User login
Hospital-Acquired Conditions & The Hospitalist
Hospitalist Neal Axon, MD, first became aware of an important change in his hospital’s policies last year while attending to an elderly patient the morning after admission to the community hospital where he works part time.
“This new form appeared in the chart requesting a urinalysis for my patient, who’d had a Foley catheter placed,” says Dr. Axon, an assistant professor of medicine at the Medical University of South Carolina in Charleston. “I didn’t know why, so I asked. I was told that it was now necessary to document that there was no UTI present on admission.” He asked the charge nurse, “So what do I do now that the catheter has been in place for 12 hours and has colonization without a true infection?”
The next thing he heard: silence.
The new form Dr. Axon encountered was an outgrowth of the requirements of the Deficit Reduction Act (DRA) of 2005, which ordered Medicare to withhold additional hospital payments for hospital-acquired complications (HAC) developed during a hospital stay. One result of the new rule is that much of a hospital’s response to these initiatives has been placed in the hands of the hospitalist. From accurate documentation of complications already present on admission (POA), to confirming that guidelines for treatment are being followed, to taking the lead on review of staff practices and education, hospitalists are in a position to have a wide-ranging impact on patient care and the financial health of their institutions.
Congress Pushes Reforms
In order for Medicare to not provide a reimbursement, an HAC has to be high-cost and/or high-volume, result in the assignment of the case to a higher payment when present as a secondary diagnosis, and “could reasonably be prevented through the application of evidence-based guidelines,” says Barry Straube, MD, chief medical officer and director of the Office of Clinical Standards and Quality at the Centers for Medicare and Medicaid Services (CMS). “CMS was to implement a process where we would not pay the hospitals additional money for these complications.”
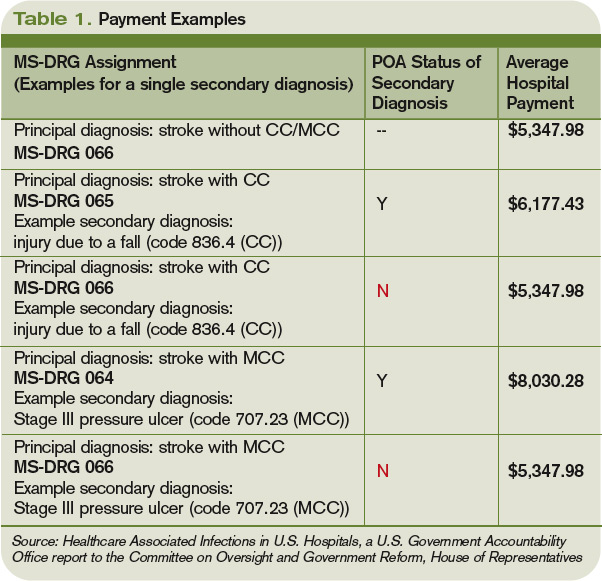
The new rules mean Medicare pays hospitals on the basis of Medicare Severity Diagnostic-Related Groups (MS-DRG), which better reflect the complexity of a patient’s illness. The biggest change was a three-tiered payment schedule: a base level for the diagnosis, a second level adding money to reflect the presence of comorbidities and complications, and a third for major complications and comorbidities (see Table 1, p. 31).
“Instituting HACs means that hospitals would no longer receive the comorbidity and complication payments if the only reason a case qualified for higher payment was the HAC,” Dr. Straube explains. “We did carve out a POA exception for those conditions that were acquired outside of the hospital. HACs only impact additional payments; the hospitals are still paid for the diagnosis that resulted in the hospital admission.”
CMS also identifies three “never events” it won’t reimburse for (see “A Brief History of Never Events,” p. 35): performing the wrong procedure, performing a procedure on the wrong body part, and performing a procedure on the wrong patient. “Neither hospitals nor physicians that are involved in such egregious situations would be paid,” Dr. Straube says.
Preventability: Subject of Controversy

The big questions surrounding HACs: Could they reasonably be prevented through the application of evidence-based guidelines? How preventable are HACs? Who decides if a complication is preventable, and therefore payment for services is withheld?
They’re concerns that are widespread among physicians, hospital administrators, and regulators alike.
“The legislation required the conditions to be ‘reasonably preventable’ using established clinical guidelines,” Dr. Straube says. “We did not have to show 100% prevention. In an imperfect world, they might still take place occasionally, but with good medical care, almost all of these are preventable in this day and age.”
For CMS, the preventable conditions are an either/or situation: Either they existed prior to admission and are subject to payment, or they did not exist at admission and additional payment for the complication will not be made. “HACs do not currently consider a patient’s individual risk for complications,” says Jennifer Meddings, MD, MSc, clinical lecturer and health researcher in the Department of Internal Medicine at the University of Michigan Health System in Ann Arbor. “We know the best strategies to prevent complications in ideal patients, and these are reflected in the HACs. In real life, many of our patients just don’t fit into the guidelines for many reasons—and you have to individualize care.”
Dr. Meddings points to DVT as a prime example. For a certain number of inpatients, the guidelines can be followed to perfection. In other patients (e.g., those with kidney conditions), previous reactions to a medication or an individual’s predisposition to clotting might interfere with treatment. However, CMS doesn’t allow appeals of nonpayment decisions for HACs based on individual circumstances.
Some experts think the rigidness of the payment policy forces physicians to treat patients exactly to guidelines. Even then, payment could be declined if an HAC develops.
“One of the points of most discussion is how preventable some of these are, particularly when choosing those you are no longer going to pay for,” Dr. Meddings says. “Many of the complications currently under review have patients that are at higher risk than others. How much our prevention strategies can alleviate or reduce the risk varies widely among patients.”
Impact on HM Practice
Many of the preventable conditions outlined by CMS do not directly affect hospitalist payment. However, hospitalists often find themselves responsible for properly documenting admission and care.
“The rule changes regarding payment for HACs are only related to hospital payments, and to date, most physicians, including hospitalists, are not directly at financial risk,” says Heidi Wald, MD, MSPH, hospitalist and assistant professor of medicine in the divisions of Health Care Policy Research and General Internal Medicine at the University of Colorado Denver School of Medicine. “Although hospitalists have no financial skin in the game, there are plenty of reasons they would take an interest in addressing HACs in their hospital. In particular, they are often seen as the ‘go-to’ group for quality improvement in their hospitals.”
For example, some HM groups have been active in working with teams of physicians, nurses, and other healthcare providers to address local policies and procedures on prevention of catheter-associated urinary tract infections (UTIs) and DVT.
“This has certainly necessitated a team approach,” says Shaun Frost, MD, FHM, an SHM board member and regional medical director for Cogent Healthcare in St. Paul, Minn. “For many of the HACs that apply to our population of patients, the hospitalist alone cannot be expected to solely execute effective quality improvements. It takes a team effort in that regard, and one that includes many different disciplines.”
The Cogent-affiliated hospitalist group at Temple University Hospital in Philadelphia formed a task force to address issues with catheter-associated UTI. One initiative focused on educating all providers involved in the proper care of the catheters and similar interventions. A secondary focus of the project was an inventory of current practices and procedures.
“It was discovered that we did not have an automatic stop order for Foley catheters, so in some situations, they were likely being left in longer than needed while nursing [staff] tried to contact a physician,” Dr. Frost explains. “We created standardized order sets that include criteria for continuing the catheter. Once the criteria are no longer applicable, nursing will be able to discontinue it.”
Although CMS has only recently turned the spotlight on HACs and never events, hospitalists have been heavily involved in the patient-safety arena for years. “It is not a new phenomenon that hospitalists work for healthcare delivery and healthcare system improvement,” Dr. Meddings says.
Hospital administration at Temple University Hospital recognized the HM group’s quality-improvement (QI) work, and has “specifically charged us with spreading the work we have done in patient safety to the entire house,” Dr. Frost says. “That speaks to the administration’s opinion of the power of the HM program to assist with institution-wide QI initiatives.”
Documentation Is Key

Beyond applying proven methods to avoid HACs, hospitalists can make a difference through documentation. If the hospitalist notes all conditions when the patient first presents to the hospital, additional comorbidity and complication payments should be made.
“The part that probably has the greatest impact on the day-to-day practice of a hospitalist is the increased importance of documentation throughout the hospital episode,” Dr. Meddings says. “If complications are occurring and they are not present in the chart, the coders may not recognize that it has occurred and will not know to include it in the bill. This can have an adverse impact on the hospital and its finances.”
Documentation issues can impact hospital payment in several ways:
- Hospitals might receive additional payment by default if certain HACs are described incorrectly or without sufficient detail (e.g., receiving overpayment because the physician did not indicate a UTI was in fact a catheter-associated UTI);
- As more attention is invested in documenting all conditions POA, hospitals might be coding more comorbidities overall than previously, which also will generate additional payment for hospitals as any POA condition is eligible for increased payment; and
- Hospitals might lose payment when admitting providers fail to adequately document the condition as POA (e.g., a pre-existing decubitus ulcer not detected until the second day of the hospital stay).
The descriptions to be used in coding are very detailed. UTIs, for example, have one code to document the POA assessment, another code to show that a UTI occurred, and a third code to indicate it was catheter-associated. Each code requires appropriate documentation in the chart (see Table 1, above).
The impact hospitalists have on care and payment is not the same across the HAC spectrum. For instance, documenting the presence of pressure ulcers might be easier than distinguishing colonization from infection in those admitted with in-dwelling urinary catheters. Others, such as DVT or vascular catheter-associated infections, are rarely POA unless they are part of the admitting diagnosis.
“This new focus on hospital-acquired conditions may work to the patient’s benefit,” Dr. Meddings says. “The inclusion of pressure ulcers has led to increased attention to skin exams on admission and preventive measures during hospitalizations. In the past, skin exams upon admission may have been given a lower priority, but that has changed.”
Dr. Meddings is concerned that the new rules could force the shifting of resources to areas where the hospital could lose money. If, when, and how many changes will actually take place is still up in the air. “Resource shifting is a concern whenever there is any sort of pay-for-performance attention directed toward one particular complication,” she says. “To balance this, many of the strategies hospitals used to prevent complications are not specific to just the diagnosis that is covered by the HAC.”
Dr. Meddings also hopes the new focus on preventable conditions will have a “halo effect” in the healthcare community. For instance, CMS mandating DVT prevention following orthopedic operations will, hopefully, result in a greater awareness of the problem in other susceptible patients.
POA Indicators

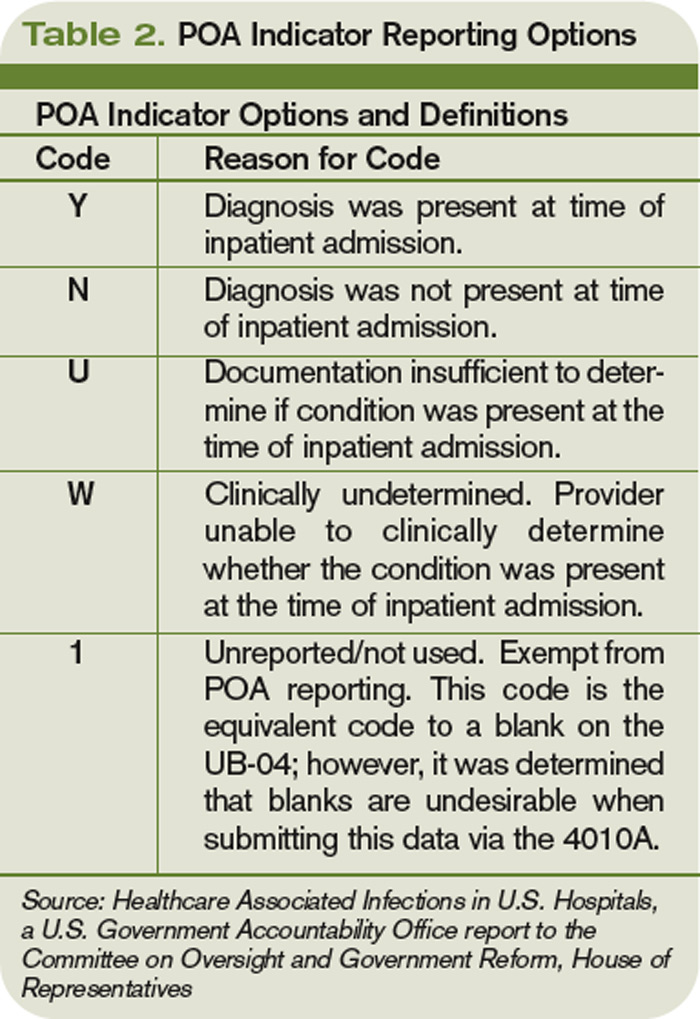
Since hospitalists often perform the initial patient history, physical, and other admission work, they are in the best position to find and document POA indicators (see Table 2, p. below). Proper notes on such things as UTIs present and the state of skin integrity are an important part of making sure the hospital is paid correctly for the care it provides.
Education on the specific definition of each potential HAC is required to help physicians avoid overtreatment of certain conditions, especially UTIs. For example, the Centers for Disease Control and Prevention (CDC) defines all UTIs as symptomatic. Therefore, the screening of all admitted patients, regardless of symptoms, is wasteful and unlikely to help the hospital’s bottom line.
“If you start screening everyone that comes through the door so you don’t miss any pre-existing UTIs, you are going to find a lot of asymptomatic colonization,” Dr. Wald says. “You are also going to spend a lot of money and time on studies and possibly treatments that may not yield many true infections. It is important that physicians know the definition of these HACs to help avoid needless interventions.”
Minimal Loss

Many hospital administrators and physicians were worried when the HAC program was first announced. Much of the stress and concern, however, seems to have dissipated. CMS estimated the HAC program would save Medicare $21 million in fiscal year 2009. Others, such as Peter McNair and colleagues writing in Health Affairs, suggest the actual impact is closer to $1.1 million.1 The CMS-projected impact of the HAC provision in fiscal-year 2009 was $21 million, out of more than $100 billion in payments.
“I think the HACs will not have a major impact because of the way payments are made,” says internist Robert Berenson, MD, a fellow at the Urban Institute in Washington, D.C., who has studied Medicare policy issues extensively, and for two years was in charge of Medicare payment policies at the Health Care Finance Administration, the precursor to CMS. “Patients who have HACs often have another comorbidity that would kick them into a higher payment category regardless of the presence of a hospital-acquired complication. In the end, it is probably more symbolic and unlikely to make a major dent in hospital income—at least at this point.”
Another limitation to CMS nonpayment for HACs is the issue of deciding which conditions are truly preventable. Dr. Berenson questions the ability of the current system to identify many additional complications for which this approach will be feasible.
“CMS has laid out its strategy, suggesting that we should be able to continue increasing the number of conditions for which providers would be paid differently based on quality,” he says. “Many observers question whether there will ever be measurement tools that are robust enough, and there will be a wide agreement on the preventability of enough conditions that this initiative will go very far.”
Although hospitalists might not face a direct financial risk, they still have their hospitals’ best interest—and their reputations—on the line. “Hospitalists care about preventing complications,” Dr. Wald says. “We are very engaged in working with our hospitals to improve care, maximize quality, and minimize cost.” TH
Kurt Ullman is a freelance medical writer based in Indiana.
Reference
- McNair PD, Luft HS, Bindman AB. Medicare’s policy not to pay for treating hospital-acquired conditions: the impact. Health Aff (Millwood). 2009;28(5):1485-1493.
TOP IMAGE SOURCE: KAREEM RIZKHALLA/ISTOCKPHOTO.COM
Hospitalist Neal Axon, MD, first became aware of an important change in his hospital’s policies last year while attending to an elderly patient the morning after admission to the community hospital where he works part time.
“This new form appeared in the chart requesting a urinalysis for my patient, who’d had a Foley catheter placed,” says Dr. Axon, an assistant professor of medicine at the Medical University of South Carolina in Charleston. “I didn’t know why, so I asked. I was told that it was now necessary to document that there was no UTI present on admission.” He asked the charge nurse, “So what do I do now that the catheter has been in place for 12 hours and has colonization without a true infection?”
The next thing he heard: silence.
The new form Dr. Axon encountered was an outgrowth of the requirements of the Deficit Reduction Act (DRA) of 2005, which ordered Medicare to withhold additional hospital payments for hospital-acquired complications (HAC) developed during a hospital stay. One result of the new rule is that much of a hospital’s response to these initiatives has been placed in the hands of the hospitalist. From accurate documentation of complications already present on admission (POA), to confirming that guidelines for treatment are being followed, to taking the lead on review of staff practices and education, hospitalists are in a position to have a wide-ranging impact on patient care and the financial health of their institutions.
Congress Pushes Reforms
In order for Medicare to not provide a reimbursement, an HAC has to be high-cost and/or high-volume, result in the assignment of the case to a higher payment when present as a secondary diagnosis, and “could reasonably be prevented through the application of evidence-based guidelines,” says Barry Straube, MD, chief medical officer and director of the Office of Clinical Standards and Quality at the Centers for Medicare and Medicaid Services (CMS). “CMS was to implement a process where we would not pay the hospitals additional money for these complications.”
The new rules mean Medicare pays hospitals on the basis of Medicare Severity Diagnostic-Related Groups (MS-DRG), which better reflect the complexity of a patient’s illness. The biggest change was a three-tiered payment schedule: a base level for the diagnosis, a second level adding money to reflect the presence of comorbidities and complications, and a third for major complications and comorbidities (see Table 1, p. 31).
“Instituting HACs means that hospitals would no longer receive the comorbidity and complication payments if the only reason a case qualified for higher payment was the HAC,” Dr. Straube explains. “We did carve out a POA exception for those conditions that were acquired outside of the hospital. HACs only impact additional payments; the hospitals are still paid for the diagnosis that resulted in the hospital admission.”
CMS also identifies three “never events” it won’t reimburse for (see “A Brief History of Never Events,” p. 35): performing the wrong procedure, performing a procedure on the wrong body part, and performing a procedure on the wrong patient. “Neither hospitals nor physicians that are involved in such egregious situations would be paid,” Dr. Straube says.
Preventability: Subject of Controversy
The big questions surrounding HACs: Could they reasonably be prevented through the application of evidence-based guidelines? How preventable are HACs? Who decides if a complication is preventable, and therefore payment for services is withheld?
They’re concerns that are widespread among physicians, hospital administrators, and regulators alike.
“The legislation required the conditions to be ‘reasonably preventable’ using established clinical guidelines,” Dr. Straube says. “We did not have to show 100% prevention. In an imperfect world, they might still take place occasionally, but with good medical care, almost all of these are preventable in this day and age.”
For CMS, the preventable conditions are an either/or situation: Either they existed prior to admission and are subject to payment, or they did not exist at admission and additional payment for the complication will not be made. “HACs do not currently consider a patient’s individual risk for complications,” says Jennifer Meddings, MD, MSc, clinical lecturer and health researcher in the Department of Internal Medicine at the University of Michigan Health System in Ann Arbor. “We know the best strategies to prevent complications in ideal patients, and these are reflected in the HACs. In real life, many of our patients just don’t fit into the guidelines for many reasons—and you have to individualize care.”
Dr. Meddings points to DVT as a prime example. For a certain number of inpatients, the guidelines can be followed to perfection. In other patients (e.g., those with kidney conditions), previous reactions to a medication or an individual’s predisposition to clotting might interfere with treatment. However, CMS doesn’t allow appeals of nonpayment decisions for HACs based on individual circumstances.
Some experts think the rigidness of the payment policy forces physicians to treat patients exactly to guidelines. Even then, payment could be declined if an HAC develops.
“One of the points of most discussion is how preventable some of these are, particularly when choosing those you are no longer going to pay for,” Dr. Meddings says. “Many of the complications currently under review have patients that are at higher risk than others. How much our prevention strategies can alleviate or reduce the risk varies widely among patients.”
Impact on HM Practice
Many of the preventable conditions outlined by CMS do not directly affect hospitalist payment. However, hospitalists often find themselves responsible for properly documenting admission and care.
“The rule changes regarding payment for HACs are only related to hospital payments, and to date, most physicians, including hospitalists, are not directly at financial risk,” says Heidi Wald, MD, MSPH, hospitalist and assistant professor of medicine in the divisions of Health Care Policy Research and General Internal Medicine at the University of Colorado Denver School of Medicine. “Although hospitalists have no financial skin in the game, there are plenty of reasons they would take an interest in addressing HACs in their hospital. In particular, they are often seen as the ‘go-to’ group for quality improvement in their hospitals.”
For example, some HM groups have been active in working with teams of physicians, nurses, and other healthcare providers to address local policies and procedures on prevention of catheter-associated urinary tract infections (UTIs) and DVT.
“This has certainly necessitated a team approach,” says Shaun Frost, MD, FHM, an SHM board member and regional medical director for Cogent Healthcare in St. Paul, Minn. “For many of the HACs that apply to our population of patients, the hospitalist alone cannot be expected to solely execute effective quality improvements. It takes a team effort in that regard, and one that includes many different disciplines.”
The Cogent-affiliated hospitalist group at Temple University Hospital in Philadelphia formed a task force to address issues with catheter-associated UTI. One initiative focused on educating all providers involved in the proper care of the catheters and similar interventions. A secondary focus of the project was an inventory of current practices and procedures.
“It was discovered that we did not have an automatic stop order for Foley catheters, so in some situations, they were likely being left in longer than needed while nursing [staff] tried to contact a physician,” Dr. Frost explains. “We created standardized order sets that include criteria for continuing the catheter. Once the criteria are no longer applicable, nursing will be able to discontinue it.”
Although CMS has only recently turned the spotlight on HACs and never events, hospitalists have been heavily involved in the patient-safety arena for years. “It is not a new phenomenon that hospitalists work for healthcare delivery and healthcare system improvement,” Dr. Meddings says.
Hospital administration at Temple University Hospital recognized the HM group’s quality-improvement (QI) work, and has “specifically charged us with spreading the work we have done in patient safety to the entire house,” Dr. Frost says. “That speaks to the administration’s opinion of the power of the HM program to assist with institution-wide QI initiatives.”
Documentation Is Key
Beyond applying proven methods to avoid HACs, hospitalists can make a difference through documentation. If the hospitalist notes all conditions when the patient first presents to the hospital, additional comorbidity and complication payments should be made.
“The part that probably has the greatest impact on the day-to-day practice of a hospitalist is the increased importance of documentation throughout the hospital episode,” Dr. Meddings says. “If complications are occurring and they are not present in the chart, the coders may not recognize that it has occurred and will not know to include it in the bill. This can have an adverse impact on the hospital and its finances.”
Documentation issues can impact hospital payment in several ways:
- Hospitals might receive additional payment by default if certain HACs are described incorrectly or without sufficient detail (e.g., receiving overpayment because the physician did not indicate a UTI was in fact a catheter-associated UTI);
- As more attention is invested in documenting all conditions POA, hospitals might be coding more comorbidities overall than previously, which also will generate additional payment for hospitals as any POA condition is eligible for increased payment; and
- Hospitals might lose payment when admitting providers fail to adequately document the condition as POA (e.g., a pre-existing decubitus ulcer not detected until the second day of the hospital stay).
The descriptions to be used in coding are very detailed. UTIs, for example, have one code to document the POA assessment, another code to show that a UTI occurred, and a third code to indicate it was catheter-associated. Each code requires appropriate documentation in the chart (see Table 1, above).
The impact hospitalists have on care and payment is not the same across the HAC spectrum. For instance, documenting the presence of pressure ulcers might be easier than distinguishing colonization from infection in those admitted with in-dwelling urinary catheters. Others, such as DVT or vascular catheter-associated infections, are rarely POA unless they are part of the admitting diagnosis.
“This new focus on hospital-acquired conditions may work to the patient’s benefit,” Dr. Meddings says. “The inclusion of pressure ulcers has led to increased attention to skin exams on admission and preventive measures during hospitalizations. In the past, skin exams upon admission may have been given a lower priority, but that has changed.”
Dr. Meddings is concerned that the new rules could force the shifting of resources to areas where the hospital could lose money. If, when, and how many changes will actually take place is still up in the air. “Resource shifting is a concern whenever there is any sort of pay-for-performance attention directed toward one particular complication,” she says. “To balance this, many of the strategies hospitals used to prevent complications are not specific to just the diagnosis that is covered by the HAC.”
Dr. Meddings also hopes the new focus on preventable conditions will have a “halo effect” in the healthcare community. For instance, CMS mandating DVT prevention following orthopedic operations will, hopefully, result in a greater awareness of the problem in other susceptible patients.
POA Indicators
Since hospitalists often perform the initial patient history, physical, and other admission work, they are in the best position to find and document POA indicators (see Table 2, p. below). Proper notes on such things as UTIs present and the state of skin integrity are an important part of making sure the hospital is paid correctly for the care it provides.
Education on the specific definition of each potential HAC is required to help physicians avoid overtreatment of certain conditions, especially UTIs. For example, the Centers for Disease Control and Prevention (CDC) defines all UTIs as symptomatic. Therefore, the screening of all admitted patients, regardless of symptoms, is wasteful and unlikely to help the hospital’s bottom line.
“If you start screening everyone that comes through the door so you don’t miss any pre-existing UTIs, you are going to find a lot of asymptomatic colonization,” Dr. Wald says. “You are also going to spend a lot of money and time on studies and possibly treatments that may not yield many true infections. It is important that physicians know the definition of these HACs to help avoid needless interventions.”
Minimal Loss
Many hospital administrators and physicians were worried when the HAC program was first announced. Much of the stress and concern, however, seems to have dissipated. CMS estimated the HAC program would save Medicare $21 million in fiscal year 2009. Others, such as Peter McNair and colleagues writing in Health Affairs, suggest the actual impact is closer to $1.1 million.1 The CMS-projected impact of the HAC provision in fiscal-year 2009 was $21 million, out of more than $100 billion in payments.
“I think the HACs will not have a major impact because of the way payments are made,” says internist Robert Berenson, MD, a fellow at the Urban Institute in Washington, D.C., who has studied Medicare policy issues extensively, and for two years was in charge of Medicare payment policies at the Health Care Finance Administration, the precursor to CMS. “Patients who have HACs often have another comorbidity that would kick them into a higher payment category regardless of the presence of a hospital-acquired complication. In the end, it is probably more symbolic and unlikely to make a major dent in hospital income—at least at this point.”
Another limitation to CMS nonpayment for HACs is the issue of deciding which conditions are truly preventable. Dr. Berenson questions the ability of the current system to identify many additional complications for which this approach will be feasible.
“CMS has laid out its strategy, suggesting that we should be able to continue increasing the number of conditions for which providers would be paid differently based on quality,” he says. “Many observers question whether there will ever be measurement tools that are robust enough, and there will be a wide agreement on the preventability of enough conditions that this initiative will go very far.”
Although hospitalists might not face a direct financial risk, they still have their hospitals’ best interest—and their reputations—on the line. “Hospitalists care about preventing complications,” Dr. Wald says. “We are very engaged in working with our hospitals to improve care, maximize quality, and minimize cost.” TH
Kurt Ullman is a freelance medical writer based in Indiana.
Reference
- McNair PD, Luft HS, Bindman AB. Medicare’s policy not to pay for treating hospital-acquired conditions: the impact. Health Aff (Millwood). 2009;28(5):1485-1493.
TOP IMAGE SOURCE: KAREEM RIZKHALLA/ISTOCKPHOTO.COM
Hospitalist Neal Axon, MD, first became aware of an important change in his hospital’s policies last year while attending to an elderly patient the morning after admission to the community hospital where he works part time.
“This new form appeared in the chart requesting a urinalysis for my patient, who’d had a Foley catheter placed,” says Dr. Axon, an assistant professor of medicine at the Medical University of South Carolina in Charleston. “I didn’t know why, so I asked. I was told that it was now necessary to document that there was no UTI present on admission.” He asked the charge nurse, “So what do I do now that the catheter has been in place for 12 hours and has colonization without a true infection?”
The next thing he heard: silence.
The new form Dr. Axon encountered was an outgrowth of the requirements of the Deficit Reduction Act (DRA) of 2005, which ordered Medicare to withhold additional hospital payments for hospital-acquired complications (HAC) developed during a hospital stay. One result of the new rule is that much of a hospital’s response to these initiatives has been placed in the hands of the hospitalist. From accurate documentation of complications already present on admission (POA), to confirming that guidelines for treatment are being followed, to taking the lead on review of staff practices and education, hospitalists are in a position to have a wide-ranging impact on patient care and the financial health of their institutions.
Congress Pushes Reforms
In order for Medicare to not provide a reimbursement, an HAC has to be high-cost and/or high-volume, result in the assignment of the case to a higher payment when present as a secondary diagnosis, and “could reasonably be prevented through the application of evidence-based guidelines,” says Barry Straube, MD, chief medical officer and director of the Office of Clinical Standards and Quality at the Centers for Medicare and Medicaid Services (CMS). “CMS was to implement a process where we would not pay the hospitals additional money for these complications.”
The new rules mean Medicare pays hospitals on the basis of Medicare Severity Diagnostic-Related Groups (MS-DRG), which better reflect the complexity of a patient’s illness. The biggest change was a three-tiered payment schedule: a base level for the diagnosis, a second level adding money to reflect the presence of comorbidities and complications, and a third for major complications and comorbidities (see Table 1, p. 31).
“Instituting HACs means that hospitals would no longer receive the comorbidity and complication payments if the only reason a case qualified for higher payment was the HAC,” Dr. Straube explains. “We did carve out a POA exception for those conditions that were acquired outside of the hospital. HACs only impact additional payments; the hospitals are still paid for the diagnosis that resulted in the hospital admission.”
CMS also identifies three “never events” it won’t reimburse for (see “A Brief History of Never Events,” p. 35): performing the wrong procedure, performing a procedure on the wrong body part, and performing a procedure on the wrong patient. “Neither hospitals nor physicians that are involved in such egregious situations would be paid,” Dr. Straube says.
Preventability: Subject of Controversy
The big questions surrounding HACs: Could they reasonably be prevented through the application of evidence-based guidelines? How preventable are HACs? Who decides if a complication is preventable, and therefore payment for services is withheld?
They’re concerns that are widespread among physicians, hospital administrators, and regulators alike.
“The legislation required the conditions to be ‘reasonably preventable’ using established clinical guidelines,” Dr. Straube says. “We did not have to show 100% prevention. In an imperfect world, they might still take place occasionally, but with good medical care, almost all of these are preventable in this day and age.”
For CMS, the preventable conditions are an either/or situation: Either they existed prior to admission and are subject to payment, or they did not exist at admission and additional payment for the complication will not be made. “HACs do not currently consider a patient’s individual risk for complications,” says Jennifer Meddings, MD, MSc, clinical lecturer and health researcher in the Department of Internal Medicine at the University of Michigan Health System in Ann Arbor. “We know the best strategies to prevent complications in ideal patients, and these are reflected in the HACs. In real life, many of our patients just don’t fit into the guidelines for many reasons—and you have to individualize care.”
Dr. Meddings points to DVT as a prime example. For a certain number of inpatients, the guidelines can be followed to perfection. In other patients (e.g., those with kidney conditions), previous reactions to a medication or an individual’s predisposition to clotting might interfere with treatment. However, CMS doesn’t allow appeals of nonpayment decisions for HACs based on individual circumstances.
Some experts think the rigidness of the payment policy forces physicians to treat patients exactly to guidelines. Even then, payment could be declined if an HAC develops.
“One of the points of most discussion is how preventable some of these are, particularly when choosing those you are no longer going to pay for,” Dr. Meddings says. “Many of the complications currently under review have patients that are at higher risk than others. How much our prevention strategies can alleviate or reduce the risk varies widely among patients.”
Impact on HM Practice
Many of the preventable conditions outlined by CMS do not directly affect hospitalist payment. However, hospitalists often find themselves responsible for properly documenting admission and care.
“The rule changes regarding payment for HACs are only related to hospital payments, and to date, most physicians, including hospitalists, are not directly at financial risk,” says Heidi Wald, MD, MSPH, hospitalist and assistant professor of medicine in the divisions of Health Care Policy Research and General Internal Medicine at the University of Colorado Denver School of Medicine. “Although hospitalists have no financial skin in the game, there are plenty of reasons they would take an interest in addressing HACs in their hospital. In particular, they are often seen as the ‘go-to’ group for quality improvement in their hospitals.”
For example, some HM groups have been active in working with teams of physicians, nurses, and other healthcare providers to address local policies and procedures on prevention of catheter-associated urinary tract infections (UTIs) and DVT.
“This has certainly necessitated a team approach,” says Shaun Frost, MD, FHM, an SHM board member and regional medical director for Cogent Healthcare in St. Paul, Minn. “For many of the HACs that apply to our population of patients, the hospitalist alone cannot be expected to solely execute effective quality improvements. It takes a team effort in that regard, and one that includes many different disciplines.”
The Cogent-affiliated hospitalist group at Temple University Hospital in Philadelphia formed a task force to address issues with catheter-associated UTI. One initiative focused on educating all providers involved in the proper care of the catheters and similar interventions. A secondary focus of the project was an inventory of current practices and procedures.
“It was discovered that we did not have an automatic stop order for Foley catheters, so in some situations, they were likely being left in longer than needed while nursing [staff] tried to contact a physician,” Dr. Frost explains. “We created standardized order sets that include criteria for continuing the catheter. Once the criteria are no longer applicable, nursing will be able to discontinue it.”
Although CMS has only recently turned the spotlight on HACs and never events, hospitalists have been heavily involved in the patient-safety arena for years. “It is not a new phenomenon that hospitalists work for healthcare delivery and healthcare system improvement,” Dr. Meddings says.
Hospital administration at Temple University Hospital recognized the HM group’s quality-improvement (QI) work, and has “specifically charged us with spreading the work we have done in patient safety to the entire house,” Dr. Frost says. “That speaks to the administration’s opinion of the power of the HM program to assist with institution-wide QI initiatives.”
Documentation Is Key
Beyond applying proven methods to avoid HACs, hospitalists can make a difference through documentation. If the hospitalist notes all conditions when the patient first presents to the hospital, additional comorbidity and complication payments should be made.
“The part that probably has the greatest impact on the day-to-day practice of a hospitalist is the increased importance of documentation throughout the hospital episode,” Dr. Meddings says. “If complications are occurring and they are not present in the chart, the coders may not recognize that it has occurred and will not know to include it in the bill. This can have an adverse impact on the hospital and its finances.”
Documentation issues can impact hospital payment in several ways:
- Hospitals might receive additional payment by default if certain HACs are described incorrectly or without sufficient detail (e.g., receiving overpayment because the physician did not indicate a UTI was in fact a catheter-associated UTI);
- As more attention is invested in documenting all conditions POA, hospitals might be coding more comorbidities overall than previously, which also will generate additional payment for hospitals as any POA condition is eligible for increased payment; and
- Hospitals might lose payment when admitting providers fail to adequately document the condition as POA (e.g., a pre-existing decubitus ulcer not detected until the second day of the hospital stay).
The descriptions to be used in coding are very detailed. UTIs, for example, have one code to document the POA assessment, another code to show that a UTI occurred, and a third code to indicate it was catheter-associated. Each code requires appropriate documentation in the chart (see Table 1, above).
The impact hospitalists have on care and payment is not the same across the HAC spectrum. For instance, documenting the presence of pressure ulcers might be easier than distinguishing colonization from infection in those admitted with in-dwelling urinary catheters. Others, such as DVT or vascular catheter-associated infections, are rarely POA unless they are part of the admitting diagnosis.
“This new focus on hospital-acquired conditions may work to the patient’s benefit,” Dr. Meddings says. “The inclusion of pressure ulcers has led to increased attention to skin exams on admission and preventive measures during hospitalizations. In the past, skin exams upon admission may have been given a lower priority, but that has changed.”
Dr. Meddings is concerned that the new rules could force the shifting of resources to areas where the hospital could lose money. If, when, and how many changes will actually take place is still up in the air. “Resource shifting is a concern whenever there is any sort of pay-for-performance attention directed toward one particular complication,” she says. “To balance this, many of the strategies hospitals used to prevent complications are not specific to just the diagnosis that is covered by the HAC.”
Dr. Meddings also hopes the new focus on preventable conditions will have a “halo effect” in the healthcare community. For instance, CMS mandating DVT prevention following orthopedic operations will, hopefully, result in a greater awareness of the problem in other susceptible patients.
POA Indicators
Since hospitalists often perform the initial patient history, physical, and other admission work, they are in the best position to find and document POA indicators (see Table 2, p. below). Proper notes on such things as UTIs present and the state of skin integrity are an important part of making sure the hospital is paid correctly for the care it provides.
Education on the specific definition of each potential HAC is required to help physicians avoid overtreatment of certain conditions, especially UTIs. For example, the Centers for Disease Control and Prevention (CDC) defines all UTIs as symptomatic. Therefore, the screening of all admitted patients, regardless of symptoms, is wasteful and unlikely to help the hospital’s bottom line.
“If you start screening everyone that comes through the door so you don’t miss any pre-existing UTIs, you are going to find a lot of asymptomatic colonization,” Dr. Wald says. “You are also going to spend a lot of money and time on studies and possibly treatments that may not yield many true infections. It is important that physicians know the definition of these HACs to help avoid needless interventions.”
Minimal Loss
Many hospital administrators and physicians were worried when the HAC program was first announced. Much of the stress and concern, however, seems to have dissipated. CMS estimated the HAC program would save Medicare $21 million in fiscal year 2009. Others, such as Peter McNair and colleagues writing in Health Affairs, suggest the actual impact is closer to $1.1 million.1 The CMS-projected impact of the HAC provision in fiscal-year 2009 was $21 million, out of more than $100 billion in payments.
“I think the HACs will not have a major impact because of the way payments are made,” says internist Robert Berenson, MD, a fellow at the Urban Institute in Washington, D.C., who has studied Medicare policy issues extensively, and for two years was in charge of Medicare payment policies at the Health Care Finance Administration, the precursor to CMS. “Patients who have HACs often have another comorbidity that would kick them into a higher payment category regardless of the presence of a hospital-acquired complication. In the end, it is probably more symbolic and unlikely to make a major dent in hospital income—at least at this point.”
Another limitation to CMS nonpayment for HACs is the issue of deciding which conditions are truly preventable. Dr. Berenson questions the ability of the current system to identify many additional complications for which this approach will be feasible.
“CMS has laid out its strategy, suggesting that we should be able to continue increasing the number of conditions for which providers would be paid differently based on quality,” he says. “Many observers question whether there will ever be measurement tools that are robust enough, and there will be a wide agreement on the preventability of enough conditions that this initiative will go very far.”
Although hospitalists might not face a direct financial risk, they still have their hospitals’ best interest—and their reputations—on the line. “Hospitalists care about preventing complications,” Dr. Wald says. “We are very engaged in working with our hospitals to improve care, maximize quality, and minimize cost.” TH
Kurt Ullman is a freelance medical writer based in Indiana.
Reference
- McNair PD, Luft HS, Bindman AB. Medicare’s policy not to pay for treating hospital-acquired conditions: the impact. Health Aff (Millwood). 2009;28(5):1485-1493.
TOP IMAGE SOURCE: KAREEM RIZKHALLA/ISTOCKPHOTO.COM
Get Well Now

Four eyes staring, boring through me, unblinking. Locked in a pose holding a hand-scrawled sign commanding their father to ♥♥GET WELL NOW♥♥, the photo of the 14-month-old twin girls was reproduced off a cheap color printer and taped to the window, backlit by the Christmas Eve morning sun. Both the sun and the daughters demanded my attention—the former a brilliant reminder of the glories of the day, the latter the sobering reality of a family rocked by illness.
Mr. Jasper, an otherwise healthy 36-year-old male who recently was diagnosed with a rare, life-threatening disease, would not be spending this holiday with his daughters. In fact, because of our hospital’s flu precautions, he hadn’t seen them in the six weeks he’d been an inpatient. In that time, one of his girls had learned to talk; the other had learned to walk. Mr. Jasper was a distant bystander. He was upset but understanding of his situation—even optimistic, remarkably. However, those girls’ eyes told a different story. What weeks ago shone as the cute countenances of toddlers—silly, carefree, cheerful—now articulated a different tone. “Let my father come home!” they beseeched.
Staring into those eyes on rounds that morning, I was haunted by a thought that had gnawed at my subconscious for weeks. It was likely, albeit not guaranteed, that we’d get Mr. Jasper home to his wife and daughters. However, it would be at a cost. Of course, there would be psychological costs, but I was more acutely concerned with the financial costs. Mr. Jasper, you see, is uninsured.
Healthcare Reform: Too Late for Many
Thousands of miles away, the U.S. Senate was, at that exact time, voting for legislation to greatly reform and expand the U.S. healthcare system. Passed along partisan lines, the bill now awaits reconciliation with the House of Representatives’ bill. From there, it will go before President Obama for signature into law. If passed, this legislation promises to give healthcare coverage to another 30 million Americans.
For Mr. Jasper, this new law will come too late.
It’ll also be too late for Mrs. Anderson, a middle-aged asthmatic now intubated in our ICU, wheezing against constricted bronchioles. Three days earlier, she was seen in the ED for worsening dyspnea, cough, and sputum production. Her symptoms resolved after a few courses of nebulized albuterol and IV steroids, and she was sent home with a prescription for prednisone and inhalers. Unable to afford to fill those prescriptions, her disease progressed, eventually strangling her breathing and tangling her in a healthcare system more willing to pay for the care of disease complications than disease prevention.
Face-to-Face with Catastrophe
Later that morning, I was asked by one of our ED physicians to see Mr. Reynolds and “persuade” him to be admitted to the hospital. Mr. Reynolds has insurance. In fact, of the 11 patients I saw that day, he was one of only three who did. One had Medicaid, the other Medicare.
Mr. Reynolds had a high-deductible, catastrophic-insurance policy. As such, he was wrestling with the decision of whether to come into the hospital to treat his severe cellulitis with IV antibiotics (our formal recommendation), or treat this at home with oral antibiotics. His face wore the torment of the trade-offs. The former surely would cost him his entire $5,000 deductible; the latter, perhaps his life, or at least a limb. As the erythema glared at me, I struggled to recollect a medical school lecture applicable to this situation.
My last patient of the day was Mr. Ramon. He, too, was uninsured. Felled by diabetic ketoacidosis, he was admitted and, as 19-year-olds are wont to do, rebounded quickly. New-onset diabetes, however, was the least of his concerns. With a girlfriend and young child at home, he had to get out of the hospital and return to his job as soon as possible: mouths to feed. Having seen his father lose limbs, kidneys, eyes, and ultimately his life to diabetes, he was motivated to do the right thing.
Unfortunately, motivation doesn’t pay for insulin. I wondered what would come of him in the next 30 years. Would he be able to care for his disease and live a long and prosperous life, or would this admission be just one in a long series of hospital stays?
Broken System
Every hospitalist is aware of these issues and could no doubt fill pages with similarly horrific stories of a healthcare system long broken. It’s remarkable how much of my time I spend trying to figure out a way to cobble together a passable (the notion of “gold standard” therapy long gone) therapeutic plan for my patients—the Walmart list of $4 drugs has taken white-coat prominence over my “Pocket Pharmacopoeia.”
This isn’t to say the U.S. healthcare system doesn’t do a lot of great things. It does, and that cannot be discounted. It’s also not to say that the bill before Congress is the answer. Still, the fact that medical costs limit many Americans from accessing needed care and have become the leading cause of bankruptcy in the U.S. should arouse concern in even the most ardent opponents of healthcare reform. Regardless of one’s political leanings and feelings about the current attempts at healthcare reform, it’s difficult to stand by and helplessly watch our patients struggle to maneuver within a system that so often seems to work against so many of them.
What’s easy to lose in the D.C. rhetoric and town-hall warfare is that every day, we delay healthcare reform results in undue patient suffering, both physical and financial. It is a system that is broken and needs, in the words of Mr. Jasper’s daughters, to “get well now.”
Before leaving to celebrate the holiday with my family, I was compelled to return to Mr. Jasper’s room. Unfortunately, the patient was off getting a treatment. But his daughters were still there, faces unchanged. Again, drawn to those eyes, I wondered what would become of this situation.
Would he make it home?
How would his family pay the bills?
What would this mean for his daughters’ future?
Would he and his family be forced to declare bankruptcy?
Would the family ever truly recover?
Staring at the picture in the window, I couldn’t help but think of my own children, also waiting for their father to come home from the hospital to celebrate the holidays.
As I turned to leave, my mind lost in thoughts of untimely illness, ill-fated outcomes, and financial devastation, I realized that in America today, nothing more than circumstances kept me from seeing my own children’s eyes staring back at me from that window. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Four eyes staring, boring through me, unblinking. Locked in a pose holding a hand-scrawled sign commanding their father to ♥♥GET WELL NOW♥♥, the photo of the 14-month-old twin girls was reproduced off a cheap color printer and taped to the window, backlit by the Christmas Eve morning sun. Both the sun and the daughters demanded my attention—the former a brilliant reminder of the glories of the day, the latter the sobering reality of a family rocked by illness.
Mr. Jasper, an otherwise healthy 36-year-old male who recently was diagnosed with a rare, life-threatening disease, would not be spending this holiday with his daughters. In fact, because of our hospital’s flu precautions, he hadn’t seen them in the six weeks he’d been an inpatient. In that time, one of his girls had learned to talk; the other had learned to walk. Mr. Jasper was a distant bystander. He was upset but understanding of his situation—even optimistic, remarkably. However, those girls’ eyes told a different story. What weeks ago shone as the cute countenances of toddlers—silly, carefree, cheerful—now articulated a different tone. “Let my father come home!” they beseeched.
Staring into those eyes on rounds that morning, I was haunted by a thought that had gnawed at my subconscious for weeks. It was likely, albeit not guaranteed, that we’d get Mr. Jasper home to his wife and daughters. However, it would be at a cost. Of course, there would be psychological costs, but I was more acutely concerned with the financial costs. Mr. Jasper, you see, is uninsured.
Healthcare Reform: Too Late for Many
Thousands of miles away, the U.S. Senate was, at that exact time, voting for legislation to greatly reform and expand the U.S. healthcare system. Passed along partisan lines, the bill now awaits reconciliation with the House of Representatives’ bill. From there, it will go before President Obama for signature into law. If passed, this legislation promises to give healthcare coverage to another 30 million Americans.
For Mr. Jasper, this new law will come too late.
It’ll also be too late for Mrs. Anderson, a middle-aged asthmatic now intubated in our ICU, wheezing against constricted bronchioles. Three days earlier, she was seen in the ED for worsening dyspnea, cough, and sputum production. Her symptoms resolved after a few courses of nebulized albuterol and IV steroids, and she was sent home with a prescription for prednisone and inhalers. Unable to afford to fill those prescriptions, her disease progressed, eventually strangling her breathing and tangling her in a healthcare system more willing to pay for the care of disease complications than disease prevention.
Face-to-Face with Catastrophe
Later that morning, I was asked by one of our ED physicians to see Mr. Reynolds and “persuade” him to be admitted to the hospital. Mr. Reynolds has insurance. In fact, of the 11 patients I saw that day, he was one of only three who did. One had Medicaid, the other Medicare.
Mr. Reynolds had a high-deductible, catastrophic-insurance policy. As such, he was wrestling with the decision of whether to come into the hospital to treat his severe cellulitis with IV antibiotics (our formal recommendation), or treat this at home with oral antibiotics. His face wore the torment of the trade-offs. The former surely would cost him his entire $5,000 deductible; the latter, perhaps his life, or at least a limb. As the erythema glared at me, I struggled to recollect a medical school lecture applicable to this situation.
My last patient of the day was Mr. Ramon. He, too, was uninsured. Felled by diabetic ketoacidosis, he was admitted and, as 19-year-olds are wont to do, rebounded quickly. New-onset diabetes, however, was the least of his concerns. With a girlfriend and young child at home, he had to get out of the hospital and return to his job as soon as possible: mouths to feed. Having seen his father lose limbs, kidneys, eyes, and ultimately his life to diabetes, he was motivated to do the right thing.
Unfortunately, motivation doesn’t pay for insulin. I wondered what would come of him in the next 30 years. Would he be able to care for his disease and live a long and prosperous life, or would this admission be just one in a long series of hospital stays?
Broken System
Every hospitalist is aware of these issues and could no doubt fill pages with similarly horrific stories of a healthcare system long broken. It’s remarkable how much of my time I spend trying to figure out a way to cobble together a passable (the notion of “gold standard” therapy long gone) therapeutic plan for my patients—the Walmart list of $4 drugs has taken white-coat prominence over my “Pocket Pharmacopoeia.”
This isn’t to say the U.S. healthcare system doesn’t do a lot of great things. It does, and that cannot be discounted. It’s also not to say that the bill before Congress is the answer. Still, the fact that medical costs limit many Americans from accessing needed care and have become the leading cause of bankruptcy in the U.S. should arouse concern in even the most ardent opponents of healthcare reform. Regardless of one’s political leanings and feelings about the current attempts at healthcare reform, it’s difficult to stand by and helplessly watch our patients struggle to maneuver within a system that so often seems to work against so many of them.
What’s easy to lose in the D.C. rhetoric and town-hall warfare is that every day, we delay healthcare reform results in undue patient suffering, both physical and financial. It is a system that is broken and needs, in the words of Mr. Jasper’s daughters, to “get well now.”
Before leaving to celebrate the holiday with my family, I was compelled to return to Mr. Jasper’s room. Unfortunately, the patient was off getting a treatment. But his daughters were still there, faces unchanged. Again, drawn to those eyes, I wondered what would become of this situation.
Would he make it home?
How would his family pay the bills?
What would this mean for his daughters’ future?
Would he and his family be forced to declare bankruptcy?
Would the family ever truly recover?
Staring at the picture in the window, I couldn’t help but think of my own children, also waiting for their father to come home from the hospital to celebrate the holidays.
As I turned to leave, my mind lost in thoughts of untimely illness, ill-fated outcomes, and financial devastation, I realized that in America today, nothing more than circumstances kept me from seeing my own children’s eyes staring back at me from that window. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Four eyes staring, boring through me, unblinking. Locked in a pose holding a hand-scrawled sign commanding their father to ♥♥GET WELL NOW♥♥, the photo of the 14-month-old twin girls was reproduced off a cheap color printer and taped to the window, backlit by the Christmas Eve morning sun. Both the sun and the daughters demanded my attention—the former a brilliant reminder of the glories of the day, the latter the sobering reality of a family rocked by illness.
Mr. Jasper, an otherwise healthy 36-year-old male who recently was diagnosed with a rare, life-threatening disease, would not be spending this holiday with his daughters. In fact, because of our hospital’s flu precautions, he hadn’t seen them in the six weeks he’d been an inpatient. In that time, one of his girls had learned to talk; the other had learned to walk. Mr. Jasper was a distant bystander. He was upset but understanding of his situation—even optimistic, remarkably. However, those girls’ eyes told a different story. What weeks ago shone as the cute countenances of toddlers—silly, carefree, cheerful—now articulated a different tone. “Let my father come home!” they beseeched.
Staring into those eyes on rounds that morning, I was haunted by a thought that had gnawed at my subconscious for weeks. It was likely, albeit not guaranteed, that we’d get Mr. Jasper home to his wife and daughters. However, it would be at a cost. Of course, there would be psychological costs, but I was more acutely concerned with the financial costs. Mr. Jasper, you see, is uninsured.
Healthcare Reform: Too Late for Many
Thousands of miles away, the U.S. Senate was, at that exact time, voting for legislation to greatly reform and expand the U.S. healthcare system. Passed along partisan lines, the bill now awaits reconciliation with the House of Representatives’ bill. From there, it will go before President Obama for signature into law. If passed, this legislation promises to give healthcare coverage to another 30 million Americans.
For Mr. Jasper, this new law will come too late.
It’ll also be too late for Mrs. Anderson, a middle-aged asthmatic now intubated in our ICU, wheezing against constricted bronchioles. Three days earlier, she was seen in the ED for worsening dyspnea, cough, and sputum production. Her symptoms resolved after a few courses of nebulized albuterol and IV steroids, and she was sent home with a prescription for prednisone and inhalers. Unable to afford to fill those prescriptions, her disease progressed, eventually strangling her breathing and tangling her in a healthcare system more willing to pay for the care of disease complications than disease prevention.
Face-to-Face with Catastrophe
Later that morning, I was asked by one of our ED physicians to see Mr. Reynolds and “persuade” him to be admitted to the hospital. Mr. Reynolds has insurance. In fact, of the 11 patients I saw that day, he was one of only three who did. One had Medicaid, the other Medicare.
Mr. Reynolds had a high-deductible, catastrophic-insurance policy. As such, he was wrestling with the decision of whether to come into the hospital to treat his severe cellulitis with IV antibiotics (our formal recommendation), or treat this at home with oral antibiotics. His face wore the torment of the trade-offs. The former surely would cost him his entire $5,000 deductible; the latter, perhaps his life, or at least a limb. As the erythema glared at me, I struggled to recollect a medical school lecture applicable to this situation.
My last patient of the day was Mr. Ramon. He, too, was uninsured. Felled by diabetic ketoacidosis, he was admitted and, as 19-year-olds are wont to do, rebounded quickly. New-onset diabetes, however, was the least of his concerns. With a girlfriend and young child at home, he had to get out of the hospital and return to his job as soon as possible: mouths to feed. Having seen his father lose limbs, kidneys, eyes, and ultimately his life to diabetes, he was motivated to do the right thing.
Unfortunately, motivation doesn’t pay for insulin. I wondered what would come of him in the next 30 years. Would he be able to care for his disease and live a long and prosperous life, or would this admission be just one in a long series of hospital stays?
Broken System
Every hospitalist is aware of these issues and could no doubt fill pages with similarly horrific stories of a healthcare system long broken. It’s remarkable how much of my time I spend trying to figure out a way to cobble together a passable (the notion of “gold standard” therapy long gone) therapeutic plan for my patients—the Walmart list of $4 drugs has taken white-coat prominence over my “Pocket Pharmacopoeia.”
This isn’t to say the U.S. healthcare system doesn’t do a lot of great things. It does, and that cannot be discounted. It’s also not to say that the bill before Congress is the answer. Still, the fact that medical costs limit many Americans from accessing needed care and have become the leading cause of bankruptcy in the U.S. should arouse concern in even the most ardent opponents of healthcare reform. Regardless of one’s political leanings and feelings about the current attempts at healthcare reform, it’s difficult to stand by and helplessly watch our patients struggle to maneuver within a system that so often seems to work against so many of them.
What’s easy to lose in the D.C. rhetoric and town-hall warfare is that every day, we delay healthcare reform results in undue patient suffering, both physical and financial. It is a system that is broken and needs, in the words of Mr. Jasper’s daughters, to “get well now.”
Before leaving to celebrate the holiday with my family, I was compelled to return to Mr. Jasper’s room. Unfortunately, the patient was off getting a treatment. But his daughters were still there, faces unchanged. Again, drawn to those eyes, I wondered what would become of this situation.
Would he make it home?
How would his family pay the bills?
What would this mean for his daughters’ future?
Would he and his family be forced to declare bankruptcy?
Would the family ever truly recover?
Staring at the picture in the window, I couldn’t help but think of my own children, also waiting for their father to come home from the hospital to celebrate the holidays.
As I turned to leave, my mind lost in thoughts of untimely illness, ill-fated outcomes, and financial devastation, I realized that in America today, nothing more than circumstances kept me from seeing my own children’s eyes staring back at me from that window. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
The Year Ahead
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
Necessary Evil: Change

The amount and complexity of medical knowledge we need to keep up with is changing and growing at a remarkable rate. I was trained in an era in which it was taken as a given that congestive heart failure patients should not receive beta-blockers; now it is a big mistake if we don’t prescribe them in most cases. But even before starting medical school, most of us realize that things will change a lot, and many of us see that as a good thing. It keeps our work interesting. Just recently, our hospital had a guest speaker who talked about potential medical applications of nanotechnology. It was way over my head, but it sounded pretty cool.
While I was prepared for ongoing changes in medical knowledge, I failed to anticipate how quickly the business of medicine would change during my career. I think the need to keep up with ever-increasing financial and regulatory issues siphons a lot of time and energy that could be used to keep up with the medical knowledge base. I wasn’t prepared for this when I started my career.
Because it is the start of a new year, I thought I would highlight one issue related to CPT coding: Medicare stopped recognizing consult codes as of Jan. 1 (see “Consultation Elimination,” p. 31).
What It Means for Hospitalists
The good news is that we can just use initial hospital visit codes, inpatient or observation, for all new visits. For example, it won’t matter anymore whether I’m admitting and serving as attending for a patient, or whether a surgeon admitted the patient and asked me to consult for preoperative medical evaluation (“clearance”). I should use the same CPT code in either situation, simply appending a modifier if I’m the admitting physician. And for billing purposes, we won’t have to worry about documenting which doctor requested that we see the patient, though it is a good idea to document it as part of the clinical record anyway.
But it gets a little more complicated. The codes aren’t going away or being removed from the CPT “bible” published by the American Medical Association (AMA). Instead, Medicare simply won’t recognize them anymore. Other payors probably will follow suit within a few months, but that isn’t certain. So it is possible that when asked by a surgeon to provide a preoperative evaluation, you will need to bill an initial hospital (or office or nursing facility) care visit if the patient is on Medicare but bill a consult code if the patient has other insurance. You should check with your billers to ensure you’re doing this correctly.
Medicare-paid consults are at a slightly higher rate than the equivalent service billed as initial hospital care (e.g., when the hospitalist is attending). So a higher reimbursing code has been replaced with one that pays a little less. For example, a 99253 consultation code requires a detailed history, detailed examination, and medical decision-making of low complexity; last year, 99253 was reimbursed by Medicare at an average rate of $114.69. The equivalent admission code for a detailed history, detailed examination, and low-complexity medical decision-making is a 99221 code, for which Medicare pays about $99.90. This represents a difference of about 14%.
However, the net financial impact of this change probably will be positive for most HM groups because you probably bill very few initial consult codes, and instead were stuck billing a follow-up visit code when seeing co-management “consults” (i.e., a patient admitted by a surgeon who asks you to follow and manage diabetes and other medical issues). Now, at least in the case of Medicare, it is appropriate for us to bill an initial hospital visit code, which provides significantly higher reimbursement than follow-up codes.
In addition, there is a modest (about 0.3%) proposed increase in work relative value units attached to the initial hospital visit codes, which will benefit us not only when we’re consulting, but also when we admit and serve as a patient’s attending.
Some specialists may be less interested in consulting on our patients because the initial visit codes will reimburse a little less than similar consultation codes. I don’t anticipate this will be a significant problem for most of us, particularly since many specialists bill the highest level of consultation code (99255), which pays about the same as the equivalent admission code (99223).
Although I think elimination of the use of consultation codes seems like a reasonable step toward simplifying how hospitalists bill for our services, keeping up with these frequent coding changes requires a high level of diligence on our part, and on the part of our administrative and clerical staffs. And it consumes time and resources that I—and my team—could better spend keeping up with changes in clinical practice.
Perhaps when all the dust settles around the healthcare reform debate, we will begin to move toward new, more creative payment models that will allow us to focus on what we do best. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
The amount and complexity of medical knowledge we need to keep up with is changing and growing at a remarkable rate. I was trained in an era in which it was taken as a given that congestive heart failure patients should not receive beta-blockers; now it is a big mistake if we don’t prescribe them in most cases. But even before starting medical school, most of us realize that things will change a lot, and many of us see that as a good thing. It keeps our work interesting. Just recently, our hospital had a guest speaker who talked about potential medical applications of nanotechnology. It was way over my head, but it sounded pretty cool.
While I was prepared for ongoing changes in medical knowledge, I failed to anticipate how quickly the business of medicine would change during my career. I think the need to keep up with ever-increasing financial and regulatory issues siphons a lot of time and energy that could be used to keep up with the medical knowledge base. I wasn’t prepared for this when I started my career.
Because it is the start of a new year, I thought I would highlight one issue related to CPT coding: Medicare stopped recognizing consult codes as of Jan. 1 (see “Consultation Elimination,” p. 31).
What It Means for Hospitalists
The good news is that we can just use initial hospital visit codes, inpatient or observation, for all new visits. For example, it won’t matter anymore whether I’m admitting and serving as attending for a patient, or whether a surgeon admitted the patient and asked me to consult for preoperative medical evaluation (“clearance”). I should use the same CPT code in either situation, simply appending a modifier if I’m the admitting physician. And for billing purposes, we won’t have to worry about documenting which doctor requested that we see the patient, though it is a good idea to document it as part of the clinical record anyway.
But it gets a little more complicated. The codes aren’t going away or being removed from the CPT “bible” published by the American Medical Association (AMA). Instead, Medicare simply won’t recognize them anymore. Other payors probably will follow suit within a few months, but that isn’t certain. So it is possible that when asked by a surgeon to provide a preoperative evaluation, you will need to bill an initial hospital (or office or nursing facility) care visit if the patient is on Medicare but bill a consult code if the patient has other insurance. You should check with your billers to ensure you’re doing this correctly.
Medicare-paid consults are at a slightly higher rate than the equivalent service billed as initial hospital care (e.g., when the hospitalist is attending). So a higher reimbursing code has been replaced with one that pays a little less. For example, a 99253 consultation code requires a detailed history, detailed examination, and medical decision-making of low complexity; last year, 99253 was reimbursed by Medicare at an average rate of $114.69. The equivalent admission code for a detailed history, detailed examination, and low-complexity medical decision-making is a 99221 code, for which Medicare pays about $99.90. This represents a difference of about 14%.
However, the net financial impact of this change probably will be positive for most HM groups because you probably bill very few initial consult codes, and instead were stuck billing a follow-up visit code when seeing co-management “consults” (i.e., a patient admitted by a surgeon who asks you to follow and manage diabetes and other medical issues). Now, at least in the case of Medicare, it is appropriate for us to bill an initial hospital visit code, which provides significantly higher reimbursement than follow-up codes.
In addition, there is a modest (about 0.3%) proposed increase in work relative value units attached to the initial hospital visit codes, which will benefit us not only when we’re consulting, but also when we admit and serve as a patient’s attending.
Some specialists may be less interested in consulting on our patients because the initial visit codes will reimburse a little less than similar consultation codes. I don’t anticipate this will be a significant problem for most of us, particularly since many specialists bill the highest level of consultation code (99255), which pays about the same as the equivalent admission code (99223).
Although I think elimination of the use of consultation codes seems like a reasonable step toward simplifying how hospitalists bill for our services, keeping up with these frequent coding changes requires a high level of diligence on our part, and on the part of our administrative and clerical staffs. And it consumes time and resources that I—and my team—could better spend keeping up with changes in clinical practice.
Perhaps when all the dust settles around the healthcare reform debate, we will begin to move toward new, more creative payment models that will allow us to focus on what we do best. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
The amount and complexity of medical knowledge we need to keep up with is changing and growing at a remarkable rate. I was trained in an era in which it was taken as a given that congestive heart failure patients should not receive beta-blockers; now it is a big mistake if we don’t prescribe them in most cases. But even before starting medical school, most of us realize that things will change a lot, and many of us see that as a good thing. It keeps our work interesting. Just recently, our hospital had a guest speaker who talked about potential medical applications of nanotechnology. It was way over my head, but it sounded pretty cool.
While I was prepared for ongoing changes in medical knowledge, I failed to anticipate how quickly the business of medicine would change during my career. I think the need to keep up with ever-increasing financial and regulatory issues siphons a lot of time and energy that could be used to keep up with the medical knowledge base. I wasn’t prepared for this when I started my career.
Because it is the start of a new year, I thought I would highlight one issue related to CPT coding: Medicare stopped recognizing consult codes as of Jan. 1 (see “Consultation Elimination,” p. 31).
What It Means for Hospitalists
The good news is that we can just use initial hospital visit codes, inpatient or observation, for all new visits. For example, it won’t matter anymore whether I’m admitting and serving as attending for a patient, or whether a surgeon admitted the patient and asked me to consult for preoperative medical evaluation (“clearance”). I should use the same CPT code in either situation, simply appending a modifier if I’m the admitting physician. And for billing purposes, we won’t have to worry about documenting which doctor requested that we see the patient, though it is a good idea to document it as part of the clinical record anyway.
But it gets a little more complicated. The codes aren’t going away or being removed from the CPT “bible” published by the American Medical Association (AMA). Instead, Medicare simply won’t recognize them anymore. Other payors probably will follow suit within a few months, but that isn’t certain. So it is possible that when asked by a surgeon to provide a preoperative evaluation, you will need to bill an initial hospital (or office or nursing facility) care visit if the patient is on Medicare but bill a consult code if the patient has other insurance. You should check with your billers to ensure you’re doing this correctly.
Medicare-paid consults are at a slightly higher rate than the equivalent service billed as initial hospital care (e.g., when the hospitalist is attending). So a higher reimbursing code has been replaced with one that pays a little less. For example, a 99253 consultation code requires a detailed history, detailed examination, and medical decision-making of low complexity; last year, 99253 was reimbursed by Medicare at an average rate of $114.69. The equivalent admission code for a detailed history, detailed examination, and low-complexity medical decision-making is a 99221 code, for which Medicare pays about $99.90. This represents a difference of about 14%.
However, the net financial impact of this change probably will be positive for most HM groups because you probably bill very few initial consult codes, and instead were stuck billing a follow-up visit code when seeing co-management “consults” (i.e., a patient admitted by a surgeon who asks you to follow and manage diabetes and other medical issues). Now, at least in the case of Medicare, it is appropriate for us to bill an initial hospital visit code, which provides significantly higher reimbursement than follow-up codes.
In addition, there is a modest (about 0.3%) proposed increase in work relative value units attached to the initial hospital visit codes, which will benefit us not only when we’re consulting, but also when we admit and serve as a patient’s attending.
Some specialists may be less interested in consulting on our patients because the initial visit codes will reimburse a little less than similar consultation codes. I don’t anticipate this will be a significant problem for most of us, particularly since many specialists bill the highest level of consultation code (99255), which pays about the same as the equivalent admission code (99223).
Although I think elimination of the use of consultation codes seems like a reasonable step toward simplifying how hospitalists bill for our services, keeping up with these frequent coding changes requires a high level of diligence on our part, and on the part of our administrative and clerical staffs. And it consumes time and resources that I—and my team—could better spend keeping up with changes in clinical practice.
Perhaps when all the dust settles around the healthcare reform debate, we will begin to move toward new, more creative payment models that will allow us to focus on what we do best. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
An Imperfect Solution

There is no doubt we are getting healthcare reform, and in the end, Democrats will declare victory for the first meaningful progress since the 1960s, when Medicare and Medicaid were passed. Of course, in the interim, we have had legislation facilitating the development of HMOs under President Nixon and a senior pharmacy benefit under President George W. Bush, but many presidents have flailed at taking a crack at making major changes.
Republicans will declare victory, too, for stopping many bad ideas and trying to hold the line on costs. And everyone will complain about all the things that are not in the bill President Obama will sign this year.
And everyone will be right.
One Out of Three
To oversimplify things, all of the talk about healthcare reform has focused on three main areas:
- Increasing access for the uninsured and underinsured;
- Reigning in healthcare costs; and
- Designing a new system that rewards performance and safety.
At best, all we are getting is a down payment on access—and it will come with a substantial cost.
But what we are more likely beginning is an unraveling of business as usual and a reshuffling of the deck—and some key stakeholders won’t like the cards they will be dealt. The best way to think of what is happening in 2010 is that this is the first step toward having the healthcare system we will have in 2020.
Civic Obligation
It is a national embarrassment for the U.S. to be the only developed country that has not come up with a solution that offers most of its citizens access to healthcare. As a culture, we have decided that every child deserves a free education, that all families should have access to fire and police protection, and that we all should have access to due process and “an attorney who will be appointed to you if you cannot afford one.”
But right now in our country, about 47 million people live sicker and die quicker because of a healthcare system that doesn’t include them. A more sorry aspect is the “underinsured,” the constantly employed person with “good” insurance who is unfortunate enough to be diagnosed with cancer only to find out that their $1 million lifetime benefit runs out in year two or three. Those families face the tough choices between bankruptcy and foreclosure, or allowing Mom or Dad to give up another year or two or three of life. Is this the America we are living in?
Reform, Part I
To get this partial loaf of healthcare reform, Obama and Congressional leaders had to be creative. What has torpedoed previous efforts has been the vast power and reach of large, well-funded stakeholders who see any change as a threat and take a “what’s in it for me” approach. These industries have not been shy about using power and money to influence Congress and the White House, and even more insidiously have gone “direct” with advertisements and commentators who use “Harry and Louise” tactics to frighten an underinformed public about this complex process.
But this time, Obama promised the doctors, the insurance industry, the pharmaceutical companies, the hospitals, the device-makers, and just about anybody who would listen that “they” would not be hurt by these reforms. In fact, in the access discussion for many of these stakeholders, the initial result would be 47 million more customers paying for healthcare products and services. Is it any wonder that the price tag must go up, and by trillions of dollars?
It is the price of admission, at least to get the ball rolling. Now we all are in the box. With a price tag approaching $3 trillion a year, and an aging population and a taxpaying workforce shrinking relative to those they must support with entitlements (think Medicare and Social Security), the die is cast for “Healthcare Reform: The Sequel.”
Trust me—the next round of change will be more cataclysmic. In the aggregate, physicians will make less than the nearly $500 billion we make now. Sure, the primary-care physicians (PCPs) and lower-paid specialties might not be hit (and could even move up), but some physicians will see a marked change in their compensation.
Hospitals will need to adapt as well. They must become more efficient. We saw this in California, Washington, Oregon, Massachusetts, and elsewhere, as capitation and managed care ratcheted down on the old “cost-plus” payment method and moved the industry to reward value and efficiency. Those who are efficient and effective will do very well. Those who have lived by just doing more and more without demonstrating their performance or achieving standards will suffer and be dissatisfied.
More Reforms Possible
The future of the insurance industry will be very different as well, maybe because of government’s more intrusive role (think Medicare for most people) or by evolving to a model like Germany’s, where 200 nonprofit insurance companies compete for business. We will demand that insurance companies return $0.95 on the dollar for patient care, not $0.75 or less, as is common practice today.
Device-makers and Big Pharma might start to see a glimpse into the future as comparative-effectiveness research looks at the value of new, expensive technology and advances in treatments. As medications become “included” in the standard benefits bundle, just like physician fees and hospitalizations, we will see a relentless push downward on pricing. Drugs will become just one more line item to be budgeted for, especially if MedPAC and Congress are involved. We will get what we can afford, not everything that is possible or available.
Because this is 21st-century America, under the cacophony of Glenn Beck and Keith Olbermann and Rush Limbaugh and Rachel Maddow, the potential losers will be loud. They will trumpet any fact or pseudo-fact to alarm the populace. Phrases like “government takeover” and “you will lose the great healthcare you have,” and “death squads” and “illegal immigrants” and “back to 19th-century healthcare,” will bounce around the 24-hour news cycle. They will make real, positive change difficult.
But the beauty of what we are passing now, in 2010, is that the train is leaving the station. We are burning the boats. The healthcare system shakeup officially is under way. There is no turning back.
HM was not borne of a new law or mandate. We are an innovation of a system that must change and evolve. And while HM is not all it eventually will be, there are hints of what we can become. For a new healthcare system that offers greater access and is grounded in documented performance and efficiency, HM will be a solution for hospitals with hospitalist groups.
A lot of uncertainty remains out there, and the next decade promises to be even more turbulent, but hospitalists are as well positioned as any stakeholder in healthcare.
We are ready to be an active, contributing, and solution-oriented profession that will add value to our patients and our healthcare communities.
Stay tuned. TH
Dr. Wellikson is CEO of SHM.
There is no doubt we are getting healthcare reform, and in the end, Democrats will declare victory for the first meaningful progress since the 1960s, when Medicare and Medicaid were passed. Of course, in the interim, we have had legislation facilitating the development of HMOs under President Nixon and a senior pharmacy benefit under President George W. Bush, but many presidents have flailed at taking a crack at making major changes.
Republicans will declare victory, too, for stopping many bad ideas and trying to hold the line on costs. And everyone will complain about all the things that are not in the bill President Obama will sign this year.
And everyone will be right.
One Out of Three
To oversimplify things, all of the talk about healthcare reform has focused on three main areas:
- Increasing access for the uninsured and underinsured;
- Reigning in healthcare costs; and
- Designing a new system that rewards performance and safety.
At best, all we are getting is a down payment on access—and it will come with a substantial cost.
But what we are more likely beginning is an unraveling of business as usual and a reshuffling of the deck—and some key stakeholders won’t like the cards they will be dealt. The best way to think of what is happening in 2010 is that this is the first step toward having the healthcare system we will have in 2020.
Civic Obligation
It is a national embarrassment for the U.S. to be the only developed country that has not come up with a solution that offers most of its citizens access to healthcare. As a culture, we have decided that every child deserves a free education, that all families should have access to fire and police protection, and that we all should have access to due process and “an attorney who will be appointed to you if you cannot afford one.”
But right now in our country, about 47 million people live sicker and die quicker because of a healthcare system that doesn’t include them. A more sorry aspect is the “underinsured,” the constantly employed person with “good” insurance who is unfortunate enough to be diagnosed with cancer only to find out that their $1 million lifetime benefit runs out in year two or three. Those families face the tough choices between bankruptcy and foreclosure, or allowing Mom or Dad to give up another year or two or three of life. Is this the America we are living in?
Reform, Part I
To get this partial loaf of healthcare reform, Obama and Congressional leaders had to be creative. What has torpedoed previous efforts has been the vast power and reach of large, well-funded stakeholders who see any change as a threat and take a “what’s in it for me” approach. These industries have not been shy about using power and money to influence Congress and the White House, and even more insidiously have gone “direct” with advertisements and commentators who use “Harry and Louise” tactics to frighten an underinformed public about this complex process.
But this time, Obama promised the doctors, the insurance industry, the pharmaceutical companies, the hospitals, the device-makers, and just about anybody who would listen that “they” would not be hurt by these reforms. In fact, in the access discussion for many of these stakeholders, the initial result would be 47 million more customers paying for healthcare products and services. Is it any wonder that the price tag must go up, and by trillions of dollars?
It is the price of admission, at least to get the ball rolling. Now we all are in the box. With a price tag approaching $3 trillion a year, and an aging population and a taxpaying workforce shrinking relative to those they must support with entitlements (think Medicare and Social Security), the die is cast for “Healthcare Reform: The Sequel.”
Trust me—the next round of change will be more cataclysmic. In the aggregate, physicians will make less than the nearly $500 billion we make now. Sure, the primary-care physicians (PCPs) and lower-paid specialties might not be hit (and could even move up), but some physicians will see a marked change in their compensation.
Hospitals will need to adapt as well. They must become more efficient. We saw this in California, Washington, Oregon, Massachusetts, and elsewhere, as capitation and managed care ratcheted down on the old “cost-plus” payment method and moved the industry to reward value and efficiency. Those who are efficient and effective will do very well. Those who have lived by just doing more and more without demonstrating their performance or achieving standards will suffer and be dissatisfied.
More Reforms Possible
The future of the insurance industry will be very different as well, maybe because of government’s more intrusive role (think Medicare for most people) or by evolving to a model like Germany’s, where 200 nonprofit insurance companies compete for business. We will demand that insurance companies return $0.95 on the dollar for patient care, not $0.75 or less, as is common practice today.
Device-makers and Big Pharma might start to see a glimpse into the future as comparative-effectiveness research looks at the value of new, expensive technology and advances in treatments. As medications become “included” in the standard benefits bundle, just like physician fees and hospitalizations, we will see a relentless push downward on pricing. Drugs will become just one more line item to be budgeted for, especially if MedPAC and Congress are involved. We will get what we can afford, not everything that is possible or available.
Because this is 21st-century America, under the cacophony of Glenn Beck and Keith Olbermann and Rush Limbaugh and Rachel Maddow, the potential losers will be loud. They will trumpet any fact or pseudo-fact to alarm the populace. Phrases like “government takeover” and “you will lose the great healthcare you have,” and “death squads” and “illegal immigrants” and “back to 19th-century healthcare,” will bounce around the 24-hour news cycle. They will make real, positive change difficult.
But the beauty of what we are passing now, in 2010, is that the train is leaving the station. We are burning the boats. The healthcare system shakeup officially is under way. There is no turning back.
HM was not borne of a new law or mandate. We are an innovation of a system that must change and evolve. And while HM is not all it eventually will be, there are hints of what we can become. For a new healthcare system that offers greater access and is grounded in documented performance and efficiency, HM will be a solution for hospitals with hospitalist groups.
A lot of uncertainty remains out there, and the next decade promises to be even more turbulent, but hospitalists are as well positioned as any stakeholder in healthcare.
We are ready to be an active, contributing, and solution-oriented profession that will add value to our patients and our healthcare communities.
Stay tuned. TH
Dr. Wellikson is CEO of SHM.
There is no doubt we are getting healthcare reform, and in the end, Democrats will declare victory for the first meaningful progress since the 1960s, when Medicare and Medicaid were passed. Of course, in the interim, we have had legislation facilitating the development of HMOs under President Nixon and a senior pharmacy benefit under President George W. Bush, but many presidents have flailed at taking a crack at making major changes.
Republicans will declare victory, too, for stopping many bad ideas and trying to hold the line on costs. And everyone will complain about all the things that are not in the bill President Obama will sign this year.
And everyone will be right.
One Out of Three
To oversimplify things, all of the talk about healthcare reform has focused on three main areas:
- Increasing access for the uninsured and underinsured;
- Reigning in healthcare costs; and
- Designing a new system that rewards performance and safety.
At best, all we are getting is a down payment on access—and it will come with a substantial cost.
But what we are more likely beginning is an unraveling of business as usual and a reshuffling of the deck—and some key stakeholders won’t like the cards they will be dealt. The best way to think of what is happening in 2010 is that this is the first step toward having the healthcare system we will have in 2020.
Civic Obligation
It is a national embarrassment for the U.S. to be the only developed country that has not come up with a solution that offers most of its citizens access to healthcare. As a culture, we have decided that every child deserves a free education, that all families should have access to fire and police protection, and that we all should have access to due process and “an attorney who will be appointed to you if you cannot afford one.”
But right now in our country, about 47 million people live sicker and die quicker because of a healthcare system that doesn’t include them. A more sorry aspect is the “underinsured,” the constantly employed person with “good” insurance who is unfortunate enough to be diagnosed with cancer only to find out that their $1 million lifetime benefit runs out in year two or three. Those families face the tough choices between bankruptcy and foreclosure, or allowing Mom or Dad to give up another year or two or three of life. Is this the America we are living in?
Reform, Part I
To get this partial loaf of healthcare reform, Obama and Congressional leaders had to be creative. What has torpedoed previous efforts has been the vast power and reach of large, well-funded stakeholders who see any change as a threat and take a “what’s in it for me” approach. These industries have not been shy about using power and money to influence Congress and the White House, and even more insidiously have gone “direct” with advertisements and commentators who use “Harry and Louise” tactics to frighten an underinformed public about this complex process.
But this time, Obama promised the doctors, the insurance industry, the pharmaceutical companies, the hospitals, the device-makers, and just about anybody who would listen that “they” would not be hurt by these reforms. In fact, in the access discussion for many of these stakeholders, the initial result would be 47 million more customers paying for healthcare products and services. Is it any wonder that the price tag must go up, and by trillions of dollars?
It is the price of admission, at least to get the ball rolling. Now we all are in the box. With a price tag approaching $3 trillion a year, and an aging population and a taxpaying workforce shrinking relative to those they must support with entitlements (think Medicare and Social Security), the die is cast for “Healthcare Reform: The Sequel.”
Trust me—the next round of change will be more cataclysmic. In the aggregate, physicians will make less than the nearly $500 billion we make now. Sure, the primary-care physicians (PCPs) and lower-paid specialties might not be hit (and could even move up), but some physicians will see a marked change in their compensation.
Hospitals will need to adapt as well. They must become more efficient. We saw this in California, Washington, Oregon, Massachusetts, and elsewhere, as capitation and managed care ratcheted down on the old “cost-plus” payment method and moved the industry to reward value and efficiency. Those who are efficient and effective will do very well. Those who have lived by just doing more and more without demonstrating their performance or achieving standards will suffer and be dissatisfied.
More Reforms Possible
The future of the insurance industry will be very different as well, maybe because of government’s more intrusive role (think Medicare for most people) or by evolving to a model like Germany’s, where 200 nonprofit insurance companies compete for business. We will demand that insurance companies return $0.95 on the dollar for patient care, not $0.75 or less, as is common practice today.
Device-makers and Big Pharma might start to see a glimpse into the future as comparative-effectiveness research looks at the value of new, expensive technology and advances in treatments. As medications become “included” in the standard benefits bundle, just like physician fees and hospitalizations, we will see a relentless push downward on pricing. Drugs will become just one more line item to be budgeted for, especially if MedPAC and Congress are involved. We will get what we can afford, not everything that is possible or available.
Because this is 21st-century America, under the cacophony of Glenn Beck and Keith Olbermann and Rush Limbaugh and Rachel Maddow, the potential losers will be loud. They will trumpet any fact or pseudo-fact to alarm the populace. Phrases like “government takeover” and “you will lose the great healthcare you have,” and “death squads” and “illegal immigrants” and “back to 19th-century healthcare,” will bounce around the 24-hour news cycle. They will make real, positive change difficult.
But the beauty of what we are passing now, in 2010, is that the train is leaving the station. We are burning the boats. The healthcare system shakeup officially is under way. There is no turning back.
HM was not borne of a new law or mandate. We are an innovation of a system that must change and evolve. And while HM is not all it eventually will be, there are hints of what we can become. For a new healthcare system that offers greater access and is grounded in documented performance and efficiency, HM will be a solution for hospitals with hospitalist groups.
A lot of uncertainty remains out there, and the next decade promises to be even more turbulent, but hospitalists are as well positioned as any stakeholder in healthcare.
We are ready to be an active, contributing, and solution-oriented profession that will add value to our patients and our healthcare communities.
Stay tuned. TH
Dr. Wellikson is CEO of SHM.
Medicare Fee Inspection
No one can call 2009 a dull year for healthcare policy. And 2010 already is shaping up as another humdinger, with several issues bubbling to the surface. One of the biggest comes courtesy of the Dartmouth Atlas of Health Care (www.dartmouthatlas.org), as politicians, analysts, researchers, and physicians grapple over how to resolve the contentious issue of geographical disparities in healthcare spending.
One of the main bodies of evidence driving the debate, the interactive Dartmouth map, depicts a color-coded nation in which wide swaths of the Midwest and West are colored with a pale green hue, which represents a significantly reduced amount of Medicare reimbursements. Meanwhile, states such as New York, New Jersey, Massachusetts, Florida, Texas, and Louisiana are marked by a darker shade of green—representing the nation’s most expensive per capita reimbursement rates.
Tucked within 2009’s massive Affordable Health Care for America Act passed by the House is a provision calling for a study of “geographic variation in healthcare spending and promoting high-value healthcare,” which is aiming for a more evenly colored landscape.
More than 50 legislators, hailing primarily from the Midwest and Pacific Northwest and calling themselves the Quality Care Coalition, pushed through the wording as a condition for supporting the larger healthcare reform bill. One measure would direct the nonpartisan Institute of Medicine (IOM) to check the accuracy of the geographic adjustment factors that underlie existing Medicare reimbursements and suggest necessary revisions. The second would call upon the IOM “to conduct a study on geographic variation and growth in volume and intensity of services in per capita healthcare spending among the Medicare, Medicaid, privately insured, and uninsured populations.”
Recommendations to Secretary of Health and Human Services Kathleen Sebelius as a result of that study would go into effect unless the House and Senate passed a joint resolution of disapproval with a two-thirds vote.
Reimbursement Battles
The implicit message is that some states, cities, and health providers have been shortchanged in their reimbursements—a complaint that flows into the larger meme that the country’s dysfunctional payment system rewards quantity, not quality. Officials at the Mayo Clinic in Rochester, Minn., have suggested in media accounts that the current Medicare formula cost the clinic $840 million in lost reimbursements in 2008 alone.
Rep. Jay Inslee (D-Washington), whose district lies northwest of Seattle, served as one of the lead negotiators on the issue. According to Inslee spokesman Robert Kellar, the geographical disparity in healthcare spending has been a perennial concern for the Washington delegation due to reimbursement rates that lag by as much as 50%, depending on the procedure. “Hospitals haven’t been able to keep or attract the personnel that they could have because of this issue,” Kellar says. In Washington state, per capita Medicare reimbursements in 2006 hovered about $1,200 below the national average, though 15 other states, led by Hawaii, received even less.
Despite the specter of a skirmish between urban and rural states and hospitals, however, the Dartmouth Atlas suggests that many disparities are more geographically nuanced. In 2006, for example, the Miami hospital referral region received more than $16,300 in Medicare reimbursements per enrollee, while nearby Fort Lauderdale received $9,800 and Atlanta less than $7,400. By comparison, New York netted $12,100, Seattle received $7,200, Rochester, Minn., received $6,700, and Honolulu was reimbursed only $5,300.
Representatives of higher-spending areas have complained that the atlas doesn’t tell the whole story—that steep living costs, poorer populations seeking medical care, and infrastructure necessary for teaching institutions can drive up Medicare expenses. As part of a compromise negotiated with the Quality Care Coalition, the examination of per capita spending will not include expenses related to graduate medical education, disproportionate share hospital (DSH) payments, and health information technology.
In attempting to get at the source of remaining cost disparities, however, the IOM has been charged with considering such factors as a local population’s relative health and socioeconomic status (race, ethnicity, gender, age, income, and education). The study will scrutinize healthcare providers’ organizational models, practice patterns, healthcare outcomes, quality benchmarks, and doctors’ discretion in making treatment decisions, among other criteria.
Differences of Opinion
Dylan Roby, an assistant professor at the UCLA Center for Health Policy Research, says the general expectation among healthcare analysts is that significant differences will remain even with additional sophisticated modeling techniques. “The main hypothesis by most people in the field is that it’s differences in practice patterns that are really driving this, not differences in need or differences in disease burden,” he says.
But what about outcomes? A recent study of heart failure patients at six California hospitals seemed to throw cold water on the notion that higher resource use doesn’t equate with better results with patients.1 The study found more treatment did lead to higher odds of survival.
Roby thinks the study’s results lay the framework for looking at hospital-to-hospital differences in how providers deliver care and allocate resources, but he cautions that they shouldn’t be overanalyzed. All six of the California hospitals in the study are linked to universities and have ample access to resources, he points out.
HM at the Forefront
As for hospitalists, Roby hopes they will be increasingly called upon as focal points for improving efficiencies within provider networks. He concedes that plenty of challenges remain: An institution’s internal politics, for instance, could stymie even the most efficient and proactive physician. Even so, Roby is hopeful that an independent study could at least spur a dialogue about best practices. “I think what the study could potentially do, rather than just act as a way to penalize hospitals that might not be efficient with care, is really offer the ability for us to look at the characteristics of hospitals, in terms of how the care is delivered,” he says.
Ideally, the ability to learn would be followed by the impetus to change. But as analysts have noted, a panel’s recommendations on how to improve healthcare delivery don’t always neatly translate into federal policy.
Consider November’s uproar over mammogram recommendations. When the 16-member U.S. Preventive Services Task Force recommended that women wait until age 50 for routine mammograms instead of starting the screening process at 40, in large part to prevent overtreatment, the fallout was fast and furious. Sebelius quickly signaled in a strongly worded statement that federal policy wasn’t about to change, despite the evidence-based conclusions of a panel convened by her department’s Agency for Healthcare Research and Quality. A group of Republican legislators decried the recommendation as evidence of bureaucrats intruding on healthcare decisions, and even Rep. Debbie Wasserman Schulz (D-Florida), herself a breast-cancer survivor, called the panel’s recommendations “disturbing” and considered Congressional hearings.
The take-home message is readily transferrable to hospitalists: The perception that patients might receive less care can spark public upheaval and force policy makers to beat a hasty retreat away from evidence-based medicine.
Despite the best intentions, a federal panel’s recommendations over resolving geographical disparities in spending could unleash far more drama. Inevitably, such a study will identify both winners and losers, the latter of whom might not accept reduced payments willingly or quietly. TH
Bryn Nelson is a freelance writer based in Seattle.
Reference
- Ellis SG, Miller D, Keys TF. Comparing physician-specific two-year patient outcomes after coronary angiography. J Am Coll Cardiol. 1999;33:1278-1285.
No one can call 2009 a dull year for healthcare policy. And 2010 already is shaping up as another humdinger, with several issues bubbling to the surface. One of the biggest comes courtesy of the Dartmouth Atlas of Health Care (www.dartmouthatlas.org), as politicians, analysts, researchers, and physicians grapple over how to resolve the contentious issue of geographical disparities in healthcare spending.
One of the main bodies of evidence driving the debate, the interactive Dartmouth map, depicts a color-coded nation in which wide swaths of the Midwest and West are colored with a pale green hue, which represents a significantly reduced amount of Medicare reimbursements. Meanwhile, states such as New York, New Jersey, Massachusetts, Florida, Texas, and Louisiana are marked by a darker shade of green—representing the nation’s most expensive per capita reimbursement rates.
Tucked within 2009’s massive Affordable Health Care for America Act passed by the House is a provision calling for a study of “geographic variation in healthcare spending and promoting high-value healthcare,” which is aiming for a more evenly colored landscape.
More than 50 legislators, hailing primarily from the Midwest and Pacific Northwest and calling themselves the Quality Care Coalition, pushed through the wording as a condition for supporting the larger healthcare reform bill. One measure would direct the nonpartisan Institute of Medicine (IOM) to check the accuracy of the geographic adjustment factors that underlie existing Medicare reimbursements and suggest necessary revisions. The second would call upon the IOM “to conduct a study on geographic variation and growth in volume and intensity of services in per capita healthcare spending among the Medicare, Medicaid, privately insured, and uninsured populations.”
Recommendations to Secretary of Health and Human Services Kathleen Sebelius as a result of that study would go into effect unless the House and Senate passed a joint resolution of disapproval with a two-thirds vote.
Reimbursement Battles
The implicit message is that some states, cities, and health providers have been shortchanged in their reimbursements—a complaint that flows into the larger meme that the country’s dysfunctional payment system rewards quantity, not quality. Officials at the Mayo Clinic in Rochester, Minn., have suggested in media accounts that the current Medicare formula cost the clinic $840 million in lost reimbursements in 2008 alone.
Rep. Jay Inslee (D-Washington), whose district lies northwest of Seattle, served as one of the lead negotiators on the issue. According to Inslee spokesman Robert Kellar, the geographical disparity in healthcare spending has been a perennial concern for the Washington delegation due to reimbursement rates that lag by as much as 50%, depending on the procedure. “Hospitals haven’t been able to keep or attract the personnel that they could have because of this issue,” Kellar says. In Washington state, per capita Medicare reimbursements in 2006 hovered about $1,200 below the national average, though 15 other states, led by Hawaii, received even less.
Despite the specter of a skirmish between urban and rural states and hospitals, however, the Dartmouth Atlas suggests that many disparities are more geographically nuanced. In 2006, for example, the Miami hospital referral region received more than $16,300 in Medicare reimbursements per enrollee, while nearby Fort Lauderdale received $9,800 and Atlanta less than $7,400. By comparison, New York netted $12,100, Seattle received $7,200, Rochester, Minn., received $6,700, and Honolulu was reimbursed only $5,300.
Representatives of higher-spending areas have complained that the atlas doesn’t tell the whole story—that steep living costs, poorer populations seeking medical care, and infrastructure necessary for teaching institutions can drive up Medicare expenses. As part of a compromise negotiated with the Quality Care Coalition, the examination of per capita spending will not include expenses related to graduate medical education, disproportionate share hospital (DSH) payments, and health information technology.
In attempting to get at the source of remaining cost disparities, however, the IOM has been charged with considering such factors as a local population’s relative health and socioeconomic status (race, ethnicity, gender, age, income, and education). The study will scrutinize healthcare providers’ organizational models, practice patterns, healthcare outcomes, quality benchmarks, and doctors’ discretion in making treatment decisions, among other criteria.
Differences of Opinion
Dylan Roby, an assistant professor at the UCLA Center for Health Policy Research, says the general expectation among healthcare analysts is that significant differences will remain even with additional sophisticated modeling techniques. “The main hypothesis by most people in the field is that it’s differences in practice patterns that are really driving this, not differences in need or differences in disease burden,” he says.
But what about outcomes? A recent study of heart failure patients at six California hospitals seemed to throw cold water on the notion that higher resource use doesn’t equate with better results with patients.1 The study found more treatment did lead to higher odds of survival.
Roby thinks the study’s results lay the framework for looking at hospital-to-hospital differences in how providers deliver care and allocate resources, but he cautions that they shouldn’t be overanalyzed. All six of the California hospitals in the study are linked to universities and have ample access to resources, he points out.
HM at the Forefront
As for hospitalists, Roby hopes they will be increasingly called upon as focal points for improving efficiencies within provider networks. He concedes that plenty of challenges remain: An institution’s internal politics, for instance, could stymie even the most efficient and proactive physician. Even so, Roby is hopeful that an independent study could at least spur a dialogue about best practices. “I think what the study could potentially do, rather than just act as a way to penalize hospitals that might not be efficient with care, is really offer the ability for us to look at the characteristics of hospitals, in terms of how the care is delivered,” he says.
Ideally, the ability to learn would be followed by the impetus to change. But as analysts have noted, a panel’s recommendations on how to improve healthcare delivery don’t always neatly translate into federal policy.
Consider November’s uproar over mammogram recommendations. When the 16-member U.S. Preventive Services Task Force recommended that women wait until age 50 for routine mammograms instead of starting the screening process at 40, in large part to prevent overtreatment, the fallout was fast and furious. Sebelius quickly signaled in a strongly worded statement that federal policy wasn’t about to change, despite the evidence-based conclusions of a panel convened by her department’s Agency for Healthcare Research and Quality. A group of Republican legislators decried the recommendation as evidence of bureaucrats intruding on healthcare decisions, and even Rep. Debbie Wasserman Schulz (D-Florida), herself a breast-cancer survivor, called the panel’s recommendations “disturbing” and considered Congressional hearings.
The take-home message is readily transferrable to hospitalists: The perception that patients might receive less care can spark public upheaval and force policy makers to beat a hasty retreat away from evidence-based medicine.
Despite the best intentions, a federal panel’s recommendations over resolving geographical disparities in spending could unleash far more drama. Inevitably, such a study will identify both winners and losers, the latter of whom might not accept reduced payments willingly or quietly. TH
Bryn Nelson is a freelance writer based in Seattle.
Reference
- Ellis SG, Miller D, Keys TF. Comparing physician-specific two-year patient outcomes after coronary angiography. J Am Coll Cardiol. 1999;33:1278-1285.
No one can call 2009 a dull year for healthcare policy. And 2010 already is shaping up as another humdinger, with several issues bubbling to the surface. One of the biggest comes courtesy of the Dartmouth Atlas of Health Care (www.dartmouthatlas.org), as politicians, analysts, researchers, and physicians grapple over how to resolve the contentious issue of geographical disparities in healthcare spending.
One of the main bodies of evidence driving the debate, the interactive Dartmouth map, depicts a color-coded nation in which wide swaths of the Midwest and West are colored with a pale green hue, which represents a significantly reduced amount of Medicare reimbursements. Meanwhile, states such as New York, New Jersey, Massachusetts, Florida, Texas, and Louisiana are marked by a darker shade of green—representing the nation’s most expensive per capita reimbursement rates.
Tucked within 2009’s massive Affordable Health Care for America Act passed by the House is a provision calling for a study of “geographic variation in healthcare spending and promoting high-value healthcare,” which is aiming for a more evenly colored landscape.
More than 50 legislators, hailing primarily from the Midwest and Pacific Northwest and calling themselves the Quality Care Coalition, pushed through the wording as a condition for supporting the larger healthcare reform bill. One measure would direct the nonpartisan Institute of Medicine (IOM) to check the accuracy of the geographic adjustment factors that underlie existing Medicare reimbursements and suggest necessary revisions. The second would call upon the IOM “to conduct a study on geographic variation and growth in volume and intensity of services in per capita healthcare spending among the Medicare, Medicaid, privately insured, and uninsured populations.”
Recommendations to Secretary of Health and Human Services Kathleen Sebelius as a result of that study would go into effect unless the House and Senate passed a joint resolution of disapproval with a two-thirds vote.
Reimbursement Battles
The implicit message is that some states, cities, and health providers have been shortchanged in their reimbursements—a complaint that flows into the larger meme that the country’s dysfunctional payment system rewards quantity, not quality. Officials at the Mayo Clinic in Rochester, Minn., have suggested in media accounts that the current Medicare formula cost the clinic $840 million in lost reimbursements in 2008 alone.
Rep. Jay Inslee (D-Washington), whose district lies northwest of Seattle, served as one of the lead negotiators on the issue. According to Inslee spokesman Robert Kellar, the geographical disparity in healthcare spending has been a perennial concern for the Washington delegation due to reimbursement rates that lag by as much as 50%, depending on the procedure. “Hospitals haven’t been able to keep or attract the personnel that they could have because of this issue,” Kellar says. In Washington state, per capita Medicare reimbursements in 2006 hovered about $1,200 below the national average, though 15 other states, led by Hawaii, received even less.
Despite the specter of a skirmish between urban and rural states and hospitals, however, the Dartmouth Atlas suggests that many disparities are more geographically nuanced. In 2006, for example, the Miami hospital referral region received more than $16,300 in Medicare reimbursements per enrollee, while nearby Fort Lauderdale received $9,800 and Atlanta less than $7,400. By comparison, New York netted $12,100, Seattle received $7,200, Rochester, Minn., received $6,700, and Honolulu was reimbursed only $5,300.
Representatives of higher-spending areas have complained that the atlas doesn’t tell the whole story—that steep living costs, poorer populations seeking medical care, and infrastructure necessary for teaching institutions can drive up Medicare expenses. As part of a compromise negotiated with the Quality Care Coalition, the examination of per capita spending will not include expenses related to graduate medical education, disproportionate share hospital (DSH) payments, and health information technology.
In attempting to get at the source of remaining cost disparities, however, the IOM has been charged with considering such factors as a local population’s relative health and socioeconomic status (race, ethnicity, gender, age, income, and education). The study will scrutinize healthcare providers’ organizational models, practice patterns, healthcare outcomes, quality benchmarks, and doctors’ discretion in making treatment decisions, among other criteria.
Differences of Opinion
Dylan Roby, an assistant professor at the UCLA Center for Health Policy Research, says the general expectation among healthcare analysts is that significant differences will remain even with additional sophisticated modeling techniques. “The main hypothesis by most people in the field is that it’s differences in practice patterns that are really driving this, not differences in need or differences in disease burden,” he says.
But what about outcomes? A recent study of heart failure patients at six California hospitals seemed to throw cold water on the notion that higher resource use doesn’t equate with better results with patients.1 The study found more treatment did lead to higher odds of survival.
Roby thinks the study’s results lay the framework for looking at hospital-to-hospital differences in how providers deliver care and allocate resources, but he cautions that they shouldn’t be overanalyzed. All six of the California hospitals in the study are linked to universities and have ample access to resources, he points out.
HM at the Forefront
As for hospitalists, Roby hopes they will be increasingly called upon as focal points for improving efficiencies within provider networks. He concedes that plenty of challenges remain: An institution’s internal politics, for instance, could stymie even the most efficient and proactive physician. Even so, Roby is hopeful that an independent study could at least spur a dialogue about best practices. “I think what the study could potentially do, rather than just act as a way to penalize hospitals that might not be efficient with care, is really offer the ability for us to look at the characteristics of hospitals, in terms of how the care is delivered,” he says.
Ideally, the ability to learn would be followed by the impetus to change. But as analysts have noted, a panel’s recommendations on how to improve healthcare delivery don’t always neatly translate into federal policy.
Consider November’s uproar over mammogram recommendations. When the 16-member U.S. Preventive Services Task Force recommended that women wait until age 50 for routine mammograms instead of starting the screening process at 40, in large part to prevent overtreatment, the fallout was fast and furious. Sebelius quickly signaled in a strongly worded statement that federal policy wasn’t about to change, despite the evidence-based conclusions of a panel convened by her department’s Agency for Healthcare Research and Quality. A group of Republican legislators decried the recommendation as evidence of bureaucrats intruding on healthcare decisions, and even Rep. Debbie Wasserman Schulz (D-Florida), herself a breast-cancer survivor, called the panel’s recommendations “disturbing” and considered Congressional hearings.
The take-home message is readily transferrable to hospitalists: The perception that patients might receive less care can spark public upheaval and force policy makers to beat a hasty retreat away from evidence-based medicine.
Despite the best intentions, a federal panel’s recommendations over resolving geographical disparities in spending could unleash far more drama. Inevitably, such a study will identify both winners and losers, the latter of whom might not accept reduced payments willingly or quietly. TH
Bryn Nelson is a freelance writer based in Seattle.
Reference
- Ellis SG, Miller D, Keys TF. Comparing physician-specific two-year patient outcomes after coronary angiography. J Am Coll Cardiol. 1999;33:1278-1285.
Consultation Elimination
As of Jan. 1, the Centers for Medicare and Medicaid Services (CMS) ceased physician payment for consultations. The elimination of consult codes will affect physician group payments as well as relative-value-unit (RVU)-based incentive payments to individual physicians.
The Medicare-designated status of outpatient consultation (99241-99245) and inpatient consultation (99251-99255) codes has changed from “A” (separately payable under the physician fee schedule, when covered) to “I” (not valid for Medicare purposes; Medicare uses another code for the reporting of and the payment for these services). So if you submit consultation codes for Medicare beneficiaries, the result will be nonpayment.
While many physicians fear the negative impact of this ruling, hospitalists should consider its potential. Let’s take a look at a scenario hospitalists encounter on a routine basis.
Typical HM Scenario
A surgeon admits a 76-year-old man for aortic valve replacement. The patient’s history also includes well-controlled hypertension and chronic obstructive pulmonary disease (COPD). Postoperatively, the patient experiences an exacerbation of COPD related to anesthesia, elevated blood pressure, and hyperglycemia. The surgeon requests the hospitalist’s advice on appropriate medical interventions of these conditions. How should the hospitalist report the initial encounter with this Medicare beneficiary?
The hospitalist should select the CPT code that best fits the service and the payor. While most physicians regard this requested service as an inpatient consultation (99251-99255), Medicare no longer recognizes those codes. Instead, the hospitalist should report this encounter as an initial hospital care service (99221-99223).
Comanagement Issues
CMS and Medicare administrative contractors regularly uncover reporting errors for co-management requests. CMS decided the nature of these services were not consultative because the surgeon is not asking the physician or qualified nonphysician provider’s (NPP’s) opinion or advice for the surgeon’s use in treating the patient. Instead, these services constituted concurrent care and should have been billed using subsequent hospital care codes (99231-99233) in the hospital inpatient setting, subsequent NF care codes (99307-99310) in the SNF/NF setting, or office or other outpatient visit codes (99201-99215) in the office or outpatient settings.1
The new ruling simplifies coding and reduces reporting errors. The initial encounter with the patient is reported as such. Regardless of who is the attending of record or the consultant, the first physician from a particular provider group reports initial hospital care codes (i.e., 99221-99223) to represent the first patient encounter, even when this encounter does not occur on the admission date. Other physicians of the same specialty within the same provider group will not be permitted to report initial hospital care codes for their own initial encounter if someone from the group and specialty has already seen the patient during that hospitalization. In other words, the first hospitalist in the provider group reports 9922x, while the remaining hospitalists use subsequent hospital care codes (9923x).
In order to differentiate “consultant” services from “attending” services, CMS will be creating a modifier. The anticipated “AI” modifier must be appended to the attending physician’s initial encounter. Other initial hospital care codes reported throughout the hospital stay, as appropriate, are presumed to be that of “consultants” (i.e., physicians with a different specialty designation than the attending physician) participating in the case. Therefore, the hospitalist now can rightfully recover the increased work effort of the initial patient encounter (99223: 3.79 relative value units, ~$147 vs. 99233: 2.0 relative value units, ~$78, based on 2010 Medicare rates). Physicians will be required to meet the minimum documentation required for the selected visit code.
Other and Undefined Service Locations
Consultations in nursing facilities are handled much like inpatient hospital care. Physicians should report initial nursing facility services (99203-99306) for the first patient encounter, and subsequent nursing facility care codes (99307-99310) for each encounter thereafter. The attending physician of record appends the assigned modifier (presumed to be “AI”) when submitting their initial care service. All other initial care codes are presumed to be those of “consulting” physicians.
Initial information from CMS does not address observation services. Logically, these hospital-based services would follow the same methodology as inpatient care: report initial observation care (99218-99220) for the first “consulting” encounter. However, this might not be appropriate given Medicare’s existing rules for observation services, which guide physicians other than the admitting physician/group to “bill the office and other outpatient service codes or outpatient consultation codes as appropriate when they provide services to the patient.”2 With Medicare’s elimination of consultation codes, the consultant reports “office and other outpatient service codes” (i.e., new patient, 99201-99205, or established patient codes, 99212-99215) by default.
Without further clarification on observation services, hospitalists should report new or established patient service codes, depending on whether the patient has been seen by a group member within the last three years.
Medicare also has existing guidelines for the ED, which suggest that any physician not meeting the consultation criteria report ED service codes (99281-99285). Without further clarification, hospitalists should continue to follow this instruction for Medicare beneficiaries.
Nonphysician Providers
Medicare’s split/shared billing guidelines apply to most hospital inpatient, hospital outpatient, and ED evaluation and management (E/M) services, with consultations as one exception. Now, in accordance with the new ruling, hospitalists should select the appropriate initial service codes that correspond to patient’s location (e.g., 99223 for inpatients). NPPs can participate in the initial service provided to patients in these locations without the hospitalist having to replicate the entire service. The hospitalist can submit the claim in their name after selecting the visit level based upon the cumulative service personally provided on the same calendar day by both the NPP and the physician. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.10I. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/ manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8A. CMS Web site. Available at: www. cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- PFS Federal Regulation Notices: Proposed Revisions to Payment Policies Under the Physician Fee Schedule and Part B for CY 2010. CMS Web site. Available at: www.cms.hhs.gov/PhysicianFeeSched/PFSFRN/itemdetail.asp?filterType=none&filterByDID=99&sortByDID=4&sortOrder=descending&itemID=CMS1223902&intNumPerPage=10. Accessed Nov. 12, 2009.
- Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B (for CY 2010). CMS Web site. Available at: www.federalregister.gov/OFR Upload/OFRData/2009-26502_PI.pdf. Accessed Nov. 10, 2009.
The Bottom Line
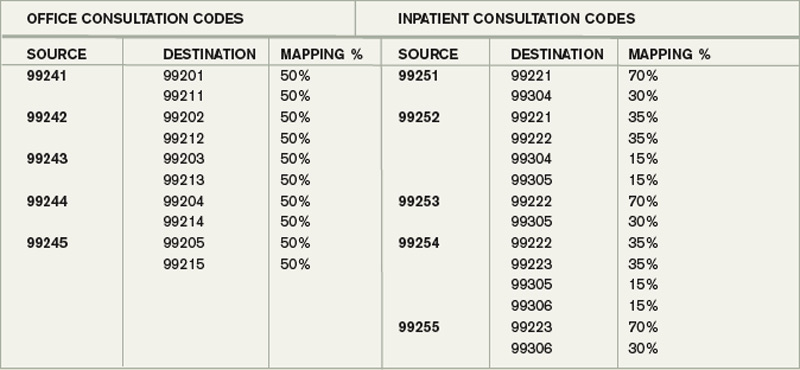
The elimination of consults will affect physician group payments as well as RVU-based incentive payments to individual physicians. HM group leaders will want to refer to the CMS formula, also known as a crosswalk. The crosswalk outlines the utilization of consult codes and E/M codes for the sole purpose of establishing aggregate budget neutrality.3
The payment differential for consultations has been redistributed to increase payments for existing E/M services.
Here’s how it works: Use the “mapping percentage” column to project the distribution of consultative services between the “replacement” (i.e., “destination”) codes. For example, presumably 70% of 99251 will now be reported as initial hospital care (99221), whereas 30% will be reported as initial nursing facility care (99304). Please note that this table does not represent billing guidance or documentation equivalencies, but it does attempt to quantify sites of consultative service and their corresponding code categories for the basis of fiscal-year projections.
Physicians should select the visit code in the appropriate code category for the service location and in accordance with CMS documentation guidelines, which are available at www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp.
As of Jan. 1, the Centers for Medicare and Medicaid Services (CMS) ceased physician payment for consultations. The elimination of consult codes will affect physician group payments as well as relative-value-unit (RVU)-based incentive payments to individual physicians.
The Medicare-designated status of outpatient consultation (99241-99245) and inpatient consultation (99251-99255) codes has changed from “A” (separately payable under the physician fee schedule, when covered) to “I” (not valid for Medicare purposes; Medicare uses another code for the reporting of and the payment for these services). So if you submit consultation codes for Medicare beneficiaries, the result will be nonpayment.
While many physicians fear the negative impact of this ruling, hospitalists should consider its potential. Let’s take a look at a scenario hospitalists encounter on a routine basis.
Typical HM Scenario
A surgeon admits a 76-year-old man for aortic valve replacement. The patient’s history also includes well-controlled hypertension and chronic obstructive pulmonary disease (COPD). Postoperatively, the patient experiences an exacerbation of COPD related to anesthesia, elevated blood pressure, and hyperglycemia. The surgeon requests the hospitalist’s advice on appropriate medical interventions of these conditions. How should the hospitalist report the initial encounter with this Medicare beneficiary?
The hospitalist should select the CPT code that best fits the service and the payor. While most physicians regard this requested service as an inpatient consultation (99251-99255), Medicare no longer recognizes those codes. Instead, the hospitalist should report this encounter as an initial hospital care service (99221-99223).
Comanagement Issues
CMS and Medicare administrative contractors regularly uncover reporting errors for co-management requests. CMS decided the nature of these services were not consultative because the surgeon is not asking the physician or qualified nonphysician provider’s (NPP’s) opinion or advice for the surgeon’s use in treating the patient. Instead, these services constituted concurrent care and should have been billed using subsequent hospital care codes (99231-99233) in the hospital inpatient setting, subsequent NF care codes (99307-99310) in the SNF/NF setting, or office or other outpatient visit codes (99201-99215) in the office or outpatient settings.1
The new ruling simplifies coding and reduces reporting errors. The initial encounter with the patient is reported as such. Regardless of who is the attending of record or the consultant, the first physician from a particular provider group reports initial hospital care codes (i.e., 99221-99223) to represent the first patient encounter, even when this encounter does not occur on the admission date. Other physicians of the same specialty within the same provider group will not be permitted to report initial hospital care codes for their own initial encounter if someone from the group and specialty has already seen the patient during that hospitalization. In other words, the first hospitalist in the provider group reports 9922x, while the remaining hospitalists use subsequent hospital care codes (9923x).
In order to differentiate “consultant” services from “attending” services, CMS will be creating a modifier. The anticipated “AI” modifier must be appended to the attending physician’s initial encounter. Other initial hospital care codes reported throughout the hospital stay, as appropriate, are presumed to be that of “consultants” (i.e., physicians with a different specialty designation than the attending physician) participating in the case. Therefore, the hospitalist now can rightfully recover the increased work effort of the initial patient encounter (99223: 3.79 relative value units, ~$147 vs. 99233: 2.0 relative value units, ~$78, based on 2010 Medicare rates). Physicians will be required to meet the minimum documentation required for the selected visit code.
Other and Undefined Service Locations
Consultations in nursing facilities are handled much like inpatient hospital care. Physicians should report initial nursing facility services (99203-99306) for the first patient encounter, and subsequent nursing facility care codes (99307-99310) for each encounter thereafter. The attending physician of record appends the assigned modifier (presumed to be “AI”) when submitting their initial care service. All other initial care codes are presumed to be those of “consulting” physicians.
Initial information from CMS does not address observation services. Logically, these hospital-based services would follow the same methodology as inpatient care: report initial observation care (99218-99220) for the first “consulting” encounter. However, this might not be appropriate given Medicare’s existing rules for observation services, which guide physicians other than the admitting physician/group to “bill the office and other outpatient service codes or outpatient consultation codes as appropriate when they provide services to the patient.”2 With Medicare’s elimination of consultation codes, the consultant reports “office and other outpatient service codes” (i.e., new patient, 99201-99205, or established patient codes, 99212-99215) by default.
Without further clarification on observation services, hospitalists should report new or established patient service codes, depending on whether the patient has been seen by a group member within the last three years.
Medicare also has existing guidelines for the ED, which suggest that any physician not meeting the consultation criteria report ED service codes (99281-99285). Without further clarification, hospitalists should continue to follow this instruction for Medicare beneficiaries.
Nonphysician Providers
Medicare’s split/shared billing guidelines apply to most hospital inpatient, hospital outpatient, and ED evaluation and management (E/M) services, with consultations as one exception. Now, in accordance with the new ruling, hospitalists should select the appropriate initial service codes that correspond to patient’s location (e.g., 99223 for inpatients). NPPs can participate in the initial service provided to patients in these locations without the hospitalist having to replicate the entire service. The hospitalist can submit the claim in their name after selecting the visit level based upon the cumulative service personally provided on the same calendar day by both the NPP and the physician. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.10I. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/ manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8A. CMS Web site. Available at: www. cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- PFS Federal Regulation Notices: Proposed Revisions to Payment Policies Under the Physician Fee Schedule and Part B for CY 2010. CMS Web site. Available at: www.cms.hhs.gov/PhysicianFeeSched/PFSFRN/itemdetail.asp?filterType=none&filterByDID=99&sortByDID=4&sortOrder=descending&itemID=CMS1223902&intNumPerPage=10. Accessed Nov. 12, 2009.
- Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B (for CY 2010). CMS Web site. Available at: www.federalregister.gov/OFR Upload/OFRData/2009-26502_PI.pdf. Accessed Nov. 10, 2009.
The Bottom Line
The elimination of consults will affect physician group payments as well as RVU-based incentive payments to individual physicians. HM group leaders will want to refer to the CMS formula, also known as a crosswalk. The crosswalk outlines the utilization of consult codes and E/M codes for the sole purpose of establishing aggregate budget neutrality.3
The payment differential for consultations has been redistributed to increase payments for existing E/M services.
Here’s how it works: Use the “mapping percentage” column to project the distribution of consultative services between the “replacement” (i.e., “destination”) codes. For example, presumably 70% of 99251 will now be reported as initial hospital care (99221), whereas 30% will be reported as initial nursing facility care (99304). Please note that this table does not represent billing guidance or documentation equivalencies, but it does attempt to quantify sites of consultative service and their corresponding code categories for the basis of fiscal-year projections.
Physicians should select the visit code in the appropriate code category for the service location and in accordance with CMS documentation guidelines, which are available at www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp.
As of Jan. 1, the Centers for Medicare and Medicaid Services (CMS) ceased physician payment for consultations. The elimination of consult codes will affect physician group payments as well as relative-value-unit (RVU)-based incentive payments to individual physicians.
The Medicare-designated status of outpatient consultation (99241-99245) and inpatient consultation (99251-99255) codes has changed from “A” (separately payable under the physician fee schedule, when covered) to “I” (not valid for Medicare purposes; Medicare uses another code for the reporting of and the payment for these services). So if you submit consultation codes for Medicare beneficiaries, the result will be nonpayment.
While many physicians fear the negative impact of this ruling, hospitalists should consider its potential. Let’s take a look at a scenario hospitalists encounter on a routine basis.
Typical HM Scenario
A surgeon admits a 76-year-old man for aortic valve replacement. The patient’s history also includes well-controlled hypertension and chronic obstructive pulmonary disease (COPD). Postoperatively, the patient experiences an exacerbation of COPD related to anesthesia, elevated blood pressure, and hyperglycemia. The surgeon requests the hospitalist’s advice on appropriate medical interventions of these conditions. How should the hospitalist report the initial encounter with this Medicare beneficiary?
The hospitalist should select the CPT code that best fits the service and the payor. While most physicians regard this requested service as an inpatient consultation (99251-99255), Medicare no longer recognizes those codes. Instead, the hospitalist should report this encounter as an initial hospital care service (99221-99223).
Comanagement Issues
CMS and Medicare administrative contractors regularly uncover reporting errors for co-management requests. CMS decided the nature of these services were not consultative because the surgeon is not asking the physician or qualified nonphysician provider’s (NPP’s) opinion or advice for the surgeon’s use in treating the patient. Instead, these services constituted concurrent care and should have been billed using subsequent hospital care codes (99231-99233) in the hospital inpatient setting, subsequent NF care codes (99307-99310) in the SNF/NF setting, or office or other outpatient visit codes (99201-99215) in the office or outpatient settings.1
The new ruling simplifies coding and reduces reporting errors. The initial encounter with the patient is reported as such. Regardless of who is the attending of record or the consultant, the first physician from a particular provider group reports initial hospital care codes (i.e., 99221-99223) to represent the first patient encounter, even when this encounter does not occur on the admission date. Other physicians of the same specialty within the same provider group will not be permitted to report initial hospital care codes for their own initial encounter if someone from the group and specialty has already seen the patient during that hospitalization. In other words, the first hospitalist in the provider group reports 9922x, while the remaining hospitalists use subsequent hospital care codes (9923x).
In order to differentiate “consultant” services from “attending” services, CMS will be creating a modifier. The anticipated “AI” modifier must be appended to the attending physician’s initial encounter. Other initial hospital care codes reported throughout the hospital stay, as appropriate, are presumed to be that of “consultants” (i.e., physicians with a different specialty designation than the attending physician) participating in the case. Therefore, the hospitalist now can rightfully recover the increased work effort of the initial patient encounter (99223: 3.79 relative value units, ~$147 vs. 99233: 2.0 relative value units, ~$78, based on 2010 Medicare rates). Physicians will be required to meet the minimum documentation required for the selected visit code.
Other and Undefined Service Locations
Consultations in nursing facilities are handled much like inpatient hospital care. Physicians should report initial nursing facility services (99203-99306) for the first patient encounter, and subsequent nursing facility care codes (99307-99310) for each encounter thereafter. The attending physician of record appends the assigned modifier (presumed to be “AI”) when submitting their initial care service. All other initial care codes are presumed to be those of “consulting” physicians.
Initial information from CMS does not address observation services. Logically, these hospital-based services would follow the same methodology as inpatient care: report initial observation care (99218-99220) for the first “consulting” encounter. However, this might not be appropriate given Medicare’s existing rules for observation services, which guide physicians other than the admitting physician/group to “bill the office and other outpatient service codes or outpatient consultation codes as appropriate when they provide services to the patient.”2 With Medicare’s elimination of consultation codes, the consultant reports “office and other outpatient service codes” (i.e., new patient, 99201-99205, or established patient codes, 99212-99215) by default.
Without further clarification on observation services, hospitalists should report new or established patient service codes, depending on whether the patient has been seen by a group member within the last three years.
Medicare also has existing guidelines for the ED, which suggest that any physician not meeting the consultation criteria report ED service codes (99281-99285). Without further clarification, hospitalists should continue to follow this instruction for Medicare beneficiaries.
Nonphysician Providers
Medicare’s split/shared billing guidelines apply to most hospital inpatient, hospital outpatient, and ED evaluation and management (E/M) services, with consultations as one exception. Now, in accordance with the new ruling, hospitalists should select the appropriate initial service codes that correspond to patient’s location (e.g., 99223 for inpatients). NPPs can participate in the initial service provided to patients in these locations without the hospitalist having to replicate the entire service. The hospitalist can submit the claim in their name after selecting the visit level based upon the cumulative service personally provided on the same calendar day by both the NPP and the physician. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.10I. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/ manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8A. CMS Web site. Available at: www. cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- PFS Federal Regulation Notices: Proposed Revisions to Payment Policies Under the Physician Fee Schedule and Part B for CY 2010. CMS Web site. Available at: www.cms.hhs.gov/PhysicianFeeSched/PFSFRN/itemdetail.asp?filterType=none&filterByDID=99&sortByDID=4&sortOrder=descending&itemID=CMS1223902&intNumPerPage=10. Accessed Nov. 12, 2009.
- Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B (for CY 2010). CMS Web site. Available at: www.federalregister.gov/OFR Upload/OFRData/2009-26502_PI.pdf. Accessed Nov. 10, 2009.
The Bottom Line
The elimination of consults will affect physician group payments as well as RVU-based incentive payments to individual physicians. HM group leaders will want to refer to the CMS formula, also known as a crosswalk. The crosswalk outlines the utilization of consult codes and E/M codes for the sole purpose of establishing aggregate budget neutrality.3
The payment differential for consultations has been redistributed to increase payments for existing E/M services.
Here’s how it works: Use the “mapping percentage” column to project the distribution of consultative services between the “replacement” (i.e., “destination”) codes. For example, presumably 70% of 99251 will now be reported as initial hospital care (99221), whereas 30% will be reported as initial nursing facility care (99304). Please note that this table does not represent billing guidance or documentation equivalencies, but it does attempt to quantify sites of consultative service and their corresponding code categories for the basis of fiscal-year projections.
Physicians should select the visit code in the appropriate code category for the service location and in accordance with CMS documentation guidelines, which are available at www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp.
Market Watch
New Generics
- Tamsulosin (generic Flomax) capsules should be available March 2, 20101
New Drugs, Indications, Dosage Forms, and Approvals
- C1 Esterase inhibitor [human] (Berinert) has been approved by the Food and Drug Administration (FDA) to treat acute abdominal attacks and facial edema associated with hereditary angioedema (HAE) in adolescents and adults. It is derived from human plasma and regulates clotting and inflammatory reactions. HAE, a genetic disorder affecting 6,000 to 10,000 Americans, is caused by a deficit of C1-INH.2
- Colesevelam HCl tablets (Welchol) have been approved by the FDA as an adjunct to diet and exercise for reducing LDL-C levels in boys and postmenarchal girls ages 10 to 17, with heterozygous familial hypercholesterolemia as monotherapy, or in combination with a statin after failing an adequate trial of diet therapy.3
- Colesevelam HCl (Welchol) has been approved by the FDA as an oral solution providing an alternate dosage form to the large oral tablets currently available.3
- Oxycodone HCl has been recommended for FDA approval. When this new formulation is dissolved in water, it forms a gel, which makes it difficult to abuse. If approved, the new formulation will keep the OxyContin name and will be available in seven dosages. The older product will be phased out and only the newer product will be available.4
- Peginterferon alpha-2b injection (PegIntron) has been recommended for FDA approval for the treatment of patients with stage-III malignant melanoma. Peginterferon alpha-2b currently is approved for treating hepatitis C in combination with ribavirin. It is a once-weekly, subcutaneous injection.5
- Ustekinumab (Stelara) has been approved by the FDA for treating moderate to severe plaque psoriasis by disabling two interleukin (IL) cytokines, IL-12 and IL-23.6 It is a monoclonal antibody administered via subcutaneous injection. Recommended dosing is a baseline injection followed by another injection at week four, followed by subsequent injections every 12 weeks.7 Serious infections have been reported in clinical trials. Therefore, the company has developed a Risk Evaluation and Mitigation Strategy (REMS), as well as targeted healthcare provider education and a patient guide. The product label also contains cautions related to potential immunosuppression, as well as information on avoiding live vaccines while being treated with the agent.
Pipeline
- Cladribine, originally approved by the FDA in an intravenous formulation in the 1990s to treat hairy cell leukemia, has been reformulated as an oral product to manage patients with multiple sclerosis.8 Merck has submitted oral cladribine as a disease-modifying therapy for multiple sclerosis. If approved, it will be the first oral disease modifying agent for treating multiple sclerosis patients.9
- Dapagliflozin, a new mechanism renal sodium-glucose co-transporter 2 (SGLT2) inhibitor, has been shown to reduce fasting plasma glucose and significantly reduce HbA1c levels in patients with Type 2 diabetes mellitus, compared with patients treated with a metformin and placebo combination.10,11 Additionally, about 25% of patients treated with dapagliflozin (vs. 6% of the placebo-metformin-treated patients) had at least a 5% decrease in body weight. Diastolic blood pressure and uric acid level also decreased but not significantly. Serious adverse events were similar between the two treated groups.
- Fingolimod, an oral, disease-modifying agent to treat multiple sclerosis, is the first in a new class of agents known as sphingosine 1-phosphate receptor modulators (S1P-R). A recent two-year study showed it significantly reduced both relapses and disability progression (compared with placebo) in patients with relapsing remitting multiple sclerosis.12,13 More information will be available on this agent.
- Naproxcinod is a cyclo-oxygenase-inhibiting nitric oxide donator (CINOD) anti-inflammatory agent.14 The proposed indication is for the relief of the signs and symptoms of osteoarthritis, predominantly for pain management.
Safety Information
- Promethazine injection has undergone a label change to include a boxed warning. The warning is to emphasize the risk of serious tissue injury when promethazine is incorrectly administered.15 The preferred route is deep intramuscular injection; if administered in or near a vein, severe tissue injury might occur. The FDA previously informed healthcare professionals about the risks of incorrectly administered promethazine in December 2006 and again in February 2008. Post-marketing adverse events reported from 1969 to 2009 have identified cases of gangrene requiring amputation associated with administration of injectable promethazine.
- Since its original FDA approval in October 2006, sitagliptin, the first oral dipeptidyl peptidase-4 (DPP-4) inhibitor, is undergoing a safety label change.16 There have been 88 post-marketing cases reported of acute pancreatitis, including two cases of necrotizing or hemorrhagic pancreatitis reported between Oct. 16, 2006, and Feb. 9, 2009.17 The updated labeling discusses more information on the pancreatitis cases reported, and recommends that healthcare professionals carefully monitor patients for the development of pancreatitis, either upon beginning therapy or around dose increases. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Japan’s Astellas settles with Impax on prostate drug. Reuters Web site. Available at: http://www.reuters.com/article/rbssPharmaceuticals%20-%20Generic%20&%20Specialty/idUST28251320091007. Accessed Oct. 13, 2009.
- FDA approves Berinert. Drugs.com Web site. Available at: http://www.drugs.com/newdrugs/csl-behring-announces-fda-approval-berinert-first-only-therapy-approved-acute-abdominal-facial-1681.html. Accessed Oct. 13, 2009.
- Welchol package label. FDA Web site. Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/022362lbl.pdf. Accessed Oct. 13, 2009.
- Walker E. FDA Panel recommends approval of new oxycodone formulation. Medpage Today Web site. Available at: http://www.medpagetoday.com/Neurology/PainManagement/16132?utm_source=breaking-news&utm_medium=email&utm_campaign=breaking-news. Accessed Oct. 13, 2009.
- Todoruk M. FDA panel supports approval of Schering-Plough’s PegIntron for patients with melanoma. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=8E68078692384C8A8249EA4A4C036635&logRowId=330581. Accessed Oct. 13, 2009.
- Gever J, Agus ZS. FDA approves biologic drug for psoriasis. Medpage Today Web site. Available at: http://www.medpagetoday.com/InfectiousDisease/PublicHealth/16147?utm_source=breaking-news&utm_medium=email&utm_campaign=breaking-news. Accessed Oct. 13, 2009.
- Stelara package label. FDA Web site. Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/125261lbl.pdf. Accessed Oct. 13, 2009.
- Leustatin package label. FDA Web site. Available at: http://www.cancerconsultants.com/druginserts/Cladribine.pdf. Accessed Oct. 13, 2009.
- Todoruk M. Merck KGaA files cladribine for FDA approval. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=08CF20114B2A4F1DA8FD33AAC7240AB8&logRowId=329839. Accessed Oct. 2, 2009.
- Dennis M. AstraZeneca, Bristol-Myers Squibb’s dapagliflozin meets endpoints in Phase III study. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=3B158484CA7A47B99CEA373CB2ABFFA2&logRowId=330336. Accessed Oct. 13, 2009.
- Gever J, Zaleznik DF, Caputo D. EASD: Phase III data look good for novel diabetes drug. Medpage Today Web site. Available at: http://www.medpagetoday.com/MeetingCoverage/EASD/16270. Accessed Oct. 11, 2009.
- Dennis M. Novartis: Phase III study shows oral MS drug fingolimod reduces relapses, disability progression. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=EDBA0E3366E2477DB714674E9C19821D&logRowId=329838. Accessed Oct. 13, 2009.
- Multiple sclerosis therapy FTY720 reduces relapses and disability progression. The Multiple Sclerosis Resource Centre Web site. Available at: http://www.msrc.co.uk/printable.cfm?pageid=1309. Accessed Oct. 13, 2009.
- NicOx submits New Drug Application (NDA) for naproxcinod to the US FDA. NicOx Web site. Available at: http://www.nicox.com/upload/PR_NDA_submission-250909__EN.pdf. Accessed Oct. 13, 2009.
- Riley K. FDA requires boxed warning for promethazine hydrochloride injection. FDA Web site. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm182498.htm. Accessed Oct. 13, 2009.
- Januvia package label. FDA Web site. Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2006/021995lbl.pdf. Accessed Oct. 13, 2009.
- Information for healthcare professionals—acute pancreatitis and sitagliptin (marketed as Januvia and Janumet). FDA Web site. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm183764.htm. Accessed Sept. 26, 2009.
New Generics
- Tamsulosin (generic Flomax) capsules should be available March 2, 20101
New Drugs, Indications, Dosage Forms, and Approvals
- C1 Esterase inhibitor [human] (Berinert) has been approved by the Food and Drug Administration (FDA) to treat acute abdominal attacks and facial edema associated with hereditary angioedema (HAE) in adolescents and adults. It is derived from human plasma and regulates clotting and inflammatory reactions. HAE, a genetic disorder affecting 6,000 to 10,000 Americans, is caused by a deficit of C1-INH.2
- Colesevelam HCl tablets (Welchol) have been approved by the FDA as an adjunct to diet and exercise for reducing LDL-C levels in boys and postmenarchal girls ages 10 to 17, with heterozygous familial hypercholesterolemia as monotherapy, or in combination with a statin after failing an adequate trial of diet therapy.3
- Colesevelam HCl (Welchol) has been approved by the FDA as an oral solution providing an alternate dosage form to the large oral tablets currently available.3
- Oxycodone HCl has been recommended for FDA approval. When this new formulation is dissolved in water, it forms a gel, which makes it difficult to abuse. If approved, the new formulation will keep the OxyContin name and will be available in seven dosages. The older product will be phased out and only the newer product will be available.4
- Peginterferon alpha-2b injection (PegIntron) has been recommended for FDA approval for the treatment of patients with stage-III malignant melanoma. Peginterferon alpha-2b currently is approved for treating hepatitis C in combination with ribavirin. It is a once-weekly, subcutaneous injection.5
- Ustekinumab (Stelara) has been approved by the FDA for treating moderate to severe plaque psoriasis by disabling two interleukin (IL) cytokines, IL-12 and IL-23.6 It is a monoclonal antibody administered via subcutaneous injection. Recommended dosing is a baseline injection followed by another injection at week four, followed by subsequent injections every 12 weeks.7 Serious infections have been reported in clinical trials. Therefore, the company has developed a Risk Evaluation and Mitigation Strategy (REMS), as well as targeted healthcare provider education and a patient guide. The product label also contains cautions related to potential immunosuppression, as well as information on avoiding live vaccines while being treated with the agent.
Pipeline
- Cladribine, originally approved by the FDA in an intravenous formulation in the 1990s to treat hairy cell leukemia, has been reformulated as an oral product to manage patients with multiple sclerosis.8 Merck has submitted oral cladribine as a disease-modifying therapy for multiple sclerosis. If approved, it will be the first oral disease modifying agent for treating multiple sclerosis patients.9
- Dapagliflozin, a new mechanism renal sodium-glucose co-transporter 2 (SGLT2) inhibitor, has been shown to reduce fasting plasma glucose and significantly reduce HbA1c levels in patients with Type 2 diabetes mellitus, compared with patients treated with a metformin and placebo combination.10,11 Additionally, about 25% of patients treated with dapagliflozin (vs. 6% of the placebo-metformin-treated patients) had at least a 5% decrease in body weight. Diastolic blood pressure and uric acid level also decreased but not significantly. Serious adverse events were similar between the two treated groups.
- Fingolimod, an oral, disease-modifying agent to treat multiple sclerosis, is the first in a new class of agents known as sphingosine 1-phosphate receptor modulators (S1P-R). A recent two-year study showed it significantly reduced both relapses and disability progression (compared with placebo) in patients with relapsing remitting multiple sclerosis.12,13 More information will be available on this agent.
- Naproxcinod is a cyclo-oxygenase-inhibiting nitric oxide donator (CINOD) anti-inflammatory agent.14 The proposed indication is for the relief of the signs and symptoms of osteoarthritis, predominantly for pain management.
Safety Information
- Promethazine injection has undergone a label change to include a boxed warning. The warning is to emphasize the risk of serious tissue injury when promethazine is incorrectly administered.15 The preferred route is deep intramuscular injection; if administered in or near a vein, severe tissue injury might occur. The FDA previously informed healthcare professionals about the risks of incorrectly administered promethazine in December 2006 and again in February 2008. Post-marketing adverse events reported from 1969 to 2009 have identified cases of gangrene requiring amputation associated with administration of injectable promethazine.
- Since its original FDA approval in October 2006, sitagliptin, the first oral dipeptidyl peptidase-4 (DPP-4) inhibitor, is undergoing a safety label change.16 There have been 88 post-marketing cases reported of acute pancreatitis, including two cases of necrotizing or hemorrhagic pancreatitis reported between Oct. 16, 2006, and Feb. 9, 2009.17 The updated labeling discusses more information on the pancreatitis cases reported, and recommends that healthcare professionals carefully monitor patients for the development of pancreatitis, either upon beginning therapy or around dose increases. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Japan’s Astellas settles with Impax on prostate drug. Reuters Web site. Available at: http://www.reuters.com/article/rbssPharmaceuticals%20-%20Generic%20&%20Specialty/idUST28251320091007. Accessed Oct. 13, 2009.
- FDA approves Berinert. Drugs.com Web site. Available at: http://www.drugs.com/newdrugs/csl-behring-announces-fda-approval-berinert-first-only-therapy-approved-acute-abdominal-facial-1681.html. Accessed Oct. 13, 2009.
- Welchol package label. FDA Web site. Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/022362lbl.pdf. Accessed Oct. 13, 2009.
- Walker E. FDA Panel recommends approval of new oxycodone formulation. Medpage Today Web site. Available at: http://www.medpagetoday.com/Neurology/PainManagement/16132?utm_source=breaking-news&utm_medium=email&utm_campaign=breaking-news. Accessed Oct. 13, 2009.
- Todoruk M. FDA panel supports approval of Schering-Plough’s PegIntron for patients with melanoma. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=8E68078692384C8A8249EA4A4C036635&logRowId=330581. Accessed Oct. 13, 2009.
- Gever J, Agus ZS. FDA approves biologic drug for psoriasis. Medpage Today Web site. Available at: http://www.medpagetoday.com/InfectiousDisease/PublicHealth/16147?utm_source=breaking-news&utm_medium=email&utm_campaign=breaking-news. Accessed Oct. 13, 2009.
- Stelara package label. FDA Web site. Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/125261lbl.pdf. Accessed Oct. 13, 2009.
- Leustatin package label. FDA Web site. Available at: http://www.cancerconsultants.com/druginserts/Cladribine.pdf. Accessed Oct. 13, 2009.
- Todoruk M. Merck KGaA files cladribine for FDA approval. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=08CF20114B2A4F1DA8FD33AAC7240AB8&logRowId=329839. Accessed Oct. 2, 2009.
- Dennis M. AstraZeneca, Bristol-Myers Squibb’s dapagliflozin meets endpoints in Phase III study. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=3B158484CA7A47B99CEA373CB2ABFFA2&logRowId=330336. Accessed Oct. 13, 2009.
- Gever J, Zaleznik DF, Caputo D. EASD: Phase III data look good for novel diabetes drug. Medpage Today Web site. Available at: http://www.medpagetoday.com/MeetingCoverage/EASD/16270. Accessed Oct. 11, 2009.
- Dennis M. Novartis: Phase III study shows oral MS drug fingolimod reduces relapses, disability progression. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=EDBA0E3366E2477DB714674E9C19821D&logRowId=329838. Accessed Oct. 13, 2009.
- Multiple sclerosis therapy FTY720 reduces relapses and disability progression. The Multiple Sclerosis Resource Centre Web site. Available at: http://www.msrc.co.uk/printable.cfm?pageid=1309. Accessed Oct. 13, 2009.
- NicOx submits New Drug Application (NDA) for naproxcinod to the US FDA. NicOx Web site. Available at: http://www.nicox.com/upload/PR_NDA_submission-250909__EN.pdf. Accessed Oct. 13, 2009.
- Riley K. FDA requires boxed warning for promethazine hydrochloride injection. FDA Web site. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm182498.htm. Accessed Oct. 13, 2009.
- Januvia package label. FDA Web site. Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2006/021995lbl.pdf. Accessed Oct. 13, 2009.
- Information for healthcare professionals—acute pancreatitis and sitagliptin (marketed as Januvia and Janumet). FDA Web site. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm183764.htm. Accessed Sept. 26, 2009.
New Generics
- Tamsulosin (generic Flomax) capsules should be available March 2, 20101
New Drugs, Indications, Dosage Forms, and Approvals
- C1 Esterase inhibitor [human] (Berinert) has been approved by the Food and Drug Administration (FDA) to treat acute abdominal attacks and facial edema associated with hereditary angioedema (HAE) in adolescents and adults. It is derived from human plasma and regulates clotting and inflammatory reactions. HAE, a genetic disorder affecting 6,000 to 10,000 Americans, is caused by a deficit of C1-INH.2
- Colesevelam HCl tablets (Welchol) have been approved by the FDA as an adjunct to diet and exercise for reducing LDL-C levels in boys and postmenarchal girls ages 10 to 17, with heterozygous familial hypercholesterolemia as monotherapy, or in combination with a statin after failing an adequate trial of diet therapy.3
- Colesevelam HCl (Welchol) has been approved by the FDA as an oral solution providing an alternate dosage form to the large oral tablets currently available.3
- Oxycodone HCl has been recommended for FDA approval. When this new formulation is dissolved in water, it forms a gel, which makes it difficult to abuse. If approved, the new formulation will keep the OxyContin name and will be available in seven dosages. The older product will be phased out and only the newer product will be available.4
- Peginterferon alpha-2b injection (PegIntron) has been recommended for FDA approval for the treatment of patients with stage-III malignant melanoma. Peginterferon alpha-2b currently is approved for treating hepatitis C in combination with ribavirin. It is a once-weekly, subcutaneous injection.5
- Ustekinumab (Stelara) has been approved by the FDA for treating moderate to severe plaque psoriasis by disabling two interleukin (IL) cytokines, IL-12 and IL-23.6 It is a monoclonal antibody administered via subcutaneous injection. Recommended dosing is a baseline injection followed by another injection at week four, followed by subsequent injections every 12 weeks.7 Serious infections have been reported in clinical trials. Therefore, the company has developed a Risk Evaluation and Mitigation Strategy (REMS), as well as targeted healthcare provider education and a patient guide. The product label also contains cautions related to potential immunosuppression, as well as information on avoiding live vaccines while being treated with the agent.
Pipeline
- Cladribine, originally approved by the FDA in an intravenous formulation in the 1990s to treat hairy cell leukemia, has been reformulated as an oral product to manage patients with multiple sclerosis.8 Merck has submitted oral cladribine as a disease-modifying therapy for multiple sclerosis. If approved, it will be the first oral disease modifying agent for treating multiple sclerosis patients.9
- Dapagliflozin, a new mechanism renal sodium-glucose co-transporter 2 (SGLT2) inhibitor, has been shown to reduce fasting plasma glucose and significantly reduce HbA1c levels in patients with Type 2 diabetes mellitus, compared with patients treated with a metformin and placebo combination.10,11 Additionally, about 25% of patients treated with dapagliflozin (vs. 6% of the placebo-metformin-treated patients) had at least a 5% decrease in body weight. Diastolic blood pressure and uric acid level also decreased but not significantly. Serious adverse events were similar between the two treated groups.
- Fingolimod, an oral, disease-modifying agent to treat multiple sclerosis, is the first in a new class of agents known as sphingosine 1-phosphate receptor modulators (S1P-R). A recent two-year study showed it significantly reduced both relapses and disability progression (compared with placebo) in patients with relapsing remitting multiple sclerosis.12,13 More information will be available on this agent.
- Naproxcinod is a cyclo-oxygenase-inhibiting nitric oxide donator (CINOD) anti-inflammatory agent.14 The proposed indication is for the relief of the signs and symptoms of osteoarthritis, predominantly for pain management.
Safety Information
- Promethazine injection has undergone a label change to include a boxed warning. The warning is to emphasize the risk of serious tissue injury when promethazine is incorrectly administered.15 The preferred route is deep intramuscular injection; if administered in or near a vein, severe tissue injury might occur. The FDA previously informed healthcare professionals about the risks of incorrectly administered promethazine in December 2006 and again in February 2008. Post-marketing adverse events reported from 1969 to 2009 have identified cases of gangrene requiring amputation associated with administration of injectable promethazine.
- Since its original FDA approval in October 2006, sitagliptin, the first oral dipeptidyl peptidase-4 (DPP-4) inhibitor, is undergoing a safety label change.16 There have been 88 post-marketing cases reported of acute pancreatitis, including two cases of necrotizing or hemorrhagic pancreatitis reported between Oct. 16, 2006, and Feb. 9, 2009.17 The updated labeling discusses more information on the pancreatitis cases reported, and recommends that healthcare professionals carefully monitor patients for the development of pancreatitis, either upon beginning therapy or around dose increases. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Japan’s Astellas settles with Impax on prostate drug. Reuters Web site. Available at: http://www.reuters.com/article/rbssPharmaceuticals%20-%20Generic%20&%20Specialty/idUST28251320091007. Accessed Oct. 13, 2009.
- FDA approves Berinert. Drugs.com Web site. Available at: http://www.drugs.com/newdrugs/csl-behring-announces-fda-approval-berinert-first-only-therapy-approved-acute-abdominal-facial-1681.html. Accessed Oct. 13, 2009.
- Welchol package label. FDA Web site. Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/022362lbl.pdf. Accessed Oct. 13, 2009.
- Walker E. FDA Panel recommends approval of new oxycodone formulation. Medpage Today Web site. Available at: http://www.medpagetoday.com/Neurology/PainManagement/16132?utm_source=breaking-news&utm_medium=email&utm_campaign=breaking-news. Accessed Oct. 13, 2009.
- Todoruk M. FDA panel supports approval of Schering-Plough’s PegIntron for patients with melanoma. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=8E68078692384C8A8249EA4A4C036635&logRowId=330581. Accessed Oct. 13, 2009.
- Gever J, Agus ZS. FDA approves biologic drug for psoriasis. Medpage Today Web site. Available at: http://www.medpagetoday.com/InfectiousDisease/PublicHealth/16147?utm_source=breaking-news&utm_medium=email&utm_campaign=breaking-news. Accessed Oct. 13, 2009.
- Stelara package label. FDA Web site. Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/125261lbl.pdf. Accessed Oct. 13, 2009.
- Leustatin package label. FDA Web site. Available at: http://www.cancerconsultants.com/druginserts/Cladribine.pdf. Accessed Oct. 13, 2009.
- Todoruk M. Merck KGaA files cladribine for FDA approval. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=08CF20114B2A4F1DA8FD33AAC7240AB8&logRowId=329839. Accessed Oct. 2, 2009.
- Dennis M. AstraZeneca, Bristol-Myers Squibb’s dapagliflozin meets endpoints in Phase III study. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=3B158484CA7A47B99CEA373CB2ABFFA2&logRowId=330336. Accessed Oct. 13, 2009.
- Gever J, Zaleznik DF, Caputo D. EASD: Phase III data look good for novel diabetes drug. Medpage Today Web site. Available at: http://www.medpagetoday.com/MeetingCoverage/EASD/16270. Accessed Oct. 11, 2009.
- Dennis M. Novartis: Phase III study shows oral MS drug fingolimod reduces relapses, disability progression. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=EDBA0E3366E2477DB714674E9C19821D&logRowId=329838. Accessed Oct. 13, 2009.
- Multiple sclerosis therapy FTY720 reduces relapses and disability progression. The Multiple Sclerosis Resource Centre Web site. Available at: http://www.msrc.co.uk/printable.cfm?pageid=1309. Accessed Oct. 13, 2009.
- NicOx submits New Drug Application (NDA) for naproxcinod to the US FDA. NicOx Web site. Available at: http://www.nicox.com/upload/PR_NDA_submission-250909__EN.pdf. Accessed Oct. 13, 2009.
- Riley K. FDA requires boxed warning for promethazine hydrochloride injection. FDA Web site. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm182498.htm. Accessed Oct. 13, 2009.
- Januvia package label. FDA Web site. Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2006/021995lbl.pdf. Accessed Oct. 13, 2009.
- Information for healthcare professionals—acute pancreatitis and sitagliptin (marketed as Januvia and Janumet). FDA Web site. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm183764.htm. Accessed Sept. 26, 2009.