User login
Official Newspaper of the American College of Surgeons
Esophagectomy treatment response nodes provide prognostic information
ORLANDO – Tumor response nodes obtained from patients who undergo esophagectomy for early-stage adenocarcinoma provide valuable prognostic information, according to Dr. Dylan Nieman.
Such nodes – lymph nodes with evidence of neoadjuvant treatment effect without residual cancer cells – may mark the prior spread of tumor, and should be counted as positive, Dr. Nieman of the University of Rochester (N.Y.) said at the annual meeting of the Society of Thoracic Surgeons.
The current practice of ignoring these nodes likely results in systematic pathologic understaging, he explained.
In 90 patients who underwent esophagectomy after neoadjuvant therapy for esophageal adenocarcinoma, the median number of nodes found per resection specimen was 18. A total of 100 tumor response nodes without viable malignant cells were identified in 38 (42%) of the patients.
The majority of the patients with treatment response nodes had only one node detected, Dr. Nieman said.
The median survival for the entire cohort was 55.6 months, and the 5-year survival was 35%. The median survival of patients with evidence of treatment response nodes was poorer, but not significantly different from those without treatment response nodes (45.9 vs. 55.6 months), he noted.
"However, for a subset of 62 patients classified as having limited or no nodal involvement – that is, AJCC N0 or N1 – the presence of treatment response nodes was associated with significantly poorer survival. This effect remained when adjusting for patient age and [American Joint Committee on Cancer] stage (hazard ratio, 2.7)," he said.
In a subset of 46 patients with pathologic AJCC stage 2B or less, the presence of treatment response nodes was still associated with poorer survival, even after adjustment for age and AJCC stage.
"To look at this a different way, if tumor response nodes were to be counted as positive, the nodal status of 29 of these patients would be upstaged. This includes 18 of 39 patients, or 46%, who were classified as node negative, and 8 of 23 patients, or 34%, who were classified as N1 by AJCC pathological assessment," he said.
The recategorization of those 29 patients resulted in better survival for the entire group, but particularly for those in the lowest-stage group, he noted.
When investigators modeled stage-adjusted survival, the counting of tumor response nodes as positive offered a better model fit, compared with following the current practice of ignoring tumor response nodes, he explained.
Patients included in the study were identified from a prospectively collected clinical database of esophagectomy patients, and were treated with neoadjuvant therapy for esophageal adenocarcinoma between 2006 and 2011. Most (82 of 90) were men. The patients had a mean age of 62 years, and were followed for a median of 27 months. Forty patients received preoperative chemotherapy, and 50 received preoperative chemoradiation.
In all cases, pathologic resection margins were negative.
On pathologic review, the majority had T3 tumors. More than 40% were staged as node negative, and more than two-thirds were staged with N0 or N1 disease.
"Prior to neoadjuvant therapy, all of these patients were clinically staged stage 2 or stage 3, but at the time of resection after neoadjuvant therapy, by AJCC staging, 24% of the patients were stage 0 or 1, 27% were stage 2, and almost half were stage 3," he said.
The findings are notable, because the current AJCC pathologic staging for esophageal adenocarcinoma is derived from the experience of patients undergoing esophagectomy alone. This approach has unclear relevance in patients who receive multimodality therapy, which has supplanted primary surgery as the standard of care for locoregionally advanced esophageal adenocarcinoma, he said.
"Future efforts at revising the staging system for esophageal adenocarcinoma should consider treatment response lymph nodes. ... We currently have pathological staging models that are of limited usefulness for our neoadjuvantly treated population. Perhaps consideration of these nodes can help improve that," he concluded.
Dr. Nieman reported having no financial disclosures.
ORLANDO – Tumor response nodes obtained from patients who undergo esophagectomy for early-stage adenocarcinoma provide valuable prognostic information, according to Dr. Dylan Nieman.
Such nodes – lymph nodes with evidence of neoadjuvant treatment effect without residual cancer cells – may mark the prior spread of tumor, and should be counted as positive, Dr. Nieman of the University of Rochester (N.Y.) said at the annual meeting of the Society of Thoracic Surgeons.
The current practice of ignoring these nodes likely results in systematic pathologic understaging, he explained.
In 90 patients who underwent esophagectomy after neoadjuvant therapy for esophageal adenocarcinoma, the median number of nodes found per resection specimen was 18. A total of 100 tumor response nodes without viable malignant cells were identified in 38 (42%) of the patients.
The majority of the patients with treatment response nodes had only one node detected, Dr. Nieman said.
The median survival for the entire cohort was 55.6 months, and the 5-year survival was 35%. The median survival of patients with evidence of treatment response nodes was poorer, but not significantly different from those without treatment response nodes (45.9 vs. 55.6 months), he noted.
"However, for a subset of 62 patients classified as having limited or no nodal involvement – that is, AJCC N0 or N1 – the presence of treatment response nodes was associated with significantly poorer survival. This effect remained when adjusting for patient age and [American Joint Committee on Cancer] stage (hazard ratio, 2.7)," he said.
In a subset of 46 patients with pathologic AJCC stage 2B or less, the presence of treatment response nodes was still associated with poorer survival, even after adjustment for age and AJCC stage.
"To look at this a different way, if tumor response nodes were to be counted as positive, the nodal status of 29 of these patients would be upstaged. This includes 18 of 39 patients, or 46%, who were classified as node negative, and 8 of 23 patients, or 34%, who were classified as N1 by AJCC pathological assessment," he said.
The recategorization of those 29 patients resulted in better survival for the entire group, but particularly for those in the lowest-stage group, he noted.
When investigators modeled stage-adjusted survival, the counting of tumor response nodes as positive offered a better model fit, compared with following the current practice of ignoring tumor response nodes, he explained.
Patients included in the study were identified from a prospectively collected clinical database of esophagectomy patients, and were treated with neoadjuvant therapy for esophageal adenocarcinoma between 2006 and 2011. Most (82 of 90) were men. The patients had a mean age of 62 years, and were followed for a median of 27 months. Forty patients received preoperative chemotherapy, and 50 received preoperative chemoradiation.
In all cases, pathologic resection margins were negative.
On pathologic review, the majority had T3 tumors. More than 40% were staged as node negative, and more than two-thirds were staged with N0 or N1 disease.
"Prior to neoadjuvant therapy, all of these patients were clinically staged stage 2 or stage 3, but at the time of resection after neoadjuvant therapy, by AJCC staging, 24% of the patients were stage 0 or 1, 27% were stage 2, and almost half were stage 3," he said.
The findings are notable, because the current AJCC pathologic staging for esophageal adenocarcinoma is derived from the experience of patients undergoing esophagectomy alone. This approach has unclear relevance in patients who receive multimodality therapy, which has supplanted primary surgery as the standard of care for locoregionally advanced esophageal adenocarcinoma, he said.
"Future efforts at revising the staging system for esophageal adenocarcinoma should consider treatment response lymph nodes. ... We currently have pathological staging models that are of limited usefulness for our neoadjuvantly treated population. Perhaps consideration of these nodes can help improve that," he concluded.
Dr. Nieman reported having no financial disclosures.
ORLANDO – Tumor response nodes obtained from patients who undergo esophagectomy for early-stage adenocarcinoma provide valuable prognostic information, according to Dr. Dylan Nieman.
Such nodes – lymph nodes with evidence of neoadjuvant treatment effect without residual cancer cells – may mark the prior spread of tumor, and should be counted as positive, Dr. Nieman of the University of Rochester (N.Y.) said at the annual meeting of the Society of Thoracic Surgeons.
The current practice of ignoring these nodes likely results in systematic pathologic understaging, he explained.
In 90 patients who underwent esophagectomy after neoadjuvant therapy for esophageal adenocarcinoma, the median number of nodes found per resection specimen was 18. A total of 100 tumor response nodes without viable malignant cells were identified in 38 (42%) of the patients.
The majority of the patients with treatment response nodes had only one node detected, Dr. Nieman said.
The median survival for the entire cohort was 55.6 months, and the 5-year survival was 35%. The median survival of patients with evidence of treatment response nodes was poorer, but not significantly different from those without treatment response nodes (45.9 vs. 55.6 months), he noted.
"However, for a subset of 62 patients classified as having limited or no nodal involvement – that is, AJCC N0 or N1 – the presence of treatment response nodes was associated with significantly poorer survival. This effect remained when adjusting for patient age and [American Joint Committee on Cancer] stage (hazard ratio, 2.7)," he said.
In a subset of 46 patients with pathologic AJCC stage 2B or less, the presence of treatment response nodes was still associated with poorer survival, even after adjustment for age and AJCC stage.
"To look at this a different way, if tumor response nodes were to be counted as positive, the nodal status of 29 of these patients would be upstaged. This includes 18 of 39 patients, or 46%, who were classified as node negative, and 8 of 23 patients, or 34%, who were classified as N1 by AJCC pathological assessment," he said.
The recategorization of those 29 patients resulted in better survival for the entire group, but particularly for those in the lowest-stage group, he noted.
When investigators modeled stage-adjusted survival, the counting of tumor response nodes as positive offered a better model fit, compared with following the current practice of ignoring tumor response nodes, he explained.
Patients included in the study were identified from a prospectively collected clinical database of esophagectomy patients, and were treated with neoadjuvant therapy for esophageal adenocarcinoma between 2006 and 2011. Most (82 of 90) were men. The patients had a mean age of 62 years, and were followed for a median of 27 months. Forty patients received preoperative chemotherapy, and 50 received preoperative chemoradiation.
In all cases, pathologic resection margins were negative.
On pathologic review, the majority had T3 tumors. More than 40% were staged as node negative, and more than two-thirds were staged with N0 or N1 disease.
"Prior to neoadjuvant therapy, all of these patients were clinically staged stage 2 or stage 3, but at the time of resection after neoadjuvant therapy, by AJCC staging, 24% of the patients were stage 0 or 1, 27% were stage 2, and almost half were stage 3," he said.
The findings are notable, because the current AJCC pathologic staging for esophageal adenocarcinoma is derived from the experience of patients undergoing esophagectomy alone. This approach has unclear relevance in patients who receive multimodality therapy, which has supplanted primary surgery as the standard of care for locoregionally advanced esophageal adenocarcinoma, he said.
"Future efforts at revising the staging system for esophageal adenocarcinoma should consider treatment response lymph nodes. ... We currently have pathological staging models that are of limited usefulness for our neoadjuvantly treated population. Perhaps consideration of these nodes can help improve that," he concluded.
Dr. Nieman reported having no financial disclosures.
AT THE STS ANNUAL MEETING
Major finding: In 62 patients classified as having limited or no nodal involvement, the presence of treatment response nodes was associated with significantly poorer survival (adjusted hazard ratio, 2.7).
Data source: A review of 90 prospectively collected cases.
Disclosures: Dr. Nieman reported having no financial disclosures.
Cryopreserved blood transfusions making a comeback
NAPLES, FLA. – Transfusions using cryopreserved red blood cells may be superior to those using standard blood storage techniques, updated analyses of a prospective study showed.
Cryopreservation minimizes the biochemical insult associated with transfusions and also appears to reduce the storage lesion, or the biochemical and structural changes that occur during refrigeration and adversely affect perfusion and oxygen off-loading, Dr. David A. Hampton said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
Cryopreserved red blood cells (CPRBCs), which are Food and Drug Administration approved for a 10-year storage life, had a median shelf life of 588 days vs. just 14 days for standard liquid preserved packed red blood cells (LPRBCs) (P less than .01).
CPRBC transfusions were used by the U.S. Navy during the Vietnam War and extensively in civilian hospitals until the FDA extended the shelf life of LPRBCs from 21 to 42 days. Secondary to concerns of poor screening practices and the rise in hepatitis and HIV in the 1980s, CPRBCs fell out of favor for routine transfusion and are currently used for patients with rare blood types or if liquid stores run out.

Researchers at five U.S. centers, however, are currently investigating the efficacy and clinical outcomes of CPRBC transfusions as compared with LPRBCs, with results expected later this summer, according to Dr. Hampton, a fourth-year surgery resident at Oregon Health and Science University (OHSU), Portland.
"There haven’t been large, robust studies of this issue, but once that’s been done, we hope the paradigm will shift from LPRBCs to an increase in CPRBC usage," he said in an interview. "All of the current studies are quite favorable and support this change."
European investigators have already shown that autologous CPRBC transfusions do not elicit an inflammatory response in healthy controls (Transfusion 2013;53:28-33), while OHSU previously reported that tissue oxygenation is superior in trauma patients receiving cryopreserved rather than standard blood transfusions during the first 3 hours after transfusion (J. Trauma Acute Care Surg. 2013;74:371-6).
The results presented at EAST were based on biochemical analyses performed on the same 57 adult trauma patients with an Injury Severity Score (ISS) of more than 4 randomized to receive 1-2 U of CPRBCs or LPRBCs.
The standard and cryopreserved groups were similar with respect to age (44 years vs. 50 years), male gender (66% vs. 73%), blunt injury mechanism (97% vs. 86%), ISS (26 vs. 17), APACHE II scores (11 for both), and number of units transfused (3.1 vs. 3.6).
The correction of anemia was similar between the CPRBC and LPRBC groups 12 hours post transfusion (hemoglobin level at 24.6 g/dL vs. 24.8 g/dL) and at discharge (26.0 g/dL vs. 25.8 g/dL), Dr. Hampton said.
The CPRBC group, however, had significantly increased concentrations of 2,3-diphosphoglycerate (DPG) (P less than .04), a protein that enhances oxygen delivery and is virtually undetectable in LPRBCs after 3 weeks of storage.
The CPRBC group had significantly lower levels of serum amyloid P (1.8 mg/dL vs. 34 mg/dL; P less than .01) and C-reactive protein (0.16 mg/dL vs. 5 mg/dL; P less than .01). Elevated levels of these proteins can potentiate anticoagulation, making it difficult to dose heparin, which in turn increases bleeding risk, Dr. Hampton explained.

CPRBC patients also had significantly lower levels of interleukin-8 (P less than .04) and tumor necrosis factor–alpha (P less than .05). Elevated levels of these proinflammatory cytokines are directly associated with transfusion-related acute lung injury.
Clinical outcomes were mixed in the study, which won the Raymond H. Alexander resident paper competition at the meeting. The cryopreserved group tended to have less acute renal failure (5% vs. 9%), multiple organ failure (9% vs. 12%), and posttransfusion fever (0% vs. 3%), but were twice as likely to experience deep vein thrombosis (32% vs. 15%) and stayed longer in the hospital (16 days vs. 11 days). Respiratory failure occurred in 32% of patients in both groups. None of the differences reached statistical significance, he said.
The results clearly show that cryopreserved RBCs increase 2,3-DPG concentrations, but the oxygen metric of real interest is whether they can increase end-organ oxygen consumption, said Dr. Levi Procter of the University of Kentucky Medical Center, Lexington, who was invited to discuss the study.
He also noted that cryopreserved blood is more expensive than standard refrigerated blood and requires time to thaw, which can be problematic when patients arrive in shock and need an immediate transfusion.
Cryopreserved blood costs about $400 vs. $200 for standard blood, but the differential is negligible given the longer shelf life, Dr. Hampton said. The FDA has approved a 14-day postthaw shelf life, so cryopreserved blood can be thawed and kept on hand in the trauma bay. In a busy level I trauma center, this pre-positioned blood will be used fairly quickly by incoming patients or those within the wards.
"Any hospital that performs transfusions is a candidate for frozen blood," he told this publication. "However, the tertiary referral centers with larger patient populations are where you will most likely see the best results."
Dr. Hampton reported study sponsorship from the U.S. Air Force Research Laboratory. Dr. Procter reported no financial disclosures.
NAPLES, FLA. – Transfusions using cryopreserved red blood cells may be superior to those using standard blood storage techniques, updated analyses of a prospective study showed.
Cryopreservation minimizes the biochemical insult associated with transfusions and also appears to reduce the storage lesion, or the biochemical and structural changes that occur during refrigeration and adversely affect perfusion and oxygen off-loading, Dr. David A. Hampton said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
Cryopreserved red blood cells (CPRBCs), which are Food and Drug Administration approved for a 10-year storage life, had a median shelf life of 588 days vs. just 14 days for standard liquid preserved packed red blood cells (LPRBCs) (P less than .01).
CPRBC transfusions were used by the U.S. Navy during the Vietnam War and extensively in civilian hospitals until the FDA extended the shelf life of LPRBCs from 21 to 42 days. Secondary to concerns of poor screening practices and the rise in hepatitis and HIV in the 1980s, CPRBCs fell out of favor for routine transfusion and are currently used for patients with rare blood types or if liquid stores run out.
Researchers at five U.S. centers, however, are currently investigating the efficacy and clinical outcomes of CPRBC transfusions as compared with LPRBCs, with results expected later this summer, according to Dr. Hampton, a fourth-year surgery resident at Oregon Health and Science University (OHSU), Portland.
"There haven’t been large, robust studies of this issue, but once that’s been done, we hope the paradigm will shift from LPRBCs to an increase in CPRBC usage," he said in an interview. "All of the current studies are quite favorable and support this change."
European investigators have already shown that autologous CPRBC transfusions do not elicit an inflammatory response in healthy controls (Transfusion 2013;53:28-33), while OHSU previously reported that tissue oxygenation is superior in trauma patients receiving cryopreserved rather than standard blood transfusions during the first 3 hours after transfusion (J. Trauma Acute Care Surg. 2013;74:371-6).
The results presented at EAST were based on biochemical analyses performed on the same 57 adult trauma patients with an Injury Severity Score (ISS) of more than 4 randomized to receive 1-2 U of CPRBCs or LPRBCs.
The standard and cryopreserved groups were similar with respect to age (44 years vs. 50 years), male gender (66% vs. 73%), blunt injury mechanism (97% vs. 86%), ISS (26 vs. 17), APACHE II scores (11 for both), and number of units transfused (3.1 vs. 3.6).
The correction of anemia was similar between the CPRBC and LPRBC groups 12 hours post transfusion (hemoglobin level at 24.6 g/dL vs. 24.8 g/dL) and at discharge (26.0 g/dL vs. 25.8 g/dL), Dr. Hampton said.
The CPRBC group, however, had significantly increased concentrations of 2,3-diphosphoglycerate (DPG) (P less than .04), a protein that enhances oxygen delivery and is virtually undetectable in LPRBCs after 3 weeks of storage.
The CPRBC group had significantly lower levels of serum amyloid P (1.8 mg/dL vs. 34 mg/dL; P less than .01) and C-reactive protein (0.16 mg/dL vs. 5 mg/dL; P less than .01). Elevated levels of these proteins can potentiate anticoagulation, making it difficult to dose heparin, which in turn increases bleeding risk, Dr. Hampton explained.
CPRBC patients also had significantly lower levels of interleukin-8 (P less than .04) and tumor necrosis factor–alpha (P less than .05). Elevated levels of these proinflammatory cytokines are directly associated with transfusion-related acute lung injury.
Clinical outcomes were mixed in the study, which won the Raymond H. Alexander resident paper competition at the meeting. The cryopreserved group tended to have less acute renal failure (5% vs. 9%), multiple organ failure (9% vs. 12%), and posttransfusion fever (0% vs. 3%), but were twice as likely to experience deep vein thrombosis (32% vs. 15%) and stayed longer in the hospital (16 days vs. 11 days). Respiratory failure occurred in 32% of patients in both groups. None of the differences reached statistical significance, he said.
The results clearly show that cryopreserved RBCs increase 2,3-DPG concentrations, but the oxygen metric of real interest is whether they can increase end-organ oxygen consumption, said Dr. Levi Procter of the University of Kentucky Medical Center, Lexington, who was invited to discuss the study.
He also noted that cryopreserved blood is more expensive than standard refrigerated blood and requires time to thaw, which can be problematic when patients arrive in shock and need an immediate transfusion.
Cryopreserved blood costs about $400 vs. $200 for standard blood, but the differential is negligible given the longer shelf life, Dr. Hampton said. The FDA has approved a 14-day postthaw shelf life, so cryopreserved blood can be thawed and kept on hand in the trauma bay. In a busy level I trauma center, this pre-positioned blood will be used fairly quickly by incoming patients or those within the wards.
"Any hospital that performs transfusions is a candidate for frozen blood," he told this publication. "However, the tertiary referral centers with larger patient populations are where you will most likely see the best results."
Dr. Hampton reported study sponsorship from the U.S. Air Force Research Laboratory. Dr. Procter reported no financial disclosures.
NAPLES, FLA. – Transfusions using cryopreserved red blood cells may be superior to those using standard blood storage techniques, updated analyses of a prospective study showed.
Cryopreservation minimizes the biochemical insult associated with transfusions and also appears to reduce the storage lesion, or the biochemical and structural changes that occur during refrigeration and adversely affect perfusion and oxygen off-loading, Dr. David A. Hampton said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
Cryopreserved red blood cells (CPRBCs), which are Food and Drug Administration approved for a 10-year storage life, had a median shelf life of 588 days vs. just 14 days for standard liquid preserved packed red blood cells (LPRBCs) (P less than .01).
CPRBC transfusions were used by the U.S. Navy during the Vietnam War and extensively in civilian hospitals until the FDA extended the shelf life of LPRBCs from 21 to 42 days. Secondary to concerns of poor screening practices and the rise in hepatitis and HIV in the 1980s, CPRBCs fell out of favor for routine transfusion and are currently used for patients with rare blood types or if liquid stores run out.
Researchers at five U.S. centers, however, are currently investigating the efficacy and clinical outcomes of CPRBC transfusions as compared with LPRBCs, with results expected later this summer, according to Dr. Hampton, a fourth-year surgery resident at Oregon Health and Science University (OHSU), Portland.
"There haven’t been large, robust studies of this issue, but once that’s been done, we hope the paradigm will shift from LPRBCs to an increase in CPRBC usage," he said in an interview. "All of the current studies are quite favorable and support this change."
European investigators have already shown that autologous CPRBC transfusions do not elicit an inflammatory response in healthy controls (Transfusion 2013;53:28-33), while OHSU previously reported that tissue oxygenation is superior in trauma patients receiving cryopreserved rather than standard blood transfusions during the first 3 hours after transfusion (J. Trauma Acute Care Surg. 2013;74:371-6).
The results presented at EAST were based on biochemical analyses performed on the same 57 adult trauma patients with an Injury Severity Score (ISS) of more than 4 randomized to receive 1-2 U of CPRBCs or LPRBCs.
The standard and cryopreserved groups were similar with respect to age (44 years vs. 50 years), male gender (66% vs. 73%), blunt injury mechanism (97% vs. 86%), ISS (26 vs. 17), APACHE II scores (11 for both), and number of units transfused (3.1 vs. 3.6).
The correction of anemia was similar between the CPRBC and LPRBC groups 12 hours post transfusion (hemoglobin level at 24.6 g/dL vs. 24.8 g/dL) and at discharge (26.0 g/dL vs. 25.8 g/dL), Dr. Hampton said.
The CPRBC group, however, had significantly increased concentrations of 2,3-diphosphoglycerate (DPG) (P less than .04), a protein that enhances oxygen delivery and is virtually undetectable in LPRBCs after 3 weeks of storage.
The CPRBC group had significantly lower levels of serum amyloid P (1.8 mg/dL vs. 34 mg/dL; P less than .01) and C-reactive protein (0.16 mg/dL vs. 5 mg/dL; P less than .01). Elevated levels of these proteins can potentiate anticoagulation, making it difficult to dose heparin, which in turn increases bleeding risk, Dr. Hampton explained.
CPRBC patients also had significantly lower levels of interleukin-8 (P less than .04) and tumor necrosis factor–alpha (P less than .05). Elevated levels of these proinflammatory cytokines are directly associated with transfusion-related acute lung injury.
Clinical outcomes were mixed in the study, which won the Raymond H. Alexander resident paper competition at the meeting. The cryopreserved group tended to have less acute renal failure (5% vs. 9%), multiple organ failure (9% vs. 12%), and posttransfusion fever (0% vs. 3%), but were twice as likely to experience deep vein thrombosis (32% vs. 15%) and stayed longer in the hospital (16 days vs. 11 days). Respiratory failure occurred in 32% of patients in both groups. None of the differences reached statistical significance, he said.
The results clearly show that cryopreserved RBCs increase 2,3-DPG concentrations, but the oxygen metric of real interest is whether they can increase end-organ oxygen consumption, said Dr. Levi Procter of the University of Kentucky Medical Center, Lexington, who was invited to discuss the study.
He also noted that cryopreserved blood is more expensive than standard refrigerated blood and requires time to thaw, which can be problematic when patients arrive in shock and need an immediate transfusion.
Cryopreserved blood costs about $400 vs. $200 for standard blood, but the differential is negligible given the longer shelf life, Dr. Hampton said. The FDA has approved a 14-day postthaw shelf life, so cryopreserved blood can be thawed and kept on hand in the trauma bay. In a busy level I trauma center, this pre-positioned blood will be used fairly quickly by incoming patients or those within the wards.
"Any hospital that performs transfusions is a candidate for frozen blood," he told this publication. "However, the tertiary referral centers with larger patient populations are where you will most likely see the best results."
Dr. Hampton reported study sponsorship from the U.S. Air Force Research Laboratory. Dr. Procter reported no financial disclosures.
At EAST SCIENTIFIC ASSEMBLY 2014
Major finding: Patients receiving cryopreserved red blood cells had higher 2,3 DPG concentrations (P less than .04), compared with patients receiving liquid preserved red blood cells.
Data source: A prospective double blind study of 57 adult trauma patients.
Disclosures: Dr. Hampton reported study sponsorship from the U.S. Air Force Research Laboratory. Dr. Procter reported no financial disclosures.

Enrollment in ACA plans exceeds 3 million
More than 3 million Americans signed up for insurance through the Affordable Care Act’s state and federal marketplaces as of Feb. 1, according to the latest official enrollment figures from the Health & Human Services department.
Of the approximately 3.3 million individuals who have enrolled since the online marketplaces launched on Oct. 1, 2013, 1.1 million enrolled in the month of January alone.
Federal officials said the enrollment trends to date are encouraging, especially the interest from young adults, the group most sought after by health insurers.

Overall, about 25% of the 3.3 million enrollees are young adults between the ages of 18 and 34 years. Enrollment from that group grew the fastest of all ages in January, according to the Health & Human Services department.
"The covered population is getting younger," HHS Secretary Kathleen Sebelius said during a Feb. 12 press briefing.
While federal officials cheered the enrollment by younger Americans, they declined to set a goal for how many young adults they want to enroll by the time the Affordable Care Act’s open enrollment closes on March 31.
More women continue to enroll in the marketplaces than men – 55% vs. 45% as of Feb. 1; similar trends were seen in the first 3 months of open enrollment.
Silver plans continue to the most popular types of health plans in the state and federal marketplaces, with 62% of enrollees choosing them. Bronze plans, selected by 19%, were the second most popular choice. Only 1% of enrollees selected catastrophic plans; most of those were young adults, according to HHS.
Most individuals who enrolled in private health plans through the marketplaces also qualified for federal subsidies. Through the first 4 months of enrollment, 82% of people who selected health plans also received financial assistance for their premium, according to the HHS data.
On Twitter @maryellenny
More than 3 million Americans signed up for insurance through the Affordable Care Act’s state and federal marketplaces as of Feb. 1, according to the latest official enrollment figures from the Health & Human Services department.
Of the approximately 3.3 million individuals who have enrolled since the online marketplaces launched on Oct. 1, 2013, 1.1 million enrolled in the month of January alone.
Federal officials said the enrollment trends to date are encouraging, especially the interest from young adults, the group most sought after by health insurers.
Overall, about 25% of the 3.3 million enrollees are young adults between the ages of 18 and 34 years. Enrollment from that group grew the fastest of all ages in January, according to the Health & Human Services department.
"The covered population is getting younger," HHS Secretary Kathleen Sebelius said during a Feb. 12 press briefing.
While federal officials cheered the enrollment by younger Americans, they declined to set a goal for how many young adults they want to enroll by the time the Affordable Care Act’s open enrollment closes on March 31.
More women continue to enroll in the marketplaces than men – 55% vs. 45% as of Feb. 1; similar trends were seen in the first 3 months of open enrollment.
Silver plans continue to the most popular types of health plans in the state and federal marketplaces, with 62% of enrollees choosing them. Bronze plans, selected by 19%, were the second most popular choice. Only 1% of enrollees selected catastrophic plans; most of those were young adults, according to HHS.
Most individuals who enrolled in private health plans through the marketplaces also qualified for federal subsidies. Through the first 4 months of enrollment, 82% of people who selected health plans also received financial assistance for their premium, according to the HHS data.
On Twitter @maryellenny
More than 3 million Americans signed up for insurance through the Affordable Care Act’s state and federal marketplaces as of Feb. 1, according to the latest official enrollment figures from the Health & Human Services department.
Of the approximately 3.3 million individuals who have enrolled since the online marketplaces launched on Oct. 1, 2013, 1.1 million enrolled in the month of January alone.
Federal officials said the enrollment trends to date are encouraging, especially the interest from young adults, the group most sought after by health insurers.
Overall, about 25% of the 3.3 million enrollees are young adults between the ages of 18 and 34 years. Enrollment from that group grew the fastest of all ages in January, according to the Health & Human Services department.
"The covered population is getting younger," HHS Secretary Kathleen Sebelius said during a Feb. 12 press briefing.
While federal officials cheered the enrollment by younger Americans, they declined to set a goal for how many young adults they want to enroll by the time the Affordable Care Act’s open enrollment closes on March 31.
More women continue to enroll in the marketplaces than men – 55% vs. 45% as of Feb. 1; similar trends were seen in the first 3 months of open enrollment.
Silver plans continue to the most popular types of health plans in the state and federal marketplaces, with 62% of enrollees choosing them. Bronze plans, selected by 19%, were the second most popular choice. Only 1% of enrollees selected catastrophic plans; most of those were young adults, according to HHS.
Most individuals who enrolled in private health plans through the marketplaces also qualified for federal subsidies. Through the first 4 months of enrollment, 82% of people who selected health plans also received financial assistance for their premium, according to the HHS data.
On Twitter @maryellenny
Spot-check Hgb testing transforming trauma blood draws
NAPLES, FLA. – Spot-check hemoglobin testing can provide immediate and accurate hemoglobin measurements in trauma patients without removing a drop of blood, a prospective cohort study shows.
"The noninvasive hemoglobin monitor, I think, will change the way we practice," Dr. Bellal Joseph said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.

Continuous, noninvasive hemoglobin (Hgb) devices have been around for years, but studies showed poor correlation with invasive Hgb blood draws in trauma patients. Advances in technology, including more sensitive sensors and a wider range of sensor sizes, allow new spot-check devices to more accurately measure a broader range of patients with a wider range of finger diameters.
Dr. Joseph, a trauma and critical care surgeon at the University of Arizona Medical Center, Tucson, and his colleagues simultaneously obtained invasive and spot-check Hgb measurements in a prospective cohort of 525 trauma patients. Spot-check Hgb was measured three times upon presentation to the Level 1 trauma center using the Pronto-7 pulse CO-oximeter device and correlated with each invasive Hgb measurement.
According to the analysis, the success rate for spot-check Hgb testing was 86% in the mostly male cohort (74%), with a mean Injury Severity Score of 20, and average age of 41 years.
The mean hemoglobin for the 450 invasive Hgb measurements was 11.5 g/dL and 11.4 g/dL for the 1,350 Pronto-7 spot-checks, Dr. Joseph said.
Sensitivity for the spot-check device was 96%, specificity 44%, positive predictive value 73%, and negative predictive value 88% in patients with a hemoglobin above and below 8 g/dL. In all, 38% of patients had a hemoglobin level of less than 8 g/dL.
A Bland-Altman plot showed that 98.7% of readings were within two standard deviations. Spearman’s rank correlation coefficient revealed spot-check Hgb had a strong correlation with invasive Hgb testing (R2 = 0.77; R = 0.86), Dr. Joseph said.
"This device is a lot better than the continuous one we used to have, which they use in the operating room a lot," he said during the poster presentation. "We’re currently looking at it in patients who have blunt spleen or blunt liver injuries. Instead of ordering q6 hour, invasive hemoglobins, we’re just putting the monitor on and seeing if we can make clinical decisions based on that."
The palm-sized Pronto-7 spot-check device also has a perfusion index to help identify patients with early shock, but this has yet to be studied or integrated into practice.
"The one concern that I still have with this device is that 14% of our patients didn’t pick up a hemoglobin, and why is that?" Dr. Joseph said. Fashion may be, in part, to blame, with readings more likely to fail in patients with nail polish on, he added.
The next phase of the study will include implementation of the spot-check device on the floors and in the ICU with the nursing staff and direct uploading of results into patient charts. A time-savings analysis also will be done.
Dr. Joseph and his coauthors reported having no financial disclosures or study support.
NAPLES, FLA. – Spot-check hemoglobin testing can provide immediate and accurate hemoglobin measurements in trauma patients without removing a drop of blood, a prospective cohort study shows.
"The noninvasive hemoglobin monitor, I think, will change the way we practice," Dr. Bellal Joseph said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Continuous, noninvasive hemoglobin (Hgb) devices have been around for years, but studies showed poor correlation with invasive Hgb blood draws in trauma patients. Advances in technology, including more sensitive sensors and a wider range of sensor sizes, allow new spot-check devices to more accurately measure a broader range of patients with a wider range of finger diameters.
Dr. Joseph, a trauma and critical care surgeon at the University of Arizona Medical Center, Tucson, and his colleagues simultaneously obtained invasive and spot-check Hgb measurements in a prospective cohort of 525 trauma patients. Spot-check Hgb was measured three times upon presentation to the Level 1 trauma center using the Pronto-7 pulse CO-oximeter device and correlated with each invasive Hgb measurement.
According to the analysis, the success rate for spot-check Hgb testing was 86% in the mostly male cohort (74%), with a mean Injury Severity Score of 20, and average age of 41 years.
The mean hemoglobin for the 450 invasive Hgb measurements was 11.5 g/dL and 11.4 g/dL for the 1,350 Pronto-7 spot-checks, Dr. Joseph said.
Sensitivity for the spot-check device was 96%, specificity 44%, positive predictive value 73%, and negative predictive value 88% in patients with a hemoglobin above and below 8 g/dL. In all, 38% of patients had a hemoglobin level of less than 8 g/dL.
A Bland-Altman plot showed that 98.7% of readings were within two standard deviations. Spearman’s rank correlation coefficient revealed spot-check Hgb had a strong correlation with invasive Hgb testing (R2 = 0.77; R = 0.86), Dr. Joseph said.
"This device is a lot better than the continuous one we used to have, which they use in the operating room a lot," he said during the poster presentation. "We’re currently looking at it in patients who have blunt spleen or blunt liver injuries. Instead of ordering q6 hour, invasive hemoglobins, we’re just putting the monitor on and seeing if we can make clinical decisions based on that."
The palm-sized Pronto-7 spot-check device also has a perfusion index to help identify patients with early shock, but this has yet to be studied or integrated into practice.
"The one concern that I still have with this device is that 14% of our patients didn’t pick up a hemoglobin, and why is that?" Dr. Joseph said. Fashion may be, in part, to blame, with readings more likely to fail in patients with nail polish on, he added.
The next phase of the study will include implementation of the spot-check device on the floors and in the ICU with the nursing staff and direct uploading of results into patient charts. A time-savings analysis also will be done.
Dr. Joseph and his coauthors reported having no financial disclosures or study support.
NAPLES, FLA. – Spot-check hemoglobin testing can provide immediate and accurate hemoglobin measurements in trauma patients without removing a drop of blood, a prospective cohort study shows.
"The noninvasive hemoglobin monitor, I think, will change the way we practice," Dr. Bellal Joseph said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Continuous, noninvasive hemoglobin (Hgb) devices have been around for years, but studies showed poor correlation with invasive Hgb blood draws in trauma patients. Advances in technology, including more sensitive sensors and a wider range of sensor sizes, allow new spot-check devices to more accurately measure a broader range of patients with a wider range of finger diameters.
Dr. Joseph, a trauma and critical care surgeon at the University of Arizona Medical Center, Tucson, and his colleagues simultaneously obtained invasive and spot-check Hgb measurements in a prospective cohort of 525 trauma patients. Spot-check Hgb was measured three times upon presentation to the Level 1 trauma center using the Pronto-7 pulse CO-oximeter device and correlated with each invasive Hgb measurement.
According to the analysis, the success rate for spot-check Hgb testing was 86% in the mostly male cohort (74%), with a mean Injury Severity Score of 20, and average age of 41 years.
The mean hemoglobin for the 450 invasive Hgb measurements was 11.5 g/dL and 11.4 g/dL for the 1,350 Pronto-7 spot-checks, Dr. Joseph said.
Sensitivity for the spot-check device was 96%, specificity 44%, positive predictive value 73%, and negative predictive value 88% in patients with a hemoglobin above and below 8 g/dL. In all, 38% of patients had a hemoglobin level of less than 8 g/dL.
A Bland-Altman plot showed that 98.7% of readings were within two standard deviations. Spearman’s rank correlation coefficient revealed spot-check Hgb had a strong correlation with invasive Hgb testing (R2 = 0.77; R = 0.86), Dr. Joseph said.
"This device is a lot better than the continuous one we used to have, which they use in the operating room a lot," he said during the poster presentation. "We’re currently looking at it in patients who have blunt spleen or blunt liver injuries. Instead of ordering q6 hour, invasive hemoglobins, we’re just putting the monitor on and seeing if we can make clinical decisions based on that."
The palm-sized Pronto-7 spot-check device also has a perfusion index to help identify patients with early shock, but this has yet to be studied or integrated into practice.
"The one concern that I still have with this device is that 14% of our patients didn’t pick up a hemoglobin, and why is that?" Dr. Joseph said. Fashion may be, in part, to blame, with readings more likely to fail in patients with nail polish on, he added.
The next phase of the study will include implementation of the spot-check device on the floors and in the ICU with the nursing staff and direct uploading of results into patient charts. A time-savings analysis also will be done.
Dr. Joseph and his coauthors reported having no financial disclosures or study support.
AT EAST SCIENTIFIC ASSEMBLY
Major finding: The mean hemoglobin was 11.5 g/dL for invasive hemoglobin testing and 11.4 g/dL for noninvasive, spot-check testing.
Data source: Prospective cohort study of 525 trauma patients.
Disclosures: Dr. Joseph and his coauthors reported having no financial disclosures or study support.

Guidelines: No ink on tumor is adequate surgical margin for early-stage breast cancer
Negative surgical margins defined by the absence of any ink on the excised tumor are adequate in most cases of early-stage breast cancer treated with breast-conserving therapy, suggest new consensus guidelines from the Society of Surgical Oncology and American Society for Radiation Oncology.
"The use of no ink on tumor as the standard for an adequate margin in invasive cancer in the era of multidisciplinary therapy is associated with low rates of ipsilateral breast tumor recurrence and has the potential to decrease re-excision rates, improve cosmetic outcomes, and decrease health care costs," concludes the 12-member multidisciplinary panel. "The routine practice to obtain negative margin widths wider than no ink on tumor is not indicated" (J. Clin. Oncol. 2014 Feb. 10 [doi:10.1200/JCO.2013.53.3935]).

The panel used as their evidence a systematic review and a meta-analysis based on 33 studies having a total of 28,162 patients with stage I or II breast cancer who were treated with breast-conserving surgery plus whole-breast radiation therapy.
Results showed that, compared with peers having negative margins, patients having positive margins were twice as likely to experience an ipsilateral recurrence, regardless of whether they had favorable tumor biology, were given a radiation boost, or received endocrine therapy (Int. J. Radiation Oncol. Biol. Phys. 2014;88:553-64).
But taking wider margins beyond the point of no ink on tumor did not further reduce the risk of ipsilateral recurrence in the patients overall or in a variety of subsets having unfavorable features (young age, aggressive biology, lobular cancers, or tumors with an extensive intraductal component).
"Our hope is that this guideline will ultimately lead to significant reductions in the high re-excision rate for women with early-stage breast cancer undergoing breast-conserving surgery. Based on the consensus panel’s extensive review of the literature, the vast majority of re-excisions are unnecessary because disease control in the breast is excellent for women with early-stage disease when radiation and hormonal therapy and/or chemotherapy are added to a women’s treatment plan," panel cochair Dr. Meena S. Moran of Yale University, New Haven, Conn., commented in a prepared statement.
In an accompanying editorial, Dr. Reshma Jagsi, University of Michigan, Ann Arbor, and her colleagues write, "We agree with the general idea that routine reexcision of close margins (beyond no ink on tumor) is not necessary, and we expect that these guidelines will have a substantial impact on the community of practicing surgeons. Therefore, radiation oncologists should be prepared to encounter an increasing number of patients with microscopically close margins who might have undergone re-excision in previous years" (Int. J. Radiation Oncol. Biol. Phys. 2014;88:535-36).
At the same time, they note that the wording of the new guidelines gives physicians and patients latitude in individualizing decisions about whether re-excision is warranted.
"Physicians applying these guidelines must have an appreciation of the rationale for the recommendations, as well as the limitations of the evidence available, so that they can interpret and apply the guidelines appropriately. Only with a sophisticated understanding of these issues can we, as a profession, continue to deliver individualized care of consistently high quality, avoiding the sort of ‘cookbook medicine’ that serves well neither physicians nor patients," the editorialists conclude.
The studies included in the meta-analysis were published between 1965 and early 2013 and had a median or mean follow-up of at least 4 years. Patients were excluded if they received neoadjuvant chemotherapy or had only ductal carcinoma in situ.

Overall, 78% of the patients studied had negative margins, defined as no ink on the invasive tumor or any ductal carcinoma in situ component. After a median follow-up of 6.6 years, the median prevalence of ipsilateral recurrence was 5.3% overall.
Patients with positive or close margins were twice as likely to have an ipsilateral recurrence (odds ratio, 1.96). In the subset of studies that were able to separate out close margins, risk was elevated with both positive margins (OR, 2.44) and close margins (OR, 1.74).
The adverse impact of positive margins was still evident in analyses taking into account use of a radiation boost (OR, 2.45) and receipt of endocrine therapy (OR, 2.53), and among patients with favorable biology in the form of estrogen receptor–positive tumors (OR, 2.66).
When the impact of the width of the negative margin was evaluated, the risks of ipsilateral recurrence with 2-mm and 5-mm margins were statistically indistinguishable from those with 1-mm margins.
The analysis confirmed that giving systemic therapy (endocrine therapy, chemotherapy, and/or biologic therapy) reduces the risk of ipsilateral recurrence. But the evidence also suggested that in the small number of patients who do not receive this therapy, wider margins beyond no ink on tumor do not further reduce that risk.
In additional findings, there was no evidence that wider margins beyond no ink on tumor are indicated in patients having more aggressive biological subtypes of breast cancer, invasive lobular carcinoma, or tumors with an extensive intraductal component, or in patients aged 40 years or younger.
The panel also concluded that margin width should not dictate the choice of whole-breast radiation therapy delivery technique, fractionation, and boost dose.
Negative surgical margins defined by the absence of any ink on the excised tumor are adequate in most cases of early-stage breast cancer treated with breast-conserving therapy, suggest new consensus guidelines from the Society of Surgical Oncology and American Society for Radiation Oncology.
"The use of no ink on tumor as the standard for an adequate margin in invasive cancer in the era of multidisciplinary therapy is associated with low rates of ipsilateral breast tumor recurrence and has the potential to decrease re-excision rates, improve cosmetic outcomes, and decrease health care costs," concludes the 12-member multidisciplinary panel. "The routine practice to obtain negative margin widths wider than no ink on tumor is not indicated" (J. Clin. Oncol. 2014 Feb. 10 [doi:10.1200/JCO.2013.53.3935]).
The panel used as their evidence a systematic review and a meta-analysis based on 33 studies having a total of 28,162 patients with stage I or II breast cancer who were treated with breast-conserving surgery plus whole-breast radiation therapy.
Results showed that, compared with peers having negative margins, patients having positive margins were twice as likely to experience an ipsilateral recurrence, regardless of whether they had favorable tumor biology, were given a radiation boost, or received endocrine therapy (Int. J. Radiation Oncol. Biol. Phys. 2014;88:553-64).
But taking wider margins beyond the point of no ink on tumor did not further reduce the risk of ipsilateral recurrence in the patients overall or in a variety of subsets having unfavorable features (young age, aggressive biology, lobular cancers, or tumors with an extensive intraductal component).
"Our hope is that this guideline will ultimately lead to significant reductions in the high re-excision rate for women with early-stage breast cancer undergoing breast-conserving surgery. Based on the consensus panel’s extensive review of the literature, the vast majority of re-excisions are unnecessary because disease control in the breast is excellent for women with early-stage disease when radiation and hormonal therapy and/or chemotherapy are added to a women’s treatment plan," panel cochair Dr. Meena S. Moran of Yale University, New Haven, Conn., commented in a prepared statement.
In an accompanying editorial, Dr. Reshma Jagsi, University of Michigan, Ann Arbor, and her colleagues write, "We agree with the general idea that routine reexcision of close margins (beyond no ink on tumor) is not necessary, and we expect that these guidelines will have a substantial impact on the community of practicing surgeons. Therefore, radiation oncologists should be prepared to encounter an increasing number of patients with microscopically close margins who might have undergone re-excision in previous years" (Int. J. Radiation Oncol. Biol. Phys. 2014;88:535-36).
At the same time, they note that the wording of the new guidelines gives physicians and patients latitude in individualizing decisions about whether re-excision is warranted.
"Physicians applying these guidelines must have an appreciation of the rationale for the recommendations, as well as the limitations of the evidence available, so that they can interpret and apply the guidelines appropriately. Only with a sophisticated understanding of these issues can we, as a profession, continue to deliver individualized care of consistently high quality, avoiding the sort of ‘cookbook medicine’ that serves well neither physicians nor patients," the editorialists conclude.
The studies included in the meta-analysis were published between 1965 and early 2013 and had a median or mean follow-up of at least 4 years. Patients were excluded if they received neoadjuvant chemotherapy or had only ductal carcinoma in situ.
Overall, 78% of the patients studied had negative margins, defined as no ink on the invasive tumor or any ductal carcinoma in situ component. After a median follow-up of 6.6 years, the median prevalence of ipsilateral recurrence was 5.3% overall.
Patients with positive or close margins were twice as likely to have an ipsilateral recurrence (odds ratio, 1.96). In the subset of studies that were able to separate out close margins, risk was elevated with both positive margins (OR, 2.44) and close margins (OR, 1.74).
The adverse impact of positive margins was still evident in analyses taking into account use of a radiation boost (OR, 2.45) and receipt of endocrine therapy (OR, 2.53), and among patients with favorable biology in the form of estrogen receptor–positive tumors (OR, 2.66).
When the impact of the width of the negative margin was evaluated, the risks of ipsilateral recurrence with 2-mm and 5-mm margins were statistically indistinguishable from those with 1-mm margins.
The analysis confirmed that giving systemic therapy (endocrine therapy, chemotherapy, and/or biologic therapy) reduces the risk of ipsilateral recurrence. But the evidence also suggested that in the small number of patients who do not receive this therapy, wider margins beyond no ink on tumor do not further reduce that risk.
In additional findings, there was no evidence that wider margins beyond no ink on tumor are indicated in patients having more aggressive biological subtypes of breast cancer, invasive lobular carcinoma, or tumors with an extensive intraductal component, or in patients aged 40 years or younger.
The panel also concluded that margin width should not dictate the choice of whole-breast radiation therapy delivery technique, fractionation, and boost dose.
Negative surgical margins defined by the absence of any ink on the excised tumor are adequate in most cases of early-stage breast cancer treated with breast-conserving therapy, suggest new consensus guidelines from the Society of Surgical Oncology and American Society for Radiation Oncology.
"The use of no ink on tumor as the standard for an adequate margin in invasive cancer in the era of multidisciplinary therapy is associated with low rates of ipsilateral breast tumor recurrence and has the potential to decrease re-excision rates, improve cosmetic outcomes, and decrease health care costs," concludes the 12-member multidisciplinary panel. "The routine practice to obtain negative margin widths wider than no ink on tumor is not indicated" (J. Clin. Oncol. 2014 Feb. 10 [doi:10.1200/JCO.2013.53.3935]).
The panel used as their evidence a systematic review and a meta-analysis based on 33 studies having a total of 28,162 patients with stage I or II breast cancer who were treated with breast-conserving surgery plus whole-breast radiation therapy.
Results showed that, compared with peers having negative margins, patients having positive margins were twice as likely to experience an ipsilateral recurrence, regardless of whether they had favorable tumor biology, were given a radiation boost, or received endocrine therapy (Int. J. Radiation Oncol. Biol. Phys. 2014;88:553-64).
But taking wider margins beyond the point of no ink on tumor did not further reduce the risk of ipsilateral recurrence in the patients overall or in a variety of subsets having unfavorable features (young age, aggressive biology, lobular cancers, or tumors with an extensive intraductal component).
"Our hope is that this guideline will ultimately lead to significant reductions in the high re-excision rate for women with early-stage breast cancer undergoing breast-conserving surgery. Based on the consensus panel’s extensive review of the literature, the vast majority of re-excisions are unnecessary because disease control in the breast is excellent for women with early-stage disease when radiation and hormonal therapy and/or chemotherapy are added to a women’s treatment plan," panel cochair Dr. Meena S. Moran of Yale University, New Haven, Conn., commented in a prepared statement.
In an accompanying editorial, Dr. Reshma Jagsi, University of Michigan, Ann Arbor, and her colleagues write, "We agree with the general idea that routine reexcision of close margins (beyond no ink on tumor) is not necessary, and we expect that these guidelines will have a substantial impact on the community of practicing surgeons. Therefore, radiation oncologists should be prepared to encounter an increasing number of patients with microscopically close margins who might have undergone re-excision in previous years" (Int. J. Radiation Oncol. Biol. Phys. 2014;88:535-36).
At the same time, they note that the wording of the new guidelines gives physicians and patients latitude in individualizing decisions about whether re-excision is warranted.
"Physicians applying these guidelines must have an appreciation of the rationale for the recommendations, as well as the limitations of the evidence available, so that they can interpret and apply the guidelines appropriately. Only with a sophisticated understanding of these issues can we, as a profession, continue to deliver individualized care of consistently high quality, avoiding the sort of ‘cookbook medicine’ that serves well neither physicians nor patients," the editorialists conclude.
The studies included in the meta-analysis were published between 1965 and early 2013 and had a median or mean follow-up of at least 4 years. Patients were excluded if they received neoadjuvant chemotherapy or had only ductal carcinoma in situ.
Overall, 78% of the patients studied had negative margins, defined as no ink on the invasive tumor or any ductal carcinoma in situ component. After a median follow-up of 6.6 years, the median prevalence of ipsilateral recurrence was 5.3% overall.
Patients with positive or close margins were twice as likely to have an ipsilateral recurrence (odds ratio, 1.96). In the subset of studies that were able to separate out close margins, risk was elevated with both positive margins (OR, 2.44) and close margins (OR, 1.74).
The adverse impact of positive margins was still evident in analyses taking into account use of a radiation boost (OR, 2.45) and receipt of endocrine therapy (OR, 2.53), and among patients with favorable biology in the form of estrogen receptor–positive tumors (OR, 2.66).
When the impact of the width of the negative margin was evaluated, the risks of ipsilateral recurrence with 2-mm and 5-mm margins were statistically indistinguishable from those with 1-mm margins.
The analysis confirmed that giving systemic therapy (endocrine therapy, chemotherapy, and/or biologic therapy) reduces the risk of ipsilateral recurrence. But the evidence also suggested that in the small number of patients who do not receive this therapy, wider margins beyond no ink on tumor do not further reduce that risk.
In additional findings, there was no evidence that wider margins beyond no ink on tumor are indicated in patients having more aggressive biological subtypes of breast cancer, invasive lobular carcinoma, or tumors with an extensive intraductal component, or in patients aged 40 years or younger.
The panel also concluded that margin width should not dictate the choice of whole-breast radiation therapy delivery technique, fractionation, and boost dose.
ICD-10 price tag going up for doctors
Making the switch from the ICD-9 to the ICD-10 diagnosis code set could cost as much as $225,000 for some small practices and up to $8 million in some large practices, according to a study from the American Medical Association.
Physician offices and hospitals must use the ICD-10 code sets beginning Oct. 1, but the preparation for the switch is taking years and involves hours of staff training, the purchase of new hardware and software, and testing with vendors and payers.

A follow-up report prepared for the AMA by Nachimson Advisors found that in certain cases, implementation costs are nearly three times higher than what the firm predicted in 2008.
In their original report, Nachimson Advisors estimated that it would cost more than $83,000 for a typical small practice (3 physicians, 2 administrative staff) to implement ICD-10, rising to $285,000 for a typical medium-size practice (10 physicians, 1 full-time coder, 6 administrative staff), and about $2.7 million for a typical large practice (100 physicians, 10 full-time coders, 64 administrative staff).
Now those costs are estimated to range from $56,000 to $226,000 for small practices and $213,000 to $824,000 for medium-size practices. And for large practices, implementing ICD-10 could cost anywhere from $2 million to $8 million.
About two-thirds of physician practices are expected to have costs in the upper range of those estimates, according to the AMA.
One reason for the increased cost is new requirements related to the adoption of electronic health records (EHRs). Nachimson Advisors also projects a larger potential for payment disruptions, estimating that 2%-6% of claims could be denied after the Oct. 1 implementation date.
"The markedly higher implementation costs for ICD-10 place a crushing burden on physicians, straining vital resources needed to invest in new health care delivery models and well-developed technology that promotes care coordination with real value to patients," Dr. Ardis Dee Hoven, AMA president, said in a statement. "Continuing to compel physicians to adopt this new coding structure threatens to disrupt innovations by diverting resources away from areas that are expected to help lower costs and improve the quality of care."
The AMA is calling on Health & Human Services secretary Kathleen Sebelius to reconsider ICD-10 implementation. But if the agency sticks to its plan, the AMA has requested several changes to mitigate some of the costs.
For example, the AMA recommends that Medicare provide a 2-year implementation period during which the agency would not be allowed to deny payments based on the specificity of the ICD-10 code provided. And the agency would provide feedback on coding to physicians during this time.
The AMA also is asking Medicare to simplify its claims requirements by adopting a policy that when the most specific ICD-10 code is used, no additional information or attachments will be required before paying the claim.
On Twitter @maryellenny
Making the switch from the ICD-9 to the ICD-10 diagnosis code set could cost as much as $225,000 for some small practices and up to $8 million in some large practices, according to a study from the American Medical Association.
Physician offices and hospitals must use the ICD-10 code sets beginning Oct. 1, but the preparation for the switch is taking years and involves hours of staff training, the purchase of new hardware and software, and testing with vendors and payers.
A follow-up report prepared for the AMA by Nachimson Advisors found that in certain cases, implementation costs are nearly three times higher than what the firm predicted in 2008.
In their original report, Nachimson Advisors estimated that it would cost more than $83,000 for a typical small practice (3 physicians, 2 administrative staff) to implement ICD-10, rising to $285,000 for a typical medium-size practice (10 physicians, 1 full-time coder, 6 administrative staff), and about $2.7 million for a typical large practice (100 physicians, 10 full-time coders, 64 administrative staff).
Now those costs are estimated to range from $56,000 to $226,000 for small practices and $213,000 to $824,000 for medium-size practices. And for large practices, implementing ICD-10 could cost anywhere from $2 million to $8 million.
About two-thirds of physician practices are expected to have costs in the upper range of those estimates, according to the AMA.
One reason for the increased cost is new requirements related to the adoption of electronic health records (EHRs). Nachimson Advisors also projects a larger potential for payment disruptions, estimating that 2%-6% of claims could be denied after the Oct. 1 implementation date.
"The markedly higher implementation costs for ICD-10 place a crushing burden on physicians, straining vital resources needed to invest in new health care delivery models and well-developed technology that promotes care coordination with real value to patients," Dr. Ardis Dee Hoven, AMA president, said in a statement. "Continuing to compel physicians to adopt this new coding structure threatens to disrupt innovations by diverting resources away from areas that are expected to help lower costs and improve the quality of care."
The AMA is calling on Health & Human Services secretary Kathleen Sebelius to reconsider ICD-10 implementation. But if the agency sticks to its plan, the AMA has requested several changes to mitigate some of the costs.
For example, the AMA recommends that Medicare provide a 2-year implementation period during which the agency would not be allowed to deny payments based on the specificity of the ICD-10 code provided. And the agency would provide feedback on coding to physicians during this time.
The AMA also is asking Medicare to simplify its claims requirements by adopting a policy that when the most specific ICD-10 code is used, no additional information or attachments will be required before paying the claim.
On Twitter @maryellenny
Making the switch from the ICD-9 to the ICD-10 diagnosis code set could cost as much as $225,000 for some small practices and up to $8 million in some large practices, according to a study from the American Medical Association.
Physician offices and hospitals must use the ICD-10 code sets beginning Oct. 1, but the preparation for the switch is taking years and involves hours of staff training, the purchase of new hardware and software, and testing with vendors and payers.
A follow-up report prepared for the AMA by Nachimson Advisors found that in certain cases, implementation costs are nearly three times higher than what the firm predicted in 2008.
In their original report, Nachimson Advisors estimated that it would cost more than $83,000 for a typical small practice (3 physicians, 2 administrative staff) to implement ICD-10, rising to $285,000 for a typical medium-size practice (10 physicians, 1 full-time coder, 6 administrative staff), and about $2.7 million for a typical large practice (100 physicians, 10 full-time coders, 64 administrative staff).
Now those costs are estimated to range from $56,000 to $226,000 for small practices and $213,000 to $824,000 for medium-size practices. And for large practices, implementing ICD-10 could cost anywhere from $2 million to $8 million.
About two-thirds of physician practices are expected to have costs in the upper range of those estimates, according to the AMA.
One reason for the increased cost is new requirements related to the adoption of electronic health records (EHRs). Nachimson Advisors also projects a larger potential for payment disruptions, estimating that 2%-6% of claims could be denied after the Oct. 1 implementation date.
"The markedly higher implementation costs for ICD-10 place a crushing burden on physicians, straining vital resources needed to invest in new health care delivery models and well-developed technology that promotes care coordination with real value to patients," Dr. Ardis Dee Hoven, AMA president, said in a statement. "Continuing to compel physicians to adopt this new coding structure threatens to disrupt innovations by diverting resources away from areas that are expected to help lower costs and improve the quality of care."
The AMA is calling on Health & Human Services secretary Kathleen Sebelius to reconsider ICD-10 implementation. But if the agency sticks to its plan, the AMA has requested several changes to mitigate some of the costs.
For example, the AMA recommends that Medicare provide a 2-year implementation period during which the agency would not be allowed to deny payments based on the specificity of the ICD-10 code provided. And the agency would provide feedback on coding to physicians during this time.
The AMA also is asking Medicare to simplify its claims requirements by adopting a policy that when the most specific ICD-10 code is used, no additional information or attachments will be required before paying the claim.
On Twitter @maryellenny

Learning and feedback reduce cesarean section rate
NEW ORLEANS – A training program that continually reinforced best practices for labor and delivery reduced the risk of cesarean section by 10% overall, and by up to 32% in a subgroup of high-risk pregnancies.
The program also significantly improved newborn outcomes, with a 12% decrease in the rate of major neonatal morbidity, Dr. Nils Chaillet reported at the Pregnancy Meeting, sponsored by the Society of Maternal-Fetal Medicine. The neonatal benefit remained significant even after excluding all preterm births from the analysis, said Dr. Chaillet of the Sainte-Justine University Hospital Research Center, Montreal.
The QUARISMA (Quality of Care, Management of Obstetrical Risk, and Mode of Delivery in Quebec) study examined the effects of a clinician training program designed to promote optimal management of labor and delivery. QUARISMA was a multifaceted evidence-medicine program based on audit, feedback, and educational activities that followed the World Health Organization guidelines for quality obstetrical care.

A 2-day training session at each participating hospital introduced the program. Throughout the 3.5-year study, a local audit committee, headed by a peer-selected leader, regularly evaluated performance and provided feedback on results and suggestions on quality improvement. These audits were conducted every 3 months. They included an analysis of each cesarean case, centering on whether and how it could have been prevented.
The study randomized 32 public hospitals in Quebec to the intervention or to a control arm of usual practice. The hospitals all had a cesarean section rate of at least 17% and no prior program aimed at reducing that rate. They had to perform more than 300 deliveries annually. All women who gave birth to an infant of at least 500 grams and 24 weeks’ gestation were included in the study.
A total of 105,351 deliveries occurred. In the control group, the baseline rate of cesarean section was 23%; that remained unchanged. The rate did decrease in the intervention group, dropping from 22.5% at baseline to 21.8% at study’s end – a 10% risk reduction that was statistically significant.
Women with low-risk pregnancies experienced a considerable benefit, Dr. Chaillet noted, with an overall risk reduction of 20%. That varied among hospital type. It was smallest (2%) at community hospitals, followed by 21% at regional hospitals and 24% at tertiary care hospitals.
Among high-risk pregnancies, the risk of a cesarean decreased by 4% overall. It did not change in tertiary care centers, but decreased by 5% at regional hospitals and 32% at community hospitals.
Medical interventions were a secondary endpoint. There were no changes in the rates of episiotomy, epidurals, or artificial rupture of membranes. However, the risk of operative vaginal delivery dropped by 12%, and pharmacologic labor induction by 18%. The odds of using oxytocin during labor increased by16%.
There were no significant changes in the composite measures of minor or major maternal morbidities. But neonatal outcomes did improve. The risk of a minor neonatal morbidity decreased by a significant 12%; the risk of a major problem decreased by 19%.
Dr. Chaillet made no financial disclosures.
On Twitter @alz_gal
NEW ORLEANS – A training program that continually reinforced best practices for labor and delivery reduced the risk of cesarean section by 10% overall, and by up to 32% in a subgroup of high-risk pregnancies.
The program also significantly improved newborn outcomes, with a 12% decrease in the rate of major neonatal morbidity, Dr. Nils Chaillet reported at the Pregnancy Meeting, sponsored by the Society of Maternal-Fetal Medicine. The neonatal benefit remained significant even after excluding all preterm births from the analysis, said Dr. Chaillet of the Sainte-Justine University Hospital Research Center, Montreal.
The QUARISMA (Quality of Care, Management of Obstetrical Risk, and Mode of Delivery in Quebec) study examined the effects of a clinician training program designed to promote optimal management of labor and delivery. QUARISMA was a multifaceted evidence-medicine program based on audit, feedback, and educational activities that followed the World Health Organization guidelines for quality obstetrical care.
A 2-day training session at each participating hospital introduced the program. Throughout the 3.5-year study, a local audit committee, headed by a peer-selected leader, regularly evaluated performance and provided feedback on results and suggestions on quality improvement. These audits were conducted every 3 months. They included an analysis of each cesarean case, centering on whether and how it could have been prevented.
The study randomized 32 public hospitals in Quebec to the intervention or to a control arm of usual practice. The hospitals all had a cesarean section rate of at least 17% and no prior program aimed at reducing that rate. They had to perform more than 300 deliveries annually. All women who gave birth to an infant of at least 500 grams and 24 weeks’ gestation were included in the study.
A total of 105,351 deliveries occurred. In the control group, the baseline rate of cesarean section was 23%; that remained unchanged. The rate did decrease in the intervention group, dropping from 22.5% at baseline to 21.8% at study’s end – a 10% risk reduction that was statistically significant.
Women with low-risk pregnancies experienced a considerable benefit, Dr. Chaillet noted, with an overall risk reduction of 20%. That varied among hospital type. It was smallest (2%) at community hospitals, followed by 21% at regional hospitals and 24% at tertiary care hospitals.
Among high-risk pregnancies, the risk of a cesarean decreased by 4% overall. It did not change in tertiary care centers, but decreased by 5% at regional hospitals and 32% at community hospitals.
Medical interventions were a secondary endpoint. There were no changes in the rates of episiotomy, epidurals, or artificial rupture of membranes. However, the risk of operative vaginal delivery dropped by 12%, and pharmacologic labor induction by 18%. The odds of using oxytocin during labor increased by16%.
There were no significant changes in the composite measures of minor or major maternal morbidities. But neonatal outcomes did improve. The risk of a minor neonatal morbidity decreased by a significant 12%; the risk of a major problem decreased by 19%.
Dr. Chaillet made no financial disclosures.
On Twitter @alz_gal
NEW ORLEANS – A training program that continually reinforced best practices for labor and delivery reduced the risk of cesarean section by 10% overall, and by up to 32% in a subgroup of high-risk pregnancies.
The program also significantly improved newborn outcomes, with a 12% decrease in the rate of major neonatal morbidity, Dr. Nils Chaillet reported at the Pregnancy Meeting, sponsored by the Society of Maternal-Fetal Medicine. The neonatal benefit remained significant even after excluding all preterm births from the analysis, said Dr. Chaillet of the Sainte-Justine University Hospital Research Center, Montreal.
The QUARISMA (Quality of Care, Management of Obstetrical Risk, and Mode of Delivery in Quebec) study examined the effects of a clinician training program designed to promote optimal management of labor and delivery. QUARISMA was a multifaceted evidence-medicine program based on audit, feedback, and educational activities that followed the World Health Organization guidelines for quality obstetrical care.
A 2-day training session at each participating hospital introduced the program. Throughout the 3.5-year study, a local audit committee, headed by a peer-selected leader, regularly evaluated performance and provided feedback on results and suggestions on quality improvement. These audits were conducted every 3 months. They included an analysis of each cesarean case, centering on whether and how it could have been prevented.
The study randomized 32 public hospitals in Quebec to the intervention or to a control arm of usual practice. The hospitals all had a cesarean section rate of at least 17% and no prior program aimed at reducing that rate. They had to perform more than 300 deliveries annually. All women who gave birth to an infant of at least 500 grams and 24 weeks’ gestation were included in the study.
A total of 105,351 deliveries occurred. In the control group, the baseline rate of cesarean section was 23%; that remained unchanged. The rate did decrease in the intervention group, dropping from 22.5% at baseline to 21.8% at study’s end – a 10% risk reduction that was statistically significant.
Women with low-risk pregnancies experienced a considerable benefit, Dr. Chaillet noted, with an overall risk reduction of 20%. That varied among hospital type. It was smallest (2%) at community hospitals, followed by 21% at regional hospitals and 24% at tertiary care hospitals.
Among high-risk pregnancies, the risk of a cesarean decreased by 4% overall. It did not change in tertiary care centers, but decreased by 5% at regional hospitals and 32% at community hospitals.
Medical interventions were a secondary endpoint. There were no changes in the rates of episiotomy, epidurals, or artificial rupture of membranes. However, the risk of operative vaginal delivery dropped by 12%, and pharmacologic labor induction by 18%. The odds of using oxytocin during labor increased by16%.
There were no significant changes in the composite measures of minor or major maternal morbidities. But neonatal outcomes did improve. The risk of a minor neonatal morbidity decreased by a significant 12%; the risk of a major problem decreased by 19%.
Dr. Chaillet made no financial disclosures.
On Twitter @alz_gal
AT THE PREGNANCY MEETING
Major finding: Among high-risk pregnancies, the risk of a cesarean decreased by 4% overall. It did not change in tertiary care centers, but decreased by 5% at regional hospitals and 32% at community hospitals.
Data source: The study randomized 32 hospitals and tracked outcomes in more than 100,000 births.
Disclosures: Dr. Chaillet had no financial disclosures.

Palliative care shortens ICU, hospital stays, review data show
SAN FRANCISCO – Palliative care in the intensive care unit reduces the length of stay in the ICU and the hospital without changing mortality rates or family satisfaction, according to a review of the literature.
Although measurements of family satisfaction overall didn’t change much from palliative care of a loved one in the ICU, some measures of components of satisfaction increased with palliative care, such as improved communication with the physician, better consensus around the goals of care, and decreased anxiety and depression in family members, reported Dr. Rebecca A. Aslakson of Johns Hopkins University, Baltimore.
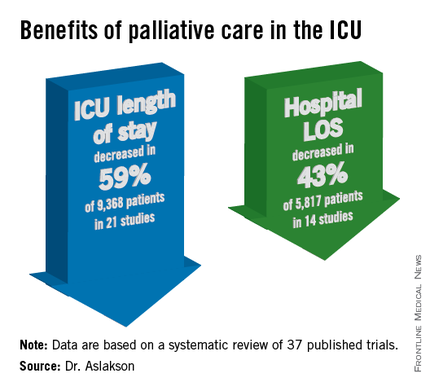
The findings have been submitted for publication, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Dr. Aslakson and her associates were unable to perform a formal meta-analysis of the 37 published trials of palliative care in the ICU because of the heterogeneity of the studies, which looked at more than 40 different outcomes. Instead, their systematic review grouped results under four outcomes that commonly were measured, and assessed those either by the number of studies or by the number of patients studied.
ICU length of stay decreased with palliative care in 13 of 21 studies (62%) that used this outcome and in 59% of 9,368 patients in those studies. Hospital length of stay decreased with palliative care in 8 of 14 studies (57%) and in 43% of 5,817 patients. Family satisfaction did not decrease in any studies or families and increased in only 1 of 14 studies (7%) and in 2% of families of 4,927 patients, Dr. Aslakson reported.
Mortality rates did not change with palliative care in 14 of 16 studies (88%) that assessed mortality and in 57% of 5,969 patients in those studies. Mortality increased in one small study (6%) and decreased in one larger study (6%).
"Talking about big-picture issues and goals of care doesn’t lead to people dying," Dr. Aslakson said. "No harm came in any of these studies." Some separate studies of palliative care outside of ICUs reported that this increases hope, "because people feel that they have more control over their choices and what’s happening to their loved ones," she added.
Integrative vs. consultative model
Dr. Aslakson and her associates also reviewed studies based on whether the interventions used integrative or consultative models of palliative care.
Generally, consultative models bring outsiders into the ICU to help provide palliative care, and integrative models train the ICU team to be the palliative care providers. In reality, the two models may overlap. For this review, the investigators applied mutually exclusive definitions to 36 of the studies. In 18 studies of integrative interventions, members of the ICU team were the only caregivers in face-to-face interactions with the patient and families. In 18 studies of consultative interventions, palliative care providers included others besides the ICU team.
In the studies of integrative palliative care, ICU length of stay decreased with palliative care in four of nine studies (44%) that measured this outcome and in 52% of 6,963 patients in those studies, she reported. Hospital length of stay decreased in two of five studies (40%) and in 24% of 3,812 patients. Family satisfaction changed in none of 15 studies, and mortality decreased in 1 of 5 studies (20%) and in 34% of 3,807 patients.
In the studies of consultative care, ICU length of stay decreased with palliative care in 9 of 12 studies (75%) that measured this outcome and in 79% of 2,405 patients in those studies. Hospital length of stay decreased in six of nine studies (67%) and in 79% of 2,005 patients. Family satisfaction increased in one of four studies (25%) and in 21% of 429 patients. Mortality increased in 1 of 11 studies (9%) and in 5% of 2,162 patients.
One model isn’t necessarily better than the other, Dr. Aslakson said. Integrative palliative care may work best in a closed ICU with perhaps four or five intensivists in a relatively small unit. An integrative approach can be much more difficult in open or semiopen ICUs that have "40 different doctors floating around," she said. "We tried that in my unit, and it didn’t work that well."

Different ICUs need palliative care models that fit them. "Look at your unit, the way it works, and who the providers are, then look at the literature and see what matches that and what might work for your unit," she said.
Outcomes of improved communication
A previous, separate review of the medical literature identified 21 controlled trials of 16 interventions to improve communication in ICUs between families and care providers. Overall, the interventions improved emotional outcomes for families and reduced ICU length of stay and treatment intensity (Chest 2011;139:543-54), she noted.
Yet another prior review of the literature reported that interventions to promote family meetings, use empathetic communication skills, and employ palliative care consultations improved family satisfaction and reduced ICU length of stay and the adverse effects of family bereavement (Curr. Opin. Crit. Care 2009;15:569-77).
Dr. Aslakson reported having no financial disclosures.
[email protected]
On Twitter @sherryboschert
SAN FRANCISCO – Palliative care in the intensive care unit reduces the length of stay in the ICU and the hospital without changing mortality rates or family satisfaction, according to a review of the literature.
Although measurements of family satisfaction overall didn’t change much from palliative care of a loved one in the ICU, some measures of components of satisfaction increased with palliative care, such as improved communication with the physician, better consensus around the goals of care, and decreased anxiety and depression in family members, reported Dr. Rebecca A. Aslakson of Johns Hopkins University, Baltimore.
The findings have been submitted for publication, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Dr. Aslakson and her associates were unable to perform a formal meta-analysis of the 37 published trials of palliative care in the ICU because of the heterogeneity of the studies, which looked at more than 40 different outcomes. Instead, their systematic review grouped results under four outcomes that commonly were measured, and assessed those either by the number of studies or by the number of patients studied.
ICU length of stay decreased with palliative care in 13 of 21 studies (62%) that used this outcome and in 59% of 9,368 patients in those studies. Hospital length of stay decreased with palliative care in 8 of 14 studies (57%) and in 43% of 5,817 patients. Family satisfaction did not decrease in any studies or families and increased in only 1 of 14 studies (7%) and in 2% of families of 4,927 patients, Dr. Aslakson reported.
Mortality rates did not change with palliative care in 14 of 16 studies (88%) that assessed mortality and in 57% of 5,969 patients in those studies. Mortality increased in one small study (6%) and decreased in one larger study (6%).
"Talking about big-picture issues and goals of care doesn’t lead to people dying," Dr. Aslakson said. "No harm came in any of these studies." Some separate studies of palliative care outside of ICUs reported that this increases hope, "because people feel that they have more control over their choices and what’s happening to their loved ones," she added.
Integrative vs. consultative model
Dr. Aslakson and her associates also reviewed studies based on whether the interventions used integrative or consultative models of palliative care.
Generally, consultative models bring outsiders into the ICU to help provide palliative care, and integrative models train the ICU team to be the palliative care providers. In reality, the two models may overlap. For this review, the investigators applied mutually exclusive definitions to 36 of the studies. In 18 studies of integrative interventions, members of the ICU team were the only caregivers in face-to-face interactions with the patient and families. In 18 studies of consultative interventions, palliative care providers included others besides the ICU team.
In the studies of integrative palliative care, ICU length of stay decreased with palliative care in four of nine studies (44%) that measured this outcome and in 52% of 6,963 patients in those studies, she reported. Hospital length of stay decreased in two of five studies (40%) and in 24% of 3,812 patients. Family satisfaction changed in none of 15 studies, and mortality decreased in 1 of 5 studies (20%) and in 34% of 3,807 patients.
In the studies of consultative care, ICU length of stay decreased with palliative care in 9 of 12 studies (75%) that measured this outcome and in 79% of 2,405 patients in those studies. Hospital length of stay decreased in six of nine studies (67%) and in 79% of 2,005 patients. Family satisfaction increased in one of four studies (25%) and in 21% of 429 patients. Mortality increased in 1 of 11 studies (9%) and in 5% of 2,162 patients.
One model isn’t necessarily better than the other, Dr. Aslakson said. Integrative palliative care may work best in a closed ICU with perhaps four or five intensivists in a relatively small unit. An integrative approach can be much more difficult in open or semiopen ICUs that have "40 different doctors floating around," she said. "We tried that in my unit, and it didn’t work that well."
Different ICUs need palliative care models that fit them. "Look at your unit, the way it works, and who the providers are, then look at the literature and see what matches that and what might work for your unit," she said.
Outcomes of improved communication
A previous, separate review of the medical literature identified 21 controlled trials of 16 interventions to improve communication in ICUs between families and care providers. Overall, the interventions improved emotional outcomes for families and reduced ICU length of stay and treatment intensity (Chest 2011;139:543-54), she noted.
Yet another prior review of the literature reported that interventions to promote family meetings, use empathetic communication skills, and employ palliative care consultations improved family satisfaction and reduced ICU length of stay and the adverse effects of family bereavement (Curr. Opin. Crit. Care 2009;15:569-77).
Dr. Aslakson reported having no financial disclosures.
[email protected]
On Twitter @sherryboschert
SAN FRANCISCO – Palliative care in the intensive care unit reduces the length of stay in the ICU and the hospital without changing mortality rates or family satisfaction, according to a review of the literature.
Although measurements of family satisfaction overall didn’t change much from palliative care of a loved one in the ICU, some measures of components of satisfaction increased with palliative care, such as improved communication with the physician, better consensus around the goals of care, and decreased anxiety and depression in family members, reported Dr. Rebecca A. Aslakson of Johns Hopkins University, Baltimore.
The findings have been submitted for publication, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Dr. Aslakson and her associates were unable to perform a formal meta-analysis of the 37 published trials of palliative care in the ICU because of the heterogeneity of the studies, which looked at more than 40 different outcomes. Instead, their systematic review grouped results under four outcomes that commonly were measured, and assessed those either by the number of studies or by the number of patients studied.
ICU length of stay decreased with palliative care in 13 of 21 studies (62%) that used this outcome and in 59% of 9,368 patients in those studies. Hospital length of stay decreased with palliative care in 8 of 14 studies (57%) and in 43% of 5,817 patients. Family satisfaction did not decrease in any studies or families and increased in only 1 of 14 studies (7%) and in 2% of families of 4,927 patients, Dr. Aslakson reported.
Mortality rates did not change with palliative care in 14 of 16 studies (88%) that assessed mortality and in 57% of 5,969 patients in those studies. Mortality increased in one small study (6%) and decreased in one larger study (6%).
"Talking about big-picture issues and goals of care doesn’t lead to people dying," Dr. Aslakson said. "No harm came in any of these studies." Some separate studies of palliative care outside of ICUs reported that this increases hope, "because people feel that they have more control over their choices and what’s happening to their loved ones," she added.
Integrative vs. consultative model
Dr. Aslakson and her associates also reviewed studies based on whether the interventions used integrative or consultative models of palliative care.
Generally, consultative models bring outsiders into the ICU to help provide palliative care, and integrative models train the ICU team to be the palliative care providers. In reality, the two models may overlap. For this review, the investigators applied mutually exclusive definitions to 36 of the studies. In 18 studies of integrative interventions, members of the ICU team were the only caregivers in face-to-face interactions with the patient and families. In 18 studies of consultative interventions, palliative care providers included others besides the ICU team.
In the studies of integrative palliative care, ICU length of stay decreased with palliative care in four of nine studies (44%) that measured this outcome and in 52% of 6,963 patients in those studies, she reported. Hospital length of stay decreased in two of five studies (40%) and in 24% of 3,812 patients. Family satisfaction changed in none of 15 studies, and mortality decreased in 1 of 5 studies (20%) and in 34% of 3,807 patients.
In the studies of consultative care, ICU length of stay decreased with palliative care in 9 of 12 studies (75%) that measured this outcome and in 79% of 2,405 patients in those studies. Hospital length of stay decreased in six of nine studies (67%) and in 79% of 2,005 patients. Family satisfaction increased in one of four studies (25%) and in 21% of 429 patients. Mortality increased in 1 of 11 studies (9%) and in 5% of 2,162 patients.
One model isn’t necessarily better than the other, Dr. Aslakson said. Integrative palliative care may work best in a closed ICU with perhaps four or five intensivists in a relatively small unit. An integrative approach can be much more difficult in open or semiopen ICUs that have "40 different doctors floating around," she said. "We tried that in my unit, and it didn’t work that well."
Different ICUs need palliative care models that fit them. "Look at your unit, the way it works, and who the providers are, then look at the literature and see what matches that and what might work for your unit," she said.
Outcomes of improved communication
A previous, separate review of the medical literature identified 21 controlled trials of 16 interventions to improve communication in ICUs between families and care providers. Overall, the interventions improved emotional outcomes for families and reduced ICU length of stay and treatment intensity (Chest 2011;139:543-54), she noted.
Yet another prior review of the literature reported that interventions to promote family meetings, use empathetic communication skills, and employ palliative care consultations improved family satisfaction and reduced ICU length of stay and the adverse effects of family bereavement (Curr. Opin. Crit. Care 2009;15:569-77).
Dr. Aslakson reported having no financial disclosures.
[email protected]
On Twitter @sherryboschert
AT THE CRITICAL CARE CONGRESS
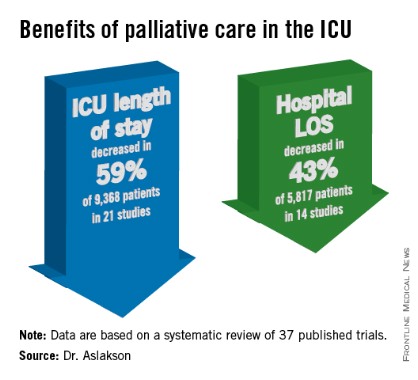
Feds spend $19 billion on EHR bonuses
The federal government has spent more than $19 billion over the last 3 years on bonuses to health care providers and hospitals to jump-start the use of electronic health records, according to figures released by the Centers for Medicare & Medicaid Services.
The money, which was paid out as part of the Medicare and Medicaid Electronic Health Records (EHR) Incentive Programs, went to physicians and other health care providers, hospitals, and Medicare Advantage organizations starting in 2011. Under the program, physicians can earn up to $44,000 over 5 years through Medicare or $63,750 over 6 years through Medicaid.

Since its launch in 2011 through the end of last year, more than 268,000 physicians have received incentive payments through the Medicare or Medicaid programs. In total, physicians took home more than $5.5 billion in bonuses over the first 3 years of the program.
But hospitals earned even more. About 4,400 hospitals earned more than $12.2 billion in EHR incentive payments from 2011 through 2013.
The government cut its biggest checks in the first 2 years of the program. And by May 2013, more than half of all physicians and other eligible providers had received bonuses through the program, according to the CMS.
In 2013 alone, more than 28,000 physicians received incentive payments through Medicare or Medicaid totaling more than $421 million.
On Twitter @maryellenny
The federal government has spent more than $19 billion over the last 3 years on bonuses to health care providers and hospitals to jump-start the use of electronic health records, according to figures released by the Centers for Medicare & Medicaid Services.
The money, which was paid out as part of the Medicare and Medicaid Electronic Health Records (EHR) Incentive Programs, went to physicians and other health care providers, hospitals, and Medicare Advantage organizations starting in 2011. Under the program, physicians can earn up to $44,000 over 5 years through Medicare or $63,750 over 6 years through Medicaid.
Since its launch in 2011 through the end of last year, more than 268,000 physicians have received incentive payments through the Medicare or Medicaid programs. In total, physicians took home more than $5.5 billion in bonuses over the first 3 years of the program.
But hospitals earned even more. About 4,400 hospitals earned more than $12.2 billion in EHR incentive payments from 2011 through 2013.
The government cut its biggest checks in the first 2 years of the program. And by May 2013, more than half of all physicians and other eligible providers had received bonuses through the program, according to the CMS.
In 2013 alone, more than 28,000 physicians received incentive payments through Medicare or Medicaid totaling more than $421 million.
On Twitter @maryellenny
The federal government has spent more than $19 billion over the last 3 years on bonuses to health care providers and hospitals to jump-start the use of electronic health records, according to figures released by the Centers for Medicare & Medicaid Services.
The money, which was paid out as part of the Medicare and Medicaid Electronic Health Records (EHR) Incentive Programs, went to physicians and other health care providers, hospitals, and Medicare Advantage organizations starting in 2011. Under the program, physicians can earn up to $44,000 over 5 years through Medicare or $63,750 over 6 years through Medicaid.
Since its launch in 2011 through the end of last year, more than 268,000 physicians have received incentive payments through the Medicare or Medicaid programs. In total, physicians took home more than $5.5 billion in bonuses over the first 3 years of the program.
But hospitals earned even more. About 4,400 hospitals earned more than $12.2 billion in EHR incentive payments from 2011 through 2013.
The government cut its biggest checks in the first 2 years of the program. And by May 2013, more than half of all physicians and other eligible providers had received bonuses through the program, according to the CMS.
In 2013 alone, more than 28,000 physicians received incentive payments through Medicare or Medicaid totaling more than $421 million.
On Twitter @maryellenny

The Surgeon of the Future: Anchoring Innovation and Science with Moral Values
Throughout the last year, Fellows of the American College of Surgeons (ACS) had many opportunities to reflect on our rich history as an organization and as a profession. Having assumed office at the conclusion of the College’s Centennial celebration, I felt that it was appropriate to shift the focus from our past to the future. The future promises to deliver innovation and advances in science. and I think it is important that, before we adopt them. we check them against our values. Thus, I have chosen as the theme of my presidential year "The Surgeon of the Future: Anchoring Innovation and Science with Moral Values.”

Several forces are shaping the future of surgery. First, the introduction and adoption of new ideas, techniques, and devices have resulted in monumental progress in surgery. For many years, the pace of innovation included intervals of time to test and validate new ideas and, when useful, to design educational and training methods to ensure their safe implementation. The pace of change has increased substantially, however, and will likely accelerate in the future.
The College is constantly scanning the horizon for new ideas and developing appropriate programs to train Fellows in the safe adoption of new devices and techniques. I encourage Fellows to take advantage of these opportunities as innovation is causing the boundaries between the specialties to blur. When I started practice, there was a clear delineation between what I did as a surgeon—primarily open operations—and what most medical specialists did—primarily diagnostic and noninvasive therapy. However, because of advances in medical technology and techniques, many services that only a surgeon once could provide are now delivered by non-surgical medical specialists. To maintain active practices in the future, surgeons will need to be skilled in all diagnostic and therapeutic aspects of disease, including interventions done via open, endoscopic, percutaneous, or natural orifice approaches
Another force affecting surgery is society’s increased concern with health care quality and costs. Value in health care is often defined as the ratio between outcomes and costs. I urge surgeons to focus on outcomes, in particular outcomes of relevance to patients and employers, including the relief of pain, ability to return to work quickly, and other quality of life issues. This is the “new” accountability of our craft: accountability for quality, for safety, for costs, and for outcomes.
Value-based care cannot be rendered by individuals acting alone; it requires high-performance teams. These teams need leadership that fosters exceptional communication, mutual respect and support, and the development of best practices.
As we face all these forces impacting our practices let us not forget that each of us has the opportunity to shape the future. True, external influences are at play, but our direct involvement will help to modulate those forces. The pessimists will tell you that the sky is falling, and there is nothing you can do about it. Don’t believe them. The future is not predetermined. You may not be able to achieve everything you want, but you should set for yourselves the highest goals and travel in that direction for as far and as long as you can. Next time you see something that needs fixing, get involved, then exercise your leadership and illuminate a path toward a better future.
The College has developed the infrastructure to help surgeons effect change. Whether it is through the Division of Education filling the gap between your practice and the current state of knowledge; or through the Division of Research and Optimal Patient Care with its measurements of quality, safety, and costs; or through the Division of Advocacy and Health Policy’s efforts to help modulate the implementation of sound socioeconomic policies; or through the Division of Member Services with its focus on you, your chapters, your projects, the College provides surgeons with the right platform to exercise their leadership. I encourage you to get involved in these programs, not only because it will help you in your career, but because it is the right thing to do for our patients and our society.
Thus far we have discussed how innovation and new knowledge will change practices and how can the surgeon of the future can remain relevant through the ACS platform. As you travel this rather difficult path of constant change, adaptation and re-invention, you will need a moral compass to guide your actions and distinguish right from wrong. This is the “anchor” I refer to in my theme for this year--the one provided by moral values. The ACS staff led by example last year when they identified a set of values that now guides their work. I have examined these principles and find that they speak for me as a surgeon as well.
· Professionalism exemplified through the highest standards of honesty, responsibility, respect, and accountability.
· Excellence demonstrated as the desire to exceed internal and external standards and expectations and the relentless pursuit of perfection.
· Innovation through the pursuit of creative and forward-thinking improvements to transform what we do for the better.
· Introspection manifested through continuous self-improvement, professional development, self-assessment, and self-awareness.
· Inclusion centered on the active engagement of all appropriate individuals and entities to collaboratively harness collective intelligence and creativity.
The value of inclusion in today’s world cannot be overemphasized. We must respect, embrace, and celebrate all cultures and incorporate our differences in our design of new things to improve creativity and respond to the needs of all. At the same time, we must stay true to ourselves and our own beliefs. Respecting and embracing others is best done when we respect ourselves and our values. The ACS is striving to embrace and collaborate with other like-minded organizations. It is only by gathering the minds and the energy of all involved that we shall succeed as a profession and as a society.
Many challenges lie ahead, but we can face them and succeed by working together, trusting ourselves, and embracing necessary change. Thank you for the privilege of serving as your President during this exciting, transformative time.
Dr. Pellegrini is President of the American College of Surgeons.
Throughout the last year, Fellows of the American College of Surgeons (ACS) had many opportunities to reflect on our rich history as an organization and as a profession. Having assumed office at the conclusion of the College’s Centennial celebration, I felt that it was appropriate to shift the focus from our past to the future. The future promises to deliver innovation and advances in science. and I think it is important that, before we adopt them. we check them against our values. Thus, I have chosen as the theme of my presidential year "The Surgeon of the Future: Anchoring Innovation and Science with Moral Values.”
Several forces are shaping the future of surgery. First, the introduction and adoption of new ideas, techniques, and devices have resulted in monumental progress in surgery. For many years, the pace of innovation included intervals of time to test and validate new ideas and, when useful, to design educational and training methods to ensure their safe implementation. The pace of change has increased substantially, however, and will likely accelerate in the future.
The College is constantly scanning the horizon for new ideas and developing appropriate programs to train Fellows in the safe adoption of new devices and techniques. I encourage Fellows to take advantage of these opportunities as innovation is causing the boundaries between the specialties to blur. When I started practice, there was a clear delineation between what I did as a surgeon—primarily open operations—and what most medical specialists did—primarily diagnostic and noninvasive therapy. However, because of advances in medical technology and techniques, many services that only a surgeon once could provide are now delivered by non-surgical medical specialists. To maintain active practices in the future, surgeons will need to be skilled in all diagnostic and therapeutic aspects of disease, including interventions done via open, endoscopic, percutaneous, or natural orifice approaches
Another force affecting surgery is society’s increased concern with health care quality and costs. Value in health care is often defined as the ratio between outcomes and costs. I urge surgeons to focus on outcomes, in particular outcomes of relevance to patients and employers, including the relief of pain, ability to return to work quickly, and other quality of life issues. This is the “new” accountability of our craft: accountability for quality, for safety, for costs, and for outcomes.
Value-based care cannot be rendered by individuals acting alone; it requires high-performance teams. These teams need leadership that fosters exceptional communication, mutual respect and support, and the development of best practices.
As we face all these forces impacting our practices let us not forget that each of us has the opportunity to shape the future. True, external influences are at play, but our direct involvement will help to modulate those forces. The pessimists will tell you that the sky is falling, and there is nothing you can do about it. Don’t believe them. The future is not predetermined. You may not be able to achieve everything you want, but you should set for yourselves the highest goals and travel in that direction for as far and as long as you can. Next time you see something that needs fixing, get involved, then exercise your leadership and illuminate a path toward a better future.
The College has developed the infrastructure to help surgeons effect change. Whether it is through the Division of Education filling the gap between your practice and the current state of knowledge; or through the Division of Research and Optimal Patient Care with its measurements of quality, safety, and costs; or through the Division of Advocacy and Health Policy’s efforts to help modulate the implementation of sound socioeconomic policies; or through the Division of Member Services with its focus on you, your chapters, your projects, the College provides surgeons with the right platform to exercise their leadership. I encourage you to get involved in these programs, not only because it will help you in your career, but because it is the right thing to do for our patients and our society.
Thus far we have discussed how innovation and new knowledge will change practices and how can the surgeon of the future can remain relevant through the ACS platform. As you travel this rather difficult path of constant change, adaptation and re-invention, you will need a moral compass to guide your actions and distinguish right from wrong. This is the “anchor” I refer to in my theme for this year--the one provided by moral values. The ACS staff led by example last year when they identified a set of values that now guides their work. I have examined these principles and find that they speak for me as a surgeon as well.
· Professionalism exemplified through the highest standards of honesty, responsibility, respect, and accountability.
· Excellence demonstrated as the desire to exceed internal and external standards and expectations and the relentless pursuit of perfection.
· Innovation through the pursuit of creative and forward-thinking improvements to transform what we do for the better.
· Introspection manifested through continuous self-improvement, professional development, self-assessment, and self-awareness.
· Inclusion centered on the active engagement of all appropriate individuals and entities to collaboratively harness collective intelligence and creativity.
The value of inclusion in today’s world cannot be overemphasized. We must respect, embrace, and celebrate all cultures and incorporate our differences in our design of new things to improve creativity and respond to the needs of all. At the same time, we must stay true to ourselves and our own beliefs. Respecting and embracing others is best done when we respect ourselves and our values. The ACS is striving to embrace and collaborate with other like-minded organizations. It is only by gathering the minds and the energy of all involved that we shall succeed as a profession and as a society.
Many challenges lie ahead, but we can face them and succeed by working together, trusting ourselves, and embracing necessary change. Thank you for the privilege of serving as your President during this exciting, transformative time.
Dr. Pellegrini is President of the American College of Surgeons.
Throughout the last year, Fellows of the American College of Surgeons (ACS) had many opportunities to reflect on our rich history as an organization and as a profession. Having assumed office at the conclusion of the College’s Centennial celebration, I felt that it was appropriate to shift the focus from our past to the future. The future promises to deliver innovation and advances in science. and I think it is important that, before we adopt them. we check them against our values. Thus, I have chosen as the theme of my presidential year "The Surgeon of the Future: Anchoring Innovation and Science with Moral Values.”
Several forces are shaping the future of surgery. First, the introduction and adoption of new ideas, techniques, and devices have resulted in monumental progress in surgery. For many years, the pace of innovation included intervals of time to test and validate new ideas and, when useful, to design educational and training methods to ensure their safe implementation. The pace of change has increased substantially, however, and will likely accelerate in the future.
The College is constantly scanning the horizon for new ideas and developing appropriate programs to train Fellows in the safe adoption of new devices and techniques. I encourage Fellows to take advantage of these opportunities as innovation is causing the boundaries between the specialties to blur. When I started practice, there was a clear delineation between what I did as a surgeon—primarily open operations—and what most medical specialists did—primarily diagnostic and noninvasive therapy. However, because of advances in medical technology and techniques, many services that only a surgeon once could provide are now delivered by non-surgical medical specialists. To maintain active practices in the future, surgeons will need to be skilled in all diagnostic and therapeutic aspects of disease, including interventions done via open, endoscopic, percutaneous, or natural orifice approaches
Another force affecting surgery is society’s increased concern with health care quality and costs. Value in health care is often defined as the ratio between outcomes and costs. I urge surgeons to focus on outcomes, in particular outcomes of relevance to patients and employers, including the relief of pain, ability to return to work quickly, and other quality of life issues. This is the “new” accountability of our craft: accountability for quality, for safety, for costs, and for outcomes.
Value-based care cannot be rendered by individuals acting alone; it requires high-performance teams. These teams need leadership that fosters exceptional communication, mutual respect and support, and the development of best practices.
As we face all these forces impacting our practices let us not forget that each of us has the opportunity to shape the future. True, external influences are at play, but our direct involvement will help to modulate those forces. The pessimists will tell you that the sky is falling, and there is nothing you can do about it. Don’t believe them. The future is not predetermined. You may not be able to achieve everything you want, but you should set for yourselves the highest goals and travel in that direction for as far and as long as you can. Next time you see something that needs fixing, get involved, then exercise your leadership and illuminate a path toward a better future.
The College has developed the infrastructure to help surgeons effect change. Whether it is through the Division of Education filling the gap between your practice and the current state of knowledge; or through the Division of Research and Optimal Patient Care with its measurements of quality, safety, and costs; or through the Division of Advocacy and Health Policy’s efforts to help modulate the implementation of sound socioeconomic policies; or through the Division of Member Services with its focus on you, your chapters, your projects, the College provides surgeons with the right platform to exercise their leadership. I encourage you to get involved in these programs, not only because it will help you in your career, but because it is the right thing to do for our patients and our society.
Thus far we have discussed how innovation and new knowledge will change practices and how can the surgeon of the future can remain relevant through the ACS platform. As you travel this rather difficult path of constant change, adaptation and re-invention, you will need a moral compass to guide your actions and distinguish right from wrong. This is the “anchor” I refer to in my theme for this year--the one provided by moral values. The ACS staff led by example last year when they identified a set of values that now guides their work. I have examined these principles and find that they speak for me as a surgeon as well.
· Professionalism exemplified through the highest standards of honesty, responsibility, respect, and accountability.
· Excellence demonstrated as the desire to exceed internal and external standards and expectations and the relentless pursuit of perfection.
· Innovation through the pursuit of creative and forward-thinking improvements to transform what we do for the better.
· Introspection manifested through continuous self-improvement, professional development, self-assessment, and self-awareness.
· Inclusion centered on the active engagement of all appropriate individuals and entities to collaboratively harness collective intelligence and creativity.
The value of inclusion in today’s world cannot be overemphasized. We must respect, embrace, and celebrate all cultures and incorporate our differences in our design of new things to improve creativity and respond to the needs of all. At the same time, we must stay true to ourselves and our own beliefs. Respecting and embracing others is best done when we respect ourselves and our values. The ACS is striving to embrace and collaborate with other like-minded organizations. It is only by gathering the minds and the energy of all involved that we shall succeed as a profession and as a society.
Many challenges lie ahead, but we can face them and succeed by working together, trusting ourselves, and embracing necessary change. Thank you for the privilege of serving as your President during this exciting, transformative time.
Dr. Pellegrini is President of the American College of Surgeons.
