User login
Ibrutinib continues to wow in CLL/SLL
SAN DIEGO – More than 90% of the first patients with previously untreated chronic lymphocytic leukemia who received ibrutinib in an early study are alive and without disease progression 5 years later, investigators reported.
Among 31 treatment-naive patients with chronic lymphocytic leukemia/small lymphocytic leukemia (CLL/SLL) who were started on the Bruton’s tyrosine kinase inhibitor ibrutinib (Imbruvica) in the phase Ib/II PCYC-1102/1103 study, the 5-year progression-free survival (PFS) rate was 92%, with the median PFS not reached. Estimated 5-year overall survival (OS) among these patients was also 92%, with the median not reached, Susan O’Brien, MD, of the University of California, Irvine, reported at the annual meeting of the American Society of Hematology.
The 5-year PFS rate for patients with relapsed/refractory disease who had received a median of four prior lines of therapy before starting on single-agent ibrutinib was 43%, with a median PFS of 52 months. In this group, the overall survival (OS) rate was 57%, with the median not reached.
“At 5 years of follow-up, there are very durable responses in treatment-naive and relapsed refractory patients. You saw that, in the treatment-naive group, there is, in fact, only one patient who has progressed so far,” Dr. O’Brien said.
In a separate study, investigators from the phase III RESONATE-2 trial reported updated safety and efficacy data showing that in first-line therapy for patients aged 65 years and older with CLL/SLL with active disease, ibrutinib was associated with significantly better PFS at 24 months, compared with chlorambucil.
In this study by Dr. O’Brien and colleagues, 31 patients with previously untreated CLL/SLL and 101 patients with relapsed/refractory disease (progression or no objective response within 24 months of starting on chemoimmunotherapy) were treated with oral ibrutinib once daily at doses of 420 mg or 840 mg until disease progression or unacceptable toxicity.
After 5 years of follow-up, 20 of the 31 treatment-naive patients (65%) and 30 of the 101 relapsed/refractory patients (30%) remained on ibrutinib therapy. The primary reasons for discontinuation among relapsed/refractory patients included progressive disease in 33%, adverse events in 21%, and investigator decision in 11%.
Best response rates in treatment-naive patients were 87% (29% complete response, 55% partial response, 3% partial response-L) and 89% in relapsed/refractory patients (10%, 76%, and 3%, respectively).
An analysis of survival by IGHV (immunoglobulin heavy chain variable) mutational status in patients with relapsed/refractory disease showed a 53% 5-year PFS rate among patients with mutated IGHV and a median PFS of 63 months, compared with 38% and 43 months for patients with unmutated IGHV. Respective 5-year overall survival rates were 66% (median OS, 63 months) and 55% (median not reached).
In an analysis of survival outcomes by chromosomal abnormalities detected by FISH (fluorescent in situ hybridization) among patients with relapsed/refractory disease, median PFS and OS rates were highest among patients with the 13q deletion, at 91% for both PFS and OS, compared with 80% for each in patients with trisomy 12, 33% and 61% for patients with deletion 11q, and 19% and 32% for patients with deletion 17p. In patients with no chromosomal abnormalities, the 5-year PFS rate was 66% (median not reached), and the 5-year OS rate was 83% (median not reached).
Among patients with complex karyotype, 90% of whom had relapsed refractory disease, the 5-year PFS rate was 36% (median 33 months), and the OS rate was 46% (median 57 months). In contrast, respective PFS and OS rates for patients without complex karyotype were 69% and 84%, with the median not reached in either survival category.
In multivariate analysis, only deletion 17p was identified as a significant predictor of PFS and OS.
Grade 3 or greater treatment-emergent adverse events occurred mostly frequently in the first year of therapy and declined thereafter. The most common grade 3 or greater events were hypertension, (26% of all patients), pneumonia (22%), neutropenia (17%), and atrial fibrillation (9%).
Paul M. Barr, MD, of the University of Rochester presented updated data from RESONATE-2, comparing ibrutinib with chlorambucil in patients 65 and older with newly diagnosed, active CLL/SLL.
At a median follow-up of 29 months, the rates of 2-year PFS were 89% for patients treated with ibrutinib (median PFS not reached) vs. 34% for chlorambucil (median PFS 15 months). This translated into a hazard ratio for ibrutinib of 0.121 (P less than .0001). The benefit of ibrutinib occurred without regard to IGHV status, and ibrutinib continues to demonstrate an OS benefit over chlorambucil with longer follow-up and crossover. Overall survival at 24 months was 95% for patients treated with ibrutinib (included 55 patients who were crossed over from chlorambucil) vs. 84% for patients treated with chlorambucil only.
“The depth of the responses has improved over time, now with 18% of patients achieving a CR with ibrutinib, and lastly, ibrutinib remains tolerable in this elderly population, with 79% of patients that are continuing on therapy,” Dr. Barr said.
Both studies were funded by Pharmacyclics. Dr. Barr and Dr. O’Brien disclosed serving as consultants to the company, and Dr. O’Brien further disclosed honoraria and research funding from Pharmacyclics.
SAN DIEGO – More than 90% of the first patients with previously untreated chronic lymphocytic leukemia who received ibrutinib in an early study are alive and without disease progression 5 years later, investigators reported.
Among 31 treatment-naive patients with chronic lymphocytic leukemia/small lymphocytic leukemia (CLL/SLL) who were started on the Bruton’s tyrosine kinase inhibitor ibrutinib (Imbruvica) in the phase Ib/II PCYC-1102/1103 study, the 5-year progression-free survival (PFS) rate was 92%, with the median PFS not reached. Estimated 5-year overall survival (OS) among these patients was also 92%, with the median not reached, Susan O’Brien, MD, of the University of California, Irvine, reported at the annual meeting of the American Society of Hematology.
The 5-year PFS rate for patients with relapsed/refractory disease who had received a median of four prior lines of therapy before starting on single-agent ibrutinib was 43%, with a median PFS of 52 months. In this group, the overall survival (OS) rate was 57%, with the median not reached.
“At 5 years of follow-up, there are very durable responses in treatment-naive and relapsed refractory patients. You saw that, in the treatment-naive group, there is, in fact, only one patient who has progressed so far,” Dr. O’Brien said.
In a separate study, investigators from the phase III RESONATE-2 trial reported updated safety and efficacy data showing that in first-line therapy for patients aged 65 years and older with CLL/SLL with active disease, ibrutinib was associated with significantly better PFS at 24 months, compared with chlorambucil.
In this study by Dr. O’Brien and colleagues, 31 patients with previously untreated CLL/SLL and 101 patients with relapsed/refractory disease (progression or no objective response within 24 months of starting on chemoimmunotherapy) were treated with oral ibrutinib once daily at doses of 420 mg or 840 mg until disease progression or unacceptable toxicity.
After 5 years of follow-up, 20 of the 31 treatment-naive patients (65%) and 30 of the 101 relapsed/refractory patients (30%) remained on ibrutinib therapy. The primary reasons for discontinuation among relapsed/refractory patients included progressive disease in 33%, adverse events in 21%, and investigator decision in 11%.
Best response rates in treatment-naive patients were 87% (29% complete response, 55% partial response, 3% partial response-L) and 89% in relapsed/refractory patients (10%, 76%, and 3%, respectively).
An analysis of survival by IGHV (immunoglobulin heavy chain variable) mutational status in patients with relapsed/refractory disease showed a 53% 5-year PFS rate among patients with mutated IGHV and a median PFS of 63 months, compared with 38% and 43 months for patients with unmutated IGHV. Respective 5-year overall survival rates were 66% (median OS, 63 months) and 55% (median not reached).
In an analysis of survival outcomes by chromosomal abnormalities detected by FISH (fluorescent in situ hybridization) among patients with relapsed/refractory disease, median PFS and OS rates were highest among patients with the 13q deletion, at 91% for both PFS and OS, compared with 80% for each in patients with trisomy 12, 33% and 61% for patients with deletion 11q, and 19% and 32% for patients with deletion 17p. In patients with no chromosomal abnormalities, the 5-year PFS rate was 66% (median not reached), and the 5-year OS rate was 83% (median not reached).
Among patients with complex karyotype, 90% of whom had relapsed refractory disease, the 5-year PFS rate was 36% (median 33 months), and the OS rate was 46% (median 57 months). In contrast, respective PFS and OS rates for patients without complex karyotype were 69% and 84%, with the median not reached in either survival category.
In multivariate analysis, only deletion 17p was identified as a significant predictor of PFS and OS.
Grade 3 or greater treatment-emergent adverse events occurred mostly frequently in the first year of therapy and declined thereafter. The most common grade 3 or greater events were hypertension, (26% of all patients), pneumonia (22%), neutropenia (17%), and atrial fibrillation (9%).
Paul M. Barr, MD, of the University of Rochester presented updated data from RESONATE-2, comparing ibrutinib with chlorambucil in patients 65 and older with newly diagnosed, active CLL/SLL.
At a median follow-up of 29 months, the rates of 2-year PFS were 89% for patients treated with ibrutinib (median PFS not reached) vs. 34% for chlorambucil (median PFS 15 months). This translated into a hazard ratio for ibrutinib of 0.121 (P less than .0001). The benefit of ibrutinib occurred without regard to IGHV status, and ibrutinib continues to demonstrate an OS benefit over chlorambucil with longer follow-up and crossover. Overall survival at 24 months was 95% for patients treated with ibrutinib (included 55 patients who were crossed over from chlorambucil) vs. 84% for patients treated with chlorambucil only.
“The depth of the responses has improved over time, now with 18% of patients achieving a CR with ibrutinib, and lastly, ibrutinib remains tolerable in this elderly population, with 79% of patients that are continuing on therapy,” Dr. Barr said.
Both studies were funded by Pharmacyclics. Dr. Barr and Dr. O’Brien disclosed serving as consultants to the company, and Dr. O’Brien further disclosed honoraria and research funding from Pharmacyclics.
SAN DIEGO – More than 90% of the first patients with previously untreated chronic lymphocytic leukemia who received ibrutinib in an early study are alive and without disease progression 5 years later, investigators reported.
Among 31 treatment-naive patients with chronic lymphocytic leukemia/small lymphocytic leukemia (CLL/SLL) who were started on the Bruton’s tyrosine kinase inhibitor ibrutinib (Imbruvica) in the phase Ib/II PCYC-1102/1103 study, the 5-year progression-free survival (PFS) rate was 92%, with the median PFS not reached. Estimated 5-year overall survival (OS) among these patients was also 92%, with the median not reached, Susan O’Brien, MD, of the University of California, Irvine, reported at the annual meeting of the American Society of Hematology.
The 5-year PFS rate for patients with relapsed/refractory disease who had received a median of four prior lines of therapy before starting on single-agent ibrutinib was 43%, with a median PFS of 52 months. In this group, the overall survival (OS) rate was 57%, with the median not reached.
“At 5 years of follow-up, there are very durable responses in treatment-naive and relapsed refractory patients. You saw that, in the treatment-naive group, there is, in fact, only one patient who has progressed so far,” Dr. O’Brien said.
In a separate study, investigators from the phase III RESONATE-2 trial reported updated safety and efficacy data showing that in first-line therapy for patients aged 65 years and older with CLL/SLL with active disease, ibrutinib was associated with significantly better PFS at 24 months, compared with chlorambucil.
In this study by Dr. O’Brien and colleagues, 31 patients with previously untreated CLL/SLL and 101 patients with relapsed/refractory disease (progression or no objective response within 24 months of starting on chemoimmunotherapy) were treated with oral ibrutinib once daily at doses of 420 mg or 840 mg until disease progression or unacceptable toxicity.
After 5 years of follow-up, 20 of the 31 treatment-naive patients (65%) and 30 of the 101 relapsed/refractory patients (30%) remained on ibrutinib therapy. The primary reasons for discontinuation among relapsed/refractory patients included progressive disease in 33%, adverse events in 21%, and investigator decision in 11%.
Best response rates in treatment-naive patients were 87% (29% complete response, 55% partial response, 3% partial response-L) and 89% in relapsed/refractory patients (10%, 76%, and 3%, respectively).
An analysis of survival by IGHV (immunoglobulin heavy chain variable) mutational status in patients with relapsed/refractory disease showed a 53% 5-year PFS rate among patients with mutated IGHV and a median PFS of 63 months, compared with 38% and 43 months for patients with unmutated IGHV. Respective 5-year overall survival rates were 66% (median OS, 63 months) and 55% (median not reached).
In an analysis of survival outcomes by chromosomal abnormalities detected by FISH (fluorescent in situ hybridization) among patients with relapsed/refractory disease, median PFS and OS rates were highest among patients with the 13q deletion, at 91% for both PFS and OS, compared with 80% for each in patients with trisomy 12, 33% and 61% for patients with deletion 11q, and 19% and 32% for patients with deletion 17p. In patients with no chromosomal abnormalities, the 5-year PFS rate was 66% (median not reached), and the 5-year OS rate was 83% (median not reached).
Among patients with complex karyotype, 90% of whom had relapsed refractory disease, the 5-year PFS rate was 36% (median 33 months), and the OS rate was 46% (median 57 months). In contrast, respective PFS and OS rates for patients without complex karyotype were 69% and 84%, with the median not reached in either survival category.
In multivariate analysis, only deletion 17p was identified as a significant predictor of PFS and OS.
Grade 3 or greater treatment-emergent adverse events occurred mostly frequently in the first year of therapy and declined thereafter. The most common grade 3 or greater events were hypertension, (26% of all patients), pneumonia (22%), neutropenia (17%), and atrial fibrillation (9%).
Paul M. Barr, MD, of the University of Rochester presented updated data from RESONATE-2, comparing ibrutinib with chlorambucil in patients 65 and older with newly diagnosed, active CLL/SLL.
At a median follow-up of 29 months, the rates of 2-year PFS were 89% for patients treated with ibrutinib (median PFS not reached) vs. 34% for chlorambucil (median PFS 15 months). This translated into a hazard ratio for ibrutinib of 0.121 (P less than .0001). The benefit of ibrutinib occurred without regard to IGHV status, and ibrutinib continues to demonstrate an OS benefit over chlorambucil with longer follow-up and crossover. Overall survival at 24 months was 95% for patients treated with ibrutinib (included 55 patients who were crossed over from chlorambucil) vs. 84% for patients treated with chlorambucil only.
“The depth of the responses has improved over time, now with 18% of patients achieving a CR with ibrutinib, and lastly, ibrutinib remains tolerable in this elderly population, with 79% of patients that are continuing on therapy,” Dr. Barr said.
Both studies were funded by Pharmacyclics. Dr. Barr and Dr. O’Brien disclosed serving as consultants to the company, and Dr. O’Brien further disclosed honoraria and research funding from Pharmacyclics.
AT ASH 2016
Key clinical point: Long-term follow-up of two studies shows a progression-free and overall survival advantage with ibrutinib in chronic lymphocytic leukemia/small lymphocytic leukemia.
Major finding: 5-year PFS and OS rates were 92% for treatment-naive patients with CLL/SLL treated with ibrutinib.
Data source: Phase Ib/II study and randomized phase III study of ibrutinib for treatment-naive and relapsed/refractory CLL/SLL.
Disclosures: Both studies were funded by Pharmacyclics. Dr. Barr and Dr. O’Brien disclosed serving as consultants to the company; Dr. O’Brien disclosed honoraria and research funding from the company.
Lenalidomide improves PFS after 1st and 2nd line CLL therapy
SAN DIEGO – Lenalidomide, a mainstay of maintenance therapy for multiple myeloma, is now making inroads into maintenance therapy following first- and second-line therapy for chronic lymphocytic leukemia (CLL), investigators reported in two phase III studies.
Among patients with previously untreated CLL who were at high risk for early disease progression following standard chemotherapy, lenalidomide (Revlimid) maintenance therapy was associated with an 80% reduction in the relative risk for disease progression compared with placebo, reported Anna Fink, MD, of the University of Cologne, Germany, and her colleagues in the German CLL Study Group.
Similarly, lenalidomide maintenance significantly improved progression-free survival (PFS) compared with placebo among patients with CLL who had at least partial responses to second-line therapy, reported Anna Schuh, MD, of the University of Oxford, England, and her colleagues in the CONTINUUM trial.
“Lenalidomide maintenance therapy significantly improved progression-free survival, from just about 9 months to almost 40 months when given to patients with CLL who responded to second-line therapy,” Dr. Schuh said at the American Society of Hematology annual meeting.
Both studies were unblinded because of the superiority of lenalidomide after prespecified analyses, on the recommendation of the respective data safety monitoring boards (DSMBs).
The PFS advantage with lenalidomide seen in each study did not translate into differences in overall survival in either study, however.
Maintenance after first-line therapy
In the CLLM1 trial, Dr. Fink and her colleagues enrolled physically fit, previously untreated patients with CLL and delivered chemoimmunotherapy at the investigator’s choice: either FCR (fludarabine, cyclophosphamide, and rituximab), FR (fludarabine and rituximab), FC (fludarabine and cyclophosphamide), or BR (bendamustine and rituximab).
Patients who had at least a partial response after a minimum of four cycles were identified as being at high risk for progression if they had minimal residual disease (MRD) levels of at least 10-2 cells, or MRD levels from 10-4 to less than 10-2 combined with either an unmutated IGHV gene status, del(17p) or TP53 mutation at baseline.
Of 468 screened patients, 89 were deemed to have high risk disease, and these patients were randomly assigned on a 2:1 basis to maintenance with lenalidomide given 5 mg orally for the first cycle and escalated to a target dose of 15 mg by the seventh cycle, or to placebo.
Additional dose escalations could be performed based on MRD assessments every 6 months, with the drug continued until progression or unacceptable toxicity. Patients also were assigned to daily low-dose aspirin or to an anticoagulation agent depending on their individual risk for thromboembolic events.
The study was stopped and unblinded after a planned interim analysis showed that the difference in PFS met the stopping boundary for efficacy.
Ultimately, 56 patients assigned to lenalidomide received study treatment, as did 29 assigned to placebo.
At a median follow-up of 17.5 months, the median PFS according to independent review was not reached for lenalidomide, vs. 13.3 months for placebo. Lenalidomide was associated with a hazard ratio (HR) for progression of 0.148 (P less than .00001), and a relative risk reduction of 80%.
Lenalidomide was also significantly better for PFS in analysis by MRD at baseline, with a PFS of 19.4 months for placebo vs. not reached among patients with less than 10-2 but more than 10-4 cells (HR, 0.125) and 3.7 vs. 32.3 months, respectively, for patients with MRD greater than 10-2 (HR 0.165).
There were three deaths (two in patients on placebo), and at the last analysis there was no difference in overall survival. In all, 42.9% of patients on lenalidomide discontinued because of adverse events, compared with 72.4% of those on placebo.
Maintenance after second-line therapy
In CONTINUUM, patients with at least a partial response after two prior lines of therapy and an Eastern Cooperative Oncology Group performance score of 0-2 were enrolled and randomized to receive either lenalidomide (160 patients) at a starting dose of 2.5 mg/day for the first 28-day cycle, 5 mg/day from cycle 2, and, if well tolerated, up to 10 mg/day from cycle 7 on, or to placebo (154 patients).
This study, as noted before, was also unblinded at the time of the primary analysis as recommended by the DSMB, after a prespecified number of events had occurred.
At a median follow-up of 31.5 months, the median PFS, a co-primary endpoint with OS, was 33.9 months in the lenalidomide arm, compared with 9.2 months in the placebo arm, translating into a HR for lenalidomide of 0.40 (P less than .001).
The lenalidomide advantage also was seen in a subgroup analysis by age, prior response to chemotherapy, and number of factors for poor prognosis. Of note, among patients older than age 70, the PFS with lenalidomide was 52.5 months, compared with 7.3 months for placebo (HR 0.34, P = .005).
In a second PFS analysis conducted after 71 months of follow-up, lenalidomide remained superior, with a median PFS of 57.5 months vs. 32.7 months in the placebo arm. As noted, there was no difference in overall survival in this study.
Grade 3 or greater adverse events occurring more frequently with lenalidomide were neutropenia, thrombocytopenia, diarrhea, pneumonia, fatigue, hypokalemia, pulmonary embolism, and sepsis. There was no difference in the incidence of second primary malignancies, however.
CLLM1 was sponsored by the German CLL Study Group with support from Celgene. CONTINUUM was supported by Celgene. Dr. Fink disclosed research funding from the company, and travel grants and honoraria from others. Dr. Schuh disclosed honoraria from and consulting with Celgene and other companies.
SAN DIEGO – Lenalidomide, a mainstay of maintenance therapy for multiple myeloma, is now making inroads into maintenance therapy following first- and second-line therapy for chronic lymphocytic leukemia (CLL), investigators reported in two phase III studies.
Among patients with previously untreated CLL who were at high risk for early disease progression following standard chemotherapy, lenalidomide (Revlimid) maintenance therapy was associated with an 80% reduction in the relative risk for disease progression compared with placebo, reported Anna Fink, MD, of the University of Cologne, Germany, and her colleagues in the German CLL Study Group.
Similarly, lenalidomide maintenance significantly improved progression-free survival (PFS) compared with placebo among patients with CLL who had at least partial responses to second-line therapy, reported Anna Schuh, MD, of the University of Oxford, England, and her colleagues in the CONTINUUM trial.
“Lenalidomide maintenance therapy significantly improved progression-free survival, from just about 9 months to almost 40 months when given to patients with CLL who responded to second-line therapy,” Dr. Schuh said at the American Society of Hematology annual meeting.
Both studies were unblinded because of the superiority of lenalidomide after prespecified analyses, on the recommendation of the respective data safety monitoring boards (DSMBs).
The PFS advantage with lenalidomide seen in each study did not translate into differences in overall survival in either study, however.
Maintenance after first-line therapy
In the CLLM1 trial, Dr. Fink and her colleagues enrolled physically fit, previously untreated patients with CLL and delivered chemoimmunotherapy at the investigator’s choice: either FCR (fludarabine, cyclophosphamide, and rituximab), FR (fludarabine and rituximab), FC (fludarabine and cyclophosphamide), or BR (bendamustine and rituximab).
Patients who had at least a partial response after a minimum of four cycles were identified as being at high risk for progression if they had minimal residual disease (MRD) levels of at least 10-2 cells, or MRD levels from 10-4 to less than 10-2 combined with either an unmutated IGHV gene status, del(17p) or TP53 mutation at baseline.
Of 468 screened patients, 89 were deemed to have high risk disease, and these patients were randomly assigned on a 2:1 basis to maintenance with lenalidomide given 5 mg orally for the first cycle and escalated to a target dose of 15 mg by the seventh cycle, or to placebo.
Additional dose escalations could be performed based on MRD assessments every 6 months, with the drug continued until progression or unacceptable toxicity. Patients also were assigned to daily low-dose aspirin or to an anticoagulation agent depending on their individual risk for thromboembolic events.
The study was stopped and unblinded after a planned interim analysis showed that the difference in PFS met the stopping boundary for efficacy.
Ultimately, 56 patients assigned to lenalidomide received study treatment, as did 29 assigned to placebo.
At a median follow-up of 17.5 months, the median PFS according to independent review was not reached for lenalidomide, vs. 13.3 months for placebo. Lenalidomide was associated with a hazard ratio (HR) for progression of 0.148 (P less than .00001), and a relative risk reduction of 80%.
Lenalidomide was also significantly better for PFS in analysis by MRD at baseline, with a PFS of 19.4 months for placebo vs. not reached among patients with less than 10-2 but more than 10-4 cells (HR, 0.125) and 3.7 vs. 32.3 months, respectively, for patients with MRD greater than 10-2 (HR 0.165).
There were three deaths (two in patients on placebo), and at the last analysis there was no difference in overall survival. In all, 42.9% of patients on lenalidomide discontinued because of adverse events, compared with 72.4% of those on placebo.
Maintenance after second-line therapy
In CONTINUUM, patients with at least a partial response after two prior lines of therapy and an Eastern Cooperative Oncology Group performance score of 0-2 were enrolled and randomized to receive either lenalidomide (160 patients) at a starting dose of 2.5 mg/day for the first 28-day cycle, 5 mg/day from cycle 2, and, if well tolerated, up to 10 mg/day from cycle 7 on, or to placebo (154 patients).
This study, as noted before, was also unblinded at the time of the primary analysis as recommended by the DSMB, after a prespecified number of events had occurred.
At a median follow-up of 31.5 months, the median PFS, a co-primary endpoint with OS, was 33.9 months in the lenalidomide arm, compared with 9.2 months in the placebo arm, translating into a HR for lenalidomide of 0.40 (P less than .001).
The lenalidomide advantage also was seen in a subgroup analysis by age, prior response to chemotherapy, and number of factors for poor prognosis. Of note, among patients older than age 70, the PFS with lenalidomide was 52.5 months, compared with 7.3 months for placebo (HR 0.34, P = .005).
In a second PFS analysis conducted after 71 months of follow-up, lenalidomide remained superior, with a median PFS of 57.5 months vs. 32.7 months in the placebo arm. As noted, there was no difference in overall survival in this study.
Grade 3 or greater adverse events occurring more frequently with lenalidomide were neutropenia, thrombocytopenia, diarrhea, pneumonia, fatigue, hypokalemia, pulmonary embolism, and sepsis. There was no difference in the incidence of second primary malignancies, however.
CLLM1 was sponsored by the German CLL Study Group with support from Celgene. CONTINUUM was supported by Celgene. Dr. Fink disclosed research funding from the company, and travel grants and honoraria from others. Dr. Schuh disclosed honoraria from and consulting with Celgene and other companies.
SAN DIEGO – Lenalidomide, a mainstay of maintenance therapy for multiple myeloma, is now making inroads into maintenance therapy following first- and second-line therapy for chronic lymphocytic leukemia (CLL), investigators reported in two phase III studies.
Among patients with previously untreated CLL who were at high risk for early disease progression following standard chemotherapy, lenalidomide (Revlimid) maintenance therapy was associated with an 80% reduction in the relative risk for disease progression compared with placebo, reported Anna Fink, MD, of the University of Cologne, Germany, and her colleagues in the German CLL Study Group.
Similarly, lenalidomide maintenance significantly improved progression-free survival (PFS) compared with placebo among patients with CLL who had at least partial responses to second-line therapy, reported Anna Schuh, MD, of the University of Oxford, England, and her colleagues in the CONTINUUM trial.
“Lenalidomide maintenance therapy significantly improved progression-free survival, from just about 9 months to almost 40 months when given to patients with CLL who responded to second-line therapy,” Dr. Schuh said at the American Society of Hematology annual meeting.
Both studies were unblinded because of the superiority of lenalidomide after prespecified analyses, on the recommendation of the respective data safety monitoring boards (DSMBs).
The PFS advantage with lenalidomide seen in each study did not translate into differences in overall survival in either study, however.
Maintenance after first-line therapy
In the CLLM1 trial, Dr. Fink and her colleagues enrolled physically fit, previously untreated patients with CLL and delivered chemoimmunotherapy at the investigator’s choice: either FCR (fludarabine, cyclophosphamide, and rituximab), FR (fludarabine and rituximab), FC (fludarabine and cyclophosphamide), or BR (bendamustine and rituximab).
Patients who had at least a partial response after a minimum of four cycles were identified as being at high risk for progression if they had minimal residual disease (MRD) levels of at least 10-2 cells, or MRD levels from 10-4 to less than 10-2 combined with either an unmutated IGHV gene status, del(17p) or TP53 mutation at baseline.
Of 468 screened patients, 89 were deemed to have high risk disease, and these patients were randomly assigned on a 2:1 basis to maintenance with lenalidomide given 5 mg orally for the first cycle and escalated to a target dose of 15 mg by the seventh cycle, or to placebo.
Additional dose escalations could be performed based on MRD assessments every 6 months, with the drug continued until progression or unacceptable toxicity. Patients also were assigned to daily low-dose aspirin or to an anticoagulation agent depending on their individual risk for thromboembolic events.
The study was stopped and unblinded after a planned interim analysis showed that the difference in PFS met the stopping boundary for efficacy.
Ultimately, 56 patients assigned to lenalidomide received study treatment, as did 29 assigned to placebo.
At a median follow-up of 17.5 months, the median PFS according to independent review was not reached for lenalidomide, vs. 13.3 months for placebo. Lenalidomide was associated with a hazard ratio (HR) for progression of 0.148 (P less than .00001), and a relative risk reduction of 80%.
Lenalidomide was also significantly better for PFS in analysis by MRD at baseline, with a PFS of 19.4 months for placebo vs. not reached among patients with less than 10-2 but more than 10-4 cells (HR, 0.125) and 3.7 vs. 32.3 months, respectively, for patients with MRD greater than 10-2 (HR 0.165).
There were three deaths (two in patients on placebo), and at the last analysis there was no difference in overall survival. In all, 42.9% of patients on lenalidomide discontinued because of adverse events, compared with 72.4% of those on placebo.
Maintenance after second-line therapy
In CONTINUUM, patients with at least a partial response after two prior lines of therapy and an Eastern Cooperative Oncology Group performance score of 0-2 were enrolled and randomized to receive either lenalidomide (160 patients) at a starting dose of 2.5 mg/day for the first 28-day cycle, 5 mg/day from cycle 2, and, if well tolerated, up to 10 mg/day from cycle 7 on, or to placebo (154 patients).
This study, as noted before, was also unblinded at the time of the primary analysis as recommended by the DSMB, after a prespecified number of events had occurred.
At a median follow-up of 31.5 months, the median PFS, a co-primary endpoint with OS, was 33.9 months in the lenalidomide arm, compared with 9.2 months in the placebo arm, translating into a HR for lenalidomide of 0.40 (P less than .001).
The lenalidomide advantage also was seen in a subgroup analysis by age, prior response to chemotherapy, and number of factors for poor prognosis. Of note, among patients older than age 70, the PFS with lenalidomide was 52.5 months, compared with 7.3 months for placebo (HR 0.34, P = .005).
In a second PFS analysis conducted after 71 months of follow-up, lenalidomide remained superior, with a median PFS of 57.5 months vs. 32.7 months in the placebo arm. As noted, there was no difference in overall survival in this study.
Grade 3 or greater adverse events occurring more frequently with lenalidomide were neutropenia, thrombocytopenia, diarrhea, pneumonia, fatigue, hypokalemia, pulmonary embolism, and sepsis. There was no difference in the incidence of second primary malignancies, however.
CLLM1 was sponsored by the German CLL Study Group with support from Celgene. CONTINUUM was supported by Celgene. Dr. Fink disclosed research funding from the company, and travel grants and honoraria from others. Dr. Schuh disclosed honoraria from and consulting with Celgene and other companies.
AT ASH 2016
Key clinical point: Lenalidomide (Revlimid) maintenance improves progression free survival following first- and second-line therapies for chronic lymphocytic leukemia.
Major finding: Median PFS vs. placebo was not reached vs. 13.3 months in CLLM1, and 33.9 vs. 9.2 months in CONTINUUM.
Data source: Phase III randomized studies of lenalidomide maintenance following first-line therapy (CLLM1) and second-line therapy (CONTINUUM).
Disclosures: CLLM1 was sponsored by the German CLL Study Group with support from Celgene. CONTINUUM was supported by Celgene. Dr. Fink disclosed research funding from Celgene, and travel grants and honoraria from other drug companies. Dr. Schuh disclosed honoraria from and consulting with Celgene and other companies.
Idelalisib held unlikely to become frontline therapy for CLL
NEW YORK – Safety issues with idelalisib, a first-in-class PI3K delta inhibitor, are an important concern in patients with chronic lymphocytic leukemia – particularly those aged 65 years and younger, according to Steven Coutre, MD.
Findings from the second interim analysis of the pivotal trial for idelalisib as reported at the 2014 annual meeting of the American Society of Hematology (Sharman J., et al. Abstract 330) and a recent update from an open-label extension represent the longest reported follow-up of idelalisib-treated patients to date. Those analyses showed substantial progression-free and overall survival advantages with idelalisib plus rituximab vs. placebo plus rituximab (progression-free survival in the latest update was 19.4 vs. 7.3 months, respectively; hazard ratio 0.25), said Dr. Coutre, professor of medicine at Stanford (Calif.) University.
“Still, even with that report, the follow-up on that initial study was relatively short, and I think it really underreports some of the safety issues of the toxicities that we see,” he said at an international congress on hematologic malignancies.
To further investigate those safety issues, Dr. Coutre and his colleagues performed an integrated analysis of eight clinical trials, including the pivotal trial. That analysis found idelalisib to be efficacious, but significant toxicities were noted, “particularly in younger less heavily-pretreated patients. [Idelalisib] should not be used as frontline therapy ... and I don’t think it will be developed in the future as frontline therapy,” Dr. Coutre said.
“At least in the relapse setting, idelalisib plus rituximab is a choice for all of our patients, but it has to be a considered choice; you have to put it in the context of other therapies that the patients have available to them and make a decision based on your individual patient.”
In the analysis, Dr. Coutre and his colleagues found numerous adverse events occurring in 15% or more of idelalisib-treated patients. These included diarrhea/colitis – with median onset at 7.1 months – in 37% who received monotherapy and 40% who received combination therapy (grade 3 or greater diarrhea/colitis in 11% and 17%, respectively), and pneumonia in 13% and 18% of patients (grade 3 or greater in 11% and 14%, respectively), Dr. Coutre said.
Transaminitis – which was observed early in the studies, usually within the first 8 weeks of treatment – also was common, occurring in 50% and 47% of those with monotherapy and combination therapy, respectively (grade 3 or greater, 16% and 13%, respectively).
Pneumonitis occurred in about 3% of patients, and usually within the first 6 months of therapy.
“So that’s sort of where things were until earlier this year when we learned from several ongoing studies, very important studies in both previously treated patients with low-grade lymphomas and previously untreated patients, that there was a further problem – and that is a difference in mortality,” he said.
Patients in many of these studies, including all of those where it was being used for previously untreated patients, were taken off the drug because of this finding.
“As a result of further analysis of these studies, there’s a new safety label indication,” he said.
Of note, in another idelalisib study reported at ASH 2015 an age-related toxicity concern emerged.
“Idelalisib was used for previously untreated patients. But the distinction here is that for the first time it was being used in younger patients – patients under the age of 65,” he said, noting that severe transaminitis occurred in a significant number of the younger patients.
More than half (52%) of patients had grade 3 or greater hepatotoxicity and all 7 subjects aged 65 years and younger required systemic steroids for toxicities.
Age was found in the study to be a significant risk factor for early hepatotoxicity.
“We’re finally starting to understand the mechanisms behind this, or at least the likely mechanisms, and this seems to be immune mediated,” he said, adding, “you see a lymphocytic infiltrate on liver biopsies, you see a lymphocytic colitis in patients who receive idelalisib.”
Typically, toxicities in these patients can be managed with corticosteroids, but in some cases of severe toxicity even steroids seem to be insufficient, he said.
Further, rapid recurrence is often seen upon re-exposure to the drug, especially with respect to hepatotoxicity, he added.
Preclinical data from mouse models supports this mechanism.
“And importantly [those models] demonstrated a decrease in regulatory T cells in patients treated with idelalisib,” he said.
Dr. Coutre reported consulting for Abbvie, Celgene, Gilead, Janssen, and Pharmacyclics.
NEW YORK – Safety issues with idelalisib, a first-in-class PI3K delta inhibitor, are an important concern in patients with chronic lymphocytic leukemia – particularly those aged 65 years and younger, according to Steven Coutre, MD.
Findings from the second interim analysis of the pivotal trial for idelalisib as reported at the 2014 annual meeting of the American Society of Hematology (Sharman J., et al. Abstract 330) and a recent update from an open-label extension represent the longest reported follow-up of idelalisib-treated patients to date. Those analyses showed substantial progression-free and overall survival advantages with idelalisib plus rituximab vs. placebo plus rituximab (progression-free survival in the latest update was 19.4 vs. 7.3 months, respectively; hazard ratio 0.25), said Dr. Coutre, professor of medicine at Stanford (Calif.) University.
“Still, even with that report, the follow-up on that initial study was relatively short, and I think it really underreports some of the safety issues of the toxicities that we see,” he said at an international congress on hematologic malignancies.
To further investigate those safety issues, Dr. Coutre and his colleagues performed an integrated analysis of eight clinical trials, including the pivotal trial. That analysis found idelalisib to be efficacious, but significant toxicities were noted, “particularly in younger less heavily-pretreated patients. [Idelalisib] should not be used as frontline therapy ... and I don’t think it will be developed in the future as frontline therapy,” Dr. Coutre said.
“At least in the relapse setting, idelalisib plus rituximab is a choice for all of our patients, but it has to be a considered choice; you have to put it in the context of other therapies that the patients have available to them and make a decision based on your individual patient.”
In the analysis, Dr. Coutre and his colleagues found numerous adverse events occurring in 15% or more of idelalisib-treated patients. These included diarrhea/colitis – with median onset at 7.1 months – in 37% who received monotherapy and 40% who received combination therapy (grade 3 or greater diarrhea/colitis in 11% and 17%, respectively), and pneumonia in 13% and 18% of patients (grade 3 or greater in 11% and 14%, respectively), Dr. Coutre said.
Transaminitis – which was observed early in the studies, usually within the first 8 weeks of treatment – also was common, occurring in 50% and 47% of those with monotherapy and combination therapy, respectively (grade 3 or greater, 16% and 13%, respectively).
Pneumonitis occurred in about 3% of patients, and usually within the first 6 months of therapy.
“So that’s sort of where things were until earlier this year when we learned from several ongoing studies, very important studies in both previously treated patients with low-grade lymphomas and previously untreated patients, that there was a further problem – and that is a difference in mortality,” he said.
Patients in many of these studies, including all of those where it was being used for previously untreated patients, were taken off the drug because of this finding.
“As a result of further analysis of these studies, there’s a new safety label indication,” he said.
Of note, in another idelalisib study reported at ASH 2015 an age-related toxicity concern emerged.
“Idelalisib was used for previously untreated patients. But the distinction here is that for the first time it was being used in younger patients – patients under the age of 65,” he said, noting that severe transaminitis occurred in a significant number of the younger patients.
More than half (52%) of patients had grade 3 or greater hepatotoxicity and all 7 subjects aged 65 years and younger required systemic steroids for toxicities.
Age was found in the study to be a significant risk factor for early hepatotoxicity.
“We’re finally starting to understand the mechanisms behind this, or at least the likely mechanisms, and this seems to be immune mediated,” he said, adding, “you see a lymphocytic infiltrate on liver biopsies, you see a lymphocytic colitis in patients who receive idelalisib.”
Typically, toxicities in these patients can be managed with corticosteroids, but in some cases of severe toxicity even steroids seem to be insufficient, he said.
Further, rapid recurrence is often seen upon re-exposure to the drug, especially with respect to hepatotoxicity, he added.
Preclinical data from mouse models supports this mechanism.
“And importantly [those models] demonstrated a decrease in regulatory T cells in patients treated with idelalisib,” he said.
Dr. Coutre reported consulting for Abbvie, Celgene, Gilead, Janssen, and Pharmacyclics.
NEW YORK – Safety issues with idelalisib, a first-in-class PI3K delta inhibitor, are an important concern in patients with chronic lymphocytic leukemia – particularly those aged 65 years and younger, according to Steven Coutre, MD.
Findings from the second interim analysis of the pivotal trial for idelalisib as reported at the 2014 annual meeting of the American Society of Hematology (Sharman J., et al. Abstract 330) and a recent update from an open-label extension represent the longest reported follow-up of idelalisib-treated patients to date. Those analyses showed substantial progression-free and overall survival advantages with idelalisib plus rituximab vs. placebo plus rituximab (progression-free survival in the latest update was 19.4 vs. 7.3 months, respectively; hazard ratio 0.25), said Dr. Coutre, professor of medicine at Stanford (Calif.) University.
“Still, even with that report, the follow-up on that initial study was relatively short, and I think it really underreports some of the safety issues of the toxicities that we see,” he said at an international congress on hematologic malignancies.
To further investigate those safety issues, Dr. Coutre and his colleagues performed an integrated analysis of eight clinical trials, including the pivotal trial. That analysis found idelalisib to be efficacious, but significant toxicities were noted, “particularly in younger less heavily-pretreated patients. [Idelalisib] should not be used as frontline therapy ... and I don’t think it will be developed in the future as frontline therapy,” Dr. Coutre said.
“At least in the relapse setting, idelalisib plus rituximab is a choice for all of our patients, but it has to be a considered choice; you have to put it in the context of other therapies that the patients have available to them and make a decision based on your individual patient.”
In the analysis, Dr. Coutre and his colleagues found numerous adverse events occurring in 15% or more of idelalisib-treated patients. These included diarrhea/colitis – with median onset at 7.1 months – in 37% who received monotherapy and 40% who received combination therapy (grade 3 or greater diarrhea/colitis in 11% and 17%, respectively), and pneumonia in 13% and 18% of patients (grade 3 or greater in 11% and 14%, respectively), Dr. Coutre said.
Transaminitis – which was observed early in the studies, usually within the first 8 weeks of treatment – also was common, occurring in 50% and 47% of those with monotherapy and combination therapy, respectively (grade 3 or greater, 16% and 13%, respectively).
Pneumonitis occurred in about 3% of patients, and usually within the first 6 months of therapy.
“So that’s sort of where things were until earlier this year when we learned from several ongoing studies, very important studies in both previously treated patients with low-grade lymphomas and previously untreated patients, that there was a further problem – and that is a difference in mortality,” he said.
Patients in many of these studies, including all of those where it was being used for previously untreated patients, were taken off the drug because of this finding.
“As a result of further analysis of these studies, there’s a new safety label indication,” he said.
Of note, in another idelalisib study reported at ASH 2015 an age-related toxicity concern emerged.
“Idelalisib was used for previously untreated patients. But the distinction here is that for the first time it was being used in younger patients – patients under the age of 65,” he said, noting that severe transaminitis occurred in a significant number of the younger patients.
More than half (52%) of patients had grade 3 or greater hepatotoxicity and all 7 subjects aged 65 years and younger required systemic steroids for toxicities.
Age was found in the study to be a significant risk factor for early hepatotoxicity.
“We’re finally starting to understand the mechanisms behind this, or at least the likely mechanisms, and this seems to be immune mediated,” he said, adding, “you see a lymphocytic infiltrate on liver biopsies, you see a lymphocytic colitis in patients who receive idelalisib.”
Typically, toxicities in these patients can be managed with corticosteroids, but in some cases of severe toxicity even steroids seem to be insufficient, he said.
Further, rapid recurrence is often seen upon re-exposure to the drug, especially with respect to hepatotoxicity, he added.
Preclinical data from mouse models supports this mechanism.
“And importantly [those models] demonstrated a decrease in regulatory T cells in patients treated with idelalisib,” he said.
Dr. Coutre reported consulting for Abbvie, Celgene, Gilead, Janssen, and Pharmacyclics.
EXPERT ANALYSIS FROM LYMPHOMA & MYELOMA
Targeted therapies predicted to blow out costs for CLL
The lifetime cost of treating chronic lymphocytic leukemia is forecast to rise precipitously for patients diagnosed today, as oral targeted therapies take over as the first-line treatment option, according to a study published November 21 in the Journal of Clinical Oncology.
The conclusion is based on economic models that also indicated the annual cost in the United States of managing chronic lymphocytic leukemia (CLL) will increase from its current level of $0.74 billion to $5.13 billion by 2025 (J Clin Oncol. 2016 Nov 21. doi: 10.1200/JCO.2016.68.2856).
While the majority of patients with CLL are covered by Medicare in the United States, they still currently pay $9,200 in out-of-pocket costs for oral agents. This figure is forecast to increase to $57,000 for those who start treatment in 2016 due to the increased costs of oral targeted therapeutics.
“Such an economic impact could result in financial toxicity, limited access, and lower adherence to the oral therapies, which may undermine their clinical effectiveness,” Qiushi Chen, from the Georgia Institute of Technology, Atlanta, and his coauthors wrote. They called for a more sustainable pricing strategy for oral targeted therapies, rather than have clinicians be forced to choose less effective but more affordable management strategies.
The researchers developed a microsimulation model of CLL, simulating the dynamics of the patient population under given management strategies from 2011-2025.
Around 130,000 patients live with CLL in the United States and around 15,000 new cases are diagnosed each year. By 2025, the authors forecast that 199,000 people will be living with the disease; a 55% increase that is both the result of new diagnoses and of improved survival with new oral targeted therapies.
Chemoimmunotherapy regimens – such as fludarabine, cyclophosphamide, and rituximab – have long been the standard first-line approach to CLL. But in recent years, new oral targeted agents such as ibrutinib and idelalisib have significantly improved progression-free survival and overall survival in CLL.
Ibrutinib is approved for first-line management of CLL, idelalisib is approved in combination with rituximab for patients with relapsed/refractory chronic lymphocytic leukemia, and venetoclax is approved for patients with relapsed chronic lymphocytic leukemia with del(17p).
“Both ibrutinib and idelalisib are priced at approximately $130,000 per [CLL patient per] year and are recommended until patients have progressive disease or significant toxicities,” the authors wrote. “In contrast, the costs for chemoimmunotherapy-based treatments range from $60,000 to $100,000 for a finite duration, that is, a typical six-cycle course that lasts for approximately 6 months.”
The higher costs will add up to additional annual spending of $29 billion to 2025, compared with around $1.12 billion annually for chemoimmunotherapy alone.
“Compared with the CIT scenario, the oral targeted therapy scenario resulted in an increase of 107,000 person–quality-adjusted life-years (149,000 person–life years), with additional discounted costs of $20.2 billion,” the authors reported.
The annual cost of cancer care in the United States is increasing across the board, from $143 billion in 2010 to $180 billion in 2020, but the cost of care for CLL is increasing more significantly than for other cancers. For example, breast and prostate cancers are forecast to have a 24%-38% increase in annual cost by 2020, while CLL is predicted to increase by 500%.
Seven authors declared research funding, honoraria and consultancy funding from a range of pharmaceutical companies including those involved in the manufacture of therapies for chronic lymphocytic leukemia. Two authors had no conflicts to declare.
The lifetime cost of treating chronic lymphocytic leukemia is forecast to rise precipitously for patients diagnosed today, as oral targeted therapies take over as the first-line treatment option, according to a study published November 21 in the Journal of Clinical Oncology.
The conclusion is based on economic models that also indicated the annual cost in the United States of managing chronic lymphocytic leukemia (CLL) will increase from its current level of $0.74 billion to $5.13 billion by 2025 (J Clin Oncol. 2016 Nov 21. doi: 10.1200/JCO.2016.68.2856).
While the majority of patients with CLL are covered by Medicare in the United States, they still currently pay $9,200 in out-of-pocket costs for oral agents. This figure is forecast to increase to $57,000 for those who start treatment in 2016 due to the increased costs of oral targeted therapeutics.
“Such an economic impact could result in financial toxicity, limited access, and lower adherence to the oral therapies, which may undermine their clinical effectiveness,” Qiushi Chen, from the Georgia Institute of Technology, Atlanta, and his coauthors wrote. They called for a more sustainable pricing strategy for oral targeted therapies, rather than have clinicians be forced to choose less effective but more affordable management strategies.
The researchers developed a microsimulation model of CLL, simulating the dynamics of the patient population under given management strategies from 2011-2025.
Around 130,000 patients live with CLL in the United States and around 15,000 new cases are diagnosed each year. By 2025, the authors forecast that 199,000 people will be living with the disease; a 55% increase that is both the result of new diagnoses and of improved survival with new oral targeted therapies.
Chemoimmunotherapy regimens – such as fludarabine, cyclophosphamide, and rituximab – have long been the standard first-line approach to CLL. But in recent years, new oral targeted agents such as ibrutinib and idelalisib have significantly improved progression-free survival and overall survival in CLL.
Ibrutinib is approved for first-line management of CLL, idelalisib is approved in combination with rituximab for patients with relapsed/refractory chronic lymphocytic leukemia, and venetoclax is approved for patients with relapsed chronic lymphocytic leukemia with del(17p).
“Both ibrutinib and idelalisib are priced at approximately $130,000 per [CLL patient per] year and are recommended until patients have progressive disease or significant toxicities,” the authors wrote. “In contrast, the costs for chemoimmunotherapy-based treatments range from $60,000 to $100,000 for a finite duration, that is, a typical six-cycle course that lasts for approximately 6 months.”
The higher costs will add up to additional annual spending of $29 billion to 2025, compared with around $1.12 billion annually for chemoimmunotherapy alone.
“Compared with the CIT scenario, the oral targeted therapy scenario resulted in an increase of 107,000 person–quality-adjusted life-years (149,000 person–life years), with additional discounted costs of $20.2 billion,” the authors reported.
The annual cost of cancer care in the United States is increasing across the board, from $143 billion in 2010 to $180 billion in 2020, but the cost of care for CLL is increasing more significantly than for other cancers. For example, breast and prostate cancers are forecast to have a 24%-38% increase in annual cost by 2020, while CLL is predicted to increase by 500%.
Seven authors declared research funding, honoraria and consultancy funding from a range of pharmaceutical companies including those involved in the manufacture of therapies for chronic lymphocytic leukemia. Two authors had no conflicts to declare.
The lifetime cost of treating chronic lymphocytic leukemia is forecast to rise precipitously for patients diagnosed today, as oral targeted therapies take over as the first-line treatment option, according to a study published November 21 in the Journal of Clinical Oncology.
The conclusion is based on economic models that also indicated the annual cost in the United States of managing chronic lymphocytic leukemia (CLL) will increase from its current level of $0.74 billion to $5.13 billion by 2025 (J Clin Oncol. 2016 Nov 21. doi: 10.1200/JCO.2016.68.2856).
While the majority of patients with CLL are covered by Medicare in the United States, they still currently pay $9,200 in out-of-pocket costs for oral agents. This figure is forecast to increase to $57,000 for those who start treatment in 2016 due to the increased costs of oral targeted therapeutics.
“Such an economic impact could result in financial toxicity, limited access, and lower adherence to the oral therapies, which may undermine their clinical effectiveness,” Qiushi Chen, from the Georgia Institute of Technology, Atlanta, and his coauthors wrote. They called for a more sustainable pricing strategy for oral targeted therapies, rather than have clinicians be forced to choose less effective but more affordable management strategies.
The researchers developed a microsimulation model of CLL, simulating the dynamics of the patient population under given management strategies from 2011-2025.
Around 130,000 patients live with CLL in the United States and around 15,000 new cases are diagnosed each year. By 2025, the authors forecast that 199,000 people will be living with the disease; a 55% increase that is both the result of new diagnoses and of improved survival with new oral targeted therapies.
Chemoimmunotherapy regimens – such as fludarabine, cyclophosphamide, and rituximab – have long been the standard first-line approach to CLL. But in recent years, new oral targeted agents such as ibrutinib and idelalisib have significantly improved progression-free survival and overall survival in CLL.
Ibrutinib is approved for first-line management of CLL, idelalisib is approved in combination with rituximab for patients with relapsed/refractory chronic lymphocytic leukemia, and venetoclax is approved for patients with relapsed chronic lymphocytic leukemia with del(17p).
“Both ibrutinib and idelalisib are priced at approximately $130,000 per [CLL patient per] year and are recommended until patients have progressive disease or significant toxicities,” the authors wrote. “In contrast, the costs for chemoimmunotherapy-based treatments range from $60,000 to $100,000 for a finite duration, that is, a typical six-cycle course that lasts for approximately 6 months.”
The higher costs will add up to additional annual spending of $29 billion to 2025, compared with around $1.12 billion annually for chemoimmunotherapy alone.
“Compared with the CIT scenario, the oral targeted therapy scenario resulted in an increase of 107,000 person–quality-adjusted life-years (149,000 person–life years), with additional discounted costs of $20.2 billion,” the authors reported.
The annual cost of cancer care in the United States is increasing across the board, from $143 billion in 2010 to $180 billion in 2020, but the cost of care for CLL is increasing more significantly than for other cancers. For example, breast and prostate cancers are forecast to have a 24%-38% increase in annual cost by 2020, while CLL is predicted to increase by 500%.
Seven authors declared research funding, honoraria and consultancy funding from a range of pharmaceutical companies including those involved in the manufacture of therapies for chronic lymphocytic leukemia. Two authors had no conflicts to declare.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: The high cost of oral therapies for chronic lymphocytic leukemia could result in financial toxicity, limited access, and lower adherence, which may undermine their clinical effectiveness.
Major finding: The cost of treating chronic lymphocytic leukemia is forecast to increase from its current level of $0.74 billion to $5.13 billion by 2025.
Data source: Microsimulation model of chronic lymphocytic leukemia treatment from 2010-2025.
Disclosures: Seven authors declared research funding, honoraria, and consultancy funding from a range of pharmaceutical companies including those involved in the manufacture of therapies for chronic lymphocytic leukemia. Two authors had no conflicts to declare.
Minimal residual disease status predicts 10-year survival in CLL
Patients who have chronic lymphocytic leukemia and achieve minimal residual disease negativity have a high probability of long-term progression-free and overall survival, irrespective of the type of therapy they receive, reported Marwan Kwok, MD, of Queen Elizabeth Hospital Birmingham (England) and colleagues.
Minimal residual disease (MRD) negativity, defined as less than 1 chronic lymphocytic leukemic (CLL) cell detectable per 10,000 leukocytes, has been shown to independently predict clinical outcome in the front line setting, but the long-term prognostic value of MRD status in other therapeutic settings remains unclear. “Our results demonstrate the long-term benefit of achieving MRD negativity regardless of the therapeutic setting and treatment modality, and support its use as a prognostic marker for long-term PFS (progression-free survival) and as a potential therapeutic goal in CLL,” the authors wrote (Blood. 2016 Oct 3. doi: 10.1182/blood-2016-05-714162).
The researchers retrospectively analyzed, with up to 18 years of follow-up, all 133 CLL patients at St. James’s University Hospital in Leeds, England, who achieved at least a partial response with various therapies between 1996 and 2007 and who received a bone marrow MRD assessment at the end of treatment, according to the international harmonized approach.
MRD negativity correlated with progression-free and overall survival, and the association was independent of the type and line of treatment, as well as adverse cytogenetic findings, the investigators said.
For those who achieved MRD negativity in front-line treatment, the 10-year progression-free survival was 65%; survival in patients who did not achieve MRD negativity was 10%. Overall survival at 10 years was 70% for those who achieved MRD negativity and 30% for MRD-positive patients.
The authors had no relevant financial disclosures.
Patients who have chronic lymphocytic leukemia and achieve minimal residual disease negativity have a high probability of long-term progression-free and overall survival, irrespective of the type of therapy they receive, reported Marwan Kwok, MD, of Queen Elizabeth Hospital Birmingham (England) and colleagues.
Minimal residual disease (MRD) negativity, defined as less than 1 chronic lymphocytic leukemic (CLL) cell detectable per 10,000 leukocytes, has been shown to independently predict clinical outcome in the front line setting, but the long-term prognostic value of MRD status in other therapeutic settings remains unclear. “Our results demonstrate the long-term benefit of achieving MRD negativity regardless of the therapeutic setting and treatment modality, and support its use as a prognostic marker for long-term PFS (progression-free survival) and as a potential therapeutic goal in CLL,” the authors wrote (Blood. 2016 Oct 3. doi: 10.1182/blood-2016-05-714162).
The researchers retrospectively analyzed, with up to 18 years of follow-up, all 133 CLL patients at St. James’s University Hospital in Leeds, England, who achieved at least a partial response with various therapies between 1996 and 2007 and who received a bone marrow MRD assessment at the end of treatment, according to the international harmonized approach.
MRD negativity correlated with progression-free and overall survival, and the association was independent of the type and line of treatment, as well as adverse cytogenetic findings, the investigators said.
For those who achieved MRD negativity in front-line treatment, the 10-year progression-free survival was 65%; survival in patients who did not achieve MRD negativity was 10%. Overall survival at 10 years was 70% for those who achieved MRD negativity and 30% for MRD-positive patients.
The authors had no relevant financial disclosures.
Patients who have chronic lymphocytic leukemia and achieve minimal residual disease negativity have a high probability of long-term progression-free and overall survival, irrespective of the type of therapy they receive, reported Marwan Kwok, MD, of Queen Elizabeth Hospital Birmingham (England) and colleagues.
Minimal residual disease (MRD) negativity, defined as less than 1 chronic lymphocytic leukemic (CLL) cell detectable per 10,000 leukocytes, has been shown to independently predict clinical outcome in the front line setting, but the long-term prognostic value of MRD status in other therapeutic settings remains unclear. “Our results demonstrate the long-term benefit of achieving MRD negativity regardless of the therapeutic setting and treatment modality, and support its use as a prognostic marker for long-term PFS (progression-free survival) and as a potential therapeutic goal in CLL,” the authors wrote (Blood. 2016 Oct 3. doi: 10.1182/blood-2016-05-714162).
The researchers retrospectively analyzed, with up to 18 years of follow-up, all 133 CLL patients at St. James’s University Hospital in Leeds, England, who achieved at least a partial response with various therapies between 1996 and 2007 and who received a bone marrow MRD assessment at the end of treatment, according to the international harmonized approach.
MRD negativity correlated with progression-free and overall survival, and the association was independent of the type and line of treatment, as well as adverse cytogenetic findings, the investigators said.
For those who achieved MRD negativity in front-line treatment, the 10-year progression-free survival was 65%; survival in patients who did not achieve MRD negativity was 10%. Overall survival at 10 years was 70% for those who achieved MRD negativity and 30% for MRD-positive patients.
The authors had no relevant financial disclosures.
FROM BLOOD
Key clinical point:
Major finding: Overall survival at 10 years was 70% for those who achieved MRD negativity and 30% for those who did not.
Data source: Retrospective, single-center study of 133 patients with chronic lymphocytic leukemia.
Disclosures: The authors had no relevant financial disclosures.
CD49d trumps novel recurrent mutations for predicting overall survival in CLL
CD49d was a strong predictor of overall survival in a cohort of 778 unselected patients with chronic lymphocytic leukemia, reported Michele Dal Bo, MD, of Centro di Riferimento Oncologico, in Aviano, Italy, and colleagues.

High CD49d expression was an independent predictor of poor overall survival in a multivariate Cox analysis (hazard ratio = 1.88, P less than .0001) and in each category of a risk stratification model. Among other biological prognosticators, CD49d was among the top predictors of overall survival (variable importance = 0.0410) along with immunoglobulin heavy chain variable (IGHV) gene mutational status and TP53 abnormalities. “In this context, TP53 disruption and NOTCH1 mutations retained prognostic relevance, in keeping with their roles in CLL cell immuno-chemoresistance,” the authors wrote.
CD49d was a strong predictor of overall survival in a cohort of 778 unselected patients with chronic lymphocytic leukemia, reported Michele Dal Bo, MD, of Centro di Riferimento Oncologico, in Aviano, Italy, and colleagues.
High CD49d expression was an independent predictor of poor overall survival in a multivariate Cox analysis (hazard ratio = 1.88, P less than .0001) and in each category of a risk stratification model. Among other biological prognosticators, CD49d was among the top predictors of overall survival (variable importance = 0.0410) along with immunoglobulin heavy chain variable (IGHV) gene mutational status and TP53 abnormalities. “In this context, TP53 disruption and NOTCH1 mutations retained prognostic relevance, in keeping with their roles in CLL cell immuno-chemoresistance,” the authors wrote.
CD49d was a strong predictor of overall survival in a cohort of 778 unselected patients with chronic lymphocytic leukemia, reported Michele Dal Bo, MD, of Centro di Riferimento Oncologico, in Aviano, Italy, and colleagues.
High CD49d expression was an independent predictor of poor overall survival in a multivariate Cox analysis (hazard ratio = 1.88, P less than .0001) and in each category of a risk stratification model. Among other biological prognosticators, CD49d was among the top predictors of overall survival (variable importance = 0.0410) along with immunoglobulin heavy chain variable (IGHV) gene mutational status and TP53 abnormalities. “In this context, TP53 disruption and NOTCH1 mutations retained prognostic relevance, in keeping with their roles in CLL cell immuno-chemoresistance,” the authors wrote.
Survival in CLL predicted by minimum residual disease
The presence or absence of minimal residual disease predicted progression-free and, to a lesser degree, overall survival among chronic lymphocytic leukemia (CLL) patients who achieved complete or partial remission with six courses of chemoimmunotherapy, based on two randomized phase III trials.
These findings underscore the value of measuring minimal residual disease (MRD) in patients who respond to a defined period of CLL therapy, Dr. Gabor Kovacs of the University of Cologne (Germany) and his associates wrote Aug. 29 in the Journal of Clinical Oncology.
The investigators examined the predictive value of measuring MRD in peripheral blood by using four-color flow cytometry at a threshold of 10-4 by analyzing data from 554 adult CLL patients who achieved complete or partial remission during two phase III trials – one (CLL8) comparing fludarabine and cyclophosphamide with fludarabine, cyclophosphamide, and rituximab (FCR) and a second (CLL10) comparing FCR with bendamustine plus rituximab (J Clin Oncol. 2016 Aug 29. doi:10.1200/JCO.2016.67.1305).
The median progression-free survival (PFS) after the end of treatment was 61 months for the 34% (186 patients) who attained MRD-negative complete remission (CR), 54 months for the 29% of patients who attained MRD-negative partial remission (PR), 35 months for the 7% of patients who attained MRD-positive CR, and 21 months for the 30% of patients who attained MRD-positive PR. Progression-free survival did not differ significantly between MRD-negative CR and MRD-negative PR patients, but was significantly longer for MRD-negative PR patients than for MRD-positive CR patients (P = .048).
Progression-free survival was even more distinct for MRD-positive CR patients, compared with those who attained MRD-positive PR (P = .002). Overall survival was significantly shorter only when patients had MRD-positive PR rather than MRD-negative CR (72 months vs. not reached, P = .001).
Among the MRD-negative PR patients, 16% had only residual lymphadenopathy, 11% had only bone marrow involvement, 48% had only splenomegaly, and 25% had more than one organ system affected, the researchers noted. Importantly, PFS for MRD-negative PR with residual splenomegaly (63 months) was similar to that for MRD-negative CR (61 months, P = .354).
In contrast, patients with MRD-negative PR and residual lymphadenopathy had shorter PFS than did MRD-negative CR patients (31 months, P = .001). “We hypothesize that residual splenomegaly after chemoimmunotherapy often represents tissue that does not contribute to a subsequent clinical progression,” the researchers commented.
They also noted an important caveat – their findings are only valid for patients who received a defined period of CLL treatment followed by observation (without maintenance), not for patients who are treated indefinitely until progression.
The CLL8 and CLL10 trials were funded by Roche, Mundipharma, and the German Federal Ministry of Education and Research. Dr. Kavocs disclosed support for travel, accommodations, and expenses from Roche and Celgene.
The report by Kovacs et al. is important because it further establishes minimal residual disease–free status as a meaningful clinical endpoint. Today, MRD-free remission as a treatment endpoint is most relevant for clinical trials as a means to demonstrate improved outcomes; MRD status is not yet a standard of care for patients with chronic lymphocytic leukemia. Data such as that reported by Kovacs et al. confirm the correlation of MRD-free status at the end of treatment with time-to-event endpoints (progression-free survival and overall survival), which require years of follow-up.

|
Dr. William G. Wierda |
MRD status as a surrogate endpoint may allow for earlier determination of more effective therapy and, in work by the German CLL Study Group, was used to model PFS hazard ratios in randomized trials. The role of MRD status in maintained remission, such as with small-molecule inhibitors, will likely be to identify opportunities for treatment-free intervals. In addition, it will certainly be a useful tool in developing curative strategies, such as in pediatric acute lymphocytic leukemia; it is unlikely that cure will be possible without an MRD-negative remission in CLL. MRD status is an important and meaningful clinical endpoint that will likely guide future clinical trials and developments for patients with CLL.
Dr. William G. Wierda is at the University of Texas MD Anderson Cancer Center, Houston. He disclosed ties to Sanofi, Genentech, Pharmacyclics, Celgene, Gilead Sciences, Novartis, Abbvie, and several other companies. These comments are from his editorial (J Clin Oncol. 2016 Aug 29. doi:10.1200/JCO.2016.69.1972).
The report by Kovacs et al. is important because it further establishes minimal residual disease–free status as a meaningful clinical endpoint. Today, MRD-free remission as a treatment endpoint is most relevant for clinical trials as a means to demonstrate improved outcomes; MRD status is not yet a standard of care for patients with chronic lymphocytic leukemia. Data such as that reported by Kovacs et al. confirm the correlation of MRD-free status at the end of treatment with time-to-event endpoints (progression-free survival and overall survival), which require years of follow-up.
|
|
Dr. William G. Wierda |
MRD status as a surrogate endpoint may allow for earlier determination of more effective therapy and, in work by the German CLL Study Group, was used to model PFS hazard ratios in randomized trials. The role of MRD status in maintained remission, such as with small-molecule inhibitors, will likely be to identify opportunities for treatment-free intervals. In addition, it will certainly be a useful tool in developing curative strategies, such as in pediatric acute lymphocytic leukemia; it is unlikely that cure will be possible without an MRD-negative remission in CLL. MRD status is an important and meaningful clinical endpoint that will likely guide future clinical trials and developments for patients with CLL.
Dr. William G. Wierda is at the University of Texas MD Anderson Cancer Center, Houston. He disclosed ties to Sanofi, Genentech, Pharmacyclics, Celgene, Gilead Sciences, Novartis, Abbvie, and several other companies. These comments are from his editorial (J Clin Oncol. 2016 Aug 29. doi:10.1200/JCO.2016.69.1972).
The report by Kovacs et al. is important because it further establishes minimal residual disease–free status as a meaningful clinical endpoint. Today, MRD-free remission as a treatment endpoint is most relevant for clinical trials as a means to demonstrate improved outcomes; MRD status is not yet a standard of care for patients with chronic lymphocytic leukemia. Data such as that reported by Kovacs et al. confirm the correlation of MRD-free status at the end of treatment with time-to-event endpoints (progression-free survival and overall survival), which require years of follow-up.
|
|
Dr. William G. Wierda |
MRD status as a surrogate endpoint may allow for earlier determination of more effective therapy and, in work by the German CLL Study Group, was used to model PFS hazard ratios in randomized trials. The role of MRD status in maintained remission, such as with small-molecule inhibitors, will likely be to identify opportunities for treatment-free intervals. In addition, it will certainly be a useful tool in developing curative strategies, such as in pediatric acute lymphocytic leukemia; it is unlikely that cure will be possible without an MRD-negative remission in CLL. MRD status is an important and meaningful clinical endpoint that will likely guide future clinical trials and developments for patients with CLL.
Dr. William G. Wierda is at the University of Texas MD Anderson Cancer Center, Houston. He disclosed ties to Sanofi, Genentech, Pharmacyclics, Celgene, Gilead Sciences, Novartis, Abbvie, and several other companies. These comments are from his editorial (J Clin Oncol. 2016 Aug 29. doi:10.1200/JCO.2016.69.1972).
The presence or absence of minimal residual disease predicted progression-free and, to a lesser degree, overall survival among chronic lymphocytic leukemia (CLL) patients who achieved complete or partial remission with six courses of chemoimmunotherapy, based on two randomized phase III trials.
These findings underscore the value of measuring minimal residual disease (MRD) in patients who respond to a defined period of CLL therapy, Dr. Gabor Kovacs of the University of Cologne (Germany) and his associates wrote Aug. 29 in the Journal of Clinical Oncology.
The investigators examined the predictive value of measuring MRD in peripheral blood by using four-color flow cytometry at a threshold of 10-4 by analyzing data from 554 adult CLL patients who achieved complete or partial remission during two phase III trials – one (CLL8) comparing fludarabine and cyclophosphamide with fludarabine, cyclophosphamide, and rituximab (FCR) and a second (CLL10) comparing FCR with bendamustine plus rituximab (J Clin Oncol. 2016 Aug 29. doi:10.1200/JCO.2016.67.1305).
The median progression-free survival (PFS) after the end of treatment was 61 months for the 34% (186 patients) who attained MRD-negative complete remission (CR), 54 months for the 29% of patients who attained MRD-negative partial remission (PR), 35 months for the 7% of patients who attained MRD-positive CR, and 21 months for the 30% of patients who attained MRD-positive PR. Progression-free survival did not differ significantly between MRD-negative CR and MRD-negative PR patients, but was significantly longer for MRD-negative PR patients than for MRD-positive CR patients (P = .048).
Progression-free survival was even more distinct for MRD-positive CR patients, compared with those who attained MRD-positive PR (P = .002). Overall survival was significantly shorter only when patients had MRD-positive PR rather than MRD-negative CR (72 months vs. not reached, P = .001).
Among the MRD-negative PR patients, 16% had only residual lymphadenopathy, 11% had only bone marrow involvement, 48% had only splenomegaly, and 25% had more than one organ system affected, the researchers noted. Importantly, PFS for MRD-negative PR with residual splenomegaly (63 months) was similar to that for MRD-negative CR (61 months, P = .354).
In contrast, patients with MRD-negative PR and residual lymphadenopathy had shorter PFS than did MRD-negative CR patients (31 months, P = .001). “We hypothesize that residual splenomegaly after chemoimmunotherapy often represents tissue that does not contribute to a subsequent clinical progression,” the researchers commented.
They also noted an important caveat – their findings are only valid for patients who received a defined period of CLL treatment followed by observation (without maintenance), not for patients who are treated indefinitely until progression.
The CLL8 and CLL10 trials were funded by Roche, Mundipharma, and the German Federal Ministry of Education and Research. Dr. Kavocs disclosed support for travel, accommodations, and expenses from Roche and Celgene.
The presence or absence of minimal residual disease predicted progression-free and, to a lesser degree, overall survival among chronic lymphocytic leukemia (CLL) patients who achieved complete or partial remission with six courses of chemoimmunotherapy, based on two randomized phase III trials.
These findings underscore the value of measuring minimal residual disease (MRD) in patients who respond to a defined period of CLL therapy, Dr. Gabor Kovacs of the University of Cologne (Germany) and his associates wrote Aug. 29 in the Journal of Clinical Oncology.
The investigators examined the predictive value of measuring MRD in peripheral blood by using four-color flow cytometry at a threshold of 10-4 by analyzing data from 554 adult CLL patients who achieved complete or partial remission during two phase III trials – one (CLL8) comparing fludarabine and cyclophosphamide with fludarabine, cyclophosphamide, and rituximab (FCR) and a second (CLL10) comparing FCR with bendamustine plus rituximab (J Clin Oncol. 2016 Aug 29. doi:10.1200/JCO.2016.67.1305).
The median progression-free survival (PFS) after the end of treatment was 61 months for the 34% (186 patients) who attained MRD-negative complete remission (CR), 54 months for the 29% of patients who attained MRD-negative partial remission (PR), 35 months for the 7% of patients who attained MRD-positive CR, and 21 months for the 30% of patients who attained MRD-positive PR. Progression-free survival did not differ significantly between MRD-negative CR and MRD-negative PR patients, but was significantly longer for MRD-negative PR patients than for MRD-positive CR patients (P = .048).
Progression-free survival was even more distinct for MRD-positive CR patients, compared with those who attained MRD-positive PR (P = .002). Overall survival was significantly shorter only when patients had MRD-positive PR rather than MRD-negative CR (72 months vs. not reached, P = .001).
Among the MRD-negative PR patients, 16% had only residual lymphadenopathy, 11% had only bone marrow involvement, 48% had only splenomegaly, and 25% had more than one organ system affected, the researchers noted. Importantly, PFS for MRD-negative PR with residual splenomegaly (63 months) was similar to that for MRD-negative CR (61 months, P = .354).
In contrast, patients with MRD-negative PR and residual lymphadenopathy had shorter PFS than did MRD-negative CR patients (31 months, P = .001). “We hypothesize that residual splenomegaly after chemoimmunotherapy often represents tissue that does not contribute to a subsequent clinical progression,” the researchers commented.
They also noted an important caveat – their findings are only valid for patients who received a defined period of CLL treatment followed by observation (without maintenance), not for patients who are treated indefinitely until progression.
The CLL8 and CLL10 trials were funded by Roche, Mundipharma, and the German Federal Ministry of Education and Research. Dr. Kavocs disclosed support for travel, accommodations, and expenses from Roche and Celgene.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Quantifying minimum residual disease significantly improved the accuracy of progression-free survival estimates in patients with chronic lymphocytic leukemia who achieved complete or partial remission after a defined period of chemoimmunotherapy.
Major finding: Progression-free survival was significantly longer for MRD-negative partially remitted patients, compared with MRD-positive completely remitted patients (P = .048), and was even more distinct for MRD-positive completely remitted patients, compared with MRD-positive partially remitted patients (P = .002).
Data source: An analysis of 554 patients achieving complete or partial remission during two randomized phase III trials (CLL8 and CLL10).Disclosures: The CLL8 and CLL10 trials were funded by Roche, Mundipharma, and the German Ministry of Education and Research. Dr. Kavocs disclosed support for travel, accommodations, and expenses from Roche and Celgene.

CLL: Genetic aberrations predict poor treatment response in elderly
In elderly patients with chronic lymphocytic leukemia, complex karyotype abnormalities, certain KRAS and POT1 mutations, and newly discovered mutations in genes involved in the DNA damage response were found to predict a poor response to chlorambucil-based chemotherapy or chemoimmunotherapy and poor survival, according to a report in Blood.
These findings are from what the investigators described as the first comprehensive prospective analysis of chromosomal aberrations (including complex karyotype abnormalities), gene mutations, and clinical and biological features in elderly CLL patients who had multiple comorbidities. This patient population is generally considered ineligible for aggressive first-line agents such as fludarabine and cyclophosphamide, said Carmen Diana Herling, MD, of the Laboratory of Functional Genomics in Lymphoid Malignancies, University of Cologne (Germany), and her associates.
For their analysis, investigators studied 161 such patients enrolled in a clinical trial in which all were treated with chlorambucil alone, chlorambucil plus obinutuzumab, or chlorambucil plus rituximab. The median patient age was 75 years. Comprehensive genetic analyses were performed using peripheral blood drawn before the patients underwent treatment.
Karyotyping detected chromosomal aberrations in 68.68% of patients, while 31.2% carried translocations and 19.5% showed complex karyotypes. Gene sequencing detected 198 missense/nonsense mutations and other abnormalities in 76.4% of patients.
Dr. Herling and her associates found that complex karyotype abnormalities independently predicted poor response to chlorambucil and poor survival. “Thus, global karyotyping (i.e., by chromosome banding analysis) seems to substantially contribute to the identification of CLL patients with most adverse prognoses and should be considered a standard assessment in future CLL trials,” they said (Blood. 2016;128:395-404).
In addition, KRAS mutations correlated with a poor treatment response, particularly to rituximab. Targeting such patients for MEK, BRAF, or ERK inhibitors “might offer personalized treatment strategies to be investigated in such cases.”
Mutations in the POT1 gene also correlated with shorter survival after chlorambucil treatment. And finally, poor treatment response also correlated with previously unknown mutations in genes involved with the response to DNA damage. This “might contribute to the accumulation of genomic alterations and clonal evolution of CLL,” Dr. Herling and her associates said.
In elderly patients with chronic lymphocytic leukemia, complex karyotype abnormalities, certain KRAS and POT1 mutations, and newly discovered mutations in genes involved in the DNA damage response were found to predict a poor response to chlorambucil-based chemotherapy or chemoimmunotherapy and poor survival, according to a report in Blood.
These findings are from what the investigators described as the first comprehensive prospective analysis of chromosomal aberrations (including complex karyotype abnormalities), gene mutations, and clinical and biological features in elderly CLL patients who had multiple comorbidities. This patient population is generally considered ineligible for aggressive first-line agents such as fludarabine and cyclophosphamide, said Carmen Diana Herling, MD, of the Laboratory of Functional Genomics in Lymphoid Malignancies, University of Cologne (Germany), and her associates.
For their analysis, investigators studied 161 such patients enrolled in a clinical trial in which all were treated with chlorambucil alone, chlorambucil plus obinutuzumab, or chlorambucil plus rituximab. The median patient age was 75 years. Comprehensive genetic analyses were performed using peripheral blood drawn before the patients underwent treatment.
Karyotyping detected chromosomal aberrations in 68.68% of patients, while 31.2% carried translocations and 19.5% showed complex karyotypes. Gene sequencing detected 198 missense/nonsense mutations and other abnormalities in 76.4% of patients.
Dr. Herling and her associates found that complex karyotype abnormalities independently predicted poor response to chlorambucil and poor survival. “Thus, global karyotyping (i.e., by chromosome banding analysis) seems to substantially contribute to the identification of CLL patients with most adverse prognoses and should be considered a standard assessment in future CLL trials,” they said (Blood. 2016;128:395-404).
In addition, KRAS mutations correlated with a poor treatment response, particularly to rituximab. Targeting such patients for MEK, BRAF, or ERK inhibitors “might offer personalized treatment strategies to be investigated in such cases.”
Mutations in the POT1 gene also correlated with shorter survival after chlorambucil treatment. And finally, poor treatment response also correlated with previously unknown mutations in genes involved with the response to DNA damage. This “might contribute to the accumulation of genomic alterations and clonal evolution of CLL,” Dr. Herling and her associates said.
In elderly patients with chronic lymphocytic leukemia, complex karyotype abnormalities, certain KRAS and POT1 mutations, and newly discovered mutations in genes involved in the DNA damage response were found to predict a poor response to chlorambucil-based chemotherapy or chemoimmunotherapy and poor survival, according to a report in Blood.
These findings are from what the investigators described as the first comprehensive prospective analysis of chromosomal aberrations (including complex karyotype abnormalities), gene mutations, and clinical and biological features in elderly CLL patients who had multiple comorbidities. This patient population is generally considered ineligible for aggressive first-line agents such as fludarabine and cyclophosphamide, said Carmen Diana Herling, MD, of the Laboratory of Functional Genomics in Lymphoid Malignancies, University of Cologne (Germany), and her associates.
For their analysis, investigators studied 161 such patients enrolled in a clinical trial in which all were treated with chlorambucil alone, chlorambucil plus obinutuzumab, or chlorambucil plus rituximab. The median patient age was 75 years. Comprehensive genetic analyses were performed using peripheral blood drawn before the patients underwent treatment.
Karyotyping detected chromosomal aberrations in 68.68% of patients, while 31.2% carried translocations and 19.5% showed complex karyotypes. Gene sequencing detected 198 missense/nonsense mutations and other abnormalities in 76.4% of patients.
Dr. Herling and her associates found that complex karyotype abnormalities independently predicted poor response to chlorambucil and poor survival. “Thus, global karyotyping (i.e., by chromosome banding analysis) seems to substantially contribute to the identification of CLL patients with most adverse prognoses and should be considered a standard assessment in future CLL trials,” they said (Blood. 2016;128:395-404).
In addition, KRAS mutations correlated with a poor treatment response, particularly to rituximab. Targeting such patients for MEK, BRAF, or ERK inhibitors “might offer personalized treatment strategies to be investigated in such cases.”
Mutations in the POT1 gene also correlated with shorter survival after chlorambucil treatment. And finally, poor treatment response also correlated with previously unknown mutations in genes involved with the response to DNA damage. This “might contribute to the accumulation of genomic alterations and clonal evolution of CLL,” Dr. Herling and her associates said.
FROM BLOOD
Key clinical point: In elderly patients who have chronic lymphocytic leukemia and comorbidities, several genetic abnormalities predict a poor response to chlorambucil-based chemotherapy or chemoimmunotherapy.
Major finding: Complex karyotype abnormalities independently predicted poor response to chlorambucil and poor survival.
Data source: A series of karyotyping and other genetic studies involving 161 elderly patients with CLL and multiple comorbidities.
Disclosures: The participants in this study were drawn from a clinical trial funded by Hoffmann–La Roche; this analysis was supported by Volkswagenstiftung and grants from Deutsche Forschungsgemeinschaft, Deutsche Jose Carreras Leukamie Foundation, Helmholtz-Gemeinschaft, Else Kroner–Fresenius Foundation, and Deutsche Krebshilfe. Dr. Herling reported having no relevant financial disclosures; her associates reported ties to Hoffmann–La Roche.
CAR T-cell therapy eyed for CLL patients with residual disease
Four of eight patients with residual chronic lymphocytic leukemia (CLL) following initial chemotherapy had complete or partial responses to an outpatient therapy that used autologous T cells genetically targeted to the B cell–specific antigen CD19, Mark Blaine Geyer, MD, of Memorial Sloan Kettering Cancer Center, New York, reported at the annual meeting of the American Society of Clinical Oncology.
The therapy employing T cells genetically modified to express CD19-targeted 19-28z chimeric antigen receptors (CARs) was well tolerated but had limited observed efficacy, especially in patients with enlarged lymph nodes. The study goal was to find a safe dose of modified T cells for patients who have disease remaining after initial chemotherapy.
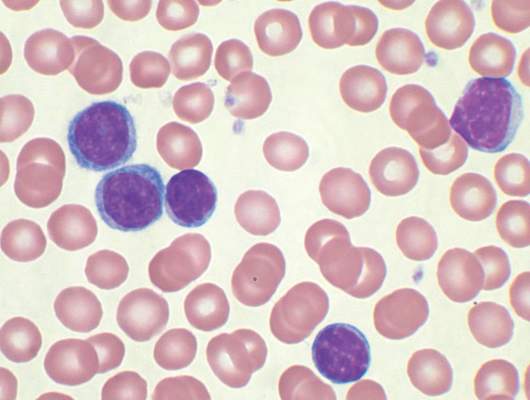
For the phase I dose escalation study (NCT01416974), Dr. Geyer and his associates enrolled eight CLL patients who had residual disease after upfront therapy consisting of six cycles of pentostatin, cyclophosphamide, and rituximab.
Five patients had clearly enlarged lymph nodes prior to T cell infusion.
Patients received cyclophosphamide 600 mg/m2 followed 2 days later by escalating doses of 19-28z T cells. Four of the five patients who received at least a 1 × 107 dose of 19-28z T cells/kg were admitted with fevers and mild cytokine release syndrome.
Maximal levels of CAR T cell persistence were detected at 8 weeks. With a median patient follow-up of 32 months, clinical complete response has been seen in two patients, partial response in two patients, and stable disease in one patient. Disease has progressed in three patients: one had a rising absolute lymphocyte count by the time of infusion and two had marrow response with progressive disease in lymph nodes. The median time to disease progression was 13.6 months, Dr. Geyer said.
Five of seven evaluable patients have received further CLL-directed therapy.
The researchers speculated that low-dose cyclophosphamide monotherapy, used before the CAR T-cell therapy, may be insufficient for lymphodepletion. Additionally, CAR T cell expansion and antitumor efficacy may be limited by a hostile CLL microenvironment. Strategies to enhance CAR T cell expansion and efficacy in patients with CLL are in preparation, Dr. Geyer reported.
Dr. Geyer had no financial disclosures. His colleagues reported various financial relationships with Juno Therapeutics, a developer of CAR technology.
On Twitter @maryjodales
Four of eight patients with residual chronic lymphocytic leukemia (CLL) following initial chemotherapy had complete or partial responses to an outpatient therapy that used autologous T cells genetically targeted to the B cell–specific antigen CD19, Mark Blaine Geyer, MD, of Memorial Sloan Kettering Cancer Center, New York, reported at the annual meeting of the American Society of Clinical Oncology.
The therapy employing T cells genetically modified to express CD19-targeted 19-28z chimeric antigen receptors (CARs) was well tolerated but had limited observed efficacy, especially in patients with enlarged lymph nodes. The study goal was to find a safe dose of modified T cells for patients who have disease remaining after initial chemotherapy.
For the phase I dose escalation study (NCT01416974), Dr. Geyer and his associates enrolled eight CLL patients who had residual disease after upfront therapy consisting of six cycles of pentostatin, cyclophosphamide, and rituximab.
Five patients had clearly enlarged lymph nodes prior to T cell infusion.
Patients received cyclophosphamide 600 mg/m2 followed 2 days later by escalating doses of 19-28z T cells. Four of the five patients who received at least a 1 × 107 dose of 19-28z T cells/kg were admitted with fevers and mild cytokine release syndrome.
Maximal levels of CAR T cell persistence were detected at 8 weeks. With a median patient follow-up of 32 months, clinical complete response has been seen in two patients, partial response in two patients, and stable disease in one patient. Disease has progressed in three patients: one had a rising absolute lymphocyte count by the time of infusion and two had marrow response with progressive disease in lymph nodes. The median time to disease progression was 13.6 months, Dr. Geyer said.
Five of seven evaluable patients have received further CLL-directed therapy.
The researchers speculated that low-dose cyclophosphamide monotherapy, used before the CAR T-cell therapy, may be insufficient for lymphodepletion. Additionally, CAR T cell expansion and antitumor efficacy may be limited by a hostile CLL microenvironment. Strategies to enhance CAR T cell expansion and efficacy in patients with CLL are in preparation, Dr. Geyer reported.
Dr. Geyer had no financial disclosures. His colleagues reported various financial relationships with Juno Therapeutics, a developer of CAR technology.
On Twitter @maryjodales
Four of eight patients with residual chronic lymphocytic leukemia (CLL) following initial chemotherapy had complete or partial responses to an outpatient therapy that used autologous T cells genetically targeted to the B cell–specific antigen CD19, Mark Blaine Geyer, MD, of Memorial Sloan Kettering Cancer Center, New York, reported at the annual meeting of the American Society of Clinical Oncology.
The therapy employing T cells genetically modified to express CD19-targeted 19-28z chimeric antigen receptors (CARs) was well tolerated but had limited observed efficacy, especially in patients with enlarged lymph nodes. The study goal was to find a safe dose of modified T cells for patients who have disease remaining after initial chemotherapy.
For the phase I dose escalation study (NCT01416974), Dr. Geyer and his associates enrolled eight CLL patients who had residual disease after upfront therapy consisting of six cycles of pentostatin, cyclophosphamide, and rituximab.
Five patients had clearly enlarged lymph nodes prior to T cell infusion.
Patients received cyclophosphamide 600 mg/m2 followed 2 days later by escalating doses of 19-28z T cells. Four of the five patients who received at least a 1 × 107 dose of 19-28z T cells/kg were admitted with fevers and mild cytokine release syndrome.
Maximal levels of CAR T cell persistence were detected at 8 weeks. With a median patient follow-up of 32 months, clinical complete response has been seen in two patients, partial response in two patients, and stable disease in one patient. Disease has progressed in three patients: one had a rising absolute lymphocyte count by the time of infusion and two had marrow response with progressive disease in lymph nodes. The median time to disease progression was 13.6 months, Dr. Geyer said.
Five of seven evaluable patients have received further CLL-directed therapy.
The researchers speculated that low-dose cyclophosphamide monotherapy, used before the CAR T-cell therapy, may be insufficient for lymphodepletion. Additionally, CAR T cell expansion and antitumor efficacy may be limited by a hostile CLL microenvironment. Strategies to enhance CAR T cell expansion and efficacy in patients with CLL are in preparation, Dr. Geyer reported.
Dr. Geyer had no financial disclosures. His colleagues reported various financial relationships with Juno Therapeutics, a developer of CAR technology.
On Twitter @maryjodales
FROM THE 2016 ASCO ANNUAL MEETING
Key clinical point: CAR T-cell therapy may be an option for chronic lymphocytic leukemia patients with residual disease after upfront therapy.
Major finding: Four of eight patients with residual CLL following initial chemotherapy had complete or partial responses to an outpatient therapy that used autologous T cells genetically targeted to the B cell–specific antigen CD19.
Data source: A phase I dose-finding and efficacy study in 8 patients with CLL.
Disclosures: Dr. Geyer had no financial disclosures. His colleagues reported various financial relationships with Juno Therapeutics, a developer of CAR technology.
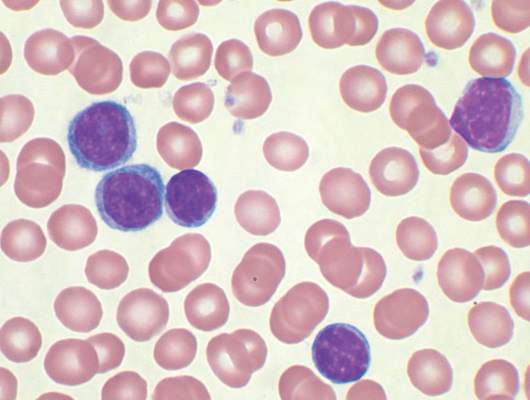
Three-drug regimen boosts progression-free survival in patients with relapsed CLL and adverse prognostic features
Progression-free survival was improved for poor prognosis patients with relapsed chronic lymphocytic leukemia when idelalisib was added to bendamustine and rituximab, based on the results of a randomized, double-blind, placebo-controlled phase III study.
The findings support the three-drug approach as an important treatment option for patients with relapsed CLL and adverse prognostic features, but the regimen also was associated with more grade 3 or greater adverse events, primarily neutropenia and opportunistic infections, that led to more study drug discontinuation, Jacqueline Claudia Barrientos, M.D., and her colleagues reported at the annual meeting of the American Society of Clinical Oncology.
The overall response rates were 68% in the three-drug group and 45% in the two-drug plus placebo group.
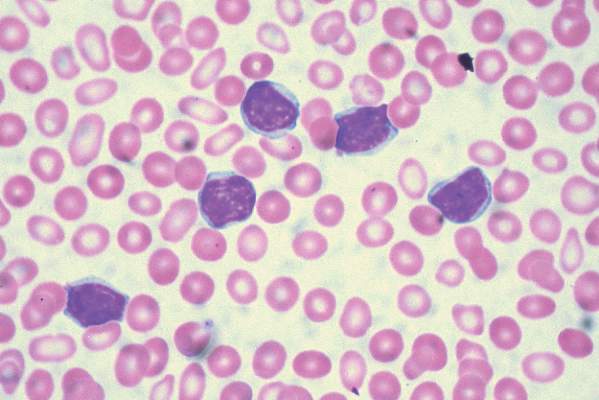
For the study, 416 patients were stratified based on whether they had 17p deletions or TP53 mutations, their IGHV mutation status, and whether they had refractory or relapsed disease. The 207 patients who received idelalisib, bendamustine, and rituximab had consistently better progression-free survival than the 209 patients who received placebo, bendamustine, and rituximab. The median progression-free survival was 23 months in the group that received idelalisib and 11 months in the group that received placebo, with an overall hazard ratio of 0.33 at a median follow-up of 12 months.
For those with 17p deletions or TP53 mutations, the median progression-free survival was 11 months with the three-drug regimen and 8 months for the two-drug plus placebo regimen. For those with neither of these abnormalities, progression-free survival was more than 24 months for patients given the three active drugs and 11 months for patients given two drugs plus placebo.
For those with the 11q deletion, median progression-free survival was 23 months with idelalisib, bendamustine, and rituximab and 9 months with placebo, bendamustine, and rituximab, said Dr. Barrientos of Hofstra University, Hempstead, N.Y.
For those with IGHV mutations, the median progression-free survival has not been reached in the idelalisib, bendamustine, and rituximab group and was 11 months in the placebo, bendamustine, and rituximab group.
Among patients with tumor burdens exceeding 5 cm, median progression-free survival was 23 months with idelalisib, bendamustine, and rituximab and about 10 months with placebo, bendamustine, and rituximab.
Grade 3 or greater adverse events affected 97% of patients given the three active drugs and 76% of patients given bendamustine and rituximab plus placebo. Adverse events resulted in drug dose reductions in 11% of those given the three active drugs and in 6% of those given bendamustine and rituximab plus placebo. The study drug was discontinued in 26% of those in the idelalisib, bendamustine, and rituximab group and in 13% of the placebo, bendamustine, and rituximab group. Death occurred in 10% of the study patients given idelalisib, bendamustine, and rituximab and in 7% of the patients given placebo, bendamustine, and rituximab.
To be eligible for the study (NCT01569295), patients needed to have previously treated recurrent CLL, have measurable lymphadenopathy, require therapy for CLL, and have experienced CLL progression for less than 36 months since the completion of their last prior therapy.
The treatment regimen consisted of 6 cycles every 28 days of bendamustine (70 mg/m2 on day 1 and day 2 of each cycle), rituximab (375 mg/m2 in cycle 1 and 500 mg/m2 in cycles 2-6), and idelalisib (150 mg twice daily) or placebo. Idelalisib or placebo was continued until an independent review committee confirmed disease progression, death, intolerable toxicity, or withdrawal of consent.
The study was sponsored by Gilead Sciences, the maker of idelalisib (Zydelig). Dr. Barrientos receives research funding from Gilead Sciences and Abbvie, and serves as a consultant or adviser to Celgene, Genentech, and Pharmacyclics.
On Twitter @maryjodales
Progression-free survival was improved for poor prognosis patients with relapsed chronic lymphocytic leukemia when idelalisib was added to bendamustine and rituximab, based on the results of a randomized, double-blind, placebo-controlled phase III study.
The findings support the three-drug approach as an important treatment option for patients with relapsed CLL and adverse prognostic features, but the regimen also was associated with more grade 3 or greater adverse events, primarily neutropenia and opportunistic infections, that led to more study drug discontinuation, Jacqueline Claudia Barrientos, M.D., and her colleagues reported at the annual meeting of the American Society of Clinical Oncology.
The overall response rates were 68% in the three-drug group and 45% in the two-drug plus placebo group.
For the study, 416 patients were stratified based on whether they had 17p deletions or TP53 mutations, their IGHV mutation status, and whether they had refractory or relapsed disease. The 207 patients who received idelalisib, bendamustine, and rituximab had consistently better progression-free survival than the 209 patients who received placebo, bendamustine, and rituximab. The median progression-free survival was 23 months in the group that received idelalisib and 11 months in the group that received placebo, with an overall hazard ratio of 0.33 at a median follow-up of 12 months.
For those with 17p deletions or TP53 mutations, the median progression-free survival was 11 months with the three-drug regimen and 8 months for the two-drug plus placebo regimen. For those with neither of these abnormalities, progression-free survival was more than 24 months for patients given the three active drugs and 11 months for patients given two drugs plus placebo.
For those with the 11q deletion, median progression-free survival was 23 months with idelalisib, bendamustine, and rituximab and 9 months with placebo, bendamustine, and rituximab, said Dr. Barrientos of Hofstra University, Hempstead, N.Y.
For those with IGHV mutations, the median progression-free survival has not been reached in the idelalisib, bendamustine, and rituximab group and was 11 months in the placebo, bendamustine, and rituximab group.
Among patients with tumor burdens exceeding 5 cm, median progression-free survival was 23 months with idelalisib, bendamustine, and rituximab and about 10 months with placebo, bendamustine, and rituximab.
Grade 3 or greater adverse events affected 97% of patients given the three active drugs and 76% of patients given bendamustine and rituximab plus placebo. Adverse events resulted in drug dose reductions in 11% of those given the three active drugs and in 6% of those given bendamustine and rituximab plus placebo. The study drug was discontinued in 26% of those in the idelalisib, bendamustine, and rituximab group and in 13% of the placebo, bendamustine, and rituximab group. Death occurred in 10% of the study patients given idelalisib, bendamustine, and rituximab and in 7% of the patients given placebo, bendamustine, and rituximab.
To be eligible for the study (NCT01569295), patients needed to have previously treated recurrent CLL, have measurable lymphadenopathy, require therapy for CLL, and have experienced CLL progression for less than 36 months since the completion of their last prior therapy.
The treatment regimen consisted of 6 cycles every 28 days of bendamustine (70 mg/m2 on day 1 and day 2 of each cycle), rituximab (375 mg/m2 in cycle 1 and 500 mg/m2 in cycles 2-6), and idelalisib (150 mg twice daily) or placebo. Idelalisib or placebo was continued until an independent review committee confirmed disease progression, death, intolerable toxicity, or withdrawal of consent.
The study was sponsored by Gilead Sciences, the maker of idelalisib (Zydelig). Dr. Barrientos receives research funding from Gilead Sciences and Abbvie, and serves as a consultant or adviser to Celgene, Genentech, and Pharmacyclics.
On Twitter @maryjodales
Progression-free survival was improved for poor prognosis patients with relapsed chronic lymphocytic leukemia when idelalisib was added to bendamustine and rituximab, based on the results of a randomized, double-blind, placebo-controlled phase III study.
The findings support the three-drug approach as an important treatment option for patients with relapsed CLL and adverse prognostic features, but the regimen also was associated with more grade 3 or greater adverse events, primarily neutropenia and opportunistic infections, that led to more study drug discontinuation, Jacqueline Claudia Barrientos, M.D., and her colleagues reported at the annual meeting of the American Society of Clinical Oncology.
The overall response rates were 68% in the three-drug group and 45% in the two-drug plus placebo group.
For the study, 416 patients were stratified based on whether they had 17p deletions or TP53 mutations, their IGHV mutation status, and whether they had refractory or relapsed disease. The 207 patients who received idelalisib, bendamustine, and rituximab had consistently better progression-free survival than the 209 patients who received placebo, bendamustine, and rituximab. The median progression-free survival was 23 months in the group that received idelalisib and 11 months in the group that received placebo, with an overall hazard ratio of 0.33 at a median follow-up of 12 months.
For those with 17p deletions or TP53 mutations, the median progression-free survival was 11 months with the three-drug regimen and 8 months for the two-drug plus placebo regimen. For those with neither of these abnormalities, progression-free survival was more than 24 months for patients given the three active drugs and 11 months for patients given two drugs plus placebo.
For those with the 11q deletion, median progression-free survival was 23 months with idelalisib, bendamustine, and rituximab and 9 months with placebo, bendamustine, and rituximab, said Dr. Barrientos of Hofstra University, Hempstead, N.Y.
For those with IGHV mutations, the median progression-free survival has not been reached in the idelalisib, bendamustine, and rituximab group and was 11 months in the placebo, bendamustine, and rituximab group.
Among patients with tumor burdens exceeding 5 cm, median progression-free survival was 23 months with idelalisib, bendamustine, and rituximab and about 10 months with placebo, bendamustine, and rituximab.
Grade 3 or greater adverse events affected 97% of patients given the three active drugs and 76% of patients given bendamustine and rituximab plus placebo. Adverse events resulted in drug dose reductions in 11% of those given the three active drugs and in 6% of those given bendamustine and rituximab plus placebo. The study drug was discontinued in 26% of those in the idelalisib, bendamustine, and rituximab group and in 13% of the placebo, bendamustine, and rituximab group. Death occurred in 10% of the study patients given idelalisib, bendamustine, and rituximab and in 7% of the patients given placebo, bendamustine, and rituximab.
To be eligible for the study (NCT01569295), patients needed to have previously treated recurrent CLL, have measurable lymphadenopathy, require therapy for CLL, and have experienced CLL progression for less than 36 months since the completion of their last prior therapy.
The treatment regimen consisted of 6 cycles every 28 days of bendamustine (70 mg/m2 on day 1 and day 2 of each cycle), rituximab (375 mg/m2 in cycle 1 and 500 mg/m2 in cycles 2-6), and idelalisib (150 mg twice daily) or placebo. Idelalisib or placebo was continued until an independent review committee confirmed disease progression, death, intolerable toxicity, or withdrawal of consent.
The study was sponsored by Gilead Sciences, the maker of idelalisib (Zydelig). Dr. Barrientos receives research funding from Gilead Sciences and Abbvie, and serves as a consultant or adviser to Celgene, Genentech, and Pharmacyclics.
On Twitter @maryjodales
FROM 2016 ASCO ANNUAL MEETING
Key clinical point: Progression-free survival was improved for poor prognosis patients with relapsed chronic lymphocytic leukemia when idelalisib was added to bendamustine, and rituximab.
Major finding: The median progression-free survival was 23 months in the group that received idelalisib and 11 months in the group that received placebo, with an overall hazard ratio of 0.33 at a median follow-up of 12 months.
Data source: A randomized, double-blind, placebo-controlled phase III study of 416 patients stratified on the basis of 17p deletions or TP53 mutations, IGHV mutation status, and whether they had refractory or relapsed disease.
Disclosures: The study was sponsored by Gilead Sciences, the maker of idelalisib (Zydelig). Dr. Barrientos receives research funding from Gilead Sciences and Abbvie, and serves as a consultant or adviser to Celgene, Genentech, and Pharmacyclics.