User login
The Hospitalist only
Medicare Outlines Anticipated Funding Changes Under Affordable Care Act


The Centers for Medicare & Medicaid Services (CMS) recently released a few Fact Sheets on how they anticipate funding changes on a few of their programs that were implemented (or sustained) under the Affordable Care Act. As a background, CMS pays most acute-care hospitals by prospectively determining payment based on a patient’s diagnosis and the severity of illness within that diagnosis (e.g. “MS-DRG”). These payment amounts are updated annually after evaluating several factors, including the costs associated with the delivery of care.
One of the most major changes described in the Fact Sheet that will affect hospitalists is how CMS will review inpatient stays based on the number of nights in the hospital. CMS has proposed that any patient who stays in the hospital for two or more “midnights” should be appropriate for payment under Medicare Part A. For those who stay in the hospital for only one (or zero) midnights, payment under Medicare Part A will only be appropriate if:
- There is sufficient documentation at the time of admission that the anticipated length of stay is two or more nights; and.
- Further documentation that circumstances changed, and the hospital stay ended prematurely because of those changes.
Overall for hospitalists, this should substantially simplify the admitting process, whereby most inpatients being admitted with the anticipation of two or more nights should qualify for an inpatient stay. This also reduces the administrative burden of correcting the “inpatient” versus “observation” designation, which keeps many hospital staffs entirely too busy. This change also should relieve a significant burden from the patients and their families, who if kept in observation for a period of time, may have to pay substantially out of pocket to make up for the difference between the cost of the stay and the reimbursement from CMS for observation status. So this is one of the moves that CMS is making to simplify (and not complicate) an already too-complicated payment system. This should go into effect October 2013 and will be a sigh of much relief from many of us.
A few other anticipated changes that will affect hospitalists include:
Payments for Unfunded Care
Another major change that will go into affect October 2013 is the amount of monies received by hospitals that care for unfunded patients. These payments historically have been made to “Disproportionate Share Hospitals” (DSH), which are hospitals that care for a higher percentage of unfunded patients. Under the Affordable Care Act, only 25% of these payments will be distributed to DSH hospitals; the remaining 75% will be reduced based on the number of uninsured in the U.S., then redistributed to DSH hospitals based on their portion of uninsured care delivered.
Most DSH hospitals should expect a decrease in DSH payments, the amount of which will depend on their share of unfunded patients.
Any reduction in the “bottom line” to the hospital can affect hospitalists, especially those who are directly employed by the hospital.
Hospital-Acquired Conditions
CMS has long had the Hospital-Acquired Condition (HAC) program in effect, which has the ability to reduce the amount of payment for inpatients who acquire a HAC during their hospital stay. Starting in October 2014, CMS will impose additional financial penalties for hospitals with high HAC rates.
Specifically, those hospitals in the highest 25th percentile of HAC rates will be penalized 1% of their overall CMS payments. Another proposed change is that the following be included in the HAC reduction plan (two “domains” of measures):
- Domain No. 1: Six of the AHRQ Patient Safety Indicators (PSIs), including pressure ulcers, foreign bodies left in after surgery, iatrogenic pneumothorax, postoperative physiologic or metabolic derangements, postoperative VTE, and accidental puncture/laceration.
- Domain No. 2: Central-line-associated bloodstream infections (CLABSI) and catheter-associated urinary tract infections (CAUTIs).
The domains will be weighted equally, and an average score will determine the total score. There will be some methodology for risk adjustment, and hospitals will be given a review and comment period to validate their own scores.
Most hospitalists have at least indirect control over many of these HACs,and all need to pay very close attention to their hospital’s rates of these now and in the future.
Readmissions
As we all know, the Hospital Readmission Reduction program went into effect October 2012; it placed 1% of CMS payments at risk. This will increase to 2% of payments as of October 2013. CMS will continue to use AMI, CHF, and pneumonia as the three conditions under which the readmissions are measured but will put in some methodology to account for planned readmissions.
In addition, in October 2014, they plan to add readmission rates for COPD and for hip/knee arthroplasty.
Hospitalists will continue to need to progress their transitions of care programs, at least for these five patients conditions but more likely (and more effectively) for all hospital discharges.
Quality Measures
Currently more than 99% of acute-care hospitals participate in the pay-for-reporting quality program through CMS, the results of which have been displayed on the Hospital Compare website (www.hospitalcompare.hhs.gov) for years. The program started in 2004 with 10 quality metrics and now includes 57 metrics. These include process and outcome measures for AMI, CHF, and pneumonia, as well as process measures for surgical care, HACs, and patient-satisfaction surveys, among others.
This program will continue to expand over time, including hospital-acquired MRSA and Clostridium difficile rates. The few hospitals not participating will have their CMS annual payments reduced by 2%.
EHR Incentives
CMS is evaluating ways to reduce the burden of reporting by aligning EHR incentives with the Inpatient Quality Reporting program.
Summary
After an open commentary period, the Final Rule will be published Aug. 1, and will become effective for discharges on or after Oct. 1. Although CMS will continue to expand the total number of measures that need to be reported, and the penalties for non-reporting or low performance will continue to escalate, CMS is at least attempting to reduce the overall burden of reporting by combining measures and programs over time and using EHRs to facilitate the bulk of reporting over time.
The global message to hospitalists is: Continue to focus on reducing the burden of HACs, enhance throughput, and carefully and thoughtfully transition patients to the next provider after their hospital discharge. All in all, although at times this can feel overwhelming, these changes represent the right direction to move for high-quality and safe patient care.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Reference
The Centers for Medicare & Medicaid Services (CMS) recently released a few Fact Sheets on how they anticipate funding changes on a few of their programs that were implemented (or sustained) under the Affordable Care Act. As a background, CMS pays most acute-care hospitals by prospectively determining payment based on a patient’s diagnosis and the severity of illness within that diagnosis (e.g. “MS-DRG”). These payment amounts are updated annually after evaluating several factors, including the costs associated with the delivery of care.
One of the most major changes described in the Fact Sheet that will affect hospitalists is how CMS will review inpatient stays based on the number of nights in the hospital. CMS has proposed that any patient who stays in the hospital for two or more “midnights” should be appropriate for payment under Medicare Part A. For those who stay in the hospital for only one (or zero) midnights, payment under Medicare Part A will only be appropriate if:
- There is sufficient documentation at the time of admission that the anticipated length of stay is two or more nights; and.
- Further documentation that circumstances changed, and the hospital stay ended prematurely because of those changes.
Overall for hospitalists, this should substantially simplify the admitting process, whereby most inpatients being admitted with the anticipation of two or more nights should qualify for an inpatient stay. This also reduces the administrative burden of correcting the “inpatient” versus “observation” designation, which keeps many hospital staffs entirely too busy. This change also should relieve a significant burden from the patients and their families, who if kept in observation for a period of time, may have to pay substantially out of pocket to make up for the difference between the cost of the stay and the reimbursement from CMS for observation status. So this is one of the moves that CMS is making to simplify (and not complicate) an already too-complicated payment system. This should go into effect October 2013 and will be a sigh of much relief from many of us.
A few other anticipated changes that will affect hospitalists include:
Payments for Unfunded Care
Another major change that will go into affect October 2013 is the amount of monies received by hospitals that care for unfunded patients. These payments historically have been made to “Disproportionate Share Hospitals” (DSH), which are hospitals that care for a higher percentage of unfunded patients. Under the Affordable Care Act, only 25% of these payments will be distributed to DSH hospitals; the remaining 75% will be reduced based on the number of uninsured in the U.S., then redistributed to DSH hospitals based on their portion of uninsured care delivered.
Most DSH hospitals should expect a decrease in DSH payments, the amount of which will depend on their share of unfunded patients.
Any reduction in the “bottom line” to the hospital can affect hospitalists, especially those who are directly employed by the hospital.
Hospital-Acquired Conditions
CMS has long had the Hospital-Acquired Condition (HAC) program in effect, which has the ability to reduce the amount of payment for inpatients who acquire a HAC during their hospital stay. Starting in October 2014, CMS will impose additional financial penalties for hospitals with high HAC rates.
Specifically, those hospitals in the highest 25th percentile of HAC rates will be penalized 1% of their overall CMS payments. Another proposed change is that the following be included in the HAC reduction plan (two “domains” of measures):
- Domain No. 1: Six of the AHRQ Patient Safety Indicators (PSIs), including pressure ulcers, foreign bodies left in after surgery, iatrogenic pneumothorax, postoperative physiologic or metabolic derangements, postoperative VTE, and accidental puncture/laceration.
- Domain No. 2: Central-line-associated bloodstream infections (CLABSI) and catheter-associated urinary tract infections (CAUTIs).
The domains will be weighted equally, and an average score will determine the total score. There will be some methodology for risk adjustment, and hospitals will be given a review and comment period to validate their own scores.
Most hospitalists have at least indirect control over many of these HACs,and all need to pay very close attention to their hospital’s rates of these now and in the future.
Readmissions
As we all know, the Hospital Readmission Reduction program went into effect October 2012; it placed 1% of CMS payments at risk. This will increase to 2% of payments as of October 2013. CMS will continue to use AMI, CHF, and pneumonia as the three conditions under which the readmissions are measured but will put in some methodology to account for planned readmissions.
In addition, in October 2014, they plan to add readmission rates for COPD and for hip/knee arthroplasty.
Hospitalists will continue to need to progress their transitions of care programs, at least for these five patients conditions but more likely (and more effectively) for all hospital discharges.
Quality Measures
Currently more than 99% of acute-care hospitals participate in the pay-for-reporting quality program through CMS, the results of which have been displayed on the Hospital Compare website (www.hospitalcompare.hhs.gov) for years. The program started in 2004 with 10 quality metrics and now includes 57 metrics. These include process and outcome measures for AMI, CHF, and pneumonia, as well as process measures for surgical care, HACs, and patient-satisfaction surveys, among others.
This program will continue to expand over time, including hospital-acquired MRSA and Clostridium difficile rates. The few hospitals not participating will have their CMS annual payments reduced by 2%.
EHR Incentives
CMS is evaluating ways to reduce the burden of reporting by aligning EHR incentives with the Inpatient Quality Reporting program.
Summary
After an open commentary period, the Final Rule will be published Aug. 1, and will become effective for discharges on or after Oct. 1. Although CMS will continue to expand the total number of measures that need to be reported, and the penalties for non-reporting or low performance will continue to escalate, CMS is at least attempting to reduce the overall burden of reporting by combining measures and programs over time and using EHRs to facilitate the bulk of reporting over time.
The global message to hospitalists is: Continue to focus on reducing the burden of HACs, enhance throughput, and carefully and thoughtfully transition patients to the next provider after their hospital discharge. All in all, although at times this can feel overwhelming, these changes represent the right direction to move for high-quality and safe patient care.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Reference
The Centers for Medicare & Medicaid Services (CMS) recently released a few Fact Sheets on how they anticipate funding changes on a few of their programs that were implemented (or sustained) under the Affordable Care Act. As a background, CMS pays most acute-care hospitals by prospectively determining payment based on a patient’s diagnosis and the severity of illness within that diagnosis (e.g. “MS-DRG”). These payment amounts are updated annually after evaluating several factors, including the costs associated with the delivery of care.
One of the most major changes described in the Fact Sheet that will affect hospitalists is how CMS will review inpatient stays based on the number of nights in the hospital. CMS has proposed that any patient who stays in the hospital for two or more “midnights” should be appropriate for payment under Medicare Part A. For those who stay in the hospital for only one (or zero) midnights, payment under Medicare Part A will only be appropriate if:
- There is sufficient documentation at the time of admission that the anticipated length of stay is two or more nights; and.
- Further documentation that circumstances changed, and the hospital stay ended prematurely because of those changes.
Overall for hospitalists, this should substantially simplify the admitting process, whereby most inpatients being admitted with the anticipation of two or more nights should qualify for an inpatient stay. This also reduces the administrative burden of correcting the “inpatient” versus “observation” designation, which keeps many hospital staffs entirely too busy. This change also should relieve a significant burden from the patients and their families, who if kept in observation for a period of time, may have to pay substantially out of pocket to make up for the difference between the cost of the stay and the reimbursement from CMS for observation status. So this is one of the moves that CMS is making to simplify (and not complicate) an already too-complicated payment system. This should go into effect October 2013 and will be a sigh of much relief from many of us.
A few other anticipated changes that will affect hospitalists include:
Payments for Unfunded Care
Another major change that will go into affect October 2013 is the amount of monies received by hospitals that care for unfunded patients. These payments historically have been made to “Disproportionate Share Hospitals” (DSH), which are hospitals that care for a higher percentage of unfunded patients. Under the Affordable Care Act, only 25% of these payments will be distributed to DSH hospitals; the remaining 75% will be reduced based on the number of uninsured in the U.S., then redistributed to DSH hospitals based on their portion of uninsured care delivered.
Most DSH hospitals should expect a decrease in DSH payments, the amount of which will depend on their share of unfunded patients.
Any reduction in the “bottom line” to the hospital can affect hospitalists, especially those who are directly employed by the hospital.
Hospital-Acquired Conditions
CMS has long had the Hospital-Acquired Condition (HAC) program in effect, which has the ability to reduce the amount of payment for inpatients who acquire a HAC during their hospital stay. Starting in October 2014, CMS will impose additional financial penalties for hospitals with high HAC rates.
Specifically, those hospitals in the highest 25th percentile of HAC rates will be penalized 1% of their overall CMS payments. Another proposed change is that the following be included in the HAC reduction plan (two “domains” of measures):
- Domain No. 1: Six of the AHRQ Patient Safety Indicators (PSIs), including pressure ulcers, foreign bodies left in after surgery, iatrogenic pneumothorax, postoperative physiologic or metabolic derangements, postoperative VTE, and accidental puncture/laceration.
- Domain No. 2: Central-line-associated bloodstream infections (CLABSI) and catheter-associated urinary tract infections (CAUTIs).
The domains will be weighted equally, and an average score will determine the total score. There will be some methodology for risk adjustment, and hospitals will be given a review and comment period to validate their own scores.
Most hospitalists have at least indirect control over many of these HACs,and all need to pay very close attention to their hospital’s rates of these now and in the future.
Readmissions
As we all know, the Hospital Readmission Reduction program went into effect October 2012; it placed 1% of CMS payments at risk. This will increase to 2% of payments as of October 2013. CMS will continue to use AMI, CHF, and pneumonia as the three conditions under which the readmissions are measured but will put in some methodology to account for planned readmissions.
In addition, in October 2014, they plan to add readmission rates for COPD and for hip/knee arthroplasty.
Hospitalists will continue to need to progress their transitions of care programs, at least for these five patients conditions but more likely (and more effectively) for all hospital discharges.
Quality Measures
Currently more than 99% of acute-care hospitals participate in the pay-for-reporting quality program through CMS, the results of which have been displayed on the Hospital Compare website (www.hospitalcompare.hhs.gov) for years. The program started in 2004 with 10 quality metrics and now includes 57 metrics. These include process and outcome measures for AMI, CHF, and pneumonia, as well as process measures for surgical care, HACs, and patient-satisfaction surveys, among others.
This program will continue to expand over time, including hospital-acquired MRSA and Clostridium difficile rates. The few hospitals not participating will have their CMS annual payments reduced by 2%.
EHR Incentives
CMS is evaluating ways to reduce the burden of reporting by aligning EHR incentives with the Inpatient Quality Reporting program.
Summary
After an open commentary period, the Final Rule will be published Aug. 1, and will become effective for discharges on or after Oct. 1. Although CMS will continue to expand the total number of measures that need to be reported, and the penalties for non-reporting or low performance will continue to escalate, CMS is at least attempting to reduce the overall burden of reporting by combining measures and programs over time and using EHRs to facilitate the bulk of reporting over time.
The global message to hospitalists is: Continue to focus on reducing the burden of HACs, enhance throughput, and carefully and thoughtfully transition patients to the next provider after their hospital discharge. All in all, although at times this can feel overwhelming, these changes represent the right direction to move for high-quality and safe patient care.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Reference
Steps Hospitalists Should Take to Reduce Turnaround Time of Death Certificates

Funeral-home representatives sometimes make multiple trips to a hospital or doctor’s office to get a death certificate signed, often waiting in the lobby for hours. I first realized this in the 1980s when starting post-residency practice as a hospitalist. I began asking these guys (they are nearly always men, in my experience) how much time they typically invest getting each certificate signed. They told of walking halfway across a golf course to catch the doctor on the 13th hole or making the 90-minute drive (each way) to a doctor’s office, sometimes finding the doctor had just left, only to repeat the process several times before getting the signature.
When the Clinton administration made electronic signatures via the Internet valid, I thought about starting a business charging funeral homes something like $200 for getting the doctor to sign it electronically within 48 hours. I would use about half of the $200 to provide an incentive for the doctor to sign quickly (sign within 48 hours, and you’ll get a $100 gift card!), then use the rest to fund the company. Since funeral homes probably spend much more than $200 per certificate paying their staff to drive around getting signatures on paper, I thought they would jump at this idea.
I never pursued it, but that doesn’t stop me from loudly proclaiming to friends and family that it was a “can’t-miss” blockbuster Internet business idea. Of course, I never tested that theory, but it makes for fun chest-thumping at parties.
A number of states, including Florida, Texas, and others, now have in place online completion of death certificates. Indiana has required use of its online death certificate since 2011; there is no option to use paper. I suspect nearly every state will do the same before long. But that alone won’t ensure timely completion. Doctors and others who complete the certificates need to ensure they respond quickly, something they often fail to do.
It Really Matters
Lack of a death certificate can hold up burial or cremation, and things like life-insurance payouts and estate settlement are delayed. For a grieving family, these things only add to their pain.
I’m aware of a tragic case from a few years ago in which a certificate was passed around to a number of doctors, each of whom thought with some justification that someone else should sign it. It sat in two different mailboxes for many days while the intended recipients were vacationing. All of this delayed the burial, and the poor family had to send updates to loved ones saying, “We don’t know when Dad’s funeral will be.” About three weeks later, the certificate was completed and the funeral held. What a terribly sad story!
Some states have laws governing how quickly certificates must be signed. A thought-provoking 2004 Medical Staff Update from Stanford University says that California requires a signature within 15 hours of death, though I wonder how often this is enforced.
Improving Turnaround Time
There are several things hospitalists could consider to improve timely completion of death certificates:
- Ensure doctors liberally complete them for one another. Don’t let one doctor’s absence delay, even for a day, getting it completed and signed. This means the “covering” doctor has access to the discharge (death) summary in the medical record.
- When several doctors in different specialties are caring for a patient at the time of death, nearly any of them could reasonably sign the certificate. It might be appropriate to adopt a policy that whichever doctor (e.g. hospitalist, intensivist, or oncologist) who had contact with the patient and is presented with the certificate should go ahead and sign it rather than passing it along to one of the other specialties, regardless of which served as attending.
- Consider creating a central access point at your hospital for receipt of death certificates. Ideally, a funeral-home representative can deliver it to one person at the hospital who will do the leg work of getting a doctor to sign it quickly. Delays are likely if the funeral-home representative has to “shop it around” to different departments and physician offices. A hospital staffer should be able to navigate this quickly.
- Pressure EMR vendors to include some sort of death-certificate functionality in the future. I don’t know if some have it already, but it seems like it shouldn’t be too difficult for an EMR to spit out a prefilled certificate in much the same way e-prescribing works. It could even be delivered electronically to the funeral home.
- For hospitalists with 24-hour, on-site presence, it could be reasonable to have an on-duty hospitalist complete the certificate at the time of death rather than waiting for the funeral home to initiate the process. This was standard when I was a resident, and it may be a practical approach in many settings.
- Consider copying one hospital I worked with previously: They created a hospitalist salary bonus for timely completion. I assure you this policy was very effective.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Funeral-home representatives sometimes make multiple trips to a hospital or doctor’s office to get a death certificate signed, often waiting in the lobby for hours. I first realized this in the 1980s when starting post-residency practice as a hospitalist. I began asking these guys (they are nearly always men, in my experience) how much time they typically invest getting each certificate signed. They told of walking halfway across a golf course to catch the doctor on the 13th hole or making the 90-minute drive (each way) to a doctor’s office, sometimes finding the doctor had just left, only to repeat the process several times before getting the signature.
When the Clinton administration made electronic signatures via the Internet valid, I thought about starting a business charging funeral homes something like $200 for getting the doctor to sign it electronically within 48 hours. I would use about half of the $200 to provide an incentive for the doctor to sign quickly (sign within 48 hours, and you’ll get a $100 gift card!), then use the rest to fund the company. Since funeral homes probably spend much more than $200 per certificate paying their staff to drive around getting signatures on paper, I thought they would jump at this idea.
I never pursued it, but that doesn’t stop me from loudly proclaiming to friends and family that it was a “can’t-miss” blockbuster Internet business idea. Of course, I never tested that theory, but it makes for fun chest-thumping at parties.
A number of states, including Florida, Texas, and others, now have in place online completion of death certificates. Indiana has required use of its online death certificate since 2011; there is no option to use paper. I suspect nearly every state will do the same before long. But that alone won’t ensure timely completion. Doctors and others who complete the certificates need to ensure they respond quickly, something they often fail to do.
It Really Matters
Lack of a death certificate can hold up burial or cremation, and things like life-insurance payouts and estate settlement are delayed. For a grieving family, these things only add to their pain.
I’m aware of a tragic case from a few years ago in which a certificate was passed around to a number of doctors, each of whom thought with some justification that someone else should sign it. It sat in two different mailboxes for many days while the intended recipients were vacationing. All of this delayed the burial, and the poor family had to send updates to loved ones saying, “We don’t know when Dad’s funeral will be.” About three weeks later, the certificate was completed and the funeral held. What a terribly sad story!
Some states have laws governing how quickly certificates must be signed. A thought-provoking 2004 Medical Staff Update from Stanford University says that California requires a signature within 15 hours of death, though I wonder how often this is enforced.
Improving Turnaround Time
There are several things hospitalists could consider to improve timely completion of death certificates:
- Ensure doctors liberally complete them for one another. Don’t let one doctor’s absence delay, even for a day, getting it completed and signed. This means the “covering” doctor has access to the discharge (death) summary in the medical record.
- When several doctors in different specialties are caring for a patient at the time of death, nearly any of them could reasonably sign the certificate. It might be appropriate to adopt a policy that whichever doctor (e.g. hospitalist, intensivist, or oncologist) who had contact with the patient and is presented with the certificate should go ahead and sign it rather than passing it along to one of the other specialties, regardless of which served as attending.
- Consider creating a central access point at your hospital for receipt of death certificates. Ideally, a funeral-home representative can deliver it to one person at the hospital who will do the leg work of getting a doctor to sign it quickly. Delays are likely if the funeral-home representative has to “shop it around” to different departments and physician offices. A hospital staffer should be able to navigate this quickly.
- Pressure EMR vendors to include some sort of death-certificate functionality in the future. I don’t know if some have it already, but it seems like it shouldn’t be too difficult for an EMR to spit out a prefilled certificate in much the same way e-prescribing works. It could even be delivered electronically to the funeral home.
- For hospitalists with 24-hour, on-site presence, it could be reasonable to have an on-duty hospitalist complete the certificate at the time of death rather than waiting for the funeral home to initiate the process. This was standard when I was a resident, and it may be a practical approach in many settings.
- Consider copying one hospital I worked with previously: They created a hospitalist salary bonus for timely completion. I assure you this policy was very effective.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Funeral-home representatives sometimes make multiple trips to a hospital or doctor’s office to get a death certificate signed, often waiting in the lobby for hours. I first realized this in the 1980s when starting post-residency practice as a hospitalist. I began asking these guys (they are nearly always men, in my experience) how much time they typically invest getting each certificate signed. They told of walking halfway across a golf course to catch the doctor on the 13th hole or making the 90-minute drive (each way) to a doctor’s office, sometimes finding the doctor had just left, only to repeat the process several times before getting the signature.
When the Clinton administration made electronic signatures via the Internet valid, I thought about starting a business charging funeral homes something like $200 for getting the doctor to sign it electronically within 48 hours. I would use about half of the $200 to provide an incentive for the doctor to sign quickly (sign within 48 hours, and you’ll get a $100 gift card!), then use the rest to fund the company. Since funeral homes probably spend much more than $200 per certificate paying their staff to drive around getting signatures on paper, I thought they would jump at this idea.
I never pursued it, but that doesn’t stop me from loudly proclaiming to friends and family that it was a “can’t-miss” blockbuster Internet business idea. Of course, I never tested that theory, but it makes for fun chest-thumping at parties.
A number of states, including Florida, Texas, and others, now have in place online completion of death certificates. Indiana has required use of its online death certificate since 2011; there is no option to use paper. I suspect nearly every state will do the same before long. But that alone won’t ensure timely completion. Doctors and others who complete the certificates need to ensure they respond quickly, something they often fail to do.
It Really Matters
Lack of a death certificate can hold up burial or cremation, and things like life-insurance payouts and estate settlement are delayed. For a grieving family, these things only add to their pain.
I’m aware of a tragic case from a few years ago in which a certificate was passed around to a number of doctors, each of whom thought with some justification that someone else should sign it. It sat in two different mailboxes for many days while the intended recipients were vacationing. All of this delayed the burial, and the poor family had to send updates to loved ones saying, “We don’t know when Dad’s funeral will be.” About three weeks later, the certificate was completed and the funeral held. What a terribly sad story!
Some states have laws governing how quickly certificates must be signed. A thought-provoking 2004 Medical Staff Update from Stanford University says that California requires a signature within 15 hours of death, though I wonder how often this is enforced.
Improving Turnaround Time
There are several things hospitalists could consider to improve timely completion of death certificates:
- Ensure doctors liberally complete them for one another. Don’t let one doctor’s absence delay, even for a day, getting it completed and signed. This means the “covering” doctor has access to the discharge (death) summary in the medical record.
- When several doctors in different specialties are caring for a patient at the time of death, nearly any of them could reasonably sign the certificate. It might be appropriate to adopt a policy that whichever doctor (e.g. hospitalist, intensivist, or oncologist) who had contact with the patient and is presented with the certificate should go ahead and sign it rather than passing it along to one of the other specialties, regardless of which served as attending.
- Consider creating a central access point at your hospital for receipt of death certificates. Ideally, a funeral-home representative can deliver it to one person at the hospital who will do the leg work of getting a doctor to sign it quickly. Delays are likely if the funeral-home representative has to “shop it around” to different departments and physician offices. A hospital staffer should be able to navigate this quickly.
- Pressure EMR vendors to include some sort of death-certificate functionality in the future. I don’t know if some have it already, but it seems like it shouldn’t be too difficult for an EMR to spit out a prefilled certificate in much the same way e-prescribing works. It could even be delivered electronically to the funeral home.
- For hospitalists with 24-hour, on-site presence, it could be reasonable to have an on-duty hospitalist complete the certificate at the time of death rather than waiting for the funeral home to initiate the process. This was standard when I was a resident, and it may be a practical approach in many settings.
- Consider copying one hospital I worked with previously: They created a hospitalist salary bonus for timely completion. I assure you this policy was very effective.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Hospitalists Should Research Salary Range by Market Before Negotiating a Job Offer

I am a third-year internal-medicine resident and currently looking for a nocturnist opportunity. I have no experience in negotiating a job or salary. When I interview for a job, should I negotiate for salary? How do I know that the salary is correct and what others in the same group are getting? Thanks for the help.
–Santhosh Mannem, New York City
Dr. Hospitalist responds:
Salary discussions are always intriguing, mainly because you won’t really know what everyone else is getting paid. There are several places to get some information. To begin, find out the general salary range for the market in which you want to work. Just because an annual salary might be $240,000 in Emporia, Kan., doesn’t mean a thing if you are looking for a job in Salt Lake City or Seattle. You can use the online resources through SHM (www.hospitalmedicine.org/survey) to paint a pretty good picture of salary by region, but remember that these are ranges only.
When I think of job offers, I like to take total compensation and break it down by category. For example, benefits are not negotiable—your employer cannot vary the health insurance coverage they provide by physician. Still, you need to consider benefits as an important part of the package. A good health insurance plan won’t mean as much to a single physician as it would to one with a family, so consider your individual needs. I strongly encourage you to make a line item for every potential benefit: health, dental, disability, life, continuing medical education (CME), professional dues, retirement plans (potentially with an employer match), malpractice insurance costs, and so on. A job with a “salary” of $300,000 but no benefits would pale in comparison to a job paying $250,000 with full benefits.
Don’t discount the value of benefits; get the numbers and assign a dollar amount. If the group is not being transparent on benefits, walk away.
With strict regard to salary, you probably will get little to no information as to what the rest of the group members are paid. Feel free to ask, but expect some vague answers. Most often, there is a fairly tight convergence of salaries within a given market, and it’s always better to interview for more than one job in the same location. You mentioned that you’d like to work as a nocturnist, which is good. These positions are recruited heavily and tend to command a higher initial salary.
Overall, your ability to negotiate a higher salary is going to be rather limited. However, there is another calculation worth mentioning: You need to find out how much you are being paid per unit of work so you can compare jobs. Here are some of the items to help you figure out a formula that works for you: annual salary, contracted shifts per year/month, pay per shift, admits/census per shift, number of weekends, and potential bonus thresholds. Use these numbers (metrics) to more accurately compare different jobs. There is no magic formula; it just depends on what is important to you, but you will get a much better picture if you combine these metrics with your benefit analysis.
As a nocturnist, I would not expect to hit any productivity metrics. If you are that busy, it’s probably a miserable job. In a business sense, nights almost always lose money.
One thing that can always be negotiated: a signing bonus and/or loan forgiveness. Often, a practice won’t want to continually offer higher starting salaries since eventually this causes wage creep across the practice. However, they can be much more flexible when it comes to “one-time” payments. This keeps the overall salary structure for the practice intact and is usually much more agreeable for your employer. As always, it’s a supply-and-demand issue, but if you are a nocturnist looking at a high-demand area, I would negotiate hard for a signing bonus and maybe even a contract-renewal bonus after your first year.
It never hurts to get creative, either. I remember negotiating my first job; I offered to sign a two-year contract (instead of one) if they would let me take off six months the first year. They said yes, I did some traveling that first year on my new salary, and I stayed with the practice for 11 years. Don’t get so caught up in salary numbers that you lose sight of what’s really important to you and whether the job would be the right fit.
Good luck and welcome to hospital medicine. You’ll love it.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to [email protected].
I am a third-year internal-medicine resident and currently looking for a nocturnist opportunity. I have no experience in negotiating a job or salary. When I interview for a job, should I negotiate for salary? How do I know that the salary is correct and what others in the same group are getting? Thanks for the help.
–Santhosh Mannem, New York City
Dr. Hospitalist responds:
Salary discussions are always intriguing, mainly because you won’t really know what everyone else is getting paid. There are several places to get some information. To begin, find out the general salary range for the market in which you want to work. Just because an annual salary might be $240,000 in Emporia, Kan., doesn’t mean a thing if you are looking for a job in Salt Lake City or Seattle. You can use the online resources through SHM (www.hospitalmedicine.org/survey) to paint a pretty good picture of salary by region, but remember that these are ranges only.
When I think of job offers, I like to take total compensation and break it down by category. For example, benefits are not negotiable—your employer cannot vary the health insurance coverage they provide by physician. Still, you need to consider benefits as an important part of the package. A good health insurance plan won’t mean as much to a single physician as it would to one with a family, so consider your individual needs. I strongly encourage you to make a line item for every potential benefit: health, dental, disability, life, continuing medical education (CME), professional dues, retirement plans (potentially with an employer match), malpractice insurance costs, and so on. A job with a “salary” of $300,000 but no benefits would pale in comparison to a job paying $250,000 with full benefits.
Don’t discount the value of benefits; get the numbers and assign a dollar amount. If the group is not being transparent on benefits, walk away.
With strict regard to salary, you probably will get little to no information as to what the rest of the group members are paid. Feel free to ask, but expect some vague answers. Most often, there is a fairly tight convergence of salaries within a given market, and it’s always better to interview for more than one job in the same location. You mentioned that you’d like to work as a nocturnist, which is good. These positions are recruited heavily and tend to command a higher initial salary.
Overall, your ability to negotiate a higher salary is going to be rather limited. However, there is another calculation worth mentioning: You need to find out how much you are being paid per unit of work so you can compare jobs. Here are some of the items to help you figure out a formula that works for you: annual salary, contracted shifts per year/month, pay per shift, admits/census per shift, number of weekends, and potential bonus thresholds. Use these numbers (metrics) to more accurately compare different jobs. There is no magic formula; it just depends on what is important to you, but you will get a much better picture if you combine these metrics with your benefit analysis.
As a nocturnist, I would not expect to hit any productivity metrics. If you are that busy, it’s probably a miserable job. In a business sense, nights almost always lose money.
One thing that can always be negotiated: a signing bonus and/or loan forgiveness. Often, a practice won’t want to continually offer higher starting salaries since eventually this causes wage creep across the practice. However, they can be much more flexible when it comes to “one-time” payments. This keeps the overall salary structure for the practice intact and is usually much more agreeable for your employer. As always, it’s a supply-and-demand issue, but if you are a nocturnist looking at a high-demand area, I would negotiate hard for a signing bonus and maybe even a contract-renewal bonus after your first year.
It never hurts to get creative, either. I remember negotiating my first job; I offered to sign a two-year contract (instead of one) if they would let me take off six months the first year. They said yes, I did some traveling that first year on my new salary, and I stayed with the practice for 11 years. Don’t get so caught up in salary numbers that you lose sight of what’s really important to you and whether the job would be the right fit.
Good luck and welcome to hospital medicine. You’ll love it.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to [email protected].
I am a third-year internal-medicine resident and currently looking for a nocturnist opportunity. I have no experience in negotiating a job or salary. When I interview for a job, should I negotiate for salary? How do I know that the salary is correct and what others in the same group are getting? Thanks for the help.
–Santhosh Mannem, New York City
Dr. Hospitalist responds:
Salary discussions are always intriguing, mainly because you won’t really know what everyone else is getting paid. There are several places to get some information. To begin, find out the general salary range for the market in which you want to work. Just because an annual salary might be $240,000 in Emporia, Kan., doesn’t mean a thing if you are looking for a job in Salt Lake City or Seattle. You can use the online resources through SHM (www.hospitalmedicine.org/survey) to paint a pretty good picture of salary by region, but remember that these are ranges only.
When I think of job offers, I like to take total compensation and break it down by category. For example, benefits are not negotiable—your employer cannot vary the health insurance coverage they provide by physician. Still, you need to consider benefits as an important part of the package. A good health insurance plan won’t mean as much to a single physician as it would to one with a family, so consider your individual needs. I strongly encourage you to make a line item for every potential benefit: health, dental, disability, life, continuing medical education (CME), professional dues, retirement plans (potentially with an employer match), malpractice insurance costs, and so on. A job with a “salary” of $300,000 but no benefits would pale in comparison to a job paying $250,000 with full benefits.
Don’t discount the value of benefits; get the numbers and assign a dollar amount. If the group is not being transparent on benefits, walk away.
With strict regard to salary, you probably will get little to no information as to what the rest of the group members are paid. Feel free to ask, but expect some vague answers. Most often, there is a fairly tight convergence of salaries within a given market, and it’s always better to interview for more than one job in the same location. You mentioned that you’d like to work as a nocturnist, which is good. These positions are recruited heavily and tend to command a higher initial salary.
Overall, your ability to negotiate a higher salary is going to be rather limited. However, there is another calculation worth mentioning: You need to find out how much you are being paid per unit of work so you can compare jobs. Here are some of the items to help you figure out a formula that works for you: annual salary, contracted shifts per year/month, pay per shift, admits/census per shift, number of weekends, and potential bonus thresholds. Use these numbers (metrics) to more accurately compare different jobs. There is no magic formula; it just depends on what is important to you, but you will get a much better picture if you combine these metrics with your benefit analysis.
As a nocturnist, I would not expect to hit any productivity metrics. If you are that busy, it’s probably a miserable job. In a business sense, nights almost always lose money.
One thing that can always be negotiated: a signing bonus and/or loan forgiveness. Often, a practice won’t want to continually offer higher starting salaries since eventually this causes wage creep across the practice. However, they can be much more flexible when it comes to “one-time” payments. This keeps the overall salary structure for the practice intact and is usually much more agreeable for your employer. As always, it’s a supply-and-demand issue, but if you are a nocturnist looking at a high-demand area, I would negotiate hard for a signing bonus and maybe even a contract-renewal bonus after your first year.
It never hurts to get creative, either. I remember negotiating my first job; I offered to sign a two-year contract (instead of one) if they would let me take off six months the first year. They said yes, I did some traveling that first year on my new salary, and I stayed with the practice for 11 years. Don’t get so caught up in salary numbers that you lose sight of what’s really important to you and whether the job would be the right fit.
Good luck and welcome to hospital medicine. You’ll love it.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to [email protected].
Should Skyrocketing Health Care Costs Concern Hospitalists?
Median hospitalist compensation has grown steadily over the past decade, but physicians aren’t immune to the sting of accelerated premiums, copays, and contributions imposed by health insurers.
According to the Hay Group’s 2011 Physician Compensation Survey, the number of physicians who contributing to health insurance premiums increased to 68% in 2011 from 58% in 2010. The survey showed only 9% of physicians did not pay anything for medical coverage, down from 19% in 2010.
Moreover, the expected physician contribution was between 1% and 25% of the premium.
Dan Fuller, president and cofounder of Alpharetta, Ga.-based IN Compass Health, has noticed an uptick in candidates’ interest in their health-care benefits. “Especially for physicians who have families, health benefits have become one of the top issues in recruiting,” the SHM Practice Analysis Committee (PAC) member says.
Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America in Nashville, Tenn., reports that he is seeing an upward trend in employees’ contributions to premiums and out-of-pocket costs. He’s also observed colleagues becoming more selective when choosing their own health-care plans and how they use those plans.
Gretchen Henkel is a freelance writer in California.
Median hospitalist compensation has grown steadily over the past decade, but physicians aren’t immune to the sting of accelerated premiums, copays, and contributions imposed by health insurers.
According to the Hay Group’s 2011 Physician Compensation Survey, the number of physicians who contributing to health insurance premiums increased to 68% in 2011 from 58% in 2010. The survey showed only 9% of physicians did not pay anything for medical coverage, down from 19% in 2010.
Moreover, the expected physician contribution was between 1% and 25% of the premium.
Dan Fuller, president and cofounder of Alpharetta, Ga.-based IN Compass Health, has noticed an uptick in candidates’ interest in their health-care benefits. “Especially for physicians who have families, health benefits have become one of the top issues in recruiting,” the SHM Practice Analysis Committee (PAC) member says.
Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America in Nashville, Tenn., reports that he is seeing an upward trend in employees’ contributions to premiums and out-of-pocket costs. He’s also observed colleagues becoming more selective when choosing their own health-care plans and how they use those plans.
Gretchen Henkel is a freelance writer in California.
Median hospitalist compensation has grown steadily over the past decade, but physicians aren’t immune to the sting of accelerated premiums, copays, and contributions imposed by health insurers.
According to the Hay Group’s 2011 Physician Compensation Survey, the number of physicians who contributing to health insurance premiums increased to 68% in 2011 from 58% in 2010. The survey showed only 9% of physicians did not pay anything for medical coverage, down from 19% in 2010.
Moreover, the expected physician contribution was between 1% and 25% of the premium.
Dan Fuller, president and cofounder of Alpharetta, Ga.-based IN Compass Health, has noticed an uptick in candidates’ interest in their health-care benefits. “Especially for physicians who have families, health benefits have become one of the top issues in recruiting,” the SHM Practice Analysis Committee (PAC) member says.
Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America in Nashville, Tenn., reports that he is seeing an upward trend in employees’ contributions to premiums and out-of-pocket costs. He’s also observed colleagues becoming more selective when choosing their own health-care plans and how they use those plans.
Gretchen Henkel is a freelance writer in California.
Advanced-Practice Providers Have More to Offer Hospital Medicine Groups

Advanced-practice providers (APPs) continue to make their presence felt in the world of hospital medicine. According to survey data from the 2012 State of Hospital Medicine report, more than half (53.9%) of respondent groups serving adults have nurse practitioners (NP) and/or physician assistants (PA) integrated into their practices. The median ratio of APPs to hospitalist physicians in these groups has remained about the same as in previous surveys, with respondents reporting 0.2 FTE NPs per FTE physician, and 0.1 FTE PAs per FTE physician. We’ve also learned that APPs tend to be stable members of most hospitalist practices, with more than 70% of groups reporting no turnover among their APPs during the survey period.
Unfortunately, we don’t yet have much information on the specific roles APPs are filling in HM practices; hopefully, this will be a subject for the next State of Hospital Medicine survey, scheduled to launch in January 2014.
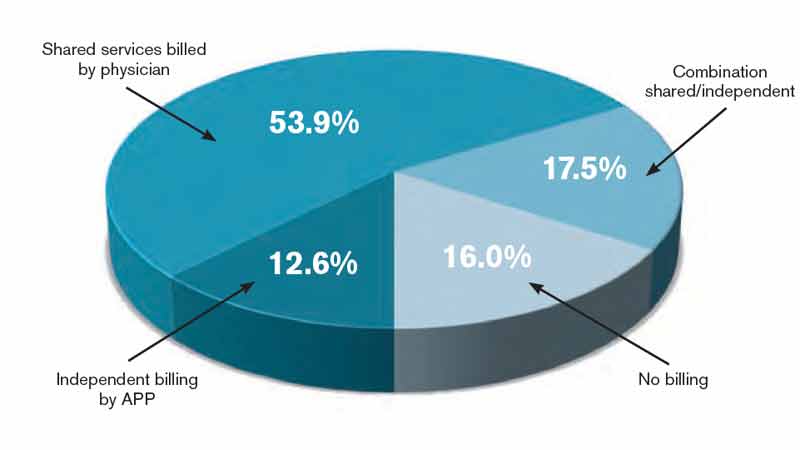
The 2012 survey did provide new information about how APP work is billed by HM groups. More than half the time, APP work is billed as a shared service under a physician’s provider number (see Table 1). Only on rare occasions is APP work billed separately under the APP’s provider number.
Perhaps most surprising of all, 16% of adult HM groups with APPs reported that their APPs don’t generally provide billable services, or no charges were submitted to payors for their services. This figure rose to 23% for hospital-employed groups.
Almost everywhere I go in my consulting work, we are asked about the value APPs can provide to hospitalist practice, and what their optimal roles are. I am extremely supportive of integrating APPs into hospitalist practice and believe they can play valuable roles supporting both excellent patient care and overall group efficiency.
But in my experience, many HM groups fail to execute well on this promise. As the survey results suggest, sometimes APPs are relegated to nonbillable tasks that could be performed by individuals at a lower skill level. Sometimes the hospitalists tend to think of the APPs as “free” help, and no real attempt is made to account for their contribution or capture their billable work. And some groups are so focused on ensuring they capture the 100% reimbursement available by billing under the physician’s name (rather than the 85% reimbursement typically available to APPs) that they lose sight of the fact that the extra physician time and effort involved might cost more than the incremental additional reimbursement received.
As a specialty, we still have a lot to learn about the optimal ways to deploy APPs to support high-quality, effective hospitalist practice. In the meantime, it can be valuable for HM groups to ensure that APPs are functioning in roles that take advantage of their advanced skills and licensure scope, and that efforts are being made to ensure the capture of all billable services provided.
I hope you will plan to participate in the 2014 State of Hospital Medicine survey and share your own practice’s experience with APPs.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
Advanced-practice providers (APPs) continue to make their presence felt in the world of hospital medicine. According to survey data from the 2012 State of Hospital Medicine report, more than half (53.9%) of respondent groups serving adults have nurse practitioners (NP) and/or physician assistants (PA) integrated into their practices. The median ratio of APPs to hospitalist physicians in these groups has remained about the same as in previous surveys, with respondents reporting 0.2 FTE NPs per FTE physician, and 0.1 FTE PAs per FTE physician. We’ve also learned that APPs tend to be stable members of most hospitalist practices, with more than 70% of groups reporting no turnover among their APPs during the survey period.
Unfortunately, we don’t yet have much information on the specific roles APPs are filling in HM practices; hopefully, this will be a subject for the next State of Hospital Medicine survey, scheduled to launch in January 2014.
The 2012 survey did provide new information about how APP work is billed by HM groups. More than half the time, APP work is billed as a shared service under a physician’s provider number (see Table 1). Only on rare occasions is APP work billed separately under the APP’s provider number.
Perhaps most surprising of all, 16% of adult HM groups with APPs reported that their APPs don’t generally provide billable services, or no charges were submitted to payors for their services. This figure rose to 23% for hospital-employed groups.
Almost everywhere I go in my consulting work, we are asked about the value APPs can provide to hospitalist practice, and what their optimal roles are. I am extremely supportive of integrating APPs into hospitalist practice and believe they can play valuable roles supporting both excellent patient care and overall group efficiency.
But in my experience, many HM groups fail to execute well on this promise. As the survey results suggest, sometimes APPs are relegated to nonbillable tasks that could be performed by individuals at a lower skill level. Sometimes the hospitalists tend to think of the APPs as “free” help, and no real attempt is made to account for their contribution or capture their billable work. And some groups are so focused on ensuring they capture the 100% reimbursement available by billing under the physician’s name (rather than the 85% reimbursement typically available to APPs) that they lose sight of the fact that the extra physician time and effort involved might cost more than the incremental additional reimbursement received.
As a specialty, we still have a lot to learn about the optimal ways to deploy APPs to support high-quality, effective hospitalist practice. In the meantime, it can be valuable for HM groups to ensure that APPs are functioning in roles that take advantage of their advanced skills and licensure scope, and that efforts are being made to ensure the capture of all billable services provided.
I hope you will plan to participate in the 2014 State of Hospital Medicine survey and share your own practice’s experience with APPs.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
Advanced-practice providers (APPs) continue to make their presence felt in the world of hospital medicine. According to survey data from the 2012 State of Hospital Medicine report, more than half (53.9%) of respondent groups serving adults have nurse practitioners (NP) and/or physician assistants (PA) integrated into their practices. The median ratio of APPs to hospitalist physicians in these groups has remained about the same as in previous surveys, with respondents reporting 0.2 FTE NPs per FTE physician, and 0.1 FTE PAs per FTE physician. We’ve also learned that APPs tend to be stable members of most hospitalist practices, with more than 70% of groups reporting no turnover among their APPs during the survey period.
Unfortunately, we don’t yet have much information on the specific roles APPs are filling in HM practices; hopefully, this will be a subject for the next State of Hospital Medicine survey, scheduled to launch in January 2014.
The 2012 survey did provide new information about how APP work is billed by HM groups. More than half the time, APP work is billed as a shared service under a physician’s provider number (see Table 1). Only on rare occasions is APP work billed separately under the APP’s provider number.
Perhaps most surprising of all, 16% of adult HM groups with APPs reported that their APPs don’t generally provide billable services, or no charges were submitted to payors for their services. This figure rose to 23% for hospital-employed groups.
Almost everywhere I go in my consulting work, we are asked about the value APPs can provide to hospitalist practice, and what their optimal roles are. I am extremely supportive of integrating APPs into hospitalist practice and believe they can play valuable roles supporting both excellent patient care and overall group efficiency.
But in my experience, many HM groups fail to execute well on this promise. As the survey results suggest, sometimes APPs are relegated to nonbillable tasks that could be performed by individuals at a lower skill level. Sometimes the hospitalists tend to think of the APPs as “free” help, and no real attempt is made to account for their contribution or capture their billable work. And some groups are so focused on ensuring they capture the 100% reimbursement available by billing under the physician’s name (rather than the 85% reimbursement typically available to APPs) that they lose sight of the fact that the extra physician time and effort involved might cost more than the incremental additional reimbursement received.
As a specialty, we still have a lot to learn about the optimal ways to deploy APPs to support high-quality, effective hospitalist practice. In the meantime, it can be valuable for HM groups to ensure that APPs are functioning in roles that take advantage of their advanced skills and licensure scope, and that efforts are being made to ensure the capture of all billable services provided.
I hope you will plan to participate in the 2014 State of Hospital Medicine survey and share your own practice’s experience with APPs.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
RIV Presenters at HM13 Explore Common Hospitalist Concerns
Two oral research poster presentations at HM13 explored malpractice concerns of hospitalists and the issue of defensive-medicine-related overutilization—popular topics considering how policymakers are attempting to bend the cost curve in the direction of greater efficiency and value.
Hospitalist Alan Kachalia, MD, JD, and colleagues at Brigham and Women’s Hospital in Boston conducted a randomized national survey of 1,020 hospitalists and analyzed their responses to common clinical scenarios. They found evidence of inappropriate overutilization and deviance from scientific evidence or recognized treatment guidelines, which the research team pegged to the practice of defensive medicine.
Dr. Kachalia’s presentation, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists,” was named best of the oral presentations in the research category.
“Our survey found substantial overutilization, frequently caused by defensive medicine,” in response to questions about practice patterns for two common clinical scenarios: preoperative evaluation and syncope, Dr. Kachalia said. Physicians who practiced at Veterans Affairs medical centers had less association with defensive medicine, while those who paid for their own liability insurance reported more. Overall, defensive medicine was reported for 37% of preoperative evaluations and 58% of the syncope scenarios.
More than 800 abstracts were submitted for HM13’s Research, Innovations, and Clinical Vignettes (RIV) competition. Nearly 600 were accepted, put on display at the annual meeting, and published online (www.shmabstracts.com). More than 100 abstracts were judged, with 15 of the Research and Innovations entries invited to make oral presentations of their projects. Three others gave “Best of RIV” plenary presentations at the conference.
The diversity and richness of HM13’s oral and poster presentations also will be highlighted in the Innovations department of The Hospitalist over the next year.
Asked to suggest policy responses to these findings, Dr. Kachalia said reform of the malpractice system is needed. “What a lot of us argue is that to get physicians to follow treatment guidelines, make them more clear and practical,” he said. “We’d also like to see safe harbors [from lawsuits] for following recognized guidelines.”
Adam Schaffer, MD, also a hospitalist at Brigham and Women’s Hospital in Boston, and colleagues reviewed a medical liability insurance carrier’s database of more than 30,000 closed claims for those in which a hospitalist was the attending of record. Dr. Schaffer’s retrospective, observational analysis, “Medical Malpractice: Causes and Outcomes of Claims Against Hospitalists,” of the claims database from 1997 to 2011 found 272 claims—almost 1%—for which the attending was a hospitalist.
“The claims rate was almost four times lower for hospitalists than for nonhospitalist internal-medicine physicians,” he said.
The average payment for claims against hospitalists also was smaller. He noted that the types of claims were similar and tended to fall in three general categories: errors in medical treatment, missed or delayed diagnoses, and medication-related errors (although claims also tended to have multiple contributing factors).
Research like Dr. Schaffer’s could help to inform patient-safety efforts and reduce legal malpractice risk, he said. If hospitalists have fewer malpractice claims, that information might also be used to argue for lower malpractice premium rates.
Larry Beresford is a freelance writer in Oakland, Calif.
Two oral research poster presentations at HM13 explored malpractice concerns of hospitalists and the issue of defensive-medicine-related overutilization—popular topics considering how policymakers are attempting to bend the cost curve in the direction of greater efficiency and value.
Hospitalist Alan Kachalia, MD, JD, and colleagues at Brigham and Women’s Hospital in Boston conducted a randomized national survey of 1,020 hospitalists and analyzed their responses to common clinical scenarios. They found evidence of inappropriate overutilization and deviance from scientific evidence or recognized treatment guidelines, which the research team pegged to the practice of defensive medicine.
Dr. Kachalia’s presentation, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists,” was named best of the oral presentations in the research category.
“Our survey found substantial overutilization, frequently caused by defensive medicine,” in response to questions about practice patterns for two common clinical scenarios: preoperative evaluation and syncope, Dr. Kachalia said. Physicians who practiced at Veterans Affairs medical centers had less association with defensive medicine, while those who paid for their own liability insurance reported more. Overall, defensive medicine was reported for 37% of preoperative evaluations and 58% of the syncope scenarios.
More than 800 abstracts were submitted for HM13’s Research, Innovations, and Clinical Vignettes (RIV) competition. Nearly 600 were accepted, put on display at the annual meeting, and published online (www.shmabstracts.com). More than 100 abstracts were judged, with 15 of the Research and Innovations entries invited to make oral presentations of their projects. Three others gave “Best of RIV” plenary presentations at the conference.
The diversity and richness of HM13’s oral and poster presentations also will be highlighted in the Innovations department of The Hospitalist over the next year.
Asked to suggest policy responses to these findings, Dr. Kachalia said reform of the malpractice system is needed. “What a lot of us argue is that to get physicians to follow treatment guidelines, make them more clear and practical,” he said. “We’d also like to see safe harbors [from lawsuits] for following recognized guidelines.”
Adam Schaffer, MD, also a hospitalist at Brigham and Women’s Hospital in Boston, and colleagues reviewed a medical liability insurance carrier’s database of more than 30,000 closed claims for those in which a hospitalist was the attending of record. Dr. Schaffer’s retrospective, observational analysis, “Medical Malpractice: Causes and Outcomes of Claims Against Hospitalists,” of the claims database from 1997 to 2011 found 272 claims—almost 1%—for which the attending was a hospitalist.
“The claims rate was almost four times lower for hospitalists than for nonhospitalist internal-medicine physicians,” he said.
The average payment for claims against hospitalists also was smaller. He noted that the types of claims were similar and tended to fall in three general categories: errors in medical treatment, missed or delayed diagnoses, and medication-related errors (although claims also tended to have multiple contributing factors).
Research like Dr. Schaffer’s could help to inform patient-safety efforts and reduce legal malpractice risk, he said. If hospitalists have fewer malpractice claims, that information might also be used to argue for lower malpractice premium rates.
Larry Beresford is a freelance writer in Oakland, Calif.
Two oral research poster presentations at HM13 explored malpractice concerns of hospitalists and the issue of defensive-medicine-related overutilization—popular topics considering how policymakers are attempting to bend the cost curve in the direction of greater efficiency and value.
Hospitalist Alan Kachalia, MD, JD, and colleagues at Brigham and Women’s Hospital in Boston conducted a randomized national survey of 1,020 hospitalists and analyzed their responses to common clinical scenarios. They found evidence of inappropriate overutilization and deviance from scientific evidence or recognized treatment guidelines, which the research team pegged to the practice of defensive medicine.
Dr. Kachalia’s presentation, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists,” was named best of the oral presentations in the research category.
“Our survey found substantial overutilization, frequently caused by defensive medicine,” in response to questions about practice patterns for two common clinical scenarios: preoperative evaluation and syncope, Dr. Kachalia said. Physicians who practiced at Veterans Affairs medical centers had less association with defensive medicine, while those who paid for their own liability insurance reported more. Overall, defensive medicine was reported for 37% of preoperative evaluations and 58% of the syncope scenarios.
More than 800 abstracts were submitted for HM13’s Research, Innovations, and Clinical Vignettes (RIV) competition. Nearly 600 were accepted, put on display at the annual meeting, and published online (www.shmabstracts.com). More than 100 abstracts were judged, with 15 of the Research and Innovations entries invited to make oral presentations of their projects. Three others gave “Best of RIV” plenary presentations at the conference.
The diversity and richness of HM13’s oral and poster presentations also will be highlighted in the Innovations department of The Hospitalist over the next year.
Asked to suggest policy responses to these findings, Dr. Kachalia said reform of the malpractice system is needed. “What a lot of us argue is that to get physicians to follow treatment guidelines, make them more clear and practical,” he said. “We’d also like to see safe harbors [from lawsuits] for following recognized guidelines.”
Adam Schaffer, MD, also a hospitalist at Brigham and Women’s Hospital in Boston, and colleagues reviewed a medical liability insurance carrier’s database of more than 30,000 closed claims for those in which a hospitalist was the attending of record. Dr. Schaffer’s retrospective, observational analysis, “Medical Malpractice: Causes and Outcomes of Claims Against Hospitalists,” of the claims database from 1997 to 2011 found 272 claims—almost 1%—for which the attending was a hospitalist.
“The claims rate was almost four times lower for hospitalists than for nonhospitalist internal-medicine physicians,” he said.
The average payment for claims against hospitalists also was smaller. He noted that the types of claims were similar and tended to fall in three general categories: errors in medical treatment, missed or delayed diagnoses, and medication-related errors (although claims also tended to have multiple contributing factors).
Research like Dr. Schaffer’s could help to inform patient-safety efforts and reduce legal malpractice risk, he said. If hospitalists have fewer malpractice claims, that information might also be used to argue for lower malpractice premium rates.
Larry Beresford is a freelance writer in Oakland, Calif.
Hospital Medicine Leaders Flock to HM13 for Answers, Encouragement

Ibe Mbanu, MD, MBA, MPH, became medical director of the adult hospitalist department at Bon Secours St. Mary’s Hospital in Richmond, Va., about six months ago. Since then, he’s been besieged by a torrent of reform-based challenges he says make his job exponentially more difficult than that of medical directors just a few years ago.
Accountable-care organizations (ACOs), value-based purchasing, and discussions about bundled payments for episodic care are changing rapidly, and as a new administrator in a group with 24 hospitalists and three nonphysician providers (NPPs), he felt he needed to attend his first SHM annual meeting to keep up.
“The landscape in health care is rapidly evolving, at a frantic pace,” Dr. Mbanu says. “I essentially came here to just try to get a condensed source of information on how to manage the changes that are coming through the pipeline, and how to effectively run my department.”
Managing a practice is a challenge, and many of the more than 2,700 attendees at HM13 said the four-day confab’s focus on the topic was a major draw. From a rebooted continuing medical education (CME) pre-course appropriately named “What Keeps You Awake at Night? Hot Topics in Hospitalist Practice Management” to dozens of breakout sessions on the topic, it’s clear that successful practice management is a concern for many hospitalists.
“Before, the drivers were pretty clear,” Dr. Mbanu says. “Volume, productivity. Now we’re switching more toward a business model that’s changing from volume to value. Trying to adapt to that change is pretty challenging.
“Now it’s critical to really understand the environment.”
Comanagement Conundrum
One particularly hot topic this year was the trend of hospitalists taking on more comanagement responsibilities for patients previously managed by other specialties, including neurology, surgery, and others. Frank Volpicelli, MD, a first-year hospitalist and instructor at New York University (NYU) Langone Medical Center in New York, was one of three members of his HM group that attended the “Perioperative Medicine: Medical Consultation and Co-Management” pre-course. This summer, his group is going to establish a presence in the preoperative clinic.
“We hope very strongly that we can prevent some complications, identify patients that we should be following when they come into the hospital, and help the surgeons out,” he says. “No. 1, keep them in the [operating room] more, and No. 2, get in front of some of the complications that they are less comfortable managing.”
Ralph Velazquez, MD, senior vice president of care management for OSF Healthcare System in Peoria, Ill., isn’t so sure comanagement of more and more patients is the best practice-management model moving forward. For example, as physician compensation is tied more to how much their care costs to deliver, a hospitalist comanaging a surgical patient’s elective knee replacement could be financially penalized for the cost of that person’s stay, despite having nothing to do with the most expensive portion of the bill.
“You have a financial model that says do more billings, but as you start developing analytics … you may see there is no difference between the model that’s doing more billing, in terms of improving quality, and the one that is doing less,” Dr. Velazquez says. “So if you’re getting the same amount of quality, and the only thing you’re doing is generating more cost by doing more billing, you need to reevaluate your strategy.”
He believes some patients benefit from comanagement, but HM groups have to be diligent in seeking them out.
“We look for simple solutions and one-size-fits-all,” he adds. “Comanagement in complex patients—definitely there’s a need for that. Comanagement in noncomplex patients, elective patients—there’s no need for that. It’s just additional cost. I don’t think it’s going to produce any value.”
Startup Academy
John Colombo, MD, FACP, a 30-year veteran of internal medicine who moved to HM a few years ago when one of the hospitals he worked at asked him to launch a hospitalist group, thinks bundled payments might alleviate that value conundrum. Then again, he’s not quite sure. That’s why attended his first annual meeting.
“I found it difficult starting a new program from scratch,” says Dr. Colombo, of Crozer Keystone Health System in Drexel Hill, Pa. “Even with the materials available, there’s not a lot of ‘how to do it’ out there. There’s no ‘Starting Hospitals for Dummies’ book.”
Dr. Colombo spent much of his meeting focused on recruiting, compensation, bonus structures, and scheduling concerns. He said all are important in the hospital-heavy metropolitan Philadelphia region where he works. Plus, with departures and retirements at other programs in his health system, Dr. Colombo went from no HM experience three years ago to being in charge of four HM programs.
“The biggest thing is, I wanted to make sure I hadn’t stepped in something that I shouldn’t have already,” he adds. “There’s many different ways to do things. So I’ve learned a few different ways. I found value.”
Demonstrate Value
Another way to discover value in running a practice is looking at the business side of the house, says Denice Cora-Bramble, MD, MBA, chief medical officer and executive vice president of Ambulatory & Community Health Services at the Children’s National Medical Center in Washington, D.C.
Dr. Bramble says many hospitalists need to understand that while clinical care is what brought them to medicine, their future paychecks depend on recognizing how to provide that care in a way that demonstrates business value.
“When you finish residency, if you have not intentionally sought out those courses or those seminars, you need to recognize that as a blind spot,” she says. “You need to fill that toolkit as it relates to the business side of medicine.
“You don’t necessarily have to know all the answers, but you need to know the right questions to ask,” she says.
Dr. Bramble adds that hospitalist leaders should take advantage of certificate programs, leadership courses, basic budgeting classes, or anything that gives them added education about the economics of healthcare.
“It all comes down to demonstrating your outcomes, demonstrating the value that you bring to that institution,” she says. “And with health-care reform, I think hospitalists are uniquely positioned to be able to partner with other areas of the hospital to look at this value-based approach.”
Gary Gammon, MD, FHM, the newly named medical director of the Hospitalist Service at FirstHealth Moore Regional Hospital in Pinehurst, N.C., is doing his part to demonstrate value to his administrators. While his group does multidisciplinary rounds on patients, one of his questions for the pre-course faculty was to make sure that system of rounding is an evidence-based practice. He’s also looking for ways to establish more hegemony to his practice to ensure the rounds are effective, regardless of which physicians and others are participating.
The feedback he received was that most people view multidisciplinary rounds as a best practice. Now, Dr. Gammon can feel more authoritative that he and his 32 hospitalists and 12 extenders are practicing HM the way it should be practiced.
“I wanted to hear just what I heard, which is the leaders in the community feel that it’s helping, feel that it’s the right thing to do, feel that there’s objective data,” he says. “This is the stuff that makes me say, ‘OK, I’ve got the same problems everybody else has.’”
Richard Quinn is a freelance writer in New Jersey.
Ibe Mbanu, MD, MBA, MPH, became medical director of the adult hospitalist department at Bon Secours St. Mary’s Hospital in Richmond, Va., about six months ago. Since then, he’s been besieged by a torrent of reform-based challenges he says make his job exponentially more difficult than that of medical directors just a few years ago.
Accountable-care organizations (ACOs), value-based purchasing, and discussions about bundled payments for episodic care are changing rapidly, and as a new administrator in a group with 24 hospitalists and three nonphysician providers (NPPs), he felt he needed to attend his first SHM annual meeting to keep up.
“The landscape in health care is rapidly evolving, at a frantic pace,” Dr. Mbanu says. “I essentially came here to just try to get a condensed source of information on how to manage the changes that are coming through the pipeline, and how to effectively run my department.”
Managing a practice is a challenge, and many of the more than 2,700 attendees at HM13 said the four-day confab’s focus on the topic was a major draw. From a rebooted continuing medical education (CME) pre-course appropriately named “What Keeps You Awake at Night? Hot Topics in Hospitalist Practice Management” to dozens of breakout sessions on the topic, it’s clear that successful practice management is a concern for many hospitalists.
“Before, the drivers were pretty clear,” Dr. Mbanu says. “Volume, productivity. Now we’re switching more toward a business model that’s changing from volume to value. Trying to adapt to that change is pretty challenging.
“Now it’s critical to really understand the environment.”
Comanagement Conundrum
One particularly hot topic this year was the trend of hospitalists taking on more comanagement responsibilities for patients previously managed by other specialties, including neurology, surgery, and others. Frank Volpicelli, MD, a first-year hospitalist and instructor at New York University (NYU) Langone Medical Center in New York, was one of three members of his HM group that attended the “Perioperative Medicine: Medical Consultation and Co-Management” pre-course. This summer, his group is going to establish a presence in the preoperative clinic.
“We hope very strongly that we can prevent some complications, identify patients that we should be following when they come into the hospital, and help the surgeons out,” he says. “No. 1, keep them in the [operating room] more, and No. 2, get in front of some of the complications that they are less comfortable managing.”
Ralph Velazquez, MD, senior vice president of care management for OSF Healthcare System in Peoria, Ill., isn’t so sure comanagement of more and more patients is the best practice-management model moving forward. For example, as physician compensation is tied more to how much their care costs to deliver, a hospitalist comanaging a surgical patient’s elective knee replacement could be financially penalized for the cost of that person’s stay, despite having nothing to do with the most expensive portion of the bill.
“You have a financial model that says do more billings, but as you start developing analytics … you may see there is no difference between the model that’s doing more billing, in terms of improving quality, and the one that is doing less,” Dr. Velazquez says. “So if you’re getting the same amount of quality, and the only thing you’re doing is generating more cost by doing more billing, you need to reevaluate your strategy.”
He believes some patients benefit from comanagement, but HM groups have to be diligent in seeking them out.
“We look for simple solutions and one-size-fits-all,” he adds. “Comanagement in complex patients—definitely there’s a need for that. Comanagement in noncomplex patients, elective patients—there’s no need for that. It’s just additional cost. I don’t think it’s going to produce any value.”
Startup Academy
John Colombo, MD, FACP, a 30-year veteran of internal medicine who moved to HM a few years ago when one of the hospitals he worked at asked him to launch a hospitalist group, thinks bundled payments might alleviate that value conundrum. Then again, he’s not quite sure. That’s why attended his first annual meeting.
“I found it difficult starting a new program from scratch,” says Dr. Colombo, of Crozer Keystone Health System in Drexel Hill, Pa. “Even with the materials available, there’s not a lot of ‘how to do it’ out there. There’s no ‘Starting Hospitals for Dummies’ book.”
Dr. Colombo spent much of his meeting focused on recruiting, compensation, bonus structures, and scheduling concerns. He said all are important in the hospital-heavy metropolitan Philadelphia region where he works. Plus, with departures and retirements at other programs in his health system, Dr. Colombo went from no HM experience three years ago to being in charge of four HM programs.
“The biggest thing is, I wanted to make sure I hadn’t stepped in something that I shouldn’t have already,” he adds. “There’s many different ways to do things. So I’ve learned a few different ways. I found value.”
Demonstrate Value
Another way to discover value in running a practice is looking at the business side of the house, says Denice Cora-Bramble, MD, MBA, chief medical officer and executive vice president of Ambulatory & Community Health Services at the Children’s National Medical Center in Washington, D.C.
Dr. Bramble says many hospitalists need to understand that while clinical care is what brought them to medicine, their future paychecks depend on recognizing how to provide that care in a way that demonstrates business value.
“When you finish residency, if you have not intentionally sought out those courses or those seminars, you need to recognize that as a blind spot,” she says. “You need to fill that toolkit as it relates to the business side of medicine.
“You don’t necessarily have to know all the answers, but you need to know the right questions to ask,” she says.
Dr. Bramble adds that hospitalist leaders should take advantage of certificate programs, leadership courses, basic budgeting classes, or anything that gives them added education about the economics of healthcare.
“It all comes down to demonstrating your outcomes, demonstrating the value that you bring to that institution,” she says. “And with health-care reform, I think hospitalists are uniquely positioned to be able to partner with other areas of the hospital to look at this value-based approach.”
Gary Gammon, MD, FHM, the newly named medical director of the Hospitalist Service at FirstHealth Moore Regional Hospital in Pinehurst, N.C., is doing his part to demonstrate value to his administrators. While his group does multidisciplinary rounds on patients, one of his questions for the pre-course faculty was to make sure that system of rounding is an evidence-based practice. He’s also looking for ways to establish more hegemony to his practice to ensure the rounds are effective, regardless of which physicians and others are participating.
The feedback he received was that most people view multidisciplinary rounds as a best practice. Now, Dr. Gammon can feel more authoritative that he and his 32 hospitalists and 12 extenders are practicing HM the way it should be practiced.
“I wanted to hear just what I heard, which is the leaders in the community feel that it’s helping, feel that it’s the right thing to do, feel that there’s objective data,” he says. “This is the stuff that makes me say, ‘OK, I’ve got the same problems everybody else has.’”
Richard Quinn is a freelance writer in New Jersey.
Ibe Mbanu, MD, MBA, MPH, became medical director of the adult hospitalist department at Bon Secours St. Mary’s Hospital in Richmond, Va., about six months ago. Since then, he’s been besieged by a torrent of reform-based challenges he says make his job exponentially more difficult than that of medical directors just a few years ago.
Accountable-care organizations (ACOs), value-based purchasing, and discussions about bundled payments for episodic care are changing rapidly, and as a new administrator in a group with 24 hospitalists and three nonphysician providers (NPPs), he felt he needed to attend his first SHM annual meeting to keep up.
“The landscape in health care is rapidly evolving, at a frantic pace,” Dr. Mbanu says. “I essentially came here to just try to get a condensed source of information on how to manage the changes that are coming through the pipeline, and how to effectively run my department.”
Managing a practice is a challenge, and many of the more than 2,700 attendees at HM13 said the four-day confab’s focus on the topic was a major draw. From a rebooted continuing medical education (CME) pre-course appropriately named “What Keeps You Awake at Night? Hot Topics in Hospitalist Practice Management” to dozens of breakout sessions on the topic, it’s clear that successful practice management is a concern for many hospitalists.
“Before, the drivers were pretty clear,” Dr. Mbanu says. “Volume, productivity. Now we’re switching more toward a business model that’s changing from volume to value. Trying to adapt to that change is pretty challenging.
“Now it’s critical to really understand the environment.”
Comanagement Conundrum
One particularly hot topic this year was the trend of hospitalists taking on more comanagement responsibilities for patients previously managed by other specialties, including neurology, surgery, and others. Frank Volpicelli, MD, a first-year hospitalist and instructor at New York University (NYU) Langone Medical Center in New York, was one of three members of his HM group that attended the “Perioperative Medicine: Medical Consultation and Co-Management” pre-course. This summer, his group is going to establish a presence in the preoperative clinic.
“We hope very strongly that we can prevent some complications, identify patients that we should be following when they come into the hospital, and help the surgeons out,” he says. “No. 1, keep them in the [operating room] more, and No. 2, get in front of some of the complications that they are less comfortable managing.”
Ralph Velazquez, MD, senior vice president of care management for OSF Healthcare System in Peoria, Ill., isn’t so sure comanagement of more and more patients is the best practice-management model moving forward. For example, as physician compensation is tied more to how much their care costs to deliver, a hospitalist comanaging a surgical patient’s elective knee replacement could be financially penalized for the cost of that person’s stay, despite having nothing to do with the most expensive portion of the bill.
“You have a financial model that says do more billings, but as you start developing analytics … you may see there is no difference between the model that’s doing more billing, in terms of improving quality, and the one that is doing less,” Dr. Velazquez says. “So if you’re getting the same amount of quality, and the only thing you’re doing is generating more cost by doing more billing, you need to reevaluate your strategy.”
He believes some patients benefit from comanagement, but HM groups have to be diligent in seeking them out.
“We look for simple solutions and one-size-fits-all,” he adds. “Comanagement in complex patients—definitely there’s a need for that. Comanagement in noncomplex patients, elective patients—there’s no need for that. It’s just additional cost. I don’t think it’s going to produce any value.”
Startup Academy
John Colombo, MD, FACP, a 30-year veteran of internal medicine who moved to HM a few years ago when one of the hospitals he worked at asked him to launch a hospitalist group, thinks bundled payments might alleviate that value conundrum. Then again, he’s not quite sure. That’s why attended his first annual meeting.
“I found it difficult starting a new program from scratch,” says Dr. Colombo, of Crozer Keystone Health System in Drexel Hill, Pa. “Even with the materials available, there’s not a lot of ‘how to do it’ out there. There’s no ‘Starting Hospitals for Dummies’ book.”
Dr. Colombo spent much of his meeting focused on recruiting, compensation, bonus structures, and scheduling concerns. He said all are important in the hospital-heavy metropolitan Philadelphia region where he works. Plus, with departures and retirements at other programs in his health system, Dr. Colombo went from no HM experience three years ago to being in charge of four HM programs.
“The biggest thing is, I wanted to make sure I hadn’t stepped in something that I shouldn’t have already,” he adds. “There’s many different ways to do things. So I’ve learned a few different ways. I found value.”
Demonstrate Value
Another way to discover value in running a practice is looking at the business side of the house, says Denice Cora-Bramble, MD, MBA, chief medical officer and executive vice president of Ambulatory & Community Health Services at the Children’s National Medical Center in Washington, D.C.
Dr. Bramble says many hospitalists need to understand that while clinical care is what brought them to medicine, their future paychecks depend on recognizing how to provide that care in a way that demonstrates business value.
“When you finish residency, if you have not intentionally sought out those courses or those seminars, you need to recognize that as a blind spot,” she says. “You need to fill that toolkit as it relates to the business side of medicine.
“You don’t necessarily have to know all the answers, but you need to know the right questions to ask,” she says.
Dr. Bramble adds that hospitalist leaders should take advantage of certificate programs, leadership courses, basic budgeting classes, or anything that gives them added education about the economics of healthcare.
“It all comes down to demonstrating your outcomes, demonstrating the value that you bring to that institution,” she says. “And with health-care reform, I think hospitalists are uniquely positioned to be able to partner with other areas of the hospital to look at this value-based approach.”
Gary Gammon, MD, FHM, the newly named medical director of the Hospitalist Service at FirstHealth Moore Regional Hospital in Pinehurst, N.C., is doing his part to demonstrate value to his administrators. While his group does multidisciplinary rounds on patients, one of his questions for the pre-course faculty was to make sure that system of rounding is an evidence-based practice. He’s also looking for ways to establish more hegemony to his practice to ensure the rounds are effective, regardless of which physicians and others are participating.
The feedback he received was that most people view multidisciplinary rounds as a best practice. Now, Dr. Gammon can feel more authoritative that he and his 32 hospitalists and 12 extenders are practicing HM the way it should be practiced.
“I wanted to hear just what I heard, which is the leaders in the community feel that it’s helping, feel that it’s the right thing to do, feel that there’s objective data,” he says. “This is the stuff that makes me say, ‘OK, I’ve got the same problems everybody else has.’”
Richard Quinn is a freelance writer in New Jersey.
Most Health-Care Professionals Use Personal Smartphones for Work
Proportion of U.S. health-care workers who used their personal smartphones for work in the past year.5 The survey, conducted by Cisco Systems Inc., found that 36% of workers believe their employers are ready for “bring your own device” policies, while 41% say their devices are not password-protected and 53% access unsecure wi-fi networks at work. Additionally, 9 out of 10 workers receive no financial support from employers for using their smartphones at work.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Proportion of U.S. health-care workers who used their personal smartphones for work in the past year.5 The survey, conducted by Cisco Systems Inc., found that 36% of workers believe their employers are ready for “bring your own device” policies, while 41% say their devices are not password-protected and 53% access unsecure wi-fi networks at work. Additionally, 9 out of 10 workers receive no financial support from employers for using their smartphones at work.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Proportion of U.S. health-care workers who used their personal smartphones for work in the past year.5 The survey, conducted by Cisco Systems Inc., found that 36% of workers believe their employers are ready for “bring your own device” policies, while 41% say their devices are not password-protected and 53% access unsecure wi-fi networks at work. Additionally, 9 out of 10 workers receive no financial support from employers for using their smartphones at work.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Digital Schedule Boards Improve Outcomes at South Carolina Hospitals

The Greenville (S.C.) Health System in 2011 instituted a unique patient tracking and surgery scheduling system developed with Integrated Business Systems and Services, also based in South Carolina. The new system, called OR-Max, replaces the ubiquitous, giant dry-erase schedule board with digital displays. The system is connected to pre- and post-op departments, as well as to another electronic board in the family waiting areas. A radio frequency identification number assigned to each new patient tracks the patient’s status through the perioperative process. Text messages update status changes to staff.
“The display boards operate like arrival and departure boards at an airport,” says Gilbert Ritchie, PhD, director of anesthesia and perfusion services. “Instead of a flight number, staff follows a case number” as they watch for status changes.
OR-Max helps to pinpoint delays, facilitates rescheduling, improves workflow, and increases patient satisfaction while reducing costs, according to the health system. GHS says it has seen a 13% increase in staff productivity under the digital scheduling system.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
The Greenville (S.C.) Health System in 2011 instituted a unique patient tracking and surgery scheduling system developed with Integrated Business Systems and Services, also based in South Carolina. The new system, called OR-Max, replaces the ubiquitous, giant dry-erase schedule board with digital displays. The system is connected to pre- and post-op departments, as well as to another electronic board in the family waiting areas. A radio frequency identification number assigned to each new patient tracks the patient’s status through the perioperative process. Text messages update status changes to staff.
“The display boards operate like arrival and departure boards at an airport,” says Gilbert Ritchie, PhD, director of anesthesia and perfusion services. “Instead of a flight number, staff follows a case number” as they watch for status changes.
OR-Max helps to pinpoint delays, facilitates rescheduling, improves workflow, and increases patient satisfaction while reducing costs, according to the health system. GHS says it has seen a 13% increase in staff productivity under the digital scheduling system.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
The Greenville (S.C.) Health System in 2011 instituted a unique patient tracking and surgery scheduling system developed with Integrated Business Systems and Services, also based in South Carolina. The new system, called OR-Max, replaces the ubiquitous, giant dry-erase schedule board with digital displays. The system is connected to pre- and post-op departments, as well as to another electronic board in the family waiting areas. A radio frequency identification number assigned to each new patient tracks the patient’s status through the perioperative process. Text messages update status changes to staff.
“The display boards operate like arrival and departure boards at an airport,” says Gilbert Ritchie, PhD, director of anesthesia and perfusion services. “Instead of a flight number, staff follows a case number” as they watch for status changes.
OR-Max helps to pinpoint delays, facilitates rescheduling, improves workflow, and increases patient satisfaction while reducing costs, according to the health system. GHS says it has seen a 13% increase in staff productivity under the digital scheduling system.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Effective Clinical Documentation Can Influence Medicare Reimbursement

Back in the 1980s, I would go by medical records every day or two and find, on the front of the charts of my recently discharged patients, a form listing the diagnoses the hospital was billing to Medicare. Before the hospital could submit a patient’s bill, the attending physician was required to review the form and, by signing it, indicate agreement.
The requirement for this signature by the physician went away a long time ago and in my memory is one of the very few examples of reducing a doctor’s paperwork.
For my first few months in practice, I regularly would seek out the people who completed the form and explain they had misunderstood the patient’s clinical situation. “The main issue was a urinary tract infection,” I would say, “but you listed diabetes as the principal diagnosis.”
I don’t ever remember them changing anything based on my feedback. Instead, they explained to me that, for billing purposes, it was legitimate to list diabetes as the principal diagnosis because it had the additional benefit of resulting in a higher payment to the hospital than having “urinary tract infection” listed first.
Such was my introduction to the world of documentation and coding for hospital billing purposes and how it can sometimes differ significantly from the way a doctor sees the clinical picture. Things have evolved a lot since then, but the way doctors document medical conditions still has a huge influence on hospital reimbursement.
Hospital CDI Programs
About 80% of hospitals have formal clinical documentation improvement (CDI) programs to help ensure all clinical conditions are captured and described in the medical record in ways that are valuable for billing and other recordkeeping purposes. These programs might lead to you receive queries about your documentation. For example, you might be asked to clarify whether your patient’s pneumonia might be on the basis of aspiration.
Within SHM’s Code-H program, Dr. Richard Pinson, a former ED physician who now works with Houston-based HCQ Consulting, has a good presentation explaining these documentation issues. In it, he makes the point that, in addition to influencing how hospitals are paid, the way various conditions are documented also influences quality ratings.
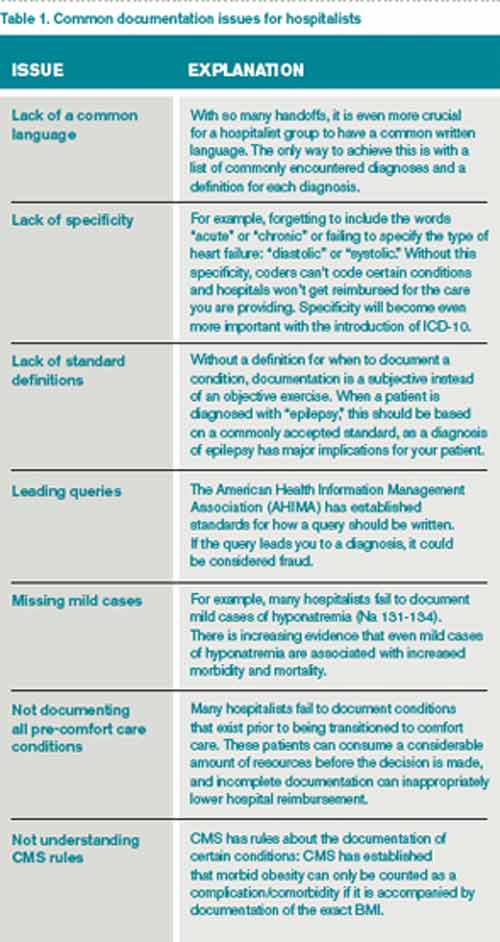
Novel Approach
The most common approach to engaging hospitalists in CDI initiatives is to have them attend a presentation on the topic, then put in place documentation specialists who generate queries asking the doctor to clarify diagnoses when it might influence payment, severity of illness determination, etc. Dr. Kenji Asakura, a Seattle hospitalist, and Erik Ordal, MBA, have a company called ClinIntell that analyzes each hospitalist (or other specialty) group’s historical patient mix and trains them on the documentation issues that they see most often. The idea of this focused approach is to make “documentation queries” unnecessary, or at least much less necessary. The benefits of this approach are many, including reducing or eliminating the risk of “leading queries”—that is, queries that seem to encourage the doctor to document a diagnosis because it is an advantage to the hospital rather than a well-considered medical opinion. Leading queries can be regarded as fraudulent and can get a lot of people in trouble.
I asked Kenji and Erik if they could provide me with a list of common documentation issues that most hospitalists need to know more about. Table 1 is what they came up with. I hope it helps you and your practice.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at [email protected].
Back in the 1980s, I would go by medical records every day or two and find, on the front of the charts of my recently discharged patients, a form listing the diagnoses the hospital was billing to Medicare. Before the hospital could submit a patient’s bill, the attending physician was required to review the form and, by signing it, indicate agreement.
The requirement for this signature by the physician went away a long time ago and in my memory is one of the very few examples of reducing a doctor’s paperwork.
For my first few months in practice, I regularly would seek out the people who completed the form and explain they had misunderstood the patient’s clinical situation. “The main issue was a urinary tract infection,” I would say, “but you listed diabetes as the principal diagnosis.”
I don’t ever remember them changing anything based on my feedback. Instead, they explained to me that, for billing purposes, it was legitimate to list diabetes as the principal diagnosis because it had the additional benefit of resulting in a higher payment to the hospital than having “urinary tract infection” listed first.
Such was my introduction to the world of documentation and coding for hospital billing purposes and how it can sometimes differ significantly from the way a doctor sees the clinical picture. Things have evolved a lot since then, but the way doctors document medical conditions still has a huge influence on hospital reimbursement.
Hospital CDI Programs
About 80% of hospitals have formal clinical documentation improvement (CDI) programs to help ensure all clinical conditions are captured and described in the medical record in ways that are valuable for billing and other recordkeeping purposes. These programs might lead to you receive queries about your documentation. For example, you might be asked to clarify whether your patient’s pneumonia might be on the basis of aspiration.
Within SHM’s Code-H program, Dr. Richard Pinson, a former ED physician who now works with Houston-based HCQ Consulting, has a good presentation explaining these documentation issues. In it, he makes the point that, in addition to influencing how hospitals are paid, the way various conditions are documented also influences quality ratings.
Novel Approach
The most common approach to engaging hospitalists in CDI initiatives is to have them attend a presentation on the topic, then put in place documentation specialists who generate queries asking the doctor to clarify diagnoses when it might influence payment, severity of illness determination, etc. Dr. Kenji Asakura, a Seattle hospitalist, and Erik Ordal, MBA, have a company called ClinIntell that analyzes each hospitalist (or other specialty) group’s historical patient mix and trains them on the documentation issues that they see most often. The idea of this focused approach is to make “documentation queries” unnecessary, or at least much less necessary. The benefits of this approach are many, including reducing or eliminating the risk of “leading queries”—that is, queries that seem to encourage the doctor to document a diagnosis because it is an advantage to the hospital rather than a well-considered medical opinion. Leading queries can be regarded as fraudulent and can get a lot of people in trouble.
I asked Kenji and Erik if they could provide me with a list of common documentation issues that most hospitalists need to know more about. Table 1 is what they came up with. I hope it helps you and your practice.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at [email protected].
Back in the 1980s, I would go by medical records every day or two and find, on the front of the charts of my recently discharged patients, a form listing the diagnoses the hospital was billing to Medicare. Before the hospital could submit a patient’s bill, the attending physician was required to review the form and, by signing it, indicate agreement.
The requirement for this signature by the physician went away a long time ago and in my memory is one of the very few examples of reducing a doctor’s paperwork.
For my first few months in practice, I regularly would seek out the people who completed the form and explain they had misunderstood the patient’s clinical situation. “The main issue was a urinary tract infection,” I would say, “but you listed diabetes as the principal diagnosis.”
I don’t ever remember them changing anything based on my feedback. Instead, they explained to me that, for billing purposes, it was legitimate to list diabetes as the principal diagnosis because it had the additional benefit of resulting in a higher payment to the hospital than having “urinary tract infection” listed first.
Such was my introduction to the world of documentation and coding for hospital billing purposes and how it can sometimes differ significantly from the way a doctor sees the clinical picture. Things have evolved a lot since then, but the way doctors document medical conditions still has a huge influence on hospital reimbursement.
Hospital CDI Programs
About 80% of hospitals have formal clinical documentation improvement (CDI) programs to help ensure all clinical conditions are captured and described in the medical record in ways that are valuable for billing and other recordkeeping purposes. These programs might lead to you receive queries about your documentation. For example, you might be asked to clarify whether your patient’s pneumonia might be on the basis of aspiration.
Within SHM’s Code-H program, Dr. Richard Pinson, a former ED physician who now works with Houston-based HCQ Consulting, has a good presentation explaining these documentation issues. In it, he makes the point that, in addition to influencing how hospitals are paid, the way various conditions are documented also influences quality ratings.
Novel Approach
The most common approach to engaging hospitalists in CDI initiatives is to have them attend a presentation on the topic, then put in place documentation specialists who generate queries asking the doctor to clarify diagnoses when it might influence payment, severity of illness determination, etc. Dr. Kenji Asakura, a Seattle hospitalist, and Erik Ordal, MBA, have a company called ClinIntell that analyzes each hospitalist (or other specialty) group’s historical patient mix and trains them on the documentation issues that they see most often. The idea of this focused approach is to make “documentation queries” unnecessary, or at least much less necessary. The benefits of this approach are many, including reducing or eliminating the risk of “leading queries”—that is, queries that seem to encourage the doctor to document a diagnosis because it is an advantage to the hospital rather than a well-considered medical opinion. Leading queries can be regarded as fraudulent and can get a lot of people in trouble.
I asked Kenji and Erik if they could provide me with a list of common documentation issues that most hospitalists need to know more about. Table 1 is what they came up with. I hope it helps you and your practice.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at [email protected].