User login
Q Does venlafaxine reduce hot flashes?
Expert Commentary
For 12 weeks, Evans et al examined the effect of venlafaxine, a serotonin noradrenergic reuptake inhibitor, on patient-perceived hot flash scores. The authors randomized 80 healthy postmenopausal women with at least 14 hot flashes per week to receive placebo or extended-release venlafaxine 37.5 mg daily for 1 week followed by 75 mg daily for 11 weeks. Sixty-one women completed the study.
Drug effect sustained, placebo effect fades. Both venlafaxine and placebo decreased the hot flash score at 1 month. However, unlike placebo, venlafaxine produced a further drop in hot flashes at 2 months, which was sustained at 3 months. All told, patient-perceived mean hot flash scores dropped 51% from baseline with venlafaxine compared with a 15% drop with placebo. Most women (93%) on venlafaxine planned to continue the treatment after the study concluded.
Confirms previous trials
These findings reinforce data from previous venlafaxine studies, in which an approximately 60% drop in hot flash score was seen with venlafaxine compared with an approximately 30% drop with placebo,1 and add to our knowledge by offering a longer study period. Prior venlafaxine studies included women with a history of breast cancer, as well as those who simply had a fear of the disease.
How does venlafaxine compare with other options?
Fewer sides effects than clonidine, whose side-effect profile limits use in many women, according to a 2004 position statement on vasomotor symptoms from the North American Menopause Society.2 Thus far, research has found venlafaxine to have fewer adverse effects, which include decreased appetite, dry mouth, and initially nausea.
On par with paroxetine. The reduction in hot flashes with venlafaxine 75 mg in this and previous studies is comparable with findings from a study of controlled-release paroxetine, a selective serotonin reuptake inhibitor, at doses of 12.5 mg or 25 mg.3
Probably less effective than estrogen. Evans et al did not directly compare venlafaxine with estrogen, but their findings suggest that venlafaxine is probably not as effective as estrogen for vasomotor symptoms.
1. Loprinzi CL, Kugler JW, Sloan JA, Mailliard JA, et al. Venlafaxine in management of hot flashes in survivors of breast cancer: a randomised controlled trial. Lancet 2000;356:2059-2063.
2. North American Menopause Society. Treatment of menopause-associated vasomotor symptoms: position statement of The North American Menopause Society. Menopause. 2004;11:11-33.
3. Stearns V, Beebe KL, Iyengar M, Dube E. Paroxetine controlled release in the treatment of menopausal hot flashes. JAMA. 2003;289:2827-2834.
Expert Commentary
For 12 weeks, Evans et al examined the effect of venlafaxine, a serotonin noradrenergic reuptake inhibitor, on patient-perceived hot flash scores. The authors randomized 80 healthy postmenopausal women with at least 14 hot flashes per week to receive placebo or extended-release venlafaxine 37.5 mg daily for 1 week followed by 75 mg daily for 11 weeks. Sixty-one women completed the study.
Drug effect sustained, placebo effect fades. Both venlafaxine and placebo decreased the hot flash score at 1 month. However, unlike placebo, venlafaxine produced a further drop in hot flashes at 2 months, which was sustained at 3 months. All told, patient-perceived mean hot flash scores dropped 51% from baseline with venlafaxine compared with a 15% drop with placebo. Most women (93%) on venlafaxine planned to continue the treatment after the study concluded.
Confirms previous trials
These findings reinforce data from previous venlafaxine studies, in which an approximately 60% drop in hot flash score was seen with venlafaxine compared with an approximately 30% drop with placebo,1 and add to our knowledge by offering a longer study period. Prior venlafaxine studies included women with a history of breast cancer, as well as those who simply had a fear of the disease.
How does venlafaxine compare with other options?
Fewer sides effects than clonidine, whose side-effect profile limits use in many women, according to a 2004 position statement on vasomotor symptoms from the North American Menopause Society.2 Thus far, research has found venlafaxine to have fewer adverse effects, which include decreased appetite, dry mouth, and initially nausea.
On par with paroxetine. The reduction in hot flashes with venlafaxine 75 mg in this and previous studies is comparable with findings from a study of controlled-release paroxetine, a selective serotonin reuptake inhibitor, at doses of 12.5 mg or 25 mg.3
Probably less effective than estrogen. Evans et al did not directly compare venlafaxine with estrogen, but their findings suggest that venlafaxine is probably not as effective as estrogen for vasomotor symptoms.
Expert Commentary
For 12 weeks, Evans et al examined the effect of venlafaxine, a serotonin noradrenergic reuptake inhibitor, on patient-perceived hot flash scores. The authors randomized 80 healthy postmenopausal women with at least 14 hot flashes per week to receive placebo or extended-release venlafaxine 37.5 mg daily for 1 week followed by 75 mg daily for 11 weeks. Sixty-one women completed the study.
Drug effect sustained, placebo effect fades. Both venlafaxine and placebo decreased the hot flash score at 1 month. However, unlike placebo, venlafaxine produced a further drop in hot flashes at 2 months, which was sustained at 3 months. All told, patient-perceived mean hot flash scores dropped 51% from baseline with venlafaxine compared with a 15% drop with placebo. Most women (93%) on venlafaxine planned to continue the treatment after the study concluded.
Confirms previous trials
These findings reinforce data from previous venlafaxine studies, in which an approximately 60% drop in hot flash score was seen with venlafaxine compared with an approximately 30% drop with placebo,1 and add to our knowledge by offering a longer study period. Prior venlafaxine studies included women with a history of breast cancer, as well as those who simply had a fear of the disease.
How does venlafaxine compare with other options?
Fewer sides effects than clonidine, whose side-effect profile limits use in many women, according to a 2004 position statement on vasomotor symptoms from the North American Menopause Society.2 Thus far, research has found venlafaxine to have fewer adverse effects, which include decreased appetite, dry mouth, and initially nausea.
On par with paroxetine. The reduction in hot flashes with venlafaxine 75 mg in this and previous studies is comparable with findings from a study of controlled-release paroxetine, a selective serotonin reuptake inhibitor, at doses of 12.5 mg or 25 mg.3
Probably less effective than estrogen. Evans et al did not directly compare venlafaxine with estrogen, but their findings suggest that venlafaxine is probably not as effective as estrogen for vasomotor symptoms.
1. Loprinzi CL, Kugler JW, Sloan JA, Mailliard JA, et al. Venlafaxine in management of hot flashes in survivors of breast cancer: a randomised controlled trial. Lancet 2000;356:2059-2063.
2. North American Menopause Society. Treatment of menopause-associated vasomotor symptoms: position statement of The North American Menopause Society. Menopause. 2004;11:11-33.
3. Stearns V, Beebe KL, Iyengar M, Dube E. Paroxetine controlled release in the treatment of menopausal hot flashes. JAMA. 2003;289:2827-2834.
1. Loprinzi CL, Kugler JW, Sloan JA, Mailliard JA, et al. Venlafaxine in management of hot flashes in survivors of breast cancer: a randomised controlled trial. Lancet 2000;356:2059-2063.
2. North American Menopause Society. Treatment of menopause-associated vasomotor symptoms: position statement of The North American Menopause Society. Menopause. 2004;11:11-33.
3. Stearns V, Beebe KL, Iyengar M, Dube E. Paroxetine controlled release in the treatment of menopausal hot flashes. JAMA. 2003;289:2827-2834.
Avoiding legal pitfalls of hysteroscopy
IN THIS ARTICLE
- Managing and minimizing operative complications
Over the course of our careers, at least 75% of Ob/Gyns will have 1 or more medical liability claims filed against us. This naturally makes us cautious, sometimes overly so.
Though hysteroscopy is usually an effective—as well as safe—alternative to hysterectomy, many Ob/Gyns have not yet integrated this technology routinely into patient care, partly because of the fear of litigation.
In this roundtable, legal and medical experts comment on ways to minimize legal risks in 3 hypothetical cases.
- Steven R. Lindheim, MD, moderator, is associate professor, department of obstetrics and gynecology, University of Wisconsin Medical School, Madison
- Daniel Williams, MD, is associate professor, department of obstetrics and gynecology, University of Cincinnati College of Medicine
- Ira Newman, Esq, is an attorney at Sanocki, Newman, Turret, LLP, New York City
- Eric H. Weitz, Esq, is an attorney at Layser & Freiwald, PC, Philadelphia
- Jerry A. Lindheim, Esq, is an attorney at Locks Law Firm, Philadelphia
Case 1: fluid overload
“Abby” is a 30-year-old nulligravida who presents with menometorrhagia and symptomatic anemia. Sonohysterography reveals a 3-cm submucous fibroid. After 3 months of pretreatment with a GnRH agonist to decrease the size of the fibroid and relieve her anemia, Abby undergoes hysteroscopic resection of the fibroid with a monopolar instrument and 1.5% glycine as the distention medium. The surgery is prolonged, and the fluid deficit at the end of the case is 1,700 mL.
Serial labs are drawn in the recovery room, and Abby is hospitalized overnight for observation. Her fluid intake is restricted and a diuretic is administered. The next day her electrolytes are normal, and she is discharged from the hospital.
When assessing clinical risk, watch fluid deficit, large myomas
DR. LINDHEIM: Clinically speaking, the choice of distention fluid in this case is appropriate, since the surgeon is using monopolar electrical current, and glycine has low molecular viscosity. However, it is imperative to strictly monitor the fluid deficit and, whenever possible, limit infusion pressure to 60 to 75 mm Hg and keep operating time below 1 hour.
Also be aware that larger submucosal myomas may have sizeable venous channels. When these channels are opened during resection, significant fluid intravasation can result.
Dr. Lindheim:As a front-page article in the Wall Street Journal8 observed, a doctor’s best tool in fighting lawsuits may simply be owning up to errors. Yet this concept has been somewhat taboo in the medical community. What are your thoughts on a physician giving a simple apology?
Mr. Lindheim: It is in the heat of passion, usually involving anger, that families seek vindication against a physician simply because the physician wasn’t nice or failed to address questions posed by the family about an unfortunate outcome. In everyday life, when emotion clouds reason, it is hard to think logically and understand complex explanations. When a physician comes across as arrogant at such a time, the patient and her family are often motivated to contact an attorney to evaluate the standard of care.
Of course, an unfortunate outcome is not always the result of medical negligence. This is difficult to explain to a family angered by a doctor’s “attitude.” An apology may somewhat soothe the anger that drives many lawsuits, but it may not be enough to deflect litigation unless the physician is prepared to take responsibility for the adverse outcome.
Mr. Newman: Patients usually seek the advice of a lawyer out of anger or mistrust. They may believe their doctor has been evasive or inaccessible.
In cases where medical negligence may have caused injury to the patient, or complications associated with the nature of the procedure result in injury, it is my opinion that the treating doctor should forthrightly address any questions and concerns the patient has. This includes making oneself available in person or by telephone on a daily basis. In fact, picking up the phone and calling a patient who feels “wronged” may be the single most effective tool the doctor has to prevent a medical malpractice lawsuit.
Complications associated with glycine solution include water intoxication with hypervolemia and hyponatremia. Once a fluid deficit reaches 750 mL, the surgeon should check electrolytes, give a diuretic, and complete the procedure as soon as possible. When deficits exceed 1,500 mL, stop the procedure immediately (assuming adequate hemostasis) and give another diuretic.
When using bipolar technology, isotonic distention media is suitable, and the deficit can safely reach up to 2,000 mL.1-3
Managing water intoxication
Treating patients with water intoxication involves removing excess fluid and correcting serum sodium levels.
Some experts have argued the case for expectant management, which consists of water restriction and spontaneous diuresis. Others counter that patients with severe hyponatremia warrant immediate therapy, since they can deteriorate rapidly with little warning of seizures and respiratory arrest.
Legal outlook: Informed consent, thorough documentation are key
MR. LINDHEIM: I assume a proper informed consent document has been signed. Only the risks and complications listed on that document can be assumed to have the patient’s consent.
To avoid a claim associated with the consent process, the form should describe the exact procedure and alternatives, as well as the potential risks and complications, and it should be signed by the patient. Remember that informed consent is not just the physician’s recitation of this information, but the patient’s articulation of her understanding in response.
In this case, the facts surrounding all events should be well documented. The OR nurse should record the time, amount, and concentration of distention media given, preferably initialized by the person actually administering the medium. If this is not possible, the nurse should note that she was present at the time of administration and observed the medium being given. If a nurse or physician is later asked to explain what medications or fluids were administered, and this information was not documented, it opens the door to fanciful speculation on their part and cross-examination by the plaintiff’s attorney.
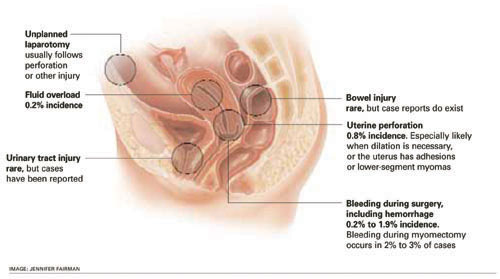
FIGURE Which complications are most common? Bleeding and perforation lead the pack, but others warrant vigilance, too
Do not attempt to insert these entries later. Handwriting specialists and other experts can detect when a record has been altered. Never try to change entries or erase them—by hand or using correction fluid. The chart is the first thing the plaintiff’s attorney will request and receive once a suit is initiated. Tampering with it is a surefire way to incur punitive damages.
Since this patient was kept for observation, the reasons for doing so may warrant an entry (eg, to monitor fluid intake and output [I/O]). If serial labs are drawn, each one should find its way into the chart.
Thorough recordkeeping is essential. Any time an item is lost or not included, the plaintiff’s attorney will argue that something is being hidden. Fluid levels are just as important as lab studies. Make sure the I/O chart is properly filled in, especially when fluid overload could give rise to litigation. These I/O sheets and medication (diuretic) forms should include the time of each assessment or administration.
Key ingredients of informed consent
DR. WILLIAMS: Could you describe an adequate informed consent form?
MR. LINDHEIM: In general, the body of the document should list all benefits and risks of the procedure, including anesthetic risk, infection, injury to organs and the need to repair them surgically, fluid overload and specific complications related to the type of distention media to be used, air emboli and their treatment, and long-term complications such as scarring and infertility.
Consent forms are usually signed at the end of the document, but you may want to insert a line next to each risk for initialing or signing by the patient, as well as a witnessing line at the end. This would make it clear the patient agreed to the procedure and was aware of all benefits and risks, and would present a strong defense to a later claim of lack of consent. I also recommend a notation in the progress records reemphasizing the consent process.
Provide patient-education articles
MR. WEITZ: Another effective technique is to mail or provide the woman with patient-oriented articles about the procedure and risks. Since most patients undergo hysteroscopy on a scheduled basis rather than emergently, they have an opportunity to read these articles before signing the consent form. Reference to these materials in the form is also an effective way to minimize medicolegal risk.
Factors leading to litigation
DR. LINDHEIM: Under what conditions would a legal action be initiated?
MR. WEITZ: All negligence claims require 4 elements:
- duty arising out of the physician-patient relationship,
- a breach of that duty (ie, deviation from the accepted standard of care),
- a link between that breach of duty and
- a specific harm.
MR. NEWMAN:In this case I believe the standards of care have been met. There is no legal case here.
MR. WEITZ: I agree. The complications that occurred did not result from deviation from the standard of care, but from the patient’s reaction to the procedure.
Should a law firm decide to proceed with this case, which seems doubtful, it would be hard to show any damage the patient suffered as a result of any alleged improper conduct.
Case 2: later finding of bowel injury
“Cathy” is a 40-year-old mother of 2 who is found to have a 10-mm polyp as part of her evaluation for abnormal uterine bleeding. She is scheduled to undergo hysteroscopic removal of the polyp with endometrial ablation. However, her uterus is severely retroverted, making serial cervical dilation necessary for entry. During the surgery, a pressure of 90 mm Hg is required for optimum visualization. The polyp is easily removed with a grasping instrument, and endometrial ablation is performed with a monopolar rollerball using 2.7% sorbitol for distention. Cathy is discharged the same day without complications.
Two days after the surgery, she calls with complaints of nausea, vomiting, and abdominal distention. She is told to go to the emergency room, where upright abdominal radiography shows free air in the abdomen. Cathy undergoes an exploratory laparotomy for small bowel perforation with end-to-end anastomosis and is discharged 1 week later without sequelae.
Factors that raise risk of perforation
DR. WILLIAMS: Uterine perforation is the most common complication of operative hysteroscopy. It is especially likely with cervical stenosis or severe anteflexion or retroflexion of the uterus; with lower-segment myomas or intrauterine synechiae; and when the operator is inexperienced.3-5
When perforation occurs without an electrical source, hysteroscopy usually is discontinued because of the inability to achieve uterine distention.
Terminate the procedure even if the perforation is small and distention is possible, since fluid will be lost into the peritoneal cavity. Usually, the patient can be observed and discharged home if there is no vaginal or intraperitoneal bleeding.3,4
When perforation occurs during use of electrical energy, laparoscopy is advised to rule out bowel injury.
Patients with unrecognized bowel injury after hysteroscopy frequently are not symptomatic until 2 to 10 days after the procedure due to the thermal nature of the injury, as this case illustrates.
Value of a photographic record
In this case, unrecognized perforation with later bowel injury could raise questions about adequate visualization throughout the case. Use of video or photography may be helpful to document that visualization.
Bowel injury also can occur in the absence of uterine perforation. With lower coagulating currents, it may take longer to achieve the desired endometrial effect, and this can sometimes lead to transmural thermal damage. This heat effect has been reported to cause bowel injury.6,7
Justify procedures in advance
DR. LINDHEIM:An expert also might question whether the ablation was necessary. Was the option of doing a simple polypectomy versus doing both a polypectomy and ablation discussed and documented?
DR. WILLIAMS: With such a small polyp, it was reasonable to perform the ablation, provided consent was given and recorded.
DR. LINDHEIM: What is the legal perspective on this issue?
MR. LINDHEIM: The physician will have to explain why it was necessary to perform an ablation when the treatment possibly required only simple polyp removal. Is it documented that the patient was refractory to medical therapy?
Whenever surgery entails any complication or additional procedures that could have been treated with simpler, less invasive methods, the surgeon is exposed to scrutiny, questioning, and accountability. For this reason, more is better than less when it comes to documentation.
MR. WEITZ: Most juries weighing treatment options are sympathetic when the patient testifies that she chose the procedure recommended by her physician. Thus, the doctor may be held accountable if something goes wrong with a riskier procedure.
If the physician wants to use informed consent as a defense, he or she should consider giving all patients articles about the various procedures so a woman cannot complain she was inadequately informed.
MR. NEWMAN: In a case like this, the plaintiff’s attorney likely would focus on documentation in the operative report as well as in the operative, anesthesia, postoperativecare, and pathology records.
Does the case have merit?
It depends on the type of injury and when it was found.
The location, size, and nature of the perforation, as described by pathology, may be pivotal in determining whether this case has merit. If the perforation can be described as a hole, tear, or laceration and is larger than a few millimeters, the doctor will have a harder time defending this case, since no perforation was discovered at surgery or before the patient’s discharge.
Following the surgery, all health-care providers should document abdominal examinations and findings at regular intervals, and should note that the patient was assessed and offered no complaints of nausea, vomiting, abdominal pain, or fever.
Should a perforation occur, finding and repairing it at the time of the original surgery is critical in preventing a lawsuit, since, in these cases, no additional injuries would be sustained by the patient—hence, no legally cognizable damages.
DR. LINDHEIM:Is our liability different if a bowel perforation is detected postopera-tively within the standard of care?
MR. WEITZ: Some physicians do not believe perforation of the bowel itself is negligent, but a failure to identify and remedy it prior to completing the original procedure is.
Of course, the timing of identifying the bowel perforation after surgery may determine whether any damage can be attributed to the delay. If the perforation is identified soon after surgery and easily repaired, it will not be easy for the patient to establish a case of additional harm.
Listen to a patient’s complaints
Another important point: Many plaintiffs complain that when they called their physician with postoperative complaints, they were ignored. One of the best liability-avoidance measures is to actively listen to patients and be responsive to their needs, even if treatment will remain the same.
As for the use of photos and video as defense, wholesale reliance on them and pathology reports is risky. Depending on how this evidence is presented, a jury may conclude the physician chose not to photograph the site where the injury occurred or intentionally took tissue samples from a different area. If a jury senses a cover-up, the defense can be undermined.
Case 3: air embolism
“Elaine” is a 35-year-old mother of 1 with secondary amenorrhea for 6 months. She delivered her son vaginally at term, but had bleeding 5 weeks postpartum that required D&C for retained placenta. After a hysterosalpingogram reveals severe Asherman’s syndrome, she is scheduled for hysteroscopic adhesiolysis.
At surgery, the cervical canal is serially dilated. On entry into the uterine cavity with a 5-mm hysteroscope, severe adhesions are visible throughout the entire cavity. Through the operating channel of the hysteroscope, a bipolar tip is used for lysis, with saline distending medium.
Shortly into the procedure, the anesthesiologist observes a decrease in oxygen saturation and a drop in end-tidal CO2, as well as hypotension. An air embolism is suspected. The gynecologist immediately stops the procedure while the anesthesiologist repositions Elaine in the left lateral decubitus position and administers 100% oxygen. The cardiac team is called, and Elaine requires invasive monitoring and catheterization of the subclavian vein. She fully recovers within 24 hours and is discharged from the hospital.
Clinical signs of collapse
DR. WILLIAMS: The most common sign of impending cardiovascular collapse is a sudden drop in end-tidal carbon dioxide, as seen in this case. Both the surgeon and the anesthesiologist acted properly.
MR. WEITZ: I assume the procedure was thoroughly discussed with the patient during the consent process, with the risk of gas emboli emphasized, and that this discussion was documented.
Advise the patient of risky techniques
If hysteroscopic placement or repetitive removal and replacement of the hysteroscope can create air bubbles, the physician should clearly document why the patient should be exposed to this risk. Most times, as in this case, there are valid explanations, but without a notation in the record, the physician is exposed to legal risk.
Standards are a double-edged sword
Perhaps industry organizations such as the American College of Obstetricians and Gynecologists should consider creating industry-wide standards for the proper use of hysteroscopes. Even with a negative outcome, including significant injury, it is difficult to prosecute a case when the medical community recognizes that the steps followed by the physician adhered to the standard of care.
Another benefit of industry-wide standards is that they provide practitioners and health-care insurers with a common framework by which to evaluate the necessity and effectiveness of hysteroscopic procedures.
MR. LINDHEIM: There are both positive and negative aspects to standards. When they exist, they increase the level of expectation, usually thought of as a minimum. When this minimum is adhered to, the risk of medicolegal liability is low. But when care deviates from it—regardless of the reason—the patient can argue that malpractice occurred. Conversely, without standards, the physician’s actions are viewed as a “judgment call,” and it is harder to argue that a deviation occurred.
Dr. Lindheim is a speaker and nonpaid consultant for Cooper-Surgical. The other panelists report no relevant financial relationships.
1. Bradley LD. Cutting the risk of hysteroscopic complications. OBG Management. 2004;16(1):44-52.
2. Witz CA, Silverberg KM, Burns WN, Schenken RS, Olive DL. Complications associated with the absorption of hysteroscopic fluid media. Fertil Steril. 1993;60:745-756.
3. Isaacson KB. Complications of hysteroscopy. Obstet Gynecol Clin North Am. 1999;26:39-51.
4. Cooper JM, Brady RM. Intraoperative and early postoperative complications of operative hysteroscopy. Obstet Gynecol Clin North Am. 2000;27:347-366.
5. Jansen FW, Vredevoogd CB, Van Ulzen K, Hermans J, Trimbos JB, Trimbos-Kemper TCM. Complications of hysteroscopy: a prospective, multicenter study. Obstet Gynecol. 2000;96:266-270.
6. Perry CP, Daniell JF, Gimpelson RJ. Bowel injury from Nd:YAG endometrial ablation. J Gynecol Surg. 1990;6:199-203.
7. Kivnick S, Kanter MH. Bowel injury from rollerball ablation of the endometrium. Obstet Gynecol. 1992;79:833-834.
8. Doctors’ new tool to fight lawsuits: saying “I’m sorry.” Wall Street Journal. May 18, 2004; page A1.
IN THIS ARTICLE
- Managing and minimizing operative complications
Over the course of our careers, at least 75% of Ob/Gyns will have 1 or more medical liability claims filed against us. This naturally makes us cautious, sometimes overly so.
Though hysteroscopy is usually an effective—as well as safe—alternative to hysterectomy, many Ob/Gyns have not yet integrated this technology routinely into patient care, partly because of the fear of litigation.
In this roundtable, legal and medical experts comment on ways to minimize legal risks in 3 hypothetical cases.
- Steven R. Lindheim, MD, moderator, is associate professor, department of obstetrics and gynecology, University of Wisconsin Medical School, Madison
- Daniel Williams, MD, is associate professor, department of obstetrics and gynecology, University of Cincinnati College of Medicine
- Ira Newman, Esq, is an attorney at Sanocki, Newman, Turret, LLP, New York City
- Eric H. Weitz, Esq, is an attorney at Layser & Freiwald, PC, Philadelphia
- Jerry A. Lindheim, Esq, is an attorney at Locks Law Firm, Philadelphia
Case 1: fluid overload
“Abby” is a 30-year-old nulligravida who presents with menometorrhagia and symptomatic anemia. Sonohysterography reveals a 3-cm submucous fibroid. After 3 months of pretreatment with a GnRH agonist to decrease the size of the fibroid and relieve her anemia, Abby undergoes hysteroscopic resection of the fibroid with a monopolar instrument and 1.5% glycine as the distention medium. The surgery is prolonged, and the fluid deficit at the end of the case is 1,700 mL.
Serial labs are drawn in the recovery room, and Abby is hospitalized overnight for observation. Her fluid intake is restricted and a diuretic is administered. The next day her electrolytes are normal, and she is discharged from the hospital.
When assessing clinical risk, watch fluid deficit, large myomas
DR. LINDHEIM: Clinically speaking, the choice of distention fluid in this case is appropriate, since the surgeon is using monopolar electrical current, and glycine has low molecular viscosity. However, it is imperative to strictly monitor the fluid deficit and, whenever possible, limit infusion pressure to 60 to 75 mm Hg and keep operating time below 1 hour.
Also be aware that larger submucosal myomas may have sizeable venous channels. When these channels are opened during resection, significant fluid intravasation can result.
Dr. Lindheim:As a front-page article in the Wall Street Journal8 observed, a doctor’s best tool in fighting lawsuits may simply be owning up to errors. Yet this concept has been somewhat taboo in the medical community. What are your thoughts on a physician giving a simple apology?
Mr. Lindheim: It is in the heat of passion, usually involving anger, that families seek vindication against a physician simply because the physician wasn’t nice or failed to address questions posed by the family about an unfortunate outcome. In everyday life, when emotion clouds reason, it is hard to think logically and understand complex explanations. When a physician comes across as arrogant at such a time, the patient and her family are often motivated to contact an attorney to evaluate the standard of care.
Of course, an unfortunate outcome is not always the result of medical negligence. This is difficult to explain to a family angered by a doctor’s “attitude.” An apology may somewhat soothe the anger that drives many lawsuits, but it may not be enough to deflect litigation unless the physician is prepared to take responsibility for the adverse outcome.
Mr. Newman: Patients usually seek the advice of a lawyer out of anger or mistrust. They may believe their doctor has been evasive or inaccessible.
In cases where medical negligence may have caused injury to the patient, or complications associated with the nature of the procedure result in injury, it is my opinion that the treating doctor should forthrightly address any questions and concerns the patient has. This includes making oneself available in person or by telephone on a daily basis. In fact, picking up the phone and calling a patient who feels “wronged” may be the single most effective tool the doctor has to prevent a medical malpractice lawsuit.
Complications associated with glycine solution include water intoxication with hypervolemia and hyponatremia. Once a fluid deficit reaches 750 mL, the surgeon should check electrolytes, give a diuretic, and complete the procedure as soon as possible. When deficits exceed 1,500 mL, stop the procedure immediately (assuming adequate hemostasis) and give another diuretic.
When using bipolar technology, isotonic distention media is suitable, and the deficit can safely reach up to 2,000 mL.1-3
Managing water intoxication
Treating patients with water intoxication involves removing excess fluid and correcting serum sodium levels.
Some experts have argued the case for expectant management, which consists of water restriction and spontaneous diuresis. Others counter that patients with severe hyponatremia warrant immediate therapy, since they can deteriorate rapidly with little warning of seizures and respiratory arrest.
Legal outlook: Informed consent, thorough documentation are key
MR. LINDHEIM: I assume a proper informed consent document has been signed. Only the risks and complications listed on that document can be assumed to have the patient’s consent.
To avoid a claim associated with the consent process, the form should describe the exact procedure and alternatives, as well as the potential risks and complications, and it should be signed by the patient. Remember that informed consent is not just the physician’s recitation of this information, but the patient’s articulation of her understanding in response.
In this case, the facts surrounding all events should be well documented. The OR nurse should record the time, amount, and concentration of distention media given, preferably initialized by the person actually administering the medium. If this is not possible, the nurse should note that she was present at the time of administration and observed the medium being given. If a nurse or physician is later asked to explain what medications or fluids were administered, and this information was not documented, it opens the door to fanciful speculation on their part and cross-examination by the plaintiff’s attorney.
FIGURE Which complications are most common? Bleeding and perforation lead the pack, but others warrant vigilance, too
Do not attempt to insert these entries later. Handwriting specialists and other experts can detect when a record has been altered. Never try to change entries or erase them—by hand or using correction fluid. The chart is the first thing the plaintiff’s attorney will request and receive once a suit is initiated. Tampering with it is a surefire way to incur punitive damages.
Since this patient was kept for observation, the reasons for doing so may warrant an entry (eg, to monitor fluid intake and output [I/O]). If serial labs are drawn, each one should find its way into the chart.
Thorough recordkeeping is essential. Any time an item is lost or not included, the plaintiff’s attorney will argue that something is being hidden. Fluid levels are just as important as lab studies. Make sure the I/O chart is properly filled in, especially when fluid overload could give rise to litigation. These I/O sheets and medication (diuretic) forms should include the time of each assessment or administration.
Key ingredients of informed consent
DR. WILLIAMS: Could you describe an adequate informed consent form?
MR. LINDHEIM: In general, the body of the document should list all benefits and risks of the procedure, including anesthetic risk, infection, injury to organs and the need to repair them surgically, fluid overload and specific complications related to the type of distention media to be used, air emboli and their treatment, and long-term complications such as scarring and infertility.
Consent forms are usually signed at the end of the document, but you may want to insert a line next to each risk for initialing or signing by the patient, as well as a witnessing line at the end. This would make it clear the patient agreed to the procedure and was aware of all benefits and risks, and would present a strong defense to a later claim of lack of consent. I also recommend a notation in the progress records reemphasizing the consent process.
Provide patient-education articles
MR. WEITZ: Another effective technique is to mail or provide the woman with patient-oriented articles about the procedure and risks. Since most patients undergo hysteroscopy on a scheduled basis rather than emergently, they have an opportunity to read these articles before signing the consent form. Reference to these materials in the form is also an effective way to minimize medicolegal risk.
Factors leading to litigation
DR. LINDHEIM: Under what conditions would a legal action be initiated?
MR. WEITZ: All negligence claims require 4 elements:
- duty arising out of the physician-patient relationship,
- a breach of that duty (ie, deviation from the accepted standard of care),
- a link between that breach of duty and
- a specific harm.
MR. NEWMAN:In this case I believe the standards of care have been met. There is no legal case here.
MR. WEITZ: I agree. The complications that occurred did not result from deviation from the standard of care, but from the patient’s reaction to the procedure.
Should a law firm decide to proceed with this case, which seems doubtful, it would be hard to show any damage the patient suffered as a result of any alleged improper conduct.
Case 2: later finding of bowel injury
“Cathy” is a 40-year-old mother of 2 who is found to have a 10-mm polyp as part of her evaluation for abnormal uterine bleeding. She is scheduled to undergo hysteroscopic removal of the polyp with endometrial ablation. However, her uterus is severely retroverted, making serial cervical dilation necessary for entry. During the surgery, a pressure of 90 mm Hg is required for optimum visualization. The polyp is easily removed with a grasping instrument, and endometrial ablation is performed with a monopolar rollerball using 2.7% sorbitol for distention. Cathy is discharged the same day without complications.
Two days after the surgery, she calls with complaints of nausea, vomiting, and abdominal distention. She is told to go to the emergency room, where upright abdominal radiography shows free air in the abdomen. Cathy undergoes an exploratory laparotomy for small bowel perforation with end-to-end anastomosis and is discharged 1 week later without sequelae.
Factors that raise risk of perforation
DR. WILLIAMS: Uterine perforation is the most common complication of operative hysteroscopy. It is especially likely with cervical stenosis or severe anteflexion or retroflexion of the uterus; with lower-segment myomas or intrauterine synechiae; and when the operator is inexperienced.3-5
When perforation occurs without an electrical source, hysteroscopy usually is discontinued because of the inability to achieve uterine distention.
Terminate the procedure even if the perforation is small and distention is possible, since fluid will be lost into the peritoneal cavity. Usually, the patient can be observed and discharged home if there is no vaginal or intraperitoneal bleeding.3,4
When perforation occurs during use of electrical energy, laparoscopy is advised to rule out bowel injury.
Patients with unrecognized bowel injury after hysteroscopy frequently are not symptomatic until 2 to 10 days after the procedure due to the thermal nature of the injury, as this case illustrates.
Value of a photographic record
In this case, unrecognized perforation with later bowel injury could raise questions about adequate visualization throughout the case. Use of video or photography may be helpful to document that visualization.
Bowel injury also can occur in the absence of uterine perforation. With lower coagulating currents, it may take longer to achieve the desired endometrial effect, and this can sometimes lead to transmural thermal damage. This heat effect has been reported to cause bowel injury.6,7
Justify procedures in advance
DR. LINDHEIM:An expert also might question whether the ablation was necessary. Was the option of doing a simple polypectomy versus doing both a polypectomy and ablation discussed and documented?
DR. WILLIAMS: With such a small polyp, it was reasonable to perform the ablation, provided consent was given and recorded.
DR. LINDHEIM: What is the legal perspective on this issue?
MR. LINDHEIM: The physician will have to explain why it was necessary to perform an ablation when the treatment possibly required only simple polyp removal. Is it documented that the patient was refractory to medical therapy?
Whenever surgery entails any complication or additional procedures that could have been treated with simpler, less invasive methods, the surgeon is exposed to scrutiny, questioning, and accountability. For this reason, more is better than less when it comes to documentation.
MR. WEITZ: Most juries weighing treatment options are sympathetic when the patient testifies that she chose the procedure recommended by her physician. Thus, the doctor may be held accountable if something goes wrong with a riskier procedure.
If the physician wants to use informed consent as a defense, he or she should consider giving all patients articles about the various procedures so a woman cannot complain she was inadequately informed.
MR. NEWMAN: In a case like this, the plaintiff’s attorney likely would focus on documentation in the operative report as well as in the operative, anesthesia, postoperativecare, and pathology records.
Does the case have merit?
It depends on the type of injury and when it was found.
The location, size, and nature of the perforation, as described by pathology, may be pivotal in determining whether this case has merit. If the perforation can be described as a hole, tear, or laceration and is larger than a few millimeters, the doctor will have a harder time defending this case, since no perforation was discovered at surgery or before the patient’s discharge.
Following the surgery, all health-care providers should document abdominal examinations and findings at regular intervals, and should note that the patient was assessed and offered no complaints of nausea, vomiting, abdominal pain, or fever.
Should a perforation occur, finding and repairing it at the time of the original surgery is critical in preventing a lawsuit, since, in these cases, no additional injuries would be sustained by the patient—hence, no legally cognizable damages.
DR. LINDHEIM:Is our liability different if a bowel perforation is detected postopera-tively within the standard of care?
MR. WEITZ: Some physicians do not believe perforation of the bowel itself is negligent, but a failure to identify and remedy it prior to completing the original procedure is.
Of course, the timing of identifying the bowel perforation after surgery may determine whether any damage can be attributed to the delay. If the perforation is identified soon after surgery and easily repaired, it will not be easy for the patient to establish a case of additional harm.
Listen to a patient’s complaints
Another important point: Many plaintiffs complain that when they called their physician with postoperative complaints, they were ignored. One of the best liability-avoidance measures is to actively listen to patients and be responsive to their needs, even if treatment will remain the same.
As for the use of photos and video as defense, wholesale reliance on them and pathology reports is risky. Depending on how this evidence is presented, a jury may conclude the physician chose not to photograph the site where the injury occurred or intentionally took tissue samples from a different area. If a jury senses a cover-up, the defense can be undermined.
Case 3: air embolism
“Elaine” is a 35-year-old mother of 1 with secondary amenorrhea for 6 months. She delivered her son vaginally at term, but had bleeding 5 weeks postpartum that required D&C for retained placenta. After a hysterosalpingogram reveals severe Asherman’s syndrome, she is scheduled for hysteroscopic adhesiolysis.
At surgery, the cervical canal is serially dilated. On entry into the uterine cavity with a 5-mm hysteroscope, severe adhesions are visible throughout the entire cavity. Through the operating channel of the hysteroscope, a bipolar tip is used for lysis, with saline distending medium.
Shortly into the procedure, the anesthesiologist observes a decrease in oxygen saturation and a drop in end-tidal CO2, as well as hypotension. An air embolism is suspected. The gynecologist immediately stops the procedure while the anesthesiologist repositions Elaine in the left lateral decubitus position and administers 100% oxygen. The cardiac team is called, and Elaine requires invasive monitoring and catheterization of the subclavian vein. She fully recovers within 24 hours and is discharged from the hospital.
Clinical signs of collapse
DR. WILLIAMS: The most common sign of impending cardiovascular collapse is a sudden drop in end-tidal carbon dioxide, as seen in this case. Both the surgeon and the anesthesiologist acted properly.
MR. WEITZ: I assume the procedure was thoroughly discussed with the patient during the consent process, with the risk of gas emboli emphasized, and that this discussion was documented.
Advise the patient of risky techniques
If hysteroscopic placement or repetitive removal and replacement of the hysteroscope can create air bubbles, the physician should clearly document why the patient should be exposed to this risk. Most times, as in this case, there are valid explanations, but without a notation in the record, the physician is exposed to legal risk.
Standards are a double-edged sword
Perhaps industry organizations such as the American College of Obstetricians and Gynecologists should consider creating industry-wide standards for the proper use of hysteroscopes. Even with a negative outcome, including significant injury, it is difficult to prosecute a case when the medical community recognizes that the steps followed by the physician adhered to the standard of care.
Another benefit of industry-wide standards is that they provide practitioners and health-care insurers with a common framework by which to evaluate the necessity and effectiveness of hysteroscopic procedures.
MR. LINDHEIM: There are both positive and negative aspects to standards. When they exist, they increase the level of expectation, usually thought of as a minimum. When this minimum is adhered to, the risk of medicolegal liability is low. But when care deviates from it—regardless of the reason—the patient can argue that malpractice occurred. Conversely, without standards, the physician’s actions are viewed as a “judgment call,” and it is harder to argue that a deviation occurred.
Dr. Lindheim is a speaker and nonpaid consultant for Cooper-Surgical. The other panelists report no relevant financial relationships.
IN THIS ARTICLE
- Managing and minimizing operative complications
Over the course of our careers, at least 75% of Ob/Gyns will have 1 or more medical liability claims filed against us. This naturally makes us cautious, sometimes overly so.
Though hysteroscopy is usually an effective—as well as safe—alternative to hysterectomy, many Ob/Gyns have not yet integrated this technology routinely into patient care, partly because of the fear of litigation.
In this roundtable, legal and medical experts comment on ways to minimize legal risks in 3 hypothetical cases.
- Steven R. Lindheim, MD, moderator, is associate professor, department of obstetrics and gynecology, University of Wisconsin Medical School, Madison
- Daniel Williams, MD, is associate professor, department of obstetrics and gynecology, University of Cincinnati College of Medicine
- Ira Newman, Esq, is an attorney at Sanocki, Newman, Turret, LLP, New York City
- Eric H. Weitz, Esq, is an attorney at Layser & Freiwald, PC, Philadelphia
- Jerry A. Lindheim, Esq, is an attorney at Locks Law Firm, Philadelphia
Case 1: fluid overload
“Abby” is a 30-year-old nulligravida who presents with menometorrhagia and symptomatic anemia. Sonohysterography reveals a 3-cm submucous fibroid. After 3 months of pretreatment with a GnRH agonist to decrease the size of the fibroid and relieve her anemia, Abby undergoes hysteroscopic resection of the fibroid with a monopolar instrument and 1.5% glycine as the distention medium. The surgery is prolonged, and the fluid deficit at the end of the case is 1,700 mL.
Serial labs are drawn in the recovery room, and Abby is hospitalized overnight for observation. Her fluid intake is restricted and a diuretic is administered. The next day her electrolytes are normal, and she is discharged from the hospital.
When assessing clinical risk, watch fluid deficit, large myomas
DR. LINDHEIM: Clinically speaking, the choice of distention fluid in this case is appropriate, since the surgeon is using monopolar electrical current, and glycine has low molecular viscosity. However, it is imperative to strictly monitor the fluid deficit and, whenever possible, limit infusion pressure to 60 to 75 mm Hg and keep operating time below 1 hour.
Also be aware that larger submucosal myomas may have sizeable venous channels. When these channels are opened during resection, significant fluid intravasation can result.
Dr. Lindheim:As a front-page article in the Wall Street Journal8 observed, a doctor’s best tool in fighting lawsuits may simply be owning up to errors. Yet this concept has been somewhat taboo in the medical community. What are your thoughts on a physician giving a simple apology?
Mr. Lindheim: It is in the heat of passion, usually involving anger, that families seek vindication against a physician simply because the physician wasn’t nice or failed to address questions posed by the family about an unfortunate outcome. In everyday life, when emotion clouds reason, it is hard to think logically and understand complex explanations. When a physician comes across as arrogant at such a time, the patient and her family are often motivated to contact an attorney to evaluate the standard of care.
Of course, an unfortunate outcome is not always the result of medical negligence. This is difficult to explain to a family angered by a doctor’s “attitude.” An apology may somewhat soothe the anger that drives many lawsuits, but it may not be enough to deflect litigation unless the physician is prepared to take responsibility for the adverse outcome.
Mr. Newman: Patients usually seek the advice of a lawyer out of anger or mistrust. They may believe their doctor has been evasive or inaccessible.
In cases where medical negligence may have caused injury to the patient, or complications associated with the nature of the procedure result in injury, it is my opinion that the treating doctor should forthrightly address any questions and concerns the patient has. This includes making oneself available in person or by telephone on a daily basis. In fact, picking up the phone and calling a patient who feels “wronged” may be the single most effective tool the doctor has to prevent a medical malpractice lawsuit.
Complications associated with glycine solution include water intoxication with hypervolemia and hyponatremia. Once a fluid deficit reaches 750 mL, the surgeon should check electrolytes, give a diuretic, and complete the procedure as soon as possible. When deficits exceed 1,500 mL, stop the procedure immediately (assuming adequate hemostasis) and give another diuretic.
When using bipolar technology, isotonic distention media is suitable, and the deficit can safely reach up to 2,000 mL.1-3
Managing water intoxication
Treating patients with water intoxication involves removing excess fluid and correcting serum sodium levels.
Some experts have argued the case for expectant management, which consists of water restriction and spontaneous diuresis. Others counter that patients with severe hyponatremia warrant immediate therapy, since they can deteriorate rapidly with little warning of seizures and respiratory arrest.
Legal outlook: Informed consent, thorough documentation are key
MR. LINDHEIM: I assume a proper informed consent document has been signed. Only the risks and complications listed on that document can be assumed to have the patient’s consent.
To avoid a claim associated with the consent process, the form should describe the exact procedure and alternatives, as well as the potential risks and complications, and it should be signed by the patient. Remember that informed consent is not just the physician’s recitation of this information, but the patient’s articulation of her understanding in response.
In this case, the facts surrounding all events should be well documented. The OR nurse should record the time, amount, and concentration of distention media given, preferably initialized by the person actually administering the medium. If this is not possible, the nurse should note that she was present at the time of administration and observed the medium being given. If a nurse or physician is later asked to explain what medications or fluids were administered, and this information was not documented, it opens the door to fanciful speculation on their part and cross-examination by the plaintiff’s attorney.
FIGURE Which complications are most common? Bleeding and perforation lead the pack, but others warrant vigilance, too
Do not attempt to insert these entries later. Handwriting specialists and other experts can detect when a record has been altered. Never try to change entries or erase them—by hand or using correction fluid. The chart is the first thing the plaintiff’s attorney will request and receive once a suit is initiated. Tampering with it is a surefire way to incur punitive damages.
Since this patient was kept for observation, the reasons for doing so may warrant an entry (eg, to monitor fluid intake and output [I/O]). If serial labs are drawn, each one should find its way into the chart.
Thorough recordkeeping is essential. Any time an item is lost or not included, the plaintiff’s attorney will argue that something is being hidden. Fluid levels are just as important as lab studies. Make sure the I/O chart is properly filled in, especially when fluid overload could give rise to litigation. These I/O sheets and medication (diuretic) forms should include the time of each assessment or administration.
Key ingredients of informed consent
DR. WILLIAMS: Could you describe an adequate informed consent form?
MR. LINDHEIM: In general, the body of the document should list all benefits and risks of the procedure, including anesthetic risk, infection, injury to organs and the need to repair them surgically, fluid overload and specific complications related to the type of distention media to be used, air emboli and their treatment, and long-term complications such as scarring and infertility.
Consent forms are usually signed at the end of the document, but you may want to insert a line next to each risk for initialing or signing by the patient, as well as a witnessing line at the end. This would make it clear the patient agreed to the procedure and was aware of all benefits and risks, and would present a strong defense to a later claim of lack of consent. I also recommend a notation in the progress records reemphasizing the consent process.
Provide patient-education articles
MR. WEITZ: Another effective technique is to mail or provide the woman with patient-oriented articles about the procedure and risks. Since most patients undergo hysteroscopy on a scheduled basis rather than emergently, they have an opportunity to read these articles before signing the consent form. Reference to these materials in the form is also an effective way to minimize medicolegal risk.
Factors leading to litigation
DR. LINDHEIM: Under what conditions would a legal action be initiated?
MR. WEITZ: All negligence claims require 4 elements:
- duty arising out of the physician-patient relationship,
- a breach of that duty (ie, deviation from the accepted standard of care),
- a link between that breach of duty and
- a specific harm.
MR. NEWMAN:In this case I believe the standards of care have been met. There is no legal case here.
MR. WEITZ: I agree. The complications that occurred did not result from deviation from the standard of care, but from the patient’s reaction to the procedure.
Should a law firm decide to proceed with this case, which seems doubtful, it would be hard to show any damage the patient suffered as a result of any alleged improper conduct.
Case 2: later finding of bowel injury
“Cathy” is a 40-year-old mother of 2 who is found to have a 10-mm polyp as part of her evaluation for abnormal uterine bleeding. She is scheduled to undergo hysteroscopic removal of the polyp with endometrial ablation. However, her uterus is severely retroverted, making serial cervical dilation necessary for entry. During the surgery, a pressure of 90 mm Hg is required for optimum visualization. The polyp is easily removed with a grasping instrument, and endometrial ablation is performed with a monopolar rollerball using 2.7% sorbitol for distention. Cathy is discharged the same day without complications.
Two days after the surgery, she calls with complaints of nausea, vomiting, and abdominal distention. She is told to go to the emergency room, where upright abdominal radiography shows free air in the abdomen. Cathy undergoes an exploratory laparotomy for small bowel perforation with end-to-end anastomosis and is discharged 1 week later without sequelae.
Factors that raise risk of perforation
DR. WILLIAMS: Uterine perforation is the most common complication of operative hysteroscopy. It is especially likely with cervical stenosis or severe anteflexion or retroflexion of the uterus; with lower-segment myomas or intrauterine synechiae; and when the operator is inexperienced.3-5
When perforation occurs without an electrical source, hysteroscopy usually is discontinued because of the inability to achieve uterine distention.
Terminate the procedure even if the perforation is small and distention is possible, since fluid will be lost into the peritoneal cavity. Usually, the patient can be observed and discharged home if there is no vaginal or intraperitoneal bleeding.3,4
When perforation occurs during use of electrical energy, laparoscopy is advised to rule out bowel injury.
Patients with unrecognized bowel injury after hysteroscopy frequently are not symptomatic until 2 to 10 days after the procedure due to the thermal nature of the injury, as this case illustrates.
Value of a photographic record
In this case, unrecognized perforation with later bowel injury could raise questions about adequate visualization throughout the case. Use of video or photography may be helpful to document that visualization.
Bowel injury also can occur in the absence of uterine perforation. With lower coagulating currents, it may take longer to achieve the desired endometrial effect, and this can sometimes lead to transmural thermal damage. This heat effect has been reported to cause bowel injury.6,7
Justify procedures in advance
DR. LINDHEIM:An expert also might question whether the ablation was necessary. Was the option of doing a simple polypectomy versus doing both a polypectomy and ablation discussed and documented?
DR. WILLIAMS: With such a small polyp, it was reasonable to perform the ablation, provided consent was given and recorded.
DR. LINDHEIM: What is the legal perspective on this issue?
MR. LINDHEIM: The physician will have to explain why it was necessary to perform an ablation when the treatment possibly required only simple polyp removal. Is it documented that the patient was refractory to medical therapy?
Whenever surgery entails any complication or additional procedures that could have been treated with simpler, less invasive methods, the surgeon is exposed to scrutiny, questioning, and accountability. For this reason, more is better than less when it comes to documentation.
MR. WEITZ: Most juries weighing treatment options are sympathetic when the patient testifies that she chose the procedure recommended by her physician. Thus, the doctor may be held accountable if something goes wrong with a riskier procedure.
If the physician wants to use informed consent as a defense, he or she should consider giving all patients articles about the various procedures so a woman cannot complain she was inadequately informed.
MR. NEWMAN: In a case like this, the plaintiff’s attorney likely would focus on documentation in the operative report as well as in the operative, anesthesia, postoperativecare, and pathology records.
Does the case have merit?
It depends on the type of injury and when it was found.
The location, size, and nature of the perforation, as described by pathology, may be pivotal in determining whether this case has merit. If the perforation can be described as a hole, tear, or laceration and is larger than a few millimeters, the doctor will have a harder time defending this case, since no perforation was discovered at surgery or before the patient’s discharge.
Following the surgery, all health-care providers should document abdominal examinations and findings at regular intervals, and should note that the patient was assessed and offered no complaints of nausea, vomiting, abdominal pain, or fever.
Should a perforation occur, finding and repairing it at the time of the original surgery is critical in preventing a lawsuit, since, in these cases, no additional injuries would be sustained by the patient—hence, no legally cognizable damages.
DR. LINDHEIM:Is our liability different if a bowel perforation is detected postopera-tively within the standard of care?
MR. WEITZ: Some physicians do not believe perforation of the bowel itself is negligent, but a failure to identify and remedy it prior to completing the original procedure is.
Of course, the timing of identifying the bowel perforation after surgery may determine whether any damage can be attributed to the delay. If the perforation is identified soon after surgery and easily repaired, it will not be easy for the patient to establish a case of additional harm.
Listen to a patient’s complaints
Another important point: Many plaintiffs complain that when they called their physician with postoperative complaints, they were ignored. One of the best liability-avoidance measures is to actively listen to patients and be responsive to their needs, even if treatment will remain the same.
As for the use of photos and video as defense, wholesale reliance on them and pathology reports is risky. Depending on how this evidence is presented, a jury may conclude the physician chose not to photograph the site where the injury occurred or intentionally took tissue samples from a different area. If a jury senses a cover-up, the defense can be undermined.
Case 3: air embolism
“Elaine” is a 35-year-old mother of 1 with secondary amenorrhea for 6 months. She delivered her son vaginally at term, but had bleeding 5 weeks postpartum that required D&C for retained placenta. After a hysterosalpingogram reveals severe Asherman’s syndrome, she is scheduled for hysteroscopic adhesiolysis.
At surgery, the cervical canal is serially dilated. On entry into the uterine cavity with a 5-mm hysteroscope, severe adhesions are visible throughout the entire cavity. Through the operating channel of the hysteroscope, a bipolar tip is used for lysis, with saline distending medium.
Shortly into the procedure, the anesthesiologist observes a decrease in oxygen saturation and a drop in end-tidal CO2, as well as hypotension. An air embolism is suspected. The gynecologist immediately stops the procedure while the anesthesiologist repositions Elaine in the left lateral decubitus position and administers 100% oxygen. The cardiac team is called, and Elaine requires invasive monitoring and catheterization of the subclavian vein. She fully recovers within 24 hours and is discharged from the hospital.
Clinical signs of collapse
DR. WILLIAMS: The most common sign of impending cardiovascular collapse is a sudden drop in end-tidal carbon dioxide, as seen in this case. Both the surgeon and the anesthesiologist acted properly.
MR. WEITZ: I assume the procedure was thoroughly discussed with the patient during the consent process, with the risk of gas emboli emphasized, and that this discussion was documented.
Advise the patient of risky techniques
If hysteroscopic placement or repetitive removal and replacement of the hysteroscope can create air bubbles, the physician should clearly document why the patient should be exposed to this risk. Most times, as in this case, there are valid explanations, but without a notation in the record, the physician is exposed to legal risk.
Standards are a double-edged sword
Perhaps industry organizations such as the American College of Obstetricians and Gynecologists should consider creating industry-wide standards for the proper use of hysteroscopes. Even with a negative outcome, including significant injury, it is difficult to prosecute a case when the medical community recognizes that the steps followed by the physician adhered to the standard of care.
Another benefit of industry-wide standards is that they provide practitioners and health-care insurers with a common framework by which to evaluate the necessity and effectiveness of hysteroscopic procedures.
MR. LINDHEIM: There are both positive and negative aspects to standards. When they exist, they increase the level of expectation, usually thought of as a minimum. When this minimum is adhered to, the risk of medicolegal liability is low. But when care deviates from it—regardless of the reason—the patient can argue that malpractice occurred. Conversely, without standards, the physician’s actions are viewed as a “judgment call,” and it is harder to argue that a deviation occurred.
Dr. Lindheim is a speaker and nonpaid consultant for Cooper-Surgical. The other panelists report no relevant financial relationships.
1. Bradley LD. Cutting the risk of hysteroscopic complications. OBG Management. 2004;16(1):44-52.
2. Witz CA, Silverberg KM, Burns WN, Schenken RS, Olive DL. Complications associated with the absorption of hysteroscopic fluid media. Fertil Steril. 1993;60:745-756.
3. Isaacson KB. Complications of hysteroscopy. Obstet Gynecol Clin North Am. 1999;26:39-51.
4. Cooper JM, Brady RM. Intraoperative and early postoperative complications of operative hysteroscopy. Obstet Gynecol Clin North Am. 2000;27:347-366.
5. Jansen FW, Vredevoogd CB, Van Ulzen K, Hermans J, Trimbos JB, Trimbos-Kemper TCM. Complications of hysteroscopy: a prospective, multicenter study. Obstet Gynecol. 2000;96:266-270.
6. Perry CP, Daniell JF, Gimpelson RJ. Bowel injury from Nd:YAG endometrial ablation. J Gynecol Surg. 1990;6:199-203.
7. Kivnick S, Kanter MH. Bowel injury from rollerball ablation of the endometrium. Obstet Gynecol. 1992;79:833-834.
8. Doctors’ new tool to fight lawsuits: saying “I’m sorry.” Wall Street Journal. May 18, 2004; page A1.
1. Bradley LD. Cutting the risk of hysteroscopic complications. OBG Management. 2004;16(1):44-52.
2. Witz CA, Silverberg KM, Burns WN, Schenken RS, Olive DL. Complications associated with the absorption of hysteroscopic fluid media. Fertil Steril. 1993;60:745-756.
3. Isaacson KB. Complications of hysteroscopy. Obstet Gynecol Clin North Am. 1999;26:39-51.
4. Cooper JM, Brady RM. Intraoperative and early postoperative complications of operative hysteroscopy. Obstet Gynecol Clin North Am. 2000;27:347-366.
5. Jansen FW, Vredevoogd CB, Van Ulzen K, Hermans J, Trimbos JB, Trimbos-Kemper TCM. Complications of hysteroscopy: a prospective, multicenter study. Obstet Gynecol. 2000;96:266-270.
6. Perry CP, Daniell JF, Gimpelson RJ. Bowel injury from Nd:YAG endometrial ablation. J Gynecol Surg. 1990;6:199-203.
7. Kivnick S, Kanter MH. Bowel injury from rollerball ablation of the endometrium. Obstet Gynecol. 1992;79:833-834.
8. Doctors’ new tool to fight lawsuits: saying “I’m sorry.” Wall Street Journal. May 18, 2004; page A1.
Aromatase inhibitors and breast cancer? Don’t write off tamoxifen
What are the findings of 3 large randomized, controlled trials on adjuvant use of aromatase inhibitors?
Results
All 3 trials found improved disease-free survival with aromatase inhibitors in women with early-stage breast carcinoma, compared with tamoxifen.
Expert commentary
Each aromatase inhibitor should be offered in clinical scenarios similar to those in the studies, the investigators concluded from their analysis. Each of the 3 trials focused on a single aromatase inhibitor:
- Anastrozole: 4-year disease-free survival of 86.9%, versus 84.5% in the tamoxifen group. Arimidex, Tamoxifen Alone or in Combination study
- Exemestane: 3-year disease-free survival of 91.5% for women already disease-free after 2 to 3 years of tamoxifen, versus 86.8% with 3 years of additional tamoxifen. Intergroup Exemestane Study
- Letrozole: 4-year survival of 93% for women who had completed 5 years of tamoxifen, versus 87% for no further treatment. MA-17 trial
Too little long-term data
Morandi and colleagues acknowledge the immaturity of their safety data, but give short shrift to osteoporotic fractures. With more and more women diagnosed with stage I—and even stage 0—breast tumors, I believe we must consider long-term safety data, especially in terms of osteoporotic fractures, before we make a wholesale change from selective estrogen receptor modulators (ie, tamoxifen) to aromatase inhibitors.
Match the patient to the study
While aromatase inhibitors are clearly superior in women with advanced breast cancer and probably superior in women at highest risk of recurrence, I am concerned about using them in women at extremely low risk for recurrence or mortality. We must make certain, however, that the patient we are treating has the same characteristics as the patients in the study upon which we are basing our management.
Furthermore, the American Society of Clinical Oncology Technology Assessment Working Group1,2 found that the evidence of tamoxifen’s safety and efficacy is “compelling, extensive, and long-term.” When it came to anastrozole, however, they found “extensive supporting data very promising, but insufficient to change the standard of practice at this time.”
Bottom line
A 5-year course of adjuvant tamoxifen remains the standard for women with hormone-receptor–positive breast cancer.
1. Winer EP, Hudis C, Burstein HJ, et al. American Society of Clinical Oncology technology assessment on the use of aromatase inhibitors as adjuvant therapy for women with hormone receptor-positive breast cancer: status report 2002. J Clin Oncol. 2002;20:3317-3327.
2. Winer EP, Hudis C, Burstein HJ, et al. American Society of Clinical Oncology technology assessment working group update: use of aromatase inhibitors in the adjuvant setting. J Clin Oncol. 2003;21:2597-2599.
What are the findings of 3 large randomized, controlled trials on adjuvant use of aromatase inhibitors?
Results
All 3 trials found improved disease-free survival with aromatase inhibitors in women with early-stage breast carcinoma, compared with tamoxifen.
Expert commentary
Each aromatase inhibitor should be offered in clinical scenarios similar to those in the studies, the investigators concluded from their analysis. Each of the 3 trials focused on a single aromatase inhibitor:
- Anastrozole: 4-year disease-free survival of 86.9%, versus 84.5% in the tamoxifen group. Arimidex, Tamoxifen Alone or in Combination study
- Exemestane: 3-year disease-free survival of 91.5% for women already disease-free after 2 to 3 years of tamoxifen, versus 86.8% with 3 years of additional tamoxifen. Intergroup Exemestane Study
- Letrozole: 4-year survival of 93% for women who had completed 5 years of tamoxifen, versus 87% for no further treatment. MA-17 trial
Too little long-term data
Morandi and colleagues acknowledge the immaturity of their safety data, but give short shrift to osteoporotic fractures. With more and more women diagnosed with stage I—and even stage 0—breast tumors, I believe we must consider long-term safety data, especially in terms of osteoporotic fractures, before we make a wholesale change from selective estrogen receptor modulators (ie, tamoxifen) to aromatase inhibitors.
Match the patient to the study
While aromatase inhibitors are clearly superior in women with advanced breast cancer and probably superior in women at highest risk of recurrence, I am concerned about using them in women at extremely low risk for recurrence or mortality. We must make certain, however, that the patient we are treating has the same characteristics as the patients in the study upon which we are basing our management.
Furthermore, the American Society of Clinical Oncology Technology Assessment Working Group1,2 found that the evidence of tamoxifen’s safety and efficacy is “compelling, extensive, and long-term.” When it came to anastrozole, however, they found “extensive supporting data very promising, but insufficient to change the standard of practice at this time.”
Bottom line
A 5-year course of adjuvant tamoxifen remains the standard for women with hormone-receptor–positive breast cancer.
What are the findings of 3 large randomized, controlled trials on adjuvant use of aromatase inhibitors?
Results
All 3 trials found improved disease-free survival with aromatase inhibitors in women with early-stage breast carcinoma, compared with tamoxifen.
Expert commentary
Each aromatase inhibitor should be offered in clinical scenarios similar to those in the studies, the investigators concluded from their analysis. Each of the 3 trials focused on a single aromatase inhibitor:
- Anastrozole: 4-year disease-free survival of 86.9%, versus 84.5% in the tamoxifen group. Arimidex, Tamoxifen Alone or in Combination study
- Exemestane: 3-year disease-free survival of 91.5% for women already disease-free after 2 to 3 years of tamoxifen, versus 86.8% with 3 years of additional tamoxifen. Intergroup Exemestane Study
- Letrozole: 4-year survival of 93% for women who had completed 5 years of tamoxifen, versus 87% for no further treatment. MA-17 trial
Too little long-term data
Morandi and colleagues acknowledge the immaturity of their safety data, but give short shrift to osteoporotic fractures. With more and more women diagnosed with stage I—and even stage 0—breast tumors, I believe we must consider long-term safety data, especially in terms of osteoporotic fractures, before we make a wholesale change from selective estrogen receptor modulators (ie, tamoxifen) to aromatase inhibitors.
Match the patient to the study
While aromatase inhibitors are clearly superior in women with advanced breast cancer and probably superior in women at highest risk of recurrence, I am concerned about using them in women at extremely low risk for recurrence or mortality. We must make certain, however, that the patient we are treating has the same characteristics as the patients in the study upon which we are basing our management.
Furthermore, the American Society of Clinical Oncology Technology Assessment Working Group1,2 found that the evidence of tamoxifen’s safety and efficacy is “compelling, extensive, and long-term.” When it came to anastrozole, however, they found “extensive supporting data very promising, but insufficient to change the standard of practice at this time.”
Bottom line
A 5-year course of adjuvant tamoxifen remains the standard for women with hormone-receptor–positive breast cancer.
1. Winer EP, Hudis C, Burstein HJ, et al. American Society of Clinical Oncology technology assessment on the use of aromatase inhibitors as adjuvant therapy for women with hormone receptor-positive breast cancer: status report 2002. J Clin Oncol. 2002;20:3317-3327.
2. Winer EP, Hudis C, Burstein HJ, et al. American Society of Clinical Oncology technology assessment working group update: use of aromatase inhibitors in the adjuvant setting. J Clin Oncol. 2003;21:2597-2599.
1. Winer EP, Hudis C, Burstein HJ, et al. American Society of Clinical Oncology technology assessment on the use of aromatase inhibitors as adjuvant therapy for women with hormone receptor-positive breast cancer: status report 2002. J Clin Oncol. 2002;20:3317-3327.
2. Winer EP, Hudis C, Burstein HJ, et al. American Society of Clinical Oncology technology assessment working group update: use of aromatase inhibitors in the adjuvant setting. J Clin Oncol. 2003;21:2597-2599.
OBG Management ©2005 Dowden Health Media
Pelvic floor exercises really do work
Do pelvic floor muscle exercise regimens improve persistent postnatal stress urinary incontinence, compared to no treatment?
Results
More than 70% of parous women in 2 treatment groups were continent on pad testing, versus 0% in the control group: Pelvic floor muscle rehabilitation, 14 of 20 continent (70%); pelvic floor plus abdominal rehabilitation, 17 of 23 (74%).
Expert Commentary
This well-designed study had important strengths: blinded outcome assessment, randomized design, and a proper control group.
A total of 64 women were randomized to a group that underwent fairly intensive instruction and assistance in pelvic floor muscle exercise (n = 21), a group following a similar physical therapy program plus abdominal training (n = 23), or a control group that received massage but no pelvic floor muscle exercise (n = 20). All subjects had 8 weekly therapy sessions under the supervision of a physiotherapist. The primary endpoint was a 20-minute pad test.
Everybody had a coach
Several weaknesses are notable. First, the setting was highly optimized: Every woman had a personal physiotherapy coach to oversee the rehabilitation program.
The small sample size and the fact that outcomes were reported only 1 week after treatment ended are problematic, as are the strict exclusion criteria, which make results difficult to generalize. Further, some outcomes were reported as “cure” when urine leakage persisted. Why not divide out those who were “dry” versus “improved”?
It is unclear why the authors used “postnatal” in the title, since women were several years remote from delivery. The power calculation is also unclear, as the authors failed to document the effect size they used to derive their needed sample size.
What about the long term?
Short-term results are encouraging, but the more pertinent issue is whether outcomes will persist. Still, with more than 200,000 surgeries performed each year in the United States for female stress incontinence—with their many well-recognized complications—it is encouraging to see such excellent science applied to evaluating nonsurgical care.
Bottom Line
Whenever possible, attempt nonsurgical treatment of persistent stress urinary incontinence. It is less invasive and less expensive than surgery, and stands a good chance of easing a patient’s symptoms.
Do pelvic floor muscle exercise regimens improve persistent postnatal stress urinary incontinence, compared to no treatment?
Results
More than 70% of parous women in 2 treatment groups were continent on pad testing, versus 0% in the control group: Pelvic floor muscle rehabilitation, 14 of 20 continent (70%); pelvic floor plus abdominal rehabilitation, 17 of 23 (74%).
Expert Commentary
This well-designed study had important strengths: blinded outcome assessment, randomized design, and a proper control group.
A total of 64 women were randomized to a group that underwent fairly intensive instruction and assistance in pelvic floor muscle exercise (n = 21), a group following a similar physical therapy program plus abdominal training (n = 23), or a control group that received massage but no pelvic floor muscle exercise (n = 20). All subjects had 8 weekly therapy sessions under the supervision of a physiotherapist. The primary endpoint was a 20-minute pad test.
Everybody had a coach
Several weaknesses are notable. First, the setting was highly optimized: Every woman had a personal physiotherapy coach to oversee the rehabilitation program.
The small sample size and the fact that outcomes were reported only 1 week after treatment ended are problematic, as are the strict exclusion criteria, which make results difficult to generalize. Further, some outcomes were reported as “cure” when urine leakage persisted. Why not divide out those who were “dry” versus “improved”?
It is unclear why the authors used “postnatal” in the title, since women were several years remote from delivery. The power calculation is also unclear, as the authors failed to document the effect size they used to derive their needed sample size.
What about the long term?
Short-term results are encouraging, but the more pertinent issue is whether outcomes will persist. Still, with more than 200,000 surgeries performed each year in the United States for female stress incontinence—with their many well-recognized complications—it is encouraging to see such excellent science applied to evaluating nonsurgical care.
Bottom Line
Whenever possible, attempt nonsurgical treatment of persistent stress urinary incontinence. It is less invasive and less expensive than surgery, and stands a good chance of easing a patient’s symptoms.
Do pelvic floor muscle exercise regimens improve persistent postnatal stress urinary incontinence, compared to no treatment?
Results
More than 70% of parous women in 2 treatment groups were continent on pad testing, versus 0% in the control group: Pelvic floor muscle rehabilitation, 14 of 20 continent (70%); pelvic floor plus abdominal rehabilitation, 17 of 23 (74%).
Expert Commentary
This well-designed study had important strengths: blinded outcome assessment, randomized design, and a proper control group.
A total of 64 women were randomized to a group that underwent fairly intensive instruction and assistance in pelvic floor muscle exercise (n = 21), a group following a similar physical therapy program plus abdominal training (n = 23), or a control group that received massage but no pelvic floor muscle exercise (n = 20). All subjects had 8 weekly therapy sessions under the supervision of a physiotherapist. The primary endpoint was a 20-minute pad test.
Everybody had a coach
Several weaknesses are notable. First, the setting was highly optimized: Every woman had a personal physiotherapy coach to oversee the rehabilitation program.
The small sample size and the fact that outcomes were reported only 1 week after treatment ended are problematic, as are the strict exclusion criteria, which make results difficult to generalize. Further, some outcomes were reported as “cure” when urine leakage persisted. Why not divide out those who were “dry” versus “improved”?
It is unclear why the authors used “postnatal” in the title, since women were several years remote from delivery. The power calculation is also unclear, as the authors failed to document the effect size they used to derive their needed sample size.
What about the long term?
Short-term results are encouraging, but the more pertinent issue is whether outcomes will persist. Still, with more than 200,000 surgeries performed each year in the United States for female stress incontinence—with their many well-recognized complications—it is encouraging to see such excellent science applied to evaluating nonsurgical care.
Bottom Line
Whenever possible, attempt nonsurgical treatment of persistent stress urinary incontinence. It is less invasive and less expensive than surgery, and stands a good chance of easing a patient’s symptoms.
Previous SGA or preterm infant increases stillbirth risk
To investigate the association between small-for-gestational-age (SGA) or preterm birth and subsequent risk of stillbirth.
Results
Odds ratios for subsequent stillbirth were 2.1 (95% confidence interval [CI], 1.6–2.8) in women with a first infant born SGA at term; 3.4 (95% CI, 2.1–5.6) in women with a first infant born SGA between 32 and 36 weeks; and 5.0 (95% CI, 2.5 to 9.8) in women with a first infant born SGA before 32 weeks.
Expert Commentary
In this population-based, retrospective, observational study utilizing the Swedish Birth Registry, which included 410,021 women who delivered first and second consecutive singleton infants between 1983 and 1997, stillbirth rates ranged from 2.4 per 1,000 women who previously delivered an infant of “normal” size to 19.0 per 1,000 women who previously delivered a very preterm, SGA infant.
The association between fetal growth restriction and adverse perinatal outcome, including death, is well known. A recent hospital-based cohort study1 showed that a significant proportion of unexplained antepartum fetal deaths can be related to growth restriction. A population-based study2 found approximately 4 in 10 stillbirths have no known cause; fetal growth restriction comprised more than a third of this group.2 This study shows that risk extends to the second pregnancy, implying a continuum of the underlying condition.
Abnormal uteroplacental and fetoplacental angiogenesis have been implicated in fetal growth restriction and preeclampsia. Randomized trials and meta-analyses provide strong evidence that antepartum fetal surveillance with umbilical arterial Doppler ultrasound in conjunction with fetal heart rate monitoring and biophysical profile can substantially reduce unexplained stillbirths in prenatally recognized growth-restricted fetuses. Surkan et al acknowledge this, and a recent review in this journal3 addressed this issue in terms of clinical practice.
Strengths and weaknesses of the study
The study population included nearly all the births in Sweden over a decade and a half; thus, sampling bias was not an issue.
The main limitation was that it was a retrospective study based on the Birth Registry and therefore could not provide all information relevant to fetal growth restriction and death in utero. Moreover, these databases are often incomplete.
A persistent challenge is our inability to reliably distinguish a baby who is growth-restricted from one who is merely small.
Bottom Line
The birth of an SGA infant in the first pregnancy substantially increases the risk of antepartum fetal death in the subsequent pregnancy. Timely diagnosis of fetal growth restriction and appropriate evidence-based management may reduce this risk.
1. Huang DY, Usher RH, Kramer MS, Yang H, Morin L, Fretts RC. Determinants of unexplained antepartum fetal deaths. Obstet Gynecol. 2000;95:215-221.
2. Kunzel W, Misselwitz B. Unexpected fetal death during pregnancy—a problem of unrecognized fetal disorders during antenatal care? Eur J Obstet Gynecol Reprod Biol. 2003;110 Suppl 1:S86-92.
3. Maulik D, Sicuranza G, Lysikiewicz A, Figueroa R. Fetal growth restriction. OBG Management. 2004;16(6):48-64.
To investigate the association between small-for-gestational-age (SGA) or preterm birth and subsequent risk of stillbirth.
Results
Odds ratios for subsequent stillbirth were 2.1 (95% confidence interval [CI], 1.6–2.8) in women with a first infant born SGA at term; 3.4 (95% CI, 2.1–5.6) in women with a first infant born SGA between 32 and 36 weeks; and 5.0 (95% CI, 2.5 to 9.8) in women with a first infant born SGA before 32 weeks.
Expert Commentary
In this population-based, retrospective, observational study utilizing the Swedish Birth Registry, which included 410,021 women who delivered first and second consecutive singleton infants between 1983 and 1997, stillbirth rates ranged from 2.4 per 1,000 women who previously delivered an infant of “normal” size to 19.0 per 1,000 women who previously delivered a very preterm, SGA infant.
The association between fetal growth restriction and adverse perinatal outcome, including death, is well known. A recent hospital-based cohort study1 showed that a significant proportion of unexplained antepartum fetal deaths can be related to growth restriction. A population-based study2 found approximately 4 in 10 stillbirths have no known cause; fetal growth restriction comprised more than a third of this group.2 This study shows that risk extends to the second pregnancy, implying a continuum of the underlying condition.
Abnormal uteroplacental and fetoplacental angiogenesis have been implicated in fetal growth restriction and preeclampsia. Randomized trials and meta-analyses provide strong evidence that antepartum fetal surveillance with umbilical arterial Doppler ultrasound in conjunction with fetal heart rate monitoring and biophysical profile can substantially reduce unexplained stillbirths in prenatally recognized growth-restricted fetuses. Surkan et al acknowledge this, and a recent review in this journal3 addressed this issue in terms of clinical practice.
Strengths and weaknesses of the study
The study population included nearly all the births in Sweden over a decade and a half; thus, sampling bias was not an issue.
The main limitation was that it was a retrospective study based on the Birth Registry and therefore could not provide all information relevant to fetal growth restriction and death in utero. Moreover, these databases are often incomplete.
A persistent challenge is our inability to reliably distinguish a baby who is growth-restricted from one who is merely small.
Bottom Line
The birth of an SGA infant in the first pregnancy substantially increases the risk of antepartum fetal death in the subsequent pregnancy. Timely diagnosis of fetal growth restriction and appropriate evidence-based management may reduce this risk.
To investigate the association between small-for-gestational-age (SGA) or preterm birth and subsequent risk of stillbirth.
Results
Odds ratios for subsequent stillbirth were 2.1 (95% confidence interval [CI], 1.6–2.8) in women with a first infant born SGA at term; 3.4 (95% CI, 2.1–5.6) in women with a first infant born SGA between 32 and 36 weeks; and 5.0 (95% CI, 2.5 to 9.8) in women with a first infant born SGA before 32 weeks.
Expert Commentary
In this population-based, retrospective, observational study utilizing the Swedish Birth Registry, which included 410,021 women who delivered first and second consecutive singleton infants between 1983 and 1997, stillbirth rates ranged from 2.4 per 1,000 women who previously delivered an infant of “normal” size to 19.0 per 1,000 women who previously delivered a very preterm, SGA infant.
The association between fetal growth restriction and adverse perinatal outcome, including death, is well known. A recent hospital-based cohort study1 showed that a significant proportion of unexplained antepartum fetal deaths can be related to growth restriction. A population-based study2 found approximately 4 in 10 stillbirths have no known cause; fetal growth restriction comprised more than a third of this group.2 This study shows that risk extends to the second pregnancy, implying a continuum of the underlying condition.
Abnormal uteroplacental and fetoplacental angiogenesis have been implicated in fetal growth restriction and preeclampsia. Randomized trials and meta-analyses provide strong evidence that antepartum fetal surveillance with umbilical arterial Doppler ultrasound in conjunction with fetal heart rate monitoring and biophysical profile can substantially reduce unexplained stillbirths in prenatally recognized growth-restricted fetuses. Surkan et al acknowledge this, and a recent review in this journal3 addressed this issue in terms of clinical practice.
Strengths and weaknesses of the study
The study population included nearly all the births in Sweden over a decade and a half; thus, sampling bias was not an issue.
The main limitation was that it was a retrospective study based on the Birth Registry and therefore could not provide all information relevant to fetal growth restriction and death in utero. Moreover, these databases are often incomplete.
A persistent challenge is our inability to reliably distinguish a baby who is growth-restricted from one who is merely small.
Bottom Line
The birth of an SGA infant in the first pregnancy substantially increases the risk of antepartum fetal death in the subsequent pregnancy. Timely diagnosis of fetal growth restriction and appropriate evidence-based management may reduce this risk.
1. Huang DY, Usher RH, Kramer MS, Yang H, Morin L, Fretts RC. Determinants of unexplained antepartum fetal deaths. Obstet Gynecol. 2000;95:215-221.
2. Kunzel W, Misselwitz B. Unexpected fetal death during pregnancy—a problem of unrecognized fetal disorders during antenatal care? Eur J Obstet Gynecol Reprod Biol. 2003;110 Suppl 1:S86-92.
3. Maulik D, Sicuranza G, Lysikiewicz A, Figueroa R. Fetal growth restriction. OBG Management. 2004;16(6):48-64.
1. Huang DY, Usher RH, Kramer MS, Yang H, Morin L, Fretts RC. Determinants of unexplained antepartum fetal deaths. Obstet Gynecol. 2000;95:215-221.
2. Kunzel W, Misselwitz B. Unexpected fetal death during pregnancy—a problem of unrecognized fetal disorders during antenatal care? Eur J Obstet Gynecol Reprod Biol. 2003;110 Suppl 1:S86-92.
3. Maulik D, Sicuranza G, Lysikiewicz A, Figueroa R. Fetal growth restriction. OBG Management. 2004;16(6):48-64.
Weekly fluconazole reduces recurrent candidiasis
To evaluate weekly fluconazole (150 mg orally for 6 months) to prevent recurrent vulvovaginal candidiasis.
Results
Immediately before randomization, all patients had a culture-proven episode of candidiasis, which was successfully treated with 3 doses of fluconazole (150 mg each) given orally at 72-hour intervals. Six months of weekly maintenance followed, with 150 mg fluconazole or placebo.
At the end of 6 months, 13/141 (9%) of the fluconazole group and 91/142 (64%) of the placebo group had suffered recurrent candidiasis (P.001 however of the fluconazole-treated patients who were disease-free after months maintenance fluconazole developed a recurrence over next months.>
Expert commentary
For the gynecologist, recurrent candidiasis is one of those niggling, but pervasive, challenges of practice. But for the woman subject to repeated outbreaks, it is a major obstacle to quality of life, even though episodic antifungal treatment is readily available with or without a visit to the office. As physicians, we just don’t appreciate the negative impact that recurrent candidiasis has on a woman’s daily functioning.
Although prolonged (6-month) antifungal therapy has proven effective against recurrent candidiasis, some women object to the extended use of topical antifungals, and oral therapy with ketoconazole is associated with hepatotoxicity. This study showed that weekly oral fluconazole for 6 months is an effective and acceptably safe way to suppress recurrences. It also leads to a prolonged disease-free interval after treatment in almost half of treated women.
Good study design, but applies mainly to Candida albicans
The strengths of this study lie in the randomized, double-blind, placebo-controlled design and the use of culture to identify and speciate fungal isolates.
However, it should be stressed that the initial treatment to clear active infection (three 150-mg doses of fluconazole every 72 hours) was more intensive than the norm.
Furthermore, since most of these women (94%) had Candida albicans infections, the applicability of these results to non-albicans species is unclear.
Bottom line
Despite frequent recurrences after stopping treatment, maintenance fluconazole prevented most symptomatic episodes of recurrent vulvovaginal candidiasis caused by C. albicans.
To evaluate weekly fluconazole (150 mg orally for 6 months) to prevent recurrent vulvovaginal candidiasis.
Results
Immediately before randomization, all patients had a culture-proven episode of candidiasis, which was successfully treated with 3 doses of fluconazole (150 mg each) given orally at 72-hour intervals. Six months of weekly maintenance followed, with 150 mg fluconazole or placebo.
At the end of 6 months, 13/141 (9%) of the fluconazole group and 91/142 (64%) of the placebo group had suffered recurrent candidiasis (P.001 however of the fluconazole-treated patients who were disease-free after months maintenance fluconazole developed a recurrence over next months.>
Expert commentary
For the gynecologist, recurrent candidiasis is one of those niggling, but pervasive, challenges of practice. But for the woman subject to repeated outbreaks, it is a major obstacle to quality of life, even though episodic antifungal treatment is readily available with or without a visit to the office. As physicians, we just don’t appreciate the negative impact that recurrent candidiasis has on a woman’s daily functioning.
Although prolonged (6-month) antifungal therapy has proven effective against recurrent candidiasis, some women object to the extended use of topical antifungals, and oral therapy with ketoconazole is associated with hepatotoxicity. This study showed that weekly oral fluconazole for 6 months is an effective and acceptably safe way to suppress recurrences. It also leads to a prolonged disease-free interval after treatment in almost half of treated women.
Good study design, but applies mainly to Candida albicans
The strengths of this study lie in the randomized, double-blind, placebo-controlled design and the use of culture to identify and speciate fungal isolates.
However, it should be stressed that the initial treatment to clear active infection (three 150-mg doses of fluconazole every 72 hours) was more intensive than the norm.
Furthermore, since most of these women (94%) had Candida albicans infections, the applicability of these results to non-albicans species is unclear.
Bottom line
Despite frequent recurrences after stopping treatment, maintenance fluconazole prevented most symptomatic episodes of recurrent vulvovaginal candidiasis caused by C. albicans.
To evaluate weekly fluconazole (150 mg orally for 6 months) to prevent recurrent vulvovaginal candidiasis.
Results
Immediately before randomization, all patients had a culture-proven episode of candidiasis, which was successfully treated with 3 doses of fluconazole (150 mg each) given orally at 72-hour intervals. Six months of weekly maintenance followed, with 150 mg fluconazole or placebo.
At the end of 6 months, 13/141 (9%) of the fluconazole group and 91/142 (64%) of the placebo group had suffered recurrent candidiasis (P.001 however of the fluconazole-treated patients who were disease-free after months maintenance fluconazole developed a recurrence over next months.>
Expert commentary
For the gynecologist, recurrent candidiasis is one of those niggling, but pervasive, challenges of practice. But for the woman subject to repeated outbreaks, it is a major obstacle to quality of life, even though episodic antifungal treatment is readily available with or without a visit to the office. As physicians, we just don’t appreciate the negative impact that recurrent candidiasis has on a woman’s daily functioning.
Although prolonged (6-month) antifungal therapy has proven effective against recurrent candidiasis, some women object to the extended use of topical antifungals, and oral therapy with ketoconazole is associated with hepatotoxicity. This study showed that weekly oral fluconazole for 6 months is an effective and acceptably safe way to suppress recurrences. It also leads to a prolonged disease-free interval after treatment in almost half of treated women.
Good study design, but applies mainly to Candida albicans
The strengths of this study lie in the randomized, double-blind, placebo-controlled design and the use of culture to identify and speciate fungal isolates.
However, it should be stressed that the initial treatment to clear active infection (three 150-mg doses of fluconazole every 72 hours) was more intensive than the norm.
Furthermore, since most of these women (94%) had Candida albicans infections, the applicability of these results to non-albicans species is unclear.
Bottom line
Despite frequent recurrences after stopping treatment, maintenance fluconazole prevented most symptomatic episodes of recurrent vulvovaginal candidiasis caused by C. albicans.
Putting new guidelines into practice is easier said than done
The field is still evolving, and it is evolving so rapidly that I believe the changed recommendations may be premature. As our understanding of the high-risk types of human papillomavirus evolves, the time may soon come when exfoliative cytology as we know it may not be the screening method of choice. The introduction of liquid-based Pap smears and reflex high-risk HPV testing has caused tremendous change in how we collect and interpret smears.
But the task of putting new technologies into practice can be somewhat daunting.
Application of the new guidelines depends in part on an accurate sexual history, past and present. Even in this era of awareness and “safe sex,” we often cannot pinpoint at what age a patient became sexually active or whether her history includes multiple partners. Furthermore, use of Viagra among men, and the soon-to-be available testosterone patch for women mean we cannot assume that our graying population is sexually inactive, monogamous, or “safe.” To apply the guidelines consistently, we may need to adjust our own thinking and recognize today’s realities.
Patients need a clear message
But most important is the mixed message to patients. As Dr. Waxman acknowledges, patients have come to equate their annual visit with a Pap test—evidence of a successful public awareness effort since 1975, when an ACOG Technical Bulletin recommended the annual test. Every clinician would agree with Dr. Waxman that we must teach our patients that the value of the annual exam is not limited to cervical cytology screening.
But that is easier said than done. A massive campaign to raise awareness of the importance of annual exams is needed before we can expect patients to be comfortable with less frequent Pap testing.
As with most controversies, the answer probably lies somewhere in the middle.
Tell patients: Don’t stop annual exams
I use a hybrid approach. For a patient who has no history of cervical disease, I suggest that we forgo the Pap test for 1 year if she is older than 65 and sexually inactive, or, if she is younger than 65 and sexually active with a single partner.
However, I carefully point out to these patients that, although their risk is low, their annual visit is still important.
The field is still evolving, and it is evolving so rapidly that I believe the changed recommendations may be premature. As our understanding of the high-risk types of human papillomavirus evolves, the time may soon come when exfoliative cytology as we know it may not be the screening method of choice. The introduction of liquid-based Pap smears and reflex high-risk HPV testing has caused tremendous change in how we collect and interpret smears.
But the task of putting new technologies into practice can be somewhat daunting.
Application of the new guidelines depends in part on an accurate sexual history, past and present. Even in this era of awareness and “safe sex,” we often cannot pinpoint at what age a patient became sexually active or whether her history includes multiple partners. Furthermore, use of Viagra among men, and the soon-to-be available testosterone patch for women mean we cannot assume that our graying population is sexually inactive, monogamous, or “safe.” To apply the guidelines consistently, we may need to adjust our own thinking and recognize today’s realities.
Patients need a clear message
But most important is the mixed message to patients. As Dr. Waxman acknowledges, patients have come to equate their annual visit with a Pap test—evidence of a successful public awareness effort since 1975, when an ACOG Technical Bulletin recommended the annual test. Every clinician would agree with Dr. Waxman that we must teach our patients that the value of the annual exam is not limited to cervical cytology screening.
But that is easier said than done. A massive campaign to raise awareness of the importance of annual exams is needed before we can expect patients to be comfortable with less frequent Pap testing.
As with most controversies, the answer probably lies somewhere in the middle.
Tell patients: Don’t stop annual exams
I use a hybrid approach. For a patient who has no history of cervical disease, I suggest that we forgo the Pap test for 1 year if she is older than 65 and sexually inactive, or, if she is younger than 65 and sexually active with a single partner.
However, I carefully point out to these patients that, although their risk is low, their annual visit is still important.
The field is still evolving, and it is evolving so rapidly that I believe the changed recommendations may be premature. As our understanding of the high-risk types of human papillomavirus evolves, the time may soon come when exfoliative cytology as we know it may not be the screening method of choice. The introduction of liquid-based Pap smears and reflex high-risk HPV testing has caused tremendous change in how we collect and interpret smears.
But the task of putting new technologies into practice can be somewhat daunting.
Application of the new guidelines depends in part on an accurate sexual history, past and present. Even in this era of awareness and “safe sex,” we often cannot pinpoint at what age a patient became sexually active or whether her history includes multiple partners. Furthermore, use of Viagra among men, and the soon-to-be available testosterone patch for women mean we cannot assume that our graying population is sexually inactive, monogamous, or “safe.” To apply the guidelines consistently, we may need to adjust our own thinking and recognize today’s realities.
Patients need a clear message
But most important is the mixed message to patients. As Dr. Waxman acknowledges, patients have come to equate their annual visit with a Pap test—evidence of a successful public awareness effort since 1975, when an ACOG Technical Bulletin recommended the annual test. Every clinician would agree with Dr. Waxman that we must teach our patients that the value of the annual exam is not limited to cervical cytology screening.
But that is easier said than done. A massive campaign to raise awareness of the importance of annual exams is needed before we can expect patients to be comfortable with less frequent Pap testing.
As with most controversies, the answer probably lies somewhere in the middle.
Tell patients: Don’t stop annual exams
I use a hybrid approach. For a patient who has no history of cervical disease, I suggest that we forgo the Pap test for 1 year if she is older than 65 and sexually inactive, or, if she is younger than 65 and sexually active with a single partner.
However, I carefully point out to these patients that, although their risk is low, their annual visit is still important.
Fetal loss linked to excess thyroid hormone
To study the fetal effects of excess maternal thyroid hormone (TH).
Results
Of the 36 couples in this study, 9 included women with TH resistance (RTH) who were euthyroid despite high TH levels, 9 included men with this condition, and 18 were unaffected. Mean miscarriage rates were 22.9%, 2.0%, and 4.4%, respectively. Infants without RTH who were born to mothers with the condition were significantly smaller than infants who shared their mother’s TH status.
Expert Commentary
Animal studies suggest that both hyperand hypothyroidism are associated with increased numbers of malformations and poor reproductive outcomes. In humans, hyperthyroidism is usually associated with thyroid autoantibodies, so it is unclear whether the increased rate of miscarriages seen with this condition is related to the elevated circulating thyroid hormone, to autoantibodies, or to both. To explore this, Anselmo et al took advantage of a “natural experiment” in a large extended family. This family harbored a single gene mutation, inherited autosomally, that made the TH receptor resistant to thyroid hormone.
Women with this mutation have, on average, twice the circulating TH level and normal thyroid-stimulating hormone (TSH). They are clinically euthyroid, without autoantibodies, but elevated TH levels pass to the fetus, which may or may not be genetically affected by the same condition.
Infants with mutation are protected
Anselmo et al found normal birth weight among babies affected by the same mutation as their mother. Presumably, these infants are euthyroid and grow normally despite elevated circulating TH. In contrast, infants who lack the mutation are significantly smaller due to the maternal environment of elevated circulating TH.
Unfortunately, although Anselmo and colleagues performed a thorough and thoughtful analysis, they did not indicate how prevalent this condition is in the general population.
Bottom Line
This study supports other evidence that elevated TH is associated with early fetal loss. This information can be generalized to patients with thyroid disease. Women on thyroid replacement should be monitored to ensure that their TH is in the normal range, and physicians should make every attempt to normalize TH in women with thyrotoxicosis.
To study the fetal effects of excess maternal thyroid hormone (TH).
Results
Of the 36 couples in this study, 9 included women with TH resistance (RTH) who were euthyroid despite high TH levels, 9 included men with this condition, and 18 were unaffected. Mean miscarriage rates were 22.9%, 2.0%, and 4.4%, respectively. Infants without RTH who were born to mothers with the condition were significantly smaller than infants who shared their mother’s TH status.
Expert Commentary
Animal studies suggest that both hyperand hypothyroidism are associated with increased numbers of malformations and poor reproductive outcomes. In humans, hyperthyroidism is usually associated with thyroid autoantibodies, so it is unclear whether the increased rate of miscarriages seen with this condition is related to the elevated circulating thyroid hormone, to autoantibodies, or to both. To explore this, Anselmo et al took advantage of a “natural experiment” in a large extended family. This family harbored a single gene mutation, inherited autosomally, that made the TH receptor resistant to thyroid hormone.
Women with this mutation have, on average, twice the circulating TH level and normal thyroid-stimulating hormone (TSH). They are clinically euthyroid, without autoantibodies, but elevated TH levels pass to the fetus, which may or may not be genetically affected by the same condition.
Infants with mutation are protected
Anselmo et al found normal birth weight among babies affected by the same mutation as their mother. Presumably, these infants are euthyroid and grow normally despite elevated circulating TH. In contrast, infants who lack the mutation are significantly smaller due to the maternal environment of elevated circulating TH.
Unfortunately, although Anselmo and colleagues performed a thorough and thoughtful analysis, they did not indicate how prevalent this condition is in the general population.
Bottom Line
This study supports other evidence that elevated TH is associated with early fetal loss. This information can be generalized to patients with thyroid disease. Women on thyroid replacement should be monitored to ensure that their TH is in the normal range, and physicians should make every attempt to normalize TH in women with thyrotoxicosis.
To study the fetal effects of excess maternal thyroid hormone (TH).
Results
Of the 36 couples in this study, 9 included women with TH resistance (RTH) who were euthyroid despite high TH levels, 9 included men with this condition, and 18 were unaffected. Mean miscarriage rates were 22.9%, 2.0%, and 4.4%, respectively. Infants without RTH who were born to mothers with the condition were significantly smaller than infants who shared their mother’s TH status.
Expert Commentary
Animal studies suggest that both hyperand hypothyroidism are associated with increased numbers of malformations and poor reproductive outcomes. In humans, hyperthyroidism is usually associated with thyroid autoantibodies, so it is unclear whether the increased rate of miscarriages seen with this condition is related to the elevated circulating thyroid hormone, to autoantibodies, or to both. To explore this, Anselmo et al took advantage of a “natural experiment” in a large extended family. This family harbored a single gene mutation, inherited autosomally, that made the TH receptor resistant to thyroid hormone.
Women with this mutation have, on average, twice the circulating TH level and normal thyroid-stimulating hormone (TSH). They are clinically euthyroid, without autoantibodies, but elevated TH levels pass to the fetus, which may or may not be genetically affected by the same condition.
Infants with mutation are protected
Anselmo et al found normal birth weight among babies affected by the same mutation as their mother. Presumably, these infants are euthyroid and grow normally despite elevated circulating TH. In contrast, infants who lack the mutation are significantly smaller due to the maternal environment of elevated circulating TH.
Unfortunately, although Anselmo and colleagues performed a thorough and thoughtful analysis, they did not indicate how prevalent this condition is in the general population.
Bottom Line
This study supports other evidence that elevated TH is associated with early fetal loss. This information can be generalized to patients with thyroid disease. Women on thyroid replacement should be monitored to ensure that their TH is in the normal range, and physicians should make every attempt to normalize TH in women with thyrotoxicosis.
OBG Management ©2004 Dowden Health Media
2 menorrhagia treatments: Which is better?
To compare outcomes, quality of life, and expenses for the levonorgestrel-releasing intrauterine system (LNG-IUS) versus hysterectomy in women with menorrhagia.
Results
After 5 years, the LNG-IUS and hysterectomy groups did not differ substantially in health-related quality of life, psychosocial well-being, or satisfaction with treatment. The LNG-IUS group had significantly lower costs ($2,817 versus $4,660 per woman).
Expert Commentary
This well-executed study compared 119 women who received LNG-IUS with 117 participants who underwent hysterectomy. Follow-up visits took place at 6 months, 12 months, and 5 years after randomization. Enrollment details and 1-year follow-up data were published in 2001.1 At the time of that report, 24 women with the LNG-IUS had undergone hysterectomy (20%).
The current study presents 5-year follow-up data and reports that hysterectomy was ultimately performed in 50 women (42%) originally treated with the LNG-IUS. For comparison, note that 25% of women who undergo myomectomy and approximately 50% of those who undergo endometrial ablation present for hysterectomy within 5 years.
Unanswered questions
Unfortunately, Hurskainen et al provide no information on why the 236 women were enrolled in this protocol, except that they all had menorrhagia. Uterine fibroids and endometrial polyps, for example, cause anatomical abnormal bleeding, and thyroid dysfunction or acquired bleeding diathesis can cause functional bleeding. It would be important to learn that these conditions did not exist in the women prior to the study.
Assessing costs in practical terms
The authors translated medical and hysterectomy expenses into US dollars. However, the cost of hysterectomy in the United States is substantially higher than the figures quoted in the article. Thus, the cost-efficiency of medical therapy is even greater than this study suggests.
In assessing costs cited in the literature, each physician must decide how his or her patients compare to the study population. I suspect that only a few US populations (well-educated, non-obese) would match the women in this trial. Nevertheless, the authors offer an objective report that medical therapy is less expensive.
Bottom Line
This study presents 3 novel facts: (1) Women who accept LNG-IUS must understand that there is a 42% chance they will need hysterectomy within 5 years; (2) the cost reduction with medical therapy in women with menorrhagia is a founded premise; and (3) health-related quality of life is improved during treatment with either medical therapy and hysterectomy.
REFERENCE
1. Hurskainen R, Teperi J, Rissanen P, et al. Quality of life and cost-effectiveness of levonorgestrel-releasing intrauterine system versus hysterectomy for treatment of menorrhagia: a randomized trial. Lancet. 2001;357:273-277.
To compare outcomes, quality of life, and expenses for the levonorgestrel-releasing intrauterine system (LNG-IUS) versus hysterectomy in women with menorrhagia.
Results
After 5 years, the LNG-IUS and hysterectomy groups did not differ substantially in health-related quality of life, psychosocial well-being, or satisfaction with treatment. The LNG-IUS group had significantly lower costs ($2,817 versus $4,660 per woman).
Expert Commentary
This well-executed study compared 119 women who received LNG-IUS with 117 participants who underwent hysterectomy. Follow-up visits took place at 6 months, 12 months, and 5 years after randomization. Enrollment details and 1-year follow-up data were published in 2001.1 At the time of that report, 24 women with the LNG-IUS had undergone hysterectomy (20%).
The current study presents 5-year follow-up data and reports that hysterectomy was ultimately performed in 50 women (42%) originally treated with the LNG-IUS. For comparison, note that 25% of women who undergo myomectomy and approximately 50% of those who undergo endometrial ablation present for hysterectomy within 5 years.
Unanswered questions
Unfortunately, Hurskainen et al provide no information on why the 236 women were enrolled in this protocol, except that they all had menorrhagia. Uterine fibroids and endometrial polyps, for example, cause anatomical abnormal bleeding, and thyroid dysfunction or acquired bleeding diathesis can cause functional bleeding. It would be important to learn that these conditions did not exist in the women prior to the study.
Assessing costs in practical terms
The authors translated medical and hysterectomy expenses into US dollars. However, the cost of hysterectomy in the United States is substantially higher than the figures quoted in the article. Thus, the cost-efficiency of medical therapy is even greater than this study suggests.
In assessing costs cited in the literature, each physician must decide how his or her patients compare to the study population. I suspect that only a few US populations (well-educated, non-obese) would match the women in this trial. Nevertheless, the authors offer an objective report that medical therapy is less expensive.
Bottom Line
This study presents 3 novel facts: (1) Women who accept LNG-IUS must understand that there is a 42% chance they will need hysterectomy within 5 years; (2) the cost reduction with medical therapy in women with menorrhagia is a founded premise; and (3) health-related quality of life is improved during treatment with either medical therapy and hysterectomy.
To compare outcomes, quality of life, and expenses for the levonorgestrel-releasing intrauterine system (LNG-IUS) versus hysterectomy in women with menorrhagia.
Results
After 5 years, the LNG-IUS and hysterectomy groups did not differ substantially in health-related quality of life, psychosocial well-being, or satisfaction with treatment. The LNG-IUS group had significantly lower costs ($2,817 versus $4,660 per woman).
Expert Commentary
This well-executed study compared 119 women who received LNG-IUS with 117 participants who underwent hysterectomy. Follow-up visits took place at 6 months, 12 months, and 5 years after randomization. Enrollment details and 1-year follow-up data were published in 2001.1 At the time of that report, 24 women with the LNG-IUS had undergone hysterectomy (20%).
The current study presents 5-year follow-up data and reports that hysterectomy was ultimately performed in 50 women (42%) originally treated with the LNG-IUS. For comparison, note that 25% of women who undergo myomectomy and approximately 50% of those who undergo endometrial ablation present for hysterectomy within 5 years.
Unanswered questions
Unfortunately, Hurskainen et al provide no information on why the 236 women were enrolled in this protocol, except that they all had menorrhagia. Uterine fibroids and endometrial polyps, for example, cause anatomical abnormal bleeding, and thyroid dysfunction or acquired bleeding diathesis can cause functional bleeding. It would be important to learn that these conditions did not exist in the women prior to the study.
Assessing costs in practical terms
The authors translated medical and hysterectomy expenses into US dollars. However, the cost of hysterectomy in the United States is substantially higher than the figures quoted in the article. Thus, the cost-efficiency of medical therapy is even greater than this study suggests.
In assessing costs cited in the literature, each physician must decide how his or her patients compare to the study population. I suspect that only a few US populations (well-educated, non-obese) would match the women in this trial. Nevertheless, the authors offer an objective report that medical therapy is less expensive.
Bottom Line
This study presents 3 novel facts: (1) Women who accept LNG-IUS must understand that there is a 42% chance they will need hysterectomy within 5 years; (2) the cost reduction with medical therapy in women with menorrhagia is a founded premise; and (3) health-related quality of life is improved during treatment with either medical therapy and hysterectomy.
REFERENCE
1. Hurskainen R, Teperi J, Rissanen P, et al. Quality of life and cost-effectiveness of levonorgestrel-releasing intrauterine system versus hysterectomy for treatment of menorrhagia: a randomized trial. Lancet. 2001;357:273-277.
REFERENCE
1. Hurskainen R, Teperi J, Rissanen P, et al. Quality of life and cost-effectiveness of levonorgestrel-releasing intrauterine system versus hysterectomy for treatment of menorrhagia: a randomized trial. Lancet. 2001;357:273-277.
First-trimester levels of sex hormone binding globulin predict gestational diabetes
To explore the association between first-trimester levels of sex hormone binding globulin (SHBG) and subsequent gestational diabetes mellitus.
Results
SHBG levels were lower among women who subsequently developed gestational diabetes than among those who didn’t (187±82 nmol/L versus 233±92 nmol/L; P .01 for every increase of nmol in shbg the odds gestational diabetes fell by ratio confidence interval>
Expert commentary
Gestational diabetes or glucose intolerance first recognized during pregnancy complicates approximately 4% of all pregnancies, varying by population studied.1 Although the best management strategy for these patients has yet to be determined, particularly for patients with only mildly elevated blood sugars, certain fetal and maternal risks are well documented. For example, women with a history of gestational diabetes face an increased risk for type 2 diabetes, with a lifetime risk of approximately 50%.2
This nested case-control study included 44 women documented to have gestational diabetes in the third trimester by the 2-step screening process (50-g screen followed by a 100-g glucose tolerance test in women with a positive screen of 140 mg/dL), as well as 94 women who had negative screening.
Serum samples that had been collected in the first trimester were examined to determine SHBG levels.
Need for earlier detection
By definition, gestational diabetes includes women who—though they are first diagnosed during pregnancy—may have had varying degrees of glucose intolerance prior to conception.
Therapeutic intervention may benefit these women and their babies. Unfortunately, women traditionally are screened for gestational diabetes between 24 and 28 weeks’ gestation, when many of the metabolic consequences have already occurred. Thus, investigators have attempted to find a method of earlier diagnosis and treatment.
SHBG and insulin resistance
SHBG is a glycoprotein produced by the liver; it binds to circulating estradiol and testosterone. Secretion is suppressed by insulin, and SHBG levels are inversely related to insulin concentrations and insulin resistance. Lower concentrations of SHBG are predictive of the development of type 2 diabetes.3 During pregnancy, SHBG concentrations are lower in women with gestational diabetes and in those who require insulin therapy.4,5
Bottom line
Measuring SHBG levels in the first trimester may allow earlier intervention or identify a population appropriate for earlier diabetes testing. However, although an association has been established between low first-trimester SHBG and the development of gestational diabetes, this marker has not been fully explored as a screening test. A larger prospective study is required to establish optimal cut points of SHBG for predicting gestational diabetes.
1. King H. Epidemiology of glucose intolerance and gestational diabetes in women of childbearing age. Diabetes Care 1998;21:B9-13.
2. Dornhorst A, Rossi M. Risk and prevention of type 2 diabetes in women with gestational diabetes. Diabetes Care. 1998;21:B43-49.
3. Haffner SM, Valdez RA, Morales PA, Hazuda HP, Stern MP. Decreased sex hormone-binding globulin predicts noninsulin-dependent diabetes mellitus in women but not in men. J Clin Endocrinol Metab. 1993;77:56-60.
4. Bartha JL, Comino-Delgado R, Romero-Carmona R, Gomez-Jaen MC. Sex hormone-binding globulin in gestational diabetes. Acta Obstet Gynecol Scand. 2000;79:839-845.
5. Kopp HP, Festa A, Krugluger W, Schernthaner G. Low levels of sex-hormone-binding globulin predict insulin requirement in patients with gestational diabetes mellitus. Exp Clin Endocrinol Diabetes. 2001;109:365-369.
To explore the association between first-trimester levels of sex hormone binding globulin (SHBG) and subsequent gestational diabetes mellitus.
Results
SHBG levels were lower among women who subsequently developed gestational diabetes than among those who didn’t (187±82 nmol/L versus 233±92 nmol/L; P .01 for every increase of nmol in shbg the odds gestational diabetes fell by ratio confidence interval>
Expert commentary
Gestational diabetes or glucose intolerance first recognized during pregnancy complicates approximately 4% of all pregnancies, varying by population studied.1 Although the best management strategy for these patients has yet to be determined, particularly for patients with only mildly elevated blood sugars, certain fetal and maternal risks are well documented. For example, women with a history of gestational diabetes face an increased risk for type 2 diabetes, with a lifetime risk of approximately 50%.2
This nested case-control study included 44 women documented to have gestational diabetes in the third trimester by the 2-step screening process (50-g screen followed by a 100-g glucose tolerance test in women with a positive screen of 140 mg/dL), as well as 94 women who had negative screening.
Serum samples that had been collected in the first trimester were examined to determine SHBG levels.
Need for earlier detection
By definition, gestational diabetes includes women who—though they are first diagnosed during pregnancy—may have had varying degrees of glucose intolerance prior to conception.
Therapeutic intervention may benefit these women and their babies. Unfortunately, women traditionally are screened for gestational diabetes between 24 and 28 weeks’ gestation, when many of the metabolic consequences have already occurred. Thus, investigators have attempted to find a method of earlier diagnosis and treatment.
SHBG and insulin resistance
SHBG is a glycoprotein produced by the liver; it binds to circulating estradiol and testosterone. Secretion is suppressed by insulin, and SHBG levels are inversely related to insulin concentrations and insulin resistance. Lower concentrations of SHBG are predictive of the development of type 2 diabetes.3 During pregnancy, SHBG concentrations are lower in women with gestational diabetes and in those who require insulin therapy.4,5
Bottom line
Measuring SHBG levels in the first trimester may allow earlier intervention or identify a population appropriate for earlier diabetes testing. However, although an association has been established between low first-trimester SHBG and the development of gestational diabetes, this marker has not been fully explored as a screening test. A larger prospective study is required to establish optimal cut points of SHBG for predicting gestational diabetes.
To explore the association between first-trimester levels of sex hormone binding globulin (SHBG) and subsequent gestational diabetes mellitus.
Results
SHBG levels were lower among women who subsequently developed gestational diabetes than among those who didn’t (187±82 nmol/L versus 233±92 nmol/L; P .01 for every increase of nmol in shbg the odds gestational diabetes fell by ratio confidence interval>
Expert commentary
Gestational diabetes or glucose intolerance first recognized during pregnancy complicates approximately 4% of all pregnancies, varying by population studied.1 Although the best management strategy for these patients has yet to be determined, particularly for patients with only mildly elevated blood sugars, certain fetal and maternal risks are well documented. For example, women with a history of gestational diabetes face an increased risk for type 2 diabetes, with a lifetime risk of approximately 50%.2
This nested case-control study included 44 women documented to have gestational diabetes in the third trimester by the 2-step screening process (50-g screen followed by a 100-g glucose tolerance test in women with a positive screen of 140 mg/dL), as well as 94 women who had negative screening.
Serum samples that had been collected in the first trimester were examined to determine SHBG levels.
Need for earlier detection
By definition, gestational diabetes includes women who—though they are first diagnosed during pregnancy—may have had varying degrees of glucose intolerance prior to conception.
Therapeutic intervention may benefit these women and their babies. Unfortunately, women traditionally are screened for gestational diabetes between 24 and 28 weeks’ gestation, when many of the metabolic consequences have already occurred. Thus, investigators have attempted to find a method of earlier diagnosis and treatment.
SHBG and insulin resistance
SHBG is a glycoprotein produced by the liver; it binds to circulating estradiol and testosterone. Secretion is suppressed by insulin, and SHBG levels are inversely related to insulin concentrations and insulin resistance. Lower concentrations of SHBG are predictive of the development of type 2 diabetes.3 During pregnancy, SHBG concentrations are lower in women with gestational diabetes and in those who require insulin therapy.4,5
Bottom line
Measuring SHBG levels in the first trimester may allow earlier intervention or identify a population appropriate for earlier diabetes testing. However, although an association has been established between low first-trimester SHBG and the development of gestational diabetes, this marker has not been fully explored as a screening test. A larger prospective study is required to establish optimal cut points of SHBG for predicting gestational diabetes.
1. King H. Epidemiology of glucose intolerance and gestational diabetes in women of childbearing age. Diabetes Care 1998;21:B9-13.
2. Dornhorst A, Rossi M. Risk and prevention of type 2 diabetes in women with gestational diabetes. Diabetes Care. 1998;21:B43-49.
3. Haffner SM, Valdez RA, Morales PA, Hazuda HP, Stern MP. Decreased sex hormone-binding globulin predicts noninsulin-dependent diabetes mellitus in women but not in men. J Clin Endocrinol Metab. 1993;77:56-60.
4. Bartha JL, Comino-Delgado R, Romero-Carmona R, Gomez-Jaen MC. Sex hormone-binding globulin in gestational diabetes. Acta Obstet Gynecol Scand. 2000;79:839-845.
5. Kopp HP, Festa A, Krugluger W, Schernthaner G. Low levels of sex-hormone-binding globulin predict insulin requirement in patients with gestational diabetes mellitus. Exp Clin Endocrinol Diabetes. 2001;109:365-369.
1. King H. Epidemiology of glucose intolerance and gestational diabetes in women of childbearing age. Diabetes Care 1998;21:B9-13.
2. Dornhorst A, Rossi M. Risk and prevention of type 2 diabetes in women with gestational diabetes. Diabetes Care. 1998;21:B43-49.
3. Haffner SM, Valdez RA, Morales PA, Hazuda HP, Stern MP. Decreased sex hormone-binding globulin predicts noninsulin-dependent diabetes mellitus in women but not in men. J Clin Endocrinol Metab. 1993;77:56-60.
4. Bartha JL, Comino-Delgado R, Romero-Carmona R, Gomez-Jaen MC. Sex hormone-binding globulin in gestational diabetes. Acta Obstet Gynecol Scand. 2000;79:839-845.
5. Kopp HP, Festa A, Krugluger W, Schernthaner G. Low levels of sex-hormone-binding globulin predict insulin requirement in patients with gestational diabetes mellitus. Exp Clin Endocrinol Diabetes. 2001;109:365-369.