User login
Key Keynotes

The 10-year anniversary of SHM was an occasion not for looking back on the first decade of the organization, but for looking ahead.
In addition to seven tracks of educational sessions and ample opportunities for networking, SHM’s 10th Annual Meeting, held May 23-25 in Dallas, provided opportunities to get a big-picture glimpse into the future of hospital medicine, in the form of some eye-opening plenary sessions.
Coming Soon: Hospital Medicine Certification
Annual Meeting attendees heard from Robert M. Wachter, MD, and past-SHM President Mary Jo Gorman, MD, MBA, on “Certification in Hospital Medicine: What Does This Mean to Hospitalists? To Employers? To Patients?” The two outlined how the American Board of Internal Medicine (ABIM) is developing a Focused Recognition for Hospital Medicine through its Maintenance of Certification (MOC) system.
Dr. Wachter, who chairs the ABIM Committee on Hospital Medicine Focused Recognition, explained that the focused recognition would give hospitalists a formal credential that recognizes hospital medicine as a distinct field within internal medicine. This is the first time ABIM has offered focused recognition for any subset of internal medicine—and, if approved, the first time the umbrella organization, the American Board of Medical Specialties (ABMS), will offer a focused recognition for a subset of any specialty.
“This is a brand new idea,” stressed Dr. Wachter. “One of the exciting things—the challenging things—is that this is a first step toward the broader issue of how to certify based on experience rather than just training.”
A Look at Digital Medicine
Informally known as the “health technology czar,” David J. Brailer, MD, PhD, served as the first national coordinator for Health Information Technology, at the Department of Health and Human Services until he resigned in April 2006. He is vice chairman of the American Health Information Community, and based on his plenary session “Health Care’s Digital Era: Implications for Hospitalists,” he is obviously familiar with hospital medicine.
“Hospitalists and health IT are co-factors in the same equation of change in healthcare,” said Dr. Brailer. “I can’t see how one can exist without the other.”
He went on to explain that hospitals must lead the way for digital medicine, as they are the institutions with the most opportunity for cost reductions in healthcare, the most opportunity for error reduction (“I’m not saying hospitals have the most errors, but that the corporatized process allows them to reduce errors that occur there,” he clarified), and the best site for innovation to move to a virtual model such as e-ICUs and new tele-specialties.
“And who can we turn to who ‘gets it,’ who can make all this happen?” asked Dr. Brailer of the innovations. “It won’t be the cardiologists, or the emergency department doctors. The obvious answer is that it will be the hospitalists.”
He warned that in order for hospitalists to be change agents, they must first take on the role of leaders of other doctors in inpatient care. “Some [hospitalists] don’t want to take on this role; others are already doing it,” he said. “I think that doctors need this leadership and I can’t think of a better group to do it than hospitalists. They’re going to have to step up to the plate on this.”
Dr. Brailer listed big issues coming up for hospitals, predicting that they will become “the hub of chronic-care management, leaders in adopting state-of-the-art technology, and leaders in quality improvement. Hospitalists are attached to each of these.” He explained that in chronic-care management, patients with chronic illnesses are cared for in a continuum-based way. Currently, inpatient care is the anchor not just for treatment, but for monitoring weight or assessing daily function levels. With chronic-care management, doctors can monitor patients without having them come into the office or the hospital.
“Primary-care doctors won’t be able to perform this off-site monitoring; they don’t have the time or the infrastructure,” explained Dr. Brailer. “But this is exactly what hospitals already do. Electronic monitoring is a real opportunity for them—and for hospitalists—to expand their care offerings.”
In spite of this expansion, he warned that hospitals will be in danger if they don’t change with the times. “The world is moving away from hospital-based care and toward [patient]-centered care,” he stated. “This is apparent in the current push for portability of patient-care information, and in today’s healthcare transparency issues. These are not hospital-friendly measures; in fact, they threaten hospitals to some degree. I hope that these trends will challenge hospitals to question how changes apply to them.”
Dr. Brailer ended with an update on public policy regarding healthcare—not a pretty picture from his insider’s view.
“Not much will happen in the next two years,” he predicted. “The FDA will pass the Prescription Drug User Fee program, and SCHIP [State Children’s Health Insurance Program] will pass in Washington D.C. I don’t think anything else will make it through the thicket of everything else going on.”
He also warned that regardless of who the next president of the U.S. is, nothing much will happen with healthcare reform. “It’s a high-priority item, but not high enough to warrant significant attention,” he said. “In the long term, it will get major attention, but probably only as a result of a catastrophe.”
Factors That Will Shape Our Future
On Friday morning, attendees heard from Jonathan B. Perlin, MD, PhD, MSHA, former under secretary for health at the Veterans Affairs, and currently the chief medical officer and senior vice-president of quality for Hospital Corporation of America (HCA) in Nashville, Tenn.—the nation’s largest hospital group.
In presenting, “Healthcare 2015: Challenges and Opportunities in the Decade Ahead,” Dr. Perlin threaded together the factors that will drive healthcare to a new level in the next eight years: the health needs of the population, including aging and the complications of diabetes, the increased requirements for delivering value, the economic pressures, and the technological changes and decentralization of healthcare delivery. Dr. Perlin, a leader in healthcare transformation and health information technology who has been termed a “clinical futurist,” pointed out that the result of these factors will be a transformation from an industrial to an information age model of healthcare.
Dr. Perlin traced the path being shaped by these challenges and opportunities, explaining that the economics of healthcare are creating pressure on the environment and disrupting the status quo. “Costs are increasing rapidly,” he stated. “It’s pretty clear that we’ve already hit some statutory alarms in the Medicare trust fund. Estimates now indicate that the trust fund will be bankrupt by 2018; we can either limit what we do or we can find better value in delivery of care.”
Response to economic pressure by Medicare and private insurers, said Dr. Perlin, provides a construct for change.
“The private sector, the government, and employers are all saying that we’re not going to buy units of healthcare services any more, we’re going to buy outcomes,” stressed Dr. Perlin. “The result is that performance becomes a gate function for even doing business in the new world.”
Toying with modest incentives in current pay-for-performance models will soon be trumped. “Medicare is changing from an incentive for simply reporting [with the current “Reporting Hospital Quality Data for Annual Payment Update” program] to value-based purchasing,” Dr. Perlin pointed out. Similarly, private insurers are differentiating performance levels and using lower co-pays to direct patients to better performers and high co-pays to redirect patients away from lower performers.
To participate in this new world of value-based purchasing and what Dr. Perlin termed “tiering and steering,” the healthcare industry must reorganize ways that it has traditionally provided care. Pen and paper are replaced by electronic health records. A locus of care is replaced by an interoperable, coordinated cooperative information network.
“The patient is the point of care in the new system, whether supported by glucometers that feed data into a central system,” said Dr. Perlin, “or a heart failure patient is tracked after discharge with a digital scale … or whether it is a hospitalist who reaches into the traditional healthcare setting with remote monitoring to provide round-the-clock support to a critically ill patient.”
In addition to providing enhanced safety, quality, continuity, and efficiency, new systems like these will provide central information sources, powerful in providing real-time, clinical decision-support, as well as generating new knowledge about disease, treatment and service delivery. The tremendous data available will reveal previously unnoticed patterns and provide more support for evidence-based care.
“Medicare and private insurers are focusing more on evidence-based care and are increasingly ambivalent about decisions not supported by evidence,” observed Dr. Perlin.
His view of the near future of healthcare was followed later that day with another plenary session that mulled how hospital medicine might look a decade from now.
Now It’s Time to Say Goodbye …
Dr. Wachter traditionally closes each Annual Meeting with a review of how far the young field of hospital medicine has come.
But at the 10th Annual Meeting, Dr. Wachter chose not to look back but to peer into his crystal ball. His presentation, “The Hospitalist Movement Two Decades Later: A Letter from the Future,” took the form of a letter from his future self, written in 2017, to SHM CEO Larry Wellikson, MD, as each man settles into a long-term care facility.
Dr. Wachter outlined the major forces starting to affect hospital medicine and imagined where they would lead us. And he couldn’t resist one glimpse back in time: “Think about the change we’ve seen already,” he marveled. “There’s no field in modern medical history that’s grown this quickly. We’re both leading the way and riding the waves.”
Dr. Wachter admitted his initial estimates for phenomenal growth of the field are already surpassed. “We originally projected that there would be 20,000 or 30,000 hospitalists,” he said. “Well, we’re already over 20,000. Now I’m thinking the final number will be around 50,000 or 60,000.”
He attributed part of that growth to several changes, including the additional responsibility of hospitalists for caring for surgical patients—something he sees as eventually becoming the norm. Another factor is the role hospitalists play in replacing residents in teaching hospitals, an area that has seen unplanned growth.
And finally, Dr. Wachter speculated that the quality measures movement will also boost the ranks of hospitalists. “We’re already seeing tremendous pressure on hospitalists to help their hospitals achieve success in pay-for-performance programs and in publicly reported measures,” he said. “This type of responsibility was originally considered a nice add-on for using hospitalists, but now it’s getting to be a crucial part. There’s a building expectation that hospitalists will guarantee superb performance.”
Dr. Wachter also touched on how information technology might change hospital medicine. “IT will definitely have an impact, in some exciting ways, and in other ways that have not been thought through,” he warned. “For example, consultation may be very different.” For example, a hospitalist in 2017 may be able to use a video link at a patient’s bedside to consult with one of 100 cardiologists around the country or around the world.
Following Dr. Wachter’s view of the future, Sylvia C. McKean, MD, had the last word at the meeting. As the chair in charge of next year’s Annual Meeting in San Diego, she presented the wrap-up on Friday afternoon, covering “What Have We Learned.”
Looking back on the previous three days, Dr. McKean pronounced, “The future is now.” Pointing to the number of meeting sessions, abstracts and poster presentations that emphasized recent innovations in hospital medicine, she said, “The Annual Meeting helps us find our expertise as hospitalists.” The Annual Meeting, along with SHM’s published Core Competencies helps define the role that hospitalists play in patient-centered care and in patient safety.
Dr. McKean thanked Chad Whelan, chair of the Annual Meeting Committee, for all his work, and said she was looking forward to 2008.
SHM Elects New Members to Board of Directors
Two new members announced; one member re-elected
SHM is pleased to announce the election of Joseph Li, MD, and Mahalakshmi Halasyamani, MD, and the re-election of Patrick Cawley, MD, to its board of directors for terms that began at the SHM Annual Meeting May 23-25 in Dallas.
“One of the strengths that keeps SHM on the cutting edge is the infusion of new talent on the board. SHM is fortunate to have a continued source of hospitalist leaders who willingly share their time and talents to help SHM shape and grow the hospital medicine specialty,” says Larry Wellikson, MD, CEO of SHM.
Each of the newly elected SHM board members comes from distinguished programs and institutions.

Dr. Li is the director of the hospital medicine program at Beth Israel Deaconess Medical Center in Boston and an assistant professor of medicine at the Harvard Medical School. He has been an active member of SHM, serving on the Education and Annual Meeting Committees, as well as the Procedures Task Force. Dr. Li earned his bachelor’s degree in pharmacy at the University of Oklahoma College of Pharmacy and his medical degree at the University of Oklahoma College of Medicine. He completed his residency at the Beth Israel Deaconess Medical Center.

Dr. Cawley is executive medical director at the Medical University Hospital of South Carolina. Prior to this, he was chief of staff at Conway Medical Center, S.C. He has served on the SHM board of directors since 2004 and is its treasurer. As an active member of SHM, he serves on the Public Policy Committee, Leadership Task Force, and on the advisory board for the Practice Management and Coding Courses. Dr. Cawley earned his bachelor’s degree in biology and chemistry from the University of Scranton (Penn.) and his medical degree from Georgetown University School of Medicine in Wash., D.C. He completed his residency at the Duke University Medical Center in Durham, N.C.

Dr. Halasyamani is the medical director of the heart failure program at Saint Joseph Mercy Hospital in Ann Arbor, Mich. Before that, she served as director of academic internal medicine inpatient services. She is also a clinical instructor of internal medicine at the University of Michigan and associate chair of the department of internal medicine at Saint Joseph Mercy Hospital. Dr. Halasyamani earned her bachelor’s degree in English and chemistry from Saint Louis University (Mo.) and her medical degree from Harvard Medical School, Boston. She completed her residency at Brigham and Women’s Hospital.
Congratulations to the newest members of the SHM Board of Directors.
The 10-year anniversary of SHM was an occasion not for looking back on the first decade of the organization, but for looking ahead.
In addition to seven tracks of educational sessions and ample opportunities for networking, SHM’s 10th Annual Meeting, held May 23-25 in Dallas, provided opportunities to get a big-picture glimpse into the future of hospital medicine, in the form of some eye-opening plenary sessions.
Coming Soon: Hospital Medicine Certification
Annual Meeting attendees heard from Robert M. Wachter, MD, and past-SHM President Mary Jo Gorman, MD, MBA, on “Certification in Hospital Medicine: What Does This Mean to Hospitalists? To Employers? To Patients?” The two outlined how the American Board of Internal Medicine (ABIM) is developing a Focused Recognition for Hospital Medicine through its Maintenance of Certification (MOC) system.
Dr. Wachter, who chairs the ABIM Committee on Hospital Medicine Focused Recognition, explained that the focused recognition would give hospitalists a formal credential that recognizes hospital medicine as a distinct field within internal medicine. This is the first time ABIM has offered focused recognition for any subset of internal medicine—and, if approved, the first time the umbrella organization, the American Board of Medical Specialties (ABMS), will offer a focused recognition for a subset of any specialty.
“This is a brand new idea,” stressed Dr. Wachter. “One of the exciting things—the challenging things—is that this is a first step toward the broader issue of how to certify based on experience rather than just training.”
A Look at Digital Medicine
Informally known as the “health technology czar,” David J. Brailer, MD, PhD, served as the first national coordinator for Health Information Technology, at the Department of Health and Human Services until he resigned in April 2006. He is vice chairman of the American Health Information Community, and based on his plenary session “Health Care’s Digital Era: Implications for Hospitalists,” he is obviously familiar with hospital medicine.
“Hospitalists and health IT are co-factors in the same equation of change in healthcare,” said Dr. Brailer. “I can’t see how one can exist without the other.”
He went on to explain that hospitals must lead the way for digital medicine, as they are the institutions with the most opportunity for cost reductions in healthcare, the most opportunity for error reduction (“I’m not saying hospitals have the most errors, but that the corporatized process allows them to reduce errors that occur there,” he clarified), and the best site for innovation to move to a virtual model such as e-ICUs and new tele-specialties.
“And who can we turn to who ‘gets it,’ who can make all this happen?” asked Dr. Brailer of the innovations. “It won’t be the cardiologists, or the emergency department doctors. The obvious answer is that it will be the hospitalists.”
He warned that in order for hospitalists to be change agents, they must first take on the role of leaders of other doctors in inpatient care. “Some [hospitalists] don’t want to take on this role; others are already doing it,” he said. “I think that doctors need this leadership and I can’t think of a better group to do it than hospitalists. They’re going to have to step up to the plate on this.”
Dr. Brailer listed big issues coming up for hospitals, predicting that they will become “the hub of chronic-care management, leaders in adopting state-of-the-art technology, and leaders in quality improvement. Hospitalists are attached to each of these.” He explained that in chronic-care management, patients with chronic illnesses are cared for in a continuum-based way. Currently, inpatient care is the anchor not just for treatment, but for monitoring weight or assessing daily function levels. With chronic-care management, doctors can monitor patients without having them come into the office or the hospital.
“Primary-care doctors won’t be able to perform this off-site monitoring; they don’t have the time or the infrastructure,” explained Dr. Brailer. “But this is exactly what hospitals already do. Electronic monitoring is a real opportunity for them—and for hospitalists—to expand their care offerings.”
In spite of this expansion, he warned that hospitals will be in danger if they don’t change with the times. “The world is moving away from hospital-based care and toward [patient]-centered care,” he stated. “This is apparent in the current push for portability of patient-care information, and in today’s healthcare transparency issues. These are not hospital-friendly measures; in fact, they threaten hospitals to some degree. I hope that these trends will challenge hospitals to question how changes apply to them.”
Dr. Brailer ended with an update on public policy regarding healthcare—not a pretty picture from his insider’s view.
“Not much will happen in the next two years,” he predicted. “The FDA will pass the Prescription Drug User Fee program, and SCHIP [State Children’s Health Insurance Program] will pass in Washington D.C. I don’t think anything else will make it through the thicket of everything else going on.”
He also warned that regardless of who the next president of the U.S. is, nothing much will happen with healthcare reform. “It’s a high-priority item, but not high enough to warrant significant attention,” he said. “In the long term, it will get major attention, but probably only as a result of a catastrophe.”
Factors That Will Shape Our Future
On Friday morning, attendees heard from Jonathan B. Perlin, MD, PhD, MSHA, former under secretary for health at the Veterans Affairs, and currently the chief medical officer and senior vice-president of quality for Hospital Corporation of America (HCA) in Nashville, Tenn.—the nation’s largest hospital group.
In presenting, “Healthcare 2015: Challenges and Opportunities in the Decade Ahead,” Dr. Perlin threaded together the factors that will drive healthcare to a new level in the next eight years: the health needs of the population, including aging and the complications of diabetes, the increased requirements for delivering value, the economic pressures, and the technological changes and decentralization of healthcare delivery. Dr. Perlin, a leader in healthcare transformation and health information technology who has been termed a “clinical futurist,” pointed out that the result of these factors will be a transformation from an industrial to an information age model of healthcare.
Dr. Perlin traced the path being shaped by these challenges and opportunities, explaining that the economics of healthcare are creating pressure on the environment and disrupting the status quo. “Costs are increasing rapidly,” he stated. “It’s pretty clear that we’ve already hit some statutory alarms in the Medicare trust fund. Estimates now indicate that the trust fund will be bankrupt by 2018; we can either limit what we do or we can find better value in delivery of care.”
Response to economic pressure by Medicare and private insurers, said Dr. Perlin, provides a construct for change.
“The private sector, the government, and employers are all saying that we’re not going to buy units of healthcare services any more, we’re going to buy outcomes,” stressed Dr. Perlin. “The result is that performance becomes a gate function for even doing business in the new world.”
Toying with modest incentives in current pay-for-performance models will soon be trumped. “Medicare is changing from an incentive for simply reporting [with the current “Reporting Hospital Quality Data for Annual Payment Update” program] to value-based purchasing,” Dr. Perlin pointed out. Similarly, private insurers are differentiating performance levels and using lower co-pays to direct patients to better performers and high co-pays to redirect patients away from lower performers.
To participate in this new world of value-based purchasing and what Dr. Perlin termed “tiering and steering,” the healthcare industry must reorganize ways that it has traditionally provided care. Pen and paper are replaced by electronic health records. A locus of care is replaced by an interoperable, coordinated cooperative information network.
“The patient is the point of care in the new system, whether supported by glucometers that feed data into a central system,” said Dr. Perlin, “or a heart failure patient is tracked after discharge with a digital scale … or whether it is a hospitalist who reaches into the traditional healthcare setting with remote monitoring to provide round-the-clock support to a critically ill patient.”
In addition to providing enhanced safety, quality, continuity, and efficiency, new systems like these will provide central information sources, powerful in providing real-time, clinical decision-support, as well as generating new knowledge about disease, treatment and service delivery. The tremendous data available will reveal previously unnoticed patterns and provide more support for evidence-based care.
“Medicare and private insurers are focusing more on evidence-based care and are increasingly ambivalent about decisions not supported by evidence,” observed Dr. Perlin.
His view of the near future of healthcare was followed later that day with another plenary session that mulled how hospital medicine might look a decade from now.
Now It’s Time to Say Goodbye …
Dr. Wachter traditionally closes each Annual Meeting with a review of how far the young field of hospital medicine has come.
But at the 10th Annual Meeting, Dr. Wachter chose not to look back but to peer into his crystal ball. His presentation, “The Hospitalist Movement Two Decades Later: A Letter from the Future,” took the form of a letter from his future self, written in 2017, to SHM CEO Larry Wellikson, MD, as each man settles into a long-term care facility.
Dr. Wachter outlined the major forces starting to affect hospital medicine and imagined where they would lead us. And he couldn’t resist one glimpse back in time: “Think about the change we’ve seen already,” he marveled. “There’s no field in modern medical history that’s grown this quickly. We’re both leading the way and riding the waves.”
Dr. Wachter admitted his initial estimates for phenomenal growth of the field are already surpassed. “We originally projected that there would be 20,000 or 30,000 hospitalists,” he said. “Well, we’re already over 20,000. Now I’m thinking the final number will be around 50,000 or 60,000.”
He attributed part of that growth to several changes, including the additional responsibility of hospitalists for caring for surgical patients—something he sees as eventually becoming the norm. Another factor is the role hospitalists play in replacing residents in teaching hospitals, an area that has seen unplanned growth.
And finally, Dr. Wachter speculated that the quality measures movement will also boost the ranks of hospitalists. “We’re already seeing tremendous pressure on hospitalists to help their hospitals achieve success in pay-for-performance programs and in publicly reported measures,” he said. “This type of responsibility was originally considered a nice add-on for using hospitalists, but now it’s getting to be a crucial part. There’s a building expectation that hospitalists will guarantee superb performance.”
Dr. Wachter also touched on how information technology might change hospital medicine. “IT will definitely have an impact, in some exciting ways, and in other ways that have not been thought through,” he warned. “For example, consultation may be very different.” For example, a hospitalist in 2017 may be able to use a video link at a patient’s bedside to consult with one of 100 cardiologists around the country or around the world.
Following Dr. Wachter’s view of the future, Sylvia C. McKean, MD, had the last word at the meeting. As the chair in charge of next year’s Annual Meeting in San Diego, she presented the wrap-up on Friday afternoon, covering “What Have We Learned.”
Looking back on the previous three days, Dr. McKean pronounced, “The future is now.” Pointing to the number of meeting sessions, abstracts and poster presentations that emphasized recent innovations in hospital medicine, she said, “The Annual Meeting helps us find our expertise as hospitalists.” The Annual Meeting, along with SHM’s published Core Competencies helps define the role that hospitalists play in patient-centered care and in patient safety.
Dr. McKean thanked Chad Whelan, chair of the Annual Meeting Committee, for all his work, and said she was looking forward to 2008.
SHM Elects New Members to Board of Directors
Two new members announced; one member re-elected
SHM is pleased to announce the election of Joseph Li, MD, and Mahalakshmi Halasyamani, MD, and the re-election of Patrick Cawley, MD, to its board of directors for terms that began at the SHM Annual Meeting May 23-25 in Dallas.
“One of the strengths that keeps SHM on the cutting edge is the infusion of new talent on the board. SHM is fortunate to have a continued source of hospitalist leaders who willingly share their time and talents to help SHM shape and grow the hospital medicine specialty,” says Larry Wellikson, MD, CEO of SHM.
Each of the newly elected SHM board members comes from distinguished programs and institutions.
Dr. Li is the director of the hospital medicine program at Beth Israel Deaconess Medical Center in Boston and an assistant professor of medicine at the Harvard Medical School. He has been an active member of SHM, serving on the Education and Annual Meeting Committees, as well as the Procedures Task Force. Dr. Li earned his bachelor’s degree in pharmacy at the University of Oklahoma College of Pharmacy and his medical degree at the University of Oklahoma College of Medicine. He completed his residency at the Beth Israel Deaconess Medical Center.
Dr. Cawley is executive medical director at the Medical University Hospital of South Carolina. Prior to this, he was chief of staff at Conway Medical Center, S.C. He has served on the SHM board of directors since 2004 and is its treasurer. As an active member of SHM, he serves on the Public Policy Committee, Leadership Task Force, and on the advisory board for the Practice Management and Coding Courses. Dr. Cawley earned his bachelor’s degree in biology and chemistry from the University of Scranton (Penn.) and his medical degree from Georgetown University School of Medicine in Wash., D.C. He completed his residency at the Duke University Medical Center in Durham, N.C.
Dr. Halasyamani is the medical director of the heart failure program at Saint Joseph Mercy Hospital in Ann Arbor, Mich. Before that, she served as director of academic internal medicine inpatient services. She is also a clinical instructor of internal medicine at the University of Michigan and associate chair of the department of internal medicine at Saint Joseph Mercy Hospital. Dr. Halasyamani earned her bachelor’s degree in English and chemistry from Saint Louis University (Mo.) and her medical degree from Harvard Medical School, Boston. She completed her residency at Brigham and Women’s Hospital.
Congratulations to the newest members of the SHM Board of Directors.
The 10-year anniversary of SHM was an occasion not for looking back on the first decade of the organization, but for looking ahead.
In addition to seven tracks of educational sessions and ample opportunities for networking, SHM’s 10th Annual Meeting, held May 23-25 in Dallas, provided opportunities to get a big-picture glimpse into the future of hospital medicine, in the form of some eye-opening plenary sessions.
Coming Soon: Hospital Medicine Certification
Annual Meeting attendees heard from Robert M. Wachter, MD, and past-SHM President Mary Jo Gorman, MD, MBA, on “Certification in Hospital Medicine: What Does This Mean to Hospitalists? To Employers? To Patients?” The two outlined how the American Board of Internal Medicine (ABIM) is developing a Focused Recognition for Hospital Medicine through its Maintenance of Certification (MOC) system.
Dr. Wachter, who chairs the ABIM Committee on Hospital Medicine Focused Recognition, explained that the focused recognition would give hospitalists a formal credential that recognizes hospital medicine as a distinct field within internal medicine. This is the first time ABIM has offered focused recognition for any subset of internal medicine—and, if approved, the first time the umbrella organization, the American Board of Medical Specialties (ABMS), will offer a focused recognition for a subset of any specialty.
“This is a brand new idea,” stressed Dr. Wachter. “One of the exciting things—the challenging things—is that this is a first step toward the broader issue of how to certify based on experience rather than just training.”
A Look at Digital Medicine
Informally known as the “health technology czar,” David J. Brailer, MD, PhD, served as the first national coordinator for Health Information Technology, at the Department of Health and Human Services until he resigned in April 2006. He is vice chairman of the American Health Information Community, and based on his plenary session “Health Care’s Digital Era: Implications for Hospitalists,” he is obviously familiar with hospital medicine.
“Hospitalists and health IT are co-factors in the same equation of change in healthcare,” said Dr. Brailer. “I can’t see how one can exist without the other.”
He went on to explain that hospitals must lead the way for digital medicine, as they are the institutions with the most opportunity for cost reductions in healthcare, the most opportunity for error reduction (“I’m not saying hospitals have the most errors, but that the corporatized process allows them to reduce errors that occur there,” he clarified), and the best site for innovation to move to a virtual model such as e-ICUs and new tele-specialties.
“And who can we turn to who ‘gets it,’ who can make all this happen?” asked Dr. Brailer of the innovations. “It won’t be the cardiologists, or the emergency department doctors. The obvious answer is that it will be the hospitalists.”
He warned that in order for hospitalists to be change agents, they must first take on the role of leaders of other doctors in inpatient care. “Some [hospitalists] don’t want to take on this role; others are already doing it,” he said. “I think that doctors need this leadership and I can’t think of a better group to do it than hospitalists. They’re going to have to step up to the plate on this.”
Dr. Brailer listed big issues coming up for hospitals, predicting that they will become “the hub of chronic-care management, leaders in adopting state-of-the-art technology, and leaders in quality improvement. Hospitalists are attached to each of these.” He explained that in chronic-care management, patients with chronic illnesses are cared for in a continuum-based way. Currently, inpatient care is the anchor not just for treatment, but for monitoring weight or assessing daily function levels. With chronic-care management, doctors can monitor patients without having them come into the office or the hospital.
“Primary-care doctors won’t be able to perform this off-site monitoring; they don’t have the time or the infrastructure,” explained Dr. Brailer. “But this is exactly what hospitals already do. Electronic monitoring is a real opportunity for them—and for hospitalists—to expand their care offerings.”
In spite of this expansion, he warned that hospitals will be in danger if they don’t change with the times. “The world is moving away from hospital-based care and toward [patient]-centered care,” he stated. “This is apparent in the current push for portability of patient-care information, and in today’s healthcare transparency issues. These are not hospital-friendly measures; in fact, they threaten hospitals to some degree. I hope that these trends will challenge hospitals to question how changes apply to them.”
Dr. Brailer ended with an update on public policy regarding healthcare—not a pretty picture from his insider’s view.
“Not much will happen in the next two years,” he predicted. “The FDA will pass the Prescription Drug User Fee program, and SCHIP [State Children’s Health Insurance Program] will pass in Washington D.C. I don’t think anything else will make it through the thicket of everything else going on.”
He also warned that regardless of who the next president of the U.S. is, nothing much will happen with healthcare reform. “It’s a high-priority item, but not high enough to warrant significant attention,” he said. “In the long term, it will get major attention, but probably only as a result of a catastrophe.”
Factors That Will Shape Our Future
On Friday morning, attendees heard from Jonathan B. Perlin, MD, PhD, MSHA, former under secretary for health at the Veterans Affairs, and currently the chief medical officer and senior vice-president of quality for Hospital Corporation of America (HCA) in Nashville, Tenn.—the nation’s largest hospital group.
In presenting, “Healthcare 2015: Challenges and Opportunities in the Decade Ahead,” Dr. Perlin threaded together the factors that will drive healthcare to a new level in the next eight years: the health needs of the population, including aging and the complications of diabetes, the increased requirements for delivering value, the economic pressures, and the technological changes and decentralization of healthcare delivery. Dr. Perlin, a leader in healthcare transformation and health information technology who has been termed a “clinical futurist,” pointed out that the result of these factors will be a transformation from an industrial to an information age model of healthcare.
Dr. Perlin traced the path being shaped by these challenges and opportunities, explaining that the economics of healthcare are creating pressure on the environment and disrupting the status quo. “Costs are increasing rapidly,” he stated. “It’s pretty clear that we’ve already hit some statutory alarms in the Medicare trust fund. Estimates now indicate that the trust fund will be bankrupt by 2018; we can either limit what we do or we can find better value in delivery of care.”
Response to economic pressure by Medicare and private insurers, said Dr. Perlin, provides a construct for change.
“The private sector, the government, and employers are all saying that we’re not going to buy units of healthcare services any more, we’re going to buy outcomes,” stressed Dr. Perlin. “The result is that performance becomes a gate function for even doing business in the new world.”
Toying with modest incentives in current pay-for-performance models will soon be trumped. “Medicare is changing from an incentive for simply reporting [with the current “Reporting Hospital Quality Data for Annual Payment Update” program] to value-based purchasing,” Dr. Perlin pointed out. Similarly, private insurers are differentiating performance levels and using lower co-pays to direct patients to better performers and high co-pays to redirect patients away from lower performers.
To participate in this new world of value-based purchasing and what Dr. Perlin termed “tiering and steering,” the healthcare industry must reorganize ways that it has traditionally provided care. Pen and paper are replaced by electronic health records. A locus of care is replaced by an interoperable, coordinated cooperative information network.
“The patient is the point of care in the new system, whether supported by glucometers that feed data into a central system,” said Dr. Perlin, “or a heart failure patient is tracked after discharge with a digital scale … or whether it is a hospitalist who reaches into the traditional healthcare setting with remote monitoring to provide round-the-clock support to a critically ill patient.”
In addition to providing enhanced safety, quality, continuity, and efficiency, new systems like these will provide central information sources, powerful in providing real-time, clinical decision-support, as well as generating new knowledge about disease, treatment and service delivery. The tremendous data available will reveal previously unnoticed patterns and provide more support for evidence-based care.
“Medicare and private insurers are focusing more on evidence-based care and are increasingly ambivalent about decisions not supported by evidence,” observed Dr. Perlin.
His view of the near future of healthcare was followed later that day with another plenary session that mulled how hospital medicine might look a decade from now.
Now It’s Time to Say Goodbye …
Dr. Wachter traditionally closes each Annual Meeting with a review of how far the young field of hospital medicine has come.
But at the 10th Annual Meeting, Dr. Wachter chose not to look back but to peer into his crystal ball. His presentation, “The Hospitalist Movement Two Decades Later: A Letter from the Future,” took the form of a letter from his future self, written in 2017, to SHM CEO Larry Wellikson, MD, as each man settles into a long-term care facility.
Dr. Wachter outlined the major forces starting to affect hospital medicine and imagined where they would lead us. And he couldn’t resist one glimpse back in time: “Think about the change we’ve seen already,” he marveled. “There’s no field in modern medical history that’s grown this quickly. We’re both leading the way and riding the waves.”
Dr. Wachter admitted his initial estimates for phenomenal growth of the field are already surpassed. “We originally projected that there would be 20,000 or 30,000 hospitalists,” he said. “Well, we’re already over 20,000. Now I’m thinking the final number will be around 50,000 or 60,000.”
He attributed part of that growth to several changes, including the additional responsibility of hospitalists for caring for surgical patients—something he sees as eventually becoming the norm. Another factor is the role hospitalists play in replacing residents in teaching hospitals, an area that has seen unplanned growth.
And finally, Dr. Wachter speculated that the quality measures movement will also boost the ranks of hospitalists. “We’re already seeing tremendous pressure on hospitalists to help their hospitals achieve success in pay-for-performance programs and in publicly reported measures,” he said. “This type of responsibility was originally considered a nice add-on for using hospitalists, but now it’s getting to be a crucial part. There’s a building expectation that hospitalists will guarantee superb performance.”
Dr. Wachter also touched on how information technology might change hospital medicine. “IT will definitely have an impact, in some exciting ways, and in other ways that have not been thought through,” he warned. “For example, consultation may be very different.” For example, a hospitalist in 2017 may be able to use a video link at a patient’s bedside to consult with one of 100 cardiologists around the country or around the world.
Following Dr. Wachter’s view of the future, Sylvia C. McKean, MD, had the last word at the meeting. As the chair in charge of next year’s Annual Meeting in San Diego, she presented the wrap-up on Friday afternoon, covering “What Have We Learned.”
Looking back on the previous three days, Dr. McKean pronounced, “The future is now.” Pointing to the number of meeting sessions, abstracts and poster presentations that emphasized recent innovations in hospital medicine, she said, “The Annual Meeting helps us find our expertise as hospitalists.” The Annual Meeting, along with SHM’s published Core Competencies helps define the role that hospitalists play in patient-centered care and in patient safety.
Dr. McKean thanked Chad Whelan, chair of the Annual Meeting Committee, for all his work, and said she was looking forward to 2008.
SHM Elects New Members to Board of Directors
Two new members announced; one member re-elected
SHM is pleased to announce the election of Joseph Li, MD, and Mahalakshmi Halasyamani, MD, and the re-election of Patrick Cawley, MD, to its board of directors for terms that began at the SHM Annual Meeting May 23-25 in Dallas.
“One of the strengths that keeps SHM on the cutting edge is the infusion of new talent on the board. SHM is fortunate to have a continued source of hospitalist leaders who willingly share their time and talents to help SHM shape and grow the hospital medicine specialty,” says Larry Wellikson, MD, CEO of SHM.
Each of the newly elected SHM board members comes from distinguished programs and institutions.
Dr. Li is the director of the hospital medicine program at Beth Israel Deaconess Medical Center in Boston and an assistant professor of medicine at the Harvard Medical School. He has been an active member of SHM, serving on the Education and Annual Meeting Committees, as well as the Procedures Task Force. Dr. Li earned his bachelor’s degree in pharmacy at the University of Oklahoma College of Pharmacy and his medical degree at the University of Oklahoma College of Medicine. He completed his residency at the Beth Israel Deaconess Medical Center.
Dr. Cawley is executive medical director at the Medical University Hospital of South Carolina. Prior to this, he was chief of staff at Conway Medical Center, S.C. He has served on the SHM board of directors since 2004 and is its treasurer. As an active member of SHM, he serves on the Public Policy Committee, Leadership Task Force, and on the advisory board for the Practice Management and Coding Courses. Dr. Cawley earned his bachelor’s degree in biology and chemistry from the University of Scranton (Penn.) and his medical degree from Georgetown University School of Medicine in Wash., D.C. He completed his residency at the Duke University Medical Center in Durham, N.C.
Dr. Halasyamani is the medical director of the heart failure program at Saint Joseph Mercy Hospital in Ann Arbor, Mich. Before that, she served as director of academic internal medicine inpatient services. She is also a clinical instructor of internal medicine at the University of Michigan and associate chair of the department of internal medicine at Saint Joseph Mercy Hospital. Dr. Halasyamani earned her bachelor’s degree in English and chemistry from Saint Louis University (Mo.) and her medical degree from Harvard Medical School, Boston. She completed her residency at Brigham and Women’s Hospital.
Congratulations to the newest members of the SHM Board of Directors.
What's Your Diagnosis?

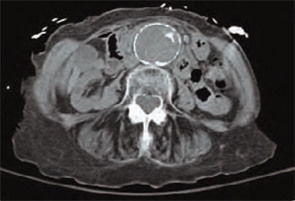
An 84-year-old white female, a former smoker with a medical history significant for coronary artery disease, chronic renal insufficiency, hypertension, and hyperlipidemia, presented to our hospital with two weeks of progressively worsening lower-back pain.
A detailed review of systems was negative for other symptoms. The patient was normotensive with stable vital signs. A physical examination found a 4 cm nontender, pulsatile mass above umbilicus, but a neurovascular exam of her lower extremities was normal. Laboratory testing revealed an elevated serum creatinine of 4.8 mg/dL (0.8-1.2 mg/dL). An abdominal computed tomography (CT) scan without contrast was performed. (See figure 1, below). TH
What should be your next appropriate
a) Obtain additional imaging studies
b) Initiate intravenous beta-blocker therapy to keep systolic blood pressure < 90 mm Hg
c) Initiate intravenous heparin therapy
d) Observation
e) Perform surgery emergently
Discussion
The answer is “d”: Observation. A CT scan of the abdomen without contrast shows a calcified abdominal aorta with aneurysmal dilatation measuring 4.4 cm in greatest diameter. No dissection or aneurysmal rupture is seen.
The abdominal aorta is the most common site for an arterial aneurysm, occurring below the origin of renal vessels in majority of cases. A diameter greater than 3.0 cm is considered aneurysmal.1 The prevalence increases markedly in individuals older than 60.2 Known risk factors include age, smoking, gender, atherosclerosis, hypertension, and family history of abdominal aneurysm.
The vast majority of the individuals with abdominal aortic aneurysms are asymptomatic. Abdominal or back pain is the most common complain in symptomatic patients. Often, patients have a ruptured aneurysm on presentation, along with pain in the abdomen, back or groin, hypotension with a tender, pulsatile abdominal mass seen on physical examination. In addition to history and examination, several imaging modalities are utilized for diagnosis. Most aneurysms are picked up incidentally on imaging studies performed for other purposes. Abdominal ultrasonography, CT scan, magnetic resonance imaging/magnetic resonance angiography and angiography are all used for diagnosis.
The size of the aneurysm is important when making management decisions. Risk of rupture increases dramatically for aneurysm diameter greater than 5-5.5 cm.3 Elective repair is generally indicated for asymptomatic aneurysms this size because mortality for emergency repair in case of rupture is extremely high. For asymptomatic aneurysms between 3.0-5.5 cm in diameter, the choice between surgery and surveillance depends on the patient’s preference, co-morbidities, presence of risk factors and the risk of surgery. For surveillance, monitor with ultrasound or CT scan every six to 24 months.1 Smoking cessation and treatment of hypertension and hyperlipidemia are important in medical management. Surgical repair is done either by the traditional transabdominal route or retroperitoneal approach. Endovascular stent grafts have also been introduced more recently. Symptomatic aneurysms require repair, regardless of the diameter.
Our patient had several risk factors, including age, smoking, hypertension, and atherosclerosis for developing an abdominal aortic aneurysm. After discussion of findings and management options, patient did not elect to undergo surgical repair. Smoking cessation, continued medical therapy for risk factors and surveillance was advised on discharge. TH
Drs. Aijaz and Newman practice at the Department of Medicine, Mayo Graduate School of Medical Education, Mayo Clinic, Rochester, Minn.
References
- Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation 2006 Mar 21;113(11):e463-654.
- Singh K, Bønaa KH, Jacobsen BK, Bjørk L, Solberg S. Prevalence of and risk factors for abdominal aortic aneurysms in a population-based study: The Tromso Study. Am J Epidemiol. 2001 Aug 1;154(3): 236-244.
- Powell JT, Greenhalgh RM. Clinical practice. Small abdominal aortic aneurysms. N Engl J Med. 2003 May 8;348(19):1895-1901.
An 84-year-old white female, a former smoker with a medical history significant for coronary artery disease, chronic renal insufficiency, hypertension, and hyperlipidemia, presented to our hospital with two weeks of progressively worsening lower-back pain.
A detailed review of systems was negative for other symptoms. The patient was normotensive with stable vital signs. A physical examination found a 4 cm nontender, pulsatile mass above umbilicus, but a neurovascular exam of her lower extremities was normal. Laboratory testing revealed an elevated serum creatinine of 4.8 mg/dL (0.8-1.2 mg/dL). An abdominal computed tomography (CT) scan without contrast was performed. (See figure 1, below). TH
What should be your next appropriate
a) Obtain additional imaging studies
b) Initiate intravenous beta-blocker therapy to keep systolic blood pressure < 90 mm Hg
c) Initiate intravenous heparin therapy
d) Observation
e) Perform surgery emergently
Discussion
The answer is “d”: Observation. A CT scan of the abdomen without contrast shows a calcified abdominal aorta with aneurysmal dilatation measuring 4.4 cm in greatest diameter. No dissection or aneurysmal rupture is seen.
The abdominal aorta is the most common site for an arterial aneurysm, occurring below the origin of renal vessels in majority of cases. A diameter greater than 3.0 cm is considered aneurysmal.1 The prevalence increases markedly in individuals older than 60.2 Known risk factors include age, smoking, gender, atherosclerosis, hypertension, and family history of abdominal aneurysm.
The vast majority of the individuals with abdominal aortic aneurysms are asymptomatic. Abdominal or back pain is the most common complain in symptomatic patients. Often, patients have a ruptured aneurysm on presentation, along with pain in the abdomen, back or groin, hypotension with a tender, pulsatile abdominal mass seen on physical examination. In addition to history and examination, several imaging modalities are utilized for diagnosis. Most aneurysms are picked up incidentally on imaging studies performed for other purposes. Abdominal ultrasonography, CT scan, magnetic resonance imaging/magnetic resonance angiography and angiography are all used for diagnosis.
The size of the aneurysm is important when making management decisions. Risk of rupture increases dramatically for aneurysm diameter greater than 5-5.5 cm.3 Elective repair is generally indicated for asymptomatic aneurysms this size because mortality for emergency repair in case of rupture is extremely high. For asymptomatic aneurysms between 3.0-5.5 cm in diameter, the choice between surgery and surveillance depends on the patient’s preference, co-morbidities, presence of risk factors and the risk of surgery. For surveillance, monitor with ultrasound or CT scan every six to 24 months.1 Smoking cessation and treatment of hypertension and hyperlipidemia are important in medical management. Surgical repair is done either by the traditional transabdominal route or retroperitoneal approach. Endovascular stent grafts have also been introduced more recently. Symptomatic aneurysms require repair, regardless of the diameter.
Our patient had several risk factors, including age, smoking, hypertension, and atherosclerosis for developing an abdominal aortic aneurysm. After discussion of findings and management options, patient did not elect to undergo surgical repair. Smoking cessation, continued medical therapy for risk factors and surveillance was advised on discharge. TH
Drs. Aijaz and Newman practice at the Department of Medicine, Mayo Graduate School of Medical Education, Mayo Clinic, Rochester, Minn.
References
- Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation 2006 Mar 21;113(11):e463-654.
- Singh K, Bønaa KH, Jacobsen BK, Bjørk L, Solberg S. Prevalence of and risk factors for abdominal aortic aneurysms in a population-based study: The Tromso Study. Am J Epidemiol. 2001 Aug 1;154(3): 236-244.
- Powell JT, Greenhalgh RM. Clinical practice. Small abdominal aortic aneurysms. N Engl J Med. 2003 May 8;348(19):1895-1901.
An 84-year-old white female, a former smoker with a medical history significant for coronary artery disease, chronic renal insufficiency, hypertension, and hyperlipidemia, presented to our hospital with two weeks of progressively worsening lower-back pain.
A detailed review of systems was negative for other symptoms. The patient was normotensive with stable vital signs. A physical examination found a 4 cm nontender, pulsatile mass above umbilicus, but a neurovascular exam of her lower extremities was normal. Laboratory testing revealed an elevated serum creatinine of 4.8 mg/dL (0.8-1.2 mg/dL). An abdominal computed tomography (CT) scan without contrast was performed. (See figure 1, below). TH
What should be your next appropriate
a) Obtain additional imaging studies
b) Initiate intravenous beta-blocker therapy to keep systolic blood pressure < 90 mm Hg
c) Initiate intravenous heparin therapy
d) Observation
e) Perform surgery emergently
Discussion
The answer is “d”: Observation. A CT scan of the abdomen without contrast shows a calcified abdominal aorta with aneurysmal dilatation measuring 4.4 cm in greatest diameter. No dissection or aneurysmal rupture is seen.
The abdominal aorta is the most common site for an arterial aneurysm, occurring below the origin of renal vessels in majority of cases. A diameter greater than 3.0 cm is considered aneurysmal.1 The prevalence increases markedly in individuals older than 60.2 Known risk factors include age, smoking, gender, atherosclerosis, hypertension, and family history of abdominal aneurysm.
The vast majority of the individuals with abdominal aortic aneurysms are asymptomatic. Abdominal or back pain is the most common complain in symptomatic patients. Often, patients have a ruptured aneurysm on presentation, along with pain in the abdomen, back or groin, hypotension with a tender, pulsatile abdominal mass seen on physical examination. In addition to history and examination, several imaging modalities are utilized for diagnosis. Most aneurysms are picked up incidentally on imaging studies performed for other purposes. Abdominal ultrasonography, CT scan, magnetic resonance imaging/magnetic resonance angiography and angiography are all used for diagnosis.
The size of the aneurysm is important when making management decisions. Risk of rupture increases dramatically for aneurysm diameter greater than 5-5.5 cm.3 Elective repair is generally indicated for asymptomatic aneurysms this size because mortality for emergency repair in case of rupture is extremely high. For asymptomatic aneurysms between 3.0-5.5 cm in diameter, the choice between surgery and surveillance depends on the patient’s preference, co-morbidities, presence of risk factors and the risk of surgery. For surveillance, monitor with ultrasound or CT scan every six to 24 months.1 Smoking cessation and treatment of hypertension and hyperlipidemia are important in medical management. Surgical repair is done either by the traditional transabdominal route or retroperitoneal approach. Endovascular stent grafts have also been introduced more recently. Symptomatic aneurysms require repair, regardless of the diameter.
Our patient had several risk factors, including age, smoking, hypertension, and atherosclerosis for developing an abdominal aortic aneurysm. After discussion of findings and management options, patient did not elect to undergo surgical repair. Smoking cessation, continued medical therapy for risk factors and surveillance was advised on discharge. TH
Drs. Aijaz and Newman practice at the Department of Medicine, Mayo Graduate School of Medical Education, Mayo Clinic, Rochester, Minn.
References
- Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation 2006 Mar 21;113(11):e463-654.
- Singh K, Bønaa KH, Jacobsen BK, Bjørk L, Solberg S. Prevalence of and risk factors for abdominal aortic aneurysms in a population-based study: The Tromso Study. Am J Epidemiol. 2001 Aug 1;154(3): 236-244.
- Powell JT, Greenhalgh RM. Clinical practice. Small abdominal aortic aneurysms. N Engl J Med. 2003 May 8;348(19):1895-1901.
Malpractice risk management: Be thorough—and involved—in obtaining informed consent
This article is the final one of 4 derived from a symposium on malpractice risk management at the 91st Clinical Congress of the American College of Surgeons, San Francisco, Calif., in October 2005. Mr. Nelson updated his comments in February 2007.
Part 1 March 2007 Informed refusal
James M. Goodman, JD
Part 2 April 2007 Common errors in self-defense
Claudia Dobbs, MA
Part 3 May 2007 Patient safety as risk management tool
Thomas J. Donnelly, JD
Part 4 THIS ISSUE
Responsibilities in obtaining informed consent
James M. Nelson, JD
You the physician—not a medical assistant, not a clerk, not a nurse—must initiate and complete the process of informed consent. You must personally obtain the patient’s consent before performing any operation, minor or major, in the office, surgical center, or operating room.
The setting should be an examining room or hospital room, not a waiting room, nursing station counter, or gurney in the operating room holding area. Exceptions occur, but considering how litigious society is today, these criteria represent the ideal.
Does the patient understand?
You must feel assured that the patient is capable of participating in the discussion, both receptively and expressively, and that she can make a sound and reasoned decision. Exceptions can apply in emergencies and for minors or adults who are otherwise not competent to grant informed consent.
If the patient wants to have a loved one or close friend join the discussion, invite that person into the room. However, he or she should play a peripheral role only.
You initiate the informed consent process, but the patient must conclude it by granting or refusing consent.
Focus the discussion
The preeminent case law on informed consent is Cobbs v. Grant, which the California Supreme Court handed down in 1972. Even today, many states follow this law. The California justices held that a patient’s “right of self-decision” was a measure of the doctor’s “duty to reveal.”
In other words, presenting information to the patient and receiving her consent requires both the physician and patient to participate. The process may require a few office contacts and perhaps 1 or 2 office visits or hospital calls. The seminal event is a focused discussion between you and the patient.
The physician describes the proposed treatment or procedure in language the patient can understand. That is, the information must be conveyed in a way that a reasonable person in the patient’s position would expect to hear it.
A situation that I recently confronted was a lapse of 8 months between the time the patient gave informed consent and the actual surgery. Here’s how that case unfolded:
- A couple of months after the surgeon obtained informed consent from the patient, and just before the day of the scheduled surgery, the patient called the surgeon and said: “I feel better. I don’t want to have the surgery.”
- A couple of months after that, the patient again called: “I’ve changed my mind,” she said. “I don’t feel well. I want the surgery.” So the surgeon performed the operation that the patient had consented to more than 8 months earlier.
Was the surgeon obligated to conduct another history, physical examination, and informed-consent discussion with the patient—long before the patient is on the gurney under preanesthesia and ready to go into the operating room? In this case, the surgeon should have—and did—talk briefly with the patient, reminding her of their earlier discussion. The patient confirmed her intent to have the surgery.
But the patient later alleged: “I lost the documents I was given and I wasn’t really prepared for the surgery.” She sued for negligence, claiming the surgery resulted in continuing severe pain. Informed consent was an issue at trial because:
- the surgeon did not document the final informed-consent discussion
- the patient denied that the discussion took place.
This situation doesn’t happen often, but it had significant consequences for my client.
Explain the likely outcome
Express the likelihood of success in general terms, not as a percentage. Courts have frowned on such statements as, “The failure rate for this procedure is 1% to 2%.” They’ve preferred that the physician simply state that a successful outcome is likely.
Another mandatory point of communication is the expected benefit and outcome. This includes a discussion of potential risks or complications that a reasonable person would consider important: any risk of death, serious injury, or significant complication—but not necessarily minor or trivial side effects.
You must tell the patient about any reasonable alternatives to the planned treatment or procedure, along with their potential risks, complications, and outcomes. We’ve found that physicians who satisfied their responsibility to discuss alternative treatments or operations sometimes failed to explain the risks, benefits, and complications.
Do not draw conclusions or speak cryptically. Never make assumptions about the patient’s knowledge or understanding of a proposed operation or its alternatives. Instead, invite the patient to ask questions. Be receptive and thoughtful when those questions are posed.
The patient should receive a clear, concise explanation of his or her condition or diagnosis and how that might affect the outcome. For example, discuss proposed surgery for pelvic prolapse in the context of the patient’s presentation.
There’s more to do afterward
The process does not necessarily end after you’ve answered all the patient’s questions and she has given informed consent (or has declined to consent). For selected treatments or operations, some states require a presentation of risks, benefits, and alternatives more specific than the “reasonable person” communication.
In many states, for example, a patient who grants consent for a hysterectomy or sterilization must be told specific points or complete a form. Some states apply similar protocols for breast cancer surgery or chemotherapy.
Handouts and videos are no substitute!
More and more, physicians are using videotapes, CDs, Web-based sources, and handouts to help patients understand procedures. But these resources cannot supplant the role of even a very busy physician. Such materials can supplement a focused discussion between physician and patient, but do not legally serve the purpose of obtaining informed consent.
A nurse or other nonphysician provider can convey some information or provide materials to the patient about the treatment or procedure toward the goal of obtaining informed consent, but, again, it is you who must then come in and complete the discussion. Whether a court accepts this system depends on the quality of the materials.
An informative handout (or video, etc.) can have a big impact on a jury’s impression of whether the patient was informed adequately. However, sometimes a busy physician relies too heavily on nonmedical staff and fails to participate sufficiently in deciding what the staff hands out. Furthermore, the physician is responsible for any information that a staff member provides to a patient.
You don’t need to volunteer information that you’ve done a certain procedure only a few times. If the patient or a family member asks this question, however, answer honestly. Even the most aggressive plaintiff’s experts acknowledge that physicians do not have to provide a tabulation of procedures they’ve performed.
Often, in a university hospital or large medical center, a surgeon who discusses a procedure with the patient is not the one who is scheduled to perform it. That situation should be included in the informed consent: “I will be the second assistant surgeon, but it’s Dr. Smith who will perform your operation.”
When a proposed therapy or procedure will involve off-label use of a drug or medical device, tell that to the patient, too, and document the discussion in the chart.
At the end of the informed-consent process, you must be satisfied that you’ve complied with the court’s mandate to meet the patient’s protected interest in autonomous decision making.
This article is the final one of 4 derived from a symposium on malpractice risk management at the 91st Clinical Congress of the American College of Surgeons, San Francisco, Calif., in October 2005. Mr. Nelson updated his comments in February 2007.
Part 1 March 2007 Informed refusal
James M. Goodman, JD
Part 2 April 2007 Common errors in self-defense
Claudia Dobbs, MA
Part 3 May 2007 Patient safety as risk management tool
Thomas J. Donnelly, JD
Part 4 THIS ISSUE
Responsibilities in obtaining informed consent
James M. Nelson, JD
You the physician—not a medical assistant, not a clerk, not a nurse—must initiate and complete the process of informed consent. You must personally obtain the patient’s consent before performing any operation, minor or major, in the office, surgical center, or operating room.
The setting should be an examining room or hospital room, not a waiting room, nursing station counter, or gurney in the operating room holding area. Exceptions occur, but considering how litigious society is today, these criteria represent the ideal.
Does the patient understand?
You must feel assured that the patient is capable of participating in the discussion, both receptively and expressively, and that she can make a sound and reasoned decision. Exceptions can apply in emergencies and for minors or adults who are otherwise not competent to grant informed consent.
If the patient wants to have a loved one or close friend join the discussion, invite that person into the room. However, he or she should play a peripheral role only.
You initiate the informed consent process, but the patient must conclude it by granting or refusing consent.
Focus the discussion
The preeminent case law on informed consent is Cobbs v. Grant, which the California Supreme Court handed down in 1972. Even today, many states follow this law. The California justices held that a patient’s “right of self-decision” was a measure of the doctor’s “duty to reveal.”
In other words, presenting information to the patient and receiving her consent requires both the physician and patient to participate. The process may require a few office contacts and perhaps 1 or 2 office visits or hospital calls. The seminal event is a focused discussion between you and the patient.
The physician describes the proposed treatment or procedure in language the patient can understand. That is, the information must be conveyed in a way that a reasonable person in the patient’s position would expect to hear it.
A situation that I recently confronted was a lapse of 8 months between the time the patient gave informed consent and the actual surgery. Here’s how that case unfolded:
- A couple of months after the surgeon obtained informed consent from the patient, and just before the day of the scheduled surgery, the patient called the surgeon and said: “I feel better. I don’t want to have the surgery.”
- A couple of months after that, the patient again called: “I’ve changed my mind,” she said. “I don’t feel well. I want the surgery.” So the surgeon performed the operation that the patient had consented to more than 8 months earlier.
Was the surgeon obligated to conduct another history, physical examination, and informed-consent discussion with the patient—long before the patient is on the gurney under preanesthesia and ready to go into the operating room? In this case, the surgeon should have—and did—talk briefly with the patient, reminding her of their earlier discussion. The patient confirmed her intent to have the surgery.
But the patient later alleged: “I lost the documents I was given and I wasn’t really prepared for the surgery.” She sued for negligence, claiming the surgery resulted in continuing severe pain. Informed consent was an issue at trial because:
- the surgeon did not document the final informed-consent discussion
- the patient denied that the discussion took place.
This situation doesn’t happen often, but it had significant consequences for my client.
Explain the likely outcome
Express the likelihood of success in general terms, not as a percentage. Courts have frowned on such statements as, “The failure rate for this procedure is 1% to 2%.” They’ve preferred that the physician simply state that a successful outcome is likely.
Another mandatory point of communication is the expected benefit and outcome. This includes a discussion of potential risks or complications that a reasonable person would consider important: any risk of death, serious injury, or significant complication—but not necessarily minor or trivial side effects.
You must tell the patient about any reasonable alternatives to the planned treatment or procedure, along with their potential risks, complications, and outcomes. We’ve found that physicians who satisfied their responsibility to discuss alternative treatments or operations sometimes failed to explain the risks, benefits, and complications.
Do not draw conclusions or speak cryptically. Never make assumptions about the patient’s knowledge or understanding of a proposed operation or its alternatives. Instead, invite the patient to ask questions. Be receptive and thoughtful when those questions are posed.
The patient should receive a clear, concise explanation of his or her condition or diagnosis and how that might affect the outcome. For example, discuss proposed surgery for pelvic prolapse in the context of the patient’s presentation.
There’s more to do afterward
The process does not necessarily end after you’ve answered all the patient’s questions and she has given informed consent (or has declined to consent). For selected treatments or operations, some states require a presentation of risks, benefits, and alternatives more specific than the “reasonable person” communication.
In many states, for example, a patient who grants consent for a hysterectomy or sterilization must be told specific points or complete a form. Some states apply similar protocols for breast cancer surgery or chemotherapy.
Handouts and videos are no substitute!
More and more, physicians are using videotapes, CDs, Web-based sources, and handouts to help patients understand procedures. But these resources cannot supplant the role of even a very busy physician. Such materials can supplement a focused discussion between physician and patient, but do not legally serve the purpose of obtaining informed consent.
A nurse or other nonphysician provider can convey some information or provide materials to the patient about the treatment or procedure toward the goal of obtaining informed consent, but, again, it is you who must then come in and complete the discussion. Whether a court accepts this system depends on the quality of the materials.
An informative handout (or video, etc.) can have a big impact on a jury’s impression of whether the patient was informed adequately. However, sometimes a busy physician relies too heavily on nonmedical staff and fails to participate sufficiently in deciding what the staff hands out. Furthermore, the physician is responsible for any information that a staff member provides to a patient.
You don’t need to volunteer information that you’ve done a certain procedure only a few times. If the patient or a family member asks this question, however, answer honestly. Even the most aggressive plaintiff’s experts acknowledge that physicians do not have to provide a tabulation of procedures they’ve performed.
Often, in a university hospital or large medical center, a surgeon who discusses a procedure with the patient is not the one who is scheduled to perform it. That situation should be included in the informed consent: “I will be the second assistant surgeon, but it’s Dr. Smith who will perform your operation.”
When a proposed therapy or procedure will involve off-label use of a drug or medical device, tell that to the patient, too, and document the discussion in the chart.
At the end of the informed-consent process, you must be satisfied that you’ve complied with the court’s mandate to meet the patient’s protected interest in autonomous decision making.
This article is the final one of 4 derived from a symposium on malpractice risk management at the 91st Clinical Congress of the American College of Surgeons, San Francisco, Calif., in October 2005. Mr. Nelson updated his comments in February 2007.
Part 1 March 2007 Informed refusal
James M. Goodman, JD
Part 2 April 2007 Common errors in self-defense
Claudia Dobbs, MA
Part 3 May 2007 Patient safety as risk management tool
Thomas J. Donnelly, JD
Part 4 THIS ISSUE
Responsibilities in obtaining informed consent
James M. Nelson, JD
You the physician—not a medical assistant, not a clerk, not a nurse—must initiate and complete the process of informed consent. You must personally obtain the patient’s consent before performing any operation, minor or major, in the office, surgical center, or operating room.
The setting should be an examining room or hospital room, not a waiting room, nursing station counter, or gurney in the operating room holding area. Exceptions occur, but considering how litigious society is today, these criteria represent the ideal.
Does the patient understand?
You must feel assured that the patient is capable of participating in the discussion, both receptively and expressively, and that she can make a sound and reasoned decision. Exceptions can apply in emergencies and for minors or adults who are otherwise not competent to grant informed consent.
If the patient wants to have a loved one or close friend join the discussion, invite that person into the room. However, he or she should play a peripheral role only.
You initiate the informed consent process, but the patient must conclude it by granting or refusing consent.
Focus the discussion
The preeminent case law on informed consent is Cobbs v. Grant, which the California Supreme Court handed down in 1972. Even today, many states follow this law. The California justices held that a patient’s “right of self-decision” was a measure of the doctor’s “duty to reveal.”
In other words, presenting information to the patient and receiving her consent requires both the physician and patient to participate. The process may require a few office contacts and perhaps 1 or 2 office visits or hospital calls. The seminal event is a focused discussion between you and the patient.
The physician describes the proposed treatment or procedure in language the patient can understand. That is, the information must be conveyed in a way that a reasonable person in the patient’s position would expect to hear it.
A situation that I recently confronted was a lapse of 8 months between the time the patient gave informed consent and the actual surgery. Here’s how that case unfolded:
- A couple of months after the surgeon obtained informed consent from the patient, and just before the day of the scheduled surgery, the patient called the surgeon and said: “I feel better. I don’t want to have the surgery.”
- A couple of months after that, the patient again called: “I’ve changed my mind,” she said. “I don’t feel well. I want the surgery.” So the surgeon performed the operation that the patient had consented to more than 8 months earlier.
Was the surgeon obligated to conduct another history, physical examination, and informed-consent discussion with the patient—long before the patient is on the gurney under preanesthesia and ready to go into the operating room? In this case, the surgeon should have—and did—talk briefly with the patient, reminding her of their earlier discussion. The patient confirmed her intent to have the surgery.
But the patient later alleged: “I lost the documents I was given and I wasn’t really prepared for the surgery.” She sued for negligence, claiming the surgery resulted in continuing severe pain. Informed consent was an issue at trial because:
- the surgeon did not document the final informed-consent discussion
- the patient denied that the discussion took place.
This situation doesn’t happen often, but it had significant consequences for my client.
Explain the likely outcome
Express the likelihood of success in general terms, not as a percentage. Courts have frowned on such statements as, “The failure rate for this procedure is 1% to 2%.” They’ve preferred that the physician simply state that a successful outcome is likely.
Another mandatory point of communication is the expected benefit and outcome. This includes a discussion of potential risks or complications that a reasonable person would consider important: any risk of death, serious injury, or significant complication—but not necessarily minor or trivial side effects.
You must tell the patient about any reasonable alternatives to the planned treatment or procedure, along with their potential risks, complications, and outcomes. We’ve found that physicians who satisfied their responsibility to discuss alternative treatments or operations sometimes failed to explain the risks, benefits, and complications.
Do not draw conclusions or speak cryptically. Never make assumptions about the patient’s knowledge or understanding of a proposed operation or its alternatives. Instead, invite the patient to ask questions. Be receptive and thoughtful when those questions are posed.
The patient should receive a clear, concise explanation of his or her condition or diagnosis and how that might affect the outcome. For example, discuss proposed surgery for pelvic prolapse in the context of the patient’s presentation.
There’s more to do afterward
The process does not necessarily end after you’ve answered all the patient’s questions and she has given informed consent (or has declined to consent). For selected treatments or operations, some states require a presentation of risks, benefits, and alternatives more specific than the “reasonable person” communication.
In many states, for example, a patient who grants consent for a hysterectomy or sterilization must be told specific points or complete a form. Some states apply similar protocols for breast cancer surgery or chemotherapy.
Handouts and videos are no substitute!
More and more, physicians are using videotapes, CDs, Web-based sources, and handouts to help patients understand procedures. But these resources cannot supplant the role of even a very busy physician. Such materials can supplement a focused discussion between physician and patient, but do not legally serve the purpose of obtaining informed consent.
A nurse or other nonphysician provider can convey some information or provide materials to the patient about the treatment or procedure toward the goal of obtaining informed consent, but, again, it is you who must then come in and complete the discussion. Whether a court accepts this system depends on the quality of the materials.
An informative handout (or video, etc.) can have a big impact on a jury’s impression of whether the patient was informed adequately. However, sometimes a busy physician relies too heavily on nonmedical staff and fails to participate sufficiently in deciding what the staff hands out. Furthermore, the physician is responsible for any information that a staff member provides to a patient.
You don’t need to volunteer information that you’ve done a certain procedure only a few times. If the patient or a family member asks this question, however, answer honestly. Even the most aggressive plaintiff’s experts acknowledge that physicians do not have to provide a tabulation of procedures they’ve performed.
Often, in a university hospital or large medical center, a surgeon who discusses a procedure with the patient is not the one who is scheduled to perform it. That situation should be included in the informed consent: “I will be the second assistant surgeon, but it’s Dr. Smith who will perform your operation.”
When a proposed therapy or procedure will involve off-label use of a drug or medical device, tell that to the patient, too, and document the discussion in the chart.
At the end of the informed-consent process, you must be satisfied that you’ve complied with the court’s mandate to meet the patient’s protected interest in autonomous decision making.
Failing the 15-minute suicide watch: Guidelines to monitor inpatients
Patient commits suicide after 15-minute checks are stopped
Honolulu County (HI) Circuit Court
A patient was brought to a hospital and interviewed by a psychiatrist. She was found to be at moderate risk for suicide, was admitted, and ordered to be monitored every 15 minutes. The patient attempted suicide 2 days later by closing a drawer on her neck. She died from the injuries the following day.
The patient’s family claimed that a hospital nurse misread the psychiatrist’s instructions and stopped the 15-minute checks on the morning of the incident, believing that the order was limited to 15-minute checks for the first 24 hours, even though they had been done for almost 2 days. The patient refused medication on the first day of admission, and the psychiatrist had started the procedure to obtain a court order committing the patient and allowing injection of necessary medication. The claims against the hospital were settled for a confidential amount.
The patient’s family claimed the psychiatrist diagnosed the patient with major depression with recurrent suicide ideation but failed to properly assess her for suicide monitoring. The family also said the patient should have been determined to be at least at high risk and required to be within sight of staff.
The psychiatrist claimed to be unaware the 15-minute monitoring had ceased. The psychiatrist saw the patient 30 minutes before she was found collapsed with her head in the drawer. The hospital staff checked the patient approximately 15 to 30 minutes before she was found.
- A defense verdict was returned
Reduced observation blamed for suicide by hanging
Kings County (NY) Supreme Court
A 45-year-old police lieutenant who suffered from alcohol abuse and depression was admitted to a psychiatric care facility. He was classiffied “Q15,” a category assigned to patients who must be visually inspected every 15 minutes, cannot have access to sharp objects or any other material or object they can use to inflict bodily harm, and must request permission to use restrooms. The next day the psychiatrist examined the patient and moved him to a “Q30” status, which halved the frequency of visual inspections, gave him unrestricted access to restrooms, and allowed him to have a bathrobe with a belt. The patient hanged himself the next day, using a restroom door to support a noose he made from the bathrobe belt.
The patient’s family faulted the hospital and psychiatrist for prematurely advancing the patient to “Q30” status. The hospital and psychiatrist claimed the suicide could not have been predicted and argued that given his background as a police lieutenant, the patient would have interpreted more stringent restrictions as incarceration. The psychiatrist argued that such a perception would have impeded the patient’s progress.
- A $71,989 verdict was returned, apportioning fault 65% to the hospital and 35% to the psychiatrist
Constant patient observation—such as one-to-one staffing or 15-minute checks—is used to protect patients from harming themselves or others. One study of a psychiatric hospital1 reported that 13% of psychiatric inpatients required constant observation.
Even 15 minutes is sufficient time to complete a suicide.3 Common methods of inpatient suicide include hanging, overdosing, and jumping from high places.4,5 One study found that 73% of inpatient suicides in a psychiatric ward occurred after 28 days of admission.5
The cost of constant observation may account for as much as 20% of the total nursing budget at a psychiatric hospital and up to 10% at a long-term care facility or general hospital.6 The annual cost of constant observation can exceed $500,000, depending on the hospital’s size and monitoring frequency.6
Determining responsibility
The outcomes of these 2 cases may appear inconsistent. In the first, the psychiatrist who assessed the patient as a moderate suicide risk was not negligent, even though the family claimed the patient was at high risk. In the second case, the psychiatrist was found partly liable for not maintaining a higher vigilance of suicide risk assessment.
Physicians cannot put every patient on one-to-one monitoring or 15-minute checks because of fear of suicide and malpractice litigation. These 2 cases demonstrate that if a suicide occurs, the courts will look for clinical reasons for the level of observation. The level of suicide precautions—one-to-one vs 15-minute checks—should be based on the patient’s clinical presentation and supported by clinical rationale.7
Risk analysis
The courts look to see if the suicide assessment was “clinically reasonable”.8 To meet this standard, perform a “suicide risk-benefit analysis” each time you make a significant clinical decision, such as ordering 15-minute checks. The record should include information sources you used (such as family members or previous medical records), factors that entered the clinical decision, and how you balanced these factors in a risk-benefit assessment (Box 1).9
Document decisions. Mistakes in clinical judgment do not necessarily constitute negligence,8 but deviations in the standard of care cannot be adequately determined in a court of law unless the clinician had documented his or her thought processes at the time of the decision.
Predicting which patients will re-experience or deny suicidal ideation is impossible,7 but if the patient is determined to be at high risk for suicide, then implement and document a plan to address this risk. In addition, communicate information regarding the risk-benefit assessment to staff responsible for implementing these precautions.
- Suicidal thoughts or behaviors—ideas, plans, attempts
- Psychiatric diagnoses—depression, bipolar disorder, schizophrenia, substance use, Cluster B personality disorders
- Physical illnesses—HIV, malignant cancers, pain syndromes
- Psychosocial features—lack of support, unemployment
- Childhood traumas
- Genetic and familial effects—family history of suicide
- Psychological features—hopelessness, agitation, impulsiveness
- Cognitive features—polarized thinking
- Demographic features—adolescents, young adults, and elderly patients
- Other factors—access to firearms, intoxication.
Source: Reference 7
- a patient is admitted for inpatient treatment
- observation status changes
- a patient’s clinical condition changes substantially
- acute psychosocial stressors are discovered during the hospitalization.7
1. Shugar G, Rehaluk R. Continuous observation for psychiatric inpatients. Compr Psychiatry 1990;30:48-55.
2. Busch KA, Fawcett J, Jacobs DG. Clinical correlates of inpatient suicide. J Clin Psychiatry 2003;64:14-9.
3. Bowers L, Gournay K, Dufy D. Suicide and self-harm in inpatient psychiatric units: a national survey of observation policies. J Adv Nursing 2000;32:437-44.
4. Proulx F, Lesage AD, Grunberg F. One hundred in-patient suicides. Br J Psychiatry 1997;171:247-50.
5. Shah AK, Ganesvaran T. Inpatient suicides in an Australian mental hospital. Aust NZ J Psychiatr 1997;31:291-8.
6. Moore P, Berman K, Knight M, Devine J. Constant observation: implications for nursing practice. J Psychosoc Nurs Ment Health Serv 1995;33:46-50.
7. American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. Available at: http://www.psych.org/psych_pract/treatg/pg/SuicidalBehavior_05-15-06.pdf. Accessed April 19, 2007.
8. Simon RI. The suicidal patient. In Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:166-86.
9. Abille v United States, 482 F Supp 703 (ND Cal 1980).
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Patient commits suicide after 15-minute checks are stopped
Honolulu County (HI) Circuit Court
A patient was brought to a hospital and interviewed by a psychiatrist. She was found to be at moderate risk for suicide, was admitted, and ordered to be monitored every 15 minutes. The patient attempted suicide 2 days later by closing a drawer on her neck. She died from the injuries the following day.
The patient’s family claimed that a hospital nurse misread the psychiatrist’s instructions and stopped the 15-minute checks on the morning of the incident, believing that the order was limited to 15-minute checks for the first 24 hours, even though they had been done for almost 2 days. The patient refused medication on the first day of admission, and the psychiatrist had started the procedure to obtain a court order committing the patient and allowing injection of necessary medication. The claims against the hospital were settled for a confidential amount.
The patient’s family claimed the psychiatrist diagnosed the patient with major depression with recurrent suicide ideation but failed to properly assess her for suicide monitoring. The family also said the patient should have been determined to be at least at high risk and required to be within sight of staff.
The psychiatrist claimed to be unaware the 15-minute monitoring had ceased. The psychiatrist saw the patient 30 minutes before she was found collapsed with her head in the drawer. The hospital staff checked the patient approximately 15 to 30 minutes before she was found.
- A defense verdict was returned
Reduced observation blamed for suicide by hanging
Kings County (NY) Supreme Court
A 45-year-old police lieutenant who suffered from alcohol abuse and depression was admitted to a psychiatric care facility. He was classiffied “Q15,” a category assigned to patients who must be visually inspected every 15 minutes, cannot have access to sharp objects or any other material or object they can use to inflict bodily harm, and must request permission to use restrooms. The next day the psychiatrist examined the patient and moved him to a “Q30” status, which halved the frequency of visual inspections, gave him unrestricted access to restrooms, and allowed him to have a bathrobe with a belt. The patient hanged himself the next day, using a restroom door to support a noose he made from the bathrobe belt.
The patient’s family faulted the hospital and psychiatrist for prematurely advancing the patient to “Q30” status. The hospital and psychiatrist claimed the suicide could not have been predicted and argued that given his background as a police lieutenant, the patient would have interpreted more stringent restrictions as incarceration. The psychiatrist argued that such a perception would have impeded the patient’s progress.
- A $71,989 verdict was returned, apportioning fault 65% to the hospital and 35% to the psychiatrist
Constant patient observation—such as one-to-one staffing or 15-minute checks—is used to protect patients from harming themselves or others. One study of a psychiatric hospital1 reported that 13% of psychiatric inpatients required constant observation.
Even 15 minutes is sufficient time to complete a suicide.3 Common methods of inpatient suicide include hanging, overdosing, and jumping from high places.4,5 One study found that 73% of inpatient suicides in a psychiatric ward occurred after 28 days of admission.5
The cost of constant observation may account for as much as 20% of the total nursing budget at a psychiatric hospital and up to 10% at a long-term care facility or general hospital.6 The annual cost of constant observation can exceed $500,000, depending on the hospital’s size and monitoring frequency.6
Determining responsibility
The outcomes of these 2 cases may appear inconsistent. In the first, the psychiatrist who assessed the patient as a moderate suicide risk was not negligent, even though the family claimed the patient was at high risk. In the second case, the psychiatrist was found partly liable for not maintaining a higher vigilance of suicide risk assessment.
Physicians cannot put every patient on one-to-one monitoring or 15-minute checks because of fear of suicide and malpractice litigation. These 2 cases demonstrate that if a suicide occurs, the courts will look for clinical reasons for the level of observation. The level of suicide precautions—one-to-one vs 15-minute checks—should be based on the patient’s clinical presentation and supported by clinical rationale.7
Risk analysis
The courts look to see if the suicide assessment was “clinically reasonable”.8 To meet this standard, perform a “suicide risk-benefit analysis” each time you make a significant clinical decision, such as ordering 15-minute checks. The record should include information sources you used (such as family members or previous medical records), factors that entered the clinical decision, and how you balanced these factors in a risk-benefit assessment (Box 1).9
Document decisions. Mistakes in clinical judgment do not necessarily constitute negligence,8 but deviations in the standard of care cannot be adequately determined in a court of law unless the clinician had documented his or her thought processes at the time of the decision.
Predicting which patients will re-experience or deny suicidal ideation is impossible,7 but if the patient is determined to be at high risk for suicide, then implement and document a plan to address this risk. In addition, communicate information regarding the risk-benefit assessment to staff responsible for implementing these precautions.
- Suicidal thoughts or behaviors—ideas, plans, attempts
- Psychiatric diagnoses—depression, bipolar disorder, schizophrenia, substance use, Cluster B personality disorders
- Physical illnesses—HIV, malignant cancers, pain syndromes
- Psychosocial features—lack of support, unemployment
- Childhood traumas
- Genetic and familial effects—family history of suicide
- Psychological features—hopelessness, agitation, impulsiveness
- Cognitive features—polarized thinking
- Demographic features—adolescents, young adults, and elderly patients
- Other factors—access to firearms, intoxication.
Source: Reference 7
- a patient is admitted for inpatient treatment
- observation status changes
- a patient’s clinical condition changes substantially
- acute psychosocial stressors are discovered during the hospitalization.7
Patient commits suicide after 15-minute checks are stopped
Honolulu County (HI) Circuit Court
A patient was brought to a hospital and interviewed by a psychiatrist. She was found to be at moderate risk for suicide, was admitted, and ordered to be monitored every 15 minutes. The patient attempted suicide 2 days later by closing a drawer on her neck. She died from the injuries the following day.
The patient’s family claimed that a hospital nurse misread the psychiatrist’s instructions and stopped the 15-minute checks on the morning of the incident, believing that the order was limited to 15-minute checks for the first 24 hours, even though they had been done for almost 2 days. The patient refused medication on the first day of admission, and the psychiatrist had started the procedure to obtain a court order committing the patient and allowing injection of necessary medication. The claims against the hospital were settled for a confidential amount.
The patient’s family claimed the psychiatrist diagnosed the patient with major depression with recurrent suicide ideation but failed to properly assess her for suicide monitoring. The family also said the patient should have been determined to be at least at high risk and required to be within sight of staff.
The psychiatrist claimed to be unaware the 15-minute monitoring had ceased. The psychiatrist saw the patient 30 minutes before she was found collapsed with her head in the drawer. The hospital staff checked the patient approximately 15 to 30 minutes before she was found.
- A defense verdict was returned
Reduced observation blamed for suicide by hanging
Kings County (NY) Supreme Court
A 45-year-old police lieutenant who suffered from alcohol abuse and depression was admitted to a psychiatric care facility. He was classiffied “Q15,” a category assigned to patients who must be visually inspected every 15 minutes, cannot have access to sharp objects or any other material or object they can use to inflict bodily harm, and must request permission to use restrooms. The next day the psychiatrist examined the patient and moved him to a “Q30” status, which halved the frequency of visual inspections, gave him unrestricted access to restrooms, and allowed him to have a bathrobe with a belt. The patient hanged himself the next day, using a restroom door to support a noose he made from the bathrobe belt.
The patient’s family faulted the hospital and psychiatrist for prematurely advancing the patient to “Q30” status. The hospital and psychiatrist claimed the suicide could not have been predicted and argued that given his background as a police lieutenant, the patient would have interpreted more stringent restrictions as incarceration. The psychiatrist argued that such a perception would have impeded the patient’s progress.
- A $71,989 verdict was returned, apportioning fault 65% to the hospital and 35% to the psychiatrist
Constant patient observation—such as one-to-one staffing or 15-minute checks—is used to protect patients from harming themselves or others. One study of a psychiatric hospital1 reported that 13% of psychiatric inpatients required constant observation.
Even 15 minutes is sufficient time to complete a suicide.3 Common methods of inpatient suicide include hanging, overdosing, and jumping from high places.4,5 One study found that 73% of inpatient suicides in a psychiatric ward occurred after 28 days of admission.5
The cost of constant observation may account for as much as 20% of the total nursing budget at a psychiatric hospital and up to 10% at a long-term care facility or general hospital.6 The annual cost of constant observation can exceed $500,000, depending on the hospital’s size and monitoring frequency.6
Determining responsibility
The outcomes of these 2 cases may appear inconsistent. In the first, the psychiatrist who assessed the patient as a moderate suicide risk was not negligent, even though the family claimed the patient was at high risk. In the second case, the psychiatrist was found partly liable for not maintaining a higher vigilance of suicide risk assessment.
Physicians cannot put every patient on one-to-one monitoring or 15-minute checks because of fear of suicide and malpractice litigation. These 2 cases demonstrate that if a suicide occurs, the courts will look for clinical reasons for the level of observation. The level of suicide precautions—one-to-one vs 15-minute checks—should be based on the patient’s clinical presentation and supported by clinical rationale.7
Risk analysis
The courts look to see if the suicide assessment was “clinically reasonable”.8 To meet this standard, perform a “suicide risk-benefit analysis” each time you make a significant clinical decision, such as ordering 15-minute checks. The record should include information sources you used (such as family members or previous medical records), factors that entered the clinical decision, and how you balanced these factors in a risk-benefit assessment (Box 1).9
Document decisions. Mistakes in clinical judgment do not necessarily constitute negligence,8 but deviations in the standard of care cannot be adequately determined in a court of law unless the clinician had documented his or her thought processes at the time of the decision.
Predicting which patients will re-experience or deny suicidal ideation is impossible,7 but if the patient is determined to be at high risk for suicide, then implement and document a plan to address this risk. In addition, communicate information regarding the risk-benefit assessment to staff responsible for implementing these precautions.
- Suicidal thoughts or behaviors—ideas, plans, attempts
- Psychiatric diagnoses—depression, bipolar disorder, schizophrenia, substance use, Cluster B personality disorders
- Physical illnesses—HIV, malignant cancers, pain syndromes
- Psychosocial features—lack of support, unemployment
- Childhood traumas
- Genetic and familial effects—family history of suicide
- Psychological features—hopelessness, agitation, impulsiveness
- Cognitive features—polarized thinking
- Demographic features—adolescents, young adults, and elderly patients
- Other factors—access to firearms, intoxication.
Source: Reference 7
- a patient is admitted for inpatient treatment
- observation status changes
- a patient’s clinical condition changes substantially
- acute psychosocial stressors are discovered during the hospitalization.7
1. Shugar G, Rehaluk R. Continuous observation for psychiatric inpatients. Compr Psychiatry 1990;30:48-55.
2. Busch KA, Fawcett J, Jacobs DG. Clinical correlates of inpatient suicide. J Clin Psychiatry 2003;64:14-9.
3. Bowers L, Gournay K, Dufy D. Suicide and self-harm in inpatient psychiatric units: a national survey of observation policies. J Adv Nursing 2000;32:437-44.
4. Proulx F, Lesage AD, Grunberg F. One hundred in-patient suicides. Br J Psychiatry 1997;171:247-50.
5. Shah AK, Ganesvaran T. Inpatient suicides in an Australian mental hospital. Aust NZ J Psychiatr 1997;31:291-8.
6. Moore P, Berman K, Knight M, Devine J. Constant observation: implications for nursing practice. J Psychosoc Nurs Ment Health Serv 1995;33:46-50.
7. American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. Available at: http://www.psych.org/psych_pract/treatg/pg/SuicidalBehavior_05-15-06.pdf. Accessed April 19, 2007.
8. Simon RI. The suicidal patient. In Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:166-86.
9. Abille v United States, 482 F Supp 703 (ND Cal 1980).
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
1. Shugar G, Rehaluk R. Continuous observation for psychiatric inpatients. Compr Psychiatry 1990;30:48-55.
2. Busch KA, Fawcett J, Jacobs DG. Clinical correlates of inpatient suicide. J Clin Psychiatry 2003;64:14-9.
3. Bowers L, Gournay K, Dufy D. Suicide and self-harm in inpatient psychiatric units: a national survey of observation policies. J Adv Nursing 2000;32:437-44.
4. Proulx F, Lesage AD, Grunberg F. One hundred in-patient suicides. Br J Psychiatry 1997;171:247-50.
5. Shah AK, Ganesvaran T. Inpatient suicides in an Australian mental hospital. Aust NZ J Psychiatr 1997;31:291-8.
6. Moore P, Berman K, Knight M, Devine J. Constant observation: implications for nursing practice. J Psychosoc Nurs Ment Health Serv 1995;33:46-50.
7. American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. Available at: http://www.psych.org/psych_pract/treatg/pg/SuicidalBehavior_05-15-06.pdf. Accessed April 19, 2007.
8. Simon RI. The suicidal patient. In Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:166-86.
9. Abille v United States, 482 F Supp 703 (ND Cal 1980).
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Town & Gown
Centers of academia and learning have been physically located within urban communities since the time of the ancient Greeks. During the Middle Ages, church-supported universities were established in Italian cities, in Paris, and in Britain at Oxford. Typically, the university community resided in a sequestered segment of the city. As a result of financial endowment and protection granted by the Church, they were largely independent of civil laws and regulations.
In the Middle Ages, students and teachers wore gowns over their attire for warmth in the drafty libraries as well as to identify themselves as scholars; hence the distinction of “town,” a term referring to the townspeople, from “gown,” the people associated with the university.1 For a host of reasons, the traditional relationship between the local community and associated centers of academia has been one of suspicion and hostility.
Establishing Alliances
Over the years, better communication and cooperation between the academic communities and their host cities has eased some of these tensions and—in some cases—has resulted in positive and cordial relationships. Some academic institutions endeavor to contribute to the general community by providing access to evening study events and lectures and by inviting the community to participate in fine arts performances.
These overtures are welcome, but it is important to recognize the potential for universities to exert a dominating influence within a community. The impact of a university on the local community can vary, depending on the size and reputation of the university as well as the size of the town. A large, powerful university has a more profound influence when it is located in a moderate-size city (one with a population less than 250,000) than if it is located in a major metropolitan community. In this situation, the onus is upon the university to recognize its position with respect to the local community and its obligation to contribute to the general societal good.
Most universities recognize the value of establishing strong alliances and trusting relationships with their host communities. Located in Gainesville, Fla., a city with a population of 186,000, the University of Florida is a large university with a major medical school and a 576-bed teaching hospital. In response to community concerns about neighborhood issues, the university’s president appointed a University of Florida Town/Gown Task Force to identify problems and make recommendations to initiate change.2 The task force members included individuals representing the student body, the university faculty, and various representatives of the local community.
Other universities also recognize the importance of working together for the common good. Situated in a town of 13,000, South Carolina’s Clemson University, which has 17,100 students, developed a town-and-gown symposium in 2006 called Community Is a Contact Sport: Universities and Cities Reaching Common Ground. Designed to address neighborhood issues, it also provided a forum for concerns, as well as an opportunity for conflict resolution (www.clemson.edu/town-gown).
From Concern to Conflict
The conflict escalates on multiple levels when town-and-gown issues are set in the context of academic versus private practice medicine. University physicians and community doctors compete for the same patient population. Primary care physicians across the country have complained that when they refer their patients to academic teaching hospitals for specialized care, the patients are absorbed by the university hospitals. They complain that they are not afforded the courtesy of a follow-up letter, nor does the patient return to their care when the acute event is resolved.3 Private practice physicians and community-based hospitals provide important services and are necessary within any community. When the local, private medical community becomes concerned that a university-based medical center seeks to usurp their patients and their livelihood, a heated conflict may ensue.
University-based, research-oriented academic medical centers, with training programs involved in cutting edge technology and highly specialized patient care services, are clearly a positive adjunct to any local community’s—or state’s, for that matter—capability to provide top-notch patient care and services. No one can deny the benefits afforded by this level of expertise. Problems arise when university-based medical centers set a powerful and lustful gaze upon the medical community at large.
During the 1990s, large medical centers across the country bought up community hospitals and medical practices. At that time, and continuing into the present, office overhead—building costs, liability insurance, personnel costs—for private practice groups has often exceeded the ability of these primary care groups to survive. Not unexpectedly, once incorporated into the system, these practices are used to support the subspecialty services at the university medical center, bypassing the community-based subspecialty physicians.
Additionally, large, academic medical centers set up funded and university-supported subspecialty groups that compete head-on with independent practitioners. Private practitioners view these circumstances as stacked competition. The primary-care doctor’s decision in selecting a subspecialty doctor for a patient is no longer based on service, timeliness, and competence, but is instead a result of proscribed referral patterns delineated by the academic institution. Discriminatory referral patterns—not based on merit—result in local discontent, frustration, and unhealthy competition.
Short-Term Savings, Long-Term Loss
These issues are complex. A case can always be made to consolidate resources at the university hospital and avoid duplication of services by stripping away departments in the community hospitals. If pursued to its logical end, this operational model effectively starves community hospitals until they evolve into low acuity, “feeder” stations for the main academic hospital facility. On paper, this plan presents economic advantages. In practice, it not only deprives the metropolitan area of community-based hospital options, but it also results in a dwindling population base and the general decline and disenchantment of the local medical community. As the medical community contracts, so does the patient-base referral radius.
University-owned community hospitals are subject to the discretion of the university medical center. Decision making is attributed to maximum utilization of resources and certification of need, but most observers see the basic principle as economic: ways of garnering a larger portion of the healthcare dollar in the university coffers. Services and even departments provided by community hospitals are likewise subject to the benevolence of the university medical system. Hospitals function like living organisms: If a department such as pediatrics is withdrawn, the hospital continues—but with a limp. Few children can be seen and evaluated in the emergency department; likewise, high-risk obstetrics must be transferred to a major university hospital because the patient may need a neonatal intensive care unit. Hospitalists and internists who happen to be double boarded in medicine and pediatrics steer away from hospitals without a pediatric department. The changes are subtle but, over time, the effects of the loss are apparent.
Hospitalists need to be cognizant of these issues when pursuing employment opportunities. Many career-minded hospitalists seek employment in community-based, full-service hospitals with university medical center affiliations. This combination can provide the best of both worlds: autonomy, opportunities for growth and development, and opportunities for working with house staff and teaching. Checking the status of the relationship between the community hospital and the affiliated university medical center may be an important factor in pre-contract negotiations and decision-making for career hospitalists.
The Bottom Line
The turf battle between community medicine and academic medicine is primarily one of economics. Interesting parallels may be drawn between this conflict and the teachings of Adam Smith. Prior to Smith, economic theory was based on the idea that every dollar you have is one less dollar for me. Smith proposed an entirely different concept: If I help you earn dollars, the economic house will grow, and I, too, will make more dollars, and then you will make more dollars. In this way, the entire system generates more than anyone could have previously imagined. This economic concept extrapolates well to the present discussion of the university medical center versus community medicine.
University health systems do not seem to realize that real growth happens when communities grow together. A robust and vibrant community hospital supports a university medical center with more vigor than an anemic, waning, and disenchanted community hospital that perceives its woes as a result of the powerful—and perhaps dogmatic—university health system. There are enough patients to grow both systems together—the patient base radius grows wider with cooperation and growth—but this cannot happen if the university engenders distrust among local practitioners and the local community. This is a situation that will either be win-win or lose-lose.
Although the crux of the conflict is economic, other aspects of town-and-gown medicine can contribute to better cooperation and understanding. Some academic medical centers have explored ways to incorporate local physicians in university-based clinical trials. These programs offer cutting edge medicine and an opportunity to participate in intellectually stimulating work; at the same time, physicians retain their private practices.
This research opportunity is being offered and supported by a number of academic institutions, including Columbia-Presbyterian in New York City, Duke in Durham, N.C., Partners HealthCare in Boston, the University of Pittsburgh, the University of Rochester (N.Y.), and Washington University (St. Louis, Mo.).4 This is a good-faith start in mending the relationship between the academic and private medical sectors. To achieve a lasting positive relationship, community physicians must trust the academic community to respect their autonomy and to recognize that they have the right to provide full-service care to their patients and to serve their patients without the fear of being unfairly disenfranchised.
The lack of integration of the academic medical community and private practitioners of medicine—the proverbial town and gown—is an old dilemma. It is time to lay it to rest. The solutions are straightforward. Empowering community hospitals and physicians will not diminish the influence of university-based hospitals, nor will there be loss of reimbursement. Just the opposite will occur. In the end, with cooperation, everyone wins; with adversarial actions, all parties lose, especially the patients. TH
Dr. Brezina is a member of the consulting clinical faculty at Duke University, Durham, N.C.
References
- Town and gown in the Middle Ages. Available at: http://en.wikipedia.org/wiki/Town_and_gown. Last accessed March 29, 2007.
- University of Florida Web site. Town/gown task force. Available at: www.facilities.ufl.edu/cp/towngown.htm. Last accessed March 29, 2007.
- Adams D, Croasdale M. Town and gown: turning rivalries into relationships [American Medical News Web site]. January 13, 2003. Available at: www.ama-assn.org/amednews/2003/01/13/prsa0113.htm. Last accessed March 20, 2007.
- Maguire P. Marriage of town and gown brings clinical research to busy practices [ACP-ASIM Observer Web site]. February 2001. Available at: www.acponline.org/journals/news/feb01/clinresearch.htm. Last accessed March 20, 2007.
Centers of academia and learning have been physically located within urban communities since the time of the ancient Greeks. During the Middle Ages, church-supported universities were established in Italian cities, in Paris, and in Britain at Oxford. Typically, the university community resided in a sequestered segment of the city. As a result of financial endowment and protection granted by the Church, they were largely independent of civil laws and regulations.
In the Middle Ages, students and teachers wore gowns over their attire for warmth in the drafty libraries as well as to identify themselves as scholars; hence the distinction of “town,” a term referring to the townspeople, from “gown,” the people associated with the university.1 For a host of reasons, the traditional relationship between the local community and associated centers of academia has been one of suspicion and hostility.
Establishing Alliances
Over the years, better communication and cooperation between the academic communities and their host cities has eased some of these tensions and—in some cases—has resulted in positive and cordial relationships. Some academic institutions endeavor to contribute to the general community by providing access to evening study events and lectures and by inviting the community to participate in fine arts performances.
These overtures are welcome, but it is important to recognize the potential for universities to exert a dominating influence within a community. The impact of a university on the local community can vary, depending on the size and reputation of the university as well as the size of the town. A large, powerful university has a more profound influence when it is located in a moderate-size city (one with a population less than 250,000) than if it is located in a major metropolitan community. In this situation, the onus is upon the university to recognize its position with respect to the local community and its obligation to contribute to the general societal good.
Most universities recognize the value of establishing strong alliances and trusting relationships with their host communities. Located in Gainesville, Fla., a city with a population of 186,000, the University of Florida is a large university with a major medical school and a 576-bed teaching hospital. In response to community concerns about neighborhood issues, the university’s president appointed a University of Florida Town/Gown Task Force to identify problems and make recommendations to initiate change.2 The task force members included individuals representing the student body, the university faculty, and various representatives of the local community.
Other universities also recognize the importance of working together for the common good. Situated in a town of 13,000, South Carolina’s Clemson University, which has 17,100 students, developed a town-and-gown symposium in 2006 called Community Is a Contact Sport: Universities and Cities Reaching Common Ground. Designed to address neighborhood issues, it also provided a forum for concerns, as well as an opportunity for conflict resolution (www.clemson.edu/town-gown).
From Concern to Conflict
The conflict escalates on multiple levels when town-and-gown issues are set in the context of academic versus private practice medicine. University physicians and community doctors compete for the same patient population. Primary care physicians across the country have complained that when they refer their patients to academic teaching hospitals for specialized care, the patients are absorbed by the university hospitals. They complain that they are not afforded the courtesy of a follow-up letter, nor does the patient return to their care when the acute event is resolved.3 Private practice physicians and community-based hospitals provide important services and are necessary within any community. When the local, private medical community becomes concerned that a university-based medical center seeks to usurp their patients and their livelihood, a heated conflict may ensue.
University-based, research-oriented academic medical centers, with training programs involved in cutting edge technology and highly specialized patient care services, are clearly a positive adjunct to any local community’s—or state’s, for that matter—capability to provide top-notch patient care and services. No one can deny the benefits afforded by this level of expertise. Problems arise when university-based medical centers set a powerful and lustful gaze upon the medical community at large.
During the 1990s, large medical centers across the country bought up community hospitals and medical practices. At that time, and continuing into the present, office overhead—building costs, liability insurance, personnel costs—for private practice groups has often exceeded the ability of these primary care groups to survive. Not unexpectedly, once incorporated into the system, these practices are used to support the subspecialty services at the university medical center, bypassing the community-based subspecialty physicians.
Additionally, large, academic medical centers set up funded and university-supported subspecialty groups that compete head-on with independent practitioners. Private practitioners view these circumstances as stacked competition. The primary-care doctor’s decision in selecting a subspecialty doctor for a patient is no longer based on service, timeliness, and competence, but is instead a result of proscribed referral patterns delineated by the academic institution. Discriminatory referral patterns—not based on merit—result in local discontent, frustration, and unhealthy competition.
Short-Term Savings, Long-Term Loss
These issues are complex. A case can always be made to consolidate resources at the university hospital and avoid duplication of services by stripping away departments in the community hospitals. If pursued to its logical end, this operational model effectively starves community hospitals until they evolve into low acuity, “feeder” stations for the main academic hospital facility. On paper, this plan presents economic advantages. In practice, it not only deprives the metropolitan area of community-based hospital options, but it also results in a dwindling population base and the general decline and disenchantment of the local medical community. As the medical community contracts, so does the patient-base referral radius.
University-owned community hospitals are subject to the discretion of the university medical center. Decision making is attributed to maximum utilization of resources and certification of need, but most observers see the basic principle as economic: ways of garnering a larger portion of the healthcare dollar in the university coffers. Services and even departments provided by community hospitals are likewise subject to the benevolence of the university medical system. Hospitals function like living organisms: If a department such as pediatrics is withdrawn, the hospital continues—but with a limp. Few children can be seen and evaluated in the emergency department; likewise, high-risk obstetrics must be transferred to a major university hospital because the patient may need a neonatal intensive care unit. Hospitalists and internists who happen to be double boarded in medicine and pediatrics steer away from hospitals without a pediatric department. The changes are subtle but, over time, the effects of the loss are apparent.
Hospitalists need to be cognizant of these issues when pursuing employment opportunities. Many career-minded hospitalists seek employment in community-based, full-service hospitals with university medical center affiliations. This combination can provide the best of both worlds: autonomy, opportunities for growth and development, and opportunities for working with house staff and teaching. Checking the status of the relationship between the community hospital and the affiliated university medical center may be an important factor in pre-contract negotiations and decision-making for career hospitalists.
The Bottom Line
The turf battle between community medicine and academic medicine is primarily one of economics. Interesting parallels may be drawn between this conflict and the teachings of Adam Smith. Prior to Smith, economic theory was based on the idea that every dollar you have is one less dollar for me. Smith proposed an entirely different concept: If I help you earn dollars, the economic house will grow, and I, too, will make more dollars, and then you will make more dollars. In this way, the entire system generates more than anyone could have previously imagined. This economic concept extrapolates well to the present discussion of the university medical center versus community medicine.
University health systems do not seem to realize that real growth happens when communities grow together. A robust and vibrant community hospital supports a university medical center with more vigor than an anemic, waning, and disenchanted community hospital that perceives its woes as a result of the powerful—and perhaps dogmatic—university health system. There are enough patients to grow both systems together—the patient base radius grows wider with cooperation and growth—but this cannot happen if the university engenders distrust among local practitioners and the local community. This is a situation that will either be win-win or lose-lose.
Although the crux of the conflict is economic, other aspects of town-and-gown medicine can contribute to better cooperation and understanding. Some academic medical centers have explored ways to incorporate local physicians in university-based clinical trials. These programs offer cutting edge medicine and an opportunity to participate in intellectually stimulating work; at the same time, physicians retain their private practices.
This research opportunity is being offered and supported by a number of academic institutions, including Columbia-Presbyterian in New York City, Duke in Durham, N.C., Partners HealthCare in Boston, the University of Pittsburgh, the University of Rochester (N.Y.), and Washington University (St. Louis, Mo.).4 This is a good-faith start in mending the relationship between the academic and private medical sectors. To achieve a lasting positive relationship, community physicians must trust the academic community to respect their autonomy and to recognize that they have the right to provide full-service care to their patients and to serve their patients without the fear of being unfairly disenfranchised.
The lack of integration of the academic medical community and private practitioners of medicine—the proverbial town and gown—is an old dilemma. It is time to lay it to rest. The solutions are straightforward. Empowering community hospitals and physicians will not diminish the influence of university-based hospitals, nor will there be loss of reimbursement. Just the opposite will occur. In the end, with cooperation, everyone wins; with adversarial actions, all parties lose, especially the patients. TH
Dr. Brezina is a member of the consulting clinical faculty at Duke University, Durham, N.C.
References
- Town and gown in the Middle Ages. Available at: http://en.wikipedia.org/wiki/Town_and_gown. Last accessed March 29, 2007.
- University of Florida Web site. Town/gown task force. Available at: www.facilities.ufl.edu/cp/towngown.htm. Last accessed March 29, 2007.
- Adams D, Croasdale M. Town and gown: turning rivalries into relationships [American Medical News Web site]. January 13, 2003. Available at: www.ama-assn.org/amednews/2003/01/13/prsa0113.htm. Last accessed March 20, 2007.
- Maguire P. Marriage of town and gown brings clinical research to busy practices [ACP-ASIM Observer Web site]. February 2001. Available at: www.acponline.org/journals/news/feb01/clinresearch.htm. Last accessed March 20, 2007.
Centers of academia and learning have been physically located within urban communities since the time of the ancient Greeks. During the Middle Ages, church-supported universities were established in Italian cities, in Paris, and in Britain at Oxford. Typically, the university community resided in a sequestered segment of the city. As a result of financial endowment and protection granted by the Church, they were largely independent of civil laws and regulations.
In the Middle Ages, students and teachers wore gowns over their attire for warmth in the drafty libraries as well as to identify themselves as scholars; hence the distinction of “town,” a term referring to the townspeople, from “gown,” the people associated with the university.1 For a host of reasons, the traditional relationship between the local community and associated centers of academia has been one of suspicion and hostility.
Establishing Alliances
Over the years, better communication and cooperation between the academic communities and their host cities has eased some of these tensions and—in some cases—has resulted in positive and cordial relationships. Some academic institutions endeavor to contribute to the general community by providing access to evening study events and lectures and by inviting the community to participate in fine arts performances.
These overtures are welcome, but it is important to recognize the potential for universities to exert a dominating influence within a community. The impact of a university on the local community can vary, depending on the size and reputation of the university as well as the size of the town. A large, powerful university has a more profound influence when it is located in a moderate-size city (one with a population less than 250,000) than if it is located in a major metropolitan community. In this situation, the onus is upon the university to recognize its position with respect to the local community and its obligation to contribute to the general societal good.
Most universities recognize the value of establishing strong alliances and trusting relationships with their host communities. Located in Gainesville, Fla., a city with a population of 186,000, the University of Florida is a large university with a major medical school and a 576-bed teaching hospital. In response to community concerns about neighborhood issues, the university’s president appointed a University of Florida Town/Gown Task Force to identify problems and make recommendations to initiate change.2 The task force members included individuals representing the student body, the university faculty, and various representatives of the local community.
Other universities also recognize the importance of working together for the common good. Situated in a town of 13,000, South Carolina’s Clemson University, which has 17,100 students, developed a town-and-gown symposium in 2006 called Community Is a Contact Sport: Universities and Cities Reaching Common Ground. Designed to address neighborhood issues, it also provided a forum for concerns, as well as an opportunity for conflict resolution (www.clemson.edu/town-gown).
From Concern to Conflict
The conflict escalates on multiple levels when town-and-gown issues are set in the context of academic versus private practice medicine. University physicians and community doctors compete for the same patient population. Primary care physicians across the country have complained that when they refer their patients to academic teaching hospitals for specialized care, the patients are absorbed by the university hospitals. They complain that they are not afforded the courtesy of a follow-up letter, nor does the patient return to their care when the acute event is resolved.3 Private practice physicians and community-based hospitals provide important services and are necessary within any community. When the local, private medical community becomes concerned that a university-based medical center seeks to usurp their patients and their livelihood, a heated conflict may ensue.
University-based, research-oriented academic medical centers, with training programs involved in cutting edge technology and highly specialized patient care services, are clearly a positive adjunct to any local community’s—or state’s, for that matter—capability to provide top-notch patient care and services. No one can deny the benefits afforded by this level of expertise. Problems arise when university-based medical centers set a powerful and lustful gaze upon the medical community at large.
During the 1990s, large medical centers across the country bought up community hospitals and medical practices. At that time, and continuing into the present, office overhead—building costs, liability insurance, personnel costs—for private practice groups has often exceeded the ability of these primary care groups to survive. Not unexpectedly, once incorporated into the system, these practices are used to support the subspecialty services at the university medical center, bypassing the community-based subspecialty physicians.
Additionally, large, academic medical centers set up funded and university-supported subspecialty groups that compete head-on with independent practitioners. Private practitioners view these circumstances as stacked competition. The primary-care doctor’s decision in selecting a subspecialty doctor for a patient is no longer based on service, timeliness, and competence, but is instead a result of proscribed referral patterns delineated by the academic institution. Discriminatory referral patterns—not based on merit—result in local discontent, frustration, and unhealthy competition.
Short-Term Savings, Long-Term Loss
These issues are complex. A case can always be made to consolidate resources at the university hospital and avoid duplication of services by stripping away departments in the community hospitals. If pursued to its logical end, this operational model effectively starves community hospitals until they evolve into low acuity, “feeder” stations for the main academic hospital facility. On paper, this plan presents economic advantages. In practice, it not only deprives the metropolitan area of community-based hospital options, but it also results in a dwindling population base and the general decline and disenchantment of the local medical community. As the medical community contracts, so does the patient-base referral radius.
University-owned community hospitals are subject to the discretion of the university medical center. Decision making is attributed to maximum utilization of resources and certification of need, but most observers see the basic principle as economic: ways of garnering a larger portion of the healthcare dollar in the university coffers. Services and even departments provided by community hospitals are likewise subject to the benevolence of the university medical system. Hospitals function like living organisms: If a department such as pediatrics is withdrawn, the hospital continues—but with a limp. Few children can be seen and evaluated in the emergency department; likewise, high-risk obstetrics must be transferred to a major university hospital because the patient may need a neonatal intensive care unit. Hospitalists and internists who happen to be double boarded in medicine and pediatrics steer away from hospitals without a pediatric department. The changes are subtle but, over time, the effects of the loss are apparent.
Hospitalists need to be cognizant of these issues when pursuing employment opportunities. Many career-minded hospitalists seek employment in community-based, full-service hospitals with university medical center affiliations. This combination can provide the best of both worlds: autonomy, opportunities for growth and development, and opportunities for working with house staff and teaching. Checking the status of the relationship between the community hospital and the affiliated university medical center may be an important factor in pre-contract negotiations and decision-making for career hospitalists.
The Bottom Line
The turf battle between community medicine and academic medicine is primarily one of economics. Interesting parallels may be drawn between this conflict and the teachings of Adam Smith. Prior to Smith, economic theory was based on the idea that every dollar you have is one less dollar for me. Smith proposed an entirely different concept: If I help you earn dollars, the economic house will grow, and I, too, will make more dollars, and then you will make more dollars. In this way, the entire system generates more than anyone could have previously imagined. This economic concept extrapolates well to the present discussion of the university medical center versus community medicine.
University health systems do not seem to realize that real growth happens when communities grow together. A robust and vibrant community hospital supports a university medical center with more vigor than an anemic, waning, and disenchanted community hospital that perceives its woes as a result of the powerful—and perhaps dogmatic—university health system. There are enough patients to grow both systems together—the patient base radius grows wider with cooperation and growth—but this cannot happen if the university engenders distrust among local practitioners and the local community. This is a situation that will either be win-win or lose-lose.
Although the crux of the conflict is economic, other aspects of town-and-gown medicine can contribute to better cooperation and understanding. Some academic medical centers have explored ways to incorporate local physicians in university-based clinical trials. These programs offer cutting edge medicine and an opportunity to participate in intellectually stimulating work; at the same time, physicians retain their private practices.
This research opportunity is being offered and supported by a number of academic institutions, including Columbia-Presbyterian in New York City, Duke in Durham, N.C., Partners HealthCare in Boston, the University of Pittsburgh, the University of Rochester (N.Y.), and Washington University (St. Louis, Mo.).4 This is a good-faith start in mending the relationship between the academic and private medical sectors. To achieve a lasting positive relationship, community physicians must trust the academic community to respect their autonomy and to recognize that they have the right to provide full-service care to their patients and to serve their patients without the fear of being unfairly disenfranchised.
The lack of integration of the academic medical community and private practitioners of medicine—the proverbial town and gown—is an old dilemma. It is time to lay it to rest. The solutions are straightforward. Empowering community hospitals and physicians will not diminish the influence of university-based hospitals, nor will there be loss of reimbursement. Just the opposite will occur. In the end, with cooperation, everyone wins; with adversarial actions, all parties lose, especially the patients. TH
Dr. Brezina is a member of the consulting clinical faculty at Duke University, Durham, N.C.
References
- Town and gown in the Middle Ages. Available at: http://en.wikipedia.org/wiki/Town_and_gown. Last accessed March 29, 2007.
- University of Florida Web site. Town/gown task force. Available at: www.facilities.ufl.edu/cp/towngown.htm. Last accessed March 29, 2007.
- Adams D, Croasdale M. Town and gown: turning rivalries into relationships [American Medical News Web site]. January 13, 2003. Available at: www.ama-assn.org/amednews/2003/01/13/prsa0113.htm. Last accessed March 20, 2007.
- Maguire P. Marriage of town and gown brings clinical research to busy practices [ACP-ASIM Observer Web site]. February 2001. Available at: www.acponline.org/journals/news/feb01/clinresearch.htm. Last accessed March 20, 2007.
Scapular Pain
Case
A 67-year-old female was referred for two weeks of left shoulder pain that kept her from sleeping and moving her arm and interfered with her job as a typist. The pain was located in the posterior shoulder just medial to the scapula, radiated down her left arm, and was positional. She had not noticed a decreased range of motion.
After failure of steroids and NSAIDs, she was referred to a chiropractor, who did not improve her shoulder pain. When she got up from the table, she noticed that she was having crushing chest pain bilaterally on each side of the sternum at the level of the first and second ribs. Since then, she had been on significant doses of opiates and oral steroids without pain resolution.
Physical Exam
A shoulder exam revealed bilateral normal range of motion with no crepitus. The patient’s head was slightly tilted, her back laterally rotated. There was a palpable tender mass over the medial aspect of her left scapula. Palpation of the rhomboid muscle caused intense acute pain that radiated down her arm and reproduced her symptoms (See sample photos 1 & 2).

Rhomboid Spasm
Etiology: A rhomboid muscle strain or spasm is usually caused by overuse of the shoulder and arm, especially during repetitive overhead activities like serving a tennis ball or reaching to put objects on a high shelf. It can also result from activities such as the prolonged use of a computer, the problem experienced by this patient.
Anatomy: The rhomboids originate on the last (seventh) cervical and first five thoracic vertebrae and insert on the medial border of the scapula. They work with the levator scapulae and the upper trapezius to elevate and retract the scapula. Spasms of the rhomboids refer pain to a local and limited area, as well as down the lateral aspect of the arm, and are often accompanied by trigger points in levator scapulae, trapezius, and pectoralis major and minor. (See photos 3a, 3b, and 4).
Treatment
Rhomboid spasm should be treated by local lidocaine injection and a depot corticosteroid into the rhomboid muscle. The lidocaine provides the direct effect of reducing the current spasm, and the anti-inflammatory effect of the steroid reduces recurrence.


Rhomboid Injection
To administer a rhomboid injection, first locate the rhomboid muscle just medial to the scapula on the posterior shoulder. A rhomboid muscle in spasm often presents as a painful, palpable mass. Next, identify an area of point tenderness. Inject lidocaine and a corticosteroid. The correct location will be confirmed by immediate pain relief; the steroid, however, may take up to a week to provide pain relief.
Three-Month Follow-Up
The patient returned three months after her rhomboid muscle was injected with lidocaine and a depo-steroid preparation. She has resumed her job as a typist and performs rhomboid spasm prevention exercises. She sleeps well and can move her arm without pain. She is active in her daily activities and enjoys shopping with her friends.

Prevention
Prevention can be achieved through the following rhomboid exercises:
- Sit with your legs stretched in front of you. Bend your right knee and place your right foot on the left/outside of your left knee. With your right hand, grab and hold on to your right ankle. Holding on to your right ankle, lean back. (See 5A.)
- The key: Press your right elbow into your right knee and point/push your right shoulder toward the floor in front of you. (See 5B.)
- Stand with your arms at your sides. Stretch one arm across your body and pull it in toward your body with your other hand. (See 5C.)
- Sit on a chair firmly planted on the floor. Lift your right leg and put the right ankle onto the knee of the left leg. Grab your right ankle with your right hand and rest your right elbow on your right knee. With your left hand, grasp the chair back behind you and rotate your torso to the left to look over your left hand. (See 5D.)




Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Case
A 67-year-old female was referred for two weeks of left shoulder pain that kept her from sleeping and moving her arm and interfered with her job as a typist. The pain was located in the posterior shoulder just medial to the scapula, radiated down her left arm, and was positional. She had not noticed a decreased range of motion.
After failure of steroids and NSAIDs, she was referred to a chiropractor, who did not improve her shoulder pain. When she got up from the table, she noticed that she was having crushing chest pain bilaterally on each side of the sternum at the level of the first and second ribs. Since then, she had been on significant doses of opiates and oral steroids without pain resolution.
Physical Exam
A shoulder exam revealed bilateral normal range of motion with no crepitus. The patient’s head was slightly tilted, her back laterally rotated. There was a palpable tender mass over the medial aspect of her left scapula. Palpation of the rhomboid muscle caused intense acute pain that radiated down her arm and reproduced her symptoms (See sample photos 1 & 2).
Rhomboid Spasm
Etiology: A rhomboid muscle strain or spasm is usually caused by overuse of the shoulder and arm, especially during repetitive overhead activities like serving a tennis ball or reaching to put objects on a high shelf. It can also result from activities such as the prolonged use of a computer, the problem experienced by this patient.
Anatomy: The rhomboids originate on the last (seventh) cervical and first five thoracic vertebrae and insert on the medial border of the scapula. They work with the levator scapulae and the upper trapezius to elevate and retract the scapula. Spasms of the rhomboids refer pain to a local and limited area, as well as down the lateral aspect of the arm, and are often accompanied by trigger points in levator scapulae, trapezius, and pectoralis major and minor. (See photos 3a, 3b, and 4).
Treatment
Rhomboid spasm should be treated by local lidocaine injection and a depot corticosteroid into the rhomboid muscle. The lidocaine provides the direct effect of reducing the current spasm, and the anti-inflammatory effect of the steroid reduces recurrence.
Rhomboid Injection
To administer a rhomboid injection, first locate the rhomboid muscle just medial to the scapula on the posterior shoulder. A rhomboid muscle in spasm often presents as a painful, palpable mass. Next, identify an area of point tenderness. Inject lidocaine and a corticosteroid. The correct location will be confirmed by immediate pain relief; the steroid, however, may take up to a week to provide pain relief.
Three-Month Follow-Up
The patient returned three months after her rhomboid muscle was injected with lidocaine and a depo-steroid preparation. She has resumed her job as a typist and performs rhomboid spasm prevention exercises. She sleeps well and can move her arm without pain. She is active in her daily activities and enjoys shopping with her friends.
Prevention
Prevention can be achieved through the following rhomboid exercises:
- Sit with your legs stretched in front of you. Bend your right knee and place your right foot on the left/outside of your left knee. With your right hand, grab and hold on to your right ankle. Holding on to your right ankle, lean back. (See 5A.)
- The key: Press your right elbow into your right knee and point/push your right shoulder toward the floor in front of you. (See 5B.)
- Stand with your arms at your sides. Stretch one arm across your body and pull it in toward your body with your other hand. (See 5C.)
- Sit on a chair firmly planted on the floor. Lift your right leg and put the right ankle onto the knee of the left leg. Grab your right ankle with your right hand and rest your right elbow on your right knee. With your left hand, grasp the chair back behind you and rotate your torso to the left to look over your left hand. (See 5D.)
Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Case
A 67-year-old female was referred for two weeks of left shoulder pain that kept her from sleeping and moving her arm and interfered with her job as a typist. The pain was located in the posterior shoulder just medial to the scapula, radiated down her left arm, and was positional. She had not noticed a decreased range of motion.
After failure of steroids and NSAIDs, she was referred to a chiropractor, who did not improve her shoulder pain. When she got up from the table, she noticed that she was having crushing chest pain bilaterally on each side of the sternum at the level of the first and second ribs. Since then, she had been on significant doses of opiates and oral steroids without pain resolution.
Physical Exam
A shoulder exam revealed bilateral normal range of motion with no crepitus. The patient’s head was slightly tilted, her back laterally rotated. There was a palpable tender mass over the medial aspect of her left scapula. Palpation of the rhomboid muscle caused intense acute pain that radiated down her arm and reproduced her symptoms (See sample photos 1 & 2).
Rhomboid Spasm
Etiology: A rhomboid muscle strain or spasm is usually caused by overuse of the shoulder and arm, especially during repetitive overhead activities like serving a tennis ball or reaching to put objects on a high shelf. It can also result from activities such as the prolonged use of a computer, the problem experienced by this patient.
Anatomy: The rhomboids originate on the last (seventh) cervical and first five thoracic vertebrae and insert on the medial border of the scapula. They work with the levator scapulae and the upper trapezius to elevate and retract the scapula. Spasms of the rhomboids refer pain to a local and limited area, as well as down the lateral aspect of the arm, and are often accompanied by trigger points in levator scapulae, trapezius, and pectoralis major and minor. (See photos 3a, 3b, and 4).
Treatment
Rhomboid spasm should be treated by local lidocaine injection and a depot corticosteroid into the rhomboid muscle. The lidocaine provides the direct effect of reducing the current spasm, and the anti-inflammatory effect of the steroid reduces recurrence.
Rhomboid Injection
To administer a rhomboid injection, first locate the rhomboid muscle just medial to the scapula on the posterior shoulder. A rhomboid muscle in spasm often presents as a painful, palpable mass. Next, identify an area of point tenderness. Inject lidocaine and a corticosteroid. The correct location will be confirmed by immediate pain relief; the steroid, however, may take up to a week to provide pain relief.
Three-Month Follow-Up
The patient returned three months after her rhomboid muscle was injected with lidocaine and a depo-steroid preparation. She has resumed her job as a typist and performs rhomboid spasm prevention exercises. She sleeps well and can move her arm without pain. She is active in her daily activities and enjoys shopping with her friends.
Prevention
Prevention can be achieved through the following rhomboid exercises:
- Sit with your legs stretched in front of you. Bend your right knee and place your right foot on the left/outside of your left knee. With your right hand, grab and hold on to your right ankle. Holding on to your right ankle, lean back. (See 5A.)
- The key: Press your right elbow into your right knee and point/push your right shoulder toward the floor in front of you. (See 5B.)
- Stand with your arms at your sides. Stretch one arm across your body and pull it in toward your body with your other hand. (See 5C.)
- Sit on a chair firmly planted on the floor. Lift your right leg and put the right ankle onto the knee of the left leg. Grab your right ankle with your right hand and rest your right elbow on your right knee. With your left hand, grasp the chair back behind you and rotate your torso to the left to look over your left hand. (See 5D.)
Dr. Ficalora is an associate professor of medicine at the Mayo Clinic College of Medicine, and Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
SHM Behind the Scenes

Remember the classic episod-es of “Star Trek” where a new cast member went on a mission? Chances were that guy would be the one to fall off a cliff or get zapped with a laser gun and would not make it back safely to the starship Enterprise.
Recently I was in a meeting focused on what happens when older adults are discharged from the hospital. I thought to myself: “Those are the patients wearing the red uniforms. But what if we could make the experience of older adults more like that of Spock and Captain Kirk, where luck and good preparation are on their side and the data to make informed decisions follow them everywhere?”
The transition of patients in and out of the hospital has become a key patient-safety concern. Patients frequently arrive at the hospital with incomplete medical histories and uncertain or missing medication lists. During a typical hospitalization, patients receive less than optimal preparation before their discharge and often leave the hospital without a clear understanding of how to care for themselves, identify new symptoms that require immediate medical attention, or take their medications. Further, it is often unclear whom patients should call with questions while they are in “the white space”—that time period between hospital discharge and follow-up care. Do they call the hospital? The hospitalist? Their primary care physician? Their cardiologist?
Safety related to transitions of care is a concern frequently raised about the hospital medicine movement. The use of hospitalists forces physician discontinuity at admission and discharge. However, SHM plans to make discharge planning an issue that brings hospitalists and hospital medicine the greatest praise. SHM is taking a clear, proactive leadership role to define safe transitions, create toolkits for hospitals to improve their current transition practices, and develop technical assistance programs to build quality improvement capacity at local institutions.
Safe Transitions
SHM is participating in two major initiatives to define safe transitions. As a member of the American Board of Internal Medicine (ABIM) Foundation Stepping Up To The Plate Initiative (SUTTP), we are helping to develop sets of principles of and standards for safe and effective transitions.
SHM also co-chaired a Transitions of Care Consensus Conference (TOCCC) in partnership with the American College of Physicians and Society of General Internal Medicine. The TOCCC further reviewed the work of the SUTTP conference and focused more specifically on issues that arise as patients transfer in and out of the hospital.
In these meetings and others, SHM’s messages were clear:
- Improvements in transitions are needed now, and shouldn’t wait for other movements such as creation of medical homes or national electronic medical records to become a reality;
- Safe transitions require teams of medical professionals on both sides of the transfer and patients and their families working together;
- Patients and their families/ caregivers must be included and prepared for transfers of care;
- Better information on patient history and medications needs to follow patients into the hospital; and
- A small subset of information from the care plan, or transition record, should follow patients through each transfer, and be made available to them in lay terms.
Both the SUTTP and TOCCC documents are under review for endorsement by multiple medical professional societies. SHM is pursuing the development of related performance measures for safe care transitions.
Technical Assistance
SHM has for years distinguished its educational offerings by offering “implementation education.” We focus on translating best practices into actual practices. To that end, with generous support from the John A. Hartford Foundation, we are developing a discharge planning toolkit.
The toolkit will provide a step-wise approach to plan, implement, and evaluate interventions to improve discharge planning. The toolkit will help quality teams establish goals, garner internal support for interventions, educate support staff, and evaluate their results.
The interventional approaches and tools are focused on:
- Improving communication among sending and receiving physicians;
- Better preparing patients for post-discharge medication management and other self-care; and
- Facilitating follow-up care and transfer of patient information.
On Sept. 7, SHM convened an advisory board in Chicago to review and provide feedback on our proposed interventional strategies, technical support offerings, and evaluation plan. An impressive group of key stakeholders attended, including:
- Representatives from major payer groups such as the Centers for Medicare and Medicaid Services, Blue Cross Blue Shield, and Kaiser Permanente;
- Professional societies including the American Geriatrics Society, the Society of General Internal Medicine, the Case Management Society of America, and the American Society of Health System Pharmacists.
- Representation from the John A. Hartford Foundation, patient advocates from The Families and Health Care Project, and leaders and practicing professionals in nursing, social work, case management, patient advocacy, geriatrics, primary care, quality improvement and, of course, hospital medicine.
While not at the September meeting, the advisory board also includes representatives from the Agency for Healthcare Research and Quality and the Joint Commission.
The advisory board provided valuable feedback on SHM’s proposed toolkit and applauded our efforts to lead teams to make substantial local hospital improvements. Participants also had the opportunity to share existing resources and strategize opportunities to encourage wide-scale adoption of the toolkit. In February the advisory board plans to reconvene to review the completed toolkit.
SHM is developing training opportunities for institutions adopting the toolkit, designed to meet the full spectrum of technical assistance needs. The full toolkit will be available free on SHM’s Web site in the spring. At the April 2008 SHM Annual Meeting in San Diego, quality teams can participate in a daylong pre-course on general quality improvement principles and hands-on application of the toolkit.
In May, SHM will begin reviewing applications for sites wishing to participate in the yearlong mentoring program or a more intensive short-term, on-site consultant service. For more information on these technical assistance programs, visit the SHM Web site at www.hospitalmedicine.org and select the “Quality Improvement” link, then “Current Initiatives.”
We hope you and your institution will join our journey into the white space to improve discharge planning and help our patients “live long and prosper.” TH
Remember the classic episod-es of “Star Trek” where a new cast member went on a mission? Chances were that guy would be the one to fall off a cliff or get zapped with a laser gun and would not make it back safely to the starship Enterprise.
Recently I was in a meeting focused on what happens when older adults are discharged from the hospital. I thought to myself: “Those are the patients wearing the red uniforms. But what if we could make the experience of older adults more like that of Spock and Captain Kirk, where luck and good preparation are on their side and the data to make informed decisions follow them everywhere?”
The transition of patients in and out of the hospital has become a key patient-safety concern. Patients frequently arrive at the hospital with incomplete medical histories and uncertain or missing medication lists. During a typical hospitalization, patients receive less than optimal preparation before their discharge and often leave the hospital without a clear understanding of how to care for themselves, identify new symptoms that require immediate medical attention, or take their medications. Further, it is often unclear whom patients should call with questions while they are in “the white space”—that time period between hospital discharge and follow-up care. Do they call the hospital? The hospitalist? Their primary care physician? Their cardiologist?
Safety related to transitions of care is a concern frequently raised about the hospital medicine movement. The use of hospitalists forces physician discontinuity at admission and discharge. However, SHM plans to make discharge planning an issue that brings hospitalists and hospital medicine the greatest praise. SHM is taking a clear, proactive leadership role to define safe transitions, create toolkits for hospitals to improve their current transition practices, and develop technical assistance programs to build quality improvement capacity at local institutions.
Safe Transitions
SHM is participating in two major initiatives to define safe transitions. As a member of the American Board of Internal Medicine (ABIM) Foundation Stepping Up To The Plate Initiative (SUTTP), we are helping to develop sets of principles of and standards for safe and effective transitions.
SHM also co-chaired a Transitions of Care Consensus Conference (TOCCC) in partnership with the American College of Physicians and Society of General Internal Medicine. The TOCCC further reviewed the work of the SUTTP conference and focused more specifically on issues that arise as patients transfer in and out of the hospital.
In these meetings and others, SHM’s messages were clear:
- Improvements in transitions are needed now, and shouldn’t wait for other movements such as creation of medical homes or national electronic medical records to become a reality;
- Safe transitions require teams of medical professionals on both sides of the transfer and patients and their families working together;
- Patients and their families/ caregivers must be included and prepared for transfers of care;
- Better information on patient history and medications needs to follow patients into the hospital; and
- A small subset of information from the care plan, or transition record, should follow patients through each transfer, and be made available to them in lay terms.
Both the SUTTP and TOCCC documents are under review for endorsement by multiple medical professional societies. SHM is pursuing the development of related performance measures for safe care transitions.
Technical Assistance
SHM has for years distinguished its educational offerings by offering “implementation education.” We focus on translating best practices into actual practices. To that end, with generous support from the John A. Hartford Foundation, we are developing a discharge planning toolkit.
The toolkit will provide a step-wise approach to plan, implement, and evaluate interventions to improve discharge planning. The toolkit will help quality teams establish goals, garner internal support for interventions, educate support staff, and evaluate their results.
The interventional approaches and tools are focused on:
- Improving communication among sending and receiving physicians;
- Better preparing patients for post-discharge medication management and other self-care; and
- Facilitating follow-up care and transfer of patient information.
On Sept. 7, SHM convened an advisory board in Chicago to review and provide feedback on our proposed interventional strategies, technical support offerings, and evaluation plan. An impressive group of key stakeholders attended, including:
- Representatives from major payer groups such as the Centers for Medicare and Medicaid Services, Blue Cross Blue Shield, and Kaiser Permanente;
- Professional societies including the American Geriatrics Society, the Society of General Internal Medicine, the Case Management Society of America, and the American Society of Health System Pharmacists.
- Representation from the John A. Hartford Foundation, patient advocates from The Families and Health Care Project, and leaders and practicing professionals in nursing, social work, case management, patient advocacy, geriatrics, primary care, quality improvement and, of course, hospital medicine.
While not at the September meeting, the advisory board also includes representatives from the Agency for Healthcare Research and Quality and the Joint Commission.
The advisory board provided valuable feedback on SHM’s proposed toolkit and applauded our efforts to lead teams to make substantial local hospital improvements. Participants also had the opportunity to share existing resources and strategize opportunities to encourage wide-scale adoption of the toolkit. In February the advisory board plans to reconvene to review the completed toolkit.
SHM is developing training opportunities for institutions adopting the toolkit, designed to meet the full spectrum of technical assistance needs. The full toolkit will be available free on SHM’s Web site in the spring. At the April 2008 SHM Annual Meeting in San Diego, quality teams can participate in a daylong pre-course on general quality improvement principles and hands-on application of the toolkit.
In May, SHM will begin reviewing applications for sites wishing to participate in the yearlong mentoring program or a more intensive short-term, on-site consultant service. For more information on these technical assistance programs, visit the SHM Web site at www.hospitalmedicine.org and select the “Quality Improvement” link, then “Current Initiatives.”
We hope you and your institution will join our journey into the white space to improve discharge planning and help our patients “live long and prosper.” TH
Remember the classic episod-es of “Star Trek” where a new cast member went on a mission? Chances were that guy would be the one to fall off a cliff or get zapped with a laser gun and would not make it back safely to the starship Enterprise.
Recently I was in a meeting focused on what happens when older adults are discharged from the hospital. I thought to myself: “Those are the patients wearing the red uniforms. But what if we could make the experience of older adults more like that of Spock and Captain Kirk, where luck and good preparation are on their side and the data to make informed decisions follow them everywhere?”
The transition of patients in and out of the hospital has become a key patient-safety concern. Patients frequently arrive at the hospital with incomplete medical histories and uncertain or missing medication lists. During a typical hospitalization, patients receive less than optimal preparation before their discharge and often leave the hospital without a clear understanding of how to care for themselves, identify new symptoms that require immediate medical attention, or take their medications. Further, it is often unclear whom patients should call with questions while they are in “the white space”—that time period between hospital discharge and follow-up care. Do they call the hospital? The hospitalist? Their primary care physician? Their cardiologist?
Safety related to transitions of care is a concern frequently raised about the hospital medicine movement. The use of hospitalists forces physician discontinuity at admission and discharge. However, SHM plans to make discharge planning an issue that brings hospitalists and hospital medicine the greatest praise. SHM is taking a clear, proactive leadership role to define safe transitions, create toolkits for hospitals to improve their current transition practices, and develop technical assistance programs to build quality improvement capacity at local institutions.
Safe Transitions
SHM is participating in two major initiatives to define safe transitions. As a member of the American Board of Internal Medicine (ABIM) Foundation Stepping Up To The Plate Initiative (SUTTP), we are helping to develop sets of principles of and standards for safe and effective transitions.
SHM also co-chaired a Transitions of Care Consensus Conference (TOCCC) in partnership with the American College of Physicians and Society of General Internal Medicine. The TOCCC further reviewed the work of the SUTTP conference and focused more specifically on issues that arise as patients transfer in and out of the hospital.
In these meetings and others, SHM’s messages were clear:
- Improvements in transitions are needed now, and shouldn’t wait for other movements such as creation of medical homes or national electronic medical records to become a reality;
- Safe transitions require teams of medical professionals on both sides of the transfer and patients and their families working together;
- Patients and their families/ caregivers must be included and prepared for transfers of care;
- Better information on patient history and medications needs to follow patients into the hospital; and
- A small subset of information from the care plan, or transition record, should follow patients through each transfer, and be made available to them in lay terms.
Both the SUTTP and TOCCC documents are under review for endorsement by multiple medical professional societies. SHM is pursuing the development of related performance measures for safe care transitions.
Technical Assistance
SHM has for years distinguished its educational offerings by offering “implementation education.” We focus on translating best practices into actual practices. To that end, with generous support from the John A. Hartford Foundation, we are developing a discharge planning toolkit.
The toolkit will provide a step-wise approach to plan, implement, and evaluate interventions to improve discharge planning. The toolkit will help quality teams establish goals, garner internal support for interventions, educate support staff, and evaluate their results.
The interventional approaches and tools are focused on:
- Improving communication among sending and receiving physicians;
- Better preparing patients for post-discharge medication management and other self-care; and
- Facilitating follow-up care and transfer of patient information.
On Sept. 7, SHM convened an advisory board in Chicago to review and provide feedback on our proposed interventional strategies, technical support offerings, and evaluation plan. An impressive group of key stakeholders attended, including:
- Representatives from major payer groups such as the Centers for Medicare and Medicaid Services, Blue Cross Blue Shield, and Kaiser Permanente;
- Professional societies including the American Geriatrics Society, the Society of General Internal Medicine, the Case Management Society of America, and the American Society of Health System Pharmacists.
- Representation from the John A. Hartford Foundation, patient advocates from The Families and Health Care Project, and leaders and practicing professionals in nursing, social work, case management, patient advocacy, geriatrics, primary care, quality improvement and, of course, hospital medicine.
While not at the September meeting, the advisory board also includes representatives from the Agency for Healthcare Research and Quality and the Joint Commission.
The advisory board provided valuable feedback on SHM’s proposed toolkit and applauded our efforts to lead teams to make substantial local hospital improvements. Participants also had the opportunity to share existing resources and strategize opportunities to encourage wide-scale adoption of the toolkit. In February the advisory board plans to reconvene to review the completed toolkit.
SHM is developing training opportunities for institutions adopting the toolkit, designed to meet the full spectrum of technical assistance needs. The full toolkit will be available free on SHM’s Web site in the spring. At the April 2008 SHM Annual Meeting in San Diego, quality teams can participate in a daylong pre-course on general quality improvement principles and hands-on application of the toolkit.
In May, SHM will begin reviewing applications for sites wishing to participate in the yearlong mentoring program or a more intensive short-term, on-site consultant service. For more information on these technical assistance programs, visit the SHM Web site at www.hospitalmedicine.org and select the “Quality Improvement” link, then “Current Initiatives.”
We hope you and your institution will join our journey into the white space to improve discharge planning and help our patients “live long and prosper.” TH
SHM Launches Geriatric Special Interest Group

At the 2006 SHM Annual Meeting Geriatrics Special Interest Forum, participants asked, “Can we create an area on the SHM Web site focused on our unique interests and needs?” Last month, SHM answered with a resounding “Yes!” as we launched the Geriatrics Special Interest Group on www.hospitalmedicine.org.
The SHM Geriatrics Special Interest Group provides a portal for SHM members to access relevant, timely information about and resources for geriatric medicine. The Community Forums provide a mechanism for participants to communicate with each other about issues in geriatric medicine and other areas of interest. In particular, the Geriatrics Special Interest Group allows users to post information about training and career development opportunities, professional meetings and forums, and funding opportunities. Users can access a wealth of geriatric-medicine resources, including breaking medical news, clinical and quality improvement tools, key publications, and archived SHM Annual Meeting presentations. The Geriatrics Special Interest Group will serve as a template for future member-requested special interest groups, including palliative care, pediatrics, and others.
The Geriatrics Special Interest Group was developed by SHM members, other experts from the community of geriatric medicine, and a team of SHM staffers. SHM member Melissa Mattison, MD, (Beth Israel Deaconess) serves as medical editor for the site and helped shape its vision, along with members Param Dedhia, MD, (Johns Hopkins, Bayview) and Jason Stein, MD (Emory University). The group also benefited from reviews and contributions made by John Degelau, MD, at HealthPartners Medical Group, Gavin W. Hougham, MD, PhD, at The John A. Hartford Foundation, Nancy Lundebjerg, MPA, and Jane Potter, MD, at the American Geriatrics Society, Odette van der Willik at the American Federation for Aging Research, and Paula M. Podrazik, MD, at the Case Management Society of America. The internal SHM development team was led by Shannon Roach and included Bruce Hanson, Travis Kamps, and Tina Budnitz.
To view the Geriatrics Special Interest Group, go to SHM’s Web site or type the address into your browser: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=12369.
We hope SHM members will utilize the Geriatrics Special Interest Group to share ideas and resources, to network, and to improve inpatient geriatric medicine. Let us know if the site meets your needs by sending your comments and suggestions to Shannon Roach at [email protected]. Have an idea for another special interest group? E-mail us that suggestion, too.
SHM: BEHIND THE SCENES
Education and quality improvement: Reflections of a New Staff Member
By Kristin Beck

It’s nice to come to work every day and focus on education and quality improvement. Ensuring that hospitalists have the most up to date information as well as support and encouragement for implementing positive change are good reasons for leaving the house in the morning.
Only three weeks into my role as senior project manager, I have had the sincere pleasure of being involved with updating quality improvement resource rooms (common Web site areas that house tools for implementing quality improvement programs) by initiating a grant-supported program for examining observation units as they relate to treating the number one reason people are hospitalized. I have also accomplished writing and submitting a grant for the Quality Improvement Pre-Course, as well as, working with a committee that looks at patient quality care and projects to enhance it.
Our work here focuses on examining what has been done, how we can improve it, and how we can institute best practices. Not bad for three weeks’ work!
Conversations in our department focus on whether members get what they need and want. People meet regularly to discuss how we can refine and improve the services we offer. Strategies for securing funding and developing programs are reviewed, not for this calendar or fiscal year but for years to come. In one of my final interviews for this job, I was reminded that we don’t deliver here—we over-deliver. Looking through The Hospitalist, titles that stand out include the words unforgettable, safety, expert, leader, admire, and smart.
When people ask what I do in my new job, I tell them that hospital medicine looks at the total experience of being a doctor. It focuses not only on medical care but also on the complete experience of being a working professional: the arts of research, negotiation, best practices, team-focused care, conflict resolution, and systems change. I explain that we do life-saving work, for it is far more than the practice of just day-to-day medicine that improves all of our lives. I tell people that it is work that makes sense.
When you come to work every day and are surrounded by a dynamic, positive energy, the work you produce is likely to mirror the hospital medicine movement: You will reflect, revise, and grow stronger. Sincere, well-planned initiatives are infectious. Continually participating in an environment that asks the questions, “Where can we take this?” and “What can we do better?” is a pretty good reason to get out of bed in the morning.
Beck is the senior project manager at SHM.
VTE Prevention Collaborative off to a Great Start
The VTE Prevention Collaborative (VTE PC) is the latest SHM initiative to support hospitalist-led efforts to reduce the incidence of preventable, hospital-acquired VTE. Launched in January 2007, the program offers individualized assistance to hospitalists who want to take the lead on this critical quality and patient safety issue.
Hospital-Acquired Venous Thromboembolism
The problem of hospital-acquired VTE is huge. More than 2 million Americans suffer from VTE each year. Most hospitalized patients have at least one risk factor for VTE. In a large registry trial capturing more than 5,451 patients at 183 sites in a six-month period, 50% (2,726) developed their VTE during hospitalization.1 A 400-bed hospital with an average rate of VTE prophylaxis can expect that 200 patients will suffer from hospital-acquired VTE each year; around half of these cases are potentially preventable.1,2
The good news is that effective and safe measures to prevent hospital-acquired VTE exist. Pharmacologic prophylaxis reduces the incidence of asymptomatic and symptomatic DVT and pulmonary embolism (PE) by 50%-65%.3, 4-11 Prevention of DVT also prevents PE and fatalities from PE. The chief concern of prophylaxis is bleeding, but bleeding risk secondary to pharmacologic prophylaxis is a rare event, as is shown in abundant data from meta-analyses and placebo-controlled, randomized controlled trials.3,4
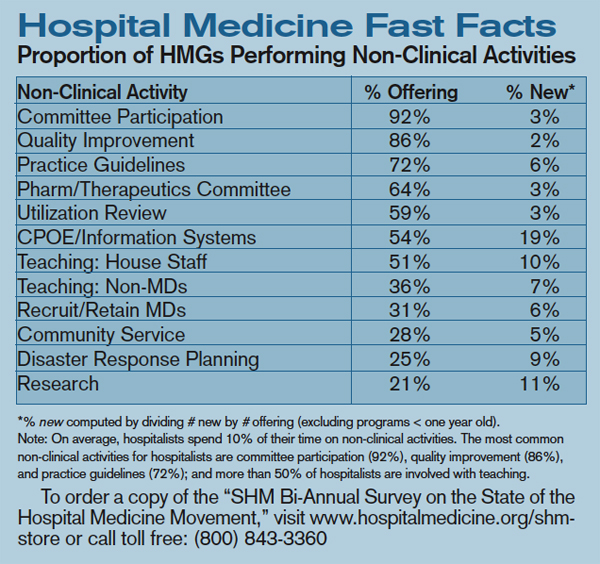
Close the Gap
Reliably preventing VTE in the hospital is inherently complex. VTE risk and bleeding risks vary within patient populations, and these risks may change for an individual patient several times in the course of the hospital stay. Weight, age, renal function, medication changes, and recent or impending invasive interventions may all influence decisions about the best VTE prevention options. Transitions across care providers and locations translate into multiple opportunities for breakdown in the delivery of optimal VTE prophylaxis. Thoughtful, evidence-based protocols, multidisciplinary system changes, and comprehensive educational efforts are required to achieve optimal VTE prophylaxis in the complex hospital setting.
How the VTE PC Can Help
The VTE PC program builds on and complements the VTE prevention materials and educational resources that SHM has produced in recent years. “Our Quality Improvement Resource Rooms have the information and resources needed to tackle a number of key quality issues,” says SHM CEO Larry Wellikson. “The VTE PC project takes this one step further by providing individualized mentorship. SHM is committed to supporting these forward-thinking, unique strategies that will allow hospitalists to lead their hospitals into a better future.”
VTE PC participants can choose the type of support that best fits their needs: a full year of distance mentoring or a one-day evaluation and consultation visit to their site.
The mentoring program presents a perfect option for individuals interested in ongoing support for their planned or active VTE prevention projects. Through the project, SHM mentors with VTE and QI experts who work with participants during eight telephone calls scheduled throughout a yearlong mentoring period. During the calls, mentors offer individualized assistance on any topics, tasks, and barriers that are encountered in the course of designing, implementing, and evaluating a VTE prevention project. Instruction and assistance are tailored to participant needs and commonly focus on:
- Working with medical center administration;
- Using practical methods to assess institutional performance in VTE prophylaxis;
- Identifying and tracking patients with hospital-acquired VTE;
- Constructing a VTE risk-assessment model and integrating it into workflow, order sets, and protocols;
- Enhancing selection of appropriate prophylaxis by linking the VTE risk assessment to a corresponding menu of proven options; and
- Bolstering your chances of success by utilizing high-reliability design features and effective implementation techniques.
The on-site consultation program is a good option for individuals interested in securing expert evaluation and input on a VTE prevention program but who don’t need ongoing support. Through the on-site consultation program, SHM consultants with VTE and QI expertise visit applicants’ hospitals to evaluate active or planned VTE prevention programs. The visits are especially helpful to participants with existing VTE prevention programs that they wish to expand or improve upon.
The consultation visits feature a structured evaluation of the site’s strengths and resources, barriers to improvement, and the design and functioning of active or proposed VTE prevention interventions. Specific consultation-visit activities vary according to participant goals and needs but may include meeting with the local project team, QI leaders, hospital administrators, and hospital medicine group leaders, as well as reviewing project documents—order sets, policies, and procedures—data, and data collection/management tools. Following the visits, SHM consultants provide participants with a written report of findings and recommendations. Participants also receive one follow-up telephone consultation.
Collaborative Members
SHM membership has responded enthusiastically to the VTE PC project. Early enrollees have a wide range of experience with VTE prevention and QI in general. Some fill QI leadership roles in their hospitals or hospital medicine groups; for others, the VTE prevention project is their first experience leading a QI effort. Enrollees represent a range of hospital types (academic centers, community teaching hospitals, community hospitals) and sizes (staffed beds range from 135 to 650) and are located in every U.S. geographic region in multiple hospital systems.
Several participants represent hospitals where VTE prevention programs have been implemented, while most have active projects in which no intervention has yet been implemented; a handful are still in the planning/initial exploration phase of work. Nearly half of the enrolled sites have a history of failed QI efforts in VTE prevention.
Many enrollees are looking to their VTE prevention efforts as a means of positioning their hospital medicine group as a local QI force. “This is the first large project the hospitalist group has undertaken since getting up and running,” reports one attendee. “I would really like to make a positive impact on patient care and lay the groundwork with this project that would allow us to be successful with future undertakings.”
Applying to the Programs
Participation in both the mentoring and on-site consultation programs is open to hospitalists who lead proposed or active VTE prevention projects. Participation is free, but enrollment is limited, so interested individuals are encouraged to apply early. SHM members can apply to either program by completing the online application available on the VTE Prevention Collaborative Web site: www.hospitalmedicine.org/vte-pc.
Direct your questions about VTE Prevention Collaborative programs to [email protected].
Bibliography
- Goldhaber SZ, Tapson VF; DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan;93(2):259-262.
- Maynard G. Workbook for Improvement: optimize prevention of venous thromboembolism at your medical center [SHM Web site, VTE Quality Improvement Resource Room]. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms&Template=/CM/ContentDisplay.cfm&ContentID=6092. Last accessed March 19, 2007.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S. Review. Comment in Chest. 2005 Jun;127(6):2297-2298.
- Shojania KG, Duncan BW, McDonald KM, et al. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment No. 43 [Agency for Healthcare Research and Quality Web site]. July 2001;332–346;AHRQ Publication No. 01-E058. Available at: www.ahrq.gov/clinic/ptsafety/. Last accessed March 19, 2007.
- Belch JJ, Lowe GD, Ward AG, et al. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115–117.
- Gardlund B. Randomised, controlled trial of low-dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The Heparin Prophylaxis Study Group. Lancet. 1996 May 18;347(9021):1357–1361. Comment in: ACP J Club. 1996 Nov-Dec;125(3):64 & Lancet. 1996 Jul 20; 348(9021):205-206.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793–800.
- Leizorovicz A, Cohen AT, Turpie AG, et al. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Kleber FX, Witt C, Vogel G, et al. Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease. Am Heart J. 2003 Apr;145(4):614–621.
- Lechler E, Schramm W, Flosbach CW. The venous thrombotic risk in non-surgical patients: epidemiological data and efficacy/safety profile of a low-molecular-weight heparin (enoxaparin). The Prime Study Group. Haemostasis. 1996;26(Suppl):49–56.
- Cohen AT, Davidson BL, Gallus AS, et al. Fondaparinux for the prevention of VTE in acutely ill medical patients (abstract 42). Blood. 2003;102:15a.
Awards Ceremony Preview
SHM created the Awards of Excellence program to honor members whose contributions to the hospital medicine movement deserve acknowledgment and respect. Award winners will receive complimentary registration and paid airfare to SHM’s Annual Meeting, which is being held this month in Dallas and will be presented during the President’s luncheon. Any physician member whose focus is the general medical care of hospitalized patients is eligible for nomination of the four awards. Award winners have been selected for the following categories: Clinical Excellence, Excellence in Teaching, Outstanding Service, and Research.
The SHM Award for Clinical Excellence will be presented to an individual for recognition of exemplary clinical service in hospital medicine. The Awards Committee has evaluated the candidates according to their outstanding contributions to patient care, their advancement of clinical knowledge, including their leadership and professionalism in medicine, as well as personal excellence in practice management.
The SHM Award for Excellence in Teaching is presented in recognition of outstanding teaching and mentorship in hospital medicine, most specifically within the academic and community practice settings. Consideration was given to those nominees who demonstrated outstanding teaching ability and who served as role models and mentored other hospitalists, residents, medical students, or other healthcare professionals.
The SHM Award for Outstanding Service in Hospital Medicine is presented in recognition of exceptional service to the discipline of hospital medicine. The winning candidate has displayed exemplary organizational and leadership activities within organized medicine and has shown contributing support in public policy.
The SHM Excellence in Research Award is presented in recognition of outstanding achievement by a researcher in the discipline of hospital medicine. The candidate selected presented peer-reviewed publications and continued education with additional research and training that provided for both intra- and extramural funding for research.
For additional information regarding SHM’s Awards Program, please e-mail [email protected]. TH
At the 2006 SHM Annual Meeting Geriatrics Special Interest Forum, participants asked, “Can we create an area on the SHM Web site focused on our unique interests and needs?” Last month, SHM answered with a resounding “Yes!” as we launched the Geriatrics Special Interest Group on www.hospitalmedicine.org.
The SHM Geriatrics Special Interest Group provides a portal for SHM members to access relevant, timely information about and resources for geriatric medicine. The Community Forums provide a mechanism for participants to communicate with each other about issues in geriatric medicine and other areas of interest. In particular, the Geriatrics Special Interest Group allows users to post information about training and career development opportunities, professional meetings and forums, and funding opportunities. Users can access a wealth of geriatric-medicine resources, including breaking medical news, clinical and quality improvement tools, key publications, and archived SHM Annual Meeting presentations. The Geriatrics Special Interest Group will serve as a template for future member-requested special interest groups, including palliative care, pediatrics, and others.
The Geriatrics Special Interest Group was developed by SHM members, other experts from the community of geriatric medicine, and a team of SHM staffers. SHM member Melissa Mattison, MD, (Beth Israel Deaconess) serves as medical editor for the site and helped shape its vision, along with members Param Dedhia, MD, (Johns Hopkins, Bayview) and Jason Stein, MD (Emory University). The group also benefited from reviews and contributions made by John Degelau, MD, at HealthPartners Medical Group, Gavin W. Hougham, MD, PhD, at The John A. Hartford Foundation, Nancy Lundebjerg, MPA, and Jane Potter, MD, at the American Geriatrics Society, Odette van der Willik at the American Federation for Aging Research, and Paula M. Podrazik, MD, at the Case Management Society of America. The internal SHM development team was led by Shannon Roach and included Bruce Hanson, Travis Kamps, and Tina Budnitz.
To view the Geriatrics Special Interest Group, go to SHM’s Web site or type the address into your browser: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=12369.
We hope SHM members will utilize the Geriatrics Special Interest Group to share ideas and resources, to network, and to improve inpatient geriatric medicine. Let us know if the site meets your needs by sending your comments and suggestions to Shannon Roach at [email protected]. Have an idea for another special interest group? E-mail us that suggestion, too.
SHM: BEHIND THE SCENES
Education and quality improvement: Reflections of a New Staff Member
By Kristin Beck
It’s nice to come to work every day and focus on education and quality improvement. Ensuring that hospitalists have the most up to date information as well as support and encouragement for implementing positive change are good reasons for leaving the house in the morning.
Only three weeks into my role as senior project manager, I have had the sincere pleasure of being involved with updating quality improvement resource rooms (common Web site areas that house tools for implementing quality improvement programs) by initiating a grant-supported program for examining observation units as they relate to treating the number one reason people are hospitalized. I have also accomplished writing and submitting a grant for the Quality Improvement Pre-Course, as well as, working with a committee that looks at patient quality care and projects to enhance it.
Our work here focuses on examining what has been done, how we can improve it, and how we can institute best practices. Not bad for three weeks’ work!
Conversations in our department focus on whether members get what they need and want. People meet regularly to discuss how we can refine and improve the services we offer. Strategies for securing funding and developing programs are reviewed, not for this calendar or fiscal year but for years to come. In one of my final interviews for this job, I was reminded that we don’t deliver here—we over-deliver. Looking through The Hospitalist, titles that stand out include the words unforgettable, safety, expert, leader, admire, and smart.
When people ask what I do in my new job, I tell them that hospital medicine looks at the total experience of being a doctor. It focuses not only on medical care but also on the complete experience of being a working professional: the arts of research, negotiation, best practices, team-focused care, conflict resolution, and systems change. I explain that we do life-saving work, for it is far more than the practice of just day-to-day medicine that improves all of our lives. I tell people that it is work that makes sense.
When you come to work every day and are surrounded by a dynamic, positive energy, the work you produce is likely to mirror the hospital medicine movement: You will reflect, revise, and grow stronger. Sincere, well-planned initiatives are infectious. Continually participating in an environment that asks the questions, “Where can we take this?” and “What can we do better?” is a pretty good reason to get out of bed in the morning.
Beck is the senior project manager at SHM.
VTE Prevention Collaborative off to a Great Start
The VTE Prevention Collaborative (VTE PC) is the latest SHM initiative to support hospitalist-led efforts to reduce the incidence of preventable, hospital-acquired VTE. Launched in January 2007, the program offers individualized assistance to hospitalists who want to take the lead on this critical quality and patient safety issue.
Hospital-Acquired Venous Thromboembolism
The problem of hospital-acquired VTE is huge. More than 2 million Americans suffer from VTE each year. Most hospitalized patients have at least one risk factor for VTE. In a large registry trial capturing more than 5,451 patients at 183 sites in a six-month period, 50% (2,726) developed their VTE during hospitalization.1 A 400-bed hospital with an average rate of VTE prophylaxis can expect that 200 patients will suffer from hospital-acquired VTE each year; around half of these cases are potentially preventable.1,2
The good news is that effective and safe measures to prevent hospital-acquired VTE exist. Pharmacologic prophylaxis reduces the incidence of asymptomatic and symptomatic DVT and pulmonary embolism (PE) by 50%-65%.3, 4-11 Prevention of DVT also prevents PE and fatalities from PE. The chief concern of prophylaxis is bleeding, but bleeding risk secondary to pharmacologic prophylaxis is a rare event, as is shown in abundant data from meta-analyses and placebo-controlled, randomized controlled trials.3,4
Close the Gap
Reliably preventing VTE in the hospital is inherently complex. VTE risk and bleeding risks vary within patient populations, and these risks may change for an individual patient several times in the course of the hospital stay. Weight, age, renal function, medication changes, and recent or impending invasive interventions may all influence decisions about the best VTE prevention options. Transitions across care providers and locations translate into multiple opportunities for breakdown in the delivery of optimal VTE prophylaxis. Thoughtful, evidence-based protocols, multidisciplinary system changes, and comprehensive educational efforts are required to achieve optimal VTE prophylaxis in the complex hospital setting.
How the VTE PC Can Help
The VTE PC program builds on and complements the VTE prevention materials and educational resources that SHM has produced in recent years. “Our Quality Improvement Resource Rooms have the information and resources needed to tackle a number of key quality issues,” says SHM CEO Larry Wellikson. “The VTE PC project takes this one step further by providing individualized mentorship. SHM is committed to supporting these forward-thinking, unique strategies that will allow hospitalists to lead their hospitals into a better future.”
VTE PC participants can choose the type of support that best fits their needs: a full year of distance mentoring or a one-day evaluation and consultation visit to their site.
The mentoring program presents a perfect option for individuals interested in ongoing support for their planned or active VTE prevention projects. Through the project, SHM mentors with VTE and QI experts who work with participants during eight telephone calls scheduled throughout a yearlong mentoring period. During the calls, mentors offer individualized assistance on any topics, tasks, and barriers that are encountered in the course of designing, implementing, and evaluating a VTE prevention project. Instruction and assistance are tailored to participant needs and commonly focus on:
- Working with medical center administration;
- Using practical methods to assess institutional performance in VTE prophylaxis;
- Identifying and tracking patients with hospital-acquired VTE;
- Constructing a VTE risk-assessment model and integrating it into workflow, order sets, and protocols;
- Enhancing selection of appropriate prophylaxis by linking the VTE risk assessment to a corresponding menu of proven options; and
- Bolstering your chances of success by utilizing high-reliability design features and effective implementation techniques.
The on-site consultation program is a good option for individuals interested in securing expert evaluation and input on a VTE prevention program but who don’t need ongoing support. Through the on-site consultation program, SHM consultants with VTE and QI expertise visit applicants’ hospitals to evaluate active or planned VTE prevention programs. The visits are especially helpful to participants with existing VTE prevention programs that they wish to expand or improve upon.
The consultation visits feature a structured evaluation of the site’s strengths and resources, barriers to improvement, and the design and functioning of active or proposed VTE prevention interventions. Specific consultation-visit activities vary according to participant goals and needs but may include meeting with the local project team, QI leaders, hospital administrators, and hospital medicine group leaders, as well as reviewing project documents—order sets, policies, and procedures—data, and data collection/management tools. Following the visits, SHM consultants provide participants with a written report of findings and recommendations. Participants also receive one follow-up telephone consultation.
Collaborative Members
SHM membership has responded enthusiastically to the VTE PC project. Early enrollees have a wide range of experience with VTE prevention and QI in general. Some fill QI leadership roles in their hospitals or hospital medicine groups; for others, the VTE prevention project is their first experience leading a QI effort. Enrollees represent a range of hospital types (academic centers, community teaching hospitals, community hospitals) and sizes (staffed beds range from 135 to 650) and are located in every U.S. geographic region in multiple hospital systems.
Several participants represent hospitals where VTE prevention programs have been implemented, while most have active projects in which no intervention has yet been implemented; a handful are still in the planning/initial exploration phase of work. Nearly half of the enrolled sites have a history of failed QI efforts in VTE prevention.
Many enrollees are looking to their VTE prevention efforts as a means of positioning their hospital medicine group as a local QI force. “This is the first large project the hospitalist group has undertaken since getting up and running,” reports one attendee. “I would really like to make a positive impact on patient care and lay the groundwork with this project that would allow us to be successful with future undertakings.”
Applying to the Programs
Participation in both the mentoring and on-site consultation programs is open to hospitalists who lead proposed or active VTE prevention projects. Participation is free, but enrollment is limited, so interested individuals are encouraged to apply early. SHM members can apply to either program by completing the online application available on the VTE Prevention Collaborative Web site: www.hospitalmedicine.org/vte-pc.
Direct your questions about VTE Prevention Collaborative programs to [email protected].
Bibliography
- Goldhaber SZ, Tapson VF; DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan;93(2):259-262.
- Maynard G. Workbook for Improvement: optimize prevention of venous thromboembolism at your medical center [SHM Web site, VTE Quality Improvement Resource Room]. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms&Template=/CM/ContentDisplay.cfm&ContentID=6092. Last accessed March 19, 2007.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S. Review. Comment in Chest. 2005 Jun;127(6):2297-2298.
- Shojania KG, Duncan BW, McDonald KM, et al. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment No. 43 [Agency for Healthcare Research and Quality Web site]. July 2001;332–346;AHRQ Publication No. 01-E058. Available at: www.ahrq.gov/clinic/ptsafety/. Last accessed March 19, 2007.
- Belch JJ, Lowe GD, Ward AG, et al. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115–117.
- Gardlund B. Randomised, controlled trial of low-dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The Heparin Prophylaxis Study Group. Lancet. 1996 May 18;347(9021):1357–1361. Comment in: ACP J Club. 1996 Nov-Dec;125(3):64 & Lancet. 1996 Jul 20; 348(9021):205-206.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793–800.
- Leizorovicz A, Cohen AT, Turpie AG, et al. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Kleber FX, Witt C, Vogel G, et al. Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease. Am Heart J. 2003 Apr;145(4):614–621.
- Lechler E, Schramm W, Flosbach CW. The venous thrombotic risk in non-surgical patients: epidemiological data and efficacy/safety profile of a low-molecular-weight heparin (enoxaparin). The Prime Study Group. Haemostasis. 1996;26(Suppl):49–56.
- Cohen AT, Davidson BL, Gallus AS, et al. Fondaparinux for the prevention of VTE in acutely ill medical patients (abstract 42). Blood. 2003;102:15a.
Awards Ceremony Preview
SHM created the Awards of Excellence program to honor members whose contributions to the hospital medicine movement deserve acknowledgment and respect. Award winners will receive complimentary registration and paid airfare to SHM’s Annual Meeting, which is being held this month in Dallas and will be presented during the President’s luncheon. Any physician member whose focus is the general medical care of hospitalized patients is eligible for nomination of the four awards. Award winners have been selected for the following categories: Clinical Excellence, Excellence in Teaching, Outstanding Service, and Research.
The SHM Award for Clinical Excellence will be presented to an individual for recognition of exemplary clinical service in hospital medicine. The Awards Committee has evaluated the candidates according to their outstanding contributions to patient care, their advancement of clinical knowledge, including their leadership and professionalism in medicine, as well as personal excellence in practice management.
The SHM Award for Excellence in Teaching is presented in recognition of outstanding teaching and mentorship in hospital medicine, most specifically within the academic and community practice settings. Consideration was given to those nominees who demonstrated outstanding teaching ability and who served as role models and mentored other hospitalists, residents, medical students, or other healthcare professionals.
The SHM Award for Outstanding Service in Hospital Medicine is presented in recognition of exceptional service to the discipline of hospital medicine. The winning candidate has displayed exemplary organizational and leadership activities within organized medicine and has shown contributing support in public policy.
The SHM Excellence in Research Award is presented in recognition of outstanding achievement by a researcher in the discipline of hospital medicine. The candidate selected presented peer-reviewed publications and continued education with additional research and training that provided for both intra- and extramural funding for research.
For additional information regarding SHM’s Awards Program, please e-mail [email protected]. TH
At the 2006 SHM Annual Meeting Geriatrics Special Interest Forum, participants asked, “Can we create an area on the SHM Web site focused on our unique interests and needs?” Last month, SHM answered with a resounding “Yes!” as we launched the Geriatrics Special Interest Group on www.hospitalmedicine.org.
The SHM Geriatrics Special Interest Group provides a portal for SHM members to access relevant, timely information about and resources for geriatric medicine. The Community Forums provide a mechanism for participants to communicate with each other about issues in geriatric medicine and other areas of interest. In particular, the Geriatrics Special Interest Group allows users to post information about training and career development opportunities, professional meetings and forums, and funding opportunities. Users can access a wealth of geriatric-medicine resources, including breaking medical news, clinical and quality improvement tools, key publications, and archived SHM Annual Meeting presentations. The Geriatrics Special Interest Group will serve as a template for future member-requested special interest groups, including palliative care, pediatrics, and others.
The Geriatrics Special Interest Group was developed by SHM members, other experts from the community of geriatric medicine, and a team of SHM staffers. SHM member Melissa Mattison, MD, (Beth Israel Deaconess) serves as medical editor for the site and helped shape its vision, along with members Param Dedhia, MD, (Johns Hopkins, Bayview) and Jason Stein, MD (Emory University). The group also benefited from reviews and contributions made by John Degelau, MD, at HealthPartners Medical Group, Gavin W. Hougham, MD, PhD, at The John A. Hartford Foundation, Nancy Lundebjerg, MPA, and Jane Potter, MD, at the American Geriatrics Society, Odette van der Willik at the American Federation for Aging Research, and Paula M. Podrazik, MD, at the Case Management Society of America. The internal SHM development team was led by Shannon Roach and included Bruce Hanson, Travis Kamps, and Tina Budnitz.
To view the Geriatrics Special Interest Group, go to SHM’s Web site or type the address into your browser: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=12369.
We hope SHM members will utilize the Geriatrics Special Interest Group to share ideas and resources, to network, and to improve inpatient geriatric medicine. Let us know if the site meets your needs by sending your comments and suggestions to Shannon Roach at [email protected]. Have an idea for another special interest group? E-mail us that suggestion, too.
SHM: BEHIND THE SCENES
Education and quality improvement: Reflections of a New Staff Member
By Kristin Beck
It’s nice to come to work every day and focus on education and quality improvement. Ensuring that hospitalists have the most up to date information as well as support and encouragement for implementing positive change are good reasons for leaving the house in the morning.
Only three weeks into my role as senior project manager, I have had the sincere pleasure of being involved with updating quality improvement resource rooms (common Web site areas that house tools for implementing quality improvement programs) by initiating a grant-supported program for examining observation units as they relate to treating the number one reason people are hospitalized. I have also accomplished writing and submitting a grant for the Quality Improvement Pre-Course, as well as, working with a committee that looks at patient quality care and projects to enhance it.
Our work here focuses on examining what has been done, how we can improve it, and how we can institute best practices. Not bad for three weeks’ work!
Conversations in our department focus on whether members get what they need and want. People meet regularly to discuss how we can refine and improve the services we offer. Strategies for securing funding and developing programs are reviewed, not for this calendar or fiscal year but for years to come. In one of my final interviews for this job, I was reminded that we don’t deliver here—we over-deliver. Looking through The Hospitalist, titles that stand out include the words unforgettable, safety, expert, leader, admire, and smart.
When people ask what I do in my new job, I tell them that hospital medicine looks at the total experience of being a doctor. It focuses not only on medical care but also on the complete experience of being a working professional: the arts of research, negotiation, best practices, team-focused care, conflict resolution, and systems change. I explain that we do life-saving work, for it is far more than the practice of just day-to-day medicine that improves all of our lives. I tell people that it is work that makes sense.
When you come to work every day and are surrounded by a dynamic, positive energy, the work you produce is likely to mirror the hospital medicine movement: You will reflect, revise, and grow stronger. Sincere, well-planned initiatives are infectious. Continually participating in an environment that asks the questions, “Where can we take this?” and “What can we do better?” is a pretty good reason to get out of bed in the morning.
Beck is the senior project manager at SHM.
VTE Prevention Collaborative off to a Great Start
The VTE Prevention Collaborative (VTE PC) is the latest SHM initiative to support hospitalist-led efforts to reduce the incidence of preventable, hospital-acquired VTE. Launched in January 2007, the program offers individualized assistance to hospitalists who want to take the lead on this critical quality and patient safety issue.
Hospital-Acquired Venous Thromboembolism
The problem of hospital-acquired VTE is huge. More than 2 million Americans suffer from VTE each year. Most hospitalized patients have at least one risk factor for VTE. In a large registry trial capturing more than 5,451 patients at 183 sites in a six-month period, 50% (2,726) developed their VTE during hospitalization.1 A 400-bed hospital with an average rate of VTE prophylaxis can expect that 200 patients will suffer from hospital-acquired VTE each year; around half of these cases are potentially preventable.1,2
The good news is that effective and safe measures to prevent hospital-acquired VTE exist. Pharmacologic prophylaxis reduces the incidence of asymptomatic and symptomatic DVT and pulmonary embolism (PE) by 50%-65%.3, 4-11 Prevention of DVT also prevents PE and fatalities from PE. The chief concern of prophylaxis is bleeding, but bleeding risk secondary to pharmacologic prophylaxis is a rare event, as is shown in abundant data from meta-analyses and placebo-controlled, randomized controlled trials.3,4
Close the Gap
Reliably preventing VTE in the hospital is inherently complex. VTE risk and bleeding risks vary within patient populations, and these risks may change for an individual patient several times in the course of the hospital stay. Weight, age, renal function, medication changes, and recent or impending invasive interventions may all influence decisions about the best VTE prevention options. Transitions across care providers and locations translate into multiple opportunities for breakdown in the delivery of optimal VTE prophylaxis. Thoughtful, evidence-based protocols, multidisciplinary system changes, and comprehensive educational efforts are required to achieve optimal VTE prophylaxis in the complex hospital setting.
How the VTE PC Can Help
The VTE PC program builds on and complements the VTE prevention materials and educational resources that SHM has produced in recent years. “Our Quality Improvement Resource Rooms have the information and resources needed to tackle a number of key quality issues,” says SHM CEO Larry Wellikson. “The VTE PC project takes this one step further by providing individualized mentorship. SHM is committed to supporting these forward-thinking, unique strategies that will allow hospitalists to lead their hospitals into a better future.”
VTE PC participants can choose the type of support that best fits their needs: a full year of distance mentoring or a one-day evaluation and consultation visit to their site.
The mentoring program presents a perfect option for individuals interested in ongoing support for their planned or active VTE prevention projects. Through the project, SHM mentors with VTE and QI experts who work with participants during eight telephone calls scheduled throughout a yearlong mentoring period. During the calls, mentors offer individualized assistance on any topics, tasks, and barriers that are encountered in the course of designing, implementing, and evaluating a VTE prevention project. Instruction and assistance are tailored to participant needs and commonly focus on:
- Working with medical center administration;
- Using practical methods to assess institutional performance in VTE prophylaxis;
- Identifying and tracking patients with hospital-acquired VTE;
- Constructing a VTE risk-assessment model and integrating it into workflow, order sets, and protocols;
- Enhancing selection of appropriate prophylaxis by linking the VTE risk assessment to a corresponding menu of proven options; and
- Bolstering your chances of success by utilizing high-reliability design features and effective implementation techniques.
The on-site consultation program is a good option for individuals interested in securing expert evaluation and input on a VTE prevention program but who don’t need ongoing support. Through the on-site consultation program, SHM consultants with VTE and QI expertise visit applicants’ hospitals to evaluate active or planned VTE prevention programs. The visits are especially helpful to participants with existing VTE prevention programs that they wish to expand or improve upon.
The consultation visits feature a structured evaluation of the site’s strengths and resources, barriers to improvement, and the design and functioning of active or proposed VTE prevention interventions. Specific consultation-visit activities vary according to participant goals and needs but may include meeting with the local project team, QI leaders, hospital administrators, and hospital medicine group leaders, as well as reviewing project documents—order sets, policies, and procedures—data, and data collection/management tools. Following the visits, SHM consultants provide participants with a written report of findings and recommendations. Participants also receive one follow-up telephone consultation.
Collaborative Members
SHM membership has responded enthusiastically to the VTE PC project. Early enrollees have a wide range of experience with VTE prevention and QI in general. Some fill QI leadership roles in their hospitals or hospital medicine groups; for others, the VTE prevention project is their first experience leading a QI effort. Enrollees represent a range of hospital types (academic centers, community teaching hospitals, community hospitals) and sizes (staffed beds range from 135 to 650) and are located in every U.S. geographic region in multiple hospital systems.
Several participants represent hospitals where VTE prevention programs have been implemented, while most have active projects in which no intervention has yet been implemented; a handful are still in the planning/initial exploration phase of work. Nearly half of the enrolled sites have a history of failed QI efforts in VTE prevention.
Many enrollees are looking to their VTE prevention efforts as a means of positioning their hospital medicine group as a local QI force. “This is the first large project the hospitalist group has undertaken since getting up and running,” reports one attendee. “I would really like to make a positive impact on patient care and lay the groundwork with this project that would allow us to be successful with future undertakings.”
Applying to the Programs
Participation in both the mentoring and on-site consultation programs is open to hospitalists who lead proposed or active VTE prevention projects. Participation is free, but enrollment is limited, so interested individuals are encouraged to apply early. SHM members can apply to either program by completing the online application available on the VTE Prevention Collaborative Web site: www.hospitalmedicine.org/vte-pc.
Direct your questions about VTE Prevention Collaborative programs to [email protected].
Bibliography
- Goldhaber SZ, Tapson VF; DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan;93(2):259-262.
- Maynard G. Workbook for Improvement: optimize prevention of venous thromboembolism at your medical center [SHM Web site, VTE Quality Improvement Resource Room]. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms&Template=/CM/ContentDisplay.cfm&ContentID=6092. Last accessed March 19, 2007.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S. Review. Comment in Chest. 2005 Jun;127(6):2297-2298.
- Shojania KG, Duncan BW, McDonald KM, et al. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment No. 43 [Agency for Healthcare Research and Quality Web site]. July 2001;332–346;AHRQ Publication No. 01-E058. Available at: www.ahrq.gov/clinic/ptsafety/. Last accessed March 19, 2007.
- Belch JJ, Lowe GD, Ward AG, et al. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115–117.
- Gardlund B. Randomised, controlled trial of low-dose heparin for prevention of fatal pulmonary embolism in patients with infectious diseases. The Heparin Prophylaxis Study Group. Lancet. 1996 May 18;347(9021):1357–1361. Comment in: ACP J Club. 1996 Nov-Dec;125(3):64 & Lancet. 1996 Jul 20; 348(9021):205-206.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793–800.
- Leizorovicz A, Cohen AT, Turpie AG, et al. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Kleber FX, Witt C, Vogel G, et al. Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease. Am Heart J. 2003 Apr;145(4):614–621.
- Lechler E, Schramm W, Flosbach CW. The venous thrombotic risk in non-surgical patients: epidemiological data and efficacy/safety profile of a low-molecular-weight heparin (enoxaparin). The Prime Study Group. Haemostasis. 1996;26(Suppl):49–56.
- Cohen AT, Davidson BL, Gallus AS, et al. Fondaparinux for the prevention of VTE in acutely ill medical patients (abstract 42). Blood. 2003;102:15a.
Awards Ceremony Preview
SHM created the Awards of Excellence program to honor members whose contributions to the hospital medicine movement deserve acknowledgment and respect. Award winners will receive complimentary registration and paid airfare to SHM’s Annual Meeting, which is being held this month in Dallas and will be presented during the President’s luncheon. Any physician member whose focus is the general medical care of hospitalized patients is eligible for nomination of the four awards. Award winners have been selected for the following categories: Clinical Excellence, Excellence in Teaching, Outstanding Service, and Research.
The SHM Award for Clinical Excellence will be presented to an individual for recognition of exemplary clinical service in hospital medicine. The Awards Committee has evaluated the candidates according to their outstanding contributions to patient care, their advancement of clinical knowledge, including their leadership and professionalism in medicine, as well as personal excellence in practice management.
The SHM Award for Excellence in Teaching is presented in recognition of outstanding teaching and mentorship in hospital medicine, most specifically within the academic and community practice settings. Consideration was given to those nominees who demonstrated outstanding teaching ability and who served as role models and mentored other hospitalists, residents, medical students, or other healthcare professionals.
The SHM Award for Outstanding Service in Hospital Medicine is presented in recognition of exceptional service to the discipline of hospital medicine. The winning candidate has displayed exemplary organizational and leadership activities within organized medicine and has shown contributing support in public policy.
The SHM Excellence in Research Award is presented in recognition of outstanding achievement by a researcher in the discipline of hospital medicine. The candidate selected presented peer-reviewed publications and continued education with additional research and training that provided for both intra- and extramural funding for research.
For additional information regarding SHM’s Awards Program, please e-mail [email protected]. TH
Malpractice risk management: Make patient safety a tool to keep risk in check
This article is the third in a series of 4 derived from a symposium on malpractice risk management at the 91st Clinical Congress of the American College of Surgeons, San Francisco, Calif., in October 2005. Mr. Donnelly updated his comments in August 2006.
Part 1 March 2007 Informed refusal
James M. Goodman, JD
Part 2 April 2007 Common errors in self-defense
Claudia Dobbs, MA
Part 3 THIS ISSUE - Patient safety as risk management tool
Thomas J. Donnelly, JD
Part 4 Responsibilities in obtaining informed consent
James M. Nelson, JD
Lawsuit filings have increased substantially in medicine over the past 10 to 15 years. So have indemnity payments—money spent in case settlements or in verdicts and awards in favor of plaintiffs. Specifically, there has been a rise in malpractice payouts higher than $1 million.1
Statistics on medical errors that are often the basis of actions are revealing:
- Deaths in the thousands. A 1999 report from the Institute of Medicine (IOM) concluded that 44,000 to 98,000 patients die annually from “preventable medical errors” in US hospitals.2
- Dollars in the billions. The annual cost of medical error has been estimated at $38 billion to $50 billion.
- Surgery at center stage. Subsequent studies suggested that more than half of deaths from preventable errors were related to surgical errors and failures.
- Prevention is a lifesaver. Other studies have supported IOM statistics, and suggested that as many as 70% of surgical adverse events are preventable.3
Received by the public as an indictment of the medical system, the IOM report and its offspring fostered a spate of research on public safety. Some invoked conclusions of NASA studies in the 1970s: Namely, it is a breakdown in communication, leadership, and teamwork that causes most commercial airline crashes—not a lack of skill.
Lesson from anesthesiology
The first transfer of NASA study methods to medicine involved anesthesiology. In the 1980s, one in 10,000 patients died in a manner related to anesthesia.4 Once anesthesiologists had implemented safety programs and made patient safety a high priority, patient mortality from anesthesia fell—dramatically. The rate is now 1 in 200,000 and approaching 1 in 300,000.4
Trends in claims paid out by medical malpractice defense insurers support that emphasis on safety and quality of care improves outcomes and reduces lawsuits. Malpractice insurance premiums for anesthesiologists in many states have decreased significantly. Other medical specialties can expect to see similar results as they focus on patient safety and risk management.5
Fatigue and patient risk
Myriad risk-management issues come into play for physicians. Long hours for residents on duty, for example, are under scrutiny. We are starting to recognize the role of fatigue in surgical error, such as wrong-site surgery, and related issues, such as inaccurate transfusion.
Surgeons must keep up to date on innovations and advancements, including technical skills and equipment modifications. From a risk-management perspective, there is no excuse for not practicing surgery in a modern, effective way.
Specialty organizations are increasingly publishing and promulgating clinical guidelines. Most states allow documents such as clinical guidelines to be introduced before a jury; the defendant surgeon who has neglected to follow an approach to a procedure that is advocated by a relevant specialty organization will face an uphill battle in court.
In selecting and preparing a candidate for surgery, these steps are integral for managing one’s malpractice risk:
- Patient selection. Improper patient selection is an obvious arena for lawsuits. If you have any doubt about which approach to take, don’t hesitate to refer the patient for a second opinion. Regardless of the conclusion, obtaining a second opinion in a difficult situation can only help you.
- Documentation. Informed consent and adequate documentation are crucial risk-management tools. The patient must understand exactly what you are recommending (see “If you can’t read your writing…”).
- Laboratory work-up. Making sure the patient obtains the requisite preoperative laboratory tests is vital (see “What do you do when managed care won’t pay for a test?”).
- Know the results. If a patient has other health issues that require medical clearance or warrant referral to an internist or primary-care physician, it’s ultimately the surgeon’s responsibility to see the patient gets the appropriate laboratory tests and to personally learn the results. Don’t assume that someone else—a primary-care physician, an internist, another specialist—will do it. Don’t be forced to say, “I referred the patient to somebody else for a work-up and assumed everything that happened was all right.”
A defendant physician who cannot read his or her own handwriting in a chart or notes is giving the plaintiff a gift. Illegible handwriting does not convey good organization, clear thinking, or an ability to communicate one’s intent to others. The plaintiff’s side may use this to make the physician seem poorly organized, rushed, and uncaring.
Surgeons must trust other staff members, including nurses, assistants, technicians, technologists, and physician-colleagues. Risk management, like good care, requires the surgical team to work in concert.
Collaboration should start no later than the patient’s hospital admission and continue through discharge. Effective communication, both verbal and written, exhibits that.
Medical notes
One of the biggest problems in malpractice suits is the abysmal quality of a physician’s written notes. This holds true in the hospital and especially after discharge and for follow-up office visits. Often such notes consist of single-line entries.
Lawyers see many cases in which the patient left a phone message explicitly stating that he or she was worried about something. The doctor’s notes read, in full: “Talked to patient.”
I’m handling 4 or 5 cases now in which physicians have not helped themselves at all—by acting as if anything that happened after surgery was an afterthought.
On-call notes made on nights and weekends provide equally poor evidence because they rarely exist. The absence of such notes presents problems from a risk-management and defensibility standpoint.
Surgeons do themselves a disservice by failing to document properly the advice they give to patients. Jurors accept timely notes made in the patient’s record. They struggle a year after the fact to accept testimony such as, “I told the nurse X, Y, and Z. I know I told the patient to come in, or get something done, or go to the emergency room.”
Even in managed care, the surgeon bears responsibility for any delay in obtaining approval for recommended tests. A surgeon who wants a test done but anticipates a roadblock from a managed-care company can’t say, weeks later, “The insurance carrier didn’t approve it.”
You may not have much input, but blaming the system is a poor legal argument. You may have to ask the patient to do more to obtain approval or offer the patient the option to pay for the test out of pocket.
If managed care refuses initially or repeatedly to pay for important tests or procedures, you must document that you or your staff explained the situation to the patient and extended the patient an opportunity to pay for the test without reimbursement.
Plaintiff patients in this situation typically say, “Of course I would have paid X dollars for that CT scan.” Such assertions ring true with jurors. Patients will never say, “I support the doctor who never told me about something because he thought my insurance wouldn’t cover it.”
In court, you can’t blame managed care or remove an option simply because you personally thought some entity ought to pay for it.
Intraoperative concerns
Most claims against surgeons focus on what happens in the operating room or immediately postoperatively. The Physician Insurance Association of America recommends several strategies to reduce or avoid operating room claims6:
- Obtain adequate training and supervision when using new surgical equipment
- Ensure that the patient gives informed consent for a procedure and that you have provided adequate information regarding risks and alternatives
- When working as an attending physician with residents or internists, make sure they are under proper supervision
- Participate in any hospital-sponsored risk-management program.
Postoperative concerns
Your liability continues after surgery. In the hospital, you must communicate clearly with nurses. Use the chart as a tool to enhance patient safety. Document your observations thoroughly.
If you bring in consultant physicians to deal with a preexisting problem or one that arose after surgery, be aware that all clinicians involved must communicate. “I never talked with my consultants. We communicated through progress notes,” will not help a defendant-physician’s case. Such notes, which tend to be terse and hard to read, should never serve as the main method of communication.
A surgeon must communicate fully with the patient, and with the family as well. At least a dozen reports have established that patients, or their family, filed a lawsuit simply because they felt that was the only way to find out what happened.7,8
The author has no affiliations to disclose.
1. The Large Loss Claim Trend. PIAA Research Notes. Rockville, MD: Physicians Insurers Association of America; 2005.
2. Committee on Quality of Health Care in America. To Err is Human: Building a safer health system. Washington, DC: National Academy Press; 1999.
3. Gawande AA, Thomas EJ, Zinner MJ, Brennan TA. The incidence and nature of surgical adverse events in Colorado and Utah in 1992. Surgery. 1999;126:66-75.
4. Gawande A. Complications, a Surgeon’s Notes on an Imperfect Science. New York, NY: Picador USA; 2003.
5. Hallinan JT. Once seen as risky, one group of doctors changes its ways. Wall Street Journal. June 21, 2005:A1.
6. Operating Room Claims, PIAA Research Notes. Rockville, MD: Physicians Insurers Association of America; 2004.
7. Moore PJ, Adler NE, Robertson PA. The effect of doctor-patient relations on medical patient perceptions and malpractice intentions. West J Med. 2000;173:244-250.
8. Hickson GB, Federspiel CF, Pichert JW, Miller CS, Gauld-Jaeger J, Bost P. Patient complaints and malpractice risk. JAMA. 2002;287:2951-2957.
This article is the third in a series of 4 derived from a symposium on malpractice risk management at the 91st Clinical Congress of the American College of Surgeons, San Francisco, Calif., in October 2005. Mr. Donnelly updated his comments in August 2006.
Part 1 March 2007 Informed refusal
James M. Goodman, JD
Part 2 April 2007 Common errors in self-defense
Claudia Dobbs, MA
Part 3 THIS ISSUE - Patient safety as risk management tool
Thomas J. Donnelly, JD
Part 4 Responsibilities in obtaining informed consent
James M. Nelson, JD
Lawsuit filings have increased substantially in medicine over the past 10 to 15 years. So have indemnity payments—money spent in case settlements or in verdicts and awards in favor of plaintiffs. Specifically, there has been a rise in malpractice payouts higher than $1 million.1
Statistics on medical errors that are often the basis of actions are revealing:
- Deaths in the thousands. A 1999 report from the Institute of Medicine (IOM) concluded that 44,000 to 98,000 patients die annually from “preventable medical errors” in US hospitals.2
- Dollars in the billions. The annual cost of medical error has been estimated at $38 billion to $50 billion.
- Surgery at center stage. Subsequent studies suggested that more than half of deaths from preventable errors were related to surgical errors and failures.
- Prevention is a lifesaver. Other studies have supported IOM statistics, and suggested that as many as 70% of surgical adverse events are preventable.3
Received by the public as an indictment of the medical system, the IOM report and its offspring fostered a spate of research on public safety. Some invoked conclusions of NASA studies in the 1970s: Namely, it is a breakdown in communication, leadership, and teamwork that causes most commercial airline crashes—not a lack of skill.
Lesson from anesthesiology
The first transfer of NASA study methods to medicine involved anesthesiology. In the 1980s, one in 10,000 patients died in a manner related to anesthesia.4 Once anesthesiologists had implemented safety programs and made patient safety a high priority, patient mortality from anesthesia fell—dramatically. The rate is now 1 in 200,000 and approaching 1 in 300,000.4
Trends in claims paid out by medical malpractice defense insurers support that emphasis on safety and quality of care improves outcomes and reduces lawsuits. Malpractice insurance premiums for anesthesiologists in many states have decreased significantly. Other medical specialties can expect to see similar results as they focus on patient safety and risk management.5
Fatigue and patient risk
Myriad risk-management issues come into play for physicians. Long hours for residents on duty, for example, are under scrutiny. We are starting to recognize the role of fatigue in surgical error, such as wrong-site surgery, and related issues, such as inaccurate transfusion.
Surgeons must keep up to date on innovations and advancements, including technical skills and equipment modifications. From a risk-management perspective, there is no excuse for not practicing surgery in a modern, effective way.
Specialty organizations are increasingly publishing and promulgating clinical guidelines. Most states allow documents such as clinical guidelines to be introduced before a jury; the defendant surgeon who has neglected to follow an approach to a procedure that is advocated by a relevant specialty organization will face an uphill battle in court.
In selecting and preparing a candidate for surgery, these steps are integral for managing one’s malpractice risk:
- Patient selection. Improper patient selection is an obvious arena for lawsuits. If you have any doubt about which approach to take, don’t hesitate to refer the patient for a second opinion. Regardless of the conclusion, obtaining a second opinion in a difficult situation can only help you.
- Documentation. Informed consent and adequate documentation are crucial risk-management tools. The patient must understand exactly what you are recommending (see “If you can’t read your writing…”).
- Laboratory work-up. Making sure the patient obtains the requisite preoperative laboratory tests is vital (see “What do you do when managed care won’t pay for a test?”).
- Know the results. If a patient has other health issues that require medical clearance or warrant referral to an internist or primary-care physician, it’s ultimately the surgeon’s responsibility to see the patient gets the appropriate laboratory tests and to personally learn the results. Don’t assume that someone else—a primary-care physician, an internist, another specialist—will do it. Don’t be forced to say, “I referred the patient to somebody else for a work-up and assumed everything that happened was all right.”
A defendant physician who cannot read his or her own handwriting in a chart or notes is giving the plaintiff a gift. Illegible handwriting does not convey good organization, clear thinking, or an ability to communicate one’s intent to others. The plaintiff’s side may use this to make the physician seem poorly organized, rushed, and uncaring.
Surgeons must trust other staff members, including nurses, assistants, technicians, technologists, and physician-colleagues. Risk management, like good care, requires the surgical team to work in concert.
Collaboration should start no later than the patient’s hospital admission and continue through discharge. Effective communication, both verbal and written, exhibits that.
Medical notes
One of the biggest problems in malpractice suits is the abysmal quality of a physician’s written notes. This holds true in the hospital and especially after discharge and for follow-up office visits. Often such notes consist of single-line entries.
Lawyers see many cases in which the patient left a phone message explicitly stating that he or she was worried about something. The doctor’s notes read, in full: “Talked to patient.”
I’m handling 4 or 5 cases now in which physicians have not helped themselves at all—by acting as if anything that happened after surgery was an afterthought.
On-call notes made on nights and weekends provide equally poor evidence because they rarely exist. The absence of such notes presents problems from a risk-management and defensibility standpoint.
Surgeons do themselves a disservice by failing to document properly the advice they give to patients. Jurors accept timely notes made in the patient’s record. They struggle a year after the fact to accept testimony such as, “I told the nurse X, Y, and Z. I know I told the patient to come in, or get something done, or go to the emergency room.”
Even in managed care, the surgeon bears responsibility for any delay in obtaining approval for recommended tests. A surgeon who wants a test done but anticipates a roadblock from a managed-care company can’t say, weeks later, “The insurance carrier didn’t approve it.”
You may not have much input, but blaming the system is a poor legal argument. You may have to ask the patient to do more to obtain approval or offer the patient the option to pay for the test out of pocket.
If managed care refuses initially or repeatedly to pay for important tests or procedures, you must document that you or your staff explained the situation to the patient and extended the patient an opportunity to pay for the test without reimbursement.
Plaintiff patients in this situation typically say, “Of course I would have paid X dollars for that CT scan.” Such assertions ring true with jurors. Patients will never say, “I support the doctor who never told me about something because he thought my insurance wouldn’t cover it.”
In court, you can’t blame managed care or remove an option simply because you personally thought some entity ought to pay for it.
Intraoperative concerns
Most claims against surgeons focus on what happens in the operating room or immediately postoperatively. The Physician Insurance Association of America recommends several strategies to reduce or avoid operating room claims6:
- Obtain adequate training and supervision when using new surgical equipment
- Ensure that the patient gives informed consent for a procedure and that you have provided adequate information regarding risks and alternatives
- When working as an attending physician with residents or internists, make sure they are under proper supervision
- Participate in any hospital-sponsored risk-management program.
Postoperative concerns
Your liability continues after surgery. In the hospital, you must communicate clearly with nurses. Use the chart as a tool to enhance patient safety. Document your observations thoroughly.
If you bring in consultant physicians to deal with a preexisting problem or one that arose after surgery, be aware that all clinicians involved must communicate. “I never talked with my consultants. We communicated through progress notes,” will not help a defendant-physician’s case. Such notes, which tend to be terse and hard to read, should never serve as the main method of communication.
A surgeon must communicate fully with the patient, and with the family as well. At least a dozen reports have established that patients, or their family, filed a lawsuit simply because they felt that was the only way to find out what happened.7,8
The author has no affiliations to disclose.
This article is the third in a series of 4 derived from a symposium on malpractice risk management at the 91st Clinical Congress of the American College of Surgeons, San Francisco, Calif., in October 2005. Mr. Donnelly updated his comments in August 2006.
Part 1 March 2007 Informed refusal
James M. Goodman, JD
Part 2 April 2007 Common errors in self-defense
Claudia Dobbs, MA
Part 3 THIS ISSUE - Patient safety as risk management tool
Thomas J. Donnelly, JD
Part 4 Responsibilities in obtaining informed consent
James M. Nelson, JD
Lawsuit filings have increased substantially in medicine over the past 10 to 15 years. So have indemnity payments—money spent in case settlements or in verdicts and awards in favor of plaintiffs. Specifically, there has been a rise in malpractice payouts higher than $1 million.1
Statistics on medical errors that are often the basis of actions are revealing:
- Deaths in the thousands. A 1999 report from the Institute of Medicine (IOM) concluded that 44,000 to 98,000 patients die annually from “preventable medical errors” in US hospitals.2
- Dollars in the billions. The annual cost of medical error has been estimated at $38 billion to $50 billion.
- Surgery at center stage. Subsequent studies suggested that more than half of deaths from preventable errors were related to surgical errors and failures.
- Prevention is a lifesaver. Other studies have supported IOM statistics, and suggested that as many as 70% of surgical adverse events are preventable.3
Received by the public as an indictment of the medical system, the IOM report and its offspring fostered a spate of research on public safety. Some invoked conclusions of NASA studies in the 1970s: Namely, it is a breakdown in communication, leadership, and teamwork that causes most commercial airline crashes—not a lack of skill.
Lesson from anesthesiology
The first transfer of NASA study methods to medicine involved anesthesiology. In the 1980s, one in 10,000 patients died in a manner related to anesthesia.4 Once anesthesiologists had implemented safety programs and made patient safety a high priority, patient mortality from anesthesia fell—dramatically. The rate is now 1 in 200,000 and approaching 1 in 300,000.4
Trends in claims paid out by medical malpractice defense insurers support that emphasis on safety and quality of care improves outcomes and reduces lawsuits. Malpractice insurance premiums for anesthesiologists in many states have decreased significantly. Other medical specialties can expect to see similar results as they focus on patient safety and risk management.5
Fatigue and patient risk
Myriad risk-management issues come into play for physicians. Long hours for residents on duty, for example, are under scrutiny. We are starting to recognize the role of fatigue in surgical error, such as wrong-site surgery, and related issues, such as inaccurate transfusion.
Surgeons must keep up to date on innovations and advancements, including technical skills and equipment modifications. From a risk-management perspective, there is no excuse for not practicing surgery in a modern, effective way.
Specialty organizations are increasingly publishing and promulgating clinical guidelines. Most states allow documents such as clinical guidelines to be introduced before a jury; the defendant surgeon who has neglected to follow an approach to a procedure that is advocated by a relevant specialty organization will face an uphill battle in court.
In selecting and preparing a candidate for surgery, these steps are integral for managing one’s malpractice risk:
- Patient selection. Improper patient selection is an obvious arena for lawsuits. If you have any doubt about which approach to take, don’t hesitate to refer the patient for a second opinion. Regardless of the conclusion, obtaining a second opinion in a difficult situation can only help you.
- Documentation. Informed consent and adequate documentation are crucial risk-management tools. The patient must understand exactly what you are recommending (see “If you can’t read your writing…”).
- Laboratory work-up. Making sure the patient obtains the requisite preoperative laboratory tests is vital (see “What do you do when managed care won’t pay for a test?”).
- Know the results. If a patient has other health issues that require medical clearance or warrant referral to an internist or primary-care physician, it’s ultimately the surgeon’s responsibility to see the patient gets the appropriate laboratory tests and to personally learn the results. Don’t assume that someone else—a primary-care physician, an internist, another specialist—will do it. Don’t be forced to say, “I referred the patient to somebody else for a work-up and assumed everything that happened was all right.”
A defendant physician who cannot read his or her own handwriting in a chart or notes is giving the plaintiff a gift. Illegible handwriting does not convey good organization, clear thinking, or an ability to communicate one’s intent to others. The plaintiff’s side may use this to make the physician seem poorly organized, rushed, and uncaring.
Surgeons must trust other staff members, including nurses, assistants, technicians, technologists, and physician-colleagues. Risk management, like good care, requires the surgical team to work in concert.
Collaboration should start no later than the patient’s hospital admission and continue through discharge. Effective communication, both verbal and written, exhibits that.
Medical notes
One of the biggest problems in malpractice suits is the abysmal quality of a physician’s written notes. This holds true in the hospital and especially after discharge and for follow-up office visits. Often such notes consist of single-line entries.
Lawyers see many cases in which the patient left a phone message explicitly stating that he or she was worried about something. The doctor’s notes read, in full: “Talked to patient.”
I’m handling 4 or 5 cases now in which physicians have not helped themselves at all—by acting as if anything that happened after surgery was an afterthought.
On-call notes made on nights and weekends provide equally poor evidence because they rarely exist. The absence of such notes presents problems from a risk-management and defensibility standpoint.
Surgeons do themselves a disservice by failing to document properly the advice they give to patients. Jurors accept timely notes made in the patient’s record. They struggle a year after the fact to accept testimony such as, “I told the nurse X, Y, and Z. I know I told the patient to come in, or get something done, or go to the emergency room.”
Even in managed care, the surgeon bears responsibility for any delay in obtaining approval for recommended tests. A surgeon who wants a test done but anticipates a roadblock from a managed-care company can’t say, weeks later, “The insurance carrier didn’t approve it.”
You may not have much input, but blaming the system is a poor legal argument. You may have to ask the patient to do more to obtain approval or offer the patient the option to pay for the test out of pocket.
If managed care refuses initially or repeatedly to pay for important tests or procedures, you must document that you or your staff explained the situation to the patient and extended the patient an opportunity to pay for the test without reimbursement.
Plaintiff patients in this situation typically say, “Of course I would have paid X dollars for that CT scan.” Such assertions ring true with jurors. Patients will never say, “I support the doctor who never told me about something because he thought my insurance wouldn’t cover it.”
In court, you can’t blame managed care or remove an option simply because you personally thought some entity ought to pay for it.
Intraoperative concerns
Most claims against surgeons focus on what happens in the operating room or immediately postoperatively. The Physician Insurance Association of America recommends several strategies to reduce or avoid operating room claims6:
- Obtain adequate training and supervision when using new surgical equipment
- Ensure that the patient gives informed consent for a procedure and that you have provided adequate information regarding risks and alternatives
- When working as an attending physician with residents or internists, make sure they are under proper supervision
- Participate in any hospital-sponsored risk-management program.
Postoperative concerns
Your liability continues after surgery. In the hospital, you must communicate clearly with nurses. Use the chart as a tool to enhance patient safety. Document your observations thoroughly.
If you bring in consultant physicians to deal with a preexisting problem or one that arose after surgery, be aware that all clinicians involved must communicate. “I never talked with my consultants. We communicated through progress notes,” will not help a defendant-physician’s case. Such notes, which tend to be terse and hard to read, should never serve as the main method of communication.
A surgeon must communicate fully with the patient, and with the family as well. At least a dozen reports have established that patients, or their family, filed a lawsuit simply because they felt that was the only way to find out what happened.7,8
The author has no affiliations to disclose.
1. The Large Loss Claim Trend. PIAA Research Notes. Rockville, MD: Physicians Insurers Association of America; 2005.
2. Committee on Quality of Health Care in America. To Err is Human: Building a safer health system. Washington, DC: National Academy Press; 1999.
3. Gawande AA, Thomas EJ, Zinner MJ, Brennan TA. The incidence and nature of surgical adverse events in Colorado and Utah in 1992. Surgery. 1999;126:66-75.
4. Gawande A. Complications, a Surgeon’s Notes on an Imperfect Science. New York, NY: Picador USA; 2003.
5. Hallinan JT. Once seen as risky, one group of doctors changes its ways. Wall Street Journal. June 21, 2005:A1.
6. Operating Room Claims, PIAA Research Notes. Rockville, MD: Physicians Insurers Association of America; 2004.
7. Moore PJ, Adler NE, Robertson PA. The effect of doctor-patient relations on medical patient perceptions and malpractice intentions. West J Med. 2000;173:244-250.
8. Hickson GB, Federspiel CF, Pichert JW, Miller CS, Gauld-Jaeger J, Bost P. Patient complaints and malpractice risk. JAMA. 2002;287:2951-2957.
1. The Large Loss Claim Trend. PIAA Research Notes. Rockville, MD: Physicians Insurers Association of America; 2005.
2. Committee on Quality of Health Care in America. To Err is Human: Building a safer health system. Washington, DC: National Academy Press; 1999.
3. Gawande AA, Thomas EJ, Zinner MJ, Brennan TA. The incidence and nature of surgical adverse events in Colorado and Utah in 1992. Surgery. 1999;126:66-75.
4. Gawande A. Complications, a Surgeon’s Notes on an Imperfect Science. New York, NY: Picador USA; 2003.
5. Hallinan JT. Once seen as risky, one group of doctors changes its ways. Wall Street Journal. June 21, 2005:A1.
6. Operating Room Claims, PIAA Research Notes. Rockville, MD: Physicians Insurers Association of America; 2004.
7. Moore PJ, Adler NE, Robertson PA. The effect of doctor-patient relations on medical patient perceptions and malpractice intentions. West J Med. 2000;173:244-250.
8. Hickson GB, Federspiel CF, Pichert JW, Miller CS, Gauld-Jaeger J, Bost P. Patient complaints and malpractice risk. JAMA. 2002;287:2951-2957.
Caring for your patient after discharge
Improper treatment of depression,
psychosis blamed for suicide
Kings County (NY) Supreme Court
A 52-year-old patient with a history of mental illness was hospitalized for treatment of major depression with recurrent psychotic features. After release she underwent counseling with a psychiatrist at a mental health center.
One month after discharge the patient was rehospitalized for 2 weeks. After this release she resumed counseling at the mental health center.
Six months later the patient’s husband telephoned the center and reported that the patient needed further treatment. The husband was instructed to bring the patient to a hospital, but he did not do so. The next day the patient committed suicide by jumping from a fourth-floor window.
The case went to trial against the psychiatrist, a social worker, and the mental health center. The patient’s family claimed that she should have been prescribed antidepressant medication, enrolled in family therapy, and received immediate care when her husband telephoned the mental health center with concerns. The psychiatrist, a social worker, and the mental health center argued that the patient was properly treated and medication was prescribed. They counterclaimed that the husband was negligent toward his wife by failing to take her to the hospital as instructed.
A $75,000 settlement was reached with the social worker prior to the verdict. Remaining parties reached a $650,000/$250,000 high/low agreement.
- A defense verdict was returned
A woman with prescription drug abuse
commits suicide 19 days after discharge
Floyd County (GA) Superior Court
A patient, in her early 40s, was under a psychiatrist’s care and admitted to an acute care psychiatric facility for prescription drug abuse. The patient was discharged from the psychiatric facility with instructions to continue outpatient therapy with the psychiatrist. The patient committed suicide 19 days later.
The patient’s family alleged that the psychiatrist failed to properly diagnose and treat the patient’s mental condition, arguing that the clinician should not have discharged the patient from the acute care psychiatric facility while she experienced drug withdrawal symptoms and depression. The psychiatrist claimed that the patient was treated properly for substance abuse, and depression was secondary and related to drug abuse. The psychiatrist also said that the patient received a comprehensive discharge plan, which included follow-up treatment with him and counselors.
- A defense verdict was returned
Suicide rates are highest immediately after hospital discharge.1,2 Inadequate follow-up care or discharge planning may increase the risk for suicide.3 A recent study of 121,933 psychiatric patients at VA hospitals found that 481 (0.4%) died of suicide within 1 year of discharge; 46% of those deaths occurred within the first 3 months. Patients who stayed less than 14 days or had poor continuity of care had a higher risk of suicide.4
Discharge may form the basis for a negligence claim if the release is not a valid exercise in professional judgment. In Bell vs New York City Health and Hospitals Corporation, a patient attempted suicide after hospital discharge. He was released despite suicidal ideation and psychosis. Citing the lack of a well documented psychiatric examination, the court found the hospital negligent because the psychiatrist failed to investigate the patient’s psychiatric history and delusions or an incident when the patient was restrained the night before.5,6
The courts have not found psychiatrists negligent when they perform a risk assessment and reasonably conclude that the benefits of release outweigh the risks.7
Reasonable protection
Two factors determine liability in suicide cases: forseeability and reasonable care.
Forseeability refers to the reasonable evaluation of suicide potential based on a risk assessment. Failure to perform and document this assessment may be evidence of negligence.
Document in your risk assessment the patient’s:
- short-term suicide risk factors (Box 1)
- suicidal thoughts, plans, intents, and actions
- feelings of hopelessness
- substance abuse
- evidence of poor impulse control8,9
- protective factors such as coping and survival skills, family responsibilities, child-related concerns, and moral/ religious beliefs.10,11
- Panic attacks
- Anxiety
- Loss of pleasure
- Diminished concentration
- Depressive turmoil
- Insomnia
Source: Reference 12
In the second case, reasonable care encompasses a discharge plan and continuity of care. Discharge plans should include safety precautions and treatment. Follow-up after discharge ensures that the treatment plan has been carried out. Educate family members about monitoring the patient, communicating observations about changes or concerns, and safeguarding the home, such as removing firearms (Box 2).13
- Emphasize the need for follow-up therapy and/or medication adherence
- Inform the patient and family of crisis management procedures and steps. Patient needs to know how to the contact treatment provider and what to do when the clinician is not immediately accessible in an emergency
- Obtain the patient’s permission for you to talk with family members as is clinically necessary
- Instruct the family to monitor the patient and communicate changes or concerns to the outpatient providers
- Enlist the family to help safeguard the home, for example, removing firearms
- Evaluate the patient’s understanding and acceptance of the aftercare plan.
Family members should be aware of any problems in the patient’s understanding or acceptance of the plan.
Source: Reference 9
- information sources (such as patient report, family report) the psychiatrist used when deciding to discharge the patient
- factors that went into the decision to discharge (such as response to medications)
- how these factors were balanced against the option of keeping the patient in the hospital.
Comparative negligence. In some suicide cases, courts have allowed a comparative negligence defense, either against the family or the patient. In Maunz vs Perales, the psychiatrist instructed the patient’s family to remove all guns from the home, referred the patient to an outpatient clinic, advised the family to make an appointment 1 week later, and then discharged the patient. The next day, the patient bought a gun and shot himself.
The court held that “people generally have a duty to exercise ordinary care for their own safety. To rule otherwise would make the doctor the absolute insurer of any patient exhibiting suicidal tendencies. The consequence of such a ruling would be that no health care provider would want to risk the liability exposure in treating such a patient, and, thus, suicidal persons would be denied necessary treatment.”5,15
1. Geddes JR, Juszczak E, O’Brien F, et al. Suicide in the 12 months after discharge from psychiatric hospital in Scotland, 1968-1992. BMJ 1995;311:357-60.
2. Roy A. Risk factors for suicide in psychiatric patients. Arch Gen Psychiatry 1982;39:1089-95.
3. Oquendo MA, Kamali M, Ellis SP, et al. Adequacy of antidepressant treatment after discharge and the occurrence of suicidal acts in major depression: a prospective study. Am J Psychiatry 2002;159:1746-51.
4. Desai RA, Dausey DJ, Rosenheck RA. Mental health service delivery and suicide risk: the role of individual patient and facility factors. Am J Psychiatry 2005;162:311-18.
5. Packman WL, Pennuto TO, Bongar B, et al. Legal issues of professional negligence in suicide cases. Behav Sci Law 2004;22:697-713.
6. Bell v. New York City Health and Hospitals Corporation 456 NYS2d 787 (1982).
7. Johnson v. United States, 409 F. Supp. 1283 (D Fla 1981).
8. Simon RI. Commentary: medical errors, sentinel events, and malpractice. J Am Acad Psychiatry Law 2006;34:99-100.
9. Berman AL. Risk management with suicidal patients. J Clin Psychol 2006;62:171-84.
10. Linehan MM, Goodstein JL, Nielsen SL, et al. Reasons for staying alive when you are thinking of killing yourself: the reasons for living inventory. J Consult Clin Psychol 1983;51:276-86.
11. Simon RI. Suicide risk assessment: is clinical experience enough? J Am Acad Psychiatry Law 2006;34:276-8.
12. Fawcett J, Scheftner WA, Fogg I, et al. Time-related predictors of suicide in major affective disorder. Am J Psychiatry 1990;147:1189-45.
13. Abille v. United States, 482 F. Supp. 703 (ND Cal 1980).
14. Simon RI. The suicidal patient. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law: a comprehensive handbook. Cambridge, MA: Harvard University Press; 1998:166-86.
15. Maunz v. Perales, 276 Kan. 313, 76 P.3d 1027 (Kan 2003).
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Dr. Grant is associate professor of psychiatry, University of Minnesota Medical Center, Minneapolis
Improper treatment of depression,
psychosis blamed for suicide
Kings County (NY) Supreme Court
A 52-year-old patient with a history of mental illness was hospitalized for treatment of major depression with recurrent psychotic features. After release she underwent counseling with a psychiatrist at a mental health center.
One month after discharge the patient was rehospitalized for 2 weeks. After this release she resumed counseling at the mental health center.
Six months later the patient’s husband telephoned the center and reported that the patient needed further treatment. The husband was instructed to bring the patient to a hospital, but he did not do so. The next day the patient committed suicide by jumping from a fourth-floor window.
The case went to trial against the psychiatrist, a social worker, and the mental health center. The patient’s family claimed that she should have been prescribed antidepressant medication, enrolled in family therapy, and received immediate care when her husband telephoned the mental health center with concerns. The psychiatrist, a social worker, and the mental health center argued that the patient was properly treated and medication was prescribed. They counterclaimed that the husband was negligent toward his wife by failing to take her to the hospital as instructed.
A $75,000 settlement was reached with the social worker prior to the verdict. Remaining parties reached a $650,000/$250,000 high/low agreement.
- A defense verdict was returned
A woman with prescription drug abuse
commits suicide 19 days after discharge
Floyd County (GA) Superior Court
A patient, in her early 40s, was under a psychiatrist’s care and admitted to an acute care psychiatric facility for prescription drug abuse. The patient was discharged from the psychiatric facility with instructions to continue outpatient therapy with the psychiatrist. The patient committed suicide 19 days later.
The patient’s family alleged that the psychiatrist failed to properly diagnose and treat the patient’s mental condition, arguing that the clinician should not have discharged the patient from the acute care psychiatric facility while she experienced drug withdrawal symptoms and depression. The psychiatrist claimed that the patient was treated properly for substance abuse, and depression was secondary and related to drug abuse. The psychiatrist also said that the patient received a comprehensive discharge plan, which included follow-up treatment with him and counselors.
- A defense verdict was returned
Suicide rates are highest immediately after hospital discharge.1,2 Inadequate follow-up care or discharge planning may increase the risk for suicide.3 A recent study of 121,933 psychiatric patients at VA hospitals found that 481 (0.4%) died of suicide within 1 year of discharge; 46% of those deaths occurred within the first 3 months. Patients who stayed less than 14 days or had poor continuity of care had a higher risk of suicide.4
Discharge may form the basis for a negligence claim if the release is not a valid exercise in professional judgment. In Bell vs New York City Health and Hospitals Corporation, a patient attempted suicide after hospital discharge. He was released despite suicidal ideation and psychosis. Citing the lack of a well documented psychiatric examination, the court found the hospital negligent because the psychiatrist failed to investigate the patient’s psychiatric history and delusions or an incident when the patient was restrained the night before.5,6
The courts have not found psychiatrists negligent when they perform a risk assessment and reasonably conclude that the benefits of release outweigh the risks.7
Reasonable protection
Two factors determine liability in suicide cases: forseeability and reasonable care.
Forseeability refers to the reasonable evaluation of suicide potential based on a risk assessment. Failure to perform and document this assessment may be evidence of negligence.
Document in your risk assessment the patient’s:
- short-term suicide risk factors (Box 1)
- suicidal thoughts, plans, intents, and actions
- feelings of hopelessness
- substance abuse
- evidence of poor impulse control8,9
- protective factors such as coping and survival skills, family responsibilities, child-related concerns, and moral/ religious beliefs.10,11
- Panic attacks
- Anxiety
- Loss of pleasure
- Diminished concentration
- Depressive turmoil
- Insomnia
Source: Reference 12
In the second case, reasonable care encompasses a discharge plan and continuity of care. Discharge plans should include safety precautions and treatment. Follow-up after discharge ensures that the treatment plan has been carried out. Educate family members about monitoring the patient, communicating observations about changes or concerns, and safeguarding the home, such as removing firearms (Box 2).13
- Emphasize the need for follow-up therapy and/or medication adherence
- Inform the patient and family of crisis management procedures and steps. Patient needs to know how to the contact treatment provider and what to do when the clinician is not immediately accessible in an emergency
- Obtain the patient’s permission for you to talk with family members as is clinically necessary
- Instruct the family to monitor the patient and communicate changes or concerns to the outpatient providers
- Enlist the family to help safeguard the home, for example, removing firearms
- Evaluate the patient’s understanding and acceptance of the aftercare plan.
Family members should be aware of any problems in the patient’s understanding or acceptance of the plan.
Source: Reference 9
- information sources (such as patient report, family report) the psychiatrist used when deciding to discharge the patient
- factors that went into the decision to discharge (such as response to medications)
- how these factors were balanced against the option of keeping the patient in the hospital.
Comparative negligence. In some suicide cases, courts have allowed a comparative negligence defense, either against the family or the patient. In Maunz vs Perales, the psychiatrist instructed the patient’s family to remove all guns from the home, referred the patient to an outpatient clinic, advised the family to make an appointment 1 week later, and then discharged the patient. The next day, the patient bought a gun and shot himself.
The court held that “people generally have a duty to exercise ordinary care for their own safety. To rule otherwise would make the doctor the absolute insurer of any patient exhibiting suicidal tendencies. The consequence of such a ruling would be that no health care provider would want to risk the liability exposure in treating such a patient, and, thus, suicidal persons would be denied necessary treatment.”5,15
Improper treatment of depression,
psychosis blamed for suicide
Kings County (NY) Supreme Court
A 52-year-old patient with a history of mental illness was hospitalized for treatment of major depression with recurrent psychotic features. After release she underwent counseling with a psychiatrist at a mental health center.
One month after discharge the patient was rehospitalized for 2 weeks. After this release she resumed counseling at the mental health center.
Six months later the patient’s husband telephoned the center and reported that the patient needed further treatment. The husband was instructed to bring the patient to a hospital, but he did not do so. The next day the patient committed suicide by jumping from a fourth-floor window.
The case went to trial against the psychiatrist, a social worker, and the mental health center. The patient’s family claimed that she should have been prescribed antidepressant medication, enrolled in family therapy, and received immediate care when her husband telephoned the mental health center with concerns. The psychiatrist, a social worker, and the mental health center argued that the patient was properly treated and medication was prescribed. They counterclaimed that the husband was negligent toward his wife by failing to take her to the hospital as instructed.
A $75,000 settlement was reached with the social worker prior to the verdict. Remaining parties reached a $650,000/$250,000 high/low agreement.
- A defense verdict was returned
A woman with prescription drug abuse
commits suicide 19 days after discharge
Floyd County (GA) Superior Court
A patient, in her early 40s, was under a psychiatrist’s care and admitted to an acute care psychiatric facility for prescription drug abuse. The patient was discharged from the psychiatric facility with instructions to continue outpatient therapy with the psychiatrist. The patient committed suicide 19 days later.
The patient’s family alleged that the psychiatrist failed to properly diagnose and treat the patient’s mental condition, arguing that the clinician should not have discharged the patient from the acute care psychiatric facility while she experienced drug withdrawal symptoms and depression. The psychiatrist claimed that the patient was treated properly for substance abuse, and depression was secondary and related to drug abuse. The psychiatrist also said that the patient received a comprehensive discharge plan, which included follow-up treatment with him and counselors.
- A defense verdict was returned
Suicide rates are highest immediately after hospital discharge.1,2 Inadequate follow-up care or discharge planning may increase the risk for suicide.3 A recent study of 121,933 psychiatric patients at VA hospitals found that 481 (0.4%) died of suicide within 1 year of discharge; 46% of those deaths occurred within the first 3 months. Patients who stayed less than 14 days or had poor continuity of care had a higher risk of suicide.4
Discharge may form the basis for a negligence claim if the release is not a valid exercise in professional judgment. In Bell vs New York City Health and Hospitals Corporation, a patient attempted suicide after hospital discharge. He was released despite suicidal ideation and psychosis. Citing the lack of a well documented psychiatric examination, the court found the hospital negligent because the psychiatrist failed to investigate the patient’s psychiatric history and delusions or an incident when the patient was restrained the night before.5,6
The courts have not found psychiatrists negligent when they perform a risk assessment and reasonably conclude that the benefits of release outweigh the risks.7
Reasonable protection
Two factors determine liability in suicide cases: forseeability and reasonable care.
Forseeability refers to the reasonable evaluation of suicide potential based on a risk assessment. Failure to perform and document this assessment may be evidence of negligence.
Document in your risk assessment the patient’s:
- short-term suicide risk factors (Box 1)
- suicidal thoughts, plans, intents, and actions
- feelings of hopelessness
- substance abuse
- evidence of poor impulse control8,9
- protective factors such as coping and survival skills, family responsibilities, child-related concerns, and moral/ religious beliefs.10,11
- Panic attacks
- Anxiety
- Loss of pleasure
- Diminished concentration
- Depressive turmoil
- Insomnia
Source: Reference 12
In the second case, reasonable care encompasses a discharge plan and continuity of care. Discharge plans should include safety precautions and treatment. Follow-up after discharge ensures that the treatment plan has been carried out. Educate family members about monitoring the patient, communicating observations about changes or concerns, and safeguarding the home, such as removing firearms (Box 2).13
- Emphasize the need for follow-up therapy and/or medication adherence
- Inform the patient and family of crisis management procedures and steps. Patient needs to know how to the contact treatment provider and what to do when the clinician is not immediately accessible in an emergency
- Obtain the patient’s permission for you to talk with family members as is clinically necessary
- Instruct the family to monitor the patient and communicate changes or concerns to the outpatient providers
- Enlist the family to help safeguard the home, for example, removing firearms
- Evaluate the patient’s understanding and acceptance of the aftercare plan.
Family members should be aware of any problems in the patient’s understanding or acceptance of the plan.
Source: Reference 9
- information sources (such as patient report, family report) the psychiatrist used when deciding to discharge the patient
- factors that went into the decision to discharge (such as response to medications)
- how these factors were balanced against the option of keeping the patient in the hospital.
Comparative negligence. In some suicide cases, courts have allowed a comparative negligence defense, either against the family or the patient. In Maunz vs Perales, the psychiatrist instructed the patient’s family to remove all guns from the home, referred the patient to an outpatient clinic, advised the family to make an appointment 1 week later, and then discharged the patient. The next day, the patient bought a gun and shot himself.
The court held that “people generally have a duty to exercise ordinary care for their own safety. To rule otherwise would make the doctor the absolute insurer of any patient exhibiting suicidal tendencies. The consequence of such a ruling would be that no health care provider would want to risk the liability exposure in treating such a patient, and, thus, suicidal persons would be denied necessary treatment.”5,15
1. Geddes JR, Juszczak E, O’Brien F, et al. Suicide in the 12 months after discharge from psychiatric hospital in Scotland, 1968-1992. BMJ 1995;311:357-60.
2. Roy A. Risk factors for suicide in psychiatric patients. Arch Gen Psychiatry 1982;39:1089-95.
3. Oquendo MA, Kamali M, Ellis SP, et al. Adequacy of antidepressant treatment after discharge and the occurrence of suicidal acts in major depression: a prospective study. Am J Psychiatry 2002;159:1746-51.
4. Desai RA, Dausey DJ, Rosenheck RA. Mental health service delivery and suicide risk: the role of individual patient and facility factors. Am J Psychiatry 2005;162:311-18.
5. Packman WL, Pennuto TO, Bongar B, et al. Legal issues of professional negligence in suicide cases. Behav Sci Law 2004;22:697-713.
6. Bell v. New York City Health and Hospitals Corporation 456 NYS2d 787 (1982).
7. Johnson v. United States, 409 F. Supp. 1283 (D Fla 1981).
8. Simon RI. Commentary: medical errors, sentinel events, and malpractice. J Am Acad Psychiatry Law 2006;34:99-100.
9. Berman AL. Risk management with suicidal patients. J Clin Psychol 2006;62:171-84.
10. Linehan MM, Goodstein JL, Nielsen SL, et al. Reasons for staying alive when you are thinking of killing yourself: the reasons for living inventory. J Consult Clin Psychol 1983;51:276-86.
11. Simon RI. Suicide risk assessment: is clinical experience enough? J Am Acad Psychiatry Law 2006;34:276-8.
12. Fawcett J, Scheftner WA, Fogg I, et al. Time-related predictors of suicide in major affective disorder. Am J Psychiatry 1990;147:1189-45.
13. Abille v. United States, 482 F. Supp. 703 (ND Cal 1980).
14. Simon RI. The suicidal patient. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law: a comprehensive handbook. Cambridge, MA: Harvard University Press; 1998:166-86.
15. Maunz v. Perales, 276 Kan. 313, 76 P.3d 1027 (Kan 2003).
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Dr. Grant is associate professor of psychiatry, University of Minnesota Medical Center, Minneapolis
1. Geddes JR, Juszczak E, O’Brien F, et al. Suicide in the 12 months after discharge from psychiatric hospital in Scotland, 1968-1992. BMJ 1995;311:357-60.
2. Roy A. Risk factors for suicide in psychiatric patients. Arch Gen Psychiatry 1982;39:1089-95.
3. Oquendo MA, Kamali M, Ellis SP, et al. Adequacy of antidepressant treatment after discharge and the occurrence of suicidal acts in major depression: a prospective study. Am J Psychiatry 2002;159:1746-51.
4. Desai RA, Dausey DJ, Rosenheck RA. Mental health service delivery and suicide risk: the role of individual patient and facility factors. Am J Psychiatry 2005;162:311-18.
5. Packman WL, Pennuto TO, Bongar B, et al. Legal issues of professional negligence in suicide cases. Behav Sci Law 2004;22:697-713.
6. Bell v. New York City Health and Hospitals Corporation 456 NYS2d 787 (1982).
7. Johnson v. United States, 409 F. Supp. 1283 (D Fla 1981).
8. Simon RI. Commentary: medical errors, sentinel events, and malpractice. J Am Acad Psychiatry Law 2006;34:99-100.
9. Berman AL. Risk management with suicidal patients. J Clin Psychol 2006;62:171-84.
10. Linehan MM, Goodstein JL, Nielsen SL, et al. Reasons for staying alive when you are thinking of killing yourself: the reasons for living inventory. J Consult Clin Psychol 1983;51:276-86.
11. Simon RI. Suicide risk assessment: is clinical experience enough? J Am Acad Psychiatry Law 2006;34:276-8.
12. Fawcett J, Scheftner WA, Fogg I, et al. Time-related predictors of suicide in major affective disorder. Am J Psychiatry 1990;147:1189-45.
13. Abille v. United States, 482 F. Supp. 703 (ND Cal 1980).
14. Simon RI. The suicidal patient. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law: a comprehensive handbook. Cambridge, MA: Harvard University Press; 1998:166-86.
15. Maunz v. Perales, 276 Kan. 313, 76 P.3d 1027 (Kan 2003).
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Dr. Grant is associate professor of psychiatry, University of Minnesota Medical Center, Minneapolis