User login
Radical vs. Sensible

Hospital medicine had grown rapidly and provided the platform for change in our nation’s hospitals long before there was any meaningful healthcare legislation in Washington. With President Obama’s appointment of an innovator—Don Berwick—to head the Centers for Medicare and Medicaid Services (CMS), there is increased opportunity to ramp up revisions, large and small, to provide the incentives and the impetus to create a healthcare system for the 21st century.
With that in mind, I thought I’d offer a few ideas that Don could institute on Day 1, which could start us in the right direction, or throw us all into chaos, depending on how it plays out. While most of my attention is directed to the Medicare population, all of these ideas would be equally applicable to the commercially insured population.
Advanced Directives
We all know that too few people in this country have taken the opportunity to discuss with their families and their personal physicians how they want their care managed at critical junctures, whether it comes on suddenly with an accident or with aging. The suggestion that Medicare would pay for an office visit with your doctor to discuss this imploded with the news media’s fanning of the “death panel” flames first stoked by Sarah Palin, which sidetracked all rational discussion.
Besides setting up people for unwarranted and unwanted assaults and protracted misery, mismanaging the end stages of life leads to an enormous misallocation of physicians’ focus at a time when we all need to be mindful stewards of our limited healthcare resources.
It is acceptable if, after careful consideration, anyone chooses to not have any advanced directive, but it should be a cognitive directed choice, not just a failure to engage.
Therefore, I am proposing that Medicare offer an incentive (e.g., waiving co-payments or deductibles) to have all Medicare beneficiaries complete an advanced directive annually, or sign a form indicating they were offered an advanced directive and declined to have one invoked. In addition, Medicare could set up a system that would allow physicians (or facilities) who would manage the patient’s healthcare to have access to the conditions of the advance directives. The forms could be attached to individual Medicare profiles, possibly on the Web, in addition to being held by a patient’s PCP or medical home, if they have one.
Personal Health Records
Most people in this country can access most of the information about their personal financial status in real time from any computer in the world. Less than 10% of Americans can retrieve meaningful personal medical information. This is in spite of the prevalence of Web-based personal health record (PHR) software from Microsoft, Revolution Health, and other software vendors, along with Kaiser Permanente and a handful of insurance companies.
PHRs allow for an initial baseline set of data to be recorded and updated as new tests, diagnoses, and medications are employed. It allows for a composite knowledge of what has been tried in the past and what is being utilized in the present. This can be under patients’ control, but it would allow for appropriate access at times of acute need (e.g., an ED visit or a hospital admission).
Too often, patients with a long-term relationship with a local PCP present to the hospital and all of the healthcare professionals are forced to make critical decisions in the first few hours with insufficient or inaccurate information. This leads to needless repetition of tests or inability to compare current data with previous data (wouldn’t it be nice to have the last EKG or labs?), or in retrying a treatment regimen that hasn’t worked in the past.
And if you are in another city or if you don’t have a local physician with all of your old records, the information gap is far worse.
Once again, we could incentivize patients to have an up-to-date PHR with reduced premiums, or lower deductibles or copayments. We could look for ways to incentivize PCPs and hospitals to help patients build and maintain their PHR. We could make it a matter of course that a patient’s PHR would be updated at each intersection with healthcare information (e.g., the pharmacy or the lab or each office visit).
Physician Accountability
Somehow, we have evolved into a fragmented health system. We need to repair the disconnect between patients and physicians. The professional pact between the patient and their primary physician needs to be in place until the patient and the “next” physician agree to the handoff of responsibility. As hospitalists, we see this at both ends of the continuum. Patients shouldn’t just be “sent” to the ED or the hospital, especially not when they are acutely ill. Their personal physician, their medical home, should “arrange” for an orderly transfer of care. This would involve a transfer of information (possibly facilitated by an updated PHR), but as much by the assurance that the accepting physician or institution is prepared for the handoff, acknowledges this to the PCP, and that the patient understands the handoff has taken place.
In the same way, patients would not be just “sent out” from the hospital. The treating physician (it could be the hospitalist, but also the surgeon or cardiologist) would remain the doctor of record—the first resource for patients’ question and issues—until another “receiving” physician has accepted the handoff, acknowledges this role, and the patient agrees.
We could rapidly shift this process by allowing the patient to decide when the hospitalization has ended. We could change the system overnight by making one of the conditions for payment for a hospitalization (to the physicians and the hospital) that the patient has signed off that indeed the hospitalization has ended.
This might include a discussion of chronic medications to continue, acute therapies to complete, understanding by the patient of where and when to receive follow-up testing and evaluation, and a clear understanding of which physician is now accountable for future issues and questions as patients travel from acute illness to normal function.
There certainly are economic and societal issues. Not everyone has a PCP or can pay for their outpatient care, and this could be a full-employment plan for liability attorneys, but in the end I am confident medical professionals would create the linkages that would minimize the deep white space patients find themselves in once they are wheeled to the front door of their hospitals.
Creatively Complete the Hospitalization
In a perfect world, everyone would have a functional, robust medical home to return to after an acute hospitalization. Unfortunately, a patient-centered medical home (PCMH) is much more of a hope than a reality for most Americans. While we are working to create a better “horizontal” hospitalization, there are clear gaps in the vertical-care world.
If we are going to be responsible for bundled care that encompasses pre-admit and post-discharge care (e.g., 30 days after discharge), then we must beef up our outpatient capabilities.
Hopefully in the long run, this can be supplied by a reinvigorated and reinvented medical home, but it is still a long way off. If payment and accountability continue to blur just when the hospitalization ends, then hospitals (and hospitalists) and Medicare and insurers will need to be creative in how and who will manage the patient. We’ll need to solve the issues around patients who are no longer sick enough to require a hospital bed but clearly are not back to their steady state.
This ties in with the accountability gap that vexes our patients every day. Very likely, hospitalists will have to assume a role in managing the patients after hospital discharge. This might take the form of a few follow-up visits and continued support systems via the Web and telephone. It will probably require a new class of hospitalist—the ambulist or the subacutist—supported by dedicated ancillary staff and systems.
Once again, Medicare and insurers can drive to a better system of post-acute care by supplying incentives: a more robust discharge payment or rewarding successful completion of a hospitalization, possibly by bundled payment incentives. In addition, there could be clear standards set that would define when this is done well with associated rewards.
I know some of these ideas are radical and make us uncomfortable. They seem to assign more responsibilities to an already overburdened profession. To be successful, these innovations require an active participation and accountability of our patients. We as the providers of healthcare cannot do this alone. It also requires the evolution of the hospital as an institution from just the healthcare provider for the acutely ill, horizontal patient, but as more a part of a continuum from acute illness to return to function. And it cries out for a robust, capable, outpatient partner in a medical home or accountable care organization (ACO) that is equally dedicated, incentivized, and accountable.
We won’t get there tomorrow, even if Dr. Berwick reads this and acts on all of the ideas on his first day at CMS.
But if we don’t get started, we know we definitely won’t get there at any time in our future. TH
Dr. Wellikson is CEO of SHM.
Hospital medicine had grown rapidly and provided the platform for change in our nation’s hospitals long before there was any meaningful healthcare legislation in Washington. With President Obama’s appointment of an innovator—Don Berwick—to head the Centers for Medicare and Medicaid Services (CMS), there is increased opportunity to ramp up revisions, large and small, to provide the incentives and the impetus to create a healthcare system for the 21st century.
With that in mind, I thought I’d offer a few ideas that Don could institute on Day 1, which could start us in the right direction, or throw us all into chaos, depending on how it plays out. While most of my attention is directed to the Medicare population, all of these ideas would be equally applicable to the commercially insured population.
Advanced Directives
We all know that too few people in this country have taken the opportunity to discuss with their families and their personal physicians how they want their care managed at critical junctures, whether it comes on suddenly with an accident or with aging. The suggestion that Medicare would pay for an office visit with your doctor to discuss this imploded with the news media’s fanning of the “death panel” flames first stoked by Sarah Palin, which sidetracked all rational discussion.
Besides setting up people for unwarranted and unwanted assaults and protracted misery, mismanaging the end stages of life leads to an enormous misallocation of physicians’ focus at a time when we all need to be mindful stewards of our limited healthcare resources.
It is acceptable if, after careful consideration, anyone chooses to not have any advanced directive, but it should be a cognitive directed choice, not just a failure to engage.
Therefore, I am proposing that Medicare offer an incentive (e.g., waiving co-payments or deductibles) to have all Medicare beneficiaries complete an advanced directive annually, or sign a form indicating they were offered an advanced directive and declined to have one invoked. In addition, Medicare could set up a system that would allow physicians (or facilities) who would manage the patient’s healthcare to have access to the conditions of the advance directives. The forms could be attached to individual Medicare profiles, possibly on the Web, in addition to being held by a patient’s PCP or medical home, if they have one.
Personal Health Records
Most people in this country can access most of the information about their personal financial status in real time from any computer in the world. Less than 10% of Americans can retrieve meaningful personal medical information. This is in spite of the prevalence of Web-based personal health record (PHR) software from Microsoft, Revolution Health, and other software vendors, along with Kaiser Permanente and a handful of insurance companies.
PHRs allow for an initial baseline set of data to be recorded and updated as new tests, diagnoses, and medications are employed. It allows for a composite knowledge of what has been tried in the past and what is being utilized in the present. This can be under patients’ control, but it would allow for appropriate access at times of acute need (e.g., an ED visit or a hospital admission).
Too often, patients with a long-term relationship with a local PCP present to the hospital and all of the healthcare professionals are forced to make critical decisions in the first few hours with insufficient or inaccurate information. This leads to needless repetition of tests or inability to compare current data with previous data (wouldn’t it be nice to have the last EKG or labs?), or in retrying a treatment regimen that hasn’t worked in the past.
And if you are in another city or if you don’t have a local physician with all of your old records, the information gap is far worse.
Once again, we could incentivize patients to have an up-to-date PHR with reduced premiums, or lower deductibles or copayments. We could look for ways to incentivize PCPs and hospitals to help patients build and maintain their PHR. We could make it a matter of course that a patient’s PHR would be updated at each intersection with healthcare information (e.g., the pharmacy or the lab or each office visit).
Physician Accountability
Somehow, we have evolved into a fragmented health system. We need to repair the disconnect between patients and physicians. The professional pact between the patient and their primary physician needs to be in place until the patient and the “next” physician agree to the handoff of responsibility. As hospitalists, we see this at both ends of the continuum. Patients shouldn’t just be “sent” to the ED or the hospital, especially not when they are acutely ill. Their personal physician, their medical home, should “arrange” for an orderly transfer of care. This would involve a transfer of information (possibly facilitated by an updated PHR), but as much by the assurance that the accepting physician or institution is prepared for the handoff, acknowledges this to the PCP, and that the patient understands the handoff has taken place.
In the same way, patients would not be just “sent out” from the hospital. The treating physician (it could be the hospitalist, but also the surgeon or cardiologist) would remain the doctor of record—the first resource for patients’ question and issues—until another “receiving” physician has accepted the handoff, acknowledges this role, and the patient agrees.
We could rapidly shift this process by allowing the patient to decide when the hospitalization has ended. We could change the system overnight by making one of the conditions for payment for a hospitalization (to the physicians and the hospital) that the patient has signed off that indeed the hospitalization has ended.
This might include a discussion of chronic medications to continue, acute therapies to complete, understanding by the patient of where and when to receive follow-up testing and evaluation, and a clear understanding of which physician is now accountable for future issues and questions as patients travel from acute illness to normal function.
There certainly are economic and societal issues. Not everyone has a PCP or can pay for their outpatient care, and this could be a full-employment plan for liability attorneys, but in the end I am confident medical professionals would create the linkages that would minimize the deep white space patients find themselves in once they are wheeled to the front door of their hospitals.
Creatively Complete the Hospitalization
In a perfect world, everyone would have a functional, robust medical home to return to after an acute hospitalization. Unfortunately, a patient-centered medical home (PCMH) is much more of a hope than a reality for most Americans. While we are working to create a better “horizontal” hospitalization, there are clear gaps in the vertical-care world.
If we are going to be responsible for bundled care that encompasses pre-admit and post-discharge care (e.g., 30 days after discharge), then we must beef up our outpatient capabilities.
Hopefully in the long run, this can be supplied by a reinvigorated and reinvented medical home, but it is still a long way off. If payment and accountability continue to blur just when the hospitalization ends, then hospitals (and hospitalists) and Medicare and insurers will need to be creative in how and who will manage the patient. We’ll need to solve the issues around patients who are no longer sick enough to require a hospital bed but clearly are not back to their steady state.
This ties in with the accountability gap that vexes our patients every day. Very likely, hospitalists will have to assume a role in managing the patients after hospital discharge. This might take the form of a few follow-up visits and continued support systems via the Web and telephone. It will probably require a new class of hospitalist—the ambulist or the subacutist—supported by dedicated ancillary staff and systems.
Once again, Medicare and insurers can drive to a better system of post-acute care by supplying incentives: a more robust discharge payment or rewarding successful completion of a hospitalization, possibly by bundled payment incentives. In addition, there could be clear standards set that would define when this is done well with associated rewards.
I know some of these ideas are radical and make us uncomfortable. They seem to assign more responsibilities to an already overburdened profession. To be successful, these innovations require an active participation and accountability of our patients. We as the providers of healthcare cannot do this alone. It also requires the evolution of the hospital as an institution from just the healthcare provider for the acutely ill, horizontal patient, but as more a part of a continuum from acute illness to return to function. And it cries out for a robust, capable, outpatient partner in a medical home or accountable care organization (ACO) that is equally dedicated, incentivized, and accountable.
We won’t get there tomorrow, even if Dr. Berwick reads this and acts on all of the ideas on his first day at CMS.
But if we don’t get started, we know we definitely won’t get there at any time in our future. TH
Dr. Wellikson is CEO of SHM.
Hospital medicine had grown rapidly and provided the platform for change in our nation’s hospitals long before there was any meaningful healthcare legislation in Washington. With President Obama’s appointment of an innovator—Don Berwick—to head the Centers for Medicare and Medicaid Services (CMS), there is increased opportunity to ramp up revisions, large and small, to provide the incentives and the impetus to create a healthcare system for the 21st century.
With that in mind, I thought I’d offer a few ideas that Don could institute on Day 1, which could start us in the right direction, or throw us all into chaos, depending on how it plays out. While most of my attention is directed to the Medicare population, all of these ideas would be equally applicable to the commercially insured population.
Advanced Directives
We all know that too few people in this country have taken the opportunity to discuss with their families and their personal physicians how they want their care managed at critical junctures, whether it comes on suddenly with an accident or with aging. The suggestion that Medicare would pay for an office visit with your doctor to discuss this imploded with the news media’s fanning of the “death panel” flames first stoked by Sarah Palin, which sidetracked all rational discussion.
Besides setting up people for unwarranted and unwanted assaults and protracted misery, mismanaging the end stages of life leads to an enormous misallocation of physicians’ focus at a time when we all need to be mindful stewards of our limited healthcare resources.
It is acceptable if, after careful consideration, anyone chooses to not have any advanced directive, but it should be a cognitive directed choice, not just a failure to engage.
Therefore, I am proposing that Medicare offer an incentive (e.g., waiving co-payments or deductibles) to have all Medicare beneficiaries complete an advanced directive annually, or sign a form indicating they were offered an advanced directive and declined to have one invoked. In addition, Medicare could set up a system that would allow physicians (or facilities) who would manage the patient’s healthcare to have access to the conditions of the advance directives. The forms could be attached to individual Medicare profiles, possibly on the Web, in addition to being held by a patient’s PCP or medical home, if they have one.
Personal Health Records
Most people in this country can access most of the information about their personal financial status in real time from any computer in the world. Less than 10% of Americans can retrieve meaningful personal medical information. This is in spite of the prevalence of Web-based personal health record (PHR) software from Microsoft, Revolution Health, and other software vendors, along with Kaiser Permanente and a handful of insurance companies.
PHRs allow for an initial baseline set of data to be recorded and updated as new tests, diagnoses, and medications are employed. It allows for a composite knowledge of what has been tried in the past and what is being utilized in the present. This can be under patients’ control, but it would allow for appropriate access at times of acute need (e.g., an ED visit or a hospital admission).
Too often, patients with a long-term relationship with a local PCP present to the hospital and all of the healthcare professionals are forced to make critical decisions in the first few hours with insufficient or inaccurate information. This leads to needless repetition of tests or inability to compare current data with previous data (wouldn’t it be nice to have the last EKG or labs?), or in retrying a treatment regimen that hasn’t worked in the past.
And if you are in another city or if you don’t have a local physician with all of your old records, the information gap is far worse.
Once again, we could incentivize patients to have an up-to-date PHR with reduced premiums, or lower deductibles or copayments. We could look for ways to incentivize PCPs and hospitals to help patients build and maintain their PHR. We could make it a matter of course that a patient’s PHR would be updated at each intersection with healthcare information (e.g., the pharmacy or the lab or each office visit).
Physician Accountability
Somehow, we have evolved into a fragmented health system. We need to repair the disconnect between patients and physicians. The professional pact between the patient and their primary physician needs to be in place until the patient and the “next” physician agree to the handoff of responsibility. As hospitalists, we see this at both ends of the continuum. Patients shouldn’t just be “sent” to the ED or the hospital, especially not when they are acutely ill. Their personal physician, their medical home, should “arrange” for an orderly transfer of care. This would involve a transfer of information (possibly facilitated by an updated PHR), but as much by the assurance that the accepting physician or institution is prepared for the handoff, acknowledges this to the PCP, and that the patient understands the handoff has taken place.
In the same way, patients would not be just “sent out” from the hospital. The treating physician (it could be the hospitalist, but also the surgeon or cardiologist) would remain the doctor of record—the first resource for patients’ question and issues—until another “receiving” physician has accepted the handoff, acknowledges this role, and the patient agrees.
We could rapidly shift this process by allowing the patient to decide when the hospitalization has ended. We could change the system overnight by making one of the conditions for payment for a hospitalization (to the physicians and the hospital) that the patient has signed off that indeed the hospitalization has ended.
This might include a discussion of chronic medications to continue, acute therapies to complete, understanding by the patient of where and when to receive follow-up testing and evaluation, and a clear understanding of which physician is now accountable for future issues and questions as patients travel from acute illness to normal function.
There certainly are economic and societal issues. Not everyone has a PCP or can pay for their outpatient care, and this could be a full-employment plan for liability attorneys, but in the end I am confident medical professionals would create the linkages that would minimize the deep white space patients find themselves in once they are wheeled to the front door of their hospitals.
Creatively Complete the Hospitalization
In a perfect world, everyone would have a functional, robust medical home to return to after an acute hospitalization. Unfortunately, a patient-centered medical home (PCMH) is much more of a hope than a reality for most Americans. While we are working to create a better “horizontal” hospitalization, there are clear gaps in the vertical-care world.
If we are going to be responsible for bundled care that encompasses pre-admit and post-discharge care (e.g., 30 days after discharge), then we must beef up our outpatient capabilities.
Hopefully in the long run, this can be supplied by a reinvigorated and reinvented medical home, but it is still a long way off. If payment and accountability continue to blur just when the hospitalization ends, then hospitals (and hospitalists) and Medicare and insurers will need to be creative in how and who will manage the patient. We’ll need to solve the issues around patients who are no longer sick enough to require a hospital bed but clearly are not back to their steady state.
This ties in with the accountability gap that vexes our patients every day. Very likely, hospitalists will have to assume a role in managing the patients after hospital discharge. This might take the form of a few follow-up visits and continued support systems via the Web and telephone. It will probably require a new class of hospitalist—the ambulist or the subacutist—supported by dedicated ancillary staff and systems.
Once again, Medicare and insurers can drive to a better system of post-acute care by supplying incentives: a more robust discharge payment or rewarding successful completion of a hospitalization, possibly by bundled payment incentives. In addition, there could be clear standards set that would define when this is done well with associated rewards.
I know some of these ideas are radical and make us uncomfortable. They seem to assign more responsibilities to an already overburdened profession. To be successful, these innovations require an active participation and accountability of our patients. We as the providers of healthcare cannot do this alone. It also requires the evolution of the hospital as an institution from just the healthcare provider for the acutely ill, horizontal patient, but as more a part of a continuum from acute illness to return to function. And it cries out for a robust, capable, outpatient partner in a medical home or accountable care organization (ACO) that is equally dedicated, incentivized, and accountable.
We won’t get there tomorrow, even if Dr. Berwick reads this and acts on all of the ideas on his first day at CMS.
But if we don’t get started, we know we definitely won’t get there at any time in our future. TH
Dr. Wellikson is CEO of SHM.
Financial Risk

When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Observation Care
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Rule Proposes Electronic Prescription of Controlled Substances, Doesn’t Scrap Pen-and-Paper Method

Is it true that the Drug Enforcement Administration (DEA) is going to allow doctors to prescribe controlled drugs electronically?
Will I still be able to prescribe on my prescription pads, or is this big government forcing me to use a computer for prescriptions?
J. Hockenstein, DO
Des Moines, Iowa
Dr. Hospitalist responds: On March 31, the DEA published in the Federal Register an interim final rule regarding the “electronic prescription for controlled substances.” (View the entire rule at www.gpoaccess.gov/fr.) The DEA is seeking comment on the proposed rule for the next 60 days. Some of us might remember that the DEA proposed a similar rule for electronic prescribing in June 2008, but that rule did not meet the security requirements already in place at federal healthcare facilities.
Under the current system, providers can create prescriptions electronically, but the prescription has to be printed on paper. The new rule proposes a system of true electronic prescribing; data can be transmitted electronically from the hospital or doctor’s office to the pharmacy without the use of a printer or fax.
This proposed rule does not eliminate the traditional method of paper and pen for prescriptions but allows providers the voluntary option of prescribing controlled substances electronically. This proposed rule also allows pharmacies to receive, dispense, and archive these electronic prescriptions.
For those providers who choose to prescribe electronically, there will be specific requirements to prevent diversion and maintain privacy. Providers must utilize software that meets the rule’s specific requirements. For example, the software system will require a two-step process to authenticate the prescribing provider. These measures might include a password, a token, or the use of biometric identifier (e.g., fingerprint or handprint). For some of us, this might sound space-aged, but such biometric systems are commonplace in other industries. For example, I provided my fingerprint as part of the test center security system when I checked in for my American Board of Internal Medicine (ABIM) recertification examination.
There are several other issues with the proposed rule that one should consider. The new proposal does not affect the existing rule regarding emergency prescriptions. The current law allows physicians to prescribe a Schedule II controlled substance by telephone and the pharmacist to dispense this substance, provided that the amount being dispensed is limited to what is reasonably required during the emergency time period and that the provider provides a hard copy of the prescription to the pharmacist within seven days of the telephone prescription. Under the proposed rule, providers will still be able to prescribe Schedule II substances by telephone under emergency situations but will have the option of providing an electronic copy of the prescription, rather than a paper one, within seven days.
There are other components of the proposed rule that could change your practice. The rule clearly states that an electronic prescription cannot be changed after transmission and that any change to the content of the prescription will render it invalid. This might be important in a handful of situations. For example, if the provider electronically prescribes a brand-name drug, the pharmacist would not be able to make a generic substitution.
Another component of the proposed rule is that it precludes the printing of an electronic prescription, which already has been transmitted and precludes the electronic transmission of a prescription that already has been printed. This situation might arise if the electronic prescription did not transmit due to a computer problem. The provider would not be able to print or fax a copy of the electronic prescription.
The proposed rule has the potential to reduce medical errors, reduce prescription forgeries, and help providers and hospitals integrate their medical records. True electronic prescribing is long overdue. In the future, I envision hospitalists prescribing from their handheld devices.
The key to success, like any computerized system, will be the ability to keep the system running and continuously maintaining and upgrading security measures. For more information regarding electronic prescriptions for controlled substances, visit www.DEAdiversion.usdoj.gov. TH
Is it true that the Drug Enforcement Administration (DEA) is going to allow doctors to prescribe controlled drugs electronically?
Will I still be able to prescribe on my prescription pads, or is this big government forcing me to use a computer for prescriptions?
J. Hockenstein, DO
Des Moines, Iowa
Dr. Hospitalist responds: On March 31, the DEA published in the Federal Register an interim final rule regarding the “electronic prescription for controlled substances.” (View the entire rule at www.gpoaccess.gov/fr.) The DEA is seeking comment on the proposed rule for the next 60 days. Some of us might remember that the DEA proposed a similar rule for electronic prescribing in June 2008, but that rule did not meet the security requirements already in place at federal healthcare facilities.
Under the current system, providers can create prescriptions electronically, but the prescription has to be printed on paper. The new rule proposes a system of true electronic prescribing; data can be transmitted electronically from the hospital or doctor’s office to the pharmacy without the use of a printer or fax.
This proposed rule does not eliminate the traditional method of paper and pen for prescriptions but allows providers the voluntary option of prescribing controlled substances electronically. This proposed rule also allows pharmacies to receive, dispense, and archive these electronic prescriptions.
For those providers who choose to prescribe electronically, there will be specific requirements to prevent diversion and maintain privacy. Providers must utilize software that meets the rule’s specific requirements. For example, the software system will require a two-step process to authenticate the prescribing provider. These measures might include a password, a token, or the use of biometric identifier (e.g., fingerprint or handprint). For some of us, this might sound space-aged, but such biometric systems are commonplace in other industries. For example, I provided my fingerprint as part of the test center security system when I checked in for my American Board of Internal Medicine (ABIM) recertification examination.
There are several other issues with the proposed rule that one should consider. The new proposal does not affect the existing rule regarding emergency prescriptions. The current law allows physicians to prescribe a Schedule II controlled substance by telephone and the pharmacist to dispense this substance, provided that the amount being dispensed is limited to what is reasonably required during the emergency time period and that the provider provides a hard copy of the prescription to the pharmacist within seven days of the telephone prescription. Under the proposed rule, providers will still be able to prescribe Schedule II substances by telephone under emergency situations but will have the option of providing an electronic copy of the prescription, rather than a paper one, within seven days.
There are other components of the proposed rule that could change your practice. The rule clearly states that an electronic prescription cannot be changed after transmission and that any change to the content of the prescription will render it invalid. This might be important in a handful of situations. For example, if the provider electronically prescribes a brand-name drug, the pharmacist would not be able to make a generic substitution.
Another component of the proposed rule is that it precludes the printing of an electronic prescription, which already has been transmitted and precludes the electronic transmission of a prescription that already has been printed. This situation might arise if the electronic prescription did not transmit due to a computer problem. The provider would not be able to print or fax a copy of the electronic prescription.
The proposed rule has the potential to reduce medical errors, reduce prescription forgeries, and help providers and hospitals integrate their medical records. True electronic prescribing is long overdue. In the future, I envision hospitalists prescribing from their handheld devices.
The key to success, like any computerized system, will be the ability to keep the system running and continuously maintaining and upgrading security measures. For more information regarding electronic prescriptions for controlled substances, visit www.DEAdiversion.usdoj.gov. TH
Is it true that the Drug Enforcement Administration (DEA) is going to allow doctors to prescribe controlled drugs electronically?
Will I still be able to prescribe on my prescription pads, or is this big government forcing me to use a computer for prescriptions?
J. Hockenstein, DO
Des Moines, Iowa
Dr. Hospitalist responds: On March 31, the DEA published in the Federal Register an interim final rule regarding the “electronic prescription for controlled substances.” (View the entire rule at www.gpoaccess.gov/fr.) The DEA is seeking comment on the proposed rule for the next 60 days. Some of us might remember that the DEA proposed a similar rule for electronic prescribing in June 2008, but that rule did not meet the security requirements already in place at federal healthcare facilities.
Under the current system, providers can create prescriptions electronically, but the prescription has to be printed on paper. The new rule proposes a system of true electronic prescribing; data can be transmitted electronically from the hospital or doctor’s office to the pharmacy without the use of a printer or fax.
This proposed rule does not eliminate the traditional method of paper and pen for prescriptions but allows providers the voluntary option of prescribing controlled substances electronically. This proposed rule also allows pharmacies to receive, dispense, and archive these electronic prescriptions.
For those providers who choose to prescribe electronically, there will be specific requirements to prevent diversion and maintain privacy. Providers must utilize software that meets the rule’s specific requirements. For example, the software system will require a two-step process to authenticate the prescribing provider. These measures might include a password, a token, or the use of biometric identifier (e.g., fingerprint or handprint). For some of us, this might sound space-aged, but such biometric systems are commonplace in other industries. For example, I provided my fingerprint as part of the test center security system when I checked in for my American Board of Internal Medicine (ABIM) recertification examination.
There are several other issues with the proposed rule that one should consider. The new proposal does not affect the existing rule regarding emergency prescriptions. The current law allows physicians to prescribe a Schedule II controlled substance by telephone and the pharmacist to dispense this substance, provided that the amount being dispensed is limited to what is reasonably required during the emergency time period and that the provider provides a hard copy of the prescription to the pharmacist within seven days of the telephone prescription. Under the proposed rule, providers will still be able to prescribe Schedule II substances by telephone under emergency situations but will have the option of providing an electronic copy of the prescription, rather than a paper one, within seven days.
There are other components of the proposed rule that could change your practice. The rule clearly states that an electronic prescription cannot be changed after transmission and that any change to the content of the prescription will render it invalid. This might be important in a handful of situations. For example, if the provider electronically prescribes a brand-name drug, the pharmacist would not be able to make a generic substitution.
Another component of the proposed rule is that it precludes the printing of an electronic prescription, which already has been transmitted and precludes the electronic transmission of a prescription that already has been printed. This situation might arise if the electronic prescription did not transmit due to a computer problem. The provider would not be able to print or fax a copy of the electronic prescription.
The proposed rule has the potential to reduce medical errors, reduce prescription forgeries, and help providers and hospitals integrate their medical records. True electronic prescribing is long overdue. In the future, I envision hospitalists prescribing from their handheld devices.
The key to success, like any computerized system, will be the ability to keep the system running and continuously maintaining and upgrading security measures. For more information regarding electronic prescriptions for controlled substances, visit www.DEAdiversion.usdoj.gov. TH
Focused Practice in Hospital Medicine Worth the Additional Cost

Focused Practice in Hospital Medicine Worth the Additional Cost
Why are we being required to fork over an extra $380 for the Focused Practice in Hospital Medicine MOC? This feels like the icing on the cake of already a major ripoff.
Dr. Ragan
Grass Valley, Calif.
Dr. Hospitalist responds: Thank you for your frank reaction to the much-anticipated American Board of Internal Medicine (ABIM) Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) program. As you noted, an additional fee is required to participate in this recertification program.
To my knowledge, any and all fees associated with recertification are paid to ABIM. No other organization benefits from the added cost, so your question might be more appropriately addressed to ABIM (see “Focused Practice in Hospital Medicine,” May 2010, p. 1). But because you asked the question, I am happy to respond with my thoughts.
Participation in the FPHM MOC program is not mandatory. I am not aware of any organization that is requiring hospitalists to participate. I don’t expect that your lack of participation will affect your ability to obtain hospital privileges. Like any new MOC program, I would expect some up-front administrative costs associated with developing and administering the practice-improvement modules and the secure examination.
It’s up to you and others to decide whether this added recognition is worth the cost. I can tell you that I have made the decision to participate. I fully expect to be part of the inaugural class of ABIM diplomates with this added recognition by the end of the year.
What went into my own decision to participate? I can tell you that I am a practicing hospitalist who makes a salary typical of most hospitalists. I am frugal with my money and certainly do not view the added cost as an insignificant amount of money. Like most hospitalists, I am not only busy with my professional life, but I have plenty of family commitments as well.
I expect the exam will be rigorous, and the requirements of the practice-improvement modules will be demanding. I would not want it any other way. In the fast-changing healthcare environment, I believe that hospitalists will be challenged to think about what it means to care for a hospitalized patient. To succeed in the future, hospitalists will be expected to not only participate, but also lead QI efforts at their institutions. The FPHM MOC will distinguish me as a hospitalist with added qualifications in the field of QI.
So how about it, Dr. Ragan? Will you join me?
What Certification Requirements Should a Hospitalist Program Have for Its Physicians?
I hope you can help me with some questions I have concerning starting a hospitalist program at my medical center. Are there certain requirements (e.g., board certification in internal medicine, ACLS, etc.) that need to be met, or is that up to the facility? The physician interested in the position is board-certified in infectious disease. Any direction you can give me on this would be greatly appreciated.
Marisa Sellers,
Medical Staff Coordinator,
Hartselle Medical Center,
Hartselle, Ala.
Dr. Hospitalist responds: Congratulations on your medical center’s decision to establish a hospitalist program. Over the past decade, HM has been the fastest-growing field in all of American medicine. The majority of the country’s acute-care hospitals have hospitalists on staff.
Approximately 85% of the country’s hospitalists received training in internal medicine. Most of the other hospitalists received training in pediatrics or family medicine. While most hospitalists are general internists, some also have additional subspecialty training, which seems to be the case of the physician at your medical center. As you know, different medical facilities have different requirements of their medical staff. At the acute-care hospital where I work clinically, maintenance of board certification is required of all medical staff. I know that is not the case for all hospitals, yet I’m not aware of any hospitals with hospitalist-specific medical staff requirements.
Most of the hospitalists who are internists will be either board-eligible or board-certified with the American Board of Internal Medicine (ABIM). You should be aware that ABIM has developed a new program, the Recognition of Focused Practice (RFP) in Hospital Medicine. As part of this maintenance of certification (MOC) program, ABIM diplomates will have the opportunity to take the first ABIM Hospital Medicine examination in October. For more information about this exam, ABIM’s rationale for recognizing a focused practice in HM, and any other questions about this program, please visit the ABIM Web site at www.abim.org/news/news/focused-
practice-hospital-medicine-qa.aspx.
I have heard from hospitalists trained as family physicians who are interested in RFP as hospitalists. It is my understanding that the American Board of Family Medicine is studying the ABIM program and working to develop a similar program for hospitalists with family medicine board certifications.
Regarding your question about hospitalists and the American Heart Association’s advanced cardiac life support (ACLS) training and certification: While I think it is a great idea for hospitalists to receive this training and maintain this certification, I am not aware of any mandate for hospitalists to be uniformly ACLS-certified. I think this is an issue the medical staff at your medical center will have to decide; basically, what is in the best interests of your patients?
Focused Practice in Hospital Medicine Worth the Additional Cost
Why are we being required to fork over an extra $380 for the Focused Practice in Hospital Medicine MOC? This feels like the icing on the cake of already a major ripoff.
Dr. Ragan
Grass Valley, Calif.
Dr. Hospitalist responds: Thank you for your frank reaction to the much-anticipated American Board of Internal Medicine (ABIM) Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) program. As you noted, an additional fee is required to participate in this recertification program.
To my knowledge, any and all fees associated with recertification are paid to ABIM. No other organization benefits from the added cost, so your question might be more appropriately addressed to ABIM (see “Focused Practice in Hospital Medicine,” May 2010, p. 1). But because you asked the question, I am happy to respond with my thoughts.
Participation in the FPHM MOC program is not mandatory. I am not aware of any organization that is requiring hospitalists to participate. I don’t expect that your lack of participation will affect your ability to obtain hospital privileges. Like any new MOC program, I would expect some up-front administrative costs associated with developing and administering the practice-improvement modules and the secure examination.
It’s up to you and others to decide whether this added recognition is worth the cost. I can tell you that I have made the decision to participate. I fully expect to be part of the inaugural class of ABIM diplomates with this added recognition by the end of the year.
What went into my own decision to participate? I can tell you that I am a practicing hospitalist who makes a salary typical of most hospitalists. I am frugal with my money and certainly do not view the added cost as an insignificant amount of money. Like most hospitalists, I am not only busy with my professional life, but I have plenty of family commitments as well.
I expect the exam will be rigorous, and the requirements of the practice-improvement modules will be demanding. I would not want it any other way. In the fast-changing healthcare environment, I believe that hospitalists will be challenged to think about what it means to care for a hospitalized patient. To succeed in the future, hospitalists will be expected to not only participate, but also lead QI efforts at their institutions. The FPHM MOC will distinguish me as a hospitalist with added qualifications in the field of QI.
So how about it, Dr. Ragan? Will you join me?
What Certification Requirements Should a Hospitalist Program Have for Its Physicians?
I hope you can help me with some questions I have concerning starting a hospitalist program at my medical center. Are there certain requirements (e.g., board certification in internal medicine, ACLS, etc.) that need to be met, or is that up to the facility? The physician interested in the position is board-certified in infectious disease. Any direction you can give me on this would be greatly appreciated.
Marisa Sellers,
Medical Staff Coordinator,
Hartselle Medical Center,
Hartselle, Ala.
Dr. Hospitalist responds: Congratulations on your medical center’s decision to establish a hospitalist program. Over the past decade, HM has been the fastest-growing field in all of American medicine. The majority of the country’s acute-care hospitals have hospitalists on staff.
Approximately 85% of the country’s hospitalists received training in internal medicine. Most of the other hospitalists received training in pediatrics or family medicine. While most hospitalists are general internists, some also have additional subspecialty training, which seems to be the case of the physician at your medical center. As you know, different medical facilities have different requirements of their medical staff. At the acute-care hospital where I work clinically, maintenance of board certification is required of all medical staff. I know that is not the case for all hospitals, yet I’m not aware of any hospitals with hospitalist-specific medical staff requirements.
Most of the hospitalists who are internists will be either board-eligible or board-certified with the American Board of Internal Medicine (ABIM). You should be aware that ABIM has developed a new program, the Recognition of Focused Practice (RFP) in Hospital Medicine. As part of this maintenance of certification (MOC) program, ABIM diplomates will have the opportunity to take the first ABIM Hospital Medicine examination in October. For more information about this exam, ABIM’s rationale for recognizing a focused practice in HM, and any other questions about this program, please visit the ABIM Web site at www.abim.org/news/news/focused-
practice-hospital-medicine-qa.aspx.
I have heard from hospitalists trained as family physicians who are interested in RFP as hospitalists. It is my understanding that the American Board of Family Medicine is studying the ABIM program and working to develop a similar program for hospitalists with family medicine board certifications.
Regarding your question about hospitalists and the American Heart Association’s advanced cardiac life support (ACLS) training and certification: While I think it is a great idea for hospitalists to receive this training and maintain this certification, I am not aware of any mandate for hospitalists to be uniformly ACLS-certified. I think this is an issue the medical staff at your medical center will have to decide; basically, what is in the best interests of your patients?
Focused Practice in Hospital Medicine Worth the Additional Cost
Why are we being required to fork over an extra $380 for the Focused Practice in Hospital Medicine MOC? This feels like the icing on the cake of already a major ripoff.
Dr. Ragan
Grass Valley, Calif.
Dr. Hospitalist responds: Thank you for your frank reaction to the much-anticipated American Board of Internal Medicine (ABIM) Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) program. As you noted, an additional fee is required to participate in this recertification program.
To my knowledge, any and all fees associated with recertification are paid to ABIM. No other organization benefits from the added cost, so your question might be more appropriately addressed to ABIM (see “Focused Practice in Hospital Medicine,” May 2010, p. 1). But because you asked the question, I am happy to respond with my thoughts.
Participation in the FPHM MOC program is not mandatory. I am not aware of any organization that is requiring hospitalists to participate. I don’t expect that your lack of participation will affect your ability to obtain hospital privileges. Like any new MOC program, I would expect some up-front administrative costs associated with developing and administering the practice-improvement modules and the secure examination.
It’s up to you and others to decide whether this added recognition is worth the cost. I can tell you that I have made the decision to participate. I fully expect to be part of the inaugural class of ABIM diplomates with this added recognition by the end of the year.
What went into my own decision to participate? I can tell you that I am a practicing hospitalist who makes a salary typical of most hospitalists. I am frugal with my money and certainly do not view the added cost as an insignificant amount of money. Like most hospitalists, I am not only busy with my professional life, but I have plenty of family commitments as well.
I expect the exam will be rigorous, and the requirements of the practice-improvement modules will be demanding. I would not want it any other way. In the fast-changing healthcare environment, I believe that hospitalists will be challenged to think about what it means to care for a hospitalized patient. To succeed in the future, hospitalists will be expected to not only participate, but also lead QI efforts at their institutions. The FPHM MOC will distinguish me as a hospitalist with added qualifications in the field of QI.
So how about it, Dr. Ragan? Will you join me?
What Certification Requirements Should a Hospitalist Program Have for Its Physicians?
I hope you can help me with some questions I have concerning starting a hospitalist program at my medical center. Are there certain requirements (e.g., board certification in internal medicine, ACLS, etc.) that need to be met, or is that up to the facility? The physician interested in the position is board-certified in infectious disease. Any direction you can give me on this would be greatly appreciated.
Marisa Sellers,
Medical Staff Coordinator,
Hartselle Medical Center,
Hartselle, Ala.
Dr. Hospitalist responds: Congratulations on your medical center’s decision to establish a hospitalist program. Over the past decade, HM has been the fastest-growing field in all of American medicine. The majority of the country’s acute-care hospitals have hospitalists on staff.
Approximately 85% of the country’s hospitalists received training in internal medicine. Most of the other hospitalists received training in pediatrics or family medicine. While most hospitalists are general internists, some also have additional subspecialty training, which seems to be the case of the physician at your medical center. As you know, different medical facilities have different requirements of their medical staff. At the acute-care hospital where I work clinically, maintenance of board certification is required of all medical staff. I know that is not the case for all hospitals, yet I’m not aware of any hospitals with hospitalist-specific medical staff requirements.
Most of the hospitalists who are internists will be either board-eligible or board-certified with the American Board of Internal Medicine (ABIM). You should be aware that ABIM has developed a new program, the Recognition of Focused Practice (RFP) in Hospital Medicine. As part of this maintenance of certification (MOC) program, ABIM diplomates will have the opportunity to take the first ABIM Hospital Medicine examination in October. For more information about this exam, ABIM’s rationale for recognizing a focused practice in HM, and any other questions about this program, please visit the ABIM Web site at www.abim.org/news/news/focused-
practice-hospital-medicine-qa.aspx.
I have heard from hospitalists trained as family physicians who are interested in RFP as hospitalists. It is my understanding that the American Board of Family Medicine is studying the ABIM program and working to develop a similar program for hospitalists with family medicine board certifications.
Regarding your question about hospitalists and the American Heart Association’s advanced cardiac life support (ACLS) training and certification: While I think it is a great idea for hospitalists to receive this training and maintain this certification, I am not aware of any mandate for hospitalists to be uniformly ACLS-certified. I think this is an issue the medical staff at your medical center will have to decide; basically, what is in the best interests of your patients?
Square Peg, Square Hole

I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
Variable Rate
Are states doing enough to discipline problem doctors? The sensitive question has flared again with the release of an annual report by Washington, D.C.-based consumer advocacy group Public Citizen.
The report analyzed statistics released by the Federation of State Medical Boards on serious disciplinary actions taken by the boards of all 50 states and the District of Columbia in 2009. Those actions include revocations, surrenders, suspensions, and probations or restrictions. Public Citizen used a three-year average (2007 to 2009) to arrive at its rate of actions per 1,000 physicians licensed in each state.
For the fourth year in a row, Alaska had the most actions, 7.89 per 1,000 doctors. Meanwhile, Minnesota had the fewest actions (1.07 per 1,000 doctors) for the second year running. For the record, the numbers aren’t broken down by specialty (see Table 1, p. 5).
So what does it all mean? Do Alaska’s doctors really require more punitive measures than those in other states, or is the state board simply more vigilant? Are Minnesota doctors that much better, or is that state failing in its duty to provide adequate oversight? Is such a ranking system even warranted?
Nearly everyone agrees on the importance of protecting the public and the integrity of the medical profession. But the aggressive jousting over what the new numbers do or do not mean suggests just how difficult it can be to come up with a metric for medical accountability that everyone agrees is both fair and reliable.
Sidney Wolfe, MD, director of Public Citizen’s Health Research Group and the lead author of the new report, dismisses the notion that Minnesota’s doctors are so good that they don’t require as many disciplinary actions. “There is not a shred of evidence for that,” he says. Instead, he calls out what he views as an ineffective board.
In turn, Robert Leach, executive director of the Minnesota Board of Medical Practice, dismisses the significance of the report’s findings. “It’s a fair ranking the way their formula applies. It’s the formula we disagree with,” he says. “It’s fairly simplistic and indicative of nothing.”
And Lisa Robin, senior vice president for advocacy and member services at the Federation of State Medical Boards, says the federation doesn’t even encourage rankings because of the variable laws and sanctions from state to state. “It doesn’t give you a true picture of what boards do, to rank them,” she says.

A Row Over Rankings
Minnesota’s Leach has a detailed list of grievances against the report. But his biggest beef is with the fact that it ranks medical boards on the number of serious disciplinary actions per 1,000 physicians licensed by the state. “The more precise number should be the number of licensed physicians who are actually practicing in the state,” he says.
From 2008 to 2009, for example, more than 19,000 physicians were licensed in Minnesota. Yet Leach says that only a little more than 14,000 were actually practicing within the state, which he describes as a large exporter of trained doctors. “So we had 5,000 physicians who weren’t even practicing here that were counted against our one disciplinary action per thousand physicians,” he says.
Public Citizen, he says, also doesn’t recognize other interventions, such as Minnesota’s “agreements for corrective action,” that normally include training or remedial coursework for doctors with an identified weakness in subject areas such as prescribing or chronic-pain management. “Not every doctor needs to be hit over the head with a hammer of serious disciplinary action to address a problem,” Leach says.
And then there’s the sticky matter of peer review. In Minnesota, “virtually every physician now practicing works for a large health plan or a facility,” he says. “We have virtually no solo practice or isolated practice in Minnesota, and those are the physicians who get in trouble: the ones who don’t have the advantage of periodic peer review, who don’t have the advantage of adequate supervision to help keep them out of trouble.”
Doctors like those in Alaska? “You always see Alaska is rated real high,” Leach says. “You have a bunch of people out there practicing in the wilderness, out in solo practice. Physicians need to have that ability to have peer review, to be able to address problem cases with their colleagues. In Minnesota, a lot of these facilities and health plans address these problems at the practice level before they even reach the board.”
A Call To Action
Dr. Wolfe isn’t buying the notion that Minnesota doctors require less formal discipline while their colleagues in Alaska need more. Whenever other low-ranking states have provided sufficient funding, replaced ineffective leadership, granted more independence, and met the other conditions necessary for a better medical board, he notes, their rate of disciplinary actions often “rockets up.”
The medical boards of North Carolina and Washington, D.C., have risen dramatically in the rankings in recent years, and Dr. Wolfe cites effective intervention in both cases. In formerly low-ranking Arizona, he says, similar corrective action in the late 1990s led to a tripling of the rate of serious disciplinary action within three years. “That’s obviously not a period of time that’s long enough to be explained by some inward migration of bad doctors or outward migration of good doctors,” he says. “It’s because the board started functioning better.”
Meanwhile, boards in South Carolina and Massachusetts have slumped in the ratings—a decline he attributes to the loss of leadership and funds.
“One area I can agree with Dr. Wolfe on is that medical boards need resources; they need adequate structure, resources, and authority to do their job and be able to protect the public,” says Robin, of the Federation of State Medical Boards. “If they’re in a big umbrella agency and they’re just one of many and share their pool of investigators with everyone, as you can imagine, that’s probably not as efficient.”
Hospitals also share in the blame, according to a separate Public Citizen report released last year that cites a chronic underreporting of doctor misconduct or incompetence to the National Practitioner Data Bank by hospitals. Robin agrees that more diligence is needed to ensure that medical boards have the information they need to properly do their jobs. As one of her board members told her, “They can’t gain information by osmosis.”
Hospitalists, however, might be well suited for addressing the underreporting issue. HM is in a “really good position to observe behavior that needs to be brought to the attention of hospital medical staff,” Dr. Wolfe says.
He recommends that one or more hospitalists should sit on each hospital’s medical peer review committee, where they can put their expertise to good use. “Hospitalists really need to get more active in this,” he says. “It’s for the betterment of the patients in the hospital, it’s for the betterment for the reputation of the hospital and the medical staff.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Are states doing enough to discipline problem doctors? The sensitive question has flared again with the release of an annual report by Washington, D.C.-based consumer advocacy group Public Citizen.
The report analyzed statistics released by the Federation of State Medical Boards on serious disciplinary actions taken by the boards of all 50 states and the District of Columbia in 2009. Those actions include revocations, surrenders, suspensions, and probations or restrictions. Public Citizen used a three-year average (2007 to 2009) to arrive at its rate of actions per 1,000 physicians licensed in each state.
For the fourth year in a row, Alaska had the most actions, 7.89 per 1,000 doctors. Meanwhile, Minnesota had the fewest actions (1.07 per 1,000 doctors) for the second year running. For the record, the numbers aren’t broken down by specialty (see Table 1, p. 5).
So what does it all mean? Do Alaska’s doctors really require more punitive measures than those in other states, or is the state board simply more vigilant? Are Minnesota doctors that much better, or is that state failing in its duty to provide adequate oversight? Is such a ranking system even warranted?
Nearly everyone agrees on the importance of protecting the public and the integrity of the medical profession. But the aggressive jousting over what the new numbers do or do not mean suggests just how difficult it can be to come up with a metric for medical accountability that everyone agrees is both fair and reliable.
Sidney Wolfe, MD, director of Public Citizen’s Health Research Group and the lead author of the new report, dismisses the notion that Minnesota’s doctors are so good that they don’t require as many disciplinary actions. “There is not a shred of evidence for that,” he says. Instead, he calls out what he views as an ineffective board.
In turn, Robert Leach, executive director of the Minnesota Board of Medical Practice, dismisses the significance of the report’s findings. “It’s a fair ranking the way their formula applies. It’s the formula we disagree with,” he says. “It’s fairly simplistic and indicative of nothing.”
And Lisa Robin, senior vice president for advocacy and member services at the Federation of State Medical Boards, says the federation doesn’t even encourage rankings because of the variable laws and sanctions from state to state. “It doesn’t give you a true picture of what boards do, to rank them,” she says.
A Row Over Rankings
Minnesota’s Leach has a detailed list of grievances against the report. But his biggest beef is with the fact that it ranks medical boards on the number of serious disciplinary actions per 1,000 physicians licensed by the state. “The more precise number should be the number of licensed physicians who are actually practicing in the state,” he says.
From 2008 to 2009, for example, more than 19,000 physicians were licensed in Minnesota. Yet Leach says that only a little more than 14,000 were actually practicing within the state, which he describes as a large exporter of trained doctors. “So we had 5,000 physicians who weren’t even practicing here that were counted against our one disciplinary action per thousand physicians,” he says.
Public Citizen, he says, also doesn’t recognize other interventions, such as Minnesota’s “agreements for corrective action,” that normally include training or remedial coursework for doctors with an identified weakness in subject areas such as prescribing or chronic-pain management. “Not every doctor needs to be hit over the head with a hammer of serious disciplinary action to address a problem,” Leach says.
And then there’s the sticky matter of peer review. In Minnesota, “virtually every physician now practicing works for a large health plan or a facility,” he says. “We have virtually no solo practice or isolated practice in Minnesota, and those are the physicians who get in trouble: the ones who don’t have the advantage of periodic peer review, who don’t have the advantage of adequate supervision to help keep them out of trouble.”
Doctors like those in Alaska? “You always see Alaska is rated real high,” Leach says. “You have a bunch of people out there practicing in the wilderness, out in solo practice. Physicians need to have that ability to have peer review, to be able to address problem cases with their colleagues. In Minnesota, a lot of these facilities and health plans address these problems at the practice level before they even reach the board.”
A Call To Action
Dr. Wolfe isn’t buying the notion that Minnesota doctors require less formal discipline while their colleagues in Alaska need more. Whenever other low-ranking states have provided sufficient funding, replaced ineffective leadership, granted more independence, and met the other conditions necessary for a better medical board, he notes, their rate of disciplinary actions often “rockets up.”
The medical boards of North Carolina and Washington, D.C., have risen dramatically in the rankings in recent years, and Dr. Wolfe cites effective intervention in both cases. In formerly low-ranking Arizona, he says, similar corrective action in the late 1990s led to a tripling of the rate of serious disciplinary action within three years. “That’s obviously not a period of time that’s long enough to be explained by some inward migration of bad doctors or outward migration of good doctors,” he says. “It’s because the board started functioning better.”
Meanwhile, boards in South Carolina and Massachusetts have slumped in the ratings—a decline he attributes to the loss of leadership and funds.
“One area I can agree with Dr. Wolfe on is that medical boards need resources; they need adequate structure, resources, and authority to do their job and be able to protect the public,” says Robin, of the Federation of State Medical Boards. “If they’re in a big umbrella agency and they’re just one of many and share their pool of investigators with everyone, as you can imagine, that’s probably not as efficient.”
Hospitals also share in the blame, according to a separate Public Citizen report released last year that cites a chronic underreporting of doctor misconduct or incompetence to the National Practitioner Data Bank by hospitals. Robin agrees that more diligence is needed to ensure that medical boards have the information they need to properly do their jobs. As one of her board members told her, “They can’t gain information by osmosis.”
Hospitalists, however, might be well suited for addressing the underreporting issue. HM is in a “really good position to observe behavior that needs to be brought to the attention of hospital medical staff,” Dr. Wolfe says.
He recommends that one or more hospitalists should sit on each hospital’s medical peer review committee, where they can put their expertise to good use. “Hospitalists really need to get more active in this,” he says. “It’s for the betterment of the patients in the hospital, it’s for the betterment for the reputation of the hospital and the medical staff.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Are states doing enough to discipline problem doctors? The sensitive question has flared again with the release of an annual report by Washington, D.C.-based consumer advocacy group Public Citizen.
The report analyzed statistics released by the Federation of State Medical Boards on serious disciplinary actions taken by the boards of all 50 states and the District of Columbia in 2009. Those actions include revocations, surrenders, suspensions, and probations or restrictions. Public Citizen used a three-year average (2007 to 2009) to arrive at its rate of actions per 1,000 physicians licensed in each state.
For the fourth year in a row, Alaska had the most actions, 7.89 per 1,000 doctors. Meanwhile, Minnesota had the fewest actions (1.07 per 1,000 doctors) for the second year running. For the record, the numbers aren’t broken down by specialty (see Table 1, p. 5).
So what does it all mean? Do Alaska’s doctors really require more punitive measures than those in other states, or is the state board simply more vigilant? Are Minnesota doctors that much better, or is that state failing in its duty to provide adequate oversight? Is such a ranking system even warranted?
Nearly everyone agrees on the importance of protecting the public and the integrity of the medical profession. But the aggressive jousting over what the new numbers do or do not mean suggests just how difficult it can be to come up with a metric for medical accountability that everyone agrees is both fair and reliable.
Sidney Wolfe, MD, director of Public Citizen’s Health Research Group and the lead author of the new report, dismisses the notion that Minnesota’s doctors are so good that they don’t require as many disciplinary actions. “There is not a shred of evidence for that,” he says. Instead, he calls out what he views as an ineffective board.
In turn, Robert Leach, executive director of the Minnesota Board of Medical Practice, dismisses the significance of the report’s findings. “It’s a fair ranking the way their formula applies. It’s the formula we disagree with,” he says. “It’s fairly simplistic and indicative of nothing.”
And Lisa Robin, senior vice president for advocacy and member services at the Federation of State Medical Boards, says the federation doesn’t even encourage rankings because of the variable laws and sanctions from state to state. “It doesn’t give you a true picture of what boards do, to rank them,” she says.
A Row Over Rankings
Minnesota’s Leach has a detailed list of grievances against the report. But his biggest beef is with the fact that it ranks medical boards on the number of serious disciplinary actions per 1,000 physicians licensed by the state. “The more precise number should be the number of licensed physicians who are actually practicing in the state,” he says.
From 2008 to 2009, for example, more than 19,000 physicians were licensed in Minnesota. Yet Leach says that only a little more than 14,000 were actually practicing within the state, which he describes as a large exporter of trained doctors. “So we had 5,000 physicians who weren’t even practicing here that were counted against our one disciplinary action per thousand physicians,” he says.
Public Citizen, he says, also doesn’t recognize other interventions, such as Minnesota’s “agreements for corrective action,” that normally include training or remedial coursework for doctors with an identified weakness in subject areas such as prescribing or chronic-pain management. “Not every doctor needs to be hit over the head with a hammer of serious disciplinary action to address a problem,” Leach says.
And then there’s the sticky matter of peer review. In Minnesota, “virtually every physician now practicing works for a large health plan or a facility,” he says. “We have virtually no solo practice or isolated practice in Minnesota, and those are the physicians who get in trouble: the ones who don’t have the advantage of periodic peer review, who don’t have the advantage of adequate supervision to help keep them out of trouble.”
Doctors like those in Alaska? “You always see Alaska is rated real high,” Leach says. “You have a bunch of people out there practicing in the wilderness, out in solo practice. Physicians need to have that ability to have peer review, to be able to address problem cases with their colleagues. In Minnesota, a lot of these facilities and health plans address these problems at the practice level before they even reach the board.”
A Call To Action
Dr. Wolfe isn’t buying the notion that Minnesota doctors require less formal discipline while their colleagues in Alaska need more. Whenever other low-ranking states have provided sufficient funding, replaced ineffective leadership, granted more independence, and met the other conditions necessary for a better medical board, he notes, their rate of disciplinary actions often “rockets up.”
The medical boards of North Carolina and Washington, D.C., have risen dramatically in the rankings in recent years, and Dr. Wolfe cites effective intervention in both cases. In formerly low-ranking Arizona, he says, similar corrective action in the late 1990s led to a tripling of the rate of serious disciplinary action within three years. “That’s obviously not a period of time that’s long enough to be explained by some inward migration of bad doctors or outward migration of good doctors,” he says. “It’s because the board started functioning better.”
Meanwhile, boards in South Carolina and Massachusetts have slumped in the ratings—a decline he attributes to the loss of leadership and funds.
“One area I can agree with Dr. Wolfe on is that medical boards need resources; they need adequate structure, resources, and authority to do their job and be able to protect the public,” says Robin, of the Federation of State Medical Boards. “If they’re in a big umbrella agency and they’re just one of many and share their pool of investigators with everyone, as you can imagine, that’s probably not as efficient.”
Hospitals also share in the blame, according to a separate Public Citizen report released last year that cites a chronic underreporting of doctor misconduct or incompetence to the National Practitioner Data Bank by hospitals. Robin agrees that more diligence is needed to ensure that medical boards have the information they need to properly do their jobs. As one of her board members told her, “They can’t gain information by osmosis.”
Hospitalists, however, might be well suited for addressing the underreporting issue. HM is in a “really good position to observe behavior that needs to be brought to the attention of hospital medical staff,” Dr. Wolfe says.
He recommends that one or more hospitalists should sit on each hospital’s medical peer review committee, where they can put their expertise to good use. “Hospitalists really need to get more active in this,” he says. “It’s for the betterment of the patients in the hospital, it’s for the betterment for the reputation of the hospital and the medical staff.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
The Cost of Regulation
The impact of last summer’s new restrictions from the Accreditation Council for Graduate Medical Education (ACGME) on how many hospitalized patients a first-year resident can treat on an internal-medicine (IM) rotation was as immediate as it was evident at Monmouth Medical Center, a 527-bed teaching hospital in Long Branch, N.J. The institution had a class of eight rookie residents whose caseloads were cut from 12 to the new threshold of 10.
Physicians “had to find some other way of getting attention . . . for 16 patients,” says Sarah Wallach, MD, FACP, director of Monmouth’s IM residency program and vice chair of the department of medicine at the hospital. At Monmouth, the solution came in the form of a new hire—a nurse practitioner (NP)—to handle the overflow. The NP service is used predominantly for referral patients from primary-care physicians (PCPs), as opposed to independent hospital admissions.
But because the NP service does not provide 24-hour coverage, the hospital can get away with only one person in the position. To extend coverage all day long, Dr. Wallach estimates she would need to hire two or three additional NPs, plus another one or two administrative positions to provide relief on holidays and vacations. “You would need five people,” she says. “I can’t afford that.”
Few hospitals or HM groups can afford new hires in today’s world of Medicare reimbursement cuts, shrinking budgets, and—courtesy of the newest rules—restricting patient caps for residents. The latest rules took hold about a year ago, but hospitalists in both academic and community settings say the impact already is noticeable.
Many hospitals have had to craft solutions, which have included burdening academic hospitals with more clinical responsibilities, turning to private HM groups (HMGs) to assume the patients residents can no longer care for, or hiring nonphysician providers (NPPs) to pick up the slack. As Dr. Wallach pointedly notes, the latter two solutions cost money at a time when hospitals have less to go around.
Already, teaching hospitals have begun discussions about how the newest rules—and the future changes they presage—will change the playing field. Will a wave of academics flee their classroom (the teaching hospital), as nonteaching duties become an intrusion? Will teaching hospitals face financial pressure as they struggle to replace the low-cost labor force that residents represent?
Perhaps most importantly from a medical perspective, will graduate trainees be as prepared as their predecessors when they enter practice?

The answers will have a direct correlation to private HMGs, which are poised to see more patients in the wake of residency restrictions, particularly on overnight services. The cost of hospital care will increase for hospitals, putting more pressure on hospitalist groups that tout themselves to C-suites as engines for cost savings. Long-term implications, unfortunately, remain murky, as the newest rules have been in place for a relatively short time. Plus, ACGME is expected—at the end of this month, according to a recent memo to program directors—to announce more changes to residency guidelines.
“Hospitalists will always be involved in teaching—it will never go away,” says Julia Wright, MD, FHM, clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison and a member of Team Hospitalist. “But it will be a very different balance, a different kind of feel.”
The Past to the Future
To understand the concerns moving forward, it’s important to first look back. In July 2003, new ACGME rules went into place capping the workweeks of residents at 80 hours. Rules were put into place that regulated the number of patients that residents could be assigned, and those thresholds were further tightened on July 1, 2009. The most notable 2009 change: A first-year resident’s patient census must not exceed 10 patients. ACGME CEO Thomas J. Nasca, MD, MACP, sent a letter to program directors in early May announcing more changes to resident work hours. The letter indicates proposals will be announced by the end of this month, and public comment will follow. At the earliest, new rules changes would go into effect in 2011. “The board may adopt a modification to the duty-hours standard,” says Julie Jacob, a spokeswoman for Chicago-based ACGME. “Any proposed standards would get a public comment.”
Jacob declined further comment, but various hospitalists and academics say they wouldn’t be surprised if new rules reflect 2008 Institute of Medicine (IOM) recommendations.1 The IOM report called for a maximum resident shift length of 30 hours, with admission of patients for up to 16 hours, plus a five-hour uninterrupted sleep period between 10 p.m. and 8 a.m. It also suggested the remaining workweek hours be used for transitional and educational activities.
However those IOM recommendations are incorporated, one thing is clear: Any adoption of those standards will have a financial impact. In fact, a study published last year reported that annual labor costs from implementing the IOM standards was estimated to be $1.6 billion in 2006 dollars (see “The Cost of Progress,” p. 25).2
“Any replacement of a resident costs more than a resident, whether it’s an NP, a PA (physician assistant), an MD, or a DO,” says Kevin O’Leary, MD, MS, associate program director of the IM residency program at Northwestern University’s Feinberg School of Medicine in Chicago. “Everybody costs more.”
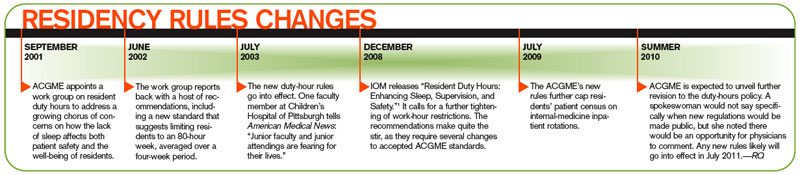
The Fate of Teachers
Some of the largest academic centers, including the Feinberg School, the University of Michigan, and the teaching service at St. Luke’s-Roosevelt Hospital in New York City, reduced patient caseloads ahead of the 2009 round of residency rule changes. Hospitalists and educators at those institutions say the proactive approach helped them adjust to the newest rules, which by some estimates reduce resident productivity by 20%.
But the changes shift the workload to academic hospitalists, many of whom forego higher-paying positions to pursue teaching and research. According to the latest SHM survey data, academic hospitalists make about $50,000 less per year than the average community hospitalist. But as clinical work intrudes further, as residents are unable to assume the patient care they once did, educators are put into positions of having to balance the educational portion of their job with patient care, says John Del Valle, MD, professor and residency program director in the department of internal medicine at the University of Michigan Health System in Ann Arbor.
“This is where difficult decisions have to be made,” Dr. Del Valle says. “This is not the blend of activities that traditional academics signed up for.”
Solutions to relieve current and impending pressure on teaching hospitalists have presented themselves in different ways. In Dr. Del Valle’s hospital, there is a split between the hospitalist service and the house staff, which is aimed at keeping up with the growth in IM admissions. That tally has climbed an average of 4% per year for the past five years, reaching some 18,000 admissions last year. To handle that workload, the nonresident service last year added three clinical full-time equivalents (FTEs) to bring its total to nearly 30 FTEs.
Dr. Del Valle notes his institution has been fortunate to be able to afford growth, thanks in large part to a payor mix with a relatively low percentage of charity care and high level of activity.
At Brigham and Women’s Hospital in Boston, the answer is a freestanding PA service that has been in place since 2005. Last summer, the program went to a 24-hour rotation to increase continuity for overnight services and to provide coverage on night shifts, an area most in the industry agree will be hit hardest by the resident caps. Physicians at Brigham’s, a teaching affiliate of Harvard Medical School, are now discussing an expansion of the PA service, or perhaps even an overhaul to a more cost-efficient solution, says Danielle Scheurer, MD, MSc, FHM, assistant professor of medicine at Harvard and director of Brigham’s general medicine service.

At Medical Center Hospital (MCH) in Odessa, Texas, the hospitalists were added to the ED call schedule once every five nights. The plan was under discussion before the new residency rules went into place; however, it was implemented to keep the IM residency program within the new limits, says Bruce Becker, MD, MCH’s chief medical officer.
And at St. Luke’s-Roosevelt Hospital, discussions are under way on how to best extend the nonteaching staff, says Ethan Fried, MD, MS, FACP, assistant professor of clinical medicine at Columbia University, vice chair for education in the department of medicine and director of graduate medical education at St. Luke’s-Roosevelt. “The adjustment has to come from the nonteaching side because the house staff at this point is saturated,” says Dr. Fried, president-elect of the Association of Program Directors in Internal Medicine (APDIM). “You can’t be cheap about acquiring your nonteaching staff.”
The Fate of Students
Perhaps paramount to the fears of how teaching hospitalists will react to current or future restrictions is the effect those limits have on the residents they safeguard. Some physicians think the new rules will produce crops of ill-prepared residents because they have been coddled with limited patient censuses. Other physicians argue that the new thresholds will actually better prepare physicians when HM groups are hiring residents for full-time positions.
Dr. Del Valle acknowledges there is as yet no rigorous data to show the impact of the current restrictions, but he agrees it’s a simple equation of patient-care mathematics. “You can’t [easily] replace 100-110 hours [of care per week],” he says.
Others say patient caps and rules to limit how much work residents do are in line with the purpose of medical training programs. “I’ve bought into the fact that these programs exist to train residents, not to provide clinical care,” Dr. O’Leary says. “I’ve drunk that Kool-Aid. … I think there’s more variation, person to person, than ‘my era vs. the current era.’ Like any new hospitalist that you hire, you need to give an orientation and give enough support to them so when they begin to see patients that they are not overwhelmed.”
Shaun Frost, MD, FACP, FHM, might be best described as halfway between those two extremes. A regional director for the eastern U.S. for Cogent Healthcare, he says duty-hour restrictions have had deleterious impacts but also create learning opportunities.
“The residency work-hour restrictions have inhibited our ability to train people to work as efficiently as trainees who were taught in the past,” says Dr. Frost, an SHM board member. “That doesn’t necessarily mean you can’t teach people to work more efficiently . . . but in the future, my hope is that residency training programs will recognize the deficit that exists in personal work efficiencies between their completion and their responsibilities as a hospitalist.”
To that end, Dr. Frost works with others to develop both structured curriculum and classroom didactics that help new hospitalists make up for gaps in preparation that weren’t addressed in residency. In some cases, that can be practice management and billing issues, but often, according to Dr. Frost, it is addressing personal workflow and bridging the “unnatural discontinuity” in patient care from residency to the real world.
“There is a cost to this investment for the future,” Dr. Frost adds. “If people don’t recognize the potential return on investment as being critical to the development of an educated workforce—an efficient and competent workforce—and thus critical to the retention of high-performing hospitalists, they are selling themselves, unfortunately, significantly short.”
Caught in the Middle
One man’s trash is another man’s treasure, the axiom tells us. Well, in healthcare circles, that could just as easily read: The woes of academic hospitalists are the wealth of community hospitalists.
The new rules “may result in more opportunities for hospitalists to provide needed clinical services,” Dr. Wright says.
The long-term implications, though, remain to be seen. While academic hospitalists say they have seen preliminary increases in care-delivery costs because of the latest rules changes, many say it’s too soon to tell just how high those costs might climb and what ripple effect might follow.
Some physicians, including Dr. Del Valle, note that while the 2009 changes and the expectation of more changes in 2011 are cause for attention, that doesn’t translate to cause for concern. In 2003, months before the 80-hour workweek rules were first put in place by ACGME, many of the same debates were already under way: How will the faculty of IM residency programs cope? How will institutions pay the bills while putting money aside for other physicians picking up the slack?
“This is a pendulum,” Dr. Del Valle says. “I think it will come back to a balanced place.”
Dr. Fried, who is more optimistic that the residency rules can have a positive, long-term effect, agrees. He says residency caps and limits should not be viewed as “things that limit education. We [should] look at them as things that ensure education continues while patient care continues.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Ulmer C, Wolman DM, Johns MM, eds. Washington, D.C.: The National Academies Press; 2008.
- Nuckols TK, Bhattacharya J, Wolman DM, Ulmer C, Escarce JJ. Cost implications of reduced work hours and workloads for resident physicians. N Engl J Med. 2009:360(21):2202-2215.
The impact of last summer’s new restrictions from the Accreditation Council for Graduate Medical Education (ACGME) on how many hospitalized patients a first-year resident can treat on an internal-medicine (IM) rotation was as immediate as it was evident at Monmouth Medical Center, a 527-bed teaching hospital in Long Branch, N.J. The institution had a class of eight rookie residents whose caseloads were cut from 12 to the new threshold of 10.
Physicians “had to find some other way of getting attention . . . for 16 patients,” says Sarah Wallach, MD, FACP, director of Monmouth’s IM residency program and vice chair of the department of medicine at the hospital. At Monmouth, the solution came in the form of a new hire—a nurse practitioner (NP)—to handle the overflow. The NP service is used predominantly for referral patients from primary-care physicians (PCPs), as opposed to independent hospital admissions.
But because the NP service does not provide 24-hour coverage, the hospital can get away with only one person in the position. To extend coverage all day long, Dr. Wallach estimates she would need to hire two or three additional NPs, plus another one or two administrative positions to provide relief on holidays and vacations. “You would need five people,” she says. “I can’t afford that.”
Few hospitals or HM groups can afford new hires in today’s world of Medicare reimbursement cuts, shrinking budgets, and—courtesy of the newest rules—restricting patient caps for residents. The latest rules took hold about a year ago, but hospitalists in both academic and community settings say the impact already is noticeable.
Many hospitals have had to craft solutions, which have included burdening academic hospitals with more clinical responsibilities, turning to private HM groups (HMGs) to assume the patients residents can no longer care for, or hiring nonphysician providers (NPPs) to pick up the slack. As Dr. Wallach pointedly notes, the latter two solutions cost money at a time when hospitals have less to go around.
Already, teaching hospitals have begun discussions about how the newest rules—and the future changes they presage—will change the playing field. Will a wave of academics flee their classroom (the teaching hospital), as nonteaching duties become an intrusion? Will teaching hospitals face financial pressure as they struggle to replace the low-cost labor force that residents represent?
Perhaps most importantly from a medical perspective, will graduate trainees be as prepared as their predecessors when they enter practice?
The answers will have a direct correlation to private HMGs, which are poised to see more patients in the wake of residency restrictions, particularly on overnight services. The cost of hospital care will increase for hospitals, putting more pressure on hospitalist groups that tout themselves to C-suites as engines for cost savings. Long-term implications, unfortunately, remain murky, as the newest rules have been in place for a relatively short time. Plus, ACGME is expected—at the end of this month, according to a recent memo to program directors—to announce more changes to residency guidelines.
“Hospitalists will always be involved in teaching—it will never go away,” says Julia Wright, MD, FHM, clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison and a member of Team Hospitalist. “But it will be a very different balance, a different kind of feel.”
The Past to the Future
To understand the concerns moving forward, it’s important to first look back. In July 2003, new ACGME rules went into place capping the workweeks of residents at 80 hours. Rules were put into place that regulated the number of patients that residents could be assigned, and those thresholds were further tightened on July 1, 2009. The most notable 2009 change: A first-year resident’s patient census must not exceed 10 patients. ACGME CEO Thomas J. Nasca, MD, MACP, sent a letter to program directors in early May announcing more changes to resident work hours. The letter indicates proposals will be announced by the end of this month, and public comment will follow. At the earliest, new rules changes would go into effect in 2011. “The board may adopt a modification to the duty-hours standard,” says Julie Jacob, a spokeswoman for Chicago-based ACGME. “Any proposed standards would get a public comment.”
Jacob declined further comment, but various hospitalists and academics say they wouldn’t be surprised if new rules reflect 2008 Institute of Medicine (IOM) recommendations.1 The IOM report called for a maximum resident shift length of 30 hours, with admission of patients for up to 16 hours, plus a five-hour uninterrupted sleep period between 10 p.m. and 8 a.m. It also suggested the remaining workweek hours be used for transitional and educational activities.
However those IOM recommendations are incorporated, one thing is clear: Any adoption of those standards will have a financial impact. In fact, a study published last year reported that annual labor costs from implementing the IOM standards was estimated to be $1.6 billion in 2006 dollars (see “The Cost of Progress,” p. 25).2
“Any replacement of a resident costs more than a resident, whether it’s an NP, a PA (physician assistant), an MD, or a DO,” says Kevin O’Leary, MD, MS, associate program director of the IM residency program at Northwestern University’s Feinberg School of Medicine in Chicago. “Everybody costs more.”
The Fate of Teachers
Some of the largest academic centers, including the Feinberg School, the University of Michigan, and the teaching service at St. Luke’s-Roosevelt Hospital in New York City, reduced patient caseloads ahead of the 2009 round of residency rule changes. Hospitalists and educators at those institutions say the proactive approach helped them adjust to the newest rules, which by some estimates reduce resident productivity by 20%.
But the changes shift the workload to academic hospitalists, many of whom forego higher-paying positions to pursue teaching and research. According to the latest SHM survey data, academic hospitalists make about $50,000 less per year than the average community hospitalist. But as clinical work intrudes further, as residents are unable to assume the patient care they once did, educators are put into positions of having to balance the educational portion of their job with patient care, says John Del Valle, MD, professor and residency program director in the department of internal medicine at the University of Michigan Health System in Ann Arbor.
“This is where difficult decisions have to be made,” Dr. Del Valle says. “This is not the blend of activities that traditional academics signed up for.”
Solutions to relieve current and impending pressure on teaching hospitalists have presented themselves in different ways. In Dr. Del Valle’s hospital, there is a split between the hospitalist service and the house staff, which is aimed at keeping up with the growth in IM admissions. That tally has climbed an average of 4% per year for the past five years, reaching some 18,000 admissions last year. To handle that workload, the nonresident service last year added three clinical full-time equivalents (FTEs) to bring its total to nearly 30 FTEs.
Dr. Del Valle notes his institution has been fortunate to be able to afford growth, thanks in large part to a payor mix with a relatively low percentage of charity care and high level of activity.
At Brigham and Women’s Hospital in Boston, the answer is a freestanding PA service that has been in place since 2005. Last summer, the program went to a 24-hour rotation to increase continuity for overnight services and to provide coverage on night shifts, an area most in the industry agree will be hit hardest by the resident caps. Physicians at Brigham’s, a teaching affiliate of Harvard Medical School, are now discussing an expansion of the PA service, or perhaps even an overhaul to a more cost-efficient solution, says Danielle Scheurer, MD, MSc, FHM, assistant professor of medicine at Harvard and director of Brigham’s general medicine service.
At Medical Center Hospital (MCH) in Odessa, Texas, the hospitalists were added to the ED call schedule once every five nights. The plan was under discussion before the new residency rules went into place; however, it was implemented to keep the IM residency program within the new limits, says Bruce Becker, MD, MCH’s chief medical officer.
And at St. Luke’s-Roosevelt Hospital, discussions are under way on how to best extend the nonteaching staff, says Ethan Fried, MD, MS, FACP, assistant professor of clinical medicine at Columbia University, vice chair for education in the department of medicine and director of graduate medical education at St. Luke’s-Roosevelt. “The adjustment has to come from the nonteaching side because the house staff at this point is saturated,” says Dr. Fried, president-elect of the Association of Program Directors in Internal Medicine (APDIM). “You can’t be cheap about acquiring your nonteaching staff.”
The Fate of Students
Perhaps paramount to the fears of how teaching hospitalists will react to current or future restrictions is the effect those limits have on the residents they safeguard. Some physicians think the new rules will produce crops of ill-prepared residents because they have been coddled with limited patient censuses. Other physicians argue that the new thresholds will actually better prepare physicians when HM groups are hiring residents for full-time positions.
Dr. Del Valle acknowledges there is as yet no rigorous data to show the impact of the current restrictions, but he agrees it’s a simple equation of patient-care mathematics. “You can’t [easily] replace 100-110 hours [of care per week],” he says.
Others say patient caps and rules to limit how much work residents do are in line with the purpose of medical training programs. “I’ve bought into the fact that these programs exist to train residents, not to provide clinical care,” Dr. O’Leary says. “I’ve drunk that Kool-Aid. … I think there’s more variation, person to person, than ‘my era vs. the current era.’ Like any new hospitalist that you hire, you need to give an orientation and give enough support to them so when they begin to see patients that they are not overwhelmed.”
Shaun Frost, MD, FACP, FHM, might be best described as halfway between those two extremes. A regional director for the eastern U.S. for Cogent Healthcare, he says duty-hour restrictions have had deleterious impacts but also create learning opportunities.
“The residency work-hour restrictions have inhibited our ability to train people to work as efficiently as trainees who were taught in the past,” says Dr. Frost, an SHM board member. “That doesn’t necessarily mean you can’t teach people to work more efficiently . . . but in the future, my hope is that residency training programs will recognize the deficit that exists in personal work efficiencies between their completion and their responsibilities as a hospitalist.”
To that end, Dr. Frost works with others to develop both structured curriculum and classroom didactics that help new hospitalists make up for gaps in preparation that weren’t addressed in residency. In some cases, that can be practice management and billing issues, but often, according to Dr. Frost, it is addressing personal workflow and bridging the “unnatural discontinuity” in patient care from residency to the real world.
“There is a cost to this investment for the future,” Dr. Frost adds. “If people don’t recognize the potential return on investment as being critical to the development of an educated workforce—an efficient and competent workforce—and thus critical to the retention of high-performing hospitalists, they are selling themselves, unfortunately, significantly short.”
Caught in the Middle
One man’s trash is another man’s treasure, the axiom tells us. Well, in healthcare circles, that could just as easily read: The woes of academic hospitalists are the wealth of community hospitalists.
The new rules “may result in more opportunities for hospitalists to provide needed clinical services,” Dr. Wright says.
The long-term implications, though, remain to be seen. While academic hospitalists say they have seen preliminary increases in care-delivery costs because of the latest rules changes, many say it’s too soon to tell just how high those costs might climb and what ripple effect might follow.
Some physicians, including Dr. Del Valle, note that while the 2009 changes and the expectation of more changes in 2011 are cause for attention, that doesn’t translate to cause for concern. In 2003, months before the 80-hour workweek rules were first put in place by ACGME, many of the same debates were already under way: How will the faculty of IM residency programs cope? How will institutions pay the bills while putting money aside for other physicians picking up the slack?
“This is a pendulum,” Dr. Del Valle says. “I think it will come back to a balanced place.”
Dr. Fried, who is more optimistic that the residency rules can have a positive, long-term effect, agrees. He says residency caps and limits should not be viewed as “things that limit education. We [should] look at them as things that ensure education continues while patient care continues.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Ulmer C, Wolman DM, Johns MM, eds. Washington, D.C.: The National Academies Press; 2008.
- Nuckols TK, Bhattacharya J, Wolman DM, Ulmer C, Escarce JJ. Cost implications of reduced work hours and workloads for resident physicians. N Engl J Med. 2009:360(21):2202-2215.
The impact of last summer’s new restrictions from the Accreditation Council for Graduate Medical Education (ACGME) on how many hospitalized patients a first-year resident can treat on an internal-medicine (IM) rotation was as immediate as it was evident at Monmouth Medical Center, a 527-bed teaching hospital in Long Branch, N.J. The institution had a class of eight rookie residents whose caseloads were cut from 12 to the new threshold of 10.
Physicians “had to find some other way of getting attention . . . for 16 patients,” says Sarah Wallach, MD, FACP, director of Monmouth’s IM residency program and vice chair of the department of medicine at the hospital. At Monmouth, the solution came in the form of a new hire—a nurse practitioner (NP)—to handle the overflow. The NP service is used predominantly for referral patients from primary-care physicians (PCPs), as opposed to independent hospital admissions.
But because the NP service does not provide 24-hour coverage, the hospital can get away with only one person in the position. To extend coverage all day long, Dr. Wallach estimates she would need to hire two or three additional NPs, plus another one or two administrative positions to provide relief on holidays and vacations. “You would need five people,” she says. “I can’t afford that.”
Few hospitals or HM groups can afford new hires in today’s world of Medicare reimbursement cuts, shrinking budgets, and—courtesy of the newest rules—restricting patient caps for residents. The latest rules took hold about a year ago, but hospitalists in both academic and community settings say the impact already is noticeable.
Many hospitals have had to craft solutions, which have included burdening academic hospitals with more clinical responsibilities, turning to private HM groups (HMGs) to assume the patients residents can no longer care for, or hiring nonphysician providers (NPPs) to pick up the slack. As Dr. Wallach pointedly notes, the latter two solutions cost money at a time when hospitals have less to go around.
Already, teaching hospitals have begun discussions about how the newest rules—and the future changes they presage—will change the playing field. Will a wave of academics flee their classroom (the teaching hospital), as nonteaching duties become an intrusion? Will teaching hospitals face financial pressure as they struggle to replace the low-cost labor force that residents represent?
Perhaps most importantly from a medical perspective, will graduate trainees be as prepared as their predecessors when they enter practice?
The answers will have a direct correlation to private HMGs, which are poised to see more patients in the wake of residency restrictions, particularly on overnight services. The cost of hospital care will increase for hospitals, putting more pressure on hospitalist groups that tout themselves to C-suites as engines for cost savings. Long-term implications, unfortunately, remain murky, as the newest rules have been in place for a relatively short time. Plus, ACGME is expected—at the end of this month, according to a recent memo to program directors—to announce more changes to residency guidelines.
“Hospitalists will always be involved in teaching—it will never go away,” says Julia Wright, MD, FHM, clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison and a member of Team Hospitalist. “But it will be a very different balance, a different kind of feel.”
The Past to the Future
To understand the concerns moving forward, it’s important to first look back. In July 2003, new ACGME rules went into place capping the workweeks of residents at 80 hours. Rules were put into place that regulated the number of patients that residents could be assigned, and those thresholds were further tightened on July 1, 2009. The most notable 2009 change: A first-year resident’s patient census must not exceed 10 patients. ACGME CEO Thomas J. Nasca, MD, MACP, sent a letter to program directors in early May announcing more changes to resident work hours. The letter indicates proposals will be announced by the end of this month, and public comment will follow. At the earliest, new rules changes would go into effect in 2011. “The board may adopt a modification to the duty-hours standard,” says Julie Jacob, a spokeswoman for Chicago-based ACGME. “Any proposed standards would get a public comment.”
Jacob declined further comment, but various hospitalists and academics say they wouldn’t be surprised if new rules reflect 2008 Institute of Medicine (IOM) recommendations.1 The IOM report called for a maximum resident shift length of 30 hours, with admission of patients for up to 16 hours, plus a five-hour uninterrupted sleep period between 10 p.m. and 8 a.m. It also suggested the remaining workweek hours be used for transitional and educational activities.
However those IOM recommendations are incorporated, one thing is clear: Any adoption of those standards will have a financial impact. In fact, a study published last year reported that annual labor costs from implementing the IOM standards was estimated to be $1.6 billion in 2006 dollars (see “The Cost of Progress,” p. 25).2
“Any replacement of a resident costs more than a resident, whether it’s an NP, a PA (physician assistant), an MD, or a DO,” says Kevin O’Leary, MD, MS, associate program director of the IM residency program at Northwestern University’s Feinberg School of Medicine in Chicago. “Everybody costs more.”
The Fate of Teachers
Some of the largest academic centers, including the Feinberg School, the University of Michigan, and the teaching service at St. Luke’s-Roosevelt Hospital in New York City, reduced patient caseloads ahead of the 2009 round of residency rule changes. Hospitalists and educators at those institutions say the proactive approach helped them adjust to the newest rules, which by some estimates reduce resident productivity by 20%.
But the changes shift the workload to academic hospitalists, many of whom forego higher-paying positions to pursue teaching and research. According to the latest SHM survey data, academic hospitalists make about $50,000 less per year than the average community hospitalist. But as clinical work intrudes further, as residents are unable to assume the patient care they once did, educators are put into positions of having to balance the educational portion of their job with patient care, says John Del Valle, MD, professor and residency program director in the department of internal medicine at the University of Michigan Health System in Ann Arbor.
“This is where difficult decisions have to be made,” Dr. Del Valle says. “This is not the blend of activities that traditional academics signed up for.”
Solutions to relieve current and impending pressure on teaching hospitalists have presented themselves in different ways. In Dr. Del Valle’s hospital, there is a split between the hospitalist service and the house staff, which is aimed at keeping up with the growth in IM admissions. That tally has climbed an average of 4% per year for the past five years, reaching some 18,000 admissions last year. To handle that workload, the nonresident service last year added three clinical full-time equivalents (FTEs) to bring its total to nearly 30 FTEs.
Dr. Del Valle notes his institution has been fortunate to be able to afford growth, thanks in large part to a payor mix with a relatively low percentage of charity care and high level of activity.
At Brigham and Women’s Hospital in Boston, the answer is a freestanding PA service that has been in place since 2005. Last summer, the program went to a 24-hour rotation to increase continuity for overnight services and to provide coverage on night shifts, an area most in the industry agree will be hit hardest by the resident caps. Physicians at Brigham’s, a teaching affiliate of Harvard Medical School, are now discussing an expansion of the PA service, or perhaps even an overhaul to a more cost-efficient solution, says Danielle Scheurer, MD, MSc, FHM, assistant professor of medicine at Harvard and director of Brigham’s general medicine service.
At Medical Center Hospital (MCH) in Odessa, Texas, the hospitalists were added to the ED call schedule once every five nights. The plan was under discussion before the new residency rules went into place; however, it was implemented to keep the IM residency program within the new limits, says Bruce Becker, MD, MCH’s chief medical officer.
And at St. Luke’s-Roosevelt Hospital, discussions are under way on how to best extend the nonteaching staff, says Ethan Fried, MD, MS, FACP, assistant professor of clinical medicine at Columbia University, vice chair for education in the department of medicine and director of graduate medical education at St. Luke’s-Roosevelt. “The adjustment has to come from the nonteaching side because the house staff at this point is saturated,” says Dr. Fried, president-elect of the Association of Program Directors in Internal Medicine (APDIM). “You can’t be cheap about acquiring your nonteaching staff.”
The Fate of Students
Perhaps paramount to the fears of how teaching hospitalists will react to current or future restrictions is the effect those limits have on the residents they safeguard. Some physicians think the new rules will produce crops of ill-prepared residents because they have been coddled with limited patient censuses. Other physicians argue that the new thresholds will actually better prepare physicians when HM groups are hiring residents for full-time positions.
Dr. Del Valle acknowledges there is as yet no rigorous data to show the impact of the current restrictions, but he agrees it’s a simple equation of patient-care mathematics. “You can’t [easily] replace 100-110 hours [of care per week],” he says.
Others say patient caps and rules to limit how much work residents do are in line with the purpose of medical training programs. “I’ve bought into the fact that these programs exist to train residents, not to provide clinical care,” Dr. O’Leary says. “I’ve drunk that Kool-Aid. … I think there’s more variation, person to person, than ‘my era vs. the current era.’ Like any new hospitalist that you hire, you need to give an orientation and give enough support to them so when they begin to see patients that they are not overwhelmed.”
Shaun Frost, MD, FACP, FHM, might be best described as halfway between those two extremes. A regional director for the eastern U.S. for Cogent Healthcare, he says duty-hour restrictions have had deleterious impacts but also create learning opportunities.
“The residency work-hour restrictions have inhibited our ability to train people to work as efficiently as trainees who were taught in the past,” says Dr. Frost, an SHM board member. “That doesn’t necessarily mean you can’t teach people to work more efficiently . . . but in the future, my hope is that residency training programs will recognize the deficit that exists in personal work efficiencies between their completion and their responsibilities as a hospitalist.”
To that end, Dr. Frost works with others to develop both structured curriculum and classroom didactics that help new hospitalists make up for gaps in preparation that weren’t addressed in residency. In some cases, that can be practice management and billing issues, but often, according to Dr. Frost, it is addressing personal workflow and bridging the “unnatural discontinuity” in patient care from residency to the real world.
“There is a cost to this investment for the future,” Dr. Frost adds. “If people don’t recognize the potential return on investment as being critical to the development of an educated workforce—an efficient and competent workforce—and thus critical to the retention of high-performing hospitalists, they are selling themselves, unfortunately, significantly short.”
Caught in the Middle
One man’s trash is another man’s treasure, the axiom tells us. Well, in healthcare circles, that could just as easily read: The woes of academic hospitalists are the wealth of community hospitalists.
The new rules “may result in more opportunities for hospitalists to provide needed clinical services,” Dr. Wright says.
The long-term implications, though, remain to be seen. While academic hospitalists say they have seen preliminary increases in care-delivery costs because of the latest rules changes, many say it’s too soon to tell just how high those costs might climb and what ripple effect might follow.
Some physicians, including Dr. Del Valle, note that while the 2009 changes and the expectation of more changes in 2011 are cause for attention, that doesn’t translate to cause for concern. In 2003, months before the 80-hour workweek rules were first put in place by ACGME, many of the same debates were already under way: How will the faculty of IM residency programs cope? How will institutions pay the bills while putting money aside for other physicians picking up the slack?
“This is a pendulum,” Dr. Del Valle says. “I think it will come back to a balanced place.”
Dr. Fried, who is more optimistic that the residency rules can have a positive, long-term effect, agrees. He says residency caps and limits should not be viewed as “things that limit education. We [should] look at them as things that ensure education continues while patient care continues.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Ulmer C, Wolman DM, Johns MM, eds. Washington, D.C.: The National Academies Press; 2008.
- Nuckols TK, Bhattacharya J, Wolman DM, Ulmer C, Escarce JJ. Cost implications of reduced work hours and workloads for resident physicians. N Engl J Med. 2009:360(21):2202-2215.
What I Learned

As I write, I’m fighting the jet stream from Washington, D.C., to Denver, midflight on my return from HM10. I’m 30,000 feet above the ground—literally and figuratively—my mind spinning with the thoughts, ideas, and memories from the largest gathering of hospitalists ever. In the end, 2,500 hospitalists descended on our nation’s capital. Shrouded by the din of healthcare reform, we discussed, deliberated, and discovered what’s new in the clinical, political, and programmatic world of HM. Out of this churn, I learned a lot. Here’s but a small sample.
Smart People = Smart Solutions
I learned that if you put really smart people in a room and give them a problem to grapple with, they come up with really smart solutions. At the inaugural Academic Hospital Medicine Leadership Summit, 100 of the brightest, most influential academic hospitalists convened to tackle the problems facing our field.
The output was an amazing crop of inventive ideas aimed at taming the vexing issues surrounding clinical sustainability, academic viability, and career satisfaction. SHM leadership has heard the cry and promises to work closely with the academic community to transform these smart solutions into future initiatives.
Hospitalists Support Healthcare Reform, Should Collude with Hospitals
I learned that most of us support the recently passed healthcare reform legislation, with a few notable dissenters. In response to a question from the chair of SHM’s Public Policy Committee, the vast majority of attendees at the opening plenary session raised their hands affirmatively in response to the question of whether they support the reform bill. Meanwhile, nearly everyone in the crowd felt it is important that SHM have an opinion regarding the legislation and continue to work closely with Congress to ensure its implementation helps our most important constituent—our patients.
Finally, I learned that Ron Greeno, CMO of Brentwood, Tenn.-based Cogent Healthcare, believes that the development of accountable-care organizations might lead hospitalists to align with hospitals to keep costs down. In fact, he saw this as a welcome, intended consequence. In his opinion, this “collusion” promises to raise the quality of care and reduce waste in the system—a statement that was met with applause from the plenary crowd.
The Healthcare Paradox
I learned that blogs save lives. Paul Levy, CEO of Beth Israel Deaconess Medical Center in Boston, roused the crowd during his keynote address by relating the power of transparency. Bothered by the paradox that the medical profession, comprising the most well-intentioned people in the world, could kill so many people through errors (ranked the No. 4 public health hazard in the U.S.), Levy decided to make his hospital’s struggles public.
On his blog, Running a Hospital (runningahospital.blogspot.com), he took the extraordinary step of publically documenting the rates of harm caused at his medical center for the world to see. Additionally, he set audacious goals to reduce the amount of harm to zero. He encouraged hospital staff to raise issues of safety and efficiency as a way to avoid the workarounds—shortcuts—that ultimately increase variability and reduce quality without addressing the core problem.
In response, the staff swarms the problem to rapidly improve the process and ultimately return the system back to homeostasis. The results of this effort can be viewed at Levy’s hospital’s website (www.bidmc.org/QualityandSafety.aspx).
Which Hill Will You Climb?
I learned that leadership is the ability to help people address problems that make the world better. At a much-anticipated presentation, Peter Pronovost, MD, of Johns Hopkins Hospital in Baltimore related a transformative story from his youth. At a summer camp, each boy was assigned to one of three groups and tasked with climbing a seemingly insurmountable hill. The first camp counselor pummeled the group with overbearing directions, directives, and derision, and in the end the group failed to conquer the hill. The second counselor took a more relaxed approach, giving the group essentially no direction. They, too, failed.
The final counselor offered nothing but the inspiration of how marvelous the view from the top of the hill would be and how they’d all have to pull together and work as a team if they wanted to attain that greatness. Dr. Pronovost was in this last group, and has been summiting insurmountable peaks ever since.
You likely are familiar with Dr. Pronovost’s work on ICU line infections. He elaborated on how he accomplished a rate of zero line infections, first at his hospital and then throughout the entire state of Michigan. The key was an inspiring vision and, once again, removal of workarounds. After compiling a checklist of the five most crucial components of line placement and management, Hopkins personnel discovered they were only compliant with the checklist 30% of the time—mostly due to shortcuts caused by inefficient systems that placed supplies too far from the clinical-care setting. After removing those barriers, the compliance rate went to 70%. It was only after empowering the nursing staff to stop physicians from proceeding with line placement unless the checklist was followed that the team was able to achieve 100% compliance.
Today, patients in the Johns Hopkins cardiovascular unit have not suffered a line infection for 87 consecutive weeks. That’s a hill worth climbing.
Saving Lives and Canine Castaways
I learned that the SHM annual meeting is attracting the highest echelon of clinical speakers. Whether it was Dr. Pronovost speaking about line infections, Dr. Greg Fonarow discussing congestive heart failure, or Dr. John Bartlett presenting on Clostrium difficile infections, HM10 featured world-class speakers.
For example, Dr. Bartlett’s work has defined the C. diff field, and the opportunity to hear him was incredible. I learned from him that severe C. diff infections are on the rise and that recurrences are tougher than ever to treat. I also learned that there are mixed data on whether nurses can detect C. diff based on stool smell alone; that up to 10% of dogs carry C. diff (out of the bed, Hogan and Grady!); and that stool transplants are becoming a quality- and quantity-of-life-saving treatment for those with severe bouts of recurrent C. diff.
To quote Dr. Bartlett, “pathophysiologically, it’s a dream; aesthetically, it sucks.”
Homeward Bound
Finally, I learned that every year, SHM feels more and more like my second family, with the annual meeting its family reunion. I saw tons of friends, made dozens more, and look forward to next year in Dallas.
Mostly, however, I was reminded of the emotional tug of being away from home, the emotive power of a few e-mailed photos of your kids, and how great if feels to turn off your electronic devices and return your folding tray and seat back to the upright and locked position. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
As I write, I’m fighting the jet stream from Washington, D.C., to Denver, midflight on my return from HM10. I’m 30,000 feet above the ground—literally and figuratively—my mind spinning with the thoughts, ideas, and memories from the largest gathering of hospitalists ever. In the end, 2,500 hospitalists descended on our nation’s capital. Shrouded by the din of healthcare reform, we discussed, deliberated, and discovered what’s new in the clinical, political, and programmatic world of HM. Out of this churn, I learned a lot. Here’s but a small sample.
Smart People = Smart Solutions
I learned that if you put really smart people in a room and give them a problem to grapple with, they come up with really smart solutions. At the inaugural Academic Hospital Medicine Leadership Summit, 100 of the brightest, most influential academic hospitalists convened to tackle the problems facing our field.
The output was an amazing crop of inventive ideas aimed at taming the vexing issues surrounding clinical sustainability, academic viability, and career satisfaction. SHM leadership has heard the cry and promises to work closely with the academic community to transform these smart solutions into future initiatives.
Hospitalists Support Healthcare Reform, Should Collude with Hospitals
I learned that most of us support the recently passed healthcare reform legislation, with a few notable dissenters. In response to a question from the chair of SHM’s Public Policy Committee, the vast majority of attendees at the opening plenary session raised their hands affirmatively in response to the question of whether they support the reform bill. Meanwhile, nearly everyone in the crowd felt it is important that SHM have an opinion regarding the legislation and continue to work closely with Congress to ensure its implementation helps our most important constituent—our patients.
Finally, I learned that Ron Greeno, CMO of Brentwood, Tenn.-based Cogent Healthcare, believes that the development of accountable-care organizations might lead hospitalists to align with hospitals to keep costs down. In fact, he saw this as a welcome, intended consequence. In his opinion, this “collusion” promises to raise the quality of care and reduce waste in the system—a statement that was met with applause from the plenary crowd.
The Healthcare Paradox
I learned that blogs save lives. Paul Levy, CEO of Beth Israel Deaconess Medical Center in Boston, roused the crowd during his keynote address by relating the power of transparency. Bothered by the paradox that the medical profession, comprising the most well-intentioned people in the world, could kill so many people through errors (ranked the No. 4 public health hazard in the U.S.), Levy decided to make his hospital’s struggles public.
On his blog, Running a Hospital (runningahospital.blogspot.com), he took the extraordinary step of publically documenting the rates of harm caused at his medical center for the world to see. Additionally, he set audacious goals to reduce the amount of harm to zero. He encouraged hospital staff to raise issues of safety and efficiency as a way to avoid the workarounds—shortcuts—that ultimately increase variability and reduce quality without addressing the core problem.
In response, the staff swarms the problem to rapidly improve the process and ultimately return the system back to homeostasis. The results of this effort can be viewed at Levy’s hospital’s website (www.bidmc.org/QualityandSafety.aspx).
Which Hill Will You Climb?
I learned that leadership is the ability to help people address problems that make the world better. At a much-anticipated presentation, Peter Pronovost, MD, of Johns Hopkins Hospital in Baltimore related a transformative story from his youth. At a summer camp, each boy was assigned to one of three groups and tasked with climbing a seemingly insurmountable hill. The first camp counselor pummeled the group with overbearing directions, directives, and derision, and in the end the group failed to conquer the hill. The second counselor took a more relaxed approach, giving the group essentially no direction. They, too, failed.
The final counselor offered nothing but the inspiration of how marvelous the view from the top of the hill would be and how they’d all have to pull together and work as a team if they wanted to attain that greatness. Dr. Pronovost was in this last group, and has been summiting insurmountable peaks ever since.
You likely are familiar with Dr. Pronovost’s work on ICU line infections. He elaborated on how he accomplished a rate of zero line infections, first at his hospital and then throughout the entire state of Michigan. The key was an inspiring vision and, once again, removal of workarounds. After compiling a checklist of the five most crucial components of line placement and management, Hopkins personnel discovered they were only compliant with the checklist 30% of the time—mostly due to shortcuts caused by inefficient systems that placed supplies too far from the clinical-care setting. After removing those barriers, the compliance rate went to 70%. It was only after empowering the nursing staff to stop physicians from proceeding with line placement unless the checklist was followed that the team was able to achieve 100% compliance.
Today, patients in the Johns Hopkins cardiovascular unit have not suffered a line infection for 87 consecutive weeks. That’s a hill worth climbing.
Saving Lives and Canine Castaways
I learned that the SHM annual meeting is attracting the highest echelon of clinical speakers. Whether it was Dr. Pronovost speaking about line infections, Dr. Greg Fonarow discussing congestive heart failure, or Dr. John Bartlett presenting on Clostrium difficile infections, HM10 featured world-class speakers.
For example, Dr. Bartlett’s work has defined the C. diff field, and the opportunity to hear him was incredible. I learned from him that severe C. diff infections are on the rise and that recurrences are tougher than ever to treat. I also learned that there are mixed data on whether nurses can detect C. diff based on stool smell alone; that up to 10% of dogs carry C. diff (out of the bed, Hogan and Grady!); and that stool transplants are becoming a quality- and quantity-of-life-saving treatment for those with severe bouts of recurrent C. diff.
To quote Dr. Bartlett, “pathophysiologically, it’s a dream; aesthetically, it sucks.”
Homeward Bound
Finally, I learned that every year, SHM feels more and more like my second family, with the annual meeting its family reunion. I saw tons of friends, made dozens more, and look forward to next year in Dallas.
Mostly, however, I was reminded of the emotional tug of being away from home, the emotive power of a few e-mailed photos of your kids, and how great if feels to turn off your electronic devices and return your folding tray and seat back to the upright and locked position. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
As I write, I’m fighting the jet stream from Washington, D.C., to Denver, midflight on my return from HM10. I’m 30,000 feet above the ground—literally and figuratively—my mind spinning with the thoughts, ideas, and memories from the largest gathering of hospitalists ever. In the end, 2,500 hospitalists descended on our nation’s capital. Shrouded by the din of healthcare reform, we discussed, deliberated, and discovered what’s new in the clinical, political, and programmatic world of HM. Out of this churn, I learned a lot. Here’s but a small sample.
Smart People = Smart Solutions
I learned that if you put really smart people in a room and give them a problem to grapple with, they come up with really smart solutions. At the inaugural Academic Hospital Medicine Leadership Summit, 100 of the brightest, most influential academic hospitalists convened to tackle the problems facing our field.
The output was an amazing crop of inventive ideas aimed at taming the vexing issues surrounding clinical sustainability, academic viability, and career satisfaction. SHM leadership has heard the cry and promises to work closely with the academic community to transform these smart solutions into future initiatives.
Hospitalists Support Healthcare Reform, Should Collude with Hospitals
I learned that most of us support the recently passed healthcare reform legislation, with a few notable dissenters. In response to a question from the chair of SHM’s Public Policy Committee, the vast majority of attendees at the opening plenary session raised their hands affirmatively in response to the question of whether they support the reform bill. Meanwhile, nearly everyone in the crowd felt it is important that SHM have an opinion regarding the legislation and continue to work closely with Congress to ensure its implementation helps our most important constituent—our patients.
Finally, I learned that Ron Greeno, CMO of Brentwood, Tenn.-based Cogent Healthcare, believes that the development of accountable-care organizations might lead hospitalists to align with hospitals to keep costs down. In fact, he saw this as a welcome, intended consequence. In his opinion, this “collusion” promises to raise the quality of care and reduce waste in the system—a statement that was met with applause from the plenary crowd.
The Healthcare Paradox
I learned that blogs save lives. Paul Levy, CEO of Beth Israel Deaconess Medical Center in Boston, roused the crowd during his keynote address by relating the power of transparency. Bothered by the paradox that the medical profession, comprising the most well-intentioned people in the world, could kill so many people through errors (ranked the No. 4 public health hazard in the U.S.), Levy decided to make his hospital’s struggles public.
On his blog, Running a Hospital (runningahospital.blogspot.com), he took the extraordinary step of publically documenting the rates of harm caused at his medical center for the world to see. Additionally, he set audacious goals to reduce the amount of harm to zero. He encouraged hospital staff to raise issues of safety and efficiency as a way to avoid the workarounds—shortcuts—that ultimately increase variability and reduce quality without addressing the core problem.
In response, the staff swarms the problem to rapidly improve the process and ultimately return the system back to homeostasis. The results of this effort can be viewed at Levy’s hospital’s website (www.bidmc.org/QualityandSafety.aspx).
Which Hill Will You Climb?
I learned that leadership is the ability to help people address problems that make the world better. At a much-anticipated presentation, Peter Pronovost, MD, of Johns Hopkins Hospital in Baltimore related a transformative story from his youth. At a summer camp, each boy was assigned to one of three groups and tasked with climbing a seemingly insurmountable hill. The first camp counselor pummeled the group with overbearing directions, directives, and derision, and in the end the group failed to conquer the hill. The second counselor took a more relaxed approach, giving the group essentially no direction. They, too, failed.
The final counselor offered nothing but the inspiration of how marvelous the view from the top of the hill would be and how they’d all have to pull together and work as a team if they wanted to attain that greatness. Dr. Pronovost was in this last group, and has been summiting insurmountable peaks ever since.
You likely are familiar with Dr. Pronovost’s work on ICU line infections. He elaborated on how he accomplished a rate of zero line infections, first at his hospital and then throughout the entire state of Michigan. The key was an inspiring vision and, once again, removal of workarounds. After compiling a checklist of the five most crucial components of line placement and management, Hopkins personnel discovered they were only compliant with the checklist 30% of the time—mostly due to shortcuts caused by inefficient systems that placed supplies too far from the clinical-care setting. After removing those barriers, the compliance rate went to 70%. It was only after empowering the nursing staff to stop physicians from proceeding with line placement unless the checklist was followed that the team was able to achieve 100% compliance.
Today, patients in the Johns Hopkins cardiovascular unit have not suffered a line infection for 87 consecutive weeks. That’s a hill worth climbing.
Saving Lives and Canine Castaways
I learned that the SHM annual meeting is attracting the highest echelon of clinical speakers. Whether it was Dr. Pronovost speaking about line infections, Dr. Greg Fonarow discussing congestive heart failure, or Dr. John Bartlett presenting on Clostrium difficile infections, HM10 featured world-class speakers.
For example, Dr. Bartlett’s work has defined the C. diff field, and the opportunity to hear him was incredible. I learned from him that severe C. diff infections are on the rise and that recurrences are tougher than ever to treat. I also learned that there are mixed data on whether nurses can detect C. diff based on stool smell alone; that up to 10% of dogs carry C. diff (out of the bed, Hogan and Grady!); and that stool transplants are becoming a quality- and quantity-of-life-saving treatment for those with severe bouts of recurrent C. diff.
To quote Dr. Bartlett, “pathophysiologically, it’s a dream; aesthetically, it sucks.”
Homeward Bound
Finally, I learned that every year, SHM feels more and more like my second family, with the annual meeting its family reunion. I saw tons of friends, made dozens more, and look forward to next year in Dallas.
Mostly, however, I was reminded of the emotional tug of being away from home, the emotive power of a few e-mailed photos of your kids, and how great if feels to turn off your electronic devices and return your folding tray and seat back to the upright and locked position. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Physicians Could Be Eligible to Receive IRS Refund

Physicians Could Be Eligible to Receive IRS Refund
I heard the Internal Revenue Service is going to refund the employment taxes physicians paid when they were residents. Is this true? If so, how do I go about filing for this?
J. Byrne, MD
New YorkRe
Dr. Hospitalist responds: On March 2, the IRS announced that it had “made an administrative determination to accept the position that medical residents are excepted from FICA taxes based on the student exception for tax periods ending before April 1, 2005, when new IRS regulations went into effect.”1 For folks like me, who have a hard time understanding the different numbers on my paycheck, here is an explanation. (I am neither an attorney nor an accountant; for any such counsel, I suggest you visit a professional.)
Federal Insurance Contributions Act, or FICA, taxes are the payroll taxes collected for Medicare and Social Security programs. These taxes fund insurance programs for the elderly, disabled, survivors (Social Security), and for healthcare (Medicare). This tax originated in 1935. Employees and employers are required to make regular contributions to FICA through payroll deductions. For 2010, the FICA tax rate is 7.65% (6.2% for Social Security and 1.45% for Medicare) on gross earnings (earnings before any deductions). The individual contribution limit for the Social Security program is 6.2% of wages up to $106,800 (a $6,621.60 cap per individual). Unlike Social Security, there is no cap on contributions to the Medicare program. Individuals and employers each contribute 1.45% of wages earned (for a total of 2.9%) to fund the Medicare program.
House staff traditionally participate in this government insurance program by contributing FICA taxes. But in the 1990s, employers and individuals began filing FICA refund claims to the IRS based on the student exception (Internal Revenue Code section 3121(b)(10)). It is my understanding that this section of the IRS code exempts students from the FICA tax.
So are house staff recognized as students under the eyes of the law? In the 1998 court case State of Minnesota vs. Apfel, the court opined that University of Minnesota house staff exist for the primary purpose of education, rather than for earning a livelihood. Based on that ruling, the IRS chief counsel issued a memorandum in July 2000 that stated house staff could meet the FICA student exemption if 1) the house staff’s employer is a school, and 2) the house staffer is considered a student by the employer.
So why has it taken so long for the IRS to decide to refund these dollars? Over the past decade, there have been other court cases with conflicting interpretations of the IRS code. In January 2005, the IRS implemented new regulations that did not require house staff to contribute FICA taxes. But this new regulation did nothing about past house-staff contributions. Last year, in another Minnesota case, Mayo Foundation for Medical Education and Research vs. the United States, the court again interpreted the IRS regulations as limiting the student FICA exception to students who are not full-time employees. Despite other ongoing lawsuits, the IRS has decided that individuals who were house staff prior to April 2005 and meet the criteria are excepted from FICA taxes.
So who is eligible to receive these FICA taxes refund? It is my understanding that if you are a house officer who contributed to FICA taxes prior to April 2005, you are eligible for a refund only if you or the institution where you trained filed a claim in a timely fashion. The period of limitation for filing a claim has expired. If you think that you are covered by a claim, the IRS states that you should expect to hear from the institution where you trained about the refund process. You will not be hearing from the IRS directly.
For more information, call 800-919-1703 or visit www.irs.gov/charities and click on “Medical Resident FICA Refund.”
Is the Economy Having a Negative Effect on Hospitalist Jobs?
I will start my senior year as a medical resident in a few months. I am interested in a career as a hospitalist. While I hear that there are a lot of hospitalists out there, one of my friends has been looking for a hospitalist job in the Northeast and has had some difficulty landing a position. Is the problem the area or the economy? Is there anything I can do to make myself a more attractive candidate?
Reza Mohan, MD
Seattle
Dr. Hospitalist responds: Congratul-ations on reaching this stage in your training as a physician; this is the time you can start thinking about your career as a hospitalist. While I understand your desire to land a plum job upon completion of training, I want to encourage you to focus your efforts during your last year of training. Becoming the best doctor possible might be the best preparation to land the ideal HM job.
It is true that since 1996, when the term “hospitalist” was first coined, it has been easy to land HM jobs. The field exploded out of nowhere, and now boasts more than 30,000 hospitalists after little more than a decade. Atlanta, Boston, San Diego, Seattle … hospitalist jobs were plentiful.
While it has been good for physicians looking for jobs, I am not sure it has been ideal for patients. I would argue that the easy availability of jobs has attracted people to our profession who probably are not ideally suited to be hospitalists. From a quality perspective, wouldn’t we be better off if there were more competition for hospitalist jobs? In fact, I am hearing talk from colleagues around the country that there are a few places where it is increasingly more difficult to land a hospitalist job. Seattle and Boston are two such places.
That said, one only has to look at the job ads in the preceding pages of The Hospitalist and the SHM Career Center (www.hospitalmedicine.org/careers) to see that HM jobs are still plentiful in most parts of the country. I would not worry about not being able to land a job as a hospitalist when you finish training. However, you might not be able to find a great job in the city of your choice.
If you are interested in networking, I encourage you to speak with HM physicians at your hospital and in your community. Don’t pass up the opportunity to attend a local SHM chapter meeting or a regional conference; both are great for connecting with hospitalists and hiring managers. Another option is to sign up with an SHM e-mail listserv, so you have the opportunity to participate in online discussions with hospitalists. TH
Reference
- IRS to honor medical resident FICA refund claims. IRS Web site. Available at www.irs.gov/charities/article/ 0,,id=219548,00.html. Published March 2, 2010. Accessed April 14, 2010.
Physicians Could Be Eligible to Receive IRS Refund
I heard the Internal Revenue Service is going to refund the employment taxes physicians paid when they were residents. Is this true? If so, how do I go about filing for this?
J. Byrne, MD
New YorkRe
Dr. Hospitalist responds: On March 2, the IRS announced that it had “made an administrative determination to accept the position that medical residents are excepted from FICA taxes based on the student exception for tax periods ending before April 1, 2005, when new IRS regulations went into effect.”1 For folks like me, who have a hard time understanding the different numbers on my paycheck, here is an explanation. (I am neither an attorney nor an accountant; for any such counsel, I suggest you visit a professional.)
Federal Insurance Contributions Act, or FICA, taxes are the payroll taxes collected for Medicare and Social Security programs. These taxes fund insurance programs for the elderly, disabled, survivors (Social Security), and for healthcare (Medicare). This tax originated in 1935. Employees and employers are required to make regular contributions to FICA through payroll deductions. For 2010, the FICA tax rate is 7.65% (6.2% for Social Security and 1.45% for Medicare) on gross earnings (earnings before any deductions). The individual contribution limit for the Social Security program is 6.2% of wages up to $106,800 (a $6,621.60 cap per individual). Unlike Social Security, there is no cap on contributions to the Medicare program. Individuals and employers each contribute 1.45% of wages earned (for a total of 2.9%) to fund the Medicare program.
House staff traditionally participate in this government insurance program by contributing FICA taxes. But in the 1990s, employers and individuals began filing FICA refund claims to the IRS based on the student exception (Internal Revenue Code section 3121(b)(10)). It is my understanding that this section of the IRS code exempts students from the FICA tax.
So are house staff recognized as students under the eyes of the law? In the 1998 court case State of Minnesota vs. Apfel, the court opined that University of Minnesota house staff exist for the primary purpose of education, rather than for earning a livelihood. Based on that ruling, the IRS chief counsel issued a memorandum in July 2000 that stated house staff could meet the FICA student exemption if 1) the house staff’s employer is a school, and 2) the house staffer is considered a student by the employer.
So why has it taken so long for the IRS to decide to refund these dollars? Over the past decade, there have been other court cases with conflicting interpretations of the IRS code. In January 2005, the IRS implemented new regulations that did not require house staff to contribute FICA taxes. But this new regulation did nothing about past house-staff contributions. Last year, in another Minnesota case, Mayo Foundation for Medical Education and Research vs. the United States, the court again interpreted the IRS regulations as limiting the student FICA exception to students who are not full-time employees. Despite other ongoing lawsuits, the IRS has decided that individuals who were house staff prior to April 2005 and meet the criteria are excepted from FICA taxes.
So who is eligible to receive these FICA taxes refund? It is my understanding that if you are a house officer who contributed to FICA taxes prior to April 2005, you are eligible for a refund only if you or the institution where you trained filed a claim in a timely fashion. The period of limitation for filing a claim has expired. If you think that you are covered by a claim, the IRS states that you should expect to hear from the institution where you trained about the refund process. You will not be hearing from the IRS directly.
For more information, call 800-919-1703 or visit www.irs.gov/charities and click on “Medical Resident FICA Refund.”
Is the Economy Having a Negative Effect on Hospitalist Jobs?
I will start my senior year as a medical resident in a few months. I am interested in a career as a hospitalist. While I hear that there are a lot of hospitalists out there, one of my friends has been looking for a hospitalist job in the Northeast and has had some difficulty landing a position. Is the problem the area or the economy? Is there anything I can do to make myself a more attractive candidate?
Reza Mohan, MD
Seattle
Dr. Hospitalist responds: Congratul-ations on reaching this stage in your training as a physician; this is the time you can start thinking about your career as a hospitalist. While I understand your desire to land a plum job upon completion of training, I want to encourage you to focus your efforts during your last year of training. Becoming the best doctor possible might be the best preparation to land the ideal HM job.
It is true that since 1996, when the term “hospitalist” was first coined, it has been easy to land HM jobs. The field exploded out of nowhere, and now boasts more than 30,000 hospitalists after little more than a decade. Atlanta, Boston, San Diego, Seattle … hospitalist jobs were plentiful.
While it has been good for physicians looking for jobs, I am not sure it has been ideal for patients. I would argue that the easy availability of jobs has attracted people to our profession who probably are not ideally suited to be hospitalists. From a quality perspective, wouldn’t we be better off if there were more competition for hospitalist jobs? In fact, I am hearing talk from colleagues around the country that there are a few places where it is increasingly more difficult to land a hospitalist job. Seattle and Boston are two such places.
That said, one only has to look at the job ads in the preceding pages of The Hospitalist and the SHM Career Center (www.hospitalmedicine.org/careers) to see that HM jobs are still plentiful in most parts of the country. I would not worry about not being able to land a job as a hospitalist when you finish training. However, you might not be able to find a great job in the city of your choice.
If you are interested in networking, I encourage you to speak with HM physicians at your hospital and in your community. Don’t pass up the opportunity to attend a local SHM chapter meeting or a regional conference; both are great for connecting with hospitalists and hiring managers. Another option is to sign up with an SHM e-mail listserv, so you have the opportunity to participate in online discussions with hospitalists. TH
Reference
- IRS to honor medical resident FICA refund claims. IRS Web site. Available at www.irs.gov/charities/article/ 0,,id=219548,00.html. Published March 2, 2010. Accessed April 14, 2010.
Physicians Could Be Eligible to Receive IRS Refund
I heard the Internal Revenue Service is going to refund the employment taxes physicians paid when they were residents. Is this true? If so, how do I go about filing for this?
J. Byrne, MD
New YorkRe
Dr. Hospitalist responds: On March 2, the IRS announced that it had “made an administrative determination to accept the position that medical residents are excepted from FICA taxes based on the student exception for tax periods ending before April 1, 2005, when new IRS regulations went into effect.”1 For folks like me, who have a hard time understanding the different numbers on my paycheck, here is an explanation. (I am neither an attorney nor an accountant; for any such counsel, I suggest you visit a professional.)
Federal Insurance Contributions Act, or FICA, taxes are the payroll taxes collected for Medicare and Social Security programs. These taxes fund insurance programs for the elderly, disabled, survivors (Social Security), and for healthcare (Medicare). This tax originated in 1935. Employees and employers are required to make regular contributions to FICA through payroll deductions. For 2010, the FICA tax rate is 7.65% (6.2% for Social Security and 1.45% for Medicare) on gross earnings (earnings before any deductions). The individual contribution limit for the Social Security program is 6.2% of wages up to $106,800 (a $6,621.60 cap per individual). Unlike Social Security, there is no cap on contributions to the Medicare program. Individuals and employers each contribute 1.45% of wages earned (for a total of 2.9%) to fund the Medicare program.
House staff traditionally participate in this government insurance program by contributing FICA taxes. But in the 1990s, employers and individuals began filing FICA refund claims to the IRS based on the student exception (Internal Revenue Code section 3121(b)(10)). It is my understanding that this section of the IRS code exempts students from the FICA tax.
So are house staff recognized as students under the eyes of the law? In the 1998 court case State of Minnesota vs. Apfel, the court opined that University of Minnesota house staff exist for the primary purpose of education, rather than for earning a livelihood. Based on that ruling, the IRS chief counsel issued a memorandum in July 2000 that stated house staff could meet the FICA student exemption if 1) the house staff’s employer is a school, and 2) the house staffer is considered a student by the employer.
So why has it taken so long for the IRS to decide to refund these dollars? Over the past decade, there have been other court cases with conflicting interpretations of the IRS code. In January 2005, the IRS implemented new regulations that did not require house staff to contribute FICA taxes. But this new regulation did nothing about past house-staff contributions. Last year, in another Minnesota case, Mayo Foundation for Medical Education and Research vs. the United States, the court again interpreted the IRS regulations as limiting the student FICA exception to students who are not full-time employees. Despite other ongoing lawsuits, the IRS has decided that individuals who were house staff prior to April 2005 and meet the criteria are excepted from FICA taxes.
So who is eligible to receive these FICA taxes refund? It is my understanding that if you are a house officer who contributed to FICA taxes prior to April 2005, you are eligible for a refund only if you or the institution where you trained filed a claim in a timely fashion. The period of limitation for filing a claim has expired. If you think that you are covered by a claim, the IRS states that you should expect to hear from the institution where you trained about the refund process. You will not be hearing from the IRS directly.
For more information, call 800-919-1703 or visit www.irs.gov/charities and click on “Medical Resident FICA Refund.”
Is the Economy Having a Negative Effect on Hospitalist Jobs?
I will start my senior year as a medical resident in a few months. I am interested in a career as a hospitalist. While I hear that there are a lot of hospitalists out there, one of my friends has been looking for a hospitalist job in the Northeast and has had some difficulty landing a position. Is the problem the area or the economy? Is there anything I can do to make myself a more attractive candidate?
Reza Mohan, MD
Seattle
Dr. Hospitalist responds: Congratul-ations on reaching this stage in your training as a physician; this is the time you can start thinking about your career as a hospitalist. While I understand your desire to land a plum job upon completion of training, I want to encourage you to focus your efforts during your last year of training. Becoming the best doctor possible might be the best preparation to land the ideal HM job.
It is true that since 1996, when the term “hospitalist” was first coined, it has been easy to land HM jobs. The field exploded out of nowhere, and now boasts more than 30,000 hospitalists after little more than a decade. Atlanta, Boston, San Diego, Seattle … hospitalist jobs were plentiful.
While it has been good for physicians looking for jobs, I am not sure it has been ideal for patients. I would argue that the easy availability of jobs has attracted people to our profession who probably are not ideally suited to be hospitalists. From a quality perspective, wouldn’t we be better off if there were more competition for hospitalist jobs? In fact, I am hearing talk from colleagues around the country that there are a few places where it is increasingly more difficult to land a hospitalist job. Seattle and Boston are two such places.
That said, one only has to look at the job ads in the preceding pages of The Hospitalist and the SHM Career Center (www.hospitalmedicine.org/careers) to see that HM jobs are still plentiful in most parts of the country. I would not worry about not being able to land a job as a hospitalist when you finish training. However, you might not be able to find a great job in the city of your choice.
If you are interested in networking, I encourage you to speak with HM physicians at your hospital and in your community. Don’t pass up the opportunity to attend a local SHM chapter meeting or a regional conference; both are great for connecting with hospitalists and hiring managers. Another option is to sign up with an SHM e-mail listserv, so you have the opportunity to participate in online discussions with hospitalists. TH
Reference
- IRS to honor medical resident FICA refund claims. IRS Web site. Available at www.irs.gov/charities/article/ 0,,id=219548,00.html. Published March 2, 2010. Accessed April 14, 2010.