies such as encryption, web-based messaging, and integrated online communication should go a long way toward assuaging privacy concerns.
Encryption software is now inexpensive, readily available, and easily added to most e-mail systems. Packages are available from companies such as EMC, Hilgraeve, Kryptiq, Proofpoint, Axway, and ZixCorp, among many others. (As always, I have no financial interest in any company mentioned in this column.)
Rather than simply encrypting their e-mail, increasing numbers of physicians are opting for the route taken by most online banking and shopping sites: a secure website. Patients sign onto it and send a message to your office. Physicians or staffers are notified in their regular e-mail of messages on the website, and then they post a reply to the patient on the site that can only be accessed by the patient. The patient is notified of the practice’s reply in his or her regular e-mail. Web-based messaging services can be incorporated into existing practice sites or can stand on their own. Medfusion, MyDocOnline, and RelayHealth are among the many vendors that offer secure cloud-based messaging services.
A big advantage of using such a service is that you’re partnering with a vendor who has to stay on top of HIPAA and other privacy requirements. Another is the option of using electronic forms, or templates. Templates ensure that patients’ messages include the information needed to process prescription refill requests, or to adequately describe their problems and provide some clinical assessment data for the physician or nurse. They also can be designed to triage messages to the front- and back-office staff, so that time is not wasted bouncing messages around the office until the proper responder is found.
Many electronic health record systems now allow you to integrate a web-based messaging system. Advantages here include the ability to view the patient’s medical record from home or anywhere else before answering the communication, and the fact that all messages automatically become a part of the patient’s record. Electronic health record vendors that provide this type of system include Allscripts, CompuGroup Medical, Cerner, Epic, GE Medical Systems, NextGen, McKesson, and Siemens.
As with any cloud-based service, insist on multiple layers of security, uninterruptible power sources, instant switchover to backup hardware in the event of a crash, and frequent, reliable backups.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is a clinical associate professor of dermatology at Seton Hall University School of Graduate Medical Education in South Orange, N.J. Dr. Eastern is a two-time past president of the Dermatological Society of New Jersey, and currently serves on its executive board. He holds teaching positions at several hospitals and has delivered more than 500 academic speaking presentations. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.
A lot of mythology regarding the new Health Insurance Portability and Accountability Act rules (which I discussed in detail a few months ago) continues to circulate. One of the biggest myths is that e-mail communication with patients is now forbidden, so let’s debunk that one right now.
Here is a statement lifted verbatim from the official HIPAA web site (FAQ section):
"Patients may initiate communications with a provider using e-mail. If this situation occurs, the health care provider can assume (unless the patient has explicitly stated otherwise) that e-mail communications are acceptable to the individual.
"If the provider feels the patient may not be aware of the possible risks of using unencrypted e-mail, or has concerns about potential liability, the provider can alert the patient of those risks, and let the patient decide whether to continue e-mail communications."
Okay, so it’s permissible – but is it a good idea? Aside from the obvious privacy issues, many physicians balk at taking on one more unreimbursed demand on their time. While no one denies that these concerns are real, there also are real benefits to be gained from properly managed online communication – among them increased practice efficiency, and increased quality of care and satisfaction for patients.
I started giving one of my e-mail addresses to selected patients several years ago as an experiment, hoping to take some pressure off of our overloaded telephone system. The patients were grateful for simplified and more direct access, and I appreciated the decrease in phone messages and interruptions while I was seeing patients. I also noticed a decrease in those frustrating, unnecessary office visits – you know, "The rash is completely gone, but you told me to come back ..."
In general, I have found that the advantages for everyone involved (not least my nurses and receptionists) far outweigh the problems. And now, newer technologies such as encryption, web-based messaging, and integrated online communication should go a long way toward assuaging privacy concerns.
Encryption software is now inexpensive, readily available, and easily added to most e-mail systems. Packages are available from companies such as EMC, Hilgraeve, Kryptiq, Proofpoint, Axway, and ZixCorp, among many others. (As always, I have no financial interest in any company mentioned in this column.)
Rather than simply encrypting their e-mail, increasing numbers of physicians are opting for the route taken by most online banking and shopping sites: a secure website. Patients sign onto it and send a message to your office. Physicians or staffers are notified in their regular e-mail of messages on the website, and then they post a reply to the patient on the site that can only be accessed by the patient. The patient is notified of the practice’s reply in his or her regular e-mail. Web-based messaging services can be incorporated into existing practice sites or can stand on their own. Medfusion, MyDocOnline, and RelayHealth are among the many vendors that offer secure cloud-based messaging services.
A big advantage of using such a service is that you’re partnering with a vendor who has to stay on top of HIPAA and other privacy requirements. Another is the option of using electronic forms, or templates. Templates ensure that patients’ messages include the information needed to process prescription refill requests, or to adequately describe their problems and provide some clinical assessment data for the physician or nurse. They also can be designed to triage messages to the front- and back-office staff, so that time is not wasted bouncing messages around the office until the proper responder is found.
Many electronic health record systems now allow you to integrate a web-based messaging system. Advantages here include the ability to view the patient’s medical record from home or anywhere else before answering the communication, and the fact that all messages automatically become a part of the patient’s record. Electronic health record vendors that provide this type of system include Allscripts, CompuGroup Medical, Cerner, Epic, GE Medical Systems, NextGen, McKesson, and Siemens.
As with any cloud-based service, insist on multiple layers of security, uninterruptible power sources, instant switchover to backup hardware in the event of a crash, and frequent, reliable backups.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is a clinical associate professor of dermatology at Seton Hall University School of Graduate Medical Education in South Orange, N.J. Dr. Eastern is a two-time past president of the Dermatological Society of New Jersey, and currently serves on its executive board. He holds teaching positions at several hospitals and has delivered more than 500 academic speaking presentations. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.
A lot of mythology regarding the new Health Insurance Portability and Accountability Act rules (which I discussed in detail a few months ago) continues to circulate. One of the biggest myths is that e-mail communication with patients is now forbidden, so let’s debunk that one right now.
Here is a statement lifted verbatim from the official HIPAA web site (FAQ section):
"Patients may initiate communications with a provider using e-mail. If this situation occurs, the health care provider can assume (unless the patient has explicitly stated otherwise) that e-mail communications are acceptable to the individual.
"If the provider feels the patient may not be aware of the possible risks of using unencrypted e-mail, or has concerns about potential liability, the provider can alert the patient of those risks, and let the patient decide whether to continue e-mail communications."
Okay, so it’s permissible – but is it a good idea? Aside from the obvious privacy issues, many physicians balk at taking on one more unreimbursed demand on their time. While no one denies that these concerns are real, there also are real benefits to be gained from properly managed online communication – among them increased practice efficiency, and increased quality of care and satisfaction for patients.
I started giving one of my e-mail addresses to selected patients several years ago as an experiment, hoping to take some pressure off of our overloaded telephone system. The patients were grateful for simplified and more direct access, and I appreciated the decrease in phone messages and interruptions while I was seeing patients. I also noticed a decrease in those frustrating, unnecessary office visits – you know, "The rash is completely gone, but you told me to come back ..."
In general, I have found that the advantages for everyone involved (not least my nurses and receptionists) far outweigh the problems. And now, newer technologies such as encryption, web-based messaging, and integrated online communication should go a long way toward assuaging privacy concerns.
Encryption software is now inexpensive, readily available, and easily added to most e-mail systems. Packages are available from companies such as EMC, Hilgraeve, Kryptiq, Proofpoint, Axway, and ZixCorp, among many others. (As always, I have no financial interest in any company mentioned in this column.)
Rather than simply encrypting their e-mail, increasing numbers of physicians are opting for the route taken by most online banking and shopping sites: a secure website. Patients sign onto it and send a message to your office. Physicians or staffers are notified in their regular e-mail of messages on the website, and then they post a reply to the patient on the site that can only be accessed by the patient. The patient is notified of the practice’s reply in his or her regular e-mail. Web-based messaging services can be incorporated into existing practice sites or can stand on their own. Medfusion, MyDocOnline, and RelayHealth are among the many vendors that offer secure cloud-based messaging services.
A big advantage of using such a service is that you’re partnering with a vendor who has to stay on top of HIPAA and other privacy requirements. Another is the option of using electronic forms, or templates. Templates ensure that patients’ messages include the information needed to process prescription refill requests, or to adequately describe their problems and provide some clinical assessment data for the physician or nurse. They also can be designed to triage messages to the front- and back-office staff, so that time is not wasted bouncing messages around the office until the proper responder is found.
Many electronic health record systems now allow you to integrate a web-based messaging system. Advantages here include the ability to view the patient’s medical record from home or anywhere else before answering the communication, and the fact that all messages automatically become a part of the patient’s record. Electronic health record vendors that provide this type of system include Allscripts, CompuGroup Medical, Cerner, Epic, GE Medical Systems, NextGen, McKesson, and Siemens.
As with any cloud-based service, insist on multiple layers of security, uninterruptible power sources, instant switchover to backup hardware in the event of a crash, and frequent, reliable backups.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is a clinical associate professor of dermatology at Seton Hall University School of Graduate Medical Education in South Orange, N.J. Dr. Eastern is a two-time past president of the Dermatological Society of New Jersey, and currently serves on its executive board. He holds teaching positions at several hospitals and has delivered more than 500 academic speaking presentations. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.

2014 budget reduces spending for ACA, IPAB
A $1 trillion spending bill that funds the government through Sept. 30 restores money for some health programs but delivers a blow to the Affordable Care Act.
Even so, President Obama is expected to sign it.
The House approved the Consolidated Appropriations Act for FY 2014 (H.R. 3547) on Jan. 15 by a vote of 359-67, and the Senate approved it a day later 72-26.
Republican members of the House Appropriations Committee added language to the bill that puts a hold on any new funding for the ACA in fiscal 2014 and takes $1 billion out of the law’s Prevention and Public Health Fund. The fund is hotly contested and has been labeled a "slush fund," by opponents.

The House Appropriations panel also succeeded in cutting $10 million in funding for the Independent Payment Advisory Board (IPAB). The IPAB was due to make its first recommendations by mid-January; however, the Obama administration has yet to appoint any members.
The spending bill continues to ban the use federal funds for needle exchanges; for research that creates or uses embryos; and for abortion, except in the case of rape, incest, or endangerment of the life of the mother.
The bill includes a $3.7 billion budget for the Centers for Medicare and Medicaid Services – almost $200 million less than it received in fiscal year 2013 but equal to what it would receive under sequestration. Some $305 million is earmarked for the timely processing and payment of benefits.
The bill increases funding for other federal health-related agencies. The National Institutes of Health budget was increased $1 billion, which should allow it to begin 385 clinical trials, according to the Senate Appropriations Committee.
There is new funding for the Brain Research through Advancing of Innovative Neurotechnologies (BRAIN) Initiative, and funding for an initiative to study prevention and treatments for Alzheimer’s disease.
Mental health programs at various labor, health, and education agencies will receive $1.13 billion, an increase of $213 million, according to the Senate panel. Those programs include violence prevention and grants to schools to help train teachers and to help build a mental health workforce. The Senate Committee estimates that new training will help add 4,375 social workers, psychologists, therapists and other mental health professionals to the behavioral health workforce. The Substance Abuse and Mental Health Services Administration received a $144 million increase in its budget, bringing it to $3.6 billion.
Funding for the Centers for Disease Control and Prevention was increased $567 million to $6.9 billion. That budget includes $30 million to support the Advanced Molecular Detection initiative, which helps the agency detect and stop infectious disease outbreaks and $160 million for the Preventive Health & Health Services Block Grant.
The legislation also includes $3.6 billion to improve the quantity and quality of health care services in medically underserved areas and populations. As part of that, $350 million is appropriated to create more than 450 new community health centers and expand services at existing ones.
On Twitter @aliciaault
A $1 trillion spending bill that funds the government through Sept. 30 restores money for some health programs but delivers a blow to the Affordable Care Act.
Even so, President Obama is expected to sign it.
The House approved the Consolidated Appropriations Act for FY 2014 (H.R. 3547) on Jan. 15 by a vote of 359-67, and the Senate approved it a day later 72-26.
Republican members of the House Appropriations Committee added language to the bill that puts a hold on any new funding for the ACA in fiscal 2014 and takes $1 billion out of the law’s Prevention and Public Health Fund. The fund is hotly contested and has been labeled a "slush fund," by opponents.
The House Appropriations panel also succeeded in cutting $10 million in funding for the Independent Payment Advisory Board (IPAB). The IPAB was due to make its first recommendations by mid-January; however, the Obama administration has yet to appoint any members.
The spending bill continues to ban the use federal funds for needle exchanges; for research that creates or uses embryos; and for abortion, except in the case of rape, incest, or endangerment of the life of the mother.
The bill includes a $3.7 billion budget for the Centers for Medicare and Medicaid Services – almost $200 million less than it received in fiscal year 2013 but equal to what it would receive under sequestration. Some $305 million is earmarked for the timely processing and payment of benefits.
The bill increases funding for other federal health-related agencies. The National Institutes of Health budget was increased $1 billion, which should allow it to begin 385 clinical trials, according to the Senate Appropriations Committee.
There is new funding for the Brain Research through Advancing of Innovative Neurotechnologies (BRAIN) Initiative, and funding for an initiative to study prevention and treatments for Alzheimer’s disease.
Mental health programs at various labor, health, and education agencies will receive $1.13 billion, an increase of $213 million, according to the Senate panel. Those programs include violence prevention and grants to schools to help train teachers and to help build a mental health workforce. The Senate Committee estimates that new training will help add 4,375 social workers, psychologists, therapists and other mental health professionals to the behavioral health workforce. The Substance Abuse and Mental Health Services Administration received a $144 million increase in its budget, bringing it to $3.6 billion.
Funding for the Centers for Disease Control and Prevention was increased $567 million to $6.9 billion. That budget includes $30 million to support the Advanced Molecular Detection initiative, which helps the agency detect and stop infectious disease outbreaks and $160 million for the Preventive Health & Health Services Block Grant.
The legislation also includes $3.6 billion to improve the quantity and quality of health care services in medically underserved areas and populations. As part of that, $350 million is appropriated to create more than 450 new community health centers and expand services at existing ones.
On Twitter @aliciaault
A $1 trillion spending bill that funds the government through Sept. 30 restores money for some health programs but delivers a blow to the Affordable Care Act.
Even so, President Obama is expected to sign it.
The House approved the Consolidated Appropriations Act for FY 2014 (H.R. 3547) on Jan. 15 by a vote of 359-67, and the Senate approved it a day later 72-26.
Republican members of the House Appropriations Committee added language to the bill that puts a hold on any new funding for the ACA in fiscal 2014 and takes $1 billion out of the law’s Prevention and Public Health Fund. The fund is hotly contested and has been labeled a "slush fund," by opponents.
The House Appropriations panel also succeeded in cutting $10 million in funding for the Independent Payment Advisory Board (IPAB). The IPAB was due to make its first recommendations by mid-January; however, the Obama administration has yet to appoint any members.
The spending bill continues to ban the use federal funds for needle exchanges; for research that creates or uses embryos; and for abortion, except in the case of rape, incest, or endangerment of the life of the mother.
The bill includes a $3.7 billion budget for the Centers for Medicare and Medicaid Services – almost $200 million less than it received in fiscal year 2013 but equal to what it would receive under sequestration. Some $305 million is earmarked for the timely processing and payment of benefits.
The bill increases funding for other federal health-related agencies. The National Institutes of Health budget was increased $1 billion, which should allow it to begin 385 clinical trials, according to the Senate Appropriations Committee.
There is new funding for the Brain Research through Advancing of Innovative Neurotechnologies (BRAIN) Initiative, and funding for an initiative to study prevention and treatments for Alzheimer’s disease.
Mental health programs at various labor, health, and education agencies will receive $1.13 billion, an increase of $213 million, according to the Senate panel. Those programs include violence prevention and grants to schools to help train teachers and to help build a mental health workforce. The Senate Committee estimates that new training will help add 4,375 social workers, psychologists, therapists and other mental health professionals to the behavioral health workforce. The Substance Abuse and Mental Health Services Administration received a $144 million increase in its budget, bringing it to $3.6 billion.
Funding for the Centers for Disease Control and Prevention was increased $567 million to $6.9 billion. That budget includes $30 million to support the Advanced Molecular Detection initiative, which helps the agency detect and stop infectious disease outbreaks and $160 million for the Preventive Health & Health Services Block Grant.
The legislation also includes $3.6 billion to improve the quantity and quality of health care services in medically underserved areas and populations. As part of that, $350 million is appropriated to create more than 450 new community health centers and expand services at existing ones.
On Twitter @aliciaault

OSHA launches hospital worker safety initiative
Improving hospital worker safety will result in improved patient safety, according to the Occupational Safety and Health Administration, which has unveiled a hospital worker safety online resource center.
Worker Safety in Hospitals: Caring for our Caregivers, OSHA's new website aimed at curbing hospital worker injury rates, was introduced during a media teleconference Jan. 16. According to OSHA, injuries occur at a rate of 158 times per 10,000 workers, making hospitals more hazardous work environments than either construction or manufacturing sites.
National workers’ compensation losses from hospital workers total $2 billion annually, said OSHA assistant secretary Dr. David Michaels.
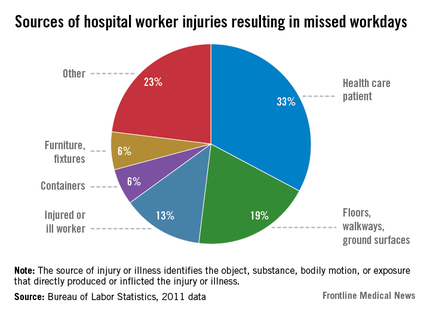
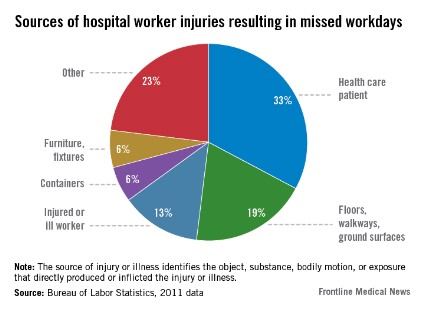
Musculoskeletal injuries, primarily from lifting and shifting patients, are the single biggest worker injury in hospitals, he said. According to OSHA, 16,680 hospital workers missed work because of a musculoskeletal injury sustained while handling a patient.
"Other hazards facing hospital workers include workplace violence, slips and falls, exposure to chemicals including hazardous drugs, exposure to infectious diseases, and needle sticks," said Dr. Michaels.
As part of a joint effort to promote the website, also on the conference call were Dr. John Howard, director of the National Institute for Occupational Safety and Health, and Dr. Erin DuPree, chief medical officer and vice president of the Joint Commission Center for Transforming Healthcare, and Dr. Lucian Leape, chairman of the Lucian Leape Institute at the National Patient Safety Foundation.
The OSHA website offers educational materials on avoiding injury when handling patients, as well as on workplace safety needs and the implementation of safety and health management systems.
The materials were culled from best practices employed at hospitals around the country deemed by OSHA to be "high-reliability organizations," and include tips such as having a daily "safety huddle" that includes a discussion of "great catches" and "near misses" that occurred during daily operations.
"One of the major barriers in making progress in patient safety is that when people report that they’ve made a mistake, they often get punished for it," said Dr. Leape. "What we’ve been trying to get people to understand is that mistakes happen because of bad systems, not bad people. You have to create an environment where you really believe that, and make it safe for people to talk about their errors so you can understand what you need to fix."
Dr. DuPree said the OSHA resources align with Joint Commission requirements such as those for hospitals to have a written plan for managing environmental safety for patients and all persons in hospitals. The Joint Commission expects that all individuals who work in the hospital should not fear retribution for speaking up about their safety concerns, Dr. DuPree said. "Leaders need to value and empower their workers. They need to understand that fear of reprisal and failure to share knowledge can compromise an organization’s ability to improve safety for all," he said.
As part of its efforts to advise hospital administrators on how to create safer work environments for their employees, the U.S. Department of Labor Occupational Safety and Health Administration has created a list of attributes of what it calls "high-reliability organizations."
Self-assessment tools, tip sheets, and other materials intended to help hospitals become high-reliability organizations (HROs) are available at OSHA's new website, Worker Safety in Hospitals: Caring for our Caregivers.
"The heart of these new materials are real life lessons from high-performing hospitals [that] have implemented best practices to reduce workplace injuries while also improving patient safety," said OSHA assistant secretary Dr. David Michaels in a press briefing.
The website emphasizes principles endorsed by the Joint Commission, particularly the promotion of a "no-blame" culture to destigmatize safety interventions. Operational strategies derived from the distillation of these best practices and endorsed by OSHA include the following:
• Sensitivity to operations. That means hospital workers should know what the standard procedures are, and follow them.
• Reluctance to simplify. This tenet calls upon hospital administrators to explore the larger context in which safety failures occur.
• Preoccupation with failure. OSHA warns administrators to "never let success breed complacency" and impels hospital leaders to "focus unceasingly on ways the system can fail" and to encourage staff to "listen to their ‘inner voice’ of concern."
• Deference to expertise. Pulling rank rather than going to the one who has the most direct experience in a situation is discouraged by OSHA.
• Resilience. Basically, know there will be failures, but hopefully only small ones; learn from them and rebound.
Dr. Michaels, Dr. Howard, Dr. DuPree, and Dr. Leape did not report any relevant financial disclosures.
*This article has been updated 1/16/2014.
Improving hospital worker safety will result in improved patient safety, according to the Occupational Safety and Health Administration, which has unveiled a hospital worker safety online resource center.
Worker Safety in Hospitals: Caring for our Caregivers, OSHA's new website aimed at curbing hospital worker injury rates, was introduced during a media teleconference Jan. 16. According to OSHA, injuries occur at a rate of 158 times per 10,000 workers, making hospitals more hazardous work environments than either construction or manufacturing sites.
National workers’ compensation losses from hospital workers total $2 billion annually, said OSHA assistant secretary Dr. David Michaels.
Musculoskeletal injuries, primarily from lifting and shifting patients, are the single biggest worker injury in hospitals, he said. According to OSHA, 16,680 hospital workers missed work because of a musculoskeletal injury sustained while handling a patient.
"Other hazards facing hospital workers include workplace violence, slips and falls, exposure to chemicals including hazardous drugs, exposure to infectious diseases, and needle sticks," said Dr. Michaels.
As part of a joint effort to promote the website, also on the conference call were Dr. John Howard, director of the National Institute for Occupational Safety and Health, and Dr. Erin DuPree, chief medical officer and vice president of the Joint Commission Center for Transforming Healthcare, and Dr. Lucian Leape, chairman of the Lucian Leape Institute at the National Patient Safety Foundation.
The OSHA website offers educational materials on avoiding injury when handling patients, as well as on workplace safety needs and the implementation of safety and health management systems.
The materials were culled from best practices employed at hospitals around the country deemed by OSHA to be "high-reliability organizations," and include tips such as having a daily "safety huddle" that includes a discussion of "great catches" and "near misses" that occurred during daily operations.
"One of the major barriers in making progress in patient safety is that when people report that they’ve made a mistake, they often get punished for it," said Dr. Leape. "What we’ve been trying to get people to understand is that mistakes happen because of bad systems, not bad people. You have to create an environment where you really believe that, and make it safe for people to talk about their errors so you can understand what you need to fix."
Dr. DuPree said the OSHA resources align with Joint Commission requirements such as those for hospitals to have a written plan for managing environmental safety for patients and all persons in hospitals. The Joint Commission expects that all individuals who work in the hospital should not fear retribution for speaking up about their safety concerns, Dr. DuPree said. "Leaders need to value and empower their workers. They need to understand that fear of reprisal and failure to share knowledge can compromise an organization’s ability to improve safety for all," he said.
As part of its efforts to advise hospital administrators on how to create safer work environments for their employees, the U.S. Department of Labor Occupational Safety and Health Administration has created a list of attributes of what it calls "high-reliability organizations."
Self-assessment tools, tip sheets, and other materials intended to help hospitals become high-reliability organizations (HROs) are available at OSHA's new website, Worker Safety in Hospitals: Caring for our Caregivers.
"The heart of these new materials are real life lessons from high-performing hospitals [that] have implemented best practices to reduce workplace injuries while also improving patient safety," said OSHA assistant secretary Dr. David Michaels in a press briefing.
The website emphasizes principles endorsed by the Joint Commission, particularly the promotion of a "no-blame" culture to destigmatize safety interventions. Operational strategies derived from the distillation of these best practices and endorsed by OSHA include the following:
• Sensitivity to operations. That means hospital workers should know what the standard procedures are, and follow them.
• Reluctance to simplify. This tenet calls upon hospital administrators to explore the larger context in which safety failures occur.
• Preoccupation with failure. OSHA warns administrators to "never let success breed complacency" and impels hospital leaders to "focus unceasingly on ways the system can fail" and to encourage staff to "listen to their ‘inner voice’ of concern."
• Deference to expertise. Pulling rank rather than going to the one who has the most direct experience in a situation is discouraged by OSHA.
• Resilience. Basically, know there will be failures, but hopefully only small ones; learn from them and rebound.
Dr. Michaels, Dr. Howard, Dr. DuPree, and Dr. Leape did not report any relevant financial disclosures.
*This article has been updated 1/16/2014.
Improving hospital worker safety will result in improved patient safety, according to the Occupational Safety and Health Administration, which has unveiled a hospital worker safety online resource center.
Worker Safety in Hospitals: Caring for our Caregivers, OSHA's new website aimed at curbing hospital worker injury rates, was introduced during a media teleconference Jan. 16. According to OSHA, injuries occur at a rate of 158 times per 10,000 workers, making hospitals more hazardous work environments than either construction or manufacturing sites.
National workers’ compensation losses from hospital workers total $2 billion annually, said OSHA assistant secretary Dr. David Michaels.
Musculoskeletal injuries, primarily from lifting and shifting patients, are the single biggest worker injury in hospitals, he said. According to OSHA, 16,680 hospital workers missed work because of a musculoskeletal injury sustained while handling a patient.
"Other hazards facing hospital workers include workplace violence, slips and falls, exposure to chemicals including hazardous drugs, exposure to infectious diseases, and needle sticks," said Dr. Michaels.
As part of a joint effort to promote the website, also on the conference call were Dr. John Howard, director of the National Institute for Occupational Safety and Health, and Dr. Erin DuPree, chief medical officer and vice president of the Joint Commission Center for Transforming Healthcare, and Dr. Lucian Leape, chairman of the Lucian Leape Institute at the National Patient Safety Foundation.
The OSHA website offers educational materials on avoiding injury when handling patients, as well as on workplace safety needs and the implementation of safety and health management systems.
The materials were culled from best practices employed at hospitals around the country deemed by OSHA to be "high-reliability organizations," and include tips such as having a daily "safety huddle" that includes a discussion of "great catches" and "near misses" that occurred during daily operations.
"One of the major barriers in making progress in patient safety is that when people report that they’ve made a mistake, they often get punished for it," said Dr. Leape. "What we’ve been trying to get people to understand is that mistakes happen because of bad systems, not bad people. You have to create an environment where you really believe that, and make it safe for people to talk about their errors so you can understand what you need to fix."
Dr. DuPree said the OSHA resources align with Joint Commission requirements such as those for hospitals to have a written plan for managing environmental safety for patients and all persons in hospitals. The Joint Commission expects that all individuals who work in the hospital should not fear retribution for speaking up about their safety concerns, Dr. DuPree said. "Leaders need to value and empower their workers. They need to understand that fear of reprisal and failure to share knowledge can compromise an organization’s ability to improve safety for all," he said.
As part of its efforts to advise hospital administrators on how to create safer work environments for their employees, the U.S. Department of Labor Occupational Safety and Health Administration has created a list of attributes of what it calls "high-reliability organizations."
Self-assessment tools, tip sheets, and other materials intended to help hospitals become high-reliability organizations (HROs) are available at OSHA's new website, Worker Safety in Hospitals: Caring for our Caregivers.
"The heart of these new materials are real life lessons from high-performing hospitals [that] have implemented best practices to reduce workplace injuries while also improving patient safety," said OSHA assistant secretary Dr. David Michaels in a press briefing.
The website emphasizes principles endorsed by the Joint Commission, particularly the promotion of a "no-blame" culture to destigmatize safety interventions. Operational strategies derived from the distillation of these best practices and endorsed by OSHA include the following:
• Sensitivity to operations. That means hospital workers should know what the standard procedures are, and follow them.
• Reluctance to simplify. This tenet calls upon hospital administrators to explore the larger context in which safety failures occur.
• Preoccupation with failure. OSHA warns administrators to "never let success breed complacency" and impels hospital leaders to "focus unceasingly on ways the system can fail" and to encourage staff to "listen to their ‘inner voice’ of concern."
• Deference to expertise. Pulling rank rather than going to the one who has the most direct experience in a situation is discouraged by OSHA.
• Resilience. Basically, know there will be failures, but hopefully only small ones; learn from them and rebound.
Dr. Michaels, Dr. Howard, Dr. DuPree, and Dr. Leape did not report any relevant financial disclosures.
*This article has been updated 1/16/2014.
2014 Volunteerism and Humanitarian Award Nominations due February 28
The American College of Surgeons (ACS), in association with Pfizer, Inc., is accepting nominations for the 2014 Surgical Volunteerism Awards and Surgical Humanitarian Award until Friday, February 28.
The ACS/Pfizer Surgical Volunteerism Award, offered in four categories, recognizes surgeons who give back to society and contribute to surgical care through organized volunteer activities. ACS Fellows in active surgical practice whose volunteer activities exceed professional commitments, or retired Fellows who have been involved in volunteerism during their active practice and into retirement are eligible for domestic, international, and military outreach awards. Resident Members and Associate Fellows (ACS Members) who have been involved in significant surgical volunteer activities during their postgraduate surgical training are eligible for the Resident award. Surgeons of all specialties are eligible for each of these awards.
The ACS/Pfizer Surgical Humanitarian Award honors surgeons who have dedicated a significant portion of their surgical careers to full-time or near full-time humanitarian efforts beyond routine surgical practice. Examples include a missionary career surgery, the founding and ongoing operations of a charitable organization that provides surgical care to the underserved, or surgical volunteer outreach during retirement. Compensation for this work may be expected and does not preclude a nominee from consideration.
The ACS Board of Governors (B/G) Surgical Volunteerism and Humanitarian Awards Workgroup will evaluate the nominations, and the B/G Executive Committee will approve the final award winners.
Self-nominations are permissible but require at least one outside letter of support.
Re-nomination of previous nominees is acceptable but requires an updated application.
Supplemental materials should be kept to a minimum and will not be returned.
The nomination website is open for electronic submissions and may be accessed through the "Announcements" section of the Operation Giving Back website at http://www.operationgivingback.facs.org. Please contact [email protected] with any questions.
The American College of Surgeons (ACS), in association with Pfizer, Inc., is accepting nominations for the 2014 Surgical Volunteerism Awards and Surgical Humanitarian Award until Friday, February 28.
The ACS/Pfizer Surgical Volunteerism Award, offered in four categories, recognizes surgeons who give back to society and contribute to surgical care through organized volunteer activities. ACS Fellows in active surgical practice whose volunteer activities exceed professional commitments, or retired Fellows who have been involved in volunteerism during their active practice and into retirement are eligible for domestic, international, and military outreach awards. Resident Members and Associate Fellows (ACS Members) who have been involved in significant surgical volunteer activities during their postgraduate surgical training are eligible for the Resident award. Surgeons of all specialties are eligible for each of these awards.
The ACS/Pfizer Surgical Humanitarian Award honors surgeons who have dedicated a significant portion of their surgical careers to full-time or near full-time humanitarian efforts beyond routine surgical practice. Examples include a missionary career surgery, the founding and ongoing operations of a charitable organization that provides surgical care to the underserved, or surgical volunteer outreach during retirement. Compensation for this work may be expected and does not preclude a nominee from consideration.
The ACS Board of Governors (B/G) Surgical Volunteerism and Humanitarian Awards Workgroup will evaluate the nominations, and the B/G Executive Committee will approve the final award winners.
Self-nominations are permissible but require at least one outside letter of support.
Re-nomination of previous nominees is acceptable but requires an updated application.
Supplemental materials should be kept to a minimum and will not be returned.
The nomination website is open for electronic submissions and may be accessed through the "Announcements" section of the Operation Giving Back website at http://www.operationgivingback.facs.org. Please contact [email protected] with any questions.
The American College of Surgeons (ACS), in association with Pfizer, Inc., is accepting nominations for the 2014 Surgical Volunteerism Awards and Surgical Humanitarian Award until Friday, February 28.
The ACS/Pfizer Surgical Volunteerism Award, offered in four categories, recognizes surgeons who give back to society and contribute to surgical care through organized volunteer activities. ACS Fellows in active surgical practice whose volunteer activities exceed professional commitments, or retired Fellows who have been involved in volunteerism during their active practice and into retirement are eligible for domestic, international, and military outreach awards. Resident Members and Associate Fellows (ACS Members) who have been involved in significant surgical volunteer activities during their postgraduate surgical training are eligible for the Resident award. Surgeons of all specialties are eligible for each of these awards.
The ACS/Pfizer Surgical Humanitarian Award honors surgeons who have dedicated a significant portion of their surgical careers to full-time or near full-time humanitarian efforts beyond routine surgical practice. Examples include a missionary career surgery, the founding and ongoing operations of a charitable organization that provides surgical care to the underserved, or surgical volunteer outreach during retirement. Compensation for this work may be expected and does not preclude a nominee from consideration.
The ACS Board of Governors (B/G) Surgical Volunteerism and Humanitarian Awards Workgroup will evaluate the nominations, and the B/G Executive Committee will approve the final award winners.
Self-nominations are permissible but require at least one outside letter of support.
Re-nomination of previous nominees is acceptable but requires an updated application.
Supplemental materials should be kept to a minimum and will not be returned.
The nomination website is open for electronic submissions and may be accessed through the "Announcements" section of the Operation Giving Back website at http://www.operationgivingback.facs.org. Please contact [email protected] with any questions.
Ronald M. Stewart, MD, FACS, to head Committee on Trauma
The Board of Regents of the American College of Surgeons (ACS) recently appointed Ronald M. Stewart, MD, FACS, as the next Chair of the ACS Committee on Trauma (COT). Dr. Stewart is professor and chair of the department of surgery at the University of Texas (UT) Health Science Center at San Antonio.
Dr. Stewart will take office in March after the COT’s 2014 Annual Meeting, when he will become the 19th Chair of the committee, succeeding Michael F. Rotondo, MD, FACS, of Rochester, NY.

"We congratulate Dr. Stewart and look forward to his leadership and direction as the COT enters its 92nd year of work to improve the care of injured patients," said Dr. Rotondo of the appointment.
Dr. Stewart received his medical degree and completed his surgical residency at from the UT Health Science Center at San Antonio. He completed a two-year trauma and surgical critical care fellowship at the University of Tennessee Health Science Center in Memphis and then served as the director of trauma at University Hospital in San Antonio.
In May 2000, then Texas Gov. George W. Bush appointed Dr. Stewart to the Governor’s Emergency Medical Services and Trauma Advisory Council. He was the recipient of the 2013 National Safety Council Surgeon\'s Award for Service to Safety and the ACS Arthur Ellenberger Award for Excellence in State Advocacy.
Dr. Stewart also served as Chair of the South Texas Chapter of the ACS COT and later as the ACS COT Region 6 Chief (Texas, New Mexico, Louisiana, and Arkansas). In addition, he is the Southern Surgical Society’s representative to the ACS Board of Governors.
The Board of Regents of the American College of Surgeons (ACS) recently appointed Ronald M. Stewart, MD, FACS, as the next Chair of the ACS Committee on Trauma (COT). Dr. Stewart is professor and chair of the department of surgery at the University of Texas (UT) Health Science Center at San Antonio.
Dr. Stewart will take office in March after the COT’s 2014 Annual Meeting, when he will become the 19th Chair of the committee, succeeding Michael F. Rotondo, MD, FACS, of Rochester, NY.
"We congratulate Dr. Stewart and look forward to his leadership and direction as the COT enters its 92nd year of work to improve the care of injured patients," said Dr. Rotondo of the appointment.
Dr. Stewart received his medical degree and completed his surgical residency at from the UT Health Science Center at San Antonio. He completed a two-year trauma and surgical critical care fellowship at the University of Tennessee Health Science Center in Memphis and then served as the director of trauma at University Hospital in San Antonio.
In May 2000, then Texas Gov. George W. Bush appointed Dr. Stewart to the Governor’s Emergency Medical Services and Trauma Advisory Council. He was the recipient of the 2013 National Safety Council Surgeon\'s Award for Service to Safety and the ACS Arthur Ellenberger Award for Excellence in State Advocacy.
Dr. Stewart also served as Chair of the South Texas Chapter of the ACS COT and later as the ACS COT Region 6 Chief (Texas, New Mexico, Louisiana, and Arkansas). In addition, he is the Southern Surgical Society’s representative to the ACS Board of Governors.
The Board of Regents of the American College of Surgeons (ACS) recently appointed Ronald M. Stewart, MD, FACS, as the next Chair of the ACS Committee on Trauma (COT). Dr. Stewart is professor and chair of the department of surgery at the University of Texas (UT) Health Science Center at San Antonio.
Dr. Stewart will take office in March after the COT’s 2014 Annual Meeting, when he will become the 19th Chair of the committee, succeeding Michael F. Rotondo, MD, FACS, of Rochester, NY.
"We congratulate Dr. Stewart and look forward to his leadership and direction as the COT enters its 92nd year of work to improve the care of injured patients," said Dr. Rotondo of the appointment.
Dr. Stewart received his medical degree and completed his surgical residency at from the UT Health Science Center at San Antonio. He completed a two-year trauma and surgical critical care fellowship at the University of Tennessee Health Science Center in Memphis and then served as the director of trauma at University Hospital in San Antonio.
In May 2000, then Texas Gov. George W. Bush appointed Dr. Stewart to the Governor’s Emergency Medical Services and Trauma Advisory Council. He was the recipient of the 2013 National Safety Council Surgeon\'s Award for Service to Safety and the ACS Arthur Ellenberger Award for Excellence in State Advocacy.
Dr. Stewart also served as Chair of the South Texas Chapter of the ACS COT and later as the ACS COT Region 6 Chief (Texas, New Mexico, Louisiana, and Arkansas). In addition, he is the Southern Surgical Society’s representative to the ACS Board of Governors.

Scholarship applications due February 1
The American Association for the Surgery of Trauma (AAST) Research and Education Foundation is accepting applications until February 1 for 2014 Trauma, Surgical Critical Care, and Emergency General Surgery Scholarships. The one-year, $50,000 awards, which will run from July 1, 2014, to June 30, 2015, will support post-residency research by young surgeons who have completed their training within the last seven years and are committed to a career in acute care surgery, including trauma, surgical critical care, and emergency general surgery. For more information and an application, visit the AAST website at www.aast.org or contact Jermica Smith, AAST Project Specialist, at [email protected].
The American Association for the Surgery of Trauma (AAST) Research and Education Foundation is accepting applications until February 1 for 2014 Trauma, Surgical Critical Care, and Emergency General Surgery Scholarships. The one-year, $50,000 awards, which will run from July 1, 2014, to June 30, 2015, will support post-residency research by young surgeons who have completed their training within the last seven years and are committed to a career in acute care surgery, including trauma, surgical critical care, and emergency general surgery. For more information and an application, visit the AAST website at www.aast.org or contact Jermica Smith, AAST Project Specialist, at [email protected].
The American Association for the Surgery of Trauma (AAST) Research and Education Foundation is accepting applications until February 1 for 2014 Trauma, Surgical Critical Care, and Emergency General Surgery Scholarships. The one-year, $50,000 awards, which will run from July 1, 2014, to June 30, 2015, will support post-residency research by young surgeons who have completed their training within the last seven years and are committed to a career in acute care surgery, including trauma, surgical critical care, and emergency general surgery. For more information and an application, visit the AAST website at www.aast.org or contact Jermica Smith, AAST Project Specialist, at [email protected].
Call for Nominations for Officers-Elect
The 2014 Nominating Committee of the Fellows (NCF) will select nominees for the three Officer-Elect positions of the American College of Surgeons (ACS): President-Elect, First Vice-President Elect, and Second Vice-President Elect. The NCF will use the following guidelines:
• Nominees must be loyal members of the College who have demonstrated outstanding integrity and medical statesmanship, along with an unquestioned devotion to the highest principles of surgical practice.
• Nominees must have demonstrated leadership qualities that might be reflected by service and active participation on ACS Committees or in other components of the College.
• Members of the Nominating Committee recognize the importance of achieving representation of all who practice surgery.
• The College encourages consideration of women and other under-represented minorities.
All nominations must include:
• A letter of recommendation
• A personal statement from the candidate detailing ACS service (for president-elect position only)
• A current curriculum vitae
• The name of one individual who can serve as a reference.
In addition, nominating entities, such as surgical special societies, ACS Advisory Councils, and ACS Chapters, must provide a description of their selection process and the total list of applicants reviewed. Any attempt to contact members of the NCF by a candidate or on behalf of a candidate will be viewed negatively and may result in disqualification. Applications submitted without the requested information will not be considered.
The deadline for submitting nominations is Friday, February 28. Submit nominations to [email protected]. If you have questions, call 312-202-5360.
The 2014 Nominating Committee of the Fellows (NCF) will select nominees for the three Officer-Elect positions of the American College of Surgeons (ACS): President-Elect, First Vice-President Elect, and Second Vice-President Elect. The NCF will use the following guidelines:
• Nominees must be loyal members of the College who have demonstrated outstanding integrity and medical statesmanship, along with an unquestioned devotion to the highest principles of surgical practice.
• Nominees must have demonstrated leadership qualities that might be reflected by service and active participation on ACS Committees or in other components of the College.
• Members of the Nominating Committee recognize the importance of achieving representation of all who practice surgery.
• The College encourages consideration of women and other under-represented minorities.
All nominations must include:
• A letter of recommendation
• A personal statement from the candidate detailing ACS service (for president-elect position only)
• A current curriculum vitae
• The name of one individual who can serve as a reference.
In addition, nominating entities, such as surgical special societies, ACS Advisory Councils, and ACS Chapters, must provide a description of their selection process and the total list of applicants reviewed. Any attempt to contact members of the NCF by a candidate or on behalf of a candidate will be viewed negatively and may result in disqualification. Applications submitted without the requested information will not be considered.
The deadline for submitting nominations is Friday, February 28. Submit nominations to [email protected]. If you have questions, call 312-202-5360.
The 2014 Nominating Committee of the Fellows (NCF) will select nominees for the three Officer-Elect positions of the American College of Surgeons (ACS): President-Elect, First Vice-President Elect, and Second Vice-President Elect. The NCF will use the following guidelines:
• Nominees must be loyal members of the College who have demonstrated outstanding integrity and medical statesmanship, along with an unquestioned devotion to the highest principles of surgical practice.
• Nominees must have demonstrated leadership qualities that might be reflected by service and active participation on ACS Committees or in other components of the College.
• Members of the Nominating Committee recognize the importance of achieving representation of all who practice surgery.
• The College encourages consideration of women and other under-represented minorities.
All nominations must include:
• A letter of recommendation
• A personal statement from the candidate detailing ACS service (for president-elect position only)
• A current curriculum vitae
• The name of one individual who can serve as a reference.
In addition, nominating entities, such as surgical special societies, ACS Advisory Councils, and ACS Chapters, must provide a description of their selection process and the total list of applicants reviewed. Any attempt to contact members of the NCF by a candidate or on behalf of a candidate will be viewed negatively and may result in disqualification. Applications submitted without the requested information will not be considered.
The deadline for submitting nominations is Friday, February 28. Submit nominations to [email protected]. If you have questions, call 312-202-5360.
Call for nominations for ACS Board of Governors
Help the American College of Surgeons (ACS) keep pace in a changing health care environment and meet the goals of its Inspiring Quality: Highest Standards, Better Outcomes initiative by nominating your chapter’s brightest, most engaged, responsible and forthright members to serve a three-year term on the ACS Board of Governors. Nominations for 2014 appointments must be submitted to your local ACS Chapter or surgical specialty society by February 28, 2014.
The Board of Governors is the representative body of the ACS. The membership-at-large nominates two-thirds of the Governors, who are elected during the Annual Meeting of the Members at the ACS Clinical Congress. Certain surgical specialty societies, ACS Chapters, and federal medical services nominate one-third of the Board of Governors.
The Governors shall act as a liaison between the Board of Regents and the Fellows, and serve as a clearinghouse for the Regents on general assigned subjects and local problems.
A Governor’s duties include:
• Provide bi-directional communication between the Board of Governors and the Fellows
• Actively participate in a minimum of one Board of Governors Workgroup
• Attend the spring Leadership Summit (spring meeting attendance is not required for international governors)
• Participate in Board of Governors’ meetings, Convocation, and the Annual Meeting of Members at the annual Clinical Congress
• Complete an Annual Survey
• Attend Chapter or Specialty Society meetings
• Assist in establishing an ACS Chapter and serve on the Chapter governing board
• Participate in local Committee on Applicants meetings and interviews
• Provide reports to the ACS Chapter or specialty society and the Board of Governors Communications Pillar
• Promote ACS Fellowship in state and specialty society
Welcome new Fellows into the ACS
An inclusive, transparent Board of Governors depends upon members who can actively serve as a link to their local community and as a resource for the ACS. For more information, go to http://www.facs.org/about/governors/candidates.html. If you have questions, call Betty Sanders, ACS Senior Administrator, Board of Governors, at 312-202-5360.
Help the American College of Surgeons (ACS) keep pace in a changing health care environment and meet the goals of its Inspiring Quality: Highest Standards, Better Outcomes initiative by nominating your chapter’s brightest, most engaged, responsible and forthright members to serve a three-year term on the ACS Board of Governors. Nominations for 2014 appointments must be submitted to your local ACS Chapter or surgical specialty society by February 28, 2014.
The Board of Governors is the representative body of the ACS. The membership-at-large nominates two-thirds of the Governors, who are elected during the Annual Meeting of the Members at the ACS Clinical Congress. Certain surgical specialty societies, ACS Chapters, and federal medical services nominate one-third of the Board of Governors.
The Governors shall act as a liaison between the Board of Regents and the Fellows, and serve as a clearinghouse for the Regents on general assigned subjects and local problems.
A Governor’s duties include:
• Provide bi-directional communication between the Board of Governors and the Fellows
• Actively participate in a minimum of one Board of Governors Workgroup
• Attend the spring Leadership Summit (spring meeting attendance is not required for international governors)
• Participate in Board of Governors’ meetings, Convocation, and the Annual Meeting of Members at the annual Clinical Congress
• Complete an Annual Survey
• Attend Chapter or Specialty Society meetings
• Assist in establishing an ACS Chapter and serve on the Chapter governing board
• Participate in local Committee on Applicants meetings and interviews
• Provide reports to the ACS Chapter or specialty society and the Board of Governors Communications Pillar
• Promote ACS Fellowship in state and specialty society
Welcome new Fellows into the ACS
An inclusive, transparent Board of Governors depends upon members who can actively serve as a link to their local community and as a resource for the ACS. For more information, go to http://www.facs.org/about/governors/candidates.html. If you have questions, call Betty Sanders, ACS Senior Administrator, Board of Governors, at 312-202-5360.
Help the American College of Surgeons (ACS) keep pace in a changing health care environment and meet the goals of its Inspiring Quality: Highest Standards, Better Outcomes initiative by nominating your chapter’s brightest, most engaged, responsible and forthright members to serve a three-year term on the ACS Board of Governors. Nominations for 2014 appointments must be submitted to your local ACS Chapter or surgical specialty society by February 28, 2014.
The Board of Governors is the representative body of the ACS. The membership-at-large nominates two-thirds of the Governors, who are elected during the Annual Meeting of the Members at the ACS Clinical Congress. Certain surgical specialty societies, ACS Chapters, and federal medical services nominate one-third of the Board of Governors.
The Governors shall act as a liaison between the Board of Regents and the Fellows, and serve as a clearinghouse for the Regents on general assigned subjects and local problems.
A Governor’s duties include:
• Provide bi-directional communication between the Board of Governors and the Fellows
• Actively participate in a minimum of one Board of Governors Workgroup
• Attend the spring Leadership Summit (spring meeting attendance is not required for international governors)
• Participate in Board of Governors’ meetings, Convocation, and the Annual Meeting of Members at the annual Clinical Congress
• Complete an Annual Survey
• Attend Chapter or Specialty Society meetings
• Assist in establishing an ACS Chapter and serve on the Chapter governing board
• Participate in local Committee on Applicants meetings and interviews
• Provide reports to the ACS Chapter or specialty society and the Board of Governors Communications Pillar
• Promote ACS Fellowship in state and specialty society
Welcome new Fellows into the ACS
An inclusive, transparent Board of Governors depends upon members who can actively serve as a link to their local community and as a resource for the ACS. For more information, go to http://www.facs.org/about/governors/candidates.html. If you have questions, call Betty Sanders, ACS Senior Administrator, Board of Governors, at 312-202-5360.
COT to host 33rd Point/Counterpoint Surgery Conference June 1-4
The American College of Surgeons (ACS) Committee on Trauma (COT) will present its 33rd annual Point/Counterpoint Acute Care Surgery Conference, June 1–4, 2014, at the Gaylord National Resort and Convention Center in National Harbor, MD. ACS Past-President L. D. Britt, MD, MPH, FACS, FCCM, is the Course Director. The conference is designed for general surgeons and other specialty surgeons, as well as emergency physicians and intensivists, residents, nurses, and paramedics who participate in a high-performance acute care team.
Using the point/counterpoint format, a speaker offers a case in favor of a specific treatment option, and another speaker offers evidence against it. An audience discussion then follows. For more information on the conference and to register online, visit the course website at http://www.pointcounterpoint-acs.com/.
The American College of Surgeons (ACS) Committee on Trauma (COT) will present its 33rd annual Point/Counterpoint Acute Care Surgery Conference, June 1–4, 2014, at the Gaylord National Resort and Convention Center in National Harbor, MD. ACS Past-President L. D. Britt, MD, MPH, FACS, FCCM, is the Course Director. The conference is designed for general surgeons and other specialty surgeons, as well as emergency physicians and intensivists, residents, nurses, and paramedics who participate in a high-performance acute care team.
Using the point/counterpoint format, a speaker offers a case in favor of a specific treatment option, and another speaker offers evidence against it. An audience discussion then follows. For more information on the conference and to register online, visit the course website at http://www.pointcounterpoint-acs.com/.
The American College of Surgeons (ACS) Committee on Trauma (COT) will present its 33rd annual Point/Counterpoint Acute Care Surgery Conference, June 1–4, 2014, at the Gaylord National Resort and Convention Center in National Harbor, MD. ACS Past-President L. D. Britt, MD, MPH, FACS, FCCM, is the Course Director. The conference is designed for general surgeons and other specialty surgeons, as well as emergency physicians and intensivists, residents, nurses, and paramedics who participate in a high-performance acute care team.
Using the point/counterpoint format, a speaker offers a case in favor of a specific treatment option, and another speaker offers evidence against it. An audience discussion then follows. For more information on the conference and to register online, visit the course website at http://www.pointcounterpoint-acs.com/.
2014 International ACS NSQIP Scholarship applications due February 14
The American College of Surgeons National Surgical Quality Improvement Program® (ACS NSQIP®) with the International Relations Committee co-sponsor International ACS NSQIP Scholarships for two surgeons from countries other than the U.S. or Canada who demonstrate strong interests in surgical quality improvement. Completed applications for the 2014 scholarships and all of the supporting documentation must be received by the International Liaison Section no later than February 14.
The scholarships of $10,000 each provide the recipients with an opportunity to attend the 2014 ACS NSQIP National Conference July 26-29 in New York, NY, and meet with program leadership and surgeon champions from ACS NSQIP participating hospitals. Following the ACS NSQIP conference, the candidate is encouraged to visit one to two hospitals reflecting the candidate’s specific clinical interests. These hospitals should also have strong quality programs.
The scholarship requirements are:
• Applicants must be graduates of schools of medicine.
• Applicants must submit their applications from their intended permanent institution.
• Applications will be accepted for processing only when the applicants have been in surgical practice, teaching, or research for a minimum of one year at their intended permanent location, following completion of all formal training (including fellowships and scholarships).
• Applicants must be younger than 55 years of age at the time of application.
• Applicants must have demonstrated a commitment to surgical quality improvement.
• Applicants must submit a fully completed application form provided by the College on its website. The application and accompanying materials must be typewritten and in English. Submission of a curriculum vitae only is unacceptable.
• Applicants must provide information regarding their work setting, including their hospital and the patients they see, as well as their participation in quality improvement activities in this setting. They must also indicate their career goals, indicating how they plan to transfer their newly acquired learning to their current workplace.
• Applicants must submit letters of recommendation from three of their colleagues. One letter must be from the chair of the department of their hospital or in the program in which they hold academic appointment, or an ACS Fellow residing in their country. The chair’s or the Fellow’s letter is to include a specific statement detailing the nature and extent of the quality improvement involvement of the applicant. Letters recommendation should be submitted separately by the the references.
• Applicants must submit a curriculum vitae of 10 or fewer pages.
The International ACS NSQIP Scholarships must be used in the year for which they are designated. They cannot be postponed.
Applicants who are awarded scholarships will submit a full written report of the experiences provided through the scholarships upon completion of their scholarships.
An unsuccessful applicant may reapply only twice and only by completing and submitting a current application form provided by the College, together with new supporting documentation.
The scholarships provide successful applicants with the privilege of participating in the ACS NSQIP National Conference. Assistance will be provided in arranging hotel accommodations during the conference.
More information regarding the ACS National Surgical Quality Improvement Program can be found at http://www.acsnsqip.org.
To qualify for consideration by the selection committee, applicants must fulfill all requirements. The formal International ACS NSQIP Scholar application appears on the ACS Scholarships web page at http://www.facs.org/memberservices/isnsqip.html. Supporting materials and questions should be sent to the International Liaison, Kate Early, via e-mail at [email protected].
All submissions must be received by the February 14 deadline for the selection committee to consider each application. All applicants will be notified of the selection committee’s decision by April 30.
The American College of Surgeons National Surgical Quality Improvement Program® (ACS NSQIP®) with the International Relations Committee co-sponsor International ACS NSQIP Scholarships for two surgeons from countries other than the U.S. or Canada who demonstrate strong interests in surgical quality improvement. Completed applications for the 2014 scholarships and all of the supporting documentation must be received by the International Liaison Section no later than February 14.
The scholarships of $10,000 each provide the recipients with an opportunity to attend the 2014 ACS NSQIP National Conference July 26-29 in New York, NY, and meet with program leadership and surgeon champions from ACS NSQIP participating hospitals. Following the ACS NSQIP conference, the candidate is encouraged to visit one to two hospitals reflecting the candidate’s specific clinical interests. These hospitals should also have strong quality programs.
The scholarship requirements are:
• Applicants must be graduates of schools of medicine.
• Applicants must submit their applications from their intended permanent institution.
• Applications will be accepted for processing only when the applicants have been in surgical practice, teaching, or research for a minimum of one year at their intended permanent location, following completion of all formal training (including fellowships and scholarships).
• Applicants must be younger than 55 years of age at the time of application.
• Applicants must have demonstrated a commitment to surgical quality improvement.
• Applicants must submit a fully completed application form provided by the College on its website. The application and accompanying materials must be typewritten and in English. Submission of a curriculum vitae only is unacceptable.
• Applicants must provide information regarding their work setting, including their hospital and the patients they see, as well as their participation in quality improvement activities in this setting. They must also indicate their career goals, indicating how they plan to transfer their newly acquired learning to their current workplace.
• Applicants must submit letters of recommendation from three of their colleagues. One letter must be from the chair of the department of their hospital or in the program in which they hold academic appointment, or an ACS Fellow residing in their country. The chair’s or the Fellow’s letter is to include a specific statement detailing the nature and extent of the quality improvement involvement of the applicant. Letters recommendation should be submitted separately by the the references.
• Applicants must submit a curriculum vitae of 10 or fewer pages.
The International ACS NSQIP Scholarships must be used in the year for which they are designated. They cannot be postponed.
Applicants who are awarded scholarships will submit a full written report of the experiences provided through the scholarships upon completion of their scholarships.
An unsuccessful applicant may reapply only twice and only by completing and submitting a current application form provided by the College, together with new supporting documentation.
The scholarships provide successful applicants with the privilege of participating in the ACS NSQIP National Conference. Assistance will be provided in arranging hotel accommodations during the conference.
More information regarding the ACS National Surgical Quality Improvement Program can be found at http://www.acsnsqip.org.
To qualify for consideration by the selection committee, applicants must fulfill all requirements. The formal International ACS NSQIP Scholar application appears on the ACS Scholarships web page at http://www.facs.org/memberservices/isnsqip.html. Supporting materials and questions should be sent to the International Liaison, Kate Early, via e-mail at [email protected].
All submissions must be received by the February 14 deadline for the selection committee to consider each application. All applicants will be notified of the selection committee’s decision by April 30.
The American College of Surgeons National Surgical Quality Improvement Program® (ACS NSQIP®) with the International Relations Committee co-sponsor International ACS NSQIP Scholarships for two surgeons from countries other than the U.S. or Canada who demonstrate strong interests in surgical quality improvement. Completed applications for the 2014 scholarships and all of the supporting documentation must be received by the International Liaison Section no later than February 14.
The scholarships of $10,000 each provide the recipients with an opportunity to attend the 2014 ACS NSQIP National Conference July 26-29 in New York, NY, and meet with program leadership and surgeon champions from ACS NSQIP participating hospitals. Following the ACS NSQIP conference, the candidate is encouraged to visit one to two hospitals reflecting the candidate’s specific clinical interests. These hospitals should also have strong quality programs.
The scholarship requirements are:
• Applicants must be graduates of schools of medicine.
• Applicants must submit their applications from their intended permanent institution.
• Applications will be accepted for processing only when the applicants have been in surgical practice, teaching, or research for a minimum of one year at their intended permanent location, following completion of all formal training (including fellowships and scholarships).
• Applicants must be younger than 55 years of age at the time of application.
• Applicants must have demonstrated a commitment to surgical quality improvement.
• Applicants must submit a fully completed application form provided by the College on its website. The application and accompanying materials must be typewritten and in English. Submission of a curriculum vitae only is unacceptable.
• Applicants must provide information regarding their work setting, including their hospital and the patients they see, as well as their participation in quality improvement activities in this setting. They must also indicate their career goals, indicating how they plan to transfer their newly acquired learning to their current workplace.
• Applicants must submit letters of recommendation from three of their colleagues. One letter must be from the chair of the department of their hospital or in the program in which they hold academic appointment, or an ACS Fellow residing in their country. The chair’s or the Fellow’s letter is to include a specific statement detailing the nature and extent of the quality improvement involvement of the applicant. Letters recommendation should be submitted separately by the the references.
• Applicants must submit a curriculum vitae of 10 or fewer pages.
The International ACS NSQIP Scholarships must be used in the year for which they are designated. They cannot be postponed.
Applicants who are awarded scholarships will submit a full written report of the experiences provided through the scholarships upon completion of their scholarships.
An unsuccessful applicant may reapply only twice and only by completing and submitting a current application form provided by the College, together with new supporting documentation.
The scholarships provide successful applicants with the privilege of participating in the ACS NSQIP National Conference. Assistance will be provided in arranging hotel accommodations during the conference.
More information regarding the ACS National Surgical Quality Improvement Program can be found at http://www.acsnsqip.org.
To qualify for consideration by the selection committee, applicants must fulfill all requirements. The formal International ACS NSQIP Scholar application appears on the ACS Scholarships web page at http://www.facs.org/memberservices/isnsqip.html. Supporting materials and questions should be sent to the International Liaison, Kate Early, via e-mail at [email protected].
All submissions must be received by the February 14 deadline for the selection committee to consider each application. All applicants will be notified of the selection committee’s decision by April 30.