User login
Engaging Veterans With Serious Mental Illness in Primary Care
People with serious mental illness (SMI) are at substantial risk for premature mortality, dying on average 10 to 20 years earlier than others.1 The reasons for this disparity are complex; however, the high prevalence of chronic disease and physical comorbidities in the SMI population have been identified as prominent factors.2 Engagement and reengagement in care, including primary care for medical comorbidities, can mitigate these mortality risks.2-4 Among veterans with SMI lost to follow-up care for more than 12 months, those not successfully reengaged in care were more likely to die compared with those reengaged in care.2,3
Given this evidence, health care systems, including the US Department of Veterans Affairs (VA), have looked to better engage these patients in care. These efforts have included mental health population health management, colocation of mental health with primary care, designation of primary care teams specializing in SMI, and integration of mental health and primary care services for patients experiencing homelessness.5-8
As part of a national approach to encourage locally driven quality improvement (QI), the VA compiles performance metrics for each facility, across a gamut of care settings, conditions, and veteran populations.9 Quarterly facility report cards, with longitudinal data and cross-facility comparisons, enable facilities to identify targets for QI and track improvement progress. One metric reports on the proportion of enrolled veterans with SMI who have primary care engagement, defined as having an assigned primary care practitioner (PCP) and a primary care visit in the prior 12 months.
In support of a QI initiative at the VA Greater Los Angeles Healthcare System (VAGLAHS), we sought to describe promising practices being utilized by VA facilities with higher levels of primary care engagement among their veterans with SMI populations.
Methods
We conducted semistructured telephone interviews with a purposeful sample of key informants at VA facilities with high levels of engagement in primary care among veterans with SMI. All project components were conducted by an interdisciplinary team, which included a medical anthropologist (JM), a mental health physician (PR), an internal medicine physician (KC), and other health services researchers (JB, AG). Because the primary objective of the project was QI, this project was designated as nonresearch by the VAGLAHS Institutional Review Board.
The VA Facility Complexity Model classifies facilities into 5 tiers: 1a (most complex), 1b, 1c, 2, and 3 (least complex), based on patient care volume, patient risk, complexity of clinical programs, and size of research and teaching programs. We sampled informants at VA facilities with complexity ratings of 1a or 1b with better than median scores for primary care engagement of veterans with SMI based on report cards from January 2019 to March 2019. To increase the likelihood of identifying lessons that can generalize to the VAGLAHS with its large population of veterans experiencing homelessness, we selected facilities serving populations consisting of more than 1000 veterans experiencing homelessness.
At each selected facility, we first aimed to interview mental health leaders responsible for quality measurement and improvement identified from a national VA database. We then used snowball sampling to identify other informants at these VA facilities who were knowledgeable about relevant processes. Potential interviewees were contacted via email.
Interviews
The interview guide was developed by the interdisciplinary team and based on published literature about strategies for engaging patients with SMI in care. Interview guide questions focused on local practice arrangements, panel management, population health practices, and quality measurement and improvement efforts for engaging veterans with SMI in primary care (Appendix). Interviews were conducted by telephone, from May 2019 through July 2019, by experienced qualitative interviewers (JM, JB). Interviewees were assured confidentiality of their responses.
Interview audio recordings were used to generate detailed notes (AG). Structured summaries were prepared from these notes, using a template based on the interview guide. We organized these summaries into matrices for analysis, grouping summarized points by interview domains to facilitate comparison across interviews.10-11 Our team reviewed and discussed the matrices, and iteratively identified and defined themes to identify the common engagement approaches and the nature of the connections between mental health and primary care. To ensure rigor, findings were checked by the senior qualitative lead (JM).
Results
The median SMI engagement score—defined as the proportion of veterans with SMI who have had a primary care visit in the prior 12 months and who have an assigned PCP—was 75.6% across 1a and 1b VA facilities. We identified 16 VA facilities that had a median or higher score and more than 1000 enrolled veterans experiencing homelessness. From these16 facilities, we emailed 31 potential interviewees, 14 of whom were identified from a VA database and 17 referred by other interviewees. In total, we interviewed 18 key informants across 11 (69%) facilities, including chiefs of psychology and mental health services, PCPs with mental health expertise, QI specialists, a psychosocial rehabilitation leader, and a local recovery coordinator, who helps veterans with SMI access recovery-oriented services. Characteristics of the facilities and interviewees are shown in Table 1. Interviews lasted a mean 35 (range, 26-50) minutes.

Engagement Approaches
The strategies used to engage veterans with SMI were heterogenous, with no single strategy common across all facilities. However, we identified 2 categories of engagement approaches: targeted outreach and routine practices.
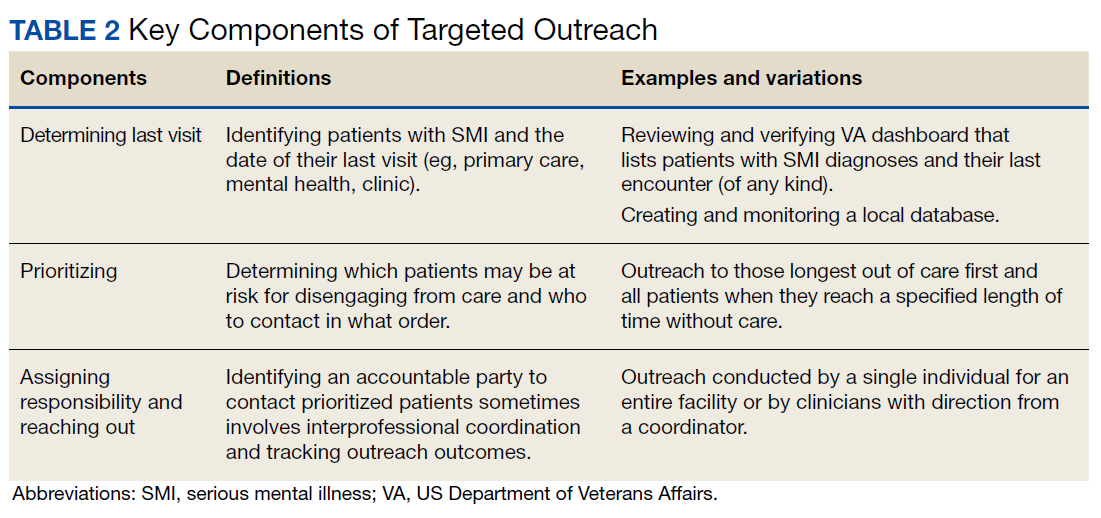
Targeted outreach strategies included deliberate, systematic approaches to reach veterans with SMI outside of regularly scheduled visits. These strategies were designed to be proactive, often prioritizing veterans at risk of disengaging from care. Designated VA care team members identified and reached out to veterans well before 12 months had passed since their prior visit (the VA definition of disengagement from care); visits included any care at VA, including, but not exclusively, primary care. Table 2 describes the key components of targeted outreach strategies: (1) identifying veterans’ last visit; (2) prioritizing which veterans to outreach to; and (3) assigning responsibility and reaching out. A key defining feature of targeted outreach is that veterans were identified and prioritized for outreach independent from any visits with mental health or other VA services.
In identifying veterans at risk for disengagement, a designated employee in mental health or primary care (eg, local recovery coordinator) reviewed a VA dashboard or locally developed report that identified veterans who have not engaged in care for several months. This process was repeated regularly. The designated employee either contacted those veterans directly or coordinated with other clinicians and support staff. When possible, a clinician or nurse with an existing relationship with the veteran would call them. If no such relationship existed, an administrative staff member made a cold call, sometimes accompanied by mailed outreach materials.
Routine practices were business-as-usual activities embedded in regular clinical workflows that facilitated engagement or reengagement of veterans with SMI in care. Of note, and in contrast to targeted outreach, these activities were tied to veteran visits with mental health practitioners. These practices were typically described as being at least as important as targeted outreach efforts. For example, during mental health visits, clinicians routinely checked the VA electronic health record to assess whether veterans had an assigned primary care team. If not, they would contact the primary care service to refer the patient for a primary care visit and assignment. If the patient already had a primary care team assigned, the mental health practitioner checked for recent primary care visits. If none were evident, the mental health practitioner might email the assigned PCP or contact them via instant message.
At some facilities, mental health support staff were able to directly schedule primary care appointments, which was identified as an important enabling factor in promoting mental health patient engagement in primary care. Some interviewees seemed to take for granted the idea that mental health practitioners would help engage patients in primary care—suggesting that these practices had perhaps become a cultural norm within their facility. However, some interviewees identified clear strategies for making these practices a consistent part of care—for example, by designing a protocol for initial mental health assessments to include a routine check for primary care engagement.
Mental Health/Primary Care Connections
Interviewees characterized the nature of the connections between mental health and primary care at their facilities. Nearly all interviewees described that their medical centers had extensive ties, formal and informal, between mental health and primary care.
Formal ties may include the reverse integration care model, in which primary care services are embedded in mental health settings. Interviewees at sites with programs based on this model noted that these programs enabled warm hand-offs from mental health to primary care and suggested that it can foster integration between primary care and mental health care for patients with SMI. However, the size, scope, and structure of these programs varied, sometimes serving a small proportion of a facility’s population of SMI patients. Other examples of formal ties included written agreements, establishing frequent, regular meetings between mental health and primary care leadership and front-line staff, and giving mental health clerks the ability to directly schedule primary care appointments.
Informal ties between mental health and primary care included communication and personal working relationships between mental health and PCPs, facilitated by mental health and primary care leaders working together in workgroups and other administrative activities. Some participants described a history of collaboration between mental health and primary care leaders yielding productive and trusting working relationships. Some interviewees described frequent direct communication between individual mental health practitioners and PCPs—either face-to-face or via secure messaging.
Discussion
VA facilities with high levels of primary care engagement among veterans with SMI used extensive engagement strategies, including a diverse array of targeted outreach and routine practices. In both approaches, intentional organizational structural and process decisions, as well as formal and informal ties between mental health and primary care, established and supported them. In addition, organizational cultural factors were especially relevant to routine practice strategies.
To enable targeted outreach, a bevy of organizational resources, both local and national were required. Large accountable care organizations and integrated delivery systems, like the VA, are often better able to create dashboards and other informational resources for population health management compared with smaller, less integrated health care systems. Though these resources are difficult to create in fragmented systems, comparable tools have been explored by multiple state health departments.12 Our findings suggest that these data tools, though resource intensive to develop, may enable facilities to be more methodical and reliable in conducting outreach to vulnerable patients.
In contrast to targeted outreach, routine practices depend less on population health management resources and more on cultural norms. Such norms are notoriously difficult to change, but intentional structural decisions like embedding primary care engagement in mental health protocols may signal that primary care engagement is an important and legitimate consideration for mental health care.13
We identified extensive and heterogenous connections between mental health and primary care in our sample of VA facilities with high engagement of patients with SMI in primary care. A growing body of literature on relational coordination studies the factors that contribute to organizational siloing and mechanisms for breaking down those silos so work can be coordinated across boundaries (eg, the organizational boundary between mental health and primary care).14 Coordinating care across these boundaries, through good relational coordination practices has been shown to improve outcomes in health care and other sectors. Notably, VA facilities in our sample had several of the defining characteristics of good relational coordination: relationships between mental health and primary care that include shared goals, shared knowledge, and mutual respect, all reinforced by frequent communication structured around problem solving.15 The relational coordination literature also offers a way to identify evidence-based interventions for facilitating relational coordination in places where it is lacking, for example, with information systems, boundary-spanning individuals, facility design, and formal conflict resolution.15 Future work might explore how relational coordination can be further used to optimize mental health and primary care connections to keep veterans with SMI engaged in care.
Our approach of interviewing informants in higher-performing facilities draws heavily on the idea of positive deviance, which holds that information on what works in health care is available from organizations that already are demonstrating “consistently exceptional performance.”16 This approach works best when high performance and organizational characteristics are observable for a large number of facilities, and when high-performing facilities are willing to share their strategies. These features allow investigators to identify promising practices and hypotheses that can then be empirically tested and compared. Such testing, including assessing for unintended consequences, is needed for the approaches we identified. Research is also needed to assess for factors that would promote the implementation of effective strategies.
Limitations
As a QI project seeking to identify promising practices, our interviews were limited to 18 key informants across 11 VA facilities with high engagement of care among veterans with SMI. No inferences can be made that these practices are directly related to this high level of engagement, nor the differential impact of different practices. Future work is needed to assess for these relationships. We also did not interview veterans to understand their perspectives on these strategies, which is an additional important topic for future work. In addition, these interviews were performed before the start of the COVID-19 pandemic. Further work is needed to understand how these strategies may have been modified in response to changes in practice. The shift to care from in-person to virtual services may have impacted both clinical interactions with veterans, as well as between clinicians.
Conclusions
Interviews with key informants demonstrate that while engaging and retaining veterans with SMI in primary care is vital, it also requires intentional and potentially resource-intensive practices, including targeted outreach and routine engagement strategies embedded into mental health visits. These promising practices can provide valuable insights for both VA and community health care systems providing care to patients with SMI.
Acknowledgments
We thank Gracielle J. Tan, MD for administrative assistance in preparing this manuscript.
1. Liu NH, Daumit GL, Dua T, et al. Excess mortality in persons with severe mental disorders: a multilevel intervention framework and priorities for clinical practice, policy and research agendas. World Psychiatry. 2017;16(1):30-40. doi:10.1002/wps.20384
2. Bowersox NW, Kilbourne AM, Abraham KM, et al. Cause-specific mortality among veterans with serious mental illness lost to follow-up. Gen Hosp Psychiatry. 2012;34(6):651-653. doi:10.1016/j.genhosppsych.2012.05.014
3. Davis CL, Kilbourne AM, Blow FC, et al. Reduced mortality among Department of Veterans Affairs patients with schizophrenia or bipolar disorder lost to follow-up and engaged in active outreach to return for care. Am J Public Health. 2012;102(suppl 1):S74-S79. doi:10.2105/AJPH.2011.300502
4. Copeland LA, Zeber JE, Wang CP, et al. Patterns of primary care and mortality among patients with schizophrenia or diabetes: a cluster analysis approach to the retrospective study of healthcare utilization. BMC Health Serv Res. 2009;9:127. doi:10.1186/1472-6963-9-127
5. Abraham KM, Mach J, Visnic S, McCarthy JF. Enhancing treatment reengagement for veterans with serious mental illness: evaluating the effectiveness of SMI re-engage. Psychiatr Serv. 2018;69(8):887-895. doi:10.1176/appi.ps.201700407
6. Ward MC, Druss BG. Reverse integration initiatives for individuals with serious mental illness. Focus (Am Psychiatr Publ). 2017;15(3):271-278. doi:10.1176/appi.focus.20170011
7. Chang ET, Vinzon M, Cohen AN, Young AS. Effective models urgently needed to improve physical care for people with serious mental illnesses. Health Serv Insights. 2019;12:1178632919837628. Published 2019 Apr 2. doi:10.1177/1178632919837628
8. Gabrielian S, Gordon AJ, Gelberg L, et al. Primary care medical services for homeless veterans. Fed Pract. 2014;31(10):10-19.
9. Lemke S, Boden MT, Kearney LK, et al. Measurement-based management of mental health quality and access in VHA: SAIL mental health domain. Psychol Serv. 2017;14(1):1-12. doi:10.1037/ser0000097
10. Averill JB. Matrix analysis as a complementary analytic strategy in qualitative inquiry. Qual Health Res. 2002;12(6):855-866. doi:10.1177/104973230201200611
11. Zuchowski JL, Chrystal JG, Hamilton AB, et al. Coordinating care across health care systems for Veterans with gynecologic malignancies: a qualitative analysis. Med Care. 2017;55(suppl 1):S53-S60. doi:10.1097/MLR.0000000000000737
12. Daumit GL, Stone EM, Kennedy-Hendricks A, Choksy S, Marsteller JA, McGinty EE. Care coordination and population health management strategies and challenges in a behavioral health home model. Med Care. 2019;57(1):79-84. doi:10.1097/MLR.0000000000001023
13. Parmelli E, Flodgren G, Beyer F, et al. The effectiveness of strategies to change organisational culture to improve healthcare performance: a systematic review. Implement Sci. 2011;6(33):1-8. doi:10.1186/1748-5908-6-33
14. Bolton R, Logan C, Gittell JH. Revisiting relational coordination: a systematic review. J Appl Behav Sci. 2021;57(3):290-322. doi:10.1177/0021886321991597
15. Gittell JH, Godfrey M, Thistlethwaite J. Interprofessional collaborative practice and relational coordination: improving healthcare through relationships. J Interprof Care. 2013;27(3):210-13. doi:10.3109/13561820.2012.730564
16. Bradley EH, Curry LA, Ramanadhan S, Rowe L, Nembhard IM, Krumholz HM. Research in action: using positive deviance to improve quality of health care. Implement Sci. 2009;4:25. Published 2009 May 8. doi:10.1186/1748-5908-4-25
People with serious mental illness (SMI) are at substantial risk for premature mortality, dying on average 10 to 20 years earlier than others.1 The reasons for this disparity are complex; however, the high prevalence of chronic disease and physical comorbidities in the SMI population have been identified as prominent factors.2 Engagement and reengagement in care, including primary care for medical comorbidities, can mitigate these mortality risks.2-4 Among veterans with SMI lost to follow-up care for more than 12 months, those not successfully reengaged in care were more likely to die compared with those reengaged in care.2,3
Given this evidence, health care systems, including the US Department of Veterans Affairs (VA), have looked to better engage these patients in care. These efforts have included mental health population health management, colocation of mental health with primary care, designation of primary care teams specializing in SMI, and integration of mental health and primary care services for patients experiencing homelessness.5-8
As part of a national approach to encourage locally driven quality improvement (QI), the VA compiles performance metrics for each facility, across a gamut of care settings, conditions, and veteran populations.9 Quarterly facility report cards, with longitudinal data and cross-facility comparisons, enable facilities to identify targets for QI and track improvement progress. One metric reports on the proportion of enrolled veterans with SMI who have primary care engagement, defined as having an assigned primary care practitioner (PCP) and a primary care visit in the prior 12 months.
In support of a QI initiative at the VA Greater Los Angeles Healthcare System (VAGLAHS), we sought to describe promising practices being utilized by VA facilities with higher levels of primary care engagement among their veterans with SMI populations.
Methods
We conducted semistructured telephone interviews with a purposeful sample of key informants at VA facilities with high levels of engagement in primary care among veterans with SMI. All project components were conducted by an interdisciplinary team, which included a medical anthropologist (JM), a mental health physician (PR), an internal medicine physician (KC), and other health services researchers (JB, AG). Because the primary objective of the project was QI, this project was designated as nonresearch by the VAGLAHS Institutional Review Board.
The VA Facility Complexity Model classifies facilities into 5 tiers: 1a (most complex), 1b, 1c, 2, and 3 (least complex), based on patient care volume, patient risk, complexity of clinical programs, and size of research and teaching programs. We sampled informants at VA facilities with complexity ratings of 1a or 1b with better than median scores for primary care engagement of veterans with SMI based on report cards from January 2019 to March 2019. To increase the likelihood of identifying lessons that can generalize to the VAGLAHS with its large population of veterans experiencing homelessness, we selected facilities serving populations consisting of more than 1000 veterans experiencing homelessness.
At each selected facility, we first aimed to interview mental health leaders responsible for quality measurement and improvement identified from a national VA database. We then used snowball sampling to identify other informants at these VA facilities who were knowledgeable about relevant processes. Potential interviewees were contacted via email.
Interviews
The interview guide was developed by the interdisciplinary team and based on published literature about strategies for engaging patients with SMI in care. Interview guide questions focused on local practice arrangements, panel management, population health practices, and quality measurement and improvement efforts for engaging veterans with SMI in primary care (Appendix). Interviews were conducted by telephone, from May 2019 through July 2019, by experienced qualitative interviewers (JM, JB). Interviewees were assured confidentiality of their responses.
Interview audio recordings were used to generate detailed notes (AG). Structured summaries were prepared from these notes, using a template based on the interview guide. We organized these summaries into matrices for analysis, grouping summarized points by interview domains to facilitate comparison across interviews.10-11 Our team reviewed and discussed the matrices, and iteratively identified and defined themes to identify the common engagement approaches and the nature of the connections between mental health and primary care. To ensure rigor, findings were checked by the senior qualitative lead (JM).
Results
The median SMI engagement score—defined as the proportion of veterans with SMI who have had a primary care visit in the prior 12 months and who have an assigned PCP—was 75.6% across 1a and 1b VA facilities. We identified 16 VA facilities that had a median or higher score and more than 1000 enrolled veterans experiencing homelessness. From these16 facilities, we emailed 31 potential interviewees, 14 of whom were identified from a VA database and 17 referred by other interviewees. In total, we interviewed 18 key informants across 11 (69%) facilities, including chiefs of psychology and mental health services, PCPs with mental health expertise, QI specialists, a psychosocial rehabilitation leader, and a local recovery coordinator, who helps veterans with SMI access recovery-oriented services. Characteristics of the facilities and interviewees are shown in Table 1. Interviews lasted a mean 35 (range, 26-50) minutes.
Engagement Approaches
The strategies used to engage veterans with SMI were heterogenous, with no single strategy common across all facilities. However, we identified 2 categories of engagement approaches: targeted outreach and routine practices.
Targeted outreach strategies included deliberate, systematic approaches to reach veterans with SMI outside of regularly scheduled visits. These strategies were designed to be proactive, often prioritizing veterans at risk of disengaging from care. Designated VA care team members identified and reached out to veterans well before 12 months had passed since their prior visit (the VA definition of disengagement from care); visits included any care at VA, including, but not exclusively, primary care. Table 2 describes the key components of targeted outreach strategies: (1) identifying veterans’ last visit; (2) prioritizing which veterans to outreach to; and (3) assigning responsibility and reaching out. A key defining feature of targeted outreach is that veterans were identified and prioritized for outreach independent from any visits with mental health or other VA services.
In identifying veterans at risk for disengagement, a designated employee in mental health or primary care (eg, local recovery coordinator) reviewed a VA dashboard or locally developed report that identified veterans who have not engaged in care for several months. This process was repeated regularly. The designated employee either contacted those veterans directly or coordinated with other clinicians and support staff. When possible, a clinician or nurse with an existing relationship with the veteran would call them. If no such relationship existed, an administrative staff member made a cold call, sometimes accompanied by mailed outreach materials.
Routine practices were business-as-usual activities embedded in regular clinical workflows that facilitated engagement or reengagement of veterans with SMI in care. Of note, and in contrast to targeted outreach, these activities were tied to veteran visits with mental health practitioners. These practices were typically described as being at least as important as targeted outreach efforts. For example, during mental health visits, clinicians routinely checked the VA electronic health record to assess whether veterans had an assigned primary care team. If not, they would contact the primary care service to refer the patient for a primary care visit and assignment. If the patient already had a primary care team assigned, the mental health practitioner checked for recent primary care visits. If none were evident, the mental health practitioner might email the assigned PCP or contact them via instant message.
At some facilities, mental health support staff were able to directly schedule primary care appointments, which was identified as an important enabling factor in promoting mental health patient engagement in primary care. Some interviewees seemed to take for granted the idea that mental health practitioners would help engage patients in primary care—suggesting that these practices had perhaps become a cultural norm within their facility. However, some interviewees identified clear strategies for making these practices a consistent part of care—for example, by designing a protocol for initial mental health assessments to include a routine check for primary care engagement.
Mental Health/Primary Care Connections
Interviewees characterized the nature of the connections between mental health and primary care at their facilities. Nearly all interviewees described that their medical centers had extensive ties, formal and informal, between mental health and primary care.
Formal ties may include the reverse integration care model, in which primary care services are embedded in mental health settings. Interviewees at sites with programs based on this model noted that these programs enabled warm hand-offs from mental health to primary care and suggested that it can foster integration between primary care and mental health care for patients with SMI. However, the size, scope, and structure of these programs varied, sometimes serving a small proportion of a facility’s population of SMI patients. Other examples of formal ties included written agreements, establishing frequent, regular meetings between mental health and primary care leadership and front-line staff, and giving mental health clerks the ability to directly schedule primary care appointments.
Informal ties between mental health and primary care included communication and personal working relationships between mental health and PCPs, facilitated by mental health and primary care leaders working together in workgroups and other administrative activities. Some participants described a history of collaboration between mental health and primary care leaders yielding productive and trusting working relationships. Some interviewees described frequent direct communication between individual mental health practitioners and PCPs—either face-to-face or via secure messaging.
Discussion
VA facilities with high levels of primary care engagement among veterans with SMI used extensive engagement strategies, including a diverse array of targeted outreach and routine practices. In both approaches, intentional organizational structural and process decisions, as well as formal and informal ties between mental health and primary care, established and supported them. In addition, organizational cultural factors were especially relevant to routine practice strategies.
To enable targeted outreach, a bevy of organizational resources, both local and national were required. Large accountable care organizations and integrated delivery systems, like the VA, are often better able to create dashboards and other informational resources for population health management compared with smaller, less integrated health care systems. Though these resources are difficult to create in fragmented systems, comparable tools have been explored by multiple state health departments.12 Our findings suggest that these data tools, though resource intensive to develop, may enable facilities to be more methodical and reliable in conducting outreach to vulnerable patients.
In contrast to targeted outreach, routine practices depend less on population health management resources and more on cultural norms. Such norms are notoriously difficult to change, but intentional structural decisions like embedding primary care engagement in mental health protocols may signal that primary care engagement is an important and legitimate consideration for mental health care.13
We identified extensive and heterogenous connections between mental health and primary care in our sample of VA facilities with high engagement of patients with SMI in primary care. A growing body of literature on relational coordination studies the factors that contribute to organizational siloing and mechanisms for breaking down those silos so work can be coordinated across boundaries (eg, the organizational boundary between mental health and primary care).14 Coordinating care across these boundaries, through good relational coordination practices has been shown to improve outcomes in health care and other sectors. Notably, VA facilities in our sample had several of the defining characteristics of good relational coordination: relationships between mental health and primary care that include shared goals, shared knowledge, and mutual respect, all reinforced by frequent communication structured around problem solving.15 The relational coordination literature also offers a way to identify evidence-based interventions for facilitating relational coordination in places where it is lacking, for example, with information systems, boundary-spanning individuals, facility design, and formal conflict resolution.15 Future work might explore how relational coordination can be further used to optimize mental health and primary care connections to keep veterans with SMI engaged in care.
Our approach of interviewing informants in higher-performing facilities draws heavily on the idea of positive deviance, which holds that information on what works in health care is available from organizations that already are demonstrating “consistently exceptional performance.”16 This approach works best when high performance and organizational characteristics are observable for a large number of facilities, and when high-performing facilities are willing to share their strategies. These features allow investigators to identify promising practices and hypotheses that can then be empirically tested and compared. Such testing, including assessing for unintended consequences, is needed for the approaches we identified. Research is also needed to assess for factors that would promote the implementation of effective strategies.
Limitations
As a QI project seeking to identify promising practices, our interviews were limited to 18 key informants across 11 VA facilities with high engagement of care among veterans with SMI. No inferences can be made that these practices are directly related to this high level of engagement, nor the differential impact of different practices. Future work is needed to assess for these relationships. We also did not interview veterans to understand their perspectives on these strategies, which is an additional important topic for future work. In addition, these interviews were performed before the start of the COVID-19 pandemic. Further work is needed to understand how these strategies may have been modified in response to changes in practice. The shift to care from in-person to virtual services may have impacted both clinical interactions with veterans, as well as between clinicians.
Conclusions
Interviews with key informants demonstrate that while engaging and retaining veterans with SMI in primary care is vital, it also requires intentional and potentially resource-intensive practices, including targeted outreach and routine engagement strategies embedded into mental health visits. These promising practices can provide valuable insights for both VA and community health care systems providing care to patients with SMI.
Acknowledgments
We thank Gracielle J. Tan, MD for administrative assistance in preparing this manuscript.
People with serious mental illness (SMI) are at substantial risk for premature mortality, dying on average 10 to 20 years earlier than others.1 The reasons for this disparity are complex; however, the high prevalence of chronic disease and physical comorbidities in the SMI population have been identified as prominent factors.2 Engagement and reengagement in care, including primary care for medical comorbidities, can mitigate these mortality risks.2-4 Among veterans with SMI lost to follow-up care for more than 12 months, those not successfully reengaged in care were more likely to die compared with those reengaged in care.2,3
Given this evidence, health care systems, including the US Department of Veterans Affairs (VA), have looked to better engage these patients in care. These efforts have included mental health population health management, colocation of mental health with primary care, designation of primary care teams specializing in SMI, and integration of mental health and primary care services for patients experiencing homelessness.5-8
As part of a national approach to encourage locally driven quality improvement (QI), the VA compiles performance metrics for each facility, across a gamut of care settings, conditions, and veteran populations.9 Quarterly facility report cards, with longitudinal data and cross-facility comparisons, enable facilities to identify targets for QI and track improvement progress. One metric reports on the proportion of enrolled veterans with SMI who have primary care engagement, defined as having an assigned primary care practitioner (PCP) and a primary care visit in the prior 12 months.
In support of a QI initiative at the VA Greater Los Angeles Healthcare System (VAGLAHS), we sought to describe promising practices being utilized by VA facilities with higher levels of primary care engagement among their veterans with SMI populations.
Methods
We conducted semistructured telephone interviews with a purposeful sample of key informants at VA facilities with high levels of engagement in primary care among veterans with SMI. All project components were conducted by an interdisciplinary team, which included a medical anthropologist (JM), a mental health physician (PR), an internal medicine physician (KC), and other health services researchers (JB, AG). Because the primary objective of the project was QI, this project was designated as nonresearch by the VAGLAHS Institutional Review Board.
The VA Facility Complexity Model classifies facilities into 5 tiers: 1a (most complex), 1b, 1c, 2, and 3 (least complex), based on patient care volume, patient risk, complexity of clinical programs, and size of research and teaching programs. We sampled informants at VA facilities with complexity ratings of 1a or 1b with better than median scores for primary care engagement of veterans with SMI based on report cards from January 2019 to March 2019. To increase the likelihood of identifying lessons that can generalize to the VAGLAHS with its large population of veterans experiencing homelessness, we selected facilities serving populations consisting of more than 1000 veterans experiencing homelessness.
At each selected facility, we first aimed to interview mental health leaders responsible for quality measurement and improvement identified from a national VA database. We then used snowball sampling to identify other informants at these VA facilities who were knowledgeable about relevant processes. Potential interviewees were contacted via email.
Interviews
The interview guide was developed by the interdisciplinary team and based on published literature about strategies for engaging patients with SMI in care. Interview guide questions focused on local practice arrangements, panel management, population health practices, and quality measurement and improvement efforts for engaging veterans with SMI in primary care (Appendix). Interviews were conducted by telephone, from May 2019 through July 2019, by experienced qualitative interviewers (JM, JB). Interviewees were assured confidentiality of their responses.
Interview audio recordings were used to generate detailed notes (AG). Structured summaries were prepared from these notes, using a template based on the interview guide. We organized these summaries into matrices for analysis, grouping summarized points by interview domains to facilitate comparison across interviews.10-11 Our team reviewed and discussed the matrices, and iteratively identified and defined themes to identify the common engagement approaches and the nature of the connections between mental health and primary care. To ensure rigor, findings were checked by the senior qualitative lead (JM).
Results
The median SMI engagement score—defined as the proportion of veterans with SMI who have had a primary care visit in the prior 12 months and who have an assigned PCP—was 75.6% across 1a and 1b VA facilities. We identified 16 VA facilities that had a median or higher score and more than 1000 enrolled veterans experiencing homelessness. From these16 facilities, we emailed 31 potential interviewees, 14 of whom were identified from a VA database and 17 referred by other interviewees. In total, we interviewed 18 key informants across 11 (69%) facilities, including chiefs of psychology and mental health services, PCPs with mental health expertise, QI specialists, a psychosocial rehabilitation leader, and a local recovery coordinator, who helps veterans with SMI access recovery-oriented services. Characteristics of the facilities and interviewees are shown in Table 1. Interviews lasted a mean 35 (range, 26-50) minutes.
Engagement Approaches
The strategies used to engage veterans with SMI were heterogenous, with no single strategy common across all facilities. However, we identified 2 categories of engagement approaches: targeted outreach and routine practices.
Targeted outreach strategies included deliberate, systematic approaches to reach veterans with SMI outside of regularly scheduled visits. These strategies were designed to be proactive, often prioritizing veterans at risk of disengaging from care. Designated VA care team members identified and reached out to veterans well before 12 months had passed since their prior visit (the VA definition of disengagement from care); visits included any care at VA, including, but not exclusively, primary care. Table 2 describes the key components of targeted outreach strategies: (1) identifying veterans’ last visit; (2) prioritizing which veterans to outreach to; and (3) assigning responsibility and reaching out. A key defining feature of targeted outreach is that veterans were identified and prioritized for outreach independent from any visits with mental health or other VA services.
In identifying veterans at risk for disengagement, a designated employee in mental health or primary care (eg, local recovery coordinator) reviewed a VA dashboard or locally developed report that identified veterans who have not engaged in care for several months. This process was repeated regularly. The designated employee either contacted those veterans directly or coordinated with other clinicians and support staff. When possible, a clinician or nurse with an existing relationship with the veteran would call them. If no such relationship existed, an administrative staff member made a cold call, sometimes accompanied by mailed outreach materials.
Routine practices were business-as-usual activities embedded in regular clinical workflows that facilitated engagement or reengagement of veterans with SMI in care. Of note, and in contrast to targeted outreach, these activities were tied to veteran visits with mental health practitioners. These practices were typically described as being at least as important as targeted outreach efforts. For example, during mental health visits, clinicians routinely checked the VA electronic health record to assess whether veterans had an assigned primary care team. If not, they would contact the primary care service to refer the patient for a primary care visit and assignment. If the patient already had a primary care team assigned, the mental health practitioner checked for recent primary care visits. If none were evident, the mental health practitioner might email the assigned PCP or contact them via instant message.
At some facilities, mental health support staff were able to directly schedule primary care appointments, which was identified as an important enabling factor in promoting mental health patient engagement in primary care. Some interviewees seemed to take for granted the idea that mental health practitioners would help engage patients in primary care—suggesting that these practices had perhaps become a cultural norm within their facility. However, some interviewees identified clear strategies for making these practices a consistent part of care—for example, by designing a protocol for initial mental health assessments to include a routine check for primary care engagement.
Mental Health/Primary Care Connections
Interviewees characterized the nature of the connections between mental health and primary care at their facilities. Nearly all interviewees described that their medical centers had extensive ties, formal and informal, between mental health and primary care.
Formal ties may include the reverse integration care model, in which primary care services are embedded in mental health settings. Interviewees at sites with programs based on this model noted that these programs enabled warm hand-offs from mental health to primary care and suggested that it can foster integration between primary care and mental health care for patients with SMI. However, the size, scope, and structure of these programs varied, sometimes serving a small proportion of a facility’s population of SMI patients. Other examples of formal ties included written agreements, establishing frequent, regular meetings between mental health and primary care leadership and front-line staff, and giving mental health clerks the ability to directly schedule primary care appointments.
Informal ties between mental health and primary care included communication and personal working relationships between mental health and PCPs, facilitated by mental health and primary care leaders working together in workgroups and other administrative activities. Some participants described a history of collaboration between mental health and primary care leaders yielding productive and trusting working relationships. Some interviewees described frequent direct communication between individual mental health practitioners and PCPs—either face-to-face or via secure messaging.
Discussion
VA facilities with high levels of primary care engagement among veterans with SMI used extensive engagement strategies, including a diverse array of targeted outreach and routine practices. In both approaches, intentional organizational structural and process decisions, as well as formal and informal ties between mental health and primary care, established and supported them. In addition, organizational cultural factors were especially relevant to routine practice strategies.
To enable targeted outreach, a bevy of organizational resources, both local and national were required. Large accountable care organizations and integrated delivery systems, like the VA, are often better able to create dashboards and other informational resources for population health management compared with smaller, less integrated health care systems. Though these resources are difficult to create in fragmented systems, comparable tools have been explored by multiple state health departments.12 Our findings suggest that these data tools, though resource intensive to develop, may enable facilities to be more methodical and reliable in conducting outreach to vulnerable patients.
In contrast to targeted outreach, routine practices depend less on population health management resources and more on cultural norms. Such norms are notoriously difficult to change, but intentional structural decisions like embedding primary care engagement in mental health protocols may signal that primary care engagement is an important and legitimate consideration for mental health care.13
We identified extensive and heterogenous connections between mental health and primary care in our sample of VA facilities with high engagement of patients with SMI in primary care. A growing body of literature on relational coordination studies the factors that contribute to organizational siloing and mechanisms for breaking down those silos so work can be coordinated across boundaries (eg, the organizational boundary between mental health and primary care).14 Coordinating care across these boundaries, through good relational coordination practices has been shown to improve outcomes in health care and other sectors. Notably, VA facilities in our sample had several of the defining characteristics of good relational coordination: relationships between mental health and primary care that include shared goals, shared knowledge, and mutual respect, all reinforced by frequent communication structured around problem solving.15 The relational coordination literature also offers a way to identify evidence-based interventions for facilitating relational coordination in places where it is lacking, for example, with information systems, boundary-spanning individuals, facility design, and formal conflict resolution.15 Future work might explore how relational coordination can be further used to optimize mental health and primary care connections to keep veterans with SMI engaged in care.
Our approach of interviewing informants in higher-performing facilities draws heavily on the idea of positive deviance, which holds that information on what works in health care is available from organizations that already are demonstrating “consistently exceptional performance.”16 This approach works best when high performance and organizational characteristics are observable for a large number of facilities, and when high-performing facilities are willing to share their strategies. These features allow investigators to identify promising practices and hypotheses that can then be empirically tested and compared. Such testing, including assessing for unintended consequences, is needed for the approaches we identified. Research is also needed to assess for factors that would promote the implementation of effective strategies.
Limitations
As a QI project seeking to identify promising practices, our interviews were limited to 18 key informants across 11 VA facilities with high engagement of care among veterans with SMI. No inferences can be made that these practices are directly related to this high level of engagement, nor the differential impact of different practices. Future work is needed to assess for these relationships. We also did not interview veterans to understand their perspectives on these strategies, which is an additional important topic for future work. In addition, these interviews were performed before the start of the COVID-19 pandemic. Further work is needed to understand how these strategies may have been modified in response to changes in practice. The shift to care from in-person to virtual services may have impacted both clinical interactions with veterans, as well as between clinicians.
Conclusions
Interviews with key informants demonstrate that while engaging and retaining veterans with SMI in primary care is vital, it also requires intentional and potentially resource-intensive practices, including targeted outreach and routine engagement strategies embedded into mental health visits. These promising practices can provide valuable insights for both VA and community health care systems providing care to patients with SMI.
Acknowledgments
We thank Gracielle J. Tan, MD for administrative assistance in preparing this manuscript.
1. Liu NH, Daumit GL, Dua T, et al. Excess mortality in persons with severe mental disorders: a multilevel intervention framework and priorities for clinical practice, policy and research agendas. World Psychiatry. 2017;16(1):30-40. doi:10.1002/wps.20384
2. Bowersox NW, Kilbourne AM, Abraham KM, et al. Cause-specific mortality among veterans with serious mental illness lost to follow-up. Gen Hosp Psychiatry. 2012;34(6):651-653. doi:10.1016/j.genhosppsych.2012.05.014
3. Davis CL, Kilbourne AM, Blow FC, et al. Reduced mortality among Department of Veterans Affairs patients with schizophrenia or bipolar disorder lost to follow-up and engaged in active outreach to return for care. Am J Public Health. 2012;102(suppl 1):S74-S79. doi:10.2105/AJPH.2011.300502
4. Copeland LA, Zeber JE, Wang CP, et al. Patterns of primary care and mortality among patients with schizophrenia or diabetes: a cluster analysis approach to the retrospective study of healthcare utilization. BMC Health Serv Res. 2009;9:127. doi:10.1186/1472-6963-9-127
5. Abraham KM, Mach J, Visnic S, McCarthy JF. Enhancing treatment reengagement for veterans with serious mental illness: evaluating the effectiveness of SMI re-engage. Psychiatr Serv. 2018;69(8):887-895. doi:10.1176/appi.ps.201700407
6. Ward MC, Druss BG. Reverse integration initiatives for individuals with serious mental illness. Focus (Am Psychiatr Publ). 2017;15(3):271-278. doi:10.1176/appi.focus.20170011
7. Chang ET, Vinzon M, Cohen AN, Young AS. Effective models urgently needed to improve physical care for people with serious mental illnesses. Health Serv Insights. 2019;12:1178632919837628. Published 2019 Apr 2. doi:10.1177/1178632919837628
8. Gabrielian S, Gordon AJ, Gelberg L, et al. Primary care medical services for homeless veterans. Fed Pract. 2014;31(10):10-19.
9. Lemke S, Boden MT, Kearney LK, et al. Measurement-based management of mental health quality and access in VHA: SAIL mental health domain. Psychol Serv. 2017;14(1):1-12. doi:10.1037/ser0000097
10. Averill JB. Matrix analysis as a complementary analytic strategy in qualitative inquiry. Qual Health Res. 2002;12(6):855-866. doi:10.1177/104973230201200611
11. Zuchowski JL, Chrystal JG, Hamilton AB, et al. Coordinating care across health care systems for Veterans with gynecologic malignancies: a qualitative analysis. Med Care. 2017;55(suppl 1):S53-S60. doi:10.1097/MLR.0000000000000737
12. Daumit GL, Stone EM, Kennedy-Hendricks A, Choksy S, Marsteller JA, McGinty EE. Care coordination and population health management strategies and challenges in a behavioral health home model. Med Care. 2019;57(1):79-84. doi:10.1097/MLR.0000000000001023
13. Parmelli E, Flodgren G, Beyer F, et al. The effectiveness of strategies to change organisational culture to improve healthcare performance: a systematic review. Implement Sci. 2011;6(33):1-8. doi:10.1186/1748-5908-6-33
14. Bolton R, Logan C, Gittell JH. Revisiting relational coordination: a systematic review. J Appl Behav Sci. 2021;57(3):290-322. doi:10.1177/0021886321991597
15. Gittell JH, Godfrey M, Thistlethwaite J. Interprofessional collaborative practice and relational coordination: improving healthcare through relationships. J Interprof Care. 2013;27(3):210-13. doi:10.3109/13561820.2012.730564
16. Bradley EH, Curry LA, Ramanadhan S, Rowe L, Nembhard IM, Krumholz HM. Research in action: using positive deviance to improve quality of health care. Implement Sci. 2009;4:25. Published 2009 May 8. doi:10.1186/1748-5908-4-25
1. Liu NH, Daumit GL, Dua T, et al. Excess mortality in persons with severe mental disorders: a multilevel intervention framework and priorities for clinical practice, policy and research agendas. World Psychiatry. 2017;16(1):30-40. doi:10.1002/wps.20384
2. Bowersox NW, Kilbourne AM, Abraham KM, et al. Cause-specific mortality among veterans with serious mental illness lost to follow-up. Gen Hosp Psychiatry. 2012;34(6):651-653. doi:10.1016/j.genhosppsych.2012.05.014
3. Davis CL, Kilbourne AM, Blow FC, et al. Reduced mortality among Department of Veterans Affairs patients with schizophrenia or bipolar disorder lost to follow-up and engaged in active outreach to return for care. Am J Public Health. 2012;102(suppl 1):S74-S79. doi:10.2105/AJPH.2011.300502
4. Copeland LA, Zeber JE, Wang CP, et al. Patterns of primary care and mortality among patients with schizophrenia or diabetes: a cluster analysis approach to the retrospective study of healthcare utilization. BMC Health Serv Res. 2009;9:127. doi:10.1186/1472-6963-9-127
5. Abraham KM, Mach J, Visnic S, McCarthy JF. Enhancing treatment reengagement for veterans with serious mental illness: evaluating the effectiveness of SMI re-engage. Psychiatr Serv. 2018;69(8):887-895. doi:10.1176/appi.ps.201700407
6. Ward MC, Druss BG. Reverse integration initiatives for individuals with serious mental illness. Focus (Am Psychiatr Publ). 2017;15(3):271-278. doi:10.1176/appi.focus.20170011
7. Chang ET, Vinzon M, Cohen AN, Young AS. Effective models urgently needed to improve physical care for people with serious mental illnesses. Health Serv Insights. 2019;12:1178632919837628. Published 2019 Apr 2. doi:10.1177/1178632919837628
8. Gabrielian S, Gordon AJ, Gelberg L, et al. Primary care medical services for homeless veterans. Fed Pract. 2014;31(10):10-19.
9. Lemke S, Boden MT, Kearney LK, et al. Measurement-based management of mental health quality and access in VHA: SAIL mental health domain. Psychol Serv. 2017;14(1):1-12. doi:10.1037/ser0000097
10. Averill JB. Matrix analysis as a complementary analytic strategy in qualitative inquiry. Qual Health Res. 2002;12(6):855-866. doi:10.1177/104973230201200611
11. Zuchowski JL, Chrystal JG, Hamilton AB, et al. Coordinating care across health care systems for Veterans with gynecologic malignancies: a qualitative analysis. Med Care. 2017;55(suppl 1):S53-S60. doi:10.1097/MLR.0000000000000737
12. Daumit GL, Stone EM, Kennedy-Hendricks A, Choksy S, Marsteller JA, McGinty EE. Care coordination and population health management strategies and challenges in a behavioral health home model. Med Care. 2019;57(1):79-84. doi:10.1097/MLR.0000000000001023
13. Parmelli E, Flodgren G, Beyer F, et al. The effectiveness of strategies to change organisational culture to improve healthcare performance: a systematic review. Implement Sci. 2011;6(33):1-8. doi:10.1186/1748-5908-6-33
14. Bolton R, Logan C, Gittell JH. Revisiting relational coordination: a systematic review. J Appl Behav Sci. 2021;57(3):290-322. doi:10.1177/0021886321991597
15. Gittell JH, Godfrey M, Thistlethwaite J. Interprofessional collaborative practice and relational coordination: improving healthcare through relationships. J Interprof Care. 2013;27(3):210-13. doi:10.3109/13561820.2012.730564
16. Bradley EH, Curry LA, Ramanadhan S, Rowe L, Nembhard IM, Krumholz HM. Research in action: using positive deviance to improve quality of health care. Implement Sci. 2009;4:25. Published 2009 May 8. doi:10.1186/1748-5908-4-25
Parent training pays off for children with autism
“Referrals for parent training should now be considered the expected standard for medical practice,” said a member of the research team, Timothy B. Smith, PhD, a professor of psychology at Brigham Young University, Provo, Utah.

Programs that show parents how to teach functional skills and address maladaptive behaviors, also known as parent-mediated or parent-implemented interventions, offer an alternative to one-on-one professional services, which are in short supply, according to the paper, which was published in the Journal of Autism and Developmental Disorders.
Methods and results
The meta-analysis included 54 papers based on randomized clinical trials involving 2,895 children, which compared the effects of various parent interventions with professional treatment, treatment as usual, or being on a wait-list to receive an intervention.
Overall the research team reported “moderately strong” average benefits from the parent-mediated interventions (Hedges’ g, 0.553), indicating a medium effect size. Parent interventions had the greatest effect on outcomes involving positive behavior and social skills (0.603), followed by language and communication (0.545), maladaptive behavior (0.519), and life skills (0.239).
Similar benefits were observed regardless of a child’s age or sex or which parent or parents implemented an intervention. The effects also appeared to be consistent regardless of intervention characteristics, such as the number of training sessions parents received, although the researchers noted that many studies did not provide data on such details.
Paul Carbone, MD, a professor of pediatrics at the University of Utah, Salt Lake City, who was not involved in the review, said it demonstrates that such parental engagement is “vitally important” and pediatricians “should not hesitate to refer interested families.”

Dr. Carbone, who is the medical director of an assessment program for children with suspected developmental disabilities, said many training programs for parents have adopted telehealth, adding to their convenience. To make appropriate referrals, primary care clinicians should become acquainted with local programs and learn which outcomes they target, he said.
Dr. Smith noted that primary care physicians are “better trained now than ever” to identify autism spectrum disorder and therefore are among the first to identify those conditions and help parents understand “that their actions at home absolutely make a difference in the child’s development.”
Overcoming limitations, future research needs
The research team attempted to overcome limitations with previous reviews by using comprehensive search terms and other methods to identify relevant studies, including some that had not been published. They included only studies that reflect common practice of training multiple parents simultaneously, they wrote.
Dr. Smith noted that long-term outcomes data and further study to compare effects on children with mild, moderate, and severe autism are needed.
Although logic would suggest greater benefits for children with severe disease, there are no data to demonstrate that, he said.
The authors of the study and Dr. Carbone reported no relevant competing interests.
“Referrals for parent training should now be considered the expected standard for medical practice,” said a member of the research team, Timothy B. Smith, PhD, a professor of psychology at Brigham Young University, Provo, Utah.
Programs that show parents how to teach functional skills and address maladaptive behaviors, also known as parent-mediated or parent-implemented interventions, offer an alternative to one-on-one professional services, which are in short supply, according to the paper, which was published in the Journal of Autism and Developmental Disorders.
Methods and results
The meta-analysis included 54 papers based on randomized clinical trials involving 2,895 children, which compared the effects of various parent interventions with professional treatment, treatment as usual, or being on a wait-list to receive an intervention.
Overall the research team reported “moderately strong” average benefits from the parent-mediated interventions (Hedges’ g, 0.553), indicating a medium effect size. Parent interventions had the greatest effect on outcomes involving positive behavior and social skills (0.603), followed by language and communication (0.545), maladaptive behavior (0.519), and life skills (0.239).
Similar benefits were observed regardless of a child’s age or sex or which parent or parents implemented an intervention. The effects also appeared to be consistent regardless of intervention characteristics, such as the number of training sessions parents received, although the researchers noted that many studies did not provide data on such details.
Paul Carbone, MD, a professor of pediatrics at the University of Utah, Salt Lake City, who was not involved in the review, said it demonstrates that such parental engagement is “vitally important” and pediatricians “should not hesitate to refer interested families.”
Dr. Carbone, who is the medical director of an assessment program for children with suspected developmental disabilities, said many training programs for parents have adopted telehealth, adding to their convenience. To make appropriate referrals, primary care clinicians should become acquainted with local programs and learn which outcomes they target, he said.
Dr. Smith noted that primary care physicians are “better trained now than ever” to identify autism spectrum disorder and therefore are among the first to identify those conditions and help parents understand “that their actions at home absolutely make a difference in the child’s development.”
Overcoming limitations, future research needs
The research team attempted to overcome limitations with previous reviews by using comprehensive search terms and other methods to identify relevant studies, including some that had not been published. They included only studies that reflect common practice of training multiple parents simultaneously, they wrote.
Dr. Smith noted that long-term outcomes data and further study to compare effects on children with mild, moderate, and severe autism are needed.
Although logic would suggest greater benefits for children with severe disease, there are no data to demonstrate that, he said.
The authors of the study and Dr. Carbone reported no relevant competing interests.
“Referrals for parent training should now be considered the expected standard for medical practice,” said a member of the research team, Timothy B. Smith, PhD, a professor of psychology at Brigham Young University, Provo, Utah.
Programs that show parents how to teach functional skills and address maladaptive behaviors, also known as parent-mediated or parent-implemented interventions, offer an alternative to one-on-one professional services, which are in short supply, according to the paper, which was published in the Journal of Autism and Developmental Disorders.
Methods and results
The meta-analysis included 54 papers based on randomized clinical trials involving 2,895 children, which compared the effects of various parent interventions with professional treatment, treatment as usual, or being on a wait-list to receive an intervention.
Overall the research team reported “moderately strong” average benefits from the parent-mediated interventions (Hedges’ g, 0.553), indicating a medium effect size. Parent interventions had the greatest effect on outcomes involving positive behavior and social skills (0.603), followed by language and communication (0.545), maladaptive behavior (0.519), and life skills (0.239).
Similar benefits were observed regardless of a child’s age or sex or which parent or parents implemented an intervention. The effects also appeared to be consistent regardless of intervention characteristics, such as the number of training sessions parents received, although the researchers noted that many studies did not provide data on such details.
Paul Carbone, MD, a professor of pediatrics at the University of Utah, Salt Lake City, who was not involved in the review, said it demonstrates that such parental engagement is “vitally important” and pediatricians “should not hesitate to refer interested families.”
Dr. Carbone, who is the medical director of an assessment program for children with suspected developmental disabilities, said many training programs for parents have adopted telehealth, adding to their convenience. To make appropriate referrals, primary care clinicians should become acquainted with local programs and learn which outcomes they target, he said.
Dr. Smith noted that primary care physicians are “better trained now than ever” to identify autism spectrum disorder and therefore are among the first to identify those conditions and help parents understand “that their actions at home absolutely make a difference in the child’s development.”
Overcoming limitations, future research needs
The research team attempted to overcome limitations with previous reviews by using comprehensive search terms and other methods to identify relevant studies, including some that had not been published. They included only studies that reflect common practice of training multiple parents simultaneously, they wrote.
Dr. Smith noted that long-term outcomes data and further study to compare effects on children with mild, moderate, and severe autism are needed.
Although logic would suggest greater benefits for children with severe disease, there are no data to demonstrate that, he said.
The authors of the study and Dr. Carbone reported no relevant competing interests.
FROM JOURNAL OF AUTISM AND DEVELOPMENTAL DISORDERS
Subtle visual dysfunctions often precede early-stage psychosis
A multinational group of investigators found that VisDys were reported considerably more often by patients with recent-onset psychosis and CHR than by those with recent-onset depression or a group acting as healthy control participants.
In addition, vision problems of higher severity were associated with less functional remission both for patients at CHR and those with recent-onset psychosis. Among patients with CHR, VisDys was also linked to lower quality of life (QOL), higher depressiveness, and more severe impairment of visuospatial constructability.
The researchers used fMRI imaging to compare resting-state functional brain connectivity in participants with recent-onset psychosis, CHR, and recent-onset depression. They found that the occipital (ON) and frontoparietal (FPN) subnetworks were particularly implicated in VisDys.
“Subtle VisDys should be regarded as a frequent phenomenon across the psychosis spectrum, impinging negatively on patients’ current ability to function in several settings of their daily and social life, their QOL, and visuospatial abilities,” write investigators led by Johanna Schwarzer, Institute for Translational Psychiatry, University of Muenster (Germany).
“These large-sample study findings suggest that VisDys are clinically highly relevant not only in [recent-onset psychosis] but especially in CHR,” they stated.
The findings were published online in Neuropsychopharmacology.
Subtle, underrecognized
Unlike patients with nonpsychotic disorders, approximately 50%-60% of patients diagnosed with schizophrenia report VisDys involving brightness, motion, form, color perception, or distorted perception of their own face, the researchers reported.
These “subtle” VisDys are “often underrecognized during clinical examination, despite their clinical relevance related to suicidal ideation, cognitive impairment, or poorer treatment response,” they wrote.
Most research into these vision problems in patients with schizophrenia has focused on patients in which the illness is in a stable, chronic state – although VisDys often appear years before the diagnosis of a psychotic disorder.
Moreover, there has been little research into the neurobiological underpinnings of VisDys, specifically in early states of psychosis and/or in comparison to other disorders, such as depression.
The Personalised Prognostic Indicators for Early Psychosis Management (PRONIA) Consortium studied the psychophysiological phenomenon of VisDys in a large sample of adolescents and young adults. The sample consisted of three diagnostic groups: those with recent-onset psychosis, those with CHR, and those with recent-onset depression.
VisDys in daily life were measured using the Schizophrenia Proneness Instrument–Adult Scale (SPI-A), which assesses basic symptoms that indicate increased risk for psychosis.
Visual information processing
Resting-state imaging data on intrinsic brain networks were also assessed in the PRONIA sample and were analyzed across 12,720 functional connectivities between 160 regions of interest across the whole brain.
In particular, the researchers were interested in the primary networks involved in visual information processing, especially the dorsal visual stream, with further focus on the ON and FPN intrinsic subnetworks.
The ON was chosen because it comprises “primary visual processing pathways,” while the FPN is “widely suggested to modulate attention related to visual information processing at higher cognitive levels.”
The investigators used a machine-learning multivariate pattern analysis approach that “enables the consideration of multiple interactions within brain systems.”
The current study involved 721 participants from the PRONIA database, including 147 participants with recent-onset psychosis (mean age, 28.45 years; 60.5% men), 143 with CHR (mean age, 26.97 years; about 50% men), 151 with recent-onset depression (mean age, 29.13 years; 47% men), and 280 in the healthy-controls group (mean age, 28.54 years; 39.4% men).
The researchers selected 14 items to assess from the SPI-A that represented different aspects of VisDys. Severity was defined by the maximum frequency within the past 3 months – from 1 (never) to 6 (daily).
The 14 items were as follows: oversensitivity to light and/or certain visual perception objects, photopsia, micropsia/macropsia, near and tele-vision, metamorphopsia, changes in color vision, altered perception of a patient’s own face, pseudomovements of optic stimuli, diplopia or oblique vision, disturbances of the estimation of distances or sizes, disturbances of the perception of straight lines/contours, maintenance of optic stimuli “visual echoes,” partial seeing (including tubular vision), and captivation of attention by details of the visual field.
Participants also completed the Beck Depression Inventory–II scale (BDI-II), the Positive and Negative Syndrome Scale (PANSS), the Functional Remission in General Schizophrenia, and several other scales that measure global and social functioning.
Other assessments included QOL and the Rey-Osterrieth Complex Figure Test, which is a neuropsychological measurement of visuospatial constructability.
Specific to early-stage psychosis?
Results showed that VisDys were reported more frequently in both recent-onset psychosis and CHR groups compared with the recent-onset depression and healthy control groups (50.34% and 55.94% vs. 16.56% and 4.28%, respectively).
The investigators noted that VisDys sum scores “showed high internal consistency” (Cronbachs alpha, 0.78 over all participants).
Among those with recent-onset psychosis, a higher VisDys sum score was correlated with lower scores for functional remission (P = .036) and social functioning (P = .014).
In CHR, higher VisDys sum scores were associated with lower scores for health-related functional remission (P = .024), lower physical and psychological QOL (P = .004 and P = .015, respectively), more severe depression on the BDI-II (P = .021), and more impaired visuospatial constructability (P = .027).
Among those with recent-onset depression and their healthy peers, “no relevant correlations were found between VisDys sum scores and any parameters representing functional remission, QOL, depressiveness, or visuospatial constructability,” the researchers wrote.
A total of 135 participants with recent-onset psychosis, 128 with CHR, and 134 with recent-onset depression also underwent resting-state fMRI.
ON functional connectivity predicted presence of VisDys in patients with recent-onset psychosis and those with CHR, with a balanced accuracy of 60.17% (P = .0001) and 67.38% (P = .029), respectively. In the combined recent-onset psychosis plus CHR sample, VisDys were predicted by FPN functional connectivity (balanced accuracy, 61.1%; P = .006).
“Findings from multivariate pattern analysis support a model of functional integrity within ON and FPN driving the VisDys phenomenon and being implicated in core disease mechanisms of early psychosis states,” the investigators noted.
“The main findings from this large sample study support the idea of VisDys being specific to the psychosis spectrum already at early stages,” while being less frequently reported in recent-onset depression, they wrote. VisDys also “appeared negligible” among those without psychiatric disorders.
Regular assessment needed
Steven Silverstein, PhD, professor of biopsychosocial medicine and professor of psychiatry, neuroscience, and ophthalmology, Center for Visual Science, University of Rochester (N.Y.) Medical Center, called the findings “important” because “they will increase appreciation in the field of mental health for the frequency and disabling nature of visual symptoms and the need for regular assessment in routine clinical practice with people at risk for or with psychotic disorders.”

In addition, “the brain imaging findings are providing needed information that could lead to treatments that target the brain networks generating the visual symptoms,” such as neurofeedback or brain stimulation, said Dr. Silverstein, who was not involved with the research.
The study was funded by a grant for the PRONIA Consortium. Individual researchers received funding from NARSAD Young Investigator Award of the Brain and Behavior Research Foundation, the Koeln Fortune Program/Faculty of Medicine, the University of Cologne, and the European Union’s Horizon 2020 research and innovation program. Open Access funding was enabled and organized by Projekt DEAL. Ms. Schwarzer and Dr. Silverstein reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A multinational group of investigators found that VisDys were reported considerably more often by patients with recent-onset psychosis and CHR than by those with recent-onset depression or a group acting as healthy control participants.
In addition, vision problems of higher severity were associated with less functional remission both for patients at CHR and those with recent-onset psychosis. Among patients with CHR, VisDys was also linked to lower quality of life (QOL), higher depressiveness, and more severe impairment of visuospatial constructability.
The researchers used fMRI imaging to compare resting-state functional brain connectivity in participants with recent-onset psychosis, CHR, and recent-onset depression. They found that the occipital (ON) and frontoparietal (FPN) subnetworks were particularly implicated in VisDys.
“Subtle VisDys should be regarded as a frequent phenomenon across the psychosis spectrum, impinging negatively on patients’ current ability to function in several settings of their daily and social life, their QOL, and visuospatial abilities,” write investigators led by Johanna Schwarzer, Institute for Translational Psychiatry, University of Muenster (Germany).
“These large-sample study findings suggest that VisDys are clinically highly relevant not only in [recent-onset psychosis] but especially in CHR,” they stated.
The findings were published online in Neuropsychopharmacology.
Subtle, underrecognized
Unlike patients with nonpsychotic disorders, approximately 50%-60% of patients diagnosed with schizophrenia report VisDys involving brightness, motion, form, color perception, or distorted perception of their own face, the researchers reported.
These “subtle” VisDys are “often underrecognized during clinical examination, despite their clinical relevance related to suicidal ideation, cognitive impairment, or poorer treatment response,” they wrote.
Most research into these vision problems in patients with schizophrenia has focused on patients in which the illness is in a stable, chronic state – although VisDys often appear years before the diagnosis of a psychotic disorder.
Moreover, there has been little research into the neurobiological underpinnings of VisDys, specifically in early states of psychosis and/or in comparison to other disorders, such as depression.
The Personalised Prognostic Indicators for Early Psychosis Management (PRONIA) Consortium studied the psychophysiological phenomenon of VisDys in a large sample of adolescents and young adults. The sample consisted of three diagnostic groups: those with recent-onset psychosis, those with CHR, and those with recent-onset depression.
VisDys in daily life were measured using the Schizophrenia Proneness Instrument–Adult Scale (SPI-A), which assesses basic symptoms that indicate increased risk for psychosis.
Visual information processing
Resting-state imaging data on intrinsic brain networks were also assessed in the PRONIA sample and were analyzed across 12,720 functional connectivities between 160 regions of interest across the whole brain.
In particular, the researchers were interested in the primary networks involved in visual information processing, especially the dorsal visual stream, with further focus on the ON and FPN intrinsic subnetworks.
The ON was chosen because it comprises “primary visual processing pathways,” while the FPN is “widely suggested to modulate attention related to visual information processing at higher cognitive levels.”
The investigators used a machine-learning multivariate pattern analysis approach that “enables the consideration of multiple interactions within brain systems.”
The current study involved 721 participants from the PRONIA database, including 147 participants with recent-onset psychosis (mean age, 28.45 years; 60.5% men), 143 with CHR (mean age, 26.97 years; about 50% men), 151 with recent-onset depression (mean age, 29.13 years; 47% men), and 280 in the healthy-controls group (mean age, 28.54 years; 39.4% men).
The researchers selected 14 items to assess from the SPI-A that represented different aspects of VisDys. Severity was defined by the maximum frequency within the past 3 months – from 1 (never) to 6 (daily).
The 14 items were as follows: oversensitivity to light and/or certain visual perception objects, photopsia, micropsia/macropsia, near and tele-vision, metamorphopsia, changes in color vision, altered perception of a patient’s own face, pseudomovements of optic stimuli, diplopia or oblique vision, disturbances of the estimation of distances or sizes, disturbances of the perception of straight lines/contours, maintenance of optic stimuli “visual echoes,” partial seeing (including tubular vision), and captivation of attention by details of the visual field.
Participants also completed the Beck Depression Inventory–II scale (BDI-II), the Positive and Negative Syndrome Scale (PANSS), the Functional Remission in General Schizophrenia, and several other scales that measure global and social functioning.
Other assessments included QOL and the Rey-Osterrieth Complex Figure Test, which is a neuropsychological measurement of visuospatial constructability.
Specific to early-stage psychosis?
Results showed that VisDys were reported more frequently in both recent-onset psychosis and CHR groups compared with the recent-onset depression and healthy control groups (50.34% and 55.94% vs. 16.56% and 4.28%, respectively).
The investigators noted that VisDys sum scores “showed high internal consistency” (Cronbachs alpha, 0.78 over all participants).
Among those with recent-onset psychosis, a higher VisDys sum score was correlated with lower scores for functional remission (P = .036) and social functioning (P = .014).
In CHR, higher VisDys sum scores were associated with lower scores for health-related functional remission (P = .024), lower physical and psychological QOL (P = .004 and P = .015, respectively), more severe depression on the BDI-II (P = .021), and more impaired visuospatial constructability (P = .027).
Among those with recent-onset depression and their healthy peers, “no relevant correlations were found between VisDys sum scores and any parameters representing functional remission, QOL, depressiveness, or visuospatial constructability,” the researchers wrote.
A total of 135 participants with recent-onset psychosis, 128 with CHR, and 134 with recent-onset depression also underwent resting-state fMRI.
ON functional connectivity predicted presence of VisDys in patients with recent-onset psychosis and those with CHR, with a balanced accuracy of 60.17% (P = .0001) and 67.38% (P = .029), respectively. In the combined recent-onset psychosis plus CHR sample, VisDys were predicted by FPN functional connectivity (balanced accuracy, 61.1%; P = .006).
“Findings from multivariate pattern analysis support a model of functional integrity within ON and FPN driving the VisDys phenomenon and being implicated in core disease mechanisms of early psychosis states,” the investigators noted.
“The main findings from this large sample study support the idea of VisDys being specific to the psychosis spectrum already at early stages,” while being less frequently reported in recent-onset depression, they wrote. VisDys also “appeared negligible” among those without psychiatric disorders.
Regular assessment needed
Steven Silverstein, PhD, professor of biopsychosocial medicine and professor of psychiatry, neuroscience, and ophthalmology, Center for Visual Science, University of Rochester (N.Y.) Medical Center, called the findings “important” because “they will increase appreciation in the field of mental health for the frequency and disabling nature of visual symptoms and the need for regular assessment in routine clinical practice with people at risk for or with psychotic disorders.”
In addition, “the brain imaging findings are providing needed information that could lead to treatments that target the brain networks generating the visual symptoms,” such as neurofeedback or brain stimulation, said Dr. Silverstein, who was not involved with the research.
The study was funded by a grant for the PRONIA Consortium. Individual researchers received funding from NARSAD Young Investigator Award of the Brain and Behavior Research Foundation, the Koeln Fortune Program/Faculty of Medicine, the University of Cologne, and the European Union’s Horizon 2020 research and innovation program. Open Access funding was enabled and organized by Projekt DEAL. Ms. Schwarzer and Dr. Silverstein reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A multinational group of investigators found that VisDys were reported considerably more often by patients with recent-onset psychosis and CHR than by those with recent-onset depression or a group acting as healthy control participants.
In addition, vision problems of higher severity were associated with less functional remission both for patients at CHR and those with recent-onset psychosis. Among patients with CHR, VisDys was also linked to lower quality of life (QOL), higher depressiveness, and more severe impairment of visuospatial constructability.
The researchers used fMRI imaging to compare resting-state functional brain connectivity in participants with recent-onset psychosis, CHR, and recent-onset depression. They found that the occipital (ON) and frontoparietal (FPN) subnetworks were particularly implicated in VisDys.
“Subtle VisDys should be regarded as a frequent phenomenon across the psychosis spectrum, impinging negatively on patients’ current ability to function in several settings of their daily and social life, their QOL, and visuospatial abilities,” write investigators led by Johanna Schwarzer, Institute for Translational Psychiatry, University of Muenster (Germany).
“These large-sample study findings suggest that VisDys are clinically highly relevant not only in [recent-onset psychosis] but especially in CHR,” they stated.
The findings were published online in Neuropsychopharmacology.
Subtle, underrecognized
Unlike patients with nonpsychotic disorders, approximately 50%-60% of patients diagnosed with schizophrenia report VisDys involving brightness, motion, form, color perception, or distorted perception of their own face, the researchers reported.
These “subtle” VisDys are “often underrecognized during clinical examination, despite their clinical relevance related to suicidal ideation, cognitive impairment, or poorer treatment response,” they wrote.
Most research into these vision problems in patients with schizophrenia has focused on patients in which the illness is in a stable, chronic state – although VisDys often appear years before the diagnosis of a psychotic disorder.
Moreover, there has been little research into the neurobiological underpinnings of VisDys, specifically in early states of psychosis and/or in comparison to other disorders, such as depression.
The Personalised Prognostic Indicators for Early Psychosis Management (PRONIA) Consortium studied the psychophysiological phenomenon of VisDys in a large sample of adolescents and young adults. The sample consisted of three diagnostic groups: those with recent-onset psychosis, those with CHR, and those with recent-onset depression.
VisDys in daily life were measured using the Schizophrenia Proneness Instrument–Adult Scale (SPI-A), which assesses basic symptoms that indicate increased risk for psychosis.
Visual information processing
Resting-state imaging data on intrinsic brain networks were also assessed in the PRONIA sample and were analyzed across 12,720 functional connectivities between 160 regions of interest across the whole brain.
In particular, the researchers were interested in the primary networks involved in visual information processing, especially the dorsal visual stream, with further focus on the ON and FPN intrinsic subnetworks.
The ON was chosen because it comprises “primary visual processing pathways,” while the FPN is “widely suggested to modulate attention related to visual information processing at higher cognitive levels.”
The investigators used a machine-learning multivariate pattern analysis approach that “enables the consideration of multiple interactions within brain systems.”
The current study involved 721 participants from the PRONIA database, including 147 participants with recent-onset psychosis (mean age, 28.45 years; 60.5% men), 143 with CHR (mean age, 26.97 years; about 50% men), 151 with recent-onset depression (mean age, 29.13 years; 47% men), and 280 in the healthy-controls group (mean age, 28.54 years; 39.4% men).
The researchers selected 14 items to assess from the SPI-A that represented different aspects of VisDys. Severity was defined by the maximum frequency within the past 3 months – from 1 (never) to 6 (daily).
The 14 items were as follows: oversensitivity to light and/or certain visual perception objects, photopsia, micropsia/macropsia, near and tele-vision, metamorphopsia, changes in color vision, altered perception of a patient’s own face, pseudomovements of optic stimuli, diplopia or oblique vision, disturbances of the estimation of distances or sizes, disturbances of the perception of straight lines/contours, maintenance of optic stimuli “visual echoes,” partial seeing (including tubular vision), and captivation of attention by details of the visual field.
Participants also completed the Beck Depression Inventory–II scale (BDI-II), the Positive and Negative Syndrome Scale (PANSS), the Functional Remission in General Schizophrenia, and several other scales that measure global and social functioning.
Other assessments included QOL and the Rey-Osterrieth Complex Figure Test, which is a neuropsychological measurement of visuospatial constructability.
Specific to early-stage psychosis?
Results showed that VisDys were reported more frequently in both recent-onset psychosis and CHR groups compared with the recent-onset depression and healthy control groups (50.34% and 55.94% vs. 16.56% and 4.28%, respectively).
The investigators noted that VisDys sum scores “showed high internal consistency” (Cronbachs alpha, 0.78 over all participants).
Among those with recent-onset psychosis, a higher VisDys sum score was correlated with lower scores for functional remission (P = .036) and social functioning (P = .014).
In CHR, higher VisDys sum scores were associated with lower scores for health-related functional remission (P = .024), lower physical and psychological QOL (P = .004 and P = .015, respectively), more severe depression on the BDI-II (P = .021), and more impaired visuospatial constructability (P = .027).
Among those with recent-onset depression and their healthy peers, “no relevant correlations were found between VisDys sum scores and any parameters representing functional remission, QOL, depressiveness, or visuospatial constructability,” the researchers wrote.
A total of 135 participants with recent-onset psychosis, 128 with CHR, and 134 with recent-onset depression also underwent resting-state fMRI.
ON functional connectivity predicted presence of VisDys in patients with recent-onset psychosis and those with CHR, with a balanced accuracy of 60.17% (P = .0001) and 67.38% (P = .029), respectively. In the combined recent-onset psychosis plus CHR sample, VisDys were predicted by FPN functional connectivity (balanced accuracy, 61.1%; P = .006).
“Findings from multivariate pattern analysis support a model of functional integrity within ON and FPN driving the VisDys phenomenon and being implicated in core disease mechanisms of early psychosis states,” the investigators noted.
“The main findings from this large sample study support the idea of VisDys being specific to the psychosis spectrum already at early stages,” while being less frequently reported in recent-onset depression, they wrote. VisDys also “appeared negligible” among those without psychiatric disorders.
Regular assessment needed
Steven Silverstein, PhD, professor of biopsychosocial medicine and professor of psychiatry, neuroscience, and ophthalmology, Center for Visual Science, University of Rochester (N.Y.) Medical Center, called the findings “important” because “they will increase appreciation in the field of mental health for the frequency and disabling nature of visual symptoms and the need for regular assessment in routine clinical practice with people at risk for or with psychotic disorders.”
In addition, “the brain imaging findings are providing needed information that could lead to treatments that target the brain networks generating the visual symptoms,” such as neurofeedback or brain stimulation, said Dr. Silverstein, who was not involved with the research.
The study was funded by a grant for the PRONIA Consortium. Individual researchers received funding from NARSAD Young Investigator Award of the Brain and Behavior Research Foundation, the Koeln Fortune Program/Faculty of Medicine, the University of Cologne, and the European Union’s Horizon 2020 research and innovation program. Open Access funding was enabled and organized by Projekt DEAL. Ms. Schwarzer and Dr. Silverstein reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NEUROPSYCHOPHARMACOLOGY
Psychiatrists’ views on psychoactive drugs clash with U.S. policy
“The consensus among experts, including psychiatrists, about specific drugs is not consistent or congruent with the schedule of these drugs” in the United States, lead author Adam Levin, MD, third-year psychiatry resident, Ohio State University, Columbus, and affiliate scholar at the Center for Psychedelic Drug Research and Education, Ohio State College of Social Work, told this news organization.

Dr. Levin stressed the importance of appropriate drug scheduling to improve access to treatments such as psilocybin (psychedelic mushrooms) and 4-methylenedioxy methamphetamine (MDMA), which are now being tested for psychiatric disorders.
“We are in the middle of a mental health crisis so having any new tools would be really important,” he said.
The survey findings were published online in the International Journal of Drug Policy.
Five drug schedules
The Controlled Substances Act of 1970 created five “schedules” that organized drugs from most to least dangerous (schedule I-V). However, Dr. Levin said that the schedules do not accurately reflect the harms or therapeutic benefits of the various drugs.
Some drugs in lower, less restrictive schedules have greater potential for harm than do those in higher schedules, he noted. For example, methamphetamine, which has been recalled in multiple formulations because of concerns about abuse and limited medical use, remains a schedule II drug.
In addition, several schedule I drugs, including psilocybin and MDMA that are deemed dangerous and of no medical value, have shown therapeutic potential and low rates of misuse, addiction, or physical harm, the investigators noted.
In fact, the Food and Drug Administration has granted breakthrough therapy status to psilocybin for treatment-resistant depression and major depressive disorder (MDD) and to MDMA for posttraumatic stress disorder. This has positioned these drugs for possible FDA approval within the next few years.
Access to schedule I drugs for research purposes is tightly controlled. “Once psilocybin was placed in schedule I, there was this massive drop-off in the research funding and amount of research; and we’re just now starting to understand the potential therapeutic value of this drug,” said Dr. Levin.
Even with a recent research resurgence, most studies are funded by charitable donations or for-profit companies because of continued hesitancy on the part of grant-making organizations, he added.
Apparent contradictions
Given the pending approval of several schedule I drugs and escalating abuse of drugs in lower schedules, there is a growing need to understand physician attitudes surrounding the apparent contradictions in the drug schedule, the investigators noted.
Their survey included a geographically diverse group of 181 mostly middle-aged psychiatrists (65.2% were men) with an average of 16.2 years of practice after residency.
Participants were randomly assigned to respond to a vignette depicting a clinical scenario where a patient wants one of four drugs to help treat severe depression: psilocybin, a schedule I drug; methamphetamine (Desoxyn), a schedule II drug; ketamine, a Schedule III drug; or alprazolam (Xanax), a schedule IV drug.
Each of these therapies has established antidepressant properties, but none are FDA approved for treatment of MDD. However, an intranasal formulation of the ketamine enantiomer Spravato (esketamine) was recently approved for treatment-resistant depression.
There were significant differences among the groups presented with different vignettes. Participants were more likely to warn against repeated use of and development of a new psychiatric problem with methamphetamine and alprazolam compared with psilocybin or ketamine.
Respondents were most concerned about increased suicide risk after the nonprescribed use of alprazolam compared with psilocybin and ketamine.
Compared with all other drugs, ketamine was more likely to be integrated into treatment plans.
Therapeutic value, abuse potential
Participants were asked to rate the safety, therapeutic value, and abuse potential of the four drugs as well as alcohol, a nonscheduled legal drug, if used properly or as directed.
Respondents viewed psilocybin and ketamine as similarly safe – and safer than methamphetamine and alprazolam. They considered ketamine as having the highest therapeutic potential, followed by psilocybin, and then alprazolam and methamphetamine. “Last was alcohol, which we expected because alcohol is not used therapeutically,” said Dr. Levin.
Survey completers viewed methamphetamine, alprazolam, and alcohol as having similarly high abuse potential, and ketamine as having mid-level abuse potential. Psilocybin was rated as having the lowest abuse potential, “which is exactly the opposite of what is implied by its schedule I status,” noted Dr. Levin.
The results provide evidence these drugs “are incorrectly scheduled,” he said.
“This suggests the schedule does not reflect current evidence, which I think is really important to understand because there are consequences to the drug schedule,” including criminal justice and research consequences, he added.
Dr. Levin pointed out that possession of drugs in more harmful schedules is linked to sometimes lengthy prison sentences.
The psychiatrists’ perceptions of the drugs “overlaps pretty significantly” with recent surveys of other mental health professionals, including psychologists and addiction experts, he noted.
The study was funded by the Drug Enforcement and Policy Center, Moritz College of Law, and The Ohio State University. Dr. Levin reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“The consensus among experts, including psychiatrists, about specific drugs is not consistent or congruent with the schedule of these drugs” in the United States, lead author Adam Levin, MD, third-year psychiatry resident, Ohio State University, Columbus, and affiliate scholar at the Center for Psychedelic Drug Research and Education, Ohio State College of Social Work, told this news organization.
Dr. Levin stressed the importance of appropriate drug scheduling to improve access to treatments such as psilocybin (psychedelic mushrooms) and 4-methylenedioxy methamphetamine (MDMA), which are now being tested for psychiatric disorders.
“We are in the middle of a mental health crisis so having any new tools would be really important,” he said.
The survey findings were published online in the International Journal of Drug Policy.
Five drug schedules
The Controlled Substances Act of 1970 created five “schedules” that organized drugs from most to least dangerous (schedule I-V). However, Dr. Levin said that the schedules do not accurately reflect the harms or therapeutic benefits of the various drugs.
Some drugs in lower, less restrictive schedules have greater potential for harm than do those in higher schedules, he noted. For example, methamphetamine, which has been recalled in multiple formulations because of concerns about abuse and limited medical use, remains a schedule II drug.
In addition, several schedule I drugs, including psilocybin and MDMA that are deemed dangerous and of no medical value, have shown therapeutic potential and low rates of misuse, addiction, or physical harm, the investigators noted.
In fact, the Food and Drug Administration has granted breakthrough therapy status to psilocybin for treatment-resistant depression and major depressive disorder (MDD) and to MDMA for posttraumatic stress disorder. This has positioned these drugs for possible FDA approval within the next few years.
Access to schedule I drugs for research purposes is tightly controlled. “Once psilocybin was placed in schedule I, there was this massive drop-off in the research funding and amount of research; and we’re just now starting to understand the potential therapeutic value of this drug,” said Dr. Levin.
Even with a recent research resurgence, most studies are funded by charitable donations or for-profit companies because of continued hesitancy on the part of grant-making organizations, he added.
Apparent contradictions
Given the pending approval of several schedule I drugs and escalating abuse of drugs in lower schedules, there is a growing need to understand physician attitudes surrounding the apparent contradictions in the drug schedule, the investigators noted.
Their survey included a geographically diverse group of 181 mostly middle-aged psychiatrists (65.2% were men) with an average of 16.2 years of practice after residency.
Participants were randomly assigned to respond to a vignette depicting a clinical scenario where a patient wants one of four drugs to help treat severe depression: psilocybin, a schedule I drug; methamphetamine (Desoxyn), a schedule II drug; ketamine, a Schedule III drug; or alprazolam (Xanax), a schedule IV drug.
Each of these therapies has established antidepressant properties, but none are FDA approved for treatment of MDD. However, an intranasal formulation of the ketamine enantiomer Spravato (esketamine) was recently approved for treatment-resistant depression.
There were significant differences among the groups presented with different vignettes. Participants were more likely to warn against repeated use of and development of a new psychiatric problem with methamphetamine and alprazolam compared with psilocybin or ketamine.
Respondents were most concerned about increased suicide risk after the nonprescribed use of alprazolam compared with psilocybin and ketamine.
Compared with all other drugs, ketamine was more likely to be integrated into treatment plans.
Therapeutic value, abuse potential
Participants were asked to rate the safety, therapeutic value, and abuse potential of the four drugs as well as alcohol, a nonscheduled legal drug, if used properly or as directed.
Respondents viewed psilocybin and ketamine as similarly safe – and safer than methamphetamine and alprazolam. They considered ketamine as having the highest therapeutic potential, followed by psilocybin, and then alprazolam and methamphetamine. “Last was alcohol, which we expected because alcohol is not used therapeutically,” said Dr. Levin.
Survey completers viewed methamphetamine, alprazolam, and alcohol as having similarly high abuse potential, and ketamine as having mid-level abuse potential. Psilocybin was rated as having the lowest abuse potential, “which is exactly the opposite of what is implied by its schedule I status,” noted Dr. Levin.
The results provide evidence these drugs “are incorrectly scheduled,” he said.
“This suggests the schedule does not reflect current evidence, which I think is really important to understand because there are consequences to the drug schedule,” including criminal justice and research consequences, he added.
Dr. Levin pointed out that possession of drugs in more harmful schedules is linked to sometimes lengthy prison sentences.
The psychiatrists’ perceptions of the drugs “overlaps pretty significantly” with recent surveys of other mental health professionals, including psychologists and addiction experts, he noted.
The study was funded by the Drug Enforcement and Policy Center, Moritz College of Law, and The Ohio State University. Dr. Levin reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“The consensus among experts, including psychiatrists, about specific drugs is not consistent or congruent with the schedule of these drugs” in the United States, lead author Adam Levin, MD, third-year psychiatry resident, Ohio State University, Columbus, and affiliate scholar at the Center for Psychedelic Drug Research and Education, Ohio State College of Social Work, told this news organization.
Dr. Levin stressed the importance of appropriate drug scheduling to improve access to treatments such as psilocybin (psychedelic mushrooms) and 4-methylenedioxy methamphetamine (MDMA), which are now being tested for psychiatric disorders.
“We are in the middle of a mental health crisis so having any new tools would be really important,” he said.
The survey findings were published online in the International Journal of Drug Policy.
Five drug schedules
The Controlled Substances Act of 1970 created five “schedules” that organized drugs from most to least dangerous (schedule I-V). However, Dr. Levin said that the schedules do not accurately reflect the harms or therapeutic benefits of the various drugs.
Some drugs in lower, less restrictive schedules have greater potential for harm than do those in higher schedules, he noted. For example, methamphetamine, which has been recalled in multiple formulations because of concerns about abuse and limited medical use, remains a schedule II drug.
In addition, several schedule I drugs, including psilocybin and MDMA that are deemed dangerous and of no medical value, have shown therapeutic potential and low rates of misuse, addiction, or physical harm, the investigators noted.
In fact, the Food and Drug Administration has granted breakthrough therapy status to psilocybin for treatment-resistant depression and major depressive disorder (MDD) and to MDMA for posttraumatic stress disorder. This has positioned these drugs for possible FDA approval within the next few years.
Access to schedule I drugs for research purposes is tightly controlled. “Once psilocybin was placed in schedule I, there was this massive drop-off in the research funding and amount of research; and we’re just now starting to understand the potential therapeutic value of this drug,” said Dr. Levin.
Even with a recent research resurgence, most studies are funded by charitable donations or for-profit companies because of continued hesitancy on the part of grant-making organizations, he added.
Apparent contradictions
Given the pending approval of several schedule I drugs and escalating abuse of drugs in lower schedules, there is a growing need to understand physician attitudes surrounding the apparent contradictions in the drug schedule, the investigators noted.
Their survey included a geographically diverse group of 181 mostly middle-aged psychiatrists (65.2% were men) with an average of 16.2 years of practice after residency.
Participants were randomly assigned to respond to a vignette depicting a clinical scenario where a patient wants one of four drugs to help treat severe depression: psilocybin, a schedule I drug; methamphetamine (Desoxyn), a schedule II drug; ketamine, a Schedule III drug; or alprazolam (Xanax), a schedule IV drug.
Each of these therapies has established antidepressant properties, but none are FDA approved for treatment of MDD. However, an intranasal formulation of the ketamine enantiomer Spravato (esketamine) was recently approved for treatment-resistant depression.
There were significant differences among the groups presented with different vignettes. Participants were more likely to warn against repeated use of and development of a new psychiatric problem with methamphetamine and alprazolam compared with psilocybin or ketamine.
Respondents were most concerned about increased suicide risk after the nonprescribed use of alprazolam compared with psilocybin and ketamine.
Compared with all other drugs, ketamine was more likely to be integrated into treatment plans.
Therapeutic value, abuse potential
Participants were asked to rate the safety, therapeutic value, and abuse potential of the four drugs as well as alcohol, a nonscheduled legal drug, if used properly or as directed.
Respondents viewed psilocybin and ketamine as similarly safe – and safer than methamphetamine and alprazolam. They considered ketamine as having the highest therapeutic potential, followed by psilocybin, and then alprazolam and methamphetamine. “Last was alcohol, which we expected because alcohol is not used therapeutically,” said Dr. Levin.
Survey completers viewed methamphetamine, alprazolam, and alcohol as having similarly high abuse potential, and ketamine as having mid-level abuse potential. Psilocybin was rated as having the lowest abuse potential, “which is exactly the opposite of what is implied by its schedule I status,” noted Dr. Levin.
The results provide evidence these drugs “are incorrectly scheduled,” he said.
“This suggests the schedule does not reflect current evidence, which I think is really important to understand because there are consequences to the drug schedule,” including criminal justice and research consequences, he added.
Dr. Levin pointed out that possession of drugs in more harmful schedules is linked to sometimes lengthy prison sentences.
The psychiatrists’ perceptions of the drugs “overlaps pretty significantly” with recent surveys of other mental health professionals, including psychologists and addiction experts, he noted.
The study was funded by the Drug Enforcement and Policy Center, Moritz College of Law, and The Ohio State University. Dr. Levin reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE INTERNATIONAL JOURNAL OF DRUG POLICY
Where a child eats breakfast is important
We’ve been told for decades that a child who doesn’t start the day with a good breakfast is entering school at a serious disadvantage. The brain needs a good supply of energy to learn optimally. So the standard wisdom goes. Subsidized school breakfast programs have been built around this chestnut. But, is there solid evidence to support the notion that simply adding a morning meal to a child’s schedule will improve his or her school performance? It sounds like common sense, but is it just one of those old grandmother’s nuggets that doesn’t stand up under close scrutiny?
A recent study from Spain suggests that the relationship between breakfast and school performance is not merely related to the nutritional needs of a growing brain. Using data from nearly 4,000 Spanish children aged 4-14 collected in a 2017 national health survey, the investigators found “skipping breakfast and eating breakfast out of the home were linked to greater odds of psychosocial behavioral problems than eating breakfast at home.” And, we already know that, in general, children who misbehave in school don’t thrive academically.

There were also associations between the absence or presence of certain food groups in the morning meal with behavioral problems. But the data lacked the granularity to draw any firm conclusions – although the authors felt that what they consider a healthy Spanish diet may have had a positive influence on behavior.
The findings in this study may simply be another example of the many positive influences that have been associated with family meals and have little to do with what is actually consumed. The association may not have much to do with the family gathering together at a single Norman Rockwell sitting, a reality that I suspect seldom occurs. The apparent positive influence of breakfast may be that it reflects a family’s priorities: that food is important, that sleep is important, and that school is important – so important that scheduling the morning should focus on sending the child off well prepared. The child who is allowed to stay up to an unhealthy hour is likely to be difficult to arouse in the morning for breakfast and getting off to school.
It may be that the child’s behavior problems are so disruptive and taxing for the family that even with their best efforts, the parents can’t find the time and energy to provide a breakfast in the home.
On the other hand, the study doesn’t tell us how many children aren’t offered breakfast at home because their families simply can’t afford it. Obviously, the answer depends on the socioeconomic mix of a given community. In some localities this may represent a sizable percentage of the population.
So where does this leave us? Unfortunately, as I read through the discussion at the end of this paper I felt that the authors were leaning too much toward further research based on the potential associations between behavior and specific food groups their data suggested.
For me, the take-home message from this paper is that our existing efforts to improve academic success with food offered in school should also include strategies that promote eating breakfast at home. For example, the backpack take-home food distribution programs that seem to have been effective could include breakfast-targeted items packaged in a way that encourage families to provide breakfast at home.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
We’ve been told for decades that a child who doesn’t start the day with a good breakfast is entering school at a serious disadvantage. The brain needs a good supply of energy to learn optimally. So the standard wisdom goes. Subsidized school breakfast programs have been built around this chestnut. But, is there solid evidence to support the notion that simply adding a morning meal to a child’s schedule will improve his or her school performance? It sounds like common sense, but is it just one of those old grandmother’s nuggets that doesn’t stand up under close scrutiny?
A recent study from Spain suggests that the relationship between breakfast and school performance is not merely related to the nutritional needs of a growing brain. Using data from nearly 4,000 Spanish children aged 4-14 collected in a 2017 national health survey, the investigators found “skipping breakfast and eating breakfast out of the home were linked to greater odds of psychosocial behavioral problems than eating breakfast at home.” And, we already know that, in general, children who misbehave in school don’t thrive academically.
There were also associations between the absence or presence of certain food groups in the morning meal with behavioral problems. But the data lacked the granularity to draw any firm conclusions – although the authors felt that what they consider a healthy Spanish diet may have had a positive influence on behavior.
The findings in this study may simply be another example of the many positive influences that have been associated with family meals and have little to do with what is actually consumed. The association may not have much to do with the family gathering together at a single Norman Rockwell sitting, a reality that I suspect seldom occurs. The apparent positive influence of breakfast may be that it reflects a family’s priorities: that food is important, that sleep is important, and that school is important – so important that scheduling the morning should focus on sending the child off well prepared. The child who is allowed to stay up to an unhealthy hour is likely to be difficult to arouse in the morning for breakfast and getting off to school.
It may be that the child’s behavior problems are so disruptive and taxing for the family that even with their best efforts, the parents can’t find the time and energy to provide a breakfast in the home.
On the other hand, the study doesn’t tell us how many children aren’t offered breakfast at home because their families simply can’t afford it. Obviously, the answer depends on the socioeconomic mix of a given community. In some localities this may represent a sizable percentage of the population.
So where does this leave us? Unfortunately, as I read through the discussion at the end of this paper I felt that the authors were leaning too much toward further research based on the potential associations between behavior and specific food groups their data suggested.
For me, the take-home message from this paper is that our existing efforts to improve academic success with food offered in school should also include strategies that promote eating breakfast at home. For example, the backpack take-home food distribution programs that seem to have been effective could include breakfast-targeted items packaged in a way that encourage families to provide breakfast at home.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
We’ve been told for decades that a child who doesn’t start the day with a good breakfast is entering school at a serious disadvantage. The brain needs a good supply of energy to learn optimally. So the standard wisdom goes. Subsidized school breakfast programs have been built around this chestnut. But, is there solid evidence to support the notion that simply adding a morning meal to a child’s schedule will improve his or her school performance? It sounds like common sense, but is it just one of those old grandmother’s nuggets that doesn’t stand up under close scrutiny?
A recent study from Spain suggests that the relationship between breakfast and school performance is not merely related to the nutritional needs of a growing brain. Using data from nearly 4,000 Spanish children aged 4-14 collected in a 2017 national health survey, the investigators found “skipping breakfast and eating breakfast out of the home were linked to greater odds of psychosocial behavioral problems than eating breakfast at home.” And, we already know that, in general, children who misbehave in school don’t thrive academically.
There were also associations between the absence or presence of certain food groups in the morning meal with behavioral problems. But the data lacked the granularity to draw any firm conclusions – although the authors felt that what they consider a healthy Spanish diet may have had a positive influence on behavior.
The findings in this study may simply be another example of the many positive influences that have been associated with family meals and have little to do with what is actually consumed. The association may not have much to do with the family gathering together at a single Norman Rockwell sitting, a reality that I suspect seldom occurs. The apparent positive influence of breakfast may be that it reflects a family’s priorities: that food is important, that sleep is important, and that school is important – so important that scheduling the morning should focus on sending the child off well prepared. The child who is allowed to stay up to an unhealthy hour is likely to be difficult to arouse in the morning for breakfast and getting off to school.
It may be that the child’s behavior problems are so disruptive and taxing for the family that even with their best efforts, the parents can’t find the time and energy to provide a breakfast in the home.
On the other hand, the study doesn’t tell us how many children aren’t offered breakfast at home because their families simply can’t afford it. Obviously, the answer depends on the socioeconomic mix of a given community. In some localities this may represent a sizable percentage of the population.
So where does this leave us? Unfortunately, as I read through the discussion at the end of this paper I felt that the authors were leaning too much toward further research based on the potential associations between behavior and specific food groups their data suggested.
For me, the take-home message from this paper is that our existing efforts to improve academic success with food offered in school should also include strategies that promote eating breakfast at home. For example, the backpack take-home food distribution programs that seem to have been effective could include breakfast-targeted items packaged in a way that encourage families to provide breakfast at home.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
How to identify and treat patients with substance use disorders
When Michael McGrath, MD, medical director of the Ohana Luxury Alcohol Rehab on the Big Island of Hawaii, trains primary care physicians, he tells them that talking with patients about substance use disorders is like having a stressful, weird conversation. But it’s a courageous one, because of the stigma associated with drug and alcohol disorders.
Dr. McGrath starts the conversation with patients by expressing that physicians now understand that addiction is a disease – one for which the patient isn’t responsible. He explains that there’s both a genetic and a nature/nurture component of the disorder and assures them that he won’t judge or abandon them but rather help them find treatment and make sure they get on the path to wellness.
It’s all too common to see patients with a substance use disorder in today’s primary care population. According to Medscape’s Physicians’ Views on Today’s Divisive Social Issues Report 2022,
According to the Recovery Research Institute, a leading nonprofit orgnaization from Massachusetts General Hospital dedicated to advancing addiction treatment and recovery, about 20 million people in the United States suffer from a substance use disorder. More than half (54%) need assistance with their recovery. The National Institute on Drug Abuse reports that substance abuse and addiction cost society more than $740 billion annually in workplace productivity, health care, and crime-related expenses.
Despite the challenges, physician experts provide advice on how to treat and help patients who have substance use disorders more effectively.
A courageous conversation
Often, the primary care physician or emergency physician is the first to be aware of a patient’s problem with a substance or a relapse. In many communities where shortages of specialized physicians and nonphysician treatment options for substance use disorders aren’t available, there’s usually limited time and resources to help patients with these disorders.
Patients often sense doctors are rushed and may not be interested in hearing about their drug or alcohol problems. Reddit threads are filled with stories like that of user “Cyralek,” who say that the two doctors they’ve seen since quitting drinking didn’t show much interest in the problem beyond ordering liver function tests.
In a nationwide study by researchers at Washington University School of Medicine, St. Louis, 80% of patients who met the diagnostic criteria for substance use disorder visited a doctor, hospital, or clinic for some reason over the past year. Only 1 in 10 were encouraged to cut back on drinking or receive any form of treatment or referral for substance misuse.
Emma Gordon, founder of a salvage yard in Los Angeles, says she used to abuse alcohol and that it affected every aspect of her life. Her brother tried to intervene, but nothing worked until she finally told a physician. “I admitted my problem and felt incredibly calm when she reacted as though it was all normal. I believe that was my first step to becoming a better me. I was thankful I had gone to see a doctor,” says Ms. Gordon.
Though physicians in primary care may not have more than a 15-minute appointment slot, seizing the opportunity to initiate a substance use disorder conversation when warranted is crucial, says Dr. McGrath. The CAGE-AID screening tool, which includes questions such as, “Have you ever felt you ought to cut down on your drinking or drug use?” is an excellent starter. Dr. McGrath also advises primary care clinicians to lower the threshold of concern to a single positive answer rather than several.
Doctors aren’t necessarily rewarded for the time it takes to develop a rapport with patients and to have a conversation that leads to asking, “How much are you drinking?”
“The system in primary care isn’t set up that way,” said Lucy McBride, MD, an internist in Washington, D.C.
Patients don’t often ask for help
In a perfect world, patients struggling with a substance use disorder would present with a request to discontinue using drugs or alcohol, as Ms. Gordon did. While that does happen sometimes, the onus is on the physician to screen for substance misuse.
“Remember, this is the disease that tells you that you don’t have a disease,” Dr. McGrath says. He also says that the use of screening instruments is a bare minimum. When patients are in the throes of a substance use disorder, the prefrontal cortex doesn’t work effectively. Dr. McGrath says there’s an alteration of consciousness so that the patient doesn’t realize the extent of the disease. “Often simply asking the patient is falling far short. It’s the biggest mistake I see,” he says.
Self-reporting from the patient may be unreliable. “That would be like a patient coming in and saying, ‘My blood sugar is 700, and I want you to give me some insulin,’ ” Dr. McGrath says. Instead, clinicians in the field need a more objective measurement.
Perhaps that means asking the patient to bring in a significant other at the next visit or digging deeper into the conversation about alcohol and drugs and their role in the patient’s life. And to really have an impact, Dr. McGrath said, the clinician should talk to the patient about referral for further evaluation.
“You have to get collateral history; that’s the goldmine for the clinician,” Dr. McGrath says. “It may take a few more minutes or mean talking to a family member, but it can make the difference between life and death.”
“I am thankful to my doctor who discussed this [substance use disorder] with me in detail,” says Ronald Williams, another Angeleno who braved the difficult discussion with his doctor. Mr. Williams says his doctor explained it in a good way and that if the doctor hadn’t guided him empathetically, the conversation might not have gone as well.
“We check patients’ cholesterol. We get them on the scale. But there is no blood test to discover how much they’re drinking, no PCR to test for social anxiety, no MRI that distinguishes between their recreational marijuana use and marijuana abuse,” said Dr. McBride.
Check the prescription drugs they’re taking
Another thing Dr. McGrath recommends is for primary care physicians to check the prescription drug monitoring program (PDMP) database in their state to help be alerted to a patient with a substance use disorder. The CDC’s PMPD guidelines recommend that the clinician check on a patient every 3 months or each time they write an opioid prescription. Assigning a staff member or a nurse to check the database can help uncover a history of doctor-shopping or use of controlled substances.
“There’s been a lot of times I’ve gone on self-report, and I’ve been bamboozled because I don’t have a truth-o-meter, and I can’t tell when a patient is telling the truth,” says Dr. McGrath.
He is also a huge proponent of point-of-service screening. Patients can urinate in a cup that has amino assay strips on the side, like an immediate COVID-19 test, or they can spit into a saliva cup. “It’s really beneficial for the patient and the clinician to know right then at the point of service if there is a substance present and what it is,” Dr. McGrath said.
It can be part of the larger conversation once a problem with substances has been uncovered. The clinician can say something like, “Let’s see where you are right now today as far as what you have in your system and where we should go from here.”
Other barriers physicians face
Many physicians may feel unprepared to meet the needs of patients with substance use disorders or prescribe medication that blunts cravings and reduces the urge to drink without the need for special training. Scientists at the National Institutes of Health found that only 1.6% of people with a substance use disorder were prescribed medication to help control it.
In the largest study on how primary care physicians address substance use disorders, fewer than 20% described themselves as very prepared to identify alcoholism or illegal drug use. Since most patients prefer to seek treatment from their primary care doctor, at least initially, not being prepared is a problem.
Although referral for specialty addiction treatment is recommended for patients with severe substance use disorders, primary care physicians with appropriate experience, training, and support can provide some of these services. “In an ideal world I wouldn’t have to refer patients out, since they’re much more likely to talk with their primary care provider about sensitive, intimate topics,” says Dr. McBride.
The issue of reimbursement
Billing for substance use disorder counseling or coordination of care is still challenging, and how to get compensated remains a conundrum for many physicians. Reimbursement may not adequately compensate providers for the additional time and staff needed, but some changes have been positive.
For instance, the American Society for Addiction Medicine reports that in 2022, Medicare expanded the physician fee schedule for opioid and SUD counseling to include reimbursement for telemedicine services.
Learning the billing CPT codes for various addiction treatments and counseling, or having a billing service that understands them, is crucial to reimbursement and keeping revenue running smoothly.
At the very least, developing relationships with treatment centers and specialists in the community can help physicians with referrals and with determining the level of care needed. Physicians can help facilitate that care with routine reassessment and frequent follow-ups, as well as by requesting reports from the treatment facility, continuing treatment of medical conditions, and reinforcing the importance of continued substance use disorder treatment.
Dr. McBride says that primary care physicians can and should make their office a safe, blame-free medical home for patients with substance use disorders. “Patients also need to understand they should bring their whole selves to the doctor – to talk about their sleep, what they consume, their depression, and not just about alcohol, but their relationship with it, and other substances,” she says.
“There needs to be time to talk about it.”
A version of this article first appeared on Medscape.com.
When Michael McGrath, MD, medical director of the Ohana Luxury Alcohol Rehab on the Big Island of Hawaii, trains primary care physicians, he tells them that talking with patients about substance use disorders is like having a stressful, weird conversation. But it’s a courageous one, because of the stigma associated with drug and alcohol disorders.
Dr. McGrath starts the conversation with patients by expressing that physicians now understand that addiction is a disease – one for which the patient isn’t responsible. He explains that there’s both a genetic and a nature/nurture component of the disorder and assures them that he won’t judge or abandon them but rather help them find treatment and make sure they get on the path to wellness.
It’s all too common to see patients with a substance use disorder in today’s primary care population. According to Medscape’s Physicians’ Views on Today’s Divisive Social Issues Report 2022,
According to the Recovery Research Institute, a leading nonprofit orgnaization from Massachusetts General Hospital dedicated to advancing addiction treatment and recovery, about 20 million people in the United States suffer from a substance use disorder. More than half (54%) need assistance with their recovery. The National Institute on Drug Abuse reports that substance abuse and addiction cost society more than $740 billion annually in workplace productivity, health care, and crime-related expenses.
Despite the challenges, physician experts provide advice on how to treat and help patients who have substance use disorders more effectively.
A courageous conversation
Often, the primary care physician or emergency physician is the first to be aware of a patient’s problem with a substance or a relapse. In many communities where shortages of specialized physicians and nonphysician treatment options for substance use disorders aren’t available, there’s usually limited time and resources to help patients with these disorders.
Patients often sense doctors are rushed and may not be interested in hearing about their drug or alcohol problems. Reddit threads are filled with stories like that of user “Cyralek,” who say that the two doctors they’ve seen since quitting drinking didn’t show much interest in the problem beyond ordering liver function tests.
In a nationwide study by researchers at Washington University School of Medicine, St. Louis, 80% of patients who met the diagnostic criteria for substance use disorder visited a doctor, hospital, or clinic for some reason over the past year. Only 1 in 10 were encouraged to cut back on drinking or receive any form of treatment or referral for substance misuse.
Emma Gordon, founder of a salvage yard in Los Angeles, says she used to abuse alcohol and that it affected every aspect of her life. Her brother tried to intervene, but nothing worked until she finally told a physician. “I admitted my problem and felt incredibly calm when she reacted as though it was all normal. I believe that was my first step to becoming a better me. I was thankful I had gone to see a doctor,” says Ms. Gordon.
Though physicians in primary care may not have more than a 15-minute appointment slot, seizing the opportunity to initiate a substance use disorder conversation when warranted is crucial, says Dr. McGrath. The CAGE-AID screening tool, which includes questions such as, “Have you ever felt you ought to cut down on your drinking or drug use?” is an excellent starter. Dr. McGrath also advises primary care clinicians to lower the threshold of concern to a single positive answer rather than several.
Doctors aren’t necessarily rewarded for the time it takes to develop a rapport with patients and to have a conversation that leads to asking, “How much are you drinking?”
“The system in primary care isn’t set up that way,” said Lucy McBride, MD, an internist in Washington, D.C.
Patients don’t often ask for help
In a perfect world, patients struggling with a substance use disorder would present with a request to discontinue using drugs or alcohol, as Ms. Gordon did. While that does happen sometimes, the onus is on the physician to screen for substance misuse.
“Remember, this is the disease that tells you that you don’t have a disease,” Dr. McGrath says. He also says that the use of screening instruments is a bare minimum. When patients are in the throes of a substance use disorder, the prefrontal cortex doesn’t work effectively. Dr. McGrath says there’s an alteration of consciousness so that the patient doesn’t realize the extent of the disease. “Often simply asking the patient is falling far short. It’s the biggest mistake I see,” he says.
Self-reporting from the patient may be unreliable. “That would be like a patient coming in and saying, ‘My blood sugar is 700, and I want you to give me some insulin,’ ” Dr. McGrath says. Instead, clinicians in the field need a more objective measurement.
Perhaps that means asking the patient to bring in a significant other at the next visit or digging deeper into the conversation about alcohol and drugs and their role in the patient’s life. And to really have an impact, Dr. McGrath said, the clinician should talk to the patient about referral for further evaluation.
“You have to get collateral history; that’s the goldmine for the clinician,” Dr. McGrath says. “It may take a few more minutes or mean talking to a family member, but it can make the difference between life and death.”
“I am thankful to my doctor who discussed this [substance use disorder] with me in detail,” says Ronald Williams, another Angeleno who braved the difficult discussion with his doctor. Mr. Williams says his doctor explained it in a good way and that if the doctor hadn’t guided him empathetically, the conversation might not have gone as well.
“We check patients’ cholesterol. We get them on the scale. But there is no blood test to discover how much they’re drinking, no PCR to test for social anxiety, no MRI that distinguishes between their recreational marijuana use and marijuana abuse,” said Dr. McBride.
Check the prescription drugs they’re taking
Another thing Dr. McGrath recommends is for primary care physicians to check the prescription drug monitoring program (PDMP) database in their state to help be alerted to a patient with a substance use disorder. The CDC’s PMPD guidelines recommend that the clinician check on a patient every 3 months or each time they write an opioid prescription. Assigning a staff member or a nurse to check the database can help uncover a history of doctor-shopping or use of controlled substances.
“There’s been a lot of times I’ve gone on self-report, and I’ve been bamboozled because I don’t have a truth-o-meter, and I can’t tell when a patient is telling the truth,” says Dr. McGrath.
He is also a huge proponent of point-of-service screening. Patients can urinate in a cup that has amino assay strips on the side, like an immediate COVID-19 test, or they can spit into a saliva cup. “It’s really beneficial for the patient and the clinician to know right then at the point of service if there is a substance present and what it is,” Dr. McGrath said.
It can be part of the larger conversation once a problem with substances has been uncovered. The clinician can say something like, “Let’s see where you are right now today as far as what you have in your system and where we should go from here.”
Other barriers physicians face
Many physicians may feel unprepared to meet the needs of patients with substance use disorders or prescribe medication that blunts cravings and reduces the urge to drink without the need for special training. Scientists at the National Institutes of Health found that only 1.6% of people with a substance use disorder were prescribed medication to help control it.
In the largest study on how primary care physicians address substance use disorders, fewer than 20% described themselves as very prepared to identify alcoholism or illegal drug use. Since most patients prefer to seek treatment from their primary care doctor, at least initially, not being prepared is a problem.
Although referral for specialty addiction treatment is recommended for patients with severe substance use disorders, primary care physicians with appropriate experience, training, and support can provide some of these services. “In an ideal world I wouldn’t have to refer patients out, since they’re much more likely to talk with their primary care provider about sensitive, intimate topics,” says Dr. McBride.
The issue of reimbursement
Billing for substance use disorder counseling or coordination of care is still challenging, and how to get compensated remains a conundrum for many physicians. Reimbursement may not adequately compensate providers for the additional time and staff needed, but some changes have been positive.
For instance, the American Society for Addiction Medicine reports that in 2022, Medicare expanded the physician fee schedule for opioid and SUD counseling to include reimbursement for telemedicine services.
Learning the billing CPT codes for various addiction treatments and counseling, or having a billing service that understands them, is crucial to reimbursement and keeping revenue running smoothly.
At the very least, developing relationships with treatment centers and specialists in the community can help physicians with referrals and with determining the level of care needed. Physicians can help facilitate that care with routine reassessment and frequent follow-ups, as well as by requesting reports from the treatment facility, continuing treatment of medical conditions, and reinforcing the importance of continued substance use disorder treatment.
Dr. McBride says that primary care physicians can and should make their office a safe, blame-free medical home for patients with substance use disorders. “Patients also need to understand they should bring their whole selves to the doctor – to talk about their sleep, what they consume, their depression, and not just about alcohol, but their relationship with it, and other substances,” she says.
“There needs to be time to talk about it.”
A version of this article first appeared on Medscape.com.
When Michael McGrath, MD, medical director of the Ohana Luxury Alcohol Rehab on the Big Island of Hawaii, trains primary care physicians, he tells them that talking with patients about substance use disorders is like having a stressful, weird conversation. But it’s a courageous one, because of the stigma associated with drug and alcohol disorders.
Dr. McGrath starts the conversation with patients by expressing that physicians now understand that addiction is a disease – one for which the patient isn’t responsible. He explains that there’s both a genetic and a nature/nurture component of the disorder and assures them that he won’t judge or abandon them but rather help them find treatment and make sure they get on the path to wellness.
It’s all too common to see patients with a substance use disorder in today’s primary care population. According to Medscape’s Physicians’ Views on Today’s Divisive Social Issues Report 2022,
According to the Recovery Research Institute, a leading nonprofit orgnaization from Massachusetts General Hospital dedicated to advancing addiction treatment and recovery, about 20 million people in the United States suffer from a substance use disorder. More than half (54%) need assistance with their recovery. The National Institute on Drug Abuse reports that substance abuse and addiction cost society more than $740 billion annually in workplace productivity, health care, and crime-related expenses.
Despite the challenges, physician experts provide advice on how to treat and help patients who have substance use disorders more effectively.
A courageous conversation
Often, the primary care physician or emergency physician is the first to be aware of a patient’s problem with a substance or a relapse. In many communities where shortages of specialized physicians and nonphysician treatment options for substance use disorders aren’t available, there’s usually limited time and resources to help patients with these disorders.
Patients often sense doctors are rushed and may not be interested in hearing about their drug or alcohol problems. Reddit threads are filled with stories like that of user “Cyralek,” who say that the two doctors they’ve seen since quitting drinking didn’t show much interest in the problem beyond ordering liver function tests.
In a nationwide study by researchers at Washington University School of Medicine, St. Louis, 80% of patients who met the diagnostic criteria for substance use disorder visited a doctor, hospital, or clinic for some reason over the past year. Only 1 in 10 were encouraged to cut back on drinking or receive any form of treatment or referral for substance misuse.
Emma Gordon, founder of a salvage yard in Los Angeles, says she used to abuse alcohol and that it affected every aspect of her life. Her brother tried to intervene, but nothing worked until she finally told a physician. “I admitted my problem and felt incredibly calm when she reacted as though it was all normal. I believe that was my first step to becoming a better me. I was thankful I had gone to see a doctor,” says Ms. Gordon.
Though physicians in primary care may not have more than a 15-minute appointment slot, seizing the opportunity to initiate a substance use disorder conversation when warranted is crucial, says Dr. McGrath. The CAGE-AID screening tool, which includes questions such as, “Have you ever felt you ought to cut down on your drinking or drug use?” is an excellent starter. Dr. McGrath also advises primary care clinicians to lower the threshold of concern to a single positive answer rather than several.
Doctors aren’t necessarily rewarded for the time it takes to develop a rapport with patients and to have a conversation that leads to asking, “How much are you drinking?”
“The system in primary care isn’t set up that way,” said Lucy McBride, MD, an internist in Washington, D.C.
Patients don’t often ask for help
In a perfect world, patients struggling with a substance use disorder would present with a request to discontinue using drugs or alcohol, as Ms. Gordon did. While that does happen sometimes, the onus is on the physician to screen for substance misuse.
“Remember, this is the disease that tells you that you don’t have a disease,” Dr. McGrath says. He also says that the use of screening instruments is a bare minimum. When patients are in the throes of a substance use disorder, the prefrontal cortex doesn’t work effectively. Dr. McGrath says there’s an alteration of consciousness so that the patient doesn’t realize the extent of the disease. “Often simply asking the patient is falling far short. It’s the biggest mistake I see,” he says.
Self-reporting from the patient may be unreliable. “That would be like a patient coming in and saying, ‘My blood sugar is 700, and I want you to give me some insulin,’ ” Dr. McGrath says. Instead, clinicians in the field need a more objective measurement.
Perhaps that means asking the patient to bring in a significant other at the next visit or digging deeper into the conversation about alcohol and drugs and their role in the patient’s life. And to really have an impact, Dr. McGrath said, the clinician should talk to the patient about referral for further evaluation.
“You have to get collateral history; that’s the goldmine for the clinician,” Dr. McGrath says. “It may take a few more minutes or mean talking to a family member, but it can make the difference between life and death.”
“I am thankful to my doctor who discussed this [substance use disorder] with me in detail,” says Ronald Williams, another Angeleno who braved the difficult discussion with his doctor. Mr. Williams says his doctor explained it in a good way and that if the doctor hadn’t guided him empathetically, the conversation might not have gone as well.
“We check patients’ cholesterol. We get them on the scale. But there is no blood test to discover how much they’re drinking, no PCR to test for social anxiety, no MRI that distinguishes between their recreational marijuana use and marijuana abuse,” said Dr. McBride.
Check the prescription drugs they’re taking
Another thing Dr. McGrath recommends is for primary care physicians to check the prescription drug monitoring program (PDMP) database in their state to help be alerted to a patient with a substance use disorder. The CDC’s PMPD guidelines recommend that the clinician check on a patient every 3 months or each time they write an opioid prescription. Assigning a staff member or a nurse to check the database can help uncover a history of doctor-shopping or use of controlled substances.
“There’s been a lot of times I’ve gone on self-report, and I’ve been bamboozled because I don’t have a truth-o-meter, and I can’t tell when a patient is telling the truth,” says Dr. McGrath.
He is also a huge proponent of point-of-service screening. Patients can urinate in a cup that has amino assay strips on the side, like an immediate COVID-19 test, or they can spit into a saliva cup. “It’s really beneficial for the patient and the clinician to know right then at the point of service if there is a substance present and what it is,” Dr. McGrath said.
It can be part of the larger conversation once a problem with substances has been uncovered. The clinician can say something like, “Let’s see where you are right now today as far as what you have in your system and where we should go from here.”
Other barriers physicians face
Many physicians may feel unprepared to meet the needs of patients with substance use disorders or prescribe medication that blunts cravings and reduces the urge to drink without the need for special training. Scientists at the National Institutes of Health found that only 1.6% of people with a substance use disorder were prescribed medication to help control it.
In the largest study on how primary care physicians address substance use disorders, fewer than 20% described themselves as very prepared to identify alcoholism or illegal drug use. Since most patients prefer to seek treatment from their primary care doctor, at least initially, not being prepared is a problem.
Although referral for specialty addiction treatment is recommended for patients with severe substance use disorders, primary care physicians with appropriate experience, training, and support can provide some of these services. “In an ideal world I wouldn’t have to refer patients out, since they’re much more likely to talk with their primary care provider about sensitive, intimate topics,” says Dr. McBride.
The issue of reimbursement
Billing for substance use disorder counseling or coordination of care is still challenging, and how to get compensated remains a conundrum for many physicians. Reimbursement may not adequately compensate providers for the additional time and staff needed, but some changes have been positive.
For instance, the American Society for Addiction Medicine reports that in 2022, Medicare expanded the physician fee schedule for opioid and SUD counseling to include reimbursement for telemedicine services.
Learning the billing CPT codes for various addiction treatments and counseling, or having a billing service that understands them, is crucial to reimbursement and keeping revenue running smoothly.
At the very least, developing relationships with treatment centers and specialists in the community can help physicians with referrals and with determining the level of care needed. Physicians can help facilitate that care with routine reassessment and frequent follow-ups, as well as by requesting reports from the treatment facility, continuing treatment of medical conditions, and reinforcing the importance of continued substance use disorder treatment.
Dr. McBride says that primary care physicians can and should make their office a safe, blame-free medical home for patients with substance use disorders. “Patients also need to understand they should bring their whole selves to the doctor – to talk about their sleep, what they consume, their depression, and not just about alcohol, but their relationship with it, and other substances,” she says.
“There needs to be time to talk about it.”
A version of this article first appeared on Medscape.com.
Robots better than humans at detecting mental well-being issues in children
Robots can be better at detecting mental well-being issues in children than parent-reported or self-reported testing, say U.K. researchers.
The researchers behind a new study, presented at the 31st IEEE International Conference on Robot & Human Interactive Communication (RO-MAN) in Naples, Italy, have suggested that robots could be a useful addition to traditional methods of mental health assessment.
“There are times when traditional methods aren’t able to catch mental well-being lapses in children, as sometimes the changes are incredibly subtle,” said Nida Itrat Abbasi, a PhD student at Cambridge (England) Affective Computing and Robotics Group, University of Cambridge, and the study’s first author. “We wanted to see whether robots might be able to help with this process,” she explained.
The authors highlighted how, during the COVID-19 pandemic, home schooling, financial pressures, and isolation from peers and friends impacted the mental health of many children. Even before the pandemic however, anxiety and depression among children in the United Kingdom has been on the rise, but the resources and support to address mental well-being are severely limited.
Children engage with robots
For their study the research team – which comprised roboticists, computer scientists, and psychiatrists from the University of Cambridge – enrolled 28 participants between ages 8 and 13 years. While being observed from an adjacent room by a parent or guardian, along with members of the research team, the participants took part in a one-to-one 45-minute session with a Nao robot – a humanoid robot about 60 cm tall – that administered a series of standard psychological questionnaires to assess the mental well-being of each participant.
Participants interacted with the robot throughout the session by speaking with it or by touching sensors on the robot’s hands and feet. Additional sensors tracked participants’ heartbeat, head, and eye movements during the session.
Professor Hatice Gunes, affective intelligence and robotics laboratory, department of computer science, University of Cambridge, said: “Children are quite tactile, and they’re drawn to technology. If they’re using a screen-based tool, they’re withdrawn from the physical world,” she said. “But robots are perfect because they’re in the physical world – they’re more interactive, so the children are more engaged.”
Prior to each session the children and their parent or guardian completed standard online questionnaires to assess each child’s mental well-being.
During each session, the robot performed four different tasks:
- Asked open-ended questions about happy and sad memories over the last week.
- Administered the Short Mood and Feelings Questionnaire (SMFQ).
- Administered a picture task inspired by the Children’s Apperception Test (CAT), where children are asked to answer questions related to pictures shown.
- Administered the Revised Children’s Anxiety and Depression Scale (RCADS) for generalized anxiety, panic disorder, and low mood.
Following the SMFQ children were divided into three different groups according to how likely they were to be struggling with their mental well-being.
The researchers found that children with varying levels of well-being concerns interacted differently with the robot. For children that might not be experiencing mental well-being–related problems, the researchers found that interacting with the robot led to more positive response ratings to the questionnaires. However, for children that might be experiencing well-being–related concerns, the robot may have enabled them to divulge their true feelings and experiences, leading to more negative response ratings to the questionnaire.
Robots an addition not a replacement
“Since the robot we use is child-sized, and completely nonthreatening, children might see the robot as a confidant – they feel like they won’t get into trouble if they share secrets with it,” said Ms. Abbasi. “Other researchers have found that children are more likely to divulge private information – like that they’re being bullied, for example – to a robot than they would be to an adult,” she said.
Study participants all said they “enjoyed talking with the robot,” commented the authors, who added that, “the children were willing to confide in the robot, in some cases sharing information with the robot that they had not yet shared via the standard assessment method of online or in-person questionnaires.”
This is the first time that robots have been used to assess mental well-being in children, the researchers pointed out. “Robots could be a useful addition to traditional methods of mental health assessment,” they said, though they emphasized that robots are “not intended to be a substitute for professional mental health support.”
“We don’t have any intention of replacing psychologists or other mental health professionals with robots, since their expertise far surpasses anything a robot can do,” said Dr. Micol Spitale, affective computing and robotics laboratory, University of Cambridge, and study coauthor. “However, our work suggests that robots could be a useful tool in helping children to open up and share things they might not be comfortable sharing at first.”
The researchers say that they hope to expand their survey in future by including more participants and following them over time. They are also investigating whether similar results could be achieved if children interact with the robot via video chat.
A version of this article first appeared on Medscape UK.
Robots can be better at detecting mental well-being issues in children than parent-reported or self-reported testing, say U.K. researchers.
The researchers behind a new study, presented at the 31st IEEE International Conference on Robot & Human Interactive Communication (RO-MAN) in Naples, Italy, have suggested that robots could be a useful addition to traditional methods of mental health assessment.
“There are times when traditional methods aren’t able to catch mental well-being lapses in children, as sometimes the changes are incredibly subtle,” said Nida Itrat Abbasi, a PhD student at Cambridge (England) Affective Computing and Robotics Group, University of Cambridge, and the study’s first author. “We wanted to see whether robots might be able to help with this process,” she explained.
The authors highlighted how, during the COVID-19 pandemic, home schooling, financial pressures, and isolation from peers and friends impacted the mental health of many children. Even before the pandemic however, anxiety and depression among children in the United Kingdom has been on the rise, but the resources and support to address mental well-being are severely limited.
Children engage with robots
For their study the research team – which comprised roboticists, computer scientists, and psychiatrists from the University of Cambridge – enrolled 28 participants between ages 8 and 13 years. While being observed from an adjacent room by a parent or guardian, along with members of the research team, the participants took part in a one-to-one 45-minute session with a Nao robot – a humanoid robot about 60 cm tall – that administered a series of standard psychological questionnaires to assess the mental well-being of each participant.
Participants interacted with the robot throughout the session by speaking with it or by touching sensors on the robot’s hands and feet. Additional sensors tracked participants’ heartbeat, head, and eye movements during the session.
Professor Hatice Gunes, affective intelligence and robotics laboratory, department of computer science, University of Cambridge, said: “Children are quite tactile, and they’re drawn to technology. If they’re using a screen-based tool, they’re withdrawn from the physical world,” she said. “But robots are perfect because they’re in the physical world – they’re more interactive, so the children are more engaged.”
Prior to each session the children and their parent or guardian completed standard online questionnaires to assess each child’s mental well-being.
During each session, the robot performed four different tasks:
- Asked open-ended questions about happy and sad memories over the last week.
- Administered the Short Mood and Feelings Questionnaire (SMFQ).
- Administered a picture task inspired by the Children’s Apperception Test (CAT), where children are asked to answer questions related to pictures shown.
- Administered the Revised Children’s Anxiety and Depression Scale (RCADS) for generalized anxiety, panic disorder, and low mood.
Following the SMFQ children were divided into three different groups according to how likely they were to be struggling with their mental well-being.
The researchers found that children with varying levels of well-being concerns interacted differently with the robot. For children that might not be experiencing mental well-being–related problems, the researchers found that interacting with the robot led to more positive response ratings to the questionnaires. However, for children that might be experiencing well-being–related concerns, the robot may have enabled them to divulge their true feelings and experiences, leading to more negative response ratings to the questionnaire.
Robots an addition not a replacement
“Since the robot we use is child-sized, and completely nonthreatening, children might see the robot as a confidant – they feel like they won’t get into trouble if they share secrets with it,” said Ms. Abbasi. “Other researchers have found that children are more likely to divulge private information – like that they’re being bullied, for example – to a robot than they would be to an adult,” she said.
Study participants all said they “enjoyed talking with the robot,” commented the authors, who added that, “the children were willing to confide in the robot, in some cases sharing information with the robot that they had not yet shared via the standard assessment method of online or in-person questionnaires.”
This is the first time that robots have been used to assess mental well-being in children, the researchers pointed out. “Robots could be a useful addition to traditional methods of mental health assessment,” they said, though they emphasized that robots are “not intended to be a substitute for professional mental health support.”
“We don’t have any intention of replacing psychologists or other mental health professionals with robots, since their expertise far surpasses anything a robot can do,” said Dr. Micol Spitale, affective computing and robotics laboratory, University of Cambridge, and study coauthor. “However, our work suggests that robots could be a useful tool in helping children to open up and share things they might not be comfortable sharing at first.”
The researchers say that they hope to expand their survey in future by including more participants and following them over time. They are also investigating whether similar results could be achieved if children interact with the robot via video chat.
A version of this article first appeared on Medscape UK.
Robots can be better at detecting mental well-being issues in children than parent-reported or self-reported testing, say U.K. researchers.
The researchers behind a new study, presented at the 31st IEEE International Conference on Robot & Human Interactive Communication (RO-MAN) in Naples, Italy, have suggested that robots could be a useful addition to traditional methods of mental health assessment.
“There are times when traditional methods aren’t able to catch mental well-being lapses in children, as sometimes the changes are incredibly subtle,” said Nida Itrat Abbasi, a PhD student at Cambridge (England) Affective Computing and Robotics Group, University of Cambridge, and the study’s first author. “We wanted to see whether robots might be able to help with this process,” she explained.
The authors highlighted how, during the COVID-19 pandemic, home schooling, financial pressures, and isolation from peers and friends impacted the mental health of many children. Even before the pandemic however, anxiety and depression among children in the United Kingdom has been on the rise, but the resources and support to address mental well-being are severely limited.
Children engage with robots
For their study the research team – which comprised roboticists, computer scientists, and psychiatrists from the University of Cambridge – enrolled 28 participants between ages 8 and 13 years. While being observed from an adjacent room by a parent or guardian, along with members of the research team, the participants took part in a one-to-one 45-minute session with a Nao robot – a humanoid robot about 60 cm tall – that administered a series of standard psychological questionnaires to assess the mental well-being of each participant.
Participants interacted with the robot throughout the session by speaking with it or by touching sensors on the robot’s hands and feet. Additional sensors tracked participants’ heartbeat, head, and eye movements during the session.
Professor Hatice Gunes, affective intelligence and robotics laboratory, department of computer science, University of Cambridge, said: “Children are quite tactile, and they’re drawn to technology. If they’re using a screen-based tool, they’re withdrawn from the physical world,” she said. “But robots are perfect because they’re in the physical world – they’re more interactive, so the children are more engaged.”
Prior to each session the children and their parent or guardian completed standard online questionnaires to assess each child’s mental well-being.
During each session, the robot performed four different tasks:
- Asked open-ended questions about happy and sad memories over the last week.
- Administered the Short Mood and Feelings Questionnaire (SMFQ).
- Administered a picture task inspired by the Children’s Apperception Test (CAT), where children are asked to answer questions related to pictures shown.
- Administered the Revised Children’s Anxiety and Depression Scale (RCADS) for generalized anxiety, panic disorder, and low mood.
Following the SMFQ children were divided into three different groups according to how likely they were to be struggling with their mental well-being.
The researchers found that children with varying levels of well-being concerns interacted differently with the robot. For children that might not be experiencing mental well-being–related problems, the researchers found that interacting with the robot led to more positive response ratings to the questionnaires. However, for children that might be experiencing well-being–related concerns, the robot may have enabled them to divulge their true feelings and experiences, leading to more negative response ratings to the questionnaire.
Robots an addition not a replacement
“Since the robot we use is child-sized, and completely nonthreatening, children might see the robot as a confidant – they feel like they won’t get into trouble if they share secrets with it,” said Ms. Abbasi. “Other researchers have found that children are more likely to divulge private information – like that they’re being bullied, for example – to a robot than they would be to an adult,” she said.
Study participants all said they “enjoyed talking with the robot,” commented the authors, who added that, “the children were willing to confide in the robot, in some cases sharing information with the robot that they had not yet shared via the standard assessment method of online or in-person questionnaires.”
This is the first time that robots have been used to assess mental well-being in children, the researchers pointed out. “Robots could be a useful addition to traditional methods of mental health assessment,” they said, though they emphasized that robots are “not intended to be a substitute for professional mental health support.”
“We don’t have any intention of replacing psychologists or other mental health professionals with robots, since their expertise far surpasses anything a robot can do,” said Dr. Micol Spitale, affective computing and robotics laboratory, University of Cambridge, and study coauthor. “However, our work suggests that robots could be a useful tool in helping children to open up and share things they might not be comfortable sharing at first.”
The researchers say that they hope to expand their survey in future by including more participants and following them over time. They are also investigating whether similar results could be achieved if children interact with the robot via video chat.
A version of this article first appeared on Medscape UK.
Implementation of a Pilot Study Evaluating the Feasibility of Delivery of Attune, a Digital Cognitive-Behavioral Stress Management (CBSM) Software Application for Treatment of Anxiety and Depressive Symptoms in Veterans with Cancer
Purpose
To assess promoters and obstacles of enrollment in a decentralized clinical research study, where veterans with cancer-related depressive symptoms are electronically prescribed a 10-session digitally administered Cognitive-Behavioral Stress Management (CBSM) program, called Attune.
Background
The US Department of Veterans Affairs (VA) National TeleOncology (NTO) Program has served 5688 veterans since inception, 3100 of which reside in rural areas (55%). Previous studies demonstrate clinically significant levels of psychosocial distress in up to 52% of patients with cancer. It is unknown if veterans with cancer experiencing psychosocial distress will benefit from a CBSM app. Traditional research studies often underrepresent rural cancer patients, so the VA-Attune clinical trial was designed for implementation in a decentralized fashion for NTO VA facilities serving a more predominant rural population.
Methods
We manually screened veteran appointments to identify potentially eligible veterans. NTO providers were notified if their patients were potentially eligible, providers asked patients if they wanted more information. Research staff then contacted veterans by telephone to confirm eligibility. Consent and HIPAA authorization were mailed to interested veterans and the consent process occurred via telephone. Descriptive statistics were used to summarize the patient population screened and consented.
Results
Between January and May 2022, there were 467 veterans screened and 15 veterans enrolled (mean [SD] age, 67.2 [8.28] years; 12 men and 3 women). 15 veterans received the electronic prescription of the Attune App and providers viewed the CBSM App as feasible. Promotors of implementation included convenience of a virtual format and use of the veteran’s mobile device to deliver the digital CBSM. Barriers identified by veterans were not having an appropriate mobile device, inadequate knowledge on using a mobile device, and insufficient time to commit to regularly using the Attune app.
Conclusions/Implications
This VA-Attune study demonstrated that clinical trials can be implemented in the VA in a decentralized fashion, enrolling rural and urban veterans. We identified significant barriers to enrollment and engagement despite our approach of remote consent. The VA-Attune research study continues to enroll veterans nationally, highlighting best practices and opportunities to improve the implementation of decentralized cancer clinical trials in the VA.
Purpose
To assess promoters and obstacles of enrollment in a decentralized clinical research study, where veterans with cancer-related depressive symptoms are electronically prescribed a 10-session digitally administered Cognitive-Behavioral Stress Management (CBSM) program, called Attune.
Background
The US Department of Veterans Affairs (VA) National TeleOncology (NTO) Program has served 5688 veterans since inception, 3100 of which reside in rural areas (55%). Previous studies demonstrate clinically significant levels of psychosocial distress in up to 52% of patients with cancer. It is unknown if veterans with cancer experiencing psychosocial distress will benefit from a CBSM app. Traditional research studies often underrepresent rural cancer patients, so the VA-Attune clinical trial was designed for implementation in a decentralized fashion for NTO VA facilities serving a more predominant rural population.
Methods
We manually screened veteran appointments to identify potentially eligible veterans. NTO providers were notified if their patients were potentially eligible, providers asked patients if they wanted more information. Research staff then contacted veterans by telephone to confirm eligibility. Consent and HIPAA authorization were mailed to interested veterans and the consent process occurred via telephone. Descriptive statistics were used to summarize the patient population screened and consented.
Results
Between January and May 2022, there were 467 veterans screened and 15 veterans enrolled (mean [SD] age, 67.2 [8.28] years; 12 men and 3 women). 15 veterans received the electronic prescription of the Attune App and providers viewed the CBSM App as feasible. Promotors of implementation included convenience of a virtual format and use of the veteran’s mobile device to deliver the digital CBSM. Barriers identified by veterans were not having an appropriate mobile device, inadequate knowledge on using a mobile device, and insufficient time to commit to regularly using the Attune app.
Conclusions/Implications
This VA-Attune study demonstrated that clinical trials can be implemented in the VA in a decentralized fashion, enrolling rural and urban veterans. We identified significant barriers to enrollment and engagement despite our approach of remote consent. The VA-Attune research study continues to enroll veterans nationally, highlighting best practices and opportunities to improve the implementation of decentralized cancer clinical trials in the VA.
Purpose
To assess promoters and obstacles of enrollment in a decentralized clinical research study, where veterans with cancer-related depressive symptoms are electronically prescribed a 10-session digitally administered Cognitive-Behavioral Stress Management (CBSM) program, called Attune.
Background
The US Department of Veterans Affairs (VA) National TeleOncology (NTO) Program has served 5688 veterans since inception, 3100 of which reside in rural areas (55%). Previous studies demonstrate clinically significant levels of psychosocial distress in up to 52% of patients with cancer. It is unknown if veterans with cancer experiencing psychosocial distress will benefit from a CBSM app. Traditional research studies often underrepresent rural cancer patients, so the VA-Attune clinical trial was designed for implementation in a decentralized fashion for NTO VA facilities serving a more predominant rural population.
Methods
We manually screened veteran appointments to identify potentially eligible veterans. NTO providers were notified if their patients were potentially eligible, providers asked patients if they wanted more information. Research staff then contacted veterans by telephone to confirm eligibility. Consent and HIPAA authorization were mailed to interested veterans and the consent process occurred via telephone. Descriptive statistics were used to summarize the patient population screened and consented.
Results
Between January and May 2022, there were 467 veterans screened and 15 veterans enrolled (mean [SD] age, 67.2 [8.28] years; 12 men and 3 women). 15 veterans received the electronic prescription of the Attune App and providers viewed the CBSM App as feasible. Promotors of implementation included convenience of a virtual format and use of the veteran’s mobile device to deliver the digital CBSM. Barriers identified by veterans were not having an appropriate mobile device, inadequate knowledge on using a mobile device, and insufficient time to commit to regularly using the Attune app.
Conclusions/Implications
This VA-Attune study demonstrated that clinical trials can be implemented in the VA in a decentralized fashion, enrolling rural and urban veterans. We identified significant barriers to enrollment and engagement despite our approach of remote consent. The VA-Attune research study continues to enroll veterans nationally, highlighting best practices and opportunities to improve the implementation of decentralized cancer clinical trials in the VA.
Are mass shootings contagious?
That’s not just a feeling – it’s a fact.
The devastating shooting on May 24 in Uvalde, Tex., which killed 19 children, two teachers, and injured 17 others, occurred 10 days after a supermarket shooting in Buffalo, N.Y., which resulted in 10 deaths. In 2021, a shooting at a massage parlor in Atlanta, which left eight dead, came less than a week before a shooting at a supermarket in Boulder, Colo., that killed 10. And a 2019 shooting in Dayton, Ohio, on Aug. 4 that killed nine people took place only a day after a Walmart shooting in El Paso, Tex., which claimed 22 lives.
Contagion theory
Researchers argue that the clustering of mass shootings suggests that this type of violence spreads like a virus and should be treated as one.
This theory – called the “contagion effect” – has been examined at length in cases of suicide, especially among teens and young adults. Studies have demonstrated that the majority of adolescents who attempt suicide have previously been exposed to the suicidal behavior of a peer.
In many cases, mass shootings are also suicides, with shooters taking their own lives at the time of the shooting or not long after.
“They have literally and figuratively given up on their life as they know it.” said Joel Dvoskin, PhD, a clinical and forensic psychologist at the University of Arizona, Tucson, and former acting commissioner of mental health for New York state.
According to contagion theory, mass shootings – and the round-the-clock media coverage they generate – lead to even more killings.
A team of researchers at Arizona State University led by Sherry Towers, PhD, analyzed mass shooting data in 2015 to find out whether those events followed a similar pattern. Dr. Towers spent much of her career modeling the spread of infectious diseases, such as influenza, Ebola, and Zika.
Dr. Towers and colleagues discovered that a mass killing tended to give rise to more killings in its immediate aftermath. According to her evaluation of USA Today’s mass shooting database, a second incident was most likely to occur within 13 days of the initial event.
What defines a mass shooting?
The FBI defines a mass shooting as any incident in which four or more people die by gunfire. That definition, however, is not universally accepted. The lack of a standard definition complicates the work of researchers who study contagion theory.
Mother Jones magazine created an open-source database of mass killings that employs a similar definition but that includes only incidents that involve a person shooting indiscriminately in a public place.
With this narrower definition, shootings involving organized crime, robberies, and domestic violence – which make up the vast majority of shootings in which multiple fatalities occur in this country – are excluded. Events such as those that occurred in Sandy Hook or the killings in Highland Park, Ill., this past July would be included.
The Gun Violence Archive categorizes mass shootings as any incident in which four or more people are shot but not necessarily killed, while Everytown for Gun Safety tallies mass shootings that take at least four lives.
James Meindl, PhD, a professor of behavioral analysis at the University of Memphis who studies mass shootings, said parsing the differences between what happened in Uvalde and what happens during a shooting involving organized crime or domestic violence is crucial when thinking about intervention and prevention.
“If you want to intervene, you have to know why the person engaged in this behavior in the first place,” Dr. Meindl said. “The factors that led a person to commit gang violence, the factors in domestic violence, the factors in indiscriminate mass shootings – those are all very different factors that would call for very different interventions.”
So, should mass shootings be treated like an infectious disease?
Rather than using contagion theory, Dr. Meindl said he prefers to view mass shootings through the lens of “generalized imitation,” a psychological concept involving the learned ability to mimic behaviors observed either in person or through the media. Behaviors “are not diseases that can spread on contact.”
Gary Slutkin, MD, is an epidemiologist who pivoted from studying the spread of diseases such as tuberculosis, HIV, and cholera to trying to understand the epidemic of gun violence.
“The more you’re exposed [to violence], the more likely you are to repeat it, just like the more you’re exposed to COVID, the more likely you are to get it and give it to somebody else,” Dr. Slutkin said. And just as people have varying degrees of susceptibility to COVID-19 and other infectious diseases, he argued that some are more susceptible to committing a mass shooting, depending on their level of isolation, personal “grievances, and their need for belonging or credit.”
To Dr. Slutkin, mass shootings, and other forms of violence, should be treated with the standard methods that public health officials would use to stop the spread of a contagious disease: detection and interdiction that would put a stop to potential events. The nonprofit organization that he founded, Cure Violence Global, employs “violence interrupters” to reach out to and engage with community members who might be at risk of being a victim of violence or of committing an act of violence, much as a public health worker would approach epidemic control.
Research conducted on the effects of this method of reducing rates of violence suggests the approach works. In 2017, New York City saw a 63% reduction in gun injuries, according to a study from the John Jay College of Criminal Justice. And after evaluating the effects of this approach in Chicago in 2014, researchers from the University of Illinois and the University of Chicago determined that there was a 19% reduction in shootings in the city.
“The results of stopping an epidemic come really fast,” Dr. Slutkin said. “But getting people to switch gears to the right kind of treatment happens really slowly.”
A version of this article first appeared on Medscape.com.
That’s not just a feeling – it’s a fact.
The devastating shooting on May 24 in Uvalde, Tex., which killed 19 children, two teachers, and injured 17 others, occurred 10 days after a supermarket shooting in Buffalo, N.Y., which resulted in 10 deaths. In 2021, a shooting at a massage parlor in Atlanta, which left eight dead, came less than a week before a shooting at a supermarket in Boulder, Colo., that killed 10. And a 2019 shooting in Dayton, Ohio, on Aug. 4 that killed nine people took place only a day after a Walmart shooting in El Paso, Tex., which claimed 22 lives.
Contagion theory
Researchers argue that the clustering of mass shootings suggests that this type of violence spreads like a virus and should be treated as one.
This theory – called the “contagion effect” – has been examined at length in cases of suicide, especially among teens and young adults. Studies have demonstrated that the majority of adolescents who attempt suicide have previously been exposed to the suicidal behavior of a peer.
In many cases, mass shootings are also suicides, with shooters taking their own lives at the time of the shooting or not long after.
“They have literally and figuratively given up on their life as they know it.” said Joel Dvoskin, PhD, a clinical and forensic psychologist at the University of Arizona, Tucson, and former acting commissioner of mental health for New York state.
According to contagion theory, mass shootings – and the round-the-clock media coverage they generate – lead to even more killings.
A team of researchers at Arizona State University led by Sherry Towers, PhD, analyzed mass shooting data in 2015 to find out whether those events followed a similar pattern. Dr. Towers spent much of her career modeling the spread of infectious diseases, such as influenza, Ebola, and Zika.
Dr. Towers and colleagues discovered that a mass killing tended to give rise to more killings in its immediate aftermath. According to her evaluation of USA Today’s mass shooting database, a second incident was most likely to occur within 13 days of the initial event.
What defines a mass shooting?
The FBI defines a mass shooting as any incident in which four or more people die by gunfire. That definition, however, is not universally accepted. The lack of a standard definition complicates the work of researchers who study contagion theory.
Mother Jones magazine created an open-source database of mass killings that employs a similar definition but that includes only incidents that involve a person shooting indiscriminately in a public place.
With this narrower definition, shootings involving organized crime, robberies, and domestic violence – which make up the vast majority of shootings in which multiple fatalities occur in this country – are excluded. Events such as those that occurred in Sandy Hook or the killings in Highland Park, Ill., this past July would be included.
The Gun Violence Archive categorizes mass shootings as any incident in which four or more people are shot but not necessarily killed, while Everytown for Gun Safety tallies mass shootings that take at least four lives.
James Meindl, PhD, a professor of behavioral analysis at the University of Memphis who studies mass shootings, said parsing the differences between what happened in Uvalde and what happens during a shooting involving organized crime or domestic violence is crucial when thinking about intervention and prevention.
“If you want to intervene, you have to know why the person engaged in this behavior in the first place,” Dr. Meindl said. “The factors that led a person to commit gang violence, the factors in domestic violence, the factors in indiscriminate mass shootings – those are all very different factors that would call for very different interventions.”
So, should mass shootings be treated like an infectious disease?
Rather than using contagion theory, Dr. Meindl said he prefers to view mass shootings through the lens of “generalized imitation,” a psychological concept involving the learned ability to mimic behaviors observed either in person or through the media. Behaviors “are not diseases that can spread on contact.”
Gary Slutkin, MD, is an epidemiologist who pivoted from studying the spread of diseases such as tuberculosis, HIV, and cholera to trying to understand the epidemic of gun violence.
“The more you’re exposed [to violence], the more likely you are to repeat it, just like the more you’re exposed to COVID, the more likely you are to get it and give it to somebody else,” Dr. Slutkin said. And just as people have varying degrees of susceptibility to COVID-19 and other infectious diseases, he argued that some are more susceptible to committing a mass shooting, depending on their level of isolation, personal “grievances, and their need for belonging or credit.”
To Dr. Slutkin, mass shootings, and other forms of violence, should be treated with the standard methods that public health officials would use to stop the spread of a contagious disease: detection and interdiction that would put a stop to potential events. The nonprofit organization that he founded, Cure Violence Global, employs “violence interrupters” to reach out to and engage with community members who might be at risk of being a victim of violence or of committing an act of violence, much as a public health worker would approach epidemic control.
Research conducted on the effects of this method of reducing rates of violence suggests the approach works. In 2017, New York City saw a 63% reduction in gun injuries, according to a study from the John Jay College of Criminal Justice. And after evaluating the effects of this approach in Chicago in 2014, researchers from the University of Illinois and the University of Chicago determined that there was a 19% reduction in shootings in the city.
“The results of stopping an epidemic come really fast,” Dr. Slutkin said. “But getting people to switch gears to the right kind of treatment happens really slowly.”
A version of this article first appeared on Medscape.com.
That’s not just a feeling – it’s a fact.
The devastating shooting on May 24 in Uvalde, Tex., which killed 19 children, two teachers, and injured 17 others, occurred 10 days after a supermarket shooting in Buffalo, N.Y., which resulted in 10 deaths. In 2021, a shooting at a massage parlor in Atlanta, which left eight dead, came less than a week before a shooting at a supermarket in Boulder, Colo., that killed 10. And a 2019 shooting in Dayton, Ohio, on Aug. 4 that killed nine people took place only a day after a Walmart shooting in El Paso, Tex., which claimed 22 lives.
Contagion theory
Researchers argue that the clustering of mass shootings suggests that this type of violence spreads like a virus and should be treated as one.
This theory – called the “contagion effect” – has been examined at length in cases of suicide, especially among teens and young adults. Studies have demonstrated that the majority of adolescents who attempt suicide have previously been exposed to the suicidal behavior of a peer.
In many cases, mass shootings are also suicides, with shooters taking their own lives at the time of the shooting or not long after.
“They have literally and figuratively given up on their life as they know it.” said Joel Dvoskin, PhD, a clinical and forensic psychologist at the University of Arizona, Tucson, and former acting commissioner of mental health for New York state.
According to contagion theory, mass shootings – and the round-the-clock media coverage they generate – lead to even more killings.
A team of researchers at Arizona State University led by Sherry Towers, PhD, analyzed mass shooting data in 2015 to find out whether those events followed a similar pattern. Dr. Towers spent much of her career modeling the spread of infectious diseases, such as influenza, Ebola, and Zika.
Dr. Towers and colleagues discovered that a mass killing tended to give rise to more killings in its immediate aftermath. According to her evaluation of USA Today’s mass shooting database, a second incident was most likely to occur within 13 days of the initial event.
What defines a mass shooting?
The FBI defines a mass shooting as any incident in which four or more people die by gunfire. That definition, however, is not universally accepted. The lack of a standard definition complicates the work of researchers who study contagion theory.
Mother Jones magazine created an open-source database of mass killings that employs a similar definition but that includes only incidents that involve a person shooting indiscriminately in a public place.
With this narrower definition, shootings involving organized crime, robberies, and domestic violence – which make up the vast majority of shootings in which multiple fatalities occur in this country – are excluded. Events such as those that occurred in Sandy Hook or the killings in Highland Park, Ill., this past July would be included.
The Gun Violence Archive categorizes mass shootings as any incident in which four or more people are shot but not necessarily killed, while Everytown for Gun Safety tallies mass shootings that take at least four lives.
James Meindl, PhD, a professor of behavioral analysis at the University of Memphis who studies mass shootings, said parsing the differences between what happened in Uvalde and what happens during a shooting involving organized crime or domestic violence is crucial when thinking about intervention and prevention.
“If you want to intervene, you have to know why the person engaged in this behavior in the first place,” Dr. Meindl said. “The factors that led a person to commit gang violence, the factors in domestic violence, the factors in indiscriminate mass shootings – those are all very different factors that would call for very different interventions.”
So, should mass shootings be treated like an infectious disease?
Rather than using contagion theory, Dr. Meindl said he prefers to view mass shootings through the lens of “generalized imitation,” a psychological concept involving the learned ability to mimic behaviors observed either in person or through the media. Behaviors “are not diseases that can spread on contact.”
Gary Slutkin, MD, is an epidemiologist who pivoted from studying the spread of diseases such as tuberculosis, HIV, and cholera to trying to understand the epidemic of gun violence.
“The more you’re exposed [to violence], the more likely you are to repeat it, just like the more you’re exposed to COVID, the more likely you are to get it and give it to somebody else,” Dr. Slutkin said. And just as people have varying degrees of susceptibility to COVID-19 and other infectious diseases, he argued that some are more susceptible to committing a mass shooting, depending on their level of isolation, personal “grievances, and their need for belonging or credit.”
To Dr. Slutkin, mass shootings, and other forms of violence, should be treated with the standard methods that public health officials would use to stop the spread of a contagious disease: detection and interdiction that would put a stop to potential events. The nonprofit organization that he founded, Cure Violence Global, employs “violence interrupters” to reach out to and engage with community members who might be at risk of being a victim of violence or of committing an act of violence, much as a public health worker would approach epidemic control.
Research conducted on the effects of this method of reducing rates of violence suggests the approach works. In 2017, New York City saw a 63% reduction in gun injuries, according to a study from the John Jay College of Criminal Justice. And after evaluating the effects of this approach in Chicago in 2014, researchers from the University of Illinois and the University of Chicago determined that there was a 19% reduction in shootings in the city.
“The results of stopping an epidemic come really fast,” Dr. Slutkin said. “But getting people to switch gears to the right kind of treatment happens really slowly.”
A version of this article first appeared on Medscape.com.
Inhaled, systemic steroids linked to changes in brain structure
New research links the use of glucocorticoids with changes in white matter microstructure – which may explain the development of anxiety, depression, and other neuropsychiatric side effects related to these drugs, investigators say.
Results from a cross-sectional study showed that use of both systemic and inhaled glucocorticoids was associated with widespread reductions in fractional anisotropy (FA) and increases in mean diffusivity.
Glucocorticoids have “a whole catalogue” of adverse events, and effects on brain structure “adds to the list,” co-investigator Onno C. Meijer, PhD, professor of molecular neuroendocrinology of corticosteroids, department of medicine, Leiden University Medical Center, the Netherlands, told this news organization.

The findings should encourage clinicians to consider whether doses they are prescribing are too high, said Dr. Meijer. He added that the negative effect of glucocorticoids on the brain was also found in those using inhalers, such as patients with asthma.
The findings were published online in the BMJ Open.
Serious side effects
Glucocorticoids, a class of synthetic steroids with immunosuppressive properties, are prescribed for a wide range of conditions, including rheumatoid arthritis and asthma.
However, they are also associated with potentially serious metabolic, cardiovascular, and musculoskeletal side effects as well as neuropsychiatric side effects such as depression, mania, and cognitive impairment.
About 1 in 3 patients exposed to “quite a lot of these drugs” will experience neuropsychiatric symptoms, Dr. Meijer said.
Most previous studies that investigated effects from high levels of glucocorticoids on brain structure have been small and involved selected populations, such as those with Cushing disease.
The new study included participants from the UK Biobank, a large population-based cohort. Participants had undergone imaging and did not have a history of psychiatric disease – although they could have conditions associated with glucocorticoid use, including anxiety, depression, mania, or delirium.
The analysis included 222 patients using oral or parenteral glucocorticoids at the time of imaging (systemic group), 557 using inhaled glucocorticoids, and 24,106 not using glucocorticoids (the control group).
Inhaled steroids target the lungs, whereas a steroid in pill form “travels in the blood and reaches each and every organ and cell in the body and typically requires higher doses,” Dr. Meijer noted.
The groups were similar with respect to sex, education, and smoking status. However, the systemic glucocorticoid group was slightly older (mean age, 66.1 years vs. 63.3 years for inhaled glucocorticoid users and 63.5 years for the control group).
In addition to age, researchers adjusted for sex, education level, head position in the scanner, head size, assessment center, and year of imaging.
Imaging analyses
Imaging analyses showed systemic glucocorticoid use was associated with reduced global FA (adjusted mean difference, -3.7e-3; 95% confidence interval, -6.4e-3 to 1.0e-3), and reductions in regional FA in the body and genu of the corpus callosum versus the control group.
Inhaled glucocorticoid use was associated with reduced global FA (AMD, -2.3e-3; 95% CI, -4.0e-3 to -5.7e-4), and lower FA in the splenium of the corpus callosum and the cingulum of the hippocampus.
Global mean diffusivity was higher in systemic glucocorticoid users (AMD, 7.2e-6; 95% CI, 3.2e-6 to 1.1e-5) and inhaled glucocorticoid users (AMD, 2.7e-6; 95% CI, 1.7e-7 to 5.2e-6), compared with the control group.
The effects of glucocorticoids on white matter were “pervasive,” and the “most important finding” of the study, Dr. Meijer said. “We were impressed by the fact white matter is so sensitive to these drugs.”
He noted that it is likely that functional connectivity between brain regions is affected by use of glucocorticoids. “You could say communication between brain regions is probably somewhat impaired or challenged,” he said.
Subgroup analyses among participants using glucocorticoids chronically, defined as reported at two consecutive visits, suggested a potential dose-dependent or duration-dependent effect of glucocorticoids on white matter microstructure.
Systemic glucocorticoid use was also associated with an increase in total and grey matter volume of the caudate nucleus.
In addition, there was a significant association between inhaled glucocorticoid use and decreased grey matter volume of the amygdala, which Dr. Meijer said was surprising because studies have shown that glucocorticoids “can drive amygdala big time.”
Move away from ‘one dose for all’?
Another surprise was that the results showed no hippocampal volume differences with steroid use, Dr. Meijer noted.
The modest association between glucocorticoid use and brain volumes could indicate that white matter integrity is more sensitive to glucocorticoids than is grey matter volume, “at least at the structural level,” he said.
He added that longer use or higher doses may be necessary to also induce volumetric changes.
Participants also completed a questionnaire to assess mood over the previous 2 weeks. Systemic glucocorticoid users had more depressive symptoms, disinterest, tenseness/restlessness, and tiredness/lethargy, compared with the control group. Inhaled glucocorticoid users only reported more tiredness/lethargy.
The investigators note that mood-related effects could be linked to the condition for which glucocorticoids were prescribed: for example, rheumatoid arthritis or chronic obstructive pulmonary disease.
In terms of cognition, systemic glucocorticoid users performed significantly worse on the symbol digit substitution task, compared with participants in the control group.
In light of these findings, pharmaceutical companies that make inhaled corticosteroids “should perhaps find out if glucocorticoids can be dosed by kilogram body weight rather than simply one dose fits all,” which is currently the case, Dr. Meijer said.
Impressive, but several limitations
Commenting on the findings, E. Sherwood Brown, MD, PhD, Distinguished Chair in Psychiatric Research and professor and vice chair for clinical research, department of psychiatry, The University of Texas Southwestern Medical Center, Dallas, called the study sample size “impressive.”
In addition, the study is the first to look at systemic as well as inhaled corticosteroids, said Dr. Brown, who was not involved with the research. He noted that previously, there had been only case reports of psychiatric symptoms with inhaled corticosteroids.
That results are in the same direction but greater with systemic, compared with inhaled corticosteroids, is “particularly interesting” because this might suggest dose-dependent effects, Dr. Brown said.
He noted that cognitive differences were also only observed with systemic corticosteroids.
Some study observations, such as smaller amygdala volume with inhaled but not systemic corticosteroids, “are harder to understand,” said Dr. Brown.
However, he pointed out some study limitations. For example, data were apparently unavailable for verbal and declarative memory test data, despite corticosteroids probably affecting the hippocampus and causing memory changes.
Other drawbacks were that the dose and duration of corticosteroid use, as well as the medical histories of study participants, were not available, Dr. Brown said.
No study funding was reported. Dr. Meijer has received research grants and honorariums from Corcept Therapeutics and a speakers’ fee from Ipsen. Dr. Brown is on an advisory board for Sage Pharmaceuticals, which is developing neurosteroids (not corticosteroids) for mood disorders. He is also on a Medscape advisory board related to bipolar disorder.
A version of this article first appeared on Medscape.com.
New research links the use of glucocorticoids with changes in white matter microstructure – which may explain the development of anxiety, depression, and other neuropsychiatric side effects related to these drugs, investigators say.
Results from a cross-sectional study showed that use of both systemic and inhaled glucocorticoids was associated with widespread reductions in fractional anisotropy (FA) and increases in mean diffusivity.
Glucocorticoids have “a whole catalogue” of adverse events, and effects on brain structure “adds to the list,” co-investigator Onno C. Meijer, PhD, professor of molecular neuroendocrinology of corticosteroids, department of medicine, Leiden University Medical Center, the Netherlands, told this news organization.
The findings should encourage clinicians to consider whether doses they are prescribing are too high, said Dr. Meijer. He added that the negative effect of glucocorticoids on the brain was also found in those using inhalers, such as patients with asthma.
The findings were published online in the BMJ Open.
Serious side effects
Glucocorticoids, a class of synthetic steroids with immunosuppressive properties, are prescribed for a wide range of conditions, including rheumatoid arthritis and asthma.
However, they are also associated with potentially serious metabolic, cardiovascular, and musculoskeletal side effects as well as neuropsychiatric side effects such as depression, mania, and cognitive impairment.
About 1 in 3 patients exposed to “quite a lot of these drugs” will experience neuropsychiatric symptoms, Dr. Meijer said.
Most previous studies that investigated effects from high levels of glucocorticoids on brain structure have been small and involved selected populations, such as those with Cushing disease.
The new study included participants from the UK Biobank, a large population-based cohort. Participants had undergone imaging and did not have a history of psychiatric disease – although they could have conditions associated with glucocorticoid use, including anxiety, depression, mania, or delirium.
The analysis included 222 patients using oral or parenteral glucocorticoids at the time of imaging (systemic group), 557 using inhaled glucocorticoids, and 24,106 not using glucocorticoids (the control group).
Inhaled steroids target the lungs, whereas a steroid in pill form “travels in the blood and reaches each and every organ and cell in the body and typically requires higher doses,” Dr. Meijer noted.
The groups were similar with respect to sex, education, and smoking status. However, the systemic glucocorticoid group was slightly older (mean age, 66.1 years vs. 63.3 years for inhaled glucocorticoid users and 63.5 years for the control group).
In addition to age, researchers adjusted for sex, education level, head position in the scanner, head size, assessment center, and year of imaging.
Imaging analyses
Imaging analyses showed systemic glucocorticoid use was associated with reduced global FA (adjusted mean difference, -3.7e-3; 95% confidence interval, -6.4e-3 to 1.0e-3), and reductions in regional FA in the body and genu of the corpus callosum versus the control group.
Inhaled glucocorticoid use was associated with reduced global FA (AMD, -2.3e-3; 95% CI, -4.0e-3 to -5.7e-4), and lower FA in the splenium of the corpus callosum and the cingulum of the hippocampus.
Global mean diffusivity was higher in systemic glucocorticoid users (AMD, 7.2e-6; 95% CI, 3.2e-6 to 1.1e-5) and inhaled glucocorticoid users (AMD, 2.7e-6; 95% CI, 1.7e-7 to 5.2e-6), compared with the control group.
The effects of glucocorticoids on white matter were “pervasive,” and the “most important finding” of the study, Dr. Meijer said. “We were impressed by the fact white matter is so sensitive to these drugs.”
He noted that it is likely that functional connectivity between brain regions is affected by use of glucocorticoids. “You could say communication between brain regions is probably somewhat impaired or challenged,” he said.
Subgroup analyses among participants using glucocorticoids chronically, defined as reported at two consecutive visits, suggested a potential dose-dependent or duration-dependent effect of glucocorticoids on white matter microstructure.
Systemic glucocorticoid use was also associated with an increase in total and grey matter volume of the caudate nucleus.
In addition, there was a significant association between inhaled glucocorticoid use and decreased grey matter volume of the amygdala, which Dr. Meijer said was surprising because studies have shown that glucocorticoids “can drive amygdala big time.”
Move away from ‘one dose for all’?
Another surprise was that the results showed no hippocampal volume differences with steroid use, Dr. Meijer noted.
The modest association between glucocorticoid use and brain volumes could indicate that white matter integrity is more sensitive to glucocorticoids than is grey matter volume, “at least at the structural level,” he said.
He added that longer use or higher doses may be necessary to also induce volumetric changes.
Participants also completed a questionnaire to assess mood over the previous 2 weeks. Systemic glucocorticoid users had more depressive symptoms, disinterest, tenseness/restlessness, and tiredness/lethargy, compared with the control group. Inhaled glucocorticoid users only reported more tiredness/lethargy.
The investigators note that mood-related effects could be linked to the condition for which glucocorticoids were prescribed: for example, rheumatoid arthritis or chronic obstructive pulmonary disease.
In terms of cognition, systemic glucocorticoid users performed significantly worse on the symbol digit substitution task, compared with participants in the control group.
In light of these findings, pharmaceutical companies that make inhaled corticosteroids “should perhaps find out if glucocorticoids can be dosed by kilogram body weight rather than simply one dose fits all,” which is currently the case, Dr. Meijer said.
Impressive, but several limitations
Commenting on the findings, E. Sherwood Brown, MD, PhD, Distinguished Chair in Psychiatric Research and professor and vice chair for clinical research, department of psychiatry, The University of Texas Southwestern Medical Center, Dallas, called the study sample size “impressive.”
In addition, the study is the first to look at systemic as well as inhaled corticosteroids, said Dr. Brown, who was not involved with the research. He noted that previously, there had been only case reports of psychiatric symptoms with inhaled corticosteroids.
That results are in the same direction but greater with systemic, compared with inhaled corticosteroids, is “particularly interesting” because this might suggest dose-dependent effects, Dr. Brown said.
He noted that cognitive differences were also only observed with systemic corticosteroids.
Some study observations, such as smaller amygdala volume with inhaled but not systemic corticosteroids, “are harder to understand,” said Dr. Brown.
However, he pointed out some study limitations. For example, data were apparently unavailable for verbal and declarative memory test data, despite corticosteroids probably affecting the hippocampus and causing memory changes.
Other drawbacks were that the dose and duration of corticosteroid use, as well as the medical histories of study participants, were not available, Dr. Brown said.
No study funding was reported. Dr. Meijer has received research grants and honorariums from Corcept Therapeutics and a speakers’ fee from Ipsen. Dr. Brown is on an advisory board for Sage Pharmaceuticals, which is developing neurosteroids (not corticosteroids) for mood disorders. He is also on a Medscape advisory board related to bipolar disorder.
A version of this article first appeared on Medscape.com.
New research links the use of glucocorticoids with changes in white matter microstructure – which may explain the development of anxiety, depression, and other neuropsychiatric side effects related to these drugs, investigators say.
Results from a cross-sectional study showed that use of both systemic and inhaled glucocorticoids was associated with widespread reductions in fractional anisotropy (FA) and increases in mean diffusivity.
Glucocorticoids have “a whole catalogue” of adverse events, and effects on brain structure “adds to the list,” co-investigator Onno C. Meijer, PhD, professor of molecular neuroendocrinology of corticosteroids, department of medicine, Leiden University Medical Center, the Netherlands, told this news organization.
The findings should encourage clinicians to consider whether doses they are prescribing are too high, said Dr. Meijer. He added that the negative effect of glucocorticoids on the brain was also found in those using inhalers, such as patients with asthma.
The findings were published online in the BMJ Open.
Serious side effects
Glucocorticoids, a class of synthetic steroids with immunosuppressive properties, are prescribed for a wide range of conditions, including rheumatoid arthritis and asthma.
However, they are also associated with potentially serious metabolic, cardiovascular, and musculoskeletal side effects as well as neuropsychiatric side effects such as depression, mania, and cognitive impairment.
About 1 in 3 patients exposed to “quite a lot of these drugs” will experience neuropsychiatric symptoms, Dr. Meijer said.
Most previous studies that investigated effects from high levels of glucocorticoids on brain structure have been small and involved selected populations, such as those with Cushing disease.
The new study included participants from the UK Biobank, a large population-based cohort. Participants had undergone imaging and did not have a history of psychiatric disease – although they could have conditions associated with glucocorticoid use, including anxiety, depression, mania, or delirium.
The analysis included 222 patients using oral or parenteral glucocorticoids at the time of imaging (systemic group), 557 using inhaled glucocorticoids, and 24,106 not using glucocorticoids (the control group).
Inhaled steroids target the lungs, whereas a steroid in pill form “travels in the blood and reaches each and every organ and cell in the body and typically requires higher doses,” Dr. Meijer noted.
The groups were similar with respect to sex, education, and smoking status. However, the systemic glucocorticoid group was slightly older (mean age, 66.1 years vs. 63.3 years for inhaled glucocorticoid users and 63.5 years for the control group).
In addition to age, researchers adjusted for sex, education level, head position in the scanner, head size, assessment center, and year of imaging.
Imaging analyses
Imaging analyses showed systemic glucocorticoid use was associated with reduced global FA (adjusted mean difference, -3.7e-3; 95% confidence interval, -6.4e-3 to 1.0e-3), and reductions in regional FA in the body and genu of the corpus callosum versus the control group.
Inhaled glucocorticoid use was associated with reduced global FA (AMD, -2.3e-3; 95% CI, -4.0e-3 to -5.7e-4), and lower FA in the splenium of the corpus callosum and the cingulum of the hippocampus.
Global mean diffusivity was higher in systemic glucocorticoid users (AMD, 7.2e-6; 95% CI, 3.2e-6 to 1.1e-5) and inhaled glucocorticoid users (AMD, 2.7e-6; 95% CI, 1.7e-7 to 5.2e-6), compared with the control group.
The effects of glucocorticoids on white matter were “pervasive,” and the “most important finding” of the study, Dr. Meijer said. “We were impressed by the fact white matter is so sensitive to these drugs.”
He noted that it is likely that functional connectivity between brain regions is affected by use of glucocorticoids. “You could say communication between brain regions is probably somewhat impaired or challenged,” he said.
Subgroup analyses among participants using glucocorticoids chronically, defined as reported at two consecutive visits, suggested a potential dose-dependent or duration-dependent effect of glucocorticoids on white matter microstructure.
Systemic glucocorticoid use was also associated with an increase in total and grey matter volume of the caudate nucleus.
In addition, there was a significant association between inhaled glucocorticoid use and decreased grey matter volume of the amygdala, which Dr. Meijer said was surprising because studies have shown that glucocorticoids “can drive amygdala big time.”
Move away from ‘one dose for all’?
Another surprise was that the results showed no hippocampal volume differences with steroid use, Dr. Meijer noted.
The modest association between glucocorticoid use and brain volumes could indicate that white matter integrity is more sensitive to glucocorticoids than is grey matter volume, “at least at the structural level,” he said.
He added that longer use or higher doses may be necessary to also induce volumetric changes.
Participants also completed a questionnaire to assess mood over the previous 2 weeks. Systemic glucocorticoid users had more depressive symptoms, disinterest, tenseness/restlessness, and tiredness/lethargy, compared with the control group. Inhaled glucocorticoid users only reported more tiredness/lethargy.
The investigators note that mood-related effects could be linked to the condition for which glucocorticoids were prescribed: for example, rheumatoid arthritis or chronic obstructive pulmonary disease.
In terms of cognition, systemic glucocorticoid users performed significantly worse on the symbol digit substitution task, compared with participants in the control group.
In light of these findings, pharmaceutical companies that make inhaled corticosteroids “should perhaps find out if glucocorticoids can be dosed by kilogram body weight rather than simply one dose fits all,” which is currently the case, Dr. Meijer said.
Impressive, but several limitations
Commenting on the findings, E. Sherwood Brown, MD, PhD, Distinguished Chair in Psychiatric Research and professor and vice chair for clinical research, department of psychiatry, The University of Texas Southwestern Medical Center, Dallas, called the study sample size “impressive.”
In addition, the study is the first to look at systemic as well as inhaled corticosteroids, said Dr. Brown, who was not involved with the research. He noted that previously, there had been only case reports of psychiatric symptoms with inhaled corticosteroids.
That results are in the same direction but greater with systemic, compared with inhaled corticosteroids, is “particularly interesting” because this might suggest dose-dependent effects, Dr. Brown said.
He noted that cognitive differences were also only observed with systemic corticosteroids.
Some study observations, such as smaller amygdala volume with inhaled but not systemic corticosteroids, “are harder to understand,” said Dr. Brown.
However, he pointed out some study limitations. For example, data were apparently unavailable for verbal and declarative memory test data, despite corticosteroids probably affecting the hippocampus and causing memory changes.
Other drawbacks were that the dose and duration of corticosteroid use, as well as the medical histories of study participants, were not available, Dr. Brown said.
No study funding was reported. Dr. Meijer has received research grants and honorariums from Corcept Therapeutics and a speakers’ fee from Ipsen. Dr. Brown is on an advisory board for Sage Pharmaceuticals, which is developing neurosteroids (not corticosteroids) for mood disorders. He is also on a Medscape advisory board related to bipolar disorder.
A version of this article first appeared on Medscape.com.
FROM BMJ OPEN