Summary: Delirium is a common problem in hospitalized patients, and all too often delirium is iatrogenic. Delirium is associated with poor outcomes such as prolonged hospitalization and functional decline, and it increases the risk of nursing home admission. The most common tool to assess the presence of delirium is the Confusion Assessment Method (CAM). Dr. Cumbler educated the audience on a more refined tool, the 3D CAM [PDF], and provided the algorithm for diagnosis and evaluation of hospital-onset delirium.
Where delirium is concerned (as with most conditions), “an ounce of prevention is worth a pound of cure.” Namely, avoid prescribing problem medications such as anticholinergics, sedative/hypnotics (except benzodiazepines for treatment of alcohol withdrawal), and antihistamines; and minimize narcotics, but don’t undertreat pain as uncontrolled pain is a more potent delirium trigger than narcotics.
Avoid sleep deprivation. Do we really require vital signs and phlebotomy between midnight and 6 a.m.? Make sure patients have their glasses and hearing aids, and keep them up and moving during daylight hours. Sleep and sensory deprivation are effective forms of human torture and are known to be rather disorienting.
Finally, antipsychotics are associated with increased mortality in dementia. Patients with agitated delirium may benefit from a low dose of haloperidol. When prescribing haloperidol, remember IV administration requires EKG monitoring (FDA black box warning), and a reasonable starting dose is 0.5 mg, NOT 5 mg.
Summary: Delirium is a common problem in hospitalized patients, and all too often delirium is iatrogenic. Delirium is associated with poor outcomes such as prolonged hospitalization and functional decline, and it increases the risk of nursing home admission. The most common tool to assess the presence of delirium is the Confusion Assessment Method (CAM). Dr. Cumbler educated the audience on a more refined tool, the 3D CAM [PDF], and provided the algorithm for diagnosis and evaluation of hospital-onset delirium.
Where delirium is concerned (as with most conditions), “an ounce of prevention is worth a pound of cure.” Namely, avoid prescribing problem medications such as anticholinergics, sedative/hypnotics (except benzodiazepines for treatment of alcohol withdrawal), and antihistamines; and minimize narcotics, but don’t undertreat pain as uncontrolled pain is a more potent delirium trigger than narcotics.
Avoid sleep deprivation. Do we really require vital signs and phlebotomy between midnight and 6 a.m.? Make sure patients have their glasses and hearing aids, and keep them up and moving during daylight hours. Sleep and sensory deprivation are effective forms of human torture and are known to be rather disorienting.
Finally, antipsychotics are associated with increased mortality in dementia. Patients with agitated delirium may benefit from a low dose of haloperidol. When prescribing haloperidol, remember IV administration requires EKG monitoring (FDA black box warning), and a reasonable starting dose is 0.5 mg, NOT 5 mg.
Minimize, but do not avoid, narcotics in patients with both pain and delirium;
Use low-dose antipsychotics, not benzodiazepines, for agitated delirium; and
STOP antipsychotics ASAP, ideally prior to discharge; if not prior to discharge, then include discontinuation date on discharge medication list. TH
HM15 Presenter: Ethan Cumbler, MD, FHM, FACP
Summary: Delirium is a common problem in hospitalized patients, and all too often delirium is iatrogenic. Delirium is associated with poor outcomes such as prolonged hospitalization and functional decline, and it increases the risk of nursing home admission. The most common tool to assess the presence of delirium is the Confusion Assessment Method (CAM). Dr. Cumbler educated the audience on a more refined tool, the 3D CAM [PDF], and provided the algorithm for diagnosis and evaluation of hospital-onset delirium.
Where delirium is concerned (as with most conditions), “an ounce of prevention is worth a pound of cure.” Namely, avoid prescribing problem medications such as anticholinergics, sedative/hypnotics (except benzodiazepines for treatment of alcohol withdrawal), and antihistamines; and minimize narcotics, but don’t undertreat pain as uncontrolled pain is a more potent delirium trigger than narcotics.
Avoid sleep deprivation. Do we really require vital signs and phlebotomy between midnight and 6 a.m.? Make sure patients have their glasses and hearing aids, and keep them up and moving during daylight hours. Sleep and sensory deprivation are effective forms of human torture and are known to be rather disorienting.
Finally, antipsychotics are associated with increased mortality in dementia. Patients with agitated delirium may benefit from a low dose of haloperidol. When prescribing haloperidol, remember IV administration requires EKG monitoring (FDA black box warning), and a reasonable starting dose is 0.5 mg, NOT 5 mg.
HM15 presenters: Joshua D. Lenchus, DO, FACP, SFHM, and Nilam Soni, MD, FHM
Summary: Drs. Lenchus and Soni focused on the forces that are driving the value and success of established procedure teams in hospital medicine groups (HMGs). These stem from a need to rapidly address the growing shortage of skilled internists who can perform diagnostic and therapeutic procedures, thus leading to a subset of hospitalists who are willing to provide these services, particularly with the assistance of bedside ultrasonography.
They stressed the importance of providing a platform that is preemptive, proprietary, and scalable. With a defined set of value-creating metrics such as faster turn-around times, a reduction in complication rates, and ultimately a reduction in cost, LOS, and utilization, data must be collected to adequately measure the impact of these services on the institution.
They also discussed the key components necessary to create a procedure service, starting with the logistics of adequate training and demonstration of competence, proper staffing, supplies and equipment, ultrasound image archiving, and the use of documentation templates. The process is followed by the development of pre-procedure and post-procedure guidelines, as well as standardized procedural techniques.
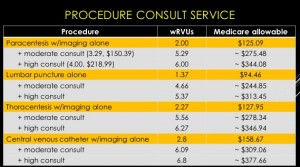
The session also reviewed billing practices and professional fees. An analysis was made comparing Medicare reimbursement and work RVUs for each procedure service with and without a full procedure consultation. A complete consultation significantly increases the allowable fee and associated wRVU. The caveat is that billing for consults is limited to services rendered for patients that are not cared for by the same hospitalist group.
Furthermore, sub-specialists historically perform these procedures. The argument can be made that hospitalists will reduce an unnecessary burden on interventional radiologists, thereby enabling them to focus on more acomplex invasive and highly technical procedures.
The key to success is the ability to find a strategic partner in the C-suite who will directly or indirectly provide the financial and political support. Other sources of funding include private foundations, medical schools, the Department of Veteran Affairs, and such patient safety organizations as AHRQ, IOM, and IHI. HMG leaders also should consider scalability across other hospitalist groups.
“If you build it, they will come."
HM takeaways
Create a business plan;
Find institutional financial and political support;
Start small and selective;
Plan for standardization and training of colleagues;
Create a credentialing/privileging process;
Bill for services and consider billing for full consults; and
HM15 presenters: Joshua D. Lenchus, DO, FACP, SFHM, and Nilam Soni, MD, FHM
Summary: Drs. Lenchus and Soni focused on the forces that are driving the value and success of established procedure teams in hospital medicine groups (HMGs). These stem from a need to rapidly address the growing shortage of skilled internists who can perform diagnostic and therapeutic procedures, thus leading to a subset of hospitalists who are willing to provide these services, particularly with the assistance of bedside ultrasonography.
They stressed the importance of providing a platform that is preemptive, proprietary, and scalable. With a defined set of value-creating metrics such as faster turn-around times, a reduction in complication rates, and ultimately a reduction in cost, LOS, and utilization, data must be collected to adequately measure the impact of these services on the institution.
They also discussed the key components necessary to create a procedure service, starting with the logistics of adequate training and demonstration of competence, proper staffing, supplies and equipment, ultrasound image archiving, and the use of documentation templates. The process is followed by the development of pre-procedure and post-procedure guidelines, as well as standardized procedural techniques.
The session also reviewed billing practices and professional fees. An analysis was made comparing Medicare reimbursement and work RVUs for each procedure service with and without a full procedure consultation. A complete consultation significantly increases the allowable fee and associated wRVU. The caveat is that billing for consults is limited to services rendered for patients that are not cared for by the same hospitalist group.
Furthermore, sub-specialists historically perform these procedures. The argument can be made that hospitalists will reduce an unnecessary burden on interventional radiologists, thereby enabling them to focus on more acomplex invasive and highly technical procedures.
The key to success is the ability to find a strategic partner in the C-suite who will directly or indirectly provide the financial and political support. Other sources of funding include private foundations, medical schools, the Department of Veteran Affairs, and such patient safety organizations as AHRQ, IOM, and IHI. HMG leaders also should consider scalability across other hospitalist groups.
“If you build it, they will come."
HM takeaways
Create a business plan;
Find institutional financial and political support;
Start small and selective;
Plan for standardization and training of colleagues;
Create a credentialing/privileging process;
Bill for services and consider billing for full consults; and
Gather baseline and follow-up data.
HM15 presenters: Joshua D. Lenchus, DO, FACP, SFHM, and Nilam Soni, MD, FHM
Summary: Drs. Lenchus and Soni focused on the forces that are driving the value and success of established procedure teams in hospital medicine groups (HMGs). These stem from a need to rapidly address the growing shortage of skilled internists who can perform diagnostic and therapeutic procedures, thus leading to a subset of hospitalists who are willing to provide these services, particularly with the assistance of bedside ultrasonography.
They stressed the importance of providing a platform that is preemptive, proprietary, and scalable. With a defined set of value-creating metrics such as faster turn-around times, a reduction in complication rates, and ultimately a reduction in cost, LOS, and utilization, data must be collected to adequately measure the impact of these services on the institution.
They also discussed the key components necessary to create a procedure service, starting with the logistics of adequate training and demonstration of competence, proper staffing, supplies and equipment, ultrasound image archiving, and the use of documentation templates. The process is followed by the development of pre-procedure and post-procedure guidelines, as well as standardized procedural techniques.
The session also reviewed billing practices and professional fees. An analysis was made comparing Medicare reimbursement and work RVUs for each procedure service with and without a full procedure consultation. A complete consultation significantly increases the allowable fee and associated wRVU. The caveat is that billing for consults is limited to services rendered for patients that are not cared for by the same hospitalist group.
Furthermore, sub-specialists historically perform these procedures. The argument can be made that hospitalists will reduce an unnecessary burden on interventional radiologists, thereby enabling them to focus on more acomplex invasive and highly technical procedures.
The key to success is the ability to find a strategic partner in the C-suite who will directly or indirectly provide the financial and political support. Other sources of funding include private foundations, medical schools, the Department of Veteran Affairs, and such patient safety organizations as AHRQ, IOM, and IHI. HMG leaders also should consider scalability across other hospitalist groups.
“If you build it, they will come."
HM takeaways
Create a business plan;
Find institutional financial and political support;
Start small and selective;
Plan for standardization and training of colleagues;
Create a credentialing/privileging process;
Bill for services and consider billing for full consults; and
HM15 presenters: Verity Schaye, Michael Janjigian, Frank Volpicelli, Susan Hunt.
Performing a physical exam is the standard of care for evaluating patients. It has been shown to have higher diagnostic utility than many technology based tests. The physical exam is the Gold Standard for dermatological and mental status assessment for which technological tests are not readily available. The tradition “laying on of hands” has important benefits for the physician patient relationship.
The teaching of physical exam skills is increasingly problematic. Barriers include attending time, comfort and skill level as well as challenges of patient comfort and potential isolation issues.
The Peyton Model provides a better means of teaching physical exam skills than the traditional “See one, do one, teach one” model. The Peyton Model has four steps:
Demonstration. The teacher performs the exam at normal speed without commentary.
Deconstruction. The teacher performs the exam while describing the steps.
Comprehension. The teacher performs the exam while the learner describes the steps.
Performance. The learner performs the exam while also describing the steps.
This approach can be abbreviated for more advanced learners with the middle two steps being combined to a discussion between the teacher and learner to highlight any differences or changes in technique. TH
HM15 presenters: Verity Schaye, Michael Janjigian, Frank Volpicelli, Susan Hunt.
Performing a physical exam is the standard of care for evaluating patients. It has been shown to have higher diagnostic utility than many technology based tests. The physical exam is the Gold Standard for dermatological and mental status assessment for which technological tests are not readily available. The tradition “laying on of hands” has important benefits for the physician patient relationship.
The teaching of physical exam skills is increasingly problematic. Barriers include attending time, comfort and skill level as well as challenges of patient comfort and potential isolation issues.
The Peyton Model provides a better means of teaching physical exam skills than the traditional “See one, do one, teach one” model. The Peyton Model has four steps:
Demonstration. The teacher performs the exam at normal speed without commentary.
Deconstruction. The teacher performs the exam while describing the steps.
Comprehension. The teacher performs the exam while the learner describes the steps.
Performance. The learner performs the exam while also describing the steps.
This approach can be abbreviated for more advanced learners with the middle two steps being combined to a discussion between the teacher and learner to highlight any differences or changes in technique. TH
HM15 presenters: Verity Schaye, Michael Janjigian, Frank Volpicelli, Susan Hunt.
Performing a physical exam is the standard of care for evaluating patients. It has been shown to have higher diagnostic utility than many technology based tests. The physical exam is the Gold Standard for dermatological and mental status assessment for which technological tests are not readily available. The tradition “laying on of hands” has important benefits for the physician patient relationship.
The teaching of physical exam skills is increasingly problematic. Barriers include attending time, comfort and skill level as well as challenges of patient comfort and potential isolation issues.
The Peyton Model provides a better means of teaching physical exam skills than the traditional “See one, do one, teach one” model. The Peyton Model has four steps:
Demonstration. The teacher performs the exam at normal speed without commentary.
Deconstruction. The teacher performs the exam while describing the steps.
Comprehension. The teacher performs the exam while the learner describes the steps.
Performance. The learner performs the exam while also describing the steps.
This approach can be abbreviated for more advanced learners with the middle two steps being combined to a discussion between the teacher and learner to highlight any differences or changes in technique. TH
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
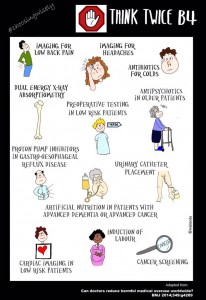
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
Every day, health care providers (HCPs) care for patients with advanced chronic illnesses. At times, HCPs make critical treatment decisions without input from the patient. As a result, patients are often confused about their disease trajectory, prognosis, benefits and burdens of treatments, and outcome preferences.1 Unfortunately, limited research has been conducted on patients who have chronic illnesses, such as congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD), regarding early discussion of advance care planning (ACP) and advance directives (ADs). This gap in the knowledge base has contributed to a delay in the initiation of ACP for patients with COPD or CHF, especially for those with end-stage illness.
Background
The Patient Self-Determination Act (PSDA) was passed in 1990 to inform patients of their rights about health care choices while in the hospital, but the completion rate for ADs remains poor.2 The 3 key elements include the right of patients to facilitate their own health care decisions, the right to refuse or accept treatment, and the right to make an AD.
One of the reasons for the poor AD completion rate may be increased confusion about the difference between ACP and an AD.3 Advance care planning is a discussion about overall goals of care related to health care and progression through the life cycle. Advance directives focus on more specific information, including who will be designated as health care proxy, which health care interventions would be requested and which would be declined, and decisions regarding code status and organ donation.
A case study was conducted at a long-term care facility to test beliefs that residents who made their wishes known through ACP would have a positive experience at the end of life (EOL).3 The study allowed the residents to provide direction on what are and are not acceptable treatments at EOL. Before this study, most residents did not have a health care proxy and had not discussed the topic of EOL care with their HCP. Treatment choices were also not designated.3 Results demonstrated that ACP had positive outcomes for residents and family members, including documentation of an AD, autonomy in decision making, person-centered approaches to care, and dying with dignity.
Much of the research regarding ADs has been conducted with seniors, hospitalized patients, and those with critical or terminal illnesses. A study by Jackson and colleagues examined attitudes, experiences, and preferences about ADs among adults of all ages. The study used an age-stratified random sample of patients from a large managed care organization.4 Findings revealed that older subjects were likely to be comfortable with and complete an AD. The most valuable outcome was the discussion of personal wishes with family and loved ones. Overall, the findings of this study concurred with the findings of other studies demonstrating that patients wanted control over EOL care decisions or wanted family members or loved ones to make those decisions. Consequently, patients not only believe the decisions are their responsibility, but also feel comfortable if their HCP initiates this conversation.4
Open and direct discussion regarding care planning can ease many of the fears related to EOL care. Discussion of an AD is a way to prepare for death and dying, rather than just a preparation for being incapacitated in the future. The process allows improved communication between patients, surrogates, and HCPs.3
The importance of communication with the patient’s primary care provider (PCP) regarding discussion of ACP or an AD is demonstrated in a longitudinal study completed by Ramsaroop and colleagues from January 1991 through July 2005. This systematic review of studies was designed to increase the completion of an AD in primary care settings.5 The study reviewed interventions that were most successful in improving the AD completion rate. The investigators extracted physician and patient barriers to completion of an AD. Findings suggested that the most successful intervention for completion of an AD were conversations that took place between patients and HCPs about ACP and occurred over multiple visits. By contrast, passive education using written materials without any direct counseling was relatively ineffective.5 The study also demonstrated the importance of completion of an AD in the primary care setting, gauging patient readiness to complete an AD, and having the PCP initiate the AD conversation.5
If communication does not occur between patients and HCPs, care preferences are often not documented. Without this documentation many patients do not receive appropriate palliative care services when needed. Palliative care is not available to and therefore often not used with patients with nononcologic diseases.6 A study by Mahtani-Chugani and colleagues evaluated barriers to providing palliative care to nononcologic patients and proposed strategies to overcome them. Findings suggested 4 barriers: (1) lack of clarity about illness and prognosis; (2) discussion limited exclusively to the curative approach; (3) avoiding terms such as “terminal illness”; and (4) cheating death, including linking nononcologic disease and death.6 A strategy to overcoming these barriers highlighted improved communication between HCP and patient and understanding that the communication process is as important as the content of the message. Therefore, equitable palliative care services should be offered to both nononcologic and oncologic patients.6
One life-limiting nononcologic disease is COPD. Chronic obstructive pulmonary disease remains a major public health problem. It is the fourth leading cause of chronic morbidity and mortality in the U.S. and is projected to rank fifth in 2020 in disease burden worldwide.7 Given its prevalence, COPD is found in all adult health care settings.
Among hospitalized veterans in the VHA in 2005, COPD was the fourth most common discharge diagnosis.8 In the veteran population, a high prevalence for developing COPD also exists due to high-risk factors including tobacco use in the military. According to a study conducted at the Cincinnati VAMC in Ohio, a 40% greater prevalence of COPD existed in this veteran population than in the general U.S. population.8
Another nononcologic, life-limiting disease is CHF. Both the prevalence and hospitalization rates for CHF show an upward trend since the 1970s, resulting in a continued increase in CHF death rates.9 According to 2008 estimates from the National Institutes of Health, there are 5 million CHF patients in the U.S. and hospitalization rates approach 1 million per year.9 Congestive heart failure affects 2.4% of the adult population and > 11% of the expanding population aged > 80 years. Existing care may slow the progression of the disease but can rarely reverse it, which usually results in a prolonged period of advanced illness. As a result of the increasing prevalence, there remains a high symptom burden for patients living with advanced CHF.10
In managing the high symptom burden of CHF and COPD, patient-centered care must be acknowledged and used. Patient-centered care mandates that beneficial therapies and recommended guidelines be offered and discussed with the patient, giving attention to patient preferences.10
Study Design
The theoretical framework for the development and implementation of this project is based on Ruland and Moore’s Peaceful End of Life Theory.11 This theory is based on 2 assumptions. The first is that each person’s approach to EOL is personal. The second is that nursing care plays a major role in making EOL a peaceful experience. The 5 outcome measures include: (1) not experiencing pain; (2) the experience of comfort; (3) the experience of dignity and respect; (4) being at peace; and (5) closeness to significant others or other caring persons.
The outcome indicator of the Peaceful End of Life Theory— experience of dignity/respect with its related criteria and prescriptors—provided structure for the development and implementation of this project. The prescriptors related to the experience of dignity/respect include involving the patient and significant others in decision making; treating the patient with dignity, empathy, and respect; and being attentive to the patient’s expressed needs, wishes, and preferences.11
Due to the increased prevalence of chronic illnesses in the VA system, veterans need encouragement to complete ADs. The VA instituted a national directive guiding education and implementation of an AD.12 These discussions occur at the first contact a veteran has with the system and at other times when appropriate. The purpose of the directive is to allow veterans to guide the course of their treatment and to assure that they are aware of the ability to refuse treatment at any time.12
Inconsistencies in Advance Directive Completion
Inconsistencies were noted with how ADs were completed at the VA Northern Indiana Health Care System in Muncie. For outpatients, the clinic nursing staff received an electronic medical record (EMR) reminder if the veteran did not have an AD. This reminder prompted the nurse to ask the veteran about completing an AD. If the veteran agreed, a social work consult was initiated by nursing. Of concern, the social worker is usually responsible for several clinics so it is unlikely the process of completing the AD would be accomplished on the day the veteran was already in the clinic.
Discussions in the inpatient setting included a physician, a nurse practitioner, or a social worker and were often disease specific and patient oriented. However, in an acute hospitalization, it was less likely that patients initiated ADs due to acute illness and rapid nature of treatment.
Another concern was related to the amount of clinical knowledge the social worker had about the specifics of each patient’s case. Without specifics, a social worker can make the AD discussion very broad. Patients want information regarding disease progression and prognosis specific to their own condition to be able to make an informed choice regarding ADs.13
A study population with the diagnoses of CHF and COPD was selected due to the prevalence in the facility and at the request of facility leadership.
Methods
The primary aim of this quality improvement (QI) project was to educate the PCP about the importance of allowing veterans to express their care goals in the form of ADs and to understand that veterans would prefer to discuss these goals with their PCP. A secondary aim was to improve goal-directed care for veterans with COPD or CHF by increasing the number of completed ADs.
By using a systems approach, ACP can be addressed in a uniform manner. This approach allows veterans to discuss their goals of care prior to the need for emergent interventions, avoiding burdensome and unwanted treatments. Through the completion of ADs, veterans are able to designate a surrogate decision maker and identify specific desired treatments and interventions as their illness advances.
Two physicians and 3 nurse practitioners volunteered to contribute to this study. In the participating clinics, veterans with a diagnosis of CHF or COPD were identified. Each veteran had 20 to 30 minutes per appointment to discuss concerns, be examined, have HCPs address concerns, and complete all clinical reminders.
The study design was a QI project focused on evaluating the following process: An EMR reminder alerted the clinic nurse who asked the veteran if he or she was interested in completing an AD. If the patient agreed, a consult was placed to the social worker for completion of the VA national form for AD. The completion rate for a sample of primary care clinics at the facility was 10% to 12%, with no participation from the PCP in the process.
The providers were educated in 5 areas: (1) the prevalence of CHF and COPD in the U.S.; (2) the difference between ACP and AD; (3) the percentage of ADs completed in the U.S. adult population and in the facility; (4) the importance of addressing ACP early in the disease trajectory of this population; and (5) the use of the EMR reminder and the template to guide discussion of ACP ( eAppendix A
The template was developed following the literature review and addressed the reoccurring themes that patients wanted to discuss concerning their specific diagnosis and treatment. The template was formatted to include 3 components: (1) health care surrogate; (2) code status; and (3) organ donation preference ( eAppendix B
). When EMR reminders appear, the PCP initiated a discussion regarding COPD or CHF and the likely progression of the illness. The provider opened a separate note entitled AD Discussion and uses the template. The provider could then guide the discussion to the veteran’s goals of care.
The natural progression from discussion of goals of care led to the discussion regarding the initiation of an AD. When completed, the note automatically appeared in the Postings section of the EMR, making it easily accessible to all other providers in different care settings.
The project time was 3 months (December 2012 through February 2013). The education was completed and the EMR reminder was turned on at the beginning of the project for veterans with a diagnosis of CHF or COPD who had not completed an AD. At the conclusion of the project, the PCPs completed a post project survey to provide information regarding their opinions on facilitators and barriers in the AD completion process ( eAppendix C
). The intervention of the PCP-initiated discussion of ACP was assessed by the percentage increase in completed ADs.
Results
Five different primary care clinics in 4 different locations throughout the health care system provided a total of 294 veterans with diagnoses of CHF or COPD. On completion of the project, 35 veterans had completed ADs. These 35 veterans represent an additional 12% of patients who previously did not complete an AD despite being approached multiple times. The veterans completed an AD following PCP-initiated discussion due to this QI project.
All 5 providers completed the post project survey and agreed that it would be beneficial to have the information regarding ADs easily accessible in the EMR. Four out of 5 providers admitted to cutting corners by not opening a new note every time to complete the AD template. They reported completing the EMR reminder within the clinic note, making it difficult to locate the information. Providers also reported on the various facilitators and barriers to AD discussion with patients (Table).
Discussion
The completion of an AD remains an important part of health care that is often neglected. When patients receive care and treatments, they often do not desire an AD, because the goals of care have not been clearly communicated and clearly documented. This can lead to poor quality of care with increased dissatisfaction and burden on the patient and health care system.14 However, if goals of care are discussed and documented, the veteran may avoid these burdensome treatments, and health care will be congruent with patient wishes. Better communication and documentation promotes increased patient satisfaction and improved quality of health care.1
This project endorses findings from a previous case study that demonstrated better patient-centered, goal-directed care results when patients have the opportunity to complete an AD, thereby improving health care quality and patient/family satisfaction.3 Previous studies suggested one way to increase the AD completion rate involves the PCP initiating a discussion with the patient.5 This project supports that conclusion.
Limitations
All the project providers expressed support regarding the importance of discussing ACPs with their patients. The major limitation identified by the project providers was time constraints in a busy primary care clinic. One provider suggested initiation of an EMR reminder once per year to prompt discussion. The same provider also recommended rescheduling an additional clinic visit to have an in-depth discussion regarding ACP.
Another limitation to this project involved the EMR. Currently, there is no way to have information in the postings section without a separate note. The project providers all agreed that it was not always possible to open a new note to use the template due to limited clinic time. This allowed information regarding health care surrogates and discussions regarding code status and organ donation to be embedded in a clinic note, which can make it difficult for other providers at different levels of care to effectively locate. Incorporating a method to allow information from an EMR reminder to be automatically placed in the postings section would alleviate this limitation.
A further limitation involved the setting. The VA provides care only to veterans. The project can be generalized to other VA primary care clinics, but generalizability beyond the VA may be limited.
This QI project took place over 3 months, another potential limitation due to the limited study period. Also, due to the short time frame of the project, a small sample size was used. Further investigation of this topic by expanding the time frame and sample size would further develop this body of knowledge.
The VA uses an EMR that is accessible to all VA providers locally and nationwide. Due to the nationwide network, expansion of the project would be possible with the support of facility leadership and the EMR reminder staff. By using the education and the template for discussion, the project could be replicated throughout the system.
Conclusion
Advance care planning and ADs should be a regular part of the health care process, especially for veterans with noncancer diagnoses, such as CHF and COPD. Clear communication about disease trajectory and prognosis are an important part of this discussion. Primary care providers are in the optimal setting to initiate this discussion.
This project supports previous findings that a PCP initiating or participating in the ACP discussion would result in an improved completion rate for ADs.5 Theoretically, improved AD completions result in patient-centered care, leading to higher patient satisfaction.
Acknowledgements The authors would like to acknowledge the VA Northern Indiana Health Care System for its support of this project.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. Pautex S, Herrmann FR, Zulian GB. Role of advance directives in palliative care units: A prospective study. Palliat Med. 2008;22(7):835-841.
2. Cohen MJ, McCannon JB, Edgman-Levitan S, Kormos WA. Exploring attitudes toward advance care directives in two diverse settings. J Palliat Med. 2010;13(12):1427-1432.
3. Jeong SY-S, Higgins I, McMillan M. The essentials of Advance Care Planning for end-of-life care for older people. J Clin Nurs. 2010;19(3-4):389-397.
4. Jackson JM, Rolnick SJ, Asche SE, Heinrich RL. Knowledge, attitudes, and p regarding advance directives among patients of a managed care organization. Am J Manag Care. 2009;15(3):177-186.
5. Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: What do we need for success? J Am Geriatr Soc. 2007;55(2):277-283.
6. Mahtani-Chugani V, González-Castro I, de Ormijana-Hernández AS, Martín-Fernández R, de la Vega EF. How to provide care for patients suffering from terminal non-oncological diseases: Barriers to a palliative care approach. Palliat Med. 2010;24(8):787-795.
7. Rabe KF, Hurd S, Anzueto A, et al; Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532-555.
8. Murphy DE, Chaudhry Z, Almoosa KF, Panos RJ. High prevalence of chronic obstructive pulmonary disease among veterans in the urban midwest. Mil Med. 2011;176(5):552-560.
9. National Institutes of Health. Division of cardiovascular disease strategic plan. National Heart, Lung, and Blood Institute Website. http://www .nhlbi.nih.gov/about/org/dcvs/sp/goal-2.4b. 2012. Accessed January 29, 2015.
10. Allen LA, Stevenson LW, Grady KL; American Heart Association; Council on Quality of Care and Outcomes Research; Council on Cardiovascular Nursing; Council on Clinical Cardiology; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Surgery and Anesthesia. Decision making in advanced heart failure: A scientific statement from the American Heart Association. Circulation. 2012;125(15):1928-1952.
11. Ruland CM, Moore SM. Theory construction based on standards of care: A proposed theory of the peaceful end of life. Nurs Outlook. 1998;46(4):169-175.
12. US Department of Veterans Affairs, Veterans Health Administration . VHA Handbook 1004.02 transmittal sheet. Published July 2, 2009. http://www.ethics.va.gov/docs/policy/ADTraining /vha_handbk_1004_02.pdf. Accessed January 29, 2015.
13. Gott M, Gardiner C, Small N, et al. Barriers to advance care planning in chronic obstructive pulmonary disease. Palliat Med. 2009;23(7): 642-648.
14. Teno JM, Gruneir A, Schwartz Z, Nanda A, Wetle T. Association between advance directives and quality end-of-life care: A national study. J Am Geriatr Soc. 2007;55(2):189-194.
Dr. Sipes is a palliative care nurse practitioner in the Department of Geriatrics and Extended Care at the VA Northern Indiana Health Care System in Marion, Indiana. Dr. Siela is an associate professor of nursing at Ball State University in Muncie, Indiana. Dr. Rogers is the clinical pharmacy coordinator for the VA Northern Indiana Health Care System.
advance care planning, advance directive, chronic illness, end-stage illness, end of life, EOL, patient-centered care, physician-patient communication, patient case documentation, electronic medical record, EMR, patient satisfaction, improve quality of health care, Elizabeth Sipes, Debra Siela, Shannon E Rogers
Dr. Sipes is a palliative care nurse practitioner in the Department of Geriatrics and Extended Care at the VA Northern Indiana Health Care System in Marion, Indiana. Dr. Siela is an associate professor of nursing at Ball State University in Muncie, Indiana. Dr. Rogers is the clinical pharmacy coordinator for the VA Northern Indiana Health Care System.
Author and Disclosure Information
Dr. Sipes is a palliative care nurse practitioner in the Department of Geriatrics and Extended Care at the VA Northern Indiana Health Care System in Marion, Indiana. Dr. Siela is an associate professor of nursing at Ball State University in Muncie, Indiana. Dr. Rogers is the clinical pharmacy coordinator for the VA Northern Indiana Health Care System.
When treating patients with chronic illnesses, health care providers should involve patients in the decision-making process.
When treating patients with chronic illnesses, health care providers should involve patients in the decision-making process.
Every day, health care providers (HCPs) care for patients with advanced chronic illnesses. At times, HCPs make critical treatment decisions without input from the patient. As a result, patients are often confused about their disease trajectory, prognosis, benefits and burdens of treatments, and outcome preferences.1 Unfortunately, limited research has been conducted on patients who have chronic illnesses, such as congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD), regarding early discussion of advance care planning (ACP) and advance directives (ADs). This gap in the knowledge base has contributed to a delay in the initiation of ACP for patients with COPD or CHF, especially for those with end-stage illness.
Background
The Patient Self-Determination Act (PSDA) was passed in 1990 to inform patients of their rights about health care choices while in the hospital, but the completion rate for ADs remains poor.2 The 3 key elements include the right of patients to facilitate their own health care decisions, the right to refuse or accept treatment, and the right to make an AD.
One of the reasons for the poor AD completion rate may be increased confusion about the difference between ACP and an AD.3 Advance care planning is a discussion about overall goals of care related to health care and progression through the life cycle. Advance directives focus on more specific information, including who will be designated as health care proxy, which health care interventions would be requested and which would be declined, and decisions regarding code status and organ donation.
A case study was conducted at a long-term care facility to test beliefs that residents who made their wishes known through ACP would have a positive experience at the end of life (EOL).3 The study allowed the residents to provide direction on what are and are not acceptable treatments at EOL. Before this study, most residents did not have a health care proxy and had not discussed the topic of EOL care with their HCP. Treatment choices were also not designated.3 Results demonstrated that ACP had positive outcomes for residents and family members, including documentation of an AD, autonomy in decision making, person-centered approaches to care, and dying with dignity.
Much of the research regarding ADs has been conducted with seniors, hospitalized patients, and those with critical or terminal illnesses. A study by Jackson and colleagues examined attitudes, experiences, and preferences about ADs among adults of all ages. The study used an age-stratified random sample of patients from a large managed care organization.4 Findings revealed that older subjects were likely to be comfortable with and complete an AD. The most valuable outcome was the discussion of personal wishes with family and loved ones. Overall, the findings of this study concurred with the findings of other studies demonstrating that patients wanted control over EOL care decisions or wanted family members or loved ones to make those decisions. Consequently, patients not only believe the decisions are their responsibility, but also feel comfortable if their HCP initiates this conversation.4
Open and direct discussion regarding care planning can ease many of the fears related to EOL care. Discussion of an AD is a way to prepare for death and dying, rather than just a preparation for being incapacitated in the future. The process allows improved communication between patients, surrogates, and HCPs.3
The importance of communication with the patient’s primary care provider (PCP) regarding discussion of ACP or an AD is demonstrated in a longitudinal study completed by Ramsaroop and colleagues from January 1991 through July 2005. This systematic review of studies was designed to increase the completion of an AD in primary care settings.5 The study reviewed interventions that were most successful in improving the AD completion rate. The investigators extracted physician and patient barriers to completion of an AD. Findings suggested that the most successful intervention for completion of an AD were conversations that took place between patients and HCPs about ACP and occurred over multiple visits. By contrast, passive education using written materials without any direct counseling was relatively ineffective.5 The study also demonstrated the importance of completion of an AD in the primary care setting, gauging patient readiness to complete an AD, and having the PCP initiate the AD conversation.5
If communication does not occur between patients and HCPs, care preferences are often not documented. Without this documentation many patients do not receive appropriate palliative care services when needed. Palliative care is not available to and therefore often not used with patients with nononcologic diseases.6 A study by Mahtani-Chugani and colleagues evaluated barriers to providing palliative care to nononcologic patients and proposed strategies to overcome them. Findings suggested 4 barriers: (1) lack of clarity about illness and prognosis; (2) discussion limited exclusively to the curative approach; (3) avoiding terms such as “terminal illness”; and (4) cheating death, including linking nononcologic disease and death.6 A strategy to overcoming these barriers highlighted improved communication between HCP and patient and understanding that the communication process is as important as the content of the message. Therefore, equitable palliative care services should be offered to both nononcologic and oncologic patients.6
One life-limiting nononcologic disease is COPD. Chronic obstructive pulmonary disease remains a major public health problem. It is the fourth leading cause of chronic morbidity and mortality in the U.S. and is projected to rank fifth in 2020 in disease burden worldwide.7 Given its prevalence, COPD is found in all adult health care settings.
Among hospitalized veterans in the VHA in 2005, COPD was the fourth most common discharge diagnosis.8 In the veteran population, a high prevalence for developing COPD also exists due to high-risk factors including tobacco use in the military. According to a study conducted at the Cincinnati VAMC in Ohio, a 40% greater prevalence of COPD existed in this veteran population than in the general U.S. population.8
Another nononcologic, life-limiting disease is CHF. Both the prevalence and hospitalization rates for CHF show an upward trend since the 1970s, resulting in a continued increase in CHF death rates.9 According to 2008 estimates from the National Institutes of Health, there are 5 million CHF patients in the U.S. and hospitalization rates approach 1 million per year.9 Congestive heart failure affects 2.4% of the adult population and > 11% of the expanding population aged > 80 years. Existing care may slow the progression of the disease but can rarely reverse it, which usually results in a prolonged period of advanced illness. As a result of the increasing prevalence, there remains a high symptom burden for patients living with advanced CHF.10
In managing the high symptom burden of CHF and COPD, patient-centered care must be acknowledged and used. Patient-centered care mandates that beneficial therapies and recommended guidelines be offered and discussed with the patient, giving attention to patient preferences.10
Study Design
The theoretical framework for the development and implementation of this project is based on Ruland and Moore’s Peaceful End of Life Theory.11 This theory is based on 2 assumptions. The first is that each person’s approach to EOL is personal. The second is that nursing care plays a major role in making EOL a peaceful experience. The 5 outcome measures include: (1) not experiencing pain; (2) the experience of comfort; (3) the experience of dignity and respect; (4) being at peace; and (5) closeness to significant others or other caring persons.
The outcome indicator of the Peaceful End of Life Theory— experience of dignity/respect with its related criteria and prescriptors—provided structure for the development and implementation of this project. The prescriptors related to the experience of dignity/respect include involving the patient and significant others in decision making; treating the patient with dignity, empathy, and respect; and being attentive to the patient’s expressed needs, wishes, and preferences.11
Due to the increased prevalence of chronic illnesses in the VA system, veterans need encouragement to complete ADs. The VA instituted a national directive guiding education and implementation of an AD.12 These discussions occur at the first contact a veteran has with the system and at other times when appropriate. The purpose of the directive is to allow veterans to guide the course of their treatment and to assure that they are aware of the ability to refuse treatment at any time.12
Inconsistencies in Advance Directive Completion
Inconsistencies were noted with how ADs were completed at the VA Northern Indiana Health Care System in Muncie. For outpatients, the clinic nursing staff received an electronic medical record (EMR) reminder if the veteran did not have an AD. This reminder prompted the nurse to ask the veteran about completing an AD. If the veteran agreed, a social work consult was initiated by nursing. Of concern, the social worker is usually responsible for several clinics so it is unlikely the process of completing the AD would be accomplished on the day the veteran was already in the clinic.
Discussions in the inpatient setting included a physician, a nurse practitioner, or a social worker and were often disease specific and patient oriented. However, in an acute hospitalization, it was less likely that patients initiated ADs due to acute illness and rapid nature of treatment.
Another concern was related to the amount of clinical knowledge the social worker had about the specifics of each patient’s case. Without specifics, a social worker can make the AD discussion very broad. Patients want information regarding disease progression and prognosis specific to their own condition to be able to make an informed choice regarding ADs.13
A study population with the diagnoses of CHF and COPD was selected due to the prevalence in the facility and at the request of facility leadership.
Methods
The primary aim of this quality improvement (QI) project was to educate the PCP about the importance of allowing veterans to express their care goals in the form of ADs and to understand that veterans would prefer to discuss these goals with their PCP. A secondary aim was to improve goal-directed care for veterans with COPD or CHF by increasing the number of completed ADs.
By using a systems approach, ACP can be addressed in a uniform manner. This approach allows veterans to discuss their goals of care prior to the need for emergent interventions, avoiding burdensome and unwanted treatments. Through the completion of ADs, veterans are able to designate a surrogate decision maker and identify specific desired treatments and interventions as their illness advances.
Two physicians and 3 nurse practitioners volunteered to contribute to this study. In the participating clinics, veterans with a diagnosis of CHF or COPD were identified. Each veteran had 20 to 30 minutes per appointment to discuss concerns, be examined, have HCPs address concerns, and complete all clinical reminders.
The study design was a QI project focused on evaluating the following process: An EMR reminder alerted the clinic nurse who asked the veteran if he or she was interested in completing an AD. If the patient agreed, a consult was placed to the social worker for completion of the VA national form for AD. The completion rate for a sample of primary care clinics at the facility was 10% to 12%, with no participation from the PCP in the process.
The providers were educated in 5 areas: (1) the prevalence of CHF and COPD in the U.S.; (2) the difference between ACP and AD; (3) the percentage of ADs completed in the U.S. adult population and in the facility; (4) the importance of addressing ACP early in the disease trajectory of this population; and (5) the use of the EMR reminder and the template to guide discussion of ACP ( eAppendix A
The template was developed following the literature review and addressed the reoccurring themes that patients wanted to discuss concerning their specific diagnosis and treatment. The template was formatted to include 3 components: (1) health care surrogate; (2) code status; and (3) organ donation preference ( eAppendix B
). When EMR reminders appear, the PCP initiated a discussion regarding COPD or CHF and the likely progression of the illness. The provider opened a separate note entitled AD Discussion and uses the template. The provider could then guide the discussion to the veteran’s goals of care.
The natural progression from discussion of goals of care led to the discussion regarding the initiation of an AD. When completed, the note automatically appeared in the Postings section of the EMR, making it easily accessible to all other providers in different care settings.
The project time was 3 months (December 2012 through February 2013). The education was completed and the EMR reminder was turned on at the beginning of the project for veterans with a diagnosis of CHF or COPD who had not completed an AD. At the conclusion of the project, the PCPs completed a post project survey to provide information regarding their opinions on facilitators and barriers in the AD completion process ( eAppendix C
). The intervention of the PCP-initiated discussion of ACP was assessed by the percentage increase in completed ADs.
Results
Five different primary care clinics in 4 different locations throughout the health care system provided a total of 294 veterans with diagnoses of CHF or COPD. On completion of the project, 35 veterans had completed ADs. These 35 veterans represent an additional 12% of patients who previously did not complete an AD despite being approached multiple times. The veterans completed an AD following PCP-initiated discussion due to this QI project.
All 5 providers completed the post project survey and agreed that it would be beneficial to have the information regarding ADs easily accessible in the EMR. Four out of 5 providers admitted to cutting corners by not opening a new note every time to complete the AD template. They reported completing the EMR reminder within the clinic note, making it difficult to locate the information. Providers also reported on the various facilitators and barriers to AD discussion with patients (Table).
Discussion
The completion of an AD remains an important part of health care that is often neglected. When patients receive care and treatments, they often do not desire an AD, because the goals of care have not been clearly communicated and clearly documented. This can lead to poor quality of care with increased dissatisfaction and burden on the patient and health care system.14 However, if goals of care are discussed and documented, the veteran may avoid these burdensome treatments, and health care will be congruent with patient wishes. Better communication and documentation promotes increased patient satisfaction and improved quality of health care.1
This project endorses findings from a previous case study that demonstrated better patient-centered, goal-directed care results when patients have the opportunity to complete an AD, thereby improving health care quality and patient/family satisfaction.3 Previous studies suggested one way to increase the AD completion rate involves the PCP initiating a discussion with the patient.5 This project supports that conclusion.
Limitations
All the project providers expressed support regarding the importance of discussing ACPs with their patients. The major limitation identified by the project providers was time constraints in a busy primary care clinic. One provider suggested initiation of an EMR reminder once per year to prompt discussion. The same provider also recommended rescheduling an additional clinic visit to have an in-depth discussion regarding ACP.
Another limitation to this project involved the EMR. Currently, there is no way to have information in the postings section without a separate note. The project providers all agreed that it was not always possible to open a new note to use the template due to limited clinic time. This allowed information regarding health care surrogates and discussions regarding code status and organ donation to be embedded in a clinic note, which can make it difficult for other providers at different levels of care to effectively locate. Incorporating a method to allow information from an EMR reminder to be automatically placed in the postings section would alleviate this limitation.
A further limitation involved the setting. The VA provides care only to veterans. The project can be generalized to other VA primary care clinics, but generalizability beyond the VA may be limited.
This QI project took place over 3 months, another potential limitation due to the limited study period. Also, due to the short time frame of the project, a small sample size was used. Further investigation of this topic by expanding the time frame and sample size would further develop this body of knowledge.
The VA uses an EMR that is accessible to all VA providers locally and nationwide. Due to the nationwide network, expansion of the project would be possible with the support of facility leadership and the EMR reminder staff. By using the education and the template for discussion, the project could be replicated throughout the system.
Conclusion
Advance care planning and ADs should be a regular part of the health care process, especially for veterans with noncancer diagnoses, such as CHF and COPD. Clear communication about disease trajectory and prognosis are an important part of this discussion. Primary care providers are in the optimal setting to initiate this discussion.
This project supports previous findings that a PCP initiating or participating in the ACP discussion would result in an improved completion rate for ADs.5 Theoretically, improved AD completions result in patient-centered care, leading to higher patient satisfaction.
Acknowledgements The authors would like to acknowledge the VA Northern Indiana Health Care System for its support of this project.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Every day, health care providers (HCPs) care for patients with advanced chronic illnesses. At times, HCPs make critical treatment decisions without input from the patient. As a result, patients are often confused about their disease trajectory, prognosis, benefits and burdens of treatments, and outcome preferences.1 Unfortunately, limited research has been conducted on patients who have chronic illnesses, such as congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD), regarding early discussion of advance care planning (ACP) and advance directives (ADs). This gap in the knowledge base has contributed to a delay in the initiation of ACP for patients with COPD or CHF, especially for those with end-stage illness.
Background
The Patient Self-Determination Act (PSDA) was passed in 1990 to inform patients of their rights about health care choices while in the hospital, but the completion rate for ADs remains poor.2 The 3 key elements include the right of patients to facilitate their own health care decisions, the right to refuse or accept treatment, and the right to make an AD.
One of the reasons for the poor AD completion rate may be increased confusion about the difference between ACP and an AD.3 Advance care planning is a discussion about overall goals of care related to health care and progression through the life cycle. Advance directives focus on more specific information, including who will be designated as health care proxy, which health care interventions would be requested and which would be declined, and decisions regarding code status and organ donation.
A case study was conducted at a long-term care facility to test beliefs that residents who made their wishes known through ACP would have a positive experience at the end of life (EOL).3 The study allowed the residents to provide direction on what are and are not acceptable treatments at EOL. Before this study, most residents did not have a health care proxy and had not discussed the topic of EOL care with their HCP. Treatment choices were also not designated.3 Results demonstrated that ACP had positive outcomes for residents and family members, including documentation of an AD, autonomy in decision making, person-centered approaches to care, and dying with dignity.
Much of the research regarding ADs has been conducted with seniors, hospitalized patients, and those with critical or terminal illnesses. A study by Jackson and colleagues examined attitudes, experiences, and preferences about ADs among adults of all ages. The study used an age-stratified random sample of patients from a large managed care organization.4 Findings revealed that older subjects were likely to be comfortable with and complete an AD. The most valuable outcome was the discussion of personal wishes with family and loved ones. Overall, the findings of this study concurred with the findings of other studies demonstrating that patients wanted control over EOL care decisions or wanted family members or loved ones to make those decisions. Consequently, patients not only believe the decisions are their responsibility, but also feel comfortable if their HCP initiates this conversation.4
Open and direct discussion regarding care planning can ease many of the fears related to EOL care. Discussion of an AD is a way to prepare for death and dying, rather than just a preparation for being incapacitated in the future. The process allows improved communication between patients, surrogates, and HCPs.3
The importance of communication with the patient’s primary care provider (PCP) regarding discussion of ACP or an AD is demonstrated in a longitudinal study completed by Ramsaroop and colleagues from January 1991 through July 2005. This systematic review of studies was designed to increase the completion of an AD in primary care settings.5 The study reviewed interventions that were most successful in improving the AD completion rate. The investigators extracted physician and patient barriers to completion of an AD. Findings suggested that the most successful intervention for completion of an AD were conversations that took place between patients and HCPs about ACP and occurred over multiple visits. By contrast, passive education using written materials without any direct counseling was relatively ineffective.5 The study also demonstrated the importance of completion of an AD in the primary care setting, gauging patient readiness to complete an AD, and having the PCP initiate the AD conversation.5
If communication does not occur between patients and HCPs, care preferences are often not documented. Without this documentation many patients do not receive appropriate palliative care services when needed. Palliative care is not available to and therefore often not used with patients with nononcologic diseases.6 A study by Mahtani-Chugani and colleagues evaluated barriers to providing palliative care to nononcologic patients and proposed strategies to overcome them. Findings suggested 4 barriers: (1) lack of clarity about illness and prognosis; (2) discussion limited exclusively to the curative approach; (3) avoiding terms such as “terminal illness”; and (4) cheating death, including linking nononcologic disease and death.6 A strategy to overcoming these barriers highlighted improved communication between HCP and patient and understanding that the communication process is as important as the content of the message. Therefore, equitable palliative care services should be offered to both nononcologic and oncologic patients.6
One life-limiting nononcologic disease is COPD. Chronic obstructive pulmonary disease remains a major public health problem. It is the fourth leading cause of chronic morbidity and mortality in the U.S. and is projected to rank fifth in 2020 in disease burden worldwide.7 Given its prevalence, COPD is found in all adult health care settings.
Among hospitalized veterans in the VHA in 2005, COPD was the fourth most common discharge diagnosis.8 In the veteran population, a high prevalence for developing COPD also exists due to high-risk factors including tobacco use in the military. According to a study conducted at the Cincinnati VAMC in Ohio, a 40% greater prevalence of COPD existed in this veteran population than in the general U.S. population.8
Another nononcologic, life-limiting disease is CHF. Both the prevalence and hospitalization rates for CHF show an upward trend since the 1970s, resulting in a continued increase in CHF death rates.9 According to 2008 estimates from the National Institutes of Health, there are 5 million CHF patients in the U.S. and hospitalization rates approach 1 million per year.9 Congestive heart failure affects 2.4% of the adult population and > 11% of the expanding population aged > 80 years. Existing care may slow the progression of the disease but can rarely reverse it, which usually results in a prolonged period of advanced illness. As a result of the increasing prevalence, there remains a high symptom burden for patients living with advanced CHF.10
In managing the high symptom burden of CHF and COPD, patient-centered care must be acknowledged and used. Patient-centered care mandates that beneficial therapies and recommended guidelines be offered and discussed with the patient, giving attention to patient preferences.10
Study Design
The theoretical framework for the development and implementation of this project is based on Ruland and Moore’s Peaceful End of Life Theory.11 This theory is based on 2 assumptions. The first is that each person’s approach to EOL is personal. The second is that nursing care plays a major role in making EOL a peaceful experience. The 5 outcome measures include: (1) not experiencing pain; (2) the experience of comfort; (3) the experience of dignity and respect; (4) being at peace; and (5) closeness to significant others or other caring persons.
The outcome indicator of the Peaceful End of Life Theory— experience of dignity/respect with its related criteria and prescriptors—provided structure for the development and implementation of this project. The prescriptors related to the experience of dignity/respect include involving the patient and significant others in decision making; treating the patient with dignity, empathy, and respect; and being attentive to the patient’s expressed needs, wishes, and preferences.11
Due to the increased prevalence of chronic illnesses in the VA system, veterans need encouragement to complete ADs. The VA instituted a national directive guiding education and implementation of an AD.12 These discussions occur at the first contact a veteran has with the system and at other times when appropriate. The purpose of the directive is to allow veterans to guide the course of their treatment and to assure that they are aware of the ability to refuse treatment at any time.12
Inconsistencies in Advance Directive Completion
Inconsistencies were noted with how ADs were completed at the VA Northern Indiana Health Care System in Muncie. For outpatients, the clinic nursing staff received an electronic medical record (EMR) reminder if the veteran did not have an AD. This reminder prompted the nurse to ask the veteran about completing an AD. If the veteran agreed, a social work consult was initiated by nursing. Of concern, the social worker is usually responsible for several clinics so it is unlikely the process of completing the AD would be accomplished on the day the veteran was already in the clinic.
Discussions in the inpatient setting included a physician, a nurse practitioner, or a social worker and were often disease specific and patient oriented. However, in an acute hospitalization, it was less likely that patients initiated ADs due to acute illness and rapid nature of treatment.
Another concern was related to the amount of clinical knowledge the social worker had about the specifics of each patient’s case. Without specifics, a social worker can make the AD discussion very broad. Patients want information regarding disease progression and prognosis specific to their own condition to be able to make an informed choice regarding ADs.13
A study population with the diagnoses of CHF and COPD was selected due to the prevalence in the facility and at the request of facility leadership.
Methods
The primary aim of this quality improvement (QI) project was to educate the PCP about the importance of allowing veterans to express their care goals in the form of ADs and to understand that veterans would prefer to discuss these goals with their PCP. A secondary aim was to improve goal-directed care for veterans with COPD or CHF by increasing the number of completed ADs.
By using a systems approach, ACP can be addressed in a uniform manner. This approach allows veterans to discuss their goals of care prior to the need for emergent interventions, avoiding burdensome and unwanted treatments. Through the completion of ADs, veterans are able to designate a surrogate decision maker and identify specific desired treatments and interventions as their illness advances.
Two physicians and 3 nurse practitioners volunteered to contribute to this study. In the participating clinics, veterans with a diagnosis of CHF or COPD were identified. Each veteran had 20 to 30 minutes per appointment to discuss concerns, be examined, have HCPs address concerns, and complete all clinical reminders.
The study design was a QI project focused on evaluating the following process: An EMR reminder alerted the clinic nurse who asked the veteran if he or she was interested in completing an AD. If the patient agreed, a consult was placed to the social worker for completion of the VA national form for AD. The completion rate for a sample of primary care clinics at the facility was 10% to 12%, with no participation from the PCP in the process.
The providers were educated in 5 areas: (1) the prevalence of CHF and COPD in the U.S.; (2) the difference between ACP and AD; (3) the percentage of ADs completed in the U.S. adult population and in the facility; (4) the importance of addressing ACP early in the disease trajectory of this population; and (5) the use of the EMR reminder and the template to guide discussion of ACP ( eAppendix A
The template was developed following the literature review and addressed the reoccurring themes that patients wanted to discuss concerning their specific diagnosis and treatment. The template was formatted to include 3 components: (1) health care surrogate; (2) code status; and (3) organ donation preference ( eAppendix B
). When EMR reminders appear, the PCP initiated a discussion regarding COPD or CHF and the likely progression of the illness. The provider opened a separate note entitled AD Discussion and uses the template. The provider could then guide the discussion to the veteran’s goals of care.
The natural progression from discussion of goals of care led to the discussion regarding the initiation of an AD. When completed, the note automatically appeared in the Postings section of the EMR, making it easily accessible to all other providers in different care settings.
The project time was 3 months (December 2012 through February 2013). The education was completed and the EMR reminder was turned on at the beginning of the project for veterans with a diagnosis of CHF or COPD who had not completed an AD. At the conclusion of the project, the PCPs completed a post project survey to provide information regarding their opinions on facilitators and barriers in the AD completion process ( eAppendix C
). The intervention of the PCP-initiated discussion of ACP was assessed by the percentage increase in completed ADs.
Results
Five different primary care clinics in 4 different locations throughout the health care system provided a total of 294 veterans with diagnoses of CHF or COPD. On completion of the project, 35 veterans had completed ADs. These 35 veterans represent an additional 12% of patients who previously did not complete an AD despite being approached multiple times. The veterans completed an AD following PCP-initiated discussion due to this QI project.
All 5 providers completed the post project survey and agreed that it would be beneficial to have the information regarding ADs easily accessible in the EMR. Four out of 5 providers admitted to cutting corners by not opening a new note every time to complete the AD template. They reported completing the EMR reminder within the clinic note, making it difficult to locate the information. Providers also reported on the various facilitators and barriers to AD discussion with patients (Table).
Discussion
The completion of an AD remains an important part of health care that is often neglected. When patients receive care and treatments, they often do not desire an AD, because the goals of care have not been clearly communicated and clearly documented. This can lead to poor quality of care with increased dissatisfaction and burden on the patient and health care system.14 However, if goals of care are discussed and documented, the veteran may avoid these burdensome treatments, and health care will be congruent with patient wishes. Better communication and documentation promotes increased patient satisfaction and improved quality of health care.1
This project endorses findings from a previous case study that demonstrated better patient-centered, goal-directed care results when patients have the opportunity to complete an AD, thereby improving health care quality and patient/family satisfaction.3 Previous studies suggested one way to increase the AD completion rate involves the PCP initiating a discussion with the patient.5 This project supports that conclusion.
Limitations
All the project providers expressed support regarding the importance of discussing ACPs with their patients. The major limitation identified by the project providers was time constraints in a busy primary care clinic. One provider suggested initiation of an EMR reminder once per year to prompt discussion. The same provider also recommended rescheduling an additional clinic visit to have an in-depth discussion regarding ACP.
Another limitation to this project involved the EMR. Currently, there is no way to have information in the postings section without a separate note. The project providers all agreed that it was not always possible to open a new note to use the template due to limited clinic time. This allowed information regarding health care surrogates and discussions regarding code status and organ donation to be embedded in a clinic note, which can make it difficult for other providers at different levels of care to effectively locate. Incorporating a method to allow information from an EMR reminder to be automatically placed in the postings section would alleviate this limitation.
A further limitation involved the setting. The VA provides care only to veterans. The project can be generalized to other VA primary care clinics, but generalizability beyond the VA may be limited.
This QI project took place over 3 months, another potential limitation due to the limited study period. Also, due to the short time frame of the project, a small sample size was used. Further investigation of this topic by expanding the time frame and sample size would further develop this body of knowledge.
The VA uses an EMR that is accessible to all VA providers locally and nationwide. Due to the nationwide network, expansion of the project would be possible with the support of facility leadership and the EMR reminder staff. By using the education and the template for discussion, the project could be replicated throughout the system.
Conclusion
Advance care planning and ADs should be a regular part of the health care process, especially for veterans with noncancer diagnoses, such as CHF and COPD. Clear communication about disease trajectory and prognosis are an important part of this discussion. Primary care providers are in the optimal setting to initiate this discussion.
This project supports previous findings that a PCP initiating or participating in the ACP discussion would result in an improved completion rate for ADs.5 Theoretically, improved AD completions result in patient-centered care, leading to higher patient satisfaction.
Acknowledgements The authors would like to acknowledge the VA Northern Indiana Health Care System for its support of this project.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. Pautex S, Herrmann FR, Zulian GB. Role of advance directives in palliative care units: A prospective study. Palliat Med. 2008;22(7):835-841.
2. Cohen MJ, McCannon JB, Edgman-Levitan S, Kormos WA. Exploring attitudes toward advance care directives in two diverse settings. J Palliat Med. 2010;13(12):1427-1432.
3. Jeong SY-S, Higgins I, McMillan M. The essentials of Advance Care Planning for end-of-life care for older people. J Clin Nurs. 2010;19(3-4):389-397.
4. Jackson JM, Rolnick SJ, Asche SE, Heinrich RL. Knowledge, attitudes, and p regarding advance directives among patients of a managed care organization. Am J Manag Care. 2009;15(3):177-186.
5. Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: What do we need for success? J Am Geriatr Soc. 2007;55(2):277-283.
6. Mahtani-Chugani V, González-Castro I, de Ormijana-Hernández AS, Martín-Fernández R, de la Vega EF. How to provide care for patients suffering from terminal non-oncological diseases: Barriers to a palliative care approach. Palliat Med. 2010;24(8):787-795.
7. Rabe KF, Hurd S, Anzueto A, et al; Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532-555.
8. Murphy DE, Chaudhry Z, Almoosa KF, Panos RJ. High prevalence of chronic obstructive pulmonary disease among veterans in the urban midwest. Mil Med. 2011;176(5):552-560.
9. National Institutes of Health. Division of cardiovascular disease strategic plan. National Heart, Lung, and Blood Institute Website. http://www .nhlbi.nih.gov/about/org/dcvs/sp/goal-2.4b. 2012. Accessed January 29, 2015.
10. Allen LA, Stevenson LW, Grady KL; American Heart Association; Council on Quality of Care and Outcomes Research; Council on Cardiovascular Nursing; Council on Clinical Cardiology; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Surgery and Anesthesia. Decision making in advanced heart failure: A scientific statement from the American Heart Association. Circulation. 2012;125(15):1928-1952.
11. Ruland CM, Moore SM. Theory construction based on standards of care: A proposed theory of the peaceful end of life. Nurs Outlook. 1998;46(4):169-175.
12. US Department of Veterans Affairs, Veterans Health Administration . VHA Handbook 1004.02 transmittal sheet. Published July 2, 2009. http://www.ethics.va.gov/docs/policy/ADTraining /vha_handbk_1004_02.pdf. Accessed January 29, 2015.
13. Gott M, Gardiner C, Small N, et al. Barriers to advance care planning in chronic obstructive pulmonary disease. Palliat Med. 2009;23(7): 642-648.
14. Teno JM, Gruneir A, Schwartz Z, Nanda A, Wetle T. Association between advance directives and quality end-of-life care: A national study. J Am Geriatr Soc. 2007;55(2):189-194.
References
1. Pautex S, Herrmann FR, Zulian GB. Role of advance directives in palliative care units: A prospective study. Palliat Med. 2008;22(7):835-841.
2. Cohen MJ, McCannon JB, Edgman-Levitan S, Kormos WA. Exploring attitudes toward advance care directives in two diverse settings. J Palliat Med. 2010;13(12):1427-1432.
3. Jeong SY-S, Higgins I, McMillan M. The essentials of Advance Care Planning for end-of-life care for older people. J Clin Nurs. 2010;19(3-4):389-397.
4. Jackson JM, Rolnick SJ, Asche SE, Heinrich RL. Knowledge, attitudes, and p regarding advance directives among patients of a managed care organization. Am J Manag Care. 2009;15(3):177-186.
5. Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: What do we need for success? J Am Geriatr Soc. 2007;55(2):277-283.
6. Mahtani-Chugani V, González-Castro I, de Ormijana-Hernández AS, Martín-Fernández R, de la Vega EF. How to provide care for patients suffering from terminal non-oncological diseases: Barriers to a palliative care approach. Palliat Med. 2010;24(8):787-795.
7. Rabe KF, Hurd S, Anzueto A, et al; Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532-555.
8. Murphy DE, Chaudhry Z, Almoosa KF, Panos RJ. High prevalence of chronic obstructive pulmonary disease among veterans in the urban midwest. Mil Med. 2011;176(5):552-560.
9. National Institutes of Health. Division of cardiovascular disease strategic plan. National Heart, Lung, and Blood Institute Website. http://www .nhlbi.nih.gov/about/org/dcvs/sp/goal-2.4b. 2012. Accessed January 29, 2015.
10. Allen LA, Stevenson LW, Grady KL; American Heart Association; Council on Quality of Care and Outcomes Research; Council on Cardiovascular Nursing; Council on Clinical Cardiology; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Surgery and Anesthesia. Decision making in advanced heart failure: A scientific statement from the American Heart Association. Circulation. 2012;125(15):1928-1952.
11. Ruland CM, Moore SM. Theory construction based on standards of care: A proposed theory of the peaceful end of life. Nurs Outlook. 1998;46(4):169-175.
12. US Department of Veterans Affairs, Veterans Health Administration . VHA Handbook 1004.02 transmittal sheet. Published July 2, 2009. http://www.ethics.va.gov/docs/policy/ADTraining /vha_handbk_1004_02.pdf. Accessed January 29, 2015.
13. Gott M, Gardiner C, Small N, et al. Barriers to advance care planning in chronic obstructive pulmonary disease. Palliat Med. 2009;23(7): 642-648.
14. Teno JM, Gruneir A, Schwartz Z, Nanda A, Wetle T. Association between advance directives and quality end-of-life care: A national study. J Am Geriatr Soc. 2007;55(2):189-194.
advance care planning, advance directive, chronic illness, end-stage illness, end of life, EOL, patient-centered care, physician-patient communication, patient case documentation, electronic medical record, EMR, patient satisfaction, improve quality of health care, Elizabeth Sipes, Debra Siela, Shannon E Rogers
Legacy Keywords
advance care planning, advance directive, chronic illness, end-stage illness, end of life, EOL, patient-centered care, physician-patient communication, patient case documentation, electronic medical record, EMR, patient satisfaction, improve quality of health care, Elizabeth Sipes, Debra Siela, Shannon E Rogers
Although patients with blood clots are oftentimes not admitted to the hospital, there are some exceptions. Monal Shah, MD, physician advisor for Parkland Hospital in Dallas, Texas, and the former section head of hospital medicine at the University of Texas Southwestern Medical Center, discusses some exceptions.
Although patients with blood clots are oftentimes not admitted to the hospital, there are some exceptions. Monal Shah, MD, physician advisor for Parkland Hospital in Dallas, Texas, and the former section head of hospital medicine at the University of Texas Southwestern Medical Center, discusses some exceptions.
Although patients with blood clots are oftentimes not admitted to the hospital, there are some exceptions. Monal Shah, MD, physician advisor for Parkland Hospital in Dallas, Texas, and the former section head of hospital medicine at the University of Texas Southwestern Medical Center, discusses some exceptions.
Adam E. Fall, MD, SFHM, who recently worked as the senior regional medical director for hospital medicine at TeamHealth in Chattanooga, Tenn., discusses the importance of allowing nuance and gradation to govern patient care in the treatment of thromboembolism in an era where hospitalists can be overly reliant on electronic medical records.
Adam E. Fall, MD, SFHM, who recently worked as the senior regional medical director for hospital medicine at TeamHealth in Chattanooga, Tenn., discusses the importance of allowing nuance and gradation to govern patient care in the treatment of thromboembolism in an era where hospitalists can be overly reliant on electronic medical records.
Adam E. Fall, MD, SFHM, who recently worked as the senior regional medical director for hospital medicine at TeamHealth in Chattanooga, Tenn., discusses the importance of allowing nuance and gradation to govern patient care in the treatment of thromboembolism in an era where hospitalists can be overly reliant on electronic medical records.
David Lichtman, PA, director of the Johns Hopkins Central Procedure Service in Baltimore, Md., says bedside procedure training should be consistent and thorough, regardless of whether the trainee is a medical student, a resident, a fellow, or an established physician. He is a strong advocate for training that includes well-designed computer coursework, evaluates practitioners from start to finish, and demonstrates that they are meeting established benchmarks.
“That’s what keeps patients safe,” he says.
Experienced, capable, and proven educators are also critical.
“Let’s face it: Not everybody is a very good teacher,” he adds.
Currently, many medical residents can do rotations that will give them hands-on experience. But some physicians question why certain procedures are still being taught to internal medicine residents if the ABIM no longer requires hands-on experience. Other programs may simply lack the resources, including experienced supervisors, to provide proper training.
The demand for more training is clearly there, however. Sally Wang, MD, FHM, director of procedure education at Brigham and Women’s Hospital and a clinical instructor at Harvard Medical School in Boston, co-leads the procedures pre-course at the SHM annual meeting. She compares the logistically complicated event to throwing a wedding. It consistently sells out despite having doubled in size, to 60 slots for a basic procedure course and 60 slots for a second course that emphasizes ultrasound. At the HM14 pre-course in Las Vegas, Dr. Wang counted enough people on the waiting list to fill an additional course.
“It was mind-boggling,” she says.
Several companies have taken notice of the pent-up demand and are offering their own courses and workshops. Joshua Lenchus, DO, RPh, FACP, SFHM, medical director of the University of Miami-Jackson Memorial Hospital’s procedure service, and others see many of these offerings as introductions only, however. At the University of Miami, he says, his rigorous, simulation-based invasive bedside procedures curriculum is mandatory for all internal medicine residents. The curriculum includes central line, thoracentesis, paracentesis, lumbar puncture, and sometimes arthrocentesis as its core procedures, though Dr. Lenchus says others can easily be added. This fall, for instance, he plans to add chest tube and arterial line placement.
He notes a dramatic reduction in central line placement and thoracentesis complications after his team began performing them to the “four pillars” of his program. Rigorous simulation-based training, strict adherence to a critical skills checklist, consistent use of ultrasound, and direct supervision can form a very effective bundle of safety measures, he says, just like a combination of seat belts, speed reduction, and other precautions can lead to fewer automobile-associated injuries and deaths. TH
David Lichtman, PA, director of the Johns Hopkins Central Procedure Service in Baltimore, Md., says bedside procedure training should be consistent and thorough, regardless of whether the trainee is a medical student, a resident, a fellow, or an established physician. He is a strong advocate for training that includes well-designed computer coursework, evaluates practitioners from start to finish, and demonstrates that they are meeting established benchmarks.
“That’s what keeps patients safe,” he says.
Experienced, capable, and proven educators are also critical.
“Let’s face it: Not everybody is a very good teacher,” he adds.
Currently, many medical residents can do rotations that will give them hands-on experience. But some physicians question why certain procedures are still being taught to internal medicine residents if the ABIM no longer requires hands-on experience. Other programs may simply lack the resources, including experienced supervisors, to provide proper training.
The demand for more training is clearly there, however. Sally Wang, MD, FHM, director of procedure education at Brigham and Women’s Hospital and a clinical instructor at Harvard Medical School in Boston, co-leads the procedures pre-course at the SHM annual meeting. She compares the logistically complicated event to throwing a wedding. It consistently sells out despite having doubled in size, to 60 slots for a basic procedure course and 60 slots for a second course that emphasizes ultrasound. At the HM14 pre-course in Las Vegas, Dr. Wang counted enough people on the waiting list to fill an additional course.
“It was mind-boggling,” she says.
Several companies have taken notice of the pent-up demand and are offering their own courses and workshops. Joshua Lenchus, DO, RPh, FACP, SFHM, medical director of the University of Miami-Jackson Memorial Hospital’s procedure service, and others see many of these offerings as introductions only, however. At the University of Miami, he says, his rigorous, simulation-based invasive bedside procedures curriculum is mandatory for all internal medicine residents. The curriculum includes central line, thoracentesis, paracentesis, lumbar puncture, and sometimes arthrocentesis as its core procedures, though Dr. Lenchus says others can easily be added. This fall, for instance, he plans to add chest tube and arterial line placement.
He notes a dramatic reduction in central line placement and thoracentesis complications after his team began performing them to the “four pillars” of his program. Rigorous simulation-based training, strict adherence to a critical skills checklist, consistent use of ultrasound, and direct supervision can form a very effective bundle of safety measures, he says, just like a combination of seat belts, speed reduction, and other precautions can lead to fewer automobile-associated injuries and deaths. TH
David Lichtman, PA, director of the Johns Hopkins Central Procedure Service in Baltimore, Md., says bedside procedure training should be consistent and thorough, regardless of whether the trainee is a medical student, a resident, a fellow, or an established physician. He is a strong advocate for training that includes well-designed computer coursework, evaluates practitioners from start to finish, and demonstrates that they are meeting established benchmarks.
“That’s what keeps patients safe,” he says.
Experienced, capable, and proven educators are also critical.
“Let’s face it: Not everybody is a very good teacher,” he adds.
Currently, many medical residents can do rotations that will give them hands-on experience. But some physicians question why certain procedures are still being taught to internal medicine residents if the ABIM no longer requires hands-on experience. Other programs may simply lack the resources, including experienced supervisors, to provide proper training.
The demand for more training is clearly there, however. Sally Wang, MD, FHM, director of procedure education at Brigham and Women’s Hospital and a clinical instructor at Harvard Medical School in Boston, co-leads the procedures pre-course at the SHM annual meeting. She compares the logistically complicated event to throwing a wedding. It consistently sells out despite having doubled in size, to 60 slots for a basic procedure course and 60 slots for a second course that emphasizes ultrasound. At the HM14 pre-course in Las Vegas, Dr. Wang counted enough people on the waiting list to fill an additional course.
“It was mind-boggling,” she says.
Several companies have taken notice of the pent-up demand and are offering their own courses and workshops. Joshua Lenchus, DO, RPh, FACP, SFHM, medical director of the University of Miami-Jackson Memorial Hospital’s procedure service, and others see many of these offerings as introductions only, however. At the University of Miami, he says, his rigorous, simulation-based invasive bedside procedures curriculum is mandatory for all internal medicine residents. The curriculum includes central line, thoracentesis, paracentesis, lumbar puncture, and sometimes arthrocentesis as its core procedures, though Dr. Lenchus says others can easily be added. This fall, for instance, he plans to add chest tube and arterial line placement.
He notes a dramatic reduction in central line placement and thoracentesis complications after his team began performing them to the “four pillars” of his program. Rigorous simulation-based training, strict adherence to a critical skills checklist, consistent use of ultrasound, and direct supervision can form a very effective bundle of safety measures, he says, just like a combination of seat belts, speed reduction, and other precautions can lead to fewer automobile-associated injuries and deaths. TH