User login
Official Newspaper of the American College of Surgeons
How to reduce early readmissions after bariatric surgery
NEW ORLEANS – A couple of home nursing visits early after bariatric surgery halved emergency department visits and hospital readmissions within the first 30 days in a case-control study, Linden A. Karas, MD, reported at Obesity Week 2016.
“Home nursing visits during the month following surgery, between doctor’s office visits, are a simple and inexpensive intervention that drastically decreases hospital revisits,” she declared at the meeting presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.

These early revisits to the hospital following bariatric surgery are not only common, they carry a substantial cost. An ED visit for hydration runs about $3,000 and a 2-day inpatient admission about $18,000. In contrast, the price tag for two home nursing visits in this study was $300, noted Dr. Karas, a surgeon at Mercy Catholic Medical Center in Philadelphia.
The triad of dehydration, nausea, and vomiting in addition to abdominal pain account for up to 40% of early readmissions following bariatric surgery. Because most hospital revisits for these reasons entail very little intervention other than IV fluids, Dr. Karas and her coinvestigators decided to investigate whether preemptive structured home visits by nurses prepared to administer IV fluids on the spot would cut down on hospital revisits. They found that indeed this strategy was successful.
Mercy Catholic Medical Center serves a largely low-income Medicare/Medicaid population. Part of the local culture is for many patients to obtain their primary care in the ED, so bariatric surgery patients are generally not reluctant to show up there if they don’t feel well in the first few weeks post surgery. That’s why in the year prior to the study the 30-day readmission rate was 23.6%, she explained.
The study included 193 consecutive prospectively followed adult participants in the home nursing program who underwent Roux-en-Y gastric bypass, laparoscopic adjustable banding, or revision surgery in 2014 and a control group of 267 matched bariatric surgery patients who underwent the same procedures in 2013, before introduction of the home nursing visits.
The first home visit occurred roughly 3 days after hospital discharge. The second one bridged the period between the first scheduled postoperative office visit at 2 weeks and the next office visit at 4 weeks. At discharge, patients were given a checklist concerning the signs and symptoms of dehydration, dietary recommendations, and lifestyle choices. Patients were encouraged to use the checklist to self-evaluate for dehydration and hand it over to the visiting nurses. The same checklist was provided to the home nurses. If the nurses found that patients met three or more criteria on the dehydration checklist, which included dry mucus membranes, heart rate greater than 90 beats/minute, headache, going more than 8 hours without urination, weakness, abdominal pain, and roughly a dozen other well-known criteria, they were instructed to initiate home hydration therapy with a banana bag and 2 L of normal saline.
If 1-2 days of home hydration failed to resolve the symptoms, the home care nurse was supposed to refer the patient to the ED. If the patient improved in response to home hydration therapy, the home nurse informed the surgeon’s office, which then set up a follow-up office visit to take place within the next 24 hours. Also, if the patient’s responses on the nutrition and behavioral health questionnaire raised any red flags regarding inadequate food and fluid intake, nonadherence to the recommended daily minimum of 30 minutes of physical activity, or depressive symptoms, the nurse was supposed to notify the surgeon to schedule a behavioral or nutrition appointment at the patient’s next scheduled visit.
The 30-day rate of all-cause hospital revisits in the home nursing care group was 11.9%, compared with 23.6% in controls. The rate of hospital revisits specifically for dehydration was 6.2% in the home visit group vs. 8.6% in controls, a 28% relative risk reduction in the home treatment group, which didn’t achieve statistical significance. However, in hindsight, it was evident that some of the visiting nurses didn’t fully understand the treatment protocol; they sent patients straight to the ED without first providing home hydration therapy. The visiting nurses were subcontracted out and weren’t part of the hospital’s bariatric surgery program.
Among those patients who did receive the therapy, however, it prevented readmission in 77% of cases. The 23% of patients who didn’t improve were referred to the hospital for further workup and treatment.
Patients with early hospital readmission had an average of 4.38 comorbid conditions, significantly more than the average 3.46 comorbidities in patients who weren’t readmitted. Several specific comorbid conditions were independently associated with significantly increased risk of hospital readmission: asthma, chronic obstructive pulmonary disease, anxiety, heart failure, and gastroesophageal reflux disease.
“Patients with those comorbidities are the ones to watch aggressively in the postop period,” according to Dr. Karas.
Insurers have paid for the home nursing visits without hesitation.
Her presentation met with an enthusiastic audience reception.
“I think it’s important that you’ve shown a return on investment for this initiative,” one surgeon commented.
Session cochair John J. Kelly, MD, chief of general and minimally invasive surgery at the University of Massachusetts in Worcester, declared, “I think this is a very-important paper. We’re obviously all faced with this dilemma in terms of readmission rates. If you can prevent them, it’s to be commended.”
Dr. Karas reported having no financial conflicts of interest regarding her study.
NEW ORLEANS – A couple of home nursing visits early after bariatric surgery halved emergency department visits and hospital readmissions within the first 30 days in a case-control study, Linden A. Karas, MD, reported at Obesity Week 2016.
“Home nursing visits during the month following surgery, between doctor’s office visits, are a simple and inexpensive intervention that drastically decreases hospital revisits,” she declared at the meeting presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
These early revisits to the hospital following bariatric surgery are not only common, they carry a substantial cost. An ED visit for hydration runs about $3,000 and a 2-day inpatient admission about $18,000. In contrast, the price tag for two home nursing visits in this study was $300, noted Dr. Karas, a surgeon at Mercy Catholic Medical Center in Philadelphia.
The triad of dehydration, nausea, and vomiting in addition to abdominal pain account for up to 40% of early readmissions following bariatric surgery. Because most hospital revisits for these reasons entail very little intervention other than IV fluids, Dr. Karas and her coinvestigators decided to investigate whether preemptive structured home visits by nurses prepared to administer IV fluids on the spot would cut down on hospital revisits. They found that indeed this strategy was successful.
Mercy Catholic Medical Center serves a largely low-income Medicare/Medicaid population. Part of the local culture is for many patients to obtain their primary care in the ED, so bariatric surgery patients are generally not reluctant to show up there if they don’t feel well in the first few weeks post surgery. That’s why in the year prior to the study the 30-day readmission rate was 23.6%, she explained.
The study included 193 consecutive prospectively followed adult participants in the home nursing program who underwent Roux-en-Y gastric bypass, laparoscopic adjustable banding, or revision surgery in 2014 and a control group of 267 matched bariatric surgery patients who underwent the same procedures in 2013, before introduction of the home nursing visits.
The first home visit occurred roughly 3 days after hospital discharge. The second one bridged the period between the first scheduled postoperative office visit at 2 weeks and the next office visit at 4 weeks. At discharge, patients were given a checklist concerning the signs and symptoms of dehydration, dietary recommendations, and lifestyle choices. Patients were encouraged to use the checklist to self-evaluate for dehydration and hand it over to the visiting nurses. The same checklist was provided to the home nurses. If the nurses found that patients met three or more criteria on the dehydration checklist, which included dry mucus membranes, heart rate greater than 90 beats/minute, headache, going more than 8 hours without urination, weakness, abdominal pain, and roughly a dozen other well-known criteria, they were instructed to initiate home hydration therapy with a banana bag and 2 L of normal saline.
If 1-2 days of home hydration failed to resolve the symptoms, the home care nurse was supposed to refer the patient to the ED. If the patient improved in response to home hydration therapy, the home nurse informed the surgeon’s office, which then set up a follow-up office visit to take place within the next 24 hours. Also, if the patient’s responses on the nutrition and behavioral health questionnaire raised any red flags regarding inadequate food and fluid intake, nonadherence to the recommended daily minimum of 30 minutes of physical activity, or depressive symptoms, the nurse was supposed to notify the surgeon to schedule a behavioral or nutrition appointment at the patient’s next scheduled visit.
The 30-day rate of all-cause hospital revisits in the home nursing care group was 11.9%, compared with 23.6% in controls. The rate of hospital revisits specifically for dehydration was 6.2% in the home visit group vs. 8.6% in controls, a 28% relative risk reduction in the home treatment group, which didn’t achieve statistical significance. However, in hindsight, it was evident that some of the visiting nurses didn’t fully understand the treatment protocol; they sent patients straight to the ED without first providing home hydration therapy. The visiting nurses were subcontracted out and weren’t part of the hospital’s bariatric surgery program.
Among those patients who did receive the therapy, however, it prevented readmission in 77% of cases. The 23% of patients who didn’t improve were referred to the hospital for further workup and treatment.
Patients with early hospital readmission had an average of 4.38 comorbid conditions, significantly more than the average 3.46 comorbidities in patients who weren’t readmitted. Several specific comorbid conditions were independently associated with significantly increased risk of hospital readmission: asthma, chronic obstructive pulmonary disease, anxiety, heart failure, and gastroesophageal reflux disease.
“Patients with those comorbidities are the ones to watch aggressively in the postop period,” according to Dr. Karas.
Insurers have paid for the home nursing visits without hesitation.
Her presentation met with an enthusiastic audience reception.
“I think it’s important that you’ve shown a return on investment for this initiative,” one surgeon commented.
Session cochair John J. Kelly, MD, chief of general and minimally invasive surgery at the University of Massachusetts in Worcester, declared, “I think this is a very-important paper. We’re obviously all faced with this dilemma in terms of readmission rates. If you can prevent them, it’s to be commended.”
Dr. Karas reported having no financial conflicts of interest regarding her study.
NEW ORLEANS – A couple of home nursing visits early after bariatric surgery halved emergency department visits and hospital readmissions within the first 30 days in a case-control study, Linden A. Karas, MD, reported at Obesity Week 2016.
“Home nursing visits during the month following surgery, between doctor’s office visits, are a simple and inexpensive intervention that drastically decreases hospital revisits,” she declared at the meeting presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
These early revisits to the hospital following bariatric surgery are not only common, they carry a substantial cost. An ED visit for hydration runs about $3,000 and a 2-day inpatient admission about $18,000. In contrast, the price tag for two home nursing visits in this study was $300, noted Dr. Karas, a surgeon at Mercy Catholic Medical Center in Philadelphia.
The triad of dehydration, nausea, and vomiting in addition to abdominal pain account for up to 40% of early readmissions following bariatric surgery. Because most hospital revisits for these reasons entail very little intervention other than IV fluids, Dr. Karas and her coinvestigators decided to investigate whether preemptive structured home visits by nurses prepared to administer IV fluids on the spot would cut down on hospital revisits. They found that indeed this strategy was successful.
Mercy Catholic Medical Center serves a largely low-income Medicare/Medicaid population. Part of the local culture is for many patients to obtain their primary care in the ED, so bariatric surgery patients are generally not reluctant to show up there if they don’t feel well in the first few weeks post surgery. That’s why in the year prior to the study the 30-day readmission rate was 23.6%, she explained.
The study included 193 consecutive prospectively followed adult participants in the home nursing program who underwent Roux-en-Y gastric bypass, laparoscopic adjustable banding, or revision surgery in 2014 and a control group of 267 matched bariatric surgery patients who underwent the same procedures in 2013, before introduction of the home nursing visits.
The first home visit occurred roughly 3 days after hospital discharge. The second one bridged the period between the first scheduled postoperative office visit at 2 weeks and the next office visit at 4 weeks. At discharge, patients were given a checklist concerning the signs and symptoms of dehydration, dietary recommendations, and lifestyle choices. Patients were encouraged to use the checklist to self-evaluate for dehydration and hand it over to the visiting nurses. The same checklist was provided to the home nurses. If the nurses found that patients met three or more criteria on the dehydration checklist, which included dry mucus membranes, heart rate greater than 90 beats/minute, headache, going more than 8 hours without urination, weakness, abdominal pain, and roughly a dozen other well-known criteria, they were instructed to initiate home hydration therapy with a banana bag and 2 L of normal saline.
If 1-2 days of home hydration failed to resolve the symptoms, the home care nurse was supposed to refer the patient to the ED. If the patient improved in response to home hydration therapy, the home nurse informed the surgeon’s office, which then set up a follow-up office visit to take place within the next 24 hours. Also, if the patient’s responses on the nutrition and behavioral health questionnaire raised any red flags regarding inadequate food and fluid intake, nonadherence to the recommended daily minimum of 30 minutes of physical activity, or depressive symptoms, the nurse was supposed to notify the surgeon to schedule a behavioral or nutrition appointment at the patient’s next scheduled visit.
The 30-day rate of all-cause hospital revisits in the home nursing care group was 11.9%, compared with 23.6% in controls. The rate of hospital revisits specifically for dehydration was 6.2% in the home visit group vs. 8.6% in controls, a 28% relative risk reduction in the home treatment group, which didn’t achieve statistical significance. However, in hindsight, it was evident that some of the visiting nurses didn’t fully understand the treatment protocol; they sent patients straight to the ED without first providing home hydration therapy. The visiting nurses were subcontracted out and weren’t part of the hospital’s bariatric surgery program.
Among those patients who did receive the therapy, however, it prevented readmission in 77% of cases. The 23% of patients who didn’t improve were referred to the hospital for further workup and treatment.
Patients with early hospital readmission had an average of 4.38 comorbid conditions, significantly more than the average 3.46 comorbidities in patients who weren’t readmitted. Several specific comorbid conditions were independently associated with significantly increased risk of hospital readmission: asthma, chronic obstructive pulmonary disease, anxiety, heart failure, and gastroesophageal reflux disease.
“Patients with those comorbidities are the ones to watch aggressively in the postop period,” according to Dr. Karas.
Insurers have paid for the home nursing visits without hesitation.
Her presentation met with an enthusiastic audience reception.
“I think it’s important that you’ve shown a return on investment for this initiative,” one surgeon commented.
Session cochair John J. Kelly, MD, chief of general and minimally invasive surgery at the University of Massachusetts in Worcester, declared, “I think this is a very-important paper. We’re obviously all faced with this dilemma in terms of readmission rates. If you can prevent them, it’s to be commended.”
Dr. Karas reported having no financial conflicts of interest regarding her study.
AT OBESITY WEEK 2016
Key clinical point:
Major finding: The combined rate of ED visits and hospital readmissions within 30 days post–bariatric surgery was 11.9% in a group of patients who received two home nursing visits that included home hydration therapy as indicated, compared with 23.6% in bariatric surgery patients who weren’t involved in the home visit program.
Data source: This study compared 30-day hospital readmission rates in 193 consecutive prospectively followed bariatric surgery patients who received two structured home nursing visits in the first 4 postoperative weeks to readmissions in 267 matched controls whose surgery occurred prior to implementation of the home nursing program.
Disclosures: The presenter reported having no financial conflicts of interest regarding the study.
Mitral valve disease often missed in pulmonary hypertension
LOS ANGELES – Dyspnea in pulmonary hypertension is caused by mitral valve disease until proven otherwise, according to Paul Forfia, MD, director of pulmonary hypertension, right heart failure, and pulmonary thromboendarterectomy at Temple University, Philadelphia.
Although mitral valve disease is a well-recognized cause of pulmonary hypertension, its significance is often underestimated in practice.
“Whether the valve is regurgitant or stenotic makes absolutely no difference. When you delay” repair or replacement, “the patient keeps getting sicker,” he said. In time, “everyone is standing around wringing their hands going, ‘Oh my god, what are we going to do? Are you serious? Fix the valve.’ We see this type of patient a couple times a month,” Dr. Forfia said at the American College of Chest Physicians annual meeting.
“I have seen lifesaving mitral valve surgery put off for many years in patients with pulmonary hypertension, when all they needed was to have their valve fixed,” he said.

Whatever the case, pulmonologists who want the valve fixed often end up playing patient ping pong with cardiologists who want the hypertension controlled beforehand, but “if I treat the pulmonary circulation first, all I am going to do is unmask the left heart failure. There will be no functional improvement whatsoever,” Dr. Forfia said.
Surgery is the best solution as long as patients are well enough to recover. “With pulmonary hypertension in the setting of severe mitral valve regurgitation or stenosis, whether the pulmonary hypertension is related to passive left heart congestion or associated with pulmonary arteriopathy, the only sensible option is to correct the underlying valvular abnormality,” he said. The surgery should be done at an institution capable of managing postop pulmonary arteriopathy, if present.
The ping pong solution is to send patients to an expert pulmonology center; the mitral valve problem will be spotted right away.
“There is no pulmonary pressure cutoff that should prohibit surgery” in patients able to recover. “There is no such thing as a pulmonary artery pressure too high to be explained by mitral valve disease. The pulmonary pressure can be as high as it wants to be. You will get nowhere by thinking the pressure is too high to address the valve,” Dr. Forfia said.
Often “you hear, ‘I’m afraid the person is going to die on the table.’ I always say ‘if the patient is not going to die on the table, they are going to die in their living room of progressive heart failure because you [didn’t] fix their valve. I have never had a patient with pulmonary hypertension not separate from cardiopulmonary bypass. It’s a myth,” he said.
When there’s a “question if the dyspnea is coming from the mitral valve, we routinely use exercise right heart catheterization to probe the situation. We have a recumbent bike in the cath lab. You’ll often provoke significant left heart congestion with a low workload. It’s very revealing to the significance of mitral valve disease,” he said.
Aortic valve disease is also missed in pulmonary hypertension. “It’s not [a] similar” problem; “it’s the same” problem, Dr. Forfia said.
Dr. Forfia is a consultant for Bayer, Actelion, and United Therapeutics.
LOS ANGELES – Dyspnea in pulmonary hypertension is caused by mitral valve disease until proven otherwise, according to Paul Forfia, MD, director of pulmonary hypertension, right heart failure, and pulmonary thromboendarterectomy at Temple University, Philadelphia.
Although mitral valve disease is a well-recognized cause of pulmonary hypertension, its significance is often underestimated in practice.
“Whether the valve is regurgitant or stenotic makes absolutely no difference. When you delay” repair or replacement, “the patient keeps getting sicker,” he said. In time, “everyone is standing around wringing their hands going, ‘Oh my god, what are we going to do? Are you serious? Fix the valve.’ We see this type of patient a couple times a month,” Dr. Forfia said at the American College of Chest Physicians annual meeting.
“I have seen lifesaving mitral valve surgery put off for many years in patients with pulmonary hypertension, when all they needed was to have their valve fixed,” he said.
Whatever the case, pulmonologists who want the valve fixed often end up playing patient ping pong with cardiologists who want the hypertension controlled beforehand, but “if I treat the pulmonary circulation first, all I am going to do is unmask the left heart failure. There will be no functional improvement whatsoever,” Dr. Forfia said.
Surgery is the best solution as long as patients are well enough to recover. “With pulmonary hypertension in the setting of severe mitral valve regurgitation or stenosis, whether the pulmonary hypertension is related to passive left heart congestion or associated with pulmonary arteriopathy, the only sensible option is to correct the underlying valvular abnormality,” he said. The surgery should be done at an institution capable of managing postop pulmonary arteriopathy, if present.
The ping pong solution is to send patients to an expert pulmonology center; the mitral valve problem will be spotted right away.
“There is no pulmonary pressure cutoff that should prohibit surgery” in patients able to recover. “There is no such thing as a pulmonary artery pressure too high to be explained by mitral valve disease. The pulmonary pressure can be as high as it wants to be. You will get nowhere by thinking the pressure is too high to address the valve,” Dr. Forfia said.
Often “you hear, ‘I’m afraid the person is going to die on the table.’ I always say ‘if the patient is not going to die on the table, they are going to die in their living room of progressive heart failure because you [didn’t] fix their valve. I have never had a patient with pulmonary hypertension not separate from cardiopulmonary bypass. It’s a myth,” he said.
When there’s a “question if the dyspnea is coming from the mitral valve, we routinely use exercise right heart catheterization to probe the situation. We have a recumbent bike in the cath lab. You’ll often provoke significant left heart congestion with a low workload. It’s very revealing to the significance of mitral valve disease,” he said.
Aortic valve disease is also missed in pulmonary hypertension. “It’s not [a] similar” problem; “it’s the same” problem, Dr. Forfia said.
Dr. Forfia is a consultant for Bayer, Actelion, and United Therapeutics.
LOS ANGELES – Dyspnea in pulmonary hypertension is caused by mitral valve disease until proven otherwise, according to Paul Forfia, MD, director of pulmonary hypertension, right heart failure, and pulmonary thromboendarterectomy at Temple University, Philadelphia.
Although mitral valve disease is a well-recognized cause of pulmonary hypertension, its significance is often underestimated in practice.
“Whether the valve is regurgitant or stenotic makes absolutely no difference. When you delay” repair or replacement, “the patient keeps getting sicker,” he said. In time, “everyone is standing around wringing their hands going, ‘Oh my god, what are we going to do? Are you serious? Fix the valve.’ We see this type of patient a couple times a month,” Dr. Forfia said at the American College of Chest Physicians annual meeting.
“I have seen lifesaving mitral valve surgery put off for many years in patients with pulmonary hypertension, when all they needed was to have their valve fixed,” he said.
Whatever the case, pulmonologists who want the valve fixed often end up playing patient ping pong with cardiologists who want the hypertension controlled beforehand, but “if I treat the pulmonary circulation first, all I am going to do is unmask the left heart failure. There will be no functional improvement whatsoever,” Dr. Forfia said.
Surgery is the best solution as long as patients are well enough to recover. “With pulmonary hypertension in the setting of severe mitral valve regurgitation or stenosis, whether the pulmonary hypertension is related to passive left heart congestion or associated with pulmonary arteriopathy, the only sensible option is to correct the underlying valvular abnormality,” he said. The surgery should be done at an institution capable of managing postop pulmonary arteriopathy, if present.
The ping pong solution is to send patients to an expert pulmonology center; the mitral valve problem will be spotted right away.
“There is no pulmonary pressure cutoff that should prohibit surgery” in patients able to recover. “There is no such thing as a pulmonary artery pressure too high to be explained by mitral valve disease. The pulmonary pressure can be as high as it wants to be. You will get nowhere by thinking the pressure is too high to address the valve,” Dr. Forfia said.
Often “you hear, ‘I’m afraid the person is going to die on the table.’ I always say ‘if the patient is not going to die on the table, they are going to die in their living room of progressive heart failure because you [didn’t] fix their valve. I have never had a patient with pulmonary hypertension not separate from cardiopulmonary bypass. It’s a myth,” he said.
When there’s a “question if the dyspnea is coming from the mitral valve, we routinely use exercise right heart catheterization to probe the situation. We have a recumbent bike in the cath lab. You’ll often provoke significant left heart congestion with a low workload. It’s very revealing to the significance of mitral valve disease,” he said.
Aortic valve disease is also missed in pulmonary hypertension. “It’s not [a] similar” problem; “it’s the same” problem, Dr. Forfia said.
Dr. Forfia is a consultant for Bayer, Actelion, and United Therapeutics.
EXPERT ANALYSIS FROM CHEST 2016
Weight loss procedure is linked to subsequent substance misuse
NEW ORLEANS – Severely obese patients who undergo Roux-en-Y gastric bypass surgery are subsequently at sharply increased risk for new-onset alcohol use disorder as well as for treatment of substance use disorder, compared with others who opt for a laparoscopic adjustable banding procedure for weight loss, Wendy C. King, PhD, reported at a meeting presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
This new finding from the NIH-sponsored Longitudinal Assessment of Bariatric Surgery–2 study (LABS-2) has important implications for clinical practice.
“Patients considering bariatric surgery really should be informed of this surgery-specific risk. Also, alcohol use disorder screening, evaluation, intervention, and referral should be incorporated as part of regular presurgical and definitely also postoperative care. And because many patients don’t return to their surgeon for long-term postoperative care, it’s important that clinicians in primary care and other specialties are really looking for this problem in long-term follow-up,” said Dr. King, an epidemiologist at the University of Pittsburgh.
LABS-2 is an observational cohort study of patients undergoing first-time bariatric surgery at 10 participating U.S. hospitals, all of which have academic ties and are rated as bariatric surgery centers of excellence. Dr. King presented 5-year postsurgical follow-up data on 1,481 patients who had Roux-en-Y gastric bypass (RYGB) and 522 with laparoscopic adjustable gastric banding (LAGB). Independently of their regular clinical care visits, participants were assessed annually for their alcohol use and its consequences using the Alcohol Use Disorders Identification Test (AUDIT), use of illicit drugs within the past year, and whether they had undergone hospitalization or counseling for alcohol or drug problems. A score of 8 or more points on the AUDIT was deemed an indication of symptoms of alcohol use disorder (AUD),
After eliminating from consideration the 7% of patients with AUD symptoms at baseline, the cumulative incidence of AUD symptoms in the RYGB patients climbed from zero to 20.8% by the end of the fifth year of follow-up. Treatment for a substance use disorder occurred in 3.5% of RYGB patients during their first 5 years postsurgery, and 7.5% admitted to illicit drug use, said Dr. King.
In contrast, the cumulative incidence of AUD symptoms through 5 years in the LAGB patients was only 11.3%, less than 1% underwent treatment for a substance use disorder, and 4.9% said they had used illicit drugs.
But LABS-2 is not a randomized trial. Patients chose their bariatric procedure together with their surgeon. For this reason, it was important to perform a multivariate regression analysis adjusted for sociodemographics, social support, psychiatric treatment, lifetime history of psychiatric hospitalization, baseline smoking and alcohol consumption, and other potential confounders.
After performing this statistical exercise, the RYGB patients remained at an adjusted 2.05-fold increased risk of AUD symptoms, compared with the LAGB patients, as well as at 3.83-fold greater risk of treatment for a substance use disorder.
The 1.6-fold increased rate of illicit drug use in the RYGB group didn’t achieve statistical significance. Moreover, on closer examination, most of this illicit drug use involved marijuana, and its use in the post–bariatric surgery population appeared to mirror secular trends in the United States as a whole, according to Dr. King.
With her coinvestigators, Dr. King searched for presurgical risk factors that might predict postsurgical substance misuse. Perhaps the most interesting finding concerned the factors that weren’t predictive, including education, unemployment, score on the Beck Depression Inventory, SF-36 mental component summary score, race, marital status, binge eating, loss of control eating, and body mass index.
Lower social support prior to surgery was associated with increased risk for developing AUD symptoms during the first 5 years after bariatric surgery. Younger age and smoking at baseline were associated with increased rates of postoperative AUD symptoms, substance use disorder treatment, and illicit drug use. A history of psychiatric treatment was associated with increased rates of substance use disorder treatment and illicit drug use.
“That could indicate greater medical surveillance among those patients or greater willingness to get treatment, since they’d had treatment for other psychiatric issues in the past,” Dr. King speculated.
She described the study’s strengths as its large size, geographically diverse patient population, unusually high retention over time, compared with other bariatric surgery studies, and the use of AUDIT, a validated and reliable screening tool. The major limitations are that investigators didn’t inquire about illicit use of opioids and benzodiazepines, and recipients of gastric sleeve procedures weren’t included in the long-term follow-up analysis because LABS-2 began before the gastric sleeve boomed in popularity.
John M. Morton, MD, a former president of the American Society for Metabolic and Bariatric Surgery, predicted that a similar study that included gastric sleeve patients would show them to have the same unremarkable postoperative rates of substance misuse as the LAGB group.
“I want to emphasize that this increased incidence of alcohol problems in the Roux-en-Y gastric bypass patients is maybe not so much a psychological issue as it is a physiologic one,” added Dr. Morton, chief of bariatric and minimally invasive surgery at Stanford (Calif.) School of Medicine.
Dr. King agreed. “Just in the last year and a half there have been some great pharmacokinetic studies showing that the Roux-en-Y affects alcohol metabolism and absorption, as well as studies in rodent models that suggest alcohol produces increased neurobiologic reward,” she noted.
The LABS-2 study is funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. King reported having no relevant financial interests.
NEW ORLEANS – Severely obese patients who undergo Roux-en-Y gastric bypass surgery are subsequently at sharply increased risk for new-onset alcohol use disorder as well as for treatment of substance use disorder, compared with others who opt for a laparoscopic adjustable banding procedure for weight loss, Wendy C. King, PhD, reported at a meeting presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
This new finding from the NIH-sponsored Longitudinal Assessment of Bariatric Surgery–2 study (LABS-2) has important implications for clinical practice.
“Patients considering bariatric surgery really should be informed of this surgery-specific risk. Also, alcohol use disorder screening, evaluation, intervention, and referral should be incorporated as part of regular presurgical and definitely also postoperative care. And because many patients don’t return to their surgeon for long-term postoperative care, it’s important that clinicians in primary care and other specialties are really looking for this problem in long-term follow-up,” said Dr. King, an epidemiologist at the University of Pittsburgh.
LABS-2 is an observational cohort study of patients undergoing first-time bariatric surgery at 10 participating U.S. hospitals, all of which have academic ties and are rated as bariatric surgery centers of excellence. Dr. King presented 5-year postsurgical follow-up data on 1,481 patients who had Roux-en-Y gastric bypass (RYGB) and 522 with laparoscopic adjustable gastric banding (LAGB). Independently of their regular clinical care visits, participants were assessed annually for their alcohol use and its consequences using the Alcohol Use Disorders Identification Test (AUDIT), use of illicit drugs within the past year, and whether they had undergone hospitalization or counseling for alcohol or drug problems. A score of 8 or more points on the AUDIT was deemed an indication of symptoms of alcohol use disorder (AUD),
After eliminating from consideration the 7% of patients with AUD symptoms at baseline, the cumulative incidence of AUD symptoms in the RYGB patients climbed from zero to 20.8% by the end of the fifth year of follow-up. Treatment for a substance use disorder occurred in 3.5% of RYGB patients during their first 5 years postsurgery, and 7.5% admitted to illicit drug use, said Dr. King.
In contrast, the cumulative incidence of AUD symptoms through 5 years in the LAGB patients was only 11.3%, less than 1% underwent treatment for a substance use disorder, and 4.9% said they had used illicit drugs.
But LABS-2 is not a randomized trial. Patients chose their bariatric procedure together with their surgeon. For this reason, it was important to perform a multivariate regression analysis adjusted for sociodemographics, social support, psychiatric treatment, lifetime history of psychiatric hospitalization, baseline smoking and alcohol consumption, and other potential confounders.
After performing this statistical exercise, the RYGB patients remained at an adjusted 2.05-fold increased risk of AUD symptoms, compared with the LAGB patients, as well as at 3.83-fold greater risk of treatment for a substance use disorder.
The 1.6-fold increased rate of illicit drug use in the RYGB group didn’t achieve statistical significance. Moreover, on closer examination, most of this illicit drug use involved marijuana, and its use in the post–bariatric surgery population appeared to mirror secular trends in the United States as a whole, according to Dr. King.
With her coinvestigators, Dr. King searched for presurgical risk factors that might predict postsurgical substance misuse. Perhaps the most interesting finding concerned the factors that weren’t predictive, including education, unemployment, score on the Beck Depression Inventory, SF-36 mental component summary score, race, marital status, binge eating, loss of control eating, and body mass index.
Lower social support prior to surgery was associated with increased risk for developing AUD symptoms during the first 5 years after bariatric surgery. Younger age and smoking at baseline were associated with increased rates of postoperative AUD symptoms, substance use disorder treatment, and illicit drug use. A history of psychiatric treatment was associated with increased rates of substance use disorder treatment and illicit drug use.
“That could indicate greater medical surveillance among those patients or greater willingness to get treatment, since they’d had treatment for other psychiatric issues in the past,” Dr. King speculated.
She described the study’s strengths as its large size, geographically diverse patient population, unusually high retention over time, compared with other bariatric surgery studies, and the use of AUDIT, a validated and reliable screening tool. The major limitations are that investigators didn’t inquire about illicit use of opioids and benzodiazepines, and recipients of gastric sleeve procedures weren’t included in the long-term follow-up analysis because LABS-2 began before the gastric sleeve boomed in popularity.
John M. Morton, MD, a former president of the American Society for Metabolic and Bariatric Surgery, predicted that a similar study that included gastric sleeve patients would show them to have the same unremarkable postoperative rates of substance misuse as the LAGB group.
“I want to emphasize that this increased incidence of alcohol problems in the Roux-en-Y gastric bypass patients is maybe not so much a psychological issue as it is a physiologic one,” added Dr. Morton, chief of bariatric and minimally invasive surgery at Stanford (Calif.) School of Medicine.
Dr. King agreed. “Just in the last year and a half there have been some great pharmacokinetic studies showing that the Roux-en-Y affects alcohol metabolism and absorption, as well as studies in rodent models that suggest alcohol produces increased neurobiologic reward,” she noted.
The LABS-2 study is funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. King reported having no relevant financial interests.
NEW ORLEANS – Severely obese patients who undergo Roux-en-Y gastric bypass surgery are subsequently at sharply increased risk for new-onset alcohol use disorder as well as for treatment of substance use disorder, compared with others who opt for a laparoscopic adjustable banding procedure for weight loss, Wendy C. King, PhD, reported at a meeting presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
This new finding from the NIH-sponsored Longitudinal Assessment of Bariatric Surgery–2 study (LABS-2) has important implications for clinical practice.
“Patients considering bariatric surgery really should be informed of this surgery-specific risk. Also, alcohol use disorder screening, evaluation, intervention, and referral should be incorporated as part of regular presurgical and definitely also postoperative care. And because many patients don’t return to their surgeon for long-term postoperative care, it’s important that clinicians in primary care and other specialties are really looking for this problem in long-term follow-up,” said Dr. King, an epidemiologist at the University of Pittsburgh.
LABS-2 is an observational cohort study of patients undergoing first-time bariatric surgery at 10 participating U.S. hospitals, all of which have academic ties and are rated as bariatric surgery centers of excellence. Dr. King presented 5-year postsurgical follow-up data on 1,481 patients who had Roux-en-Y gastric bypass (RYGB) and 522 with laparoscopic adjustable gastric banding (LAGB). Independently of their regular clinical care visits, participants were assessed annually for their alcohol use and its consequences using the Alcohol Use Disorders Identification Test (AUDIT), use of illicit drugs within the past year, and whether they had undergone hospitalization or counseling for alcohol or drug problems. A score of 8 or more points on the AUDIT was deemed an indication of symptoms of alcohol use disorder (AUD),
After eliminating from consideration the 7% of patients with AUD symptoms at baseline, the cumulative incidence of AUD symptoms in the RYGB patients climbed from zero to 20.8% by the end of the fifth year of follow-up. Treatment for a substance use disorder occurred in 3.5% of RYGB patients during their first 5 years postsurgery, and 7.5% admitted to illicit drug use, said Dr. King.
In contrast, the cumulative incidence of AUD symptoms through 5 years in the LAGB patients was only 11.3%, less than 1% underwent treatment for a substance use disorder, and 4.9% said they had used illicit drugs.
But LABS-2 is not a randomized trial. Patients chose their bariatric procedure together with their surgeon. For this reason, it was important to perform a multivariate regression analysis adjusted for sociodemographics, social support, psychiatric treatment, lifetime history of psychiatric hospitalization, baseline smoking and alcohol consumption, and other potential confounders.
After performing this statistical exercise, the RYGB patients remained at an adjusted 2.05-fold increased risk of AUD symptoms, compared with the LAGB patients, as well as at 3.83-fold greater risk of treatment for a substance use disorder.
The 1.6-fold increased rate of illicit drug use in the RYGB group didn’t achieve statistical significance. Moreover, on closer examination, most of this illicit drug use involved marijuana, and its use in the post–bariatric surgery population appeared to mirror secular trends in the United States as a whole, according to Dr. King.
With her coinvestigators, Dr. King searched for presurgical risk factors that might predict postsurgical substance misuse. Perhaps the most interesting finding concerned the factors that weren’t predictive, including education, unemployment, score on the Beck Depression Inventory, SF-36 mental component summary score, race, marital status, binge eating, loss of control eating, and body mass index.
Lower social support prior to surgery was associated with increased risk for developing AUD symptoms during the first 5 years after bariatric surgery. Younger age and smoking at baseline were associated with increased rates of postoperative AUD symptoms, substance use disorder treatment, and illicit drug use. A history of psychiatric treatment was associated with increased rates of substance use disorder treatment and illicit drug use.
“That could indicate greater medical surveillance among those patients or greater willingness to get treatment, since they’d had treatment for other psychiatric issues in the past,” Dr. King speculated.
She described the study’s strengths as its large size, geographically diverse patient population, unusually high retention over time, compared with other bariatric surgery studies, and the use of AUDIT, a validated and reliable screening tool. The major limitations are that investigators didn’t inquire about illicit use of opioids and benzodiazepines, and recipients of gastric sleeve procedures weren’t included in the long-term follow-up analysis because LABS-2 began before the gastric sleeve boomed in popularity.
John M. Morton, MD, a former president of the American Society for Metabolic and Bariatric Surgery, predicted that a similar study that included gastric sleeve patients would show them to have the same unremarkable postoperative rates of substance misuse as the LAGB group.
“I want to emphasize that this increased incidence of alcohol problems in the Roux-en-Y gastric bypass patients is maybe not so much a psychological issue as it is a physiologic one,” added Dr. Morton, chief of bariatric and minimally invasive surgery at Stanford (Calif.) School of Medicine.
Dr. King agreed. “Just in the last year and a half there have been some great pharmacokinetic studies showing that the Roux-en-Y affects alcohol metabolism and absorption, as well as studies in rodent models that suggest alcohol produces increased neurobiologic reward,” she noted.
The LABS-2 study is funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. King reported having no relevant financial interests.
AT OBESITY WEEK 2016
Key clinical point:
Major finding: In the first 5 years following bariatric surgery, patients who underwent Roux-en-Y gastric bypass were twice as likely to develop new-onset alcohol use disorder and nearly four times more likely to be treated for substance use disorder, compared with recipients of laparoscopic gastric banding.
Data source: The LABS-2 study is an observational cohort study involving more than 2,000 patients in long-term follow-up after undergoing Roux-en-Y gastric bypass or laparoscopic adjustable banding.
Disclosures: LABS-2 is funded by the National Institute of Diabetes and Digestive and Kidney Diseases. The presenter reported having no relevant financial interests.
Can carotid interventions affect cognitive function?
COLUMBUS, OHIO – The primary goal of carotid artery revascularization is to prevent stroke, heart attack or death, but carotid artery stenting and carotid endarterectomy may also cause changes in cognitive skills, according Raghu Motaganahalli, MD, of the Indiana University, Indianapolis.
“What about cognitive dysfunction as a result of carotid artery stenting (CAS) or carotid endarterectomy (CEA)?” Dr. Motaganahalli asked at the annual meeting of the Midwestern Vascular Surgical Society. “I think this is real, that there’s some truth to the matter. The question is how much and what domains of cognitive functions are affected?”

“Cerebrovascular hemodynamics status plays a role in cognitive function, but we need a better understanding of cerebrovascular hemodynamic failure and either improvement or decline of cognitive function after CAS or CEA,” he said.
A review of published trials shows that 10%-20% of patients who have either CAS or CEA have some degree of cognitive dysfunction as early as a day after the procedure. “It’s not a small number, compared to stoke, risk of myocardial infarction and death,” he said.
Some series have reported up to 40% of patients showed some cognitive dysfunction, and post–carotid endarterectomy cognitive dysfunction has been associated with early death, Dr. Motaganahalli said.
Cognitive dysfunction manifests in various forms, ranging from level of consciousness and memory to mood and ability to make calculations. Although the Mini-Mental State Examination Global Cognitive Assessment tool provides a method for evaluating cognitive function, “There is no uniformly accepted neurocognition test,” Dr. Motaganahalli said. That explains the wide variability of findings among published studies.
Vascular surgeons take a somewhat casual approach to their patients’ cognitive abilities after carotid revascularization, Dr. Motaganahalli said. “We don’t evaluate their memory and their cognitive functions on post-op day one; we just look to see whether they have neurologic dysfunction up front and that they’re capable of going home after that.”
But predicting in advance which patients are predisposed to cognitive decline after the procedures is difficult, he said. He cited a systematic review of 32 studies published between 1990-2007 that showed variable results (Stroke. 2008;39:3116-27): 11 studies during 1990-2005 suggested cognition actually improved after CEA; 9 studies during 1994-2006 suggested the opposite; 4 trials during 1992-2005 suggested no change in cognition after CEA; 5 studies during 2003-2007 showed improvement in cognition after CAS; and 3 trials comparing CAS and CEA and cognition found no differences in how the two procedures affect cognition.
Dr. Motaganahalli also cited a systematic review of 37 studies, 18 of which examined CEA, 12 CAS and seven compared CEA and CAS, found that either cognitive improvement or impairment for CEA and CAS separately were 10–15% of patients (Cerebrovasc Dis Extra. 2014;4:132-48).
“We have 69 papers that looked at cognitive function alone, but unfortunately, we don’t know whether cognitive function really improved based on this data set,” he said. “None of them are making the argument so clearly that there is cognitive improvement after revascularization.”
The variability in study findings can be due to differences in methodologies, the types of psychometric tests used, statistical analyses and the timing of cognitive assessments, Dr. Motaganahalli said.
Cognitive impairment after stroke caused by carotid disease is better understood than is cognitive impairment in the absence of a major stroke, Dr. Motaganahalli said.
“The mechanisms of how carotid disease can cause the cognitive impairment are threefold: It could be microembolism and hypoperfusion, which together can cause white matter disease and thereby some cognitive dysfunction in the long term,” he said (Neuroimaging Clin N Am. 2007 Aug;17:313-24).
Functional neurons may be a biomarker of cognitive outcome, he said. Hypoperfusion of functional neurons may lead to hypofunctional neurons, which can increase cerebral blood flow and cerebral metabolic rate for oxygen (CMRO2), and thus improve cognition. However, when additional variables are introduced to the hypofunctional neurons – such as microembolism, white matter disease, and prolonged hypoperfusion – that can lead to neuronal infarction that, while increasing cerebral blood flow, causes no change in CMRO2 and, thus, no cognitive improvement. The interval between hypofunctional neurons and neuronal infarction “is the time to do the revascularization, as long as you can demonstrate that there may be some truth to matter that it influences cognition,” Dr. Motaganahalli said.
While vascular surgeons may not be able to predict who will have cognitive decline after carotid interventions, “There are some pointers for possibly picking those patients who may benefit,” Dr. Motaganahalli said.
That choice of patients revolves around recognizing that chronic ischemia induces and increases the severity of cognitive dysfunction. Therefore, incorporating the pathophysiology of chronic ischemia into the algorithm for carotid artery disease may provide an opportunity to extend the goals of carotid artery revascularization to include preventing or reversing cognitive decline, he said.
Dr. Motaganahalli disclosed he is a consultant to Silk Road Medical.
COLUMBUS, OHIO – The primary goal of carotid artery revascularization is to prevent stroke, heart attack or death, but carotid artery stenting and carotid endarterectomy may also cause changes in cognitive skills, according Raghu Motaganahalli, MD, of the Indiana University, Indianapolis.
“What about cognitive dysfunction as a result of carotid artery stenting (CAS) or carotid endarterectomy (CEA)?” Dr. Motaganahalli asked at the annual meeting of the Midwestern Vascular Surgical Society. “I think this is real, that there’s some truth to the matter. The question is how much and what domains of cognitive functions are affected?”
“Cerebrovascular hemodynamics status plays a role in cognitive function, but we need a better understanding of cerebrovascular hemodynamic failure and either improvement or decline of cognitive function after CAS or CEA,” he said.
A review of published trials shows that 10%-20% of patients who have either CAS or CEA have some degree of cognitive dysfunction as early as a day after the procedure. “It’s not a small number, compared to stoke, risk of myocardial infarction and death,” he said.
Some series have reported up to 40% of patients showed some cognitive dysfunction, and post–carotid endarterectomy cognitive dysfunction has been associated with early death, Dr. Motaganahalli said.
Cognitive dysfunction manifests in various forms, ranging from level of consciousness and memory to mood and ability to make calculations. Although the Mini-Mental State Examination Global Cognitive Assessment tool provides a method for evaluating cognitive function, “There is no uniformly accepted neurocognition test,” Dr. Motaganahalli said. That explains the wide variability of findings among published studies.
Vascular surgeons take a somewhat casual approach to their patients’ cognitive abilities after carotid revascularization, Dr. Motaganahalli said. “We don’t evaluate their memory and their cognitive functions on post-op day one; we just look to see whether they have neurologic dysfunction up front and that they’re capable of going home after that.”
But predicting in advance which patients are predisposed to cognitive decline after the procedures is difficult, he said. He cited a systematic review of 32 studies published between 1990-2007 that showed variable results (Stroke. 2008;39:3116-27): 11 studies during 1990-2005 suggested cognition actually improved after CEA; 9 studies during 1994-2006 suggested the opposite; 4 trials during 1992-2005 suggested no change in cognition after CEA; 5 studies during 2003-2007 showed improvement in cognition after CAS; and 3 trials comparing CAS and CEA and cognition found no differences in how the two procedures affect cognition.
Dr. Motaganahalli also cited a systematic review of 37 studies, 18 of which examined CEA, 12 CAS and seven compared CEA and CAS, found that either cognitive improvement or impairment for CEA and CAS separately were 10–15% of patients (Cerebrovasc Dis Extra. 2014;4:132-48).
“We have 69 papers that looked at cognitive function alone, but unfortunately, we don’t know whether cognitive function really improved based on this data set,” he said. “None of them are making the argument so clearly that there is cognitive improvement after revascularization.”
The variability in study findings can be due to differences in methodologies, the types of psychometric tests used, statistical analyses and the timing of cognitive assessments, Dr. Motaganahalli said.
Cognitive impairment after stroke caused by carotid disease is better understood than is cognitive impairment in the absence of a major stroke, Dr. Motaganahalli said.
“The mechanisms of how carotid disease can cause the cognitive impairment are threefold: It could be microembolism and hypoperfusion, which together can cause white matter disease and thereby some cognitive dysfunction in the long term,” he said (Neuroimaging Clin N Am. 2007 Aug;17:313-24).
Functional neurons may be a biomarker of cognitive outcome, he said. Hypoperfusion of functional neurons may lead to hypofunctional neurons, which can increase cerebral blood flow and cerebral metabolic rate for oxygen (CMRO2), and thus improve cognition. However, when additional variables are introduced to the hypofunctional neurons – such as microembolism, white matter disease, and prolonged hypoperfusion – that can lead to neuronal infarction that, while increasing cerebral blood flow, causes no change in CMRO2 and, thus, no cognitive improvement. The interval between hypofunctional neurons and neuronal infarction “is the time to do the revascularization, as long as you can demonstrate that there may be some truth to matter that it influences cognition,” Dr. Motaganahalli said.
While vascular surgeons may not be able to predict who will have cognitive decline after carotid interventions, “There are some pointers for possibly picking those patients who may benefit,” Dr. Motaganahalli said.
That choice of patients revolves around recognizing that chronic ischemia induces and increases the severity of cognitive dysfunction. Therefore, incorporating the pathophysiology of chronic ischemia into the algorithm for carotid artery disease may provide an opportunity to extend the goals of carotid artery revascularization to include preventing or reversing cognitive decline, he said.
Dr. Motaganahalli disclosed he is a consultant to Silk Road Medical.
COLUMBUS, OHIO – The primary goal of carotid artery revascularization is to prevent stroke, heart attack or death, but carotid artery stenting and carotid endarterectomy may also cause changes in cognitive skills, according Raghu Motaganahalli, MD, of the Indiana University, Indianapolis.
“What about cognitive dysfunction as a result of carotid artery stenting (CAS) or carotid endarterectomy (CEA)?” Dr. Motaganahalli asked at the annual meeting of the Midwestern Vascular Surgical Society. “I think this is real, that there’s some truth to the matter. The question is how much and what domains of cognitive functions are affected?”
“Cerebrovascular hemodynamics status plays a role in cognitive function, but we need a better understanding of cerebrovascular hemodynamic failure and either improvement or decline of cognitive function after CAS or CEA,” he said.
A review of published trials shows that 10%-20% of patients who have either CAS or CEA have some degree of cognitive dysfunction as early as a day after the procedure. “It’s not a small number, compared to stoke, risk of myocardial infarction and death,” he said.
Some series have reported up to 40% of patients showed some cognitive dysfunction, and post–carotid endarterectomy cognitive dysfunction has been associated with early death, Dr. Motaganahalli said.
Cognitive dysfunction manifests in various forms, ranging from level of consciousness and memory to mood and ability to make calculations. Although the Mini-Mental State Examination Global Cognitive Assessment tool provides a method for evaluating cognitive function, “There is no uniformly accepted neurocognition test,” Dr. Motaganahalli said. That explains the wide variability of findings among published studies.
Vascular surgeons take a somewhat casual approach to their patients’ cognitive abilities after carotid revascularization, Dr. Motaganahalli said. “We don’t evaluate their memory and their cognitive functions on post-op day one; we just look to see whether they have neurologic dysfunction up front and that they’re capable of going home after that.”
But predicting in advance which patients are predisposed to cognitive decline after the procedures is difficult, he said. He cited a systematic review of 32 studies published between 1990-2007 that showed variable results (Stroke. 2008;39:3116-27): 11 studies during 1990-2005 suggested cognition actually improved after CEA; 9 studies during 1994-2006 suggested the opposite; 4 trials during 1992-2005 suggested no change in cognition after CEA; 5 studies during 2003-2007 showed improvement in cognition after CAS; and 3 trials comparing CAS and CEA and cognition found no differences in how the two procedures affect cognition.
Dr. Motaganahalli also cited a systematic review of 37 studies, 18 of which examined CEA, 12 CAS and seven compared CEA and CAS, found that either cognitive improvement or impairment for CEA and CAS separately were 10–15% of patients (Cerebrovasc Dis Extra. 2014;4:132-48).
“We have 69 papers that looked at cognitive function alone, but unfortunately, we don’t know whether cognitive function really improved based on this data set,” he said. “None of them are making the argument so clearly that there is cognitive improvement after revascularization.”
The variability in study findings can be due to differences in methodologies, the types of psychometric tests used, statistical analyses and the timing of cognitive assessments, Dr. Motaganahalli said.
Cognitive impairment after stroke caused by carotid disease is better understood than is cognitive impairment in the absence of a major stroke, Dr. Motaganahalli said.
“The mechanisms of how carotid disease can cause the cognitive impairment are threefold: It could be microembolism and hypoperfusion, which together can cause white matter disease and thereby some cognitive dysfunction in the long term,” he said (Neuroimaging Clin N Am. 2007 Aug;17:313-24).
Functional neurons may be a biomarker of cognitive outcome, he said. Hypoperfusion of functional neurons may lead to hypofunctional neurons, which can increase cerebral blood flow and cerebral metabolic rate for oxygen (CMRO2), and thus improve cognition. However, when additional variables are introduced to the hypofunctional neurons – such as microembolism, white matter disease, and prolonged hypoperfusion – that can lead to neuronal infarction that, while increasing cerebral blood flow, causes no change in CMRO2 and, thus, no cognitive improvement. The interval between hypofunctional neurons and neuronal infarction “is the time to do the revascularization, as long as you can demonstrate that there may be some truth to matter that it influences cognition,” Dr. Motaganahalli said.
While vascular surgeons may not be able to predict who will have cognitive decline after carotid interventions, “There are some pointers for possibly picking those patients who may benefit,” Dr. Motaganahalli said.
That choice of patients revolves around recognizing that chronic ischemia induces and increases the severity of cognitive dysfunction. Therefore, incorporating the pathophysiology of chronic ischemia into the algorithm for carotid artery disease may provide an opportunity to extend the goals of carotid artery revascularization to include preventing or reversing cognitive decline, he said.
Dr. Motaganahalli disclosed he is a consultant to Silk Road Medical.
AT THE ANNUAL MEETING OF THE MIDWESTERN VASCULAR SURGERY SOCIETY
Key clinical point: Incorporating the pathophysiology of chronic ischemia into the algorithm for carotid artery disease could expand the goals of revascularization to encompass cognitive decline.
Major finding: Cerebrovascular hemodynamic status plays a role in cognitive function after carotid artery interventions, but the mechanisms of either improvement or decline need better understanding.
Data source: Systematic review of 32 papers on neurocognition after carotid interventions published between 1990-2007 and analysis of 37 studies of CAS or CEA or both published since 2007.
Disclosures: Dr. Motaganahalli disclosed he is a consultant to Silk Road Medical Inc.
Balancing speed, safety in device approvals
WASHINGTON – Regulators from two continents are slowly inching toward more common ground when it comes to device approvals, a move that should strike a better balance between the time to approval and safety of the products.
It is no surprise that for devices to be approved in the United States, a much more rigorous evidence standard exists than it does in Europe, but the Food and Drug Administration is looking for ways to make changes to allow for quicker approval times without compromising safety.
Meanwhile, across the Atlantic, European regulators are looking for increased evidence requirements that will not stifle innovation.

However, health information technology may help relieve some inefficiencies going forward.
“If we combine quality registries, claims data, the evolving improving electronic health records, and the data warehouses that all of our health systems have, we can conduct prospective, observational, and clinical trials at a dramatically lower cost, answering many more questions per unit of time,” Dr. Califf added.
Other areas that will help improve the efficiency of the U.S. approval process is the work on developing a framework to bring feasibility studies back to America.
“I want to really accelerate that because we are hearing from a lot of people that they want to access the technology early; it’s the right thing to do, and we are hearing from industry that they’d like to work in the United States,” he said.
However, that is going to require one group that is generally more risk adverse to be willing to participate more in the process.
“The main limiting factors at this point in time are the health systems that we are all working in,” Dr. Califf noted. “They are very risk adverse. So while it is nice to argue and advertise that your interventional cardiologists are the best in town on your billboard, protecting those interventional cardiologists to do the high-risk, early studies that are really needed to develop devices is a different matter.”
He called on doctors to go back to their health systems to help better develop those early feasibility pathways to help bring some of that innovation back the United States.
Finally, Dr. Califf addressed the idea of developing evidence that can function not only for device approval, but for payment as well, especially as reimbursement systems are becoming more value driven.
“We are going to move to a system where reimbursement will increasingly move away from fee for service and increasingly gravitate to payment for value,” Dr. Califf said. “In order for this to work, we’ve got to develop the kinds of clinical trials [that include] the calculation of value, so the winners can be promoted on a wider scale and the procedures and technologies that don’t provide incremental value are left behind.”
He continued: “We need your help in figuring out the common source of information so that the FDA can make its decision – which is different from CMS’s decision – but where there’s a continuum of knowledge that allows for products to be approved if they are worthwhile, and then to be paid for and allowed to be marketed.”
Meanwhile, developers are facing a different situation in Europe, where more regulation and more stringent evidence standards could be coming down the pike.
Dr. Fraser noted research that has shown that devices first approved in Europe, compared with their U.S. counterparts, are associated with an increased incidence of recalls or safety alerts.
That being said, he noted that there are several proposed regulations that would increase the evidence requirements related to regulatory approval that manufacturers could face in the coming year, a challenge as it will require some level of harmonization across countries and regulatory systems within each country.
“In Europe, we are on the dawn of a new era regarding medical device assessment, but it is going to pose a very large challenge for our colleagues in the regulatory agencies because of their personnel, funding, and the integration between all these bodies and national systems. There are also tremendous challenges for us as physicians to ensure that we seek the evidence, we assess and contribute to it, and particularly now, that we also routinely take part in new systems for postmarket surveillance,” he said.
WASHINGTON – Regulators from two continents are slowly inching toward more common ground when it comes to device approvals, a move that should strike a better balance between the time to approval and safety of the products.
It is no surprise that for devices to be approved in the United States, a much more rigorous evidence standard exists than it does in Europe, but the Food and Drug Administration is looking for ways to make changes to allow for quicker approval times without compromising safety.
Meanwhile, across the Atlantic, European regulators are looking for increased evidence requirements that will not stifle innovation.
However, health information technology may help relieve some inefficiencies going forward.
“If we combine quality registries, claims data, the evolving improving electronic health records, and the data warehouses that all of our health systems have, we can conduct prospective, observational, and clinical trials at a dramatically lower cost, answering many more questions per unit of time,” Dr. Califf added.
Other areas that will help improve the efficiency of the U.S. approval process is the work on developing a framework to bring feasibility studies back to America.
“I want to really accelerate that because we are hearing from a lot of people that they want to access the technology early; it’s the right thing to do, and we are hearing from industry that they’d like to work in the United States,” he said.
However, that is going to require one group that is generally more risk adverse to be willing to participate more in the process.
“The main limiting factors at this point in time are the health systems that we are all working in,” Dr. Califf noted. “They are very risk adverse. So while it is nice to argue and advertise that your interventional cardiologists are the best in town on your billboard, protecting those interventional cardiologists to do the high-risk, early studies that are really needed to develop devices is a different matter.”
He called on doctors to go back to their health systems to help better develop those early feasibility pathways to help bring some of that innovation back the United States.
Finally, Dr. Califf addressed the idea of developing evidence that can function not only for device approval, but for payment as well, especially as reimbursement systems are becoming more value driven.
“We are going to move to a system where reimbursement will increasingly move away from fee for service and increasingly gravitate to payment for value,” Dr. Califf said. “In order for this to work, we’ve got to develop the kinds of clinical trials [that include] the calculation of value, so the winners can be promoted on a wider scale and the procedures and technologies that don’t provide incremental value are left behind.”
He continued: “We need your help in figuring out the common source of information so that the FDA can make its decision – which is different from CMS’s decision – but where there’s a continuum of knowledge that allows for products to be approved if they are worthwhile, and then to be paid for and allowed to be marketed.”
Meanwhile, developers are facing a different situation in Europe, where more regulation and more stringent evidence standards could be coming down the pike.
Dr. Fraser noted research that has shown that devices first approved in Europe, compared with their U.S. counterparts, are associated with an increased incidence of recalls or safety alerts.
That being said, he noted that there are several proposed regulations that would increase the evidence requirements related to regulatory approval that manufacturers could face in the coming year, a challenge as it will require some level of harmonization across countries and regulatory systems within each country.
“In Europe, we are on the dawn of a new era regarding medical device assessment, but it is going to pose a very large challenge for our colleagues in the regulatory agencies because of their personnel, funding, and the integration between all these bodies and national systems. There are also tremendous challenges for us as physicians to ensure that we seek the evidence, we assess and contribute to it, and particularly now, that we also routinely take part in new systems for postmarket surveillance,” he said.
WASHINGTON – Regulators from two continents are slowly inching toward more common ground when it comes to device approvals, a move that should strike a better balance between the time to approval and safety of the products.
It is no surprise that for devices to be approved in the United States, a much more rigorous evidence standard exists than it does in Europe, but the Food and Drug Administration is looking for ways to make changes to allow for quicker approval times without compromising safety.
Meanwhile, across the Atlantic, European regulators are looking for increased evidence requirements that will not stifle innovation.
However, health information technology may help relieve some inefficiencies going forward.
“If we combine quality registries, claims data, the evolving improving electronic health records, and the data warehouses that all of our health systems have, we can conduct prospective, observational, and clinical trials at a dramatically lower cost, answering many more questions per unit of time,” Dr. Califf added.
Other areas that will help improve the efficiency of the U.S. approval process is the work on developing a framework to bring feasibility studies back to America.
“I want to really accelerate that because we are hearing from a lot of people that they want to access the technology early; it’s the right thing to do, and we are hearing from industry that they’d like to work in the United States,” he said.
However, that is going to require one group that is generally more risk adverse to be willing to participate more in the process.
“The main limiting factors at this point in time are the health systems that we are all working in,” Dr. Califf noted. “They are very risk adverse. So while it is nice to argue and advertise that your interventional cardiologists are the best in town on your billboard, protecting those interventional cardiologists to do the high-risk, early studies that are really needed to develop devices is a different matter.”
He called on doctors to go back to their health systems to help better develop those early feasibility pathways to help bring some of that innovation back the United States.
Finally, Dr. Califf addressed the idea of developing evidence that can function not only for device approval, but for payment as well, especially as reimbursement systems are becoming more value driven.
“We are going to move to a system where reimbursement will increasingly move away from fee for service and increasingly gravitate to payment for value,” Dr. Califf said. “In order for this to work, we’ve got to develop the kinds of clinical trials [that include] the calculation of value, so the winners can be promoted on a wider scale and the procedures and technologies that don’t provide incremental value are left behind.”
He continued: “We need your help in figuring out the common source of information so that the FDA can make its decision – which is different from CMS’s decision – but where there’s a continuum of knowledge that allows for products to be approved if they are worthwhile, and then to be paid for and allowed to be marketed.”
Meanwhile, developers are facing a different situation in Europe, where more regulation and more stringent evidence standards could be coming down the pike.
Dr. Fraser noted research that has shown that devices first approved in Europe, compared with their U.S. counterparts, are associated with an increased incidence of recalls or safety alerts.
That being said, he noted that there are several proposed regulations that would increase the evidence requirements related to regulatory approval that manufacturers could face in the coming year, a challenge as it will require some level of harmonization across countries and regulatory systems within each country.
“In Europe, we are on the dawn of a new era regarding medical device assessment, but it is going to pose a very large challenge for our colleagues in the regulatory agencies because of their personnel, funding, and the integration between all these bodies and national systems. There are also tremendous challenges for us as physicians to ensure that we seek the evidence, we assess and contribute to it, and particularly now, that we also routinely take part in new systems for postmarket surveillance,” he said.
AT TCT 2016
Employer-provided insurance stable after ACA implementation
Concerns that Affordable Care Act (ACA) provisions implemented in 2014 would lead large numbers of employers to drop health insurance coverage appear to have been unfounded, according to a study published in the journal Health Affairs.
More than 95% of employers did not change their insurance coverage policy between 2013 and 2014: 46.4% offered coverage in 2013 and continued it in 2014 and 49.1% did not offer coverage either year. Of the 21,900 private-sector employers included in the analysis, 3.5% provided coverage in 2013 but not in 2014 and 1.1% did not offer it in 2013 but did in 2014, reported Jean Abraham, PhD, of the University of Minnesota, Minneapolis, and her associates (Health Aff. 2016 Oct 26;35[11]. doi: 10.1377/hlthaff.2016.0631).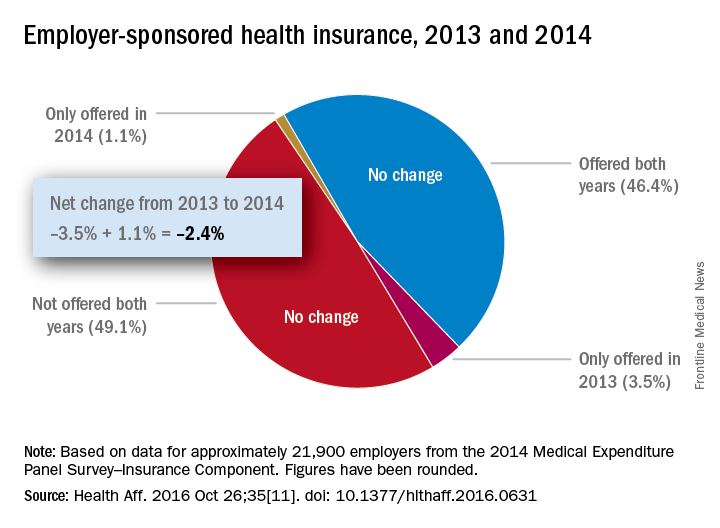
The analysis of data from the 2014 Medical Expenditure Panel Survey–Insurance Component, however, did show associations between coverage changes and several workforce and employer characteristics. “Small firms were more likely to drop coverage compared to large ones, as were those with more low-wage workers compared to those with fewer such workers, newer establishments compared to older ones, and those in the service sector compared to those in blue- and white-collar industries,” Dr. Abraham and her associates wrote.
The Robert Wood Johnson Foundation’s State Health Access Reform Evaluation program supported the study. No other financial disclosures were provided.
Concerns that Affordable Care Act (ACA) provisions implemented in 2014 would lead large numbers of employers to drop health insurance coverage appear to have been unfounded, according to a study published in the journal Health Affairs.
More than 95% of employers did not change their insurance coverage policy between 2013 and 2014: 46.4% offered coverage in 2013 and continued it in 2014 and 49.1% did not offer coverage either year. Of the 21,900 private-sector employers included in the analysis, 3.5% provided coverage in 2013 but not in 2014 and 1.1% did not offer it in 2013 but did in 2014, reported Jean Abraham, PhD, of the University of Minnesota, Minneapolis, and her associates (Health Aff. 2016 Oct 26;35[11]. doi: 10.1377/hlthaff.2016.0631).
The analysis of data from the 2014 Medical Expenditure Panel Survey–Insurance Component, however, did show associations between coverage changes and several workforce and employer characteristics. “Small firms were more likely to drop coverage compared to large ones, as were those with more low-wage workers compared to those with fewer such workers, newer establishments compared to older ones, and those in the service sector compared to those in blue- and white-collar industries,” Dr. Abraham and her associates wrote.
The Robert Wood Johnson Foundation’s State Health Access Reform Evaluation program supported the study. No other financial disclosures were provided.
Concerns that Affordable Care Act (ACA) provisions implemented in 2014 would lead large numbers of employers to drop health insurance coverage appear to have been unfounded, according to a study published in the journal Health Affairs.
More than 95% of employers did not change their insurance coverage policy between 2013 and 2014: 46.4% offered coverage in 2013 and continued it in 2014 and 49.1% did not offer coverage either year. Of the 21,900 private-sector employers included in the analysis, 3.5% provided coverage in 2013 but not in 2014 and 1.1% did not offer it in 2013 but did in 2014, reported Jean Abraham, PhD, of the University of Minnesota, Minneapolis, and her associates (Health Aff. 2016 Oct 26;35[11]. doi: 10.1377/hlthaff.2016.0631).
The analysis of data from the 2014 Medical Expenditure Panel Survey–Insurance Component, however, did show associations between coverage changes and several workforce and employer characteristics. “Small firms were more likely to drop coverage compared to large ones, as were those with more low-wage workers compared to those with fewer such workers, newer establishments compared to older ones, and those in the service sector compared to those in blue- and white-collar industries,” Dr. Abraham and her associates wrote.
The Robert Wood Johnson Foundation’s State Health Access Reform Evaluation program supported the study. No other financial disclosures were provided.
Number of Medicare part D drug plans continues to decline
There will be 16% fewer Medicare part D prescription drug plans available in 2017, compared with 2016, according to an analysis by the Kaiser Family Foundation.
In 2017, there will be 746 stand-alone prescription drug plans available to Medicare beneficiaries in the 50 states and the District of Columbia, which is 140 (16%) less than were available in 2016 and 1,129 (60%) less than the peak in 2007, Kaiser reported.
Of the nearly 41 million people enrolled in Medicare part D plans in 2016, about 12 million receive the low-income subsidy. The Congressional Budget Office estimates that spending on part D benefits will be $94 billion in 2017, which is 15.6% of overall Medicare costs. Medicare actuaries have projected that the cost per enrollee will increase by 5.8% annually from 2015 to 2025, Kaiser reported.
There will be 16% fewer Medicare part D prescription drug plans available in 2017, compared with 2016, according to an analysis by the Kaiser Family Foundation.
In 2017, there will be 746 stand-alone prescription drug plans available to Medicare beneficiaries in the 50 states and the District of Columbia, which is 140 (16%) less than were available in 2016 and 1,129 (60%) less than the peak in 2007, Kaiser reported.
Of the nearly 41 million people enrolled in Medicare part D plans in 2016, about 12 million receive the low-income subsidy. The Congressional Budget Office estimates that spending on part D benefits will be $94 billion in 2017, which is 15.6% of overall Medicare costs. Medicare actuaries have projected that the cost per enrollee will increase by 5.8% annually from 2015 to 2025, Kaiser reported.
There will be 16% fewer Medicare part D prescription drug plans available in 2017, compared with 2016, according to an analysis by the Kaiser Family Foundation.
In 2017, there will be 746 stand-alone prescription drug plans available to Medicare beneficiaries in the 50 states and the District of Columbia, which is 140 (16%) less than were available in 2016 and 1,129 (60%) less than the peak in 2007, Kaiser reported.
Of the nearly 41 million people enrolled in Medicare part D plans in 2016, about 12 million receive the low-income subsidy. The Congressional Budget Office estimates that spending on part D benefits will be $94 billion in 2017, which is 15.6% of overall Medicare costs. Medicare actuaries have projected that the cost per enrollee will increase by 5.8% annually from 2015 to 2025, Kaiser reported.
7 tips for successful value-based care contracts
During a recent webinar presented by the American Bar Association, legal experts provided guidance on how doctors can successfully draft pay-for-performance contracts and prevent disputes with payers.
1. Clearly define terms
Contract terms and definitions should be clearly outlined and understood by both parties before value-based agreements are signed, said Melissa J. Hulke, a director in the Berkeley Research Group, LLC health analytics practice.

“Contract terms become central to resolving differences, so it’s important the contract is well defined, especially when moving away from fee for service,” she said. “These are more complex arrangements.”
Another area that needs thorough definition surrounds referral volume. Contracts can include the phrases, “predominately refer” or “primarily refer,” without defining the meaning of “predominately” or “primarily,” Ms. Hulke said.
“If that’s not defined in the contract, it’s hard to establish a benchmark to not only project the provider’s performance under the arrangement and how much revenue they can expect to receive, but it’s hard to know if you’re meeting that benchmark, as well,” she said. “I strongly encourage that if [a term states] “primarily, predominately, [or] mostly refer,” that you have a specific percentage benchmark included. That will help to avoid any disagreement later on.”
2. Review payment calculations
Ensure that payment formulas are examined and agreed upon.

“I think that should be baked into the contracts of today because they are so complex and there is so much money at stake,” she said. “Walk through that compensation exhibit, walk through the examples of what’s supposed to happen.
If not in agreement with calculations, talk to the payer’s financial personnel about how the numbers were reached and try to resolve any differences.
3. Monitor results
Actively monitor projected-to-actual financial performance under the contract. If performance is not being monitored and results are not being tested, it’s impossible to tell whether the contract is succeeding or failing, Ms. Hulke said.
It’s a good idea to monitor projected-to-actual financial performance monthly or at least quarterly, she advised.
“Tracking budget to actual performance and investigating successes and failures are important if the contracts are material to the provider’s business,” Ms. Hulke said.
4. Institute time frames for government methodologies
Be specific about when contracts are linked to Medicare reimbursement methodologies.
If commercial payers are tying payment rates to government programs, which often occurs, contracts should include whether the reimbursement is based on Medicare rates and methodologies as of a particular date and time, according to Ms. Hulke. For instance, the contract could specify that rates are tied to Medicare methodologies at the time the contract was executed. Alternatively, contracts could allow the physician payment rate to fluctuate depending on changes the government makes to Medicare rates and methodologies during the span of the contract.
“If this is not defined, when Medicare makes a change, the parties may have differing opinions on the appropriate rate of reimbursement that’s being paid,” she said.
5. Structure around state and federal laws
Conduct a regulatory analysis before inking any value based payment arrangement/transaction, and structure and document around potential legal constraints, Ms. Hanna said.
Know the laws in your state, she advised. Some states have requirements for provider incentive programs, while others may have rules for provider organizations or intermediaries that assume certain financial risk. When working with federal health care payers, review the Stark Law and Anti-Kickback regulations and ensure that if triggered by the arrangement, the venture falls within an exception of the statutes. Other legal considerations when drafting contracts include:
• HIPAA and state privacy laws.
• Antitrust laws.
• Telemedicine and telehealth laws.
• Medicare Advantage benefit guidelines for programs designed for specific Medicare Advantage populations.
• Scope of practice laws applicable to mid-level medical providers.
6. Design a dispute-resolution strategy
Include a thorough dispute-resolution strategy within the contract. The strategies help facilitate an orderly process for resolving disputes cost effectively, Ms. Hanna said. She suggested that policies start with an informal dispute-resolution process that sends unresolved matters to senior executives at each organization.
“This allows business leaders – and not the lawyers – to find a business solution to a thorny and potentially costly problem before each party gets entrenched in its own position and own sense of having been wronged,” she said in an interview. “The business solution may or may not rely on contract language but may be tailored to keep the relationship moving forward. However, if the informal process proves unsuccessful, then the process gets punted to the legal system – whether in a court proceeding or arbitration.”
7. Have an exit strategy
Include an exit strategy that ensures an end to the arrangement goes as smoothly and fairly as possible. The strategy will depend on the nature and structure of the payer-provider alignment and the value-based payment arrangement, Ms. Hanna said in an interview.
For example, in a true, corporate joint venture, the exit strategy may include buyout rights of the newly formed entity. In this case, it’s important to consider and negotiate the price of the buyout and what circumstances that will trigger the buyout. Termination rights should also be included in an exit strategy, Ms. Hanna said. One option is to allow termination “without case,” by either party.
“Clients often do not like this approach because the intention of the parties going in is to build a strong, long-term relationship where provider and payer benefit,” she said. “A ‘without cause’ termination rights gives the parties a safety valve if circumstances change or the relationship is just not successful.”
An alternative is to allow the relationship time to mature and grow before either party can exercise a without cause termination. A related approach is to develop triggering events that would give one or both parties the right to terminate the agreement, without the other party “having committed a bad act,” Ms. Hanna said in the interview.
“For instance, if the relationship does not meet certain financial or other benchmarks within an agreed-upon time frame, this may be a sufficient reason to terminate the relationship, abandon, or renegotiate the value-based purchasing payment formula or, perhaps, end an exclusive or other preferential relationship,” she said.
[email protected]
On Twitter @legal_med
During a recent webinar presented by the American Bar Association, legal experts provided guidance on how doctors can successfully draft pay-for-performance contracts and prevent disputes with payers.
1. Clearly define terms
Contract terms and definitions should be clearly outlined and understood by both parties before value-based agreements are signed, said Melissa J. Hulke, a director in the Berkeley Research Group, LLC health analytics practice.
“Contract terms become central to resolving differences, so it’s important the contract is well defined, especially when moving away from fee for service,” she said. “These are more complex arrangements.”
Another area that needs thorough definition surrounds referral volume. Contracts can include the phrases, “predominately refer” or “primarily refer,” without defining the meaning of “predominately” or “primarily,” Ms. Hulke said.
“If that’s not defined in the contract, it’s hard to establish a benchmark to not only project the provider’s performance under the arrangement and how much revenue they can expect to receive, but it’s hard to know if you’re meeting that benchmark, as well,” she said. “I strongly encourage that if [a term states] “primarily, predominately, [or] mostly refer,” that you have a specific percentage benchmark included. That will help to avoid any disagreement later on.”
2. Review payment calculations
Ensure that payment formulas are examined and agreed upon.
“I think that should be baked into the contracts of today because they are so complex and there is so much money at stake,” she said. “Walk through that compensation exhibit, walk through the examples of what’s supposed to happen.
If not in agreement with calculations, talk to the payer’s financial personnel about how the numbers were reached and try to resolve any differences.
3. Monitor results
Actively monitor projected-to-actual financial performance under the contract. If performance is not being monitored and results are not being tested, it’s impossible to tell whether the contract is succeeding or failing, Ms. Hulke said.
It’s a good idea to monitor projected-to-actual financial performance monthly or at least quarterly, she advised.
“Tracking budget to actual performance and investigating successes and failures are important if the contracts are material to the provider’s business,” Ms. Hulke said.
4. Institute time frames for government methodologies
Be specific about when contracts are linked to Medicare reimbursement methodologies.
If commercial payers are tying payment rates to government programs, which often occurs, contracts should include whether the reimbursement is based on Medicare rates and methodologies as of a particular date and time, according to Ms. Hulke. For instance, the contract could specify that rates are tied to Medicare methodologies at the time the contract was executed. Alternatively, contracts could allow the physician payment rate to fluctuate depending on changes the government makes to Medicare rates and methodologies during the span of the contract.
“If this is not defined, when Medicare makes a change, the parties may have differing opinions on the appropriate rate of reimbursement that’s being paid,” she said.
5. Structure around state and federal laws
Conduct a regulatory analysis before inking any value based payment arrangement/transaction, and structure and document around potential legal constraints, Ms. Hanna said.
Know the laws in your state, she advised. Some states have requirements for provider incentive programs, while others may have rules for provider organizations or intermediaries that assume certain financial risk. When working with federal health care payers, review the Stark Law and Anti-Kickback regulations and ensure that if triggered by the arrangement, the venture falls within an exception of the statutes. Other legal considerations when drafting contracts include:
• HIPAA and state privacy laws.
• Antitrust laws.
• Telemedicine and telehealth laws.
• Medicare Advantage benefit guidelines for programs designed for specific Medicare Advantage populations.
• Scope of practice laws applicable to mid-level medical providers.
6. Design a dispute-resolution strategy
Include a thorough dispute-resolution strategy within the contract. The strategies help facilitate an orderly process for resolving disputes cost effectively, Ms. Hanna said. She suggested that policies start with an informal dispute-resolution process that sends unresolved matters to senior executives at each organization.
“This allows business leaders – and not the lawyers – to find a business solution to a thorny and potentially costly problem before each party gets entrenched in its own position and own sense of having been wronged,” she said in an interview. “The business solution may or may not rely on contract language but may be tailored to keep the relationship moving forward. However, if the informal process proves unsuccessful, then the process gets punted to the legal system – whether in a court proceeding or arbitration.”
7. Have an exit strategy
Include an exit strategy that ensures an end to the arrangement goes as smoothly and fairly as possible. The strategy will depend on the nature and structure of the payer-provider alignment and the value-based payment arrangement, Ms. Hanna said in an interview.
For example, in a true, corporate joint venture, the exit strategy may include buyout rights of the newly formed entity. In this case, it’s important to consider and negotiate the price of the buyout and what circumstances that will trigger the buyout. Termination rights should also be included in an exit strategy, Ms. Hanna said. One option is to allow termination “without case,” by either party.
“Clients often do not like this approach because the intention of the parties going in is to build a strong, long-term relationship where provider and payer benefit,” she said. “A ‘without cause’ termination rights gives the parties a safety valve if circumstances change or the relationship is just not successful.”
An alternative is to allow the relationship time to mature and grow before either party can exercise a without cause termination. A related approach is to develop triggering events that would give one or both parties the right to terminate the agreement, without the other party “having committed a bad act,” Ms. Hanna said in the interview.
“For instance, if the relationship does not meet certain financial or other benchmarks within an agreed-upon time frame, this may be a sufficient reason to terminate the relationship, abandon, or renegotiate the value-based purchasing payment formula or, perhaps, end an exclusive or other preferential relationship,” she said.
[email protected]
On Twitter @legal_med
During a recent webinar presented by the American Bar Association, legal experts provided guidance on how doctors can successfully draft pay-for-performance contracts and prevent disputes with payers.
1. Clearly define terms
Contract terms and definitions should be clearly outlined and understood by both parties before value-based agreements are signed, said Melissa J. Hulke, a director in the Berkeley Research Group, LLC health analytics practice.
“Contract terms become central to resolving differences, so it’s important the contract is well defined, especially when moving away from fee for service,” she said. “These are more complex arrangements.”
Another area that needs thorough definition surrounds referral volume. Contracts can include the phrases, “predominately refer” or “primarily refer,” without defining the meaning of “predominately” or “primarily,” Ms. Hulke said.
“If that’s not defined in the contract, it’s hard to establish a benchmark to not only project the provider’s performance under the arrangement and how much revenue they can expect to receive, but it’s hard to know if you’re meeting that benchmark, as well,” she said. “I strongly encourage that if [a term states] “primarily, predominately, [or] mostly refer,” that you have a specific percentage benchmark included. That will help to avoid any disagreement later on.”
2. Review payment calculations
Ensure that payment formulas are examined and agreed upon.
“I think that should be baked into the contracts of today because they are so complex and there is so much money at stake,” she said. “Walk through that compensation exhibit, walk through the examples of what’s supposed to happen.
If not in agreement with calculations, talk to the payer’s financial personnel about how the numbers were reached and try to resolve any differences.
3. Monitor results
Actively monitor projected-to-actual financial performance under the contract. If performance is not being monitored and results are not being tested, it’s impossible to tell whether the contract is succeeding or failing, Ms. Hulke said.
It’s a good idea to monitor projected-to-actual financial performance monthly or at least quarterly, she advised.
“Tracking budget to actual performance and investigating successes and failures are important if the contracts are material to the provider’s business,” Ms. Hulke said.
4. Institute time frames for government methodologies
Be specific about when contracts are linked to Medicare reimbursement methodologies.
If commercial payers are tying payment rates to government programs, which often occurs, contracts should include whether the reimbursement is based on Medicare rates and methodologies as of a particular date and time, according to Ms. Hulke. For instance, the contract could specify that rates are tied to Medicare methodologies at the time the contract was executed. Alternatively, contracts could allow the physician payment rate to fluctuate depending on changes the government makes to Medicare rates and methodologies during the span of the contract.
“If this is not defined, when Medicare makes a change, the parties may have differing opinions on the appropriate rate of reimbursement that’s being paid,” she said.
5. Structure around state and federal laws
Conduct a regulatory analysis before inking any value based payment arrangement/transaction, and structure and document around potential legal constraints, Ms. Hanna said.
Know the laws in your state, she advised. Some states have requirements for provider incentive programs, while others may have rules for provider organizations or intermediaries that assume certain financial risk. When working with federal health care payers, review the Stark Law and Anti-Kickback regulations and ensure that if triggered by the arrangement, the venture falls within an exception of the statutes. Other legal considerations when drafting contracts include:
• HIPAA and state privacy laws.
• Antitrust laws.
• Telemedicine and telehealth laws.
• Medicare Advantage benefit guidelines for programs designed for specific Medicare Advantage populations.
• Scope of practice laws applicable to mid-level medical providers.
6. Design a dispute-resolution strategy
Include a thorough dispute-resolution strategy within the contract. The strategies help facilitate an orderly process for resolving disputes cost effectively, Ms. Hanna said. She suggested that policies start with an informal dispute-resolution process that sends unresolved matters to senior executives at each organization.
“This allows business leaders – and not the lawyers – to find a business solution to a thorny and potentially costly problem before each party gets entrenched in its own position and own sense of having been wronged,” she said in an interview. “The business solution may or may not rely on contract language but may be tailored to keep the relationship moving forward. However, if the informal process proves unsuccessful, then the process gets punted to the legal system – whether in a court proceeding or arbitration.”
7. Have an exit strategy
Include an exit strategy that ensures an end to the arrangement goes as smoothly and fairly as possible. The strategy will depend on the nature and structure of the payer-provider alignment and the value-based payment arrangement, Ms. Hanna said in an interview.
For example, in a true, corporate joint venture, the exit strategy may include buyout rights of the newly formed entity. In this case, it’s important to consider and negotiate the price of the buyout and what circumstances that will trigger the buyout. Termination rights should also be included in an exit strategy, Ms. Hanna said. One option is to allow termination “without case,” by either party.
“Clients often do not like this approach because the intention of the parties going in is to build a strong, long-term relationship where provider and payer benefit,” she said. “A ‘without cause’ termination rights gives the parties a safety valve if circumstances change or the relationship is just not successful.”
An alternative is to allow the relationship time to mature and grow before either party can exercise a without cause termination. A related approach is to develop triggering events that would give one or both parties the right to terminate the agreement, without the other party “having committed a bad act,” Ms. Hanna said in the interview.
“For instance, if the relationship does not meet certain financial or other benchmarks within an agreed-upon time frame, this may be a sufficient reason to terminate the relationship, abandon, or renegotiate the value-based purchasing payment formula or, perhaps, end an exclusive or other preferential relationship,” she said.
[email protected]
On Twitter @legal_med
Staple line reinforcement linked to increased leak risk in bariatric surgery
Laparoscopic sleeve gastrectomy is safe and effective overall, but staple line reinforcement appears to increase the rate of postsurgical leaks – which were associated with readmissions and, in some cases, reoperations.
A large review of quality improvement data found that staple line reinforcement – an extremely common technique – was associated with a 60% increased risk of leak, compared with closures without staple line reinforcement, Elizabeth R. Berger, MD, and her colleagues reported in the October issue of the Annals of Surgery (2016;264:464-73).
“This study also demonstrates that leaks were significantly more morbid than bleeding with higher readmission and reoperation rates in patients with a leak vs. a bleed,” wrote Dr. Berger of Loyola University, Chicago, and her coauthors. “Therefore, a surgeon should consider the benefits, risks, and costs of each surgical technique in performing a laparoscopic sleeve gastrectomy and selectively utilize those that, in their hands, minimize morbidity while maximizing clinical effectiveness.”
The team examined outcomes in 189,477 laparoscopic sleeve gastrectomies performed by 1,634 surgeons at 720 centers from 2012 to 2014. All of the data were extracted from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program, created in 2012 by the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery.
They examined the impact of staple line reinforcement, oversewing the staple line, bougie size, and distance of the staple line from the pylorus on 30-day outcomes, and their effect on weight loss and weight-related comorbidities at 1 year. Outcomes included morbidity, leak rates, and bleeding, which were examined at both the patient and surgeon levels.
Most patients (126,904; 67%) patients had some type of staple line reinforcement (SLR); the rest had only oversewn staple lines (OSL) or no reinforcement. Leaks occurred in 1,703 patients and bleeds in 1,436 patients. Leaks were more serious than bleeds: Patients with a leak were almost 28% more likely to readmitted and 11% more likely to need a reoperation than were patients who had only a bleed.
At the patient level, those with SLR with or without OSL were 20%-46% more likely to experience a leak than were those who had neither. Bleeding rates were about 70% lower in the SLR groups.
Most surgeons in the analysis (80%) used some type of SLR; almost 20% routinely used only OSL, and 30% routinely used only SLR. At the surgeon level, SLR was associated with a 60% increased risk of a postoperative leak, compared with no reinforcement. There was no association between SLR and bleeding risk, however.
Oversewing had an effect on 1-year weight loss. Patients with oversewn staple lines lost an additional 1.3 points on the body mass index (BMI) scale, compared with patients with no type of reinforcement.
“The reason for increased leaks from SLR is relatively unclear,” the authors wrote. “The two layers of material that are placed within the staple line could increase ischemia or decrease the relative staple heights. At the notches, where one staple firing ends and the next one begins, there is sandwiching of the two layers of staples and a combined four layers of SLR. This bulk may predispose to leaks.”
Larger bougie sizes (BS) seemed more beneficial than did smaller ones, in both the surgeon- and patient-level analyses. A BS of at least 38 French was associated with a 28% decreased risk of a leak (odds ratio 0.72) at the patient level and a 10% decreased risk at the surgeon level (OR 0.90). There were no associations with bleeding.
“Our findings support literature that describes narrower BSs leads to increased ischemia secondary to increased intraluminal pressure, causing more leaks,” the authors wrote.
A BS of at least 40 French had a significant impact on weight loss. At 1 year, patients with the larger BS had lost 2.45 points more on the BMI scale than did those with smaller sizes.
This finding is in accord with other studies, including one that found the best weight-loss outcomes associated with a BS of more than 60 French. “Perhaps the sleeve works because of more rapid emptying, which is favored by a relatively larger BS, rather than because of restriction,” they said.
The distance to the pylorus (DP) from the staple line initiation point was divided into four sections: less than 4 cm; 4-5 cm; 5-6 cm; and 6 cm or more.
On a patient level, there was no association between DP and leak rates. There was, however, an association with bleeding. A DP of 4-4.99 cm had the highest rate, 90%, while a DP of 5-5.99 cm had the lowest (71%). DP was also associated with weight loss on this level, with a distance of more than 6 cm being associated with the biggest BMI decrease (3.7 points).
“Our data show significantly increased excess weight loss in a stepwise fashion as the DP increases,” the authors said. “Our data suggest that as DP increased, there was an increased excess weight loss, possibly explained by preserving the ‘antral mill.’ Stapling further from the pylorus perhaps keeps the antrum’s functional component intact and allows food to enter the distal gut more quickly, leading to earlier satiety and increased weight loss.”
Only 114 surgeons (8%) used a DP of less than 4 cm. There were no significant associations with any 30-day outcomes and DP after adjustment.
The authors had no financial disclosures.
Before drawing overarching conclusions and implementing recommendations based on this study, there are several limitations that must be borne in mind when considering data-mining exercises such as this one:
• It should be taken into account that there was significant intraoperative variation in technique and experience among the surgeons that was not captured through the data acquisition.
• Similarly, the true distance between the stapler and the selected bougie is also variable, adding an inherent lack of accuracy of the true real diameter of the completed gastric tube.
• There is a lack of granular information, including the type of SLR or staplers used, thereby also limiting any reliable conclusions that could be drawn.
• There are additional techniques, such as omental buttressing, and the use of clips, sutures, or hemostatic agents that are not reported, yet may have an impact on leak and bleeding rates.
• The reported follow-up rate of 39.4% at 1 year is typically considered to be suboptimal.
• SLR techniques may also include oversewing, and these are also subject to wide variation, including the type of suture material used, and the actual suturing technique that was implemented.
• Only those patients whose bleeding was severe enough to warrant transfusions were included, such that lower level bleeding would have not been represented in this report.
• There were also deficiencies in correlating leaks or bleeding rates with staple height selection, or the experience and learning curve of the surgeon.

Samer Mattar, MD, is a bariatric surgeon and professor of surgery at Oregon Health and Science University, Portland. Dr. Mattar has no disclosures.
Before drawing overarching conclusions and implementing recommendations based on this study, there are several limitations that must be borne in mind when considering data-mining exercises such as this one:
• It should be taken into account that there was significant intraoperative variation in technique and experience among the surgeons that was not captured through the data acquisition.
• Similarly, the true distance between the stapler and the selected bougie is also variable, adding an inherent lack of accuracy of the true real diameter of the completed gastric tube.
• There is a lack of granular information, including the type of SLR or staplers used, thereby also limiting any reliable conclusions that could be drawn.
• There are additional techniques, such as omental buttressing, and the use of clips, sutures, or hemostatic agents that are not reported, yet may have an impact on leak and bleeding rates.
• The reported follow-up rate of 39.4% at 1 year is typically considered to be suboptimal.
• SLR techniques may also include oversewing, and these are also subject to wide variation, including the type of suture material used, and the actual suturing technique that was implemented.
• Only those patients whose bleeding was severe enough to warrant transfusions were included, such that lower level bleeding would have not been represented in this report.
• There were also deficiencies in correlating leaks or bleeding rates with staple height selection, or the experience and learning curve of the surgeon.
Samer Mattar, MD, is a bariatric surgeon and professor of surgery at Oregon Health and Science University, Portland. Dr. Mattar has no disclosures.
Before drawing overarching conclusions and implementing recommendations based on this study, there are several limitations that must be borne in mind when considering data-mining exercises such as this one:
• It should be taken into account that there was significant intraoperative variation in technique and experience among the surgeons that was not captured through the data acquisition.
• Similarly, the true distance between the stapler and the selected bougie is also variable, adding an inherent lack of accuracy of the true real diameter of the completed gastric tube.
• There is a lack of granular information, including the type of SLR or staplers used, thereby also limiting any reliable conclusions that could be drawn.
• There are additional techniques, such as omental buttressing, and the use of clips, sutures, or hemostatic agents that are not reported, yet may have an impact on leak and bleeding rates.
• The reported follow-up rate of 39.4% at 1 year is typically considered to be suboptimal.
• SLR techniques may also include oversewing, and these are also subject to wide variation, including the type of suture material used, and the actual suturing technique that was implemented.
• Only those patients whose bleeding was severe enough to warrant transfusions were included, such that lower level bleeding would have not been represented in this report.
• There were also deficiencies in correlating leaks or bleeding rates with staple height selection, or the experience and learning curve of the surgeon.
Samer Mattar, MD, is a bariatric surgeon and professor of surgery at Oregon Health and Science University, Portland. Dr. Mattar has no disclosures.
Laparoscopic sleeve gastrectomy is safe and effective overall, but staple line reinforcement appears to increase the rate of postsurgical leaks – which were associated with readmissions and, in some cases, reoperations.
A large review of quality improvement data found that staple line reinforcement – an extremely common technique – was associated with a 60% increased risk of leak, compared with closures without staple line reinforcement, Elizabeth R. Berger, MD, and her colleagues reported in the October issue of the Annals of Surgery (2016;264:464-73).
“This study also demonstrates that leaks were significantly more morbid than bleeding with higher readmission and reoperation rates in patients with a leak vs. a bleed,” wrote Dr. Berger of Loyola University, Chicago, and her coauthors. “Therefore, a surgeon should consider the benefits, risks, and costs of each surgical technique in performing a laparoscopic sleeve gastrectomy and selectively utilize those that, in their hands, minimize morbidity while maximizing clinical effectiveness.”
The team examined outcomes in 189,477 laparoscopic sleeve gastrectomies performed by 1,634 surgeons at 720 centers from 2012 to 2014. All of the data were extracted from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program, created in 2012 by the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery.
They examined the impact of staple line reinforcement, oversewing the staple line, bougie size, and distance of the staple line from the pylorus on 30-day outcomes, and their effect on weight loss and weight-related comorbidities at 1 year. Outcomes included morbidity, leak rates, and bleeding, which were examined at both the patient and surgeon levels.
Most patients (126,904; 67%) patients had some type of staple line reinforcement (SLR); the rest had only oversewn staple lines (OSL) or no reinforcement. Leaks occurred in 1,703 patients and bleeds in 1,436 patients. Leaks were more serious than bleeds: Patients with a leak were almost 28% more likely to readmitted and 11% more likely to need a reoperation than were patients who had only a bleed.
At the patient level, those with SLR with or without OSL were 20%-46% more likely to experience a leak than were those who had neither. Bleeding rates were about 70% lower in the SLR groups.
Most surgeons in the analysis (80%) used some type of SLR; almost 20% routinely used only OSL, and 30% routinely used only SLR. At the surgeon level, SLR was associated with a 60% increased risk of a postoperative leak, compared with no reinforcement. There was no association between SLR and bleeding risk, however.
Oversewing had an effect on 1-year weight loss. Patients with oversewn staple lines lost an additional 1.3 points on the body mass index (BMI) scale, compared with patients with no type of reinforcement.
“The reason for increased leaks from SLR is relatively unclear,” the authors wrote. “The two layers of material that are placed within the staple line could increase ischemia or decrease the relative staple heights. At the notches, where one staple firing ends and the next one begins, there is sandwiching of the two layers of staples and a combined four layers of SLR. This bulk may predispose to leaks.”
Larger bougie sizes (BS) seemed more beneficial than did smaller ones, in both the surgeon- and patient-level analyses. A BS of at least 38 French was associated with a 28% decreased risk of a leak (odds ratio 0.72) at the patient level and a 10% decreased risk at the surgeon level (OR 0.90). There were no associations with bleeding.
“Our findings support literature that describes narrower BSs leads to increased ischemia secondary to increased intraluminal pressure, causing more leaks,” the authors wrote.
A BS of at least 40 French had a significant impact on weight loss. At 1 year, patients with the larger BS had lost 2.45 points more on the BMI scale than did those with smaller sizes.
This finding is in accord with other studies, including one that found the best weight-loss outcomes associated with a BS of more than 60 French. “Perhaps the sleeve works because of more rapid emptying, which is favored by a relatively larger BS, rather than because of restriction,” they said.
The distance to the pylorus (DP) from the staple line initiation point was divided into four sections: less than 4 cm; 4-5 cm; 5-6 cm; and 6 cm or more.
On a patient level, there was no association between DP and leak rates. There was, however, an association with bleeding. A DP of 4-4.99 cm had the highest rate, 90%, while a DP of 5-5.99 cm had the lowest (71%). DP was also associated with weight loss on this level, with a distance of more than 6 cm being associated with the biggest BMI decrease (3.7 points).
“Our data show significantly increased excess weight loss in a stepwise fashion as the DP increases,” the authors said. “Our data suggest that as DP increased, there was an increased excess weight loss, possibly explained by preserving the ‘antral mill.’ Stapling further from the pylorus perhaps keeps the antrum’s functional component intact and allows food to enter the distal gut more quickly, leading to earlier satiety and increased weight loss.”
Only 114 surgeons (8%) used a DP of less than 4 cm. There were no significant associations with any 30-day outcomes and DP after adjustment.
The authors had no financial disclosures.
Laparoscopic sleeve gastrectomy is safe and effective overall, but staple line reinforcement appears to increase the rate of postsurgical leaks – which were associated with readmissions and, in some cases, reoperations.
A large review of quality improvement data found that staple line reinforcement – an extremely common technique – was associated with a 60% increased risk of leak, compared with closures without staple line reinforcement, Elizabeth R. Berger, MD, and her colleagues reported in the October issue of the Annals of Surgery (2016;264:464-73).
“This study also demonstrates that leaks were significantly more morbid than bleeding with higher readmission and reoperation rates in patients with a leak vs. a bleed,” wrote Dr. Berger of Loyola University, Chicago, and her coauthors. “Therefore, a surgeon should consider the benefits, risks, and costs of each surgical technique in performing a laparoscopic sleeve gastrectomy and selectively utilize those that, in their hands, minimize morbidity while maximizing clinical effectiveness.”
The team examined outcomes in 189,477 laparoscopic sleeve gastrectomies performed by 1,634 surgeons at 720 centers from 2012 to 2014. All of the data were extracted from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program, created in 2012 by the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery.
They examined the impact of staple line reinforcement, oversewing the staple line, bougie size, and distance of the staple line from the pylorus on 30-day outcomes, and their effect on weight loss and weight-related comorbidities at 1 year. Outcomes included morbidity, leak rates, and bleeding, which were examined at both the patient and surgeon levels.
Most patients (126,904; 67%) patients had some type of staple line reinforcement (SLR); the rest had only oversewn staple lines (OSL) or no reinforcement. Leaks occurred in 1,703 patients and bleeds in 1,436 patients. Leaks were more serious than bleeds: Patients with a leak were almost 28% more likely to readmitted and 11% more likely to need a reoperation than were patients who had only a bleed.
At the patient level, those with SLR with or without OSL were 20%-46% more likely to experience a leak than were those who had neither. Bleeding rates were about 70% lower in the SLR groups.
Most surgeons in the analysis (80%) used some type of SLR; almost 20% routinely used only OSL, and 30% routinely used only SLR. At the surgeon level, SLR was associated with a 60% increased risk of a postoperative leak, compared with no reinforcement. There was no association between SLR and bleeding risk, however.
Oversewing had an effect on 1-year weight loss. Patients with oversewn staple lines lost an additional 1.3 points on the body mass index (BMI) scale, compared with patients with no type of reinforcement.
“The reason for increased leaks from SLR is relatively unclear,” the authors wrote. “The two layers of material that are placed within the staple line could increase ischemia or decrease the relative staple heights. At the notches, where one staple firing ends and the next one begins, there is sandwiching of the two layers of staples and a combined four layers of SLR. This bulk may predispose to leaks.”
Larger bougie sizes (BS) seemed more beneficial than did smaller ones, in both the surgeon- and patient-level analyses. A BS of at least 38 French was associated with a 28% decreased risk of a leak (odds ratio 0.72) at the patient level and a 10% decreased risk at the surgeon level (OR 0.90). There were no associations with bleeding.
“Our findings support literature that describes narrower BSs leads to increased ischemia secondary to increased intraluminal pressure, causing more leaks,” the authors wrote.
A BS of at least 40 French had a significant impact on weight loss. At 1 year, patients with the larger BS had lost 2.45 points more on the BMI scale than did those with smaller sizes.
This finding is in accord with other studies, including one that found the best weight-loss outcomes associated with a BS of more than 60 French. “Perhaps the sleeve works because of more rapid emptying, which is favored by a relatively larger BS, rather than because of restriction,” they said.
The distance to the pylorus (DP) from the staple line initiation point was divided into four sections: less than 4 cm; 4-5 cm; 5-6 cm; and 6 cm or more.
On a patient level, there was no association between DP and leak rates. There was, however, an association with bleeding. A DP of 4-4.99 cm had the highest rate, 90%, while a DP of 5-5.99 cm had the lowest (71%). DP was also associated with weight loss on this level, with a distance of more than 6 cm being associated with the biggest BMI decrease (3.7 points).
“Our data show significantly increased excess weight loss in a stepwise fashion as the DP increases,” the authors said. “Our data suggest that as DP increased, there was an increased excess weight loss, possibly explained by preserving the ‘antral mill.’ Stapling further from the pylorus perhaps keeps the antrum’s functional component intact and allows food to enter the distal gut more quickly, leading to earlier satiety and increased weight loss.”
Only 114 surgeons (8%) used a DP of less than 4 cm. There were no significant associations with any 30-day outcomes and DP after adjustment.
The authors had no financial disclosures.
FROM THE ANNALS OF SURGERY
Key clinical point:
Major finding: Compared to not reinforcing the staple line, doing sow as associated with up to a 60% increase in the risk of a postsurgical leak.
Data source: The database review contained outcomes on 189,477 laparoscopic sleeve gastrectomies.
Disclosures: None of the study authors had any financial disclosures.
