User login
The Hospitalist only
Hospitalists Should Refrain from Texting Patient Information

Refrain from Texting about Your Patients
Can I text my partners patient information?
–Stephen Henry, San Luis Obispo, Calif.
Dr. Hospitalist responds:
Can you? Sure. Do you? Probably. Should you? No.
Texting any patient information falls under the category of ePHI (Electronic Protected Health Information) as part of HIPAA. Technically, such patient-specific information must be protected at all times. Once you send a text, at least three copies are known to exist: one on each of the devices, plus one copy on the network it went through, adding for each network it has to cross. Sure, your phone may be password-protected, but is your partner’s? What about the carrier? How protected is their data?
HIPAA goes into excruciating technical detail about all the safeguards that must be present. You are more than welcome to read it (www.hhs.gov/ocr/privacy/hipaa/administrative/securityrule) to see if you meet all the standards. Or you can take my word for it: You don’t.
So you can see why most health organizations expressly prohibit the texting of patient information. If you rang up your local health-care or hospital lawyer, I’m sure they would tell you to never text patient information. Is that reasonable advice? In 2013, I doubt it.
So what’s the practical advice to follow? For starters, password-protect your phone, if you haven’t already. Nothing worse than losing your phone and having patient information on it. A lot of the OCR (Office for Civil Rights, a branch of Health and Human Services) fines for HIPAA violations stem from folks misplacing unencrypted devices with patient information on them.
Just as important, don’t text anything that you wouldn’t want to see blown up on a lawyer’s display board in court. I’ve seen some really egregious examples of communication between doctors that have no business being preserved electronically. Texting “Mr. X in Room 2101 is a meth-using, narcotic-seeking, half-naked, lunatic troll” is an absolutely stupid thing to do. For that matter, so are remarks that seem less offensive: “And his son is completely unreasonable.” Save your commentary and stick to the facts, because you just generated three copies forever.
If you receive an insensitive text, don’t reply. Simply call the sending physician to discuss any issues. Even being on a “secure” texting network won’t protect you from errors of commission.
If I were to text about a patient (purely hypothetically, mind you), I would limit the information as much as possible. Keep it simple and generic (what HIPAA likes to call “de-identified information”)—for example, “Room 428 is ready for discharge.”
Please, hold the subjective commentary. There is no good reason to have an extended text exchange about a patient; you are creating an electronic trail that has no good reason to exist and never really goes away. It’s just the same as writing in the chart, except that it has the illusion of privacy. And that’s all it is: an illusion.
At the end of the day, I’d probably worry more about the discoverable aspect of your text messages in a lawsuit than the possibility of a HIPAA fine, but neither one sounds like much fun to me.
Refrain from Texting about Your Patients
Can I text my partners patient information?
–Stephen Henry, San Luis Obispo, Calif.
Dr. Hospitalist responds:
Can you? Sure. Do you? Probably. Should you? No.
Texting any patient information falls under the category of ePHI (Electronic Protected Health Information) as part of HIPAA. Technically, such patient-specific information must be protected at all times. Once you send a text, at least three copies are known to exist: one on each of the devices, plus one copy on the network it went through, adding for each network it has to cross. Sure, your phone may be password-protected, but is your partner’s? What about the carrier? How protected is their data?
HIPAA goes into excruciating technical detail about all the safeguards that must be present. You are more than welcome to read it (www.hhs.gov/ocr/privacy/hipaa/administrative/securityrule) to see if you meet all the standards. Or you can take my word for it: You don’t.
So you can see why most health organizations expressly prohibit the texting of patient information. If you rang up your local health-care or hospital lawyer, I’m sure they would tell you to never text patient information. Is that reasonable advice? In 2013, I doubt it.
So what’s the practical advice to follow? For starters, password-protect your phone, if you haven’t already. Nothing worse than losing your phone and having patient information on it. A lot of the OCR (Office for Civil Rights, a branch of Health and Human Services) fines for HIPAA violations stem from folks misplacing unencrypted devices with patient information on them.
Just as important, don’t text anything that you wouldn’t want to see blown up on a lawyer’s display board in court. I’ve seen some really egregious examples of communication between doctors that have no business being preserved electronically. Texting “Mr. X in Room 2101 is a meth-using, narcotic-seeking, half-naked, lunatic troll” is an absolutely stupid thing to do. For that matter, so are remarks that seem less offensive: “And his son is completely unreasonable.” Save your commentary and stick to the facts, because you just generated three copies forever.
If you receive an insensitive text, don’t reply. Simply call the sending physician to discuss any issues. Even being on a “secure” texting network won’t protect you from errors of commission.
If I were to text about a patient (purely hypothetically, mind you), I would limit the information as much as possible. Keep it simple and generic (what HIPAA likes to call “de-identified information”)—for example, “Room 428 is ready for discharge.”
Please, hold the subjective commentary. There is no good reason to have an extended text exchange about a patient; you are creating an electronic trail that has no good reason to exist and never really goes away. It’s just the same as writing in the chart, except that it has the illusion of privacy. And that’s all it is: an illusion.
At the end of the day, I’d probably worry more about the discoverable aspect of your text messages in a lawsuit than the possibility of a HIPAA fine, but neither one sounds like much fun to me.
Refrain from Texting about Your Patients
Can I text my partners patient information?
–Stephen Henry, San Luis Obispo, Calif.
Dr. Hospitalist responds:
Can you? Sure. Do you? Probably. Should you? No.
Texting any patient information falls under the category of ePHI (Electronic Protected Health Information) as part of HIPAA. Technically, such patient-specific information must be protected at all times. Once you send a text, at least three copies are known to exist: one on each of the devices, plus one copy on the network it went through, adding for each network it has to cross. Sure, your phone may be password-protected, but is your partner’s? What about the carrier? How protected is their data?
HIPAA goes into excruciating technical detail about all the safeguards that must be present. You are more than welcome to read it (www.hhs.gov/ocr/privacy/hipaa/administrative/securityrule) to see if you meet all the standards. Or you can take my word for it: You don’t.
So you can see why most health organizations expressly prohibit the texting of patient information. If you rang up your local health-care or hospital lawyer, I’m sure they would tell you to never text patient information. Is that reasonable advice? In 2013, I doubt it.
So what’s the practical advice to follow? For starters, password-protect your phone, if you haven’t already. Nothing worse than losing your phone and having patient information on it. A lot of the OCR (Office for Civil Rights, a branch of Health and Human Services) fines for HIPAA violations stem from folks misplacing unencrypted devices with patient information on them.
Just as important, don’t text anything that you wouldn’t want to see blown up on a lawyer’s display board in court. I’ve seen some really egregious examples of communication between doctors that have no business being preserved electronically. Texting “Mr. X in Room 2101 is a meth-using, narcotic-seeking, half-naked, lunatic troll” is an absolutely stupid thing to do. For that matter, so are remarks that seem less offensive: “And his son is completely unreasonable.” Save your commentary and stick to the facts, because you just generated three copies forever.
If you receive an insensitive text, don’t reply. Simply call the sending physician to discuss any issues. Even being on a “secure” texting network won’t protect you from errors of commission.
If I were to text about a patient (purely hypothetically, mind you), I would limit the information as much as possible. Keep it simple and generic (what HIPAA likes to call “de-identified information”)—for example, “Room 428 is ready for discharge.”
Please, hold the subjective commentary. There is no good reason to have an extended text exchange about a patient; you are creating an electronic trail that has no good reason to exist and never really goes away. It’s just the same as writing in the chart, except that it has the illusion of privacy. And that’s all it is: an illusion.
At the end of the day, I’d probably worry more about the discoverable aspect of your text messages in a lawsuit than the possibility of a HIPAA fine, but neither one sounds like much fun to me.
Work-Hour Restrictions Impact Staffing, Education for Academic Hospital Medicine
Source: 2012 State of Hospital Medicine report


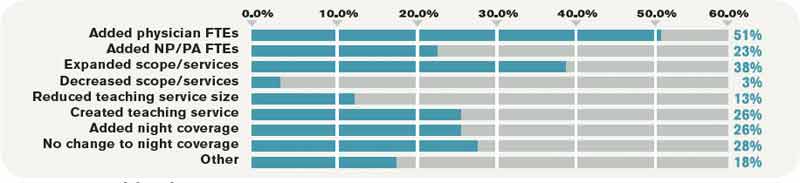
In July 2011, the Accreditation Council for Graduate Medical Education (ACGME) implemented new duty-hour restrictions on resident physicians. Among other changes, interns were restricted to a maximum of 16 hours of continuous duty. New rules also limited second-year residents and above to 24 hours of continuous duty, plus up to four additional hours for transition and educational activities. Recommendations were made for strategic napping, greater supervision requirements, and a minimum of eight to 10 hours off between shifts.
The 2012 State of Hospital Medicine report, which is based on 2011 data encompassing the period of these duty-hour changes, takes a systematic look at how academic HM practices have adjusted to the new resident rules. The most notable changes have been the addition of physician FTEs (51.3% of adult academic HM practices have done so) and nurse practitioners or physician assistants (23%). Additional common responses to resident work-hour limitations are listed in Table 1.
Source: 2012 State of Hospital Medicine report
These data underscore the immensity of changes academic HM groups have faced as a result of new work-hour limitations, as the majority of internal-medicine residents work with hospitalist attendings on inpatient medicine rotations. House staff no longer can be used as an inexpensive source of labor, given limitations on service and new expectations for resident education and supervision.
As others have commented on this topic in The Hospitalist, the role of the academic hospitalist is being redefined. No longer is academic HM synonymous with teaching alone; the clinical duties of many academic hospitalists now include a combination of teaching and non-teaching services, often with some night coverage. At our hospitals in San Diego and Boston, for instance, changes incurred due to work-hour restrictions include elimination of house staff coverage from one of the medical center’s hospitals and a significant increase in nonteaching service responsibilities across all hospitalists. An alternative approach that some programs have embraced is the recruitment of separate cadres of teaching and nonteaching hospitalists, which might result in markedly different professional expectations within the same group or institution.
Trends shifting clinical work from residents to hospitalists are likely to continue, no doubt increasing demand for hospitalists and physician extenders. In the past, the combination of less expensive resident labor and lower salaries in academia was financially favorable for hospitals. Due to resident duty-hour limitations, academic hospitalist groups have had to negotiate not only for additional hires, but, in many instances, also higher salaries commensurate with nonteaching work.
Given the impact on a hospital’s finances, academic HM practices have had to look more closely at clinical volumes and productivity, making protected time for nonclinical pursuits more difficult to come by. Alignment of hospitalists’ interests with those of hospital administrators through performance-improvement projects (e.g. reducing length of stay, readmissions, or nosocomial infections) will be crucial to the financial viability of the academic HM practice, and leadership in these areas will define and differentiate academic hospitalists in the future.
Dr. Bryan Huang, who works in Boston, and Dr. Grace Huang, who works in San Diego, both are members of SHM’s Practice Analysis Committee.
Source: 2012 State of Hospital Medicine report
In July 2011, the Accreditation Council for Graduate Medical Education (ACGME) implemented new duty-hour restrictions on resident physicians. Among other changes, interns were restricted to a maximum of 16 hours of continuous duty. New rules also limited second-year residents and above to 24 hours of continuous duty, plus up to four additional hours for transition and educational activities. Recommendations were made for strategic napping, greater supervision requirements, and a minimum of eight to 10 hours off between shifts.
The 2012 State of Hospital Medicine report, which is based on 2011 data encompassing the period of these duty-hour changes, takes a systematic look at how academic HM practices have adjusted to the new resident rules. The most notable changes have been the addition of physician FTEs (51.3% of adult academic HM practices have done so) and nurse practitioners or physician assistants (23%). Additional common responses to resident work-hour limitations are listed in Table 1.
Source: 2012 State of Hospital Medicine report
These data underscore the immensity of changes academic HM groups have faced as a result of new work-hour limitations, as the majority of internal-medicine residents work with hospitalist attendings on inpatient medicine rotations. House staff no longer can be used as an inexpensive source of labor, given limitations on service and new expectations for resident education and supervision.
As others have commented on this topic in The Hospitalist, the role of the academic hospitalist is being redefined. No longer is academic HM synonymous with teaching alone; the clinical duties of many academic hospitalists now include a combination of teaching and non-teaching services, often with some night coverage. At our hospitals in San Diego and Boston, for instance, changes incurred due to work-hour restrictions include elimination of house staff coverage from one of the medical center’s hospitals and a significant increase in nonteaching service responsibilities across all hospitalists. An alternative approach that some programs have embraced is the recruitment of separate cadres of teaching and nonteaching hospitalists, which might result in markedly different professional expectations within the same group or institution.
Trends shifting clinical work from residents to hospitalists are likely to continue, no doubt increasing demand for hospitalists and physician extenders. In the past, the combination of less expensive resident labor and lower salaries in academia was financially favorable for hospitals. Due to resident duty-hour limitations, academic hospitalist groups have had to negotiate not only for additional hires, but, in many instances, also higher salaries commensurate with nonteaching work.
Given the impact on a hospital’s finances, academic HM practices have had to look more closely at clinical volumes and productivity, making protected time for nonclinical pursuits more difficult to come by. Alignment of hospitalists’ interests with those of hospital administrators through performance-improvement projects (e.g. reducing length of stay, readmissions, or nosocomial infections) will be crucial to the financial viability of the academic HM practice, and leadership in these areas will define and differentiate academic hospitalists in the future.
Dr. Bryan Huang, who works in Boston, and Dr. Grace Huang, who works in San Diego, both are members of SHM’s Practice Analysis Committee.
Source: 2012 State of Hospital Medicine report
In July 2011, the Accreditation Council for Graduate Medical Education (ACGME) implemented new duty-hour restrictions on resident physicians. Among other changes, interns were restricted to a maximum of 16 hours of continuous duty. New rules also limited second-year residents and above to 24 hours of continuous duty, plus up to four additional hours for transition and educational activities. Recommendations were made for strategic napping, greater supervision requirements, and a minimum of eight to 10 hours off between shifts.
The 2012 State of Hospital Medicine report, which is based on 2011 data encompassing the period of these duty-hour changes, takes a systematic look at how academic HM practices have adjusted to the new resident rules. The most notable changes have been the addition of physician FTEs (51.3% of adult academic HM practices have done so) and nurse practitioners or physician assistants (23%). Additional common responses to resident work-hour limitations are listed in Table 1.
Source: 2012 State of Hospital Medicine report
These data underscore the immensity of changes academic HM groups have faced as a result of new work-hour limitations, as the majority of internal-medicine residents work with hospitalist attendings on inpatient medicine rotations. House staff no longer can be used as an inexpensive source of labor, given limitations on service and new expectations for resident education and supervision.
As others have commented on this topic in The Hospitalist, the role of the academic hospitalist is being redefined. No longer is academic HM synonymous with teaching alone; the clinical duties of many academic hospitalists now include a combination of teaching and non-teaching services, often with some night coverage. At our hospitals in San Diego and Boston, for instance, changes incurred due to work-hour restrictions include elimination of house staff coverage from one of the medical center’s hospitals and a significant increase in nonteaching service responsibilities across all hospitalists. An alternative approach that some programs have embraced is the recruitment of separate cadres of teaching and nonteaching hospitalists, which might result in markedly different professional expectations within the same group or institution.
Trends shifting clinical work from residents to hospitalists are likely to continue, no doubt increasing demand for hospitalists and physician extenders. In the past, the combination of less expensive resident labor and lower salaries in academia was financially favorable for hospitals. Due to resident duty-hour limitations, academic hospitalist groups have had to negotiate not only for additional hires, but, in many instances, also higher salaries commensurate with nonteaching work.
Given the impact on a hospital’s finances, academic HM practices have had to look more closely at clinical volumes and productivity, making protected time for nonclinical pursuits more difficult to come by. Alignment of hospitalists’ interests with those of hospital administrators through performance-improvement projects (e.g. reducing length of stay, readmissions, or nosocomial infections) will be crucial to the financial viability of the academic HM practice, and leadership in these areas will define and differentiate academic hospitalists in the future.
Dr. Bryan Huang, who works in Boston, and Dr. Grace Huang, who works in San Diego, both are members of SHM’s Practice Analysis Committee.
SHM To Award First Certificates of Leadership at HM13
This month, Thomas McIlraith, MD, SFHM, will be on stage at HM13 accepting one of the first SHM Certificates in Leadership. As chair of hospital medicine at Sacramento, Calif.-based Mercy Medical Group, Dr. McIlraith already is familiar with the need for leadership in our specialty and shares why SHM’s Leadership Academy and new certification have helped his hospital and his career.
Question: What made you apply for the Certificate in Leadership in the first place?
Answer: I have always felt that a young field like hospital medicine needs to have resources to develop leadership; I don’t think there is another place in the field of medicine that has more shared responsibility requiring coordinated response than hospital medicine.
I have always been impressed and grateful that SHM recognized this and put forth the considerable effort required to create and develop the Leadership Academies into the premiere institution that they have evolved into. That is why I not only got involved in the leadership academies personally, but also had my entire leadership team complete the curriculum.
Certification is the culmination of that experience for me; I am hoping it is not the end, however. I have had other leadership training course work, and while the SHM Leadership Academies and the certification process were the best experience, I have learned that you can never have too much leadership training.
There are always new challenges a leader will be called on to face, and leadership skills need to continually grow.
Q: What’s been the biggest impact on your career so far? How do you plan on using it in the future?
A: It is not enough to be successful; you have to be able to tell the story of your success. Most of us want to be humble and focus on serving our patients, but the tree that falls in the woods is applicable to successful hospital medicine programs: If nobody hears about it, are you really successful? Can you really drive change?
Lenny Marcus put it best in his SHM Leadership Academy session on meta-leadership: Learning how to communicate to your boss is leading up; communicating across the silos of your organization is meta-leadership. The academies teach you about the skills you need for leadership; certification allows you to put those skills into action.
I vividly remember the day that academy instructor Eric Rice called me up to give me feedback on the first draft of my project. I was already stressed out because in four days I knew I had to give a critical presentation to top hospital leadership and health plan medical directors about our group. We had two new hospital presidents and a new service area senior vice president that had already terminated their contract with the ED group that covered three of the four hospitals. I knew they were scrutinizing my group; the pressure was on.
Eric gave the feedback that I had been focusing on the clinical aspects of my project and said I needed to tell the economic story—to measure the economic impact of my intervention. Further, he advised me on how to get the data to tell that story. I knew that he had just given me the material I needed to blow away the upcoming presentation to the hospital presidents, but would I get the data in time? I called up the CFO of the hospital as Eric advised, told him that I needed the data for a presentation I was giving to his boss in four days.
I got the data in time and blew away the presentation. I got to inform one of the new presidents that we had improved the contribution margin in his ICU by half a million dollars and cut length of stay by 0.9 days, while dramatically improving sepsis mortality. I was then able to go on and tell the HM leaders of our entire hospital system about our intervention and encouraged them to take similar steps.
Someday I hope I get the chance to tell Lenny Marcus this story; I hope he will consider me a meta-leader.
After the dust settled from those successes, I went back to my computer to write up the final draft of my project and I was able to tell a much better story than I ever could have without that advice Eric Rice and the committee [gave me].
My new boss was at the presentation that I gave. We went to the American Medical Group Association conference recently, and he did not hesitate to walk around bragging about what we had done, often quoting the numbers I delivered in my presentation. In another coda to the story, the new service area senior vice president asked my wife and I to join him and his wife for dinner; we have struck up a very valuable friendship.
—Thomas McIlraith, MD, SFHM
Q: What would you say to others who are thinking about applying for the certificate?
A: What are you waiting for?
On a more serious note, we are all engaged with important projects to make our hospitals run better, to keep our patients safer, and give our patients better experience. In the certification process, you continue with that work while top leaders from the field of hospital medicine coach and advise you.
Not only do you come out with a better product in the short term, but also you have better skills for taking on projects in the future; you know what questions to ask and what stories to tell and to whom. That stays with you long after the certification project is over.
Q: How are the results of your project benefiting your institution?
A: My hospitalists are seeing increased productivity and my hospitals are seeing stronger contribution margin in tough economic times. Further, the successful completion of the project has elevated the reputation of my department.
This month, Thomas McIlraith, MD, SFHM, will be on stage at HM13 accepting one of the first SHM Certificates in Leadership. As chair of hospital medicine at Sacramento, Calif.-based Mercy Medical Group, Dr. McIlraith already is familiar with the need for leadership in our specialty and shares why SHM’s Leadership Academy and new certification have helped his hospital and his career.
Question: What made you apply for the Certificate in Leadership in the first place?
Answer: I have always felt that a young field like hospital medicine needs to have resources to develop leadership; I don’t think there is another place in the field of medicine that has more shared responsibility requiring coordinated response than hospital medicine.
I have always been impressed and grateful that SHM recognized this and put forth the considerable effort required to create and develop the Leadership Academies into the premiere institution that they have evolved into. That is why I not only got involved in the leadership academies personally, but also had my entire leadership team complete the curriculum.
Certification is the culmination of that experience for me; I am hoping it is not the end, however. I have had other leadership training course work, and while the SHM Leadership Academies and the certification process were the best experience, I have learned that you can never have too much leadership training.
There are always new challenges a leader will be called on to face, and leadership skills need to continually grow.
Q: What’s been the biggest impact on your career so far? How do you plan on using it in the future?
A: It is not enough to be successful; you have to be able to tell the story of your success. Most of us want to be humble and focus on serving our patients, but the tree that falls in the woods is applicable to successful hospital medicine programs: If nobody hears about it, are you really successful? Can you really drive change?
Lenny Marcus put it best in his SHM Leadership Academy session on meta-leadership: Learning how to communicate to your boss is leading up; communicating across the silos of your organization is meta-leadership. The academies teach you about the skills you need for leadership; certification allows you to put those skills into action.
I vividly remember the day that academy instructor Eric Rice called me up to give me feedback on the first draft of my project. I was already stressed out because in four days I knew I had to give a critical presentation to top hospital leadership and health plan medical directors about our group. We had two new hospital presidents and a new service area senior vice president that had already terminated their contract with the ED group that covered three of the four hospitals. I knew they were scrutinizing my group; the pressure was on.
Eric gave the feedback that I had been focusing on the clinical aspects of my project and said I needed to tell the economic story—to measure the economic impact of my intervention. Further, he advised me on how to get the data to tell that story. I knew that he had just given me the material I needed to blow away the upcoming presentation to the hospital presidents, but would I get the data in time? I called up the CFO of the hospital as Eric advised, told him that I needed the data for a presentation I was giving to his boss in four days.
I got the data in time and blew away the presentation. I got to inform one of the new presidents that we had improved the contribution margin in his ICU by half a million dollars and cut length of stay by 0.9 days, while dramatically improving sepsis mortality. I was then able to go on and tell the HM leaders of our entire hospital system about our intervention and encouraged them to take similar steps.
Someday I hope I get the chance to tell Lenny Marcus this story; I hope he will consider me a meta-leader.
After the dust settled from those successes, I went back to my computer to write up the final draft of my project and I was able to tell a much better story than I ever could have without that advice Eric Rice and the committee [gave me].
My new boss was at the presentation that I gave. We went to the American Medical Group Association conference recently, and he did not hesitate to walk around bragging about what we had done, often quoting the numbers I delivered in my presentation. In another coda to the story, the new service area senior vice president asked my wife and I to join him and his wife for dinner; we have struck up a very valuable friendship.
—Thomas McIlraith, MD, SFHM
Q: What would you say to others who are thinking about applying for the certificate?
A: What are you waiting for?
On a more serious note, we are all engaged with important projects to make our hospitals run better, to keep our patients safer, and give our patients better experience. In the certification process, you continue with that work while top leaders from the field of hospital medicine coach and advise you.
Not only do you come out with a better product in the short term, but also you have better skills for taking on projects in the future; you know what questions to ask and what stories to tell and to whom. That stays with you long after the certification project is over.
Q: How are the results of your project benefiting your institution?
A: My hospitalists are seeing increased productivity and my hospitals are seeing stronger contribution margin in tough economic times. Further, the successful completion of the project has elevated the reputation of my department.
This month, Thomas McIlraith, MD, SFHM, will be on stage at HM13 accepting one of the first SHM Certificates in Leadership. As chair of hospital medicine at Sacramento, Calif.-based Mercy Medical Group, Dr. McIlraith already is familiar with the need for leadership in our specialty and shares why SHM’s Leadership Academy and new certification have helped his hospital and his career.
Question: What made you apply for the Certificate in Leadership in the first place?
Answer: I have always felt that a young field like hospital medicine needs to have resources to develop leadership; I don’t think there is another place in the field of medicine that has more shared responsibility requiring coordinated response than hospital medicine.
I have always been impressed and grateful that SHM recognized this and put forth the considerable effort required to create and develop the Leadership Academies into the premiere institution that they have evolved into. That is why I not only got involved in the leadership academies personally, but also had my entire leadership team complete the curriculum.
Certification is the culmination of that experience for me; I am hoping it is not the end, however. I have had other leadership training course work, and while the SHM Leadership Academies and the certification process were the best experience, I have learned that you can never have too much leadership training.
There are always new challenges a leader will be called on to face, and leadership skills need to continually grow.
Q: What’s been the biggest impact on your career so far? How do you plan on using it in the future?
A: It is not enough to be successful; you have to be able to tell the story of your success. Most of us want to be humble and focus on serving our patients, but the tree that falls in the woods is applicable to successful hospital medicine programs: If nobody hears about it, are you really successful? Can you really drive change?
Lenny Marcus put it best in his SHM Leadership Academy session on meta-leadership: Learning how to communicate to your boss is leading up; communicating across the silos of your organization is meta-leadership. The academies teach you about the skills you need for leadership; certification allows you to put those skills into action.
I vividly remember the day that academy instructor Eric Rice called me up to give me feedback on the first draft of my project. I was already stressed out because in four days I knew I had to give a critical presentation to top hospital leadership and health plan medical directors about our group. We had two new hospital presidents and a new service area senior vice president that had already terminated their contract with the ED group that covered three of the four hospitals. I knew they were scrutinizing my group; the pressure was on.
Eric gave the feedback that I had been focusing on the clinical aspects of my project and said I needed to tell the economic story—to measure the economic impact of my intervention. Further, he advised me on how to get the data to tell that story. I knew that he had just given me the material I needed to blow away the upcoming presentation to the hospital presidents, but would I get the data in time? I called up the CFO of the hospital as Eric advised, told him that I needed the data for a presentation I was giving to his boss in four days.
I got the data in time and blew away the presentation. I got to inform one of the new presidents that we had improved the contribution margin in his ICU by half a million dollars and cut length of stay by 0.9 days, while dramatically improving sepsis mortality. I was then able to go on and tell the HM leaders of our entire hospital system about our intervention and encouraged them to take similar steps.
Someday I hope I get the chance to tell Lenny Marcus this story; I hope he will consider me a meta-leader.
After the dust settled from those successes, I went back to my computer to write up the final draft of my project and I was able to tell a much better story than I ever could have without that advice Eric Rice and the committee [gave me].
My new boss was at the presentation that I gave. We went to the American Medical Group Association conference recently, and he did not hesitate to walk around bragging about what we had done, often quoting the numbers I delivered in my presentation. In another coda to the story, the new service area senior vice president asked my wife and I to join him and his wife for dinner; we have struck up a very valuable friendship.
—Thomas McIlraith, MD, SFHM
Q: What would you say to others who are thinking about applying for the certificate?
A: What are you waiting for?
On a more serious note, we are all engaged with important projects to make our hospitals run better, to keep our patients safer, and give our patients better experience. In the certification process, you continue with that work while top leaders from the field of hospital medicine coach and advise you.
Not only do you come out with a better product in the short term, but also you have better skills for taking on projects in the future; you know what questions to ask and what stories to tell and to whom. That stays with you long after the certification project is over.
Q: How are the results of your project benefiting your institution?
A: My hospitalists are seeing increased productivity and my hospitals are seeing stronger contribution margin in tough economic times. Further, the successful completion of the project has elevated the reputation of my department.
SHM Welcomes Nonphysician Fellows to Hospital Medicine
This year marks the first in which nonphysicians will be inducted as Fellows and senior Fellows in Hospital Medicine. SHM welcomes those nurse practitioners, physician assistants, and practice administrators who practice as hospitalists to the growing ranks of individuals committing their time and talent to the specialty.
NonPhysician SHM Fellows 2013
PRACTICE ADMINISTRATORS
- Kim Dickinson, SFHM
- Leslie L. Flores, MHA, SFHM
- Vicky-Lynne Gloger, MS, SFHM
- Roberta P. Himebaugh, MBA, SFHM
- Ajay Kharbanda, MBA, CMPE, SFHM
- Dave K. Dookeeram, MPH, FACHE, FHM
- Bradley J. Eshbaugh, MBA, FACMPE, FHM
- Lara Hauslaib, MPH, FHM
- Holly A. Hammond, MBA, FHM
NURSE PRACTITIONERS & PHYSICIAN ASSISTANTS
- Lorraine L. Britting, ANP, SFHM
- Jeanette Ann Kalupa, DNP, SFHM
- Mikkii Swanson, DNP, MSN, RN, SFHM
- Deborah Haywood, RN, MBA, FHM
- Julie Lepzinski, RN, BSN, MBA, FHM
- James W. Levy, PA-C, FHM
- Susan Willis, PhD, PA-C, FHM
This year marks the first in which nonphysicians will be inducted as Fellows and senior Fellows in Hospital Medicine. SHM welcomes those nurse practitioners, physician assistants, and practice administrators who practice as hospitalists to the growing ranks of individuals committing their time and talent to the specialty.
NonPhysician SHM Fellows 2013
PRACTICE ADMINISTRATORS
- Kim Dickinson, SFHM
- Leslie L. Flores, MHA, SFHM
- Vicky-Lynne Gloger, MS, SFHM
- Roberta P. Himebaugh, MBA, SFHM
- Ajay Kharbanda, MBA, CMPE, SFHM
- Dave K. Dookeeram, MPH, FACHE, FHM
- Bradley J. Eshbaugh, MBA, FACMPE, FHM
- Lara Hauslaib, MPH, FHM
- Holly A. Hammond, MBA, FHM
NURSE PRACTITIONERS & PHYSICIAN ASSISTANTS
- Lorraine L. Britting, ANP, SFHM
- Jeanette Ann Kalupa, DNP, SFHM
- Mikkii Swanson, DNP, MSN, RN, SFHM
- Deborah Haywood, RN, MBA, FHM
- Julie Lepzinski, RN, BSN, MBA, FHM
- James W. Levy, PA-C, FHM
- Susan Willis, PhD, PA-C, FHM
This year marks the first in which nonphysicians will be inducted as Fellows and senior Fellows in Hospital Medicine. SHM welcomes those nurse practitioners, physician assistants, and practice administrators who practice as hospitalists to the growing ranks of individuals committing their time and talent to the specialty.
NonPhysician SHM Fellows 2013
PRACTICE ADMINISTRATORS
- Kim Dickinson, SFHM
- Leslie L. Flores, MHA, SFHM
- Vicky-Lynne Gloger, MS, SFHM
- Roberta P. Himebaugh, MBA, SFHM
- Ajay Kharbanda, MBA, CMPE, SFHM
- Dave K. Dookeeram, MPH, FACHE, FHM
- Bradley J. Eshbaugh, MBA, FACMPE, FHM
- Lara Hauslaib, MPH, FHM
- Holly A. Hammond, MBA, FHM
NURSE PRACTITIONERS & PHYSICIAN ASSISTANTS
- Lorraine L. Britting, ANP, SFHM
- Jeanette Ann Kalupa, DNP, SFHM
- Mikkii Swanson, DNP, MSN, RN, SFHM
- Deborah Haywood, RN, MBA, FHM
- Julie Lepzinski, RN, BSN, MBA, FHM
- James W. Levy, PA-C, FHM
- Susan Willis, PhD, PA-C, FHM
Sunshine Rule Requires Physicians to Report Gifts from Drug, Medical Device Companies


—Joshua Lenchus, DO, RPh, FACP, SFHM
Hospitalist leaders are taking a wait-and-see approach to the Physician Payment Sunshine Act, which requires reporting of payments and gifts from drug and medical device companies. But as wary as many are after publication of the Final Rule 1 in February, SHM and other groups already have claimed at least one victory in tweaking the new rules.
The Sunshine Rule, as it’s known, was included in the Affordable Care Act of 2010. The rule, created by the Centers for Medicaid & Medicare Services (CMS), requires manufacturers to publicly report gifts, payments, or other transfers of value to physicians from pharmaceutical and medical device manufacturers worth more than $10 (see “Dos and Don’ts,” below).1
One major change to the law sought by SHM and others was tied to the reporting of indirect payments to speakers at accredited continuing medical education (CME) classes or courses. The proposed rule required reporting of those payments even if a particular industry group did not select the speakers or pay them. SHM and three dozen other societies lobbied CMS to change the rule.2 The final rule says indirect payments don’t have to be reported if the CME program meets widely accepted accreditation standards and the industry participant is neither directly paid nor selected by the vendor.
CME Coalition, a Washington, D.C.-based advocacy group, said in a statement the caveat recognizes that CMS “is sending a strong message to commercial supporters: Underwriting accredited continuing education programs for health-care providers is to be applauded, not restricted.”
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, FACP, SFHM, said the initial rule was too restrictive and could have reduced physician participation in important CME activities. He said the Accreditation Council for Continuing Medical Education (ACCME) and other industry groups already govern the ethical issue of accepting direct payments that could imply bias to patients.
“I’m not so sure we needed the Sunshine Act as part of the ACA at all because these same things were in effect from the ACCME and other CME accrediting organizations,” said Dr. Lenchus, a Team Hospitalist member and president of the medical staff at Jackson Health System in Miami. “What this has done is impose additional administrative requirements that now take time away from our seeing patients or doing clinical activity.”
Those costs will add up quickly, according to figures from the Federal Register, Dr. Lenchus said. CMS projects the administrative costs of reviewing reports at $1.9 million for teaching hospital staff—the category Dr. Lenchus says is most applicable to hospitalists.
Dr. Lenchus says there was discussion within the Public Policy Committee about how much information needed to be publicly reported in relation to CME. Some members “wanted nothing recorded” and “some people wanted everything recorded.”
“The rule that has been implemented strikes a nice balance between the two,” he said.
Transparent Process
Industry groups and group purchasing organizations (GPOs) currently are working to put in place systems and procedures to begin collecting the data in August. Data will be collected through the end of 2013 and must be reported to CMS by March 31, 2014. CMS will then unveil a public website showcasing the information by Sept. 30, 2014.
Public Policy Committee member Jack Percelay, MD, MPH, FAAP, SFHM, said some hospitalists might feel they are “being picked on again” by having to report the added information. He instead looks at the intended push toward added transparency as “a set of obligations we have as physicians.”
“We have tremendous discretion about how health-care dollars are spent and with that comes a fiduciary responsibility, both to the patient and to the public,” he said. “This does not seem terribly burdensome to me. If I was getting nickel and dimed for every piece of candy I took through the exhibit hall during a meeting, that would be ridiculous. I’m happy to do this in a reasoned way.”
Dr. Percelay noted that the Sunshine Rule does not prevent industry payments to physicians or groups, but simply requires the public reporting and display of the remuneration. In that vein, he likened it to ethical rules that govern those who hold elected office.
“Someone should be able to Google and see that I’ve [received] funds from market research,” he said. “It’s not much different from politicians. It’s then up to the public and the media to do their due diligence.”
Dr. Lenchus said the public database has the potential to be misinterpreted by a public unfamiliar with how health care works. In particular, patients might not be able to discern the differences between the value of lunches, the payments for being on advisory boards, and industry-funded research.
“I really fear the public will look at this website, see there is any financial inducement to any physician, and erroneously conclude that any prescription of that company’s medication means that person is getting a kickback,” he says. “And we know that’s absolutely false.”
Richard Quinn is a freelance writer in New Jersey.
References
- Centers for Medicare & Medicaid Services. Medicare, Medicaid, Children’s Health Insurance Programs; transparency reports and reporting of physician ownership or investment interests. Federal Register website. Available at: https://www.federalregister.gov/articles/2013/02/08/2013-02572/medicare-mediaid-childrens-health-insurance-programs-transparency-reports-and-reporting-of. Accessed March 24, 2013.
- Council of Medical Specialty Societies. Letter to CMS. SHM website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_ and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=30674. Accessed March 24, 2013.
—Joshua Lenchus, DO, RPh, FACP, SFHM
Hospitalist leaders are taking a wait-and-see approach to the Physician Payment Sunshine Act, which requires reporting of payments and gifts from drug and medical device companies. But as wary as many are after publication of the Final Rule 1 in February, SHM and other groups already have claimed at least one victory in tweaking the new rules.
The Sunshine Rule, as it’s known, was included in the Affordable Care Act of 2010. The rule, created by the Centers for Medicaid & Medicare Services (CMS), requires manufacturers to publicly report gifts, payments, or other transfers of value to physicians from pharmaceutical and medical device manufacturers worth more than $10 (see “Dos and Don’ts,” below).1
One major change to the law sought by SHM and others was tied to the reporting of indirect payments to speakers at accredited continuing medical education (CME) classes or courses. The proposed rule required reporting of those payments even if a particular industry group did not select the speakers or pay them. SHM and three dozen other societies lobbied CMS to change the rule.2 The final rule says indirect payments don’t have to be reported if the CME program meets widely accepted accreditation standards and the industry participant is neither directly paid nor selected by the vendor.
CME Coalition, a Washington, D.C.-based advocacy group, said in a statement the caveat recognizes that CMS “is sending a strong message to commercial supporters: Underwriting accredited continuing education programs for health-care providers is to be applauded, not restricted.”
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, FACP, SFHM, said the initial rule was too restrictive and could have reduced physician participation in important CME activities. He said the Accreditation Council for Continuing Medical Education (ACCME) and other industry groups already govern the ethical issue of accepting direct payments that could imply bias to patients.
“I’m not so sure we needed the Sunshine Act as part of the ACA at all because these same things were in effect from the ACCME and other CME accrediting organizations,” said Dr. Lenchus, a Team Hospitalist member and president of the medical staff at Jackson Health System in Miami. “What this has done is impose additional administrative requirements that now take time away from our seeing patients or doing clinical activity.”
Those costs will add up quickly, according to figures from the Federal Register, Dr. Lenchus said. CMS projects the administrative costs of reviewing reports at $1.9 million for teaching hospital staff—the category Dr. Lenchus says is most applicable to hospitalists.
Dr. Lenchus says there was discussion within the Public Policy Committee about how much information needed to be publicly reported in relation to CME. Some members “wanted nothing recorded” and “some people wanted everything recorded.”
“The rule that has been implemented strikes a nice balance between the two,” he said.
Transparent Process
Industry groups and group purchasing organizations (GPOs) currently are working to put in place systems and procedures to begin collecting the data in August. Data will be collected through the end of 2013 and must be reported to CMS by March 31, 2014. CMS will then unveil a public website showcasing the information by Sept. 30, 2014.
Public Policy Committee member Jack Percelay, MD, MPH, FAAP, SFHM, said some hospitalists might feel they are “being picked on again” by having to report the added information. He instead looks at the intended push toward added transparency as “a set of obligations we have as physicians.”
“We have tremendous discretion about how health-care dollars are spent and with that comes a fiduciary responsibility, both to the patient and to the public,” he said. “This does not seem terribly burdensome to me. If I was getting nickel and dimed for every piece of candy I took through the exhibit hall during a meeting, that would be ridiculous. I’m happy to do this in a reasoned way.”
Dr. Percelay noted that the Sunshine Rule does not prevent industry payments to physicians or groups, but simply requires the public reporting and display of the remuneration. In that vein, he likened it to ethical rules that govern those who hold elected office.
“Someone should be able to Google and see that I’ve [received] funds from market research,” he said. “It’s not much different from politicians. It’s then up to the public and the media to do their due diligence.”
Dr. Lenchus said the public database has the potential to be misinterpreted by a public unfamiliar with how health care works. In particular, patients might not be able to discern the differences between the value of lunches, the payments for being on advisory boards, and industry-funded research.
“I really fear the public will look at this website, see there is any financial inducement to any physician, and erroneously conclude that any prescription of that company’s medication means that person is getting a kickback,” he says. “And we know that’s absolutely false.”
Richard Quinn is a freelance writer in New Jersey.
References
- Centers for Medicare & Medicaid Services. Medicare, Medicaid, Children’s Health Insurance Programs; transparency reports and reporting of physician ownership or investment interests. Federal Register website. Available at: https://www.federalregister.gov/articles/2013/02/08/2013-02572/medicare-mediaid-childrens-health-insurance-programs-transparency-reports-and-reporting-of. Accessed March 24, 2013.
- Council of Medical Specialty Societies. Letter to CMS. SHM website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_ and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=30674. Accessed March 24, 2013.
—Joshua Lenchus, DO, RPh, FACP, SFHM
Hospitalist leaders are taking a wait-and-see approach to the Physician Payment Sunshine Act, which requires reporting of payments and gifts from drug and medical device companies. But as wary as many are after publication of the Final Rule 1 in February, SHM and other groups already have claimed at least one victory in tweaking the new rules.
The Sunshine Rule, as it’s known, was included in the Affordable Care Act of 2010. The rule, created by the Centers for Medicaid & Medicare Services (CMS), requires manufacturers to publicly report gifts, payments, or other transfers of value to physicians from pharmaceutical and medical device manufacturers worth more than $10 (see “Dos and Don’ts,” below).1
One major change to the law sought by SHM and others was tied to the reporting of indirect payments to speakers at accredited continuing medical education (CME) classes or courses. The proposed rule required reporting of those payments even if a particular industry group did not select the speakers or pay them. SHM and three dozen other societies lobbied CMS to change the rule.2 The final rule says indirect payments don’t have to be reported if the CME program meets widely accepted accreditation standards and the industry participant is neither directly paid nor selected by the vendor.
CME Coalition, a Washington, D.C.-based advocacy group, said in a statement the caveat recognizes that CMS “is sending a strong message to commercial supporters: Underwriting accredited continuing education programs for health-care providers is to be applauded, not restricted.”
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, FACP, SFHM, said the initial rule was too restrictive and could have reduced physician participation in important CME activities. He said the Accreditation Council for Continuing Medical Education (ACCME) and other industry groups already govern the ethical issue of accepting direct payments that could imply bias to patients.
“I’m not so sure we needed the Sunshine Act as part of the ACA at all because these same things were in effect from the ACCME and other CME accrediting organizations,” said Dr. Lenchus, a Team Hospitalist member and president of the medical staff at Jackson Health System in Miami. “What this has done is impose additional administrative requirements that now take time away from our seeing patients or doing clinical activity.”
Those costs will add up quickly, according to figures from the Federal Register, Dr. Lenchus said. CMS projects the administrative costs of reviewing reports at $1.9 million for teaching hospital staff—the category Dr. Lenchus says is most applicable to hospitalists.
Dr. Lenchus says there was discussion within the Public Policy Committee about how much information needed to be publicly reported in relation to CME. Some members “wanted nothing recorded” and “some people wanted everything recorded.”
“The rule that has been implemented strikes a nice balance between the two,” he said.
Transparent Process
Industry groups and group purchasing organizations (GPOs) currently are working to put in place systems and procedures to begin collecting the data in August. Data will be collected through the end of 2013 and must be reported to CMS by March 31, 2014. CMS will then unveil a public website showcasing the information by Sept. 30, 2014.
Public Policy Committee member Jack Percelay, MD, MPH, FAAP, SFHM, said some hospitalists might feel they are “being picked on again” by having to report the added information. He instead looks at the intended push toward added transparency as “a set of obligations we have as physicians.”
“We have tremendous discretion about how health-care dollars are spent and with that comes a fiduciary responsibility, both to the patient and to the public,” he said. “This does not seem terribly burdensome to me. If I was getting nickel and dimed for every piece of candy I took through the exhibit hall during a meeting, that would be ridiculous. I’m happy to do this in a reasoned way.”
Dr. Percelay noted that the Sunshine Rule does not prevent industry payments to physicians or groups, but simply requires the public reporting and display of the remuneration. In that vein, he likened it to ethical rules that govern those who hold elected office.
“Someone should be able to Google and see that I’ve [received] funds from market research,” he said. “It’s not much different from politicians. It’s then up to the public and the media to do their due diligence.”
Dr. Lenchus said the public database has the potential to be misinterpreted by a public unfamiliar with how health care works. In particular, patients might not be able to discern the differences between the value of lunches, the payments for being on advisory boards, and industry-funded research.
“I really fear the public will look at this website, see there is any financial inducement to any physician, and erroneously conclude that any prescription of that company’s medication means that person is getting a kickback,” he says. “And we know that’s absolutely false.”
Richard Quinn is a freelance writer in New Jersey.
References
- Centers for Medicare & Medicaid Services. Medicare, Medicaid, Children’s Health Insurance Programs; transparency reports and reporting of physician ownership or investment interests. Federal Register website. Available at: https://www.federalregister.gov/articles/2013/02/08/2013-02572/medicare-mediaid-childrens-health-insurance-programs-transparency-reports-and-reporting-of. Accessed March 24, 2013.
- Council of Medical Specialty Societies. Letter to CMS. SHM website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_ and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=30674. Accessed March 24, 2013.
'Systems,' Not 'Points,' Is Correct Terminology for ROS Statements
The “Billing and Coding Bandwagon” article in the May 2011 issue of The Hospitalist (p. 26) recently was brought to my attention and I have some concerns that the following statement gives a false impression of acceptable documentation: “When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
In fact, that would still not be considered acceptable documentation for services that require a complete review of systems (99222, 99223, 99219, 99220, 99235, and 99236). The documentation guidelines clearly state: “A complete ROS [review of systems] inquires about the system(s) directly related to the problem(s) identified in the HPI plus all additional body systems.” At least 10 organ systems must be reviewed. Those systems with positive or pertinent negative responses must be individually documented. For the remaining systems, a notation indicating all other systems are negative is permissible. In the absence of such a notation, at least 10 systems must be individually documented.
What Medicare is saying is the provider must have inquired about all 14 systems, not just 10 or 12. The term “point” means nothing in an ROS statement. “Systems” is the correct terminology, not “points.”
I am afraid the article is misleading and could be providing inappropriate documentation advice to hospitalists dealing with CMS and AMA guidelines.
The “Billing and Coding Bandwagon” article in the May 2011 issue of The Hospitalist (p. 26) recently was brought to my attention and I have some concerns that the following statement gives a false impression of acceptable documentation: “When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
In fact, that would still not be considered acceptable documentation for services that require a complete review of systems (99222, 99223, 99219, 99220, 99235, and 99236). The documentation guidelines clearly state: “A complete ROS [review of systems] inquires about the system(s) directly related to the problem(s) identified in the HPI plus all additional body systems.” At least 10 organ systems must be reviewed. Those systems with positive or pertinent negative responses must be individually documented. For the remaining systems, a notation indicating all other systems are negative is permissible. In the absence of such a notation, at least 10 systems must be individually documented.
What Medicare is saying is the provider must have inquired about all 14 systems, not just 10 or 12. The term “point” means nothing in an ROS statement. “Systems” is the correct terminology, not “points.”
I am afraid the article is misleading and could be providing inappropriate documentation advice to hospitalists dealing with CMS and AMA guidelines.
The “Billing and Coding Bandwagon” article in the May 2011 issue of The Hospitalist (p. 26) recently was brought to my attention and I have some concerns that the following statement gives a false impression of acceptable documentation: “When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
In fact, that would still not be considered acceptable documentation for services that require a complete review of systems (99222, 99223, 99219, 99220, 99235, and 99236). The documentation guidelines clearly state: “A complete ROS [review of systems] inquires about the system(s) directly related to the problem(s) identified in the HPI plus all additional body systems.” At least 10 organ systems must be reviewed. Those systems with positive or pertinent negative responses must be individually documented. For the remaining systems, a notation indicating all other systems are negative is permissible. In the absence of such a notation, at least 10 systems must be individually documented.
What Medicare is saying is the provider must have inquired about all 14 systems, not just 10 or 12. The term “point” means nothing in an ROS statement. “Systems” is the correct terminology, not “points.”
I am afraid the article is misleading and could be providing inappropriate documentation advice to hospitalists dealing with CMS and AMA guidelines.
Some Thoughts on the Patient-Doctor Relationship
There is an inherent power differential in the patient-doctor relationship: The patient comes to the doctor as an authority on his/her physical or emotional state and is thus either intellectually or emotionally dependent on the doctor’s treatment plan and advice. It is therefore absolutely essential that the doctor respect the patient as an equal participant in the treatment. Although the doctor certainly has knowledge about how similar conditions were successfully treated in the past, hopefully a medical professional will display an attitude of respect and mutual collaboration with the patient to resolve his/her problem.
Listening is a key component of conveying an attitude of respect toward the patient. Nowadays practitioners are most often taking notes at their computers while speaking with the patient. This is certainly time-efficient and may in fact be necessary in order for a medical practice to remain solvent with the demands of Medicare and insurance companies. However, multitasking does not convey to the patient that they are connecting with the doctor. Listening is a complex action, which not only involves the ears, but the eyes, the kinesthetic responses of the whole body, and attention to the patient’s nonverbal communication.
Some of the key faux pas to avoid when listening to the patient include:
- Not centering oneself before engaging in a “crucial conversation”;
- Not listening because one is thinking ahead to his/her own response;
- Not maintaining eye contact;
- Not being aware of when one feels challenged and/or defensive;
- Discouraging the patient from contributing his/her own ideas;
- Not allowing the patient to give feedback on what s/he heard as instructions; and
- Taking phone calls or allowing interruptions during a consultation.
It is always helpful to give a patient clear, written instructions about medications, diet, exercise, etc., that result from the consultation. Some doctors send this report via secure email to the patient for review, which is an excellent technique.
The art of apology is another topic that greatly impacts the doctor-patient relationship, as well as the doctor’s relationship with the patient’s family members. This art is a process that has recently emerged in the medical and medical insurance industries. Kaiser Permanente’s director of medical-legal affairs has adopted the practice of asking permission to videotape the actual conversation in which a physician apologizes to a patient for a mistake in a procedure. These conversations are meant to help medical professionals learn how to admit mistakes and ask for forgiveness. Oftentimes patients are looking for just such a communication, which may allow them to put to rest feelings of resentment, bitterness, and regret.
Our patients’ well-being is our ideal goal. Knowing that they have been heard and their feelings understood may in the long run allow patients and their families to heal mind/body/soul more powerfully than we had ever thought. Of course, in our litigious society this may well be an art that remains to be developed over the long term.
There is an inherent power differential in the patient-doctor relationship: The patient comes to the doctor as an authority on his/her physical or emotional state and is thus either intellectually or emotionally dependent on the doctor’s treatment plan and advice. It is therefore absolutely essential that the doctor respect the patient as an equal participant in the treatment. Although the doctor certainly has knowledge about how similar conditions were successfully treated in the past, hopefully a medical professional will display an attitude of respect and mutual collaboration with the patient to resolve his/her problem.
Listening is a key component of conveying an attitude of respect toward the patient. Nowadays practitioners are most often taking notes at their computers while speaking with the patient. This is certainly time-efficient and may in fact be necessary in order for a medical practice to remain solvent with the demands of Medicare and insurance companies. However, multitasking does not convey to the patient that they are connecting with the doctor. Listening is a complex action, which not only involves the ears, but the eyes, the kinesthetic responses of the whole body, and attention to the patient’s nonverbal communication.
Some of the key faux pas to avoid when listening to the patient include:
- Not centering oneself before engaging in a “crucial conversation”;
- Not listening because one is thinking ahead to his/her own response;
- Not maintaining eye contact;
- Not being aware of when one feels challenged and/or defensive;
- Discouraging the patient from contributing his/her own ideas;
- Not allowing the patient to give feedback on what s/he heard as instructions; and
- Taking phone calls or allowing interruptions during a consultation.
It is always helpful to give a patient clear, written instructions about medications, diet, exercise, etc., that result from the consultation. Some doctors send this report via secure email to the patient for review, which is an excellent technique.
The art of apology is another topic that greatly impacts the doctor-patient relationship, as well as the doctor’s relationship with the patient’s family members. This art is a process that has recently emerged in the medical and medical insurance industries. Kaiser Permanente’s director of medical-legal affairs has adopted the practice of asking permission to videotape the actual conversation in which a physician apologizes to a patient for a mistake in a procedure. These conversations are meant to help medical professionals learn how to admit mistakes and ask for forgiveness. Oftentimes patients are looking for just such a communication, which may allow them to put to rest feelings of resentment, bitterness, and regret.
Our patients’ well-being is our ideal goal. Knowing that they have been heard and their feelings understood may in the long run allow patients and their families to heal mind/body/soul more powerfully than we had ever thought. Of course, in our litigious society this may well be an art that remains to be developed over the long term.
There is an inherent power differential in the patient-doctor relationship: The patient comes to the doctor as an authority on his/her physical or emotional state and is thus either intellectually or emotionally dependent on the doctor’s treatment plan and advice. It is therefore absolutely essential that the doctor respect the patient as an equal participant in the treatment. Although the doctor certainly has knowledge about how similar conditions were successfully treated in the past, hopefully a medical professional will display an attitude of respect and mutual collaboration with the patient to resolve his/her problem.
Listening is a key component of conveying an attitude of respect toward the patient. Nowadays practitioners are most often taking notes at their computers while speaking with the patient. This is certainly time-efficient and may in fact be necessary in order for a medical practice to remain solvent with the demands of Medicare and insurance companies. However, multitasking does not convey to the patient that they are connecting with the doctor. Listening is a complex action, which not only involves the ears, but the eyes, the kinesthetic responses of the whole body, and attention to the patient’s nonverbal communication.
Some of the key faux pas to avoid when listening to the patient include:
- Not centering oneself before engaging in a “crucial conversation”;
- Not listening because one is thinking ahead to his/her own response;
- Not maintaining eye contact;
- Not being aware of when one feels challenged and/or defensive;
- Discouraging the patient from contributing his/her own ideas;
- Not allowing the patient to give feedback on what s/he heard as instructions; and
- Taking phone calls or allowing interruptions during a consultation.
It is always helpful to give a patient clear, written instructions about medications, diet, exercise, etc., that result from the consultation. Some doctors send this report via secure email to the patient for review, which is an excellent technique.
The art of apology is another topic that greatly impacts the doctor-patient relationship, as well as the doctor’s relationship with the patient’s family members. This art is a process that has recently emerged in the medical and medical insurance industries. Kaiser Permanente’s director of medical-legal affairs has adopted the practice of asking permission to videotape the actual conversation in which a physician apologizes to a patient for a mistake in a procedure. These conversations are meant to help medical professionals learn how to admit mistakes and ask for forgiveness. Oftentimes patients are looking for just such a communication, which may allow them to put to rest feelings of resentment, bitterness, and regret.
Our patients’ well-being is our ideal goal. Knowing that they have been heard and their feelings understood may in the long run allow patients and their families to heal mind/body/soul more powerfully than we had ever thought. Of course, in our litigious society this may well be an art that remains to be developed over the long term.
Coordinated Approach May Help in Caring for Hospitals’ Neediest Patients

To my way of thinking, a person’s diagnosis or pathophysiology is not as strong a predictor of needing inpatient hospital care as it might have been 10 or 20 years ago. Rather than the clinical diagnosis (e.g. pneumonia), it seems to me that frailty or social complexity often are the principal determinants of which patients are admitted to a hospital for medical conditions.
Some of these patients are admitted frequently but appear to realize little or no benefit from hospitalization. These patients typically have little or no social support, and they often have either significant mental health disorders or substance abuse, or both. Much has been written about these patients, and I recommend an article by Dr. Atul Gawande in the Jan. 24, 2011, issue of The New Yorker titled “The Hot Spotters: Can We Lower Medical Costs by Giving the Neediest Patients Better Care?”
The Agency for Healthcare Research and Quality’s “Statistical Brief 354” on how health-care expenditures are allocated across the population reported that 1% of the population accounted for more than 22% of health-care spending in 2008. One in 5 of those were in that category again in 2009. Some of these patients would benefit from care plans.
The Role of Care Plans
It seems that there may be few effective inpatient interventions that will benefit these patients. After all, they have chronic issues that require ongoing relationships with outpatient providers, something that many of these patients lack. But for some (most?) of these patients, it seems clear that frequent hospitalizations don’t help and sometimes just perpetuate or worsen the patient’s dependence on the hospital at a high financial cost to society—and significant frustration and burnout on the part of hospital caregivers, including hospitalists.
For most hospitals, this problem is significant enough to require some sort of coordinated approach to the care of the dozens of types of patients in this category. Implementing whatever plan of care seems appropriate to the caregivers during each admission is frustrating, ensures lots of variation in care, and makes it easier for manipulative patients to abuse the hospital resources and personnel.
A better approach is to follow the same plan of care from one hospital visit to the next. You already knew that. But developing a care plan to follow during each ED visit and admission is time-consuming and often fraught with uncertainty about where boundaries should be set. So if you’re like me, you might just try to guide the patient to discharge this time and hope that whoever sees the patient on the next admission will take the initiative to develop the care plan. The result is that few such plans are developed.
Your Hospital Needs a Care Plan
Relying on individual doctors or nurses to take the initiative to develop care plans will almost always mean few plans are developed, they will vary in their effectiveness, and other providers may not be aware a plan exists. This was the case at the hospital where I practice until I heard Dr. Rick Hilger, MD, SFHM, a hospitalist at Regions Hospital in Minneapolis, present on this topic at HM12 in San Diego.
Dr. Hilger led a multidisciplinary team to develop care plans (they call them “restriction care plans”) and found that they dramatically reduced the rate of hospital admissions and ED visits for these patients. Hearing about this experience served as a kick in the pants for me, so I did much the same thing at “my” hospital. We have now developed plans for more than 20 patients and found that they visit our ED and are admitted less often. And, anecdotally at least, hospitalists and other hospital staff find that the care plans reduce, at least a little, the stress of caring for these patients.
Unanswered Questions
Although it seems clear that care plans reduce visits to the hospital that develops them, I suspect that some of these patients aren’t consuming any fewer health-care resources. They may just seek care from a different hospital.
My home state of Washington is working to develop individual patient care plans available to all hospitals in the state. A system called the Emergency Department Information Exchange (EDIE) has been adopted by nearly all the hospitals in the state. It allows them to share information on ED visits and such things as care plans with one another. For example, through EDIE, each hospital could see the opiate dosing schedule and admission criteria agreed to by patient and primary-care physician.
So it seems that care plans and the technology to share them can make it more difficult for patients to harm themselves by visiting many hospitals to get excessive opiate prescriptions, for example. This should benefit the patient and lower ED and hospital expenditures for these patients. But we don’t know what portion of costs simply is shifted to other settings, so there is no easy way to know the net effect on health-care costs.
An important unanswered question is whether these care plans improve patient well-being. It seems clear they do in some cases, but it is hard to know whether some patients may be worse off because of the plan.
Conclusion
I think nearly every hospital would benefit from a care plan committee composed of at least one hospitalist, ED physician, a nursing representative, and potentially other disciplines (see “Care Plan Attributes,” above). Our committee includes our inpatient psychiatrist, a really valuable contributor.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
To my way of thinking, a person’s diagnosis or pathophysiology is not as strong a predictor of needing inpatient hospital care as it might have been 10 or 20 years ago. Rather than the clinical diagnosis (e.g. pneumonia), it seems to me that frailty or social complexity often are the principal determinants of which patients are admitted to a hospital for medical conditions.
Some of these patients are admitted frequently but appear to realize little or no benefit from hospitalization. These patients typically have little or no social support, and they often have either significant mental health disorders or substance abuse, or both. Much has been written about these patients, and I recommend an article by Dr. Atul Gawande in the Jan. 24, 2011, issue of The New Yorker titled “The Hot Spotters: Can We Lower Medical Costs by Giving the Neediest Patients Better Care?”
The Agency for Healthcare Research and Quality’s “Statistical Brief 354” on how health-care expenditures are allocated across the population reported that 1% of the population accounted for more than 22% of health-care spending in 2008. One in 5 of those were in that category again in 2009. Some of these patients would benefit from care plans.
The Role of Care Plans
It seems that there may be few effective inpatient interventions that will benefit these patients. After all, they have chronic issues that require ongoing relationships with outpatient providers, something that many of these patients lack. But for some (most?) of these patients, it seems clear that frequent hospitalizations don’t help and sometimes just perpetuate or worsen the patient’s dependence on the hospital at a high financial cost to society—and significant frustration and burnout on the part of hospital caregivers, including hospitalists.
For most hospitals, this problem is significant enough to require some sort of coordinated approach to the care of the dozens of types of patients in this category. Implementing whatever plan of care seems appropriate to the caregivers during each admission is frustrating, ensures lots of variation in care, and makes it easier for manipulative patients to abuse the hospital resources and personnel.
A better approach is to follow the same plan of care from one hospital visit to the next. You already knew that. But developing a care plan to follow during each ED visit and admission is time-consuming and often fraught with uncertainty about where boundaries should be set. So if you’re like me, you might just try to guide the patient to discharge this time and hope that whoever sees the patient on the next admission will take the initiative to develop the care plan. The result is that few such plans are developed.
Your Hospital Needs a Care Plan
Relying on individual doctors or nurses to take the initiative to develop care plans will almost always mean few plans are developed, they will vary in their effectiveness, and other providers may not be aware a plan exists. This was the case at the hospital where I practice until I heard Dr. Rick Hilger, MD, SFHM, a hospitalist at Regions Hospital in Minneapolis, present on this topic at HM12 in San Diego.
Dr. Hilger led a multidisciplinary team to develop care plans (they call them “restriction care plans”) and found that they dramatically reduced the rate of hospital admissions and ED visits for these patients. Hearing about this experience served as a kick in the pants for me, so I did much the same thing at “my” hospital. We have now developed plans for more than 20 patients and found that they visit our ED and are admitted less often. And, anecdotally at least, hospitalists and other hospital staff find that the care plans reduce, at least a little, the stress of caring for these patients.
Unanswered Questions
Although it seems clear that care plans reduce visits to the hospital that develops them, I suspect that some of these patients aren’t consuming any fewer health-care resources. They may just seek care from a different hospital.
My home state of Washington is working to develop individual patient care plans available to all hospitals in the state. A system called the Emergency Department Information Exchange (EDIE) has been adopted by nearly all the hospitals in the state. It allows them to share information on ED visits and such things as care plans with one another. For example, through EDIE, each hospital could see the opiate dosing schedule and admission criteria agreed to by patient and primary-care physician.
So it seems that care plans and the technology to share them can make it more difficult for patients to harm themselves by visiting many hospitals to get excessive opiate prescriptions, for example. This should benefit the patient and lower ED and hospital expenditures for these patients. But we don’t know what portion of costs simply is shifted to other settings, so there is no easy way to know the net effect on health-care costs.
An important unanswered question is whether these care plans improve patient well-being. It seems clear they do in some cases, but it is hard to know whether some patients may be worse off because of the plan.
Conclusion
I think nearly every hospital would benefit from a care plan committee composed of at least one hospitalist, ED physician, a nursing representative, and potentially other disciplines (see “Care Plan Attributes,” above). Our committee includes our inpatient psychiatrist, a really valuable contributor.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
To my way of thinking, a person’s diagnosis or pathophysiology is not as strong a predictor of needing inpatient hospital care as it might have been 10 or 20 years ago. Rather than the clinical diagnosis (e.g. pneumonia), it seems to me that frailty or social complexity often are the principal determinants of which patients are admitted to a hospital for medical conditions.
Some of these patients are admitted frequently but appear to realize little or no benefit from hospitalization. These patients typically have little or no social support, and they often have either significant mental health disorders or substance abuse, or both. Much has been written about these patients, and I recommend an article by Dr. Atul Gawande in the Jan. 24, 2011, issue of The New Yorker titled “The Hot Spotters: Can We Lower Medical Costs by Giving the Neediest Patients Better Care?”
The Agency for Healthcare Research and Quality’s “Statistical Brief 354” on how health-care expenditures are allocated across the population reported that 1% of the population accounted for more than 22% of health-care spending in 2008. One in 5 of those were in that category again in 2009. Some of these patients would benefit from care plans.
The Role of Care Plans
It seems that there may be few effective inpatient interventions that will benefit these patients. After all, they have chronic issues that require ongoing relationships with outpatient providers, something that many of these patients lack. But for some (most?) of these patients, it seems clear that frequent hospitalizations don’t help and sometimes just perpetuate or worsen the patient’s dependence on the hospital at a high financial cost to society—and significant frustration and burnout on the part of hospital caregivers, including hospitalists.
For most hospitals, this problem is significant enough to require some sort of coordinated approach to the care of the dozens of types of patients in this category. Implementing whatever plan of care seems appropriate to the caregivers during each admission is frustrating, ensures lots of variation in care, and makes it easier for manipulative patients to abuse the hospital resources and personnel.
A better approach is to follow the same plan of care from one hospital visit to the next. You already knew that. But developing a care plan to follow during each ED visit and admission is time-consuming and often fraught with uncertainty about where boundaries should be set. So if you’re like me, you might just try to guide the patient to discharge this time and hope that whoever sees the patient on the next admission will take the initiative to develop the care plan. The result is that few such plans are developed.
Your Hospital Needs a Care Plan
Relying on individual doctors or nurses to take the initiative to develop care plans will almost always mean few plans are developed, they will vary in their effectiveness, and other providers may not be aware a plan exists. This was the case at the hospital where I practice until I heard Dr. Rick Hilger, MD, SFHM, a hospitalist at Regions Hospital in Minneapolis, present on this topic at HM12 in San Diego.
Dr. Hilger led a multidisciplinary team to develop care plans (they call them “restriction care plans”) and found that they dramatically reduced the rate of hospital admissions and ED visits for these patients. Hearing about this experience served as a kick in the pants for me, so I did much the same thing at “my” hospital. We have now developed plans for more than 20 patients and found that they visit our ED and are admitted less often. And, anecdotally at least, hospitalists and other hospital staff find that the care plans reduce, at least a little, the stress of caring for these patients.
Unanswered Questions
Although it seems clear that care plans reduce visits to the hospital that develops them, I suspect that some of these patients aren’t consuming any fewer health-care resources. They may just seek care from a different hospital.
My home state of Washington is working to develop individual patient care plans available to all hospitals in the state. A system called the Emergency Department Information Exchange (EDIE) has been adopted by nearly all the hospitals in the state. It allows them to share information on ED visits and such things as care plans with one another. For example, through EDIE, each hospital could see the opiate dosing schedule and admission criteria agreed to by patient and primary-care physician.
So it seems that care plans and the technology to share them can make it more difficult for patients to harm themselves by visiting many hospitals to get excessive opiate prescriptions, for example. This should benefit the patient and lower ED and hospital expenditures for these patients. But we don’t know what portion of costs simply is shifted to other settings, so there is no easy way to know the net effect on health-care costs.
An important unanswered question is whether these care plans improve patient well-being. It seems clear they do in some cases, but it is hard to know whether some patients may be worse off because of the plan.
Conclusion
I think nearly every hospital would benefit from a care plan committee composed of at least one hospitalist, ED physician, a nursing representative, and potentially other disciplines (see “Care Plan Attributes,” above). Our committee includes our inpatient psychiatrist, a really valuable contributor.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Hybrid Nocturnist Solution is Key to Lehigh Valley Hospitalist Program’s Success

Twenty-four-hour coverage is standard practice for all successful hospitalist groups. At Lehigh Valley Hospital in Allentown, Pa., the hospitalist group features 17 FTEs that split time in a traditional seven-on/seven-off schedule. Five doctors per week round on units seeing patients; one works triage/admitting in the morning and sees some follow-ups in the afternoon; and one works a middle shift for admissions, consults, and ICU transfers.
The foundation of this coverage comes at night. We employ an overnight doctor—a nocturnist—every day of the year. This doctor’s sole responsibility is to cover night admissions, rapid responses, floor calls, and transfers.
Change Is Necessary, Difficult
Lehigh Valley’s change to a nocturnist model came about when members of the group asked for it. We needed to put a model in place that could help the group, improve morale, and improve our care at night. Of all of our shifts, nobody wanted to work overnight. Each clinician was working about four weeks of nights per year, and we started to notice that our new hires from residency were the only ones truly capable of handling the sleep challenges—or, more truthfully, our veteran hospitalists were having difficulty with the nights.
For such a large group, having a nocturnist makes sense. However, there are a few issues to contend with in hiring a nocturnist. Most notably, nocturnists are hard to come by. It takes a special type of person to come in and work the opposite schedule from everyone else. Nocturnists are typically alone in the hospital and don’t always have the support of other hospitalists when times get tough. They usually are at the mercy of other stakeholders. Namely, they are at the mercy of the ED. If the ED is busy, then so is the nocturnist. That special type of person knows the balance and becomes a specialist in ED dynamics, as well as in ED night staffing.
Nocturnists are expensive; we looked at MGMA and SHM data and realized that we would have to pay a 20% to 50% premium if we wanted to employ a true seven-on nocturnist. And if we wanted all nights covered, we would have to hire two of these doctors.
Another point of contention is the buy-in from administration. CEOs and CMOs often don’t understand the need to pay for a nocturnist, and more often than not, they fail to see the need to have a nocturnist employed in the first place.
Finally, in the event of sick time, holidays, or vacation time, the hospitalist team is at the mercy of the nocturnist in terms of necessitating coverage.
Internal Solution=Perfect Remedy
In addition to the aforementioned concerns, I recently experienced a “what’s most important to me?” moment at work with the expectation of my first child. I planned on returning to work after my maternity leave, but I was reassessing just exactly how much I wanted to come back to work. It was in this setting that I began to brainstorm ways to help the group with our concerns regarding working nights, as well as my own feelings of being torn with such a grueling schedule while having a new baby at home.
Then the solution hit me: a new nocturnist model.
After long discussions with the group and group leadership, we found, not surprisingly, there were a good number of people who valued time more than money. I fell into the category of desiring more time away over a premium salary. We also found two others like me who fit this same category. None of us were considered “nocturnists” up to this point, and none of us would have gone for the idea of being seven-on/seven-off nocturnists, either. So we needed a new plan.
And with a little brainstorming and schedule-wrenching, the new nocturnist was born at Lehigh Valley. We are a group of 17. By taking the three willing participants out of the pool of 17 hospitalists and asking them to exclusively work nights, rotating in a one-week-on, two-weeks-off rotation, we were able to still leave 14 doctors to run the day shifts. The daytime hospitalists would no longer have to work nights, drastically improving their quality of work life.
This was a huge step forward for our group. It was a morale boost for the daytime doctors and actually allowed the group to save money. We were looking for doctors 18 and 19, and instead found internal solutions to our night problems. The schedule fit together like a patchwork quilt.
In exchange for two weeks off, the three nocturnists agreed to no additional vacation time. Our salaries stayed the same, too. So from a budgetary standpoint, nothing changed. From a quality-of-life standpoint, everyone was happy. My nocturnist colleagues and I were happy to exchange working nights every third week for the same salary in exchange for more days off.
The new schedule even allowed the group to eliminate the middle shift, creating an additional hospitalist available for daytime rounding. And having three nocturnists creates a pool of night doctors who are readily available to cover each other’s sick or personal time.
In all fairness, this new model was not an easy sell to administration. But as the group became more stable and morale increased, we, as members of the group, relied on this stability. We also noticed an increase in recruitment. Veterans and rookies wanted to start in a practice that had its nights covered. Ultimately, increasing our daytime capacity increased our inpatient encounters, and by increasing recruitment and retaining our current staff, our administration saw the benefits.
Employing a team of nocturnists maintains group stability, is cost-effective, helps with retention, boosts morale, and is attractive new recruits. Hospitalist programs that are struggling with staffing should consider a similar approach—and remember that they might be able to change everyday life without changing the ever-important bottom line.
Dr. Verdetti-Healy is a nocturnist at Lehigh Valley Hospital in Allentown, Pa.
Daniel Bitetto, MD, SFHM, chief of the section of hospital medicine at Lehigh Valley Hospital in Allentown, Pa., contributed to this report.
Twenty-four-hour coverage is standard practice for all successful hospitalist groups. At Lehigh Valley Hospital in Allentown, Pa., the hospitalist group features 17 FTEs that split time in a traditional seven-on/seven-off schedule. Five doctors per week round on units seeing patients; one works triage/admitting in the morning and sees some follow-ups in the afternoon; and one works a middle shift for admissions, consults, and ICU transfers.
The foundation of this coverage comes at night. We employ an overnight doctor—a nocturnist—every day of the year. This doctor’s sole responsibility is to cover night admissions, rapid responses, floor calls, and transfers.
Change Is Necessary, Difficult
Lehigh Valley’s change to a nocturnist model came about when members of the group asked for it. We needed to put a model in place that could help the group, improve morale, and improve our care at night. Of all of our shifts, nobody wanted to work overnight. Each clinician was working about four weeks of nights per year, and we started to notice that our new hires from residency were the only ones truly capable of handling the sleep challenges—or, more truthfully, our veteran hospitalists were having difficulty with the nights.
For such a large group, having a nocturnist makes sense. However, there are a few issues to contend with in hiring a nocturnist. Most notably, nocturnists are hard to come by. It takes a special type of person to come in and work the opposite schedule from everyone else. Nocturnists are typically alone in the hospital and don’t always have the support of other hospitalists when times get tough. They usually are at the mercy of other stakeholders. Namely, they are at the mercy of the ED. If the ED is busy, then so is the nocturnist. That special type of person knows the balance and becomes a specialist in ED dynamics, as well as in ED night staffing.
Nocturnists are expensive; we looked at MGMA and SHM data and realized that we would have to pay a 20% to 50% premium if we wanted to employ a true seven-on nocturnist. And if we wanted all nights covered, we would have to hire two of these doctors.
Another point of contention is the buy-in from administration. CEOs and CMOs often don’t understand the need to pay for a nocturnist, and more often than not, they fail to see the need to have a nocturnist employed in the first place.
Finally, in the event of sick time, holidays, or vacation time, the hospitalist team is at the mercy of the nocturnist in terms of necessitating coverage.
Internal Solution=Perfect Remedy
In addition to the aforementioned concerns, I recently experienced a “what’s most important to me?” moment at work with the expectation of my first child. I planned on returning to work after my maternity leave, but I was reassessing just exactly how much I wanted to come back to work. It was in this setting that I began to brainstorm ways to help the group with our concerns regarding working nights, as well as my own feelings of being torn with such a grueling schedule while having a new baby at home.
Then the solution hit me: a new nocturnist model.
After long discussions with the group and group leadership, we found, not surprisingly, there were a good number of people who valued time more than money. I fell into the category of desiring more time away over a premium salary. We also found two others like me who fit this same category. None of us were considered “nocturnists” up to this point, and none of us would have gone for the idea of being seven-on/seven-off nocturnists, either. So we needed a new plan.
And with a little brainstorming and schedule-wrenching, the new nocturnist was born at Lehigh Valley. We are a group of 17. By taking the three willing participants out of the pool of 17 hospitalists and asking them to exclusively work nights, rotating in a one-week-on, two-weeks-off rotation, we were able to still leave 14 doctors to run the day shifts. The daytime hospitalists would no longer have to work nights, drastically improving their quality of work life.
This was a huge step forward for our group. It was a morale boost for the daytime doctors and actually allowed the group to save money. We were looking for doctors 18 and 19, and instead found internal solutions to our night problems. The schedule fit together like a patchwork quilt.
In exchange for two weeks off, the three nocturnists agreed to no additional vacation time. Our salaries stayed the same, too. So from a budgetary standpoint, nothing changed. From a quality-of-life standpoint, everyone was happy. My nocturnist colleagues and I were happy to exchange working nights every third week for the same salary in exchange for more days off.
The new schedule even allowed the group to eliminate the middle shift, creating an additional hospitalist available for daytime rounding. And having three nocturnists creates a pool of night doctors who are readily available to cover each other’s sick or personal time.
In all fairness, this new model was not an easy sell to administration. But as the group became more stable and morale increased, we, as members of the group, relied on this stability. We also noticed an increase in recruitment. Veterans and rookies wanted to start in a practice that had its nights covered. Ultimately, increasing our daytime capacity increased our inpatient encounters, and by increasing recruitment and retaining our current staff, our administration saw the benefits.
Employing a team of nocturnists maintains group stability, is cost-effective, helps with retention, boosts morale, and is attractive new recruits. Hospitalist programs that are struggling with staffing should consider a similar approach—and remember that they might be able to change everyday life without changing the ever-important bottom line.
Dr. Verdetti-Healy is a nocturnist at Lehigh Valley Hospital in Allentown, Pa.
Daniel Bitetto, MD, SFHM, chief of the section of hospital medicine at Lehigh Valley Hospital in Allentown, Pa., contributed to this report.
Twenty-four-hour coverage is standard practice for all successful hospitalist groups. At Lehigh Valley Hospital in Allentown, Pa., the hospitalist group features 17 FTEs that split time in a traditional seven-on/seven-off schedule. Five doctors per week round on units seeing patients; one works triage/admitting in the morning and sees some follow-ups in the afternoon; and one works a middle shift for admissions, consults, and ICU transfers.
The foundation of this coverage comes at night. We employ an overnight doctor—a nocturnist—every day of the year. This doctor’s sole responsibility is to cover night admissions, rapid responses, floor calls, and transfers.
Change Is Necessary, Difficult
Lehigh Valley’s change to a nocturnist model came about when members of the group asked for it. We needed to put a model in place that could help the group, improve morale, and improve our care at night. Of all of our shifts, nobody wanted to work overnight. Each clinician was working about four weeks of nights per year, and we started to notice that our new hires from residency were the only ones truly capable of handling the sleep challenges—or, more truthfully, our veteran hospitalists were having difficulty with the nights.
For such a large group, having a nocturnist makes sense. However, there are a few issues to contend with in hiring a nocturnist. Most notably, nocturnists are hard to come by. It takes a special type of person to come in and work the opposite schedule from everyone else. Nocturnists are typically alone in the hospital and don’t always have the support of other hospitalists when times get tough. They usually are at the mercy of other stakeholders. Namely, they are at the mercy of the ED. If the ED is busy, then so is the nocturnist. That special type of person knows the balance and becomes a specialist in ED dynamics, as well as in ED night staffing.
Nocturnists are expensive; we looked at MGMA and SHM data and realized that we would have to pay a 20% to 50% premium if we wanted to employ a true seven-on nocturnist. And if we wanted all nights covered, we would have to hire two of these doctors.
Another point of contention is the buy-in from administration. CEOs and CMOs often don’t understand the need to pay for a nocturnist, and more often than not, they fail to see the need to have a nocturnist employed in the first place.
Finally, in the event of sick time, holidays, or vacation time, the hospitalist team is at the mercy of the nocturnist in terms of necessitating coverage.
Internal Solution=Perfect Remedy
In addition to the aforementioned concerns, I recently experienced a “what’s most important to me?” moment at work with the expectation of my first child. I planned on returning to work after my maternity leave, but I was reassessing just exactly how much I wanted to come back to work. It was in this setting that I began to brainstorm ways to help the group with our concerns regarding working nights, as well as my own feelings of being torn with such a grueling schedule while having a new baby at home.
Then the solution hit me: a new nocturnist model.
After long discussions with the group and group leadership, we found, not surprisingly, there were a good number of people who valued time more than money. I fell into the category of desiring more time away over a premium salary. We also found two others like me who fit this same category. None of us were considered “nocturnists” up to this point, and none of us would have gone for the idea of being seven-on/seven-off nocturnists, either. So we needed a new plan.
And with a little brainstorming and schedule-wrenching, the new nocturnist was born at Lehigh Valley. We are a group of 17. By taking the three willing participants out of the pool of 17 hospitalists and asking them to exclusively work nights, rotating in a one-week-on, two-weeks-off rotation, we were able to still leave 14 doctors to run the day shifts. The daytime hospitalists would no longer have to work nights, drastically improving their quality of work life.
This was a huge step forward for our group. It was a morale boost for the daytime doctors and actually allowed the group to save money. We were looking for doctors 18 and 19, and instead found internal solutions to our night problems. The schedule fit together like a patchwork quilt.
In exchange for two weeks off, the three nocturnists agreed to no additional vacation time. Our salaries stayed the same, too. So from a budgetary standpoint, nothing changed. From a quality-of-life standpoint, everyone was happy. My nocturnist colleagues and I were happy to exchange working nights every third week for the same salary in exchange for more days off.
The new schedule even allowed the group to eliminate the middle shift, creating an additional hospitalist available for daytime rounding. And having three nocturnists creates a pool of night doctors who are readily available to cover each other’s sick or personal time.
In all fairness, this new model was not an easy sell to administration. But as the group became more stable and morale increased, we, as members of the group, relied on this stability. We also noticed an increase in recruitment. Veterans and rookies wanted to start in a practice that had its nights covered. Ultimately, increasing our daytime capacity increased our inpatient encounters, and by increasing recruitment and retaining our current staff, our administration saw the benefits.
Employing a team of nocturnists maintains group stability, is cost-effective, helps with retention, boosts morale, and is attractive new recruits. Hospitalist programs that are struggling with staffing should consider a similar approach—and remember that they might be able to change everyday life without changing the ever-important bottom line.
Dr. Verdetti-Healy is a nocturnist at Lehigh Valley Hospital in Allentown, Pa.
Daniel Bitetto, MD, SFHM, chief of the section of hospital medicine at Lehigh Valley Hospital in Allentown, Pa., contributed to this report.
Communication Key to Peaceful Coexistence for Competing Hospital Medicine Groups

Experienced hospitalists and medical directors agree that the key to multiple hospitalist groups coexisting effectively under one roof—whether directly competing or not—is good communication. Effective communication can take time to build.
“Start by working together on something—anything, [such as] a hospital committee of some sort where there’s not likely to be much tension,” says hospitalist pioneer and practice consultant John Nelson, MD, MHM.
Dr. Nelson practices at Overlake Hospital in Bellevue, Wash., which has a hospitalist group employed by the hospital and another employed by Group Health Cooperative, a nonprofit health system in Washington state. It is important to put some trust in the trust bank, he says, “and that’s hard if you have no social connections at all. At my hospital, we enjoy each other’s company, we visit each other at lunch, and we even tried to have a journal club.” The two hospitalist groups work together on developing care protocols. Dr. Nelson says it also makes sense for the groups’ leaders to sit down together on a regular basis and have a venue for discussing important issues and solving problems that may arise.
Other suggestions for hospitalist groups working together under one roof include:
- Clearly define each group’s territory. The groups’ representatives can go out and try to persuade health plans or physician groups to shift their hospitalist allegiances, but there should be no “trolling” or “poaching” of patients going on inside the hospital’s walls. That will only confuse patients and disrupt the hospital’s larger service goals.
- Inform the ED and other key staff of your schedules. It’s important that everyone know exactly who is supposed to get which patients, and how these referrals get made. But recognize that mistakes happen and, hopefully, these will even out between the groups over time.
- Transparency, honesty, and even-handed treatment of all hospitalists can prevent resentment. Clearly defined guidelines and expectations are helpful. If the policy spells out transfers for an incorrectly referred patient, both sides should be accessible and cooperative with that process.
- Identify areas of common interest and agree to work together on these areas (i.e. competition-free zones). It might be possible, for example, for competing groups to take each others’ after-hours call on a rotating basis, with a firm commitment not to steal patients along the way.
- Spell out responsibilities in a way that everyone can agree is fair, such as alternating referrals or taking call on alternating days. For example, if subsidies are paid to more than one hospitalist group, is this done equitably, such as based on the number of hospitalist FTEs or shifts?
- Restrictive covenants and contractual noncompete clauses could become an issue in areas where multiple groups practice. Rather than using overly broad, blanket language, it could be clarified that such pacts apply only to the hospital where the physician currently works, and within a reasonable time frame. But everyone involved should be aware of what these covenants contain and, if they appear unreasonable, don’t sign them.
—Larry Beresford
Experienced hospitalists and medical directors agree that the key to multiple hospitalist groups coexisting effectively under one roof—whether directly competing or not—is good communication. Effective communication can take time to build.
“Start by working together on something—anything, [such as] a hospital committee of some sort where there’s not likely to be much tension,” says hospitalist pioneer and practice consultant John Nelson, MD, MHM.
Dr. Nelson practices at Overlake Hospital in Bellevue, Wash., which has a hospitalist group employed by the hospital and another employed by Group Health Cooperative, a nonprofit health system in Washington state. It is important to put some trust in the trust bank, he says, “and that’s hard if you have no social connections at all. At my hospital, we enjoy each other’s company, we visit each other at lunch, and we even tried to have a journal club.” The two hospitalist groups work together on developing care protocols. Dr. Nelson says it also makes sense for the groups’ leaders to sit down together on a regular basis and have a venue for discussing important issues and solving problems that may arise.
Other suggestions for hospitalist groups working together under one roof include:
- Clearly define each group’s territory. The groups’ representatives can go out and try to persuade health plans or physician groups to shift their hospitalist allegiances, but there should be no “trolling” or “poaching” of patients going on inside the hospital’s walls. That will only confuse patients and disrupt the hospital’s larger service goals.
- Inform the ED and other key staff of your schedules. It’s important that everyone know exactly who is supposed to get which patients, and how these referrals get made. But recognize that mistakes happen and, hopefully, these will even out between the groups over time.
- Transparency, honesty, and even-handed treatment of all hospitalists can prevent resentment. Clearly defined guidelines and expectations are helpful. If the policy spells out transfers for an incorrectly referred patient, both sides should be accessible and cooperative with that process.
- Identify areas of common interest and agree to work together on these areas (i.e. competition-free zones). It might be possible, for example, for competing groups to take each others’ after-hours call on a rotating basis, with a firm commitment not to steal patients along the way.
- Spell out responsibilities in a way that everyone can agree is fair, such as alternating referrals or taking call on alternating days. For example, if subsidies are paid to more than one hospitalist group, is this done equitably, such as based on the number of hospitalist FTEs or shifts?
- Restrictive covenants and contractual noncompete clauses could become an issue in areas where multiple groups practice. Rather than using overly broad, blanket language, it could be clarified that such pacts apply only to the hospital where the physician currently works, and within a reasonable time frame. But everyone involved should be aware of what these covenants contain and, if they appear unreasonable, don’t sign them.
—Larry Beresford
Experienced hospitalists and medical directors agree that the key to multiple hospitalist groups coexisting effectively under one roof—whether directly competing or not—is good communication. Effective communication can take time to build.
“Start by working together on something—anything, [such as] a hospital committee of some sort where there’s not likely to be much tension,” says hospitalist pioneer and practice consultant John Nelson, MD, MHM.
Dr. Nelson practices at Overlake Hospital in Bellevue, Wash., which has a hospitalist group employed by the hospital and another employed by Group Health Cooperative, a nonprofit health system in Washington state. It is important to put some trust in the trust bank, he says, “and that’s hard if you have no social connections at all. At my hospital, we enjoy each other’s company, we visit each other at lunch, and we even tried to have a journal club.” The two hospitalist groups work together on developing care protocols. Dr. Nelson says it also makes sense for the groups’ leaders to sit down together on a regular basis and have a venue for discussing important issues and solving problems that may arise.
Other suggestions for hospitalist groups working together under one roof include:
- Clearly define each group’s territory. The groups’ representatives can go out and try to persuade health plans or physician groups to shift their hospitalist allegiances, but there should be no “trolling” or “poaching” of patients going on inside the hospital’s walls. That will only confuse patients and disrupt the hospital’s larger service goals.
- Inform the ED and other key staff of your schedules. It’s important that everyone know exactly who is supposed to get which patients, and how these referrals get made. But recognize that mistakes happen and, hopefully, these will even out between the groups over time.
- Transparency, honesty, and even-handed treatment of all hospitalists can prevent resentment. Clearly defined guidelines and expectations are helpful. If the policy spells out transfers for an incorrectly referred patient, both sides should be accessible and cooperative with that process.
- Identify areas of common interest and agree to work together on these areas (i.e. competition-free zones). It might be possible, for example, for competing groups to take each others’ after-hours call on a rotating basis, with a firm commitment not to steal patients along the way.
- Spell out responsibilities in a way that everyone can agree is fair, such as alternating referrals or taking call on alternating days. For example, if subsidies are paid to more than one hospitalist group, is this done equitably, such as based on the number of hospitalist FTEs or shifts?
- Restrictive covenants and contractual noncompete clauses could become an issue in areas where multiple groups practice. Rather than using overly broad, blanket language, it could be clarified that such pacts apply only to the hospital where the physician currently works, and within a reasonable time frame. But everyone involved should be aware of what these covenants contain and, if they appear unreasonable, don’t sign them.
—Larry Beresford