User login
Official Newspaper of the American College of Surgeons
VIDEO: Surgical quality measures boost survival in cancer patients
BALTIMORE – Surgeons’ adherence to select quality measures when treating stage IIIA non–small-cell lung cancer patients led to improved patient survival, according to a study presented at the 2016 annual meeting of the American Association for Thoracic Surgery.
Researchers at Washington University in St. Louis identified 10,323 patients who received surgery for Stage IIIA NSCLC in the National Cancer Data Base from 2006 to 2010, and chose four quality measures that should have been met by surgeons: delivery of neoadjuvant multiagent chemotherapy (with or without radiation therapy); performing a lobectomy or greater resection; obtaining more than 10 lymph nodes, and achieving an R0 resection.
The researchers said 12.8% of patients met all four quality measures. Kaplan-Meier analysis demonstrated improved overall median survival by number of quality measures obtained: 0 quality measures, 12.7 months; 1 quality measure, 25.0 months; 2 quality measures, 31.4 months; 3 quality measures, 36.6 months; and 4 quality measures, 43.5 months.
In an interview, Dr. Mark S. Allen, professor of surgery at the Mayo Clinic in Rochester, Minn., and a discussant on the paper at AATS 2016, said the most striking result of the study was that such a low percentage of patients had all four quality measures performed for stage IIIA cancer. He called that finding “disappointing.”
“In general, [the study] shows there is still some work to be done to improve the quality when we operate on stage IIIA patients,” Dr. Allen said. “I’m not sure we do the greatest job of staging them clinically. When they are staged properly they probably do need preoperative chemotherapy, and I’m not sure we do that all the time.” He added that surgeon education about quality outcomes was critical to process improvement and patient outcomes.
Dr. Allen reported no relevant financial disclosures.
On Twitter @richpizzi
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
BALTIMORE – Surgeons’ adherence to select quality measures when treating stage IIIA non–small-cell lung cancer patients led to improved patient survival, according to a study presented at the 2016 annual meeting of the American Association for Thoracic Surgery.
Researchers at Washington University in St. Louis identified 10,323 patients who received surgery for Stage IIIA NSCLC in the National Cancer Data Base from 2006 to 2010, and chose four quality measures that should have been met by surgeons: delivery of neoadjuvant multiagent chemotherapy (with or without radiation therapy); performing a lobectomy or greater resection; obtaining more than 10 lymph nodes, and achieving an R0 resection.
The researchers said 12.8% of patients met all four quality measures. Kaplan-Meier analysis demonstrated improved overall median survival by number of quality measures obtained: 0 quality measures, 12.7 months; 1 quality measure, 25.0 months; 2 quality measures, 31.4 months; 3 quality measures, 36.6 months; and 4 quality measures, 43.5 months.
In an interview, Dr. Mark S. Allen, professor of surgery at the Mayo Clinic in Rochester, Minn., and a discussant on the paper at AATS 2016, said the most striking result of the study was that such a low percentage of patients had all four quality measures performed for stage IIIA cancer. He called that finding “disappointing.”
“In general, [the study] shows there is still some work to be done to improve the quality when we operate on stage IIIA patients,” Dr. Allen said. “I’m not sure we do the greatest job of staging them clinically. When they are staged properly they probably do need preoperative chemotherapy, and I’m not sure we do that all the time.” He added that surgeon education about quality outcomes was critical to process improvement and patient outcomes.
Dr. Allen reported no relevant financial disclosures.
On Twitter @richpizzi
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
BALTIMORE – Surgeons’ adherence to select quality measures when treating stage IIIA non–small-cell lung cancer patients led to improved patient survival, according to a study presented at the 2016 annual meeting of the American Association for Thoracic Surgery.
Researchers at Washington University in St. Louis identified 10,323 patients who received surgery for Stage IIIA NSCLC in the National Cancer Data Base from 2006 to 2010, and chose four quality measures that should have been met by surgeons: delivery of neoadjuvant multiagent chemotherapy (with or without radiation therapy); performing a lobectomy or greater resection; obtaining more than 10 lymph nodes, and achieving an R0 resection.
The researchers said 12.8% of patients met all four quality measures. Kaplan-Meier analysis demonstrated improved overall median survival by number of quality measures obtained: 0 quality measures, 12.7 months; 1 quality measure, 25.0 months; 2 quality measures, 31.4 months; 3 quality measures, 36.6 months; and 4 quality measures, 43.5 months.
In an interview, Dr. Mark S. Allen, professor of surgery at the Mayo Clinic in Rochester, Minn., and a discussant on the paper at AATS 2016, said the most striking result of the study was that such a low percentage of patients had all four quality measures performed for stage IIIA cancer. He called that finding “disappointing.”
“In general, [the study] shows there is still some work to be done to improve the quality when we operate on stage IIIA patients,” Dr. Allen said. “I’m not sure we do the greatest job of staging them clinically. When they are staged properly they probably do need preoperative chemotherapy, and I’m not sure we do that all the time.” He added that surgeon education about quality outcomes was critical to process improvement and patient outcomes.
Dr. Allen reported no relevant financial disclosures.
On Twitter @richpizzi
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE AATS ANNUAL MEETING

Gyn. oncologists are in demand for robotic hysterectomy
SAN DIEGO – The demand for gynecologic oncologists to perform robotic hysterectomies – even for benign indications – has increased to the point that additional fellowship training spots will be necessary to meet the need, Dr. Kayla M. Wishall said at the annual meeting of the Society of Gynecologic Oncology.
More and more patients want their hysterectomies performed robotically. They find the high-quality optics and minimally invasive nature of the robotic procedure appealing – smaller incisions, less blood loss, shorter hospital stay, and faster recovery. And gynecologic oncologists are getting an increasing number of referrals because of their special expertise in robotic surgery and extensive experience with higher-risk patients, explained Dr. Wishall, a gynecologic oncologist at Hahnemann University Hospital/Drexel University in Philadelphia.
“This trend will likely tax the limited resources of gynecologic oncologists,” she added.
Another possible reason for the growing demand for gynecologic oncologist–performed robotic hysterectomies is that these subspecialists achieve better outcomes than gynecologists who do robotic hysterectomies, at least according to the findings of a retrospective study performed by Dr. Wishall, which included all of the 468 robotic hysterectomies performed at a large academic medical center in a recent 5-year period.
Gynecologic oncologists performed 64 (16.5%) of the 387 robotic hysterectomies done for benign indications. All told, gynecologists did 254 of the robotic hysterectomies; gynecologic oncologists performed 214.
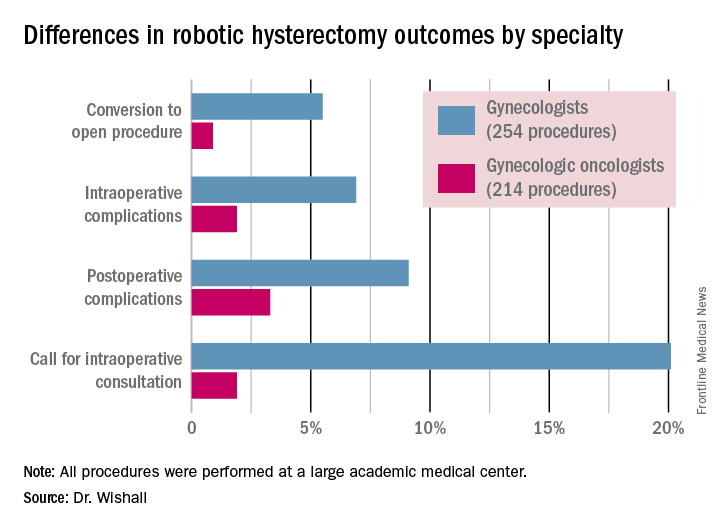
Even though patients referred to gynecologic oncologists for these procedures were older, heavier, more likely to have had previous abdominal surgery, more often members of racial minorities, and had a higher prevalence of cardiac comorbidities, they experienced significantly fewer intra- and postoperative complications than patients whose robotic hysterectomies were performed by gynecologists, Dr. Wishall reported.
The combined intraoperative and postoperative complication rate for robotic hysterectomies performed by gynecologic oncologists was 5.2%, compared with 16% for gynecologists. But the rate of cardiac comorbidities, for instance, was 36.4% among patients seeing gynecologic oncologists, compared with 23.6% among those seeing gynecologists.
Moreover, gynecologists were about 10-fold more likely than gynecologic oncologists to call for an intraoperative consultation and sixfold more likely to convert their robotic hysterectomy to an open procedure. Their average operating room time was about 40% longer (244 minutes versus 171 minutes), too, in this single-center experience.
Dr. Wishall reported having no financial conflicts related to her study, which was conducted free of commercial support.
I read this article initially with amusement and then with outrage and disdain. This article summarizes the single-site, retrospective study by Dr. Kayla Wishall at the annual meeting of the Society of Gynecologic Oncology. Not only is this nonscience, but nonsensical science. As a single center retrospective study, conclusions must be suspect.

|
Dr. Charles E. Miller |
The comparison numbers of the two groups are small. While confounders would appear to be greater in the oncology group, we know nothing about the difficulty of the surgeries themselves – size of uterus, adnexal disease, endometriosis, pelvic adhesions, etc. Oftentimes, gynecologic oncologists dealing with endometrial carcinoma are going to face a less difficult challenge than a generalist dealing with an 18-weeks–size uterus in a woman who has undergone three prior C-sections, an open myomectomy, or stage IV endometriosis.
We are also not privy to the experience of the surgeons involved; that is, the number of procedures performed by each surgeon in the compared groups. It is certainly well known that complications decrease with surgeon experience. In a multicenter analysis by Peter Lim et al., looking at robotic assisted hysterectomies performed by high-volume surgeons (60 or more prior procedures), the intraoperative complication rate was only 0.7% and the postoperative complication rate 6.3% (Int J Gynaecol Obstet. 2016 Jun;133[3]:359-64).
As a benign gynecologist who has been performing minimally invasive gynecologic surgery for 30 years and more recently, robotic surgery, I am shocked with the tenor of this study, as it would imply that unless someone is boarded in gynecologic oncology, he or she should not be performing robotic hysterectomies.
I would advise Dr. Wishall to reevaluate her surgeon population and look at the impact of experience as well as procedure difficultly. I am absolutely sure that she will find that many of the surgeons with excellent outcomes will be generalists, who are well experienced in robotic hysterectomy.
Dr. Charles E. Miller is a clinical associate professor at the University of Illinois at Chicago, and a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill. He reported having no financial disclosures relevant to this article.
I read this article initially with amusement and then with outrage and disdain. This article summarizes the single-site, retrospective study by Dr. Kayla Wishall at the annual meeting of the Society of Gynecologic Oncology. Not only is this nonscience, but nonsensical science. As a single center retrospective study, conclusions must be suspect.
|
|
Dr. Charles E. Miller |
The comparison numbers of the two groups are small. While confounders would appear to be greater in the oncology group, we know nothing about the difficulty of the surgeries themselves – size of uterus, adnexal disease, endometriosis, pelvic adhesions, etc. Oftentimes, gynecologic oncologists dealing with endometrial carcinoma are going to face a less difficult challenge than a generalist dealing with an 18-weeks–size uterus in a woman who has undergone three prior C-sections, an open myomectomy, or stage IV endometriosis.
We are also not privy to the experience of the surgeons involved; that is, the number of procedures performed by each surgeon in the compared groups. It is certainly well known that complications decrease with surgeon experience. In a multicenter analysis by Peter Lim et al., looking at robotic assisted hysterectomies performed by high-volume surgeons (60 or more prior procedures), the intraoperative complication rate was only 0.7% and the postoperative complication rate 6.3% (Int J Gynaecol Obstet. 2016 Jun;133[3]:359-64).
As a benign gynecologist who has been performing minimally invasive gynecologic surgery for 30 years and more recently, robotic surgery, I am shocked with the tenor of this study, as it would imply that unless someone is boarded in gynecologic oncology, he or she should not be performing robotic hysterectomies.
I would advise Dr. Wishall to reevaluate her surgeon population and look at the impact of experience as well as procedure difficultly. I am absolutely sure that she will find that many of the surgeons with excellent outcomes will be generalists, who are well experienced in robotic hysterectomy.
Dr. Charles E. Miller is a clinical associate professor at the University of Illinois at Chicago, and a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill. He reported having no financial disclosures relevant to this article.
I read this article initially with amusement and then with outrage and disdain. This article summarizes the single-site, retrospective study by Dr. Kayla Wishall at the annual meeting of the Society of Gynecologic Oncology. Not only is this nonscience, but nonsensical science. As a single center retrospective study, conclusions must be suspect.
|
|
Dr. Charles E. Miller |
The comparison numbers of the two groups are small. While confounders would appear to be greater in the oncology group, we know nothing about the difficulty of the surgeries themselves – size of uterus, adnexal disease, endometriosis, pelvic adhesions, etc. Oftentimes, gynecologic oncologists dealing with endometrial carcinoma are going to face a less difficult challenge than a generalist dealing with an 18-weeks–size uterus in a woman who has undergone three prior C-sections, an open myomectomy, or stage IV endometriosis.
We are also not privy to the experience of the surgeons involved; that is, the number of procedures performed by each surgeon in the compared groups. It is certainly well known that complications decrease with surgeon experience. In a multicenter analysis by Peter Lim et al., looking at robotic assisted hysterectomies performed by high-volume surgeons (60 or more prior procedures), the intraoperative complication rate was only 0.7% and the postoperative complication rate 6.3% (Int J Gynaecol Obstet. 2016 Jun;133[3]:359-64).
As a benign gynecologist who has been performing minimally invasive gynecologic surgery for 30 years and more recently, robotic surgery, I am shocked with the tenor of this study, as it would imply that unless someone is boarded in gynecologic oncology, he or she should not be performing robotic hysterectomies.
I would advise Dr. Wishall to reevaluate her surgeon population and look at the impact of experience as well as procedure difficultly. I am absolutely sure that she will find that many of the surgeons with excellent outcomes will be generalists, who are well experienced in robotic hysterectomy.
Dr. Charles E. Miller is a clinical associate professor at the University of Illinois at Chicago, and a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville and Schaumburg, Ill. He reported having no financial disclosures relevant to this article.
SAN DIEGO – The demand for gynecologic oncologists to perform robotic hysterectomies – even for benign indications – has increased to the point that additional fellowship training spots will be necessary to meet the need, Dr. Kayla M. Wishall said at the annual meeting of the Society of Gynecologic Oncology.
More and more patients want their hysterectomies performed robotically. They find the high-quality optics and minimally invasive nature of the robotic procedure appealing – smaller incisions, less blood loss, shorter hospital stay, and faster recovery. And gynecologic oncologists are getting an increasing number of referrals because of their special expertise in robotic surgery and extensive experience with higher-risk patients, explained Dr. Wishall, a gynecologic oncologist at Hahnemann University Hospital/Drexel University in Philadelphia.
“This trend will likely tax the limited resources of gynecologic oncologists,” she added.
Another possible reason for the growing demand for gynecologic oncologist–performed robotic hysterectomies is that these subspecialists achieve better outcomes than gynecologists who do robotic hysterectomies, at least according to the findings of a retrospective study performed by Dr. Wishall, which included all of the 468 robotic hysterectomies performed at a large academic medical center in a recent 5-year period.
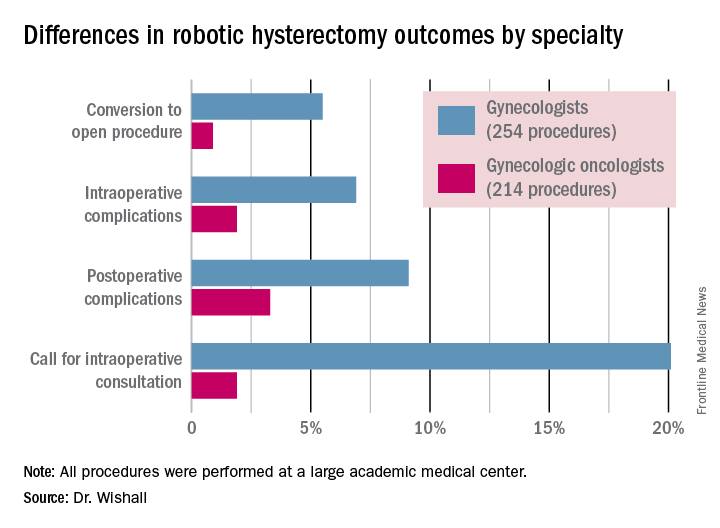
Gynecologic oncologists performed 64 (16.5%) of the 387 robotic hysterectomies done for benign indications. All told, gynecologists did 254 of the robotic hysterectomies; gynecologic oncologists performed 214.
Even though patients referred to gynecologic oncologists for these procedures were older, heavier, more likely to have had previous abdominal surgery, more often members of racial minorities, and had a higher prevalence of cardiac comorbidities, they experienced significantly fewer intra- and postoperative complications than patients whose robotic hysterectomies were performed by gynecologists, Dr. Wishall reported.
The combined intraoperative and postoperative complication rate for robotic hysterectomies performed by gynecologic oncologists was 5.2%, compared with 16% for gynecologists. But the rate of cardiac comorbidities, for instance, was 36.4% among patients seeing gynecologic oncologists, compared with 23.6% among those seeing gynecologists.
Moreover, gynecologists were about 10-fold more likely than gynecologic oncologists to call for an intraoperative consultation and sixfold more likely to convert their robotic hysterectomy to an open procedure. Their average operating room time was about 40% longer (244 minutes versus 171 minutes), too, in this single-center experience.
Dr. Wishall reported having no financial conflicts related to her study, which was conducted free of commercial support.
SAN DIEGO – The demand for gynecologic oncologists to perform robotic hysterectomies – even for benign indications – has increased to the point that additional fellowship training spots will be necessary to meet the need, Dr. Kayla M. Wishall said at the annual meeting of the Society of Gynecologic Oncology.
More and more patients want their hysterectomies performed robotically. They find the high-quality optics and minimally invasive nature of the robotic procedure appealing – smaller incisions, less blood loss, shorter hospital stay, and faster recovery. And gynecologic oncologists are getting an increasing number of referrals because of their special expertise in robotic surgery and extensive experience with higher-risk patients, explained Dr. Wishall, a gynecologic oncologist at Hahnemann University Hospital/Drexel University in Philadelphia.
“This trend will likely tax the limited resources of gynecologic oncologists,” she added.
Another possible reason for the growing demand for gynecologic oncologist–performed robotic hysterectomies is that these subspecialists achieve better outcomes than gynecologists who do robotic hysterectomies, at least according to the findings of a retrospective study performed by Dr. Wishall, which included all of the 468 robotic hysterectomies performed at a large academic medical center in a recent 5-year period.
Gynecologic oncologists performed 64 (16.5%) of the 387 robotic hysterectomies done for benign indications. All told, gynecologists did 254 of the robotic hysterectomies; gynecologic oncologists performed 214.
Even though patients referred to gynecologic oncologists for these procedures were older, heavier, more likely to have had previous abdominal surgery, more often members of racial minorities, and had a higher prevalence of cardiac comorbidities, they experienced significantly fewer intra- and postoperative complications than patients whose robotic hysterectomies were performed by gynecologists, Dr. Wishall reported.
The combined intraoperative and postoperative complication rate for robotic hysterectomies performed by gynecologic oncologists was 5.2%, compared with 16% for gynecologists. But the rate of cardiac comorbidities, for instance, was 36.4% among patients seeing gynecologic oncologists, compared with 23.6% among those seeing gynecologists.
Moreover, gynecologists were about 10-fold more likely than gynecologic oncologists to call for an intraoperative consultation and sixfold more likely to convert their robotic hysterectomy to an open procedure. Their average operating room time was about 40% longer (244 minutes versus 171 minutes), too, in this single-center experience.
Dr. Wishall reported having no financial conflicts related to her study, which was conducted free of commercial support.
AT THE ANNUAL MEETING ON WOMEN’S CANCER
Key clinical point: Gynecologic oncologists achieved better robotic hysterectomy outcomes than gynecologists despite challenging referrals.
Major finding: The combined intraoperative and postoperative complication rate for robotic hysterectomies performed by gynecologic oncologists was 5.2%, compared with 16% for gynecologists.
Data source: A retrospective observational study conducted at a single center included 254 women whose robotic hysterectomies were performed by gynecologists and 214 done by gynecologic oncologists.
Disclosures: Dr. Wishall reported having no financial conflicts related to the study, which was conducted free of commercial support.
VIDEO: Endoscopic pyloromyotomy works for gastroparesis when meds don’t
SAN DIEGO – Gastric peroral endoscopic myotomy, a novel procedure for gastroparesis, restored gastric emptying in 30 refractory patients at Johns Hopkins University, Baltimore, and elsewhere in the largest series to date for the technique.
Drug therapy had failed, and Botox injections and transpyloric stenting weren’t helping much. On gastric emptying scans (GES), patients had around 40% of solid meals in their stomachs at 4 hours. Their gastroparesis was related mostly to diabetes and postoperative complications, but about a quarter of the cases were idiopathic.
Twenty-six patients (87%) responded to gastric peroral endoscopic myotomy (G-POEM) during a median follow-up of 5.5 months. Nausea, vomiting, and abdominal pain resolved or improved in most. On repeat GES in 17 patients, emptying time normalized in about half and improved in a third. Overall, patients had 17% of solid meals in their stomachs at 4 hours. G-POEM took an average of 72 minutes, and patients were in the hospital for about 3 days. One patient in the series developed pneumoperitoneum, and another had a prepyloric ulcer.
“The problem with transpyloric stents is that they migrate,” said investigator Dr. Mouen A. Khashab, director of therapeutic endoscopy at Johns Hopkins University. “G-POEM offers a permanent solution with few side effects. You have to be good at doing POEM in the esophagus first, as a prerequisite.”
In an interview at the annual Digestive Disease Week, Dr. Khashab explained the procedure in detail, as well as how he incorporates it into his practice and the patient population most likely to benefit.
SAN DIEGO – Gastric peroral endoscopic myotomy, a novel procedure for gastroparesis, restored gastric emptying in 30 refractory patients at Johns Hopkins University, Baltimore, and elsewhere in the largest series to date for the technique.
Drug therapy had failed, and Botox injections and transpyloric stenting weren’t helping much. On gastric emptying scans (GES), patients had around 40% of solid meals in their stomachs at 4 hours. Their gastroparesis was related mostly to diabetes and postoperative complications, but about a quarter of the cases were idiopathic.
Twenty-six patients (87%) responded to gastric peroral endoscopic myotomy (G-POEM) during a median follow-up of 5.5 months. Nausea, vomiting, and abdominal pain resolved or improved in most. On repeat GES in 17 patients, emptying time normalized in about half and improved in a third. Overall, patients had 17% of solid meals in their stomachs at 4 hours. G-POEM took an average of 72 minutes, and patients were in the hospital for about 3 days. One patient in the series developed pneumoperitoneum, and another had a prepyloric ulcer.
“The problem with transpyloric stents is that they migrate,” said investigator Dr. Mouen A. Khashab, director of therapeutic endoscopy at Johns Hopkins University. “G-POEM offers a permanent solution with few side effects. You have to be good at doing POEM in the esophagus first, as a prerequisite.”
In an interview at the annual Digestive Disease Week, Dr. Khashab explained the procedure in detail, as well as how he incorporates it into his practice and the patient population most likely to benefit.
SAN DIEGO – Gastric peroral endoscopic myotomy, a novel procedure for gastroparesis, restored gastric emptying in 30 refractory patients at Johns Hopkins University, Baltimore, and elsewhere in the largest series to date for the technique.
Drug therapy had failed, and Botox injections and transpyloric stenting weren’t helping much. On gastric emptying scans (GES), patients had around 40% of solid meals in their stomachs at 4 hours. Their gastroparesis was related mostly to diabetes and postoperative complications, but about a quarter of the cases were idiopathic.
Twenty-six patients (87%) responded to gastric peroral endoscopic myotomy (G-POEM) during a median follow-up of 5.5 months. Nausea, vomiting, and abdominal pain resolved or improved in most. On repeat GES in 17 patients, emptying time normalized in about half and improved in a third. Overall, patients had 17% of solid meals in their stomachs at 4 hours. G-POEM took an average of 72 minutes, and patients were in the hospital for about 3 days. One patient in the series developed pneumoperitoneum, and another had a prepyloric ulcer.
“The problem with transpyloric stents is that they migrate,” said investigator Dr. Mouen A. Khashab, director of therapeutic endoscopy at Johns Hopkins University. “G-POEM offers a permanent solution with few side effects. You have to be good at doing POEM in the esophagus first, as a prerequisite.”
In an interview at the annual Digestive Disease Week, Dr. Khashab explained the procedure in detail, as well as how he incorporates it into his practice and the patient population most likely to benefit.
AT DDW® 2016

Most people who undergo gender reassignment surgery appreciate the results
ORLANDO – Gender reassignment surgery is the most extreme step for those transgender individuals who wish to complete the transformation to the opposite sex. While many transgender people do not opt to take this step, it may be an option for people who still have gender dysphoria after a thorough diagnostic work-up by a mental health professional, hormonal treatment, and having lived in the desired gender role as a “real-life test.”
Dr. Stan Monstrey, of Ghent University Hospital, Belgium, is an experienced gender reassignment surgeon and reported at the annual meeting of the American Academy of Clinical Endocrinology that between 1995 and 2005, he saw about 20-30 new patients a year. But now, he said, “We operate on a weekly basis between a minimum of three and sometimes six or seven transsexuals, so ... in our practice, probably between 90% and 95% are still going the whole way, still want what was called initially binary surgery.”

Transwomen: Male to female
The transformation procedure for male to female begins with feminizing aesthetic procedures, such as reducing the Adam’s apple (laryngeal prominence of the thyroid cartilage) and chin, frontal boss of the forehead, and possibly other facial work such as rhinoplasty. “Sometimes minor changes can have a huge effect on the face of the patient,” Dr. Monstrey said. “This is becoming, in our opinion, increasingly important for transwomen.”
Then, in about 75% of cases, Dr. Monstrey performs at least two surgeries under the same anesthesia – breast augmentation and perineal transformation. He said even after years of hormone therapy, most such patients have only a limited amount of breast tissue but want more prominent breasts. Implants can be placed behind or in front of the pectoralis muscle via inframammary, transaxillary, or occasionally periareolar approaches. Results are immediate, and complications are rare.
Another technique, which has become very popular over the past 5-10 years, is lipofilling to fill defects and depressions in the breasts. Stem cells contained in the fat may help soften scars. But when faced with a patient who had a BRCA1 mutation, the surgeons would not use lipofilling, fearing the potential for breast cancer, and would use prostheses instead (J Sex Med. 2014 Oct;11:2496-9). Still, questions remain about even using hormone treatments in such a patient.
Dr. Monstrey mentioned that in Belgium, breast augmentation for transwomen is considered reconstructive surgery and is always reimbursed whereas it is considered aesthetic surgery and never reimbursed for non-transwomen who want larger breasts. (For transmen, breast amputation is similarly reimbursed.)
The second operation is genital transformation. Basically, the interior of the penis is removed and the skin is invaginated to form a vagina of 8-18.5 cm and a scrotal flap, along with castration and removal of the penile bulb erectile tissue (corpus spongiosum) posteriorly. It is important to protect the rectal wall, which is not very strong. The foreskin becomes the new clitoral hood and inner side of the labia minora, and the clitoris is formed by reducing and transposing the penile glans. If the patient had a small penis and not enough tissue for the reconstruction, skin flaps from various other sites can be used.
Among more than 1,200 patients, 92% could achieve orgasm. Rectovaginal fistulas occurred in 4 patients, 19 needed repositioning of the urethra, 21 needed an operation to lengthen the vagina, and 95 needed aesthetic correction of the vulva. Dr. Monstrey said many patients have asked him when they should tell their new boyfriends about their transformation, meaning that the surgery was quite convincing even with penetrative sex.
If the first operation does not work, another technique is to use an isolated piece of colon or sigmoid bowel, which has been performed completely laparoscopically by a very skilled gastroenterologic surgeon at the hospital in Ghent.
Speaking to a roomful of endocrinologists, Dr. Monstrey told them, “I’ll be the first one to agree with you that indeed puberty blockers are a very good thing. However, we as surgeons are not so enthusiastic about them because … it is impossible to create a normal vagina” because of a lack of available tissue from the underdeveloped penis.
Transmen: Female to male
“Transmen react much better to hormonal therapy than do transwomen,” he said. “If they hide their breasts they really look like men. The disadvantage is that the surgical treatment is much more complex.” The most important operation for them is subcutaneous mastectomy and male contouring. A small, semiareolar incision leaves almost no scar. Most patients still require excision of redundant skin of the breasts.
Phalloplasty is a complex operation aimed at giving the patient an aesthetic phallus, a normal scrotum, the ability to void while standing, and to perform sexual intercourse, all while protecting erogenous sensation, with minimal morbidity and mortality. Dr. Monstrey reported that he has performed 600-700 phalloplasties.
The most common technique has been to use a free vascularized flap from another bodily site with the artery, vein, and nerves to reconnect at the phalloplasty site. Because the skin is very thin on the inner forearm, it is often used and allows forming an inner tube for the urethra and an outer tube for the penis. The surgery may have to be done in three or four stages for the best results. From pictures that Dr. Monstrey showed, it was obvious that the constructed penises were not absolutely natural in appearance, but he said most patients were “rather happy” with them, despite many of these patients being quite demanding. A scrotum is constructed from transposition of the labia minora.
Unfortunately, voiding while standing is often a problem, with 197 out of 562 patients (35%) having a fistula and urine leakage, but this issue frequently corrects itself. “More difficult to treat are the strictures with stenosis, which can be a problem voiding,” he said (occurring in 78/562). Other complications were 5 complete and 43 partial flap failures, 4 cases of compression syndrome, 58 cases of delayed wound healing, and 15 cases of transient ischemia. Flap failures occurred mainly in smokers, “so we don’t operate on smokers anymore,” he said.
One year after the constructive surgery, a penile prosthesis is implanted for those who want it, allowing sexual intercourse. Most individuals had orgasmic function, not because of reconnected nerves in the flap, but, Dr. Monstrey said he believes, because the clitoris, placed beneath the phallus, is denuded and stimulated during sexual activity. He said the problem is that the prostheses are usually intended for elderly men “who have sex a couple of times a month and who have a normal anatomy.” Young transmen may engage in more sexual activity, “so we have a lot of problems with exposure [of the prosthesis], infection, technical defects, and so on,” he said.
A technique gaining popularity is to use a skin flap from the groin area to make a urethra and one from the thigh to construct a penis. Although a penile transplant has recently been performed for a patient who had lost his penis to cancer, transplants are not being considered at this point, both for surgical technical reasons and because of a need for lifelong immunosuppressive drugs.
Proper referrals and counseling
The World Professional Association for Transgender Health in its Standard of Care guidelines 7 recommends one mental health professional referral for the breast surgery and two such referrals for genital surgery. The issue of possible parenthood should be discussed with patients, along with early counseling about fertility options. The age of majority and consent in different countries is important. Dr. Monstrey said genital surgery may be possible before the age of 18 years if all members of a multidisciplinary team of health professionals agree on a case by case basis that the adolescent can understand the risks, benefits, and alternatives to the surgery with the same degree of competence as someone 18 years of age or older.
Dr. Monstrey reported having no financial disclosures.
ORLANDO – Gender reassignment surgery is the most extreme step for those transgender individuals who wish to complete the transformation to the opposite sex. While many transgender people do not opt to take this step, it may be an option for people who still have gender dysphoria after a thorough diagnostic work-up by a mental health professional, hormonal treatment, and having lived in the desired gender role as a “real-life test.”
Dr. Stan Monstrey, of Ghent University Hospital, Belgium, is an experienced gender reassignment surgeon and reported at the annual meeting of the American Academy of Clinical Endocrinology that between 1995 and 2005, he saw about 20-30 new patients a year. But now, he said, “We operate on a weekly basis between a minimum of three and sometimes six or seven transsexuals, so ... in our practice, probably between 90% and 95% are still going the whole way, still want what was called initially binary surgery.”
Transwomen: Male to female
The transformation procedure for male to female begins with feminizing aesthetic procedures, such as reducing the Adam’s apple (laryngeal prominence of the thyroid cartilage) and chin, frontal boss of the forehead, and possibly other facial work such as rhinoplasty. “Sometimes minor changes can have a huge effect on the face of the patient,” Dr. Monstrey said. “This is becoming, in our opinion, increasingly important for transwomen.”
Then, in about 75% of cases, Dr. Monstrey performs at least two surgeries under the same anesthesia – breast augmentation and perineal transformation. He said even after years of hormone therapy, most such patients have only a limited amount of breast tissue but want more prominent breasts. Implants can be placed behind or in front of the pectoralis muscle via inframammary, transaxillary, or occasionally periareolar approaches. Results are immediate, and complications are rare.
Another technique, which has become very popular over the past 5-10 years, is lipofilling to fill defects and depressions in the breasts. Stem cells contained in the fat may help soften scars. But when faced with a patient who had a BRCA1 mutation, the surgeons would not use lipofilling, fearing the potential for breast cancer, and would use prostheses instead (J Sex Med. 2014 Oct;11:2496-9). Still, questions remain about even using hormone treatments in such a patient.
Dr. Monstrey mentioned that in Belgium, breast augmentation for transwomen is considered reconstructive surgery and is always reimbursed whereas it is considered aesthetic surgery and never reimbursed for non-transwomen who want larger breasts. (For transmen, breast amputation is similarly reimbursed.)
The second operation is genital transformation. Basically, the interior of the penis is removed and the skin is invaginated to form a vagina of 8-18.5 cm and a scrotal flap, along with castration and removal of the penile bulb erectile tissue (corpus spongiosum) posteriorly. It is important to protect the rectal wall, which is not very strong. The foreskin becomes the new clitoral hood and inner side of the labia minora, and the clitoris is formed by reducing and transposing the penile glans. If the patient had a small penis and not enough tissue for the reconstruction, skin flaps from various other sites can be used.
Among more than 1,200 patients, 92% could achieve orgasm. Rectovaginal fistulas occurred in 4 patients, 19 needed repositioning of the urethra, 21 needed an operation to lengthen the vagina, and 95 needed aesthetic correction of the vulva. Dr. Monstrey said many patients have asked him when they should tell their new boyfriends about their transformation, meaning that the surgery was quite convincing even with penetrative sex.
If the first operation does not work, another technique is to use an isolated piece of colon or sigmoid bowel, which has been performed completely laparoscopically by a very skilled gastroenterologic surgeon at the hospital in Ghent.
Speaking to a roomful of endocrinologists, Dr. Monstrey told them, “I’ll be the first one to agree with you that indeed puberty blockers are a very good thing. However, we as surgeons are not so enthusiastic about them because … it is impossible to create a normal vagina” because of a lack of available tissue from the underdeveloped penis.
Transmen: Female to male
“Transmen react much better to hormonal therapy than do transwomen,” he said. “If they hide their breasts they really look like men. The disadvantage is that the surgical treatment is much more complex.” The most important operation for them is subcutaneous mastectomy and male contouring. A small, semiareolar incision leaves almost no scar. Most patients still require excision of redundant skin of the breasts.
Phalloplasty is a complex operation aimed at giving the patient an aesthetic phallus, a normal scrotum, the ability to void while standing, and to perform sexual intercourse, all while protecting erogenous sensation, with minimal morbidity and mortality. Dr. Monstrey reported that he has performed 600-700 phalloplasties.
The most common technique has been to use a free vascularized flap from another bodily site with the artery, vein, and nerves to reconnect at the phalloplasty site. Because the skin is very thin on the inner forearm, it is often used and allows forming an inner tube for the urethra and an outer tube for the penis. The surgery may have to be done in three or four stages for the best results. From pictures that Dr. Monstrey showed, it was obvious that the constructed penises were not absolutely natural in appearance, but he said most patients were “rather happy” with them, despite many of these patients being quite demanding. A scrotum is constructed from transposition of the labia minora.
Unfortunately, voiding while standing is often a problem, with 197 out of 562 patients (35%) having a fistula and urine leakage, but this issue frequently corrects itself. “More difficult to treat are the strictures with stenosis, which can be a problem voiding,” he said (occurring in 78/562). Other complications were 5 complete and 43 partial flap failures, 4 cases of compression syndrome, 58 cases of delayed wound healing, and 15 cases of transient ischemia. Flap failures occurred mainly in smokers, “so we don’t operate on smokers anymore,” he said.
One year after the constructive surgery, a penile prosthesis is implanted for those who want it, allowing sexual intercourse. Most individuals had orgasmic function, not because of reconnected nerves in the flap, but, Dr. Monstrey said he believes, because the clitoris, placed beneath the phallus, is denuded and stimulated during sexual activity. He said the problem is that the prostheses are usually intended for elderly men “who have sex a couple of times a month and who have a normal anatomy.” Young transmen may engage in more sexual activity, “so we have a lot of problems with exposure [of the prosthesis], infection, technical defects, and so on,” he said.
A technique gaining popularity is to use a skin flap from the groin area to make a urethra and one from the thigh to construct a penis. Although a penile transplant has recently been performed for a patient who had lost his penis to cancer, transplants are not being considered at this point, both for surgical technical reasons and because of a need for lifelong immunosuppressive drugs.
Proper referrals and counseling
The World Professional Association for Transgender Health in its Standard of Care guidelines 7 recommends one mental health professional referral for the breast surgery and two such referrals for genital surgery. The issue of possible parenthood should be discussed with patients, along with early counseling about fertility options. The age of majority and consent in different countries is important. Dr. Monstrey said genital surgery may be possible before the age of 18 years if all members of a multidisciplinary team of health professionals agree on a case by case basis that the adolescent can understand the risks, benefits, and alternatives to the surgery with the same degree of competence as someone 18 years of age or older.
Dr. Monstrey reported having no financial disclosures.
ORLANDO – Gender reassignment surgery is the most extreme step for those transgender individuals who wish to complete the transformation to the opposite sex. While many transgender people do not opt to take this step, it may be an option for people who still have gender dysphoria after a thorough diagnostic work-up by a mental health professional, hormonal treatment, and having lived in the desired gender role as a “real-life test.”
Dr. Stan Monstrey, of Ghent University Hospital, Belgium, is an experienced gender reassignment surgeon and reported at the annual meeting of the American Academy of Clinical Endocrinology that between 1995 and 2005, he saw about 20-30 new patients a year. But now, he said, “We operate on a weekly basis between a minimum of three and sometimes six or seven transsexuals, so ... in our practice, probably between 90% and 95% are still going the whole way, still want what was called initially binary surgery.”
Transwomen: Male to female
The transformation procedure for male to female begins with feminizing aesthetic procedures, such as reducing the Adam’s apple (laryngeal prominence of the thyroid cartilage) and chin, frontal boss of the forehead, and possibly other facial work such as rhinoplasty. “Sometimes minor changes can have a huge effect on the face of the patient,” Dr. Monstrey said. “This is becoming, in our opinion, increasingly important for transwomen.”
Then, in about 75% of cases, Dr. Monstrey performs at least two surgeries under the same anesthesia – breast augmentation and perineal transformation. He said even after years of hormone therapy, most such patients have only a limited amount of breast tissue but want more prominent breasts. Implants can be placed behind or in front of the pectoralis muscle via inframammary, transaxillary, or occasionally periareolar approaches. Results are immediate, and complications are rare.
Another technique, which has become very popular over the past 5-10 years, is lipofilling to fill defects and depressions in the breasts. Stem cells contained in the fat may help soften scars. But when faced with a patient who had a BRCA1 mutation, the surgeons would not use lipofilling, fearing the potential for breast cancer, and would use prostheses instead (J Sex Med. 2014 Oct;11:2496-9). Still, questions remain about even using hormone treatments in such a patient.
Dr. Monstrey mentioned that in Belgium, breast augmentation for transwomen is considered reconstructive surgery and is always reimbursed whereas it is considered aesthetic surgery and never reimbursed for non-transwomen who want larger breasts. (For transmen, breast amputation is similarly reimbursed.)
The second operation is genital transformation. Basically, the interior of the penis is removed and the skin is invaginated to form a vagina of 8-18.5 cm and a scrotal flap, along with castration and removal of the penile bulb erectile tissue (corpus spongiosum) posteriorly. It is important to protect the rectal wall, which is not very strong. The foreskin becomes the new clitoral hood and inner side of the labia minora, and the clitoris is formed by reducing and transposing the penile glans. If the patient had a small penis and not enough tissue for the reconstruction, skin flaps from various other sites can be used.
Among more than 1,200 patients, 92% could achieve orgasm. Rectovaginal fistulas occurred in 4 patients, 19 needed repositioning of the urethra, 21 needed an operation to lengthen the vagina, and 95 needed aesthetic correction of the vulva. Dr. Monstrey said many patients have asked him when they should tell their new boyfriends about their transformation, meaning that the surgery was quite convincing even with penetrative sex.
If the first operation does not work, another technique is to use an isolated piece of colon or sigmoid bowel, which has been performed completely laparoscopically by a very skilled gastroenterologic surgeon at the hospital in Ghent.
Speaking to a roomful of endocrinologists, Dr. Monstrey told them, “I’ll be the first one to agree with you that indeed puberty blockers are a very good thing. However, we as surgeons are not so enthusiastic about them because … it is impossible to create a normal vagina” because of a lack of available tissue from the underdeveloped penis.
Transmen: Female to male
“Transmen react much better to hormonal therapy than do transwomen,” he said. “If they hide their breasts they really look like men. The disadvantage is that the surgical treatment is much more complex.” The most important operation for them is subcutaneous mastectomy and male contouring. A small, semiareolar incision leaves almost no scar. Most patients still require excision of redundant skin of the breasts.
Phalloplasty is a complex operation aimed at giving the patient an aesthetic phallus, a normal scrotum, the ability to void while standing, and to perform sexual intercourse, all while protecting erogenous sensation, with minimal morbidity and mortality. Dr. Monstrey reported that he has performed 600-700 phalloplasties.
The most common technique has been to use a free vascularized flap from another bodily site with the artery, vein, and nerves to reconnect at the phalloplasty site. Because the skin is very thin on the inner forearm, it is often used and allows forming an inner tube for the urethra and an outer tube for the penis. The surgery may have to be done in three or four stages for the best results. From pictures that Dr. Monstrey showed, it was obvious that the constructed penises were not absolutely natural in appearance, but he said most patients were “rather happy” with them, despite many of these patients being quite demanding. A scrotum is constructed from transposition of the labia minora.
Unfortunately, voiding while standing is often a problem, with 197 out of 562 patients (35%) having a fistula and urine leakage, but this issue frequently corrects itself. “More difficult to treat are the strictures with stenosis, which can be a problem voiding,” he said (occurring in 78/562). Other complications were 5 complete and 43 partial flap failures, 4 cases of compression syndrome, 58 cases of delayed wound healing, and 15 cases of transient ischemia. Flap failures occurred mainly in smokers, “so we don’t operate on smokers anymore,” he said.
One year after the constructive surgery, a penile prosthesis is implanted for those who want it, allowing sexual intercourse. Most individuals had orgasmic function, not because of reconnected nerves in the flap, but, Dr. Monstrey said he believes, because the clitoris, placed beneath the phallus, is denuded and stimulated during sexual activity. He said the problem is that the prostheses are usually intended for elderly men “who have sex a couple of times a month and who have a normal anatomy.” Young transmen may engage in more sexual activity, “so we have a lot of problems with exposure [of the prosthesis], infection, technical defects, and so on,” he said.
A technique gaining popularity is to use a skin flap from the groin area to make a urethra and one from the thigh to construct a penis. Although a penile transplant has recently been performed for a patient who had lost his penis to cancer, transplants are not being considered at this point, both for surgical technical reasons and because of a need for lifelong immunosuppressive drugs.
Proper referrals and counseling
The World Professional Association for Transgender Health in its Standard of Care guidelines 7 recommends one mental health professional referral for the breast surgery and two such referrals for genital surgery. The issue of possible parenthood should be discussed with patients, along with early counseling about fertility options. The age of majority and consent in different countries is important. Dr. Monstrey said genital surgery may be possible before the age of 18 years if all members of a multidisciplinary team of health professionals agree on a case by case basis that the adolescent can understand the risks, benefits, and alternatives to the surgery with the same degree of competence as someone 18 years of age or older.
Dr. Monstrey reported having no financial disclosures.
AACE 2016

Low hematocrit in elderly portends increased bleeding post PCI
PARIS – A low hematocrit in an elderly patient who’s going to undergo percutaneous coronary intervention signals a markedly increased risk of major bleeding within 30 days of the procedure, according to Dr. David Marti.
“Analysis of hematocrit in elderly patients can guide important procedural characteristics, such as access site and antithrombotic regimen,” he said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.

For example, studies have established that transradial artery access percutaneous coronary intervention (PCI) results in significantly less bleeding than the transfemoral route, said Dr. Marti, an interventional cardiologist at the University of Alcalá in Madrid.
He presented a prospective study of 212 consecutive patients aged 75 or older who underwent PCI at a single university hospital. Their mean age was 81.4 years, and slightly over half of them presented with an acute coronary syndrome.
All patients received dual-antiplatelet therapy in accord with current guidelines. Stent type and procedural anticoagulant regimen were left to the discretion of the cardiologist; 80% of the subjects received bivalirudin-based anticoagulation.
The primary study outcome was the 30-day incidence of major bleeding, as defined by a Bleeding Academic Research Consortium (BARC) type 3-5 event. The overall rate in this elderly PCI population was 5.5%. However, the rate varied markedly by baseline hematocrit tertile, in accord with the investigators’ study hypothesis.
Major bleeding occurred in 2.9% of patients with an Hct greater than 42% and 3.1% in those with an Hct of 38%-52%, and jumped to 10.6% in the one-third of subjects whose baseline Hct was below 38%, Dr. Marti reported.
Thus, a preprocedural Hct below 38% was associated with a 4.1-fold increased risk of major bleeding within 30 days following PCI. An Hct in this range was a stronger predictor of BARC type 3-5 bleeding risk than were other factors better known as being important, including advanced age, greater body weight, female sex, or an elevated serum creatinine indicative of chronic kidney disease. Indeed, an Hct below 38% was the only statistically significant predictor of major bleeding in this elderly population.
The likely explanation for the observed results is that a low Hct level in elderly patients usually reflects subclinical blood loss that can be worsened by antithrombotic therapies, the cardiologist explained.
The presenter reported having no financial conflicts regarding this study, conducted without commercial support.
PARIS – A low hematocrit in an elderly patient who’s going to undergo percutaneous coronary intervention signals a markedly increased risk of major bleeding within 30 days of the procedure, according to Dr. David Marti.
“Analysis of hematocrit in elderly patients can guide important procedural characteristics, such as access site and antithrombotic regimen,” he said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
For example, studies have established that transradial artery access percutaneous coronary intervention (PCI) results in significantly less bleeding than the transfemoral route, said Dr. Marti, an interventional cardiologist at the University of Alcalá in Madrid.
He presented a prospective study of 212 consecutive patients aged 75 or older who underwent PCI at a single university hospital. Their mean age was 81.4 years, and slightly over half of them presented with an acute coronary syndrome.
All patients received dual-antiplatelet therapy in accord with current guidelines. Stent type and procedural anticoagulant regimen were left to the discretion of the cardiologist; 80% of the subjects received bivalirudin-based anticoagulation.
The primary study outcome was the 30-day incidence of major bleeding, as defined by a Bleeding Academic Research Consortium (BARC) type 3-5 event. The overall rate in this elderly PCI population was 5.5%. However, the rate varied markedly by baseline hematocrit tertile, in accord with the investigators’ study hypothesis.
Major bleeding occurred in 2.9% of patients with an Hct greater than 42% and 3.1% in those with an Hct of 38%-52%, and jumped to 10.6% in the one-third of subjects whose baseline Hct was below 38%, Dr. Marti reported.
Thus, a preprocedural Hct below 38% was associated with a 4.1-fold increased risk of major bleeding within 30 days following PCI. An Hct in this range was a stronger predictor of BARC type 3-5 bleeding risk than were other factors better known as being important, including advanced age, greater body weight, female sex, or an elevated serum creatinine indicative of chronic kidney disease. Indeed, an Hct below 38% was the only statistically significant predictor of major bleeding in this elderly population.
The likely explanation for the observed results is that a low Hct level in elderly patients usually reflects subclinical blood loss that can be worsened by antithrombotic therapies, the cardiologist explained.
The presenter reported having no financial conflicts regarding this study, conducted without commercial support.
PARIS – A low hematocrit in an elderly patient who’s going to undergo percutaneous coronary intervention signals a markedly increased risk of major bleeding within 30 days of the procedure, according to Dr. David Marti.
“Analysis of hematocrit in elderly patients can guide important procedural characteristics, such as access site and antithrombotic regimen,” he said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
For example, studies have established that transradial artery access percutaneous coronary intervention (PCI) results in significantly less bleeding than the transfemoral route, said Dr. Marti, an interventional cardiologist at the University of Alcalá in Madrid.
He presented a prospective study of 212 consecutive patients aged 75 or older who underwent PCI at a single university hospital. Their mean age was 81.4 years, and slightly over half of them presented with an acute coronary syndrome.
All patients received dual-antiplatelet therapy in accord with current guidelines. Stent type and procedural anticoagulant regimen were left to the discretion of the cardiologist; 80% of the subjects received bivalirudin-based anticoagulation.
The primary study outcome was the 30-day incidence of major bleeding, as defined by a Bleeding Academic Research Consortium (BARC) type 3-5 event. The overall rate in this elderly PCI population was 5.5%. However, the rate varied markedly by baseline hematocrit tertile, in accord with the investigators’ study hypothesis.
Major bleeding occurred in 2.9% of patients with an Hct greater than 42% and 3.1% in those with an Hct of 38%-52%, and jumped to 10.6% in the one-third of subjects whose baseline Hct was below 38%, Dr. Marti reported.
Thus, a preprocedural Hct below 38% was associated with a 4.1-fold increased risk of major bleeding within 30 days following PCI. An Hct in this range was a stronger predictor of BARC type 3-5 bleeding risk than were other factors better known as being important, including advanced age, greater body weight, female sex, or an elevated serum creatinine indicative of chronic kidney disease. Indeed, an Hct below 38% was the only statistically significant predictor of major bleeding in this elderly population.
The likely explanation for the observed results is that a low Hct level in elderly patients usually reflects subclinical blood loss that can be worsened by antithrombotic therapies, the cardiologist explained.
The presenter reported having no financial conflicts regarding this study, conducted without commercial support.
AT EUROPCR 2016
Key clinical point: Elderly patients scheduled for PCI have a fourfold greater risk of major bleeding within 30 days if their Hct is less than 38%.
Major finding: The 30-day incidence of BARC types 3-5 major bleeding was 10.9% in elderly patients with a pre-PCI Hct below 38%, compared with 2.9% in those in the top Hct tertile.
Data source: A prospective study of 212 consecutive patients aged 75 or older who underwent PCI at a single university hospital.
Disclosures: The presenter reported having no financial conflicts regarding this study, conducted without commercial support.

Transcatheter aortic valve implantation equivalent to surgical replacement
Transcatheter aortic valve implantation shows reductions in early and mid-term all-cause mortality similar to those with surgical aortic valve replacement, even in patients with low to intermediate surgical risk, a meta-analysis and systematic review has shown.
Dr. Giuseppe Gargiulo of Federico II University in Naples, Italy, and coauthors analyzed data from five randomized trials and 31 observational matched studies comparing mortality outcomes in 16,638 patients undergoing transcatheter aortic valve implantation (TAVI) or surgical aortic valve replacement (SAVR).
Their analysis found no statistically significant difference between the two procedures in terms of early or midterm all-cause mortality, even among patients judged as being at low to intermediate surgical risk (Ann Intern Med. 2016 Jun 7. doi: 10.7326/M16-0060).
In terms of 2- to 5-year mortality, overall there was a statistically nonsignificant increase in the risk of all-cause mortality with TAVI (odds ratio, 1.28; 95% confidence interval, 0.97-1.69), although the long-term mortality outcomes in patients in the low to intermediate surgical risk subgroup were inconclusive.
However, the authors did note significantly reduced early all-cause mortality in individuals who underwent transfemoral TAVI compared to those who underwent SAVR (OR 0.68, 95%CI, 0.53 to 0.87).
The analysis also showed that individuals who underwent TAVI had a higher incidence of permanent pacemaker implantation, vascular complications, and moderate to severe paravalvular leak, while those who underwent SAVR had more frequent incidence of major bleeding, acute kidney injury, and new-onset atrial fibrillation.
“These findings, which apply to adults with severe aortic stenosis, consolidate the role of TAVI as an alternative to SAVR,” the authors wrote. “Indeed, TAVI techniques continue to improve, newer valves address the issue of paravalvular leak, the percentage of pacemakers is decreasing, and the rate of vascular complications is expected to be lowered as the result of smaller sheaths and improved procedural techniques.”
The researchers noted that elderly patients and those with coronary artery disease showed a greater benefit from TAVI than from SAVR, suggesting that this may be because these groups have a heightened risk that favors less invasive surgical approaches.
They also found greater reductions in early mortality with TAVI when a Sapien valve was implanted, compared to a CoreValve. They noted that this was due mostly to a single large study and the effect did not persist through to the midterm follow-up.
One author reported grants from the CardioPath PhD Program, Federico II University of Naples, and from the European Association of Percutaneous Coronary Interventions, outside the submitted work. Another author declared a consultancy for Edwards Lifesciences. There were no other conflicts of interest declared.
Transcatheter aortic valve implantation shows reductions in early and mid-term all-cause mortality similar to those with surgical aortic valve replacement, even in patients with low to intermediate surgical risk, a meta-analysis and systematic review has shown.
Dr. Giuseppe Gargiulo of Federico II University in Naples, Italy, and coauthors analyzed data from five randomized trials and 31 observational matched studies comparing mortality outcomes in 16,638 patients undergoing transcatheter aortic valve implantation (TAVI) or surgical aortic valve replacement (SAVR).
Their analysis found no statistically significant difference between the two procedures in terms of early or midterm all-cause mortality, even among patients judged as being at low to intermediate surgical risk (Ann Intern Med. 2016 Jun 7. doi: 10.7326/M16-0060).
In terms of 2- to 5-year mortality, overall there was a statistically nonsignificant increase in the risk of all-cause mortality with TAVI (odds ratio, 1.28; 95% confidence interval, 0.97-1.69), although the long-term mortality outcomes in patients in the low to intermediate surgical risk subgroup were inconclusive.
However, the authors did note significantly reduced early all-cause mortality in individuals who underwent transfemoral TAVI compared to those who underwent SAVR (OR 0.68, 95%CI, 0.53 to 0.87).
The analysis also showed that individuals who underwent TAVI had a higher incidence of permanent pacemaker implantation, vascular complications, and moderate to severe paravalvular leak, while those who underwent SAVR had more frequent incidence of major bleeding, acute kidney injury, and new-onset atrial fibrillation.
“These findings, which apply to adults with severe aortic stenosis, consolidate the role of TAVI as an alternative to SAVR,” the authors wrote. “Indeed, TAVI techniques continue to improve, newer valves address the issue of paravalvular leak, the percentage of pacemakers is decreasing, and the rate of vascular complications is expected to be lowered as the result of smaller sheaths and improved procedural techniques.”
The researchers noted that elderly patients and those with coronary artery disease showed a greater benefit from TAVI than from SAVR, suggesting that this may be because these groups have a heightened risk that favors less invasive surgical approaches.
They also found greater reductions in early mortality with TAVI when a Sapien valve was implanted, compared to a CoreValve. They noted that this was due mostly to a single large study and the effect did not persist through to the midterm follow-up.
One author reported grants from the CardioPath PhD Program, Federico II University of Naples, and from the European Association of Percutaneous Coronary Interventions, outside the submitted work. Another author declared a consultancy for Edwards Lifesciences. There were no other conflicts of interest declared.
Transcatheter aortic valve implantation shows reductions in early and mid-term all-cause mortality similar to those with surgical aortic valve replacement, even in patients with low to intermediate surgical risk, a meta-analysis and systematic review has shown.
Dr. Giuseppe Gargiulo of Federico II University in Naples, Italy, and coauthors analyzed data from five randomized trials and 31 observational matched studies comparing mortality outcomes in 16,638 patients undergoing transcatheter aortic valve implantation (TAVI) or surgical aortic valve replacement (SAVR).
Their analysis found no statistically significant difference between the two procedures in terms of early or midterm all-cause mortality, even among patients judged as being at low to intermediate surgical risk (Ann Intern Med. 2016 Jun 7. doi: 10.7326/M16-0060).
In terms of 2- to 5-year mortality, overall there was a statistically nonsignificant increase in the risk of all-cause mortality with TAVI (odds ratio, 1.28; 95% confidence interval, 0.97-1.69), although the long-term mortality outcomes in patients in the low to intermediate surgical risk subgroup were inconclusive.
However, the authors did note significantly reduced early all-cause mortality in individuals who underwent transfemoral TAVI compared to those who underwent SAVR (OR 0.68, 95%CI, 0.53 to 0.87).
The analysis also showed that individuals who underwent TAVI had a higher incidence of permanent pacemaker implantation, vascular complications, and moderate to severe paravalvular leak, while those who underwent SAVR had more frequent incidence of major bleeding, acute kidney injury, and new-onset atrial fibrillation.
“These findings, which apply to adults with severe aortic stenosis, consolidate the role of TAVI as an alternative to SAVR,” the authors wrote. “Indeed, TAVI techniques continue to improve, newer valves address the issue of paravalvular leak, the percentage of pacemakers is decreasing, and the rate of vascular complications is expected to be lowered as the result of smaller sheaths and improved procedural techniques.”
The researchers noted that elderly patients and those with coronary artery disease showed a greater benefit from TAVI than from SAVR, suggesting that this may be because these groups have a heightened risk that favors less invasive surgical approaches.
They also found greater reductions in early mortality with TAVI when a Sapien valve was implanted, compared to a CoreValve. They noted that this was due mostly to a single large study and the effect did not persist through to the midterm follow-up.
One author reported grants from the CardioPath PhD Program, Federico II University of Naples, and from the European Association of Percutaneous Coronary Interventions, outside the submitted work. Another author declared a consultancy for Edwards Lifesciences. There were no other conflicts of interest declared.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical point: Transcatheter aortic valve implantation shows reductions in early and mid-term all-cause mortality similar to those of surgical aortic valve replacement.
Major finding: Transcatheter aortic valve implantation and surgical aortic valve replacement show similar reductions in mortality, even in patients at low to intermediate surgical risk.
Data source: Systematic review and meta-analysis.
Disclosures: One author reported grants from the CardioPath PhD Program, Federico II University of Naples, and from the European Association of Percutaneous Coronary Interventions, outside the submitted work. Another author declared a consultancy for Edwards Lifesciences. There were no other conflicts of interest declared.
Infliximab fails as salvage treatment for severe ulcerative colitis
LOS ANGELES – The inpatient use of infliximab for severe ulcerative colitis does not avoid the need for colectomy in patients who fail steroid therapy, results from a single-center study demonstrated.
In an interview at the annual meeting of the American Society of Colon and Rectal Surgeons, lead study author Dr. Rachel E. Andrew, a third-year resident in the department of surgery at Penn State Hershey Medical Center in Hershey, Pa., said that despite recent interest in providing inpatient infliximab as an alternative to surgery for those with steroid-refractory disease, 82% of those who received salvage infliximab went on to undergo a total abdominal colectomy during the same admission.

“Our findings suggest that inpatient infliximab was not effective at improving the severity of colitis in these patients,” she said. “Further, infliximab was unreliable in avoiding the need for a total colectomy in this population of ulcerative colitis patients. One difference between our study and those previously published on this subject is that our study focuses on patients with a severity of colitis that resulted in their admission to a surgery service. In terms of evaluating the benefit of infliximab and providing a reliable avoidance of colectomy, we feel that this population of ulcerative colitis patients would be most appropriate to evaluate this issue. This possible difference in patient population may explain the difference in our study findings and those previously published.”
The researchers compared colectomy rates in 173 patients with severe ulcerative colitis who were admitted to the colorectal surgery service at Penn State Hershey Medical Center. Their mean age was 41 years, with 155 (90%) treated with high-dose steroids alone, and with 18 (10%) having received inpatient infliximab as salvage therapy due to a lack of response to steroids alone. Of the patients who received high-dose steroids alone, 81 (52%) required total colectomy, compared with 14 (82%) who received infliximab salvage therapy (P = .046).
The researchers observed no statistically significant differences between the two groups regarding rates of hospital readmission, superficial, deep and organ space surgical-site infections, unplanned return to the operating room, and all complication rates (P greater than .05). Among patients who required total colectomy, hospital costs were 27% higher among those who received infliximab compared with those who received high-dose steroids alone (a mean of $19,880 vs. $14,492, respectively), but because of the small sample size of the infliximab cohort this difference did not reach statistical significance.
“In our institution, salvage infliximab has not been shown to be effective,” Dr. Andrew said. “One key difference between our findings and other studies is that our study population had a high colectomy rate; 82% is much higher than the approximately 30% colectomy rate described in many reports from colleagues in gastroenterology. While there are several potential explanations for our higher rate of colectomy, including the potential concerns that surgeons might be inclined to opt for surgery more readily than non-surgical providers, it is likely that the patients in our study had more severe forms of colitis. It might be the case that there are certain severities of colitis that are beyond the ability of infliximab to salvage, which would be an important issue in selecting which patients to provide inpatient infliximab, so as to not unnecessarily delay surgery, increase hospital costs and to avoid escalating the degree of immunosuppression without a reasonable likelihood of clinical improvement.”
Dr. Andrew reported having no financial disclosures.
LOS ANGELES – The inpatient use of infliximab for severe ulcerative colitis does not avoid the need for colectomy in patients who fail steroid therapy, results from a single-center study demonstrated.
In an interview at the annual meeting of the American Society of Colon and Rectal Surgeons, lead study author Dr. Rachel E. Andrew, a third-year resident in the department of surgery at Penn State Hershey Medical Center in Hershey, Pa., said that despite recent interest in providing inpatient infliximab as an alternative to surgery for those with steroid-refractory disease, 82% of those who received salvage infliximab went on to undergo a total abdominal colectomy during the same admission.
“Our findings suggest that inpatient infliximab was not effective at improving the severity of colitis in these patients,” she said. “Further, infliximab was unreliable in avoiding the need for a total colectomy in this population of ulcerative colitis patients. One difference between our study and those previously published on this subject is that our study focuses on patients with a severity of colitis that resulted in their admission to a surgery service. In terms of evaluating the benefit of infliximab and providing a reliable avoidance of colectomy, we feel that this population of ulcerative colitis patients would be most appropriate to evaluate this issue. This possible difference in patient population may explain the difference in our study findings and those previously published.”
The researchers compared colectomy rates in 173 patients with severe ulcerative colitis who were admitted to the colorectal surgery service at Penn State Hershey Medical Center. Their mean age was 41 years, with 155 (90%) treated with high-dose steroids alone, and with 18 (10%) having received inpatient infliximab as salvage therapy due to a lack of response to steroids alone. Of the patients who received high-dose steroids alone, 81 (52%) required total colectomy, compared with 14 (82%) who received infliximab salvage therapy (P = .046).
The researchers observed no statistically significant differences between the two groups regarding rates of hospital readmission, superficial, deep and organ space surgical-site infections, unplanned return to the operating room, and all complication rates (P greater than .05). Among patients who required total colectomy, hospital costs were 27% higher among those who received infliximab compared with those who received high-dose steroids alone (a mean of $19,880 vs. $14,492, respectively), but because of the small sample size of the infliximab cohort this difference did not reach statistical significance.
“In our institution, salvage infliximab has not been shown to be effective,” Dr. Andrew said. “One key difference between our findings and other studies is that our study population had a high colectomy rate; 82% is much higher than the approximately 30% colectomy rate described in many reports from colleagues in gastroenterology. While there are several potential explanations for our higher rate of colectomy, including the potential concerns that surgeons might be inclined to opt for surgery more readily than non-surgical providers, it is likely that the patients in our study had more severe forms of colitis. It might be the case that there are certain severities of colitis that are beyond the ability of infliximab to salvage, which would be an important issue in selecting which patients to provide inpatient infliximab, so as to not unnecessarily delay surgery, increase hospital costs and to avoid escalating the degree of immunosuppression without a reasonable likelihood of clinical improvement.”
Dr. Andrew reported having no financial disclosures.
LOS ANGELES – The inpatient use of infliximab for severe ulcerative colitis does not avoid the need for colectomy in patients who fail steroid therapy, results from a single-center study demonstrated.
In an interview at the annual meeting of the American Society of Colon and Rectal Surgeons, lead study author Dr. Rachel E. Andrew, a third-year resident in the department of surgery at Penn State Hershey Medical Center in Hershey, Pa., said that despite recent interest in providing inpatient infliximab as an alternative to surgery for those with steroid-refractory disease, 82% of those who received salvage infliximab went on to undergo a total abdominal colectomy during the same admission.
“Our findings suggest that inpatient infliximab was not effective at improving the severity of colitis in these patients,” she said. “Further, infliximab was unreliable in avoiding the need for a total colectomy in this population of ulcerative colitis patients. One difference between our study and those previously published on this subject is that our study focuses on patients with a severity of colitis that resulted in their admission to a surgery service. In terms of evaluating the benefit of infliximab and providing a reliable avoidance of colectomy, we feel that this population of ulcerative colitis patients would be most appropriate to evaluate this issue. This possible difference in patient population may explain the difference in our study findings and those previously published.”
The researchers compared colectomy rates in 173 patients with severe ulcerative colitis who were admitted to the colorectal surgery service at Penn State Hershey Medical Center. Their mean age was 41 years, with 155 (90%) treated with high-dose steroids alone, and with 18 (10%) having received inpatient infliximab as salvage therapy due to a lack of response to steroids alone. Of the patients who received high-dose steroids alone, 81 (52%) required total colectomy, compared with 14 (82%) who received infliximab salvage therapy (P = .046).
The researchers observed no statistically significant differences between the two groups regarding rates of hospital readmission, superficial, deep and organ space surgical-site infections, unplanned return to the operating room, and all complication rates (P greater than .05). Among patients who required total colectomy, hospital costs were 27% higher among those who received infliximab compared with those who received high-dose steroids alone (a mean of $19,880 vs. $14,492, respectively), but because of the small sample size of the infliximab cohort this difference did not reach statistical significance.
“In our institution, salvage infliximab has not been shown to be effective,” Dr. Andrew said. “One key difference between our findings and other studies is that our study population had a high colectomy rate; 82% is much higher than the approximately 30% colectomy rate described in many reports from colleagues in gastroenterology. While there are several potential explanations for our higher rate of colectomy, including the potential concerns that surgeons might be inclined to opt for surgery more readily than non-surgical providers, it is likely that the patients in our study had more severe forms of colitis. It might be the case that there are certain severities of colitis that are beyond the ability of infliximab to salvage, which would be an important issue in selecting which patients to provide inpatient infliximab, so as to not unnecessarily delay surgery, increase hospital costs and to avoid escalating the degree of immunosuppression without a reasonable likelihood of clinical improvement.”
Dr. Andrew reported having no financial disclosures.
AT THE ASCRS ANNUAL MEETING
Key clinical point: Infliximab was not effective as inpatient salvage therapy for severe ulcerative colitis.
Major finding: Of patients who received high-dose steroids alone, 81 (52%) required total colectomy, compared with 14 (82%) who received infliximab salvage therapy (P = .046).
Data source: A study of 173 patients with severe ulcerative colitis who were admitted to the colorectal surgery service at Penn State Hershey Medical Center.
Disclosures: Dr. Andrew reported having no financial disclosures.

Experts endorse metabolic surgery for diabetes intervention
Metabolic surgery should be recommended for obese patients with type 2 diabetes mellitus, according to an international consensus statement from 48 clinicians and scholars issued after the Second Diabetes Surgery Summit held as part of the World Congress on Interventional Therapies for Type 2 Diabetes in London in 2015.
Current treatment plans for patients with type 2 diabetes do no include bariatric/metabolic surgery, despite increasing evidence of improved glycemic control and reduced cardiovascular risk factors in surgically treated patients, wrote Dr. Francesco Rubino and colleagues on behalf of members of the Second Diabetes Surgery Summit (DSS-II). The guidelines were endorsed by 45 global medical and scientific societies at the time of publication. The statement was published in a special edition of Diabetes Care (Diabetes Care. 2016;39:861-77. doi:10.2337/dc16-0236).

The guidelines recommend metabolic surgery for patients with type 2 diabetes who have class III obesity (defined as a body mass index of at least 40 kg/m2) or class II obesity (defined as a BMI of 35 kg/m2-39.9 kg/m2). In addition, metabolic surgery should be considered as a option for those patients with type 2 diabetes whose BMI falls within the 30 kg/m2-34.9 kg/m2 range if hyperglycemia remains uncontrolled after treatment attempts with oral or injectable medications. For Asian patients, the BMI thresholds for surgery should be reduced by 2.5 kg/m2, the researchers noted.
The conclusions are based on a review of published evidence on metabolic surgery and type 2 diabetes from January 1, 2005, through September 30, 2015.
The researchers assessed the evidence based on factors including long-term effects of surgery on glycemic control, effectiveness of surgery compared with nonsurgical interventions, comparisons of surgical procedures, and effects of surgery on diabetes complications, cardiovascular risk factors, and mortality. They also considered the short- and long-term safety of different procedures. The recommendations offer guidance on patient selection, pre- and postoperative workups, choice of procedure, and defining goals and success of surgery.
“The success of metabolic surgery needs to be defined in the larger context of comprehensive diabetes care plans,” the researchers noted. “Metabolic surgery should be considered a means to achieve the glycemic control necessary to reduce risk of microvascular complications and CVD.”
The researchers acknowledged that complications from metabolic surgery may require reoperations and rehospitalizations. Other limitations include a lack of evidence in several areas including: cost-effectiveness, optimal nutrition management after surgery, postoperative lifestyle interventions, and long-term effects of surgery, and further research is needed.
However, “there is now sufficient clinical and mechanistic evidence to support inclusion of GI surgery among antidiabetes interventions for people with type 2 diabetes and obesity,” the researchers said. They called for collaboration between clinicians and regulators to recognize the potential value of metabolic surgery for type 2 diabetes and develop appropriate reimbursement plans.
The DSS-II and WCITD 2015 were sponsored by the International Diabetes Society Task Force, King’s College London, King’s College Hospital, Johnson & Johnson, Medtronic, Medimmune, Fractyl, DIAMOND MetaCure, Gore, Novo Nordisk, and NGM Biopharmaceuticals. The researchers reported no relevant conflicts.
“The new guidelines provide much needed guidance for general practitioners, endocrinologists, and diabetes specialists about the use of metabolic surgery in the treatment of obese patients with type 2 diabetes,” wrote Dr. William T. Cefalu and colleagues in an accompanying editorial.
However, “one of the many issues that remains unanswered for metabolic surgery pertains to the exact mechanism of action. Specifically, we now recognize that postoperative improvements in metabolic control occur rapidly and out of proportion to weight loss, yet the physiological and molecular mechanisms underlying these beneficial glycemic effects remain incompletely elucidated,” they wrote. In addition, “before we can fully appreciate the role of metabolic surgery in becoming a readily available, viable option in our treatment algorithm and expand the appropriate candidate pool, we need to fully understand the efficacy, complications, long-term clinical outcomes, and costs. In particular, it will be important to clarify the financial implications to patients, providers, and insurers (both private and government sectors) and to appreciate that these barriers may be hard to overcome in resource poor areas of the world,” they said.
“It is an exciting time for those of us in diabetes research, and the ability to be part of a paradigm change in the understanding, approach, and management of the disease will keep us focused on the next steps to address the larger issue of prevention,” they noted (Diabetes Care. 2016;39:857-60. doi:10.2337/dc16-0686) .
Dr. Cefalu is affiliated with the Pennington Biomedical Research Center at Louisiana State University in Baton Rouge, La. He disclosed financial relationships with multiple companies including AstraZeneca, Janssen, MannKind Corp., Intarcia Therapeutics, and Sanofi.
“The new guidelines provide much needed guidance for general practitioners, endocrinologists, and diabetes specialists about the use of metabolic surgery in the treatment of obese patients with type 2 diabetes,” wrote Dr. William T. Cefalu and colleagues in an accompanying editorial.
However, “one of the many issues that remains unanswered for metabolic surgery pertains to the exact mechanism of action. Specifically, we now recognize that postoperative improvements in metabolic control occur rapidly and out of proportion to weight loss, yet the physiological and molecular mechanisms underlying these beneficial glycemic effects remain incompletely elucidated,” they wrote. In addition, “before we can fully appreciate the role of metabolic surgery in becoming a readily available, viable option in our treatment algorithm and expand the appropriate candidate pool, we need to fully understand the efficacy, complications, long-term clinical outcomes, and costs. In particular, it will be important to clarify the financial implications to patients, providers, and insurers (both private and government sectors) and to appreciate that these barriers may be hard to overcome in resource poor areas of the world,” they said.
“It is an exciting time for those of us in diabetes research, and the ability to be part of a paradigm change in the understanding, approach, and management of the disease will keep us focused on the next steps to address the larger issue of prevention,” they noted (Diabetes Care. 2016;39:857-60. doi:10.2337/dc16-0686) .
Dr. Cefalu is affiliated with the Pennington Biomedical Research Center at Louisiana State University in Baton Rouge, La. He disclosed financial relationships with multiple companies including AstraZeneca, Janssen, MannKind Corp., Intarcia Therapeutics, and Sanofi.
“The new guidelines provide much needed guidance for general practitioners, endocrinologists, and diabetes specialists about the use of metabolic surgery in the treatment of obese patients with type 2 diabetes,” wrote Dr. William T. Cefalu and colleagues in an accompanying editorial.
However, “one of the many issues that remains unanswered for metabolic surgery pertains to the exact mechanism of action. Specifically, we now recognize that postoperative improvements in metabolic control occur rapidly and out of proportion to weight loss, yet the physiological and molecular mechanisms underlying these beneficial glycemic effects remain incompletely elucidated,” they wrote. In addition, “before we can fully appreciate the role of metabolic surgery in becoming a readily available, viable option in our treatment algorithm and expand the appropriate candidate pool, we need to fully understand the efficacy, complications, long-term clinical outcomes, and costs. In particular, it will be important to clarify the financial implications to patients, providers, and insurers (both private and government sectors) and to appreciate that these barriers may be hard to overcome in resource poor areas of the world,” they said.
“It is an exciting time for those of us in diabetes research, and the ability to be part of a paradigm change in the understanding, approach, and management of the disease will keep us focused on the next steps to address the larger issue of prevention,” they noted (Diabetes Care. 2016;39:857-60. doi:10.2337/dc16-0686) .
Dr. Cefalu is affiliated with the Pennington Biomedical Research Center at Louisiana State University in Baton Rouge, La. He disclosed financial relationships with multiple companies including AstraZeneca, Janssen, MannKind Corp., Intarcia Therapeutics, and Sanofi.
Metabolic surgery should be recommended for obese patients with type 2 diabetes mellitus, according to an international consensus statement from 48 clinicians and scholars issued after the Second Diabetes Surgery Summit held as part of the World Congress on Interventional Therapies for Type 2 Diabetes in London in 2015.
Current treatment plans for patients with type 2 diabetes do no include bariatric/metabolic surgery, despite increasing evidence of improved glycemic control and reduced cardiovascular risk factors in surgically treated patients, wrote Dr. Francesco Rubino and colleagues on behalf of members of the Second Diabetes Surgery Summit (DSS-II). The guidelines were endorsed by 45 global medical and scientific societies at the time of publication. The statement was published in a special edition of Diabetes Care (Diabetes Care. 2016;39:861-77. doi:10.2337/dc16-0236).
The guidelines recommend metabolic surgery for patients with type 2 diabetes who have class III obesity (defined as a body mass index of at least 40 kg/m2) or class II obesity (defined as a BMI of 35 kg/m2-39.9 kg/m2). In addition, metabolic surgery should be considered as a option for those patients with type 2 diabetes whose BMI falls within the 30 kg/m2-34.9 kg/m2 range if hyperglycemia remains uncontrolled after treatment attempts with oral or injectable medications. For Asian patients, the BMI thresholds for surgery should be reduced by 2.5 kg/m2, the researchers noted.
The conclusions are based on a review of published evidence on metabolic surgery and type 2 diabetes from January 1, 2005, through September 30, 2015.
The researchers assessed the evidence based on factors including long-term effects of surgery on glycemic control, effectiveness of surgery compared with nonsurgical interventions, comparisons of surgical procedures, and effects of surgery on diabetes complications, cardiovascular risk factors, and mortality. They also considered the short- and long-term safety of different procedures. The recommendations offer guidance on patient selection, pre- and postoperative workups, choice of procedure, and defining goals and success of surgery.
“The success of metabolic surgery needs to be defined in the larger context of comprehensive diabetes care plans,” the researchers noted. “Metabolic surgery should be considered a means to achieve the glycemic control necessary to reduce risk of microvascular complications and CVD.”
The researchers acknowledged that complications from metabolic surgery may require reoperations and rehospitalizations. Other limitations include a lack of evidence in several areas including: cost-effectiveness, optimal nutrition management after surgery, postoperative lifestyle interventions, and long-term effects of surgery, and further research is needed.
However, “there is now sufficient clinical and mechanistic evidence to support inclusion of GI surgery among antidiabetes interventions for people with type 2 diabetes and obesity,” the researchers said. They called for collaboration between clinicians and regulators to recognize the potential value of metabolic surgery for type 2 diabetes and develop appropriate reimbursement plans.
The DSS-II and WCITD 2015 were sponsored by the International Diabetes Society Task Force, King’s College London, King’s College Hospital, Johnson & Johnson, Medtronic, Medimmune, Fractyl, DIAMOND MetaCure, Gore, Novo Nordisk, and NGM Biopharmaceuticals. The researchers reported no relevant conflicts.
Metabolic surgery should be recommended for obese patients with type 2 diabetes mellitus, according to an international consensus statement from 48 clinicians and scholars issued after the Second Diabetes Surgery Summit held as part of the World Congress on Interventional Therapies for Type 2 Diabetes in London in 2015.
Current treatment plans for patients with type 2 diabetes do no include bariatric/metabolic surgery, despite increasing evidence of improved glycemic control and reduced cardiovascular risk factors in surgically treated patients, wrote Dr. Francesco Rubino and colleagues on behalf of members of the Second Diabetes Surgery Summit (DSS-II). The guidelines were endorsed by 45 global medical and scientific societies at the time of publication. The statement was published in a special edition of Diabetes Care (Diabetes Care. 2016;39:861-77. doi:10.2337/dc16-0236).
The guidelines recommend metabolic surgery for patients with type 2 diabetes who have class III obesity (defined as a body mass index of at least 40 kg/m2) or class II obesity (defined as a BMI of 35 kg/m2-39.9 kg/m2). In addition, metabolic surgery should be considered as a option for those patients with type 2 diabetes whose BMI falls within the 30 kg/m2-34.9 kg/m2 range if hyperglycemia remains uncontrolled after treatment attempts with oral or injectable medications. For Asian patients, the BMI thresholds for surgery should be reduced by 2.5 kg/m2, the researchers noted.
The conclusions are based on a review of published evidence on metabolic surgery and type 2 diabetes from January 1, 2005, through September 30, 2015.
The researchers assessed the evidence based on factors including long-term effects of surgery on glycemic control, effectiveness of surgery compared with nonsurgical interventions, comparisons of surgical procedures, and effects of surgery on diabetes complications, cardiovascular risk factors, and mortality. They also considered the short- and long-term safety of different procedures. The recommendations offer guidance on patient selection, pre- and postoperative workups, choice of procedure, and defining goals and success of surgery.
“The success of metabolic surgery needs to be defined in the larger context of comprehensive diabetes care plans,” the researchers noted. “Metabolic surgery should be considered a means to achieve the glycemic control necessary to reduce risk of microvascular complications and CVD.”
The researchers acknowledged that complications from metabolic surgery may require reoperations and rehospitalizations. Other limitations include a lack of evidence in several areas including: cost-effectiveness, optimal nutrition management after surgery, postoperative lifestyle interventions, and long-term effects of surgery, and further research is needed.
However, “there is now sufficient clinical and mechanistic evidence to support inclusion of GI surgery among antidiabetes interventions for people with type 2 diabetes and obesity,” the researchers said. They called for collaboration between clinicians and regulators to recognize the potential value of metabolic surgery for type 2 diabetes and develop appropriate reimbursement plans.
The DSS-II and WCITD 2015 were sponsored by the International Diabetes Society Task Force, King’s College London, King’s College Hospital, Johnson & Johnson, Medtronic, Medimmune, Fractyl, DIAMOND MetaCure, Gore, Novo Nordisk, and NGM Biopharmaceuticals. The researchers reported no relevant conflicts.
FROM DIABETES CARE
Key clinical point: Metabolic surgery should be recommended for obese patients with type 2 diabetes mellitus.
Major finding: Surgery is recommended for patients with type 2 diabetes who have a BMI of 35 kg/m2 or higher and should be considered for patients with a BMI of 30 kg/m2-34.9 kg/m2 with uncontrolled hyperglycemia.
Data source: Published evidence on metabolic surgery and type 2 diabetes identified on Medline between January 1, 2005 and September 30, 2015.
Disclosures: The DSS-II and WCITD 2015 were sponsored by the International Diabetes Society Task Force, King’s College London, King’s College Hospital, Johnson & Johnson, Medtronic, Medimmune, Fractyl, DIAMOND MetaCure, Gore, Novo Nordisk, and NGM Biopharmaceuticals. The researchers reported no relevant conflicts.

Study eyes impact of surgical safety checklists on mortality
After implementation of surgical safety checklists in a tertiary care hospital, researchers observed a 27% reduction of risk-adjusted all-cause 90-day mortality, but adjusted all-cause 30-day mortality remained unchanged.
In addition, length of stay was reduced but 30-day readmission rate was not, according to the study published online in JAMA Surgery. Those key findings are from an effort to assess the association between the implementation of surgical safety checklists (SSCs) and rates of all-cause 90- and 30-day mortality.

Previous studies have analyzed in-hospital mortality or 30-day mortality “but not intermediate-term outcome variables,” said lead author Dr. Matthias Bock of the department of anesthesiology and intensive care medicine at Merano Hospital, Merano, Italy. “Almost one-quarter (23.6%) of the deaths within 30 days after surgery occurred after discharge, and 39.7% of patients undergoing surgery experienced only post-discharge complications. Ninety-day mortality often doubles 30-day mortality. In-hospital mortality and 30-day mortality might therefore underreport the real risk to these patients, especially after tumor surgery or among the elderly. Studies of the effect or the association of the implementation of surgical safety checklists (SSCs) on 90-day mortality are lacking.”
Dr. Bock and his associates retrospectively evaluated the outcomes of surgical procedures performed during the six months before and six months after implementation of SSCs at the 715-bed Central Hospital of Bolzano (CHB) in Italy (Jan. 1-June 30, 2010, and Jan. 1-June 30, 2013, respectively). The key outcome measures were risk-adjusted rates of 90- and 30-day mortality, readmission rate, and LOS (JAMA Surg. 2016 Feb 3. doi:10.1001/jamasurg.2015.5490).
The study sample consisted of 10,741 patients, including 5,444 pre-intervention and 5,297 post-intervention patients. Of these, 53% were female and their mean age was 53 years.
The researchers reported that 90-day all-cause mortality was 2.4% before SSC implementation, compared with 2.2% after implementation, for an adjusted odds ratio (AOR) of 0.73 (P = .02). However, 30-day all-cause mortality was 1.36% before SSC implementation, compared with 1.32% after implementation, for an AOR of 0.79 (P = .17), remaining essentially unchanged.
Dr. Bock and his associates also found that 30-day readmission rates were similar in the pre-implementation and post-implementation groups (14.6% vs. 14.5%, respectively: P = .90), but the adjusted length of stay favored the post-implementation group (a mean of 9.6 days, compared with a mean of 10.4 days in the in the pre-implementation group; P less than .001).
The researchers acknowledged certain limitations of the study, including its single-center design and the lack of a control group. “The study design highly reduces the risk for observation bias (Hawthorne effect),” they wrote. “Furthermore, we did not inform the staff about the purpose of our study. We analyzed only objective outcome data to reduce reporting bias as much as possible.”
The finding of a decline in LOS “suggests potential cost savings after the implementation of SSCs,” they concluded. “Further trials should address this hypothesis and the effect on quality of care owing to a reduction of the costs of complications or unplanned reoperations.”
The study was supported by the Public Health Care Company of South Tyrol, Italy, and by the Autonomous Province of Bolzano, Italy. The researchers reported having no financial disclosures.
We commend the authors for choosing to focus on the 90-day postoperative all-cause mortality rate, and we are reassured that they saw a statistically significant decrease. However, we should also consider why no statistically significant change in the 30-day postoperative all-cause mortality rate was observed. This finding could be attributable to inherent differences in the population studied, to the case mix, or to insufficient power to detect change related to sample size.
This article also highlights the ongoing challenges of checklist implementation and measurement of the impact of the SSC. First, whether SSC performance underwent direct observation during implementation and whether that observation compared with reported performance are unclear. Checklist performance appears to be measured primarily by checking whether a form was completed. Significant discordance between paper checklist completion and actual completion has been described. Second, 80% completion was considered the threshold for complete implementation in this study, whereas recent literature supports that full rather than partial checklist completion provides an opportunity for significant improvement of the effect of the SSC on the quality of patient care and surgical safety. With more effective implementation and full SSC use in every case, the improvement in outcomes seen could have been even. If the SSC is not used, it cannot help.
These comments were extracted from an editorial that appeared online in JAMA Surgery (JAMA Surg. 2016 Feb 3. doi:10.1001/jamasurg.2015.5551). Dr. William Berry is with the department of health policy and management at Harvard School of Public Health, Boston; Dr. Alex Haynes is with the department of surgical oncology at Massachusetts General Hospital, Boston; and Dr. Janaka Lagoo is with the Harvard School of Public Health and Brigham and Women’s Hospital, Boston. The authors reported having no financial disclosures.
We commend the authors for choosing to focus on the 90-day postoperative all-cause mortality rate, and we are reassured that they saw a statistically significant decrease. However, we should also consider why no statistically significant change in the 30-day postoperative all-cause mortality rate was observed. This finding could be attributable to inherent differences in the population studied, to the case mix, or to insufficient power to detect change related to sample size.
This article also highlights the ongoing challenges of checklist implementation and measurement of the impact of the SSC. First, whether SSC performance underwent direct observation during implementation and whether that observation compared with reported performance are unclear. Checklist performance appears to be measured primarily by checking whether a form was completed. Significant discordance between paper checklist completion and actual completion has been described. Second, 80% completion was considered the threshold for complete implementation in this study, whereas recent literature supports that full rather than partial checklist completion provides an opportunity for significant improvement of the effect of the SSC on the quality of patient care and surgical safety. With more effective implementation and full SSC use in every case, the improvement in outcomes seen could have been even. If the SSC is not used, it cannot help.
These comments were extracted from an editorial that appeared online in JAMA Surgery (JAMA Surg. 2016 Feb 3. doi:10.1001/jamasurg.2015.5551). Dr. William Berry is with the department of health policy and management at Harvard School of Public Health, Boston; Dr. Alex Haynes is with the department of surgical oncology at Massachusetts General Hospital, Boston; and Dr. Janaka Lagoo is with the Harvard School of Public Health and Brigham and Women’s Hospital, Boston. The authors reported having no financial disclosures.
We commend the authors for choosing to focus on the 90-day postoperative all-cause mortality rate, and we are reassured that they saw a statistically significant decrease. However, we should also consider why no statistically significant change in the 30-day postoperative all-cause mortality rate was observed. This finding could be attributable to inherent differences in the population studied, to the case mix, or to insufficient power to detect change related to sample size.
This article also highlights the ongoing challenges of checklist implementation and measurement of the impact of the SSC. First, whether SSC performance underwent direct observation during implementation and whether that observation compared with reported performance are unclear. Checklist performance appears to be measured primarily by checking whether a form was completed. Significant discordance between paper checklist completion and actual completion has been described. Second, 80% completion was considered the threshold for complete implementation in this study, whereas recent literature supports that full rather than partial checklist completion provides an opportunity for significant improvement of the effect of the SSC on the quality of patient care and surgical safety. With more effective implementation and full SSC use in every case, the improvement in outcomes seen could have been even. If the SSC is not used, it cannot help.
These comments were extracted from an editorial that appeared online in JAMA Surgery (JAMA Surg. 2016 Feb 3. doi:10.1001/jamasurg.2015.5551). Dr. William Berry is with the department of health policy and management at Harvard School of Public Health, Boston; Dr. Alex Haynes is with the department of surgical oncology at Massachusetts General Hospital, Boston; and Dr. Janaka Lagoo is with the Harvard School of Public Health and Brigham and Women’s Hospital, Boston. The authors reported having no financial disclosures.
After implementation of surgical safety checklists in a tertiary care hospital, researchers observed a 27% reduction of risk-adjusted all-cause 90-day mortality, but adjusted all-cause 30-day mortality remained unchanged.
In addition, length of stay was reduced but 30-day readmission rate was not, according to the study published online in JAMA Surgery. Those key findings are from an effort to assess the association between the implementation of surgical safety checklists (SSCs) and rates of all-cause 90- and 30-day mortality.
Previous studies have analyzed in-hospital mortality or 30-day mortality “but not intermediate-term outcome variables,” said lead author Dr. Matthias Bock of the department of anesthesiology and intensive care medicine at Merano Hospital, Merano, Italy. “Almost one-quarter (23.6%) of the deaths within 30 days after surgery occurred after discharge, and 39.7% of patients undergoing surgery experienced only post-discharge complications. Ninety-day mortality often doubles 30-day mortality. In-hospital mortality and 30-day mortality might therefore underreport the real risk to these patients, especially after tumor surgery or among the elderly. Studies of the effect or the association of the implementation of surgical safety checklists (SSCs) on 90-day mortality are lacking.”
Dr. Bock and his associates retrospectively evaluated the outcomes of surgical procedures performed during the six months before and six months after implementation of SSCs at the 715-bed Central Hospital of Bolzano (CHB) in Italy (Jan. 1-June 30, 2010, and Jan. 1-June 30, 2013, respectively). The key outcome measures were risk-adjusted rates of 90- and 30-day mortality, readmission rate, and LOS (JAMA Surg. 2016 Feb 3. doi:10.1001/jamasurg.2015.5490).
The study sample consisted of 10,741 patients, including 5,444 pre-intervention and 5,297 post-intervention patients. Of these, 53% were female and their mean age was 53 years.
The researchers reported that 90-day all-cause mortality was 2.4% before SSC implementation, compared with 2.2% after implementation, for an adjusted odds ratio (AOR) of 0.73 (P = .02). However, 30-day all-cause mortality was 1.36% before SSC implementation, compared with 1.32% after implementation, for an AOR of 0.79 (P = .17), remaining essentially unchanged.
Dr. Bock and his associates also found that 30-day readmission rates were similar in the pre-implementation and post-implementation groups (14.6% vs. 14.5%, respectively: P = .90), but the adjusted length of stay favored the post-implementation group (a mean of 9.6 days, compared with a mean of 10.4 days in the in the pre-implementation group; P less than .001).
The researchers acknowledged certain limitations of the study, including its single-center design and the lack of a control group. “The study design highly reduces the risk for observation bias (Hawthorne effect),” they wrote. “Furthermore, we did not inform the staff about the purpose of our study. We analyzed only objective outcome data to reduce reporting bias as much as possible.”
The finding of a decline in LOS “suggests potential cost savings after the implementation of SSCs,” they concluded. “Further trials should address this hypothesis and the effect on quality of care owing to a reduction of the costs of complications or unplanned reoperations.”
The study was supported by the Public Health Care Company of South Tyrol, Italy, and by the Autonomous Province of Bolzano, Italy. The researchers reported having no financial disclosures.
After implementation of surgical safety checklists in a tertiary care hospital, researchers observed a 27% reduction of risk-adjusted all-cause 90-day mortality, but adjusted all-cause 30-day mortality remained unchanged.
In addition, length of stay was reduced but 30-day readmission rate was not, according to the study published online in JAMA Surgery. Those key findings are from an effort to assess the association between the implementation of surgical safety checklists (SSCs) and rates of all-cause 90- and 30-day mortality.
Previous studies have analyzed in-hospital mortality or 30-day mortality “but not intermediate-term outcome variables,” said lead author Dr. Matthias Bock of the department of anesthesiology and intensive care medicine at Merano Hospital, Merano, Italy. “Almost one-quarter (23.6%) of the deaths within 30 days after surgery occurred after discharge, and 39.7% of patients undergoing surgery experienced only post-discharge complications. Ninety-day mortality often doubles 30-day mortality. In-hospital mortality and 30-day mortality might therefore underreport the real risk to these patients, especially after tumor surgery or among the elderly. Studies of the effect or the association of the implementation of surgical safety checklists (SSCs) on 90-day mortality are lacking.”
Dr. Bock and his associates retrospectively evaluated the outcomes of surgical procedures performed during the six months before and six months after implementation of SSCs at the 715-bed Central Hospital of Bolzano (CHB) in Italy (Jan. 1-June 30, 2010, and Jan. 1-June 30, 2013, respectively). The key outcome measures were risk-adjusted rates of 90- and 30-day mortality, readmission rate, and LOS (JAMA Surg. 2016 Feb 3. doi:10.1001/jamasurg.2015.5490).
The study sample consisted of 10,741 patients, including 5,444 pre-intervention and 5,297 post-intervention patients. Of these, 53% were female and their mean age was 53 years.
The researchers reported that 90-day all-cause mortality was 2.4% before SSC implementation, compared with 2.2% after implementation, for an adjusted odds ratio (AOR) of 0.73 (P = .02). However, 30-day all-cause mortality was 1.36% before SSC implementation, compared with 1.32% after implementation, for an AOR of 0.79 (P = .17), remaining essentially unchanged.
Dr. Bock and his associates also found that 30-day readmission rates were similar in the pre-implementation and post-implementation groups (14.6% vs. 14.5%, respectively: P = .90), but the adjusted length of stay favored the post-implementation group (a mean of 9.6 days, compared with a mean of 10.4 days in the in the pre-implementation group; P less than .001).
The researchers acknowledged certain limitations of the study, including its single-center design and the lack of a control group. “The study design highly reduces the risk for observation bias (Hawthorne effect),” they wrote. “Furthermore, we did not inform the staff about the purpose of our study. We analyzed only objective outcome data to reduce reporting bias as much as possible.”
The finding of a decline in LOS “suggests potential cost savings after the implementation of SSCs,” they concluded. “Further trials should address this hypothesis and the effect on quality of care owing to a reduction of the costs of complications or unplanned reoperations.”
The study was supported by the Public Health Care Company of South Tyrol, Italy, and by the Autonomous Province of Bolzano, Italy. The researchers reported having no financial disclosures.
FROM JAMA SURGERY
Key clinical point: Implementation of surgical safety checklists (SSCs) at a hospital led to reduced risk of mortality at 90 days, but not at 30 days.
Major finding: Ninety-day all-cause mortality was 2.4% before implementation of SSCs, compared with 2.2% after implementation, for an adjusted odds ratio (AOR) of 0.73 (P = .02).
Data source: A retrospective evaluation of surgical procedures performed on 10,741 patients during the 6 months before and 6 months after implementation of SSCs at the 715-bed Central Hospital of Bolzano in Italy.
Disclosures: The study was supported by the Public Health Care Company of South Tyrol, Italy, and by the Autonomous Province of Bolzano, Italy. The researchers reported having no financial disclosures.

Neoadjuvant chemo found to benefit locally advanced colon cancer
LOS ANGELES – Treatment with neoadjuvant chemotherapy leads to significant downstaging in a selected group of patients with advanced colon cancer, results from a large registry study showed.
“Neoadjuvant chemotherapy is already established as a treatment strategy in several other types of cancers, such as breast cancer, gastric cancer, and rectal cancer,” lead study author Dr. Moniek Verstegen said at the annual meeting of the American Society of Colon and Rectal Surgeons. “It reduces tumor size and promotes resectability. In colon cancer, however, this treatment strategy is relatively new and not applied very often.”

Preliminary results from the ongoing FOxTROT trial in the United Kingdom showed that preoperative chemotherapy for radiologically staged, locally advanced, operable primary colon cancer is feasible, with acceptable toxicity and perioperative morbidity, but long-term results are not yet available. The aim of the current study was to see how often neoadjuvant chemotherapy is used in the Netherlands for stage II and III colon cancer and to assess the tumor and nodal downsizing effects. Moreover, perioperative results and long-term outcomes were compared between those treated with neoadjuvant chemotherapy and those who were treated with adjuvant chemotherapy for locally advanced colon cancer.
The researchers searched the Netherlands Cancer Registry from 2008-2012 to identify 24,944 patients diagnosed with stage II and III colon cancer. Dr. Verstegen, a researcher in the department of surgery at Radboud University Medical Center, Nijmegen, Netherlands, reported results from 85 patients who received neoadjuvant chemotherapy and 2,216 who received adjuvant chemotherapy (the control group). Both groups were similar in terms of age (a median of about 65 years), gender, localization of the primary tumor, differentiation grade, morphology, and clinical T and N stage. Multivisceral resections were performed significantly more often in the neoadjuvant group, compared with the control group (21% vs. 5%, respectively; P less than .001). There were no differences between groups in the number of complete resections, nor in the rate of complications. Furthermore, no patient died within 30 days of neoadjuvant chemotherapy after surgery.
Tumor downstaging was observed in 47% of patients treated with neoadjuvant chemotherapy and there were three complete responses. At the same time, nodal downstaging was observed in 50% of patients treated with neoadjuvant chemotherapy. The 3-year overall survival was 73% in both groups.
Dr. Verstegen acknowledged certain limitations of the study, including its retrospective design and the lack of data on recurrences and disease-free survival. “Neoadjuvant chemotherapy seems to be a safe treatment strategy, since we have low postoperative morbidity and mortality rates,” she concluded. “We see comparable outcomes compared to the control group. Prospective trials are needed to confirm the safety and value of neoadjuvant chemotherapy.”
Dr. Verstegen reported having no financial disclosures.
LOS ANGELES – Treatment with neoadjuvant chemotherapy leads to significant downstaging in a selected group of patients with advanced colon cancer, results from a large registry study showed.
“Neoadjuvant chemotherapy is already established as a treatment strategy in several other types of cancers, such as breast cancer, gastric cancer, and rectal cancer,” lead study author Dr. Moniek Verstegen said at the annual meeting of the American Society of Colon and Rectal Surgeons. “It reduces tumor size and promotes resectability. In colon cancer, however, this treatment strategy is relatively new and not applied very often.”
Preliminary results from the ongoing FOxTROT trial in the United Kingdom showed that preoperative chemotherapy for radiologically staged, locally advanced, operable primary colon cancer is feasible, with acceptable toxicity and perioperative morbidity, but long-term results are not yet available. The aim of the current study was to see how often neoadjuvant chemotherapy is used in the Netherlands for stage II and III colon cancer and to assess the tumor and nodal downsizing effects. Moreover, perioperative results and long-term outcomes were compared between those treated with neoadjuvant chemotherapy and those who were treated with adjuvant chemotherapy for locally advanced colon cancer.
The researchers searched the Netherlands Cancer Registry from 2008-2012 to identify 24,944 patients diagnosed with stage II and III colon cancer. Dr. Verstegen, a researcher in the department of surgery at Radboud University Medical Center, Nijmegen, Netherlands, reported results from 85 patients who received neoadjuvant chemotherapy and 2,216 who received adjuvant chemotherapy (the control group). Both groups were similar in terms of age (a median of about 65 years), gender, localization of the primary tumor, differentiation grade, morphology, and clinical T and N stage. Multivisceral resections were performed significantly more often in the neoadjuvant group, compared with the control group (21% vs. 5%, respectively; P less than .001). There were no differences between groups in the number of complete resections, nor in the rate of complications. Furthermore, no patient died within 30 days of neoadjuvant chemotherapy after surgery.
Tumor downstaging was observed in 47% of patients treated with neoadjuvant chemotherapy and there were three complete responses. At the same time, nodal downstaging was observed in 50% of patients treated with neoadjuvant chemotherapy. The 3-year overall survival was 73% in both groups.
Dr. Verstegen acknowledged certain limitations of the study, including its retrospective design and the lack of data on recurrences and disease-free survival. “Neoadjuvant chemotherapy seems to be a safe treatment strategy, since we have low postoperative morbidity and mortality rates,” she concluded. “We see comparable outcomes compared to the control group. Prospective trials are needed to confirm the safety and value of neoadjuvant chemotherapy.”
Dr. Verstegen reported having no financial disclosures.
LOS ANGELES – Treatment with neoadjuvant chemotherapy leads to significant downstaging in a selected group of patients with advanced colon cancer, results from a large registry study showed.
“Neoadjuvant chemotherapy is already established as a treatment strategy in several other types of cancers, such as breast cancer, gastric cancer, and rectal cancer,” lead study author Dr. Moniek Verstegen said at the annual meeting of the American Society of Colon and Rectal Surgeons. “It reduces tumor size and promotes resectability. In colon cancer, however, this treatment strategy is relatively new and not applied very often.”
Preliminary results from the ongoing FOxTROT trial in the United Kingdom showed that preoperative chemotherapy for radiologically staged, locally advanced, operable primary colon cancer is feasible, with acceptable toxicity and perioperative morbidity, but long-term results are not yet available. The aim of the current study was to see how often neoadjuvant chemotherapy is used in the Netherlands for stage II and III colon cancer and to assess the tumor and nodal downsizing effects. Moreover, perioperative results and long-term outcomes were compared between those treated with neoadjuvant chemotherapy and those who were treated with adjuvant chemotherapy for locally advanced colon cancer.
The researchers searched the Netherlands Cancer Registry from 2008-2012 to identify 24,944 patients diagnosed with stage II and III colon cancer. Dr. Verstegen, a researcher in the department of surgery at Radboud University Medical Center, Nijmegen, Netherlands, reported results from 85 patients who received neoadjuvant chemotherapy and 2,216 who received adjuvant chemotherapy (the control group). Both groups were similar in terms of age (a median of about 65 years), gender, localization of the primary tumor, differentiation grade, morphology, and clinical T and N stage. Multivisceral resections were performed significantly more often in the neoadjuvant group, compared with the control group (21% vs. 5%, respectively; P less than .001). There were no differences between groups in the number of complete resections, nor in the rate of complications. Furthermore, no patient died within 30 days of neoadjuvant chemotherapy after surgery.
Tumor downstaging was observed in 47% of patients treated with neoadjuvant chemotherapy and there were three complete responses. At the same time, nodal downstaging was observed in 50% of patients treated with neoadjuvant chemotherapy. The 3-year overall survival was 73% in both groups.
Dr. Verstegen acknowledged certain limitations of the study, including its retrospective design and the lack of data on recurrences and disease-free survival. “Neoadjuvant chemotherapy seems to be a safe treatment strategy, since we have low postoperative morbidity and mortality rates,” she concluded. “We see comparable outcomes compared to the control group. Prospective trials are needed to confirm the safety and value of neoadjuvant chemotherapy.”
Dr. Verstegen reported having no financial disclosures.
AT THE ASCRS ANNUAL MEETING
Key clinical point: Patients with locally advanced colon cancer may benefit from neoadjuvant chemotherapy.
Major finding: Tumor downstaging was observed in 47% of patients treated with neoadjuvant chemotherapy and there were three complete responses.
Data source: An analysis of 85 patients with stage II or III colon cancer who received neoadjuvant chemotherapy and 2,216 who received adjuvant chemotherapy.
Disclosures: Dr. Verstegen reported having no financial disclosures.
