User login
Quality tool tied to improved adherence
CHICAGO – A multifaceted quality initiative that consists of staff education, patient reminders and a feedback loop may help to improve therapy adherence and encourage lifestyle changes of at-risk cardiovascular patients in settings with limited resources, according to results of a clinical trial from Brazil presented at the American Heart Association scientific sessions 2018.
“In patients at high cardiovascular risk – in this case patients with established cardiovascular disease – a multifaceted quality-improvement intervention resulted in significant improvement in the use of evidence-based therapies,” said Otavio Berwanger, MD, PhD, of the Heart Hospital in Sao Paolo. He reported results of the BRIDGE Cardiovascular Prevention Cluster Randomized Trial. “The tools used in our trial can become the basis for developing quality-improvement programs to maximize the use of evidence-based therapies for the management of these high-risk patients with, especially in limited-resource settings.”
BRIDGE-CV included 1,619 patients from 40 care settings. Institutions that adopted the multifaceted intervention adhered to 73.5% of the evidence-based therapies (antiplatelet agents, statins and ACE inhibitors) while those in the control group adhered to 58.7% of the performance measures, Dr. Berwanger said. That represents a gain of 25%. The study employed an “all-or-none” model. That is, participating sites were required to adopt all components of the quality-improvement initiative or none.

He noted that although the evidence supporting the use of platelet therapies, statins, and ACE inhibitors is strong, “translation of these findings in practice is clearly suboptimal.” He added, “It seems to be an even larger problem in settings like mine in Brazil, so quality-improvement interventions, especially in lower-resource settings such as low- and middle-income countries, are definitely needed.”
The quality-improvement model the trial evaluated involved two levels of intervention. The first level comprised three steps: a case manager evaluating the patient’s treatment needs with the aid of a checklist; then an evaluation by the physician; and then providing physicians with what Dr. Berwanger described as “a physician support tool” – a one-page summary of major guideline recommendations. The second level comprised monthly audit and feedback reports to the providers and patient education about lifestyle modification. Staff education and training was also provided to sites that adopted the model. “Our intervention was sort of based on behavioral marketing,” Dr. Berwanger said.
The trial also identified a number of trends among secondary endpoints, although the populations were too small to reach statistical significance. For example, Dr. Berwanger noted that intervention sites had higher use of high-dose statins and more than double the rate of smoking cessation. He also noted a 24% relative risk reduction in major cardiovascular events in the intervention group vs. controls. Among the intervention sites, teaching institutions seems to have a notable improvement in adherence outcomes than other settings, Dr. Berwanger said, but the study did not fully analyze that trend.
“We see this study not as the final word but as the first step,” he said. “More studies are needed.”
Dr. Berwanger reported receiving research support and/or honoraria from Astra Zeneca, Amgen, Bayer, Eurofarma, Servier, Novartis and NovoNordisk. Amgen sponsored the investigator-initiated trial.
SOURCE: Berwanger O, et al. AHA 2018 Abstr.19360.
CHICAGO – A multifaceted quality initiative that consists of staff education, patient reminders and a feedback loop may help to improve therapy adherence and encourage lifestyle changes of at-risk cardiovascular patients in settings with limited resources, according to results of a clinical trial from Brazil presented at the American Heart Association scientific sessions 2018.
“In patients at high cardiovascular risk – in this case patients with established cardiovascular disease – a multifaceted quality-improvement intervention resulted in significant improvement in the use of evidence-based therapies,” said Otavio Berwanger, MD, PhD, of the Heart Hospital in Sao Paolo. He reported results of the BRIDGE Cardiovascular Prevention Cluster Randomized Trial. “The tools used in our trial can become the basis for developing quality-improvement programs to maximize the use of evidence-based therapies for the management of these high-risk patients with, especially in limited-resource settings.”
BRIDGE-CV included 1,619 patients from 40 care settings. Institutions that adopted the multifaceted intervention adhered to 73.5% of the evidence-based therapies (antiplatelet agents, statins and ACE inhibitors) while those in the control group adhered to 58.7% of the performance measures, Dr. Berwanger said. That represents a gain of 25%. The study employed an “all-or-none” model. That is, participating sites were required to adopt all components of the quality-improvement initiative or none.
He noted that although the evidence supporting the use of platelet therapies, statins, and ACE inhibitors is strong, “translation of these findings in practice is clearly suboptimal.” He added, “It seems to be an even larger problem in settings like mine in Brazil, so quality-improvement interventions, especially in lower-resource settings such as low- and middle-income countries, are definitely needed.”
The quality-improvement model the trial evaluated involved two levels of intervention. The first level comprised three steps: a case manager evaluating the patient’s treatment needs with the aid of a checklist; then an evaluation by the physician; and then providing physicians with what Dr. Berwanger described as “a physician support tool” – a one-page summary of major guideline recommendations. The second level comprised monthly audit and feedback reports to the providers and patient education about lifestyle modification. Staff education and training was also provided to sites that adopted the model. “Our intervention was sort of based on behavioral marketing,” Dr. Berwanger said.
The trial also identified a number of trends among secondary endpoints, although the populations were too small to reach statistical significance. For example, Dr. Berwanger noted that intervention sites had higher use of high-dose statins and more than double the rate of smoking cessation. He also noted a 24% relative risk reduction in major cardiovascular events in the intervention group vs. controls. Among the intervention sites, teaching institutions seems to have a notable improvement in adherence outcomes than other settings, Dr. Berwanger said, but the study did not fully analyze that trend.
“We see this study not as the final word but as the first step,” he said. “More studies are needed.”
Dr. Berwanger reported receiving research support and/or honoraria from Astra Zeneca, Amgen, Bayer, Eurofarma, Servier, Novartis and NovoNordisk. Amgen sponsored the investigator-initiated trial.
SOURCE: Berwanger O, et al. AHA 2018 Abstr.19360.
CHICAGO – A multifaceted quality initiative that consists of staff education, patient reminders and a feedback loop may help to improve therapy adherence and encourage lifestyle changes of at-risk cardiovascular patients in settings with limited resources, according to results of a clinical trial from Brazil presented at the American Heart Association scientific sessions 2018.
“In patients at high cardiovascular risk – in this case patients with established cardiovascular disease – a multifaceted quality-improvement intervention resulted in significant improvement in the use of evidence-based therapies,” said Otavio Berwanger, MD, PhD, of the Heart Hospital in Sao Paolo. He reported results of the BRIDGE Cardiovascular Prevention Cluster Randomized Trial. “The tools used in our trial can become the basis for developing quality-improvement programs to maximize the use of evidence-based therapies for the management of these high-risk patients with, especially in limited-resource settings.”
BRIDGE-CV included 1,619 patients from 40 care settings. Institutions that adopted the multifaceted intervention adhered to 73.5% of the evidence-based therapies (antiplatelet agents, statins and ACE inhibitors) while those in the control group adhered to 58.7% of the performance measures, Dr. Berwanger said. That represents a gain of 25%. The study employed an “all-or-none” model. That is, participating sites were required to adopt all components of the quality-improvement initiative or none.
He noted that although the evidence supporting the use of platelet therapies, statins, and ACE inhibitors is strong, “translation of these findings in practice is clearly suboptimal.” He added, “It seems to be an even larger problem in settings like mine in Brazil, so quality-improvement interventions, especially in lower-resource settings such as low- and middle-income countries, are definitely needed.”
The quality-improvement model the trial evaluated involved two levels of intervention. The first level comprised three steps: a case manager evaluating the patient’s treatment needs with the aid of a checklist; then an evaluation by the physician; and then providing physicians with what Dr. Berwanger described as “a physician support tool” – a one-page summary of major guideline recommendations. The second level comprised monthly audit and feedback reports to the providers and patient education about lifestyle modification. Staff education and training was also provided to sites that adopted the model. “Our intervention was sort of based on behavioral marketing,” Dr. Berwanger said.
The trial also identified a number of trends among secondary endpoints, although the populations were too small to reach statistical significance. For example, Dr. Berwanger noted that intervention sites had higher use of high-dose statins and more than double the rate of smoking cessation. He also noted a 24% relative risk reduction in major cardiovascular events in the intervention group vs. controls. Among the intervention sites, teaching institutions seems to have a notable improvement in adherence outcomes than other settings, Dr. Berwanger said, but the study did not fully analyze that trend.
“We see this study not as the final word but as the first step,” he said. “More studies are needed.”
Dr. Berwanger reported receiving research support and/or honoraria from Astra Zeneca, Amgen, Bayer, Eurofarma, Servier, Novartis and NovoNordisk. Amgen sponsored the investigator-initiated trial.
SOURCE: Berwanger O, et al. AHA 2018 Abstr.19360.
REPORTING FROM AMERICAN HEART ASSOCIATION SCIENTIFIC SESSIONS 2018
Key clinical point: A multifaceted quality-improvement initiative led to improved adherence to evidence-based therapies.
Major finding: Sites that adopted the intervention had adherence rates 25% higher than control sites.
Study details: Two-arm, cluster-randomized, controlled trial of 1,619 high-risk, stable patients with established CVD from 40 sites.
Disclosures: Dr. Berwanger disclosed receiving research support and/or honoraria from AstraZeneca, Amgen, Bayer, Eurofarma, Servier, Novartis and NovoNordisk. Amgen sponsored the investigator-initiated trial.
Source: Berwanger O, et al. 2018-LBCT-19360-AHA.
ICYMI: Alirocumab improves cardiovascular outcomes
Among patients in the ODYSSEY Outcomes trial who’d had an acute coronary syndrome, only 9.5% of the alirocumab group versus 11.1% of the placebo group experienced composite primary endpoint events – death from coronary heart disease, nonfatal MI, fatal or nonfatal ischemic stroke, or unstable angina requiring hospitalization. Furthermore, the incidence of adverse events in both groups was similar, although the alirocumab group experienced more local injection-site reactions.
The ODYSSEY Outcomes primary results were published in the New England Journal of Medicine (2018 Nov 7; doi: 10.1056/NEJMoa1801174).
We covered the story last March, from the American College of Cardiology scientific sessions. Find our coverage at the link below:
https://www.mdedge.com/ecardiologynews/article/160512/acc-conference-coverage/odyssey-outcomes-trial-redefines-secondary.
Among patients in the ODYSSEY Outcomes trial who’d had an acute coronary syndrome, only 9.5% of the alirocumab group versus 11.1% of the placebo group experienced composite primary endpoint events – death from coronary heart disease, nonfatal MI, fatal or nonfatal ischemic stroke, or unstable angina requiring hospitalization. Furthermore, the incidence of adverse events in both groups was similar, although the alirocumab group experienced more local injection-site reactions.
The ODYSSEY Outcomes primary results were published in the New England Journal of Medicine (2018 Nov 7; doi: 10.1056/NEJMoa1801174).
We covered the story last March, from the American College of Cardiology scientific sessions. Find our coverage at the link below:
https://www.mdedge.com/ecardiologynews/article/160512/acc-conference-coverage/odyssey-outcomes-trial-redefines-secondary.
Among patients in the ODYSSEY Outcomes trial who’d had an acute coronary syndrome, only 9.5% of the alirocumab group versus 11.1% of the placebo group experienced composite primary endpoint events – death from coronary heart disease, nonfatal MI, fatal or nonfatal ischemic stroke, or unstable angina requiring hospitalization. Furthermore, the incidence of adverse events in both groups was similar, although the alirocumab group experienced more local injection-site reactions.
The ODYSSEY Outcomes primary results were published in the New England Journal of Medicine (2018 Nov 7; doi: 10.1056/NEJMoa1801174).
We covered the story last March, from the American College of Cardiology scientific sessions. Find our coverage at the link below:
https://www.mdedge.com/ecardiologynews/article/160512/acc-conference-coverage/odyssey-outcomes-trial-redefines-secondary.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
AHA promises practice-changing late breakers
Of the trials chosen for the six Late-Breaking Clinical Trial sessions, all being presented in the first 2 days of the American Heart Association scientific sessions in Chicago Nov. 10-12. Here are some of the most potentially practice-changing studies to look out for.

Saturday
- REDUCE-IT: Relative to placebo, the fish oil derivative AMR101 (icosapent-ethyl) evaluated in the REDUCE-IT trial was associated with a 25% reduction in a primary composite endpoint of major adverse cardiovascular events (MACE), according top-line data released in September. A highly purified ethyl ester of eicosapentaenoic acid (EPA), AMR101 (Vascepa, Amarin) was studied on top of statin therapy in both primary and secondary prevention cohorts among the 8,000 patients randomized. Relative efficacy for primary and secondary prevention was not described in the initial release of data and will be of particular when the full results are released on Saturday, Nov. 10 at 2:00 p.m.
- DECLARE TIMI58: In top line results from DECLARE TIMI58, which randomized more than 17,000 participants with type 2 diabetes an experimental arm or placebo, the SGLT2 inhibitor dapagliflozin (Farxiga, AstraZeneca) was linked to a reduction in the composite endpoint of hospitalization for heart failure or cardiovascular death. In the early release of results, no mention was made of the effect of this agent on a composite of cardiovascular death, MI, or ischemic stroke, which was a secondary co-primary endpoint. This and the impact of dapagliflozin on an array of secondary endpoints will be revealed when the full results are made available in the Saturday late-breaker session at 2:00 p.m.
- VITAL: The relative effect of vitamin D, fish oil, or both on body composition was compared in the VITAL study, which randomized more than 20,000 patients. Fish oil plus vitamin D, fish oil plus placebo, vitamin D plus placebo, and two placebos were compared in a 2 x 2 factorial design. The primary outcome includes total body fat and lean mass as well as these components in the abdomen and other anatomic sites. Body mass index, waist circumference, and waist-to-hip ratio are among secondary outcomes. In addition, the relative effects of these treatments on lipids, blood glucose, and other aspects of metabolism were followed over the 2 years of the study, to presented at 2 p.m. on Saturday.
- CIRT: Responding to the evidence that inflammation is a crucial contributor to atherothrombosis, the CIRT trial tested whether the anti-inflammatory agent methotrexate reduces rates of MI, stroke, and cardiovascular death relative to placebo in patients with stable coronary artery disease and either type 2 diabetes or metabolic syndrome. The study enrolled about 7,000 patients and will have follow-up of nearly 6 years. Secondary endpoints, such as the impact of methotrexate on rates of coronary revascularization, peripheral artery disease, venous thromboembolism, and aortic stenosis, may provide insight about the ways in which control of inflammation affects vascular pathology. The presentation is at 2 p.m. on Saturday.
- Also on Saturday, diverse trial hypotheses are being tested. For example, the cost effectiveness of a PCSK9 inhibitor will be the focus of the ODYSSEY OUTCOMES economics study, presented at the 2:00 session. The results of YOGA-CaRe, a multicenter trial of a yoga-based cardiac rehabilitation program, will be presented in a subsequent Saturday late-breaking session. Of highlights of the third Saturday late-breaking session, ALERT-AF will determine whether a computerized decision protocol affected anticoagulation management in hospitalized patients with atrial fibrillation.
Sunday
- PIONEER-HF: It has been previously shown that sacubitril/valsartan improves outcome in stable heart failure patients with a reduced ejection fraction (HRrEF), but PIONEER-HF will test the tolerability of this strategy when this treatment is initiated prior to hospital discharge. Patients with a left ventricular ejection fraction of 40% or less and elevated N-terminal pro hormone BNP (NT-proBNP) will be randomized to sacubitril/valsartan (Entresto, Novartis) or the ACE inhibitor enalapril. The primary outcome of the trial, which enrolled more than 700 patients, is the time-averaged percentage change in NT-proBNP from baseline. Secondary outcome measures included the proportion of patients with symptomatic hypotension, hyperkalemia, and angioedema. Presentation will be at the Sunday 10:45 a.m. session.
- TICAB: The hypothesis that ticagrelor is superior to aspirin for preventing a composite MACE endpoint of CV death, myocardial infarction, target vessel revascularization, and stroke in patients undergoing coronary artery bypass grafting is the basis for the TICAB trial. The nearly 1,900 patients were randomized to 90 mg of ticagrelor twice daily or 100 mg of aspirin twice daily. Major bleeding events, CV death, and all cause death are key secondary outcomes. Relative benefit in context of safety, particularly bleeding risk, will be of interest when the final results are revealed at 5:30 p.m. on Sunday.
All-in-all, the Sunday late-breaking sessions are no less crowded with potentially practice-changing studies, including T-TIME, an evaluation of low-dose alteplase during primary percutaneous intervention at 9:00 a.m., TRED-HF, a study of withdrawal of heart failure therapy in patients who have recovered from dilated cardiomyopathy at 10:45 a.m., and ISAR TEST 4, which will provide 10-year outcomes after coronary stents with biodegradable versus permanent polymer coated devices, at 5:30 p.m.
Of the trials chosen for the six Late-Breaking Clinical Trial sessions, all being presented in the first 2 days of the American Heart Association scientific sessions in Chicago Nov. 10-12. Here are some of the most potentially practice-changing studies to look out for.
Saturday
- REDUCE-IT: Relative to placebo, the fish oil derivative AMR101 (icosapent-ethyl) evaluated in the REDUCE-IT trial was associated with a 25% reduction in a primary composite endpoint of major adverse cardiovascular events (MACE), according top-line data released in September. A highly purified ethyl ester of eicosapentaenoic acid (EPA), AMR101 (Vascepa, Amarin) was studied on top of statin therapy in both primary and secondary prevention cohorts among the 8,000 patients randomized. Relative efficacy for primary and secondary prevention was not described in the initial release of data and will be of particular when the full results are released on Saturday, Nov. 10 at 2:00 p.m.
- DECLARE TIMI58: In top line results from DECLARE TIMI58, which randomized more than 17,000 participants with type 2 diabetes an experimental arm or placebo, the SGLT2 inhibitor dapagliflozin (Farxiga, AstraZeneca) was linked to a reduction in the composite endpoint of hospitalization for heart failure or cardiovascular death. In the early release of results, no mention was made of the effect of this agent on a composite of cardiovascular death, MI, or ischemic stroke, which was a secondary co-primary endpoint. This and the impact of dapagliflozin on an array of secondary endpoints will be revealed when the full results are made available in the Saturday late-breaker session at 2:00 p.m.
- VITAL: The relative effect of vitamin D, fish oil, or both on body composition was compared in the VITAL study, which randomized more than 20,000 patients. Fish oil plus vitamin D, fish oil plus placebo, vitamin D plus placebo, and two placebos were compared in a 2 x 2 factorial design. The primary outcome includes total body fat and lean mass as well as these components in the abdomen and other anatomic sites. Body mass index, waist circumference, and waist-to-hip ratio are among secondary outcomes. In addition, the relative effects of these treatments on lipids, blood glucose, and other aspects of metabolism were followed over the 2 years of the study, to presented at 2 p.m. on Saturday.
- CIRT: Responding to the evidence that inflammation is a crucial contributor to atherothrombosis, the CIRT trial tested whether the anti-inflammatory agent methotrexate reduces rates of MI, stroke, and cardiovascular death relative to placebo in patients with stable coronary artery disease and either type 2 diabetes or metabolic syndrome. The study enrolled about 7,000 patients and will have follow-up of nearly 6 years. Secondary endpoints, such as the impact of methotrexate on rates of coronary revascularization, peripheral artery disease, venous thromboembolism, and aortic stenosis, may provide insight about the ways in which control of inflammation affects vascular pathology. The presentation is at 2 p.m. on Saturday.
- Also on Saturday, diverse trial hypotheses are being tested. For example, the cost effectiveness of a PCSK9 inhibitor will be the focus of the ODYSSEY OUTCOMES economics study, presented at the 2:00 session. The results of YOGA-CaRe, a multicenter trial of a yoga-based cardiac rehabilitation program, will be presented in a subsequent Saturday late-breaking session. Of highlights of the third Saturday late-breaking session, ALERT-AF will determine whether a computerized decision protocol affected anticoagulation management in hospitalized patients with atrial fibrillation.
Sunday
- PIONEER-HF: It has been previously shown that sacubitril/valsartan improves outcome in stable heart failure patients with a reduced ejection fraction (HRrEF), but PIONEER-HF will test the tolerability of this strategy when this treatment is initiated prior to hospital discharge. Patients with a left ventricular ejection fraction of 40% or less and elevated N-terminal pro hormone BNP (NT-proBNP) will be randomized to sacubitril/valsartan (Entresto, Novartis) or the ACE inhibitor enalapril. The primary outcome of the trial, which enrolled more than 700 patients, is the time-averaged percentage change in NT-proBNP from baseline. Secondary outcome measures included the proportion of patients with symptomatic hypotension, hyperkalemia, and angioedema. Presentation will be at the Sunday 10:45 a.m. session.
- TICAB: The hypothesis that ticagrelor is superior to aspirin for preventing a composite MACE endpoint of CV death, myocardial infarction, target vessel revascularization, and stroke in patients undergoing coronary artery bypass grafting is the basis for the TICAB trial. The nearly 1,900 patients were randomized to 90 mg of ticagrelor twice daily or 100 mg of aspirin twice daily. Major bleeding events, CV death, and all cause death are key secondary outcomes. Relative benefit in context of safety, particularly bleeding risk, will be of interest when the final results are revealed at 5:30 p.m. on Sunday.
All-in-all, the Sunday late-breaking sessions are no less crowded with potentially practice-changing studies, including T-TIME, an evaluation of low-dose alteplase during primary percutaneous intervention at 9:00 a.m., TRED-HF, a study of withdrawal of heart failure therapy in patients who have recovered from dilated cardiomyopathy at 10:45 a.m., and ISAR TEST 4, which will provide 10-year outcomes after coronary stents with biodegradable versus permanent polymer coated devices, at 5:30 p.m.
Of the trials chosen for the six Late-Breaking Clinical Trial sessions, all being presented in the first 2 days of the American Heart Association scientific sessions in Chicago Nov. 10-12. Here are some of the most potentially practice-changing studies to look out for.
Saturday
- REDUCE-IT: Relative to placebo, the fish oil derivative AMR101 (icosapent-ethyl) evaluated in the REDUCE-IT trial was associated with a 25% reduction in a primary composite endpoint of major adverse cardiovascular events (MACE), according top-line data released in September. A highly purified ethyl ester of eicosapentaenoic acid (EPA), AMR101 (Vascepa, Amarin) was studied on top of statin therapy in both primary and secondary prevention cohorts among the 8,000 patients randomized. Relative efficacy for primary and secondary prevention was not described in the initial release of data and will be of particular when the full results are released on Saturday, Nov. 10 at 2:00 p.m.
- DECLARE TIMI58: In top line results from DECLARE TIMI58, which randomized more than 17,000 participants with type 2 diabetes an experimental arm or placebo, the SGLT2 inhibitor dapagliflozin (Farxiga, AstraZeneca) was linked to a reduction in the composite endpoint of hospitalization for heart failure or cardiovascular death. In the early release of results, no mention was made of the effect of this agent on a composite of cardiovascular death, MI, or ischemic stroke, which was a secondary co-primary endpoint. This and the impact of dapagliflozin on an array of secondary endpoints will be revealed when the full results are made available in the Saturday late-breaker session at 2:00 p.m.
- VITAL: The relative effect of vitamin D, fish oil, or both on body composition was compared in the VITAL study, which randomized more than 20,000 patients. Fish oil plus vitamin D, fish oil plus placebo, vitamin D plus placebo, and two placebos were compared in a 2 x 2 factorial design. The primary outcome includes total body fat and lean mass as well as these components in the abdomen and other anatomic sites. Body mass index, waist circumference, and waist-to-hip ratio are among secondary outcomes. In addition, the relative effects of these treatments on lipids, blood glucose, and other aspects of metabolism were followed over the 2 years of the study, to presented at 2 p.m. on Saturday.
- CIRT: Responding to the evidence that inflammation is a crucial contributor to atherothrombosis, the CIRT trial tested whether the anti-inflammatory agent methotrexate reduces rates of MI, stroke, and cardiovascular death relative to placebo in patients with stable coronary artery disease and either type 2 diabetes or metabolic syndrome. The study enrolled about 7,000 patients and will have follow-up of nearly 6 years. Secondary endpoints, such as the impact of methotrexate on rates of coronary revascularization, peripheral artery disease, venous thromboembolism, and aortic stenosis, may provide insight about the ways in which control of inflammation affects vascular pathology. The presentation is at 2 p.m. on Saturday.
- Also on Saturday, diverse trial hypotheses are being tested. For example, the cost effectiveness of a PCSK9 inhibitor will be the focus of the ODYSSEY OUTCOMES economics study, presented at the 2:00 session. The results of YOGA-CaRe, a multicenter trial of a yoga-based cardiac rehabilitation program, will be presented in a subsequent Saturday late-breaking session. Of highlights of the third Saturday late-breaking session, ALERT-AF will determine whether a computerized decision protocol affected anticoagulation management in hospitalized patients with atrial fibrillation.
Sunday
- PIONEER-HF: It has been previously shown that sacubitril/valsartan improves outcome in stable heart failure patients with a reduced ejection fraction (HRrEF), but PIONEER-HF will test the tolerability of this strategy when this treatment is initiated prior to hospital discharge. Patients with a left ventricular ejection fraction of 40% or less and elevated N-terminal pro hormone BNP (NT-proBNP) will be randomized to sacubitril/valsartan (Entresto, Novartis) or the ACE inhibitor enalapril. The primary outcome of the trial, which enrolled more than 700 patients, is the time-averaged percentage change in NT-proBNP from baseline. Secondary outcome measures included the proportion of patients with symptomatic hypotension, hyperkalemia, and angioedema. Presentation will be at the Sunday 10:45 a.m. session.
- TICAB: The hypothesis that ticagrelor is superior to aspirin for preventing a composite MACE endpoint of CV death, myocardial infarction, target vessel revascularization, and stroke in patients undergoing coronary artery bypass grafting is the basis for the TICAB trial. The nearly 1,900 patients were randomized to 90 mg of ticagrelor twice daily or 100 mg of aspirin twice daily. Major bleeding events, CV death, and all cause death are key secondary outcomes. Relative benefit in context of safety, particularly bleeding risk, will be of interest when the final results are revealed at 5:30 p.m. on Sunday.
All-in-all, the Sunday late-breaking sessions are no less crowded with potentially practice-changing studies, including T-TIME, an evaluation of low-dose alteplase during primary percutaneous intervention at 9:00 a.m., TRED-HF, a study of withdrawal of heart failure therapy in patients who have recovered from dilated cardiomyopathy at 10:45 a.m., and ISAR TEST 4, which will provide 10-year outcomes after coronary stents with biodegradable versus permanent polymer coated devices, at 5:30 p.m.
CT opens extended window for stroke thrombolysis
MONTREAL – An extended time window for thrombolytic treatment of acute ischemic stroke patients using tissue plasminogen activator out to 9 hours from stroke onset was safe and effective using CT perfusion imaging and automated imaging processing software to select suitable patients in the EXTEND trial. This result matches the groundbreaking finding reported earlier in 2018 that used MRI to select patients for extended thrombolysis.

“To reproduce our results you need to set up CT perfusion” as well as the RAPID software for automated image processing to identify patients with a small infarct core and a large area of salvageable brain, said Henry Ma, MD, a stroke neurologist at Monash University, Melbourne, as he reported results from the trial at the World Stroke Congress. “EXTEND is the first positive thrombolysis trial in an extended time window using automated penumbral imaging.”
The new finding, from a trial with 225 randomized stroke patients, was especially notable because, by showing the validity of CT imaging for patient selection, it makes applying the extended time window for thrombolytic therapy more feasible for U.S. and Canadian stroke centers where CT imaging is much more common than MRI. A report from European investigators published in August 2018 from the WAKE-UP trial showed that thrombolysis with tissue plasminogen activator (tPA) was safe and effective when administered to patients who woke up with an acute ischemic stroke that had occurred more than 4.5 hours before treatment, but this study exclusively used MRI for patient selection (N Engl J Med. 2018 Aug 16;379[7]:611-22).
“In North America, our systems are more equipped for using CT,” commented Ashfaq Shuaib, MD, a professor of medicine and neurologist at the University of Alberta, Edmonton. Based on the WAKE-UP results, “MR would be preferred, but what we’ve been doing [since the WAKE-UP report] is if we see a CT scan that’s good we go ahead” with thrombolysis.

“Biologically, it doesn’t matter whether you use MR or CT; they both index the same underlying pathology. We’ve been hesitant to go beyond the MR finding from WAKE-UP, where there were data, but the findings from EXTEND were right in line with the WAKE-UP results, and that’s all we need to be reassured” that CT perfusion imaging also works for patient selection, commented Jeffrey L. Saver, MD, professor of medicine and director of the Comprehensive Stroke Center at the University of California, Los Angeles.
CT perfusion imaging and automated image processing “worked to select stroke patients” for an extended time window for treatment with mechanical thrombectomy in the DAWN (N Engl J Med. 2018 Jan 4;378[1]:11-21) and DEFUSE 3 (N Engl J Med. 2018 Feb 22;378[8]:308-18) trials, a history that makes the new finding of successfully using CT imaging to select patients who qualify for extended use of thrombolysis “a convincing result,” Dr. Saver said in an interview. The new EXTEND findings “will have a major impact” on using an extended time window for thrombolysis in U.S. practice, he predicted.
The EXTEND trial (Int J Stroke. 2012 Jan 1;7[1]:74-80) ran at 22 sites in Australia, 11 sites in Taiwan, and 1 center in New Zealand. Recruitment of patients into the study stopped early, after enrolling 225 patients, in June 2018, when results from WAKE-UP came out.
The EXTEND investigators enrolled patients who were either 4.5-9 hours out from the onset of their stroke or patients with a wake-up stroke with an uncertain onset. Participating centers could use either CT perfusion or MRI to identify candidates for treatment, and all used the RAPID software for image processing to identify patients with a perfusion lesion of at least 10 mL and an ischemic core volume no greater than 70 mL. Dr. Ma did not report what percentage of patients underwent imaging with each of these methods, but hinted that clinicians had used CT for a majority of the cases. The study randomized patients to receive either 0.9 mg/kg tPA or placebo, and by the trial protocol none of the enrolled patients received treatment with mechanical thrombectomy.
The trial’s primary endpoint was the percentage of patients with a modified Rankin Scale score of 0 or 1 at 90 days after their stroke, which was achieved by 44% more patients in the tPA group relative to the placebo arm after adjustment for age and baseline stroke severity, a statistically significant difference. The results were also positive for several secondary endpoints, such as recanalization 24 hours after treatment, which occurred in 67% of patients treated with tPA and 37% of the control patients, a statistically significant 68% relative improvement with thrombolysis.
Mortality at 90 days was similar in the two arms – 9% among the placebo patients and 12% among those who received tPA. The rate of symptomatic intracranial hemorrhage 36 hours after treatment was significantly higher among patients treated with tPA at 6%, compared with 1% in the placebo group, but the magnitude of this adverse effect was consistent with rates of intracranial hemorrhages previously reported in other studies of thrombolytic treatment for acute ischemic stroke, Dr. Ma said. The small number of increased intracranial hemorrhages “was not associated with increased mortality, and did not negate the positive result of an improved rate of excellent functional outcomes.”
These findings will likely spur further adoption of imaging processing software of the type used in EXTEND by U.S. stroke centers, Dr. Saver predicted.
“More and more centers have been getting this [software], and now they have two reasons to have it: to identify patients for an extended window for mechanical thrombectomy and to identify patients for an extended window for thrombolysis. It is a compelling case to have the imaging software as widely disseminated as possible. Centers that want to do the best for patients should have this imaging-processing software,” Dr. Saver said.
Dr. Ma and Dr. Shuaib reported no disclosures. Dr. Saver has received research funding and personal fees from Medtronic-Abbott and Neuravia.
SOURCE: Ma H et al. Int J. Stroke. 2018 Oct;13(2S):235, Abstract 1014.
Ever since results from the WAKE-UP trial came out earlier in 2018, we at the University of Cincinnati have been imaging acute ischemic stroke patients who presented outside the standard 4.5-hour time limit for thrombolysis with MRI to see if they qualify for an extended window for thrombolysis. But this has been a cumbersome and redundant process because our default imaging method is CT, so we have been imaging potential candidates for an extended thrombolytic window twice, first with CT and then later with MRI.

The EXTEND findings also provide a further reason for U.S. stroke centers to purchase and use some type of imaging processing software if they don’t already have it, either the RAPID software that was used in EXTEND or one of the several similar software packages that are now available. Several primary stroke centers in my area still do not currently use this software, although its use has been quickly spreading and it will now be increasingly hard for these centers to hold off acquiring it. Fortunately the increased competition among software vendors who sell this type of software has meant that the price has been dropping.
Pooja Khatri, MD , is a professor of neurology and director of acute stroke at the University of Cincinnati. She has been a consultant to Biogen, Greenwich, and PTC Therapeutics. She made these comments in an interview.
Ever since results from the WAKE-UP trial came out earlier in 2018, we at the University of Cincinnati have been imaging acute ischemic stroke patients who presented outside the standard 4.5-hour time limit for thrombolysis with MRI to see if they qualify for an extended window for thrombolysis. But this has been a cumbersome and redundant process because our default imaging method is CT, so we have been imaging potential candidates for an extended thrombolytic window twice, first with CT and then later with MRI.
The EXTEND findings also provide a further reason for U.S. stroke centers to purchase and use some type of imaging processing software if they don’t already have it, either the RAPID software that was used in EXTEND or one of the several similar software packages that are now available. Several primary stroke centers in my area still do not currently use this software, although its use has been quickly spreading and it will now be increasingly hard for these centers to hold off acquiring it. Fortunately the increased competition among software vendors who sell this type of software has meant that the price has been dropping.
Pooja Khatri, MD , is a professor of neurology and director of acute stroke at the University of Cincinnati. She has been a consultant to Biogen, Greenwich, and PTC Therapeutics. She made these comments in an interview.
Ever since results from the WAKE-UP trial came out earlier in 2018, we at the University of Cincinnati have been imaging acute ischemic stroke patients who presented outside the standard 4.5-hour time limit for thrombolysis with MRI to see if they qualify for an extended window for thrombolysis. But this has been a cumbersome and redundant process because our default imaging method is CT, so we have been imaging potential candidates for an extended thrombolytic window twice, first with CT and then later with MRI.
The EXTEND findings also provide a further reason for U.S. stroke centers to purchase and use some type of imaging processing software if they don’t already have it, either the RAPID software that was used in EXTEND or one of the several similar software packages that are now available. Several primary stroke centers in my area still do not currently use this software, although its use has been quickly spreading and it will now be increasingly hard for these centers to hold off acquiring it. Fortunately the increased competition among software vendors who sell this type of software has meant that the price has been dropping.
Pooja Khatri, MD , is a professor of neurology and director of acute stroke at the University of Cincinnati. She has been a consultant to Biogen, Greenwich, and PTC Therapeutics. She made these comments in an interview.
MONTREAL – An extended time window for thrombolytic treatment of acute ischemic stroke patients using tissue plasminogen activator out to 9 hours from stroke onset was safe and effective using CT perfusion imaging and automated imaging processing software to select suitable patients in the EXTEND trial. This result matches the groundbreaking finding reported earlier in 2018 that used MRI to select patients for extended thrombolysis.
“To reproduce our results you need to set up CT perfusion” as well as the RAPID software for automated image processing to identify patients with a small infarct core and a large area of salvageable brain, said Henry Ma, MD, a stroke neurologist at Monash University, Melbourne, as he reported results from the trial at the World Stroke Congress. “EXTEND is the first positive thrombolysis trial in an extended time window using automated penumbral imaging.”
The new finding, from a trial with 225 randomized stroke patients, was especially notable because, by showing the validity of CT imaging for patient selection, it makes applying the extended time window for thrombolytic therapy more feasible for U.S. and Canadian stroke centers where CT imaging is much more common than MRI. A report from European investigators published in August 2018 from the WAKE-UP trial showed that thrombolysis with tissue plasminogen activator (tPA) was safe and effective when administered to patients who woke up with an acute ischemic stroke that had occurred more than 4.5 hours before treatment, but this study exclusively used MRI for patient selection (N Engl J Med. 2018 Aug 16;379[7]:611-22).
“In North America, our systems are more equipped for using CT,” commented Ashfaq Shuaib, MD, a professor of medicine and neurologist at the University of Alberta, Edmonton. Based on the WAKE-UP results, “MR would be preferred, but what we’ve been doing [since the WAKE-UP report] is if we see a CT scan that’s good we go ahead” with thrombolysis.
“Biologically, it doesn’t matter whether you use MR or CT; they both index the same underlying pathology. We’ve been hesitant to go beyond the MR finding from WAKE-UP, where there were data, but the findings from EXTEND were right in line with the WAKE-UP results, and that’s all we need to be reassured” that CT perfusion imaging also works for patient selection, commented Jeffrey L. Saver, MD, professor of medicine and director of the Comprehensive Stroke Center at the University of California, Los Angeles.
CT perfusion imaging and automated image processing “worked to select stroke patients” for an extended time window for treatment with mechanical thrombectomy in the DAWN (N Engl J Med. 2018 Jan 4;378[1]:11-21) and DEFUSE 3 (N Engl J Med. 2018 Feb 22;378[8]:308-18) trials, a history that makes the new finding of successfully using CT imaging to select patients who qualify for extended use of thrombolysis “a convincing result,” Dr. Saver said in an interview. The new EXTEND findings “will have a major impact” on using an extended time window for thrombolysis in U.S. practice, he predicted.
The EXTEND trial (Int J Stroke. 2012 Jan 1;7[1]:74-80) ran at 22 sites in Australia, 11 sites in Taiwan, and 1 center in New Zealand. Recruitment of patients into the study stopped early, after enrolling 225 patients, in June 2018, when results from WAKE-UP came out.
The EXTEND investigators enrolled patients who were either 4.5-9 hours out from the onset of their stroke or patients with a wake-up stroke with an uncertain onset. Participating centers could use either CT perfusion or MRI to identify candidates for treatment, and all used the RAPID software for image processing to identify patients with a perfusion lesion of at least 10 mL and an ischemic core volume no greater than 70 mL. Dr. Ma did not report what percentage of patients underwent imaging with each of these methods, but hinted that clinicians had used CT for a majority of the cases. The study randomized patients to receive either 0.9 mg/kg tPA or placebo, and by the trial protocol none of the enrolled patients received treatment with mechanical thrombectomy.
The trial’s primary endpoint was the percentage of patients with a modified Rankin Scale score of 0 or 1 at 90 days after their stroke, which was achieved by 44% more patients in the tPA group relative to the placebo arm after adjustment for age and baseline stroke severity, a statistically significant difference. The results were also positive for several secondary endpoints, such as recanalization 24 hours after treatment, which occurred in 67% of patients treated with tPA and 37% of the control patients, a statistically significant 68% relative improvement with thrombolysis.
Mortality at 90 days was similar in the two arms – 9% among the placebo patients and 12% among those who received tPA. The rate of symptomatic intracranial hemorrhage 36 hours after treatment was significantly higher among patients treated with tPA at 6%, compared with 1% in the placebo group, but the magnitude of this adverse effect was consistent with rates of intracranial hemorrhages previously reported in other studies of thrombolytic treatment for acute ischemic stroke, Dr. Ma said. The small number of increased intracranial hemorrhages “was not associated with increased mortality, and did not negate the positive result of an improved rate of excellent functional outcomes.”
These findings will likely spur further adoption of imaging processing software of the type used in EXTEND by U.S. stroke centers, Dr. Saver predicted.
“More and more centers have been getting this [software], and now they have two reasons to have it: to identify patients for an extended window for mechanical thrombectomy and to identify patients for an extended window for thrombolysis. It is a compelling case to have the imaging software as widely disseminated as possible. Centers that want to do the best for patients should have this imaging-processing software,” Dr. Saver said.
Dr. Ma and Dr. Shuaib reported no disclosures. Dr. Saver has received research funding and personal fees from Medtronic-Abbott and Neuravia.
SOURCE: Ma H et al. Int J. Stroke. 2018 Oct;13(2S):235, Abstract 1014.
MONTREAL – An extended time window for thrombolytic treatment of acute ischemic stroke patients using tissue plasminogen activator out to 9 hours from stroke onset was safe and effective using CT perfusion imaging and automated imaging processing software to select suitable patients in the EXTEND trial. This result matches the groundbreaking finding reported earlier in 2018 that used MRI to select patients for extended thrombolysis.
“To reproduce our results you need to set up CT perfusion” as well as the RAPID software for automated image processing to identify patients with a small infarct core and a large area of salvageable brain, said Henry Ma, MD, a stroke neurologist at Monash University, Melbourne, as he reported results from the trial at the World Stroke Congress. “EXTEND is the first positive thrombolysis trial in an extended time window using automated penumbral imaging.”
The new finding, from a trial with 225 randomized stroke patients, was especially notable because, by showing the validity of CT imaging for patient selection, it makes applying the extended time window for thrombolytic therapy more feasible for U.S. and Canadian stroke centers where CT imaging is much more common than MRI. A report from European investigators published in August 2018 from the WAKE-UP trial showed that thrombolysis with tissue plasminogen activator (tPA) was safe and effective when administered to patients who woke up with an acute ischemic stroke that had occurred more than 4.5 hours before treatment, but this study exclusively used MRI for patient selection (N Engl J Med. 2018 Aug 16;379[7]:611-22).
“In North America, our systems are more equipped for using CT,” commented Ashfaq Shuaib, MD, a professor of medicine and neurologist at the University of Alberta, Edmonton. Based on the WAKE-UP results, “MR would be preferred, but what we’ve been doing [since the WAKE-UP report] is if we see a CT scan that’s good we go ahead” with thrombolysis.
“Biologically, it doesn’t matter whether you use MR or CT; they both index the same underlying pathology. We’ve been hesitant to go beyond the MR finding from WAKE-UP, where there were data, but the findings from EXTEND were right in line with the WAKE-UP results, and that’s all we need to be reassured” that CT perfusion imaging also works for patient selection, commented Jeffrey L. Saver, MD, professor of medicine and director of the Comprehensive Stroke Center at the University of California, Los Angeles.
CT perfusion imaging and automated image processing “worked to select stroke patients” for an extended time window for treatment with mechanical thrombectomy in the DAWN (N Engl J Med. 2018 Jan 4;378[1]:11-21) and DEFUSE 3 (N Engl J Med. 2018 Feb 22;378[8]:308-18) trials, a history that makes the new finding of successfully using CT imaging to select patients who qualify for extended use of thrombolysis “a convincing result,” Dr. Saver said in an interview. The new EXTEND findings “will have a major impact” on using an extended time window for thrombolysis in U.S. practice, he predicted.
The EXTEND trial (Int J Stroke. 2012 Jan 1;7[1]:74-80) ran at 22 sites in Australia, 11 sites in Taiwan, and 1 center in New Zealand. Recruitment of patients into the study stopped early, after enrolling 225 patients, in June 2018, when results from WAKE-UP came out.
The EXTEND investigators enrolled patients who were either 4.5-9 hours out from the onset of their stroke or patients with a wake-up stroke with an uncertain onset. Participating centers could use either CT perfusion or MRI to identify candidates for treatment, and all used the RAPID software for image processing to identify patients with a perfusion lesion of at least 10 mL and an ischemic core volume no greater than 70 mL. Dr. Ma did not report what percentage of patients underwent imaging with each of these methods, but hinted that clinicians had used CT for a majority of the cases. The study randomized patients to receive either 0.9 mg/kg tPA or placebo, and by the trial protocol none of the enrolled patients received treatment with mechanical thrombectomy.
The trial’s primary endpoint was the percentage of patients with a modified Rankin Scale score of 0 or 1 at 90 days after their stroke, which was achieved by 44% more patients in the tPA group relative to the placebo arm after adjustment for age and baseline stroke severity, a statistically significant difference. The results were also positive for several secondary endpoints, such as recanalization 24 hours after treatment, which occurred in 67% of patients treated with tPA and 37% of the control patients, a statistically significant 68% relative improvement with thrombolysis.
Mortality at 90 days was similar in the two arms – 9% among the placebo patients and 12% among those who received tPA. The rate of symptomatic intracranial hemorrhage 36 hours after treatment was significantly higher among patients treated with tPA at 6%, compared with 1% in the placebo group, but the magnitude of this adverse effect was consistent with rates of intracranial hemorrhages previously reported in other studies of thrombolytic treatment for acute ischemic stroke, Dr. Ma said. The small number of increased intracranial hemorrhages “was not associated with increased mortality, and did not negate the positive result of an improved rate of excellent functional outcomes.”
These findings will likely spur further adoption of imaging processing software of the type used in EXTEND by U.S. stroke centers, Dr. Saver predicted.
“More and more centers have been getting this [software], and now they have two reasons to have it: to identify patients for an extended window for mechanical thrombectomy and to identify patients for an extended window for thrombolysis. It is a compelling case to have the imaging software as widely disseminated as possible. Centers that want to do the best for patients should have this imaging-processing software,” Dr. Saver said.
Dr. Ma and Dr. Shuaib reported no disclosures. Dr. Saver has received research funding and personal fees from Medtronic-Abbott and Neuravia.
SOURCE: Ma H et al. Int J. Stroke. 2018 Oct;13(2S):235, Abstract 1014.
REPORTING FROM THE WORLD STROKE CONGRESS
Key clinical point:
Major finding: Patients who received thrombolysis 4.5-9 hours after stroke onset had a 44% increased rate of good outcomes, compared with controls.
Study details: EXTEND, a multicenter, controlled trial with 225 patients.
Disclosures: Dr. Ma and Dr. Shuaib had no disclosures. Dr. Saver has received research funding and personal fees from Medtronic-Abbott and Neuravia.
Source: Ma H et al. Int J. Stroke. 2018 Oct;13(2S):235, Abstract 1014.
Data support revising ASCVD cardiovascular risk threshold
MUNICH – Revising the threshold for actionable high cardiovascular risk from the current 7.5% or greater risk of an event within 10 years as defined in American College of Cardiology/American Heart Association guidelines using the Atherosclerotic Cardiovascular Disease (ASCVD ) Risk Calculator to a 10% or greater 10-year risk would provide the optimal balance of sensitivity and specificity for discriminating future risk of cardiovascular events, according to Robert S. Rosenman, MD.

“I think this is very important from a public health policy perspective,” Dr. Rosenman, a cardiologist who is professor of medicine at Mount Sinai School of Medicine in New York, said at the annual congress of the European Society of Cardiology.
He elaborated: “This would eliminate 11.4 million people who are currently candidates for a statin but may not be getting the benefits of statin therapy. We feel that this information is actually quite important for the primary prevention population because there’s been a lot of pushback from our primary care physician colleagues about the overtreatment of low-risk individuals” under the current guidelines (Circulation. 2014 Jun 24;129[25 Suppl 2]:S49-73).
Dr. Rosenman and his coinvestigators conducted a secondary analysis of data on 21,343 adults in the REGARDS (Reasons for Geographic and Racial Differences in Stroke) study. All participants were free of a baseline history of heart disease or stroke. During a median 8.5 years of follow-up, 1,717 of them experienced adjudicated coronary heart disease or stroke events.
In multivariate analyses adjusted for standard cardiovascular risk factors, socioeconomic and demographic factors, and the use of statins and/or antihypertensive drugs, the higher the baseline 10-year predicted risk using the ACC/AHA ASCVD Risk Calculator based on the Pooled Cohort risk equations, the higher the incidence rate of cardiovascular events. No surprise there.
What was impressive, however, was that the optimal combination of sensitivity and specificity as captured in a statistic known as Youden’s index occurred at a 10-year predicted risk of 10%-12%. The biggest net improvement obtained through reclassification resulted from moving the threshold for elevated 10-year cardiovascular risk warranting statin therapy from 7.5% or greater to 10% or more, rather than using thresholds of 15% or 20%.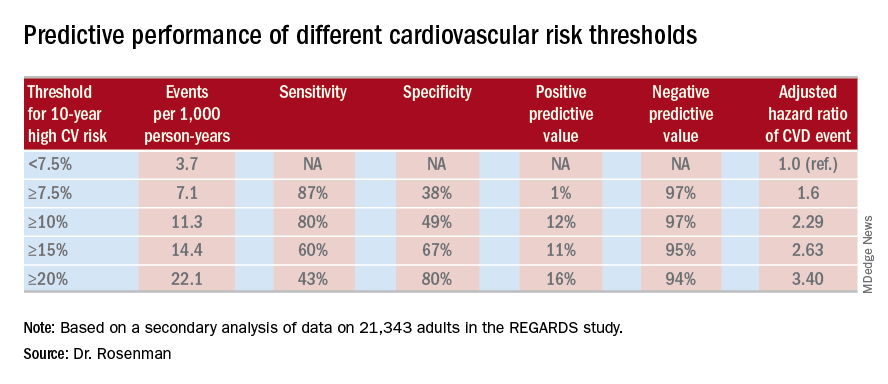
He cited data from the 2011-2014 National Health and Nutrition Examination Survey in support of his estimate that switching to a 10% threshold from the current 7.5% threshold would reduce the number of Americans deemed at high cardiovascular risk from 57.1 million to 45.8 million.
“This cutoff value of 10%, by the way, is the same cutoff value used in the recently published ACC/AHA guideline on hypertension. And it’s also the same cutoff value used for antiplatelet therapy in looking at the benefit/risk ratio. So this value of 10% is, I think, really the right number. Our study is the first effort that has been shown to validate that number, and it brings the cutoff values in the various guidelines in line,” the cardiologist observed.
Asked if these new findings are likely to result in a revision of the ACC/AHA cardiovascular risk assessment guidelines, Dr. Rosenman replied that the guidelines are under revision, with the draft update now circulating for comment. So the timing is dicey: His study is now in prepublication peer review, but hasn’t yet been published and thus may not carry persuasive weight.
“Hopefully, the guideline panel is going to make an adjustment to make the 10% figure in line with the blood pressure guidelines,” he said.
The new analysis of the REGARDS study was funded by a collaboration between Amgen, Mount Sinai School of Medicine, and the University of Alabama. Dr. Rosenman reported receiving research funding from and serving as an advisor to Amgen and a handful of other companies.
MUNICH – Revising the threshold for actionable high cardiovascular risk from the current 7.5% or greater risk of an event within 10 years as defined in American College of Cardiology/American Heart Association guidelines using the Atherosclerotic Cardiovascular Disease (ASCVD ) Risk Calculator to a 10% or greater 10-year risk would provide the optimal balance of sensitivity and specificity for discriminating future risk of cardiovascular events, according to Robert S. Rosenman, MD.
“I think this is very important from a public health policy perspective,” Dr. Rosenman, a cardiologist who is professor of medicine at Mount Sinai School of Medicine in New York, said at the annual congress of the European Society of Cardiology.
He elaborated: “This would eliminate 11.4 million people who are currently candidates for a statin but may not be getting the benefits of statin therapy. We feel that this information is actually quite important for the primary prevention population because there’s been a lot of pushback from our primary care physician colleagues about the overtreatment of low-risk individuals” under the current guidelines (Circulation. 2014 Jun 24;129[25 Suppl 2]:S49-73).
Dr. Rosenman and his coinvestigators conducted a secondary analysis of data on 21,343 adults in the REGARDS (Reasons for Geographic and Racial Differences in Stroke) study. All participants were free of a baseline history of heart disease or stroke. During a median 8.5 years of follow-up, 1,717 of them experienced adjudicated coronary heart disease or stroke events.
In multivariate analyses adjusted for standard cardiovascular risk factors, socioeconomic and demographic factors, and the use of statins and/or antihypertensive drugs, the higher the baseline 10-year predicted risk using the ACC/AHA ASCVD Risk Calculator based on the Pooled Cohort risk equations, the higher the incidence rate of cardiovascular events. No surprise there.
What was impressive, however, was that the optimal combination of sensitivity and specificity as captured in a statistic known as Youden’s index occurred at a 10-year predicted risk of 10%-12%. The biggest net improvement obtained through reclassification resulted from moving the threshold for elevated 10-year cardiovascular risk warranting statin therapy from 7.5% or greater to 10% or more, rather than using thresholds of 15% or 20%.
He cited data from the 2011-2014 National Health and Nutrition Examination Survey in support of his estimate that switching to a 10% threshold from the current 7.5% threshold would reduce the number of Americans deemed at high cardiovascular risk from 57.1 million to 45.8 million.
“This cutoff value of 10%, by the way, is the same cutoff value used in the recently published ACC/AHA guideline on hypertension. And it’s also the same cutoff value used for antiplatelet therapy in looking at the benefit/risk ratio. So this value of 10% is, I think, really the right number. Our study is the first effort that has been shown to validate that number, and it brings the cutoff values in the various guidelines in line,” the cardiologist observed.
Asked if these new findings are likely to result in a revision of the ACC/AHA cardiovascular risk assessment guidelines, Dr. Rosenman replied that the guidelines are under revision, with the draft update now circulating for comment. So the timing is dicey: His study is now in prepublication peer review, but hasn’t yet been published and thus may not carry persuasive weight.
“Hopefully, the guideline panel is going to make an adjustment to make the 10% figure in line with the blood pressure guidelines,” he said.
The new analysis of the REGARDS study was funded by a collaboration between Amgen, Mount Sinai School of Medicine, and the University of Alabama. Dr. Rosenman reported receiving research funding from and serving as an advisor to Amgen and a handful of other companies.
MUNICH – Revising the threshold for actionable high cardiovascular risk from the current 7.5% or greater risk of an event within 10 years as defined in American College of Cardiology/American Heart Association guidelines using the Atherosclerotic Cardiovascular Disease (ASCVD ) Risk Calculator to a 10% or greater 10-year risk would provide the optimal balance of sensitivity and specificity for discriminating future risk of cardiovascular events, according to Robert S. Rosenman, MD.
“I think this is very important from a public health policy perspective,” Dr. Rosenman, a cardiologist who is professor of medicine at Mount Sinai School of Medicine in New York, said at the annual congress of the European Society of Cardiology.
He elaborated: “This would eliminate 11.4 million people who are currently candidates for a statin but may not be getting the benefits of statin therapy. We feel that this information is actually quite important for the primary prevention population because there’s been a lot of pushback from our primary care physician colleagues about the overtreatment of low-risk individuals” under the current guidelines (Circulation. 2014 Jun 24;129[25 Suppl 2]:S49-73).
Dr. Rosenman and his coinvestigators conducted a secondary analysis of data on 21,343 adults in the REGARDS (Reasons for Geographic and Racial Differences in Stroke) study. All participants were free of a baseline history of heart disease or stroke. During a median 8.5 years of follow-up, 1,717 of them experienced adjudicated coronary heart disease or stroke events.
In multivariate analyses adjusted for standard cardiovascular risk factors, socioeconomic and demographic factors, and the use of statins and/or antihypertensive drugs, the higher the baseline 10-year predicted risk using the ACC/AHA ASCVD Risk Calculator based on the Pooled Cohort risk equations, the higher the incidence rate of cardiovascular events. No surprise there.
What was impressive, however, was that the optimal combination of sensitivity and specificity as captured in a statistic known as Youden’s index occurred at a 10-year predicted risk of 10%-12%. The biggest net improvement obtained through reclassification resulted from moving the threshold for elevated 10-year cardiovascular risk warranting statin therapy from 7.5% or greater to 10% or more, rather than using thresholds of 15% or 20%.
He cited data from the 2011-2014 National Health and Nutrition Examination Survey in support of his estimate that switching to a 10% threshold from the current 7.5% threshold would reduce the number of Americans deemed at high cardiovascular risk from 57.1 million to 45.8 million.
“This cutoff value of 10%, by the way, is the same cutoff value used in the recently published ACC/AHA guideline on hypertension. And it’s also the same cutoff value used for antiplatelet therapy in looking at the benefit/risk ratio. So this value of 10% is, I think, really the right number. Our study is the first effort that has been shown to validate that number, and it brings the cutoff values in the various guidelines in line,” the cardiologist observed.
Asked if these new findings are likely to result in a revision of the ACC/AHA cardiovascular risk assessment guidelines, Dr. Rosenman replied that the guidelines are under revision, with the draft update now circulating for comment. So the timing is dicey: His study is now in prepublication peer review, but hasn’t yet been published and thus may not carry persuasive weight.
“Hopefully, the guideline panel is going to make an adjustment to make the 10% figure in line with the blood pressure guidelines,” he said.
The new analysis of the REGARDS study was funded by a collaboration between Amgen, Mount Sinai School of Medicine, and the University of Alabama. Dr. Rosenman reported receiving research funding from and serving as an advisor to Amgen and a handful of other companies.
REPORTING FROM THE ESC CONGRESS 2018
Key clinical point:
Major finding: Redefining the threshold for high 10-year cardiovascular risk from the current 7.5% to 10% would reduce the number of Americans warranting statin therapy by 11.4 million.
Study details: This was a secondary analysis of data on 21,343 adults in the REGARDS study, 1,717 of whom experienced coronary heart disease or stroke events during a median 8.5 years of prospective follow-up.
Disclosures: The new analysis of the REGARDS study was funded by a collaboration between Amgen, Mount Sinai School of Medicine, and the University of Alabama. The presenter reported ties to Amgen and a handful of other companies.
Antiphospholipid antibodies are surprisingly common in first-MI patients
CHICAGO – Patients with a first MI were nearly nine times more likely to have detectable IgG antiphospholipid antibodies than were matched controls in a cross-sectional cohort study, Elisabet Svenungsson, MD, PhD, reported at the annual meeting of the American College of Rheumatology.
Her case-control study included 805 Swedish patients tested for antiphospholipid antibodies 6-10 weeks after experiencing their first MI and an equal number of age-, sex-, and location-matched controls. Prior to their MIs, none of the patients had been diagnosed with antiphospholipid syndrome, which requires both positive antiphospholipid antibodies and a vascular thrombotic event or obstetric morbidity.
A positive test for IgG anti-cardiolipin antibody was present in 10.9% of the first-MI patients, compared with 0.9% of controls. Similarly, 10.4% of acute MI patients and 0.9% of controls were positive for anti-beta2-glycoprotein-1 antibodies. Most patients who tested positive for one were positive for both. Thus, it’s possible that IgG antiphospholipid antibody positivity is an important silent risk factor that’s present in 1 in 10 MI patients, according to Dr. Svenungsson, professor of rheumatology at the Karolinska Institute in Stockholm.
If these results are confirmed and expanded upon in additional studies, testing for antiphospholipid antibodies could become part of the routine care in patients with an acute MI. Those who test positive would meet the criteria for antiphospholipid syndrome and qualify for long-term oral anticoagulation to reduce their elevated risk of further vascular events, she explained in this video interview.
The study was published in Annals of Internal Medicine simultaneously with the presentation at the ACR annual meeting (Ann Int Med. 2018 Oct 23. doi: 10.7326/M18-2130).
SOURCE: Grosso G et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 855.
CHICAGO – Patients with a first MI were nearly nine times more likely to have detectable IgG antiphospholipid antibodies than were matched controls in a cross-sectional cohort study, Elisabet Svenungsson, MD, PhD, reported at the annual meeting of the American College of Rheumatology.
Her case-control study included 805 Swedish patients tested for antiphospholipid antibodies 6-10 weeks after experiencing their first MI and an equal number of age-, sex-, and location-matched controls. Prior to their MIs, none of the patients had been diagnosed with antiphospholipid syndrome, which requires both positive antiphospholipid antibodies and a vascular thrombotic event or obstetric morbidity.
A positive test for IgG anti-cardiolipin antibody was present in 10.9% of the first-MI patients, compared with 0.9% of controls. Similarly, 10.4% of acute MI patients and 0.9% of controls were positive for anti-beta2-glycoprotein-1 antibodies. Most patients who tested positive for one were positive for both. Thus, it’s possible that IgG antiphospholipid antibody positivity is an important silent risk factor that’s present in 1 in 10 MI patients, according to Dr. Svenungsson, professor of rheumatology at the Karolinska Institute in Stockholm.
If these results are confirmed and expanded upon in additional studies, testing for antiphospholipid antibodies could become part of the routine care in patients with an acute MI. Those who test positive would meet the criteria for antiphospholipid syndrome and qualify for long-term oral anticoagulation to reduce their elevated risk of further vascular events, she explained in this video interview.
The study was published in Annals of Internal Medicine simultaneously with the presentation at the ACR annual meeting (Ann Int Med. 2018 Oct 23. doi: 10.7326/M18-2130).
SOURCE: Grosso G et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 855.
CHICAGO – Patients with a first MI were nearly nine times more likely to have detectable IgG antiphospholipid antibodies than were matched controls in a cross-sectional cohort study, Elisabet Svenungsson, MD, PhD, reported at the annual meeting of the American College of Rheumatology.
Her case-control study included 805 Swedish patients tested for antiphospholipid antibodies 6-10 weeks after experiencing their first MI and an equal number of age-, sex-, and location-matched controls. Prior to their MIs, none of the patients had been diagnosed with antiphospholipid syndrome, which requires both positive antiphospholipid antibodies and a vascular thrombotic event or obstetric morbidity.
A positive test for IgG anti-cardiolipin antibody was present in 10.9% of the first-MI patients, compared with 0.9% of controls. Similarly, 10.4% of acute MI patients and 0.9% of controls were positive for anti-beta2-glycoprotein-1 antibodies. Most patients who tested positive for one were positive for both. Thus, it’s possible that IgG antiphospholipid antibody positivity is an important silent risk factor that’s present in 1 in 10 MI patients, according to Dr. Svenungsson, professor of rheumatology at the Karolinska Institute in Stockholm.
If these results are confirmed and expanded upon in additional studies, testing for antiphospholipid antibodies could become part of the routine care in patients with an acute MI. Those who test positive would meet the criteria for antiphospholipid syndrome and qualify for long-term oral anticoagulation to reduce their elevated risk of further vascular events, she explained in this video interview.
The study was published in Annals of Internal Medicine simultaneously with the presentation at the ACR annual meeting (Ann Int Med. 2018 Oct 23. doi: 10.7326/M18-2130).
SOURCE: Grosso G et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 855.
REPORTING FROM THE ACR ANNUAL MEETING

Risk score validated for major NSAID adverse events
CHICAGO – Researchers have derived and validated a 10-item formula to estimate a patient’s risk for developing a major adverse event while on NSAID treatment.
The calculator could “help guide use of NSAIDs in clinical practice,” said Daniel H. Solomon, MD, at the annual meeting of the American College of Rheumatology. Although he called for further validation of the risk-score formula using other databases, he noted that it uses readily available data and could easily be calculated with standard inputs in an electronic medical record. The formula predicts the risk for a major adverse effect during 1 year of daily NSAID use.
Dr. Solomon and his associates devised the risk-score calculator with data collected in the PRECISION (Prospective Randomized Evaluation of Celecoxib Integrated Safety vs Ibuprofen or Naproxen) trial, a safety study designed to test whether treatment with celecoxib was noninferior to treatment with naproxen or ibuprofen for producing cardiovascular adverse events, a hypothesis proven by the study’s results (N Engl J Med. 2016 Dec 29;375[26]:2519-29). They had full data available for 23,950 of the more than 24,000 enrolled patients. The patients averaged 63 years old, just over a third were men, their average body mass index was 31 kg/m2, and 90% had osteoarthritis and 10% had rheumatoid arthritis. The study enrolled patients with an elevated risk for a cardiovascular event, so 63% had hypertension and 36% had diabetes.
The adverse events included as possible outcomes estimated by the formula were all-cause death, major adverse cardiovascular events, clinically significant GI events, or renal insufficiency or failure. The investigators used data from more than 15,000 patients enrolled during the first 4 years of the study to derive the risk-score formula, and data from the nearly 9,000 patients enrolled during the next 5 years to validate it.
The analysis identified and validated 10 baseline items that, when plugged into the formula, calculated a predicted rate for the subsequent development of a major averse event during 1 year of NSAID treatment. The 10 parameters are: age, sex, known cardiovascular disease, hypertension, diabetes, current cigarette use, on treatment with a statin, baseline serum creatinine level, rheumatoid arthritis, and hematocrit.
As examples of the accuracy of the prediction score, Dr. Solomon reported that, among the patients with a predicted risk for a major adverse event of less than 1%, the observed rate was 0.4%; among people with a predicted rate of 1%-4%, the observed rate was 1.7%; and among those with a predicted risk of more than 4% the observed rate was 5.6%. Major cardiovascular events were the most common type of adverse events observed among the nearly 24,000 patients enrolled in PRECISION. A total of 5% of the patients fell into the lowest risk category, with a risk of less than 1%; 70% were in the intermediate risk category, with a predicted risk of 1%-4%; and 25% had a predicted risk of more than 4%, reported Dr. Solomon, a professor of medicine at Harvard Medical School and a rheumatologist at Brigham and Women’s Hospital in Boston.
Age is a major driver of risk, he noted. A patient who is at least 65 years old would have a greater than 1% risk for an adverse event regardless of the other nine risk factors in the scoring formula.
PRECISION was funded by Pfizer. Dr. Solomon has received research funding from AbbVie, Amgen, Bristol-Myers Squibb, Genentech, and Pfizer.
SOURCE: Solomon D et al. ACR Annual Meeting, Abstract 2952. Arthritis Rheumatol. 2018;70(Suppl 10).
CHICAGO – Researchers have derived and validated a 10-item formula to estimate a patient’s risk for developing a major adverse event while on NSAID treatment.
The calculator could “help guide use of NSAIDs in clinical practice,” said Daniel H. Solomon, MD, at the annual meeting of the American College of Rheumatology. Although he called for further validation of the risk-score formula using other databases, he noted that it uses readily available data and could easily be calculated with standard inputs in an electronic medical record. The formula predicts the risk for a major adverse effect during 1 year of daily NSAID use.
Dr. Solomon and his associates devised the risk-score calculator with data collected in the PRECISION (Prospective Randomized Evaluation of Celecoxib Integrated Safety vs Ibuprofen or Naproxen) trial, a safety study designed to test whether treatment with celecoxib was noninferior to treatment with naproxen or ibuprofen for producing cardiovascular adverse events, a hypothesis proven by the study’s results (N Engl J Med. 2016 Dec 29;375[26]:2519-29). They had full data available for 23,950 of the more than 24,000 enrolled patients. The patients averaged 63 years old, just over a third were men, their average body mass index was 31 kg/m2, and 90% had osteoarthritis and 10% had rheumatoid arthritis. The study enrolled patients with an elevated risk for a cardiovascular event, so 63% had hypertension and 36% had diabetes.
The adverse events included as possible outcomes estimated by the formula were all-cause death, major adverse cardiovascular events, clinically significant GI events, or renal insufficiency or failure. The investigators used data from more than 15,000 patients enrolled during the first 4 years of the study to derive the risk-score formula, and data from the nearly 9,000 patients enrolled during the next 5 years to validate it.
The analysis identified and validated 10 baseline items that, when plugged into the formula, calculated a predicted rate for the subsequent development of a major averse event during 1 year of NSAID treatment. The 10 parameters are: age, sex, known cardiovascular disease, hypertension, diabetes, current cigarette use, on treatment with a statin, baseline serum creatinine level, rheumatoid arthritis, and hematocrit.
As examples of the accuracy of the prediction score, Dr. Solomon reported that, among the patients with a predicted risk for a major adverse event of less than 1%, the observed rate was 0.4%; among people with a predicted rate of 1%-4%, the observed rate was 1.7%; and among those with a predicted risk of more than 4% the observed rate was 5.6%. Major cardiovascular events were the most common type of adverse events observed among the nearly 24,000 patients enrolled in PRECISION. A total of 5% of the patients fell into the lowest risk category, with a risk of less than 1%; 70% were in the intermediate risk category, with a predicted risk of 1%-4%; and 25% had a predicted risk of more than 4%, reported Dr. Solomon, a professor of medicine at Harvard Medical School and a rheumatologist at Brigham and Women’s Hospital in Boston.
Age is a major driver of risk, he noted. A patient who is at least 65 years old would have a greater than 1% risk for an adverse event regardless of the other nine risk factors in the scoring formula.
PRECISION was funded by Pfizer. Dr. Solomon has received research funding from AbbVie, Amgen, Bristol-Myers Squibb, Genentech, and Pfizer.
SOURCE: Solomon D et al. ACR Annual Meeting, Abstract 2952. Arthritis Rheumatol. 2018;70(Suppl 10).
CHICAGO – Researchers have derived and validated a 10-item formula to estimate a patient’s risk for developing a major adverse event while on NSAID treatment.
The calculator could “help guide use of NSAIDs in clinical practice,” said Daniel H. Solomon, MD, at the annual meeting of the American College of Rheumatology. Although he called for further validation of the risk-score formula using other databases, he noted that it uses readily available data and could easily be calculated with standard inputs in an electronic medical record. The formula predicts the risk for a major adverse effect during 1 year of daily NSAID use.
Dr. Solomon and his associates devised the risk-score calculator with data collected in the PRECISION (Prospective Randomized Evaluation of Celecoxib Integrated Safety vs Ibuprofen or Naproxen) trial, a safety study designed to test whether treatment with celecoxib was noninferior to treatment with naproxen or ibuprofen for producing cardiovascular adverse events, a hypothesis proven by the study’s results (N Engl J Med. 2016 Dec 29;375[26]:2519-29). They had full data available for 23,950 of the more than 24,000 enrolled patients. The patients averaged 63 years old, just over a third were men, their average body mass index was 31 kg/m2, and 90% had osteoarthritis and 10% had rheumatoid arthritis. The study enrolled patients with an elevated risk for a cardiovascular event, so 63% had hypertension and 36% had diabetes.
The adverse events included as possible outcomes estimated by the formula were all-cause death, major adverse cardiovascular events, clinically significant GI events, or renal insufficiency or failure. The investigators used data from more than 15,000 patients enrolled during the first 4 years of the study to derive the risk-score formula, and data from the nearly 9,000 patients enrolled during the next 5 years to validate it.
The analysis identified and validated 10 baseline items that, when plugged into the formula, calculated a predicted rate for the subsequent development of a major averse event during 1 year of NSAID treatment. The 10 parameters are: age, sex, known cardiovascular disease, hypertension, diabetes, current cigarette use, on treatment with a statin, baseline serum creatinine level, rheumatoid arthritis, and hematocrit.
As examples of the accuracy of the prediction score, Dr. Solomon reported that, among the patients with a predicted risk for a major adverse event of less than 1%, the observed rate was 0.4%; among people with a predicted rate of 1%-4%, the observed rate was 1.7%; and among those with a predicted risk of more than 4% the observed rate was 5.6%. Major cardiovascular events were the most common type of adverse events observed among the nearly 24,000 patients enrolled in PRECISION. A total of 5% of the patients fell into the lowest risk category, with a risk of less than 1%; 70% were in the intermediate risk category, with a predicted risk of 1%-4%; and 25% had a predicted risk of more than 4%, reported Dr. Solomon, a professor of medicine at Harvard Medical School and a rheumatologist at Brigham and Women’s Hospital in Boston.
Age is a major driver of risk, he noted. A patient who is at least 65 years old would have a greater than 1% risk for an adverse event regardless of the other nine risk factors in the scoring formula.
PRECISION was funded by Pfizer. Dr. Solomon has received research funding from AbbVie, Amgen, Bristol-Myers Squibb, Genentech, and Pfizer.
SOURCE: Solomon D et al. ACR Annual Meeting, Abstract 2952. Arthritis Rheumatol. 2018;70(Suppl 10).
REPORTING FROM THE ACR ANNUAL MEETING
Key clinical point:
Major finding: Five percent of patients had a predicted risk below 1%; 70% had 1%-4% risk; 25% had greater than 4% risk.
Study details: Derivation and validation of the risk score used data from 23,950 patients in the PRECISION trial.
Disclosures: PRECISION was funded by Pfizer. Dr. Solomon has received research funding from AbbVie, Amgen, Bristol-Myers Squibb, Genentech, and Pfizer.
Source: Solomon D et al. ACR Annual Meeting, Abstract 2952. Arthritis Rheumatol. 2018;70(Suppl 10).
Transition to high-sensitivity troponin T assay helped boost ED discharge rates
SAN DIEGO – After transitioning to using the high-sensitivity troponin T assay for patients over the age of 35 years who presented to the ED with chest pain or tightness, an increased number of patients were discharged, yet no impact was observed on the time to admission and/or observation, according to a study conducted at two Philadelphia-based hospitals.

“Biomarkers have been a cornerstone of evaluating patients who present with chest pain,” Frederick T. Randolph, MD, said at the annual meeting of the American College of Emergency Physicians. “Recently in the United States, fifth-generation or high-sensitivity troponin [assays] have been approved for use. Our institution made the plan to transition to utilization of high-sensitivity troponins. At that time, we were aware of European studies that they were able to discharge a higher percentage of patients from the ED. There have been no prior studies of the clinical impact of transition to high-sensitivity troponin [assays] in the U.S.”
Dr. Randolph, director of the Chest Pain Center at Thomas Jefferson University, Philadelphia, and his colleagues performed a before and after study assessing all patients over age 35 years who presented to two hospitals with chest pain or tightness and who received a troponin assay draw in the ED. They conducted two town halls, in-services with cardiology and emergency medicine, and distributed a slide set to all providers. “There was no guidance as to who to order the troponin on,” said Dr. Randolph, who is also vice chief of emergency medicine at the university. “Essentially, the recommendation was, ‘Keep using troponins the same way you’ve been using troponins for years.’ The education was centered on how frequently we were going to order repeat troponins and how to interpret those results.”
The researchers used a 0- and 2-hour sampling strategy (unless the first value was less than 6 ng/L) and used a cut-point of 19 ng/L to define “ruled out” and a cut-point of 53 ng/L to define “consistent with acute myocardial infarction.” Indeterminate values were repeated every 2 hours. Dr. Randolph and his associates collected data for 1 year prior to transition to high-sensitivity troponins in 4,295 patients, and 2 months post transition in 769 patients. The primary outcome was discharge rate from the ED. Secondary outcome was time from presentation to admission/observation decision.
There were no statistically significant differences between the pre- and posttransition groups in the percentage of those aged 36-64 years (74% vs. 76%, respectively) or in the percentage of those who were nonwhite (61% vs. 59%). The only statistically significant difference was a higher percentage of females in the preimplementation group (49% vs. 46%; P = .02).
In all, the researchers were able to discharge 45.2% of all patients during the pretransition period, compared with 58.7% of patients in the posttransition period, for an absolute increase of 13% (P less than .001). There was no difference between the two groups in time to decision to admit or to observe (a mean of 199.1 vs. 192.2 minutes, respectively; P = .96). “Areas of future study would be to evaluate those patients who were discharged and monitor them for any changes in outcomes, to see if there is any increase in morbidity or complications,” said Dr. Randolph. “An additional research curiosity would be the downstream consequences on cost or revenue to the institution given the increased number of admissions and the decreased use of diagnostic testing such as coronary computed tomography angiography and stress testing.”
Dr. Randolph disclosed that some of the study authors have participated in multiple biomarker studies over the years. He reported having no financial disclosures.
Source: Randolph FT et al. Ann Emerg Med. 2018 Oct;72;4:S2-3. doi. 10.1016/j.annemergmed.2018.08.009.
SAN DIEGO – After transitioning to using the high-sensitivity troponin T assay for patients over the age of 35 years who presented to the ED with chest pain or tightness, an increased number of patients were discharged, yet no impact was observed on the time to admission and/or observation, according to a study conducted at two Philadelphia-based hospitals.
“Biomarkers have been a cornerstone of evaluating patients who present with chest pain,” Frederick T. Randolph, MD, said at the annual meeting of the American College of Emergency Physicians. “Recently in the United States, fifth-generation or high-sensitivity troponin [assays] have been approved for use. Our institution made the plan to transition to utilization of high-sensitivity troponins. At that time, we were aware of European studies that they were able to discharge a higher percentage of patients from the ED. There have been no prior studies of the clinical impact of transition to high-sensitivity troponin [assays] in the U.S.”
Dr. Randolph, director of the Chest Pain Center at Thomas Jefferson University, Philadelphia, and his colleagues performed a before and after study assessing all patients over age 35 years who presented to two hospitals with chest pain or tightness and who received a troponin assay draw in the ED. They conducted two town halls, in-services with cardiology and emergency medicine, and distributed a slide set to all providers. “There was no guidance as to who to order the troponin on,” said Dr. Randolph, who is also vice chief of emergency medicine at the university. “Essentially, the recommendation was, ‘Keep using troponins the same way you’ve been using troponins for years.’ The education was centered on how frequently we were going to order repeat troponins and how to interpret those results.”
The researchers used a 0- and 2-hour sampling strategy (unless the first value was less than 6 ng/L) and used a cut-point of 19 ng/L to define “ruled out” and a cut-point of 53 ng/L to define “consistent with acute myocardial infarction.” Indeterminate values were repeated every 2 hours. Dr. Randolph and his associates collected data for 1 year prior to transition to high-sensitivity troponins in 4,295 patients, and 2 months post transition in 769 patients. The primary outcome was discharge rate from the ED. Secondary outcome was time from presentation to admission/observation decision.
There were no statistically significant differences between the pre- and posttransition groups in the percentage of those aged 36-64 years (74% vs. 76%, respectively) or in the percentage of those who were nonwhite (61% vs. 59%). The only statistically significant difference was a higher percentage of females in the preimplementation group (49% vs. 46%; P = .02).
In all, the researchers were able to discharge 45.2% of all patients during the pretransition period, compared with 58.7% of patients in the posttransition period, for an absolute increase of 13% (P less than .001). There was no difference between the two groups in time to decision to admit or to observe (a mean of 199.1 vs. 192.2 minutes, respectively; P = .96). “Areas of future study would be to evaluate those patients who were discharged and monitor them for any changes in outcomes, to see if there is any increase in morbidity or complications,” said Dr. Randolph. “An additional research curiosity would be the downstream consequences on cost or revenue to the institution given the increased number of admissions and the decreased use of diagnostic testing such as coronary computed tomography angiography and stress testing.”
Dr. Randolph disclosed that some of the study authors have participated in multiple biomarker studies over the years. He reported having no financial disclosures.
Source: Randolph FT et al. Ann Emerg Med. 2018 Oct;72;4:S2-3. doi. 10.1016/j.annemergmed.2018.08.009.
SAN DIEGO – After transitioning to using the high-sensitivity troponin T assay for patients over the age of 35 years who presented to the ED with chest pain or tightness, an increased number of patients were discharged, yet no impact was observed on the time to admission and/or observation, according to a study conducted at two Philadelphia-based hospitals.
“Biomarkers have been a cornerstone of evaluating patients who present with chest pain,” Frederick T. Randolph, MD, said at the annual meeting of the American College of Emergency Physicians. “Recently in the United States, fifth-generation or high-sensitivity troponin [assays] have been approved for use. Our institution made the plan to transition to utilization of high-sensitivity troponins. At that time, we were aware of European studies that they were able to discharge a higher percentage of patients from the ED. There have been no prior studies of the clinical impact of transition to high-sensitivity troponin [assays] in the U.S.”
Dr. Randolph, director of the Chest Pain Center at Thomas Jefferson University, Philadelphia, and his colleagues performed a before and after study assessing all patients over age 35 years who presented to two hospitals with chest pain or tightness and who received a troponin assay draw in the ED. They conducted two town halls, in-services with cardiology and emergency medicine, and distributed a slide set to all providers. “There was no guidance as to who to order the troponin on,” said Dr. Randolph, who is also vice chief of emergency medicine at the university. “Essentially, the recommendation was, ‘Keep using troponins the same way you’ve been using troponins for years.’ The education was centered on how frequently we were going to order repeat troponins and how to interpret those results.”
The researchers used a 0- and 2-hour sampling strategy (unless the first value was less than 6 ng/L) and used a cut-point of 19 ng/L to define “ruled out” and a cut-point of 53 ng/L to define “consistent with acute myocardial infarction.” Indeterminate values were repeated every 2 hours. Dr. Randolph and his associates collected data for 1 year prior to transition to high-sensitivity troponins in 4,295 patients, and 2 months post transition in 769 patients. The primary outcome was discharge rate from the ED. Secondary outcome was time from presentation to admission/observation decision.
There were no statistically significant differences between the pre- and posttransition groups in the percentage of those aged 36-64 years (74% vs. 76%, respectively) or in the percentage of those who were nonwhite (61% vs. 59%). The only statistically significant difference was a higher percentage of females in the preimplementation group (49% vs. 46%; P = .02).
In all, the researchers were able to discharge 45.2% of all patients during the pretransition period, compared with 58.7% of patients in the posttransition period, for an absolute increase of 13% (P less than .001). There was no difference between the two groups in time to decision to admit or to observe (a mean of 199.1 vs. 192.2 minutes, respectively; P = .96). “Areas of future study would be to evaluate those patients who were discharged and monitor them for any changes in outcomes, to see if there is any increase in morbidity or complications,” said Dr. Randolph. “An additional research curiosity would be the downstream consequences on cost or revenue to the institution given the increased number of admissions and the decreased use of diagnostic testing such as coronary computed tomography angiography and stress testing.”
Dr. Randolph disclosed that some of the study authors have participated in multiple biomarker studies over the years. He reported having no financial disclosures.
Source: Randolph FT et al. Ann Emerg Med. 2018 Oct;72;4:S2-3. doi. 10.1016/j.annemergmed.2018.08.009.
AT ACEP18
Key clinical point: .
Major finding: After conversion to using the high-sensitivity troponin T assay, the ED discharge rate increased to 58.7%, from 45.2% (P less than 0.001).
Study details: A before and after study of 5,064 patients aged 35 and older who presented to the ED with chest pain or tightness.
Disclosures: Dr. Randolph disclosed that some of the study authors have participated in multiple biomarker studies over the years. He reported having no financial disclosures.
Source: Randolph FT et al. Ann Emerg Med. 2018 Oct;72;4:S2-3. doi: 10.1016/j.annemergmed.2018.08.009.
Stroke risk in elderly following AMI extends to 12 weeks
ATLANTA – Acute myocardial infarction is associated with a risk of stroke that extends beyond the 1-month time window currently considered the at-risk period, according to an analysis of Medicare data.

“The results of our study may allow clinicians to more accurately counsel patients regarding their stroke etiology and may allow refinement of stroke etiology classification systems and clinical trial selection criteria,” lead study author Alexander E. Merkler, MD, said in an interview in advance of the annual meeting of the American Neurological Association.
In an effort to better understand the duration of heightened stroke risk after acute myocardial infarction, Dr. Merkler, a neurologist at New York–based Weill Cornell Medicine, and his colleagues conducted a retrospective cohort study using inpatient and outpatient claims during 2008-2015 from a nationally representative 5% sample of Medicare beneficiaries who were at least 66 years old. They used previously validated ICD-9-CM diagnosis codes to ascertain the exposure variable of acute MI and the outcome of ischemic stroke but excluded strokes that occurred during an acute MI hospitalization.
Patients were censored at the time of ischemic stroke, death, end of Medicare coverage, or by Sept. 30, 2015. The researchers fit Cox regression models separately for the groups with and without acute MI to examine its association with ischemic stroke after adjusting for demographics, stroke risk factors, and Charlson comorbidities. Next, they used the corresponding survival probabilities to compute the hazard ratio (HR) in each 4-week interval after discharge, up to week 12. They also conducted a subgroup analysis to evaluate the duration of heightened ischemic stroke risk by MI type: ST-segment elevation MI (STEMI) versus non-STEMI (NSTEMI).
Dr. Merkler and his colleagues drew from data on 1.7 million eligible beneficiaries. Of these, 46,182 were hospitalized for acute MI and 80,466 for ischemic stroke. After they adjusted for demographics, stroke risk factors, and Charlson comorbidities, the researchers found that the risk of ischemic stroke was highest in the first 4 weeks after discharge from the MI hospitalization (HR, 2.7), yet remained elevated during weeks 5-8 (HR, 2.0) and weeks 9-12 (HR, 1.6). It was no longer significantly elevated afterward. The prolonged period of heightened ischemic stroke risk was evident in patients with both STEMI and NSTEMI.
“We were surprised by how long the risk of stroke lasts after MI,” Dr. Merkler said. He acknowledged certain limitations of the analysis, including the fact that patients were all over the age of 65 years. “In addition, we lack granular detail such as severity of MI [and] the extent of stroke work-up,” he said.
Dr. Merkler disclosed that he is supported by a grant from the National Institutes of Health and by the Leon Levy Foundation in Neuroscience. Most of his coauthors are also supported by NIH grants.
[email protected]
Source: Ann Neurol. 2018;84[S22]:S146-7, Abstract M122.
ATLANTA – Acute myocardial infarction is associated with a risk of stroke that extends beyond the 1-month time window currently considered the at-risk period, according to an analysis of Medicare data.
“The results of our study may allow clinicians to more accurately counsel patients regarding their stroke etiology and may allow refinement of stroke etiology classification systems and clinical trial selection criteria,” lead study author Alexander E. Merkler, MD, said in an interview in advance of the annual meeting of the American Neurological Association.
In an effort to better understand the duration of heightened stroke risk after acute myocardial infarction, Dr. Merkler, a neurologist at New York–based Weill Cornell Medicine, and his colleagues conducted a retrospective cohort study using inpatient and outpatient claims during 2008-2015 from a nationally representative 5% sample of Medicare beneficiaries who were at least 66 years old. They used previously validated ICD-9-CM diagnosis codes to ascertain the exposure variable of acute MI and the outcome of ischemic stroke but excluded strokes that occurred during an acute MI hospitalization.
Patients were censored at the time of ischemic stroke, death, end of Medicare coverage, or by Sept. 30, 2015. The researchers fit Cox regression models separately for the groups with and without acute MI to examine its association with ischemic stroke after adjusting for demographics, stroke risk factors, and Charlson comorbidities. Next, they used the corresponding survival probabilities to compute the hazard ratio (HR) in each 4-week interval after discharge, up to week 12. They also conducted a subgroup analysis to evaluate the duration of heightened ischemic stroke risk by MI type: ST-segment elevation MI (STEMI) versus non-STEMI (NSTEMI).
Dr. Merkler and his colleagues drew from data on 1.7 million eligible beneficiaries. Of these, 46,182 were hospitalized for acute MI and 80,466 for ischemic stroke. After they adjusted for demographics, stroke risk factors, and Charlson comorbidities, the researchers found that the risk of ischemic stroke was highest in the first 4 weeks after discharge from the MI hospitalization (HR, 2.7), yet remained elevated during weeks 5-8 (HR, 2.0) and weeks 9-12 (HR, 1.6). It was no longer significantly elevated afterward. The prolonged period of heightened ischemic stroke risk was evident in patients with both STEMI and NSTEMI.
“We were surprised by how long the risk of stroke lasts after MI,” Dr. Merkler said. He acknowledged certain limitations of the analysis, including the fact that patients were all over the age of 65 years. “In addition, we lack granular detail such as severity of MI [and] the extent of stroke work-up,” he said.
Dr. Merkler disclosed that he is supported by a grant from the National Institutes of Health and by the Leon Levy Foundation in Neuroscience. Most of his coauthors are also supported by NIH grants.
[email protected]
Source: Ann Neurol. 2018;84[S22]:S146-7, Abstract M122.
ATLANTA – Acute myocardial infarction is associated with a risk of stroke that extends beyond the 1-month time window currently considered the at-risk period, according to an analysis of Medicare data.
“The results of our study may allow clinicians to more accurately counsel patients regarding their stroke etiology and may allow refinement of stroke etiology classification systems and clinical trial selection criteria,” lead study author Alexander E. Merkler, MD, said in an interview in advance of the annual meeting of the American Neurological Association.
In an effort to better understand the duration of heightened stroke risk after acute myocardial infarction, Dr. Merkler, a neurologist at New York–based Weill Cornell Medicine, and his colleagues conducted a retrospective cohort study using inpatient and outpatient claims during 2008-2015 from a nationally representative 5% sample of Medicare beneficiaries who were at least 66 years old. They used previously validated ICD-9-CM diagnosis codes to ascertain the exposure variable of acute MI and the outcome of ischemic stroke but excluded strokes that occurred during an acute MI hospitalization.
Patients were censored at the time of ischemic stroke, death, end of Medicare coverage, or by Sept. 30, 2015. The researchers fit Cox regression models separately for the groups with and without acute MI to examine its association with ischemic stroke after adjusting for demographics, stroke risk factors, and Charlson comorbidities. Next, they used the corresponding survival probabilities to compute the hazard ratio (HR) in each 4-week interval after discharge, up to week 12. They also conducted a subgroup analysis to evaluate the duration of heightened ischemic stroke risk by MI type: ST-segment elevation MI (STEMI) versus non-STEMI (NSTEMI).
Dr. Merkler and his colleagues drew from data on 1.7 million eligible beneficiaries. Of these, 46,182 were hospitalized for acute MI and 80,466 for ischemic stroke. After they adjusted for demographics, stroke risk factors, and Charlson comorbidities, the researchers found that the risk of ischemic stroke was highest in the first 4 weeks after discharge from the MI hospitalization (HR, 2.7), yet remained elevated during weeks 5-8 (HR, 2.0) and weeks 9-12 (HR, 1.6). It was no longer significantly elevated afterward. The prolonged period of heightened ischemic stroke risk was evident in patients with both STEMI and NSTEMI.
“We were surprised by how long the risk of stroke lasts after MI,” Dr. Merkler said. He acknowledged certain limitations of the analysis, including the fact that patients were all over the age of 65 years. “In addition, we lack granular detail such as severity of MI [and] the extent of stroke work-up,” he said.
Dr. Merkler disclosed that he is supported by a grant from the National Institutes of Health and by the Leon Levy Foundation in Neuroscience. Most of his coauthors are also supported by NIH grants.
[email protected]
Source: Ann Neurol. 2018;84[S22]:S146-7, Abstract M122.
AT ANA 2018
Key clinical point: .
Major finding: The risk of ischemic stroke was highest in the first 4 weeks after discharge from the MI hospitalization (HR, 2.7), yet remained elevated during weeks 5-8 (HR, 2.0) and weeks 9-12 (HR, 1.6).
Study details: An analysis of 46,182 Medicare beneficiaries who were hospitalized for acute MI and 80,466 who were hospitalized for ischemic stroke.
Disclosures: Dr. Merkler disclosed that he is supported by a grant from the National Institutes of Health and by the Leon Levy Foundation in Neuroscience. Most of his coauthors are also supported by NIH grants.
Source: Ann Neurol. 2018;84[S22]:S146-7, Abstract M122.
Fat attenuation index boosts coronary CT prognostication
MUNICH – The perivascular fat attenuation index, a new measure of coronary plaque inflammation using data collected by a conventional coronary CT scan, identified an elevated risk for future cardiovascular death that was independent of standard risk factors in both derivation and validation studies with prospective data from more than 3,900 patients.

Patients with a high fat attenuation index (FAI) in the perivascular fat surrounding their right coronary artery had a five- to ninefold higher risk of cardiac mortality during 4-6 years of follow-up than did those with lower scores, after adjustment for conventional risk factors and standard findings from the coronary CT, Charalambos Antoniades, MD, said at the annual congress of the European Society of Cardiology.
The FAI is a “powerful, novel technology for cardiovascular disease risk stratification. It has striking prognostic value for cardiac death and nonfatal MI over and above other risk scores and state-of-the-art interpretation of coronary CT angiography,” said Dr. Antoniades, professor of cardiovascular medicine at the University of Oxford (England). He also highlighted that the data he reported suggested a protective effect in patients with a high FAI who received treatment with aspirin or a statin, and he suggested that FAI might be a way to better target an anti-inflammatory agent such as canakinumab (Ilaris), which showed cardiovascular protective effects in the CANTOS trial (N Engl J Med. 2017 Sep 21;377[12]:1119-31).
Another key feature of the FAI analysis is that it uses data collected by “any standard” coronary CT angiogram, Dr. Antoniades said. He is a founder of, shareholder in, and chief scientific officer of Caristo Diagnostics, the company developing the software that uses coronary CT data to calculate the FAI.
Dr. Antoniades and his associates derived the FAI using data collected from 1,872 patients who underwent planned coronary CT angiography at a clinic in Erlangen, Germany, during 2005-2009. The researchers correlated FAI scores with cardiovascular disease outcomes during a median follow-up of 72 months. They then validated the FAI using data collected from 2,040 patients who underwent a planned coronary CT exam at the Cleveland Clinic during 2008-2016 and then had a median follow-up of 54 months. The researchers called this overall post-hoc analysis of prospectively collected CT and outcomes data the Cardiovascular Risk Prediction using Computed Tomography (CRISP-CT) study.
Using the derivation data, FAI measurements taken from fat around the proximal right coronary artery that met or exceeded the specified cutoff value of –70.1 Hounsfield units were tied to a 9.04-fold greater rate of cardiac death during follow-up, compared with patients with a lower FAI, and after adjustment for several demographic, clinical, and CT-angiography variables. When the researchers ran this analysis using data from the validation patients and the same cutoff value they found that an elevated FAI linked with a 5.6-fold higher rate of cardiac death. Concurrently with Dr. Antoniades’ talk the results appeared in an online article that was later published (Lancet. 2018 Sep 15;392[10151]:929-39).
Calculating a patient’s FAI offers the prospect for “better use of CT information,” Dr. Antoniades said during the discussion of his report. After a coronary CT scan and conventional data processing, about half the patients have no finding that warrants intervention, but about 10% of these patients actually have an inflamed coronary plaque that is at high risk for rupture that could trigger a cardiac event. The FAI provides a way to use coronary CT angiography to identify these at-risk patients, he explained.
MUNICH – The perivascular fat attenuation index, a new measure of coronary plaque inflammation using data collected by a conventional coronary CT scan, identified an elevated risk for future cardiovascular death that was independent of standard risk factors in both derivation and validation studies with prospective data from more than 3,900 patients.
Patients with a high fat attenuation index (FAI) in the perivascular fat surrounding their right coronary artery had a five- to ninefold higher risk of cardiac mortality during 4-6 years of follow-up than did those with lower scores, after adjustment for conventional risk factors and standard findings from the coronary CT, Charalambos Antoniades, MD, said at the annual congress of the European Society of Cardiology.
The FAI is a “powerful, novel technology for cardiovascular disease risk stratification. It has striking prognostic value for cardiac death and nonfatal MI over and above other risk scores and state-of-the-art interpretation of coronary CT angiography,” said Dr. Antoniades, professor of cardiovascular medicine at the University of Oxford (England). He also highlighted that the data he reported suggested a protective effect in patients with a high FAI who received treatment with aspirin or a statin, and he suggested that FAI might be a way to better target an anti-inflammatory agent such as canakinumab (Ilaris), which showed cardiovascular protective effects in the CANTOS trial (N Engl J Med. 2017 Sep 21;377[12]:1119-31).
Another key feature of the FAI analysis is that it uses data collected by “any standard” coronary CT angiogram, Dr. Antoniades said. He is a founder of, shareholder in, and chief scientific officer of Caristo Diagnostics, the company developing the software that uses coronary CT data to calculate the FAI.
Dr. Antoniades and his associates derived the FAI using data collected from 1,872 patients who underwent planned coronary CT angiography at a clinic in Erlangen, Germany, during 2005-2009. The researchers correlated FAI scores with cardiovascular disease outcomes during a median follow-up of 72 months. They then validated the FAI using data collected from 2,040 patients who underwent a planned coronary CT exam at the Cleveland Clinic during 2008-2016 and then had a median follow-up of 54 months. The researchers called this overall post-hoc analysis of prospectively collected CT and outcomes data the Cardiovascular Risk Prediction using Computed Tomography (CRISP-CT) study.
Using the derivation data, FAI measurements taken from fat around the proximal right coronary artery that met or exceeded the specified cutoff value of –70.1 Hounsfield units were tied to a 9.04-fold greater rate of cardiac death during follow-up, compared with patients with a lower FAI, and after adjustment for several demographic, clinical, and CT-angiography variables. When the researchers ran this analysis using data from the validation patients and the same cutoff value they found that an elevated FAI linked with a 5.6-fold higher rate of cardiac death. Concurrently with Dr. Antoniades’ talk the results appeared in an online article that was later published (Lancet. 2018 Sep 15;392[10151]:929-39).
Calculating a patient’s FAI offers the prospect for “better use of CT information,” Dr. Antoniades said during the discussion of his report. After a coronary CT scan and conventional data processing, about half the patients have no finding that warrants intervention, but about 10% of these patients actually have an inflamed coronary plaque that is at high risk for rupture that could trigger a cardiac event. The FAI provides a way to use coronary CT angiography to identify these at-risk patients, he explained.
MUNICH – The perivascular fat attenuation index, a new measure of coronary plaque inflammation using data collected by a conventional coronary CT scan, identified an elevated risk for future cardiovascular death that was independent of standard risk factors in both derivation and validation studies with prospective data from more than 3,900 patients.
Patients with a high fat attenuation index (FAI) in the perivascular fat surrounding their right coronary artery had a five- to ninefold higher risk of cardiac mortality during 4-6 years of follow-up than did those with lower scores, after adjustment for conventional risk factors and standard findings from the coronary CT, Charalambos Antoniades, MD, said at the annual congress of the European Society of Cardiology.
The FAI is a “powerful, novel technology for cardiovascular disease risk stratification. It has striking prognostic value for cardiac death and nonfatal MI over and above other risk scores and state-of-the-art interpretation of coronary CT angiography,” said Dr. Antoniades, professor of cardiovascular medicine at the University of Oxford (England). He also highlighted that the data he reported suggested a protective effect in patients with a high FAI who received treatment with aspirin or a statin, and he suggested that FAI might be a way to better target an anti-inflammatory agent such as canakinumab (Ilaris), which showed cardiovascular protective effects in the CANTOS trial (N Engl J Med. 2017 Sep 21;377[12]:1119-31).
Another key feature of the FAI analysis is that it uses data collected by “any standard” coronary CT angiogram, Dr. Antoniades said. He is a founder of, shareholder in, and chief scientific officer of Caristo Diagnostics, the company developing the software that uses coronary CT data to calculate the FAI.
Dr. Antoniades and his associates derived the FAI using data collected from 1,872 patients who underwent planned coronary CT angiography at a clinic in Erlangen, Germany, during 2005-2009. The researchers correlated FAI scores with cardiovascular disease outcomes during a median follow-up of 72 months. They then validated the FAI using data collected from 2,040 patients who underwent a planned coronary CT exam at the Cleveland Clinic during 2008-2016 and then had a median follow-up of 54 months. The researchers called this overall post-hoc analysis of prospectively collected CT and outcomes data the Cardiovascular Risk Prediction using Computed Tomography (CRISP-CT) study.
Using the derivation data, FAI measurements taken from fat around the proximal right coronary artery that met or exceeded the specified cutoff value of –70.1 Hounsfield units were tied to a 9.04-fold greater rate of cardiac death during follow-up, compared with patients with a lower FAI, and after adjustment for several demographic, clinical, and CT-angiography variables. When the researchers ran this analysis using data from the validation patients and the same cutoff value they found that an elevated FAI linked with a 5.6-fold higher rate of cardiac death. Concurrently with Dr. Antoniades’ talk the results appeared in an online article that was later published (Lancet. 2018 Sep 15;392[10151]:929-39).
Calculating a patient’s FAI offers the prospect for “better use of CT information,” Dr. Antoniades said during the discussion of his report. After a coronary CT scan and conventional data processing, about half the patients have no finding that warrants intervention, but about 10% of these patients actually have an inflamed coronary plaque that is at high risk for rupture that could trigger a cardiac event. The FAI provides a way to use coronary CT angiography to identify these at-risk patients, he explained.
REPORTING FROM THE ESC CONGRESS 2018
Key clinical point:
Major finding: Patients with a fat attenuation index at or above the selected cutoff had a five- to ninefold increased rate of cardiac death.
Study details: The CRISP-CT study, which ran a post-hoc analysis of CT angiography data from 3,912 patients.
Disclosures: Dr. Antoniades is a founder of, shareholder in, and chief scientific officer of Caristo Diagnostics, the company developing fat attenuation index software.