User login
Official Newspaper of the American College of Surgeons
Why consults don’t happen
Today our team saw an 89-year-old gentleman on the hospitalist service with dementia, heart failure, atrial fibrillation, chronic kidney disease, and problems falling. His last known fall was less than 3 months ago and resulted in a broken hip requiring surgical intervention. This was his fourth hospitalization in 6 months, yet it was the first time he was seen by our service.
The frequency at which palliative care (PC) consults are ordered in a particular hospital varies widely. Some reasons for this are not easy fixes – PC is not available in each hospital (as was the case in two of this gentleman’s four hospitalizations), many PC teams are available only Monday-Friday, and patient volumes within a hospital ebb and flow with much less predictability than the tides.
However, some of the reasons are amenable to change. These might include the particular group of hospitalists, or one attending physician, utilizing PC consults less frequently than another. Or it may simply be that the connection was not made between the patient’s experience and the usefulness of an early PC consults. Screening tools are one method of decreasing variability in PC involvement as well as increasing the appropriateness of our service for a particular patient.
There are quite a few palliative care screening tools available. Many of them focus on what most of us would expect, which are the most common diagnoses we see (late-stage cancer, HF, cirrhosis, end-stage renal disease, dementia, etc.). Multiple studies have estimated that mature PC programs in large hospitals are consulted on 1%-2% of live discharges. However, we estimate that more than 10% of these discharged patients have palliative needs that go unmet. While it is true that we wish PC could be involved in all of these lives, this large number of people who spend time in the hospital with these diagnoses, coupled with a national shortage of PC providers, translates into an unbalanced equation.
Rather than looking at a specific diagnosis, we suggest incorporating inquiries on the presence of "palliative care–related problems." While these might require more thought or investigation into a patient’s situation, we find them to be more fruitful than using diagnosis alone.
Some examples? Mismatch between the expectations of the medical team vs. patient/family when it comes to prognosis or the goals of care would be one of them. Another might be persistent uncontrolled symptoms despite usual medical management. Family members disagreeing or demonstrating concerns about the goals of care is still another.
Having used various screening tools in multiple hospitals and clinical settings, we suggest the following considerations in setting up your own:
• Stakeholder management: The right services and staff need to agree on this being a way to improve quality of care (we always provide an "opt-out" option for those who don’t want us involved for some reason).
• Start small: Implement these on one unit at a time or limit the diagnoses to one or two conditions only. You can make the criteria less stringent if the PC team’s bandwidth is not too narrow.
• Be flexible: Even by starting small, there will be times that the PC teams are overwhelmed on a particular day leaving the occasional patient who meets criteria unseen. If the consult is urgent, a phone call is appropriate so that an assumption isn’t made that the screening tool will catch 100% of the patients.
• Track data: When using these tools, palliative care teams have been able to show things such as improved Hospital Consumer Assessment of Healthcare Providers and Systems survey results and decreased readmissions. Demonstrate what you’re doing for your institution so that you can expand the units or patients served.
PC screening tools are an effective way to decrease variability and improve quality. For examples of tools that we use, please get in touch. Find our contact info and read earlier columns at ehospitalistnews/Palliatively.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.
Today our team saw an 89-year-old gentleman on the hospitalist service with dementia, heart failure, atrial fibrillation, chronic kidney disease, and problems falling. His last known fall was less than 3 months ago and resulted in a broken hip requiring surgical intervention. This was his fourth hospitalization in 6 months, yet it was the first time he was seen by our service.
The frequency at which palliative care (PC) consults are ordered in a particular hospital varies widely. Some reasons for this are not easy fixes – PC is not available in each hospital (as was the case in two of this gentleman’s four hospitalizations), many PC teams are available only Monday-Friday, and patient volumes within a hospital ebb and flow with much less predictability than the tides.
However, some of the reasons are amenable to change. These might include the particular group of hospitalists, or one attending physician, utilizing PC consults less frequently than another. Or it may simply be that the connection was not made between the patient’s experience and the usefulness of an early PC consults. Screening tools are one method of decreasing variability in PC involvement as well as increasing the appropriateness of our service for a particular patient.
There are quite a few palliative care screening tools available. Many of them focus on what most of us would expect, which are the most common diagnoses we see (late-stage cancer, HF, cirrhosis, end-stage renal disease, dementia, etc.). Multiple studies have estimated that mature PC programs in large hospitals are consulted on 1%-2% of live discharges. However, we estimate that more than 10% of these discharged patients have palliative needs that go unmet. While it is true that we wish PC could be involved in all of these lives, this large number of people who spend time in the hospital with these diagnoses, coupled with a national shortage of PC providers, translates into an unbalanced equation.
Rather than looking at a specific diagnosis, we suggest incorporating inquiries on the presence of "palliative care–related problems." While these might require more thought or investigation into a patient’s situation, we find them to be more fruitful than using diagnosis alone.
Some examples? Mismatch between the expectations of the medical team vs. patient/family when it comes to prognosis or the goals of care would be one of them. Another might be persistent uncontrolled symptoms despite usual medical management. Family members disagreeing or demonstrating concerns about the goals of care is still another.
Having used various screening tools in multiple hospitals and clinical settings, we suggest the following considerations in setting up your own:
• Stakeholder management: The right services and staff need to agree on this being a way to improve quality of care (we always provide an "opt-out" option for those who don’t want us involved for some reason).
• Start small: Implement these on one unit at a time or limit the diagnoses to one or two conditions only. You can make the criteria less stringent if the PC team’s bandwidth is not too narrow.
• Be flexible: Even by starting small, there will be times that the PC teams are overwhelmed on a particular day leaving the occasional patient who meets criteria unseen. If the consult is urgent, a phone call is appropriate so that an assumption isn’t made that the screening tool will catch 100% of the patients.
• Track data: When using these tools, palliative care teams have been able to show things such as improved Hospital Consumer Assessment of Healthcare Providers and Systems survey results and decreased readmissions. Demonstrate what you’re doing for your institution so that you can expand the units or patients served.
PC screening tools are an effective way to decrease variability and improve quality. For examples of tools that we use, please get in touch. Find our contact info and read earlier columns at ehospitalistnews/Palliatively.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.
Today our team saw an 89-year-old gentleman on the hospitalist service with dementia, heart failure, atrial fibrillation, chronic kidney disease, and problems falling. His last known fall was less than 3 months ago and resulted in a broken hip requiring surgical intervention. This was his fourth hospitalization in 6 months, yet it was the first time he was seen by our service.
The frequency at which palliative care (PC) consults are ordered in a particular hospital varies widely. Some reasons for this are not easy fixes – PC is not available in each hospital (as was the case in two of this gentleman’s four hospitalizations), many PC teams are available only Monday-Friday, and patient volumes within a hospital ebb and flow with much less predictability than the tides.
However, some of the reasons are amenable to change. These might include the particular group of hospitalists, or one attending physician, utilizing PC consults less frequently than another. Or it may simply be that the connection was not made between the patient’s experience and the usefulness of an early PC consults. Screening tools are one method of decreasing variability in PC involvement as well as increasing the appropriateness of our service for a particular patient.
There are quite a few palliative care screening tools available. Many of them focus on what most of us would expect, which are the most common diagnoses we see (late-stage cancer, HF, cirrhosis, end-stage renal disease, dementia, etc.). Multiple studies have estimated that mature PC programs in large hospitals are consulted on 1%-2% of live discharges. However, we estimate that more than 10% of these discharged patients have palliative needs that go unmet. While it is true that we wish PC could be involved in all of these lives, this large number of people who spend time in the hospital with these diagnoses, coupled with a national shortage of PC providers, translates into an unbalanced equation.
Rather than looking at a specific diagnosis, we suggest incorporating inquiries on the presence of "palliative care–related problems." While these might require more thought or investigation into a patient’s situation, we find them to be more fruitful than using diagnosis alone.
Some examples? Mismatch between the expectations of the medical team vs. patient/family when it comes to prognosis or the goals of care would be one of them. Another might be persistent uncontrolled symptoms despite usual medical management. Family members disagreeing or demonstrating concerns about the goals of care is still another.
Having used various screening tools in multiple hospitals and clinical settings, we suggest the following considerations in setting up your own:
• Stakeholder management: The right services and staff need to agree on this being a way to improve quality of care (we always provide an "opt-out" option for those who don’t want us involved for some reason).
• Start small: Implement these on one unit at a time or limit the diagnoses to one or two conditions only. You can make the criteria less stringent if the PC team’s bandwidth is not too narrow.
• Be flexible: Even by starting small, there will be times that the PC teams are overwhelmed on a particular day leaving the occasional patient who meets criteria unseen. If the consult is urgent, a phone call is appropriate so that an assumption isn’t made that the screening tool will catch 100% of the patients.
• Track data: When using these tools, palliative care teams have been able to show things such as improved Hospital Consumer Assessment of Healthcare Providers and Systems survey results and decreased readmissions. Demonstrate what you’re doing for your institution so that you can expand the units or patients served.
PC screening tools are an effective way to decrease variability and improve quality. For examples of tools that we use, please get in touch. Find our contact info and read earlier columns at ehospitalistnews/Palliatively.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.

Thrombolysis may offer benefit in stable pulmonary embolism
Thrombolytic therapy decreased all-cause mortality in patients with hemodynamically stable pulmonary embolism associated with right ventricular dysfunction – those at "intermediate risk," according to a meta-analysis published online June 17 in JAMA.
The investigators described their study of 16 randomized, controlled clinical trials involving 2,115 patients as "the first analysis of thrombolysis in PE that has sufficient statistical power to detect associations with a meaningful mortality reduction." If their findings are confirmed in future randomized clinical trials, "there may be a shift in the treatment of selected patients with intermediate-risk PE using thrombolytics."
However, "the optimism regarding this clinical advantage must be tempered by [our] finding of significantly increased risk of major bleeding and intracranial hemorrhage associated with thrombolytic therapy, particularly for patients older than 65 years," said Dr. Saurav Chatterjee of the division of cardiology, St. Luke’s-Roosevelt Hospital Center of the Mount Sinai Health System, New York, and his associates (JAMA 2014;311:2414-21).
The study population included 1,499 patients who had hemodynamically stable PE associated with right ventricular dysfunction, the largest subset of patients seen in clinical practice and the group for whom the risks and benefits of thrombolysis are the most unclear.
After a mean follow-up of 82 days, overall mortality was 2.17% in patients who received thrombolysis, compared with 3.89% in those who received anticoagulation. In addition, the risk of recurrent PE was significantly lower with thrombolytic therapy (1.17%) than with anticoagulation (3.04%).
However, the rate of major bleeding was 9.24% for thrombolytic therapy, compared with 3.42% for anticoagulation. And the rate of intracranial hemorrhage was 1.46% for thrombolysis, compared with 0.19% for anticoagulation, the investigators said.
The bleeding risk was especially high in patients aged 65 years and older. Attenuation of this risk in younger patients suggests that they may be considered stronger candidates for thrombolytic therapy, Dr. Chatterjee and his associates said.
Dr. Chatterjee reported no financial conflicts; his associates reported ties to AstraZeneca, Boston Scientific, Cardiostem, Cordis, EKOS Corporation, Embolitech, GenWay, Johnson & Johnson, Soteria, and Vascular Magnetics.

|
|
Dr. Chatterjee and his associates calculated the net clinical benefit of thrombolysis, and their result "suggests evidence of modest efficacy in intermediate-risk PE," said Dr. Joshua A. Beckman.
But their findings do not yet add up to a change in the standard of care. Each clinician must decide on an individualized basis which of these patients should receive thrombolytic therapy, based on clinical presentation, comorbid conditions, and both the physician’s and the patient’s tolerance of risk.
Dr. Beckman is in the cardiovascular division at Brigham and Women’s Hospital, Boston. He reported being a board member for Vascular Interventional Advances; receiving grant funding from Bristol-Myers Squibb; and consulting for AstraZeneca, Boston Scientific, Ferring, Merck, and Novartis. These remarks were taken from his editorial accompanying Dr. Chatterjee’s report (JAMA 2014;311:2385-6).
|
|
|
Dr. Chatterjee and his associates calculated the net clinical benefit of thrombolysis, and their result "suggests evidence of modest efficacy in intermediate-risk PE," said Dr. Joshua A. Beckman.
But their findings do not yet add up to a change in the standard of care. Each clinician must decide on an individualized basis which of these patients should receive thrombolytic therapy, based on clinical presentation, comorbid conditions, and both the physician’s and the patient’s tolerance of risk.
Dr. Beckman is in the cardiovascular division at Brigham and Women’s Hospital, Boston. He reported being a board member for Vascular Interventional Advances; receiving grant funding from Bristol-Myers Squibb; and consulting for AstraZeneca, Boston Scientific, Ferring, Merck, and Novartis. These remarks were taken from his editorial accompanying Dr. Chatterjee’s report (JAMA 2014;311:2385-6).
|
|
|
Dr. Chatterjee and his associates calculated the net clinical benefit of thrombolysis, and their result "suggests evidence of modest efficacy in intermediate-risk PE," said Dr. Joshua A. Beckman.
But their findings do not yet add up to a change in the standard of care. Each clinician must decide on an individualized basis which of these patients should receive thrombolytic therapy, based on clinical presentation, comorbid conditions, and both the physician’s and the patient’s tolerance of risk.
Dr. Beckman is in the cardiovascular division at Brigham and Women’s Hospital, Boston. He reported being a board member for Vascular Interventional Advances; receiving grant funding from Bristol-Myers Squibb; and consulting for AstraZeneca, Boston Scientific, Ferring, Merck, and Novartis. These remarks were taken from his editorial accompanying Dr. Chatterjee’s report (JAMA 2014;311:2385-6).
Thrombolytic therapy decreased all-cause mortality in patients with hemodynamically stable pulmonary embolism associated with right ventricular dysfunction – those at "intermediate risk," according to a meta-analysis published online June 17 in JAMA.
The investigators described their study of 16 randomized, controlled clinical trials involving 2,115 patients as "the first analysis of thrombolysis in PE that has sufficient statistical power to detect associations with a meaningful mortality reduction." If their findings are confirmed in future randomized clinical trials, "there may be a shift in the treatment of selected patients with intermediate-risk PE using thrombolytics."
However, "the optimism regarding this clinical advantage must be tempered by [our] finding of significantly increased risk of major bleeding and intracranial hemorrhage associated with thrombolytic therapy, particularly for patients older than 65 years," said Dr. Saurav Chatterjee of the division of cardiology, St. Luke’s-Roosevelt Hospital Center of the Mount Sinai Health System, New York, and his associates (JAMA 2014;311:2414-21).
The study population included 1,499 patients who had hemodynamically stable PE associated with right ventricular dysfunction, the largest subset of patients seen in clinical practice and the group for whom the risks and benefits of thrombolysis are the most unclear.
After a mean follow-up of 82 days, overall mortality was 2.17% in patients who received thrombolysis, compared with 3.89% in those who received anticoagulation. In addition, the risk of recurrent PE was significantly lower with thrombolytic therapy (1.17%) than with anticoagulation (3.04%).
However, the rate of major bleeding was 9.24% for thrombolytic therapy, compared with 3.42% for anticoagulation. And the rate of intracranial hemorrhage was 1.46% for thrombolysis, compared with 0.19% for anticoagulation, the investigators said.
The bleeding risk was especially high in patients aged 65 years and older. Attenuation of this risk in younger patients suggests that they may be considered stronger candidates for thrombolytic therapy, Dr. Chatterjee and his associates said.
Dr. Chatterjee reported no financial conflicts; his associates reported ties to AstraZeneca, Boston Scientific, Cardiostem, Cordis, EKOS Corporation, Embolitech, GenWay, Johnson & Johnson, Soteria, and Vascular Magnetics.
Thrombolytic therapy decreased all-cause mortality in patients with hemodynamically stable pulmonary embolism associated with right ventricular dysfunction – those at "intermediate risk," according to a meta-analysis published online June 17 in JAMA.
The investigators described their study of 16 randomized, controlled clinical trials involving 2,115 patients as "the first analysis of thrombolysis in PE that has sufficient statistical power to detect associations with a meaningful mortality reduction." If their findings are confirmed in future randomized clinical trials, "there may be a shift in the treatment of selected patients with intermediate-risk PE using thrombolytics."
However, "the optimism regarding this clinical advantage must be tempered by [our] finding of significantly increased risk of major bleeding and intracranial hemorrhage associated with thrombolytic therapy, particularly for patients older than 65 years," said Dr. Saurav Chatterjee of the division of cardiology, St. Luke’s-Roosevelt Hospital Center of the Mount Sinai Health System, New York, and his associates (JAMA 2014;311:2414-21).
The study population included 1,499 patients who had hemodynamically stable PE associated with right ventricular dysfunction, the largest subset of patients seen in clinical practice and the group for whom the risks and benefits of thrombolysis are the most unclear.
After a mean follow-up of 82 days, overall mortality was 2.17% in patients who received thrombolysis, compared with 3.89% in those who received anticoagulation. In addition, the risk of recurrent PE was significantly lower with thrombolytic therapy (1.17%) than with anticoagulation (3.04%).
However, the rate of major bleeding was 9.24% for thrombolytic therapy, compared with 3.42% for anticoagulation. And the rate of intracranial hemorrhage was 1.46% for thrombolysis, compared with 0.19% for anticoagulation, the investigators said.
The bleeding risk was especially high in patients aged 65 years and older. Attenuation of this risk in younger patients suggests that they may be considered stronger candidates for thrombolytic therapy, Dr. Chatterjee and his associates said.
Dr. Chatterjee reported no financial conflicts; his associates reported ties to AstraZeneca, Boston Scientific, Cardiostem, Cordis, EKOS Corporation, Embolitech, GenWay, Johnson & Johnson, Soteria, and Vascular Magnetics.
FROM JAMA
Key clinical point: Thrombolysis may be a therapeutic alternative to anticoagulation in some patients with stable, intermediate-risk pulmonary embolism.
Major finding: Mortality was 2.17% in PE patients who received thrombolysis, compared with 3.89% in those who received anticoagulation; the risk of recurrent PE also was significantly lower with thrombolytic therapy (1.17%) than with anticoagulation (3.04%).
Data source: A meta-analysis of 16 randomized, controlled trials involving 2,115 patients with PE, including 1,499 with intermediate-risk PE, who were followed for a mean of 82 days.
Disclosures: Dr. Chatterjee reported no financial conflicts; his associates reported ties to AstraZeneca, Boston Scientific, Cardiostem, Cordis, EKOS Corporation, Embolitech, GenWay, Johnson & Johnson, Soteria, and Vascular Magnetics.

Point/Counterpoint: Is accreditation necessary to maintain quality in bariatric surgery?
Yes: Accreditation is why bariatric surgery outcomes are so good.
In the early days of bariatric surgery, there were very high mortality rates, up to 21% at 1 year in some studies. Because of that level of risk to patients, accreditation was implemented. Currently, mortality rates for bariatric surgery are at 0.15%, an extraordinary achievement in less than a decade. There are now 729 accredited hospitals in the United States, and that number says much about the level of access for patients. It is not unfettered access to bariatric surgery that is important, but rather access by patients to quality care. That’s what matters at the end of the day.

Accreditation isn’t keeping patients from gaining access to bariatric surgery. The bigger problem in access is making sure the federal and state health exchanges provide coverage for bariatric surgery among the essential health benefits. Fewer than half the states have this coverage.
Since accreditation started, there have been six studies with findings supporting it and three with findings that did not. Among the papers supporting it, Flum et al. is most persuasive because it looks at the Medicare population before and after the implementation of accreditation. It shows a big improvement in deaths, complications, and readmissions after the accreditation mandate despite an increase in the number of patients undergoing bariatric surgery (Ann. Surg. 2011;254:860-5).
The question that always comes up is whether it is volume (the number of cases you’re doing) or accreditation that matters for outcomes. A 2013 study found that accreditation status rendered a benefit independent of volume (Surg. Endosc. 2013;27:4539-46).
If we look at the three papers that found against accreditation, I would dismiss one study because it preceded the accreditation movement (Arch. Surg. 2009;144:319-25).
A study of Michigan patients reported similar complication rates at Centers of Excellence (COEs) and non-COEs (JAMA 2010;304:435-42). The problem with that study is that all of the hospitals in the study essentially are COEs, with the same components that come out of the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP). They have a registry. They have volume requirements. They have quality improvement. So, essentially, they’re all COEs, and I’m glad that they embrace the same concepts that we espouse.
The final paper, by Dr. Dimick, takes an econometric approach using differences within differences analysis, which means you look at the differential rate of change to see if the experimental group (in this case, the Medicare population) is different in some way from the control group (non-Medicare). Here’s the problem: That is not a true control. Non-Medicare patients were exposed to accreditation. All of the major insurers embraced accreditation then and continue to do so.
The paper didn’t look at mortality and failure to rescue patients from complications (JAMA 2013;309:792-9). Even though mortality may be low, it still matters. It’s what I would call a sentinel event. It’s become so rare that when it happens, it’s a signal of an issue around quality. We see improvements in both the Medicare and non-Medicare populations. Do two rights make a wrong? Does that mean that accreditation doesn’t work? I think it points out that we’re seeing important changes for the better for all groups.
We presented findings at the American Surgical Association this year showing that accredited hospitals had lower total charges with lower rates of complications, mortality, and failure to rescue. What accreditation provides is a safety net. If something goes wrong, the difference is the ability to recover from complications. There was not a big difference between accredited and non-accredited hospitals in complications in general, but a bigger difference in mortality. Mortality still counts. Failure to rescue is a very important metric that we all need to pay attention to.
Some of our other data show a halo effect from accreditation. In the accredited centers, outcomes were better for non-bariatric procedures. Why? Because they had more experience with obese patients. It’s a collateral benefit.
Without accreditation, I wonder what will happen at hospitals that aren’t required to be accredited. Will they still have the registry? Will they still have the resources they need? Not everybody has the advantages that Michigan has with major insurer support to pay for accreditation efforts. And it’s critical that we have those data. You can’t manage what you don’t measure. Accreditation is vital for bariatric surgery.
Dr. Morton is director of both bariatric surgery and surgical quality at Stanford (Calif.) University Medical Center. He disclosed financial associations with Vivus, Covidien, and Ethicon.
No: The data do not show that outcomes are better in COEs.
The Centers of Excellence has evolved into the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP), which is an outcomes benchmarking and quality improvement program. So we are, in many ways, looking in the rear-view mirror when we talk about whether or not the historical accreditation process improved outcomes.
I’m going to make two arguments against the historical way it was done. The first argument is that limiting care to Centers of Excellence (COEs) as they were defined had very little benefit on outcomes and may have caused some harm.

A lot of the data out there to evaluate the COE program are a little misleading. They looked at Medicare data for outcomes before and after the Medicare COE mandate was put in place requiring that bariatric surgery be performed in a COE to qualify for coverage. The problem with that is the outcomes are improving so quickly that you can’t just do a before and after study. You need to adjust for that time frame to make sure you’re not getting a spurious finding.
We did a study comparing improvement trends for any complications, serious complications, and reoperations before and after Medicare implemented its coverage decision. Surgeons were already getting better before that. There was no change in the trajectory of improvements when the policy was implemented. We concluded that the policy that selectively referred patients to Centers of Excellence didn’t have any benefit (JAMA 2013;309:792-9). We originally included mortality in our analysis but deaths were so rare that it didn’t meet power specifications set by the journal.
In that paper, we did a head-to-head comparison of COEs vs. non-COEs in 12 large states. It’s hard to do a randomized controlled trial for this, so we did an instrumental variable analysis, a sophisticated analysis that takes out a lot of the unmeasured confounding in selection bias. We found that there was no benefit to having bariatric surgery in a COE.
We noticed that many hospitals that traditionally served minorities did not achieve accreditation. One can assume that’s because they probably didn’t have the resources to participate in the program. After the policy was implemented, the rate of bariatric surgery in minorities dropped substantially, whereas it went up in non-minority patients (JAMA 2013;310:1399-1400). So, there’s potential evidence of harm with these policies.
Medicare eliminated their facility accreditation requirement for bariatric surgery last September.
My second argument is that we could be doing something so much better than accreditation to improve bariatric surgery outcomes. Michigan’s approach is a large quality improvement collaborative funded by Blue Cross Blue Shield. We’re using lessons learned in Michigan to implement change on a broader scale without the involvement of payers. We have 70 surgeons and 32 bariatric surgery programs benchmarking outcomes and using those in strategic ways to learn from each other, hopefully improving everybody’s outcomes.
We standardized venous thromboembolism (VTE) prophylaxis across the state and implemented decision support. VTE rates fell by half. We saw a 90% improvement in mortality and a 24% drop in overall complications. Yes, bariatric surgery centers everywhere were improving at that same time, but when we compared Michigan hospitals participating in our collaborative to non-Michigan hospitals, we saw steeper declines in adverse outcomes in Michigan. That’s very robust evidence that this approach is effective for improving perioperative care.
We have launched a technical skill initiative in which surgeons participating in the collaborative give us a video of a typical procedure that gets rated in a blinded fashion by their peers. We just got funded to use these videos in a coaching program to help surgeons in Michigan improve our technique.
Doing this kind of collaborative work doesn’t take a ton of money. It does take time, strategy, and social capital – developing networks of surgeons that work together and learn together. The historical Centers of Excellence program wasn’t a bad idea, but it wasn’t correlated with perioperative outcomes, and it did have harms.
Dr. Dimick is chief of minimally invasive surgery at the University of Michigan Health System, Ann Arbor. He disclosed being a stockholder in ArborMetrix.
Yes: Accreditation is why bariatric surgery outcomes are so good.
In the early days of bariatric surgery, there were very high mortality rates, up to 21% at 1 year in some studies. Because of that level of risk to patients, accreditation was implemented. Currently, mortality rates for bariatric surgery are at 0.15%, an extraordinary achievement in less than a decade. There are now 729 accredited hospitals in the United States, and that number says much about the level of access for patients. It is not unfettered access to bariatric surgery that is important, but rather access by patients to quality care. That’s what matters at the end of the day.
Accreditation isn’t keeping patients from gaining access to bariatric surgery. The bigger problem in access is making sure the federal and state health exchanges provide coverage for bariatric surgery among the essential health benefits. Fewer than half the states have this coverage.
Since accreditation started, there have been six studies with findings supporting it and three with findings that did not. Among the papers supporting it, Flum et al. is most persuasive because it looks at the Medicare population before and after the implementation of accreditation. It shows a big improvement in deaths, complications, and readmissions after the accreditation mandate despite an increase in the number of patients undergoing bariatric surgery (Ann. Surg. 2011;254:860-5).
The question that always comes up is whether it is volume (the number of cases you’re doing) or accreditation that matters for outcomes. A 2013 study found that accreditation status rendered a benefit independent of volume (Surg. Endosc. 2013;27:4539-46).
If we look at the three papers that found against accreditation, I would dismiss one study because it preceded the accreditation movement (Arch. Surg. 2009;144:319-25).
A study of Michigan patients reported similar complication rates at Centers of Excellence (COEs) and non-COEs (JAMA 2010;304:435-42). The problem with that study is that all of the hospitals in the study essentially are COEs, with the same components that come out of the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP). They have a registry. They have volume requirements. They have quality improvement. So, essentially, they’re all COEs, and I’m glad that they embrace the same concepts that we espouse.
The final paper, by Dr. Dimick, takes an econometric approach using differences within differences analysis, which means you look at the differential rate of change to see if the experimental group (in this case, the Medicare population) is different in some way from the control group (non-Medicare). Here’s the problem: That is not a true control. Non-Medicare patients were exposed to accreditation. All of the major insurers embraced accreditation then and continue to do so.
The paper didn’t look at mortality and failure to rescue patients from complications (JAMA 2013;309:792-9). Even though mortality may be low, it still matters. It’s what I would call a sentinel event. It’s become so rare that when it happens, it’s a signal of an issue around quality. We see improvements in both the Medicare and non-Medicare populations. Do two rights make a wrong? Does that mean that accreditation doesn’t work? I think it points out that we’re seeing important changes for the better for all groups.
We presented findings at the American Surgical Association this year showing that accredited hospitals had lower total charges with lower rates of complications, mortality, and failure to rescue. What accreditation provides is a safety net. If something goes wrong, the difference is the ability to recover from complications. There was not a big difference between accredited and non-accredited hospitals in complications in general, but a bigger difference in mortality. Mortality still counts. Failure to rescue is a very important metric that we all need to pay attention to.
Some of our other data show a halo effect from accreditation. In the accredited centers, outcomes were better for non-bariatric procedures. Why? Because they had more experience with obese patients. It’s a collateral benefit.
Without accreditation, I wonder what will happen at hospitals that aren’t required to be accredited. Will they still have the registry? Will they still have the resources they need? Not everybody has the advantages that Michigan has with major insurer support to pay for accreditation efforts. And it’s critical that we have those data. You can’t manage what you don’t measure. Accreditation is vital for bariatric surgery.
Dr. Morton is director of both bariatric surgery and surgical quality at Stanford (Calif.) University Medical Center. He disclosed financial associations with Vivus, Covidien, and Ethicon.
No: The data do not show that outcomes are better in COEs.
The Centers of Excellence has evolved into the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP), which is an outcomes benchmarking and quality improvement program. So we are, in many ways, looking in the rear-view mirror when we talk about whether or not the historical accreditation process improved outcomes.
I’m going to make two arguments against the historical way it was done. The first argument is that limiting care to Centers of Excellence (COEs) as they were defined had very little benefit on outcomes and may have caused some harm.
A lot of the data out there to evaluate the COE program are a little misleading. They looked at Medicare data for outcomes before and after the Medicare COE mandate was put in place requiring that bariatric surgery be performed in a COE to qualify for coverage. The problem with that is the outcomes are improving so quickly that you can’t just do a before and after study. You need to adjust for that time frame to make sure you’re not getting a spurious finding.
We did a study comparing improvement trends for any complications, serious complications, and reoperations before and after Medicare implemented its coverage decision. Surgeons were already getting better before that. There was no change in the trajectory of improvements when the policy was implemented. We concluded that the policy that selectively referred patients to Centers of Excellence didn’t have any benefit (JAMA 2013;309:792-9). We originally included mortality in our analysis but deaths were so rare that it didn’t meet power specifications set by the journal.
In that paper, we did a head-to-head comparison of COEs vs. non-COEs in 12 large states. It’s hard to do a randomized controlled trial for this, so we did an instrumental variable analysis, a sophisticated analysis that takes out a lot of the unmeasured confounding in selection bias. We found that there was no benefit to having bariatric surgery in a COE.
We noticed that many hospitals that traditionally served minorities did not achieve accreditation. One can assume that’s because they probably didn’t have the resources to participate in the program. After the policy was implemented, the rate of bariatric surgery in minorities dropped substantially, whereas it went up in non-minority patients (JAMA 2013;310:1399-1400). So, there’s potential evidence of harm with these policies.
Medicare eliminated their facility accreditation requirement for bariatric surgery last September.
My second argument is that we could be doing something so much better than accreditation to improve bariatric surgery outcomes. Michigan’s approach is a large quality improvement collaborative funded by Blue Cross Blue Shield. We’re using lessons learned in Michigan to implement change on a broader scale without the involvement of payers. We have 70 surgeons and 32 bariatric surgery programs benchmarking outcomes and using those in strategic ways to learn from each other, hopefully improving everybody’s outcomes.
We standardized venous thromboembolism (VTE) prophylaxis across the state and implemented decision support. VTE rates fell by half. We saw a 90% improvement in mortality and a 24% drop in overall complications. Yes, bariatric surgery centers everywhere were improving at that same time, but when we compared Michigan hospitals participating in our collaborative to non-Michigan hospitals, we saw steeper declines in adverse outcomes in Michigan. That’s very robust evidence that this approach is effective for improving perioperative care.
We have launched a technical skill initiative in which surgeons participating in the collaborative give us a video of a typical procedure that gets rated in a blinded fashion by their peers. We just got funded to use these videos in a coaching program to help surgeons in Michigan improve our technique.
Doing this kind of collaborative work doesn’t take a ton of money. It does take time, strategy, and social capital – developing networks of surgeons that work together and learn together. The historical Centers of Excellence program wasn’t a bad idea, but it wasn’t correlated with perioperative outcomes, and it did have harms.
Dr. Dimick is chief of minimally invasive surgery at the University of Michigan Health System, Ann Arbor. He disclosed being a stockholder in ArborMetrix.
Yes: Accreditation is why bariatric surgery outcomes are so good.
In the early days of bariatric surgery, there were very high mortality rates, up to 21% at 1 year in some studies. Because of that level of risk to patients, accreditation was implemented. Currently, mortality rates for bariatric surgery are at 0.15%, an extraordinary achievement in less than a decade. There are now 729 accredited hospitals in the United States, and that number says much about the level of access for patients. It is not unfettered access to bariatric surgery that is important, but rather access by patients to quality care. That’s what matters at the end of the day.
Accreditation isn’t keeping patients from gaining access to bariatric surgery. The bigger problem in access is making sure the federal and state health exchanges provide coverage for bariatric surgery among the essential health benefits. Fewer than half the states have this coverage.
Since accreditation started, there have been six studies with findings supporting it and three with findings that did not. Among the papers supporting it, Flum et al. is most persuasive because it looks at the Medicare population before and after the implementation of accreditation. It shows a big improvement in deaths, complications, and readmissions after the accreditation mandate despite an increase in the number of patients undergoing bariatric surgery (Ann. Surg. 2011;254:860-5).
The question that always comes up is whether it is volume (the number of cases you’re doing) or accreditation that matters for outcomes. A 2013 study found that accreditation status rendered a benefit independent of volume (Surg. Endosc. 2013;27:4539-46).
If we look at the three papers that found against accreditation, I would dismiss one study because it preceded the accreditation movement (Arch. Surg. 2009;144:319-25).
A study of Michigan patients reported similar complication rates at Centers of Excellence (COEs) and non-COEs (JAMA 2010;304:435-42). The problem with that study is that all of the hospitals in the study essentially are COEs, with the same components that come out of the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP). They have a registry. They have volume requirements. They have quality improvement. So, essentially, they’re all COEs, and I’m glad that they embrace the same concepts that we espouse.
The final paper, by Dr. Dimick, takes an econometric approach using differences within differences analysis, which means you look at the differential rate of change to see if the experimental group (in this case, the Medicare population) is different in some way from the control group (non-Medicare). Here’s the problem: That is not a true control. Non-Medicare patients were exposed to accreditation. All of the major insurers embraced accreditation then and continue to do so.
The paper didn’t look at mortality and failure to rescue patients from complications (JAMA 2013;309:792-9). Even though mortality may be low, it still matters. It’s what I would call a sentinel event. It’s become so rare that when it happens, it’s a signal of an issue around quality. We see improvements in both the Medicare and non-Medicare populations. Do two rights make a wrong? Does that mean that accreditation doesn’t work? I think it points out that we’re seeing important changes for the better for all groups.
We presented findings at the American Surgical Association this year showing that accredited hospitals had lower total charges with lower rates of complications, mortality, and failure to rescue. What accreditation provides is a safety net. If something goes wrong, the difference is the ability to recover from complications. There was not a big difference between accredited and non-accredited hospitals in complications in general, but a bigger difference in mortality. Mortality still counts. Failure to rescue is a very important metric that we all need to pay attention to.
Some of our other data show a halo effect from accreditation. In the accredited centers, outcomes were better for non-bariatric procedures. Why? Because they had more experience with obese patients. It’s a collateral benefit.
Without accreditation, I wonder what will happen at hospitals that aren’t required to be accredited. Will they still have the registry? Will they still have the resources they need? Not everybody has the advantages that Michigan has with major insurer support to pay for accreditation efforts. And it’s critical that we have those data. You can’t manage what you don’t measure. Accreditation is vital for bariatric surgery.
Dr. Morton is director of both bariatric surgery and surgical quality at Stanford (Calif.) University Medical Center. He disclosed financial associations with Vivus, Covidien, and Ethicon.
No: The data do not show that outcomes are better in COEs.
The Centers of Excellence has evolved into the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP), which is an outcomes benchmarking and quality improvement program. So we are, in many ways, looking in the rear-view mirror when we talk about whether or not the historical accreditation process improved outcomes.
I’m going to make two arguments against the historical way it was done. The first argument is that limiting care to Centers of Excellence (COEs) as they were defined had very little benefit on outcomes and may have caused some harm.
A lot of the data out there to evaluate the COE program are a little misleading. They looked at Medicare data for outcomes before and after the Medicare COE mandate was put in place requiring that bariatric surgery be performed in a COE to qualify for coverage. The problem with that is the outcomes are improving so quickly that you can’t just do a before and after study. You need to adjust for that time frame to make sure you’re not getting a spurious finding.
We did a study comparing improvement trends for any complications, serious complications, and reoperations before and after Medicare implemented its coverage decision. Surgeons were already getting better before that. There was no change in the trajectory of improvements when the policy was implemented. We concluded that the policy that selectively referred patients to Centers of Excellence didn’t have any benefit (JAMA 2013;309:792-9). We originally included mortality in our analysis but deaths were so rare that it didn’t meet power specifications set by the journal.
In that paper, we did a head-to-head comparison of COEs vs. non-COEs in 12 large states. It’s hard to do a randomized controlled trial for this, so we did an instrumental variable analysis, a sophisticated analysis that takes out a lot of the unmeasured confounding in selection bias. We found that there was no benefit to having bariatric surgery in a COE.
We noticed that many hospitals that traditionally served minorities did not achieve accreditation. One can assume that’s because they probably didn’t have the resources to participate in the program. After the policy was implemented, the rate of bariatric surgery in minorities dropped substantially, whereas it went up in non-minority patients (JAMA 2013;310:1399-1400). So, there’s potential evidence of harm with these policies.
Medicare eliminated their facility accreditation requirement for bariatric surgery last September.
My second argument is that we could be doing something so much better than accreditation to improve bariatric surgery outcomes. Michigan’s approach is a large quality improvement collaborative funded by Blue Cross Blue Shield. We’re using lessons learned in Michigan to implement change on a broader scale without the involvement of payers. We have 70 surgeons and 32 bariatric surgery programs benchmarking outcomes and using those in strategic ways to learn from each other, hopefully improving everybody’s outcomes.
We standardized venous thromboembolism (VTE) prophylaxis across the state and implemented decision support. VTE rates fell by half. We saw a 90% improvement in mortality and a 24% drop in overall complications. Yes, bariatric surgery centers everywhere were improving at that same time, but when we compared Michigan hospitals participating in our collaborative to non-Michigan hospitals, we saw steeper declines in adverse outcomes in Michigan. That’s very robust evidence that this approach is effective for improving perioperative care.
We have launched a technical skill initiative in which surgeons participating in the collaborative give us a video of a typical procedure that gets rated in a blinded fashion by their peers. We just got funded to use these videos in a coaching program to help surgeons in Michigan improve our technique.
Doing this kind of collaborative work doesn’t take a ton of money. It does take time, strategy, and social capital – developing networks of surgeons that work together and learn together. The historical Centers of Excellence program wasn’t a bad idea, but it wasn’t correlated with perioperative outcomes, and it did have harms.
Dr. Dimick is chief of minimally invasive surgery at the University of Michigan Health System, Ann Arbor. He disclosed being a stockholder in ArborMetrix.

Ensure business associate agreements comply with HIPAA rule, attorneys advise
CHICAGO – A new HIPAA rule means physicians face broader liability for protected health information breaches by their business associates.
The final omnibus rule on the Health Insurance Portability and Accountability Act broadens the definition of who and what is considered a business associate and places more responsibility on doctors for protected health information (PHI) acts or omissions by such associates.

About "28%-49% of breaches in the health care industry are associated with business associates and how they’re using data," health law attorney Clinton R. Mikel said at a physicians’ legal issues conference held by the American Bar Association.
"It’s important to know who your business associates are, how you’re [interacting] with them and what they’re doing with your data."
The final HIPAA omnibus rule went into effect in September 2013, but allowed covered entities and businesses to continue operating under some existing contracts for up to 1 year. Grandfathered business agreements must be revised to meet the new HIPAA requirements by Sept. 22, 2014.
Under the omnibus rule, a business associate is defined as any person or entity that creates, receives, maintains, or transmits PHI on behalf of a covered entity. The regulation means that business associates now include patient safety organizations, data transmission organizations, personal health record vendors, entities that transmit and need routine access to PHI, and data storage vendors – paper based and cloud based.
On physicians’ immediate checklist of things to be reviewed and updated is their existing business-associate agreement template, said Mr. Mikel, a partner at The Health Law Partners, PC, in Southfield, Mich. The revised agreement should ensure that associates comply with all measures of the Security Rule for electronic PHI and that business associates report any breach of unsecured PHI.
In addition, business associates should enter into contracts only with subcontractors that comply with such agreements and restrict subcontractors from disclosing PHI in an inappropriate manner.
Distribute the new template as soon as possible for all new contracts and evaluate outstanding business associate relationships, Mr. Mikel advised.
Proper data security from cloud-based vendors is especially important in light of the new HIPAA rule, said Hemant Pathak, assistant general counsel for Microsoft. Make certain they are told where and how their data is stored in "the cloud" and have clear data maps and geographic boundary information.
Vendors should be "transparent about what their operations are, have a breach procedure, and be willing to share" their policies, Mr. Pathak added. "It should not be something that is obtuse. It should be something that is clear and transparent."
Under the omnibus rule, both the doctor and vendor are on the hook if PHI is exposed.
"It’s important for both of us in protecting our reputations and understanding what the needs are from a compliance" standpoint, Mr. Pathak said.
CHICAGO – A new HIPAA rule means physicians face broader liability for protected health information breaches by their business associates.
The final omnibus rule on the Health Insurance Portability and Accountability Act broadens the definition of who and what is considered a business associate and places more responsibility on doctors for protected health information (PHI) acts or omissions by such associates.
About "28%-49% of breaches in the health care industry are associated with business associates and how they’re using data," health law attorney Clinton R. Mikel said at a physicians’ legal issues conference held by the American Bar Association.
"It’s important to know who your business associates are, how you’re [interacting] with them and what they’re doing with your data."
The final HIPAA omnibus rule went into effect in September 2013, but allowed covered entities and businesses to continue operating under some existing contracts for up to 1 year. Grandfathered business agreements must be revised to meet the new HIPAA requirements by Sept. 22, 2014.
Under the omnibus rule, a business associate is defined as any person or entity that creates, receives, maintains, or transmits PHI on behalf of a covered entity. The regulation means that business associates now include patient safety organizations, data transmission organizations, personal health record vendors, entities that transmit and need routine access to PHI, and data storage vendors – paper based and cloud based.
On physicians’ immediate checklist of things to be reviewed and updated is their existing business-associate agreement template, said Mr. Mikel, a partner at The Health Law Partners, PC, in Southfield, Mich. The revised agreement should ensure that associates comply with all measures of the Security Rule for electronic PHI and that business associates report any breach of unsecured PHI.
In addition, business associates should enter into contracts only with subcontractors that comply with such agreements and restrict subcontractors from disclosing PHI in an inappropriate manner.
Distribute the new template as soon as possible for all new contracts and evaluate outstanding business associate relationships, Mr. Mikel advised.
Proper data security from cloud-based vendors is especially important in light of the new HIPAA rule, said Hemant Pathak, assistant general counsel for Microsoft. Make certain they are told where and how their data is stored in "the cloud" and have clear data maps and geographic boundary information.
Vendors should be "transparent about what their operations are, have a breach procedure, and be willing to share" their policies, Mr. Pathak added. "It should not be something that is obtuse. It should be something that is clear and transparent."
Under the omnibus rule, both the doctor and vendor are on the hook if PHI is exposed.
"It’s important for both of us in protecting our reputations and understanding what the needs are from a compliance" standpoint, Mr. Pathak said.
CHICAGO – A new HIPAA rule means physicians face broader liability for protected health information breaches by their business associates.
The final omnibus rule on the Health Insurance Portability and Accountability Act broadens the definition of who and what is considered a business associate and places more responsibility on doctors for protected health information (PHI) acts or omissions by such associates.
About "28%-49% of breaches in the health care industry are associated with business associates and how they’re using data," health law attorney Clinton R. Mikel said at a physicians’ legal issues conference held by the American Bar Association.
"It’s important to know who your business associates are, how you’re [interacting] with them and what they’re doing with your data."
The final HIPAA omnibus rule went into effect in September 2013, but allowed covered entities and businesses to continue operating under some existing contracts for up to 1 year. Grandfathered business agreements must be revised to meet the new HIPAA requirements by Sept. 22, 2014.
Under the omnibus rule, a business associate is defined as any person or entity that creates, receives, maintains, or transmits PHI on behalf of a covered entity. The regulation means that business associates now include patient safety organizations, data transmission organizations, personal health record vendors, entities that transmit and need routine access to PHI, and data storage vendors – paper based and cloud based.
On physicians’ immediate checklist of things to be reviewed and updated is their existing business-associate agreement template, said Mr. Mikel, a partner at The Health Law Partners, PC, in Southfield, Mich. The revised agreement should ensure that associates comply with all measures of the Security Rule for electronic PHI and that business associates report any breach of unsecured PHI.
In addition, business associates should enter into contracts only with subcontractors that comply with such agreements and restrict subcontractors from disclosing PHI in an inappropriate manner.
Distribute the new template as soon as possible for all new contracts and evaluate outstanding business associate relationships, Mr. Mikel advised.
Proper data security from cloud-based vendors is especially important in light of the new HIPAA rule, said Hemant Pathak, assistant general counsel for Microsoft. Make certain they are told where and how their data is stored in "the cloud" and have clear data maps and geographic boundary information.
Vendors should be "transparent about what their operations are, have a breach procedure, and be willing to share" their policies, Mr. Pathak added. "It should not be something that is obtuse. It should be something that is clear and transparent."
Under the omnibus rule, both the doctor and vendor are on the hook if PHI is exposed.
"It’s important for both of us in protecting our reputations and understanding what the needs are from a compliance" standpoint, Mr. Pathak said.
AT AN ABA CONFERENCE

Adding age to stage better predicts adrenocortical carcinoma prognosis
BOSTON – A proposed system for staging adrenocortical carcinomas appears to more accurately predict prognoses across all age and stage groups, but the system is not quite ready for prime time, investigators say.
The system combines information on patient age, tumor stage, and nodal and metastatic (TNM) status. In a retrospective study, the TNM-age system was better at predicting 5-year overall survival than was the European Network for the Study of Adrenal Tumors (ENSAT) staging system, which was in turn a modification of another system, said Dr. Elliot Asare, a research resident in the department of surgical education at the Medical College of Wisconsin in Milwaukee.

The improved predictive power of the TNM-age system may be due to differences in tumor biology between older and younger patients, Dr. Asare noted.
"Improved staging allows for a more accurate assessment of the natural history of the disease," he said at the annual meeting of the American Association of Endocrine Surgeons.
The two main staging systems currently used for adrenocortical carcinoma (ACC) are the American Joint Committee on Cancer/International Union Against Cancer (AJCC/UICC) system, and ENSAT, which was proposed in 2009 as a modified version of the AJCC/UICC staging system. Under the ENSAT modification, stage IV disease would be limited to patients with distant metastases.
However, the ENSAT criteria were not good at discriminating between stage I and stage II disease, and failed to show a significant survival difference, Dr. Asare noted.
The investigators undertook to see whether the ENSAT’s prognostic accuracy might improve with a larger data set, and to determine whether adding age as a variable to staging ACC could improve the accuracy of survival predictions.
They drew data on patients with a histologic diagnosis of ACC from 1985 through 2006 in the National Cancer Database, and used Surveillance, Epidemiology and End Results (SEER) summary stage information to establish TNM stage according to ENSAT criteria.
They considered tumor size, resection margin status, histologic grade, lymph node status, SEER summary stage, vital status, and age of diagnosis.
Out of a total of 3,263 patients with ACC, sufficient data were available on 1,597.
When they applied the staging criteria, they were able to validate the ENSAT system for stage III vs. stage IV (P less than .0001), and for stage II vs. state III (P less than .0001), but no significant differences between I and II (P =.04). The 5-year overall survival rates under ENSAT were 68% for stage I and 61% for stage II.
They then developed their alternative staging system by adding age to the mix, as follows:
• Stage 1: T1-T2, N0, M0, age 55 or younger.
• Stage II: T1-T2, N0, M0, age over 55.
• Stage III: T1-T2, N1, M0, any age, or T3-T4, any N, M0, any age.
• Stage IV: any T, any N, M1.
By using this system applied to the same cohort, they found that the respective 5-year overall survival rates (stage I-IV) were 70%, 53%, 37%, and 9.7%, respectively. In addition, the survival rates were significantly different between stages I and II (P less than .0001), stages II and III (P = .0004), and stages III and IV (P less than .0001).
Significant predictors of death under the TNM-age staging were stage II and above, positive tumor resection margins, and grade.
Dr. Asare noted that the study was limited by the lack of some variables in the database and an absence of information on cause-specific mortality, and by the fact that age cannot be used as a continuous variable in a classification system.
The staging system needs to be tested in a validation study with information from an independent database, he added.
Dr. Asare disclosed receiving support from the American College of Surgeons Clinical Scholars in Residence fellowship, partially supported by an unrestricted education grant from Genentech.
BOSTON – A proposed system for staging adrenocortical carcinomas appears to more accurately predict prognoses across all age and stage groups, but the system is not quite ready for prime time, investigators say.
The system combines information on patient age, tumor stage, and nodal and metastatic (TNM) status. In a retrospective study, the TNM-age system was better at predicting 5-year overall survival than was the European Network for the Study of Adrenal Tumors (ENSAT) staging system, which was in turn a modification of another system, said Dr. Elliot Asare, a research resident in the department of surgical education at the Medical College of Wisconsin in Milwaukee.
The improved predictive power of the TNM-age system may be due to differences in tumor biology between older and younger patients, Dr. Asare noted.
"Improved staging allows for a more accurate assessment of the natural history of the disease," he said at the annual meeting of the American Association of Endocrine Surgeons.
The two main staging systems currently used for adrenocortical carcinoma (ACC) are the American Joint Committee on Cancer/International Union Against Cancer (AJCC/UICC) system, and ENSAT, which was proposed in 2009 as a modified version of the AJCC/UICC staging system. Under the ENSAT modification, stage IV disease would be limited to patients with distant metastases.
However, the ENSAT criteria were not good at discriminating between stage I and stage II disease, and failed to show a significant survival difference, Dr. Asare noted.
The investigators undertook to see whether the ENSAT’s prognostic accuracy might improve with a larger data set, and to determine whether adding age as a variable to staging ACC could improve the accuracy of survival predictions.
They drew data on patients with a histologic diagnosis of ACC from 1985 through 2006 in the National Cancer Database, and used Surveillance, Epidemiology and End Results (SEER) summary stage information to establish TNM stage according to ENSAT criteria.
They considered tumor size, resection margin status, histologic grade, lymph node status, SEER summary stage, vital status, and age of diagnosis.
Out of a total of 3,263 patients with ACC, sufficient data were available on 1,597.
When they applied the staging criteria, they were able to validate the ENSAT system for stage III vs. stage IV (P less than .0001), and for stage II vs. state III (P less than .0001), but no significant differences between I and II (P =.04). The 5-year overall survival rates under ENSAT were 68% for stage I and 61% for stage II.
They then developed their alternative staging system by adding age to the mix, as follows:
• Stage 1: T1-T2, N0, M0, age 55 or younger.
• Stage II: T1-T2, N0, M0, age over 55.
• Stage III: T1-T2, N1, M0, any age, or T3-T4, any N, M0, any age.
• Stage IV: any T, any N, M1.
By using this system applied to the same cohort, they found that the respective 5-year overall survival rates (stage I-IV) were 70%, 53%, 37%, and 9.7%, respectively. In addition, the survival rates were significantly different between stages I and II (P less than .0001), stages II and III (P = .0004), and stages III and IV (P less than .0001).
Significant predictors of death under the TNM-age staging were stage II and above, positive tumor resection margins, and grade.
Dr. Asare noted that the study was limited by the lack of some variables in the database and an absence of information on cause-specific mortality, and by the fact that age cannot be used as a continuous variable in a classification system.
The staging system needs to be tested in a validation study with information from an independent database, he added.
Dr. Asare disclosed receiving support from the American College of Surgeons Clinical Scholars in Residence fellowship, partially supported by an unrestricted education grant from Genentech.
BOSTON – A proposed system for staging adrenocortical carcinomas appears to more accurately predict prognoses across all age and stage groups, but the system is not quite ready for prime time, investigators say.
The system combines information on patient age, tumor stage, and nodal and metastatic (TNM) status. In a retrospective study, the TNM-age system was better at predicting 5-year overall survival than was the European Network for the Study of Adrenal Tumors (ENSAT) staging system, which was in turn a modification of another system, said Dr. Elliot Asare, a research resident in the department of surgical education at the Medical College of Wisconsin in Milwaukee.
The improved predictive power of the TNM-age system may be due to differences in tumor biology between older and younger patients, Dr. Asare noted.
"Improved staging allows for a more accurate assessment of the natural history of the disease," he said at the annual meeting of the American Association of Endocrine Surgeons.
The two main staging systems currently used for adrenocortical carcinoma (ACC) are the American Joint Committee on Cancer/International Union Against Cancer (AJCC/UICC) system, and ENSAT, which was proposed in 2009 as a modified version of the AJCC/UICC staging system. Under the ENSAT modification, stage IV disease would be limited to patients with distant metastases.
However, the ENSAT criteria were not good at discriminating between stage I and stage II disease, and failed to show a significant survival difference, Dr. Asare noted.
The investigators undertook to see whether the ENSAT’s prognostic accuracy might improve with a larger data set, and to determine whether adding age as a variable to staging ACC could improve the accuracy of survival predictions.
They drew data on patients with a histologic diagnosis of ACC from 1985 through 2006 in the National Cancer Database, and used Surveillance, Epidemiology and End Results (SEER) summary stage information to establish TNM stage according to ENSAT criteria.
They considered tumor size, resection margin status, histologic grade, lymph node status, SEER summary stage, vital status, and age of diagnosis.
Out of a total of 3,263 patients with ACC, sufficient data were available on 1,597.
When they applied the staging criteria, they were able to validate the ENSAT system for stage III vs. stage IV (P less than .0001), and for stage II vs. state III (P less than .0001), but no significant differences between I and II (P =.04). The 5-year overall survival rates under ENSAT were 68% for stage I and 61% for stage II.
They then developed their alternative staging system by adding age to the mix, as follows:
• Stage 1: T1-T2, N0, M0, age 55 or younger.
• Stage II: T1-T2, N0, M0, age over 55.
• Stage III: T1-T2, N1, M0, any age, or T3-T4, any N, M0, any age.
• Stage IV: any T, any N, M1.
By using this system applied to the same cohort, they found that the respective 5-year overall survival rates (stage I-IV) were 70%, 53%, 37%, and 9.7%, respectively. In addition, the survival rates were significantly different between stages I and II (P less than .0001), stages II and III (P = .0004), and stages III and IV (P less than .0001).
Significant predictors of death under the TNM-age staging were stage II and above, positive tumor resection margins, and grade.
Dr. Asare noted that the study was limited by the lack of some variables in the database and an absence of information on cause-specific mortality, and by the fact that age cannot be used as a continuous variable in a classification system.
The staging system needs to be tested in a validation study with information from an independent database, he added.
Dr. Asare disclosed receiving support from the American College of Surgeons Clinical Scholars in Residence fellowship, partially supported by an unrestricted education grant from Genentech.
AT AAES 2014
Key clinical point: Adding age to the ENSAT staging system improved prediction of adrenocortical carcinoma prognosis.
Major finding: A modified staging system showed significant differences in 5-year overall survival between all stages of adrenocortical carcinoma; the ENSAT staging system did not.
Data source: Retrospective study of 1,597 patients with adrenocortical carcinoma in the National Cancer Database.
Disclosures: Dr. Asare disclosed receiving support from the American College of Surgeons Clinical Scholars in Residence fellowship, partially supported by an unrestricted education grant from Genentech.

EHR Report: Across the ages
Eighty percent of physicians are now using electronic health records in their offices. We have been impressed that the younger physicians to whom we have spoken often view their experience with EHRs very differently from older physicians. Is such a difference inevitable, perhaps, not just because change is more difficult for many people as they get older but also because expectations are influenced by experience. Noticing these different thoughts and feelings, we’ve asked two physicians more than 55 years old and two younger physicians to share some thoughts on their experiences with electronic records.
Mathew Clark (family physician)
I’ve been in practice for 31 years and using an EHR system for just under 5. I’m not thrilled with it, but I accept that it’s an unavoidable part of my practice now, and so I don’t waste energy being upset about it. I’ve learned to function efficiently with an EHR, doing the best I can. I remember physicians, before the days of SOAP notes, who would write pithy, useful notes such as "probable strep, Pen VK 500 bid for 10 days" on 3x5 index cards. Such notes lacked detail, and it’s not hard to imagine the problems this lack of detail might create, but they were readable at a glance, and told you what you needed to know. On the other hand, the massively detailed, bloated notes we see with our EHRs, obscured by "copy-forward" text and fictional (in other words, never really asked or examined) information, present very significant practical and legal issues of their own, and take hours of physician time to complete. Given a choice, I’d probably go for the index cards.
Natalie McGann (family physician)
I have been a family physician in practice for 4 years since graduating from residency. The advent of the EHR hasn’t been an overwhelming transition for those of us in the early stages of our careers. Much of our schooling to date has included laptops and other electronic devices that for many prove an easier means of communication. Despite that fact that EHRs require a host of extraneous clicks and check boxes, it is still less cumbersome than documenting encounters on paper. For the generation of young physicians accustomed to having answers at their fingertips, the idea of flipping through paper charts to collate a patient’s medical record seems far more complicated than clicking a few tabs without ever leaving your chair. I, and most colleagues in my peer group to whom I’ve spoken, agree that we would not be likely to a join a practice that doesn’t utilize an EHR or have a current plan to adopt one. Anything less would feel like a step back at this point.
Danielle Carcia (intern, family medicine residency)
Overall, I enjoy using electronic medical records. I feel that it places all pertinent information about the patient in an easy-to-follow and concise manner. The ability to read through past providers and even at times specialists visits with a patient can be very helpful when navigating an appointment with a new patient. As a young physician, electronics have been an extension of myself for my entire adult life, so a computer in front of me during an office visit is comforting. I do not feel it distracts from my interaction with patients, or takes away from their experience at all, just the opposite, it allows me to more confidently care for them with up to date, and organized information at my fingertips.
Dave Depietro (family physician)
I have been a family physician for 25 years and feel that the EHRs have affected my office in a number of ways. It has definitely improved the efficacy of office tasks such as doing prescription refills, interoffice communication, and scheduling. Also before EHRs, the turnaround time for a dictated note was about a week, and now most notes are completed by the end of the day. This makes it easier if I am taking care of one of my partner’s patients or dealing with a patient I recently saw. Also in this day of pay for performance we can now gather data much easier. This would be almost impossible to do if we still had paper charts.
EHRs unfortunately also have their downsides. The main problem I see is that they add a significant amount of time for providers to complete tasks. When I dictated a note, I could have completed a note within 1-2 minutes where now with EHRs, it can take maybe 3-5 minutes/patient. Also to approve labs, x-rays, etc. it just takes longer. I feel that EHRs have added about 1½ hr to my day. I feel most of my colleagues have the same complaint. They routinely take work home at night and spend 1-2 hours at home completing notes. Many of my peers seem stressed and frustrated. Even though EHRs make the office more efficient, I feel that the provider pays the price. My other complaint is the cost of IT support to keep the EHRs running smoothly. The promise of EHRs is that they would save physicians’ money and reduce staffing, however I have not seen that happen.
I ask myself, at the end of the day, would I go back to paper charts? The answer is no. Despite their downsides, I feel that the positives of EHRs outweigh the negatives. Older doctors just need to adapt to this new way of practicing medicine.
The Bottom Line
Clearly there is a range of opinion about the effect of electronic health records on our practices and our lives, with those opinions at least partly segregated by age. We are interested in your thoughts and plan to publish some of those thoughts in future columns, so please let us know at [email protected]. Thanks.
Dr. Notte is a family physician and clinical informaticist for Abington Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is editor in chief of Redi-Reference Inc., a software company that creates mobile apps.
Eighty percent of physicians are now using electronic health records in their offices. We have been impressed that the younger physicians to whom we have spoken often view their experience with EHRs very differently from older physicians. Is such a difference inevitable, perhaps, not just because change is more difficult for many people as they get older but also because expectations are influenced by experience. Noticing these different thoughts and feelings, we’ve asked two physicians more than 55 years old and two younger physicians to share some thoughts on their experiences with electronic records.
Mathew Clark (family physician)
I’ve been in practice for 31 years and using an EHR system for just under 5. I’m not thrilled with it, but I accept that it’s an unavoidable part of my practice now, and so I don’t waste energy being upset about it. I’ve learned to function efficiently with an EHR, doing the best I can. I remember physicians, before the days of SOAP notes, who would write pithy, useful notes such as "probable strep, Pen VK 500 bid for 10 days" on 3x5 index cards. Such notes lacked detail, and it’s not hard to imagine the problems this lack of detail might create, but they were readable at a glance, and told you what you needed to know. On the other hand, the massively detailed, bloated notes we see with our EHRs, obscured by "copy-forward" text and fictional (in other words, never really asked or examined) information, present very significant practical and legal issues of their own, and take hours of physician time to complete. Given a choice, I’d probably go for the index cards.
Natalie McGann (family physician)
I have been a family physician in practice for 4 years since graduating from residency. The advent of the EHR hasn’t been an overwhelming transition for those of us in the early stages of our careers. Much of our schooling to date has included laptops and other electronic devices that for many prove an easier means of communication. Despite that fact that EHRs require a host of extraneous clicks and check boxes, it is still less cumbersome than documenting encounters on paper. For the generation of young physicians accustomed to having answers at their fingertips, the idea of flipping through paper charts to collate a patient’s medical record seems far more complicated than clicking a few tabs without ever leaving your chair. I, and most colleagues in my peer group to whom I’ve spoken, agree that we would not be likely to a join a practice that doesn’t utilize an EHR or have a current plan to adopt one. Anything less would feel like a step back at this point.
Danielle Carcia (intern, family medicine residency)
Overall, I enjoy using electronic medical records. I feel that it places all pertinent information about the patient in an easy-to-follow and concise manner. The ability to read through past providers and even at times specialists visits with a patient can be very helpful when navigating an appointment with a new patient. As a young physician, electronics have been an extension of myself for my entire adult life, so a computer in front of me during an office visit is comforting. I do not feel it distracts from my interaction with patients, or takes away from their experience at all, just the opposite, it allows me to more confidently care for them with up to date, and organized information at my fingertips.
Dave Depietro (family physician)
I have been a family physician for 25 years and feel that the EHRs have affected my office in a number of ways. It has definitely improved the efficacy of office tasks such as doing prescription refills, interoffice communication, and scheduling. Also before EHRs, the turnaround time for a dictated note was about a week, and now most notes are completed by the end of the day. This makes it easier if I am taking care of one of my partner’s patients or dealing with a patient I recently saw. Also in this day of pay for performance we can now gather data much easier. This would be almost impossible to do if we still had paper charts.
EHRs unfortunately also have their downsides. The main problem I see is that they add a significant amount of time for providers to complete tasks. When I dictated a note, I could have completed a note within 1-2 minutes where now with EHRs, it can take maybe 3-5 minutes/patient. Also to approve labs, x-rays, etc. it just takes longer. I feel that EHRs have added about 1½ hr to my day. I feel most of my colleagues have the same complaint. They routinely take work home at night and spend 1-2 hours at home completing notes. Many of my peers seem stressed and frustrated. Even though EHRs make the office more efficient, I feel that the provider pays the price. My other complaint is the cost of IT support to keep the EHRs running smoothly. The promise of EHRs is that they would save physicians’ money and reduce staffing, however I have not seen that happen.
I ask myself, at the end of the day, would I go back to paper charts? The answer is no. Despite their downsides, I feel that the positives of EHRs outweigh the negatives. Older doctors just need to adapt to this new way of practicing medicine.
The Bottom Line
Clearly there is a range of opinion about the effect of electronic health records on our practices and our lives, with those opinions at least partly segregated by age. We are interested in your thoughts and plan to publish some of those thoughts in future columns, so please let us know at [email protected]. Thanks.
Dr. Notte is a family physician and clinical informaticist for Abington Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is editor in chief of Redi-Reference Inc., a software company that creates mobile apps.
Eighty percent of physicians are now using electronic health records in their offices. We have been impressed that the younger physicians to whom we have spoken often view their experience with EHRs very differently from older physicians. Is such a difference inevitable, perhaps, not just because change is more difficult for many people as they get older but also because expectations are influenced by experience. Noticing these different thoughts and feelings, we’ve asked two physicians more than 55 years old and two younger physicians to share some thoughts on their experiences with electronic records.
Mathew Clark (family physician)
I’ve been in practice for 31 years and using an EHR system for just under 5. I’m not thrilled with it, but I accept that it’s an unavoidable part of my practice now, and so I don’t waste energy being upset about it. I’ve learned to function efficiently with an EHR, doing the best I can. I remember physicians, before the days of SOAP notes, who would write pithy, useful notes such as "probable strep, Pen VK 500 bid for 10 days" on 3x5 index cards. Such notes lacked detail, and it’s not hard to imagine the problems this lack of detail might create, but they were readable at a glance, and told you what you needed to know. On the other hand, the massively detailed, bloated notes we see with our EHRs, obscured by "copy-forward" text and fictional (in other words, never really asked or examined) information, present very significant practical and legal issues of their own, and take hours of physician time to complete. Given a choice, I’d probably go for the index cards.
Natalie McGann (family physician)
I have been a family physician in practice for 4 years since graduating from residency. The advent of the EHR hasn’t been an overwhelming transition for those of us in the early stages of our careers. Much of our schooling to date has included laptops and other electronic devices that for many prove an easier means of communication. Despite that fact that EHRs require a host of extraneous clicks and check boxes, it is still less cumbersome than documenting encounters on paper. For the generation of young physicians accustomed to having answers at their fingertips, the idea of flipping through paper charts to collate a patient’s medical record seems far more complicated than clicking a few tabs without ever leaving your chair. I, and most colleagues in my peer group to whom I’ve spoken, agree that we would not be likely to a join a practice that doesn’t utilize an EHR or have a current plan to adopt one. Anything less would feel like a step back at this point.
Danielle Carcia (intern, family medicine residency)
Overall, I enjoy using electronic medical records. I feel that it places all pertinent information about the patient in an easy-to-follow and concise manner. The ability to read through past providers and even at times specialists visits with a patient can be very helpful when navigating an appointment with a new patient. As a young physician, electronics have been an extension of myself for my entire adult life, so a computer in front of me during an office visit is comforting. I do not feel it distracts from my interaction with patients, or takes away from their experience at all, just the opposite, it allows me to more confidently care for them with up to date, and organized information at my fingertips.
Dave Depietro (family physician)
I have been a family physician for 25 years and feel that the EHRs have affected my office in a number of ways. It has definitely improved the efficacy of office tasks such as doing prescription refills, interoffice communication, and scheduling. Also before EHRs, the turnaround time for a dictated note was about a week, and now most notes are completed by the end of the day. This makes it easier if I am taking care of one of my partner’s patients or dealing with a patient I recently saw. Also in this day of pay for performance we can now gather data much easier. This would be almost impossible to do if we still had paper charts.
EHRs unfortunately also have their downsides. The main problem I see is that they add a significant amount of time for providers to complete tasks. When I dictated a note, I could have completed a note within 1-2 minutes where now with EHRs, it can take maybe 3-5 minutes/patient. Also to approve labs, x-rays, etc. it just takes longer. I feel that EHRs have added about 1½ hr to my day. I feel most of my colleagues have the same complaint. They routinely take work home at night and spend 1-2 hours at home completing notes. Many of my peers seem stressed and frustrated. Even though EHRs make the office more efficient, I feel that the provider pays the price. My other complaint is the cost of IT support to keep the EHRs running smoothly. The promise of EHRs is that they would save physicians’ money and reduce staffing, however I have not seen that happen.
I ask myself, at the end of the day, would I go back to paper charts? The answer is no. Despite their downsides, I feel that the positives of EHRs outweigh the negatives. Older doctors just need to adapt to this new way of practicing medicine.
The Bottom Line
Clearly there is a range of opinion about the effect of electronic health records on our practices and our lives, with those opinions at least partly segregated by age. We are interested in your thoughts and plan to publish some of those thoughts in future columns, so please let us know at [email protected]. Thanks.
Dr. Notte is a family physician and clinical informaticist for Abington Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is editor in chief of Redi-Reference Inc., a software company that creates mobile apps.

Republicans more likely to report being hurt by health reform
Six out of 10 Americans say that they have not been affected by the Affordable Care Act, with an unsurprising political split among those who say it has either helped or hurt them, according to a report from the Kaiser Family Foundation.
Among Republicans, 37% say that they have been hurt by the health reform law and 5% say that they have been helped. The numbers were basically reversed for Democrats, with 26% saying that they have been helped and 8% reporting that they been hurt. Independents lean more toward the Republicans, with 27% saying that they have been hurt and 11% saying that they have been helped, Kaiser reported in its latest Health Tracking Poll.
Those who report being hurt by the law were most likely to cite their increased health care costs (14% of the public overall), while those who say they have been helped most often say that someone in their family was able to get or keep coverage (5% of the public overall), Kaiser said.
The survey involved a nationally representative sample of 1,505 adults and was conducted May 13-19.

Six out of 10 Americans say that they have not been affected by the Affordable Care Act, with an unsurprising political split among those who say it has either helped or hurt them, according to a report from the Kaiser Family Foundation.
Among Republicans, 37% say that they have been hurt by the health reform law and 5% say that they have been helped. The numbers were basically reversed for Democrats, with 26% saying that they have been helped and 8% reporting that they been hurt. Independents lean more toward the Republicans, with 27% saying that they have been hurt and 11% saying that they have been helped, Kaiser reported in its latest Health Tracking Poll.
Those who report being hurt by the law were most likely to cite their increased health care costs (14% of the public overall), while those who say they have been helped most often say that someone in their family was able to get or keep coverage (5% of the public overall), Kaiser said.
The survey involved a nationally representative sample of 1,505 adults and was conducted May 13-19.
Six out of 10 Americans say that they have not been affected by the Affordable Care Act, with an unsurprising political split among those who say it has either helped or hurt them, according to a report from the Kaiser Family Foundation.
Among Republicans, 37% say that they have been hurt by the health reform law and 5% say that they have been helped. The numbers were basically reversed for Democrats, with 26% saying that they have been helped and 8% reporting that they been hurt. Independents lean more toward the Republicans, with 27% saying that they have been hurt and 11% saying that they have been helped, Kaiser reported in its latest Health Tracking Poll.
Those who report being hurt by the law were most likely to cite their increased health care costs (14% of the public overall), while those who say they have been helped most often say that someone in their family was able to get or keep coverage (5% of the public overall), Kaiser said.
The survey involved a nationally representative sample of 1,505 adults and was conducted May 13-19.
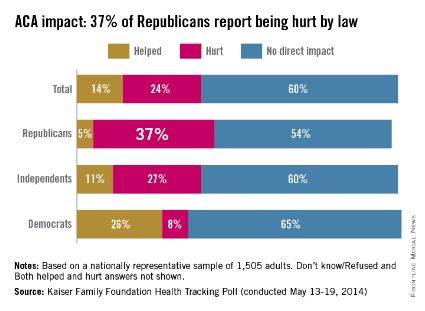
Critical Care Commentary: Brain death – patient, law, and family
Perhaps no other concept in modern medicine is surrounded by as much misunderstanding and controversy as that of death by neurologic criteria, or brain death.
Legal challenges to brain death have spanned the gamut of continuing life support for a legally dead patient to denying a family’s request to continue support for their dead child.

Two recent, highly publicized cases highlight the poles of these controversies and concerns. In November 2013, Marlise Muñoz was declared brain dead. She was 33 years old and 14 weeks’ pregnant. Concordant with the patient’s wishes, the husband requested that the hospital remove the patient from mechanical ventilatory support. Citing Texas law that precludes the withholding of life-sustaining treatment to a pregnant patient, the hospital refused, despite the logical fallacy of withholding life support from a person declared dead.
In December 2013, 13-year-old Jahi McMath was declared brain dead. Her parents obtained a court order to prevent the hospital from discontinuing ventilatory support. A better understanding of the development of the concept of brain death and the incorporation of recent evidence into its determination may reduce the confusion and misunderstandings surrounding the determination of brain death.
Three reports in 1959 describe death of the nervous system and brain death (coma dépassé) building upon clinical and laboratory data from the 1930s relating the cessation of brain blood flow and EEG activity to ensuing apnea and subsequent cardiac arrest (Machado et al. J Med Ethics. 2007;33[4]:197). With the increasing sophistication of critical care support, especially mechanical ventilation, the loss of central respiratory drive no longer meant imminent death, and patients could be supported for long periods of time without recovery of brain function.
In 1968, an ad hoc committee at Harvard Medical School proposed a definition of irreversible coma and brain death (Beecher et al. JAMA. 1968;205[6]:337). They posited that any organ that no longer functions and has no possibility of functioning again was "for all practical purposes dead." The goals of the committee were (1) to reduce the suffering of patients and families and the care burden of hospitals; and (2) mitigate the controversies that surrounded obtaining organs for transplantation.
The committee then set out their rationale for their proposed characteristics of the permanently nonfunctioning brain. Subsequently, in 1976, The Conference of the Medical Royal Colleges and their Faculties in the United Kingdom required a deeply comatose state, irremediable structural brain damage, and irreversible cessation of brain stem function to ascertain brain death (Spinello. J Intensive Care Med. May 2014, in press).
In 1981, the National Conference of Commissioners on Uniform State Laws approved the Uniform Determination of Death Act (UDDA), codifying the legal concept of brain death. Thirty-six states and the District of Columbia have enacted the UDDA, but legal precedent and statutes in the remaining states are consistent with the UDDA. New York and New Jersey require that a family’s religious or moral views be considered in the process following the determination of brain death (Gostin. JAMA. 2014;311[9]:903); in all other states, clinicians are not required to consult with family prior to withdrawing ventilatory support from the brain dead patient.
‘No reports of clinical recovery’
However, the UDDA does not define brain death but rather states that "a determination of death must be made with accepted medical standards" (Wijdicks et al. Neurology. 2010;74[23]:1911). The American Academy of Neurology (AAN) published a practice parameter in 1995 to guide clinicians in the determination of brain death; this was updated by their Quality Standards Committee in 2010 (Wijdicks et al. Neurology. 2010;74[23]:1911). In the updated guidance document, the committee stated: "There are no reports of clinical recovery in patients after the clinical diagnosis of brain death has been determined using the AAN practice parameter."
It is striking, however, that there appears to be an inconsistent approach and criteria for the determination of brain death across hospitals, and even amongst specialties within a hospital (Powner et al. Crit Care Med. 2004;32[6]:1284). Further, in most states, any physician is permitted to ascertain brain death, though some states have now added requirements for specific qualifications and/or confirmation by a second physician (Spinello IM. J Intensive Care Med. May 2014, in press).
These inconsistencies in criteria, process, and experience may be responsible for reports in the lay press of recovery following pronouncement of brain death. Every hospital should have a validated, well-defined process for the evaluation of brain death guided by the AAN practice parameter.
A single exam
In most states, a single exam is required to determine brain death. The clinical setting and the results of imaging studies should be used to determine the duration of observation needed to exclude the possibility of recovery. Given that the patient should be normothermic, have a normal systolic blood pressure, have both a history and imaging studies supporting an irreversible cause of coma, and that drugs and toxins must be excluded as a cause of coma, this observation period is uncommonly less than several hours.
Confounded by movement
Movement of the patient with devastating brain injury is often a confounder in the determination of brain death.
This is also a source of confusion and concern for the family. Plantar reflexes have been commonly reported in patients pronounced brain dead. Head turning in response to noxious stimuli, repetitive leg movements, facial myokymia, and other movements have been observed (Wu et al. Crit Care. 2013;17[4]:440; Wijdicks et al. Neurology. 2010;74[23]:1911). When this is observed, knowledge of the potential reflex arcs is needed, and consultation with a neurologist or other physician skilled in brain death determination is usually appropriate.
Movement can sometimes extend to apparent respiratory activity. This can be caused by ventilator autocycling due to variations in circuit pressure (especially in a noncompliant lung or with large tidal volumes) or triggering due to cardiac-induced alterations in transpulmonary pressure. The latter is most common in a hyperdynamic circulatory state.
Apnea is a critical criterion for the determination of brain death and is most reliably assessed when the patient has been removed from the mechanical ventilator. During testing, apnea should be present despite achieving a PaCO2 of greater than or equal to 60 mm Hg, or 20 mm Hg above the baseline to support the diagnosis of brain death.
Some patients, especially those who are hemodynamically unstable or who require high levels of PEEP to support oxygenation, may not tolerate the apnea test without oxygen desaturation or hypotension.
Most commonly, the apnea test is performed with the patient off the ventilator and 6 L/min of oxygen flowing through an insufflation catheter placed near the carina. We prefer to use a modified Mapleson circuit with enough flow to only partially distend the anesthesia bag in the circuit. With this arrangement, one can look not only at the patient’s chest wall and abdomen for signs of respiratory activity but also look for cyclic changes in the level of bag inflation.
In patients with ARDS, trauma involving the chest or other causes of oxygenation failure, CPAP, with or without an antecedent recruitment maneuver may facilitate successful completion of the apnea test (Hocker et al. Neurocrit Care. 2014;20[2]:298).
Controversy over ancillary testing
There are no well-designed prospective studies examining the accuracy of ancillary tests for the determination of brain death using the appropriate control group of patients with coma but who are not brain dead and with blinding of the interpretation of the study results to the clinical setting.
Brain death is not synonymous with complete neuronal death. While cortical areas exhibit moderate to severe histopathologic ischemic changes in the large majority (but not all) of brain dead patients, the basal ganglia and diencephalon inconsistently demonstrate these changes (Wijdicks et al. Neurology. 2008;70[15]:1234). Thus, it may not be surprising that both false-positive (test positive for brain death – clinically not brain dead) and false-negative (test negative for brain death – clinically brain dead) results have been reported for virtually all tests proposed for confirmatory testing, including CT angiography, transcranial Doppler, and nuclear brain scan. Confirmatory testing is most commonly used in patients who cannot complete an apnea test.
It has been forcefully argued that, in adults, confirmatory tests should not be done (Wijdicks. Neurology. 2010;75[1]:77). There will be some patients in whom brain death cannot be definitively determined. When all criteria of the AAN guidelines cannot be fulfilled, clinicians should err on the side of concluding that the patient is not brain dead and turn their efforts toward counseling the family regarding the likelihood of neurologic recovery and assisting the family in ascertaining the desires of the patient under these circumstances.
It is vital that care providers not lose perspective on the plight of the family in these settings. The symbolic power of a beating heart to a parent, spouse, or loved one cannot be underestimated. Family members who observe resuscitation efforts have been shown to have a lower incidence of posttraumatic stress disorder symptoms (Jabre et al. N Engl J Med. 2013;368[11]:1008).
A recent trial demonstrated that family presence during the brain death determination had an increased understanding of brain death without an adverse impact on emotional well being (Tawil et al. Crit Care Med. 2013;42[4]:934). A consistent process for determination of brain death, engagement of the family in the brain death evaluation and helping them understand the meaning of patient movements that can be distressingly misinterpreted, and honesty when a definitive determination of brain death cannot be determined will not remove the misunderstanding or controversy surrounding a diagnosis of brain death but will serve to ensure its accurate and humane application.
Dr. Bowton is Professor, Section on Critical Care, Department of Anesthesiology, Wake Forest Baptist Health, Winston-Salem, North Carolina. Read previous Critical Care Commentaries online.
|
|
In this thorough and somber commentary, Dr. Bowton clearly points out how much gray remains in a world that demands black and white certainty.
Brain death, and its implication, is not an exact diagnosis, which impacts the family, society, and the care-giving team, but most of all, the patient.
As there are times that brain death cannot be truly determined, we must be mindful that our primary goal is always the patient, then the families, society, and others. As a practitioner in New York, where family discussion is the law, I have not found this to be a great impediment; with palliative care and pastoral support, most issues can be resolved. As we progress in our knowledge, a more global unified approach would be welcomed.
Dr. Peter Spiro, FCCP Section Editor
|
|
|
In this thorough and somber commentary, Dr. Bowton clearly points out how much gray remains in a world that demands black and white certainty.
Brain death, and its implication, is not an exact diagnosis, which impacts the family, society, and the care-giving team, but most of all, the patient.
As there are times that brain death cannot be truly determined, we must be mindful that our primary goal is always the patient, then the families, society, and others. As a practitioner in New York, where family discussion is the law, I have not found this to be a great impediment; with palliative care and pastoral support, most issues can be resolved. As we progress in our knowledge, a more global unified approach would be welcomed.
Dr. Peter Spiro, FCCP Section Editor
|
|
|
In this thorough and somber commentary, Dr. Bowton clearly points out how much gray remains in a world that demands black and white certainty.
Brain death, and its implication, is not an exact diagnosis, which impacts the family, society, and the care-giving team, but most of all, the patient.
As there are times that brain death cannot be truly determined, we must be mindful that our primary goal is always the patient, then the families, society, and others. As a practitioner in New York, where family discussion is the law, I have not found this to be a great impediment; with palliative care and pastoral support, most issues can be resolved. As we progress in our knowledge, a more global unified approach would be welcomed.
Dr. Peter Spiro, FCCP Section Editor
Perhaps no other concept in modern medicine is surrounded by as much misunderstanding and controversy as that of death by neurologic criteria, or brain death.
Legal challenges to brain death have spanned the gamut of continuing life support for a legally dead patient to denying a family’s request to continue support for their dead child.
Two recent, highly publicized cases highlight the poles of these controversies and concerns. In November 2013, Marlise Muñoz was declared brain dead. She was 33 years old and 14 weeks’ pregnant. Concordant with the patient’s wishes, the husband requested that the hospital remove the patient from mechanical ventilatory support. Citing Texas law that precludes the withholding of life-sustaining treatment to a pregnant patient, the hospital refused, despite the logical fallacy of withholding life support from a person declared dead.
In December 2013, 13-year-old Jahi McMath was declared brain dead. Her parents obtained a court order to prevent the hospital from discontinuing ventilatory support. A better understanding of the development of the concept of brain death and the incorporation of recent evidence into its determination may reduce the confusion and misunderstandings surrounding the determination of brain death.
Three reports in 1959 describe death of the nervous system and brain death (coma dépassé) building upon clinical and laboratory data from the 1930s relating the cessation of brain blood flow and EEG activity to ensuing apnea and subsequent cardiac arrest (Machado et al. J Med Ethics. 2007;33[4]:197). With the increasing sophistication of critical care support, especially mechanical ventilation, the loss of central respiratory drive no longer meant imminent death, and patients could be supported for long periods of time without recovery of brain function.
In 1968, an ad hoc committee at Harvard Medical School proposed a definition of irreversible coma and brain death (Beecher et al. JAMA. 1968;205[6]:337). They posited that any organ that no longer functions and has no possibility of functioning again was "for all practical purposes dead." The goals of the committee were (1) to reduce the suffering of patients and families and the care burden of hospitals; and (2) mitigate the controversies that surrounded obtaining organs for transplantation.
The committee then set out their rationale for their proposed characteristics of the permanently nonfunctioning brain. Subsequently, in 1976, The Conference of the Medical Royal Colleges and their Faculties in the United Kingdom required a deeply comatose state, irremediable structural brain damage, and irreversible cessation of brain stem function to ascertain brain death (Spinello. J Intensive Care Med. May 2014, in press).
In 1981, the National Conference of Commissioners on Uniform State Laws approved the Uniform Determination of Death Act (UDDA), codifying the legal concept of brain death. Thirty-six states and the District of Columbia have enacted the UDDA, but legal precedent and statutes in the remaining states are consistent with the UDDA. New York and New Jersey require that a family’s religious or moral views be considered in the process following the determination of brain death (Gostin. JAMA. 2014;311[9]:903); in all other states, clinicians are not required to consult with family prior to withdrawing ventilatory support from the brain dead patient.
‘No reports of clinical recovery’
However, the UDDA does not define brain death but rather states that "a determination of death must be made with accepted medical standards" (Wijdicks et al. Neurology. 2010;74[23]:1911). The American Academy of Neurology (AAN) published a practice parameter in 1995 to guide clinicians in the determination of brain death; this was updated by their Quality Standards Committee in 2010 (Wijdicks et al. Neurology. 2010;74[23]:1911). In the updated guidance document, the committee stated: "There are no reports of clinical recovery in patients after the clinical diagnosis of brain death has been determined using the AAN practice parameter."
It is striking, however, that there appears to be an inconsistent approach and criteria for the determination of brain death across hospitals, and even amongst specialties within a hospital (Powner et al. Crit Care Med. 2004;32[6]:1284). Further, in most states, any physician is permitted to ascertain brain death, though some states have now added requirements for specific qualifications and/or confirmation by a second physician (Spinello IM. J Intensive Care Med. May 2014, in press).
These inconsistencies in criteria, process, and experience may be responsible for reports in the lay press of recovery following pronouncement of brain death. Every hospital should have a validated, well-defined process for the evaluation of brain death guided by the AAN practice parameter.
A single exam
In most states, a single exam is required to determine brain death. The clinical setting and the results of imaging studies should be used to determine the duration of observation needed to exclude the possibility of recovery. Given that the patient should be normothermic, have a normal systolic blood pressure, have both a history and imaging studies supporting an irreversible cause of coma, and that drugs and toxins must be excluded as a cause of coma, this observation period is uncommonly less than several hours.
Confounded by movement
Movement of the patient with devastating brain injury is often a confounder in the determination of brain death.
This is also a source of confusion and concern for the family. Plantar reflexes have been commonly reported in patients pronounced brain dead. Head turning in response to noxious stimuli, repetitive leg movements, facial myokymia, and other movements have been observed (Wu et al. Crit Care. 2013;17[4]:440; Wijdicks et al. Neurology. 2010;74[23]:1911). When this is observed, knowledge of the potential reflex arcs is needed, and consultation with a neurologist or other physician skilled in brain death determination is usually appropriate.
Movement can sometimes extend to apparent respiratory activity. This can be caused by ventilator autocycling due to variations in circuit pressure (especially in a noncompliant lung or with large tidal volumes) or triggering due to cardiac-induced alterations in transpulmonary pressure. The latter is most common in a hyperdynamic circulatory state.
Apnea is a critical criterion for the determination of brain death and is most reliably assessed when the patient has been removed from the mechanical ventilator. During testing, apnea should be present despite achieving a PaCO2 of greater than or equal to 60 mm Hg, or 20 mm Hg above the baseline to support the diagnosis of brain death.
Some patients, especially those who are hemodynamically unstable or who require high levels of PEEP to support oxygenation, may not tolerate the apnea test without oxygen desaturation or hypotension.
Most commonly, the apnea test is performed with the patient off the ventilator and 6 L/min of oxygen flowing through an insufflation catheter placed near the carina. We prefer to use a modified Mapleson circuit with enough flow to only partially distend the anesthesia bag in the circuit. With this arrangement, one can look not only at the patient’s chest wall and abdomen for signs of respiratory activity but also look for cyclic changes in the level of bag inflation.
In patients with ARDS, trauma involving the chest or other causes of oxygenation failure, CPAP, with or without an antecedent recruitment maneuver may facilitate successful completion of the apnea test (Hocker et al. Neurocrit Care. 2014;20[2]:298).
Controversy over ancillary testing
There are no well-designed prospective studies examining the accuracy of ancillary tests for the determination of brain death using the appropriate control group of patients with coma but who are not brain dead and with blinding of the interpretation of the study results to the clinical setting.
Brain death is not synonymous with complete neuronal death. While cortical areas exhibit moderate to severe histopathologic ischemic changes in the large majority (but not all) of brain dead patients, the basal ganglia and diencephalon inconsistently demonstrate these changes (Wijdicks et al. Neurology. 2008;70[15]:1234). Thus, it may not be surprising that both false-positive (test positive for brain death – clinically not brain dead) and false-negative (test negative for brain death – clinically brain dead) results have been reported for virtually all tests proposed for confirmatory testing, including CT angiography, transcranial Doppler, and nuclear brain scan. Confirmatory testing is most commonly used in patients who cannot complete an apnea test.
It has been forcefully argued that, in adults, confirmatory tests should not be done (Wijdicks. Neurology. 2010;75[1]:77). There will be some patients in whom brain death cannot be definitively determined. When all criteria of the AAN guidelines cannot be fulfilled, clinicians should err on the side of concluding that the patient is not brain dead and turn their efforts toward counseling the family regarding the likelihood of neurologic recovery and assisting the family in ascertaining the desires of the patient under these circumstances.
It is vital that care providers not lose perspective on the plight of the family in these settings. The symbolic power of a beating heart to a parent, spouse, or loved one cannot be underestimated. Family members who observe resuscitation efforts have been shown to have a lower incidence of posttraumatic stress disorder symptoms (Jabre et al. N Engl J Med. 2013;368[11]:1008).
A recent trial demonstrated that family presence during the brain death determination had an increased understanding of brain death without an adverse impact on emotional well being (Tawil et al. Crit Care Med. 2013;42[4]:934). A consistent process for determination of brain death, engagement of the family in the brain death evaluation and helping them understand the meaning of patient movements that can be distressingly misinterpreted, and honesty when a definitive determination of brain death cannot be determined will not remove the misunderstanding or controversy surrounding a diagnosis of brain death but will serve to ensure its accurate and humane application.
Dr. Bowton is Professor, Section on Critical Care, Department of Anesthesiology, Wake Forest Baptist Health, Winston-Salem, North Carolina. Read previous Critical Care Commentaries online.
Perhaps no other concept in modern medicine is surrounded by as much misunderstanding and controversy as that of death by neurologic criteria, or brain death.
Legal challenges to brain death have spanned the gamut of continuing life support for a legally dead patient to denying a family’s request to continue support for their dead child.
Two recent, highly publicized cases highlight the poles of these controversies and concerns. In November 2013, Marlise Muñoz was declared brain dead. She was 33 years old and 14 weeks’ pregnant. Concordant with the patient’s wishes, the husband requested that the hospital remove the patient from mechanical ventilatory support. Citing Texas law that precludes the withholding of life-sustaining treatment to a pregnant patient, the hospital refused, despite the logical fallacy of withholding life support from a person declared dead.
In December 2013, 13-year-old Jahi McMath was declared brain dead. Her parents obtained a court order to prevent the hospital from discontinuing ventilatory support. A better understanding of the development of the concept of brain death and the incorporation of recent evidence into its determination may reduce the confusion and misunderstandings surrounding the determination of brain death.
Three reports in 1959 describe death of the nervous system and brain death (coma dépassé) building upon clinical and laboratory data from the 1930s relating the cessation of brain blood flow and EEG activity to ensuing apnea and subsequent cardiac arrest (Machado et al. J Med Ethics. 2007;33[4]:197). With the increasing sophistication of critical care support, especially mechanical ventilation, the loss of central respiratory drive no longer meant imminent death, and patients could be supported for long periods of time without recovery of brain function.
In 1968, an ad hoc committee at Harvard Medical School proposed a definition of irreversible coma and brain death (Beecher et al. JAMA. 1968;205[6]:337). They posited that any organ that no longer functions and has no possibility of functioning again was "for all practical purposes dead." The goals of the committee were (1) to reduce the suffering of patients and families and the care burden of hospitals; and (2) mitigate the controversies that surrounded obtaining organs for transplantation.
The committee then set out their rationale for their proposed characteristics of the permanently nonfunctioning brain. Subsequently, in 1976, The Conference of the Medical Royal Colleges and their Faculties in the United Kingdom required a deeply comatose state, irremediable structural brain damage, and irreversible cessation of brain stem function to ascertain brain death (Spinello. J Intensive Care Med. May 2014, in press).
In 1981, the National Conference of Commissioners on Uniform State Laws approved the Uniform Determination of Death Act (UDDA), codifying the legal concept of brain death. Thirty-six states and the District of Columbia have enacted the UDDA, but legal precedent and statutes in the remaining states are consistent with the UDDA. New York and New Jersey require that a family’s religious or moral views be considered in the process following the determination of brain death (Gostin. JAMA. 2014;311[9]:903); in all other states, clinicians are not required to consult with family prior to withdrawing ventilatory support from the brain dead patient.
‘No reports of clinical recovery’
However, the UDDA does not define brain death but rather states that "a determination of death must be made with accepted medical standards" (Wijdicks et al. Neurology. 2010;74[23]:1911). The American Academy of Neurology (AAN) published a practice parameter in 1995 to guide clinicians in the determination of brain death; this was updated by their Quality Standards Committee in 2010 (Wijdicks et al. Neurology. 2010;74[23]:1911). In the updated guidance document, the committee stated: "There are no reports of clinical recovery in patients after the clinical diagnosis of brain death has been determined using the AAN practice parameter."
It is striking, however, that there appears to be an inconsistent approach and criteria for the determination of brain death across hospitals, and even amongst specialties within a hospital (Powner et al. Crit Care Med. 2004;32[6]:1284). Further, in most states, any physician is permitted to ascertain brain death, though some states have now added requirements for specific qualifications and/or confirmation by a second physician (Spinello IM. J Intensive Care Med. May 2014, in press).
These inconsistencies in criteria, process, and experience may be responsible for reports in the lay press of recovery following pronouncement of brain death. Every hospital should have a validated, well-defined process for the evaluation of brain death guided by the AAN practice parameter.
A single exam
In most states, a single exam is required to determine brain death. The clinical setting and the results of imaging studies should be used to determine the duration of observation needed to exclude the possibility of recovery. Given that the patient should be normothermic, have a normal systolic blood pressure, have both a history and imaging studies supporting an irreversible cause of coma, and that drugs and toxins must be excluded as a cause of coma, this observation period is uncommonly less than several hours.
Confounded by movement
Movement of the patient with devastating brain injury is often a confounder in the determination of brain death.
This is also a source of confusion and concern for the family. Plantar reflexes have been commonly reported in patients pronounced brain dead. Head turning in response to noxious stimuli, repetitive leg movements, facial myokymia, and other movements have been observed (Wu et al. Crit Care. 2013;17[4]:440; Wijdicks et al. Neurology. 2010;74[23]:1911). When this is observed, knowledge of the potential reflex arcs is needed, and consultation with a neurologist or other physician skilled in brain death determination is usually appropriate.
Movement can sometimes extend to apparent respiratory activity. This can be caused by ventilator autocycling due to variations in circuit pressure (especially in a noncompliant lung or with large tidal volumes) or triggering due to cardiac-induced alterations in transpulmonary pressure. The latter is most common in a hyperdynamic circulatory state.
Apnea is a critical criterion for the determination of brain death and is most reliably assessed when the patient has been removed from the mechanical ventilator. During testing, apnea should be present despite achieving a PaCO2 of greater than or equal to 60 mm Hg, or 20 mm Hg above the baseline to support the diagnosis of brain death.
Some patients, especially those who are hemodynamically unstable or who require high levels of PEEP to support oxygenation, may not tolerate the apnea test without oxygen desaturation or hypotension.
Most commonly, the apnea test is performed with the patient off the ventilator and 6 L/min of oxygen flowing through an insufflation catheter placed near the carina. We prefer to use a modified Mapleson circuit with enough flow to only partially distend the anesthesia bag in the circuit. With this arrangement, one can look not only at the patient’s chest wall and abdomen for signs of respiratory activity but also look for cyclic changes in the level of bag inflation.
In patients with ARDS, trauma involving the chest or other causes of oxygenation failure, CPAP, with or without an antecedent recruitment maneuver may facilitate successful completion of the apnea test (Hocker et al. Neurocrit Care. 2014;20[2]:298).
Controversy over ancillary testing
There are no well-designed prospective studies examining the accuracy of ancillary tests for the determination of brain death using the appropriate control group of patients with coma but who are not brain dead and with blinding of the interpretation of the study results to the clinical setting.
Brain death is not synonymous with complete neuronal death. While cortical areas exhibit moderate to severe histopathologic ischemic changes in the large majority (but not all) of brain dead patients, the basal ganglia and diencephalon inconsistently demonstrate these changes (Wijdicks et al. Neurology. 2008;70[15]:1234). Thus, it may not be surprising that both false-positive (test positive for brain death – clinically not brain dead) and false-negative (test negative for brain death – clinically brain dead) results have been reported for virtually all tests proposed for confirmatory testing, including CT angiography, transcranial Doppler, and nuclear brain scan. Confirmatory testing is most commonly used in patients who cannot complete an apnea test.
It has been forcefully argued that, in adults, confirmatory tests should not be done (Wijdicks. Neurology. 2010;75[1]:77). There will be some patients in whom brain death cannot be definitively determined. When all criteria of the AAN guidelines cannot be fulfilled, clinicians should err on the side of concluding that the patient is not brain dead and turn their efforts toward counseling the family regarding the likelihood of neurologic recovery and assisting the family in ascertaining the desires of the patient under these circumstances.
It is vital that care providers not lose perspective on the plight of the family in these settings. The symbolic power of a beating heart to a parent, spouse, or loved one cannot be underestimated. Family members who observe resuscitation efforts have been shown to have a lower incidence of posttraumatic stress disorder symptoms (Jabre et al. N Engl J Med. 2013;368[11]:1008).
A recent trial demonstrated that family presence during the brain death determination had an increased understanding of brain death without an adverse impact on emotional well being (Tawil et al. Crit Care Med. 2013;42[4]:934). A consistent process for determination of brain death, engagement of the family in the brain death evaluation and helping them understand the meaning of patient movements that can be distressingly misinterpreted, and honesty when a definitive determination of brain death cannot be determined will not remove the misunderstanding or controversy surrounding a diagnosis of brain death but will serve to ensure its accurate and humane application.
Dr. Bowton is Professor, Section on Critical Care, Department of Anesthesiology, Wake Forest Baptist Health, Winston-Salem, North Carolina. Read previous Critical Care Commentaries online.

Doing it right
“It is concluded that nasogastric suction should not be used routinely following abdominal surgery." This is the concluding statement from a paper presented at the Pacific Coast Surgical Association and published in the American Journal of Surgery more than 50 years ago (Am. J. Surg 1957;94:257-61).
Since then innumerable randomized controlled trials and meta-analyses have confirmed that nasogastric tubes inserted prophylactically after abdominal surgery, even when gastrointestinal anastomoses have been constructed, are unnecessary. So how did this incontrovertible evidence impact my practice and that of most of my surgical colleagues? Not at all, at least not for many years. We continued our routine of torturing postoperative patients with nasogastric tubes because it had been drummed into us during residency and because we were uncomfortable not doing so. But why did we persist after convincing evidence to the contrary emerged?
Unfortunately it is not uncommon that even when good evidence exists, we fail to incorporate it into decision-making. The comfort we enjoy with our standard way of doing things is often preferred to the discomfort – cognitive dissonance – we experience when confronted with mounting empirical evidence that challenges our beliefs. All too often, the cognitive dissonance is reduced by holding on to those notions with which we are most comfortable and ignoring or rejecting new information no matter how valid.
What is the harm? In the case of prophylactic nasogastric tubes, considerable discomfort has unnecessarily complicated the postoperative courses of millions of patients. Many trials have shown that aspiration and pneumonia, the adverse events for which the tubes were placed to prevent, occurred more frequently in patients with than those without nasogastric tubes.
Prophylactic gastric decompression is but one of many practices that have been continued long after their efficacy was disproven. How many radical mastectomies were performed after modified radical mastectomy, and then later partial mastectomy with radiation were shown with irrefutable data to provide equal survival with less disfigurement and fewer complications such as arm lymphedema? For many years after the indications for tonsillectomy were narrowed, this procedure continued to be more commonly done than was appropriate based on the evidence available.
Some hold on to their cherished habits more persistently and longer than others. In order to maintain consonance and avoid the stress of dissonance, I have known surgeons who have retained nearly all of the practices they learned from their mentors during residency long past their utility. Such individuals may insist that they alone prep their patients and that long outmoded suture and instruments be maintained on the operating room supply list. When new, and often proven to be superior, instruments, sutures, and pathways of care for their patients are introduced in their institutions, they find it difficult or even impossible to change.
In an era when the few controlled trials and meta-analyses available were buried within a surgical literature that was difficult to access and the term evidence-based surgery was not yet a part of our lexicon, such a rigid posture was often tolerated. I would hope that in most institutions and departments of surgery this is no longer the case. We live in a time when the imperatives of renewal and reevaluation of our practices are increasing. Therefore, reviewing new evidence, even that which goes against our established notions, and incorporating new proven methods, are essential to maintaining the highest standard of patient care.
Although many gray areas remain and there is often more than one best way to manage a surgical patient, our treatments should be based on the best evidence available rather than on what we learned 5, 10, or even 30 years ago. Fortunately, such evidence is now readily accessible. A notable example is “Evidence-based decisions in surgery,” surgical practice guidelines recently introduced by the American College of Surgeons (ACS) under the guidance of Dr. Lewis Flint.
“Evidence-based decisions in surgery” presently consists of 15 modules of the most common diseases and conditions encountered by general surgeons. These modules can be easily accessed by ACS Fellows on any mobile device at the point-of-care (http://ebds.facs.org). Surgical recommendations along with the strength of evidence (weak, moderate, or strong) for each are presented in an easy-to-interpret format. The modules have been developed by American College of Surgeons staff and been peer-reviewed by the Best Practices Workgroup of the College’s Board of Governors and by representatives of the Advisory Council for General Surgery. A consensus of the reviewers was used to determine the content of each module. It is emphasized that the purpose of these modules is to guide rather than dictate decision-making.
In addition to the strength of evidence for each recommendation, a clinical decision algorithm for a typical patient, suggested talking points for patient education, and key references on which the recommendations are based are also provided. Although clinical practice guidelines have been developed by a number of specialty surgical societies, I have found none that are as easy to digest and use in a busy clinical practice as “Evidence-based decisions in surgery.
So we no longer have an excuse to hold on to our cherished and venerable practices that are outmoded and possibly not in the best interest of our patients. The information needed to do it right is virtually one click of a mouse away. Try applying “Evidence-based decisions in surgery” in your practice. I am convinced you will find them valuable as you make decisions for the most appropriate care of your patients.
Dr. Rikkers is Editor in Chief of ACS Surgery News
“It is concluded that nasogastric suction should not be used routinely following abdominal surgery." This is the concluding statement from a paper presented at the Pacific Coast Surgical Association and published in the American Journal of Surgery more than 50 years ago (Am. J. Surg 1957;94:257-61).
Since then innumerable randomized controlled trials and meta-analyses have confirmed that nasogastric tubes inserted prophylactically after abdominal surgery, even when gastrointestinal anastomoses have been constructed, are unnecessary. So how did this incontrovertible evidence impact my practice and that of most of my surgical colleagues? Not at all, at least not for many years. We continued our routine of torturing postoperative patients with nasogastric tubes because it had been drummed into us during residency and because we were uncomfortable not doing so. But why did we persist after convincing evidence to the contrary emerged?
Unfortunately it is not uncommon that even when good evidence exists, we fail to incorporate it into decision-making. The comfort we enjoy with our standard way of doing things is often preferred to the discomfort – cognitive dissonance – we experience when confronted with mounting empirical evidence that challenges our beliefs. All too often, the cognitive dissonance is reduced by holding on to those notions with which we are most comfortable and ignoring or rejecting new information no matter how valid.
What is the harm? In the case of prophylactic nasogastric tubes, considerable discomfort has unnecessarily complicated the postoperative courses of millions of patients. Many trials have shown that aspiration and pneumonia, the adverse events for which the tubes were placed to prevent, occurred more frequently in patients with than those without nasogastric tubes.
Prophylactic gastric decompression is but one of many practices that have been continued long after their efficacy was disproven. How many radical mastectomies were performed after modified radical mastectomy, and then later partial mastectomy with radiation were shown with irrefutable data to provide equal survival with less disfigurement and fewer complications such as arm lymphedema? For many years after the indications for tonsillectomy were narrowed, this procedure continued to be more commonly done than was appropriate based on the evidence available.
Some hold on to their cherished habits more persistently and longer than others. In order to maintain consonance and avoid the stress of dissonance, I have known surgeons who have retained nearly all of the practices they learned from their mentors during residency long past their utility. Such individuals may insist that they alone prep their patients and that long outmoded suture and instruments be maintained on the operating room supply list. When new, and often proven to be superior, instruments, sutures, and pathways of care for their patients are introduced in their institutions, they find it difficult or even impossible to change.
In an era when the few controlled trials and meta-analyses available were buried within a surgical literature that was difficult to access and the term evidence-based surgery was not yet a part of our lexicon, such a rigid posture was often tolerated. I would hope that in most institutions and departments of surgery this is no longer the case. We live in a time when the imperatives of renewal and reevaluation of our practices are increasing. Therefore, reviewing new evidence, even that which goes against our established notions, and incorporating new proven methods, are essential to maintaining the highest standard of patient care.
Although many gray areas remain and there is often more than one best way to manage a surgical patient, our treatments should be based on the best evidence available rather than on what we learned 5, 10, or even 30 years ago. Fortunately, such evidence is now readily accessible. A notable example is “Evidence-based decisions in surgery,” surgical practice guidelines recently introduced by the American College of Surgeons (ACS) under the guidance of Dr. Lewis Flint.
“Evidence-based decisions in surgery” presently consists of 15 modules of the most common diseases and conditions encountered by general surgeons. These modules can be easily accessed by ACS Fellows on any mobile device at the point-of-care (http://ebds.facs.org). Surgical recommendations along with the strength of evidence (weak, moderate, or strong) for each are presented in an easy-to-interpret format. The modules have been developed by American College of Surgeons staff and been peer-reviewed by the Best Practices Workgroup of the College’s Board of Governors and by representatives of the Advisory Council for General Surgery. A consensus of the reviewers was used to determine the content of each module. It is emphasized that the purpose of these modules is to guide rather than dictate decision-making.
In addition to the strength of evidence for each recommendation, a clinical decision algorithm for a typical patient, suggested talking points for patient education, and key references on which the recommendations are based are also provided. Although clinical practice guidelines have been developed by a number of specialty surgical societies, I have found none that are as easy to digest and use in a busy clinical practice as “Evidence-based decisions in surgery.
So we no longer have an excuse to hold on to our cherished and venerable practices that are outmoded and possibly not in the best interest of our patients. The information needed to do it right is virtually one click of a mouse away. Try applying “Evidence-based decisions in surgery” in your practice. I am convinced you will find them valuable as you make decisions for the most appropriate care of your patients.
Dr. Rikkers is Editor in Chief of ACS Surgery News
“It is concluded that nasogastric suction should not be used routinely following abdominal surgery." This is the concluding statement from a paper presented at the Pacific Coast Surgical Association and published in the American Journal of Surgery more than 50 years ago (Am. J. Surg 1957;94:257-61).
Since then innumerable randomized controlled trials and meta-analyses have confirmed that nasogastric tubes inserted prophylactically after abdominal surgery, even when gastrointestinal anastomoses have been constructed, are unnecessary. So how did this incontrovertible evidence impact my practice and that of most of my surgical colleagues? Not at all, at least not for many years. We continued our routine of torturing postoperative patients with nasogastric tubes because it had been drummed into us during residency and because we were uncomfortable not doing so. But why did we persist after convincing evidence to the contrary emerged?
Unfortunately it is not uncommon that even when good evidence exists, we fail to incorporate it into decision-making. The comfort we enjoy with our standard way of doing things is often preferred to the discomfort – cognitive dissonance – we experience when confronted with mounting empirical evidence that challenges our beliefs. All too often, the cognitive dissonance is reduced by holding on to those notions with which we are most comfortable and ignoring or rejecting new information no matter how valid.
What is the harm? In the case of prophylactic nasogastric tubes, considerable discomfort has unnecessarily complicated the postoperative courses of millions of patients. Many trials have shown that aspiration and pneumonia, the adverse events for which the tubes were placed to prevent, occurred more frequently in patients with than those without nasogastric tubes.
Prophylactic gastric decompression is but one of many practices that have been continued long after their efficacy was disproven. How many radical mastectomies were performed after modified radical mastectomy, and then later partial mastectomy with radiation were shown with irrefutable data to provide equal survival with less disfigurement and fewer complications such as arm lymphedema? For many years after the indications for tonsillectomy were narrowed, this procedure continued to be more commonly done than was appropriate based on the evidence available.
Some hold on to their cherished habits more persistently and longer than others. In order to maintain consonance and avoid the stress of dissonance, I have known surgeons who have retained nearly all of the practices they learned from their mentors during residency long past their utility. Such individuals may insist that they alone prep their patients and that long outmoded suture and instruments be maintained on the operating room supply list. When new, and often proven to be superior, instruments, sutures, and pathways of care for their patients are introduced in their institutions, they find it difficult or even impossible to change.
In an era when the few controlled trials and meta-analyses available were buried within a surgical literature that was difficult to access and the term evidence-based surgery was not yet a part of our lexicon, such a rigid posture was often tolerated. I would hope that in most institutions and departments of surgery this is no longer the case. We live in a time when the imperatives of renewal and reevaluation of our practices are increasing. Therefore, reviewing new evidence, even that which goes against our established notions, and incorporating new proven methods, are essential to maintaining the highest standard of patient care.
Although many gray areas remain and there is often more than one best way to manage a surgical patient, our treatments should be based on the best evidence available rather than on what we learned 5, 10, or even 30 years ago. Fortunately, such evidence is now readily accessible. A notable example is “Evidence-based decisions in surgery,” surgical practice guidelines recently introduced by the American College of Surgeons (ACS) under the guidance of Dr. Lewis Flint.
“Evidence-based decisions in surgery” presently consists of 15 modules of the most common diseases and conditions encountered by general surgeons. These modules can be easily accessed by ACS Fellows on any mobile device at the point-of-care (http://ebds.facs.org). Surgical recommendations along with the strength of evidence (weak, moderate, or strong) for each are presented in an easy-to-interpret format. The modules have been developed by American College of Surgeons staff and been peer-reviewed by the Best Practices Workgroup of the College’s Board of Governors and by representatives of the Advisory Council for General Surgery. A consensus of the reviewers was used to determine the content of each module. It is emphasized that the purpose of these modules is to guide rather than dictate decision-making.
In addition to the strength of evidence for each recommendation, a clinical decision algorithm for a typical patient, suggested talking points for patient education, and key references on which the recommendations are based are also provided. Although clinical practice guidelines have been developed by a number of specialty surgical societies, I have found none that are as easy to digest and use in a busy clinical practice as “Evidence-based decisions in surgery.
So we no longer have an excuse to hold on to our cherished and venerable practices that are outmoded and possibly not in the best interest of our patients. The information needed to do it right is virtually one click of a mouse away. Try applying “Evidence-based decisions in surgery” in your practice. I am convinced you will find them valuable as you make decisions for the most appropriate care of your patients.
Dr. Rikkers is Editor in Chief of ACS Surgery News

Three miRNA biomarkers predicted osteoarthritis severity
PARIS – Three micro RNAs have been shown to be associated with disease severity in patients with hip or knee osteoarthritis, based on data from a large population-based cohort in Italy*.
The presence of three specific miRNAs are biomarkers that might prove to be useful for predicting OA severity if validated in other cohorts and diverse populations of OA patients, Dr. Christian Beyer reported at a press conference during the annual European Congress of Rheumatology (Ann. Rheum. Dis. 2014 [doi:10.1136/annrheumdis-2013-204698]).

The miRNAs could also be a first step toward finding new OA therapies, such as approaches that avert cartilage loss, said Dr. Beyer of the University of Erlangen–Nuremberg (Germany).
For the study, serum samples from 816 cohort members who had osteoarthritis and were followed for at least 15 years were analyzed for the presence of any of the 374 miRNAs. A microarray screening identified 12 candidate miRNAs, validated in the entire cohort. Based on a regression analysis, the 67 cohort members who went on to have knee or hip arthroplasty were found to differentially express three of the miRNAs: let-7e, miR-454, and miR-885-5p. The most promising of the markers appears to be let-7e.
Let-7e was a negative predictor for total joint arthroplasty with an adjusted hazard ratio of 0.75 (95% confidence interval, 0.58-0.96; P = .021) when normalized to U6, and 0.76 (95% CI, 0.6-0.97; P = .026) after normalization to the Ct-average. However, miR-454 was inversely correlated with severe knee or hip osteoarthritis with an adjusted HR of 0.77 (95% CI, 0.61-0.97; P = .028) when normalized to U6. This correlation was lost when data were normalized to Ct-average (P = .118). Finally, miR-885-5p showed a trend toward a positive relationship with arthroplasty when normalized to U6 (HR, 1.24; 95% CI, 0.95-1.62; P = .107) or to Ct-average (HR, 1.30; 95% CI, 0.99-1.70; P = .056).
If specific miRNAs prove to be biomarkers to predict OA severity, it would offer the ability to use markers that are found in the peripheral circulation, stable over time, and not sex dependent. Such markers also could prove useful for finding new OA therapies, he said.
Next steps for further study include validation of the miRNA biomarkers in other OA cohorts, Dr. Beyer said. The well-defined Bruneck cohort is a stable community that has been extensively studied similar to the Framingham cohort in the United States. The Bruneck cohort is all white, however, and the results of this study need to be validated in diverse populations.
Dr. Beyer declared having no relevant financial disclosures.
On Twitter@maryjodales
CORRECTION, 6/12/2014: An earlier version of the article misstated the location of the study cohort.
PARIS – Three micro RNAs have been shown to be associated with disease severity in patients with hip or knee osteoarthritis, based on data from a large population-based cohort in Italy*.
The presence of three specific miRNAs are biomarkers that might prove to be useful for predicting OA severity if validated in other cohorts and diverse populations of OA patients, Dr. Christian Beyer reported at a press conference during the annual European Congress of Rheumatology (Ann. Rheum. Dis. 2014 [doi:10.1136/annrheumdis-2013-204698]).
The miRNAs could also be a first step toward finding new OA therapies, such as approaches that avert cartilage loss, said Dr. Beyer of the University of Erlangen–Nuremberg (Germany).
For the study, serum samples from 816 cohort members who had osteoarthritis and were followed for at least 15 years were analyzed for the presence of any of the 374 miRNAs. A microarray screening identified 12 candidate miRNAs, validated in the entire cohort. Based on a regression analysis, the 67 cohort members who went on to have knee or hip arthroplasty were found to differentially express three of the miRNAs: let-7e, miR-454, and miR-885-5p. The most promising of the markers appears to be let-7e.
Let-7e was a negative predictor for total joint arthroplasty with an adjusted hazard ratio of 0.75 (95% confidence interval, 0.58-0.96; P = .021) when normalized to U6, and 0.76 (95% CI, 0.6-0.97; P = .026) after normalization to the Ct-average. However, miR-454 was inversely correlated with severe knee or hip osteoarthritis with an adjusted HR of 0.77 (95% CI, 0.61-0.97; P = .028) when normalized to U6. This correlation was lost when data were normalized to Ct-average (P = .118). Finally, miR-885-5p showed a trend toward a positive relationship with arthroplasty when normalized to U6 (HR, 1.24; 95% CI, 0.95-1.62; P = .107) or to Ct-average (HR, 1.30; 95% CI, 0.99-1.70; P = .056).
If specific miRNAs prove to be biomarkers to predict OA severity, it would offer the ability to use markers that are found in the peripheral circulation, stable over time, and not sex dependent. Such markers also could prove useful for finding new OA therapies, he said.
Next steps for further study include validation of the miRNA biomarkers in other OA cohorts, Dr. Beyer said. The well-defined Bruneck cohort is a stable community that has been extensively studied similar to the Framingham cohort in the United States. The Bruneck cohort is all white, however, and the results of this study need to be validated in diverse populations.
Dr. Beyer declared having no relevant financial disclosures.
On Twitter@maryjodales
CORRECTION, 6/12/2014: An earlier version of the article misstated the location of the study cohort.
PARIS – Three micro RNAs have been shown to be associated with disease severity in patients with hip or knee osteoarthritis, based on data from a large population-based cohort in Italy*.
The presence of three specific miRNAs are biomarkers that might prove to be useful for predicting OA severity if validated in other cohorts and diverse populations of OA patients, Dr. Christian Beyer reported at a press conference during the annual European Congress of Rheumatology (Ann. Rheum. Dis. 2014 [doi:10.1136/annrheumdis-2013-204698]).
The miRNAs could also be a first step toward finding new OA therapies, such as approaches that avert cartilage loss, said Dr. Beyer of the University of Erlangen–Nuremberg (Germany).
For the study, serum samples from 816 cohort members who had osteoarthritis and were followed for at least 15 years were analyzed for the presence of any of the 374 miRNAs. A microarray screening identified 12 candidate miRNAs, validated in the entire cohort. Based on a regression analysis, the 67 cohort members who went on to have knee or hip arthroplasty were found to differentially express three of the miRNAs: let-7e, miR-454, and miR-885-5p. The most promising of the markers appears to be let-7e.
Let-7e was a negative predictor for total joint arthroplasty with an adjusted hazard ratio of 0.75 (95% confidence interval, 0.58-0.96; P = .021) when normalized to U6, and 0.76 (95% CI, 0.6-0.97; P = .026) after normalization to the Ct-average. However, miR-454 was inversely correlated with severe knee or hip osteoarthritis with an adjusted HR of 0.77 (95% CI, 0.61-0.97; P = .028) when normalized to U6. This correlation was lost when data were normalized to Ct-average (P = .118). Finally, miR-885-5p showed a trend toward a positive relationship with arthroplasty when normalized to U6 (HR, 1.24; 95% CI, 0.95-1.62; P = .107) or to Ct-average (HR, 1.30; 95% CI, 0.99-1.70; P = .056).
If specific miRNAs prove to be biomarkers to predict OA severity, it would offer the ability to use markers that are found in the peripheral circulation, stable over time, and not sex dependent. Such markers also could prove useful for finding new OA therapies, he said.
Next steps for further study include validation of the miRNA biomarkers in other OA cohorts, Dr. Beyer said. The well-defined Bruneck cohort is a stable community that has been extensively studied similar to the Framingham cohort in the United States. The Bruneck cohort is all white, however, and the results of this study need to be validated in diverse populations.
Dr. Beyer declared having no relevant financial disclosures.
On Twitter@maryjodales
CORRECTION, 6/12/2014: An earlier version of the article misstated the location of the study cohort.
AT THE EULAR CONGRESS 2014
Key clinical point: Biomarkers may allow early interventions to limit osteoarthritis risks, such as cartilage damage.
Major finding: Let-7e was a negative predictor for total joint arthroplasty with an adjusted HR of 0.75 (95% CI, 0.58-0.96; P = .021) when normalized to U6, and 0.76 (95% CI, 0.6-0.97; P = .026) after normalization to the Ct-average.
Data source: The large population-based Bruneck cohort in Italy.
Disclosures: Dr. Beyer had no relevant financial disclosures.
