User login
Malpractice Chronicle
Reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
Was Follow-Up Adequate After Neurosurgery in Cancún?
Shortly after arriving in Mexico for a brief stay, a 44-year-old woman collapsed in the customs area. She was taken to a hospital in Cancún, where she underwent emergency neurosurgery for a brain bleed. After several days of hospitalization, she was stabilized and returned to Michigan with instructions to see her family clinician.
Her appointment was delayed by an ice storm, which interrupted power to the office of the defendant internist, Dr. M. That Saturday, the woman visited the office's clinic and was examined by the defendant family practitioner, Dr. P. She presented with a shaved head and a neurosurgical scar on the left side of her head; she complained of headache and some blurred or double vision. She gave Dr. P. a list of medications and medical records (in Spanish) from the Mexican hospital.
Findings on her physical examination were normal. She was instructed to return to see Dr. M., and she did so at the clinic on the following Monday. She repeated her complaints of double vision, headache, and fatigue. Dr. M. charged his office staff with attempting to have the Mexican records translated and to arrange for a neurosurgery appointment.
The patient was ultimately scheduled for head CT and an office visit with a neurosurgeon six days later. The day after those arrangements were made, however, she experienced a massive brain bleed and died.
According to the plaintiff, the surgeons in Mexico drained the blood from the initial bleed but did not detect its source—an aneurysm in the subarachnoid space. The plaintiff alleged that the defendants should have hospitalized the decedent immediately upon her return from Mexico or sent her for an immediate neurosurgical consult. Had the decedent undergone CT immediately, it was argued, the aneurysm would have been detected, surgery would have been performed, and she would have survived.
The defendants argued that the neurosurgical follow-up was out of their area of expertise and that they made appropriate arrangements for the decedent to be seen by a neurosurgeon. They maintained that the decedent appeared stable and seemed to be improving and that it was possible that the fatal bleed was not related to the first bleed. The defendants also claimed that definitive treatment should have been given in Mexico.
According to a published report, a defense verdict was returned.
Ultrasound Misplaced, Diagnosis Delayed for a Year
In March 2003 at age 2, the minor plaintiff was admitted to the defendant hospital under the care of the defendant pediatric urologist, who was treating her for bilateral vesicoureteral urinary reflux and frequent urinary tract infections (UTIs). The defendant surgically reimplanted both ureters to stop urinary reflux. The toddler was discharged to home in her parents' care two days after the procedure.
The child continued to experience UTIs. Renal ultrasonography revealed a blockage in the left ureter, but the ultrasound was lost by the defendant hospital. Results were never conveyed to the ordering physicians, who failed to follow up to obtain them.
In April 2004, the defendant urologist diagnosed the condition and determined that it had gone untreated for a year. Repeat renal ultrasonography demonstrated the blockage, and a nuclear renal scan confirmed that the child's left kidney was no longer functioning at all as a result of urinary backup. In addition to losing all function of the left kidney, the child has compromised function in the right kidney. She is expected to require dialysis in the future and eventually kidney transplantation.
A $9.75 million settlement was reached.
Complications of Undiagnosed Diverticulitis
A 62-year-old woman visited the defendant internist with complaints of abdominal pressure, poor appetite, weakness, and dizziness. Her medical history included hypertension, diverticulitis, hysterectomy, and tonsillectomy.
The defendant ordered a chest x-ray, complete blood count, and urinalysis. After reviewing test results, the defendant made a diagnosis of urinary tract infection and prescribed ceftriaxone by intramuscular injection and oral ciprofloxacin.
After receiving the first injection of ceftriaxone, the patient called the defendant's office, complaining of increased discomfort. She requested admission to the hospital, which was allegedly refused by a member of the office staff. The following day, the plaintiff was transported to the hospital by ambulance with complaints of left lower quadrant pain, intermittent for one week and worsening that evening. The plaintiff reported no nausea or diarrhea but was belching.
The emergency department physician identified tender palpation in the abdomen with no rebounding and decreased bowel sounds. The defendant internist's answering service was contacted, and the covering physician ordered admission with a diagnosis of diverticulitis. CT of the abdomen and pelvis revealed evidence of free air under the hemidiaphragm, ascites, and phlegmonous reaction; the results also suggested diverticulitis with perforation in the rectosigmoid region and inflammatory changes.
Five hours later, the patient was taken to surgery for an exploratory laparotomy and colostomy to address the apparent perforated diverticulum. Her immediate postoperative course included profound hypotension with narrow-complex tachycardia. These developments, allegedly resulting from abdominal sepsis due to the delay in diagnosing the perforated diverticulum, necessitated pressors and dopamine.
Soon thereafter, the patient developed right-leg ischemia. She underwent embolectomy and thrombectomy to the right common femoral artery and the superficial femoral artery, with repair to the right profunda by use of a saphenous vein patch angioplasty. Two days later, the patient was taken to surgery for an above-knee amputation.
The plaintiff claimed that the defendant was negligent in failing to recognize early manifestations of diverticulitis and to order CT or MRl. The plaintiff also claimed that she should have been hospitalized when she requested admission.
The defendant maintained that the patient's history and the laboratory study results suggested that she had the flu or a urinary tract infection and that hospitalization was not needed. The defendant also maintained that when he called for a surgical consultation, the surgeon did not arrive for four and one-half hours.
According to a published report, a defense verdict was returned. A motion for a new trial was pending.
Surgery Continued Despite Patient's Deteriorating Condition
In 1986, the patient, then age 8, was found to be mildly mentally retarded (IQ, 59 to 70). He also had paranoid schizophrenia, causing him to hear voices in his head. The patient lived with his sister, who served as his guardian.
At age 19, the patient was scheduled to undergo surgery to correct curvature of the spine. The operation was to be performed by Dr. R., assisted by Dr. M. and by an anesthesiologist, Dr. L.
About one hour into the surgery, the patient began to manifest decreased urinary output with no known cause, but the procedure continued. About 90 minutes later, an equipment malfunction made it impossible for the medical team to monitor the patient's nerve responses and oxygen levels, but the surgery still continued.
At some point during the surgery, the patient had an unexplained blood loss and his serum calcium level dropped below normal. He also experienced a loss of oxygen to the brain, then went into cardiac arrest. At that point, the surgery was discontinued, uncompleted.
The patient was comatose for several days, during which he displayed prolonged seizure activity. After regaining consciousness, he remained in the hospital for nearly four weeks before being transferred to another facility for rehabilitation.
The patient continues to have symptoms of various neurologic problems, including athetoid-choreiform movement, which causes a general loss of balance and muscular control and cognitive deficits, which make him unable to communicate.
The plaintiff claimed that the surgery should have been stopped when the problems arose. The plaintiff also claimed that Dr. R. should have ordered intraoperative lab work when the plaintiff's condition deteriorated.
The matter was ultimately tried against Drs. R. and L. only. They denied any negligence.
According to a published report, a $3 million verdict was returned.
Reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
Was Follow-Up Adequate After Neurosurgery in Cancún?
Shortly after arriving in Mexico for a brief stay, a 44-year-old woman collapsed in the customs area. She was taken to a hospital in Cancún, where she underwent emergency neurosurgery for a brain bleed. After several days of hospitalization, she was stabilized and returned to Michigan with instructions to see her family clinician.
Her appointment was delayed by an ice storm, which interrupted power to the office of the defendant internist, Dr. M. That Saturday, the woman visited the office's clinic and was examined by the defendant family practitioner, Dr. P. She presented with a shaved head and a neurosurgical scar on the left side of her head; she complained of headache and some blurred or double vision. She gave Dr. P. a list of medications and medical records (in Spanish) from the Mexican hospital.
Findings on her physical examination were normal. She was instructed to return to see Dr. M., and she did so at the clinic on the following Monday. She repeated her complaints of double vision, headache, and fatigue. Dr. M. charged his office staff with attempting to have the Mexican records translated and to arrange for a neurosurgery appointment.
The patient was ultimately scheduled for head CT and an office visit with a neurosurgeon six days later. The day after those arrangements were made, however, she experienced a massive brain bleed and died.
According to the plaintiff, the surgeons in Mexico drained the blood from the initial bleed but did not detect its source—an aneurysm in the subarachnoid space. The plaintiff alleged that the defendants should have hospitalized the decedent immediately upon her return from Mexico or sent her for an immediate neurosurgical consult. Had the decedent undergone CT immediately, it was argued, the aneurysm would have been detected, surgery would have been performed, and she would have survived.
The defendants argued that the neurosurgical follow-up was out of their area of expertise and that they made appropriate arrangements for the decedent to be seen by a neurosurgeon. They maintained that the decedent appeared stable and seemed to be improving and that it was possible that the fatal bleed was not related to the first bleed. The defendants also claimed that definitive treatment should have been given in Mexico.
According to a published report, a defense verdict was returned.
Ultrasound Misplaced, Diagnosis Delayed for a Year
In March 2003 at age 2, the minor plaintiff was admitted to the defendant hospital under the care of the defendant pediatric urologist, who was treating her for bilateral vesicoureteral urinary reflux and frequent urinary tract infections (UTIs). The defendant surgically reimplanted both ureters to stop urinary reflux. The toddler was discharged to home in her parents' care two days after the procedure.
The child continued to experience UTIs. Renal ultrasonography revealed a blockage in the left ureter, but the ultrasound was lost by the defendant hospital. Results were never conveyed to the ordering physicians, who failed to follow up to obtain them.
In April 2004, the defendant urologist diagnosed the condition and determined that it had gone untreated for a year. Repeat renal ultrasonography demonstrated the blockage, and a nuclear renal scan confirmed that the child's left kidney was no longer functioning at all as a result of urinary backup. In addition to losing all function of the left kidney, the child has compromised function in the right kidney. She is expected to require dialysis in the future and eventually kidney transplantation.
A $9.75 million settlement was reached.
Complications of Undiagnosed Diverticulitis
A 62-year-old woman visited the defendant internist with complaints of abdominal pressure, poor appetite, weakness, and dizziness. Her medical history included hypertension, diverticulitis, hysterectomy, and tonsillectomy.
The defendant ordered a chest x-ray, complete blood count, and urinalysis. After reviewing test results, the defendant made a diagnosis of urinary tract infection and prescribed ceftriaxone by intramuscular injection and oral ciprofloxacin.
After receiving the first injection of ceftriaxone, the patient called the defendant's office, complaining of increased discomfort. She requested admission to the hospital, which was allegedly refused by a member of the office staff. The following day, the plaintiff was transported to the hospital by ambulance with complaints of left lower quadrant pain, intermittent for one week and worsening that evening. The plaintiff reported no nausea or diarrhea but was belching.
The emergency department physician identified tender palpation in the abdomen with no rebounding and decreased bowel sounds. The defendant internist's answering service was contacted, and the covering physician ordered admission with a diagnosis of diverticulitis. CT of the abdomen and pelvis revealed evidence of free air under the hemidiaphragm, ascites, and phlegmonous reaction; the results also suggested diverticulitis with perforation in the rectosigmoid region and inflammatory changes.
Five hours later, the patient was taken to surgery for an exploratory laparotomy and colostomy to address the apparent perforated diverticulum. Her immediate postoperative course included profound hypotension with narrow-complex tachycardia. These developments, allegedly resulting from abdominal sepsis due to the delay in diagnosing the perforated diverticulum, necessitated pressors and dopamine.
Soon thereafter, the patient developed right-leg ischemia. She underwent embolectomy and thrombectomy to the right common femoral artery and the superficial femoral artery, with repair to the right profunda by use of a saphenous vein patch angioplasty. Two days later, the patient was taken to surgery for an above-knee amputation.
The plaintiff claimed that the defendant was negligent in failing to recognize early manifestations of diverticulitis and to order CT or MRl. The plaintiff also claimed that she should have been hospitalized when she requested admission.
The defendant maintained that the patient's history and the laboratory study results suggested that she had the flu or a urinary tract infection and that hospitalization was not needed. The defendant also maintained that when he called for a surgical consultation, the surgeon did not arrive for four and one-half hours.
According to a published report, a defense verdict was returned. A motion for a new trial was pending.
Surgery Continued Despite Patient's Deteriorating Condition
In 1986, the patient, then age 8, was found to be mildly mentally retarded (IQ, 59 to 70). He also had paranoid schizophrenia, causing him to hear voices in his head. The patient lived with his sister, who served as his guardian.
At age 19, the patient was scheduled to undergo surgery to correct curvature of the spine. The operation was to be performed by Dr. R., assisted by Dr. M. and by an anesthesiologist, Dr. L.
About one hour into the surgery, the patient began to manifest decreased urinary output with no known cause, but the procedure continued. About 90 minutes later, an equipment malfunction made it impossible for the medical team to monitor the patient's nerve responses and oxygen levels, but the surgery still continued.
At some point during the surgery, the patient had an unexplained blood loss and his serum calcium level dropped below normal. He also experienced a loss of oxygen to the brain, then went into cardiac arrest. At that point, the surgery was discontinued, uncompleted.
The patient was comatose for several days, during which he displayed prolonged seizure activity. After regaining consciousness, he remained in the hospital for nearly four weeks before being transferred to another facility for rehabilitation.
The patient continues to have symptoms of various neurologic problems, including athetoid-choreiform movement, which causes a general loss of balance and muscular control and cognitive deficits, which make him unable to communicate.
The plaintiff claimed that the surgery should have been stopped when the problems arose. The plaintiff also claimed that Dr. R. should have ordered intraoperative lab work when the plaintiff's condition deteriorated.
The matter was ultimately tried against Drs. R. and L. only. They denied any negligence.
According to a published report, a $3 million verdict was returned.
Reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
Was Follow-Up Adequate After Neurosurgery in Cancún?
Shortly after arriving in Mexico for a brief stay, a 44-year-old woman collapsed in the customs area. She was taken to a hospital in Cancún, where she underwent emergency neurosurgery for a brain bleed. After several days of hospitalization, she was stabilized and returned to Michigan with instructions to see her family clinician.
Her appointment was delayed by an ice storm, which interrupted power to the office of the defendant internist, Dr. M. That Saturday, the woman visited the office's clinic and was examined by the defendant family practitioner, Dr. P. She presented with a shaved head and a neurosurgical scar on the left side of her head; she complained of headache and some blurred or double vision. She gave Dr. P. a list of medications and medical records (in Spanish) from the Mexican hospital.
Findings on her physical examination were normal. She was instructed to return to see Dr. M., and she did so at the clinic on the following Monday. She repeated her complaints of double vision, headache, and fatigue. Dr. M. charged his office staff with attempting to have the Mexican records translated and to arrange for a neurosurgery appointment.
The patient was ultimately scheduled for head CT and an office visit with a neurosurgeon six days later. The day after those arrangements were made, however, she experienced a massive brain bleed and died.
According to the plaintiff, the surgeons in Mexico drained the blood from the initial bleed but did not detect its source—an aneurysm in the subarachnoid space. The plaintiff alleged that the defendants should have hospitalized the decedent immediately upon her return from Mexico or sent her for an immediate neurosurgical consult. Had the decedent undergone CT immediately, it was argued, the aneurysm would have been detected, surgery would have been performed, and she would have survived.
The defendants argued that the neurosurgical follow-up was out of their area of expertise and that they made appropriate arrangements for the decedent to be seen by a neurosurgeon. They maintained that the decedent appeared stable and seemed to be improving and that it was possible that the fatal bleed was not related to the first bleed. The defendants also claimed that definitive treatment should have been given in Mexico.
According to a published report, a defense verdict was returned.
Ultrasound Misplaced, Diagnosis Delayed for a Year
In March 2003 at age 2, the minor plaintiff was admitted to the defendant hospital under the care of the defendant pediatric urologist, who was treating her for bilateral vesicoureteral urinary reflux and frequent urinary tract infections (UTIs). The defendant surgically reimplanted both ureters to stop urinary reflux. The toddler was discharged to home in her parents' care two days after the procedure.
The child continued to experience UTIs. Renal ultrasonography revealed a blockage in the left ureter, but the ultrasound was lost by the defendant hospital. Results were never conveyed to the ordering physicians, who failed to follow up to obtain them.
In April 2004, the defendant urologist diagnosed the condition and determined that it had gone untreated for a year. Repeat renal ultrasonography demonstrated the blockage, and a nuclear renal scan confirmed that the child's left kidney was no longer functioning at all as a result of urinary backup. In addition to losing all function of the left kidney, the child has compromised function in the right kidney. She is expected to require dialysis in the future and eventually kidney transplantation.
A $9.75 million settlement was reached.
Complications of Undiagnosed Diverticulitis
A 62-year-old woman visited the defendant internist with complaints of abdominal pressure, poor appetite, weakness, and dizziness. Her medical history included hypertension, diverticulitis, hysterectomy, and tonsillectomy.
The defendant ordered a chest x-ray, complete blood count, and urinalysis. After reviewing test results, the defendant made a diagnosis of urinary tract infection and prescribed ceftriaxone by intramuscular injection and oral ciprofloxacin.
After receiving the first injection of ceftriaxone, the patient called the defendant's office, complaining of increased discomfort. She requested admission to the hospital, which was allegedly refused by a member of the office staff. The following day, the plaintiff was transported to the hospital by ambulance with complaints of left lower quadrant pain, intermittent for one week and worsening that evening. The plaintiff reported no nausea or diarrhea but was belching.
The emergency department physician identified tender palpation in the abdomen with no rebounding and decreased bowel sounds. The defendant internist's answering service was contacted, and the covering physician ordered admission with a diagnosis of diverticulitis. CT of the abdomen and pelvis revealed evidence of free air under the hemidiaphragm, ascites, and phlegmonous reaction; the results also suggested diverticulitis with perforation in the rectosigmoid region and inflammatory changes.
Five hours later, the patient was taken to surgery for an exploratory laparotomy and colostomy to address the apparent perforated diverticulum. Her immediate postoperative course included profound hypotension with narrow-complex tachycardia. These developments, allegedly resulting from abdominal sepsis due to the delay in diagnosing the perforated diverticulum, necessitated pressors and dopamine.
Soon thereafter, the patient developed right-leg ischemia. She underwent embolectomy and thrombectomy to the right common femoral artery and the superficial femoral artery, with repair to the right profunda by use of a saphenous vein patch angioplasty. Two days later, the patient was taken to surgery for an above-knee amputation.
The plaintiff claimed that the defendant was negligent in failing to recognize early manifestations of diverticulitis and to order CT or MRl. The plaintiff also claimed that she should have been hospitalized when she requested admission.
The defendant maintained that the patient's history and the laboratory study results suggested that she had the flu or a urinary tract infection and that hospitalization was not needed. The defendant also maintained that when he called for a surgical consultation, the surgeon did not arrive for four and one-half hours.
According to a published report, a defense verdict was returned. A motion for a new trial was pending.
Surgery Continued Despite Patient's Deteriorating Condition
In 1986, the patient, then age 8, was found to be mildly mentally retarded (IQ, 59 to 70). He also had paranoid schizophrenia, causing him to hear voices in his head. The patient lived with his sister, who served as his guardian.
At age 19, the patient was scheduled to undergo surgery to correct curvature of the spine. The operation was to be performed by Dr. R., assisted by Dr. M. and by an anesthesiologist, Dr. L.
About one hour into the surgery, the patient began to manifest decreased urinary output with no known cause, but the procedure continued. About 90 minutes later, an equipment malfunction made it impossible for the medical team to monitor the patient's nerve responses and oxygen levels, but the surgery still continued.
At some point during the surgery, the patient had an unexplained blood loss and his serum calcium level dropped below normal. He also experienced a loss of oxygen to the brain, then went into cardiac arrest. At that point, the surgery was discontinued, uncompleted.
The patient was comatose for several days, during which he displayed prolonged seizure activity. After regaining consciousness, he remained in the hospital for nearly four weeks before being transferred to another facility for rehabilitation.
The patient continues to have symptoms of various neurologic problems, including athetoid-choreiform movement, which causes a general loss of balance and muscular control and cognitive deficits, which make him unable to communicate.
The plaintiff claimed that the surgery should have been stopped when the problems arose. The plaintiff also claimed that Dr. R. should have ordered intraoperative lab work when the plaintiff's condition deteriorated.
The matter was ultimately tried against Drs. R. and L. only. They denied any negligence.
According to a published report, a $3 million verdict was returned.
Ensuring Patient Safety and Quality Care
In addition to the longstanding issues of patients’ lack of access to health care and the increasing costs of that care, there continue to be concerns about the safety and quality of care being delivered in the United States. This is especially true as more information on the nature and extent of errors in health care has been brought to the forefront.
Since 1990, the National Practitioner Data Bank (NPDB) has been collecting information on health care practitioners, including NPs and PAs, with regard to disciplinary actions such as monetary judgments (both by settlement and jury decision), loss of licensure, and limitation of practice. Over the years, PAs and NPs have experienced increased liability (mostly as a result of their expanding scope of practice), greater patient care responsibilities, and more autonomy. However, according to an article in the March 20, 2000, edition of Medical Economics, “Judging from the actual number of malpractice cases settled, PAs and NPs are in court much less often than their doctor colleagues.”
Information from the NPDB, in fact, reveals that NPs and PAs still incur a remarkably low rate of malpractice judgments. Moreover, anecdotal data support the possibility that hiring a PA or NP may even reduce the risk of malpractice liability.
The Health Care Quality Improvement Act, passed by Congress in 1986, requires that all malpractice payments made on behalf of any clinician who is licensed, registered, or certified by the state must be reported to the NPDB. Since the data bank began collecting statistics, it has recorded a total of 235,797 paid claims for all physicians of every type, with an average paid claim (inflation adjusted) of $282,782. During that same period, the NPDB recorded a total of 1,130 paid claims for PAs, with an average paid claim of $86,568. The total number of NP claims was 470, but average claim data were not available.
You can get some perspective on these data by keeping in mind that in 2006, there were 633,000 physicians, 125,000 NPs, and 70,000 PAs practicing in the US. There are five physicians for every NP in the country; nine physicians for every PA. Can we surmise then that the number of physician-related paid claims should be five times that of NP-related paid claims and nine times that of PA-related claims?
In reality, the number of physician-related paid claims approaches 100 times that of PA-related paid claims. A further disparity is noted when mean losses are compared: The 2006 mean physician-related losses are 33% higher than PA-related losses ($312,000 for physicians vs $234,000 for PAs). Unfortunately, it should be noted that the mean rate for PAs is approaching that of the physician.
Another way of examining the differences among the malpractice experiences of NPs, PAs, and physicians is to calculate how many providers of each type exist for each malpractice paid claim. Data from 2006 show that one claim was paid for every 2.68 physicians, compared to one for every 210.43 NPs and one for every 619.5 PAs.
It is true that we don’t know for sure how accurate the data reported to the NPDB are. Variations in NP practice—whether independent, collaborative, or phys-ician-supervised—exist from state to state, which may affect the reliability of the data. Also, differences exist among states in the way NPs are licensed. In some states, an NP is licensed as a nurse while in others he or she would be licensed as an NP, which can similarly alter the reporting. And because prescriptive authority by PAs and NPs varies from state to state, it may be true that states are not on an equal footing when it comes to their settlement of claims against NPs or PAs.
Lastly, NPs are reported to the NPDB separately from certified nurse midwives (596 paid claims) and advanced practice nurses (1,181 claims including CRNAs). If they were reported as one group, that would also affect the numbers.
It must be remembered that each health care provider is responsible for his or her own negligent acts. Even if you are a dependent practitioner with a supervising physician who is responsible for your actions, that does not exonerate you from the risk of individual liability.
To win a negligence case and recover damages from an NP or PA, a patient must prove three things: that the PA or NP owed the patient a duty of care, that he or she breached that duty, and that the patient was harmed as a result of the NP’s or PA’s action or failure to act. Conduct that may lead to liability includes failure to properly diagnose, failure to refer, exceeding one’s scope of practice, negligent monitoring, failure to question a physician’s abnormal order, or failure to properly follow up.
In most cases, PAs and NPs are covered under their employer’s policy. In spite of that, they may still be liable for their own negligence and for all or part of a plaintiff’s award or settlement. It is important, in my experience, that NPs and PAs maintain their own personal medical liability insurance.
There are plenty of articles and handbooks that discuss methods to avoid medical liability, such as the Physician Assistant Legal Handbook by Aspen Health Law and Compliance Center and The Advanced Practice Nurse’s Legal Handbook by Rebecca F. Cady, RNC, BSN, JD. But in my opinion, they all boil down to the following basic principles:
• Know and understand your scope of practice under state law.
• Know and understand your hospital or institutional policies.
• Know and understand the importance of communicating honestly with your patients and your supervising or collaborating physician.
Ensuring patient safety and improving quality of care are steadfast goals for all NPs and PAs. We need to continue our discussions on best practices for preventing medical errors as well as finding ways to remove barriers to effective practice. I would love to hear from you about these matters. Please e-mail me at [email protected].
In addition to the longstanding issues of patients’ lack of access to health care and the increasing costs of that care, there continue to be concerns about the safety and quality of care being delivered in the United States. This is especially true as more information on the nature and extent of errors in health care has been brought to the forefront.
Since 1990, the National Practitioner Data Bank (NPDB) has been collecting information on health care practitioners, including NPs and PAs, with regard to disciplinary actions such as monetary judgments (both by settlement and jury decision), loss of licensure, and limitation of practice. Over the years, PAs and NPs have experienced increased liability (mostly as a result of their expanding scope of practice), greater patient care responsibilities, and more autonomy. However, according to an article in the March 20, 2000, edition of Medical Economics, “Judging from the actual number of malpractice cases settled, PAs and NPs are in court much less often than their doctor colleagues.”
Information from the NPDB, in fact, reveals that NPs and PAs still incur a remarkably low rate of malpractice judgments. Moreover, anecdotal data support the possibility that hiring a PA or NP may even reduce the risk of malpractice liability.
The Health Care Quality Improvement Act, passed by Congress in 1986, requires that all malpractice payments made on behalf of any clinician who is licensed, registered, or certified by the state must be reported to the NPDB. Since the data bank began collecting statistics, it has recorded a total of 235,797 paid claims for all physicians of every type, with an average paid claim (inflation adjusted) of $282,782. During that same period, the NPDB recorded a total of 1,130 paid claims for PAs, with an average paid claim of $86,568. The total number of NP claims was 470, but average claim data were not available.
You can get some perspective on these data by keeping in mind that in 2006, there were 633,000 physicians, 125,000 NPs, and 70,000 PAs practicing in the US. There are five physicians for every NP in the country; nine physicians for every PA. Can we surmise then that the number of physician-related paid claims should be five times that of NP-related paid claims and nine times that of PA-related claims?
In reality, the number of physician-related paid claims approaches 100 times that of PA-related paid claims. A further disparity is noted when mean losses are compared: The 2006 mean physician-related losses are 33% higher than PA-related losses ($312,000 for physicians vs $234,000 for PAs). Unfortunately, it should be noted that the mean rate for PAs is approaching that of the physician.
Another way of examining the differences among the malpractice experiences of NPs, PAs, and physicians is to calculate how many providers of each type exist for each malpractice paid claim. Data from 2006 show that one claim was paid for every 2.68 physicians, compared to one for every 210.43 NPs and one for every 619.5 PAs.
It is true that we don’t know for sure how accurate the data reported to the NPDB are. Variations in NP practice—whether independent, collaborative, or phys-ician-supervised—exist from state to state, which may affect the reliability of the data. Also, differences exist among states in the way NPs are licensed. In some states, an NP is licensed as a nurse while in others he or she would be licensed as an NP, which can similarly alter the reporting. And because prescriptive authority by PAs and NPs varies from state to state, it may be true that states are not on an equal footing when it comes to their settlement of claims against NPs or PAs.
Lastly, NPs are reported to the NPDB separately from certified nurse midwives (596 paid claims) and advanced practice nurses (1,181 claims including CRNAs). If they were reported as one group, that would also affect the numbers.
It must be remembered that each health care provider is responsible for his or her own negligent acts. Even if you are a dependent practitioner with a supervising physician who is responsible for your actions, that does not exonerate you from the risk of individual liability.
To win a negligence case and recover damages from an NP or PA, a patient must prove three things: that the PA or NP owed the patient a duty of care, that he or she breached that duty, and that the patient was harmed as a result of the NP’s or PA’s action or failure to act. Conduct that may lead to liability includes failure to properly diagnose, failure to refer, exceeding one’s scope of practice, negligent monitoring, failure to question a physician’s abnormal order, or failure to properly follow up.
In most cases, PAs and NPs are covered under their employer’s policy. In spite of that, they may still be liable for their own negligence and for all or part of a plaintiff’s award or settlement. It is important, in my experience, that NPs and PAs maintain their own personal medical liability insurance.
There are plenty of articles and handbooks that discuss methods to avoid medical liability, such as the Physician Assistant Legal Handbook by Aspen Health Law and Compliance Center and The Advanced Practice Nurse’s Legal Handbook by Rebecca F. Cady, RNC, BSN, JD. But in my opinion, they all boil down to the following basic principles:
• Know and understand your scope of practice under state law.
• Know and understand your hospital or institutional policies.
• Know and understand the importance of communicating honestly with your patients and your supervising or collaborating physician.
Ensuring patient safety and improving quality of care are steadfast goals for all NPs and PAs. We need to continue our discussions on best practices for preventing medical errors as well as finding ways to remove barriers to effective practice. I would love to hear from you about these matters. Please e-mail me at [email protected].
In addition to the longstanding issues of patients’ lack of access to health care and the increasing costs of that care, there continue to be concerns about the safety and quality of care being delivered in the United States. This is especially true as more information on the nature and extent of errors in health care has been brought to the forefront.
Since 1990, the National Practitioner Data Bank (NPDB) has been collecting information on health care practitioners, including NPs and PAs, with regard to disciplinary actions such as monetary judgments (both by settlement and jury decision), loss of licensure, and limitation of practice. Over the years, PAs and NPs have experienced increased liability (mostly as a result of their expanding scope of practice), greater patient care responsibilities, and more autonomy. However, according to an article in the March 20, 2000, edition of Medical Economics, “Judging from the actual number of malpractice cases settled, PAs and NPs are in court much less often than their doctor colleagues.”
Information from the NPDB, in fact, reveals that NPs and PAs still incur a remarkably low rate of malpractice judgments. Moreover, anecdotal data support the possibility that hiring a PA or NP may even reduce the risk of malpractice liability.
The Health Care Quality Improvement Act, passed by Congress in 1986, requires that all malpractice payments made on behalf of any clinician who is licensed, registered, or certified by the state must be reported to the NPDB. Since the data bank began collecting statistics, it has recorded a total of 235,797 paid claims for all physicians of every type, with an average paid claim (inflation adjusted) of $282,782. During that same period, the NPDB recorded a total of 1,130 paid claims for PAs, with an average paid claim of $86,568. The total number of NP claims was 470, but average claim data were not available.
You can get some perspective on these data by keeping in mind that in 2006, there were 633,000 physicians, 125,000 NPs, and 70,000 PAs practicing in the US. There are five physicians for every NP in the country; nine physicians for every PA. Can we surmise then that the number of physician-related paid claims should be five times that of NP-related paid claims and nine times that of PA-related claims?
In reality, the number of physician-related paid claims approaches 100 times that of PA-related paid claims. A further disparity is noted when mean losses are compared: The 2006 mean physician-related losses are 33% higher than PA-related losses ($312,000 for physicians vs $234,000 for PAs). Unfortunately, it should be noted that the mean rate for PAs is approaching that of the physician.
Another way of examining the differences among the malpractice experiences of NPs, PAs, and physicians is to calculate how many providers of each type exist for each malpractice paid claim. Data from 2006 show that one claim was paid for every 2.68 physicians, compared to one for every 210.43 NPs and one for every 619.5 PAs.
It is true that we don’t know for sure how accurate the data reported to the NPDB are. Variations in NP practice—whether independent, collaborative, or phys-ician-supervised—exist from state to state, which may affect the reliability of the data. Also, differences exist among states in the way NPs are licensed. In some states, an NP is licensed as a nurse while in others he or she would be licensed as an NP, which can similarly alter the reporting. And because prescriptive authority by PAs and NPs varies from state to state, it may be true that states are not on an equal footing when it comes to their settlement of claims against NPs or PAs.
Lastly, NPs are reported to the NPDB separately from certified nurse midwives (596 paid claims) and advanced practice nurses (1,181 claims including CRNAs). If they were reported as one group, that would also affect the numbers.
It must be remembered that each health care provider is responsible for his or her own negligent acts. Even if you are a dependent practitioner with a supervising physician who is responsible for your actions, that does not exonerate you from the risk of individual liability.
To win a negligence case and recover damages from an NP or PA, a patient must prove three things: that the PA or NP owed the patient a duty of care, that he or she breached that duty, and that the patient was harmed as a result of the NP’s or PA’s action or failure to act. Conduct that may lead to liability includes failure to properly diagnose, failure to refer, exceeding one’s scope of practice, negligent monitoring, failure to question a physician’s abnormal order, or failure to properly follow up.
In most cases, PAs and NPs are covered under their employer’s policy. In spite of that, they may still be liable for their own negligence and for all or part of a plaintiff’s award or settlement. It is important, in my experience, that NPs and PAs maintain their own personal medical liability insurance.
There are plenty of articles and handbooks that discuss methods to avoid medical liability, such as the Physician Assistant Legal Handbook by Aspen Health Law and Compliance Center and The Advanced Practice Nurse’s Legal Handbook by Rebecca F. Cady, RNC, BSN, JD. But in my opinion, they all boil down to the following basic principles:
• Know and understand your scope of practice under state law.
• Know and understand your hospital or institutional policies.
• Know and understand the importance of communicating honestly with your patients and your supervising or collaborating physician.
Ensuring patient safety and improving quality of care are steadfast goals for all NPs and PAs. We need to continue our discussions on best practices for preventing medical errors as well as finding ways to remove barriers to effective practice. I would love to hear from you about these matters. Please e-mail me at [email protected].
Malpractice minute
Could a patient’s violent act
have been prevented?
THE PATIENT. A man under outpatient care of the state’s regional behavioral health authority was diagnosed with schizophrenia, paranoid type.
CASE FACTS. The patient killed his developmentally disabled niece, age 26.
THE VICTIM’S FAMILY’S CLAIM. The death would not have occurred if the patient had been civilly committed or heavily medicated.
THE BEHAVIORAL HEALTH AUTHORITY’S DEFENSE. The violent act was unforeseeable, and the patient was compliant with treatment. The victim’s mother should not have left the disabled woman alone with the patient.
Submit your verdict and find out how the court ruled. Click on “Have more to say about this topic?” to comment.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Could a patient’s violent act
have been prevented?
THE PATIENT. A man under outpatient care of the state’s regional behavioral health authority was diagnosed with schizophrenia, paranoid type.
CASE FACTS. The patient killed his developmentally disabled niece, age 26.
THE VICTIM’S FAMILY’S CLAIM. The death would not have occurred if the patient had been civilly committed or heavily medicated.
THE BEHAVIORAL HEALTH AUTHORITY’S DEFENSE. The violent act was unforeseeable, and the patient was compliant with treatment. The victim’s mother should not have left the disabled woman alone with the patient.
Submit your verdict and find out how the court ruled. Click on “Have more to say about this topic?” to comment.
Could a patient’s violent act
have been prevented?
THE PATIENT. A man under outpatient care of the state’s regional behavioral health authority was diagnosed with schizophrenia, paranoid type.
CASE FACTS. The patient killed his developmentally disabled niece, age 26.
THE VICTIM’S FAMILY’S CLAIM. The death would not have occurred if the patient had been civilly committed or heavily medicated.
THE BEHAVIORAL HEALTH AUTHORITY’S DEFENSE. The violent act was unforeseeable, and the patient was compliant with treatment. The victim’s mother should not have left the disabled woman alone with the patient.
Submit your verdict and find out how the court ruled. Click on “Have more to say about this topic?” to comment.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Violence risk: Is clinical judgment enough?
Dear Dr. Mossman:
Multiple studies support the reliability and validity of actuarial measures—such as the Historical, Clinical, and Risk Management (HCR-20) risk assessment scheme—to assess violence risk, whereas physicians’ clinical judgment is highly variable. Should clinicians use actuarial measures to assess a patient’s risk of violence? Could it be considered negligent not to use actuarial measures?—Submitted by “Dr. S”
In the 30 years since the Tarasoff decision—which held that psychiatrists have a duty to protect individuals who are being threatened with bodily harm by a patient1—assessing patients’ risk of future violence has become an accepted part of mental health practice.2 Dr. S has asked 2 sophisticated questions about risk assessment. The short answer is that although so-called “actuarial” techniques for assessing risk are valuable, psychiatrists who do not use them are not practicing negligently. To explain why, this article discusses:
- the difference between “clinical” and “actuarial” judgment
- the HCR-20’s strengths and weaknesses
- actuarial measures and negligence.
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
Clinical vs actuarial judgment
In the 1970s and 1980s, mental health professionals believed they could not accurately predict violence.3 We now know this is not correct. Since the 1990s, when researchers adopted better methods for gauging the accuracy of risk assessments,4-6 research has shown that mental health clinicians can assess dangerousness with clearly-better-than-chance accuracy, whether the assessment covers just the next few days, several months, or years.4
Over the same period, psychologists recognized that when it comes to making predictions, clinical judgment—making predictions by putting together information in one’s head—often is inferior to using simple formulae derived from empirically demonstrated relationships between data and outcome.7 This approach—“actuarial” judgment—is how insurance companies use data to calculate risk.
By the late 1990s, psychologists had developed actuarial risk assessment instruments (ARAIs)8 that could accurately rank the likelihood of various forms of violence. Table 1 lists some well-known ARAIs and the populations for which they were designed. In clinical practice, psychiatrists usually focus on risk posed by psychiatric patients. The HCR-209 was designed to help evaluate this type of risk.
Table 1
Examples of actuarial risk assessment instruments (ARAIs)
| ARAI | Risk assessed |
|---|---|
| HCR-209 | Violence in psychiatric populations, such as formerly hospitalized patients |
| Classification Of Violence Risk (COVR) | Violence by civil psychiatric patients following discharge into the community |
| Violence Risk Assessment Guide (VRAG) | Violent recidivism by formerly incarcerated offenders |
| Static-99 | Recidivism by sex offenders |
HCR-20’s pros and cons
The HCR-20 has 20 items:
- 10 concerning the patient’s history
- 5 related to clinical factors
- 5 that deal with risk management (Table 2).
To use the HCR-20 as an exercise of true actuarial judgment, you would base your opinion of a patient’s risk of violence solely on the HCR-20 score, without regard for other patient factors. However, the HCR-20’s developers think this approach “may be unreasonable, unethical, and illegal.”9 One reason is that the HCR-20 omits obvious signs of potential violence, such as a clearly stated threat with unambiguous intent to act.
For example, if a patient is doing well in the hospital (and has a low score on HCR-20 clinical items), a psychiatrist might assume the patient will cause few problems after discharge. But if the risk management items generate a high score, the psychiatrist should realize that these factors raise the patient’s violence risk and may require additional intervention—perhaps a different type of community placement or special effort to help the patient follow up with out-patient treatment.
Table 2
Items from the Historical, Clinical, and Risk Management (HCR-20)
| Historical items | Clinical items | Risk management items |
|---|---|---|
| H1 Previous violence | C1 Lack of insight | R1 Plans lack feasibility |
| H2 Young age at first incident | C2 Negative attitudes | R2 Exposure to destabilizers |
| H3 Relationship instability | C3 Active symptoms of major mental illness | R3 Lack of personal support |
| H4 Employment problems | C4 Impulsivity | R4 Noncompliance with remediation attempts |
| H5 Substance use problems | C5 Unresponsive to treatment | R5 Stress |
| H6 Major mental illness | ||
| H7 Psychopathy | ||
| H8 Early maladjustment | ||
| H9 Personality disorder | ||
| H10 Prior supervision failure | ||
| Score each item 0, 1, or 2, depending on how closely the patient matches the described characteristic. For example, when scoring item C3 (active symptoms of major mental illness), a patient gets 0 for “no active symptoms,” 1 for “possible/less serious active symptoms,” or 2 for “definite/serious active symptoms.” An individual can receive a total HCR-20 score of 0 to 40. The higher the score, the higher likelihood of violence in the coming months. | ||
| Source: Reprinted with permission from Webster CD, Douglas KS, Eaves D, Hart SD. HCR-20: assessing risk for violence, version 2. Burnaby, British Columbia, Canada: Simon Fraser University, Mental Health, Law, and Policy Institute; 1997 | ||
Is not using ARAIs negligent?
Some writers believe that using ARAIs should12 or may soon13 become the standard of care. Why, then, do psychiatrists seldom use ARAIs in their clinical work? Partly it is because clinicians rarely receive adequate training in assessing violence risk or the science supporting it. After a 5-hour training module featuring the HCR-20, psychiatry residents could better identify factors that affect violence risk, organize their reasoning, and come up with risk management strategies.2
Psychiatrists may have other reasons for not using ARAIs that make clinical sense. Although ARAIs can rank individuals’ violence risk, the probabilities of violence associated with each rank aren’t substantial enough to justify differences in management.14 Scientifically, it’s interesting to know that we can separate patients into groups with “low” (9%) and “high” (49%) risks of violence.15 But would you want to manage these patients differently? Most psychiatrists probably would not feel comfortable ignoring a 9% risk of violence.
To avoid negligence, psychiatrists need only “exercise the skill, knowledge, and care normally possessed and exercised by other members of their profession.”17 Psychiatrists seldom use ARAIs,12 so failing to use them cannot constitute malpractice. As Simon points out, a practicing psychiatrist’s role is to treat patients, not predict violence. He concludes, “at this time, the standard of care does not require the average or reasonable psychiatrist to use actuarial assessment instruments in the evaluation and treatment of potentially violent patients.”16
1. Tarasoff vs Regents of the University of California, 551 P. 2d 334 (Cal. 1976).
2. McNiel DE, Chamberlain JR, Weaver CM, et al. Impact of clinical training on violence risk assessment. Am J Psychiatry 2008;165:195-200.
3. Monahan J. The clinical prediction of violent behavior. Washington, DC: National Institute of Mental Health; 1981.
4. Mossman D. Assessing predictions of violence: being accurate about accuracy. J Consult Clin Psychol 1994;62:783-92.
5. Rice ME, Harris GT. Violent recidivism: assessing predictive validity. J Consult Clin Psychol 1995;63:737-48.
6. Gardner W, Lidz CW, Mulvey EP, Shaw EC. Clinical versus actuarial predictions of violence in patients with mental illness. J Consult Clin Psychol 1996;64:602-9.
7. Dawes RM, Faust D, Meehl PE. Clinical versus actuarial judgment. Science 1989;243:1668-74.
8. Hart SD, Michie C, Cooke DJ. Precision of actuarial risk assessment instruments: evaluating the ‘margins of error’ of group v. individual predictions of violence. Brit J Psychiatry 2007;190:60-5.
9. Webster CD, Douglas KS, Eaves D, Hart SD. HCR-20: assessing risk for violence, version 2. Burnaby, British Columbia: Simon Fraser University, Mental Health, Law, and Policy Institute; 1997.
10. Quinsey VL, Harris GT, Rice ME, Cormier CA. Violent offenders: appraising and managing risk. 2nd ed. Washington, DC: American Psychological Association; 2006.
11. Hanson RK, Morton-Bourgon KE. The accuracy of recidivism risk assessments for sexual offenders: a meta-analysis. Ottawa, Canada: Public Safety Canada; 2007. Available at: http://www.publicsafety.gc.ca/res/cor/rep/_fl/crp2007-01-en.pdf. Accessed April 21, 2008.
12. Swanson JW. Preventing the unpredicted: managing violence risk in mental health care. Psychiatr Serv 2008;59:191-3.
13. Lamberg L. New tools aid violence risk assessment. JAMA 2007;298(5):499-501.
14. Mossman D. Commentary: assessing the risk of violence—are “accurate” predictions useful? J Am Acad Psychiatry Law 2000;28:272-81.
15. Monahan J, Steadman HJ, Robbins PC, et al. An actuarial model of violence risk assessment for persons with mental disorders. Psychiatr Serv 2005;56:810-15.
16. Simon RI. The myth of “imminent” violence in psychiatry and the law. Univ Cincinnati L Rev 2006;75:631-43.
17. Dobbs DB. The law of torts. St. Paul, MN: West Group; 2000:269.
Dear Dr. Mossman:
Multiple studies support the reliability and validity of actuarial measures—such as the Historical, Clinical, and Risk Management (HCR-20) risk assessment scheme—to assess violence risk, whereas physicians’ clinical judgment is highly variable. Should clinicians use actuarial measures to assess a patient’s risk of violence? Could it be considered negligent not to use actuarial measures?—Submitted by “Dr. S”
In the 30 years since the Tarasoff decision—which held that psychiatrists have a duty to protect individuals who are being threatened with bodily harm by a patient1—assessing patients’ risk of future violence has become an accepted part of mental health practice.2 Dr. S has asked 2 sophisticated questions about risk assessment. The short answer is that although so-called “actuarial” techniques for assessing risk are valuable, psychiatrists who do not use them are not practicing negligently. To explain why, this article discusses:
- the difference between “clinical” and “actuarial” judgment
- the HCR-20’s strengths and weaknesses
- actuarial measures and negligence.
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
Clinical vs actuarial judgment
In the 1970s and 1980s, mental health professionals believed they could not accurately predict violence.3 We now know this is not correct. Since the 1990s, when researchers adopted better methods for gauging the accuracy of risk assessments,4-6 research has shown that mental health clinicians can assess dangerousness with clearly-better-than-chance accuracy, whether the assessment covers just the next few days, several months, or years.4
Over the same period, psychologists recognized that when it comes to making predictions, clinical judgment—making predictions by putting together information in one’s head—often is inferior to using simple formulae derived from empirically demonstrated relationships between data and outcome.7 This approach—“actuarial” judgment—is how insurance companies use data to calculate risk.
By the late 1990s, psychologists had developed actuarial risk assessment instruments (ARAIs)8 that could accurately rank the likelihood of various forms of violence. Table 1 lists some well-known ARAIs and the populations for which they were designed. In clinical practice, psychiatrists usually focus on risk posed by psychiatric patients. The HCR-209 was designed to help evaluate this type of risk.
Table 1
Examples of actuarial risk assessment instruments (ARAIs)
| ARAI | Risk assessed |
|---|---|
| HCR-209 | Violence in psychiatric populations, such as formerly hospitalized patients |
| Classification Of Violence Risk (COVR) | Violence by civil psychiatric patients following discharge into the community |
| Violence Risk Assessment Guide (VRAG) | Violent recidivism by formerly incarcerated offenders |
| Static-99 | Recidivism by sex offenders |
HCR-20’s pros and cons
The HCR-20 has 20 items:
- 10 concerning the patient’s history
- 5 related to clinical factors
- 5 that deal with risk management (Table 2).
To use the HCR-20 as an exercise of true actuarial judgment, you would base your opinion of a patient’s risk of violence solely on the HCR-20 score, without regard for other patient factors. However, the HCR-20’s developers think this approach “may be unreasonable, unethical, and illegal.”9 One reason is that the HCR-20 omits obvious signs of potential violence, such as a clearly stated threat with unambiguous intent to act.
For example, if a patient is doing well in the hospital (and has a low score on HCR-20 clinical items), a psychiatrist might assume the patient will cause few problems after discharge. But if the risk management items generate a high score, the psychiatrist should realize that these factors raise the patient’s violence risk and may require additional intervention—perhaps a different type of community placement or special effort to help the patient follow up with out-patient treatment.
Table 2
Items from the Historical, Clinical, and Risk Management (HCR-20)
| Historical items | Clinical items | Risk management items |
|---|---|---|
| H1 Previous violence | C1 Lack of insight | R1 Plans lack feasibility |
| H2 Young age at first incident | C2 Negative attitudes | R2 Exposure to destabilizers |
| H3 Relationship instability | C3 Active symptoms of major mental illness | R3 Lack of personal support |
| H4 Employment problems | C4 Impulsivity | R4 Noncompliance with remediation attempts |
| H5 Substance use problems | C5 Unresponsive to treatment | R5 Stress |
| H6 Major mental illness | ||
| H7 Psychopathy | ||
| H8 Early maladjustment | ||
| H9 Personality disorder | ||
| H10 Prior supervision failure | ||
| Score each item 0, 1, or 2, depending on how closely the patient matches the described characteristic. For example, when scoring item C3 (active symptoms of major mental illness), a patient gets 0 for “no active symptoms,” 1 for “possible/less serious active symptoms,” or 2 for “definite/serious active symptoms.” An individual can receive a total HCR-20 score of 0 to 40. The higher the score, the higher likelihood of violence in the coming months. | ||
| Source: Reprinted with permission from Webster CD, Douglas KS, Eaves D, Hart SD. HCR-20: assessing risk for violence, version 2. Burnaby, British Columbia, Canada: Simon Fraser University, Mental Health, Law, and Policy Institute; 1997 | ||
Is not using ARAIs negligent?
Some writers believe that using ARAIs should12 or may soon13 become the standard of care. Why, then, do psychiatrists seldom use ARAIs in their clinical work? Partly it is because clinicians rarely receive adequate training in assessing violence risk or the science supporting it. After a 5-hour training module featuring the HCR-20, psychiatry residents could better identify factors that affect violence risk, organize their reasoning, and come up with risk management strategies.2
Psychiatrists may have other reasons for not using ARAIs that make clinical sense. Although ARAIs can rank individuals’ violence risk, the probabilities of violence associated with each rank aren’t substantial enough to justify differences in management.14 Scientifically, it’s interesting to know that we can separate patients into groups with “low” (9%) and “high” (49%) risks of violence.15 But would you want to manage these patients differently? Most psychiatrists probably would not feel comfortable ignoring a 9% risk of violence.
To avoid negligence, psychiatrists need only “exercise the skill, knowledge, and care normally possessed and exercised by other members of their profession.”17 Psychiatrists seldom use ARAIs,12 so failing to use them cannot constitute malpractice. As Simon points out, a practicing psychiatrist’s role is to treat patients, not predict violence. He concludes, “at this time, the standard of care does not require the average or reasonable psychiatrist to use actuarial assessment instruments in the evaluation and treatment of potentially violent patients.”16
Dear Dr. Mossman:
Multiple studies support the reliability and validity of actuarial measures—such as the Historical, Clinical, and Risk Management (HCR-20) risk assessment scheme—to assess violence risk, whereas physicians’ clinical judgment is highly variable. Should clinicians use actuarial measures to assess a patient’s risk of violence? Could it be considered negligent not to use actuarial measures?—Submitted by “Dr. S”
In the 30 years since the Tarasoff decision—which held that psychiatrists have a duty to protect individuals who are being threatened with bodily harm by a patient1—assessing patients’ risk of future violence has become an accepted part of mental health practice.2 Dr. S has asked 2 sophisticated questions about risk assessment. The short answer is that although so-called “actuarial” techniques for assessing risk are valuable, psychiatrists who do not use them are not practicing negligently. To explain why, this article discusses:
- the difference between “clinical” and “actuarial” judgment
- the HCR-20’s strengths and weaknesses
- actuarial measures and negligence.
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online marketplace of risk management publications and resources (www.prms.com).
Clinical vs actuarial judgment
In the 1970s and 1980s, mental health professionals believed they could not accurately predict violence.3 We now know this is not correct. Since the 1990s, when researchers adopted better methods for gauging the accuracy of risk assessments,4-6 research has shown that mental health clinicians can assess dangerousness with clearly-better-than-chance accuracy, whether the assessment covers just the next few days, several months, or years.4
Over the same period, psychologists recognized that when it comes to making predictions, clinical judgment—making predictions by putting together information in one’s head—often is inferior to using simple formulae derived from empirically demonstrated relationships between data and outcome.7 This approach—“actuarial” judgment—is how insurance companies use data to calculate risk.
By the late 1990s, psychologists had developed actuarial risk assessment instruments (ARAIs)8 that could accurately rank the likelihood of various forms of violence. Table 1 lists some well-known ARAIs and the populations for which they were designed. In clinical practice, psychiatrists usually focus on risk posed by psychiatric patients. The HCR-209 was designed to help evaluate this type of risk.
Table 1
Examples of actuarial risk assessment instruments (ARAIs)
| ARAI | Risk assessed |
|---|---|
| HCR-209 | Violence in psychiatric populations, such as formerly hospitalized patients |
| Classification Of Violence Risk (COVR) | Violence by civil psychiatric patients following discharge into the community |
| Violence Risk Assessment Guide (VRAG) | Violent recidivism by formerly incarcerated offenders |
| Static-99 | Recidivism by sex offenders |
HCR-20’s pros and cons
The HCR-20 has 20 items:
- 10 concerning the patient’s history
- 5 related to clinical factors
- 5 that deal with risk management (Table 2).
To use the HCR-20 as an exercise of true actuarial judgment, you would base your opinion of a patient’s risk of violence solely on the HCR-20 score, without regard for other patient factors. However, the HCR-20’s developers think this approach “may be unreasonable, unethical, and illegal.”9 One reason is that the HCR-20 omits obvious signs of potential violence, such as a clearly stated threat with unambiguous intent to act.
For example, if a patient is doing well in the hospital (and has a low score on HCR-20 clinical items), a psychiatrist might assume the patient will cause few problems after discharge. But if the risk management items generate a high score, the psychiatrist should realize that these factors raise the patient’s violence risk and may require additional intervention—perhaps a different type of community placement or special effort to help the patient follow up with out-patient treatment.
Table 2
Items from the Historical, Clinical, and Risk Management (HCR-20)
| Historical items | Clinical items | Risk management items |
|---|---|---|
| H1 Previous violence | C1 Lack of insight | R1 Plans lack feasibility |
| H2 Young age at first incident | C2 Negative attitudes | R2 Exposure to destabilizers |
| H3 Relationship instability | C3 Active symptoms of major mental illness | R3 Lack of personal support |
| H4 Employment problems | C4 Impulsivity | R4 Noncompliance with remediation attempts |
| H5 Substance use problems | C5 Unresponsive to treatment | R5 Stress |
| H6 Major mental illness | ||
| H7 Psychopathy | ||
| H8 Early maladjustment | ||
| H9 Personality disorder | ||
| H10 Prior supervision failure | ||
| Score each item 0, 1, or 2, depending on how closely the patient matches the described characteristic. For example, when scoring item C3 (active symptoms of major mental illness), a patient gets 0 for “no active symptoms,” 1 for “possible/less serious active symptoms,” or 2 for “definite/serious active symptoms.” An individual can receive a total HCR-20 score of 0 to 40. The higher the score, the higher likelihood of violence in the coming months. | ||
| Source: Reprinted with permission from Webster CD, Douglas KS, Eaves D, Hart SD. HCR-20: assessing risk for violence, version 2. Burnaby, British Columbia, Canada: Simon Fraser University, Mental Health, Law, and Policy Institute; 1997 | ||
Is not using ARAIs negligent?
Some writers believe that using ARAIs should12 or may soon13 become the standard of care. Why, then, do psychiatrists seldom use ARAIs in their clinical work? Partly it is because clinicians rarely receive adequate training in assessing violence risk or the science supporting it. After a 5-hour training module featuring the HCR-20, psychiatry residents could better identify factors that affect violence risk, organize their reasoning, and come up with risk management strategies.2
Psychiatrists may have other reasons for not using ARAIs that make clinical sense. Although ARAIs can rank individuals’ violence risk, the probabilities of violence associated with each rank aren’t substantial enough to justify differences in management.14 Scientifically, it’s interesting to know that we can separate patients into groups with “low” (9%) and “high” (49%) risks of violence.15 But would you want to manage these patients differently? Most psychiatrists probably would not feel comfortable ignoring a 9% risk of violence.
To avoid negligence, psychiatrists need only “exercise the skill, knowledge, and care normally possessed and exercised by other members of their profession.”17 Psychiatrists seldom use ARAIs,12 so failing to use them cannot constitute malpractice. As Simon points out, a practicing psychiatrist’s role is to treat patients, not predict violence. He concludes, “at this time, the standard of care does not require the average or reasonable psychiatrist to use actuarial assessment instruments in the evaluation and treatment of potentially violent patients.”16
1. Tarasoff vs Regents of the University of California, 551 P. 2d 334 (Cal. 1976).
2. McNiel DE, Chamberlain JR, Weaver CM, et al. Impact of clinical training on violence risk assessment. Am J Psychiatry 2008;165:195-200.
3. Monahan J. The clinical prediction of violent behavior. Washington, DC: National Institute of Mental Health; 1981.
4. Mossman D. Assessing predictions of violence: being accurate about accuracy. J Consult Clin Psychol 1994;62:783-92.
5. Rice ME, Harris GT. Violent recidivism: assessing predictive validity. J Consult Clin Psychol 1995;63:737-48.
6. Gardner W, Lidz CW, Mulvey EP, Shaw EC. Clinical versus actuarial predictions of violence in patients with mental illness. J Consult Clin Psychol 1996;64:602-9.
7. Dawes RM, Faust D, Meehl PE. Clinical versus actuarial judgment. Science 1989;243:1668-74.
8. Hart SD, Michie C, Cooke DJ. Precision of actuarial risk assessment instruments: evaluating the ‘margins of error’ of group v. individual predictions of violence. Brit J Psychiatry 2007;190:60-5.
9. Webster CD, Douglas KS, Eaves D, Hart SD. HCR-20: assessing risk for violence, version 2. Burnaby, British Columbia: Simon Fraser University, Mental Health, Law, and Policy Institute; 1997.
10. Quinsey VL, Harris GT, Rice ME, Cormier CA. Violent offenders: appraising and managing risk. 2nd ed. Washington, DC: American Psychological Association; 2006.
11. Hanson RK, Morton-Bourgon KE. The accuracy of recidivism risk assessments for sexual offenders: a meta-analysis. Ottawa, Canada: Public Safety Canada; 2007. Available at: http://www.publicsafety.gc.ca/res/cor/rep/_fl/crp2007-01-en.pdf. Accessed April 21, 2008.
12. Swanson JW. Preventing the unpredicted: managing violence risk in mental health care. Psychiatr Serv 2008;59:191-3.
13. Lamberg L. New tools aid violence risk assessment. JAMA 2007;298(5):499-501.
14. Mossman D. Commentary: assessing the risk of violence—are “accurate” predictions useful? J Am Acad Psychiatry Law 2000;28:272-81.
15. Monahan J, Steadman HJ, Robbins PC, et al. An actuarial model of violence risk assessment for persons with mental disorders. Psychiatr Serv 2005;56:810-15.
16. Simon RI. The myth of “imminent” violence in psychiatry and the law. Univ Cincinnati L Rev 2006;75:631-43.
17. Dobbs DB. The law of torts. St. Paul, MN: West Group; 2000:269.
1. Tarasoff vs Regents of the University of California, 551 P. 2d 334 (Cal. 1976).
2. McNiel DE, Chamberlain JR, Weaver CM, et al. Impact of clinical training on violence risk assessment. Am J Psychiatry 2008;165:195-200.
3. Monahan J. The clinical prediction of violent behavior. Washington, DC: National Institute of Mental Health; 1981.
4. Mossman D. Assessing predictions of violence: being accurate about accuracy. J Consult Clin Psychol 1994;62:783-92.
5. Rice ME, Harris GT. Violent recidivism: assessing predictive validity. J Consult Clin Psychol 1995;63:737-48.
6. Gardner W, Lidz CW, Mulvey EP, Shaw EC. Clinical versus actuarial predictions of violence in patients with mental illness. J Consult Clin Psychol 1996;64:602-9.
7. Dawes RM, Faust D, Meehl PE. Clinical versus actuarial judgment. Science 1989;243:1668-74.
8. Hart SD, Michie C, Cooke DJ. Precision of actuarial risk assessment instruments: evaluating the ‘margins of error’ of group v. individual predictions of violence. Brit J Psychiatry 2007;190:60-5.
9. Webster CD, Douglas KS, Eaves D, Hart SD. HCR-20: assessing risk for violence, version 2. Burnaby, British Columbia: Simon Fraser University, Mental Health, Law, and Policy Institute; 1997.
10. Quinsey VL, Harris GT, Rice ME, Cormier CA. Violent offenders: appraising and managing risk. 2nd ed. Washington, DC: American Psychological Association; 2006.
11. Hanson RK, Morton-Bourgon KE. The accuracy of recidivism risk assessments for sexual offenders: a meta-analysis. Ottawa, Canada: Public Safety Canada; 2007. Available at: http://www.publicsafety.gc.ca/res/cor/rep/_fl/crp2007-01-en.pdf. Accessed April 21, 2008.
12. Swanson JW. Preventing the unpredicted: managing violence risk in mental health care. Psychiatr Serv 2008;59:191-3.
13. Lamberg L. New tools aid violence risk assessment. JAMA 2007;298(5):499-501.
14. Mossman D. Commentary: assessing the risk of violence—are “accurate” predictions useful? J Am Acad Psychiatry Law 2000;28:272-81.
15. Monahan J, Steadman HJ, Robbins PC, et al. An actuarial model of violence risk assessment for persons with mental disorders. Psychiatr Serv 2005;56:810-15.
16. Simon RI. The myth of “imminent” violence in psychiatry and the law. Univ Cincinnati L Rev 2006;75:631-43.
17. Dobbs DB. The law of torts. St. Paul, MN: West Group; 2000:269.
What is the best choice for prophylaxis against VTE in medical inpatients?
Case
A 76-year-old gentleman is admitted for progressively worsening dyspnea, cough, and bilateral leg edema. Upon admission, his blood pressure is 150/90 mm/Hg, pulse 90 beats per minute, and respiration is 24 per minute.
Pertinent physical findings include jugular venous distension, bilateral crackles, S3 gallop, and 2+ bilateral lower extremity edema. The chest radiograph shows cardiomegaly and pulmonary edema. He is admitted to the hospital with a diagnosis of acute decompensated heart failure and starts aggressive medical therapy.
Overview
Approximately 2 million cases of deep-vein thrombosis (DVT) occur annually in the United States. Based on studies utilizing ventilation-perfusion scanning, half these patients likely have a silent pulmonary embolism (PE); of these, approximately 250,000 die.
The spectrum of venous thromboembolism (VTE), which includes DVT and PE, can vary from being asymptomatic to sudden death. Autopsy studies suggest a leading cause of sudden death in hospitalized medical patients is often a PE. There also are sequelae, such as chronic pulmonary hypertension, occurring in approximately 5% of PE cases, and post-thrombotic syndrome, occurring in approximately 40% of patients with DVT at two years.1
A recent study suggests DVT occurs three times more commonly in the outpatient setting. However, more than half of these patients were hospitalized in the three months prior.2 This is likely due to inadequate in-hospital prevention because of absence of prophylaxis, use of an unsuitable modality, insufficient dose of the drug, or ineffective duration of therapy. Inadequate and omitted VTE prophylaxis for medical patients was clearly demonstrated in the DVT Free Registry. This registry was created by 183 U.S. hospitals and included 5,451 patients, inpatients, and outpatients with ultrasound-confirmed DVT.
The number of medical inpatients who received prophylaxis in the 30 days prior to diagnosis was 28%—lower than the 48% of surgical patients.3 In a recent international registry, IMPROVE, only approximately 50% of hospitalized patients received prophylaxis.4
Virchow’s triad describes three underlying etiologic factors for thrombosis: stasis of blood flow, endothelial injury, and hypercoagulability. Established VTE risk factors reflect these underlying pathophysiologic processes. Important risk factors for VTE include increasing age, prolonged immobility, malignancy, major surgery, multiple trauma, prior VTE, and chronic heart failure.5
However, the magnitude of risk conferred by these and other risk factors varies (see Table 1, p. 35). It is not known how these factors interact to determine a patient’s individual VTE risk, but there is evidence it increases in proportion to the number of predisposing factors present.
In a recent systematic review of nine studies, including approximately 20,000 patients, prophylaxis reduced the rate of symptomatic VTE in at-risk hospitalized medical patients without increasing major bleeding.6
Multiple healthcare organizations, such as the National Quality Forum (NQF), Joint Commission on Accreditation of Healthcare Organizations (JCAHO), and Agency for Healthcare Research and Quality (AHRQ) have identified VTE as a preventable condition in hospitalized patients. Formal risk assessment must be conducted as a first step, followed by the initiation of timely prophylaxis to improve patient safety.
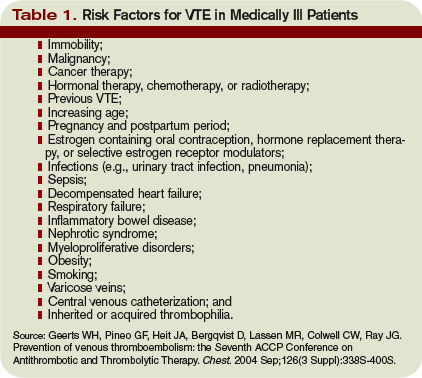
Review of the Data
Mechanical forms of prophylaxis, such as graduated compression stockings, have been evaluated in patients with stroke and myocardial infarction. Intermittent pneumatic compression stockings and venous foot pumps have not been studied in randomized controlled trials (RCTs) in general medical patients.
Although there is data supporting the efficacy of these devices in surgical patients, the American College of Chest Physicians’ (ACCP) guidelines recommend against the use of mechanical forms of prophylaxis in medical patients unless there is a contraindication to pharmacologic prophylaxis.7
The ideal prophylactic agent is cost-effective and has no side effects. Available pharmacologic options for prevention of VTE in medical patients include unfractionated heparin (UFH), low molecular weight heparins (LMWHs), and the synthetic pentasaccharide, fondaparinux. Oral anticoagulants, (e.g., vitamin K antagonists [VKA]), have not been adequately studied in medical inpatients. Since VKA take several days to achieve therapeutic anticoagulation, we do not recommend using them de novo as VTE prophylaxis.
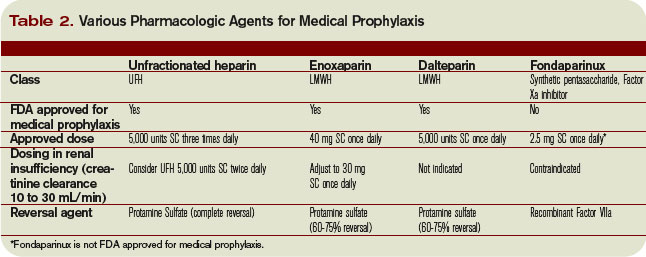
However, patients taking an oral VKA in the outpatient setting who have a therapeutic international normalized ratio (INR) during hospitalization probably are adequately protected from VTE and do not need additional pharmacologic prophylaxis. Newer anticoagulants in phase III testing for prevention of VTE in medically ill patients include oral direct thrombin inhibitors and anti-Xa inhibitors. ACCP guidelines recommend either low-dose UFH or LMWH as first-line agents for VTE prevention in medical inpatients.
Unfractionated heparin: UFH is a heterogeneous mixture of repeating polysaccharide chains of varying sizes, averaging about 15,000 Daltons. It binds anti-thrombin III (AT-III) and facilitates AT-III-mediated inactivation of factors IIa, IXa, Xa, and XIIa; of these, IIa and Xa are most responsive to inhibition.
Due to its large size, UFH only is partially absorbed from subcutaneous (SC) tissue, and it has a variable anticoagulant response due to interactions with plasma proteins, macrophages, and endothelial cells.8 However, in prophylactic SC doses (5,000 units two or three times daily), monitoring of the activated partial thromboplastin time (aPTT) is not required. In some cases, (e.g., frail or elderly patients), prophylactic SC doses may slightly prolong the aPTT.
UFH also binds to platelets and platelet factor 4 (PF4), and may precipitate heparin-induced thrombocytopenia (HIT). At least three clinical trials have compared the efficacy of SC UFH with a placebo and found prophylactic doses of UFH decrease the relative risk of DVT as detected by fibrinogen uptake test by about 70% without increasing the risk of bleeding.9-11
Low molecular weight heparins: LMWHs are derived from UFH through a chemical depolymerization, or fractionation, process. They are about one-third the size of UFH, with a molecular weight of approximately 5,000 Daltons.
These smaller molecules are readily absorbed from the SC tissue, eliciting a more predictable anticoagulant response than UFH. Unlike UFH, LMWHs have only minimal nonspecific binding to plasma proteins, endothelial cells, and monocytes, resulting in a predictable dose response. This obviates the need for lab monitoring, even when used in full, therapeutic dosing.
Compared with UFH, these agents have a longer plasma half-life, allowing them to be dosed SC once or twice daily. Also, they don’t bind platelets as readily as UFH resulting in a lower risk of HIT. Because they’re smaller, LMWHs tend to preferentially inhibit factor Xa, whereas UFH tends to inhibit factors Xa and IIa equally.
LMWHs have been evaluated in two large, placebo-controlled clinical trials for the prevention of VTE in medical inpatients.
In the first trial, MEDENOX, almost half the patients were older than 75 (mean age approximately 73). Inclusion criteria were NYHA class 3 or 4 heart failure, acute respiratory failure without mechanical ventilation, acute infection without septic shock, acute rheumatic disease, or inflammatory bowel disease. The primary outcome was assessed in 866 patients. Enoxaparin 40 mg SC once daily decreased the rate of VTE by two-thirds, from 15% to 5% (p=0.0002), without increased bleeding or thrombocytopenia compared with placebo.12 Enoxaparin 40 mg SC once daily is approved by the Food and Drug Administration (FDA) for VTE prophylaxis in medically ill patients.
PREVENT was an international, multicenter, randomized, double-blind, placebo-controlled trial evaluating dalteparin’s efficacy and safety. The inclusion criteria in this trial were acute congestive heart failure, non-ventilator-requiring acute respiratory failure, infection without septic shock, acute rheumatologic disorders, or inflammatory bowel disease. It studied 2,991 patients, and the primary outcome was VTE incidence and sudden death at day 21.
Dalteparin at 5,000 units decreased the rate of VTE, as detected by compression ultrasound, from 5% in the placebo group to 2.8%, a relative risk reduction of 45% (p=0.0015). The authors concluded the use of dalteparin reduced the incidence of VTE without increased risk of bleeding.13 Dalteparin is FDA approved for VTE prophylaxis in medical inpatients.
At least two meta-analyses have evaluated LMWHs compared with UFH. In the first, nine trials comparing LMWH to UFH (4,669 patients) were included. No significant effect was observed on DVT, clinical PE, or mortality. However, LMWH reduced the risk of major hemorrhage by 52% (p=0.049).14
In a more recent meta-analysis, 36 studies were included comparing placebos with UFH and LMWH. Both agents were associated with a reduced risk of VTE. A UFH dosage of 5,000 units three times daily was more effective in preventing DVT than a dosage of 5,000 units twice daily when compared with the control (risk ratio [RR], 0.27; 95% confidence interval [CI], 0.20-0.36; vs. RR, 0.52; 95% CI, 0.28-0.96). Neither UFH nor LMWH reduced mortality. When directly compared with UFH, LMWH was associated with a lower risk of DVT (RR, 0.68; 95% CI, 0.52-0.88) and injection-site hematoma (RR, 0.47; 95% CI, 0.36-0.62), but no difference was seen between the two agents in the risk of bleeding or thrombocytopenia.
This contemporary meta-analysis clearly illustrates that UFH and LMWH reduce VTE risk in hospitalized medical patients, but neither agent alters mortality. When directly compared, LMWH is more effective in preventing DVT.15
Despite the higher drug acquisition costs, LMWHs are more cost-effective than UFH for prophylaxis in medical patients because of their lower complication rates of HIT. LMWH reduces incremental costs by $13.88 per day compared with UFH.16, 17
Synthetic pentasaccharide: Fondaparinux is a synthetic analogue of the unique pentasaccharide sequence that mediates the interaction of heparin with antithrombin. It inhibits both free and platelet-bound factor Xa. It binds antithrombin with high affinity, has close to 100% bioavailability, and has a plasma half-life of 17 hours that permits once-daily administration.
The drug is excreted unchanged in the urine and therefore contraindicated in patients with severe renal impairment (e.g., creatinine clearance less than 30 mL/min). It does not bind PF4 in vitro and thus should not cause HIT.
Fondaparinux has been evaluated in medical inpatients in a randomized placebo controlled trial, ARTEMIS. Fondaparinux 2.5 mg SC once daily decreased the rate of venographically-confirmed DVT from 10.5% to 5.6% (p=0.029); there was also a decrease in fatal PE from 1.7% to 0.7% (p=0.029). A reduction in overall mortality from 6% to 3.3% (P=NS) was observed. Major bleeding occurred in 0.2% of patients in both groups. The drug is not FDA approved to prevent VTE in medical inpatients.18
Duration of therapy: Most clinical trials have used prophylaxis for seven to 14 days. The Extended Clinical Prophylaxis in Acutely Ill Medical Patients (EXCLAIM) trial evaluated duration of therapy, the results of which were presented recently at the 21st Congress of the International Society on Thrombosis and Haemostasis (ISTH).
Of the 5,105 patients who met inclusion criteria, 5,049, or 99%, received open-label prophylaxis with enoxaparin (10 ± four days); 2,013 patients subsequently received extended-duration enoxaparin; and 2,027 received placebo (each for 28 ± four days). Subjects were at least 40 years old, had been recently immobilized (for at least 3 days) and had a predefined acute medical illness. Mobility was defined as level 1 (total bed rest or sedentary) or level 2 (bathroom privileges). After a planned blinded interim analysis, the trial’s data safety monitoring board recommended an amendment to the inclusion criteria, changing level 2 mobility to include age >75 years, and/or prior VTE, and/or diagnosed cancer.
When compared with placebo, extended-duration enoxaparin following the open-label, standard-duration enoxaparin reduced the relative risk of VTE by 44% (2.8% vs. 4.9%; p=0.0011). There was major bleeding in 12 subjects who received extended-duration enoxaparin and three subjects receiving placebo (0.6% vs. 0.1%; p=0.0192).
There was no difference in all-cause mortality between the extended-duration enoxaparin and placebo groups at six months (10.1% vs. 8.9%, p=0.179). The authors concluded 38 days of enoxaparin 40 mg SC once daily significantly reduced the overall incidence of VTE compared with a 10-day regimen in acutely ill medical patients with reduced mobility. This reduction in overall risk for VTE was consistent with a reduction in risk for asymptomatic proximal DVT and symptomatic VTE.
Based on this trial, we would recommend five weeks of prophylaxis for those older than 75 years with prior history of VTE or with active cancer. In the absence of these criteria, we recommend up to 14 days of therapy.
For many patients, this will mean prophylaxis after discharge from the hospital. While this represents a change in practice for many and may significantly complicate some discharge care plans we believe the significant burden of post-hospital VTE mandates a more aggressive approach to peri-hospitalization prophylaxis.
Back to the Case
Our patient has acute decompensated heart failure and likely will be limited in his ability to ambulate. All the clinical trials discussed above included similar patients and support the use of pharmacological prophylaxis. All hospitalized medical patients should undergo VTE risk assessment and implementation of pharmacologic prophylaxis in the absence of contraindications. TH
Dr. Lenchus is an assistant professor of medicine at the University of Miami School of Medicine. Dr. Jaffer is an associate professor of medicine at the University of Miami School of Medicine, where he serves as the chief of the division of hospital medicine.
References
- Hirsh J, Hoak J. Management of deep vein thrombosis and pulmonary embolism. A statement for healthcare professionals. Council on Thrombosis (in consultation with the Council on Cardiovascular Radiology), American Heart Association. Circulation. 1996 Jun 15;93(12):2212-2245.
- Spencer FA, Lessard D, Emery C, Reed G, Goldberg RJ. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007 Jul 23;167(14):1471-1475.
- Goldhaber SZ, Tapson VF. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan 15;93(2):259-262.
- Tapson VF, Decousus H, Pini M, et al. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism. Chest. Sep 2007;132(3):936-945.
- Anderson FA, Jr., Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003 Jun 17;107(23 Suppl 1):I9-16.
- Dentali F, Douketis JD, Gianni M, Lim W, Crowther MA. Meta-analysis: anticoagulant prophylaxis to prevent symptomatic venous thromboembolism in hospitalized medical patients. Ann Intern Med. 2007 Feb 20;146(4):278-288.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S.
- Hirsh J, Raschke R. Heparin and low-molecular-weight heparin: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):188S-203S.
- Cade JF, Andrews JT, Stubbs AE. Comparison of sodium and calcium heparin in prevention of venous thromboembolism. Aust N Z J Med. 1982 Oct;12(5):501-504.
- Gallus AS, Hirsh J, Tutle RJ, et al. Small subcutaneous doses of heparin in prevention of venous thrombosis. N Engl J Med. 1973 Mar 15;288(11):545-551.
- Belch JJ, Lowe GD, Ward AG, Forbes CD, Prentice CR. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115-117.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793-800.
- Leizorovicz A, Cohen AT, Turpie AG, Olsson CG, Vaitkus PT, Goldhaber SZ. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Mismetti P, Laporte-Simitsidis S, Tardy B, et al. Prevention of venous thromboembolism in internal medicine with unfractionated or low-molecular-weight heparins: a meta-analysis of randomised clinical trials. Thromb Haemost. Jan 2000;83(1):14-19.
- Wein L, Wein S, Haas SJ, Shaw J, Krum H. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2007 Jul 23;167(14):1476-1486.
- McGarry LJ, Thompson D, Weinstein MC, Goldhaber SZ. Cost effectiveness of thromboprophylaxis with a low-molecular-weight heparin versus unfractionated heparin in acutely ill medical inpatients. Am J Manag Care. 2004 Sep;10(9):632-642.
- Creekmore FM, Oderda GM, Pendleton RC, Brixner DI. Incidence and economic implications of heparin-induced thrombocytopenia in medical patients receiving prophylaxis for venous thromboembolism. Pharmacotherapy. 2006 Oct;26(10):1438-1445.
- Cohen AT, Davidson BL, Gallus AS, et al. Efficacy and safety of fondaparinux for the prevention of venous thromboembolism in older acute medical patients: randomised placebo controlled trial. BMJ. 2006 Feb 11;332(7537):325-329.
Case
A 76-year-old gentleman is admitted for progressively worsening dyspnea, cough, and bilateral leg edema. Upon admission, his blood pressure is 150/90 mm/Hg, pulse 90 beats per minute, and respiration is 24 per minute.
Pertinent physical findings include jugular venous distension, bilateral crackles, S3 gallop, and 2+ bilateral lower extremity edema. The chest radiograph shows cardiomegaly and pulmonary edema. He is admitted to the hospital with a diagnosis of acute decompensated heart failure and starts aggressive medical therapy.
Overview
Approximately 2 million cases of deep-vein thrombosis (DVT) occur annually in the United States. Based on studies utilizing ventilation-perfusion scanning, half these patients likely have a silent pulmonary embolism (PE); of these, approximately 250,000 die.
The spectrum of venous thromboembolism (VTE), which includes DVT and PE, can vary from being asymptomatic to sudden death. Autopsy studies suggest a leading cause of sudden death in hospitalized medical patients is often a PE. There also are sequelae, such as chronic pulmonary hypertension, occurring in approximately 5% of PE cases, and post-thrombotic syndrome, occurring in approximately 40% of patients with DVT at two years.1
A recent study suggests DVT occurs three times more commonly in the outpatient setting. However, more than half of these patients were hospitalized in the three months prior.2 This is likely due to inadequate in-hospital prevention because of absence of prophylaxis, use of an unsuitable modality, insufficient dose of the drug, or ineffective duration of therapy. Inadequate and omitted VTE prophylaxis for medical patients was clearly demonstrated in the DVT Free Registry. This registry was created by 183 U.S. hospitals and included 5,451 patients, inpatients, and outpatients with ultrasound-confirmed DVT.
The number of medical inpatients who received prophylaxis in the 30 days prior to diagnosis was 28%—lower than the 48% of surgical patients.3 In a recent international registry, IMPROVE, only approximately 50% of hospitalized patients received prophylaxis.4
Virchow’s triad describes three underlying etiologic factors for thrombosis: stasis of blood flow, endothelial injury, and hypercoagulability. Established VTE risk factors reflect these underlying pathophysiologic processes. Important risk factors for VTE include increasing age, prolonged immobility, malignancy, major surgery, multiple trauma, prior VTE, and chronic heart failure.5
However, the magnitude of risk conferred by these and other risk factors varies (see Table 1, p. 35). It is not known how these factors interact to determine a patient’s individual VTE risk, but there is evidence it increases in proportion to the number of predisposing factors present.
In a recent systematic review of nine studies, including approximately 20,000 patients, prophylaxis reduced the rate of symptomatic VTE in at-risk hospitalized medical patients without increasing major bleeding.6
Multiple healthcare organizations, such as the National Quality Forum (NQF), Joint Commission on Accreditation of Healthcare Organizations (JCAHO), and Agency for Healthcare Research and Quality (AHRQ) have identified VTE as a preventable condition in hospitalized patients. Formal risk assessment must be conducted as a first step, followed by the initiation of timely prophylaxis to improve patient safety.
Review of the Data
Mechanical forms of prophylaxis, such as graduated compression stockings, have been evaluated in patients with stroke and myocardial infarction. Intermittent pneumatic compression stockings and venous foot pumps have not been studied in randomized controlled trials (RCTs) in general medical patients.
Although there is data supporting the efficacy of these devices in surgical patients, the American College of Chest Physicians’ (ACCP) guidelines recommend against the use of mechanical forms of prophylaxis in medical patients unless there is a contraindication to pharmacologic prophylaxis.7
The ideal prophylactic agent is cost-effective and has no side effects. Available pharmacologic options for prevention of VTE in medical patients include unfractionated heparin (UFH), low molecular weight heparins (LMWHs), and the synthetic pentasaccharide, fondaparinux. Oral anticoagulants, (e.g., vitamin K antagonists [VKA]), have not been adequately studied in medical inpatients. Since VKA take several days to achieve therapeutic anticoagulation, we do not recommend using them de novo as VTE prophylaxis.
However, patients taking an oral VKA in the outpatient setting who have a therapeutic international normalized ratio (INR) during hospitalization probably are adequately protected from VTE and do not need additional pharmacologic prophylaxis. Newer anticoagulants in phase III testing for prevention of VTE in medically ill patients include oral direct thrombin inhibitors and anti-Xa inhibitors. ACCP guidelines recommend either low-dose UFH or LMWH as first-line agents for VTE prevention in medical inpatients.
Unfractionated heparin: UFH is a heterogeneous mixture of repeating polysaccharide chains of varying sizes, averaging about 15,000 Daltons. It binds anti-thrombin III (AT-III) and facilitates AT-III-mediated inactivation of factors IIa, IXa, Xa, and XIIa; of these, IIa and Xa are most responsive to inhibition.
Due to its large size, UFH only is partially absorbed from subcutaneous (SC) tissue, and it has a variable anticoagulant response due to interactions with plasma proteins, macrophages, and endothelial cells.8 However, in prophylactic SC doses (5,000 units two or three times daily), monitoring of the activated partial thromboplastin time (aPTT) is not required. In some cases, (e.g., frail or elderly patients), prophylactic SC doses may slightly prolong the aPTT.
UFH also binds to platelets and platelet factor 4 (PF4), and may precipitate heparin-induced thrombocytopenia (HIT). At least three clinical trials have compared the efficacy of SC UFH with a placebo and found prophylactic doses of UFH decrease the relative risk of DVT as detected by fibrinogen uptake test by about 70% without increasing the risk of bleeding.9-11
Low molecular weight heparins: LMWHs are derived from UFH through a chemical depolymerization, or fractionation, process. They are about one-third the size of UFH, with a molecular weight of approximately 5,000 Daltons.
These smaller molecules are readily absorbed from the SC tissue, eliciting a more predictable anticoagulant response than UFH. Unlike UFH, LMWHs have only minimal nonspecific binding to plasma proteins, endothelial cells, and monocytes, resulting in a predictable dose response. This obviates the need for lab monitoring, even when used in full, therapeutic dosing.
Compared with UFH, these agents have a longer plasma half-life, allowing them to be dosed SC once or twice daily. Also, they don’t bind platelets as readily as UFH resulting in a lower risk of HIT. Because they’re smaller, LMWHs tend to preferentially inhibit factor Xa, whereas UFH tends to inhibit factors Xa and IIa equally.
LMWHs have been evaluated in two large, placebo-controlled clinical trials for the prevention of VTE in medical inpatients.
In the first trial, MEDENOX, almost half the patients were older than 75 (mean age approximately 73). Inclusion criteria were NYHA class 3 or 4 heart failure, acute respiratory failure without mechanical ventilation, acute infection without septic shock, acute rheumatic disease, or inflammatory bowel disease. The primary outcome was assessed in 866 patients. Enoxaparin 40 mg SC once daily decreased the rate of VTE by two-thirds, from 15% to 5% (p=0.0002), without increased bleeding or thrombocytopenia compared with placebo.12 Enoxaparin 40 mg SC once daily is approved by the Food and Drug Administration (FDA) for VTE prophylaxis in medically ill patients.
PREVENT was an international, multicenter, randomized, double-blind, placebo-controlled trial evaluating dalteparin’s efficacy and safety. The inclusion criteria in this trial were acute congestive heart failure, non-ventilator-requiring acute respiratory failure, infection without septic shock, acute rheumatologic disorders, or inflammatory bowel disease. It studied 2,991 patients, and the primary outcome was VTE incidence and sudden death at day 21.
Dalteparin at 5,000 units decreased the rate of VTE, as detected by compression ultrasound, from 5% in the placebo group to 2.8%, a relative risk reduction of 45% (p=0.0015). The authors concluded the use of dalteparin reduced the incidence of VTE without increased risk of bleeding.13 Dalteparin is FDA approved for VTE prophylaxis in medical inpatients.
At least two meta-analyses have evaluated LMWHs compared with UFH. In the first, nine trials comparing LMWH to UFH (4,669 patients) were included. No significant effect was observed on DVT, clinical PE, or mortality. However, LMWH reduced the risk of major hemorrhage by 52% (p=0.049).14
In a more recent meta-analysis, 36 studies were included comparing placebos with UFH and LMWH. Both agents were associated with a reduced risk of VTE. A UFH dosage of 5,000 units three times daily was more effective in preventing DVT than a dosage of 5,000 units twice daily when compared with the control (risk ratio [RR], 0.27; 95% confidence interval [CI], 0.20-0.36; vs. RR, 0.52; 95% CI, 0.28-0.96). Neither UFH nor LMWH reduced mortality. When directly compared with UFH, LMWH was associated with a lower risk of DVT (RR, 0.68; 95% CI, 0.52-0.88) and injection-site hematoma (RR, 0.47; 95% CI, 0.36-0.62), but no difference was seen between the two agents in the risk of bleeding or thrombocytopenia.
This contemporary meta-analysis clearly illustrates that UFH and LMWH reduce VTE risk in hospitalized medical patients, but neither agent alters mortality. When directly compared, LMWH is more effective in preventing DVT.15
Despite the higher drug acquisition costs, LMWHs are more cost-effective than UFH for prophylaxis in medical patients because of their lower complication rates of HIT. LMWH reduces incremental costs by $13.88 per day compared with UFH.16, 17
Synthetic pentasaccharide: Fondaparinux is a synthetic analogue of the unique pentasaccharide sequence that mediates the interaction of heparin with antithrombin. It inhibits both free and platelet-bound factor Xa. It binds antithrombin with high affinity, has close to 100% bioavailability, and has a plasma half-life of 17 hours that permits once-daily administration.
The drug is excreted unchanged in the urine and therefore contraindicated in patients with severe renal impairment (e.g., creatinine clearance less than 30 mL/min). It does not bind PF4 in vitro and thus should not cause HIT.
Fondaparinux has been evaluated in medical inpatients in a randomized placebo controlled trial, ARTEMIS. Fondaparinux 2.5 mg SC once daily decreased the rate of venographically-confirmed DVT from 10.5% to 5.6% (p=0.029); there was also a decrease in fatal PE from 1.7% to 0.7% (p=0.029). A reduction in overall mortality from 6% to 3.3% (P=NS) was observed. Major bleeding occurred in 0.2% of patients in both groups. The drug is not FDA approved to prevent VTE in medical inpatients.18
Duration of therapy: Most clinical trials have used prophylaxis for seven to 14 days. The Extended Clinical Prophylaxis in Acutely Ill Medical Patients (EXCLAIM) trial evaluated duration of therapy, the results of which were presented recently at the 21st Congress of the International Society on Thrombosis and Haemostasis (ISTH).
Of the 5,105 patients who met inclusion criteria, 5,049, or 99%, received open-label prophylaxis with enoxaparin (10 ± four days); 2,013 patients subsequently received extended-duration enoxaparin; and 2,027 received placebo (each for 28 ± four days). Subjects were at least 40 years old, had been recently immobilized (for at least 3 days) and had a predefined acute medical illness. Mobility was defined as level 1 (total bed rest or sedentary) or level 2 (bathroom privileges). After a planned blinded interim analysis, the trial’s data safety monitoring board recommended an amendment to the inclusion criteria, changing level 2 mobility to include age >75 years, and/or prior VTE, and/or diagnosed cancer.
When compared with placebo, extended-duration enoxaparin following the open-label, standard-duration enoxaparin reduced the relative risk of VTE by 44% (2.8% vs. 4.9%; p=0.0011). There was major bleeding in 12 subjects who received extended-duration enoxaparin and three subjects receiving placebo (0.6% vs. 0.1%; p=0.0192).
There was no difference in all-cause mortality between the extended-duration enoxaparin and placebo groups at six months (10.1% vs. 8.9%, p=0.179). The authors concluded 38 days of enoxaparin 40 mg SC once daily significantly reduced the overall incidence of VTE compared with a 10-day regimen in acutely ill medical patients with reduced mobility. This reduction in overall risk for VTE was consistent with a reduction in risk for asymptomatic proximal DVT and symptomatic VTE.
Based on this trial, we would recommend five weeks of prophylaxis for those older than 75 years with prior history of VTE or with active cancer. In the absence of these criteria, we recommend up to 14 days of therapy.
For many patients, this will mean prophylaxis after discharge from the hospital. While this represents a change in practice for many and may significantly complicate some discharge care plans we believe the significant burden of post-hospital VTE mandates a more aggressive approach to peri-hospitalization prophylaxis.
Back to the Case
Our patient has acute decompensated heart failure and likely will be limited in his ability to ambulate. All the clinical trials discussed above included similar patients and support the use of pharmacological prophylaxis. All hospitalized medical patients should undergo VTE risk assessment and implementation of pharmacologic prophylaxis in the absence of contraindications. TH
Dr. Lenchus is an assistant professor of medicine at the University of Miami School of Medicine. Dr. Jaffer is an associate professor of medicine at the University of Miami School of Medicine, where he serves as the chief of the division of hospital medicine.
References
- Hirsh J, Hoak J. Management of deep vein thrombosis and pulmonary embolism. A statement for healthcare professionals. Council on Thrombosis (in consultation with the Council on Cardiovascular Radiology), American Heart Association. Circulation. 1996 Jun 15;93(12):2212-2245.
- Spencer FA, Lessard D, Emery C, Reed G, Goldberg RJ. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007 Jul 23;167(14):1471-1475.
- Goldhaber SZ, Tapson VF. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan 15;93(2):259-262.
- Tapson VF, Decousus H, Pini M, et al. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism. Chest. Sep 2007;132(3):936-945.
- Anderson FA, Jr., Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003 Jun 17;107(23 Suppl 1):I9-16.
- Dentali F, Douketis JD, Gianni M, Lim W, Crowther MA. Meta-analysis: anticoagulant prophylaxis to prevent symptomatic venous thromboembolism in hospitalized medical patients. Ann Intern Med. 2007 Feb 20;146(4):278-288.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S.
- Hirsh J, Raschke R. Heparin and low-molecular-weight heparin: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):188S-203S.
- Cade JF, Andrews JT, Stubbs AE. Comparison of sodium and calcium heparin in prevention of venous thromboembolism. Aust N Z J Med. 1982 Oct;12(5):501-504.
- Gallus AS, Hirsh J, Tutle RJ, et al. Small subcutaneous doses of heparin in prevention of venous thrombosis. N Engl J Med. 1973 Mar 15;288(11):545-551.
- Belch JJ, Lowe GD, Ward AG, Forbes CD, Prentice CR. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115-117.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793-800.
- Leizorovicz A, Cohen AT, Turpie AG, Olsson CG, Vaitkus PT, Goldhaber SZ. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Mismetti P, Laporte-Simitsidis S, Tardy B, et al. Prevention of venous thromboembolism in internal medicine with unfractionated or low-molecular-weight heparins: a meta-analysis of randomised clinical trials. Thromb Haemost. Jan 2000;83(1):14-19.
- Wein L, Wein S, Haas SJ, Shaw J, Krum H. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2007 Jul 23;167(14):1476-1486.
- McGarry LJ, Thompson D, Weinstein MC, Goldhaber SZ. Cost effectiveness of thromboprophylaxis with a low-molecular-weight heparin versus unfractionated heparin in acutely ill medical inpatients. Am J Manag Care. 2004 Sep;10(9):632-642.
- Creekmore FM, Oderda GM, Pendleton RC, Brixner DI. Incidence and economic implications of heparin-induced thrombocytopenia in medical patients receiving prophylaxis for venous thromboembolism. Pharmacotherapy. 2006 Oct;26(10):1438-1445.
- Cohen AT, Davidson BL, Gallus AS, et al. Efficacy and safety of fondaparinux for the prevention of venous thromboembolism in older acute medical patients: randomised placebo controlled trial. BMJ. 2006 Feb 11;332(7537):325-329.
Case
A 76-year-old gentleman is admitted for progressively worsening dyspnea, cough, and bilateral leg edema. Upon admission, his blood pressure is 150/90 mm/Hg, pulse 90 beats per minute, and respiration is 24 per minute.
Pertinent physical findings include jugular venous distension, bilateral crackles, S3 gallop, and 2+ bilateral lower extremity edema. The chest radiograph shows cardiomegaly and pulmonary edema. He is admitted to the hospital with a diagnosis of acute decompensated heart failure and starts aggressive medical therapy.
Overview
Approximately 2 million cases of deep-vein thrombosis (DVT) occur annually in the United States. Based on studies utilizing ventilation-perfusion scanning, half these patients likely have a silent pulmonary embolism (PE); of these, approximately 250,000 die.
The spectrum of venous thromboembolism (VTE), which includes DVT and PE, can vary from being asymptomatic to sudden death. Autopsy studies suggest a leading cause of sudden death in hospitalized medical patients is often a PE. There also are sequelae, such as chronic pulmonary hypertension, occurring in approximately 5% of PE cases, and post-thrombotic syndrome, occurring in approximately 40% of patients with DVT at two years.1
A recent study suggests DVT occurs three times more commonly in the outpatient setting. However, more than half of these patients were hospitalized in the three months prior.2 This is likely due to inadequate in-hospital prevention because of absence of prophylaxis, use of an unsuitable modality, insufficient dose of the drug, or ineffective duration of therapy. Inadequate and omitted VTE prophylaxis for medical patients was clearly demonstrated in the DVT Free Registry. This registry was created by 183 U.S. hospitals and included 5,451 patients, inpatients, and outpatients with ultrasound-confirmed DVT.
The number of medical inpatients who received prophylaxis in the 30 days prior to diagnosis was 28%—lower than the 48% of surgical patients.3 In a recent international registry, IMPROVE, only approximately 50% of hospitalized patients received prophylaxis.4
Virchow’s triad describes three underlying etiologic factors for thrombosis: stasis of blood flow, endothelial injury, and hypercoagulability. Established VTE risk factors reflect these underlying pathophysiologic processes. Important risk factors for VTE include increasing age, prolonged immobility, malignancy, major surgery, multiple trauma, prior VTE, and chronic heart failure.5
However, the magnitude of risk conferred by these and other risk factors varies (see Table 1, p. 35). It is not known how these factors interact to determine a patient’s individual VTE risk, but there is evidence it increases in proportion to the number of predisposing factors present.
In a recent systematic review of nine studies, including approximately 20,000 patients, prophylaxis reduced the rate of symptomatic VTE in at-risk hospitalized medical patients without increasing major bleeding.6
Multiple healthcare organizations, such as the National Quality Forum (NQF), Joint Commission on Accreditation of Healthcare Organizations (JCAHO), and Agency for Healthcare Research and Quality (AHRQ) have identified VTE as a preventable condition in hospitalized patients. Formal risk assessment must be conducted as a first step, followed by the initiation of timely prophylaxis to improve patient safety.
Review of the Data
Mechanical forms of prophylaxis, such as graduated compression stockings, have been evaluated in patients with stroke and myocardial infarction. Intermittent pneumatic compression stockings and venous foot pumps have not been studied in randomized controlled trials (RCTs) in general medical patients.
Although there is data supporting the efficacy of these devices in surgical patients, the American College of Chest Physicians’ (ACCP) guidelines recommend against the use of mechanical forms of prophylaxis in medical patients unless there is a contraindication to pharmacologic prophylaxis.7
The ideal prophylactic agent is cost-effective and has no side effects. Available pharmacologic options for prevention of VTE in medical patients include unfractionated heparin (UFH), low molecular weight heparins (LMWHs), and the synthetic pentasaccharide, fondaparinux. Oral anticoagulants, (e.g., vitamin K antagonists [VKA]), have not been adequately studied in medical inpatients. Since VKA take several days to achieve therapeutic anticoagulation, we do not recommend using them de novo as VTE prophylaxis.
However, patients taking an oral VKA in the outpatient setting who have a therapeutic international normalized ratio (INR) during hospitalization probably are adequately protected from VTE and do not need additional pharmacologic prophylaxis. Newer anticoagulants in phase III testing for prevention of VTE in medically ill patients include oral direct thrombin inhibitors and anti-Xa inhibitors. ACCP guidelines recommend either low-dose UFH or LMWH as first-line agents for VTE prevention in medical inpatients.
Unfractionated heparin: UFH is a heterogeneous mixture of repeating polysaccharide chains of varying sizes, averaging about 15,000 Daltons. It binds anti-thrombin III (AT-III) and facilitates AT-III-mediated inactivation of factors IIa, IXa, Xa, and XIIa; of these, IIa and Xa are most responsive to inhibition.
Due to its large size, UFH only is partially absorbed from subcutaneous (SC) tissue, and it has a variable anticoagulant response due to interactions with plasma proteins, macrophages, and endothelial cells.8 However, in prophylactic SC doses (5,000 units two or three times daily), monitoring of the activated partial thromboplastin time (aPTT) is not required. In some cases, (e.g., frail or elderly patients), prophylactic SC doses may slightly prolong the aPTT.
UFH also binds to platelets and platelet factor 4 (PF4), and may precipitate heparin-induced thrombocytopenia (HIT). At least three clinical trials have compared the efficacy of SC UFH with a placebo and found prophylactic doses of UFH decrease the relative risk of DVT as detected by fibrinogen uptake test by about 70% without increasing the risk of bleeding.9-11
Low molecular weight heparins: LMWHs are derived from UFH through a chemical depolymerization, or fractionation, process. They are about one-third the size of UFH, with a molecular weight of approximately 5,000 Daltons.
These smaller molecules are readily absorbed from the SC tissue, eliciting a more predictable anticoagulant response than UFH. Unlike UFH, LMWHs have only minimal nonspecific binding to plasma proteins, endothelial cells, and monocytes, resulting in a predictable dose response. This obviates the need for lab monitoring, even when used in full, therapeutic dosing.
Compared with UFH, these agents have a longer plasma half-life, allowing them to be dosed SC once or twice daily. Also, they don’t bind platelets as readily as UFH resulting in a lower risk of HIT. Because they’re smaller, LMWHs tend to preferentially inhibit factor Xa, whereas UFH tends to inhibit factors Xa and IIa equally.
LMWHs have been evaluated in two large, placebo-controlled clinical trials for the prevention of VTE in medical inpatients.
In the first trial, MEDENOX, almost half the patients were older than 75 (mean age approximately 73). Inclusion criteria were NYHA class 3 or 4 heart failure, acute respiratory failure without mechanical ventilation, acute infection without septic shock, acute rheumatic disease, or inflammatory bowel disease. The primary outcome was assessed in 866 patients. Enoxaparin 40 mg SC once daily decreased the rate of VTE by two-thirds, from 15% to 5% (p=0.0002), without increased bleeding or thrombocytopenia compared with placebo.12 Enoxaparin 40 mg SC once daily is approved by the Food and Drug Administration (FDA) for VTE prophylaxis in medically ill patients.
PREVENT was an international, multicenter, randomized, double-blind, placebo-controlled trial evaluating dalteparin’s efficacy and safety. The inclusion criteria in this trial were acute congestive heart failure, non-ventilator-requiring acute respiratory failure, infection without septic shock, acute rheumatologic disorders, or inflammatory bowel disease. It studied 2,991 patients, and the primary outcome was VTE incidence and sudden death at day 21.
Dalteparin at 5,000 units decreased the rate of VTE, as detected by compression ultrasound, from 5% in the placebo group to 2.8%, a relative risk reduction of 45% (p=0.0015). The authors concluded the use of dalteparin reduced the incidence of VTE without increased risk of bleeding.13 Dalteparin is FDA approved for VTE prophylaxis in medical inpatients.
At least two meta-analyses have evaluated LMWHs compared with UFH. In the first, nine trials comparing LMWH to UFH (4,669 patients) were included. No significant effect was observed on DVT, clinical PE, or mortality. However, LMWH reduced the risk of major hemorrhage by 52% (p=0.049).14
In a more recent meta-analysis, 36 studies were included comparing placebos with UFH and LMWH. Both agents were associated with a reduced risk of VTE. A UFH dosage of 5,000 units three times daily was more effective in preventing DVT than a dosage of 5,000 units twice daily when compared with the control (risk ratio [RR], 0.27; 95% confidence interval [CI], 0.20-0.36; vs. RR, 0.52; 95% CI, 0.28-0.96). Neither UFH nor LMWH reduced mortality. When directly compared with UFH, LMWH was associated with a lower risk of DVT (RR, 0.68; 95% CI, 0.52-0.88) and injection-site hematoma (RR, 0.47; 95% CI, 0.36-0.62), but no difference was seen between the two agents in the risk of bleeding or thrombocytopenia.
This contemporary meta-analysis clearly illustrates that UFH and LMWH reduce VTE risk in hospitalized medical patients, but neither agent alters mortality. When directly compared, LMWH is more effective in preventing DVT.15
Despite the higher drug acquisition costs, LMWHs are more cost-effective than UFH for prophylaxis in medical patients because of their lower complication rates of HIT. LMWH reduces incremental costs by $13.88 per day compared with UFH.16, 17
Synthetic pentasaccharide: Fondaparinux is a synthetic analogue of the unique pentasaccharide sequence that mediates the interaction of heparin with antithrombin. It inhibits both free and platelet-bound factor Xa. It binds antithrombin with high affinity, has close to 100% bioavailability, and has a plasma half-life of 17 hours that permits once-daily administration.
The drug is excreted unchanged in the urine and therefore contraindicated in patients with severe renal impairment (e.g., creatinine clearance less than 30 mL/min). It does not bind PF4 in vitro and thus should not cause HIT.
Fondaparinux has been evaluated in medical inpatients in a randomized placebo controlled trial, ARTEMIS. Fondaparinux 2.5 mg SC once daily decreased the rate of venographically-confirmed DVT from 10.5% to 5.6% (p=0.029); there was also a decrease in fatal PE from 1.7% to 0.7% (p=0.029). A reduction in overall mortality from 6% to 3.3% (P=NS) was observed. Major bleeding occurred in 0.2% of patients in both groups. The drug is not FDA approved to prevent VTE in medical inpatients.18
Duration of therapy: Most clinical trials have used prophylaxis for seven to 14 days. The Extended Clinical Prophylaxis in Acutely Ill Medical Patients (EXCLAIM) trial evaluated duration of therapy, the results of which were presented recently at the 21st Congress of the International Society on Thrombosis and Haemostasis (ISTH).
Of the 5,105 patients who met inclusion criteria, 5,049, or 99%, received open-label prophylaxis with enoxaparin (10 ± four days); 2,013 patients subsequently received extended-duration enoxaparin; and 2,027 received placebo (each for 28 ± four days). Subjects were at least 40 years old, had been recently immobilized (for at least 3 days) and had a predefined acute medical illness. Mobility was defined as level 1 (total bed rest or sedentary) or level 2 (bathroom privileges). After a planned blinded interim analysis, the trial’s data safety monitoring board recommended an amendment to the inclusion criteria, changing level 2 mobility to include age >75 years, and/or prior VTE, and/or diagnosed cancer.
When compared with placebo, extended-duration enoxaparin following the open-label, standard-duration enoxaparin reduced the relative risk of VTE by 44% (2.8% vs. 4.9%; p=0.0011). There was major bleeding in 12 subjects who received extended-duration enoxaparin and three subjects receiving placebo (0.6% vs. 0.1%; p=0.0192).
There was no difference in all-cause mortality between the extended-duration enoxaparin and placebo groups at six months (10.1% vs. 8.9%, p=0.179). The authors concluded 38 days of enoxaparin 40 mg SC once daily significantly reduced the overall incidence of VTE compared with a 10-day regimen in acutely ill medical patients with reduced mobility. This reduction in overall risk for VTE was consistent with a reduction in risk for asymptomatic proximal DVT and symptomatic VTE.
Based on this trial, we would recommend five weeks of prophylaxis for those older than 75 years with prior history of VTE or with active cancer. In the absence of these criteria, we recommend up to 14 days of therapy.
For many patients, this will mean prophylaxis after discharge from the hospital. While this represents a change in practice for many and may significantly complicate some discharge care plans we believe the significant burden of post-hospital VTE mandates a more aggressive approach to peri-hospitalization prophylaxis.
Back to the Case
Our patient has acute decompensated heart failure and likely will be limited in his ability to ambulate. All the clinical trials discussed above included similar patients and support the use of pharmacological prophylaxis. All hospitalized medical patients should undergo VTE risk assessment and implementation of pharmacologic prophylaxis in the absence of contraindications. TH
Dr. Lenchus is an assistant professor of medicine at the University of Miami School of Medicine. Dr. Jaffer is an associate professor of medicine at the University of Miami School of Medicine, where he serves as the chief of the division of hospital medicine.
References
- Hirsh J, Hoak J. Management of deep vein thrombosis and pulmonary embolism. A statement for healthcare professionals. Council on Thrombosis (in consultation with the Council on Cardiovascular Radiology), American Heart Association. Circulation. 1996 Jun 15;93(12):2212-2245.
- Spencer FA, Lessard D, Emery C, Reed G, Goldberg RJ. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007 Jul 23;167(14):1471-1475.
- Goldhaber SZ, Tapson VF. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004 Jan 15;93(2):259-262.
- Tapson VF, Decousus H, Pini M, et al. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism. Chest. Sep 2007;132(3):936-945.
- Anderson FA, Jr., Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003 Jun 17;107(23 Suppl 1):I9-16.
- Dentali F, Douketis JD, Gianni M, Lim W, Crowther MA. Meta-analysis: anticoagulant prophylaxis to prevent symptomatic venous thromboembolism in hospitalized medical patients. Ann Intern Med. 2007 Feb 20;146(4):278-288.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S.
- Hirsh J, Raschke R. Heparin and low-molecular-weight heparin: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):188S-203S.
- Cade JF, Andrews JT, Stubbs AE. Comparison of sodium and calcium heparin in prevention of venous thromboembolism. Aust N Z J Med. 1982 Oct;12(5):501-504.
- Gallus AS, Hirsh J, Tutle RJ, et al. Small subcutaneous doses of heparin in prevention of venous thrombosis. N Engl J Med. 1973 Mar 15;288(11):545-551.
- Belch JJ, Lowe GD, Ward AG, Forbes CD, Prentice CR. Prevention of deep vein thrombosis in medical patients by low-dose heparin. Scott Med J. 1981 Apr;26(2):115-117.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999 Sep 9;341(11):793-800.
- Leizorovicz A, Cohen AT, Turpie AG, Olsson CG, Vaitkus PT, Goldhaber SZ. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004 Aug 17;110(7):874-879.
- Mismetti P, Laporte-Simitsidis S, Tardy B, et al. Prevention of venous thromboembolism in internal medicine with unfractionated or low-molecular-weight heparins: a meta-analysis of randomised clinical trials. Thromb Haemost. Jan 2000;83(1):14-19.
- Wein L, Wein S, Haas SJ, Shaw J, Krum H. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2007 Jul 23;167(14):1476-1486.
- McGarry LJ, Thompson D, Weinstein MC, Goldhaber SZ. Cost effectiveness of thromboprophylaxis with a low-molecular-weight heparin versus unfractionated heparin in acutely ill medical inpatients. Am J Manag Care. 2004 Sep;10(9):632-642.
- Creekmore FM, Oderda GM, Pendleton RC, Brixner DI. Incidence and economic implications of heparin-induced thrombocytopenia in medical patients receiving prophylaxis for venous thromboembolism. Pharmacotherapy. 2006 Oct;26(10):1438-1445.
- Cohen AT, Davidson BL, Gallus AS, et al. Efficacy and safety of fondaparinux for the prevention of venous thromboembolism in older acute medical patients: randomised placebo controlled trial. BMJ. 2006 Feb 11;332(7537):325-329.
Choose Your Exam Rules
Physicians only should perform patient examinations based upon the presenting problem and the standard of care. As mentioned in my previous column (April 2008, p. 21), the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA) set forth two sets of documentation guidelines. The biggest difference between them is the exam component.
1995 Guidelines
The 1995 guidelines distinguish 10 body areas (head and face; neck; chest, breast, and axillae; abdomen; genitalia, groin, and buttocks; back and spine; right upper extremity; left upper extremity; right lower extremity; and left lower extremity) from 12 organ systems (constitutional; eyes; ears, nose, mouth, and throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary; neurological; psychiatric; hematologic, lymphatic, and immunologic).
Further, these guidelines let physicians document their findings in any manner while adhering to some simple rules:
- Document relevant negative findings. Commenting that a system or area is “negative” or “normal” is acceptable when referring to unaffected areas or asymptomatic organ systems; and
- Elaborate on abnormal findings. Commenting that a system or area is “abnormal” is not sufficient unless additional comments describing the abnormality are documented.
1997 Guidelines
The 1997 guidelines comprise bulleted items—referred to as elements—that correspond to each organ system. Some elements specify numeric criterion that must be met to credit the physician for documentation of that element.
For example, the physician only receives credit for documentation of vital signs (an element of the constitutional system) when three measurements are referenced (e.g., blood pressure, heart rate, and respiratory rate). Documentation that does not include three measurements or only contains a single generalized comment (e.g., vital signs stable) cannot be credited to the physician in the 1997 guidelines—even though these same comments are credited when applying the 1995 guidelines.
This logic also applies to the lymphatic system. The physician must identify findings associated with at least two lymphatic areas examined (e.g., “no lymphadenopathy of the neck or axillae”).
Elements that do not contain numeric criterion but identify multiple components require documentation of at least one component. For example, one psychiatric element involves the assessment of the patient’s “mood and affect.” If the physician comments that the patient appears depressed but does not comment on a flat (or normal) affect, the physician still receives credit for this exam element.
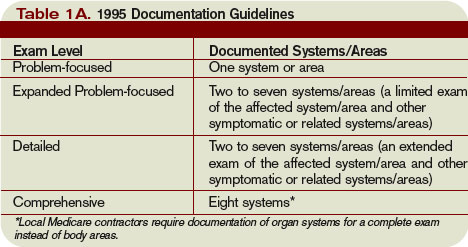
Levels of Exam
There are four levels of exam, determined by the number of elements documented in the progress note (see Tables 1A and 1B, p. below).
As with the history component, the physician must meet the requirements for a particular level of exam before assigning it. The most problematic feature of the 1995 guidelines involves the “detailed” exam. Both the expanded problem-focused and detailed exams involve two to seven systems/areas, but the detailed exam requires an “extended” exam of the affected system/area related to the presenting problem. Questions surround the number of elements needed to qualify as an “extended” exam of the affected system/area.
Does “regular rate and rhythm; normal S1, S2; no jugular venous distention; no murmur, gallop, or rub; peripheral pulses intact; no edema noted” constitute an “extended” exam of the cardiovascular system, or should there be an additional comment regarding the abdominal aorta? This decision is left to the discretion of the local Medicare contractor and/or the medical reviewer.
Since no other CMS directive has been provided, documentation of the detailed exam continues to be inconsistent. More importantly, review and audit of the detailed exam remains arbitrary. Some Medicare contractors suggest using the 1997 requirements for the detailed exam, while others create their own definition and corresponding number of exam elements needed for documentation of the detailed exam. This issue exemplifies the ambiguity for which the 1995 guidelines often are criticized.
Meanwhile, the 1997 guidelines often are criticized as too specific. While this may help the medical reviewer/auditor, it hinders the physician. Physicians are frequently frustrated trying to remember the explicit comments and number of elements associated with a particular level of exam.
One solution is documentation templates. Physicians can use paper or electronic templates that incorporate cues and prompts for normal exam findings, incorporating adequate space to elaborate abnormal findings.
Remember the physician has the option of utilizing either the 1995 or 1997 guidelines, depending upon which set he perceives as easier to implement.
Additionally, auditors must review physician documentation using both the 1995 and 1997 guidelines, and apply the most favorable result to the final audit score.
Each type of evaluation and management service identifies a specific level of exam that must be documented in the medical record before the associated CPT code is submitted on a claim.
The most common visit categories provided by hospitalists and corresponding exam levels are outlined in Table 2 (above). Similar to the history component, other visit categories, such as critical care and discharge day management, do not have specified levels of exam or associated documentation requirements for physical exam elements. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Physicians only should perform patient examinations based upon the presenting problem and the standard of care. As mentioned in my previous column (April 2008, p. 21), the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA) set forth two sets of documentation guidelines. The biggest difference between them is the exam component.
1995 Guidelines
The 1995 guidelines distinguish 10 body areas (head and face; neck; chest, breast, and axillae; abdomen; genitalia, groin, and buttocks; back and spine; right upper extremity; left upper extremity; right lower extremity; and left lower extremity) from 12 organ systems (constitutional; eyes; ears, nose, mouth, and throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary; neurological; psychiatric; hematologic, lymphatic, and immunologic).
Further, these guidelines let physicians document their findings in any manner while adhering to some simple rules:
- Document relevant negative findings. Commenting that a system or area is “negative” or “normal” is acceptable when referring to unaffected areas or asymptomatic organ systems; and
- Elaborate on abnormal findings. Commenting that a system or area is “abnormal” is not sufficient unless additional comments describing the abnormality are documented.
1997 Guidelines
The 1997 guidelines comprise bulleted items—referred to as elements—that correspond to each organ system. Some elements specify numeric criterion that must be met to credit the physician for documentation of that element.
For example, the physician only receives credit for documentation of vital signs (an element of the constitutional system) when three measurements are referenced (e.g., blood pressure, heart rate, and respiratory rate). Documentation that does not include three measurements or only contains a single generalized comment (e.g., vital signs stable) cannot be credited to the physician in the 1997 guidelines—even though these same comments are credited when applying the 1995 guidelines.
This logic also applies to the lymphatic system. The physician must identify findings associated with at least two lymphatic areas examined (e.g., “no lymphadenopathy of the neck or axillae”).
Elements that do not contain numeric criterion but identify multiple components require documentation of at least one component. For example, one psychiatric element involves the assessment of the patient’s “mood and affect.” If the physician comments that the patient appears depressed but does not comment on a flat (or normal) affect, the physician still receives credit for this exam element.
Levels of Exam
There are four levels of exam, determined by the number of elements documented in the progress note (see Tables 1A and 1B, p. below).
As with the history component, the physician must meet the requirements for a particular level of exam before assigning it. The most problematic feature of the 1995 guidelines involves the “detailed” exam. Both the expanded problem-focused and detailed exams involve two to seven systems/areas, but the detailed exam requires an “extended” exam of the affected system/area related to the presenting problem. Questions surround the number of elements needed to qualify as an “extended” exam of the affected system/area.
Does “regular rate and rhythm; normal S1, S2; no jugular venous distention; no murmur, gallop, or rub; peripheral pulses intact; no edema noted” constitute an “extended” exam of the cardiovascular system, or should there be an additional comment regarding the abdominal aorta? This decision is left to the discretion of the local Medicare contractor and/or the medical reviewer.
Since no other CMS directive has been provided, documentation of the detailed exam continues to be inconsistent. More importantly, review and audit of the detailed exam remains arbitrary. Some Medicare contractors suggest using the 1997 requirements for the detailed exam, while others create their own definition and corresponding number of exam elements needed for documentation of the detailed exam. This issue exemplifies the ambiguity for which the 1995 guidelines often are criticized.
Meanwhile, the 1997 guidelines often are criticized as too specific. While this may help the medical reviewer/auditor, it hinders the physician. Physicians are frequently frustrated trying to remember the explicit comments and number of elements associated with a particular level of exam.
One solution is documentation templates. Physicians can use paper or electronic templates that incorporate cues and prompts for normal exam findings, incorporating adequate space to elaborate abnormal findings.
Remember the physician has the option of utilizing either the 1995 or 1997 guidelines, depending upon which set he perceives as easier to implement.
Additionally, auditors must review physician documentation using both the 1995 and 1997 guidelines, and apply the most favorable result to the final audit score.
Each type of evaluation and management service identifies a specific level of exam that must be documented in the medical record before the associated CPT code is submitted on a claim.
The most common visit categories provided by hospitalists and corresponding exam levels are outlined in Table 2 (above). Similar to the history component, other visit categories, such as critical care and discharge day management, do not have specified levels of exam or associated documentation requirements for physical exam elements. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Physicians only should perform patient examinations based upon the presenting problem and the standard of care. As mentioned in my previous column (April 2008, p. 21), the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA) set forth two sets of documentation guidelines. The biggest difference between them is the exam component.
1995 Guidelines
The 1995 guidelines distinguish 10 body areas (head and face; neck; chest, breast, and axillae; abdomen; genitalia, groin, and buttocks; back and spine; right upper extremity; left upper extremity; right lower extremity; and left lower extremity) from 12 organ systems (constitutional; eyes; ears, nose, mouth, and throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary; neurological; psychiatric; hematologic, lymphatic, and immunologic).
Further, these guidelines let physicians document their findings in any manner while adhering to some simple rules:
- Document relevant negative findings. Commenting that a system or area is “negative” or “normal” is acceptable when referring to unaffected areas or asymptomatic organ systems; and
- Elaborate on abnormal findings. Commenting that a system or area is “abnormal” is not sufficient unless additional comments describing the abnormality are documented.
1997 Guidelines
The 1997 guidelines comprise bulleted items—referred to as elements—that correspond to each organ system. Some elements specify numeric criterion that must be met to credit the physician for documentation of that element.
For example, the physician only receives credit for documentation of vital signs (an element of the constitutional system) when three measurements are referenced (e.g., blood pressure, heart rate, and respiratory rate). Documentation that does not include three measurements or only contains a single generalized comment (e.g., vital signs stable) cannot be credited to the physician in the 1997 guidelines—even though these same comments are credited when applying the 1995 guidelines.
This logic also applies to the lymphatic system. The physician must identify findings associated with at least two lymphatic areas examined (e.g., “no lymphadenopathy of the neck or axillae”).
Elements that do not contain numeric criterion but identify multiple components require documentation of at least one component. For example, one psychiatric element involves the assessment of the patient’s “mood and affect.” If the physician comments that the patient appears depressed but does not comment on a flat (or normal) affect, the physician still receives credit for this exam element.
Levels of Exam
There are four levels of exam, determined by the number of elements documented in the progress note (see Tables 1A and 1B, p. below).
As with the history component, the physician must meet the requirements for a particular level of exam before assigning it. The most problematic feature of the 1995 guidelines involves the “detailed” exam. Both the expanded problem-focused and detailed exams involve two to seven systems/areas, but the detailed exam requires an “extended” exam of the affected system/area related to the presenting problem. Questions surround the number of elements needed to qualify as an “extended” exam of the affected system/area.
Does “regular rate and rhythm; normal S1, S2; no jugular venous distention; no murmur, gallop, or rub; peripheral pulses intact; no edema noted” constitute an “extended” exam of the cardiovascular system, or should there be an additional comment regarding the abdominal aorta? This decision is left to the discretion of the local Medicare contractor and/or the medical reviewer.
Since no other CMS directive has been provided, documentation of the detailed exam continues to be inconsistent. More importantly, review and audit of the detailed exam remains arbitrary. Some Medicare contractors suggest using the 1997 requirements for the detailed exam, while others create their own definition and corresponding number of exam elements needed for documentation of the detailed exam. This issue exemplifies the ambiguity for which the 1995 guidelines often are criticized.
Meanwhile, the 1997 guidelines often are criticized as too specific. While this may help the medical reviewer/auditor, it hinders the physician. Physicians are frequently frustrated trying to remember the explicit comments and number of elements associated with a particular level of exam.
One solution is documentation templates. Physicians can use paper or electronic templates that incorporate cues and prompts for normal exam findings, incorporating adequate space to elaborate abnormal findings.
Remember the physician has the option of utilizing either the 1995 or 1997 guidelines, depending upon which set he perceives as easier to implement.
Additionally, auditors must review physician documentation using both the 1995 and 1997 guidelines, and apply the most favorable result to the final audit score.
Each type of evaluation and management service identifies a specific level of exam that must be documented in the medical record before the associated CPT code is submitted on a claim.
The most common visit categories provided by hospitalists and corresponding exam levels are outlined in Table 2 (above). Similar to the history component, other visit categories, such as critical care and discharge day management, do not have specified levels of exam or associated documentation requirements for physical exam elements. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
No Fee for Errors
State governments, private payors, Medicare, and hospitals have reached the same conclusion: Hospitals should not charge for preventable medical errors.
One of the latest entities to join this trend is Washington state. Early this year, healthcare associations there passed a resolution saying Washington healthcare providers no longer will charge for preventable hospital errors. The resolution applies to 28 “never events” published by the National Quality Forum (NQF). These are medical errors that clearly are identifiable, preventable, serious in their consequences for patients, and indicative of a real problem in the safety and credibility of a healthcare facility. (For a complete list of events, visit NQF’s Web site (www.qualityforum.org/pdf/news/prSeriousReportableEvents10-15-06.pdf).
Hospitals in Massachusetts, Minnesota, Pennsylvania, and Vermont have adopted similar policies. Private insurers Aetna, Wellpoint, and Blue Cross Blue Shield each are taking steps toward refusing payment for treatment resulting from serious medical errors in hospitals.
Amid these decisions, the American Hospital Association (AHA) released a quality advisory Feb. 12, recommending hospitals implement a no-charge policy for serious adverse errors.
“There’s certainly been a lot of conversation about aligning payment around outcomes,” says Nancy E. Foster, the AHA’s vice president for quality and patient safety policy. “Most of those conversations have focused on reward for doing the right thing, but there were certainly parts of those conversations based on the notion of who’s responsible and who pays when something that was preventable did happen.”
Even the federal government has gotten involved. Beginning in October, the Centers for Medicare and Medicaid Services (CMS) plans to no longer reimburse for specific preventable conditions.
CMS “Stop Payments”
If Congress approves Medicare’s plan, the CMS will not pay any extra-care costs for eight conditions unless they were present upon admission—and it prohibits hospitals from charging patients for such conditions. The conditions include three “never events”:
- Objects left in the body during surgery (“never event”);
- Air embolism (“never event”);
- Blood incompatibility (“never event”);
- Falls;
- Catheter-associated urinary tract infections;
- Pressure ulcers (decubitus ulcers);
- Vascular catheter-associated infection; and
- Surgical site infection after coronary artery bypass graft surgery (mediastinitis).
Next year, the CMS plans to add more conditions to the no-pay list. The most likely additions are ventilator-associated pneumonia, staphylococcus aureus septicemia, deep-vein thrombosis (DVT), and pulmonary embolism.
The CMS rule obviously directly affects hospital income, which will affect hospital processes and staff.
“As hospitalists, this affects us,” says Winthrop F. Whitcomb, MD, director of clinical performance improvement at Mercy Medical Center in Springfield, Mass., director of hospital medicine at Catholic Health East, and co-founder of SHM. “It’s another thing showcasing the value of hospitalists because we tend to document well. When a patient comes in with DVT or a pressure ulcer, we tend to document that, and that will help our hospitals.”
Other physicians may balk at hospital requests to amend or add to their notes to ensure payment, but, says Dr. Whitcomb: “Hospitalists understand the requirement for documentation. If you’re not a hospitalist, you may not be happy to be asked to change your documentation so that the hospital can get paid more, but we understand how important this is.”
Hospitals likely will continue to closely oversee physician documentation on Medicare patients.
“At our hospital, we [already] work with coders,” Dr. Whitcomb says. “I’ve heard of this more and more. They round with us now on every Medicare patient and review the charts. They actually write a formal note that prompts us to document accurately—they may ask us to amend that something was present on admission.” Dr. Whitcomb’s hospital has a paper-based system for this information; an electronic system will include this type of prompt. “Electronic prompts can be customized, but they can also be ignored; prompt fatigue is a big issue,” Dr. Whitcomb warns.
Another potential effect on hospitalists will be involvement in hospital efforts to prevent the eight conditions.
“The CMS change is definitely going to up the ante for quality improvement and patient safety work, no matter who undertakes it,” Dr. Whitcomb says. “It should expand opportunities for hospitalists to work in [quality improvement]. Hospitalists may end up leading teams to specifically address certain never events. The good news is, it gets right at the bottom line of the hospital, so nonclinicians like administrators in the financial office will immediately understand the importance of work like this.”
Leaving a sponge inside a patient is clearly a preventable medical error—but what about pressure ulcers? Or DVT?
In his “Wachter’s World” blog post of Feb. 11 (www.wachtersworld.org), Robert Wachter, MD, professor and associate chairman of the Department of Medicine at the University of California, San Francisco, addressed the CMS rule.
“For some of the events on the Medicare list, particularly the infections (such as catheter-related bloodstream infections), there is good evidence that the vast majority of events can be prevented,” Dr. Wachter wrote. “For others, such as pressure ulcers and falls, although some commonsensical practices have been widely promoted (particularly through IHI’s 5 Million Lives campaign), the evidence linking adherence to ‘prevention practices’ and reductions in adverse events is tenuous. These adverse events should stay off the list until the evidence is stronger.”
In spite of his misgivings, Dr. Wachter is a strong proponent of the trend toward nonpayment for preventable errors. “We’ve already seen hospitals putting far more resources into trying to prevent line infections, falls, and [pressure ulcers] than they were before,” he says. “And remember that the dollars at stake are relatively small. The extra payments for “Complicating Conditions” (CC) are not enormous, and many patients who have one CC have more than one; in which case, the hospital will still receive the extra payment even if the adverse event-related payment is denied. So, in essence the policy is creating an unusual amount of patient safety momentum for a relatively small displacement of dollars – a pretty clever trick.”
For more information on the CMS rule, read “Medicare’s decision to withhold payment for hospital errors: the devil is in the details,” by Dr. Wachter, Nancy Foster, and Adams Dudley, MD, in the February 2008 Joint Commission Journal of Quality and Patient Safety. TH
Jane Jerrard is a medical writer based in Chicago.
State governments, private payors, Medicare, and hospitals have reached the same conclusion: Hospitals should not charge for preventable medical errors.
One of the latest entities to join this trend is Washington state. Early this year, healthcare associations there passed a resolution saying Washington healthcare providers no longer will charge for preventable hospital errors. The resolution applies to 28 “never events” published by the National Quality Forum (NQF). These are medical errors that clearly are identifiable, preventable, serious in their consequences for patients, and indicative of a real problem in the safety and credibility of a healthcare facility. (For a complete list of events, visit NQF’s Web site (www.qualityforum.org/pdf/news/prSeriousReportableEvents10-15-06.pdf).
Hospitals in Massachusetts, Minnesota, Pennsylvania, and Vermont have adopted similar policies. Private insurers Aetna, Wellpoint, and Blue Cross Blue Shield each are taking steps toward refusing payment for treatment resulting from serious medical errors in hospitals.
Amid these decisions, the American Hospital Association (AHA) released a quality advisory Feb. 12, recommending hospitals implement a no-charge policy for serious adverse errors.
“There’s certainly been a lot of conversation about aligning payment around outcomes,” says Nancy E. Foster, the AHA’s vice president for quality and patient safety policy. “Most of those conversations have focused on reward for doing the right thing, but there were certainly parts of those conversations based on the notion of who’s responsible and who pays when something that was preventable did happen.”
Even the federal government has gotten involved. Beginning in October, the Centers for Medicare and Medicaid Services (CMS) plans to no longer reimburse for specific preventable conditions.
CMS “Stop Payments”
If Congress approves Medicare’s plan, the CMS will not pay any extra-care costs for eight conditions unless they were present upon admission—and it prohibits hospitals from charging patients for such conditions. The conditions include three “never events”:
- Objects left in the body during surgery (“never event”);
- Air embolism (“never event”);
- Blood incompatibility (“never event”);
- Falls;
- Catheter-associated urinary tract infections;
- Pressure ulcers (decubitus ulcers);
- Vascular catheter-associated infection; and
- Surgical site infection after coronary artery bypass graft surgery (mediastinitis).
Next year, the CMS plans to add more conditions to the no-pay list. The most likely additions are ventilator-associated pneumonia, staphylococcus aureus septicemia, deep-vein thrombosis (DVT), and pulmonary embolism.
The CMS rule obviously directly affects hospital income, which will affect hospital processes and staff.
“As hospitalists, this affects us,” says Winthrop F. Whitcomb, MD, director of clinical performance improvement at Mercy Medical Center in Springfield, Mass., director of hospital medicine at Catholic Health East, and co-founder of SHM. “It’s another thing showcasing the value of hospitalists because we tend to document well. When a patient comes in with DVT or a pressure ulcer, we tend to document that, and that will help our hospitals.”
Other physicians may balk at hospital requests to amend or add to their notes to ensure payment, but, says Dr. Whitcomb: “Hospitalists understand the requirement for documentation. If you’re not a hospitalist, you may not be happy to be asked to change your documentation so that the hospital can get paid more, but we understand how important this is.”
Hospitals likely will continue to closely oversee physician documentation on Medicare patients.
“At our hospital, we [already] work with coders,” Dr. Whitcomb says. “I’ve heard of this more and more. They round with us now on every Medicare patient and review the charts. They actually write a formal note that prompts us to document accurately—they may ask us to amend that something was present on admission.” Dr. Whitcomb’s hospital has a paper-based system for this information; an electronic system will include this type of prompt. “Electronic prompts can be customized, but they can also be ignored; prompt fatigue is a big issue,” Dr. Whitcomb warns.
Another potential effect on hospitalists will be involvement in hospital efforts to prevent the eight conditions.
“The CMS change is definitely going to up the ante for quality improvement and patient safety work, no matter who undertakes it,” Dr. Whitcomb says. “It should expand opportunities for hospitalists to work in [quality improvement]. Hospitalists may end up leading teams to specifically address certain never events. The good news is, it gets right at the bottom line of the hospital, so nonclinicians like administrators in the financial office will immediately understand the importance of work like this.”
Leaving a sponge inside a patient is clearly a preventable medical error—but what about pressure ulcers? Or DVT?
In his “Wachter’s World” blog post of Feb. 11 (www.wachtersworld.org), Robert Wachter, MD, professor and associate chairman of the Department of Medicine at the University of California, San Francisco, addressed the CMS rule.
“For some of the events on the Medicare list, particularly the infections (such as catheter-related bloodstream infections), there is good evidence that the vast majority of events can be prevented,” Dr. Wachter wrote. “For others, such as pressure ulcers and falls, although some commonsensical practices have been widely promoted (particularly through IHI’s 5 Million Lives campaign), the evidence linking adherence to ‘prevention practices’ and reductions in adverse events is tenuous. These adverse events should stay off the list until the evidence is stronger.”
In spite of his misgivings, Dr. Wachter is a strong proponent of the trend toward nonpayment for preventable errors. “We’ve already seen hospitals putting far more resources into trying to prevent line infections, falls, and [pressure ulcers] than they were before,” he says. “And remember that the dollars at stake are relatively small. The extra payments for “Complicating Conditions” (CC) are not enormous, and many patients who have one CC have more than one; in which case, the hospital will still receive the extra payment even if the adverse event-related payment is denied. So, in essence the policy is creating an unusual amount of patient safety momentum for a relatively small displacement of dollars – a pretty clever trick.”
For more information on the CMS rule, read “Medicare’s decision to withhold payment for hospital errors: the devil is in the details,” by Dr. Wachter, Nancy Foster, and Adams Dudley, MD, in the February 2008 Joint Commission Journal of Quality and Patient Safety. TH
Jane Jerrard is a medical writer based in Chicago.
State governments, private payors, Medicare, and hospitals have reached the same conclusion: Hospitals should not charge for preventable medical errors.
One of the latest entities to join this trend is Washington state. Early this year, healthcare associations there passed a resolution saying Washington healthcare providers no longer will charge for preventable hospital errors. The resolution applies to 28 “never events” published by the National Quality Forum (NQF). These are medical errors that clearly are identifiable, preventable, serious in their consequences for patients, and indicative of a real problem in the safety and credibility of a healthcare facility. (For a complete list of events, visit NQF’s Web site (www.qualityforum.org/pdf/news/prSeriousReportableEvents10-15-06.pdf).
Hospitals in Massachusetts, Minnesota, Pennsylvania, and Vermont have adopted similar policies. Private insurers Aetna, Wellpoint, and Blue Cross Blue Shield each are taking steps toward refusing payment for treatment resulting from serious medical errors in hospitals.
Amid these decisions, the American Hospital Association (AHA) released a quality advisory Feb. 12, recommending hospitals implement a no-charge policy for serious adverse errors.
“There’s certainly been a lot of conversation about aligning payment around outcomes,” says Nancy E. Foster, the AHA’s vice president for quality and patient safety policy. “Most of those conversations have focused on reward for doing the right thing, but there were certainly parts of those conversations based on the notion of who’s responsible and who pays when something that was preventable did happen.”
Even the federal government has gotten involved. Beginning in October, the Centers for Medicare and Medicaid Services (CMS) plans to no longer reimburse for specific preventable conditions.
CMS “Stop Payments”
If Congress approves Medicare’s plan, the CMS will not pay any extra-care costs for eight conditions unless they were present upon admission—and it prohibits hospitals from charging patients for such conditions. The conditions include three “never events”:
- Objects left in the body during surgery (“never event”);
- Air embolism (“never event”);
- Blood incompatibility (“never event”);
- Falls;
- Catheter-associated urinary tract infections;
- Pressure ulcers (decubitus ulcers);
- Vascular catheter-associated infection; and
- Surgical site infection after coronary artery bypass graft surgery (mediastinitis).
Next year, the CMS plans to add more conditions to the no-pay list. The most likely additions are ventilator-associated pneumonia, staphylococcus aureus septicemia, deep-vein thrombosis (DVT), and pulmonary embolism.
The CMS rule obviously directly affects hospital income, which will affect hospital processes and staff.
“As hospitalists, this affects us,” says Winthrop F. Whitcomb, MD, director of clinical performance improvement at Mercy Medical Center in Springfield, Mass., director of hospital medicine at Catholic Health East, and co-founder of SHM. “It’s another thing showcasing the value of hospitalists because we tend to document well. When a patient comes in with DVT or a pressure ulcer, we tend to document that, and that will help our hospitals.”
Other physicians may balk at hospital requests to amend or add to their notes to ensure payment, but, says Dr. Whitcomb: “Hospitalists understand the requirement for documentation. If you’re not a hospitalist, you may not be happy to be asked to change your documentation so that the hospital can get paid more, but we understand how important this is.”
Hospitals likely will continue to closely oversee physician documentation on Medicare patients.
“At our hospital, we [already] work with coders,” Dr. Whitcomb says. “I’ve heard of this more and more. They round with us now on every Medicare patient and review the charts. They actually write a formal note that prompts us to document accurately—they may ask us to amend that something was present on admission.” Dr. Whitcomb’s hospital has a paper-based system for this information; an electronic system will include this type of prompt. “Electronic prompts can be customized, but they can also be ignored; prompt fatigue is a big issue,” Dr. Whitcomb warns.
Another potential effect on hospitalists will be involvement in hospital efforts to prevent the eight conditions.
“The CMS change is definitely going to up the ante for quality improvement and patient safety work, no matter who undertakes it,” Dr. Whitcomb says. “It should expand opportunities for hospitalists to work in [quality improvement]. Hospitalists may end up leading teams to specifically address certain never events. The good news is, it gets right at the bottom line of the hospital, so nonclinicians like administrators in the financial office will immediately understand the importance of work like this.”
Leaving a sponge inside a patient is clearly a preventable medical error—but what about pressure ulcers? Or DVT?
In his “Wachter’s World” blog post of Feb. 11 (www.wachtersworld.org), Robert Wachter, MD, professor and associate chairman of the Department of Medicine at the University of California, San Francisco, addressed the CMS rule.
“For some of the events on the Medicare list, particularly the infections (such as catheter-related bloodstream infections), there is good evidence that the vast majority of events can be prevented,” Dr. Wachter wrote. “For others, such as pressure ulcers and falls, although some commonsensical practices have been widely promoted (particularly through IHI’s 5 Million Lives campaign), the evidence linking adherence to ‘prevention practices’ and reductions in adverse events is tenuous. These adverse events should stay off the list until the evidence is stronger.”
In spite of his misgivings, Dr. Wachter is a strong proponent of the trend toward nonpayment for preventable errors. “We’ve already seen hospitals putting far more resources into trying to prevent line infections, falls, and [pressure ulcers] than they were before,” he says. “And remember that the dollars at stake are relatively small. The extra payments for “Complicating Conditions” (CC) are not enormous, and many patients who have one CC have more than one; in which case, the hospital will still receive the extra payment even if the adverse event-related payment is denied. So, in essence the policy is creating an unusual amount of patient safety momentum for a relatively small displacement of dollars – a pretty clever trick.”
For more information on the CMS rule, read “Medicare’s decision to withhold payment for hospital errors: the devil is in the details,” by Dr. Wachter, Nancy Foster, and Adams Dudley, MD, in the February 2008 Joint Commission Journal of Quality and Patient Safety. TH
Jane Jerrard is a medical writer based in Chicago.
Mentorship Essentials
You may have had a mentor as a resident and possibly in your first year as a hospitalist, but don’t count out these valuable resources as you continue in your career. And don’t count out mentors who may come from other walks of life.
“It’s natural for physicians to look toward other physicians for guidance,” says Russell L. Holman, MD, chief operating officer for Cogent Healthcare, Nashville. “For physicians, including hospitalists, their natural inclination is to seek mentors who are physicians or have a similar training background. While there are many great physician mentors, you may be limiting yourself and missing opportunities that come from broader mentoring.”
Informal mentoring relationships are an excellent way to learn all sorts of leadership skills, from the subtle—like handling complains about a physician’s constant body odor—to hard skills, such as putting together a budget for your department or practice.
—Russell L. Holman, MD, chief operating officer, Cogent Healthcare, Nashville
Management Mentors
Dr. Holman identified people at various stages in his career who could impart skills he sought, from a vice president of [human relations] for an integrated health system who steered him on personnel management and leadership development, to a carpenter-turned-attorney who helped him hone critical thinking skills.
“Talking to a mentor can show you the fresh side of new or old situations,” says Dr. Holman. “And you can feel comfortable telling them things that you wouldn’t tell anyone else. [When] you don’t work together, it provides a safe harbor to express ideas and opinions you normally wouldn’t.”
Mary Jo Gorman, MD, MBA, chief executive officer of Advanced ICU Care in St. Louis, Mo., agrees. “If you want someone to bounce ideas off of, try to find someone outside your organization,” she advises. She recommends physician organizations such as SHM: “Find someone who will listen, can keep their mouth shut and give you some honest feedback. For that reason, I’m a fan of professional coaches and career counselors. They provide an objective and unbiased audience and can suggest straightforward ways to manage sensitive issues.”
You also can find valuable mentors inside your workplace. “An often overlooked resource for hospitalist leaders is the other managers in their facilities,” says Dr. Gorman. “When I was a new manager, one of my mentors was the director of nursing. We could toss ideas back and forth, and she knew the politics and the personalities of the place, knew what mattered and what didn’t, and could steer me in the right direction.”
The managers and directors you work with, regardless of whether they’re physicians, are likely to have a lot of management experience, and can be resources for on-the-spot advice and guidance.
“Depending on the situation, even a chief operating officer or CEO of your hospital can give you good ideas and help you,” adds Dr. Gorman. “You’re a hospitalist; they’re supposed to be on your side. And they may be just five or 10 years older than you, but they have a lot of people management experience under their belts.”
They’re Everywhere
If you look beyond physicians and other healthcare professionals, finding an informal mentor is simply a matter of keeping your eyes and your mind open.
“You find a mentor by being in different situations,” Dr. Holman says. “Take advantage of getting to know people in different spheres, see what makes them tick that you can learn and apply to yourself.”
Consider all aspects of your life outside the workplace—your neighborhood, your church, your children’s school, any organizations you volunteer for, or social venues. Even your family—does anyone have management or business experience?
Keep your options open for learning from others, but if you have a specific area where you want to gain knowledge, you can search your circle of acquaintances to see who might be able to fill in that gap.
“Outside of healthcare, my personal accountant was a huge help,” says Dr. Gorman. “He sat down with me and helped me understand the financials I was supposed to do. You may have to pay for this service, but if you’re just asking for a few hours of their time and you have a good relationship, they’ll help you out.”
Regardless of what you want to learn, keep in mind that mentors can come in any shape and form. “A mentor can be someone younger than you, someone less well educated,” Dr. Holman points out. “What matters is when you recognize the value of the perspectives they bring.”
In fact, Dr. Holman says, he deliberately looks for people who are a little different from himself. “We tend to gravitate to those who are like us, but [in mentoring] this doesn’t lend itself to the greatest growth long-term,” he explains.
Make Mentoring Work
When you target someone as a potential mentor, it’s best to start with occasional questions and keep the relationship casual.
“My experience—and this is supported by literature—is that mentoring relationships are most solid when they form naturally,” Dr. Holman says. “The mentorship arena lends itself to flexibility and informal structure.”
Dr. Gorman agrees, suggesting that you not even mention “the M word.” “In my experience, asking someone flat out if they’ll be your mentor doesn’t really work,” Dr. Gorman says. “It sounds like a big commitment, and they shy away from it. Instead, I’d say just keep going back to the same people for guidance. Find those people who will listen to you and give you some help.”
Once you establish a mentoring relationship, try to find a way to return the favor—at least by being a good mentee.
“It’s particularly rewarding when mentoring is not one-sided, when each person has something to bring to the table,” Dr. Holman says. “Though it may be mostly one-sided, it’s good to be able to give some advice or counsel in return.”
Dr. Gorman adds that a good mentee either will act on advice or address why they didn’t. “No one likes to give advice just to see you blow it off, or head straight into a situation they warned you against,” she stresses. “Be respectful of their time, and be prepared when you present a problem. And be sure to thank them. You don’t have to send flowers or anything, just a verbal thank you for their time.”
No matter what stage your career is in, you can always pick up new skills and perspectives—particularly if you’re in a leadership position. Even if you feel you’re well established, finding new mentors can only make you better at what you do.
“You should always look for someone to learn from,” Dr. Gorman says. “They’re out there, no matter where you are or what you’re doing. Throw out some questions and see who you hit it off with, who gives you sound advice.” TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
You may have had a mentor as a resident and possibly in your first year as a hospitalist, but don’t count out these valuable resources as you continue in your career. And don’t count out mentors who may come from other walks of life.
“It’s natural for physicians to look toward other physicians for guidance,” says Russell L. Holman, MD, chief operating officer for Cogent Healthcare, Nashville. “For physicians, including hospitalists, their natural inclination is to seek mentors who are physicians or have a similar training background. While there are many great physician mentors, you may be limiting yourself and missing opportunities that come from broader mentoring.”
Informal mentoring relationships are an excellent way to learn all sorts of leadership skills, from the subtle—like handling complains about a physician’s constant body odor—to hard skills, such as putting together a budget for your department or practice.
—Russell L. Holman, MD, chief operating officer, Cogent Healthcare, Nashville
Management Mentors
Dr. Holman identified people at various stages in his career who could impart skills he sought, from a vice president of [human relations] for an integrated health system who steered him on personnel management and leadership development, to a carpenter-turned-attorney who helped him hone critical thinking skills.
“Talking to a mentor can show you the fresh side of new or old situations,” says Dr. Holman. “And you can feel comfortable telling them things that you wouldn’t tell anyone else. [When] you don’t work together, it provides a safe harbor to express ideas and opinions you normally wouldn’t.”
Mary Jo Gorman, MD, MBA, chief executive officer of Advanced ICU Care in St. Louis, Mo., agrees. “If you want someone to bounce ideas off of, try to find someone outside your organization,” she advises. She recommends physician organizations such as SHM: “Find someone who will listen, can keep their mouth shut and give you some honest feedback. For that reason, I’m a fan of professional coaches and career counselors. They provide an objective and unbiased audience and can suggest straightforward ways to manage sensitive issues.”
You also can find valuable mentors inside your workplace. “An often overlooked resource for hospitalist leaders is the other managers in their facilities,” says Dr. Gorman. “When I was a new manager, one of my mentors was the director of nursing. We could toss ideas back and forth, and she knew the politics and the personalities of the place, knew what mattered and what didn’t, and could steer me in the right direction.”
The managers and directors you work with, regardless of whether they’re physicians, are likely to have a lot of management experience, and can be resources for on-the-spot advice and guidance.
“Depending on the situation, even a chief operating officer or CEO of your hospital can give you good ideas and help you,” adds Dr. Gorman. “You’re a hospitalist; they’re supposed to be on your side. And they may be just five or 10 years older than you, but they have a lot of people management experience under their belts.”
They’re Everywhere
If you look beyond physicians and other healthcare professionals, finding an informal mentor is simply a matter of keeping your eyes and your mind open.
“You find a mentor by being in different situations,” Dr. Holman says. “Take advantage of getting to know people in different spheres, see what makes them tick that you can learn and apply to yourself.”
Consider all aspects of your life outside the workplace—your neighborhood, your church, your children’s school, any organizations you volunteer for, or social venues. Even your family—does anyone have management or business experience?
Keep your options open for learning from others, but if you have a specific area where you want to gain knowledge, you can search your circle of acquaintances to see who might be able to fill in that gap.
“Outside of healthcare, my personal accountant was a huge help,” says Dr. Gorman. “He sat down with me and helped me understand the financials I was supposed to do. You may have to pay for this service, but if you’re just asking for a few hours of their time and you have a good relationship, they’ll help you out.”
Regardless of what you want to learn, keep in mind that mentors can come in any shape and form. “A mentor can be someone younger than you, someone less well educated,” Dr. Holman points out. “What matters is when you recognize the value of the perspectives they bring.”
In fact, Dr. Holman says, he deliberately looks for people who are a little different from himself. “We tend to gravitate to those who are like us, but [in mentoring] this doesn’t lend itself to the greatest growth long-term,” he explains.
Make Mentoring Work
When you target someone as a potential mentor, it’s best to start with occasional questions and keep the relationship casual.
“My experience—and this is supported by literature—is that mentoring relationships are most solid when they form naturally,” Dr. Holman says. “The mentorship arena lends itself to flexibility and informal structure.”
Dr. Gorman agrees, suggesting that you not even mention “the M word.” “In my experience, asking someone flat out if they’ll be your mentor doesn’t really work,” Dr. Gorman says. “It sounds like a big commitment, and they shy away from it. Instead, I’d say just keep going back to the same people for guidance. Find those people who will listen to you and give you some help.”
Once you establish a mentoring relationship, try to find a way to return the favor—at least by being a good mentee.
“It’s particularly rewarding when mentoring is not one-sided, when each person has something to bring to the table,” Dr. Holman says. “Though it may be mostly one-sided, it’s good to be able to give some advice or counsel in return.”
Dr. Gorman adds that a good mentee either will act on advice or address why they didn’t. “No one likes to give advice just to see you blow it off, or head straight into a situation they warned you against,” she stresses. “Be respectful of their time, and be prepared when you present a problem. And be sure to thank them. You don’t have to send flowers or anything, just a verbal thank you for their time.”
No matter what stage your career is in, you can always pick up new skills and perspectives—particularly if you’re in a leadership position. Even if you feel you’re well established, finding new mentors can only make you better at what you do.
“You should always look for someone to learn from,” Dr. Gorman says. “They’re out there, no matter where you are or what you’re doing. Throw out some questions and see who you hit it off with, who gives you sound advice.” TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
You may have had a mentor as a resident and possibly in your first year as a hospitalist, but don’t count out these valuable resources as you continue in your career. And don’t count out mentors who may come from other walks of life.
“It’s natural for physicians to look toward other physicians for guidance,” says Russell L. Holman, MD, chief operating officer for Cogent Healthcare, Nashville. “For physicians, including hospitalists, their natural inclination is to seek mentors who are physicians or have a similar training background. While there are many great physician mentors, you may be limiting yourself and missing opportunities that come from broader mentoring.”
Informal mentoring relationships are an excellent way to learn all sorts of leadership skills, from the subtle—like handling complains about a physician’s constant body odor—to hard skills, such as putting together a budget for your department or practice.
—Russell L. Holman, MD, chief operating officer, Cogent Healthcare, Nashville
Management Mentors
Dr. Holman identified people at various stages in his career who could impart skills he sought, from a vice president of [human relations] for an integrated health system who steered him on personnel management and leadership development, to a carpenter-turned-attorney who helped him hone critical thinking skills.
“Talking to a mentor can show you the fresh side of new or old situations,” says Dr. Holman. “And you can feel comfortable telling them things that you wouldn’t tell anyone else. [When] you don’t work together, it provides a safe harbor to express ideas and opinions you normally wouldn’t.”
Mary Jo Gorman, MD, MBA, chief executive officer of Advanced ICU Care in St. Louis, Mo., agrees. “If you want someone to bounce ideas off of, try to find someone outside your organization,” she advises. She recommends physician organizations such as SHM: “Find someone who will listen, can keep their mouth shut and give you some honest feedback. For that reason, I’m a fan of professional coaches and career counselors. They provide an objective and unbiased audience and can suggest straightforward ways to manage sensitive issues.”
You also can find valuable mentors inside your workplace. “An often overlooked resource for hospitalist leaders is the other managers in their facilities,” says Dr. Gorman. “When I was a new manager, one of my mentors was the director of nursing. We could toss ideas back and forth, and she knew the politics and the personalities of the place, knew what mattered and what didn’t, and could steer me in the right direction.”
The managers and directors you work with, regardless of whether they’re physicians, are likely to have a lot of management experience, and can be resources for on-the-spot advice and guidance.
“Depending on the situation, even a chief operating officer or CEO of your hospital can give you good ideas and help you,” adds Dr. Gorman. “You’re a hospitalist; they’re supposed to be on your side. And they may be just five or 10 years older than you, but they have a lot of people management experience under their belts.”
They’re Everywhere
If you look beyond physicians and other healthcare professionals, finding an informal mentor is simply a matter of keeping your eyes and your mind open.
“You find a mentor by being in different situations,” Dr. Holman says. “Take advantage of getting to know people in different spheres, see what makes them tick that you can learn and apply to yourself.”
Consider all aspects of your life outside the workplace—your neighborhood, your church, your children’s school, any organizations you volunteer for, or social venues. Even your family—does anyone have management or business experience?
Keep your options open for learning from others, but if you have a specific area where you want to gain knowledge, you can search your circle of acquaintances to see who might be able to fill in that gap.
“Outside of healthcare, my personal accountant was a huge help,” says Dr. Gorman. “He sat down with me and helped me understand the financials I was supposed to do. You may have to pay for this service, but if you’re just asking for a few hours of their time and you have a good relationship, they’ll help you out.”
Regardless of what you want to learn, keep in mind that mentors can come in any shape and form. “A mentor can be someone younger than you, someone less well educated,” Dr. Holman points out. “What matters is when you recognize the value of the perspectives they bring.”
In fact, Dr. Holman says, he deliberately looks for people who are a little different from himself. “We tend to gravitate to those who are like us, but [in mentoring] this doesn’t lend itself to the greatest growth long-term,” he explains.
Make Mentoring Work
When you target someone as a potential mentor, it’s best to start with occasional questions and keep the relationship casual.
“My experience—and this is supported by literature—is that mentoring relationships are most solid when they form naturally,” Dr. Holman says. “The mentorship arena lends itself to flexibility and informal structure.”
Dr. Gorman agrees, suggesting that you not even mention “the M word.” “In my experience, asking someone flat out if they’ll be your mentor doesn’t really work,” Dr. Gorman says. “It sounds like a big commitment, and they shy away from it. Instead, I’d say just keep going back to the same people for guidance. Find those people who will listen to you and give you some help.”
Once you establish a mentoring relationship, try to find a way to return the favor—at least by being a good mentee.
“It’s particularly rewarding when mentoring is not one-sided, when each person has something to bring to the table,” Dr. Holman says. “Though it may be mostly one-sided, it’s good to be able to give some advice or counsel in return.”
Dr. Gorman adds that a good mentee either will act on advice or address why they didn’t. “No one likes to give advice just to see you blow it off, or head straight into a situation they warned you against,” she stresses. “Be respectful of their time, and be prepared when you present a problem. And be sure to thank them. You don’t have to send flowers or anything, just a verbal thank you for their time.”
No matter what stage your career is in, you can always pick up new skills and perspectives—particularly if you’re in a leadership position. Even if you feel you’re well established, finding new mentors can only make you better at what you do.
“You should always look for someone to learn from,” Dr. Gorman says. “They’re out there, no matter where you are or what you’re doing. Throw out some questions and see who you hit it off with, who gives you sound advice.” TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
Nurse Ratios Suffer
Several studies have linked lower nurse-to-patient ratios with fewer medical errors and deaths, better overall treatment, and reduced rates of nurse burnout. These findings led California, in 1999, to pass the country’s first law mandating a minimum nurse-to-patient staffing ratio.
By 2004, the mandated ratio was one licensed nurse for every six patients; that was decreased in 2005 to one nurse for every five patients. Since then, similar bills have been passed or proposed in at least 25 more states. The benefits to patients and nurses of these improved ratios are clear. However, their effect on hospitalists, other staff members, and hospitals have not been widely studied. Further, the mandates often do not come with additional money to implement them.
In this month’s issue of the Journal of Hospital Medicine, Patrick Conway, MD, and colleagues examine nurse staffing trends in California hospitals since the mandate went into effect. They were particularly interested in what they called “safety net” hospitals: urban, government-owned, resource-poor institutions with at least 36% of patients uninsured or on Medicaid.
Dr. Conway, a pediatric hospitalist and assistant professor of pediatrics at the Cincinnati Children’s Hospital Medical Center, and his coauthors hypothesized that cash-strapped hospitals would find it hard to meet the mandate and might shortchange other programs in an effort to comply. Laudable as such legislation might be, “we wanted to make it clear to hospitalists and hospitals that the ratios could have an impact on other goals they wanted to achieve, such as meeting pay-for-performance targets,” he says.
Using financial data from the California Office of Statewide Health Planning and Development, they examined staffing trends on adult general medical surgical units in short-term, acute-care general hospitals from 1993 to 2004, the most recent years for which complete data was available. For 2003 and 2004, they also analyzed staff ratios according to five characteristics: hospital ownership (profit, nonprofit, government-owned), market competitiveness, teaching status, location (urban vs. rural), and whether or not the hospital met the definition of a safety net facility.
From 1993-99, nurse staffing ratios remained flat; they rose steadily thereafter. Not surprisingly, the largest increase occurred between 2003 and 2004, the year implementation was slated to go into effect. During that period, the median ratio for all hospitals studied went from less than one nurse per four patients to more than 1:4, exceeding the mandated figure. Fewer than 25% of hospitals fell short of the minimum mandate of 1:5.

However, further analysis reveals more nuances. The mandate requires a minimum ratio of licensed nurses to patients; those nurses can be registered nurses (RNs), licensed vocational nurses (LVNs), or a combination. In 2004, only 2.4% of hospitals fell below the mandated minimum for that year of 1:6, compared with 5% from the year before—but 11.4% were below 1:5 (RNs plus LVNs). When RNs only were considered, 29.5% of hospitals fell short of one for every five patients.
Further, some states are considering a minimum mandate of one licensed nurse per every four patients—yet 40.4% of the hospitals in this study did not meet that standard. “This demonstrates the substantial increase in the proportion of hospitals that are below minimum ratios as the number of nurses or required training level of nurses is increased,” the authors point out.
The finding that nearly 30% of hospitals had less than one registered nurse for every five patients was surprising, says Dr. Conway, whose wife is a registered nurse. In other words, “if you or I or our parents were admitted to a hospital, your chances are about one in three that they will have less than one nurse for every five patients. That means each nurse has less time to spend per patient.”
For-profit hospitals, non-teaching hospitals, and hospitals in urban or more competitive locations fared best at achieving the mandated ratios. However, hospitals with high Medicaid or uninsured populations were significantly more likely to fall below the minimum ratios than their more affluent counterparts and did not achieve the marked gains in staffing ratios achieved in other facilities.
All in all, more than 20% of safety net hospitals failed to achieve the 2004 mandate of 1:5, compared with about 12% of the other types of hospitals.
Of the safety net hospitals that did achieve the mandate, one wonders what types of tradeoffs they had to make, Dr. Conway adds: “Are they closing emergency rooms? Investing less in new equipment and facilities? Hiring less-trained staff? This study raises those questions, although it doesn’t answer them.”
More and more, hospitalists are being held responsible for quality improvement programs and outcomes measures within hospitals. The targets monitored often are those most strongly influenced by nurse presence, such as the number of central line infections, pressure ulcers, urinary tract infections, ventilator-acquired pneumonia, and similar conditions.
On the other hand, “no one has yet studied what happens when a hospital goes from a ratio of 1:5 to 1:4,” Dr. Conway says. It is possible that the [patient] gains realized may not be large enough to justify the compromises a hospital might have to make in other areas to meet that goal. “We must determine what the tradeoffs are and identify optimal nurse staffing ratios. Adequate nurse staffing is a significant key to achieving a successful team management approach in a hospital.” TH
Norra MacReady is a medical writer based in California.
Editor’s note: Dr. Conway was featured in the February 2008 issue (p. 28) as a member of the White House Fellows Program.
Several studies have linked lower nurse-to-patient ratios with fewer medical errors and deaths, better overall treatment, and reduced rates of nurse burnout. These findings led California, in 1999, to pass the country’s first law mandating a minimum nurse-to-patient staffing ratio.
By 2004, the mandated ratio was one licensed nurse for every six patients; that was decreased in 2005 to one nurse for every five patients. Since then, similar bills have been passed or proposed in at least 25 more states. The benefits to patients and nurses of these improved ratios are clear. However, their effect on hospitalists, other staff members, and hospitals have not been widely studied. Further, the mandates often do not come with additional money to implement them.
In this month’s issue of the Journal of Hospital Medicine, Patrick Conway, MD, and colleagues examine nurse staffing trends in California hospitals since the mandate went into effect. They were particularly interested in what they called “safety net” hospitals: urban, government-owned, resource-poor institutions with at least 36% of patients uninsured or on Medicaid.
Dr. Conway, a pediatric hospitalist and assistant professor of pediatrics at the Cincinnati Children’s Hospital Medical Center, and his coauthors hypothesized that cash-strapped hospitals would find it hard to meet the mandate and might shortchange other programs in an effort to comply. Laudable as such legislation might be, “we wanted to make it clear to hospitalists and hospitals that the ratios could have an impact on other goals they wanted to achieve, such as meeting pay-for-performance targets,” he says.
Using financial data from the California Office of Statewide Health Planning and Development, they examined staffing trends on adult general medical surgical units in short-term, acute-care general hospitals from 1993 to 2004, the most recent years for which complete data was available. For 2003 and 2004, they also analyzed staff ratios according to five characteristics: hospital ownership (profit, nonprofit, government-owned), market competitiveness, teaching status, location (urban vs. rural), and whether or not the hospital met the definition of a safety net facility.
From 1993-99, nurse staffing ratios remained flat; they rose steadily thereafter. Not surprisingly, the largest increase occurred between 2003 and 2004, the year implementation was slated to go into effect. During that period, the median ratio for all hospitals studied went from less than one nurse per four patients to more than 1:4, exceeding the mandated figure. Fewer than 25% of hospitals fell short of the minimum mandate of 1:5.
However, further analysis reveals more nuances. The mandate requires a minimum ratio of licensed nurses to patients; those nurses can be registered nurses (RNs), licensed vocational nurses (LVNs), or a combination. In 2004, only 2.4% of hospitals fell below the mandated minimum for that year of 1:6, compared with 5% from the year before—but 11.4% were below 1:5 (RNs plus LVNs). When RNs only were considered, 29.5% of hospitals fell short of one for every five patients.
Further, some states are considering a minimum mandate of one licensed nurse per every four patients—yet 40.4% of the hospitals in this study did not meet that standard. “This demonstrates the substantial increase in the proportion of hospitals that are below minimum ratios as the number of nurses or required training level of nurses is increased,” the authors point out.
The finding that nearly 30% of hospitals had less than one registered nurse for every five patients was surprising, says Dr. Conway, whose wife is a registered nurse. In other words, “if you or I or our parents were admitted to a hospital, your chances are about one in three that they will have less than one nurse for every five patients. That means each nurse has less time to spend per patient.”
For-profit hospitals, non-teaching hospitals, and hospitals in urban or more competitive locations fared best at achieving the mandated ratios. However, hospitals with high Medicaid or uninsured populations were significantly more likely to fall below the minimum ratios than their more affluent counterparts and did not achieve the marked gains in staffing ratios achieved in other facilities.
All in all, more than 20% of safety net hospitals failed to achieve the 2004 mandate of 1:5, compared with about 12% of the other types of hospitals.
Of the safety net hospitals that did achieve the mandate, one wonders what types of tradeoffs they had to make, Dr. Conway adds: “Are they closing emergency rooms? Investing less in new equipment and facilities? Hiring less-trained staff? This study raises those questions, although it doesn’t answer them.”
More and more, hospitalists are being held responsible for quality improvement programs and outcomes measures within hospitals. The targets monitored often are those most strongly influenced by nurse presence, such as the number of central line infections, pressure ulcers, urinary tract infections, ventilator-acquired pneumonia, and similar conditions.
On the other hand, “no one has yet studied what happens when a hospital goes from a ratio of 1:5 to 1:4,” Dr. Conway says. It is possible that the [patient] gains realized may not be large enough to justify the compromises a hospital might have to make in other areas to meet that goal. “We must determine what the tradeoffs are and identify optimal nurse staffing ratios. Adequate nurse staffing is a significant key to achieving a successful team management approach in a hospital.” TH
Norra MacReady is a medical writer based in California.
Editor’s note: Dr. Conway was featured in the February 2008 issue (p. 28) as a member of the White House Fellows Program.
Several studies have linked lower nurse-to-patient ratios with fewer medical errors and deaths, better overall treatment, and reduced rates of nurse burnout. These findings led California, in 1999, to pass the country’s first law mandating a minimum nurse-to-patient staffing ratio.
By 2004, the mandated ratio was one licensed nurse for every six patients; that was decreased in 2005 to one nurse for every five patients. Since then, similar bills have been passed or proposed in at least 25 more states. The benefits to patients and nurses of these improved ratios are clear. However, their effect on hospitalists, other staff members, and hospitals have not been widely studied. Further, the mandates often do not come with additional money to implement them.
In this month’s issue of the Journal of Hospital Medicine, Patrick Conway, MD, and colleagues examine nurse staffing trends in California hospitals since the mandate went into effect. They were particularly interested in what they called “safety net” hospitals: urban, government-owned, resource-poor institutions with at least 36% of patients uninsured or on Medicaid.
Dr. Conway, a pediatric hospitalist and assistant professor of pediatrics at the Cincinnati Children’s Hospital Medical Center, and his coauthors hypothesized that cash-strapped hospitals would find it hard to meet the mandate and might shortchange other programs in an effort to comply. Laudable as such legislation might be, “we wanted to make it clear to hospitalists and hospitals that the ratios could have an impact on other goals they wanted to achieve, such as meeting pay-for-performance targets,” he says.
Using financial data from the California Office of Statewide Health Planning and Development, they examined staffing trends on adult general medical surgical units in short-term, acute-care general hospitals from 1993 to 2004, the most recent years for which complete data was available. For 2003 and 2004, they also analyzed staff ratios according to five characteristics: hospital ownership (profit, nonprofit, government-owned), market competitiveness, teaching status, location (urban vs. rural), and whether or not the hospital met the definition of a safety net facility.
From 1993-99, nurse staffing ratios remained flat; they rose steadily thereafter. Not surprisingly, the largest increase occurred between 2003 and 2004, the year implementation was slated to go into effect. During that period, the median ratio for all hospitals studied went from less than one nurse per four patients to more than 1:4, exceeding the mandated figure. Fewer than 25% of hospitals fell short of the minimum mandate of 1:5.
However, further analysis reveals more nuances. The mandate requires a minimum ratio of licensed nurses to patients; those nurses can be registered nurses (RNs), licensed vocational nurses (LVNs), or a combination. In 2004, only 2.4% of hospitals fell below the mandated minimum for that year of 1:6, compared with 5% from the year before—but 11.4% were below 1:5 (RNs plus LVNs). When RNs only were considered, 29.5% of hospitals fell short of one for every five patients.
Further, some states are considering a minimum mandate of one licensed nurse per every four patients—yet 40.4% of the hospitals in this study did not meet that standard. “This demonstrates the substantial increase in the proportion of hospitals that are below minimum ratios as the number of nurses or required training level of nurses is increased,” the authors point out.
The finding that nearly 30% of hospitals had less than one registered nurse for every five patients was surprising, says Dr. Conway, whose wife is a registered nurse. In other words, “if you or I or our parents were admitted to a hospital, your chances are about one in three that they will have less than one nurse for every five patients. That means each nurse has less time to spend per patient.”
For-profit hospitals, non-teaching hospitals, and hospitals in urban or more competitive locations fared best at achieving the mandated ratios. However, hospitals with high Medicaid or uninsured populations were significantly more likely to fall below the minimum ratios than their more affluent counterparts and did not achieve the marked gains in staffing ratios achieved in other facilities.
All in all, more than 20% of safety net hospitals failed to achieve the 2004 mandate of 1:5, compared with about 12% of the other types of hospitals.
Of the safety net hospitals that did achieve the mandate, one wonders what types of tradeoffs they had to make, Dr. Conway adds: “Are they closing emergency rooms? Investing less in new equipment and facilities? Hiring less-trained staff? This study raises those questions, although it doesn’t answer them.”
More and more, hospitalists are being held responsible for quality improvement programs and outcomes measures within hospitals. The targets monitored often are those most strongly influenced by nurse presence, such as the number of central line infections, pressure ulcers, urinary tract infections, ventilator-acquired pneumonia, and similar conditions.
On the other hand, “no one has yet studied what happens when a hospital goes from a ratio of 1:5 to 1:4,” Dr. Conway says. It is possible that the [patient] gains realized may not be large enough to justify the compromises a hospital might have to make in other areas to meet that goal. “We must determine what the tradeoffs are and identify optimal nurse staffing ratios. Adequate nurse staffing is a significant key to achieving a successful team management approach in a hospital.” TH
Norra MacReady is a medical writer based in California.
Editor’s note: Dr. Conway was featured in the February 2008 issue (p. 28) as a member of the White House Fellows Program.
Protect the Platelets
The frequency of drug-induced thrombocytopenia (DIT) in acutely ill patients is thought to be up to 25%, making it a common problem.1,2
Hundreds of drugs have been identified as causing DIT, due to either accelerated immune-mediated platelet destruction, decreased platelet production (bone marrow suppression), or platelet aggregation. The latter is the case in heparin-induced thrombocytopenia and thrombosis (HITT). DIT should be suspected in any patient who presents with acute thrombocytopenia from an unknown cause.3
Normal adult platelet counts usually are in the range of 140,000 to 450,000/mm3. A patient who presents with severe thrombocytopenia (less than 20,000 platelets/mm3) should strongly be suspected as having a drug-induced cause.
A patient also can present with moderate to severe thrombocytopenia (less than 50,000 platelets/mm3) and spontaneous bleeding from a drug-induced cause. The spontaneous bleeding can take the form of simple petechiae or ecchymoses, as well as mucosal bleeding or life-threatening intracranial or gastrointestinal hemorrhage. It may also present itself as bleeding around catheter insertion sites.
When DIT occurs, platelet count usually falls within two to three days of taking a drug that’s been taken before, or seven or more days after starting a drug the patient has not been exposed to. Once the offending drug is discontinued, platelet counts usually recover within 10 days.
Exclusions of other causes of thrombocytopenia, such as inflammatory processes and congenital disorders, as well as nondrug causes including sepsis, malignancy, extensive burns, chronic alcoholism, human immunodeficiency virus, splenomegaly, and disseminated intravascular coagulation, become part of the differential diagnosis.
Generally, the frequency and severity of bleeding manifestations correlate with the actual platelet count. Patients with a platelet count of less than 50,000/mm3 have an increased risk of spontaneous hemorrhage, but the severity may vary. Other risk factors include advanced age, bleeding history, and general bleeding diatheses.
A thorough physical examination and drug history are essential. Agents commonly associated with thrombocytopenia should be identified first followed by a more extensive review for other causes. A careful drug history should include prescriptions, over-the-counter medications (specifically quinine and acetaminophen), dietary supplements, folk remedies, other complementary and alternative therapies, and vaccinations.
The Agents
The top two suspects for DIT are antineoplastic agents and heparin. After these two, the agents most frequently associated with DIT development include:
- Quinine/quinidine;
- Phenytoin;
- Sulfonamide antibiotics;
- Cimetidine;
- Ranitidine;
- Rifampin/rifampicin;
- Carbamazepine;
- Thiazide diuretics;
- Penicillin;
- Oral antidiabetic drugs;
- Nonsteroidal anti-inflammatory drugs;
- Gold salts; and
- Procainamide.
A complete list of all case reports describing DIT, organized by generic
drug names, is available online at http://w3.ouhsc.edu/platelets/ditp.html.4
Management
Removal of the potentially offending agent, if known, is prudent before clinically significant bleeding occurs. If the offending agent is not discontinued, the platelet count will continue to decrease and bleeding will become more severe. If necessary, an alternate agent with a similar pharmacologic effect can be started. Daily platelet count monitoring is also recommended for management. Rare cases may require platelet transfusions, intravenous immunoglobulin therapy or plasmapheresis.
A complete blood count and peripheral blood smear may provide important indications into the mechanism of the disorder, but they’re not necessary for patient management. TH
Michele B Kaufman, PharmD, BSc, is a registere pharmacist based in New York City.
References
- Visentin GP, Liu CY. Drug-induced thrombocytopenia. Hematol Oncol Clin N Am. 2007;21:685-696.
- Wazny LD, Ariano RE. Evaluation and management of drug-induced thrombocytopenia in the acutely ill patient. Pharmacother. 2000;20(3):292-307.
- Aster RH, Bougie DW. Drug-induced thrombocytopenia. N Engl J Med. 2007;357(6):580-587.
- Majhail NS, Lichtin AE. What is the best way to determine if thrombocytopenia in a patient on multiple medications is drug-induced? Cleve Clin J Med. 2002;69(3):259-262.
The frequency of drug-induced thrombocytopenia (DIT) in acutely ill patients is thought to be up to 25%, making it a common problem.1,2
Hundreds of drugs have been identified as causing DIT, due to either accelerated immune-mediated platelet destruction, decreased platelet production (bone marrow suppression), or platelet aggregation. The latter is the case in heparin-induced thrombocytopenia and thrombosis (HITT). DIT should be suspected in any patient who presents with acute thrombocytopenia from an unknown cause.3
Normal adult platelet counts usually are in the range of 140,000 to 450,000/mm3. A patient who presents with severe thrombocytopenia (less than 20,000 platelets/mm3) should strongly be suspected as having a drug-induced cause.
A patient also can present with moderate to severe thrombocytopenia (less than 50,000 platelets/mm3) and spontaneous bleeding from a drug-induced cause. The spontaneous bleeding can take the form of simple petechiae or ecchymoses, as well as mucosal bleeding or life-threatening intracranial or gastrointestinal hemorrhage. It may also present itself as bleeding around catheter insertion sites.
When DIT occurs, platelet count usually falls within two to three days of taking a drug that’s been taken before, or seven or more days after starting a drug the patient has not been exposed to. Once the offending drug is discontinued, platelet counts usually recover within 10 days.
Exclusions of other causes of thrombocytopenia, such as inflammatory processes and congenital disorders, as well as nondrug causes including sepsis, malignancy, extensive burns, chronic alcoholism, human immunodeficiency virus, splenomegaly, and disseminated intravascular coagulation, become part of the differential diagnosis.
Generally, the frequency and severity of bleeding manifestations correlate with the actual platelet count. Patients with a platelet count of less than 50,000/mm3 have an increased risk of spontaneous hemorrhage, but the severity may vary. Other risk factors include advanced age, bleeding history, and general bleeding diatheses.
A thorough physical examination and drug history are essential. Agents commonly associated with thrombocytopenia should be identified first followed by a more extensive review for other causes. A careful drug history should include prescriptions, over-the-counter medications (specifically quinine and acetaminophen), dietary supplements, folk remedies, other complementary and alternative therapies, and vaccinations.
The Agents
The top two suspects for DIT are antineoplastic agents and heparin. After these two, the agents most frequently associated with DIT development include:
- Quinine/quinidine;
- Phenytoin;
- Sulfonamide antibiotics;
- Cimetidine;
- Ranitidine;
- Rifampin/rifampicin;
- Carbamazepine;
- Thiazide diuretics;
- Penicillin;
- Oral antidiabetic drugs;
- Nonsteroidal anti-inflammatory drugs;
- Gold salts; and
- Procainamide.
A complete list of all case reports describing DIT, organized by generic
drug names, is available online at http://w3.ouhsc.edu/platelets/ditp.html.4
Management
Removal of the potentially offending agent, if known, is prudent before clinically significant bleeding occurs. If the offending agent is not discontinued, the platelet count will continue to decrease and bleeding will become more severe. If necessary, an alternate agent with a similar pharmacologic effect can be started. Daily platelet count monitoring is also recommended for management. Rare cases may require platelet transfusions, intravenous immunoglobulin therapy or plasmapheresis.
A complete blood count and peripheral blood smear may provide important indications into the mechanism of the disorder, but they’re not necessary for patient management. TH
Michele B Kaufman, PharmD, BSc, is a registere pharmacist based in New York City.
References
- Visentin GP, Liu CY. Drug-induced thrombocytopenia. Hematol Oncol Clin N Am. 2007;21:685-696.
- Wazny LD, Ariano RE. Evaluation and management of drug-induced thrombocytopenia in the acutely ill patient. Pharmacother. 2000;20(3):292-307.
- Aster RH, Bougie DW. Drug-induced thrombocytopenia. N Engl J Med. 2007;357(6):580-587.
- Majhail NS, Lichtin AE. What is the best way to determine if thrombocytopenia in a patient on multiple medications is drug-induced? Cleve Clin J Med. 2002;69(3):259-262.
The frequency of drug-induced thrombocytopenia (DIT) in acutely ill patients is thought to be up to 25%, making it a common problem.1,2
Hundreds of drugs have been identified as causing DIT, due to either accelerated immune-mediated platelet destruction, decreased platelet production (bone marrow suppression), or platelet aggregation. The latter is the case in heparin-induced thrombocytopenia and thrombosis (HITT). DIT should be suspected in any patient who presents with acute thrombocytopenia from an unknown cause.3
Normal adult platelet counts usually are in the range of 140,000 to 450,000/mm3. A patient who presents with severe thrombocytopenia (less than 20,000 platelets/mm3) should strongly be suspected as having a drug-induced cause.
A patient also can present with moderate to severe thrombocytopenia (less than 50,000 platelets/mm3) and spontaneous bleeding from a drug-induced cause. The spontaneous bleeding can take the form of simple petechiae or ecchymoses, as well as mucosal bleeding or life-threatening intracranial or gastrointestinal hemorrhage. It may also present itself as bleeding around catheter insertion sites.
When DIT occurs, platelet count usually falls within two to three days of taking a drug that’s been taken before, or seven or more days after starting a drug the patient has not been exposed to. Once the offending drug is discontinued, platelet counts usually recover within 10 days.
Exclusions of other causes of thrombocytopenia, such as inflammatory processes and congenital disorders, as well as nondrug causes including sepsis, malignancy, extensive burns, chronic alcoholism, human immunodeficiency virus, splenomegaly, and disseminated intravascular coagulation, become part of the differential diagnosis.
Generally, the frequency and severity of bleeding manifestations correlate with the actual platelet count. Patients with a platelet count of less than 50,000/mm3 have an increased risk of spontaneous hemorrhage, but the severity may vary. Other risk factors include advanced age, bleeding history, and general bleeding diatheses.
A thorough physical examination and drug history are essential. Agents commonly associated with thrombocytopenia should be identified first followed by a more extensive review for other causes. A careful drug history should include prescriptions, over-the-counter medications (specifically quinine and acetaminophen), dietary supplements, folk remedies, other complementary and alternative therapies, and vaccinations.
The Agents
The top two suspects for DIT are antineoplastic agents and heparin. After these two, the agents most frequently associated with DIT development include:
- Quinine/quinidine;
- Phenytoin;
- Sulfonamide antibiotics;
- Cimetidine;
- Ranitidine;
- Rifampin/rifampicin;
- Carbamazepine;
- Thiazide diuretics;
- Penicillin;
- Oral antidiabetic drugs;
- Nonsteroidal anti-inflammatory drugs;
- Gold salts; and
- Procainamide.
A complete list of all case reports describing DIT, organized by generic
drug names, is available online at http://w3.ouhsc.edu/platelets/ditp.html.4
Management
Removal of the potentially offending agent, if known, is prudent before clinically significant bleeding occurs. If the offending agent is not discontinued, the platelet count will continue to decrease and bleeding will become more severe. If necessary, an alternate agent with a similar pharmacologic effect can be started. Daily platelet count monitoring is also recommended for management. Rare cases may require platelet transfusions, intravenous immunoglobulin therapy or plasmapheresis.
A complete blood count and peripheral blood smear may provide important indications into the mechanism of the disorder, but they’re not necessary for patient management. TH
Michele B Kaufman, PharmD, BSc, is a registere pharmacist based in New York City.
References
- Visentin GP, Liu CY. Drug-induced thrombocytopenia. Hematol Oncol Clin N Am. 2007;21:685-696.
- Wazny LD, Ariano RE. Evaluation and management of drug-induced thrombocytopenia in the acutely ill patient. Pharmacother. 2000;20(3):292-307.
- Aster RH, Bougie DW. Drug-induced thrombocytopenia. N Engl J Med. 2007;357(6):580-587.
- Majhail NS, Lichtin AE. What is the best way to determine if thrombocytopenia in a patient on multiple medications is drug-induced? Cleve Clin J Med. 2002;69(3):259-262.