User login
Bowel resection for endometriosis restores fertility in many women
NATIONAL HARBOR, MD. – Pregnancy occurred in more than half of infertile women who had a segmental laparoscopic bowel resection for endometriosis.
Of 155 women, 96 (62%) conceived after the surgery. Most of these pregnancies (71 of 96; 74%) were spontaneous, Dr. Rosa Maria Neme reported at a meeting sponsored by AAGL.
The prospective study included women treated during 2009-2012 at the University of São Paulo, Brazil, said Dr. Neme, director of the university’s endometriosis center. The patients were a mean of 32 years old.
Most (92%) had bowel symptoms, including pain during defecation, diarrhea and constipation, abdominal bloating, and dyschezia. Endometriosis-related symptoms were present in all, and included dysmenorrhea, nonmenstrual pelvic pain and dyspareunia, tenesmus, cyclic rectal bleeding, lower back pain, and asthenia.
An associated infertility was present in 62% (155), with a mean duration of 18 months. Most patients (78%) had already undergone some form of fertility treatment before surgery and 69% had undergone a previous surgery for pelvic pain.
All of the patients had a torus bowel resection. A number of other procedures also were performed during the surgery, including extensive ureterolysis (80%), ovarian cystectomy (70%), partial vaginal resection (20%), and appendectomy (20%).
The mean operative time was 117 minutes. There were no conversions to open surgery, no transfusions, and no intra- or postoperative complications. The mean length of stay was 3 days. The pathology of all resected lesions was stromal and glandular endometriosis.
After the surgery, 96 pregnancies occurred among the subgroup with infertility (62%). The median time to conception was 8 months. The majority of pregnancies were spontaneous (71), with the rest achieved by in vitro fertilization. There were four miscarriages.
A quality of life survey was conducted at 6 months. By that time, dysmenorrhea, dyspareunia and pain on defecation, intestinal cramping, diarrhea and constipation had disappeared in all women.
Dr. Neme had no financial disclosures.
NATIONAL HARBOR, MD. – Pregnancy occurred in more than half of infertile women who had a segmental laparoscopic bowel resection for endometriosis.
Of 155 women, 96 (62%) conceived after the surgery. Most of these pregnancies (71 of 96; 74%) were spontaneous, Dr. Rosa Maria Neme reported at a meeting sponsored by AAGL.
The prospective study included women treated during 2009-2012 at the University of São Paulo, Brazil, said Dr. Neme, director of the university’s endometriosis center. The patients were a mean of 32 years old.
Most (92%) had bowel symptoms, including pain during defecation, diarrhea and constipation, abdominal bloating, and dyschezia. Endometriosis-related symptoms were present in all, and included dysmenorrhea, nonmenstrual pelvic pain and dyspareunia, tenesmus, cyclic rectal bleeding, lower back pain, and asthenia.
An associated infertility was present in 62% (155), with a mean duration of 18 months. Most patients (78%) had already undergone some form of fertility treatment before surgery and 69% had undergone a previous surgery for pelvic pain.
All of the patients had a torus bowel resection. A number of other procedures also were performed during the surgery, including extensive ureterolysis (80%), ovarian cystectomy (70%), partial vaginal resection (20%), and appendectomy (20%).
The mean operative time was 117 minutes. There were no conversions to open surgery, no transfusions, and no intra- or postoperative complications. The mean length of stay was 3 days. The pathology of all resected lesions was stromal and glandular endometriosis.
After the surgery, 96 pregnancies occurred among the subgroup with infertility (62%). The median time to conception was 8 months. The majority of pregnancies were spontaneous (71), with the rest achieved by in vitro fertilization. There were four miscarriages.
A quality of life survey was conducted at 6 months. By that time, dysmenorrhea, dyspareunia and pain on defecation, intestinal cramping, diarrhea and constipation had disappeared in all women.
Dr. Neme had no financial disclosures.
NATIONAL HARBOR, MD. – Pregnancy occurred in more than half of infertile women who had a segmental laparoscopic bowel resection for endometriosis.
Of 155 women, 96 (62%) conceived after the surgery. Most of these pregnancies (71 of 96; 74%) were spontaneous, Dr. Rosa Maria Neme reported at a meeting sponsored by AAGL.
The prospective study included women treated during 2009-2012 at the University of São Paulo, Brazil, said Dr. Neme, director of the university’s endometriosis center. The patients were a mean of 32 years old.
Most (92%) had bowel symptoms, including pain during defecation, diarrhea and constipation, abdominal bloating, and dyschezia. Endometriosis-related symptoms were present in all, and included dysmenorrhea, nonmenstrual pelvic pain and dyspareunia, tenesmus, cyclic rectal bleeding, lower back pain, and asthenia.
An associated infertility was present in 62% (155), with a mean duration of 18 months. Most patients (78%) had already undergone some form of fertility treatment before surgery and 69% had undergone a previous surgery for pelvic pain.
All of the patients had a torus bowel resection. A number of other procedures also were performed during the surgery, including extensive ureterolysis (80%), ovarian cystectomy (70%), partial vaginal resection (20%), and appendectomy (20%).
The mean operative time was 117 minutes. There were no conversions to open surgery, no transfusions, and no intra- or postoperative complications. The mean length of stay was 3 days. The pathology of all resected lesions was stromal and glandular endometriosis.
After the surgery, 96 pregnancies occurred among the subgroup with infertility (62%). The median time to conception was 8 months. The majority of pregnancies were spontaneous (71), with the rest achieved by in vitro fertilization. There were four miscarriages.
A quality of life survey was conducted at 6 months. By that time, dysmenorrhea, dyspareunia and pain on defecation, intestinal cramping, diarrhea and constipation had disappeared in all women.
Dr. Neme had no financial disclosures.
AT THE AAGL GLOBAL CONGRESS
Major finding: Pregnancy occurred in 62% of women with bowel endometriosis who underwent a bowel resection.
Data source: The prospective study involved 250 women, 155 of whom had infertility.
Disclosures: Dr. Neme had no financial disclosures.
New model predicts risk of ureteral injury related to colorectal surgery
PHOENIX – A new model based on clinical, hospital, and operative factors predicted the risk of ureteral injury among patients undergoing colorectal surgery.
Using data from the Nationwide Inpatient Sample, which includes more than 2 million patients in the United States, researchers retrospectively studied patients undergoing surgery in the United States between 2001 and 2010 for colorectal cancer, polyps, diverticular disease, or inflammatory bowel disease.
Less than 1% of patients sustained a ureteral injury, but the incidence rose significantly during the study period and injured patients had sharply higher rates of complications, researchers reported at the annual meeting of the American Society of Colon and Rectal Surgeons.
Eight factors were independently associated with the risk of ureteral injury. A predictive model incorporating these factors had an area under the receiver operating characteristic curve of 0.73. The model-predicted probability of injury ranged from 0.1% to 1.65%, depending on hospital factors, disease type, and procedure type, said Dr. Wissam J. Halabi, a research fellow at the University of California-Irvine, Orange.
Patients had higher adjusted odds of ureteral injury if they had rectal cancer (odds ratio, 1.85), adhesions (OR, 1.83), and metastatic cancer (OR, 1.76); if they had lost weight (OR, 1.08); and if they underwent surgery at a teaching hospital (OR, 1.05). On the other hand, patients had lower odds of injury if they had a laparoscopic procedure (OR, 0.91), a transverse colectomy (OR, 0.90), or a right hemicolectomy (OR, 0.43).
With the new predictive model incorporating these factors, the probability of injury ranged from 0.1% for patients undergoing laparoscopic right hemicolectomy to 1.65% for patients having all five adverse risk factors.
"Diverticulitis did not appear as a predictor in our model," Dr. Halabi said. "As for radiation, one of our predictors was metastatic cancer. So this goes for any cancer at advanced stage that has spread to lymph nodes or distant organ metastasis. In the case of rectal cancer, those are most likely to have received radiation therapy. So part of this effect of radiation therapy was apparent in the metastatic cancer group predictor."
Analyses were based on 2,165,848 colorectal surgery procedures. The overall rate of ureteral injury was 0.28%, he reported.
There was a significant 24% increase in the rate during the study period, from 2.5 per 1,000 cases in 2001-2005 to 3.1 per 1,000 cases in 2006-2010.
On average, the patients sustaining injury were younger and were more likely to be female and to have metastatic cancer, to be immunosuppressed, and to have had weight loss. They were less likely to have certain major comorbidities, such as diabetes and hypertension.
"Interestingly, obesity was similar in the two groups," Dr. Halabi commented.
Patients who sustained ureteral injuries had longer hospital stays and higher rates of a variety of postoperative complications, such as anastomotic leak and acute renal failure, but in-hospital mortality was statistically indistinguishable.
In adjusted analysis, patients with ureteral injury were significantly more likely to die (OR, 1.45) and to experience complications (OR, 1.66), and they had a longer hospital stay (+3.65 days) and total hospital charges (+$31,497).
Ureteral injuries "affect a relatively younger and healthier population. However, they have a significant and dramatic impact on outcomes," he added. "This predictive model can be used for risk stratification and counseling."
Dr. Halabi disclosed no relevant conflicts of interest.

|
|
I thought it was an interesting study to look specifically at the ureter in colorectal surgical patients because we sort of extrapolate from the gynecologic world.
One of the things I took away from the study was that risk is really related to the complexity of the case. The researchers talked about adhesions, but I really think that adhesions are a surrogate for complexity. I think the study reinforces for those of us who believe in ureteral stents to help us avoid the ureteral injury, or identify the injury when it occurs, that reoperation is another important factor to look at.
Dr. Mark Welton is with Stanford (Calif.) University. He was the session comoderator and made his comments in an interview. He had no relevant disclosures.
|
|
|
I thought it was an interesting study to look specifically at the ureter in colorectal surgical patients because we sort of extrapolate from the gynecologic world.
One of the things I took away from the study was that risk is really related to the complexity of the case. The researchers talked about adhesions, but I really think that adhesions are a surrogate for complexity. I think the study reinforces for those of us who believe in ureteral stents to help us avoid the ureteral injury, or identify the injury when it occurs, that reoperation is another important factor to look at.
Dr. Mark Welton is with Stanford (Calif.) University. He was the session comoderator and made his comments in an interview. He had no relevant disclosures.
|
|
|
I thought it was an interesting study to look specifically at the ureter in colorectal surgical patients because we sort of extrapolate from the gynecologic world.
One of the things I took away from the study was that risk is really related to the complexity of the case. The researchers talked about adhesions, but I really think that adhesions are a surrogate for complexity. I think the study reinforces for those of us who believe in ureteral stents to help us avoid the ureteral injury, or identify the injury when it occurs, that reoperation is another important factor to look at.
Dr. Mark Welton is with Stanford (Calif.) University. He was the session comoderator and made his comments in an interview. He had no relevant disclosures.
PHOENIX – A new model based on clinical, hospital, and operative factors predicted the risk of ureteral injury among patients undergoing colorectal surgery.
Using data from the Nationwide Inpatient Sample, which includes more than 2 million patients in the United States, researchers retrospectively studied patients undergoing surgery in the United States between 2001 and 2010 for colorectal cancer, polyps, diverticular disease, or inflammatory bowel disease.
Less than 1% of patients sustained a ureteral injury, but the incidence rose significantly during the study period and injured patients had sharply higher rates of complications, researchers reported at the annual meeting of the American Society of Colon and Rectal Surgeons.
Eight factors were independently associated with the risk of ureteral injury. A predictive model incorporating these factors had an area under the receiver operating characteristic curve of 0.73. The model-predicted probability of injury ranged from 0.1% to 1.65%, depending on hospital factors, disease type, and procedure type, said Dr. Wissam J. Halabi, a research fellow at the University of California-Irvine, Orange.
Patients had higher adjusted odds of ureteral injury if they had rectal cancer (odds ratio, 1.85), adhesions (OR, 1.83), and metastatic cancer (OR, 1.76); if they had lost weight (OR, 1.08); and if they underwent surgery at a teaching hospital (OR, 1.05). On the other hand, patients had lower odds of injury if they had a laparoscopic procedure (OR, 0.91), a transverse colectomy (OR, 0.90), or a right hemicolectomy (OR, 0.43).
With the new predictive model incorporating these factors, the probability of injury ranged from 0.1% for patients undergoing laparoscopic right hemicolectomy to 1.65% for patients having all five adverse risk factors.
"Diverticulitis did not appear as a predictor in our model," Dr. Halabi said. "As for radiation, one of our predictors was metastatic cancer. So this goes for any cancer at advanced stage that has spread to lymph nodes or distant organ metastasis. In the case of rectal cancer, those are most likely to have received radiation therapy. So part of this effect of radiation therapy was apparent in the metastatic cancer group predictor."
Analyses were based on 2,165,848 colorectal surgery procedures. The overall rate of ureteral injury was 0.28%, he reported.
There was a significant 24% increase in the rate during the study period, from 2.5 per 1,000 cases in 2001-2005 to 3.1 per 1,000 cases in 2006-2010.
On average, the patients sustaining injury were younger and were more likely to be female and to have metastatic cancer, to be immunosuppressed, and to have had weight loss. They were less likely to have certain major comorbidities, such as diabetes and hypertension.
"Interestingly, obesity was similar in the two groups," Dr. Halabi commented.
Patients who sustained ureteral injuries had longer hospital stays and higher rates of a variety of postoperative complications, such as anastomotic leak and acute renal failure, but in-hospital mortality was statistically indistinguishable.
In adjusted analysis, patients with ureteral injury were significantly more likely to die (OR, 1.45) and to experience complications (OR, 1.66), and they had a longer hospital stay (+3.65 days) and total hospital charges (+$31,497).
Ureteral injuries "affect a relatively younger and healthier population. However, they have a significant and dramatic impact on outcomes," he added. "This predictive model can be used for risk stratification and counseling."
Dr. Halabi disclosed no relevant conflicts of interest.
PHOENIX – A new model based on clinical, hospital, and operative factors predicted the risk of ureteral injury among patients undergoing colorectal surgery.
Using data from the Nationwide Inpatient Sample, which includes more than 2 million patients in the United States, researchers retrospectively studied patients undergoing surgery in the United States between 2001 and 2010 for colorectal cancer, polyps, diverticular disease, or inflammatory bowel disease.
Less than 1% of patients sustained a ureteral injury, but the incidence rose significantly during the study period and injured patients had sharply higher rates of complications, researchers reported at the annual meeting of the American Society of Colon and Rectal Surgeons.
Eight factors were independently associated with the risk of ureteral injury. A predictive model incorporating these factors had an area under the receiver operating characteristic curve of 0.73. The model-predicted probability of injury ranged from 0.1% to 1.65%, depending on hospital factors, disease type, and procedure type, said Dr. Wissam J. Halabi, a research fellow at the University of California-Irvine, Orange.
Patients had higher adjusted odds of ureteral injury if they had rectal cancer (odds ratio, 1.85), adhesions (OR, 1.83), and metastatic cancer (OR, 1.76); if they had lost weight (OR, 1.08); and if they underwent surgery at a teaching hospital (OR, 1.05). On the other hand, patients had lower odds of injury if they had a laparoscopic procedure (OR, 0.91), a transverse colectomy (OR, 0.90), or a right hemicolectomy (OR, 0.43).
With the new predictive model incorporating these factors, the probability of injury ranged from 0.1% for patients undergoing laparoscopic right hemicolectomy to 1.65% for patients having all five adverse risk factors.
"Diverticulitis did not appear as a predictor in our model," Dr. Halabi said. "As for radiation, one of our predictors was metastatic cancer. So this goes for any cancer at advanced stage that has spread to lymph nodes or distant organ metastasis. In the case of rectal cancer, those are most likely to have received radiation therapy. So part of this effect of radiation therapy was apparent in the metastatic cancer group predictor."
Analyses were based on 2,165,848 colorectal surgery procedures. The overall rate of ureteral injury was 0.28%, he reported.
There was a significant 24% increase in the rate during the study period, from 2.5 per 1,000 cases in 2001-2005 to 3.1 per 1,000 cases in 2006-2010.
On average, the patients sustaining injury were younger and were more likely to be female and to have metastatic cancer, to be immunosuppressed, and to have had weight loss. They were less likely to have certain major comorbidities, such as diabetes and hypertension.
"Interestingly, obesity was similar in the two groups," Dr. Halabi commented.
Patients who sustained ureteral injuries had longer hospital stays and higher rates of a variety of postoperative complications, such as anastomotic leak and acute renal failure, but in-hospital mortality was statistically indistinguishable.
In adjusted analysis, patients with ureteral injury were significantly more likely to die (OR, 1.45) and to experience complications (OR, 1.66), and they had a longer hospital stay (+3.65 days) and total hospital charges (+$31,497).
Ureteral injuries "affect a relatively younger and healthier population. However, they have a significant and dramatic impact on outcomes," he added. "This predictive model can be used for risk stratification and counseling."
Dr. Halabi disclosed no relevant conflicts of interest.
AT THE ASCRS ANNUAL MEETING
Major Finding: The predictive model had an area under the receiver operating characteristic curve of 0.73. The model-predicted probability of injury ranged from 0.1% to 1.65%, depending on the presence of various factors.
Data Source: A retrospective study of 2.1 million patients undergoing colorectal surgery between 2001 and 2010.
Disclosures: Dr. Halabi disclosed no relevant conflicts of interest.

Transversus abdominis plane block added to ERP reduced hospital stay
The addition of a transversus abdominis plane block to standard enhanced recovery pathway protocols decreased lengths of stay to less than 3 days in roughly two-thirds of patients who underwent laparoscopic colectomy, findings from a small study showed.
To determine the impact of a TAP block on rates of discharge for colorectal laparoscopic surgery, researchers at University Hospitals Case Medical Center in Cleveland observed 100 consecutive patients who underwent the elective procedure performed over a 1-year period by the same experienced laparoscopic colorectal surgeon. The TAP block was administered at the conclusion of the laparoscopic procedure.
The mean age of the study population was 60.5 years, and 62 were female. The mean body mass index was 28.4 kg/m². Surgical indications in two-thirds of patients included colorectal cancer or polyp. One-third of patients had an inflammatory condition such as diverticulitis, ulcerative colitis, or Crohn’s disease, said Dr. Joanne Favuzza and Dr. Conor P. Delaney (J. Am. Coll. Surg. 2013;217:503-6).
The investigators found that 62% of patients were discharged within 48 hours, with 27% being discharged on day 1. No operative mortality was reported, and only one patient experienced a complication post discharge. Two patients were readmitted, both having had lengths of stay exceeding 48 hours.
Incidence rates of complication or readmission were not significantly affected by the block. Eight patients experienced postoperative complications: one patient on the second day post surgery, another patient on the third day, and the rest after the fourth day. Three patients had complications involving the ileus or lower-bowel obstruction, four patients had anastomotic or gastrointestinal bleed, and one had a urinary tract infection.
"This study demonstrated that the addition of a TAP block to an established ERP can reproducibly reduce length of stay to less than 3 days," wrote Dr. Favuzza and Dr. Delaney, who also noted that a prospective randomized controlled trial is underway to further evaluate the benefits of TAP blocks to ERP in colorectal surgery.
Dr. Favuzza reported no relevant disclosures. Dr. Delaney is a paid a consultant to Adolor Corp., Ferring Pharmaceuticals, and Pacira Pharmaceuticals.
The addition of a transversus abdominis plane block to standard enhanced recovery pathway protocols decreased lengths of stay to less than 3 days in roughly two-thirds of patients who underwent laparoscopic colectomy, findings from a small study showed.
To determine the impact of a TAP block on rates of discharge for colorectal laparoscopic surgery, researchers at University Hospitals Case Medical Center in Cleveland observed 100 consecutive patients who underwent the elective procedure performed over a 1-year period by the same experienced laparoscopic colorectal surgeon. The TAP block was administered at the conclusion of the laparoscopic procedure.
The mean age of the study population was 60.5 years, and 62 were female. The mean body mass index was 28.4 kg/m². Surgical indications in two-thirds of patients included colorectal cancer or polyp. One-third of patients had an inflammatory condition such as diverticulitis, ulcerative colitis, or Crohn’s disease, said Dr. Joanne Favuzza and Dr. Conor P. Delaney (J. Am. Coll. Surg. 2013;217:503-6).
The investigators found that 62% of patients were discharged within 48 hours, with 27% being discharged on day 1. No operative mortality was reported, and only one patient experienced a complication post discharge. Two patients were readmitted, both having had lengths of stay exceeding 48 hours.
Incidence rates of complication or readmission were not significantly affected by the block. Eight patients experienced postoperative complications: one patient on the second day post surgery, another patient on the third day, and the rest after the fourth day. Three patients had complications involving the ileus or lower-bowel obstruction, four patients had anastomotic or gastrointestinal bleed, and one had a urinary tract infection.
"This study demonstrated that the addition of a TAP block to an established ERP can reproducibly reduce length of stay to less than 3 days," wrote Dr. Favuzza and Dr. Delaney, who also noted that a prospective randomized controlled trial is underway to further evaluate the benefits of TAP blocks to ERP in colorectal surgery.
Dr. Favuzza reported no relevant disclosures. Dr. Delaney is a paid a consultant to Adolor Corp., Ferring Pharmaceuticals, and Pacira Pharmaceuticals.
The addition of a transversus abdominis plane block to standard enhanced recovery pathway protocols decreased lengths of stay to less than 3 days in roughly two-thirds of patients who underwent laparoscopic colectomy, findings from a small study showed.
To determine the impact of a TAP block on rates of discharge for colorectal laparoscopic surgery, researchers at University Hospitals Case Medical Center in Cleveland observed 100 consecutive patients who underwent the elective procedure performed over a 1-year period by the same experienced laparoscopic colorectal surgeon. The TAP block was administered at the conclusion of the laparoscopic procedure.
The mean age of the study population was 60.5 years, and 62 were female. The mean body mass index was 28.4 kg/m². Surgical indications in two-thirds of patients included colorectal cancer or polyp. One-third of patients had an inflammatory condition such as diverticulitis, ulcerative colitis, or Crohn’s disease, said Dr. Joanne Favuzza and Dr. Conor P. Delaney (J. Am. Coll. Surg. 2013;217:503-6).
The investigators found that 62% of patients were discharged within 48 hours, with 27% being discharged on day 1. No operative mortality was reported, and only one patient experienced a complication post discharge. Two patients were readmitted, both having had lengths of stay exceeding 48 hours.
Incidence rates of complication or readmission were not significantly affected by the block. Eight patients experienced postoperative complications: one patient on the second day post surgery, another patient on the third day, and the rest after the fourth day. Three patients had complications involving the ileus or lower-bowel obstruction, four patients had anastomotic or gastrointestinal bleed, and one had a urinary tract infection.
"This study demonstrated that the addition of a TAP block to an established ERP can reproducibly reduce length of stay to less than 3 days," wrote Dr. Favuzza and Dr. Delaney, who also noted that a prospective randomized controlled trial is underway to further evaluate the benefits of TAP blocks to ERP in colorectal surgery.
Dr. Favuzza reported no relevant disclosures. Dr. Delaney is a paid a consultant to Adolor Corp., Ferring Pharmaceuticals, and Pacira Pharmaceuticals.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Major finding: The addition of a transversus abdominis plane block to enhanced recovery pathways accelerated discharge rates in two-thirds of colorectal laparoscopy patients, with no added complications.
Data source: Consecutive observational study of 100 elective laparoscopic colectomy patients treated by same surgeon.
Disclosures: Dr. Favuzza reported no relevant disclosures. Dr. Delaney is a paid a consultant to Adolor Corp., Ferring Pharmaceuticals, and Pacira Pharmaceuticals.
A one-size-fits-all fenestrated graft for iliac aneurysms?
CHICAGO – A novel bifurcated covered stent graft limb that uses an off-the-shelf graft can treat large common iliac aneurysms, while preserving good pelvic blood flow.
The alternative endovascular approach has been performed on 15 patients since April 2011, with a success rate of 100%. Bilateral stent grafts were placed in four patients.
The all-male cohort has been able to maintain appropriate exercise tolerance and remains free from erectile dysfunction, pelvic ischemia, buttock claudication, and paralysis.
"These people do well," extremely well, Dr. Patrick Kelly said at the annual meeting of the Midwestern Vascular Surgical Society*.
Several iliac branch grafts are currently under investigation, including the Cook Zenith Branch iliac endovascular graft. They promise to preserve flow to the internal iliac artery and thus reduce the potential for ischemic sequelae resulting from iliac embolization. Depending on patient anatomy, however, the internal iliac may become jailed upon deployment of the main body graft, said Dr. Kelly of Sanford Health, Sioux Falls, S.D. The fenestrated systems are also limited by bridging stent technology and the relatively short bridging stent.

His alternative modified bifurcated limb divides the common iliac flow into the internal and external iliac arteries, while excluding the common iliac artery aneurysm.
"The pros are that it uses an off the shelf [graft], should be able to handle virtually any anatomy, can be used to treat either existing EVAR [endovascular aneurysm repair] or previous open repairs, and has multiple off-ramps, so you don’t jail yourself," he said. "The cons: It requires arm access – although I’m not sure that’s a con – and it requires three stents."
Operative details
The bifurcated limb is created by sewing an 8-mm and 10-mm covered stent graft to the distal end of a standard 16 x 20 x 82-mm stent graft limb. The distal ends of both the 8-mm and 10-mm grafts are left free, allowing flexibility and easier selection of the internal iliac artery, he said.
Once the graft is resheathed using a spiral wire technique, a traditional infrarenal abdominal aneurysm repair is performed. In order to exclude the common iliac aneurysm, the graft is oriented with the 8-mm limb toward the internal iliac and with the distal end of the 8-mm limb being deployed 2-3 cm above the origin of the internal iliac artery. The internal iliac artery is selected from an arm approach, through the 8-mm limb of the bifurcated stent graft limb.
Angiograms are performed and a 3-cm covered, self-expanding bridge stent graft is deployed. The 10-mm limb is used to extend the graft into the external iliac, thus completing exclusion of the common iliac aneurysm, while preserving both the internal and external iliac arteries, Dr. Kelly said.
Thus far, occlusion of the external iliac artery has been reported in one patient, and there were no recurring endoleaks. There was a type-3 endoleak between the main body and bridging stent that was visible on diagnostic angiography, but it resolved after being reballooned and patent flow was established upon completion angiography, Dr. Kelly explained. There was also a retrograde fill that was fixed 1 year postoperatively by extending the limb to obtain a healthy seal.
The average patient age was 65.4 years (range, 46-87 years); fluoroscopy time, 46 minutes (range, 29-91 minutes); and average length of stay 3.1 days (range, 1-9 days).
This compares with an average hospital stay of 4-7 days for the tried-and-true method of open aneurysm repair, which has bleeding rates of 30% or more, colonic ischemia in 20%-30%, and paraplegia in 2%-3%, Dr. Kelly noted.
Audience reaction
Dr. Rebecca Kelso of the Cleveland Clinic, who comoderated the session, was enthusiastic about the novel approach.
"The potential for it is quite significant, because the other main competitive device he mentioned that’s on the market still has anatomic limitations for use," she said in an interview. "So if he has something that can be used in any patient, no matter what the circumstances, well then that has significant implications for being available commercially for everyone."
Fellow moderator Dr. Patrick J. Geraghty of Washington University, St. Louis, remarked that while the approach uses a standardized graft, it is somewhat tailored since the length and the diameter of the Bivon grafts extending into the external and internal iliac arteries can be chosen separately. That said, the one-size-fits-all approach is particularly appealing because it could simplify treatment planning and reduce treatment delays.
"If you have a patient who is symptomatic and you have an off-the-shelf component, you could potentially treat them within the next 24 hours," he said in an interview. "The current turnaround time for the fenestrated system is about a month or so, so it would shorten treatment delays and might lead to a broader application of the technology."
A potentially shorter hospital length of stay could also reduce hospital costs, Dr. Kelso noted.
While the audience appeared equally enthusiastic about the results, some members questioned whether results on a physician-modified graft without an Investigational Device Exemption (IDE) should be presented at the meeting in light of recent warnings by the U.S. Food and Drug Administration that such interventions involve the use of significant-risk devices and need to be conducted under an IDE. Dr. Kelly responded that he is currently working with the FDA to obtain an IDE.
Earlier this year, the Society of Thoracic Surgeons and the American College of Cardiology became the first medical societies to receive an IDE to study alternative access for transcatheter aortic valve replacement using the STS/ACC TVT Registry
Dr. Kelly and Dr. Kelso reported having no financial disclosures. Dr. Geraghty disclosed relationships with Cook Medical and Bard/Lutonix.
*CORRECTION, 10/29/2013: An earlier version of this article misstated the name of the annual meeting of the Midwestern Vascular Surgical Society.
Vascular surgeons are like cobblers – we try to make the perfect pair of shoes for each customer. While all aneurysm operations are similar in principle, in reality each successful operation depends on a unique blend of surgical skill and experience applied to the individual anatomy of each patient. By combining endovascular and open surgical skills, vascular surgeons are enticed to develop ever more innovative solutions for complex problems. Dr. Kelly should be congratulated for thinking outside the box and applying his imagination and skill to the solution of this common clinical scenario. While I am intrigued by the technique, I will reserve my enthusiastic endorsement because of the relatively high cost and the fact the common iliac artery must be sufficiently large to accommodate the physician-modified bifurcated graft. Others have described the use of "stacked" Gore Excluder device to achieve a similar result. And the Cook Iliac Branched Device is nearing approval. In the long run, the FDA needs to adopt policies that encourage rather discourage innovation in the development of novel surgical treatments. The current onerous IDE process is excessively complex and expensive. Physician-modified endografts fill an important gap in our ability to deliver quality, customized care for every patient. And there is no evidence that innovation in vascular surgery has been harmful to patients. After all, every operation is "physician modified."
Dr. John F. Eidt is a vascular surgeon at the Greenville (South Carolina) Health System, and an associate medical editor for Vascular Specialist.
Vascular surgeons are like cobblers – we try to make the perfect pair of shoes for each customer. While all aneurysm operations are similar in principle, in reality each successful operation depends on a unique blend of surgical skill and experience applied to the individual anatomy of each patient. By combining endovascular and open surgical skills, vascular surgeons are enticed to develop ever more innovative solutions for complex problems. Dr. Kelly should be congratulated for thinking outside the box and applying his imagination and skill to the solution of this common clinical scenario. While I am intrigued by the technique, I will reserve my enthusiastic endorsement because of the relatively high cost and the fact the common iliac artery must be sufficiently large to accommodate the physician-modified bifurcated graft. Others have described the use of "stacked" Gore Excluder device to achieve a similar result. And the Cook Iliac Branched Device is nearing approval. In the long run, the FDA needs to adopt policies that encourage rather discourage innovation in the development of novel surgical treatments. The current onerous IDE process is excessively complex and expensive. Physician-modified endografts fill an important gap in our ability to deliver quality, customized care for every patient. And there is no evidence that innovation in vascular surgery has been harmful to patients. After all, every operation is "physician modified."
Dr. John F. Eidt is a vascular surgeon at the Greenville (South Carolina) Health System, and an associate medical editor for Vascular Specialist.
Vascular surgeons are like cobblers – we try to make the perfect pair of shoes for each customer. While all aneurysm operations are similar in principle, in reality each successful operation depends on a unique blend of surgical skill and experience applied to the individual anatomy of each patient. By combining endovascular and open surgical skills, vascular surgeons are enticed to develop ever more innovative solutions for complex problems. Dr. Kelly should be congratulated for thinking outside the box and applying his imagination and skill to the solution of this common clinical scenario. While I am intrigued by the technique, I will reserve my enthusiastic endorsement because of the relatively high cost and the fact the common iliac artery must be sufficiently large to accommodate the physician-modified bifurcated graft. Others have described the use of "stacked" Gore Excluder device to achieve a similar result. And the Cook Iliac Branched Device is nearing approval. In the long run, the FDA needs to adopt policies that encourage rather discourage innovation in the development of novel surgical treatments. The current onerous IDE process is excessively complex and expensive. Physician-modified endografts fill an important gap in our ability to deliver quality, customized care for every patient. And there is no evidence that innovation in vascular surgery has been harmful to patients. After all, every operation is "physician modified."
Dr. John F. Eidt is a vascular surgeon at the Greenville (South Carolina) Health System, and an associate medical editor for Vascular Specialist.
CHICAGO – A novel bifurcated covered stent graft limb that uses an off-the-shelf graft can treat large common iliac aneurysms, while preserving good pelvic blood flow.
The alternative endovascular approach has been performed on 15 patients since April 2011, with a success rate of 100%. Bilateral stent grafts were placed in four patients.
The all-male cohort has been able to maintain appropriate exercise tolerance and remains free from erectile dysfunction, pelvic ischemia, buttock claudication, and paralysis.
"These people do well," extremely well, Dr. Patrick Kelly said at the annual meeting of the Midwestern Vascular Surgical Society*.
Several iliac branch grafts are currently under investigation, including the Cook Zenith Branch iliac endovascular graft. They promise to preserve flow to the internal iliac artery and thus reduce the potential for ischemic sequelae resulting from iliac embolization. Depending on patient anatomy, however, the internal iliac may become jailed upon deployment of the main body graft, said Dr. Kelly of Sanford Health, Sioux Falls, S.D. The fenestrated systems are also limited by bridging stent technology and the relatively short bridging stent.
His alternative modified bifurcated limb divides the common iliac flow into the internal and external iliac arteries, while excluding the common iliac artery aneurysm.
"The pros are that it uses an off the shelf [graft], should be able to handle virtually any anatomy, can be used to treat either existing EVAR [endovascular aneurysm repair] or previous open repairs, and has multiple off-ramps, so you don’t jail yourself," he said. "The cons: It requires arm access – although I’m not sure that’s a con – and it requires three stents."
Operative details
The bifurcated limb is created by sewing an 8-mm and 10-mm covered stent graft to the distal end of a standard 16 x 20 x 82-mm stent graft limb. The distal ends of both the 8-mm and 10-mm grafts are left free, allowing flexibility and easier selection of the internal iliac artery, he said.
Once the graft is resheathed using a spiral wire technique, a traditional infrarenal abdominal aneurysm repair is performed. In order to exclude the common iliac aneurysm, the graft is oriented with the 8-mm limb toward the internal iliac and with the distal end of the 8-mm limb being deployed 2-3 cm above the origin of the internal iliac artery. The internal iliac artery is selected from an arm approach, through the 8-mm limb of the bifurcated stent graft limb.
Angiograms are performed and a 3-cm covered, self-expanding bridge stent graft is deployed. The 10-mm limb is used to extend the graft into the external iliac, thus completing exclusion of the common iliac aneurysm, while preserving both the internal and external iliac arteries, Dr. Kelly said.
Thus far, occlusion of the external iliac artery has been reported in one patient, and there were no recurring endoleaks. There was a type-3 endoleak between the main body and bridging stent that was visible on diagnostic angiography, but it resolved after being reballooned and patent flow was established upon completion angiography, Dr. Kelly explained. There was also a retrograde fill that was fixed 1 year postoperatively by extending the limb to obtain a healthy seal.
The average patient age was 65.4 years (range, 46-87 years); fluoroscopy time, 46 minutes (range, 29-91 minutes); and average length of stay 3.1 days (range, 1-9 days).
This compares with an average hospital stay of 4-7 days for the tried-and-true method of open aneurysm repair, which has bleeding rates of 30% or more, colonic ischemia in 20%-30%, and paraplegia in 2%-3%, Dr. Kelly noted.
Audience reaction
Dr. Rebecca Kelso of the Cleveland Clinic, who comoderated the session, was enthusiastic about the novel approach.
"The potential for it is quite significant, because the other main competitive device he mentioned that’s on the market still has anatomic limitations for use," she said in an interview. "So if he has something that can be used in any patient, no matter what the circumstances, well then that has significant implications for being available commercially for everyone."
Fellow moderator Dr. Patrick J. Geraghty of Washington University, St. Louis, remarked that while the approach uses a standardized graft, it is somewhat tailored since the length and the diameter of the Bivon grafts extending into the external and internal iliac arteries can be chosen separately. That said, the one-size-fits-all approach is particularly appealing because it could simplify treatment planning and reduce treatment delays.
"If you have a patient who is symptomatic and you have an off-the-shelf component, you could potentially treat them within the next 24 hours," he said in an interview. "The current turnaround time for the fenestrated system is about a month or so, so it would shorten treatment delays and might lead to a broader application of the technology."
A potentially shorter hospital length of stay could also reduce hospital costs, Dr. Kelso noted.
While the audience appeared equally enthusiastic about the results, some members questioned whether results on a physician-modified graft without an Investigational Device Exemption (IDE) should be presented at the meeting in light of recent warnings by the U.S. Food and Drug Administration that such interventions involve the use of significant-risk devices and need to be conducted under an IDE. Dr. Kelly responded that he is currently working with the FDA to obtain an IDE.
Earlier this year, the Society of Thoracic Surgeons and the American College of Cardiology became the first medical societies to receive an IDE to study alternative access for transcatheter aortic valve replacement using the STS/ACC TVT Registry
Dr. Kelly and Dr. Kelso reported having no financial disclosures. Dr. Geraghty disclosed relationships with Cook Medical and Bard/Lutonix.
*CORRECTION, 10/29/2013: An earlier version of this article misstated the name of the annual meeting of the Midwestern Vascular Surgical Society.
CHICAGO – A novel bifurcated covered stent graft limb that uses an off-the-shelf graft can treat large common iliac aneurysms, while preserving good pelvic blood flow.
The alternative endovascular approach has been performed on 15 patients since April 2011, with a success rate of 100%. Bilateral stent grafts were placed in four patients.
The all-male cohort has been able to maintain appropriate exercise tolerance and remains free from erectile dysfunction, pelvic ischemia, buttock claudication, and paralysis.
"These people do well," extremely well, Dr. Patrick Kelly said at the annual meeting of the Midwestern Vascular Surgical Society*.
Several iliac branch grafts are currently under investigation, including the Cook Zenith Branch iliac endovascular graft. They promise to preserve flow to the internal iliac artery and thus reduce the potential for ischemic sequelae resulting from iliac embolization. Depending on patient anatomy, however, the internal iliac may become jailed upon deployment of the main body graft, said Dr. Kelly of Sanford Health, Sioux Falls, S.D. The fenestrated systems are also limited by bridging stent technology and the relatively short bridging stent.
His alternative modified bifurcated limb divides the common iliac flow into the internal and external iliac arteries, while excluding the common iliac artery aneurysm.
"The pros are that it uses an off the shelf [graft], should be able to handle virtually any anatomy, can be used to treat either existing EVAR [endovascular aneurysm repair] or previous open repairs, and has multiple off-ramps, so you don’t jail yourself," he said. "The cons: It requires arm access – although I’m not sure that’s a con – and it requires three stents."
Operative details
The bifurcated limb is created by sewing an 8-mm and 10-mm covered stent graft to the distal end of a standard 16 x 20 x 82-mm stent graft limb. The distal ends of both the 8-mm and 10-mm grafts are left free, allowing flexibility and easier selection of the internal iliac artery, he said.
Once the graft is resheathed using a spiral wire technique, a traditional infrarenal abdominal aneurysm repair is performed. In order to exclude the common iliac aneurysm, the graft is oriented with the 8-mm limb toward the internal iliac and with the distal end of the 8-mm limb being deployed 2-3 cm above the origin of the internal iliac artery. The internal iliac artery is selected from an arm approach, through the 8-mm limb of the bifurcated stent graft limb.
Angiograms are performed and a 3-cm covered, self-expanding bridge stent graft is deployed. The 10-mm limb is used to extend the graft into the external iliac, thus completing exclusion of the common iliac aneurysm, while preserving both the internal and external iliac arteries, Dr. Kelly said.
Thus far, occlusion of the external iliac artery has been reported in one patient, and there were no recurring endoleaks. There was a type-3 endoleak between the main body and bridging stent that was visible on diagnostic angiography, but it resolved after being reballooned and patent flow was established upon completion angiography, Dr. Kelly explained. There was also a retrograde fill that was fixed 1 year postoperatively by extending the limb to obtain a healthy seal.
The average patient age was 65.4 years (range, 46-87 years); fluoroscopy time, 46 minutes (range, 29-91 minutes); and average length of stay 3.1 days (range, 1-9 days).
This compares with an average hospital stay of 4-7 days for the tried-and-true method of open aneurysm repair, which has bleeding rates of 30% or more, colonic ischemia in 20%-30%, and paraplegia in 2%-3%, Dr. Kelly noted.
Audience reaction
Dr. Rebecca Kelso of the Cleveland Clinic, who comoderated the session, was enthusiastic about the novel approach.
"The potential for it is quite significant, because the other main competitive device he mentioned that’s on the market still has anatomic limitations for use," she said in an interview. "So if he has something that can be used in any patient, no matter what the circumstances, well then that has significant implications for being available commercially for everyone."
Fellow moderator Dr. Patrick J. Geraghty of Washington University, St. Louis, remarked that while the approach uses a standardized graft, it is somewhat tailored since the length and the diameter of the Bivon grafts extending into the external and internal iliac arteries can be chosen separately. That said, the one-size-fits-all approach is particularly appealing because it could simplify treatment planning and reduce treatment delays.
"If you have a patient who is symptomatic and you have an off-the-shelf component, you could potentially treat them within the next 24 hours," he said in an interview. "The current turnaround time for the fenestrated system is about a month or so, so it would shorten treatment delays and might lead to a broader application of the technology."
A potentially shorter hospital length of stay could also reduce hospital costs, Dr. Kelso noted.
While the audience appeared equally enthusiastic about the results, some members questioned whether results on a physician-modified graft without an Investigational Device Exemption (IDE) should be presented at the meeting in light of recent warnings by the U.S. Food and Drug Administration that such interventions involve the use of significant-risk devices and need to be conducted under an IDE. Dr. Kelly responded that he is currently working with the FDA to obtain an IDE.
Earlier this year, the Society of Thoracic Surgeons and the American College of Cardiology became the first medical societies to receive an IDE to study alternative access for transcatheter aortic valve replacement using the STS/ACC TVT Registry
Dr. Kelly and Dr. Kelso reported having no financial disclosures. Dr. Geraghty disclosed relationships with Cook Medical and Bard/Lutonix.
*CORRECTION, 10/29/2013: An earlier version of this article misstated the name of the annual meeting of the Midwestern Vascular Surgical Society.
THE ANNUAL MEETING OF THE MIDWESTERN VASCULAR SURGICAL SOCIETY
Major finding: All patients are able to maintain appropriate exercise tolerance and are free of erectile dysfunction, pelvic ischemia, buttock claudication, and paralysis.
Data source: Two-year experience with a physician-modified fenestrated graft in 15 men with abdominal and iliac aneurysm.
Disclosures: Dr. Kelly and Dr. Kelso reported having no financial disclosures. Dr. Geraghty disclosed relationships with Cook Medical and Bard/Lutonix.

Laparoscopic colon surgery may keep older patients independent longer
WASHINGTON – Elderly patients who undergo laparoscopic colon surgery are significantly more likely to be discharged back to their homes than to a long-term care facility.
In a retrospective study of almost 10,000 elderly patients, 12.5% of those who had a laparoscopic procedure went to a nursing home, compared with 20% of those who had open surgery. In a multivariate analysis, laparoscopic surgery was associated with a significant, 39% decrease in the risk of being discharged to a nursing home, Dr. Richard Liu said at the annual clinical congress of the American College of Surgeons.
"For patients in their early 70s who do not have advanced disease or significant comorbidities, laparoscopic colon cancer resection is an option not only to prolong survival but also to preserve quality of life," said Dr. Liu, a surgical resident at Dalhousie University, Halifax, N.S.
The study highlights some important differences in the ways surgeons and patients perceive surgical outcomes. Surgeons and researchers often focus on 5-year survival rates and short-term morbidity and mortality, Dr. Liu said. But prior research done by his group found that immediate quality of life was at least as important to elderly patients – and sometimes more so.
"We have looked at elderly patients in our emergency services and followed up with them several times after admission," he said in an interview. "A common theme that came up was quality of life after hospitalization. Some were actually refusing to have operations for fear of what might become of them afterward."
Dr. Liu’s study comprised 9,416 patients from the U.S. National Inpatient Sample database. All were older than 70 years (mean age 79) and all were living independently at home. They underwent elective colon surgery during 2009-2010 for either cancer or a resection. The primary outcome was discharge back to home or to a long-term care facility. None of the patients were discharged to home health care or to hospice.
Most of the group (61%) had open surgery; the remainder had laparoscopy. Of those who had open surgery, 20% were discharged to a nursing facility, compared with 12.5% of the laparoscopy group – a significant difference.
Laparoscopy significantly decreased the chance of a nursing home admission by 39% in a multivariate analysis that controlled for age, sex, race, comorbidity score, cancer stage, income and insurance, and hospital size.
Factors significantly associated with nursing home discharge included advancing age and cancer stage.
Generally speaking, open surgery is physically more trying for elderly patients. A difficult recovery could be just enough to tip them over the edge from independent living, Dr. Liu said.
Dr. Liu had no financial disclosures.
WASHINGTON – Elderly patients who undergo laparoscopic colon surgery are significantly more likely to be discharged back to their homes than to a long-term care facility.
In a retrospective study of almost 10,000 elderly patients, 12.5% of those who had a laparoscopic procedure went to a nursing home, compared with 20% of those who had open surgery. In a multivariate analysis, laparoscopic surgery was associated with a significant, 39% decrease in the risk of being discharged to a nursing home, Dr. Richard Liu said at the annual clinical congress of the American College of Surgeons.
"For patients in their early 70s who do not have advanced disease or significant comorbidities, laparoscopic colon cancer resection is an option not only to prolong survival but also to preserve quality of life," said Dr. Liu, a surgical resident at Dalhousie University, Halifax, N.S.
The study highlights some important differences in the ways surgeons and patients perceive surgical outcomes. Surgeons and researchers often focus on 5-year survival rates and short-term morbidity and mortality, Dr. Liu said. But prior research done by his group found that immediate quality of life was at least as important to elderly patients – and sometimes more so.
"We have looked at elderly patients in our emergency services and followed up with them several times after admission," he said in an interview. "A common theme that came up was quality of life after hospitalization. Some were actually refusing to have operations for fear of what might become of them afterward."
Dr. Liu’s study comprised 9,416 patients from the U.S. National Inpatient Sample database. All were older than 70 years (mean age 79) and all were living independently at home. They underwent elective colon surgery during 2009-2010 for either cancer or a resection. The primary outcome was discharge back to home or to a long-term care facility. None of the patients were discharged to home health care or to hospice.
Most of the group (61%) had open surgery; the remainder had laparoscopy. Of those who had open surgery, 20% were discharged to a nursing facility, compared with 12.5% of the laparoscopy group – a significant difference.
Laparoscopy significantly decreased the chance of a nursing home admission by 39% in a multivariate analysis that controlled for age, sex, race, comorbidity score, cancer stage, income and insurance, and hospital size.
Factors significantly associated with nursing home discharge included advancing age and cancer stage.
Generally speaking, open surgery is physically more trying for elderly patients. A difficult recovery could be just enough to tip them over the edge from independent living, Dr. Liu said.
Dr. Liu had no financial disclosures.
WASHINGTON – Elderly patients who undergo laparoscopic colon surgery are significantly more likely to be discharged back to their homes than to a long-term care facility.
In a retrospective study of almost 10,000 elderly patients, 12.5% of those who had a laparoscopic procedure went to a nursing home, compared with 20% of those who had open surgery. In a multivariate analysis, laparoscopic surgery was associated with a significant, 39% decrease in the risk of being discharged to a nursing home, Dr. Richard Liu said at the annual clinical congress of the American College of Surgeons.
"For patients in their early 70s who do not have advanced disease or significant comorbidities, laparoscopic colon cancer resection is an option not only to prolong survival but also to preserve quality of life," said Dr. Liu, a surgical resident at Dalhousie University, Halifax, N.S.
The study highlights some important differences in the ways surgeons and patients perceive surgical outcomes. Surgeons and researchers often focus on 5-year survival rates and short-term morbidity and mortality, Dr. Liu said. But prior research done by his group found that immediate quality of life was at least as important to elderly patients – and sometimes more so.
"We have looked at elderly patients in our emergency services and followed up with them several times after admission," he said in an interview. "A common theme that came up was quality of life after hospitalization. Some were actually refusing to have operations for fear of what might become of them afterward."
Dr. Liu’s study comprised 9,416 patients from the U.S. National Inpatient Sample database. All were older than 70 years (mean age 79) and all were living independently at home. They underwent elective colon surgery during 2009-2010 for either cancer or a resection. The primary outcome was discharge back to home or to a long-term care facility. None of the patients were discharged to home health care or to hospice.
Most of the group (61%) had open surgery; the remainder had laparoscopy. Of those who had open surgery, 20% were discharged to a nursing facility, compared with 12.5% of the laparoscopy group – a significant difference.
Laparoscopy significantly decreased the chance of a nursing home admission by 39% in a multivariate analysis that controlled for age, sex, race, comorbidity score, cancer stage, income and insurance, and hospital size.
Factors significantly associated with nursing home discharge included advancing age and cancer stage.
Generally speaking, open surgery is physically more trying for elderly patients. A difficult recovery could be just enough to tip them over the edge from independent living, Dr. Liu said.
Dr. Liu had no financial disclosures.
AT THE ACS CLINICAL CONGRESS
Major finding: Of those older patients who had open surgery, 20% were discharged to a nursing facility, compared with 12.5% of the laparoscopy group, a significant difference.
Data source: The study included data on 9,416 patients.
Disclosures: Dr. Richard Liu had no financial disclosures.

Colorectal surgeons post better rectal surgery outcomes than general surgeons
WASHINGTON – Although general surgeons perform the majority of rectal resections in the United States, their patients have more severe postoperative complications, longer lengths of stay, higher hospital costs, and higher mortality rates than do those of colorectal surgeons.
A review of more than 60,000 cases over a 6-year period found that patients who had been operated on by a general surgeon had a 42% increase in the risk of mortality. They stayed in the hospital an average 1 day longer than the patients of colorectal surgeons, and had bills more than $1,000 higher. Although their overall complication rate was lower, general surgeons’ patients tended to have more severe complications, including pulmonary complications and surgical site infections, Dr. Marc Casasanta said at the annual clinical congress of the American College of Surgeons.

Dr. Casasanta of the University of Texas, Houston, extracted his data from the Premier Perspective database, the largest inpatient database in the United States. His analysis included 60,412 nonemergent rectal resections performed from 2005 to 2011.
Most of these (74%) were performed by general surgeons, with colorectal surgeons performing the remainder. Adverse outcomes examined included length and cost of hospital admission, overall complications and severe complications, and mortality.
There were several significant differences in the patient populations. General surgeons had older patients (63 vs. 61 years), and their patients tended to be sicker, with less minor disease severity (31% vs. 35%) and more major (29% vs. 17%) and extreme disease severity (8% vs. 6%).
Colorectal surgeons treated significantly more patients with inflammatory bowel disease (10% vs. 4%). They worked exclusively in urban hospitals, compared with 87% of general surgeons. Half of colorectal surgeons worked in teaching hospitals versus 37% of general surgeons.
The mean overall length of stay was a little more than 8 days. The mean hospital cost was $19,093.The overall complication rate was 29%, and mortality was 1.5%.
Complications varied significantly by surgeon specialty. General surgeons had significantly higher rates of digestive complications (including anastomotic problems), as well as pulmonary complications, lower-extremity thromboembolism, shock, and surgical site infections, including intra-abdominal infections.
The univariate analysis identified several patient characteristics significantly associated with poor outcomes, including age older than 62 years (odds ratio, 1.43), female gender (OR, 1.23), major disease severity (OR, 4.7), extreme disease severity (OR, 23), and a diagnosis of inflammatory bowel disease (OR, 1.41).
Other significant risk factors were being treated in a rural hospital (OR 1.29), being treated in a teaching hospital (OR, 1.08), and having a general surgeon (OR, 1.16). Having a colorectal surgeon decreased the risk of a poor outcome by 14%.
In the multivariate analysis, patients of general surgeons were 13% less likely to have any complication and 20% less likely to have ileus. But these patients were also significantly more likely to have severe complications, including pulmonary problems (13%) and surgical site infections (11%).
The length of stay was about 1 day longer, and hospitals costs were $1,122 more expensive. Patients of general surgeons were 42% more likely to die.
Dr. Casasanta said he had no relevant financial disclosures. However, Dr. Eric Haas, the primary investigator, said he has been a consultant for Applied Medical; and has received consulting fees, research funding, and honoraria from Intuitive Surgical.
WASHINGTON – Although general surgeons perform the majority of rectal resections in the United States, their patients have more severe postoperative complications, longer lengths of stay, higher hospital costs, and higher mortality rates than do those of colorectal surgeons.
A review of more than 60,000 cases over a 6-year period found that patients who had been operated on by a general surgeon had a 42% increase in the risk of mortality. They stayed in the hospital an average 1 day longer than the patients of colorectal surgeons, and had bills more than $1,000 higher. Although their overall complication rate was lower, general surgeons’ patients tended to have more severe complications, including pulmonary complications and surgical site infections, Dr. Marc Casasanta said at the annual clinical congress of the American College of Surgeons.
Dr. Casasanta of the University of Texas, Houston, extracted his data from the Premier Perspective database, the largest inpatient database in the United States. His analysis included 60,412 nonemergent rectal resections performed from 2005 to 2011.
Most of these (74%) were performed by general surgeons, with colorectal surgeons performing the remainder. Adverse outcomes examined included length and cost of hospital admission, overall complications and severe complications, and mortality.
There were several significant differences in the patient populations. General surgeons had older patients (63 vs. 61 years), and their patients tended to be sicker, with less minor disease severity (31% vs. 35%) and more major (29% vs. 17%) and extreme disease severity (8% vs. 6%).
Colorectal surgeons treated significantly more patients with inflammatory bowel disease (10% vs. 4%). They worked exclusively in urban hospitals, compared with 87% of general surgeons. Half of colorectal surgeons worked in teaching hospitals versus 37% of general surgeons.
The mean overall length of stay was a little more than 8 days. The mean hospital cost was $19,093.The overall complication rate was 29%, and mortality was 1.5%.
Complications varied significantly by surgeon specialty. General surgeons had significantly higher rates of digestive complications (including anastomotic problems), as well as pulmonary complications, lower-extremity thromboembolism, shock, and surgical site infections, including intra-abdominal infections.
The univariate analysis identified several patient characteristics significantly associated with poor outcomes, including age older than 62 years (odds ratio, 1.43), female gender (OR, 1.23), major disease severity (OR, 4.7), extreme disease severity (OR, 23), and a diagnosis of inflammatory bowel disease (OR, 1.41).
Other significant risk factors were being treated in a rural hospital (OR 1.29), being treated in a teaching hospital (OR, 1.08), and having a general surgeon (OR, 1.16). Having a colorectal surgeon decreased the risk of a poor outcome by 14%.
In the multivariate analysis, patients of general surgeons were 13% less likely to have any complication and 20% less likely to have ileus. But these patients were also significantly more likely to have severe complications, including pulmonary problems (13%) and surgical site infections (11%).
The length of stay was about 1 day longer, and hospitals costs were $1,122 more expensive. Patients of general surgeons were 42% more likely to die.
Dr. Casasanta said he had no relevant financial disclosures. However, Dr. Eric Haas, the primary investigator, said he has been a consultant for Applied Medical; and has received consulting fees, research funding, and honoraria from Intuitive Surgical.
WASHINGTON – Although general surgeons perform the majority of rectal resections in the United States, their patients have more severe postoperative complications, longer lengths of stay, higher hospital costs, and higher mortality rates than do those of colorectal surgeons.
A review of more than 60,000 cases over a 6-year period found that patients who had been operated on by a general surgeon had a 42% increase in the risk of mortality. They stayed in the hospital an average 1 day longer than the patients of colorectal surgeons, and had bills more than $1,000 higher. Although their overall complication rate was lower, general surgeons’ patients tended to have more severe complications, including pulmonary complications and surgical site infections, Dr. Marc Casasanta said at the annual clinical congress of the American College of Surgeons.
Dr. Casasanta of the University of Texas, Houston, extracted his data from the Premier Perspective database, the largest inpatient database in the United States. His analysis included 60,412 nonemergent rectal resections performed from 2005 to 2011.
Most of these (74%) were performed by general surgeons, with colorectal surgeons performing the remainder. Adverse outcomes examined included length and cost of hospital admission, overall complications and severe complications, and mortality.
There were several significant differences in the patient populations. General surgeons had older patients (63 vs. 61 years), and their patients tended to be sicker, with less minor disease severity (31% vs. 35%) and more major (29% vs. 17%) and extreme disease severity (8% vs. 6%).
Colorectal surgeons treated significantly more patients with inflammatory bowel disease (10% vs. 4%). They worked exclusively in urban hospitals, compared with 87% of general surgeons. Half of colorectal surgeons worked in teaching hospitals versus 37% of general surgeons.
The mean overall length of stay was a little more than 8 days. The mean hospital cost was $19,093.The overall complication rate was 29%, and mortality was 1.5%.
Complications varied significantly by surgeon specialty. General surgeons had significantly higher rates of digestive complications (including anastomotic problems), as well as pulmonary complications, lower-extremity thromboembolism, shock, and surgical site infections, including intra-abdominal infections.
The univariate analysis identified several patient characteristics significantly associated with poor outcomes, including age older than 62 years (odds ratio, 1.43), female gender (OR, 1.23), major disease severity (OR, 4.7), extreme disease severity (OR, 23), and a diagnosis of inflammatory bowel disease (OR, 1.41).
Other significant risk factors were being treated in a rural hospital (OR 1.29), being treated in a teaching hospital (OR, 1.08), and having a general surgeon (OR, 1.16). Having a colorectal surgeon decreased the risk of a poor outcome by 14%.
In the multivariate analysis, patients of general surgeons were 13% less likely to have any complication and 20% less likely to have ileus. But these patients were also significantly more likely to have severe complications, including pulmonary problems (13%) and surgical site infections (11%).
The length of stay was about 1 day longer, and hospitals costs were $1,122 more expensive. Patients of general surgeons were 42% more likely to die.
Dr. Casasanta said he had no relevant financial disclosures. However, Dr. Eric Haas, the primary investigator, said he has been a consultant for Applied Medical; and has received consulting fees, research funding, and honoraria from Intuitive Surgical.
AT THE ACS CLINICAL CONGRESS
Major finding: Patients undergoing a rectal resection had more serious complications, and were 42% more likely to die if they had a general surgeon than if they had a colorectal surgeon.
Data source: The study included more than 60,000 surgeries performed over a 6-year period.
Disclosures: Dr. Marc Casasanta said he had no relevant financial disclosures. However, Dr. Eric Haas, the primary investigator, said he has been a consultant for Applied Medical, and has received consulting fees, research funding, and honoraria from Intuitive Surgical.

Sigmoidoscopy may not be enough for older patients
WASHINGTON – Colon cancer screening with sigmoidoscopy alone could miss up to 50% of colon polyps in older patients.
As people age, polyps seem to develop more and more proximally, Dr. Victor Tsirline said at the annual clinical congress of the American College of Surgeons. His review of more than 120,000 colonoscopies found that a flexible sigmoidoscopy alone could miss 44% of polyps in patients aged 60-69 years and 50% in those aged 70-79 years.
"We found that proximal colon polyps are more frequent with advanced age than previously considered," said Dr. Tsirline of Carolinas Medical Center, Charlotte, N.C. "So if this is true, what happens if we use sigmoidoscopy instead of colonoscopy? If we had, we would have missed 22,800 polyps, and 16,800 of those would have been adenomatous. In [patients 59 and younger] 32%-36% would be missed and in the older patients, 45%-50%."
Dr. Tsirline obtained his data from the Provation MD endoscopy transcription system. He obtained information on 120,365 colonoscopies that were performed from 2003 to 2011.
He cross-referenced this with CoPathPlus, a pathology reporting system. This allowed him to cross-reference polyp pathology (adenoma vs. hyperplasia) by computer algorithm. There was complete information available on 43,833 polyps.
Because of the large sample size, he set his level of statistical significance at P = less than 0.01.
The patients in the study were aged 20-90 years. Of the entire group of procedures, 53,492 colonoscopies (44%) identified polyps. Most studies (64%) found a single polyp; 25% found two, and 11% found three or more. A subset of the colonoscopies was only for average risk screening (44,806). Of these, 46% identified polyps.
Overall, 48% of polyps were adenomatous; 37% were hyperplastic. Pathology was not available for the remainder.
The polyps were fairly evenly distributed throughout the colon: rectum, 18%; sigmoid, 26%; descending, 14%; transverse, 16%; ascending, 15%; cecum, 11%.
However, when broken down by patient age, the distribution changed significantly. With every advancing decade of life, patients were:
• 22% less likely to have polyps in the rectum or sigmoid.
• 7% more likely to have polyps in the descending colon.
• 19% more likely to have polyps in the transverse colon.
• 30% more likely to have polyps in the ascending colon.
• 22% more likely to have polyps in the cecum.
All of these risks were statistically significant, and they held for both adenomatous and hyperplastic polyps.
The findings led Dr. Tsirline to conclude that flexible sigmoidoscopy should not be relied upon as an effective colon cancer screening method in patients older than 60 years. The U.S. Preventive Services Task Force states that sigmoidoscopy every 5 years combined with high-sensitivity fecal occult blood testing every 3 years is an adequate screening alternative.
"From this study, it’s pretty apparent that sigmoidoscopy should not be used for colon cancer screening in older patients," he said.
During a discussion, Dr. Tsirline fielded a question about screening the very elderly – patients in their 80s and 90s. The study group did include a small number of these patients, he said.
"I think the argument for not screening older individuals is based on the question of whether finding a colon cancer would change anything. Most people think the risks of screening and treatment would outweigh the benefits. Yes, you may find anything, but what are you going to do about it?"
Dr. Tsirline had no financial disclosures.
WASHINGTON – Colon cancer screening with sigmoidoscopy alone could miss up to 50% of colon polyps in older patients.
As people age, polyps seem to develop more and more proximally, Dr. Victor Tsirline said at the annual clinical congress of the American College of Surgeons. His review of more than 120,000 colonoscopies found that a flexible sigmoidoscopy alone could miss 44% of polyps in patients aged 60-69 years and 50% in those aged 70-79 years.
"We found that proximal colon polyps are more frequent with advanced age than previously considered," said Dr. Tsirline of Carolinas Medical Center, Charlotte, N.C. "So if this is true, what happens if we use sigmoidoscopy instead of colonoscopy? If we had, we would have missed 22,800 polyps, and 16,800 of those would have been adenomatous. In [patients 59 and younger] 32%-36% would be missed and in the older patients, 45%-50%."
Dr. Tsirline obtained his data from the Provation MD endoscopy transcription system. He obtained information on 120,365 colonoscopies that were performed from 2003 to 2011.
He cross-referenced this with CoPathPlus, a pathology reporting system. This allowed him to cross-reference polyp pathology (adenoma vs. hyperplasia) by computer algorithm. There was complete information available on 43,833 polyps.
Because of the large sample size, he set his level of statistical significance at P = less than 0.01.
The patients in the study were aged 20-90 years. Of the entire group of procedures, 53,492 colonoscopies (44%) identified polyps. Most studies (64%) found a single polyp; 25% found two, and 11% found three or more. A subset of the colonoscopies was only for average risk screening (44,806). Of these, 46% identified polyps.
Overall, 48% of polyps were adenomatous; 37% were hyperplastic. Pathology was not available for the remainder.
The polyps were fairly evenly distributed throughout the colon: rectum, 18%; sigmoid, 26%; descending, 14%; transverse, 16%; ascending, 15%; cecum, 11%.
However, when broken down by patient age, the distribution changed significantly. With every advancing decade of life, patients were:
• 22% less likely to have polyps in the rectum or sigmoid.
• 7% more likely to have polyps in the descending colon.
• 19% more likely to have polyps in the transverse colon.
• 30% more likely to have polyps in the ascending colon.
• 22% more likely to have polyps in the cecum.
All of these risks were statistically significant, and they held for both adenomatous and hyperplastic polyps.
The findings led Dr. Tsirline to conclude that flexible sigmoidoscopy should not be relied upon as an effective colon cancer screening method in patients older than 60 years. The U.S. Preventive Services Task Force states that sigmoidoscopy every 5 years combined with high-sensitivity fecal occult blood testing every 3 years is an adequate screening alternative.
"From this study, it’s pretty apparent that sigmoidoscopy should not be used for colon cancer screening in older patients," he said.
During a discussion, Dr. Tsirline fielded a question about screening the very elderly – patients in their 80s and 90s. The study group did include a small number of these patients, he said.
"I think the argument for not screening older individuals is based on the question of whether finding a colon cancer would change anything. Most people think the risks of screening and treatment would outweigh the benefits. Yes, you may find anything, but what are you going to do about it?"
Dr. Tsirline had no financial disclosures.
WASHINGTON – Colon cancer screening with sigmoidoscopy alone could miss up to 50% of colon polyps in older patients.
As people age, polyps seem to develop more and more proximally, Dr. Victor Tsirline said at the annual clinical congress of the American College of Surgeons. His review of more than 120,000 colonoscopies found that a flexible sigmoidoscopy alone could miss 44% of polyps in patients aged 60-69 years and 50% in those aged 70-79 years.
"We found that proximal colon polyps are more frequent with advanced age than previously considered," said Dr. Tsirline of Carolinas Medical Center, Charlotte, N.C. "So if this is true, what happens if we use sigmoidoscopy instead of colonoscopy? If we had, we would have missed 22,800 polyps, and 16,800 of those would have been adenomatous. In [patients 59 and younger] 32%-36% would be missed and in the older patients, 45%-50%."
Dr. Tsirline obtained his data from the Provation MD endoscopy transcription system. He obtained information on 120,365 colonoscopies that were performed from 2003 to 2011.
He cross-referenced this with CoPathPlus, a pathology reporting system. This allowed him to cross-reference polyp pathology (adenoma vs. hyperplasia) by computer algorithm. There was complete information available on 43,833 polyps.
Because of the large sample size, he set his level of statistical significance at P = less than 0.01.
The patients in the study were aged 20-90 years. Of the entire group of procedures, 53,492 colonoscopies (44%) identified polyps. Most studies (64%) found a single polyp; 25% found two, and 11% found three or more. A subset of the colonoscopies was only for average risk screening (44,806). Of these, 46% identified polyps.
Overall, 48% of polyps were adenomatous; 37% were hyperplastic. Pathology was not available for the remainder.
The polyps were fairly evenly distributed throughout the colon: rectum, 18%; sigmoid, 26%; descending, 14%; transverse, 16%; ascending, 15%; cecum, 11%.
However, when broken down by patient age, the distribution changed significantly. With every advancing decade of life, patients were:
• 22% less likely to have polyps in the rectum or sigmoid.
• 7% more likely to have polyps in the descending colon.
• 19% more likely to have polyps in the transverse colon.
• 30% more likely to have polyps in the ascending colon.
• 22% more likely to have polyps in the cecum.
All of these risks were statistically significant, and they held for both adenomatous and hyperplastic polyps.
The findings led Dr. Tsirline to conclude that flexible sigmoidoscopy should not be relied upon as an effective colon cancer screening method in patients older than 60 years. The U.S. Preventive Services Task Force states that sigmoidoscopy every 5 years combined with high-sensitivity fecal occult blood testing every 3 years is an adequate screening alternative.
"From this study, it’s pretty apparent that sigmoidoscopy should not be used for colon cancer screening in older patients," he said.
During a discussion, Dr. Tsirline fielded a question about screening the very elderly – patients in their 80s and 90s. The study group did include a small number of these patients, he said.
"I think the argument for not screening older individuals is based on the question of whether finding a colon cancer would change anything. Most people think the risks of screening and treatment would outweigh the benefits. Yes, you may find anything, but what are you going to do about it?"
Dr. Tsirline had no financial disclosures.
AT THE ACS CLINICAL CONGRESS
Major finding: Because people are 30% more likely to have polyps in the ascending colon and 22% more likely to have polyps in the cecum as they age, sigmoidoscopy may not be an adequate screening method.
Data source: Study of 120,000 colonoscopies.
Disclosures: Dr. Victor Tsirline had no financial disclosures.
Early walking and eating improve outcomes for bowel surgery patients
WASHINGTON – A program to enhance recovery from bowel surgery significantly decreased the incidence rate of both postoperative ileus and 30-day readmission.
Early walking and postoperative alimentation, beginning with three times on postop day 1, drove the improved outcomes, Dr. Terrence Loftus reported at the annual clinical congress of the American College of Surgeons.
His 3-year retrospective study compared outcomes before and after the program was implemented. In addition to confirming the benefits, the study says something about how change becomes part of a systemwide culture, said Dr. Loftus, medical director of surgical services and clinical resources for Banner Health, Phoenix.
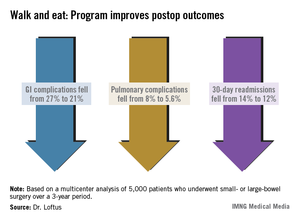
"When you see a before-and-after picture, it gives you the sense that change is like clicking on a light switch, and then everything starts happening. In reality, it’s not. It’s something that catches on over time. It’s a social process that gets passed along. It’s not Dr. Loftus coming in and showing a few slides and saying, ‘Okay, now this is what you have to do.’ It’s surgeons having conversations in the lounge and saying, ‘I tried this and it worked. You should try it too.’ "
In 2010, Banner Health System’s Surgery Clinical Consensus Group decided to tackle the system’s less-than-stellar rates of postoperative ileus and readmission among patients who had bowel surgery.
While there are a number of published enhanced-care pathways, Dr. Loftus found a wide variety of applications over Banner Health’s large medical system. "In some places, people didn’t even know about them, and in others they were using their own version," he said. "We needed a systemwide approach to recovery – something that would be useful over a large, heterogeneous health care system."
The Banner consensus group came up with the Bowel Surgery Strategic Initiative, a program implemented in 19 hospitals spread over six states, covered by 119 surgeons. The system was widely diversified, including everything from an 18-bed critical access unit to a large 600-bed level I trauma center.

"The surgeons ranged from solo private practice, to group practices, hospital employed, and locum tenens, so you can begin to understand the wide diversity of practices and environments we were trying to implement this in," Dr. Loftus said.
The first step was to develop a literature-based GI care pathway that could be widely implemented. The group’s first version had 80 steps – vastly too many.
The final program was based on just two drivers: early alimentation and early ambulation. Eating began with the earliest possible removal of the nasogastric tube (if present), 200-250 cc of oral intake on postoperative day 1, and a progressively advancing diet. Ambulation started with getting up and walking three times on postop day 1, with progressively increasing physical activity.
The team studied a 3-year period spanning 18 months on either side of the implementation date of July 2011. The analysis included 5,000 patients who had undergone elective small- or large-bowel surgery during that time period.
Dr. Loftus said there was a significant increase in both ambulation and alimentation. Before the program, the mean ambulation rate was 53%; that increased to 73% afterward. Alimentation increased from 51% to 71%. The composite of both drivers increased from 53% to 72%.
There were associated improvements in most of the clinical outcomes assessed. Overall, the complication rate decreased significantly, from 36% to 29%. Gastrointestinal complications fell from 27% to 21%, with the incidence of postoperative ileus declining from 27% to 21%. Pulmonary complications also decreased significantly, from 8% to 5.6%.
Thirty-day readmission declined from 14% to 12% – also a significant decrease. This was expected, Dr. Loftus said, because most of the readmissions were due to paralytic ileus.
Length of stay, however, was not significantly affected. There was no change in mortality.
The project also illuminated the importance of a facility’s own professional culture. Chart audits found that some facilities were only ambulating patients about a third of the time that it was ordered – even though nursing estimated the rate at 80% and surgeons at 70%.
Facilities that had particularly good postintervention outcomes were already ahead of the game before the project. "These already had a culture of activity. Nursing was getting patients up on day 1, and they set up their schedules in a way that says, ‘These patients will get up. We are going to do this no matter what.’ "
Dr. Loftus had no financial disclosures.
WASHINGTON – A program to enhance recovery from bowel surgery significantly decreased the incidence rate of both postoperative ileus and 30-day readmission.
Early walking and postoperative alimentation, beginning with three times on postop day 1, drove the improved outcomes, Dr. Terrence Loftus reported at the annual clinical congress of the American College of Surgeons.
His 3-year retrospective study compared outcomes before and after the program was implemented. In addition to confirming the benefits, the study says something about how change becomes part of a systemwide culture, said Dr. Loftus, medical director of surgical services and clinical resources for Banner Health, Phoenix.
"When you see a before-and-after picture, it gives you the sense that change is like clicking on a light switch, and then everything starts happening. In reality, it’s not. It’s something that catches on over time. It’s a social process that gets passed along. It’s not Dr. Loftus coming in and showing a few slides and saying, ‘Okay, now this is what you have to do.’ It’s surgeons having conversations in the lounge and saying, ‘I tried this and it worked. You should try it too.’ "
In 2010, Banner Health System’s Surgery Clinical Consensus Group decided to tackle the system’s less-than-stellar rates of postoperative ileus and readmission among patients who had bowel surgery.
While there are a number of published enhanced-care pathways, Dr. Loftus found a wide variety of applications over Banner Health’s large medical system. "In some places, people didn’t even know about them, and in others they were using their own version," he said. "We needed a systemwide approach to recovery – something that would be useful over a large, heterogeneous health care system."
The Banner consensus group came up with the Bowel Surgery Strategic Initiative, a program implemented in 19 hospitals spread over six states, covered by 119 surgeons. The system was widely diversified, including everything from an 18-bed critical access unit to a large 600-bed level I trauma center.
"The surgeons ranged from solo private practice, to group practices, hospital employed, and locum tenens, so you can begin to understand the wide diversity of practices and environments we were trying to implement this in," Dr. Loftus said.
The first step was to develop a literature-based GI care pathway that could be widely implemented. The group’s first version had 80 steps – vastly too many.
The final program was based on just two drivers: early alimentation and early ambulation. Eating began with the earliest possible removal of the nasogastric tube (if present), 200-250 cc of oral intake on postoperative day 1, and a progressively advancing diet. Ambulation started with getting up and walking three times on postop day 1, with progressively increasing physical activity.
The team studied a 3-year period spanning 18 months on either side of the implementation date of July 2011. The analysis included 5,000 patients who had undergone elective small- or large-bowel surgery during that time period.
Dr. Loftus said there was a significant increase in both ambulation and alimentation. Before the program, the mean ambulation rate was 53%; that increased to 73% afterward. Alimentation increased from 51% to 71%. The composite of both drivers increased from 53% to 72%.
There were associated improvements in most of the clinical outcomes assessed. Overall, the complication rate decreased significantly, from 36% to 29%. Gastrointestinal complications fell from 27% to 21%, with the incidence of postoperative ileus declining from 27% to 21%. Pulmonary complications also decreased significantly, from 8% to 5.6%.
Thirty-day readmission declined from 14% to 12% – also a significant decrease. This was expected, Dr. Loftus said, because most of the readmissions were due to paralytic ileus.
Length of stay, however, was not significantly affected. There was no change in mortality.
The project also illuminated the importance of a facility’s own professional culture. Chart audits found that some facilities were only ambulating patients about a third of the time that it was ordered – even though nursing estimated the rate at 80% and surgeons at 70%.
Facilities that had particularly good postintervention outcomes were already ahead of the game before the project. "These already had a culture of activity. Nursing was getting patients up on day 1, and they set up their schedules in a way that says, ‘These patients will get up. We are going to do this no matter what.’ "
Dr. Loftus had no financial disclosures.
WASHINGTON – A program to enhance recovery from bowel surgery significantly decreased the incidence rate of both postoperative ileus and 30-day readmission.
Early walking and postoperative alimentation, beginning with three times on postop day 1, drove the improved outcomes, Dr. Terrence Loftus reported at the annual clinical congress of the American College of Surgeons.
His 3-year retrospective study compared outcomes before and after the program was implemented. In addition to confirming the benefits, the study says something about how change becomes part of a systemwide culture, said Dr. Loftus, medical director of surgical services and clinical resources for Banner Health, Phoenix.
"When you see a before-and-after picture, it gives you the sense that change is like clicking on a light switch, and then everything starts happening. In reality, it’s not. It’s something that catches on over time. It’s a social process that gets passed along. It’s not Dr. Loftus coming in and showing a few slides and saying, ‘Okay, now this is what you have to do.’ It’s surgeons having conversations in the lounge and saying, ‘I tried this and it worked. You should try it too.’ "
In 2010, Banner Health System’s Surgery Clinical Consensus Group decided to tackle the system’s less-than-stellar rates of postoperative ileus and readmission among patients who had bowel surgery.
While there are a number of published enhanced-care pathways, Dr. Loftus found a wide variety of applications over Banner Health’s large medical system. "In some places, people didn’t even know about them, and in others they were using their own version," he said. "We needed a systemwide approach to recovery – something that would be useful over a large, heterogeneous health care system."
The Banner consensus group came up with the Bowel Surgery Strategic Initiative, a program implemented in 19 hospitals spread over six states, covered by 119 surgeons. The system was widely diversified, including everything from an 18-bed critical access unit to a large 600-bed level I trauma center.
"The surgeons ranged from solo private practice, to group practices, hospital employed, and locum tenens, so you can begin to understand the wide diversity of practices and environments we were trying to implement this in," Dr. Loftus said.
The first step was to develop a literature-based GI care pathway that could be widely implemented. The group’s first version had 80 steps – vastly too many.
The final program was based on just two drivers: early alimentation and early ambulation. Eating began with the earliest possible removal of the nasogastric tube (if present), 200-250 cc of oral intake on postoperative day 1, and a progressively advancing diet. Ambulation started with getting up and walking three times on postop day 1, with progressively increasing physical activity.
The team studied a 3-year period spanning 18 months on either side of the implementation date of July 2011. The analysis included 5,000 patients who had undergone elective small- or large-bowel surgery during that time period.
Dr. Loftus said there was a significant increase in both ambulation and alimentation. Before the program, the mean ambulation rate was 53%; that increased to 73% afterward. Alimentation increased from 51% to 71%. The composite of both drivers increased from 53% to 72%.
There were associated improvements in most of the clinical outcomes assessed. Overall, the complication rate decreased significantly, from 36% to 29%. Gastrointestinal complications fell from 27% to 21%, with the incidence of postoperative ileus declining from 27% to 21%. Pulmonary complications also decreased significantly, from 8% to 5.6%.
Thirty-day readmission declined from 14% to 12% – also a significant decrease. This was expected, Dr. Loftus said, because most of the readmissions were due to paralytic ileus.
Length of stay, however, was not significantly affected. There was no change in mortality.
The project also illuminated the importance of a facility’s own professional culture. Chart audits found that some facilities were only ambulating patients about a third of the time that it was ordered – even though nursing estimated the rate at 80% and surgeons at 70%.
Facilities that had particularly good postintervention outcomes were already ahead of the game before the project. "These already had a culture of activity. Nursing was getting patients up on day 1, and they set up their schedules in a way that says, ‘These patients will get up. We are going to do this no matter what.’ "
Dr. Loftus had no financial disclosures.
AT THE ACS CLINICAL CONGRESS
Major finding: A recovery program based on early ambulation and alimentation for patients with bowel surgery decreased readmission from 14% to 12%, and postoperative complications from 36% to 29%.
Data source: The retrospective study contained 5,000 patients who had elective small- or large-bowel surgery.
Disclosures: Dr. Loftus had no financial disclosures.
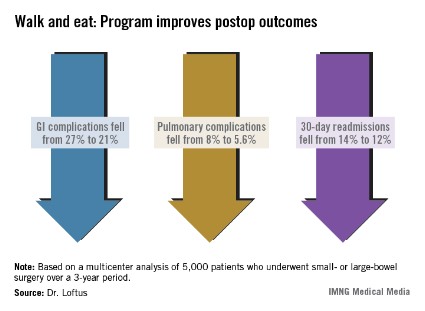
Alvimopan reduces ileus, cuts hospital time in bowel surgery
WASHINGTON – The nonopioid pain reliever alvimopan significantly decreased the incidence of postoperative ileus and shortened hospital stay among bowel surgery patients who took the drug as part of an existing accelerated recovery program.
Compared with patients who took placebo, those who took alvimopan left the hospital about 1 day sooner. In addition to the decrease in ileus, patients experienced a quicker return to normal bowel function, including time to first flatus and first bowel movement, Dr. Robert Moesinger said at the annual clinical congress of the American College of Surgeons.
"Alvimopan augmented the already improved outcomes we had seen with our validated recovery pathway, in both laparoscopic- and open-surgery patients," said Dr. Moesinger of Intermountain Healthcare, Salt Lake City. "Given the very diverse nature of our health care system, with multiple types of hospitals and surgeons, we feel these data are widely applicable and we are very comfortable recommending its routine use for patients having elective bowel surgery."

Dr. Moesinger and his colleagues conducted a randomized, placebo-controlled trial of alvimopan in 248 such patients. Those taking the study drug received 12 mg before surgery; after surgery, they received 12 mg twice a day until discharge.
The primary endpoint was postoperative length of stay. Secondary endpoints included the incidence of postoperative ileus, time to first flatus and first bowel movement, tolerance of solid food, total hospital and pharmacy costs, nasogastric tube reinsertion, 30-day readmission rates, and anastomotic leak.
The patients’ mean age was 61 years. There were no significant differences in any of their baseline demographics or clinical characteristics. Because of a statistical fluke, the placebo group did contain significantly more open-surgery patients than the alvimopan group (34% vs. 20%). The rest of the patients had laparoscopic surgery. Patients had an average of nine doses of the study drug.
The mean length of stay was 4 days in the alvimopan group and 5 in the placebo group – a significant difference.
There was significantly less postoperative ileus in the alvimopan group (2% vs. 10%). Significantly fewer of those taking the study drug needed a nasogastric tube reinserted (2% vs. 9%). The rates of 30-day readmission, reoperation, and anastomotic leak were similar in both groups. The mean time to first bowel movement was about 1 day sooner in the alvimopan group.
The median hospital cost was $10,832 for the alvimopan group and $11,924 for the placebo group – a significant difference. The median total pharmacy cost was $476 vs. $501; this difference was not significant.
Because Cubist Pharmaceuticals, which makes alvimopan, provided the study drug at no cost, the overall cost analysis cannot be considered complete, Dr. Moesinger noted. However, the pharmacy cost for a similar course of the drug would be $84. Figuring that cost into the total saved for each admission ($1,686) still yielded a net financial benefit of $930 per patient, he said.
Dr. Moesinger had no financial disclosures.
Alvimopan (Entereg, Cubist Pharmaceuticals) is an orally administered, peripherally acting mu-opioid receptor antagonist that does not cross the blood-brain barrier. It is designed to reverse opioid-induced changes in the gastrointestinal tract without adversely affecting opioid-induced analgesia.

|
| Dr. Brian E. Lacy |
Alvimopan, the first FDA-approved medication for the treatment of postoperative ileus (POI), was approved in May 2008 with a Risk Evaluation and Mitigation Strategy in place, due to concerns over an increased number of myocardial infarctions in one research study.
Postoperative ileus is the impairment of gastrointestinal motility after abdominal or pelvic surgery, and is an expected complication of major abdominal surgery. It can affect all segments of the gastrointestinal tract and may lead to symptoms of nausea, vomiting, bloating, distention, constipation, and inability to evacuate flatus. Several studies have demonstrated that POI delays hospital discharges, increases the rate of hospital readmission after abdominal surgery, and increases the risk of postoperative complications. As such, POI imposes a significant economic impact on the health care system.
The current study confirms earlier studies involving over 2,000 patients that led to the approval of alvimopan. The current study was a single-center, randomized, double-blind study comparing placebo to alvimopan. Patients randomized to alvimopan (12 mg preoperatively; 12 mg twice daily until discharge) were discharged from the hospital 1 day earlier, were less likely to have a nasogastric tube reinserted, and had a bowel movement 1 day earlier, compared with those patients receiving placebo. The authors reported a significant cost savings per patient.*
These findings are important given the absence of other FDA-approved medications for the treatment of POI and the lack of other effective treatments. Alvimopan is available only to patients who are in hospitals that are registered to use this medication under the EASE (Entereg Access Support and Education) program. This recent study should prompt nonparticipating hospitals to consider routine use of alvimopan in all patients undergoing elective and emergent surgeries at risk for development of POI.
Dr. Brian E. Lacy is a professor of medicine at the Geisel School of Medicine at Dartmouth, Hanover, N.H., and chief of the section of gastroenterology and hepatology at Dartmouth-Hitchcock Medical Center. He has no relevant conflicts of interest.
*CORRECTION 11/21/13: The original version of this story misstated the cost savings per patient.
Alvimopan (Entereg, Cubist Pharmaceuticals) is an orally administered, peripherally acting mu-opioid receptor antagonist that does not cross the blood-brain barrier. It is designed to reverse opioid-induced changes in the gastrointestinal tract without adversely affecting opioid-induced analgesia.
|
|
| Dr. Brian E. Lacy |
Alvimopan, the first FDA-approved medication for the treatment of postoperative ileus (POI), was approved in May 2008 with a Risk Evaluation and Mitigation Strategy in place, due to concerns over an increased number of myocardial infarctions in one research study.
Postoperative ileus is the impairment of gastrointestinal motility after abdominal or pelvic surgery, and is an expected complication of major abdominal surgery. It can affect all segments of the gastrointestinal tract and may lead to symptoms of nausea, vomiting, bloating, distention, constipation, and inability to evacuate flatus. Several studies have demonstrated that POI delays hospital discharges, increases the rate of hospital readmission after abdominal surgery, and increases the risk of postoperative complications. As such, POI imposes a significant economic impact on the health care system.
The current study confirms earlier studies involving over 2,000 patients that led to the approval of alvimopan. The current study was a single-center, randomized, double-blind study comparing placebo to alvimopan. Patients randomized to alvimopan (12 mg preoperatively; 12 mg twice daily until discharge) were discharged from the hospital 1 day earlier, were less likely to have a nasogastric tube reinserted, and had a bowel movement 1 day earlier, compared with those patients receiving placebo. The authors reported a significant cost savings per patient.*
These findings are important given the absence of other FDA-approved medications for the treatment of POI and the lack of other effective treatments. Alvimopan is available only to patients who are in hospitals that are registered to use this medication under the EASE (Entereg Access Support and Education) program. This recent study should prompt nonparticipating hospitals to consider routine use of alvimopan in all patients undergoing elective and emergent surgeries at risk for development of POI.
Dr. Brian E. Lacy is a professor of medicine at the Geisel School of Medicine at Dartmouth, Hanover, N.H., and chief of the section of gastroenterology and hepatology at Dartmouth-Hitchcock Medical Center. He has no relevant conflicts of interest.
*CORRECTION 11/21/13: The original version of this story misstated the cost savings per patient.
Alvimopan (Entereg, Cubist Pharmaceuticals) is an orally administered, peripherally acting mu-opioid receptor antagonist that does not cross the blood-brain barrier. It is designed to reverse opioid-induced changes in the gastrointestinal tract without adversely affecting opioid-induced analgesia.
|
|
| Dr. Brian E. Lacy |
Alvimopan, the first FDA-approved medication for the treatment of postoperative ileus (POI), was approved in May 2008 with a Risk Evaluation and Mitigation Strategy in place, due to concerns over an increased number of myocardial infarctions in one research study.
Postoperative ileus is the impairment of gastrointestinal motility after abdominal or pelvic surgery, and is an expected complication of major abdominal surgery. It can affect all segments of the gastrointestinal tract and may lead to symptoms of nausea, vomiting, bloating, distention, constipation, and inability to evacuate flatus. Several studies have demonstrated that POI delays hospital discharges, increases the rate of hospital readmission after abdominal surgery, and increases the risk of postoperative complications. As such, POI imposes a significant economic impact on the health care system.
The current study confirms earlier studies involving over 2,000 patients that led to the approval of alvimopan. The current study was a single-center, randomized, double-blind study comparing placebo to alvimopan. Patients randomized to alvimopan (12 mg preoperatively; 12 mg twice daily until discharge) were discharged from the hospital 1 day earlier, were less likely to have a nasogastric tube reinserted, and had a bowel movement 1 day earlier, compared with those patients receiving placebo. The authors reported a significant cost savings per patient.*
These findings are important given the absence of other FDA-approved medications for the treatment of POI and the lack of other effective treatments. Alvimopan is available only to patients who are in hospitals that are registered to use this medication under the EASE (Entereg Access Support and Education) program. This recent study should prompt nonparticipating hospitals to consider routine use of alvimopan in all patients undergoing elective and emergent surgeries at risk for development of POI.
Dr. Brian E. Lacy is a professor of medicine at the Geisel School of Medicine at Dartmouth, Hanover, N.H., and chief of the section of gastroenterology and hepatology at Dartmouth-Hitchcock Medical Center. He has no relevant conflicts of interest.
*CORRECTION 11/21/13: The original version of this story misstated the cost savings per patient.
WASHINGTON – The nonopioid pain reliever alvimopan significantly decreased the incidence of postoperative ileus and shortened hospital stay among bowel surgery patients who took the drug as part of an existing accelerated recovery program.
Compared with patients who took placebo, those who took alvimopan left the hospital about 1 day sooner. In addition to the decrease in ileus, patients experienced a quicker return to normal bowel function, including time to first flatus and first bowel movement, Dr. Robert Moesinger said at the annual clinical congress of the American College of Surgeons.
"Alvimopan augmented the already improved outcomes we had seen with our validated recovery pathway, in both laparoscopic- and open-surgery patients," said Dr. Moesinger of Intermountain Healthcare, Salt Lake City. "Given the very diverse nature of our health care system, with multiple types of hospitals and surgeons, we feel these data are widely applicable and we are very comfortable recommending its routine use for patients having elective bowel surgery."
Dr. Moesinger and his colleagues conducted a randomized, placebo-controlled trial of alvimopan in 248 such patients. Those taking the study drug received 12 mg before surgery; after surgery, they received 12 mg twice a day until discharge.
The primary endpoint was postoperative length of stay. Secondary endpoints included the incidence of postoperative ileus, time to first flatus and first bowel movement, tolerance of solid food, total hospital and pharmacy costs, nasogastric tube reinsertion, 30-day readmission rates, and anastomotic leak.
The patients’ mean age was 61 years. There were no significant differences in any of their baseline demographics or clinical characteristics. Because of a statistical fluke, the placebo group did contain significantly more open-surgery patients than the alvimopan group (34% vs. 20%). The rest of the patients had laparoscopic surgery. Patients had an average of nine doses of the study drug.
The mean length of stay was 4 days in the alvimopan group and 5 in the placebo group – a significant difference.
There was significantly less postoperative ileus in the alvimopan group (2% vs. 10%). Significantly fewer of those taking the study drug needed a nasogastric tube reinserted (2% vs. 9%). The rates of 30-day readmission, reoperation, and anastomotic leak were similar in both groups. The mean time to first bowel movement was about 1 day sooner in the alvimopan group.
The median hospital cost was $10,832 for the alvimopan group and $11,924 for the placebo group – a significant difference. The median total pharmacy cost was $476 vs. $501; this difference was not significant.
Because Cubist Pharmaceuticals, which makes alvimopan, provided the study drug at no cost, the overall cost analysis cannot be considered complete, Dr. Moesinger noted. However, the pharmacy cost for a similar course of the drug would be $84. Figuring that cost into the total saved for each admission ($1,686) still yielded a net financial benefit of $930 per patient, he said.
Dr. Moesinger had no financial disclosures.
WASHINGTON – The nonopioid pain reliever alvimopan significantly decreased the incidence of postoperative ileus and shortened hospital stay among bowel surgery patients who took the drug as part of an existing accelerated recovery program.
Compared with patients who took placebo, those who took alvimopan left the hospital about 1 day sooner. In addition to the decrease in ileus, patients experienced a quicker return to normal bowel function, including time to first flatus and first bowel movement, Dr. Robert Moesinger said at the annual clinical congress of the American College of Surgeons.
"Alvimopan augmented the already improved outcomes we had seen with our validated recovery pathway, in both laparoscopic- and open-surgery patients," said Dr. Moesinger of Intermountain Healthcare, Salt Lake City. "Given the very diverse nature of our health care system, with multiple types of hospitals and surgeons, we feel these data are widely applicable and we are very comfortable recommending its routine use for patients having elective bowel surgery."
Dr. Moesinger and his colleagues conducted a randomized, placebo-controlled trial of alvimopan in 248 such patients. Those taking the study drug received 12 mg before surgery; after surgery, they received 12 mg twice a day until discharge.
The primary endpoint was postoperative length of stay. Secondary endpoints included the incidence of postoperative ileus, time to first flatus and first bowel movement, tolerance of solid food, total hospital and pharmacy costs, nasogastric tube reinsertion, 30-day readmission rates, and anastomotic leak.
The patients’ mean age was 61 years. There were no significant differences in any of their baseline demographics or clinical characteristics. Because of a statistical fluke, the placebo group did contain significantly more open-surgery patients than the alvimopan group (34% vs. 20%). The rest of the patients had laparoscopic surgery. Patients had an average of nine doses of the study drug.
The mean length of stay was 4 days in the alvimopan group and 5 in the placebo group – a significant difference.
There was significantly less postoperative ileus in the alvimopan group (2% vs. 10%). Significantly fewer of those taking the study drug needed a nasogastric tube reinserted (2% vs. 9%). The rates of 30-day readmission, reoperation, and anastomotic leak were similar in both groups. The mean time to first bowel movement was about 1 day sooner in the alvimopan group.
The median hospital cost was $10,832 for the alvimopan group and $11,924 for the placebo group – a significant difference. The median total pharmacy cost was $476 vs. $501; this difference was not significant.
Because Cubist Pharmaceuticals, which makes alvimopan, provided the study drug at no cost, the overall cost analysis cannot be considered complete, Dr. Moesinger noted. However, the pharmacy cost for a similar course of the drug would be $84. Figuring that cost into the total saved for each admission ($1,686) still yielded a net financial benefit of $930 per patient, he said.
Dr. Moesinger had no financial disclosures.
AT THE ACS CLINICAL CONGRESS
Major finding: Compared with placebo, alvimopan given before and after elective bowel surgery reduced the length of stay by 1 day and significantly decreased the incidence of postoperative ileus (2% vs. 10%).
Data source: The randomized placebo-controlled trial comprised 248 patients.
Disclosures: Dr. Moesinger had no financial disclosures.

Surgeons as proficient as gastroenterologists at colonoscopy
WASHINGTON (IMNG) – A British study suggests that it is experience, not specialty, that makes the endoscopist.
The review of more than 2,000 colonoscopies performed in 1 year determined that gastroenterologists and surgeons had identical colonoscopy completion and adverse-event outcomes, Dr. Camille Yvon reported at the annual congress of the American College of Surgeons.
Dr. Yvon, of the Medway Maritime NHS Hospital in Gillingham, England, reported the results of an audit conducted at the Kent facility from March 2011 to March 2012. It was based on prospectively collected data and was designed to compare clinical outcomes among a group of 10 physicians who were performing endoscopies during that time. Included were five consultant colorectal surgeons, one senior trust grade surgeon, and four consultant gastroenterologists.
All of the clinicians were certified by the U.K. Joint Advisory Group on Endoscopy (JAG). The group requires clinicians to complete a mentored training period and to meet specific safety and quality standards, including the following:
• 90% completion rate for colonoscopies (entering the cecum).
• Adenoma detection rate more than 10%.
• Polyp recovery more than 90%.
• Good-quality bowel prep more than 90%.
• Colonoscopy perforation rate less than 1/1,000.
• Postpolypectomy bleeding requiring transfusion less than 1/100.
• Postpolypectomy perforation rate less than 1/500.
• Flexible sigmoidoscopy perforation rate less than 1/5,000.
To become JAG accredited, physicians must be supervised by an accredited physician while performing at least 200 procedures, 100 of which were in the past year; 75% must have been colonoscopies. Certification assessment is done by two different people on two different occasions.
The audit comprised 2,058 colonoscopies. The measured outcomes were number of colonoscopies per clinician, cecal intubation rate of at least 90%, perforation rate of less than 1/1,000, and a less than 1/100 rate of postpolypectomy bleeding requiring a transfusion.
Of the total number of colonoscopies, 1,237 were done by the surgeons and the rest by the gastroenterologists. Clinicians performed an average of 205 procedures per year (range, 105-448 per year). Gastroenterologists performed an average of 205 per year, while surgeons performed an average of 206.
The overall cecal intubation rate was 94%. The average rate for both surgeons and gastroenterologists was also 94%.
There were no perforations during the study period. There were two instances of severe postpolypectomy bleeding (0.09%). However, Dr. Yvon reported, the number was too small for any meaningful statistical analysis.
Dr. Yvon had no financial disclosures.
WASHINGTON (IMNG) – A British study suggests that it is experience, not specialty, that makes the endoscopist.
The review of more than 2,000 colonoscopies performed in 1 year determined that gastroenterologists and surgeons had identical colonoscopy completion and adverse-event outcomes, Dr. Camille Yvon reported at the annual congress of the American College of Surgeons.
Dr. Yvon, of the Medway Maritime NHS Hospital in Gillingham, England, reported the results of an audit conducted at the Kent facility from March 2011 to March 2012. It was based on prospectively collected data and was designed to compare clinical outcomes among a group of 10 physicians who were performing endoscopies during that time. Included were five consultant colorectal surgeons, one senior trust grade surgeon, and four consultant gastroenterologists.
All of the clinicians were certified by the U.K. Joint Advisory Group on Endoscopy (JAG). The group requires clinicians to complete a mentored training period and to meet specific safety and quality standards, including the following:
• 90% completion rate for colonoscopies (entering the cecum).
• Adenoma detection rate more than 10%.
• Polyp recovery more than 90%.
• Good-quality bowel prep more than 90%.
• Colonoscopy perforation rate less than 1/1,000.
• Postpolypectomy bleeding requiring transfusion less than 1/100.
• Postpolypectomy perforation rate less than 1/500.
• Flexible sigmoidoscopy perforation rate less than 1/5,000.
To become JAG accredited, physicians must be supervised by an accredited physician while performing at least 200 procedures, 100 of which were in the past year; 75% must have been colonoscopies. Certification assessment is done by two different people on two different occasions.
The audit comprised 2,058 colonoscopies. The measured outcomes were number of colonoscopies per clinician, cecal intubation rate of at least 90%, perforation rate of less than 1/1,000, and a less than 1/100 rate of postpolypectomy bleeding requiring a transfusion.
Of the total number of colonoscopies, 1,237 were done by the surgeons and the rest by the gastroenterologists. Clinicians performed an average of 205 procedures per year (range, 105-448 per year). Gastroenterologists performed an average of 205 per year, while surgeons performed an average of 206.
The overall cecal intubation rate was 94%. The average rate for both surgeons and gastroenterologists was also 94%.
There were no perforations during the study period. There were two instances of severe postpolypectomy bleeding (0.09%). However, Dr. Yvon reported, the number was too small for any meaningful statistical analysis.
Dr. Yvon had no financial disclosures.
WASHINGTON (IMNG) – A British study suggests that it is experience, not specialty, that makes the endoscopist.
The review of more than 2,000 colonoscopies performed in 1 year determined that gastroenterologists and surgeons had identical colonoscopy completion and adverse-event outcomes, Dr. Camille Yvon reported at the annual congress of the American College of Surgeons.
Dr. Yvon, of the Medway Maritime NHS Hospital in Gillingham, England, reported the results of an audit conducted at the Kent facility from March 2011 to March 2012. It was based on prospectively collected data and was designed to compare clinical outcomes among a group of 10 physicians who were performing endoscopies during that time. Included were five consultant colorectal surgeons, one senior trust grade surgeon, and four consultant gastroenterologists.
All of the clinicians were certified by the U.K. Joint Advisory Group on Endoscopy (JAG). The group requires clinicians to complete a mentored training period and to meet specific safety and quality standards, including the following:
• 90% completion rate for colonoscopies (entering the cecum).
• Adenoma detection rate more than 10%.
• Polyp recovery more than 90%.
• Good-quality bowel prep more than 90%.
• Colonoscopy perforation rate less than 1/1,000.
• Postpolypectomy bleeding requiring transfusion less than 1/100.
• Postpolypectomy perforation rate less than 1/500.
• Flexible sigmoidoscopy perforation rate less than 1/5,000.
To become JAG accredited, physicians must be supervised by an accredited physician while performing at least 200 procedures, 100 of which were in the past year; 75% must have been colonoscopies. Certification assessment is done by two different people on two different occasions.
The audit comprised 2,058 colonoscopies. The measured outcomes were number of colonoscopies per clinician, cecal intubation rate of at least 90%, perforation rate of less than 1/1,000, and a less than 1/100 rate of postpolypectomy bleeding requiring a transfusion.
Of the total number of colonoscopies, 1,237 were done by the surgeons and the rest by the gastroenterologists. Clinicians performed an average of 205 procedures per year (range, 105-448 per year). Gastroenterologists performed an average of 205 per year, while surgeons performed an average of 206.
The overall cecal intubation rate was 94%. The average rate for both surgeons and gastroenterologists was also 94%.
There were no perforations during the study period. There were two instances of severe postpolypectomy bleeding (0.09%). However, Dr. Yvon reported, the number was too small for any meaningful statistical analysis.
Dr. Yvon had no financial disclosures.
AT THE ACS CLINICAL CONGRESS
Major finding: Gastroenterologists and surgeons both completed an average of 94% of colonoscopies they performed during a 1-year audit period.
Data source: The audit examined outcomes of more than 2,000 colonoscopies.
Disclosures: Dr. Yvon had no financial disclosures.