User login
Ten Clinical Decisions to Eliminate Wasteful Healthcare Spending
Have you ever prescribed stress ulcer prophylaxis therapy to patients at low risk for gastrointestinal complications? Have you ever repeated CBC or chemistry testing in the face of clinical and lab stability? Have you once or twice ordered bronchodilators for children with bronchiolitis?
If you answered “yes” to any of those questions, you might want to reconsider some of your practices. That’s the message hospitalist leaders have for adult and pediatric HM practitioners interested in curbing wasteful healthcare spending.
SHM has joined the American Board of Internal Medicine (ABIM) Foundation’s Choosing Wisely campaign, a multiyear effort to spark national dialogue about waste in the healthcare system and the kinds of common treatments that doctors and patients should think twice about before deciding to pursue. Ad hoc subcommittees of SHM’s Hospital Quality and Patient Safety Committee created lists of five adult and five pediatric treatments that hospitalists and their patients should question. Those lists were shared alongside 15 other medical specialty societies at a Feb. 21 news conference in Washington, D.C.

Choosing Wisely (www.choosingwisely.org) has been recognized by the professional and consumer media in a big way, says Daniel Wolfson, executive vice president and chief operating officer of the ABIM Foundation, which is affiliated with but distinct from the American Board of Internal Medicine (www.abim.org). “The conversation about overuse is now on the table, and people recognize that it’s an important subject to talk about—without the kind of hysterics that we’ve seen previously around, for example, rationing,” he says. “We’re talking about treatments that are not beneficial and potentially are harmful to patients … things that are ordered for many patients when the benefit does not exceed the risk. These are not absolutes; there are times when a treatment might be indicated because of a certain history or clinical finding. But be clear on what those circumstances are.”
SHM is excited to be a partner in the Choosing Wisely campaign, says Gregory Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Healthcare Improvement and Innovation. With its broad professional and consumer outreach and emphasis on informing and engaging the consumer, the Choosing Wisely effort meshes well with the center’s QI and patient safety goals.
“We acknowledge that there is waste in our system. We also believe that if you have an engaged, empowered patient, together you will make better choices, have less waste, and probably also reduce costs,” Dr. Maynard says.
Developing SHM’s “think twice” lists under a tight deadline was a challenge, says John Bulger, DO, FACP, SFHM, chief quality officer at Geisinger Medical Center in Danville, Pa., and chair of the adult committee. It was especially difficult trying to encourage the broadest possible input from experts in the field. SHM board and committee members were asked for suggested treatments that should be targeted as wasteful, and a preliminary list of 100 was grouped, whittled down, and sent to SHM members to vote on. The committee conducted two blind votes and sent a list of seven recommendations to the SHM board, which made the final choices for submission to the ABIM Foundation.
“The ABIM Foundation has fairly strict guidelines for Choosing Wisely,” Dr. Bulger says. The process was meant to be transparent and well documented, and the SHM committees will publish an article in the Journal of Hospital Medicine describing how its lists were compiled. Choices were to be made based on the evidence for treatments that lie within the specialty’s purview. “Because our practice is so diverse, you can find many core treatments that hospitalists impact on a daily basis and that are unique to the work of hospital medicine,” Dr. Bulger adds.
Fourteen pediatric hospitalists followed a similar process in developing its five suggestions.
“While this issue has been addressed in adult settings, in pediatrics, discussions about waste are almost nonexistent,” says Ricardo Quinonez, MD, FHM, a pediatric hospitalist at Texas Children’s Hospital in Houston and chair of the pediatric ad-hoc committee. “I don’t think anyone was too surprised by our list, which is heavy on respiratory illnesses. That’s what kids get admitted to the hospital for.”

Dr. Quinonez suggests pediatric hospitalists use the list to engage with their specialist colleagues about appropriate treatment choices. “If you want to improve quality, here’s a place to start,” he says.

Dr. Bulger encourages hospitalists to stop and take a long look at the lists and think about ways to improve their own practice. He encourages hospitalists to take the recommendations to their hospitals’ quality-improvement (QI) committees and start collecting baseline data, he says, adding that “we should be able to come back a year from now and show that we’ve been able to change practice using these lists.”
A full-day pre-course, “QI for High Value Healthcare: Making the ABIM Foundation’s Choosing Wisely Campaign a Reality,” co-led by Dr. Bulger and Ian Jenkins, MD, of the University of California at San Diego, is planned for HM13 in Washington, D.C., in May (www.hospitalmedicine2013.org).
“[The pre-course] will feature the Choosing Wisely list and how you can both implement and improve on it,” Dr. Maynard says. Longer-term, SHM hopes to compile protocols, order sets, checklists, and other tools for posting on its technical assistance web pages. “Eventually, there may be a mentored implementation program and toolkit, based on best practices from the field. … Lots of people have done bits and pieces of this in their local settings. What’s lacking is a cohesive, portable approach, and that’s what we have our eyes on.”
Wolfson says the ABIM Foundation plans to conduct surveys in the next six months to gauge whether physicians think they should be stewards of healthcare resources. “I think you’ll start to see at leading institutions where it’s no longer just ‘Why didn’t you order this test?’ But ‘Why did you—and what were you hoping to learn from it?’” he says. “Just asking that question is a good start—and saying to yourself: Am I choosing wisely?”
Larry Beresford is a freelance writer in Oakland, Calif.
Have you ever prescribed stress ulcer prophylaxis therapy to patients at low risk for gastrointestinal complications? Have you ever repeated CBC or chemistry testing in the face of clinical and lab stability? Have you once or twice ordered bronchodilators for children with bronchiolitis?
If you answered “yes” to any of those questions, you might want to reconsider some of your practices. That’s the message hospitalist leaders have for adult and pediatric HM practitioners interested in curbing wasteful healthcare spending.
SHM has joined the American Board of Internal Medicine (ABIM) Foundation’s Choosing Wisely campaign, a multiyear effort to spark national dialogue about waste in the healthcare system and the kinds of common treatments that doctors and patients should think twice about before deciding to pursue. Ad hoc subcommittees of SHM’s Hospital Quality and Patient Safety Committee created lists of five adult and five pediatric treatments that hospitalists and their patients should question. Those lists were shared alongside 15 other medical specialty societies at a Feb. 21 news conference in Washington, D.C.
Choosing Wisely (www.choosingwisely.org) has been recognized by the professional and consumer media in a big way, says Daniel Wolfson, executive vice president and chief operating officer of the ABIM Foundation, which is affiliated with but distinct from the American Board of Internal Medicine (www.abim.org). “The conversation about overuse is now on the table, and people recognize that it’s an important subject to talk about—without the kind of hysterics that we’ve seen previously around, for example, rationing,” he says. “We’re talking about treatments that are not beneficial and potentially are harmful to patients … things that are ordered for many patients when the benefit does not exceed the risk. These are not absolutes; there are times when a treatment might be indicated because of a certain history or clinical finding. But be clear on what those circumstances are.”
SHM is excited to be a partner in the Choosing Wisely campaign, says Gregory Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Healthcare Improvement and Innovation. With its broad professional and consumer outreach and emphasis on informing and engaging the consumer, the Choosing Wisely effort meshes well with the center’s QI and patient safety goals.
“We acknowledge that there is waste in our system. We also believe that if you have an engaged, empowered patient, together you will make better choices, have less waste, and probably also reduce costs,” Dr. Maynard says.
Developing SHM’s “think twice” lists under a tight deadline was a challenge, says John Bulger, DO, FACP, SFHM, chief quality officer at Geisinger Medical Center in Danville, Pa., and chair of the adult committee. It was especially difficult trying to encourage the broadest possible input from experts in the field. SHM board and committee members were asked for suggested treatments that should be targeted as wasteful, and a preliminary list of 100 was grouped, whittled down, and sent to SHM members to vote on. The committee conducted two blind votes and sent a list of seven recommendations to the SHM board, which made the final choices for submission to the ABIM Foundation.
“The ABIM Foundation has fairly strict guidelines for Choosing Wisely,” Dr. Bulger says. The process was meant to be transparent and well documented, and the SHM committees will publish an article in the Journal of Hospital Medicine describing how its lists were compiled. Choices were to be made based on the evidence for treatments that lie within the specialty’s purview. “Because our practice is so diverse, you can find many core treatments that hospitalists impact on a daily basis and that are unique to the work of hospital medicine,” Dr. Bulger adds.
Fourteen pediatric hospitalists followed a similar process in developing its five suggestions.
“While this issue has been addressed in adult settings, in pediatrics, discussions about waste are almost nonexistent,” says Ricardo Quinonez, MD, FHM, a pediatric hospitalist at Texas Children’s Hospital in Houston and chair of the pediatric ad-hoc committee. “I don’t think anyone was too surprised by our list, which is heavy on respiratory illnesses. That’s what kids get admitted to the hospital for.”
Dr. Quinonez suggests pediatric hospitalists use the list to engage with their specialist colleagues about appropriate treatment choices. “If you want to improve quality, here’s a place to start,” he says.
Dr. Bulger encourages hospitalists to stop and take a long look at the lists and think about ways to improve their own practice. He encourages hospitalists to take the recommendations to their hospitals’ quality-improvement (QI) committees and start collecting baseline data, he says, adding that “we should be able to come back a year from now and show that we’ve been able to change practice using these lists.”
A full-day pre-course, “QI for High Value Healthcare: Making the ABIM Foundation’s Choosing Wisely Campaign a Reality,” co-led by Dr. Bulger and Ian Jenkins, MD, of the University of California at San Diego, is planned for HM13 in Washington, D.C., in May (www.hospitalmedicine2013.org).
“[The pre-course] will feature the Choosing Wisely list and how you can both implement and improve on it,” Dr. Maynard says. Longer-term, SHM hopes to compile protocols, order sets, checklists, and other tools for posting on its technical assistance web pages. “Eventually, there may be a mentored implementation program and toolkit, based on best practices from the field. … Lots of people have done bits and pieces of this in their local settings. What’s lacking is a cohesive, portable approach, and that’s what we have our eyes on.”
Wolfson says the ABIM Foundation plans to conduct surveys in the next six months to gauge whether physicians think they should be stewards of healthcare resources. “I think you’ll start to see at leading institutions where it’s no longer just ‘Why didn’t you order this test?’ But ‘Why did you—and what were you hoping to learn from it?’” he says. “Just asking that question is a good start—and saying to yourself: Am I choosing wisely?”
Larry Beresford is a freelance writer in Oakland, Calif.
Have you ever prescribed stress ulcer prophylaxis therapy to patients at low risk for gastrointestinal complications? Have you ever repeated CBC or chemistry testing in the face of clinical and lab stability? Have you once or twice ordered bronchodilators for children with bronchiolitis?
If you answered “yes” to any of those questions, you might want to reconsider some of your practices. That’s the message hospitalist leaders have for adult and pediatric HM practitioners interested in curbing wasteful healthcare spending.
SHM has joined the American Board of Internal Medicine (ABIM) Foundation’s Choosing Wisely campaign, a multiyear effort to spark national dialogue about waste in the healthcare system and the kinds of common treatments that doctors and patients should think twice about before deciding to pursue. Ad hoc subcommittees of SHM’s Hospital Quality and Patient Safety Committee created lists of five adult and five pediatric treatments that hospitalists and their patients should question. Those lists were shared alongside 15 other medical specialty societies at a Feb. 21 news conference in Washington, D.C.
Choosing Wisely (www.choosingwisely.org) has been recognized by the professional and consumer media in a big way, says Daniel Wolfson, executive vice president and chief operating officer of the ABIM Foundation, which is affiliated with but distinct from the American Board of Internal Medicine (www.abim.org). “The conversation about overuse is now on the table, and people recognize that it’s an important subject to talk about—without the kind of hysterics that we’ve seen previously around, for example, rationing,” he says. “We’re talking about treatments that are not beneficial and potentially are harmful to patients … things that are ordered for many patients when the benefit does not exceed the risk. These are not absolutes; there are times when a treatment might be indicated because of a certain history or clinical finding. But be clear on what those circumstances are.”
SHM is excited to be a partner in the Choosing Wisely campaign, says Gregory Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Healthcare Improvement and Innovation. With its broad professional and consumer outreach and emphasis on informing and engaging the consumer, the Choosing Wisely effort meshes well with the center’s QI and patient safety goals.
“We acknowledge that there is waste in our system. We also believe that if you have an engaged, empowered patient, together you will make better choices, have less waste, and probably also reduce costs,” Dr. Maynard says.
Developing SHM’s “think twice” lists under a tight deadline was a challenge, says John Bulger, DO, FACP, SFHM, chief quality officer at Geisinger Medical Center in Danville, Pa., and chair of the adult committee. It was especially difficult trying to encourage the broadest possible input from experts in the field. SHM board and committee members were asked for suggested treatments that should be targeted as wasteful, and a preliminary list of 100 was grouped, whittled down, and sent to SHM members to vote on. The committee conducted two blind votes and sent a list of seven recommendations to the SHM board, which made the final choices for submission to the ABIM Foundation.
“The ABIM Foundation has fairly strict guidelines for Choosing Wisely,” Dr. Bulger says. The process was meant to be transparent and well documented, and the SHM committees will publish an article in the Journal of Hospital Medicine describing how its lists were compiled. Choices were to be made based on the evidence for treatments that lie within the specialty’s purview. “Because our practice is so diverse, you can find many core treatments that hospitalists impact on a daily basis and that are unique to the work of hospital medicine,” Dr. Bulger adds.
Fourteen pediatric hospitalists followed a similar process in developing its five suggestions.
“While this issue has been addressed in adult settings, in pediatrics, discussions about waste are almost nonexistent,” says Ricardo Quinonez, MD, FHM, a pediatric hospitalist at Texas Children’s Hospital in Houston and chair of the pediatric ad-hoc committee. “I don’t think anyone was too surprised by our list, which is heavy on respiratory illnesses. That’s what kids get admitted to the hospital for.”
Dr. Quinonez suggests pediatric hospitalists use the list to engage with their specialist colleagues about appropriate treatment choices. “If you want to improve quality, here’s a place to start,” he says.
Dr. Bulger encourages hospitalists to stop and take a long look at the lists and think about ways to improve their own practice. He encourages hospitalists to take the recommendations to their hospitals’ quality-improvement (QI) committees and start collecting baseline data, he says, adding that “we should be able to come back a year from now and show that we’ve been able to change practice using these lists.”
A full-day pre-course, “QI for High Value Healthcare: Making the ABIM Foundation’s Choosing Wisely Campaign a Reality,” co-led by Dr. Bulger and Ian Jenkins, MD, of the University of California at San Diego, is planned for HM13 in Washington, D.C., in May (www.hospitalmedicine2013.org).
“[The pre-course] will feature the Choosing Wisely list and how you can both implement and improve on it,” Dr. Maynard says. Longer-term, SHM hopes to compile protocols, order sets, checklists, and other tools for posting on its technical assistance web pages. “Eventually, there may be a mentored implementation program and toolkit, based on best practices from the field. … Lots of people have done bits and pieces of this in their local settings. What’s lacking is a cohesive, portable approach, and that’s what we have our eyes on.”
Wolfson says the ABIM Foundation plans to conduct surveys in the next six months to gauge whether physicians think they should be stewards of healthcare resources. “I think you’ll start to see at leading institutions where it’s no longer just ‘Why didn’t you order this test?’ But ‘Why did you—and what were you hoping to learn from it?’” he says. “Just asking that question is a good start—and saying to yourself: Am I choosing wisely?”
Larry Beresford is a freelance writer in Oakland, Calif.
Hospital Medicine Guidelines for Management of Diabetic Foot Infections
Background
In the U.S. alone, there are an estimated 25.8 million people with diabetes, or about 8.3% of the population. Due to comorbidities of peripheral neuropathy and peripheral vascular disease associated with diabetes, these patients are at higher risk for developing foot infections. Among the myriad diabetes complications, diabetic foot infections (DFI) are the main reason for diabetes-related hospitalizations and lower-extremity amputations. U.S. hospitals admit roughly 5,700 patients per year for DFI; 71,000 lower-extremity amputations are attributed to diabetes.1,2
Studies have demonstrated that DFI management according to guidelines improves survival, reduces complications, and is cost-effective with a major clinical outcome of reduced amputations.3 But prospective observational studies have shown that, in practice, guidelines often are not followed and can lead to poor outcomes.4 Studies suggest a need for more simple, straightforward guidelines.
Guidelines Update
In June 2012, the Infectious Diseases Society of America (IDSA) updated its 2004 guidelines on the management of diabetic foot infections.5 Although IDSA made no major changes to its recommendations, the 2012 guidelines were revised to be more simple and clear. These new guidelines have been reviewed and endorsed by SHM.
Specific recommendations include:
- All patients with suspected DFI should be assessed on three levels: the patient, the extremity involved, and the wound. Patients should be assessed for signs of systemic illness or metabolic derangements. The extremity should be examined for peripheral arterial disease (PAD) using the Ankle-Brachial Index (ABI), and those with an ABI <0.4 should be evaluated by a vascular surgeon.
- Uninfected wounds should be distinguished from infected wounds based on the presence of two or more classic signs of inflammation and purulence. All wounds should be classified based on validated systems, such as those established by IDSA or the International Working Group on the Diabetic Foot (IWGDF). The IDSA classification of wounds as uninfected, mild, moderate, and severe correlate well with the IWGDF’s PEDIS (Perfusion, Extent, Depth, Infection and Sensation) Grades 1, 2, 3, and 4. Wounds are distinguished by size (more or less than 2 cm in width), extent (depth of tissue involvement), and the presence of two or more signs of systemic inflammatory response syndrome.
- Whenever possible, management of DFI should involve multidisciplinary teams that include a microbiologist or ID expert, surgeon/podiatrist familiar with debridement of foot infections, and wound care experts familiar with dressings that provide pressure off-loading.
- All wounds should be debrided, and cultures should be sent from deep tissue via biopsy or curettage (scraping of the base of the ulcer). Wound surface swabs should not be sent for culture, as they often are inaccurate.
- All patients with severe infections and some patients with moderate infections with complicating features (i.e. severe PAD or inability to manage outpatient treatment due to psychosocial reasons) should be admitted. Those with mild infection or some moderate infections without complicating features can be managed as outpatients.
- All patients with suspected DFI should have plain radiographs of the affected limb to evaluate for bony abnormalities, soft-tissue gas, or foreign bodies, but they are only 54% sensitive and 68% specific for osteomyelitis. MRI is more sensitive (90%) and specific (up to 90%) for detecting osteomyelitis. When MRI is contraindicated, a bone scan coupled with a tagged white-blood count scan is the next best test for detecting osteomyelitis.
- Osteomyelitis, which is found in as many as 20% of mild to moderate DFI cases and as many as 50% of severe DFI cases, should be suspected in any patient with large (>2 cm square), deep, or chronic (>six weeks) wounds, as well as those who have wounds overlying a bony prominence or have a positive probe-to-bone (PTB) test. The most definitive diagnosis of osteomyelitis is via bone biopsy for culture and histology. Patients with osteomyelitis can be managed surgically with resection or medically with prolonged antibiotics (>four weeks). If surgical resection removes the infected bone with clean margins, the antibiotic course can be shortened to two to five days post-operatively.
- Effective treatment includes both wound care as well as antibiotic therapy. Antibiotics should be started after cultures are sent. Empiric antibiotics for mild to moderate infections in patients who have not been recently treated can be directed at gram-positive cocci (GPC), as Staphylococcus is the most common causal organism identified. Patients with severe infection can be started empirically on parenteral broad-spectrum antibiotics covering for GPC (particularly methicillin-resistant Staphylococcus aureus in at-risk patients), gram-negative bacteria, and obligate anaerobes. Antibiotics should be tailored once culture and sensitivity results are available. Generally, mild infections should be treated for one to two weeks and moderate to severe infections for two to three weeks, if there is no suspicion of osteomyelitis.
Analysis
The United Kingdom National Institute for Clinical Excellence (NICE) guideline development group published guidelines for inpatient management of diabetic foot problems in 2011.6 The NICE guidelines are largely similar to the 2012 IDSA guidelines. NICE guidelines call for each hospital to have a care pathway for all patients who present with a diabetic foot problem, and that these patients should be cared for by a multidisciplinary team, including appropriate wound care and debridement, assessment of vascular function, imaging with plain radiographs and MRI if osteomyelitis is suspected, and directed antibiotic therapy.
HM Takeaways
Diabetic foot infections are a common occurrence, and the guidelines for their management demonstrate how coordinated clinical care is important for improving patient care and outcomes. As health reimbursement moves toward a model of bundled payments for treatment and a greater emphasis on measureable outcomes, hospitalists are well positioned to be managers of such organized approaches with multidisciplinary teams.
Dr. Ly is a hospitalist in the division of hospital medicine at the University of California at San Francisco.
References
- Centers for Disease Control and Prevention. Age-Adjusted Hospital Discharge Rates for Peripheral Arterial Disease (PAD), Ulcer/Inflammation/Infection (ULCER), or Neuropathy as First-Listed Diagnosis per 1,000 Diabetic Population, United States, 1988–2007. CDC website. Available at: http://www.cdc.gov/diabetes/statistics/hosplea/diabetes_complications/fig2_pop.htm. Accessed Jan. 28, 2013.
- Centers for Disease Control and Prevention. Number (in thousands) of hospital discharges for nontraumatic lower extremity amputation with diabetes as a listed diagnosis, 1988-2006. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/diabetes/statistics/lea/fig1.htm. Accessed Jan. 28, 2013.
- Ortegon MM, Redekop WK, Niessen LW. Cost-effectiveness of prevention and treatment of the diabetic foot: a Markov analysis. Diabetes Care. 2004;27:901-907.Prompers L, Huijberts M, Apelqvist J, et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia. 2007;50:18-25.
- Lipsky BA, Berendt AR, Comia PB, et al. 2012 Infectious Diseases Society of America Clinical Practice Guideline for the Diagnosis and Treatment of Diabetic Foot Infections. Clin Infect Dis. 2012;54(12):132-173.
- Tan T, Shaw EJ, Siddiqui F, Kandaswamy P, Barry PW, Baker M. Inpatient management of diabetic foot problems: summary of NICE guidance. BMJ. 2011;342:d1280.
Background
In the U.S. alone, there are an estimated 25.8 million people with diabetes, or about 8.3% of the population. Due to comorbidities of peripheral neuropathy and peripheral vascular disease associated with diabetes, these patients are at higher risk for developing foot infections. Among the myriad diabetes complications, diabetic foot infections (DFI) are the main reason for diabetes-related hospitalizations and lower-extremity amputations. U.S. hospitals admit roughly 5,700 patients per year for DFI; 71,000 lower-extremity amputations are attributed to diabetes.1,2
Studies have demonstrated that DFI management according to guidelines improves survival, reduces complications, and is cost-effective with a major clinical outcome of reduced amputations.3 But prospective observational studies have shown that, in practice, guidelines often are not followed and can lead to poor outcomes.4 Studies suggest a need for more simple, straightforward guidelines.
Guidelines Update
In June 2012, the Infectious Diseases Society of America (IDSA) updated its 2004 guidelines on the management of diabetic foot infections.5 Although IDSA made no major changes to its recommendations, the 2012 guidelines were revised to be more simple and clear. These new guidelines have been reviewed and endorsed by SHM.
Specific recommendations include:
- All patients with suspected DFI should be assessed on three levels: the patient, the extremity involved, and the wound. Patients should be assessed for signs of systemic illness or metabolic derangements. The extremity should be examined for peripheral arterial disease (PAD) using the Ankle-Brachial Index (ABI), and those with an ABI <0.4 should be evaluated by a vascular surgeon.
- Uninfected wounds should be distinguished from infected wounds based on the presence of two or more classic signs of inflammation and purulence. All wounds should be classified based on validated systems, such as those established by IDSA or the International Working Group on the Diabetic Foot (IWGDF). The IDSA classification of wounds as uninfected, mild, moderate, and severe correlate well with the IWGDF’s PEDIS (Perfusion, Extent, Depth, Infection and Sensation) Grades 1, 2, 3, and 4. Wounds are distinguished by size (more or less than 2 cm in width), extent (depth of tissue involvement), and the presence of two or more signs of systemic inflammatory response syndrome.
- Whenever possible, management of DFI should involve multidisciplinary teams that include a microbiologist or ID expert, surgeon/podiatrist familiar with debridement of foot infections, and wound care experts familiar with dressings that provide pressure off-loading.
- All wounds should be debrided, and cultures should be sent from deep tissue via biopsy or curettage (scraping of the base of the ulcer). Wound surface swabs should not be sent for culture, as they often are inaccurate.
- All patients with severe infections and some patients with moderate infections with complicating features (i.e. severe PAD or inability to manage outpatient treatment due to psychosocial reasons) should be admitted. Those with mild infection or some moderate infections without complicating features can be managed as outpatients.
- All patients with suspected DFI should have plain radiographs of the affected limb to evaluate for bony abnormalities, soft-tissue gas, or foreign bodies, but they are only 54% sensitive and 68% specific for osteomyelitis. MRI is more sensitive (90%) and specific (up to 90%) for detecting osteomyelitis. When MRI is contraindicated, a bone scan coupled with a tagged white-blood count scan is the next best test for detecting osteomyelitis.
- Osteomyelitis, which is found in as many as 20% of mild to moderate DFI cases and as many as 50% of severe DFI cases, should be suspected in any patient with large (>2 cm square), deep, or chronic (>six weeks) wounds, as well as those who have wounds overlying a bony prominence or have a positive probe-to-bone (PTB) test. The most definitive diagnosis of osteomyelitis is via bone biopsy for culture and histology. Patients with osteomyelitis can be managed surgically with resection or medically with prolonged antibiotics (>four weeks). If surgical resection removes the infected bone with clean margins, the antibiotic course can be shortened to two to five days post-operatively.
- Effective treatment includes both wound care as well as antibiotic therapy. Antibiotics should be started after cultures are sent. Empiric antibiotics for mild to moderate infections in patients who have not been recently treated can be directed at gram-positive cocci (GPC), as Staphylococcus is the most common causal organism identified. Patients with severe infection can be started empirically on parenteral broad-spectrum antibiotics covering for GPC (particularly methicillin-resistant Staphylococcus aureus in at-risk patients), gram-negative bacteria, and obligate anaerobes. Antibiotics should be tailored once culture and sensitivity results are available. Generally, mild infections should be treated for one to two weeks and moderate to severe infections for two to three weeks, if there is no suspicion of osteomyelitis.
Analysis
The United Kingdom National Institute for Clinical Excellence (NICE) guideline development group published guidelines for inpatient management of diabetic foot problems in 2011.6 The NICE guidelines are largely similar to the 2012 IDSA guidelines. NICE guidelines call for each hospital to have a care pathway for all patients who present with a diabetic foot problem, and that these patients should be cared for by a multidisciplinary team, including appropriate wound care and debridement, assessment of vascular function, imaging with plain radiographs and MRI if osteomyelitis is suspected, and directed antibiotic therapy.
HM Takeaways
Diabetic foot infections are a common occurrence, and the guidelines for their management demonstrate how coordinated clinical care is important for improving patient care and outcomes. As health reimbursement moves toward a model of bundled payments for treatment and a greater emphasis on measureable outcomes, hospitalists are well positioned to be managers of such organized approaches with multidisciplinary teams.
Dr. Ly is a hospitalist in the division of hospital medicine at the University of California at San Francisco.
References
- Centers for Disease Control and Prevention. Age-Adjusted Hospital Discharge Rates for Peripheral Arterial Disease (PAD), Ulcer/Inflammation/Infection (ULCER), or Neuropathy as First-Listed Diagnosis per 1,000 Diabetic Population, United States, 1988–2007. CDC website. Available at: http://www.cdc.gov/diabetes/statistics/hosplea/diabetes_complications/fig2_pop.htm. Accessed Jan. 28, 2013.
- Centers for Disease Control and Prevention. Number (in thousands) of hospital discharges for nontraumatic lower extremity amputation with diabetes as a listed diagnosis, 1988-2006. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/diabetes/statistics/lea/fig1.htm. Accessed Jan. 28, 2013.
- Ortegon MM, Redekop WK, Niessen LW. Cost-effectiveness of prevention and treatment of the diabetic foot: a Markov analysis. Diabetes Care. 2004;27:901-907.Prompers L, Huijberts M, Apelqvist J, et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia. 2007;50:18-25.
- Lipsky BA, Berendt AR, Comia PB, et al. 2012 Infectious Diseases Society of America Clinical Practice Guideline for the Diagnosis and Treatment of Diabetic Foot Infections. Clin Infect Dis. 2012;54(12):132-173.
- Tan T, Shaw EJ, Siddiqui F, Kandaswamy P, Barry PW, Baker M. Inpatient management of diabetic foot problems: summary of NICE guidance. BMJ. 2011;342:d1280.
Background
In the U.S. alone, there are an estimated 25.8 million people with diabetes, or about 8.3% of the population. Due to comorbidities of peripheral neuropathy and peripheral vascular disease associated with diabetes, these patients are at higher risk for developing foot infections. Among the myriad diabetes complications, diabetic foot infections (DFI) are the main reason for diabetes-related hospitalizations and lower-extremity amputations. U.S. hospitals admit roughly 5,700 patients per year for DFI; 71,000 lower-extremity amputations are attributed to diabetes.1,2
Studies have demonstrated that DFI management according to guidelines improves survival, reduces complications, and is cost-effective with a major clinical outcome of reduced amputations.3 But prospective observational studies have shown that, in practice, guidelines often are not followed and can lead to poor outcomes.4 Studies suggest a need for more simple, straightforward guidelines.
Guidelines Update
In June 2012, the Infectious Diseases Society of America (IDSA) updated its 2004 guidelines on the management of diabetic foot infections.5 Although IDSA made no major changes to its recommendations, the 2012 guidelines were revised to be more simple and clear. These new guidelines have been reviewed and endorsed by SHM.
Specific recommendations include:
- All patients with suspected DFI should be assessed on three levels: the patient, the extremity involved, and the wound. Patients should be assessed for signs of systemic illness or metabolic derangements. The extremity should be examined for peripheral arterial disease (PAD) using the Ankle-Brachial Index (ABI), and those with an ABI <0.4 should be evaluated by a vascular surgeon.
- Uninfected wounds should be distinguished from infected wounds based on the presence of two or more classic signs of inflammation and purulence. All wounds should be classified based on validated systems, such as those established by IDSA or the International Working Group on the Diabetic Foot (IWGDF). The IDSA classification of wounds as uninfected, mild, moderate, and severe correlate well with the IWGDF’s PEDIS (Perfusion, Extent, Depth, Infection and Sensation) Grades 1, 2, 3, and 4. Wounds are distinguished by size (more or less than 2 cm in width), extent (depth of tissue involvement), and the presence of two or more signs of systemic inflammatory response syndrome.
- Whenever possible, management of DFI should involve multidisciplinary teams that include a microbiologist or ID expert, surgeon/podiatrist familiar with debridement of foot infections, and wound care experts familiar with dressings that provide pressure off-loading.
- All wounds should be debrided, and cultures should be sent from deep tissue via biopsy or curettage (scraping of the base of the ulcer). Wound surface swabs should not be sent for culture, as they often are inaccurate.
- All patients with severe infections and some patients with moderate infections with complicating features (i.e. severe PAD or inability to manage outpatient treatment due to psychosocial reasons) should be admitted. Those with mild infection or some moderate infections without complicating features can be managed as outpatients.
- All patients with suspected DFI should have plain radiographs of the affected limb to evaluate for bony abnormalities, soft-tissue gas, or foreign bodies, but they are only 54% sensitive and 68% specific for osteomyelitis. MRI is more sensitive (90%) and specific (up to 90%) for detecting osteomyelitis. When MRI is contraindicated, a bone scan coupled with a tagged white-blood count scan is the next best test for detecting osteomyelitis.
- Osteomyelitis, which is found in as many as 20% of mild to moderate DFI cases and as many as 50% of severe DFI cases, should be suspected in any patient with large (>2 cm square), deep, or chronic (>six weeks) wounds, as well as those who have wounds overlying a bony prominence or have a positive probe-to-bone (PTB) test. The most definitive diagnosis of osteomyelitis is via bone biopsy for culture and histology. Patients with osteomyelitis can be managed surgically with resection or medically with prolonged antibiotics (>four weeks). If surgical resection removes the infected bone with clean margins, the antibiotic course can be shortened to two to five days post-operatively.
- Effective treatment includes both wound care as well as antibiotic therapy. Antibiotics should be started after cultures are sent. Empiric antibiotics for mild to moderate infections in patients who have not been recently treated can be directed at gram-positive cocci (GPC), as Staphylococcus is the most common causal organism identified. Patients with severe infection can be started empirically on parenteral broad-spectrum antibiotics covering for GPC (particularly methicillin-resistant Staphylococcus aureus in at-risk patients), gram-negative bacteria, and obligate anaerobes. Antibiotics should be tailored once culture and sensitivity results are available. Generally, mild infections should be treated for one to two weeks and moderate to severe infections for two to three weeks, if there is no suspicion of osteomyelitis.
Analysis
The United Kingdom National Institute for Clinical Excellence (NICE) guideline development group published guidelines for inpatient management of diabetic foot problems in 2011.6 The NICE guidelines are largely similar to the 2012 IDSA guidelines. NICE guidelines call for each hospital to have a care pathway for all patients who present with a diabetic foot problem, and that these patients should be cared for by a multidisciplinary team, including appropriate wound care and debridement, assessment of vascular function, imaging with plain radiographs and MRI if osteomyelitis is suspected, and directed antibiotic therapy.
HM Takeaways
Diabetic foot infections are a common occurrence, and the guidelines for their management demonstrate how coordinated clinical care is important for improving patient care and outcomes. As health reimbursement moves toward a model of bundled payments for treatment and a greater emphasis on measureable outcomes, hospitalists are well positioned to be managers of such organized approaches with multidisciplinary teams.
Dr. Ly is a hospitalist in the division of hospital medicine at the University of California at San Francisco.
References
- Centers for Disease Control and Prevention. Age-Adjusted Hospital Discharge Rates for Peripheral Arterial Disease (PAD), Ulcer/Inflammation/Infection (ULCER), or Neuropathy as First-Listed Diagnosis per 1,000 Diabetic Population, United States, 1988–2007. CDC website. Available at: http://www.cdc.gov/diabetes/statistics/hosplea/diabetes_complications/fig2_pop.htm. Accessed Jan. 28, 2013.
- Centers for Disease Control and Prevention. Number (in thousands) of hospital discharges for nontraumatic lower extremity amputation with diabetes as a listed diagnosis, 1988-2006. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/diabetes/statistics/lea/fig1.htm. Accessed Jan. 28, 2013.
- Ortegon MM, Redekop WK, Niessen LW. Cost-effectiveness of prevention and treatment of the diabetic foot: a Markov analysis. Diabetes Care. 2004;27:901-907.Prompers L, Huijberts M, Apelqvist J, et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia. 2007;50:18-25.
- Lipsky BA, Berendt AR, Comia PB, et al. 2012 Infectious Diseases Society of America Clinical Practice Guideline for the Diagnosis and Treatment of Diabetic Foot Infections. Clin Infect Dis. 2012;54(12):132-173.
- Tan T, Shaw EJ, Siddiqui F, Kandaswamy P, Barry PW, Baker M. Inpatient management of diabetic foot problems: summary of NICE guidance. BMJ. 2011;342:d1280.
Medicare Billing Regulations for Nonphysician Providers Vary by State, Facility
Nurse practitioners (NPs) and physician assistants (PAs), referred to as nonphysician providers (NPPs) in billing policy, provide many different services in the hospital setting. Roles include:
- Rounding independently and following patients of varying acuity with physician supervision. The NPP may ask the physician to see the patient, as necessary, if a change in the patient’s condition arises and warrants physician evaluation.
- Providing prompt consultative
- services when the physician is not
- readily available.
- Rounding alongside the physician and expediting the work of admission services through a combined effort.
Hospitalist programs may elect one model over another, or utilize NPPs according to existing need and shifting census. Employers must be aware of state and federal regulations, facility-imposed standards of care, and billing requirements surrounding NPP services.
Medicare Enrollment and Billing Eligibility
Certified PAs and NPs may provide covered services to Medicare beneficiaries in accordance with their state scope of practice under state law and corresponding supervision/collaboration requirements. They can submit claims for these services, providing they meet enrollment qualifications.1
PAs must have:
- Graduated from a PA educational program accredited by the Accreditation Review Commission on Education for the Physician Assistant (or its predecessor agencies, the Commission on Accreditation of Allied Health Education Programs (CAAHEP) and the Committee on Allied Health Education and Accreditation (CAHEA); or
- Passed the national certification examination administered by the National Commission on Certification of Physician Assistants (NCCPA); and
- A license as a PA in the practicing state.
NPs must:
- Be a registered nurse who is authorized and licensed by the state to practice as a nurse practitioner by Dec. 31, 2000; or
- After Jan. 1, 2001, be a registered nurse who is authorized and licensed by the state to practice as an NP and be certified by a recognized national certifying body that has established standards for NPs (e.g. American Academy of Nurse Practitioners, American Nurses Credentialing Center, AACN Certification Corp., or National Board on Certification of Hospice and Palliative Nurses); and
- Possess a master’s degree in nursing.
Independent Billing
NPPs can see patients in any setting without the presence of a physician. The physician is not required to see the patient but must be available by phone or beeper in accordance with supervisory/collaborative guidelines. Physician cosignature is not required unless mandated by state law or the facility.
NPPs document and report their services according to the Centers for Medicare & Medicaid Services (CMS) Documentation Guidelines (available at www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/EMDOC.html). The NPP should be listed as the rendering provider on the claim form. Currently, insurance programs Medicare and Aetna Inc. consistently enroll and recognize NPPs as billing providers and reimburse these services at 85% of the allowable physician rate.2
Shared/Split Billing
When two providers (a physician and NPP) from the same group (direct employment or a lease arrangement contractually linking the providers) perform a service for the same patient on the same calendar day, CMS allows the combined services to be reported under a single provider’s name.
Allowable services. NPPs are only limited by the state scope of practice under state law, and the facility rules in which the NPPs practice. Services must be performed under the appropriate level of supervision or collaboration. Medicare reimburses reasonable and necessary services not otherwise excluded from coverage.
However, shared/split rules restrict the services reported under this billing model, recognizing only evaluation and management (E/M) services (and not procedures) provided in the ED, outpatient hospital clinics, or inpatient hospital (i.e. facility-based services). Shared/split rules do not involve all types of E/M services. For hospitalist programs, critical-care services (99291-99292) are excluded.3
Physician requirement. Shared/split rules require a face-to-face patient encounter by each provider on the same calendar day. There are no billing mandates requiring the NPP to see the patient before the physician does, although practice style might govern this decision.4 CMS does not specify the extent of provider involvement, but it could be established by local Medicare contractor requirements. Some contractors reference physician participation as a “substantive” service without further elaboration on specific parameters. Therefore, the physician determines the critical or key portion of his/her personal service. Minimalistic documentation can be problematic for quality or medicolegal aspects of patient care, and physicians might benefit from a more detailed notation of participation.
Documentation. Physician documentation must include an attestation that supports the physician encounter (e.g. “Patient seen and examined by me”), the individual with whom the service is shared (e.g. “Agree with note by X”), their portion of the rendered service (e.g. “Pulse oximetry 94% on room air. Audible rhonchi at bilateral lung bases. Start O2 2L nasal cannula. Obtain CXR”), the date, and a legible signature. NPP documentation should include as similar reference to the physician with whom the service is being shared for better charge capture. It alerts coders, auditors, and payor representatives to consider both notes in support of the billed service and ensures that the correct notes are sent to the payor in the event of claim denial and subsequent appeal.
Although the visit level is supported by both provider services, only one claim may be submitted for a shared/split service. The rendering provider listed on the claim can be the physician (reimbursed at 100% of the Medicare allowable physician rate) or the NPP (reimbursed at 85% of the allowable physician rate).
Non-Medicare Claims
Shared/split billing policy only applies to Medicare beneficiaries, while independent billing policy applies to Medicare and Aetna. Excessive costs prevent most other non-Medicare insurers from credentialing and enrollment NPPs. Absence of payor policy does not disqualify reimbursement for shared services, but it does require additional measures to establish recognition of NPP services and a corresponding reimbursement model.
After determining payor mix, develop a reasonable guideline for those payors who do not enroll NPPs. Delineate, in writing, a predetermined time frame for guideline implementation unless the payor can provide an alternate billing option. Some experts suggest physician groups outline the following key issues when structuring a billing option5:
- Type of NPPs involved in patient care;
- Category of services provided;
- Service location(s);
- Physician involvement;
- Mechanism for reporting services; and
- Documentation requirements.
Guidelines can be developed for any of the billing options (independent, “incident-to,” shared/split). Be sure to obtain written payor response before initiating the billing process.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
NPP Billing Reminders

Discharge day management (99238-99239) often is delegated to qualified NPPs.3 Because this service is time-based, the final code selection is based upon the total time spent with the patient, and on the patient’s unit/floor, coordinating care prior to the patient leaving the hospital on the day of discharge. If this service is solely provided by the NPP, the NPP must report the appropriate code under his/her own name on the claim form (for eligible payors). If this service is shared with the physician, report the code representing the cumulative, documented time in both notes, provided that each note identifies the face-toface service from each provider, and his/her corresponding participation.

Many questions arise about NPPs performing the admission service because NPPs might not be given “admitting” privileges by the facility in which they practice. NPPs may provide and/or participate in services according to their state scope practice and facility-imposed guidelines. Billing policy supports state law and will reimburse any “independent” service permitted by the state. Facilities may limit NPP scope of practice by disallowing independent admission service but permittin a shared service with the physician. If this service is shared with the physician, report the code representing the cumulative, documented encounter, provided that each note identifies the face-to-face service from each provider, and his/her corresponding participation

Prior to Medicare’s elimination of consultation services (99241-99245, 99251-99255), shared/split billing rules excluded consultations from this claim-reporting model.3 Since the elimination of consults, “consultations” are reported as initial hospital care services (99221-99223).3 Therefore, consultative services can be shared by NPPs and physicians, and reported as a cumulative initial hospital service through the shared/ split billing model. Other payors still accept consultation codes and do not have a specified shared/split model. This allows for the consultative service to be reported as a cumulative NPP/physician effort under the physician name, as long as a written contractual agreement exists allowing this billing option.
References
- Centers for Medicare & Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 190-200. Centers for Medicare & Medicaid website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c15.pdf. Accessed Nov. 5, 2012.
- Aetna Inc. Aetna office links updates. Reminder: Reimbursement change for mid-level practitioners. Aetna Inc. website. Available at www.aetna.com/provider/data/OLU_MA_JUN2010_final.pdf. Accessed Nov. 6, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. Centers for Medicare & Medicaid website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan 21, 2013.
- Pohlig, C. Nonphysician Providers in Your Practice. In: Coding for Chest Medicine 2011. Northbrook, Ill.: American College of Chest Physicians, 2010.
Nurse practitioners (NPs) and physician assistants (PAs), referred to as nonphysician providers (NPPs) in billing policy, provide many different services in the hospital setting. Roles include:
- Rounding independently and following patients of varying acuity with physician supervision. The NPP may ask the physician to see the patient, as necessary, if a change in the patient’s condition arises and warrants physician evaluation.
- Providing prompt consultative
- services when the physician is not
- readily available.
- Rounding alongside the physician and expediting the work of admission services through a combined effort.
Hospitalist programs may elect one model over another, or utilize NPPs according to existing need and shifting census. Employers must be aware of state and federal regulations, facility-imposed standards of care, and billing requirements surrounding NPP services.
Medicare Enrollment and Billing Eligibility
Certified PAs and NPs may provide covered services to Medicare beneficiaries in accordance with their state scope of practice under state law and corresponding supervision/collaboration requirements. They can submit claims for these services, providing they meet enrollment qualifications.1
PAs must have:
- Graduated from a PA educational program accredited by the Accreditation Review Commission on Education for the Physician Assistant (or its predecessor agencies, the Commission on Accreditation of Allied Health Education Programs (CAAHEP) and the Committee on Allied Health Education and Accreditation (CAHEA); or
- Passed the national certification examination administered by the National Commission on Certification of Physician Assistants (NCCPA); and
- A license as a PA in the practicing state.
NPs must:
- Be a registered nurse who is authorized and licensed by the state to practice as a nurse practitioner by Dec. 31, 2000; or
- After Jan. 1, 2001, be a registered nurse who is authorized and licensed by the state to practice as an NP and be certified by a recognized national certifying body that has established standards for NPs (e.g. American Academy of Nurse Practitioners, American Nurses Credentialing Center, AACN Certification Corp., or National Board on Certification of Hospice and Palliative Nurses); and
- Possess a master’s degree in nursing.
Independent Billing
NPPs can see patients in any setting without the presence of a physician. The physician is not required to see the patient but must be available by phone or beeper in accordance with supervisory/collaborative guidelines. Physician cosignature is not required unless mandated by state law or the facility.
NPPs document and report their services according to the Centers for Medicare & Medicaid Services (CMS) Documentation Guidelines (available at www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/EMDOC.html). The NPP should be listed as the rendering provider on the claim form. Currently, insurance programs Medicare and Aetna Inc. consistently enroll and recognize NPPs as billing providers and reimburse these services at 85% of the allowable physician rate.2
Shared/Split Billing
When two providers (a physician and NPP) from the same group (direct employment or a lease arrangement contractually linking the providers) perform a service for the same patient on the same calendar day, CMS allows the combined services to be reported under a single provider’s name.
Allowable services. NPPs are only limited by the state scope of practice under state law, and the facility rules in which the NPPs practice. Services must be performed under the appropriate level of supervision or collaboration. Medicare reimburses reasonable and necessary services not otherwise excluded from coverage.
However, shared/split rules restrict the services reported under this billing model, recognizing only evaluation and management (E/M) services (and not procedures) provided in the ED, outpatient hospital clinics, or inpatient hospital (i.e. facility-based services). Shared/split rules do not involve all types of E/M services. For hospitalist programs, critical-care services (99291-99292) are excluded.3
Physician requirement. Shared/split rules require a face-to-face patient encounter by each provider on the same calendar day. There are no billing mandates requiring the NPP to see the patient before the physician does, although practice style might govern this decision.4 CMS does not specify the extent of provider involvement, but it could be established by local Medicare contractor requirements. Some contractors reference physician participation as a “substantive” service without further elaboration on specific parameters. Therefore, the physician determines the critical or key portion of his/her personal service. Minimalistic documentation can be problematic for quality or medicolegal aspects of patient care, and physicians might benefit from a more detailed notation of participation.
Documentation. Physician documentation must include an attestation that supports the physician encounter (e.g. “Patient seen and examined by me”), the individual with whom the service is shared (e.g. “Agree with note by X”), their portion of the rendered service (e.g. “Pulse oximetry 94% on room air. Audible rhonchi at bilateral lung bases. Start O2 2L nasal cannula. Obtain CXR”), the date, and a legible signature. NPP documentation should include as similar reference to the physician with whom the service is being shared for better charge capture. It alerts coders, auditors, and payor representatives to consider both notes in support of the billed service and ensures that the correct notes are sent to the payor in the event of claim denial and subsequent appeal.
Although the visit level is supported by both provider services, only one claim may be submitted for a shared/split service. The rendering provider listed on the claim can be the physician (reimbursed at 100% of the Medicare allowable physician rate) or the NPP (reimbursed at 85% of the allowable physician rate).
Non-Medicare Claims
Shared/split billing policy only applies to Medicare beneficiaries, while independent billing policy applies to Medicare and Aetna. Excessive costs prevent most other non-Medicare insurers from credentialing and enrollment NPPs. Absence of payor policy does not disqualify reimbursement for shared services, but it does require additional measures to establish recognition of NPP services and a corresponding reimbursement model.
After determining payor mix, develop a reasonable guideline for those payors who do not enroll NPPs. Delineate, in writing, a predetermined time frame for guideline implementation unless the payor can provide an alternate billing option. Some experts suggest physician groups outline the following key issues when structuring a billing option5:
- Type of NPPs involved in patient care;
- Category of services provided;
- Service location(s);
- Physician involvement;
- Mechanism for reporting services; and
- Documentation requirements.
Guidelines can be developed for any of the billing options (independent, “incident-to,” shared/split). Be sure to obtain written payor response before initiating the billing process.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
NPP Billing Reminders
Discharge day management (99238-99239) often is delegated to qualified NPPs.3 Because this service is time-based, the final code selection is based upon the total time spent with the patient, and on the patient’s unit/floor, coordinating care prior to the patient leaving the hospital on the day of discharge. If this service is solely provided by the NPP, the NPP must report the appropriate code under his/her own name on the claim form (for eligible payors). If this service is shared with the physician, report the code representing the cumulative, documented time in both notes, provided that each note identifies the face-toface service from each provider, and his/her corresponding participation.
Many questions arise about NPPs performing the admission service because NPPs might not be given “admitting” privileges by the facility in which they practice. NPPs may provide and/or participate in services according to their state scope practice and facility-imposed guidelines. Billing policy supports state law and will reimburse any “independent” service permitted by the state. Facilities may limit NPP scope of practice by disallowing independent admission service but permittin a shared service with the physician. If this service is shared with the physician, report the code representing the cumulative, documented encounter, provided that each note identifies the face-to-face service from each provider, and his/her corresponding participation
Prior to Medicare’s elimination of consultation services (99241-99245, 99251-99255), shared/split billing rules excluded consultations from this claim-reporting model.3 Since the elimination of consults, “consultations” are reported as initial hospital care services (99221-99223).3 Therefore, consultative services can be shared by NPPs and physicians, and reported as a cumulative initial hospital service through the shared/ split billing model. Other payors still accept consultation codes and do not have a specified shared/split model. This allows for the consultative service to be reported as a cumulative NPP/physician effort under the physician name, as long as a written contractual agreement exists allowing this billing option.
References
- Centers for Medicare & Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 190-200. Centers for Medicare & Medicaid website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c15.pdf. Accessed Nov. 5, 2012.
- Aetna Inc. Aetna office links updates. Reminder: Reimbursement change for mid-level practitioners. Aetna Inc. website. Available at www.aetna.com/provider/data/OLU_MA_JUN2010_final.pdf. Accessed Nov. 6, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. Centers for Medicare & Medicaid website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan 21, 2013.
- Pohlig, C. Nonphysician Providers in Your Practice. In: Coding for Chest Medicine 2011. Northbrook, Ill.: American College of Chest Physicians, 2010.
Nurse practitioners (NPs) and physician assistants (PAs), referred to as nonphysician providers (NPPs) in billing policy, provide many different services in the hospital setting. Roles include:
- Rounding independently and following patients of varying acuity with physician supervision. The NPP may ask the physician to see the patient, as necessary, if a change in the patient’s condition arises and warrants physician evaluation.
- Providing prompt consultative
- services when the physician is not
- readily available.
- Rounding alongside the physician and expediting the work of admission services through a combined effort.
Hospitalist programs may elect one model over another, or utilize NPPs according to existing need and shifting census. Employers must be aware of state and federal regulations, facility-imposed standards of care, and billing requirements surrounding NPP services.
Medicare Enrollment and Billing Eligibility
Certified PAs and NPs may provide covered services to Medicare beneficiaries in accordance with their state scope of practice under state law and corresponding supervision/collaboration requirements. They can submit claims for these services, providing they meet enrollment qualifications.1
PAs must have:
- Graduated from a PA educational program accredited by the Accreditation Review Commission on Education for the Physician Assistant (or its predecessor agencies, the Commission on Accreditation of Allied Health Education Programs (CAAHEP) and the Committee on Allied Health Education and Accreditation (CAHEA); or
- Passed the national certification examination administered by the National Commission on Certification of Physician Assistants (NCCPA); and
- A license as a PA in the practicing state.
NPs must:
- Be a registered nurse who is authorized and licensed by the state to practice as a nurse practitioner by Dec. 31, 2000; or
- After Jan. 1, 2001, be a registered nurse who is authorized and licensed by the state to practice as an NP and be certified by a recognized national certifying body that has established standards for NPs (e.g. American Academy of Nurse Practitioners, American Nurses Credentialing Center, AACN Certification Corp., or National Board on Certification of Hospice and Palliative Nurses); and
- Possess a master’s degree in nursing.
Independent Billing
NPPs can see patients in any setting without the presence of a physician. The physician is not required to see the patient but must be available by phone or beeper in accordance with supervisory/collaborative guidelines. Physician cosignature is not required unless mandated by state law or the facility.
NPPs document and report their services according to the Centers for Medicare & Medicaid Services (CMS) Documentation Guidelines (available at www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/EMDOC.html). The NPP should be listed as the rendering provider on the claim form. Currently, insurance programs Medicare and Aetna Inc. consistently enroll and recognize NPPs as billing providers and reimburse these services at 85% of the allowable physician rate.2
Shared/Split Billing
When two providers (a physician and NPP) from the same group (direct employment or a lease arrangement contractually linking the providers) perform a service for the same patient on the same calendar day, CMS allows the combined services to be reported under a single provider’s name.
Allowable services. NPPs are only limited by the state scope of practice under state law, and the facility rules in which the NPPs practice. Services must be performed under the appropriate level of supervision or collaboration. Medicare reimburses reasonable and necessary services not otherwise excluded from coverage.
However, shared/split rules restrict the services reported under this billing model, recognizing only evaluation and management (E/M) services (and not procedures) provided in the ED, outpatient hospital clinics, or inpatient hospital (i.e. facility-based services). Shared/split rules do not involve all types of E/M services. For hospitalist programs, critical-care services (99291-99292) are excluded.3
Physician requirement. Shared/split rules require a face-to-face patient encounter by each provider on the same calendar day. There are no billing mandates requiring the NPP to see the patient before the physician does, although practice style might govern this decision.4 CMS does not specify the extent of provider involvement, but it could be established by local Medicare contractor requirements. Some contractors reference physician participation as a “substantive” service without further elaboration on specific parameters. Therefore, the physician determines the critical or key portion of his/her personal service. Minimalistic documentation can be problematic for quality or medicolegal aspects of patient care, and physicians might benefit from a more detailed notation of participation.
Documentation. Physician documentation must include an attestation that supports the physician encounter (e.g. “Patient seen and examined by me”), the individual with whom the service is shared (e.g. “Agree with note by X”), their portion of the rendered service (e.g. “Pulse oximetry 94% on room air. Audible rhonchi at bilateral lung bases. Start O2 2L nasal cannula. Obtain CXR”), the date, and a legible signature. NPP documentation should include as similar reference to the physician with whom the service is being shared for better charge capture. It alerts coders, auditors, and payor representatives to consider both notes in support of the billed service and ensures that the correct notes are sent to the payor in the event of claim denial and subsequent appeal.
Although the visit level is supported by both provider services, only one claim may be submitted for a shared/split service. The rendering provider listed on the claim can be the physician (reimbursed at 100% of the Medicare allowable physician rate) or the NPP (reimbursed at 85% of the allowable physician rate).
Non-Medicare Claims
Shared/split billing policy only applies to Medicare beneficiaries, while independent billing policy applies to Medicare and Aetna. Excessive costs prevent most other non-Medicare insurers from credentialing and enrollment NPPs. Absence of payor policy does not disqualify reimbursement for shared services, but it does require additional measures to establish recognition of NPP services and a corresponding reimbursement model.
After determining payor mix, develop a reasonable guideline for those payors who do not enroll NPPs. Delineate, in writing, a predetermined time frame for guideline implementation unless the payor can provide an alternate billing option. Some experts suggest physician groups outline the following key issues when structuring a billing option5:
- Type of NPPs involved in patient care;
- Category of services provided;
- Service location(s);
- Physician involvement;
- Mechanism for reporting services; and
- Documentation requirements.
Guidelines can be developed for any of the billing options (independent, “incident-to,” shared/split). Be sure to obtain written payor response before initiating the billing process.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
NPP Billing Reminders
Discharge day management (99238-99239) often is delegated to qualified NPPs.3 Because this service is time-based, the final code selection is based upon the total time spent with the patient, and on the patient’s unit/floor, coordinating care prior to the patient leaving the hospital on the day of discharge. If this service is solely provided by the NPP, the NPP must report the appropriate code under his/her own name on the claim form (for eligible payors). If this service is shared with the physician, report the code representing the cumulative, documented time in both notes, provided that each note identifies the face-toface service from each provider, and his/her corresponding participation.
Many questions arise about NPPs performing the admission service because NPPs might not be given “admitting” privileges by the facility in which they practice. NPPs may provide and/or participate in services according to their state scope practice and facility-imposed guidelines. Billing policy supports state law and will reimburse any “independent” service permitted by the state. Facilities may limit NPP scope of practice by disallowing independent admission service but permittin a shared service with the physician. If this service is shared with the physician, report the code representing the cumulative, documented encounter, provided that each note identifies the face-to-face service from each provider, and his/her corresponding participation
Prior to Medicare’s elimination of consultation services (99241-99245, 99251-99255), shared/split billing rules excluded consultations from this claim-reporting model.3 Since the elimination of consults, “consultations” are reported as initial hospital care services (99221-99223).3 Therefore, consultative services can be shared by NPPs and physicians, and reported as a cumulative initial hospital service through the shared/ split billing model. Other payors still accept consultation codes and do not have a specified shared/split model. This allows for the consultative service to be reported as a cumulative NPP/physician effort under the physician name, as long as a written contractual agreement exists allowing this billing option.
References
- Centers for Medicare & Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 190-200. Centers for Medicare & Medicaid website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c15.pdf. Accessed Nov. 5, 2012.
- Aetna Inc. Aetna office links updates. Reminder: Reimbursement change for mid-level practitioners. Aetna Inc. website. Available at www.aetna.com/provider/data/OLU_MA_JUN2010_final.pdf. Accessed Nov. 6, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. Centers for Medicare & Medicaid website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan 21, 2013.
- Pohlig, C. Nonphysician Providers in Your Practice. In: Coding for Chest Medicine 2011. Northbrook, Ill.: American College of Chest Physicians, 2010.
Hospitalwide Reductions in Pediatric Patient Harm are Achievable

Clinical question: Can a broadly constructed improvement initiative significantly reduce serious safety events (SSEs)?
Study design: Single-institution quality-improvement initiative.
Setting: Cincinnati Children’s Hospital Medical Center.
Synopsis: A multidisciplinary team supported by leadership was formed to reduce SSEs across the hospital by 80% within four years. A consulting firm with expertise in the field was also engaged for this process. Multifaceted interventions were clustered according to perceived key drivers of change in the institution: error prevention systems, improved safety governance, cause analysis programs, lessons-learned programs, and specific tactical interventions.
SSEs per 10,000 adjusted patient-days decreased significantly, to a mean of 0.3 from 0.9 (P<0.0001) after implementation, while days between SSEs increased to a mean of 55.2 from 19.4 (P<0.0001).
This work represents one of the most robust single-center approaches to improving patient safety that has been published to date. The authors attribute much of their success to culture change, which required “relentless clarity of vision by the organization.” Although this substantially limits immediate generalizability of any of the specific interventions, the work stands on its own as a prime example of what may be accomplished through focused dedication to reducing patient harm.
Bottom line: Patient harm is preventable through a widespread and multifaceted institutional initiative.
Citation: Muething SE, Goudie A, Schoettker PJ, et al. Quality improvement initiative to reduce serious safety events and improve patient safety culture. Pediatrics. 2012;130:e423-431.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: Can a broadly constructed improvement initiative significantly reduce serious safety events (SSEs)?
Study design: Single-institution quality-improvement initiative.
Setting: Cincinnati Children’s Hospital Medical Center.
Synopsis: A multidisciplinary team supported by leadership was formed to reduce SSEs across the hospital by 80% within four years. A consulting firm with expertise in the field was also engaged for this process. Multifaceted interventions were clustered according to perceived key drivers of change in the institution: error prevention systems, improved safety governance, cause analysis programs, lessons-learned programs, and specific tactical interventions.
SSEs per 10,000 adjusted patient-days decreased significantly, to a mean of 0.3 from 0.9 (P<0.0001) after implementation, while days between SSEs increased to a mean of 55.2 from 19.4 (P<0.0001).
This work represents one of the most robust single-center approaches to improving patient safety that has been published to date. The authors attribute much of their success to culture change, which required “relentless clarity of vision by the organization.” Although this substantially limits immediate generalizability of any of the specific interventions, the work stands on its own as a prime example of what may be accomplished through focused dedication to reducing patient harm.
Bottom line: Patient harm is preventable through a widespread and multifaceted institutional initiative.
Citation: Muething SE, Goudie A, Schoettker PJ, et al. Quality improvement initiative to reduce serious safety events and improve patient safety culture. Pediatrics. 2012;130:e423-431.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: Can a broadly constructed improvement initiative significantly reduce serious safety events (SSEs)?
Study design: Single-institution quality-improvement initiative.
Setting: Cincinnati Children’s Hospital Medical Center.
Synopsis: A multidisciplinary team supported by leadership was formed to reduce SSEs across the hospital by 80% within four years. A consulting firm with expertise in the field was also engaged for this process. Multifaceted interventions were clustered according to perceived key drivers of change in the institution: error prevention systems, improved safety governance, cause analysis programs, lessons-learned programs, and specific tactical interventions.
SSEs per 10,000 adjusted patient-days decreased significantly, to a mean of 0.3 from 0.9 (P<0.0001) after implementation, while days between SSEs increased to a mean of 55.2 from 19.4 (P<0.0001).
This work represents one of the most robust single-center approaches to improving patient safety that has been published to date. The authors attribute much of their success to culture change, which required “relentless clarity of vision by the organization.” Although this substantially limits immediate generalizability of any of the specific interventions, the work stands on its own as a prime example of what may be accomplished through focused dedication to reducing patient harm.
Bottom line: Patient harm is preventable through a widespread and multifaceted institutional initiative.
Citation: Muething SE, Goudie A, Schoettker PJ, et al. Quality improvement initiative to reduce serious safety events and improve patient safety culture. Pediatrics. 2012;130:e423-431.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
ITL: Physician Reviews of HM-Relevant Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- Guidelines on steroids and antivirals to treat Bell’s palsy
- Probiotics to reduce Clostridium difficile-associated diarrhea
- Rates of hemorrhage from warfarin therapy higher in clinical practice
- Less experienced doctors incur higher treatment costs
- Pay-for-performance incentive reduces mortality in England
- No benefit in ultrafiltration to treat acute heart failure
- Hospitalized patients often receive too much acetaminophen
- Longer anticoagulation therapy beneficial after bioprosthetic aortic valve replacement
- Antimicrobial-coated catheters and risk of urinary tract infection
- Patient outcomes improve after in-hospital cardiac arrest
Updated Guidelines on Steroids and Antivirals in Bell’s Palsy
Clinical question: Does the use of steroids and/or antivirals improve recovery in patients with newly diagnosed Bell’s palsy?
Background: The American Academy of Neurology’s last recommendation in 2001 stated that steroids were probably effective and antivirals possibly effective. The current review and recommendations looked at additional studies published since 2000.
Study design: Systematic review of MEDLINE and Cochrane Database of Systematic Reviews data published since June 2000.
Setting: Prospective controlled studies from Germany, Sweden, Scotland, Italy, South Korea, Japan, and Bangladesh.
Synopsis: The authors identified nine studies that fulfilled inclusion criteria. Two of these studies examined treatment with steroids alone and were judged to have the lowest risk for bias. Both studies enrolled patients within three days of symptom onset, continued treatment for 10 days, and demonstrated a significant increase in the probability of complete recovery in patients randomized to steroids (NNT 6-8). Two high-quality studies were identified that looked at the addition of antivirals to steroids. Neither study showed a statistically significant benefit.
Of note, the studies did not quantify the risk of harm from steroid use in patients with comorbidities, such as diabetes. Thus, the authors concluded that in some patients, it would be reasonable to consider limiting steroid use.
Bottom line: For patients with new-onset Bell’s palsy, steroids increase the probability of recovery of facial nerve function. Patients offered antivirals should be counseled that a benefit from antivirals has not been established, and, if there is a benefit, it is modest at best.
Citation: Gronseth GS, Paduga R. Evidence-based guideline update: steroids and antivirals for Bell palsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2012;79(22):2209-2213.
Probiotic Prophylaxis Reduces Clostridium Difficile-Associated Diarrhea
Clinical question: Are probiotics a safe and efficacious therapy for the prevention of Clostridium difficile-associated diarrhea (CDAD)?
Background: CDAD is the most common cause of hospital-acquired infectious diarrhea in high-income countries. There has been a dramatic rise in the incidence and severity of CDAD since 2002. Previous studies suggested that probiotics might reduce the incidence of CDAD with few adverse events.
Study design: Systematic review and meta-analysis of the literature.
Setting: Randomized controlled trials from the U.S., Canada, Chile, China, United Kingdom, Turkey, Poland, and Sweden.
Synopsis: Investigators identified 20 trials including 3,818 participants using a systematic search of randomized controlled trials of a specified probiotic of any strain in adults or pediatric subjects treated with antibiotics. Probiotics reduced the incidence of CDAD by 66% (risk ratio 0.34, 95% CI 0.24 to 0.49). Subgroup analyses showed similar results in both adults and children, with lower and high doses, and with different probiotic species.
Of probiotic-treated patients, 9.3% experienced an adverse event compared with 12.6% of control patients (relative risk 0.82, 95% CI 0.65 to 1.05). There was no report of any serious adverse events attributable to probiotics.
One limitation is the considerable variability in the reported risk of CDAD in the control group (0% to 40%). The absolute benefit from probiotics will depend on the risk in patients who do not receive prophylaxis.
Bottom line: Moderate-quality evidence suggests that probiotic prophylaxis results in a large reduction in C. diff-associated diarrhea without an increase in clinically important adverse events.
Citation: Johnston BC, Ma SSY, Goldenberg JZ, et al. Probiotics for the prevention of Clostridium difficile-associated diarrhea: a systematic review and meta-analysis. Ann Intern Med. 2012;157(12):878-888.
Rates of Hemorrhage from Warfarin Therapy Higher in Clinical Practice
Clinical question: What is the incidence of hemorrhage in a large population-based cohort of patients with atrial fibrillation who have started warfarin therapy?
Background: There is strong evidence that supports the use of warfarin to reduce the risk of stroke and systemic embolism in patients with atrial fibrillation. There are currently no large studies offering real-world, population-based estimates of hemorrhage rates among patients taking warfarin.
Study design: Retrospective cohort study.
Setting: Ontario.
Synopsis: This population-based, cohort study included 125,195 residents of Ontario age ≥66 years with atrial fibrillation who started taking warfarin sometime from 1997 to 2008. Hemorrhage was defined as bleeding requiring an emergency department visit or hospital admission. The overall risk of hemorrhage was 3.8% per person-year, but it was 11.8% in the first 30 days of therapy. For subjects age >75 years, the overall risk was 4.6% compared with 2.9% for those between 66 and 75 years.
Most hospital admissions involved gastrointestinal hemorrhages (63%). Almost 1 in 5 people (18%) with hospital admissions for hemorrhages died in the hospital or within seven days of discharge.
Bottom line: Rates of hemorrhage for older patients on warfarin therapy are significantly higher in clinical practice than the rates reported in clinical trials. The difference is likely due to the strict inclusion criteria, younger average age, and close monitoring of patients in clinical trials.
Citation: Gomes T, Mamdani MM, Holbrook AM, Paterson JM, Hellings C, Juurlink DN. Rates of hemorrhage during warfarin therapy for atrial fibrillation. CMAJ. 2013; Jan 21 [Epub ahead of print].
Less Experienced Doctors Incur Higher Treatment Costs
Clinical question: Which physician characteristics are associated with higher cost profiles?
Background: While both public and private insurers increasingly use physician cost profiles to identify physicians whose practice patterns account for more healthcare spending than other physicians, the individual physician characteristics associated with cost-profile performance are unknown.
Study design: Retrospective cohort study.
Setting: Four commercial health plans in Massachusetts.
Synopsis: Data collected from the insurance claims records of 1.13 million patients aged 18-65 years who were enrolled in one of four commercial health plans in Massachusetts in 2004 and 2005 were matched with the public records of 12,116 doctors who were stratified into five groups according to years of experience (<10, 10-19, 20-29, 30-39, and ≥40 years).
A strong association was found between physician experience and cost profiles, with the most experienced doctors—40 or more years of experience—providing the least costly care. Costs increased with each successively less experienced group (by 2.5%, 6.5%, 10%, and 13.2% more, respectively, to treat the same condition). No association was found between cost profiles and other physician characteristics, such as having had malpractice claims or disciplinary actions, board certification status, and practice size.
Differences appear to be driven by high-cost outlier patients. While median costs were similar between physicians with different levels of experience, the costs of treating patients at the 95 percentile of cost were much higher among physicians with less experience.
Bottom line: Doctors in this study with the least experience incurred 13.2% greater costs than their most senior counterparts.
Citation: Mehrotra A, Reid RO, Adams JL, Friedberg MW, McGlynn EA, Hussey PS. Physicians with the least experience have higher cost profiles than do physicians with the most experience. Health Aff (Millwood). 2012;31(11):2453-2463.
Pay-For-Performance Incentive Reduces Mortality in England
Clinical question: Do pay-for-performance programs improve quality of care?
Background: Pay-for-performance programs are being widely adopted both internationally and in the U.S. There is, however, limited evidence that these programs improve patient outcomes, and most prior studies have shown modest or inconsistent improvements in quality of care.
Study design: Prospective cohort study.
Setting: National Health Service (NHS) hospitals in northwest England.
Synopsis: The Advanced Quality program, the first hospital-based pay-for-performance program in England, was introduced in October 2004 in all 24 NHS hospitals in northwest England that provide emergency care. The program used a “tournament” system in which only the top-performing hospitals received bonus payments. There was no penalty for poor performers.
The primary end-point was 30-day in-hospital mortality among patients admitted for pneumonia, heart failure, or acute myocardial infarction. Over the three-year period studied (18 months before and 18 months after introduction of the program), the risk-adjusted mortality for these three conditions decreased significantly with an absolute reduction of 1.3% (95% CI 0.4 to 2.1%; P=0.006). The largest change, for pneumonia, was significant (1.9%, 95% CI 0.9 to 3.0, P<0.001), with nonsignificant reductions for acute myocardial infarction (0.6%, 95% CI -0.4 to 1.7; P=0.23) and heart failure (0.6%, 95% CI -0.6 to 1.8; P=0.30).
Bottom line: The introduction of a pay-for-performance program for all National Health Service hospitals in one region of England was associated with a significant reduction in mortality.
Citation: Sutton M, Nikolova S, Boaden R, Lester H, McDonald R, Roland M. Reduced mortality with hospital pay for performance in England. N Engl J Med. 2012;367(19):1821-1828.
Ultrafiltration Shows No Benefit in Acute Heart Failure
Clinical question: Is ultrafiltration superior to pharmacotherapy in the treatment of patients with acute heart failure and cardiorenal syndrome?
Background: Venovenous ultrafiltration is an alternative to diuretic therapy in patients with acute decompensated heart failure and worsened renal function that could allow greater control of the rate of fluid removal and improve outcomes. Little is known about the efficacy and safety of ultrafiltration compared to standard pharmacological therapy.
Study design: Multicenter randomized controlled trial.
Setting: Fourteen clinical centers in the U.S. and Canada.
Synopsis: One hundred eighty-eight patients admitted to a hospital with acute decompensated heart failure and worsened renal function were randomized to stepped pharmacological therapy or ultrafiltration. Ultrafiltration was inferior to pharmacological therapy with respect to the pre-specified primary composite endpoint, the change in serum creatinine level, and body weight at 96 hours after enrollment (P=0.003). This difference was primarily due to an increase in the serum creatinine level in the ultrafiltration group (0.23 vs. -0.04 mg/dl; P=0.003). There was no significant difference in weight loss at 96 hours (loss of 5.5 kg vs. 5.7kg; P=0.58).
A higher percentage of patients in the ultrafiltration group had a serious adverse event over the 60-day follow-up period (72% vs. 57%, P=0.03). There was no significant difference in the composite rate of death or rehospitalization for heart failure in the ultrafiltration group compared to the pharmacologic-therapy group (38% vs. 35%; P=0.96).
Bottom line: Pharmacological therapy is superior to ultrafiltration in patients with acute decompensated heart failure and worsened renal function.
Citation: Bart BA, Goldsmith SR, Lee KL, et al. Ultrafiltration in decompensated heart failure with cardiorenal syndrome. N Engl J Med. 2012;367:2296-2304.
Hospitalized Patients Often Receive Too Much Acetaminophen
Clinical question: What are the prevalence and factors associated with supratherapeutic dosing of acetaminophen in hospitalized patients?
Background: Acetaminophen is a commonly used medication that at high doses can be associated with significant adverse events, including liver failure. Considerable efforts have been made in the outpatient setting to limit the risks associated with acetaminophen. Little research has examined acetaminophen exposure in the inpatient setting.
Study design: Retrospective cohort study.
Setting: Two academic tertiary-care hospitals in the U.S.
Synopsis: The authors reviewed the electronic medication administration record of all adult patients admitted to two academic hospitals from June 1, 2010, to Aug. 31, 2010. A total of 14,411 patients (60.7%) were prescribed acetaminophen, of whom 955 (6.6%) were prescribed more than the 4g per day (the maximum recommended daily dose) at least once. In addition, 22.3% of patients >65 and 17.6% of patients with chronic liver disease exceeded the recommended limit of 3g per day. Half the supratherapeutic episodes involved doses exceeding 5g a day, often for several days. In adjusted analyses, scheduled administration (rather than as needed), a diagnosis of osteoarthritis, and higher-strength tablets were all associated with a higher risk of exposure to supratherapeutic doses.
Bottom line: A significant proportion of hospitalized patients are exposed to supratherapeutic dosing of acetaminophen.
Citation: Zhou L, Maviglia SM, Mahoney LM, et al. Supra-therapeutic dosing of acetaminophen among hospitalized patients. Arch Intern Med. 2012;172(22):1721-1728.
Longer Anticoagulation Therapy after Bioprosthetic Aortic Valve Replacement Might Be Beneficial
Clinical question: How long should anticoagulation therapy with warfarin be continued after surgical bioprosthetic aortic valve replacement?
Background: Current guidelines recommend a three-month course of anticoagulation therapy after bioprosthetic aortic valve surgery. However, the appropriate duration of post-operative anticoagulation therapy has not been well established
Study design: Retrospective cohort study.
Setting: Denmark.
Synopsis: Using data from the Danish National Registries, 4,075 subjects without atrial fibrillation who underwent bioprosthetic aortic valve implantation from 1997 to 2009 were identified. The association between different durations of warfarin therapy after aortic valve implantation and the combined end point of stroke, thromboembolic events, cardiovascular death, or bleeding episodes was examined.
The risk of adverse outcomes was substantially higher for patients not treated with warfarin compared to treated patents. The estimated adverse event rate was 7 per 100 person-years for untreated patients versus 2.7 per 100 for warfarin-treated patients (adjusted incidence rate ratio [IRR] 2.46, 95% CI 1.09 to 6.48). Patients not treated with warfarin were at higher risk of cardiovascular death within 30 to 89 days after surgery, with an event rate of 31.7 per 100 person-years versus 3.8 per 100 person-years (adjusted IRR 7.61, 95% CI 4.37 to 13.26). The difference in cardiovascular mortality continued to be significant from 90 to 179 days after surgery, with an event rate of 6.5 per 100 person-years versus 2.1 per 100 person-years (IRR 3.51, 95% CI 1.54 to 8.03).
Bottom line: Discontinuation of warfarin therapy within six months of bioprosthetic aortic valve replacement is associated with increased cardiovascular death.
Citation: Mérie C, Køber L, Skov Olsen P, et al. Association of warfarin therapy duration after bioprosthetic aortic valve replacement with risk of mortality, thromboembolic complications, and bleeding. JAMA. 2012;308(20):2118-2125.
Limited Evidence for Antimicrobial-Coated Catheters
Clinical question: Does the use of antimicrobial-coated catheters reduce the risk of catheter-associated urinary tract infection (UTI) compared to standard polytetrafluoroethylene (PTFE) catheters?
Background: UTIs associated with indwelling catheters are a major preventable cause of harm for hospitalized patients. Prior studies have shown that catheters made with antimicrobial coatings can reduce rates of bacteriuria, but their usefulness against symptomatic catheter-associated UTIs remains uncertain.
Study design: Multicenter randomized controlled trial.
Setting: Twenty-four hospitals in the United Kingdom.
Synopsis: A total of 7,102 patients >16 undergoing urethral catheterization for an anticipated duration of <14 days were randomly allocated in a 1:1:1 ratio to receive a silver-alloy-coated catheter, a nitrofural-impregnated silicone catheter, or a standard PTFE-coated catheter. The primary outcome was defined as presence of patient-reported symptoms of UTI and prescription of antibiotic for UTI. Incidence of symptomatic catheter-associated UTI up to six weeks after randomization did not differ significantly between groups and occurred in 12.6% of the PTFE control, 12.5% of the silver alloy group, and 10.6% of the nitrofural group. In secondary outcomes, the nitrofural catheter was associated with a slightly reduced incidence of culture-confirmed symptomatic UTI (absolute risk reduction of 1.4%) and lower rate of bacteriuria, but it also had greater patient-reported discomfort during use and removal.
Bottom line: Antimicrobial-coated catheters do not show a clinically significant benefit over standard PTFE catheters in preventing catheter-associated UTI.
Citation: Pickard R, Lam T, Maclennan G, et al. Antimicrobial catheters for reduction of symptomatic urinary tract infection in adults requiring short-term catheterisation in hospital: a multicentre randomized controlled trial. Lancet. 2012;380:1927-1935.
Outcomes Improve after In-Hospital Cardiac Arrest
Clinical question: Have outcomes after in-hospital cardiac arrest improved with recent advances in resuscitation care?
Background: Over the past decade, quality-improvement (QI) efforts in hospital resuscitation care have included use of mock cardiac arrests, defibrillation by nonmedical personnel, and participation in QI registries. It is unclear what effect these efforts have had on overall survival and neurologic recovery.
Study design: Retrospective cohort study.
Setting: Five hundred fifty-three hospitals in the U.S.
Synopsis: A total of 113,514 patients age >18 with a cardiac arrest occurring from Jan. 1, 2000, to Nov. 19, 2009, were identified. Analyses were separated by initial rhythm (PEA/asystole or ventricular fibrillation/tachycardia). Overall survival to discharge increased significantly to 22.3% in 2009 from 13.7% in 2000, with similar increases within each rhythm group. Rates of acute resuscitation survival (return of spontaneous circulation for at least 20 contiguous minutes after initial arrest) and post-resuscitation survival (survival to discharge among patients surviving acute resuscitation) also improved during the study period. Rates of clinically significant neurologic disability, as defined by cerebral performance scores >1, decreased over time for the overall cohort and the subset with ventricular fibrillation/tachycardia. The study was limited by including only hospitals motivated to participate in a QI registry.
Bottom line: From 2000 to 2009, survival after in-hospital cardiac arrest improved, and rates of clinically significant neurologic disability among survivors decreased.
Citation: Girotra S, Nallamothu B, Spertus J, et al. Trends in survival after in-hospital cardiac arrest. N Engl J Med. 2012;367:1912-1920.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Guidelines on steroids and antivirals to treat Bell’s palsy
- Probiotics to reduce Clostridium difficile-associated diarrhea
- Rates of hemorrhage from warfarin therapy higher in clinical practice
- Less experienced doctors incur higher treatment costs
- Pay-for-performance incentive reduces mortality in England
- No benefit in ultrafiltration to treat acute heart failure
- Hospitalized patients often receive too much acetaminophen
- Longer anticoagulation therapy beneficial after bioprosthetic aortic valve replacement
- Antimicrobial-coated catheters and risk of urinary tract infection
- Patient outcomes improve after in-hospital cardiac arrest
Updated Guidelines on Steroids and Antivirals in Bell’s Palsy
Clinical question: Does the use of steroids and/or antivirals improve recovery in patients with newly diagnosed Bell’s palsy?
Background: The American Academy of Neurology’s last recommendation in 2001 stated that steroids were probably effective and antivirals possibly effective. The current review and recommendations looked at additional studies published since 2000.
Study design: Systematic review of MEDLINE and Cochrane Database of Systematic Reviews data published since June 2000.
Setting: Prospective controlled studies from Germany, Sweden, Scotland, Italy, South Korea, Japan, and Bangladesh.
Synopsis: The authors identified nine studies that fulfilled inclusion criteria. Two of these studies examined treatment with steroids alone and were judged to have the lowest risk for bias. Both studies enrolled patients within three days of symptom onset, continued treatment for 10 days, and demonstrated a significant increase in the probability of complete recovery in patients randomized to steroids (NNT 6-8). Two high-quality studies were identified that looked at the addition of antivirals to steroids. Neither study showed a statistically significant benefit.
Of note, the studies did not quantify the risk of harm from steroid use in patients with comorbidities, such as diabetes. Thus, the authors concluded that in some patients, it would be reasonable to consider limiting steroid use.
Bottom line: For patients with new-onset Bell’s palsy, steroids increase the probability of recovery of facial nerve function. Patients offered antivirals should be counseled that a benefit from antivirals has not been established, and, if there is a benefit, it is modest at best.
Citation: Gronseth GS, Paduga R. Evidence-based guideline update: steroids and antivirals for Bell palsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2012;79(22):2209-2213.
Probiotic Prophylaxis Reduces Clostridium Difficile-Associated Diarrhea
Clinical question: Are probiotics a safe and efficacious therapy for the prevention of Clostridium difficile-associated diarrhea (CDAD)?
Background: CDAD is the most common cause of hospital-acquired infectious diarrhea in high-income countries. There has been a dramatic rise in the incidence and severity of CDAD since 2002. Previous studies suggested that probiotics might reduce the incidence of CDAD with few adverse events.
Study design: Systematic review and meta-analysis of the literature.
Setting: Randomized controlled trials from the U.S., Canada, Chile, China, United Kingdom, Turkey, Poland, and Sweden.
Synopsis: Investigators identified 20 trials including 3,818 participants using a systematic search of randomized controlled trials of a specified probiotic of any strain in adults or pediatric subjects treated with antibiotics. Probiotics reduced the incidence of CDAD by 66% (risk ratio 0.34, 95% CI 0.24 to 0.49). Subgroup analyses showed similar results in both adults and children, with lower and high doses, and with different probiotic species.
Of probiotic-treated patients, 9.3% experienced an adverse event compared with 12.6% of control patients (relative risk 0.82, 95% CI 0.65 to 1.05). There was no report of any serious adverse events attributable to probiotics.
One limitation is the considerable variability in the reported risk of CDAD in the control group (0% to 40%). The absolute benefit from probiotics will depend on the risk in patients who do not receive prophylaxis.
Bottom line: Moderate-quality evidence suggests that probiotic prophylaxis results in a large reduction in C. diff-associated diarrhea without an increase in clinically important adverse events.
Citation: Johnston BC, Ma SSY, Goldenberg JZ, et al. Probiotics for the prevention of Clostridium difficile-associated diarrhea: a systematic review and meta-analysis. Ann Intern Med. 2012;157(12):878-888.
Rates of Hemorrhage from Warfarin Therapy Higher in Clinical Practice
Clinical question: What is the incidence of hemorrhage in a large population-based cohort of patients with atrial fibrillation who have started warfarin therapy?
Background: There is strong evidence that supports the use of warfarin to reduce the risk of stroke and systemic embolism in patients with atrial fibrillation. There are currently no large studies offering real-world, population-based estimates of hemorrhage rates among patients taking warfarin.
Study design: Retrospective cohort study.
Setting: Ontario.
Synopsis: This population-based, cohort study included 125,195 residents of Ontario age ≥66 years with atrial fibrillation who started taking warfarin sometime from 1997 to 2008. Hemorrhage was defined as bleeding requiring an emergency department visit or hospital admission. The overall risk of hemorrhage was 3.8% per person-year, but it was 11.8% in the first 30 days of therapy. For subjects age >75 years, the overall risk was 4.6% compared with 2.9% for those between 66 and 75 years.
Most hospital admissions involved gastrointestinal hemorrhages (63%). Almost 1 in 5 people (18%) with hospital admissions for hemorrhages died in the hospital or within seven days of discharge.
Bottom line: Rates of hemorrhage for older patients on warfarin therapy are significantly higher in clinical practice than the rates reported in clinical trials. The difference is likely due to the strict inclusion criteria, younger average age, and close monitoring of patients in clinical trials.
Citation: Gomes T, Mamdani MM, Holbrook AM, Paterson JM, Hellings C, Juurlink DN. Rates of hemorrhage during warfarin therapy for atrial fibrillation. CMAJ. 2013; Jan 21 [Epub ahead of print].
Less Experienced Doctors Incur Higher Treatment Costs
Clinical question: Which physician characteristics are associated with higher cost profiles?
Background: While both public and private insurers increasingly use physician cost profiles to identify physicians whose practice patterns account for more healthcare spending than other physicians, the individual physician characteristics associated with cost-profile performance are unknown.
Study design: Retrospective cohort study.
Setting: Four commercial health plans in Massachusetts.
Synopsis: Data collected from the insurance claims records of 1.13 million patients aged 18-65 years who were enrolled in one of four commercial health plans in Massachusetts in 2004 and 2005 were matched with the public records of 12,116 doctors who were stratified into five groups according to years of experience (<10, 10-19, 20-29, 30-39, and ≥40 years).
A strong association was found between physician experience and cost profiles, with the most experienced doctors—40 or more years of experience—providing the least costly care. Costs increased with each successively less experienced group (by 2.5%, 6.5%, 10%, and 13.2% more, respectively, to treat the same condition). No association was found between cost profiles and other physician characteristics, such as having had malpractice claims or disciplinary actions, board certification status, and practice size.
Differences appear to be driven by high-cost outlier patients. While median costs were similar between physicians with different levels of experience, the costs of treating patients at the 95 percentile of cost were much higher among physicians with less experience.
Bottom line: Doctors in this study with the least experience incurred 13.2% greater costs than their most senior counterparts.
Citation: Mehrotra A, Reid RO, Adams JL, Friedberg MW, McGlynn EA, Hussey PS. Physicians with the least experience have higher cost profiles than do physicians with the most experience. Health Aff (Millwood). 2012;31(11):2453-2463.
Pay-For-Performance Incentive Reduces Mortality in England
Clinical question: Do pay-for-performance programs improve quality of care?
Background: Pay-for-performance programs are being widely adopted both internationally and in the U.S. There is, however, limited evidence that these programs improve patient outcomes, and most prior studies have shown modest or inconsistent improvements in quality of care.
Study design: Prospective cohort study.
Setting: National Health Service (NHS) hospitals in northwest England.
Synopsis: The Advanced Quality program, the first hospital-based pay-for-performance program in England, was introduced in October 2004 in all 24 NHS hospitals in northwest England that provide emergency care. The program used a “tournament” system in which only the top-performing hospitals received bonus payments. There was no penalty for poor performers.
The primary end-point was 30-day in-hospital mortality among patients admitted for pneumonia, heart failure, or acute myocardial infarction. Over the three-year period studied (18 months before and 18 months after introduction of the program), the risk-adjusted mortality for these three conditions decreased significantly with an absolute reduction of 1.3% (95% CI 0.4 to 2.1%; P=0.006). The largest change, for pneumonia, was significant (1.9%, 95% CI 0.9 to 3.0, P<0.001), with nonsignificant reductions for acute myocardial infarction (0.6%, 95% CI -0.4 to 1.7; P=0.23) and heart failure (0.6%, 95% CI -0.6 to 1.8; P=0.30).
Bottom line: The introduction of a pay-for-performance program for all National Health Service hospitals in one region of England was associated with a significant reduction in mortality.
Citation: Sutton M, Nikolova S, Boaden R, Lester H, McDonald R, Roland M. Reduced mortality with hospital pay for performance in England. N Engl J Med. 2012;367(19):1821-1828.
Ultrafiltration Shows No Benefit in Acute Heart Failure
Clinical question: Is ultrafiltration superior to pharmacotherapy in the treatment of patients with acute heart failure and cardiorenal syndrome?
Background: Venovenous ultrafiltration is an alternative to diuretic therapy in patients with acute decompensated heart failure and worsened renal function that could allow greater control of the rate of fluid removal and improve outcomes. Little is known about the efficacy and safety of ultrafiltration compared to standard pharmacological therapy.
Study design: Multicenter randomized controlled trial.
Setting: Fourteen clinical centers in the U.S. and Canada.
Synopsis: One hundred eighty-eight patients admitted to a hospital with acute decompensated heart failure and worsened renal function were randomized to stepped pharmacological therapy or ultrafiltration. Ultrafiltration was inferior to pharmacological therapy with respect to the pre-specified primary composite endpoint, the change in serum creatinine level, and body weight at 96 hours after enrollment (P=0.003). This difference was primarily due to an increase in the serum creatinine level in the ultrafiltration group (0.23 vs. -0.04 mg/dl; P=0.003). There was no significant difference in weight loss at 96 hours (loss of 5.5 kg vs. 5.7kg; P=0.58).
A higher percentage of patients in the ultrafiltration group had a serious adverse event over the 60-day follow-up period (72% vs. 57%, P=0.03). There was no significant difference in the composite rate of death or rehospitalization for heart failure in the ultrafiltration group compared to the pharmacologic-therapy group (38% vs. 35%; P=0.96).
Bottom line: Pharmacological therapy is superior to ultrafiltration in patients with acute decompensated heart failure and worsened renal function.
Citation: Bart BA, Goldsmith SR, Lee KL, et al. Ultrafiltration in decompensated heart failure with cardiorenal syndrome. N Engl J Med. 2012;367:2296-2304.
Hospitalized Patients Often Receive Too Much Acetaminophen
Clinical question: What are the prevalence and factors associated with supratherapeutic dosing of acetaminophen in hospitalized patients?
Background: Acetaminophen is a commonly used medication that at high doses can be associated with significant adverse events, including liver failure. Considerable efforts have been made in the outpatient setting to limit the risks associated with acetaminophen. Little research has examined acetaminophen exposure in the inpatient setting.
Study design: Retrospective cohort study.
Setting: Two academic tertiary-care hospitals in the U.S.
Synopsis: The authors reviewed the electronic medication administration record of all adult patients admitted to two academic hospitals from June 1, 2010, to Aug. 31, 2010. A total of 14,411 patients (60.7%) were prescribed acetaminophen, of whom 955 (6.6%) were prescribed more than the 4g per day (the maximum recommended daily dose) at least once. In addition, 22.3% of patients >65 and 17.6% of patients with chronic liver disease exceeded the recommended limit of 3g per day. Half the supratherapeutic episodes involved doses exceeding 5g a day, often for several days. In adjusted analyses, scheduled administration (rather than as needed), a diagnosis of osteoarthritis, and higher-strength tablets were all associated with a higher risk of exposure to supratherapeutic doses.
Bottom line: A significant proportion of hospitalized patients are exposed to supratherapeutic dosing of acetaminophen.
Citation: Zhou L, Maviglia SM, Mahoney LM, et al. Supra-therapeutic dosing of acetaminophen among hospitalized patients. Arch Intern Med. 2012;172(22):1721-1728.
Longer Anticoagulation Therapy after Bioprosthetic Aortic Valve Replacement Might Be Beneficial
Clinical question: How long should anticoagulation therapy with warfarin be continued after surgical bioprosthetic aortic valve replacement?
Background: Current guidelines recommend a three-month course of anticoagulation therapy after bioprosthetic aortic valve surgery. However, the appropriate duration of post-operative anticoagulation therapy has not been well established
Study design: Retrospective cohort study.
Setting: Denmark.
Synopsis: Using data from the Danish National Registries, 4,075 subjects without atrial fibrillation who underwent bioprosthetic aortic valve implantation from 1997 to 2009 were identified. The association between different durations of warfarin therapy after aortic valve implantation and the combined end point of stroke, thromboembolic events, cardiovascular death, or bleeding episodes was examined.
The risk of adverse outcomes was substantially higher for patients not treated with warfarin compared to treated patents. The estimated adverse event rate was 7 per 100 person-years for untreated patients versus 2.7 per 100 for warfarin-treated patients (adjusted incidence rate ratio [IRR] 2.46, 95% CI 1.09 to 6.48). Patients not treated with warfarin were at higher risk of cardiovascular death within 30 to 89 days after surgery, with an event rate of 31.7 per 100 person-years versus 3.8 per 100 person-years (adjusted IRR 7.61, 95% CI 4.37 to 13.26). The difference in cardiovascular mortality continued to be significant from 90 to 179 days after surgery, with an event rate of 6.5 per 100 person-years versus 2.1 per 100 person-years (IRR 3.51, 95% CI 1.54 to 8.03).
Bottom line: Discontinuation of warfarin therapy within six months of bioprosthetic aortic valve replacement is associated with increased cardiovascular death.
Citation: Mérie C, Køber L, Skov Olsen P, et al. Association of warfarin therapy duration after bioprosthetic aortic valve replacement with risk of mortality, thromboembolic complications, and bleeding. JAMA. 2012;308(20):2118-2125.
Limited Evidence for Antimicrobial-Coated Catheters
Clinical question: Does the use of antimicrobial-coated catheters reduce the risk of catheter-associated urinary tract infection (UTI) compared to standard polytetrafluoroethylene (PTFE) catheters?
Background: UTIs associated with indwelling catheters are a major preventable cause of harm for hospitalized patients. Prior studies have shown that catheters made with antimicrobial coatings can reduce rates of bacteriuria, but their usefulness against symptomatic catheter-associated UTIs remains uncertain.
Study design: Multicenter randomized controlled trial.
Setting: Twenty-four hospitals in the United Kingdom.
Synopsis: A total of 7,102 patients >16 undergoing urethral catheterization for an anticipated duration of <14 days were randomly allocated in a 1:1:1 ratio to receive a silver-alloy-coated catheter, a nitrofural-impregnated silicone catheter, or a standard PTFE-coated catheter. The primary outcome was defined as presence of patient-reported symptoms of UTI and prescription of antibiotic for UTI. Incidence of symptomatic catheter-associated UTI up to six weeks after randomization did not differ significantly between groups and occurred in 12.6% of the PTFE control, 12.5% of the silver alloy group, and 10.6% of the nitrofural group. In secondary outcomes, the nitrofural catheter was associated with a slightly reduced incidence of culture-confirmed symptomatic UTI (absolute risk reduction of 1.4%) and lower rate of bacteriuria, but it also had greater patient-reported discomfort during use and removal.
Bottom line: Antimicrobial-coated catheters do not show a clinically significant benefit over standard PTFE catheters in preventing catheter-associated UTI.
Citation: Pickard R, Lam T, Maclennan G, et al. Antimicrobial catheters for reduction of symptomatic urinary tract infection in adults requiring short-term catheterisation in hospital: a multicentre randomized controlled trial. Lancet. 2012;380:1927-1935.
Outcomes Improve after In-Hospital Cardiac Arrest
Clinical question: Have outcomes after in-hospital cardiac arrest improved with recent advances in resuscitation care?
Background: Over the past decade, quality-improvement (QI) efforts in hospital resuscitation care have included use of mock cardiac arrests, defibrillation by nonmedical personnel, and participation in QI registries. It is unclear what effect these efforts have had on overall survival and neurologic recovery.
Study design: Retrospective cohort study.
Setting: Five hundred fifty-three hospitals in the U.S.
Synopsis: A total of 113,514 patients age >18 with a cardiac arrest occurring from Jan. 1, 2000, to Nov. 19, 2009, were identified. Analyses were separated by initial rhythm (PEA/asystole or ventricular fibrillation/tachycardia). Overall survival to discharge increased significantly to 22.3% in 2009 from 13.7% in 2000, with similar increases within each rhythm group. Rates of acute resuscitation survival (return of spontaneous circulation for at least 20 contiguous minutes after initial arrest) and post-resuscitation survival (survival to discharge among patients surviving acute resuscitation) also improved during the study period. Rates of clinically significant neurologic disability, as defined by cerebral performance scores >1, decreased over time for the overall cohort and the subset with ventricular fibrillation/tachycardia. The study was limited by including only hospitals motivated to participate in a QI registry.
Bottom line: From 2000 to 2009, survival after in-hospital cardiac arrest improved, and rates of clinically significant neurologic disability among survivors decreased.
Citation: Girotra S, Nallamothu B, Spertus J, et al. Trends in survival after in-hospital cardiac arrest. N Engl J Med. 2012;367:1912-1920.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Guidelines on steroids and antivirals to treat Bell’s palsy
- Probiotics to reduce Clostridium difficile-associated diarrhea
- Rates of hemorrhage from warfarin therapy higher in clinical practice
- Less experienced doctors incur higher treatment costs
- Pay-for-performance incentive reduces mortality in England
- No benefit in ultrafiltration to treat acute heart failure
- Hospitalized patients often receive too much acetaminophen
- Longer anticoagulation therapy beneficial after bioprosthetic aortic valve replacement
- Antimicrobial-coated catheters and risk of urinary tract infection
- Patient outcomes improve after in-hospital cardiac arrest
Updated Guidelines on Steroids and Antivirals in Bell’s Palsy
Clinical question: Does the use of steroids and/or antivirals improve recovery in patients with newly diagnosed Bell’s palsy?
Background: The American Academy of Neurology’s last recommendation in 2001 stated that steroids were probably effective and antivirals possibly effective. The current review and recommendations looked at additional studies published since 2000.
Study design: Systematic review of MEDLINE and Cochrane Database of Systematic Reviews data published since June 2000.
Setting: Prospective controlled studies from Germany, Sweden, Scotland, Italy, South Korea, Japan, and Bangladesh.
Synopsis: The authors identified nine studies that fulfilled inclusion criteria. Two of these studies examined treatment with steroids alone and were judged to have the lowest risk for bias. Both studies enrolled patients within three days of symptom onset, continued treatment for 10 days, and demonstrated a significant increase in the probability of complete recovery in patients randomized to steroids (NNT 6-8). Two high-quality studies were identified that looked at the addition of antivirals to steroids. Neither study showed a statistically significant benefit.
Of note, the studies did not quantify the risk of harm from steroid use in patients with comorbidities, such as diabetes. Thus, the authors concluded that in some patients, it would be reasonable to consider limiting steroid use.
Bottom line: For patients with new-onset Bell’s palsy, steroids increase the probability of recovery of facial nerve function. Patients offered antivirals should be counseled that a benefit from antivirals has not been established, and, if there is a benefit, it is modest at best.
Citation: Gronseth GS, Paduga R. Evidence-based guideline update: steroids and antivirals for Bell palsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2012;79(22):2209-2213.
Probiotic Prophylaxis Reduces Clostridium Difficile-Associated Diarrhea
Clinical question: Are probiotics a safe and efficacious therapy for the prevention of Clostridium difficile-associated diarrhea (CDAD)?
Background: CDAD is the most common cause of hospital-acquired infectious diarrhea in high-income countries. There has been a dramatic rise in the incidence and severity of CDAD since 2002. Previous studies suggested that probiotics might reduce the incidence of CDAD with few adverse events.
Study design: Systematic review and meta-analysis of the literature.
Setting: Randomized controlled trials from the U.S., Canada, Chile, China, United Kingdom, Turkey, Poland, and Sweden.
Synopsis: Investigators identified 20 trials including 3,818 participants using a systematic search of randomized controlled trials of a specified probiotic of any strain in adults or pediatric subjects treated with antibiotics. Probiotics reduced the incidence of CDAD by 66% (risk ratio 0.34, 95% CI 0.24 to 0.49). Subgroup analyses showed similar results in both adults and children, with lower and high doses, and with different probiotic species.
Of probiotic-treated patients, 9.3% experienced an adverse event compared with 12.6% of control patients (relative risk 0.82, 95% CI 0.65 to 1.05). There was no report of any serious adverse events attributable to probiotics.
One limitation is the considerable variability in the reported risk of CDAD in the control group (0% to 40%). The absolute benefit from probiotics will depend on the risk in patients who do not receive prophylaxis.
Bottom line: Moderate-quality evidence suggests that probiotic prophylaxis results in a large reduction in C. diff-associated diarrhea without an increase in clinically important adverse events.
Citation: Johnston BC, Ma SSY, Goldenberg JZ, et al. Probiotics for the prevention of Clostridium difficile-associated diarrhea: a systematic review and meta-analysis. Ann Intern Med. 2012;157(12):878-888.
Rates of Hemorrhage from Warfarin Therapy Higher in Clinical Practice
Clinical question: What is the incidence of hemorrhage in a large population-based cohort of patients with atrial fibrillation who have started warfarin therapy?
Background: There is strong evidence that supports the use of warfarin to reduce the risk of stroke and systemic embolism in patients with atrial fibrillation. There are currently no large studies offering real-world, population-based estimates of hemorrhage rates among patients taking warfarin.
Study design: Retrospective cohort study.
Setting: Ontario.
Synopsis: This population-based, cohort study included 125,195 residents of Ontario age ≥66 years with atrial fibrillation who started taking warfarin sometime from 1997 to 2008. Hemorrhage was defined as bleeding requiring an emergency department visit or hospital admission. The overall risk of hemorrhage was 3.8% per person-year, but it was 11.8% in the first 30 days of therapy. For subjects age >75 years, the overall risk was 4.6% compared with 2.9% for those between 66 and 75 years.
Most hospital admissions involved gastrointestinal hemorrhages (63%). Almost 1 in 5 people (18%) with hospital admissions for hemorrhages died in the hospital or within seven days of discharge.
Bottom line: Rates of hemorrhage for older patients on warfarin therapy are significantly higher in clinical practice than the rates reported in clinical trials. The difference is likely due to the strict inclusion criteria, younger average age, and close monitoring of patients in clinical trials.
Citation: Gomes T, Mamdani MM, Holbrook AM, Paterson JM, Hellings C, Juurlink DN. Rates of hemorrhage during warfarin therapy for atrial fibrillation. CMAJ. 2013; Jan 21 [Epub ahead of print].
Less Experienced Doctors Incur Higher Treatment Costs
Clinical question: Which physician characteristics are associated with higher cost profiles?
Background: While both public and private insurers increasingly use physician cost profiles to identify physicians whose practice patterns account for more healthcare spending than other physicians, the individual physician characteristics associated with cost-profile performance are unknown.
Study design: Retrospective cohort study.
Setting: Four commercial health plans in Massachusetts.
Synopsis: Data collected from the insurance claims records of 1.13 million patients aged 18-65 years who were enrolled in one of four commercial health plans in Massachusetts in 2004 and 2005 were matched with the public records of 12,116 doctors who were stratified into five groups according to years of experience (<10, 10-19, 20-29, 30-39, and ≥40 years).
A strong association was found between physician experience and cost profiles, with the most experienced doctors—40 or more years of experience—providing the least costly care. Costs increased with each successively less experienced group (by 2.5%, 6.5%, 10%, and 13.2% more, respectively, to treat the same condition). No association was found between cost profiles and other physician characteristics, such as having had malpractice claims or disciplinary actions, board certification status, and practice size.
Differences appear to be driven by high-cost outlier patients. While median costs were similar between physicians with different levels of experience, the costs of treating patients at the 95 percentile of cost were much higher among physicians with less experience.
Bottom line: Doctors in this study with the least experience incurred 13.2% greater costs than their most senior counterparts.
Citation: Mehrotra A, Reid RO, Adams JL, Friedberg MW, McGlynn EA, Hussey PS. Physicians with the least experience have higher cost profiles than do physicians with the most experience. Health Aff (Millwood). 2012;31(11):2453-2463.
Pay-For-Performance Incentive Reduces Mortality in England
Clinical question: Do pay-for-performance programs improve quality of care?
Background: Pay-for-performance programs are being widely adopted both internationally and in the U.S. There is, however, limited evidence that these programs improve patient outcomes, and most prior studies have shown modest or inconsistent improvements in quality of care.
Study design: Prospective cohort study.
Setting: National Health Service (NHS) hospitals in northwest England.
Synopsis: The Advanced Quality program, the first hospital-based pay-for-performance program in England, was introduced in October 2004 in all 24 NHS hospitals in northwest England that provide emergency care. The program used a “tournament” system in which only the top-performing hospitals received bonus payments. There was no penalty for poor performers.
The primary end-point was 30-day in-hospital mortality among patients admitted for pneumonia, heart failure, or acute myocardial infarction. Over the three-year period studied (18 months before and 18 months after introduction of the program), the risk-adjusted mortality for these three conditions decreased significantly with an absolute reduction of 1.3% (95% CI 0.4 to 2.1%; P=0.006). The largest change, for pneumonia, was significant (1.9%, 95% CI 0.9 to 3.0, P<0.001), with nonsignificant reductions for acute myocardial infarction (0.6%, 95% CI -0.4 to 1.7; P=0.23) and heart failure (0.6%, 95% CI -0.6 to 1.8; P=0.30).
Bottom line: The introduction of a pay-for-performance program for all National Health Service hospitals in one region of England was associated with a significant reduction in mortality.
Citation: Sutton M, Nikolova S, Boaden R, Lester H, McDonald R, Roland M. Reduced mortality with hospital pay for performance in England. N Engl J Med. 2012;367(19):1821-1828.
Ultrafiltration Shows No Benefit in Acute Heart Failure
Clinical question: Is ultrafiltration superior to pharmacotherapy in the treatment of patients with acute heart failure and cardiorenal syndrome?
Background: Venovenous ultrafiltration is an alternative to diuretic therapy in patients with acute decompensated heart failure and worsened renal function that could allow greater control of the rate of fluid removal and improve outcomes. Little is known about the efficacy and safety of ultrafiltration compared to standard pharmacological therapy.
Study design: Multicenter randomized controlled trial.
Setting: Fourteen clinical centers in the U.S. and Canada.
Synopsis: One hundred eighty-eight patients admitted to a hospital with acute decompensated heart failure and worsened renal function were randomized to stepped pharmacological therapy or ultrafiltration. Ultrafiltration was inferior to pharmacological therapy with respect to the pre-specified primary composite endpoint, the change in serum creatinine level, and body weight at 96 hours after enrollment (P=0.003). This difference was primarily due to an increase in the serum creatinine level in the ultrafiltration group (0.23 vs. -0.04 mg/dl; P=0.003). There was no significant difference in weight loss at 96 hours (loss of 5.5 kg vs. 5.7kg; P=0.58).
A higher percentage of patients in the ultrafiltration group had a serious adverse event over the 60-day follow-up period (72% vs. 57%, P=0.03). There was no significant difference in the composite rate of death or rehospitalization for heart failure in the ultrafiltration group compared to the pharmacologic-therapy group (38% vs. 35%; P=0.96).
Bottom line: Pharmacological therapy is superior to ultrafiltration in patients with acute decompensated heart failure and worsened renal function.
Citation: Bart BA, Goldsmith SR, Lee KL, et al. Ultrafiltration in decompensated heart failure with cardiorenal syndrome. N Engl J Med. 2012;367:2296-2304.
Hospitalized Patients Often Receive Too Much Acetaminophen
Clinical question: What are the prevalence and factors associated with supratherapeutic dosing of acetaminophen in hospitalized patients?
Background: Acetaminophen is a commonly used medication that at high doses can be associated with significant adverse events, including liver failure. Considerable efforts have been made in the outpatient setting to limit the risks associated with acetaminophen. Little research has examined acetaminophen exposure in the inpatient setting.
Study design: Retrospective cohort study.
Setting: Two academic tertiary-care hospitals in the U.S.
Synopsis: The authors reviewed the electronic medication administration record of all adult patients admitted to two academic hospitals from June 1, 2010, to Aug. 31, 2010. A total of 14,411 patients (60.7%) were prescribed acetaminophen, of whom 955 (6.6%) were prescribed more than the 4g per day (the maximum recommended daily dose) at least once. In addition, 22.3% of patients >65 and 17.6% of patients with chronic liver disease exceeded the recommended limit of 3g per day. Half the supratherapeutic episodes involved doses exceeding 5g a day, often for several days. In adjusted analyses, scheduled administration (rather than as needed), a diagnosis of osteoarthritis, and higher-strength tablets were all associated with a higher risk of exposure to supratherapeutic doses.
Bottom line: A significant proportion of hospitalized patients are exposed to supratherapeutic dosing of acetaminophen.
Citation: Zhou L, Maviglia SM, Mahoney LM, et al. Supra-therapeutic dosing of acetaminophen among hospitalized patients. Arch Intern Med. 2012;172(22):1721-1728.
Longer Anticoagulation Therapy after Bioprosthetic Aortic Valve Replacement Might Be Beneficial
Clinical question: How long should anticoagulation therapy with warfarin be continued after surgical bioprosthetic aortic valve replacement?
Background: Current guidelines recommend a three-month course of anticoagulation therapy after bioprosthetic aortic valve surgery. However, the appropriate duration of post-operative anticoagulation therapy has not been well established
Study design: Retrospective cohort study.
Setting: Denmark.
Synopsis: Using data from the Danish National Registries, 4,075 subjects without atrial fibrillation who underwent bioprosthetic aortic valve implantation from 1997 to 2009 were identified. The association between different durations of warfarin therapy after aortic valve implantation and the combined end point of stroke, thromboembolic events, cardiovascular death, or bleeding episodes was examined.
The risk of adverse outcomes was substantially higher for patients not treated with warfarin compared to treated patents. The estimated adverse event rate was 7 per 100 person-years for untreated patients versus 2.7 per 100 for warfarin-treated patients (adjusted incidence rate ratio [IRR] 2.46, 95% CI 1.09 to 6.48). Patients not treated with warfarin were at higher risk of cardiovascular death within 30 to 89 days after surgery, with an event rate of 31.7 per 100 person-years versus 3.8 per 100 person-years (adjusted IRR 7.61, 95% CI 4.37 to 13.26). The difference in cardiovascular mortality continued to be significant from 90 to 179 days after surgery, with an event rate of 6.5 per 100 person-years versus 2.1 per 100 person-years (IRR 3.51, 95% CI 1.54 to 8.03).
Bottom line: Discontinuation of warfarin therapy within six months of bioprosthetic aortic valve replacement is associated with increased cardiovascular death.
Citation: Mérie C, Køber L, Skov Olsen P, et al. Association of warfarin therapy duration after bioprosthetic aortic valve replacement with risk of mortality, thromboembolic complications, and bleeding. JAMA. 2012;308(20):2118-2125.
Limited Evidence for Antimicrobial-Coated Catheters
Clinical question: Does the use of antimicrobial-coated catheters reduce the risk of catheter-associated urinary tract infection (UTI) compared to standard polytetrafluoroethylene (PTFE) catheters?
Background: UTIs associated with indwelling catheters are a major preventable cause of harm for hospitalized patients. Prior studies have shown that catheters made with antimicrobial coatings can reduce rates of bacteriuria, but their usefulness against symptomatic catheter-associated UTIs remains uncertain.
Study design: Multicenter randomized controlled trial.
Setting: Twenty-four hospitals in the United Kingdom.
Synopsis: A total of 7,102 patients >16 undergoing urethral catheterization for an anticipated duration of <14 days were randomly allocated in a 1:1:1 ratio to receive a silver-alloy-coated catheter, a nitrofural-impregnated silicone catheter, or a standard PTFE-coated catheter. The primary outcome was defined as presence of patient-reported symptoms of UTI and prescription of antibiotic for UTI. Incidence of symptomatic catheter-associated UTI up to six weeks after randomization did not differ significantly between groups and occurred in 12.6% of the PTFE control, 12.5% of the silver alloy group, and 10.6% of the nitrofural group. In secondary outcomes, the nitrofural catheter was associated with a slightly reduced incidence of culture-confirmed symptomatic UTI (absolute risk reduction of 1.4%) and lower rate of bacteriuria, but it also had greater patient-reported discomfort during use and removal.
Bottom line: Antimicrobial-coated catheters do not show a clinically significant benefit over standard PTFE catheters in preventing catheter-associated UTI.
Citation: Pickard R, Lam T, Maclennan G, et al. Antimicrobial catheters for reduction of symptomatic urinary tract infection in adults requiring short-term catheterisation in hospital: a multicentre randomized controlled trial. Lancet. 2012;380:1927-1935.
Outcomes Improve after In-Hospital Cardiac Arrest
Clinical question: Have outcomes after in-hospital cardiac arrest improved with recent advances in resuscitation care?
Background: Over the past decade, quality-improvement (QI) efforts in hospital resuscitation care have included use of mock cardiac arrests, defibrillation by nonmedical personnel, and participation in QI registries. It is unclear what effect these efforts have had on overall survival and neurologic recovery.
Study design: Retrospective cohort study.
Setting: Five hundred fifty-three hospitals in the U.S.
Synopsis: A total of 113,514 patients age >18 with a cardiac arrest occurring from Jan. 1, 2000, to Nov. 19, 2009, were identified. Analyses were separated by initial rhythm (PEA/asystole or ventricular fibrillation/tachycardia). Overall survival to discharge increased significantly to 22.3% in 2009 from 13.7% in 2000, with similar increases within each rhythm group. Rates of acute resuscitation survival (return of spontaneous circulation for at least 20 contiguous minutes after initial arrest) and post-resuscitation survival (survival to discharge among patients surviving acute resuscitation) also improved during the study period. Rates of clinically significant neurologic disability, as defined by cerebral performance scores >1, decreased over time for the overall cohort and the subset with ventricular fibrillation/tachycardia. The study was limited by including only hospitals motivated to participate in a QI registry.
Bottom line: From 2000 to 2009, survival after in-hospital cardiac arrest improved, and rates of clinically significant neurologic disability among survivors decreased.
Citation: Girotra S, Nallamothu B, Spertus J, et al. Trends in survival after in-hospital cardiac arrest. N Engl J Med. 2012;367:1912-1920.
Affordable Care Act Provides Two-Year Increase in Medicaid Payments for Primary-Care Services
Some hospitalist groups can expect a bump in total revenue over the next two years, thanks to the Medicaid-to-Medicare parity regulation that was included in the Affordable Care Act. But whether the increase in reimbursement lasts beyond 2014 is anyone’s guess.
The regulation, which the Centers for Medicare & Medicaid Services (CMS) released in November and made effective Jan. 1, increases Medicaid payments for certain primary-care services to 100% of Medicare levels this year and next. States will receive an estimated $11 billion over the next two years to fund the program, according to the American Academy of Family Physicians (AAFP). Eligible providers include physicians, physician assistants (PAs), and nurse practitioners (NPs), who self-attest they are board-certified in family, pediatric, or general internal medicine; it also includes those doctors, PAs, or NPs who self-attest that at least 60% of all Medicaid services they bill or provide in a managed-care environment are for specific evaluation and management (E&M) and vaccine administration codes.1
The concept is to boost Medicaid participation by improving historically lagging reimbursement rates.2 To wit, CMS’ Office of the Actuary estimates the parity rule will add more than 10,000 new primary-care physicians (PCPs) to the Medicaid participation ranks.3
SHM Public Policy Committee member Brad Flansbaum, DO, MPH, SFHM, says that hospitalists who deal with Medicaid populations can expect at least some increase in their revenue over the next two years. For example, he says, take an HM group earning $100,000 a year in Medicaid revenue. Now consider Urban Institute figures that show, in 2012, Medicaid physician fees on average were 66% of Medicare physician fees (with wide state variations). The parity rule now pays that hypothetical HM group about $150,000.
“It’s simple math,” Dr. Flansbaum says. “I would emphasize that the bump in pay is going to be proportional to the percentage of Medicaid patients that you see. There are some doctors who see an awful lot of Medicaid patients in safety-net and public hospitals, and that money, when it comes back to departments and divisions, can be used for things that a lot of these places never had the means to do before. It could be salary, but it could also mean hiring more people, more resources. It makes a difference.”
Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, says SHM advocated for the parity regulation, as Medicaid has historically paid for only about 70% of the healthcare delivered to patients. Although the parity issue has not gathered as much attention as other facets of the healthcare reform movement, having CMS recognize that delivery of primary care is not restricted to traditional offices is one he and SHM are particularly proud of.
“This is a correction long in coming,” Dr. Greeno says. “We’re happy hospitalists were included in the group of people that will achieve that parity.”

Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City, says few physicians are even aware of the provision, in part because of a widespread frustration with Medicaid’s historic reimbursements rates.
“It’s almost a foregone conclusion that Medicaid never pays, reimbursement always goes down, and the interactions with Medicaid are always increasingly difficult,” Dr. Flansbaum adds.
The question for physicians and policy wonks now is what happens to the parity regulation after its scheduled expiration Dec. 31, 2014. Several medical societies, including SHM and the American College of Physicians (ACP), lobbied Congress to make sure the parity regulation was not impacted by the “fiscal cliff” negotiations. The next step is to craft a permanent funding source to pay for it.
“Unless Congress acts to permanently extend and fund this provision, a sudden return to disparate and inadequate payment for primary services needed by Medicaid patients after only two years will again threaten to restrict their access to such needed services,” AAFP said in a statement after the rule was implemented. “It would once again shut out people who have come to know and depend on their primary care physicians. Only by extending Medicaid parity with Medicare can we ensure that these Americans continue to have uninterrupted medical care in the future.”

—Brad Flansbaum, DO, MPH, SFHM, Lenox Hill Hospital, New York City, SHM Public Policy Committee member
SHM recommended that CMS work with the states to facilitate timely data collection designed to determine the effects on the quality and efficiency of care being received under Medicaid as a result of the enhanced fees. CMS agreed with this recommendation and the resulting data, hopefully, will make the case for continuing the enhanced payment following 2014.
Dr. Flansbaum says SHM’s policy team will continue to work on the issue, but given the precarious state of federal budgets and political dysfunction in Washington, it’s too early to know whether a funding source will be identified to pay for parity in 2015 and beyond—especially as politicians have yet to craft long-term solutions to issues including the sustainable-growth rate formula and other specialists, including radiologists and obstetricians, lobby to be eligible for the parity pay. However, he is hopeful that physicians who see the added impact of parity pay in the next two years will lobby Congress to find a way to continue the higher reimbursement.
“I can’t tell you whether or not when you put on the scale of all the priorities whether it’s going to be a new Air Force bomber, another $50 billion into Medicare for physicians, or an educational system upgrade,” he says. “I don’t know where the government is going to assign its priorities. Will the money be there to extend both the two-year Medicaid and the reprieve? And if the answer is yes, will it be extended to other providers beyond just primary-care practitioners? It’s anyone’s guess.”
Richard Quinn is a freelance writer in New Jersey.
References
- FAQ: Medicaid/Medicare Parity Regulation. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Images/Advocacy_Image/pdf/Parity_FAQ_Final.pdf. Accessed Jan. 27, 2013.
- Centers for Medicare & Medicaid Services. Medicaid program; payments for services furnished by certain primary care physicians and charges for vaccine administration under the Vaccines for Children program. Federal Register website. Available at: http://www.gpo.gov/fdsys/pkg/FR-2012-11-06/pdf/2012-26507.pdf. Accessed Jan. 15, 2013.
- Bindman A. JAMA Forum: Warning: Dangerous physician payment cliffs ahead. Journal of the American Medical Association website. Available at: http://newsatjama.jama.com/2013/01/10/jama-forum-warning-dangerous-physician-payment-cliffs-ahead/.Accessed Jan. 15, 2013.
Some hospitalist groups can expect a bump in total revenue over the next two years, thanks to the Medicaid-to-Medicare parity regulation that was included in the Affordable Care Act. But whether the increase in reimbursement lasts beyond 2014 is anyone’s guess.
The regulation, which the Centers for Medicare & Medicaid Services (CMS) released in November and made effective Jan. 1, increases Medicaid payments for certain primary-care services to 100% of Medicare levels this year and next. States will receive an estimated $11 billion over the next two years to fund the program, according to the American Academy of Family Physicians (AAFP). Eligible providers include physicians, physician assistants (PAs), and nurse practitioners (NPs), who self-attest they are board-certified in family, pediatric, or general internal medicine; it also includes those doctors, PAs, or NPs who self-attest that at least 60% of all Medicaid services they bill or provide in a managed-care environment are for specific evaluation and management (E&M) and vaccine administration codes.1
The concept is to boost Medicaid participation by improving historically lagging reimbursement rates.2 To wit, CMS’ Office of the Actuary estimates the parity rule will add more than 10,000 new primary-care physicians (PCPs) to the Medicaid participation ranks.3
SHM Public Policy Committee member Brad Flansbaum, DO, MPH, SFHM, says that hospitalists who deal with Medicaid populations can expect at least some increase in their revenue over the next two years. For example, he says, take an HM group earning $100,000 a year in Medicaid revenue. Now consider Urban Institute figures that show, in 2012, Medicaid physician fees on average were 66% of Medicare physician fees (with wide state variations). The parity rule now pays that hypothetical HM group about $150,000.
“It’s simple math,” Dr. Flansbaum says. “I would emphasize that the bump in pay is going to be proportional to the percentage of Medicaid patients that you see. There are some doctors who see an awful lot of Medicaid patients in safety-net and public hospitals, and that money, when it comes back to departments and divisions, can be used for things that a lot of these places never had the means to do before. It could be salary, but it could also mean hiring more people, more resources. It makes a difference.”
Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, says SHM advocated for the parity regulation, as Medicaid has historically paid for only about 70% of the healthcare delivered to patients. Although the parity issue has not gathered as much attention as other facets of the healthcare reform movement, having CMS recognize that delivery of primary care is not restricted to traditional offices is one he and SHM are particularly proud of.
“This is a correction long in coming,” Dr. Greeno says. “We’re happy hospitalists were included in the group of people that will achieve that parity.”
Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City, says few physicians are even aware of the provision, in part because of a widespread frustration with Medicaid’s historic reimbursements rates.
“It’s almost a foregone conclusion that Medicaid never pays, reimbursement always goes down, and the interactions with Medicaid are always increasingly difficult,” Dr. Flansbaum adds.
The question for physicians and policy wonks now is what happens to the parity regulation after its scheduled expiration Dec. 31, 2014. Several medical societies, including SHM and the American College of Physicians (ACP), lobbied Congress to make sure the parity regulation was not impacted by the “fiscal cliff” negotiations. The next step is to craft a permanent funding source to pay for it.
“Unless Congress acts to permanently extend and fund this provision, a sudden return to disparate and inadequate payment for primary services needed by Medicaid patients after only two years will again threaten to restrict their access to such needed services,” AAFP said in a statement after the rule was implemented. “It would once again shut out people who have come to know and depend on their primary care physicians. Only by extending Medicaid parity with Medicare can we ensure that these Americans continue to have uninterrupted medical care in the future.”
—Brad Flansbaum, DO, MPH, SFHM, Lenox Hill Hospital, New York City, SHM Public Policy Committee member
SHM recommended that CMS work with the states to facilitate timely data collection designed to determine the effects on the quality and efficiency of care being received under Medicaid as a result of the enhanced fees. CMS agreed with this recommendation and the resulting data, hopefully, will make the case for continuing the enhanced payment following 2014.
Dr. Flansbaum says SHM’s policy team will continue to work on the issue, but given the precarious state of federal budgets and political dysfunction in Washington, it’s too early to know whether a funding source will be identified to pay for parity in 2015 and beyond—especially as politicians have yet to craft long-term solutions to issues including the sustainable-growth rate formula and other specialists, including radiologists and obstetricians, lobby to be eligible for the parity pay. However, he is hopeful that physicians who see the added impact of parity pay in the next two years will lobby Congress to find a way to continue the higher reimbursement.
“I can’t tell you whether or not when you put on the scale of all the priorities whether it’s going to be a new Air Force bomber, another $50 billion into Medicare for physicians, or an educational system upgrade,” he says. “I don’t know where the government is going to assign its priorities. Will the money be there to extend both the two-year Medicaid and the reprieve? And if the answer is yes, will it be extended to other providers beyond just primary-care practitioners? It’s anyone’s guess.”
Richard Quinn is a freelance writer in New Jersey.
References
- FAQ: Medicaid/Medicare Parity Regulation. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Images/Advocacy_Image/pdf/Parity_FAQ_Final.pdf. Accessed Jan. 27, 2013.
- Centers for Medicare & Medicaid Services. Medicaid program; payments for services furnished by certain primary care physicians and charges for vaccine administration under the Vaccines for Children program. Federal Register website. Available at: http://www.gpo.gov/fdsys/pkg/FR-2012-11-06/pdf/2012-26507.pdf. Accessed Jan. 15, 2013.
- Bindman A. JAMA Forum: Warning: Dangerous physician payment cliffs ahead. Journal of the American Medical Association website. Available at: http://newsatjama.jama.com/2013/01/10/jama-forum-warning-dangerous-physician-payment-cliffs-ahead/.Accessed Jan. 15, 2013.
Some hospitalist groups can expect a bump in total revenue over the next two years, thanks to the Medicaid-to-Medicare parity regulation that was included in the Affordable Care Act. But whether the increase in reimbursement lasts beyond 2014 is anyone’s guess.
The regulation, which the Centers for Medicare & Medicaid Services (CMS) released in November and made effective Jan. 1, increases Medicaid payments for certain primary-care services to 100% of Medicare levels this year and next. States will receive an estimated $11 billion over the next two years to fund the program, according to the American Academy of Family Physicians (AAFP). Eligible providers include physicians, physician assistants (PAs), and nurse practitioners (NPs), who self-attest they are board-certified in family, pediatric, or general internal medicine; it also includes those doctors, PAs, or NPs who self-attest that at least 60% of all Medicaid services they bill or provide in a managed-care environment are for specific evaluation and management (E&M) and vaccine administration codes.1
The concept is to boost Medicaid participation by improving historically lagging reimbursement rates.2 To wit, CMS’ Office of the Actuary estimates the parity rule will add more than 10,000 new primary-care physicians (PCPs) to the Medicaid participation ranks.3
SHM Public Policy Committee member Brad Flansbaum, DO, MPH, SFHM, says that hospitalists who deal with Medicaid populations can expect at least some increase in their revenue over the next two years. For example, he says, take an HM group earning $100,000 a year in Medicaid revenue. Now consider Urban Institute figures that show, in 2012, Medicaid physician fees on average were 66% of Medicare physician fees (with wide state variations). The parity rule now pays that hypothetical HM group about $150,000.
“It’s simple math,” Dr. Flansbaum says. “I would emphasize that the bump in pay is going to be proportional to the percentage of Medicaid patients that you see. There are some doctors who see an awful lot of Medicaid patients in safety-net and public hospitals, and that money, when it comes back to departments and divisions, can be used for things that a lot of these places never had the means to do before. It could be salary, but it could also mean hiring more people, more resources. It makes a difference.”
Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, says SHM advocated for the parity regulation, as Medicaid has historically paid for only about 70% of the healthcare delivered to patients. Although the parity issue has not gathered as much attention as other facets of the healthcare reform movement, having CMS recognize that delivery of primary care is not restricted to traditional offices is one he and SHM are particularly proud of.
“This is a correction long in coming,” Dr. Greeno says. “We’re happy hospitalists were included in the group of people that will achieve that parity.”
Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City, says few physicians are even aware of the provision, in part because of a widespread frustration with Medicaid’s historic reimbursements rates.
“It’s almost a foregone conclusion that Medicaid never pays, reimbursement always goes down, and the interactions with Medicaid are always increasingly difficult,” Dr. Flansbaum adds.
The question for physicians and policy wonks now is what happens to the parity regulation after its scheduled expiration Dec. 31, 2014. Several medical societies, including SHM and the American College of Physicians (ACP), lobbied Congress to make sure the parity regulation was not impacted by the “fiscal cliff” negotiations. The next step is to craft a permanent funding source to pay for it.
“Unless Congress acts to permanently extend and fund this provision, a sudden return to disparate and inadequate payment for primary services needed by Medicaid patients after only two years will again threaten to restrict their access to such needed services,” AAFP said in a statement after the rule was implemented. “It would once again shut out people who have come to know and depend on their primary care physicians. Only by extending Medicaid parity with Medicare can we ensure that these Americans continue to have uninterrupted medical care in the future.”
—Brad Flansbaum, DO, MPH, SFHM, Lenox Hill Hospital, New York City, SHM Public Policy Committee member
SHM recommended that CMS work with the states to facilitate timely data collection designed to determine the effects on the quality and efficiency of care being received under Medicaid as a result of the enhanced fees. CMS agreed with this recommendation and the resulting data, hopefully, will make the case for continuing the enhanced payment following 2014.
Dr. Flansbaum says SHM’s policy team will continue to work on the issue, but given the precarious state of federal budgets and political dysfunction in Washington, it’s too early to know whether a funding source will be identified to pay for parity in 2015 and beyond—especially as politicians have yet to craft long-term solutions to issues including the sustainable-growth rate formula and other specialists, including radiologists and obstetricians, lobby to be eligible for the parity pay. However, he is hopeful that physicians who see the added impact of parity pay in the next two years will lobby Congress to find a way to continue the higher reimbursement.
“I can’t tell you whether or not when you put on the scale of all the priorities whether it’s going to be a new Air Force bomber, another $50 billion into Medicare for physicians, or an educational system upgrade,” he says. “I don’t know where the government is going to assign its priorities. Will the money be there to extend both the two-year Medicaid and the reprieve? And if the answer is yes, will it be extended to other providers beyond just primary-care practitioners? It’s anyone’s guess.”
Richard Quinn is a freelance writer in New Jersey.
References
- FAQ: Medicaid/Medicare Parity Regulation. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Images/Advocacy_Image/pdf/Parity_FAQ_Final.pdf. Accessed Jan. 27, 2013.
- Centers for Medicare & Medicaid Services. Medicaid program; payments for services furnished by certain primary care physicians and charges for vaccine administration under the Vaccines for Children program. Federal Register website. Available at: http://www.gpo.gov/fdsys/pkg/FR-2012-11-06/pdf/2012-26507.pdf. Accessed Jan. 15, 2013.
- Bindman A. JAMA Forum: Warning: Dangerous physician payment cliffs ahead. Journal of the American Medical Association website. Available at: http://newsatjama.jama.com/2013/01/10/jama-forum-warning-dangerous-physician-payment-cliffs-ahead/.Accessed Jan. 15, 2013.
Multiple Patient-Safety Events Affect 1 in 1000 Hospitalizations
Patients who experienced multiple patient-safety events—co-occurring iatrogenic events during a single stay in a U.S. hospital in 2004.6 This represents 1 out of every 1,000 hospitalizations. These patients experienced four times greater average lengths of stay and eight times greater average charges per admission.
Patients who experienced multiple patient-safety events—co-occurring iatrogenic events during a single stay in a U.S. hospital in 2004.6 This represents 1 out of every 1,000 hospitalizations. These patients experienced four times greater average lengths of stay and eight times greater average charges per admission.
Patients who experienced multiple patient-safety events—co-occurring iatrogenic events during a single stay in a U.S. hospital in 2004.6 This represents 1 out of every 1,000 hospitalizations. These patients experienced four times greater average lengths of stay and eight times greater average charges per admission.
New Anticoagulation Website Offers Guidelines, Self-Assessment Tools
In January, the Anticoagulation Forum, a nonprofit in Newton, Mass., launched “Anti-Coagulation Centers of Excellence,” a searchable resource center of guidelines and tools, including up-to-date information on novel oral anticoagulants, examples of excellence submitted by other providers, and an online self-assessment tool of anticoagulation programs’ performance. In its first month, the site (www.excellence.acforum.org) had 1,200 visitors, with about 10% of visitors attempting the self-assessment. Participating centers tend to be hospital-based outpatient clinics for patients receiving anti-thrombotic medications.
In January, the Anticoagulation Forum, a nonprofit in Newton, Mass., launched “Anti-Coagulation Centers of Excellence,” a searchable resource center of guidelines and tools, including up-to-date information on novel oral anticoagulants, examples of excellence submitted by other providers, and an online self-assessment tool of anticoagulation programs’ performance. In its first month, the site (www.excellence.acforum.org) had 1,200 visitors, with about 10% of visitors attempting the self-assessment. Participating centers tend to be hospital-based outpatient clinics for patients receiving anti-thrombotic medications.
In January, the Anticoagulation Forum, a nonprofit in Newton, Mass., launched “Anti-Coagulation Centers of Excellence,” a searchable resource center of guidelines and tools, including up-to-date information on novel oral anticoagulants, examples of excellence submitted by other providers, and an online self-assessment tool of anticoagulation programs’ performance. In its first month, the site (www.excellence.acforum.org) had 1,200 visitors, with about 10% of visitors attempting the self-assessment. Participating centers tend to be hospital-based outpatient clinics for patients receiving anti-thrombotic medications.
Post-Hospital Syndrome Contributes to Readmission Risk for Elderly
Post-hospital syndrome, as labeled in a recent, widely publicized opinion piece in the New England Journal of Medicine, is not a new concept, according to one hospitalist pioneer.1
Harlan Krumholz, MD, of the Yale School of Medicine in New Haven, Conn., writes in NEJM what others previously have described as “hospitalization-associated disability,” says Mark Williams, MD, MHM, chief of hospital medicine at Northwestern University School of Medicine and principal investigator of SHM’s Project BOOST (www.hospitalmedicine.org/boost).2
Dr. Krumholz found that the majority of 30-day readmissions for elderly patients with heart failure, pneumonia, or chronic obstructive pulmonary disease are for conditions other than the diagnosis named at discharge. He attributes this phenomenon to hospitalization-related sleep deprivation, malnourishment, pain and discomfort, cognition- and physical function-altering medications, deconditioning from bed rest or inactivity, and the experience of confronting stressful, mentally challenging situations in the hospital.1 Such stressors leave elderly patients with post-hospitalization disabilities comparable to a bad case of jet lag.
For Dr. Williams, the physical deterioration leading to rehospitalizations is better attributed to the underlying serious illness and comorbidities experienced by elderly patients—a kind of high-risk, post-illness syndrome. Prior research also has demonstrated the effects of bed rest for hospitalized elderly patients.
Regardless of the origins, is there anything hospitalists can do about this syndrome? “Absolutely,” Dr. Williams says. “Get elderly, hospitalized patients out of bed as quickly as possible, and be mindful of medications and their effects on elderly patients. But most hospitalists already think about these things when managing elderly patients.”
References
Post-hospital syndrome, as labeled in a recent, widely publicized opinion piece in the New England Journal of Medicine, is not a new concept, according to one hospitalist pioneer.1
Harlan Krumholz, MD, of the Yale School of Medicine in New Haven, Conn., writes in NEJM what others previously have described as “hospitalization-associated disability,” says Mark Williams, MD, MHM, chief of hospital medicine at Northwestern University School of Medicine and principal investigator of SHM’s Project BOOST (www.hospitalmedicine.org/boost).2
Dr. Krumholz found that the majority of 30-day readmissions for elderly patients with heart failure, pneumonia, or chronic obstructive pulmonary disease are for conditions other than the diagnosis named at discharge. He attributes this phenomenon to hospitalization-related sleep deprivation, malnourishment, pain and discomfort, cognition- and physical function-altering medications, deconditioning from bed rest or inactivity, and the experience of confronting stressful, mentally challenging situations in the hospital.1 Such stressors leave elderly patients with post-hospitalization disabilities comparable to a bad case of jet lag.
For Dr. Williams, the physical deterioration leading to rehospitalizations is better attributed to the underlying serious illness and comorbidities experienced by elderly patients—a kind of high-risk, post-illness syndrome. Prior research also has demonstrated the effects of bed rest for hospitalized elderly patients.
Regardless of the origins, is there anything hospitalists can do about this syndrome? “Absolutely,” Dr. Williams says. “Get elderly, hospitalized patients out of bed as quickly as possible, and be mindful of medications and their effects on elderly patients. But most hospitalists already think about these things when managing elderly patients.”
References
Post-hospital syndrome, as labeled in a recent, widely publicized opinion piece in the New England Journal of Medicine, is not a new concept, according to one hospitalist pioneer.1
Harlan Krumholz, MD, of the Yale School of Medicine in New Haven, Conn., writes in NEJM what others previously have described as “hospitalization-associated disability,” says Mark Williams, MD, MHM, chief of hospital medicine at Northwestern University School of Medicine and principal investigator of SHM’s Project BOOST (www.hospitalmedicine.org/boost).2
Dr. Krumholz found that the majority of 30-day readmissions for elderly patients with heart failure, pneumonia, or chronic obstructive pulmonary disease are for conditions other than the diagnosis named at discharge. He attributes this phenomenon to hospitalization-related sleep deprivation, malnourishment, pain and discomfort, cognition- and physical function-altering medications, deconditioning from bed rest or inactivity, and the experience of confronting stressful, mentally challenging situations in the hospital.1 Such stressors leave elderly patients with post-hospitalization disabilities comparable to a bad case of jet lag.
For Dr. Williams, the physical deterioration leading to rehospitalizations is better attributed to the underlying serious illness and comorbidities experienced by elderly patients—a kind of high-risk, post-illness syndrome. Prior research also has demonstrated the effects of bed rest for hospitalized elderly patients.
Regardless of the origins, is there anything hospitalists can do about this syndrome? “Absolutely,” Dr. Williams says. “Get elderly, hospitalized patients out of bed as quickly as possible, and be mindful of medications and their effects on elderly patients. But most hospitalists already think about these things when managing elderly patients.”
References
How Should Physicians Assess and Manage Pressure Ulcers in the Hospitalized Patient?
The Case
An 85-year-old woman with stroke, functional quadriplegia, and diabetes mellitus presents with altered mental status. She is febrile (38.5°C) with leukocytosis (14,400 cells/mm3) and has a 5 cm x 4 cm x 2 cm Stage III malodorous sacral ulcer without surrounding erythema, tunneling, or pain. The ulcer base is partially covered by green slough. How should this pressure ulcer be evaluated and treated?
Overview
Pressure ulcers in vulnerable populations, such as the elderly and those with limited mobility, are exceedingly common. In the acute-care setting, the incidence of pressure ulcers ranges from 0.4% to 38%, with 2.5 million cases treated annually at an estimated cost of $11 billion per year.1,2 Moreover, as of Oct. 1, 2008, the Centers for Medicare & Medicaid Services (CMS) guideline states that hospitals will no longer receive additional payment when a hospitalized patient develops Stage III or IV pressure ulcers that are not present on admission.
A pressure ulcer is a localized injury to skin and underlying soft tissue over a bony prominence due to sustained external pressure.3 Prolonged pressure on these weight-bearing areas leads to reduced blood flow, ischemia, cell death, and necrosis of local tissues.4 Risk factors for developing pressure ulcers include increased external pressure, shear, friction, moisture, poor perfusion, immobility, incontinence, malnutrition, and impaired mental status.4 Inadequately treated pressure ulcers can lead to pain, tunneling, fistula formation, disfigurement, infection, prolonged hospitalization, lower quality of life, and increased mortality.4
Because of the significant morbidities and high costs associated with the care of pressure ulcers in acute care, hospitalists must be familiar with the assessment and treatment of pressure ulcers in vulnerable patients.
Review of the Data
The management of pressure ulcers in the hospitalized patient starts with a comprehensive assessment of the patient’s medical comorbidities, risk factors, and wound-staging. Considerations must be given to differentiate an infected pressure ulcer from a noninfected ulcer. These evaluations then guide the appropriate treatments of pressure ulcers, including the prevention of progression or formation of new ulcers, debridement, application of wound dressing, and antibiotic use.
Assessing pressure ulcer stage. The National Pressure Ulcer Advisory Panel (NPUAP) Classification System is the most commonly used staging tool. It describes four stages of pressure ulcers (see Table 1).3 A Stage 1 pressure ulcer is characterized by intact skin with nonblanchable erythema and may be discolored, painful, soft, firm, and warmer or cooler compared to adjacent area. A Stage II pressure ulcer presents with partial thickness skin loss with a shallow red-pink wound bed without slough, or as an intact or ruptured serum-filled blister. Stage II pressure ulcers do not include skin tears, tape burns, macerations, or excoriations. A Stage III pressure ulcer has full thickness skin loss with or without visible subcutaneous fat. Bone, tendon, or muscle are not exposed or directly palpable. Slough may be present but it does not obscure the depth of ulcer. Deep ulcers can develop in anatomical regions with high adiposity, such as the pelvic girdle. A Stage IV pressure ulcer has full thickness tissue loss with exposed and palpable bone, tendon, or muscle. Slough, eschar, undermining, and tunneling may be present. The depth of a Stage IV ulcer varies depending on anatomical location and adiposity. Stage IV ulcers also create a nidus for osteomyelitis.
NPUAP describes two additional categories of pressure ulcers: unstageable and deep tissue injury.3 An unstageable ulcer has full thickness skin or tissue loss of unknown depth because the wound base is completely obscured by slough or eschar. The ulcer can only be accurately categorized as Stage III or IV after sufficient slough or eschar is removed to identify wound depth. Lastly, suspected deep tissue injury describes a localized area of discolored intact skin (purple or maroon) or blood-filled blister due to damage of underlying tissue from pressure or shear.
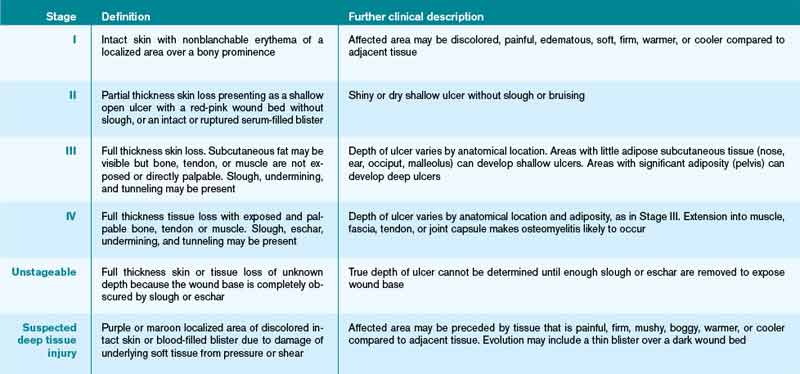
Diagnosing infected pressure ulcers. Pressure ulcer infection delays wound healing and increases risks for sepsis, cellulitis, osteomyelitis, and death.5,6 Clinical evidence of soft tissue involvement, such as erythema, warmth, tenderness, foul odor, or purulent discharge, and systemic inflammatory response (fever, tachycardia, or leukocytosis) are suggestive of a wound infection.3,5 However, these clinical signs may be absent and thus make the distinction between chronic wound and infected pressure ulcer difficult.7 Delayed healing with friable granulation tissue and increased pain in a treated wound may be the only signs of a pressure ulcer infection.3,5,7
Routine laboratory tests (i.e. white blood cell count, C-reactive protein, and erythrocyte sedimentation rate) are neither sensitive nor specific in diagnosing wound infection. Moreover, because pressure ulcers are typically colonized with ≥105 organisms/mL of normal skin flora and bacteria from adjacent gastrointestinal or urogenital environments, swab cultures identify colonizing organisms and are not recommended as a diagnostic test for pressure ulcer microbiologic evaluation.5,6 If microbiological data are needed to guide antibiotic use, cultures of blood, bone, or deep tissue biopsied from a surgically debrided wound should be used.5 Importantly, a higher index of suspicion should be maintained for infection of Stage III or IV pressure ulcers because they are more commonly infected than Stage I or II ulcers.3
Prevention. The prevention of wound progression is essential in treating acute, chronic, or infected pressure ulcers. Although management guidelines are limited by few high-quality, randomized controlled trials, NPUAP recommends a number of prevention strategies targeting risk factors that contribute to pressure ulcer development.2,3,8
For all bed-bound and chair-bound persons with impaired ability to self-reposition, risk assessment for pressure ulcer should be done on admission and repeated every 24 hours. The presence of such risk factors as immobility, shear, friction, moisture, incontinence, and malnutrition should be used to guide preventive treatments. Pressure relief on an ulcer can be achieved by repositioning the immobile patient at one- to two-hour intervals. Pressure-redistributing support surfaces (static, overlays, or dynamic) reduce tissue pressure and decrease overall incidence of pressure ulcers. Due to a lack of relative efficacy data, the selection of a support surface should be determined by the patient’s individual needs in order to reduce pressure and shear.3 For instance, dynamic support is an appropriate surface for an immobile patient with multiple or nonhealing ulcers. Shearing force and friction can be reduced by limiting head-of-bed elevation to <30° and using such transfer aids as bed linens while repositioning patients. The use of pillows, foam wedges, or other devices should be used to eliminate direct contact of bony prominences or reduce pressure on heels.8
Skin care should be optimized to limit excessive dryness or moisture. This includes using moisturizers for dry skin, particularly for the sacrum, and implementing bowel and bladder programs and absorbent underpads in patients with bowel or bladder incontinence.2 Given that patients with pressure ulcers are in a catabolic state, those who are nutritionally compromised may benefit from nutritional supplementation.3 Lastly, appropriate use of local and systemic pain regimen for painful pressure ulcers can improve patient cooperation in repositioning, dressing change, and quality of life.
Debridement. Wound debridement removes necrotic tissue often present in infected or chronic pressure ulcers, reduces risk for further infection, and promotes granulation tissue formation and wound healing. Debridement, however, is not indicated for ulcers of an ischemic limb or dry eschar of the heel, due to propensity for complications.3,4 The five common debridement methods are sharp, mechanical, autolytic, enzymatic, and biosurgical. The debridement method of choice is determined by clinician preference and availability.4
Sharp debridement results in rapid removal of large amounts of nonviable necrotic tissues and eschar using sharp instruments and, therefore, is indicated if wound infection or sepsis is present. Mechanical debridement by wet-to-dry dressing or whirlpool nonselectively removes granulation tissue and, thus, should be used cautiously. Autolytic debridement uses occlusive dressings (i.e. hydrocolloid or hydrogel) to maintain a moist wound environment in order to optimize the body’s inherent ability to selectively self-digest necrotic tissues. Enzymatic debridement with concentrated topical proteolytic enzymes (i.e. collagenase) digests necrotic tissues and achieves faster debridement than autolysis while being less invasive than surgical intervention. Biosurgery utilizes maggots (i.e. Lucilia sericata) that produce enzymes to effectively debride necrotic tissues.
Wound care and dressing. Pressure ulcers should be cleansed with each dressing change using such physiologic solutions as normal saline. Cleansing with antimicrobial solutions for ulcers with large necrotic debris or infection needs to be thoughtfully administered due to the potential impairment on wound healing.4 Wound dressing should maintain a moist wound environment to allow epithelialization and limit excessive exudates in order to prevent maceration. Although there are many categories of moisture retentive dressings, their comparative effectiveness remain unclear.4 Table 2 summarizes characteristics of common wound dressings and their applications.
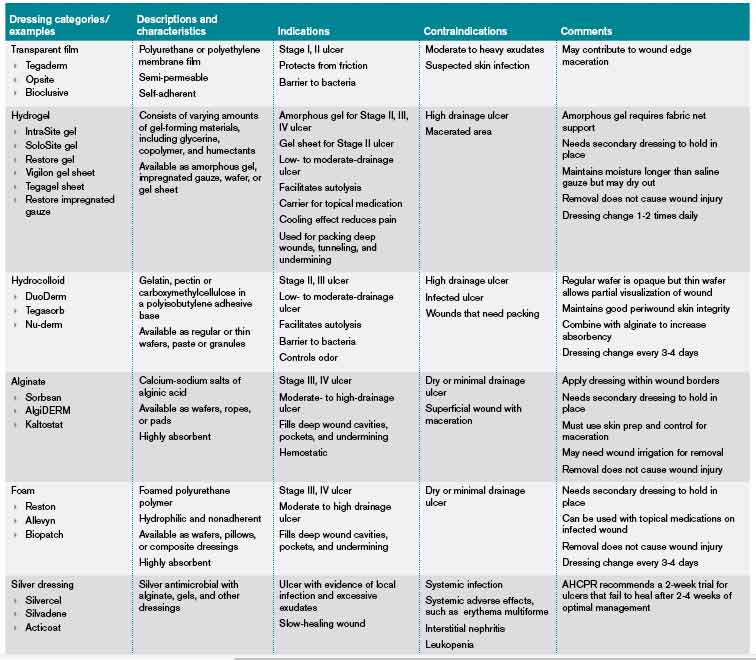
Antibiotic use. Topical antibiotics are appropriate for Stage III or IV ulcers with signs of local infection, including periwound erythema and friable granulation tissue.4 The Agency for Health Care Policy and Research recommends a two-week trial of a topical antibiotic, such as silver sulfadiazine, for pressure ulcers that fail to heal after two to four weeks of optimal care.6 Systemic antibiotics should be used for patients who demonstrate evidence of systemic infection including sepsis, osteomyelitis, or cellulitis with associated fever and leukocytosis. The choice of systemic antibiotics should be based on cultures from blood, bone, or deep tissue biopsied from a surgically debrided wound.4,6
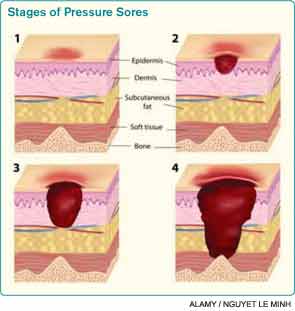
Back to the Case
The patient was hospitalized for altered mental status. She was at high risk for the progression of her sacral ulcer and the development of new pressure ulcers due to immobility, incontinence, malnutrition, and impaired mental status. The sacral wound was a chronic, Stage III pressure ulcer without evidence of local tissue infection. However, the presence of leukocytosis and fever were suggestive of an underlying infection. Her urine analysis was consistent with a urinary tract infection.
Trimethoprim/sulfamethoxazole was administered with subsequent resolution of leukocytosis, fever, and delirium. The sacral ulcer was cleansed with normal saline and covered with hydrocolloid dressing every 72 hours in order to maintain a moist wound environment and facilitate autolysis. Preventive interventions guided by her risk factors for pressure ulcer were implemented. Interventions included:
- Daily skin and wound assessment;
- Pressure relief with repositioning every two hours;
- Use of a dynamic support surface;
- Head-of-bed elevation of no more than <30° to reduce shear and friction;
- Use of transfer aids;
- Use of devices to eliminate direct contact of bony prominences;
- Optimizing skin care with moisturizers for dry skin and frequent changing of absorbent under pads for incontinence; and
- Consulting nutrition service to optimize nutritional intake.
Bottom Line
Assessments of pressure ulcer stage, wound infection, and risk factors guide targeted therapeutic interventions that facilitate wound healing and prevent new pressure ulcer formation.
Dr. Prager is a fellow in the Brookdale Department of Geriatrics and Palliative Medicine at Mount Sinai School of Medicine in New York City. Dr. Ko is a hospitalist and an assistant professor in the Brookdale Department of Geriatrics and Palliative Medicine at Mount Sinai.
References
- Pressure ulcers in America: prevalence, incidence, and implications for the future. An executive summary of the National Pressure Ulcer Advisory Panel monograph. Adv Skin Wound Care. 2001;14(4):208-215.
- Reddy M, Gill SS, Rochon PA. Preventing pressure ulcers: a systematic review. JAMA. 2006;296(8):974-984.
- European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel. Treatment of Pressure Ulcers: Quick Reference Guide. Washington, D.C.: National Pressure Ulcer Advisory Panel; 2009.
- Bates-Jensen BM. Chapter 58. Pressure Ulcers. In: Halter JB, Ouslander JG, Tinetti ME, Studenski S, High KP, Asthana S, eds. Hazzard’s Geriatric Medicine and Gerontology. 6th ed. New York: McGraw-Hill; 2009.
- Livesley NJ, Chow AW. Infected pressure ulcers in elderly individuals. Clin Infect Dis. 2002;35(11):1390-1396.
- Agency for Health Care Policy and Research (AHCPR). Treatment of Pressure Ulcers. Clinical Practice Guideline Number 15. U.S. Department of Health and Human Services. 1994.
- Reddy M, Gill SS, Wu W, Kalkar SR, Rochon PA. Does this patient have an infection of a chronic wound? JAMA. 2012;307(6):605-611.
- National Pressure Ulcer Advisory Panel. Pressure Ulcer Prevention Points. National Pressure Ulcer Advisory Panel website. Available at: http://www.npuap.org/resources/educational-and-clinical-resources/pressure-ulcer-prevention-points/. Accessed Aug. 1, 2012.
- Reuben DB, Herr KA, Pacala JT, et al. Skin Ulcers. In: Geriatrics At Your Fingertips. 12th ed. New York: The American Geriatrics Society; 2010.
The Case
An 85-year-old woman with stroke, functional quadriplegia, and diabetes mellitus presents with altered mental status. She is febrile (38.5°C) with leukocytosis (14,400 cells/mm3) and has a 5 cm x 4 cm x 2 cm Stage III malodorous sacral ulcer without surrounding erythema, tunneling, or pain. The ulcer base is partially covered by green slough. How should this pressure ulcer be evaluated and treated?
Overview
Pressure ulcers in vulnerable populations, such as the elderly and those with limited mobility, are exceedingly common. In the acute-care setting, the incidence of pressure ulcers ranges from 0.4% to 38%, with 2.5 million cases treated annually at an estimated cost of $11 billion per year.1,2 Moreover, as of Oct. 1, 2008, the Centers for Medicare & Medicaid Services (CMS) guideline states that hospitals will no longer receive additional payment when a hospitalized patient develops Stage III or IV pressure ulcers that are not present on admission.
A pressure ulcer is a localized injury to skin and underlying soft tissue over a bony prominence due to sustained external pressure.3 Prolonged pressure on these weight-bearing areas leads to reduced blood flow, ischemia, cell death, and necrosis of local tissues.4 Risk factors for developing pressure ulcers include increased external pressure, shear, friction, moisture, poor perfusion, immobility, incontinence, malnutrition, and impaired mental status.4 Inadequately treated pressure ulcers can lead to pain, tunneling, fistula formation, disfigurement, infection, prolonged hospitalization, lower quality of life, and increased mortality.4
Because of the significant morbidities and high costs associated with the care of pressure ulcers in acute care, hospitalists must be familiar with the assessment and treatment of pressure ulcers in vulnerable patients.
Review of the Data
The management of pressure ulcers in the hospitalized patient starts with a comprehensive assessment of the patient’s medical comorbidities, risk factors, and wound-staging. Considerations must be given to differentiate an infected pressure ulcer from a noninfected ulcer. These evaluations then guide the appropriate treatments of pressure ulcers, including the prevention of progression or formation of new ulcers, debridement, application of wound dressing, and antibiotic use.
Assessing pressure ulcer stage. The National Pressure Ulcer Advisory Panel (NPUAP) Classification System is the most commonly used staging tool. It describes four stages of pressure ulcers (see Table 1).3 A Stage 1 pressure ulcer is characterized by intact skin with nonblanchable erythema and may be discolored, painful, soft, firm, and warmer or cooler compared to adjacent area. A Stage II pressure ulcer presents with partial thickness skin loss with a shallow red-pink wound bed without slough, or as an intact or ruptured serum-filled blister. Stage II pressure ulcers do not include skin tears, tape burns, macerations, or excoriations. A Stage III pressure ulcer has full thickness skin loss with or without visible subcutaneous fat. Bone, tendon, or muscle are not exposed or directly palpable. Slough may be present but it does not obscure the depth of ulcer. Deep ulcers can develop in anatomical regions with high adiposity, such as the pelvic girdle. A Stage IV pressure ulcer has full thickness tissue loss with exposed and palpable bone, tendon, or muscle. Slough, eschar, undermining, and tunneling may be present. The depth of a Stage IV ulcer varies depending on anatomical location and adiposity. Stage IV ulcers also create a nidus for osteomyelitis.
NPUAP describes two additional categories of pressure ulcers: unstageable and deep tissue injury.3 An unstageable ulcer has full thickness skin or tissue loss of unknown depth because the wound base is completely obscured by slough or eschar. The ulcer can only be accurately categorized as Stage III or IV after sufficient slough or eschar is removed to identify wound depth. Lastly, suspected deep tissue injury describes a localized area of discolored intact skin (purple or maroon) or blood-filled blister due to damage of underlying tissue from pressure or shear.
Diagnosing infected pressure ulcers. Pressure ulcer infection delays wound healing and increases risks for sepsis, cellulitis, osteomyelitis, and death.5,6 Clinical evidence of soft tissue involvement, such as erythema, warmth, tenderness, foul odor, or purulent discharge, and systemic inflammatory response (fever, tachycardia, or leukocytosis) are suggestive of a wound infection.3,5 However, these clinical signs may be absent and thus make the distinction between chronic wound and infected pressure ulcer difficult.7 Delayed healing with friable granulation tissue and increased pain in a treated wound may be the only signs of a pressure ulcer infection.3,5,7
Routine laboratory tests (i.e. white blood cell count, C-reactive protein, and erythrocyte sedimentation rate) are neither sensitive nor specific in diagnosing wound infection. Moreover, because pressure ulcers are typically colonized with ≥105 organisms/mL of normal skin flora and bacteria from adjacent gastrointestinal or urogenital environments, swab cultures identify colonizing organisms and are not recommended as a diagnostic test for pressure ulcer microbiologic evaluation.5,6 If microbiological data are needed to guide antibiotic use, cultures of blood, bone, or deep tissue biopsied from a surgically debrided wound should be used.5 Importantly, a higher index of suspicion should be maintained for infection of Stage III or IV pressure ulcers because they are more commonly infected than Stage I or II ulcers.3
Prevention. The prevention of wound progression is essential in treating acute, chronic, or infected pressure ulcers. Although management guidelines are limited by few high-quality, randomized controlled trials, NPUAP recommends a number of prevention strategies targeting risk factors that contribute to pressure ulcer development.2,3,8
For all bed-bound and chair-bound persons with impaired ability to self-reposition, risk assessment for pressure ulcer should be done on admission and repeated every 24 hours. The presence of such risk factors as immobility, shear, friction, moisture, incontinence, and malnutrition should be used to guide preventive treatments. Pressure relief on an ulcer can be achieved by repositioning the immobile patient at one- to two-hour intervals. Pressure-redistributing support surfaces (static, overlays, or dynamic) reduce tissue pressure and decrease overall incidence of pressure ulcers. Due to a lack of relative efficacy data, the selection of a support surface should be determined by the patient’s individual needs in order to reduce pressure and shear.3 For instance, dynamic support is an appropriate surface for an immobile patient with multiple or nonhealing ulcers. Shearing force and friction can be reduced by limiting head-of-bed elevation to <30° and using such transfer aids as bed linens while repositioning patients. The use of pillows, foam wedges, or other devices should be used to eliminate direct contact of bony prominences or reduce pressure on heels.8
Skin care should be optimized to limit excessive dryness or moisture. This includes using moisturizers for dry skin, particularly for the sacrum, and implementing bowel and bladder programs and absorbent underpads in patients with bowel or bladder incontinence.2 Given that patients with pressure ulcers are in a catabolic state, those who are nutritionally compromised may benefit from nutritional supplementation.3 Lastly, appropriate use of local and systemic pain regimen for painful pressure ulcers can improve patient cooperation in repositioning, dressing change, and quality of life.
Debridement. Wound debridement removes necrotic tissue often present in infected or chronic pressure ulcers, reduces risk for further infection, and promotes granulation tissue formation and wound healing. Debridement, however, is not indicated for ulcers of an ischemic limb or dry eschar of the heel, due to propensity for complications.3,4 The five common debridement methods are sharp, mechanical, autolytic, enzymatic, and biosurgical. The debridement method of choice is determined by clinician preference and availability.4
Sharp debridement results in rapid removal of large amounts of nonviable necrotic tissues and eschar using sharp instruments and, therefore, is indicated if wound infection or sepsis is present. Mechanical debridement by wet-to-dry dressing or whirlpool nonselectively removes granulation tissue and, thus, should be used cautiously. Autolytic debridement uses occlusive dressings (i.e. hydrocolloid or hydrogel) to maintain a moist wound environment in order to optimize the body’s inherent ability to selectively self-digest necrotic tissues. Enzymatic debridement with concentrated topical proteolytic enzymes (i.e. collagenase) digests necrotic tissues and achieves faster debridement than autolysis while being less invasive than surgical intervention. Biosurgery utilizes maggots (i.e. Lucilia sericata) that produce enzymes to effectively debride necrotic tissues.
Wound care and dressing. Pressure ulcers should be cleansed with each dressing change using such physiologic solutions as normal saline. Cleansing with antimicrobial solutions for ulcers with large necrotic debris or infection needs to be thoughtfully administered due to the potential impairment on wound healing.4 Wound dressing should maintain a moist wound environment to allow epithelialization and limit excessive exudates in order to prevent maceration. Although there are many categories of moisture retentive dressings, their comparative effectiveness remain unclear.4 Table 2 summarizes characteristics of common wound dressings and their applications.
Antibiotic use. Topical antibiotics are appropriate for Stage III or IV ulcers with signs of local infection, including periwound erythema and friable granulation tissue.4 The Agency for Health Care Policy and Research recommends a two-week trial of a topical antibiotic, such as silver sulfadiazine, for pressure ulcers that fail to heal after two to four weeks of optimal care.6 Systemic antibiotics should be used for patients who demonstrate evidence of systemic infection including sepsis, osteomyelitis, or cellulitis with associated fever and leukocytosis. The choice of systemic antibiotics should be based on cultures from blood, bone, or deep tissue biopsied from a surgically debrided wound.4,6
Back to the Case
The patient was hospitalized for altered mental status. She was at high risk for the progression of her sacral ulcer and the development of new pressure ulcers due to immobility, incontinence, malnutrition, and impaired mental status. The sacral wound was a chronic, Stage III pressure ulcer without evidence of local tissue infection. However, the presence of leukocytosis and fever were suggestive of an underlying infection. Her urine analysis was consistent with a urinary tract infection.
Trimethoprim/sulfamethoxazole was administered with subsequent resolution of leukocytosis, fever, and delirium. The sacral ulcer was cleansed with normal saline and covered with hydrocolloid dressing every 72 hours in order to maintain a moist wound environment and facilitate autolysis. Preventive interventions guided by her risk factors for pressure ulcer were implemented. Interventions included:
- Daily skin and wound assessment;
- Pressure relief with repositioning every two hours;
- Use of a dynamic support surface;
- Head-of-bed elevation of no more than <30° to reduce shear and friction;
- Use of transfer aids;
- Use of devices to eliminate direct contact of bony prominences;
- Optimizing skin care with moisturizers for dry skin and frequent changing of absorbent under pads for incontinence; and
- Consulting nutrition service to optimize nutritional intake.
Bottom Line
Assessments of pressure ulcer stage, wound infection, and risk factors guide targeted therapeutic interventions that facilitate wound healing and prevent new pressure ulcer formation.
Dr. Prager is a fellow in the Brookdale Department of Geriatrics and Palliative Medicine at Mount Sinai School of Medicine in New York City. Dr. Ko is a hospitalist and an assistant professor in the Brookdale Department of Geriatrics and Palliative Medicine at Mount Sinai.
References
- Pressure ulcers in America: prevalence, incidence, and implications for the future. An executive summary of the National Pressure Ulcer Advisory Panel monograph. Adv Skin Wound Care. 2001;14(4):208-215.
- Reddy M, Gill SS, Rochon PA. Preventing pressure ulcers: a systematic review. JAMA. 2006;296(8):974-984.
- European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel. Treatment of Pressure Ulcers: Quick Reference Guide. Washington, D.C.: National Pressure Ulcer Advisory Panel; 2009.
- Bates-Jensen BM. Chapter 58. Pressure Ulcers. In: Halter JB, Ouslander JG, Tinetti ME, Studenski S, High KP, Asthana S, eds. Hazzard’s Geriatric Medicine and Gerontology. 6th ed. New York: McGraw-Hill; 2009.
- Livesley NJ, Chow AW. Infected pressure ulcers in elderly individuals. Clin Infect Dis. 2002;35(11):1390-1396.
- Agency for Health Care Policy and Research (AHCPR). Treatment of Pressure Ulcers. Clinical Practice Guideline Number 15. U.S. Department of Health and Human Services. 1994.
- Reddy M, Gill SS, Wu W, Kalkar SR, Rochon PA. Does this patient have an infection of a chronic wound? JAMA. 2012;307(6):605-611.
- National Pressure Ulcer Advisory Panel. Pressure Ulcer Prevention Points. National Pressure Ulcer Advisory Panel website. Available at: http://www.npuap.org/resources/educational-and-clinical-resources/pressure-ulcer-prevention-points/. Accessed Aug. 1, 2012.
- Reuben DB, Herr KA, Pacala JT, et al. Skin Ulcers. In: Geriatrics At Your Fingertips. 12th ed. New York: The American Geriatrics Society; 2010.
The Case
An 85-year-old woman with stroke, functional quadriplegia, and diabetes mellitus presents with altered mental status. She is febrile (38.5°C) with leukocytosis (14,400 cells/mm3) and has a 5 cm x 4 cm x 2 cm Stage III malodorous sacral ulcer without surrounding erythema, tunneling, or pain. The ulcer base is partially covered by green slough. How should this pressure ulcer be evaluated and treated?
Overview
Pressure ulcers in vulnerable populations, such as the elderly and those with limited mobility, are exceedingly common. In the acute-care setting, the incidence of pressure ulcers ranges from 0.4% to 38%, with 2.5 million cases treated annually at an estimated cost of $11 billion per year.1,2 Moreover, as of Oct. 1, 2008, the Centers for Medicare & Medicaid Services (CMS) guideline states that hospitals will no longer receive additional payment when a hospitalized patient develops Stage III or IV pressure ulcers that are not present on admission.
A pressure ulcer is a localized injury to skin and underlying soft tissue over a bony prominence due to sustained external pressure.3 Prolonged pressure on these weight-bearing areas leads to reduced blood flow, ischemia, cell death, and necrosis of local tissues.4 Risk factors for developing pressure ulcers include increased external pressure, shear, friction, moisture, poor perfusion, immobility, incontinence, malnutrition, and impaired mental status.4 Inadequately treated pressure ulcers can lead to pain, tunneling, fistula formation, disfigurement, infection, prolonged hospitalization, lower quality of life, and increased mortality.4
Because of the significant morbidities and high costs associated with the care of pressure ulcers in acute care, hospitalists must be familiar with the assessment and treatment of pressure ulcers in vulnerable patients.
Review of the Data
The management of pressure ulcers in the hospitalized patient starts with a comprehensive assessment of the patient’s medical comorbidities, risk factors, and wound-staging. Considerations must be given to differentiate an infected pressure ulcer from a noninfected ulcer. These evaluations then guide the appropriate treatments of pressure ulcers, including the prevention of progression or formation of new ulcers, debridement, application of wound dressing, and antibiotic use.
Assessing pressure ulcer stage. The National Pressure Ulcer Advisory Panel (NPUAP) Classification System is the most commonly used staging tool. It describes four stages of pressure ulcers (see Table 1).3 A Stage 1 pressure ulcer is characterized by intact skin with nonblanchable erythema and may be discolored, painful, soft, firm, and warmer or cooler compared to adjacent area. A Stage II pressure ulcer presents with partial thickness skin loss with a shallow red-pink wound bed without slough, or as an intact or ruptured serum-filled blister. Stage II pressure ulcers do not include skin tears, tape burns, macerations, or excoriations. A Stage III pressure ulcer has full thickness skin loss with or without visible subcutaneous fat. Bone, tendon, or muscle are not exposed or directly palpable. Slough may be present but it does not obscure the depth of ulcer. Deep ulcers can develop in anatomical regions with high adiposity, such as the pelvic girdle. A Stage IV pressure ulcer has full thickness tissue loss with exposed and palpable bone, tendon, or muscle. Slough, eschar, undermining, and tunneling may be present. The depth of a Stage IV ulcer varies depending on anatomical location and adiposity. Stage IV ulcers also create a nidus for osteomyelitis.
NPUAP describes two additional categories of pressure ulcers: unstageable and deep tissue injury.3 An unstageable ulcer has full thickness skin or tissue loss of unknown depth because the wound base is completely obscured by slough or eschar. The ulcer can only be accurately categorized as Stage III or IV after sufficient slough or eschar is removed to identify wound depth. Lastly, suspected deep tissue injury describes a localized area of discolored intact skin (purple or maroon) or blood-filled blister due to damage of underlying tissue from pressure or shear.
Diagnosing infected pressure ulcers. Pressure ulcer infection delays wound healing and increases risks for sepsis, cellulitis, osteomyelitis, and death.5,6 Clinical evidence of soft tissue involvement, such as erythema, warmth, tenderness, foul odor, or purulent discharge, and systemic inflammatory response (fever, tachycardia, or leukocytosis) are suggestive of a wound infection.3,5 However, these clinical signs may be absent and thus make the distinction between chronic wound and infected pressure ulcer difficult.7 Delayed healing with friable granulation tissue and increased pain in a treated wound may be the only signs of a pressure ulcer infection.3,5,7
Routine laboratory tests (i.e. white blood cell count, C-reactive protein, and erythrocyte sedimentation rate) are neither sensitive nor specific in diagnosing wound infection. Moreover, because pressure ulcers are typically colonized with ≥105 organisms/mL of normal skin flora and bacteria from adjacent gastrointestinal or urogenital environments, swab cultures identify colonizing organisms and are not recommended as a diagnostic test for pressure ulcer microbiologic evaluation.5,6 If microbiological data are needed to guide antibiotic use, cultures of blood, bone, or deep tissue biopsied from a surgically debrided wound should be used.5 Importantly, a higher index of suspicion should be maintained for infection of Stage III or IV pressure ulcers because they are more commonly infected than Stage I or II ulcers.3
Prevention. The prevention of wound progression is essential in treating acute, chronic, or infected pressure ulcers. Although management guidelines are limited by few high-quality, randomized controlled trials, NPUAP recommends a number of prevention strategies targeting risk factors that contribute to pressure ulcer development.2,3,8
For all bed-bound and chair-bound persons with impaired ability to self-reposition, risk assessment for pressure ulcer should be done on admission and repeated every 24 hours. The presence of such risk factors as immobility, shear, friction, moisture, incontinence, and malnutrition should be used to guide preventive treatments. Pressure relief on an ulcer can be achieved by repositioning the immobile patient at one- to two-hour intervals. Pressure-redistributing support surfaces (static, overlays, or dynamic) reduce tissue pressure and decrease overall incidence of pressure ulcers. Due to a lack of relative efficacy data, the selection of a support surface should be determined by the patient’s individual needs in order to reduce pressure and shear.3 For instance, dynamic support is an appropriate surface for an immobile patient with multiple or nonhealing ulcers. Shearing force and friction can be reduced by limiting head-of-bed elevation to <30° and using such transfer aids as bed linens while repositioning patients. The use of pillows, foam wedges, or other devices should be used to eliminate direct contact of bony prominences or reduce pressure on heels.8
Skin care should be optimized to limit excessive dryness or moisture. This includes using moisturizers for dry skin, particularly for the sacrum, and implementing bowel and bladder programs and absorbent underpads in patients with bowel or bladder incontinence.2 Given that patients with pressure ulcers are in a catabolic state, those who are nutritionally compromised may benefit from nutritional supplementation.3 Lastly, appropriate use of local and systemic pain regimen for painful pressure ulcers can improve patient cooperation in repositioning, dressing change, and quality of life.
Debridement. Wound debridement removes necrotic tissue often present in infected or chronic pressure ulcers, reduces risk for further infection, and promotes granulation tissue formation and wound healing. Debridement, however, is not indicated for ulcers of an ischemic limb or dry eschar of the heel, due to propensity for complications.3,4 The five common debridement methods are sharp, mechanical, autolytic, enzymatic, and biosurgical. The debridement method of choice is determined by clinician preference and availability.4
Sharp debridement results in rapid removal of large amounts of nonviable necrotic tissues and eschar using sharp instruments and, therefore, is indicated if wound infection or sepsis is present. Mechanical debridement by wet-to-dry dressing or whirlpool nonselectively removes granulation tissue and, thus, should be used cautiously. Autolytic debridement uses occlusive dressings (i.e. hydrocolloid or hydrogel) to maintain a moist wound environment in order to optimize the body’s inherent ability to selectively self-digest necrotic tissues. Enzymatic debridement with concentrated topical proteolytic enzymes (i.e. collagenase) digests necrotic tissues and achieves faster debridement than autolysis while being less invasive than surgical intervention. Biosurgery utilizes maggots (i.e. Lucilia sericata) that produce enzymes to effectively debride necrotic tissues.
Wound care and dressing. Pressure ulcers should be cleansed with each dressing change using such physiologic solutions as normal saline. Cleansing with antimicrobial solutions for ulcers with large necrotic debris or infection needs to be thoughtfully administered due to the potential impairment on wound healing.4 Wound dressing should maintain a moist wound environment to allow epithelialization and limit excessive exudates in order to prevent maceration. Although there are many categories of moisture retentive dressings, their comparative effectiveness remain unclear.4 Table 2 summarizes characteristics of common wound dressings and their applications.
Antibiotic use. Topical antibiotics are appropriate for Stage III or IV ulcers with signs of local infection, including periwound erythema and friable granulation tissue.4 The Agency for Health Care Policy and Research recommends a two-week trial of a topical antibiotic, such as silver sulfadiazine, for pressure ulcers that fail to heal after two to four weeks of optimal care.6 Systemic antibiotics should be used for patients who demonstrate evidence of systemic infection including sepsis, osteomyelitis, or cellulitis with associated fever and leukocytosis. The choice of systemic antibiotics should be based on cultures from blood, bone, or deep tissue biopsied from a surgically debrided wound.4,6
Back to the Case
The patient was hospitalized for altered mental status. She was at high risk for the progression of her sacral ulcer and the development of new pressure ulcers due to immobility, incontinence, malnutrition, and impaired mental status. The sacral wound was a chronic, Stage III pressure ulcer without evidence of local tissue infection. However, the presence of leukocytosis and fever were suggestive of an underlying infection. Her urine analysis was consistent with a urinary tract infection.
Trimethoprim/sulfamethoxazole was administered with subsequent resolution of leukocytosis, fever, and delirium. The sacral ulcer was cleansed with normal saline and covered with hydrocolloid dressing every 72 hours in order to maintain a moist wound environment and facilitate autolysis. Preventive interventions guided by her risk factors for pressure ulcer were implemented. Interventions included:
- Daily skin and wound assessment;
- Pressure relief with repositioning every two hours;
- Use of a dynamic support surface;
- Head-of-bed elevation of no more than <30° to reduce shear and friction;
- Use of transfer aids;
- Use of devices to eliminate direct contact of bony prominences;
- Optimizing skin care with moisturizers for dry skin and frequent changing of absorbent under pads for incontinence; and
- Consulting nutrition service to optimize nutritional intake.
Bottom Line
Assessments of pressure ulcer stage, wound infection, and risk factors guide targeted therapeutic interventions that facilitate wound healing and prevent new pressure ulcer formation.
Dr. Prager is a fellow in the Brookdale Department of Geriatrics and Palliative Medicine at Mount Sinai School of Medicine in New York City. Dr. Ko is a hospitalist and an assistant professor in the Brookdale Department of Geriatrics and Palliative Medicine at Mount Sinai.
References
- Pressure ulcers in America: prevalence, incidence, and implications for the future. An executive summary of the National Pressure Ulcer Advisory Panel monograph. Adv Skin Wound Care. 2001;14(4):208-215.
- Reddy M, Gill SS, Rochon PA. Preventing pressure ulcers: a systematic review. JAMA. 2006;296(8):974-984.
- European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel. Treatment of Pressure Ulcers: Quick Reference Guide. Washington, D.C.: National Pressure Ulcer Advisory Panel; 2009.
- Bates-Jensen BM. Chapter 58. Pressure Ulcers. In: Halter JB, Ouslander JG, Tinetti ME, Studenski S, High KP, Asthana S, eds. Hazzard’s Geriatric Medicine and Gerontology. 6th ed. New York: McGraw-Hill; 2009.
- Livesley NJ, Chow AW. Infected pressure ulcers in elderly individuals. Clin Infect Dis. 2002;35(11):1390-1396.
- Agency for Health Care Policy and Research (AHCPR). Treatment of Pressure Ulcers. Clinical Practice Guideline Number 15. U.S. Department of Health and Human Services. 1994.
- Reddy M, Gill SS, Wu W, Kalkar SR, Rochon PA. Does this patient have an infection of a chronic wound? JAMA. 2012;307(6):605-611.
- National Pressure Ulcer Advisory Panel. Pressure Ulcer Prevention Points. National Pressure Ulcer Advisory Panel website. Available at: http://www.npuap.org/resources/educational-and-clinical-resources/pressure-ulcer-prevention-points/. Accessed Aug. 1, 2012.
- Reuben DB, Herr KA, Pacala JT, et al. Skin Ulcers. In: Geriatrics At Your Fingertips. 12th ed. New York: The American Geriatrics Society; 2010.