User login
Things We Do For No Reason: Blood Cultures for Uncomplicated Skin and Soft Tissue Infections in Children
The “Things We Do for No Reason” (TWDFNR) series reviews practices that have become common parts of hospital care but may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent “black and white” conclusions or clinical practice standards but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
CLINICAL SCENARIO
An 8-year-old previously healthy girl presented to the emergency department (ED) with 2 days of warmth, swelling, and pain over her right upper thigh. Three days prior before presentation, a “pimple” appeared on her leg and drained a small amount of pus. Over the next 24 hours, the lesion became swollen, red, and painful. Her pediatrician prescribed trimethoprim-sulfamethoxazole. The patient took 3 doses of this medication but still experienced worsening pain and swelling.
In the ED, she had normal vital signs for her age except for temperature of 100.8 °F. A 2 cm × 3 cm area of fluctuance, erythema, and warmth was noted, and bedside ultrasound demonstrated a simple fluid collection. Incision and drainage was performed with expression of several milliliters of pus. The patient was referred for admission due to worsening symptoms despite outpatient antibiotic therapy. The ED providers ordered a blood culture at the time of admission.
BACKGROUND
Skin and soft tissue infections (SSTIs) are common pediatric diagnoses, which account for an estimated 390,000 ED visits annually1 and represent the 7th most common reason for pediatric hospital admission in the United States.2 The rates of SSTIs have increased over the past several decades partly due to the rise of methicillin-resistant Staphylococcus aureus (MRSA).3
Why You Might Think Blood Cultures are Helpful In Children with SSTIs?
Prior to the introduction of the Haemophilus influenzae vaccine, the rates of SSTI-associated bacteremia ranged from 8% to 20%.4,5 Although the rate of bacteremia has declined significantly, blood cultures are still commonly performed as part of the evaluation of uncomplicated SSTIs in children; studies have shown that blood culture rates are 46% in the combined outpatient/inpatient setting,6 34% in the ED setting,7 and 47%-94% in the inpatient setting.7-11 Clinicians still feel that bacteremia detection is important to guide the selection of antibiotics and treatment duration. Providers may also underestimate the risk of obtaining a contaminant result and associated charges. Lastly, clinicians may perform blood cultures due to cultural norms at their institution.
Why Blood Cultures are Unnecessary in Children with Uncomplicated SSTIs
Several decades into the post vaccine era, the current guidelines from the Infectious Diseases Society of America (IDSA) do not recommend blood cultures as part of the routine evaluation of uncomplicated SSTIs.12 Multiple single-center studies have failed to demonstrate the benefits of obtaining blood cultures in pediatric patients with uncomplicated SSTIs in the post-H. influenzae vaccine era.6–11
Sadow et al11 performed a retrospective case series of 381 children hospitalized with cellulitis to determine the rate and yield of blood cultures. Of the 266 (70%) patients who had a blood culture performed, 5 (1.9%) were true positives and 13 (5.4%) were contaminants. Notably, the true positive results included 3 children with active varicella infection and 2 children with septic joints; the latter would qualify as a complicated SSTI or as a separate infectious process altogether. No significant change in management resulted the positive blood cultures.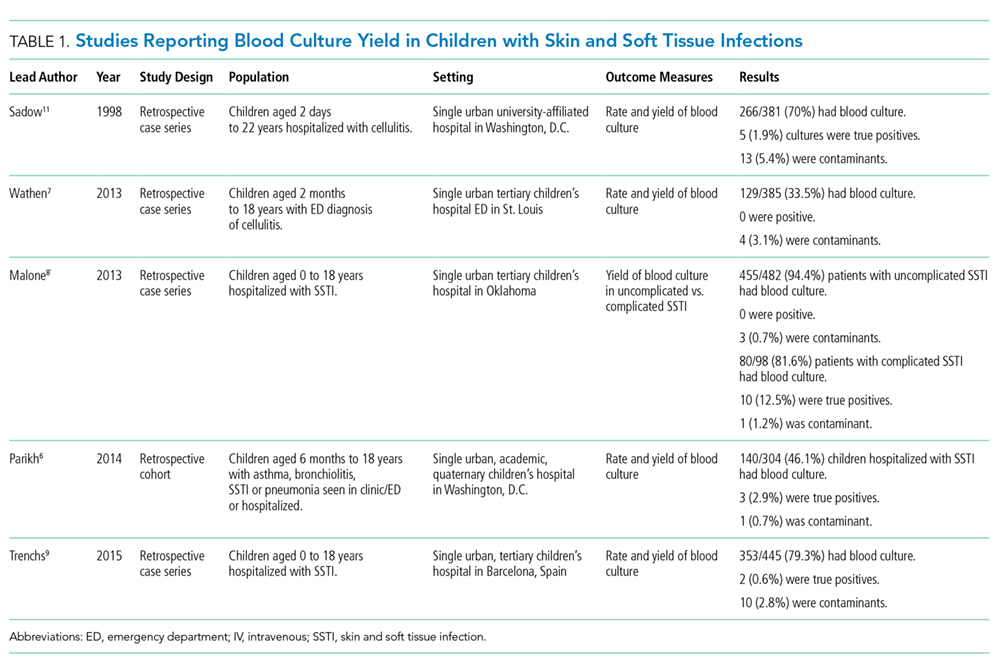
Wathen et al7 conducted a similar retrospective case series of 385 children with cellulitis who presented to the ED of a single tertiary-care children’s hospital to determine the rate and yield of blood cultures. Of the 129 (33.5%) blood cultures performed, there were no true positives and 4 (3.1%) contaminants. Obtaining a blood culture was also associated with high rates of ordering complete blood count and hospitalization.
Malone et al8 performed a retrospective case series of 580 children hospitalized with an SSTI at a single children’s hospital to determine the yield of blood cultures for uncomplicated versus complicated SSTIs. Of the 482 patients with uncomplicated SSTIs, 455 (94.4%) had a blood culture, with no true positive cultures and 3 (0.7%) contaminants. Obtaining a blood culture in this study was associated with an almost 1 day increase in length of stay (LOS; mean LOS 3.24 vs 2.33 days, P = .04).
Parikh et al6 conducted a retrospective cohort study of 304 children with SSTIs in both inpatient and outpatient settings to determine the yield and rate of blood cultures. Of this group, 140 (46.1%) patients had a blood culture performed, of which there were 3 (2.9%) true positives and 1 (0.7%) contaminant. True-positive bacteria included MRSA and Streptococcus pyogenes, neither of which was associated with a change in antibiotic regimen or increase in hospital LOS. The total charges associated with the original 140 blood cultures were estimated to be $42,450 annually in the authors’ institution.
Lastly, Trenchs et al9 performed a retrospective case series of 445 children hospitalized with SSTI in a Spanish children’s hospital and found 353 (79.3%) blood cultures with 2 (0.6%) true positives and 10 (2.8%) contaminants. Methicillin-sensitive Staphylococcus aureus (MSSA) and S. pyogenes were the sole true-positive bacteria, and no change in management was reported. Obtaining blood cultures was associated with an increased hospital LOS (median LOS 4 vs. 3 days, P
Across these studies, the reported rates of true-positive blood cultures ranged from 0%-2.9%. Of the 1997 patients included in the studies, only 10 (0.5%) had true-positive blood cultures. This rate decreased to 0.4% if the 2 patients with septic arthritis from the study of Sadow et al were excluded. Isolated organisms included MRSA, MSSA, S. pyogenes, and Streptococcus pneumoniae. No unusual organisms were isolated in uncomplicated SSTIs, and the true-positive results were not associated with any reported change in antibiotic management.6–9,11 False-positive blood culture results were found in 0%-5.4% of patients,6–9,11 accounting for 30 patients or 1.5% of the total patients.
Harms Associated With Unnecessary Blood Cultures in SSTIs
Blood cultures necessitate venipunctures, which are painful for children and families. The inevitable false-positive contaminants also lead to repeat venipunctures and, potentially, unnecessary antibiotic exposure. From a high-value care perspective, Parikh et al reported hospital charges of $300 per blood culture and $250 for identification and sensitivity of positives.6 Assuming that these single-center charges are representative of national charges and using 0.5% true positivity and 1.5% false positivity rates, subjecting all children with uncomplicated SSTIs to blood culture would result in $60,250 charges to find one true positive blood culture, with no resultant changes in management. Additionally, among the 200 children cultured to find one true positive, there would be 3 false positives, necessitating another $1650 in charges for identification, sensitivity analysis, and repeat culture. These amounts do not factor in the significant expenditures associated with increased LOS. The potential savings associated with forgoing blood cultures in children with SSTIs should be an incentive for institutional change.
When Blood Cultures May Be Reasonable
The current IDSA guidelines recommend blood cultures for SSTIs in patients with immunodeficiency, animal bites, and immersion injuries (soft tissue injuries occurring in fresh or saltwater).12 Previous studies also delineated criteria for “complicated” SSTIs, typically defined as surgical or traumatic wounds, infections requiring surgical intervention (not including simple incision and drainage), or infected ulcers or burns.8,9 In the study of Malone et al, 10 (12.5%) positives were found among 80 patients with complicated SSTIs who had blood cultures performed.8 Although this work had a single-center study design with a relatively small sample size, no unusual organisms were found; the grown cultures included MRSA, MSSA, and S. pneumoniae. In addition to patients with complicated SSTIs, immunocompromised children, such as those receiving chemotherapy or other immunosuppressive agents, were excluded from the studies of blood culture yield in SSTIs and may warrant blood cultures given the risk of overwhelming infection and susceptibility to rare or invasive organisms.12 In a study of 57 pediatric patients with leukemia and no central catheters who experienced skin or soft tissue complications, Demircioglu et al13 reported 6 positive blood cultures, including Klebsiella oxytoca, Pseudomonas aeruginosa, and Escherichia coli. These organisms would not be covered by typical SSTI antibiotic regimens, illustrating the value of blood cultures in this selected group of patients. Lastly, although the above studies included some infants, the data on utility of blood cultures in neonates are limited. Blood cultures may be reasonable in this group given the relative immunocompromised state of neonates compared with older children. Additionally, any infants aged
What You Should Do Instead Of Blood Cultures for Uncomplicated SSTIs
Gram stain and wound culture of any purulent material may assist with choice of empiric antibiotic therapy and appropriate narrowing of regimen for antibiotic stewardship. Wound cultures of purulent material can identify the causative organism in 58%-66% of the cases.9,14 The rate of wound culture varies widely from 29% to 81% in studies across different healthcare systems.9,10,15 The use of visually appealing posters advising clinicians to “culture pus, not blood” has been shown to significantly decreased the number of blood cultures performed at a single pediatric hospital.10
RECOMMENDATIONS
- Do not obtain blood cultures in pediatric patients with uncomplicated SSTIs.
- If purulent material is available spontaneously or after incision and drainage, then send it for Gram stain and bacterial culture.
- Blood cultures are reasonable in patients with complicated SSTIs and in immunocompromised patients with SSTIs.
- Despite limited data, blood cultures may be reasonable in neonates with SSTIs. Febrile infants with SSTIs aged less than 90 days should be managed under existing febrile infant guidelines.
CONCLUSIONS
Blood cultures in pediatric patients with uncomplicated SSTIs have no proven benefit and are associated with increased LOS, non-negligible false-positive rate, and associated increase in financial charges to the patient and healthcare system. The patient described in the clinical scenario would have an extremely low likelihood of having any meaningful clinical information provided by blood culture as part of her evaluation.
Do you think this is a low-value practice? Is this truly a “Thing We Do for No Reason?” Share what you do in your practice and join in the conversation online by retweeting it on Twitter (#TWDFNR) and liking it on Facebook. We invite you to propose ideas for other “Things We Do for No Reason” topics by emailing [email protected].
DISCLOSURES
The authors have no conflicts of interest relevant to this article to disclose.
1. Mistry R, Shapiro D, Goyal M, et al. Clinical management of skin and soft tissue infections in the U.S. Emergency Departments. West J Emerg Med. 2014;15(4):491-498. doi:10.5811/westjem.2014.4.20583. PubMed
2. Witt WP, Weiss AJ, Elixhauser A. Overview of hospital stays for children in the United States, 2012; Statistical Brief #187. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb187-Hospital-Stays-Children-2012.pdf.
3. Dukic VM, Lauderdale DS, Wilder J, Daum RS, David MZ. Epidemics of community-associated methicillin-resistant Staphylococcus aureus in the United States: a meta-analysis. Otto M, ed. PLoS One. 2013;8(1):e52722. doi: 10.1371/journal.pone.0052722. PubMed
4. Fleisher G, Ludwig S, Henretig F, Ruddy R, Henry W. Cellulitis: initial management. Ann Emerg Med. 1981;10(7):356-359. PubMed
5. Fleisher G, Ludwig S, Campos J. Cellulitis: bacterial etiology, clinical features, and laboratory findings. J Pediatr. 1980;97(4):591-593. doi: 10.1016/S0022-3476(80)80014-X http://www.ncbi.nlm.nih.gov/pubmed/6775063. Accessed July 26, 2017.
6. Parikh K, Davis AB, Pavuluri P. Do we need this blood culture? Hosp Pediatr. 2014;4(2):78-84. doi:10.1542/hpeds.2013-0053. PubMed
7. Wathen D, Halloran DR. Blood culture associations in children with a diagnosis of cellulitis in the era of methicillin-resistant Staphylococcus aureus. Hosp Pediatr. 2013;3(2):103-107. http://www.ncbi.nlm.nih.gov/pubmed/24340410. Accessed July 26, 2017.
8. Malone JR, Durica SR, Thompson DM, Bogie A, Naifeh M. Blood cultures in the evaluation of uncomplicated skin and soft tissue infections. Pediatrics. 2013;132(3):454-459. doi:10.1542/peds.2013-1384. PubMed
9. Trenchs V, Hernandez-Bou S, Bianchi C, Arnan M, Gene A, Luaces C. Blood cultures are not useful in the evaluation of children with uncomplicated superficial skin and soft tissue infections. Pediatr Infect Dis J. 2015;34(9):924-927. doi:10.1097/INF.0000000000000768. PubMed
10. Sloane AJ, Pressel DM. Culture pus, not blood: decreasing routine laboratory testing in patients with uncomplicated skin and soft tissue infections. Hosp Pediatr. 2016;6(7):394-398. doi:10.1542/hpeds.2015-0186. PubMed
11. Sadow KB, Chamberlain JM. Blood cultures in the evaluation of children with cellulitis. Pediatrics. 1998;101(3):E4. doi: 10.1542/peds.101.3.e4 http://www.ncbi.nlm.nih.gov/pubmed/9481023. Accessed July 26, 2017.
12. Stevens DL, Bisno AL, Chambers HF, et al. Executive Summary: practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of America. Clin Infect Dis. 2014;59(2):147-159. doi:10.1093/cid/ciu444.
13. Demircioğlu F, Ylmaz S, Oren H, Ozgüven AA, Irken G. Skin and soft tissue complications in pediatric leukemia patients with and without central venous catheters. J Pediatr Hematol Oncol. 2008;30(1):32-35. doi:10.1097/MPH.0b013e31815cc429. PubMed
14. Ray GT, Suaya JA, Baxter R. Microbiology of skin and soft tissue infections in the age of community-acquired methicillin-resistant Staphylococcus aureus. Diagn Microbiol Infect Dis. 2013;76(1):24-30. doi:10.1016/j.diagmicrobio.2013.02.020. PubMed
15. Baumann BM, Russo CJ, Pavlik D, et al. Management of pediatric skin abscesses in pediatric, general academic and community emergency departments. West J Emerg Med. 2011;12(2):159-167. http://www.ncbi.nlm.nih.gov/pubmed/21691519. Accessed July 26, 2017.
The “Things We Do for No Reason” (TWDFNR) series reviews practices that have become common parts of hospital care but may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent “black and white” conclusions or clinical practice standards but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
CLINICAL SCENARIO
An 8-year-old previously healthy girl presented to the emergency department (ED) with 2 days of warmth, swelling, and pain over her right upper thigh. Three days prior before presentation, a “pimple” appeared on her leg and drained a small amount of pus. Over the next 24 hours, the lesion became swollen, red, and painful. Her pediatrician prescribed trimethoprim-sulfamethoxazole. The patient took 3 doses of this medication but still experienced worsening pain and swelling.
In the ED, she had normal vital signs for her age except for temperature of 100.8 °F. A 2 cm × 3 cm area of fluctuance, erythema, and warmth was noted, and bedside ultrasound demonstrated a simple fluid collection. Incision and drainage was performed with expression of several milliliters of pus. The patient was referred for admission due to worsening symptoms despite outpatient antibiotic therapy. The ED providers ordered a blood culture at the time of admission.
BACKGROUND
Skin and soft tissue infections (SSTIs) are common pediatric diagnoses, which account for an estimated 390,000 ED visits annually1 and represent the 7th most common reason for pediatric hospital admission in the United States.2 The rates of SSTIs have increased over the past several decades partly due to the rise of methicillin-resistant Staphylococcus aureus (MRSA).3
Why You Might Think Blood Cultures are Helpful In Children with SSTIs?
Prior to the introduction of the Haemophilus influenzae vaccine, the rates of SSTI-associated bacteremia ranged from 8% to 20%.4,5 Although the rate of bacteremia has declined significantly, blood cultures are still commonly performed as part of the evaluation of uncomplicated SSTIs in children; studies have shown that blood culture rates are 46% in the combined outpatient/inpatient setting,6 34% in the ED setting,7 and 47%-94% in the inpatient setting.7-11 Clinicians still feel that bacteremia detection is important to guide the selection of antibiotics and treatment duration. Providers may also underestimate the risk of obtaining a contaminant result and associated charges. Lastly, clinicians may perform blood cultures due to cultural norms at their institution.
Why Blood Cultures are Unnecessary in Children with Uncomplicated SSTIs
Several decades into the post vaccine era, the current guidelines from the Infectious Diseases Society of America (IDSA) do not recommend blood cultures as part of the routine evaluation of uncomplicated SSTIs.12 Multiple single-center studies have failed to demonstrate the benefits of obtaining blood cultures in pediatric patients with uncomplicated SSTIs in the post-H. influenzae vaccine era.6–11
Sadow et al11 performed a retrospective case series of 381 children hospitalized with cellulitis to determine the rate and yield of blood cultures. Of the 266 (70%) patients who had a blood culture performed, 5 (1.9%) were true positives and 13 (5.4%) were contaminants. Notably, the true positive results included 3 children with active varicella infection and 2 children with septic joints; the latter would qualify as a complicated SSTI or as a separate infectious process altogether. No significant change in management resulted the positive blood cultures.
Wathen et al7 conducted a similar retrospective case series of 385 children with cellulitis who presented to the ED of a single tertiary-care children’s hospital to determine the rate and yield of blood cultures. Of the 129 (33.5%) blood cultures performed, there were no true positives and 4 (3.1%) contaminants. Obtaining a blood culture was also associated with high rates of ordering complete blood count and hospitalization.
Malone et al8 performed a retrospective case series of 580 children hospitalized with an SSTI at a single children’s hospital to determine the yield of blood cultures for uncomplicated versus complicated SSTIs. Of the 482 patients with uncomplicated SSTIs, 455 (94.4%) had a blood culture, with no true positive cultures and 3 (0.7%) contaminants. Obtaining a blood culture in this study was associated with an almost 1 day increase in length of stay (LOS; mean LOS 3.24 vs 2.33 days, P = .04).
Parikh et al6 conducted a retrospective cohort study of 304 children with SSTIs in both inpatient and outpatient settings to determine the yield and rate of blood cultures. Of this group, 140 (46.1%) patients had a blood culture performed, of which there were 3 (2.9%) true positives and 1 (0.7%) contaminant. True-positive bacteria included MRSA and Streptococcus pyogenes, neither of which was associated with a change in antibiotic regimen or increase in hospital LOS. The total charges associated with the original 140 blood cultures were estimated to be $42,450 annually in the authors’ institution.
Lastly, Trenchs et al9 performed a retrospective case series of 445 children hospitalized with SSTI in a Spanish children’s hospital and found 353 (79.3%) blood cultures with 2 (0.6%) true positives and 10 (2.8%) contaminants. Methicillin-sensitive Staphylococcus aureus (MSSA) and S. pyogenes were the sole true-positive bacteria, and no change in management was reported. Obtaining blood cultures was associated with an increased hospital LOS (median LOS 4 vs. 3 days, P
Across these studies, the reported rates of true-positive blood cultures ranged from 0%-2.9%. Of the 1997 patients included in the studies, only 10 (0.5%) had true-positive blood cultures. This rate decreased to 0.4% if the 2 patients with septic arthritis from the study of Sadow et al were excluded. Isolated organisms included MRSA, MSSA, S. pyogenes, and Streptococcus pneumoniae. No unusual organisms were isolated in uncomplicated SSTIs, and the true-positive results were not associated with any reported change in antibiotic management.6–9,11 False-positive blood culture results were found in 0%-5.4% of patients,6–9,11 accounting for 30 patients or 1.5% of the total patients.
Harms Associated With Unnecessary Blood Cultures in SSTIs
Blood cultures necessitate venipunctures, which are painful for children and families. The inevitable false-positive contaminants also lead to repeat venipunctures and, potentially, unnecessary antibiotic exposure. From a high-value care perspective, Parikh et al reported hospital charges of $300 per blood culture and $250 for identification and sensitivity of positives.6 Assuming that these single-center charges are representative of national charges and using 0.5% true positivity and 1.5% false positivity rates, subjecting all children with uncomplicated SSTIs to blood culture would result in $60,250 charges to find one true positive blood culture, with no resultant changes in management. Additionally, among the 200 children cultured to find one true positive, there would be 3 false positives, necessitating another $1650 in charges for identification, sensitivity analysis, and repeat culture. These amounts do not factor in the significant expenditures associated with increased LOS. The potential savings associated with forgoing blood cultures in children with SSTIs should be an incentive for institutional change.
When Blood Cultures May Be Reasonable
The current IDSA guidelines recommend blood cultures for SSTIs in patients with immunodeficiency, animal bites, and immersion injuries (soft tissue injuries occurring in fresh or saltwater).12 Previous studies also delineated criteria for “complicated” SSTIs, typically defined as surgical or traumatic wounds, infections requiring surgical intervention (not including simple incision and drainage), or infected ulcers or burns.8,9 In the study of Malone et al, 10 (12.5%) positives were found among 80 patients with complicated SSTIs who had blood cultures performed.8 Although this work had a single-center study design with a relatively small sample size, no unusual organisms were found; the grown cultures included MRSA, MSSA, and S. pneumoniae. In addition to patients with complicated SSTIs, immunocompromised children, such as those receiving chemotherapy or other immunosuppressive agents, were excluded from the studies of blood culture yield in SSTIs and may warrant blood cultures given the risk of overwhelming infection and susceptibility to rare or invasive organisms.12 In a study of 57 pediatric patients with leukemia and no central catheters who experienced skin or soft tissue complications, Demircioglu et al13 reported 6 positive blood cultures, including Klebsiella oxytoca, Pseudomonas aeruginosa, and Escherichia coli. These organisms would not be covered by typical SSTI antibiotic regimens, illustrating the value of blood cultures in this selected group of patients. Lastly, although the above studies included some infants, the data on utility of blood cultures in neonates are limited. Blood cultures may be reasonable in this group given the relative immunocompromised state of neonates compared with older children. Additionally, any infants aged
What You Should Do Instead Of Blood Cultures for Uncomplicated SSTIs
Gram stain and wound culture of any purulent material may assist with choice of empiric antibiotic therapy and appropriate narrowing of regimen for antibiotic stewardship. Wound cultures of purulent material can identify the causative organism in 58%-66% of the cases.9,14 The rate of wound culture varies widely from 29% to 81% in studies across different healthcare systems.9,10,15 The use of visually appealing posters advising clinicians to “culture pus, not blood” has been shown to significantly decreased the number of blood cultures performed at a single pediatric hospital.10
RECOMMENDATIONS
- Do not obtain blood cultures in pediatric patients with uncomplicated SSTIs.
- If purulent material is available spontaneously or after incision and drainage, then send it for Gram stain and bacterial culture.
- Blood cultures are reasonable in patients with complicated SSTIs and in immunocompromised patients with SSTIs.
- Despite limited data, blood cultures may be reasonable in neonates with SSTIs. Febrile infants with SSTIs aged less than 90 days should be managed under existing febrile infant guidelines.
CONCLUSIONS
Blood cultures in pediatric patients with uncomplicated SSTIs have no proven benefit and are associated with increased LOS, non-negligible false-positive rate, and associated increase in financial charges to the patient and healthcare system. The patient described in the clinical scenario would have an extremely low likelihood of having any meaningful clinical information provided by blood culture as part of her evaluation.
Do you think this is a low-value practice? Is this truly a “Thing We Do for No Reason?” Share what you do in your practice and join in the conversation online by retweeting it on Twitter (#TWDFNR) and liking it on Facebook. We invite you to propose ideas for other “Things We Do for No Reason” topics by emailing [email protected].
DISCLOSURES
The authors have no conflicts of interest relevant to this article to disclose.
The “Things We Do for No Reason” (TWDFNR) series reviews practices that have become common parts of hospital care but may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent “black and white” conclusions or clinical practice standards but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
CLINICAL SCENARIO
An 8-year-old previously healthy girl presented to the emergency department (ED) with 2 days of warmth, swelling, and pain over her right upper thigh. Three days prior before presentation, a “pimple” appeared on her leg and drained a small amount of pus. Over the next 24 hours, the lesion became swollen, red, and painful. Her pediatrician prescribed trimethoprim-sulfamethoxazole. The patient took 3 doses of this medication but still experienced worsening pain and swelling.
In the ED, she had normal vital signs for her age except for temperature of 100.8 °F. A 2 cm × 3 cm area of fluctuance, erythema, and warmth was noted, and bedside ultrasound demonstrated a simple fluid collection. Incision and drainage was performed with expression of several milliliters of pus. The patient was referred for admission due to worsening symptoms despite outpatient antibiotic therapy. The ED providers ordered a blood culture at the time of admission.
BACKGROUND
Skin and soft tissue infections (SSTIs) are common pediatric diagnoses, which account for an estimated 390,000 ED visits annually1 and represent the 7th most common reason for pediatric hospital admission in the United States.2 The rates of SSTIs have increased over the past several decades partly due to the rise of methicillin-resistant Staphylococcus aureus (MRSA).3
Why You Might Think Blood Cultures are Helpful In Children with SSTIs?
Prior to the introduction of the Haemophilus influenzae vaccine, the rates of SSTI-associated bacteremia ranged from 8% to 20%.4,5 Although the rate of bacteremia has declined significantly, blood cultures are still commonly performed as part of the evaluation of uncomplicated SSTIs in children; studies have shown that blood culture rates are 46% in the combined outpatient/inpatient setting,6 34% in the ED setting,7 and 47%-94% in the inpatient setting.7-11 Clinicians still feel that bacteremia detection is important to guide the selection of antibiotics and treatment duration. Providers may also underestimate the risk of obtaining a contaminant result and associated charges. Lastly, clinicians may perform blood cultures due to cultural norms at their institution.
Why Blood Cultures are Unnecessary in Children with Uncomplicated SSTIs
Several decades into the post vaccine era, the current guidelines from the Infectious Diseases Society of America (IDSA) do not recommend blood cultures as part of the routine evaluation of uncomplicated SSTIs.12 Multiple single-center studies have failed to demonstrate the benefits of obtaining blood cultures in pediatric patients with uncomplicated SSTIs in the post-H. influenzae vaccine era.6–11
Sadow et al11 performed a retrospective case series of 381 children hospitalized with cellulitis to determine the rate and yield of blood cultures. Of the 266 (70%) patients who had a blood culture performed, 5 (1.9%) were true positives and 13 (5.4%) were contaminants. Notably, the true positive results included 3 children with active varicella infection and 2 children with septic joints; the latter would qualify as a complicated SSTI or as a separate infectious process altogether. No significant change in management resulted the positive blood cultures.
Wathen et al7 conducted a similar retrospective case series of 385 children with cellulitis who presented to the ED of a single tertiary-care children’s hospital to determine the rate and yield of blood cultures. Of the 129 (33.5%) blood cultures performed, there were no true positives and 4 (3.1%) contaminants. Obtaining a blood culture was also associated with high rates of ordering complete blood count and hospitalization.
Malone et al8 performed a retrospective case series of 580 children hospitalized with an SSTI at a single children’s hospital to determine the yield of blood cultures for uncomplicated versus complicated SSTIs. Of the 482 patients with uncomplicated SSTIs, 455 (94.4%) had a blood culture, with no true positive cultures and 3 (0.7%) contaminants. Obtaining a blood culture in this study was associated with an almost 1 day increase in length of stay (LOS; mean LOS 3.24 vs 2.33 days, P = .04).
Parikh et al6 conducted a retrospective cohort study of 304 children with SSTIs in both inpatient and outpatient settings to determine the yield and rate of blood cultures. Of this group, 140 (46.1%) patients had a blood culture performed, of which there were 3 (2.9%) true positives and 1 (0.7%) contaminant. True-positive bacteria included MRSA and Streptococcus pyogenes, neither of which was associated with a change in antibiotic regimen or increase in hospital LOS. The total charges associated with the original 140 blood cultures were estimated to be $42,450 annually in the authors’ institution.
Lastly, Trenchs et al9 performed a retrospective case series of 445 children hospitalized with SSTI in a Spanish children’s hospital and found 353 (79.3%) blood cultures with 2 (0.6%) true positives and 10 (2.8%) contaminants. Methicillin-sensitive Staphylococcus aureus (MSSA) and S. pyogenes were the sole true-positive bacteria, and no change in management was reported. Obtaining blood cultures was associated with an increased hospital LOS (median LOS 4 vs. 3 days, P
Across these studies, the reported rates of true-positive blood cultures ranged from 0%-2.9%. Of the 1997 patients included in the studies, only 10 (0.5%) had true-positive blood cultures. This rate decreased to 0.4% if the 2 patients with septic arthritis from the study of Sadow et al were excluded. Isolated organisms included MRSA, MSSA, S. pyogenes, and Streptococcus pneumoniae. No unusual organisms were isolated in uncomplicated SSTIs, and the true-positive results were not associated with any reported change in antibiotic management.6–9,11 False-positive blood culture results were found in 0%-5.4% of patients,6–9,11 accounting for 30 patients or 1.5% of the total patients.
Harms Associated With Unnecessary Blood Cultures in SSTIs
Blood cultures necessitate venipunctures, which are painful for children and families. The inevitable false-positive contaminants also lead to repeat venipunctures and, potentially, unnecessary antibiotic exposure. From a high-value care perspective, Parikh et al reported hospital charges of $300 per blood culture and $250 for identification and sensitivity of positives.6 Assuming that these single-center charges are representative of national charges and using 0.5% true positivity and 1.5% false positivity rates, subjecting all children with uncomplicated SSTIs to blood culture would result in $60,250 charges to find one true positive blood culture, with no resultant changes in management. Additionally, among the 200 children cultured to find one true positive, there would be 3 false positives, necessitating another $1650 in charges for identification, sensitivity analysis, and repeat culture. These amounts do not factor in the significant expenditures associated with increased LOS. The potential savings associated with forgoing blood cultures in children with SSTIs should be an incentive for institutional change.
When Blood Cultures May Be Reasonable
The current IDSA guidelines recommend blood cultures for SSTIs in patients with immunodeficiency, animal bites, and immersion injuries (soft tissue injuries occurring in fresh or saltwater).12 Previous studies also delineated criteria for “complicated” SSTIs, typically defined as surgical or traumatic wounds, infections requiring surgical intervention (not including simple incision and drainage), or infected ulcers or burns.8,9 In the study of Malone et al, 10 (12.5%) positives were found among 80 patients with complicated SSTIs who had blood cultures performed.8 Although this work had a single-center study design with a relatively small sample size, no unusual organisms were found; the grown cultures included MRSA, MSSA, and S. pneumoniae. In addition to patients with complicated SSTIs, immunocompromised children, such as those receiving chemotherapy or other immunosuppressive agents, were excluded from the studies of blood culture yield in SSTIs and may warrant blood cultures given the risk of overwhelming infection and susceptibility to rare or invasive organisms.12 In a study of 57 pediatric patients with leukemia and no central catheters who experienced skin or soft tissue complications, Demircioglu et al13 reported 6 positive blood cultures, including Klebsiella oxytoca, Pseudomonas aeruginosa, and Escherichia coli. These organisms would not be covered by typical SSTI antibiotic regimens, illustrating the value of blood cultures in this selected group of patients. Lastly, although the above studies included some infants, the data on utility of blood cultures in neonates are limited. Blood cultures may be reasonable in this group given the relative immunocompromised state of neonates compared with older children. Additionally, any infants aged
What You Should Do Instead Of Blood Cultures for Uncomplicated SSTIs
Gram stain and wound culture of any purulent material may assist with choice of empiric antibiotic therapy and appropriate narrowing of regimen for antibiotic stewardship. Wound cultures of purulent material can identify the causative organism in 58%-66% of the cases.9,14 The rate of wound culture varies widely from 29% to 81% in studies across different healthcare systems.9,10,15 The use of visually appealing posters advising clinicians to “culture pus, not blood” has been shown to significantly decreased the number of blood cultures performed at a single pediatric hospital.10
RECOMMENDATIONS
- Do not obtain blood cultures in pediatric patients with uncomplicated SSTIs.
- If purulent material is available spontaneously or after incision and drainage, then send it for Gram stain and bacterial culture.
- Blood cultures are reasonable in patients with complicated SSTIs and in immunocompromised patients with SSTIs.
- Despite limited data, blood cultures may be reasonable in neonates with SSTIs. Febrile infants with SSTIs aged less than 90 days should be managed under existing febrile infant guidelines.
CONCLUSIONS
Blood cultures in pediatric patients with uncomplicated SSTIs have no proven benefit and are associated with increased LOS, non-negligible false-positive rate, and associated increase in financial charges to the patient and healthcare system. The patient described in the clinical scenario would have an extremely low likelihood of having any meaningful clinical information provided by blood culture as part of her evaluation.
Do you think this is a low-value practice? Is this truly a “Thing We Do for No Reason?” Share what you do in your practice and join in the conversation online by retweeting it on Twitter (#TWDFNR) and liking it on Facebook. We invite you to propose ideas for other “Things We Do for No Reason” topics by emailing [email protected].
DISCLOSURES
The authors have no conflicts of interest relevant to this article to disclose.
1. Mistry R, Shapiro D, Goyal M, et al. Clinical management of skin and soft tissue infections in the U.S. Emergency Departments. West J Emerg Med. 2014;15(4):491-498. doi:10.5811/westjem.2014.4.20583. PubMed
2. Witt WP, Weiss AJ, Elixhauser A. Overview of hospital stays for children in the United States, 2012; Statistical Brief #187. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb187-Hospital-Stays-Children-2012.pdf.
3. Dukic VM, Lauderdale DS, Wilder J, Daum RS, David MZ. Epidemics of community-associated methicillin-resistant Staphylococcus aureus in the United States: a meta-analysis. Otto M, ed. PLoS One. 2013;8(1):e52722. doi: 10.1371/journal.pone.0052722. PubMed
4. Fleisher G, Ludwig S, Henretig F, Ruddy R, Henry W. Cellulitis: initial management. Ann Emerg Med. 1981;10(7):356-359. PubMed
5. Fleisher G, Ludwig S, Campos J. Cellulitis: bacterial etiology, clinical features, and laboratory findings. J Pediatr. 1980;97(4):591-593. doi: 10.1016/S0022-3476(80)80014-X http://www.ncbi.nlm.nih.gov/pubmed/6775063. Accessed July 26, 2017.
6. Parikh K, Davis AB, Pavuluri P. Do we need this blood culture? Hosp Pediatr. 2014;4(2):78-84. doi:10.1542/hpeds.2013-0053. PubMed
7. Wathen D, Halloran DR. Blood culture associations in children with a diagnosis of cellulitis in the era of methicillin-resistant Staphylococcus aureus. Hosp Pediatr. 2013;3(2):103-107. http://www.ncbi.nlm.nih.gov/pubmed/24340410. Accessed July 26, 2017.
8. Malone JR, Durica SR, Thompson DM, Bogie A, Naifeh M. Blood cultures in the evaluation of uncomplicated skin and soft tissue infections. Pediatrics. 2013;132(3):454-459. doi:10.1542/peds.2013-1384. PubMed
9. Trenchs V, Hernandez-Bou S, Bianchi C, Arnan M, Gene A, Luaces C. Blood cultures are not useful in the evaluation of children with uncomplicated superficial skin and soft tissue infections. Pediatr Infect Dis J. 2015;34(9):924-927. doi:10.1097/INF.0000000000000768. PubMed
10. Sloane AJ, Pressel DM. Culture pus, not blood: decreasing routine laboratory testing in patients with uncomplicated skin and soft tissue infections. Hosp Pediatr. 2016;6(7):394-398. doi:10.1542/hpeds.2015-0186. PubMed
11. Sadow KB, Chamberlain JM. Blood cultures in the evaluation of children with cellulitis. Pediatrics. 1998;101(3):E4. doi: 10.1542/peds.101.3.e4 http://www.ncbi.nlm.nih.gov/pubmed/9481023. Accessed July 26, 2017.
12. Stevens DL, Bisno AL, Chambers HF, et al. Executive Summary: practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of America. Clin Infect Dis. 2014;59(2):147-159. doi:10.1093/cid/ciu444.
13. Demircioğlu F, Ylmaz S, Oren H, Ozgüven AA, Irken G. Skin and soft tissue complications in pediatric leukemia patients with and without central venous catheters. J Pediatr Hematol Oncol. 2008;30(1):32-35. doi:10.1097/MPH.0b013e31815cc429. PubMed
14. Ray GT, Suaya JA, Baxter R. Microbiology of skin and soft tissue infections in the age of community-acquired methicillin-resistant Staphylococcus aureus. Diagn Microbiol Infect Dis. 2013;76(1):24-30. doi:10.1016/j.diagmicrobio.2013.02.020. PubMed
15. Baumann BM, Russo CJ, Pavlik D, et al. Management of pediatric skin abscesses in pediatric, general academic and community emergency departments. West J Emerg Med. 2011;12(2):159-167. http://www.ncbi.nlm.nih.gov/pubmed/21691519. Accessed July 26, 2017.
1. Mistry R, Shapiro D, Goyal M, et al. Clinical management of skin and soft tissue infections in the U.S. Emergency Departments. West J Emerg Med. 2014;15(4):491-498. doi:10.5811/westjem.2014.4.20583. PubMed
2. Witt WP, Weiss AJ, Elixhauser A. Overview of hospital stays for children in the United States, 2012; Statistical Brief #187. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb187-Hospital-Stays-Children-2012.pdf.
3. Dukic VM, Lauderdale DS, Wilder J, Daum RS, David MZ. Epidemics of community-associated methicillin-resistant Staphylococcus aureus in the United States: a meta-analysis. Otto M, ed. PLoS One. 2013;8(1):e52722. doi: 10.1371/journal.pone.0052722. PubMed
4. Fleisher G, Ludwig S, Henretig F, Ruddy R, Henry W. Cellulitis: initial management. Ann Emerg Med. 1981;10(7):356-359. PubMed
5. Fleisher G, Ludwig S, Campos J. Cellulitis: bacterial etiology, clinical features, and laboratory findings. J Pediatr. 1980;97(4):591-593. doi: 10.1016/S0022-3476(80)80014-X http://www.ncbi.nlm.nih.gov/pubmed/6775063. Accessed July 26, 2017.
6. Parikh K, Davis AB, Pavuluri P. Do we need this blood culture? Hosp Pediatr. 2014;4(2):78-84. doi:10.1542/hpeds.2013-0053. PubMed
7. Wathen D, Halloran DR. Blood culture associations in children with a diagnosis of cellulitis in the era of methicillin-resistant Staphylococcus aureus. Hosp Pediatr. 2013;3(2):103-107. http://www.ncbi.nlm.nih.gov/pubmed/24340410. Accessed July 26, 2017.
8. Malone JR, Durica SR, Thompson DM, Bogie A, Naifeh M. Blood cultures in the evaluation of uncomplicated skin and soft tissue infections. Pediatrics. 2013;132(3):454-459. doi:10.1542/peds.2013-1384. PubMed
9. Trenchs V, Hernandez-Bou S, Bianchi C, Arnan M, Gene A, Luaces C. Blood cultures are not useful in the evaluation of children with uncomplicated superficial skin and soft tissue infections. Pediatr Infect Dis J. 2015;34(9):924-927. doi:10.1097/INF.0000000000000768. PubMed
10. Sloane AJ, Pressel DM. Culture pus, not blood: decreasing routine laboratory testing in patients with uncomplicated skin and soft tissue infections. Hosp Pediatr. 2016;6(7):394-398. doi:10.1542/hpeds.2015-0186. PubMed
11. Sadow KB, Chamberlain JM. Blood cultures in the evaluation of children with cellulitis. Pediatrics. 1998;101(3):E4. doi: 10.1542/peds.101.3.e4 http://www.ncbi.nlm.nih.gov/pubmed/9481023. Accessed July 26, 2017.
12. Stevens DL, Bisno AL, Chambers HF, et al. Executive Summary: practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of America. Clin Infect Dis. 2014;59(2):147-159. doi:10.1093/cid/ciu444.
13. Demircioğlu F, Ylmaz S, Oren H, Ozgüven AA, Irken G. Skin and soft tissue complications in pediatric leukemia patients with and without central venous catheters. J Pediatr Hematol Oncol. 2008;30(1):32-35. doi:10.1097/MPH.0b013e31815cc429. PubMed
14. Ray GT, Suaya JA, Baxter R. Microbiology of skin and soft tissue infections in the age of community-acquired methicillin-resistant Staphylococcus aureus. Diagn Microbiol Infect Dis. 2013;76(1):24-30. doi:10.1016/j.diagmicrobio.2013.02.020. PubMed
15. Baumann BM, Russo CJ, Pavlik D, et al. Management of pediatric skin abscesses in pediatric, general academic and community emergency departments. West J Emerg Med. 2011;12(2):159-167. http://www.ncbi.nlm.nih.gov/pubmed/21691519. Accessed July 26, 2017.
© 2018 Society of Hospital Medicine
Mental Health Conditions and Unplanned Hospital Readmissions in Children
Readmission prevention is a focus of national efforts to improve the quality of hospital care for children.1-5 Several factors contribute to the risk of readmission for hospitalized children, including age, race or ethnicity, payer, and the type and number of comorbid health conditions.6-9 Mental health conditions (MHCs) are a prevalent comorbidity in children hospitalized for physical health reasons that could influence their postdischarge health and safety.
MHCs are increasingly common in children hospitalized for physical health indications; a comorbid MHC is currently present in 10% to 25% of hospitalized children ages 3 years and older.10,11 Hospital length of stay (LOS) and cost are higher in children with an MHC.12,13 Increased resource use may occur because MHCs can impede hospital treatment effectiveness and the child’s recovery from physical illness. MHCs are associated with a lower adherence with medications14-16 and a lower ability to cope with health events and problems.17-19 In adults, MHCs are a well-established risk factor for hospital readmission for a variety of physical health conditions.20-24 Although the influence of MHCs on readmissions in children has not been extensively investigated, higher readmission rates have been reported in adolescents hospitalized for diabetes with an MHC compared with those with no MHC.25,26
To our knowledge, no large studies have examined the relationship between the presence of a comorbid MHC and hospital readmissions in children or adolescents hospitalized for a broad array of medical or procedure conditions. Therefore, we conducted this study to (1) assess the likelihood of 30-day hospital readmission in children with versus without MHC who were hospitalized for one of 10 medical or 10 procedure conditions, and (2) to assess which MHCs are associated with the highest likelihood of hospital readmission.
METHODS
Study Design and Setting
We conducted a national, retrospective cohort study of index hospitalizations for children ages 3 to 21 years who were discharged from January 1, 2013, to November 30, 2013, in the Agency for Healthcare Research and Quality’s (AHRQ) Nationwide Readmissions Database (NRD). Admissions occurring in December 2013 were excluded because they did not have a 30-day timeframe available for readmission measurement. The 2013 NRD includes administrative data for a nationally representative sample of 14 million hospitalizations in 21 states, accounting for 49% of all US hospitalizations and weighted to represent 35.6 million hospitalizations. The database includes deidentified, verified patient linkage numbers so that patients can be tracked across multiple hospitalizations at the same institution or different institutions within a state. The NRD includes hospital information, patient demographic information, and the International Classification of Diseases, 9th Revision-Clinical Modification (ICD-9-CM) discharge diagnoses and procedures, with 1 primary diagnosis and up to 24 additional fields for comorbid diagnoses. This study was approved for exemption by the Children’s Hospital of Philadelphia Institutional Review Board.
Index Admissions
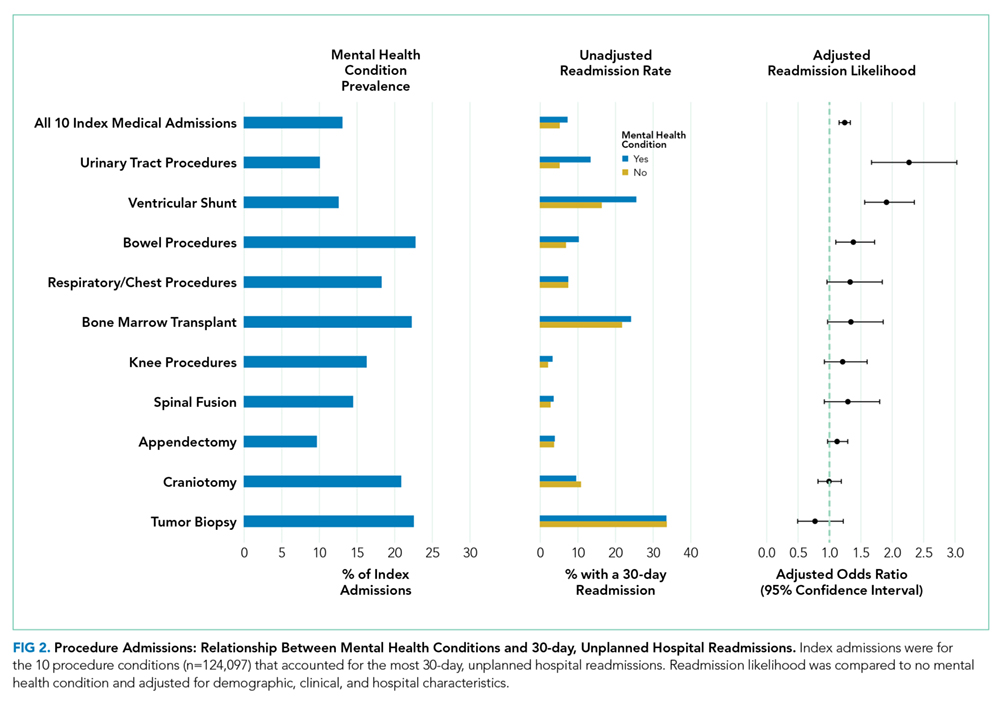
We used the methods described below to create a study cohort of the 10 medical and 10 procedure index admissions associated with the highest volume (ie, the greatest absolute number) of 30-day hospital readmissions. Conditions with a high volume of readmissions were chosen in an effort to identify conditions in which readmission-prevention interventions had the greatest potential to reduce the absolute number of readmissions. We first categorized index hospitalizations for medical and procedure conditions by using the All Patient Refined Diagnosis Related Groups (APR-DRGs; 3M Health Information Systems, Wallingford, CT).27 APR-DRGs use all diagnosis and/or procedure ICD-9-CM codes registered for a hospital discharge to assign 1 reason that best explains the need for hospitalization. We then excluded obstetric hospitalizations, psychiatric hospitalizations, and hospitalizations resulting in death or transfer from being considered as index admissions. Afterwards, we ranked each APR-DRG index hospitalization by the total number of 30-day hospital readmissions that occurred afterward and selected the 10 medical and 10 procedure index admissions with the highest number of readmissions. The APR-DRG index admissions are listed in Figures 1 and 2. For the APR-DRG “digestive system diagnoses,” the most common diagnosis was constipation, and we refer to that category as “constipation.” The most common diagnosis for the APR-DRG called “other operating room procedure for neoplasm” was tumor biopsy, and we refer to that category as “tumor biopsy.”
Main Outcome Measure
The primary study outcome was unplanned, all-cause readmission to any hospital within 30 days of index hospitalization. All-cause readmissions include any hospitalization for the same or different condition as the index admission, including conditions not eligible to be considered as index admissions (obstetric, psychiatric, and hospitalizations resulting in death or transfer). Planned readmissions, identified by using pediatric-specific measure specifications endorsed by AHRQ and the National Quality Forum,28 were excluded from measurement. For index admissions with multiple 30-day readmissions, only the first readmission was counted. Each readmission was treated as an index admission.
Main Independent Variable
The main independent variable was the presence of an MHC documented during the index hospitalization. MHCs were identified and classified into diagnosis categories derived from the AHRQ Chronic Condition Indicator system by using ICD-9-CM codes.29 MHC categories included anxiety disorders, attention-deficit/hyperactivity disorder (ADHD), autism, depression, and substance abuse. Less common MHCs included bipolar disorder, schizophrenia, disruptive behavior disorders, somatoform disorders, and eating disorders. These conditions are included in the group with any MHC, but we did not calculate the adjusted odds ratios (AORs) of readmission for these conditions. Children were identified as having multiple MHCs if they had more than 1 MHC.
Other Characteristics of Index Hospitalizations
A priori, we selected for analysis the known demographic, clinical, and hospital factors associated with the risk of readmission.20-24 The demographic characteristics included patient age, gender, payer category, urban or rural residence, and the median income quartile for a patient’s ZIP code. The hospital characteristics included location, ownership, and teaching hospital designation. The clinical characteristics included the number of chronic conditions30 and indicators for the presence of a complex chronic condition in each of 12 organ systems.31
Statistical Analysis
We calculated descriptive summary statistics for the characteristics of index hospitalizations. We compared characteristics in index admissions of children with versus without MHC by using Wilcoxon Rank-Sum tests for continuous variables and Wald χ2 tests for categorical variables. In the multivariable analysis, we derived logistic regression models to assess the relationship of 30-day hospital readmission with each type of MHC, adjusting for index admission demographic, hospital, and clinical characteristics. MHCs were modeled as binary indicator variables with the presence of any MHC, more than 1 MHC, or each of 5 MHC categories (anxiety disorders, ADHD, autism, depression, substance abuse) compared with no MHC. Four types of logistic regression models were derived (1) for the combined sample of all 10 index medical admissions with each MHC category versus no MHC as a primary predictor, (2) for each medical index admission with any MHC versus no MHC as the primary predictor, (3) for the combined sample of all 10 index procedure admissions with each MHC category versus no MHC as a primary predictor, and (4) for each procedure index admission with any MHC versus no MHC as the primary predictor. All analyses were weighted to achieve national estimates and clustered by hospital by using AHRQ-recommended survey procedures. SAS version 9.4 (SAS Institute, Cary, NC) was used for all analyses. All tests were two-sided, and a P < .05 was
considered statistically significant.
RESULTS
Study Population
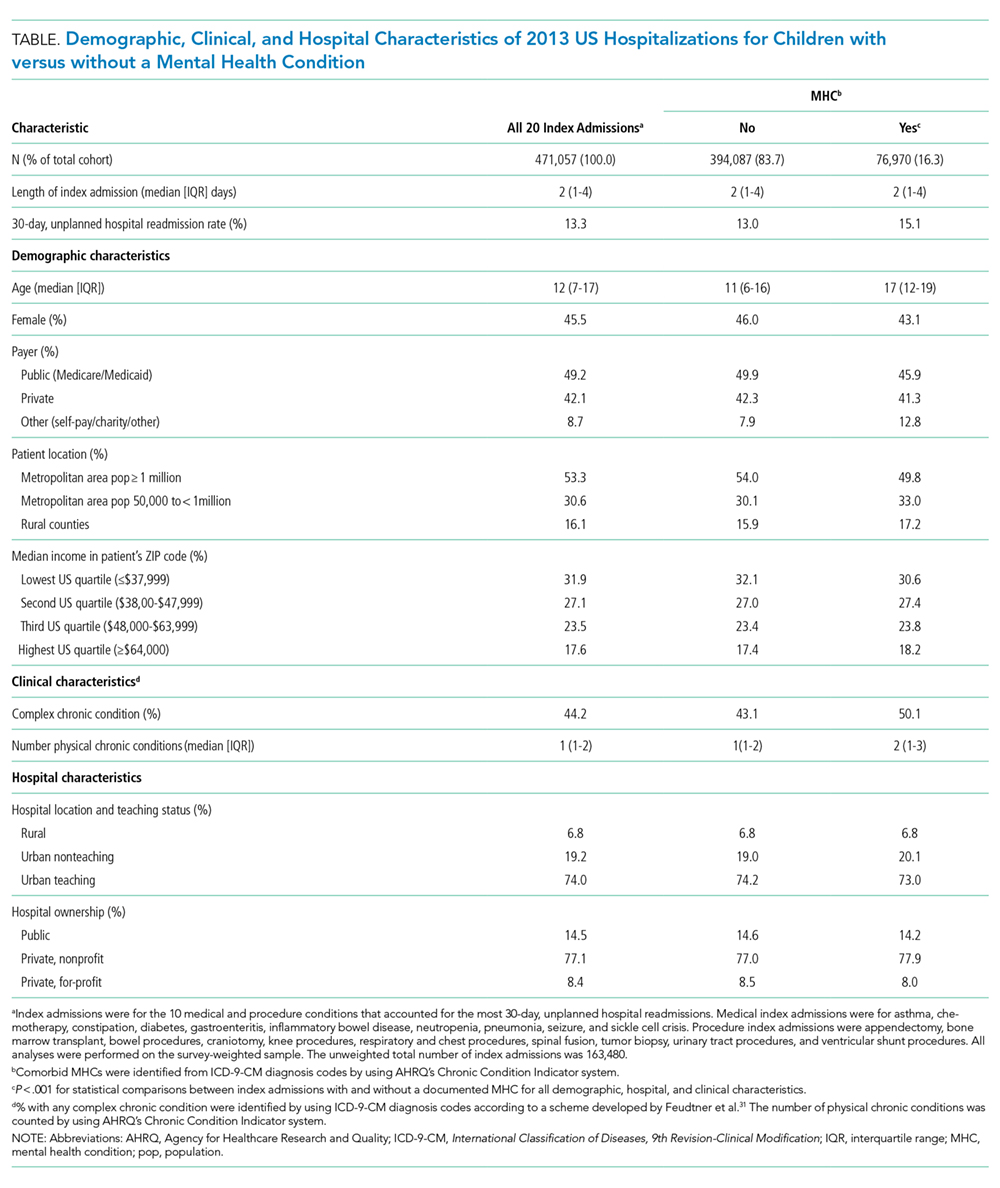
Across all index admissions, 16.3% were for children with an MHC. Overall, children with MHCs were older and more likely to have a chronic30 or complex chronic31 physical health condition than children with no MHCs (Table).
Index Medical Admissions, Mental Health Conditions, and Hospital Readmission
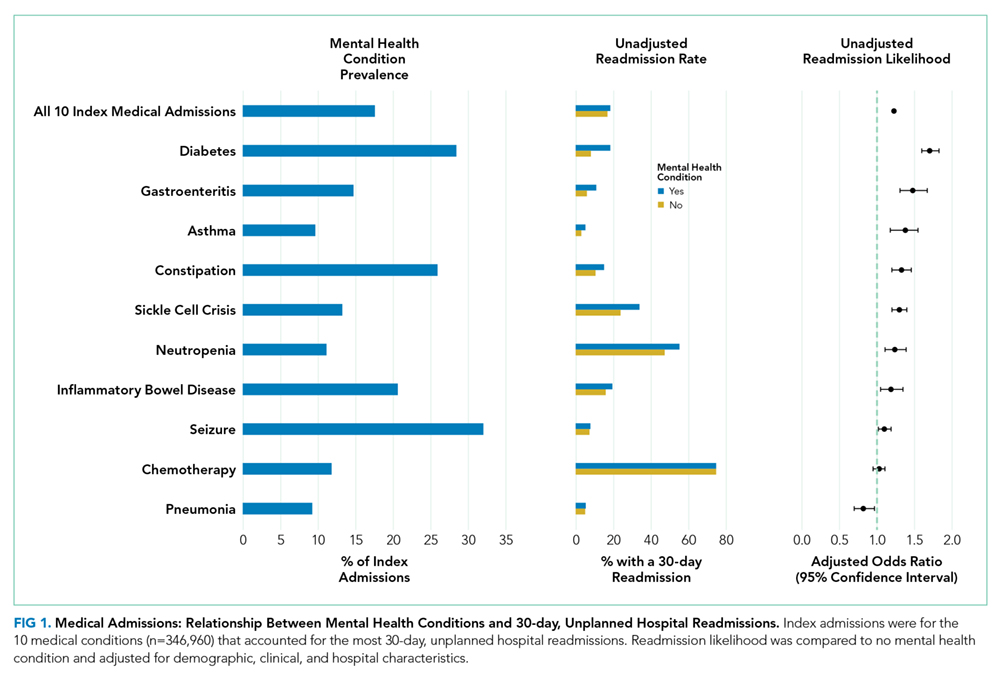
The 10 index medical hospitalizations with the most readmissions for children ages 3 to 20 years were asthma, chemotherapy, constipation, diabetes, gastroenteritis, inflammatory bowel disease, neutropenia, pneumonia, seizure, and sickle cell crisis. Across all index medical hospitalizations, 17.5% were for patients with an MHC (Figure 1). Of index medical admissions with any MHC, 26.3% had ADHD, 22.9% had an anxiety disorder, 14.9% had autism, 18.3% had depression, and 30.9% had substance abuse. Among all admissions with MHCs, 28.9% had 2 or more MHCs.
Index Medical Admissions Combined
For all index medical hospitalizations combined, 17.0% (n = 59,138) had an unplanned, 30-day hospital readmission. The rate of 30-day hospital readmissions was higher with versus without an MHC (17.5 vs 16.8%; P < .001). In a multivariable analysis, presence of an MHC was associated with a higher likelihood of hospital readmission following an index medical admission (AOR, 1.23; 95% confidence interval [CI], 1.19-1.26); Figure 1). All MHCs except autism and ADHD had a higher likelihood of readmission (Figure 3).
Specific Index Medical Admissions
Index Procedure Admissions, Mental Health Conditions, and Hospital Readmission
Index Procedure Admissions Combined

Specific Index Procedure Admissions
For specific index procedure admissions, the rate of 30-day hospital readmission ranged from 2.2% for knee procedures to 33.6% for tumor biopsy. For 3 (ie, urinary tract, ventricular shunt, and bowel procedures) of the 10 specific index procedure hospitalizations, having an MHC was associated with higher adjusted odds of 30-day readmission (AOR range, 1.38-2.27; Figure 2).
In total, adjusting for sociodemographic, clinical, and hospital characteristics, MHCs were associated with an additional 2501 medical readmissions and 217 procedure readmissions beyond what would have been expected if MHCs were not associated with readmissions.
DISCUSSION
MHCs are common among pediatric hospitalizations with the highest volume of readmissions; MHCs were present in approximately 1 in 5 medical and 1 in 7 procedure index hospitalizations. Across medical and procedure admissions, the adjusted likelihood of unplanned, all-cause 30-day readmission was 25% higher for children with versus without an MHC. The readmission likelihood varied by the type of medical or procedure admission and by the type of MHC. MHCs had the strongest associations with readmissions following hospitalization for diabetes and urinary tract procedures. The MHC categories associated with the highest readmission likelihood were depression, substance abuse, and multiple MHCs.
The current study complements existing literature by helping establish MHCs as a prevalent and important risk factor for hospital readmission in children. Estimates of the prevalence of MHCs in hospitalized children are between 10% and 25%,10,11,32 and prevalence has increased by as much as 160% over the last 10 years.29 Prior investigations have found that children with an MHC tend to stay longer in the hospital compared with children with no MHC.32 Results from the present study suggest that children with MHCs also experience more inpatient days because of rehospitalizations. Subsequent investigations should strive to understand the mechanisms in the hospital, community, and family environment that are responsible for the increased inpatient utilization in children with MHCs. Understanding how the receipt of mental health services before, during, and after hospitalization influences readmissions could help identify opportunities for practice improvement. Families report the need for better coordination of their child’s medical and mental health care,33 and opportunities exist to improve attendance at mental health visits after acute care encounters.34 Among adults, interventions that address posthospital access to mental healthcare have prevented readmissions.35
Depression was associated with an increased risk of readmission in medical and procedure hospitalizations. As a well-known risk factor for readmission in adult patients,21 depression can adversely affect and exacerbate the physical health recovery of patients experiencing acute and chronic illnesses.14,36,37 Depression is considered a modifiable contributor that, when controlled, may help lower readmission risk. Optimal adherence with behavior and medication treatment for depression is associated with a lower risk of unplanned 30-day readmissions.14-16,19 Emerging evidence demonstrates how multifaceted, psychosocial approaches can improve patients’ adherence with depression treatment plans.38 Increased attention to depression in hospitalized children may uncover new ways to manage symptoms as children transition from hospital to home.
Other MHCs were associated with a different risk of readmission among medical and procedure hospitalizations. For example, ADHD or autism documented during index hospitalization was associated with an increased risk of readmission following procedure hospitalizations and a decreased risk following medical hospitalizations. Perhaps children with ADHD or autism who exhibit hyperactive, impulsive, or repetitive behaviors39,40 are at risk for disrupting their postprocedure wound healing, nutrition recovery, or pain tolerance, which might contribute to increased readmission risk.
MHCs were associated with different readmission risks across specific types of medical or procedure hospitalizations. For example, among medical conditions, the association of readmissions with MHCs was highest for diabetes, which is consistent with prior research.26 Factors that might mediate this relationship include changes in diet and appetite, difficulty with diabetes care plan adherence, and intentional nonadherence as a form of self-harm. Similarly, a higher risk of readmission in chronic medical conditions like asthma, constipation, and sickle cell disease might be mediated by difficulty adhering to medical plans or managing exacerbations at home. In contrast, MHCs had no association with readmission following chemotherapy. In our clinical experience, readmissions following chemotherapy are driven by physiologic problems, such as thrombocytopenia, fever, and/or neutropenia. MHCs might have limited influence over those health issues. For procedure hospitalizations, MHCs had 1 of the strongest associations with ventricular shunt procedures. We hypothesize that MHCs might lead some children to experience general health symptoms that might be associated with shunt malfunction (eg, fatigue, headache, behavior change), which could lead to an increased risk of readmission to evaluate for shunt malfunction. Conversely, we found no relationship between MHCs and readmissions following appendectomy. For appendectomy, MHCs might have limited influence over the development of postsurgical complications (eg, wound infection or ileus). Future research to better elucidate mediators of increased risk of readmission associated with MHCs in certain medical and procedure conditions could help explain these relationships and identify possible future intervention targets to prevent readmissions.
This study has several limitations. The administrative data are not positioned to discover the mechanisms by which MHCs are associated with a higher likelihood of readmission. We used hospital ICD-9-CM codes to identify patients with MHCs. Other methods using more clinically rich data (eg, chart review, prescription medications, etc.) may be preferable to identify patients with MHCs. Although the use of ICD-9-CM codes may have sufficient specificity, some hospitalized children may have an MHC that is not coded. Patients identified by using diagnosis codes could represent patients with a higher severity of illness, patients using medications, or patients whose outpatient records are accessible to make the hospital team aware of the MHC. If documentation of MHCs during hospitalization represents a higher severity of illness, findings may not extrapolate to lower-severity MHCs. As hospitals transition from ICD-9 -CM to ICD-10 coding, and health systems develop more integrated inpatient and outpatient EHRs, diagnostic specificity may improve. We could not analyze the relationships with several potential confounders and explanatory variables that may be related both to the likelihood of having an MHC and the risk of readmission, including medication administration, psychiatric consultation, and parent mental health. Postdischarge health services, including access to a medical home or a usual source of mental healthcare and measures of medication adherence, were not available in the NRD.
Despite these limitations, the current study underscores the importance of MHCs in hospitalized children upon discharge. As subsequent investigations uncover the key drivers explaining the influence of MHCs on hospital readmission risk, hospitals and their local outpatient and community practices may find it useful to consider MHCs when (1) developing contingency plans and establishing follow-up care at discharge,41 (2) exploring opportunities of care integration between mental and physical health care professionals, and (3) devising strategies to reduce hospital readmissions among populations of children.
CONCLUSIONS
MHCs are prevalent in hospitalized children and are associated with an increased risk of 30-day, unplanned hospital readmission. Future readmission prevention efforts may uncover new ways to improve children’s transitions from hospital to home by investigating strategies to address their MHCs.
Acknowledgments
The authors thank Donjo Lau and Troy Richardson for their assistance with the analysis.
Disclosures
Dr. Doupnik was supported by a Ruth L. Kirschstein National Research Service Award institutional training grant (T32-HP010026), funded by the National Institutes of Health. Dr. Zima was supported by the Behavioral Health Centers of Excellence for California (SB852). Dr. Bardach was supported by the National Institute of Child Health and Human Development (K23-HD065836). Dr. Berry was supported by the Agency for Healthcare Research and Quality (R21 HS023092-01). The authors have no financial relationships relevant to this article to disclose. The authors have no potential conflicts of interest to disclose. Dr. Doupnik led the study design and analysis and drafted the initial manuscript. Mr. Lawlor performed the data analysis. Dr. Hall provided statistical consultation. All authors participated in the design of the study, interpretation of the data, revised the manuscript for key intellectual content, and all authors read and approved the final manuscript.
1. Dougherty D, Schiff J, Mangione-Smith R. The Children’s Health Insurance Program Reauthorization Act quality measures initiatives: moving forward to improve measurement, care, and child and adolescent outcomes. Acad Pediatr. 2011;11(3):S1-S10. PubMed
2. Bardach NS, Vittinghoff E, Asteria-Penaloza R, et al. Measuring Hospital Quality Using Pediatric Readmission and Revisit Rates. Pediatrics. 2013;132(3):429-436. doi:10.1542/peds.2012-3527. PubMed
3. Khan A, Nakamura MM, Zaslavsky AM, et al. Same-Hospital Readmission Rates as a Measure of Pediatric Quality of Care. JAMA Pediatr. 2015;169(10):905-912. doi:10.1001/jamapediatrics.2015.1129. PubMed
4. Fassl BA, Nkoy FL, Stone BL, et al. The Joint Commission Children’s Asthma Care quality measures and asthma readmissions. Pediatrics. 2012;130(3):482-491. doi:10.1542/peds.2011-3318. PubMed
5. Hain PD, Gay JC, Berutti TW, Whitney GM, Wang W, Saville BR. Preventability of Early Readmissions at a Children’s Hospital. Pediatrics. 2013;131(1):e171-e181. doi:10.1542/peds.2012-0820. PubMed
6. Nagasako E, Reidhead B, Waterman B, et al. Adding Socioeconomic Data to Hospital Readmissions Calculations May Produce More Useful Results. Health Aff. 2014;33(5):786-791. PubMed
7. Hu J, Gonsahn MD, Nerenz DR. Socioeconomic Status and Readmissions: Evidence from an Urban Teaching Hospital. Health Aff. 2014;33(5):778-785. doi:10.1377/hlthaff.2013.0816. PubMed
8. Sills MR, Hall M, Colvin JD, et al. Association of Social Determinants with Children’s Hospitals’ Preventable Readmissions Performance. JAMA Pediatr. 2016;170(4):350-358. doi:10.1001/jamapediatrics.2015.4440. PubMed
9. Eselius LL, Cleary PD, Zaslavsky AM, Huskamp HA, Busch SH. Case-Mix Adjustment of Consumer Reports about Managed Behavioral Health Care and Health Plans. Health Serv Res. 2008;43(6):2014-2032. doi:10.1111/j.1475-6773.2008.00894.x. PubMed
10. Doupnik SK, Henry MK, Bae H, et al. Mental Health Conditions and Symptoms in Pediatric Hospitalizations: A Single-Center Point Prevalence Study. Acad Pediatr. 2017;17(2):184-190. PubMed
11. Bardach NS, Coker TR, Zima BT, et al. Common and Costly Hospitalizations for Pediatric Mental Health Disorders. Pediatrics. 2014;133(4):602-609. doi:10.1542/peds.2013-3165. PubMed
12. Doupnik SK, Mitra N, Feudtner C, Marcus SC. The Influence of Comorbid Mood and Anxiety Disorders on Outcomes of Pediatric Patients Hospitalized for Pneumonia. Hosp Pediatr. 2016;6(3):135-142. doi:10.1542/hpeds.2015-0177. PubMed
13. Snell C, Fernandes S, Bujoreanu IS, Garcia G. Depression, illness severity, and healthcare utilization in cystic fibrosis. Pediatr Pulmonol. 2014;49(12):1177-1181. doi:10.1002/ppul.22990. PubMed
14. DiMatteo MR, Lepper HS, Croghan TW. Depression Is a Risk Factor for Noncompliance with Medical Treatment: Meta-analysis of the Effects of Anxiety and Depression on Patient Adherence. Arch Intern Med . 2000;160(14):2101-2107. doi:10.1001/archinte.160.14.2101. PubMed
15. Gray WN, Denson LA, Baldassano RN, Hommel KA. Treatment Adherence in Adolescents with Inflammatory Bowel Disease: The Collective Impact of Barriers to Adherence and Anxiety/Depressive Symptoms. J Pediatr Psychol. 2012;37(3):282-291. doi:10.1093/jpepsy/jsr092. PubMed
16. Mosnaim G, Li H, Martin M, et al. Factors associated with levels of adherence to inhaled corticosteroids in minority adolescents with asthma. Ann Allergy Asthma Immunol. 2014;112(2):116-120. doi:10.1016/j.anai.2013.11.021. PubMed
17. Compas BE, Jaser SS, Dunn MJ, Rodriguez EM. Coping with Chronic Illness in Childhood and Adolescence. Ann Rev Clin Psychol. 2012;8(1):455-480. doi:10.1146/annurev-clinpsy-032511-143108. PubMed
18. Graue M, Wentzel-Larsen T, Bru E, Hanestad BR, Søvik O. The coping styles of adolescents with type 1 diabetes are associated with degree of metabolic control. Diabetes Care. 2004;27(6):1313-1317. PubMed
19. Jaser SS, White LE. Coping and resilience in adolescents with type 1 diabetes. Child Care Health Dev. 2011;37(3):335-342. doi:10.1111/j.1365-2214.2010.01184.x. PubMed
20. Cancino RS, Culpepper L, Sadikova E, Martin J, Jack BW, Mitchell SE. Dose-response relationship between depressive symptoms and hospital readmission. J Hosp Med. 2014;9(6):358-364. doi:10.1002/jhm.2180. PubMed
21. Pederson JL, Warkentin LM, Majumdar SR, McAlister FA. Depressive symptoms are associated with higher rates of readmission or mortality after medical hospitalization: A systematic review and meta-analysis. J Hosp Med. 2016;11(5):373-380. doi:10.1002/jhm.2547. PubMed
22. Chwastiak LA, Davydow DS, McKibbin CL, et al. The Effect of Serious Mental Illness on the Risk of Rehospitalization Among Patients with Diabetes. Psychosomatics. 2014;55(2):134-143. PubMed
23. Daratha KB, Barbosa-Leiker C, H Burley M, et al. Co-occurring mood disorders among hospitalized patients and risk for subsequent medical hospitalization. Gen Hosp Psychiatry. 2012;34(5):500-505. doi:10.1016/j.genhosppsych.2012.05.001. PubMed
24. Kartha A, Anthony D, Manasseh CS, et al. Depression is a risk factor for rehospitalization in medical inpatients. Prim Care Companion J Clin Psychiatry. 2007;9(4):256-262. PubMed
25. Myrvik MP, Burks LM, Hoffman RG, Dasgupta M, Panepinto JA. Mental health disorders influence admission rates for pain in children with sickle cell disease. Pediatr Blood Cancer. 2013;60(7):1211-1214. doi:10.1002/pbc.24394. PubMed
26. Garrison MM, Katon WJ, Richardson LP. The impact of psychiatric comorbidities on readmissions for diabetes in youth. Diabetes Care. 2005;28(9):2150-2154. PubMed
27. Averill R, Goldfield N, Hughes JS, et al. All Patient Refined Diagnosis Related Groups (APR-DRGs) Version 20.0: Methodology Overview. https://www.hcup-us.ahrq.gov/db/nation/nis/APR-DRGsV20MethodologyOverviewandBibliography.pdf. Accessed on November 2, 2016.
28. Berry JG, Toomey SL, Zaslavsky AM, et al. Pediatric readmission prevalence and variability across hospitals. JAMA. 2013;309(4):372-380. PubMed
29. Zima BT, Rodean J, Hall M, Bardach NS, Coker TR, Berry JG. Psychiatric Disorders and Trends in Resource Use in Pediatric Hospitals. Pediatrics. 2016;138(5):e20160909-e20160909. doi:10.1542/peds.2016-0909. PubMed
30. Chronic Condition Indicator (CCI) for ICD-9-CM. Healthcare Cost and Utilization Project (HCUP) Tools & Software Page. http://www.hcup-us.ahrq.gov/toolssoftware/chronic/chronic.jsp. Accessed on October 30, 2015.
31. Feudtner C, Feinstein J, Zhong W, Hall M, Dai D. Pediatric complex chronic conditions classification system version 2: updated for ICD-10 and complex medical technology dependence and transplantation. BMC Pediatr. 2014;14(1):199-205. PubMed
32. Doupnik S, Lawlor J, Zima BT, et al. Mental Health Conditions and Medical and Surgical Hospital Utilization. Pediatrics. 2016;138(6):e20162416. doi:10.1542/peds.2016-2416. PubMed
33. Brown NM, Green JC, Desai MM, Weitzman CC, Rosenthal MS. Need and Unmet Need for Care Coordination Among Children with Mental Health Conditions. Pediatrics. 2014;133(3):e530-e537. doi:10.1542/peds.2013-2590. PubMed
34. Sobolewski B, Richey L, Kowatch RA, Grupp-Phelan J. Mental health follow-up among adolescents with suicidal behaviors after emergency department discharge. Arch Suicide Res. 2013;17(4):323-334. doi:10.1080/13811118.2013.801807. PubMed
35. Hansen LO, Greenwald JL, Budnitz T, et al. Project BOOST: Effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8):421-427. doi:10.1002/jhm.2054. PubMed
36. Di Marco F, Verga M, Santus P, et al. Close correlation between anxiety, depression, and asthma control. Respir Med. 2010;104(1):22-28. doi:10.1016/j.rmed.2009.08.005. PubMed
37. Ghose SS, Williams LS, Swindle RW. Depression and other mental health diagnoses after stroke increase inpatient and outpatient medical utilization three years poststroke. Med Care. 2005;43(12):1259-1264. PubMed
38. Szigethy E, Bujoreanu SI, Youk AO, et al. Randomized efficacy trial of two psychotherapies for depression in youth with inflammatory bowel disease. J Am Acad Child Adolesc Psychiatry. 2014;53(7):726-735. PubMed
39. Swensen A, Birnbaum HG, Ben Hamadi R, Greenberg P, Cremieux PY, Secnik K. Incidence and costs of accidents among attention-deficit/hyperactivity disorder patients. J Adolesc Health. 2004;35(4):346.e1-346.e9. doi:10.1016/j.jadohealth.2003.12.003. PubMed
40. Chan E, Zhan C, Homer CJ. Health Care Use and Costs for Children with Attention-Deficit/Hyperactivity Disorder: National Estimates from the Medical Expenditure Panel Survey. Arch Pediatr Adolesc Med. 2002;156(5):504-511. doi:10.1001/archpedi.156.5.504. PubMed
41. Berry JG, Blaine K, Rogers J, et al. A Framework of Pediatric Hospital Discharge Care Informed by Legislation, Research, and Practice. JAMA Pediatr. 2014;168(10):955-962. doi:10.1001/jamapediatrics.2014.891. PubMed
Readmission prevention is a focus of national efforts to improve the quality of hospital care for children.1-5 Several factors contribute to the risk of readmission for hospitalized children, including age, race or ethnicity, payer, and the type and number of comorbid health conditions.6-9 Mental health conditions (MHCs) are a prevalent comorbidity in children hospitalized for physical health reasons that could influence their postdischarge health and safety.
MHCs are increasingly common in children hospitalized for physical health indications; a comorbid MHC is currently present in 10% to 25% of hospitalized children ages 3 years and older.10,11 Hospital length of stay (LOS) and cost are higher in children with an MHC.12,13 Increased resource use may occur because MHCs can impede hospital treatment effectiveness and the child’s recovery from physical illness. MHCs are associated with a lower adherence with medications14-16 and a lower ability to cope with health events and problems.17-19 In adults, MHCs are a well-established risk factor for hospital readmission for a variety of physical health conditions.20-24 Although the influence of MHCs on readmissions in children has not been extensively investigated, higher readmission rates have been reported in adolescents hospitalized for diabetes with an MHC compared with those with no MHC.25,26
To our knowledge, no large studies have examined the relationship between the presence of a comorbid MHC and hospital readmissions in children or adolescents hospitalized for a broad array of medical or procedure conditions. Therefore, we conducted this study to (1) assess the likelihood of 30-day hospital readmission in children with versus without MHC who were hospitalized for one of 10 medical or 10 procedure conditions, and (2) to assess which MHCs are associated with the highest likelihood of hospital readmission.
METHODS
Study Design and Setting
We conducted a national, retrospective cohort study of index hospitalizations for children ages 3 to 21 years who were discharged from January 1, 2013, to November 30, 2013, in the Agency for Healthcare Research and Quality’s (AHRQ) Nationwide Readmissions Database (NRD). Admissions occurring in December 2013 were excluded because they did not have a 30-day timeframe available for readmission measurement. The 2013 NRD includes administrative data for a nationally representative sample of 14 million hospitalizations in 21 states, accounting for 49% of all US hospitalizations and weighted to represent 35.6 million hospitalizations. The database includes deidentified, verified patient linkage numbers so that patients can be tracked across multiple hospitalizations at the same institution or different institutions within a state. The NRD includes hospital information, patient demographic information, and the International Classification of Diseases, 9th Revision-Clinical Modification (ICD-9-CM) discharge diagnoses and procedures, with 1 primary diagnosis and up to 24 additional fields for comorbid diagnoses. This study was approved for exemption by the Children’s Hospital of Philadelphia Institutional Review Board.
Index Admissions
We used the methods described below to create a study cohort of the 10 medical and 10 procedure index admissions associated with the highest volume (ie, the greatest absolute number) of 30-day hospital readmissions. Conditions with a high volume of readmissions were chosen in an effort to identify conditions in which readmission-prevention interventions had the greatest potential to reduce the absolute number of readmissions. We first categorized index hospitalizations for medical and procedure conditions by using the All Patient Refined Diagnosis Related Groups (APR-DRGs; 3M Health Information Systems, Wallingford, CT).27 APR-DRGs use all diagnosis and/or procedure ICD-9-CM codes registered for a hospital discharge to assign 1 reason that best explains the need for hospitalization. We then excluded obstetric hospitalizations, psychiatric hospitalizations, and hospitalizations resulting in death or transfer from being considered as index admissions. Afterwards, we ranked each APR-DRG index hospitalization by the total number of 30-day hospital readmissions that occurred afterward and selected the 10 medical and 10 procedure index admissions with the highest number of readmissions. The APR-DRG index admissions are listed in Figures 1 and 2. For the APR-DRG “digestive system diagnoses,” the most common diagnosis was constipation, and we refer to that category as “constipation.” The most common diagnosis for the APR-DRG called “other operating room procedure for neoplasm” was tumor biopsy, and we refer to that category as “tumor biopsy.”
Main Outcome Measure
The primary study outcome was unplanned, all-cause readmission to any hospital within 30 days of index hospitalization. All-cause readmissions include any hospitalization for the same or different condition as the index admission, including conditions not eligible to be considered as index admissions (obstetric, psychiatric, and hospitalizations resulting in death or transfer). Planned readmissions, identified by using pediatric-specific measure specifications endorsed by AHRQ and the National Quality Forum,28 were excluded from measurement. For index admissions with multiple 30-day readmissions, only the first readmission was counted. Each readmission was treated as an index admission.
Main Independent Variable
The main independent variable was the presence of an MHC documented during the index hospitalization. MHCs were identified and classified into diagnosis categories derived from the AHRQ Chronic Condition Indicator system by using ICD-9-CM codes.29 MHC categories included anxiety disorders, attention-deficit/hyperactivity disorder (ADHD), autism, depression, and substance abuse. Less common MHCs included bipolar disorder, schizophrenia, disruptive behavior disorders, somatoform disorders, and eating disorders. These conditions are included in the group with any MHC, but we did not calculate the adjusted odds ratios (AORs) of readmission for these conditions. Children were identified as having multiple MHCs if they had more than 1 MHC.
Other Characteristics of Index Hospitalizations
A priori, we selected for analysis the known demographic, clinical, and hospital factors associated with the risk of readmission.20-24 The demographic characteristics included patient age, gender, payer category, urban or rural residence, and the median income quartile for a patient’s ZIP code. The hospital characteristics included location, ownership, and teaching hospital designation. The clinical characteristics included the number of chronic conditions30 and indicators for the presence of a complex chronic condition in each of 12 organ systems.31
Statistical Analysis
We calculated descriptive summary statistics for the characteristics of index hospitalizations. We compared characteristics in index admissions of children with versus without MHC by using Wilcoxon Rank-Sum tests for continuous variables and Wald χ2 tests for categorical variables. In the multivariable analysis, we derived logistic regression models to assess the relationship of 30-day hospital readmission with each type of MHC, adjusting for index admission demographic, hospital, and clinical characteristics. MHCs were modeled as binary indicator variables with the presence of any MHC, more than 1 MHC, or each of 5 MHC categories (anxiety disorders, ADHD, autism, depression, substance abuse) compared with no MHC. Four types of logistic regression models were derived (1) for the combined sample of all 10 index medical admissions with each MHC category versus no MHC as a primary predictor, (2) for each medical index admission with any MHC versus no MHC as the primary predictor, (3) for the combined sample of all 10 index procedure admissions with each MHC category versus no MHC as a primary predictor, and (4) for each procedure index admission with any MHC versus no MHC as the primary predictor. All analyses were weighted to achieve national estimates and clustered by hospital by using AHRQ-recommended survey procedures. SAS version 9.4 (SAS Institute, Cary, NC) was used for all analyses. All tests were two-sided, and a P < .05 was
considered statistically significant.
RESULTS
Study Population
Across all index admissions, 16.3% were for children with an MHC. Overall, children with MHCs were older and more likely to have a chronic30 or complex chronic31 physical health condition than children with no MHCs (Table).
Index Medical Admissions, Mental Health Conditions, and Hospital Readmission
The 10 index medical hospitalizations with the most readmissions for children ages 3 to 20 years were asthma, chemotherapy, constipation, diabetes, gastroenteritis, inflammatory bowel disease, neutropenia, pneumonia, seizure, and sickle cell crisis. Across all index medical hospitalizations, 17.5% were for patients with an MHC (Figure 1). Of index medical admissions with any MHC, 26.3% had ADHD, 22.9% had an anxiety disorder, 14.9% had autism, 18.3% had depression, and 30.9% had substance abuse. Among all admissions with MHCs, 28.9% had 2 or more MHCs.
Index Medical Admissions Combined
For all index medical hospitalizations combined, 17.0% (n = 59,138) had an unplanned, 30-day hospital readmission. The rate of 30-day hospital readmissions was higher with versus without an MHC (17.5 vs 16.8%; P < .001). In a multivariable analysis, presence of an MHC was associated with a higher likelihood of hospital readmission following an index medical admission (AOR, 1.23; 95% confidence interval [CI], 1.19-1.26); Figure 1). All MHCs except autism and ADHD had a higher likelihood of readmission (Figure 3).
Specific Index Medical Admissions
Index Procedure Admissions, Mental Health Conditions, and Hospital Readmission
Index Procedure Admissions Combined
Specific Index Procedure Admissions
For specific index procedure admissions, the rate of 30-day hospital readmission ranged from 2.2% for knee procedures to 33.6% for tumor biopsy. For 3 (ie, urinary tract, ventricular shunt, and bowel procedures) of the 10 specific index procedure hospitalizations, having an MHC was associated with higher adjusted odds of 30-day readmission (AOR range, 1.38-2.27; Figure 2).
In total, adjusting for sociodemographic, clinical, and hospital characteristics, MHCs were associated with an additional 2501 medical readmissions and 217 procedure readmissions beyond what would have been expected if MHCs were not associated with readmissions.
DISCUSSION
MHCs are common among pediatric hospitalizations with the highest volume of readmissions; MHCs were present in approximately 1 in 5 medical and 1 in 7 procedure index hospitalizations. Across medical and procedure admissions, the adjusted likelihood of unplanned, all-cause 30-day readmission was 25% higher for children with versus without an MHC. The readmission likelihood varied by the type of medical or procedure admission and by the type of MHC. MHCs had the strongest associations with readmissions following hospitalization for diabetes and urinary tract procedures. The MHC categories associated with the highest readmission likelihood were depression, substance abuse, and multiple MHCs.
The current study complements existing literature by helping establish MHCs as a prevalent and important risk factor for hospital readmission in children. Estimates of the prevalence of MHCs in hospitalized children are between 10% and 25%,10,11,32 and prevalence has increased by as much as 160% over the last 10 years.29 Prior investigations have found that children with an MHC tend to stay longer in the hospital compared with children with no MHC.32 Results from the present study suggest that children with MHCs also experience more inpatient days because of rehospitalizations. Subsequent investigations should strive to understand the mechanisms in the hospital, community, and family environment that are responsible for the increased inpatient utilization in children with MHCs. Understanding how the receipt of mental health services before, during, and after hospitalization influences readmissions could help identify opportunities for practice improvement. Families report the need for better coordination of their child’s medical and mental health care,33 and opportunities exist to improve attendance at mental health visits after acute care encounters.34 Among adults, interventions that address posthospital access to mental healthcare have prevented readmissions.35
Depression was associated with an increased risk of readmission in medical and procedure hospitalizations. As a well-known risk factor for readmission in adult patients,21 depression can adversely affect and exacerbate the physical health recovery of patients experiencing acute and chronic illnesses.14,36,37 Depression is considered a modifiable contributor that, when controlled, may help lower readmission risk. Optimal adherence with behavior and medication treatment for depression is associated with a lower risk of unplanned 30-day readmissions.14-16,19 Emerging evidence demonstrates how multifaceted, psychosocial approaches can improve patients’ adherence with depression treatment plans.38 Increased attention to depression in hospitalized children may uncover new ways to manage symptoms as children transition from hospital to home.
Other MHCs were associated with a different risk of readmission among medical and procedure hospitalizations. For example, ADHD or autism documented during index hospitalization was associated with an increased risk of readmission following procedure hospitalizations and a decreased risk following medical hospitalizations. Perhaps children with ADHD or autism who exhibit hyperactive, impulsive, or repetitive behaviors39,40 are at risk for disrupting their postprocedure wound healing, nutrition recovery, or pain tolerance, which might contribute to increased readmission risk.
MHCs were associated with different readmission risks across specific types of medical or procedure hospitalizations. For example, among medical conditions, the association of readmissions with MHCs was highest for diabetes, which is consistent with prior research.26 Factors that might mediate this relationship include changes in diet and appetite, difficulty with diabetes care plan adherence, and intentional nonadherence as a form of self-harm. Similarly, a higher risk of readmission in chronic medical conditions like asthma, constipation, and sickle cell disease might be mediated by difficulty adhering to medical plans or managing exacerbations at home. In contrast, MHCs had no association with readmission following chemotherapy. In our clinical experience, readmissions following chemotherapy are driven by physiologic problems, such as thrombocytopenia, fever, and/or neutropenia. MHCs might have limited influence over those health issues. For procedure hospitalizations, MHCs had 1 of the strongest associations with ventricular shunt procedures. We hypothesize that MHCs might lead some children to experience general health symptoms that might be associated with shunt malfunction (eg, fatigue, headache, behavior change), which could lead to an increased risk of readmission to evaluate for shunt malfunction. Conversely, we found no relationship between MHCs and readmissions following appendectomy. For appendectomy, MHCs might have limited influence over the development of postsurgical complications (eg, wound infection or ileus). Future research to better elucidate mediators of increased risk of readmission associated with MHCs in certain medical and procedure conditions could help explain these relationships and identify possible future intervention targets to prevent readmissions.
This study has several limitations. The administrative data are not positioned to discover the mechanisms by which MHCs are associated with a higher likelihood of readmission. We used hospital ICD-9-CM codes to identify patients with MHCs. Other methods using more clinically rich data (eg, chart review, prescription medications, etc.) may be preferable to identify patients with MHCs. Although the use of ICD-9-CM codes may have sufficient specificity, some hospitalized children may have an MHC that is not coded. Patients identified by using diagnosis codes could represent patients with a higher severity of illness, patients using medications, or patients whose outpatient records are accessible to make the hospital team aware of the MHC. If documentation of MHCs during hospitalization represents a higher severity of illness, findings may not extrapolate to lower-severity MHCs. As hospitals transition from ICD-9 -CM to ICD-10 coding, and health systems develop more integrated inpatient and outpatient EHRs, diagnostic specificity may improve. We could not analyze the relationships with several potential confounders and explanatory variables that may be related both to the likelihood of having an MHC and the risk of readmission, including medication administration, psychiatric consultation, and parent mental health. Postdischarge health services, including access to a medical home or a usual source of mental healthcare and measures of medication adherence, were not available in the NRD.
Despite these limitations, the current study underscores the importance of MHCs in hospitalized children upon discharge. As subsequent investigations uncover the key drivers explaining the influence of MHCs on hospital readmission risk, hospitals and their local outpatient and community practices may find it useful to consider MHCs when (1) developing contingency plans and establishing follow-up care at discharge,41 (2) exploring opportunities of care integration between mental and physical health care professionals, and (3) devising strategies to reduce hospital readmissions among populations of children.
CONCLUSIONS
MHCs are prevalent in hospitalized children and are associated with an increased risk of 30-day, unplanned hospital readmission. Future readmission prevention efforts may uncover new ways to improve children’s transitions from hospital to home by investigating strategies to address their MHCs.
Acknowledgments
The authors thank Donjo Lau and Troy Richardson for their assistance with the analysis.
Disclosures
Dr. Doupnik was supported by a Ruth L. Kirschstein National Research Service Award institutional training grant (T32-HP010026), funded by the National Institutes of Health. Dr. Zima was supported by the Behavioral Health Centers of Excellence for California (SB852). Dr. Bardach was supported by the National Institute of Child Health and Human Development (K23-HD065836). Dr. Berry was supported by the Agency for Healthcare Research and Quality (R21 HS023092-01). The authors have no financial relationships relevant to this article to disclose. The authors have no potential conflicts of interest to disclose. Dr. Doupnik led the study design and analysis and drafted the initial manuscript. Mr. Lawlor performed the data analysis. Dr. Hall provided statistical consultation. All authors participated in the design of the study, interpretation of the data, revised the manuscript for key intellectual content, and all authors read and approved the final manuscript.
Readmission prevention is a focus of national efforts to improve the quality of hospital care for children.1-5 Several factors contribute to the risk of readmission for hospitalized children, including age, race or ethnicity, payer, and the type and number of comorbid health conditions.6-9 Mental health conditions (MHCs) are a prevalent comorbidity in children hospitalized for physical health reasons that could influence their postdischarge health and safety.
MHCs are increasingly common in children hospitalized for physical health indications; a comorbid MHC is currently present in 10% to 25% of hospitalized children ages 3 years and older.10,11 Hospital length of stay (LOS) and cost are higher in children with an MHC.12,13 Increased resource use may occur because MHCs can impede hospital treatment effectiveness and the child’s recovery from physical illness. MHCs are associated with a lower adherence with medications14-16 and a lower ability to cope with health events and problems.17-19 In adults, MHCs are a well-established risk factor for hospital readmission for a variety of physical health conditions.20-24 Although the influence of MHCs on readmissions in children has not been extensively investigated, higher readmission rates have been reported in adolescents hospitalized for diabetes with an MHC compared with those with no MHC.25,26
To our knowledge, no large studies have examined the relationship between the presence of a comorbid MHC and hospital readmissions in children or adolescents hospitalized for a broad array of medical or procedure conditions. Therefore, we conducted this study to (1) assess the likelihood of 30-day hospital readmission in children with versus without MHC who were hospitalized for one of 10 medical or 10 procedure conditions, and (2) to assess which MHCs are associated with the highest likelihood of hospital readmission.
METHODS
Study Design and Setting
We conducted a national, retrospective cohort study of index hospitalizations for children ages 3 to 21 years who were discharged from January 1, 2013, to November 30, 2013, in the Agency for Healthcare Research and Quality’s (AHRQ) Nationwide Readmissions Database (NRD). Admissions occurring in December 2013 were excluded because they did not have a 30-day timeframe available for readmission measurement. The 2013 NRD includes administrative data for a nationally representative sample of 14 million hospitalizations in 21 states, accounting for 49% of all US hospitalizations and weighted to represent 35.6 million hospitalizations. The database includes deidentified, verified patient linkage numbers so that patients can be tracked across multiple hospitalizations at the same institution or different institutions within a state. The NRD includes hospital information, patient demographic information, and the International Classification of Diseases, 9th Revision-Clinical Modification (ICD-9-CM) discharge diagnoses and procedures, with 1 primary diagnosis and up to 24 additional fields for comorbid diagnoses. This study was approved for exemption by the Children’s Hospital of Philadelphia Institutional Review Board.
Index Admissions
We used the methods described below to create a study cohort of the 10 medical and 10 procedure index admissions associated with the highest volume (ie, the greatest absolute number) of 30-day hospital readmissions. Conditions with a high volume of readmissions were chosen in an effort to identify conditions in which readmission-prevention interventions had the greatest potential to reduce the absolute number of readmissions. We first categorized index hospitalizations for medical and procedure conditions by using the All Patient Refined Diagnosis Related Groups (APR-DRGs; 3M Health Information Systems, Wallingford, CT).27 APR-DRGs use all diagnosis and/or procedure ICD-9-CM codes registered for a hospital discharge to assign 1 reason that best explains the need for hospitalization. We then excluded obstetric hospitalizations, psychiatric hospitalizations, and hospitalizations resulting in death or transfer from being considered as index admissions. Afterwards, we ranked each APR-DRG index hospitalization by the total number of 30-day hospital readmissions that occurred afterward and selected the 10 medical and 10 procedure index admissions with the highest number of readmissions. The APR-DRG index admissions are listed in Figures 1 and 2. For the APR-DRG “digestive system diagnoses,” the most common diagnosis was constipation, and we refer to that category as “constipation.” The most common diagnosis for the APR-DRG called “other operating room procedure for neoplasm” was tumor biopsy, and we refer to that category as “tumor biopsy.”
Main Outcome Measure
The primary study outcome was unplanned, all-cause readmission to any hospital within 30 days of index hospitalization. All-cause readmissions include any hospitalization for the same or different condition as the index admission, including conditions not eligible to be considered as index admissions (obstetric, psychiatric, and hospitalizations resulting in death or transfer). Planned readmissions, identified by using pediatric-specific measure specifications endorsed by AHRQ and the National Quality Forum,28 were excluded from measurement. For index admissions with multiple 30-day readmissions, only the first readmission was counted. Each readmission was treated as an index admission.
Main Independent Variable
The main independent variable was the presence of an MHC documented during the index hospitalization. MHCs were identified and classified into diagnosis categories derived from the AHRQ Chronic Condition Indicator system by using ICD-9-CM codes.29 MHC categories included anxiety disorders, attention-deficit/hyperactivity disorder (ADHD), autism, depression, and substance abuse. Less common MHCs included bipolar disorder, schizophrenia, disruptive behavior disorders, somatoform disorders, and eating disorders. These conditions are included in the group with any MHC, but we did not calculate the adjusted odds ratios (AORs) of readmission for these conditions. Children were identified as having multiple MHCs if they had more than 1 MHC.
Other Characteristics of Index Hospitalizations
A priori, we selected for analysis the known demographic, clinical, and hospital factors associated with the risk of readmission.20-24 The demographic characteristics included patient age, gender, payer category, urban or rural residence, and the median income quartile for a patient’s ZIP code. The hospital characteristics included location, ownership, and teaching hospital designation. The clinical characteristics included the number of chronic conditions30 and indicators for the presence of a complex chronic condition in each of 12 organ systems.31
Statistical Analysis
We calculated descriptive summary statistics for the characteristics of index hospitalizations. We compared characteristics in index admissions of children with versus without MHC by using Wilcoxon Rank-Sum tests for continuous variables and Wald χ2 tests for categorical variables. In the multivariable analysis, we derived logistic regression models to assess the relationship of 30-day hospital readmission with each type of MHC, adjusting for index admission demographic, hospital, and clinical characteristics. MHCs were modeled as binary indicator variables with the presence of any MHC, more than 1 MHC, or each of 5 MHC categories (anxiety disorders, ADHD, autism, depression, substance abuse) compared with no MHC. Four types of logistic regression models were derived (1) for the combined sample of all 10 index medical admissions with each MHC category versus no MHC as a primary predictor, (2) for each medical index admission with any MHC versus no MHC as the primary predictor, (3) for the combined sample of all 10 index procedure admissions with each MHC category versus no MHC as a primary predictor, and (4) for each procedure index admission with any MHC versus no MHC as the primary predictor. All analyses were weighted to achieve national estimates and clustered by hospital by using AHRQ-recommended survey procedures. SAS version 9.4 (SAS Institute, Cary, NC) was used for all analyses. All tests were two-sided, and a P < .05 was
considered statistically significant.
RESULTS
Study Population
Across all index admissions, 16.3% were for children with an MHC. Overall, children with MHCs were older and more likely to have a chronic30 or complex chronic31 physical health condition than children with no MHCs (Table).
Index Medical Admissions, Mental Health Conditions, and Hospital Readmission
The 10 index medical hospitalizations with the most readmissions for children ages 3 to 20 years were asthma, chemotherapy, constipation, diabetes, gastroenteritis, inflammatory bowel disease, neutropenia, pneumonia, seizure, and sickle cell crisis. Across all index medical hospitalizations, 17.5% were for patients with an MHC (Figure 1). Of index medical admissions with any MHC, 26.3% had ADHD, 22.9% had an anxiety disorder, 14.9% had autism, 18.3% had depression, and 30.9% had substance abuse. Among all admissions with MHCs, 28.9% had 2 or more MHCs.
Index Medical Admissions Combined
For all index medical hospitalizations combined, 17.0% (n = 59,138) had an unplanned, 30-day hospital readmission. The rate of 30-day hospital readmissions was higher with versus without an MHC (17.5 vs 16.8%; P < .001). In a multivariable analysis, presence of an MHC was associated with a higher likelihood of hospital readmission following an index medical admission (AOR, 1.23; 95% confidence interval [CI], 1.19-1.26); Figure 1). All MHCs except autism and ADHD had a higher likelihood of readmission (Figure 3).
Specific Index Medical Admissions
Index Procedure Admissions, Mental Health Conditions, and Hospital Readmission
Index Procedure Admissions Combined
Specific Index Procedure Admissions
For specific index procedure admissions, the rate of 30-day hospital readmission ranged from 2.2% for knee procedures to 33.6% for tumor biopsy. For 3 (ie, urinary tract, ventricular shunt, and bowel procedures) of the 10 specific index procedure hospitalizations, having an MHC was associated with higher adjusted odds of 30-day readmission (AOR range, 1.38-2.27; Figure 2).
In total, adjusting for sociodemographic, clinical, and hospital characteristics, MHCs were associated with an additional 2501 medical readmissions and 217 procedure readmissions beyond what would have been expected if MHCs were not associated with readmissions.
DISCUSSION
MHCs are common among pediatric hospitalizations with the highest volume of readmissions; MHCs were present in approximately 1 in 5 medical and 1 in 7 procedure index hospitalizations. Across medical and procedure admissions, the adjusted likelihood of unplanned, all-cause 30-day readmission was 25% higher for children with versus without an MHC. The readmission likelihood varied by the type of medical or procedure admission and by the type of MHC. MHCs had the strongest associations with readmissions following hospitalization for diabetes and urinary tract procedures. The MHC categories associated with the highest readmission likelihood were depression, substance abuse, and multiple MHCs.
The current study complements existing literature by helping establish MHCs as a prevalent and important risk factor for hospital readmission in children. Estimates of the prevalence of MHCs in hospitalized children are between 10% and 25%,10,11,32 and prevalence has increased by as much as 160% over the last 10 years.29 Prior investigations have found that children with an MHC tend to stay longer in the hospital compared with children with no MHC.32 Results from the present study suggest that children with MHCs also experience more inpatient days because of rehospitalizations. Subsequent investigations should strive to understand the mechanisms in the hospital, community, and family environment that are responsible for the increased inpatient utilization in children with MHCs. Understanding how the receipt of mental health services before, during, and after hospitalization influences readmissions could help identify opportunities for practice improvement. Families report the need for better coordination of their child’s medical and mental health care,33 and opportunities exist to improve attendance at mental health visits after acute care encounters.34 Among adults, interventions that address posthospital access to mental healthcare have prevented readmissions.35
Depression was associated with an increased risk of readmission in medical and procedure hospitalizations. As a well-known risk factor for readmission in adult patients,21 depression can adversely affect and exacerbate the physical health recovery of patients experiencing acute and chronic illnesses.14,36,37 Depression is considered a modifiable contributor that, when controlled, may help lower readmission risk. Optimal adherence with behavior and medication treatment for depression is associated with a lower risk of unplanned 30-day readmissions.14-16,19 Emerging evidence demonstrates how multifaceted, psychosocial approaches can improve patients’ adherence with depression treatment plans.38 Increased attention to depression in hospitalized children may uncover new ways to manage symptoms as children transition from hospital to home.
Other MHCs were associated with a different risk of readmission among medical and procedure hospitalizations. For example, ADHD or autism documented during index hospitalization was associated with an increased risk of readmission following procedure hospitalizations and a decreased risk following medical hospitalizations. Perhaps children with ADHD or autism who exhibit hyperactive, impulsive, or repetitive behaviors39,40 are at risk for disrupting their postprocedure wound healing, nutrition recovery, or pain tolerance, which might contribute to increased readmission risk.
MHCs were associated with different readmission risks across specific types of medical or procedure hospitalizations. For example, among medical conditions, the association of readmissions with MHCs was highest for diabetes, which is consistent with prior research.26 Factors that might mediate this relationship include changes in diet and appetite, difficulty with diabetes care plan adherence, and intentional nonadherence as a form of self-harm. Similarly, a higher risk of readmission in chronic medical conditions like asthma, constipation, and sickle cell disease might be mediated by difficulty adhering to medical plans or managing exacerbations at home. In contrast, MHCs had no association with readmission following chemotherapy. In our clinical experience, readmissions following chemotherapy are driven by physiologic problems, such as thrombocytopenia, fever, and/or neutropenia. MHCs might have limited influence over those health issues. For procedure hospitalizations, MHCs had 1 of the strongest associations with ventricular shunt procedures. We hypothesize that MHCs might lead some children to experience general health symptoms that might be associated with shunt malfunction (eg, fatigue, headache, behavior change), which could lead to an increased risk of readmission to evaluate for shunt malfunction. Conversely, we found no relationship between MHCs and readmissions following appendectomy. For appendectomy, MHCs might have limited influence over the development of postsurgical complications (eg, wound infection or ileus). Future research to better elucidate mediators of increased risk of readmission associated with MHCs in certain medical and procedure conditions could help explain these relationships and identify possible future intervention targets to prevent readmissions.
This study has several limitations. The administrative data are not positioned to discover the mechanisms by which MHCs are associated with a higher likelihood of readmission. We used hospital ICD-9-CM codes to identify patients with MHCs. Other methods using more clinically rich data (eg, chart review, prescription medications, etc.) may be preferable to identify patients with MHCs. Although the use of ICD-9-CM codes may have sufficient specificity, some hospitalized children may have an MHC that is not coded. Patients identified by using diagnosis codes could represent patients with a higher severity of illness, patients using medications, or patients whose outpatient records are accessible to make the hospital team aware of the MHC. If documentation of MHCs during hospitalization represents a higher severity of illness, findings may not extrapolate to lower-severity MHCs. As hospitals transition from ICD-9 -CM to ICD-10 coding, and health systems develop more integrated inpatient and outpatient EHRs, diagnostic specificity may improve. We could not analyze the relationships with several potential confounders and explanatory variables that may be related both to the likelihood of having an MHC and the risk of readmission, including medication administration, psychiatric consultation, and parent mental health. Postdischarge health services, including access to a medical home or a usual source of mental healthcare and measures of medication adherence, were not available in the NRD.
Despite these limitations, the current study underscores the importance of MHCs in hospitalized children upon discharge. As subsequent investigations uncover the key drivers explaining the influence of MHCs on hospital readmission risk, hospitals and their local outpatient and community practices may find it useful to consider MHCs when (1) developing contingency plans and establishing follow-up care at discharge,41 (2) exploring opportunities of care integration between mental and physical health care professionals, and (3) devising strategies to reduce hospital readmissions among populations of children.
CONCLUSIONS
MHCs are prevalent in hospitalized children and are associated with an increased risk of 30-day, unplanned hospital readmission. Future readmission prevention efforts may uncover new ways to improve children’s transitions from hospital to home by investigating strategies to address their MHCs.
Acknowledgments
The authors thank Donjo Lau and Troy Richardson for their assistance with the analysis.
Disclosures
Dr. Doupnik was supported by a Ruth L. Kirschstein National Research Service Award institutional training grant (T32-HP010026), funded by the National Institutes of Health. Dr. Zima was supported by the Behavioral Health Centers of Excellence for California (SB852). Dr. Bardach was supported by the National Institute of Child Health and Human Development (K23-HD065836). Dr. Berry was supported by the Agency for Healthcare Research and Quality (R21 HS023092-01). The authors have no financial relationships relevant to this article to disclose. The authors have no potential conflicts of interest to disclose. Dr. Doupnik led the study design and analysis and drafted the initial manuscript. Mr. Lawlor performed the data analysis. Dr. Hall provided statistical consultation. All authors participated in the design of the study, interpretation of the data, revised the manuscript for key intellectual content, and all authors read and approved the final manuscript.
1. Dougherty D, Schiff J, Mangione-Smith R. The Children’s Health Insurance Program Reauthorization Act quality measures initiatives: moving forward to improve measurement, care, and child and adolescent outcomes. Acad Pediatr. 2011;11(3):S1-S10. PubMed
2. Bardach NS, Vittinghoff E, Asteria-Penaloza R, et al. Measuring Hospital Quality Using Pediatric Readmission and Revisit Rates. Pediatrics. 2013;132(3):429-436. doi:10.1542/peds.2012-3527. PubMed
3. Khan A, Nakamura MM, Zaslavsky AM, et al. Same-Hospital Readmission Rates as a Measure of Pediatric Quality of Care. JAMA Pediatr. 2015;169(10):905-912. doi:10.1001/jamapediatrics.2015.1129. PubMed
4. Fassl BA, Nkoy FL, Stone BL, et al. The Joint Commission Children’s Asthma Care quality measures and asthma readmissions. Pediatrics. 2012;130(3):482-491. doi:10.1542/peds.2011-3318. PubMed
5. Hain PD, Gay JC, Berutti TW, Whitney GM, Wang W, Saville BR. Preventability of Early Readmissions at a Children’s Hospital. Pediatrics. 2013;131(1):e171-e181. doi:10.1542/peds.2012-0820. PubMed
6. Nagasako E, Reidhead B, Waterman B, et al. Adding Socioeconomic Data to Hospital Readmissions Calculations May Produce More Useful Results. Health Aff. 2014;33(5):786-791. PubMed
7. Hu J, Gonsahn MD, Nerenz DR. Socioeconomic Status and Readmissions: Evidence from an Urban Teaching Hospital. Health Aff. 2014;33(5):778-785. doi:10.1377/hlthaff.2013.0816. PubMed
8. Sills MR, Hall M, Colvin JD, et al. Association of Social Determinants with Children’s Hospitals’ Preventable Readmissions Performance. JAMA Pediatr. 2016;170(4):350-358. doi:10.1001/jamapediatrics.2015.4440. PubMed
9. Eselius LL, Cleary PD, Zaslavsky AM, Huskamp HA, Busch SH. Case-Mix Adjustment of Consumer Reports about Managed Behavioral Health Care and Health Plans. Health Serv Res. 2008;43(6):2014-2032. doi:10.1111/j.1475-6773.2008.00894.x. PubMed
10. Doupnik SK, Henry MK, Bae H, et al. Mental Health Conditions and Symptoms in Pediatric Hospitalizations: A Single-Center Point Prevalence Study. Acad Pediatr. 2017;17(2):184-190. PubMed
11. Bardach NS, Coker TR, Zima BT, et al. Common and Costly Hospitalizations for Pediatric Mental Health Disorders. Pediatrics. 2014;133(4):602-609. doi:10.1542/peds.2013-3165. PubMed
12. Doupnik SK, Mitra N, Feudtner C, Marcus SC. The Influence of Comorbid Mood and Anxiety Disorders on Outcomes of Pediatric Patients Hospitalized for Pneumonia. Hosp Pediatr. 2016;6(3):135-142. doi:10.1542/hpeds.2015-0177. PubMed
13. Snell C, Fernandes S, Bujoreanu IS, Garcia G. Depression, illness severity, and healthcare utilization in cystic fibrosis. Pediatr Pulmonol. 2014;49(12):1177-1181. doi:10.1002/ppul.22990. PubMed
14. DiMatteo MR, Lepper HS, Croghan TW. Depression Is a Risk Factor for Noncompliance with Medical Treatment: Meta-analysis of the Effects of Anxiety and Depression on Patient Adherence. Arch Intern Med . 2000;160(14):2101-2107. doi:10.1001/archinte.160.14.2101. PubMed
15. Gray WN, Denson LA, Baldassano RN, Hommel KA. Treatment Adherence in Adolescents with Inflammatory Bowel Disease: The Collective Impact of Barriers to Adherence and Anxiety/Depressive Symptoms. J Pediatr Psychol. 2012;37(3):282-291. doi:10.1093/jpepsy/jsr092. PubMed
16. Mosnaim G, Li H, Martin M, et al. Factors associated with levels of adherence to inhaled corticosteroids in minority adolescents with asthma. Ann Allergy Asthma Immunol. 2014;112(2):116-120. doi:10.1016/j.anai.2013.11.021. PubMed
17. Compas BE, Jaser SS, Dunn MJ, Rodriguez EM. Coping with Chronic Illness in Childhood and Adolescence. Ann Rev Clin Psychol. 2012;8(1):455-480. doi:10.1146/annurev-clinpsy-032511-143108. PubMed
18. Graue M, Wentzel-Larsen T, Bru E, Hanestad BR, Søvik O. The coping styles of adolescents with type 1 diabetes are associated with degree of metabolic control. Diabetes Care. 2004;27(6):1313-1317. PubMed
19. Jaser SS, White LE. Coping and resilience in adolescents with type 1 diabetes. Child Care Health Dev. 2011;37(3):335-342. doi:10.1111/j.1365-2214.2010.01184.x. PubMed
20. Cancino RS, Culpepper L, Sadikova E, Martin J, Jack BW, Mitchell SE. Dose-response relationship between depressive symptoms and hospital readmission. J Hosp Med. 2014;9(6):358-364. doi:10.1002/jhm.2180. PubMed
21. Pederson JL, Warkentin LM, Majumdar SR, McAlister FA. Depressive symptoms are associated with higher rates of readmission or mortality after medical hospitalization: A systematic review and meta-analysis. J Hosp Med. 2016;11(5):373-380. doi:10.1002/jhm.2547. PubMed
22. Chwastiak LA, Davydow DS, McKibbin CL, et al. The Effect of Serious Mental Illness on the Risk of Rehospitalization Among Patients with Diabetes. Psychosomatics. 2014;55(2):134-143. PubMed
23. Daratha KB, Barbosa-Leiker C, H Burley M, et al. Co-occurring mood disorders among hospitalized patients and risk for subsequent medical hospitalization. Gen Hosp Psychiatry. 2012;34(5):500-505. doi:10.1016/j.genhosppsych.2012.05.001. PubMed
24. Kartha A, Anthony D, Manasseh CS, et al. Depression is a risk factor for rehospitalization in medical inpatients. Prim Care Companion J Clin Psychiatry. 2007;9(4):256-262. PubMed
25. Myrvik MP, Burks LM, Hoffman RG, Dasgupta M, Panepinto JA. Mental health disorders influence admission rates for pain in children with sickle cell disease. Pediatr Blood Cancer. 2013;60(7):1211-1214. doi:10.1002/pbc.24394. PubMed
26. Garrison MM, Katon WJ, Richardson LP. The impact of psychiatric comorbidities on readmissions for diabetes in youth. Diabetes Care. 2005;28(9):2150-2154. PubMed
27. Averill R, Goldfield N, Hughes JS, et al. All Patient Refined Diagnosis Related Groups (APR-DRGs) Version 20.0: Methodology Overview. https://www.hcup-us.ahrq.gov/db/nation/nis/APR-DRGsV20MethodologyOverviewandBibliography.pdf. Accessed on November 2, 2016.
28. Berry JG, Toomey SL, Zaslavsky AM, et al. Pediatric readmission prevalence and variability across hospitals. JAMA. 2013;309(4):372-380. PubMed
29. Zima BT, Rodean J, Hall M, Bardach NS, Coker TR, Berry JG. Psychiatric Disorders and Trends in Resource Use in Pediatric Hospitals. Pediatrics. 2016;138(5):e20160909-e20160909. doi:10.1542/peds.2016-0909. PubMed
30. Chronic Condition Indicator (CCI) for ICD-9-CM. Healthcare Cost and Utilization Project (HCUP) Tools & Software Page. http://www.hcup-us.ahrq.gov/toolssoftware/chronic/chronic.jsp. Accessed on October 30, 2015.
31. Feudtner C, Feinstein J, Zhong W, Hall M, Dai D. Pediatric complex chronic conditions classification system version 2: updated for ICD-10 and complex medical technology dependence and transplantation. BMC Pediatr. 2014;14(1):199-205. PubMed
32. Doupnik S, Lawlor J, Zima BT, et al. Mental Health Conditions and Medical and Surgical Hospital Utilization. Pediatrics. 2016;138(6):e20162416. doi:10.1542/peds.2016-2416. PubMed
33. Brown NM, Green JC, Desai MM, Weitzman CC, Rosenthal MS. Need and Unmet Need for Care Coordination Among Children with Mental Health Conditions. Pediatrics. 2014;133(3):e530-e537. doi:10.1542/peds.2013-2590. PubMed
34. Sobolewski B, Richey L, Kowatch RA, Grupp-Phelan J. Mental health follow-up among adolescents with suicidal behaviors after emergency department discharge. Arch Suicide Res. 2013;17(4):323-334. doi:10.1080/13811118.2013.801807. PubMed
35. Hansen LO, Greenwald JL, Budnitz T, et al. Project BOOST: Effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8):421-427. doi:10.1002/jhm.2054. PubMed
36. Di Marco F, Verga M, Santus P, et al. Close correlation between anxiety, depression, and asthma control. Respir Med. 2010;104(1):22-28. doi:10.1016/j.rmed.2009.08.005. PubMed
37. Ghose SS, Williams LS, Swindle RW. Depression and other mental health diagnoses after stroke increase inpatient and outpatient medical utilization three years poststroke. Med Care. 2005;43(12):1259-1264. PubMed
38. Szigethy E, Bujoreanu SI, Youk AO, et al. Randomized efficacy trial of two psychotherapies for depression in youth with inflammatory bowel disease. J Am Acad Child Adolesc Psychiatry. 2014;53(7):726-735. PubMed
39. Swensen A, Birnbaum HG, Ben Hamadi R, Greenberg P, Cremieux PY, Secnik K. Incidence and costs of accidents among attention-deficit/hyperactivity disorder patients. J Adolesc Health. 2004;35(4):346.e1-346.e9. doi:10.1016/j.jadohealth.2003.12.003. PubMed
40. Chan E, Zhan C, Homer CJ. Health Care Use and Costs for Children with Attention-Deficit/Hyperactivity Disorder: National Estimates from the Medical Expenditure Panel Survey. Arch Pediatr Adolesc Med. 2002;156(5):504-511. doi:10.1001/archpedi.156.5.504. PubMed
41. Berry JG, Blaine K, Rogers J, et al. A Framework of Pediatric Hospital Discharge Care Informed by Legislation, Research, and Practice. JAMA Pediatr. 2014;168(10):955-962. doi:10.1001/jamapediatrics.2014.891. PubMed
1. Dougherty D, Schiff J, Mangione-Smith R. The Children’s Health Insurance Program Reauthorization Act quality measures initiatives: moving forward to improve measurement, care, and child and adolescent outcomes. Acad Pediatr. 2011;11(3):S1-S10. PubMed
2. Bardach NS, Vittinghoff E, Asteria-Penaloza R, et al. Measuring Hospital Quality Using Pediatric Readmission and Revisit Rates. Pediatrics. 2013;132(3):429-436. doi:10.1542/peds.2012-3527. PubMed
3. Khan A, Nakamura MM, Zaslavsky AM, et al. Same-Hospital Readmission Rates as a Measure of Pediatric Quality of Care. JAMA Pediatr. 2015;169(10):905-912. doi:10.1001/jamapediatrics.2015.1129. PubMed
4. Fassl BA, Nkoy FL, Stone BL, et al. The Joint Commission Children’s Asthma Care quality measures and asthma readmissions. Pediatrics. 2012;130(3):482-491. doi:10.1542/peds.2011-3318. PubMed
5. Hain PD, Gay JC, Berutti TW, Whitney GM, Wang W, Saville BR. Preventability of Early Readmissions at a Children’s Hospital. Pediatrics. 2013;131(1):e171-e181. doi:10.1542/peds.2012-0820. PubMed
6. Nagasako E, Reidhead B, Waterman B, et al. Adding Socioeconomic Data to Hospital Readmissions Calculations May Produce More Useful Results. Health Aff. 2014;33(5):786-791. PubMed
7. Hu J, Gonsahn MD, Nerenz DR. Socioeconomic Status and Readmissions: Evidence from an Urban Teaching Hospital. Health Aff. 2014;33(5):778-785. doi:10.1377/hlthaff.2013.0816. PubMed
8. Sills MR, Hall M, Colvin JD, et al. Association of Social Determinants with Children’s Hospitals’ Preventable Readmissions Performance. JAMA Pediatr. 2016;170(4):350-358. doi:10.1001/jamapediatrics.2015.4440. PubMed
9. Eselius LL, Cleary PD, Zaslavsky AM, Huskamp HA, Busch SH. Case-Mix Adjustment of Consumer Reports about Managed Behavioral Health Care and Health Plans. Health Serv Res. 2008;43(6):2014-2032. doi:10.1111/j.1475-6773.2008.00894.x. PubMed
10. Doupnik SK, Henry MK, Bae H, et al. Mental Health Conditions and Symptoms in Pediatric Hospitalizations: A Single-Center Point Prevalence Study. Acad Pediatr. 2017;17(2):184-190. PubMed
11. Bardach NS, Coker TR, Zima BT, et al. Common and Costly Hospitalizations for Pediatric Mental Health Disorders. Pediatrics. 2014;133(4):602-609. doi:10.1542/peds.2013-3165. PubMed
12. Doupnik SK, Mitra N, Feudtner C, Marcus SC. The Influence of Comorbid Mood and Anxiety Disorders on Outcomes of Pediatric Patients Hospitalized for Pneumonia. Hosp Pediatr. 2016;6(3):135-142. doi:10.1542/hpeds.2015-0177. PubMed
13. Snell C, Fernandes S, Bujoreanu IS, Garcia G. Depression, illness severity, and healthcare utilization in cystic fibrosis. Pediatr Pulmonol. 2014;49(12):1177-1181. doi:10.1002/ppul.22990. PubMed
14. DiMatteo MR, Lepper HS, Croghan TW. Depression Is a Risk Factor for Noncompliance with Medical Treatment: Meta-analysis of the Effects of Anxiety and Depression on Patient Adherence. Arch Intern Med . 2000;160(14):2101-2107. doi:10.1001/archinte.160.14.2101. PubMed
15. Gray WN, Denson LA, Baldassano RN, Hommel KA. Treatment Adherence in Adolescents with Inflammatory Bowel Disease: The Collective Impact of Barriers to Adherence and Anxiety/Depressive Symptoms. J Pediatr Psychol. 2012;37(3):282-291. doi:10.1093/jpepsy/jsr092. PubMed
16. Mosnaim G, Li H, Martin M, et al. Factors associated with levels of adherence to inhaled corticosteroids in minority adolescents with asthma. Ann Allergy Asthma Immunol. 2014;112(2):116-120. doi:10.1016/j.anai.2013.11.021. PubMed
17. Compas BE, Jaser SS, Dunn MJ, Rodriguez EM. Coping with Chronic Illness in Childhood and Adolescence. Ann Rev Clin Psychol. 2012;8(1):455-480. doi:10.1146/annurev-clinpsy-032511-143108. PubMed
18. Graue M, Wentzel-Larsen T, Bru E, Hanestad BR, Søvik O. The coping styles of adolescents with type 1 diabetes are associated with degree of metabolic control. Diabetes Care. 2004;27(6):1313-1317. PubMed
19. Jaser SS, White LE. Coping and resilience in adolescents with type 1 diabetes. Child Care Health Dev. 2011;37(3):335-342. doi:10.1111/j.1365-2214.2010.01184.x. PubMed
20. Cancino RS, Culpepper L, Sadikova E, Martin J, Jack BW, Mitchell SE. Dose-response relationship between depressive symptoms and hospital readmission. J Hosp Med. 2014;9(6):358-364. doi:10.1002/jhm.2180. PubMed
21. Pederson JL, Warkentin LM, Majumdar SR, McAlister FA. Depressive symptoms are associated with higher rates of readmission or mortality after medical hospitalization: A systematic review and meta-analysis. J Hosp Med. 2016;11(5):373-380. doi:10.1002/jhm.2547. PubMed
22. Chwastiak LA, Davydow DS, McKibbin CL, et al. The Effect of Serious Mental Illness on the Risk of Rehospitalization Among Patients with Diabetes. Psychosomatics. 2014;55(2):134-143. PubMed
23. Daratha KB, Barbosa-Leiker C, H Burley M, et al. Co-occurring mood disorders among hospitalized patients and risk for subsequent medical hospitalization. Gen Hosp Psychiatry. 2012;34(5):500-505. doi:10.1016/j.genhosppsych.2012.05.001. PubMed
24. Kartha A, Anthony D, Manasseh CS, et al. Depression is a risk factor for rehospitalization in medical inpatients. Prim Care Companion J Clin Psychiatry. 2007;9(4):256-262. PubMed
25. Myrvik MP, Burks LM, Hoffman RG, Dasgupta M, Panepinto JA. Mental health disorders influence admission rates for pain in children with sickle cell disease. Pediatr Blood Cancer. 2013;60(7):1211-1214. doi:10.1002/pbc.24394. PubMed
26. Garrison MM, Katon WJ, Richardson LP. The impact of psychiatric comorbidities on readmissions for diabetes in youth. Diabetes Care. 2005;28(9):2150-2154. PubMed
27. Averill R, Goldfield N, Hughes JS, et al. All Patient Refined Diagnosis Related Groups (APR-DRGs) Version 20.0: Methodology Overview. https://www.hcup-us.ahrq.gov/db/nation/nis/APR-DRGsV20MethodologyOverviewandBibliography.pdf. Accessed on November 2, 2016.
28. Berry JG, Toomey SL, Zaslavsky AM, et al. Pediatric readmission prevalence and variability across hospitals. JAMA. 2013;309(4):372-380. PubMed
29. Zima BT, Rodean J, Hall M, Bardach NS, Coker TR, Berry JG. Psychiatric Disorders and Trends in Resource Use in Pediatric Hospitals. Pediatrics. 2016;138(5):e20160909-e20160909. doi:10.1542/peds.2016-0909. PubMed
30. Chronic Condition Indicator (CCI) for ICD-9-CM. Healthcare Cost and Utilization Project (HCUP) Tools & Software Page. http://www.hcup-us.ahrq.gov/toolssoftware/chronic/chronic.jsp. Accessed on October 30, 2015.
31. Feudtner C, Feinstein J, Zhong W, Hall M, Dai D. Pediatric complex chronic conditions classification system version 2: updated for ICD-10 and complex medical technology dependence and transplantation. BMC Pediatr. 2014;14(1):199-205. PubMed
32. Doupnik S, Lawlor J, Zima BT, et al. Mental Health Conditions and Medical and Surgical Hospital Utilization. Pediatrics. 2016;138(6):e20162416. doi:10.1542/peds.2016-2416. PubMed
33. Brown NM, Green JC, Desai MM, Weitzman CC, Rosenthal MS. Need and Unmet Need for Care Coordination Among Children with Mental Health Conditions. Pediatrics. 2014;133(3):e530-e537. doi:10.1542/peds.2013-2590. PubMed
34. Sobolewski B, Richey L, Kowatch RA, Grupp-Phelan J. Mental health follow-up among adolescents with suicidal behaviors after emergency department discharge. Arch Suicide Res. 2013;17(4):323-334. doi:10.1080/13811118.2013.801807. PubMed
35. Hansen LO, Greenwald JL, Budnitz T, et al. Project BOOST: Effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8):421-427. doi:10.1002/jhm.2054. PubMed
36. Di Marco F, Verga M, Santus P, et al. Close correlation between anxiety, depression, and asthma control. Respir Med. 2010;104(1):22-28. doi:10.1016/j.rmed.2009.08.005. PubMed
37. Ghose SS, Williams LS, Swindle RW. Depression and other mental health diagnoses after stroke increase inpatient and outpatient medical utilization three years poststroke. Med Care. 2005;43(12):1259-1264. PubMed
38. Szigethy E, Bujoreanu SI, Youk AO, et al. Randomized efficacy trial of two psychotherapies for depression in youth with inflammatory bowel disease. J Am Acad Child Adolesc Psychiatry. 2014;53(7):726-735. PubMed
39. Swensen A, Birnbaum HG, Ben Hamadi R, Greenberg P, Cremieux PY, Secnik K. Incidence and costs of accidents among attention-deficit/hyperactivity disorder patients. J Adolesc Health. 2004;35(4):346.e1-346.e9. doi:10.1016/j.jadohealth.2003.12.003. PubMed
40. Chan E, Zhan C, Homer CJ. Health Care Use and Costs for Children with Attention-Deficit/Hyperactivity Disorder: National Estimates from the Medical Expenditure Panel Survey. Arch Pediatr Adolesc Med. 2002;156(5):504-511. doi:10.1001/archpedi.156.5.504. PubMed
41. Berry JG, Blaine K, Rogers J, et al. A Framework of Pediatric Hospital Discharge Care Informed by Legislation, Research, and Practice. JAMA Pediatr. 2014;168(10):955-962. doi:10.1001/jamapediatrics.2014.891. PubMed
© 2018 Society of Hospital Medicine
Using Simulation to Enhance Care of Older Veterans
Enhancing patient-centered care is an important priority for caregivers in all settings but particularly in long-term care (LTC) where patients also are residents. Simulation is a potential strategy to effect cultural change for health care providers at LTC facilities. In a clinical setting, simulation is an educational model that allows staff to practice behaviors or skills without putting patients at risk. Due to limited time, staffing, and budget resources, the use of simulation for training is not common at LTC facilities.
Background
The simulation model is considered an effective teaching and learning strategy for replicating experiences in nursing practice.1,2 The interactive experience provides the learner with opportunities to engage with patients through psychomotor participation, critical thinking, reflection, and debriefing. Prelicensure nursing education programs and acute care hospitals are the most common users of simulation learning. However, there is a paucity of literature addressing the use of simulation in LTC.
One study was conducted in 2002 by P.K. Beville called the Virtual Dementia Tour, a program using evidence-based simulation. Beville found that study participants using the simulation model had a heightened awareness of the challenges of confused elderly as well as unrealistic expectations by caregivers.3 Although the Virtual Dementia Tour is available for a fee for training professional caregivers, lay people, family, and first responders, many LTC facilities do not have sufficient funding for simulation and simulation equipment, and many do not have dedicated staff for nursing education. Most staff in LTC facilities are unlicensed and may not have had simulation training experience. Additionally, due to staffing and budget constraints, staff education may be limited.
This article will describe the successful implementation of a simulation-based quality improvement project created by and used at the Louis Stokes Cleveland VA Medical Center (LSCVAMC) LTC facility. The LSCVAMC has acute care beds and is adjacent to its LTC facility. Also, a previously successful simulation educational program to improve delirium care was conducted at this acute care hospital.4
Experiential Learning Opportunity
Many residents in a LTC facility have been diagnosed with dementia. As part of a cultural transformation at LSCVAMC, a simulation program was used to help sensitize LTC caregivers to the many sensory changes that occur in older veterans with dementia. The program was guided by the Kolb model.5
The Kolb model of experiential learning includes 4 elements: abstract conceptualization (knowledge), active experimentation (application), concrete experience (engagement), and reflective observation (self-evaluation).5 A simulation program can touch all 4 elements of the Kolb model by providing an educational experience for all learning styles as well as facilitating critical thinking. Nursing homes that provide care to residents with dementia are required to include dementia education annually to staff.6 Long-term care facilities can take advantage of using simulation education along with their traditional educational programs to provide staff with exposure to realistic resident care conditions.7
Methods
The simulation learning experience was provided to all nursing, recreation therapy, and rehabilitation services staff at the LTC facility. The goal was to create an affective, psychomotor learning experience that refreshed, reminded, and sensitized the staff to the challenges that many residents face. The LSCVAMC LTC leadership was supportive of this simulation model because it was not time intensive for direct care staff, and the materials needed were inexpensive. The only equipment that was purchased were several eyeglass readers, popcorn kernels, and Vaseline, resulting in a budget of about $10. The simulation program was scheduled on all shifts. In addition to the simulation experience, the model consists of pre- and postsurveys and a dementia review handout. Staff were able to complete a pre- and postsurvey as well as a debriefing all within a 30-minute time slot.
The pre- and posteducation surveys used were designed to measure learnings and provide data for future education planning. The surveys required only a yes/no and short answers. To reduce the total time of participants’ involvement in the simulation program, an online survey was used. Presurvey questions were designed to identify basic knowledge and experience with dementia, both at work and in personal life. The postsurvey questions sought to identify affective feelings about the participants experience as well as lessons learned and how that could impact future care.
The dementia review handout that was provided to staff 2 weeks before the simulation provided an overview of dementia. It included communication techniques and care planning suggestions.8 The time spent in the simulation room was about 10 to 15 minutes but depended on the activity. The total in-service time was about 30 minutes, depending on the time allotted for debriefing. Room choice was influenced by the number of participants performing the simulation at the same time. Activity stations/tables generally provided 1 experience at a time.
The room that was used had adjustable lighting with the ability to provide a low light setting. Activities were chosen based on the goals for the physical and cognitive disabilities to be simulated. Table 1 identifies equipment used with success and chosen with consideration for ease and expense in describing the disability. 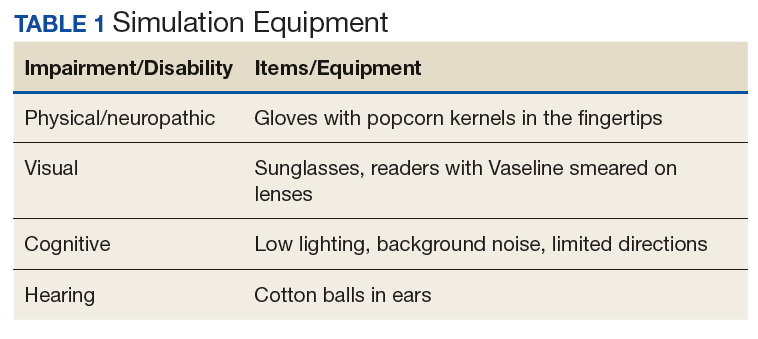
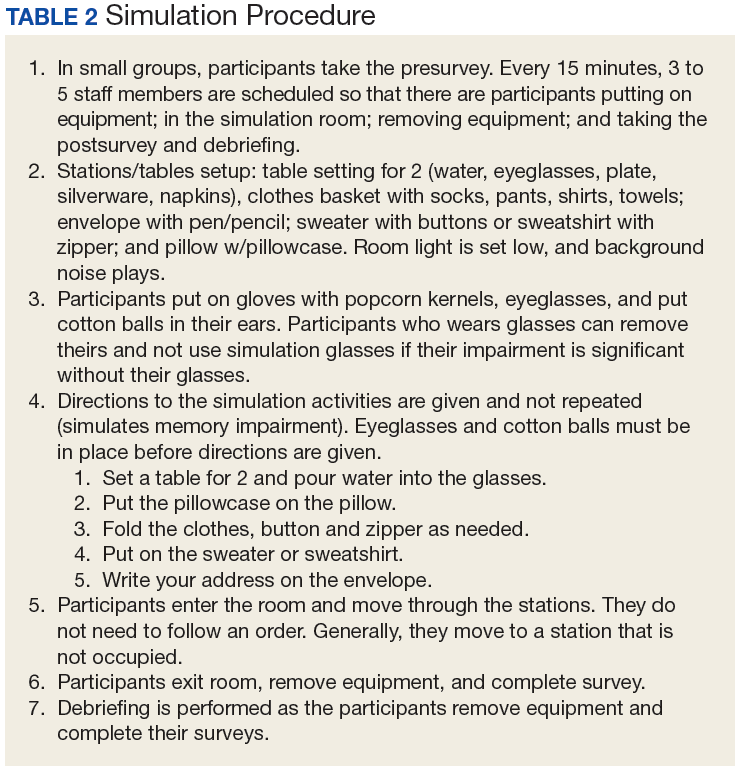
Simulation activities were based on the staff learning needs determined by the presimulation survey. Simulated deficits impacted activities of daily living, mood, and cognition. Neuropathy, arthritis, paralysis, dementia, glaucoma, cataracts, and hearing loss are conditions that are easily represented in a simulation.
Participants also gained additional knowledge of dementia through the Kolb process, which was included in the debriefing. The survey followed the completion of the simulation session to identify knowledge deficits for general remediation and program development and expansion.
Discussion
During the dementia simulation, active experimentation or application learning may be counterintuitive. Staff do not apply their knowledge of dementia directly as in other education settings where they can practice or demonstrate a skill. Instead, participants experience care from the perspective of residents. This learning transitions well into reflective observation as the participants begin to understand the challenges of the cognitively impaired resident, which are manifested in the residents’ behaviors.
Debriefing and a postsimulation survey provide a guided reflection to assimilate new knowledge and revise presimulation attitudes about dementia.9 Reflective observation or self-evaluation is a learning activity that is not a routine part of staff education but can be a powerful learning tool. The postsimulation survey incorporated Bloom’s taxonomy: the affective domain of learning by challenging staff to organize their values with the experience and resolving in their mind any conflicts.10 The goal of the process is to help internalize the education by encouraging changes in behavior (in this case dementia care) and considering the new experience.
Survey Results
The 30-minute program allowed 155 staff to experience cognitive and physical impairment while completing tasks. The pre- and postsurveys were analyzed by 2 learning and dementia survey content experts. The survey questions were open-ended with the intention of eliciting affective behavior responses and staff could provide comments (See eTables 1 and 2 at www.mdedge.com/fedprac). All participants indicated they had knowledge of dementia before the simulation, but 70% acknowledged in the postsimulation survey that they did not have the dementia knowledge that they thought they had. Patience and understanding were most commonly reported in the reflective observation/affective domain (values are internalized leading to changes in behavior).
Participants also described success in closing the loop of experiential learning as a result of the simulation. Some participants verbalized experiencing emotional distress when they realized that their temporary, frustrating impairment was a permanent condition for the residents. Postexperience comments supported the success of the Kolb model experiential learning activity.
Conclusion
Dementia simulation can augment didactic education for improving the quality of dementia care. The virtual dementia simulation was an inexpensive educational program that did not adversely impact scheduling or patient care in a LTC facility. Care providers provided anecdotal feedback that suggested that the program increased their awareness of the difficulty of performing activities of daily living for patients with dementia. The simulation touched all 4 elements of the Kolb Model. The participants had gained new knowledge or reinforced existing knowledge. The simulation activities addressed the application and engagement parts of the model. Self-evaluation resulted from the debriefing time and postsurvey questions. The virtual dementia simulation will be repeated with additional debrief time and a long-term follow-up survey to identify additional learning needs and changes in professional practice.
Acknowledgments
The author thanks Nurse Educator Lisa Weber, MSN, RN-BC, for her contribution to the manuscript.
1. Aebersold M, Tschannen D. Simulation in nursing practice: the impact on patient care. Online J Issues Nurs. 2013;18(2):6.
2. Mariani B, Doolen J. Nursing simulation research: what are the perceived gaps? Clin Simulation in Nurs. 2016;12(1):30-36.
3. Beville PK. Virtual Dementia Tour helps sensitize health care providers. Am J Alzheimers Dis Other Demen. 2002;17(3):183-190.
4. Kresevic D, Heath B, Fine-Smilovich E, et al. Simulation training, coaching, and cue cards improve delirium care. Fed Pract. 2016;33(12):22-28.
5. Chmil JV, Turk M, Adamson K, Larew C. Effects of an experiential learning simulation design on clinical nursing judgment development. Nurse Educ. 2015;40(5):228-232.
6. Centers for Medicare & Medicaid Services. Medicare and Medicaid programs; reform of requirements for long-term care facilities, final rule. https://www.federalregister.gov/documents/2016/10/04/2016-23503/medicare-and-medicaid-programs-reform-of-requirements-for-long-term-care-facilities. Published October 4, 2016. Accessed May 22, 2018.
7. Donahoe J, Moon L, VanCleave K. Increasing student empathy toward older adults using the virtual dementia tour. J Baccalaureate Soc Work. 2014;19(1):S23-S40.
8. Coggins MD. Behavioral expressions in dementia patients. http://www.todaysgeriatricmedicine.com/archive/0115p6.shtml. Published 2015. Accessed May 10, 2018.
9. Al Sabei SD, Lasater K. Simulation debriefing for clinical judgment development: a concept analysis. Nurse Educ Today. 2016;45:42-47.
10. Anderson LW, Krathwohl DR, Bloom BS, eds. A Taxonomy for Learning, Teaching, and Assessing: A revision of Bloom’s Taxonomy of Educational Objectives. New York: Longman; 2001.
Enhancing patient-centered care is an important priority for caregivers in all settings but particularly in long-term care (LTC) where patients also are residents. Simulation is a potential strategy to effect cultural change for health care providers at LTC facilities. In a clinical setting, simulation is an educational model that allows staff to practice behaviors or skills without putting patients at risk. Due to limited time, staffing, and budget resources, the use of simulation for training is not common at LTC facilities.
Background
The simulation model is considered an effective teaching and learning strategy for replicating experiences in nursing practice.1,2 The interactive experience provides the learner with opportunities to engage with patients through psychomotor participation, critical thinking, reflection, and debriefing. Prelicensure nursing education programs and acute care hospitals are the most common users of simulation learning. However, there is a paucity of literature addressing the use of simulation in LTC.
One study was conducted in 2002 by P.K. Beville called the Virtual Dementia Tour, a program using evidence-based simulation. Beville found that study participants using the simulation model had a heightened awareness of the challenges of confused elderly as well as unrealistic expectations by caregivers.3 Although the Virtual Dementia Tour is available for a fee for training professional caregivers, lay people, family, and first responders, many LTC facilities do not have sufficient funding for simulation and simulation equipment, and many do not have dedicated staff for nursing education. Most staff in LTC facilities are unlicensed and may not have had simulation training experience. Additionally, due to staffing and budget constraints, staff education may be limited.
This article will describe the successful implementation of a simulation-based quality improvement project created by and used at the Louis Stokes Cleveland VA Medical Center (LSCVAMC) LTC facility. The LSCVAMC has acute care beds and is adjacent to its LTC facility. Also, a previously successful simulation educational program to improve delirium care was conducted at this acute care hospital.4
Experiential Learning Opportunity
Many residents in a LTC facility have been diagnosed with dementia. As part of a cultural transformation at LSCVAMC, a simulation program was used to help sensitize LTC caregivers to the many sensory changes that occur in older veterans with dementia. The program was guided by the Kolb model.5
The Kolb model of experiential learning includes 4 elements: abstract conceptualization (knowledge), active experimentation (application), concrete experience (engagement), and reflective observation (self-evaluation).5 A simulation program can touch all 4 elements of the Kolb model by providing an educational experience for all learning styles as well as facilitating critical thinking. Nursing homes that provide care to residents with dementia are required to include dementia education annually to staff.6 Long-term care facilities can take advantage of using simulation education along with their traditional educational programs to provide staff with exposure to realistic resident care conditions.7
Methods
The simulation learning experience was provided to all nursing, recreation therapy, and rehabilitation services staff at the LTC facility. The goal was to create an affective, psychomotor learning experience that refreshed, reminded, and sensitized the staff to the challenges that many residents face. The LSCVAMC LTC leadership was supportive of this simulation model because it was not time intensive for direct care staff, and the materials needed were inexpensive. The only equipment that was purchased were several eyeglass readers, popcorn kernels, and Vaseline, resulting in a budget of about $10. The simulation program was scheduled on all shifts. In addition to the simulation experience, the model consists of pre- and postsurveys and a dementia review handout. Staff were able to complete a pre- and postsurvey as well as a debriefing all within a 30-minute time slot.
The pre- and posteducation surveys used were designed to measure learnings and provide data for future education planning. The surveys required only a yes/no and short answers. To reduce the total time of participants’ involvement in the simulation program, an online survey was used. Presurvey questions were designed to identify basic knowledge and experience with dementia, both at work and in personal life. The postsurvey questions sought to identify affective feelings about the participants experience as well as lessons learned and how that could impact future care.
The dementia review handout that was provided to staff 2 weeks before the simulation provided an overview of dementia. It included communication techniques and care planning suggestions.8 The time spent in the simulation room was about 10 to 15 minutes but depended on the activity. The total in-service time was about 30 minutes, depending on the time allotted for debriefing. Room choice was influenced by the number of participants performing the simulation at the same time. Activity stations/tables generally provided 1 experience at a time.
The room that was used had adjustable lighting with the ability to provide a low light setting. Activities were chosen based on the goals for the physical and cognitive disabilities to be simulated. Table 1 identifies equipment used with success and chosen with consideration for ease and expense in describing the disability.
Simulation activities were based on the staff learning needs determined by the presimulation survey. Simulated deficits impacted activities of daily living, mood, and cognition. Neuropathy, arthritis, paralysis, dementia, glaucoma, cataracts, and hearing loss are conditions that are easily represented in a simulation.
Participants also gained additional knowledge of dementia through the Kolb process, which was included in the debriefing. The survey followed the completion of the simulation session to identify knowledge deficits for general remediation and program development and expansion.
Discussion
During the dementia simulation, active experimentation or application learning may be counterintuitive. Staff do not apply their knowledge of dementia directly as in other education settings where they can practice or demonstrate a skill. Instead, participants experience care from the perspective of residents. This learning transitions well into reflective observation as the participants begin to understand the challenges of the cognitively impaired resident, which are manifested in the residents’ behaviors.
Debriefing and a postsimulation survey provide a guided reflection to assimilate new knowledge and revise presimulation attitudes about dementia.9 Reflective observation or self-evaluation is a learning activity that is not a routine part of staff education but can be a powerful learning tool. The postsimulation survey incorporated Bloom’s taxonomy: the affective domain of learning by challenging staff to organize their values with the experience and resolving in their mind any conflicts.10 The goal of the process is to help internalize the education by encouraging changes in behavior (in this case dementia care) and considering the new experience.
Survey Results
The 30-minute program allowed 155 staff to experience cognitive and physical impairment while completing tasks. The pre- and postsurveys were analyzed by 2 learning and dementia survey content experts. The survey questions were open-ended with the intention of eliciting affective behavior responses and staff could provide comments (See eTables 1 and 2 at www.mdedge.com/fedprac). All participants indicated they had knowledge of dementia before the simulation, but 70% acknowledged in the postsimulation survey that they did not have the dementia knowledge that they thought they had. Patience and understanding were most commonly reported in the reflective observation/affective domain (values are internalized leading to changes in behavior).
Participants also described success in closing the loop of experiential learning as a result of the simulation. Some participants verbalized experiencing emotional distress when they realized that their temporary, frustrating impairment was a permanent condition for the residents. Postexperience comments supported the success of the Kolb model experiential learning activity.
Conclusion
Dementia simulation can augment didactic education for improving the quality of dementia care. The virtual dementia simulation was an inexpensive educational program that did not adversely impact scheduling or patient care in a LTC facility. Care providers provided anecdotal feedback that suggested that the program increased their awareness of the difficulty of performing activities of daily living for patients with dementia. The simulation touched all 4 elements of the Kolb Model. The participants had gained new knowledge or reinforced existing knowledge. The simulation activities addressed the application and engagement parts of the model. Self-evaluation resulted from the debriefing time and postsurvey questions. The virtual dementia simulation will be repeated with additional debrief time and a long-term follow-up survey to identify additional learning needs and changes in professional practice.
Acknowledgments
The author thanks Nurse Educator Lisa Weber, MSN, RN-BC, for her contribution to the manuscript.
Enhancing patient-centered care is an important priority for caregivers in all settings but particularly in long-term care (LTC) where patients also are residents. Simulation is a potential strategy to effect cultural change for health care providers at LTC facilities. In a clinical setting, simulation is an educational model that allows staff to practice behaviors or skills without putting patients at risk. Due to limited time, staffing, and budget resources, the use of simulation for training is not common at LTC facilities.
Background
The simulation model is considered an effective teaching and learning strategy for replicating experiences in nursing practice.1,2 The interactive experience provides the learner with opportunities to engage with patients through psychomotor participation, critical thinking, reflection, and debriefing. Prelicensure nursing education programs and acute care hospitals are the most common users of simulation learning. However, there is a paucity of literature addressing the use of simulation in LTC.
One study was conducted in 2002 by P.K. Beville called the Virtual Dementia Tour, a program using evidence-based simulation. Beville found that study participants using the simulation model had a heightened awareness of the challenges of confused elderly as well as unrealistic expectations by caregivers.3 Although the Virtual Dementia Tour is available for a fee for training professional caregivers, lay people, family, and first responders, many LTC facilities do not have sufficient funding for simulation and simulation equipment, and many do not have dedicated staff for nursing education. Most staff in LTC facilities are unlicensed and may not have had simulation training experience. Additionally, due to staffing and budget constraints, staff education may be limited.
This article will describe the successful implementation of a simulation-based quality improvement project created by and used at the Louis Stokes Cleveland VA Medical Center (LSCVAMC) LTC facility. The LSCVAMC has acute care beds and is adjacent to its LTC facility. Also, a previously successful simulation educational program to improve delirium care was conducted at this acute care hospital.4
Experiential Learning Opportunity
Many residents in a LTC facility have been diagnosed with dementia. As part of a cultural transformation at LSCVAMC, a simulation program was used to help sensitize LTC caregivers to the many sensory changes that occur in older veterans with dementia. The program was guided by the Kolb model.5
The Kolb model of experiential learning includes 4 elements: abstract conceptualization (knowledge), active experimentation (application), concrete experience (engagement), and reflective observation (self-evaluation).5 A simulation program can touch all 4 elements of the Kolb model by providing an educational experience for all learning styles as well as facilitating critical thinking. Nursing homes that provide care to residents with dementia are required to include dementia education annually to staff.6 Long-term care facilities can take advantage of using simulation education along with their traditional educational programs to provide staff with exposure to realistic resident care conditions.7
Methods
The simulation learning experience was provided to all nursing, recreation therapy, and rehabilitation services staff at the LTC facility. The goal was to create an affective, psychomotor learning experience that refreshed, reminded, and sensitized the staff to the challenges that many residents face. The LSCVAMC LTC leadership was supportive of this simulation model because it was not time intensive for direct care staff, and the materials needed were inexpensive. The only equipment that was purchased were several eyeglass readers, popcorn kernels, and Vaseline, resulting in a budget of about $10. The simulation program was scheduled on all shifts. In addition to the simulation experience, the model consists of pre- and postsurveys and a dementia review handout. Staff were able to complete a pre- and postsurvey as well as a debriefing all within a 30-minute time slot.
The pre- and posteducation surveys used were designed to measure learnings and provide data for future education planning. The surveys required only a yes/no and short answers. To reduce the total time of participants’ involvement in the simulation program, an online survey was used. Presurvey questions were designed to identify basic knowledge and experience with dementia, both at work and in personal life. The postsurvey questions sought to identify affective feelings about the participants experience as well as lessons learned and how that could impact future care.
The dementia review handout that was provided to staff 2 weeks before the simulation provided an overview of dementia. It included communication techniques and care planning suggestions.8 The time spent in the simulation room was about 10 to 15 minutes but depended on the activity. The total in-service time was about 30 minutes, depending on the time allotted for debriefing. Room choice was influenced by the number of participants performing the simulation at the same time. Activity stations/tables generally provided 1 experience at a time.
The room that was used had adjustable lighting with the ability to provide a low light setting. Activities were chosen based on the goals for the physical and cognitive disabilities to be simulated. Table 1 identifies equipment used with success and chosen with consideration for ease and expense in describing the disability.
Simulation activities were based on the staff learning needs determined by the presimulation survey. Simulated deficits impacted activities of daily living, mood, and cognition. Neuropathy, arthritis, paralysis, dementia, glaucoma, cataracts, and hearing loss are conditions that are easily represented in a simulation.
Participants also gained additional knowledge of dementia through the Kolb process, which was included in the debriefing. The survey followed the completion of the simulation session to identify knowledge deficits for general remediation and program development and expansion.
Discussion
During the dementia simulation, active experimentation or application learning may be counterintuitive. Staff do not apply their knowledge of dementia directly as in other education settings where they can practice or demonstrate a skill. Instead, participants experience care from the perspective of residents. This learning transitions well into reflective observation as the participants begin to understand the challenges of the cognitively impaired resident, which are manifested in the residents’ behaviors.
Debriefing and a postsimulation survey provide a guided reflection to assimilate new knowledge and revise presimulation attitudes about dementia.9 Reflective observation or self-evaluation is a learning activity that is not a routine part of staff education but can be a powerful learning tool. The postsimulation survey incorporated Bloom’s taxonomy: the affective domain of learning by challenging staff to organize their values with the experience and resolving in their mind any conflicts.10 The goal of the process is to help internalize the education by encouraging changes in behavior (in this case dementia care) and considering the new experience.
Survey Results
The 30-minute program allowed 155 staff to experience cognitive and physical impairment while completing tasks. The pre- and postsurveys were analyzed by 2 learning and dementia survey content experts. The survey questions were open-ended with the intention of eliciting affective behavior responses and staff could provide comments (See eTables 1 and 2 at www.mdedge.com/fedprac). All participants indicated they had knowledge of dementia before the simulation, but 70% acknowledged in the postsimulation survey that they did not have the dementia knowledge that they thought they had. Patience and understanding were most commonly reported in the reflective observation/affective domain (values are internalized leading to changes in behavior).
Participants also described success in closing the loop of experiential learning as a result of the simulation. Some participants verbalized experiencing emotional distress when they realized that their temporary, frustrating impairment was a permanent condition for the residents. Postexperience comments supported the success of the Kolb model experiential learning activity.
Conclusion
Dementia simulation can augment didactic education for improving the quality of dementia care. The virtual dementia simulation was an inexpensive educational program that did not adversely impact scheduling or patient care in a LTC facility. Care providers provided anecdotal feedback that suggested that the program increased their awareness of the difficulty of performing activities of daily living for patients with dementia. The simulation touched all 4 elements of the Kolb Model. The participants had gained new knowledge or reinforced existing knowledge. The simulation activities addressed the application and engagement parts of the model. Self-evaluation resulted from the debriefing time and postsurvey questions. The virtual dementia simulation will be repeated with additional debrief time and a long-term follow-up survey to identify additional learning needs and changes in professional practice.
Acknowledgments
The author thanks Nurse Educator Lisa Weber, MSN, RN-BC, for her contribution to the manuscript.
1. Aebersold M, Tschannen D. Simulation in nursing practice: the impact on patient care. Online J Issues Nurs. 2013;18(2):6.
2. Mariani B, Doolen J. Nursing simulation research: what are the perceived gaps? Clin Simulation in Nurs. 2016;12(1):30-36.
3. Beville PK. Virtual Dementia Tour helps sensitize health care providers. Am J Alzheimers Dis Other Demen. 2002;17(3):183-190.
4. Kresevic D, Heath B, Fine-Smilovich E, et al. Simulation training, coaching, and cue cards improve delirium care. Fed Pract. 2016;33(12):22-28.
5. Chmil JV, Turk M, Adamson K, Larew C. Effects of an experiential learning simulation design on clinical nursing judgment development. Nurse Educ. 2015;40(5):228-232.
6. Centers for Medicare & Medicaid Services. Medicare and Medicaid programs; reform of requirements for long-term care facilities, final rule. https://www.federalregister.gov/documents/2016/10/04/2016-23503/medicare-and-medicaid-programs-reform-of-requirements-for-long-term-care-facilities. Published October 4, 2016. Accessed May 22, 2018.
7. Donahoe J, Moon L, VanCleave K. Increasing student empathy toward older adults using the virtual dementia tour. J Baccalaureate Soc Work. 2014;19(1):S23-S40.
8. Coggins MD. Behavioral expressions in dementia patients. http://www.todaysgeriatricmedicine.com/archive/0115p6.shtml. Published 2015. Accessed May 10, 2018.
9. Al Sabei SD, Lasater K. Simulation debriefing for clinical judgment development: a concept analysis. Nurse Educ Today. 2016;45:42-47.
10. Anderson LW, Krathwohl DR, Bloom BS, eds. A Taxonomy for Learning, Teaching, and Assessing: A revision of Bloom’s Taxonomy of Educational Objectives. New York: Longman; 2001.
1. Aebersold M, Tschannen D. Simulation in nursing practice: the impact on patient care. Online J Issues Nurs. 2013;18(2):6.
2. Mariani B, Doolen J. Nursing simulation research: what are the perceived gaps? Clin Simulation in Nurs. 2016;12(1):30-36.
3. Beville PK. Virtual Dementia Tour helps sensitize health care providers. Am J Alzheimers Dis Other Demen. 2002;17(3):183-190.
4. Kresevic D, Heath B, Fine-Smilovich E, et al. Simulation training, coaching, and cue cards improve delirium care. Fed Pract. 2016;33(12):22-28.
5. Chmil JV, Turk M, Adamson K, Larew C. Effects of an experiential learning simulation design on clinical nursing judgment development. Nurse Educ. 2015;40(5):228-232.
6. Centers for Medicare & Medicaid Services. Medicare and Medicaid programs; reform of requirements for long-term care facilities, final rule. https://www.federalregister.gov/documents/2016/10/04/2016-23503/medicare-and-medicaid-programs-reform-of-requirements-for-long-term-care-facilities. Published October 4, 2016. Accessed May 22, 2018.
7. Donahoe J, Moon L, VanCleave K. Increasing student empathy toward older adults using the virtual dementia tour. J Baccalaureate Soc Work. 2014;19(1):S23-S40.
8. Coggins MD. Behavioral expressions in dementia patients. http://www.todaysgeriatricmedicine.com/archive/0115p6.shtml. Published 2015. Accessed May 10, 2018.
9. Al Sabei SD, Lasater K. Simulation debriefing for clinical judgment development: a concept analysis. Nurse Educ Today. 2016;45:42-47.
10. Anderson LW, Krathwohl DR, Bloom BS, eds. A Taxonomy for Learning, Teaching, and Assessing: A revision of Bloom’s Taxonomy of Educational Objectives. New York: Longman; 2001.
Workforce Assessment of VA Home-Based Primary Care Pharmacists
Home-Based Primary Care (HBPC) is a unique interdisciplinary program within the Veteran’s Health Administration (VHA) that specifically targets veterans with complex, chronic disabling diseases who have difficulty traveling to a VHA facility.1 Veterans are provided comprehensive longitudinal primary care in their homes, with the goal of maximizing the veteran’s independence. Clinical pharmacists are known as medication experts and have an essential role within interdisciplinary teams, including HBPC, improving medication safety, and decreasing inappropriate prescribing practices.2,3 Clinical pharmacy specialists (CPSs) within the VHA work collaboratively but autonomously as advanced practice providers assisting with the pharmacologic management of many diseases and chronic conditions. The remainder of this article will refer to the HBPC pharmacist as a CPS.
The CPS is actively involved in providing comprehensive medication management (CMM) services across VHA and has the expertise to effectively assist veterans in achieving targeted clinical outcomes. While the value and role of CPSs in the primary care setting are described extensively in the literature, data regarding the CPS in HBPC are limited.4-6 Therefore, the purpose of the assessment was to evaluate the status of the HBPC pharmacy workforce, identify current pharmacist activities and strong practices, and clarify national variations among programs. Future use of this analysis may assist with standardization of the HBPC CPS role and development of business rules in combination with a workload-based staffing model tool.
Background
The role of the pharmacist in the HBPC setting has evolved from providing basic medication therapy reviews to an advanced role providing CMM services under a VHA scope of practice (SOP), which outlines 8 functions that may be authorized, including medication prescriptive authority.7 The SOP may be disease specific (limited) but is increasingly transitioning to have a practice-area scope (global), which is consistent with other VHA advanced practice providers.7 Effective use of a CPS in this role allows for optimization of CMM and increasing veteran access to VHA care.
The VHA employed 7,285 pharmacists in 2014.8 Many were considered CPSs with prescriptive authority. These pharmacists were responsible for ordering more than 1.7 million distinct prescriptions across the VHA in fiscal year 2014, which represented 2.6% of the total prescriptions that year.7 A 2007 VHA study also demonstrated both an increase in appropriate prescribing practices and improved medication use when CPSs worked in collaboration with the HBPC team.9 With this evolution of VHA pharmacists, there has been an increase in the use of CPSs in HBPC and changes in staffing ratios to allow for additional clinical activities and comprehensive patient care provision.1
The HBPC model serves a complex population in which each veteran has about 8 chronic conditions.1,10 An interdisciplinary team consisting of various health care professionals, such as physicians, nurse practitioners, nurses, social workers, registered dietitians, psychologists, rehabilitation therapists, pharmacists, etc, work collaboratively to care for these veterans in the patient’s home. This team is a type of patient-centered medical home (PCMH) that focuses on providing primary care services to an at-risk veteran population who have difficulty leaving the home.1 Home-based primary care has been shown to be cost-effective, reducing average annual cost of health care by up to 24%.10 Another study showed that patients using HBPC had a 27% reduction in hospital admissions and 69% reduction in inpatient hospital days when compared with patients who were not using HBPC.11
The interdisciplinary team meets at least once weekly to discuss and design individualized care plans for veterans enrolled in the program. It is desirable for pharmacists on these teams to have special expertise and certification in geriatric pharmacotherapy and chronic disease management (eg, board-certified geriatric pharmacist [BCGP], board-certified pharmacotherapy specialist [BCPS], or board-certified ambulatory care pharmacist [BCACP]) due to the complexity of comorbidities of these veterans.12 Additional education such as postgraduate pharmacy residency training also is beneficial for CPSs in this setting.
The CPS proactively performs CMM that is often greater in scope than a targeted disease review due to multiple comorbid conditions that are often present within veteran patients.1 These comprehensive medication reviews are considered a core function and must be performed on enrollment in HBPC, quarterly, and when clinically indicated or requested by the team.13 Sufficient time must be allocated to the CPS in order to provide these high-quality medication reviews. Additional core functions of the CPS are outlined in the functional statement and/or SOP, but responsibilities include CMM and disease management. This typically consists of prescribing and/or adjusting medications, as well as providing patient and caregiver education, which can be performed either face-to-face or via telehealth visits (eg, telephone and video). A CPS also may make home visits to assess the veteran, either independently or with other disciplines of the HBPC team.
The HBPC Subject Matter Expert (SME) workgroup was chartered by the Veterans Affairs Central Office (VACO) Pharmacy Benefits Management Service (PBM) Clinical Pharmacy Practice Office (CPPO) to explore pharmacy practice changes in the HBPC setting. This workgroup serves as clinical practice leadership within the HBPC setting to provide expertise and lead initiatives supporting the advanced practice role of the HBPC CPS.
As HBPC programs expanded throughout VHA, it was paramount to determine the current state of HBPC pharmacy practice by collecting necessary data points to assess uniformity and better understand opportunities for practice standardization. The SME workgroup developed a voluntary yet comprehensive survey assessment that served to proactively assess the future of HBPC pharmacy.
Methods
The HBPC SME workgroup, in conjunction with CPPO, developed the assessment. Questions were designed and tested within a small group of CPSs and then distributed electronically. In August 2014, the assessment was e-mailed to all 21 VHA service areas with an active HBPC program, and responses were collected through a Microsoft SharePoint (Redmond, WA) survey. A response was requested from chiefs of pharmacy, clinical pharmacy leadership, or a representative.
This voluntary assessment contained 24 multipart questions related to background information of HBPC programs and clinical pharmacy services. Duplicate responses were consolidated and clarified with individual sites post hoc.
Descriptive statistics were used to analyze responses. To standardize the comparison across sites with a variety of full-time equivalent employees (FTEEs), the average patient census was divided by the CPS FTEE allocated to the programs at that site. For example, if a site reported 316 patients with 0.25 CPS FTEE, a standardized ratio for this site was 1,264 patients per FTEE. If a patient census range was reported, the median number would be used.
Results
The team received responses from 130 of 141 VHA facilities (92%), encompassing 270 CPSs. A total of 168.75 FTEEs were officially designated as HBPC CPSs. All 21 VHA service areas at the time were represented. The majority of responding programs (67%) had < 1 CPS FTEE allocated to HBPC; many of these CPSs were working in other pharmacy areas but were only dedicated to HBPC part-time. 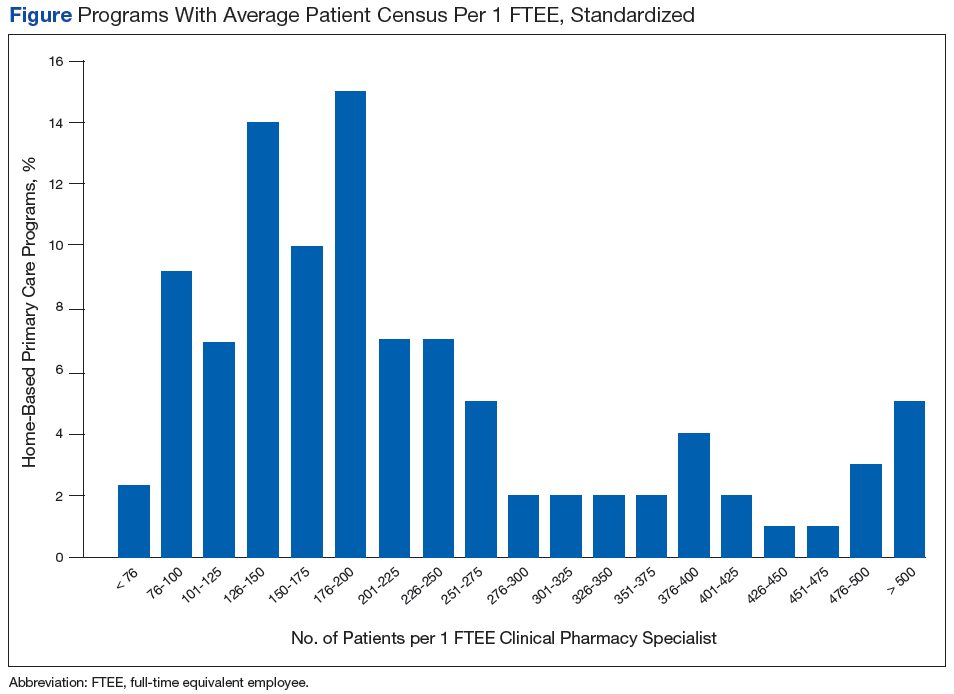
Nearly 90% of CPSs completed postgraduate year 1 residency training. Fifty-seven percent of CPSs held advanced certifications, such as BCGP, BCACP, or BCPS. Sixty-two percent of CPSs with these specialized board certifications had residency training. Use of a SOP was reported by 76% of CPSs, and 66% of these had a global practice-area scope. Table 1 outlines the functions authorized by a global or limited SOP.6 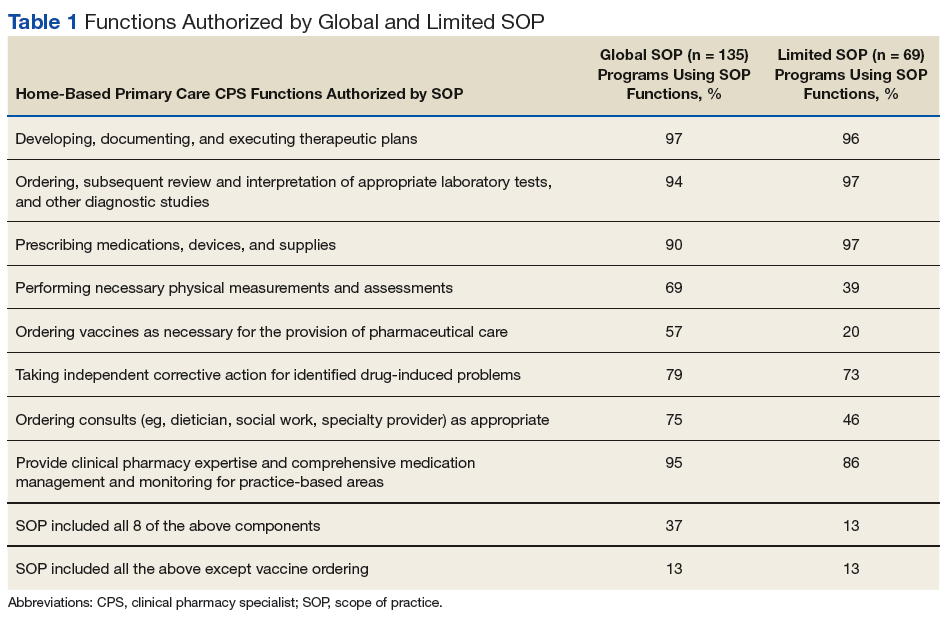
Overall, 52% of sites reported CPS involvement in CMM of primarily anticoagulation, diabetes mellitus (DM), anemia, hyperlipidemia, and hypertension. The reported average time spent for each disease encounter is delineated in Table 2. 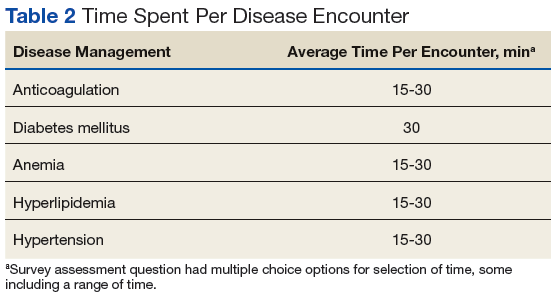
Thirty-five percent of sites reported CPS participation in home visits, and the majority of those completed between 1 and 10 home visits per month. The types of interventions provided often included medication education, assessment of medication adherence, and CMM for DM, hyperlipidemia, hypertension, etc. Multiple interventions often were made during each home visit.
The workload of medication reviews was divided among multiple CPSs in 55% of the programs. The majority of programs completed fewer than 20 initial medication reviews per month and between 21 and 80 quarterly medication reviews per month (81% and 62%, respectively). The average time for a CPS to complete initial medication reviews was 78 minutes and 42 minutes for quarterly medication reviews.
Sites with CPSs that held a SOP (76%) took an average of 83 minutes to complete an initial medication review and 48 minutes to complete a quarterly review. Sites with CPSs without a SOP (24%) took an average of 72 minutes to complete an initial medication review and 36 minutes to complete a quarterly review. Many CPSs allocate ≤ 20 hours per month on routine pharmacy functions (eg, prescription verification, dispensing activities, nonformulary medication requests) and ≤ 20 hours per month on nonpatient care activities (eg, education, medication use evaluations, training, projects), 67% and 82%, respectively.
Ninety-seven percent of CPSs actively attended weekly HBPC program interdisciplinary team (IDT) meetings, with 67% attending 1 weekly IDT meeting and 30% attending 2 to 5 weekly IDT meetings. Time spent attending IDT and roundtable discussions averaged 3.5 hours per week. Multiple programs noted growth within the 12 months preceding the survey, as 37 sites were granted approval for a total of 29.75 additional CPS FTEEs, and an additional 10 sites had a total of 9.25 FTEEs pending approval.
Discussion
Analysis of this assessment allowed the HBPC CPS SME workgroup to identify strong practices and variations in individual HBPC pharmacy programs. The majority of CPSs (66%) are using global, practice area-based SOPs, which allows more autonomy via direct patient care to veterans through CMM and home visits. This trend suggests the focus of the HBPC CPS role has expanded beyond traditional pharmacist activities. These global SOPs result in a higher yield of CPS functions, such as developing, documenting, and executing therapeutic plans and prescribing medications (Table 1). A higher percentage of CPSs with a practice area-based SOP were authorized to perform all 8 functions. Therefore, increased use of practice area-based SOPs and the expansion of the HBPC CPS role can support the team and increase clinical services available to veterans.
Clinical pharmacy specialists using SOPs take longer to complete medication reviews compared with those not using SOPs. Although the assessment was not designed to evaluate the reasons for these time differences, post-hoc follow-up clarification with individual sites determined CPS use of a SOP can lend to a more time-intensive and comprehensive medication review. This may lead to more optimized and safe medication regimens and elimination of unnecessary and/or inappropriate medications for HBPC veterans.
While only 35% of pharmacists were participating in the home visits at the time of this assessment, this is another area to explore as an opportunity to expand CMM. Although the assessment showed the majority of these home visits addressed medication education and adherence, programs may find it advantageous to provide CPS home visits for veterans identified as high risk or requiring specialized CMM. Additional data are needed regarding the ideal population to target for CPS home visits, as well as the estimated benefits of conducting home visits, such as outcomes and efficiency.
With growth noted in multiple programs, HBPC leadership should continue to encourage expanded pharmacist roles at an advanced practice level with SOPs, to provide veteran-centered care. This practice allows the team to concentrate efforts on patient acuity while increasing veteran access to VHA care. Additional CPS FTEEs are necessary to allow for expansion of the HBPC CPS role. The data also demonstrate HBPC often uses a part-time workforce where pharmacists are assigned to HBPC < 40 hours per week, and multiple pharmacists may be used to fulfill 1 CPS FTEE position. Home-Based Primary Care programs are encouraged to consolidate the number of CPSs involved as core individuals to promote continuity and avoid fragmented care.
Limitations
One limitation of the assessment is that the questions were designed and tested by a small group of CPSs, which may have led to response bias and potential misinterpretation of some questions. Time spent on medication reviews may have been underestimated, as some sites reported the maximum allowable workload credit time rather than actual time spent. Recall bias also is a limitation because the assessment relied on the recollection of the CPS or chief of pharmacy. Additionally, while the assessment focused on quantity and time spent on medication reviews, it was not designed to evaluate quality. Examination of what constitutes a high-quality medication review would be helpful to provide guidance and standardize care across the VHA.
Conclusion
Clinical pharmacy specialists practicing in the VHA HBPC setting are highly trained clinicians. A significant percentage of CPSs practice with a SOP that includes prescriptive privileges. However, variations in practice and function exist in the system. This presents an excellent opportunity for future standardization and promotion of the highest and best use of the CPS to improve quality of care for HBPC. With the expansion of the CPS role, there is potential for pharmacists to increase clinical activities and improve care for home-based veterans. The CPPO HBPC SME workgroup will continue to examine and explore the CPS role in this practice setting, develop staffing and practice guidance documents, and assess the benefit of CPS home visits.
1. US Department of Veterans Affairs. VHA Directive 1141.01: home-based primary care special population aligned care team program. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=5417. Updated September 20, 2017. Accessed April 3, 2018.
2. Brahmbhatt M, Palla K, Kossifologos A, Mitchell D, Lee T. Appropriateness of medication prescribing using the STOPP/START criteria in veterans receiving home-based primary care. Consult Pharm. 2013;28(6):361-369.
3. Hanlon JT, Weinberger M, Samsa GP, et al. A randomized, controlled trial of a clinical pharmacist intervention to improve inappropriate prescribing in elderly outpatients with polypharmacy. Am J Med. 1996;100(4):428-437.
4. Rose AJ, McCullough MB, Carter BL, Rudin RS. The clinical pharmacy specialist: part of the solution. J Gen Intern Med. 2017;32(4):375–377.
5. Giberson S, Yoder S, Lee MP. Improving patient and health system outcomes through advanced pharmacy practice: a report to the U.S. Surgeon General 2011. https://www.accp.com/docs/positions/misc/Improving_Patient_and_Health_System_Outcomes.pdf. Published December 2011. Accessed April 3, 2018.
6. Lee AJ, Boro MS, Knapp KK, Meier JL, Korman NE. Clinical and economic outcomes of pharmacist recommendations in a Veterans Affairs medical center. Am J Health Syst Pharm. 2002;59(21):2070–2077.
7. Ourth H, Groppi J, Morreale AP, Quicci-Roberts K. Clinical pharmacist prescribing activities in the Veterans Health Administration. Am J Health Syst Pharm. 2016;73(18):1406-1415.
8. US Department of Veteran Affairs, Veterans Health Administration, Healthcare Talent Management Workforce Management & Consulting Office. VHA workforce planning report 2015.https://www.vacareers.va.gov/assets/common/print/2015_VHA_Workforce_Succession_Strategic_Plan.pdf. Published 2015. Accessed April 3, 2018.
9. Davis RG, Hepfinger CA, Sauer KA, Wilhardt MS. Retrospective evaluation of medication appropriateness and clinical pharmacist drug therapy recommendations for home-based primary care veterans. Am J Geriatr Pharmacother. 2007;5(1):40-47.
10. Beales JL, Edes T. Veteran’s Affairs home based primary care. Clin Geriatr Med. 2009;25(1):149-154.
11. Cooper DF, Granadillo OR, Stacey CM. Home-based primary care: the care of the veteran at home. Home Healthc Nurse. 2007;25(5):315-322.
12. Pradel FG, Palumbo FB, Flowers L, et al. White paper: value of specialty certification in pharmacy. J Am Pharm Assoc. 2004;44(5):612-620.
13. US Department of Veterans Affairs, Veterans Health Administration. VHA Handbook 1108.11(1). Clinical pharmacy services. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=3120. Updated June 29, 2017. Accessed April 3, 2018
Home-Based Primary Care (HBPC) is a unique interdisciplinary program within the Veteran’s Health Administration (VHA) that specifically targets veterans with complex, chronic disabling diseases who have difficulty traveling to a VHA facility.1 Veterans are provided comprehensive longitudinal primary care in their homes, with the goal of maximizing the veteran’s independence. Clinical pharmacists are known as medication experts and have an essential role within interdisciplinary teams, including HBPC, improving medication safety, and decreasing inappropriate prescribing practices.2,3 Clinical pharmacy specialists (CPSs) within the VHA work collaboratively but autonomously as advanced practice providers assisting with the pharmacologic management of many diseases and chronic conditions. The remainder of this article will refer to the HBPC pharmacist as a CPS.
The CPS is actively involved in providing comprehensive medication management (CMM) services across VHA and has the expertise to effectively assist veterans in achieving targeted clinical outcomes. While the value and role of CPSs in the primary care setting are described extensively in the literature, data regarding the CPS in HBPC are limited.4-6 Therefore, the purpose of the assessment was to evaluate the status of the HBPC pharmacy workforce, identify current pharmacist activities and strong practices, and clarify national variations among programs. Future use of this analysis may assist with standardization of the HBPC CPS role and development of business rules in combination with a workload-based staffing model tool.
Background
The role of the pharmacist in the HBPC setting has evolved from providing basic medication therapy reviews to an advanced role providing CMM services under a VHA scope of practice (SOP), which outlines 8 functions that may be authorized, including medication prescriptive authority.7 The SOP may be disease specific (limited) but is increasingly transitioning to have a practice-area scope (global), which is consistent with other VHA advanced practice providers.7 Effective use of a CPS in this role allows for optimization of CMM and increasing veteran access to VHA care.
The VHA employed 7,285 pharmacists in 2014.8 Many were considered CPSs with prescriptive authority. These pharmacists were responsible for ordering more than 1.7 million distinct prescriptions across the VHA in fiscal year 2014, which represented 2.6% of the total prescriptions that year.7 A 2007 VHA study also demonstrated both an increase in appropriate prescribing practices and improved medication use when CPSs worked in collaboration with the HBPC team.9 With this evolution of VHA pharmacists, there has been an increase in the use of CPSs in HBPC and changes in staffing ratios to allow for additional clinical activities and comprehensive patient care provision.1
The HBPC model serves a complex population in which each veteran has about 8 chronic conditions.1,10 An interdisciplinary team consisting of various health care professionals, such as physicians, nurse practitioners, nurses, social workers, registered dietitians, psychologists, rehabilitation therapists, pharmacists, etc, work collaboratively to care for these veterans in the patient’s home. This team is a type of patient-centered medical home (PCMH) that focuses on providing primary care services to an at-risk veteran population who have difficulty leaving the home.1 Home-based primary care has been shown to be cost-effective, reducing average annual cost of health care by up to 24%.10 Another study showed that patients using HBPC had a 27% reduction in hospital admissions and 69% reduction in inpatient hospital days when compared with patients who were not using HBPC.11
The interdisciplinary team meets at least once weekly to discuss and design individualized care plans for veterans enrolled in the program. It is desirable for pharmacists on these teams to have special expertise and certification in geriatric pharmacotherapy and chronic disease management (eg, board-certified geriatric pharmacist [BCGP], board-certified pharmacotherapy specialist [BCPS], or board-certified ambulatory care pharmacist [BCACP]) due to the complexity of comorbidities of these veterans.12 Additional education such as postgraduate pharmacy residency training also is beneficial for CPSs in this setting.
The CPS proactively performs CMM that is often greater in scope than a targeted disease review due to multiple comorbid conditions that are often present within veteran patients.1 These comprehensive medication reviews are considered a core function and must be performed on enrollment in HBPC, quarterly, and when clinically indicated or requested by the team.13 Sufficient time must be allocated to the CPS in order to provide these high-quality medication reviews. Additional core functions of the CPS are outlined in the functional statement and/or SOP, but responsibilities include CMM and disease management. This typically consists of prescribing and/or adjusting medications, as well as providing patient and caregiver education, which can be performed either face-to-face or via telehealth visits (eg, telephone and video). A CPS also may make home visits to assess the veteran, either independently or with other disciplines of the HBPC team.
The HBPC Subject Matter Expert (SME) workgroup was chartered by the Veterans Affairs Central Office (VACO) Pharmacy Benefits Management Service (PBM) Clinical Pharmacy Practice Office (CPPO) to explore pharmacy practice changes in the HBPC setting. This workgroup serves as clinical practice leadership within the HBPC setting to provide expertise and lead initiatives supporting the advanced practice role of the HBPC CPS.
As HBPC programs expanded throughout VHA, it was paramount to determine the current state of HBPC pharmacy practice by collecting necessary data points to assess uniformity and better understand opportunities for practice standardization. The SME workgroup developed a voluntary yet comprehensive survey assessment that served to proactively assess the future of HBPC pharmacy.
Methods
The HBPC SME workgroup, in conjunction with CPPO, developed the assessment. Questions were designed and tested within a small group of CPSs and then distributed electronically. In August 2014, the assessment was e-mailed to all 21 VHA service areas with an active HBPC program, and responses were collected through a Microsoft SharePoint (Redmond, WA) survey. A response was requested from chiefs of pharmacy, clinical pharmacy leadership, or a representative.
This voluntary assessment contained 24 multipart questions related to background information of HBPC programs and clinical pharmacy services. Duplicate responses were consolidated and clarified with individual sites post hoc.
Descriptive statistics were used to analyze responses. To standardize the comparison across sites with a variety of full-time equivalent employees (FTEEs), the average patient census was divided by the CPS FTEE allocated to the programs at that site. For example, if a site reported 316 patients with 0.25 CPS FTEE, a standardized ratio for this site was 1,264 patients per FTEE. If a patient census range was reported, the median number would be used.
Results
The team received responses from 130 of 141 VHA facilities (92%), encompassing 270 CPSs. A total of 168.75 FTEEs were officially designated as HBPC CPSs. All 21 VHA service areas at the time were represented. The majority of responding programs (67%) had < 1 CPS FTEE allocated to HBPC; many of these CPSs were working in other pharmacy areas but were only dedicated to HBPC part-time.
Nearly 90% of CPSs completed postgraduate year 1 residency training. Fifty-seven percent of CPSs held advanced certifications, such as BCGP, BCACP, or BCPS. Sixty-two percent of CPSs with these specialized board certifications had residency training. Use of a SOP was reported by 76% of CPSs, and 66% of these had a global practice-area scope. Table 1 outlines the functions authorized by a global or limited SOP.6
Overall, 52% of sites reported CPS involvement in CMM of primarily anticoagulation, diabetes mellitus (DM), anemia, hyperlipidemia, and hypertension. The reported average time spent for each disease encounter is delineated in Table 2.
Thirty-five percent of sites reported CPS participation in home visits, and the majority of those completed between 1 and 10 home visits per month. The types of interventions provided often included medication education, assessment of medication adherence, and CMM for DM, hyperlipidemia, hypertension, etc. Multiple interventions often were made during each home visit.
The workload of medication reviews was divided among multiple CPSs in 55% of the programs. The majority of programs completed fewer than 20 initial medication reviews per month and between 21 and 80 quarterly medication reviews per month (81% and 62%, respectively). The average time for a CPS to complete initial medication reviews was 78 minutes and 42 minutes for quarterly medication reviews.
Sites with CPSs that held a SOP (76%) took an average of 83 minutes to complete an initial medication review and 48 minutes to complete a quarterly review. Sites with CPSs without a SOP (24%) took an average of 72 minutes to complete an initial medication review and 36 minutes to complete a quarterly review. Many CPSs allocate ≤ 20 hours per month on routine pharmacy functions (eg, prescription verification, dispensing activities, nonformulary medication requests) and ≤ 20 hours per month on nonpatient care activities (eg, education, medication use evaluations, training, projects), 67% and 82%, respectively.
Ninety-seven percent of CPSs actively attended weekly HBPC program interdisciplinary team (IDT) meetings, with 67% attending 1 weekly IDT meeting and 30% attending 2 to 5 weekly IDT meetings. Time spent attending IDT and roundtable discussions averaged 3.5 hours per week. Multiple programs noted growth within the 12 months preceding the survey, as 37 sites were granted approval for a total of 29.75 additional CPS FTEEs, and an additional 10 sites had a total of 9.25 FTEEs pending approval.
Discussion
Analysis of this assessment allowed the HBPC CPS SME workgroup to identify strong practices and variations in individual HBPC pharmacy programs. The majority of CPSs (66%) are using global, practice area-based SOPs, which allows more autonomy via direct patient care to veterans through CMM and home visits. This trend suggests the focus of the HBPC CPS role has expanded beyond traditional pharmacist activities. These global SOPs result in a higher yield of CPS functions, such as developing, documenting, and executing therapeutic plans and prescribing medications (Table 1). A higher percentage of CPSs with a practice area-based SOP were authorized to perform all 8 functions. Therefore, increased use of practice area-based SOPs and the expansion of the HBPC CPS role can support the team and increase clinical services available to veterans.
Clinical pharmacy specialists using SOPs take longer to complete medication reviews compared with those not using SOPs. Although the assessment was not designed to evaluate the reasons for these time differences, post-hoc follow-up clarification with individual sites determined CPS use of a SOP can lend to a more time-intensive and comprehensive medication review. This may lead to more optimized and safe medication regimens and elimination of unnecessary and/or inappropriate medications for HBPC veterans.
While only 35% of pharmacists were participating in the home visits at the time of this assessment, this is another area to explore as an opportunity to expand CMM. Although the assessment showed the majority of these home visits addressed medication education and adherence, programs may find it advantageous to provide CPS home visits for veterans identified as high risk or requiring specialized CMM. Additional data are needed regarding the ideal population to target for CPS home visits, as well as the estimated benefits of conducting home visits, such as outcomes and efficiency.
With growth noted in multiple programs, HBPC leadership should continue to encourage expanded pharmacist roles at an advanced practice level with SOPs, to provide veteran-centered care. This practice allows the team to concentrate efforts on patient acuity while increasing veteran access to VHA care. Additional CPS FTEEs are necessary to allow for expansion of the HBPC CPS role. The data also demonstrate HBPC often uses a part-time workforce where pharmacists are assigned to HBPC < 40 hours per week, and multiple pharmacists may be used to fulfill 1 CPS FTEE position. Home-Based Primary Care programs are encouraged to consolidate the number of CPSs involved as core individuals to promote continuity and avoid fragmented care.
Limitations
One limitation of the assessment is that the questions were designed and tested by a small group of CPSs, which may have led to response bias and potential misinterpretation of some questions. Time spent on medication reviews may have been underestimated, as some sites reported the maximum allowable workload credit time rather than actual time spent. Recall bias also is a limitation because the assessment relied on the recollection of the CPS or chief of pharmacy. Additionally, while the assessment focused on quantity and time spent on medication reviews, it was not designed to evaluate quality. Examination of what constitutes a high-quality medication review would be helpful to provide guidance and standardize care across the VHA.
Conclusion
Clinical pharmacy specialists practicing in the VHA HBPC setting are highly trained clinicians. A significant percentage of CPSs practice with a SOP that includes prescriptive privileges. However, variations in practice and function exist in the system. This presents an excellent opportunity for future standardization and promotion of the highest and best use of the CPS to improve quality of care for HBPC. With the expansion of the CPS role, there is potential for pharmacists to increase clinical activities and improve care for home-based veterans. The CPPO HBPC SME workgroup will continue to examine and explore the CPS role in this practice setting, develop staffing and practice guidance documents, and assess the benefit of CPS home visits.
Home-Based Primary Care (HBPC) is a unique interdisciplinary program within the Veteran’s Health Administration (VHA) that specifically targets veterans with complex, chronic disabling diseases who have difficulty traveling to a VHA facility.1 Veterans are provided comprehensive longitudinal primary care in their homes, with the goal of maximizing the veteran’s independence. Clinical pharmacists are known as medication experts and have an essential role within interdisciplinary teams, including HBPC, improving medication safety, and decreasing inappropriate prescribing practices.2,3 Clinical pharmacy specialists (CPSs) within the VHA work collaboratively but autonomously as advanced practice providers assisting with the pharmacologic management of many diseases and chronic conditions. The remainder of this article will refer to the HBPC pharmacist as a CPS.
The CPS is actively involved in providing comprehensive medication management (CMM) services across VHA and has the expertise to effectively assist veterans in achieving targeted clinical outcomes. While the value and role of CPSs in the primary care setting are described extensively in the literature, data regarding the CPS in HBPC are limited.4-6 Therefore, the purpose of the assessment was to evaluate the status of the HBPC pharmacy workforce, identify current pharmacist activities and strong practices, and clarify national variations among programs. Future use of this analysis may assist with standardization of the HBPC CPS role and development of business rules in combination with a workload-based staffing model tool.
Background
The role of the pharmacist in the HBPC setting has evolved from providing basic medication therapy reviews to an advanced role providing CMM services under a VHA scope of practice (SOP), which outlines 8 functions that may be authorized, including medication prescriptive authority.7 The SOP may be disease specific (limited) but is increasingly transitioning to have a practice-area scope (global), which is consistent with other VHA advanced practice providers.7 Effective use of a CPS in this role allows for optimization of CMM and increasing veteran access to VHA care.
The VHA employed 7,285 pharmacists in 2014.8 Many were considered CPSs with prescriptive authority. These pharmacists were responsible for ordering more than 1.7 million distinct prescriptions across the VHA in fiscal year 2014, which represented 2.6% of the total prescriptions that year.7 A 2007 VHA study also demonstrated both an increase in appropriate prescribing practices and improved medication use when CPSs worked in collaboration with the HBPC team.9 With this evolution of VHA pharmacists, there has been an increase in the use of CPSs in HBPC and changes in staffing ratios to allow for additional clinical activities and comprehensive patient care provision.1
The HBPC model serves a complex population in which each veteran has about 8 chronic conditions.1,10 An interdisciplinary team consisting of various health care professionals, such as physicians, nurse practitioners, nurses, social workers, registered dietitians, psychologists, rehabilitation therapists, pharmacists, etc, work collaboratively to care for these veterans in the patient’s home. This team is a type of patient-centered medical home (PCMH) that focuses on providing primary care services to an at-risk veteran population who have difficulty leaving the home.1 Home-based primary care has been shown to be cost-effective, reducing average annual cost of health care by up to 24%.10 Another study showed that patients using HBPC had a 27% reduction in hospital admissions and 69% reduction in inpatient hospital days when compared with patients who were not using HBPC.11
The interdisciplinary team meets at least once weekly to discuss and design individualized care plans for veterans enrolled in the program. It is desirable for pharmacists on these teams to have special expertise and certification in geriatric pharmacotherapy and chronic disease management (eg, board-certified geriatric pharmacist [BCGP], board-certified pharmacotherapy specialist [BCPS], or board-certified ambulatory care pharmacist [BCACP]) due to the complexity of comorbidities of these veterans.12 Additional education such as postgraduate pharmacy residency training also is beneficial for CPSs in this setting.
The CPS proactively performs CMM that is often greater in scope than a targeted disease review due to multiple comorbid conditions that are often present within veteran patients.1 These comprehensive medication reviews are considered a core function and must be performed on enrollment in HBPC, quarterly, and when clinically indicated or requested by the team.13 Sufficient time must be allocated to the CPS in order to provide these high-quality medication reviews. Additional core functions of the CPS are outlined in the functional statement and/or SOP, but responsibilities include CMM and disease management. This typically consists of prescribing and/or adjusting medications, as well as providing patient and caregiver education, which can be performed either face-to-face or via telehealth visits (eg, telephone and video). A CPS also may make home visits to assess the veteran, either independently or with other disciplines of the HBPC team.
The HBPC Subject Matter Expert (SME) workgroup was chartered by the Veterans Affairs Central Office (VACO) Pharmacy Benefits Management Service (PBM) Clinical Pharmacy Practice Office (CPPO) to explore pharmacy practice changes in the HBPC setting. This workgroup serves as clinical practice leadership within the HBPC setting to provide expertise and lead initiatives supporting the advanced practice role of the HBPC CPS.
As HBPC programs expanded throughout VHA, it was paramount to determine the current state of HBPC pharmacy practice by collecting necessary data points to assess uniformity and better understand opportunities for practice standardization. The SME workgroup developed a voluntary yet comprehensive survey assessment that served to proactively assess the future of HBPC pharmacy.
Methods
The HBPC SME workgroup, in conjunction with CPPO, developed the assessment. Questions were designed and tested within a small group of CPSs and then distributed electronically. In August 2014, the assessment was e-mailed to all 21 VHA service areas with an active HBPC program, and responses were collected through a Microsoft SharePoint (Redmond, WA) survey. A response was requested from chiefs of pharmacy, clinical pharmacy leadership, or a representative.
This voluntary assessment contained 24 multipart questions related to background information of HBPC programs and clinical pharmacy services. Duplicate responses were consolidated and clarified with individual sites post hoc.
Descriptive statistics were used to analyze responses. To standardize the comparison across sites with a variety of full-time equivalent employees (FTEEs), the average patient census was divided by the CPS FTEE allocated to the programs at that site. For example, if a site reported 316 patients with 0.25 CPS FTEE, a standardized ratio for this site was 1,264 patients per FTEE. If a patient census range was reported, the median number would be used.
Results
The team received responses from 130 of 141 VHA facilities (92%), encompassing 270 CPSs. A total of 168.75 FTEEs were officially designated as HBPC CPSs. All 21 VHA service areas at the time were represented. The majority of responding programs (67%) had < 1 CPS FTEE allocated to HBPC; many of these CPSs were working in other pharmacy areas but were only dedicated to HBPC part-time.
Nearly 90% of CPSs completed postgraduate year 1 residency training. Fifty-seven percent of CPSs held advanced certifications, such as BCGP, BCACP, or BCPS. Sixty-two percent of CPSs with these specialized board certifications had residency training. Use of a SOP was reported by 76% of CPSs, and 66% of these had a global practice-area scope. Table 1 outlines the functions authorized by a global or limited SOP.6
Overall, 52% of sites reported CPS involvement in CMM of primarily anticoagulation, diabetes mellitus (DM), anemia, hyperlipidemia, and hypertension. The reported average time spent for each disease encounter is delineated in Table 2.
Thirty-five percent of sites reported CPS participation in home visits, and the majority of those completed between 1 and 10 home visits per month. The types of interventions provided often included medication education, assessment of medication adherence, and CMM for DM, hyperlipidemia, hypertension, etc. Multiple interventions often were made during each home visit.
The workload of medication reviews was divided among multiple CPSs in 55% of the programs. The majority of programs completed fewer than 20 initial medication reviews per month and between 21 and 80 quarterly medication reviews per month (81% and 62%, respectively). The average time for a CPS to complete initial medication reviews was 78 minutes and 42 minutes for quarterly medication reviews.
Sites with CPSs that held a SOP (76%) took an average of 83 minutes to complete an initial medication review and 48 minutes to complete a quarterly review. Sites with CPSs without a SOP (24%) took an average of 72 minutes to complete an initial medication review and 36 minutes to complete a quarterly review. Many CPSs allocate ≤ 20 hours per month on routine pharmacy functions (eg, prescription verification, dispensing activities, nonformulary medication requests) and ≤ 20 hours per month on nonpatient care activities (eg, education, medication use evaluations, training, projects), 67% and 82%, respectively.
Ninety-seven percent of CPSs actively attended weekly HBPC program interdisciplinary team (IDT) meetings, with 67% attending 1 weekly IDT meeting and 30% attending 2 to 5 weekly IDT meetings. Time spent attending IDT and roundtable discussions averaged 3.5 hours per week. Multiple programs noted growth within the 12 months preceding the survey, as 37 sites were granted approval for a total of 29.75 additional CPS FTEEs, and an additional 10 sites had a total of 9.25 FTEEs pending approval.
Discussion
Analysis of this assessment allowed the HBPC CPS SME workgroup to identify strong practices and variations in individual HBPC pharmacy programs. The majority of CPSs (66%) are using global, practice area-based SOPs, which allows more autonomy via direct patient care to veterans through CMM and home visits. This trend suggests the focus of the HBPC CPS role has expanded beyond traditional pharmacist activities. These global SOPs result in a higher yield of CPS functions, such as developing, documenting, and executing therapeutic plans and prescribing medications (Table 1). A higher percentage of CPSs with a practice area-based SOP were authorized to perform all 8 functions. Therefore, increased use of practice area-based SOPs and the expansion of the HBPC CPS role can support the team and increase clinical services available to veterans.
Clinical pharmacy specialists using SOPs take longer to complete medication reviews compared with those not using SOPs. Although the assessment was not designed to evaluate the reasons for these time differences, post-hoc follow-up clarification with individual sites determined CPS use of a SOP can lend to a more time-intensive and comprehensive medication review. This may lead to more optimized and safe medication regimens and elimination of unnecessary and/or inappropriate medications for HBPC veterans.
While only 35% of pharmacists were participating in the home visits at the time of this assessment, this is another area to explore as an opportunity to expand CMM. Although the assessment showed the majority of these home visits addressed medication education and adherence, programs may find it advantageous to provide CPS home visits for veterans identified as high risk or requiring specialized CMM. Additional data are needed regarding the ideal population to target for CPS home visits, as well as the estimated benefits of conducting home visits, such as outcomes and efficiency.
With growth noted in multiple programs, HBPC leadership should continue to encourage expanded pharmacist roles at an advanced practice level with SOPs, to provide veteran-centered care. This practice allows the team to concentrate efforts on patient acuity while increasing veteran access to VHA care. Additional CPS FTEEs are necessary to allow for expansion of the HBPC CPS role. The data also demonstrate HBPC often uses a part-time workforce where pharmacists are assigned to HBPC < 40 hours per week, and multiple pharmacists may be used to fulfill 1 CPS FTEE position. Home-Based Primary Care programs are encouraged to consolidate the number of CPSs involved as core individuals to promote continuity and avoid fragmented care.
Limitations
One limitation of the assessment is that the questions were designed and tested by a small group of CPSs, which may have led to response bias and potential misinterpretation of some questions. Time spent on medication reviews may have been underestimated, as some sites reported the maximum allowable workload credit time rather than actual time spent. Recall bias also is a limitation because the assessment relied on the recollection of the CPS or chief of pharmacy. Additionally, while the assessment focused on quantity and time spent on medication reviews, it was not designed to evaluate quality. Examination of what constitutes a high-quality medication review would be helpful to provide guidance and standardize care across the VHA.
Conclusion
Clinical pharmacy specialists practicing in the VHA HBPC setting are highly trained clinicians. A significant percentage of CPSs practice with a SOP that includes prescriptive privileges. However, variations in practice and function exist in the system. This presents an excellent opportunity for future standardization and promotion of the highest and best use of the CPS to improve quality of care for HBPC. With the expansion of the CPS role, there is potential for pharmacists to increase clinical activities and improve care for home-based veterans. The CPPO HBPC SME workgroup will continue to examine and explore the CPS role in this practice setting, develop staffing and practice guidance documents, and assess the benefit of CPS home visits.
1. US Department of Veterans Affairs. VHA Directive 1141.01: home-based primary care special population aligned care team program. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=5417. Updated September 20, 2017. Accessed April 3, 2018.
2. Brahmbhatt M, Palla K, Kossifologos A, Mitchell D, Lee T. Appropriateness of medication prescribing using the STOPP/START criteria in veterans receiving home-based primary care. Consult Pharm. 2013;28(6):361-369.
3. Hanlon JT, Weinberger M, Samsa GP, et al. A randomized, controlled trial of a clinical pharmacist intervention to improve inappropriate prescribing in elderly outpatients with polypharmacy. Am J Med. 1996;100(4):428-437.
4. Rose AJ, McCullough MB, Carter BL, Rudin RS. The clinical pharmacy specialist: part of the solution. J Gen Intern Med. 2017;32(4):375–377.
5. Giberson S, Yoder S, Lee MP. Improving patient and health system outcomes through advanced pharmacy practice: a report to the U.S. Surgeon General 2011. https://www.accp.com/docs/positions/misc/Improving_Patient_and_Health_System_Outcomes.pdf. Published December 2011. Accessed April 3, 2018.
6. Lee AJ, Boro MS, Knapp KK, Meier JL, Korman NE. Clinical and economic outcomes of pharmacist recommendations in a Veterans Affairs medical center. Am J Health Syst Pharm. 2002;59(21):2070–2077.
7. Ourth H, Groppi J, Morreale AP, Quicci-Roberts K. Clinical pharmacist prescribing activities in the Veterans Health Administration. Am J Health Syst Pharm. 2016;73(18):1406-1415.
8. US Department of Veteran Affairs, Veterans Health Administration, Healthcare Talent Management Workforce Management & Consulting Office. VHA workforce planning report 2015.https://www.vacareers.va.gov/assets/common/print/2015_VHA_Workforce_Succession_Strategic_Plan.pdf. Published 2015. Accessed April 3, 2018.
9. Davis RG, Hepfinger CA, Sauer KA, Wilhardt MS. Retrospective evaluation of medication appropriateness and clinical pharmacist drug therapy recommendations for home-based primary care veterans. Am J Geriatr Pharmacother. 2007;5(1):40-47.
10. Beales JL, Edes T. Veteran’s Affairs home based primary care. Clin Geriatr Med. 2009;25(1):149-154.
11. Cooper DF, Granadillo OR, Stacey CM. Home-based primary care: the care of the veteran at home. Home Healthc Nurse. 2007;25(5):315-322.
12. Pradel FG, Palumbo FB, Flowers L, et al. White paper: value of specialty certification in pharmacy. J Am Pharm Assoc. 2004;44(5):612-620.
13. US Department of Veterans Affairs, Veterans Health Administration. VHA Handbook 1108.11(1). Clinical pharmacy services. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=3120. Updated June 29, 2017. Accessed April 3, 2018
1. US Department of Veterans Affairs. VHA Directive 1141.01: home-based primary care special population aligned care team program. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=5417. Updated September 20, 2017. Accessed April 3, 2018.
2. Brahmbhatt M, Palla K, Kossifologos A, Mitchell D, Lee T. Appropriateness of medication prescribing using the STOPP/START criteria in veterans receiving home-based primary care. Consult Pharm. 2013;28(6):361-369.
3. Hanlon JT, Weinberger M, Samsa GP, et al. A randomized, controlled trial of a clinical pharmacist intervention to improve inappropriate prescribing in elderly outpatients with polypharmacy. Am J Med. 1996;100(4):428-437.
4. Rose AJ, McCullough MB, Carter BL, Rudin RS. The clinical pharmacy specialist: part of the solution. J Gen Intern Med. 2017;32(4):375–377.
5. Giberson S, Yoder S, Lee MP. Improving patient and health system outcomes through advanced pharmacy practice: a report to the U.S. Surgeon General 2011. https://www.accp.com/docs/positions/misc/Improving_Patient_and_Health_System_Outcomes.pdf. Published December 2011. Accessed April 3, 2018.
6. Lee AJ, Boro MS, Knapp KK, Meier JL, Korman NE. Clinical and economic outcomes of pharmacist recommendations in a Veterans Affairs medical center. Am J Health Syst Pharm. 2002;59(21):2070–2077.
7. Ourth H, Groppi J, Morreale AP, Quicci-Roberts K. Clinical pharmacist prescribing activities in the Veterans Health Administration. Am J Health Syst Pharm. 2016;73(18):1406-1415.
8. US Department of Veteran Affairs, Veterans Health Administration, Healthcare Talent Management Workforce Management & Consulting Office. VHA workforce planning report 2015.https://www.vacareers.va.gov/assets/common/print/2015_VHA_Workforce_Succession_Strategic_Plan.pdf. Published 2015. Accessed April 3, 2018.
9. Davis RG, Hepfinger CA, Sauer KA, Wilhardt MS. Retrospective evaluation of medication appropriateness and clinical pharmacist drug therapy recommendations for home-based primary care veterans. Am J Geriatr Pharmacother. 2007;5(1):40-47.
10. Beales JL, Edes T. Veteran’s Affairs home based primary care. Clin Geriatr Med. 2009;25(1):149-154.
11. Cooper DF, Granadillo OR, Stacey CM. Home-based primary care: the care of the veteran at home. Home Healthc Nurse. 2007;25(5):315-322.
12. Pradel FG, Palumbo FB, Flowers L, et al. White paper: value of specialty certification in pharmacy. J Am Pharm Assoc. 2004;44(5):612-620.
13. US Department of Veterans Affairs, Veterans Health Administration. VHA Handbook 1108.11(1). Clinical pharmacy services. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=3120. Updated June 29, 2017. Accessed April 3, 2018
Acute Kidney Injury. 2017 Hospital Medicine Revised Core Competencies
Acute kidney injury (AKI), also known as acute renal failure (ARF), is a decline in renal function over a period of hours or days that results in the accumulation of nitrogenous waste products and an impaired ability to maintain fluid/electrolyte/acid-base homeostasis. Epidemiologic studies of AKI are confounded by inconsistent definitions and underreporting. The average incidence is estimated to be 23.8 cases per 1000 hospital discharges.1Approximately 5% to 20% of critically ill patients experience AKI during the course of their illness.2 AKI may present in isolation, develop as a complication of other comorbid illness, or result as a deleterious adverse effect of treatment or diagnostic interventions. Uncomplicated AKI is associated with a mortality rate of up to 10%.3-6 Patients with AKI and multiorgan failure have mortality rates higher than 50%.3-6 AKI is associated with an increased length of hospital stay; a rise in serum creatinine of 0.5 mg/dL or greater while hospitalized confers a 3.5-day increase in length of stay.7 Hospitalists facilitate the expeditious evaluation and management of AKI to improve patient outcomes, optimize resource use, and reduce length of stay. Hospitalists can also advocate and initiate preventive strategies to reduce the incidence of secondary AKI.
KNOWLEDGE
Hospitalists should be able to:
Describe the symptoms and signs of AKI.
Describe and differentiate pathophysiologic causes of AKI including prerenal, intrinsic renal, and postrenal processes.
Differentiate among the causes of prerenal, intrinsic renal, and postrenal types of AKI.
Describe a logical sequence of indicated tests required to evaluate etiologies of AKI based on classification of AKI type.
List common potentially nephrotoxic agents that can cause or worsen AKI.
Explain the indications, contraindications, and mechanisms of action of the interventions used to treat AKI.
Explain the indications, contraindications, benefits, and risks of acute hemodialysis.
Recognize indications for specialty consultation for AKI and the role of nephrology and/or urology specialists.
Describe criteria, including specific measures of clinical stability, that must be met before discharging patients with AKI.
Explain the specific goals that should be met to ensure safe transitions of care for patients with AKI.
SKILLS
Hospitalists should be able to:
Assess patients with suspected AKI in a timely manner and manage or comanage the patient with the primary requesting service.
Elicit a thorough and relevant medical history with emphasis on factors predisposing or contributing to the development of AKI.
Review all drug use including prescription and over-the-counter medications, herbal remedies, nutritional supplements, and illicit drugs to identify common potential nephrotoxins.
Perform a physical examination to assess volume status and to identify underlying comorbid states that may predispose to the development of AKI.
Order and interpret results of indicated diagnostic studies that may include urinalysis and microscopic sediment analysis, urinary diagnostic indices, urinary protein excretion, serologic evaluation, and renal imaging.
Interpret common clinical, laboratory, and imaging findings used to evaluate and follow the severity of AKI.
Diagnose common complications, such as electrolyte abnormalities, that occur with AKI and institute corrective measures.
Calculate estimated creatinine clearance for medication dosage adjustments when indicated.
Identify patients at risk for developing AKI and institute appropriate preventive measures including avoidance of unnecessary radiographic contrast exposure and adherence to evidence-based interventions to reduce the risk of contrast-induced nephropathy.
Coordinate appropriate nutritional and metabolic interventions.
Formulate an AKI treatment plan tailored to the individual patient, which may include fluid management, pharmacologic agents, nutritional recommendations, and patient education.
Identify and treat factors that may complicate the management of AKI, including extreme blood pressure, underlying infections, and the sequelae of electrolyte abnormalities.
Communicate with patients and families to explain the cause and prognosis of AKI.
Communicate with patients and families to explain the rationale for the use of radiographic tests and procedures and the benefit and potential adverse effects of radiographic contrast agents.
Facilitate discharge planning early during hospitalization.
Communicate with patients and families to explain the goals of care, discharge instructions, and management after hospital discharge to ensure safe follow-up and transitions of care.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include nursing, nutrition, and pharmacy services, in the care of patients with AKI that begins at admission and continues through all care transitions.
Follow evidence-based recommendations, protocols, and risk-stratification tools for the treatment of AKI.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Advocate for, establish, and support initiatives to reduce the incidence of iatrogenic AKI.
Lead, coordinate, and/or participate in multidisciplinary teams (including nephrology, nursing, pharmacy, and nutrition services) to improve processes that facilitate early identification of AKI and improved patient outcomes.
Lead, coordinate, and/or participate in multidisciplinary initiatives to promote patient safety and optimize management strategies for AKI.
1. Xue JL, Daniels F, Star RA, Kimmel PL, Eggers PW, Molitoris BA, et al. Incidence and mortality of acute renal failure in Medicare beneficiaries, 1992-2001. J Am Soc Nephrol. 2006;17(4):1135-1142.
2. Metnitz PG, Krenn CG, Steltzer H, Lang T, Ploder J, Lenz K, et al. Effect of acute renal failure requiring renal replacement therapy on outcome in critically ill patients. Crit Care Med. 2002;30(9):2051-2058.
3. Cosentino F, Chaff C, Piedmonte M. Risk factors influencing survival in ICU acute renal failure. Nephrol Dial Transplant. 1994;9(Suppl 4):179-182.
4. Hou SH, Bushinsky DA, Wish JB, Cohen JJ, Harrington JT. Hospital-acquired renal insufficiency: a prospective study. Am H Med. 1983;74(2):243-248.
5. Liano F, Junco E, Pascual J, Madero R, Verde E. The spectrum of acute renal failure in the intensive care unit compared with that seen in other settings. The Madrid Acute Renal Failure Study Group. Kidney Int Suppl. 1998;66:S16-S24.
6. Shusterman N, Strom BL, Murray TG, Morrison G, West SL, Maislin G. Risk factors and outcome of hospital-acquired acute renal failure. Clinical epidemiologic study. Am J Med. 1987;83(1):65-71.
7. Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16(11):3365-3370.
Acute kidney injury (AKI), also known as acute renal failure (ARF), is a decline in renal function over a period of hours or days that results in the accumulation of nitrogenous waste products and an impaired ability to maintain fluid/electrolyte/acid-base homeostasis. Epidemiologic studies of AKI are confounded by inconsistent definitions and underreporting. The average incidence is estimated to be 23.8 cases per 1000 hospital discharges.1Approximately 5% to 20% of critically ill patients experience AKI during the course of their illness.2 AKI may present in isolation, develop as a complication of other comorbid illness, or result as a deleterious adverse effect of treatment or diagnostic interventions. Uncomplicated AKI is associated with a mortality rate of up to 10%.3-6 Patients with AKI and multiorgan failure have mortality rates higher than 50%.3-6 AKI is associated with an increased length of hospital stay; a rise in serum creatinine of 0.5 mg/dL or greater while hospitalized confers a 3.5-day increase in length of stay.7 Hospitalists facilitate the expeditious evaluation and management of AKI to improve patient outcomes, optimize resource use, and reduce length of stay. Hospitalists can also advocate and initiate preventive strategies to reduce the incidence of secondary AKI.
KNOWLEDGE
Hospitalists should be able to:
Describe the symptoms and signs of AKI.
Describe and differentiate pathophysiologic causes of AKI including prerenal, intrinsic renal, and postrenal processes.
Differentiate among the causes of prerenal, intrinsic renal, and postrenal types of AKI.
Describe a logical sequence of indicated tests required to evaluate etiologies of AKI based on classification of AKI type.
List common potentially nephrotoxic agents that can cause or worsen AKI.
Explain the indications, contraindications, and mechanisms of action of the interventions used to treat AKI.
Explain the indications, contraindications, benefits, and risks of acute hemodialysis.
Recognize indications for specialty consultation for AKI and the role of nephrology and/or urology specialists.
Describe criteria, including specific measures of clinical stability, that must be met before discharging patients with AKI.
Explain the specific goals that should be met to ensure safe transitions of care for patients with AKI.
SKILLS
Hospitalists should be able to:
Assess patients with suspected AKI in a timely manner and manage or comanage the patient with the primary requesting service.
Elicit a thorough and relevant medical history with emphasis on factors predisposing or contributing to the development of AKI.
Review all drug use including prescription and over-the-counter medications, herbal remedies, nutritional supplements, and illicit drugs to identify common potential nephrotoxins.
Perform a physical examination to assess volume status and to identify underlying comorbid states that may predispose to the development of AKI.
Order and interpret results of indicated diagnostic studies that may include urinalysis and microscopic sediment analysis, urinary diagnostic indices, urinary protein excretion, serologic evaluation, and renal imaging.
Interpret common clinical, laboratory, and imaging findings used to evaluate and follow the severity of AKI.
Diagnose common complications, such as electrolyte abnormalities, that occur with AKI and institute corrective measures.
Calculate estimated creatinine clearance for medication dosage adjustments when indicated.
Identify patients at risk for developing AKI and institute appropriate preventive measures including avoidance of unnecessary radiographic contrast exposure and adherence to evidence-based interventions to reduce the risk of contrast-induced nephropathy.
Coordinate appropriate nutritional and metabolic interventions.
Formulate an AKI treatment plan tailored to the individual patient, which may include fluid management, pharmacologic agents, nutritional recommendations, and patient education.
Identify and treat factors that may complicate the management of AKI, including extreme blood pressure, underlying infections, and the sequelae of electrolyte abnormalities.
Communicate with patients and families to explain the cause and prognosis of AKI.
Communicate with patients and families to explain the rationale for the use of radiographic tests and procedures and the benefit and potential adverse effects of radiographic contrast agents.
Facilitate discharge planning early during hospitalization.
Communicate with patients and families to explain the goals of care, discharge instructions, and management after hospital discharge to ensure safe follow-up and transitions of care.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include nursing, nutrition, and pharmacy services, in the care of patients with AKI that begins at admission and continues through all care transitions.
Follow evidence-based recommendations, protocols, and risk-stratification tools for the treatment of AKI.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Advocate for, establish, and support initiatives to reduce the incidence of iatrogenic AKI.
Lead, coordinate, and/or participate in multidisciplinary teams (including nephrology, nursing, pharmacy, and nutrition services) to improve processes that facilitate early identification of AKI and improved patient outcomes.
Lead, coordinate, and/or participate in multidisciplinary initiatives to promote patient safety and optimize management strategies for AKI.
Acute kidney injury (AKI), also known as acute renal failure (ARF), is a decline in renal function over a period of hours or days that results in the accumulation of nitrogenous waste products and an impaired ability to maintain fluid/electrolyte/acid-base homeostasis. Epidemiologic studies of AKI are confounded by inconsistent definitions and underreporting. The average incidence is estimated to be 23.8 cases per 1000 hospital discharges.1Approximately 5% to 20% of critically ill patients experience AKI during the course of their illness.2 AKI may present in isolation, develop as a complication of other comorbid illness, or result as a deleterious adverse effect of treatment or diagnostic interventions. Uncomplicated AKI is associated with a mortality rate of up to 10%.3-6 Patients with AKI and multiorgan failure have mortality rates higher than 50%.3-6 AKI is associated with an increased length of hospital stay; a rise in serum creatinine of 0.5 mg/dL or greater while hospitalized confers a 3.5-day increase in length of stay.7 Hospitalists facilitate the expeditious evaluation and management of AKI to improve patient outcomes, optimize resource use, and reduce length of stay. Hospitalists can also advocate and initiate preventive strategies to reduce the incidence of secondary AKI.
KNOWLEDGE
Hospitalists should be able to:
Describe the symptoms and signs of AKI.
Describe and differentiate pathophysiologic causes of AKI including prerenal, intrinsic renal, and postrenal processes.
Differentiate among the causes of prerenal, intrinsic renal, and postrenal types of AKI.
Describe a logical sequence of indicated tests required to evaluate etiologies of AKI based on classification of AKI type.
List common potentially nephrotoxic agents that can cause or worsen AKI.
Explain the indications, contraindications, and mechanisms of action of the interventions used to treat AKI.
Explain the indications, contraindications, benefits, and risks of acute hemodialysis.
Recognize indications for specialty consultation for AKI and the role of nephrology and/or urology specialists.
Describe criteria, including specific measures of clinical stability, that must be met before discharging patients with AKI.
Explain the specific goals that should be met to ensure safe transitions of care for patients with AKI.
SKILLS
Hospitalists should be able to:
Assess patients with suspected AKI in a timely manner and manage or comanage the patient with the primary requesting service.
Elicit a thorough and relevant medical history with emphasis on factors predisposing or contributing to the development of AKI.
Review all drug use including prescription and over-the-counter medications, herbal remedies, nutritional supplements, and illicit drugs to identify common potential nephrotoxins.
Perform a physical examination to assess volume status and to identify underlying comorbid states that may predispose to the development of AKI.
Order and interpret results of indicated diagnostic studies that may include urinalysis and microscopic sediment analysis, urinary diagnostic indices, urinary protein excretion, serologic evaluation, and renal imaging.
Interpret common clinical, laboratory, and imaging findings used to evaluate and follow the severity of AKI.
Diagnose common complications, such as electrolyte abnormalities, that occur with AKI and institute corrective measures.
Calculate estimated creatinine clearance for medication dosage adjustments when indicated.
Identify patients at risk for developing AKI and institute appropriate preventive measures including avoidance of unnecessary radiographic contrast exposure and adherence to evidence-based interventions to reduce the risk of contrast-induced nephropathy.
Coordinate appropriate nutritional and metabolic interventions.
Formulate an AKI treatment plan tailored to the individual patient, which may include fluid management, pharmacologic agents, nutritional recommendations, and patient education.
Identify and treat factors that may complicate the management of AKI, including extreme blood pressure, underlying infections, and the sequelae of electrolyte abnormalities.
Communicate with patients and families to explain the cause and prognosis of AKI.
Communicate with patients and families to explain the rationale for the use of radiographic tests and procedures and the benefit and potential adverse effects of radiographic contrast agents.
Facilitate discharge planning early during hospitalization.
Communicate with patients and families to explain the goals of care, discharge instructions, and management after hospital discharge to ensure safe follow-up and transitions of care.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include nursing, nutrition, and pharmacy services, in the care of patients with AKI that begins at admission and continues through all care transitions.
Follow evidence-based recommendations, protocols, and risk-stratification tools for the treatment of AKI.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Advocate for, establish, and support initiatives to reduce the incidence of iatrogenic AKI.
Lead, coordinate, and/or participate in multidisciplinary teams (including nephrology, nursing, pharmacy, and nutrition services) to improve processes that facilitate early identification of AKI and improved patient outcomes.
Lead, coordinate, and/or participate in multidisciplinary initiatives to promote patient safety and optimize management strategies for AKI.
1. Xue JL, Daniels F, Star RA, Kimmel PL, Eggers PW, Molitoris BA, et al. Incidence and mortality of acute renal failure in Medicare beneficiaries, 1992-2001. J Am Soc Nephrol. 2006;17(4):1135-1142.
2. Metnitz PG, Krenn CG, Steltzer H, Lang T, Ploder J, Lenz K, et al. Effect of acute renal failure requiring renal replacement therapy on outcome in critically ill patients. Crit Care Med. 2002;30(9):2051-2058.
3. Cosentino F, Chaff C, Piedmonte M. Risk factors influencing survival in ICU acute renal failure. Nephrol Dial Transplant. 1994;9(Suppl 4):179-182.
4. Hou SH, Bushinsky DA, Wish JB, Cohen JJ, Harrington JT. Hospital-acquired renal insufficiency: a prospective study. Am H Med. 1983;74(2):243-248.
5. Liano F, Junco E, Pascual J, Madero R, Verde E. The spectrum of acute renal failure in the intensive care unit compared with that seen in other settings. The Madrid Acute Renal Failure Study Group. Kidney Int Suppl. 1998;66:S16-S24.
6. Shusterman N, Strom BL, Murray TG, Morrison G, West SL, Maislin G. Risk factors and outcome of hospital-acquired acute renal failure. Clinical epidemiologic study. Am J Med. 1987;83(1):65-71.
7. Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16(11):3365-3370.
1. Xue JL, Daniels F, Star RA, Kimmel PL, Eggers PW, Molitoris BA, et al. Incidence and mortality of acute renal failure in Medicare beneficiaries, 1992-2001. J Am Soc Nephrol. 2006;17(4):1135-1142.
2. Metnitz PG, Krenn CG, Steltzer H, Lang T, Ploder J, Lenz K, et al. Effect of acute renal failure requiring renal replacement therapy on outcome in critically ill patients. Crit Care Med. 2002;30(9):2051-2058.
3. Cosentino F, Chaff C, Piedmonte M. Risk factors influencing survival in ICU acute renal failure. Nephrol Dial Transplant. 1994;9(Suppl 4):179-182.
4. Hou SH, Bushinsky DA, Wish JB, Cohen JJ, Harrington JT. Hospital-acquired renal insufficiency: a prospective study. Am H Med. 1983;74(2):243-248.
5. Liano F, Junco E, Pascual J, Madero R, Verde E. The spectrum of acute renal failure in the intensive care unit compared with that seen in other settings. The Madrid Acute Renal Failure Study Group. Kidney Int Suppl. 1998;66:S16-S24.
6. Shusterman N, Strom BL, Murray TG, Morrison G, West SL, Maislin G. Risk factors and outcome of hospital-acquired acute renal failure. Clinical epidemiologic study. Am J Med. 1987;83(1):65-71.
7. Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16(11):3365-3370.
© 2017 Society of Hospital Medicine
Alcohol and Drug Withdrawal. 2017 Hospital Medicine Revised Core Competencies
Alcohol and drug withdrawal is a set of signs and symptoms that develops in association with sudden cessation or reduction in the use of alcohol or a number of prescription (particularly opioids and benzodiazepines), over-the-counter (OTC), or illicit drugs. Withdrawal syndromes encompass a broad range of symptoms from mild anxiety and tremulousness to more serious manifestations such as delirium tremens, which occurs in up to 5% of alcohol-dependent persons who undergo withdrawal.1 Withdrawal may occur before hospitalization or during the course of hospitalization. Alcohol- and substance-related disorders account for more than 400,000 hospital discharges each year and are associated with a mean length of stay of approximately 4.6 days.2 Alcohol and drug dependence is often an end product of a combination of biopsychosocial influences, and in most cases, a multidisciplinary approach is necessary to successfully treat affected individuals. Hospitalists can lead their institutions in evidence-based treatment protocols that improve care, reduce costs and length of stay, and facilitate better overall outcomes in patients with substance-related withdrawal syndromes.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Describe the effects of drug and alcohol withdrawal on medical illness and the effects of medical illness on substance withdrawal.
Recognize the symptoms and signs of alcohol and drug withdrawal, including withdrawal from prescription and OTC drugs.
Recognize the medical complications from substance use and dependence.
Determine when consultation with a medical toxicologist or expert is necessary.
Distinguish alcohol or drug withdrawal from other causes of delirium.
Differentiate delirium tremens from other alcohol withdrawal syndromes.
Differentiate the clinical manifestations of alcohol or drug intoxication from those of withdrawal.
Recognize different characteristic withdrawal syndromes, such as abstinence syndrome of opioid withdrawal and delirium tremens of alcohol withdrawal.
Describe the tests indicated to evaluate alcohol or drug withdrawal.
Identify patients at increased risk for drug and alcohol withdrawal according to current diagnostic criteria.
Explain indications, contraindications, and mechanisms of action of pharmacologic agents used to treat acute alcohol and drug withdrawal.
Identify local trends in illicit drug use.
Determine the best setting within the hospital to initiate, monitor, evaluate, and treat patients with drug or alcohol withdrawal.
Explain patient characteristics that portend a poor prognosis.
Explain patient characteristics that indicate a requirement for a higher level of care and/or monitoring.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transitions.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history, with emphasis on substance use.
Assess patients with suspected alcohol or drug withdrawal in a timely manner, identify the level of care required, and manage or comanage the patient with the primary requesting service.
Perform a rapid, efficient, and targeted physical examination to assess for alcohol or drug withdrawal and determine whether life-threatening comorbidities are present.
Assess for common comorbidities in patients with a history of alcohol and drug use.
Formulate a treatment plan tailored to the individual patient, which may include appropriate pharmacologic agents and dosing, route of administration, and nutritional supplementation.
Integrate existing literature and federal regulations into the management of patients with opioid withdrawal syndromes. For patients who are undergoing existing treatment for opioid dependency, communicate with outpatient treatment centers and integrate dosing regimens into care management.
Manage withdrawal syndromes in patients with concomitant medical or surgical issues.
Diagnose oversedation and other complications associated with withdrawal therapies.
Recommend the use of restraints and direct observation to ensure patient safety when appropriate.
Reassure, reorient, and frequently monitor patients in a calm environment.
Use the acute hospitalization as an opportunity to counsel patients about abstinence, recovery, and the medical risks of drug and alcohol use.
Initiate preventive measures before discharge, including alcohol and drug cessation measures.
Facilitate discharge planning early in the hospitalization, including communicating with the primary care provider and presenting the patient with contact information for follow-up care, support, and rehabilitation.
Communicate with patients and families to explain the goals of care, discharge instructions, and management after hospital discharge to ensure safe follow-up and transition of care.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include psychiatry, pharmacy, nursing, and social services, in the treatment of patients with substance use or dependency.
Follow evidence-based national recommendations to guide diagnosis, monitoring, and treatment of withdrawal symptoms.
Act in a nonjudgmental manner when managing the hospitalized patient with substance use.
Establish and maintain an open dialogue with patients and families regarding care goals and limitations.
Appreciate and document the value of appropriate treatment in reducing mortality, duration of delirium, time required to control agitation, adequate control of delirium, treatment of complications, and cost.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate, and/or participate in multidisciplinary teams, which may include psychiatry and toxicology, to improve patient safety and management strategies for patients with substance abuse.
Lead, coordinate, and/or participate in the development and promotion of guidelines and/or pathways that facilitate efficient and timely evaluation and treatment of patients with alcohol and drug withdrawal.
Promote the development and use of evidence-based guidelines and protocols for the treatment of withdrawal syndromes.
Advocate for hospital resources to improve the care of patients with substance withdrawal and the environment in which the care is delivered.
Establish relationships with and develop knowledge of community-based organizations that provide support to patients with substance use disorders.
Promote awareness of substance use disorders and screening for them.
Coordinate initiatives to address the increased risk of readmissions associated with substance and polysubstance abuse.
1. Mayo-Smith MF. Pharmacological management of alcohol withdrawal. A meta-analysis and evidence-based practice guideline. American Society of Addiction Medicine Working Group on Pharmacological Management of Alcohol Withdrawal. JAMA. 1997;278(2):144-151.
2. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. U.S. Department of Health & Human Services. Available at: http://hcupnet.ahrq.gov/. Accessed May 2015.
Alcohol and drug withdrawal is a set of signs and symptoms that develops in association with sudden cessation or reduction in the use of alcohol or a number of prescription (particularly opioids and benzodiazepines), over-the-counter (OTC), or illicit drugs. Withdrawal syndromes encompass a broad range of symptoms from mild anxiety and tremulousness to more serious manifestations such as delirium tremens, which occurs in up to 5% of alcohol-dependent persons who undergo withdrawal.1 Withdrawal may occur before hospitalization or during the course of hospitalization. Alcohol- and substance-related disorders account for more than 400,000 hospital discharges each year and are associated with a mean length of stay of approximately 4.6 days.2 Alcohol and drug dependence is often an end product of a combination of biopsychosocial influences, and in most cases, a multidisciplinary approach is necessary to successfully treat affected individuals. Hospitalists can lead their institutions in evidence-based treatment protocols that improve care, reduce costs and length of stay, and facilitate better overall outcomes in patients with substance-related withdrawal syndromes.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Describe the effects of drug and alcohol withdrawal on medical illness and the effects of medical illness on substance withdrawal.
Recognize the symptoms and signs of alcohol and drug withdrawal, including withdrawal from prescription and OTC drugs.
Recognize the medical complications from substance use and dependence.
Determine when consultation with a medical toxicologist or expert is necessary.
Distinguish alcohol or drug withdrawal from other causes of delirium.
Differentiate delirium tremens from other alcohol withdrawal syndromes.
Differentiate the clinical manifestations of alcohol or drug intoxication from those of withdrawal.
Recognize different characteristic withdrawal syndromes, such as abstinence syndrome of opioid withdrawal and delirium tremens of alcohol withdrawal.
Describe the tests indicated to evaluate alcohol or drug withdrawal.
Identify patients at increased risk for drug and alcohol withdrawal according to current diagnostic criteria.
Explain indications, contraindications, and mechanisms of action of pharmacologic agents used to treat acute alcohol and drug withdrawal.
Identify local trends in illicit drug use.
Determine the best setting within the hospital to initiate, monitor, evaluate, and treat patients with drug or alcohol withdrawal.
Explain patient characteristics that portend a poor prognosis.
Explain patient characteristics that indicate a requirement for a higher level of care and/or monitoring.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transitions.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history, with emphasis on substance use.
Assess patients with suspected alcohol or drug withdrawal in a timely manner, identify the level of care required, and manage or comanage the patient with the primary requesting service.
Perform a rapid, efficient, and targeted physical examination to assess for alcohol or drug withdrawal and determine whether life-threatening comorbidities are present.
Assess for common comorbidities in patients with a history of alcohol and drug use.
Formulate a treatment plan tailored to the individual patient, which may include appropriate pharmacologic agents and dosing, route of administration, and nutritional supplementation.
Integrate existing literature and federal regulations into the management of patients with opioid withdrawal syndromes. For patients who are undergoing existing treatment for opioid dependency, communicate with outpatient treatment centers and integrate dosing regimens into care management.
Manage withdrawal syndromes in patients with concomitant medical or surgical issues.
Diagnose oversedation and other complications associated with withdrawal therapies.
Recommend the use of restraints and direct observation to ensure patient safety when appropriate.
Reassure, reorient, and frequently monitor patients in a calm environment.
Use the acute hospitalization as an opportunity to counsel patients about abstinence, recovery, and the medical risks of drug and alcohol use.
Initiate preventive measures before discharge, including alcohol and drug cessation measures.
Facilitate discharge planning early in the hospitalization, including communicating with the primary care provider and presenting the patient with contact information for follow-up care, support, and rehabilitation.
Communicate with patients and families to explain the goals of care, discharge instructions, and management after hospital discharge to ensure safe follow-up and transition of care.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include psychiatry, pharmacy, nursing, and social services, in the treatment of patients with substance use or dependency.
Follow evidence-based national recommendations to guide diagnosis, monitoring, and treatment of withdrawal symptoms.
Act in a nonjudgmental manner when managing the hospitalized patient with substance use.
Establish and maintain an open dialogue with patients and families regarding care goals and limitations.
Appreciate and document the value of appropriate treatment in reducing mortality, duration of delirium, time required to control agitation, adequate control of delirium, treatment of complications, and cost.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate, and/or participate in multidisciplinary teams, which may include psychiatry and toxicology, to improve patient safety and management strategies for patients with substance abuse.
Lead, coordinate, and/or participate in the development and promotion of guidelines and/or pathways that facilitate efficient and timely evaluation and treatment of patients with alcohol and drug withdrawal.
Promote the development and use of evidence-based guidelines and protocols for the treatment of withdrawal syndromes.
Advocate for hospital resources to improve the care of patients with substance withdrawal and the environment in which the care is delivered.
Establish relationships with and develop knowledge of community-based organizations that provide support to patients with substance use disorders.
Promote awareness of substance use disorders and screening for them.
Coordinate initiatives to address the increased risk of readmissions associated with substance and polysubstance abuse.
Alcohol and drug withdrawal is a set of signs and symptoms that develops in association with sudden cessation or reduction in the use of alcohol or a number of prescription (particularly opioids and benzodiazepines), over-the-counter (OTC), or illicit drugs. Withdrawal syndromes encompass a broad range of symptoms from mild anxiety and tremulousness to more serious manifestations such as delirium tremens, which occurs in up to 5% of alcohol-dependent persons who undergo withdrawal.1 Withdrawal may occur before hospitalization or during the course of hospitalization. Alcohol- and substance-related disorders account for more than 400,000 hospital discharges each year and are associated with a mean length of stay of approximately 4.6 days.2 Alcohol and drug dependence is often an end product of a combination of biopsychosocial influences, and in most cases, a multidisciplinary approach is necessary to successfully treat affected individuals. Hospitalists can lead their institutions in evidence-based treatment protocols that improve care, reduce costs and length of stay, and facilitate better overall outcomes in patients with substance-related withdrawal syndromes.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Describe the effects of drug and alcohol withdrawal on medical illness and the effects of medical illness on substance withdrawal.
Recognize the symptoms and signs of alcohol and drug withdrawal, including withdrawal from prescription and OTC drugs.
Recognize the medical complications from substance use and dependence.
Determine when consultation with a medical toxicologist or expert is necessary.
Distinguish alcohol or drug withdrawal from other causes of delirium.
Differentiate delirium tremens from other alcohol withdrawal syndromes.
Differentiate the clinical manifestations of alcohol or drug intoxication from those of withdrawal.
Recognize different characteristic withdrawal syndromes, such as abstinence syndrome of opioid withdrawal and delirium tremens of alcohol withdrawal.
Describe the tests indicated to evaluate alcohol or drug withdrawal.
Identify patients at increased risk for drug and alcohol withdrawal according to current diagnostic criteria.
Explain indications, contraindications, and mechanisms of action of pharmacologic agents used to treat acute alcohol and drug withdrawal.
Identify local trends in illicit drug use.
Determine the best setting within the hospital to initiate, monitor, evaluate, and treat patients with drug or alcohol withdrawal.
Explain patient characteristics that portend a poor prognosis.
Explain patient characteristics that indicate a requirement for a higher level of care and/or monitoring.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transitions.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history, with emphasis on substance use.
Assess patients with suspected alcohol or drug withdrawal in a timely manner, identify the level of care required, and manage or comanage the patient with the primary requesting service.
Perform a rapid, efficient, and targeted physical examination to assess for alcohol or drug withdrawal and determine whether life-threatening comorbidities are present.
Assess for common comorbidities in patients with a history of alcohol and drug use.
Formulate a treatment plan tailored to the individual patient, which may include appropriate pharmacologic agents and dosing, route of administration, and nutritional supplementation.
Integrate existing literature and federal regulations into the management of patients with opioid withdrawal syndromes. For patients who are undergoing existing treatment for opioid dependency, communicate with outpatient treatment centers and integrate dosing regimens into care management.
Manage withdrawal syndromes in patients with concomitant medical or surgical issues.
Diagnose oversedation and other complications associated with withdrawal therapies.
Recommend the use of restraints and direct observation to ensure patient safety when appropriate.
Reassure, reorient, and frequently monitor patients in a calm environment.
Use the acute hospitalization as an opportunity to counsel patients about abstinence, recovery, and the medical risks of drug and alcohol use.
Initiate preventive measures before discharge, including alcohol and drug cessation measures.
Facilitate discharge planning early in the hospitalization, including communicating with the primary care provider and presenting the patient with contact information for follow-up care, support, and rehabilitation.
Communicate with patients and families to explain the goals of care, discharge instructions, and management after hospital discharge to ensure safe follow-up and transition of care.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include psychiatry, pharmacy, nursing, and social services, in the treatment of patients with substance use or dependency.
Follow evidence-based national recommendations to guide diagnosis, monitoring, and treatment of withdrawal symptoms.
Act in a nonjudgmental manner when managing the hospitalized patient with substance use.
Establish and maintain an open dialogue with patients and families regarding care goals and limitations.
Appreciate and document the value of appropriate treatment in reducing mortality, duration of delirium, time required to control agitation, adequate control of delirium, treatment of complications, and cost.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate, and/or participate in multidisciplinary teams, which may include psychiatry and toxicology, to improve patient safety and management strategies for patients with substance abuse.
Lead, coordinate, and/or participate in the development and promotion of guidelines and/or pathways that facilitate efficient and timely evaluation and treatment of patients with alcohol and drug withdrawal.
Promote the development and use of evidence-based guidelines and protocols for the treatment of withdrawal syndromes.
Advocate for hospital resources to improve the care of patients with substance withdrawal and the environment in which the care is delivered.
Establish relationships with and develop knowledge of community-based organizations that provide support to patients with substance use disorders.
Promote awareness of substance use disorders and screening for them.
Coordinate initiatives to address the increased risk of readmissions associated with substance and polysubstance abuse.
1. Mayo-Smith MF. Pharmacological management of alcohol withdrawal. A meta-analysis and evidence-based practice guideline. American Society of Addiction Medicine Working Group on Pharmacological Management of Alcohol Withdrawal. JAMA. 1997;278(2):144-151.
2. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. U.S. Department of Health & Human Services. Available at: http://hcupnet.ahrq.gov/. Accessed May 2015.
1. Mayo-Smith MF. Pharmacological management of alcohol withdrawal. A meta-analysis and evidence-based practice guideline. American Society of Addiction Medicine Working Group on Pharmacological Management of Alcohol Withdrawal. JAMA. 1997;278(2):144-151.
2. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. U.S. Department of Health & Human Services. Available at: http://hcupnet.ahrq.gov/. Accessed May 2015.
© 2017 Society of Hospital Medicine
Asthma. 2017 Hospital Medicine Revised Core Competencies
Asthma is a chronic disease characterized by airway inflammation and reversible airflow limitation. It is one of the most common chronic conditions and it leads to marked morbidity and mortality in hospitalized patients. In the United States, 1 in 12 persons has asthma and nearly 50% of affected individuals experience an asthma exacerbation each year, accounting for 1.8 million emergency department visits.1,2 Annually, more than 400,000 hospital discharges occur with asthma as the primary diagnosis, with an average length of stay of 3.2 days.2Hospitalists are central to the provision of care for patients with asthma through the use of evidence-based approaches to manage acute exacerbations and to prevent their recurrence. Hospitalists should strive to lead multidisciplinary teams to develop institutional guidelines and/or care pathways to improve efficiency and quality of care and to reduce readmission rates and morbidity and mortality from asthma.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Define asthma and describe the pathophysiologic processes that lead to reversible airway obstruction and inflammation.
Identify precipitants of asthma exacerbation, including environmental and occupational exposures.
Recognize the clinical presentation of asthma exacerbation and differentiate it from other acute respiratory and nonrespiratory syndromes.
Describe the role of diagnostic testing, including peak flow monitoring, used for evaluation of asthma exacerbation.
Recognize indications for specialty consultation, including pulmonary and allergy medicine.
Describe evidence-based therapies for the treatment of asthma exacerbations, which may include bronchodilators, systemic corticosteroids, and oxygen.
Explain indications, contraindications, and mechanisms of action of pharmacologic agents used to treat asthma.
Recognize signs and symptoms of impending respiratory failure.
Explain the indications for invasive and noninvasive ventilatory support.
List the risk factors for disease severity and death from asthma.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transition.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history to identify triggers of asthma and symptoms consistent with asthma exacerbation.
Perform a targeted physical examination to elicit signs consistent with asthma exacerbation, differentiate findings from those of other mimicking conditions, and assess illness severity.
Select appropriate diagnostic studies to evaluate severity of asthma exacerbation and interpret the results.
Recognize indications for transfer to the intensive care unit, including impending respiratory failure, and coordinate intubation or noninvasive mechanical ventilation when indicated.
Prescribe appropriate evidence-based pharmacologic therapies during asthma exacerbation, recommending the most appropriate route, dose, frequency, and duration of treatment.
Communicate with patients and families to explain the natural history and prognosis of asthma.
Facilitate discharge planning early during hospitalization.
Develop an asthma action plan in preparation for discharge.
Educate patients and families regarding the indications and appropriate use of daily use inhalers and rescue inhalers for asthmatic control.
Ensure that patients receive training of proper inhaler and peak flow techniques before hospital discharge.
Communicate with patients and families to explain symptoms and signs that should prompt emergent medical attention.
Communicate with patients and families to explain the goals of care, including clinical stability criteria, the importance of preventive measures (such as smoking cessation, avoidance of second-hand smoke, appropriate vaccinations, and modification of environmental exposures), and required follow-up care.
Communicate with patients and families to explain discharge medications, potential adverse effects, duration of therapy and dosing, and taper schedule.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
Provide and coordinate resources to ensure safe transition from the hospital to arranged follow-up care.
ATTITUDES
Hospitalists should be able to:
Work collaboratively with primary care physicians and emergency physicians in making admission decisions.
Employ a multidisciplinary approach, which may include pulmonary medicine, respiratory therapy, nursing, and social services, in the care of patients with asthma exacerbation.
Follow evidence-based recommendations for the treatment of patients with asthma exacerbations.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Contribute to and/or develop educational modules, order sets, and/or pathways that facilitate use of evidence-based strategies for asthma exacerbation in the emergency department and the hospital, with goals of improving outcomes, decreasing length of stay, and reducing rehospitalization rates.
Lead, coordinate, and/or participate in efforts to educate staff on the importance of smoking cessation counseling and other preventive measures.
Lead, coordinate, and/or participate in multidisciplinary initiatives, which may include collaborative efforts with pulmonologists and respiratory therapists, to promote patient safety and optimize cost-effective diagnostic and management strategies for patients with asthma.
1. Centers for Disease Control and Prevention. CDC Vital Signs: Asthma in the US. Available at: http://www.cdc.gov/vitalsigns/asthma/. Accessed June 2015.
2. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. U.S. Department of Health & Human Services. Available at: http://hcupnet.ahrq.gov/. Accessed June 2015.
Asthma is a chronic disease characterized by airway inflammation and reversible airflow limitation. It is one of the most common chronic conditions and it leads to marked morbidity and mortality in hospitalized patients. In the United States, 1 in 12 persons has asthma and nearly 50% of affected individuals experience an asthma exacerbation each year, accounting for 1.8 million emergency department visits.1,2 Annually, more than 400,000 hospital discharges occur with asthma as the primary diagnosis, with an average length of stay of 3.2 days.2Hospitalists are central to the provision of care for patients with asthma through the use of evidence-based approaches to manage acute exacerbations and to prevent their recurrence. Hospitalists should strive to lead multidisciplinary teams to develop institutional guidelines and/or care pathways to improve efficiency and quality of care and to reduce readmission rates and morbidity and mortality from asthma.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Define asthma and describe the pathophysiologic processes that lead to reversible airway obstruction and inflammation.
Identify precipitants of asthma exacerbation, including environmental and occupational exposures.
Recognize the clinical presentation of asthma exacerbation and differentiate it from other acute respiratory and nonrespiratory syndromes.
Describe the role of diagnostic testing, including peak flow monitoring, used for evaluation of asthma exacerbation.
Recognize indications for specialty consultation, including pulmonary and allergy medicine.
Describe evidence-based therapies for the treatment of asthma exacerbations, which may include bronchodilators, systemic corticosteroids, and oxygen.
Explain indications, contraindications, and mechanisms of action of pharmacologic agents used to treat asthma.
Recognize signs and symptoms of impending respiratory failure.
Explain the indications for invasive and noninvasive ventilatory support.
List the risk factors for disease severity and death from asthma.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transition.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history to identify triggers of asthma and symptoms consistent with asthma exacerbation.
Perform a targeted physical examination to elicit signs consistent with asthma exacerbation, differentiate findings from those of other mimicking conditions, and assess illness severity.
Select appropriate diagnostic studies to evaluate severity of asthma exacerbation and interpret the results.
Recognize indications for transfer to the intensive care unit, including impending respiratory failure, and coordinate intubation or noninvasive mechanical ventilation when indicated.
Prescribe appropriate evidence-based pharmacologic therapies during asthma exacerbation, recommending the most appropriate route, dose, frequency, and duration of treatment.
Communicate with patients and families to explain the natural history and prognosis of asthma.
Facilitate discharge planning early during hospitalization.
Develop an asthma action plan in preparation for discharge.
Educate patients and families regarding the indications and appropriate use of daily use inhalers and rescue inhalers for asthmatic control.
Ensure that patients receive training of proper inhaler and peak flow techniques before hospital discharge.
Communicate with patients and families to explain symptoms and signs that should prompt emergent medical attention.
Communicate with patients and families to explain the goals of care, including clinical stability criteria, the importance of preventive measures (such as smoking cessation, avoidance of second-hand smoke, appropriate vaccinations, and modification of environmental exposures), and required follow-up care.
Communicate with patients and families to explain discharge medications, potential adverse effects, duration of therapy and dosing, and taper schedule.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
Provide and coordinate resources to ensure safe transition from the hospital to arranged follow-up care.
ATTITUDES
Hospitalists should be able to:
Work collaboratively with primary care physicians and emergency physicians in making admission decisions.
Employ a multidisciplinary approach, which may include pulmonary medicine, respiratory therapy, nursing, and social services, in the care of patients with asthma exacerbation.
Follow evidence-based recommendations for the treatment of patients with asthma exacerbations.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Contribute to and/or develop educational modules, order sets, and/or pathways that facilitate use of evidence-based strategies for asthma exacerbation in the emergency department and the hospital, with goals of improving outcomes, decreasing length of stay, and reducing rehospitalization rates.
Lead, coordinate, and/or participate in efforts to educate staff on the importance of smoking cessation counseling and other preventive measures.
Lead, coordinate, and/or participate in multidisciplinary initiatives, which may include collaborative efforts with pulmonologists and respiratory therapists, to promote patient safety and optimize cost-effective diagnostic and management strategies for patients with asthma.
Asthma is a chronic disease characterized by airway inflammation and reversible airflow limitation. It is one of the most common chronic conditions and it leads to marked morbidity and mortality in hospitalized patients. In the United States, 1 in 12 persons has asthma and nearly 50% of affected individuals experience an asthma exacerbation each year, accounting for 1.8 million emergency department visits.1,2 Annually, more than 400,000 hospital discharges occur with asthma as the primary diagnosis, with an average length of stay of 3.2 days.2Hospitalists are central to the provision of care for patients with asthma through the use of evidence-based approaches to manage acute exacerbations and to prevent their recurrence. Hospitalists should strive to lead multidisciplinary teams to develop institutional guidelines and/or care pathways to improve efficiency and quality of care and to reduce readmission rates and morbidity and mortality from asthma.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Define asthma and describe the pathophysiologic processes that lead to reversible airway obstruction and inflammation.
Identify precipitants of asthma exacerbation, including environmental and occupational exposures.
Recognize the clinical presentation of asthma exacerbation and differentiate it from other acute respiratory and nonrespiratory syndromes.
Describe the role of diagnostic testing, including peak flow monitoring, used for evaluation of asthma exacerbation.
Recognize indications for specialty consultation, including pulmonary and allergy medicine.
Describe evidence-based therapies for the treatment of asthma exacerbations, which may include bronchodilators, systemic corticosteroids, and oxygen.
Explain indications, contraindications, and mechanisms of action of pharmacologic agents used to treat asthma.
Recognize signs and symptoms of impending respiratory failure.
Explain the indications for invasive and noninvasive ventilatory support.
List the risk factors for disease severity and death from asthma.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transition.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history to identify triggers of asthma and symptoms consistent with asthma exacerbation.
Perform a targeted physical examination to elicit signs consistent with asthma exacerbation, differentiate findings from those of other mimicking conditions, and assess illness severity.
Select appropriate diagnostic studies to evaluate severity of asthma exacerbation and interpret the results.
Recognize indications for transfer to the intensive care unit, including impending respiratory failure, and coordinate intubation or noninvasive mechanical ventilation when indicated.
Prescribe appropriate evidence-based pharmacologic therapies during asthma exacerbation, recommending the most appropriate route, dose, frequency, and duration of treatment.
Communicate with patients and families to explain the natural history and prognosis of asthma.
Facilitate discharge planning early during hospitalization.
Develop an asthma action plan in preparation for discharge.
Educate patients and families regarding the indications and appropriate use of daily use inhalers and rescue inhalers for asthmatic control.
Ensure that patients receive training of proper inhaler and peak flow techniques before hospital discharge.
Communicate with patients and families to explain symptoms and signs that should prompt emergent medical attention.
Communicate with patients and families to explain the goals of care, including clinical stability criteria, the importance of preventive measures (such as smoking cessation, avoidance of second-hand smoke, appropriate vaccinations, and modification of environmental exposures), and required follow-up care.
Communicate with patients and families to explain discharge medications, potential adverse effects, duration of therapy and dosing, and taper schedule.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
Provide and coordinate resources to ensure safe transition from the hospital to arranged follow-up care.
ATTITUDES
Hospitalists should be able to:
Work collaboratively with primary care physicians and emergency physicians in making admission decisions.
Employ a multidisciplinary approach, which may include pulmonary medicine, respiratory therapy, nursing, and social services, in the care of patients with asthma exacerbation.
Follow evidence-based recommendations for the treatment of patients with asthma exacerbations.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Contribute to and/or develop educational modules, order sets, and/or pathways that facilitate use of evidence-based strategies for asthma exacerbation in the emergency department and the hospital, with goals of improving outcomes, decreasing length of stay, and reducing rehospitalization rates.
Lead, coordinate, and/or participate in efforts to educate staff on the importance of smoking cessation counseling and other preventive measures.
Lead, coordinate, and/or participate in multidisciplinary initiatives, which may include collaborative efforts with pulmonologists and respiratory therapists, to promote patient safety and optimize cost-effective diagnostic and management strategies for patients with asthma.
1. Centers for Disease Control and Prevention. CDC Vital Signs: Asthma in the US. Available at: http://www.cdc.gov/vitalsigns/asthma/. Accessed June 2015.
2. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. U.S. Department of Health & Human Services. Available at: http://hcupnet.ahrq.gov/. Accessed June 2015.
1. Centers for Disease Control and Prevention. CDC Vital Signs: Asthma in the US. Available at: http://www.cdc.gov/vitalsigns/asthma/. Accessed June 2015.
2. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. U.S. Department of Health & Human Services. Available at: http://hcupnet.ahrq.gov/. Accessed June 2015.
© 2017 Society of Hospital Medicine
Cardiac Arrhythmia. 2017 Hospital Medicine Revised Core Competencies
Cardiac arrhythmias are a group of conditions characterized by an abnormal heart rate or rhythm. These are common and affect approximately 5% of the population in the United States. More than 250,000 Americans die each year of sudden cardiac arrest, and most cases are thought to be due to ventricular fibrillation or ventricular tachycardia.1 Several cardiac arrhythmias can cause instability, prompting hospitalization, or they may result from complications during hospitalization. Annually, more than 740,000 hospital discharges are associated with a primary diagnosis of cardiac arrhythmia.2 Hospitalists identify and treat all types of arrhythmias, coordinate specialty and primary care resources, and transition patients safely and cost-effectively through the acute hospitalization and into the outpatient setting.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Identify and differentiate the common clinical presentations of both benign and pathologic arrhythmias.
Explain the causes of atrial and ventricular arrhythmias.
Describe the indicated tests required to evaluate arrhythmias.
Explain how medications, metabolic abnormalities, and medical comorbidities may precipitate various arrhythmias.
Explain indications, contraindications, and mechanisms of action of pharmacologic agents used to treat cardiac arrhythmias. Discuss the management options and goals for patients hospitalized with arrhythmias.
Describe the patient characteristics and comorbid conditions that predict outcomes in patients with arrhythmias.
Recognize indications for specialty consultation, which may include cardiology and cardiac electrophysiology.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transitions.
Recall appropriate indications for both initiation and discontinuation of continuous telemetry monitoring in the hospitalized patient.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history, including medications, family history, and social history.
Perform a targeted physical examination with emphasis on identifying signs associated with hemodynamic instability, tissue perfusion, and occult cardiac and vascular disease.
Identify common benign and pathologic arrhythmias on electrocardiography, rhythm strips, and continuous telemetry monitoring.
Determine the appropriate level of care required based on risk stratification of patients with cardiac arrhythmias.
Identify and prioritize high-risk arrhythmias that require urgent intervention and implement emergency protocols as indicated.
Formulate patient-specific and evidence-based care plans incorporating diagnostic findings, prognosis, and patient characteristics.
Develop patient-specific care plans that may include rate-controlling interventions, cardioversion, defibrillation, or implantable medical devices.
Communicate with patients and families to explain the natural history and prognosis of cardiac arrhythmias.
Communicate with patients and families to explain tests and procedures and their indications and to obtain informed consent.
Communicate with patients and families to explain drug interactions for antiarrhythmic drugs and the importance of strict adherence to medication regimens and laboratory monitoring.
Facilitate discharge planning early during hospitalization.
Communicate with patients and families to explain the goals of care, discharge instructions, and management after hospital discharge to ensure safe follow-up and transitions of care.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include primary care, cardiology, nursing, and social services, in the care of patients with cardiac arrhythmias that begins at admission and continues through all care transitions.
Follow evidence-based recommendations to guide diagnosis, monitoring, and treatment of cardiac arrhythmias.
Acknowledge and ameliorate patient discomfort from uncontrolled arrhythmias and electrical cardioversion therapies.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate, and/or participate in multidisciplinary teams to develop patient care guidelines and/or pathways on the basis of peer-reviewed outcomes research, patient and physician satisfaction, and cost.
Implement systems to ensure hospital-wide adherence to national standards and document those measures as specified by recognized organizations (eg, The Joint Commission, American Heart Association, American College of Cardiology, Agency for Healthcare Research and Quality).
Lead, coordinate, and/or participate in quality improvement initiatives to promote early identification of arrhythmias, reduce preventable complications, and promote appropriate use of telemetry resources.
Cardiac arrhythmias are a group of conditions characterized by an abnormal heart rate or rhythm. These are common and affect approximately 5% of the population in the United States. More than 250,000 Americans die each year of sudden cardiac arrest, and most cases are thought to be due to ventricular fibrillation or ventricular tachycardia.1 Several cardiac arrhythmias can cause instability, prompting hospitalization, or they may result from complications during hospitalization. Annually, more than 740,000 hospital discharges are associated with a primary diagnosis of cardiac arrhythmia.2 Hospitalists identify and treat all types of arrhythmias, coordinate specialty and primary care resources, and transition patients safely and cost-effectively through the acute hospitalization and into the outpatient setting.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Identify and differentiate the common clinical presentations of both benign and pathologic arrhythmias.
Explain the causes of atrial and ventricular arrhythmias.
Describe the indicated tests required to evaluate arrhythmias.
Explain how medications, metabolic abnormalities, and medical comorbidities may precipitate various arrhythmias.
Explain indications, contraindications, and mechanisms of action of pharmacologic agents used to treat cardiac arrhythmias. Discuss the management options and goals for patients hospitalized with arrhythmias.
Describe the patient characteristics and comorbid conditions that predict outcomes in patients with arrhythmias.
Recognize indications for specialty consultation, which may include cardiology and cardiac electrophysiology.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transitions.
Recall appropriate indications for both initiation and discontinuation of continuous telemetry monitoring in the hospitalized patient.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history, including medications, family history, and social history.
Perform a targeted physical examination with emphasis on identifying signs associated with hemodynamic instability, tissue perfusion, and occult cardiac and vascular disease.
Identify common benign and pathologic arrhythmias on electrocardiography, rhythm strips, and continuous telemetry monitoring.
Determine the appropriate level of care required based on risk stratification of patients with cardiac arrhythmias.
Identify and prioritize high-risk arrhythmias that require urgent intervention and implement emergency protocols as indicated.
Formulate patient-specific and evidence-based care plans incorporating diagnostic findings, prognosis, and patient characteristics.
Develop patient-specific care plans that may include rate-controlling interventions, cardioversion, defibrillation, or implantable medical devices.
Communicate with patients and families to explain the natural history and prognosis of cardiac arrhythmias.
Communicate with patients and families to explain tests and procedures and their indications and to obtain informed consent.
Communicate with patients and families to explain drug interactions for antiarrhythmic drugs and the importance of strict adherence to medication regimens and laboratory monitoring.
Facilitate discharge planning early during hospitalization.
Communicate with patients and families to explain the goals of care, discharge instructions, and management after hospital discharge to ensure safe follow-up and transitions of care.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include primary care, cardiology, nursing, and social services, in the care of patients with cardiac arrhythmias that begins at admission and continues through all care transitions.
Follow evidence-based recommendations to guide diagnosis, monitoring, and treatment of cardiac arrhythmias.
Acknowledge and ameliorate patient discomfort from uncontrolled arrhythmias and electrical cardioversion therapies.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate, and/or participate in multidisciplinary teams to develop patient care guidelines and/or pathways on the basis of peer-reviewed outcomes research, patient and physician satisfaction, and cost.
Implement systems to ensure hospital-wide adherence to national standards and document those measures as specified by recognized organizations (eg, The Joint Commission, American Heart Association, American College of Cardiology, Agency for Healthcare Research and Quality).
Lead, coordinate, and/or participate in quality improvement initiatives to promote early identification of arrhythmias, reduce preventable complications, and promote appropriate use of telemetry resources.
Cardiac arrhythmias are a group of conditions characterized by an abnormal heart rate or rhythm. These are common and affect approximately 5% of the population in the United States. More than 250,000 Americans die each year of sudden cardiac arrest, and most cases are thought to be due to ventricular fibrillation or ventricular tachycardia.1 Several cardiac arrhythmias can cause instability, prompting hospitalization, or they may result from complications during hospitalization. Annually, more than 740,000 hospital discharges are associated with a primary diagnosis of cardiac arrhythmia.2 Hospitalists identify and treat all types of arrhythmias, coordinate specialty and primary care resources, and transition patients safely and cost-effectively through the acute hospitalization and into the outpatient setting.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Identify and differentiate the common clinical presentations of both benign and pathologic arrhythmias.
Explain the causes of atrial and ventricular arrhythmias.
Describe the indicated tests required to evaluate arrhythmias.
Explain how medications, metabolic abnormalities, and medical comorbidities may precipitate various arrhythmias.
Explain indications, contraindications, and mechanisms of action of pharmacologic agents used to treat cardiac arrhythmias. Discuss the management options and goals for patients hospitalized with arrhythmias.
Describe the patient characteristics and comorbid conditions that predict outcomes in patients with arrhythmias.
Recognize indications for specialty consultation, which may include cardiology and cardiac electrophysiology.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transitions.
Recall appropriate indications for both initiation and discontinuation of continuous telemetry monitoring in the hospitalized patient.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history, including medications, family history, and social history.
Perform a targeted physical examination with emphasis on identifying signs associated with hemodynamic instability, tissue perfusion, and occult cardiac and vascular disease.
Identify common benign and pathologic arrhythmias on electrocardiography, rhythm strips, and continuous telemetry monitoring.
Determine the appropriate level of care required based on risk stratification of patients with cardiac arrhythmias.
Identify and prioritize high-risk arrhythmias that require urgent intervention and implement emergency protocols as indicated.
Formulate patient-specific and evidence-based care plans incorporating diagnostic findings, prognosis, and patient characteristics.
Develop patient-specific care plans that may include rate-controlling interventions, cardioversion, defibrillation, or implantable medical devices.
Communicate with patients and families to explain the natural history and prognosis of cardiac arrhythmias.
Communicate with patients and families to explain tests and procedures and their indications and to obtain informed consent.
Communicate with patients and families to explain drug interactions for antiarrhythmic drugs and the importance of strict adherence to medication regimens and laboratory monitoring.
Facilitate discharge planning early during hospitalization.
Communicate with patients and families to explain the goals of care, discharge instructions, and management after hospital discharge to ensure safe follow-up and transitions of care.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include primary care, cardiology, nursing, and social services, in the care of patients with cardiac arrhythmias that begins at admission and continues through all care transitions.
Follow evidence-based recommendations to guide diagnosis, monitoring, and treatment of cardiac arrhythmias.
Acknowledge and ameliorate patient discomfort from uncontrolled arrhythmias and electrical cardioversion therapies.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate, and/or participate in multidisciplinary teams to develop patient care guidelines and/or pathways on the basis of peer-reviewed outcomes research, patient and physician satisfaction, and cost.
Implement systems to ensure hospital-wide adherence to national standards and document those measures as specified by recognized organizations (eg, The Joint Commission, American Heart Association, American College of Cardiology, Agency for Healthcare Research and Quality).
Lead, coordinate, and/or participate in quality improvement initiatives to promote early identification of arrhythmias, reduce preventable complications, and promote appropriate use of telemetry resources.
© 2017 Society of Hospital Medicine
Chronic Obstructive Pulmonary Disease. 2017 Hospital Medicine Revised Core Competencies
Chronic obstructive pulmonary disease (COPD) is a heterogeneous group of respiratory conditions, predominantly composed of chronic bronchitis and emphysema. COPD is defined by airflow limitation that is not completely reversible, and it is associated with an abnormal airway inflammatory response. Exposure to tobacco smoke is the main risk factor. COPD affects more than 12 million Americans and is the third leading cause of death in the United States. A COPD exacerbation is defined as an increase in the usual symptoms of COPD that is beyond day-to-day variations and leads to a change in medication and often results in hospitalization. Annually, more than 670,000 hospital discharges occur with COPD as the primary diagnosis, and nearly 1 of every 5 hospitalized patients 40 years or older has COPD.1,2The average length of stay is 4.3 days.1 COPD is a substantial cause of disability and carries a large economic burden, accounting for almost $17 billion of total hospital charges billed to Medicare each year.3 The early detection and prompt treatment of exacerbations are essential to ensure optimal outcomes and to reduce the burden of COPD. Hospitalists use evidence-based approaches to optimize care, and they should strive to lead multidisciplinary teams to develop institutional guidelines and/or care pathways to reduce readmission rates and mortality from COPD exacerbations.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Define COPD and describe the pathophysiologic processes that lead to small airway obstruction and alveolar destruction.
Describe potential precipitants of exacerbation, including both infectious and noninfectious etiologies.
Differentiate the clinical presentation of a COPD exacerbation from asthma, heart failure, and other acute respiratory and nonrespiratory syndromes.
List the indicators of disease severity.
Describe the role of diagnostic testing used for the evaluation of COPD.
Describe the role of pulmonary function tests in the treatment of a COPD exacerbation.
Distinguish the medical management of patients with COPD exacerbations from that of patients with stable COPD.
Recognize indications for specialty consultation, which may include pulmonary medicine.
Describe the evidence-based therapies for treatment of COPD exacerbations, which may include bronchodilators, systemic corticosteroids, oxygen, and antibiotics.
Identify the potential risks of supplemental oxygen therapy, including development of hypercarbia in patients with chronic respiratory acidosis.
Explain indications, contraindications, and mechanisms of action of pharmacologic agents used to treat COPD.
Describe and differentiate the means of ventilatory support, including the use of noninvasive positive pressure ventilation in COPD exacerbation.
Recognize anxiety and depression as important comorbid conditions that negatively affect outcomes.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transition.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history to identify symptoms consistent with a COPD exacerbation and etiologic precipitants.
Perform a targeted physical examination to elicit signs consistent with a COPD exacerbation, differentiate findings from those of other mimicking conditions, and assess illness severity.
Diagnose a COPD exacerbation on the basis of history, physical examination, and radiographic data.
Select and interpret appropriate diagnostic studies to evaluate the severity of a COPD exacerbation.
Recognize symptoms, signs, and severity of impending respiratory failure and select the indicated evidence-based ventilatory approach.
Select patients with COPD exacerbation who would benefit from use of positive pressure ventilation and identify those in whom this intervention is contraindicated.
Prescribe appropriate evidence-based pharmacologic therapies during COPD exacerbation, recommending the most appropriate drug route, dose, frequency, and duration of treatment.
Address treatment preferences, including advance directives early during hospital stay; implement end-of-life decisions by patients and/or families when indicated or desired.
Evaluate COPD in perioperative risk assessment, recommend measures to optimize perioperative management of COPD, and manage postoperative complications related to underlying COPD.
Identify patients with COPD who may benefit from pulmonary rehabilitation.
Communicate with patients and families to explain the natural history and prognosis of COPD.
Facilitate discharge planning early during hospitalization.
Communicate with patients and families to explain discharge medications, potential adverse effects, duration of therapy and dosing, and taper schedule.
Ensure that patients receive training on proper inhaler techniques and use before hospital discharge.
Communicate with patients and families to explain the goals of care (including clinical stability criteria, the importance of preventive measures), discharge instructions, and management after hospital discharge to ensure safe follow-up and transitions of care.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
Provide and coordinate resources to ensure safe transition from the hospital to arranged follow-up care.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include pulmonary medicine, respiratory therapy, nursing, and social services, in the care of patients with a COPD exacerbation, beginning at admission and continuing through all care transitions.
Engage in a collaborative way with primary care physicians and emergency physicians in making admission decisions.
Promote and encourage preventive strategies, including smoking cessation, vaccinations, and venous thromboembolism prophylaxis.
Establish and maintain an open dialogue with patients and/or families regarding goals and limitations of care, including palliative care and end-of-life wishes.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate, and/or participate in multidisciplinary initiatives, which may include collaborative efforts with pulmonologists, to promote patient safety and optimize cost-effective diagnostic and management strategies for patients with COPD.
Lead, coordinate, and/or participate in the development of educational modules, order sets, and/or pathways that facilitate use of evidence-based strategies for COPD exacerbation in the emergency department and the hospital, with goals of improving outcomes, decreasing length of stay, and reducing rehospitalization rates.
Lead efforts to educate patients and staff on the importance of smoking cessation and other preventive measures.
1. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. U.S. Department of Health & Human Services. Available at: http://hcupnet.ahrq.gov/. Accessed June 2015.
2. Wier LM, Elizhauser A, Pfuntner A, Au DH. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Overview of Hospitalizations Among Patients With COPD, 2008. Statistical Brief #106. Rockville, MD; Agency for Health Care Policy and Research (US). 2011. Available at: http://www.ncbi.nlm.nih.gov/books/NBK53969/. Accessed June 2015.
3. Agency for Healthcare Research and Quality. Chronic obstructive pulmonary disease (COPD): hospital 30-day, all-cause, risk-standardized mortality rate following acute exacerbation of COPD. Available at http://www.qualitymeasures.ahrq.gov/content.aspx?id=48198. Accessed June 2015.
Chronic obstructive pulmonary disease (COPD) is a heterogeneous group of respiratory conditions, predominantly composed of chronic bronchitis and emphysema. COPD is defined by airflow limitation that is not completely reversible, and it is associated with an abnormal airway inflammatory response. Exposure to tobacco smoke is the main risk factor. COPD affects more than 12 million Americans and is the third leading cause of death in the United States. A COPD exacerbation is defined as an increase in the usual symptoms of COPD that is beyond day-to-day variations and leads to a change in medication and often results in hospitalization. Annually, more than 670,000 hospital discharges occur with COPD as the primary diagnosis, and nearly 1 of every 5 hospitalized patients 40 years or older has COPD.1,2The average length of stay is 4.3 days.1 COPD is a substantial cause of disability and carries a large economic burden, accounting for almost $17 billion of total hospital charges billed to Medicare each year.3 The early detection and prompt treatment of exacerbations are essential to ensure optimal outcomes and to reduce the burden of COPD. Hospitalists use evidence-based approaches to optimize care, and they should strive to lead multidisciplinary teams to develop institutional guidelines and/or care pathways to reduce readmission rates and mortality from COPD exacerbations.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Define COPD and describe the pathophysiologic processes that lead to small airway obstruction and alveolar destruction.
Describe potential precipitants of exacerbation, including both infectious and noninfectious etiologies.
Differentiate the clinical presentation of a COPD exacerbation from asthma, heart failure, and other acute respiratory and nonrespiratory syndromes.
List the indicators of disease severity.
Describe the role of diagnostic testing used for the evaluation of COPD.
Describe the role of pulmonary function tests in the treatment of a COPD exacerbation.
Distinguish the medical management of patients with COPD exacerbations from that of patients with stable COPD.
Recognize indications for specialty consultation, which may include pulmonary medicine.
Describe the evidence-based therapies for treatment of COPD exacerbations, which may include bronchodilators, systemic corticosteroids, oxygen, and antibiotics.
Identify the potential risks of supplemental oxygen therapy, including development of hypercarbia in patients with chronic respiratory acidosis.
Explain indications, contraindications, and mechanisms of action of pharmacologic agents used to treat COPD.
Describe and differentiate the means of ventilatory support, including the use of noninvasive positive pressure ventilation in COPD exacerbation.
Recognize anxiety and depression as important comorbid conditions that negatively affect outcomes.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transition.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history to identify symptoms consistent with a COPD exacerbation and etiologic precipitants.
Perform a targeted physical examination to elicit signs consistent with a COPD exacerbation, differentiate findings from those of other mimicking conditions, and assess illness severity.
Diagnose a COPD exacerbation on the basis of history, physical examination, and radiographic data.
Select and interpret appropriate diagnostic studies to evaluate the severity of a COPD exacerbation.
Recognize symptoms, signs, and severity of impending respiratory failure and select the indicated evidence-based ventilatory approach.
Select patients with COPD exacerbation who would benefit from use of positive pressure ventilation and identify those in whom this intervention is contraindicated.
Prescribe appropriate evidence-based pharmacologic therapies during COPD exacerbation, recommending the most appropriate drug route, dose, frequency, and duration of treatment.
Address treatment preferences, including advance directives early during hospital stay; implement end-of-life decisions by patients and/or families when indicated or desired.
Evaluate COPD in perioperative risk assessment, recommend measures to optimize perioperative management of COPD, and manage postoperative complications related to underlying COPD.
Identify patients with COPD who may benefit from pulmonary rehabilitation.
Communicate with patients and families to explain the natural history and prognosis of COPD.
Facilitate discharge planning early during hospitalization.
Communicate with patients and families to explain discharge medications, potential adverse effects, duration of therapy and dosing, and taper schedule.
Ensure that patients receive training on proper inhaler techniques and use before hospital discharge.
Communicate with patients and families to explain the goals of care (including clinical stability criteria, the importance of preventive measures), discharge instructions, and management after hospital discharge to ensure safe follow-up and transitions of care.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
Provide and coordinate resources to ensure safe transition from the hospital to arranged follow-up care.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include pulmonary medicine, respiratory therapy, nursing, and social services, in the care of patients with a COPD exacerbation, beginning at admission and continuing through all care transitions.
Engage in a collaborative way with primary care physicians and emergency physicians in making admission decisions.
Promote and encourage preventive strategies, including smoking cessation, vaccinations, and venous thromboembolism prophylaxis.
Establish and maintain an open dialogue with patients and/or families regarding goals and limitations of care, including palliative care and end-of-life wishes.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate, and/or participate in multidisciplinary initiatives, which may include collaborative efforts with pulmonologists, to promote patient safety and optimize cost-effective diagnostic and management strategies for patients with COPD.
Lead, coordinate, and/or participate in the development of educational modules, order sets, and/or pathways that facilitate use of evidence-based strategies for COPD exacerbation in the emergency department and the hospital, with goals of improving outcomes, decreasing length of stay, and reducing rehospitalization rates.
Lead efforts to educate patients and staff on the importance of smoking cessation and other preventive measures.
Chronic obstructive pulmonary disease (COPD) is a heterogeneous group of respiratory conditions, predominantly composed of chronic bronchitis and emphysema. COPD is defined by airflow limitation that is not completely reversible, and it is associated with an abnormal airway inflammatory response. Exposure to tobacco smoke is the main risk factor. COPD affects more than 12 million Americans and is the third leading cause of death in the United States. A COPD exacerbation is defined as an increase in the usual symptoms of COPD that is beyond day-to-day variations and leads to a change in medication and often results in hospitalization. Annually, more than 670,000 hospital discharges occur with COPD as the primary diagnosis, and nearly 1 of every 5 hospitalized patients 40 years or older has COPD.1,2The average length of stay is 4.3 days.1 COPD is a substantial cause of disability and carries a large economic burden, accounting for almost $17 billion of total hospital charges billed to Medicare each year.3 The early detection and prompt treatment of exacerbations are essential to ensure optimal outcomes and to reduce the burden of COPD. Hospitalists use evidence-based approaches to optimize care, and they should strive to lead multidisciplinary teams to develop institutional guidelines and/or care pathways to reduce readmission rates and mortality from COPD exacerbations.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Define COPD and describe the pathophysiologic processes that lead to small airway obstruction and alveolar destruction.
Describe potential precipitants of exacerbation, including both infectious and noninfectious etiologies.
Differentiate the clinical presentation of a COPD exacerbation from asthma, heart failure, and other acute respiratory and nonrespiratory syndromes.
List the indicators of disease severity.
Describe the role of diagnostic testing used for the evaluation of COPD.
Describe the role of pulmonary function tests in the treatment of a COPD exacerbation.
Distinguish the medical management of patients with COPD exacerbations from that of patients with stable COPD.
Recognize indications for specialty consultation, which may include pulmonary medicine.
Describe the evidence-based therapies for treatment of COPD exacerbations, which may include bronchodilators, systemic corticosteroids, oxygen, and antibiotics.
Identify the potential risks of supplemental oxygen therapy, including development of hypercarbia in patients with chronic respiratory acidosis.
Explain indications, contraindications, and mechanisms of action of pharmacologic agents used to treat COPD.
Describe and differentiate the means of ventilatory support, including the use of noninvasive positive pressure ventilation in COPD exacerbation.
Recognize anxiety and depression as important comorbid conditions that negatively affect outcomes.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transition.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history to identify symptoms consistent with a COPD exacerbation and etiologic precipitants.
Perform a targeted physical examination to elicit signs consistent with a COPD exacerbation, differentiate findings from those of other mimicking conditions, and assess illness severity.
Diagnose a COPD exacerbation on the basis of history, physical examination, and radiographic data.
Select and interpret appropriate diagnostic studies to evaluate the severity of a COPD exacerbation.
Recognize symptoms, signs, and severity of impending respiratory failure and select the indicated evidence-based ventilatory approach.
Select patients with COPD exacerbation who would benefit from use of positive pressure ventilation and identify those in whom this intervention is contraindicated.
Prescribe appropriate evidence-based pharmacologic therapies during COPD exacerbation, recommending the most appropriate drug route, dose, frequency, and duration of treatment.
Address treatment preferences, including advance directives early during hospital stay; implement end-of-life decisions by patients and/or families when indicated or desired.
Evaluate COPD in perioperative risk assessment, recommend measures to optimize perioperative management of COPD, and manage postoperative complications related to underlying COPD.
Identify patients with COPD who may benefit from pulmonary rehabilitation.
Communicate with patients and families to explain the natural history and prognosis of COPD.
Facilitate discharge planning early during hospitalization.
Communicate with patients and families to explain discharge medications, potential adverse effects, duration of therapy and dosing, and taper schedule.
Ensure that patients receive training on proper inhaler techniques and use before hospital discharge.
Communicate with patients and families to explain the goals of care (including clinical stability criteria, the importance of preventive measures), discharge instructions, and management after hospital discharge to ensure safe follow-up and transitions of care.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
Provide and coordinate resources to ensure safe transition from the hospital to arranged follow-up care.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include pulmonary medicine, respiratory therapy, nursing, and social services, in the care of patients with a COPD exacerbation, beginning at admission and continuing through all care transitions.
Engage in a collaborative way with primary care physicians and emergency physicians in making admission decisions.
Promote and encourage preventive strategies, including smoking cessation, vaccinations, and venous thromboembolism prophylaxis.
Establish and maintain an open dialogue with patients and/or families regarding goals and limitations of care, including palliative care and end-of-life wishes.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate, and/or participate in multidisciplinary initiatives, which may include collaborative efforts with pulmonologists, to promote patient safety and optimize cost-effective diagnostic and management strategies for patients with COPD.
Lead, coordinate, and/or participate in the development of educational modules, order sets, and/or pathways that facilitate use of evidence-based strategies for COPD exacerbation in the emergency department and the hospital, with goals of improving outcomes, decreasing length of stay, and reducing rehospitalization rates.
Lead efforts to educate patients and staff on the importance of smoking cessation and other preventive measures.
1. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. U.S. Department of Health & Human Services. Available at: http://hcupnet.ahrq.gov/. Accessed June 2015.
2. Wier LM, Elizhauser A, Pfuntner A, Au DH. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Overview of Hospitalizations Among Patients With COPD, 2008. Statistical Brief #106. Rockville, MD; Agency for Health Care Policy and Research (US). 2011. Available at: http://www.ncbi.nlm.nih.gov/books/NBK53969/. Accessed June 2015.
3. Agency for Healthcare Research and Quality. Chronic obstructive pulmonary disease (COPD): hospital 30-day, all-cause, risk-standardized mortality rate following acute exacerbation of COPD. Available at http://www.qualitymeasures.ahrq.gov/content.aspx?id=48198. Accessed June 2015.
1. Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. U.S. Department of Health & Human Services. Available at: http://hcupnet.ahrq.gov/. Accessed June 2015.
2. Wier LM, Elizhauser A, Pfuntner A, Au DH. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Overview of Hospitalizations Among Patients With COPD, 2008. Statistical Brief #106. Rockville, MD; Agency for Health Care Policy and Research (US). 2011. Available at: http://www.ncbi.nlm.nih.gov/books/NBK53969/. Accessed June 2015.
3. Agency for Healthcare Research and Quality. Chronic obstructive pulmonary disease (COPD): hospital 30-day, all-cause, risk-standardized mortality rate following acute exacerbation of COPD. Available at http://www.qualitymeasures.ahrq.gov/content.aspx?id=48198. Accessed June 2015.
© 2017 Society of Hospital Medicine
Community-Acquired Pneumonia. 2017 Hospital Medicine Revised Core Competencies
Community-acquired pneumonia (CAP) is an infection of the lung parenchyma that occurs in the community or is diagnosed within 48 hours of hospital admission. CAP is a common and potentially life-threatening infection, and it is a leading cause of death from infectious diseases. Approximately 25% of persons with CAP require hospitalization, and 10% to 20% of these patients require admission to the intensive care unit.1-3 The mortality rate ranges from about 13% in hospitalized patients to 36% in patients admitted to the intensive care unit.1-3 CAP is a curable condition and an organized approach to management is likely to improve clinical results and reduce mortality. Pneumonia outcome measures are used to evaluate performance of healthcare providers and organizations. Hospitalists apply evidence-based guidelines to the management of patients hospitalized with pneumonia and lead initiatives to improve quality of care and reduce practice variability.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Define CAP, list the likely etiologies and the signs and symptoms, and distinguish CAP from hospital-acquired pneumonia and healthcare-associated pneumonia.
Describe other causes of pulmonary infiltrates on radiographic studies.
Describe the tests indicated to evaluate and treat CAP.
Explain indications for respiratory isolation.
Identify patients with comorbidities (such as immunocompromise, diabetes mellitus, and extremes of age) who are at high risk of a complicated course.
Identify specific pathogens that predispose patients to a complicated course.
Recognize indications for specialty consultation.
Describe indicated therapeutic modalities for CAP, including oxygen therapy, respiratory care modalities, appropriate antimicrobial selection and duration, and other evidence-based treatments.
Predict patient risk for morbidity and mortality from CAP using a validated risk score.
Explain goals for hospital discharge, including evidence-based measures of clinical stability for safe care transition.
Describe factors associated with a nonresponding pneumonia.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history to identify symptoms consistent with CAP and demographic factors that may predispose patients to CAP.
Perform a targeted physical examination to elicit signs consistent with CAP and differentiate it from other mimicking conditions.
Order and interpret laboratory, microbiologic, and radiologic studies to confirm the diagnosis of CAP and risk stratify patients.
Apply evidence-based tools (such as the Pneumonia Severity Index) to triage decisions and identify factors that support the need for intensive care unit admission.
Initiate empiric antimicrobials for CAP on the basis of illness severity and evidence-based national guidelines, incorporating local resistance patterns.
Formulate a subsequent treatment plan that includes narrowing antimicrobial therapies on the basis of available culture data and patient response to treatment.
Recognize the criteria for clinical stability, including the appropriate deescalation of treatment such as transitioning from parenteral to oral antimicrobials.
Recognize and address complications of CAP and/or inadequate response to therapy, including respiratory failure and parapneumonic effusions.
Communicate with patients and families to explain the pathophysiology and prognosis of CAP.
Communicate with patients and families to explain tests and procedures and their indications and to obtain informed consent.
Communicate with patients and families to explain the use and potential adverse effects of pharmacologic agents.
Facilitate discharge planning early during hospitalization.
Communicate with patients and families to explain the goals of care (including clinical stability criteria, the importance of preventive measures such as smoking cessation), discharge instructions, and management after hospital discharge to ensure safe follow-up and transitions of care.
Recognize and address barriers to follow-up care and anticipated postdischarge requirements.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include nursing, respiratory therapy, nutrition, and pharmacy services, to the care of patients with CAP through all care transitions.
Follow evidence-based recommendations for the treatment of patients with CAP.
Work collaboratively with primary care physicians and emergency physicians in making admission decisions.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate, and/or participate in multidisciplinary initiatives, which may include collaborative efforts with infectious disease and pulmonary specialists, to promote patient safety and cost-effective diagnostic and management strategies for patients with CAP.
Lead, coordinate, and/or participate in efforts to identify, address, and monitor quality indicators for CAP.
Implement systems to ensure hospital-wide adherence to national standards and document those measures as specified by recognized organizations (eg, Centers for Medicare & Medicaid Services, Infectious Diseases Society of America, American Thoracic Society).
Integrate evidence-based clinical severity scores and clinical judgment into admission decisions.
Lead efforts to educate staff on the importance of smoking cessation counseling, vaccinations, and other preventive measures.
1. File TM Jr, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med. 2010;122(2):130-141.
2. Fine MJ, Smith MA, Carson CA, Mutha SS, Sankey SS, Weissfeld LA, et al. Prognosis and outcomes of patients with community-acquired pneumonia. A meta-analysis. JAMA. 1996;275(2):134.
3. Niederman MS, Mandell LA, Anzueto A, Bass JB, Broughton WA, Campbell GD, et al; American Thoracic Society. Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med. 2001;163(7):1730-1754.
Community-acquired pneumonia (CAP) is an infection of the lung parenchyma that occurs in the community or is diagnosed within 48 hours of hospital admission. CAP is a common and potentially life-threatening infection, and it is a leading cause of death from infectious diseases. Approximately 25% of persons with CAP require hospitalization, and 10% to 20% of these patients require admission to the intensive care unit.1-3 The mortality rate ranges from about 13% in hospitalized patients to 36% in patients admitted to the intensive care unit.1-3 CAP is a curable condition and an organized approach to management is likely to improve clinical results and reduce mortality. Pneumonia outcome measures are used to evaluate performance of healthcare providers and organizations. Hospitalists apply evidence-based guidelines to the management of patients hospitalized with pneumonia and lead initiatives to improve quality of care and reduce practice variability.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Define CAP, list the likely etiologies and the signs and symptoms, and distinguish CAP from hospital-acquired pneumonia and healthcare-associated pneumonia.
Describe other causes of pulmonary infiltrates on radiographic studies.
Describe the tests indicated to evaluate and treat CAP.
Explain indications for respiratory isolation.
Identify patients with comorbidities (such as immunocompromise, diabetes mellitus, and extremes of age) who are at high risk of a complicated course.
Identify specific pathogens that predispose patients to a complicated course.
Recognize indications for specialty consultation.
Describe indicated therapeutic modalities for CAP, including oxygen therapy, respiratory care modalities, appropriate antimicrobial selection and duration, and other evidence-based treatments.
Predict patient risk for morbidity and mortality from CAP using a validated risk score.
Explain goals for hospital discharge, including evidence-based measures of clinical stability for safe care transition.
Describe factors associated with a nonresponding pneumonia.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history to identify symptoms consistent with CAP and demographic factors that may predispose patients to CAP.
Perform a targeted physical examination to elicit signs consistent with CAP and differentiate it from other mimicking conditions.
Order and interpret laboratory, microbiologic, and radiologic studies to confirm the diagnosis of CAP and risk stratify patients.
Apply evidence-based tools (such as the Pneumonia Severity Index) to triage decisions and identify factors that support the need for intensive care unit admission.
Initiate empiric antimicrobials for CAP on the basis of illness severity and evidence-based national guidelines, incorporating local resistance patterns.
Formulate a subsequent treatment plan that includes narrowing antimicrobial therapies on the basis of available culture data and patient response to treatment.
Recognize the criteria for clinical stability, including the appropriate deescalation of treatment such as transitioning from parenteral to oral antimicrobials.
Recognize and address complications of CAP and/or inadequate response to therapy, including respiratory failure and parapneumonic effusions.
Communicate with patients and families to explain the pathophysiology and prognosis of CAP.
Communicate with patients and families to explain tests and procedures and their indications and to obtain informed consent.
Communicate with patients and families to explain the use and potential adverse effects of pharmacologic agents.
Facilitate discharge planning early during hospitalization.
Communicate with patients and families to explain the goals of care (including clinical stability criteria, the importance of preventive measures such as smoking cessation), discharge instructions, and management after hospital discharge to ensure safe follow-up and transitions of care.
Recognize and address barriers to follow-up care and anticipated postdischarge requirements.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include nursing, respiratory therapy, nutrition, and pharmacy services, to the care of patients with CAP through all care transitions.
Follow evidence-based recommendations for the treatment of patients with CAP.
Work collaboratively with primary care physicians and emergency physicians in making admission decisions.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate, and/or participate in multidisciplinary initiatives, which may include collaborative efforts with infectious disease and pulmonary specialists, to promote patient safety and cost-effective diagnostic and management strategies for patients with CAP.
Lead, coordinate, and/or participate in efforts to identify, address, and monitor quality indicators for CAP.
Implement systems to ensure hospital-wide adherence to national standards and document those measures as specified by recognized organizations (eg, Centers for Medicare & Medicaid Services, Infectious Diseases Society of America, American Thoracic Society).
Integrate evidence-based clinical severity scores and clinical judgment into admission decisions.
Lead efforts to educate staff on the importance of smoking cessation counseling, vaccinations, and other preventive measures.
Community-acquired pneumonia (CAP) is an infection of the lung parenchyma that occurs in the community or is diagnosed within 48 hours of hospital admission. CAP is a common and potentially life-threatening infection, and it is a leading cause of death from infectious diseases. Approximately 25% of persons with CAP require hospitalization, and 10% to 20% of these patients require admission to the intensive care unit.1-3 The mortality rate ranges from about 13% in hospitalized patients to 36% in patients admitted to the intensive care unit.1-3 CAP is a curable condition and an organized approach to management is likely to improve clinical results and reduce mortality. Pneumonia outcome measures are used to evaluate performance of healthcare providers and organizations. Hospitalists apply evidence-based guidelines to the management of patients hospitalized with pneumonia and lead initiatives to improve quality of care and reduce practice variability.
Want all 52 JHM Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
KNOWLEDGE
Hospitalists should be able to:
Define CAP, list the likely etiologies and the signs and symptoms, and distinguish CAP from hospital-acquired pneumonia and healthcare-associated pneumonia.
Describe other causes of pulmonary infiltrates on radiographic studies.
Describe the tests indicated to evaluate and treat CAP.
Explain indications for respiratory isolation.
Identify patients with comorbidities (such as immunocompromise, diabetes mellitus, and extremes of age) who are at high risk of a complicated course.
Identify specific pathogens that predispose patients to a complicated course.
Recognize indications for specialty consultation.
Describe indicated therapeutic modalities for CAP, including oxygen therapy, respiratory care modalities, appropriate antimicrobial selection and duration, and other evidence-based treatments.
Predict patient risk for morbidity and mortality from CAP using a validated risk score.
Explain goals for hospital discharge, including evidence-based measures of clinical stability for safe care transition.
Describe factors associated with a nonresponding pneumonia.
SKILLS
Hospitalists should be able to:
Elicit a thorough and relevant medical history to identify symptoms consistent with CAP and demographic factors that may predispose patients to CAP.
Perform a targeted physical examination to elicit signs consistent with CAP and differentiate it from other mimicking conditions.
Order and interpret laboratory, microbiologic, and radiologic studies to confirm the diagnosis of CAP and risk stratify patients.
Apply evidence-based tools (such as the Pneumonia Severity Index) to triage decisions and identify factors that support the need for intensive care unit admission.
Initiate empiric antimicrobials for CAP on the basis of illness severity and evidence-based national guidelines, incorporating local resistance patterns.
Formulate a subsequent treatment plan that includes narrowing antimicrobial therapies on the basis of available culture data and patient response to treatment.
Recognize the criteria for clinical stability, including the appropriate deescalation of treatment such as transitioning from parenteral to oral antimicrobials.
Recognize and address complications of CAP and/or inadequate response to therapy, including respiratory failure and parapneumonic effusions.
Communicate with patients and families to explain the pathophysiology and prognosis of CAP.
Communicate with patients and families to explain tests and procedures and their indications and to obtain informed consent.
Communicate with patients and families to explain the use and potential adverse effects of pharmacologic agents.
Facilitate discharge planning early during hospitalization.
Communicate with patients and families to explain the goals of care (including clinical stability criteria, the importance of preventive measures such as smoking cessation), discharge instructions, and management after hospital discharge to ensure safe follow-up and transitions of care.
Recognize and address barriers to follow-up care and anticipated postdischarge requirements.
Document the treatment plan and provide clear discharge instructions for postdischarge clinicians.
ATTITUDES
Hospitalists should be able to:
Employ a multidisciplinary approach, which may include nursing, respiratory therapy, nutrition, and pharmacy services, to the care of patients with CAP through all care transitions.
Follow evidence-based recommendations for the treatment of patients with CAP.
Work collaboratively with primary care physicians and emergency physicians in making admission decisions.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate, and/or participate in multidisciplinary initiatives, which may include collaborative efforts with infectious disease and pulmonary specialists, to promote patient safety and cost-effective diagnostic and management strategies for patients with CAP.
Lead, coordinate, and/or participate in efforts to identify, address, and monitor quality indicators for CAP.
Implement systems to ensure hospital-wide adherence to national standards and document those measures as specified by recognized organizations (eg, Centers for Medicare & Medicaid Services, Infectious Diseases Society of America, American Thoracic Society).
Integrate evidence-based clinical severity scores and clinical judgment into admission decisions.
Lead efforts to educate staff on the importance of smoking cessation counseling, vaccinations, and other preventive measures.
1. File TM Jr, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med. 2010;122(2):130-141.
2. Fine MJ, Smith MA, Carson CA, Mutha SS, Sankey SS, Weissfeld LA, et al. Prognosis and outcomes of patients with community-acquired pneumonia. A meta-analysis. JAMA. 1996;275(2):134.
3. Niederman MS, Mandell LA, Anzueto A, Bass JB, Broughton WA, Campbell GD, et al; American Thoracic Society. Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med. 2001;163(7):1730-1754.
1. File TM Jr, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med. 2010;122(2):130-141.
2. Fine MJ, Smith MA, Carson CA, Mutha SS, Sankey SS, Weissfeld LA, et al. Prognosis and outcomes of patients with community-acquired pneumonia. A meta-analysis. JAMA. 1996;275(2):134.
3. Niederman MS, Mandell LA, Anzueto A, Bass JB, Broughton WA, Campbell GD, et al; American Thoracic Society. Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med. 2001;163(7):1730-1754.
© 2017 Society of Hospital Medicine