User login
Mentoring 101
If you’re in an HM leadership position, don’t be surprised if you’re asked to be a mentor for a less-experienced hospitalist. Why should you voluntarily spend valuable time sharing your guidance and advice? Because to lead is to mentor, and when you dive into the process it rewards all parties involved.
To Lead Is to Mentor
Whether you were just promoted or you’re a leadership veteran approached for the first time by an eager new hospitalist, don’t hesitate to add mentoring to your schedule and responsibilities.
“When you start out as a leader, you get where you want to go by being a mentor,” says Eric E. Howell, MD, director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore and faculty for SHM’s Leadership Academy. “You gather disciples, as it were, who will then see you as a leader and support you as a good leadership choice.”
Not only that, but mentoring can add to your skill set as a leader, says Joan C. Faro, MD, FACP, MBA, chief medical officer at John T. Mather Memorial Hospital, Port Jefferson, N.Y. “If you’re interested in developing leadership skills, it’s one of those things you need to do, and do well. If you can’t mentor, then you really can’t lead.”
Plus, when you mentor, you get to feel the reward inherent in helping a young physician whose shoes you once filled. “It’s like raising a kid,” says Dr. Faro. “You want to do a good job because you want to see someone succeed.” This is especially true for mentoring relationships within your HM group.
That means fully flushing out the program and dedicating the time necessary to make it a success. “If you are the de facto leader of a group, you have some obligation to people interested in career development,” says Dr. Howell. “I think it’s part of the job to help advance those people.”
The Ground Rules
Any new mentoring arrangement should start with a discussion of expectations, responsibilities, time frames, and communication. What are the mentee’s expectations for the relationship? How much time can you, the mentor, offer?
Whether the arrangement is formal (a director mentoring a new hire) or casual (an established hospitalist asking a conference speaker for a long-distance mentoring relationship), ground rules are important, Dr. Howell insists. “The mentoring relationship can be established informally, but it’s worthwhile to set some rules on responsibilities: How is the feedback going to come, how frank and honest do you want to be, when should we meet? …Rules will depend on the relationship and on the individuals involved.”
If nothing else, agree to how frequently you will meet or speak. “It could be quarterly or it could be weekly,” says Dr. Howell. “Face time is important, but e-mail and phone calls will work, too, as long as you’ve established some ground rules about this. If the mentee expects a face-to-face meeting and you’re e-mailing your answers, that could be a problem. So you need to establish how you’re going to communicate.”
Those meetings can add up to a sizeable commitment. How much time, exactly, should a new mentor expect to devote to this aspect of leadership? “It varies widely,” Dr. Howell admits. “But I will say that many younger mentees require much more time than older mentors expect. If they’re struggling or haven’t found their stride yet, it can require several hours a week, which is a lot for a busy person’s schedule. But many relationships can be handled weekly or monthly.”
Dr. Faro, who has mentored many hospitalists within her organization, says, “You need to build the relationship; you need enough contact time so that you can understand each other.” For her, that amounts to 40 to 50 hours of getting-to-know-you time, she says. “After that, maybe an hour a week.”
Tailor Mentoring
Dr. Faro tailors her guidance to the personality, capabilities, and level of independence of each person she mentors—hence her lengthy initial time frame.
“You need to start with setting up a clear set of goals and outcomes,” she says. “They really need to know what they’re doing and why they’re doing it. So, set up a plan with specific time frames. It’s your job to determine how independent they are; you may end up giving them goals rather than them stating what they’re going to do.”
—Joan C. Faro, MD, FACP, MBA, chief medical officer, John T. Mather Memorial Hospital, Port Jefferson, N.Y.
For example, she might tell one mentee to develop an order set for patients with syncope, and expect a document by an agreed-upon deadline. She might give another individual the same assignment, but walk that person through each step—within reason. “You can’t do it for them, or they’re not going to learn,” she maintains.
Each completed task is met with constructive criticism. How well was the task done? Did the physician leave out anything? If Dr. Faro senses that more guidance is necessary, she steps up her level of involvement.
What Makes a Successful Mentor?
Dr. Faro understands the mentor/mentee process because she’s been part of it for so long. How can you get to that point? Simply agreeing to be a mentor and having regular meetings with your mentee doesn’t necessarily mean you’re doing a good job.
“Good mentors probably listen more than they talk,” explains Dr. Howell. “For many people, if they can talk it out, they will reach their own conclusions and that’s much more powerful than being told something. That ‘Aha!’ moment is a big career moment.”
He also believes strong mentors can give even non-hospitalists helpful career advice. “Good mentors are able to step out of their own shoes and look at the unique situation of the other person, and give advice tailored to that situation,” he explains. “You have to be altruistic in your mentoring; you can’t do it for your own needs.”
Successful mentors also understand their mentees. For example, mentees in leadership positions should receive advice about how to invest in themselves and their careers. “I always recommend SHM’s Leadership Academy, as well as several books, including Getting to Yes and Good to Great to improve themselves as leaders,” says Dr. Howell.
Finally, a mentor who does the job well understands when the relationship isn’t working. If this is the case, “be up-front and honest, and if possible, point that person to another mentor,” Dr. Howell says. “If you can introduce them and get them started, that’s best. You can also share a mentee with someone else; you can each handle different areas. I have many different mentors in different areas. It’s more productive that way.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
If you’re in an HM leadership position, don’t be surprised if you’re asked to be a mentor for a less-experienced hospitalist. Why should you voluntarily spend valuable time sharing your guidance and advice? Because to lead is to mentor, and when you dive into the process it rewards all parties involved.
To Lead Is to Mentor
Whether you were just promoted or you’re a leadership veteran approached for the first time by an eager new hospitalist, don’t hesitate to add mentoring to your schedule and responsibilities.
“When you start out as a leader, you get where you want to go by being a mentor,” says Eric E. Howell, MD, director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore and faculty for SHM’s Leadership Academy. “You gather disciples, as it were, who will then see you as a leader and support you as a good leadership choice.”
Not only that, but mentoring can add to your skill set as a leader, says Joan C. Faro, MD, FACP, MBA, chief medical officer at John T. Mather Memorial Hospital, Port Jefferson, N.Y. “If you’re interested in developing leadership skills, it’s one of those things you need to do, and do well. If you can’t mentor, then you really can’t lead.”
Plus, when you mentor, you get to feel the reward inherent in helping a young physician whose shoes you once filled. “It’s like raising a kid,” says Dr. Faro. “You want to do a good job because you want to see someone succeed.” This is especially true for mentoring relationships within your HM group.
That means fully flushing out the program and dedicating the time necessary to make it a success. “If you are the de facto leader of a group, you have some obligation to people interested in career development,” says Dr. Howell. “I think it’s part of the job to help advance those people.”
The Ground Rules
Any new mentoring arrangement should start with a discussion of expectations, responsibilities, time frames, and communication. What are the mentee’s expectations for the relationship? How much time can you, the mentor, offer?
Whether the arrangement is formal (a director mentoring a new hire) or casual (an established hospitalist asking a conference speaker for a long-distance mentoring relationship), ground rules are important, Dr. Howell insists. “The mentoring relationship can be established informally, but it’s worthwhile to set some rules on responsibilities: How is the feedback going to come, how frank and honest do you want to be, when should we meet? …Rules will depend on the relationship and on the individuals involved.”
If nothing else, agree to how frequently you will meet or speak. “It could be quarterly or it could be weekly,” says Dr. Howell. “Face time is important, but e-mail and phone calls will work, too, as long as you’ve established some ground rules about this. If the mentee expects a face-to-face meeting and you’re e-mailing your answers, that could be a problem. So you need to establish how you’re going to communicate.”
Those meetings can add up to a sizeable commitment. How much time, exactly, should a new mentor expect to devote to this aspect of leadership? “It varies widely,” Dr. Howell admits. “But I will say that many younger mentees require much more time than older mentors expect. If they’re struggling or haven’t found their stride yet, it can require several hours a week, which is a lot for a busy person’s schedule. But many relationships can be handled weekly or monthly.”
Dr. Faro, who has mentored many hospitalists within her organization, says, “You need to build the relationship; you need enough contact time so that you can understand each other.” For her, that amounts to 40 to 50 hours of getting-to-know-you time, she says. “After that, maybe an hour a week.”
Tailor Mentoring
Dr. Faro tailors her guidance to the personality, capabilities, and level of independence of each person she mentors—hence her lengthy initial time frame.
“You need to start with setting up a clear set of goals and outcomes,” she says. “They really need to know what they’re doing and why they’re doing it. So, set up a plan with specific time frames. It’s your job to determine how independent they are; you may end up giving them goals rather than them stating what they’re going to do.”
—Joan C. Faro, MD, FACP, MBA, chief medical officer, John T. Mather Memorial Hospital, Port Jefferson, N.Y.
For example, she might tell one mentee to develop an order set for patients with syncope, and expect a document by an agreed-upon deadline. She might give another individual the same assignment, but walk that person through each step—within reason. “You can’t do it for them, or they’re not going to learn,” she maintains.
Each completed task is met with constructive criticism. How well was the task done? Did the physician leave out anything? If Dr. Faro senses that more guidance is necessary, she steps up her level of involvement.
What Makes a Successful Mentor?
Dr. Faro understands the mentor/mentee process because she’s been part of it for so long. How can you get to that point? Simply agreeing to be a mentor and having regular meetings with your mentee doesn’t necessarily mean you’re doing a good job.
“Good mentors probably listen more than they talk,” explains Dr. Howell. “For many people, if they can talk it out, they will reach their own conclusions and that’s much more powerful than being told something. That ‘Aha!’ moment is a big career moment.”
He also believes strong mentors can give even non-hospitalists helpful career advice. “Good mentors are able to step out of their own shoes and look at the unique situation of the other person, and give advice tailored to that situation,” he explains. “You have to be altruistic in your mentoring; you can’t do it for your own needs.”
Successful mentors also understand their mentees. For example, mentees in leadership positions should receive advice about how to invest in themselves and their careers. “I always recommend SHM’s Leadership Academy, as well as several books, including Getting to Yes and Good to Great to improve themselves as leaders,” says Dr. Howell.
Finally, a mentor who does the job well understands when the relationship isn’t working. If this is the case, “be up-front and honest, and if possible, point that person to another mentor,” Dr. Howell says. “If you can introduce them and get them started, that’s best. You can also share a mentee with someone else; you can each handle different areas. I have many different mentors in different areas. It’s more productive that way.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
If you’re in an HM leadership position, don’t be surprised if you’re asked to be a mentor for a less-experienced hospitalist. Why should you voluntarily spend valuable time sharing your guidance and advice? Because to lead is to mentor, and when you dive into the process it rewards all parties involved.
To Lead Is to Mentor
Whether you were just promoted or you’re a leadership veteran approached for the first time by an eager new hospitalist, don’t hesitate to add mentoring to your schedule and responsibilities.
“When you start out as a leader, you get where you want to go by being a mentor,” says Eric E. Howell, MD, director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore and faculty for SHM’s Leadership Academy. “You gather disciples, as it were, who will then see you as a leader and support you as a good leadership choice.”
Not only that, but mentoring can add to your skill set as a leader, says Joan C. Faro, MD, FACP, MBA, chief medical officer at John T. Mather Memorial Hospital, Port Jefferson, N.Y. “If you’re interested in developing leadership skills, it’s one of those things you need to do, and do well. If you can’t mentor, then you really can’t lead.”
Plus, when you mentor, you get to feel the reward inherent in helping a young physician whose shoes you once filled. “It’s like raising a kid,” says Dr. Faro. “You want to do a good job because you want to see someone succeed.” This is especially true for mentoring relationships within your HM group.
That means fully flushing out the program and dedicating the time necessary to make it a success. “If you are the de facto leader of a group, you have some obligation to people interested in career development,” says Dr. Howell. “I think it’s part of the job to help advance those people.”
The Ground Rules
Any new mentoring arrangement should start with a discussion of expectations, responsibilities, time frames, and communication. What are the mentee’s expectations for the relationship? How much time can you, the mentor, offer?
Whether the arrangement is formal (a director mentoring a new hire) or casual (an established hospitalist asking a conference speaker for a long-distance mentoring relationship), ground rules are important, Dr. Howell insists. “The mentoring relationship can be established informally, but it’s worthwhile to set some rules on responsibilities: How is the feedback going to come, how frank and honest do you want to be, when should we meet? …Rules will depend on the relationship and on the individuals involved.”
If nothing else, agree to how frequently you will meet or speak. “It could be quarterly or it could be weekly,” says Dr. Howell. “Face time is important, but e-mail and phone calls will work, too, as long as you’ve established some ground rules about this. If the mentee expects a face-to-face meeting and you’re e-mailing your answers, that could be a problem. So you need to establish how you’re going to communicate.”
Those meetings can add up to a sizeable commitment. How much time, exactly, should a new mentor expect to devote to this aspect of leadership? “It varies widely,” Dr. Howell admits. “But I will say that many younger mentees require much more time than older mentors expect. If they’re struggling or haven’t found their stride yet, it can require several hours a week, which is a lot for a busy person’s schedule. But many relationships can be handled weekly or monthly.”
Dr. Faro, who has mentored many hospitalists within her organization, says, “You need to build the relationship; you need enough contact time so that you can understand each other.” For her, that amounts to 40 to 50 hours of getting-to-know-you time, she says. “After that, maybe an hour a week.”
Tailor Mentoring
Dr. Faro tailors her guidance to the personality, capabilities, and level of independence of each person she mentors—hence her lengthy initial time frame.
“You need to start with setting up a clear set of goals and outcomes,” she says. “They really need to know what they’re doing and why they’re doing it. So, set up a plan with specific time frames. It’s your job to determine how independent they are; you may end up giving them goals rather than them stating what they’re going to do.”
—Joan C. Faro, MD, FACP, MBA, chief medical officer, John T. Mather Memorial Hospital, Port Jefferson, N.Y.
For example, she might tell one mentee to develop an order set for patients with syncope, and expect a document by an agreed-upon deadline. She might give another individual the same assignment, but walk that person through each step—within reason. “You can’t do it for them, or they’re not going to learn,” she maintains.
Each completed task is met with constructive criticism. How well was the task done? Did the physician leave out anything? If Dr. Faro senses that more guidance is necessary, she steps up her level of involvement.
What Makes a Successful Mentor?
Dr. Faro understands the mentor/mentee process because she’s been part of it for so long. How can you get to that point? Simply agreeing to be a mentor and having regular meetings with your mentee doesn’t necessarily mean you’re doing a good job.
“Good mentors probably listen more than they talk,” explains Dr. Howell. “For many people, if they can talk it out, they will reach their own conclusions and that’s much more powerful than being told something. That ‘Aha!’ moment is a big career moment.”
He also believes strong mentors can give even non-hospitalists helpful career advice. “Good mentors are able to step out of their own shoes and look at the unique situation of the other person, and give advice tailored to that situation,” he explains. “You have to be altruistic in your mentoring; you can’t do it for your own needs.”
Successful mentors also understand their mentees. For example, mentees in leadership positions should receive advice about how to invest in themselves and their careers. “I always recommend SHM’s Leadership Academy, as well as several books, including Getting to Yes and Good to Great to improve themselves as leaders,” says Dr. Howell.
Finally, a mentor who does the job well understands when the relationship isn’t working. If this is the case, “be up-front and honest, and if possible, point that person to another mentor,” Dr. Howell says. “If you can introduce them and get them started, that’s best. You can also share a mentee with someone else; you can each handle different areas. I have many different mentors in different areas. It’s more productive that way.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Serotonin Syndrome
A healthy 30-year-old female presented to the urgent care center with confusion, tremor, and a blood pressure of 160/110 mm Hg. She had no history of hypertension, diabetes, dyslipidemia, renal dysfunction, or smoking. A basic metabolic panel revealed no abnormalities.
Her medication history revealed use of paroxetine (20 mg) subsequent to a depressive episode two years prior. A source of the hypertension was not identified, and she was sent home without further follow-up. The next day, she was admitted to the hospital via the emergency department for stroke symptoms, including numbness and weakness on her right side (extremities and face), with confusion and diplopia. She remained hospitalized for four days during which time she continued to experience transient ischemic attacks. The paroxetine eventually was discontinued. She subsequently has recovered without negative sequelae.
Serotonin syndrome is a consequence of a hyperserotonergic state, due to drug-induced serotonin intensification.1 It can be mild or life-threatening and is characterized by a triad of clinical manifestations: mental status changes, autonomic hyperactivity, and neuromuscular abnormalities.2 Clinicians may miss mild symptoms, such as diarrhea, tremor, tachycardia, diaphoresis, or mydriasis. This can result in an increase in the dose of the causative agent or addition of a serotonergic agent, thus yielding a worsening clinical decline.3
Patients with a more severe clinical presentation include those with severe hypertension (as in the case above), tachycardia, muscular rigidity, and shock. Laboratory abnormalities may be present if the patient develops subsequent rhabdomyolysis, seizures, metabolic acidosis, or renal failure. Serotonin syndrome is diagnosed based on the patient’s presentation, history, and physical examination. It should be differentiated from neuroleptic malignant syndrome, which has a similar presentation.4
Serotonergic agents used alone, or in combination, may lead to serotonin syndrome.5 A recent report discussed the appearance of serotonin syndrome in patients receiving only sumatriptan. Other offenders include such antidepressants as monoamine oxidase inhibitors, buspirone, citalopram, clomipramine, escitalopram, fluoxetine, fluvoxamine, nefazodone, paroxetine, sertraline, trazodone, and venlafaxine. Other causative agents include dextromethorphan, fentanyl, granisetron, levodopa, linezolid, lithium, meperidine, metoclopramide, ondansetron, pentazocine, sibutramine, sumatriptan, tramadol, valproate, and drugs of abuse (e.g., amphetamines, cocaine, LSD, ecstasy). Additionally, ginseng, St. John’s Wort, and tryptophan have been implicated.
Many of these agents require an adequate washout period prior to beginning other serotonergic agents. Mild to moderately severe cases usually resolve within 24 to 72 hours, although most resolve within a week depending on the half-life of the medication. Serotonin syndrome carries an 11% mortality rate and is best managed by stopping the offending agent and providing supportive care. TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Sorenson S. Serotonin syndrome. UTox Update 2002;4(4):1-2. A Publication of the Utah Poison Control Center for Health Professionals. Available at http://uuhsc.utah.edu/poison/healthpros/utox/vol4_no4.pdf. Last accessed June 20, 2008.
- Soldin OP, Tonning JM. Serotonin syndrome associated with triptan monotherapy. N Engl J Med. 2008;358(20):2185-2186.
- Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med. 2005;352(11):1112-1120.
- Nolan S, Scoggin JA. Serotonin syndrome: recognition and management. US Pharm. 2002;23(2). www.uspharmacist.com/oldformat.asp?url=newlook/files/feat/acf2fa6.htm. Last accessed June 20, 2008.
- Mayo Clinic.com. Diseases and conditions. www.mayoclinic.com/health/serotonin-syndrome/DS00860. Last accessed June 20, 2008.
A healthy 30-year-old female presented to the urgent care center with confusion, tremor, and a blood pressure of 160/110 mm Hg. She had no history of hypertension, diabetes, dyslipidemia, renal dysfunction, or smoking. A basic metabolic panel revealed no abnormalities.
Her medication history revealed use of paroxetine (20 mg) subsequent to a depressive episode two years prior. A source of the hypertension was not identified, and she was sent home without further follow-up. The next day, she was admitted to the hospital via the emergency department for stroke symptoms, including numbness and weakness on her right side (extremities and face), with confusion and diplopia. She remained hospitalized for four days during which time she continued to experience transient ischemic attacks. The paroxetine eventually was discontinued. She subsequently has recovered without negative sequelae.
Serotonin syndrome is a consequence of a hyperserotonergic state, due to drug-induced serotonin intensification.1 It can be mild or life-threatening and is characterized by a triad of clinical manifestations: mental status changes, autonomic hyperactivity, and neuromuscular abnormalities.2 Clinicians may miss mild symptoms, such as diarrhea, tremor, tachycardia, diaphoresis, or mydriasis. This can result in an increase in the dose of the causative agent or addition of a serotonergic agent, thus yielding a worsening clinical decline.3
Patients with a more severe clinical presentation include those with severe hypertension (as in the case above), tachycardia, muscular rigidity, and shock. Laboratory abnormalities may be present if the patient develops subsequent rhabdomyolysis, seizures, metabolic acidosis, or renal failure. Serotonin syndrome is diagnosed based on the patient’s presentation, history, and physical examination. It should be differentiated from neuroleptic malignant syndrome, which has a similar presentation.4
Serotonergic agents used alone, or in combination, may lead to serotonin syndrome.5 A recent report discussed the appearance of serotonin syndrome in patients receiving only sumatriptan. Other offenders include such antidepressants as monoamine oxidase inhibitors, buspirone, citalopram, clomipramine, escitalopram, fluoxetine, fluvoxamine, nefazodone, paroxetine, sertraline, trazodone, and venlafaxine. Other causative agents include dextromethorphan, fentanyl, granisetron, levodopa, linezolid, lithium, meperidine, metoclopramide, ondansetron, pentazocine, sibutramine, sumatriptan, tramadol, valproate, and drugs of abuse (e.g., amphetamines, cocaine, LSD, ecstasy). Additionally, ginseng, St. John’s Wort, and tryptophan have been implicated.
Many of these agents require an adequate washout period prior to beginning other serotonergic agents. Mild to moderately severe cases usually resolve within 24 to 72 hours, although most resolve within a week depending on the half-life of the medication. Serotonin syndrome carries an 11% mortality rate and is best managed by stopping the offending agent and providing supportive care. TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Sorenson S. Serotonin syndrome. UTox Update 2002;4(4):1-2. A Publication of the Utah Poison Control Center for Health Professionals. Available at http://uuhsc.utah.edu/poison/healthpros/utox/vol4_no4.pdf. Last accessed June 20, 2008.
- Soldin OP, Tonning JM. Serotonin syndrome associated with triptan monotherapy. N Engl J Med. 2008;358(20):2185-2186.
- Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med. 2005;352(11):1112-1120.
- Nolan S, Scoggin JA. Serotonin syndrome: recognition and management. US Pharm. 2002;23(2). www.uspharmacist.com/oldformat.asp?url=newlook/files/feat/acf2fa6.htm. Last accessed June 20, 2008.
- Mayo Clinic.com. Diseases and conditions. www.mayoclinic.com/health/serotonin-syndrome/DS00860. Last accessed June 20, 2008.
A healthy 30-year-old female presented to the urgent care center with confusion, tremor, and a blood pressure of 160/110 mm Hg. She had no history of hypertension, diabetes, dyslipidemia, renal dysfunction, or smoking. A basic metabolic panel revealed no abnormalities.
Her medication history revealed use of paroxetine (20 mg) subsequent to a depressive episode two years prior. A source of the hypertension was not identified, and she was sent home without further follow-up. The next day, she was admitted to the hospital via the emergency department for stroke symptoms, including numbness and weakness on her right side (extremities and face), with confusion and diplopia. She remained hospitalized for four days during which time she continued to experience transient ischemic attacks. The paroxetine eventually was discontinued. She subsequently has recovered without negative sequelae.
Serotonin syndrome is a consequence of a hyperserotonergic state, due to drug-induced serotonin intensification.1 It can be mild or life-threatening and is characterized by a triad of clinical manifestations: mental status changes, autonomic hyperactivity, and neuromuscular abnormalities.2 Clinicians may miss mild symptoms, such as diarrhea, tremor, tachycardia, diaphoresis, or mydriasis. This can result in an increase in the dose of the causative agent or addition of a serotonergic agent, thus yielding a worsening clinical decline.3
Patients with a more severe clinical presentation include those with severe hypertension (as in the case above), tachycardia, muscular rigidity, and shock. Laboratory abnormalities may be present if the patient develops subsequent rhabdomyolysis, seizures, metabolic acidosis, or renal failure. Serotonin syndrome is diagnosed based on the patient’s presentation, history, and physical examination. It should be differentiated from neuroleptic malignant syndrome, which has a similar presentation.4
Serotonergic agents used alone, or in combination, may lead to serotonin syndrome.5 A recent report discussed the appearance of serotonin syndrome in patients receiving only sumatriptan. Other offenders include such antidepressants as monoamine oxidase inhibitors, buspirone, citalopram, clomipramine, escitalopram, fluoxetine, fluvoxamine, nefazodone, paroxetine, sertraline, trazodone, and venlafaxine. Other causative agents include dextromethorphan, fentanyl, granisetron, levodopa, linezolid, lithium, meperidine, metoclopramide, ondansetron, pentazocine, sibutramine, sumatriptan, tramadol, valproate, and drugs of abuse (e.g., amphetamines, cocaine, LSD, ecstasy). Additionally, ginseng, St. John’s Wort, and tryptophan have been implicated.
Many of these agents require an adequate washout period prior to beginning other serotonergic agents. Mild to moderately severe cases usually resolve within 24 to 72 hours, although most resolve within a week depending on the half-life of the medication. Serotonin syndrome carries an 11% mortality rate and is best managed by stopping the offending agent and providing supportive care. TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Sorenson S. Serotonin syndrome. UTox Update 2002;4(4):1-2. A Publication of the Utah Poison Control Center for Health Professionals. Available at http://uuhsc.utah.edu/poison/healthpros/utox/vol4_no4.pdf. Last accessed June 20, 2008.
- Soldin OP, Tonning JM. Serotonin syndrome associated with triptan monotherapy. N Engl J Med. 2008;358(20):2185-2186.
- Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med. 2005;352(11):1112-1120.
- Nolan S, Scoggin JA. Serotonin syndrome: recognition and management. US Pharm. 2002;23(2). www.uspharmacist.com/oldformat.asp?url=newlook/files/feat/acf2fa6.htm. Last accessed June 20, 2008.
- Mayo Clinic.com. Diseases and conditions. www.mayoclinic.com/health/serotonin-syndrome/DS00860. Last accessed June 20, 2008.
The latest research you need to know
Literature at a Glance
- ICU management by critical care physicians may increase the odds of hospital mortality
- Iatrogenic drug overdose common among patients with renal insufficiency
- An educational effort lowers hospital mortality for severe sepsis and septic shock
- SSRI and problem-solving therapy prevents post-stroke depression
- Stop orders for Foley catheters reduce the duration of inappropriate urinary catheterization
- No thromboembolism risk with interrupting anticoagulation in atrial fibrillation patients undergoing surgery
- Obese patients may be initially under-dosed with vancomycin
- Antipsychotic therapy is associated with short-term serious events in older adults with dementia
- Cardiac troponin is associated with worse outcome in acute heart failure
Does management of ICU patients by critical care physicians reduce mortality?
Background: There is variation in the extent of involvement by critical care physicians in managing patients in ICUs. Several small studies have demonstrated improved outcomes when patients are managed by critical care physicians. This study expanded these findings by examining a national database of multiple ICUs.
Study design: Retrospective database analysis.
Setting: 123 ICUs in 100 U.S. hospitals
Synopsis: Using a national database of ICU patients, 101,832 admissions were analyzed. Controlling for ICU characteristics, patient demographics, and severity of illness (SOI), the impact of critical care management (CCM) on the primary outcome of hospital mortality was analyzed. Patients who received CCM had higher SOI, received more procedures, and had higher mortality rates than those who did not receive CCM. After adjustment for these variables, hospital mortality rates were higher for those patients who received CCM.
Because this was a retrospective analysis, it is not possible to state there was a causal relationship between care by a critical care physician and worse outcome. Other unmeasured clinical differences between the patients receiving CCM and those that did not may have existed that resulted in the higher mortality. Additionally, although the database identified management by a critical care physician, it did not differentiate whether the management was by a full-time intensivist. Therefore, conclusions cannot be made regarding the value of full-time, on-site intensivist management.
Bottom line: Additional analysis is required to determine the value of intensivists in the management of critically ill patients.
Citation: Levy MM, Rapoport J, Lemeshow S, Chalfin DB, Phillips G, Danis M. Association between critical care physician management and patient mortality in the intensive care unit. Ann Int Med 2008; 148: 801-809.
What is the frequency of iatrogenic drug overdose in patients with renal insufficiency?
Background: The Institute of Medicine Report, “To Err is Human” suggested 7,000 deaths occur annually because of medication errors. Renal insufficiency is relatively common in hospitalized patients. Previous studies have suggested overdose of medications is frequent in patients with renal insufficiency. There is a lack of large-scale studies identifying the most commonly overdosed medications and the predictive physician factors for these errors.
Study design: Retrospective observational study.
Setting: A single 1,080-bed tertiary teaching hospital
Synopsis: A clinical data mart was constructed that contained 48 months of prescription data, serum creatinine levels, along with physician characteristics. 28,954 patients with renal insufficiency had 431,119 prescription orders to analyze. 3.5% of drug doses were found excessive. The overdose rate in patients with moderate to severe renal insufficiency was 28.2%. 10 drugs accounted for 85.4% of the overdoses. There was a negative correlation between physician clinical experience and overdose rate.
Study results are limited by the study’s retrospective nature. Further, the prescribed dose was presumed to be the dose actually administered, and there were no data on the actual doses given to patients. The study was limited to a single institution and may not be generalizable.
Bottom line: Iatrogenic drug overdose is quite common among inpatients with renal insufficiency. Only a few drugs are commonly responsible. The physicians’ clinical experience, workload of prescriptions, and patients’ renal function correlated with overdose.
Citation: Sheen SS, Choi JE, Park RW, Kim EY, Lee YH, Kang UG. Overdoser rate of drugs requiring renal dose adjustment: data analysis of 4 years prescriptions at a tertiary teaching hospital. J Gen Intern Med 2007;23(4):423-8
Will a national education program based on the “Surviving Sepsis Campaign” guidelines improve survival and processes of care?
Background: Sepsis is one of the most prevalent diseases and one of the main causes of death among hospitalized patients. Several single-center studies have suggested quality improvement efforts based on the Surviving Sepsis Guidelines were associated with better outcomes.
Study design: Prospective multicenter before-and-after study design.
Setting: 59 medical and surgical ICUs throughout Spain.
Synopsis: 854 patients with severe sepsis were enrolled in the pre–intervention group. The intervention consisted of education on the use of bundles of care. The treatment was organized into two bundles: a resuscitation bundle (six tasks to be performed within six hours) and a management bundle (four tasks to be completed within 24 hours). 1,465 patients were enrolled in the post-training period. Hospital mortality, adherence to the bundles, ICU mortality, 28-day mortality, hospital and ICU length of stay were measured.
Patients in the post-intervention group had lower mortality (44.0% vs. 39.5% P=0.04) and better compliance with the bundles improved. No other outcomes improved. One year later, mortality gains persisted but compliance with the resuscitation bundle had lapsed.
This study did not employ a control group, making it difficult to ascribe the improvement in compliance solely to the training given (some improvement in processes may have occurred independent of the training).
Bottom line: A national education effort to promote bundles of care for severe sepsis and septic shock was associated with improved guideline compliance and lower hospital mortality.
Citation: Ferrer R, Artigas A, Levy MM, et al. Improvement in process of care and outcomes after a multicenter severe sepsis educational program in Spain. JAMA 2008;299(19):2294-2303.
Can SSRI and problem-solving therapy reduce the incidence of depression in non-depressed patients with a recent stroke?
Background: Depression occurs in more than half of previously non-depressed patients after a stroke. Post-stroke depression is associated with impaired recovery and increased mortality.
Study design: A multicenter randomized controlled trial.
Setting: Two urban university-affiliated hospitals and a suburban rehabilitation hospital in the U.S.
Synopsis: 178 patients age 50 to 90 were enrolled within three months of an index stroke in a 12-month trial. The patients were randomized into three groups of a double-blind placebo control comparison of escitalopram with placebo, and non-blinded problem-solving therapy group.
During the period of the trial, patients on escitalopram experienced significant reductions in the incidence of depression versus placebo (23.1% vs. 34.5%). Problem-solving therapy did not result in significant benefit over the placebo.
The study results were limited by several factors. The study did not include all patients with acute stroke, employed a relatively small sample size, used a non-blinded psychological problem-solving therapy group, and had a high drop out rate.
Bottom line: Consider SSRI use to prevent depression in post-stroke patients.
Citation: Robinson RG, Jorge RE, Moser DJ, et. al. Escitalopram and problem-solving therapy for prevention of post stroke depression: a randomized controlled trial. JAMA 2008;299 (20):2391-2400
Do stop orders for indwelling urinary catheters reduce the duration of inappropriate urinary catheterization and incidence of urinary tract infection?
Background: About 25% of hospitalized patients have an indwelling urinary catheter inserted, and in 30% to 50% of these patients, urinary catheters are not indicated. Approximately 50% of patients with a catheter inserted for five days or more will develop bacteriuria with about 80% of hospital-acquired urinary tract infections occurring in patients with a urinary catheter.
Study design: A randomized controlled study.
Setting: Three tertiary care hospitals in Ontario, Canada.
Synopsis: 692 patients with indwelling urinary catheters admitted to seven general medical units in three tertiary care hospitals from January 2004 to June 2006 were randomized into two groups: 269 in the stop-order group, and 252 in the usual care group. Patients in the stop-order group had fewer days of inappropriate and total urinary catheter used (2.20 days) compared with the usual care group (3.89 days). There was no difference in the incidence of urinary tract infection between both groups.
Study results were limited by several factors, including a lack of control for exposure of participants to antimicrobials, missing urine cultures, and lack of evaluation of the effect of reducing urinary catheter use on mobility and quality of life. The 1.34-day reduction in the duration of catheterization may not be sufficient to significantly reduce bacteriuria.
Bottom line: Consider using stop orders in all patients with indwelling urinary catheters.
Citation: Loeb M, Hunt D, O’Halloran K, et. al. Stop orders to reduce inappropriate urinary catheterization in hospitalized patients: a randomized control trial. J Gen Intern Med 2008;23(6):816-820.
Does interrupting anticoagulation in patients with atrial fibrillation undergoing surgery cause an increased rate of thromboembolism?
Background: There is a known risk of thromboembolism (between 0.5% and 20% annually) in patients with atrial fibrillation. Studies are limited regarding the risk of thromboembolism with holding anticoagulation in the perioperative period for nonvalvular atrial fibrillation. This study attempted to answer this question.
Study design: Prospective cohort.
Setting: Thromboembolism clinic of the Mayo Clinic.
Synopsis: 345 patients with nonvalvular atrial fibrillation whose anticoagulation was perioperatively held were monitored for three months after surgery for thromboembolic events. Warfarin therapy was held for 5.3 days +/- three days before surgery and restarted 1.3 days +/- 3.4 days after surgery. Bridging heparin therapy was used for 204/386 procedures.
Four patients suffered six thromboembolic events; two patients while receiving bridging heparin therapy and two without heparin. The total incidence of thromboembolic events was 1.1%. This is compared with an expected incidence of 0.09% to 2.07% for patients with atrial fibrillation on warfarin. Bleeding complications rates were also low.
The authors recognized a possible selection bias and the fact patients who received bridging heparin therapy were not randomized. Despite these potential flaws, there seems to be minimal risk of holding anticoagulation in the perioperative period. Bridging heparin therapy added no additional benefit.
Bottom line: There is no increased risk of thromboembolism if anticoagulation is interrupted without bridging therapy in nonvalvular atrial fibrillation patients undergoing surgery.
Citation: Wysokinski WE, McBane RD, Daniels PR, et al. Periprocedural anticoagulation management of patients with nonvalvular atrial fibrillation. Mayo Clinic Proceedings 2008;83(6):639-645.
Are obese patients under-dosed when prescribed intravenous vancomycin?
Background: Weight-based vancomycin dosing has been recommended by the Infectious Diseases Society of America, yet flat dosing is still commonly employed. Flat dosing has the potential of increasing resistance and having adverse clinical effects.
Study design: Retrospective cohort.
Setting: Two tertiary care medical centers without pharmacy-guided vancomycin dosing programs.
Synopsis: A retrospective review was done of pharmacy prescription files at two tertiary care medical centers that did not have pharmacy-guided vancomycin programs. Patients were divided into cohorts based on their body mass index: underweight (<18.5 kg/sqm) normal weight (18.5-24.9 kg/sqm) overweight (25.0-29.9 kg/sqm) and obese (>29.9 kg/sqm). Each class was studied for rates of adequate vancomycin dosing which was defined as >10 mg/kg/dose. A total of 421 patients were included. There were no other dissimilar baseline characteristics. Total daily dose was similar for all groups with adequate initial dosing achieved in 100%, 99.0%, 93.9% and 27.7% for underweight, normal weight, overweight and obese patients, respectively.
Bottom line: Use weight-based dosing of vancomycin to limit the possibility of under-dosing in obese patients.
Citation: Hall RG, Payne KD, Bain AB, et al. Multicenter evaluation of vancomycin dosing: emphasis on obesity. Am J of Med. 2008;121:515-518.
What is the rate of adverse events with short-term antipsychotic therapy in elderly demented patients?
Study design: Population-based retrospective cohort study.
Setting: Community-dwelling cohort and nursing home cohort.
Synopsis: A cohort of patients from Ontario age 66 and older with the diagnosis of dementia and a prescription for an anti-psychotic drug between April 1, 1997, and March 31, 2004, were divided into two groups by where they lived (community or nursing home). Each cohort was further divided into three groups based on antipsychotic exposure of none, atypical, or conventional.
All serious adverse events (defined as extra-pyramidal symptoms (EPS), cerebrovascular events, and acute care hospital admission or death) were evaluated within 30 days of initiating therapy. In the community group, individuals who received conventional antipsychotic therapy were 3.8 times more likely to have an adverse event compared with the group taking no antipsychotics. The patients prescribed an atypical antipsychotic medicine were 3.2 times more likely to experience an adverse event. In the nursing home group, patients who received conventional and atypical antipsychotic therapy were 2.4 and 1.9 times more likely to have a serious adverse event, respectively.
Bottom line: Serious events are frequent following the short-term use of antipsychotic therapy in older adults with dementia. Serious adverse events were more common among those who received a prescription for conventional rather than atypical antipsychotic drugs.
Citation: Rochon PA, Normand SL, Gomes T, et al. Antipsychotic therapy and short-term serious events in older adults with dementia. Arch Intern Med. 2008;168(10):1090-1096
What is the association between troponin levels and adverse events in hospitalized patients with acute decompensated heart failure?
Background: There were more than 1 million hospitalizations for heart failure in 2007, making it the most costly medical condition based on diagnosis and treatment. Evidence suggests an initial risk stratification process allows for earlier implementation of aggressive therapy, which can affect hospital utilization.
Study design: Retrospective analysis of Acute Decompensated Heart Failure National Registry (ADHERE).
Setting: Hospitalization records from 274 hospitals from October 2001 to January 2004.
Synopsis: Evaluation of the data from ADHERE for outcomes associated with elevated troponin levels in patients with acute decompensated heart failure (ADHF). Patients who had a creatinine level above 2.0 mg per deciliter were excluded.
Cardiac troponin I was measured in 61,379 patients and cardiac troponin T in 7880 patients. Overall, 4,240 patients (6.2%) had an elevated troponin level. Troponin positive patients had a higher rate of in-hospital mortality than troponin negative patients (8.0% vs. 2.7%, P<0.001). The adjusted odds ratio for death among patients with a positive troponin test was 2.55. Ischemic heart failure was present in 53% of the troponin positive patients and was not a useful predictor of troponin status or mortality.
Bottom line: Measurement of troponin is an important prognostic indicator in the initial evaluation of patients with ADHF. This early assessment of risk should be factored into medical decisions with respect to triage and medical management.
Citation: Peacock FW, De Marco T, Fonarow GC, et al. Cardiac troponin and outcome in acute heart failure. N Engl J Med 2008;358:2117-26
Literature at a Glance
- ICU management by critical care physicians may increase the odds of hospital mortality
- Iatrogenic drug overdose common among patients with renal insufficiency
- An educational effort lowers hospital mortality for severe sepsis and septic shock
- SSRI and problem-solving therapy prevents post-stroke depression
- Stop orders for Foley catheters reduce the duration of inappropriate urinary catheterization
- No thromboembolism risk with interrupting anticoagulation in atrial fibrillation patients undergoing surgery
- Obese patients may be initially under-dosed with vancomycin
- Antipsychotic therapy is associated with short-term serious events in older adults with dementia
- Cardiac troponin is associated with worse outcome in acute heart failure
Does management of ICU patients by critical care physicians reduce mortality?
Background: There is variation in the extent of involvement by critical care physicians in managing patients in ICUs. Several small studies have demonstrated improved outcomes when patients are managed by critical care physicians. This study expanded these findings by examining a national database of multiple ICUs.
Study design: Retrospective database analysis.
Setting: 123 ICUs in 100 U.S. hospitals
Synopsis: Using a national database of ICU patients, 101,832 admissions were analyzed. Controlling for ICU characteristics, patient demographics, and severity of illness (SOI), the impact of critical care management (CCM) on the primary outcome of hospital mortality was analyzed. Patients who received CCM had higher SOI, received more procedures, and had higher mortality rates than those who did not receive CCM. After adjustment for these variables, hospital mortality rates were higher for those patients who received CCM.
Because this was a retrospective analysis, it is not possible to state there was a causal relationship between care by a critical care physician and worse outcome. Other unmeasured clinical differences between the patients receiving CCM and those that did not may have existed that resulted in the higher mortality. Additionally, although the database identified management by a critical care physician, it did not differentiate whether the management was by a full-time intensivist. Therefore, conclusions cannot be made regarding the value of full-time, on-site intensivist management.
Bottom line: Additional analysis is required to determine the value of intensivists in the management of critically ill patients.
Citation: Levy MM, Rapoport J, Lemeshow S, Chalfin DB, Phillips G, Danis M. Association between critical care physician management and patient mortality in the intensive care unit. Ann Int Med 2008; 148: 801-809.
What is the frequency of iatrogenic drug overdose in patients with renal insufficiency?
Background: The Institute of Medicine Report, “To Err is Human” suggested 7,000 deaths occur annually because of medication errors. Renal insufficiency is relatively common in hospitalized patients. Previous studies have suggested overdose of medications is frequent in patients with renal insufficiency. There is a lack of large-scale studies identifying the most commonly overdosed medications and the predictive physician factors for these errors.
Study design: Retrospective observational study.
Setting: A single 1,080-bed tertiary teaching hospital
Synopsis: A clinical data mart was constructed that contained 48 months of prescription data, serum creatinine levels, along with physician characteristics. 28,954 patients with renal insufficiency had 431,119 prescription orders to analyze. 3.5% of drug doses were found excessive. The overdose rate in patients with moderate to severe renal insufficiency was 28.2%. 10 drugs accounted for 85.4% of the overdoses. There was a negative correlation between physician clinical experience and overdose rate.
Study results are limited by the study’s retrospective nature. Further, the prescribed dose was presumed to be the dose actually administered, and there were no data on the actual doses given to patients. The study was limited to a single institution and may not be generalizable.
Bottom line: Iatrogenic drug overdose is quite common among inpatients with renal insufficiency. Only a few drugs are commonly responsible. The physicians’ clinical experience, workload of prescriptions, and patients’ renal function correlated with overdose.
Citation: Sheen SS, Choi JE, Park RW, Kim EY, Lee YH, Kang UG. Overdoser rate of drugs requiring renal dose adjustment: data analysis of 4 years prescriptions at a tertiary teaching hospital. J Gen Intern Med 2007;23(4):423-8
Will a national education program based on the “Surviving Sepsis Campaign” guidelines improve survival and processes of care?
Background: Sepsis is one of the most prevalent diseases and one of the main causes of death among hospitalized patients. Several single-center studies have suggested quality improvement efforts based on the Surviving Sepsis Guidelines were associated with better outcomes.
Study design: Prospective multicenter before-and-after study design.
Setting: 59 medical and surgical ICUs throughout Spain.
Synopsis: 854 patients with severe sepsis were enrolled in the pre–intervention group. The intervention consisted of education on the use of bundles of care. The treatment was organized into two bundles: a resuscitation bundle (six tasks to be performed within six hours) and a management bundle (four tasks to be completed within 24 hours). 1,465 patients were enrolled in the post-training period. Hospital mortality, adherence to the bundles, ICU mortality, 28-day mortality, hospital and ICU length of stay were measured.
Patients in the post-intervention group had lower mortality (44.0% vs. 39.5% P=0.04) and better compliance with the bundles improved. No other outcomes improved. One year later, mortality gains persisted but compliance with the resuscitation bundle had lapsed.
This study did not employ a control group, making it difficult to ascribe the improvement in compliance solely to the training given (some improvement in processes may have occurred independent of the training).
Bottom line: A national education effort to promote bundles of care for severe sepsis and septic shock was associated with improved guideline compliance and lower hospital mortality.
Citation: Ferrer R, Artigas A, Levy MM, et al. Improvement in process of care and outcomes after a multicenter severe sepsis educational program in Spain. JAMA 2008;299(19):2294-2303.
Can SSRI and problem-solving therapy reduce the incidence of depression in non-depressed patients with a recent stroke?
Background: Depression occurs in more than half of previously non-depressed patients after a stroke. Post-stroke depression is associated with impaired recovery and increased mortality.
Study design: A multicenter randomized controlled trial.
Setting: Two urban university-affiliated hospitals and a suburban rehabilitation hospital in the U.S.
Synopsis: 178 patients age 50 to 90 were enrolled within three months of an index stroke in a 12-month trial. The patients were randomized into three groups of a double-blind placebo control comparison of escitalopram with placebo, and non-blinded problem-solving therapy group.
During the period of the trial, patients on escitalopram experienced significant reductions in the incidence of depression versus placebo (23.1% vs. 34.5%). Problem-solving therapy did not result in significant benefit over the placebo.
The study results were limited by several factors. The study did not include all patients with acute stroke, employed a relatively small sample size, used a non-blinded psychological problem-solving therapy group, and had a high drop out rate.
Bottom line: Consider SSRI use to prevent depression in post-stroke patients.
Citation: Robinson RG, Jorge RE, Moser DJ, et. al. Escitalopram and problem-solving therapy for prevention of post stroke depression: a randomized controlled trial. JAMA 2008;299 (20):2391-2400
Do stop orders for indwelling urinary catheters reduce the duration of inappropriate urinary catheterization and incidence of urinary tract infection?
Background: About 25% of hospitalized patients have an indwelling urinary catheter inserted, and in 30% to 50% of these patients, urinary catheters are not indicated. Approximately 50% of patients with a catheter inserted for five days or more will develop bacteriuria with about 80% of hospital-acquired urinary tract infections occurring in patients with a urinary catheter.
Study design: A randomized controlled study.
Setting: Three tertiary care hospitals in Ontario, Canada.
Synopsis: 692 patients with indwelling urinary catheters admitted to seven general medical units in three tertiary care hospitals from January 2004 to June 2006 were randomized into two groups: 269 in the stop-order group, and 252 in the usual care group. Patients in the stop-order group had fewer days of inappropriate and total urinary catheter used (2.20 days) compared with the usual care group (3.89 days). There was no difference in the incidence of urinary tract infection between both groups.
Study results were limited by several factors, including a lack of control for exposure of participants to antimicrobials, missing urine cultures, and lack of evaluation of the effect of reducing urinary catheter use on mobility and quality of life. The 1.34-day reduction in the duration of catheterization may not be sufficient to significantly reduce bacteriuria.
Bottom line: Consider using stop orders in all patients with indwelling urinary catheters.
Citation: Loeb M, Hunt D, O’Halloran K, et. al. Stop orders to reduce inappropriate urinary catheterization in hospitalized patients: a randomized control trial. J Gen Intern Med 2008;23(6):816-820.
Does interrupting anticoagulation in patients with atrial fibrillation undergoing surgery cause an increased rate of thromboembolism?
Background: There is a known risk of thromboembolism (between 0.5% and 20% annually) in patients with atrial fibrillation. Studies are limited regarding the risk of thromboembolism with holding anticoagulation in the perioperative period for nonvalvular atrial fibrillation. This study attempted to answer this question.
Study design: Prospective cohort.
Setting: Thromboembolism clinic of the Mayo Clinic.
Synopsis: 345 patients with nonvalvular atrial fibrillation whose anticoagulation was perioperatively held were monitored for three months after surgery for thromboembolic events. Warfarin therapy was held for 5.3 days +/- three days before surgery and restarted 1.3 days +/- 3.4 days after surgery. Bridging heparin therapy was used for 204/386 procedures.
Four patients suffered six thromboembolic events; two patients while receiving bridging heparin therapy and two without heparin. The total incidence of thromboembolic events was 1.1%. This is compared with an expected incidence of 0.09% to 2.07% for patients with atrial fibrillation on warfarin. Bleeding complications rates were also low.
The authors recognized a possible selection bias and the fact patients who received bridging heparin therapy were not randomized. Despite these potential flaws, there seems to be minimal risk of holding anticoagulation in the perioperative period. Bridging heparin therapy added no additional benefit.
Bottom line: There is no increased risk of thromboembolism if anticoagulation is interrupted without bridging therapy in nonvalvular atrial fibrillation patients undergoing surgery.
Citation: Wysokinski WE, McBane RD, Daniels PR, et al. Periprocedural anticoagulation management of patients with nonvalvular atrial fibrillation. Mayo Clinic Proceedings 2008;83(6):639-645.
Are obese patients under-dosed when prescribed intravenous vancomycin?
Background: Weight-based vancomycin dosing has been recommended by the Infectious Diseases Society of America, yet flat dosing is still commonly employed. Flat dosing has the potential of increasing resistance and having adverse clinical effects.
Study design: Retrospective cohort.
Setting: Two tertiary care medical centers without pharmacy-guided vancomycin dosing programs.
Synopsis: A retrospective review was done of pharmacy prescription files at two tertiary care medical centers that did not have pharmacy-guided vancomycin programs. Patients were divided into cohorts based on their body mass index: underweight (<18.5 kg/sqm) normal weight (18.5-24.9 kg/sqm) overweight (25.0-29.9 kg/sqm) and obese (>29.9 kg/sqm). Each class was studied for rates of adequate vancomycin dosing which was defined as >10 mg/kg/dose. A total of 421 patients were included. There were no other dissimilar baseline characteristics. Total daily dose was similar for all groups with adequate initial dosing achieved in 100%, 99.0%, 93.9% and 27.7% for underweight, normal weight, overweight and obese patients, respectively.
Bottom line: Use weight-based dosing of vancomycin to limit the possibility of under-dosing in obese patients.
Citation: Hall RG, Payne KD, Bain AB, et al. Multicenter evaluation of vancomycin dosing: emphasis on obesity. Am J of Med. 2008;121:515-518.
What is the rate of adverse events with short-term antipsychotic therapy in elderly demented patients?
Study design: Population-based retrospective cohort study.
Setting: Community-dwelling cohort and nursing home cohort.
Synopsis: A cohort of patients from Ontario age 66 and older with the diagnosis of dementia and a prescription for an anti-psychotic drug between April 1, 1997, and March 31, 2004, were divided into two groups by where they lived (community or nursing home). Each cohort was further divided into three groups based on antipsychotic exposure of none, atypical, or conventional.
All serious adverse events (defined as extra-pyramidal symptoms (EPS), cerebrovascular events, and acute care hospital admission or death) were evaluated within 30 days of initiating therapy. In the community group, individuals who received conventional antipsychotic therapy were 3.8 times more likely to have an adverse event compared with the group taking no antipsychotics. The patients prescribed an atypical antipsychotic medicine were 3.2 times more likely to experience an adverse event. In the nursing home group, patients who received conventional and atypical antipsychotic therapy were 2.4 and 1.9 times more likely to have a serious adverse event, respectively.
Bottom line: Serious events are frequent following the short-term use of antipsychotic therapy in older adults with dementia. Serious adverse events were more common among those who received a prescription for conventional rather than atypical antipsychotic drugs.
Citation: Rochon PA, Normand SL, Gomes T, et al. Antipsychotic therapy and short-term serious events in older adults with dementia. Arch Intern Med. 2008;168(10):1090-1096
What is the association between troponin levels and adverse events in hospitalized patients with acute decompensated heart failure?
Background: There were more than 1 million hospitalizations for heart failure in 2007, making it the most costly medical condition based on diagnosis and treatment. Evidence suggests an initial risk stratification process allows for earlier implementation of aggressive therapy, which can affect hospital utilization.
Study design: Retrospective analysis of Acute Decompensated Heart Failure National Registry (ADHERE).
Setting: Hospitalization records from 274 hospitals from October 2001 to January 2004.
Synopsis: Evaluation of the data from ADHERE for outcomes associated with elevated troponin levels in patients with acute decompensated heart failure (ADHF). Patients who had a creatinine level above 2.0 mg per deciliter were excluded.
Cardiac troponin I was measured in 61,379 patients and cardiac troponin T in 7880 patients. Overall, 4,240 patients (6.2%) had an elevated troponin level. Troponin positive patients had a higher rate of in-hospital mortality than troponin negative patients (8.0% vs. 2.7%, P<0.001). The adjusted odds ratio for death among patients with a positive troponin test was 2.55. Ischemic heart failure was present in 53% of the troponin positive patients and was not a useful predictor of troponin status or mortality.
Bottom line: Measurement of troponin is an important prognostic indicator in the initial evaluation of patients with ADHF. This early assessment of risk should be factored into medical decisions with respect to triage and medical management.
Citation: Peacock FW, De Marco T, Fonarow GC, et al. Cardiac troponin and outcome in acute heart failure. N Engl J Med 2008;358:2117-26
Literature at a Glance
- ICU management by critical care physicians may increase the odds of hospital mortality
- Iatrogenic drug overdose common among patients with renal insufficiency
- An educational effort lowers hospital mortality for severe sepsis and septic shock
- SSRI and problem-solving therapy prevents post-stroke depression
- Stop orders for Foley catheters reduce the duration of inappropriate urinary catheterization
- No thromboembolism risk with interrupting anticoagulation in atrial fibrillation patients undergoing surgery
- Obese patients may be initially under-dosed with vancomycin
- Antipsychotic therapy is associated with short-term serious events in older adults with dementia
- Cardiac troponin is associated with worse outcome in acute heart failure
Does management of ICU patients by critical care physicians reduce mortality?
Background: There is variation in the extent of involvement by critical care physicians in managing patients in ICUs. Several small studies have demonstrated improved outcomes when patients are managed by critical care physicians. This study expanded these findings by examining a national database of multiple ICUs.
Study design: Retrospective database analysis.
Setting: 123 ICUs in 100 U.S. hospitals
Synopsis: Using a national database of ICU patients, 101,832 admissions were analyzed. Controlling for ICU characteristics, patient demographics, and severity of illness (SOI), the impact of critical care management (CCM) on the primary outcome of hospital mortality was analyzed. Patients who received CCM had higher SOI, received more procedures, and had higher mortality rates than those who did not receive CCM. After adjustment for these variables, hospital mortality rates were higher for those patients who received CCM.
Because this was a retrospective analysis, it is not possible to state there was a causal relationship between care by a critical care physician and worse outcome. Other unmeasured clinical differences between the patients receiving CCM and those that did not may have existed that resulted in the higher mortality. Additionally, although the database identified management by a critical care physician, it did not differentiate whether the management was by a full-time intensivist. Therefore, conclusions cannot be made regarding the value of full-time, on-site intensivist management.
Bottom line: Additional analysis is required to determine the value of intensivists in the management of critically ill patients.
Citation: Levy MM, Rapoport J, Lemeshow S, Chalfin DB, Phillips G, Danis M. Association between critical care physician management and patient mortality in the intensive care unit. Ann Int Med 2008; 148: 801-809.
What is the frequency of iatrogenic drug overdose in patients with renal insufficiency?
Background: The Institute of Medicine Report, “To Err is Human” suggested 7,000 deaths occur annually because of medication errors. Renal insufficiency is relatively common in hospitalized patients. Previous studies have suggested overdose of medications is frequent in patients with renal insufficiency. There is a lack of large-scale studies identifying the most commonly overdosed medications and the predictive physician factors for these errors.
Study design: Retrospective observational study.
Setting: A single 1,080-bed tertiary teaching hospital
Synopsis: A clinical data mart was constructed that contained 48 months of prescription data, serum creatinine levels, along with physician characteristics. 28,954 patients with renal insufficiency had 431,119 prescription orders to analyze. 3.5% of drug doses were found excessive. The overdose rate in patients with moderate to severe renal insufficiency was 28.2%. 10 drugs accounted for 85.4% of the overdoses. There was a negative correlation between physician clinical experience and overdose rate.
Study results are limited by the study’s retrospective nature. Further, the prescribed dose was presumed to be the dose actually administered, and there were no data on the actual doses given to patients. The study was limited to a single institution and may not be generalizable.
Bottom line: Iatrogenic drug overdose is quite common among inpatients with renal insufficiency. Only a few drugs are commonly responsible. The physicians’ clinical experience, workload of prescriptions, and patients’ renal function correlated with overdose.
Citation: Sheen SS, Choi JE, Park RW, Kim EY, Lee YH, Kang UG. Overdoser rate of drugs requiring renal dose adjustment: data analysis of 4 years prescriptions at a tertiary teaching hospital. J Gen Intern Med 2007;23(4):423-8
Will a national education program based on the “Surviving Sepsis Campaign” guidelines improve survival and processes of care?
Background: Sepsis is one of the most prevalent diseases and one of the main causes of death among hospitalized patients. Several single-center studies have suggested quality improvement efforts based on the Surviving Sepsis Guidelines were associated with better outcomes.
Study design: Prospective multicenter before-and-after study design.
Setting: 59 medical and surgical ICUs throughout Spain.
Synopsis: 854 patients with severe sepsis were enrolled in the pre–intervention group. The intervention consisted of education on the use of bundles of care. The treatment was organized into two bundles: a resuscitation bundle (six tasks to be performed within six hours) and a management bundle (four tasks to be completed within 24 hours). 1,465 patients were enrolled in the post-training period. Hospital mortality, adherence to the bundles, ICU mortality, 28-day mortality, hospital and ICU length of stay were measured.
Patients in the post-intervention group had lower mortality (44.0% vs. 39.5% P=0.04) and better compliance with the bundles improved. No other outcomes improved. One year later, mortality gains persisted but compliance with the resuscitation bundle had lapsed.
This study did not employ a control group, making it difficult to ascribe the improvement in compliance solely to the training given (some improvement in processes may have occurred independent of the training).
Bottom line: A national education effort to promote bundles of care for severe sepsis and septic shock was associated with improved guideline compliance and lower hospital mortality.
Citation: Ferrer R, Artigas A, Levy MM, et al. Improvement in process of care and outcomes after a multicenter severe sepsis educational program in Spain. JAMA 2008;299(19):2294-2303.
Can SSRI and problem-solving therapy reduce the incidence of depression in non-depressed patients with a recent stroke?
Background: Depression occurs in more than half of previously non-depressed patients after a stroke. Post-stroke depression is associated with impaired recovery and increased mortality.
Study design: A multicenter randomized controlled trial.
Setting: Two urban university-affiliated hospitals and a suburban rehabilitation hospital in the U.S.
Synopsis: 178 patients age 50 to 90 were enrolled within three months of an index stroke in a 12-month trial. The patients were randomized into three groups of a double-blind placebo control comparison of escitalopram with placebo, and non-blinded problem-solving therapy group.
During the period of the trial, patients on escitalopram experienced significant reductions in the incidence of depression versus placebo (23.1% vs. 34.5%). Problem-solving therapy did not result in significant benefit over the placebo.
The study results were limited by several factors. The study did not include all patients with acute stroke, employed a relatively small sample size, used a non-blinded psychological problem-solving therapy group, and had a high drop out rate.
Bottom line: Consider SSRI use to prevent depression in post-stroke patients.
Citation: Robinson RG, Jorge RE, Moser DJ, et. al. Escitalopram and problem-solving therapy for prevention of post stroke depression: a randomized controlled trial. JAMA 2008;299 (20):2391-2400
Do stop orders for indwelling urinary catheters reduce the duration of inappropriate urinary catheterization and incidence of urinary tract infection?
Background: About 25% of hospitalized patients have an indwelling urinary catheter inserted, and in 30% to 50% of these patients, urinary catheters are not indicated. Approximately 50% of patients with a catheter inserted for five days or more will develop bacteriuria with about 80% of hospital-acquired urinary tract infections occurring in patients with a urinary catheter.
Study design: A randomized controlled study.
Setting: Three tertiary care hospitals in Ontario, Canada.
Synopsis: 692 patients with indwelling urinary catheters admitted to seven general medical units in three tertiary care hospitals from January 2004 to June 2006 were randomized into two groups: 269 in the stop-order group, and 252 in the usual care group. Patients in the stop-order group had fewer days of inappropriate and total urinary catheter used (2.20 days) compared with the usual care group (3.89 days). There was no difference in the incidence of urinary tract infection between both groups.
Study results were limited by several factors, including a lack of control for exposure of participants to antimicrobials, missing urine cultures, and lack of evaluation of the effect of reducing urinary catheter use on mobility and quality of life. The 1.34-day reduction in the duration of catheterization may not be sufficient to significantly reduce bacteriuria.
Bottom line: Consider using stop orders in all patients with indwelling urinary catheters.
Citation: Loeb M, Hunt D, O’Halloran K, et. al. Stop orders to reduce inappropriate urinary catheterization in hospitalized patients: a randomized control trial. J Gen Intern Med 2008;23(6):816-820.
Does interrupting anticoagulation in patients with atrial fibrillation undergoing surgery cause an increased rate of thromboembolism?
Background: There is a known risk of thromboembolism (between 0.5% and 20% annually) in patients with atrial fibrillation. Studies are limited regarding the risk of thromboembolism with holding anticoagulation in the perioperative period for nonvalvular atrial fibrillation. This study attempted to answer this question.
Study design: Prospective cohort.
Setting: Thromboembolism clinic of the Mayo Clinic.
Synopsis: 345 patients with nonvalvular atrial fibrillation whose anticoagulation was perioperatively held were monitored for three months after surgery for thromboembolic events. Warfarin therapy was held for 5.3 days +/- three days before surgery and restarted 1.3 days +/- 3.4 days after surgery. Bridging heparin therapy was used for 204/386 procedures.
Four patients suffered six thromboembolic events; two patients while receiving bridging heparin therapy and two without heparin. The total incidence of thromboembolic events was 1.1%. This is compared with an expected incidence of 0.09% to 2.07% for patients with atrial fibrillation on warfarin. Bleeding complications rates were also low.
The authors recognized a possible selection bias and the fact patients who received bridging heparin therapy were not randomized. Despite these potential flaws, there seems to be minimal risk of holding anticoagulation in the perioperative period. Bridging heparin therapy added no additional benefit.
Bottom line: There is no increased risk of thromboembolism if anticoagulation is interrupted without bridging therapy in nonvalvular atrial fibrillation patients undergoing surgery.
Citation: Wysokinski WE, McBane RD, Daniels PR, et al. Periprocedural anticoagulation management of patients with nonvalvular atrial fibrillation. Mayo Clinic Proceedings 2008;83(6):639-645.
Are obese patients under-dosed when prescribed intravenous vancomycin?
Background: Weight-based vancomycin dosing has been recommended by the Infectious Diseases Society of America, yet flat dosing is still commonly employed. Flat dosing has the potential of increasing resistance and having adverse clinical effects.
Study design: Retrospective cohort.
Setting: Two tertiary care medical centers without pharmacy-guided vancomycin dosing programs.
Synopsis: A retrospective review was done of pharmacy prescription files at two tertiary care medical centers that did not have pharmacy-guided vancomycin programs. Patients were divided into cohorts based on their body mass index: underweight (<18.5 kg/sqm) normal weight (18.5-24.9 kg/sqm) overweight (25.0-29.9 kg/sqm) and obese (>29.9 kg/sqm). Each class was studied for rates of adequate vancomycin dosing which was defined as >10 mg/kg/dose. A total of 421 patients were included. There were no other dissimilar baseline characteristics. Total daily dose was similar for all groups with adequate initial dosing achieved in 100%, 99.0%, 93.9% and 27.7% for underweight, normal weight, overweight and obese patients, respectively.
Bottom line: Use weight-based dosing of vancomycin to limit the possibility of under-dosing in obese patients.
Citation: Hall RG, Payne KD, Bain AB, et al. Multicenter evaluation of vancomycin dosing: emphasis on obesity. Am J of Med. 2008;121:515-518.
What is the rate of adverse events with short-term antipsychotic therapy in elderly demented patients?
Study design: Population-based retrospective cohort study.
Setting: Community-dwelling cohort and nursing home cohort.
Synopsis: A cohort of patients from Ontario age 66 and older with the diagnosis of dementia and a prescription for an anti-psychotic drug between April 1, 1997, and March 31, 2004, were divided into two groups by where they lived (community or nursing home). Each cohort was further divided into three groups based on antipsychotic exposure of none, atypical, or conventional.
All serious adverse events (defined as extra-pyramidal symptoms (EPS), cerebrovascular events, and acute care hospital admission or death) were evaluated within 30 days of initiating therapy. In the community group, individuals who received conventional antipsychotic therapy were 3.8 times more likely to have an adverse event compared with the group taking no antipsychotics. The patients prescribed an atypical antipsychotic medicine were 3.2 times more likely to experience an adverse event. In the nursing home group, patients who received conventional and atypical antipsychotic therapy were 2.4 and 1.9 times more likely to have a serious adverse event, respectively.
Bottom line: Serious events are frequent following the short-term use of antipsychotic therapy in older adults with dementia. Serious adverse events were more common among those who received a prescription for conventional rather than atypical antipsychotic drugs.
Citation: Rochon PA, Normand SL, Gomes T, et al. Antipsychotic therapy and short-term serious events in older adults with dementia. Arch Intern Med. 2008;168(10):1090-1096
What is the association between troponin levels and adverse events in hospitalized patients with acute decompensated heart failure?
Background: There were more than 1 million hospitalizations for heart failure in 2007, making it the most costly medical condition based on diagnosis and treatment. Evidence suggests an initial risk stratification process allows for earlier implementation of aggressive therapy, which can affect hospital utilization.
Study design: Retrospective analysis of Acute Decompensated Heart Failure National Registry (ADHERE).
Setting: Hospitalization records from 274 hospitals from October 2001 to January 2004.
Synopsis: Evaluation of the data from ADHERE for outcomes associated with elevated troponin levels in patients with acute decompensated heart failure (ADHF). Patients who had a creatinine level above 2.0 mg per deciliter were excluded.
Cardiac troponin I was measured in 61,379 patients and cardiac troponin T in 7880 patients. Overall, 4,240 patients (6.2%) had an elevated troponin level. Troponin positive patients had a higher rate of in-hospital mortality than troponin negative patients (8.0% vs. 2.7%, P<0.001). The adjusted odds ratio for death among patients with a positive troponin test was 2.55. Ischemic heart failure was present in 53% of the troponin positive patients and was not a useful predictor of troponin status or mortality.
Bottom line: Measurement of troponin is an important prognostic indicator in the initial evaluation of patients with ADHF. This early assessment of risk should be factored into medical decisions with respect to triage and medical management.
Citation: Peacock FW, De Marco T, Fonarow GC, et al. Cardiac troponin and outcome in acute heart failure. N Engl J Med 2008;358:2117-26
Behind the Scenes

In the last year, SHM has made great strides in improving the user experience at www. hospitalmedicine.org. Now it’s easier than ever to keep up with the latest news from the fastest-growing specialty in the history of modern healthcare. In an effort to bring as much energy as possible to this cutting-edge specialty, SHM strives to expand our online tools by offering our members the latest resources in education, events and publications over the newest mediums available. Like hospital medicine, Web 2.0 is a trend on the rise. From blogs to podcasts to our new RSS feeds, you will notice many new applications throughout SHM’s site.
hospitalmedicine.org: New and Improved
The first step in setting this new approach into motion was a complete overhaul of SHM’s Web site. This major renovation set the stage for a variety of new features, including seven resource rooms focused on Quality Improvement and supplemental clinical tools, as well as the introduction of online discussion forums and the SHM Career Center.
New Event Sites
Following our Web site expansion, we introduced several specialty sites for our most popular products, including SHM’s “2007-2008 State of the Hospital Medicine Movement” survey, as well as SHM’s Leadership Academy, Annual Meeting, and (coming soon) SHM’s One Day University.
These sites offer inside information about product news, meeting topics, curricula, and exclusive member offers. This year’s Hospital Medicine 2009 (HM09) site features more than 40 presentations from Hospital Medicine 2008 (HM08) for users to view such topics as quality improvement, operations, and clinical. With year-round access to resources, information from past meetings isn’t lost. It can be retrieved daily for practicing hospitalists.
Blogs
SHM first introduced blogs to our members in 2007 with the launch of “Wachter’s World” (www.wachtersworld.org), as well as the HM07 blog, which featured an inside look at the goings-on at the annual meeting. Blogs create an interactive forum to discuss relevant issues on a daily basis and introduce readers to the perspectives of some of the most reputable hospitalists in the specialty today.
This year, we expanded our blogs to reflect on past events, offering participants a chance to share highlights and feedback from our annual meetings. Not only does this help our members keep current on hospital medicine news, but it also provides an outlet to voice opinions and help influence the direction of the society.

Podcasts
For those of you who enjoy auditory learning, you will find podcasts attached to event pages and CME listings. Our podcast library features guests, such as featured keynote speakers, industry specialists, SHM board members, and event attendees. Be on the lookout for SHM team members at upcoming events, as you may have the opportunity for a podcast interview of your own!
RSS Feeds
In June 2008 SHM created its own RSS feed, offering biweekly updates. Subscribers to SHM’s RSS feed receive up-to-the minute news streaming to their e-mail/PDAs, with updates ranging from SHM’s organizational growth and development to relative changes in legislation/public policy and anything relating to hospital medicine. Subscribe today so that you don’t miss the most current updates to hospitalmedicine.org.
Social Networking
Networking always has been one of the most important benefits of SHM membership. From communicating with local hospitalists at chapter meetings, to national and international colleagues at our annual meeting, there is a sense of community among those in the hospital medicine field. SHM recognizes the importance of building this community and has taken networking to a new level through participation in social networking sites such as Facebook and LinkedIn. If you currently are a user of these sites, join the SHM group and get connected!
All of these resources are at your fingertips. Visit us online at www.hospitalmedicine.org to try out one or all of these new features and upgrade your SHM experience. TH
In the last year, SHM has made great strides in improving the user experience at www. hospitalmedicine.org. Now it’s easier than ever to keep up with the latest news from the fastest-growing specialty in the history of modern healthcare. In an effort to bring as much energy as possible to this cutting-edge specialty, SHM strives to expand our online tools by offering our members the latest resources in education, events and publications over the newest mediums available. Like hospital medicine, Web 2.0 is a trend on the rise. From blogs to podcasts to our new RSS feeds, you will notice many new applications throughout SHM’s site.
hospitalmedicine.org: New and Improved
The first step in setting this new approach into motion was a complete overhaul of SHM’s Web site. This major renovation set the stage for a variety of new features, including seven resource rooms focused on Quality Improvement and supplemental clinical tools, as well as the introduction of online discussion forums and the SHM Career Center.
New Event Sites
Following our Web site expansion, we introduced several specialty sites for our most popular products, including SHM’s “2007-2008 State of the Hospital Medicine Movement” survey, as well as SHM’s Leadership Academy, Annual Meeting, and (coming soon) SHM’s One Day University.
These sites offer inside information about product news, meeting topics, curricula, and exclusive member offers. This year’s Hospital Medicine 2009 (HM09) site features more than 40 presentations from Hospital Medicine 2008 (HM08) for users to view such topics as quality improvement, operations, and clinical. With year-round access to resources, information from past meetings isn’t lost. It can be retrieved daily for practicing hospitalists.
Blogs
SHM first introduced blogs to our members in 2007 with the launch of “Wachter’s World” (www.wachtersworld.org), as well as the HM07 blog, which featured an inside look at the goings-on at the annual meeting. Blogs create an interactive forum to discuss relevant issues on a daily basis and introduce readers to the perspectives of some of the most reputable hospitalists in the specialty today.
This year, we expanded our blogs to reflect on past events, offering participants a chance to share highlights and feedback from our annual meetings. Not only does this help our members keep current on hospital medicine news, but it also provides an outlet to voice opinions and help influence the direction of the society.
Podcasts
For those of you who enjoy auditory learning, you will find podcasts attached to event pages and CME listings. Our podcast library features guests, such as featured keynote speakers, industry specialists, SHM board members, and event attendees. Be on the lookout for SHM team members at upcoming events, as you may have the opportunity for a podcast interview of your own!
RSS Feeds
In June 2008 SHM created its own RSS feed, offering biweekly updates. Subscribers to SHM’s RSS feed receive up-to-the minute news streaming to their e-mail/PDAs, with updates ranging from SHM’s organizational growth and development to relative changes in legislation/public policy and anything relating to hospital medicine. Subscribe today so that you don’t miss the most current updates to hospitalmedicine.org.
Social Networking
Networking always has been one of the most important benefits of SHM membership. From communicating with local hospitalists at chapter meetings, to national and international colleagues at our annual meeting, there is a sense of community among those in the hospital medicine field. SHM recognizes the importance of building this community and has taken networking to a new level through participation in social networking sites such as Facebook and LinkedIn. If you currently are a user of these sites, join the SHM group and get connected!
All of these resources are at your fingertips. Visit us online at www.hospitalmedicine.org to try out one or all of these new features and upgrade your SHM experience. TH
In the last year, SHM has made great strides in improving the user experience at www. hospitalmedicine.org. Now it’s easier than ever to keep up with the latest news from the fastest-growing specialty in the history of modern healthcare. In an effort to bring as much energy as possible to this cutting-edge specialty, SHM strives to expand our online tools by offering our members the latest resources in education, events and publications over the newest mediums available. Like hospital medicine, Web 2.0 is a trend on the rise. From blogs to podcasts to our new RSS feeds, you will notice many new applications throughout SHM’s site.
hospitalmedicine.org: New and Improved
The first step in setting this new approach into motion was a complete overhaul of SHM’s Web site. This major renovation set the stage for a variety of new features, including seven resource rooms focused on Quality Improvement and supplemental clinical tools, as well as the introduction of online discussion forums and the SHM Career Center.
New Event Sites
Following our Web site expansion, we introduced several specialty sites for our most popular products, including SHM’s “2007-2008 State of the Hospital Medicine Movement” survey, as well as SHM’s Leadership Academy, Annual Meeting, and (coming soon) SHM’s One Day University.
These sites offer inside information about product news, meeting topics, curricula, and exclusive member offers. This year’s Hospital Medicine 2009 (HM09) site features more than 40 presentations from Hospital Medicine 2008 (HM08) for users to view such topics as quality improvement, operations, and clinical. With year-round access to resources, information from past meetings isn’t lost. It can be retrieved daily for practicing hospitalists.
Blogs
SHM first introduced blogs to our members in 2007 with the launch of “Wachter’s World” (www.wachtersworld.org), as well as the HM07 blog, which featured an inside look at the goings-on at the annual meeting. Blogs create an interactive forum to discuss relevant issues on a daily basis and introduce readers to the perspectives of some of the most reputable hospitalists in the specialty today.
This year, we expanded our blogs to reflect on past events, offering participants a chance to share highlights and feedback from our annual meetings. Not only does this help our members keep current on hospital medicine news, but it also provides an outlet to voice opinions and help influence the direction of the society.
Podcasts
For those of you who enjoy auditory learning, you will find podcasts attached to event pages and CME listings. Our podcast library features guests, such as featured keynote speakers, industry specialists, SHM board members, and event attendees. Be on the lookout for SHM team members at upcoming events, as you may have the opportunity for a podcast interview of your own!
RSS Feeds
In June 2008 SHM created its own RSS feed, offering biweekly updates. Subscribers to SHM’s RSS feed receive up-to-the minute news streaming to their e-mail/PDAs, with updates ranging from SHM’s organizational growth and development to relative changes in legislation/public policy and anything relating to hospital medicine. Subscribe today so that you don’t miss the most current updates to hospitalmedicine.org.
Social Networking
Networking always has been one of the most important benefits of SHM membership. From communicating with local hospitalists at chapter meetings, to national and international colleagues at our annual meeting, there is a sense of community among those in the hospital medicine field. SHM recognizes the importance of building this community and has taken networking to a new level through participation in social networking sites such as Facebook and LinkedIn. If you currently are a user of these sites, join the SHM group and get connected!
All of these resources are at your fingertips. Visit us online at www.hospitalmedicine.org to try out one or all of these new features and upgrade your SHM experience. TH
Mixed Messages Called Out
I am a hospitalist outsider. A traditional internist, I cared for my patients in and out of the hospital, provided ICU and unassigned ED call, and later transitioned to hospital-only work. Our group developed a hospitalist program and has, hopefully, run an above-average system growing with our community. Even performing full-time hospital work, it took me a year to get over being referred to as a “hospitalist.” It seemed a confining label.
I also feel like an outsider while reading hospitalist literature’s divergent messages to hospitalists. On one hand, I hear great things about how hospitalists will revolutionize healthcare, spearheading improvements in safety, efficiency, and satisfaction, and filling administrative roles. I then see articles about negotiating out of working nights and weekends, about how the productivity of hospitalists remains stagnant but subsidy demands increase, and about how to limit caseloads. I see articles about hospitalist groups becoming privately held corporations, sending revenue that physicians generate (and hospitals subsidize) into the pockets of private investors.
There are two growing hospitalist camps. The first is filled with strategic thinkers driven to fix inefficient hospital care and save each of those 100,000 Institute of Medicine lives. These are the chief residents of yesterday, academically oriented problem solvers with IT savvy and a propensity for coffee-fueled all-nighters. You know them within your hospitalist groups and medical staffs.
The second camp consists of the lifestyle hospitalists; those for whom salary and 16 shifts a month are the goals that supersede professional loyalty to any particular group. These are the physicians who can help meet various metrics but want nothing to do with designing them.
These two groups read the literature with different eyes and career aspirations. As this division spreads, I strain to hear a drowning voice regarding another physician role: our responsibility to our patients. Drowning because both camps are swimming away from the patient, one toward a desk job, the other to a defined shift schedule.
Caring for patients is why we are in medicine in the first place. Most hospitalists came from primary care residencies, so the rewards of lifestyle and money must have been less important than direct patient contact. Primary care graduates entered traditional practices, promptly encountering the headaches of running a practice. Then suddenly a plum job with higher compensation and limited work hours was born, and, unsurprisingly, the primary care fields lost physicians to the hospitalist movement.
For new hospitalists exiting residency, there is no institutional knowledge of the old ways, and while they are not perfect, there are some noble qualities. Dedication to the profession is one, as is an enduring responsibility to one’s patient. Medicine required an occasional need to interrupt personal interests to help a sick human being—a patient—through a difficult time. For those physicians with traditional experience, can you recall articles suggesting negotiating for no nights and weekends? I’m not sure who we expect to provide this care to our patients if we can negotiate out of working.
There are certainly drawbacks to the traditional system: strained family relationships, substance abuse, and poor work-life balance—but don’t throw the baby out with the bathwater. These values elevated medicine to the position it holds today: a respected and well-compensated profession. I fear this young hospitalist specialty may not live up to its hype or responsibilities if hospitalists are motivated to focus on their “job” rather that their duties as the “doctor.” So what to do?
I think this can be a specialty that identifies members as physicians first and hospitalists second through the expectations of our peers in our own groups, medical staffs, and physician societies. We need to grow our groups with physicians dedicated not just to their partners, but the physician community at large; with those who want to improve care not just by meeting myocardial infarction guidelines, but with those who work with other physicians to help the patient manage their heart disease for 30 years; with physicians who ask about quality, teamwork, and the local community during the job interview and don’t begin with salary, patient caps, and weekend limitations.
Hospitalist group leaders need to expect these traits from their physicians. Otherwise practicing hospitalists will forever remain glorified residents and not leaders.
SHM needs to promote and recognize the values of being a physician in this field, instead of patting itself on the back for how trailblazing hospitalists could be while simultaneously ignoring what we are. TH
Edward Norman, MD, Internist/Hospitalist, Loveland, Colo.
I am a hospitalist outsider. A traditional internist, I cared for my patients in and out of the hospital, provided ICU and unassigned ED call, and later transitioned to hospital-only work. Our group developed a hospitalist program and has, hopefully, run an above-average system growing with our community. Even performing full-time hospital work, it took me a year to get over being referred to as a “hospitalist.” It seemed a confining label.
I also feel like an outsider while reading hospitalist literature’s divergent messages to hospitalists. On one hand, I hear great things about how hospitalists will revolutionize healthcare, spearheading improvements in safety, efficiency, and satisfaction, and filling administrative roles. I then see articles about negotiating out of working nights and weekends, about how the productivity of hospitalists remains stagnant but subsidy demands increase, and about how to limit caseloads. I see articles about hospitalist groups becoming privately held corporations, sending revenue that physicians generate (and hospitals subsidize) into the pockets of private investors.
There are two growing hospitalist camps. The first is filled with strategic thinkers driven to fix inefficient hospital care and save each of those 100,000 Institute of Medicine lives. These are the chief residents of yesterday, academically oriented problem solvers with IT savvy and a propensity for coffee-fueled all-nighters. You know them within your hospitalist groups and medical staffs.
The second camp consists of the lifestyle hospitalists; those for whom salary and 16 shifts a month are the goals that supersede professional loyalty to any particular group. These are the physicians who can help meet various metrics but want nothing to do with designing them.
These two groups read the literature with different eyes and career aspirations. As this division spreads, I strain to hear a drowning voice regarding another physician role: our responsibility to our patients. Drowning because both camps are swimming away from the patient, one toward a desk job, the other to a defined shift schedule.
Caring for patients is why we are in medicine in the first place. Most hospitalists came from primary care residencies, so the rewards of lifestyle and money must have been less important than direct patient contact. Primary care graduates entered traditional practices, promptly encountering the headaches of running a practice. Then suddenly a plum job with higher compensation and limited work hours was born, and, unsurprisingly, the primary care fields lost physicians to the hospitalist movement.
For new hospitalists exiting residency, there is no institutional knowledge of the old ways, and while they are not perfect, there are some noble qualities. Dedication to the profession is one, as is an enduring responsibility to one’s patient. Medicine required an occasional need to interrupt personal interests to help a sick human being—a patient—through a difficult time. For those physicians with traditional experience, can you recall articles suggesting negotiating for no nights and weekends? I’m not sure who we expect to provide this care to our patients if we can negotiate out of working.
There are certainly drawbacks to the traditional system: strained family relationships, substance abuse, and poor work-life balance—but don’t throw the baby out with the bathwater. These values elevated medicine to the position it holds today: a respected and well-compensated profession. I fear this young hospitalist specialty may not live up to its hype or responsibilities if hospitalists are motivated to focus on their “job” rather that their duties as the “doctor.” So what to do?
I think this can be a specialty that identifies members as physicians first and hospitalists second through the expectations of our peers in our own groups, medical staffs, and physician societies. We need to grow our groups with physicians dedicated not just to their partners, but the physician community at large; with those who want to improve care not just by meeting myocardial infarction guidelines, but with those who work with other physicians to help the patient manage their heart disease for 30 years; with physicians who ask about quality, teamwork, and the local community during the job interview and don’t begin with salary, patient caps, and weekend limitations.
Hospitalist group leaders need to expect these traits from their physicians. Otherwise practicing hospitalists will forever remain glorified residents and not leaders.
SHM needs to promote and recognize the values of being a physician in this field, instead of patting itself on the back for how trailblazing hospitalists could be while simultaneously ignoring what we are. TH
Edward Norman, MD, Internist/Hospitalist, Loveland, Colo.
I am a hospitalist outsider. A traditional internist, I cared for my patients in and out of the hospital, provided ICU and unassigned ED call, and later transitioned to hospital-only work. Our group developed a hospitalist program and has, hopefully, run an above-average system growing with our community. Even performing full-time hospital work, it took me a year to get over being referred to as a “hospitalist.” It seemed a confining label.
I also feel like an outsider while reading hospitalist literature’s divergent messages to hospitalists. On one hand, I hear great things about how hospitalists will revolutionize healthcare, spearheading improvements in safety, efficiency, and satisfaction, and filling administrative roles. I then see articles about negotiating out of working nights and weekends, about how the productivity of hospitalists remains stagnant but subsidy demands increase, and about how to limit caseloads. I see articles about hospitalist groups becoming privately held corporations, sending revenue that physicians generate (and hospitals subsidize) into the pockets of private investors.
There are two growing hospitalist camps. The first is filled with strategic thinkers driven to fix inefficient hospital care and save each of those 100,000 Institute of Medicine lives. These are the chief residents of yesterday, academically oriented problem solvers with IT savvy and a propensity for coffee-fueled all-nighters. You know them within your hospitalist groups and medical staffs.
The second camp consists of the lifestyle hospitalists; those for whom salary and 16 shifts a month are the goals that supersede professional loyalty to any particular group. These are the physicians who can help meet various metrics but want nothing to do with designing them.
These two groups read the literature with different eyes and career aspirations. As this division spreads, I strain to hear a drowning voice regarding another physician role: our responsibility to our patients. Drowning because both camps are swimming away from the patient, one toward a desk job, the other to a defined shift schedule.
Caring for patients is why we are in medicine in the first place. Most hospitalists came from primary care residencies, so the rewards of lifestyle and money must have been less important than direct patient contact. Primary care graduates entered traditional practices, promptly encountering the headaches of running a practice. Then suddenly a plum job with higher compensation and limited work hours was born, and, unsurprisingly, the primary care fields lost physicians to the hospitalist movement.
For new hospitalists exiting residency, there is no institutional knowledge of the old ways, and while they are not perfect, there are some noble qualities. Dedication to the profession is one, as is an enduring responsibility to one’s patient. Medicine required an occasional need to interrupt personal interests to help a sick human being—a patient—through a difficult time. For those physicians with traditional experience, can you recall articles suggesting negotiating for no nights and weekends? I’m not sure who we expect to provide this care to our patients if we can negotiate out of working.
There are certainly drawbacks to the traditional system: strained family relationships, substance abuse, and poor work-life balance—but don’t throw the baby out with the bathwater. These values elevated medicine to the position it holds today: a respected and well-compensated profession. I fear this young hospitalist specialty may not live up to its hype or responsibilities if hospitalists are motivated to focus on their “job” rather that their duties as the “doctor.” So what to do?
I think this can be a specialty that identifies members as physicians first and hospitalists second through the expectations of our peers in our own groups, medical staffs, and physician societies. We need to grow our groups with physicians dedicated not just to their partners, but the physician community at large; with those who want to improve care not just by meeting myocardial infarction guidelines, but with those who work with other physicians to help the patient manage their heart disease for 30 years; with physicians who ask about quality, teamwork, and the local community during the job interview and don’t begin with salary, patient caps, and weekend limitations.
Hospitalist group leaders need to expect these traits from their physicians. Otherwise practicing hospitalists will forever remain glorified residents and not leaders.
SHM needs to promote and recognize the values of being a physician in this field, instead of patting itself on the back for how trailblazing hospitalists could be while simultaneously ignoring what we are. TH
Edward Norman, MD, Internist/Hospitalist, Loveland, Colo.
Strategies for breaking bad news to patients
The author reports no financial relationships relevant to this article.
Editors’ note: This article appears under the “Focus on professional liability” series banner even though Dr. Bub’s discussion does not directly address matters of being sued. Our, and his, belief is that good communication brings a significant added benefit of lowering a physician’s litigation risk.
- It was tiring to try and think logically as the guy threw more and more facts at me.—An adolescent with cancer1
Consider the findings of two surveys of radiology residents and attending mammographers on breaking bad or troubling news to patients:
- 16% of residents and 4% of mammographers “didn’t feel confident communicating with patients who displayed strong emotional responses”
- 86% of residents and 81% of staff experienced “some or moderate stress communicating the need for biopsy”
- The majority of all respondents “hadn’t received feedback about their communication skills or communication training after medical school”
- 68% to 78% of respondents expressed interest in “improving their communication.”2
Breaking what you might perceive as “bad” news is never easy; even experienced practitioners may find the task stressful, as the results of these two surveys reveal. Physicians having been trained to do no harm, few find themselves at ease revealing information that has the potential to disappoint or upset, even devastate.
In this article, I offer an approach to breaking bad news in a manner that lessens the trauma to the patient and buffers you from the stress, and distress, of delivering it. The box near the end of this article gathers pearls for giving bad news based on my work and the experiences of others.
We are not unaffected by this task
Most of us find the act of breaking bad news a professional burden that we could just as soon do without. When we perceive an element of personal responsibility, our burden becomes greater: We may experience fear, guilt, or shame—and, for some, that leads to psychological stress disorders and burnout.
How do we cope, being occasional messengers of bad news?
We avoid. An obvious strategy. Consider Dr. D., a radiologist who heads a breast imaging center. He confides that many physicians ask him to inform their patients when he notes an abnormality on their mammogram. Still other physicians, Dr. D. points out, simply have their nurses call patients with troubling results.
Or we run. Another widely used strategy is to break the news and bolt. One cancer survivor lamented: “As soon as I started to cry, he ran off to fetch his nurse. Don’t you know doctors flee from suffering?”
Keeping matters in balance—that is the challenge
How do we maintain our sensitivity, humanity, and connection while, simultaneously, limiting our own vulnerability and pain? Many of us have wrestled with this issue from the earliest days of training:
- In the hospital’s predawn stillness, she confided fears about surgery to me, the medical student. I tried to reassure her. They operated. Finding extensive metastases, they closed immediately. That evening, aching for her, I cried.
- “Don’t worry,” another student reassured me. “It gets easier.”
- I hope not. If it does, I’ll have lost my humanity.3
Simultaneously, how do we handle our feelings of impotence, failure, and, perhaps, guilt—when every expression, gesture, word, and silence are potentially filled with meaning to those who are receiving the news?
David Lenz, an artist, in a commentary on his award-winning painting, “Sam and the Perfect World,” wrote:
- My wife Rosemarie had just given birth to our son Sam, and although he appeared perfectly healthy, something, nevertheless, didn’t seem right. There was an awkward silence in the room, no words of congratulation or comments about how cute he was—even though he was cute. Five minutes later the diagnosis was given: Sam has Down syndrome. “Are you going to keep him?” a nurse asked. Later that evening someone else came by to “console” us.
- “It’s every mother’s worst nightmare,” she said.
- Welcome to the world, Sam.4
5 and invest in deep and surface acting (of empathy).6 I disagree with this advice7 ; instead, I advocate that we notice, validate, and park our emotions. Later, we take time to integrate our emotions through self-care. Rather than relying on “the art of medicine” to communicate bad news, we should approach this task as a serious professional challenge and incorporate principles of trauma counseling, psychotherapy, and chaplaincy into the practice of medicine. Instead of distancing from our emotions and our patients, we draw closer.
Here is how one physician handles breaking bad news.
CASE
Dr. Bob, we’ll call him, typifies the overworked primary care physician. Yet, when a lab or imaging report that reveals an abnormal result lands on his desk, he, not a nurse, calls the patient. He waits a few days if the test or study was ordered by another physician; in that situation, he often reaches a frightened, confused person who had already been called by the specialist’s nurse.
When that happens, Dr. Bob invites the patient, and a close relative, to schedule an office visit with him. In the interim, he forms a liaison with the specialist so that they can function as a team.
At the office visit, Dr. Bob refuses to prognosticate. Instead, he recommends that they take matters “one step at a time.” His approach is positive and reassuring but not overly optimistic. His message is clear: “You are not alone. I will be a supportive presence throughout your journey.”
Two notable things about Dr. Bob: First, he does not suffer burnout or what some have called “compassion fatigue”; to the contrary, the relationship he forges with his patients and their loved ones, and the gratitude and loyalty he receives from them, sustain and reward him.
Second, Dr. Bob has never been sued.
The key to Dr. Bob’s success is that he does not shy from breaking bad news. Instead, he views the occasion as an opportunity for healing. His approach is to detach from the outcome but not from the patient. He relieves fear and isolation, and offers, as one patient said it, “candor with hope.”
Summon your personal strengths to succeed
But taking this approach requires a shift from the standard biomedical philosophy—a three-pronged cultivation of personal resources. Here is how you can make that shift.
First, cultivate equanimity—that evenness of mind
Consider that destruction is an inherent component of creation. There can’t be light without darkness, birth without death, joy without suffering, perfection without imperfection. The Sufi mystic, Rumi, said it succinctly: “A butterfly needs two wings to fly.”
Recognize that not all news is equally bad. The spectrum runs from merely inconvenient to utterly devastating; how the news is perceived and received is highly subjective. Avoid projecting your personal perspective onto the recipient:
- I was totally perplexed. I had just broken the news that Mrs. Smith had an incurable colon cancer, and they responded by nodding, then asking me whether I preferred a chocolate cake or an apple pie for their next visit because it was their custom to bring home-baked goodies for the staff.
- After her death, Mr. Smith faithfully continued this tradition. Then one day he arrived for his regular appointment unshaven, distressed and sans cake. He had lost weight and looked every bit of his 78 years. Something was very wrong.
- “She’s gone, she’s gone,” he lamented.
- At last he’s grieving flashed through my mind, so I responded: “Yes, it’s been about 9 months now, hasn’t it?”
- “No, just two weeks…she said she was my girlfriend…just 29 years old…moved in last month then left taking my money,” he cried.
- She assumed the mantle of a grieving widow. Only years later did she write that she had been secretly relieved that her husband was killed in an automobile accident. He had been abusive and she was planning to leave him anyway.
- It was my birthday, and we were about to celebrate with a dinner of leg of lamb and roast potatoes. My cell phone rang. It was my internist calling; my LDL cholesterol was mildly elevated and my dexa scan demonstrated slight osteopenia. The tone of his voice was matter-of-fact but I felt awful: I am getting old.
Realize that long-term well-being doesn’t depend on good vs. bad news:
- What do Chuck Close and Dan Gottlieb have in common? Each was a healthy young adult when suddenly becoming paraplegic—Chuck from a spinal artery thrombosis, Dan from a serious accident. Each adapted to his condition. Chuck developed a unique style of painting that established his fame as an artist. Dan, a psychotherapist, became an author, teacher, and highly regarded radio interviewer. Each has recently stated that he has never been happier.
Remind yourself of hidden opportunities. Bad news triggers a crisis—an unwelcome, unstable situation with obvious danger. Less apparent is the potential for positive personal transformation and gain:
- “It was the best thing that could have happened to me,” she said, lying with her right foot propped up, ankle heavily bandaged with pins and rods protruding. “Yes, it’s a horribly fractured ankle but I had been rushing, rushing, rushing, and when I fell down the steps, it was as if an angel was forcing me to slow down, be present to my family. I really think this fractured ankle was the best thing that could have happened—it may even have saved my marriage.”
Second, cultivate yourself as a healer
You may not always be able to cure but you can always facilitate healing. In addition to a treatment plan, remind yourself to create a parallel healing plan, listing the interventions that will help the recipient integrate losses and become as functionally whole as possible.
Your ability to heal depends as much on who you are as what you do:
- Work through your own trauma stories and you reduce the likelihood that you either attempt to rescue, or flee from engagement with, patients when their problems trigger painful memories for you
- Accept your imperfections as an inseparable aspect of your humanity
- Learn to accept life as a journey, with suffering and death being inevitable, and bad news ceases to be so exceptional
- Deepen your own joy, mindfulness, and faith and you find meaning in your work even when you cannot cure
- Have realistic expectations of your abilities and try to cultivate a realistic attitude in your patients:
- In Western culture there is a belief, conscious or not, that medicine can save us from the death that lies in wait for us… In a study conducted in 2006 among Israeli doctors, 68% of the participants reported that patients had unrealistic expectations of them. The study reflects unrealistic expectations of medicine in general.8
Third, cultivate skills to break really bad news
Sometimes news is so bad, so overwhelming, that it has the potential to trigger an acute stress reaction (ASR) and even posttraumatic stress disorder (PTSD) in the recipient. Typically, this is life-threatening news—a diagnosis of HIV infection or cancer; abortion or stillbirth; or the sudden, unexpected death of a loved one. The result is shock, horror, disorientation, and memory distortion.
So how can you approach a situation in which you must offer very bad news? To begin, the box, below “Pearls for breaking bad news…,” provides a set of skills and tools for delivering bad news.
In addition, as much as possible, break bad news in increments, so that the patient has time to cope and adjust. And there is more to keep in mind:
- Provide a safe, supportive environment
- Relieve the isolation that trauma inflicts by forging a relationship that is a partnership
- Relieve helplessness by empowering and assisting the patient to seek useful consultants, resources, and supports (One example: A patient who has breast or ovarian cancer can call the SHARE [Self-help for Women with Ovarian or Breast Cancer] hotline: [866] 891-2392)
- Over time, although not initially, help provide meaning to the experience for your patient and for you.
- Don’t have your assistant call with bad news unless she or he is trained to do this, humanely, and to handle the response. Don’t leave a message asking the patient to call back unless you are reasonably certain you will be able to take the call.
- Before you enter the room or place a call, pause, take a deep breath, acknowledge your feelings so you can set them aside, and be fully present. Remember: Empathy begins at home.
- Effective communication always begins and ends with listening. On entering a room, notice the people present, the atmosphere, and the interactions. Over the telephone, notice breath and tone of voice in addition to words spoken. Create space for the recipient to speak, even if silence is uncomfortably long.
- Begin the session by greeting everyone present by name and by shaking hands.
- Offer a general inquiry and listen. A simple “How are you?” allows the patient to express a feeling—“I’m OK but anxious,” for example. Respond with empathy early in the encounter: “Yes, it’s scary waiting for results.”
- Use simple, nontechnical language to describe the situation. Be brief, because a person in a high state of arousal has limited capacity to absorb details. Avoid harsh language (“aggressive,” “failure”) and use a calm, modulated tone.
- Listen and validate the responses you get, recognizing that you may be the recipient of an entire spectrum of emotional expression—from silence to an outburst of anger, from rage to grief. Keep in mind: Anything said in grief is acceptable.
- Remember: You are not responsible for your patients’ happiness. When a patient cries, it does not mean that you failed. An outpouring of grief is healing; your silent, supportive presence is invaluable.
- Don’t attempt to prematurely comfort; don’t try to “make it better,” because this stifles grief. Offering a box of tissues, on the other hand, is simply considerate.
- Don’t present the bleakest scenario. Later, as the patient adapts to her new reality, she will usually be able to tolerate more.
- Be forearmed with some basic treatment and referral options so that the patient isn’t left facing the dark unknown.
- Now, invite the patient’s perspective. Appreciate that she may be experiencing a sea of emotions, especially if the news is totally unexpected. It’s not sufficient to lay out options, then leave the final decision to her. Part of decision-making involves the processing of emotions. Gendlin’s technique of focusing is very useful at this point in the conversation.1
- If you are at the hospital, 1) consider having a chaplain present when the news is potentially devastating and 2) attend to privacy concerns when breaking bad news.
- Treat the person, not the pathology. Ask about her work, activities, and circle of support—all of which are relevant to her situation.
- Be clear that you will remain actively involved in her care even after you refer the patient to the best consultants available.
- Don’t limit yourself to the negative. Look for what is healthy about your patient’s situation, too, and support it.
- Give as much information as possible in writing at this time; amnesia is common. Offer to share the information with at least one family member over the telephone, or schedule a second visit at which a relative will be present.
- When you’re questioned directly, give yourself the benefit of a few moments to ground yourself before you respond.
- Ensure a safe exit for your patient. Does she have someone to drive her, keep her company, etc.?
- Consider calling her that evening to see how she is and to answer any additional questions.
- Invest in self-care. This might include debriefing, taking a break between patients for integration, and grounding and rituals that enable you to detoxify after a difficult day. Cultivate whatever spiritual and meditative practices are part of your life, even if it is simply a walk in the park.
- Empower yourself with relationship skills that enhance your ability to communicate and counsel.
- Have faith! The time that you invest in healthy practice and communication will save you much more over the course of your career.
Reference
1. Bub B. Communication skills that heal: a practical approach to a new professionalism in medicine. Abingdon, UK: Radcliffe Publishing; 2006.
Frankel E. Sacred Therapy. Boston: Shambhala; 2003.
Herman J. Trauma and Recovery. New York: Basic Books; 1992.
Schneider J. Finding My Way: Healing and Transformation Through Loss and Grief. Colfax, Wis: Seasons Press; 1994.
1. Training workshop sponsored by Melissa’s Living Legacy Foundation, April 2004 (http://www.teenslivingwithcancer.org).
2. Sasson JP, Lown BA. Communicating practices in the diagnostic mammography suite. Med Encounter. 2006;20(4):66.-
3. Christianson AL. A piece of my mind. More stories. JAMA. 2002;288:931.-
4. Bub B. Medicine and the arts. Sam and the Perfect World by David Lenz. Commentary. Acad Med. 2007;82(2):200-201.
5. Meier DE, Back AL, Morrison RS. The inner life of physicians and care of the seriously ill. JAMA. 2001;286:3007-3014.
6. Larson EB, Yao X. Clinical empathy as emotional labor in the patient–physician relationship. JAMA. 2005;293:1100-1106.
7. Bub B. Focusing and the healing sequence: reclaiming authentic emotions as an aid to communication and well-being in medicine. Explore (NY). 2007;3:413-416.
8. Schwartzman O. White Doctor, Black Gods: White Psychiatric Medicine in the Jungles of Africa. Israel: Aryeh Nir Publishing House; 256 pages. http://www.haaretz.com/hasen/spages/834952.html.
The author reports no financial relationships relevant to this article.
Editors’ note: This article appears under the “Focus on professional liability” series banner even though Dr. Bub’s discussion does not directly address matters of being sued. Our, and his, belief is that good communication brings a significant added benefit of lowering a physician’s litigation risk.
- It was tiring to try and think logically as the guy threw more and more facts at me.—An adolescent with cancer1
Consider the findings of two surveys of radiology residents and attending mammographers on breaking bad or troubling news to patients:
- 16% of residents and 4% of mammographers “didn’t feel confident communicating with patients who displayed strong emotional responses”
- 86% of residents and 81% of staff experienced “some or moderate stress communicating the need for biopsy”
- The majority of all respondents “hadn’t received feedback about their communication skills or communication training after medical school”
- 68% to 78% of respondents expressed interest in “improving their communication.”2
Breaking what you might perceive as “bad” news is never easy; even experienced practitioners may find the task stressful, as the results of these two surveys reveal. Physicians having been trained to do no harm, few find themselves at ease revealing information that has the potential to disappoint or upset, even devastate.
In this article, I offer an approach to breaking bad news in a manner that lessens the trauma to the patient and buffers you from the stress, and distress, of delivering it. The box near the end of this article gathers pearls for giving bad news based on my work and the experiences of others.
We are not unaffected by this task
Most of us find the act of breaking bad news a professional burden that we could just as soon do without. When we perceive an element of personal responsibility, our burden becomes greater: We may experience fear, guilt, or shame—and, for some, that leads to psychological stress disorders and burnout.
How do we cope, being occasional messengers of bad news?
We avoid. An obvious strategy. Consider Dr. D., a radiologist who heads a breast imaging center. He confides that many physicians ask him to inform their patients when he notes an abnormality on their mammogram. Still other physicians, Dr. D. points out, simply have their nurses call patients with troubling results.
Or we run. Another widely used strategy is to break the news and bolt. One cancer survivor lamented: “As soon as I started to cry, he ran off to fetch his nurse. Don’t you know doctors flee from suffering?”
Keeping matters in balance—that is the challenge
How do we maintain our sensitivity, humanity, and connection while, simultaneously, limiting our own vulnerability and pain? Many of us have wrestled with this issue from the earliest days of training:
- In the hospital’s predawn stillness, she confided fears about surgery to me, the medical student. I tried to reassure her. They operated. Finding extensive metastases, they closed immediately. That evening, aching for her, I cried.
- “Don’t worry,” another student reassured me. “It gets easier.”
- I hope not. If it does, I’ll have lost my humanity.3
Simultaneously, how do we handle our feelings of impotence, failure, and, perhaps, guilt—when every expression, gesture, word, and silence are potentially filled with meaning to those who are receiving the news?
David Lenz, an artist, in a commentary on his award-winning painting, “Sam and the Perfect World,” wrote:
- My wife Rosemarie had just given birth to our son Sam, and although he appeared perfectly healthy, something, nevertheless, didn’t seem right. There was an awkward silence in the room, no words of congratulation or comments about how cute he was—even though he was cute. Five minutes later the diagnosis was given: Sam has Down syndrome. “Are you going to keep him?” a nurse asked. Later that evening someone else came by to “console” us.
- “It’s every mother’s worst nightmare,” she said.
- Welcome to the world, Sam.4
5 and invest in deep and surface acting (of empathy).6 I disagree with this advice7 ; instead, I advocate that we notice, validate, and park our emotions. Later, we take time to integrate our emotions through self-care. Rather than relying on “the art of medicine” to communicate bad news, we should approach this task as a serious professional challenge and incorporate principles of trauma counseling, psychotherapy, and chaplaincy into the practice of medicine. Instead of distancing from our emotions and our patients, we draw closer.
Here is how one physician handles breaking bad news.
CASE
Dr. Bob, we’ll call him, typifies the overworked primary care physician. Yet, when a lab or imaging report that reveals an abnormal result lands on his desk, he, not a nurse, calls the patient. He waits a few days if the test or study was ordered by another physician; in that situation, he often reaches a frightened, confused person who had already been called by the specialist’s nurse.
When that happens, Dr. Bob invites the patient, and a close relative, to schedule an office visit with him. In the interim, he forms a liaison with the specialist so that they can function as a team.
At the office visit, Dr. Bob refuses to prognosticate. Instead, he recommends that they take matters “one step at a time.” His approach is positive and reassuring but not overly optimistic. His message is clear: “You are not alone. I will be a supportive presence throughout your journey.”
Two notable things about Dr. Bob: First, he does not suffer burnout or what some have called “compassion fatigue”; to the contrary, the relationship he forges with his patients and their loved ones, and the gratitude and loyalty he receives from them, sustain and reward him.
Second, Dr. Bob has never been sued.
The key to Dr. Bob’s success is that he does not shy from breaking bad news. Instead, he views the occasion as an opportunity for healing. His approach is to detach from the outcome but not from the patient. He relieves fear and isolation, and offers, as one patient said it, “candor with hope.”
Summon your personal strengths to succeed
But taking this approach requires a shift from the standard biomedical philosophy—a three-pronged cultivation of personal resources. Here is how you can make that shift.
First, cultivate equanimity—that evenness of mind
Consider that destruction is an inherent component of creation. There can’t be light without darkness, birth without death, joy without suffering, perfection without imperfection. The Sufi mystic, Rumi, said it succinctly: “A butterfly needs two wings to fly.”
Recognize that not all news is equally bad. The spectrum runs from merely inconvenient to utterly devastating; how the news is perceived and received is highly subjective. Avoid projecting your personal perspective onto the recipient:
- I was totally perplexed. I had just broken the news that Mrs. Smith had an incurable colon cancer, and they responded by nodding, then asking me whether I preferred a chocolate cake or an apple pie for their next visit because it was their custom to bring home-baked goodies for the staff.
- After her death, Mr. Smith faithfully continued this tradition. Then one day he arrived for his regular appointment unshaven, distressed and sans cake. He had lost weight and looked every bit of his 78 years. Something was very wrong.
- “She’s gone, she’s gone,” he lamented.
- At last he’s grieving flashed through my mind, so I responded: “Yes, it’s been about 9 months now, hasn’t it?”
- “No, just two weeks…she said she was my girlfriend…just 29 years old…moved in last month then left taking my money,” he cried.
- She assumed the mantle of a grieving widow. Only years later did she write that she had been secretly relieved that her husband was killed in an automobile accident. He had been abusive and she was planning to leave him anyway.
- It was my birthday, and we were about to celebrate with a dinner of leg of lamb and roast potatoes. My cell phone rang. It was my internist calling; my LDL cholesterol was mildly elevated and my dexa scan demonstrated slight osteopenia. The tone of his voice was matter-of-fact but I felt awful: I am getting old.
Realize that long-term well-being doesn’t depend on good vs. bad news:
- What do Chuck Close and Dan Gottlieb have in common? Each was a healthy young adult when suddenly becoming paraplegic—Chuck from a spinal artery thrombosis, Dan from a serious accident. Each adapted to his condition. Chuck developed a unique style of painting that established his fame as an artist. Dan, a psychotherapist, became an author, teacher, and highly regarded radio interviewer. Each has recently stated that he has never been happier.
Remind yourself of hidden opportunities. Bad news triggers a crisis—an unwelcome, unstable situation with obvious danger. Less apparent is the potential for positive personal transformation and gain:
- “It was the best thing that could have happened to me,” she said, lying with her right foot propped up, ankle heavily bandaged with pins and rods protruding. “Yes, it’s a horribly fractured ankle but I had been rushing, rushing, rushing, and when I fell down the steps, it was as if an angel was forcing me to slow down, be present to my family. I really think this fractured ankle was the best thing that could have happened—it may even have saved my marriage.”
Second, cultivate yourself as a healer
You may not always be able to cure but you can always facilitate healing. In addition to a treatment plan, remind yourself to create a parallel healing plan, listing the interventions that will help the recipient integrate losses and become as functionally whole as possible.
Your ability to heal depends as much on who you are as what you do:
- Work through your own trauma stories and you reduce the likelihood that you either attempt to rescue, or flee from engagement with, patients when their problems trigger painful memories for you
- Accept your imperfections as an inseparable aspect of your humanity
- Learn to accept life as a journey, with suffering and death being inevitable, and bad news ceases to be so exceptional
- Deepen your own joy, mindfulness, and faith and you find meaning in your work even when you cannot cure
- Have realistic expectations of your abilities and try to cultivate a realistic attitude in your patients:
- In Western culture there is a belief, conscious or not, that medicine can save us from the death that lies in wait for us… In a study conducted in 2006 among Israeli doctors, 68% of the participants reported that patients had unrealistic expectations of them. The study reflects unrealistic expectations of medicine in general.8
Third, cultivate skills to break really bad news
Sometimes news is so bad, so overwhelming, that it has the potential to trigger an acute stress reaction (ASR) and even posttraumatic stress disorder (PTSD) in the recipient. Typically, this is life-threatening news—a diagnosis of HIV infection or cancer; abortion or stillbirth; or the sudden, unexpected death of a loved one. The result is shock, horror, disorientation, and memory distortion.
So how can you approach a situation in which you must offer very bad news? To begin, the box, below “Pearls for breaking bad news…,” provides a set of skills and tools for delivering bad news.
In addition, as much as possible, break bad news in increments, so that the patient has time to cope and adjust. And there is more to keep in mind:
- Provide a safe, supportive environment
- Relieve the isolation that trauma inflicts by forging a relationship that is a partnership
- Relieve helplessness by empowering and assisting the patient to seek useful consultants, resources, and supports (One example: A patient who has breast or ovarian cancer can call the SHARE [Self-help for Women with Ovarian or Breast Cancer] hotline: [866] 891-2392)
- Over time, although not initially, help provide meaning to the experience for your patient and for you.
- Don’t have your assistant call with bad news unless she or he is trained to do this, humanely, and to handle the response. Don’t leave a message asking the patient to call back unless you are reasonably certain you will be able to take the call.
- Before you enter the room or place a call, pause, take a deep breath, acknowledge your feelings so you can set them aside, and be fully present. Remember: Empathy begins at home.
- Effective communication always begins and ends with listening. On entering a room, notice the people present, the atmosphere, and the interactions. Over the telephone, notice breath and tone of voice in addition to words spoken. Create space for the recipient to speak, even if silence is uncomfortably long.
- Begin the session by greeting everyone present by name and by shaking hands.
- Offer a general inquiry and listen. A simple “How are you?” allows the patient to express a feeling—“I’m OK but anxious,” for example. Respond with empathy early in the encounter: “Yes, it’s scary waiting for results.”
- Use simple, nontechnical language to describe the situation. Be brief, because a person in a high state of arousal has limited capacity to absorb details. Avoid harsh language (“aggressive,” “failure”) and use a calm, modulated tone.
- Listen and validate the responses you get, recognizing that you may be the recipient of an entire spectrum of emotional expression—from silence to an outburst of anger, from rage to grief. Keep in mind: Anything said in grief is acceptable.
- Remember: You are not responsible for your patients’ happiness. When a patient cries, it does not mean that you failed. An outpouring of grief is healing; your silent, supportive presence is invaluable.
- Don’t attempt to prematurely comfort; don’t try to “make it better,” because this stifles grief. Offering a box of tissues, on the other hand, is simply considerate.
- Don’t present the bleakest scenario. Later, as the patient adapts to her new reality, she will usually be able to tolerate more.
- Be forearmed with some basic treatment and referral options so that the patient isn’t left facing the dark unknown.
- Now, invite the patient’s perspective. Appreciate that she may be experiencing a sea of emotions, especially if the news is totally unexpected. It’s not sufficient to lay out options, then leave the final decision to her. Part of decision-making involves the processing of emotions. Gendlin’s technique of focusing is very useful at this point in the conversation.1
- If you are at the hospital, 1) consider having a chaplain present when the news is potentially devastating and 2) attend to privacy concerns when breaking bad news.
- Treat the person, not the pathology. Ask about her work, activities, and circle of support—all of which are relevant to her situation.
- Be clear that you will remain actively involved in her care even after you refer the patient to the best consultants available.
- Don’t limit yourself to the negative. Look for what is healthy about your patient’s situation, too, and support it.
- Give as much information as possible in writing at this time; amnesia is common. Offer to share the information with at least one family member over the telephone, or schedule a second visit at which a relative will be present.
- When you’re questioned directly, give yourself the benefit of a few moments to ground yourself before you respond.
- Ensure a safe exit for your patient. Does she have someone to drive her, keep her company, etc.?
- Consider calling her that evening to see how she is and to answer any additional questions.
- Invest in self-care. This might include debriefing, taking a break between patients for integration, and grounding and rituals that enable you to detoxify after a difficult day. Cultivate whatever spiritual and meditative practices are part of your life, even if it is simply a walk in the park.
- Empower yourself with relationship skills that enhance your ability to communicate and counsel.
- Have faith! The time that you invest in healthy practice and communication will save you much more over the course of your career.
Reference
1. Bub B. Communication skills that heal: a practical approach to a new professionalism in medicine. Abingdon, UK: Radcliffe Publishing; 2006.
Frankel E. Sacred Therapy. Boston: Shambhala; 2003.
Herman J. Trauma and Recovery. New York: Basic Books; 1992.
Schneider J. Finding My Way: Healing and Transformation Through Loss and Grief. Colfax, Wis: Seasons Press; 1994.
The author reports no financial relationships relevant to this article.
Editors’ note: This article appears under the “Focus on professional liability” series banner even though Dr. Bub’s discussion does not directly address matters of being sued. Our, and his, belief is that good communication brings a significant added benefit of lowering a physician’s litigation risk.
- It was tiring to try and think logically as the guy threw more and more facts at me.—An adolescent with cancer1
Consider the findings of two surveys of radiology residents and attending mammographers on breaking bad or troubling news to patients:
- 16% of residents and 4% of mammographers “didn’t feel confident communicating with patients who displayed strong emotional responses”
- 86% of residents and 81% of staff experienced “some or moderate stress communicating the need for biopsy”
- The majority of all respondents “hadn’t received feedback about their communication skills or communication training after medical school”
- 68% to 78% of respondents expressed interest in “improving their communication.”2
Breaking what you might perceive as “bad” news is never easy; even experienced practitioners may find the task stressful, as the results of these two surveys reveal. Physicians having been trained to do no harm, few find themselves at ease revealing information that has the potential to disappoint or upset, even devastate.
In this article, I offer an approach to breaking bad news in a manner that lessens the trauma to the patient and buffers you from the stress, and distress, of delivering it. The box near the end of this article gathers pearls for giving bad news based on my work and the experiences of others.
We are not unaffected by this task
Most of us find the act of breaking bad news a professional burden that we could just as soon do without. When we perceive an element of personal responsibility, our burden becomes greater: We may experience fear, guilt, or shame—and, for some, that leads to psychological stress disorders and burnout.
How do we cope, being occasional messengers of bad news?
We avoid. An obvious strategy. Consider Dr. D., a radiologist who heads a breast imaging center. He confides that many physicians ask him to inform their patients when he notes an abnormality on their mammogram. Still other physicians, Dr. D. points out, simply have their nurses call patients with troubling results.
Or we run. Another widely used strategy is to break the news and bolt. One cancer survivor lamented: “As soon as I started to cry, he ran off to fetch his nurse. Don’t you know doctors flee from suffering?”
Keeping matters in balance—that is the challenge
How do we maintain our sensitivity, humanity, and connection while, simultaneously, limiting our own vulnerability and pain? Many of us have wrestled with this issue from the earliest days of training:
- In the hospital’s predawn stillness, she confided fears about surgery to me, the medical student. I tried to reassure her. They operated. Finding extensive metastases, they closed immediately. That evening, aching for her, I cried.
- “Don’t worry,” another student reassured me. “It gets easier.”
- I hope not. If it does, I’ll have lost my humanity.3
Simultaneously, how do we handle our feelings of impotence, failure, and, perhaps, guilt—when every expression, gesture, word, and silence are potentially filled with meaning to those who are receiving the news?
David Lenz, an artist, in a commentary on his award-winning painting, “Sam and the Perfect World,” wrote:
- My wife Rosemarie had just given birth to our son Sam, and although he appeared perfectly healthy, something, nevertheless, didn’t seem right. There was an awkward silence in the room, no words of congratulation or comments about how cute he was—even though he was cute. Five minutes later the diagnosis was given: Sam has Down syndrome. “Are you going to keep him?” a nurse asked. Later that evening someone else came by to “console” us.
- “It’s every mother’s worst nightmare,” she said.
- Welcome to the world, Sam.4
5 and invest in deep and surface acting (of empathy).6 I disagree with this advice7 ; instead, I advocate that we notice, validate, and park our emotions. Later, we take time to integrate our emotions through self-care. Rather than relying on “the art of medicine” to communicate bad news, we should approach this task as a serious professional challenge and incorporate principles of trauma counseling, psychotherapy, and chaplaincy into the practice of medicine. Instead of distancing from our emotions and our patients, we draw closer.
Here is how one physician handles breaking bad news.
CASE
Dr. Bob, we’ll call him, typifies the overworked primary care physician. Yet, when a lab or imaging report that reveals an abnormal result lands on his desk, he, not a nurse, calls the patient. He waits a few days if the test or study was ordered by another physician; in that situation, he often reaches a frightened, confused person who had already been called by the specialist’s nurse.
When that happens, Dr. Bob invites the patient, and a close relative, to schedule an office visit with him. In the interim, he forms a liaison with the specialist so that they can function as a team.
At the office visit, Dr. Bob refuses to prognosticate. Instead, he recommends that they take matters “one step at a time.” His approach is positive and reassuring but not overly optimistic. His message is clear: “You are not alone. I will be a supportive presence throughout your journey.”
Two notable things about Dr. Bob: First, he does not suffer burnout or what some have called “compassion fatigue”; to the contrary, the relationship he forges with his patients and their loved ones, and the gratitude and loyalty he receives from them, sustain and reward him.
Second, Dr. Bob has never been sued.
The key to Dr. Bob’s success is that he does not shy from breaking bad news. Instead, he views the occasion as an opportunity for healing. His approach is to detach from the outcome but not from the patient. He relieves fear and isolation, and offers, as one patient said it, “candor with hope.”
Summon your personal strengths to succeed
But taking this approach requires a shift from the standard biomedical philosophy—a three-pronged cultivation of personal resources. Here is how you can make that shift.
First, cultivate equanimity—that evenness of mind
Consider that destruction is an inherent component of creation. There can’t be light without darkness, birth without death, joy without suffering, perfection without imperfection. The Sufi mystic, Rumi, said it succinctly: “A butterfly needs two wings to fly.”
Recognize that not all news is equally bad. The spectrum runs from merely inconvenient to utterly devastating; how the news is perceived and received is highly subjective. Avoid projecting your personal perspective onto the recipient:
- I was totally perplexed. I had just broken the news that Mrs. Smith had an incurable colon cancer, and they responded by nodding, then asking me whether I preferred a chocolate cake or an apple pie for their next visit because it was their custom to bring home-baked goodies for the staff.
- After her death, Mr. Smith faithfully continued this tradition. Then one day he arrived for his regular appointment unshaven, distressed and sans cake. He had lost weight and looked every bit of his 78 years. Something was very wrong.
- “She’s gone, she’s gone,” he lamented.
- At last he’s grieving flashed through my mind, so I responded: “Yes, it’s been about 9 months now, hasn’t it?”
- “No, just two weeks…she said she was my girlfriend…just 29 years old…moved in last month then left taking my money,” he cried.
- She assumed the mantle of a grieving widow. Only years later did she write that she had been secretly relieved that her husband was killed in an automobile accident. He had been abusive and she was planning to leave him anyway.
- It was my birthday, and we were about to celebrate with a dinner of leg of lamb and roast potatoes. My cell phone rang. It was my internist calling; my LDL cholesterol was mildly elevated and my dexa scan demonstrated slight osteopenia. The tone of his voice was matter-of-fact but I felt awful: I am getting old.
Realize that long-term well-being doesn’t depend on good vs. bad news:
- What do Chuck Close and Dan Gottlieb have in common? Each was a healthy young adult when suddenly becoming paraplegic—Chuck from a spinal artery thrombosis, Dan from a serious accident. Each adapted to his condition. Chuck developed a unique style of painting that established his fame as an artist. Dan, a psychotherapist, became an author, teacher, and highly regarded radio interviewer. Each has recently stated that he has never been happier.
Remind yourself of hidden opportunities. Bad news triggers a crisis—an unwelcome, unstable situation with obvious danger. Less apparent is the potential for positive personal transformation and gain:
- “It was the best thing that could have happened to me,” she said, lying with her right foot propped up, ankle heavily bandaged with pins and rods protruding. “Yes, it’s a horribly fractured ankle but I had been rushing, rushing, rushing, and when I fell down the steps, it was as if an angel was forcing me to slow down, be present to my family. I really think this fractured ankle was the best thing that could have happened—it may even have saved my marriage.”
Second, cultivate yourself as a healer
You may not always be able to cure but you can always facilitate healing. In addition to a treatment plan, remind yourself to create a parallel healing plan, listing the interventions that will help the recipient integrate losses and become as functionally whole as possible.
Your ability to heal depends as much on who you are as what you do:
- Work through your own trauma stories and you reduce the likelihood that you either attempt to rescue, or flee from engagement with, patients when their problems trigger painful memories for you
- Accept your imperfections as an inseparable aspect of your humanity
- Learn to accept life as a journey, with suffering and death being inevitable, and bad news ceases to be so exceptional
- Deepen your own joy, mindfulness, and faith and you find meaning in your work even when you cannot cure
- Have realistic expectations of your abilities and try to cultivate a realistic attitude in your patients:
- In Western culture there is a belief, conscious or not, that medicine can save us from the death that lies in wait for us… In a study conducted in 2006 among Israeli doctors, 68% of the participants reported that patients had unrealistic expectations of them. The study reflects unrealistic expectations of medicine in general.8
Third, cultivate skills to break really bad news
Sometimes news is so bad, so overwhelming, that it has the potential to trigger an acute stress reaction (ASR) and even posttraumatic stress disorder (PTSD) in the recipient. Typically, this is life-threatening news—a diagnosis of HIV infection or cancer; abortion or stillbirth; or the sudden, unexpected death of a loved one. The result is shock, horror, disorientation, and memory distortion.
So how can you approach a situation in which you must offer very bad news? To begin, the box, below “Pearls for breaking bad news…,” provides a set of skills and tools for delivering bad news.
In addition, as much as possible, break bad news in increments, so that the patient has time to cope and adjust. And there is more to keep in mind:
- Provide a safe, supportive environment
- Relieve the isolation that trauma inflicts by forging a relationship that is a partnership
- Relieve helplessness by empowering and assisting the patient to seek useful consultants, resources, and supports (One example: A patient who has breast or ovarian cancer can call the SHARE [Self-help for Women with Ovarian or Breast Cancer] hotline: [866] 891-2392)
- Over time, although not initially, help provide meaning to the experience for your patient and for you.
- Don’t have your assistant call with bad news unless she or he is trained to do this, humanely, and to handle the response. Don’t leave a message asking the patient to call back unless you are reasonably certain you will be able to take the call.
- Before you enter the room or place a call, pause, take a deep breath, acknowledge your feelings so you can set them aside, and be fully present. Remember: Empathy begins at home.
- Effective communication always begins and ends with listening. On entering a room, notice the people present, the atmosphere, and the interactions. Over the telephone, notice breath and tone of voice in addition to words spoken. Create space for the recipient to speak, even if silence is uncomfortably long.
- Begin the session by greeting everyone present by name and by shaking hands.
- Offer a general inquiry and listen. A simple “How are you?” allows the patient to express a feeling—“I’m OK but anxious,” for example. Respond with empathy early in the encounter: “Yes, it’s scary waiting for results.”
- Use simple, nontechnical language to describe the situation. Be brief, because a person in a high state of arousal has limited capacity to absorb details. Avoid harsh language (“aggressive,” “failure”) and use a calm, modulated tone.
- Listen and validate the responses you get, recognizing that you may be the recipient of an entire spectrum of emotional expression—from silence to an outburst of anger, from rage to grief. Keep in mind: Anything said in grief is acceptable.
- Remember: You are not responsible for your patients’ happiness. When a patient cries, it does not mean that you failed. An outpouring of grief is healing; your silent, supportive presence is invaluable.
- Don’t attempt to prematurely comfort; don’t try to “make it better,” because this stifles grief. Offering a box of tissues, on the other hand, is simply considerate.
- Don’t present the bleakest scenario. Later, as the patient adapts to her new reality, she will usually be able to tolerate more.
- Be forearmed with some basic treatment and referral options so that the patient isn’t left facing the dark unknown.
- Now, invite the patient’s perspective. Appreciate that she may be experiencing a sea of emotions, especially if the news is totally unexpected. It’s not sufficient to lay out options, then leave the final decision to her. Part of decision-making involves the processing of emotions. Gendlin’s technique of focusing is very useful at this point in the conversation.1
- If you are at the hospital, 1) consider having a chaplain present when the news is potentially devastating and 2) attend to privacy concerns when breaking bad news.
- Treat the person, not the pathology. Ask about her work, activities, and circle of support—all of which are relevant to her situation.
- Be clear that you will remain actively involved in her care even after you refer the patient to the best consultants available.
- Don’t limit yourself to the negative. Look for what is healthy about your patient’s situation, too, and support it.
- Give as much information as possible in writing at this time; amnesia is common. Offer to share the information with at least one family member over the telephone, or schedule a second visit at which a relative will be present.
- When you’re questioned directly, give yourself the benefit of a few moments to ground yourself before you respond.
- Ensure a safe exit for your patient. Does she have someone to drive her, keep her company, etc.?
- Consider calling her that evening to see how she is and to answer any additional questions.
- Invest in self-care. This might include debriefing, taking a break between patients for integration, and grounding and rituals that enable you to detoxify after a difficult day. Cultivate whatever spiritual and meditative practices are part of your life, even if it is simply a walk in the park.
- Empower yourself with relationship skills that enhance your ability to communicate and counsel.
- Have faith! The time that you invest in healthy practice and communication will save you much more over the course of your career.
Reference
1. Bub B. Communication skills that heal: a practical approach to a new professionalism in medicine. Abingdon, UK: Radcliffe Publishing; 2006.
Frankel E. Sacred Therapy. Boston: Shambhala; 2003.
Herman J. Trauma and Recovery. New York: Basic Books; 1992.
Schneider J. Finding My Way: Healing and Transformation Through Loss and Grief. Colfax, Wis: Seasons Press; 1994.
1. Training workshop sponsored by Melissa’s Living Legacy Foundation, April 2004 (http://www.teenslivingwithcancer.org).
2. Sasson JP, Lown BA. Communicating practices in the diagnostic mammography suite. Med Encounter. 2006;20(4):66.-
3. Christianson AL. A piece of my mind. More stories. JAMA. 2002;288:931.-
4. Bub B. Medicine and the arts. Sam and the Perfect World by David Lenz. Commentary. Acad Med. 2007;82(2):200-201.
5. Meier DE, Back AL, Morrison RS. The inner life of physicians and care of the seriously ill. JAMA. 2001;286:3007-3014.
6. Larson EB, Yao X. Clinical empathy as emotional labor in the patient–physician relationship. JAMA. 2005;293:1100-1106.
7. Bub B. Focusing and the healing sequence: reclaiming authentic emotions as an aid to communication and well-being in medicine. Explore (NY). 2007;3:413-416.
8. Schwartzman O. White Doctor, Black Gods: White Psychiatric Medicine in the Jungles of Africa. Israel: Aryeh Nir Publishing House; 256 pages. http://www.haaretz.com/hasen/spages/834952.html.
1. Training workshop sponsored by Melissa’s Living Legacy Foundation, April 2004 (http://www.teenslivingwithcancer.org).
2. Sasson JP, Lown BA. Communicating practices in the diagnostic mammography suite. Med Encounter. 2006;20(4):66.-
3. Christianson AL. A piece of my mind. More stories. JAMA. 2002;288:931.-
4. Bub B. Medicine and the arts. Sam and the Perfect World by David Lenz. Commentary. Acad Med. 2007;82(2):200-201.
5. Meier DE, Back AL, Morrison RS. The inner life of physicians and care of the seriously ill. JAMA. 2001;286:3007-3014.
6. Larson EB, Yao X. Clinical empathy as emotional labor in the patient–physician relationship. JAMA. 2005;293:1100-1106.
7. Bub B. Focusing and the healing sequence: reclaiming authentic emotions as an aid to communication and well-being in medicine. Explore (NY). 2007;3:413-416.
8. Schwartzman O. White Doctor, Black Gods: White Psychiatric Medicine in the Jungles of Africa. Israel: Aryeh Nir Publishing House; 256 pages. http://www.haaretz.com/hasen/spages/834952.html.
Do post-discharge telephone calls to patients reduce the rate of complications?
Case
A 75-year-old male with history of diabetes and heart disease is discharged from the hospital after treatment for pneumonia. He has eight medications on his discharge list and is given two new prescriptions at discharge. He has a primary care provider but will not be able to see her until three weeks after discharge. Will a follow-up call decrease potential complications?
Overview
Medication errors are prevalent, especially during the transition period from discharge to follow-up with primary care physicians. There are more than 700,000 emergency department (ED) visits each year for adverse drug events with nearly 120,000 of these episodes resulting in hospitalization.1
The likelihood of an adverse drug event increases in patients using more than five medications and when there is a lack of understanding of how and why they are taking certain medications, scenarios common on hospital discharge.2 Studies evaluating effective means to reduce medication errors during transitions out of the hospital offer few solutions. One effective method, however, appears to be follow-up telephone calls.
Telephone calls have been looked at in multiple studies and usually are performed in the studies by nurses, nurse practitioners, or pharmacists and occur within days of discharge from the hospital. These calls offer a mechanism to provide answers to questions about their medical condition or medications.
Review of the Data
There is a wide range of studies evaluating the benefit of a post-discharge telephone call. Unfortunately, most of the data are of low methodological quality with low patient numbers and high risk of bias.3
Much of the data are divided into subgroups of patients, including ED patients, cardiac patients, surgical patients, medicine patients, and other small groups. The end points also vary and examine areas such as patient satisfaction, reduction in medication errors, and effect on readmissions or repeat ED visits. The bulk of studies used a standardized script. These calls lasted only minutes, which could make it user-friendly, especially for a busy hospitalist’s schedule. Unfortunately, the effect of these interventions is mixed.
With ED patients, phone calls have been shown to be an effective means of communication between patients and physicians. In a study of 297 patients, the authors were only able to reach half the patients but still were able to identify medical problems needing referral or further intervention in 37% of the patients contacted.4 Another two studies revealed similar results with approximately 40% of the contacted patients requiring further clarification on their discharge instructions.5,6
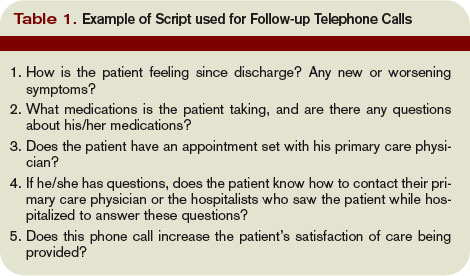
Importantly, 95% of these patients felt the call was beneficial. Thus, more than one-third of patients discharged from an ED are likely to have problems and a follow-up telephone call offers an opportunity to intervene on these potential problems. Another ED study evaluated patients older than 75 and found a nurse liaison could effectively assess the complexity of a patient’s questions and appropriately advise them over the phone or triage them to the correct care provider for further care.7
Post-discharge follow-up telephone calls also can benefit patients discharged from the hospital. A recent paper reported that approximately 12% of patients develop new or worsening symptoms within a few days post-discharge and adverse drug events can occur in between 23% to 49% of people during this transition period.8-10
Another study evaluating resource use in heart failure patients found follow-up telephone calls significantly decreased the average number of hospital days over six months time and readmission rate at six months in the call group, as well as increased patient satisfaction.11
A randomized placebo-controlled trial evaluating follow-up calls from pharmacists to discharged medical patients found the call group patients were more satisfied with their post-discharge care. Additionally, there were less ED visits within 30 days of discharge in the call group compared to placebo or standard care.12
On the other hand, several studies have questioned the utility of follow-up telephone calls for improving transitions of care. A Stanford University group divided medical and surgical patients into three groups with one receiving routine follow-up calls, another requiring a patient-initiated call and a final group without any intervention and found there was no difference between these groups in regards to patient satisfaction or 30-day readmission rates.13
An outpatient trial completed at a South Dakota Veterans Affairs clinic also determined telephone calls had little effect on decreasing resources or hospital admissions.14
Although this study did not include inpatients, it demonstrates the fact that follow-up telephone calls may not be as helpful as shown in other trials and that more thorough and well-designed trials are needed to more definitively answer this question.
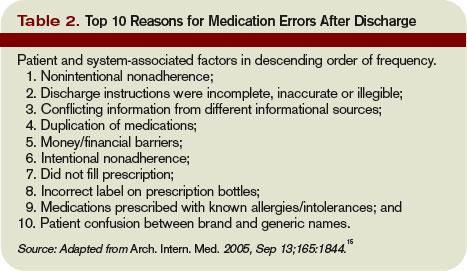
Back to the Case
The hospitalist makes a call to the patient to follow-up after he is discharged, and he says he is glad she called. He had questions about one of his medications that was discontinued while he was hospitalized and wants to know if he should restart it. He also says he is having low-grade fevers again and is not sure if he should come back in for evaluation.
The hospitalist is able to answer his questions about his medication list and instructs him to restart the metformin they had stopped while he was an inpatient. The hospitalist also is able to better explain what symptoms to be aware of and when the patient should come in for re-evaluation. The patient appreciates the five-minute call, and the hospitalist is glad she cleared up the patient’s confusion regarding his medications before a serious error or unnecessary readmission to the hospital occurred. TH
Dr. Moulds is a third-year internal medicine resident at the University of Colorado Denver. Dr. Epstein is director of medical affairs and clinical research at IPC-The Hospitalist Company.
References
- www.cdc.gov.
- Epstein K, Juarez E, Loya K, Gorman MJ, Singer A. Frequency of new or worsening symptoms in the post-hospitalization period. J Hosp Med. 2007 Mar;2(2):58-68.
- Mistiaen P, Poot E. Telephone follow-up, initiated by a hospital-based health professional, for post-discharge problems in patients discharged from hospital to home. Cochrane Database Syst Rev. 2006, Issue 4. Art. No.: CD004510. DOI:10.1002/14651858.CD004510.pub3.
- Shesser R, Smith M, Adams S, Walls R, Paxton M. The effectiveness of an organized follow-up system. Ann Emerg Med. 1986 Aug;15(8):911-915.
- Jones J, Clark W, Bradford J, Dougherty J. Efficacy of a telephone follow-up system in the emergency department. J Emerg Med. 1988 May-June;6(3):249-254.
- Jones JS, Young MS, LaFleur RA, Brown MD. Effectiveness of an organized follow-up system for elder patients released from the emergency department. Acad Emerg Med. 1997 Dec;4(12):1147-1152.
- Poncia HD, Ryan J, Carver M. Next day telephone follow up of the elderly: a needs assessment and critical incident monitoring tool for the accident and emergency department. J Accid Emerg Med. 2000 Sep;17(5):337-340.
- Kripalani S, Price M, Vigil V, Epstein K. Frequency and predictors of prescription-related issues after hospital discharge. J Hosp Med. 2008 Jan/Feb;3(1):12-19.
- Forster A, Murff H, Peterson J, Gandhi T, Bates D. Adverse drug events occurring following hospital discharge. J Gen Intern Med. 2005;20:317-323.
- Forster A, Murff H, Peterson J, Gandhi T, Bates D. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161-167.
- Riegel B, Carlson B, Kopp Z, LePetri B, Glaser D, Unger A. Effect of a standardized nurse case-management telephone intervention on resource use in patients with chronic heart failure. Arch Intern Med. 2002 Mar 25;162(6):705-712.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001 Dec 21;111(9B):26S-30S.
- Bostrom J, Caldwell J, McGuire K, Everson D. Telephone follow-up after discharge from the hospital: does it make a difference? Appl Nurs Res. 1996 May;9(2):47-52.
- Welch HG, Johnson DJ, Edson R. Telephone care as an adjunct to routine medical follow-up. A negative randomized trial. Eff Clin Pract. 2000 May-June;3(3):123-130.
- Coleman E, Smith J, Raha D, Min S. Posthospital medication discrepancies. Arch Intern Med. 2005;165:1842-1847.
Case
A 75-year-old male with history of diabetes and heart disease is discharged from the hospital after treatment for pneumonia. He has eight medications on his discharge list and is given two new prescriptions at discharge. He has a primary care provider but will not be able to see her until three weeks after discharge. Will a follow-up call decrease potential complications?
Overview
Medication errors are prevalent, especially during the transition period from discharge to follow-up with primary care physicians. There are more than 700,000 emergency department (ED) visits each year for adverse drug events with nearly 120,000 of these episodes resulting in hospitalization.1
The likelihood of an adverse drug event increases in patients using more than five medications and when there is a lack of understanding of how and why they are taking certain medications, scenarios common on hospital discharge.2 Studies evaluating effective means to reduce medication errors during transitions out of the hospital offer few solutions. One effective method, however, appears to be follow-up telephone calls.
Telephone calls have been looked at in multiple studies and usually are performed in the studies by nurses, nurse practitioners, or pharmacists and occur within days of discharge from the hospital. These calls offer a mechanism to provide answers to questions about their medical condition or medications.
Review of the Data
There is a wide range of studies evaluating the benefit of a post-discharge telephone call. Unfortunately, most of the data are of low methodological quality with low patient numbers and high risk of bias.3
Much of the data are divided into subgroups of patients, including ED patients, cardiac patients, surgical patients, medicine patients, and other small groups. The end points also vary and examine areas such as patient satisfaction, reduction in medication errors, and effect on readmissions or repeat ED visits. The bulk of studies used a standardized script. These calls lasted only minutes, which could make it user-friendly, especially for a busy hospitalist’s schedule. Unfortunately, the effect of these interventions is mixed.
With ED patients, phone calls have been shown to be an effective means of communication between patients and physicians. In a study of 297 patients, the authors were only able to reach half the patients but still were able to identify medical problems needing referral or further intervention in 37% of the patients contacted.4 Another two studies revealed similar results with approximately 40% of the contacted patients requiring further clarification on their discharge instructions.5,6
Importantly, 95% of these patients felt the call was beneficial. Thus, more than one-third of patients discharged from an ED are likely to have problems and a follow-up telephone call offers an opportunity to intervene on these potential problems. Another ED study evaluated patients older than 75 and found a nurse liaison could effectively assess the complexity of a patient’s questions and appropriately advise them over the phone or triage them to the correct care provider for further care.7
Post-discharge follow-up telephone calls also can benefit patients discharged from the hospital. A recent paper reported that approximately 12% of patients develop new or worsening symptoms within a few days post-discharge and adverse drug events can occur in between 23% to 49% of people during this transition period.8-10
Another study evaluating resource use in heart failure patients found follow-up telephone calls significantly decreased the average number of hospital days over six months time and readmission rate at six months in the call group, as well as increased patient satisfaction.11
A randomized placebo-controlled trial evaluating follow-up calls from pharmacists to discharged medical patients found the call group patients were more satisfied with their post-discharge care. Additionally, there were less ED visits within 30 days of discharge in the call group compared to placebo or standard care.12
On the other hand, several studies have questioned the utility of follow-up telephone calls for improving transitions of care. A Stanford University group divided medical and surgical patients into three groups with one receiving routine follow-up calls, another requiring a patient-initiated call and a final group without any intervention and found there was no difference between these groups in regards to patient satisfaction or 30-day readmission rates.13
An outpatient trial completed at a South Dakota Veterans Affairs clinic also determined telephone calls had little effect on decreasing resources or hospital admissions.14
Although this study did not include inpatients, it demonstrates the fact that follow-up telephone calls may not be as helpful as shown in other trials and that more thorough and well-designed trials are needed to more definitively answer this question.
Back to the Case
The hospitalist makes a call to the patient to follow-up after he is discharged, and he says he is glad she called. He had questions about one of his medications that was discontinued while he was hospitalized and wants to know if he should restart it. He also says he is having low-grade fevers again and is not sure if he should come back in for evaluation.
The hospitalist is able to answer his questions about his medication list and instructs him to restart the metformin they had stopped while he was an inpatient. The hospitalist also is able to better explain what symptoms to be aware of and when the patient should come in for re-evaluation. The patient appreciates the five-minute call, and the hospitalist is glad she cleared up the patient’s confusion regarding his medications before a serious error or unnecessary readmission to the hospital occurred. TH
Dr. Moulds is a third-year internal medicine resident at the University of Colorado Denver. Dr. Epstein is director of medical affairs and clinical research at IPC-The Hospitalist Company.
References
- www.cdc.gov.
- Epstein K, Juarez E, Loya K, Gorman MJ, Singer A. Frequency of new or worsening symptoms in the post-hospitalization period. J Hosp Med. 2007 Mar;2(2):58-68.
- Mistiaen P, Poot E. Telephone follow-up, initiated by a hospital-based health professional, for post-discharge problems in patients discharged from hospital to home. Cochrane Database Syst Rev. 2006, Issue 4. Art. No.: CD004510. DOI:10.1002/14651858.CD004510.pub3.
- Shesser R, Smith M, Adams S, Walls R, Paxton M. The effectiveness of an organized follow-up system. Ann Emerg Med. 1986 Aug;15(8):911-915.
- Jones J, Clark W, Bradford J, Dougherty J. Efficacy of a telephone follow-up system in the emergency department. J Emerg Med. 1988 May-June;6(3):249-254.
- Jones JS, Young MS, LaFleur RA, Brown MD. Effectiveness of an organized follow-up system for elder patients released from the emergency department. Acad Emerg Med. 1997 Dec;4(12):1147-1152.
- Poncia HD, Ryan J, Carver M. Next day telephone follow up of the elderly: a needs assessment and critical incident monitoring tool for the accident and emergency department. J Accid Emerg Med. 2000 Sep;17(5):337-340.
- Kripalani S, Price M, Vigil V, Epstein K. Frequency and predictors of prescription-related issues after hospital discharge. J Hosp Med. 2008 Jan/Feb;3(1):12-19.
- Forster A, Murff H, Peterson J, Gandhi T, Bates D. Adverse drug events occurring following hospital discharge. J Gen Intern Med. 2005;20:317-323.
- Forster A, Murff H, Peterson J, Gandhi T, Bates D. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161-167.
- Riegel B, Carlson B, Kopp Z, LePetri B, Glaser D, Unger A. Effect of a standardized nurse case-management telephone intervention on resource use in patients with chronic heart failure. Arch Intern Med. 2002 Mar 25;162(6):705-712.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001 Dec 21;111(9B):26S-30S.
- Bostrom J, Caldwell J, McGuire K, Everson D. Telephone follow-up after discharge from the hospital: does it make a difference? Appl Nurs Res. 1996 May;9(2):47-52.
- Welch HG, Johnson DJ, Edson R. Telephone care as an adjunct to routine medical follow-up. A negative randomized trial. Eff Clin Pract. 2000 May-June;3(3):123-130.
- Coleman E, Smith J, Raha D, Min S. Posthospital medication discrepancies. Arch Intern Med. 2005;165:1842-1847.
Case
A 75-year-old male with history of diabetes and heart disease is discharged from the hospital after treatment for pneumonia. He has eight medications on his discharge list and is given two new prescriptions at discharge. He has a primary care provider but will not be able to see her until three weeks after discharge. Will a follow-up call decrease potential complications?
Overview
Medication errors are prevalent, especially during the transition period from discharge to follow-up with primary care physicians. There are more than 700,000 emergency department (ED) visits each year for adverse drug events with nearly 120,000 of these episodes resulting in hospitalization.1
The likelihood of an adverse drug event increases in patients using more than five medications and when there is a lack of understanding of how and why they are taking certain medications, scenarios common on hospital discharge.2 Studies evaluating effective means to reduce medication errors during transitions out of the hospital offer few solutions. One effective method, however, appears to be follow-up telephone calls.
Telephone calls have been looked at in multiple studies and usually are performed in the studies by nurses, nurse practitioners, or pharmacists and occur within days of discharge from the hospital. These calls offer a mechanism to provide answers to questions about their medical condition or medications.
Review of the Data
There is a wide range of studies evaluating the benefit of a post-discharge telephone call. Unfortunately, most of the data are of low methodological quality with low patient numbers and high risk of bias.3
Much of the data are divided into subgroups of patients, including ED patients, cardiac patients, surgical patients, medicine patients, and other small groups. The end points also vary and examine areas such as patient satisfaction, reduction in medication errors, and effect on readmissions or repeat ED visits. The bulk of studies used a standardized script. These calls lasted only minutes, which could make it user-friendly, especially for a busy hospitalist’s schedule. Unfortunately, the effect of these interventions is mixed.
With ED patients, phone calls have been shown to be an effective means of communication between patients and physicians. In a study of 297 patients, the authors were only able to reach half the patients but still were able to identify medical problems needing referral or further intervention in 37% of the patients contacted.4 Another two studies revealed similar results with approximately 40% of the contacted patients requiring further clarification on their discharge instructions.5,6
Importantly, 95% of these patients felt the call was beneficial. Thus, more than one-third of patients discharged from an ED are likely to have problems and a follow-up telephone call offers an opportunity to intervene on these potential problems. Another ED study evaluated patients older than 75 and found a nurse liaison could effectively assess the complexity of a patient’s questions and appropriately advise them over the phone or triage them to the correct care provider for further care.7
Post-discharge follow-up telephone calls also can benefit patients discharged from the hospital. A recent paper reported that approximately 12% of patients develop new or worsening symptoms within a few days post-discharge and adverse drug events can occur in between 23% to 49% of people during this transition period.8-10
Another study evaluating resource use in heart failure patients found follow-up telephone calls significantly decreased the average number of hospital days over six months time and readmission rate at six months in the call group, as well as increased patient satisfaction.11
A randomized placebo-controlled trial evaluating follow-up calls from pharmacists to discharged medical patients found the call group patients were more satisfied with their post-discharge care. Additionally, there were less ED visits within 30 days of discharge in the call group compared to placebo or standard care.12
On the other hand, several studies have questioned the utility of follow-up telephone calls for improving transitions of care. A Stanford University group divided medical and surgical patients into three groups with one receiving routine follow-up calls, another requiring a patient-initiated call and a final group without any intervention and found there was no difference between these groups in regards to patient satisfaction or 30-day readmission rates.13
An outpatient trial completed at a South Dakota Veterans Affairs clinic also determined telephone calls had little effect on decreasing resources or hospital admissions.14
Although this study did not include inpatients, it demonstrates the fact that follow-up telephone calls may not be as helpful as shown in other trials and that more thorough and well-designed trials are needed to more definitively answer this question.
Back to the Case
The hospitalist makes a call to the patient to follow-up after he is discharged, and he says he is glad she called. He had questions about one of his medications that was discontinued while he was hospitalized and wants to know if he should restart it. He also says he is having low-grade fevers again and is not sure if he should come back in for evaluation.
The hospitalist is able to answer his questions about his medication list and instructs him to restart the metformin they had stopped while he was an inpatient. The hospitalist also is able to better explain what symptoms to be aware of and when the patient should come in for re-evaluation. The patient appreciates the five-minute call, and the hospitalist is glad she cleared up the patient’s confusion regarding his medications before a serious error or unnecessary readmission to the hospital occurred. TH
Dr. Moulds is a third-year internal medicine resident at the University of Colorado Denver. Dr. Epstein is director of medical affairs and clinical research at IPC-The Hospitalist Company.
References
- www.cdc.gov.
- Epstein K, Juarez E, Loya K, Gorman MJ, Singer A. Frequency of new or worsening symptoms in the post-hospitalization period. J Hosp Med. 2007 Mar;2(2):58-68.
- Mistiaen P, Poot E. Telephone follow-up, initiated by a hospital-based health professional, for post-discharge problems in patients discharged from hospital to home. Cochrane Database Syst Rev. 2006, Issue 4. Art. No.: CD004510. DOI:10.1002/14651858.CD004510.pub3.
- Shesser R, Smith M, Adams S, Walls R, Paxton M. The effectiveness of an organized follow-up system. Ann Emerg Med. 1986 Aug;15(8):911-915.
- Jones J, Clark W, Bradford J, Dougherty J. Efficacy of a telephone follow-up system in the emergency department. J Emerg Med. 1988 May-June;6(3):249-254.
- Jones JS, Young MS, LaFleur RA, Brown MD. Effectiveness of an organized follow-up system for elder patients released from the emergency department. Acad Emerg Med. 1997 Dec;4(12):1147-1152.
- Poncia HD, Ryan J, Carver M. Next day telephone follow up of the elderly: a needs assessment and critical incident monitoring tool for the accident and emergency department. J Accid Emerg Med. 2000 Sep;17(5):337-340.
- Kripalani S, Price M, Vigil V, Epstein K. Frequency and predictors of prescription-related issues after hospital discharge. J Hosp Med. 2008 Jan/Feb;3(1):12-19.
- Forster A, Murff H, Peterson J, Gandhi T, Bates D. Adverse drug events occurring following hospital discharge. J Gen Intern Med. 2005;20:317-323.
- Forster A, Murff H, Peterson J, Gandhi T, Bates D. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161-167.
- Riegel B, Carlson B, Kopp Z, LePetri B, Glaser D, Unger A. Effect of a standardized nurse case-management telephone intervention on resource use in patients with chronic heart failure. Arch Intern Med. 2002 Mar 25;162(6):705-712.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001 Dec 21;111(9B):26S-30S.
- Bostrom J, Caldwell J, McGuire K, Everson D. Telephone follow-up after discharge from the hospital: does it make a difference? Appl Nurs Res. 1996 May;9(2):47-52.
- Welch HG, Johnson DJ, Edson R. Telephone care as an adjunct to routine medical follow-up. A negative randomized trial. Eff Clin Pract. 2000 May-June;3(3):123-130.
- Coleman E, Smith J, Raha D, Min S. Posthospital medication discrepancies. Arch Intern Med. 2005;165:1842-1847.
Seek Work Wisely
Hospital medicine has come a long way since the term hospitalist was coined slightly more than a decade ago. SHM estimates the need for 30,000 practicing hospitalists within the next decade.
Filling an available hospitalist position is a two-way process that involves considerations and negotiations at various levels. When looking for the suitable hospitalist job, it is critical that you think both about what your potential employer needs and what you expect from the role you seek. The following insights provide a gauge of what an employer is looking for in a hospitalist applicant.
1) Clinical and procedural skills. Good clinical acumen is fundamental to being a successful hospitalist. As you complete residency training, your professional references are a reliable means for others to judge clinical skills. It’s important that your references comment on your clinical proficiency in their letters. Procedural skills always are welcome but by no means mandatory.
In larger facilities, where residents in training or specialists do many procedures, the program may not insist on procedural skills. On the other hand, some hospital medicine programs may require a proficiency in ICU procedures, which include intubations, central line placement, and A-line placements to mention a few. The SHM publication The Core Competencies in Hospital Medicine: A Framework for Curriculum Development is a great resource for understanding the knowledge and skills expected of a hospitalist physician.
2) Professionalism and teamwork. There are an extraordinary number of healthcare providers a hospitalist needs to work with. In addition to establishing a courteous rapport with patients and their families, good communication with primary care physicians, specialists, nursing staff, case managers, midlevel providers, and administrative and secretarial staff is essential. With this diversity of interactions, professionalism and teamwork are highly regarded and go a long way in establishing you as proficient hospitalist. An applicant’s professionalism is not only judged during the interview period but also confirmed by references. An unwavering positive attitude and commitment to a healthy work environment also are attributes that are recognized by a potential employer.
3) Quality improvement focus. Quality improvement activities and participation in such programs have rightly received unprecedented attention. SHM data indicate that 86% of hospitalist groups are active in quality improvement initiatives. Many hospital medicine programs participate in some form of Medicare pay-for-performance initiatives in order to ensure evidence-based patient care, better health outcomes, and reduce preventable complications.
A commitment to and active interest in quality improvement is highly desirable. Prior participation in and/or research for programs such as venous thromboembolism (VTE) prophylaxis, inpatient glycemic control, fall preventions, CHF optimization, medicine reconciliation pathways, and other evidence-based measures are a definite plus. In addition, specific training in areas such as perioperative care, improving safety of transitions of care, and stroke management are beneficial. Elaborating on any systems enhancement projects undertaken especially during hospital medicine clinical rotations/electives and/or fellowships will be invaluable.
4) Leadership skills. Nonclinical and administrative responsibilities are an important element of many hospitalist programs. Interest in various committees and an ability to assume leadership roles reflect favorably on your application. A good hospital medicine program will often encourage your interest in fostering the program and invite your involvement in initiatives to promote good patient care and facilitate fiscal strength.
An applicant should inquire about opportunities to participate in organizational committees and develop leadership skills, as this will be important for your professional growth. Take the time to point out any previous committee involvement in national healthcare organizations such as SHM.
5) Workflow efficiency. The ability to multitask and be organized are great skills to have as a hospitalist. Hospitalist work often involves managing several things during a short time span (i.e., rounding, admitting, teaching, holding family conferences, answering pages, and running codes). Successfully completing these responsibilities involves patience, structure, and resourcefulness during the course of any given day.
6) Teaching and research skills. In academic hospital medicine programs, good teaching and research skills can be very desirable. Chief residency or assistant chief residency experience is a good sign of teaching experience. Participation in research projects will boost your chances when looking for an academic hospitalist job. In non-academic practices, the employer may not focus much on these skills. Nevertheless, it is of significant value when the practice also hires midlevel practitioners like nurse practitioners or physician’s assistants or is thinking about how to evaluate the effects of a new program or intervention.
7) Local ties and durability. In view of the significant demand for hospitalists, recruiting can be challenging for any program. Another important aspect an employer looks at is whether you have any local ties or other compelling reasons to stay in the area for a long time. If you do have some geographic attachments or other reasons to be in the area for an extended duration, it will make the program more receptive toward you. Also, obtaining or applying for state licensure will save significant time and put you ahead of the curve.
8) Board certification. Most programs require you to be board certified or eligible when hired. Many programs expect you to obtain board certification within one to two years of starting your job. The sooner this is accomplished the more beneficial for the applicant.
Other Considerations
The diversity of hospital medicine programs provides an array of opportunities to choose from. Broadly speaking, the practice type could be academic or community based. The choice would depend upon your interest and proficiency in teaching.
In terms of schedules offered, several models exist. Many hospitalist programs are increasingly becoming 24/7, and it may be expected that you work different shifts. Also look into the licensure requirements of the state where you want to practice and be prepared with the required documentation, as some states may take longer to issue the license.
Above all, always remember: As much as it is important for you to find a befitting job, it is similarly essential for hospital medicine programs to hire worthy and valuable physicians. TH
Dr. Asudani is assistant clinical professor of medicine and a hospitalist at Baystate Medical Center, Tufts School of Medicine. Dr. Gandla is program medical director, Cogent Healthcare, High Point Regional Health System.
Hospital medicine has come a long way since the term hospitalist was coined slightly more than a decade ago. SHM estimates the need for 30,000 practicing hospitalists within the next decade.
Filling an available hospitalist position is a two-way process that involves considerations and negotiations at various levels. When looking for the suitable hospitalist job, it is critical that you think both about what your potential employer needs and what you expect from the role you seek. The following insights provide a gauge of what an employer is looking for in a hospitalist applicant.
1) Clinical and procedural skills. Good clinical acumen is fundamental to being a successful hospitalist. As you complete residency training, your professional references are a reliable means for others to judge clinical skills. It’s important that your references comment on your clinical proficiency in their letters. Procedural skills always are welcome but by no means mandatory.
In larger facilities, where residents in training or specialists do many procedures, the program may not insist on procedural skills. On the other hand, some hospital medicine programs may require a proficiency in ICU procedures, which include intubations, central line placement, and A-line placements to mention a few. The SHM publication The Core Competencies in Hospital Medicine: A Framework for Curriculum Development is a great resource for understanding the knowledge and skills expected of a hospitalist physician.
2) Professionalism and teamwork. There are an extraordinary number of healthcare providers a hospitalist needs to work with. In addition to establishing a courteous rapport with patients and their families, good communication with primary care physicians, specialists, nursing staff, case managers, midlevel providers, and administrative and secretarial staff is essential. With this diversity of interactions, professionalism and teamwork are highly regarded and go a long way in establishing you as proficient hospitalist. An applicant’s professionalism is not only judged during the interview period but also confirmed by references. An unwavering positive attitude and commitment to a healthy work environment also are attributes that are recognized by a potential employer.
3) Quality improvement focus. Quality improvement activities and participation in such programs have rightly received unprecedented attention. SHM data indicate that 86% of hospitalist groups are active in quality improvement initiatives. Many hospital medicine programs participate in some form of Medicare pay-for-performance initiatives in order to ensure evidence-based patient care, better health outcomes, and reduce preventable complications.
A commitment to and active interest in quality improvement is highly desirable. Prior participation in and/or research for programs such as venous thromboembolism (VTE) prophylaxis, inpatient glycemic control, fall preventions, CHF optimization, medicine reconciliation pathways, and other evidence-based measures are a definite plus. In addition, specific training in areas such as perioperative care, improving safety of transitions of care, and stroke management are beneficial. Elaborating on any systems enhancement projects undertaken especially during hospital medicine clinical rotations/electives and/or fellowships will be invaluable.
4) Leadership skills. Nonclinical and administrative responsibilities are an important element of many hospitalist programs. Interest in various committees and an ability to assume leadership roles reflect favorably on your application. A good hospital medicine program will often encourage your interest in fostering the program and invite your involvement in initiatives to promote good patient care and facilitate fiscal strength.
An applicant should inquire about opportunities to participate in organizational committees and develop leadership skills, as this will be important for your professional growth. Take the time to point out any previous committee involvement in national healthcare organizations such as SHM.
5) Workflow efficiency. The ability to multitask and be organized are great skills to have as a hospitalist. Hospitalist work often involves managing several things during a short time span (i.e., rounding, admitting, teaching, holding family conferences, answering pages, and running codes). Successfully completing these responsibilities involves patience, structure, and resourcefulness during the course of any given day.
6) Teaching and research skills. In academic hospital medicine programs, good teaching and research skills can be very desirable. Chief residency or assistant chief residency experience is a good sign of teaching experience. Participation in research projects will boost your chances when looking for an academic hospitalist job. In non-academic practices, the employer may not focus much on these skills. Nevertheless, it is of significant value when the practice also hires midlevel practitioners like nurse practitioners or physician’s assistants or is thinking about how to evaluate the effects of a new program or intervention.
7) Local ties and durability. In view of the significant demand for hospitalists, recruiting can be challenging for any program. Another important aspect an employer looks at is whether you have any local ties or other compelling reasons to stay in the area for a long time. If you do have some geographic attachments or other reasons to be in the area for an extended duration, it will make the program more receptive toward you. Also, obtaining or applying for state licensure will save significant time and put you ahead of the curve.
8) Board certification. Most programs require you to be board certified or eligible when hired. Many programs expect you to obtain board certification within one to two years of starting your job. The sooner this is accomplished the more beneficial for the applicant.
Other Considerations
The diversity of hospital medicine programs provides an array of opportunities to choose from. Broadly speaking, the practice type could be academic or community based. The choice would depend upon your interest and proficiency in teaching.
In terms of schedules offered, several models exist. Many hospitalist programs are increasingly becoming 24/7, and it may be expected that you work different shifts. Also look into the licensure requirements of the state where you want to practice and be prepared with the required documentation, as some states may take longer to issue the license.
Above all, always remember: As much as it is important for you to find a befitting job, it is similarly essential for hospital medicine programs to hire worthy and valuable physicians. TH
Dr. Asudani is assistant clinical professor of medicine and a hospitalist at Baystate Medical Center, Tufts School of Medicine. Dr. Gandla is program medical director, Cogent Healthcare, High Point Regional Health System.
Hospital medicine has come a long way since the term hospitalist was coined slightly more than a decade ago. SHM estimates the need for 30,000 practicing hospitalists within the next decade.
Filling an available hospitalist position is a two-way process that involves considerations and negotiations at various levels. When looking for the suitable hospitalist job, it is critical that you think both about what your potential employer needs and what you expect from the role you seek. The following insights provide a gauge of what an employer is looking for in a hospitalist applicant.
1) Clinical and procedural skills. Good clinical acumen is fundamental to being a successful hospitalist. As you complete residency training, your professional references are a reliable means for others to judge clinical skills. It’s important that your references comment on your clinical proficiency in their letters. Procedural skills always are welcome but by no means mandatory.
In larger facilities, where residents in training or specialists do many procedures, the program may not insist on procedural skills. On the other hand, some hospital medicine programs may require a proficiency in ICU procedures, which include intubations, central line placement, and A-line placements to mention a few. The SHM publication The Core Competencies in Hospital Medicine: A Framework for Curriculum Development is a great resource for understanding the knowledge and skills expected of a hospitalist physician.
2) Professionalism and teamwork. There are an extraordinary number of healthcare providers a hospitalist needs to work with. In addition to establishing a courteous rapport with patients and their families, good communication with primary care physicians, specialists, nursing staff, case managers, midlevel providers, and administrative and secretarial staff is essential. With this diversity of interactions, professionalism and teamwork are highly regarded and go a long way in establishing you as proficient hospitalist. An applicant’s professionalism is not only judged during the interview period but also confirmed by references. An unwavering positive attitude and commitment to a healthy work environment also are attributes that are recognized by a potential employer.
3) Quality improvement focus. Quality improvement activities and participation in such programs have rightly received unprecedented attention. SHM data indicate that 86% of hospitalist groups are active in quality improvement initiatives. Many hospital medicine programs participate in some form of Medicare pay-for-performance initiatives in order to ensure evidence-based patient care, better health outcomes, and reduce preventable complications.
A commitment to and active interest in quality improvement is highly desirable. Prior participation in and/or research for programs such as venous thromboembolism (VTE) prophylaxis, inpatient glycemic control, fall preventions, CHF optimization, medicine reconciliation pathways, and other evidence-based measures are a definite plus. In addition, specific training in areas such as perioperative care, improving safety of transitions of care, and stroke management are beneficial. Elaborating on any systems enhancement projects undertaken especially during hospital medicine clinical rotations/electives and/or fellowships will be invaluable.
4) Leadership skills. Nonclinical and administrative responsibilities are an important element of many hospitalist programs. Interest in various committees and an ability to assume leadership roles reflect favorably on your application. A good hospital medicine program will often encourage your interest in fostering the program and invite your involvement in initiatives to promote good patient care and facilitate fiscal strength.
An applicant should inquire about opportunities to participate in organizational committees and develop leadership skills, as this will be important for your professional growth. Take the time to point out any previous committee involvement in national healthcare organizations such as SHM.
5) Workflow efficiency. The ability to multitask and be organized are great skills to have as a hospitalist. Hospitalist work often involves managing several things during a short time span (i.e., rounding, admitting, teaching, holding family conferences, answering pages, and running codes). Successfully completing these responsibilities involves patience, structure, and resourcefulness during the course of any given day.
6) Teaching and research skills. In academic hospital medicine programs, good teaching and research skills can be very desirable. Chief residency or assistant chief residency experience is a good sign of teaching experience. Participation in research projects will boost your chances when looking for an academic hospitalist job. In non-academic practices, the employer may not focus much on these skills. Nevertheless, it is of significant value when the practice also hires midlevel practitioners like nurse practitioners or physician’s assistants or is thinking about how to evaluate the effects of a new program or intervention.
7) Local ties and durability. In view of the significant demand for hospitalists, recruiting can be challenging for any program. Another important aspect an employer looks at is whether you have any local ties or other compelling reasons to stay in the area for a long time. If you do have some geographic attachments or other reasons to be in the area for an extended duration, it will make the program more receptive toward you. Also, obtaining or applying for state licensure will save significant time and put you ahead of the curve.
8) Board certification. Most programs require you to be board certified or eligible when hired. Many programs expect you to obtain board certification within one to two years of starting your job. The sooner this is accomplished the more beneficial for the applicant.
Other Considerations
The diversity of hospital medicine programs provides an array of opportunities to choose from. Broadly speaking, the practice type could be academic or community based. The choice would depend upon your interest and proficiency in teaching.
In terms of schedules offered, several models exist. Many hospitalist programs are increasingly becoming 24/7, and it may be expected that you work different shifts. Also look into the licensure requirements of the state where you want to practice and be prepared with the required documentation, as some states may take longer to issue the license.
Above all, always remember: As much as it is important for you to find a befitting job, it is similarly essential for hospital medicine programs to hire worthy and valuable physicians. TH
Dr. Asudani is assistant clinical professor of medicine and a hospitalist at Baystate Medical Center, Tufts School of Medicine. Dr. Gandla is program medical director, Cogent Healthcare, High Point Regional Health System.
Medical Board Maneuvers
There are a few pieces of mail that bring an instant feeling of dread—an audit letter from the IRS, a credit card bill after a Las Vegas vacation, and a letter from the medical board. We have no good solutions for the first two pieces of correspondence, but we have a few suggestions when communicating with the medical board.
1) Understand the medical board’s purpose. Every state regulates the practice of medicine for the same reason: Medicine requires highly specialized knowledge, and the average patient does not have the knowledge or experience to determine which physicians are qualified to practice.
Think of the harm that could result if incompetent physicians could practice medicine without oversight. Even worse, think of the harm that could result if non-physicians could provide medical services without proper education and training. That’s why, in every state, the legislatures have passed laws to regulate and control the practice of medicine so people can be properly protected against the unauthorized, unqualified, and improper practice of medicine. Almost everyone agrees regulation of this nature serves a legitimate public purpose.
Consequently, whenever a physician deals with a medical board, they are best served by remembering that the medical board exists to protect the public from the unauthorized, unqualified and improper practice of medicine. The physician’s ultimate goal is to reassure that medical board that their practice is authorized, well-grounded in medicine, and within the standards of professional care. Even if the patient has complained because of a questionable motive, such as attempting to gain an advantage in a billing dispute, a physician cannot use the patient’s motive as grounds for defending poor medical care. Medical boards often distrust physicians who try to shift the focus from the adequacy of their medical care to a patient’s shortcomings.
2) Do I need a lawyer? In most states, the medical board will ask a physician to respond to every patient complaint—even if the complaint is outlandish. Rather than judging the complaint when it arrives, the medical board is more interested in assessing the physician’s response to the complaint. An unhappy patient may lack the acumen to explain the course of treatment and the specifics of their condition, so the medical board relies upon the physician to describe their conduct and the course of care.
Unless the patient’s complaint is in the category of “the doctor placed transmitters in my brain and now the aliens won’t leave me alone,” we always recommend a physician review the complaint and the proposed response with an attorney. In every state, there are attorneys who specialize in representing physicians before medical boards.
Because they’ve dealt with the medical board in many cases throughout a number of years, these attorneys have a good idea of what the medical board expects to see in a response, and, more importantly, what the medical board does not want to see in a response. Investing in an attorney’s services at the outset is money well spent.
Far too often, we see physicians who tried to save a couple of hundred dollars by responding to the medical board, but their response was ineffective. The physician is then faced with spending several thousand dollars defending a disciplinary proceeding. Even worse, if the physician has made a sufficiently serious mistake in the initial response, the physician is going to be stuck with that mistake, severely limiting the attorney’s ability to defend the disciplinary proceeding. Some medical malpractice insurers reimburse physicians for attorney’s fees incurred in responding to a medical board complaint, so check your policy.
3) Candor is your friend. Undoubtedly, there are occasions when a patient complains about medical care without justification. Patients have unrealistic expectations and often fail to understand that each patient’s condition presents a unique challenge. Conversely, some complaints absolutely are legitimate. Every physician makes mistakes, and the medical board will react negatively to a physician who defends an unreasonable course of care. In fact, the medical board will view the physician’s defense of unreasonable care as evidence the mistake is not an aberration in the physician’s practice.
When confronted with one of those instances where the patient’s complaint is legitimate, we doubly recommend you confer with an attorney about your response. At a minimum, however, a physician must be able to explain:
- Why a mistake occurred;
- What steps the physician took to minimize the consequences of the mistake for the patient;
- Why the mistake represents an aberration, not a reason for continued concern; and
- What changes the physician has implemented to ensure the mistake will not reoccur.
In preparing a response to the medical board, we’ve recommended physicians take continuing education in the areas of the patients’ complaints. By taking this remedial measure voluntarily, a physician reduces the likelihood the medical board will impose it as a remedial sanction.
When we first began defending healthcare professionals before their licensing agencies, we thought we’d be spending lots of time dealing with complicated medical issues. We were wrong.
By an overwhelming proportion, the majority of disciplinary actions against physicians arise from three sources:
- Allegations of improper sexual conduct;
- Allegations of substance abuse; or
- Allegations of financial impropriety.
Physicians face the same problems that affect non-physicians—but a physician’s breach of the obligations owed to patients allows a medical board to take disciplinary action. The physician-patient relationship has an inherent disparity of power that makes patients vulnerable to a physician’s abuse of trust. For this reason, medical boards view allegations of this nature quite seriously.
The first question a physician has to ask when accused of these form of misconduct is, “Is it true?” If you are tempted, to answer, “no,” even if the real answer is “yes,” think twice. If you lie to the medical board about one of these issues, you almost certainly will lose your medical license. You will have demonstrated to the board that you not only lack judgment, but that you can’t be trusted. If it even crossed your mind to alter the medical or billing records, don’t. The medical board will probably obtain copies of those records from another source.
If the answer to the question, “Is it true?” is “yes,” the physician faces the prospect that the medical board will revoke or suspend their license. In these situations, we regularly recommend physicians embark on a course of action designed to save the medical license—even if the physician will be subject to arduous probationary terms.
We will recommend the physicians engage practice monitors, seek substance abuse counseling, and repay any wrongfully obtained money. In many states, there are specialized programs that provide mental health and addiction counseling for physicians, and these programs represent potential lifelines for physicians in crisis. Your goal is demonstrate to the medical board that you’ve seen the error of your ways and have committed to a program that will return you to good standing.
Responding to the medical board is a scary proposition. The majority of complaints are dismissed without any disciplinary action against a physician—but no physician should take a complaint lightly. Be thoughtful and candid in your response to maximize the likelihood that the medical board will dismiss the complaint. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado, Denver.
There are a few pieces of mail that bring an instant feeling of dread—an audit letter from the IRS, a credit card bill after a Las Vegas vacation, and a letter from the medical board. We have no good solutions for the first two pieces of correspondence, but we have a few suggestions when communicating with the medical board.
1) Understand the medical board’s purpose. Every state regulates the practice of medicine for the same reason: Medicine requires highly specialized knowledge, and the average patient does not have the knowledge or experience to determine which physicians are qualified to practice.
Think of the harm that could result if incompetent physicians could practice medicine without oversight. Even worse, think of the harm that could result if non-physicians could provide medical services without proper education and training. That’s why, in every state, the legislatures have passed laws to regulate and control the practice of medicine so people can be properly protected against the unauthorized, unqualified, and improper practice of medicine. Almost everyone agrees regulation of this nature serves a legitimate public purpose.
Consequently, whenever a physician deals with a medical board, they are best served by remembering that the medical board exists to protect the public from the unauthorized, unqualified and improper practice of medicine. The physician’s ultimate goal is to reassure that medical board that their practice is authorized, well-grounded in medicine, and within the standards of professional care. Even if the patient has complained because of a questionable motive, such as attempting to gain an advantage in a billing dispute, a physician cannot use the patient’s motive as grounds for defending poor medical care. Medical boards often distrust physicians who try to shift the focus from the adequacy of their medical care to a patient’s shortcomings.
2) Do I need a lawyer? In most states, the medical board will ask a physician to respond to every patient complaint—even if the complaint is outlandish. Rather than judging the complaint when it arrives, the medical board is more interested in assessing the physician’s response to the complaint. An unhappy patient may lack the acumen to explain the course of treatment and the specifics of their condition, so the medical board relies upon the physician to describe their conduct and the course of care.
Unless the patient’s complaint is in the category of “the doctor placed transmitters in my brain and now the aliens won’t leave me alone,” we always recommend a physician review the complaint and the proposed response with an attorney. In every state, there are attorneys who specialize in representing physicians before medical boards.
Because they’ve dealt with the medical board in many cases throughout a number of years, these attorneys have a good idea of what the medical board expects to see in a response, and, more importantly, what the medical board does not want to see in a response. Investing in an attorney’s services at the outset is money well spent.
Far too often, we see physicians who tried to save a couple of hundred dollars by responding to the medical board, but their response was ineffective. The physician is then faced with spending several thousand dollars defending a disciplinary proceeding. Even worse, if the physician has made a sufficiently serious mistake in the initial response, the physician is going to be stuck with that mistake, severely limiting the attorney’s ability to defend the disciplinary proceeding. Some medical malpractice insurers reimburse physicians for attorney’s fees incurred in responding to a medical board complaint, so check your policy.
3) Candor is your friend. Undoubtedly, there are occasions when a patient complains about medical care without justification. Patients have unrealistic expectations and often fail to understand that each patient’s condition presents a unique challenge. Conversely, some complaints absolutely are legitimate. Every physician makes mistakes, and the medical board will react negatively to a physician who defends an unreasonable course of care. In fact, the medical board will view the physician’s defense of unreasonable care as evidence the mistake is not an aberration in the physician’s practice.
When confronted with one of those instances where the patient’s complaint is legitimate, we doubly recommend you confer with an attorney about your response. At a minimum, however, a physician must be able to explain:
- Why a mistake occurred;
- What steps the physician took to minimize the consequences of the mistake for the patient;
- Why the mistake represents an aberration, not a reason for continued concern; and
- What changes the physician has implemented to ensure the mistake will not reoccur.
In preparing a response to the medical board, we’ve recommended physicians take continuing education in the areas of the patients’ complaints. By taking this remedial measure voluntarily, a physician reduces the likelihood the medical board will impose it as a remedial sanction.
When we first began defending healthcare professionals before their licensing agencies, we thought we’d be spending lots of time dealing with complicated medical issues. We were wrong.
By an overwhelming proportion, the majority of disciplinary actions against physicians arise from three sources:
- Allegations of improper sexual conduct;
- Allegations of substance abuse; or
- Allegations of financial impropriety.
Physicians face the same problems that affect non-physicians—but a physician’s breach of the obligations owed to patients allows a medical board to take disciplinary action. The physician-patient relationship has an inherent disparity of power that makes patients vulnerable to a physician’s abuse of trust. For this reason, medical boards view allegations of this nature quite seriously.
The first question a physician has to ask when accused of these form of misconduct is, “Is it true?” If you are tempted, to answer, “no,” even if the real answer is “yes,” think twice. If you lie to the medical board about one of these issues, you almost certainly will lose your medical license. You will have demonstrated to the board that you not only lack judgment, but that you can’t be trusted. If it even crossed your mind to alter the medical or billing records, don’t. The medical board will probably obtain copies of those records from another source.
If the answer to the question, “Is it true?” is “yes,” the physician faces the prospect that the medical board will revoke or suspend their license. In these situations, we regularly recommend physicians embark on a course of action designed to save the medical license—even if the physician will be subject to arduous probationary terms.
We will recommend the physicians engage practice monitors, seek substance abuse counseling, and repay any wrongfully obtained money. In many states, there are specialized programs that provide mental health and addiction counseling for physicians, and these programs represent potential lifelines for physicians in crisis. Your goal is demonstrate to the medical board that you’ve seen the error of your ways and have committed to a program that will return you to good standing.
Responding to the medical board is a scary proposition. The majority of complaints are dismissed without any disciplinary action against a physician—but no physician should take a complaint lightly. Be thoughtful and candid in your response to maximize the likelihood that the medical board will dismiss the complaint. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado, Denver.
There are a few pieces of mail that bring an instant feeling of dread—an audit letter from the IRS, a credit card bill after a Las Vegas vacation, and a letter from the medical board. We have no good solutions for the first two pieces of correspondence, but we have a few suggestions when communicating with the medical board.
1) Understand the medical board’s purpose. Every state regulates the practice of medicine for the same reason: Medicine requires highly specialized knowledge, and the average patient does not have the knowledge or experience to determine which physicians are qualified to practice.
Think of the harm that could result if incompetent physicians could practice medicine without oversight. Even worse, think of the harm that could result if non-physicians could provide medical services without proper education and training. That’s why, in every state, the legislatures have passed laws to regulate and control the practice of medicine so people can be properly protected against the unauthorized, unqualified, and improper practice of medicine. Almost everyone agrees regulation of this nature serves a legitimate public purpose.
Consequently, whenever a physician deals with a medical board, they are best served by remembering that the medical board exists to protect the public from the unauthorized, unqualified and improper practice of medicine. The physician’s ultimate goal is to reassure that medical board that their practice is authorized, well-grounded in medicine, and within the standards of professional care. Even if the patient has complained because of a questionable motive, such as attempting to gain an advantage in a billing dispute, a physician cannot use the patient’s motive as grounds for defending poor medical care. Medical boards often distrust physicians who try to shift the focus from the adequacy of their medical care to a patient’s shortcomings.
2) Do I need a lawyer? In most states, the medical board will ask a physician to respond to every patient complaint—even if the complaint is outlandish. Rather than judging the complaint when it arrives, the medical board is more interested in assessing the physician’s response to the complaint. An unhappy patient may lack the acumen to explain the course of treatment and the specifics of their condition, so the medical board relies upon the physician to describe their conduct and the course of care.
Unless the patient’s complaint is in the category of “the doctor placed transmitters in my brain and now the aliens won’t leave me alone,” we always recommend a physician review the complaint and the proposed response with an attorney. In every state, there are attorneys who specialize in representing physicians before medical boards.
Because they’ve dealt with the medical board in many cases throughout a number of years, these attorneys have a good idea of what the medical board expects to see in a response, and, more importantly, what the medical board does not want to see in a response. Investing in an attorney’s services at the outset is money well spent.
Far too often, we see physicians who tried to save a couple of hundred dollars by responding to the medical board, but their response was ineffective. The physician is then faced with spending several thousand dollars defending a disciplinary proceeding. Even worse, if the physician has made a sufficiently serious mistake in the initial response, the physician is going to be stuck with that mistake, severely limiting the attorney’s ability to defend the disciplinary proceeding. Some medical malpractice insurers reimburse physicians for attorney’s fees incurred in responding to a medical board complaint, so check your policy.
3) Candor is your friend. Undoubtedly, there are occasions when a patient complains about medical care without justification. Patients have unrealistic expectations and often fail to understand that each patient’s condition presents a unique challenge. Conversely, some complaints absolutely are legitimate. Every physician makes mistakes, and the medical board will react negatively to a physician who defends an unreasonable course of care. In fact, the medical board will view the physician’s defense of unreasonable care as evidence the mistake is not an aberration in the physician’s practice.
When confronted with one of those instances where the patient’s complaint is legitimate, we doubly recommend you confer with an attorney about your response. At a minimum, however, a physician must be able to explain:
- Why a mistake occurred;
- What steps the physician took to minimize the consequences of the mistake for the patient;
- Why the mistake represents an aberration, not a reason for continued concern; and
- What changes the physician has implemented to ensure the mistake will not reoccur.
In preparing a response to the medical board, we’ve recommended physicians take continuing education in the areas of the patients’ complaints. By taking this remedial measure voluntarily, a physician reduces the likelihood the medical board will impose it as a remedial sanction.
When we first began defending healthcare professionals before their licensing agencies, we thought we’d be spending lots of time dealing with complicated medical issues. We were wrong.
By an overwhelming proportion, the majority of disciplinary actions against physicians arise from three sources:
- Allegations of improper sexual conduct;
- Allegations of substance abuse; or
- Allegations of financial impropriety.
Physicians face the same problems that affect non-physicians—but a physician’s breach of the obligations owed to patients allows a medical board to take disciplinary action. The physician-patient relationship has an inherent disparity of power that makes patients vulnerable to a physician’s abuse of trust. For this reason, medical boards view allegations of this nature quite seriously.
The first question a physician has to ask when accused of these form of misconduct is, “Is it true?” If you are tempted, to answer, “no,” even if the real answer is “yes,” think twice. If you lie to the medical board about one of these issues, you almost certainly will lose your medical license. You will have demonstrated to the board that you not only lack judgment, but that you can’t be trusted. If it even crossed your mind to alter the medical or billing records, don’t. The medical board will probably obtain copies of those records from another source.
If the answer to the question, “Is it true?” is “yes,” the physician faces the prospect that the medical board will revoke or suspend their license. In these situations, we regularly recommend physicians embark on a course of action designed to save the medical license—even if the physician will be subject to arduous probationary terms.
We will recommend the physicians engage practice monitors, seek substance abuse counseling, and repay any wrongfully obtained money. In many states, there are specialized programs that provide mental health and addiction counseling for physicians, and these programs represent potential lifelines for physicians in crisis. Your goal is demonstrate to the medical board that you’ve seen the error of your ways and have committed to a program that will return you to good standing.
Responding to the medical board is a scary proposition. The majority of complaints are dismissed without any disciplinary action against a physician—but no physician should take a complaint lightly. Be thoughtful and candid in your response to maximize the likelihood that the medical board will dismiss the complaint. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado, Denver.
Sort Out Surgical Cases
Hospitalists often are involved in the care of a surgical patient. Reimbursement for surgical procedures includes payment for pre-, intra-, and post-operative care.
Knowing the billing and coding responsibilities apart from those of the surgeon is imperative for the hospitalist’s accurate charge capture. There are several critical misconceptions in this regard:
- Hospitalists cannot bill for services when involved in a surgical case;
- Surgeons are not responsible for inpatient care if the patient is stable and does not require additional inpatient post-op visits; and
- Modifiers are not required for hospitalist claims unless the hospitalist reports under the same tax identification number as the surgeon.
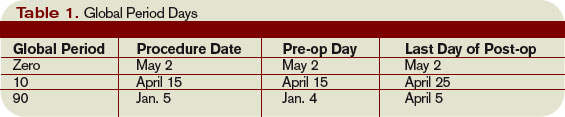
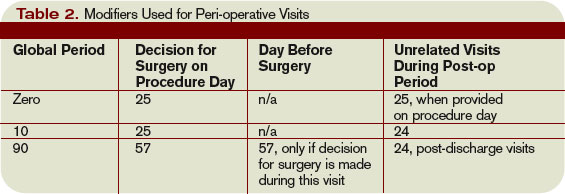
Determine Global Period
Procedures are categorized as major or minor surgery. A global period is assigned to each procedure code, designating post-operative periods of zero, 10, or 90 days. Physician services during this global period are considered part of the packaged payment and not separately reimbursed.
The global period for any given CPT code can be identified in the Medicare Physician Fee Schedule and accessed at www.cms.hhs.gov/PfsLookup. In addition to zero, 10, and 90 days, services can be noted with:
- XXX, indicating the global period concept does not apply; or
- ZZZ, indicating an “add-on” procedure that must always be reported with the relevant primary procedure code; “add-on” procedures assume the global period of the primary procedure.
Major surgery routinely is allotted 90-day global periods. Therefore, the surgeon is responsible for the patient and must provide all related care one day prior to the surgery forward thru 90 postoperative days at no additional charge. Minor surgery, including endoscopy, has zero or 10-day postoperative periods, bundling all services on the surgical day only, or the surgical day and the subsequent 10 days, respectively (see Table 1, p. above).
The Surgeon Defined
Any qualified physician able to perform “surgical” services within his scope of practice is considered a “surgeon” for billing purposes. For example, a pulmonologist, or primary care physician, must meet the surgical billing and documentation requirements when performing bronchoscopies or uncomplicated incision-and-drainage services, respectively.
Surgical services easily are identified as any code included in range 20000-69999. This code series includes major, minor, and endoscopic procedures. The “surgeon” and all physicians in the same group practice (i.e., reporting services under the same tax identification number) with the same specialty designation must adhere to the global period billing rules.
Alternately, physicians with different specialty designations in the same group practice (e.g., multispecialty group that reports services under the same tax identification number) or different group practices can perform and separately report medically necessary services during the surgeon’s global period, as long as a formal (mutually agreed upon) transfer of care did not occur. Information on physician specialty designations is available at www.highmarkmedicareservices.com/partb/refman/appendix-d.html.
Package Components
The following services are included in the surgeon’s packaged payment:
- Preoperative visits after the decision for surgery is made beginning one day prior to surgery;
- All additional post-operative medical or surgical services provided by the surgeon related to complications, but not require additional trips to the operating room;
- Post-operative visits by the surgeon related to recovery from surgery, including but not limited to dressing changes; local incisional care; removal of cutaneous sutures and staples; line removals; changes and removal of tracheostomy tubes; and discharge services; and
- Post-operative pain management provided by the surgeon.
Services not included are:
- The initial consultation or evaluation of the problem by the surgeon to determine the need for surgery. Append modifier 57 to this visit if provided the day before or day of major surgery to alert the payer that the service resulted in the decision for surgery. Append modifier 25 to this visit if provided the day of minor surgery;
- Services of other physicians except where the other physicians are providing coverage for the surgeon or agree on a transfer of care. This agreement may be in the form of a letter or an annotation in the discharge summary, hospital record, or ASC record;
- Post-operative visits by the surgeon unrelated to the diagnosis for which the surgical procedure is performed, unless the visits occur due to complications of the surgery. These services only are payable after the patient has been discharged from the hospitalization in which the surgery occurred. Append modifier 24 to these unrelated post-op visits;
- Diagnostic tests and procedures, including diagnostic radiological procedures;
- Clearly distinct surgical procedures during the post-operative period that do not result in repeat operations or treatment for complications;
- Treatment for post-operative complications that require a return trip to the operating room, catheterization lab, or endoscopy suite;
- Immunosuppressive therapy for organ transplants; and
- Critical care services (CPT codes 99291 and 99292) unrelated to the surgery in which a seriously injured or burned patient is critically ill and requires constant attendance of the surgeon. Append modifier 24 to these unrelated critical care services (see Table 2, above).
Payer Variations
While Medicare does not require modifier usage by hospitalists providing medically necessary services on surgical cases, some private payers do. Their electronic claim systems may not differentiate services by non-surgical specialists, requiring all physicians to append the appropriate modifier depending on the reason and timing of the service (see “Key Modifiers” below). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Hospitalists often are involved in the care of a surgical patient. Reimbursement for surgical procedures includes payment for pre-, intra-, and post-operative care.
Knowing the billing and coding responsibilities apart from those of the surgeon is imperative for the hospitalist’s accurate charge capture. There are several critical misconceptions in this regard:
- Hospitalists cannot bill for services when involved in a surgical case;
- Surgeons are not responsible for inpatient care if the patient is stable and does not require additional inpatient post-op visits; and
- Modifiers are not required for hospitalist claims unless the hospitalist reports under the same tax identification number as the surgeon.
Determine Global Period
Procedures are categorized as major or minor surgery. A global period is assigned to each procedure code, designating post-operative periods of zero, 10, or 90 days. Physician services during this global period are considered part of the packaged payment and not separately reimbursed.
The global period for any given CPT code can be identified in the Medicare Physician Fee Schedule and accessed at www.cms.hhs.gov/PfsLookup. In addition to zero, 10, and 90 days, services can be noted with:
- XXX, indicating the global period concept does not apply; or
- ZZZ, indicating an “add-on” procedure that must always be reported with the relevant primary procedure code; “add-on” procedures assume the global period of the primary procedure.
Major surgery routinely is allotted 90-day global periods. Therefore, the surgeon is responsible for the patient and must provide all related care one day prior to the surgery forward thru 90 postoperative days at no additional charge. Minor surgery, including endoscopy, has zero or 10-day postoperative periods, bundling all services on the surgical day only, or the surgical day and the subsequent 10 days, respectively (see Table 1, p. above).
The Surgeon Defined
Any qualified physician able to perform “surgical” services within his scope of practice is considered a “surgeon” for billing purposes. For example, a pulmonologist, or primary care physician, must meet the surgical billing and documentation requirements when performing bronchoscopies or uncomplicated incision-and-drainage services, respectively.
Surgical services easily are identified as any code included in range 20000-69999. This code series includes major, minor, and endoscopic procedures. The “surgeon” and all physicians in the same group practice (i.e., reporting services under the same tax identification number) with the same specialty designation must adhere to the global period billing rules.
Alternately, physicians with different specialty designations in the same group practice (e.g., multispecialty group that reports services under the same tax identification number) or different group practices can perform and separately report medically necessary services during the surgeon’s global period, as long as a formal (mutually agreed upon) transfer of care did not occur. Information on physician specialty designations is available at www.highmarkmedicareservices.com/partb/refman/appendix-d.html.
Package Components
The following services are included in the surgeon’s packaged payment:
- Preoperative visits after the decision for surgery is made beginning one day prior to surgery;
- All additional post-operative medical or surgical services provided by the surgeon related to complications, but not require additional trips to the operating room;
- Post-operative visits by the surgeon related to recovery from surgery, including but not limited to dressing changes; local incisional care; removal of cutaneous sutures and staples; line removals; changes and removal of tracheostomy tubes; and discharge services; and
- Post-operative pain management provided by the surgeon.
Services not included are:
- The initial consultation or evaluation of the problem by the surgeon to determine the need for surgery. Append modifier 57 to this visit if provided the day before or day of major surgery to alert the payer that the service resulted in the decision for surgery. Append modifier 25 to this visit if provided the day of minor surgery;
- Services of other physicians except where the other physicians are providing coverage for the surgeon or agree on a transfer of care. This agreement may be in the form of a letter or an annotation in the discharge summary, hospital record, or ASC record;
- Post-operative visits by the surgeon unrelated to the diagnosis for which the surgical procedure is performed, unless the visits occur due to complications of the surgery. These services only are payable after the patient has been discharged from the hospitalization in which the surgery occurred. Append modifier 24 to these unrelated post-op visits;
- Diagnostic tests and procedures, including diagnostic radiological procedures;
- Clearly distinct surgical procedures during the post-operative period that do not result in repeat operations or treatment for complications;
- Treatment for post-operative complications that require a return trip to the operating room, catheterization lab, or endoscopy suite;
- Immunosuppressive therapy for organ transplants; and
- Critical care services (CPT codes 99291 and 99292) unrelated to the surgery in which a seriously injured or burned patient is critically ill and requires constant attendance of the surgeon. Append modifier 24 to these unrelated critical care services (see Table 2, above).
Payer Variations
While Medicare does not require modifier usage by hospitalists providing medically necessary services on surgical cases, some private payers do. Their electronic claim systems may not differentiate services by non-surgical specialists, requiring all physicians to append the appropriate modifier depending on the reason and timing of the service (see “Key Modifiers” below). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Hospitalists often are involved in the care of a surgical patient. Reimbursement for surgical procedures includes payment for pre-, intra-, and post-operative care.
Knowing the billing and coding responsibilities apart from those of the surgeon is imperative for the hospitalist’s accurate charge capture. There are several critical misconceptions in this regard:
- Hospitalists cannot bill for services when involved in a surgical case;
- Surgeons are not responsible for inpatient care if the patient is stable and does not require additional inpatient post-op visits; and
- Modifiers are not required for hospitalist claims unless the hospitalist reports under the same tax identification number as the surgeon.
Determine Global Period
Procedures are categorized as major or minor surgery. A global period is assigned to each procedure code, designating post-operative periods of zero, 10, or 90 days. Physician services during this global period are considered part of the packaged payment and not separately reimbursed.
The global period for any given CPT code can be identified in the Medicare Physician Fee Schedule and accessed at www.cms.hhs.gov/PfsLookup. In addition to zero, 10, and 90 days, services can be noted with:
- XXX, indicating the global period concept does not apply; or
- ZZZ, indicating an “add-on” procedure that must always be reported with the relevant primary procedure code; “add-on” procedures assume the global period of the primary procedure.
Major surgery routinely is allotted 90-day global periods. Therefore, the surgeon is responsible for the patient and must provide all related care one day prior to the surgery forward thru 90 postoperative days at no additional charge. Minor surgery, including endoscopy, has zero or 10-day postoperative periods, bundling all services on the surgical day only, or the surgical day and the subsequent 10 days, respectively (see Table 1, p. above).
The Surgeon Defined
Any qualified physician able to perform “surgical” services within his scope of practice is considered a “surgeon” for billing purposes. For example, a pulmonologist, or primary care physician, must meet the surgical billing and documentation requirements when performing bronchoscopies or uncomplicated incision-and-drainage services, respectively.
Surgical services easily are identified as any code included in range 20000-69999. This code series includes major, minor, and endoscopic procedures. The “surgeon” and all physicians in the same group practice (i.e., reporting services under the same tax identification number) with the same specialty designation must adhere to the global period billing rules.
Alternately, physicians with different specialty designations in the same group practice (e.g., multispecialty group that reports services under the same tax identification number) or different group practices can perform and separately report medically necessary services during the surgeon’s global period, as long as a formal (mutually agreed upon) transfer of care did not occur. Information on physician specialty designations is available at www.highmarkmedicareservices.com/partb/refman/appendix-d.html.
Package Components
The following services are included in the surgeon’s packaged payment:
- Preoperative visits after the decision for surgery is made beginning one day prior to surgery;
- All additional post-operative medical or surgical services provided by the surgeon related to complications, but not require additional trips to the operating room;
- Post-operative visits by the surgeon related to recovery from surgery, including but not limited to dressing changes; local incisional care; removal of cutaneous sutures and staples; line removals; changes and removal of tracheostomy tubes; and discharge services; and
- Post-operative pain management provided by the surgeon.
Services not included are:
- The initial consultation or evaluation of the problem by the surgeon to determine the need for surgery. Append modifier 57 to this visit if provided the day before or day of major surgery to alert the payer that the service resulted in the decision for surgery. Append modifier 25 to this visit if provided the day of minor surgery;
- Services of other physicians except where the other physicians are providing coverage for the surgeon or agree on a transfer of care. This agreement may be in the form of a letter or an annotation in the discharge summary, hospital record, or ASC record;
- Post-operative visits by the surgeon unrelated to the diagnosis for which the surgical procedure is performed, unless the visits occur due to complications of the surgery. These services only are payable after the patient has been discharged from the hospitalization in which the surgery occurred. Append modifier 24 to these unrelated post-op visits;
- Diagnostic tests and procedures, including diagnostic radiological procedures;
- Clearly distinct surgical procedures during the post-operative period that do not result in repeat operations or treatment for complications;
- Treatment for post-operative complications that require a return trip to the operating room, catheterization lab, or endoscopy suite;
- Immunosuppressive therapy for organ transplants; and
- Critical care services (CPT codes 99291 and 99292) unrelated to the surgery in which a seriously injured or burned patient is critically ill and requires constant attendance of the surgeon. Append modifier 24 to these unrelated critical care services (see Table 2, above).
Payer Variations
While Medicare does not require modifier usage by hospitalists providing medically necessary services on surgical cases, some private payers do. Their electronic claim systems may not differentiate services by non-surgical specialists, requiring all physicians to append the appropriate modifier depending on the reason and timing of the service (see “Key Modifiers” below). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.