User login
MDedge latest news is breaking news from medical conferences, journals, guidelines, the FDA and CDC.
Diet Rich in Ultraprocessed Grains Increases Risk for IBD
, a large study has found.
The sweeping analysis of 124,590 adults from 21 countries found that those eating at least 19 g of ultraprocessed grains a day were about twice as likely to be diagnosed with IBD as peers eating less than 9 g daily.
“Our study adds robust evidence from a large, diverse global cohort that frequent consumption of ultraprocessed grains is associated with an increased risk of developing inflammatory bowel disease,” Neeraj Narula, MD, MPH, gastroenterologist and associate professor of medicine, McMaster University, Hamilton, Ontario, Canada, told GI & Hepatology News.

The study also “further clarifies that not all grains carry risk — minimally processed grains like fresh bread and rice were associated with lower risk even. These results build on and specify previous findings linking ultraprocessed foods more broadly to IBD,” Narula said.
The study was published in The American Journal of Gastroenterology.
Diet Matters to IBD Risk
According to the latest US data (2021-2023), ultraprocessed foods made up 62% of daily calories for young people and 53% for adults in 2021-2023.
The Prospective Urban Rural Epidemiology (PURE) study has followed participants aged 35-70 years for a median of nearly 13 years. At enrollment, volunteers completed country-specific food-frequency questionnaires, enabling researchers to quantify usual intake of more than 130 food items and track new cases of IBD reported at biennial follow-ups.
The researchers classified packaged breads, sweet breakfast cereals, crackers, pastries and ready-to-heat pizza or pasta as ultraprocessed grains because they are refined and typically contain additives such as emulsifiers and preservatives. Fresh bakery bread and plain rice were analyzed separately as minimally processed grain references.
During a median of 12.9 years, 605 participants developed IBD; 497 developed ulcerative colitis (UC) and 108 developed Crohn’s disease.
Increased intake of ultraprocessed grains was associated with a higher risk for IBD, with hazard ratios (HR) of 2.08 for intake of ≥ 50 g/d and 1.37 for 19-50 g/d compared to intake of < 19 g/d. The increased risk was largely driven by a significantly increased risk for UC (HR, 2.46) and not Crohn’s disease (HR, 0.98).
Among the different ultraprocessed grain products, packaged bread stood out: Consuming ≥ 30 g/d of packaged bread (a little more than one slice) was associated with a greater than twofold increased risk for IBD (HR, 2.11) compared to no intake of packaged bread.
In contrast, greater consumption of fresh bread was associated with a reduced risk of developing IBD (HR, 0.61 for ≥ 65 g/d and 0.45 for 16-65 g/d compared to < 16 g/d).
Increased intake of rice was also associated with a lower risk of developing IBD (HR, 0.63 for ≥ 1 serving/d and 0.99 for < 1 serving/d).
When the researchers widened the lens to all ultraprocessed foods — from sodas to salty snacks — the risk for IBD climbed further.
Participants eating at least five servings a day had nearly a fourfold greater odds of IBD than those eating fewer than one serving (HR, 3.95) — a finding consistent with other data from the PURE study cohort.
What to Tell Patients?
The authors acknowledged in their paper that it’s difficult — if not impossible — to completely avoid ultraprocessed food in the Western diet.
They said their findings support “public health strategies to promote consumption of whole and minimally processed foods while reducing the consumption of highly processed alternatives.”
“I tell my patients that emerging literature shows an association between ultraprocessed food intake and IBD risk, but it’s not yet clear whether simply cutting out those foods will improve disease activity once IBD is established,” Narula told GI & Hepatology News.
“However, I still encourage patients to reduce ultraprocessed foods and to follow a Mediterranean-style diet — focusing on minimally processed grains, fruits, vegetables, healthy fats, and lean proteins — to support overall gut and general health,” Narula said.
Reached for comment, Ashwin Ananthakrishnan, MD, MPH, AGAF, associate professor of medicine, Massachusetts General Hospital, Boston, who wasn’t part of the study, said it “adds incrementally to the growing data on how ultraprocessed foods may affect the risk of IBD.”

“They (and others) have previously shown a link between general ultraprocessed food consumption and risk of IBD. Others have shown that some of this is mediated through refined grains. This study more specifically studies that question and demonstrates an association,” said Ananthkrishnan.
“This should not be used, however, to counsel patients. It does not study the impact of grain intake on patients with IBD. It may help inform population level preventive strategies (or in high-risk individuals) but requires more confirmation since there is significant heterogeneity between the various countries in this cohort. Countries that have high refined grain intake are also enriched in several other IBD risk factors (including genetics),” Ananthkrishnan told GI & Hepatology News.
The PURE study is an investigator-initiated study funded by the Population Health Research Institute, Hamilton Health Sciences Research Institute, Canadian Institutes of Health Research, and Heart and Stroke Foundation of Ontario. It received support from Canadian Institutes of Health Research’s Strategy for Patient Oriented Research, Ontario SPOR Support Unit, and Ontario Ministry of Health and Long-Term Care and unrestricted grants from several pharmaceutical companies. Narula declared receiving honoraria from Janssen, Abbvie, Takeda, Pfizer, Sandoz, Novartis, Iterative Health, Innomar Strategies, Fresinius Kabi, Amgen, Organon, Eli Lilly, and Ferring. Ananthkrishnan declared having no relevant disclosures.
A version of this article appeared on Medscape.com.
, a large study has found.
The sweeping analysis of 124,590 adults from 21 countries found that those eating at least 19 g of ultraprocessed grains a day were about twice as likely to be diagnosed with IBD as peers eating less than 9 g daily.
“Our study adds robust evidence from a large, diverse global cohort that frequent consumption of ultraprocessed grains is associated with an increased risk of developing inflammatory bowel disease,” Neeraj Narula, MD, MPH, gastroenterologist and associate professor of medicine, McMaster University, Hamilton, Ontario, Canada, told GI & Hepatology News.
The study also “further clarifies that not all grains carry risk — minimally processed grains like fresh bread and rice were associated with lower risk even. These results build on and specify previous findings linking ultraprocessed foods more broadly to IBD,” Narula said.
The study was published in The American Journal of Gastroenterology.
Diet Matters to IBD Risk
According to the latest US data (2021-2023), ultraprocessed foods made up 62% of daily calories for young people and 53% for adults in 2021-2023.
The Prospective Urban Rural Epidemiology (PURE) study has followed participants aged 35-70 years for a median of nearly 13 years. At enrollment, volunteers completed country-specific food-frequency questionnaires, enabling researchers to quantify usual intake of more than 130 food items and track new cases of IBD reported at biennial follow-ups.
The researchers classified packaged breads, sweet breakfast cereals, crackers, pastries and ready-to-heat pizza or pasta as ultraprocessed grains because they are refined and typically contain additives such as emulsifiers and preservatives. Fresh bakery bread and plain rice were analyzed separately as minimally processed grain references.
During a median of 12.9 years, 605 participants developed IBD; 497 developed ulcerative colitis (UC) and 108 developed Crohn’s disease.
Increased intake of ultraprocessed grains was associated with a higher risk for IBD, with hazard ratios (HR) of 2.08 for intake of ≥ 50 g/d and 1.37 for 19-50 g/d compared to intake of < 19 g/d. The increased risk was largely driven by a significantly increased risk for UC (HR, 2.46) and not Crohn’s disease (HR, 0.98).
Among the different ultraprocessed grain products, packaged bread stood out: Consuming ≥ 30 g/d of packaged bread (a little more than one slice) was associated with a greater than twofold increased risk for IBD (HR, 2.11) compared to no intake of packaged bread.
In contrast, greater consumption of fresh bread was associated with a reduced risk of developing IBD (HR, 0.61 for ≥ 65 g/d and 0.45 for 16-65 g/d compared to < 16 g/d).
Increased intake of rice was also associated with a lower risk of developing IBD (HR, 0.63 for ≥ 1 serving/d and 0.99 for < 1 serving/d).
When the researchers widened the lens to all ultraprocessed foods — from sodas to salty snacks — the risk for IBD climbed further.
Participants eating at least five servings a day had nearly a fourfold greater odds of IBD than those eating fewer than one serving (HR, 3.95) — a finding consistent with other data from the PURE study cohort.
What to Tell Patients?
The authors acknowledged in their paper that it’s difficult — if not impossible — to completely avoid ultraprocessed food in the Western diet.
They said their findings support “public health strategies to promote consumption of whole and minimally processed foods while reducing the consumption of highly processed alternatives.”
“I tell my patients that emerging literature shows an association between ultraprocessed food intake and IBD risk, but it’s not yet clear whether simply cutting out those foods will improve disease activity once IBD is established,” Narula told GI & Hepatology News.
“However, I still encourage patients to reduce ultraprocessed foods and to follow a Mediterranean-style diet — focusing on minimally processed grains, fruits, vegetables, healthy fats, and lean proteins — to support overall gut and general health,” Narula said.
Reached for comment, Ashwin Ananthakrishnan, MD, MPH, AGAF, associate professor of medicine, Massachusetts General Hospital, Boston, who wasn’t part of the study, said it “adds incrementally to the growing data on how ultraprocessed foods may affect the risk of IBD.”
“They (and others) have previously shown a link between general ultraprocessed food consumption and risk of IBD. Others have shown that some of this is mediated through refined grains. This study more specifically studies that question and demonstrates an association,” said Ananthkrishnan.
“This should not be used, however, to counsel patients. It does not study the impact of grain intake on patients with IBD. It may help inform population level preventive strategies (or in high-risk individuals) but requires more confirmation since there is significant heterogeneity between the various countries in this cohort. Countries that have high refined grain intake are also enriched in several other IBD risk factors (including genetics),” Ananthkrishnan told GI & Hepatology News.
The PURE study is an investigator-initiated study funded by the Population Health Research Institute, Hamilton Health Sciences Research Institute, Canadian Institutes of Health Research, and Heart and Stroke Foundation of Ontario. It received support from Canadian Institutes of Health Research’s Strategy for Patient Oriented Research, Ontario SPOR Support Unit, and Ontario Ministry of Health and Long-Term Care and unrestricted grants from several pharmaceutical companies. Narula declared receiving honoraria from Janssen, Abbvie, Takeda, Pfizer, Sandoz, Novartis, Iterative Health, Innomar Strategies, Fresinius Kabi, Amgen, Organon, Eli Lilly, and Ferring. Ananthkrishnan declared having no relevant disclosures.
A version of this article appeared on Medscape.com.
, a large study has found.
The sweeping analysis of 124,590 adults from 21 countries found that those eating at least 19 g of ultraprocessed grains a day were about twice as likely to be diagnosed with IBD as peers eating less than 9 g daily.
“Our study adds robust evidence from a large, diverse global cohort that frequent consumption of ultraprocessed grains is associated with an increased risk of developing inflammatory bowel disease,” Neeraj Narula, MD, MPH, gastroenterologist and associate professor of medicine, McMaster University, Hamilton, Ontario, Canada, told GI & Hepatology News.
The study also “further clarifies that not all grains carry risk — minimally processed grains like fresh bread and rice were associated with lower risk even. These results build on and specify previous findings linking ultraprocessed foods more broadly to IBD,” Narula said.
The study was published in The American Journal of Gastroenterology.
Diet Matters to IBD Risk
According to the latest US data (2021-2023), ultraprocessed foods made up 62% of daily calories for young people and 53% for adults in 2021-2023.
The Prospective Urban Rural Epidemiology (PURE) study has followed participants aged 35-70 years for a median of nearly 13 years. At enrollment, volunteers completed country-specific food-frequency questionnaires, enabling researchers to quantify usual intake of more than 130 food items and track new cases of IBD reported at biennial follow-ups.
The researchers classified packaged breads, sweet breakfast cereals, crackers, pastries and ready-to-heat pizza or pasta as ultraprocessed grains because they are refined and typically contain additives such as emulsifiers and preservatives. Fresh bakery bread and plain rice were analyzed separately as minimally processed grain references.
During a median of 12.9 years, 605 participants developed IBD; 497 developed ulcerative colitis (UC) and 108 developed Crohn’s disease.
Increased intake of ultraprocessed grains was associated with a higher risk for IBD, with hazard ratios (HR) of 2.08 for intake of ≥ 50 g/d and 1.37 for 19-50 g/d compared to intake of < 19 g/d. The increased risk was largely driven by a significantly increased risk for UC (HR, 2.46) and not Crohn’s disease (HR, 0.98).
Among the different ultraprocessed grain products, packaged bread stood out: Consuming ≥ 30 g/d of packaged bread (a little more than one slice) was associated with a greater than twofold increased risk for IBD (HR, 2.11) compared to no intake of packaged bread.
In contrast, greater consumption of fresh bread was associated with a reduced risk of developing IBD (HR, 0.61 for ≥ 65 g/d and 0.45 for 16-65 g/d compared to < 16 g/d).
Increased intake of rice was also associated with a lower risk of developing IBD (HR, 0.63 for ≥ 1 serving/d and 0.99 for < 1 serving/d).
When the researchers widened the lens to all ultraprocessed foods — from sodas to salty snacks — the risk for IBD climbed further.
Participants eating at least five servings a day had nearly a fourfold greater odds of IBD than those eating fewer than one serving (HR, 3.95) — a finding consistent with other data from the PURE study cohort.
What to Tell Patients?
The authors acknowledged in their paper that it’s difficult — if not impossible — to completely avoid ultraprocessed food in the Western diet.
They said their findings support “public health strategies to promote consumption of whole and minimally processed foods while reducing the consumption of highly processed alternatives.”
“I tell my patients that emerging literature shows an association between ultraprocessed food intake and IBD risk, but it’s not yet clear whether simply cutting out those foods will improve disease activity once IBD is established,” Narula told GI & Hepatology News.
“However, I still encourage patients to reduce ultraprocessed foods and to follow a Mediterranean-style diet — focusing on minimally processed grains, fruits, vegetables, healthy fats, and lean proteins — to support overall gut and general health,” Narula said.
Reached for comment, Ashwin Ananthakrishnan, MD, MPH, AGAF, associate professor of medicine, Massachusetts General Hospital, Boston, who wasn’t part of the study, said it “adds incrementally to the growing data on how ultraprocessed foods may affect the risk of IBD.”
“They (and others) have previously shown a link between general ultraprocessed food consumption and risk of IBD. Others have shown that some of this is mediated through refined grains. This study more specifically studies that question and demonstrates an association,” said Ananthkrishnan.
“This should not be used, however, to counsel patients. It does not study the impact of grain intake on patients with IBD. It may help inform population level preventive strategies (or in high-risk individuals) but requires more confirmation since there is significant heterogeneity between the various countries in this cohort. Countries that have high refined grain intake are also enriched in several other IBD risk factors (including genetics),” Ananthkrishnan told GI & Hepatology News.
The PURE study is an investigator-initiated study funded by the Population Health Research Institute, Hamilton Health Sciences Research Institute, Canadian Institutes of Health Research, and Heart and Stroke Foundation of Ontario. It received support from Canadian Institutes of Health Research’s Strategy for Patient Oriented Research, Ontario SPOR Support Unit, and Ontario Ministry of Health and Long-Term Care and unrestricted grants from several pharmaceutical companies. Narula declared receiving honoraria from Janssen, Abbvie, Takeda, Pfizer, Sandoz, Novartis, Iterative Health, Innomar Strategies, Fresinius Kabi, Amgen, Organon, Eli Lilly, and Ferring. Ananthkrishnan declared having no relevant disclosures.
A version of this article appeared on Medscape.com.
Journal Highlights: May-July 2025
Esophagus/Motility
Nguyen AD, et al. AGA Clinical Practice Update on Incorporating Functional Lumen Imaging Probe Into Esophageal Clinical Practice: Expert Review. Gastroenterology. 2025 Jul. doi: 10.1053/j.gastro.2025.05.011.
Hartnett DA, et al. Distribution of Esophageal Eosinophilia as a Predictor of Proton Pump Inhibitor Response in Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.06.032.
Gyawali CP, et al. pH Impedance Monitoring on Proton Pump Inhibitor Therapy Impacts Management Decisions in Proven GERD but not in Unproven GERD. Clin Gastroenterol Hepatol. 2025 May. doi: 10.1016/j.cgh.2025.02.032.
Stomach
Wiklund AK, et al. Risk of Gastric Adenocarcinoma After Eradication of Helicobacter pylori. Gastroenterology. 2025 Feb. doi: 10.1053/j.gastro.2025.01.239.
Sonaiya S, et al. Over-the-Scope Clip versus Standard Endoscopic Therapy as First-Line Intervention for Nonvariceal Upper Gastrointestinal Bleeding: A Cost-Effectiveness Analysis. Tech Innov Gastrointest. 2025 Jun. doi: 10.1016/j.tige.2025.250935.
Colon
Hassan C, et al. Colon Cancer Screening, Surveillance, and Treatment: Novel Artificial Intelligence Driving Strategies in the Management of Colon Lesions. Gastroenterology. 2025 Mar. doi: 10.1053/j.gastro.2025.02.021.

Pancreas
Wilcox CM, et al; US Pancreatic Disease Study Group. Management of the Disconnected Pancreatic Duct in Pancreatic Necrosis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.05.024.
Ghimire C, et al. The effect of advances in pancreatic cancer treatment in population mortality: A SEER-based study. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100739.
Hepatology
Canivet CM, et al. Validation of the AASLD/EASL Multi-Step Screening Strategies for MASLD. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100747.
Miscellaneous
Chang L, et al. Gut Feelings: The Critical Role of Interoception in Obesity and Disorders of Gut-Brain Interaction. Gastroenterology. 2025 Aug. doi: 10.1053/j.gastro.2025.04.002.
Bashiri K, et al. Advancing Hemostatic Powder Technologies for Management of Gastrointestinal Bleeding: Challenges and Solutions. Tech Innov Gastrointest. 2025 Jul. doi: 10.1016/j.tige.2025.250940.
Dr. Trieu is assistant professor of medicine, interventional endoscopy, in the Division of Gastroenterology at Washington University in St. Louis School of Medicine, Missouri.
Esophagus/Motility
Nguyen AD, et al. AGA Clinical Practice Update on Incorporating Functional Lumen Imaging Probe Into Esophageal Clinical Practice: Expert Review. Gastroenterology. 2025 Jul. doi: 10.1053/j.gastro.2025.05.011.
Hartnett DA, et al. Distribution of Esophageal Eosinophilia as a Predictor of Proton Pump Inhibitor Response in Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.06.032.
Gyawali CP, et al. pH Impedance Monitoring on Proton Pump Inhibitor Therapy Impacts Management Decisions in Proven GERD but not in Unproven GERD. Clin Gastroenterol Hepatol. 2025 May. doi: 10.1016/j.cgh.2025.02.032.
Stomach
Wiklund AK, et al. Risk of Gastric Adenocarcinoma After Eradication of Helicobacter pylori. Gastroenterology. 2025 Feb. doi: 10.1053/j.gastro.2025.01.239.
Sonaiya S, et al. Over-the-Scope Clip versus Standard Endoscopic Therapy as First-Line Intervention for Nonvariceal Upper Gastrointestinal Bleeding: A Cost-Effectiveness Analysis. Tech Innov Gastrointest. 2025 Jun. doi: 10.1016/j.tige.2025.250935.
Colon
Hassan C, et al. Colon Cancer Screening, Surveillance, and Treatment: Novel Artificial Intelligence Driving Strategies in the Management of Colon Lesions. Gastroenterology. 2025 Mar. doi: 10.1053/j.gastro.2025.02.021.
Pancreas
Wilcox CM, et al; US Pancreatic Disease Study Group. Management of the Disconnected Pancreatic Duct in Pancreatic Necrosis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.05.024.
Ghimire C, et al. The effect of advances in pancreatic cancer treatment in population mortality: A SEER-based study. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100739.
Hepatology
Canivet CM, et al. Validation of the AASLD/EASL Multi-Step Screening Strategies for MASLD. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100747.
Miscellaneous
Chang L, et al. Gut Feelings: The Critical Role of Interoception in Obesity and Disorders of Gut-Brain Interaction. Gastroenterology. 2025 Aug. doi: 10.1053/j.gastro.2025.04.002.
Bashiri K, et al. Advancing Hemostatic Powder Technologies for Management of Gastrointestinal Bleeding: Challenges and Solutions. Tech Innov Gastrointest. 2025 Jul. doi: 10.1016/j.tige.2025.250940.
Dr. Trieu is assistant professor of medicine, interventional endoscopy, in the Division of Gastroenterology at Washington University in St. Louis School of Medicine, Missouri.
Esophagus/Motility
Nguyen AD, et al. AGA Clinical Practice Update on Incorporating Functional Lumen Imaging Probe Into Esophageal Clinical Practice: Expert Review. Gastroenterology. 2025 Jul. doi: 10.1053/j.gastro.2025.05.011.
Hartnett DA, et al. Distribution of Esophageal Eosinophilia as a Predictor of Proton Pump Inhibitor Response in Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.06.032.
Gyawali CP, et al. pH Impedance Monitoring on Proton Pump Inhibitor Therapy Impacts Management Decisions in Proven GERD but not in Unproven GERD. Clin Gastroenterol Hepatol. 2025 May. doi: 10.1016/j.cgh.2025.02.032.
Stomach
Wiklund AK, et al. Risk of Gastric Adenocarcinoma After Eradication of Helicobacter pylori. Gastroenterology. 2025 Feb. doi: 10.1053/j.gastro.2025.01.239.
Sonaiya S, et al. Over-the-Scope Clip versus Standard Endoscopic Therapy as First-Line Intervention for Nonvariceal Upper Gastrointestinal Bleeding: A Cost-Effectiveness Analysis. Tech Innov Gastrointest. 2025 Jun. doi: 10.1016/j.tige.2025.250935.
Colon
Hassan C, et al. Colon Cancer Screening, Surveillance, and Treatment: Novel Artificial Intelligence Driving Strategies in the Management of Colon Lesions. Gastroenterology. 2025 Mar. doi: 10.1053/j.gastro.2025.02.021.
Pancreas
Wilcox CM, et al; US Pancreatic Disease Study Group. Management of the Disconnected Pancreatic Duct in Pancreatic Necrosis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.05.024.
Ghimire C, et al. The effect of advances in pancreatic cancer treatment in population mortality: A SEER-based study. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100739.
Hepatology
Canivet CM, et al. Validation of the AASLD/EASL Multi-Step Screening Strategies for MASLD. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100747.
Miscellaneous
Chang L, et al. Gut Feelings: The Critical Role of Interoception in Obesity and Disorders of Gut-Brain Interaction. Gastroenterology. 2025 Aug. doi: 10.1053/j.gastro.2025.04.002.
Bashiri K, et al. Advancing Hemostatic Powder Technologies for Management of Gastrointestinal Bleeding: Challenges and Solutions. Tech Innov Gastrointest. 2025 Jul. doi: 10.1016/j.tige.2025.250940.
Dr. Trieu is assistant professor of medicine, interventional endoscopy, in the Division of Gastroenterology at Washington University in St. Louis School of Medicine, Missouri.
Federal Government Funds Program for Hepatitis C Care and Cure
, according to an HHS press release.
The program, known as the Hepatitis C Elimination Initiative Pilot, will be administered by the Substance and Mental Health Administration. “This program is designed to support communities severely affected by homelessness and to gain insights on effective ways to identify patients, complete treatment, cure infections, and reduce reinfection by hepatitis C,” according to the press release.
The upfront investment in hepatitis C management is projected to not only save lives, but also to save community health care costs in the long-term, according to the press release.
“This is a vigorous pilot program that provides the first steps toward the large goal of eliminating hepatitis C in the United States population,” said William Schaffner, MD, professor of infectious diseases at Vanderbilt University Medical Center, Nashville, Tennessee, in an interview.
Hepatitis C affects more than two million individuals in the US, and is often complicated by social and medical issues such as homelessness, substance abuse, and mental health issues, said Schaffner. Fortunately, hepatitis C can be treated with oral medications that cure the chronic viral infection, thereby ending ongoing liver injury and interrupting person-to-person transmission of the virus by sharing needles, he said.
Given that the population most affected with hepatitis C also is often homeless, with possible mental health issues and sharing of needles for illicit drug use, challenges in reaching this population include assuring them that the care they receive though this and other programs is nonjudgemental and helpful, Schaffner told GI & Hepatology News.
The oral medications that now can cure the chronic hepatitis C viral infections must be taken over a period of weeks, and patients who lead socially disorganized lives often need assistance to assure that the medicine is taken as intended, so trained and sensitive personnel who are committed to helping this population are needed to make treatment programs succeed, he said.
Looking ahead, “the purpose of the pilot studies that will be funded by this program is to explore various approaches to determine which are more successful in bringing patients in to be evaluated and then to complete treatment,” Schaffner added.
State and community-based organizations are among the entities eligible to apply for the program. Potential applicants can find information about the program and application materials on the SAMSHA website.
Schaffner had no financial conflicts to disclose.
A version of this article appeared on Medscape.com .
, according to an HHS press release.
The program, known as the Hepatitis C Elimination Initiative Pilot, will be administered by the Substance and Mental Health Administration. “This program is designed to support communities severely affected by homelessness and to gain insights on effective ways to identify patients, complete treatment, cure infections, and reduce reinfection by hepatitis C,” according to the press release.
The upfront investment in hepatitis C management is projected to not only save lives, but also to save community health care costs in the long-term, according to the press release.
“This is a vigorous pilot program that provides the first steps toward the large goal of eliminating hepatitis C in the United States population,” said William Schaffner, MD, professor of infectious diseases at Vanderbilt University Medical Center, Nashville, Tennessee, in an interview.
Hepatitis C affects more than two million individuals in the US, and is often complicated by social and medical issues such as homelessness, substance abuse, and mental health issues, said Schaffner. Fortunately, hepatitis C can be treated with oral medications that cure the chronic viral infection, thereby ending ongoing liver injury and interrupting person-to-person transmission of the virus by sharing needles, he said.
Given that the population most affected with hepatitis C also is often homeless, with possible mental health issues and sharing of needles for illicit drug use, challenges in reaching this population include assuring them that the care they receive though this and other programs is nonjudgemental and helpful, Schaffner told GI & Hepatology News.
The oral medications that now can cure the chronic hepatitis C viral infections must be taken over a period of weeks, and patients who lead socially disorganized lives often need assistance to assure that the medicine is taken as intended, so trained and sensitive personnel who are committed to helping this population are needed to make treatment programs succeed, he said.
Looking ahead, “the purpose of the pilot studies that will be funded by this program is to explore various approaches to determine which are more successful in bringing patients in to be evaluated and then to complete treatment,” Schaffner added.
State and community-based organizations are among the entities eligible to apply for the program. Potential applicants can find information about the program and application materials on the SAMSHA website.
Schaffner had no financial conflicts to disclose.
A version of this article appeared on Medscape.com .
, according to an HHS press release.
The program, known as the Hepatitis C Elimination Initiative Pilot, will be administered by the Substance and Mental Health Administration. “This program is designed to support communities severely affected by homelessness and to gain insights on effective ways to identify patients, complete treatment, cure infections, and reduce reinfection by hepatitis C,” according to the press release.
The upfront investment in hepatitis C management is projected to not only save lives, but also to save community health care costs in the long-term, according to the press release.
“This is a vigorous pilot program that provides the first steps toward the large goal of eliminating hepatitis C in the United States population,” said William Schaffner, MD, professor of infectious diseases at Vanderbilt University Medical Center, Nashville, Tennessee, in an interview.
Hepatitis C affects more than two million individuals in the US, and is often complicated by social and medical issues such as homelessness, substance abuse, and mental health issues, said Schaffner. Fortunately, hepatitis C can be treated with oral medications that cure the chronic viral infection, thereby ending ongoing liver injury and interrupting person-to-person transmission of the virus by sharing needles, he said.
Given that the population most affected with hepatitis C also is often homeless, with possible mental health issues and sharing of needles for illicit drug use, challenges in reaching this population include assuring them that the care they receive though this and other programs is nonjudgemental and helpful, Schaffner told GI & Hepatology News.
The oral medications that now can cure the chronic hepatitis C viral infections must be taken over a period of weeks, and patients who lead socially disorganized lives often need assistance to assure that the medicine is taken as intended, so trained and sensitive personnel who are committed to helping this population are needed to make treatment programs succeed, he said.
Looking ahead, “the purpose of the pilot studies that will be funded by this program is to explore various approaches to determine which are more successful in bringing patients in to be evaluated and then to complete treatment,” Schaffner added.
State and community-based organizations are among the entities eligible to apply for the program. Potential applicants can find information about the program and application materials on the SAMSHA website.
Schaffner had no financial conflicts to disclose.
A version of this article appeared on Medscape.com .
Follow-Up Colonoscopies Low After Blood-Based Screening
Positioning Yourself For Success in Private Practice

In this video, Peter Naas, MD, of Gastroenterology Associates in Greenville, South Carolina, shares insights on how young physicians can best position themselves for a successful career in private practice gastroenterology.
In this video, Peter Naas, MD, of Gastroenterology Associates in Greenville, South Carolina, shares insights on how young physicians can best position themselves for a successful career in private practice gastroenterology.
In this video, Peter Naas, MD, of Gastroenterology Associates in Greenville, South Carolina, shares insights on how young physicians can best position themselves for a successful career in private practice gastroenterology.
Most GI Service Chiefs Support POCUS Training, But Uptake Is Slow
, according to a national survey.
Low POCUS uptake may be explained by substantial barriers to implementation, including lack of trained instructors, necessary equipment, and support staff, lead author Keerthi Thallapureddy, MD, of the University of Texas Health San Antonio, and colleagues, reported.
“POCUS is being increasingly used by gastroenterologists due to its portability and real-time diagnostic ability,” the investigators wrote in Gastro Hep Advances, but “there is limited understanding of how gastroenterologists use POCUS.”
To learn more, the investigators conducted a nationwide survey of the VA healthcare system. Separate questionnaires were sent to chiefs of staff (n = 130) and GI service chiefs (n = 117), yielding response rates of 100% and 79%, respectively.
Respondents represented a wide distribution of geographic regions and institutional complexity levels, with 80% of GI groups based at high-complexity centers and 92% in urban locations. A minority (8%) reported the presence of a liver transplant program.
Data collection focused on the prevalence of POCUS use, types of clinical applications, institutional policies and training processes, and perceived or actual barriers to wider adoption. Barriers were sorted into three categories: training, equipment, and infrastructure.
Of the 93 GI service chiefs who participated in the survey, 44% reported that at least 1 gastroenterologist at their facility currently uses POCUS. Most common procedural uses were paracentesis (23%) and liver biopsy (13%), while ascites assessment (19%) and biliary visualization (7%) were the most common diagnostic uses.
Among the same respondents, 69% said they would support sending clinicians to a POCUS training course, and 37% said their teams had expressed an active interest in pursuing such training. Only 17% of facilities had a formal process in place to obtain POCUS training, and an equal proportion had implemented a facility-wide policy to guide its use.
Barriers to implementation were widespread and often multifactorial.
Most challenges related to training: 48% of sites reported a lack of trained providers, 28% cited insufficient funding for training, 24% noted a lack of training opportunities, and 14% reported difficulty securing travel funds.
Equipment limitations were also common, with 41% of sites lacking ultrasound machines and 27% lacking funding to purchase them.
Institutional infrastructure posed further hurdles. Nearly a quarter of GI chiefs (23%) reported lacking a clinician champion to lead implementation, while others cited a lack of support staff, simulation space, privileging criteria, image archiving capabilities, or standardized reporting forms.
“Our findings on current POCUS use, training, barriers, and infrastructure can guide expansion of POCUS use and training among GI groups,” Dr. Thallapureddy and colleagues wrote, noting that early efforts to expand access to GI-specific POCUS training are already underway.
They cited growing interest from national organizations such as the American Gastroenterological Association and the American Association for the Study of Liver Diseases, the latter of which piloted training workshops at the 2024 Liver Meeting. Similarly, the International Bowel Ultrasound Group now offers a 3-part certification program in intestinal ultrasound and is developing additional online and interactive modules to improve training accessibility.
The study was supported by the US Department of Veterans Affairs, Quality Enhancement Research Initiative Partnered Evaluation Initiative Grant, and the VA National Center for Patient Safety. The investigators reported no conflicts of interest.
, according to a national survey.
Low POCUS uptake may be explained by substantial barriers to implementation, including lack of trained instructors, necessary equipment, and support staff, lead author Keerthi Thallapureddy, MD, of the University of Texas Health San Antonio, and colleagues, reported.
“POCUS is being increasingly used by gastroenterologists due to its portability and real-time diagnostic ability,” the investigators wrote in Gastro Hep Advances, but “there is limited understanding of how gastroenterologists use POCUS.”
To learn more, the investigators conducted a nationwide survey of the VA healthcare system. Separate questionnaires were sent to chiefs of staff (n = 130) and GI service chiefs (n = 117), yielding response rates of 100% and 79%, respectively.
Respondents represented a wide distribution of geographic regions and institutional complexity levels, with 80% of GI groups based at high-complexity centers and 92% in urban locations. A minority (8%) reported the presence of a liver transplant program.
Data collection focused on the prevalence of POCUS use, types of clinical applications, institutional policies and training processes, and perceived or actual barriers to wider adoption. Barriers were sorted into three categories: training, equipment, and infrastructure.
Of the 93 GI service chiefs who participated in the survey, 44% reported that at least 1 gastroenterologist at their facility currently uses POCUS. Most common procedural uses were paracentesis (23%) and liver biopsy (13%), while ascites assessment (19%) and biliary visualization (7%) were the most common diagnostic uses.
Among the same respondents, 69% said they would support sending clinicians to a POCUS training course, and 37% said their teams had expressed an active interest in pursuing such training. Only 17% of facilities had a formal process in place to obtain POCUS training, and an equal proportion had implemented a facility-wide policy to guide its use.
Barriers to implementation were widespread and often multifactorial.
Most challenges related to training: 48% of sites reported a lack of trained providers, 28% cited insufficient funding for training, 24% noted a lack of training opportunities, and 14% reported difficulty securing travel funds.
Equipment limitations were also common, with 41% of sites lacking ultrasound machines and 27% lacking funding to purchase them.
Institutional infrastructure posed further hurdles. Nearly a quarter of GI chiefs (23%) reported lacking a clinician champion to lead implementation, while others cited a lack of support staff, simulation space, privileging criteria, image archiving capabilities, or standardized reporting forms.
“Our findings on current POCUS use, training, barriers, and infrastructure can guide expansion of POCUS use and training among GI groups,” Dr. Thallapureddy and colleagues wrote, noting that early efforts to expand access to GI-specific POCUS training are already underway.
They cited growing interest from national organizations such as the American Gastroenterological Association and the American Association for the Study of Liver Diseases, the latter of which piloted training workshops at the 2024 Liver Meeting. Similarly, the International Bowel Ultrasound Group now offers a 3-part certification program in intestinal ultrasound and is developing additional online and interactive modules to improve training accessibility.
The study was supported by the US Department of Veterans Affairs, Quality Enhancement Research Initiative Partnered Evaluation Initiative Grant, and the VA National Center for Patient Safety. The investigators reported no conflicts of interest.
, according to a national survey.
Low POCUS uptake may be explained by substantial barriers to implementation, including lack of trained instructors, necessary equipment, and support staff, lead author Keerthi Thallapureddy, MD, of the University of Texas Health San Antonio, and colleagues, reported.
“POCUS is being increasingly used by gastroenterologists due to its portability and real-time diagnostic ability,” the investigators wrote in Gastro Hep Advances, but “there is limited understanding of how gastroenterologists use POCUS.”
To learn more, the investigators conducted a nationwide survey of the VA healthcare system. Separate questionnaires were sent to chiefs of staff (n = 130) and GI service chiefs (n = 117), yielding response rates of 100% and 79%, respectively.
Respondents represented a wide distribution of geographic regions and institutional complexity levels, with 80% of GI groups based at high-complexity centers and 92% in urban locations. A minority (8%) reported the presence of a liver transplant program.
Data collection focused on the prevalence of POCUS use, types of clinical applications, institutional policies and training processes, and perceived or actual barriers to wider adoption. Barriers were sorted into three categories: training, equipment, and infrastructure.
Of the 93 GI service chiefs who participated in the survey, 44% reported that at least 1 gastroenterologist at their facility currently uses POCUS. Most common procedural uses were paracentesis (23%) and liver biopsy (13%), while ascites assessment (19%) and biliary visualization (7%) were the most common diagnostic uses.
Among the same respondents, 69% said they would support sending clinicians to a POCUS training course, and 37% said their teams had expressed an active interest in pursuing such training. Only 17% of facilities had a formal process in place to obtain POCUS training, and an equal proportion had implemented a facility-wide policy to guide its use.
Barriers to implementation were widespread and often multifactorial.
Most challenges related to training: 48% of sites reported a lack of trained providers, 28% cited insufficient funding for training, 24% noted a lack of training opportunities, and 14% reported difficulty securing travel funds.
Equipment limitations were also common, with 41% of sites lacking ultrasound machines and 27% lacking funding to purchase them.
Institutional infrastructure posed further hurdles. Nearly a quarter of GI chiefs (23%) reported lacking a clinician champion to lead implementation, while others cited a lack of support staff, simulation space, privileging criteria, image archiving capabilities, or standardized reporting forms.
“Our findings on current POCUS use, training, barriers, and infrastructure can guide expansion of POCUS use and training among GI groups,” Dr. Thallapureddy and colleagues wrote, noting that early efforts to expand access to GI-specific POCUS training are already underway.
They cited growing interest from national organizations such as the American Gastroenterological Association and the American Association for the Study of Liver Diseases, the latter of which piloted training workshops at the 2024 Liver Meeting. Similarly, the International Bowel Ultrasound Group now offers a 3-part certification program in intestinal ultrasound and is developing additional online and interactive modules to improve training accessibility.
The study was supported by the US Department of Veterans Affairs, Quality Enhancement Research Initiative Partnered Evaluation Initiative Grant, and the VA National Center for Patient Safety. The investigators reported no conflicts of interest.
FROM GASTRO HEP ADVANCES
AGA Women’s Committee Outlines Roadmap Towards Gender Equity
Despite the increasing number of women joining the field, GI remains one of the most male-dominated medical subspecialties. and has highlighted future directions to achieve gender equality in GI.
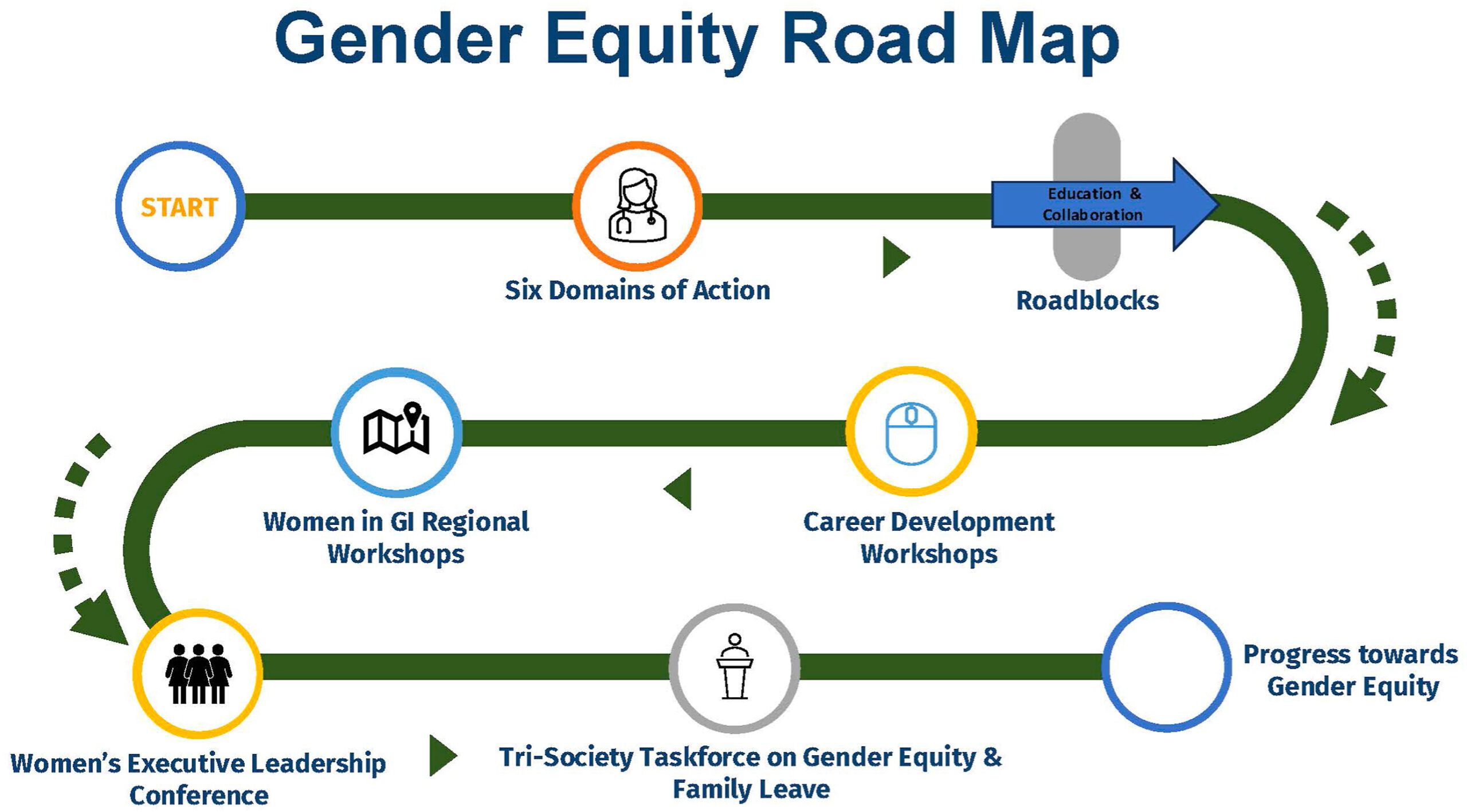
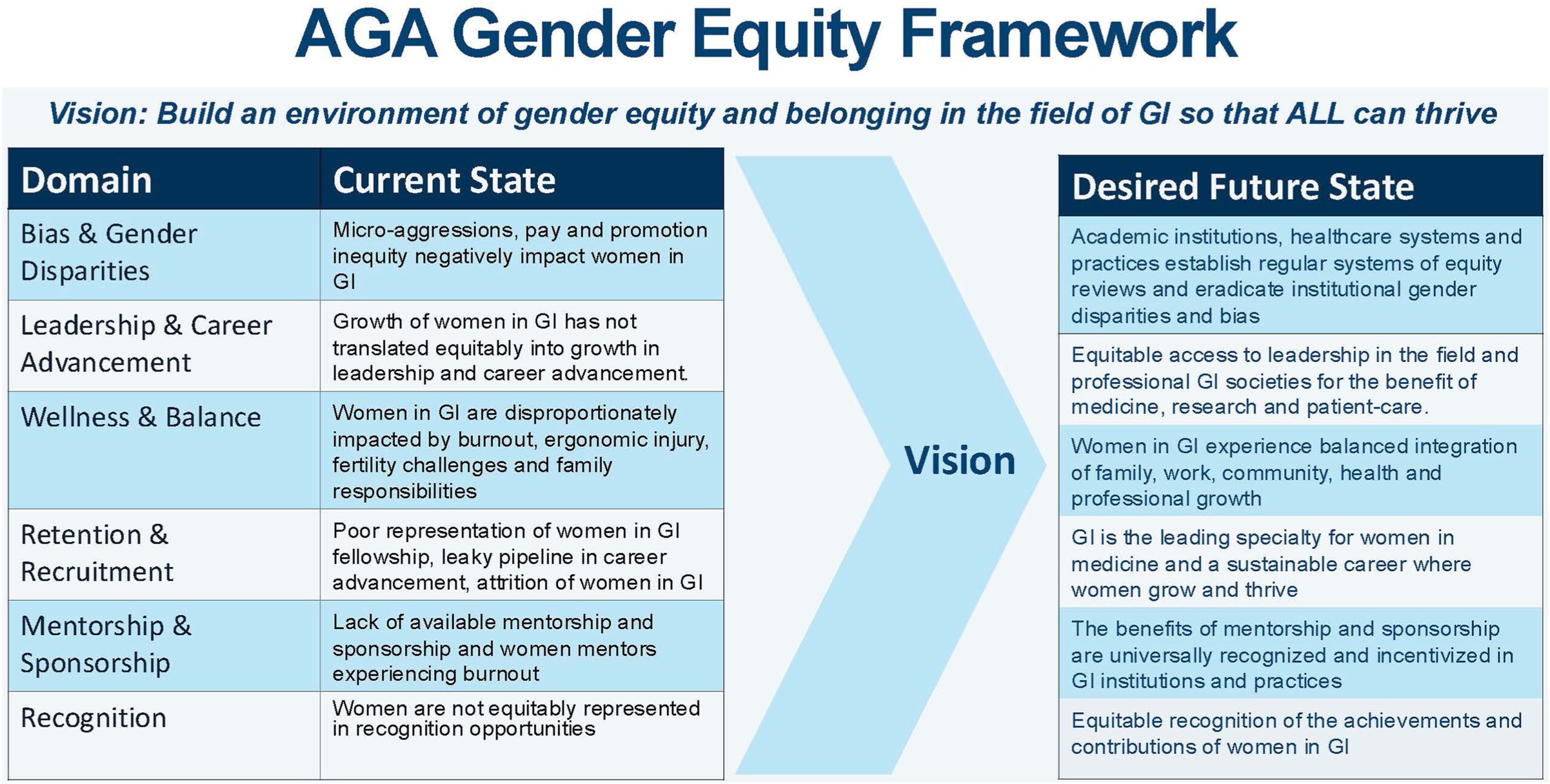
The AGA Gender Equity Framework outlines six domains of action, the current state and desired future state: bias & gender disparities, leadership & career advancement, wellness & balance, retention & recruitment, mentorship & sponsorship, and recognition.
Based on the desired future state, the group created a roadmap towards gender equity with measurable tactics. Career development workshops, including the Women in GI regional workshops and Women’s Executive Leadership Conference, are both crucial tactics.
AGA outlined a few key areas for future gender equity efforts to focus on:
- Clearer GI-specific transparency guidelines regarding recruitment, salary, promotions, funding, and leadership.
- Pathway and research programs that help students from underrepresented backgrounds get involved and stay engaged in GI.
- Support networks (through GI societies, institutions, or other organizations) that help women connect, collaborate, and grow their careers.
The AGA Women’s Committee, along with other AGA committees, will continue to work to achieve the vision laid out in the AGA Gender Equity Framework and Gender Equity Road Map.
Despite the increasing number of women joining the field, GI remains one of the most male-dominated medical subspecialties. and has highlighted future directions to achieve gender equality in GI.
The AGA Gender Equity Framework outlines six domains of action, the current state and desired future state: bias & gender disparities, leadership & career advancement, wellness & balance, retention & recruitment, mentorship & sponsorship, and recognition.
Based on the desired future state, the group created a roadmap towards gender equity with measurable tactics. Career development workshops, including the Women in GI regional workshops and Women’s Executive Leadership Conference, are both crucial tactics.
AGA outlined a few key areas for future gender equity efforts to focus on:
- Clearer GI-specific transparency guidelines regarding recruitment, salary, promotions, funding, and leadership.
- Pathway and research programs that help students from underrepresented backgrounds get involved and stay engaged in GI.
- Support networks (through GI societies, institutions, or other organizations) that help women connect, collaborate, and grow their careers.
The AGA Women’s Committee, along with other AGA committees, will continue to work to achieve the vision laid out in the AGA Gender Equity Framework and Gender Equity Road Map.
Despite the increasing number of women joining the field, GI remains one of the most male-dominated medical subspecialties. and has highlighted future directions to achieve gender equality in GI.
The AGA Gender Equity Framework outlines six domains of action, the current state and desired future state: bias & gender disparities, leadership & career advancement, wellness & balance, retention & recruitment, mentorship & sponsorship, and recognition.
Based on the desired future state, the group created a roadmap towards gender equity with measurable tactics. Career development workshops, including the Women in GI regional workshops and Women’s Executive Leadership Conference, are both crucial tactics.
AGA outlined a few key areas for future gender equity efforts to focus on:
- Clearer GI-specific transparency guidelines regarding recruitment, salary, promotions, funding, and leadership.
- Pathway and research programs that help students from underrepresented backgrounds get involved and stay engaged in GI.
- Support networks (through GI societies, institutions, or other organizations) that help women connect, collaborate, and grow their careers.
The AGA Women’s Committee, along with other AGA committees, will continue to work to achieve the vision laid out in the AGA Gender Equity Framework and Gender Equity Road Map.
Evolving Standards of Practice: Esophageal Varices and Barrett’s Esophagus
Dear colleagues,
In the dynamic field of medicine, long-held practices are being reevaluated in light of new evidence and evolving standards of practice.

Dr. Anahita Rabiee discusses the importance of prioritizing non-selective beta blockers (NSBB) over endoscopic variceal ligation (EVL) in the primary prophylaxis of variceal bleeding in patients with compensated cirrhosis. Drawing on data from the PREDESCI trial and real-world experience, she argues that NSBB address the upstream driver—portal hypertension—more broadly and effectively than EVL. In a complementary piece, Dr. Tarek Sawas explores the nuanced landscape of screening and surveillance in Barrett’s esophagus. From how to manage irregular Z-lines, to rethinking the need for 1-year follow-up endoscopies and interpreting the implications of the BOSS trial, Dr. Sawas advocates for a more personalized, risk-based approach.
We hope these perspectives spark dialogue and reflection in your own practice. Join the conversation on X at @AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, and chief of endoscopy at West Haven VA Medical Center, both in Connecticut. He is an associate editor for GI & Hepatology News.
Choose NSBBs, Not EVL, in Patients with Compensated Cirrhosis
BY ANAHITA RABIEE, MD, MHS
I strongly favor the use of non selective beta blockers (NSBBs) in patients with compensated cirrhosis, rather than endoscopy and esophageal variceal ligation (EVL) for primary prophylaxis.
Since the results of PREDESCI trial (β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (CSPH)) were published in 2019, there has been much debate on the role of screening endoscopy and EVL for primary prophylaxis. While many argue that a single randomized trial should not overturn long standing practice, several compelling reasons convince me to choose NSBBs, when possible.
Recent guidance from major liver societies now recommends NSBBs as first line therapy for CSPH. Yet, adoption in clinical practice remains inconsistent.
Here is why I believe NSBB represent a better solution:

Treating Upstream, Not Just a Local Treatment
NSBBs such as propranolol and nadolol decrease portal pressure by decreasing portal venous inflow through β1 and β2 adrenergic blockade. Carvedilol is often preferred given its additional α1 adrenergic blocking activity making it the most effective one in decreasing the portal pressure. Therefore, NSBBs address the upstream driver of decompensation by decreasing portal pressures.
EVL, in contrast, is a local fix that only prevents variceal bleeding. Ascites, not variceal bleeding, is the most common initial decompensating event and is associated with high mortality. Preventing all forms of decompensation is clearly preferable to preventing just one.
Broader Eligibility, More Patients Benefit
CSPH is defined as hepatic venous pressure gradient (HVPG)>10 mmHg, the threshold where increased portal venous inflow secondary to splanchnic vasodilation and hyperdynamic circulation drives the increase in portal hypertension. This threshold has been shown to strongly predict decompensation in patients with compensated disease.
While all patients with varices have CSPH, not all patients with CSPH have varices. They can be identified by other non invasive criteria such as cross sectional imaging showing collaterals, or liver stiffness and platelet thresholds that have been previously validated. By restricting intervention to those with large varices and offering only EVL, we miss the opportunity to intervene earlier and to a broader group that would benefit from this treatment.
Comprehensive Protection Without Repeated Endoscopies
Once on an appropriate NSBB dose, patients are protected against variceal bleeding (at least as effectively as EVL). This eliminates the need for repeated surveillance endoscopies to identify and treat large varices in otherwise compensated patients.
Better Tolerated and – In Many Cases – Overlaps With Existing Medication List!
While overtreatment is a concern, regular endoscopies every two years are also burdensome. Many patients already need beta blockers for cardiac conditions such as atrial fibrillation, ischemic heart disease or hypertension. Carvedilol, in particular, offers dual benefit for both hepatologists and cardiologists.
It is important to emphasize that these arguments apply to compensated cirrhosis. In decompensated disease, the approach changes. After a variceal bleed, both NSBBs and EVL are required for secondary prophylaxis. In patients with prior ascites but no variceal bleed, the benefit of NSBBs is less pronounced since decompensation has already occurred. In this setting, NSBBs can still be used selectively, but only if systolic blood pressure remains above 90 mmHg.
The evidence supporting NSBBs over EVL in compensated cirrhosis is not perfect, but few things in medicine are. Given current data, NSBBs should be the first line therapy in compensated cirrhosis with CSPH. Once a patient is on an appropriate and tolerated NSBB dose, routine endoscopic surveillance is unnecessary. Endoscopy should be reserved for those who cannot tolerate NSBBs, in whom EVL is then indicated if large varices are present.
Dr. Rabiee is based at the Yale School of Medicine, New Haven, Connecticut, and the Veterans Affairs Connecticut Healthcare System, West Haven, Connecticut. She has no disclosures in regard to this article.
Rethinking Screening and Surveillance in Barrett’s Esophagus: Navigating Controversies and Nuances
BY TAREK SAWAS, MD, MPH
Barrett’s esophagus (BE) is a precursor to esophageal adenocarcinoma (EAC). Despite our comprehensive guidelines, many of the day-to-day decisions still rely on clinical judgment and honest conversations with patients. This article explores common scenarios in which management decisions are nuanced and the right answer remains debatable.
Irregular Z-Line/Ultrashort Segment BE: Leave Or Watch It?
Few findings provoke more confusion than irregular Z-line or intestinal metaplasia (IM) < 1 cm at the gastroesophageal junction (GEJ). For years, we have debated whether these subtle changes represent a precursor to EAC or simply a benign variant. We have wrestled with how to handle these cases from whether we should take biopsies to how to perform surveillance.
The American College of Gastroenterology (ACG) guideline suggests that irregular Z-lines should not be routinely biopsied or surveyed. Similarly, the upcoming American Gastroenterology Association (AGA) surveillance guideline suggests against surveillance of IM<1 cm citing the low individual annual risk of progression to high-grade dysplasia (HGD) and EAC of 0.23% per year which is lower than that of non-dysplastic Barrett’s esophagus (NDBE). However, this is not the entire picture.
Despite the low per-patient risk, IM<1cm is highly prevalent with columnar mucosa observed in approximately 15% of patients undergoing upper endoscopy. This paradox is unsettling. While any one patient with IM<1 cm is unlikely to progress to EAC, the group accounts for a meaningful share of the EAC burden. Some experts have argued that this justifies routine biopsy and surveillance in all patients with visible columnar mucosa regardless of length. However, this approach risks overwhelming our surveillance infrastructure.
A recent decision modeling analysis suggested that at the lowest progression rates, either no surveillance or one-time endoscopy can be considered. Based on these data, I do not regularly biopsy ultrashort segments unless the mucosa appears suspicious. In those with IM<1 cm detected during a high-quality endoscopic exam, no follow-up is needed. However, if the exam is suboptimal, I perform a 1-time high-quality repeat exam. If there is no evidence of dysplasia then I do not pursue any further surveillance.
The One-Year Follow-Up Endoscopy: Is It Necessary?
Another controversy is the one-year follow-up endoscopy after an initial diagnosis of NDBE. Proponents of this approach cite the high proportion of post endoscopy esophageal neoplasia and cancer (PEEN/PEEC) detected in the first year after diagnosis (missed HGD/EAC). In fact, PEEN account for about a quarter of all HGD/EAC cases diagnosed during surveillance.
While this approach might mitigate PEEN/PEEC risk, it may not be necessary if the index endoscopy is high quality. To ensure high quality exams, several best practices have been proposed including:
- Use of high-definition white light endoscopy (HD-WLE) with chromoendoscopy (virtual or dye based)
- Appropriate inspection time (1 minute per cm of circumferential BE)
- Accurate documentation using the Prague criteria
- Adherence to the Seattle protocol with additional targeted biopsies
If the index endoscopy meets these quality metrics, I typically do not bring the patient back at one year. However, if the exam quality is in question, then I repeat it at one year to establish a reliable baseline and rule out prevalent neoplasia.

Surveillance In NDBE: After BOSS, Do We Rethink Everything?
The recently published BOSS trial (Barrett’s Oesophagus Surveillance Study) has reignited the debate over the value of endoscopic surveillance in NDBE. In this study, 3,453 patients with NDBE across the UK were randomized to either surveillance endoscopy every two years or endoscopy only as clinically indicated. After a median follow-up of 12.8 years, the trial found no significant difference in all-cause mortality between the two groups.
While these findings are important, they should be interpreted with caution. First, the primary endpoint, all-cause mortality, is not optimal for evaluating surveillance for EAC. Surveillance is not intended to reduce all-cause mortality but rather to reduce EAC–related mortality. Second, a substantial number of patients in the no surveillance group still underwent endoscopy at intervals that were not meaningfully different from those in the surveillance group. If both groups receive similar exposure to endoscopy, the comparison loses power. Lastly, the trial was underpowered due to overestimation of progression risk during its initial design. As we have since learned, the risk of progression of NDBE is lower than originally assumed.
So where do we stand now? For me, the BOSS trial does not negate the value of surveillance. it reminds us that a one-size-fits-all approach is inefficient, and our strategy must be risk based. For low-risk individuals, particularly older adults with short-segment NDBE, surveillance may offer little benefit. But in healthier, younger patients with longer segments or additional risk factors, surveillance remains an essential tool for early neoplasia detection.
When to Stop Surveillance
Perhaps the most under-discussed point is when to stop surveillance. Existing guidelines do not account for competing mortality risks unrelated to EAC or provide specific recommendations regarding cessation of surveillance. The desired benefits of surveillance likely diminish with advanced age and greater comorbidity because of lower life expectancy and ineligibility for definitive therapy for EAC.
A recent modeling study found that the optimal ages for last surveillance were 81, 80, 77, and 73 years for men with no, mild, moderate, and severe comorbidity respectively and 75, 73, 73, and 69 years for women. In my practice, I discuss surveillance cessation in patients older than 75 based on their comorbidities. If the risk of progression is outweighed by the risk of the procedure or by the reality of limited life expectancy, we should not hesitate to consider surveillance cessation.
In summary, high-quality endoscopic exam in appropriately selected patients remains the cornerstone of BE surveillance. A more personalized, risk-based approach is needed taking into account competing comorbidities. Emerging technology through risk stratification tools such as biomarkers and artificial intelligence may refine our approach and help address the current limitations.
Dr. Sawas is based at the University of Texas Southwestern, Dallas, Texas. He has no disclosures in regard to this article.
Dear colleagues,
In the dynamic field of medicine, long-held practices are being reevaluated in light of new evidence and evolving standards of practice.
Dr. Anahita Rabiee discusses the importance of prioritizing non-selective beta blockers (NSBB) over endoscopic variceal ligation (EVL) in the primary prophylaxis of variceal bleeding in patients with compensated cirrhosis. Drawing on data from the PREDESCI trial and real-world experience, she argues that NSBB address the upstream driver—portal hypertension—more broadly and effectively than EVL. In a complementary piece, Dr. Tarek Sawas explores the nuanced landscape of screening and surveillance in Barrett’s esophagus. From how to manage irregular Z-lines, to rethinking the need for 1-year follow-up endoscopies and interpreting the implications of the BOSS trial, Dr. Sawas advocates for a more personalized, risk-based approach.
We hope these perspectives spark dialogue and reflection in your own practice. Join the conversation on X at @AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, and chief of endoscopy at West Haven VA Medical Center, both in Connecticut. He is an associate editor for GI & Hepatology News.
Choose NSBBs, Not EVL, in Patients with Compensated Cirrhosis
BY ANAHITA RABIEE, MD, MHS
I strongly favor the use of non selective beta blockers (NSBBs) in patients with compensated cirrhosis, rather than endoscopy and esophageal variceal ligation (EVL) for primary prophylaxis.
Since the results of PREDESCI trial (β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (CSPH)) were published in 2019, there has been much debate on the role of screening endoscopy and EVL for primary prophylaxis. While many argue that a single randomized trial should not overturn long standing practice, several compelling reasons convince me to choose NSBBs, when possible.
Recent guidance from major liver societies now recommends NSBBs as first line therapy for CSPH. Yet, adoption in clinical practice remains inconsistent.
Here is why I believe NSBB represent a better solution:
Treating Upstream, Not Just a Local Treatment
NSBBs such as propranolol and nadolol decrease portal pressure by decreasing portal venous inflow through β1 and β2 adrenergic blockade. Carvedilol is often preferred given its additional α1 adrenergic blocking activity making it the most effective one in decreasing the portal pressure. Therefore, NSBBs address the upstream driver of decompensation by decreasing portal pressures.
EVL, in contrast, is a local fix that only prevents variceal bleeding. Ascites, not variceal bleeding, is the most common initial decompensating event and is associated with high mortality. Preventing all forms of decompensation is clearly preferable to preventing just one.
Broader Eligibility, More Patients Benefit
CSPH is defined as hepatic venous pressure gradient (HVPG)>10 mmHg, the threshold where increased portal venous inflow secondary to splanchnic vasodilation and hyperdynamic circulation drives the increase in portal hypertension. This threshold has been shown to strongly predict decompensation in patients with compensated disease.
While all patients with varices have CSPH, not all patients with CSPH have varices. They can be identified by other non invasive criteria such as cross sectional imaging showing collaterals, or liver stiffness and platelet thresholds that have been previously validated. By restricting intervention to those with large varices and offering only EVL, we miss the opportunity to intervene earlier and to a broader group that would benefit from this treatment.
Comprehensive Protection Without Repeated Endoscopies
Once on an appropriate NSBB dose, patients are protected against variceal bleeding (at least as effectively as EVL). This eliminates the need for repeated surveillance endoscopies to identify and treat large varices in otherwise compensated patients.
Better Tolerated and – In Many Cases – Overlaps With Existing Medication List!
While overtreatment is a concern, regular endoscopies every two years are also burdensome. Many patients already need beta blockers for cardiac conditions such as atrial fibrillation, ischemic heart disease or hypertension. Carvedilol, in particular, offers dual benefit for both hepatologists and cardiologists.
It is important to emphasize that these arguments apply to compensated cirrhosis. In decompensated disease, the approach changes. After a variceal bleed, both NSBBs and EVL are required for secondary prophylaxis. In patients with prior ascites but no variceal bleed, the benefit of NSBBs is less pronounced since decompensation has already occurred. In this setting, NSBBs can still be used selectively, but only if systolic blood pressure remains above 90 mmHg.
The evidence supporting NSBBs over EVL in compensated cirrhosis is not perfect, but few things in medicine are. Given current data, NSBBs should be the first line therapy in compensated cirrhosis with CSPH. Once a patient is on an appropriate and tolerated NSBB dose, routine endoscopic surveillance is unnecessary. Endoscopy should be reserved for those who cannot tolerate NSBBs, in whom EVL is then indicated if large varices are present.
Dr. Rabiee is based at the Yale School of Medicine, New Haven, Connecticut, and the Veterans Affairs Connecticut Healthcare System, West Haven, Connecticut. She has no disclosures in regard to this article.
Rethinking Screening and Surveillance in Barrett’s Esophagus: Navigating Controversies and Nuances
BY TAREK SAWAS, MD, MPH
Barrett’s esophagus (BE) is a precursor to esophageal adenocarcinoma (EAC). Despite our comprehensive guidelines, many of the day-to-day decisions still rely on clinical judgment and honest conversations with patients. This article explores common scenarios in which management decisions are nuanced and the right answer remains debatable.
Irregular Z-Line/Ultrashort Segment BE: Leave Or Watch It?
Few findings provoke more confusion than irregular Z-line or intestinal metaplasia (IM) < 1 cm at the gastroesophageal junction (GEJ). For years, we have debated whether these subtle changes represent a precursor to EAC or simply a benign variant. We have wrestled with how to handle these cases from whether we should take biopsies to how to perform surveillance.
The American College of Gastroenterology (ACG) guideline suggests that irregular Z-lines should not be routinely biopsied or surveyed. Similarly, the upcoming American Gastroenterology Association (AGA) surveillance guideline suggests against surveillance of IM<1 cm citing the low individual annual risk of progression to high-grade dysplasia (HGD) and EAC of 0.23% per year which is lower than that of non-dysplastic Barrett’s esophagus (NDBE). However, this is not the entire picture.
Despite the low per-patient risk, IM<1cm is highly prevalent with columnar mucosa observed in approximately 15% of patients undergoing upper endoscopy. This paradox is unsettling. While any one patient with IM<1 cm is unlikely to progress to EAC, the group accounts for a meaningful share of the EAC burden. Some experts have argued that this justifies routine biopsy and surveillance in all patients with visible columnar mucosa regardless of length. However, this approach risks overwhelming our surveillance infrastructure.
A recent decision modeling analysis suggested that at the lowest progression rates, either no surveillance or one-time endoscopy can be considered. Based on these data, I do not regularly biopsy ultrashort segments unless the mucosa appears suspicious. In those with IM<1 cm detected during a high-quality endoscopic exam, no follow-up is needed. However, if the exam is suboptimal, I perform a 1-time high-quality repeat exam. If there is no evidence of dysplasia then I do not pursue any further surveillance.
The One-Year Follow-Up Endoscopy: Is It Necessary?
Another controversy is the one-year follow-up endoscopy after an initial diagnosis of NDBE. Proponents of this approach cite the high proportion of post endoscopy esophageal neoplasia and cancer (PEEN/PEEC) detected in the first year after diagnosis (missed HGD/EAC). In fact, PEEN account for about a quarter of all HGD/EAC cases diagnosed during surveillance.
While this approach might mitigate PEEN/PEEC risk, it may not be necessary if the index endoscopy is high quality. To ensure high quality exams, several best practices have been proposed including:
- Use of high-definition white light endoscopy (HD-WLE) with chromoendoscopy (virtual or dye based)
- Appropriate inspection time (1 minute per cm of circumferential BE)
- Accurate documentation using the Prague criteria
- Adherence to the Seattle protocol with additional targeted biopsies
If the index endoscopy meets these quality metrics, I typically do not bring the patient back at one year. However, if the exam quality is in question, then I repeat it at one year to establish a reliable baseline and rule out prevalent neoplasia.
Surveillance In NDBE: After BOSS, Do We Rethink Everything?
The recently published BOSS trial (Barrett’s Oesophagus Surveillance Study) has reignited the debate over the value of endoscopic surveillance in NDBE. In this study, 3,453 patients with NDBE across the UK were randomized to either surveillance endoscopy every two years or endoscopy only as clinically indicated. After a median follow-up of 12.8 years, the trial found no significant difference in all-cause mortality between the two groups.
While these findings are important, they should be interpreted with caution. First, the primary endpoint, all-cause mortality, is not optimal for evaluating surveillance for EAC. Surveillance is not intended to reduce all-cause mortality but rather to reduce EAC–related mortality. Second, a substantial number of patients in the no surveillance group still underwent endoscopy at intervals that were not meaningfully different from those in the surveillance group. If both groups receive similar exposure to endoscopy, the comparison loses power. Lastly, the trial was underpowered due to overestimation of progression risk during its initial design. As we have since learned, the risk of progression of NDBE is lower than originally assumed.
So where do we stand now? For me, the BOSS trial does not negate the value of surveillance. it reminds us that a one-size-fits-all approach is inefficient, and our strategy must be risk based. For low-risk individuals, particularly older adults with short-segment NDBE, surveillance may offer little benefit. But in healthier, younger patients with longer segments or additional risk factors, surveillance remains an essential tool for early neoplasia detection.
When to Stop Surveillance
Perhaps the most under-discussed point is when to stop surveillance. Existing guidelines do not account for competing mortality risks unrelated to EAC or provide specific recommendations regarding cessation of surveillance. The desired benefits of surveillance likely diminish with advanced age and greater comorbidity because of lower life expectancy and ineligibility for definitive therapy for EAC.
A recent modeling study found that the optimal ages for last surveillance were 81, 80, 77, and 73 years for men with no, mild, moderate, and severe comorbidity respectively and 75, 73, 73, and 69 years for women. In my practice, I discuss surveillance cessation in patients older than 75 based on their comorbidities. If the risk of progression is outweighed by the risk of the procedure or by the reality of limited life expectancy, we should not hesitate to consider surveillance cessation.
In summary, high-quality endoscopic exam in appropriately selected patients remains the cornerstone of BE surveillance. A more personalized, risk-based approach is needed taking into account competing comorbidities. Emerging technology through risk stratification tools such as biomarkers and artificial intelligence may refine our approach and help address the current limitations.
Dr. Sawas is based at the University of Texas Southwestern, Dallas, Texas. He has no disclosures in regard to this article.
Dear colleagues,
In the dynamic field of medicine, long-held practices are being reevaluated in light of new evidence and evolving standards of practice.
Dr. Anahita Rabiee discusses the importance of prioritizing non-selective beta blockers (NSBB) over endoscopic variceal ligation (EVL) in the primary prophylaxis of variceal bleeding in patients with compensated cirrhosis. Drawing on data from the PREDESCI trial and real-world experience, she argues that NSBB address the upstream driver—portal hypertension—more broadly and effectively than EVL. In a complementary piece, Dr. Tarek Sawas explores the nuanced landscape of screening and surveillance in Barrett’s esophagus. From how to manage irregular Z-lines, to rethinking the need for 1-year follow-up endoscopies and interpreting the implications of the BOSS trial, Dr. Sawas advocates for a more personalized, risk-based approach.
We hope these perspectives spark dialogue and reflection in your own practice. Join the conversation on X at @AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, and chief of endoscopy at West Haven VA Medical Center, both in Connecticut. He is an associate editor for GI & Hepatology News.
Choose NSBBs, Not EVL, in Patients with Compensated Cirrhosis
BY ANAHITA RABIEE, MD, MHS
I strongly favor the use of non selective beta blockers (NSBBs) in patients with compensated cirrhosis, rather than endoscopy and esophageal variceal ligation (EVL) for primary prophylaxis.
Since the results of PREDESCI trial (β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (CSPH)) were published in 2019, there has been much debate on the role of screening endoscopy and EVL for primary prophylaxis. While many argue that a single randomized trial should not overturn long standing practice, several compelling reasons convince me to choose NSBBs, when possible.
Recent guidance from major liver societies now recommends NSBBs as first line therapy for CSPH. Yet, adoption in clinical practice remains inconsistent.
Here is why I believe NSBB represent a better solution:
Treating Upstream, Not Just a Local Treatment
NSBBs such as propranolol and nadolol decrease portal pressure by decreasing portal venous inflow through β1 and β2 adrenergic blockade. Carvedilol is often preferred given its additional α1 adrenergic blocking activity making it the most effective one in decreasing the portal pressure. Therefore, NSBBs address the upstream driver of decompensation by decreasing portal pressures.
EVL, in contrast, is a local fix that only prevents variceal bleeding. Ascites, not variceal bleeding, is the most common initial decompensating event and is associated with high mortality. Preventing all forms of decompensation is clearly preferable to preventing just one.
Broader Eligibility, More Patients Benefit
CSPH is defined as hepatic venous pressure gradient (HVPG)>10 mmHg, the threshold where increased portal venous inflow secondary to splanchnic vasodilation and hyperdynamic circulation drives the increase in portal hypertension. This threshold has been shown to strongly predict decompensation in patients with compensated disease.
While all patients with varices have CSPH, not all patients with CSPH have varices. They can be identified by other non invasive criteria such as cross sectional imaging showing collaterals, or liver stiffness and platelet thresholds that have been previously validated. By restricting intervention to those with large varices and offering only EVL, we miss the opportunity to intervene earlier and to a broader group that would benefit from this treatment.
Comprehensive Protection Without Repeated Endoscopies
Once on an appropriate NSBB dose, patients are protected against variceal bleeding (at least as effectively as EVL). This eliminates the need for repeated surveillance endoscopies to identify and treat large varices in otherwise compensated patients.
Better Tolerated and – In Many Cases – Overlaps With Existing Medication List!
While overtreatment is a concern, regular endoscopies every two years are also burdensome. Many patients already need beta blockers for cardiac conditions such as atrial fibrillation, ischemic heart disease or hypertension. Carvedilol, in particular, offers dual benefit for both hepatologists and cardiologists.
It is important to emphasize that these arguments apply to compensated cirrhosis. In decompensated disease, the approach changes. After a variceal bleed, both NSBBs and EVL are required for secondary prophylaxis. In patients with prior ascites but no variceal bleed, the benefit of NSBBs is less pronounced since decompensation has already occurred. In this setting, NSBBs can still be used selectively, but only if systolic blood pressure remains above 90 mmHg.
The evidence supporting NSBBs over EVL in compensated cirrhosis is not perfect, but few things in medicine are. Given current data, NSBBs should be the first line therapy in compensated cirrhosis with CSPH. Once a patient is on an appropriate and tolerated NSBB dose, routine endoscopic surveillance is unnecessary. Endoscopy should be reserved for those who cannot tolerate NSBBs, in whom EVL is then indicated if large varices are present.
Dr. Rabiee is based at the Yale School of Medicine, New Haven, Connecticut, and the Veterans Affairs Connecticut Healthcare System, West Haven, Connecticut. She has no disclosures in regard to this article.
Rethinking Screening and Surveillance in Barrett’s Esophagus: Navigating Controversies and Nuances
BY TAREK SAWAS, MD, MPH
Barrett’s esophagus (BE) is a precursor to esophageal adenocarcinoma (EAC). Despite our comprehensive guidelines, many of the day-to-day decisions still rely on clinical judgment and honest conversations with patients. This article explores common scenarios in which management decisions are nuanced and the right answer remains debatable.
Irregular Z-Line/Ultrashort Segment BE: Leave Or Watch It?
Few findings provoke more confusion than irregular Z-line or intestinal metaplasia (IM) < 1 cm at the gastroesophageal junction (GEJ). For years, we have debated whether these subtle changes represent a precursor to EAC or simply a benign variant. We have wrestled with how to handle these cases from whether we should take biopsies to how to perform surveillance.
The American College of Gastroenterology (ACG) guideline suggests that irregular Z-lines should not be routinely biopsied or surveyed. Similarly, the upcoming American Gastroenterology Association (AGA) surveillance guideline suggests against surveillance of IM<1 cm citing the low individual annual risk of progression to high-grade dysplasia (HGD) and EAC of 0.23% per year which is lower than that of non-dysplastic Barrett’s esophagus (NDBE). However, this is not the entire picture.
Despite the low per-patient risk, IM<1cm is highly prevalent with columnar mucosa observed in approximately 15% of patients undergoing upper endoscopy. This paradox is unsettling. While any one patient with IM<1 cm is unlikely to progress to EAC, the group accounts for a meaningful share of the EAC burden. Some experts have argued that this justifies routine biopsy and surveillance in all patients with visible columnar mucosa regardless of length. However, this approach risks overwhelming our surveillance infrastructure.
A recent decision modeling analysis suggested that at the lowest progression rates, either no surveillance or one-time endoscopy can be considered. Based on these data, I do not regularly biopsy ultrashort segments unless the mucosa appears suspicious. In those with IM<1 cm detected during a high-quality endoscopic exam, no follow-up is needed. However, if the exam is suboptimal, I perform a 1-time high-quality repeat exam. If there is no evidence of dysplasia then I do not pursue any further surveillance.
The One-Year Follow-Up Endoscopy: Is It Necessary?
Another controversy is the one-year follow-up endoscopy after an initial diagnosis of NDBE. Proponents of this approach cite the high proportion of post endoscopy esophageal neoplasia and cancer (PEEN/PEEC) detected in the first year after diagnosis (missed HGD/EAC). In fact, PEEN account for about a quarter of all HGD/EAC cases diagnosed during surveillance.
While this approach might mitigate PEEN/PEEC risk, it may not be necessary if the index endoscopy is high quality. To ensure high quality exams, several best practices have been proposed including:
- Use of high-definition white light endoscopy (HD-WLE) with chromoendoscopy (virtual or dye based)
- Appropriate inspection time (1 minute per cm of circumferential BE)
- Accurate documentation using the Prague criteria
- Adherence to the Seattle protocol with additional targeted biopsies
If the index endoscopy meets these quality metrics, I typically do not bring the patient back at one year. However, if the exam quality is in question, then I repeat it at one year to establish a reliable baseline and rule out prevalent neoplasia.
Surveillance In NDBE: After BOSS, Do We Rethink Everything?
The recently published BOSS trial (Barrett’s Oesophagus Surveillance Study) has reignited the debate over the value of endoscopic surveillance in NDBE. In this study, 3,453 patients with NDBE across the UK were randomized to either surveillance endoscopy every two years or endoscopy only as clinically indicated. After a median follow-up of 12.8 years, the trial found no significant difference in all-cause mortality between the two groups.
While these findings are important, they should be interpreted with caution. First, the primary endpoint, all-cause mortality, is not optimal for evaluating surveillance for EAC. Surveillance is not intended to reduce all-cause mortality but rather to reduce EAC–related mortality. Second, a substantial number of patients in the no surveillance group still underwent endoscopy at intervals that were not meaningfully different from those in the surveillance group. If both groups receive similar exposure to endoscopy, the comparison loses power. Lastly, the trial was underpowered due to overestimation of progression risk during its initial design. As we have since learned, the risk of progression of NDBE is lower than originally assumed.
So where do we stand now? For me, the BOSS trial does not negate the value of surveillance. it reminds us that a one-size-fits-all approach is inefficient, and our strategy must be risk based. For low-risk individuals, particularly older adults with short-segment NDBE, surveillance may offer little benefit. But in healthier, younger patients with longer segments or additional risk factors, surveillance remains an essential tool for early neoplasia detection.
When to Stop Surveillance
Perhaps the most under-discussed point is when to stop surveillance. Existing guidelines do not account for competing mortality risks unrelated to EAC or provide specific recommendations regarding cessation of surveillance. The desired benefits of surveillance likely diminish with advanced age and greater comorbidity because of lower life expectancy and ineligibility for definitive therapy for EAC.
A recent modeling study found that the optimal ages for last surveillance were 81, 80, 77, and 73 years for men with no, mild, moderate, and severe comorbidity respectively and 75, 73, 73, and 69 years for women. In my practice, I discuss surveillance cessation in patients older than 75 based on their comorbidities. If the risk of progression is outweighed by the risk of the procedure or by the reality of limited life expectancy, we should not hesitate to consider surveillance cessation.
In summary, high-quality endoscopic exam in appropriately selected patients remains the cornerstone of BE surveillance. A more personalized, risk-based approach is needed taking into account competing comorbidities. Emerging technology through risk stratification tools such as biomarkers and artificial intelligence may refine our approach and help address the current limitations.
Dr. Sawas is based at the University of Texas Southwestern, Dallas, Texas. He has no disclosures in regard to this article.
IBD Medications Show No Link with Breast Cancer Recurrence
, according to investigators.
These findings diminish concerns that IBD therapy could theoretically reactivate dormant micrometastases, lead author Guillaume Le Cosquer, MD, of Toulouse University Hospital, Toulouse, France, and colleagues, reported.
“In patients with IBD, medical management of subjects with a history of breast cancer is a frequent and unresolved problem for clinicians,” the investigators wrote in Clinical Gastroenterology and Hepatology (2024 Nov. doi: 10.1016/j.cgh.2024.09.034).
Previous studies have reported that conventional immunosuppressants and biologics do not increase risk of incident cancer among IBD patients with a prior nondigestive malignancy; however, recent guidelines from the European Crohn’s and Colitis Organisation (ECCO) suggest that data are insufficient to make associated recommendations, prompting the present study.
“[T]he major strength of our work is that it is the first to focus on the most frequent cancer (breast cancer) in patients with IBD only, with the longest follow-up after breast cancer in patients with IBD ever published,” Dr. Le Cosquer and colleagues noted.
The dataset included 207 patients with IBD and a history of breast cancer, drawn from 7 tertiary centers across France.
The index date was the time of breast cancer diagnosis, and patients were followed for a median of 71 months. The median time from cancer diagnosis to initiation of IBD treatment was 28 months.
First-line post-cancer treatments included conventional immunosuppressants (19.3%), anti–tumor necrosis factor (anti-TNF) agents (19.8%), vedolizumab (7.2%), and ustekinumab (1.9%). Approximately half (51.6%) received no immunosuppressive therapy during follow-up.
Over the study period, 42 incident cancers were recorded (20.3%), among which 34 were breast cancer recurrences. Adjusted incidence rates per 1000 person-years were 10.2 (95% CI, 6.0–16.4) in the untreated group and 28.9 (95% CI, 11.6–59.6) in patients exposed to immunosuppressive or biologic therapies (P = .0519). Incident cancer–free survival did not differ significantly between treated and untreated groups (P = .4796).
On multivariable analysis, independent predictors of incident cancer included T4d stage (P = .036), triple-negative status (P = .016), and follow-up duration shorter than 71 months (P = .005).
“[I]mmunosuppressant and biologic use in selected patients with IBD with prior breast cancer does not seem to increase the risk of incident cancer,” the investigators wrote, noting that the main predictors of cancer recurrence were known poor prognostic features of breast cancer.
Dr. Le Cosquer and colleagues acknowledged a lack of prospective safety data for biologic therapies among patients with prior malignancy, as these individuals are often excluded from clinical trials. Still, they underscored alignment between their findings and earlier retrospective studies, including analyses from the SAPPHIRE registry and Medicare data, which also found no significant increase in breast cancer recurrence with anti-TNF agents or newer biologics such as vedolizumab and ustekinumab.
“Our findings will help clinicians to make decisions in multidisciplinary meetings to start immunosuppressants or biologics in case of IBD flare-up in these patients,” they concluded.
The investigators disclosed relationships with AbbVie, Janssen, Takeda, and others.
Patients with inflammatory bowel disease (IBD) are at risk for a host of other illnesses, including cancer, at rates similar to or greater than the general population. When faced with uncertainty about drug safety with a cancer diagnosis, the reflex is to avoid the therapy altogether. This may lead to significant flares which may in turn lead to difficulty in tolerating cancer therapy and a shortened and lower quality life.
Le Cosquer et al. address the question of the risk of incident cancer among patients with a history of breast cancer. The authors found that the risk was related to poor prognostic factors for breast cancer and not IBD therapy. This should be interpreted with caution as the numbers, though the largest reported, are 207 patients. After propensity score matching, crude incidence rates per 1000 person years appeared greater in the treatment arm (28.9) versus the untreated arm (10.2), P = .0519. With a greater number of patients, it is conceivable the difference is significant.

On the flip side, prior to diagnosis, the majority of IBD patients received immunosuppressant or biologic therapy; however, after the index cancer, 51.6% of patients received no treatment. The survival curves show a near 25% difference in favor of treated patients after 300 months, albeit with very small numbers, raising the question of whether withholding IBD therapy is more harmful.
It is reassuring that the multiple papers cited in the article have not shown an increase in solid organ tumors to date. However, the practitioner needs to balance maintenance of IBD remission and overall health with the risk of complications in the patient with underlying malignancy. This complex decision making will shift over time and should involve the patient, the oncologist, and the gastroenterologist. In my practice, thiopurines are avoided and anti-integrins and IL-23s are preferred. However, anti-TNF agents and JAK-inhibitors are used when the patients’ overall benefit from disease control outweighs their (theoretical) risk for recurrence, infection, and thromboembolism.
Uma Mahadevan, MD, AGAF, is the Lynne and Marc Benioff Professor of Gastroenterology, and director of the Colitis and Crohn’s Disease Center at the University of California, San Francisco. She declared research support from the Leona M. and Harry B. Helmsley Trust, and has served as a consultant for multiple pharmaceutical firms.
Patients with inflammatory bowel disease (IBD) are at risk for a host of other illnesses, including cancer, at rates similar to or greater than the general population. When faced with uncertainty about drug safety with a cancer diagnosis, the reflex is to avoid the therapy altogether. This may lead to significant flares which may in turn lead to difficulty in tolerating cancer therapy and a shortened and lower quality life.
Le Cosquer et al. address the question of the risk of incident cancer among patients with a history of breast cancer. The authors found that the risk was related to poor prognostic factors for breast cancer and not IBD therapy. This should be interpreted with caution as the numbers, though the largest reported, are 207 patients. After propensity score matching, crude incidence rates per 1000 person years appeared greater in the treatment arm (28.9) versus the untreated arm (10.2), P = .0519. With a greater number of patients, it is conceivable the difference is significant.
On the flip side, prior to diagnosis, the majority of IBD patients received immunosuppressant or biologic therapy; however, after the index cancer, 51.6% of patients received no treatment. The survival curves show a near 25% difference in favor of treated patients after 300 months, albeit with very small numbers, raising the question of whether withholding IBD therapy is more harmful.
It is reassuring that the multiple papers cited in the article have not shown an increase in solid organ tumors to date. However, the practitioner needs to balance maintenance of IBD remission and overall health with the risk of complications in the patient with underlying malignancy. This complex decision making will shift over time and should involve the patient, the oncologist, and the gastroenterologist. In my practice, thiopurines are avoided and anti-integrins and IL-23s are preferred. However, anti-TNF agents and JAK-inhibitors are used when the patients’ overall benefit from disease control outweighs their (theoretical) risk for recurrence, infection, and thromboembolism.
Uma Mahadevan, MD, AGAF, is the Lynne and Marc Benioff Professor of Gastroenterology, and director of the Colitis and Crohn’s Disease Center at the University of California, San Francisco. She declared research support from the Leona M. and Harry B. Helmsley Trust, and has served as a consultant for multiple pharmaceutical firms.
Patients with inflammatory bowel disease (IBD) are at risk for a host of other illnesses, including cancer, at rates similar to or greater than the general population. When faced with uncertainty about drug safety with a cancer diagnosis, the reflex is to avoid the therapy altogether. This may lead to significant flares which may in turn lead to difficulty in tolerating cancer therapy and a shortened and lower quality life.
Le Cosquer et al. address the question of the risk of incident cancer among patients with a history of breast cancer. The authors found that the risk was related to poor prognostic factors for breast cancer and not IBD therapy. This should be interpreted with caution as the numbers, though the largest reported, are 207 patients. After propensity score matching, crude incidence rates per 1000 person years appeared greater in the treatment arm (28.9) versus the untreated arm (10.2), P = .0519. With a greater number of patients, it is conceivable the difference is significant.
On the flip side, prior to diagnosis, the majority of IBD patients received immunosuppressant or biologic therapy; however, after the index cancer, 51.6% of patients received no treatment. The survival curves show a near 25% difference in favor of treated patients after 300 months, albeit with very small numbers, raising the question of whether withholding IBD therapy is more harmful.
It is reassuring that the multiple papers cited in the article have not shown an increase in solid organ tumors to date. However, the practitioner needs to balance maintenance of IBD remission and overall health with the risk of complications in the patient with underlying malignancy. This complex decision making will shift over time and should involve the patient, the oncologist, and the gastroenterologist. In my practice, thiopurines are avoided and anti-integrins and IL-23s are preferred. However, anti-TNF agents and JAK-inhibitors are used when the patients’ overall benefit from disease control outweighs their (theoretical) risk for recurrence, infection, and thromboembolism.
Uma Mahadevan, MD, AGAF, is the Lynne and Marc Benioff Professor of Gastroenterology, and director of the Colitis and Crohn’s Disease Center at the University of California, San Francisco. She declared research support from the Leona M. and Harry B. Helmsley Trust, and has served as a consultant for multiple pharmaceutical firms.
, according to investigators.
These findings diminish concerns that IBD therapy could theoretically reactivate dormant micrometastases, lead author Guillaume Le Cosquer, MD, of Toulouse University Hospital, Toulouse, France, and colleagues, reported.
“In patients with IBD, medical management of subjects with a history of breast cancer is a frequent and unresolved problem for clinicians,” the investigators wrote in Clinical Gastroenterology and Hepatology (2024 Nov. doi: 10.1016/j.cgh.2024.09.034).
Previous studies have reported that conventional immunosuppressants and biologics do not increase risk of incident cancer among IBD patients with a prior nondigestive malignancy; however, recent guidelines from the European Crohn’s and Colitis Organisation (ECCO) suggest that data are insufficient to make associated recommendations, prompting the present study.
“[T]he major strength of our work is that it is the first to focus on the most frequent cancer (breast cancer) in patients with IBD only, with the longest follow-up after breast cancer in patients with IBD ever published,” Dr. Le Cosquer and colleagues noted.
The dataset included 207 patients with IBD and a history of breast cancer, drawn from 7 tertiary centers across France.
The index date was the time of breast cancer diagnosis, and patients were followed for a median of 71 months. The median time from cancer diagnosis to initiation of IBD treatment was 28 months.
First-line post-cancer treatments included conventional immunosuppressants (19.3%), anti–tumor necrosis factor (anti-TNF) agents (19.8%), vedolizumab (7.2%), and ustekinumab (1.9%). Approximately half (51.6%) received no immunosuppressive therapy during follow-up.
Over the study period, 42 incident cancers were recorded (20.3%), among which 34 were breast cancer recurrences. Adjusted incidence rates per 1000 person-years were 10.2 (95% CI, 6.0–16.4) in the untreated group and 28.9 (95% CI, 11.6–59.6) in patients exposed to immunosuppressive or biologic therapies (P = .0519). Incident cancer–free survival did not differ significantly between treated and untreated groups (P = .4796).
On multivariable analysis, independent predictors of incident cancer included T4d stage (P = .036), triple-negative status (P = .016), and follow-up duration shorter than 71 months (P = .005).
“[I]mmunosuppressant and biologic use in selected patients with IBD with prior breast cancer does not seem to increase the risk of incident cancer,” the investigators wrote, noting that the main predictors of cancer recurrence were known poor prognostic features of breast cancer.
Dr. Le Cosquer and colleagues acknowledged a lack of prospective safety data for biologic therapies among patients with prior malignancy, as these individuals are often excluded from clinical trials. Still, they underscored alignment between their findings and earlier retrospective studies, including analyses from the SAPPHIRE registry and Medicare data, which also found no significant increase in breast cancer recurrence with anti-TNF agents or newer biologics such as vedolizumab and ustekinumab.
“Our findings will help clinicians to make decisions in multidisciplinary meetings to start immunosuppressants or biologics in case of IBD flare-up in these patients,” they concluded.
The investigators disclosed relationships with AbbVie, Janssen, Takeda, and others.
, according to investigators.
These findings diminish concerns that IBD therapy could theoretically reactivate dormant micrometastases, lead author Guillaume Le Cosquer, MD, of Toulouse University Hospital, Toulouse, France, and colleagues, reported.
“In patients with IBD, medical management of subjects with a history of breast cancer is a frequent and unresolved problem for clinicians,” the investigators wrote in Clinical Gastroenterology and Hepatology (2024 Nov. doi: 10.1016/j.cgh.2024.09.034).
Previous studies have reported that conventional immunosuppressants and biologics do not increase risk of incident cancer among IBD patients with a prior nondigestive malignancy; however, recent guidelines from the European Crohn’s and Colitis Organisation (ECCO) suggest that data are insufficient to make associated recommendations, prompting the present study.
“[T]he major strength of our work is that it is the first to focus on the most frequent cancer (breast cancer) in patients with IBD only, with the longest follow-up after breast cancer in patients with IBD ever published,” Dr. Le Cosquer and colleagues noted.
The dataset included 207 patients with IBD and a history of breast cancer, drawn from 7 tertiary centers across France.
The index date was the time of breast cancer diagnosis, and patients were followed for a median of 71 months. The median time from cancer diagnosis to initiation of IBD treatment was 28 months.
First-line post-cancer treatments included conventional immunosuppressants (19.3%), anti–tumor necrosis factor (anti-TNF) agents (19.8%), vedolizumab (7.2%), and ustekinumab (1.9%). Approximately half (51.6%) received no immunosuppressive therapy during follow-up.
Over the study period, 42 incident cancers were recorded (20.3%), among which 34 were breast cancer recurrences. Adjusted incidence rates per 1000 person-years were 10.2 (95% CI, 6.0–16.4) in the untreated group and 28.9 (95% CI, 11.6–59.6) in patients exposed to immunosuppressive or biologic therapies (P = .0519). Incident cancer–free survival did not differ significantly between treated and untreated groups (P = .4796).
On multivariable analysis, independent predictors of incident cancer included T4d stage (P = .036), triple-negative status (P = .016), and follow-up duration shorter than 71 months (P = .005).
“[I]mmunosuppressant and biologic use in selected patients with IBD with prior breast cancer does not seem to increase the risk of incident cancer,” the investigators wrote, noting that the main predictors of cancer recurrence were known poor prognostic features of breast cancer.
Dr. Le Cosquer and colleagues acknowledged a lack of prospective safety data for biologic therapies among patients with prior malignancy, as these individuals are often excluded from clinical trials. Still, they underscored alignment between their findings and earlier retrospective studies, including analyses from the SAPPHIRE registry and Medicare data, which also found no significant increase in breast cancer recurrence with anti-TNF agents or newer biologics such as vedolizumab and ustekinumab.
“Our findings will help clinicians to make decisions in multidisciplinary meetings to start immunosuppressants or biologics in case of IBD flare-up in these patients,” they concluded.
The investigators disclosed relationships with AbbVie, Janssen, Takeda, and others.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
GLP-1 Receptor Agonist Use in Gastrointestinal Endoscopy: A Review of Current Evidence and Guidelines
The use of glucagon-like peptide-1 receptor agonists (GLP-1 RAs) has increased over the past several years and has become a cornerstone in both diabetes and weight loss management, particularly because of its unique combination of glucose control, weight reduction potential, and cardiac and metabolic benefits. However, increased use of these agents presents a dilemma in gastrointestinal endoscopy as it pertains to their safety and management during the periprocedural period.
highlighting gaps and future directions.
Pharmacology and Mechanisms of Action
GLP-1 RAs have several mechanisms of action that make them relevant in gastrointestinal endoscopy. These medications modulate glucose control via enhancement of glucose-dependent insulin secretion and reduction of postprandial glucagon, which promotes satiety and delays gastric emptying. This delay in gastric emptying mediated by vagal pathways has been postulated to increase gastric residuals, posing a risk for aspiration during anesthesia.1
It is important to also consider the pharmacokinetics of GLP-1 RAs, as some have shorter half-lives on the order of several hours, like exenatide, while others, like semaglutide, are dosed weekly. Additionally, common side effects of GLP-1 RAs include nausea, vomiting, bloating, and early satiety, which pose challenges for patients undergoing endoscopic procedures.
Current Guidelines
Various societies have published guidelines on the periprocedural use of GLP-1 RAs. The American Society of Anesthesiologist (ASA) in 2023 presented early recommendations to hold GLP-1 RAs either day of procedure or week prior depending on pharmacokinetics, because of the risk of delayed gastric emptying and increased potential for aspiration.2 Soon thereafter, a multi-gastroenterology society guideline was released stating more data is needed to decide if GLP-1 RAs need to be held prior to endoscopic procedures.3
In early 2024, the American Gastroenterological Association (AGA) published a rapid clinical update that advocated for a more individualized approach, particularly in light of limited overall data for GLP-1 RAs and endoscopic procedures.4 In asymptomatic patients who follow typical fasting protocols for procedures, it is generally safe to proceed with endoscopy without holding GLP-1 RAs. In symptomatic patients (nausea, abdominal distension, etc), the AGA advises additional precautions, including performing transabdominal ultrasound if feasible to assess retained gastric contents. The AGA also suggests placing a patient on a clear liquid diet the day prior to the procedure — rather than holding GLP-1 RAs — as another reasonable strategy.
The guidelines continue to evolve with newer multi-society guidelines establishing best practices. While initially in 2023 the ASA did recommend holding these medications prior to endoscopy, the initial guidance was based on expert opinion with limited evidence. Newer multi-society guidance published jointly by the ASA along with various gastroenterology societies, including the AGA in December 2024, takes a more nuanced approach.5
The newer guidelines include two main recommendations:
1. Periprocedural management of GLP-1 RAs should be a joint decision among the procedural, anesthesia, and prescribing team balancing metabolic needs vs patient risks.
- In a low-risk patient, one that is asymptomatic and on standard dosing, among other factors, the guidance states that GLP-1 RAs can be continued.
- In higher-risk patients, the original guidance of holding a day or a week prior to endoscopic procedures should be followed.
2. Periprocedural management of GLP-1 RAs should attempt to minimize the aspiration risks loosely associated with delayed gastric emptying.
- Consider a 24-hour clear liquid diet a day prior to the procedure and transabdominal ultrasound to check gastric contents.
- It is acknowledged that this guidance is based on limited evidence and will be evolving as new medications and data are released.
Recent Clinical Studies
Although there is very little data to guide clinicians, several recent studies have been published that can direct clinical decision-making as guidelines continue to be refined and updated.

A multicenter trial of approximately 800 patients undergoing upper endoscopy found a significant difference in rates of retained gastric contents between those that underwent endoscopy who did and did not follow the ASA guidance on periprocedural management of GLP-1 RAs (12.7% vs 4.4%; P < .0001). However, there were no significant differences in rates of aborted procedures or unplanned intubations.
Furthermore, a multivariable analysis was performed controlling for GLP-1 RA type and other factors, which found the likelihood of gastric retention increased by 36% for every 1% increase in hemoglobin A1c. This study suggests that a more individualized approach to holding GLP-1 RA would be applicable rather than a universal periprocedural hold.6
More recently, a single-center study of nearly 600 patients undergoing upper endoscopy showed that while there were slightly increased rates of retained gastric contents (OR 3.80; P = .003) and aborted procedures (1.3% vs 0%; P = .02), the rates of adverse anesthesia events (hypoxia, etc) were similar between the groups and no cases of pulmonary aspiration were noted.7
One single-center study of 57 patients evaluated the safety of GLP-1 RAs in those undergoing endoscopic sleeve gastrectomy. GLP-1 RAs were continued on all patients, but all adhered to a liquid only diet for at least 24 hours prior to the procedure. There were no instances of retained gastric solids, aspiration, or hypoxia. This study suggests that with a 24-hour clear liquid diet and routine NPO recommendations prior to endoscopy, it would be safe to continue GLP-1 RAs. This study provides rationale for the AGA recommendation for a clear liquid diet 24 hours prior to endoscopic procedures for those on GLP-1 RAs.8
A study looking at those who underwent emergency surgery and endoscopy with claims data of use of GLP-1 RAs found an overall incidence of postoperative respiratory complications of 3.5% for those with GLP-1 RAs fill history vs 4.0% for those without (P = .12). Approximately 800 of the 24,000 patients identified had undergone endoscopic procedures for GI bleeding or food impaction. The study overall showed that preoperative use of GLP-1 RAs in patients undergoing surgery or endoscopy, evaluated as a combined group, was not associated with an increased risk of pulmonary complications.9
Lastly, a systematic review and meta-analysis that included 15 studies that quantified gastric emptying using various methods, including gastric emptying scintigraphy and acetaminophen absorption test, found that there was a quantifiable delay in gastric emptying of about 36 minutes, compared to placebo (P < .01), in patients using GLP-1 RAs. However, compared to standard periprocedural fasting, this delay is clinically insignificant and standard fasting protocols would still be appropriate for patients on GLP-1 RAs.10
These studies taken together suggest that while GLP-1 RAs can mildly increase the likelihood of retained gastric contents, there is no statistically significant increase in the risk of aspiration or other anesthesia complications. Furthermore, while decreased gastric emptying is a known effect of GLP-1 RAs, this effect may not be clinically significant in the context of standard periprocedural fasting protocols particularly when combined with a 24-hour clear liquid diet. These findings support at a minimum a more patient-specific strategy for periprocedural management of GLP-1 RAs.
Clinical Implications
These most recent studies, as well as prior studies and guidelines by various societies lead to a dilemma among endoscopists on proper patient counseling on GLP-1 RAs use before endoscopic procedures. Clinicians must balance the metabolic benefits of GLP-1 RAs with potential endoscopic complications and risks.
Holding therapy theoretically decreases aspiration risk and pulmonary complications, though evidence remains low to support this. Holding medication, however, affects glycemic control leading to potential rebound hyperglycemia which may impact and delay plans for endoscopy. With growing indications for the use of GLP-1 RAs, a more tailored patient-centered treatment plan may be required, especially with consideration of procedure indication and comorbidities.
Currently, practice patterns at different institutions vary widely, making standardization much more difficult. Some centers have opted to follow ASA guidelines of holding these medications up to 1 week prior to procedures, while others have continued therapy with no pre-procedural adjustments. This leaves endoscopists to deal with the downstream effects of inconvenience to patients, care delays, and financial considerations if procedures are postponed related to GLP-1 RAs use.
Future Directions
Future studies are needed to make further evidence-based recommendations. Studies should focus on stratifying risks and recommendations based on procedure type (EGD, colonoscopy, etc). More widespread implementation of gastric ultrasound can assist in real-time decision-making, albeit this would require expertise and dedicated time within the pre-procedural workflow. Randomized controlled trials comparing outcomes of patients who continue GLP-1 RAs vs those who discontinue stratified by baseline risk will be instrumental for making concrete guidelines that provide clarity on periprocedural management of GLP-1 RAs.
Conclusion
The periprocedural management of GLP-1 RAs remains a controversial topic that presents unique challenges in endoscopy. Several guidelines have been released by various stakeholders including anesthesiologists, gastroenterologists, and other prescribing providers. Clinical data remains limited with no robust evidence available to suggest that gastric emptying delays caused by GLP-1 RAs prior to endoscopic procedures significantly increases risk of aspiration, pulmonary complications, or other comorbidities. Evolving multi-society guidelines will be important to establish more consistent practices with reassessment of the data as new studies emerge. A multidisciplinary, individualized patient approach may be the best strategy for managing GLP-1 RAs for patients undergoing endoscopic procedures.
Dr. Sekar and Dr. Asamoah are based in the department of gastroenterology at MedStar Georgetown University Hospital, Washington, D.C. Dr. Sekar reports no conflicts of interest in regard to this article. Dr. Asamoah serves on the Johnson & Johnson advisory board for inflammatory bowel disease–related therapies.
References
1. Halim MA et al. Glucagon-Like Peptide-1 Inhibits Prandial Gastrointestinal Motility Through Myenteric Neuronal Mechanisms in Humans. J Clin Endocrinol Metab. 2018 Feb. doi: 10.1210/jc.2017-02006.
2. American Society of Anesthesiologists. American Society of Anesthesiologists releases consensus-based guidance on preoperative use of GLP-1 receptor agonists. 2023 Jun 20. www.asahq.org/about-asa/newsroom/news-releases/2023/06/american-society-of-anesthesiologists-consensus-based-guidance-on-preoperative
3. American Gastroenterological Association. GI multi-society statement regarding GLP-1 agonists and endoscopy. 2023 Jul 25. gastro.org/news/gi-multi-society-statement-regarding-glp-1-agonists-and-endoscopy/.
4. Hashash JG et al. AGA Rapid Clinical Practice Update on the Management of Patients Taking GLP-1 Receptor Agonists Prior to Endoscopy: Communication. Clin Gastroenterol Hepatol. 2024 Apr. doi: 10.1016/j.cgh.2023.11.002.
5. Kindel TL et al; American Gastroenterological Association; American Society for Metabolic and Bariatric Surgery; American Society of Anesthesiologists; International Society of Perioperative Care of Patients with Obesity; Society of American Gastrointestinal and Endoscopic Surgeons. Multi-society Clinical Practice Guidance for the Safe Use of Glucagon-like Peptide-1 Receptor Agonists in the Perioperative Period. Clin Gastroenterol Hepatol. 2024 Oct. doi: 10.1016/j.cgh.2024.10.003.
6. Phan J et al. Glucagon-Like Peptide Receptor Agonists Use Before Endoscopy Is Associated With Low Retained Gastric Contents: A Multicenter Cross-Sectional Analysis. Am J Gastroenterol. 2025 Mar. doi: 10.14309/ajg.0000000000002969.
7. Panchal S et al. Endoscopy and Anesthesia Outcomes Associated With Glucagon-like Peptide-1 Receptor Agonist use in Patients Undergoing Outpatient Upper Endoscopy. Gastrointest Endosc. 2025 Aug. doi:10.1016/j.gie.2025.01.004.
8. Maselli DB et al. Safe Continuation of glucagon-like Peptide 1 Receptor Agonists at Endoscopy: A Case Series of 57 Adults Undergoing Endoscopic Sleeve Gastroplasty. Obes Surg. 2024 Jul. doi: 10.1007/s11695-024-07278-2.
9. Dixit AA et al. Preoperative GLP-1 Receptor Agonist Use and Risk of Postoperative Respiratory Complications. JAMA. 2024 Apr. doi: 10.1001/jama.2024.5003.
10. Hiramoto B et al. Quantified Metrics of Gastric Emptying Delay by Glucagon-Like Peptide-1 Agonists: A systematic review and meta-analysis with insights for periprocedural management. Am J Gastroenterol. 2024 Jun. doi: 10.14309/ajg.0000000000002820.
The use of glucagon-like peptide-1 receptor agonists (GLP-1 RAs) has increased over the past several years and has become a cornerstone in both diabetes and weight loss management, particularly because of its unique combination of glucose control, weight reduction potential, and cardiac and metabolic benefits. However, increased use of these agents presents a dilemma in gastrointestinal endoscopy as it pertains to their safety and management during the periprocedural period.
highlighting gaps and future directions.
Pharmacology and Mechanisms of Action
GLP-1 RAs have several mechanisms of action that make them relevant in gastrointestinal endoscopy. These medications modulate glucose control via enhancement of glucose-dependent insulin secretion and reduction of postprandial glucagon, which promotes satiety and delays gastric emptying. This delay in gastric emptying mediated by vagal pathways has been postulated to increase gastric residuals, posing a risk for aspiration during anesthesia.1
It is important to also consider the pharmacokinetics of GLP-1 RAs, as some have shorter half-lives on the order of several hours, like exenatide, while others, like semaglutide, are dosed weekly. Additionally, common side effects of GLP-1 RAs include nausea, vomiting, bloating, and early satiety, which pose challenges for patients undergoing endoscopic procedures.
Current Guidelines
Various societies have published guidelines on the periprocedural use of GLP-1 RAs. The American Society of Anesthesiologist (ASA) in 2023 presented early recommendations to hold GLP-1 RAs either day of procedure or week prior depending on pharmacokinetics, because of the risk of delayed gastric emptying and increased potential for aspiration.2 Soon thereafter, a multi-gastroenterology society guideline was released stating more data is needed to decide if GLP-1 RAs need to be held prior to endoscopic procedures.3
In early 2024, the American Gastroenterological Association (AGA) published a rapid clinical update that advocated for a more individualized approach, particularly in light of limited overall data for GLP-1 RAs and endoscopic procedures.4 In asymptomatic patients who follow typical fasting protocols for procedures, it is generally safe to proceed with endoscopy without holding GLP-1 RAs. In symptomatic patients (nausea, abdominal distension, etc), the AGA advises additional precautions, including performing transabdominal ultrasound if feasible to assess retained gastric contents. The AGA also suggests placing a patient on a clear liquid diet the day prior to the procedure — rather than holding GLP-1 RAs — as another reasonable strategy.
The guidelines continue to evolve with newer multi-society guidelines establishing best practices. While initially in 2023 the ASA did recommend holding these medications prior to endoscopy, the initial guidance was based on expert opinion with limited evidence. Newer multi-society guidance published jointly by the ASA along with various gastroenterology societies, including the AGA in December 2024, takes a more nuanced approach.5
The newer guidelines include two main recommendations:
1. Periprocedural management of GLP-1 RAs should be a joint decision among the procedural, anesthesia, and prescribing team balancing metabolic needs vs patient risks.
- In a low-risk patient, one that is asymptomatic and on standard dosing, among other factors, the guidance states that GLP-1 RAs can be continued.
- In higher-risk patients, the original guidance of holding a day or a week prior to endoscopic procedures should be followed.
2. Periprocedural management of GLP-1 RAs should attempt to minimize the aspiration risks loosely associated with delayed gastric emptying.
- Consider a 24-hour clear liquid diet a day prior to the procedure and transabdominal ultrasound to check gastric contents.
- It is acknowledged that this guidance is based on limited evidence and will be evolving as new medications and data are released.
Recent Clinical Studies
Although there is very little data to guide clinicians, several recent studies have been published that can direct clinical decision-making as guidelines continue to be refined and updated.
A multicenter trial of approximately 800 patients undergoing upper endoscopy found a significant difference in rates of retained gastric contents between those that underwent endoscopy who did and did not follow the ASA guidance on periprocedural management of GLP-1 RAs (12.7% vs 4.4%; P < .0001). However, there were no significant differences in rates of aborted procedures or unplanned intubations.
Furthermore, a multivariable analysis was performed controlling for GLP-1 RA type and other factors, which found the likelihood of gastric retention increased by 36% for every 1% increase in hemoglobin A1c. This study suggests that a more individualized approach to holding GLP-1 RA would be applicable rather than a universal periprocedural hold.6
More recently, a single-center study of nearly 600 patients undergoing upper endoscopy showed that while there were slightly increased rates of retained gastric contents (OR 3.80; P = .003) and aborted procedures (1.3% vs 0%; P = .02), the rates of adverse anesthesia events (hypoxia, etc) were similar between the groups and no cases of pulmonary aspiration were noted.7
One single-center study of 57 patients evaluated the safety of GLP-1 RAs in those undergoing endoscopic sleeve gastrectomy. GLP-1 RAs were continued on all patients, but all adhered to a liquid only diet for at least 24 hours prior to the procedure. There were no instances of retained gastric solids, aspiration, or hypoxia. This study suggests that with a 24-hour clear liquid diet and routine NPO recommendations prior to endoscopy, it would be safe to continue GLP-1 RAs. This study provides rationale for the AGA recommendation for a clear liquid diet 24 hours prior to endoscopic procedures for those on GLP-1 RAs.8
A study looking at those who underwent emergency surgery and endoscopy with claims data of use of GLP-1 RAs found an overall incidence of postoperative respiratory complications of 3.5% for those with GLP-1 RAs fill history vs 4.0% for those without (P = .12). Approximately 800 of the 24,000 patients identified had undergone endoscopic procedures for GI bleeding or food impaction. The study overall showed that preoperative use of GLP-1 RAs in patients undergoing surgery or endoscopy, evaluated as a combined group, was not associated with an increased risk of pulmonary complications.9
Lastly, a systematic review and meta-analysis that included 15 studies that quantified gastric emptying using various methods, including gastric emptying scintigraphy and acetaminophen absorption test, found that there was a quantifiable delay in gastric emptying of about 36 minutes, compared to placebo (P < .01), in patients using GLP-1 RAs. However, compared to standard periprocedural fasting, this delay is clinically insignificant and standard fasting protocols would still be appropriate for patients on GLP-1 RAs.10
These studies taken together suggest that while GLP-1 RAs can mildly increase the likelihood of retained gastric contents, there is no statistically significant increase in the risk of aspiration or other anesthesia complications. Furthermore, while decreased gastric emptying is a known effect of GLP-1 RAs, this effect may not be clinically significant in the context of standard periprocedural fasting protocols particularly when combined with a 24-hour clear liquid diet. These findings support at a minimum a more patient-specific strategy for periprocedural management of GLP-1 RAs.
Clinical Implications
These most recent studies, as well as prior studies and guidelines by various societies lead to a dilemma among endoscopists on proper patient counseling on GLP-1 RAs use before endoscopic procedures. Clinicians must balance the metabolic benefits of GLP-1 RAs with potential endoscopic complications and risks.
Holding therapy theoretically decreases aspiration risk and pulmonary complications, though evidence remains low to support this. Holding medication, however, affects glycemic control leading to potential rebound hyperglycemia which may impact and delay plans for endoscopy. With growing indications for the use of GLP-1 RAs, a more tailored patient-centered treatment plan may be required, especially with consideration of procedure indication and comorbidities.
Currently, practice patterns at different institutions vary widely, making standardization much more difficult. Some centers have opted to follow ASA guidelines of holding these medications up to 1 week prior to procedures, while others have continued therapy with no pre-procedural adjustments. This leaves endoscopists to deal with the downstream effects of inconvenience to patients, care delays, and financial considerations if procedures are postponed related to GLP-1 RAs use.
Future Directions
Future studies are needed to make further evidence-based recommendations. Studies should focus on stratifying risks and recommendations based on procedure type (EGD, colonoscopy, etc). More widespread implementation of gastric ultrasound can assist in real-time decision-making, albeit this would require expertise and dedicated time within the pre-procedural workflow. Randomized controlled trials comparing outcomes of patients who continue GLP-1 RAs vs those who discontinue stratified by baseline risk will be instrumental for making concrete guidelines that provide clarity on periprocedural management of GLP-1 RAs.
Conclusion
The periprocedural management of GLP-1 RAs remains a controversial topic that presents unique challenges in endoscopy. Several guidelines have been released by various stakeholders including anesthesiologists, gastroenterologists, and other prescribing providers. Clinical data remains limited with no robust evidence available to suggest that gastric emptying delays caused by GLP-1 RAs prior to endoscopic procedures significantly increases risk of aspiration, pulmonary complications, or other comorbidities. Evolving multi-society guidelines will be important to establish more consistent practices with reassessment of the data as new studies emerge. A multidisciplinary, individualized patient approach may be the best strategy for managing GLP-1 RAs for patients undergoing endoscopic procedures.
Dr. Sekar and Dr. Asamoah are based in the department of gastroenterology at MedStar Georgetown University Hospital, Washington, D.C. Dr. Sekar reports no conflicts of interest in regard to this article. Dr. Asamoah serves on the Johnson & Johnson advisory board for inflammatory bowel disease–related therapies.
References
1. Halim MA et al. Glucagon-Like Peptide-1 Inhibits Prandial Gastrointestinal Motility Through Myenteric Neuronal Mechanisms in Humans. J Clin Endocrinol Metab. 2018 Feb. doi: 10.1210/jc.2017-02006.
2. American Society of Anesthesiologists. American Society of Anesthesiologists releases consensus-based guidance on preoperative use of GLP-1 receptor agonists. 2023 Jun 20. www.asahq.org/about-asa/newsroom/news-releases/2023/06/american-society-of-anesthesiologists-consensus-based-guidance-on-preoperative
3. American Gastroenterological Association. GI multi-society statement regarding GLP-1 agonists and endoscopy. 2023 Jul 25. gastro.org/news/gi-multi-society-statement-regarding-glp-1-agonists-and-endoscopy/.
4. Hashash JG et al. AGA Rapid Clinical Practice Update on the Management of Patients Taking GLP-1 Receptor Agonists Prior to Endoscopy: Communication. Clin Gastroenterol Hepatol. 2024 Apr. doi: 10.1016/j.cgh.2023.11.002.
5. Kindel TL et al; American Gastroenterological Association; American Society for Metabolic and Bariatric Surgery; American Society of Anesthesiologists; International Society of Perioperative Care of Patients with Obesity; Society of American Gastrointestinal and Endoscopic Surgeons. Multi-society Clinical Practice Guidance for the Safe Use of Glucagon-like Peptide-1 Receptor Agonists in the Perioperative Period. Clin Gastroenterol Hepatol. 2024 Oct. doi: 10.1016/j.cgh.2024.10.003.
6. Phan J et al. Glucagon-Like Peptide Receptor Agonists Use Before Endoscopy Is Associated With Low Retained Gastric Contents: A Multicenter Cross-Sectional Analysis. Am J Gastroenterol. 2025 Mar. doi: 10.14309/ajg.0000000000002969.
7. Panchal S et al. Endoscopy and Anesthesia Outcomes Associated With Glucagon-like Peptide-1 Receptor Agonist use in Patients Undergoing Outpatient Upper Endoscopy. Gastrointest Endosc. 2025 Aug. doi:10.1016/j.gie.2025.01.004.
8. Maselli DB et al. Safe Continuation of glucagon-like Peptide 1 Receptor Agonists at Endoscopy: A Case Series of 57 Adults Undergoing Endoscopic Sleeve Gastroplasty. Obes Surg. 2024 Jul. doi: 10.1007/s11695-024-07278-2.
9. Dixit AA et al. Preoperative GLP-1 Receptor Agonist Use and Risk of Postoperative Respiratory Complications. JAMA. 2024 Apr. doi: 10.1001/jama.2024.5003.
10. Hiramoto B et al. Quantified Metrics of Gastric Emptying Delay by Glucagon-Like Peptide-1 Agonists: A systematic review and meta-analysis with insights for periprocedural management. Am J Gastroenterol. 2024 Jun. doi: 10.14309/ajg.0000000000002820.
The use of glucagon-like peptide-1 receptor agonists (GLP-1 RAs) has increased over the past several years and has become a cornerstone in both diabetes and weight loss management, particularly because of its unique combination of glucose control, weight reduction potential, and cardiac and metabolic benefits. However, increased use of these agents presents a dilemma in gastrointestinal endoscopy as it pertains to their safety and management during the periprocedural period.
highlighting gaps and future directions.
Pharmacology and Mechanisms of Action
GLP-1 RAs have several mechanisms of action that make them relevant in gastrointestinal endoscopy. These medications modulate glucose control via enhancement of glucose-dependent insulin secretion and reduction of postprandial glucagon, which promotes satiety and delays gastric emptying. This delay in gastric emptying mediated by vagal pathways has been postulated to increase gastric residuals, posing a risk for aspiration during anesthesia.1
It is important to also consider the pharmacokinetics of GLP-1 RAs, as some have shorter half-lives on the order of several hours, like exenatide, while others, like semaglutide, are dosed weekly. Additionally, common side effects of GLP-1 RAs include nausea, vomiting, bloating, and early satiety, which pose challenges for patients undergoing endoscopic procedures.
Current Guidelines
Various societies have published guidelines on the periprocedural use of GLP-1 RAs. The American Society of Anesthesiologist (ASA) in 2023 presented early recommendations to hold GLP-1 RAs either day of procedure or week prior depending on pharmacokinetics, because of the risk of delayed gastric emptying and increased potential for aspiration.2 Soon thereafter, a multi-gastroenterology society guideline was released stating more data is needed to decide if GLP-1 RAs need to be held prior to endoscopic procedures.3
In early 2024, the American Gastroenterological Association (AGA) published a rapid clinical update that advocated for a more individualized approach, particularly in light of limited overall data for GLP-1 RAs and endoscopic procedures.4 In asymptomatic patients who follow typical fasting protocols for procedures, it is generally safe to proceed with endoscopy without holding GLP-1 RAs. In symptomatic patients (nausea, abdominal distension, etc), the AGA advises additional precautions, including performing transabdominal ultrasound if feasible to assess retained gastric contents. The AGA also suggests placing a patient on a clear liquid diet the day prior to the procedure — rather than holding GLP-1 RAs — as another reasonable strategy.
The guidelines continue to evolve with newer multi-society guidelines establishing best practices. While initially in 2023 the ASA did recommend holding these medications prior to endoscopy, the initial guidance was based on expert opinion with limited evidence. Newer multi-society guidance published jointly by the ASA along with various gastroenterology societies, including the AGA in December 2024, takes a more nuanced approach.5
The newer guidelines include two main recommendations:
1. Periprocedural management of GLP-1 RAs should be a joint decision among the procedural, anesthesia, and prescribing team balancing metabolic needs vs patient risks.
- In a low-risk patient, one that is asymptomatic and on standard dosing, among other factors, the guidance states that GLP-1 RAs can be continued.
- In higher-risk patients, the original guidance of holding a day or a week prior to endoscopic procedures should be followed.
2. Periprocedural management of GLP-1 RAs should attempt to minimize the aspiration risks loosely associated with delayed gastric emptying.
- Consider a 24-hour clear liquid diet a day prior to the procedure and transabdominal ultrasound to check gastric contents.
- It is acknowledged that this guidance is based on limited evidence and will be evolving as new medications and data are released.
Recent Clinical Studies
Although there is very little data to guide clinicians, several recent studies have been published that can direct clinical decision-making as guidelines continue to be refined and updated.
A multicenter trial of approximately 800 patients undergoing upper endoscopy found a significant difference in rates of retained gastric contents between those that underwent endoscopy who did and did not follow the ASA guidance on periprocedural management of GLP-1 RAs (12.7% vs 4.4%; P < .0001). However, there were no significant differences in rates of aborted procedures or unplanned intubations.
Furthermore, a multivariable analysis was performed controlling for GLP-1 RA type and other factors, which found the likelihood of gastric retention increased by 36% for every 1% increase in hemoglobin A1c. This study suggests that a more individualized approach to holding GLP-1 RA would be applicable rather than a universal periprocedural hold.6
More recently, a single-center study of nearly 600 patients undergoing upper endoscopy showed that while there were slightly increased rates of retained gastric contents (OR 3.80; P = .003) and aborted procedures (1.3% vs 0%; P = .02), the rates of adverse anesthesia events (hypoxia, etc) were similar between the groups and no cases of pulmonary aspiration were noted.7
One single-center study of 57 patients evaluated the safety of GLP-1 RAs in those undergoing endoscopic sleeve gastrectomy. GLP-1 RAs were continued on all patients, but all adhered to a liquid only diet for at least 24 hours prior to the procedure. There were no instances of retained gastric solids, aspiration, or hypoxia. This study suggests that with a 24-hour clear liquid diet and routine NPO recommendations prior to endoscopy, it would be safe to continue GLP-1 RAs. This study provides rationale for the AGA recommendation for a clear liquid diet 24 hours prior to endoscopic procedures for those on GLP-1 RAs.8
A study looking at those who underwent emergency surgery and endoscopy with claims data of use of GLP-1 RAs found an overall incidence of postoperative respiratory complications of 3.5% for those with GLP-1 RAs fill history vs 4.0% for those without (P = .12). Approximately 800 of the 24,000 patients identified had undergone endoscopic procedures for GI bleeding or food impaction. The study overall showed that preoperative use of GLP-1 RAs in patients undergoing surgery or endoscopy, evaluated as a combined group, was not associated with an increased risk of pulmonary complications.9
Lastly, a systematic review and meta-analysis that included 15 studies that quantified gastric emptying using various methods, including gastric emptying scintigraphy and acetaminophen absorption test, found that there was a quantifiable delay in gastric emptying of about 36 minutes, compared to placebo (P < .01), in patients using GLP-1 RAs. However, compared to standard periprocedural fasting, this delay is clinically insignificant and standard fasting protocols would still be appropriate for patients on GLP-1 RAs.10
These studies taken together suggest that while GLP-1 RAs can mildly increase the likelihood of retained gastric contents, there is no statistically significant increase in the risk of aspiration or other anesthesia complications. Furthermore, while decreased gastric emptying is a known effect of GLP-1 RAs, this effect may not be clinically significant in the context of standard periprocedural fasting protocols particularly when combined with a 24-hour clear liquid diet. These findings support at a minimum a more patient-specific strategy for periprocedural management of GLP-1 RAs.
Clinical Implications
These most recent studies, as well as prior studies and guidelines by various societies lead to a dilemma among endoscopists on proper patient counseling on GLP-1 RAs use before endoscopic procedures. Clinicians must balance the metabolic benefits of GLP-1 RAs with potential endoscopic complications and risks.
Holding therapy theoretically decreases aspiration risk and pulmonary complications, though evidence remains low to support this. Holding medication, however, affects glycemic control leading to potential rebound hyperglycemia which may impact and delay plans for endoscopy. With growing indications for the use of GLP-1 RAs, a more tailored patient-centered treatment plan may be required, especially with consideration of procedure indication and comorbidities.
Currently, practice patterns at different institutions vary widely, making standardization much more difficult. Some centers have opted to follow ASA guidelines of holding these medications up to 1 week prior to procedures, while others have continued therapy with no pre-procedural adjustments. This leaves endoscopists to deal with the downstream effects of inconvenience to patients, care delays, and financial considerations if procedures are postponed related to GLP-1 RAs use.
Future Directions
Future studies are needed to make further evidence-based recommendations. Studies should focus on stratifying risks and recommendations based on procedure type (EGD, colonoscopy, etc). More widespread implementation of gastric ultrasound can assist in real-time decision-making, albeit this would require expertise and dedicated time within the pre-procedural workflow. Randomized controlled trials comparing outcomes of patients who continue GLP-1 RAs vs those who discontinue stratified by baseline risk will be instrumental for making concrete guidelines that provide clarity on periprocedural management of GLP-1 RAs.
Conclusion
The periprocedural management of GLP-1 RAs remains a controversial topic that presents unique challenges in endoscopy. Several guidelines have been released by various stakeholders including anesthesiologists, gastroenterologists, and other prescribing providers. Clinical data remains limited with no robust evidence available to suggest that gastric emptying delays caused by GLP-1 RAs prior to endoscopic procedures significantly increases risk of aspiration, pulmonary complications, or other comorbidities. Evolving multi-society guidelines will be important to establish more consistent practices with reassessment of the data as new studies emerge. A multidisciplinary, individualized patient approach may be the best strategy for managing GLP-1 RAs for patients undergoing endoscopic procedures.
Dr. Sekar and Dr. Asamoah are based in the department of gastroenterology at MedStar Georgetown University Hospital, Washington, D.C. Dr. Sekar reports no conflicts of interest in regard to this article. Dr. Asamoah serves on the Johnson & Johnson advisory board for inflammatory bowel disease–related therapies.
References
1. Halim MA et al. Glucagon-Like Peptide-1 Inhibits Prandial Gastrointestinal Motility Through Myenteric Neuronal Mechanisms in Humans. J Clin Endocrinol Metab. 2018 Feb. doi: 10.1210/jc.2017-02006.
2. American Society of Anesthesiologists. American Society of Anesthesiologists releases consensus-based guidance on preoperative use of GLP-1 receptor agonists. 2023 Jun 20. www.asahq.org/about-asa/newsroom/news-releases/2023/06/american-society-of-anesthesiologists-consensus-based-guidance-on-preoperative
3. American Gastroenterological Association. GI multi-society statement regarding GLP-1 agonists and endoscopy. 2023 Jul 25. gastro.org/news/gi-multi-society-statement-regarding-glp-1-agonists-and-endoscopy/.
4. Hashash JG et al. AGA Rapid Clinical Practice Update on the Management of Patients Taking GLP-1 Receptor Agonists Prior to Endoscopy: Communication. Clin Gastroenterol Hepatol. 2024 Apr. doi: 10.1016/j.cgh.2023.11.002.
5. Kindel TL et al; American Gastroenterological Association; American Society for Metabolic and Bariatric Surgery; American Society of Anesthesiologists; International Society of Perioperative Care of Patients with Obesity; Society of American Gastrointestinal and Endoscopic Surgeons. Multi-society Clinical Practice Guidance for the Safe Use of Glucagon-like Peptide-1 Receptor Agonists in the Perioperative Period. Clin Gastroenterol Hepatol. 2024 Oct. doi: 10.1016/j.cgh.2024.10.003.
6. Phan J et al. Glucagon-Like Peptide Receptor Agonists Use Before Endoscopy Is Associated With Low Retained Gastric Contents: A Multicenter Cross-Sectional Analysis. Am J Gastroenterol. 2025 Mar. doi: 10.14309/ajg.0000000000002969.
7. Panchal S et al. Endoscopy and Anesthesia Outcomes Associated With Glucagon-like Peptide-1 Receptor Agonist use in Patients Undergoing Outpatient Upper Endoscopy. Gastrointest Endosc. 2025 Aug. doi:10.1016/j.gie.2025.01.004.
8. Maselli DB et al. Safe Continuation of glucagon-like Peptide 1 Receptor Agonists at Endoscopy: A Case Series of 57 Adults Undergoing Endoscopic Sleeve Gastroplasty. Obes Surg. 2024 Jul. doi: 10.1007/s11695-024-07278-2.
9. Dixit AA et al. Preoperative GLP-1 Receptor Agonist Use and Risk of Postoperative Respiratory Complications. JAMA. 2024 Apr. doi: 10.1001/jama.2024.5003.
10. Hiramoto B et al. Quantified Metrics of Gastric Emptying Delay by Glucagon-Like Peptide-1 Agonists: A systematic review and meta-analysis with insights for periprocedural management. Am J Gastroenterol. 2024 Jun. doi: 10.14309/ajg.0000000000002820.