User login
Should we identify and treat hyperlipidemia in the advanced elderly?
No randomized controlled trials exist that identify and treat hyperlipidemia for advanced elderly patients (age >80 years). Expert and consensus guidelines state that hyperlipidemia found in any patient with coronary artery disease (CAD), or at risk of CAD, should be treated irrespective of age; however, evidence is limited to support lowering lipids for advanced elderly patients with and without known CAD (strength of recommendation: C, based on expert and consensus guidelines).1
When prescribing lipid-lowering therapy for older adults, assess competing risks as a function of age
Cari Levy, MD, CMD
Division of Health Care Policy and Research, University of Colorado, Aurora
Many of my patients are over age 82, and these are precisely the ones for whom additional data on the benefits of lipid-lowering would be helpful. Unfortunately, there are no data on lipid-lowering therapy in this population. Polypharmacy is a concern when caring for elderly patients, as are the practical difficulties of medication expense and taking drugs properly. Additionally, because older patients have many competing risks for death, the absolute effect of treating any one problem is relatively small. When prescribing lipid-lowering therapy for older adults, as is often the case with geriatrics, one must assess the “competing risks” as a function of age and, for now, base the treatment decision on these risks rather than evidence-based medicine for the evidence is not yet available.
Evidence summary
CAD is the leading cause of death in the United States and is a significant cause of mortality and morbidity for those aged 65 years and older. Multiple studies have demonstrated the value of lipid-lowering therapy for the primary and secondary prevention of CAD. Most of these studies have not been specifically oriented toward the elderly; however, substantial data from subgroup analyses of older subjects from major lipid treatment trials has consistently demonstrated the beneficial effects of statin therapy in reducing all cardiovascular events for patients with known CAD who are 65 and older.2-7
Unfortunately, randomized trials of hyperlipidemia treatment with statins have enrolled few people aged 80 and above. Hence, it is unclear whether the benefit of statins on cardiovascular mortality extends to advanced elderly patients. These people comprise the fastest-growing segment of the population, increasing by about 3% per year. They tend to experience concomitant chronic illness, shorter life expectancy, and physical frailty, leading to quality-of-life and end-of-life issues. Is it beneficial and cost-effective to treat these very elderly patients for hyperlipidemia?
The first prospective, randomized trial8 of the use of statins among the elderly examined the impact of pravastatin therapy on primary and secondary prevention of cardiovascular and cerebrovascular events for men and women (age 70–82 years), with a history of vascular disease or with risk factors for vascular disease. The sample of 5804 participants was randomized to receive pravastatin 40 mg or placebo, followed for an average of 3.2 years, and monitored for the combined endpoint of myocardial infarction (MI), stroke, and CAD death. The study showed 19% (95% confidence interval [CI], 6–31; P=.006) proportional reduction in the rate of coronary death or nonfatal MI. The absolute risk reduction for coronary death or nonfatal myocardial infarction or nonfatal stroke was significant (2.2%, number needed to treat [NNT]=45). Rates of adverse drug events were similar in the intervention and control groups.8
Serum cholesterol normally declines with age; so the benefit of lowering lipids with medication in this age group is unclear. Furthermore, a meta-analysis9 showed an inverse relationship between total serum cholesterol and all-cause mortality for people aged 80 and above, raising the possibility that lowering cholesterol may be detrimental in this age group. Two other cohort studies10,11 found that low cholesterol was related to all-cause mortality, even when adjusted for health status and indicators of frailty. The reasons for this relationship are not clear, but some postulated mechanisms exist. It is possible that lower cholesterol levels can increase the risk of a variety of nonatherosclerotic diseases since cholesterol may play a direct role in immune response. Alternatively, preclinical diseases, chronic inflammation, or malnutrition may suppress cholesterol levels.4
Recommendations from others
National Cholesterol Education Program Adult Treatment Panel III guidelines1 outline risk identification and management of hyperlipidemia in all age groups with no exceptions noted for the very elderly. A recent scientific statement from the American Heart Association12 outlined the data on the implementation of all primary and secondary prevention guidelines for the elderly and emphasized that the latest cholesterol treatment recommendations should be applied to all eligible adults, with no exceptions for the very elderly.
1. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486-2497.
2. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: A randomised placebo-controlled trial. Lancet 2002;360(9326):7-22.
3. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: The Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383-1389.
4. Miettinen TA, Pyorala K, Olsson AG, et al. Cholesterol-lowering therapy in women and elderly patients with myocardial infarction or angina pectoris: Findings from the Scandinavian Simvastatin Survival Study (4S). Circulation 1997;96:4211-4218.
5. Pfeffer MA, Sacks FM, Moye LA, et al. Cholesterol and Recurrent Events: A secondary prevention trial for normolipidemic patients. CARE Investigators. Am J Cardiol 1995;76:98C-106C.
6. Lewis SJ, Moye LA, Sacks FM, et al. Effect of pravastatin on cardiovascular events in older patients with myocardial infarction and cholesterol levels in the average range. Results of the Cholesterol and Recurrent Events (CARE) trial. Ann Intern Med 1998;129:681-689.
7. Hunt D, Young P, Simes J, et al. Benefits of pravastatin on cardiovascular events and mortality in older patients with coronary heart disease are equal to or exceed those seen in younger patients: Results from the LIPID trial. Ann Intern Med 2001;134:931-940.
8. Shepherd J, Blauw GJ, Murphy MB, et al. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): A randomised controlled trial. Lancet 2002;360:1623-1630.
9. Anum EA, Adera T. Hypercholesterolemia and coronary heart disease in the elderly: a meta-analysis. Ann Epidemiol 2004;14:705-721.
10. Schatz IJ, Masaki K, Yano K, et al. Cholesterol and all-cause mortality in elderly people from the Honolulu Heart Program: A cohort study. Lancet 2001;358:351-355.
11. Brescianini S, Maggi S, Farchi G, et al. Low total cholesterol and increased risk of dying: Are low levels clinical warning signs in the elderly? Results from the Italian Longitudinal Study on Aging. J Am Geriatr Soc 2003;51:991-996.
12. Secondary Prevention of Coronary Heart Disease in the Elderly (With Emphasis on Patients >=75 Years of Age): An American Heart Association Scientific Statement From the Council on Clinical Cardiology Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention. Circulation 2002;105:1735-1743.
No randomized controlled trials exist that identify and treat hyperlipidemia for advanced elderly patients (age >80 years). Expert and consensus guidelines state that hyperlipidemia found in any patient with coronary artery disease (CAD), or at risk of CAD, should be treated irrespective of age; however, evidence is limited to support lowering lipids for advanced elderly patients with and without known CAD (strength of recommendation: C, based on expert and consensus guidelines).1
When prescribing lipid-lowering therapy for older adults, assess competing risks as a function of age
Cari Levy, MD, CMD
Division of Health Care Policy and Research, University of Colorado, Aurora
Many of my patients are over age 82, and these are precisely the ones for whom additional data on the benefits of lipid-lowering would be helpful. Unfortunately, there are no data on lipid-lowering therapy in this population. Polypharmacy is a concern when caring for elderly patients, as are the practical difficulties of medication expense and taking drugs properly. Additionally, because older patients have many competing risks for death, the absolute effect of treating any one problem is relatively small. When prescribing lipid-lowering therapy for older adults, as is often the case with geriatrics, one must assess the “competing risks” as a function of age and, for now, base the treatment decision on these risks rather than evidence-based medicine for the evidence is not yet available.
Evidence summary
CAD is the leading cause of death in the United States and is a significant cause of mortality and morbidity for those aged 65 years and older. Multiple studies have demonstrated the value of lipid-lowering therapy for the primary and secondary prevention of CAD. Most of these studies have not been specifically oriented toward the elderly; however, substantial data from subgroup analyses of older subjects from major lipid treatment trials has consistently demonstrated the beneficial effects of statin therapy in reducing all cardiovascular events for patients with known CAD who are 65 and older.2-7
Unfortunately, randomized trials of hyperlipidemia treatment with statins have enrolled few people aged 80 and above. Hence, it is unclear whether the benefit of statins on cardiovascular mortality extends to advanced elderly patients. These people comprise the fastest-growing segment of the population, increasing by about 3% per year. They tend to experience concomitant chronic illness, shorter life expectancy, and physical frailty, leading to quality-of-life and end-of-life issues. Is it beneficial and cost-effective to treat these very elderly patients for hyperlipidemia?
The first prospective, randomized trial8 of the use of statins among the elderly examined the impact of pravastatin therapy on primary and secondary prevention of cardiovascular and cerebrovascular events for men and women (age 70–82 years), with a history of vascular disease or with risk factors for vascular disease. The sample of 5804 participants was randomized to receive pravastatin 40 mg or placebo, followed for an average of 3.2 years, and monitored for the combined endpoint of myocardial infarction (MI), stroke, and CAD death. The study showed 19% (95% confidence interval [CI], 6–31; P=.006) proportional reduction in the rate of coronary death or nonfatal MI. The absolute risk reduction for coronary death or nonfatal myocardial infarction or nonfatal stroke was significant (2.2%, number needed to treat [NNT]=45). Rates of adverse drug events were similar in the intervention and control groups.8
Serum cholesterol normally declines with age; so the benefit of lowering lipids with medication in this age group is unclear. Furthermore, a meta-analysis9 showed an inverse relationship between total serum cholesterol and all-cause mortality for people aged 80 and above, raising the possibility that lowering cholesterol may be detrimental in this age group. Two other cohort studies10,11 found that low cholesterol was related to all-cause mortality, even when adjusted for health status and indicators of frailty. The reasons for this relationship are not clear, but some postulated mechanisms exist. It is possible that lower cholesterol levels can increase the risk of a variety of nonatherosclerotic diseases since cholesterol may play a direct role in immune response. Alternatively, preclinical diseases, chronic inflammation, or malnutrition may suppress cholesterol levels.4
Recommendations from others
National Cholesterol Education Program Adult Treatment Panel III guidelines1 outline risk identification and management of hyperlipidemia in all age groups with no exceptions noted for the very elderly. A recent scientific statement from the American Heart Association12 outlined the data on the implementation of all primary and secondary prevention guidelines for the elderly and emphasized that the latest cholesterol treatment recommendations should be applied to all eligible adults, with no exceptions for the very elderly.
No randomized controlled trials exist that identify and treat hyperlipidemia for advanced elderly patients (age >80 years). Expert and consensus guidelines state that hyperlipidemia found in any patient with coronary artery disease (CAD), or at risk of CAD, should be treated irrespective of age; however, evidence is limited to support lowering lipids for advanced elderly patients with and without known CAD (strength of recommendation: C, based on expert and consensus guidelines).1
When prescribing lipid-lowering therapy for older adults, assess competing risks as a function of age
Cari Levy, MD, CMD
Division of Health Care Policy and Research, University of Colorado, Aurora
Many of my patients are over age 82, and these are precisely the ones for whom additional data on the benefits of lipid-lowering would be helpful. Unfortunately, there are no data on lipid-lowering therapy in this population. Polypharmacy is a concern when caring for elderly patients, as are the practical difficulties of medication expense and taking drugs properly. Additionally, because older patients have many competing risks for death, the absolute effect of treating any one problem is relatively small. When prescribing lipid-lowering therapy for older adults, as is often the case with geriatrics, one must assess the “competing risks” as a function of age and, for now, base the treatment decision on these risks rather than evidence-based medicine for the evidence is not yet available.
Evidence summary
CAD is the leading cause of death in the United States and is a significant cause of mortality and morbidity for those aged 65 years and older. Multiple studies have demonstrated the value of lipid-lowering therapy for the primary and secondary prevention of CAD. Most of these studies have not been specifically oriented toward the elderly; however, substantial data from subgroup analyses of older subjects from major lipid treatment trials has consistently demonstrated the beneficial effects of statin therapy in reducing all cardiovascular events for patients with known CAD who are 65 and older.2-7
Unfortunately, randomized trials of hyperlipidemia treatment with statins have enrolled few people aged 80 and above. Hence, it is unclear whether the benefit of statins on cardiovascular mortality extends to advanced elderly patients. These people comprise the fastest-growing segment of the population, increasing by about 3% per year. They tend to experience concomitant chronic illness, shorter life expectancy, and physical frailty, leading to quality-of-life and end-of-life issues. Is it beneficial and cost-effective to treat these very elderly patients for hyperlipidemia?
The first prospective, randomized trial8 of the use of statins among the elderly examined the impact of pravastatin therapy on primary and secondary prevention of cardiovascular and cerebrovascular events for men and women (age 70–82 years), with a history of vascular disease or with risk factors for vascular disease. The sample of 5804 participants was randomized to receive pravastatin 40 mg or placebo, followed for an average of 3.2 years, and monitored for the combined endpoint of myocardial infarction (MI), stroke, and CAD death. The study showed 19% (95% confidence interval [CI], 6–31; P=.006) proportional reduction in the rate of coronary death or nonfatal MI. The absolute risk reduction for coronary death or nonfatal myocardial infarction or nonfatal stroke was significant (2.2%, number needed to treat [NNT]=45). Rates of adverse drug events were similar in the intervention and control groups.8
Serum cholesterol normally declines with age; so the benefit of lowering lipids with medication in this age group is unclear. Furthermore, a meta-analysis9 showed an inverse relationship between total serum cholesterol and all-cause mortality for people aged 80 and above, raising the possibility that lowering cholesterol may be detrimental in this age group. Two other cohort studies10,11 found that low cholesterol was related to all-cause mortality, even when adjusted for health status and indicators of frailty. The reasons for this relationship are not clear, but some postulated mechanisms exist. It is possible that lower cholesterol levels can increase the risk of a variety of nonatherosclerotic diseases since cholesterol may play a direct role in immune response. Alternatively, preclinical diseases, chronic inflammation, or malnutrition may suppress cholesterol levels.4
Recommendations from others
National Cholesterol Education Program Adult Treatment Panel III guidelines1 outline risk identification and management of hyperlipidemia in all age groups with no exceptions noted for the very elderly. A recent scientific statement from the American Heart Association12 outlined the data on the implementation of all primary and secondary prevention guidelines for the elderly and emphasized that the latest cholesterol treatment recommendations should be applied to all eligible adults, with no exceptions for the very elderly.
1. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486-2497.
2. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: A randomised placebo-controlled trial. Lancet 2002;360(9326):7-22.
3. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: The Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383-1389.
4. Miettinen TA, Pyorala K, Olsson AG, et al. Cholesterol-lowering therapy in women and elderly patients with myocardial infarction or angina pectoris: Findings from the Scandinavian Simvastatin Survival Study (4S). Circulation 1997;96:4211-4218.
5. Pfeffer MA, Sacks FM, Moye LA, et al. Cholesterol and Recurrent Events: A secondary prevention trial for normolipidemic patients. CARE Investigators. Am J Cardiol 1995;76:98C-106C.
6. Lewis SJ, Moye LA, Sacks FM, et al. Effect of pravastatin on cardiovascular events in older patients with myocardial infarction and cholesterol levels in the average range. Results of the Cholesterol and Recurrent Events (CARE) trial. Ann Intern Med 1998;129:681-689.
7. Hunt D, Young P, Simes J, et al. Benefits of pravastatin on cardiovascular events and mortality in older patients with coronary heart disease are equal to or exceed those seen in younger patients: Results from the LIPID trial. Ann Intern Med 2001;134:931-940.
8. Shepherd J, Blauw GJ, Murphy MB, et al. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): A randomised controlled trial. Lancet 2002;360:1623-1630.
9. Anum EA, Adera T. Hypercholesterolemia and coronary heart disease in the elderly: a meta-analysis. Ann Epidemiol 2004;14:705-721.
10. Schatz IJ, Masaki K, Yano K, et al. Cholesterol and all-cause mortality in elderly people from the Honolulu Heart Program: A cohort study. Lancet 2001;358:351-355.
11. Brescianini S, Maggi S, Farchi G, et al. Low total cholesterol and increased risk of dying: Are low levels clinical warning signs in the elderly? Results from the Italian Longitudinal Study on Aging. J Am Geriatr Soc 2003;51:991-996.
12. Secondary Prevention of Coronary Heart Disease in the Elderly (With Emphasis on Patients >=75 Years of Age): An American Heart Association Scientific Statement From the Council on Clinical Cardiology Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention. Circulation 2002;105:1735-1743.
1. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486-2497.
2. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: A randomised placebo-controlled trial. Lancet 2002;360(9326):7-22.
3. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: The Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383-1389.
4. Miettinen TA, Pyorala K, Olsson AG, et al. Cholesterol-lowering therapy in women and elderly patients with myocardial infarction or angina pectoris: Findings from the Scandinavian Simvastatin Survival Study (4S). Circulation 1997;96:4211-4218.
5. Pfeffer MA, Sacks FM, Moye LA, et al. Cholesterol and Recurrent Events: A secondary prevention trial for normolipidemic patients. CARE Investigators. Am J Cardiol 1995;76:98C-106C.
6. Lewis SJ, Moye LA, Sacks FM, et al. Effect of pravastatin on cardiovascular events in older patients with myocardial infarction and cholesterol levels in the average range. Results of the Cholesterol and Recurrent Events (CARE) trial. Ann Intern Med 1998;129:681-689.
7. Hunt D, Young P, Simes J, et al. Benefits of pravastatin on cardiovascular events and mortality in older patients with coronary heart disease are equal to or exceed those seen in younger patients: Results from the LIPID trial. Ann Intern Med 2001;134:931-940.
8. Shepherd J, Blauw GJ, Murphy MB, et al. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): A randomised controlled trial. Lancet 2002;360:1623-1630.
9. Anum EA, Adera T. Hypercholesterolemia and coronary heart disease in the elderly: a meta-analysis. Ann Epidemiol 2004;14:705-721.
10. Schatz IJ, Masaki K, Yano K, et al. Cholesterol and all-cause mortality in elderly people from the Honolulu Heart Program: A cohort study. Lancet 2001;358:351-355.
11. Brescianini S, Maggi S, Farchi G, et al. Low total cholesterol and increased risk of dying: Are low levels clinical warning signs in the elderly? Results from the Italian Longitudinal Study on Aging. J Am Geriatr Soc 2003;51:991-996.
12. Secondary Prevention of Coronary Heart Disease in the Elderly (With Emphasis on Patients >=75 Years of Age): An American Heart Association Scientific Statement From the Council on Clinical Cardiology Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention. Circulation 2002;105:1735-1743.
Evidence-based answers from the Family Physicians Inquiries Network
Are oral agents effective for the treatment of verruca vulgaris?
Of the available oral therapies for common warts, none has sufficient evidence to recommend it as an effective therapy (strength of recommendation [SOR]: B). To date, no oral agent has been shown to be effective in a randomized, placebo-controlled, double-blinded trial. Very limited evidence is emerging that zinc may be effective (SOR: C).
Persistent treatment with topical/intralesional therapy should continue to be the mainstay
Christopher P. Paulson, MD
US Air Force Family Medicine Residency, Eglin Air Force Base, Eglin, Fla
Verruca vulgaris (the common wart) is frequently encountered by the family physician, often after unsuccessful topical treatment. Unfortunately, evidence is insufficient to warrant routine use of oral agents such as cimetidine, zinc, or levamisole in the treatment of refractory lesions. The added cost and potential side effects of proposed oral treatments isn’t justified until more rigorous studies show clear clinical efficacy. Persistent treatment with proven topical and intralesional therapy for refractory lesions should continue to be the mainstay of therapy for verruca vulgaris.
Evidence summary
Oral therapies for common warts suffer from a lack rigorous clinical data regarding their efficacy. A detailed literature search found multiple trials evaluating various oral agents. However, only 6 trials met the selection criteria of randomized, controlled trials published in English.
Cimetidine (Tagamet) has been compared with placebo in 3 trials1-3 and was not found superior to placebo. Levamisole (Ergamisol), used in combination with cimetidine, has been compared with cimetidine alone in 2 trials,4,5 and was found to be effective at speeding regression of warts, with patients in the combination arm showing a mean regression time of 7.8 weeks compared with 11 weeks in the cimetidine alone group. These small studies involved 48 and 44 patients, respectively. In addition, 1 nonrandomized controlled trial6 found levamisole at 5 mg/kg for 3 days every 2 weeks to be superior to placebo in achieving complete cure of warts in a group of 40 patients.
Zinc is the only agent to demonstrate efficacy in a completely randomized and placebo-controlled study.7 However, this trial was unblinded, had only 40 subjects assigned to each agent, had a dropout rate of 46%, and did not follow intention-to-treat analysis.
Recommendations from others
Clinical Evidence lists cimetidine and levamisole as therapies of unknown effectiveness.8 The commentary on both agents notes that the size of each randomized controlled trial cited may have been too small to detect clinically important differences.
1. Rogers CJ, Gibney MD, Siegfried EC, Harrsion BR, Glaser DA. Cimetidine therapy for recalcitrant warts in adults: is it any better than placebo? J Am Acad Dermatol 1999;41:123-127
2. Karabulut AA, Sahin S, Eksioglu M. Is cimetidine effective for nongenital warts: a double-blind, placebo-controlled study. Arch Dermatol 1997;133:533-534.
3. Yilmaz E, Alpsoy E, Basaran E. Cimetidine therapy for warts: a placebo-controlled, double-blind study. J Am Acad Dermatol 1996;34:1005-1007.
4. Parsad D, Pandhi R, Juneja A, Negi KS. Cimetidine and levamisole versus cimetidine alone for recalcitrant warts in children. Pediatr Dermatol 2001;18:349-352.
5. Parsad D, Saini R, Negi KS. Comparison of combination of cimetidine and levamisole with cimetidine alone in the treatment of recalcitrant warts. Australas J Dermatol 1999;40:93-95.
6. Amer M, Tosson Z, Soliman A, Selim AG, Salem A, al-Gendy AA. Verrucae treated by levamisole. Int J Dermatol 1991;30:738-740.
7. Al-Gurairi FT, Al-Waiz M, Sharqui KE. Oral zinc sulphate in the treatment of recalcitrant viral warts: randomized, placebo-controlled trial. Br J Dermatol 2002;146:423-431.
8. Bigby M, Gibbs S. Clinical Evidence [monograph online], No. 13. London: BMJ Publishing Group, 2003. Updated June 2005. Available at: clinicalevidence.com. Accessed on October 14, 2005.
Of the available oral therapies for common warts, none has sufficient evidence to recommend it as an effective therapy (strength of recommendation [SOR]: B). To date, no oral agent has been shown to be effective in a randomized, placebo-controlled, double-blinded trial. Very limited evidence is emerging that zinc may be effective (SOR: C).
Persistent treatment with topical/intralesional therapy should continue to be the mainstay
Christopher P. Paulson, MD
US Air Force Family Medicine Residency, Eglin Air Force Base, Eglin, Fla
Verruca vulgaris (the common wart) is frequently encountered by the family physician, often after unsuccessful topical treatment. Unfortunately, evidence is insufficient to warrant routine use of oral agents such as cimetidine, zinc, or levamisole in the treatment of refractory lesions. The added cost and potential side effects of proposed oral treatments isn’t justified until more rigorous studies show clear clinical efficacy. Persistent treatment with proven topical and intralesional therapy for refractory lesions should continue to be the mainstay of therapy for verruca vulgaris.
Evidence summary
Oral therapies for common warts suffer from a lack rigorous clinical data regarding their efficacy. A detailed literature search found multiple trials evaluating various oral agents. However, only 6 trials met the selection criteria of randomized, controlled trials published in English.
Cimetidine (Tagamet) has been compared with placebo in 3 trials1-3 and was not found superior to placebo. Levamisole (Ergamisol), used in combination with cimetidine, has been compared with cimetidine alone in 2 trials,4,5 and was found to be effective at speeding regression of warts, with patients in the combination arm showing a mean regression time of 7.8 weeks compared with 11 weeks in the cimetidine alone group. These small studies involved 48 and 44 patients, respectively. In addition, 1 nonrandomized controlled trial6 found levamisole at 5 mg/kg for 3 days every 2 weeks to be superior to placebo in achieving complete cure of warts in a group of 40 patients.
Zinc is the only agent to demonstrate efficacy in a completely randomized and placebo-controlled study.7 However, this trial was unblinded, had only 40 subjects assigned to each agent, had a dropout rate of 46%, and did not follow intention-to-treat analysis.
Recommendations from others
Clinical Evidence lists cimetidine and levamisole as therapies of unknown effectiveness.8 The commentary on both agents notes that the size of each randomized controlled trial cited may have been too small to detect clinically important differences.
Of the available oral therapies for common warts, none has sufficient evidence to recommend it as an effective therapy (strength of recommendation [SOR]: B). To date, no oral agent has been shown to be effective in a randomized, placebo-controlled, double-blinded trial. Very limited evidence is emerging that zinc may be effective (SOR: C).
Persistent treatment with topical/intralesional therapy should continue to be the mainstay
Christopher P. Paulson, MD
US Air Force Family Medicine Residency, Eglin Air Force Base, Eglin, Fla
Verruca vulgaris (the common wart) is frequently encountered by the family physician, often after unsuccessful topical treatment. Unfortunately, evidence is insufficient to warrant routine use of oral agents such as cimetidine, zinc, or levamisole in the treatment of refractory lesions. The added cost and potential side effects of proposed oral treatments isn’t justified until more rigorous studies show clear clinical efficacy. Persistent treatment with proven topical and intralesional therapy for refractory lesions should continue to be the mainstay of therapy for verruca vulgaris.
Evidence summary
Oral therapies for common warts suffer from a lack rigorous clinical data regarding their efficacy. A detailed literature search found multiple trials evaluating various oral agents. However, only 6 trials met the selection criteria of randomized, controlled trials published in English.
Cimetidine (Tagamet) has been compared with placebo in 3 trials1-3 and was not found superior to placebo. Levamisole (Ergamisol), used in combination with cimetidine, has been compared with cimetidine alone in 2 trials,4,5 and was found to be effective at speeding regression of warts, with patients in the combination arm showing a mean regression time of 7.8 weeks compared with 11 weeks in the cimetidine alone group. These small studies involved 48 and 44 patients, respectively. In addition, 1 nonrandomized controlled trial6 found levamisole at 5 mg/kg for 3 days every 2 weeks to be superior to placebo in achieving complete cure of warts in a group of 40 patients.
Zinc is the only agent to demonstrate efficacy in a completely randomized and placebo-controlled study.7 However, this trial was unblinded, had only 40 subjects assigned to each agent, had a dropout rate of 46%, and did not follow intention-to-treat analysis.
Recommendations from others
Clinical Evidence lists cimetidine and levamisole as therapies of unknown effectiveness.8 The commentary on both agents notes that the size of each randomized controlled trial cited may have been too small to detect clinically important differences.
1. Rogers CJ, Gibney MD, Siegfried EC, Harrsion BR, Glaser DA. Cimetidine therapy for recalcitrant warts in adults: is it any better than placebo? J Am Acad Dermatol 1999;41:123-127
2. Karabulut AA, Sahin S, Eksioglu M. Is cimetidine effective for nongenital warts: a double-blind, placebo-controlled study. Arch Dermatol 1997;133:533-534.
3. Yilmaz E, Alpsoy E, Basaran E. Cimetidine therapy for warts: a placebo-controlled, double-blind study. J Am Acad Dermatol 1996;34:1005-1007.
4. Parsad D, Pandhi R, Juneja A, Negi KS. Cimetidine and levamisole versus cimetidine alone for recalcitrant warts in children. Pediatr Dermatol 2001;18:349-352.
5. Parsad D, Saini R, Negi KS. Comparison of combination of cimetidine and levamisole with cimetidine alone in the treatment of recalcitrant warts. Australas J Dermatol 1999;40:93-95.
6. Amer M, Tosson Z, Soliman A, Selim AG, Salem A, al-Gendy AA. Verrucae treated by levamisole. Int J Dermatol 1991;30:738-740.
7. Al-Gurairi FT, Al-Waiz M, Sharqui KE. Oral zinc sulphate in the treatment of recalcitrant viral warts: randomized, placebo-controlled trial. Br J Dermatol 2002;146:423-431.
8. Bigby M, Gibbs S. Clinical Evidence [monograph online], No. 13. London: BMJ Publishing Group, 2003. Updated June 2005. Available at: clinicalevidence.com. Accessed on October 14, 2005.
1. Rogers CJ, Gibney MD, Siegfried EC, Harrsion BR, Glaser DA. Cimetidine therapy for recalcitrant warts in adults: is it any better than placebo? J Am Acad Dermatol 1999;41:123-127
2. Karabulut AA, Sahin S, Eksioglu M. Is cimetidine effective for nongenital warts: a double-blind, placebo-controlled study. Arch Dermatol 1997;133:533-534.
3. Yilmaz E, Alpsoy E, Basaran E. Cimetidine therapy for warts: a placebo-controlled, double-blind study. J Am Acad Dermatol 1996;34:1005-1007.
4. Parsad D, Pandhi R, Juneja A, Negi KS. Cimetidine and levamisole versus cimetidine alone for recalcitrant warts in children. Pediatr Dermatol 2001;18:349-352.
5. Parsad D, Saini R, Negi KS. Comparison of combination of cimetidine and levamisole with cimetidine alone in the treatment of recalcitrant warts. Australas J Dermatol 1999;40:93-95.
6. Amer M, Tosson Z, Soliman A, Selim AG, Salem A, al-Gendy AA. Verrucae treated by levamisole. Int J Dermatol 1991;30:738-740.
7. Al-Gurairi FT, Al-Waiz M, Sharqui KE. Oral zinc sulphate in the treatment of recalcitrant viral warts: randomized, placebo-controlled trial. Br J Dermatol 2002;146:423-431.
8. Bigby M, Gibbs S. Clinical Evidence [monograph online], No. 13. London: BMJ Publishing Group, 2003. Updated June 2005. Available at: clinicalevidence.com. Accessed on October 14, 2005.
Evidence-based answers from the Family Physicians Inquiries Network
What is the best way to diagnose polycystic ovarian syndrome?
Polycystic ovarian syndrome (PCOS) is diagnosed for women of childbearing age presenting with 2 of the following: 1) oligo- or anovulatory menstrual irregularities, 2) evidence of hyperandrogenism in the absence of secondary cause; 3) enlarged ovaries with multiple small follicular cysts on transvaginal ultrasound (strength of recommendation [SOR]: C, based on expert opinion).
Depending on the clinical presentation, secondary causes should be excluded (TABLE) (SOR: C, expert opinion). While not among the diagnostic criteria, insulin resistance is common, and patients with PCOS should be evaluated for metabolic abnormalities, particularly hyperlipidemia and glucose intolerance or diabetes (SOR: B, based on prospective cohort studies).
Faty liver and insulin resistance are common problems in patients with PCOS
Pouran Yousefi, MD
Baylor College of Medicine, Houston, Texas
Today we have a better understanding of the relation between obesity, insulin resistance, and polycystic ovarian syndrome (PCOS), but it is not quite clear whether the insulin resistance plays the main pathophysiologic role in this condition. As the prevalence of obesity, metabolic syndrome, and diabetes increases in our society, it is expected that the incidence of PCOS will rise as well.
Unfortunately, there is no single specific diagnostic test available for the diagnosis of PCOS. I practice in a community clinic where access to pelvic ultrasound is limited, and often I have to rely on laboratory analysis to make the diagnosis. Aside from TSH, prolactin, DHEA sulfate, 17 OHP, free testosterone, LH/FSH, and lipid panel, I calculate insulin resistance (IR) using fasting blood sugar and insulin level. If the IR level is elevated, I counsel the patient about PCOS and refer her to a dietitian for weight management while waiting for a pelvic ultrasonography appointment. However, due to multiple limitations that apply to the measurement of IR, experts in this field do not recommend its widespread use for the diagnosis of PCOS.
I also find that elevated ALT is not uncommon among my overweight patients who present with PCOS related symptoms. Further workup in this group of patients usually leads to the diagnosis of fatty infiltration of the liver.
TABLE
Differential diagnosis of hyperandrogenism in PCOS
| DIFFERENTIAL DIAGNOSES | CLINICAL FEATURES | TEST |
|---|---|---|
| Nonclassical congenital adrenal hyperplasia | Family history; more common among Ashkenazi Jews | 17-hydroxyprogesterone |
| Androgen-secreting neoplasms | Rapid virilization | DHEA-S (adrenal) Testosterone (ovary) |
| Hypothyroidism | Fatigue, dry skin, cold intolerance, weight gain, constipation, goiter | Thyroid-stimulating hormone |
| Hyperprolactinemia | Galactorrhea | Prolactin (may be mildly high in PCOS) |
| Cushing syndrome (rare) | Moon face, buffalo hump, abdominal striae, centripetal fat pattern, hypertension, easy bruising | 24 hour urine free cortisol Dexamethasone suppression test (confirmatory) |
| Acromegaly | Acral enlargement, coarse features, prognathism | Insulin-like growth factor |
| Adapted from Chang, Am J Obstet Gynecol 2004.6 | ||
Evidence summary
Polycystic ovarian syndrome is a condition of unexplained hyperandrogenic chronic anovulation that affects at least 4% of women of reproductive age.1 Because PCOS is a clinical syndrome, no single diagnostic criterion is sufficient for diagnosis.2 Clinical features include menstrual irregularities or infertility, hirsutism, male-pattern balding, acne, ovarian enlargement, and signs of insulin resistance (eg, central obesity, acanthosis nigricans). A 2003 international consensus panel concluded that the presence of 2 of 3 criteria (oligo/anovulation, hyperandrogenism, polycystic ovaries), in the absence of other secondary causes, is sufficient to make the diagnosis.2 Evidence for hyperandrogenism includes hirsutism, acne, or elevated total testosterone levels.3 A high luteinizing hormone/follicle-stimulating hormone (LH/FSH) ratio supports the diagnosis. However, because this measure varies considerably in relation to ovulation, body-mass index (BMI), and the particular measurement assay used, the consensus panel recommended against its use as a diagnostic criterion.2 Based on optimum receiver operator characteristic curve analyses, ultrasound criteria include the presence of 12 or more follicles in each ovary measuring 2 to 9 mm in diameter (sensitivity=75%, specificity=99%, positive predictive value [PPV]=75%, negative predictive value [NPV]=99%, assuming 4% prevalence) or ovarian volume over 7 mL (sensitivity=67.5%, specificity=91.2%, PPV=24%, NPV 99%).4,5
PCOS is also a diagnosis of exclusion. Secondary causes of hyperandrogenism may be suggested by clinical findings, including 1) abrupt onset, short duration, or sudden progressive worsening of hirsutism; 2) onset of symptoms in the third decade of life or later; or 3) signs of virilization (deepening voice, clitoromegaly).6 The differential diagnosis, clinical features and potentially useful diagnostic tests to rule out secondary causes are shown in the TABLE.
Women with PCOS often experience insulin resistance, and are at increased risk for developing type 2 diabetes, dyslipidemia, and cardiovascular disease. One cross-sectional study7 of 122 women with PCOS between 13.5 and 40 years of age found that 35% had impaired glucose tolerance, and another 10% had non-insulindependent diabetes. A prospective case-control study8 of young women (aged <35 years) found that compared with age- and BMI-matched controls, those with PCOS had higher levels of fasting glucose, insulin, total and low-density lipoprotein cholesterol, and altered left ventricular mass and cardiac function on echocardiogram. Once PCOS is suspected, the diagnostic work-up should include a 2-hour glucose tolerance test and lipid panel to assess cardiovascular risk, particularly among obese women.
Recommendations from others
A 2002 American College of Obstetricians and Gynecologists guideline9 adopted the 1990 National Institutes of Health consensus panel criteria for diagnosing PCOS (ie, chronic anovulation and clinical or biochemical signs of hyperandrogenism, excluding other causes), and recommends that all patients have documentation of elevated testosterone levels; thyroid-stimulating hormone (TSH), prolactin, and 17-hydroxyprogesterone levels to exclude secondary causes of hyperandrogenism; and evaluation for metabolic abnormalities with a 2-hour glucose tolerance test and fasting lipid panel.
1. Knochenhauer ES, Key TJ, Kahsar-Miller M, Waggoner W, Boots LR, Azziz R. Prevalence of the polycystic ovary syndrome in unselected black and white women of the southeastern United States: a prospective study. J Clin Endocrinol Metab 1998;83:3078-3082.
2. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril 2004;81:19-25.
3. Robinson S, Rodin DA, Deacon A, Wheeler MJ, Clayton RN. Which hormone tests for the diagnosis of polycystic ovary syndrome? Br J Obstet Gynaecol 1992;99:232-238.
4. Jonard S, Robert Y, Cortet-Rudelli C, Pigny P, Decanter C, Dewailly D. Ultrasound examination of polycystic ovaries: is it worth counting the follicles? Hum Reprod 2003;18:598-603.
5. Jonard S, Robert Y, Dewailly D. Revisiting the ovarian volume as a diagnostic criterion for polycystic ovaries. Hum Reprod 2005;20:2893-2898.
6. Chang RJ. A practical approach to the diagnosis of polycystic ovary syndrome. Am J Obstet Gynecol 2004;191:713-717.
7. Ehrmann DA, Barnes RB, Rosenfield RL, Cavaghan MK, Imperial J. Prevalence of impaired glucose tolerance and diabetes in women with polycystic ovary syndrome. Diabetes Care 1999;22:141-146.
8. Orio F, Jr, Palomba S, Spinelli L, et al. The cardiovascular risk of young women with polycystic ovary syndrome: an observational, analytical, prospective case-control study. J Clin Endocrinol Metab 2004;89:3696-3701.
9. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin #41. Clinical Management Guidelines for Obstetrician-Gynecologists: Polycystic Ovary Syndrome. Obstet Gynecol 2002;100:1389-1402.
Polycystic ovarian syndrome (PCOS) is diagnosed for women of childbearing age presenting with 2 of the following: 1) oligo- or anovulatory menstrual irregularities, 2) evidence of hyperandrogenism in the absence of secondary cause; 3) enlarged ovaries with multiple small follicular cysts on transvaginal ultrasound (strength of recommendation [SOR]: C, based on expert opinion).
Depending on the clinical presentation, secondary causes should be excluded (TABLE) (SOR: C, expert opinion). While not among the diagnostic criteria, insulin resistance is common, and patients with PCOS should be evaluated for metabolic abnormalities, particularly hyperlipidemia and glucose intolerance or diabetes (SOR: B, based on prospective cohort studies).
Faty liver and insulin resistance are common problems in patients with PCOS
Pouran Yousefi, MD
Baylor College of Medicine, Houston, Texas
Today we have a better understanding of the relation between obesity, insulin resistance, and polycystic ovarian syndrome (PCOS), but it is not quite clear whether the insulin resistance plays the main pathophysiologic role in this condition. As the prevalence of obesity, metabolic syndrome, and diabetes increases in our society, it is expected that the incidence of PCOS will rise as well.
Unfortunately, there is no single specific diagnostic test available for the diagnosis of PCOS. I practice in a community clinic where access to pelvic ultrasound is limited, and often I have to rely on laboratory analysis to make the diagnosis. Aside from TSH, prolactin, DHEA sulfate, 17 OHP, free testosterone, LH/FSH, and lipid panel, I calculate insulin resistance (IR) using fasting blood sugar and insulin level. If the IR level is elevated, I counsel the patient about PCOS and refer her to a dietitian for weight management while waiting for a pelvic ultrasonography appointment. However, due to multiple limitations that apply to the measurement of IR, experts in this field do not recommend its widespread use for the diagnosis of PCOS.
I also find that elevated ALT is not uncommon among my overweight patients who present with PCOS related symptoms. Further workup in this group of patients usually leads to the diagnosis of fatty infiltration of the liver.
TABLE
Differential diagnosis of hyperandrogenism in PCOS
| DIFFERENTIAL DIAGNOSES | CLINICAL FEATURES | TEST |
|---|---|---|
| Nonclassical congenital adrenal hyperplasia | Family history; more common among Ashkenazi Jews | 17-hydroxyprogesterone |
| Androgen-secreting neoplasms | Rapid virilization | DHEA-S (adrenal) Testosterone (ovary) |
| Hypothyroidism | Fatigue, dry skin, cold intolerance, weight gain, constipation, goiter | Thyroid-stimulating hormone |
| Hyperprolactinemia | Galactorrhea | Prolactin (may be mildly high in PCOS) |
| Cushing syndrome (rare) | Moon face, buffalo hump, abdominal striae, centripetal fat pattern, hypertension, easy bruising | 24 hour urine free cortisol Dexamethasone suppression test (confirmatory) |
| Acromegaly | Acral enlargement, coarse features, prognathism | Insulin-like growth factor |
| Adapted from Chang, Am J Obstet Gynecol 2004.6 | ||
Evidence summary
Polycystic ovarian syndrome is a condition of unexplained hyperandrogenic chronic anovulation that affects at least 4% of women of reproductive age.1 Because PCOS is a clinical syndrome, no single diagnostic criterion is sufficient for diagnosis.2 Clinical features include menstrual irregularities or infertility, hirsutism, male-pattern balding, acne, ovarian enlargement, and signs of insulin resistance (eg, central obesity, acanthosis nigricans). A 2003 international consensus panel concluded that the presence of 2 of 3 criteria (oligo/anovulation, hyperandrogenism, polycystic ovaries), in the absence of other secondary causes, is sufficient to make the diagnosis.2 Evidence for hyperandrogenism includes hirsutism, acne, or elevated total testosterone levels.3 A high luteinizing hormone/follicle-stimulating hormone (LH/FSH) ratio supports the diagnosis. However, because this measure varies considerably in relation to ovulation, body-mass index (BMI), and the particular measurement assay used, the consensus panel recommended against its use as a diagnostic criterion.2 Based on optimum receiver operator characteristic curve analyses, ultrasound criteria include the presence of 12 or more follicles in each ovary measuring 2 to 9 mm in diameter (sensitivity=75%, specificity=99%, positive predictive value [PPV]=75%, negative predictive value [NPV]=99%, assuming 4% prevalence) or ovarian volume over 7 mL (sensitivity=67.5%, specificity=91.2%, PPV=24%, NPV 99%).4,5
PCOS is also a diagnosis of exclusion. Secondary causes of hyperandrogenism may be suggested by clinical findings, including 1) abrupt onset, short duration, or sudden progressive worsening of hirsutism; 2) onset of symptoms in the third decade of life or later; or 3) signs of virilization (deepening voice, clitoromegaly).6 The differential diagnosis, clinical features and potentially useful diagnostic tests to rule out secondary causes are shown in the TABLE.
Women with PCOS often experience insulin resistance, and are at increased risk for developing type 2 diabetes, dyslipidemia, and cardiovascular disease. One cross-sectional study7 of 122 women with PCOS between 13.5 and 40 years of age found that 35% had impaired glucose tolerance, and another 10% had non-insulindependent diabetes. A prospective case-control study8 of young women (aged <35 years) found that compared with age- and BMI-matched controls, those with PCOS had higher levels of fasting glucose, insulin, total and low-density lipoprotein cholesterol, and altered left ventricular mass and cardiac function on echocardiogram. Once PCOS is suspected, the diagnostic work-up should include a 2-hour glucose tolerance test and lipid panel to assess cardiovascular risk, particularly among obese women.
Recommendations from others
A 2002 American College of Obstetricians and Gynecologists guideline9 adopted the 1990 National Institutes of Health consensus panel criteria for diagnosing PCOS (ie, chronic anovulation and clinical or biochemical signs of hyperandrogenism, excluding other causes), and recommends that all patients have documentation of elevated testosterone levels; thyroid-stimulating hormone (TSH), prolactin, and 17-hydroxyprogesterone levels to exclude secondary causes of hyperandrogenism; and evaluation for metabolic abnormalities with a 2-hour glucose tolerance test and fasting lipid panel.
Polycystic ovarian syndrome (PCOS) is diagnosed for women of childbearing age presenting with 2 of the following: 1) oligo- or anovulatory menstrual irregularities, 2) evidence of hyperandrogenism in the absence of secondary cause; 3) enlarged ovaries with multiple small follicular cysts on transvaginal ultrasound (strength of recommendation [SOR]: C, based on expert opinion).
Depending on the clinical presentation, secondary causes should be excluded (TABLE) (SOR: C, expert opinion). While not among the diagnostic criteria, insulin resistance is common, and patients with PCOS should be evaluated for metabolic abnormalities, particularly hyperlipidemia and glucose intolerance or diabetes (SOR: B, based on prospective cohort studies).
Faty liver and insulin resistance are common problems in patients with PCOS
Pouran Yousefi, MD
Baylor College of Medicine, Houston, Texas
Today we have a better understanding of the relation between obesity, insulin resistance, and polycystic ovarian syndrome (PCOS), but it is not quite clear whether the insulin resistance plays the main pathophysiologic role in this condition. As the prevalence of obesity, metabolic syndrome, and diabetes increases in our society, it is expected that the incidence of PCOS will rise as well.
Unfortunately, there is no single specific diagnostic test available for the diagnosis of PCOS. I practice in a community clinic where access to pelvic ultrasound is limited, and often I have to rely on laboratory analysis to make the diagnosis. Aside from TSH, prolactin, DHEA sulfate, 17 OHP, free testosterone, LH/FSH, and lipid panel, I calculate insulin resistance (IR) using fasting blood sugar and insulin level. If the IR level is elevated, I counsel the patient about PCOS and refer her to a dietitian for weight management while waiting for a pelvic ultrasonography appointment. However, due to multiple limitations that apply to the measurement of IR, experts in this field do not recommend its widespread use for the diagnosis of PCOS.
I also find that elevated ALT is not uncommon among my overweight patients who present with PCOS related symptoms. Further workup in this group of patients usually leads to the diagnosis of fatty infiltration of the liver.
TABLE
Differential diagnosis of hyperandrogenism in PCOS
| DIFFERENTIAL DIAGNOSES | CLINICAL FEATURES | TEST |
|---|---|---|
| Nonclassical congenital adrenal hyperplasia | Family history; more common among Ashkenazi Jews | 17-hydroxyprogesterone |
| Androgen-secreting neoplasms | Rapid virilization | DHEA-S (adrenal) Testosterone (ovary) |
| Hypothyroidism | Fatigue, dry skin, cold intolerance, weight gain, constipation, goiter | Thyroid-stimulating hormone |
| Hyperprolactinemia | Galactorrhea | Prolactin (may be mildly high in PCOS) |
| Cushing syndrome (rare) | Moon face, buffalo hump, abdominal striae, centripetal fat pattern, hypertension, easy bruising | 24 hour urine free cortisol Dexamethasone suppression test (confirmatory) |
| Acromegaly | Acral enlargement, coarse features, prognathism | Insulin-like growth factor |
| Adapted from Chang, Am J Obstet Gynecol 2004.6 | ||
Evidence summary
Polycystic ovarian syndrome is a condition of unexplained hyperandrogenic chronic anovulation that affects at least 4% of women of reproductive age.1 Because PCOS is a clinical syndrome, no single diagnostic criterion is sufficient for diagnosis.2 Clinical features include menstrual irregularities or infertility, hirsutism, male-pattern balding, acne, ovarian enlargement, and signs of insulin resistance (eg, central obesity, acanthosis nigricans). A 2003 international consensus panel concluded that the presence of 2 of 3 criteria (oligo/anovulation, hyperandrogenism, polycystic ovaries), in the absence of other secondary causes, is sufficient to make the diagnosis.2 Evidence for hyperandrogenism includes hirsutism, acne, or elevated total testosterone levels.3 A high luteinizing hormone/follicle-stimulating hormone (LH/FSH) ratio supports the diagnosis. However, because this measure varies considerably in relation to ovulation, body-mass index (BMI), and the particular measurement assay used, the consensus panel recommended against its use as a diagnostic criterion.2 Based on optimum receiver operator characteristic curve analyses, ultrasound criteria include the presence of 12 or more follicles in each ovary measuring 2 to 9 mm in diameter (sensitivity=75%, specificity=99%, positive predictive value [PPV]=75%, negative predictive value [NPV]=99%, assuming 4% prevalence) or ovarian volume over 7 mL (sensitivity=67.5%, specificity=91.2%, PPV=24%, NPV 99%).4,5
PCOS is also a diagnosis of exclusion. Secondary causes of hyperandrogenism may be suggested by clinical findings, including 1) abrupt onset, short duration, or sudden progressive worsening of hirsutism; 2) onset of symptoms in the third decade of life or later; or 3) signs of virilization (deepening voice, clitoromegaly).6 The differential diagnosis, clinical features and potentially useful diagnostic tests to rule out secondary causes are shown in the TABLE.
Women with PCOS often experience insulin resistance, and are at increased risk for developing type 2 diabetes, dyslipidemia, and cardiovascular disease. One cross-sectional study7 of 122 women with PCOS between 13.5 and 40 years of age found that 35% had impaired glucose tolerance, and another 10% had non-insulindependent diabetes. A prospective case-control study8 of young women (aged <35 years) found that compared with age- and BMI-matched controls, those with PCOS had higher levels of fasting glucose, insulin, total and low-density lipoprotein cholesterol, and altered left ventricular mass and cardiac function on echocardiogram. Once PCOS is suspected, the diagnostic work-up should include a 2-hour glucose tolerance test and lipid panel to assess cardiovascular risk, particularly among obese women.
Recommendations from others
A 2002 American College of Obstetricians and Gynecologists guideline9 adopted the 1990 National Institutes of Health consensus panel criteria for diagnosing PCOS (ie, chronic anovulation and clinical or biochemical signs of hyperandrogenism, excluding other causes), and recommends that all patients have documentation of elevated testosterone levels; thyroid-stimulating hormone (TSH), prolactin, and 17-hydroxyprogesterone levels to exclude secondary causes of hyperandrogenism; and evaluation for metabolic abnormalities with a 2-hour glucose tolerance test and fasting lipid panel.
1. Knochenhauer ES, Key TJ, Kahsar-Miller M, Waggoner W, Boots LR, Azziz R. Prevalence of the polycystic ovary syndrome in unselected black and white women of the southeastern United States: a prospective study. J Clin Endocrinol Metab 1998;83:3078-3082.
2. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril 2004;81:19-25.
3. Robinson S, Rodin DA, Deacon A, Wheeler MJ, Clayton RN. Which hormone tests for the diagnosis of polycystic ovary syndrome? Br J Obstet Gynaecol 1992;99:232-238.
4. Jonard S, Robert Y, Cortet-Rudelli C, Pigny P, Decanter C, Dewailly D. Ultrasound examination of polycystic ovaries: is it worth counting the follicles? Hum Reprod 2003;18:598-603.
5. Jonard S, Robert Y, Dewailly D. Revisiting the ovarian volume as a diagnostic criterion for polycystic ovaries. Hum Reprod 2005;20:2893-2898.
6. Chang RJ. A practical approach to the diagnosis of polycystic ovary syndrome. Am J Obstet Gynecol 2004;191:713-717.
7. Ehrmann DA, Barnes RB, Rosenfield RL, Cavaghan MK, Imperial J. Prevalence of impaired glucose tolerance and diabetes in women with polycystic ovary syndrome. Diabetes Care 1999;22:141-146.
8. Orio F, Jr, Palomba S, Spinelli L, et al. The cardiovascular risk of young women with polycystic ovary syndrome: an observational, analytical, prospective case-control study. J Clin Endocrinol Metab 2004;89:3696-3701.
9. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin #41. Clinical Management Guidelines for Obstetrician-Gynecologists: Polycystic Ovary Syndrome. Obstet Gynecol 2002;100:1389-1402.
1. Knochenhauer ES, Key TJ, Kahsar-Miller M, Waggoner W, Boots LR, Azziz R. Prevalence of the polycystic ovary syndrome in unselected black and white women of the southeastern United States: a prospective study. J Clin Endocrinol Metab 1998;83:3078-3082.
2. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril 2004;81:19-25.
3. Robinson S, Rodin DA, Deacon A, Wheeler MJ, Clayton RN. Which hormone tests for the diagnosis of polycystic ovary syndrome? Br J Obstet Gynaecol 1992;99:232-238.
4. Jonard S, Robert Y, Cortet-Rudelli C, Pigny P, Decanter C, Dewailly D. Ultrasound examination of polycystic ovaries: is it worth counting the follicles? Hum Reprod 2003;18:598-603.
5. Jonard S, Robert Y, Dewailly D. Revisiting the ovarian volume as a diagnostic criterion for polycystic ovaries. Hum Reprod 2005;20:2893-2898.
6. Chang RJ. A practical approach to the diagnosis of polycystic ovary syndrome. Am J Obstet Gynecol 2004;191:713-717.
7. Ehrmann DA, Barnes RB, Rosenfield RL, Cavaghan MK, Imperial J. Prevalence of impaired glucose tolerance and diabetes in women with polycystic ovary syndrome. Diabetes Care 1999;22:141-146.
8. Orio F, Jr, Palomba S, Spinelli L, et al. The cardiovascular risk of young women with polycystic ovary syndrome: an observational, analytical, prospective case-control study. J Clin Endocrinol Metab 2004;89:3696-3701.
9. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin #41. Clinical Management Guidelines for Obstetrician-Gynecologists: Polycystic Ovary Syndrome. Obstet Gynecol 2002;100:1389-1402.
Evidence-based answers from the Family Physicians Inquiries Network
What is the best test to detect herpes in skin lesions?
Polymerase chain reaction (PCR) techniques appear to be more sensitive and specific in detecting herpes simplex virus (HSV) in genital lesions (strength of recommendation [SOR]: A, based on 2 diagnostic cohort studies); however, viral culture remains the gold standard (SOR: C, based on expert opinion). Studies of serologic and antibody detection tests report higher sensitivities than viral culture (SOR: C, based on consensus guidelines). Cytologic tests such as the Tzanck smear and Papanicolaou (Pap) smear have poor sensitivities and specificities and should not be relied upon for a diagnosis of genital herpes (SOR: C, based on expert opinion).
Test ulcers with culture or PCR
James Holt, MD
Department of Family Medicine, East Tennessee State University, Johnson City
Genital and oral lesions consistent with herpes simplex lesions are relatively common in my practice. Before PCR testing was available, ulcers could be tested via culture—which took too long to be immediately useful—or via Tzanck smear, which helped greatly if multinucleated giant cells were seen. However, both tests were relatively insensitive. As this Clinical Inquiry demonstrates, ulcers currently should be tested either with culture or with PCR. Herpes culture is most sensitive if vesicles are still intact for unroofing.
Evidence summary
More than 50 million individuals in the United States have genital herpes. The diagnosis of genital herpes based on clinical history and physical examination is often inaccurate.1 Clinical suspicion needs to be confirmed by laboratory testing because it has a direct impact on counseling and prognosis.2
Viral culture is still the gold standard test for the detection of HSV; however, the rate of positive cultures depends on the stage of the lesion, the quality of the specimen, and the transport conditions. A British study3 found the rate of virus recovery for early vesicles to be 52% to 93%. This dropped to 41% to 72% if midstage ulcers were present. Finally, the detection for late-stage crusted lesions was only 19% to 27%. Another disadvantage is that culture is labor-intensive. A positive culture takes an average of 3 days to grow, whereas a negative culture must incubate for 10 days.3
PCR techniques are more sensitive and results can be available in less than 4 hours.3 In 110 clinical samples from dermal or genital lesions of patients with suspected HSV infection, the sensitivity of PCR was 98% (positive likelihood ratio [LR+]=∞; negative likelihood ratio [LR–]=0.02) compared with 73% (LR+ = ∞; LR– = 0.27) for culture. The specificities of both were 100%.4 In London, 233 samples from patients at a genitourinary medicine clinic were tested with both viral culture and PCR. HSV was detected in 79 samples by culture and 132 samples by PCR. The detection by PCR was higher in early as well as late stages of infection and in both first and recurrent episodes.3 The reference standard for these studies was not an independent standard, but a positive result on both tests or modified versions of the PCR test. The use of a version of the test of interest (PCR) as part of the reference standard, while probably unavoidable in this situation, will tend inflate the sensitivity and specificity.
In another study, daily sampling of lesions in patients with known HSV infections detected HSV DNA on 15 of 17 days with PCR and only 3 of 17 days with culture.1 This suggests that PCR is more effective in detecting early, as well as late, stages of infection. Currently PCR is more expensive, but it may become cheaper because of decreased labor expense when compared with culture.
Genital herpes may also be detected with enzyme immunoassay testing in as little as 5 hours. In a study5 using 275 samples from genital lesions, HSV was detected in 65% of the antigen tests and 53% of the viral cultures. The sensitivity of this method is equal to culture for early lesions, but much higher in late-stage lesions (58% vs 26%).5
Serologic tests are often used to detect HSV because they can differentiate between HSV-1 and HSV-2. There is an FDA-approved point-of-care test called POCkit that gives results from capillary blood or serum during an office visit. These tests are 80% to 98% sensitive and more than 96% specific. Unfortunately, they are not readily available in all countries.2
Other detection methods include the Tzanck smear, which is only 40% to 50% sensitive compared with culture, and the Pap smear, which is 60% to 70% sensitive.6 These tests should not be the sole method for the diagnosis of HSV. They cannot differentiate between HSV 1 and HSV 2; furthermore, the Tzanck prep will give a positive result if varicella zoster virus is present.6 If these tests are positive, confirmatory testing specific for HSV should be performed.
Recommendations from others
The Centers for Disease Control and Prevention7 recommends screening with a viral culture when a genital lesion is present, however, the sensitivity declines rapidly within a few days as the lesion begins to heal. To collect a sample the lesion must be unroofed using a Dacron swab, which is then placed in a viral transport medium and processed within 24 hours. Swabs containing calcium agglutinate are toxic to HSV.6 Type-specific antibodies develop during the first several weeks and can be detected with serologic tests; however, these may be falsely negative in the early stages of a primary infection.7
The US Preventative Services Task Force8 recommends against routine serologic screening for HSV in asymptomatic adolescents and adults. They also recommend against routine screening of asymptomatic pregnant women at any time during pregnancy as a way to decrease neonatal transmission.8
1. Albrecht MA. Clinical manifestations and diagnosis of genital herpes simplex virus infection. UpToDate [database online]. Available at: www.uptodate.com.
2. Centers for Disease Control and Prevention. Diseases characterized by genital ulcers. Sexually transmitted diseases treatment guidelines. MMWR Recomm Rep 2002;51(RR-6):11-25.
3. Ramaswamy M, McDonald C, Smith M, et al. Diagnosis of genital herpes by real time PCR in routine clinical practice. Sex Trasm Infect 2004;80:406-410.
4. Schmutzhard J, Riedel H, Wirgart B, Grillner L. Detection of herpes simplex virus type 1, herpes simplex virus type 2 and varicella-zoster virus in skin lesions. Comparison of real-time PCR, nested PCR and virus isolation. J Clin Virol 2004;29:120-126.
5. Cone RW, Swenson PD, Hobson AC, Remington M, Corey L. Herpes simplex virus detection from genital lesions: a comparative study using antigen detection (HerpChek) and culture. J Clin Microbiol 1993;31:1774-1776.
6. Herpes, genital. InfoPOEMS [online database]. Available at www.infopoems.com.
7. Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines 2002. Diseases Characterized by Genital Ulcers. Available at: www.cdc.gov/STD/treatment/2-2002TG.htm. Accessed on March 13, 2006.
8. United States Preventative Services Task Force. Screening for Genital Herpes. March 2005. Available at: www.ahrq.gov/clinic/uspstf/uspsherp.htm. Accessed on March 13, 2006.
Polymerase chain reaction (PCR) techniques appear to be more sensitive and specific in detecting herpes simplex virus (HSV) in genital lesions (strength of recommendation [SOR]: A, based on 2 diagnostic cohort studies); however, viral culture remains the gold standard (SOR: C, based on expert opinion). Studies of serologic and antibody detection tests report higher sensitivities than viral culture (SOR: C, based on consensus guidelines). Cytologic tests such as the Tzanck smear and Papanicolaou (Pap) smear have poor sensitivities and specificities and should not be relied upon for a diagnosis of genital herpes (SOR: C, based on expert opinion).
Test ulcers with culture or PCR
James Holt, MD
Department of Family Medicine, East Tennessee State University, Johnson City
Genital and oral lesions consistent with herpes simplex lesions are relatively common in my practice. Before PCR testing was available, ulcers could be tested via culture—which took too long to be immediately useful—or via Tzanck smear, which helped greatly if multinucleated giant cells were seen. However, both tests were relatively insensitive. As this Clinical Inquiry demonstrates, ulcers currently should be tested either with culture or with PCR. Herpes culture is most sensitive if vesicles are still intact for unroofing.
Evidence summary
More than 50 million individuals in the United States have genital herpes. The diagnosis of genital herpes based on clinical history and physical examination is often inaccurate.1 Clinical suspicion needs to be confirmed by laboratory testing because it has a direct impact on counseling and prognosis.2
Viral culture is still the gold standard test for the detection of HSV; however, the rate of positive cultures depends on the stage of the lesion, the quality of the specimen, and the transport conditions. A British study3 found the rate of virus recovery for early vesicles to be 52% to 93%. This dropped to 41% to 72% if midstage ulcers were present. Finally, the detection for late-stage crusted lesions was only 19% to 27%. Another disadvantage is that culture is labor-intensive. A positive culture takes an average of 3 days to grow, whereas a negative culture must incubate for 10 days.3
PCR techniques are more sensitive and results can be available in less than 4 hours.3 In 110 clinical samples from dermal or genital lesions of patients with suspected HSV infection, the sensitivity of PCR was 98% (positive likelihood ratio [LR+]=∞; negative likelihood ratio [LR–]=0.02) compared with 73% (LR+ = ∞; LR– = 0.27) for culture. The specificities of both were 100%.4 In London, 233 samples from patients at a genitourinary medicine clinic were tested with both viral culture and PCR. HSV was detected in 79 samples by culture and 132 samples by PCR. The detection by PCR was higher in early as well as late stages of infection and in both first and recurrent episodes.3 The reference standard for these studies was not an independent standard, but a positive result on both tests or modified versions of the PCR test. The use of a version of the test of interest (PCR) as part of the reference standard, while probably unavoidable in this situation, will tend inflate the sensitivity and specificity.
In another study, daily sampling of lesions in patients with known HSV infections detected HSV DNA on 15 of 17 days with PCR and only 3 of 17 days with culture.1 This suggests that PCR is more effective in detecting early, as well as late, stages of infection. Currently PCR is more expensive, but it may become cheaper because of decreased labor expense when compared with culture.
Genital herpes may also be detected with enzyme immunoassay testing in as little as 5 hours. In a study5 using 275 samples from genital lesions, HSV was detected in 65% of the antigen tests and 53% of the viral cultures. The sensitivity of this method is equal to culture for early lesions, but much higher in late-stage lesions (58% vs 26%).5
Serologic tests are often used to detect HSV because they can differentiate between HSV-1 and HSV-2. There is an FDA-approved point-of-care test called POCkit that gives results from capillary blood or serum during an office visit. These tests are 80% to 98% sensitive and more than 96% specific. Unfortunately, they are not readily available in all countries.2
Other detection methods include the Tzanck smear, which is only 40% to 50% sensitive compared with culture, and the Pap smear, which is 60% to 70% sensitive.6 These tests should not be the sole method for the diagnosis of HSV. They cannot differentiate between HSV 1 and HSV 2; furthermore, the Tzanck prep will give a positive result if varicella zoster virus is present.6 If these tests are positive, confirmatory testing specific for HSV should be performed.
Recommendations from others
The Centers for Disease Control and Prevention7 recommends screening with a viral culture when a genital lesion is present, however, the sensitivity declines rapidly within a few days as the lesion begins to heal. To collect a sample the lesion must be unroofed using a Dacron swab, which is then placed in a viral transport medium and processed within 24 hours. Swabs containing calcium agglutinate are toxic to HSV.6 Type-specific antibodies develop during the first several weeks and can be detected with serologic tests; however, these may be falsely negative in the early stages of a primary infection.7
The US Preventative Services Task Force8 recommends against routine serologic screening for HSV in asymptomatic adolescents and adults. They also recommend against routine screening of asymptomatic pregnant women at any time during pregnancy as a way to decrease neonatal transmission.8
Polymerase chain reaction (PCR) techniques appear to be more sensitive and specific in detecting herpes simplex virus (HSV) in genital lesions (strength of recommendation [SOR]: A, based on 2 diagnostic cohort studies); however, viral culture remains the gold standard (SOR: C, based on expert opinion). Studies of serologic and antibody detection tests report higher sensitivities than viral culture (SOR: C, based on consensus guidelines). Cytologic tests such as the Tzanck smear and Papanicolaou (Pap) smear have poor sensitivities and specificities and should not be relied upon for a diagnosis of genital herpes (SOR: C, based on expert opinion).
Test ulcers with culture or PCR
James Holt, MD
Department of Family Medicine, East Tennessee State University, Johnson City
Genital and oral lesions consistent with herpes simplex lesions are relatively common in my practice. Before PCR testing was available, ulcers could be tested via culture—which took too long to be immediately useful—or via Tzanck smear, which helped greatly if multinucleated giant cells were seen. However, both tests were relatively insensitive. As this Clinical Inquiry demonstrates, ulcers currently should be tested either with culture or with PCR. Herpes culture is most sensitive if vesicles are still intact for unroofing.
Evidence summary
More than 50 million individuals in the United States have genital herpes. The diagnosis of genital herpes based on clinical history and physical examination is often inaccurate.1 Clinical suspicion needs to be confirmed by laboratory testing because it has a direct impact on counseling and prognosis.2
Viral culture is still the gold standard test for the detection of HSV; however, the rate of positive cultures depends on the stage of the lesion, the quality of the specimen, and the transport conditions. A British study3 found the rate of virus recovery for early vesicles to be 52% to 93%. This dropped to 41% to 72% if midstage ulcers were present. Finally, the detection for late-stage crusted lesions was only 19% to 27%. Another disadvantage is that culture is labor-intensive. A positive culture takes an average of 3 days to grow, whereas a negative culture must incubate for 10 days.3
PCR techniques are more sensitive and results can be available in less than 4 hours.3 In 110 clinical samples from dermal or genital lesions of patients with suspected HSV infection, the sensitivity of PCR was 98% (positive likelihood ratio [LR+]=∞; negative likelihood ratio [LR–]=0.02) compared with 73% (LR+ = ∞; LR– = 0.27) for culture. The specificities of both were 100%.4 In London, 233 samples from patients at a genitourinary medicine clinic were tested with both viral culture and PCR. HSV was detected in 79 samples by culture and 132 samples by PCR. The detection by PCR was higher in early as well as late stages of infection and in both first and recurrent episodes.3 The reference standard for these studies was not an independent standard, but a positive result on both tests or modified versions of the PCR test. The use of a version of the test of interest (PCR) as part of the reference standard, while probably unavoidable in this situation, will tend inflate the sensitivity and specificity.
In another study, daily sampling of lesions in patients with known HSV infections detected HSV DNA on 15 of 17 days with PCR and only 3 of 17 days with culture.1 This suggests that PCR is more effective in detecting early, as well as late, stages of infection. Currently PCR is more expensive, but it may become cheaper because of decreased labor expense when compared with culture.
Genital herpes may also be detected with enzyme immunoassay testing in as little as 5 hours. In a study5 using 275 samples from genital lesions, HSV was detected in 65% of the antigen tests and 53% of the viral cultures. The sensitivity of this method is equal to culture for early lesions, but much higher in late-stage lesions (58% vs 26%).5
Serologic tests are often used to detect HSV because they can differentiate between HSV-1 and HSV-2. There is an FDA-approved point-of-care test called POCkit that gives results from capillary blood or serum during an office visit. These tests are 80% to 98% sensitive and more than 96% specific. Unfortunately, they are not readily available in all countries.2
Other detection methods include the Tzanck smear, which is only 40% to 50% sensitive compared with culture, and the Pap smear, which is 60% to 70% sensitive.6 These tests should not be the sole method for the diagnosis of HSV. They cannot differentiate between HSV 1 and HSV 2; furthermore, the Tzanck prep will give a positive result if varicella zoster virus is present.6 If these tests are positive, confirmatory testing specific for HSV should be performed.
Recommendations from others
The Centers for Disease Control and Prevention7 recommends screening with a viral culture when a genital lesion is present, however, the sensitivity declines rapidly within a few days as the lesion begins to heal. To collect a sample the lesion must be unroofed using a Dacron swab, which is then placed in a viral transport medium and processed within 24 hours. Swabs containing calcium agglutinate are toxic to HSV.6 Type-specific antibodies develop during the first several weeks and can be detected with serologic tests; however, these may be falsely negative in the early stages of a primary infection.7
The US Preventative Services Task Force8 recommends against routine serologic screening for HSV in asymptomatic adolescents and adults. They also recommend against routine screening of asymptomatic pregnant women at any time during pregnancy as a way to decrease neonatal transmission.8
1. Albrecht MA. Clinical manifestations and diagnosis of genital herpes simplex virus infection. UpToDate [database online]. Available at: www.uptodate.com.
2. Centers for Disease Control and Prevention. Diseases characterized by genital ulcers. Sexually transmitted diseases treatment guidelines. MMWR Recomm Rep 2002;51(RR-6):11-25.
3. Ramaswamy M, McDonald C, Smith M, et al. Diagnosis of genital herpes by real time PCR in routine clinical practice. Sex Trasm Infect 2004;80:406-410.
4. Schmutzhard J, Riedel H, Wirgart B, Grillner L. Detection of herpes simplex virus type 1, herpes simplex virus type 2 and varicella-zoster virus in skin lesions. Comparison of real-time PCR, nested PCR and virus isolation. J Clin Virol 2004;29:120-126.
5. Cone RW, Swenson PD, Hobson AC, Remington M, Corey L. Herpes simplex virus detection from genital lesions: a comparative study using antigen detection (HerpChek) and culture. J Clin Microbiol 1993;31:1774-1776.
6. Herpes, genital. InfoPOEMS [online database]. Available at www.infopoems.com.
7. Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines 2002. Diseases Characterized by Genital Ulcers. Available at: www.cdc.gov/STD/treatment/2-2002TG.htm. Accessed on March 13, 2006.
8. United States Preventative Services Task Force. Screening for Genital Herpes. March 2005. Available at: www.ahrq.gov/clinic/uspstf/uspsherp.htm. Accessed on March 13, 2006.
1. Albrecht MA. Clinical manifestations and diagnosis of genital herpes simplex virus infection. UpToDate [database online]. Available at: www.uptodate.com.
2. Centers for Disease Control and Prevention. Diseases characterized by genital ulcers. Sexually transmitted diseases treatment guidelines. MMWR Recomm Rep 2002;51(RR-6):11-25.
3. Ramaswamy M, McDonald C, Smith M, et al. Diagnosis of genital herpes by real time PCR in routine clinical practice. Sex Trasm Infect 2004;80:406-410.
4. Schmutzhard J, Riedel H, Wirgart B, Grillner L. Detection of herpes simplex virus type 1, herpes simplex virus type 2 and varicella-zoster virus in skin lesions. Comparison of real-time PCR, nested PCR and virus isolation. J Clin Virol 2004;29:120-126.
5. Cone RW, Swenson PD, Hobson AC, Remington M, Corey L. Herpes simplex virus detection from genital lesions: a comparative study using antigen detection (HerpChek) and culture. J Clin Microbiol 1993;31:1774-1776.
6. Herpes, genital. InfoPOEMS [online database]. Available at www.infopoems.com.
7. Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines 2002. Diseases Characterized by Genital Ulcers. Available at: www.cdc.gov/STD/treatment/2-2002TG.htm. Accessed on March 13, 2006.
8. United States Preventative Services Task Force. Screening for Genital Herpes. March 2005. Available at: www.ahrq.gov/clinic/uspstf/uspsherp.htm. Accessed on March 13, 2006.
Evidence-based answers from the Family Physicians Inquiries Network
When are empiric antibiotics appropriate for urinary tract infection symptoms?
Healthy, nonpregnant women presenting with the triad of frequency, dysuria, and no vaginal symptoms have about a 96% chance of having an urinary tract infection (UTI) (positive likelihood ratio [LR+]=24.6). Since no urinalysis result would substantially change the high likelihood of disease for these patients, empiric therapy is appropriate (strength of recommendation [SOR]: B).
A triage system based only on having 1 or more urinary symptoms is more sensitive but less specific: the chance of having a UTI drops to 50% (LR+=19). While empiric therapy is still likely to be appropriate, rates of false positives and inappropriate antibiotic use may rise (SOR: B).
Empiric treatment by telephone may also be considered (SOR: C). While no studies have specifically addressed the diagnostic value of UTI symptoms reported by phone, no increase in pyelonephritis or other adverse events has been seen with telephone treatment protocols. And while telephone treatment protocols can increase the use of guideline-recommended antibiotics and decrease costs, they may increase unnecessary antibiotic use overall. Contraindications to empiric therapy are listed in TABLE 1.
Telephone protocol for UTI reduces unnecessary office visits and lab testing
Robert Bonacci, MD
Mayo Clinic, Rochester, Minn
We have 10 years of experience with a telephone treatment protocol we developed for uncomplicated UTI; it has since been adopted by the Institute for Clinical Systems Improvement (ICSI). The protocol reduces unnecessary office visits and lab testing. We believe the protocol actually increases our prescribing of preferred first-line antibiotics for UTI. While it is convenient for our patients, its use has resulted in patients wanting to be treated over the phone even if they have “failed” the protocol. Overall, our patients are thankful we have a telephone protocol for uncomplicated UTI. We enjoy the use of a handful of other telephone protocols and hope to move toward web-based protocols in the future.
TABLE 1
Contraindications to empiric antibiotics for urinary tract infection (telephone treatment)
| Vaginal discharge |
| Prolonged symptoms |
| Severe or intolerable flank, side, or abdominal pain |
| Inability to urinate for more than 4 hours |
| Body temperature higher than 38.1°C (100.5°F) with flank pain, chills, nausea, or abdominal pain |
| Pregnancy |
| Recent urologic surgery, procedure, or bladder catheterization; UTI within the last 6 weeks or frequent UTI (≥3 times) in the last 12 months |
| Any symptoms that warrant urgent office-based evaluation according to the clinician |
| Adapted from Vinson and Quesenberry, Arch Intern Med 2004.6 |
Evidence summary
An evidence-based review1 found 5 high-quality studies on the diagnosis of acute uncomplicated UTI among women. (“Uncomplicated” was defined as normal urinary tract and no contributing medical problems, such as diabetes, neurogenic bladder, renal stones.) UTIs were defined as the presence of significant bacteriuria (≥104 to 105 colony-forming units) on culture. A patient presenting to a clinician with 1 or more UTI symptoms had approximately a 50% chance of having significant bacteriuria on culture.1 The authors estimated the pretest probability of UTI as 5% from the incidence of asymptomatic bacteriuria among healthy women.1,2 This produced a LR+ of 19 simply for presenting to a clinician with 1 or more UTI symptoms.1 The summary LRs for clinical signs and symptoms in the prediction of UTI after presentation to the office are found in TABLE 2. A history of a vaginal discharge or irritation has a LR– of 0.3, decreasing the probability of UTI for a patient presenting to the office from approximately 50% to 20%, so further testing would be indicated.1
No single sign or symptom accurately predicted UTI. However, the triad of dysuria with frequency but without vaginal symptoms increased the probability of significant bacteriuria on culture from 50% to 96% (LR+=24.6).1 In contrast, a 1999 review of 51 studies calculated that if both the nitrites and leukocyte esterase are positive on urine dipstick testing, the LR+ is 4.2; if both are negative the LR– is 0.3.1,3 Since the probability of UTI for patients with the symptom triad is so high, dipstick urinalysis is unlikely to alter management regardless of whether nitrites and leukocyte esterase were both positive or negative (posttest probability=98%–99% and 80%, respectively). If urine dipstick or other office-based tests are not needed to make the diagnosis of uncomplicated UTI for a patient with the classic triad of symptoms, then telephone treatment based on symptoms may be reasonable. Women who have recurrent UTIs (2 or more culture positive UTIs over the previous 12 months) can accurately self-diagnose subsequent UTIs based on symptoms (LR+=4.0).4,5
A recent retrospective case series6 evaluated a telephone guideline for the empiric treatment of UTI for 4177 women in a California HMO. UTI criteria were ≤10 days of dysuria; frequency, urgency, pressure, or increased nocturia; or gross hematuria. Women were excluded if they had any one of a variety of contraindications (TABLE 1). Upper tract infection occurred in 21 patients (1.1%) within 60 days of telephone treatment, two thirds of which likely represented treatment failures. This is similar to rates in control groups of other studies. Fourteen women (1.5%) received care for sexually transmitted diseases or other gynecologic conditions, primarily bacterial vaginitis, within 60 days of telephone treatment. Of note, 6% of the cohort were elderly, diabetic, taking glucocorticoids or early in pregnancy and are typically excluded from other studies. This higher-risk group did not have an increased incidence of either sepsis or pyelonephritis.6 No increase in adverse outcomes was seen in another study of a telephone treatment protocol.7
Several studies6-8 have noted that telephone treatment protocols increase the use of protocol-recommended antibiotics (eg, generally less expensive agents such as trimethoprim-sulfamethoxazole), which may help limit resistance to fluoroquinolones. However, specific data are not available.
McIssac et al9 reviewed a cohort of 231 women presenting to family physicians’ offices with uncomplicated cystitis symptoms. Empiric therapy resulted in approximately 40% of women unnecessarily receiving antibiotics. Treating only women with classic cystitis symptoms and pyuria would have decreased the unnecessary use of antibiotics to 26.2%, but fewer women with confirmed cystitis would have received immediate antibiotics (66.4% vs 91.8%). They derived a clinical decision rule designed to balance false positives and false negatives. It recommends immediate antibiotic treatment if women have ≥2 of 4 signs or symptoms: dysuria, leukocyte esterase (greater than trace), positive nitrites, or blood (greater than trace) on dipstick (LR+=2.29). Otherwise the rule recommends a culture to guide antibiotic therapy. This decision rule would have reduced unnecessary antibiotic use by 27.5% while ensuring that more women with confirmed UTIs received immediate antibiotics (81.3%).
In 1999, Saint et al8 estimated savings of $367,000 for 147,000 women enrolled over 1 year after widespread guideline implementation. Two cost-effectiveness studies10,11 of office treatment concluded that empiric treatment without additional testing is the least costly option in this setting. However, a recent, comprehensive cost-effectiveness study11 concluded that if a patient presents to an office, the marginal cost of performing a pelvic examination and urine culture for women with a negative dipstick was relatively low ($4 to $32 per symptom day avoided).
TABLE 2
Diagnosis of urinary tract infection
| DIAGNOSTIC CRITERIA | LR+ | LR– | SUMMARY LR |
|---|---|---|---|
| Presenting to medical care with possible UTI | 19.0 | ||
| Dysuria | 1.5 | 0.5 | |
| Frequency | 1.8 | 0.6 | |
| Hematuria | 2.0 | 0.9 | |
| Recurrent UTI symptoms for a woman with history of UTI | 4.0 | 0.0 | |
| Vaginal discharge or irritation | 0.2–0.3 | 2.7–3.1 | |
| Dysuria, frequency, and absence of vaginal discharge or irritation | 24.6 | ||
| Dysuria absent, + vaginal discharge | 0.3 | ||
| Dysuria and + vaginal discharge | 0.7 | ||
| + Leukocytes* or + nitrate on urine dipstick analysis | 4.2 | 0.3† | |
| “UTI Rule”‡ | 2.3 | ||
| * Leukocyte greater than trace on dipstick | |||
| † Leukocytes negative and nitrite negative | |||
| ‡ “UTI Rule”—positive if 2 or more present: dysuria,+ leukocytes, + nitrate, + heme (> trace) | |||
| LR, likelihood ratio; UTI, urinary tract infection. | |||
| Adapted from Bent et al, JAMA 2002.1 | |||
Recommendations from others
A 2002 Institute for Clinical Systems Improvement guideline12 advised offering telephone treatment of uncomplicated UTI for low-risk patients if preferred by both provider and patient.
1. Bent S, Nallamothu BK, Simel DL, Fihn SD, Saint S. Does this woman have an acute uncomplicated urinary tract infection? JAMA 2002;287:2701-2710.
2. Hooton T, Scholes D, Stapleton AE, et al. A prospective study of asymptomatic bacteriuria in sexually active young women. N Engl J Med 2000;343:992-997.
3. Hurlbut T, Littenberg B. The diagnostic accuracy of rapid dipstick tests to predict urinary tract infection. Am J Clin Pathol 1991;96:582-588.
4. Gupta K, Hooton TM, Roberts PL, Stamm WE. Patient-initiated treatment of uncomplicated recurrent urinary tract infections in young women. Ann Intern Med 2001;135:9-16.
5. Schaeffer AJ, Stuppy BA. Efficacy and safety of self-start therapy in women with recurrent urinary tract infections. J Urol 1999;161:207-211.
6. Vinson DR, Quesenberry CP, Jr. The safety of telephone management of presumed cystitis in women. Arch Intern Med 2004;164:1026-1029.
7. Barry HC, Hickner J, Ebell MH, Ettenhofer T. A randomized controlled trial of telephone management of suspected urinary tract infections in women. J Fam Pract 2001;50:589-594.
8. Saint S, Scholes D, Fihn SD, Farrell RG, Stamm WE. The effectiveness of a clinical practice guideline for the management of presumed uncomplicated urinary tract infection in women. Am J Med 1999;106:636-641.
9. McIsaac WJ, Low DE, Biringer A, Pimlott N, Evans M, Glazier R. The impact of empirical management of acute cystitis on unnecessary antibiotic use. Arch Intern Med 2002;162:600-605.
10. Barry HC, Ebell MH, Hickner J. Evaluation of suspected urinary tract infection in ambulatory women: a cost-utility analysis of office-based strategies. J Fam Pract 1997;44:49-60.
11. Rothberg MB, Wong JB. All dysuria is local. A cost-effectiveness model for designing site-specific management algorithms. J Gen Intern Med 2004;19(5 Pt 1):433-443.
12. Uncomplicated urinary tract infection in women. Bloomington, Minn: Institute for Clinical Systems Improvement; July 2004. Available at guidelines.gov/summary/summary.aspx?doc_id=5570. Accessed on March 7, 2006.
Healthy, nonpregnant women presenting with the triad of frequency, dysuria, and no vaginal symptoms have about a 96% chance of having an urinary tract infection (UTI) (positive likelihood ratio [LR+]=24.6). Since no urinalysis result would substantially change the high likelihood of disease for these patients, empiric therapy is appropriate (strength of recommendation [SOR]: B).
A triage system based only on having 1 or more urinary symptoms is more sensitive but less specific: the chance of having a UTI drops to 50% (LR+=19). While empiric therapy is still likely to be appropriate, rates of false positives and inappropriate antibiotic use may rise (SOR: B).
Empiric treatment by telephone may also be considered (SOR: C). While no studies have specifically addressed the diagnostic value of UTI symptoms reported by phone, no increase in pyelonephritis or other adverse events has been seen with telephone treatment protocols. And while telephone treatment protocols can increase the use of guideline-recommended antibiotics and decrease costs, they may increase unnecessary antibiotic use overall. Contraindications to empiric therapy are listed in TABLE 1.
Telephone protocol for UTI reduces unnecessary office visits and lab testing
Robert Bonacci, MD
Mayo Clinic, Rochester, Minn
We have 10 years of experience with a telephone treatment protocol we developed for uncomplicated UTI; it has since been adopted by the Institute for Clinical Systems Improvement (ICSI). The protocol reduces unnecessary office visits and lab testing. We believe the protocol actually increases our prescribing of preferred first-line antibiotics for UTI. While it is convenient for our patients, its use has resulted in patients wanting to be treated over the phone even if they have “failed” the protocol. Overall, our patients are thankful we have a telephone protocol for uncomplicated UTI. We enjoy the use of a handful of other telephone protocols and hope to move toward web-based protocols in the future.
TABLE 1
Contraindications to empiric antibiotics for urinary tract infection (telephone treatment)
| Vaginal discharge |
| Prolonged symptoms |
| Severe or intolerable flank, side, or abdominal pain |
| Inability to urinate for more than 4 hours |
| Body temperature higher than 38.1°C (100.5°F) with flank pain, chills, nausea, or abdominal pain |
| Pregnancy |
| Recent urologic surgery, procedure, or bladder catheterization; UTI within the last 6 weeks or frequent UTI (≥3 times) in the last 12 months |
| Any symptoms that warrant urgent office-based evaluation according to the clinician |
| Adapted from Vinson and Quesenberry, Arch Intern Med 2004.6 |
Evidence summary
An evidence-based review1 found 5 high-quality studies on the diagnosis of acute uncomplicated UTI among women. (“Uncomplicated” was defined as normal urinary tract and no contributing medical problems, such as diabetes, neurogenic bladder, renal stones.) UTIs were defined as the presence of significant bacteriuria (≥104 to 105 colony-forming units) on culture. A patient presenting to a clinician with 1 or more UTI symptoms had approximately a 50% chance of having significant bacteriuria on culture.1 The authors estimated the pretest probability of UTI as 5% from the incidence of asymptomatic bacteriuria among healthy women.1,2 This produced a LR+ of 19 simply for presenting to a clinician with 1 or more UTI symptoms.1 The summary LRs for clinical signs and symptoms in the prediction of UTI after presentation to the office are found in TABLE 2. A history of a vaginal discharge or irritation has a LR– of 0.3, decreasing the probability of UTI for a patient presenting to the office from approximately 50% to 20%, so further testing would be indicated.1
No single sign or symptom accurately predicted UTI. However, the triad of dysuria with frequency but without vaginal symptoms increased the probability of significant bacteriuria on culture from 50% to 96% (LR+=24.6).1 In contrast, a 1999 review of 51 studies calculated that if both the nitrites and leukocyte esterase are positive on urine dipstick testing, the LR+ is 4.2; if both are negative the LR– is 0.3.1,3 Since the probability of UTI for patients with the symptom triad is so high, dipstick urinalysis is unlikely to alter management regardless of whether nitrites and leukocyte esterase were both positive or negative (posttest probability=98%–99% and 80%, respectively). If urine dipstick or other office-based tests are not needed to make the diagnosis of uncomplicated UTI for a patient with the classic triad of symptoms, then telephone treatment based on symptoms may be reasonable. Women who have recurrent UTIs (2 or more culture positive UTIs over the previous 12 months) can accurately self-diagnose subsequent UTIs based on symptoms (LR+=4.0).4,5
A recent retrospective case series6 evaluated a telephone guideline for the empiric treatment of UTI for 4177 women in a California HMO. UTI criteria were ≤10 days of dysuria; frequency, urgency, pressure, or increased nocturia; or gross hematuria. Women were excluded if they had any one of a variety of contraindications (TABLE 1). Upper tract infection occurred in 21 patients (1.1%) within 60 days of telephone treatment, two thirds of which likely represented treatment failures. This is similar to rates in control groups of other studies. Fourteen women (1.5%) received care for sexually transmitted diseases or other gynecologic conditions, primarily bacterial vaginitis, within 60 days of telephone treatment. Of note, 6% of the cohort were elderly, diabetic, taking glucocorticoids or early in pregnancy and are typically excluded from other studies. This higher-risk group did not have an increased incidence of either sepsis or pyelonephritis.6 No increase in adverse outcomes was seen in another study of a telephone treatment protocol.7
Several studies6-8 have noted that telephone treatment protocols increase the use of protocol-recommended antibiotics (eg, generally less expensive agents such as trimethoprim-sulfamethoxazole), which may help limit resistance to fluoroquinolones. However, specific data are not available.
McIssac et al9 reviewed a cohort of 231 women presenting to family physicians’ offices with uncomplicated cystitis symptoms. Empiric therapy resulted in approximately 40% of women unnecessarily receiving antibiotics. Treating only women with classic cystitis symptoms and pyuria would have decreased the unnecessary use of antibiotics to 26.2%, but fewer women with confirmed cystitis would have received immediate antibiotics (66.4% vs 91.8%). They derived a clinical decision rule designed to balance false positives and false negatives. It recommends immediate antibiotic treatment if women have ≥2 of 4 signs or symptoms: dysuria, leukocyte esterase (greater than trace), positive nitrites, or blood (greater than trace) on dipstick (LR+=2.29). Otherwise the rule recommends a culture to guide antibiotic therapy. This decision rule would have reduced unnecessary antibiotic use by 27.5% while ensuring that more women with confirmed UTIs received immediate antibiotics (81.3%).
In 1999, Saint et al8 estimated savings of $367,000 for 147,000 women enrolled over 1 year after widespread guideline implementation. Two cost-effectiveness studies10,11 of office treatment concluded that empiric treatment without additional testing is the least costly option in this setting. However, a recent, comprehensive cost-effectiveness study11 concluded that if a patient presents to an office, the marginal cost of performing a pelvic examination and urine culture for women with a negative dipstick was relatively low ($4 to $32 per symptom day avoided).
TABLE 2
Diagnosis of urinary tract infection
| DIAGNOSTIC CRITERIA | LR+ | LR– | SUMMARY LR |
|---|---|---|---|
| Presenting to medical care with possible UTI | 19.0 | ||
| Dysuria | 1.5 | 0.5 | |
| Frequency | 1.8 | 0.6 | |
| Hematuria | 2.0 | 0.9 | |
| Recurrent UTI symptoms for a woman with history of UTI | 4.0 | 0.0 | |
| Vaginal discharge or irritation | 0.2–0.3 | 2.7–3.1 | |
| Dysuria, frequency, and absence of vaginal discharge or irritation | 24.6 | ||
| Dysuria absent, + vaginal discharge | 0.3 | ||
| Dysuria and + vaginal discharge | 0.7 | ||
| + Leukocytes* or + nitrate on urine dipstick analysis | 4.2 | 0.3† | |
| “UTI Rule”‡ | 2.3 | ||
| * Leukocyte greater than trace on dipstick | |||
| † Leukocytes negative and nitrite negative | |||
| ‡ “UTI Rule”—positive if 2 or more present: dysuria,+ leukocytes, + nitrate, + heme (> trace) | |||
| LR, likelihood ratio; UTI, urinary tract infection. | |||
| Adapted from Bent et al, JAMA 2002.1 | |||
Recommendations from others
A 2002 Institute for Clinical Systems Improvement guideline12 advised offering telephone treatment of uncomplicated UTI for low-risk patients if preferred by both provider and patient.
Healthy, nonpregnant women presenting with the triad of frequency, dysuria, and no vaginal symptoms have about a 96% chance of having an urinary tract infection (UTI) (positive likelihood ratio [LR+]=24.6). Since no urinalysis result would substantially change the high likelihood of disease for these patients, empiric therapy is appropriate (strength of recommendation [SOR]: B).
A triage system based only on having 1 or more urinary symptoms is more sensitive but less specific: the chance of having a UTI drops to 50% (LR+=19). While empiric therapy is still likely to be appropriate, rates of false positives and inappropriate antibiotic use may rise (SOR: B).
Empiric treatment by telephone may also be considered (SOR: C). While no studies have specifically addressed the diagnostic value of UTI symptoms reported by phone, no increase in pyelonephritis or other adverse events has been seen with telephone treatment protocols. And while telephone treatment protocols can increase the use of guideline-recommended antibiotics and decrease costs, they may increase unnecessary antibiotic use overall. Contraindications to empiric therapy are listed in TABLE 1.
Telephone protocol for UTI reduces unnecessary office visits and lab testing
Robert Bonacci, MD
Mayo Clinic, Rochester, Minn
We have 10 years of experience with a telephone treatment protocol we developed for uncomplicated UTI; it has since been adopted by the Institute for Clinical Systems Improvement (ICSI). The protocol reduces unnecessary office visits and lab testing. We believe the protocol actually increases our prescribing of preferred first-line antibiotics for UTI. While it is convenient for our patients, its use has resulted in patients wanting to be treated over the phone even if they have “failed” the protocol. Overall, our patients are thankful we have a telephone protocol for uncomplicated UTI. We enjoy the use of a handful of other telephone protocols and hope to move toward web-based protocols in the future.
TABLE 1
Contraindications to empiric antibiotics for urinary tract infection (telephone treatment)
| Vaginal discharge |
| Prolonged symptoms |
| Severe or intolerable flank, side, or abdominal pain |
| Inability to urinate for more than 4 hours |
| Body temperature higher than 38.1°C (100.5°F) with flank pain, chills, nausea, or abdominal pain |
| Pregnancy |
| Recent urologic surgery, procedure, or bladder catheterization; UTI within the last 6 weeks or frequent UTI (≥3 times) in the last 12 months |
| Any symptoms that warrant urgent office-based evaluation according to the clinician |
| Adapted from Vinson and Quesenberry, Arch Intern Med 2004.6 |
Evidence summary
An evidence-based review1 found 5 high-quality studies on the diagnosis of acute uncomplicated UTI among women. (“Uncomplicated” was defined as normal urinary tract and no contributing medical problems, such as diabetes, neurogenic bladder, renal stones.) UTIs were defined as the presence of significant bacteriuria (≥104 to 105 colony-forming units) on culture. A patient presenting to a clinician with 1 or more UTI symptoms had approximately a 50% chance of having significant bacteriuria on culture.1 The authors estimated the pretest probability of UTI as 5% from the incidence of asymptomatic bacteriuria among healthy women.1,2 This produced a LR+ of 19 simply for presenting to a clinician with 1 or more UTI symptoms.1 The summary LRs for clinical signs and symptoms in the prediction of UTI after presentation to the office are found in TABLE 2. A history of a vaginal discharge or irritation has a LR– of 0.3, decreasing the probability of UTI for a patient presenting to the office from approximately 50% to 20%, so further testing would be indicated.1
No single sign or symptom accurately predicted UTI. However, the triad of dysuria with frequency but without vaginal symptoms increased the probability of significant bacteriuria on culture from 50% to 96% (LR+=24.6).1 In contrast, a 1999 review of 51 studies calculated that if both the nitrites and leukocyte esterase are positive on urine dipstick testing, the LR+ is 4.2; if both are negative the LR– is 0.3.1,3 Since the probability of UTI for patients with the symptom triad is so high, dipstick urinalysis is unlikely to alter management regardless of whether nitrites and leukocyte esterase were both positive or negative (posttest probability=98%–99% and 80%, respectively). If urine dipstick or other office-based tests are not needed to make the diagnosis of uncomplicated UTI for a patient with the classic triad of symptoms, then telephone treatment based on symptoms may be reasonable. Women who have recurrent UTIs (2 or more culture positive UTIs over the previous 12 months) can accurately self-diagnose subsequent UTIs based on symptoms (LR+=4.0).4,5
A recent retrospective case series6 evaluated a telephone guideline for the empiric treatment of UTI for 4177 women in a California HMO. UTI criteria were ≤10 days of dysuria; frequency, urgency, pressure, or increased nocturia; or gross hematuria. Women were excluded if they had any one of a variety of contraindications (TABLE 1). Upper tract infection occurred in 21 patients (1.1%) within 60 days of telephone treatment, two thirds of which likely represented treatment failures. This is similar to rates in control groups of other studies. Fourteen women (1.5%) received care for sexually transmitted diseases or other gynecologic conditions, primarily bacterial vaginitis, within 60 days of telephone treatment. Of note, 6% of the cohort were elderly, diabetic, taking glucocorticoids or early in pregnancy and are typically excluded from other studies. This higher-risk group did not have an increased incidence of either sepsis or pyelonephritis.6 No increase in adverse outcomes was seen in another study of a telephone treatment protocol.7
Several studies6-8 have noted that telephone treatment protocols increase the use of protocol-recommended antibiotics (eg, generally less expensive agents such as trimethoprim-sulfamethoxazole), which may help limit resistance to fluoroquinolones. However, specific data are not available.
McIssac et al9 reviewed a cohort of 231 women presenting to family physicians’ offices with uncomplicated cystitis symptoms. Empiric therapy resulted in approximately 40% of women unnecessarily receiving antibiotics. Treating only women with classic cystitis symptoms and pyuria would have decreased the unnecessary use of antibiotics to 26.2%, but fewer women with confirmed cystitis would have received immediate antibiotics (66.4% vs 91.8%). They derived a clinical decision rule designed to balance false positives and false negatives. It recommends immediate antibiotic treatment if women have ≥2 of 4 signs or symptoms: dysuria, leukocyte esterase (greater than trace), positive nitrites, or blood (greater than trace) on dipstick (LR+=2.29). Otherwise the rule recommends a culture to guide antibiotic therapy. This decision rule would have reduced unnecessary antibiotic use by 27.5% while ensuring that more women with confirmed UTIs received immediate antibiotics (81.3%).
In 1999, Saint et al8 estimated savings of $367,000 for 147,000 women enrolled over 1 year after widespread guideline implementation. Two cost-effectiveness studies10,11 of office treatment concluded that empiric treatment without additional testing is the least costly option in this setting. However, a recent, comprehensive cost-effectiveness study11 concluded that if a patient presents to an office, the marginal cost of performing a pelvic examination and urine culture for women with a negative dipstick was relatively low ($4 to $32 per symptom day avoided).
TABLE 2
Diagnosis of urinary tract infection
| DIAGNOSTIC CRITERIA | LR+ | LR– | SUMMARY LR |
|---|---|---|---|
| Presenting to medical care with possible UTI | 19.0 | ||
| Dysuria | 1.5 | 0.5 | |
| Frequency | 1.8 | 0.6 | |
| Hematuria | 2.0 | 0.9 | |
| Recurrent UTI symptoms for a woman with history of UTI | 4.0 | 0.0 | |
| Vaginal discharge or irritation | 0.2–0.3 | 2.7–3.1 | |
| Dysuria, frequency, and absence of vaginal discharge or irritation | 24.6 | ||
| Dysuria absent, + vaginal discharge | 0.3 | ||
| Dysuria and + vaginal discharge | 0.7 | ||
| + Leukocytes* or + nitrate on urine dipstick analysis | 4.2 | 0.3† | |
| “UTI Rule”‡ | 2.3 | ||
| * Leukocyte greater than trace on dipstick | |||
| † Leukocytes negative and nitrite negative | |||
| ‡ “UTI Rule”—positive if 2 or more present: dysuria,+ leukocytes, + nitrate, + heme (> trace) | |||
| LR, likelihood ratio; UTI, urinary tract infection. | |||
| Adapted from Bent et al, JAMA 2002.1 | |||
Recommendations from others
A 2002 Institute for Clinical Systems Improvement guideline12 advised offering telephone treatment of uncomplicated UTI for low-risk patients if preferred by both provider and patient.
1. Bent S, Nallamothu BK, Simel DL, Fihn SD, Saint S. Does this woman have an acute uncomplicated urinary tract infection? JAMA 2002;287:2701-2710.
2. Hooton T, Scholes D, Stapleton AE, et al. A prospective study of asymptomatic bacteriuria in sexually active young women. N Engl J Med 2000;343:992-997.
3. Hurlbut T, Littenberg B. The diagnostic accuracy of rapid dipstick tests to predict urinary tract infection. Am J Clin Pathol 1991;96:582-588.
4. Gupta K, Hooton TM, Roberts PL, Stamm WE. Patient-initiated treatment of uncomplicated recurrent urinary tract infections in young women. Ann Intern Med 2001;135:9-16.
5. Schaeffer AJ, Stuppy BA. Efficacy and safety of self-start therapy in women with recurrent urinary tract infections. J Urol 1999;161:207-211.
6. Vinson DR, Quesenberry CP, Jr. The safety of telephone management of presumed cystitis in women. Arch Intern Med 2004;164:1026-1029.
7. Barry HC, Hickner J, Ebell MH, Ettenhofer T. A randomized controlled trial of telephone management of suspected urinary tract infections in women. J Fam Pract 2001;50:589-594.
8. Saint S, Scholes D, Fihn SD, Farrell RG, Stamm WE. The effectiveness of a clinical practice guideline for the management of presumed uncomplicated urinary tract infection in women. Am J Med 1999;106:636-641.
9. McIsaac WJ, Low DE, Biringer A, Pimlott N, Evans M, Glazier R. The impact of empirical management of acute cystitis on unnecessary antibiotic use. Arch Intern Med 2002;162:600-605.
10. Barry HC, Ebell MH, Hickner J. Evaluation of suspected urinary tract infection in ambulatory women: a cost-utility analysis of office-based strategies. J Fam Pract 1997;44:49-60.
11. Rothberg MB, Wong JB. All dysuria is local. A cost-effectiveness model for designing site-specific management algorithms. J Gen Intern Med 2004;19(5 Pt 1):433-443.
12. Uncomplicated urinary tract infection in women. Bloomington, Minn: Institute for Clinical Systems Improvement; July 2004. Available at guidelines.gov/summary/summary.aspx?doc_id=5570. Accessed on March 7, 2006.
1. Bent S, Nallamothu BK, Simel DL, Fihn SD, Saint S. Does this woman have an acute uncomplicated urinary tract infection? JAMA 2002;287:2701-2710.
2. Hooton T, Scholes D, Stapleton AE, et al. A prospective study of asymptomatic bacteriuria in sexually active young women. N Engl J Med 2000;343:992-997.
3. Hurlbut T, Littenberg B. The diagnostic accuracy of rapid dipstick tests to predict urinary tract infection. Am J Clin Pathol 1991;96:582-588.
4. Gupta K, Hooton TM, Roberts PL, Stamm WE. Patient-initiated treatment of uncomplicated recurrent urinary tract infections in young women. Ann Intern Med 2001;135:9-16.
5. Schaeffer AJ, Stuppy BA. Efficacy and safety of self-start therapy in women with recurrent urinary tract infections. J Urol 1999;161:207-211.
6. Vinson DR, Quesenberry CP, Jr. The safety of telephone management of presumed cystitis in women. Arch Intern Med 2004;164:1026-1029.
7. Barry HC, Hickner J, Ebell MH, Ettenhofer T. A randomized controlled trial of telephone management of suspected urinary tract infections in women. J Fam Pract 2001;50:589-594.
8. Saint S, Scholes D, Fihn SD, Farrell RG, Stamm WE. The effectiveness of a clinical practice guideline for the management of presumed uncomplicated urinary tract infection in women. Am J Med 1999;106:636-641.
9. McIsaac WJ, Low DE, Biringer A, Pimlott N, Evans M, Glazier R. The impact of empirical management of acute cystitis on unnecessary antibiotic use. Arch Intern Med 2002;162:600-605.
10. Barry HC, Ebell MH, Hickner J. Evaluation of suspected urinary tract infection in ambulatory women: a cost-utility analysis of office-based strategies. J Fam Pract 1997;44:49-60.
11. Rothberg MB, Wong JB. All dysuria is local. A cost-effectiveness model for designing site-specific management algorithms. J Gen Intern Med 2004;19(5 Pt 1):433-443.
12. Uncomplicated urinary tract infection in women. Bloomington, Minn: Institute for Clinical Systems Improvement; July 2004. Available at guidelines.gov/summary/summary.aspx?doc_id=5570. Accessed on March 7, 2006.
Evidence-based answers from the Family Physicians Inquiries Network
When should a child with an undescended testis be referred to a urologist?
Infants with an undescended testis should be referred between ages 6 and 15 months, since almost all who experience spontaneous descent do so by 6 months (strength of recommendation [SOR]: A, extrapolation from cohort studies).
The incidence of germ cell aplasia in undescended testes begins to rise at 15 months (SOR: C, extrapolation of observational studies); however, evidence is inconclusive that orchiopexy at this age results in higher rates of paternity success (SOR: B, retrospective cohort study).
Orchiopexy may allow earlier detection of testicular tumors (SOR: C, expert opinion), but it has not been shown to reduce the risk of testicular cancer (SOR: B, retrospective cohort study) or improve 5-year survival rates for those patients diagnosed with testicular cancer (SOR: B, retrospective cohort study).
Periodically evaluate a newborn’s scrotum for either an undescended or reascended testicle
Danny Thomason, DO
Oklahoma State University, Tulsa
This Inquiry highlights 2 important considerations regarding the child with a cryptorchid testis. First, periodically evaluate the newborn and infant patient’s scrotum for either an undescended or reascended testicle. In my practice at Oklahoma State University Family Medicine Residency, I ask residents to perform the scrotal examination at birth, at every well-child visit up to 1 year of age, and then yearly thereafter. During puberty, these exams serve as opportunities to educate patients about testicular self-examination.
Secondly, as the authors indicate, there is some disagreement in the literature as to the risk of testicular cancer following orchiopexy for cryptorchidism. However, surgical repair is likely to facilitate regular testicular self-examination, which could increase the likelihood of detection of cancer during young adulthood.
Evidence summary
Three large cohort studies determined that cryptorchidism (FIGURE) is present at birth in approximately 3% of term infants (higher in preterm infants), with spontaneous descent occurring in two thirds of cases by age 3 to 6 months. One study1 of 10,730 consecutive male term infants found cryptorchidism at birth in 2.7%, dropping to 1.22% by 6 months of age, but without further change at 1 year. A similar study2 followed 6935 infant boys, finding cryptorchidism at birth in 3.7%, which decreased to 1% at 3 months and remained unchanged at 1 year. A third study3 found cryptorchidism at birth in 90 of 6414 (2.7%) infant boys. At follow-up, 45 of 90 had testicular descent at 1 month, 60 of 90 at 3 months, 67 of 90 at 9 months and at 1 year.
The 2 main indications for orchiopexy are potential avoidance of infertility and early detection and treatment of testicular cancer. A literature review4 of fertility after orchiopexy for undescended testis found inconclusive results. While epidemiological and pathological data (testicular biopsy, hormonal analysis, and sperm counts performed after orchiopexy) predict diminished fertility potential for men with unilaterally undescended testes, studies evaluating paternity find no difference from normal men. Biopsy studies of undescended testes at the time of orchiopexy show increased incidence of germ cell aplasia with older age at surgery (0.5%, 2%, 20%, and 45% at 6, 12, 24, and 48 months, respectively).4 A retrospective cohort study5 found 87% successful paternity after orchiopexy for 24 patients with unilateral undescended testis and 33% success for 9 with bilateral undescended testes but there was no normal control group. The boys were aged 1 to 14 years (mean, 7 years) at surgery, and there was no relationship between timing of orchiopexy and paternity success.5
The benefits of orchiopexy for testicular cancer are also unclear; expert opinion suggests that orchiopexy may allow earlier detection of testicular tumors.6 A cohort study7 of boys with cryptorchidism showed an increased risk of testicular cancer (relative risk=5.2). However, risk did not decrease after orchiopexy in early childhood. A retrospective cohort study8 of 137 men with cryptorchidism who developed testicular cancer found no difference in 5-year survival between those who had orchiopexy (at ages 2 to 42) and those who had not (61% vs 63%, respectively).
FIGURE
Cryptorchidism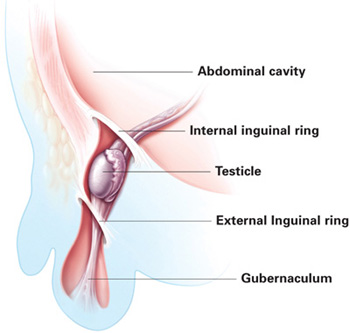
In most cases of cryptorchidism, the testis will be inguinal or prescrotal. A smaller number of cases are ectopic (have left the inguinal ring), abdominal, or absent. ILLUSTRATION BY RICH LaROCCO
Recommendations from others
The American Academy of Pediatrics policy section on urology says that spontaneous descent after 6 months is unlikely and recommends orchiopexy by 1 year of age.9
1. Ghirri P, Ciulli C, Vuerich M, et al. Incidence at birth and natural history of cryptorchidism: a study of 10,730 consecutive male infants. J Endocrinol Invest 2002;25:709-715.
2. Berkowitz GS, Lapinski RH, Dolgin MD, et al. Prevalence and natural history of cryptorchidism. Pediatrics 1993;92:44-49.
3. Scorer CG. The descent of the testis. Arch Dis Childhood 1964;39:605-609.
4. Husmann DA. Cryptorchidism. In: Belman AB, King LR, Kramer SA, eds. Clinical Pediatric Urology. 4th ed. London, UK: Martin Dunitz Ltd.; 2002: 1125–1154.
5. Cendron M, Keating MA, Huff DS, Koop CE, Snyder HM, 3rd, Duckett JW. Cryptorchidism, orchiopexy and infertility: a critical long-term retrospective analysis. J Urol 1989;142(2 pt 2):559-562.
6. Docimo SG, Silver RI, Cromie W. The undescended testicle: diagnosis and management. Am Fam Physician 2000;62:2037-2048.
7. Prener A, Engholm G, Jensen OM. Genital anomalies and risk for testicular cancer in Danish men. Epidemiology 1996;7:14-19.
8. Batata MA, Chu FC, Hilaris BS, Whitmore WF, Golbey RB. Testicular cancer in cryptorchids. Cancer 1982;49:1023-1030.
9. American Academy of Pediatrics Policy Statement. Timing of elective surgery on the genitalia of male children with particular reference to the risks, benefits, and psychological effects of surgery and anesthesia. Pediatrics 1996;97:590-594.
Infants with an undescended testis should be referred between ages 6 and 15 months, since almost all who experience spontaneous descent do so by 6 months (strength of recommendation [SOR]: A, extrapolation from cohort studies).
The incidence of germ cell aplasia in undescended testes begins to rise at 15 months (SOR: C, extrapolation of observational studies); however, evidence is inconclusive that orchiopexy at this age results in higher rates of paternity success (SOR: B, retrospective cohort study).
Orchiopexy may allow earlier detection of testicular tumors (SOR: C, expert opinion), but it has not been shown to reduce the risk of testicular cancer (SOR: B, retrospective cohort study) or improve 5-year survival rates for those patients diagnosed with testicular cancer (SOR: B, retrospective cohort study).
Periodically evaluate a newborn’s scrotum for either an undescended or reascended testicle
Danny Thomason, DO
Oklahoma State University, Tulsa
This Inquiry highlights 2 important considerations regarding the child with a cryptorchid testis. First, periodically evaluate the newborn and infant patient’s scrotum for either an undescended or reascended testicle. In my practice at Oklahoma State University Family Medicine Residency, I ask residents to perform the scrotal examination at birth, at every well-child visit up to 1 year of age, and then yearly thereafter. During puberty, these exams serve as opportunities to educate patients about testicular self-examination.
Secondly, as the authors indicate, there is some disagreement in the literature as to the risk of testicular cancer following orchiopexy for cryptorchidism. However, surgical repair is likely to facilitate regular testicular self-examination, which could increase the likelihood of detection of cancer during young adulthood.
Evidence summary
Three large cohort studies determined that cryptorchidism (FIGURE) is present at birth in approximately 3% of term infants (higher in preterm infants), with spontaneous descent occurring in two thirds of cases by age 3 to 6 months. One study1 of 10,730 consecutive male term infants found cryptorchidism at birth in 2.7%, dropping to 1.22% by 6 months of age, but without further change at 1 year. A similar study2 followed 6935 infant boys, finding cryptorchidism at birth in 3.7%, which decreased to 1% at 3 months and remained unchanged at 1 year. A third study3 found cryptorchidism at birth in 90 of 6414 (2.7%) infant boys. At follow-up, 45 of 90 had testicular descent at 1 month, 60 of 90 at 3 months, 67 of 90 at 9 months and at 1 year.
The 2 main indications for orchiopexy are potential avoidance of infertility and early detection and treatment of testicular cancer. A literature review4 of fertility after orchiopexy for undescended testis found inconclusive results. While epidemiological and pathological data (testicular biopsy, hormonal analysis, and sperm counts performed after orchiopexy) predict diminished fertility potential for men with unilaterally undescended testes, studies evaluating paternity find no difference from normal men. Biopsy studies of undescended testes at the time of orchiopexy show increased incidence of germ cell aplasia with older age at surgery (0.5%, 2%, 20%, and 45% at 6, 12, 24, and 48 months, respectively).4 A retrospective cohort study5 found 87% successful paternity after orchiopexy for 24 patients with unilateral undescended testis and 33% success for 9 with bilateral undescended testes but there was no normal control group. The boys were aged 1 to 14 years (mean, 7 years) at surgery, and there was no relationship between timing of orchiopexy and paternity success.5
The benefits of orchiopexy for testicular cancer are also unclear; expert opinion suggests that orchiopexy may allow earlier detection of testicular tumors.6 A cohort study7 of boys with cryptorchidism showed an increased risk of testicular cancer (relative risk=5.2). However, risk did not decrease after orchiopexy in early childhood. A retrospective cohort study8 of 137 men with cryptorchidism who developed testicular cancer found no difference in 5-year survival between those who had orchiopexy (at ages 2 to 42) and those who had not (61% vs 63%, respectively).
FIGURE
Cryptorchidism
In most cases of cryptorchidism, the testis will be inguinal or prescrotal. A smaller number of cases are ectopic (have left the inguinal ring), abdominal, or absent. ILLUSTRATION BY RICH LaROCCO
Recommendations from others
The American Academy of Pediatrics policy section on urology says that spontaneous descent after 6 months is unlikely and recommends orchiopexy by 1 year of age.9
Infants with an undescended testis should be referred between ages 6 and 15 months, since almost all who experience spontaneous descent do so by 6 months (strength of recommendation [SOR]: A, extrapolation from cohort studies).
The incidence of germ cell aplasia in undescended testes begins to rise at 15 months (SOR: C, extrapolation of observational studies); however, evidence is inconclusive that orchiopexy at this age results in higher rates of paternity success (SOR: B, retrospective cohort study).
Orchiopexy may allow earlier detection of testicular tumors (SOR: C, expert opinion), but it has not been shown to reduce the risk of testicular cancer (SOR: B, retrospective cohort study) or improve 5-year survival rates for those patients diagnosed with testicular cancer (SOR: B, retrospective cohort study).
Periodically evaluate a newborn’s scrotum for either an undescended or reascended testicle
Danny Thomason, DO
Oklahoma State University, Tulsa
This Inquiry highlights 2 important considerations regarding the child with a cryptorchid testis. First, periodically evaluate the newborn and infant patient’s scrotum for either an undescended or reascended testicle. In my practice at Oklahoma State University Family Medicine Residency, I ask residents to perform the scrotal examination at birth, at every well-child visit up to 1 year of age, and then yearly thereafter. During puberty, these exams serve as opportunities to educate patients about testicular self-examination.
Secondly, as the authors indicate, there is some disagreement in the literature as to the risk of testicular cancer following orchiopexy for cryptorchidism. However, surgical repair is likely to facilitate regular testicular self-examination, which could increase the likelihood of detection of cancer during young adulthood.
Evidence summary
Three large cohort studies determined that cryptorchidism (FIGURE) is present at birth in approximately 3% of term infants (higher in preterm infants), with spontaneous descent occurring in two thirds of cases by age 3 to 6 months. One study1 of 10,730 consecutive male term infants found cryptorchidism at birth in 2.7%, dropping to 1.22% by 6 months of age, but without further change at 1 year. A similar study2 followed 6935 infant boys, finding cryptorchidism at birth in 3.7%, which decreased to 1% at 3 months and remained unchanged at 1 year. A third study3 found cryptorchidism at birth in 90 of 6414 (2.7%) infant boys. At follow-up, 45 of 90 had testicular descent at 1 month, 60 of 90 at 3 months, 67 of 90 at 9 months and at 1 year.
The 2 main indications for orchiopexy are potential avoidance of infertility and early detection and treatment of testicular cancer. A literature review4 of fertility after orchiopexy for undescended testis found inconclusive results. While epidemiological and pathological data (testicular biopsy, hormonal analysis, and sperm counts performed after orchiopexy) predict diminished fertility potential for men with unilaterally undescended testes, studies evaluating paternity find no difference from normal men. Biopsy studies of undescended testes at the time of orchiopexy show increased incidence of germ cell aplasia with older age at surgery (0.5%, 2%, 20%, and 45% at 6, 12, 24, and 48 months, respectively).4 A retrospective cohort study5 found 87% successful paternity after orchiopexy for 24 patients with unilateral undescended testis and 33% success for 9 with bilateral undescended testes but there was no normal control group. The boys were aged 1 to 14 years (mean, 7 years) at surgery, and there was no relationship between timing of orchiopexy and paternity success.5
The benefits of orchiopexy for testicular cancer are also unclear; expert opinion suggests that orchiopexy may allow earlier detection of testicular tumors.6 A cohort study7 of boys with cryptorchidism showed an increased risk of testicular cancer (relative risk=5.2). However, risk did not decrease after orchiopexy in early childhood. A retrospective cohort study8 of 137 men with cryptorchidism who developed testicular cancer found no difference in 5-year survival between those who had orchiopexy (at ages 2 to 42) and those who had not (61% vs 63%, respectively).
FIGURE
Cryptorchidism
In most cases of cryptorchidism, the testis will be inguinal or prescrotal. A smaller number of cases are ectopic (have left the inguinal ring), abdominal, or absent. ILLUSTRATION BY RICH LaROCCO
Recommendations from others
The American Academy of Pediatrics policy section on urology says that spontaneous descent after 6 months is unlikely and recommends orchiopexy by 1 year of age.9
1. Ghirri P, Ciulli C, Vuerich M, et al. Incidence at birth and natural history of cryptorchidism: a study of 10,730 consecutive male infants. J Endocrinol Invest 2002;25:709-715.
2. Berkowitz GS, Lapinski RH, Dolgin MD, et al. Prevalence and natural history of cryptorchidism. Pediatrics 1993;92:44-49.
3. Scorer CG. The descent of the testis. Arch Dis Childhood 1964;39:605-609.
4. Husmann DA. Cryptorchidism. In: Belman AB, King LR, Kramer SA, eds. Clinical Pediatric Urology. 4th ed. London, UK: Martin Dunitz Ltd.; 2002: 1125–1154.
5. Cendron M, Keating MA, Huff DS, Koop CE, Snyder HM, 3rd, Duckett JW. Cryptorchidism, orchiopexy and infertility: a critical long-term retrospective analysis. J Urol 1989;142(2 pt 2):559-562.
6. Docimo SG, Silver RI, Cromie W. The undescended testicle: diagnosis and management. Am Fam Physician 2000;62:2037-2048.
7. Prener A, Engholm G, Jensen OM. Genital anomalies and risk for testicular cancer in Danish men. Epidemiology 1996;7:14-19.
8. Batata MA, Chu FC, Hilaris BS, Whitmore WF, Golbey RB. Testicular cancer in cryptorchids. Cancer 1982;49:1023-1030.
9. American Academy of Pediatrics Policy Statement. Timing of elective surgery on the genitalia of male children with particular reference to the risks, benefits, and psychological effects of surgery and anesthesia. Pediatrics 1996;97:590-594.
1. Ghirri P, Ciulli C, Vuerich M, et al. Incidence at birth and natural history of cryptorchidism: a study of 10,730 consecutive male infants. J Endocrinol Invest 2002;25:709-715.
2. Berkowitz GS, Lapinski RH, Dolgin MD, et al. Prevalence and natural history of cryptorchidism. Pediatrics 1993;92:44-49.
3. Scorer CG. The descent of the testis. Arch Dis Childhood 1964;39:605-609.
4. Husmann DA. Cryptorchidism. In: Belman AB, King LR, Kramer SA, eds. Clinical Pediatric Urology. 4th ed. London, UK: Martin Dunitz Ltd.; 2002: 1125–1154.
5. Cendron M, Keating MA, Huff DS, Koop CE, Snyder HM, 3rd, Duckett JW. Cryptorchidism, orchiopexy and infertility: a critical long-term retrospective analysis. J Urol 1989;142(2 pt 2):559-562.
6. Docimo SG, Silver RI, Cromie W. The undescended testicle: diagnosis and management. Am Fam Physician 2000;62:2037-2048.
7. Prener A, Engholm G, Jensen OM. Genital anomalies and risk for testicular cancer in Danish men. Epidemiology 1996;7:14-19.
8. Batata MA, Chu FC, Hilaris BS, Whitmore WF, Golbey RB. Testicular cancer in cryptorchids. Cancer 1982;49:1023-1030.
9. American Academy of Pediatrics Policy Statement. Timing of elective surgery on the genitalia of male children with particular reference to the risks, benefits, and psychological effects of surgery and anesthesia. Pediatrics 1996;97:590-594.
Evidence-based answers from the Family Physicians Inquiries Network
When should COX-2 selective NSAIDs be used for osteoarthritis and rheumatoid arthritis?
Cyclo-oxygenase-2 (COX-2) selective nonsteroidal anti-inflammatory drugs (NSAIDs) are as effective as acetaminophen and nonselective NSAIDs in treating of osteoarthritis, and are equally effective in reducing pain and inflammation and improving of joint function for patients with rheumatoid arthritis, when compared with nonselective NSAIDs. The COX-2 selective NSAIDs also have a better gastrointestinal safety profile in short-term (6–12 month) treatment (strength of recommendation [SOR]: A, based on meta-analysis of randomized controlled trials with patient-oriented outcomes).
However, with recent growing concern of the cardiovascular safety of COX-2 selective NSAIDs, it is imperative to select appropriate patients by considering benefit vs risks, which include serious gastrointestinal bleeding (TABLE 1), history of intolerance to nonselective NSAID, cardiovascular disease or associated risks, renal disease, patient’s preference, and cost.
Nonselective NSAIDs with misoprostol or a PPI instead of COX-2 inhibitor is a reasonable strategy
Joseph Saseen, PharmD, FCCP, BCPS
University of Colorado at Denver and Health Sciences Center, Denver, Colo
Although celecoxib is an effective NSAID, rofecoxib and lumericoxib are the only COX-2 selective inhibitors that definitively reduce gastrointestinal (GI) ulcerations/complications compared with nonselective NSAID therapy.1,2 However, neither of these are on the market. Data from the CLASS study showed no reduced risk of GI ulcerations/complications with celecoxib vs ibuprofen or diclofenac among patients receiving low-dose aspirin.3 Low-dose aspirin reduces cardiovascular events for patients with moderate or high cardiovascular risk (Framingham scores ≥10%). Therefore, using nonselective NSAID therapy in combination with either misoprostol or a proton pump inhibitor (eg, omeprazole) instead of celecoxib, is a reasonable and proven strategy to provide NSAID therapy for patients on low-dose aspirin who are at high risk for NSAID-associated gastropathy.
Evidence summary
A Cochrane review4 (6 randomized controlled trials, N=1689, mean duration 5.8 weeks) assessed the efficacy and safety of acetaminophen in the management of osteoarthritis, comparing it with placebo and NSAIDs. Acetaminophen was superior to placebo in pain reduction and global assessment (number needed to treat [NNT]=2) with a similar safety profile. NSAIDs were better than acetaminophen in pain reduction, patient (NNT=6) and physician global assessment (NNT=17), but no better for functional improvement. Compared with nonselective NSAIDs, acetaminophen led to fewer withdrawals (number needed to harm [NNH]=20) and fewer GI adverse events (NNH=9), but there was no statistical difference when compared with COX-2 selective NSAIDs.
Another Cochrane review5 (26 randomized controlled trials) found that rofecoxib (Vioxx) was more effective than placebo (NNT=5), and equally effective with other NSAIDs in the management of osteoarthritis. They reported fewer GI adverse events (endoscopically observed gastric erosion and ulcers) with rofecoxib than with other NSAIDs—naproxen (Naprosyn), ibuprofen (Motrin), diclofenac (Cataflam), nabumetone (Relafen), diclofenac/misoprostol (Arthrotec), and nimesulide. However, the withdrawal rate due to adverse events and the increase in blood pressure and edema were significantly greater with rofecoxib than placebo at 6 weeks.
Two Cochrane reviews6-7 confirmed the efficacy of celecoxib (Celebrex) and rofecoxib in treating of rheumatoid arthritis. One review included 2 RCTs (N=8734) with a placebo arm (8 weeks) and naproxen arm (9 months).7 The rofecoxib groups (25 mg, 50 mg) had more responders than the placebo group (NNT=8 and 6 respectively). Compared with naproxen (1 g), no difference was seen in efficacy in the OMERACT outcomes (Outcome Measures for Rheumatoid Arthritis Clinical Trials), but all combined GI adverse events (perforation, ulcer, obstruction, bleeding, and all episodes of GI bleeding) were significantly reduced at 9 months (NNH=20). The withdrawals were the same in the 3 groups. Compared with placebo, the rofecoxib groups had similar incidence of elevated blood pressure and edema (NNH=50 and 100, respectively). Compared with the naproxen group, no difference was seen in renal adverse events, but total cardiovascular thrombotic events (NNH=200) and nonfatal MI (NNH=300) increased at 9 months in the 50 mg rofecoxib group.
Similar cardiovascular adverse events were reported in the APPROVE trial.9 In this study, patients taking rofecoxib 25 mg daily for 18 months had increased total thrombotic events (MI, stroke, peripheral arterial and venous thrombosis, and pulmonary embolism) when compared with placebo (NNH=63). A recent study also raised the same concern of increased cardiovascular adverse events with celecoxib.10 This study demonstrated an increase risk of cardiovascular events (combined death, myocardial infarction, stroke, and heart failure) for patients taking celecoxib 200 mg twice a day (NNH=77) or 400 mg twice a day (NNH=42).
Many patients taking low-dose aspirin for cardioprotection also frequently require treatment of pain and inflammation with a NSAID. Even low-dose aspirin (75 mg/d) is known to be associated with increased GI toxicity (ulcers and hemorrhages).11 A recent double-blind, randomized placebo-controlled trial found that 12 weeks of treatment with a combination of low-dose aspirin and a COX-2 selective NSAID (rofecoxib) had more than twice the incidence of endoscopically confirmed gastric and duodenal ulcers, compared with aspirin alone, and no difference with a nonselective NSAID.12 This has raised the safety concern of concomitant use of a COX-2 selective NSAID with low-dose aspirin.
TABLE 1
Prediction of serious gastrointestinal bleeding
| RISK FACTORS PRESENT | RISK OF GI BLEEDING |
|---|---|
| 0 factor | 0.4 % |
| Any 1 factor | 1.0 % |
| All 4 factors | 9.0 % |
| Risk factors include age >75 years, history of peptic ulcer disease, history of gastrointestinal bleeding, history of cardiovascular disease | |
| Source: Silverstein et al, Ann Intern Med 1995.8 | |
Recommendations from others
The American Pain Society recommends that for patients with osteoarthritis, acetaminophen is the drug of choice for mild pain.13 For moderate to severe pain and or inflammation, a COX-2 selective NSAID is the first choice, unless the patient is at significant risk for hypertension or renal disorder. For patients with active rheumatoid arthritis and moderate to severe pain with or without inflammation, a COX-2 selective NSAID should be used concomitantly with a disease-modifying antirheumatic drug (DMARD), unless contraindicated by existing uncontrolled hypertension and renal disease. It further recommends that for a person who is at risk for a cardiovascular event, an aspirin (75–160 mg/d), should be given along with a COX-2 selective NSAID.
The American College of Rheumatology recommends that a COX-2 selective NSAID should be considered for a person with osteoarthritis and pain not relieved by an adequate dose of acetaminophen (not to exceed 4 g/d).14,15 The COX-2 selective NSAID is particularly advantageous for those who have higher risk factors for adverse GI events (TABLE 2). For a person with rheumatoid arthritis, in addition to DMARDs, NSAIDs (salicylates, nonselective NSAID, or COX-2 selective NSAID) should be used to reduce joint pain and swelling and improve joint function. Patients with additional risks for cardiovascular events should be cautioned about use of a COX-2 selective NSAID.
A recent AHRQ report on managing osteoarthritis underscores the importance of physician-patient partnership and patient’s self management of osteoarthritis, and recommends acetaminophen (up to 4 g/day) as the drug of choice.16 It further cautions the injudicious use of NSAIDs because of its greater GI toxicity when compared with acetaminophen, and its higher medical costs.
TABLE 2
Risk factors for upper gastrointestinal adverse events
| Age ≥65 years |
| Comorbid medical conditions |
| Oral glucocorticoids |
| History of peptic ulcer disease |
| History of upper gastrointestinal bleeding |
| Anticoagulants |
| Source: American College of Rheumatology, Arthritis Rheum 2000.12 |
1. Bombardier C, Laine L, Reicin A, et al. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. N Engl J Med 2000;343:1520-1528.
2. Schnitzer TJ, Burmester GR, Mysler E, et al. Comparison of lumiracoxib with naproxen and ibuprofen in the Therapeutic Arthritis Research and Gastrointestinal Event Trial (TARGET), reduction in ulcer complications: randomised controlled trial. Lancet 2004;364:665-674.
3. Silverstein FE, Faich G, Goldstein JL, et al. Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study: A randomized controlled trial. Celecoxib Long-term Arthritis Safety Study. JAMA 2000;284:1247-1255.
4. Towheed TE, Judd MG, Hochberg MC, Wells G. Acetaminophen for osteoarthritis. Cochrane Database Syst Rev 2003;(2):CD004257.-
5. Garner SE, Fidan DD, Frankish RR, Maxwell LJ. Rofecoxib for osteoarthritis. Cochrane Database Syst Rev 2005;(1):CD005115.-
6. Garner S, Fidan D, Frankish R, et al. Celecoxib for rheumatoid arthritis. Cochrane Database Syst Rev 2002;(4):CD003831.-
7. Garner SE, Fidan DD, Frankish RR, et al. Rofecoxib for rheumatoid arthritis. Cochrane Database Syst Rev 2005;(1):CD003685.-
8. Silverstein FE, Graham DY, Senior JR, et al. Misoprostol reduced serious gastrointestinal complications in patients with rheumatoid arthritis receiving nonsteroidal anti-inflammatory drugs. A randomized, double-blind, placebo-controlled trial. Ann Intern Med 1995;123:241-249.
9. Bresalier RS, Sandler RS, Quan H, et al. Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N Engl J Med 2005;352:1092-1102.
10. Solomon SD, McMurray JJ, Pfeffer MA, et al. Cardiovascular risk associated with celecoxib in clinical trial for colorectal adenoma prevention. N Engl J Med 2005;352:1071-1080.
11. Derry S, Loke YK. Risk of gastrointestinal haemorrhage with long term use of aspirin: meta-analysis. BMJ 2000;321:1183-1187.
12. Laine L, Maller ES, Yu C, Quan H, Simon T. Ulcer formation with low-dose enteric-coated aspirin and the effect of COX-2 selective inhibition: A double-blind trial. Gastroenterology 2004;127:395-402.
13. Simon LS, Lipman AG, Jacox AK, et al. Pain in Osteoarthritis, Rheumatoid Arthritis and Juvenile Chronic Arthritis. 2nd ed. Glenview, Ill: American Pain Society; 2002.
14. American College of Rheumatology (ACR) Subcommittee on Osteoarthritis Guidelines. Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum 2000;43:1905-1915.
15. American College of Rheumatology Subcommittee on Rheumatoid Arthritis Guidelines. Guidelines for the management of rheumatoid arthritis: 2002 Update. Arthritis Rheum 2002;46:328-346.
16. Managing Osteoarthritis: Helping the Elderly Maintain Function and Mobility. Issue 4, AHRQ Pub. No 02-0023, May 2002. Agency for Healthcare Research and Quality. Available at: www.ahrq.gov/research/osteoria/osteoria.htm#self-manage.
Cyclo-oxygenase-2 (COX-2) selective nonsteroidal anti-inflammatory drugs (NSAIDs) are as effective as acetaminophen and nonselective NSAIDs in treating of osteoarthritis, and are equally effective in reducing pain and inflammation and improving of joint function for patients with rheumatoid arthritis, when compared with nonselective NSAIDs. The COX-2 selective NSAIDs also have a better gastrointestinal safety profile in short-term (6–12 month) treatment (strength of recommendation [SOR]: A, based on meta-analysis of randomized controlled trials with patient-oriented outcomes).
However, with recent growing concern of the cardiovascular safety of COX-2 selective NSAIDs, it is imperative to select appropriate patients by considering benefit vs risks, which include serious gastrointestinal bleeding (TABLE 1), history of intolerance to nonselective NSAID, cardiovascular disease or associated risks, renal disease, patient’s preference, and cost.
Nonselective NSAIDs with misoprostol or a PPI instead of COX-2 inhibitor is a reasonable strategy
Joseph Saseen, PharmD, FCCP, BCPS
University of Colorado at Denver and Health Sciences Center, Denver, Colo
Although celecoxib is an effective NSAID, rofecoxib and lumericoxib are the only COX-2 selective inhibitors that definitively reduce gastrointestinal (GI) ulcerations/complications compared with nonselective NSAID therapy.1,2 However, neither of these are on the market. Data from the CLASS study showed no reduced risk of GI ulcerations/complications with celecoxib vs ibuprofen or diclofenac among patients receiving low-dose aspirin.3 Low-dose aspirin reduces cardiovascular events for patients with moderate or high cardiovascular risk (Framingham scores ≥10%). Therefore, using nonselective NSAID therapy in combination with either misoprostol or a proton pump inhibitor (eg, omeprazole) instead of celecoxib, is a reasonable and proven strategy to provide NSAID therapy for patients on low-dose aspirin who are at high risk for NSAID-associated gastropathy.
Evidence summary
A Cochrane review4 (6 randomized controlled trials, N=1689, mean duration 5.8 weeks) assessed the efficacy and safety of acetaminophen in the management of osteoarthritis, comparing it with placebo and NSAIDs. Acetaminophen was superior to placebo in pain reduction and global assessment (number needed to treat [NNT]=2) with a similar safety profile. NSAIDs were better than acetaminophen in pain reduction, patient (NNT=6) and physician global assessment (NNT=17), but no better for functional improvement. Compared with nonselective NSAIDs, acetaminophen led to fewer withdrawals (number needed to harm [NNH]=20) and fewer GI adverse events (NNH=9), but there was no statistical difference when compared with COX-2 selective NSAIDs.
Another Cochrane review5 (26 randomized controlled trials) found that rofecoxib (Vioxx) was more effective than placebo (NNT=5), and equally effective with other NSAIDs in the management of osteoarthritis. They reported fewer GI adverse events (endoscopically observed gastric erosion and ulcers) with rofecoxib than with other NSAIDs—naproxen (Naprosyn), ibuprofen (Motrin), diclofenac (Cataflam), nabumetone (Relafen), diclofenac/misoprostol (Arthrotec), and nimesulide. However, the withdrawal rate due to adverse events and the increase in blood pressure and edema were significantly greater with rofecoxib than placebo at 6 weeks.
Two Cochrane reviews6-7 confirmed the efficacy of celecoxib (Celebrex) and rofecoxib in treating of rheumatoid arthritis. One review included 2 RCTs (N=8734) with a placebo arm (8 weeks) and naproxen arm (9 months).7 The rofecoxib groups (25 mg, 50 mg) had more responders than the placebo group (NNT=8 and 6 respectively). Compared with naproxen (1 g), no difference was seen in efficacy in the OMERACT outcomes (Outcome Measures for Rheumatoid Arthritis Clinical Trials), but all combined GI adverse events (perforation, ulcer, obstruction, bleeding, and all episodes of GI bleeding) were significantly reduced at 9 months (NNH=20). The withdrawals were the same in the 3 groups. Compared with placebo, the rofecoxib groups had similar incidence of elevated blood pressure and edema (NNH=50 and 100, respectively). Compared with the naproxen group, no difference was seen in renal adverse events, but total cardiovascular thrombotic events (NNH=200) and nonfatal MI (NNH=300) increased at 9 months in the 50 mg rofecoxib group.
Similar cardiovascular adverse events were reported in the APPROVE trial.9 In this study, patients taking rofecoxib 25 mg daily for 18 months had increased total thrombotic events (MI, stroke, peripheral arterial and venous thrombosis, and pulmonary embolism) when compared with placebo (NNH=63). A recent study also raised the same concern of increased cardiovascular adverse events with celecoxib.10 This study demonstrated an increase risk of cardiovascular events (combined death, myocardial infarction, stroke, and heart failure) for patients taking celecoxib 200 mg twice a day (NNH=77) or 400 mg twice a day (NNH=42).
Many patients taking low-dose aspirin for cardioprotection also frequently require treatment of pain and inflammation with a NSAID. Even low-dose aspirin (75 mg/d) is known to be associated with increased GI toxicity (ulcers and hemorrhages).11 A recent double-blind, randomized placebo-controlled trial found that 12 weeks of treatment with a combination of low-dose aspirin and a COX-2 selective NSAID (rofecoxib) had more than twice the incidence of endoscopically confirmed gastric and duodenal ulcers, compared with aspirin alone, and no difference with a nonselective NSAID.12 This has raised the safety concern of concomitant use of a COX-2 selective NSAID with low-dose aspirin.
TABLE 1
Prediction of serious gastrointestinal bleeding
| RISK FACTORS PRESENT | RISK OF GI BLEEDING |
|---|---|
| 0 factor | 0.4 % |
| Any 1 factor | 1.0 % |
| All 4 factors | 9.0 % |
| Risk factors include age >75 years, history of peptic ulcer disease, history of gastrointestinal bleeding, history of cardiovascular disease | |
| Source: Silverstein et al, Ann Intern Med 1995.8 | |
Recommendations from others
The American Pain Society recommends that for patients with osteoarthritis, acetaminophen is the drug of choice for mild pain.13 For moderate to severe pain and or inflammation, a COX-2 selective NSAID is the first choice, unless the patient is at significant risk for hypertension or renal disorder. For patients with active rheumatoid arthritis and moderate to severe pain with or without inflammation, a COX-2 selective NSAID should be used concomitantly with a disease-modifying antirheumatic drug (DMARD), unless contraindicated by existing uncontrolled hypertension and renal disease. It further recommends that for a person who is at risk for a cardiovascular event, an aspirin (75–160 mg/d), should be given along with a COX-2 selective NSAID.
The American College of Rheumatology recommends that a COX-2 selective NSAID should be considered for a person with osteoarthritis and pain not relieved by an adequate dose of acetaminophen (not to exceed 4 g/d).14,15 The COX-2 selective NSAID is particularly advantageous for those who have higher risk factors for adverse GI events (TABLE 2). For a person with rheumatoid arthritis, in addition to DMARDs, NSAIDs (salicylates, nonselective NSAID, or COX-2 selective NSAID) should be used to reduce joint pain and swelling and improve joint function. Patients with additional risks for cardiovascular events should be cautioned about use of a COX-2 selective NSAID.
A recent AHRQ report on managing osteoarthritis underscores the importance of physician-patient partnership and patient’s self management of osteoarthritis, and recommends acetaminophen (up to 4 g/day) as the drug of choice.16 It further cautions the injudicious use of NSAIDs because of its greater GI toxicity when compared with acetaminophen, and its higher medical costs.
TABLE 2
Risk factors for upper gastrointestinal adverse events
| Age ≥65 years |
| Comorbid medical conditions |
| Oral glucocorticoids |
| History of peptic ulcer disease |
| History of upper gastrointestinal bleeding |
| Anticoagulants |
| Source: American College of Rheumatology, Arthritis Rheum 2000.12 |
Cyclo-oxygenase-2 (COX-2) selective nonsteroidal anti-inflammatory drugs (NSAIDs) are as effective as acetaminophen and nonselective NSAIDs in treating of osteoarthritis, and are equally effective in reducing pain and inflammation and improving of joint function for patients with rheumatoid arthritis, when compared with nonselective NSAIDs. The COX-2 selective NSAIDs also have a better gastrointestinal safety profile in short-term (6–12 month) treatment (strength of recommendation [SOR]: A, based on meta-analysis of randomized controlled trials with patient-oriented outcomes).
However, with recent growing concern of the cardiovascular safety of COX-2 selective NSAIDs, it is imperative to select appropriate patients by considering benefit vs risks, which include serious gastrointestinal bleeding (TABLE 1), history of intolerance to nonselective NSAID, cardiovascular disease or associated risks, renal disease, patient’s preference, and cost.
Nonselective NSAIDs with misoprostol or a PPI instead of COX-2 inhibitor is a reasonable strategy
Joseph Saseen, PharmD, FCCP, BCPS
University of Colorado at Denver and Health Sciences Center, Denver, Colo
Although celecoxib is an effective NSAID, rofecoxib and lumericoxib are the only COX-2 selective inhibitors that definitively reduce gastrointestinal (GI) ulcerations/complications compared with nonselective NSAID therapy.1,2 However, neither of these are on the market. Data from the CLASS study showed no reduced risk of GI ulcerations/complications with celecoxib vs ibuprofen or diclofenac among patients receiving low-dose aspirin.3 Low-dose aspirin reduces cardiovascular events for patients with moderate or high cardiovascular risk (Framingham scores ≥10%). Therefore, using nonselective NSAID therapy in combination with either misoprostol or a proton pump inhibitor (eg, omeprazole) instead of celecoxib, is a reasonable and proven strategy to provide NSAID therapy for patients on low-dose aspirin who are at high risk for NSAID-associated gastropathy.
Evidence summary
A Cochrane review4 (6 randomized controlled trials, N=1689, mean duration 5.8 weeks) assessed the efficacy and safety of acetaminophen in the management of osteoarthritis, comparing it with placebo and NSAIDs. Acetaminophen was superior to placebo in pain reduction and global assessment (number needed to treat [NNT]=2) with a similar safety profile. NSAIDs were better than acetaminophen in pain reduction, patient (NNT=6) and physician global assessment (NNT=17), but no better for functional improvement. Compared with nonselective NSAIDs, acetaminophen led to fewer withdrawals (number needed to harm [NNH]=20) and fewer GI adverse events (NNH=9), but there was no statistical difference when compared with COX-2 selective NSAIDs.
Another Cochrane review5 (26 randomized controlled trials) found that rofecoxib (Vioxx) was more effective than placebo (NNT=5), and equally effective with other NSAIDs in the management of osteoarthritis. They reported fewer GI adverse events (endoscopically observed gastric erosion and ulcers) with rofecoxib than with other NSAIDs—naproxen (Naprosyn), ibuprofen (Motrin), diclofenac (Cataflam), nabumetone (Relafen), diclofenac/misoprostol (Arthrotec), and nimesulide. However, the withdrawal rate due to adverse events and the increase in blood pressure and edema were significantly greater with rofecoxib than placebo at 6 weeks.
Two Cochrane reviews6-7 confirmed the efficacy of celecoxib (Celebrex) and rofecoxib in treating of rheumatoid arthritis. One review included 2 RCTs (N=8734) with a placebo arm (8 weeks) and naproxen arm (9 months).7 The rofecoxib groups (25 mg, 50 mg) had more responders than the placebo group (NNT=8 and 6 respectively). Compared with naproxen (1 g), no difference was seen in efficacy in the OMERACT outcomes (Outcome Measures for Rheumatoid Arthritis Clinical Trials), but all combined GI adverse events (perforation, ulcer, obstruction, bleeding, and all episodes of GI bleeding) were significantly reduced at 9 months (NNH=20). The withdrawals were the same in the 3 groups. Compared with placebo, the rofecoxib groups had similar incidence of elevated blood pressure and edema (NNH=50 and 100, respectively). Compared with the naproxen group, no difference was seen in renal adverse events, but total cardiovascular thrombotic events (NNH=200) and nonfatal MI (NNH=300) increased at 9 months in the 50 mg rofecoxib group.
Similar cardiovascular adverse events were reported in the APPROVE trial.9 In this study, patients taking rofecoxib 25 mg daily for 18 months had increased total thrombotic events (MI, stroke, peripheral arterial and venous thrombosis, and pulmonary embolism) when compared with placebo (NNH=63). A recent study also raised the same concern of increased cardiovascular adverse events with celecoxib.10 This study demonstrated an increase risk of cardiovascular events (combined death, myocardial infarction, stroke, and heart failure) for patients taking celecoxib 200 mg twice a day (NNH=77) or 400 mg twice a day (NNH=42).
Many patients taking low-dose aspirin for cardioprotection also frequently require treatment of pain and inflammation with a NSAID. Even low-dose aspirin (75 mg/d) is known to be associated with increased GI toxicity (ulcers and hemorrhages).11 A recent double-blind, randomized placebo-controlled trial found that 12 weeks of treatment with a combination of low-dose aspirin and a COX-2 selective NSAID (rofecoxib) had more than twice the incidence of endoscopically confirmed gastric and duodenal ulcers, compared with aspirin alone, and no difference with a nonselective NSAID.12 This has raised the safety concern of concomitant use of a COX-2 selective NSAID with low-dose aspirin.
TABLE 1
Prediction of serious gastrointestinal bleeding
| RISK FACTORS PRESENT | RISK OF GI BLEEDING |
|---|---|
| 0 factor | 0.4 % |
| Any 1 factor | 1.0 % |
| All 4 factors | 9.0 % |
| Risk factors include age >75 years, history of peptic ulcer disease, history of gastrointestinal bleeding, history of cardiovascular disease | |
| Source: Silverstein et al, Ann Intern Med 1995.8 | |
Recommendations from others
The American Pain Society recommends that for patients with osteoarthritis, acetaminophen is the drug of choice for mild pain.13 For moderate to severe pain and or inflammation, a COX-2 selective NSAID is the first choice, unless the patient is at significant risk for hypertension or renal disorder. For patients with active rheumatoid arthritis and moderate to severe pain with or without inflammation, a COX-2 selective NSAID should be used concomitantly with a disease-modifying antirheumatic drug (DMARD), unless contraindicated by existing uncontrolled hypertension and renal disease. It further recommends that for a person who is at risk for a cardiovascular event, an aspirin (75–160 mg/d), should be given along with a COX-2 selective NSAID.
The American College of Rheumatology recommends that a COX-2 selective NSAID should be considered for a person with osteoarthritis and pain not relieved by an adequate dose of acetaminophen (not to exceed 4 g/d).14,15 The COX-2 selective NSAID is particularly advantageous for those who have higher risk factors for adverse GI events (TABLE 2). For a person with rheumatoid arthritis, in addition to DMARDs, NSAIDs (salicylates, nonselective NSAID, or COX-2 selective NSAID) should be used to reduce joint pain and swelling and improve joint function. Patients with additional risks for cardiovascular events should be cautioned about use of a COX-2 selective NSAID.
A recent AHRQ report on managing osteoarthritis underscores the importance of physician-patient partnership and patient’s self management of osteoarthritis, and recommends acetaminophen (up to 4 g/day) as the drug of choice.16 It further cautions the injudicious use of NSAIDs because of its greater GI toxicity when compared with acetaminophen, and its higher medical costs.
TABLE 2
Risk factors for upper gastrointestinal adverse events
| Age ≥65 years |
| Comorbid medical conditions |
| Oral glucocorticoids |
| History of peptic ulcer disease |
| History of upper gastrointestinal bleeding |
| Anticoagulants |
| Source: American College of Rheumatology, Arthritis Rheum 2000.12 |
1. Bombardier C, Laine L, Reicin A, et al. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. N Engl J Med 2000;343:1520-1528.
2. Schnitzer TJ, Burmester GR, Mysler E, et al. Comparison of lumiracoxib with naproxen and ibuprofen in the Therapeutic Arthritis Research and Gastrointestinal Event Trial (TARGET), reduction in ulcer complications: randomised controlled trial. Lancet 2004;364:665-674.
3. Silverstein FE, Faich G, Goldstein JL, et al. Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study: A randomized controlled trial. Celecoxib Long-term Arthritis Safety Study. JAMA 2000;284:1247-1255.
4. Towheed TE, Judd MG, Hochberg MC, Wells G. Acetaminophen for osteoarthritis. Cochrane Database Syst Rev 2003;(2):CD004257.-
5. Garner SE, Fidan DD, Frankish RR, Maxwell LJ. Rofecoxib for osteoarthritis. Cochrane Database Syst Rev 2005;(1):CD005115.-
6. Garner S, Fidan D, Frankish R, et al. Celecoxib for rheumatoid arthritis. Cochrane Database Syst Rev 2002;(4):CD003831.-
7. Garner SE, Fidan DD, Frankish RR, et al. Rofecoxib for rheumatoid arthritis. Cochrane Database Syst Rev 2005;(1):CD003685.-
8. Silverstein FE, Graham DY, Senior JR, et al. Misoprostol reduced serious gastrointestinal complications in patients with rheumatoid arthritis receiving nonsteroidal anti-inflammatory drugs. A randomized, double-blind, placebo-controlled trial. Ann Intern Med 1995;123:241-249.
9. Bresalier RS, Sandler RS, Quan H, et al. Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N Engl J Med 2005;352:1092-1102.
10. Solomon SD, McMurray JJ, Pfeffer MA, et al. Cardiovascular risk associated with celecoxib in clinical trial for colorectal adenoma prevention. N Engl J Med 2005;352:1071-1080.
11. Derry S, Loke YK. Risk of gastrointestinal haemorrhage with long term use of aspirin: meta-analysis. BMJ 2000;321:1183-1187.
12. Laine L, Maller ES, Yu C, Quan H, Simon T. Ulcer formation with low-dose enteric-coated aspirin and the effect of COX-2 selective inhibition: A double-blind trial. Gastroenterology 2004;127:395-402.
13. Simon LS, Lipman AG, Jacox AK, et al. Pain in Osteoarthritis, Rheumatoid Arthritis and Juvenile Chronic Arthritis. 2nd ed. Glenview, Ill: American Pain Society; 2002.
14. American College of Rheumatology (ACR) Subcommittee on Osteoarthritis Guidelines. Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum 2000;43:1905-1915.
15. American College of Rheumatology Subcommittee on Rheumatoid Arthritis Guidelines. Guidelines for the management of rheumatoid arthritis: 2002 Update. Arthritis Rheum 2002;46:328-346.
16. Managing Osteoarthritis: Helping the Elderly Maintain Function and Mobility. Issue 4, AHRQ Pub. No 02-0023, May 2002. Agency for Healthcare Research and Quality. Available at: www.ahrq.gov/research/osteoria/osteoria.htm#self-manage.
1. Bombardier C, Laine L, Reicin A, et al. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. N Engl J Med 2000;343:1520-1528.
2. Schnitzer TJ, Burmester GR, Mysler E, et al. Comparison of lumiracoxib with naproxen and ibuprofen in the Therapeutic Arthritis Research and Gastrointestinal Event Trial (TARGET), reduction in ulcer complications: randomised controlled trial. Lancet 2004;364:665-674.
3. Silverstein FE, Faich G, Goldstein JL, et al. Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study: A randomized controlled trial. Celecoxib Long-term Arthritis Safety Study. JAMA 2000;284:1247-1255.
4. Towheed TE, Judd MG, Hochberg MC, Wells G. Acetaminophen for osteoarthritis. Cochrane Database Syst Rev 2003;(2):CD004257.-
5. Garner SE, Fidan DD, Frankish RR, Maxwell LJ. Rofecoxib for osteoarthritis. Cochrane Database Syst Rev 2005;(1):CD005115.-
6. Garner S, Fidan D, Frankish R, et al. Celecoxib for rheumatoid arthritis. Cochrane Database Syst Rev 2002;(4):CD003831.-
7. Garner SE, Fidan DD, Frankish RR, et al. Rofecoxib for rheumatoid arthritis. Cochrane Database Syst Rev 2005;(1):CD003685.-
8. Silverstein FE, Graham DY, Senior JR, et al. Misoprostol reduced serious gastrointestinal complications in patients with rheumatoid arthritis receiving nonsteroidal anti-inflammatory drugs. A randomized, double-blind, placebo-controlled trial. Ann Intern Med 1995;123:241-249.
9. Bresalier RS, Sandler RS, Quan H, et al. Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N Engl J Med 2005;352:1092-1102.
10. Solomon SD, McMurray JJ, Pfeffer MA, et al. Cardiovascular risk associated with celecoxib in clinical trial for colorectal adenoma prevention. N Engl J Med 2005;352:1071-1080.
11. Derry S, Loke YK. Risk of gastrointestinal haemorrhage with long term use of aspirin: meta-analysis. BMJ 2000;321:1183-1187.
12. Laine L, Maller ES, Yu C, Quan H, Simon T. Ulcer formation with low-dose enteric-coated aspirin and the effect of COX-2 selective inhibition: A double-blind trial. Gastroenterology 2004;127:395-402.
13. Simon LS, Lipman AG, Jacox AK, et al. Pain in Osteoarthritis, Rheumatoid Arthritis and Juvenile Chronic Arthritis. 2nd ed. Glenview, Ill: American Pain Society; 2002.
14. American College of Rheumatology (ACR) Subcommittee on Osteoarthritis Guidelines. Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum 2000;43:1905-1915.
15. American College of Rheumatology Subcommittee on Rheumatoid Arthritis Guidelines. Guidelines for the management of rheumatoid arthritis: 2002 Update. Arthritis Rheum 2002;46:328-346.
16. Managing Osteoarthritis: Helping the Elderly Maintain Function and Mobility. Issue 4, AHRQ Pub. No 02-0023, May 2002. Agency for Healthcare Research and Quality. Available at: www.ahrq.gov/research/osteoria/osteoria.htm#self-manage.
Evidence-based answers from the Family Physicians Inquiries Network
What is the best way to treat tinea cruris?
After clinical diagnosis and microscopic confirmation, tinea cruris is best treated with a topical allylamine or an azole antifungal (strength of recommendation: A, based on multiple randomized controlled trials [RCTs]). Differences in current comparison data are insufficient to stratify the 2 groups of topical antifungals. Determining which group to use depends on patient compliance, medication accessibility, and cost. The fungicidal allylamines (naftifine and terbinafine) and butenafine (allylamine derivative) are a more costly group of topical tinea treatments, yet they are more convenient as they allow for a shorter duration of treatment compared with fungistatic azoles (clotrimazole, econazole, ketoconazole, oxiconazole, miconazole, and sulconazole).
Choice of treatment should reflect cost and convenience to the patient
Dan Hunter-Smith, MD
Adventist LaGrange Family Medicine Residency, LaGrange, Ill
This review illustrates that the “best way” to treat a problem can have more to do with the needs of a given patient than intrinsic differences between treatments. All reviewed treatments were roughly therapeutically equivalent and equally safe. This leaves the choice of treatment to reflect the importance of cost and convenience to the patient. If cost is an issue for the patient, the frugal way to treat tinea cruris is to have the patient go to the vaginitis treatment section of the pharmacy and pick up a 15-g tube of miconazole or clotrimazole cream for $7 to $10. Terbinafine cream or spray costs $10 to $13 over the counter, but it reduces the onus of compliance to once-a-day for 1 week. If terbinafine 1% solution is preferred, a 30-mL bottle costs $77. Most of the time, I let the patient make their own choice.
Evidence summary
Tinea cruris (“jock itch”) is a superficial dermatophyte infection of the groin and surrounding skin. Obese adult men are affected more than women, and it is rarely seen in children. Because excessive perspiration is the most common predisposing factor, patient education on proper hygiene makes intuitive sense for successful treatment, yet it has not been studied.1Trichophyton rubrum is the most common source of tinea cruris, as well as tinea corporis (“ringworm”), in the United States.2 Most studies involving patients with tinea cruris combine data with tinea corporis.
Although more than 25 RCTs document the safety and efficacy of antifungal treatments, few head-to-head trials are available. Several topical preparations are approved for the treatment of tinea cruris. Selection should be based on patient compliance (duration of treatment), overall cost, and tolerability. The 2 main classes of antifungals are allylamines and azoles.
Allylamines. Allylamines offer a shorter duration of therapy, lower relapse rates, and work independent of the cytochrome P450 system. Multiple RCTs have documented the efficacy and safety of the 2 available allylamine antifungals, terbinafine and naftifine, when compared with placebo and various azoles.
Terbinafine is available in several 1% formulations (emulsion-gel, cream, and solution/spray), all studied and dosed once daily for 1 week. One placebo controlled trial showed the 1% emulsion-gel version (Lamisil) was effective in 89% of the study population vs 23% of the placebo group (NNT=1.5); it was particularly suitable on hairy skin. Seven weeks post-treatment, 84% of the intent-to-treat population of the Lamisil group remained mycologically negative.3 Data combined from 2 other RCTs yielded 83% efficacy 3 weeks post-treatment when 66 patients were treated with terbinafine 1% cream, compared with 12% efficacy for 73 patients using the vehicle cream (NNT=1.4).4 Another placebo-controlled study of 66 patients demonstrated 100% microscopic cure of terbinafine 1% solution by week 2 and maintaining 90% cure at 4 weeks.5
In a multicenter, double-blind RCT funded by the manufacturers of terbinafine, bifonazole 1% cream for 3 weeks was compared with terbinafine 1% cream used daily for 1 week (followed by 2 weeks of its vehicle cream). Mycological and clinical cure rates were greater than 95% in both groups at 3 weeks. At the 8-week follow-up, no statistically significant differences were seen in KOH positivity rates (20.24% of patients in the bifonazole-treated group were KOH-positive vs 11.76% in the terbinafine group). Symptom relapse rates at 8 weeks were not available.6
In a 4-week study involving 104 patients, naftifine 1% cream (Naftin) was compared with econazole 1% cream (Spectazole) (both applied twice daily). At the end of the study, naftifine 1% cream had a higher (but not statistically significant) mycological and clinical cure rate of 78% compared with 68% with econazole 1% cream.7 Similar results (79% mycological cure) were seen in a placebo-controlled trial with 70 patients using once daily naftifine 1% cream after 2 weeks of treatment (NNT=2).8
Butenafine (Mentax), a benzylamine antifungal, was 88% to 93% mycologically effective in a noncomparative study, when used twice daily for 2 weeks.9 Similar results were found in a study of 76 patients with tinea cruris; after 2 weeks of daily application, 78% (modified intent-to-treat group) were mycologically cured. Mycological cure plus “cleared” or “excellent” clinical evaluation remained for 73% at day 42 vs 5% of the placebo group (NNT=1.47).10
Azoles. Azoles are less expensive than allylamines, but require longer treatment periods, theoretically compromising patient adherence to therapy. One of the more popular azoles is clotrimazole (Lotrimin, Mycelex), one of the oldest antifungal treatments. One RCT compared cure rates for 139 patients for clotrimazole 1% cream compared with ciclopirox olamine 1% cream when both were applied twice daily for 28 days. By the end of the 4-week period, 69% of the clotrimazole group was clinically and mycologically cured compared with 64% of the ciclopirox group.11
Miconazole 2% cream (Micatin, Monistat) (used twice daily for 2 weeks by inmates in a Florida prison) demonstrated 75.5% clinical clearing (against tinea cruris, pedis, or corporis, or Candida cutaneous infections) when compared with placebo (NNT=1.57). Of the 99 patients evaluated, 48 were diagnosed with tinea cruris; however, results were not broken down into diagnostic category. The length of follow-up for these patients was not disclosed.12
Alternative therapy. Ajoene 0.6% gel (isolated from garlic), was as effective as terbinafine 1% cream (both applied twice daily for 2 weeks) in a RCT of 60 Venezuelan Army soldiers.13 Sixty days after treatment, 73% of the Ajoene-treated patients and 71% in the terbinafine group were asymptomatic. An open-pilot study of 14 patients with tinea cruris demonstrated 71% mycological cure with a honey, olive oil, and beeswax (1:1:1) mixture, applied 3 times daily up to 3 weeks, likely due to honey’s inhibitory effect on fungus and beeswax’s anti-inflammatory properties.14
Recommendations from others
The Sanford Guide to Antimicrobial Therapy (2005) recommends topical butenafine and terbinafine as primary agents of choice for tinea cruris due to their fungicidal activity.15 The American Academy of Family Physicians recommends any of the topical antifungal treatments as first-line treatment for tinea cruris.16 A systematic review on tinea pedis topical therapy acknowledges the higher cure rates by allylamines, compared with azoles, but concludes that azoles remain the most costeffective in the treatment of tinea pedis.17 No recent guidelines from the American Academy of Dermatology are available.
1. Gupta AK, Chaudhry M, Elewski BE. Tinea corporis, tinea cruris, tinea nigra, and piedra. Dermatol Clin 2003;21:395-400.
2. Foster KW, Ghannoum MA, Elewski BE. Epidemiologic surveillance of cutaneous fungal infection in the United States from 1999 to 2002. J Am Acad Dermatol 2004;30:748-752.
3. van Heerden JS, Vismer HF. Tinea corporis/cruris: new treatment options. Dermatology 1997;194(Suppl 1):14-18.
4. Zaias N, Berman B, Cordero CN, et al. Efficacy of a 1-week, once daily regimen of terbinafine 1% cream in the treatment of tinea cruris and tinea corporis. J Am Acad Dermatol 1993;29:646-648.
5. Lebwohl M, Elewski B, Eisen D, Savin RC. Efficacy and safety of terbinafine 1% solution in the treatment of interdigital tinea pedis and tinea corporis or tinea cruris. Cutis 2001;67:261-266.
6. Budimulja U. Terbinafine 1% cream vs. bifonazole 1% cream in the treatment of tinea cruris. Int J Dermatol 1998;37:871-873.
7. Millikan LE, Galen WK, Gewirtzman GB, et al. Naftifine cream 1% versus econazole cream 1% in the treatment of tinea cruris and tinea corporis. J Am Acad Dermatol 1988;18(1 Pt 1):52-56.
8. Jordan RE, Rapini RP, Rex IH, Jr, et al. Once-daily naftine cream 1% in the treatment of tinea cruris and tinea corporis. Int J Dermatol 1990;29:441-442.
9. Saple DG, Amar AK, Ravichandran G, Korde KM, Desai A. Efficacy and safety of butenafine in superficial dermatophytoses (tinea pedis, tinea cruris, tinea corporis). J Indian Med Assoc 2001;99:274-275.
10. Lescher JL, Babel DE, Stewart DM, et al. Butenafine 1% cream in the treatment of tinea cruris: A multicenter, vehicle-controlled, double-blind trial. J Am Acad Dermatol 1997;36:S20-S24.
11. Bogaert H, Cordero C, Ollague W, Savin RC, Shalita AR, Zaias N. Multicentre double-blind clinical trials of ciclopirox olamine cream 1% in the treatment of tinea corporis and tinea cruris. J Int Med Res 1986;14:210-216.
12. Fulton JE, Jr. Miconazole therapy for endemic fungal disease. Srch Dermatology 1975;111:596-598.
13. Ledezma E, Lopez JC, Marin P, et al. Ajoene in the topical short-term treatment of tinea cruris and tinea corporis in humans. Randomized comparative study with terbinafine. Arzneimittelforschung 1999;49:544-547.
14. Al-Waili NS. An alternative treatment for pityriasis versicolor, tinea cruris, tinea corporis and tinea faciei with topical application of honey, olive oil and beeswax mixture: an open pilot study. Complement Ther Med 2004;12:45-47.
15. The Sanford Guide to Antimicrobial Therapy. 35th ed. Hyde Park, Vt: Antimicrobial Therapy; 2005.
16. Noble S, Forbes R, Stamm P. Diagnosis and management of common tinea infections. Am Fam Physician 1998;58:163-178.Available at: www.aafp.org/afp/980700ap/noble.html. Accessed on February 9, 2006.
17. Crawford F, Hart R, Bell-Syer S, Togerson D, Young P, Russell I. Topical treatments for fungal infections of the skin and nails of the foot. Cochrane Database Syst Rev 1999;(3):CD001434.
After clinical diagnosis and microscopic confirmation, tinea cruris is best treated with a topical allylamine or an azole antifungal (strength of recommendation: A, based on multiple randomized controlled trials [RCTs]). Differences in current comparison data are insufficient to stratify the 2 groups of topical antifungals. Determining which group to use depends on patient compliance, medication accessibility, and cost. The fungicidal allylamines (naftifine and terbinafine) and butenafine (allylamine derivative) are a more costly group of topical tinea treatments, yet they are more convenient as they allow for a shorter duration of treatment compared with fungistatic azoles (clotrimazole, econazole, ketoconazole, oxiconazole, miconazole, and sulconazole).
Choice of treatment should reflect cost and convenience to the patient
Dan Hunter-Smith, MD
Adventist LaGrange Family Medicine Residency, LaGrange, Ill
This review illustrates that the “best way” to treat a problem can have more to do with the needs of a given patient than intrinsic differences between treatments. All reviewed treatments were roughly therapeutically equivalent and equally safe. This leaves the choice of treatment to reflect the importance of cost and convenience to the patient. If cost is an issue for the patient, the frugal way to treat tinea cruris is to have the patient go to the vaginitis treatment section of the pharmacy and pick up a 15-g tube of miconazole or clotrimazole cream for $7 to $10. Terbinafine cream or spray costs $10 to $13 over the counter, but it reduces the onus of compliance to once-a-day for 1 week. If terbinafine 1% solution is preferred, a 30-mL bottle costs $77. Most of the time, I let the patient make their own choice.
Evidence summary
Tinea cruris (“jock itch”) is a superficial dermatophyte infection of the groin and surrounding skin. Obese adult men are affected more than women, and it is rarely seen in children. Because excessive perspiration is the most common predisposing factor, patient education on proper hygiene makes intuitive sense for successful treatment, yet it has not been studied.1Trichophyton rubrum is the most common source of tinea cruris, as well as tinea corporis (“ringworm”), in the United States.2 Most studies involving patients with tinea cruris combine data with tinea corporis.
Although more than 25 RCTs document the safety and efficacy of antifungal treatments, few head-to-head trials are available. Several topical preparations are approved for the treatment of tinea cruris. Selection should be based on patient compliance (duration of treatment), overall cost, and tolerability. The 2 main classes of antifungals are allylamines and azoles.
Allylamines. Allylamines offer a shorter duration of therapy, lower relapse rates, and work independent of the cytochrome P450 system. Multiple RCTs have documented the efficacy and safety of the 2 available allylamine antifungals, terbinafine and naftifine, when compared with placebo and various azoles.
Terbinafine is available in several 1% formulations (emulsion-gel, cream, and solution/spray), all studied and dosed once daily for 1 week. One placebo controlled trial showed the 1% emulsion-gel version (Lamisil) was effective in 89% of the study population vs 23% of the placebo group (NNT=1.5); it was particularly suitable on hairy skin. Seven weeks post-treatment, 84% of the intent-to-treat population of the Lamisil group remained mycologically negative.3 Data combined from 2 other RCTs yielded 83% efficacy 3 weeks post-treatment when 66 patients were treated with terbinafine 1% cream, compared with 12% efficacy for 73 patients using the vehicle cream (NNT=1.4).4 Another placebo-controlled study of 66 patients demonstrated 100% microscopic cure of terbinafine 1% solution by week 2 and maintaining 90% cure at 4 weeks.5
In a multicenter, double-blind RCT funded by the manufacturers of terbinafine, bifonazole 1% cream for 3 weeks was compared with terbinafine 1% cream used daily for 1 week (followed by 2 weeks of its vehicle cream). Mycological and clinical cure rates were greater than 95% in both groups at 3 weeks. At the 8-week follow-up, no statistically significant differences were seen in KOH positivity rates (20.24% of patients in the bifonazole-treated group were KOH-positive vs 11.76% in the terbinafine group). Symptom relapse rates at 8 weeks were not available.6
In a 4-week study involving 104 patients, naftifine 1% cream (Naftin) was compared with econazole 1% cream (Spectazole) (both applied twice daily). At the end of the study, naftifine 1% cream had a higher (but not statistically significant) mycological and clinical cure rate of 78% compared with 68% with econazole 1% cream.7 Similar results (79% mycological cure) were seen in a placebo-controlled trial with 70 patients using once daily naftifine 1% cream after 2 weeks of treatment (NNT=2).8
Butenafine (Mentax), a benzylamine antifungal, was 88% to 93% mycologically effective in a noncomparative study, when used twice daily for 2 weeks.9 Similar results were found in a study of 76 patients with tinea cruris; after 2 weeks of daily application, 78% (modified intent-to-treat group) were mycologically cured. Mycological cure plus “cleared” or “excellent” clinical evaluation remained for 73% at day 42 vs 5% of the placebo group (NNT=1.47).10
Azoles. Azoles are less expensive than allylamines, but require longer treatment periods, theoretically compromising patient adherence to therapy. One of the more popular azoles is clotrimazole (Lotrimin, Mycelex), one of the oldest antifungal treatments. One RCT compared cure rates for 139 patients for clotrimazole 1% cream compared with ciclopirox olamine 1% cream when both were applied twice daily for 28 days. By the end of the 4-week period, 69% of the clotrimazole group was clinically and mycologically cured compared with 64% of the ciclopirox group.11
Miconazole 2% cream (Micatin, Monistat) (used twice daily for 2 weeks by inmates in a Florida prison) demonstrated 75.5% clinical clearing (against tinea cruris, pedis, or corporis, or Candida cutaneous infections) when compared with placebo (NNT=1.57). Of the 99 patients evaluated, 48 were diagnosed with tinea cruris; however, results were not broken down into diagnostic category. The length of follow-up for these patients was not disclosed.12
Alternative therapy. Ajoene 0.6% gel (isolated from garlic), was as effective as terbinafine 1% cream (both applied twice daily for 2 weeks) in a RCT of 60 Venezuelan Army soldiers.13 Sixty days after treatment, 73% of the Ajoene-treated patients and 71% in the terbinafine group were asymptomatic. An open-pilot study of 14 patients with tinea cruris demonstrated 71% mycological cure with a honey, olive oil, and beeswax (1:1:1) mixture, applied 3 times daily up to 3 weeks, likely due to honey’s inhibitory effect on fungus and beeswax’s anti-inflammatory properties.14
Recommendations from others
The Sanford Guide to Antimicrobial Therapy (2005) recommends topical butenafine and terbinafine as primary agents of choice for tinea cruris due to their fungicidal activity.15 The American Academy of Family Physicians recommends any of the topical antifungal treatments as first-line treatment for tinea cruris.16 A systematic review on tinea pedis topical therapy acknowledges the higher cure rates by allylamines, compared with azoles, but concludes that azoles remain the most costeffective in the treatment of tinea pedis.17 No recent guidelines from the American Academy of Dermatology are available.
After clinical diagnosis and microscopic confirmation, tinea cruris is best treated with a topical allylamine or an azole antifungal (strength of recommendation: A, based on multiple randomized controlled trials [RCTs]). Differences in current comparison data are insufficient to stratify the 2 groups of topical antifungals. Determining which group to use depends on patient compliance, medication accessibility, and cost. The fungicidal allylamines (naftifine and terbinafine) and butenafine (allylamine derivative) are a more costly group of topical tinea treatments, yet they are more convenient as they allow for a shorter duration of treatment compared with fungistatic azoles (clotrimazole, econazole, ketoconazole, oxiconazole, miconazole, and sulconazole).
Choice of treatment should reflect cost and convenience to the patient
Dan Hunter-Smith, MD
Adventist LaGrange Family Medicine Residency, LaGrange, Ill
This review illustrates that the “best way” to treat a problem can have more to do with the needs of a given patient than intrinsic differences between treatments. All reviewed treatments were roughly therapeutically equivalent and equally safe. This leaves the choice of treatment to reflect the importance of cost and convenience to the patient. If cost is an issue for the patient, the frugal way to treat tinea cruris is to have the patient go to the vaginitis treatment section of the pharmacy and pick up a 15-g tube of miconazole or clotrimazole cream for $7 to $10. Terbinafine cream or spray costs $10 to $13 over the counter, but it reduces the onus of compliance to once-a-day for 1 week. If terbinafine 1% solution is preferred, a 30-mL bottle costs $77. Most of the time, I let the patient make their own choice.
Evidence summary
Tinea cruris (“jock itch”) is a superficial dermatophyte infection of the groin and surrounding skin. Obese adult men are affected more than women, and it is rarely seen in children. Because excessive perspiration is the most common predisposing factor, patient education on proper hygiene makes intuitive sense for successful treatment, yet it has not been studied.1Trichophyton rubrum is the most common source of tinea cruris, as well as tinea corporis (“ringworm”), in the United States.2 Most studies involving patients with tinea cruris combine data with tinea corporis.
Although more than 25 RCTs document the safety and efficacy of antifungal treatments, few head-to-head trials are available. Several topical preparations are approved for the treatment of tinea cruris. Selection should be based on patient compliance (duration of treatment), overall cost, and tolerability. The 2 main classes of antifungals are allylamines and azoles.
Allylamines. Allylamines offer a shorter duration of therapy, lower relapse rates, and work independent of the cytochrome P450 system. Multiple RCTs have documented the efficacy and safety of the 2 available allylamine antifungals, terbinafine and naftifine, when compared with placebo and various azoles.
Terbinafine is available in several 1% formulations (emulsion-gel, cream, and solution/spray), all studied and dosed once daily for 1 week. One placebo controlled trial showed the 1% emulsion-gel version (Lamisil) was effective in 89% of the study population vs 23% of the placebo group (NNT=1.5); it was particularly suitable on hairy skin. Seven weeks post-treatment, 84% of the intent-to-treat population of the Lamisil group remained mycologically negative.3 Data combined from 2 other RCTs yielded 83% efficacy 3 weeks post-treatment when 66 patients were treated with terbinafine 1% cream, compared with 12% efficacy for 73 patients using the vehicle cream (NNT=1.4).4 Another placebo-controlled study of 66 patients demonstrated 100% microscopic cure of terbinafine 1% solution by week 2 and maintaining 90% cure at 4 weeks.5
In a multicenter, double-blind RCT funded by the manufacturers of terbinafine, bifonazole 1% cream for 3 weeks was compared with terbinafine 1% cream used daily for 1 week (followed by 2 weeks of its vehicle cream). Mycological and clinical cure rates were greater than 95% in both groups at 3 weeks. At the 8-week follow-up, no statistically significant differences were seen in KOH positivity rates (20.24% of patients in the bifonazole-treated group were KOH-positive vs 11.76% in the terbinafine group). Symptom relapse rates at 8 weeks were not available.6
In a 4-week study involving 104 patients, naftifine 1% cream (Naftin) was compared with econazole 1% cream (Spectazole) (both applied twice daily). At the end of the study, naftifine 1% cream had a higher (but not statistically significant) mycological and clinical cure rate of 78% compared with 68% with econazole 1% cream.7 Similar results (79% mycological cure) were seen in a placebo-controlled trial with 70 patients using once daily naftifine 1% cream after 2 weeks of treatment (NNT=2).8
Butenafine (Mentax), a benzylamine antifungal, was 88% to 93% mycologically effective in a noncomparative study, when used twice daily for 2 weeks.9 Similar results were found in a study of 76 patients with tinea cruris; after 2 weeks of daily application, 78% (modified intent-to-treat group) were mycologically cured. Mycological cure plus “cleared” or “excellent” clinical evaluation remained for 73% at day 42 vs 5% of the placebo group (NNT=1.47).10
Azoles. Azoles are less expensive than allylamines, but require longer treatment periods, theoretically compromising patient adherence to therapy. One of the more popular azoles is clotrimazole (Lotrimin, Mycelex), one of the oldest antifungal treatments. One RCT compared cure rates for 139 patients for clotrimazole 1% cream compared with ciclopirox olamine 1% cream when both were applied twice daily for 28 days. By the end of the 4-week period, 69% of the clotrimazole group was clinically and mycologically cured compared with 64% of the ciclopirox group.11
Miconazole 2% cream (Micatin, Monistat) (used twice daily for 2 weeks by inmates in a Florida prison) demonstrated 75.5% clinical clearing (against tinea cruris, pedis, or corporis, or Candida cutaneous infections) when compared with placebo (NNT=1.57). Of the 99 patients evaluated, 48 were diagnosed with tinea cruris; however, results were not broken down into diagnostic category. The length of follow-up for these patients was not disclosed.12
Alternative therapy. Ajoene 0.6% gel (isolated from garlic), was as effective as terbinafine 1% cream (both applied twice daily for 2 weeks) in a RCT of 60 Venezuelan Army soldiers.13 Sixty days after treatment, 73% of the Ajoene-treated patients and 71% in the terbinafine group were asymptomatic. An open-pilot study of 14 patients with tinea cruris demonstrated 71% mycological cure with a honey, olive oil, and beeswax (1:1:1) mixture, applied 3 times daily up to 3 weeks, likely due to honey’s inhibitory effect on fungus and beeswax’s anti-inflammatory properties.14
Recommendations from others
The Sanford Guide to Antimicrobial Therapy (2005) recommends topical butenafine and terbinafine as primary agents of choice for tinea cruris due to their fungicidal activity.15 The American Academy of Family Physicians recommends any of the topical antifungal treatments as first-line treatment for tinea cruris.16 A systematic review on tinea pedis topical therapy acknowledges the higher cure rates by allylamines, compared with azoles, but concludes that azoles remain the most costeffective in the treatment of tinea pedis.17 No recent guidelines from the American Academy of Dermatology are available.
1. Gupta AK, Chaudhry M, Elewski BE. Tinea corporis, tinea cruris, tinea nigra, and piedra. Dermatol Clin 2003;21:395-400.
2. Foster KW, Ghannoum MA, Elewski BE. Epidemiologic surveillance of cutaneous fungal infection in the United States from 1999 to 2002. J Am Acad Dermatol 2004;30:748-752.
3. van Heerden JS, Vismer HF. Tinea corporis/cruris: new treatment options. Dermatology 1997;194(Suppl 1):14-18.
4. Zaias N, Berman B, Cordero CN, et al. Efficacy of a 1-week, once daily regimen of terbinafine 1% cream in the treatment of tinea cruris and tinea corporis. J Am Acad Dermatol 1993;29:646-648.
5. Lebwohl M, Elewski B, Eisen D, Savin RC. Efficacy and safety of terbinafine 1% solution in the treatment of interdigital tinea pedis and tinea corporis or tinea cruris. Cutis 2001;67:261-266.
6. Budimulja U. Terbinafine 1% cream vs. bifonazole 1% cream in the treatment of tinea cruris. Int J Dermatol 1998;37:871-873.
7. Millikan LE, Galen WK, Gewirtzman GB, et al. Naftifine cream 1% versus econazole cream 1% in the treatment of tinea cruris and tinea corporis. J Am Acad Dermatol 1988;18(1 Pt 1):52-56.
8. Jordan RE, Rapini RP, Rex IH, Jr, et al. Once-daily naftine cream 1% in the treatment of tinea cruris and tinea corporis. Int J Dermatol 1990;29:441-442.
9. Saple DG, Amar AK, Ravichandran G, Korde KM, Desai A. Efficacy and safety of butenafine in superficial dermatophytoses (tinea pedis, tinea cruris, tinea corporis). J Indian Med Assoc 2001;99:274-275.
10. Lescher JL, Babel DE, Stewart DM, et al. Butenafine 1% cream in the treatment of tinea cruris: A multicenter, vehicle-controlled, double-blind trial. J Am Acad Dermatol 1997;36:S20-S24.
11. Bogaert H, Cordero C, Ollague W, Savin RC, Shalita AR, Zaias N. Multicentre double-blind clinical trials of ciclopirox olamine cream 1% in the treatment of tinea corporis and tinea cruris. J Int Med Res 1986;14:210-216.
12. Fulton JE, Jr. Miconazole therapy for endemic fungal disease. Srch Dermatology 1975;111:596-598.
13. Ledezma E, Lopez JC, Marin P, et al. Ajoene in the topical short-term treatment of tinea cruris and tinea corporis in humans. Randomized comparative study with terbinafine. Arzneimittelforschung 1999;49:544-547.
14. Al-Waili NS. An alternative treatment for pityriasis versicolor, tinea cruris, tinea corporis and tinea faciei with topical application of honey, olive oil and beeswax mixture: an open pilot study. Complement Ther Med 2004;12:45-47.
15. The Sanford Guide to Antimicrobial Therapy. 35th ed. Hyde Park, Vt: Antimicrobial Therapy; 2005.
16. Noble S, Forbes R, Stamm P. Diagnosis and management of common tinea infections. Am Fam Physician 1998;58:163-178.Available at: www.aafp.org/afp/980700ap/noble.html. Accessed on February 9, 2006.
17. Crawford F, Hart R, Bell-Syer S, Togerson D, Young P, Russell I. Topical treatments for fungal infections of the skin and nails of the foot. Cochrane Database Syst Rev 1999;(3):CD001434.
1. Gupta AK, Chaudhry M, Elewski BE. Tinea corporis, tinea cruris, tinea nigra, and piedra. Dermatol Clin 2003;21:395-400.
2. Foster KW, Ghannoum MA, Elewski BE. Epidemiologic surveillance of cutaneous fungal infection in the United States from 1999 to 2002. J Am Acad Dermatol 2004;30:748-752.
3. van Heerden JS, Vismer HF. Tinea corporis/cruris: new treatment options. Dermatology 1997;194(Suppl 1):14-18.
4. Zaias N, Berman B, Cordero CN, et al. Efficacy of a 1-week, once daily regimen of terbinafine 1% cream in the treatment of tinea cruris and tinea corporis. J Am Acad Dermatol 1993;29:646-648.
5. Lebwohl M, Elewski B, Eisen D, Savin RC. Efficacy and safety of terbinafine 1% solution in the treatment of interdigital tinea pedis and tinea corporis or tinea cruris. Cutis 2001;67:261-266.
6. Budimulja U. Terbinafine 1% cream vs. bifonazole 1% cream in the treatment of tinea cruris. Int J Dermatol 1998;37:871-873.
7. Millikan LE, Galen WK, Gewirtzman GB, et al. Naftifine cream 1% versus econazole cream 1% in the treatment of tinea cruris and tinea corporis. J Am Acad Dermatol 1988;18(1 Pt 1):52-56.
8. Jordan RE, Rapini RP, Rex IH, Jr, et al. Once-daily naftine cream 1% in the treatment of tinea cruris and tinea corporis. Int J Dermatol 1990;29:441-442.
9. Saple DG, Amar AK, Ravichandran G, Korde KM, Desai A. Efficacy and safety of butenafine in superficial dermatophytoses (tinea pedis, tinea cruris, tinea corporis). J Indian Med Assoc 2001;99:274-275.
10. Lescher JL, Babel DE, Stewart DM, et al. Butenafine 1% cream in the treatment of tinea cruris: A multicenter, vehicle-controlled, double-blind trial. J Am Acad Dermatol 1997;36:S20-S24.
11. Bogaert H, Cordero C, Ollague W, Savin RC, Shalita AR, Zaias N. Multicentre double-blind clinical trials of ciclopirox olamine cream 1% in the treatment of tinea corporis and tinea cruris. J Int Med Res 1986;14:210-216.
12. Fulton JE, Jr. Miconazole therapy for endemic fungal disease. Srch Dermatology 1975;111:596-598.
13. Ledezma E, Lopez JC, Marin P, et al. Ajoene in the topical short-term treatment of tinea cruris and tinea corporis in humans. Randomized comparative study with terbinafine. Arzneimittelforschung 1999;49:544-547.
14. Al-Waili NS. An alternative treatment for pityriasis versicolor, tinea cruris, tinea corporis and tinea faciei with topical application of honey, olive oil and beeswax mixture: an open pilot study. Complement Ther Med 2004;12:45-47.
15. The Sanford Guide to Antimicrobial Therapy. 35th ed. Hyde Park, Vt: Antimicrobial Therapy; 2005.
16. Noble S, Forbes R, Stamm P. Diagnosis and management of common tinea infections. Am Fam Physician 1998;58:163-178.Available at: www.aafp.org/afp/980700ap/noble.html. Accessed on February 9, 2006.
17. Crawford F, Hart R, Bell-Syer S, Togerson D, Young P, Russell I. Topical treatments for fungal infections of the skin and nails of the foot. Cochrane Database Syst Rev 1999;(3):CD001434.
Evidence-based answers from the Family Physicians Inquiries Network
What is the best way to manage GERD symptoms in the elderly?
No evidence supports one method over another in managing uncomplicated gastroesophageal reflux disease (GERD) for patients aged >65 years. For those with endoscopically documented esophagitis, proton pump inhibitors (PPIs) relieve symptoms faster than histamine H2 receptor antagonists (H2RAs) (strength of recommendation [SOR]: B, extrapolation from randomized controlled trials [RCTs]). Treating elderly patients with pantoprazole (Protonix) after resolution of acute esophagitis results in fewer relapses than with placebo (SOR: B, double-blind RCT). Limited evidence suggests that such maintenance therapy for prior esophagitis with either H2RAs or PPIs, at half- and full-dose strength,1 decreases the frequency of relapse (SOR: B, extrapolation from uncontrolled clinical trial).
Laparoscopic antireflux surgery for treating symptomatic GERD among elderly patients without paraesophageal hernia reduces esophageal acidity, with no apparent increase in postoperative morbidity or mortality compared with younger patients (SOR: C, nonequivalent before-after study). Upper endoscopy is recommended for elderly patients with alarm symptoms, new-onset GERD, or longstanding disease (SOR: C, expert consensus; see TABLE).
Elderly patients are at risk for more severe complications from GERD, and their relative discomfort from the disease process is often less than from comparable pathology for younger patients (SOR: C, expert consensus). Based on safety profiles and success in the general patient population, PPIs as a class are considered first-line treatment for GERD and esophagitis for the elderly (SOR: C, expert consensus).
Teasing out serious disease from routine GERD is a challenge in the elderly
Peter Danis, MD
St. John’s Mercy Medical Center, St. Louis, Mo
Who really needs the invasive workup and expensive medicine, and who needs the simple approach? Elderly patients can attribute symptoms to “just indigestion” when there are other more serious diseases present (ie, angina, severe esophagitis, stricture, cancer). The physician may need a more detailed and patient approach to get the “real” story. Lifestyle changes and over-the-counter medications will resolve the majority of GERD symptoms. If the simple things don’t work or there are warning signs/symptoms, then a further workup is needed. The older patient may then be willing to pay the cost of the long term PPI when they know that there is significant pathology and the potential for long term symptom relief.
Evidence summary
Aggregated data from 2 randomized reflux esophagitis trials conducted in the United Kingdom were analyzed with respect to patient age. Comparison of symptom relief and esophageal lesion healing showed that elderly patients treated with omeprazole (Prilosec) fared better than those treated with either cimetidine (Tagamet) or ranitidine (Zantac).2 The pooled data involved 555 patients with endoscopically proven reflux esophagitis, 154 of whom were over the age of 65. After 8 weeks, rates of esophageal healing among the elderly were 70% for those receiving omeprazole and 29% for those receiving H2RAs (41% difference; 95% confidence interval [CI], 26–55), while the rate of asymptomatic elderly patients was 79% for the omeprazole group and 51% for the H2RA group (28% difference; 95% CI, 12–44).3 Patients treated with omeprazole healed faster than those taking H2RAs, as shown by endoscopy, and more of them experienced symptom relief.
A multicenter, randomized, double-blind trial of GERD maintenance therapy started with an initial open phase in which elderly patients with GERD and documented esophagitis were treated and then had documented resolution of esophagitis by endoscopy after 6 months. The researchers then randomized 105 of these elderly patients to receive treatment with either low-dose (20 mg/d) pantoprazole or placebo for 6 months. Endoscopy was performed after 12 months for all patients, unless indicated sooner. Intention-to-treat analysis showed a disease-free rate of 79.6% (95% CI, 68.3–90.9) in the treatment group, compared with 30.4% (95% CI, 18.3–42.4) in the placebo group (number needed to treat [NNT]=2). Symptom reports concerning the same patients also suggest a marked drop in symptoms that correlated with healing.4
A prospective, nonequivalence, before-after study compared efficacy of, and complications from, laparoscopic surgery for symptomatic GERD between younger and older (≥65 years) patients. The investigators examined postoperative morbidity and mortality for 359 patients referred for laparoscopic surgery, either a partial or Nissen (full) fundoplication. They excluded those requiring more extensive surgery or repair of paraesophageal hernia. The 42 elderly patients had a higher mean American Society of Anesthesiologists score compared with the younger patients, reflecting higher preoperative comorbidity, but were similar with regard to weight and gender.
Before surgery, investigators performed 24-hour ambulatory pH monitoring. Preoperative exposure times to a pH below 4 (TpH <4) were similar for the younger and older patients (median 14.2% and 13.9%, respectively). Postoperative complication rates were similar for both groups. No deaths occurred. Minor postoperative complications involved 7% of the elderly patients and 6% of the younger group. The 24-hour pH monitoring scores showed improvement at 6 weeks after surgery for both groups, with the median TpH <4 at 1.1% (95% CL, 0.5) in the elderly vs a median of 1.8% (95% CL, 1.9) in the younger patients. At 1 year postoperatively, the values were also similar between the two groups; the median TpH <4 (95% CL) were 1.4% (1.5) in the elderly group and 1.2% (0.6) in the younger patient group.
The results of this study should be interpreted with caution, however. The study design is prone to bias, the patients had relatively low symptom scores at baseline, and sicker patients may have been excluded during the referral process.5
TABLE
Warning signs and symptoms of dyspepsia and GERD that suggest complicated disease or more serious underlying process1
| Dysphagia |
| Unexplained weight loss |
| History of gastrointestinal bleeding |
| Early satiety |
| Iron deficiency anemia |
| Vomiting |
| Odynophagia (sharp substernal pain on swallowing) |
| Initial onset of heartburn-like symptoms after the age of 50 years |
| History of immunocompromised state |
| Anorexia |
Recommendations from others
The Veterans Health Affairs/Department of Defense clinical practice guidelines recommend differentiating GERD (feelings of substernal burning associated with acid regurgitation) from dyspepsia (chronic or recurrent discomfort centered in the upper abdomen), of which GERD is a subset.6 The guidelines recommend gastroenterology consultation or upper endoscopy to rule out neoplastic or pre-neoplastic lesions if alarm symptoms (TABLE) suggesting complicated GERD are present.7
The Institute for Clinical Systems Improvement guidelines on dyspepsia and GERD recommend that all patients aged ≥50 years with symptoms of uncomplicated dyspepsia undergo upper endoscopy non-urgently because of the increased incidence of peptic ulcer disease, pre-neoplastic lesions, malignancy, and increased morbidity out of proportion to symptoms that are more common in an older patient population. The guidelines also recommend endoscopy for patients aged ≥50 years with uncomplicated GERD and the presence of symptoms for greater than 10 years because of the increased risk of pre-neoplastic and neoplastic lesions, including Barrett’s esophagus.8
1. Pilotto A, Franceschi M, Leandro G, et al. Long-term clinical outcome of elderly patients with reflux esophagitis: a six-month to three-year follow-up study. Am J Ther 2002;9:295-300.
2. James OF, Parry-Billings K. Comparison of omeprazole and histamine H2–receptor antagonists in the treatment of elderly and young patients with reflux oesophagitis. Age Aging 1994;23:121-126.
3. Omeprazole was better than H2-antagonists in reflux esophagitis. ACP Journal Club 1994;121:65.-
4. Pilotto A, Leandro G, Franceschi M. Short and long term therapy for reflux oesophagitis in the elderly: a multicentre, placebo-controlled study with pantoprazole. Aliment Pharmacol Ther 2003;17:1399-1406.
5. Trus TL, Laycock WS, Wo JM, et al. Laparoscopic antireflux surgery in the elderly. Am J Gastroenterol 1998;93:351-353.
6. Bazaldua OV, Schneider FD. Evaluation and management of dyspepsia. Am Fam Physician 1999;60:1773-1784.
7. VHA/DoD Clinical Practice Guideline for the Management of Adults with Gastroesophageal Reflux Disease in Primary Care Practice. Washington, DC: Veterans Health Administration, Department of Defense; 2003 March 12. Available at: www.guideline.gov/summary/summary.aspx?ss=15&doc_id=5188&nbr=3570#s25. Accessed on February 9, 2006.
8. Institute for Clinical Systems Improvement (ICSI). Dyspepsia and GERD. Bloomington, Minn: ICSI Guidelines; July 2004. Available at: www.guideline.gov/summary/summary.aspx?doc_id=5624. Accessed on February 9, 2006.
No evidence supports one method over another in managing uncomplicated gastroesophageal reflux disease (GERD) for patients aged >65 years. For those with endoscopically documented esophagitis, proton pump inhibitors (PPIs) relieve symptoms faster than histamine H2 receptor antagonists (H2RAs) (strength of recommendation [SOR]: B, extrapolation from randomized controlled trials [RCTs]). Treating elderly patients with pantoprazole (Protonix) after resolution of acute esophagitis results in fewer relapses than with placebo (SOR: B, double-blind RCT). Limited evidence suggests that such maintenance therapy for prior esophagitis with either H2RAs or PPIs, at half- and full-dose strength,1 decreases the frequency of relapse (SOR: B, extrapolation from uncontrolled clinical trial).
Laparoscopic antireflux surgery for treating symptomatic GERD among elderly patients without paraesophageal hernia reduces esophageal acidity, with no apparent increase in postoperative morbidity or mortality compared with younger patients (SOR: C, nonequivalent before-after study). Upper endoscopy is recommended for elderly patients with alarm symptoms, new-onset GERD, or longstanding disease (SOR: C, expert consensus; see TABLE).
Elderly patients are at risk for more severe complications from GERD, and their relative discomfort from the disease process is often less than from comparable pathology for younger patients (SOR: C, expert consensus). Based on safety profiles and success in the general patient population, PPIs as a class are considered first-line treatment for GERD and esophagitis for the elderly (SOR: C, expert consensus).
Teasing out serious disease from routine GERD is a challenge in the elderly
Peter Danis, MD
St. John’s Mercy Medical Center, St. Louis, Mo
Who really needs the invasive workup and expensive medicine, and who needs the simple approach? Elderly patients can attribute symptoms to “just indigestion” when there are other more serious diseases present (ie, angina, severe esophagitis, stricture, cancer). The physician may need a more detailed and patient approach to get the “real” story. Lifestyle changes and over-the-counter medications will resolve the majority of GERD symptoms. If the simple things don’t work or there are warning signs/symptoms, then a further workup is needed. The older patient may then be willing to pay the cost of the long term PPI when they know that there is significant pathology and the potential for long term symptom relief.
Evidence summary
Aggregated data from 2 randomized reflux esophagitis trials conducted in the United Kingdom were analyzed with respect to patient age. Comparison of symptom relief and esophageal lesion healing showed that elderly patients treated with omeprazole (Prilosec) fared better than those treated with either cimetidine (Tagamet) or ranitidine (Zantac).2 The pooled data involved 555 patients with endoscopically proven reflux esophagitis, 154 of whom were over the age of 65. After 8 weeks, rates of esophageal healing among the elderly were 70% for those receiving omeprazole and 29% for those receiving H2RAs (41% difference; 95% confidence interval [CI], 26–55), while the rate of asymptomatic elderly patients was 79% for the omeprazole group and 51% for the H2RA group (28% difference; 95% CI, 12–44).3 Patients treated with omeprazole healed faster than those taking H2RAs, as shown by endoscopy, and more of them experienced symptom relief.
A multicenter, randomized, double-blind trial of GERD maintenance therapy started with an initial open phase in which elderly patients with GERD and documented esophagitis were treated and then had documented resolution of esophagitis by endoscopy after 6 months. The researchers then randomized 105 of these elderly patients to receive treatment with either low-dose (20 mg/d) pantoprazole or placebo for 6 months. Endoscopy was performed after 12 months for all patients, unless indicated sooner. Intention-to-treat analysis showed a disease-free rate of 79.6% (95% CI, 68.3–90.9) in the treatment group, compared with 30.4% (95% CI, 18.3–42.4) in the placebo group (number needed to treat [NNT]=2). Symptom reports concerning the same patients also suggest a marked drop in symptoms that correlated with healing.4
A prospective, nonequivalence, before-after study compared efficacy of, and complications from, laparoscopic surgery for symptomatic GERD between younger and older (≥65 years) patients. The investigators examined postoperative morbidity and mortality for 359 patients referred for laparoscopic surgery, either a partial or Nissen (full) fundoplication. They excluded those requiring more extensive surgery or repair of paraesophageal hernia. The 42 elderly patients had a higher mean American Society of Anesthesiologists score compared with the younger patients, reflecting higher preoperative comorbidity, but were similar with regard to weight and gender.
Before surgery, investigators performed 24-hour ambulatory pH monitoring. Preoperative exposure times to a pH below 4 (TpH <4) were similar for the younger and older patients (median 14.2% and 13.9%, respectively). Postoperative complication rates were similar for both groups. No deaths occurred. Minor postoperative complications involved 7% of the elderly patients and 6% of the younger group. The 24-hour pH monitoring scores showed improvement at 6 weeks after surgery for both groups, with the median TpH <4 at 1.1% (95% CL, 0.5) in the elderly vs a median of 1.8% (95% CL, 1.9) in the younger patients. At 1 year postoperatively, the values were also similar between the two groups; the median TpH <4 (95% CL) were 1.4% (1.5) in the elderly group and 1.2% (0.6) in the younger patient group.
The results of this study should be interpreted with caution, however. The study design is prone to bias, the patients had relatively low symptom scores at baseline, and sicker patients may have been excluded during the referral process.5
TABLE
Warning signs and symptoms of dyspepsia and GERD that suggest complicated disease or more serious underlying process1
| Dysphagia |
| Unexplained weight loss |
| History of gastrointestinal bleeding |
| Early satiety |
| Iron deficiency anemia |
| Vomiting |
| Odynophagia (sharp substernal pain on swallowing) |
| Initial onset of heartburn-like symptoms after the age of 50 years |
| History of immunocompromised state |
| Anorexia |
Recommendations from others
The Veterans Health Affairs/Department of Defense clinical practice guidelines recommend differentiating GERD (feelings of substernal burning associated with acid regurgitation) from dyspepsia (chronic or recurrent discomfort centered in the upper abdomen), of which GERD is a subset.6 The guidelines recommend gastroenterology consultation or upper endoscopy to rule out neoplastic or pre-neoplastic lesions if alarm symptoms (TABLE) suggesting complicated GERD are present.7
The Institute for Clinical Systems Improvement guidelines on dyspepsia and GERD recommend that all patients aged ≥50 years with symptoms of uncomplicated dyspepsia undergo upper endoscopy non-urgently because of the increased incidence of peptic ulcer disease, pre-neoplastic lesions, malignancy, and increased morbidity out of proportion to symptoms that are more common in an older patient population. The guidelines also recommend endoscopy for patients aged ≥50 years with uncomplicated GERD and the presence of symptoms for greater than 10 years because of the increased risk of pre-neoplastic and neoplastic lesions, including Barrett’s esophagus.8
No evidence supports one method over another in managing uncomplicated gastroesophageal reflux disease (GERD) for patients aged >65 years. For those with endoscopically documented esophagitis, proton pump inhibitors (PPIs) relieve symptoms faster than histamine H2 receptor antagonists (H2RAs) (strength of recommendation [SOR]: B, extrapolation from randomized controlled trials [RCTs]). Treating elderly patients with pantoprazole (Protonix) after resolution of acute esophagitis results in fewer relapses than with placebo (SOR: B, double-blind RCT). Limited evidence suggests that such maintenance therapy for prior esophagitis with either H2RAs or PPIs, at half- and full-dose strength,1 decreases the frequency of relapse (SOR: B, extrapolation from uncontrolled clinical trial).
Laparoscopic antireflux surgery for treating symptomatic GERD among elderly patients without paraesophageal hernia reduces esophageal acidity, with no apparent increase in postoperative morbidity or mortality compared with younger patients (SOR: C, nonequivalent before-after study). Upper endoscopy is recommended for elderly patients with alarm symptoms, new-onset GERD, or longstanding disease (SOR: C, expert consensus; see TABLE).
Elderly patients are at risk for more severe complications from GERD, and their relative discomfort from the disease process is often less than from comparable pathology for younger patients (SOR: C, expert consensus). Based on safety profiles and success in the general patient population, PPIs as a class are considered first-line treatment for GERD and esophagitis for the elderly (SOR: C, expert consensus).
Teasing out serious disease from routine GERD is a challenge in the elderly
Peter Danis, MD
St. John’s Mercy Medical Center, St. Louis, Mo
Who really needs the invasive workup and expensive medicine, and who needs the simple approach? Elderly patients can attribute symptoms to “just indigestion” when there are other more serious diseases present (ie, angina, severe esophagitis, stricture, cancer). The physician may need a more detailed and patient approach to get the “real” story. Lifestyle changes and over-the-counter medications will resolve the majority of GERD symptoms. If the simple things don’t work or there are warning signs/symptoms, then a further workup is needed. The older patient may then be willing to pay the cost of the long term PPI when they know that there is significant pathology and the potential for long term symptom relief.
Evidence summary
Aggregated data from 2 randomized reflux esophagitis trials conducted in the United Kingdom were analyzed with respect to patient age. Comparison of symptom relief and esophageal lesion healing showed that elderly patients treated with omeprazole (Prilosec) fared better than those treated with either cimetidine (Tagamet) or ranitidine (Zantac).2 The pooled data involved 555 patients with endoscopically proven reflux esophagitis, 154 of whom were over the age of 65. After 8 weeks, rates of esophageal healing among the elderly were 70% for those receiving omeprazole and 29% for those receiving H2RAs (41% difference; 95% confidence interval [CI], 26–55), while the rate of asymptomatic elderly patients was 79% for the omeprazole group and 51% for the H2RA group (28% difference; 95% CI, 12–44).3 Patients treated with omeprazole healed faster than those taking H2RAs, as shown by endoscopy, and more of them experienced symptom relief.
A multicenter, randomized, double-blind trial of GERD maintenance therapy started with an initial open phase in which elderly patients with GERD and documented esophagitis were treated and then had documented resolution of esophagitis by endoscopy after 6 months. The researchers then randomized 105 of these elderly patients to receive treatment with either low-dose (20 mg/d) pantoprazole or placebo for 6 months. Endoscopy was performed after 12 months for all patients, unless indicated sooner. Intention-to-treat analysis showed a disease-free rate of 79.6% (95% CI, 68.3–90.9) in the treatment group, compared with 30.4% (95% CI, 18.3–42.4) in the placebo group (number needed to treat [NNT]=2). Symptom reports concerning the same patients also suggest a marked drop in symptoms that correlated with healing.4
A prospective, nonequivalence, before-after study compared efficacy of, and complications from, laparoscopic surgery for symptomatic GERD between younger and older (≥65 years) patients. The investigators examined postoperative morbidity and mortality for 359 patients referred for laparoscopic surgery, either a partial or Nissen (full) fundoplication. They excluded those requiring more extensive surgery or repair of paraesophageal hernia. The 42 elderly patients had a higher mean American Society of Anesthesiologists score compared with the younger patients, reflecting higher preoperative comorbidity, but were similar with regard to weight and gender.
Before surgery, investigators performed 24-hour ambulatory pH monitoring. Preoperative exposure times to a pH below 4 (TpH <4) were similar for the younger and older patients (median 14.2% and 13.9%, respectively). Postoperative complication rates were similar for both groups. No deaths occurred. Minor postoperative complications involved 7% of the elderly patients and 6% of the younger group. The 24-hour pH monitoring scores showed improvement at 6 weeks after surgery for both groups, with the median TpH <4 at 1.1% (95% CL, 0.5) in the elderly vs a median of 1.8% (95% CL, 1.9) in the younger patients. At 1 year postoperatively, the values were also similar between the two groups; the median TpH <4 (95% CL) were 1.4% (1.5) in the elderly group and 1.2% (0.6) in the younger patient group.
The results of this study should be interpreted with caution, however. The study design is prone to bias, the patients had relatively low symptom scores at baseline, and sicker patients may have been excluded during the referral process.5
TABLE
Warning signs and symptoms of dyspepsia and GERD that suggest complicated disease or more serious underlying process1
| Dysphagia |
| Unexplained weight loss |
| History of gastrointestinal bleeding |
| Early satiety |
| Iron deficiency anemia |
| Vomiting |
| Odynophagia (sharp substernal pain on swallowing) |
| Initial onset of heartburn-like symptoms after the age of 50 years |
| History of immunocompromised state |
| Anorexia |
Recommendations from others
The Veterans Health Affairs/Department of Defense clinical practice guidelines recommend differentiating GERD (feelings of substernal burning associated with acid regurgitation) from dyspepsia (chronic or recurrent discomfort centered in the upper abdomen), of which GERD is a subset.6 The guidelines recommend gastroenterology consultation or upper endoscopy to rule out neoplastic or pre-neoplastic lesions if alarm symptoms (TABLE) suggesting complicated GERD are present.7
The Institute for Clinical Systems Improvement guidelines on dyspepsia and GERD recommend that all patients aged ≥50 years with symptoms of uncomplicated dyspepsia undergo upper endoscopy non-urgently because of the increased incidence of peptic ulcer disease, pre-neoplastic lesions, malignancy, and increased morbidity out of proportion to symptoms that are more common in an older patient population. The guidelines also recommend endoscopy for patients aged ≥50 years with uncomplicated GERD and the presence of symptoms for greater than 10 years because of the increased risk of pre-neoplastic and neoplastic lesions, including Barrett’s esophagus.8
1. Pilotto A, Franceschi M, Leandro G, et al. Long-term clinical outcome of elderly patients with reflux esophagitis: a six-month to three-year follow-up study. Am J Ther 2002;9:295-300.
2. James OF, Parry-Billings K. Comparison of omeprazole and histamine H2–receptor antagonists in the treatment of elderly and young patients with reflux oesophagitis. Age Aging 1994;23:121-126.
3. Omeprazole was better than H2-antagonists in reflux esophagitis. ACP Journal Club 1994;121:65.-
4. Pilotto A, Leandro G, Franceschi M. Short and long term therapy for reflux oesophagitis in the elderly: a multicentre, placebo-controlled study with pantoprazole. Aliment Pharmacol Ther 2003;17:1399-1406.
5. Trus TL, Laycock WS, Wo JM, et al. Laparoscopic antireflux surgery in the elderly. Am J Gastroenterol 1998;93:351-353.
6. Bazaldua OV, Schneider FD. Evaluation and management of dyspepsia. Am Fam Physician 1999;60:1773-1784.
7. VHA/DoD Clinical Practice Guideline for the Management of Adults with Gastroesophageal Reflux Disease in Primary Care Practice. Washington, DC: Veterans Health Administration, Department of Defense; 2003 March 12. Available at: www.guideline.gov/summary/summary.aspx?ss=15&doc_id=5188&nbr=3570#s25. Accessed on February 9, 2006.
8. Institute for Clinical Systems Improvement (ICSI). Dyspepsia and GERD. Bloomington, Minn: ICSI Guidelines; July 2004. Available at: www.guideline.gov/summary/summary.aspx?doc_id=5624. Accessed on February 9, 2006.
1. Pilotto A, Franceschi M, Leandro G, et al. Long-term clinical outcome of elderly patients with reflux esophagitis: a six-month to three-year follow-up study. Am J Ther 2002;9:295-300.
2. James OF, Parry-Billings K. Comparison of omeprazole and histamine H2–receptor antagonists in the treatment of elderly and young patients with reflux oesophagitis. Age Aging 1994;23:121-126.
3. Omeprazole was better than H2-antagonists in reflux esophagitis. ACP Journal Club 1994;121:65.-
4. Pilotto A, Leandro G, Franceschi M. Short and long term therapy for reflux oesophagitis in the elderly: a multicentre, placebo-controlled study with pantoprazole. Aliment Pharmacol Ther 2003;17:1399-1406.
5. Trus TL, Laycock WS, Wo JM, et al. Laparoscopic antireflux surgery in the elderly. Am J Gastroenterol 1998;93:351-353.
6. Bazaldua OV, Schneider FD. Evaluation and management of dyspepsia. Am Fam Physician 1999;60:1773-1784.
7. VHA/DoD Clinical Practice Guideline for the Management of Adults with Gastroesophageal Reflux Disease in Primary Care Practice. Washington, DC: Veterans Health Administration, Department of Defense; 2003 March 12. Available at: www.guideline.gov/summary/summary.aspx?ss=15&doc_id=5188&nbr=3570#s25. Accessed on February 9, 2006.
8. Institute for Clinical Systems Improvement (ICSI). Dyspepsia and GERD. Bloomington, Minn: ICSI Guidelines; July 2004. Available at: www.guideline.gov/summary/summary.aspx?doc_id=5624. Accessed on February 9, 2006.
Evidence-based answers from the Family Physicians Inquiries Network
How should patients with Barrett’s esophagus be monitored?
Some patients who have been diagnosed with Barrett’s esophagus will develop dysplasia and, in some cases, esophageal carcinoma (strength of recommendation [SOR]: A, based on consistent cohort studies). Endoscopic surveillance is recommended for all patients with Barrett’s esophagus as it is superior to other methods for detecting esophageal cancer (SOR: B, based on systematic review). The degree of dysplasia noted on biopsy specimens correlates with the risk of esophageal carcinoma development and should guide the frequency of subsequent evaluations (SOR: B, based on consistent cohort studies). The optimal frequency of endoscopy has yet to be determined in any randomized trial.
Recommendations from the 2002 American College of Gastroenterology (ACG) Practice Guideline provide guidance as to the frequency of endoscopy surveillance but were not based on an explicit systematic review of the literature (SOR: C, based on expert opinion; see TABLE 1).
Reduced monitoring for most patients with Barrett’s esophagus appears safe
Paul Crawford, MD
USAF–Eglin Family Practice Residency, Eglin Air Force Base, Fla
Family physicians have long been at the mercy of expert opinion when considering how to monitor patients with Barrett’s esophagus. This review of the evidence clearly shows that the days of yearly EGD for all Barrett’s esophagus patients are over.
Unlike other conditions—such as cervical dysplasia, where monitoring and therapies to remove dysplasia are proven to save lives—Barrett’s esophagus progresses slowly and unpredictably. Thus, until technological advances allow identification of higher risk Barrett’s esophagus patients, an EGD every 3 years for those without dysplasia seems to be a reasonable monitoring interval. Perhaps most importantly, family physicians can reassure Barrett’s esophagus patients in the community that they are likely to live a normal lifespan and die of something other than esophageal cancer.
Evidence summary
Barrett’s esophagus has been defined as “a change in the esophageal epithelium of any length that can be recognized at endoscopy and is confirmed to have intestinal metaplasia by biopsy of the tubular esophagus.”1 Intestinal metaplasia is a premalignant lesion for adenocarcinoma of the esophagus. Surveillance by serial endoscopy with biopsy has been recommended in an effort to find high-grade dysplasia or carcinoma in an early, asymptomatic, and potentially curable stage.1-4 Approximately 75% of patients involved in a Barrett’s esophagus surveillance program will present with resectable tumors, compared with only 25% of those not receiving surveillance.4
A recent systematic review assessing screening tools for esophageal carcinoma found standard endoscopy to be superior (90%–100% sensitivity) to other less invasive methods such as questionnaire (60%–70%), and fecal occult blood testing (20%).4 Additional endoscopy tools such as brush and balloon cytology increased the cost of surveillance without any improvement in diagnostic yield.
The degree of dysplasia on esophageal biopsy in Barrett’s esophagus patients is currently the best indicator of risk of progression to esophageal carcinoma. The data reviewed by the ACG for the practice guideline was drawn from several prospective studies and one available registry. In sum, a total of 783 Barrett’s esophagus patients were followed for a mean of 2.9 to 7.3 years. Esophageal carcinoma developed in 2% of patients with no dysplasia, 7% of patients with low-grade dysplasia (LGD) and 22% of patients with high-grade dysplasia (HGD).1 The ACG recommendations regarding frequency of esophagogastroduodenoscopy (EGD) were not based on an explicit critical appraisal of the literature. Recent cohort studies are consistent with recommendations for graded surveillance frequency. A randomized clinical trial to determine optimal endoscopic frequency and benefit has not been reported.
Several concerns have been raised regarding the utility of degree of dysplasia in determining optimal frequency of endoscopic surveillance. First, the progression of esophageal lesions over time is unpredictable. Skacel et al5 reported a series of 34 patients with LGD at initial pathologic examination. On subsequent surveillance endoscopy with repeat biopsy, 73% no longer demonstrated dysplasia. Such patients can be allowed to return to having surveillance every 3 years.
In addition to the non-linear progression of dysplasia, inter-rater reliability of the interpretation of pathology specimens varies substantially. Adequate reliability has been demonstrated among pathologists assigning results to 2 categories (either no dysplasia and LGD or HGD and carcinoma) (κ=0.7). Assignment to four distinct pathologic grades, however, was not reliable (κ=0.46, where 1.0 is complete agreement).1 In order to make a diagnosis of HGD or carcinoma, interpretation must be independently confirmed by 2 expert pathologists.1-3
Recommendations for frequent endoscopic surveillance are also weakened by the overall low rate of mortality from esophageal carcinoma noted in Barrett’s esophagus patients. A recent population based study demonstrated that there was no difference in overall mortality in those with a Barrett’s esophagus diagnosis compared with the general population.6 An increased risk of death from esophageal carcinoma was seen in patients with Barrett’s esophagus (4.7% seen in Barrett’s esophagus patients compared with 0.8% predicted in the general population; P<.05). The overall increased effect on mortality, however, was relatively small. Esophageal carcinoma accounted for less then 5% of deaths in Barrett’s esophagus patients reported during the study’s 6-year follow-up period.
Data from prospective studies published after 2002 may better predict prognosis for Barrett’s esophagus patients.6-9 Even lower rates of progression to esophageal carcinoma (<0.5% a year or <1/220 patient-years) have been reported in these studies drawing from the general population rather than referred patients, likely stemming from differences in gender mix, patient age, and risk factors.
In addition to grade of dysplasia, the length of the dysplastic Barrett’s esophagus segment is emerging as a potentially predictive risk factor. While the ACG cautions that esophageal cancer has been reported in patients with so-called “short segment” Barrett’s esophagus (SSBE) (≤3 cm),1 recent prospective studies have shown an increased risk of carcinoma development with long segment Barrett’s esophagus (LSBE).7-9 Weston et al7 reported a 2.4% progression rate to HGD or esophageal carcinoma with SSBE and no dysplasia compared with 6.8% with LSBE (P=.002). If patients had LGD, the rate of progression to esophageal carcinoma with SSBE was 5.3% and jumped to 35% in patients with LSBE (P<.001). Conio et al8 reported that 4 of 5 cases of esophageal carcinoma noted through surveillance had LSBE. Hage et al9 reported a significantly increased risk of progression to HGD or esophageal carcinoma with long segment disease (P<.02).
While currently still considered investigational, DNA content flow cytometry may be a future tool used in risk stratification. Reid et al10 report a 5-year cumulative risk of esophageal carcinoma of 1.7% in Barrett’s esophagus patients with negative, low-grade or indefinite grades of dysplasia. Subsequent application of flow cytometry allowed for further stratification of these low-risk patients. Those with neither aneuploidy nor an increased 4N had a 5-year cumulative risk of cancer of 0% while the risk for those with abnormalities on cytometry increased to 28% (relative risk=19; P<.001).
TABLE
Grade of dysplasia and recommendations for Barrett’s esophagus surveillance as proposed by the ACG
| DYSPLASIA | DOCUMENTATION | FOLLOW-UP ENDOSCOPY |
|---|---|---|
| None | Two EGDs with biopsy | 3 years |
| Low-grade | Highest grade on repeat | 1 year until no dysplasia |
| High-grade | Repeat EGD with biopsy to rule out cancer/document high-grade dysplasia; expert pathologist confirmation | Focal: every 3 months |
| Multifocal: intervention | ||
| Mucosal irregularity: EMR | ||
| ACG, American College of Gastroenterology; EGD, esophagogastroduodenoscopy; EMR, endoscopic mucosal resection. Intervention: ie, esophagectomy. Ablative therapies only in the setting of a clinical trial or for those unable to tolerate surgery. | ||
Recommendations from others
The French Society of Digestive Endoscopy has published guidelines on monitoring Barrett’s esophagus.3 Their recommendations differ only slightly from the ACG in advocating a slightly increased frequency of EGD surveillance based on degree of dysplasia, and utilizing the length of the dysplastic segment in decision-making. Neither the American Academy of Family Physicians nor the US Preventive Services Task Force make any specific recommendations about Barrett’s esophagus surveillance.
1. Sampliner RE. Updated guidelines for the diagnosis, surveillance, and therapy of Barrett’s esophagus. Am J Gastroenterol 2002;97:1888-1895.
2. Management of Barrett’s esophagus. The Society for Surgery of the Alimentary Tract (SSAT), American Gastroenterological Association (AGA), American Society for Gastrointestinal Endoscopy (ASGE) Consensus Panel. J Gastrointest Surg 2000;4:115-116.
3. Boyer J, Robaszkiewicz M. Guidelines of the French Society of Digestive Endoscopy: Monitoring of Barrett’s esophagus. The Council of the French Society of Digestive Endoscopy. Endoscopy 2000;32:498-499.
4. Gerson LB, Triadafilopoulos G. Screening for esophageal adenocarcinoma: an evidence-based approach. Am J Med 2002;113:499-505.
5. Skacel M, Petras RE, Gramlich TL, et al. The diagnosis of low grade dysplasia in Barrett’s esophagus and its implications for disease progression. Am J Gastroenterol 2000;95:3383-3387.
6. Anderson LA, Murray LJ, Murphy SJ, et al. Mortality in Barrett’s oesophagus: results from a population based study. Gut 2003;52:1081-1084.
7. Weston AP, Sharma P, Mathur S, et al. Risk stratification of barrett’s esophagus: updated prospective multivariate analysis. Am J Gastroenterol 2004;99:1657-1666.
8. Conio M, Blanchi S, Laertosa G, et al. Long-term endoscopic surveillance of patients with Barrett’s esophagus. Incidence of dysplasia and adenocarcinoma: a prospective study. Am J Gastroenterol 2003;98:1931-1939.
9. Hage M, Siersema PD, van Dekken H, Steyerber EW, Dees J, Kuipers EJ. Oesophageal cancer incidence and mortality in patients with long-segment Barrett’s oesophagus after a mean follow-up of 12.7 years. Scand J Gastroenterol 2004;39:1175-1179.
10. Reid BJ, Levine DS, Longton G, Blount P, Rabinovitch PS. Predictors of progression to cancer in Barrett’s esophagus: baseline histology and flow cytometry identify low- and high-risk patient subsets. Am J Gastroenterol 2000;95:1669-1676.
Some patients who have been diagnosed with Barrett’s esophagus will develop dysplasia and, in some cases, esophageal carcinoma (strength of recommendation [SOR]: A, based on consistent cohort studies). Endoscopic surveillance is recommended for all patients with Barrett’s esophagus as it is superior to other methods for detecting esophageal cancer (SOR: B, based on systematic review). The degree of dysplasia noted on biopsy specimens correlates with the risk of esophageal carcinoma development and should guide the frequency of subsequent evaluations (SOR: B, based on consistent cohort studies). The optimal frequency of endoscopy has yet to be determined in any randomized trial.
Recommendations from the 2002 American College of Gastroenterology (ACG) Practice Guideline provide guidance as to the frequency of endoscopy surveillance but were not based on an explicit systematic review of the literature (SOR: C, based on expert opinion; see TABLE 1).
Reduced monitoring for most patients with Barrett’s esophagus appears safe
Paul Crawford, MD
USAF–Eglin Family Practice Residency, Eglin Air Force Base, Fla
Family physicians have long been at the mercy of expert opinion when considering how to monitor patients with Barrett’s esophagus. This review of the evidence clearly shows that the days of yearly EGD for all Barrett’s esophagus patients are over.
Unlike other conditions—such as cervical dysplasia, where monitoring and therapies to remove dysplasia are proven to save lives—Barrett’s esophagus progresses slowly and unpredictably. Thus, until technological advances allow identification of higher risk Barrett’s esophagus patients, an EGD every 3 years for those without dysplasia seems to be a reasonable monitoring interval. Perhaps most importantly, family physicians can reassure Barrett’s esophagus patients in the community that they are likely to live a normal lifespan and die of something other than esophageal cancer.
Evidence summary
Barrett’s esophagus has been defined as “a change in the esophageal epithelium of any length that can be recognized at endoscopy and is confirmed to have intestinal metaplasia by biopsy of the tubular esophagus.”1 Intestinal metaplasia is a premalignant lesion for adenocarcinoma of the esophagus. Surveillance by serial endoscopy with biopsy has been recommended in an effort to find high-grade dysplasia or carcinoma in an early, asymptomatic, and potentially curable stage.1-4 Approximately 75% of patients involved in a Barrett’s esophagus surveillance program will present with resectable tumors, compared with only 25% of those not receiving surveillance.4
A recent systematic review assessing screening tools for esophageal carcinoma found standard endoscopy to be superior (90%–100% sensitivity) to other less invasive methods such as questionnaire (60%–70%), and fecal occult blood testing (20%).4 Additional endoscopy tools such as brush and balloon cytology increased the cost of surveillance without any improvement in diagnostic yield.
The degree of dysplasia on esophageal biopsy in Barrett’s esophagus patients is currently the best indicator of risk of progression to esophageal carcinoma. The data reviewed by the ACG for the practice guideline was drawn from several prospective studies and one available registry. In sum, a total of 783 Barrett’s esophagus patients were followed for a mean of 2.9 to 7.3 years. Esophageal carcinoma developed in 2% of patients with no dysplasia, 7% of patients with low-grade dysplasia (LGD) and 22% of patients with high-grade dysplasia (HGD).1 The ACG recommendations regarding frequency of esophagogastroduodenoscopy (EGD) were not based on an explicit critical appraisal of the literature. Recent cohort studies are consistent with recommendations for graded surveillance frequency. A randomized clinical trial to determine optimal endoscopic frequency and benefit has not been reported.
Several concerns have been raised regarding the utility of degree of dysplasia in determining optimal frequency of endoscopic surveillance. First, the progression of esophageal lesions over time is unpredictable. Skacel et al5 reported a series of 34 patients with LGD at initial pathologic examination. On subsequent surveillance endoscopy with repeat biopsy, 73% no longer demonstrated dysplasia. Such patients can be allowed to return to having surveillance every 3 years.
In addition to the non-linear progression of dysplasia, inter-rater reliability of the interpretation of pathology specimens varies substantially. Adequate reliability has been demonstrated among pathologists assigning results to 2 categories (either no dysplasia and LGD or HGD and carcinoma) (κ=0.7). Assignment to four distinct pathologic grades, however, was not reliable (κ=0.46, where 1.0 is complete agreement).1 In order to make a diagnosis of HGD or carcinoma, interpretation must be independently confirmed by 2 expert pathologists.1-3
Recommendations for frequent endoscopic surveillance are also weakened by the overall low rate of mortality from esophageal carcinoma noted in Barrett’s esophagus patients. A recent population based study demonstrated that there was no difference in overall mortality in those with a Barrett’s esophagus diagnosis compared with the general population.6 An increased risk of death from esophageal carcinoma was seen in patients with Barrett’s esophagus (4.7% seen in Barrett’s esophagus patients compared with 0.8% predicted in the general population; P<.05). The overall increased effect on mortality, however, was relatively small. Esophageal carcinoma accounted for less then 5% of deaths in Barrett’s esophagus patients reported during the study’s 6-year follow-up period.
Data from prospective studies published after 2002 may better predict prognosis for Barrett’s esophagus patients.6-9 Even lower rates of progression to esophageal carcinoma (<0.5% a year or <1/220 patient-years) have been reported in these studies drawing from the general population rather than referred patients, likely stemming from differences in gender mix, patient age, and risk factors.
In addition to grade of dysplasia, the length of the dysplastic Barrett’s esophagus segment is emerging as a potentially predictive risk factor. While the ACG cautions that esophageal cancer has been reported in patients with so-called “short segment” Barrett’s esophagus (SSBE) (≤3 cm),1 recent prospective studies have shown an increased risk of carcinoma development with long segment Barrett’s esophagus (LSBE).7-9 Weston et al7 reported a 2.4% progression rate to HGD or esophageal carcinoma with SSBE and no dysplasia compared with 6.8% with LSBE (P=.002). If patients had LGD, the rate of progression to esophageal carcinoma with SSBE was 5.3% and jumped to 35% in patients with LSBE (P<.001). Conio et al8 reported that 4 of 5 cases of esophageal carcinoma noted through surveillance had LSBE. Hage et al9 reported a significantly increased risk of progression to HGD or esophageal carcinoma with long segment disease (P<.02).
While currently still considered investigational, DNA content flow cytometry may be a future tool used in risk stratification. Reid et al10 report a 5-year cumulative risk of esophageal carcinoma of 1.7% in Barrett’s esophagus patients with negative, low-grade or indefinite grades of dysplasia. Subsequent application of flow cytometry allowed for further stratification of these low-risk patients. Those with neither aneuploidy nor an increased 4N had a 5-year cumulative risk of cancer of 0% while the risk for those with abnormalities on cytometry increased to 28% (relative risk=19; P<.001).
TABLE
Grade of dysplasia and recommendations for Barrett’s esophagus surveillance as proposed by the ACG
| DYSPLASIA | DOCUMENTATION | FOLLOW-UP ENDOSCOPY |
|---|---|---|
| None | Two EGDs with biopsy | 3 years |
| Low-grade | Highest grade on repeat | 1 year until no dysplasia |
| High-grade | Repeat EGD with biopsy to rule out cancer/document high-grade dysplasia; expert pathologist confirmation | Focal: every 3 months |
| Multifocal: intervention | ||
| Mucosal irregularity: EMR | ||
| ACG, American College of Gastroenterology; EGD, esophagogastroduodenoscopy; EMR, endoscopic mucosal resection. Intervention: ie, esophagectomy. Ablative therapies only in the setting of a clinical trial or for those unable to tolerate surgery. | ||
Recommendations from others
The French Society of Digestive Endoscopy has published guidelines on monitoring Barrett’s esophagus.3 Their recommendations differ only slightly from the ACG in advocating a slightly increased frequency of EGD surveillance based on degree of dysplasia, and utilizing the length of the dysplastic segment in decision-making. Neither the American Academy of Family Physicians nor the US Preventive Services Task Force make any specific recommendations about Barrett’s esophagus surveillance.
Some patients who have been diagnosed with Barrett’s esophagus will develop dysplasia and, in some cases, esophageal carcinoma (strength of recommendation [SOR]: A, based on consistent cohort studies). Endoscopic surveillance is recommended for all patients with Barrett’s esophagus as it is superior to other methods for detecting esophageal cancer (SOR: B, based on systematic review). The degree of dysplasia noted on biopsy specimens correlates with the risk of esophageal carcinoma development and should guide the frequency of subsequent evaluations (SOR: B, based on consistent cohort studies). The optimal frequency of endoscopy has yet to be determined in any randomized trial.
Recommendations from the 2002 American College of Gastroenterology (ACG) Practice Guideline provide guidance as to the frequency of endoscopy surveillance but were not based on an explicit systematic review of the literature (SOR: C, based on expert opinion; see TABLE 1).
Reduced monitoring for most patients with Barrett’s esophagus appears safe
Paul Crawford, MD
USAF–Eglin Family Practice Residency, Eglin Air Force Base, Fla
Family physicians have long been at the mercy of expert opinion when considering how to monitor patients with Barrett’s esophagus. This review of the evidence clearly shows that the days of yearly EGD for all Barrett’s esophagus patients are over.
Unlike other conditions—such as cervical dysplasia, where monitoring and therapies to remove dysplasia are proven to save lives—Barrett’s esophagus progresses slowly and unpredictably. Thus, until technological advances allow identification of higher risk Barrett’s esophagus patients, an EGD every 3 years for those without dysplasia seems to be a reasonable monitoring interval. Perhaps most importantly, family physicians can reassure Barrett’s esophagus patients in the community that they are likely to live a normal lifespan and die of something other than esophageal cancer.
Evidence summary
Barrett’s esophagus has been defined as “a change in the esophageal epithelium of any length that can be recognized at endoscopy and is confirmed to have intestinal metaplasia by biopsy of the tubular esophagus.”1 Intestinal metaplasia is a premalignant lesion for adenocarcinoma of the esophagus. Surveillance by serial endoscopy with biopsy has been recommended in an effort to find high-grade dysplasia or carcinoma in an early, asymptomatic, and potentially curable stage.1-4 Approximately 75% of patients involved in a Barrett’s esophagus surveillance program will present with resectable tumors, compared with only 25% of those not receiving surveillance.4
A recent systematic review assessing screening tools for esophageal carcinoma found standard endoscopy to be superior (90%–100% sensitivity) to other less invasive methods such as questionnaire (60%–70%), and fecal occult blood testing (20%).4 Additional endoscopy tools such as brush and balloon cytology increased the cost of surveillance without any improvement in diagnostic yield.
The degree of dysplasia on esophageal biopsy in Barrett’s esophagus patients is currently the best indicator of risk of progression to esophageal carcinoma. The data reviewed by the ACG for the practice guideline was drawn from several prospective studies and one available registry. In sum, a total of 783 Barrett’s esophagus patients were followed for a mean of 2.9 to 7.3 years. Esophageal carcinoma developed in 2% of patients with no dysplasia, 7% of patients with low-grade dysplasia (LGD) and 22% of patients with high-grade dysplasia (HGD).1 The ACG recommendations regarding frequency of esophagogastroduodenoscopy (EGD) were not based on an explicit critical appraisal of the literature. Recent cohort studies are consistent with recommendations for graded surveillance frequency. A randomized clinical trial to determine optimal endoscopic frequency and benefit has not been reported.
Several concerns have been raised regarding the utility of degree of dysplasia in determining optimal frequency of endoscopic surveillance. First, the progression of esophageal lesions over time is unpredictable. Skacel et al5 reported a series of 34 patients with LGD at initial pathologic examination. On subsequent surveillance endoscopy with repeat biopsy, 73% no longer demonstrated dysplasia. Such patients can be allowed to return to having surveillance every 3 years.
In addition to the non-linear progression of dysplasia, inter-rater reliability of the interpretation of pathology specimens varies substantially. Adequate reliability has been demonstrated among pathologists assigning results to 2 categories (either no dysplasia and LGD or HGD and carcinoma) (κ=0.7). Assignment to four distinct pathologic grades, however, was not reliable (κ=0.46, where 1.0 is complete agreement).1 In order to make a diagnosis of HGD or carcinoma, interpretation must be independently confirmed by 2 expert pathologists.1-3
Recommendations for frequent endoscopic surveillance are also weakened by the overall low rate of mortality from esophageal carcinoma noted in Barrett’s esophagus patients. A recent population based study demonstrated that there was no difference in overall mortality in those with a Barrett’s esophagus diagnosis compared with the general population.6 An increased risk of death from esophageal carcinoma was seen in patients with Barrett’s esophagus (4.7% seen in Barrett’s esophagus patients compared with 0.8% predicted in the general population; P<.05). The overall increased effect on mortality, however, was relatively small. Esophageal carcinoma accounted for less then 5% of deaths in Barrett’s esophagus patients reported during the study’s 6-year follow-up period.
Data from prospective studies published after 2002 may better predict prognosis for Barrett’s esophagus patients.6-9 Even lower rates of progression to esophageal carcinoma (<0.5% a year or <1/220 patient-years) have been reported in these studies drawing from the general population rather than referred patients, likely stemming from differences in gender mix, patient age, and risk factors.
In addition to grade of dysplasia, the length of the dysplastic Barrett’s esophagus segment is emerging as a potentially predictive risk factor. While the ACG cautions that esophageal cancer has been reported in patients with so-called “short segment” Barrett’s esophagus (SSBE) (≤3 cm),1 recent prospective studies have shown an increased risk of carcinoma development with long segment Barrett’s esophagus (LSBE).7-9 Weston et al7 reported a 2.4% progression rate to HGD or esophageal carcinoma with SSBE and no dysplasia compared with 6.8% with LSBE (P=.002). If patients had LGD, the rate of progression to esophageal carcinoma with SSBE was 5.3% and jumped to 35% in patients with LSBE (P<.001). Conio et al8 reported that 4 of 5 cases of esophageal carcinoma noted through surveillance had LSBE. Hage et al9 reported a significantly increased risk of progression to HGD or esophageal carcinoma with long segment disease (P<.02).
While currently still considered investigational, DNA content flow cytometry may be a future tool used in risk stratification. Reid et al10 report a 5-year cumulative risk of esophageal carcinoma of 1.7% in Barrett’s esophagus patients with negative, low-grade or indefinite grades of dysplasia. Subsequent application of flow cytometry allowed for further stratification of these low-risk patients. Those with neither aneuploidy nor an increased 4N had a 5-year cumulative risk of cancer of 0% while the risk for those with abnormalities on cytometry increased to 28% (relative risk=19; P<.001).
TABLE
Grade of dysplasia and recommendations for Barrett’s esophagus surveillance as proposed by the ACG
| DYSPLASIA | DOCUMENTATION | FOLLOW-UP ENDOSCOPY |
|---|---|---|
| None | Two EGDs with biopsy | 3 years |
| Low-grade | Highest grade on repeat | 1 year until no dysplasia |
| High-grade | Repeat EGD with biopsy to rule out cancer/document high-grade dysplasia; expert pathologist confirmation | Focal: every 3 months |
| Multifocal: intervention | ||
| Mucosal irregularity: EMR | ||
| ACG, American College of Gastroenterology; EGD, esophagogastroduodenoscopy; EMR, endoscopic mucosal resection. Intervention: ie, esophagectomy. Ablative therapies only in the setting of a clinical trial or for those unable to tolerate surgery. | ||
Recommendations from others
The French Society of Digestive Endoscopy has published guidelines on monitoring Barrett’s esophagus.3 Their recommendations differ only slightly from the ACG in advocating a slightly increased frequency of EGD surveillance based on degree of dysplasia, and utilizing the length of the dysplastic segment in decision-making. Neither the American Academy of Family Physicians nor the US Preventive Services Task Force make any specific recommendations about Barrett’s esophagus surveillance.
1. Sampliner RE. Updated guidelines for the diagnosis, surveillance, and therapy of Barrett’s esophagus. Am J Gastroenterol 2002;97:1888-1895.
2. Management of Barrett’s esophagus. The Society for Surgery of the Alimentary Tract (SSAT), American Gastroenterological Association (AGA), American Society for Gastrointestinal Endoscopy (ASGE) Consensus Panel. J Gastrointest Surg 2000;4:115-116.
3. Boyer J, Robaszkiewicz M. Guidelines of the French Society of Digestive Endoscopy: Monitoring of Barrett’s esophagus. The Council of the French Society of Digestive Endoscopy. Endoscopy 2000;32:498-499.
4. Gerson LB, Triadafilopoulos G. Screening for esophageal adenocarcinoma: an evidence-based approach. Am J Med 2002;113:499-505.
5. Skacel M, Petras RE, Gramlich TL, et al. The diagnosis of low grade dysplasia in Barrett’s esophagus and its implications for disease progression. Am J Gastroenterol 2000;95:3383-3387.
6. Anderson LA, Murray LJ, Murphy SJ, et al. Mortality in Barrett’s oesophagus: results from a population based study. Gut 2003;52:1081-1084.
7. Weston AP, Sharma P, Mathur S, et al. Risk stratification of barrett’s esophagus: updated prospective multivariate analysis. Am J Gastroenterol 2004;99:1657-1666.
8. Conio M, Blanchi S, Laertosa G, et al. Long-term endoscopic surveillance of patients with Barrett’s esophagus. Incidence of dysplasia and adenocarcinoma: a prospective study. Am J Gastroenterol 2003;98:1931-1939.
9. Hage M, Siersema PD, van Dekken H, Steyerber EW, Dees J, Kuipers EJ. Oesophageal cancer incidence and mortality in patients with long-segment Barrett’s oesophagus after a mean follow-up of 12.7 years. Scand J Gastroenterol 2004;39:1175-1179.
10. Reid BJ, Levine DS, Longton G, Blount P, Rabinovitch PS. Predictors of progression to cancer in Barrett’s esophagus: baseline histology and flow cytometry identify low- and high-risk patient subsets. Am J Gastroenterol 2000;95:1669-1676.
1. Sampliner RE. Updated guidelines for the diagnosis, surveillance, and therapy of Barrett’s esophagus. Am J Gastroenterol 2002;97:1888-1895.
2. Management of Barrett’s esophagus. The Society for Surgery of the Alimentary Tract (SSAT), American Gastroenterological Association (AGA), American Society for Gastrointestinal Endoscopy (ASGE) Consensus Panel. J Gastrointest Surg 2000;4:115-116.
3. Boyer J, Robaszkiewicz M. Guidelines of the French Society of Digestive Endoscopy: Monitoring of Barrett’s esophagus. The Council of the French Society of Digestive Endoscopy. Endoscopy 2000;32:498-499.
4. Gerson LB, Triadafilopoulos G. Screening for esophageal adenocarcinoma: an evidence-based approach. Am J Med 2002;113:499-505.
5. Skacel M, Petras RE, Gramlich TL, et al. The diagnosis of low grade dysplasia in Barrett’s esophagus and its implications for disease progression. Am J Gastroenterol 2000;95:3383-3387.
6. Anderson LA, Murray LJ, Murphy SJ, et al. Mortality in Barrett’s oesophagus: results from a population based study. Gut 2003;52:1081-1084.
7. Weston AP, Sharma P, Mathur S, et al. Risk stratification of barrett’s esophagus: updated prospective multivariate analysis. Am J Gastroenterol 2004;99:1657-1666.
8. Conio M, Blanchi S, Laertosa G, et al. Long-term endoscopic surveillance of patients with Barrett’s esophagus. Incidence of dysplasia and adenocarcinoma: a prospective study. Am J Gastroenterol 2003;98:1931-1939.
9. Hage M, Siersema PD, van Dekken H, Steyerber EW, Dees J, Kuipers EJ. Oesophageal cancer incidence and mortality in patients with long-segment Barrett’s oesophagus after a mean follow-up of 12.7 years. Scand J Gastroenterol 2004;39:1175-1179.
10. Reid BJ, Levine DS, Longton G, Blount P, Rabinovitch PS. Predictors of progression to cancer in Barrett’s esophagus: baseline histology and flow cytometry identify low- and high-risk patient subsets. Am J Gastroenterol 2000;95:1669-1676.
Evidence-based answers from the Family Physicians Inquiries Network