User login
The Hospitalist only
Observation Care
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Hospitalist Salary Spike

In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
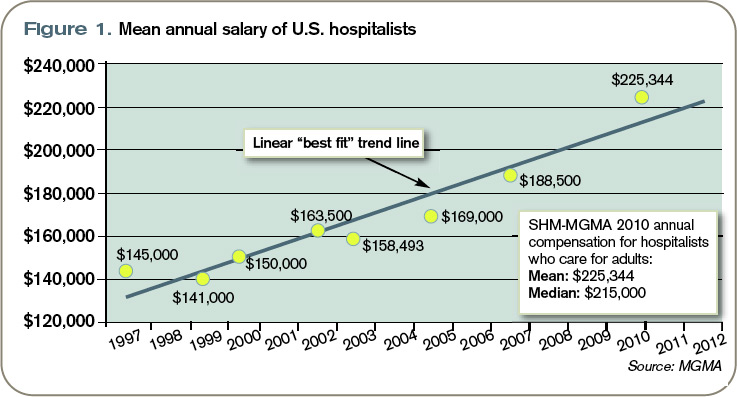
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Square Peg, Square Hole

I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
Transitions Telethon

The headline was as biting as it was inciting. “Frustrations with hospitalist care: Need to improve transitions and communication,” it screamed from the cover of a recent issue of the Annals of Internal Medicine.1 Reading on the run, I thumbed to page 469 and glanced at the first few paragraphs, my mind spinning with the implications.
The article was an editorial following a recent thought piece by a primary-care physician (PCP) frustrated with his interactions with the HM model—mainly around the lack of communication from hospitalists about his patients, his marginalized role with his patients’ hospital care, and the lack of information transfer around transitions.2
Frustrations and Slapstick Comedy
Frustration with hospitalist care? Is this how PCPs see us? Are we really “frustrating” our outpatient colleagues? To an outsider, this presented a one-sided view of the issue—the side that sounds simplistically negative. What if someone important to our group should read this article, someone like my hospital CEO? I didn’t have to wonder for long as I looked up from my elevator reading to note my hospital CEO entering.
What followed eerily resembled one of those scenes from a slapstick comedy, as the boob, played perfectly by me, obviously fumbles something he intends to hide from his boss behind his back to escape the knowing eye of said boss. And, like a pornographic-magazine-sniffing parent, my CEO knowingly diagnosed the situation.
“Whatcha reading?” he sagely queried.
“Nothing,” I replied unconvincingly.
“Nothing? It sure looks like you hastily stuffed a magazine or something down the back of your pants as I walked in.”
“Oh, this?” I responded, unearthing a large medical journal from my pants, leaving an untucked shirt in its wake. “This is just a medical journal. You know, lots of medical stuff. It’s pretty complex. Probably hard for nonmedical types to understand,” I replied, employing a bit of professorial condescension to throw him off track.
“Annals of Internal Medicine,” he replied. “What a coincidence. I just received an e-mail from a friend with an Annals article about the issues of transitions of care with the hospitalist model. Sounds like a real problem. Maybe our new electronic health records will fix that. If not, you should fix it. Let’s chat about it soon.”
“Right,” I said as the elevator doors swished behind him, leaving me disheveled in both appearance and thoughts.
Testimonials?
The more recent Annals editorial summarized—and then printed—a few of the many online responses to the original thought piece.3 The responses ranged from outrage with the HM model of care to more measured discussions of the limitations of the “old” model it replaced. However, the tone and implications were clear: At least some, if not many, PCPs are displeased with the HM model.
One writer related a recent example in which his elderly patient was admitted unbeknownst to him. After receiving a query from a family member, he called the hospitalist on duty, who was uninformed about the patient details, had made questionable therapeutic changes, and was “unapologetic” about her team’s lack of communication, arguing that the ED physician “should have called.” That led this PCP to conclude that the system is “disjointed and isolating,” leaving “patients feeling abandoned.” Another writer commented that the current system of communication results in “potentially detrimental and demoralizing degrees of separation.” A response by a hospitalist detailed how they were able to put a system in place to contact PCPs with whom they are contracted 80% of the time.
The Annals editors concluded that the letters they received in response to the first article “reflect a schism that exists in internal medicine about the positive and negative effects of hospitalist care,” noting that “the evidence is still deficient about how to deliver care optimally when complex, seriously-ill patients must transition between multiple providers in diverse health care settings.” The authors go on to call for “intensive research and productive debates” about the HM model of care.
A Challenge to You
“Disjointed and isolating”? … “Detrimental and demoralizing”? … Lauding 80% PCP contact rates? … “Intensive research and debate”?
I get that this is a complex issue and that healthcare in the U.S. is fragmented to the point of fracture. To wit, it can be agonizingly time-consuming to track down PCPs and wade through their automated phone systems. And this assumes that your patient has a PCP, can identify that PCP, and has their phone number. If they don’t, you’re left to sift through online phone books, clinic websites, or Google searches with the hopes that you can summon the right Dr. Davis, Davies, or Daves—the patient’s not quite sure of the spelling but knows “she’s a nice lady doctor.” I know firsthand the tension between taking the time to make that PCP call and getting home in time for dinner with my family—I’m often guilty of choosing dinner.
However, I’m not sure “intensive research” is the answer. Nor is this a problem that can wait for technological solutions. I don’t want to diminish the great strides that have been made or understate the need to continue to innovate around transitions—this needs to be an area of ongoing study. But this is a problem that has at least one relatively simple, short-term solution: Just pick up the phone. As one Annals writer rightly questions: “How has inter-physician communication come to be regarded as an unexpected courtesy rather than an obligation?”
Good question.
So, I have a simple challenge for you: For one week, join me in committing to calling 100% of the available PCPs on patient discharge. I can guarantee you this will prove to be a hard, time-consuming, and, at times, migraine-inducing process. But it is an intervention that will make a difference, can be launched tomorrow, and does not require “intensive research and debate.”
We’ll no doubt gain some insight into our patients’ current therapeutic regimens, enlist PCPs’ help with the treatment decisions, and ensure that our patients’ transitions are as safe as possible. My guess is that we’ll also find it valuable to the point it becomes habit.
Start by committing with me to just one week.
Then go home and have dinner. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Frustrations with hospitalist care: need to improve transitions and communication. Ann Intern Med. 2010;152(7):469.
- Beckman H. Three degrees of separation. Ann Intern Med. 2009;151(12):890-891.
- The relationship between hospitalists and primary care physicians. Ann Intern Med. 2010;152(7):474-6.
The headline was as biting as it was inciting. “Frustrations with hospitalist care: Need to improve transitions and communication,” it screamed from the cover of a recent issue of the Annals of Internal Medicine.1 Reading on the run, I thumbed to page 469 and glanced at the first few paragraphs, my mind spinning with the implications.
The article was an editorial following a recent thought piece by a primary-care physician (PCP) frustrated with his interactions with the HM model—mainly around the lack of communication from hospitalists about his patients, his marginalized role with his patients’ hospital care, and the lack of information transfer around transitions.2
Frustrations and Slapstick Comedy
Frustration with hospitalist care? Is this how PCPs see us? Are we really “frustrating” our outpatient colleagues? To an outsider, this presented a one-sided view of the issue—the side that sounds simplistically negative. What if someone important to our group should read this article, someone like my hospital CEO? I didn’t have to wonder for long as I looked up from my elevator reading to note my hospital CEO entering.
What followed eerily resembled one of those scenes from a slapstick comedy, as the boob, played perfectly by me, obviously fumbles something he intends to hide from his boss behind his back to escape the knowing eye of said boss. And, like a pornographic-magazine-sniffing parent, my CEO knowingly diagnosed the situation.
“Whatcha reading?” he sagely queried.
“Nothing,” I replied unconvincingly.
“Nothing? It sure looks like you hastily stuffed a magazine or something down the back of your pants as I walked in.”
“Oh, this?” I responded, unearthing a large medical journal from my pants, leaving an untucked shirt in its wake. “This is just a medical journal. You know, lots of medical stuff. It’s pretty complex. Probably hard for nonmedical types to understand,” I replied, employing a bit of professorial condescension to throw him off track.
“Annals of Internal Medicine,” he replied. “What a coincidence. I just received an e-mail from a friend with an Annals article about the issues of transitions of care with the hospitalist model. Sounds like a real problem. Maybe our new electronic health records will fix that. If not, you should fix it. Let’s chat about it soon.”
“Right,” I said as the elevator doors swished behind him, leaving me disheveled in both appearance and thoughts.
Testimonials?
The more recent Annals editorial summarized—and then printed—a few of the many online responses to the original thought piece.3 The responses ranged from outrage with the HM model of care to more measured discussions of the limitations of the “old” model it replaced. However, the tone and implications were clear: At least some, if not many, PCPs are displeased with the HM model.
One writer related a recent example in which his elderly patient was admitted unbeknownst to him. After receiving a query from a family member, he called the hospitalist on duty, who was uninformed about the patient details, had made questionable therapeutic changes, and was “unapologetic” about her team’s lack of communication, arguing that the ED physician “should have called.” That led this PCP to conclude that the system is “disjointed and isolating,” leaving “patients feeling abandoned.” Another writer commented that the current system of communication results in “potentially detrimental and demoralizing degrees of separation.” A response by a hospitalist detailed how they were able to put a system in place to contact PCPs with whom they are contracted 80% of the time.
The Annals editors concluded that the letters they received in response to the first article “reflect a schism that exists in internal medicine about the positive and negative effects of hospitalist care,” noting that “the evidence is still deficient about how to deliver care optimally when complex, seriously-ill patients must transition between multiple providers in diverse health care settings.” The authors go on to call for “intensive research and productive debates” about the HM model of care.
A Challenge to You
“Disjointed and isolating”? … “Detrimental and demoralizing”? … Lauding 80% PCP contact rates? … “Intensive research and debate”?
I get that this is a complex issue and that healthcare in the U.S. is fragmented to the point of fracture. To wit, it can be agonizingly time-consuming to track down PCPs and wade through their automated phone systems. And this assumes that your patient has a PCP, can identify that PCP, and has their phone number. If they don’t, you’re left to sift through online phone books, clinic websites, or Google searches with the hopes that you can summon the right Dr. Davis, Davies, or Daves—the patient’s not quite sure of the spelling but knows “she’s a nice lady doctor.” I know firsthand the tension between taking the time to make that PCP call and getting home in time for dinner with my family—I’m often guilty of choosing dinner.
However, I’m not sure “intensive research” is the answer. Nor is this a problem that can wait for technological solutions. I don’t want to diminish the great strides that have been made or understate the need to continue to innovate around transitions—this needs to be an area of ongoing study. But this is a problem that has at least one relatively simple, short-term solution: Just pick up the phone. As one Annals writer rightly questions: “How has inter-physician communication come to be regarded as an unexpected courtesy rather than an obligation?”
Good question.
So, I have a simple challenge for you: For one week, join me in committing to calling 100% of the available PCPs on patient discharge. I can guarantee you this will prove to be a hard, time-consuming, and, at times, migraine-inducing process. But it is an intervention that will make a difference, can be launched tomorrow, and does not require “intensive research and debate.”
We’ll no doubt gain some insight into our patients’ current therapeutic regimens, enlist PCPs’ help with the treatment decisions, and ensure that our patients’ transitions are as safe as possible. My guess is that we’ll also find it valuable to the point it becomes habit.
Start by committing with me to just one week.
Then go home and have dinner. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Frustrations with hospitalist care: need to improve transitions and communication. Ann Intern Med. 2010;152(7):469.
- Beckman H. Three degrees of separation. Ann Intern Med. 2009;151(12):890-891.
- The relationship between hospitalists and primary care physicians. Ann Intern Med. 2010;152(7):474-6.
The headline was as biting as it was inciting. “Frustrations with hospitalist care: Need to improve transitions and communication,” it screamed from the cover of a recent issue of the Annals of Internal Medicine.1 Reading on the run, I thumbed to page 469 and glanced at the first few paragraphs, my mind spinning with the implications.
The article was an editorial following a recent thought piece by a primary-care physician (PCP) frustrated with his interactions with the HM model—mainly around the lack of communication from hospitalists about his patients, his marginalized role with his patients’ hospital care, and the lack of information transfer around transitions.2
Frustrations and Slapstick Comedy
Frustration with hospitalist care? Is this how PCPs see us? Are we really “frustrating” our outpatient colleagues? To an outsider, this presented a one-sided view of the issue—the side that sounds simplistically negative. What if someone important to our group should read this article, someone like my hospital CEO? I didn’t have to wonder for long as I looked up from my elevator reading to note my hospital CEO entering.
What followed eerily resembled one of those scenes from a slapstick comedy, as the boob, played perfectly by me, obviously fumbles something he intends to hide from his boss behind his back to escape the knowing eye of said boss. And, like a pornographic-magazine-sniffing parent, my CEO knowingly diagnosed the situation.
“Whatcha reading?” he sagely queried.
“Nothing,” I replied unconvincingly.
“Nothing? It sure looks like you hastily stuffed a magazine or something down the back of your pants as I walked in.”
“Oh, this?” I responded, unearthing a large medical journal from my pants, leaving an untucked shirt in its wake. “This is just a medical journal. You know, lots of medical stuff. It’s pretty complex. Probably hard for nonmedical types to understand,” I replied, employing a bit of professorial condescension to throw him off track.
“Annals of Internal Medicine,” he replied. “What a coincidence. I just received an e-mail from a friend with an Annals article about the issues of transitions of care with the hospitalist model. Sounds like a real problem. Maybe our new electronic health records will fix that. If not, you should fix it. Let’s chat about it soon.”
“Right,” I said as the elevator doors swished behind him, leaving me disheveled in both appearance and thoughts.
Testimonials?
The more recent Annals editorial summarized—and then printed—a few of the many online responses to the original thought piece.3 The responses ranged from outrage with the HM model of care to more measured discussions of the limitations of the “old” model it replaced. However, the tone and implications were clear: At least some, if not many, PCPs are displeased with the HM model.
One writer related a recent example in which his elderly patient was admitted unbeknownst to him. After receiving a query from a family member, he called the hospitalist on duty, who was uninformed about the patient details, had made questionable therapeutic changes, and was “unapologetic” about her team’s lack of communication, arguing that the ED physician “should have called.” That led this PCP to conclude that the system is “disjointed and isolating,” leaving “patients feeling abandoned.” Another writer commented that the current system of communication results in “potentially detrimental and demoralizing degrees of separation.” A response by a hospitalist detailed how they were able to put a system in place to contact PCPs with whom they are contracted 80% of the time.
The Annals editors concluded that the letters they received in response to the first article “reflect a schism that exists in internal medicine about the positive and negative effects of hospitalist care,” noting that “the evidence is still deficient about how to deliver care optimally when complex, seriously-ill patients must transition between multiple providers in diverse health care settings.” The authors go on to call for “intensive research and productive debates” about the HM model of care.
A Challenge to You
“Disjointed and isolating”? … “Detrimental and demoralizing”? … Lauding 80% PCP contact rates? … “Intensive research and debate”?
I get that this is a complex issue and that healthcare in the U.S. is fragmented to the point of fracture. To wit, it can be agonizingly time-consuming to track down PCPs and wade through their automated phone systems. And this assumes that your patient has a PCP, can identify that PCP, and has their phone number. If they don’t, you’re left to sift through online phone books, clinic websites, or Google searches with the hopes that you can summon the right Dr. Davis, Davies, or Daves—the patient’s not quite sure of the spelling but knows “she’s a nice lady doctor.” I know firsthand the tension between taking the time to make that PCP call and getting home in time for dinner with my family—I’m often guilty of choosing dinner.
However, I’m not sure “intensive research” is the answer. Nor is this a problem that can wait for technological solutions. I don’t want to diminish the great strides that have been made or understate the need to continue to innovate around transitions—this needs to be an area of ongoing study. But this is a problem that has at least one relatively simple, short-term solution: Just pick up the phone. As one Annals writer rightly questions: “How has inter-physician communication come to be regarded as an unexpected courtesy rather than an obligation?”
Good question.
So, I have a simple challenge for you: For one week, join me in committing to calling 100% of the available PCPs on patient discharge. I can guarantee you this will prove to be a hard, time-consuming, and, at times, migraine-inducing process. But it is an intervention that will make a difference, can be launched tomorrow, and does not require “intensive research and debate.”
We’ll no doubt gain some insight into our patients’ current therapeutic regimens, enlist PCPs’ help with the treatment decisions, and ensure that our patients’ transitions are as safe as possible. My guess is that we’ll also find it valuable to the point it becomes habit.
Start by committing with me to just one week.
Then go home and have dinner. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Frustrations with hospitalist care: need to improve transitions and communication. Ann Intern Med. 2010;152(7):469.
- Beckman H. Three degrees of separation. Ann Intern Med. 2009;151(12):890-891.
- The relationship between hospitalists and primary care physicians. Ann Intern Med. 2010;152(7):474-6.
Variable Rate
Are states doing enough to discipline problem doctors? The sensitive question has flared again with the release of an annual report by Washington, D.C.-based consumer advocacy group Public Citizen.
The report analyzed statistics released by the Federation of State Medical Boards on serious disciplinary actions taken by the boards of all 50 states and the District of Columbia in 2009. Those actions include revocations, surrenders, suspensions, and probations or restrictions. Public Citizen used a three-year average (2007 to 2009) to arrive at its rate of actions per 1,000 physicians licensed in each state.
For the fourth year in a row, Alaska had the most actions, 7.89 per 1,000 doctors. Meanwhile, Minnesota had the fewest actions (1.07 per 1,000 doctors) for the second year running. For the record, the numbers aren’t broken down by specialty (see Table 1, p. 5).
So what does it all mean? Do Alaska’s doctors really require more punitive measures than those in other states, or is the state board simply more vigilant? Are Minnesota doctors that much better, or is that state failing in its duty to provide adequate oversight? Is such a ranking system even warranted?
Nearly everyone agrees on the importance of protecting the public and the integrity of the medical profession. But the aggressive jousting over what the new numbers do or do not mean suggests just how difficult it can be to come up with a metric for medical accountability that everyone agrees is both fair and reliable.
Sidney Wolfe, MD, director of Public Citizen’s Health Research Group and the lead author of the new report, dismisses the notion that Minnesota’s doctors are so good that they don’t require as many disciplinary actions. “There is not a shred of evidence for that,” he says. Instead, he calls out what he views as an ineffective board.
In turn, Robert Leach, executive director of the Minnesota Board of Medical Practice, dismisses the significance of the report’s findings. “It’s a fair ranking the way their formula applies. It’s the formula we disagree with,” he says. “It’s fairly simplistic and indicative of nothing.”
And Lisa Robin, senior vice president for advocacy and member services at the Federation of State Medical Boards, says the federation doesn’t even encourage rankings because of the variable laws and sanctions from state to state. “It doesn’t give you a true picture of what boards do, to rank them,” she says.

A Row Over Rankings
Minnesota’s Leach has a detailed list of grievances against the report. But his biggest beef is with the fact that it ranks medical boards on the number of serious disciplinary actions per 1,000 physicians licensed by the state. “The more precise number should be the number of licensed physicians who are actually practicing in the state,” he says.
From 2008 to 2009, for example, more than 19,000 physicians were licensed in Minnesota. Yet Leach says that only a little more than 14,000 were actually practicing within the state, which he describes as a large exporter of trained doctors. “So we had 5,000 physicians who weren’t even practicing here that were counted against our one disciplinary action per thousand physicians,” he says.
Public Citizen, he says, also doesn’t recognize other interventions, such as Minnesota’s “agreements for corrective action,” that normally include training or remedial coursework for doctors with an identified weakness in subject areas such as prescribing or chronic-pain management. “Not every doctor needs to be hit over the head with a hammer of serious disciplinary action to address a problem,” Leach says.
And then there’s the sticky matter of peer review. In Minnesota, “virtually every physician now practicing works for a large health plan or a facility,” he says. “We have virtually no solo practice or isolated practice in Minnesota, and those are the physicians who get in trouble: the ones who don’t have the advantage of periodic peer review, who don’t have the advantage of adequate supervision to help keep them out of trouble.”
Doctors like those in Alaska? “You always see Alaska is rated real high,” Leach says. “You have a bunch of people out there practicing in the wilderness, out in solo practice. Physicians need to have that ability to have peer review, to be able to address problem cases with their colleagues. In Minnesota, a lot of these facilities and health plans address these problems at the practice level before they even reach the board.”
A Call To Action
Dr. Wolfe isn’t buying the notion that Minnesota doctors require less formal discipline while their colleagues in Alaska need more. Whenever other low-ranking states have provided sufficient funding, replaced ineffective leadership, granted more independence, and met the other conditions necessary for a better medical board, he notes, their rate of disciplinary actions often “rockets up.”
The medical boards of North Carolina and Washington, D.C., have risen dramatically in the rankings in recent years, and Dr. Wolfe cites effective intervention in both cases. In formerly low-ranking Arizona, he says, similar corrective action in the late 1990s led to a tripling of the rate of serious disciplinary action within three years. “That’s obviously not a period of time that’s long enough to be explained by some inward migration of bad doctors or outward migration of good doctors,” he says. “It’s because the board started functioning better.”
Meanwhile, boards in South Carolina and Massachusetts have slumped in the ratings—a decline he attributes to the loss of leadership and funds.
“One area I can agree with Dr. Wolfe on is that medical boards need resources; they need adequate structure, resources, and authority to do their job and be able to protect the public,” says Robin, of the Federation of State Medical Boards. “If they’re in a big umbrella agency and they’re just one of many and share their pool of investigators with everyone, as you can imagine, that’s probably not as efficient.”
Hospitals also share in the blame, according to a separate Public Citizen report released last year that cites a chronic underreporting of doctor misconduct or incompetence to the National Practitioner Data Bank by hospitals. Robin agrees that more diligence is needed to ensure that medical boards have the information they need to properly do their jobs. As one of her board members told her, “They can’t gain information by osmosis.”
Hospitalists, however, might be well suited for addressing the underreporting issue. HM is in a “really good position to observe behavior that needs to be brought to the attention of hospital medical staff,” Dr. Wolfe says.
He recommends that one or more hospitalists should sit on each hospital’s medical peer review committee, where they can put their expertise to good use. “Hospitalists really need to get more active in this,” he says. “It’s for the betterment of the patients in the hospital, it’s for the betterment for the reputation of the hospital and the medical staff.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Are states doing enough to discipline problem doctors? The sensitive question has flared again with the release of an annual report by Washington, D.C.-based consumer advocacy group Public Citizen.
The report analyzed statistics released by the Federation of State Medical Boards on serious disciplinary actions taken by the boards of all 50 states and the District of Columbia in 2009. Those actions include revocations, surrenders, suspensions, and probations or restrictions. Public Citizen used a three-year average (2007 to 2009) to arrive at its rate of actions per 1,000 physicians licensed in each state.
For the fourth year in a row, Alaska had the most actions, 7.89 per 1,000 doctors. Meanwhile, Minnesota had the fewest actions (1.07 per 1,000 doctors) for the second year running. For the record, the numbers aren’t broken down by specialty (see Table 1, p. 5).
So what does it all mean? Do Alaska’s doctors really require more punitive measures than those in other states, or is the state board simply more vigilant? Are Minnesota doctors that much better, or is that state failing in its duty to provide adequate oversight? Is such a ranking system even warranted?
Nearly everyone agrees on the importance of protecting the public and the integrity of the medical profession. But the aggressive jousting over what the new numbers do or do not mean suggests just how difficult it can be to come up with a metric for medical accountability that everyone agrees is both fair and reliable.
Sidney Wolfe, MD, director of Public Citizen’s Health Research Group and the lead author of the new report, dismisses the notion that Minnesota’s doctors are so good that they don’t require as many disciplinary actions. “There is not a shred of evidence for that,” he says. Instead, he calls out what he views as an ineffective board.
In turn, Robert Leach, executive director of the Minnesota Board of Medical Practice, dismisses the significance of the report’s findings. “It’s a fair ranking the way their formula applies. It’s the formula we disagree with,” he says. “It’s fairly simplistic and indicative of nothing.”
And Lisa Robin, senior vice president for advocacy and member services at the Federation of State Medical Boards, says the federation doesn’t even encourage rankings because of the variable laws and sanctions from state to state. “It doesn’t give you a true picture of what boards do, to rank them,” she says.
A Row Over Rankings
Minnesota’s Leach has a detailed list of grievances against the report. But his biggest beef is with the fact that it ranks medical boards on the number of serious disciplinary actions per 1,000 physicians licensed by the state. “The more precise number should be the number of licensed physicians who are actually practicing in the state,” he says.
From 2008 to 2009, for example, more than 19,000 physicians were licensed in Minnesota. Yet Leach says that only a little more than 14,000 were actually practicing within the state, which he describes as a large exporter of trained doctors. “So we had 5,000 physicians who weren’t even practicing here that were counted against our one disciplinary action per thousand physicians,” he says.
Public Citizen, he says, also doesn’t recognize other interventions, such as Minnesota’s “agreements for corrective action,” that normally include training or remedial coursework for doctors with an identified weakness in subject areas such as prescribing or chronic-pain management. “Not every doctor needs to be hit over the head with a hammer of serious disciplinary action to address a problem,” Leach says.
And then there’s the sticky matter of peer review. In Minnesota, “virtually every physician now practicing works for a large health plan or a facility,” he says. “We have virtually no solo practice or isolated practice in Minnesota, and those are the physicians who get in trouble: the ones who don’t have the advantage of periodic peer review, who don’t have the advantage of adequate supervision to help keep them out of trouble.”
Doctors like those in Alaska? “You always see Alaska is rated real high,” Leach says. “You have a bunch of people out there practicing in the wilderness, out in solo practice. Physicians need to have that ability to have peer review, to be able to address problem cases with their colleagues. In Minnesota, a lot of these facilities and health plans address these problems at the practice level before they even reach the board.”
A Call To Action
Dr. Wolfe isn’t buying the notion that Minnesota doctors require less formal discipline while their colleagues in Alaska need more. Whenever other low-ranking states have provided sufficient funding, replaced ineffective leadership, granted more independence, and met the other conditions necessary for a better medical board, he notes, their rate of disciplinary actions often “rockets up.”
The medical boards of North Carolina and Washington, D.C., have risen dramatically in the rankings in recent years, and Dr. Wolfe cites effective intervention in both cases. In formerly low-ranking Arizona, he says, similar corrective action in the late 1990s led to a tripling of the rate of serious disciplinary action within three years. “That’s obviously not a period of time that’s long enough to be explained by some inward migration of bad doctors or outward migration of good doctors,” he says. “It’s because the board started functioning better.”
Meanwhile, boards in South Carolina and Massachusetts have slumped in the ratings—a decline he attributes to the loss of leadership and funds.
“One area I can agree with Dr. Wolfe on is that medical boards need resources; they need adequate structure, resources, and authority to do their job and be able to protect the public,” says Robin, of the Federation of State Medical Boards. “If they’re in a big umbrella agency and they’re just one of many and share their pool of investigators with everyone, as you can imagine, that’s probably not as efficient.”
Hospitals also share in the blame, according to a separate Public Citizen report released last year that cites a chronic underreporting of doctor misconduct or incompetence to the National Practitioner Data Bank by hospitals. Robin agrees that more diligence is needed to ensure that medical boards have the information they need to properly do their jobs. As one of her board members told her, “They can’t gain information by osmosis.”
Hospitalists, however, might be well suited for addressing the underreporting issue. HM is in a “really good position to observe behavior that needs to be brought to the attention of hospital medical staff,” Dr. Wolfe says.
He recommends that one or more hospitalists should sit on each hospital’s medical peer review committee, where they can put their expertise to good use. “Hospitalists really need to get more active in this,” he says. “It’s for the betterment of the patients in the hospital, it’s for the betterment for the reputation of the hospital and the medical staff.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Are states doing enough to discipline problem doctors? The sensitive question has flared again with the release of an annual report by Washington, D.C.-based consumer advocacy group Public Citizen.
The report analyzed statistics released by the Federation of State Medical Boards on serious disciplinary actions taken by the boards of all 50 states and the District of Columbia in 2009. Those actions include revocations, surrenders, suspensions, and probations or restrictions. Public Citizen used a three-year average (2007 to 2009) to arrive at its rate of actions per 1,000 physicians licensed in each state.
For the fourth year in a row, Alaska had the most actions, 7.89 per 1,000 doctors. Meanwhile, Minnesota had the fewest actions (1.07 per 1,000 doctors) for the second year running. For the record, the numbers aren’t broken down by specialty (see Table 1, p. 5).
So what does it all mean? Do Alaska’s doctors really require more punitive measures than those in other states, or is the state board simply more vigilant? Are Minnesota doctors that much better, or is that state failing in its duty to provide adequate oversight? Is such a ranking system even warranted?
Nearly everyone agrees on the importance of protecting the public and the integrity of the medical profession. But the aggressive jousting over what the new numbers do or do not mean suggests just how difficult it can be to come up with a metric for medical accountability that everyone agrees is both fair and reliable.
Sidney Wolfe, MD, director of Public Citizen’s Health Research Group and the lead author of the new report, dismisses the notion that Minnesota’s doctors are so good that they don’t require as many disciplinary actions. “There is not a shred of evidence for that,” he says. Instead, he calls out what he views as an ineffective board.
In turn, Robert Leach, executive director of the Minnesota Board of Medical Practice, dismisses the significance of the report’s findings. “It’s a fair ranking the way their formula applies. It’s the formula we disagree with,” he says. “It’s fairly simplistic and indicative of nothing.”
And Lisa Robin, senior vice president for advocacy and member services at the Federation of State Medical Boards, says the federation doesn’t even encourage rankings because of the variable laws and sanctions from state to state. “It doesn’t give you a true picture of what boards do, to rank them,” she says.
A Row Over Rankings
Minnesota’s Leach has a detailed list of grievances against the report. But his biggest beef is with the fact that it ranks medical boards on the number of serious disciplinary actions per 1,000 physicians licensed by the state. “The more precise number should be the number of licensed physicians who are actually practicing in the state,” he says.
From 2008 to 2009, for example, more than 19,000 physicians were licensed in Minnesota. Yet Leach says that only a little more than 14,000 were actually practicing within the state, which he describes as a large exporter of trained doctors. “So we had 5,000 physicians who weren’t even practicing here that were counted against our one disciplinary action per thousand physicians,” he says.
Public Citizen, he says, also doesn’t recognize other interventions, such as Minnesota’s “agreements for corrective action,” that normally include training or remedial coursework for doctors with an identified weakness in subject areas such as prescribing or chronic-pain management. “Not every doctor needs to be hit over the head with a hammer of serious disciplinary action to address a problem,” Leach says.
And then there’s the sticky matter of peer review. In Minnesota, “virtually every physician now practicing works for a large health plan or a facility,” he says. “We have virtually no solo practice or isolated practice in Minnesota, and those are the physicians who get in trouble: the ones who don’t have the advantage of periodic peer review, who don’t have the advantage of adequate supervision to help keep them out of trouble.”
Doctors like those in Alaska? “You always see Alaska is rated real high,” Leach says. “You have a bunch of people out there practicing in the wilderness, out in solo practice. Physicians need to have that ability to have peer review, to be able to address problem cases with their colleagues. In Minnesota, a lot of these facilities and health plans address these problems at the practice level before they even reach the board.”
A Call To Action
Dr. Wolfe isn’t buying the notion that Minnesota doctors require less formal discipline while their colleagues in Alaska need more. Whenever other low-ranking states have provided sufficient funding, replaced ineffective leadership, granted more independence, and met the other conditions necessary for a better medical board, he notes, their rate of disciplinary actions often “rockets up.”
The medical boards of North Carolina and Washington, D.C., have risen dramatically in the rankings in recent years, and Dr. Wolfe cites effective intervention in both cases. In formerly low-ranking Arizona, he says, similar corrective action in the late 1990s led to a tripling of the rate of serious disciplinary action within three years. “That’s obviously not a period of time that’s long enough to be explained by some inward migration of bad doctors or outward migration of good doctors,” he says. “It’s because the board started functioning better.”
Meanwhile, boards in South Carolina and Massachusetts have slumped in the ratings—a decline he attributes to the loss of leadership and funds.
“One area I can agree with Dr. Wolfe on is that medical boards need resources; they need adequate structure, resources, and authority to do their job and be able to protect the public,” says Robin, of the Federation of State Medical Boards. “If they’re in a big umbrella agency and they’re just one of many and share their pool of investigators with everyone, as you can imagine, that’s probably not as efficient.”
Hospitals also share in the blame, according to a separate Public Citizen report released last year that cites a chronic underreporting of doctor misconduct or incompetence to the National Practitioner Data Bank by hospitals. Robin agrees that more diligence is needed to ensure that medical boards have the information they need to properly do their jobs. As one of her board members told her, “They can’t gain information by osmosis.”
Hospitalists, however, might be well suited for addressing the underreporting issue. HM is in a “really good position to observe behavior that needs to be brought to the attention of hospital medical staff,” Dr. Wolfe says.
He recommends that one or more hospitalists should sit on each hospital’s medical peer review committee, where they can put their expertise to good use. “Hospitalists really need to get more active in this,” he says. “It’s for the betterment of the patients in the hospital, it’s for the betterment for the reputation of the hospital and the medical staff.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
The Cost of Regulation
The impact of last summer’s new restrictions from the Accreditation Council for Graduate Medical Education (ACGME) on how many hospitalized patients a first-year resident can treat on an internal-medicine (IM) rotation was as immediate as it was evident at Monmouth Medical Center, a 527-bed teaching hospital in Long Branch, N.J. The institution had a class of eight rookie residents whose caseloads were cut from 12 to the new threshold of 10.
Physicians “had to find some other way of getting attention . . . for 16 patients,” says Sarah Wallach, MD, FACP, director of Monmouth’s IM residency program and vice chair of the department of medicine at the hospital. At Monmouth, the solution came in the form of a new hire—a nurse practitioner (NP)—to handle the overflow. The NP service is used predominantly for referral patients from primary-care physicians (PCPs), as opposed to independent hospital admissions.
But because the NP service does not provide 24-hour coverage, the hospital can get away with only one person in the position. To extend coverage all day long, Dr. Wallach estimates she would need to hire two or three additional NPs, plus another one or two administrative positions to provide relief on holidays and vacations. “You would need five people,” she says. “I can’t afford that.”
Few hospitals or HM groups can afford new hires in today’s world of Medicare reimbursement cuts, shrinking budgets, and—courtesy of the newest rules—restricting patient caps for residents. The latest rules took hold about a year ago, but hospitalists in both academic and community settings say the impact already is noticeable.
Many hospitals have had to craft solutions, which have included burdening academic hospitals with more clinical responsibilities, turning to private HM groups (HMGs) to assume the patients residents can no longer care for, or hiring nonphysician providers (NPPs) to pick up the slack. As Dr. Wallach pointedly notes, the latter two solutions cost money at a time when hospitals have less to go around.
Already, teaching hospitals have begun discussions about how the newest rules—and the future changes they presage—will change the playing field. Will a wave of academics flee their classroom (the teaching hospital), as nonteaching duties become an intrusion? Will teaching hospitals face financial pressure as they struggle to replace the low-cost labor force that residents represent?
Perhaps most importantly from a medical perspective, will graduate trainees be as prepared as their predecessors when they enter practice?

The answers will have a direct correlation to private HMGs, which are poised to see more patients in the wake of residency restrictions, particularly on overnight services. The cost of hospital care will increase for hospitals, putting more pressure on hospitalist groups that tout themselves to C-suites as engines for cost savings. Long-term implications, unfortunately, remain murky, as the newest rules have been in place for a relatively short time. Plus, ACGME is expected—at the end of this month, according to a recent memo to program directors—to announce more changes to residency guidelines.
“Hospitalists will always be involved in teaching—it will never go away,” says Julia Wright, MD, FHM, clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison and a member of Team Hospitalist. “But it will be a very different balance, a different kind of feel.”
The Past to the Future
To understand the concerns moving forward, it’s important to first look back. In July 2003, new ACGME rules went into place capping the workweeks of residents at 80 hours. Rules were put into place that regulated the number of patients that residents could be assigned, and those thresholds were further tightened on July 1, 2009. The most notable 2009 change: A first-year resident’s patient census must not exceed 10 patients. ACGME CEO Thomas J. Nasca, MD, MACP, sent a letter to program directors in early May announcing more changes to resident work hours. The letter indicates proposals will be announced by the end of this month, and public comment will follow. At the earliest, new rules changes would go into effect in 2011. “The board may adopt a modification to the duty-hours standard,” says Julie Jacob, a spokeswoman for Chicago-based ACGME. “Any proposed standards would get a public comment.”
Jacob declined further comment, but various hospitalists and academics say they wouldn’t be surprised if new rules reflect 2008 Institute of Medicine (IOM) recommendations.1 The IOM report called for a maximum resident shift length of 30 hours, with admission of patients for up to 16 hours, plus a five-hour uninterrupted sleep period between 10 p.m. and 8 a.m. It also suggested the remaining workweek hours be used for transitional and educational activities.
However those IOM recommendations are incorporated, one thing is clear: Any adoption of those standards will have a financial impact. In fact, a study published last year reported that annual labor costs from implementing the IOM standards was estimated to be $1.6 billion in 2006 dollars (see “The Cost of Progress,” p. 25).2
“Any replacement of a resident costs more than a resident, whether it’s an NP, a PA (physician assistant), an MD, or a DO,” says Kevin O’Leary, MD, MS, associate program director of the IM residency program at Northwestern University’s Feinberg School of Medicine in Chicago. “Everybody costs more.”
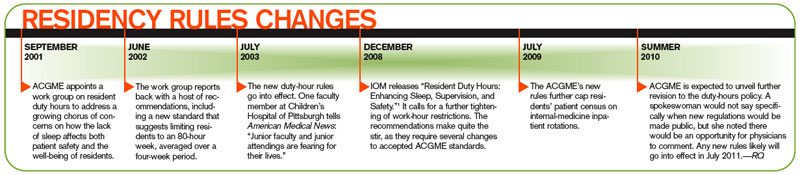
The Fate of Teachers
Some of the largest academic centers, including the Feinberg School, the University of Michigan, and the teaching service at St. Luke’s-Roosevelt Hospital in New York City, reduced patient caseloads ahead of the 2009 round of residency rule changes. Hospitalists and educators at those institutions say the proactive approach helped them adjust to the newest rules, which by some estimates reduce resident productivity by 20%.
But the changes shift the workload to academic hospitalists, many of whom forego higher-paying positions to pursue teaching and research. According to the latest SHM survey data, academic hospitalists make about $50,000 less per year than the average community hospitalist. But as clinical work intrudes further, as residents are unable to assume the patient care they once did, educators are put into positions of having to balance the educational portion of their job with patient care, says John Del Valle, MD, professor and residency program director in the department of internal medicine at the University of Michigan Health System in Ann Arbor.
“This is where difficult decisions have to be made,” Dr. Del Valle says. “This is not the blend of activities that traditional academics signed up for.”
Solutions to relieve current and impending pressure on teaching hospitalists have presented themselves in different ways. In Dr. Del Valle’s hospital, there is a split between the hospitalist service and the house staff, which is aimed at keeping up with the growth in IM admissions. That tally has climbed an average of 4% per year for the past five years, reaching some 18,000 admissions last year. To handle that workload, the nonresident service last year added three clinical full-time equivalents (FTEs) to bring its total to nearly 30 FTEs.
Dr. Del Valle notes his institution has been fortunate to be able to afford growth, thanks in large part to a payor mix with a relatively low percentage of charity care and high level of activity.
At Brigham and Women’s Hospital in Boston, the answer is a freestanding PA service that has been in place since 2005. Last summer, the program went to a 24-hour rotation to increase continuity for overnight services and to provide coverage on night shifts, an area most in the industry agree will be hit hardest by the resident caps. Physicians at Brigham’s, a teaching affiliate of Harvard Medical School, are now discussing an expansion of the PA service, or perhaps even an overhaul to a more cost-efficient solution, says Danielle Scheurer, MD, MSc, FHM, assistant professor of medicine at Harvard and director of Brigham’s general medicine service.

At Medical Center Hospital (MCH) in Odessa, Texas, the hospitalists were added to the ED call schedule once every five nights. The plan was under discussion before the new residency rules went into place; however, it was implemented to keep the IM residency program within the new limits, says Bruce Becker, MD, MCH’s chief medical officer.
And at St. Luke’s-Roosevelt Hospital, discussions are under way on how to best extend the nonteaching staff, says Ethan Fried, MD, MS, FACP, assistant professor of clinical medicine at Columbia University, vice chair for education in the department of medicine and director of graduate medical education at St. Luke’s-Roosevelt. “The adjustment has to come from the nonteaching side because the house staff at this point is saturated,” says Dr. Fried, president-elect of the Association of Program Directors in Internal Medicine (APDIM). “You can’t be cheap about acquiring your nonteaching staff.”
The Fate of Students
Perhaps paramount to the fears of how teaching hospitalists will react to current or future restrictions is the effect those limits have on the residents they safeguard. Some physicians think the new rules will produce crops of ill-prepared residents because they have been coddled with limited patient censuses. Other physicians argue that the new thresholds will actually better prepare physicians when HM groups are hiring residents for full-time positions.
Dr. Del Valle acknowledges there is as yet no rigorous data to show the impact of the current restrictions, but he agrees it’s a simple equation of patient-care mathematics. “You can’t [easily] replace 100-110 hours [of care per week],” he says.
Others say patient caps and rules to limit how much work residents do are in line with the purpose of medical training programs. “I’ve bought into the fact that these programs exist to train residents, not to provide clinical care,” Dr. O’Leary says. “I’ve drunk that Kool-Aid. … I think there’s more variation, person to person, than ‘my era vs. the current era.’ Like any new hospitalist that you hire, you need to give an orientation and give enough support to them so when they begin to see patients that they are not overwhelmed.”
Shaun Frost, MD, FACP, FHM, might be best described as halfway between those two extremes. A regional director for the eastern U.S. for Cogent Healthcare, he says duty-hour restrictions have had deleterious impacts but also create learning opportunities.
“The residency work-hour restrictions have inhibited our ability to train people to work as efficiently as trainees who were taught in the past,” says Dr. Frost, an SHM board member. “That doesn’t necessarily mean you can’t teach people to work more efficiently . . . but in the future, my hope is that residency training programs will recognize the deficit that exists in personal work efficiencies between their completion and their responsibilities as a hospitalist.”
To that end, Dr. Frost works with others to develop both structured curriculum and classroom didactics that help new hospitalists make up for gaps in preparation that weren’t addressed in residency. In some cases, that can be practice management and billing issues, but often, according to Dr. Frost, it is addressing personal workflow and bridging the “unnatural discontinuity” in patient care from residency to the real world.
“There is a cost to this investment for the future,” Dr. Frost adds. “If people don’t recognize the potential return on investment as being critical to the development of an educated workforce—an efficient and competent workforce—and thus critical to the retention of high-performing hospitalists, they are selling themselves, unfortunately, significantly short.”
Caught in the Middle
One man’s trash is another man’s treasure, the axiom tells us. Well, in healthcare circles, that could just as easily read: The woes of academic hospitalists are the wealth of community hospitalists.
The new rules “may result in more opportunities for hospitalists to provide needed clinical services,” Dr. Wright says.
The long-term implications, though, remain to be seen. While academic hospitalists say they have seen preliminary increases in care-delivery costs because of the latest rules changes, many say it’s too soon to tell just how high those costs might climb and what ripple effect might follow.
Some physicians, including Dr. Del Valle, note that while the 2009 changes and the expectation of more changes in 2011 are cause for attention, that doesn’t translate to cause for concern. In 2003, months before the 80-hour workweek rules were first put in place by ACGME, many of the same debates were already under way: How will the faculty of IM residency programs cope? How will institutions pay the bills while putting money aside for other physicians picking up the slack?
“This is a pendulum,” Dr. Del Valle says. “I think it will come back to a balanced place.”
Dr. Fried, who is more optimistic that the residency rules can have a positive, long-term effect, agrees. He says residency caps and limits should not be viewed as “things that limit education. We [should] look at them as things that ensure education continues while patient care continues.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Ulmer C, Wolman DM, Johns MM, eds. Washington, D.C.: The National Academies Press; 2008.
- Nuckols TK, Bhattacharya J, Wolman DM, Ulmer C, Escarce JJ. Cost implications of reduced work hours and workloads for resident physicians. N Engl J Med. 2009:360(21):2202-2215.
The impact of last summer’s new restrictions from the Accreditation Council for Graduate Medical Education (ACGME) on how many hospitalized patients a first-year resident can treat on an internal-medicine (IM) rotation was as immediate as it was evident at Monmouth Medical Center, a 527-bed teaching hospital in Long Branch, N.J. The institution had a class of eight rookie residents whose caseloads were cut from 12 to the new threshold of 10.
Physicians “had to find some other way of getting attention . . . for 16 patients,” says Sarah Wallach, MD, FACP, director of Monmouth’s IM residency program and vice chair of the department of medicine at the hospital. At Monmouth, the solution came in the form of a new hire—a nurse practitioner (NP)—to handle the overflow. The NP service is used predominantly for referral patients from primary-care physicians (PCPs), as opposed to independent hospital admissions.
But because the NP service does not provide 24-hour coverage, the hospital can get away with only one person in the position. To extend coverage all day long, Dr. Wallach estimates she would need to hire two or three additional NPs, plus another one or two administrative positions to provide relief on holidays and vacations. “You would need five people,” she says. “I can’t afford that.”
Few hospitals or HM groups can afford new hires in today’s world of Medicare reimbursement cuts, shrinking budgets, and—courtesy of the newest rules—restricting patient caps for residents. The latest rules took hold about a year ago, but hospitalists in both academic and community settings say the impact already is noticeable.
Many hospitals have had to craft solutions, which have included burdening academic hospitals with more clinical responsibilities, turning to private HM groups (HMGs) to assume the patients residents can no longer care for, or hiring nonphysician providers (NPPs) to pick up the slack. As Dr. Wallach pointedly notes, the latter two solutions cost money at a time when hospitals have less to go around.
Already, teaching hospitals have begun discussions about how the newest rules—and the future changes they presage—will change the playing field. Will a wave of academics flee their classroom (the teaching hospital), as nonteaching duties become an intrusion? Will teaching hospitals face financial pressure as they struggle to replace the low-cost labor force that residents represent?
Perhaps most importantly from a medical perspective, will graduate trainees be as prepared as their predecessors when they enter practice?
The answers will have a direct correlation to private HMGs, which are poised to see more patients in the wake of residency restrictions, particularly on overnight services. The cost of hospital care will increase for hospitals, putting more pressure on hospitalist groups that tout themselves to C-suites as engines for cost savings. Long-term implications, unfortunately, remain murky, as the newest rules have been in place for a relatively short time. Plus, ACGME is expected—at the end of this month, according to a recent memo to program directors—to announce more changes to residency guidelines.
“Hospitalists will always be involved in teaching—it will never go away,” says Julia Wright, MD, FHM, clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison and a member of Team Hospitalist. “But it will be a very different balance, a different kind of feel.”
The Past to the Future
To understand the concerns moving forward, it’s important to first look back. In July 2003, new ACGME rules went into place capping the workweeks of residents at 80 hours. Rules were put into place that regulated the number of patients that residents could be assigned, and those thresholds were further tightened on July 1, 2009. The most notable 2009 change: A first-year resident’s patient census must not exceed 10 patients. ACGME CEO Thomas J. Nasca, MD, MACP, sent a letter to program directors in early May announcing more changes to resident work hours. The letter indicates proposals will be announced by the end of this month, and public comment will follow. At the earliest, new rules changes would go into effect in 2011. “The board may adopt a modification to the duty-hours standard,” says Julie Jacob, a spokeswoman for Chicago-based ACGME. “Any proposed standards would get a public comment.”
Jacob declined further comment, but various hospitalists and academics say they wouldn’t be surprised if new rules reflect 2008 Institute of Medicine (IOM) recommendations.1 The IOM report called for a maximum resident shift length of 30 hours, with admission of patients for up to 16 hours, plus a five-hour uninterrupted sleep period between 10 p.m. and 8 a.m. It also suggested the remaining workweek hours be used for transitional and educational activities.
However those IOM recommendations are incorporated, one thing is clear: Any adoption of those standards will have a financial impact. In fact, a study published last year reported that annual labor costs from implementing the IOM standards was estimated to be $1.6 billion in 2006 dollars (see “The Cost of Progress,” p. 25).2
“Any replacement of a resident costs more than a resident, whether it’s an NP, a PA (physician assistant), an MD, or a DO,” says Kevin O’Leary, MD, MS, associate program director of the IM residency program at Northwestern University’s Feinberg School of Medicine in Chicago. “Everybody costs more.”
The Fate of Teachers
Some of the largest academic centers, including the Feinberg School, the University of Michigan, and the teaching service at St. Luke’s-Roosevelt Hospital in New York City, reduced patient caseloads ahead of the 2009 round of residency rule changes. Hospitalists and educators at those institutions say the proactive approach helped them adjust to the newest rules, which by some estimates reduce resident productivity by 20%.
But the changes shift the workload to academic hospitalists, many of whom forego higher-paying positions to pursue teaching and research. According to the latest SHM survey data, academic hospitalists make about $50,000 less per year than the average community hospitalist. But as clinical work intrudes further, as residents are unable to assume the patient care they once did, educators are put into positions of having to balance the educational portion of their job with patient care, says John Del Valle, MD, professor and residency program director in the department of internal medicine at the University of Michigan Health System in Ann Arbor.
“This is where difficult decisions have to be made,” Dr. Del Valle says. “This is not the blend of activities that traditional academics signed up for.”
Solutions to relieve current and impending pressure on teaching hospitalists have presented themselves in different ways. In Dr. Del Valle’s hospital, there is a split between the hospitalist service and the house staff, which is aimed at keeping up with the growth in IM admissions. That tally has climbed an average of 4% per year for the past five years, reaching some 18,000 admissions last year. To handle that workload, the nonresident service last year added three clinical full-time equivalents (FTEs) to bring its total to nearly 30 FTEs.
Dr. Del Valle notes his institution has been fortunate to be able to afford growth, thanks in large part to a payor mix with a relatively low percentage of charity care and high level of activity.
At Brigham and Women’s Hospital in Boston, the answer is a freestanding PA service that has been in place since 2005. Last summer, the program went to a 24-hour rotation to increase continuity for overnight services and to provide coverage on night shifts, an area most in the industry agree will be hit hardest by the resident caps. Physicians at Brigham’s, a teaching affiliate of Harvard Medical School, are now discussing an expansion of the PA service, or perhaps even an overhaul to a more cost-efficient solution, says Danielle Scheurer, MD, MSc, FHM, assistant professor of medicine at Harvard and director of Brigham’s general medicine service.
At Medical Center Hospital (MCH) in Odessa, Texas, the hospitalists were added to the ED call schedule once every five nights. The plan was under discussion before the new residency rules went into place; however, it was implemented to keep the IM residency program within the new limits, says Bruce Becker, MD, MCH’s chief medical officer.
And at St. Luke’s-Roosevelt Hospital, discussions are under way on how to best extend the nonteaching staff, says Ethan Fried, MD, MS, FACP, assistant professor of clinical medicine at Columbia University, vice chair for education in the department of medicine and director of graduate medical education at St. Luke’s-Roosevelt. “The adjustment has to come from the nonteaching side because the house staff at this point is saturated,” says Dr. Fried, president-elect of the Association of Program Directors in Internal Medicine (APDIM). “You can’t be cheap about acquiring your nonteaching staff.”
The Fate of Students
Perhaps paramount to the fears of how teaching hospitalists will react to current or future restrictions is the effect those limits have on the residents they safeguard. Some physicians think the new rules will produce crops of ill-prepared residents because they have been coddled with limited patient censuses. Other physicians argue that the new thresholds will actually better prepare physicians when HM groups are hiring residents for full-time positions.
Dr. Del Valle acknowledges there is as yet no rigorous data to show the impact of the current restrictions, but he agrees it’s a simple equation of patient-care mathematics. “You can’t [easily] replace 100-110 hours [of care per week],” he says.
Others say patient caps and rules to limit how much work residents do are in line with the purpose of medical training programs. “I’ve bought into the fact that these programs exist to train residents, not to provide clinical care,” Dr. O’Leary says. “I’ve drunk that Kool-Aid. … I think there’s more variation, person to person, than ‘my era vs. the current era.’ Like any new hospitalist that you hire, you need to give an orientation and give enough support to them so when they begin to see patients that they are not overwhelmed.”
Shaun Frost, MD, FACP, FHM, might be best described as halfway between those two extremes. A regional director for the eastern U.S. for Cogent Healthcare, he says duty-hour restrictions have had deleterious impacts but also create learning opportunities.
“The residency work-hour restrictions have inhibited our ability to train people to work as efficiently as trainees who were taught in the past,” says Dr. Frost, an SHM board member. “That doesn’t necessarily mean you can’t teach people to work more efficiently . . . but in the future, my hope is that residency training programs will recognize the deficit that exists in personal work efficiencies between their completion and their responsibilities as a hospitalist.”
To that end, Dr. Frost works with others to develop both structured curriculum and classroom didactics that help new hospitalists make up for gaps in preparation that weren’t addressed in residency. In some cases, that can be practice management and billing issues, but often, according to Dr. Frost, it is addressing personal workflow and bridging the “unnatural discontinuity” in patient care from residency to the real world.
“There is a cost to this investment for the future,” Dr. Frost adds. “If people don’t recognize the potential return on investment as being critical to the development of an educated workforce—an efficient and competent workforce—and thus critical to the retention of high-performing hospitalists, they are selling themselves, unfortunately, significantly short.”
Caught in the Middle
One man’s trash is another man’s treasure, the axiom tells us. Well, in healthcare circles, that could just as easily read: The woes of academic hospitalists are the wealth of community hospitalists.
The new rules “may result in more opportunities for hospitalists to provide needed clinical services,” Dr. Wright says.
The long-term implications, though, remain to be seen. While academic hospitalists say they have seen preliminary increases in care-delivery costs because of the latest rules changes, many say it’s too soon to tell just how high those costs might climb and what ripple effect might follow.
Some physicians, including Dr. Del Valle, note that while the 2009 changes and the expectation of more changes in 2011 are cause for attention, that doesn’t translate to cause for concern. In 2003, months before the 80-hour workweek rules were first put in place by ACGME, many of the same debates were already under way: How will the faculty of IM residency programs cope? How will institutions pay the bills while putting money aside for other physicians picking up the slack?
“This is a pendulum,” Dr. Del Valle says. “I think it will come back to a balanced place.”
Dr. Fried, who is more optimistic that the residency rules can have a positive, long-term effect, agrees. He says residency caps and limits should not be viewed as “things that limit education. We [should] look at them as things that ensure education continues while patient care continues.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Ulmer C, Wolman DM, Johns MM, eds. Washington, D.C.: The National Academies Press; 2008.
- Nuckols TK, Bhattacharya J, Wolman DM, Ulmer C, Escarce JJ. Cost implications of reduced work hours and workloads for resident physicians. N Engl J Med. 2009:360(21):2202-2215.
The impact of last summer’s new restrictions from the Accreditation Council for Graduate Medical Education (ACGME) on how many hospitalized patients a first-year resident can treat on an internal-medicine (IM) rotation was as immediate as it was evident at Monmouth Medical Center, a 527-bed teaching hospital in Long Branch, N.J. The institution had a class of eight rookie residents whose caseloads were cut from 12 to the new threshold of 10.
Physicians “had to find some other way of getting attention . . . for 16 patients,” says Sarah Wallach, MD, FACP, director of Monmouth’s IM residency program and vice chair of the department of medicine at the hospital. At Monmouth, the solution came in the form of a new hire—a nurse practitioner (NP)—to handle the overflow. The NP service is used predominantly for referral patients from primary-care physicians (PCPs), as opposed to independent hospital admissions.
But because the NP service does not provide 24-hour coverage, the hospital can get away with only one person in the position. To extend coverage all day long, Dr. Wallach estimates she would need to hire two or three additional NPs, plus another one or two administrative positions to provide relief on holidays and vacations. “You would need five people,” she says. “I can’t afford that.”
Few hospitals or HM groups can afford new hires in today’s world of Medicare reimbursement cuts, shrinking budgets, and—courtesy of the newest rules—restricting patient caps for residents. The latest rules took hold about a year ago, but hospitalists in both academic and community settings say the impact already is noticeable.
Many hospitals have had to craft solutions, which have included burdening academic hospitals with more clinical responsibilities, turning to private HM groups (HMGs) to assume the patients residents can no longer care for, or hiring nonphysician providers (NPPs) to pick up the slack. As Dr. Wallach pointedly notes, the latter two solutions cost money at a time when hospitals have less to go around.
Already, teaching hospitals have begun discussions about how the newest rules—and the future changes they presage—will change the playing field. Will a wave of academics flee their classroom (the teaching hospital), as nonteaching duties become an intrusion? Will teaching hospitals face financial pressure as they struggle to replace the low-cost labor force that residents represent?
Perhaps most importantly from a medical perspective, will graduate trainees be as prepared as their predecessors when they enter practice?
The answers will have a direct correlation to private HMGs, which are poised to see more patients in the wake of residency restrictions, particularly on overnight services. The cost of hospital care will increase for hospitals, putting more pressure on hospitalist groups that tout themselves to C-suites as engines for cost savings. Long-term implications, unfortunately, remain murky, as the newest rules have been in place for a relatively short time. Plus, ACGME is expected—at the end of this month, according to a recent memo to program directors—to announce more changes to residency guidelines.
“Hospitalists will always be involved in teaching—it will never go away,” says Julia Wright, MD, FHM, clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison and a member of Team Hospitalist. “But it will be a very different balance, a different kind of feel.”
The Past to the Future
To understand the concerns moving forward, it’s important to first look back. In July 2003, new ACGME rules went into place capping the workweeks of residents at 80 hours. Rules were put into place that regulated the number of patients that residents could be assigned, and those thresholds were further tightened on July 1, 2009. The most notable 2009 change: A first-year resident’s patient census must not exceed 10 patients. ACGME CEO Thomas J. Nasca, MD, MACP, sent a letter to program directors in early May announcing more changes to resident work hours. The letter indicates proposals will be announced by the end of this month, and public comment will follow. At the earliest, new rules changes would go into effect in 2011. “The board may adopt a modification to the duty-hours standard,” says Julie Jacob, a spokeswoman for Chicago-based ACGME. “Any proposed standards would get a public comment.”
Jacob declined further comment, but various hospitalists and academics say they wouldn’t be surprised if new rules reflect 2008 Institute of Medicine (IOM) recommendations.1 The IOM report called for a maximum resident shift length of 30 hours, with admission of patients for up to 16 hours, plus a five-hour uninterrupted sleep period between 10 p.m. and 8 a.m. It also suggested the remaining workweek hours be used for transitional and educational activities.
However those IOM recommendations are incorporated, one thing is clear: Any adoption of those standards will have a financial impact. In fact, a study published last year reported that annual labor costs from implementing the IOM standards was estimated to be $1.6 billion in 2006 dollars (see “The Cost of Progress,” p. 25).2
“Any replacement of a resident costs more than a resident, whether it’s an NP, a PA (physician assistant), an MD, or a DO,” says Kevin O’Leary, MD, MS, associate program director of the IM residency program at Northwestern University’s Feinberg School of Medicine in Chicago. “Everybody costs more.”
The Fate of Teachers
Some of the largest academic centers, including the Feinberg School, the University of Michigan, and the teaching service at St. Luke’s-Roosevelt Hospital in New York City, reduced patient caseloads ahead of the 2009 round of residency rule changes. Hospitalists and educators at those institutions say the proactive approach helped them adjust to the newest rules, which by some estimates reduce resident productivity by 20%.
But the changes shift the workload to academic hospitalists, many of whom forego higher-paying positions to pursue teaching and research. According to the latest SHM survey data, academic hospitalists make about $50,000 less per year than the average community hospitalist. But as clinical work intrudes further, as residents are unable to assume the patient care they once did, educators are put into positions of having to balance the educational portion of their job with patient care, says John Del Valle, MD, professor and residency program director in the department of internal medicine at the University of Michigan Health System in Ann Arbor.
“This is where difficult decisions have to be made,” Dr. Del Valle says. “This is not the blend of activities that traditional academics signed up for.”
Solutions to relieve current and impending pressure on teaching hospitalists have presented themselves in different ways. In Dr. Del Valle’s hospital, there is a split between the hospitalist service and the house staff, which is aimed at keeping up with the growth in IM admissions. That tally has climbed an average of 4% per year for the past five years, reaching some 18,000 admissions last year. To handle that workload, the nonresident service last year added three clinical full-time equivalents (FTEs) to bring its total to nearly 30 FTEs.
Dr. Del Valle notes his institution has been fortunate to be able to afford growth, thanks in large part to a payor mix with a relatively low percentage of charity care and high level of activity.
At Brigham and Women’s Hospital in Boston, the answer is a freestanding PA service that has been in place since 2005. Last summer, the program went to a 24-hour rotation to increase continuity for overnight services and to provide coverage on night shifts, an area most in the industry agree will be hit hardest by the resident caps. Physicians at Brigham’s, a teaching affiliate of Harvard Medical School, are now discussing an expansion of the PA service, or perhaps even an overhaul to a more cost-efficient solution, says Danielle Scheurer, MD, MSc, FHM, assistant professor of medicine at Harvard and director of Brigham’s general medicine service.
At Medical Center Hospital (MCH) in Odessa, Texas, the hospitalists were added to the ED call schedule once every five nights. The plan was under discussion before the new residency rules went into place; however, it was implemented to keep the IM residency program within the new limits, says Bruce Becker, MD, MCH’s chief medical officer.
And at St. Luke’s-Roosevelt Hospital, discussions are under way on how to best extend the nonteaching staff, says Ethan Fried, MD, MS, FACP, assistant professor of clinical medicine at Columbia University, vice chair for education in the department of medicine and director of graduate medical education at St. Luke’s-Roosevelt. “The adjustment has to come from the nonteaching side because the house staff at this point is saturated,” says Dr. Fried, president-elect of the Association of Program Directors in Internal Medicine (APDIM). “You can’t be cheap about acquiring your nonteaching staff.”
The Fate of Students
Perhaps paramount to the fears of how teaching hospitalists will react to current or future restrictions is the effect those limits have on the residents they safeguard. Some physicians think the new rules will produce crops of ill-prepared residents because they have been coddled with limited patient censuses. Other physicians argue that the new thresholds will actually better prepare physicians when HM groups are hiring residents for full-time positions.
Dr. Del Valle acknowledges there is as yet no rigorous data to show the impact of the current restrictions, but he agrees it’s a simple equation of patient-care mathematics. “You can’t [easily] replace 100-110 hours [of care per week],” he says.
Others say patient caps and rules to limit how much work residents do are in line with the purpose of medical training programs. “I’ve bought into the fact that these programs exist to train residents, not to provide clinical care,” Dr. O’Leary says. “I’ve drunk that Kool-Aid. … I think there’s more variation, person to person, than ‘my era vs. the current era.’ Like any new hospitalist that you hire, you need to give an orientation and give enough support to them so when they begin to see patients that they are not overwhelmed.”
Shaun Frost, MD, FACP, FHM, might be best described as halfway between those two extremes. A regional director for the eastern U.S. for Cogent Healthcare, he says duty-hour restrictions have had deleterious impacts but also create learning opportunities.
“The residency work-hour restrictions have inhibited our ability to train people to work as efficiently as trainees who were taught in the past,” says Dr. Frost, an SHM board member. “That doesn’t necessarily mean you can’t teach people to work more efficiently . . . but in the future, my hope is that residency training programs will recognize the deficit that exists in personal work efficiencies between their completion and their responsibilities as a hospitalist.”
To that end, Dr. Frost works with others to develop both structured curriculum and classroom didactics that help new hospitalists make up for gaps in preparation that weren’t addressed in residency. In some cases, that can be practice management and billing issues, but often, according to Dr. Frost, it is addressing personal workflow and bridging the “unnatural discontinuity” in patient care from residency to the real world.
“There is a cost to this investment for the future,” Dr. Frost adds. “If people don’t recognize the potential return on investment as being critical to the development of an educated workforce—an efficient and competent workforce—and thus critical to the retention of high-performing hospitalists, they are selling themselves, unfortunately, significantly short.”
Caught in the Middle
One man’s trash is another man’s treasure, the axiom tells us. Well, in healthcare circles, that could just as easily read: The woes of academic hospitalists are the wealth of community hospitalists.
The new rules “may result in more opportunities for hospitalists to provide needed clinical services,” Dr. Wright says.
The long-term implications, though, remain to be seen. While academic hospitalists say they have seen preliminary increases in care-delivery costs because of the latest rules changes, many say it’s too soon to tell just how high those costs might climb and what ripple effect might follow.
Some physicians, including Dr. Del Valle, note that while the 2009 changes and the expectation of more changes in 2011 are cause for attention, that doesn’t translate to cause for concern. In 2003, months before the 80-hour workweek rules were first put in place by ACGME, many of the same debates were already under way: How will the faculty of IM residency programs cope? How will institutions pay the bills while putting money aside for other physicians picking up the slack?
“This is a pendulum,” Dr. Del Valle says. “I think it will come back to a balanced place.”
Dr. Fried, who is more optimistic that the residency rules can have a positive, long-term effect, agrees. He says residency caps and limits should not be viewed as “things that limit education. We [should] look at them as things that ensure education continues while patient care continues.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Ulmer C, Wolman DM, Johns MM, eds. Washington, D.C.: The National Academies Press; 2008.
- Nuckols TK, Bhattacharya J, Wolman DM, Ulmer C, Escarce JJ. Cost implications of reduced work hours and workloads for resident physicians. N Engl J Med. 2009:360(21):2202-2215.
Spousal Consent
When recruiting a hospitalist for his company, Jason Stuckey makes it a point to call the candidate’s home. His goal isn’t to speak with the hospitalist the company is interested in hiring—it’s to talk with the candidate’s spouse.
“One of the top five mistakes recruiters make is to not involve the spouse in the [recruitment] process,” says Stuckey, who directs HM recruiting for TeamHealth, a Knoxville, Tenn.-based company that provides healthcare staffing and administrative services to hospitals in 14 states.
Hospitalists are generally so busy with work that the spouse is often the person in the family who takes the lead in the job search, says Tim Lary, vice president of profession staffing for IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif.
The spouse often gives final approval on a decision to accept a job offer, adds Peggy Fricke, director of physician staffing for Eagle Hospital Physicians, an Atlanta-based company that manages hospitalist practices for hospitals in the Southeast and Mid-Atlantic regions.
“The physician could be making the most money, but if their spouse and family are not happy, then they won’t stay in the position long,” Stuckey explains. “I’ve also found that if the spouse is not on board with moving and uprooting the family to a new location, then it’s not going to happen.”
As a result, recruiters and prospective employers often spend just as much time engaging the spouse as they do the actual job candidate, the recruiters say. For this reason, hospitalists who are searching for a new job would be wise to include their husband or wife as early as possible in the job hunt in order to get the most out of the recruiting process.
For example, while the hospitalist focuses on determining if the work is the right fit professionally and financially, the spouse can appraise the community to see if it meets the family’s needs in such areas as schools, neighborhoods, religious services, community groups, and entertainment/cultural outlets. If the hospitalist is invited for an on-site interview, it’s important that their spouse makes the trip as well.
“We always do a community tour, and we will do school tours when asked,” Fricke says of Eagle’s recruiting efforts. “We can introduce the families of the other hospitalists in the practice so a spouse can meet and get to know them.”
—Jason Stuckey, director, HM recruitment, TeamHealth, Knoxville, Tenn.
Upfront Inclusion
When the spouse is involved in the process, they usually are more receptive to receiving information about what opportunities exist in other communities and more open to the idea of moving to a new place, Stuckey says.
For instances in which children are involved, the spouse is most often interested in learning about the location’s school districts and private schools, and determining if the community has a good quality of life for families, Fricke says. For situations in which there are no children or the children are grown, the spouse often focuses on job prospects in their own profession.
Hospitalists with a husband or wife who works and whose career is important to them should see if the HM recruiter can help put their spouse in touch with potential employers in the community, because many times they will, says Fricke, who has connected spouses in IT and engineering fields with people who could assist them in their job search.
“It goes back to making sure everyone is happy. If the spouse can’t find work, that is going to affect their happiness,” says Darren Swenson, MD, medical affairs director for IPC of Nevada and regional chair of IPC’s national advisory board.
Aside from schools, quality of life, and their own job opportunities, spouses also ask about what their hospitalist husband or wife’s work schedule would be and how much vacation and holiday time they would have in the prospective job, Dr. Swenson says.
“It’s extremely important that we look at our hospitalists and their spouses being happy in their home life, because if they’re not, that is going to spill over into in their work life,” IPC’s Lary says.
Good Partnership, Bad Partnership
Times arise when the spouse takes a proactive role in evaluating the actual HM job offer, the recruiters say. “In all couples, there is someone who is dominant and someone who is not,” says Fricke, who has seen spouses participate in job interviews with hospital administrators. “If the spouse is dominant, we try to understand them and listen to what is important to them.”
Sometimes the spouse is an attorney or other type of professional who wants to review the hospitalist contract and has the most questions about it, Dr. Swenson says. When that happens, recruiters will often have group members sit in to answer their questions, he says.
“Absolutely, without question, the spouse has to be involved. But if the spouse is too demanding and everything has to be run through them, to an employer, that can be a big turnoff,” Stuckey says.
When it comes to business matters, the physician—not the spouse—has to take the lead, he says. If the physician doesn’t, it could make the prospective employer wonder what challenges could be ahead should the candidate be hired, Stuckey says.
Two-Physician Families
One time when it is acceptable for a spouse to get intimately involved in the contract and negotiations is when he or she is a hospitalist who also is being recruited by the same prospective employer.
“It’s a unique situation. It’s great to have two for the price of one, so to speak,” Stuckey says. “But there are challenges from the employer’s perspective—for example, scheduling—that have to be resolved on the front end rather than when they get there.”
While still relatively rare, husband-wife hospitalist couples are becoming more prevalent because there are more hospitalists, Fricke says. They tend to meet each other in medical school or residency, she says.
“Even though they are a couple, we treat them as individuals during the recruiting process,” Fricke says. “I think the most important thing is we try to do anything we can—within reason, of course—to help the hospitalist and their spouse make the best decision for themselves and their family.” TH
Lisa Ryan is a freelance writer based in New Jersey.
When recruiting a hospitalist for his company, Jason Stuckey makes it a point to call the candidate’s home. His goal isn’t to speak with the hospitalist the company is interested in hiring—it’s to talk with the candidate’s spouse.
“One of the top five mistakes recruiters make is to not involve the spouse in the [recruitment] process,” says Stuckey, who directs HM recruiting for TeamHealth, a Knoxville, Tenn.-based company that provides healthcare staffing and administrative services to hospitals in 14 states.
Hospitalists are generally so busy with work that the spouse is often the person in the family who takes the lead in the job search, says Tim Lary, vice president of profession staffing for IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif.
The spouse often gives final approval on a decision to accept a job offer, adds Peggy Fricke, director of physician staffing for Eagle Hospital Physicians, an Atlanta-based company that manages hospitalist practices for hospitals in the Southeast and Mid-Atlantic regions.
“The physician could be making the most money, but if their spouse and family are not happy, then they won’t stay in the position long,” Stuckey explains. “I’ve also found that if the spouse is not on board with moving and uprooting the family to a new location, then it’s not going to happen.”
As a result, recruiters and prospective employers often spend just as much time engaging the spouse as they do the actual job candidate, the recruiters say. For this reason, hospitalists who are searching for a new job would be wise to include their husband or wife as early as possible in the job hunt in order to get the most out of the recruiting process.
For example, while the hospitalist focuses on determining if the work is the right fit professionally and financially, the spouse can appraise the community to see if it meets the family’s needs in such areas as schools, neighborhoods, religious services, community groups, and entertainment/cultural outlets. If the hospitalist is invited for an on-site interview, it’s important that their spouse makes the trip as well.
“We always do a community tour, and we will do school tours when asked,” Fricke says of Eagle’s recruiting efforts. “We can introduce the families of the other hospitalists in the practice so a spouse can meet and get to know them.”
—Jason Stuckey, director, HM recruitment, TeamHealth, Knoxville, Tenn.
Upfront Inclusion
When the spouse is involved in the process, they usually are more receptive to receiving information about what opportunities exist in other communities and more open to the idea of moving to a new place, Stuckey says.
For instances in which children are involved, the spouse is most often interested in learning about the location’s school districts and private schools, and determining if the community has a good quality of life for families, Fricke says. For situations in which there are no children or the children are grown, the spouse often focuses on job prospects in their own profession.
Hospitalists with a husband or wife who works and whose career is important to them should see if the HM recruiter can help put their spouse in touch with potential employers in the community, because many times they will, says Fricke, who has connected spouses in IT and engineering fields with people who could assist them in their job search.
“It goes back to making sure everyone is happy. If the spouse can’t find work, that is going to affect their happiness,” says Darren Swenson, MD, medical affairs director for IPC of Nevada and regional chair of IPC’s national advisory board.
Aside from schools, quality of life, and their own job opportunities, spouses also ask about what their hospitalist husband or wife’s work schedule would be and how much vacation and holiday time they would have in the prospective job, Dr. Swenson says.
“It’s extremely important that we look at our hospitalists and their spouses being happy in their home life, because if they’re not, that is going to spill over into in their work life,” IPC’s Lary says.
Good Partnership, Bad Partnership
Times arise when the spouse takes a proactive role in evaluating the actual HM job offer, the recruiters say. “In all couples, there is someone who is dominant and someone who is not,” says Fricke, who has seen spouses participate in job interviews with hospital administrators. “If the spouse is dominant, we try to understand them and listen to what is important to them.”
Sometimes the spouse is an attorney or other type of professional who wants to review the hospitalist contract and has the most questions about it, Dr. Swenson says. When that happens, recruiters will often have group members sit in to answer their questions, he says.
“Absolutely, without question, the spouse has to be involved. But if the spouse is too demanding and everything has to be run through them, to an employer, that can be a big turnoff,” Stuckey says.
When it comes to business matters, the physician—not the spouse—has to take the lead, he says. If the physician doesn’t, it could make the prospective employer wonder what challenges could be ahead should the candidate be hired, Stuckey says.
Two-Physician Families
One time when it is acceptable for a spouse to get intimately involved in the contract and negotiations is when he or she is a hospitalist who also is being recruited by the same prospective employer.
“It’s a unique situation. It’s great to have two for the price of one, so to speak,” Stuckey says. “But there are challenges from the employer’s perspective—for example, scheduling—that have to be resolved on the front end rather than when they get there.”
While still relatively rare, husband-wife hospitalist couples are becoming more prevalent because there are more hospitalists, Fricke says. They tend to meet each other in medical school or residency, she says.
“Even though they are a couple, we treat them as individuals during the recruiting process,” Fricke says. “I think the most important thing is we try to do anything we can—within reason, of course—to help the hospitalist and their spouse make the best decision for themselves and their family.” TH
Lisa Ryan is a freelance writer based in New Jersey.
When recruiting a hospitalist for his company, Jason Stuckey makes it a point to call the candidate’s home. His goal isn’t to speak with the hospitalist the company is interested in hiring—it’s to talk with the candidate’s spouse.
“One of the top five mistakes recruiters make is to not involve the spouse in the [recruitment] process,” says Stuckey, who directs HM recruiting for TeamHealth, a Knoxville, Tenn.-based company that provides healthcare staffing and administrative services to hospitals in 14 states.
Hospitalists are generally so busy with work that the spouse is often the person in the family who takes the lead in the job search, says Tim Lary, vice president of profession staffing for IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif.
The spouse often gives final approval on a decision to accept a job offer, adds Peggy Fricke, director of physician staffing for Eagle Hospital Physicians, an Atlanta-based company that manages hospitalist practices for hospitals in the Southeast and Mid-Atlantic regions.
“The physician could be making the most money, but if their spouse and family are not happy, then they won’t stay in the position long,” Stuckey explains. “I’ve also found that if the spouse is not on board with moving and uprooting the family to a new location, then it’s not going to happen.”
As a result, recruiters and prospective employers often spend just as much time engaging the spouse as they do the actual job candidate, the recruiters say. For this reason, hospitalists who are searching for a new job would be wise to include their husband or wife as early as possible in the job hunt in order to get the most out of the recruiting process.
For example, while the hospitalist focuses on determining if the work is the right fit professionally and financially, the spouse can appraise the community to see if it meets the family’s needs in such areas as schools, neighborhoods, religious services, community groups, and entertainment/cultural outlets. If the hospitalist is invited for an on-site interview, it’s important that their spouse makes the trip as well.
“We always do a community tour, and we will do school tours when asked,” Fricke says of Eagle’s recruiting efforts. “We can introduce the families of the other hospitalists in the practice so a spouse can meet and get to know them.”
—Jason Stuckey, director, HM recruitment, TeamHealth, Knoxville, Tenn.
Upfront Inclusion
When the spouse is involved in the process, they usually are more receptive to receiving information about what opportunities exist in other communities and more open to the idea of moving to a new place, Stuckey says.
For instances in which children are involved, the spouse is most often interested in learning about the location’s school districts and private schools, and determining if the community has a good quality of life for families, Fricke says. For situations in which there are no children or the children are grown, the spouse often focuses on job prospects in their own profession.
Hospitalists with a husband or wife who works and whose career is important to them should see if the HM recruiter can help put their spouse in touch with potential employers in the community, because many times they will, says Fricke, who has connected spouses in IT and engineering fields with people who could assist them in their job search.
“It goes back to making sure everyone is happy. If the spouse can’t find work, that is going to affect their happiness,” says Darren Swenson, MD, medical affairs director for IPC of Nevada and regional chair of IPC’s national advisory board.
Aside from schools, quality of life, and their own job opportunities, spouses also ask about what their hospitalist husband or wife’s work schedule would be and how much vacation and holiday time they would have in the prospective job, Dr. Swenson says.
“It’s extremely important that we look at our hospitalists and their spouses being happy in their home life, because if they’re not, that is going to spill over into in their work life,” IPC’s Lary says.
Good Partnership, Bad Partnership
Times arise when the spouse takes a proactive role in evaluating the actual HM job offer, the recruiters say. “In all couples, there is someone who is dominant and someone who is not,” says Fricke, who has seen spouses participate in job interviews with hospital administrators. “If the spouse is dominant, we try to understand them and listen to what is important to them.”
Sometimes the spouse is an attorney or other type of professional who wants to review the hospitalist contract and has the most questions about it, Dr. Swenson says. When that happens, recruiters will often have group members sit in to answer their questions, he says.
“Absolutely, without question, the spouse has to be involved. But if the spouse is too demanding and everything has to be run through them, to an employer, that can be a big turnoff,” Stuckey says.
When it comes to business matters, the physician—not the spouse—has to take the lead, he says. If the physician doesn’t, it could make the prospective employer wonder what challenges could be ahead should the candidate be hired, Stuckey says.
Two-Physician Families
One time when it is acceptable for a spouse to get intimately involved in the contract and negotiations is when he or she is a hospitalist who also is being recruited by the same prospective employer.
“It’s a unique situation. It’s great to have two for the price of one, so to speak,” Stuckey says. “But there are challenges from the employer’s perspective—for example, scheduling—that have to be resolved on the front end rather than when they get there.”
While still relatively rare, husband-wife hospitalist couples are becoming more prevalent because there are more hospitalists, Fricke says. They tend to meet each other in medical school or residency, she says.
“Even though they are a couple, we treat them as individuals during the recruiting process,” Fricke says. “I think the most important thing is we try to do anything we can—within reason, of course—to help the hospitalist and their spouse make the best decision for themselves and their family.” TH
Lisa Ryan is a freelance writer based in New Jersey.
Discharge Services
Discharge day management services (99238-99239) seem unlikely to cause confusion in the physician community; however, continued requests for documentation involving these CPT codes prove the opposite.
Here’s an example of how a billing error might be made for discharge day management services. A patient with diabetes mellitus, hypertension, and chronic kidney disease is stable for discharge. The patient is being transferred to a skilled nursing facility (SNF). Dr. Aardsma prepares the patient for hospital discharge, and Dr. Broxton admits the patient to the SNF later that day. Dr. Aardsma and Dr. Broxton are members of the same group practice, with the same specialty designation. Can both physicians report their services?
Key Elements
Consider the basic billing principles of discharge services: what, who, and when.
Hospital discharge day management codes are used to report the physician’s total duration of time spent preparing the patient for discharge. These codes include, as appropriate:
- Final examination of the patient;
- Discussion of the hospital stay, even if the time spent by the physician on that date is not continuous;
- Instructions for continuing care to all relevant caregivers; and
- Preparation of discharge records, prescriptions, and referral forms.1
Hospitalists should report one discharge code per hospitalization, but only when the service occurs after the initial date of admission: 99238, hospital discharge day management, 30 minutes or less; or 99239, hospital discharge day management, more than 30 minutes.1,2 Select one of the two codes, depending upon the cumulative discharge service time provided on the patient’s hospital unit/floor during a single calendar day. Do not count time for services performed outside of the patient’s unit or floor (i.e., calls to the receiving physician/facility made from the physician’s private office) or services performed after the patient physically leaves the hospital.
Physician documentation must refer to the discharge status, as well as other clinically relevant information. Don’t be misled into believing that the presence of a discharge summary alone satisfies documentation requirements. In addition to the discharge groundwork, hospitalists must physically see the patient on the day he or she reports discharge management. Discharge summaries are not always useful in noting the physician’s required face-to-face encounter with the patient. Simply state, “Patient seen and examined by me on discharge day.”
Alternatively, hospitalists can elect to include details of a discharge day exam. Although a final exam isn’t mandatory for billing 99238-99239, it is the best justification of a face-to-face encounter on discharge day. Documentation of the time is required when reporting 99239 (e.g., discharge time >30 minutes). Time isn’t typically included in a discharge summary, and upon post-payment payor review, a claim involving 99239 without documented time in the patient’s medical record might result in either a service reduction to the lower level of care (99238) or a request for payment refund.3 Physicians can document all necessary details in the formal summary or a progress note.
Transfers of Care
The admitting physician or group is responsible for performing discharge services unless a formal transfer of care occurs, such as the patient’s transfer from the ICU to the standard medical floor as the patient’s condition improves. Without this transfer of care, comanaging physicians should merely report subsequent hospital-care codes (99231-99233) for the final patient encounter. An example of this is surgical comanagement: If a surgeon is identified as the attending of record, they are responsible for postoperative management of the patient, including discharge services.4,5 Providers in a different group or specialty report 99231-99233 for their medically necessary care.
As with all other time-based services, only the billing provider’s time counts. Discharge-related services performed by residents, students, or ancillary staff (i.e., RNs) do not count toward the physician’s discharge service time. Report the date of the physician’s actual discharge visit even if the patient leaves the facility on a different calendar date—for example, if a patient leaves the next day due to availability of the receiving facility.
Pronouncement of Death
Physicians might not realize that they can report discharge day management codes for pronouncement of death.7 Only the hospitalist who performs the pronouncement is allowed to report this service on the date pronouncement occurred, even if the paperwork is delayed to a subsequent date. Completion of the death certificate alone is not sufficient for billing. Hospitalists must “examine” the patient, thus satisfying the “face to face” visit requirement.
Additional services (e.g., speaking with family members, speaking with healthcare providers, filling out the necessary documentation) count toward the cumulative discharge service time, if performed on the patient’s unit or floor. Document the cumulative time when reporting 99239.
Back to the Case
Typical billing and payment rules mandate the reporting of only one E/M service per specialty, per patient, per day. One of the few exceptions involves reporting a hospital discharge code (99238-99239) with initial nursing facility care (99304-99306). Either the same physician or different physicians from the same group and specialty can report the hospital discharge and the nursing facility admission on the same day. When the same physician or group discharges the patient from any other location (e.g., observation unit) on the same day, report only one service: either the observation discharge (99217) or the initial nursing facility care (99304-99306).
When the same physician or group discharges a patient from the hospital and admits the patient to a facility other than a nursing facility on the same day, report only one service: either the hospital discharge (99228-99239) or the admission care (e.g., long-term acute-care hospital: 99221-99223). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1C. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 3, 2010.
- Highmark Medicare Services Provider Bulletins: Hospital Discharge Day Management Codes 99238 and 99239. Highmark Medicare Services Web site. Available at: www.highmarkmedicareservices.com/bulletins/partb/news02212008a.html. Accessed March 4, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.1A. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.3B. Centers for Medicare & Medicaid Services Web site, Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.2E. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1d. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Reporting inpatient hospital evaluation and management (E/M) services that could be described by current procedural terminology (CPT) consultation codes. Cigna Government Services Web site. Available at: www.cignagovernmentservices.com/partb/pubs/news/2010/0210/cope11694.html. Accessed March 5, 2010.
Discharge day management services (99238-99239) seem unlikely to cause confusion in the physician community; however, continued requests for documentation involving these CPT codes prove the opposite.
Here’s an example of how a billing error might be made for discharge day management services. A patient with diabetes mellitus, hypertension, and chronic kidney disease is stable for discharge. The patient is being transferred to a skilled nursing facility (SNF). Dr. Aardsma prepares the patient for hospital discharge, and Dr. Broxton admits the patient to the SNF later that day. Dr. Aardsma and Dr. Broxton are members of the same group practice, with the same specialty designation. Can both physicians report their services?
Key Elements
Consider the basic billing principles of discharge services: what, who, and when.
Hospital discharge day management codes are used to report the physician’s total duration of time spent preparing the patient for discharge. These codes include, as appropriate:
- Final examination of the patient;
- Discussion of the hospital stay, even if the time spent by the physician on that date is not continuous;
- Instructions for continuing care to all relevant caregivers; and
- Preparation of discharge records, prescriptions, and referral forms.1
Hospitalists should report one discharge code per hospitalization, but only when the service occurs after the initial date of admission: 99238, hospital discharge day management, 30 minutes or less; or 99239, hospital discharge day management, more than 30 minutes.1,2 Select one of the two codes, depending upon the cumulative discharge service time provided on the patient’s hospital unit/floor during a single calendar day. Do not count time for services performed outside of the patient’s unit or floor (i.e., calls to the receiving physician/facility made from the physician’s private office) or services performed after the patient physically leaves the hospital.
Physician documentation must refer to the discharge status, as well as other clinically relevant information. Don’t be misled into believing that the presence of a discharge summary alone satisfies documentation requirements. In addition to the discharge groundwork, hospitalists must physically see the patient on the day he or she reports discharge management. Discharge summaries are not always useful in noting the physician’s required face-to-face encounter with the patient. Simply state, “Patient seen and examined by me on discharge day.”
Alternatively, hospitalists can elect to include details of a discharge day exam. Although a final exam isn’t mandatory for billing 99238-99239, it is the best justification of a face-to-face encounter on discharge day. Documentation of the time is required when reporting 99239 (e.g., discharge time >30 minutes). Time isn’t typically included in a discharge summary, and upon post-payment payor review, a claim involving 99239 without documented time in the patient’s medical record might result in either a service reduction to the lower level of care (99238) or a request for payment refund.3 Physicians can document all necessary details in the formal summary or a progress note.
Transfers of Care
The admitting physician or group is responsible for performing discharge services unless a formal transfer of care occurs, such as the patient’s transfer from the ICU to the standard medical floor as the patient’s condition improves. Without this transfer of care, comanaging physicians should merely report subsequent hospital-care codes (99231-99233) for the final patient encounter. An example of this is surgical comanagement: If a surgeon is identified as the attending of record, they are responsible for postoperative management of the patient, including discharge services.4,5 Providers in a different group or specialty report 99231-99233 for their medically necessary care.
As with all other time-based services, only the billing provider’s time counts. Discharge-related services performed by residents, students, or ancillary staff (i.e., RNs) do not count toward the physician’s discharge service time. Report the date of the physician’s actual discharge visit even if the patient leaves the facility on a different calendar date—for example, if a patient leaves the next day due to availability of the receiving facility.
Pronouncement of Death
Physicians might not realize that they can report discharge day management codes for pronouncement of death.7 Only the hospitalist who performs the pronouncement is allowed to report this service on the date pronouncement occurred, even if the paperwork is delayed to a subsequent date. Completion of the death certificate alone is not sufficient for billing. Hospitalists must “examine” the patient, thus satisfying the “face to face” visit requirement.
Additional services (e.g., speaking with family members, speaking with healthcare providers, filling out the necessary documentation) count toward the cumulative discharge service time, if performed on the patient’s unit or floor. Document the cumulative time when reporting 99239.
Back to the Case
Typical billing and payment rules mandate the reporting of only one E/M service per specialty, per patient, per day. One of the few exceptions involves reporting a hospital discharge code (99238-99239) with initial nursing facility care (99304-99306). Either the same physician or different physicians from the same group and specialty can report the hospital discharge and the nursing facility admission on the same day. When the same physician or group discharges the patient from any other location (e.g., observation unit) on the same day, report only one service: either the observation discharge (99217) or the initial nursing facility care (99304-99306).
When the same physician or group discharges a patient from the hospital and admits the patient to a facility other than a nursing facility on the same day, report only one service: either the hospital discharge (99228-99239) or the admission care (e.g., long-term acute-care hospital: 99221-99223). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1C. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 3, 2010.
- Highmark Medicare Services Provider Bulletins: Hospital Discharge Day Management Codes 99238 and 99239. Highmark Medicare Services Web site. Available at: www.highmarkmedicareservices.com/bulletins/partb/news02212008a.html. Accessed March 4, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.1A. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.3B. Centers for Medicare & Medicaid Services Web site, Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.2E. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1d. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Reporting inpatient hospital evaluation and management (E/M) services that could be described by current procedural terminology (CPT) consultation codes. Cigna Government Services Web site. Available at: www.cignagovernmentservices.com/partb/pubs/news/2010/0210/cope11694.html. Accessed March 5, 2010.
Discharge day management services (99238-99239) seem unlikely to cause confusion in the physician community; however, continued requests for documentation involving these CPT codes prove the opposite.
Here’s an example of how a billing error might be made for discharge day management services. A patient with diabetes mellitus, hypertension, and chronic kidney disease is stable for discharge. The patient is being transferred to a skilled nursing facility (SNF). Dr. Aardsma prepares the patient for hospital discharge, and Dr. Broxton admits the patient to the SNF later that day. Dr. Aardsma and Dr. Broxton are members of the same group practice, with the same specialty designation. Can both physicians report their services?
Key Elements
Consider the basic billing principles of discharge services: what, who, and when.
Hospital discharge day management codes are used to report the physician’s total duration of time spent preparing the patient for discharge. These codes include, as appropriate:
- Final examination of the patient;
- Discussion of the hospital stay, even if the time spent by the physician on that date is not continuous;
- Instructions for continuing care to all relevant caregivers; and
- Preparation of discharge records, prescriptions, and referral forms.1
Hospitalists should report one discharge code per hospitalization, but only when the service occurs after the initial date of admission: 99238, hospital discharge day management, 30 minutes or less; or 99239, hospital discharge day management, more than 30 minutes.1,2 Select one of the two codes, depending upon the cumulative discharge service time provided on the patient’s hospital unit/floor during a single calendar day. Do not count time for services performed outside of the patient’s unit or floor (i.e., calls to the receiving physician/facility made from the physician’s private office) or services performed after the patient physically leaves the hospital.
Physician documentation must refer to the discharge status, as well as other clinically relevant information. Don’t be misled into believing that the presence of a discharge summary alone satisfies documentation requirements. In addition to the discharge groundwork, hospitalists must physically see the patient on the day he or she reports discharge management. Discharge summaries are not always useful in noting the physician’s required face-to-face encounter with the patient. Simply state, “Patient seen and examined by me on discharge day.”
Alternatively, hospitalists can elect to include details of a discharge day exam. Although a final exam isn’t mandatory for billing 99238-99239, it is the best justification of a face-to-face encounter on discharge day. Documentation of the time is required when reporting 99239 (e.g., discharge time >30 minutes). Time isn’t typically included in a discharge summary, and upon post-payment payor review, a claim involving 99239 without documented time in the patient’s medical record might result in either a service reduction to the lower level of care (99238) or a request for payment refund.3 Physicians can document all necessary details in the formal summary or a progress note.
Transfers of Care
The admitting physician or group is responsible for performing discharge services unless a formal transfer of care occurs, such as the patient’s transfer from the ICU to the standard medical floor as the patient’s condition improves. Without this transfer of care, comanaging physicians should merely report subsequent hospital-care codes (99231-99233) for the final patient encounter. An example of this is surgical comanagement: If a surgeon is identified as the attending of record, they are responsible for postoperative management of the patient, including discharge services.4,5 Providers in a different group or specialty report 99231-99233 for their medically necessary care.
As with all other time-based services, only the billing provider’s time counts. Discharge-related services performed by residents, students, or ancillary staff (i.e., RNs) do not count toward the physician’s discharge service time. Report the date of the physician’s actual discharge visit even if the patient leaves the facility on a different calendar date—for example, if a patient leaves the next day due to availability of the receiving facility.
Pronouncement of Death
Physicians might not realize that they can report discharge day management codes for pronouncement of death.7 Only the hospitalist who performs the pronouncement is allowed to report this service on the date pronouncement occurred, even if the paperwork is delayed to a subsequent date. Completion of the death certificate alone is not sufficient for billing. Hospitalists must “examine” the patient, thus satisfying the “face to face” visit requirement.
Additional services (e.g., speaking with family members, speaking with healthcare providers, filling out the necessary documentation) count toward the cumulative discharge service time, if performed on the patient’s unit or floor. Document the cumulative time when reporting 99239.
Back to the Case
Typical billing and payment rules mandate the reporting of only one E/M service per specialty, per patient, per day. One of the few exceptions involves reporting a hospital discharge code (99238-99239) with initial nursing facility care (99304-99306). Either the same physician or different physicians from the same group and specialty can report the hospital discharge and the nursing facility admission on the same day. When the same physician or group discharges the patient from any other location (e.g., observation unit) on the same day, report only one service: either the observation discharge (99217) or the initial nursing facility care (99304-99306).
When the same physician or group discharges a patient from the hospital and admits the patient to a facility other than a nursing facility on the same day, report only one service: either the hospital discharge (99228-99239) or the admission care (e.g., long-term acute-care hospital: 99221-99223). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1C. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 3, 2010.
- Highmark Medicare Services Provider Bulletins: Hospital Discharge Day Management Codes 99238 and 99239. Highmark Medicare Services Web site. Available at: www.highmarkmedicareservices.com/bulletins/partb/news02212008a.html. Accessed March 4, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.1A. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 40.3B. Centers for Medicare & Medicaid Services Web site, Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.2E. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1d. Centers for Medicare & Medicaid Services Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed March 5, 2010.
- Reporting inpatient hospital evaluation and management (E/M) services that could be described by current procedural terminology (CPT) consultation codes. Cigna Government Services Web site. Available at: www.cignagovernmentservices.com/partb/pubs/news/2010/0210/cope11694.html. Accessed March 5, 2010.
The Humble Approach
Bijo Chacko, MD, FHM, says the varied resources available in the multispecialty medical group in which he practices help to ensure patients receive the best possible care. The structure at Preferred Health Partners in Brooklyn, N.Y., which offers primary and specialty medical services under one roof, requires hospitalists to collaborate frequently with primary-care physicians (PCPs).
That interaction breaks down barriers, fosters communication, promotes the exchange of ideas, and ultimately improves the transition of care from outpatient to inpatient and vice versa, Dr. Chacko says.
His affinity for that environment might explain his passion for the work done by SHM’s Young Physician Task Force, and why “resources” is the word he repeats most often when describing the value of the group’s efforts. Just as experienced hospitalists can learn by interacting with PCPs and other specialists, those who are new to HM can benefit from those who have established themselves in the profession and cleared the hurdles physicians encounter early in a career, he says.
“The advantage of youth is the inherent energy that comes with it,” says Dr. Chacko, hospitalist program medical director with Preferred Health Partners, medical director of the hospitalist program at Good Samaritan Hospital in Suffern, N.Y., and a member of Team Hospitalist. “You really need that energy in your daily work routine, especially early in a career. The disadvantage is, depending on your training, you may not have the experience or been exposed to resources required to take on some of the challenges you’ll face. Hence, expanding the number of resources available to early-career hospitalists—and encouraging them to utilize what is available to them—becomes pivotal.”
Question: Two years after residency, you made the transition to hospitalist program medical director. What advice would you give to an aspiring HM leader?
Answer: Coming out of medical school or residency, you’re not provided all the tools you need to be a successful leader. Some people may achieve those skills during their training or in their first job. But going through some of the unique courses provided by SHM, such as the Leadership Academy, has been invaluable. The information, as well as the connections you make with others throughout the country, really prepares you for a leadership role and some of the challenges you may not have been taught to face in medical school.
Q: What are some of the challenges you aren’t necessarily taught how to handle?
A: Leadership roles take on a complexity of their own. You’re dealing with communications issues; you’re dealing with conflict resolution. Those are unique areas that have to be approached delicately. And one of the fundamental aspects of being a good leader is to define a shared organizational vision and set of shared values for your group that should be supported and promoted.
Q: Can you describe the vision and values you set for your group?
A: Our vision is to be the hospitalist program of choice for patients and physicians in the region. But the key aspect is, we want to provide high-quality patient care with a touch of humility. A physician who demonstrates his or her empathetic side goes a long way in what we do. Research has shown hospitalists provide efficient care—outcomes on cost savings are good. But the other issue is the patient experience, and that’s where the humility factor comes into play.
Q: How do you teach the physicians in your group to be more humble?
A: One thing we emphasize with the team is to imagine themselves or a family member in the patient’s shoes when they are communicating with them. This hits home the importance of bedside manners, and it has to be revisited at times.
Q: Any other techniques?
A: Positive feedback always translates well. We use examples from patients who say they generally had a great experience. In many cases, it amounts to a patient saying, “The doctor was able to explain things to me in a simpler language than anyone has been able to do before, or even attempted to do.” That positive reinforcement resonates well with the doctors. We also share patient scenarios where there were opportunities for improvement.
Q: Considering the demands of your leadership roles at Preferred Health Partners and Good Samaritan Hospital, why is it still a priority for you to provide inpatient clinical care?
A: The old adage is, if you don’t use it, you lose it. Because clinical care is so broad and diverse, and because it is changing so rapidly, it behooves one to stay abreast of it. Also, when you are leading members of a group, I think it’s important to walk in the trenches with them.
Q: You joined SHM’s Young Physician Task Force and served as chairman for two years. What prompted you to participate?
A: When I joined, I had already begun my leadership role as medical director and I was an early-career hospitalist, so I felt it made sense for my professional growth. I wanted an opportunity to collaborate with leading young hospitalists in the country and help shape some of the programs the (group) was working on.
Q: What issues has the group addressed?
A: Initially, the task force was focused on getting information out to early-career hospitalists and providing resources they could utilize. It redefined its section of the SHM website (www.hospitalmedicine .org/youngphysician), which now serves as a portal with information about everything from careers in hospital medicine to how to approach residency. It also introduced the Resident’s Corner (a quarterly column in The Hospitalist, see p. 25), which caters to residents and helps them make a smooth transition to a possible career in hospital medicine. The group has developed programs for early-career hospitalists at the annual SHM meetings.
Q: What major issues are on the agenda now?
A: The group is working on developing a mentorship program for early-career hospitalists, which would be a really valuable resource. The group also is working on projects to reach medical students and residents. The goal is to get them more engaged, and help them realize the diversity and rewards that accompany a career in hospital medicine.
Q: What do you see as the benefit of the mentor program?
A: The beauty of hospital medicine is there is a lot of diversity. If you have an interest in academia, quality initiatives, or research, that’s available. If you have a leadership interest, that can definitely be attained. …
But when you have someone who has had some experience in hospital medicine and can share that experience, and you can get their insights and hear about the challenges they faced and how they faced them, it can make the transition much easier. This will provide young hospitalists with pearls of wisdom and information they may not have been able to access elsewhere.
Q: So it comes back to the idea that there’s still a lot to learn, even after medical school and residency.
A: That’s exactly right. The scope of questions that can be posed or issues that can be addressed is infinite. Beyond that, someone who has already walked that pathway can help establish the fact that hospital medicine should be looked upon as a career with many opportunities, as opposed to a transition point to an alternative career. TH
Mark Leiser is a freelance writer in New Jersey.
Bijo Chacko, MD, FHM, says the varied resources available in the multispecialty medical group in which he practices help to ensure patients receive the best possible care. The structure at Preferred Health Partners in Brooklyn, N.Y., which offers primary and specialty medical services under one roof, requires hospitalists to collaborate frequently with primary-care physicians (PCPs).
That interaction breaks down barriers, fosters communication, promotes the exchange of ideas, and ultimately improves the transition of care from outpatient to inpatient and vice versa, Dr. Chacko says.
His affinity for that environment might explain his passion for the work done by SHM’s Young Physician Task Force, and why “resources” is the word he repeats most often when describing the value of the group’s efforts. Just as experienced hospitalists can learn by interacting with PCPs and other specialists, those who are new to HM can benefit from those who have established themselves in the profession and cleared the hurdles physicians encounter early in a career, he says.
“The advantage of youth is the inherent energy that comes with it,” says Dr. Chacko, hospitalist program medical director with Preferred Health Partners, medical director of the hospitalist program at Good Samaritan Hospital in Suffern, N.Y., and a member of Team Hospitalist. “You really need that energy in your daily work routine, especially early in a career. The disadvantage is, depending on your training, you may not have the experience or been exposed to resources required to take on some of the challenges you’ll face. Hence, expanding the number of resources available to early-career hospitalists—and encouraging them to utilize what is available to them—becomes pivotal.”
Question: Two years after residency, you made the transition to hospitalist program medical director. What advice would you give to an aspiring HM leader?
Answer: Coming out of medical school or residency, you’re not provided all the tools you need to be a successful leader. Some people may achieve those skills during their training or in their first job. But going through some of the unique courses provided by SHM, such as the Leadership Academy, has been invaluable. The information, as well as the connections you make with others throughout the country, really prepares you for a leadership role and some of the challenges you may not have been taught to face in medical school.
Q: What are some of the challenges you aren’t necessarily taught how to handle?
A: Leadership roles take on a complexity of their own. You’re dealing with communications issues; you’re dealing with conflict resolution. Those are unique areas that have to be approached delicately. And one of the fundamental aspects of being a good leader is to define a shared organizational vision and set of shared values for your group that should be supported and promoted.
Q: Can you describe the vision and values you set for your group?
A: Our vision is to be the hospitalist program of choice for patients and physicians in the region. But the key aspect is, we want to provide high-quality patient care with a touch of humility. A physician who demonstrates his or her empathetic side goes a long way in what we do. Research has shown hospitalists provide efficient care—outcomes on cost savings are good. But the other issue is the patient experience, and that’s where the humility factor comes into play.
Q: How do you teach the physicians in your group to be more humble?
A: One thing we emphasize with the team is to imagine themselves or a family member in the patient’s shoes when they are communicating with them. This hits home the importance of bedside manners, and it has to be revisited at times.
Q: Any other techniques?
A: Positive feedback always translates well. We use examples from patients who say they generally had a great experience. In many cases, it amounts to a patient saying, “The doctor was able to explain things to me in a simpler language than anyone has been able to do before, or even attempted to do.” That positive reinforcement resonates well with the doctors. We also share patient scenarios where there were opportunities for improvement.
Q: Considering the demands of your leadership roles at Preferred Health Partners and Good Samaritan Hospital, why is it still a priority for you to provide inpatient clinical care?
A: The old adage is, if you don’t use it, you lose it. Because clinical care is so broad and diverse, and because it is changing so rapidly, it behooves one to stay abreast of it. Also, when you are leading members of a group, I think it’s important to walk in the trenches with them.
Q: You joined SHM’s Young Physician Task Force and served as chairman for two years. What prompted you to participate?
A: When I joined, I had already begun my leadership role as medical director and I was an early-career hospitalist, so I felt it made sense for my professional growth. I wanted an opportunity to collaborate with leading young hospitalists in the country and help shape some of the programs the (group) was working on.
Q: What issues has the group addressed?
A: Initially, the task force was focused on getting information out to early-career hospitalists and providing resources they could utilize. It redefined its section of the SHM website (www.hospitalmedicine .org/youngphysician), which now serves as a portal with information about everything from careers in hospital medicine to how to approach residency. It also introduced the Resident’s Corner (a quarterly column in The Hospitalist, see p. 25), which caters to residents and helps them make a smooth transition to a possible career in hospital medicine. The group has developed programs for early-career hospitalists at the annual SHM meetings.
Q: What major issues are on the agenda now?
A: The group is working on developing a mentorship program for early-career hospitalists, which would be a really valuable resource. The group also is working on projects to reach medical students and residents. The goal is to get them more engaged, and help them realize the diversity and rewards that accompany a career in hospital medicine.
Q: What do you see as the benefit of the mentor program?
A: The beauty of hospital medicine is there is a lot of diversity. If you have an interest in academia, quality initiatives, or research, that’s available. If you have a leadership interest, that can definitely be attained. …
But when you have someone who has had some experience in hospital medicine and can share that experience, and you can get their insights and hear about the challenges they faced and how they faced them, it can make the transition much easier. This will provide young hospitalists with pearls of wisdom and information they may not have been able to access elsewhere.
Q: So it comes back to the idea that there’s still a lot to learn, even after medical school and residency.
A: That’s exactly right. The scope of questions that can be posed or issues that can be addressed is infinite. Beyond that, someone who has already walked that pathway can help establish the fact that hospital medicine should be looked upon as a career with many opportunities, as opposed to a transition point to an alternative career. TH
Mark Leiser is a freelance writer in New Jersey.
Bijo Chacko, MD, FHM, says the varied resources available in the multispecialty medical group in which he practices help to ensure patients receive the best possible care. The structure at Preferred Health Partners in Brooklyn, N.Y., which offers primary and specialty medical services under one roof, requires hospitalists to collaborate frequently with primary-care physicians (PCPs).
That interaction breaks down barriers, fosters communication, promotes the exchange of ideas, and ultimately improves the transition of care from outpatient to inpatient and vice versa, Dr. Chacko says.
His affinity for that environment might explain his passion for the work done by SHM’s Young Physician Task Force, and why “resources” is the word he repeats most often when describing the value of the group’s efforts. Just as experienced hospitalists can learn by interacting with PCPs and other specialists, those who are new to HM can benefit from those who have established themselves in the profession and cleared the hurdles physicians encounter early in a career, he says.
“The advantage of youth is the inherent energy that comes with it,” says Dr. Chacko, hospitalist program medical director with Preferred Health Partners, medical director of the hospitalist program at Good Samaritan Hospital in Suffern, N.Y., and a member of Team Hospitalist. “You really need that energy in your daily work routine, especially early in a career. The disadvantage is, depending on your training, you may not have the experience or been exposed to resources required to take on some of the challenges you’ll face. Hence, expanding the number of resources available to early-career hospitalists—and encouraging them to utilize what is available to them—becomes pivotal.”
Question: Two years after residency, you made the transition to hospitalist program medical director. What advice would you give to an aspiring HM leader?
Answer: Coming out of medical school or residency, you’re not provided all the tools you need to be a successful leader. Some people may achieve those skills during their training or in their first job. But going through some of the unique courses provided by SHM, such as the Leadership Academy, has been invaluable. The information, as well as the connections you make with others throughout the country, really prepares you for a leadership role and some of the challenges you may not have been taught to face in medical school.
Q: What are some of the challenges you aren’t necessarily taught how to handle?
A: Leadership roles take on a complexity of their own. You’re dealing with communications issues; you’re dealing with conflict resolution. Those are unique areas that have to be approached delicately. And one of the fundamental aspects of being a good leader is to define a shared organizational vision and set of shared values for your group that should be supported and promoted.
Q: Can you describe the vision and values you set for your group?
A: Our vision is to be the hospitalist program of choice for patients and physicians in the region. But the key aspect is, we want to provide high-quality patient care with a touch of humility. A physician who demonstrates his or her empathetic side goes a long way in what we do. Research has shown hospitalists provide efficient care—outcomes on cost savings are good. But the other issue is the patient experience, and that’s where the humility factor comes into play.
Q: How do you teach the physicians in your group to be more humble?
A: One thing we emphasize with the team is to imagine themselves or a family member in the patient’s shoes when they are communicating with them. This hits home the importance of bedside manners, and it has to be revisited at times.
Q: Any other techniques?
A: Positive feedback always translates well. We use examples from patients who say they generally had a great experience. In many cases, it amounts to a patient saying, “The doctor was able to explain things to me in a simpler language than anyone has been able to do before, or even attempted to do.” That positive reinforcement resonates well with the doctors. We also share patient scenarios where there were opportunities for improvement.
Q: Considering the demands of your leadership roles at Preferred Health Partners and Good Samaritan Hospital, why is it still a priority for you to provide inpatient clinical care?
A: The old adage is, if you don’t use it, you lose it. Because clinical care is so broad and diverse, and because it is changing so rapidly, it behooves one to stay abreast of it. Also, when you are leading members of a group, I think it’s important to walk in the trenches with them.
Q: You joined SHM’s Young Physician Task Force and served as chairman for two years. What prompted you to participate?
A: When I joined, I had already begun my leadership role as medical director and I was an early-career hospitalist, so I felt it made sense for my professional growth. I wanted an opportunity to collaborate with leading young hospitalists in the country and help shape some of the programs the (group) was working on.
Q: What issues has the group addressed?
A: Initially, the task force was focused on getting information out to early-career hospitalists and providing resources they could utilize. It redefined its section of the SHM website (www.hospitalmedicine .org/youngphysician), which now serves as a portal with information about everything from careers in hospital medicine to how to approach residency. It also introduced the Resident’s Corner (a quarterly column in The Hospitalist, see p. 25), which caters to residents and helps them make a smooth transition to a possible career in hospital medicine. The group has developed programs for early-career hospitalists at the annual SHM meetings.
Q: What major issues are on the agenda now?
A: The group is working on developing a mentorship program for early-career hospitalists, which would be a really valuable resource. The group also is working on projects to reach medical students and residents. The goal is to get them more engaged, and help them realize the diversity and rewards that accompany a career in hospital medicine.
Q: What do you see as the benefit of the mentor program?
A: The beauty of hospital medicine is there is a lot of diversity. If you have an interest in academia, quality initiatives, or research, that’s available. If you have a leadership interest, that can definitely be attained. …
But when you have someone who has had some experience in hospital medicine and can share that experience, and you can get their insights and hear about the challenges they faced and how they faced them, it can make the transition much easier. This will provide young hospitalists with pearls of wisdom and information they may not have been able to access elsewhere.
Q: So it comes back to the idea that there’s still a lot to learn, even after medical school and residency.
A: That’s exactly right. The scope of questions that can be posed or issues that can be addressed is infinite. Beyond that, someone who has already walked that pathway can help establish the fact that hospital medicine should be looked upon as a career with many opportunities, as opposed to a transition point to an alternative career. TH
Mark Leiser is a freelance writer in New Jersey.
The Earlier, the Better

Most hospitals work hard to increase the portion of discharges that occur early in the workday and decrease the number that occur in the afternoon or evening. In every case, hospitalists have an important role in making this happen.
In my April 2009 column (“Top O’ the Morning,” p. 53), I wrote about why this is important to hospitals and which strategies hospitalists could adopt. But this is still such a big issue for hospitalists that I thought I would elaborate on a few of the really simple ideas. Your HM group could implement most of the following strategies beginning next week, and you wouldn’t need months of meetings with other hospital departments.
But before I get to the ideas, I want to mention a couple of other things. First, I can’t resist pointing out that giving hospitalists a financial incentive for writing the majority of discharge orders by a certain time in the morning has met with mixed results, despite the fact that some institutions believe this approach is valuable. In the absence of computerized physician order entry (CPOE), it can be really difficult to track exactly when the doctor wrote the discharge order. And, more importantly, a financial incentive might discourage a hospitalist from discharging a patient this afternoon, and they might instead wait to discharge tomorrow morning—adding to length of stay and defeating the goal of the incentive.
It turns out that a lot has been written about throughput; just do an Internet search and pair “throughput” with terms like “hospital,” “hospitalist,” “ED,” etc. Remarkably, I haven’t been able to dig up much material that specifically addresses early-morning discharges, which is an important component of throughput.
Let’s turn our attention to some specific recommendations for increasing morning discharges. Remember, I’ve selected these because they’re easy to implement and won’t require HM groups to negotiate with others at the hospital.
Write “Probable Discharge Tomorrow” Orders
Letting other staff know the anticipated discharge date via an order in the chart typically is more effective than writing the same information in the progress note section of the chart. Although a hospitalist should verbally communicate the anticipated discharge date with the patient’s nurse and discharge planner, it still is worthwhile to write an order, because it increases the chance all, or nearly all, staff (e.g., night nurses) will be aware of the plan and communicate the same message to the family.
Your group could establish a rule or financial incentive, such that all charts will be reviewed after discharge, and a certain portion (e.g., 85%) must have such an order written sometime prior to discharge. It doesn’t always need to be written on the day prior to discharge; instead, an order written on Monday could say “likely discharge on Wednesday or Thursday.” And, of course, there shouldn’t be a requirement that the patient actually be discharged on the day that was forecast.
Prepare the Day Prior
Typically, hospitalized-patient discharges are very time-consuming. Most discharges are complicated by last-minute medical or social loose ends that require attention. Routinely trying to uncover and address these on the evening prior to discharge will ensure that a larger percentage of patients will be discharged—and vacate their room—earlier the next day. Here is what this might look like:
On Tuesday, Dr. Guaraldi is wrapping up most work for the day. He stops by to see his patient, Mr. Schultz, to see if he is improving as expected. Indeed, Mr. Schultz is looking better and probably will be ready for discharge Wednesday morning. So, Dr. Guaraldi talks with Mr. Schultz and calls the patient’s daughter to answer any questions and concerns, ensuring no surprises by the Wednesday-morning discharge. When the daughter asks (as nearly all family members do) what time she should plan to pick up her dad, Dr. Guaraldi can suggest a time based on when he will be able to round in the morning. He also can arrange to have the discharge planning staff alerted if there are more complicated issues (e.g., arranging for professional transport home).
Dr. Guaraldi then dictates the discharge summary, addresses the discharge medicine reconciliation, and writes the prescriptions. In doing so, he might uncover some loose ends and might end up ordering a lab or imaging test to be done in the evening so the results will be available early Wednesday morning and won’t delay the routine discharge.
On Wednesday morning, Dr. Guaraldi rounds on Mr. Schultz early, finds the patient is improving as expected, and writes the discharge order. The whole visit takes only a few minutes, as most of the time-consuming work was completed the prior evening. In fact, because it is a relatively short visit, it is a lot easier for Dr. Guaraldi to arrange to round on Mr. Schultz early in the day (e.g., even on the way to see ICU patients), as the hospital’s chief medical officer is always asking him to do.
I hope this scenario doesn’t sound too difficult. (Another benefit of dictating discharge summaries the evening before discharge is that the typed document should be available the next morning, so the patient can have a copy to take with him at discharge.) Of course, it won’t apply to all patients, such as those patients whose discharges can’t be predicted.
Many hospitalists think arranging for discharge the evening before is impossible because “I’m just too spent at the end of a long day to stay late getting patients ready for discharge tomorrow!” But realize you won’t be doing any more work; you’re rearranging when you do the work. The time you spend arranging for discharge in advance will save you time and stress tomorrow. My own experience is that it is much easier to do all the discharge work the evening before than in the morning when I’m so busy and am being pulled in 10 different directions. Most morning discharge visits are relatively quick and painless, which is really valuable for increasing the efficiency and decreasing the stress of morning rounds.
The alert reader already has figured out there is a pretty big cost to doing the discharge work the evening before. Some patients won’t be able to discharge as planned (e.g., they have a fever overnight) and the preparations will have been in vain. My experience is that such “failed” discharges are reasonably common, but even when they occur, it is usually reasonable to use most of the original prescriptions and discharge summary, with an addendum as required. For example, Dr. Guaraldi could dictate an addendum stating:
“The patient originally was planned for discharge on Wednesday but had a temperature of 38.6 degrees Celsius the night before, so stayed in the hospital for two more days for … ”
Start Rounds Earlier
This strategy might be the most difficult for you and your HM group to arrange, but I propose it because you could do it without having to negotiate with a lot of other departments in the hospital. If your group currently has a day shift that starts at 8 a.m. with a team conference, you could instead start at 7 a.m. Your group could try to shorten the duration of the morning team conference, or eliminate it. Whether the need to get patients discharged early in the day is worth the complexity of rearranging your schedule will depend on the circumstances of your hospital and your group. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Most hospitals work hard to increase the portion of discharges that occur early in the workday and decrease the number that occur in the afternoon or evening. In every case, hospitalists have an important role in making this happen.
In my April 2009 column (“Top O’ the Morning,” p. 53), I wrote about why this is important to hospitals and which strategies hospitalists could adopt. But this is still such a big issue for hospitalists that I thought I would elaborate on a few of the really simple ideas. Your HM group could implement most of the following strategies beginning next week, and you wouldn’t need months of meetings with other hospital departments.
But before I get to the ideas, I want to mention a couple of other things. First, I can’t resist pointing out that giving hospitalists a financial incentive for writing the majority of discharge orders by a certain time in the morning has met with mixed results, despite the fact that some institutions believe this approach is valuable. In the absence of computerized physician order entry (CPOE), it can be really difficult to track exactly when the doctor wrote the discharge order. And, more importantly, a financial incentive might discourage a hospitalist from discharging a patient this afternoon, and they might instead wait to discharge tomorrow morning—adding to length of stay and defeating the goal of the incentive.
It turns out that a lot has been written about throughput; just do an Internet search and pair “throughput” with terms like “hospital,” “hospitalist,” “ED,” etc. Remarkably, I haven’t been able to dig up much material that specifically addresses early-morning discharges, which is an important component of throughput.
Let’s turn our attention to some specific recommendations for increasing morning discharges. Remember, I’ve selected these because they’re easy to implement and won’t require HM groups to negotiate with others at the hospital.
Write “Probable Discharge Tomorrow” Orders
Letting other staff know the anticipated discharge date via an order in the chart typically is more effective than writing the same information in the progress note section of the chart. Although a hospitalist should verbally communicate the anticipated discharge date with the patient’s nurse and discharge planner, it still is worthwhile to write an order, because it increases the chance all, or nearly all, staff (e.g., night nurses) will be aware of the plan and communicate the same message to the family.
Your group could establish a rule or financial incentive, such that all charts will be reviewed after discharge, and a certain portion (e.g., 85%) must have such an order written sometime prior to discharge. It doesn’t always need to be written on the day prior to discharge; instead, an order written on Monday could say “likely discharge on Wednesday or Thursday.” And, of course, there shouldn’t be a requirement that the patient actually be discharged on the day that was forecast.
Prepare the Day Prior
Typically, hospitalized-patient discharges are very time-consuming. Most discharges are complicated by last-minute medical or social loose ends that require attention. Routinely trying to uncover and address these on the evening prior to discharge will ensure that a larger percentage of patients will be discharged—and vacate their room—earlier the next day. Here is what this might look like:
On Tuesday, Dr. Guaraldi is wrapping up most work for the day. He stops by to see his patient, Mr. Schultz, to see if he is improving as expected. Indeed, Mr. Schultz is looking better and probably will be ready for discharge Wednesday morning. So, Dr. Guaraldi talks with Mr. Schultz and calls the patient’s daughter to answer any questions and concerns, ensuring no surprises by the Wednesday-morning discharge. When the daughter asks (as nearly all family members do) what time she should plan to pick up her dad, Dr. Guaraldi can suggest a time based on when he will be able to round in the morning. He also can arrange to have the discharge planning staff alerted if there are more complicated issues (e.g., arranging for professional transport home).
Dr. Guaraldi then dictates the discharge summary, addresses the discharge medicine reconciliation, and writes the prescriptions. In doing so, he might uncover some loose ends and might end up ordering a lab or imaging test to be done in the evening so the results will be available early Wednesday morning and won’t delay the routine discharge.
On Wednesday morning, Dr. Guaraldi rounds on Mr. Schultz early, finds the patient is improving as expected, and writes the discharge order. The whole visit takes only a few minutes, as most of the time-consuming work was completed the prior evening. In fact, because it is a relatively short visit, it is a lot easier for Dr. Guaraldi to arrange to round on Mr. Schultz early in the day (e.g., even on the way to see ICU patients), as the hospital’s chief medical officer is always asking him to do.
I hope this scenario doesn’t sound too difficult. (Another benefit of dictating discharge summaries the evening before discharge is that the typed document should be available the next morning, so the patient can have a copy to take with him at discharge.) Of course, it won’t apply to all patients, such as those patients whose discharges can’t be predicted.
Many hospitalists think arranging for discharge the evening before is impossible because “I’m just too spent at the end of a long day to stay late getting patients ready for discharge tomorrow!” But realize you won’t be doing any more work; you’re rearranging when you do the work. The time you spend arranging for discharge in advance will save you time and stress tomorrow. My own experience is that it is much easier to do all the discharge work the evening before than in the morning when I’m so busy and am being pulled in 10 different directions. Most morning discharge visits are relatively quick and painless, which is really valuable for increasing the efficiency and decreasing the stress of morning rounds.
The alert reader already has figured out there is a pretty big cost to doing the discharge work the evening before. Some patients won’t be able to discharge as planned (e.g., they have a fever overnight) and the preparations will have been in vain. My experience is that such “failed” discharges are reasonably common, but even when they occur, it is usually reasonable to use most of the original prescriptions and discharge summary, with an addendum as required. For example, Dr. Guaraldi could dictate an addendum stating:
“The patient originally was planned for discharge on Wednesday but had a temperature of 38.6 degrees Celsius the night before, so stayed in the hospital for two more days for … ”
Start Rounds Earlier
This strategy might be the most difficult for you and your HM group to arrange, but I propose it because you could do it without having to negotiate with a lot of other departments in the hospital. If your group currently has a day shift that starts at 8 a.m. with a team conference, you could instead start at 7 a.m. Your group could try to shorten the duration of the morning team conference, or eliminate it. Whether the need to get patients discharged early in the day is worth the complexity of rearranging your schedule will depend on the circumstances of your hospital and your group. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Most hospitals work hard to increase the portion of discharges that occur early in the workday and decrease the number that occur in the afternoon or evening. In every case, hospitalists have an important role in making this happen.
In my April 2009 column (“Top O’ the Morning,” p. 53), I wrote about why this is important to hospitals and which strategies hospitalists could adopt. But this is still such a big issue for hospitalists that I thought I would elaborate on a few of the really simple ideas. Your HM group could implement most of the following strategies beginning next week, and you wouldn’t need months of meetings with other hospital departments.
But before I get to the ideas, I want to mention a couple of other things. First, I can’t resist pointing out that giving hospitalists a financial incentive for writing the majority of discharge orders by a certain time in the morning has met with mixed results, despite the fact that some institutions believe this approach is valuable. In the absence of computerized physician order entry (CPOE), it can be really difficult to track exactly when the doctor wrote the discharge order. And, more importantly, a financial incentive might discourage a hospitalist from discharging a patient this afternoon, and they might instead wait to discharge tomorrow morning—adding to length of stay and defeating the goal of the incentive.
It turns out that a lot has been written about throughput; just do an Internet search and pair “throughput” with terms like “hospital,” “hospitalist,” “ED,” etc. Remarkably, I haven’t been able to dig up much material that specifically addresses early-morning discharges, which is an important component of throughput.
Let’s turn our attention to some specific recommendations for increasing morning discharges. Remember, I’ve selected these because they’re easy to implement and won’t require HM groups to negotiate with others at the hospital.
Write “Probable Discharge Tomorrow” Orders
Letting other staff know the anticipated discharge date via an order in the chart typically is more effective than writing the same information in the progress note section of the chart. Although a hospitalist should verbally communicate the anticipated discharge date with the patient’s nurse and discharge planner, it still is worthwhile to write an order, because it increases the chance all, or nearly all, staff (e.g., night nurses) will be aware of the plan and communicate the same message to the family.
Your group could establish a rule or financial incentive, such that all charts will be reviewed after discharge, and a certain portion (e.g., 85%) must have such an order written sometime prior to discharge. It doesn’t always need to be written on the day prior to discharge; instead, an order written on Monday could say “likely discharge on Wednesday or Thursday.” And, of course, there shouldn’t be a requirement that the patient actually be discharged on the day that was forecast.
Prepare the Day Prior
Typically, hospitalized-patient discharges are very time-consuming. Most discharges are complicated by last-minute medical or social loose ends that require attention. Routinely trying to uncover and address these on the evening prior to discharge will ensure that a larger percentage of patients will be discharged—and vacate their room—earlier the next day. Here is what this might look like:
On Tuesday, Dr. Guaraldi is wrapping up most work for the day. He stops by to see his patient, Mr. Schultz, to see if he is improving as expected. Indeed, Mr. Schultz is looking better and probably will be ready for discharge Wednesday morning. So, Dr. Guaraldi talks with Mr. Schultz and calls the patient’s daughter to answer any questions and concerns, ensuring no surprises by the Wednesday-morning discharge. When the daughter asks (as nearly all family members do) what time she should plan to pick up her dad, Dr. Guaraldi can suggest a time based on when he will be able to round in the morning. He also can arrange to have the discharge planning staff alerted if there are more complicated issues (e.g., arranging for professional transport home).
Dr. Guaraldi then dictates the discharge summary, addresses the discharge medicine reconciliation, and writes the prescriptions. In doing so, he might uncover some loose ends and might end up ordering a lab or imaging test to be done in the evening so the results will be available early Wednesday morning and won’t delay the routine discharge.
On Wednesday morning, Dr. Guaraldi rounds on Mr. Schultz early, finds the patient is improving as expected, and writes the discharge order. The whole visit takes only a few minutes, as most of the time-consuming work was completed the prior evening. In fact, because it is a relatively short visit, it is a lot easier for Dr. Guaraldi to arrange to round on Mr. Schultz early in the day (e.g., even on the way to see ICU patients), as the hospital’s chief medical officer is always asking him to do.
I hope this scenario doesn’t sound too difficult. (Another benefit of dictating discharge summaries the evening before discharge is that the typed document should be available the next morning, so the patient can have a copy to take with him at discharge.) Of course, it won’t apply to all patients, such as those patients whose discharges can’t be predicted.
Many hospitalists think arranging for discharge the evening before is impossible because “I’m just too spent at the end of a long day to stay late getting patients ready for discharge tomorrow!” But realize you won’t be doing any more work; you’re rearranging when you do the work. The time you spend arranging for discharge in advance will save you time and stress tomorrow. My own experience is that it is much easier to do all the discharge work the evening before than in the morning when I’m so busy and am being pulled in 10 different directions. Most morning discharge visits are relatively quick and painless, which is really valuable for increasing the efficiency and decreasing the stress of morning rounds.
The alert reader already has figured out there is a pretty big cost to doing the discharge work the evening before. Some patients won’t be able to discharge as planned (e.g., they have a fever overnight) and the preparations will have been in vain. My experience is that such “failed” discharges are reasonably common, but even when they occur, it is usually reasonable to use most of the original prescriptions and discharge summary, with an addendum as required. For example, Dr. Guaraldi could dictate an addendum stating:
“The patient originally was planned for discharge on Wednesday but had a temperature of 38.6 degrees Celsius the night before, so stayed in the hospital for two more days for … ”
Start Rounds Earlier
This strategy might be the most difficult for you and your HM group to arrange, but I propose it because you could do it without having to negotiate with a lot of other departments in the hospital. If your group currently has a day shift that starts at 8 a.m. with a team conference, you could instead start at 7 a.m. Your group could try to shorten the duration of the morning team conference, or eliminate it. Whether the need to get patients discharged early in the day is worth the complexity of rearranging your schedule will depend on the circumstances of your hospital and your group. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.