User login
Palliative Care in Hospitals
The field of palliative care has grown rapidly in recent years in response to patient need and clinician interest in effective approaches to managing chronic life‐threatening illness.1 This article reviews the clinical, educational, demographic, and financial imperatives driving this growth, describes the clinical components of palliative care and the range of service models available, defines the relationship of hospital‐based palliative care to hospice, summarizes the literature on palliative care outcomes, and presents practical resources for clinicians seeking knowledge and skills in the field.
DEFINITION
Palliative care is medical care focused on the relief of suffering and support for the best possible quality of life for patients facing serious, life‐threatening illness and their families. It aims to identify and address the physical, psychological, and practical burdens of illness. Palliative care in the United States grew out of the hospice movement that originated in both the United Kingdom and the United States about 30 years ago. Hospice care was developed specifically to address the needs of the dying and their families and was codified in the United States by the addition in 1983 of a federal Medicare benefit for hospice care. In the last 30 years the Medicare hospice benefit has enabled more than 7 million patients and their families to receive intensive palliative care for the terminally ill, primarily in the home. The growth in the number and needs of seriously and chronically ill patients who are not clearly terminally ill has led to the development of palliative care services outside the hospice benefit provided by Medicare (and other insurers). Both hospice and nonhospice professionals have participated in extending the hospice approach through development of palliative care services. Palliative care may be delivered simultaneously with all appropriate curative and life‐prolonging interventions. In practice, palliative care practitioners provide assessment and treatment of pain and other symptom distress; employ communication skills with patients, families, and colleagues; support complex medical decision making and goal setting based on identifying and respecting patient wishes and goals; and promote medically informed care coordination, continuity, and practical support for patients, family caregivers, and professional colleagues across healthcare settings and through the trajectory of an illness.1, 2
Palliative care is both a general approach to health care and a growing practice specialty for professionals committing most or all of their time to the delivery of palliative care services.3 The term palliative medicine refers to the physician discipline within the larger field of palliative care. As of 2005, more than 1890 physicians have received specialty certification through a palliative care credentialing exam given by the American Board of Hospice and Palliative Medicine.4 Formal recognition of the subspecialty is currently being sought in collaboration with the American Board of Medical Specialties.5 As of August 2005, there were more than 50 postgraduate palliative care subspecialty fellowship programs in the United States.6 Between 2000 and 2003, the American Hospital Association (AHA) annual survey recorded a 67% growth in the number of hospital‐based palliative care programs reported, from 632 to 1027, for a total of 25% of responding AHA member hospitals.7
REASONS FOR GROWTH IN PALLIATIVE CARE
A primary justification for the rapid growth in palliative care programs in institutional settings is the abundant data demonstrating the high prevalence of pain and symptom distress in hospitals,811 nursing homes,12, 13 and community settings.14 Virtually all persons with serious illness spend at least some time in a hospital, usually on multiple occasions, in the course of their disease or condition.15 Despite the finding that when polled more than 90% of Americans say they would prefer to die at home, more than 75% of adult deaths occur in institutional settings (hospital or nursing homes)more than 50% in hospitals and 25% in nursing homesand 85% of pediatric deaths occur in hospitals.16, 17 Further, more than half of persons older than age 85 die in a nursing home and 43% of persons older than age 65 reside in a long‐term care facility at some time before they die,1821 a figure projected to rise substantially over the next several decades. The much larger number of patients who are not dying but are living with chronic, debilitating, and life‐threatening illness also need expert symptom management, communication and decision‐making support, and coordination of care across settings. In one national survey, physicians reported that poor care coordination resulted in patient communication problems, lack of emotional support for patients, adverse drug reactions, unnecessary hospitalization, patients not functioning to potential, and unnecessary pain.22 In addition to studies demonstrating high degrees of symptom distress across all age groups in hospitalized and nursing home patients,814 other works have shown high use of burdensome, nonbeneficial technologies among the seriously ill,2327 caregiver burden on families,2831 and communication problems between these patients, their families, and their treating physicians about the goals of care and the medical decisions that should follow.32, 33 Other studies have reported broad dissatisfaction with the general quality of care for the seriously ill and dying in hospitals and nursing homes,18, 34 specifically, perceptions of impersonal and indifferent care. Several studies of patients and their families have identified relief of suffering, practical support needs, open communication, and opportunities to relieve burdens on and strengthen relationships with family as the top‐priority needs from the healthcare system.3440
The growth in the number and needs of the elderly with multiple chronic conditions who will turn to the healthcare system in coming years underscores the need to create a delivery system in the United States that can be responsive to these priorities. By 2030 the number of persons with chronic conditions will exceed 157 million.4144 With the possible exception of advanced cancer conditions (accounting for 24% of adult deaths), in which prognosis is somewhat more reliably linked to performance status,4243 prognostication of outcome is a highly inexact science for the chronically ill of all ages and in a range of diagnostic categories, including stroke, dementia, and end‐stage cardiac, renal, hepatic, and pulmonary diseases. This has been a major part of the impetus for the growth in palliative care services not predicated on a link to terminal prognoses.4143 Hospitals and nursing homes are under increasing pressure to structure care processes in a manner fitted to the needs of the seriously ill because of studies demonstrating poor quality of care, demands from patients and families, accreditation requirements, and the costs of care for this patient population. More than 95% of Medicare spending goes to the 63% of Medicare patients with two or more chronic conditions, and three quarters of Medicare dollars go to hospitals.44 Hospital costs have risen nearly 10% per year in each of the last 2 years, because of both the increasing numbers of patients turning to them for care and the growth in the number and expense of effective life‐prolonging therapies. These forces have stimulated the development of new models for the efficient and effective care of patients with serious and complex illness.2227, 44
CLINICAL COMPONENTS
The three primary domains of palliative care clinical practice are assessment and treatment of pain and other symptom distress, including psychiatric symptoms64; communication about goals of care and support for complex medical decision making; and provision of practical and psychosocial support, care coordination, and continuity, as well as bereavement services if death occurs.1, 2, 65 Palliative care specialists work to support primary and specialist physicians in the care of complex and seriously ill patients by providing intensive bedside treatment and reassessment of multiple‐symptom distress, by helping with time‐consuming and difficult interactions with distressed patients and family members, and by attempting to ensure a seamless, safe, and well‐communicated discharge and follow‐up process after the patient leaves the hospital.66 Resources for physicians seeking more knowledge or training in the treatment of symptom distress and other aspects of palliative care are given in Table 1.
| Palliative care clinical competencies |
|---|
|
|
Education on Palliative and End of Life Care ( |
|
End of Life/Palliative Education Resource Center ( |
|
Department of Pain Medicine and Palliative Medicine at Beth Israel Medical Center ( |
|
|
|
American Academy of Hospice and Palliative Medicine ( |
|
American Board of Hospice and Palliative Medicine ( |
|
Center for Palliative Care at Harvard Medical School ( |
|
National Consensus Project on Quality Palliative Care ( |
|
American Geriatrics Society ( |
| Palliative care program development |
|
Center to Advance Palliative Care ( |
|
Palliative Care Leadership Centers ( |
|
Promoting Excellence in End of Life Care ( |
The core components of symptom management67, 68 include: 1) Routine and repeated formal assessment, without which most symptoms will be neither identified nor addressed; 2) Expertise in prescribing, including the safe use of opioid analgesics, adjuvant approaches to pain management, and management of a wide range of other common and distressing symptoms and syndromes including, for example, delirium, dyspnea, fatigue, nausea, bowel obstruction, and depression69; and 3) Skillful management of treatment side effects, which is required to successfully control symptoms.
Communication skills and effective support for making decisions about clinical care goals include not only fundamental physician responsibilities such as communicating bad news and elucidating patient wishes for future care, but also the ability to promote communication and consensus about care goals among multiple specialist consultants, to address and resolve disagreements and conflicts among patients, families, and providers about goals of care, and to assist in the evolving process of balancing the benefits with the burdens of various medical interventions.32, 7073
The great majority of care for an illness is provided at home by family members neither trained nor emotionally prepared for these responsibilities.51, 74 The burden on family caregivers is one of the top concerns of seriously ill patients.35 Patients and families often struggle with anxieties about doing the wrong thing, difficulty traveling to physicians' offices, social isolation, and a high prevalence of preventable suffering of all types.3440 Palliative care clinicians attempt to improve the success and sustainability of the discharge plan by providing medically informed and therefore more appropriate care management recommendations and by mobilizing a range of community resources to increase the likelihood that families will be able to manage the care at home with the necessary supports and backups in place, including appropriate screening and referrals for complicated grief and bereavement.51, 75, 76 Several small prospective studies of palliative care have suggested that palliative care has resulted in reduction in the number of emergency department visits and hospitalizations and in the length of hospital stays, presumably because of the efficacy and comprehensiveness of care coordination in averting crises.54, 55, 61, 9798
CLINICAL MODELS
Given the multifaceted approach needed to support patient quality of life throughout advanced illness, one profession or individual cannot be expected to provide all aspects of palliative care. As described in the recently completed National Consensus Project Guidelines for Quality Palliative Care,2 specialty‐level palliative care is optimally delivered through an interdisciplinary team consisting of appropriately trained and credentialed physicians, nurses, and social workers with additional support and contributions from chaplains, rehabilitative experts, psychiatrists, and other professionals as indicated. Clearly, however, the staffing of a palliative care program will depend critically on the needs and capacities of the setting. A full interdisciplinary team is needed for a large tertiary‐care teaching hospital, whereas a part‐time advance‐practice nurse with backup from colleagues as needed may suffice for a small rural hospital or long‐term care setting. Specialist‐level palliative care is delivered through a range of clinical models and settings, including inpatient consultation services, dedicated inpatient units, and outpatient practices, among others.77, 78 Programs within the United States are housed in a range of clinical subspecialties including oncology, geriatrics, nursing, case management, hospitalist, and other programs, depending on the locus of leadership and administrative support.77, 78 Most programs are supported by utilizing diverse sources,77 including physician and nurse‐practitioner billing through insurers such as Medicare Part B,53, 81 as well as hospital support typically predicated on cost avoidance analyses, foundation and other grants, and philanthropy. Detailed guidance on appropriate documentation and billing for palliative care physician services may be found in Schapiro et al.,53 von Gunten,79 and on the Web site of the Center to Advance Palliative Care (
RELATIONSHIP TO HOSPICE
Although new clinical specialties in palliative medicine and nursing are emerging, in the United States palliative care for those in the terminal stages of illness has been delivered through hospice programs for more than 30 years. Under current regulatory and payment guidelines hospice care is delivered to patients who are certified by their physicians as likely to die within 6 months if the disease follows its usual course and who are willing to give up insurance coverage for medical treatment primarily focused on cure or prolongation of life. It is noteworthy that there is great variability among United States hospices, with some able to support continued disease‐modifying treatments such as chemotherapy and radiation if a patient so desires.2 Hospice programs aim to create increased opportunity for death at home, focusing on symptom control and the psychological and spiritual issues that are paramount to persons in the terminal phases of illness. Once the hospice benefit has been accessed, patients and families receive comprehensive case‐managed services across all settings of care (although the great majority of hospice care is delivered at home) from an interdisciplinary team, coverage for medications and equipment related to the terminal illness, and practical, psychosocial, respite, and bereavement support for caregivers.80, 81 Several recent studies have confirmed the findings of an earlier work82 in demonstrating the beneficial outcomes of hospice care including reduced mortality in spouses and high levels of family satisfaction.18, 83 Palliative care programs based in both hospital and community settings have led to increases in hospice referral rates and hospice length of stay, promoting continuity of palliative care and the intensive palliation and family support needed as death approaches.55 Coordination and partnerships between palliative care and hospice programs are critical to achieving continuity of palliative care throughout the full course of an illness and across the continuum of care settings.2
IMPACT OF PALLIATIVE CARE ON QUALITY OF CARE
Reports on palliative care specialist services utilizing diverse models and approaches have suggested a range of benefits from palliative care, including reduced pain4547 and other symptom distress,45, 48, 49 improved health‐related quality of life,95 high patient and family satisfaction18, 4951, 96 with care and with physician communication, and increased likelihood of the location of death being outside a hospital.33, 49, 52, 9799
Because it can help to demonstrate care structures, processes, and outcomes associated with improved quality (such as routine assessment of pain in the hospital), a palliative care program may help hospitals measure and meet Joint Commission for Accreditation of Healthcare Organizations (JCAHO) requirements in the domains of pain management, communication, family and patient education, and continuity of care, among others.53 Several groups have reported marked increases in hospice referral rate and hospice length of stay as a result of hospital‐ and nursing‐home‐based palliative care programs, presumably as a result of enhanced case identification, counseling, and referral processes.54, 55 Case control and observational studies of palliative care and ethics consultation services have demonstrated reductions in costs per day and in hospital and ICU lengths of stay, presumably because of enhanced support for discussions about the goals of care and the resulting facilitation of patient and family decisions about the types and settings of future care.50, 5561 Hospitals have begun to invest in palliative care services, both to enhance quality of care and because of their measurable impact on reducing ICU and total bed days and their efficacy in supporting transitions from high‐intensity, high‐cost hospital settings to more appropriate and desired care settings, such as the home.5563, 9798 Observational studies have yielded no differences in mortality between patients receiving palliative care and controls receiving the usual care.48, 55, 56
EDUCATION IN PALLIATIVE CARE
Curricular content on palliative care has been noticeably lacking from medical and nursing education curricula, textbooks, and certifying examinations, although this is beginning to change.8491 Both the Liaison Committee for Medical Education (LCME) and the Accreditation Council for Graduate Medical Education (ACGME) now require or strongly encourage programs to provide under‐ and postgraduate training in palliative care in order to be accredited.89, 90 As of 2005, more than 50% of teaching hospitals had established palliative care clinical services,92 which constitute the necessary platform for clinical training. The rapid growth in the availability of postgraduate fellowship training in palliative medicine will produce the faculty leaders needed for these educational and research programs in medical school and residency training programs.93, 94 Physicians in practice may gain knowledge and skills through a range of national courses and Web‐based resources and through preparation for the certifying exam given annually by the American Board of Hospice and Palliative Medicine4 (Table 1).
CONCLUSIONS
The growth in palliative care specialists and programs in hospitals in the United States represents a grass roots professional response to the needs of a patient population with chronic advanced illnesses and family care burdens within a healthcare system structured to provide care for acute intercurrent illness. Rapid increases in the number of new hospital programs, as well as early studies indicating improved clinical, satisfaction, and utilization outcomes, suggest that palliative care services are likely to become a routine and well‐integrated part of the healthcare continuum in the United States over the next several years. A number of resources are available to healthcare professionals seeking more training as well as to hospitals or nursing homes wishing to establish their own clinical or educational programs. Such programs have provided a platform for both newly graduated and seasoned professionals to continue to serve the needs of their patients through the assessment and relief of suffering, provided simultaneously with efforts to cure or mitigate disease.
- ,.Clinical practice: palliative care.N Engl J Med.2004;350:2582–2590.
- National Consensus Project for Quality Palliative Care: The development of practice guidelines 2004. Available from URL:http://www.nationalconsensusproject.org. [accessed August 10, 2005].
- ,.Palliative medicine: an emerging field of specialization.Cancer Invest.2000;18:761–767.
- American Board of Hospice and Palliative Medicine. Available from URL:http://www.abhpm.org[accessed August 10, 2005].
- ,,, et al.Physician board certification in hospice and palliative medicine.J Palliat Med.2000;3:441–447.
- American Academy of Hospice and Palliative Medicine. Available from URL:http://www.aahpm.org[accessed August 10, 2005].
- American Hospital Association. Hospital Statistics 2004. Available from URL:http://www.ahastatistics.org[accessed August 10, 2005].
- ,,.Pain and satisfaction with pain control in hospitalized medical patients.Arch Intern Med.2004;164:175–180.
- ,,, et al.Pain and discomfort associated with common hospital procedures and experiences.J Pain Symptom Manage.1998;15:91–101.
- ,,, et al. The symptom burden of seriously ill hospitalized patients.J Pain Symptom Manage.1999;17:248–255.
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT).The SUPPORT Principal Investigators.JAMA.1995;274:1591–1598.
- ,,, et al.Persistent pain in nursing home residents.JAMA.2001;285:2081.
- ,,, et al.Management of pain in elderly patients with cancer. SAGE Study Group. Systematic assessment of geriatric drug use via epidemiology.JAMA.1998;279:1877–1882.
- ,,, et al.Pain and its treatment in outpatients with metastatic cancer.N Engl J Med.1994;330:592–596.
- Dartmouth Atlas. Available from URL: http://www.dartmouthatlas.org/endoflife/end_of_life.php[accessed August 10, 2005].
- Institute of Medicine.Approaching death: improving care at the end of life.Washington, DC:National Academy Press,1997.
- Institute of Medicine.When Children die: improving palliative and end of life care for children and their families.Washington, DC:National Academies Press,2002.
- ,,, et al.Family perspectives on end‐of‐life care at the last place of care.JAMA.2004;291:88–93.
- . Brown Atlas. Available from URL:http://www.chcr.brown.edu/dying/brownatlas.htm[accessed August 10, 2005].
- .Creating excellent palliative care in nursing homes.J Palliat Med.2003;6:7–9.
- ,,, et al.Needs of the dying in nursing homes.J Palliat Med.2002;5:895–901.
- Mathematica Policy Research, Inc.National public engagement campaign on chronic illness—physician survey, final report.Princeton, NJ:Mathematica Policy Research, Inc.,2001.
- ,,,.Patterns of use of common major procedures in medical care of older adults.J Am Geriatr Soc.1999;47:553–558.
- ,.Dying to pay: the cost of end of life care.J Palliat Care.1998;14:5–15.
- ,,, et al.Older age, aggressiveness of care, and survival for seriously ill, hospitalized adults. SUPPORT Investigators. Study to understand prognoses and preferences for outcomes and risks of treatments.Ann Intern Med.1999;131:721–728.
- .Demands of an aging population for critical care and pulmonary services.JAMA.2001;285:1016–1017.
- ,,,.Medicare beneficiaries' costs of care in the last year of life.Health Aff.2001;20:188–195.
- ,,,.Stress in caregivers of hospitalized oldest‐old patients.J Gerontol A Biol Sci Med Sci.2001;56:M231–M235.
- ,.Caregiving as a risk factor for mortality: the Caregiver Health Effects Study.JAMA.1999;282:2215–2219.
- ,,,,,.Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients.N Engl J Med.1999;341:956–963.
- ,,, et al.The impact of serious illness on patients' families.JAMA.1994;272:1839–1844.
- .Doctor–patient communication. In:Morrison RS,Meier DE, editors.Geriatric palliative care.New York:Oxford University Press,2003.
- ,.Communicating sad, bad, and difficult news in medicine.Lancet.2004;363:312–319.
- ,,,.Understanding economic and other burdens of terminal illness: the experience of patients and their caregivers.Ann Intern Med.2000;132:451–459.
- ,,.Quality end‐of‐life care: patients' perspectives.JAMA.1999;281:163–168.
- ,,, et al.Preparing for the end of life: preferences of patients, families, physicians, and other care providers.J Pain Symptom Manage.2001;22:727–737.
- ,,, et al.Factors considered important at the end of life by patients, family, physicians, and other care providers.JAMA.2000;284:2476–2482.
- ,,,,,.In search of a good death: observations of patients, families, and providers.Ann Intern Med.2000;132:825–832.
- ,,, et al.Measurement of quality of care and quality of life at the end of life.Gerontologist.2002;42:71–80.
- ,,, et al.Family reports of barriers to optimal care of the dying.Nurs Res.2000;49:310–317.
- ,,, et al.Patterns of functional decline at the end of life.JAMA.2003;289:2387–2392.
- ,, Cohn F, et al. Prognoses of seriously ill hospitalized patients on the days before death: implications for patient care and public policy.New Horizons.1997;5:56–61.
- ,,, et al.The last 2 years of life: functional trajectories of frail older people.J Am Geriatr Soc.2003;51:492–498.
- Partnership for Solutions. Chronic Conditions:Making the Case for Ongoing Care.Baltimore:Johns Hopkins University,2002.
- ,,, et al.Is there evidence that palliative care teams alter end‐of‐life experiences of patients and their caregivers?J Pain Symptom Manage.2003;25:150–168.
- ,,, et al.Implementing guidelines for cancer pain management: results of a randomized controlled clinical trial.J Clin Oncol.1999;17:361–370.
- ,,, et al.Randomized clinical trial of an implantable drug delivery system compared with comprehensive medical management for refractory cancer pain: impact on pain, drug‐related toxicity, and survival.J Clin Oncol2002;20:4040–4049.
- ,,, et al.The comprehensive care team: a controlled trial of outpatient palliative medicine consultation.Arch Intern Med.2004;164:83–91.
- ,,, et al.Palliative care consultations: how do they impact the care of hospitalized patients?J Pain Symptom Manage.2000;20:166–173.
- ,,, et al.An intensive communication intervention for the critically ill.Am J Med.2000;109:469–475.
- ,,.The moderating influence of service use on negative caregiving consequences.J Gerontol B Psychol Sci Soc Sci.1996;51:S121–131.
- ,,.Communication skills training for health care professionals working with cancer patients, their families and/or carers (Cochrane Review).The Cochrane Library. Chichester, UK:John Wiley 21:1412–1415.
- ,,, et al. Living and dying well with cancer: Successfully integrating palliative care and cancer treatment. Available from URL:http://www.promotingexcellence.org[accessed August 10, 2005].
- ,,, et al.A high‐volume specialist palliative care unit and team may reduce in‐hospital end‐of‐life care costs.J Palliat Med.2003;6:699–705.
- ,,, et al.Effect of ethics consultations on nonbeneficial life‐sustaining treatments in the intensive care setting.JAMA.2003;290:1166–1172.
- ,.Impact of a proactive approach to improve end‐of‐life care in a medical ICU.Chest.2003;123:266–271.
- ,,, et al.A randomized controlled trial of the cost‐effectiveness of a district co‐ordinating service for terminally ill cancer patients.Palliat Med.1996;10:151–161.
- ,,, et al.The impact of a regional palliative care program on the cost of palliative care delivery.J Palliat Med.1999;3:181–186.
- ,,.Effectiveness of a home‐based palliative care program for end‐of‐life.J Palliat Med.2003;6:715–724.
- ,,.A study of proactive ethics consultation for critically and terminally ill patients with extended lengths of stay.Crit Care Med.1998;26:252–259.
- ,.Experience with an end‐of‐life practice at a university hospital.Crit Care Med.1997;25:197–202.
- .Perspectives on care at the close of life. Psychological considerations, growth, and transcendence at the end of life: the art of the possible.JAMA.2001;285:2898–2905.
- ,,.Improving palliative care.Ann Intern Med.1997;127:225–230.
- .Completing the continuum of cancer care: integrating life‐prolongation and palliation.CA Cancer J Clin.2000;50:123–132.
- ,.Pain management: pharmacological approaches.Cancer Treat Res.1999;100:1–29.
- ,.Pain and symptom management in palliative care.Cancer Control.1996;3:204–213.
- .ABC of palliative care. Anorexia, cachexia, and nutrition.BMJ.1997;315:1219–1222.
- .Perspectives on care at the close of life. Initiating end‐of‐life discussions with seriously ill patients: addressing the “elephant in the room.”JAMA.2000;284:2502–2507.
- ,,.“I wish things were different”: expressing wishes in response to loss, futility, and unrealistic hopes.Ann Intern Med.2001;135:551–555.
- ,,.Discussing palliative care with patients. ACP‐ASIM End‐of‐Life Care Consensus Panel.Ann Intern Med.1999;130:744–749.
- ,,.The patient‐physician relationship. Ensuring competency in end‐of‐life care: communication and relational skills.JAMA.2000;284:3051–3057.
- .The loneliness of the long‐term care giver.N Engl J Med.1999;340:1587–1590.
- ,,,,,.Integrating case management and palliative care.J Palliat Med.2004;7:121–136.
- ,,.The influence of caregiving and bereavement support on adjusting to an older relative's death.Gerontologist.1991;31:32–42.
- Center to Advance Palliative Care. A guide to developing a hospital‐based palliative care program. Available from URL:http://www.capc.org[accessed August 10, 2005].
- .Secondary and tertiary palliative care in US hospitals.JAMA.2002;287:875–881.
- .Coding and reimbursement mechanisms for physician services in hospice and palliative care.J Palliat Med.2000;2:157–164.
- National Hospice and Palliative Care Organization. NHPCO facts and figures. Available from URL:http://www.nhpco.org[accessed August 10, 2005].
- .When pain and suffering do not require a prognosis: Working toward meaningful hospital–hospice partnership.J Palliat Med.2003;6:109–115.
- ,,, et al.An alternative in terminal care: results of the National Hospice Study.J Chronic Dis.1986;39:9–26.
- ,.The health impact of health care on families: a matched cohort study of hospice use by decedents and mortality outcomes in surviving, widowed spouses.Soc Sci Med.2003;57:465–475.
- ,.Educational programs in US medical schools, 2002–2003.JAMA.2003;290:1190–1196.
- .Medical education in end‐of‐life care: the status of reform.J Palliat Med.2002;5:243–248.
- ,.ACGME requirements for end‐of‐life training in selected residency and fellowship programs: a status report.Acad Med.2002;77:299–304.
- ,,, et al.Recommendations for incorporating palliative care education into the acute care hospital setting.Acad Med.1999;74:871–877.
- ,,.The status of medical education in end‐of‐life care: a national report.J Gen Intern Med.2003;18:685–695.
- Liaison Committee on Medical Education. Available from URL: http://www.lcme.org[accessed August 10, 2005].
- Accreditation Council for Graduate Medical Education.Program requirements for residency education in the subspecialties of internal medicine. Graduate Medical Education Directory 2000–2001. Chicago,2000.
- ,.Palliative care in undergraduate medical education. Status report and future directions.JAMA.1997;278:733–738.
- ,.Survey of palliative care programs in United States teaching hospitals.J Palliat Med.2001;4:309–314.
- ,,, et al.Initial voluntary program standards for fellowship training in palliative medicine.J Palliat Med.2002;5:23–33.
- American Academy of Hospice and Palliative Medicine. Fellowship Program Directory. Available from URL:http://www.aahpm.org/fellowship/directory/htm[accessed August 10, 2005].
- ,,, et al.Quality of life in palliative cancer care. Results from a cluster randomized trial.J Clin Oncol.2001;19:3884–3894.
- ,,.Family satisfaction with end‐of‐life care for cancer patients in a cluster randomized trial.J Pain Symptom Manage.2002;24:53–63.
- ,,, et al.A palliative care intervention and death at home: a cluster randomized trial.Lancet.2000;356:888–893.
- ,,.Impact of palliative care case management on resource use by patients dying of cancer at a Veterans Affairs medical center.J Palliat Med.2005;8:26–35.
- ,,.Family satisfaction with end‐of‐life care for cancer patients in a cluster randomized trial.J Pain Symptom Manage.2002;24:53–63
The field of palliative care has grown rapidly in recent years in response to patient need and clinician interest in effective approaches to managing chronic life‐threatening illness.1 This article reviews the clinical, educational, demographic, and financial imperatives driving this growth, describes the clinical components of palliative care and the range of service models available, defines the relationship of hospital‐based palliative care to hospice, summarizes the literature on palliative care outcomes, and presents practical resources for clinicians seeking knowledge and skills in the field.
DEFINITION
Palliative care is medical care focused on the relief of suffering and support for the best possible quality of life for patients facing serious, life‐threatening illness and their families. It aims to identify and address the physical, psychological, and practical burdens of illness. Palliative care in the United States grew out of the hospice movement that originated in both the United Kingdom and the United States about 30 years ago. Hospice care was developed specifically to address the needs of the dying and their families and was codified in the United States by the addition in 1983 of a federal Medicare benefit for hospice care. In the last 30 years the Medicare hospice benefit has enabled more than 7 million patients and their families to receive intensive palliative care for the terminally ill, primarily in the home. The growth in the number and needs of seriously and chronically ill patients who are not clearly terminally ill has led to the development of palliative care services outside the hospice benefit provided by Medicare (and other insurers). Both hospice and nonhospice professionals have participated in extending the hospice approach through development of palliative care services. Palliative care may be delivered simultaneously with all appropriate curative and life‐prolonging interventions. In practice, palliative care practitioners provide assessment and treatment of pain and other symptom distress; employ communication skills with patients, families, and colleagues; support complex medical decision making and goal setting based on identifying and respecting patient wishes and goals; and promote medically informed care coordination, continuity, and practical support for patients, family caregivers, and professional colleagues across healthcare settings and through the trajectory of an illness.1, 2
Palliative care is both a general approach to health care and a growing practice specialty for professionals committing most or all of their time to the delivery of palliative care services.3 The term palliative medicine refers to the physician discipline within the larger field of palliative care. As of 2005, more than 1890 physicians have received specialty certification through a palliative care credentialing exam given by the American Board of Hospice and Palliative Medicine.4 Formal recognition of the subspecialty is currently being sought in collaboration with the American Board of Medical Specialties.5 As of August 2005, there were more than 50 postgraduate palliative care subspecialty fellowship programs in the United States.6 Between 2000 and 2003, the American Hospital Association (AHA) annual survey recorded a 67% growth in the number of hospital‐based palliative care programs reported, from 632 to 1027, for a total of 25% of responding AHA member hospitals.7
REASONS FOR GROWTH IN PALLIATIVE CARE
A primary justification for the rapid growth in palliative care programs in institutional settings is the abundant data demonstrating the high prevalence of pain and symptom distress in hospitals,811 nursing homes,12, 13 and community settings.14 Virtually all persons with serious illness spend at least some time in a hospital, usually on multiple occasions, in the course of their disease or condition.15 Despite the finding that when polled more than 90% of Americans say they would prefer to die at home, more than 75% of adult deaths occur in institutional settings (hospital or nursing homes)more than 50% in hospitals and 25% in nursing homesand 85% of pediatric deaths occur in hospitals.16, 17 Further, more than half of persons older than age 85 die in a nursing home and 43% of persons older than age 65 reside in a long‐term care facility at some time before they die,1821 a figure projected to rise substantially over the next several decades. The much larger number of patients who are not dying but are living with chronic, debilitating, and life‐threatening illness also need expert symptom management, communication and decision‐making support, and coordination of care across settings. In one national survey, physicians reported that poor care coordination resulted in patient communication problems, lack of emotional support for patients, adverse drug reactions, unnecessary hospitalization, patients not functioning to potential, and unnecessary pain.22 In addition to studies demonstrating high degrees of symptom distress across all age groups in hospitalized and nursing home patients,814 other works have shown high use of burdensome, nonbeneficial technologies among the seriously ill,2327 caregiver burden on families,2831 and communication problems between these patients, their families, and their treating physicians about the goals of care and the medical decisions that should follow.32, 33 Other studies have reported broad dissatisfaction with the general quality of care for the seriously ill and dying in hospitals and nursing homes,18, 34 specifically, perceptions of impersonal and indifferent care. Several studies of patients and their families have identified relief of suffering, practical support needs, open communication, and opportunities to relieve burdens on and strengthen relationships with family as the top‐priority needs from the healthcare system.3440
The growth in the number and needs of the elderly with multiple chronic conditions who will turn to the healthcare system in coming years underscores the need to create a delivery system in the United States that can be responsive to these priorities. By 2030 the number of persons with chronic conditions will exceed 157 million.4144 With the possible exception of advanced cancer conditions (accounting for 24% of adult deaths), in which prognosis is somewhat more reliably linked to performance status,4243 prognostication of outcome is a highly inexact science for the chronically ill of all ages and in a range of diagnostic categories, including stroke, dementia, and end‐stage cardiac, renal, hepatic, and pulmonary diseases. This has been a major part of the impetus for the growth in palliative care services not predicated on a link to terminal prognoses.4143 Hospitals and nursing homes are under increasing pressure to structure care processes in a manner fitted to the needs of the seriously ill because of studies demonstrating poor quality of care, demands from patients and families, accreditation requirements, and the costs of care for this patient population. More than 95% of Medicare spending goes to the 63% of Medicare patients with two or more chronic conditions, and three quarters of Medicare dollars go to hospitals.44 Hospital costs have risen nearly 10% per year in each of the last 2 years, because of both the increasing numbers of patients turning to them for care and the growth in the number and expense of effective life‐prolonging therapies. These forces have stimulated the development of new models for the efficient and effective care of patients with serious and complex illness.2227, 44
CLINICAL COMPONENTS
The three primary domains of palliative care clinical practice are assessment and treatment of pain and other symptom distress, including psychiatric symptoms64; communication about goals of care and support for complex medical decision making; and provision of practical and psychosocial support, care coordination, and continuity, as well as bereavement services if death occurs.1, 2, 65 Palliative care specialists work to support primary and specialist physicians in the care of complex and seriously ill patients by providing intensive bedside treatment and reassessment of multiple‐symptom distress, by helping with time‐consuming and difficult interactions with distressed patients and family members, and by attempting to ensure a seamless, safe, and well‐communicated discharge and follow‐up process after the patient leaves the hospital.66 Resources for physicians seeking more knowledge or training in the treatment of symptom distress and other aspects of palliative care are given in Table 1.
| Palliative care clinical competencies |
|---|
|
|
Education on Palliative and End of Life Care ( |
|
End of Life/Palliative Education Resource Center ( |
|
Department of Pain Medicine and Palliative Medicine at Beth Israel Medical Center ( |
|
|
|
American Academy of Hospice and Palliative Medicine ( |
|
American Board of Hospice and Palliative Medicine ( |
|
Center for Palliative Care at Harvard Medical School ( |
|
National Consensus Project on Quality Palliative Care ( |
|
American Geriatrics Society ( |
| Palliative care program development |
|
Center to Advance Palliative Care ( |
|
Palliative Care Leadership Centers ( |
|
Promoting Excellence in End of Life Care ( |
The core components of symptom management67, 68 include: 1) Routine and repeated formal assessment, without which most symptoms will be neither identified nor addressed; 2) Expertise in prescribing, including the safe use of opioid analgesics, adjuvant approaches to pain management, and management of a wide range of other common and distressing symptoms and syndromes including, for example, delirium, dyspnea, fatigue, nausea, bowel obstruction, and depression69; and 3) Skillful management of treatment side effects, which is required to successfully control symptoms.
Communication skills and effective support for making decisions about clinical care goals include not only fundamental physician responsibilities such as communicating bad news and elucidating patient wishes for future care, but also the ability to promote communication and consensus about care goals among multiple specialist consultants, to address and resolve disagreements and conflicts among patients, families, and providers about goals of care, and to assist in the evolving process of balancing the benefits with the burdens of various medical interventions.32, 7073
The great majority of care for an illness is provided at home by family members neither trained nor emotionally prepared for these responsibilities.51, 74 The burden on family caregivers is one of the top concerns of seriously ill patients.35 Patients and families often struggle with anxieties about doing the wrong thing, difficulty traveling to physicians' offices, social isolation, and a high prevalence of preventable suffering of all types.3440 Palliative care clinicians attempt to improve the success and sustainability of the discharge plan by providing medically informed and therefore more appropriate care management recommendations and by mobilizing a range of community resources to increase the likelihood that families will be able to manage the care at home with the necessary supports and backups in place, including appropriate screening and referrals for complicated grief and bereavement.51, 75, 76 Several small prospective studies of palliative care have suggested that palliative care has resulted in reduction in the number of emergency department visits and hospitalizations and in the length of hospital stays, presumably because of the efficacy and comprehensiveness of care coordination in averting crises.54, 55, 61, 9798
CLINICAL MODELS
Given the multifaceted approach needed to support patient quality of life throughout advanced illness, one profession or individual cannot be expected to provide all aspects of palliative care. As described in the recently completed National Consensus Project Guidelines for Quality Palliative Care,2 specialty‐level palliative care is optimally delivered through an interdisciplinary team consisting of appropriately trained and credentialed physicians, nurses, and social workers with additional support and contributions from chaplains, rehabilitative experts, psychiatrists, and other professionals as indicated. Clearly, however, the staffing of a palliative care program will depend critically on the needs and capacities of the setting. A full interdisciplinary team is needed for a large tertiary‐care teaching hospital, whereas a part‐time advance‐practice nurse with backup from colleagues as needed may suffice for a small rural hospital or long‐term care setting. Specialist‐level palliative care is delivered through a range of clinical models and settings, including inpatient consultation services, dedicated inpatient units, and outpatient practices, among others.77, 78 Programs within the United States are housed in a range of clinical subspecialties including oncology, geriatrics, nursing, case management, hospitalist, and other programs, depending on the locus of leadership and administrative support.77, 78 Most programs are supported by utilizing diverse sources,77 including physician and nurse‐practitioner billing through insurers such as Medicare Part B,53, 81 as well as hospital support typically predicated on cost avoidance analyses, foundation and other grants, and philanthropy. Detailed guidance on appropriate documentation and billing for palliative care physician services may be found in Schapiro et al.,53 von Gunten,79 and on the Web site of the Center to Advance Palliative Care (
RELATIONSHIP TO HOSPICE
Although new clinical specialties in palliative medicine and nursing are emerging, in the United States palliative care for those in the terminal stages of illness has been delivered through hospice programs for more than 30 years. Under current regulatory and payment guidelines hospice care is delivered to patients who are certified by their physicians as likely to die within 6 months if the disease follows its usual course and who are willing to give up insurance coverage for medical treatment primarily focused on cure or prolongation of life. It is noteworthy that there is great variability among United States hospices, with some able to support continued disease‐modifying treatments such as chemotherapy and radiation if a patient so desires.2 Hospice programs aim to create increased opportunity for death at home, focusing on symptom control and the psychological and spiritual issues that are paramount to persons in the terminal phases of illness. Once the hospice benefit has been accessed, patients and families receive comprehensive case‐managed services across all settings of care (although the great majority of hospice care is delivered at home) from an interdisciplinary team, coverage for medications and equipment related to the terminal illness, and practical, psychosocial, respite, and bereavement support for caregivers.80, 81 Several recent studies have confirmed the findings of an earlier work82 in demonstrating the beneficial outcomes of hospice care including reduced mortality in spouses and high levels of family satisfaction.18, 83 Palliative care programs based in both hospital and community settings have led to increases in hospice referral rates and hospice length of stay, promoting continuity of palliative care and the intensive palliation and family support needed as death approaches.55 Coordination and partnerships between palliative care and hospice programs are critical to achieving continuity of palliative care throughout the full course of an illness and across the continuum of care settings.2
IMPACT OF PALLIATIVE CARE ON QUALITY OF CARE
Reports on palliative care specialist services utilizing diverse models and approaches have suggested a range of benefits from palliative care, including reduced pain4547 and other symptom distress,45, 48, 49 improved health‐related quality of life,95 high patient and family satisfaction18, 4951, 96 with care and with physician communication, and increased likelihood of the location of death being outside a hospital.33, 49, 52, 9799
Because it can help to demonstrate care structures, processes, and outcomes associated with improved quality (such as routine assessment of pain in the hospital), a palliative care program may help hospitals measure and meet Joint Commission for Accreditation of Healthcare Organizations (JCAHO) requirements in the domains of pain management, communication, family and patient education, and continuity of care, among others.53 Several groups have reported marked increases in hospice referral rate and hospice length of stay as a result of hospital‐ and nursing‐home‐based palliative care programs, presumably as a result of enhanced case identification, counseling, and referral processes.54, 55 Case control and observational studies of palliative care and ethics consultation services have demonstrated reductions in costs per day and in hospital and ICU lengths of stay, presumably because of enhanced support for discussions about the goals of care and the resulting facilitation of patient and family decisions about the types and settings of future care.50, 5561 Hospitals have begun to invest in palliative care services, both to enhance quality of care and because of their measurable impact on reducing ICU and total bed days and their efficacy in supporting transitions from high‐intensity, high‐cost hospital settings to more appropriate and desired care settings, such as the home.5563, 9798 Observational studies have yielded no differences in mortality between patients receiving palliative care and controls receiving the usual care.48, 55, 56
EDUCATION IN PALLIATIVE CARE
Curricular content on palliative care has been noticeably lacking from medical and nursing education curricula, textbooks, and certifying examinations, although this is beginning to change.8491 Both the Liaison Committee for Medical Education (LCME) and the Accreditation Council for Graduate Medical Education (ACGME) now require or strongly encourage programs to provide under‐ and postgraduate training in palliative care in order to be accredited.89, 90 As of 2005, more than 50% of teaching hospitals had established palliative care clinical services,92 which constitute the necessary platform for clinical training. The rapid growth in the availability of postgraduate fellowship training in palliative medicine will produce the faculty leaders needed for these educational and research programs in medical school and residency training programs.93, 94 Physicians in practice may gain knowledge and skills through a range of national courses and Web‐based resources and through preparation for the certifying exam given annually by the American Board of Hospice and Palliative Medicine4 (Table 1).
CONCLUSIONS
The growth in palliative care specialists and programs in hospitals in the United States represents a grass roots professional response to the needs of a patient population with chronic advanced illnesses and family care burdens within a healthcare system structured to provide care for acute intercurrent illness. Rapid increases in the number of new hospital programs, as well as early studies indicating improved clinical, satisfaction, and utilization outcomes, suggest that palliative care services are likely to become a routine and well‐integrated part of the healthcare continuum in the United States over the next several years. A number of resources are available to healthcare professionals seeking more training as well as to hospitals or nursing homes wishing to establish their own clinical or educational programs. Such programs have provided a platform for both newly graduated and seasoned professionals to continue to serve the needs of their patients through the assessment and relief of suffering, provided simultaneously with efforts to cure or mitigate disease.
The field of palliative care has grown rapidly in recent years in response to patient need and clinician interest in effective approaches to managing chronic life‐threatening illness.1 This article reviews the clinical, educational, demographic, and financial imperatives driving this growth, describes the clinical components of palliative care and the range of service models available, defines the relationship of hospital‐based palliative care to hospice, summarizes the literature on palliative care outcomes, and presents practical resources for clinicians seeking knowledge and skills in the field.
DEFINITION
Palliative care is medical care focused on the relief of suffering and support for the best possible quality of life for patients facing serious, life‐threatening illness and their families. It aims to identify and address the physical, psychological, and practical burdens of illness. Palliative care in the United States grew out of the hospice movement that originated in both the United Kingdom and the United States about 30 years ago. Hospice care was developed specifically to address the needs of the dying and their families and was codified in the United States by the addition in 1983 of a federal Medicare benefit for hospice care. In the last 30 years the Medicare hospice benefit has enabled more than 7 million patients and their families to receive intensive palliative care for the terminally ill, primarily in the home. The growth in the number and needs of seriously and chronically ill patients who are not clearly terminally ill has led to the development of palliative care services outside the hospice benefit provided by Medicare (and other insurers). Both hospice and nonhospice professionals have participated in extending the hospice approach through development of palliative care services. Palliative care may be delivered simultaneously with all appropriate curative and life‐prolonging interventions. In practice, palliative care practitioners provide assessment and treatment of pain and other symptom distress; employ communication skills with patients, families, and colleagues; support complex medical decision making and goal setting based on identifying and respecting patient wishes and goals; and promote medically informed care coordination, continuity, and practical support for patients, family caregivers, and professional colleagues across healthcare settings and through the trajectory of an illness.1, 2
Palliative care is both a general approach to health care and a growing practice specialty for professionals committing most or all of their time to the delivery of palliative care services.3 The term palliative medicine refers to the physician discipline within the larger field of palliative care. As of 2005, more than 1890 physicians have received specialty certification through a palliative care credentialing exam given by the American Board of Hospice and Palliative Medicine.4 Formal recognition of the subspecialty is currently being sought in collaboration with the American Board of Medical Specialties.5 As of August 2005, there were more than 50 postgraduate palliative care subspecialty fellowship programs in the United States.6 Between 2000 and 2003, the American Hospital Association (AHA) annual survey recorded a 67% growth in the number of hospital‐based palliative care programs reported, from 632 to 1027, for a total of 25% of responding AHA member hospitals.7
REASONS FOR GROWTH IN PALLIATIVE CARE
A primary justification for the rapid growth in palliative care programs in institutional settings is the abundant data demonstrating the high prevalence of pain and symptom distress in hospitals,811 nursing homes,12, 13 and community settings.14 Virtually all persons with serious illness spend at least some time in a hospital, usually on multiple occasions, in the course of their disease or condition.15 Despite the finding that when polled more than 90% of Americans say they would prefer to die at home, more than 75% of adult deaths occur in institutional settings (hospital or nursing homes)more than 50% in hospitals and 25% in nursing homesand 85% of pediatric deaths occur in hospitals.16, 17 Further, more than half of persons older than age 85 die in a nursing home and 43% of persons older than age 65 reside in a long‐term care facility at some time before they die,1821 a figure projected to rise substantially over the next several decades. The much larger number of patients who are not dying but are living with chronic, debilitating, and life‐threatening illness also need expert symptom management, communication and decision‐making support, and coordination of care across settings. In one national survey, physicians reported that poor care coordination resulted in patient communication problems, lack of emotional support for patients, adverse drug reactions, unnecessary hospitalization, patients not functioning to potential, and unnecessary pain.22 In addition to studies demonstrating high degrees of symptom distress across all age groups in hospitalized and nursing home patients,814 other works have shown high use of burdensome, nonbeneficial technologies among the seriously ill,2327 caregiver burden on families,2831 and communication problems between these patients, their families, and their treating physicians about the goals of care and the medical decisions that should follow.32, 33 Other studies have reported broad dissatisfaction with the general quality of care for the seriously ill and dying in hospitals and nursing homes,18, 34 specifically, perceptions of impersonal and indifferent care. Several studies of patients and their families have identified relief of suffering, practical support needs, open communication, and opportunities to relieve burdens on and strengthen relationships with family as the top‐priority needs from the healthcare system.3440
The growth in the number and needs of the elderly with multiple chronic conditions who will turn to the healthcare system in coming years underscores the need to create a delivery system in the United States that can be responsive to these priorities. By 2030 the number of persons with chronic conditions will exceed 157 million.4144 With the possible exception of advanced cancer conditions (accounting for 24% of adult deaths), in which prognosis is somewhat more reliably linked to performance status,4243 prognostication of outcome is a highly inexact science for the chronically ill of all ages and in a range of diagnostic categories, including stroke, dementia, and end‐stage cardiac, renal, hepatic, and pulmonary diseases. This has been a major part of the impetus for the growth in palliative care services not predicated on a link to terminal prognoses.4143 Hospitals and nursing homes are under increasing pressure to structure care processes in a manner fitted to the needs of the seriously ill because of studies demonstrating poor quality of care, demands from patients and families, accreditation requirements, and the costs of care for this patient population. More than 95% of Medicare spending goes to the 63% of Medicare patients with two or more chronic conditions, and three quarters of Medicare dollars go to hospitals.44 Hospital costs have risen nearly 10% per year in each of the last 2 years, because of both the increasing numbers of patients turning to them for care and the growth in the number and expense of effective life‐prolonging therapies. These forces have stimulated the development of new models for the efficient and effective care of patients with serious and complex illness.2227, 44
CLINICAL COMPONENTS
The three primary domains of palliative care clinical practice are assessment and treatment of pain and other symptom distress, including psychiatric symptoms64; communication about goals of care and support for complex medical decision making; and provision of practical and psychosocial support, care coordination, and continuity, as well as bereavement services if death occurs.1, 2, 65 Palliative care specialists work to support primary and specialist physicians in the care of complex and seriously ill patients by providing intensive bedside treatment and reassessment of multiple‐symptom distress, by helping with time‐consuming and difficult interactions with distressed patients and family members, and by attempting to ensure a seamless, safe, and well‐communicated discharge and follow‐up process after the patient leaves the hospital.66 Resources for physicians seeking more knowledge or training in the treatment of symptom distress and other aspects of palliative care are given in Table 1.
| Palliative care clinical competencies |
|---|
|
|
Education on Palliative and End of Life Care ( |
|
End of Life/Palliative Education Resource Center ( |
|
Department of Pain Medicine and Palliative Medicine at Beth Israel Medical Center ( |
|
|
|
American Academy of Hospice and Palliative Medicine ( |
|
American Board of Hospice and Palliative Medicine ( |
|
Center for Palliative Care at Harvard Medical School ( |
|
National Consensus Project on Quality Palliative Care ( |
|
American Geriatrics Society ( |
| Palliative care program development |
|
Center to Advance Palliative Care ( |
|
Palliative Care Leadership Centers ( |
|
Promoting Excellence in End of Life Care ( |
The core components of symptom management67, 68 include: 1) Routine and repeated formal assessment, without which most symptoms will be neither identified nor addressed; 2) Expertise in prescribing, including the safe use of opioid analgesics, adjuvant approaches to pain management, and management of a wide range of other common and distressing symptoms and syndromes including, for example, delirium, dyspnea, fatigue, nausea, bowel obstruction, and depression69; and 3) Skillful management of treatment side effects, which is required to successfully control symptoms.
Communication skills and effective support for making decisions about clinical care goals include not only fundamental physician responsibilities such as communicating bad news and elucidating patient wishes for future care, but also the ability to promote communication and consensus about care goals among multiple specialist consultants, to address and resolve disagreements and conflicts among patients, families, and providers about goals of care, and to assist in the evolving process of balancing the benefits with the burdens of various medical interventions.32, 7073
The great majority of care for an illness is provided at home by family members neither trained nor emotionally prepared for these responsibilities.51, 74 The burden on family caregivers is one of the top concerns of seriously ill patients.35 Patients and families often struggle with anxieties about doing the wrong thing, difficulty traveling to physicians' offices, social isolation, and a high prevalence of preventable suffering of all types.3440 Palliative care clinicians attempt to improve the success and sustainability of the discharge plan by providing medically informed and therefore more appropriate care management recommendations and by mobilizing a range of community resources to increase the likelihood that families will be able to manage the care at home with the necessary supports and backups in place, including appropriate screening and referrals for complicated grief and bereavement.51, 75, 76 Several small prospective studies of palliative care have suggested that palliative care has resulted in reduction in the number of emergency department visits and hospitalizations and in the length of hospital stays, presumably because of the efficacy and comprehensiveness of care coordination in averting crises.54, 55, 61, 9798
CLINICAL MODELS
Given the multifaceted approach needed to support patient quality of life throughout advanced illness, one profession or individual cannot be expected to provide all aspects of palliative care. As described in the recently completed National Consensus Project Guidelines for Quality Palliative Care,2 specialty‐level palliative care is optimally delivered through an interdisciplinary team consisting of appropriately trained and credentialed physicians, nurses, and social workers with additional support and contributions from chaplains, rehabilitative experts, psychiatrists, and other professionals as indicated. Clearly, however, the staffing of a palliative care program will depend critically on the needs and capacities of the setting. A full interdisciplinary team is needed for a large tertiary‐care teaching hospital, whereas a part‐time advance‐practice nurse with backup from colleagues as needed may suffice for a small rural hospital or long‐term care setting. Specialist‐level palliative care is delivered through a range of clinical models and settings, including inpatient consultation services, dedicated inpatient units, and outpatient practices, among others.77, 78 Programs within the United States are housed in a range of clinical subspecialties including oncology, geriatrics, nursing, case management, hospitalist, and other programs, depending on the locus of leadership and administrative support.77, 78 Most programs are supported by utilizing diverse sources,77 including physician and nurse‐practitioner billing through insurers such as Medicare Part B,53, 81 as well as hospital support typically predicated on cost avoidance analyses, foundation and other grants, and philanthropy. Detailed guidance on appropriate documentation and billing for palliative care physician services may be found in Schapiro et al.,53 von Gunten,79 and on the Web site of the Center to Advance Palliative Care (
RELATIONSHIP TO HOSPICE
Although new clinical specialties in palliative medicine and nursing are emerging, in the United States palliative care for those in the terminal stages of illness has been delivered through hospice programs for more than 30 years. Under current regulatory and payment guidelines hospice care is delivered to patients who are certified by their physicians as likely to die within 6 months if the disease follows its usual course and who are willing to give up insurance coverage for medical treatment primarily focused on cure or prolongation of life. It is noteworthy that there is great variability among United States hospices, with some able to support continued disease‐modifying treatments such as chemotherapy and radiation if a patient so desires.2 Hospice programs aim to create increased opportunity for death at home, focusing on symptom control and the psychological and spiritual issues that are paramount to persons in the terminal phases of illness. Once the hospice benefit has been accessed, patients and families receive comprehensive case‐managed services across all settings of care (although the great majority of hospice care is delivered at home) from an interdisciplinary team, coverage for medications and equipment related to the terminal illness, and practical, psychosocial, respite, and bereavement support for caregivers.80, 81 Several recent studies have confirmed the findings of an earlier work82 in demonstrating the beneficial outcomes of hospice care including reduced mortality in spouses and high levels of family satisfaction.18, 83 Palliative care programs based in both hospital and community settings have led to increases in hospice referral rates and hospice length of stay, promoting continuity of palliative care and the intensive palliation and family support needed as death approaches.55 Coordination and partnerships between palliative care and hospice programs are critical to achieving continuity of palliative care throughout the full course of an illness and across the continuum of care settings.2
IMPACT OF PALLIATIVE CARE ON QUALITY OF CARE
Reports on palliative care specialist services utilizing diverse models and approaches have suggested a range of benefits from palliative care, including reduced pain4547 and other symptom distress,45, 48, 49 improved health‐related quality of life,95 high patient and family satisfaction18, 4951, 96 with care and with physician communication, and increased likelihood of the location of death being outside a hospital.33, 49, 52, 9799
Because it can help to demonstrate care structures, processes, and outcomes associated with improved quality (such as routine assessment of pain in the hospital), a palliative care program may help hospitals measure and meet Joint Commission for Accreditation of Healthcare Organizations (JCAHO) requirements in the domains of pain management, communication, family and patient education, and continuity of care, among others.53 Several groups have reported marked increases in hospice referral rate and hospice length of stay as a result of hospital‐ and nursing‐home‐based palliative care programs, presumably as a result of enhanced case identification, counseling, and referral processes.54, 55 Case control and observational studies of palliative care and ethics consultation services have demonstrated reductions in costs per day and in hospital and ICU lengths of stay, presumably because of enhanced support for discussions about the goals of care and the resulting facilitation of patient and family decisions about the types and settings of future care.50, 5561 Hospitals have begun to invest in palliative care services, both to enhance quality of care and because of their measurable impact on reducing ICU and total bed days and their efficacy in supporting transitions from high‐intensity, high‐cost hospital settings to more appropriate and desired care settings, such as the home.5563, 9798 Observational studies have yielded no differences in mortality between patients receiving palliative care and controls receiving the usual care.48, 55, 56
EDUCATION IN PALLIATIVE CARE
Curricular content on palliative care has been noticeably lacking from medical and nursing education curricula, textbooks, and certifying examinations, although this is beginning to change.8491 Both the Liaison Committee for Medical Education (LCME) and the Accreditation Council for Graduate Medical Education (ACGME) now require or strongly encourage programs to provide under‐ and postgraduate training in palliative care in order to be accredited.89, 90 As of 2005, more than 50% of teaching hospitals had established palliative care clinical services,92 which constitute the necessary platform for clinical training. The rapid growth in the availability of postgraduate fellowship training in palliative medicine will produce the faculty leaders needed for these educational and research programs in medical school and residency training programs.93, 94 Physicians in practice may gain knowledge and skills through a range of national courses and Web‐based resources and through preparation for the certifying exam given annually by the American Board of Hospice and Palliative Medicine4 (Table 1).
CONCLUSIONS
The growth in palliative care specialists and programs in hospitals in the United States represents a grass roots professional response to the needs of a patient population with chronic advanced illnesses and family care burdens within a healthcare system structured to provide care for acute intercurrent illness. Rapid increases in the number of new hospital programs, as well as early studies indicating improved clinical, satisfaction, and utilization outcomes, suggest that palliative care services are likely to become a routine and well‐integrated part of the healthcare continuum in the United States over the next several years. A number of resources are available to healthcare professionals seeking more training as well as to hospitals or nursing homes wishing to establish their own clinical or educational programs. Such programs have provided a platform for both newly graduated and seasoned professionals to continue to serve the needs of their patients through the assessment and relief of suffering, provided simultaneously with efforts to cure or mitigate disease.
- ,.Clinical practice: palliative care.N Engl J Med.2004;350:2582–2590.
- National Consensus Project for Quality Palliative Care: The development of practice guidelines 2004. Available from URL:http://www.nationalconsensusproject.org. [accessed August 10, 2005].
- ,.Palliative medicine: an emerging field of specialization.Cancer Invest.2000;18:761–767.
- American Board of Hospice and Palliative Medicine. Available from URL:http://www.abhpm.org[accessed August 10, 2005].
- ,,, et al.Physician board certification in hospice and palliative medicine.J Palliat Med.2000;3:441–447.
- American Academy of Hospice and Palliative Medicine. Available from URL:http://www.aahpm.org[accessed August 10, 2005].
- American Hospital Association. Hospital Statistics 2004. Available from URL:http://www.ahastatistics.org[accessed August 10, 2005].
- ,,.Pain and satisfaction with pain control in hospitalized medical patients.Arch Intern Med.2004;164:175–180.
- ,,, et al.Pain and discomfort associated with common hospital procedures and experiences.J Pain Symptom Manage.1998;15:91–101.
- ,,, et al. The symptom burden of seriously ill hospitalized patients.J Pain Symptom Manage.1999;17:248–255.
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT).The SUPPORT Principal Investigators.JAMA.1995;274:1591–1598.
- ,,, et al.Persistent pain in nursing home residents.JAMA.2001;285:2081.
- ,,, et al.Management of pain in elderly patients with cancer. SAGE Study Group. Systematic assessment of geriatric drug use via epidemiology.JAMA.1998;279:1877–1882.
- ,,, et al.Pain and its treatment in outpatients with metastatic cancer.N Engl J Med.1994;330:592–596.
- Dartmouth Atlas. Available from URL: http://www.dartmouthatlas.org/endoflife/end_of_life.php[accessed August 10, 2005].
- Institute of Medicine.Approaching death: improving care at the end of life.Washington, DC:National Academy Press,1997.
- Institute of Medicine.When Children die: improving palliative and end of life care for children and their families.Washington, DC:National Academies Press,2002.
- ,,, et al.Family perspectives on end‐of‐life care at the last place of care.JAMA.2004;291:88–93.
- . Brown Atlas. Available from URL:http://www.chcr.brown.edu/dying/brownatlas.htm[accessed August 10, 2005].
- .Creating excellent palliative care in nursing homes.J Palliat Med.2003;6:7–9.
- ,,, et al.Needs of the dying in nursing homes.J Palliat Med.2002;5:895–901.
- Mathematica Policy Research, Inc.National public engagement campaign on chronic illness—physician survey, final report.Princeton, NJ:Mathematica Policy Research, Inc.,2001.
- ,,,.Patterns of use of common major procedures in medical care of older adults.J Am Geriatr Soc.1999;47:553–558.
- ,.Dying to pay: the cost of end of life care.J Palliat Care.1998;14:5–15.
- ,,, et al.Older age, aggressiveness of care, and survival for seriously ill, hospitalized adults. SUPPORT Investigators. Study to understand prognoses and preferences for outcomes and risks of treatments.Ann Intern Med.1999;131:721–728.
- .Demands of an aging population for critical care and pulmonary services.JAMA.2001;285:1016–1017.
- ,,,.Medicare beneficiaries' costs of care in the last year of life.Health Aff.2001;20:188–195.
- ,,,.Stress in caregivers of hospitalized oldest‐old patients.J Gerontol A Biol Sci Med Sci.2001;56:M231–M235.
- ,.Caregiving as a risk factor for mortality: the Caregiver Health Effects Study.JAMA.1999;282:2215–2219.
- ,,,,,.Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients.N Engl J Med.1999;341:956–963.
- ,,, et al.The impact of serious illness on patients' families.JAMA.1994;272:1839–1844.
- .Doctor–patient communication. In:Morrison RS,Meier DE, editors.Geriatric palliative care.New York:Oxford University Press,2003.
- ,.Communicating sad, bad, and difficult news in medicine.Lancet.2004;363:312–319.
- ,,,.Understanding economic and other burdens of terminal illness: the experience of patients and their caregivers.Ann Intern Med.2000;132:451–459.
- ,,.Quality end‐of‐life care: patients' perspectives.JAMA.1999;281:163–168.
- ,,, et al.Preparing for the end of life: preferences of patients, families, physicians, and other care providers.J Pain Symptom Manage.2001;22:727–737.
- ,,, et al.Factors considered important at the end of life by patients, family, physicians, and other care providers.JAMA.2000;284:2476–2482.
- ,,,,,.In search of a good death: observations of patients, families, and providers.Ann Intern Med.2000;132:825–832.
- ,,, et al.Measurement of quality of care and quality of life at the end of life.Gerontologist.2002;42:71–80.
- ,,, et al.Family reports of barriers to optimal care of the dying.Nurs Res.2000;49:310–317.
- ,,, et al.Patterns of functional decline at the end of life.JAMA.2003;289:2387–2392.
- ,, Cohn F, et al. Prognoses of seriously ill hospitalized patients on the days before death: implications for patient care and public policy.New Horizons.1997;5:56–61.
- ,,, et al.The last 2 years of life: functional trajectories of frail older people.J Am Geriatr Soc.2003;51:492–498.
- Partnership for Solutions. Chronic Conditions:Making the Case for Ongoing Care.Baltimore:Johns Hopkins University,2002.
- ,,, et al.Is there evidence that palliative care teams alter end‐of‐life experiences of patients and their caregivers?J Pain Symptom Manage.2003;25:150–168.
- ,,, et al.Implementing guidelines for cancer pain management: results of a randomized controlled clinical trial.J Clin Oncol.1999;17:361–370.
- ,,, et al.Randomized clinical trial of an implantable drug delivery system compared with comprehensive medical management for refractory cancer pain: impact on pain, drug‐related toxicity, and survival.J Clin Oncol2002;20:4040–4049.
- ,,, et al.The comprehensive care team: a controlled trial of outpatient palliative medicine consultation.Arch Intern Med.2004;164:83–91.
- ,,, et al.Palliative care consultations: how do they impact the care of hospitalized patients?J Pain Symptom Manage.2000;20:166–173.
- ,,, et al.An intensive communication intervention for the critically ill.Am J Med.2000;109:469–475.
- ,,.The moderating influence of service use on negative caregiving consequences.J Gerontol B Psychol Sci Soc Sci.1996;51:S121–131.
- ,,.Communication skills training for health care professionals working with cancer patients, their families and/or carers (Cochrane Review).The Cochrane Library. Chichester, UK:John Wiley 21:1412–1415.
- ,,, et al. Living and dying well with cancer: Successfully integrating palliative care and cancer treatment. Available from URL:http://www.promotingexcellence.org[accessed August 10, 2005].
- ,,, et al.A high‐volume specialist palliative care unit and team may reduce in‐hospital end‐of‐life care costs.J Palliat Med.2003;6:699–705.
- ,,, et al.Effect of ethics consultations on nonbeneficial life‐sustaining treatments in the intensive care setting.JAMA.2003;290:1166–1172.
- ,.Impact of a proactive approach to improve end‐of‐life care in a medical ICU.Chest.2003;123:266–271.
- ,,, et al.A randomized controlled trial of the cost‐effectiveness of a district co‐ordinating service for terminally ill cancer patients.Palliat Med.1996;10:151–161.
- ,,, et al.The impact of a regional palliative care program on the cost of palliative care delivery.J Palliat Med.1999;3:181–186.
- ,,.Effectiveness of a home‐based palliative care program for end‐of‐life.J Palliat Med.2003;6:715–724.
- ,,.A study of proactive ethics consultation for critically and terminally ill patients with extended lengths of stay.Crit Care Med.1998;26:252–259.
- ,.Experience with an end‐of‐life practice at a university hospital.Crit Care Med.1997;25:197–202.
- .Perspectives on care at the close of life. Psychological considerations, growth, and transcendence at the end of life: the art of the possible.JAMA.2001;285:2898–2905.
- ,,.Improving palliative care.Ann Intern Med.1997;127:225–230.
- .Completing the continuum of cancer care: integrating life‐prolongation and palliation.CA Cancer J Clin.2000;50:123–132.
- ,.Pain management: pharmacological approaches.Cancer Treat Res.1999;100:1–29.
- ,.Pain and symptom management in palliative care.Cancer Control.1996;3:204–213.
- .ABC of palliative care. Anorexia, cachexia, and nutrition.BMJ.1997;315:1219–1222.
- .Perspectives on care at the close of life. Initiating end‐of‐life discussions with seriously ill patients: addressing the “elephant in the room.”JAMA.2000;284:2502–2507.
- ,,.“I wish things were different”: expressing wishes in response to loss, futility, and unrealistic hopes.Ann Intern Med.2001;135:551–555.
- ,,.Discussing palliative care with patients. ACP‐ASIM End‐of‐Life Care Consensus Panel.Ann Intern Med.1999;130:744–749.
- ,,.The patient‐physician relationship. Ensuring competency in end‐of‐life care: communication and relational skills.JAMA.2000;284:3051–3057.
- .The loneliness of the long‐term care giver.N Engl J Med.1999;340:1587–1590.
- ,,,,,.Integrating case management and palliative care.J Palliat Med.2004;7:121–136.
- ,,.The influence of caregiving and bereavement support on adjusting to an older relative's death.Gerontologist.1991;31:32–42.
- Center to Advance Palliative Care. A guide to developing a hospital‐based palliative care program. Available from URL:http://www.capc.org[accessed August 10, 2005].
- .Secondary and tertiary palliative care in US hospitals.JAMA.2002;287:875–881.
- .Coding and reimbursement mechanisms for physician services in hospice and palliative care.J Palliat Med.2000;2:157–164.
- National Hospice and Palliative Care Organization. NHPCO facts and figures. Available from URL:http://www.nhpco.org[accessed August 10, 2005].
- .When pain and suffering do not require a prognosis: Working toward meaningful hospital–hospice partnership.J Palliat Med.2003;6:109–115.
- ,,, et al.An alternative in terminal care: results of the National Hospice Study.J Chronic Dis.1986;39:9–26.
- ,.The health impact of health care on families: a matched cohort study of hospice use by decedents and mortality outcomes in surviving, widowed spouses.Soc Sci Med.2003;57:465–475.
- ,.Educational programs in US medical schools, 2002–2003.JAMA.2003;290:1190–1196.
- .Medical education in end‐of‐life care: the status of reform.J Palliat Med.2002;5:243–248.
- ,.ACGME requirements for end‐of‐life training in selected residency and fellowship programs: a status report.Acad Med.2002;77:299–304.
- ,,, et al.Recommendations for incorporating palliative care education into the acute care hospital setting.Acad Med.1999;74:871–877.
- ,,.The status of medical education in end‐of‐life care: a national report.J Gen Intern Med.2003;18:685–695.
- Liaison Committee on Medical Education. Available from URL: http://www.lcme.org[accessed August 10, 2005].
- Accreditation Council for Graduate Medical Education.Program requirements for residency education in the subspecialties of internal medicine. Graduate Medical Education Directory 2000–2001. Chicago,2000.
- ,.Palliative care in undergraduate medical education. Status report and future directions.JAMA.1997;278:733–738.
- ,.Survey of palliative care programs in United States teaching hospitals.J Palliat Med.2001;4:309–314.
- ,,, et al.Initial voluntary program standards for fellowship training in palliative medicine.J Palliat Med.2002;5:23–33.
- American Academy of Hospice and Palliative Medicine. Fellowship Program Directory. Available from URL:http://www.aahpm.org/fellowship/directory/htm[accessed August 10, 2005].
- ,,, et al.Quality of life in palliative cancer care. Results from a cluster randomized trial.J Clin Oncol.2001;19:3884–3894.
- ,,.Family satisfaction with end‐of‐life care for cancer patients in a cluster randomized trial.J Pain Symptom Manage.2002;24:53–63.
- ,,, et al.A palliative care intervention and death at home: a cluster randomized trial.Lancet.2000;356:888–893.
- ,,.Impact of palliative care case management on resource use by patients dying of cancer at a Veterans Affairs medical center.J Palliat Med.2005;8:26–35.
- ,,.Family satisfaction with end‐of‐life care for cancer patients in a cluster randomized trial.J Pain Symptom Manage.2002;24:53–63
- ,.Clinical practice: palliative care.N Engl J Med.2004;350:2582–2590.
- National Consensus Project for Quality Palliative Care: The development of practice guidelines 2004. Available from URL:http://www.nationalconsensusproject.org. [accessed August 10, 2005].
- ,.Palliative medicine: an emerging field of specialization.Cancer Invest.2000;18:761–767.
- American Board of Hospice and Palliative Medicine. Available from URL:http://www.abhpm.org[accessed August 10, 2005].
- ,,, et al.Physician board certification in hospice and palliative medicine.J Palliat Med.2000;3:441–447.
- American Academy of Hospice and Palliative Medicine. Available from URL:http://www.aahpm.org[accessed August 10, 2005].
- American Hospital Association. Hospital Statistics 2004. Available from URL:http://www.ahastatistics.org[accessed August 10, 2005].
- ,,.Pain and satisfaction with pain control in hospitalized medical patients.Arch Intern Med.2004;164:175–180.
- ,,, et al.Pain and discomfort associated with common hospital procedures and experiences.J Pain Symptom Manage.1998;15:91–101.
- ,,, et al. The symptom burden of seriously ill hospitalized patients.J Pain Symptom Manage.1999;17:248–255.
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT).The SUPPORT Principal Investigators.JAMA.1995;274:1591–1598.
- ,,, et al.Persistent pain in nursing home residents.JAMA.2001;285:2081.
- ,,, et al.Management of pain in elderly patients with cancer. SAGE Study Group. Systematic assessment of geriatric drug use via epidemiology.JAMA.1998;279:1877–1882.
- ,,, et al.Pain and its treatment in outpatients with metastatic cancer.N Engl J Med.1994;330:592–596.
- Dartmouth Atlas. Available from URL: http://www.dartmouthatlas.org/endoflife/end_of_life.php[accessed August 10, 2005].
- Institute of Medicine.Approaching death: improving care at the end of life.Washington, DC:National Academy Press,1997.
- Institute of Medicine.When Children die: improving palliative and end of life care for children and their families.Washington, DC:National Academies Press,2002.
- ,,, et al.Family perspectives on end‐of‐life care at the last place of care.JAMA.2004;291:88–93.
- . Brown Atlas. Available from URL:http://www.chcr.brown.edu/dying/brownatlas.htm[accessed August 10, 2005].
- .Creating excellent palliative care in nursing homes.J Palliat Med.2003;6:7–9.
- ,,, et al.Needs of the dying in nursing homes.J Palliat Med.2002;5:895–901.
- Mathematica Policy Research, Inc.National public engagement campaign on chronic illness—physician survey, final report.Princeton, NJ:Mathematica Policy Research, Inc.,2001.
- ,,,.Patterns of use of common major procedures in medical care of older adults.J Am Geriatr Soc.1999;47:553–558.
- ,.Dying to pay: the cost of end of life care.J Palliat Care.1998;14:5–15.
- ,,, et al.Older age, aggressiveness of care, and survival for seriously ill, hospitalized adults. SUPPORT Investigators. Study to understand prognoses and preferences for outcomes and risks of treatments.Ann Intern Med.1999;131:721–728.
- .Demands of an aging population for critical care and pulmonary services.JAMA.2001;285:1016–1017.
- ,,,.Medicare beneficiaries' costs of care in the last year of life.Health Aff.2001;20:188–195.
- ,,,.Stress in caregivers of hospitalized oldest‐old patients.J Gerontol A Biol Sci Med Sci.2001;56:M231–M235.
- ,.Caregiving as a risk factor for mortality: the Caregiver Health Effects Study.JAMA.1999;282:2215–2219.
- ,,,,,.Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients.N Engl J Med.1999;341:956–963.
- ,,, et al.The impact of serious illness on patients' families.JAMA.1994;272:1839–1844.
- .Doctor–patient communication. In:Morrison RS,Meier DE, editors.Geriatric palliative care.New York:Oxford University Press,2003.
- ,.Communicating sad, bad, and difficult news in medicine.Lancet.2004;363:312–319.
- ,,,.Understanding economic and other burdens of terminal illness: the experience of patients and their caregivers.Ann Intern Med.2000;132:451–459.
- ,,.Quality end‐of‐life care: patients' perspectives.JAMA.1999;281:163–168.
- ,,, et al.Preparing for the end of life: preferences of patients, families, physicians, and other care providers.J Pain Symptom Manage.2001;22:727–737.
- ,,, et al.Factors considered important at the end of life by patients, family, physicians, and other care providers.JAMA.2000;284:2476–2482.
- ,,,,,.In search of a good death: observations of patients, families, and providers.Ann Intern Med.2000;132:825–832.
- ,,, et al.Measurement of quality of care and quality of life at the end of life.Gerontologist.2002;42:71–80.
- ,,, et al.Family reports of barriers to optimal care of the dying.Nurs Res.2000;49:310–317.
- ,,, et al.Patterns of functional decline at the end of life.JAMA.2003;289:2387–2392.
- ,, Cohn F, et al. Prognoses of seriously ill hospitalized patients on the days before death: implications for patient care and public policy.New Horizons.1997;5:56–61.
- ,,, et al.The last 2 years of life: functional trajectories of frail older people.J Am Geriatr Soc.2003;51:492–498.
- Partnership for Solutions. Chronic Conditions:Making the Case for Ongoing Care.Baltimore:Johns Hopkins University,2002.
- ,,, et al.Is there evidence that palliative care teams alter end‐of‐life experiences of patients and their caregivers?J Pain Symptom Manage.2003;25:150–168.
- ,,, et al.Implementing guidelines for cancer pain management: results of a randomized controlled clinical trial.J Clin Oncol.1999;17:361–370.
- ,,, et al.Randomized clinical trial of an implantable drug delivery system compared with comprehensive medical management for refractory cancer pain: impact on pain, drug‐related toxicity, and survival.J Clin Oncol2002;20:4040–4049.
- ,,, et al.The comprehensive care team: a controlled trial of outpatient palliative medicine consultation.Arch Intern Med.2004;164:83–91.
- ,,, et al.Palliative care consultations: how do they impact the care of hospitalized patients?J Pain Symptom Manage.2000;20:166–173.
- ,,, et al.An intensive communication intervention for the critically ill.Am J Med.2000;109:469–475.
- ,,.The moderating influence of service use on negative caregiving consequences.J Gerontol B Psychol Sci Soc Sci.1996;51:S121–131.
- ,,.Communication skills training for health care professionals working with cancer patients, their families and/or carers (Cochrane Review).The Cochrane Library. Chichester, UK:John Wiley 21:1412–1415.
- ,,, et al. Living and dying well with cancer: Successfully integrating palliative care and cancer treatment. Available from URL:http://www.promotingexcellence.org[accessed August 10, 2005].
- ,,, et al.A high‐volume specialist palliative care unit and team may reduce in‐hospital end‐of‐life care costs.J Palliat Med.2003;6:699–705.
- ,,, et al.Effect of ethics consultations on nonbeneficial life‐sustaining treatments in the intensive care setting.JAMA.2003;290:1166–1172.
- ,.Impact of a proactive approach to improve end‐of‐life care in a medical ICU.Chest.2003;123:266–271.
- ,,, et al.A randomized controlled trial of the cost‐effectiveness of a district co‐ordinating service for terminally ill cancer patients.Palliat Med.1996;10:151–161.
- ,,, et al.The impact of a regional palliative care program on the cost of palliative care delivery.J Palliat Med.1999;3:181–186.
- ,,.Effectiveness of a home‐based palliative care program for end‐of‐life.J Palliat Med.2003;6:715–724.
- ,,.A study of proactive ethics consultation for critically and terminally ill patients with extended lengths of stay.Crit Care Med.1998;26:252–259.
- ,.Experience with an end‐of‐life practice at a university hospital.Crit Care Med.1997;25:197–202.
- .Perspectives on care at the close of life. Psychological considerations, growth, and transcendence at the end of life: the art of the possible.JAMA.2001;285:2898–2905.
- ,,.Improving palliative care.Ann Intern Med.1997;127:225–230.
- .Completing the continuum of cancer care: integrating life‐prolongation and palliation.CA Cancer J Clin.2000;50:123–132.
- ,.Pain management: pharmacological approaches.Cancer Treat Res.1999;100:1–29.
- ,.Pain and symptom management in palliative care.Cancer Control.1996;3:204–213.
- .ABC of palliative care. Anorexia, cachexia, and nutrition.BMJ.1997;315:1219–1222.
- .Perspectives on care at the close of life. Initiating end‐of‐life discussions with seriously ill patients: addressing the “elephant in the room.”JAMA.2000;284:2502–2507.
- ,,.“I wish things were different”: expressing wishes in response to loss, futility, and unrealistic hopes.Ann Intern Med.2001;135:551–555.
- ,,.Discussing palliative care with patients. ACP‐ASIM End‐of‐Life Care Consensus Panel.Ann Intern Med.1999;130:744–749.
- ,,.The patient‐physician relationship. Ensuring competency in end‐of‐life care: communication and relational skills.JAMA.2000;284:3051–3057.
- .The loneliness of the long‐term care giver.N Engl J Med.1999;340:1587–1590.
- ,,,,,.Integrating case management and palliative care.J Palliat Med.2004;7:121–136.
- ,,.The influence of caregiving and bereavement support on adjusting to an older relative's death.Gerontologist.1991;31:32–42.
- Center to Advance Palliative Care. A guide to developing a hospital‐based palliative care program. Available from URL:http://www.capc.org[accessed August 10, 2005].
- .Secondary and tertiary palliative care in US hospitals.JAMA.2002;287:875–881.
- .Coding and reimbursement mechanisms for physician services in hospice and palliative care.J Palliat Med.2000;2:157–164.
- National Hospice and Palliative Care Organization. NHPCO facts and figures. Available from URL:http://www.nhpco.org[accessed August 10, 2005].
- .When pain and suffering do not require a prognosis: Working toward meaningful hospital–hospice partnership.J Palliat Med.2003;6:109–115.
- ,,, et al.An alternative in terminal care: results of the National Hospice Study.J Chronic Dis.1986;39:9–26.
- ,.The health impact of health care on families: a matched cohort study of hospice use by decedents and mortality outcomes in surviving, widowed spouses.Soc Sci Med.2003;57:465–475.
- ,.Educational programs in US medical schools, 2002–2003.JAMA.2003;290:1190–1196.
- .Medical education in end‐of‐life care: the status of reform.J Palliat Med.2002;5:243–248.
- ,.ACGME requirements for end‐of‐life training in selected residency and fellowship programs: a status report.Acad Med.2002;77:299–304.
- ,,, et al.Recommendations for incorporating palliative care education into the acute care hospital setting.Acad Med.1999;74:871–877.
- ,,.The status of medical education in end‐of‐life care: a national report.J Gen Intern Med.2003;18:685–695.
- Liaison Committee on Medical Education. Available from URL: http://www.lcme.org[accessed August 10, 2005].
- Accreditation Council for Graduate Medical Education.Program requirements for residency education in the subspecialties of internal medicine. Graduate Medical Education Directory 2000–2001. Chicago,2000.
- ,.Palliative care in undergraduate medical education. Status report and future directions.JAMA.1997;278:733–738.
- ,.Survey of palliative care programs in United States teaching hospitals.J Palliat Med.2001;4:309–314.
- ,,, et al.Initial voluntary program standards for fellowship training in palliative medicine.J Palliat Med.2002;5:23–33.
- American Academy of Hospice and Palliative Medicine. Fellowship Program Directory. Available from URL:http://www.aahpm.org/fellowship/directory/htm[accessed August 10, 2005].
- ,,, et al.Quality of life in palliative cancer care. Results from a cluster randomized trial.J Clin Oncol.2001;19:3884–3894.
- ,,.Family satisfaction with end‐of‐life care for cancer patients in a cluster randomized trial.J Pain Symptom Manage.2002;24:53–63.
- ,,, et al.A palliative care intervention and death at home: a cluster randomized trial.Lancet.2000;356:888–893.
- ,,.Impact of palliative care case management on resource use by patients dying of cancer at a Veterans Affairs medical center.J Palliat Med.2005;8:26–35.
- ,,.Family satisfaction with end‐of‐life care for cancer patients in a cluster randomized trial.J Pain Symptom Manage.2002;24:53–63
Handoffs
I'm used to feeling inadequate. Oftentimes, what ails my patients I'm not able to address, let alone fix. But one time I crossed the line from absorber of sorrows to active agent.
All set with my preconceived notions, I went into the hospital room to see Stan. He had severe hypertension and had had several previous transient ischemic attacks, and now he was back with another. His renal function was minimal, with dialysis coming soon. Despite our repeatedly having social work arrange outpatient appointments, he had never followed up. Last admission, they even gave him a month's worth of his antihypertensive medications, but here he was 6 weeks later off meds and admitted again.
I spoke with him but we got nowhere. He maintained that he could not afford his medication. I asked him why he didn't work. He said that he did do odd jobs, and besides, in a few months he would qualify for Social Security. I guess I was in a bad mood, so I heard myself ask, Do you realize you are playing with fire here? You will end up with a real stroke? Simply saying you want to wait for Social Security is not a plan.
Stan looked at me closely. Probably judging me to be about half his age, he said, Whatever, doc. Don't you have someone else to lecture? I sat down, took a deep breath, and tried to sound kind when I said, Do you realize that you will need dialysis soon? Stan replied that he had no intention of going on dialysis. We went in circles, with me trying to determine if he was delusional, suicidal, or trying to shock me. We left it as it was. The medical system would do its best, but his life was his to run.
Bending the HIPPA rules, I went to the nurse's station and called Stan's daughter to get some background, answers to questions like why she couldn't help him buy his medication. I was wholly in my righteous problem‐solving mode. Yet she was not alarmed by my dire prognostics. When the call was about to end, I asked if all of us could meet when she came to pick him up the next day. After a pause, she stated, I'm not coming up. Tell him to wait in the lobby for me. I'll be there to pick him up sometime after 5. Collecting her dad from the hospital on Christmas Eve, and she couldn't be bothered to enter the building? I hung up, sat back in my chair, and stared at my progress note.
I subsequently found out from the case manager that after being discharged, unlike before, he was going to a homeless shelter, not his daughter's house. I thought he must have been an awful father for a child to turn her own dad away on Christmas Eve.
Clearly, she had had no intention of picking him up from the hospital before my call; I had inadvertently shamed her into it.
I went back to talk with Stan. I decided to make inquiries of him based only on the information I was supposed to have. The case manager tells me you're going to the homeless shelter tomorrow. Don't you live with your daughter?
Not realizing that the doctors and case managers were on the same team, he seemed somewhat taken aback. I found a chair and sat down as he spoke. I wasn't always like this, you know. I'm not a drinker, nuts, or anything; I just was put out to pasture. I'm a computer programmer but not the new kind. I worked on those huge 1960s types. The personal computer revolution put me out of business. Before I had a chance to say anything, he continued, I know what you're thinking, I should have gotten trained or something to keep up, but I didn't, you know, I just didn't. I should've.
He must have seen a flicker of compassion on my face, as he went on, I've been staying with my daughter on and off for years. I'd get some job, get a place, but never for long. I don't like to stay with her. She has her own life, her own problems. She doesn't need me getting in the way, especially around Christmas. Around the holidays, I go to the shelter. My grandkids don't need me ruining the season.
He may well have been a lousy father, but I didn't see his medical noncompliance as a personal affront anymore. He should have made some different decisions in the past, but now he was a 64‐year‐old homeless man, alone. So, besides lecturing him on his blood pressure and work habits, could I do anything really helpful?
It didn't take me long to come up with something. The problem was how to approach it. Feeling like I was breaking some rule, I trailed him to the hospital lobby right after discharge. To my chagrin, he didn't so much as slow down. He saw his daughter's car, walked out, and got in her car before I knew what to do. Feeling like a fool, I stood at the window, noted how slate gray and dour the sky was, in complete contrast to the festive lobby, and thought about how useless I really was in the end. All my good intentions aside, he was no better off for having me as his doctor.
I bought myself a cup of coffee and while walking lost in thought, I literally bumped into Stan coming through the hospital's main doors. Laughing awkwardly, he said, I forgot my jacket in my room. He looked more scared now than he did after hearing my dire pronouncements of doom. He seemed like a child whose mother was angry at his forgetfulness. As he shuffled off, I couldn't stand it any longer. I didn't want him rushing around worried that his daughter would get fed up and leave. I told him to tell his daughter that I knew where his jacket was and that I'd be right back with it.
I got the coat, and when I approached him back in the lobby, I gave it to him. I then handed him the money I had set aside in my white coat. Trying to make myself sound casual, I said, Use this to take your grandkids out to dinner and buy them something. Neither wanting to give him a chance to say no nor wishing to make it more awkward for him, I quickly turned around and left without looking back.
As I resumed my $2 cup of coffee, I wondered if I had acted as a doctor, as a good Samaritan, or as an egoist? I was not deluded into believing I could buy his pride back for long with my pocket change. But maybe I could be a good person in addition to a caring, up‐to‐date doctor.
Later that day in the ER, a very sad place on Christmas Eve, I imagined Stan buying gifts or a fancy dinner for his family, just like he used to. He will need dialysis and probably will end up back in the shelter. I don't think he even knew my name, but maybe because I cared a little bit about what happened to him, he will, too.
I'm used to feeling inadequate. Oftentimes, what ails my patients I'm not able to address, let alone fix. But one time I crossed the line from absorber of sorrows to active agent.
All set with my preconceived notions, I went into the hospital room to see Stan. He had severe hypertension and had had several previous transient ischemic attacks, and now he was back with another. His renal function was minimal, with dialysis coming soon. Despite our repeatedly having social work arrange outpatient appointments, he had never followed up. Last admission, they even gave him a month's worth of his antihypertensive medications, but here he was 6 weeks later off meds and admitted again.
I spoke with him but we got nowhere. He maintained that he could not afford his medication. I asked him why he didn't work. He said that he did do odd jobs, and besides, in a few months he would qualify for Social Security. I guess I was in a bad mood, so I heard myself ask, Do you realize you are playing with fire here? You will end up with a real stroke? Simply saying you want to wait for Social Security is not a plan.
Stan looked at me closely. Probably judging me to be about half his age, he said, Whatever, doc. Don't you have someone else to lecture? I sat down, took a deep breath, and tried to sound kind when I said, Do you realize that you will need dialysis soon? Stan replied that he had no intention of going on dialysis. We went in circles, with me trying to determine if he was delusional, suicidal, or trying to shock me. We left it as it was. The medical system would do its best, but his life was his to run.
Bending the HIPPA rules, I went to the nurse's station and called Stan's daughter to get some background, answers to questions like why she couldn't help him buy his medication. I was wholly in my righteous problem‐solving mode. Yet she was not alarmed by my dire prognostics. When the call was about to end, I asked if all of us could meet when she came to pick him up the next day. After a pause, she stated, I'm not coming up. Tell him to wait in the lobby for me. I'll be there to pick him up sometime after 5. Collecting her dad from the hospital on Christmas Eve, and she couldn't be bothered to enter the building? I hung up, sat back in my chair, and stared at my progress note.
I subsequently found out from the case manager that after being discharged, unlike before, he was going to a homeless shelter, not his daughter's house. I thought he must have been an awful father for a child to turn her own dad away on Christmas Eve.
Clearly, she had had no intention of picking him up from the hospital before my call; I had inadvertently shamed her into it.
I went back to talk with Stan. I decided to make inquiries of him based only on the information I was supposed to have. The case manager tells me you're going to the homeless shelter tomorrow. Don't you live with your daughter?
Not realizing that the doctors and case managers were on the same team, he seemed somewhat taken aback. I found a chair and sat down as he spoke. I wasn't always like this, you know. I'm not a drinker, nuts, or anything; I just was put out to pasture. I'm a computer programmer but not the new kind. I worked on those huge 1960s types. The personal computer revolution put me out of business. Before I had a chance to say anything, he continued, I know what you're thinking, I should have gotten trained or something to keep up, but I didn't, you know, I just didn't. I should've.
He must have seen a flicker of compassion on my face, as he went on, I've been staying with my daughter on and off for years. I'd get some job, get a place, but never for long. I don't like to stay with her. She has her own life, her own problems. She doesn't need me getting in the way, especially around Christmas. Around the holidays, I go to the shelter. My grandkids don't need me ruining the season.
He may well have been a lousy father, but I didn't see his medical noncompliance as a personal affront anymore. He should have made some different decisions in the past, but now he was a 64‐year‐old homeless man, alone. So, besides lecturing him on his blood pressure and work habits, could I do anything really helpful?
It didn't take me long to come up with something. The problem was how to approach it. Feeling like I was breaking some rule, I trailed him to the hospital lobby right after discharge. To my chagrin, he didn't so much as slow down. He saw his daughter's car, walked out, and got in her car before I knew what to do. Feeling like a fool, I stood at the window, noted how slate gray and dour the sky was, in complete contrast to the festive lobby, and thought about how useless I really was in the end. All my good intentions aside, he was no better off for having me as his doctor.
I bought myself a cup of coffee and while walking lost in thought, I literally bumped into Stan coming through the hospital's main doors. Laughing awkwardly, he said, I forgot my jacket in my room. He looked more scared now than he did after hearing my dire pronouncements of doom. He seemed like a child whose mother was angry at his forgetfulness. As he shuffled off, I couldn't stand it any longer. I didn't want him rushing around worried that his daughter would get fed up and leave. I told him to tell his daughter that I knew where his jacket was and that I'd be right back with it.
I got the coat, and when I approached him back in the lobby, I gave it to him. I then handed him the money I had set aside in my white coat. Trying to make myself sound casual, I said, Use this to take your grandkids out to dinner and buy them something. Neither wanting to give him a chance to say no nor wishing to make it more awkward for him, I quickly turned around and left without looking back.
As I resumed my $2 cup of coffee, I wondered if I had acted as a doctor, as a good Samaritan, or as an egoist? I was not deluded into believing I could buy his pride back for long with my pocket change. But maybe I could be a good person in addition to a caring, up‐to‐date doctor.
Later that day in the ER, a very sad place on Christmas Eve, I imagined Stan buying gifts or a fancy dinner for his family, just like he used to. He will need dialysis and probably will end up back in the shelter. I don't think he even knew my name, but maybe because I cared a little bit about what happened to him, he will, too.
I'm used to feeling inadequate. Oftentimes, what ails my patients I'm not able to address, let alone fix. But one time I crossed the line from absorber of sorrows to active agent.
All set with my preconceived notions, I went into the hospital room to see Stan. He had severe hypertension and had had several previous transient ischemic attacks, and now he was back with another. His renal function was minimal, with dialysis coming soon. Despite our repeatedly having social work arrange outpatient appointments, he had never followed up. Last admission, they even gave him a month's worth of his antihypertensive medications, but here he was 6 weeks later off meds and admitted again.
I spoke with him but we got nowhere. He maintained that he could not afford his medication. I asked him why he didn't work. He said that he did do odd jobs, and besides, in a few months he would qualify for Social Security. I guess I was in a bad mood, so I heard myself ask, Do you realize you are playing with fire here? You will end up with a real stroke? Simply saying you want to wait for Social Security is not a plan.
Stan looked at me closely. Probably judging me to be about half his age, he said, Whatever, doc. Don't you have someone else to lecture? I sat down, took a deep breath, and tried to sound kind when I said, Do you realize that you will need dialysis soon? Stan replied that he had no intention of going on dialysis. We went in circles, with me trying to determine if he was delusional, suicidal, or trying to shock me. We left it as it was. The medical system would do its best, but his life was his to run.
Bending the HIPPA rules, I went to the nurse's station and called Stan's daughter to get some background, answers to questions like why she couldn't help him buy his medication. I was wholly in my righteous problem‐solving mode. Yet she was not alarmed by my dire prognostics. When the call was about to end, I asked if all of us could meet when she came to pick him up the next day. After a pause, she stated, I'm not coming up. Tell him to wait in the lobby for me. I'll be there to pick him up sometime after 5. Collecting her dad from the hospital on Christmas Eve, and she couldn't be bothered to enter the building? I hung up, sat back in my chair, and stared at my progress note.
I subsequently found out from the case manager that after being discharged, unlike before, he was going to a homeless shelter, not his daughter's house. I thought he must have been an awful father for a child to turn her own dad away on Christmas Eve.
Clearly, she had had no intention of picking him up from the hospital before my call; I had inadvertently shamed her into it.
I went back to talk with Stan. I decided to make inquiries of him based only on the information I was supposed to have. The case manager tells me you're going to the homeless shelter tomorrow. Don't you live with your daughter?
Not realizing that the doctors and case managers were on the same team, he seemed somewhat taken aback. I found a chair and sat down as he spoke. I wasn't always like this, you know. I'm not a drinker, nuts, or anything; I just was put out to pasture. I'm a computer programmer but not the new kind. I worked on those huge 1960s types. The personal computer revolution put me out of business. Before I had a chance to say anything, he continued, I know what you're thinking, I should have gotten trained or something to keep up, but I didn't, you know, I just didn't. I should've.
He must have seen a flicker of compassion on my face, as he went on, I've been staying with my daughter on and off for years. I'd get some job, get a place, but never for long. I don't like to stay with her. She has her own life, her own problems. She doesn't need me getting in the way, especially around Christmas. Around the holidays, I go to the shelter. My grandkids don't need me ruining the season.
He may well have been a lousy father, but I didn't see his medical noncompliance as a personal affront anymore. He should have made some different decisions in the past, but now he was a 64‐year‐old homeless man, alone. So, besides lecturing him on his blood pressure and work habits, could I do anything really helpful?
It didn't take me long to come up with something. The problem was how to approach it. Feeling like I was breaking some rule, I trailed him to the hospital lobby right after discharge. To my chagrin, he didn't so much as slow down. He saw his daughter's car, walked out, and got in her car before I knew what to do. Feeling like a fool, I stood at the window, noted how slate gray and dour the sky was, in complete contrast to the festive lobby, and thought about how useless I really was in the end. All my good intentions aside, he was no better off for having me as his doctor.
I bought myself a cup of coffee and while walking lost in thought, I literally bumped into Stan coming through the hospital's main doors. Laughing awkwardly, he said, I forgot my jacket in my room. He looked more scared now than he did after hearing my dire pronouncements of doom. He seemed like a child whose mother was angry at his forgetfulness. As he shuffled off, I couldn't stand it any longer. I didn't want him rushing around worried that his daughter would get fed up and leave. I told him to tell his daughter that I knew where his jacket was and that I'd be right back with it.
I got the coat, and when I approached him back in the lobby, I gave it to him. I then handed him the money I had set aside in my white coat. Trying to make myself sound casual, I said, Use this to take your grandkids out to dinner and buy them something. Neither wanting to give him a chance to say no nor wishing to make it more awkward for him, I quickly turned around and left without looking back.
As I resumed my $2 cup of coffee, I wondered if I had acted as a doctor, as a good Samaritan, or as an egoist? I was not deluded into believing I could buy his pride back for long with my pocket change. But maybe I could be a good person in addition to a caring, up‐to‐date doctor.
Later that day in the ER, a very sad place on Christmas Eve, I imagined Stan buying gifts or a fancy dinner for his family, just like he used to. He will need dialysis and probably will end up back in the shelter. I don't think he even knew my name, but maybe because I cared a little bit about what happened to him, he will, too.
Geriatric Care Approaches in Hospitalist Programs
Between 1996with the first appearance of hospitalists in the medical literatureand the present, the hospitalist workforce has grown to nearly 10,000.1, 2 More remarkable is the estimate that the number of hospitalists will double in the next 5 years.2 The rapid growth of hospital medicine raises significant issues for the care of older patients, who are hospitalized at high rates3 and suffer numerous complications from hospitalization including functional decline,4 delirium,5 and a disproportionate share of adverse events.6 Conversely, the needs of patients older than 65 years of age, whose hospital stays make up nearly 50% of acute‐care bed days, will shape the future of hospital medicine.3
To date, the hospital medicine literature has failed to address the particular challenges of treating older patients, focusing primarily on opportunities for reductions in costs and length of stay for hospitalists' Medicare patients (of about $1000 per admission and 0.5 days, respectively7, 8) when compared with those cared for by other physicians. This focus on economic efficiency reflects the early orientation of the hospitalist movement. More recently, leaders of the hospitalist professional organization, the Society of Hospital Medicine (SHM), have increasingly recognized that caring for the older population will require additional knowledge and clinical skills beyond that taught in internal medicine residencies.9 Beyond educational initiatives, however, hospitalists must reconsider the paradigms of hospital care that make the hospital setting so dangerous for the older patient.
Given the aging population and the predicted growth of hospital medicine, it is essential to develop an understanding of the impact of hospitalists on the care of older patients and to encourage clinical innovation at the intersection of hospital medicine and geriatrics. Consequently, this article 1) identifies and summarizes geriatric care approaches in hospitalist programs, 2) presents a case study of geriatric hospital care by a hospitalist group, and 3) highlights opportunities for innovation and further research.
METHODS
Sample
We conducted a cross‐sectional survey of the hospitalist community via two mailings to SHM Listservs in September 2003 and September 2004. To encourage responses, the e‐mails used terms such as innovating, developing, providing hospitalist services, and caring for the geriatric patient or Medicare population. Respondents to the e‐mail solicitations (n = 14), leaders of SHM and academic hospitalist groups (n = 14), and leaders of the American Geriatrics Society specializing in acute care (n = 3) were queried about additional contacts who might know about programs utilizing geriatric care approaches. Each of these contacts was subsequently solicited and queried.10 Thirteen of the respondents described the current use by their hospitalist groups of one or more geriatric care approaches that represented a departure from usual care. We subsequently refer to these approaches as innovations. The 13 respondents completed in‐depth telephone interviews with one of the authors (H.W.). All respondents were recontacted in the spring of 2005 to update their responses. Two of the 13 programs were eliminated from the analysis after the interviews were completed. The first of these programs was identified in 2003 but had been discontinued by 2004. The second program was eliminated because the innovation was not implemented.
Data Collection
We developed a data collection tool to gather descriptive information from respondents regarding characteristics of the hospitalist group, the clinical program, the primary hospital, and the innovation (focus, target patients, organization, staffing, training, rounding, other). In addition, respondents were queried about motivations for the innovation; successes, opportunities, and future plans; and failures and barriers to implementation.
Analysis
First, we summarized the characteristics of the 11 innovations (Table 1). Second, geriatric care approaches were identified from the innovations on the basis of their objectives and the types of responses we encountered most frequently. The approaches were not mutually exclusive. For instance, a program providing postdischarge care at a skilled nursing facility (SNF) might also use a geriatrician‐hospitalist staffing model.
| Site | A | B | C | D | E | F | G | H | I | J | K |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Focus | |||||||||||
| Medical care | x | x | x | x | |||||||
| Postdischarge care | x | x | |||||||||
| Perioperative care | x | x | x | ||||||||
| Geriatric assessment | x | x | x | ||||||||
| Quality improvement | x | x | x | x | |||||||
| Staffing | x | ||||||||||
| Generalist‐hospitalist | x | x | x | x | x | x | |||||
| Geriatrician‐hospitalist | x | x | x | x | x | x | |||||
| Advanced‐practice nurse | x | x | x | x | |||||||
| Patient targeting | |||||||||||
| By age | x | x | x | x | x | x | x | x | x | ||
| By diagnosis | x | x | x | x | x | x | |||||
| By location | x | x | x | x | x | x | |||||
| Organization | |||||||||||
| Unit | x | x | x | x | x | x | |||||
| Service | x | x | x | x | x | x | |||||
| Interdisciplinary rounds | x | x | x | x | x | x | |||||
| Geriatrics training | x | x | x | x | x | x | x |
RESULTS
In 2003 the annual survey of the American Hospital Association identified 1415 hospitalist groups in the United States (Joe Miller, SHM senior vice‐president, personal communication). Remarkably, our query identified only 11 hospitalist groups with clinical innovations aimed at the older population. These innovations ranged from single individuals involved in targeted quality‐improvement projects to highly developed programs addressing an array of clinical needs for the hospitalized older patient. These 11 programs are summarized in Table 1 and described below.
Focus
Hospitalists' programs targeted to the older patient were designed to meet various needs arising from an episode of hospital care. These included innovations designed around their core clinical activities in providing acute medical care (four innovations), as well as innovations targeted to postdischarge care at SNFs (two innovations), perioperative care in consultative or comanagement models (four innovations), comprehensive geriatric assessment (three innovations), and clinical quality improvement such as audit tools (four innovations).
Staffing
Four innovations employed physicians without specific geriatrics training (generalist‐hospitalists), four innovations employed 16 fellowship‐trained geriatricians (geriatrician‐hospitalists), and two programs employed both geriatricians and generalist hospitalists. Four innovations employed advanced‐practice nurses, both with and without gerontology training.
Patients
Nine of the 11 innovations targeted patients by age (older than 65, 70, or 75 years). Of the two innovations that did not target patients by age, one focused on improving the quality of care for all patients on a medical ward by focusing on geriatric issues (Site I), and a second was concerned with postdischarge care for all patients discharged to affiliated SNFs (Site K). In addition to targeting by age, six innovations targeted patients on the basis of diagnosis, four of which focused on surgical diagnosis. Finally, patient selection by location occurred in six of the innovations, as described in the next section.
Organization
Six of the innovations were organized to operate within a clinical service (such as a medical or surgical team). In contrast to the service‐based innovations, six clinical innovations for older patients operated in geographic units including acute care for elders (ACE) units (n = 2), SNFs (n = 2), a medical nursing unit (n = 1), and an emergency department (ED; n = 1). Of the two ACE units, one (Site G) existed prior to the establishment of the hospitalist group. In this instance, a geriatrician‐hospitalist appointed jointly by the hospitalist group and the Division of Geriatrics staffed ACE unit patients of select private physicians and unassigned patients. The second ACE unit (Site H), established with the formation of the hospitalist group, was staffed by two hospitalists among eight physicians in a private geriatrics group. Regarding SNFs, one hospitalist group for a large health care organization (Site K) rounded at contract SNFs at which group members held medical directorships; another hospitalist program took over rounding at an SNF owned by its health system (Site A).
Rounding
Six of the innovations incorporated interdisciplinary rounds, including all three innovations with medical care as their focus. Four of the six innovations with interdisciplinary rounds were based in ACE units or SNFs. One of these six innovations (Site C), a perioperative initiative, incorporated twice‐weekly multidisciplinary rounds attended by an attending surgeon, surgical residents, and a hospitalistin addition to the nurses, case managers, and therapists.
Training
Seven of the 11 innovations involved geriatrics training. Four of the training innovations targeted nursing staff, four targeted hospitalist physicians, and one targeted both nurses and physicians. Most institutions developed their own curricula. Three hospitalist groups, however, modified preexisting curricula, struggling to adapt them to the needs of hospital‐based staff. Two innovations (Sites A and K) used a clinical mentoring model in which generalist‐hospitalists learned geriatrics principles while working side by side with geriatrician‐hospitalists.
Case Study
We selected the most comprehensive program for further description. This case illustrates the power of integrating geriatric and hospital medicine paradigms.
Hospital Internal Medicine, Mayo Clinic, Rochester, MN (Site A)
The Mayo Clinic established the Hospital Internal Medicine Group (HIM) in 1998 in response to changing resident workload regulations. The practice initially focused on perioperative medical care for a busy orthopedic trauma surgery (OTS) service. In 2000, noting the average age of the elective orthopedic population was 81, the leadership of HIM made a strategic decision to recruit physicians with geriatrics training. By 2005, 6 of the 22 physicians the group employed were geriatricians.
In mid‐2005 the group's members covered eight services in 1‐ to 2‐week block rotations. Three of the services are uniquely focused on the older patient: the Geriatric Medicine Service (GeM), the OTS, and the SNF. On the GeM, a geriatrician‐hospitalist works alongside a generalist‐hospitalist to for care medical patients triaged to the service based on age (older than 75) and frailty. Although the GeM is based on a medical nursing unit, the unit is neither configured nor staffed like an ACE unit, and up to 20% of the GeM's patients overflow to other units. In addition to providing acute care, the GeM employs standardized documentation to facilitate universal comprehensive geriatric assessment. On the OTS, HIM hospitalists care for postoperative patients in a comanagement model, descriptions of which have been published elsewhere.11, 12 As a reflection of its orientation toward the older surgical patient, every OTS patient is assessed for delirium with the confusion assessment method instrument.13 Finally, the 30‐bed SNF service (on which 75% of admissions are postoperative for subacute rehabilitation) is supervised by a HIM physician and a nurse‐practitioner.
Additional activities of HIM physicians are clinical quality improvement including participation in the creation of inpatient care pathways, revision of the hospital's discharge processes, ongoing review of adverse events, and use of standardized tools for intrahospital transfers. In addition, the HIM group prioritizes geriatrics education for its physicians and hospital medicine fellows. In turn, geriatrics fellows rotate through the GeM, SNF, and OTS services.
DISCUSSION
Although SHM increasingly recognizes the challenges inherent in caring for older patients, few hospitalists are adapting their care for this vulnerable population. We identified only 11 innovations in geriatric care despite there being more than 1000 hospitalist groups. This apparent paucity of innovation in geriatrics might be explained by the relatively recent introduction of hospital medicine. As no hospitalist program is more than 10 years old, most programs are still focused on building core clinical activities or on other competing demands. In addition to time, funding may limit the typical program's ability to innovate without directly increasing revenue. Although the geriatrics literature supports that specialized inpatient care for older patients can result in increased physical functioning and quality of life at no additional cost, it may be that geriatricians have yet to make this case effectively to the hospitalist community.14, 15
The findings of this study were limited by our survey methodology. Specifically, our sample was limited to professional contacts and those using SHM listservs. In addition, some innovative hospitalists may not consider their programs to be geriatric programs and so may not have responded to our queries. Therefore, the reported innovations are not representative of geriatric care among all hospitalist groups, and we are unable to provide a comprehensive picture of geriatric care in hospitalist programs. In addition, we cannot comment on the effectiveness of the care approaches at participating institutions. For example, interdisciplinary care is an important tenet of geriatric medicine. Although six of our programs reported interdisciplinary rounds, it is unclear if these rounds are models of effective collaborative practice. Nonetheless, the information obtained from the structured interviews allowed the identification of several instructive themes discussed below.
Opportunities
The growth of the hospitalist movement provides an opportunity to reconsider clinical paradigms for the hospitalized older population. Hospitalists bring clinical skills in treating acute illness, preventing hospital complications, and providing perioperative care.16, 17 As leaders in institutional quality, safety, and utilization initiatives, hospitalists are often given protected time for such endeavors.18, 19 In so doing, the incentives of hospitalists are aligned with those of hospital administrators. This orientation makes hospitalists open to innovation in clinical care improvement.
The opportunity for hospitalists to bring fresh approaches to acute care geriatrics need not happen in a vacuum. More than 30 years of geriatrics research has provided a framework, literature, and expertise to inform hospitalist groups. The common goal of clinical excellence for the hospitalized older patient should motivate cooperation, collaborative approaches, and a joint clinical research agenda. From our inquiry to hospitalist groups, it appears that this sort of interaction occurs infrequently. The innovations identified and the case study described highlight several ways in which the geriatric medicine and hospital medicine experiences inform one another. These include approaches to staffing, organization, and quality improvement, as well as to clinical areas amenable to innovation.
Approaches
Staffing and Organization
The employment of geriatrics‐trained clinicians by hospitalist programs is one approach to supporting generalist‐hospitalists and inclining group culture toward clinical geriatric concerns. Programs that purposefully hired geriatricians and gerontology nurse‐practitioners used them to staff geriatrics services including ACE units, SNFs and, in the case of HIM, a GeM service that was a modification of a medical service. In addition, two programs relied on geriatrician‐hospitalists to serve as clinical mentors to generalist‐hospitalists.
In particular, the use of geriatrics‐trained staff on specialized services such as ACE units is encouraging, as specialized geriatric units remain an underutilized care model,20 despite compelling evidence of their effectiveness in improving physical functioning and reducing nursing home admissions.14 Although the factors undermining the success of ACE units in the past may also pose challenges for hospitalists, hospitalist groups may be better positioned to maintain the interest and financial commitment of hospital administrators. The HIM's GeM Service is also of interest, given the need to disseminate best practices in geriatrics throughout the hospital. The benefits to older patients of such a service, however, have not been demonstrated. Likewise, comprehensive geriatric assessment and geriatric consultation in the inpatient setting are reported to have had mixed results in the absence of targeting individuals at highest risk for adverse outcomes.21
Patient Safety and Quality Improvement
Hospital medicine has rapidly integrated principles of quality improvement and patient safety, having grown up contemporaneously with the patient safety movement. Several of the hospitalist programs we identified spearheaded quality improvement efforts directed at the particular needs of older patients such as delirium prevention, provision of immunizations, and removal of indwelling Foley catheters.
These efforts can be seen in the context of the many hospitalist programs focusing on standardizing care, understanding iatrogenesis, adopting safe technologies, and generally moving hospital culture forward.22 In choosing to embrace patient safety practices such as medication reconciliation (endorsed by the Institute for Healthcare Improvement),23 hospitalists may confer disproportionate benefits to older patients, who frequently require multiple medications and are at high risk for adverse drug events.6 As the efficacy of many of these interventions is poorly understood, hospitalist and geriatricians (whose work on the hazards of hospitalization anticipated the patient safety movement by many years24) may find a shared clinical research agenda with patient safety as its focus.
Areas of Clinical Opportunity
Perioperative Care
Commentators have noted hospitalists' growing participation in perioperative care,17 much of which concerns the older orthopedic surgery patient.12 Through their embedding in surgical wards, hospitalists may become actual or de facto members of surgical teams with a significant impact on team culture and care delivery. For example, hospitalists at one program implemented a perioperative beta‐blocker protocol for older orthopedic surgery patients, leading to a marked decrease in postoperative cardiac events (Site B).
Although many hospitalist programs participate in similar initiatives, it is likely that additional attention to the needs of older patients will augment the effectiveness of their interventions. For instance, structured geriatrics consultation can reduce the incidence of postoperative delirium among hip fracture patients by 46% (NNT = 5.6).25 Increased attention to postoperative pain control and early mobilization, among others, may affect the functional recovery of the older surgical patient.26, 27
Postdischarge care and care transitions
The hallmark of the hospitalist modelthe handoff of care from a primary care provider to an inpatient provideris commonly considered the major limitation of the hospitalist model because of the risk of lost clinical information.1 Because older patients are particularly susceptible to postdischarge adverse events, their care transitions may require specialized attention.28 Two of the innovations we identified (Sites A and K) have extended care of older patients into the postacute setting by integrating SNF care into their programs as a way to streamline discharge processes, decrease miscommunication, and underscore the limitations of postacute care.
A growing body of evidence supports the role of discharge strategies in improving care transitions. In one study, postdischarge follow‐up with a hospital physician rather than a community physician resulted in a reduction of the combined end point of 30‐day mortality and nonelective readmission.29 In a randomized trial, postdischarge phone calls by a pharmacist reduced the number of ED visits within 30 days of discharge.30 In another trial, older patients receiving a multifactorial intervention aimed at providing the skills for active participation in care transitions resulted in a reduced number of readmissions within 30 days.31 Understanding and implementing these activities may be crucial to both the care of older patients and the success of the hospitalist enterprise.
Barriers
Part of the challenge of treating older patients in hospitals is that the paradigms of geriatrics and hospital medicine differ substantially.32 Notably, geriatric medicine goals of maximizing function and quality of life may conflict with traditional medical goals of diagnosis and cure. This dichotomy is amplified in the hospital setting because hospitals are organized to maximize the physician's ability to stabilize, diagnose, cure, and discharge.33
By design, the hospitalist model introduces additional challenges into the hospital paradigm that affect the older patient, such as the discontinuities addressed above. Additional factors that hospitalists identified as barriers to the effective care of older patients include: 1) poor communication skills, 2) ineffective interdisciplinary collaboration, 3) limited geriatrics knowledge base, and 4) insufficient support for care coordination.34 Despite these recognized challenges, our query to hospitalist groups identified few that had made clinical excellence in geriatrics a focus of their activities.
Even with its prioritization of geriatric medicine, the well‐developed HIM model faces challenges. In particular, the feasibility of the geriatrician‐hospitalist is limited by the many geriatricians who, because of the scarcity of those who are fellowship trained, may be unprepared to care for acutely ill older patients, as their training has not focused on the hospital setting.35, 36 In addition, the surgical comanagement model depends on a unique collaboration with surgical colleagues. Finally, the ability of the HIM group to incorporate geriatrics paradigms into the hospital setting depends on extensive support from the hospital in the form of resources and a shared vision that is unlikely to be found at most institutions.
CONCLUSIONS
The rapid growth of the hospitalist movement will significantly affect clinical care in American hospitals. As most hospital patients are older, the impact on acute care geriatrics cannot be overlooked. In our study, we identified only a small number of hospitalist groups that have made geriatric medicine a priority. These programs prioritize geriatric medicine through the employment of geriatrics‐trained staff, adaptation of geriatric care models such as ACE units, and commitment to clinical quality improvement and patient safety. They also focus on common clinical challenges for older patients, including postoperative and postdischarge care. Although much can be learned from these examples, programs at other institutions will need to be individualized to meet the specific needs of each hospital and community. The common goal of clinical excellence shared by hospitalists and geriatricians should motivate cooperation, collaborative approaches, and a joint clinical research agenda at all levels, as the current paradigm of hospital care remains inadequate to meet the needs of the acutely ill older patient.
- ,.The emerging role of hospitalists in the American health care system.N Engl J Med.1996;335:514–517.
- Society of Hospital Medicine. Growth of hospital medicine nationwide. Available at URL: http://www.hospitalmedicine.org/Content/NavigationMenu/Media/GrowthofHospitalMedicineNationwide/Growth_of_Hospital_M.htm[accessed January 20, 2005].
- ,.2002 National Hospital Discharge Survey.Advance data from Vital And Health Statistics. No. 342.Hyattsville (MD):National Center for Health Statistics,2002.
- ,,, et al.Functional outcomes of acute medical illness and hospitalization in older persons.Arch Intern Med.1996;156,:645–652.
- ,,.Delirium: a symptom of how hospital care is failing older persons and a window to improve the quality of hospital care.Am J Med.1999;106:565–573.
- ,.Incidence and types of preventable adverse events in elderly patients: population based review of medical records.BMJ.2000;320:741–744.
- ,,.The effect of full‐time faculty hospitalists on the efficiency of care at a community teaching hospital.Ann Intern Med.1998;129:197–203.
- ,,,,,.The value of a hospitalist service: efficient care for the aging population?Chest.2001;119:580–589.year="2001"2001.
- .Improving care for older adults: SHM educational initiatives.Hospitalist.2004;8(Suppl):45–47.
- .Qualitative evaluation and research methods.2nd ed.Thousand Oaks (CA):Sage Publications,1990:176.
- ,,, et al.Effects of a hospitalist model on elderly patients with hip fracture.Arch Intern Med.2005;165:796–801.
- ,,, et al.Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial.Ann Intern Med.2004;141:28–38.
- ,,, et al.Clarifying confusion: the confusion assessment method. A new method for the detection of delirium.Ann Intern Med.1990;113:941–948.
- ,,Geriatric evaluation and management units for hospitalized patients. In:Making healthcare safer: a critical analysis of Patient Safety Practices Evidence Report/Technology AssessmentNo. 43.2001. AHRQ Publication No. 01‐E058.
- ,,, et al.A controlled trial of inpatient and outpatient geriatric evaluation and management.N Engl J Med.2002;346:905–912.
- ,.The hospitalist movement five years later.JAMA.2002;287:487–494.
- .The hospitalist joins the surgical team.Ann Intern Med.2004;141:67–69.
- .The end of the beginning: patient safety five years after ‘To Err Is Human.’Health Aff.2004;23S2:W534–W545.
- .How hospitalists add value.Hospitalist.2005;9(Suppl 1):6–7.
- ,,, et al.Dissemination and characteristics of acute care of elders (ACE) units in the United States.Int J Technol Assess Health Care.2003;19:220–227.
- ,,, et al.Multidisciplinary geriatric consultation services,Chap. 29.Evidence Report/Technology Assessment No. 43.2001. AHRQ Publication No. 01‐E058.
- .Hospitalists spearhead a wide range of patient safety improvement projects.Hospitalist.2004;8(Suppl.):33–35.
- Institute for Healthcare Improvement.100k Lives campaign. 10‐20‐2005.
- .Hazards of hospitalization of the elderly.Ann Intern Med.1993;118:219–223.
- ,,, et al.Reducing delirium after hip fracture: a randomized trial.J Am Geriatr Soc.2001;49:516–522.
- ,,, et al.The impact of postoperative pain on outcomes following hip fracture.Pain.2003;103:303–311.
- ,,, et al.Physical therapy and mobility 2 and 6 months after hip fracture.J Am Geriatr Soc.2004;52:1114–1120.
- .Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex needs.J Am Geriatr Soc.2003;51:549–555.
- ,,, et al.Continuity of care and patient outcomes after hospital discharge.J Gen Intern Med.2004;19:624–631.
- ,,, et al.The impact of follow‐up telephone calls to patients after hospitalization.Dis Mon.2002;48:239–248.
- ,,, et al.The care transitions intervention: results from a randomized controlled trial. Society of Hospital Medicine Annual Meeting, Chicago, IL,2005.
- .Case management: high intensity care for frail patients with complex needs.Geriatrics.1998;53:62–68.
- .The care of strangers: the rise of America's hospital system.New York:Basic Books,1987.
- ,,.Hospitalists' role in caring for older Americans: Executive Summary.2002. San Francisco, prepared for the John Hartford Foundation.
- Geriatric medicine training and practice in the United States at the beginning of the 21st century.New York:Association of Directors of Geriatric Academic Programs,2002.
- AGS Education Committee.Guidelines for fellowship training in geriatrics.1998;46:1473–1477.
Between 1996with the first appearance of hospitalists in the medical literatureand the present, the hospitalist workforce has grown to nearly 10,000.1, 2 More remarkable is the estimate that the number of hospitalists will double in the next 5 years.2 The rapid growth of hospital medicine raises significant issues for the care of older patients, who are hospitalized at high rates3 and suffer numerous complications from hospitalization including functional decline,4 delirium,5 and a disproportionate share of adverse events.6 Conversely, the needs of patients older than 65 years of age, whose hospital stays make up nearly 50% of acute‐care bed days, will shape the future of hospital medicine.3
To date, the hospital medicine literature has failed to address the particular challenges of treating older patients, focusing primarily on opportunities for reductions in costs and length of stay for hospitalists' Medicare patients (of about $1000 per admission and 0.5 days, respectively7, 8) when compared with those cared for by other physicians. This focus on economic efficiency reflects the early orientation of the hospitalist movement. More recently, leaders of the hospitalist professional organization, the Society of Hospital Medicine (SHM), have increasingly recognized that caring for the older population will require additional knowledge and clinical skills beyond that taught in internal medicine residencies.9 Beyond educational initiatives, however, hospitalists must reconsider the paradigms of hospital care that make the hospital setting so dangerous for the older patient.
Given the aging population and the predicted growth of hospital medicine, it is essential to develop an understanding of the impact of hospitalists on the care of older patients and to encourage clinical innovation at the intersection of hospital medicine and geriatrics. Consequently, this article 1) identifies and summarizes geriatric care approaches in hospitalist programs, 2) presents a case study of geriatric hospital care by a hospitalist group, and 3) highlights opportunities for innovation and further research.
METHODS
Sample
We conducted a cross‐sectional survey of the hospitalist community via two mailings to SHM Listservs in September 2003 and September 2004. To encourage responses, the e‐mails used terms such as innovating, developing, providing hospitalist services, and caring for the geriatric patient or Medicare population. Respondents to the e‐mail solicitations (n = 14), leaders of SHM and academic hospitalist groups (n = 14), and leaders of the American Geriatrics Society specializing in acute care (n = 3) were queried about additional contacts who might know about programs utilizing geriatric care approaches. Each of these contacts was subsequently solicited and queried.10 Thirteen of the respondents described the current use by their hospitalist groups of one or more geriatric care approaches that represented a departure from usual care. We subsequently refer to these approaches as innovations. The 13 respondents completed in‐depth telephone interviews with one of the authors (H.W.). All respondents were recontacted in the spring of 2005 to update their responses. Two of the 13 programs were eliminated from the analysis after the interviews were completed. The first of these programs was identified in 2003 but had been discontinued by 2004. The second program was eliminated because the innovation was not implemented.
Data Collection
We developed a data collection tool to gather descriptive information from respondents regarding characteristics of the hospitalist group, the clinical program, the primary hospital, and the innovation (focus, target patients, organization, staffing, training, rounding, other). In addition, respondents were queried about motivations for the innovation; successes, opportunities, and future plans; and failures and barriers to implementation.
Analysis
First, we summarized the characteristics of the 11 innovations (Table 1). Second, geriatric care approaches were identified from the innovations on the basis of their objectives and the types of responses we encountered most frequently. The approaches were not mutually exclusive. For instance, a program providing postdischarge care at a skilled nursing facility (SNF) might also use a geriatrician‐hospitalist staffing model.
| Site | A | B | C | D | E | F | G | H | I | J | K |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Focus | |||||||||||
| Medical care | x | x | x | x | |||||||
| Postdischarge care | x | x | |||||||||
| Perioperative care | x | x | x | ||||||||
| Geriatric assessment | x | x | x | ||||||||
| Quality improvement | x | x | x | x | |||||||
| Staffing | x | ||||||||||
| Generalist‐hospitalist | x | x | x | x | x | x | |||||
| Geriatrician‐hospitalist | x | x | x | x | x | x | |||||
| Advanced‐practice nurse | x | x | x | x | |||||||
| Patient targeting | |||||||||||
| By age | x | x | x | x | x | x | x | x | x | ||
| By diagnosis | x | x | x | x | x | x | |||||
| By location | x | x | x | x | x | x | |||||
| Organization | |||||||||||
| Unit | x | x | x | x | x | x | |||||
| Service | x | x | x | x | x | x | |||||
| Interdisciplinary rounds | x | x | x | x | x | x | |||||
| Geriatrics training | x | x | x | x | x | x | x |
RESULTS
In 2003 the annual survey of the American Hospital Association identified 1415 hospitalist groups in the United States (Joe Miller, SHM senior vice‐president, personal communication). Remarkably, our query identified only 11 hospitalist groups with clinical innovations aimed at the older population. These innovations ranged from single individuals involved in targeted quality‐improvement projects to highly developed programs addressing an array of clinical needs for the hospitalized older patient. These 11 programs are summarized in Table 1 and described below.
Focus
Hospitalists' programs targeted to the older patient were designed to meet various needs arising from an episode of hospital care. These included innovations designed around their core clinical activities in providing acute medical care (four innovations), as well as innovations targeted to postdischarge care at SNFs (two innovations), perioperative care in consultative or comanagement models (four innovations), comprehensive geriatric assessment (three innovations), and clinical quality improvement such as audit tools (four innovations).
Staffing
Four innovations employed physicians without specific geriatrics training (generalist‐hospitalists), four innovations employed 16 fellowship‐trained geriatricians (geriatrician‐hospitalists), and two programs employed both geriatricians and generalist hospitalists. Four innovations employed advanced‐practice nurses, both with and without gerontology training.
Patients
Nine of the 11 innovations targeted patients by age (older than 65, 70, or 75 years). Of the two innovations that did not target patients by age, one focused on improving the quality of care for all patients on a medical ward by focusing on geriatric issues (Site I), and a second was concerned with postdischarge care for all patients discharged to affiliated SNFs (Site K). In addition to targeting by age, six innovations targeted patients on the basis of diagnosis, four of which focused on surgical diagnosis. Finally, patient selection by location occurred in six of the innovations, as described in the next section.
Organization
Six of the innovations were organized to operate within a clinical service (such as a medical or surgical team). In contrast to the service‐based innovations, six clinical innovations for older patients operated in geographic units including acute care for elders (ACE) units (n = 2), SNFs (n = 2), a medical nursing unit (n = 1), and an emergency department (ED; n = 1). Of the two ACE units, one (Site G) existed prior to the establishment of the hospitalist group. In this instance, a geriatrician‐hospitalist appointed jointly by the hospitalist group and the Division of Geriatrics staffed ACE unit patients of select private physicians and unassigned patients. The second ACE unit (Site H), established with the formation of the hospitalist group, was staffed by two hospitalists among eight physicians in a private geriatrics group. Regarding SNFs, one hospitalist group for a large health care organization (Site K) rounded at contract SNFs at which group members held medical directorships; another hospitalist program took over rounding at an SNF owned by its health system (Site A).
Rounding
Six of the innovations incorporated interdisciplinary rounds, including all three innovations with medical care as their focus. Four of the six innovations with interdisciplinary rounds were based in ACE units or SNFs. One of these six innovations (Site C), a perioperative initiative, incorporated twice‐weekly multidisciplinary rounds attended by an attending surgeon, surgical residents, and a hospitalistin addition to the nurses, case managers, and therapists.
Training
Seven of the 11 innovations involved geriatrics training. Four of the training innovations targeted nursing staff, four targeted hospitalist physicians, and one targeted both nurses and physicians. Most institutions developed their own curricula. Three hospitalist groups, however, modified preexisting curricula, struggling to adapt them to the needs of hospital‐based staff. Two innovations (Sites A and K) used a clinical mentoring model in which generalist‐hospitalists learned geriatrics principles while working side by side with geriatrician‐hospitalists.
Case Study
We selected the most comprehensive program for further description. This case illustrates the power of integrating geriatric and hospital medicine paradigms.
Hospital Internal Medicine, Mayo Clinic, Rochester, MN (Site A)
The Mayo Clinic established the Hospital Internal Medicine Group (HIM) in 1998 in response to changing resident workload regulations. The practice initially focused on perioperative medical care for a busy orthopedic trauma surgery (OTS) service. In 2000, noting the average age of the elective orthopedic population was 81, the leadership of HIM made a strategic decision to recruit physicians with geriatrics training. By 2005, 6 of the 22 physicians the group employed were geriatricians.
In mid‐2005 the group's members covered eight services in 1‐ to 2‐week block rotations. Three of the services are uniquely focused on the older patient: the Geriatric Medicine Service (GeM), the OTS, and the SNF. On the GeM, a geriatrician‐hospitalist works alongside a generalist‐hospitalist to for care medical patients triaged to the service based on age (older than 75) and frailty. Although the GeM is based on a medical nursing unit, the unit is neither configured nor staffed like an ACE unit, and up to 20% of the GeM's patients overflow to other units. In addition to providing acute care, the GeM employs standardized documentation to facilitate universal comprehensive geriatric assessment. On the OTS, HIM hospitalists care for postoperative patients in a comanagement model, descriptions of which have been published elsewhere.11, 12 As a reflection of its orientation toward the older surgical patient, every OTS patient is assessed for delirium with the confusion assessment method instrument.13 Finally, the 30‐bed SNF service (on which 75% of admissions are postoperative for subacute rehabilitation) is supervised by a HIM physician and a nurse‐practitioner.
Additional activities of HIM physicians are clinical quality improvement including participation in the creation of inpatient care pathways, revision of the hospital's discharge processes, ongoing review of adverse events, and use of standardized tools for intrahospital transfers. In addition, the HIM group prioritizes geriatrics education for its physicians and hospital medicine fellows. In turn, geriatrics fellows rotate through the GeM, SNF, and OTS services.
DISCUSSION
Although SHM increasingly recognizes the challenges inherent in caring for older patients, few hospitalists are adapting their care for this vulnerable population. We identified only 11 innovations in geriatric care despite there being more than 1000 hospitalist groups. This apparent paucity of innovation in geriatrics might be explained by the relatively recent introduction of hospital medicine. As no hospitalist program is more than 10 years old, most programs are still focused on building core clinical activities or on other competing demands. In addition to time, funding may limit the typical program's ability to innovate without directly increasing revenue. Although the geriatrics literature supports that specialized inpatient care for older patients can result in increased physical functioning and quality of life at no additional cost, it may be that geriatricians have yet to make this case effectively to the hospitalist community.14, 15
The findings of this study were limited by our survey methodology. Specifically, our sample was limited to professional contacts and those using SHM listservs. In addition, some innovative hospitalists may not consider their programs to be geriatric programs and so may not have responded to our queries. Therefore, the reported innovations are not representative of geriatric care among all hospitalist groups, and we are unable to provide a comprehensive picture of geriatric care in hospitalist programs. In addition, we cannot comment on the effectiveness of the care approaches at participating institutions. For example, interdisciplinary care is an important tenet of geriatric medicine. Although six of our programs reported interdisciplinary rounds, it is unclear if these rounds are models of effective collaborative practice. Nonetheless, the information obtained from the structured interviews allowed the identification of several instructive themes discussed below.
Opportunities
The growth of the hospitalist movement provides an opportunity to reconsider clinical paradigms for the hospitalized older population. Hospitalists bring clinical skills in treating acute illness, preventing hospital complications, and providing perioperative care.16, 17 As leaders in institutional quality, safety, and utilization initiatives, hospitalists are often given protected time for such endeavors.18, 19 In so doing, the incentives of hospitalists are aligned with those of hospital administrators. This orientation makes hospitalists open to innovation in clinical care improvement.
The opportunity for hospitalists to bring fresh approaches to acute care geriatrics need not happen in a vacuum. More than 30 years of geriatrics research has provided a framework, literature, and expertise to inform hospitalist groups. The common goal of clinical excellence for the hospitalized older patient should motivate cooperation, collaborative approaches, and a joint clinical research agenda. From our inquiry to hospitalist groups, it appears that this sort of interaction occurs infrequently. The innovations identified and the case study described highlight several ways in which the geriatric medicine and hospital medicine experiences inform one another. These include approaches to staffing, organization, and quality improvement, as well as to clinical areas amenable to innovation.
Approaches
Staffing and Organization
The employment of geriatrics‐trained clinicians by hospitalist programs is one approach to supporting generalist‐hospitalists and inclining group culture toward clinical geriatric concerns. Programs that purposefully hired geriatricians and gerontology nurse‐practitioners used them to staff geriatrics services including ACE units, SNFs and, in the case of HIM, a GeM service that was a modification of a medical service. In addition, two programs relied on geriatrician‐hospitalists to serve as clinical mentors to generalist‐hospitalists.
In particular, the use of geriatrics‐trained staff on specialized services such as ACE units is encouraging, as specialized geriatric units remain an underutilized care model,20 despite compelling evidence of their effectiveness in improving physical functioning and reducing nursing home admissions.14 Although the factors undermining the success of ACE units in the past may also pose challenges for hospitalists, hospitalist groups may be better positioned to maintain the interest and financial commitment of hospital administrators. The HIM's GeM Service is also of interest, given the need to disseminate best practices in geriatrics throughout the hospital. The benefits to older patients of such a service, however, have not been demonstrated. Likewise, comprehensive geriatric assessment and geriatric consultation in the inpatient setting are reported to have had mixed results in the absence of targeting individuals at highest risk for adverse outcomes.21
Patient Safety and Quality Improvement
Hospital medicine has rapidly integrated principles of quality improvement and patient safety, having grown up contemporaneously with the patient safety movement. Several of the hospitalist programs we identified spearheaded quality improvement efforts directed at the particular needs of older patients such as delirium prevention, provision of immunizations, and removal of indwelling Foley catheters.
These efforts can be seen in the context of the many hospitalist programs focusing on standardizing care, understanding iatrogenesis, adopting safe technologies, and generally moving hospital culture forward.22 In choosing to embrace patient safety practices such as medication reconciliation (endorsed by the Institute for Healthcare Improvement),23 hospitalists may confer disproportionate benefits to older patients, who frequently require multiple medications and are at high risk for adverse drug events.6 As the efficacy of many of these interventions is poorly understood, hospitalist and geriatricians (whose work on the hazards of hospitalization anticipated the patient safety movement by many years24) may find a shared clinical research agenda with patient safety as its focus.
Areas of Clinical Opportunity
Perioperative Care
Commentators have noted hospitalists' growing participation in perioperative care,17 much of which concerns the older orthopedic surgery patient.12 Through their embedding in surgical wards, hospitalists may become actual or de facto members of surgical teams with a significant impact on team culture and care delivery. For example, hospitalists at one program implemented a perioperative beta‐blocker protocol for older orthopedic surgery patients, leading to a marked decrease in postoperative cardiac events (Site B).
Although many hospitalist programs participate in similar initiatives, it is likely that additional attention to the needs of older patients will augment the effectiveness of their interventions. For instance, structured geriatrics consultation can reduce the incidence of postoperative delirium among hip fracture patients by 46% (NNT = 5.6).25 Increased attention to postoperative pain control and early mobilization, among others, may affect the functional recovery of the older surgical patient.26, 27
Postdischarge care and care transitions
The hallmark of the hospitalist modelthe handoff of care from a primary care provider to an inpatient provideris commonly considered the major limitation of the hospitalist model because of the risk of lost clinical information.1 Because older patients are particularly susceptible to postdischarge adverse events, their care transitions may require specialized attention.28 Two of the innovations we identified (Sites A and K) have extended care of older patients into the postacute setting by integrating SNF care into their programs as a way to streamline discharge processes, decrease miscommunication, and underscore the limitations of postacute care.
A growing body of evidence supports the role of discharge strategies in improving care transitions. In one study, postdischarge follow‐up with a hospital physician rather than a community physician resulted in a reduction of the combined end point of 30‐day mortality and nonelective readmission.29 In a randomized trial, postdischarge phone calls by a pharmacist reduced the number of ED visits within 30 days of discharge.30 In another trial, older patients receiving a multifactorial intervention aimed at providing the skills for active participation in care transitions resulted in a reduced number of readmissions within 30 days.31 Understanding and implementing these activities may be crucial to both the care of older patients and the success of the hospitalist enterprise.
Barriers
Part of the challenge of treating older patients in hospitals is that the paradigms of geriatrics and hospital medicine differ substantially.32 Notably, geriatric medicine goals of maximizing function and quality of life may conflict with traditional medical goals of diagnosis and cure. This dichotomy is amplified in the hospital setting because hospitals are organized to maximize the physician's ability to stabilize, diagnose, cure, and discharge.33
By design, the hospitalist model introduces additional challenges into the hospital paradigm that affect the older patient, such as the discontinuities addressed above. Additional factors that hospitalists identified as barriers to the effective care of older patients include: 1) poor communication skills, 2) ineffective interdisciplinary collaboration, 3) limited geriatrics knowledge base, and 4) insufficient support for care coordination.34 Despite these recognized challenges, our query to hospitalist groups identified few that had made clinical excellence in geriatrics a focus of their activities.
Even with its prioritization of geriatric medicine, the well‐developed HIM model faces challenges. In particular, the feasibility of the geriatrician‐hospitalist is limited by the many geriatricians who, because of the scarcity of those who are fellowship trained, may be unprepared to care for acutely ill older patients, as their training has not focused on the hospital setting.35, 36 In addition, the surgical comanagement model depends on a unique collaboration with surgical colleagues. Finally, the ability of the HIM group to incorporate geriatrics paradigms into the hospital setting depends on extensive support from the hospital in the form of resources and a shared vision that is unlikely to be found at most institutions.
CONCLUSIONS
The rapid growth of the hospitalist movement will significantly affect clinical care in American hospitals. As most hospital patients are older, the impact on acute care geriatrics cannot be overlooked. In our study, we identified only a small number of hospitalist groups that have made geriatric medicine a priority. These programs prioritize geriatric medicine through the employment of geriatrics‐trained staff, adaptation of geriatric care models such as ACE units, and commitment to clinical quality improvement and patient safety. They also focus on common clinical challenges for older patients, including postoperative and postdischarge care. Although much can be learned from these examples, programs at other institutions will need to be individualized to meet the specific needs of each hospital and community. The common goal of clinical excellence shared by hospitalists and geriatricians should motivate cooperation, collaborative approaches, and a joint clinical research agenda at all levels, as the current paradigm of hospital care remains inadequate to meet the needs of the acutely ill older patient.
Between 1996with the first appearance of hospitalists in the medical literatureand the present, the hospitalist workforce has grown to nearly 10,000.1, 2 More remarkable is the estimate that the number of hospitalists will double in the next 5 years.2 The rapid growth of hospital medicine raises significant issues for the care of older patients, who are hospitalized at high rates3 and suffer numerous complications from hospitalization including functional decline,4 delirium,5 and a disproportionate share of adverse events.6 Conversely, the needs of patients older than 65 years of age, whose hospital stays make up nearly 50% of acute‐care bed days, will shape the future of hospital medicine.3
To date, the hospital medicine literature has failed to address the particular challenges of treating older patients, focusing primarily on opportunities for reductions in costs and length of stay for hospitalists' Medicare patients (of about $1000 per admission and 0.5 days, respectively7, 8) when compared with those cared for by other physicians. This focus on economic efficiency reflects the early orientation of the hospitalist movement. More recently, leaders of the hospitalist professional organization, the Society of Hospital Medicine (SHM), have increasingly recognized that caring for the older population will require additional knowledge and clinical skills beyond that taught in internal medicine residencies.9 Beyond educational initiatives, however, hospitalists must reconsider the paradigms of hospital care that make the hospital setting so dangerous for the older patient.
Given the aging population and the predicted growth of hospital medicine, it is essential to develop an understanding of the impact of hospitalists on the care of older patients and to encourage clinical innovation at the intersection of hospital medicine and geriatrics. Consequently, this article 1) identifies and summarizes geriatric care approaches in hospitalist programs, 2) presents a case study of geriatric hospital care by a hospitalist group, and 3) highlights opportunities for innovation and further research.
METHODS
Sample
We conducted a cross‐sectional survey of the hospitalist community via two mailings to SHM Listservs in September 2003 and September 2004. To encourage responses, the e‐mails used terms such as innovating, developing, providing hospitalist services, and caring for the geriatric patient or Medicare population. Respondents to the e‐mail solicitations (n = 14), leaders of SHM and academic hospitalist groups (n = 14), and leaders of the American Geriatrics Society specializing in acute care (n = 3) were queried about additional contacts who might know about programs utilizing geriatric care approaches. Each of these contacts was subsequently solicited and queried.10 Thirteen of the respondents described the current use by their hospitalist groups of one or more geriatric care approaches that represented a departure from usual care. We subsequently refer to these approaches as innovations. The 13 respondents completed in‐depth telephone interviews with one of the authors (H.W.). All respondents were recontacted in the spring of 2005 to update their responses. Two of the 13 programs were eliminated from the analysis after the interviews were completed. The first of these programs was identified in 2003 but had been discontinued by 2004. The second program was eliminated because the innovation was not implemented.
Data Collection
We developed a data collection tool to gather descriptive information from respondents regarding characteristics of the hospitalist group, the clinical program, the primary hospital, and the innovation (focus, target patients, organization, staffing, training, rounding, other). In addition, respondents were queried about motivations for the innovation; successes, opportunities, and future plans; and failures and barriers to implementation.
Analysis
First, we summarized the characteristics of the 11 innovations (Table 1). Second, geriatric care approaches were identified from the innovations on the basis of their objectives and the types of responses we encountered most frequently. The approaches were not mutually exclusive. For instance, a program providing postdischarge care at a skilled nursing facility (SNF) might also use a geriatrician‐hospitalist staffing model.
| Site | A | B | C | D | E | F | G | H | I | J | K |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Focus | |||||||||||
| Medical care | x | x | x | x | |||||||
| Postdischarge care | x | x | |||||||||
| Perioperative care | x | x | x | ||||||||
| Geriatric assessment | x | x | x | ||||||||
| Quality improvement | x | x | x | x | |||||||
| Staffing | x | ||||||||||
| Generalist‐hospitalist | x | x | x | x | x | x | |||||
| Geriatrician‐hospitalist | x | x | x | x | x | x | |||||
| Advanced‐practice nurse | x | x | x | x | |||||||
| Patient targeting | |||||||||||
| By age | x | x | x | x | x | x | x | x | x | ||
| By diagnosis | x | x | x | x | x | x | |||||
| By location | x | x | x | x | x | x | |||||
| Organization | |||||||||||
| Unit | x | x | x | x | x | x | |||||
| Service | x | x | x | x | x | x | |||||
| Interdisciplinary rounds | x | x | x | x | x | x | |||||
| Geriatrics training | x | x | x | x | x | x | x |
RESULTS
In 2003 the annual survey of the American Hospital Association identified 1415 hospitalist groups in the United States (Joe Miller, SHM senior vice‐president, personal communication). Remarkably, our query identified only 11 hospitalist groups with clinical innovations aimed at the older population. These innovations ranged from single individuals involved in targeted quality‐improvement projects to highly developed programs addressing an array of clinical needs for the hospitalized older patient. These 11 programs are summarized in Table 1 and described below.
Focus
Hospitalists' programs targeted to the older patient were designed to meet various needs arising from an episode of hospital care. These included innovations designed around their core clinical activities in providing acute medical care (four innovations), as well as innovations targeted to postdischarge care at SNFs (two innovations), perioperative care in consultative or comanagement models (four innovations), comprehensive geriatric assessment (three innovations), and clinical quality improvement such as audit tools (four innovations).
Staffing
Four innovations employed physicians without specific geriatrics training (generalist‐hospitalists), four innovations employed 16 fellowship‐trained geriatricians (geriatrician‐hospitalists), and two programs employed both geriatricians and generalist hospitalists. Four innovations employed advanced‐practice nurses, both with and without gerontology training.
Patients
Nine of the 11 innovations targeted patients by age (older than 65, 70, or 75 years). Of the two innovations that did not target patients by age, one focused on improving the quality of care for all patients on a medical ward by focusing on geriatric issues (Site I), and a second was concerned with postdischarge care for all patients discharged to affiliated SNFs (Site K). In addition to targeting by age, six innovations targeted patients on the basis of diagnosis, four of which focused on surgical diagnosis. Finally, patient selection by location occurred in six of the innovations, as described in the next section.
Organization
Six of the innovations were organized to operate within a clinical service (such as a medical or surgical team). In contrast to the service‐based innovations, six clinical innovations for older patients operated in geographic units including acute care for elders (ACE) units (n = 2), SNFs (n = 2), a medical nursing unit (n = 1), and an emergency department (ED; n = 1). Of the two ACE units, one (Site G) existed prior to the establishment of the hospitalist group. In this instance, a geriatrician‐hospitalist appointed jointly by the hospitalist group and the Division of Geriatrics staffed ACE unit patients of select private physicians and unassigned patients. The second ACE unit (Site H), established with the formation of the hospitalist group, was staffed by two hospitalists among eight physicians in a private geriatrics group. Regarding SNFs, one hospitalist group for a large health care organization (Site K) rounded at contract SNFs at which group members held medical directorships; another hospitalist program took over rounding at an SNF owned by its health system (Site A).
Rounding
Six of the innovations incorporated interdisciplinary rounds, including all three innovations with medical care as their focus. Four of the six innovations with interdisciplinary rounds were based in ACE units or SNFs. One of these six innovations (Site C), a perioperative initiative, incorporated twice‐weekly multidisciplinary rounds attended by an attending surgeon, surgical residents, and a hospitalistin addition to the nurses, case managers, and therapists.
Training
Seven of the 11 innovations involved geriatrics training. Four of the training innovations targeted nursing staff, four targeted hospitalist physicians, and one targeted both nurses and physicians. Most institutions developed their own curricula. Three hospitalist groups, however, modified preexisting curricula, struggling to adapt them to the needs of hospital‐based staff. Two innovations (Sites A and K) used a clinical mentoring model in which generalist‐hospitalists learned geriatrics principles while working side by side with geriatrician‐hospitalists.
Case Study
We selected the most comprehensive program for further description. This case illustrates the power of integrating geriatric and hospital medicine paradigms.
Hospital Internal Medicine, Mayo Clinic, Rochester, MN (Site A)
The Mayo Clinic established the Hospital Internal Medicine Group (HIM) in 1998 in response to changing resident workload regulations. The practice initially focused on perioperative medical care for a busy orthopedic trauma surgery (OTS) service. In 2000, noting the average age of the elective orthopedic population was 81, the leadership of HIM made a strategic decision to recruit physicians with geriatrics training. By 2005, 6 of the 22 physicians the group employed were geriatricians.
In mid‐2005 the group's members covered eight services in 1‐ to 2‐week block rotations. Three of the services are uniquely focused on the older patient: the Geriatric Medicine Service (GeM), the OTS, and the SNF. On the GeM, a geriatrician‐hospitalist works alongside a generalist‐hospitalist to for care medical patients triaged to the service based on age (older than 75) and frailty. Although the GeM is based on a medical nursing unit, the unit is neither configured nor staffed like an ACE unit, and up to 20% of the GeM's patients overflow to other units. In addition to providing acute care, the GeM employs standardized documentation to facilitate universal comprehensive geriatric assessment. On the OTS, HIM hospitalists care for postoperative patients in a comanagement model, descriptions of which have been published elsewhere.11, 12 As a reflection of its orientation toward the older surgical patient, every OTS patient is assessed for delirium with the confusion assessment method instrument.13 Finally, the 30‐bed SNF service (on which 75% of admissions are postoperative for subacute rehabilitation) is supervised by a HIM physician and a nurse‐practitioner.
Additional activities of HIM physicians are clinical quality improvement including participation in the creation of inpatient care pathways, revision of the hospital's discharge processes, ongoing review of adverse events, and use of standardized tools for intrahospital transfers. In addition, the HIM group prioritizes geriatrics education for its physicians and hospital medicine fellows. In turn, geriatrics fellows rotate through the GeM, SNF, and OTS services.
DISCUSSION
Although SHM increasingly recognizes the challenges inherent in caring for older patients, few hospitalists are adapting their care for this vulnerable population. We identified only 11 innovations in geriatric care despite there being more than 1000 hospitalist groups. This apparent paucity of innovation in geriatrics might be explained by the relatively recent introduction of hospital medicine. As no hospitalist program is more than 10 years old, most programs are still focused on building core clinical activities or on other competing demands. In addition to time, funding may limit the typical program's ability to innovate without directly increasing revenue. Although the geriatrics literature supports that specialized inpatient care for older patients can result in increased physical functioning and quality of life at no additional cost, it may be that geriatricians have yet to make this case effectively to the hospitalist community.14, 15
The findings of this study were limited by our survey methodology. Specifically, our sample was limited to professional contacts and those using SHM listservs. In addition, some innovative hospitalists may not consider their programs to be geriatric programs and so may not have responded to our queries. Therefore, the reported innovations are not representative of geriatric care among all hospitalist groups, and we are unable to provide a comprehensive picture of geriatric care in hospitalist programs. In addition, we cannot comment on the effectiveness of the care approaches at participating institutions. For example, interdisciplinary care is an important tenet of geriatric medicine. Although six of our programs reported interdisciplinary rounds, it is unclear if these rounds are models of effective collaborative practice. Nonetheless, the information obtained from the structured interviews allowed the identification of several instructive themes discussed below.
Opportunities
The growth of the hospitalist movement provides an opportunity to reconsider clinical paradigms for the hospitalized older population. Hospitalists bring clinical skills in treating acute illness, preventing hospital complications, and providing perioperative care.16, 17 As leaders in institutional quality, safety, and utilization initiatives, hospitalists are often given protected time for such endeavors.18, 19 In so doing, the incentives of hospitalists are aligned with those of hospital administrators. This orientation makes hospitalists open to innovation in clinical care improvement.
The opportunity for hospitalists to bring fresh approaches to acute care geriatrics need not happen in a vacuum. More than 30 years of geriatrics research has provided a framework, literature, and expertise to inform hospitalist groups. The common goal of clinical excellence for the hospitalized older patient should motivate cooperation, collaborative approaches, and a joint clinical research agenda. From our inquiry to hospitalist groups, it appears that this sort of interaction occurs infrequently. The innovations identified and the case study described highlight several ways in which the geriatric medicine and hospital medicine experiences inform one another. These include approaches to staffing, organization, and quality improvement, as well as to clinical areas amenable to innovation.
Approaches
Staffing and Organization
The employment of geriatrics‐trained clinicians by hospitalist programs is one approach to supporting generalist‐hospitalists and inclining group culture toward clinical geriatric concerns. Programs that purposefully hired geriatricians and gerontology nurse‐practitioners used them to staff geriatrics services including ACE units, SNFs and, in the case of HIM, a GeM service that was a modification of a medical service. In addition, two programs relied on geriatrician‐hospitalists to serve as clinical mentors to generalist‐hospitalists.
In particular, the use of geriatrics‐trained staff on specialized services such as ACE units is encouraging, as specialized geriatric units remain an underutilized care model,20 despite compelling evidence of their effectiveness in improving physical functioning and reducing nursing home admissions.14 Although the factors undermining the success of ACE units in the past may also pose challenges for hospitalists, hospitalist groups may be better positioned to maintain the interest and financial commitment of hospital administrators. The HIM's GeM Service is also of interest, given the need to disseminate best practices in geriatrics throughout the hospital. The benefits to older patients of such a service, however, have not been demonstrated. Likewise, comprehensive geriatric assessment and geriatric consultation in the inpatient setting are reported to have had mixed results in the absence of targeting individuals at highest risk for adverse outcomes.21
Patient Safety and Quality Improvement
Hospital medicine has rapidly integrated principles of quality improvement and patient safety, having grown up contemporaneously with the patient safety movement. Several of the hospitalist programs we identified spearheaded quality improvement efforts directed at the particular needs of older patients such as delirium prevention, provision of immunizations, and removal of indwelling Foley catheters.
These efforts can be seen in the context of the many hospitalist programs focusing on standardizing care, understanding iatrogenesis, adopting safe technologies, and generally moving hospital culture forward.22 In choosing to embrace patient safety practices such as medication reconciliation (endorsed by the Institute for Healthcare Improvement),23 hospitalists may confer disproportionate benefits to older patients, who frequently require multiple medications and are at high risk for adverse drug events.6 As the efficacy of many of these interventions is poorly understood, hospitalist and geriatricians (whose work on the hazards of hospitalization anticipated the patient safety movement by many years24) may find a shared clinical research agenda with patient safety as its focus.
Areas of Clinical Opportunity
Perioperative Care
Commentators have noted hospitalists' growing participation in perioperative care,17 much of which concerns the older orthopedic surgery patient.12 Through their embedding in surgical wards, hospitalists may become actual or de facto members of surgical teams with a significant impact on team culture and care delivery. For example, hospitalists at one program implemented a perioperative beta‐blocker protocol for older orthopedic surgery patients, leading to a marked decrease in postoperative cardiac events (Site B).
Although many hospitalist programs participate in similar initiatives, it is likely that additional attention to the needs of older patients will augment the effectiveness of their interventions. For instance, structured geriatrics consultation can reduce the incidence of postoperative delirium among hip fracture patients by 46% (NNT = 5.6).25 Increased attention to postoperative pain control and early mobilization, among others, may affect the functional recovery of the older surgical patient.26, 27
Postdischarge care and care transitions
The hallmark of the hospitalist modelthe handoff of care from a primary care provider to an inpatient provideris commonly considered the major limitation of the hospitalist model because of the risk of lost clinical information.1 Because older patients are particularly susceptible to postdischarge adverse events, their care transitions may require specialized attention.28 Two of the innovations we identified (Sites A and K) have extended care of older patients into the postacute setting by integrating SNF care into their programs as a way to streamline discharge processes, decrease miscommunication, and underscore the limitations of postacute care.
A growing body of evidence supports the role of discharge strategies in improving care transitions. In one study, postdischarge follow‐up with a hospital physician rather than a community physician resulted in a reduction of the combined end point of 30‐day mortality and nonelective readmission.29 In a randomized trial, postdischarge phone calls by a pharmacist reduced the number of ED visits within 30 days of discharge.30 In another trial, older patients receiving a multifactorial intervention aimed at providing the skills for active participation in care transitions resulted in a reduced number of readmissions within 30 days.31 Understanding and implementing these activities may be crucial to both the care of older patients and the success of the hospitalist enterprise.
Barriers
Part of the challenge of treating older patients in hospitals is that the paradigms of geriatrics and hospital medicine differ substantially.32 Notably, geriatric medicine goals of maximizing function and quality of life may conflict with traditional medical goals of diagnosis and cure. This dichotomy is amplified in the hospital setting because hospitals are organized to maximize the physician's ability to stabilize, diagnose, cure, and discharge.33
By design, the hospitalist model introduces additional challenges into the hospital paradigm that affect the older patient, such as the discontinuities addressed above. Additional factors that hospitalists identified as barriers to the effective care of older patients include: 1) poor communication skills, 2) ineffective interdisciplinary collaboration, 3) limited geriatrics knowledge base, and 4) insufficient support for care coordination.34 Despite these recognized challenges, our query to hospitalist groups identified few that had made clinical excellence in geriatrics a focus of their activities.
Even with its prioritization of geriatric medicine, the well‐developed HIM model faces challenges. In particular, the feasibility of the geriatrician‐hospitalist is limited by the many geriatricians who, because of the scarcity of those who are fellowship trained, may be unprepared to care for acutely ill older patients, as their training has not focused on the hospital setting.35, 36 In addition, the surgical comanagement model depends on a unique collaboration with surgical colleagues. Finally, the ability of the HIM group to incorporate geriatrics paradigms into the hospital setting depends on extensive support from the hospital in the form of resources and a shared vision that is unlikely to be found at most institutions.
CONCLUSIONS
The rapid growth of the hospitalist movement will significantly affect clinical care in American hospitals. As most hospital patients are older, the impact on acute care geriatrics cannot be overlooked. In our study, we identified only a small number of hospitalist groups that have made geriatric medicine a priority. These programs prioritize geriatric medicine through the employment of geriatrics‐trained staff, adaptation of geriatric care models such as ACE units, and commitment to clinical quality improvement and patient safety. They also focus on common clinical challenges for older patients, including postoperative and postdischarge care. Although much can be learned from these examples, programs at other institutions will need to be individualized to meet the specific needs of each hospital and community. The common goal of clinical excellence shared by hospitalists and geriatricians should motivate cooperation, collaborative approaches, and a joint clinical research agenda at all levels, as the current paradigm of hospital care remains inadequate to meet the needs of the acutely ill older patient.
- ,.The emerging role of hospitalists in the American health care system.N Engl J Med.1996;335:514–517.
- Society of Hospital Medicine. Growth of hospital medicine nationwide. Available at URL: http://www.hospitalmedicine.org/Content/NavigationMenu/Media/GrowthofHospitalMedicineNationwide/Growth_of_Hospital_M.htm[accessed January 20, 2005].
- ,.2002 National Hospital Discharge Survey.Advance data from Vital And Health Statistics. No. 342.Hyattsville (MD):National Center for Health Statistics,2002.
- ,,, et al.Functional outcomes of acute medical illness and hospitalization in older persons.Arch Intern Med.1996;156,:645–652.
- ,,.Delirium: a symptom of how hospital care is failing older persons and a window to improve the quality of hospital care.Am J Med.1999;106:565–573.
- ,.Incidence and types of preventable adverse events in elderly patients: population based review of medical records.BMJ.2000;320:741–744.
- ,,.The effect of full‐time faculty hospitalists on the efficiency of care at a community teaching hospital.Ann Intern Med.1998;129:197–203.
- ,,,,,.The value of a hospitalist service: efficient care for the aging population?Chest.2001;119:580–589.year="2001"2001.
- .Improving care for older adults: SHM educational initiatives.Hospitalist.2004;8(Suppl):45–47.
- .Qualitative evaluation and research methods.2nd ed.Thousand Oaks (CA):Sage Publications,1990:176.
- ,,, et al.Effects of a hospitalist model on elderly patients with hip fracture.Arch Intern Med.2005;165:796–801.
- ,,, et al.Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial.Ann Intern Med.2004;141:28–38.
- ,,, et al.Clarifying confusion: the confusion assessment method. A new method for the detection of delirium.Ann Intern Med.1990;113:941–948.
- ,,Geriatric evaluation and management units for hospitalized patients. In:Making healthcare safer: a critical analysis of Patient Safety Practices Evidence Report/Technology AssessmentNo. 43.2001. AHRQ Publication No. 01‐E058.
- ,,, et al.A controlled trial of inpatient and outpatient geriatric evaluation and management.N Engl J Med.2002;346:905–912.
- ,.The hospitalist movement five years later.JAMA.2002;287:487–494.
- .The hospitalist joins the surgical team.Ann Intern Med.2004;141:67–69.
- .The end of the beginning: patient safety five years after ‘To Err Is Human.’Health Aff.2004;23S2:W534–W545.
- .How hospitalists add value.Hospitalist.2005;9(Suppl 1):6–7.
- ,,, et al.Dissemination and characteristics of acute care of elders (ACE) units in the United States.Int J Technol Assess Health Care.2003;19:220–227.
- ,,, et al.Multidisciplinary geriatric consultation services,Chap. 29.Evidence Report/Technology Assessment No. 43.2001. AHRQ Publication No. 01‐E058.
- .Hospitalists spearhead a wide range of patient safety improvement projects.Hospitalist.2004;8(Suppl.):33–35.
- Institute for Healthcare Improvement.100k Lives campaign. 10‐20‐2005.
- .Hazards of hospitalization of the elderly.Ann Intern Med.1993;118:219–223.
- ,,, et al.Reducing delirium after hip fracture: a randomized trial.J Am Geriatr Soc.2001;49:516–522.
- ,,, et al.The impact of postoperative pain on outcomes following hip fracture.Pain.2003;103:303–311.
- ,,, et al.Physical therapy and mobility 2 and 6 months after hip fracture.J Am Geriatr Soc.2004;52:1114–1120.
- .Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex needs.J Am Geriatr Soc.2003;51:549–555.
- ,,, et al.Continuity of care and patient outcomes after hospital discharge.J Gen Intern Med.2004;19:624–631.
- ,,, et al.The impact of follow‐up telephone calls to patients after hospitalization.Dis Mon.2002;48:239–248.
- ,,, et al.The care transitions intervention: results from a randomized controlled trial. Society of Hospital Medicine Annual Meeting, Chicago, IL,2005.
- .Case management: high intensity care for frail patients with complex needs.Geriatrics.1998;53:62–68.
- .The care of strangers: the rise of America's hospital system.New York:Basic Books,1987.
- ,,.Hospitalists' role in caring for older Americans: Executive Summary.2002. San Francisco, prepared for the John Hartford Foundation.
- Geriatric medicine training and practice in the United States at the beginning of the 21st century.New York:Association of Directors of Geriatric Academic Programs,2002.
- AGS Education Committee.Guidelines for fellowship training in geriatrics.1998;46:1473–1477.
- ,.The emerging role of hospitalists in the American health care system.N Engl J Med.1996;335:514–517.
- Society of Hospital Medicine. Growth of hospital medicine nationwide. Available at URL: http://www.hospitalmedicine.org/Content/NavigationMenu/Media/GrowthofHospitalMedicineNationwide/Growth_of_Hospital_M.htm[accessed January 20, 2005].
- ,.2002 National Hospital Discharge Survey.Advance data from Vital And Health Statistics. No. 342.Hyattsville (MD):National Center for Health Statistics,2002.
- ,,, et al.Functional outcomes of acute medical illness and hospitalization in older persons.Arch Intern Med.1996;156,:645–652.
- ,,.Delirium: a symptom of how hospital care is failing older persons and a window to improve the quality of hospital care.Am J Med.1999;106:565–573.
- ,.Incidence and types of preventable adverse events in elderly patients: population based review of medical records.BMJ.2000;320:741–744.
- ,,.The effect of full‐time faculty hospitalists on the efficiency of care at a community teaching hospital.Ann Intern Med.1998;129:197–203.
- ,,,,,.The value of a hospitalist service: efficient care for the aging population?Chest.2001;119:580–589.year="2001"2001.
- .Improving care for older adults: SHM educational initiatives.Hospitalist.2004;8(Suppl):45–47.
- .Qualitative evaluation and research methods.2nd ed.Thousand Oaks (CA):Sage Publications,1990:176.
- ,,, et al.Effects of a hospitalist model on elderly patients with hip fracture.Arch Intern Med.2005;165:796–801.
- ,,, et al.Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial.Ann Intern Med.2004;141:28–38.
- ,,, et al.Clarifying confusion: the confusion assessment method. A new method for the detection of delirium.Ann Intern Med.1990;113:941–948.
- ,,Geriatric evaluation and management units for hospitalized patients. In:Making healthcare safer: a critical analysis of Patient Safety Practices Evidence Report/Technology AssessmentNo. 43.2001. AHRQ Publication No. 01‐E058.
- ,,, et al.A controlled trial of inpatient and outpatient geriatric evaluation and management.N Engl J Med.2002;346:905–912.
- ,.The hospitalist movement five years later.JAMA.2002;287:487–494.
- .The hospitalist joins the surgical team.Ann Intern Med.2004;141:67–69.
- .The end of the beginning: patient safety five years after ‘To Err Is Human.’Health Aff.2004;23S2:W534–W545.
- .How hospitalists add value.Hospitalist.2005;9(Suppl 1):6–7.
- ,,, et al.Dissemination and characteristics of acute care of elders (ACE) units in the United States.Int J Technol Assess Health Care.2003;19:220–227.
- ,,, et al.Multidisciplinary geriatric consultation services,Chap. 29.Evidence Report/Technology Assessment No. 43.2001. AHRQ Publication No. 01‐E058.
- .Hospitalists spearhead a wide range of patient safety improvement projects.Hospitalist.2004;8(Suppl.):33–35.
- Institute for Healthcare Improvement.100k Lives campaign. 10‐20‐2005.
- .Hazards of hospitalization of the elderly.Ann Intern Med.1993;118:219–223.
- ,,, et al.Reducing delirium after hip fracture: a randomized trial.J Am Geriatr Soc.2001;49:516–522.
- ,,, et al.The impact of postoperative pain on outcomes following hip fracture.Pain.2003;103:303–311.
- ,,, et al.Physical therapy and mobility 2 and 6 months after hip fracture.J Am Geriatr Soc.2004;52:1114–1120.
- .Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex needs.J Am Geriatr Soc.2003;51:549–555.
- ,,, et al.Continuity of care and patient outcomes after hospital discharge.J Gen Intern Med.2004;19:624–631.
- ,,, et al.The impact of follow‐up telephone calls to patients after hospitalization.Dis Mon.2002;48:239–248.
- ,,, et al.The care transitions intervention: results from a randomized controlled trial. Society of Hospital Medicine Annual Meeting, Chicago, IL,2005.
- .Case management: high intensity care for frail patients with complex needs.Geriatrics.1998;53:62–68.
- .The care of strangers: the rise of America's hospital system.New York:Basic Books,1987.
- ,,.Hospitalists' role in caring for older Americans: Executive Summary.2002. San Francisco, prepared for the John Hartford Foundation.
- Geriatric medicine training and practice in the United States at the beginning of the 21st century.New York:Association of Directors of Geriatric Academic Programs,2002.
- AGS Education Committee.Guidelines for fellowship training in geriatrics.1998;46:1473–1477.
Treatment of Community‐Acquired Pneumonia
In the United States, community‐acquired pneumonia (CAP) leads to nearly 1 million hospitalizations annually, with aggregate costs of hospitalization approaching $9 billion.1, 2 In an effort to improve the appropriate, cost‐effective care for patients with CAP, several professional societies have developed clinical practice guidelines and pathways for pneumonia.37 Although the guidelines address all aspects of care, they devote substantial attention to antibiotic recommendations. Most U.S. guidelines recommend treatment of hospitalized patients with an intravenous beta‐lactam combined with a macrolide, or a fluoroquinolone with activity against Streptococcus pneumoniae. Of the major U.S. CAP practice guidelines, only one6 recommends doxycycline as an alternative to a macrolide for inpatients.
Doxycycline is an attractive alternative to macrolides. Similar to macrolides, doxycycline is active against a wide variety of organisms including atypical bacteria (Chlamydia pneumoniae, Legionella pneumophilus, and Mycoplasma pneumoniae) and is well tolerated.810 In addition, it is inexpensive (cost of $1.00/day [awp] for 100 mg p.o. bid), and rates of tetracycline/doxycycline resistance among S. pneumoniae isolates have remained low, in contrast to the increasing rates of resistance to macrolides and fluoroquinolones.11, 12 The most recent guidelines from the Infectious Diseases Society of America cited limited published clinical data on the effectiveness of doxycycline in CAP as a barrier to increased use.7 Only one study of hospitalized patients has been published in the era of penicillin‐resistant pneumococcus, and this study included only 43 low‐risk patients treated with doxycycline.13 At the university hospital affiliated with the University of California, San Francisco, ceftriaxone plus doxycycline is generally recommended as initial empiric antibiotic therapy for patients hospitalized with CAP, but significant variability in prescribing exists, allowing for comparisons between patients treated with different initial empiric antibiotic regimens. We compared outcomes of hospitalized patients with CAP treated with ceftriaxone plus doxycycline to those of patients treated with alternative initial empiric therapy at an academic medical center.
METHODS
Study Population
A retrospective cohort study of all adults (age 18 years) discharged from the inpatient general medicine service of Moffitt‐Long Hospital at the University of California, San Francisco, was conducted from January 1999 through July 2001. Eligibility criteria included a principal discharge diagnosis of CAP and a chest radiograph demonstrating an infiltrate within 48 hours of admission. Exclusion criteria included infection with the human immunodeficiency virus, history of organ transplantation or use of immunosuppressive therapy (including prednisone > 15 mg/day), cystic fibrosis, postobstructive pneumonia, active tuberculosis, recent hospitalization (within 10 days), or admission for comfort care. The study protocol and procedures were reviewed and approved by the UCSF Committee for Human Research.
Data Collection
Medical record review by trained research assistants blinded to the research question was used to gather demographic data, comorbid illnesses, physical examination findings on initial presentation, and laboratory or radiographic results on initial presentation. The pneumonia severity index (PSI) score was calculated for each patient using the above data.14 In addition, data were collected on antibiotic allergies, antibiotics used within the 30 days prior to admission, results of sputum or blood cultures, and admission location (intensive care unit [ICU] versus medical floor).
Data from TSI (Transition Systems Inc., Boston, MA), the hospital administrative database, were used to identify the initial empiric antibiotic regimen. All antibiotics prescribed within the first 48 hours of hospitalization were considered initial empiric therapy with few exceptions. Initial empiric therapy was classified as 1) ceftriaxone plus doxycycline (including patients treated with these agents alone in the first 48 hours, as well as patients treated with both agents in the first 24 hours who were switched to alternative therapy [broader coverage] on the second day), or 2) other appropriate therapy (treatment consistent with current national guideline recommendations including at least a beta‐lactam plus a macrolide or a beta‐lactam plus a fluoroquinolone, or fluoroquinolone monotherapy). Patients receiving therapy inconsistent with current national guideline recommendations were excluded.
Outcomes
TSI data were used to identify length of stay, death during the index hospitalization, and return to the emergency department or readmission within 30 days of discharge. The National Death Index was used to identify all deaths that occurred after hospital discharge. The 30‐day mortality data included deaths occurring during the index hospitalization and in the 30 days after the index hospitalization discharge.
Statistical Analysis
For the purposes of this analysis we compared patients treated with ceftriaxone plus doxycycline to patients treated with other appropriate therapy. To examine demographic and clinical differences between the two groups, statistical tests of comparison were performed using chi‐square tests for the dichotomous variables and t tests for the numeric variables, all of which were normally distributed (after log transformation in the case of length of stay).
To adjust for clinical variables that might contribute to differences in outcomes between the two groups, we used backward stepwise logistic regression analysis to construct a propensity score15 for the likelihood of ceftriaxone plus doxycycline use. The propensity score reflected the conditional probability of exposure to ceftriaxone plus doxycycline and allowed for stratification and, subsequently, comparisons by quintiles of propensity score. Propensity scores often have distinct advantages over direct adjustment for a large number of confounding variables and allow direct comparisons between groups with a similar propensity for receiving ceftriaxone plus doxycycline.15 Unlike random assignment of treatment, however, the propensity score cannot balance unmeasured variables that may affect treatment assignment. Thus, the possibility of bias remains. The variables used to build the score included age, presence of comorbid illness, admission from a nursing home or long‐term care facility, antibiotic allergy, prior antibiotic use, PSI score, PSI risk class, diagnosis of aspiration, admission to the ICU, and positive blood cultures. The propensity score was then stratified and used as an adjustment variable in comparisons between groups for in‐hospital mortality, 30‐day mortality, and 30‐day readmission rates. As expected, length of stay was highly skewed and was therefore log‐transformed and compared between groups with adjustment for the propensity score.
To further address issues related to potential selection bias, a separate analysis was performed on a subset of the original cohort that excluded patients for whom ceftriaxone plus doxycycline would not generally be recommended as first‐line therapy. For this analysis, patients admitted from a nursing home or long‐term care facility, patients admitted to the ICU, and patients with a principal diagnosis of aspiration pneumonia were excluded. A propensity score was rederived for this subset, which was used to adjust for differences in outcomes. All statistical procedures were performed using STATA (Ver. 7.0, Stata Corporation, College Station TX).
RESULTS
Patient Characteristics
A total of 341 patients were eligible for analysis. Of this group, 216 were treated with ceftriaxone plus doxycycline and 125 received other appropriate therapy. Both groups of patients were similar in age. Patients treated with ceftriaxone plus doxycycline had a lower median PSI score and fewer comorbid illnesses than did patients treated with other appropriate therapy (Table 1). Blood cultures were positive in 30 (8.8%) of the 341 patients included in the analysis, with S. pneumoniae the most commonly isolated organism (n = 17, 5.0%). Of S. pneumoniae isolates, 4 (24%) were resistant to penicillin (MIC 1 g/mL), and 2 (12%) were resistant to tetracycline (MIC 8 g/mL).
| Ceftriaxone/doxycycline | Other appropriate therapy | |
|---|---|---|
| ||
| Patients (n) | 216 | 125 |
| Age (median) | 76 | 74 |
| PSI Score (median)a | 97 | 108 |
| PSI Risk Class (%)a | ||
| Class I | 9.3 | 5.6 |
| Class II | 11.1 | 8.8 |
| Class III | 21.8 | 13.6 |
| Class IV | 40.7 | 40.0 |
| Class V | 17.1 | 32.0 |
| Comorbid Illness (%)a | 36.1 | 47.2 |
| Nursing Home/LCF (%)a | 5.1 | 14.4 |
| Aspiration (%)a | 3.2 | 20.0 |
| Admission to ICU (%)a | 6.0 | 28.0 |
Common antibiotic choices in patients receiving other appropriate therapy included a beta‐lactam/beta‐lactamase inhibitor plus doxycycline or a macrolide (n = 36, 29%), fluoroquinolone monotherapy (n = 16, 13%), and a variety of other antibiotic combinations with activity against S. pneumoniae and atypical bacteria (n = 52, 42%).
Clinical Outcomes
Analyses of unadjusted outcomes showed that patients treated with ceftriaxone plus doxycycline had significantly lower inpatient (2% vs. 14%, P < .001) and 30‐day (6% vs. 20%, P < .001) mortality compared to patients treated with other regimens (Table 2). Multivariable logistic regression analysis identified three variables (diagnosis of congestive heart failure, admission to the ICU, and the presence of comorbid illness) associated with initial antibiotic selection, which were used to build a propensity score. After adjustment for the propensity score, use of ceftriaxone plus doxycycline remained significantly associated with lower inpatient mortality (OR = 0.26, 95% CI: 0.080.81) and 30‐day mortality (OR = 0.37, 95% CI: 0.170.81). Differences in length of stay and 30‐day readmission rates between the treatment groups were not significant (Table 2).
| Ceftriaxone + doxycycline (n = 216) | Other appropriate therapy (n = 125) | Adjusted odds ratio (95% confidence interval) | |
|---|---|---|---|
| |||
| Inpatient Mortality | 2.3% | 14.4% | 0.26 (0.080.81) |
| 30‐day mortality | 6.0% | 20.0% | 0.37 (0.170.81) |
| Length of stay (median days) | 3.0 | 4.0 | 0.09 (0.250.06)a |
| 30‐day readmission | 10.7% | 12.0% | 0.87 (0.421.81) |
Subset Analysis
To address issues related to selection bias, we performed an analysis of a subset of the patients after excluding those admitted from a nursing home, diagnosed with aspiration, or admitted to the ICU, for whom ceftriaxone plus doxycycline would not be considered recommended (or first‐line) therapy. The two resulting groups were similar, except there were fewer patients with comorbid illness in the ceftriaxone plus doxycycline group (34% vs. 50%, P = .015). The propensity score was rederived for this subset and used for adjustment. Unadjusted and adjusted outcomes are shown in Table 3. Use of ceftriaxone plus doxycycline in this subset also was associated with reduced odds of inpatient mortality (OR = 0.17, 95% CI: 0.040.77). The odds of 30‐day mortality also were reduced but not significantly, as the confidence interval included 1.0 (OR = 0.43, 95% CI: 0.141.31). There were no differences between groups in length of stay or in 30‐day readmission rate.
| Ceftriaxone + doxycycline (n = 188) | Other appropriate therapy (n = 70) | Adjusted odds ratio (95% CI) | |
|---|---|---|---|
| |||
| Age (median years) | 75 | 71 | |
| PSI score (mean) | 95 | 98 | |
| Comorbid illness (%)a | 33.5 | 50.0 | |
| Inpatient mortality | 1.6% | 7.1% | 0.17 (0.040.77) |
| 30‐day mortality | 4.8% | 8.6% | 0.43 (0.141.31) |
| LOS (median days) | 3 | 3 | 0.06 (0.240.12)b |
| 30‐day readmission | 11.9% | 10.0% | 1.31 (0.523.28) |
DISCUSSION
In our hospital setting, the use of ceftriaxone plus doxycycline as the initial empiric antibiotic therapy for patients hospitalized with community‐acquired pneumonia was associated with significantly lower inpatient and 30‐day mortality, even after adjusting for clinical differences between groups. We did not find a difference between regimens in hospital length of stay or 30‐day readmission rate. In case the multivariable model was insufficient to account for the clinical differences (i.e., selection bias) between groups, we also performed an analysis of a subgroup of less severely ill patients by excluding those admitted from nursing homes, those admitted to the intensive care unit, and those with aspiration pneumonia. In this subset, use of ceftriaxone plus doxycycline remained associated with lower inpatient mortality but not with lower 30‐day mortality. Although, as an observational study, the results of our findings could still be a result of residual confounding, we believe the results provide valuable information regarding doxycycline.
Combination therapy with a macrolide, but not doxycycline, is advocated by the practice guidelines of several major U.S. professional societies,3, 4, 7 apparently because of a lack of data on the effectiveness of combination therapy with doxycycline.7 Only one randomized, unblinded study, in 87 low‐risk patients hospitalized with CAP, that compared monotherapy with IV doxycycline versus physician‐determined therapy has been conducted.13 This study found no differences between treatment groups in clinical outcomes but did find that use of doxycycline was associated with shorter hospital stays and reduced costs. Our results, achieved in a real‐world setting in relatively ill hospitalized patients (58% were in PSI risk class IV or V), provide further support for the use of combination therapy with doxycycline.
Hospitalized patients treated with a beta‐lactam in combination with a macrolide are often discharged on macrolide monotherapy. In our population most patients treated with ceftriaxone plus doxycycline were discharged on doxycycline if they required continued therapy (data not shown). In the current era of resistance of Streptococcus pneumoniae to antibiotics, there is good reason to believe doxycycline may perform as well, if not better, than macrolides when hospitalized patients with CAP are discharged on oral monotherapy. Macrolide resistance rates among invasive pneumococcal isolates in the United States doubled from 10% to 20% during a period in which prescriptions for macrolides increased by 13%.12 In addition, a large surveillance study of more than 1500 isolates collected in 1999 and 2000 found that 26% of the isolates were resistant to macrolides, whereas only 16% were resistant to tetracycline.16 In vitro testing against S. Pneumoniae has also suggested that tetracycline resistance overestimates doxycycline resistance.17, 18 More recently, Streptococcus pneumoniae susceptibility data from the SENTRY Antimicrobial Surveillance program reaffirmed doxycycline's in vitro superiority over macrolides.17
Our study had several limitations. The study design adopted precluded determining whether favorable results with the use of ceftriaxone plus doxycycline resulted from an effect unique to this combination of antibiotics, the possible anti‐inflammatory properties of doxycycline alone,19, 20 or unmeasured confounders. For example, processes of care that affect clinical outcomes for patients hospitalized with CAP, such as the timing of antibiotic delivery, the timing of blood cultures, and stability assessment on discharge were not measured in this study. To affect outcomes, these processes of care would need to be differentially distributed between our comparison groups. However, because this study was performed in a single institution during a single interval, it is likely that the performance of these processes of care would be similar for all patients.
In conclusion, ceftriaxone plus doxycycline appears to be an effective, and possibly superior, therapy for patients hospitalized with CAP. Randomized controlled trials of doxycycline‐containing regimens versus other regimens are warranted.
- ,,, et al.Hospitalized pneumonia. Outcomes, treatment patterns, and costs in urban and rural areas.J Gen Intern Med.1996;11:415–421.
- ,,, et al.The cost of treating community‐acquired pneumonia.Clin Ther.1998;20:820–837.
- ,,, et al.Practice guidelines for the management of community‐acquired pneumonia in adults. Infectious Diseases Society of America.Clin Infect Dis.2000;31:347–382.
- ,,, et al.Management of community‐acquired pneumonia in the era of pneumococcal resistance: a report from the Drug‐Resistant Streptococcus pneumoniae Therapeutic Working Group.Arch Intern Med.2000;160:1399–1408.
- ,,, et al.Canadian guidelines for the initial management of community‐acquired pneumonia: an evidence‐based update by the Canadian Infectious Diseases Society and the Canadian Thoracic Society. The Canadian Community‐Acquired Pneumonia Working Group.Clin Infect Dis.2000;31:383–421.
- ,,, et al.Guidelines for the management of adults with community‐acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention.Am J Respir Crit Care Med.2001;163:1730–1754.
- ,,, et al.Update of practice guidelines for the management of community‐acquired pneumonia in immunocompetent adults.Clin Infect Dis.2003;37:1405–1433
- ,,.Doxycycline.Ther Drug Monit1982;4:115–135
- ,.Chloramphenicol and tetracyclines.Med Clin North Am.1987;71:1155–1168
- ,.Tetracyclines.Med Clin North Am.1995;79:789–801
- ,,, et al.Antibiotic resistance among gram‐negative bacilli in US intensive care units: implications for fluoroquinolone use.JAMA.2003;289:885–888
- ,,, et al.Macrolide resistance among invasive Streptococcus pneumoniae isolates.JAMA.2001;286:1857–1862.
- ,,, et al.Doxycycline is a cost‐effective therapy for hospitalized patients with community‐acquired pneumonia.Arch Intern Med.1999;159:266–270.
- ,,, et al.A prediction rule to identify low‐risk patients with community‐acquired pneumonia.N Engl J Med.1997;336:243–250.
- .Reducing bias in observational studies using subclassification on the propensity score.J Am Stat Assoc.1984;79:516–524
- ,,, et al.Antimicrobial resistance among clinical isolates of Streptococcus pneumoniae in the United States during 1999—2000, including a comparison of resistance rates since 1994—1995.Antimicrob Agents Chemother.2001;45:1721–1729
- ,,.Doxycycline use for community‐acquired pneumonia: contemporary in vitro spectrum of activity against Streptococcus pneumoniae (1999–2002).Diagn Microbiol Infect Dis.2004;49:147–149
- ,,, et al.Doxycycline activity against Streptococcus pneumoniae.Chest.1995;108:1775–1776.
- ,,, et al.Inhibition of enzymatic activity of phospholipases A2 by minocycline and doxycycline.Biochem Pharmacol.1992;44:1165–1170.
- ,,, et al.Doxycycline reduces mortality to lethal endotoxemia by reducing nitric oxide synthesis via an interleukin‐10‐independent mechanism.J Infect Dis.1998;177:489–492.
In the United States, community‐acquired pneumonia (CAP) leads to nearly 1 million hospitalizations annually, with aggregate costs of hospitalization approaching $9 billion.1, 2 In an effort to improve the appropriate, cost‐effective care for patients with CAP, several professional societies have developed clinical practice guidelines and pathways for pneumonia.37 Although the guidelines address all aspects of care, they devote substantial attention to antibiotic recommendations. Most U.S. guidelines recommend treatment of hospitalized patients with an intravenous beta‐lactam combined with a macrolide, or a fluoroquinolone with activity against Streptococcus pneumoniae. Of the major U.S. CAP practice guidelines, only one6 recommends doxycycline as an alternative to a macrolide for inpatients.
Doxycycline is an attractive alternative to macrolides. Similar to macrolides, doxycycline is active against a wide variety of organisms including atypical bacteria (Chlamydia pneumoniae, Legionella pneumophilus, and Mycoplasma pneumoniae) and is well tolerated.810 In addition, it is inexpensive (cost of $1.00/day [awp] for 100 mg p.o. bid), and rates of tetracycline/doxycycline resistance among S. pneumoniae isolates have remained low, in contrast to the increasing rates of resistance to macrolides and fluoroquinolones.11, 12 The most recent guidelines from the Infectious Diseases Society of America cited limited published clinical data on the effectiveness of doxycycline in CAP as a barrier to increased use.7 Only one study of hospitalized patients has been published in the era of penicillin‐resistant pneumococcus, and this study included only 43 low‐risk patients treated with doxycycline.13 At the university hospital affiliated with the University of California, San Francisco, ceftriaxone plus doxycycline is generally recommended as initial empiric antibiotic therapy for patients hospitalized with CAP, but significant variability in prescribing exists, allowing for comparisons between patients treated with different initial empiric antibiotic regimens. We compared outcomes of hospitalized patients with CAP treated with ceftriaxone plus doxycycline to those of patients treated with alternative initial empiric therapy at an academic medical center.
METHODS
Study Population
A retrospective cohort study of all adults (age 18 years) discharged from the inpatient general medicine service of Moffitt‐Long Hospital at the University of California, San Francisco, was conducted from January 1999 through July 2001. Eligibility criteria included a principal discharge diagnosis of CAP and a chest radiograph demonstrating an infiltrate within 48 hours of admission. Exclusion criteria included infection with the human immunodeficiency virus, history of organ transplantation or use of immunosuppressive therapy (including prednisone > 15 mg/day), cystic fibrosis, postobstructive pneumonia, active tuberculosis, recent hospitalization (within 10 days), or admission for comfort care. The study protocol and procedures were reviewed and approved by the UCSF Committee for Human Research.
Data Collection
Medical record review by trained research assistants blinded to the research question was used to gather demographic data, comorbid illnesses, physical examination findings on initial presentation, and laboratory or radiographic results on initial presentation. The pneumonia severity index (PSI) score was calculated for each patient using the above data.14 In addition, data were collected on antibiotic allergies, antibiotics used within the 30 days prior to admission, results of sputum or blood cultures, and admission location (intensive care unit [ICU] versus medical floor).
Data from TSI (Transition Systems Inc., Boston, MA), the hospital administrative database, were used to identify the initial empiric antibiotic regimen. All antibiotics prescribed within the first 48 hours of hospitalization were considered initial empiric therapy with few exceptions. Initial empiric therapy was classified as 1) ceftriaxone plus doxycycline (including patients treated with these agents alone in the first 48 hours, as well as patients treated with both agents in the first 24 hours who were switched to alternative therapy [broader coverage] on the second day), or 2) other appropriate therapy (treatment consistent with current national guideline recommendations including at least a beta‐lactam plus a macrolide or a beta‐lactam plus a fluoroquinolone, or fluoroquinolone monotherapy). Patients receiving therapy inconsistent with current national guideline recommendations were excluded.
Outcomes
TSI data were used to identify length of stay, death during the index hospitalization, and return to the emergency department or readmission within 30 days of discharge. The National Death Index was used to identify all deaths that occurred after hospital discharge. The 30‐day mortality data included deaths occurring during the index hospitalization and in the 30 days after the index hospitalization discharge.
Statistical Analysis
For the purposes of this analysis we compared patients treated with ceftriaxone plus doxycycline to patients treated with other appropriate therapy. To examine demographic and clinical differences between the two groups, statistical tests of comparison were performed using chi‐square tests for the dichotomous variables and t tests for the numeric variables, all of which were normally distributed (after log transformation in the case of length of stay).
To adjust for clinical variables that might contribute to differences in outcomes between the two groups, we used backward stepwise logistic regression analysis to construct a propensity score15 for the likelihood of ceftriaxone plus doxycycline use. The propensity score reflected the conditional probability of exposure to ceftriaxone plus doxycycline and allowed for stratification and, subsequently, comparisons by quintiles of propensity score. Propensity scores often have distinct advantages over direct adjustment for a large number of confounding variables and allow direct comparisons between groups with a similar propensity for receiving ceftriaxone plus doxycycline.15 Unlike random assignment of treatment, however, the propensity score cannot balance unmeasured variables that may affect treatment assignment. Thus, the possibility of bias remains. The variables used to build the score included age, presence of comorbid illness, admission from a nursing home or long‐term care facility, antibiotic allergy, prior antibiotic use, PSI score, PSI risk class, diagnosis of aspiration, admission to the ICU, and positive blood cultures. The propensity score was then stratified and used as an adjustment variable in comparisons between groups for in‐hospital mortality, 30‐day mortality, and 30‐day readmission rates. As expected, length of stay was highly skewed and was therefore log‐transformed and compared between groups with adjustment for the propensity score.
To further address issues related to potential selection bias, a separate analysis was performed on a subset of the original cohort that excluded patients for whom ceftriaxone plus doxycycline would not generally be recommended as first‐line therapy. For this analysis, patients admitted from a nursing home or long‐term care facility, patients admitted to the ICU, and patients with a principal diagnosis of aspiration pneumonia were excluded. A propensity score was rederived for this subset, which was used to adjust for differences in outcomes. All statistical procedures were performed using STATA (Ver. 7.0, Stata Corporation, College Station TX).
RESULTS
Patient Characteristics
A total of 341 patients were eligible for analysis. Of this group, 216 were treated with ceftriaxone plus doxycycline and 125 received other appropriate therapy. Both groups of patients were similar in age. Patients treated with ceftriaxone plus doxycycline had a lower median PSI score and fewer comorbid illnesses than did patients treated with other appropriate therapy (Table 1). Blood cultures were positive in 30 (8.8%) of the 341 patients included in the analysis, with S. pneumoniae the most commonly isolated organism (n = 17, 5.0%). Of S. pneumoniae isolates, 4 (24%) were resistant to penicillin (MIC 1 g/mL), and 2 (12%) were resistant to tetracycline (MIC 8 g/mL).
| Ceftriaxone/doxycycline | Other appropriate therapy | |
|---|---|---|
| ||
| Patients (n) | 216 | 125 |
| Age (median) | 76 | 74 |
| PSI Score (median)a | 97 | 108 |
| PSI Risk Class (%)a | ||
| Class I | 9.3 | 5.6 |
| Class II | 11.1 | 8.8 |
| Class III | 21.8 | 13.6 |
| Class IV | 40.7 | 40.0 |
| Class V | 17.1 | 32.0 |
| Comorbid Illness (%)a | 36.1 | 47.2 |
| Nursing Home/LCF (%)a | 5.1 | 14.4 |
| Aspiration (%)a | 3.2 | 20.0 |
| Admission to ICU (%)a | 6.0 | 28.0 |
Common antibiotic choices in patients receiving other appropriate therapy included a beta‐lactam/beta‐lactamase inhibitor plus doxycycline or a macrolide (n = 36, 29%), fluoroquinolone monotherapy (n = 16, 13%), and a variety of other antibiotic combinations with activity against S. pneumoniae and atypical bacteria (n = 52, 42%).
Clinical Outcomes
Analyses of unadjusted outcomes showed that patients treated with ceftriaxone plus doxycycline had significantly lower inpatient (2% vs. 14%, P < .001) and 30‐day (6% vs. 20%, P < .001) mortality compared to patients treated with other regimens (Table 2). Multivariable logistic regression analysis identified three variables (diagnosis of congestive heart failure, admission to the ICU, and the presence of comorbid illness) associated with initial antibiotic selection, which were used to build a propensity score. After adjustment for the propensity score, use of ceftriaxone plus doxycycline remained significantly associated with lower inpatient mortality (OR = 0.26, 95% CI: 0.080.81) and 30‐day mortality (OR = 0.37, 95% CI: 0.170.81). Differences in length of stay and 30‐day readmission rates between the treatment groups were not significant (Table 2).
| Ceftriaxone + doxycycline (n = 216) | Other appropriate therapy (n = 125) | Adjusted odds ratio (95% confidence interval) | |
|---|---|---|---|
| |||
| Inpatient Mortality | 2.3% | 14.4% | 0.26 (0.080.81) |
| 30‐day mortality | 6.0% | 20.0% | 0.37 (0.170.81) |
| Length of stay (median days) | 3.0 | 4.0 | 0.09 (0.250.06)a |
| 30‐day readmission | 10.7% | 12.0% | 0.87 (0.421.81) |
Subset Analysis
To address issues related to selection bias, we performed an analysis of a subset of the patients after excluding those admitted from a nursing home, diagnosed with aspiration, or admitted to the ICU, for whom ceftriaxone plus doxycycline would not be considered recommended (or first‐line) therapy. The two resulting groups were similar, except there were fewer patients with comorbid illness in the ceftriaxone plus doxycycline group (34% vs. 50%, P = .015). The propensity score was rederived for this subset and used for adjustment. Unadjusted and adjusted outcomes are shown in Table 3. Use of ceftriaxone plus doxycycline in this subset also was associated with reduced odds of inpatient mortality (OR = 0.17, 95% CI: 0.040.77). The odds of 30‐day mortality also were reduced but not significantly, as the confidence interval included 1.0 (OR = 0.43, 95% CI: 0.141.31). There were no differences between groups in length of stay or in 30‐day readmission rate.
| Ceftriaxone + doxycycline (n = 188) | Other appropriate therapy (n = 70) | Adjusted odds ratio (95% CI) | |
|---|---|---|---|
| |||
| Age (median years) | 75 | 71 | |
| PSI score (mean) | 95 | 98 | |
| Comorbid illness (%)a | 33.5 | 50.0 | |
| Inpatient mortality | 1.6% | 7.1% | 0.17 (0.040.77) |
| 30‐day mortality | 4.8% | 8.6% | 0.43 (0.141.31) |
| LOS (median days) | 3 | 3 | 0.06 (0.240.12)b |
| 30‐day readmission | 11.9% | 10.0% | 1.31 (0.523.28) |
DISCUSSION
In our hospital setting, the use of ceftriaxone plus doxycycline as the initial empiric antibiotic therapy for patients hospitalized with community‐acquired pneumonia was associated with significantly lower inpatient and 30‐day mortality, even after adjusting for clinical differences between groups. We did not find a difference between regimens in hospital length of stay or 30‐day readmission rate. In case the multivariable model was insufficient to account for the clinical differences (i.e., selection bias) between groups, we also performed an analysis of a subgroup of less severely ill patients by excluding those admitted from nursing homes, those admitted to the intensive care unit, and those with aspiration pneumonia. In this subset, use of ceftriaxone plus doxycycline remained associated with lower inpatient mortality but not with lower 30‐day mortality. Although, as an observational study, the results of our findings could still be a result of residual confounding, we believe the results provide valuable information regarding doxycycline.
Combination therapy with a macrolide, but not doxycycline, is advocated by the practice guidelines of several major U.S. professional societies,3, 4, 7 apparently because of a lack of data on the effectiveness of combination therapy with doxycycline.7 Only one randomized, unblinded study, in 87 low‐risk patients hospitalized with CAP, that compared monotherapy with IV doxycycline versus physician‐determined therapy has been conducted.13 This study found no differences between treatment groups in clinical outcomes but did find that use of doxycycline was associated with shorter hospital stays and reduced costs. Our results, achieved in a real‐world setting in relatively ill hospitalized patients (58% were in PSI risk class IV or V), provide further support for the use of combination therapy with doxycycline.
Hospitalized patients treated with a beta‐lactam in combination with a macrolide are often discharged on macrolide monotherapy. In our population most patients treated with ceftriaxone plus doxycycline were discharged on doxycycline if they required continued therapy (data not shown). In the current era of resistance of Streptococcus pneumoniae to antibiotics, there is good reason to believe doxycycline may perform as well, if not better, than macrolides when hospitalized patients with CAP are discharged on oral monotherapy. Macrolide resistance rates among invasive pneumococcal isolates in the United States doubled from 10% to 20% during a period in which prescriptions for macrolides increased by 13%.12 In addition, a large surveillance study of more than 1500 isolates collected in 1999 and 2000 found that 26% of the isolates were resistant to macrolides, whereas only 16% were resistant to tetracycline.16 In vitro testing against S. Pneumoniae has also suggested that tetracycline resistance overestimates doxycycline resistance.17, 18 More recently, Streptococcus pneumoniae susceptibility data from the SENTRY Antimicrobial Surveillance program reaffirmed doxycycline's in vitro superiority over macrolides.17
Our study had several limitations. The study design adopted precluded determining whether favorable results with the use of ceftriaxone plus doxycycline resulted from an effect unique to this combination of antibiotics, the possible anti‐inflammatory properties of doxycycline alone,19, 20 or unmeasured confounders. For example, processes of care that affect clinical outcomes for patients hospitalized with CAP, such as the timing of antibiotic delivery, the timing of blood cultures, and stability assessment on discharge were not measured in this study. To affect outcomes, these processes of care would need to be differentially distributed between our comparison groups. However, because this study was performed in a single institution during a single interval, it is likely that the performance of these processes of care would be similar for all patients.
In conclusion, ceftriaxone plus doxycycline appears to be an effective, and possibly superior, therapy for patients hospitalized with CAP. Randomized controlled trials of doxycycline‐containing regimens versus other regimens are warranted.
In the United States, community‐acquired pneumonia (CAP) leads to nearly 1 million hospitalizations annually, with aggregate costs of hospitalization approaching $9 billion.1, 2 In an effort to improve the appropriate, cost‐effective care for patients with CAP, several professional societies have developed clinical practice guidelines and pathways for pneumonia.37 Although the guidelines address all aspects of care, they devote substantial attention to antibiotic recommendations. Most U.S. guidelines recommend treatment of hospitalized patients with an intravenous beta‐lactam combined with a macrolide, or a fluoroquinolone with activity against Streptococcus pneumoniae. Of the major U.S. CAP practice guidelines, only one6 recommends doxycycline as an alternative to a macrolide for inpatients.
Doxycycline is an attractive alternative to macrolides. Similar to macrolides, doxycycline is active against a wide variety of organisms including atypical bacteria (Chlamydia pneumoniae, Legionella pneumophilus, and Mycoplasma pneumoniae) and is well tolerated.810 In addition, it is inexpensive (cost of $1.00/day [awp] for 100 mg p.o. bid), and rates of tetracycline/doxycycline resistance among S. pneumoniae isolates have remained low, in contrast to the increasing rates of resistance to macrolides and fluoroquinolones.11, 12 The most recent guidelines from the Infectious Diseases Society of America cited limited published clinical data on the effectiveness of doxycycline in CAP as a barrier to increased use.7 Only one study of hospitalized patients has been published in the era of penicillin‐resistant pneumococcus, and this study included only 43 low‐risk patients treated with doxycycline.13 At the university hospital affiliated with the University of California, San Francisco, ceftriaxone plus doxycycline is generally recommended as initial empiric antibiotic therapy for patients hospitalized with CAP, but significant variability in prescribing exists, allowing for comparisons between patients treated with different initial empiric antibiotic regimens. We compared outcomes of hospitalized patients with CAP treated with ceftriaxone plus doxycycline to those of patients treated with alternative initial empiric therapy at an academic medical center.
METHODS
Study Population
A retrospective cohort study of all adults (age 18 years) discharged from the inpatient general medicine service of Moffitt‐Long Hospital at the University of California, San Francisco, was conducted from January 1999 through July 2001. Eligibility criteria included a principal discharge diagnosis of CAP and a chest radiograph demonstrating an infiltrate within 48 hours of admission. Exclusion criteria included infection with the human immunodeficiency virus, history of organ transplantation or use of immunosuppressive therapy (including prednisone > 15 mg/day), cystic fibrosis, postobstructive pneumonia, active tuberculosis, recent hospitalization (within 10 days), or admission for comfort care. The study protocol and procedures were reviewed and approved by the UCSF Committee for Human Research.
Data Collection
Medical record review by trained research assistants blinded to the research question was used to gather demographic data, comorbid illnesses, physical examination findings on initial presentation, and laboratory or radiographic results on initial presentation. The pneumonia severity index (PSI) score was calculated for each patient using the above data.14 In addition, data were collected on antibiotic allergies, antibiotics used within the 30 days prior to admission, results of sputum or blood cultures, and admission location (intensive care unit [ICU] versus medical floor).
Data from TSI (Transition Systems Inc., Boston, MA), the hospital administrative database, were used to identify the initial empiric antibiotic regimen. All antibiotics prescribed within the first 48 hours of hospitalization were considered initial empiric therapy with few exceptions. Initial empiric therapy was classified as 1) ceftriaxone plus doxycycline (including patients treated with these agents alone in the first 48 hours, as well as patients treated with both agents in the first 24 hours who were switched to alternative therapy [broader coverage] on the second day), or 2) other appropriate therapy (treatment consistent with current national guideline recommendations including at least a beta‐lactam plus a macrolide or a beta‐lactam plus a fluoroquinolone, or fluoroquinolone monotherapy). Patients receiving therapy inconsistent with current national guideline recommendations were excluded.
Outcomes
TSI data were used to identify length of stay, death during the index hospitalization, and return to the emergency department or readmission within 30 days of discharge. The National Death Index was used to identify all deaths that occurred after hospital discharge. The 30‐day mortality data included deaths occurring during the index hospitalization and in the 30 days after the index hospitalization discharge.
Statistical Analysis
For the purposes of this analysis we compared patients treated with ceftriaxone plus doxycycline to patients treated with other appropriate therapy. To examine demographic and clinical differences between the two groups, statistical tests of comparison were performed using chi‐square tests for the dichotomous variables and t tests for the numeric variables, all of which were normally distributed (after log transformation in the case of length of stay).
To adjust for clinical variables that might contribute to differences in outcomes between the two groups, we used backward stepwise logistic regression analysis to construct a propensity score15 for the likelihood of ceftriaxone plus doxycycline use. The propensity score reflected the conditional probability of exposure to ceftriaxone plus doxycycline and allowed for stratification and, subsequently, comparisons by quintiles of propensity score. Propensity scores often have distinct advantages over direct adjustment for a large number of confounding variables and allow direct comparisons between groups with a similar propensity for receiving ceftriaxone plus doxycycline.15 Unlike random assignment of treatment, however, the propensity score cannot balance unmeasured variables that may affect treatment assignment. Thus, the possibility of bias remains. The variables used to build the score included age, presence of comorbid illness, admission from a nursing home or long‐term care facility, antibiotic allergy, prior antibiotic use, PSI score, PSI risk class, diagnosis of aspiration, admission to the ICU, and positive blood cultures. The propensity score was then stratified and used as an adjustment variable in comparisons between groups for in‐hospital mortality, 30‐day mortality, and 30‐day readmission rates. As expected, length of stay was highly skewed and was therefore log‐transformed and compared between groups with adjustment for the propensity score.
To further address issues related to potential selection bias, a separate analysis was performed on a subset of the original cohort that excluded patients for whom ceftriaxone plus doxycycline would not generally be recommended as first‐line therapy. For this analysis, patients admitted from a nursing home or long‐term care facility, patients admitted to the ICU, and patients with a principal diagnosis of aspiration pneumonia were excluded. A propensity score was rederived for this subset, which was used to adjust for differences in outcomes. All statistical procedures were performed using STATA (Ver. 7.0, Stata Corporation, College Station TX).
RESULTS
Patient Characteristics
A total of 341 patients were eligible for analysis. Of this group, 216 were treated with ceftriaxone plus doxycycline and 125 received other appropriate therapy. Both groups of patients were similar in age. Patients treated with ceftriaxone plus doxycycline had a lower median PSI score and fewer comorbid illnesses than did patients treated with other appropriate therapy (Table 1). Blood cultures were positive in 30 (8.8%) of the 341 patients included in the analysis, with S. pneumoniae the most commonly isolated organism (n = 17, 5.0%). Of S. pneumoniae isolates, 4 (24%) were resistant to penicillin (MIC 1 g/mL), and 2 (12%) were resistant to tetracycline (MIC 8 g/mL).
| Ceftriaxone/doxycycline | Other appropriate therapy | |
|---|---|---|
| ||
| Patients (n) | 216 | 125 |
| Age (median) | 76 | 74 |
| PSI Score (median)a | 97 | 108 |
| PSI Risk Class (%)a | ||
| Class I | 9.3 | 5.6 |
| Class II | 11.1 | 8.8 |
| Class III | 21.8 | 13.6 |
| Class IV | 40.7 | 40.0 |
| Class V | 17.1 | 32.0 |
| Comorbid Illness (%)a | 36.1 | 47.2 |
| Nursing Home/LCF (%)a | 5.1 | 14.4 |
| Aspiration (%)a | 3.2 | 20.0 |
| Admission to ICU (%)a | 6.0 | 28.0 |
Common antibiotic choices in patients receiving other appropriate therapy included a beta‐lactam/beta‐lactamase inhibitor plus doxycycline or a macrolide (n = 36, 29%), fluoroquinolone monotherapy (n = 16, 13%), and a variety of other antibiotic combinations with activity against S. pneumoniae and atypical bacteria (n = 52, 42%).
Clinical Outcomes
Analyses of unadjusted outcomes showed that patients treated with ceftriaxone plus doxycycline had significantly lower inpatient (2% vs. 14%, P < .001) and 30‐day (6% vs. 20%, P < .001) mortality compared to patients treated with other regimens (Table 2). Multivariable logistic regression analysis identified three variables (diagnosis of congestive heart failure, admission to the ICU, and the presence of comorbid illness) associated with initial antibiotic selection, which were used to build a propensity score. After adjustment for the propensity score, use of ceftriaxone plus doxycycline remained significantly associated with lower inpatient mortality (OR = 0.26, 95% CI: 0.080.81) and 30‐day mortality (OR = 0.37, 95% CI: 0.170.81). Differences in length of stay and 30‐day readmission rates between the treatment groups were not significant (Table 2).
| Ceftriaxone + doxycycline (n = 216) | Other appropriate therapy (n = 125) | Adjusted odds ratio (95% confidence interval) | |
|---|---|---|---|
| |||
| Inpatient Mortality | 2.3% | 14.4% | 0.26 (0.080.81) |
| 30‐day mortality | 6.0% | 20.0% | 0.37 (0.170.81) |
| Length of stay (median days) | 3.0 | 4.0 | 0.09 (0.250.06)a |
| 30‐day readmission | 10.7% | 12.0% | 0.87 (0.421.81) |
Subset Analysis
To address issues related to selection bias, we performed an analysis of a subset of the patients after excluding those admitted from a nursing home, diagnosed with aspiration, or admitted to the ICU, for whom ceftriaxone plus doxycycline would not be considered recommended (or first‐line) therapy. The two resulting groups were similar, except there were fewer patients with comorbid illness in the ceftriaxone plus doxycycline group (34% vs. 50%, P = .015). The propensity score was rederived for this subset and used for adjustment. Unadjusted and adjusted outcomes are shown in Table 3. Use of ceftriaxone plus doxycycline in this subset also was associated with reduced odds of inpatient mortality (OR = 0.17, 95% CI: 0.040.77). The odds of 30‐day mortality also were reduced but not significantly, as the confidence interval included 1.0 (OR = 0.43, 95% CI: 0.141.31). There were no differences between groups in length of stay or in 30‐day readmission rate.
| Ceftriaxone + doxycycline (n = 188) | Other appropriate therapy (n = 70) | Adjusted odds ratio (95% CI) | |
|---|---|---|---|
| |||
| Age (median years) | 75 | 71 | |
| PSI score (mean) | 95 | 98 | |
| Comorbid illness (%)a | 33.5 | 50.0 | |
| Inpatient mortality | 1.6% | 7.1% | 0.17 (0.040.77) |
| 30‐day mortality | 4.8% | 8.6% | 0.43 (0.141.31) |
| LOS (median days) | 3 | 3 | 0.06 (0.240.12)b |
| 30‐day readmission | 11.9% | 10.0% | 1.31 (0.523.28) |
DISCUSSION
In our hospital setting, the use of ceftriaxone plus doxycycline as the initial empiric antibiotic therapy for patients hospitalized with community‐acquired pneumonia was associated with significantly lower inpatient and 30‐day mortality, even after adjusting for clinical differences between groups. We did not find a difference between regimens in hospital length of stay or 30‐day readmission rate. In case the multivariable model was insufficient to account for the clinical differences (i.e., selection bias) between groups, we also performed an analysis of a subgroup of less severely ill patients by excluding those admitted from nursing homes, those admitted to the intensive care unit, and those with aspiration pneumonia. In this subset, use of ceftriaxone plus doxycycline remained associated with lower inpatient mortality but not with lower 30‐day mortality. Although, as an observational study, the results of our findings could still be a result of residual confounding, we believe the results provide valuable information regarding doxycycline.
Combination therapy with a macrolide, but not doxycycline, is advocated by the practice guidelines of several major U.S. professional societies,3, 4, 7 apparently because of a lack of data on the effectiveness of combination therapy with doxycycline.7 Only one randomized, unblinded study, in 87 low‐risk patients hospitalized with CAP, that compared monotherapy with IV doxycycline versus physician‐determined therapy has been conducted.13 This study found no differences between treatment groups in clinical outcomes but did find that use of doxycycline was associated with shorter hospital stays and reduced costs. Our results, achieved in a real‐world setting in relatively ill hospitalized patients (58% were in PSI risk class IV or V), provide further support for the use of combination therapy with doxycycline.
Hospitalized patients treated with a beta‐lactam in combination with a macrolide are often discharged on macrolide monotherapy. In our population most patients treated with ceftriaxone plus doxycycline were discharged on doxycycline if they required continued therapy (data not shown). In the current era of resistance of Streptococcus pneumoniae to antibiotics, there is good reason to believe doxycycline may perform as well, if not better, than macrolides when hospitalized patients with CAP are discharged on oral monotherapy. Macrolide resistance rates among invasive pneumococcal isolates in the United States doubled from 10% to 20% during a period in which prescriptions for macrolides increased by 13%.12 In addition, a large surveillance study of more than 1500 isolates collected in 1999 and 2000 found that 26% of the isolates were resistant to macrolides, whereas only 16% were resistant to tetracycline.16 In vitro testing against S. Pneumoniae has also suggested that tetracycline resistance overestimates doxycycline resistance.17, 18 More recently, Streptococcus pneumoniae susceptibility data from the SENTRY Antimicrobial Surveillance program reaffirmed doxycycline's in vitro superiority over macrolides.17
Our study had several limitations. The study design adopted precluded determining whether favorable results with the use of ceftriaxone plus doxycycline resulted from an effect unique to this combination of antibiotics, the possible anti‐inflammatory properties of doxycycline alone,19, 20 or unmeasured confounders. For example, processes of care that affect clinical outcomes for patients hospitalized with CAP, such as the timing of antibiotic delivery, the timing of blood cultures, and stability assessment on discharge were not measured in this study. To affect outcomes, these processes of care would need to be differentially distributed between our comparison groups. However, because this study was performed in a single institution during a single interval, it is likely that the performance of these processes of care would be similar for all patients.
In conclusion, ceftriaxone plus doxycycline appears to be an effective, and possibly superior, therapy for patients hospitalized with CAP. Randomized controlled trials of doxycycline‐containing regimens versus other regimens are warranted.
- ,,, et al.Hospitalized pneumonia. Outcomes, treatment patterns, and costs in urban and rural areas.J Gen Intern Med.1996;11:415–421.
- ,,, et al.The cost of treating community‐acquired pneumonia.Clin Ther.1998;20:820–837.
- ,,, et al.Practice guidelines for the management of community‐acquired pneumonia in adults. Infectious Diseases Society of America.Clin Infect Dis.2000;31:347–382.
- ,,, et al.Management of community‐acquired pneumonia in the era of pneumococcal resistance: a report from the Drug‐Resistant Streptococcus pneumoniae Therapeutic Working Group.Arch Intern Med.2000;160:1399–1408.
- ,,, et al.Canadian guidelines for the initial management of community‐acquired pneumonia: an evidence‐based update by the Canadian Infectious Diseases Society and the Canadian Thoracic Society. The Canadian Community‐Acquired Pneumonia Working Group.Clin Infect Dis.2000;31:383–421.
- ,,, et al.Guidelines for the management of adults with community‐acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention.Am J Respir Crit Care Med.2001;163:1730–1754.
- ,,, et al.Update of practice guidelines for the management of community‐acquired pneumonia in immunocompetent adults.Clin Infect Dis.2003;37:1405–1433
- ,,.Doxycycline.Ther Drug Monit1982;4:115–135
- ,.Chloramphenicol and tetracyclines.Med Clin North Am.1987;71:1155–1168
- ,.Tetracyclines.Med Clin North Am.1995;79:789–801
- ,,, et al.Antibiotic resistance among gram‐negative bacilli in US intensive care units: implications for fluoroquinolone use.JAMA.2003;289:885–888
- ,,, et al.Macrolide resistance among invasive Streptococcus pneumoniae isolates.JAMA.2001;286:1857–1862.
- ,,, et al.Doxycycline is a cost‐effective therapy for hospitalized patients with community‐acquired pneumonia.Arch Intern Med.1999;159:266–270.
- ,,, et al.A prediction rule to identify low‐risk patients with community‐acquired pneumonia.N Engl J Med.1997;336:243–250.
- .Reducing bias in observational studies using subclassification on the propensity score.J Am Stat Assoc.1984;79:516–524
- ,,, et al.Antimicrobial resistance among clinical isolates of Streptococcus pneumoniae in the United States during 1999—2000, including a comparison of resistance rates since 1994—1995.Antimicrob Agents Chemother.2001;45:1721–1729
- ,,.Doxycycline use for community‐acquired pneumonia: contemporary in vitro spectrum of activity against Streptococcus pneumoniae (1999–2002).Diagn Microbiol Infect Dis.2004;49:147–149
- ,,, et al.Doxycycline activity against Streptococcus pneumoniae.Chest.1995;108:1775–1776.
- ,,, et al.Inhibition of enzymatic activity of phospholipases A2 by minocycline and doxycycline.Biochem Pharmacol.1992;44:1165–1170.
- ,,, et al.Doxycycline reduces mortality to lethal endotoxemia by reducing nitric oxide synthesis via an interleukin‐10‐independent mechanism.J Infect Dis.1998;177:489–492.
- ,,, et al.Hospitalized pneumonia. Outcomes, treatment patterns, and costs in urban and rural areas.J Gen Intern Med.1996;11:415–421.
- ,,, et al.The cost of treating community‐acquired pneumonia.Clin Ther.1998;20:820–837.
- ,,, et al.Practice guidelines for the management of community‐acquired pneumonia in adults. Infectious Diseases Society of America.Clin Infect Dis.2000;31:347–382.
- ,,, et al.Management of community‐acquired pneumonia in the era of pneumococcal resistance: a report from the Drug‐Resistant Streptococcus pneumoniae Therapeutic Working Group.Arch Intern Med.2000;160:1399–1408.
- ,,, et al.Canadian guidelines for the initial management of community‐acquired pneumonia: an evidence‐based update by the Canadian Infectious Diseases Society and the Canadian Thoracic Society. The Canadian Community‐Acquired Pneumonia Working Group.Clin Infect Dis.2000;31:383–421.
- ,,, et al.Guidelines for the management of adults with community‐acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention.Am J Respir Crit Care Med.2001;163:1730–1754.
- ,,, et al.Update of practice guidelines for the management of community‐acquired pneumonia in immunocompetent adults.Clin Infect Dis.2003;37:1405–1433
- ,,.Doxycycline.Ther Drug Monit1982;4:115–135
- ,.Chloramphenicol and tetracyclines.Med Clin North Am.1987;71:1155–1168
- ,.Tetracyclines.Med Clin North Am.1995;79:789–801
- ,,, et al.Antibiotic resistance among gram‐negative bacilli in US intensive care units: implications for fluoroquinolone use.JAMA.2003;289:885–888
- ,,, et al.Macrolide resistance among invasive Streptococcus pneumoniae isolates.JAMA.2001;286:1857–1862.
- ,,, et al.Doxycycline is a cost‐effective therapy for hospitalized patients with community‐acquired pneumonia.Arch Intern Med.1999;159:266–270.
- ,,, et al.A prediction rule to identify low‐risk patients with community‐acquired pneumonia.N Engl J Med.1997;336:243–250.
- .Reducing bias in observational studies using subclassification on the propensity score.J Am Stat Assoc.1984;79:516–524
- ,,, et al.Antimicrobial resistance among clinical isolates of Streptococcus pneumoniae in the United States during 1999—2000, including a comparison of resistance rates since 1994—1995.Antimicrob Agents Chemother.2001;45:1721–1729
- ,,.Doxycycline use for community‐acquired pneumonia: contemporary in vitro spectrum of activity against Streptococcus pneumoniae (1999–2002).Diagn Microbiol Infect Dis.2004;49:147–149
- ,,, et al.Doxycycline activity against Streptococcus pneumoniae.Chest.1995;108:1775–1776.
- ,,, et al.Inhibition of enzymatic activity of phospholipases A2 by minocycline and doxycycline.Biochem Pharmacol.1992;44:1165–1170.
- ,,, et al.Doxycycline reduces mortality to lethal endotoxemia by reducing nitric oxide synthesis via an interleukin‐10‐independent mechanism.J Infect Dis.1998;177:489–492.
Copyright © 2006 Society of Hospital Medicine
Editorial
You hold in your hands the inaugural issue of the Journal of Hospital Medicine (JHM). Our goal is for JHM to become the premier forum for peer‐reviewed research articles and evidence‐based reviews in the specialty of hospital medicine.
Yes, the specialty of hospital medicine. This official publication of the Society of Hospital Medicine signifies another step forward in the evolution of this specialty. With the publication of JHM the Society of Hospital Medicine continues its pivotal educational and leadership role in shaping the practice of hospital medicine. The Society is dedicated to promoting the highest‐quality care for all hospitalized patients and excellence in hospital medicine through education, advocacy, and research. As part of the Society's effort to improve care and standards, it is providing JHM to all members as part of their membership. We hope that our readership will grow to include individuals involved in all aspects of hospital care.
Packed with the results of new studies and state‐of‐the‐art reviews, JHM is not aimed solely at academicians and voracious readers of the medical literature. Rather, we hope that it fills a practical need to promote lifelong learning in both hospitalists and their hospital colleagues. For example, in this issue, national experts in palliative care and geriatrics summarize the pertinent literature and the important role of such care for hospitalized patients. JHM will also serve as a key venue for hospital medicine researchers to disseminate their findings and for educators to share their knowledge and techniques.
Why bother to create yet another journal? Given the stacks of journals that adorn many of our desks (and some of our chairs and windowsills), do we really need another to get lost among the mail that inundates us? We believe the field of hospital medicine involves a growing body of knowledge deserving of a journal focused solely on it. Hospital medicine evolved from efforts to fill a need identified by overstretched primary care physicians in the late 1980s. Physicians like the cofounders of SHM, John Nelson in Florida and Win Whitcomb in Massachusetts, began careers in a field that today numbers more than 12,000 physicians. Labeled with the moniker hospitalist given us by Bob Wachter and Lee Goldman,1 we now make up the fastest‐growing medical specialty in the United States.2 Yet, until now, no journal was devoted solely to this specialty.
The Journal of Hospital Medicine aims to provide physicians and other health care professionals with continuing insight into the basic and clinical sciences to support informed clinical decision making in the hospital. As hospitalists increasingly take an active role in the successful delivery of bench research discoveries to the bedside and become vigorous participants in the translational and clinical research sought by the National Institutes of Health,3 JHM will disseminate their findings. In addition, we hope to foster balanced debates on medical issues and health care trends that affect hospital medicine and patient care. Nonclinical aspects of hospital medicine also will be featured, including public health and the political, philosophic, ethical, legal, environmental, economic, historical, and cultural issues surrounding hospital care. We especially want to encourage submissions that evaluate projects involving the entire hospital care team: physicians and our colleagues in the hospitalnurses, pharmacists, administrators, physical and occupational therapists, social workers, and case managers.
Two articles (see pages 48 and 57) highlight this inaugural issue. One describes the development of The Core Competencies in Hospital Medicine: A Framework for Curriculum Development (a supplement to this issue), and the other demonstrates how this document can be applied to curriculum development.4, 5 This milestone in the evolution of hospital medicine provides an initial structural framework to guide medical educators in developing curricula that incorporate these competencies into the training and evaluation of students, clinicians‐in‐training, and practicing hospitalists.4 The president and CEO of the American Board of Internal Medicine (ABIM), Christine Cassel, offers her perspective on this landmark document.6 Its timeliness is reflected by the current efforts of the American College of Physicians, the ABIM, and others to redesign the training and the certification requirements of internists. As this supplement demonstrates, the Society of Hospital Medicine will be intimately involved in this process.
After this auspicious start, subsequent issues will include articles in the following categories. Original research articles will report results of randomized controlled trials, evaluations of diagnostic tests, prospective cohort studies, casecontrol studies, and high‐quality observational studies. We are interested in publishing both quantitative and qualitative research. Review articles, especially those targeting the hospital medicine core competencies, are eagerly sought. We also seek descriptions of interventions that transform hospital care delivery in the hospital. For example, accounts of the implementation of quality‐improvement projects and outcomes, including barriers that were overcome or that blocked implementation, would be invaluable to hospitalists throughout the country. Clinical conundrums should describe clinical cases that present diagnostic dilemmas or involve issues of medical errors. To facilitate the professional development of hospitalists, we seek articles focused on their professional development in community, academic, and administrative settings. Examples of leadership topics are managing physician performance, leading and managing change, and self‐evaluation. Teaching tips or descriptions of educational programs or curricula also are desired. For researchers, potential topics include descriptions of specific techniques used for surveys, meta‐analyses, economic evaluations, and statistical analyses.Penetrating point manuscripts, those that go beyond the cutting edge to explain the next potential breakthrough or intervention in the developing field of hospital medicine, may be authored by thought leaders inside and outside the health care field as well as by hospitalists with novel ideas. Equally vital, I want to share the illuminating perspectives of physicians, patients, and families of patients as they reflect on the experience of being in the hospitalhospitalists can enlighten us through their handoffs, and patients and their families can inform us about their view from the hospital bed.
Finally, never forget that this is your journal. Let me know what you like and what changes you think can make it better. Please e‐mail your suggestions, comments, criticisms, and ideas to us at JHMeditor@ hospitalmedicine.org. This is your chance to help shape the practice of hospital medicine and the future of hospital care. I look forward to your guidance. Together we can expand our knowledge and continue to grow in our careers.
The more you see the less you know
The less you find out as you grow
I knew much more then than I do now.
U2, City of Blinding Lights,
How to Dismantle an Atomic Bomb
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- .The future of hospital medicine: evolution or revolution?Am J Med.2004;117:446–450.
- .Translational and clinical science—time for a new vision.N Engl J Med2005;35:1621‐1623.
- ,,,,, eds.The core competencies in hospital medicine: development and methodology.J Hosp Med.2006;1:48–56.
- ,,,,.How to use The Core Competencies in Hospital Medicine: A Framework for Curriculum Development.J Hosp Med.2006;1:57–67.
- .Hospital medicine: early successes and challenges ahead.J Hosp Med.2006;1:3–4.
You hold in your hands the inaugural issue of the Journal of Hospital Medicine (JHM). Our goal is for JHM to become the premier forum for peer‐reviewed research articles and evidence‐based reviews in the specialty of hospital medicine.
Yes, the specialty of hospital medicine. This official publication of the Society of Hospital Medicine signifies another step forward in the evolution of this specialty. With the publication of JHM the Society of Hospital Medicine continues its pivotal educational and leadership role in shaping the practice of hospital medicine. The Society is dedicated to promoting the highest‐quality care for all hospitalized patients and excellence in hospital medicine through education, advocacy, and research. As part of the Society's effort to improve care and standards, it is providing JHM to all members as part of their membership. We hope that our readership will grow to include individuals involved in all aspects of hospital care.
Packed with the results of new studies and state‐of‐the‐art reviews, JHM is not aimed solely at academicians and voracious readers of the medical literature. Rather, we hope that it fills a practical need to promote lifelong learning in both hospitalists and their hospital colleagues. For example, in this issue, national experts in palliative care and geriatrics summarize the pertinent literature and the important role of such care for hospitalized patients. JHM will also serve as a key venue for hospital medicine researchers to disseminate their findings and for educators to share their knowledge and techniques.
Why bother to create yet another journal? Given the stacks of journals that adorn many of our desks (and some of our chairs and windowsills), do we really need another to get lost among the mail that inundates us? We believe the field of hospital medicine involves a growing body of knowledge deserving of a journal focused solely on it. Hospital medicine evolved from efforts to fill a need identified by overstretched primary care physicians in the late 1980s. Physicians like the cofounders of SHM, John Nelson in Florida and Win Whitcomb in Massachusetts, began careers in a field that today numbers more than 12,000 physicians. Labeled with the moniker hospitalist given us by Bob Wachter and Lee Goldman,1 we now make up the fastest‐growing medical specialty in the United States.2 Yet, until now, no journal was devoted solely to this specialty.
The Journal of Hospital Medicine aims to provide physicians and other health care professionals with continuing insight into the basic and clinical sciences to support informed clinical decision making in the hospital. As hospitalists increasingly take an active role in the successful delivery of bench research discoveries to the bedside and become vigorous participants in the translational and clinical research sought by the National Institutes of Health,3 JHM will disseminate their findings. In addition, we hope to foster balanced debates on medical issues and health care trends that affect hospital medicine and patient care. Nonclinical aspects of hospital medicine also will be featured, including public health and the political, philosophic, ethical, legal, environmental, economic, historical, and cultural issues surrounding hospital care. We especially want to encourage submissions that evaluate projects involving the entire hospital care team: physicians and our colleagues in the hospitalnurses, pharmacists, administrators, physical and occupational therapists, social workers, and case managers.
Two articles (see pages 48 and 57) highlight this inaugural issue. One describes the development of The Core Competencies in Hospital Medicine: A Framework for Curriculum Development (a supplement to this issue), and the other demonstrates how this document can be applied to curriculum development.4, 5 This milestone in the evolution of hospital medicine provides an initial structural framework to guide medical educators in developing curricula that incorporate these competencies into the training and evaluation of students, clinicians‐in‐training, and practicing hospitalists.4 The president and CEO of the American Board of Internal Medicine (ABIM), Christine Cassel, offers her perspective on this landmark document.6 Its timeliness is reflected by the current efforts of the American College of Physicians, the ABIM, and others to redesign the training and the certification requirements of internists. As this supplement demonstrates, the Society of Hospital Medicine will be intimately involved in this process.
After this auspicious start, subsequent issues will include articles in the following categories. Original research articles will report results of randomized controlled trials, evaluations of diagnostic tests, prospective cohort studies, casecontrol studies, and high‐quality observational studies. We are interested in publishing both quantitative and qualitative research. Review articles, especially those targeting the hospital medicine core competencies, are eagerly sought. We also seek descriptions of interventions that transform hospital care delivery in the hospital. For example, accounts of the implementation of quality‐improvement projects and outcomes, including barriers that were overcome or that blocked implementation, would be invaluable to hospitalists throughout the country. Clinical conundrums should describe clinical cases that present diagnostic dilemmas or involve issues of medical errors. To facilitate the professional development of hospitalists, we seek articles focused on their professional development in community, academic, and administrative settings. Examples of leadership topics are managing physician performance, leading and managing change, and self‐evaluation. Teaching tips or descriptions of educational programs or curricula also are desired. For researchers, potential topics include descriptions of specific techniques used for surveys, meta‐analyses, economic evaluations, and statistical analyses.Penetrating point manuscripts, those that go beyond the cutting edge to explain the next potential breakthrough or intervention in the developing field of hospital medicine, may be authored by thought leaders inside and outside the health care field as well as by hospitalists with novel ideas. Equally vital, I want to share the illuminating perspectives of physicians, patients, and families of patients as they reflect on the experience of being in the hospitalhospitalists can enlighten us through their handoffs, and patients and their families can inform us about their view from the hospital bed.
Finally, never forget that this is your journal. Let me know what you like and what changes you think can make it better. Please e‐mail your suggestions, comments, criticisms, and ideas to us at JHMeditor@ hospitalmedicine.org. This is your chance to help shape the practice of hospital medicine and the future of hospital care. I look forward to your guidance. Together we can expand our knowledge and continue to grow in our careers.
The more you see the less you know
The less you find out as you grow
I knew much more then than I do now.
U2, City of Blinding Lights,
How to Dismantle an Atomic Bomb
You hold in your hands the inaugural issue of the Journal of Hospital Medicine (JHM). Our goal is for JHM to become the premier forum for peer‐reviewed research articles and evidence‐based reviews in the specialty of hospital medicine.
Yes, the specialty of hospital medicine. This official publication of the Society of Hospital Medicine signifies another step forward in the evolution of this specialty. With the publication of JHM the Society of Hospital Medicine continues its pivotal educational and leadership role in shaping the practice of hospital medicine. The Society is dedicated to promoting the highest‐quality care for all hospitalized patients and excellence in hospital medicine through education, advocacy, and research. As part of the Society's effort to improve care and standards, it is providing JHM to all members as part of their membership. We hope that our readership will grow to include individuals involved in all aspects of hospital care.
Packed with the results of new studies and state‐of‐the‐art reviews, JHM is not aimed solely at academicians and voracious readers of the medical literature. Rather, we hope that it fills a practical need to promote lifelong learning in both hospitalists and their hospital colleagues. For example, in this issue, national experts in palliative care and geriatrics summarize the pertinent literature and the important role of such care for hospitalized patients. JHM will also serve as a key venue for hospital medicine researchers to disseminate their findings and for educators to share their knowledge and techniques.
Why bother to create yet another journal? Given the stacks of journals that adorn many of our desks (and some of our chairs and windowsills), do we really need another to get lost among the mail that inundates us? We believe the field of hospital medicine involves a growing body of knowledge deserving of a journal focused solely on it. Hospital medicine evolved from efforts to fill a need identified by overstretched primary care physicians in the late 1980s. Physicians like the cofounders of SHM, John Nelson in Florida and Win Whitcomb in Massachusetts, began careers in a field that today numbers more than 12,000 physicians. Labeled with the moniker hospitalist given us by Bob Wachter and Lee Goldman,1 we now make up the fastest‐growing medical specialty in the United States.2 Yet, until now, no journal was devoted solely to this specialty.
The Journal of Hospital Medicine aims to provide physicians and other health care professionals with continuing insight into the basic and clinical sciences to support informed clinical decision making in the hospital. As hospitalists increasingly take an active role in the successful delivery of bench research discoveries to the bedside and become vigorous participants in the translational and clinical research sought by the National Institutes of Health,3 JHM will disseminate their findings. In addition, we hope to foster balanced debates on medical issues and health care trends that affect hospital medicine and patient care. Nonclinical aspects of hospital medicine also will be featured, including public health and the political, philosophic, ethical, legal, environmental, economic, historical, and cultural issues surrounding hospital care. We especially want to encourage submissions that evaluate projects involving the entire hospital care team: physicians and our colleagues in the hospitalnurses, pharmacists, administrators, physical and occupational therapists, social workers, and case managers.
Two articles (see pages 48 and 57) highlight this inaugural issue. One describes the development of The Core Competencies in Hospital Medicine: A Framework for Curriculum Development (a supplement to this issue), and the other demonstrates how this document can be applied to curriculum development.4, 5 This milestone in the evolution of hospital medicine provides an initial structural framework to guide medical educators in developing curricula that incorporate these competencies into the training and evaluation of students, clinicians‐in‐training, and practicing hospitalists.4 The president and CEO of the American Board of Internal Medicine (ABIM), Christine Cassel, offers her perspective on this landmark document.6 Its timeliness is reflected by the current efforts of the American College of Physicians, the ABIM, and others to redesign the training and the certification requirements of internists. As this supplement demonstrates, the Society of Hospital Medicine will be intimately involved in this process.
After this auspicious start, subsequent issues will include articles in the following categories. Original research articles will report results of randomized controlled trials, evaluations of diagnostic tests, prospective cohort studies, casecontrol studies, and high‐quality observational studies. We are interested in publishing both quantitative and qualitative research. Review articles, especially those targeting the hospital medicine core competencies, are eagerly sought. We also seek descriptions of interventions that transform hospital care delivery in the hospital. For example, accounts of the implementation of quality‐improvement projects and outcomes, including barriers that were overcome or that blocked implementation, would be invaluable to hospitalists throughout the country. Clinical conundrums should describe clinical cases that present diagnostic dilemmas or involve issues of medical errors. To facilitate the professional development of hospitalists, we seek articles focused on their professional development in community, academic, and administrative settings. Examples of leadership topics are managing physician performance, leading and managing change, and self‐evaluation. Teaching tips or descriptions of educational programs or curricula also are desired. For researchers, potential topics include descriptions of specific techniques used for surveys, meta‐analyses, economic evaluations, and statistical analyses.Penetrating point manuscripts, those that go beyond the cutting edge to explain the next potential breakthrough or intervention in the developing field of hospital medicine, may be authored by thought leaders inside and outside the health care field as well as by hospitalists with novel ideas. Equally vital, I want to share the illuminating perspectives of physicians, patients, and families of patients as they reflect on the experience of being in the hospitalhospitalists can enlighten us through their handoffs, and patients and their families can inform us about their view from the hospital bed.
Finally, never forget that this is your journal. Let me know what you like and what changes you think can make it better. Please e‐mail your suggestions, comments, criticisms, and ideas to us at JHMeditor@ hospitalmedicine.org. This is your chance to help shape the practice of hospital medicine and the future of hospital care. I look forward to your guidance. Together we can expand our knowledge and continue to grow in our careers.
The more you see the less you know
The less you find out as you grow
I knew much more then than I do now.
U2, City of Blinding Lights,
How to Dismantle an Atomic Bomb
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- .The future of hospital medicine: evolution or revolution?Am J Med.2004;117:446–450.
- .Translational and clinical science—time for a new vision.N Engl J Med2005;35:1621‐1623.
- ,,,,, eds.The core competencies in hospital medicine: development and methodology.J Hosp Med.2006;1:48–56.
- ,,,,.How to use The Core Competencies in Hospital Medicine: A Framework for Curriculum Development.J Hosp Med.2006;1:57–67.
- .Hospital medicine: early successes and challenges ahead.J Hosp Med.2006;1:3–4.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- .The future of hospital medicine: evolution or revolution?Am J Med.2004;117:446–450.
- .Translational and clinical science—time for a new vision.N Engl J Med2005;35:1621‐1623.
- ,,,,, eds.The core competencies in hospital medicine: development and methodology.J Hosp Med.2006;1:48–56.
- ,,,,.How to use The Core Competencies in Hospital Medicine: A Framework for Curriculum Development.J Hosp Med.2006;1:57–67.
- .Hospital medicine: early successes and challenges ahead.J Hosp Med.2006;1:3–4.
Care of Hospitalized Older Patients
An emergency room resident once was instructing a medical student in how to place a nasogastric tube in order to evaluate a patient with melena and postural hypotension. When the tube came to a stop, the student connected a syringe to the tube and aspirated. Then, to the consternation of the resident, the student yanked out the tube as soon as he saw blood flowing into the syringe. Why'd you do that? the surprised resident asked. There's blood down there! came the quick reply.
Like that medical student, hospital‐based physicianshospitalists, geriatricians, and othersmay miss the boat when caring for hospitalized older patients. Hospitals are full, and they're filled largely with older patients. These patients, like those who are younger, generally want to be treated and sent home. Older patients, however, frequently pose specific challenges. They may talk and move more slowly, stay longer, and be more likely to die. They more often need help in caring for themselves, and many have lost the support necessary to remain at home, making it difficult for them to return there. In short, older patients often need more care and more time.
It may be tempting to ignore the challenges that arise in caring for older patients. An avoidance strategy is expedient, at least in the short term. Ultimately, however, ignoring the challenges of caring for older patients will prove no wiser than yanking the nasogastric tube. Instead, we can recognize the challenges and use this opportunity to learn to improve their care.
This article describes the state of the science in hospital care for older patients, opportunities awaiting those who care for these patients, and barriers to seizing those opportunities. I conclude with five recommendations for physicians who care for hospitalized older patients.
STATE OF THE SCIENCE
Older patients shape hospital medicine and will determine its future. In 2002 the 12% of the population age 65 years or older accounted for roughly 50% of all hospitalizations unrelated to childbirth.1, 2 Hospital admissions of older persons will balloon as the number of persons older than age 65 rises by a million a year, increasing from 13% of the population today to 21% by 2030.2
Older persons in hospitals pose substantial clinical challenges. Many have multiple comorbid diseases and virtually all have complex medical regimens.1, 35 Many have cognitive impairment or dementia, often accompanied by delirium, which hinder communication and can lead to behaviors that require extra attention and impede diagnostic tests and treatment.611 Some have difficulty walking and caring for themselves, and a third leave the hospital without having recovered to their baseline level of function, with those age 85 years or older at highest risk for this decline independent of the reason for admission.1215 These characteristics increase the care, resources, and staff time older patients need, prolong their stays, and increase their hospital costs beyond those expected for their diagnosis.16 They also are at higher risk for iatrogenic complications, death, and rehospitalization,1720 and the risk of errors may be increased by frequent transitions in providers and sites of care.2125 Older persons require greater assistance at home, and yet they have often lost much of the support needed to live at home.10, 13, 20
Despite the magnitude of these challenges, we know surprisingly little about how best to care for hospitalized older persons, especially those older than age 75. The evidence base for treatment of specific common diseases is inadequate. The very old are underrepresented in clinical trials,26, 27 and the majority of older patients with common conditions such as heart failure may not meet the enrollment criteria for clinical trials.28 Thus, what is known about treating diseases in younger patients may be extrapolated to determine treatments in older persons based only on a leap of faith, which may be misguided.29, 30 In fact, the efficacy of conventional treatments for common conditions (e.g., acute myocardial infarction and hypertension) may diminish with age,31, 32 indicating that clinical trials targeted specifically to older patients may be necessary.
Despite the dearth of evidence about the management of common diseases in hospitalized older patients, hospital‐based geriatricians have developed substantial high‐grade evidence about the prevention of two geriatric syndromes, functional disability and delirium. The incidence of both syndromes can be reduced (without increasing hospital or health care costs) by multicomponent interventions that include comprehensive assessment, targeted treatment, and environmental modification to promote independence and safety.3, 3335 Moreover, the randomized trials that evaluated these interventions have provided models for how other innovations by hospital‐based physicians can be evaluated. Despite the evidence that these approaches are effective and either cost saving or cost neutral, these models have not been widely adopted.36
Many challenges in the prevention and management of geriatric syndromes in the hospital remain. For example, sophisticated approaches to the management of delirium are disappointingonce delirium has developed, intensive state‐of‐the‐art approaches to its management are no more effective than standard care in shortening its duration or ameliorating its sequelae.37, 38 The indiscriminate use of indwelling urinary catheters is decried, but there is no evidence that their use is declining, even in patients without an indication for catheterization.3942 Malnutrition and falls can be prevented and depression treated in patients outside the hospital,4345 but it is unclear whether these maladies can be prevented or treated effectively in hospitalized elders. Finally, intriguing evidence suggests that geriatric syndromes and their sequelae may be prevented and outcomes improved by caring for patients at home whenever possible, bringing intensive nursing and physician care into the home without some of the adverse effects of hospitalization.46
The physician workforce is not prepared to provide optimal care to hospitalized older persons. Few hospitalists or other hospital‐based physicians have received more than minimal training in geriatric medicine, and few geriatricians practice extensively in the hospital. At the same time that the ranks of physicians who consider themselves hospitalists have been expanding by 1000 or more a year in the United States, the number of certified geriatricians has been decreasing as hundreds decide each year not to renew their certificates.47, 48 Fewer than 300 geriatricians complete training each year and enter the workforce, and most new geriatricians practice in ambulatory or long‐term‐care settings. Wald's study in this issue indicates the paucity of geriatricians in hospital medicine (with the apparently single exception of the Mayo Clinic's Hospital Internal Medicine Group) and a relative lack of interest among hospitalists in developing knowledge about the effective and efficient treatment of older persons, in particular.49
OPPORTUNITIES
Opportunities to improve the care of hospitalized older patients arise from the state of the science in their care and from the common ground that hospitalists and geriatricians share. The older patients of both hospitalists and geriatricians are seriously ill, with annual mortality rates of 20%30% for patients with common conditions such as myocardial infarction or colon cancer and mortality rates of 50% or higher for patients with dementia or severe disability.5, 5053 We should view the care of our patients in the context of their prognoses,5, 54 recognizing that patients' preferences for the goals, style, and site of care vary widely.55, 56 The substantial association of mortality with geriatric syndromes such as disability, dementia, delirium, and depressionan association that is independent of pathophysiologic indicators of disease severitysuggests that substantial benefits may accrue by targeting interventions to the prevention or amelioration of these syndromes.5, 9, 10, 53, 57, 58
Hospitalists and geriatricians also share the perspective of working in complex systems in which the effectiveness, efficiency, and safety of care depend on system functions as well as on their technical expertise as individuals.5961 Together, and with colleagues in other disciplines, they may redesign how hospitals and the systems around them work to reduce errors, increase attention to aspects of care that are easily overlooked, and improve patient outcomes.
BARRIERS
Hospitalists and geriatricians face barriers to improving care for hospitalized older patients. First, gaps in knowledge limit the capacity to provide the care and achieve the outcomes desired. Fundamental discoveries in clinical science are needed to prevent or treat geriatric syndromes, to treat common diseases in the very old, and to put into practice what is known. Addressing these gaps in knowledge will require a sustained effort that spans methods and disciplines.
Second, the dominant reductionist paradigm values discovery of the mechanism of disease over discovery of ways to manage illness effectively and efficiently.6267 Similarly, diagnostic tests and therapies based on beliefs about the mechanism of diseasefor example, PET scans in persons with memory disorders and chemotherapy in persons with refractory cancersare pursued aggressively and paid handsomely, whereas efforts to reduce errors or improve continuity of care receive little attention or reward. The challenges of caring for hospitalized older patients will require advances on both fronts: in our knowledge of the pathogenesis of disorders that have proven resistant to current therapies (such as delirium) and in our knowledge of how to structure clinical care that engages patients and families and achieves desired outcomes effectively, consistently, and efficiently.
The structure and styles of our practices provide the third challenge. Hospitalists pride themselves on their efficient management of patients while maintaining or improving patient outcomes. A focus on efficient management can, however, lead to an assembly‐line approach, turning each patient into a series of do‐order‐call‐check tasks to get the patient out of the hospital as quickly as possible. This approach has advantages but may also blind physicians to the scope and complexity of issues that arise in caring for the very old through the course of an illness that often extends beyond hospitalization.25 Geriatricians pride themselves on their comprehensive management of patients, gathering clinical information from many sources (especially in the many patients with cognitive impairment), exploring and articulating goals of care, and assessing self‐care and neurologic, psychological, and social domains in addition to conventional pathophysiology. Yet too often, geriatricians are not available in hospitals, and as Wald found, they have rarely been integrated into hospitalist groups.
FIVE RECOMMENDATIONS FOR HOSPITALISTS AND GERIATRICIANS
I conclude with five recommendations for hospital‐based physicians who care for older patients and for geriatricians. First, step back, look at your patients, and note their predicament in its full complexity. Once hospitalists start looking for cognitive impairment, weakness, and difficulty walking and the difficulty of finding a good situation after leaving the hospital, it will be easy to see these problems. And once geriatricians start looking at why their patients are going into the hospital and what happens to them, it will be easy to see the need to become engaged. Seeing the full range of patients' problems won't address them, but we certainly won't address them if we don't look.
Second, learn what is known about how best to care for the aged and integrate this learning into your hospital practice. For hospitalists, learning how to identify each patient's goals of care, what works to prevent delirium and promote mobility, which drugs to avoid and which doses to modify, and how to access resources to help patients and families achieve their goals after they leave the hospital will benefit older patients. Pocket and PDA resources to extend learning are readily available.68 For geriatricians, learning how to avoid hospitalization (especially when resources can be mobilized to provide a hospital at home), how to work within the timeframe of hospitalization, and what current disease‐specific management strategies have been shown to be effective in the aged will benefit their patients. Maintaining the distinction between what is believed and what is known on the basis of high‐quality evidence will enhance learning and decrease the risk of stubbornly pursuing harmful or wasteful practices. This is especially important in situations where the evidence is weak and opinions are strong.
Third, to provide the best care for our older patients, we must embrace aging, not deny it. Most hospitalized older patients, and most patients of geriatricians, will decline and die in a few years. The inevitability of these outcomes may tempt us either to abandon our incurable patients or to focus single‐mindedly on treatable problems one at a time, rather than on the interplay of multiple problems in an individual person. Either choice is mistaken. Although we are powerless to prevent decline and death in the long run, we have a tremendous capacity to delay and ameliorate decline, to enhance comfort and joy, to protect from harm, and, often, to delay death.
Fourth, ask questions about what you do not know or understand. The risk, of course, is that your curiosity will be sparked, possibly slowing you in completing the myriad tasks to be donea risk worth taking. Will ACE inhibitors and beta‐blockers benefit patients with heart failure without systolic dysfunction? Why do so many older patients become delirious, and are features of hospitalization catalyzing the effects of disease in causing delirium? Why do we continue to send cognitively impaired patients home without scheduled follow‐up and with instruction sheets they cannot read, and how can we change the system to prevent this? If you cannot find answers to your questions grounded in strong evidence, maintain your skepticism about answers given easily.
Finally, consider discovering the answers to some of your questions. Part of the excitement of caring for the very old is that we have so much to learn and that what we do learn can be so powerful.
- ,.Hospitalization in the United States, 2002. Publication 05‐056.Washington (DC):AHRQ,2005.
- .Improving health care for older persons.Ann Intern Med.2003;139:421–424.
- ,,, et al.A controlled trial of inpatient and outpatient geriatric evaluation and management.N Engl J Med.2002;346:905–912.
- ,,, et al.Hospital diagnoses, Medicare charges, and nursing home admissions in the year when older persons become severely disabled.JAMA.1997;277:728–734.
- ,,, et al.Development and validation of a prognostic index for 1‐year mortality in older adults after hospitalization.JAMA.2001;285:2987–2994.
- ,,,.Delirium is independently associated with poor functional recovery after hip fracture.J Am Geriatr Soc.2000;48:618–624.
- ,,, et al.The course of delirium in older medical inpatients: a prospective study.J Gen Intern Med.2003;18:696–704.
- ,,,.Does delirium increase hospital stay?J Am Geriatr Soc.2003;51:1539–1546.
- ,,, et al.Does delirium contribute to poor hospital outcomes? A three‐site epidemiologic study.J Gen Intern Med.1998;13:234–242.
- ,,, et al.A predictive index for functional decline in hospitalized elderly medical patients.J Gen Intern Med.1993;8:645–652.
- ,,.A prospective study of delirium in hospitalized elderly.JAMA.1990;263:1097–1101.
- ,,, et al.Unsteadiness reported by older hospitalized patients predicts functional decline.J Am Geriatr Soc.2003;51:621–626.
- ,,, et al.Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: increased vulnerability with age.J Am Geriatr Soc.2003;51:451–458.
- ,,, et al.Functional outcomes of acute medical illness and hospitalization in older persons.Arch Intern Med.1996;156:645–652.
- ,,, et al.Functional disability in the hospitalized elderly.JAMA.1982;248:847–850.
- ,,, et al.Diagnosis‐related group‐adjusted hospital costs are higher in older medical patients with lower functional status.J Am Geriatr Soc.2003;51:1729–1734.
- ,.Adverse events, negligence in hospitalized patients: results from the Harvard Medical Practice Study.Perspect Healthc Risk Manage.1991;11(2):2–8.
- ,,, et al.Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I.N Engl J Med.1991;324:370–376.
- ,,, et al.The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II.N Engl J Med.1991;324:377–384.
- ,,,.Effects of functional status changes before and during hospitalization on nursing home admission of older adults.J Gerontol A Biol Sci Med Sci.1999;54:M521–M526.
- ,,.Characterization of geriatric drug‐related hospital readmissions.Med Care.1991;29:989–1003.
- ,,,.The impact of clinical pharmacists' consultations on physicians' geriatric drug prescribing. A randomized controlled trial.Med Care.1992;30:646–658.
- ,,,.Posthospital medication discrepancies: prevalence and contributing factors.Arch Intern Med.2005;165:1842–1847.
- ,,.A new tool for identifying discrepancies in postacute medications for community‐dwelling older adults.Am J Geriatr Pharmacother.2004;2(2):141–147.
- ,.Lost in transition: challenges and opportunities for improving the quality of transitional care.Ann Intern Med.2004;141:533–536.
- ,,, et al.Enrollment of older persons in cancer trials after the medicare reimbursement policy change.Arch Intern Med.2005;165:1514–1520.
- ,,, et al.Underrepresentation of patients 65 years of age or older in cancer‐treatment trials.N Engl J Med.1999;341:2061–2067.
- ,,, et al.Most hospitalized older persons do not meet the enrollment criteria for clinical trials in heart failure.Am Heart J.2003;146(2):250–257.
- ,.Problems in the “evidence” of “evidence‐based medicine.”Am J Med.1997;103:529–535.
- .National initiatives in ageing research in the United Kingdom.Age Ageing.2002;31(2):93–95.
- .Embracing complexity: A consideration of hypertension in the very old.J Gerontol A Biol Sci Med Sci.2003;58:653–658.
- ,,, et al.Lack of benefit for intravenous thrombolysis in patients with myocardial infarction who are older than 75 years.Circulation.2000;101:2239–2246.
- ,,, et al.A randomized trial of care in a hospital medical unit especially designed to improve the functional outcomes of acutely ill older patients.N Engl J Med.1995;332:1338–1344.
- ,,, et al.A multicomponent intervention to prevent delirium in hospitalized older patients.N Engl J Med.1999;340:669–676.
- ,,,.Reducing delirium after hip fracture: a randomized trial.J Am Geriatr Soc.2001;49:516–522.
- ,,,.Dissemination and characteristics of acute care for elders (ACE) units in the United States.Int J Technol Assess Health Care.2003;19(1):220–227.
- ,.Treatment of delirium in older medical inpatients: a challenge for geriatric specialists.J Am Geriatr Soc.2002;50:2101–2103.
- ,,, et al.Systematic detection and multidisciplinary care of delirium in older medical inpatients: a randomized trial.CMAJ.2002;167:753–759.
- .Clinical and economic consequences of nosocomial catheter‐related bacteriuria.Am J Infect Control.2000;28(1):68–75.
- ,.Preventing catheter‐related bacteriuria: should we? Can we? How?Arch Intern Med.1999;159:800–808.
- ,,.Indwelling urinary catheters: a one‐point restraint?Ann Intern Med.2002;137(2):125–127.
- ,, et al.Risk factors for indwelling urinary catheterization among older hospitalized patients without a specific medical indication for catheterization.J Patient Saf.2005. In press.
- ,,.Protein and energy supplementation in elderly people at risk from malnutrition.Cochrane Database Syst Rev.2005(2):CD003288.
- .Clinical practice. Preventing falls in elderly persons.N Engl J Med.2003;348(1):42–49.
- ,,, et al.Collaborative care management of late‐life depression in the primary care setting: a randomized controlled trial.JAMA.2002;288:2836–2845.
- ,,,,,.Hospital in the home: a randomised controlled trial.Med J Aust.1999;170(4):156–160.
- .Hospitalists in the United States—mission accomplished or work in progress?N Engl J Med.2004;350:1935–1936.
- ,,,.Academic geriatric programs in US allopathic and osteopathic medical schools.JAMA.2002;288:2313–2319.
- ,,.Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs.J Hosp Med.2006;1:29–35.
- ,,, et al.The implications of regional variations in Medicare spending. Part 1: the content, quality, and accessibility of care.Ann Intern Med.2003;138:273–287.
- ,,, et al.The implications of regional variations in Medicare spending. Part 2: health outcomes and satisfaction with care.Ann Intern Med.2003;138:288–298.
- ,.Mortality from pneumonia and hip fractures in patients with advanced dementia.JAMA.2000;284:2447–2448.
- ,.Survival in end‐stage dementia following acute illness.JAMA.2000;284(1):47–52.
- ,.Cancer screening in elderly patients: a framework for individualized decision making.JAMA.2001;285:2750–2756.
- ,,,.Understanding the treatment preferences of seriously ill patients.N Engl J Med.2002;346:1061–1066.
- ,,, et al.Health values of hospitalized patients 80 years or older. HELP Investigators. Hospitalized Elderly Longitudinal Project.JAMA.1998;279:371–375.
- ,,, et al.Depressive symptoms and 3‐year mortality in older hospitalized medical patients.Ann Intern Med.1999;130:563–569.
- ,,, et al.Relation between symptoms of depression and health status outcomes in acutely ill hospitalized older persons.Ann Intern Med.1997;126:417–425.
- ,,,.Five system barriers to achieving ultrasafe health care.Ann Intern Med.2005;142:756–764.
- .Specialized care for elderly patients.N Engl J Med.2002;346:874.
- .The end of the beginning: patient safety five years after ‘To Err Is Human.’Health Aff (Millwood).2004;Suppl Web Exclusives:W4–534–545.
- .An additional basic science for clinical medicine: II. The limitations of randomized trials.Ann Intern Med.1983;99:544–550.
- .An additional basic science for clinical medicine: III. The challenges of comparison and measurement.Ann Intern Med.1983;99:705–712.
- .An additional basic science for clinical medicine: IV. The development of clinimetrics.Ann Intern Med.1983;99:843–848.
- .An additional basic science for clinical medicine: I. The constraining fundamental paradigms.Ann Intern Med.1983;99:393–397.
- ,.The end of the disease era.Am J Med.2004;116(3):179–185.
- ,, Agostini JV. Potential pitfalls of disease‐specific guidelines for patients with multiple conditions.N Engl J Med.2004;351:2870–2874.
- ,,, et al.Geriatrics at your fingertips: 2005.7th ed.Malden (MA):Blackwell Publishing, for the American Geriatrics Society,2005.
An emergency room resident once was instructing a medical student in how to place a nasogastric tube in order to evaluate a patient with melena and postural hypotension. When the tube came to a stop, the student connected a syringe to the tube and aspirated. Then, to the consternation of the resident, the student yanked out the tube as soon as he saw blood flowing into the syringe. Why'd you do that? the surprised resident asked. There's blood down there! came the quick reply.
Like that medical student, hospital‐based physicianshospitalists, geriatricians, and othersmay miss the boat when caring for hospitalized older patients. Hospitals are full, and they're filled largely with older patients. These patients, like those who are younger, generally want to be treated and sent home. Older patients, however, frequently pose specific challenges. They may talk and move more slowly, stay longer, and be more likely to die. They more often need help in caring for themselves, and many have lost the support necessary to remain at home, making it difficult for them to return there. In short, older patients often need more care and more time.
It may be tempting to ignore the challenges that arise in caring for older patients. An avoidance strategy is expedient, at least in the short term. Ultimately, however, ignoring the challenges of caring for older patients will prove no wiser than yanking the nasogastric tube. Instead, we can recognize the challenges and use this opportunity to learn to improve their care.
This article describes the state of the science in hospital care for older patients, opportunities awaiting those who care for these patients, and barriers to seizing those opportunities. I conclude with five recommendations for physicians who care for hospitalized older patients.
STATE OF THE SCIENCE
Older patients shape hospital medicine and will determine its future. In 2002 the 12% of the population age 65 years or older accounted for roughly 50% of all hospitalizations unrelated to childbirth.1, 2 Hospital admissions of older persons will balloon as the number of persons older than age 65 rises by a million a year, increasing from 13% of the population today to 21% by 2030.2
Older persons in hospitals pose substantial clinical challenges. Many have multiple comorbid diseases and virtually all have complex medical regimens.1, 35 Many have cognitive impairment or dementia, often accompanied by delirium, which hinder communication and can lead to behaviors that require extra attention and impede diagnostic tests and treatment.611 Some have difficulty walking and caring for themselves, and a third leave the hospital without having recovered to their baseline level of function, with those age 85 years or older at highest risk for this decline independent of the reason for admission.1215 These characteristics increase the care, resources, and staff time older patients need, prolong their stays, and increase their hospital costs beyond those expected for their diagnosis.16 They also are at higher risk for iatrogenic complications, death, and rehospitalization,1720 and the risk of errors may be increased by frequent transitions in providers and sites of care.2125 Older persons require greater assistance at home, and yet they have often lost much of the support needed to live at home.10, 13, 20
Despite the magnitude of these challenges, we know surprisingly little about how best to care for hospitalized older persons, especially those older than age 75. The evidence base for treatment of specific common diseases is inadequate. The very old are underrepresented in clinical trials,26, 27 and the majority of older patients with common conditions such as heart failure may not meet the enrollment criteria for clinical trials.28 Thus, what is known about treating diseases in younger patients may be extrapolated to determine treatments in older persons based only on a leap of faith, which may be misguided.29, 30 In fact, the efficacy of conventional treatments for common conditions (e.g., acute myocardial infarction and hypertension) may diminish with age,31, 32 indicating that clinical trials targeted specifically to older patients may be necessary.
Despite the dearth of evidence about the management of common diseases in hospitalized older patients, hospital‐based geriatricians have developed substantial high‐grade evidence about the prevention of two geriatric syndromes, functional disability and delirium. The incidence of both syndromes can be reduced (without increasing hospital or health care costs) by multicomponent interventions that include comprehensive assessment, targeted treatment, and environmental modification to promote independence and safety.3, 3335 Moreover, the randomized trials that evaluated these interventions have provided models for how other innovations by hospital‐based physicians can be evaluated. Despite the evidence that these approaches are effective and either cost saving or cost neutral, these models have not been widely adopted.36
Many challenges in the prevention and management of geriatric syndromes in the hospital remain. For example, sophisticated approaches to the management of delirium are disappointingonce delirium has developed, intensive state‐of‐the‐art approaches to its management are no more effective than standard care in shortening its duration or ameliorating its sequelae.37, 38 The indiscriminate use of indwelling urinary catheters is decried, but there is no evidence that their use is declining, even in patients without an indication for catheterization.3942 Malnutrition and falls can be prevented and depression treated in patients outside the hospital,4345 but it is unclear whether these maladies can be prevented or treated effectively in hospitalized elders. Finally, intriguing evidence suggests that geriatric syndromes and their sequelae may be prevented and outcomes improved by caring for patients at home whenever possible, bringing intensive nursing and physician care into the home without some of the adverse effects of hospitalization.46
The physician workforce is not prepared to provide optimal care to hospitalized older persons. Few hospitalists or other hospital‐based physicians have received more than minimal training in geriatric medicine, and few geriatricians practice extensively in the hospital. At the same time that the ranks of physicians who consider themselves hospitalists have been expanding by 1000 or more a year in the United States, the number of certified geriatricians has been decreasing as hundreds decide each year not to renew their certificates.47, 48 Fewer than 300 geriatricians complete training each year and enter the workforce, and most new geriatricians practice in ambulatory or long‐term‐care settings. Wald's study in this issue indicates the paucity of geriatricians in hospital medicine (with the apparently single exception of the Mayo Clinic's Hospital Internal Medicine Group) and a relative lack of interest among hospitalists in developing knowledge about the effective and efficient treatment of older persons, in particular.49
OPPORTUNITIES
Opportunities to improve the care of hospitalized older patients arise from the state of the science in their care and from the common ground that hospitalists and geriatricians share. The older patients of both hospitalists and geriatricians are seriously ill, with annual mortality rates of 20%30% for patients with common conditions such as myocardial infarction or colon cancer and mortality rates of 50% or higher for patients with dementia or severe disability.5, 5053 We should view the care of our patients in the context of their prognoses,5, 54 recognizing that patients' preferences for the goals, style, and site of care vary widely.55, 56 The substantial association of mortality with geriatric syndromes such as disability, dementia, delirium, and depressionan association that is independent of pathophysiologic indicators of disease severitysuggests that substantial benefits may accrue by targeting interventions to the prevention or amelioration of these syndromes.5, 9, 10, 53, 57, 58
Hospitalists and geriatricians also share the perspective of working in complex systems in which the effectiveness, efficiency, and safety of care depend on system functions as well as on their technical expertise as individuals.5961 Together, and with colleagues in other disciplines, they may redesign how hospitals and the systems around them work to reduce errors, increase attention to aspects of care that are easily overlooked, and improve patient outcomes.
BARRIERS
Hospitalists and geriatricians face barriers to improving care for hospitalized older patients. First, gaps in knowledge limit the capacity to provide the care and achieve the outcomes desired. Fundamental discoveries in clinical science are needed to prevent or treat geriatric syndromes, to treat common diseases in the very old, and to put into practice what is known. Addressing these gaps in knowledge will require a sustained effort that spans methods and disciplines.
Second, the dominant reductionist paradigm values discovery of the mechanism of disease over discovery of ways to manage illness effectively and efficiently.6267 Similarly, diagnostic tests and therapies based on beliefs about the mechanism of diseasefor example, PET scans in persons with memory disorders and chemotherapy in persons with refractory cancersare pursued aggressively and paid handsomely, whereas efforts to reduce errors or improve continuity of care receive little attention or reward. The challenges of caring for hospitalized older patients will require advances on both fronts: in our knowledge of the pathogenesis of disorders that have proven resistant to current therapies (such as delirium) and in our knowledge of how to structure clinical care that engages patients and families and achieves desired outcomes effectively, consistently, and efficiently.
The structure and styles of our practices provide the third challenge. Hospitalists pride themselves on their efficient management of patients while maintaining or improving patient outcomes. A focus on efficient management can, however, lead to an assembly‐line approach, turning each patient into a series of do‐order‐call‐check tasks to get the patient out of the hospital as quickly as possible. This approach has advantages but may also blind physicians to the scope and complexity of issues that arise in caring for the very old through the course of an illness that often extends beyond hospitalization.25 Geriatricians pride themselves on their comprehensive management of patients, gathering clinical information from many sources (especially in the many patients with cognitive impairment), exploring and articulating goals of care, and assessing self‐care and neurologic, psychological, and social domains in addition to conventional pathophysiology. Yet too often, geriatricians are not available in hospitals, and as Wald found, they have rarely been integrated into hospitalist groups.
FIVE RECOMMENDATIONS FOR HOSPITALISTS AND GERIATRICIANS
I conclude with five recommendations for hospital‐based physicians who care for older patients and for geriatricians. First, step back, look at your patients, and note their predicament in its full complexity. Once hospitalists start looking for cognitive impairment, weakness, and difficulty walking and the difficulty of finding a good situation after leaving the hospital, it will be easy to see these problems. And once geriatricians start looking at why their patients are going into the hospital and what happens to them, it will be easy to see the need to become engaged. Seeing the full range of patients' problems won't address them, but we certainly won't address them if we don't look.
Second, learn what is known about how best to care for the aged and integrate this learning into your hospital practice. For hospitalists, learning how to identify each patient's goals of care, what works to prevent delirium and promote mobility, which drugs to avoid and which doses to modify, and how to access resources to help patients and families achieve their goals after they leave the hospital will benefit older patients. Pocket and PDA resources to extend learning are readily available.68 For geriatricians, learning how to avoid hospitalization (especially when resources can be mobilized to provide a hospital at home), how to work within the timeframe of hospitalization, and what current disease‐specific management strategies have been shown to be effective in the aged will benefit their patients. Maintaining the distinction between what is believed and what is known on the basis of high‐quality evidence will enhance learning and decrease the risk of stubbornly pursuing harmful or wasteful practices. This is especially important in situations where the evidence is weak and opinions are strong.
Third, to provide the best care for our older patients, we must embrace aging, not deny it. Most hospitalized older patients, and most patients of geriatricians, will decline and die in a few years. The inevitability of these outcomes may tempt us either to abandon our incurable patients or to focus single‐mindedly on treatable problems one at a time, rather than on the interplay of multiple problems in an individual person. Either choice is mistaken. Although we are powerless to prevent decline and death in the long run, we have a tremendous capacity to delay and ameliorate decline, to enhance comfort and joy, to protect from harm, and, often, to delay death.
Fourth, ask questions about what you do not know or understand. The risk, of course, is that your curiosity will be sparked, possibly slowing you in completing the myriad tasks to be donea risk worth taking. Will ACE inhibitors and beta‐blockers benefit patients with heart failure without systolic dysfunction? Why do so many older patients become delirious, and are features of hospitalization catalyzing the effects of disease in causing delirium? Why do we continue to send cognitively impaired patients home without scheduled follow‐up and with instruction sheets they cannot read, and how can we change the system to prevent this? If you cannot find answers to your questions grounded in strong evidence, maintain your skepticism about answers given easily.
Finally, consider discovering the answers to some of your questions. Part of the excitement of caring for the very old is that we have so much to learn and that what we do learn can be so powerful.
An emergency room resident once was instructing a medical student in how to place a nasogastric tube in order to evaluate a patient with melena and postural hypotension. When the tube came to a stop, the student connected a syringe to the tube and aspirated. Then, to the consternation of the resident, the student yanked out the tube as soon as he saw blood flowing into the syringe. Why'd you do that? the surprised resident asked. There's blood down there! came the quick reply.
Like that medical student, hospital‐based physicianshospitalists, geriatricians, and othersmay miss the boat when caring for hospitalized older patients. Hospitals are full, and they're filled largely with older patients. These patients, like those who are younger, generally want to be treated and sent home. Older patients, however, frequently pose specific challenges. They may talk and move more slowly, stay longer, and be more likely to die. They more often need help in caring for themselves, and many have lost the support necessary to remain at home, making it difficult for them to return there. In short, older patients often need more care and more time.
It may be tempting to ignore the challenges that arise in caring for older patients. An avoidance strategy is expedient, at least in the short term. Ultimately, however, ignoring the challenges of caring for older patients will prove no wiser than yanking the nasogastric tube. Instead, we can recognize the challenges and use this opportunity to learn to improve their care.
This article describes the state of the science in hospital care for older patients, opportunities awaiting those who care for these patients, and barriers to seizing those opportunities. I conclude with five recommendations for physicians who care for hospitalized older patients.
STATE OF THE SCIENCE
Older patients shape hospital medicine and will determine its future. In 2002 the 12% of the population age 65 years or older accounted for roughly 50% of all hospitalizations unrelated to childbirth.1, 2 Hospital admissions of older persons will balloon as the number of persons older than age 65 rises by a million a year, increasing from 13% of the population today to 21% by 2030.2
Older persons in hospitals pose substantial clinical challenges. Many have multiple comorbid diseases and virtually all have complex medical regimens.1, 35 Many have cognitive impairment or dementia, often accompanied by delirium, which hinder communication and can lead to behaviors that require extra attention and impede diagnostic tests and treatment.611 Some have difficulty walking and caring for themselves, and a third leave the hospital without having recovered to their baseline level of function, with those age 85 years or older at highest risk for this decline independent of the reason for admission.1215 These characteristics increase the care, resources, and staff time older patients need, prolong their stays, and increase their hospital costs beyond those expected for their diagnosis.16 They also are at higher risk for iatrogenic complications, death, and rehospitalization,1720 and the risk of errors may be increased by frequent transitions in providers and sites of care.2125 Older persons require greater assistance at home, and yet they have often lost much of the support needed to live at home.10, 13, 20
Despite the magnitude of these challenges, we know surprisingly little about how best to care for hospitalized older persons, especially those older than age 75. The evidence base for treatment of specific common diseases is inadequate. The very old are underrepresented in clinical trials,26, 27 and the majority of older patients with common conditions such as heart failure may not meet the enrollment criteria for clinical trials.28 Thus, what is known about treating diseases in younger patients may be extrapolated to determine treatments in older persons based only on a leap of faith, which may be misguided.29, 30 In fact, the efficacy of conventional treatments for common conditions (e.g., acute myocardial infarction and hypertension) may diminish with age,31, 32 indicating that clinical trials targeted specifically to older patients may be necessary.
Despite the dearth of evidence about the management of common diseases in hospitalized older patients, hospital‐based geriatricians have developed substantial high‐grade evidence about the prevention of two geriatric syndromes, functional disability and delirium. The incidence of both syndromes can be reduced (without increasing hospital or health care costs) by multicomponent interventions that include comprehensive assessment, targeted treatment, and environmental modification to promote independence and safety.3, 3335 Moreover, the randomized trials that evaluated these interventions have provided models for how other innovations by hospital‐based physicians can be evaluated. Despite the evidence that these approaches are effective and either cost saving or cost neutral, these models have not been widely adopted.36
Many challenges in the prevention and management of geriatric syndromes in the hospital remain. For example, sophisticated approaches to the management of delirium are disappointingonce delirium has developed, intensive state‐of‐the‐art approaches to its management are no more effective than standard care in shortening its duration or ameliorating its sequelae.37, 38 The indiscriminate use of indwelling urinary catheters is decried, but there is no evidence that their use is declining, even in patients without an indication for catheterization.3942 Malnutrition and falls can be prevented and depression treated in patients outside the hospital,4345 but it is unclear whether these maladies can be prevented or treated effectively in hospitalized elders. Finally, intriguing evidence suggests that geriatric syndromes and their sequelae may be prevented and outcomes improved by caring for patients at home whenever possible, bringing intensive nursing and physician care into the home without some of the adverse effects of hospitalization.46
The physician workforce is not prepared to provide optimal care to hospitalized older persons. Few hospitalists or other hospital‐based physicians have received more than minimal training in geriatric medicine, and few geriatricians practice extensively in the hospital. At the same time that the ranks of physicians who consider themselves hospitalists have been expanding by 1000 or more a year in the United States, the number of certified geriatricians has been decreasing as hundreds decide each year not to renew their certificates.47, 48 Fewer than 300 geriatricians complete training each year and enter the workforce, and most new geriatricians practice in ambulatory or long‐term‐care settings. Wald's study in this issue indicates the paucity of geriatricians in hospital medicine (with the apparently single exception of the Mayo Clinic's Hospital Internal Medicine Group) and a relative lack of interest among hospitalists in developing knowledge about the effective and efficient treatment of older persons, in particular.49
OPPORTUNITIES
Opportunities to improve the care of hospitalized older patients arise from the state of the science in their care and from the common ground that hospitalists and geriatricians share. The older patients of both hospitalists and geriatricians are seriously ill, with annual mortality rates of 20%30% for patients with common conditions such as myocardial infarction or colon cancer and mortality rates of 50% or higher for patients with dementia or severe disability.5, 5053 We should view the care of our patients in the context of their prognoses,5, 54 recognizing that patients' preferences for the goals, style, and site of care vary widely.55, 56 The substantial association of mortality with geriatric syndromes such as disability, dementia, delirium, and depressionan association that is independent of pathophysiologic indicators of disease severitysuggests that substantial benefits may accrue by targeting interventions to the prevention or amelioration of these syndromes.5, 9, 10, 53, 57, 58
Hospitalists and geriatricians also share the perspective of working in complex systems in which the effectiveness, efficiency, and safety of care depend on system functions as well as on their technical expertise as individuals.5961 Together, and with colleagues in other disciplines, they may redesign how hospitals and the systems around them work to reduce errors, increase attention to aspects of care that are easily overlooked, and improve patient outcomes.
BARRIERS
Hospitalists and geriatricians face barriers to improving care for hospitalized older patients. First, gaps in knowledge limit the capacity to provide the care and achieve the outcomes desired. Fundamental discoveries in clinical science are needed to prevent or treat geriatric syndromes, to treat common diseases in the very old, and to put into practice what is known. Addressing these gaps in knowledge will require a sustained effort that spans methods and disciplines.
Second, the dominant reductionist paradigm values discovery of the mechanism of disease over discovery of ways to manage illness effectively and efficiently.6267 Similarly, diagnostic tests and therapies based on beliefs about the mechanism of diseasefor example, PET scans in persons with memory disorders and chemotherapy in persons with refractory cancersare pursued aggressively and paid handsomely, whereas efforts to reduce errors or improve continuity of care receive little attention or reward. The challenges of caring for hospitalized older patients will require advances on both fronts: in our knowledge of the pathogenesis of disorders that have proven resistant to current therapies (such as delirium) and in our knowledge of how to structure clinical care that engages patients and families and achieves desired outcomes effectively, consistently, and efficiently.
The structure and styles of our practices provide the third challenge. Hospitalists pride themselves on their efficient management of patients while maintaining or improving patient outcomes. A focus on efficient management can, however, lead to an assembly‐line approach, turning each patient into a series of do‐order‐call‐check tasks to get the patient out of the hospital as quickly as possible. This approach has advantages but may also blind physicians to the scope and complexity of issues that arise in caring for the very old through the course of an illness that often extends beyond hospitalization.25 Geriatricians pride themselves on their comprehensive management of patients, gathering clinical information from many sources (especially in the many patients with cognitive impairment), exploring and articulating goals of care, and assessing self‐care and neurologic, psychological, and social domains in addition to conventional pathophysiology. Yet too often, geriatricians are not available in hospitals, and as Wald found, they have rarely been integrated into hospitalist groups.
FIVE RECOMMENDATIONS FOR HOSPITALISTS AND GERIATRICIANS
I conclude with five recommendations for hospital‐based physicians who care for older patients and for geriatricians. First, step back, look at your patients, and note their predicament in its full complexity. Once hospitalists start looking for cognitive impairment, weakness, and difficulty walking and the difficulty of finding a good situation after leaving the hospital, it will be easy to see these problems. And once geriatricians start looking at why their patients are going into the hospital and what happens to them, it will be easy to see the need to become engaged. Seeing the full range of patients' problems won't address them, but we certainly won't address them if we don't look.
Second, learn what is known about how best to care for the aged and integrate this learning into your hospital practice. For hospitalists, learning how to identify each patient's goals of care, what works to prevent delirium and promote mobility, which drugs to avoid and which doses to modify, and how to access resources to help patients and families achieve their goals after they leave the hospital will benefit older patients. Pocket and PDA resources to extend learning are readily available.68 For geriatricians, learning how to avoid hospitalization (especially when resources can be mobilized to provide a hospital at home), how to work within the timeframe of hospitalization, and what current disease‐specific management strategies have been shown to be effective in the aged will benefit their patients. Maintaining the distinction between what is believed and what is known on the basis of high‐quality evidence will enhance learning and decrease the risk of stubbornly pursuing harmful or wasteful practices. This is especially important in situations where the evidence is weak and opinions are strong.
Third, to provide the best care for our older patients, we must embrace aging, not deny it. Most hospitalized older patients, and most patients of geriatricians, will decline and die in a few years. The inevitability of these outcomes may tempt us either to abandon our incurable patients or to focus single‐mindedly on treatable problems one at a time, rather than on the interplay of multiple problems in an individual person. Either choice is mistaken. Although we are powerless to prevent decline and death in the long run, we have a tremendous capacity to delay and ameliorate decline, to enhance comfort and joy, to protect from harm, and, often, to delay death.
Fourth, ask questions about what you do not know or understand. The risk, of course, is that your curiosity will be sparked, possibly slowing you in completing the myriad tasks to be donea risk worth taking. Will ACE inhibitors and beta‐blockers benefit patients with heart failure without systolic dysfunction? Why do so many older patients become delirious, and are features of hospitalization catalyzing the effects of disease in causing delirium? Why do we continue to send cognitively impaired patients home without scheduled follow‐up and with instruction sheets they cannot read, and how can we change the system to prevent this? If you cannot find answers to your questions grounded in strong evidence, maintain your skepticism about answers given easily.
Finally, consider discovering the answers to some of your questions. Part of the excitement of caring for the very old is that we have so much to learn and that what we do learn can be so powerful.
- ,.Hospitalization in the United States, 2002. Publication 05‐056.Washington (DC):AHRQ,2005.
- .Improving health care for older persons.Ann Intern Med.2003;139:421–424.
- ,,, et al.A controlled trial of inpatient and outpatient geriatric evaluation and management.N Engl J Med.2002;346:905–912.
- ,,, et al.Hospital diagnoses, Medicare charges, and nursing home admissions in the year when older persons become severely disabled.JAMA.1997;277:728–734.
- ,,, et al.Development and validation of a prognostic index for 1‐year mortality in older adults after hospitalization.JAMA.2001;285:2987–2994.
- ,,,.Delirium is independently associated with poor functional recovery after hip fracture.J Am Geriatr Soc.2000;48:618–624.
- ,,, et al.The course of delirium in older medical inpatients: a prospective study.J Gen Intern Med.2003;18:696–704.
- ,,,.Does delirium increase hospital stay?J Am Geriatr Soc.2003;51:1539–1546.
- ,,, et al.Does delirium contribute to poor hospital outcomes? A three‐site epidemiologic study.J Gen Intern Med.1998;13:234–242.
- ,,, et al.A predictive index for functional decline in hospitalized elderly medical patients.J Gen Intern Med.1993;8:645–652.
- ,,.A prospective study of delirium in hospitalized elderly.JAMA.1990;263:1097–1101.
- ,,, et al.Unsteadiness reported by older hospitalized patients predicts functional decline.J Am Geriatr Soc.2003;51:621–626.
- ,,, et al.Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: increased vulnerability with age.J Am Geriatr Soc.2003;51:451–458.
- ,,, et al.Functional outcomes of acute medical illness and hospitalization in older persons.Arch Intern Med.1996;156:645–652.
- ,,, et al.Functional disability in the hospitalized elderly.JAMA.1982;248:847–850.
- ,,, et al.Diagnosis‐related group‐adjusted hospital costs are higher in older medical patients with lower functional status.J Am Geriatr Soc.2003;51:1729–1734.
- ,.Adverse events, negligence in hospitalized patients: results from the Harvard Medical Practice Study.Perspect Healthc Risk Manage.1991;11(2):2–8.
- ,,, et al.Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I.N Engl J Med.1991;324:370–376.
- ,,, et al.The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II.N Engl J Med.1991;324:377–384.
- ,,,.Effects of functional status changes before and during hospitalization on nursing home admission of older adults.J Gerontol A Biol Sci Med Sci.1999;54:M521–M526.
- ,,.Characterization of geriatric drug‐related hospital readmissions.Med Care.1991;29:989–1003.
- ,,,.The impact of clinical pharmacists' consultations on physicians' geriatric drug prescribing. A randomized controlled trial.Med Care.1992;30:646–658.
- ,,,.Posthospital medication discrepancies: prevalence and contributing factors.Arch Intern Med.2005;165:1842–1847.
- ,,.A new tool for identifying discrepancies in postacute medications for community‐dwelling older adults.Am J Geriatr Pharmacother.2004;2(2):141–147.
- ,.Lost in transition: challenges and opportunities for improving the quality of transitional care.Ann Intern Med.2004;141:533–536.
- ,,, et al.Enrollment of older persons in cancer trials after the medicare reimbursement policy change.Arch Intern Med.2005;165:1514–1520.
- ,,, et al.Underrepresentation of patients 65 years of age or older in cancer‐treatment trials.N Engl J Med.1999;341:2061–2067.
- ,,, et al.Most hospitalized older persons do not meet the enrollment criteria for clinical trials in heart failure.Am Heart J.2003;146(2):250–257.
- ,.Problems in the “evidence” of “evidence‐based medicine.”Am J Med.1997;103:529–535.
- .National initiatives in ageing research in the United Kingdom.Age Ageing.2002;31(2):93–95.
- .Embracing complexity: A consideration of hypertension in the very old.J Gerontol A Biol Sci Med Sci.2003;58:653–658.
- ,,, et al.Lack of benefit for intravenous thrombolysis in patients with myocardial infarction who are older than 75 years.Circulation.2000;101:2239–2246.
- ,,, et al.A randomized trial of care in a hospital medical unit especially designed to improve the functional outcomes of acutely ill older patients.N Engl J Med.1995;332:1338–1344.
- ,,, et al.A multicomponent intervention to prevent delirium in hospitalized older patients.N Engl J Med.1999;340:669–676.
- ,,,.Reducing delirium after hip fracture: a randomized trial.J Am Geriatr Soc.2001;49:516–522.
- ,,,.Dissemination and characteristics of acute care for elders (ACE) units in the United States.Int J Technol Assess Health Care.2003;19(1):220–227.
- ,.Treatment of delirium in older medical inpatients: a challenge for geriatric specialists.J Am Geriatr Soc.2002;50:2101–2103.
- ,,, et al.Systematic detection and multidisciplinary care of delirium in older medical inpatients: a randomized trial.CMAJ.2002;167:753–759.
- .Clinical and economic consequences of nosocomial catheter‐related bacteriuria.Am J Infect Control.2000;28(1):68–75.
- ,.Preventing catheter‐related bacteriuria: should we? Can we? How?Arch Intern Med.1999;159:800–808.
- ,,.Indwelling urinary catheters: a one‐point restraint?Ann Intern Med.2002;137(2):125–127.
- ,, et al.Risk factors for indwelling urinary catheterization among older hospitalized patients without a specific medical indication for catheterization.J Patient Saf.2005. In press.
- ,,.Protein and energy supplementation in elderly people at risk from malnutrition.Cochrane Database Syst Rev.2005(2):CD003288.
- .Clinical practice. Preventing falls in elderly persons.N Engl J Med.2003;348(1):42–49.
- ,,, et al.Collaborative care management of late‐life depression in the primary care setting: a randomized controlled trial.JAMA.2002;288:2836–2845.
- ,,,,,.Hospital in the home: a randomised controlled trial.Med J Aust.1999;170(4):156–160.
- .Hospitalists in the United States—mission accomplished or work in progress?N Engl J Med.2004;350:1935–1936.
- ,,,.Academic geriatric programs in US allopathic and osteopathic medical schools.JAMA.2002;288:2313–2319.
- ,,.Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs.J Hosp Med.2006;1:29–35.
- ,,, et al.The implications of regional variations in Medicare spending. Part 1: the content, quality, and accessibility of care.Ann Intern Med.2003;138:273–287.
- ,,, et al.The implications of regional variations in Medicare spending. Part 2: health outcomes and satisfaction with care.Ann Intern Med.2003;138:288–298.
- ,.Mortality from pneumonia and hip fractures in patients with advanced dementia.JAMA.2000;284:2447–2448.
- ,.Survival in end‐stage dementia following acute illness.JAMA.2000;284(1):47–52.
- ,.Cancer screening in elderly patients: a framework for individualized decision making.JAMA.2001;285:2750–2756.
- ,,,.Understanding the treatment preferences of seriously ill patients.N Engl J Med.2002;346:1061–1066.
- ,,, et al.Health values of hospitalized patients 80 years or older. HELP Investigators. Hospitalized Elderly Longitudinal Project.JAMA.1998;279:371–375.
- ,,, et al.Depressive symptoms and 3‐year mortality in older hospitalized medical patients.Ann Intern Med.1999;130:563–569.
- ,,, et al.Relation between symptoms of depression and health status outcomes in acutely ill hospitalized older persons.Ann Intern Med.1997;126:417–425.
- ,,,.Five system barriers to achieving ultrasafe health care.Ann Intern Med.2005;142:756–764.
- .Specialized care for elderly patients.N Engl J Med.2002;346:874.
- .The end of the beginning: patient safety five years after ‘To Err Is Human.’Health Aff (Millwood).2004;Suppl Web Exclusives:W4–534–545.
- .An additional basic science for clinical medicine: II. The limitations of randomized trials.Ann Intern Med.1983;99:544–550.
- .An additional basic science for clinical medicine: III. The challenges of comparison and measurement.Ann Intern Med.1983;99:705–712.
- .An additional basic science for clinical medicine: IV. The development of clinimetrics.Ann Intern Med.1983;99:843–848.
- .An additional basic science for clinical medicine: I. The constraining fundamental paradigms.Ann Intern Med.1983;99:393–397.
- ,.The end of the disease era.Am J Med.2004;116(3):179–185.
- ,, Agostini JV. Potential pitfalls of disease‐specific guidelines for patients with multiple conditions.N Engl J Med.2004;351:2870–2874.
- ,,, et al.Geriatrics at your fingertips: 2005.7th ed.Malden (MA):Blackwell Publishing, for the American Geriatrics Society,2005.
- ,.Hospitalization in the United States, 2002. Publication 05‐056.Washington (DC):AHRQ,2005.
- .Improving health care for older persons.Ann Intern Med.2003;139:421–424.
- ,,, et al.A controlled trial of inpatient and outpatient geriatric evaluation and management.N Engl J Med.2002;346:905–912.
- ,,, et al.Hospital diagnoses, Medicare charges, and nursing home admissions in the year when older persons become severely disabled.JAMA.1997;277:728–734.
- ,,, et al.Development and validation of a prognostic index for 1‐year mortality in older adults after hospitalization.JAMA.2001;285:2987–2994.
- ,,,.Delirium is independently associated with poor functional recovery after hip fracture.J Am Geriatr Soc.2000;48:618–624.
- ,,, et al.The course of delirium in older medical inpatients: a prospective study.J Gen Intern Med.2003;18:696–704.
- ,,,.Does delirium increase hospital stay?J Am Geriatr Soc.2003;51:1539–1546.
- ,,, et al.Does delirium contribute to poor hospital outcomes? A three‐site epidemiologic study.J Gen Intern Med.1998;13:234–242.
- ,,, et al.A predictive index for functional decline in hospitalized elderly medical patients.J Gen Intern Med.1993;8:645–652.
- ,,.A prospective study of delirium in hospitalized elderly.JAMA.1990;263:1097–1101.
- ,,, et al.Unsteadiness reported by older hospitalized patients predicts functional decline.J Am Geriatr Soc.2003;51:621–626.
- ,,, et al.Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: increased vulnerability with age.J Am Geriatr Soc.2003;51:451–458.
- ,,, et al.Functional outcomes of acute medical illness and hospitalization in older persons.Arch Intern Med.1996;156:645–652.
- ,,, et al.Functional disability in the hospitalized elderly.JAMA.1982;248:847–850.
- ,,, et al.Diagnosis‐related group‐adjusted hospital costs are higher in older medical patients with lower functional status.J Am Geriatr Soc.2003;51:1729–1734.
- ,.Adverse events, negligence in hospitalized patients: results from the Harvard Medical Practice Study.Perspect Healthc Risk Manage.1991;11(2):2–8.
- ,,, et al.Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I.N Engl J Med.1991;324:370–376.
- ,,, et al.The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II.N Engl J Med.1991;324:377–384.
- ,,,.Effects of functional status changes before and during hospitalization on nursing home admission of older adults.J Gerontol A Biol Sci Med Sci.1999;54:M521–M526.
- ,,.Characterization of geriatric drug‐related hospital readmissions.Med Care.1991;29:989–1003.
- ,,,.The impact of clinical pharmacists' consultations on physicians' geriatric drug prescribing. A randomized controlled trial.Med Care.1992;30:646–658.
- ,,,.Posthospital medication discrepancies: prevalence and contributing factors.Arch Intern Med.2005;165:1842–1847.
- ,,.A new tool for identifying discrepancies in postacute medications for community‐dwelling older adults.Am J Geriatr Pharmacother.2004;2(2):141–147.
- ,.Lost in transition: challenges and opportunities for improving the quality of transitional care.Ann Intern Med.2004;141:533–536.
- ,,, et al.Enrollment of older persons in cancer trials after the medicare reimbursement policy change.Arch Intern Med.2005;165:1514–1520.
- ,,, et al.Underrepresentation of patients 65 years of age or older in cancer‐treatment trials.N Engl J Med.1999;341:2061–2067.
- ,,, et al.Most hospitalized older persons do not meet the enrollment criteria for clinical trials in heart failure.Am Heart J.2003;146(2):250–257.
- ,.Problems in the “evidence” of “evidence‐based medicine.”Am J Med.1997;103:529–535.
- .National initiatives in ageing research in the United Kingdom.Age Ageing.2002;31(2):93–95.
- .Embracing complexity: A consideration of hypertension in the very old.J Gerontol A Biol Sci Med Sci.2003;58:653–658.
- ,,, et al.Lack of benefit for intravenous thrombolysis in patients with myocardial infarction who are older than 75 years.Circulation.2000;101:2239–2246.
- ,,, et al.A randomized trial of care in a hospital medical unit especially designed to improve the functional outcomes of acutely ill older patients.N Engl J Med.1995;332:1338–1344.
- ,,, et al.A multicomponent intervention to prevent delirium in hospitalized older patients.N Engl J Med.1999;340:669–676.
- ,,,.Reducing delirium after hip fracture: a randomized trial.J Am Geriatr Soc.2001;49:516–522.
- ,,,.Dissemination and characteristics of acute care for elders (ACE) units in the United States.Int J Technol Assess Health Care.2003;19(1):220–227.
- ,.Treatment of delirium in older medical inpatients: a challenge for geriatric specialists.J Am Geriatr Soc.2002;50:2101–2103.
- ,,, et al.Systematic detection and multidisciplinary care of delirium in older medical inpatients: a randomized trial.CMAJ.2002;167:753–759.
- .Clinical and economic consequences of nosocomial catheter‐related bacteriuria.Am J Infect Control.2000;28(1):68–75.
- ,.Preventing catheter‐related bacteriuria: should we? Can we? How?Arch Intern Med.1999;159:800–808.
- ,,.Indwelling urinary catheters: a one‐point restraint?Ann Intern Med.2002;137(2):125–127.
- ,, et al.Risk factors for indwelling urinary catheterization among older hospitalized patients without a specific medical indication for catheterization.J Patient Saf.2005. In press.
- ,,.Protein and energy supplementation in elderly people at risk from malnutrition.Cochrane Database Syst Rev.2005(2):CD003288.
- .Clinical practice. Preventing falls in elderly persons.N Engl J Med.2003;348(1):42–49.
- ,,, et al.Collaborative care management of late‐life depression in the primary care setting: a randomized controlled trial.JAMA.2002;288:2836–2845.
- ,,,,,.Hospital in the home: a randomised controlled trial.Med J Aust.1999;170(4):156–160.
- .Hospitalists in the United States—mission accomplished or work in progress?N Engl J Med.2004;350:1935–1936.
- ,,,.Academic geriatric programs in US allopathic and osteopathic medical schools.JAMA.2002;288:2313–2319.
- ,,.Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs.J Hosp Med.2006;1:29–35.
- ,,, et al.The implications of regional variations in Medicare spending. Part 1: the content, quality, and accessibility of care.Ann Intern Med.2003;138:273–287.
- ,,, et al.The implications of regional variations in Medicare spending. Part 2: health outcomes and satisfaction with care.Ann Intern Med.2003;138:288–298.
- ,.Mortality from pneumonia and hip fractures in patients with advanced dementia.JAMA.2000;284:2447–2448.
- ,.Survival in end‐stage dementia following acute illness.JAMA.2000;284(1):47–52.
- ,.Cancer screening in elderly patients: a framework for individualized decision making.JAMA.2001;285:2750–2756.
- ,,,.Understanding the treatment preferences of seriously ill patients.N Engl J Med.2002;346:1061–1066.
- ,,, et al.Health values of hospitalized patients 80 years or older. HELP Investigators. Hospitalized Elderly Longitudinal Project.JAMA.1998;279:371–375.
- ,,, et al.Depressive symptoms and 3‐year mortality in older hospitalized medical patients.Ann Intern Med.1999;130:563–569.
- ,,, et al.Relation between symptoms of depression and health status outcomes in acutely ill hospitalized older persons.Ann Intern Med.1997;126:417–425.
- ,,,.Five system barriers to achieving ultrasafe health care.Ann Intern Med.2005;142:756–764.
- .Specialized care for elderly patients.N Engl J Med.2002;346:874.
- .The end of the beginning: patient safety five years after ‘To Err Is Human.’Health Aff (Millwood).2004;Suppl Web Exclusives:W4–534–545.
- .An additional basic science for clinical medicine: II. The limitations of randomized trials.Ann Intern Med.1983;99:544–550.
- .An additional basic science for clinical medicine: III. The challenges of comparison and measurement.Ann Intern Med.1983;99:705–712.
- .An additional basic science for clinical medicine: IV. The development of clinimetrics.Ann Intern Med.1983;99:843–848.
- .An additional basic science for clinical medicine: I. The constraining fundamental paradigms.Ann Intern Med.1983;99:393–397.
- ,.The end of the disease era.Am J Med.2004;116(3):179–185.
- ,, Agostini JV. Potential pitfalls of disease‐specific guidelines for patients with multiple conditions.N Engl J Med.2004;351:2870–2874.
- ,,, et al.Geriatrics at your fingertips: 2005.7th ed.Malden (MA):Blackwell Publishing, for the American Geriatrics Society,2005.
View from the Hospital Bed
For many of you, the hospital has by now become your home away from home. You spend a great deal of time there. You know your way from the ER to the ICU and the morgue. You've learned the hierarchy of who can tell whom what to do, and when it's your turn to do so, you can rattle off an impressive string of acronyms and medspeak in rapid fire. And then, there's that white coat that gives you added stature and authority.
We, the patients, family members, and other concerned visitors, are babes in the woods in this setting. If we've been lucky in life heretofore, we find that visiting a hospital can be like stepping off a hijacked plane into a foreign country we never planned to visit. Few things look familiar. We don't fully understand what we're being made to do. We don't speak the language well enough to communicate with those surrounding us, and we're not certain how friendly they are or what might provoke them into hurting us or our loved ones.
The signs we see don't mean much to usthe few words we recognize tend to scare us more than anything else. We don't know how to interpret the various uniforms people are wearing, other than the white coats we're all familiar with. Quite a few of the busy people moving with confidence around us have the aura of authority figures, no matter what they're wearing. When it's our turn, they focus on us or our loved ones, freely taking samples of blood, attaching instruments, probing private body parts, and asking intensely personal questions. But they don't really say much at all directly to us, and they don't seem interested in a lot of what we try to tell them. We're left feeling confused, humiliated, and somewhat stupid. Obviously, we're not astute enough to figure out what they want us to tell them. Why couldn't we remember everything we'd eaten or taken in the last 24 hours? We failed the test, and the consequences could be life threatening.
I am not exaggerating the situation. Last winter, my husbandwho had some chronic health issues but was still able to hold down a demanding job and carry on a fairly normal lifewas taken down by a nasty anonymous virus that attacked several major organ systems. We thought it was a bad case of the flu. I only took him to the emergency room because his weakness failed to pass in a few days and listening to him struggle to breathe scared me badly. It was the doctor's answering service (not the doctor on call, who never returned my call) that advised me to take him to the ER.
Within the first 24 hours at the hospital, I lost all ability to communicate with my husband when he was sedated and hooked up to a ventilator. For the next three and a half weeks, he lay unconscious, struggling for survival, and I lived on what his doctors and nurses chose to tell me. And they weren't saying a lot that I could make sense of.
For one thing, as his condition worsened he was in the care of eight specialists. Each would tell me something different, and I wasn't equipped to put all these pieces of information together in a meaningful way. For example, early on, I heard the following statements from different doctors all in the same day: He has a virus. His lungs are in really bad shape, and he could die. There are some indications he had a heart attack. His kidneys are failing, and he's going to need dialysis.
I knew that viruses can kill people. I knew that my husband was considered a high risk for heart attacks and that his lungs had been compromised by years of smoking. But I could not fathom how all of these things were related, let alone what was causing the kidneys to fail at this particular time. It took a very long timedays, maybe a week or morebefore I had both the courage and opportunity to pester my husband's infectious disease specialist with so many questions that he explained that the virus had attacked the heart, lungs, and kidneys and that most of what we were seeing was the aftermath of that battle.
This same doctor also helped me by shedding light on why the brief reports I was receiving from different specialists often seemed, to my layman's ears, to contradict each other. (One day the cardiologist told me, His heart's basically in pretty good shape. Yet, a scant hour later, the pulmonary specialist informed me, He's getting worse. He could die.) Each specialist, he told me, tends to focus on the area of the body he or she specializes in, not the patient's overall condition, and their comments reflect that narrow focus. How long would it have taken me to figure that out, if not for this man?
A lot of the frustration I felt as I chased after valuable tidbits of information about my husband's condition could have been alleviated with just a few words. Some days it would have been enough just to have had my anguish acknowledged with something as simple as I know you're frustrated and tired of hearing that we have no clear answers. Believe me, we want a better understanding of what's happening to your husband, too.
Aside from having to assemble the comments my husband's many doctors gave me into a comprehensive picture, I grew very weary of trying to catch these men and women as they came through on their rounds. Some routinely came through the ICU before the start of visiting hours each day. A few had no discernable routine at allI was as likely to encounter them at 8:30 p.m. as at 3 p.m. or 10 a.m. Yet if I was not at my husband's bedside or in the ICU waiting room, I'd get no report from them that day. This system forces the family to forgo any semblance of a normal life. In my case, there were no other family members with which to trade off this vigil, so I missed doctors whenever I went home or out of the room for a bite to eat.
I do not believe that our local hospital is unusual in any of these respects. In talking to people in other parts of the country who've been through a hospital experience, I have heard similar complaints voiced over and over.
And I do not question the quality of the medical care my husband received. As far as I know, everyone involved did their best to save him. Sadly, they did not succeed. Doug died on March 16, 2005, after five and a half weeks in the ICU. Many very good‐hearted, caring people worked on him during that time.
But some, though pleasant, didn't go out of their way to help me one iota. The day my husband started waking up after 25 days in a comalike state, I was in a funk and had found excuses to stay home until midafternoon, figuring there'd be no change in his condition. When I finally dragged myself into his room and spoke to him, I was astonished to see him react with a very slight head movement. Overjoyed, I immediately informed his nurse that he had responded to me, and she replied with a smile, Yes, I know. He's been responsive all day!
Now, these people knew that I'd been hovering at his bedside for 25 days, anxiously waiting for him to wake up, pestering them about why he wasn't and asking what was wrong. Did no one think this development worth a phone call to me?
Since my husband's death, I have heard that some hospitals have patient advocates and hospitalists, but my impression is that a fairly small percentage of hospitals have invested in these types of positions. And I question how well one or two such people in a hospital full of sick patients can help everyone who needs their services. It was hard enough for me to connect with the one woman in our hospital who, during the short time my husband seemed to be on the way to recovering, could help to arrange his transfer to a long‐term care facility.
My point is, the system that is routinely followed in most hospitalsthe system that determines doctors' routines, the system that causes health care workers to tend to treat patients and their families more like objects than human beingsdoes not do service to those it was set up to serve.
My point is, when it's everyone's responsibility to communicate with a patient's family, it winds up being no one's responsibility. Hospitals need to assign this responsibility to a specific person when a critically ill patient is in the care of a team of specialists.
My point is, please think of us wandering lost and scared in that foreign land you call home the next time you encounter one of us there.
For many of you, the hospital has by now become your home away from home. You spend a great deal of time there. You know your way from the ER to the ICU and the morgue. You've learned the hierarchy of who can tell whom what to do, and when it's your turn to do so, you can rattle off an impressive string of acronyms and medspeak in rapid fire. And then, there's that white coat that gives you added stature and authority.
We, the patients, family members, and other concerned visitors, are babes in the woods in this setting. If we've been lucky in life heretofore, we find that visiting a hospital can be like stepping off a hijacked plane into a foreign country we never planned to visit. Few things look familiar. We don't fully understand what we're being made to do. We don't speak the language well enough to communicate with those surrounding us, and we're not certain how friendly they are or what might provoke them into hurting us or our loved ones.
The signs we see don't mean much to usthe few words we recognize tend to scare us more than anything else. We don't know how to interpret the various uniforms people are wearing, other than the white coats we're all familiar with. Quite a few of the busy people moving with confidence around us have the aura of authority figures, no matter what they're wearing. When it's our turn, they focus on us or our loved ones, freely taking samples of blood, attaching instruments, probing private body parts, and asking intensely personal questions. But they don't really say much at all directly to us, and they don't seem interested in a lot of what we try to tell them. We're left feeling confused, humiliated, and somewhat stupid. Obviously, we're not astute enough to figure out what they want us to tell them. Why couldn't we remember everything we'd eaten or taken in the last 24 hours? We failed the test, and the consequences could be life threatening.
I am not exaggerating the situation. Last winter, my husbandwho had some chronic health issues but was still able to hold down a demanding job and carry on a fairly normal lifewas taken down by a nasty anonymous virus that attacked several major organ systems. We thought it was a bad case of the flu. I only took him to the emergency room because his weakness failed to pass in a few days and listening to him struggle to breathe scared me badly. It was the doctor's answering service (not the doctor on call, who never returned my call) that advised me to take him to the ER.
Within the first 24 hours at the hospital, I lost all ability to communicate with my husband when he was sedated and hooked up to a ventilator. For the next three and a half weeks, he lay unconscious, struggling for survival, and I lived on what his doctors and nurses chose to tell me. And they weren't saying a lot that I could make sense of.
For one thing, as his condition worsened he was in the care of eight specialists. Each would tell me something different, and I wasn't equipped to put all these pieces of information together in a meaningful way. For example, early on, I heard the following statements from different doctors all in the same day: He has a virus. His lungs are in really bad shape, and he could die. There are some indications he had a heart attack. His kidneys are failing, and he's going to need dialysis.
I knew that viruses can kill people. I knew that my husband was considered a high risk for heart attacks and that his lungs had been compromised by years of smoking. But I could not fathom how all of these things were related, let alone what was causing the kidneys to fail at this particular time. It took a very long timedays, maybe a week or morebefore I had both the courage and opportunity to pester my husband's infectious disease specialist with so many questions that he explained that the virus had attacked the heart, lungs, and kidneys and that most of what we were seeing was the aftermath of that battle.
This same doctor also helped me by shedding light on why the brief reports I was receiving from different specialists often seemed, to my layman's ears, to contradict each other. (One day the cardiologist told me, His heart's basically in pretty good shape. Yet, a scant hour later, the pulmonary specialist informed me, He's getting worse. He could die.) Each specialist, he told me, tends to focus on the area of the body he or she specializes in, not the patient's overall condition, and their comments reflect that narrow focus. How long would it have taken me to figure that out, if not for this man?
A lot of the frustration I felt as I chased after valuable tidbits of information about my husband's condition could have been alleviated with just a few words. Some days it would have been enough just to have had my anguish acknowledged with something as simple as I know you're frustrated and tired of hearing that we have no clear answers. Believe me, we want a better understanding of what's happening to your husband, too.
Aside from having to assemble the comments my husband's many doctors gave me into a comprehensive picture, I grew very weary of trying to catch these men and women as they came through on their rounds. Some routinely came through the ICU before the start of visiting hours each day. A few had no discernable routine at allI was as likely to encounter them at 8:30 p.m. as at 3 p.m. or 10 a.m. Yet if I was not at my husband's bedside or in the ICU waiting room, I'd get no report from them that day. This system forces the family to forgo any semblance of a normal life. In my case, there were no other family members with which to trade off this vigil, so I missed doctors whenever I went home or out of the room for a bite to eat.
I do not believe that our local hospital is unusual in any of these respects. In talking to people in other parts of the country who've been through a hospital experience, I have heard similar complaints voiced over and over.
And I do not question the quality of the medical care my husband received. As far as I know, everyone involved did their best to save him. Sadly, they did not succeed. Doug died on March 16, 2005, after five and a half weeks in the ICU. Many very good‐hearted, caring people worked on him during that time.
But some, though pleasant, didn't go out of their way to help me one iota. The day my husband started waking up after 25 days in a comalike state, I was in a funk and had found excuses to stay home until midafternoon, figuring there'd be no change in his condition. When I finally dragged myself into his room and spoke to him, I was astonished to see him react with a very slight head movement. Overjoyed, I immediately informed his nurse that he had responded to me, and she replied with a smile, Yes, I know. He's been responsive all day!
Now, these people knew that I'd been hovering at his bedside for 25 days, anxiously waiting for him to wake up, pestering them about why he wasn't and asking what was wrong. Did no one think this development worth a phone call to me?
Since my husband's death, I have heard that some hospitals have patient advocates and hospitalists, but my impression is that a fairly small percentage of hospitals have invested in these types of positions. And I question how well one or two such people in a hospital full of sick patients can help everyone who needs their services. It was hard enough for me to connect with the one woman in our hospital who, during the short time my husband seemed to be on the way to recovering, could help to arrange his transfer to a long‐term care facility.
My point is, the system that is routinely followed in most hospitalsthe system that determines doctors' routines, the system that causes health care workers to tend to treat patients and their families more like objects than human beingsdoes not do service to those it was set up to serve.
My point is, when it's everyone's responsibility to communicate with a patient's family, it winds up being no one's responsibility. Hospitals need to assign this responsibility to a specific person when a critically ill patient is in the care of a team of specialists.
My point is, please think of us wandering lost and scared in that foreign land you call home the next time you encounter one of us there.
For many of you, the hospital has by now become your home away from home. You spend a great deal of time there. You know your way from the ER to the ICU and the morgue. You've learned the hierarchy of who can tell whom what to do, and when it's your turn to do so, you can rattle off an impressive string of acronyms and medspeak in rapid fire. And then, there's that white coat that gives you added stature and authority.
We, the patients, family members, and other concerned visitors, are babes in the woods in this setting. If we've been lucky in life heretofore, we find that visiting a hospital can be like stepping off a hijacked plane into a foreign country we never planned to visit. Few things look familiar. We don't fully understand what we're being made to do. We don't speak the language well enough to communicate with those surrounding us, and we're not certain how friendly they are or what might provoke them into hurting us or our loved ones.
The signs we see don't mean much to usthe few words we recognize tend to scare us more than anything else. We don't know how to interpret the various uniforms people are wearing, other than the white coats we're all familiar with. Quite a few of the busy people moving with confidence around us have the aura of authority figures, no matter what they're wearing. When it's our turn, they focus on us or our loved ones, freely taking samples of blood, attaching instruments, probing private body parts, and asking intensely personal questions. But they don't really say much at all directly to us, and they don't seem interested in a lot of what we try to tell them. We're left feeling confused, humiliated, and somewhat stupid. Obviously, we're not astute enough to figure out what they want us to tell them. Why couldn't we remember everything we'd eaten or taken in the last 24 hours? We failed the test, and the consequences could be life threatening.
I am not exaggerating the situation. Last winter, my husbandwho had some chronic health issues but was still able to hold down a demanding job and carry on a fairly normal lifewas taken down by a nasty anonymous virus that attacked several major organ systems. We thought it was a bad case of the flu. I only took him to the emergency room because his weakness failed to pass in a few days and listening to him struggle to breathe scared me badly. It was the doctor's answering service (not the doctor on call, who never returned my call) that advised me to take him to the ER.
Within the first 24 hours at the hospital, I lost all ability to communicate with my husband when he was sedated and hooked up to a ventilator. For the next three and a half weeks, he lay unconscious, struggling for survival, and I lived on what his doctors and nurses chose to tell me. And they weren't saying a lot that I could make sense of.
For one thing, as his condition worsened he was in the care of eight specialists. Each would tell me something different, and I wasn't equipped to put all these pieces of information together in a meaningful way. For example, early on, I heard the following statements from different doctors all in the same day: He has a virus. His lungs are in really bad shape, and he could die. There are some indications he had a heart attack. His kidneys are failing, and he's going to need dialysis.
I knew that viruses can kill people. I knew that my husband was considered a high risk for heart attacks and that his lungs had been compromised by years of smoking. But I could not fathom how all of these things were related, let alone what was causing the kidneys to fail at this particular time. It took a very long timedays, maybe a week or morebefore I had both the courage and opportunity to pester my husband's infectious disease specialist with so many questions that he explained that the virus had attacked the heart, lungs, and kidneys and that most of what we were seeing was the aftermath of that battle.
This same doctor also helped me by shedding light on why the brief reports I was receiving from different specialists often seemed, to my layman's ears, to contradict each other. (One day the cardiologist told me, His heart's basically in pretty good shape. Yet, a scant hour later, the pulmonary specialist informed me, He's getting worse. He could die.) Each specialist, he told me, tends to focus on the area of the body he or she specializes in, not the patient's overall condition, and their comments reflect that narrow focus. How long would it have taken me to figure that out, if not for this man?
A lot of the frustration I felt as I chased after valuable tidbits of information about my husband's condition could have been alleviated with just a few words. Some days it would have been enough just to have had my anguish acknowledged with something as simple as I know you're frustrated and tired of hearing that we have no clear answers. Believe me, we want a better understanding of what's happening to your husband, too.
Aside from having to assemble the comments my husband's many doctors gave me into a comprehensive picture, I grew very weary of trying to catch these men and women as they came through on their rounds. Some routinely came through the ICU before the start of visiting hours each day. A few had no discernable routine at allI was as likely to encounter them at 8:30 p.m. as at 3 p.m. or 10 a.m. Yet if I was not at my husband's bedside or in the ICU waiting room, I'd get no report from them that day. This system forces the family to forgo any semblance of a normal life. In my case, there were no other family members with which to trade off this vigil, so I missed doctors whenever I went home or out of the room for a bite to eat.
I do not believe that our local hospital is unusual in any of these respects. In talking to people in other parts of the country who've been through a hospital experience, I have heard similar complaints voiced over and over.
And I do not question the quality of the medical care my husband received. As far as I know, everyone involved did their best to save him. Sadly, they did not succeed. Doug died on March 16, 2005, after five and a half weeks in the ICU. Many very good‐hearted, caring people worked on him during that time.
But some, though pleasant, didn't go out of their way to help me one iota. The day my husband started waking up after 25 days in a comalike state, I was in a funk and had found excuses to stay home until midafternoon, figuring there'd be no change in his condition. When I finally dragged myself into his room and spoke to him, I was astonished to see him react with a very slight head movement. Overjoyed, I immediately informed his nurse that he had responded to me, and she replied with a smile, Yes, I know. He's been responsive all day!
Now, these people knew that I'd been hovering at his bedside for 25 days, anxiously waiting for him to wake up, pestering them about why he wasn't and asking what was wrong. Did no one think this development worth a phone call to me?
Since my husband's death, I have heard that some hospitals have patient advocates and hospitalists, but my impression is that a fairly small percentage of hospitals have invested in these types of positions. And I question how well one or two such people in a hospital full of sick patients can help everyone who needs their services. It was hard enough for me to connect with the one woman in our hospital who, during the short time my husband seemed to be on the way to recovering, could help to arrange his transfer to a long‐term care facility.
My point is, the system that is routinely followed in most hospitalsthe system that determines doctors' routines, the system that causes health care workers to tend to treat patients and their families more like objects than human beingsdoes not do service to those it was set up to serve.
My point is, when it's everyone's responsibility to communicate with a patient's family, it winds up being no one's responsibility. Hospitals need to assign this responsibility to a specific person when a critically ill patient is in the care of a team of specialists.
My point is, please think of us wandering lost and scared in that foreign land you call home the next time you encounter one of us there.
Clinical Conundrum
A 49‐year‐old man presented with 2 days of chills, fever, anorexia, and increased cough and dyspnea. The patient had a history of chronic obstructive pulmonary disease (COPD) and noted that his cough and dyspnea had increased above normal for several days. He was now dyspneic with minimal activity and had slept at a 45‐degree incline the night prior to evaluation due to dyspnea. He noted less improvement than usual with the use of his metered dose inhaler. His cough was occasionally productive of small amounts of white phlegm. He had vomited once. During a coughing episode the patient experienced a sudden onset of sharp right upper quadrant abdominal pain that worsened with coughing and sudden position changes. The patient denied a prior history of abdominal pain or surgery. The patient's last bowel movement was 2 days prior to admission. He denied melena or bright red blood per rectum.
My initial differential diagnosis for this patient's dyspnea and cough is pneumonia, acute exacerbation of COPD, or congestive heart failure. The presence of fever and anorexia increases the likelihood of infectious etiologies, whereas the presence of orthopnea points toward congestive heart failure. Noncardiac processessuch as a large pleural effusion or apical lung diseasecould also cause orthopnea. His abdominal pain could be a result of pneumonia alone (perhaps in the right lower lobe with diaphragmatic irritation), but I am also considering complications of pneumonia such as empyema. Although his abdominal pain, dyspnea, and cough could also be a result of hepatobiliary disease, a perforated viscus, or pancreatitis, we currently have little reason to suspect a direct abdominal etiology. My top diagnosis is community‐acquired pneumonia, perhaps accompanied by pleural effusion.
His medical history was significant for dilated cardiomyopathy and heavy alcohol use. His medications included various meter‐dosed inhalers, bupropion, digoxin, spironolactone, lisinopril, and metoprolol. He had never received corticosteroid therapy and had not previously been hospitalized for COPD‐related problems. He had smoked one pack of cigarettes daily for 40 years.
Heavy alcohol use is associated with an increased risk of several pulmonary infections such as gram‐negative necrotizing pneumonia (classically, Klebsiella pneumoniae), pneumococcal pneumonia, aspiration pneumonia, anaerobic lung abscesses, and tuberculosis. Given his right upper quadrant pain, acute alcoholic hepatitis and alcohol‐related pancreatitis enter the differential. His history of cardiomyopathy makes me consider congestive heart failure as more likely than before, and perhaps his abdominal pain is a result of hepatic congestion from right heart failure. His fever, however, cannot be attributed to cardiac failure. Less likely diagnoses include ischemic conditions related to his cardiomyopathy such as mesenteric ischemia from low perfusion or embolism from a cardiac thrombus. A pulmonary infection remains the most likely diagnosis.
He was an ill‐appearing man in moderate respiratory distress, looking older than his stated age. His temperature was 38.4C, heart rate 129 beats/minute, blood pressure 85/56 mm Hg, respiratory rate 24 breaths/minute, and oxygen saturation 92% on room air. A cardiovascular exam revealed no murmur, gallop, or rub. The jugular venous pulse was not elevated. His lungs were clear to auscultation. Abdominal exam revealed right‐sided abdominal tenderness that appeared to localize to the rectus sheath. Otherwise, the abdomen was soft, with normal bowel sounds and no organomegaly. Rectal examination revealed guaiac negative stool and no focal tenderness. His extremities were normal.
His vital signs are worrisome for impending cardiovascular collapse and shock, possibly due to sepsis. The relatively nonfocal cardiopulmonary exam is surprising given his initial symptoms and makes me wonder if his dyspnea is primarily related to an abdominal process leading to diaphragmatic irritation rather than to a thoracic process. Congestive heart failure seems unlikely given the lack of supportive physical examination findings. His abdominal exam findings are puzzling. Although his abdominal wall tenderness could be benignperhaps from muscular strain or a tear from coughingit could represent a more worrisome process such as infection or a hematoma in the abdominal wall muscles. Mesenteric ischemia is still possible, as the exam is often unimpressive. A hepatic abscess or subphrenic abscess should be considered, as physical exam findings in these conditions can be subtle.
My differential remains relatively unchanged, but I have now put consideration of a hepatic or subphrenic abscess higher on my list. Early empiric broad‐spectrum antibiotics seem necessary.
He had a white blood cell count of 26,700/mL with 92% neutrophils, a hemoglobin of 14.6 g/dL, and a platelet count of 312,000/mL. Sodium was 134 mmol/L, potassium was 4.3 mmol/L, chloride was 94 mmol/L, bicarbonate was 23 mmol/L, blood urea nitrogen was 23 mg/dL, and creatinine was 2.1 mg/dL. The results of the calcium, protein, albumin, and liver function tests were normal. Urinalysis was negative for protein and red blood cells. An electrocardiogram revealed sinus tachycardia. A chest radiograph at admission revealed mild opacities in both lower lobes and the right middle lobe consistent with either atelectasis or pneumonia (Fig. 1). A very small left effusion was also identified.
The additional data reinforce my clinical impression that this process is likely to be infectious. The chest radiograph is consistent with community‐acquired pneumonia, possibly from an atypical pathogen. Given his elevated creatinine, I am also considering a pulmonary‐renal syndrome such as vasculitis, though hematuria was not present. A subphrenic abscess, mesenteric ischemia, or an abdominal wall process (because his abdominal tenderness on exam still needs an explanation) remain possibilities; my suspicion would increase if he does not respond appropriately to therapy for community‐acquired pneumonia.
The clinical team's working diagnosis also was community‐acquired pneumonia. Blood and sputum cultures were obtained, and the patient was treated with intravenous ceftriaxone, azithromycin, and intravenous fluid. By the second day, his creatinine had normalized; however, his hypoxemia had worsened, and he now required supplemental oxygen. His temperature was 39.3C, and his heart rate was 150 beats/minute. The findings of an abdominal ultrasound of the kidneys, spleen, and right upper quadrant were normal.
It is too early to say the patient has failed therapy because a patient can get worse before getting better during the course of antibiotic therapy for community‐acquired pneumonia. Fever, for example, may take up to 7 days to resolve, depending on host factors and the pathogen. Though I typically wait about 72 hours before assuming a patient is not appropriately responding to therapy, the additional information has made me concerned. The degree of tachycardia is significant and warrants an EKG to exclude an arrthymia. I would also repeat the chest radiograph to evaluate for worsening infiltrates or increased pleural effusion.
On the third hospital day, the patient's abdominal pain had decreased with analgesia, but his fever, cough, and dyspnea remained largely unchanged. Antibiotics were changed to intravenous levofloxacin. A repeat chest radiograph revealed elevation of the right hemidiaphragm and bilateral effusions (Fig. 2). An electrocardiogram revealed sinus tachycardia. Blood cultures revealed no growth, and sputum cultures grew oral flora.
A significantly elevated right hemidiaphragm makes me reconsider the diagnosis of simple community‐acquired pneumonia. The differential diagnosis for an elevated hemidiaphragm is best considered by location in relation to the diaphragm. Causes above the diaphragm include rib fracture, atelectasis, pleural thickening, and volume loss of the lung for another reason (e.g., surgery, bronchial obstruction due to tumor or mucus plugging), as well as mimics such as a densely consolidated pneumonia, pulmonary infarction, or a subpulmonary effusion. Diaphragmatic causes include eventration, rupture, phrenic nerve weakness, and intrinsic weakness because of neuromuscular disease (usually bilateral). Causes below the diaphragm that must be considered are subphrenic or liver abscess, liver (and other abdominal) malignancy, pancreatic pseudocyst, and distended bowel. Given the clinical picture, I am focusing below the diaphragmespecially on a possible hepatic or subphrenic abscess (which could be missed on ultrasound) and mimics of it such as dense consolidation or a subpulmonary effusion. Given the lack of response to antibiotics, I need to consider an infection that is not being treated, either because of location (abscess, effusion) or microbiology (tuberculosis, a parasite, a fungus, resistant bacteria). After confirming that the patient has a substantive pleural effusion, he needs a thoracentesis.
On the fourth hospital day, his temperature was 38.8C, and his white blood cell count was 21,000/mL. A right‐sided thoracentesis was performed; approximately 250 cc of fluid was obtained. Pleural fluid analysis revealed bloody fluid, with a white blood cell count of 16,750/mL with 94% neutrophils, 40,000 red blood cells/mL, lactate dehydrogenase of 278 U/L (normal serum value 80200 U/L), protein of 3.7 g/dL, and glucose of 81 mg/dL. A pleural fluid pH was not obtained. A gram stain revealed many white blood cells with no organisms noted. Serum protein was 7.4 g/dL. These results were thought to represent an exudative parapneumonic effusion; levofloxacin and supplemental oxygen were continued.
The pleural fluid appears exudative, but I am not sure this man has a parapneumonic effusion because, despite clinical deterioration, an obvious infiltrate is not seen on interval chest radiography. We must look closely at the fluid because this is a bloody effusion and somewhat atypical for a parapneumonic effusion. Also, the effusion does not appear large enough to explain why he has not improved on the current antibiotics. We should thus reconsider our diagnosis and management. I would obtain additional imaging (such as an abdominal and chest computed tomography [CT]) and perhaps obtain a consultation from the pulmonary team regarding the postulated initial diagnosis of pneumonia with effusion.
On the fifth day of hospitalization, the patient's dyspnea and cough persisted but were improved. His abdominal pain was minimal and felt improved with flatus. Fever continued to 38.8C, and the white blood cell count was 20,000/mL. On examination the patient had decreased breath sounds at the right base and bibasilar crackles. His abdomen was soft, with tenderness in his right upper quadrant only with deep palpation; bowel sounds remained. An ultrasound of the chest was performed to look for a loculated effusion; however, no fluid was identified. The pulmonary consultant thought it likely that the patient had a subpulmonic effusion and recommended CT of the abdomen and chest.
His right upper quadrant tenderness is still unexplained. I would agree with the CT, primarily to evaluate other causes of his elevated diaphragm such as subphrenic or hepatic abscess. For now, I would make no change in antibiotic therapy.
On the sixth hospital day, the patient had an episode of bilious emesis. Chest and abdominal CT revealed collapse of the right middle and lower lobes with a small adjacent effusion, and a 6 6 16 cm abscess intimately opposed to the right lobe of the liver. Extending from the inferior extent of the abscess was a tubular thick‐walled structure connecting to the cecum that was suspicious of a thickened inflamed appendix. There was periappendiceal stranding suggesting inflammation. The small bowel was diffusely dilated up to 4.5 cm, suggesting a small bowel obstruction.
I suspect that his abscess is related to a perforated appendix and that the dilated small bowel is most likely a result of localized irritation of the bowel by the abscess and appendicitis. The collapsed lung is most likely due to local inflammation from the subdiaphragmatic abscess. Treatment should now be changed substantially. I would ask a surgeon to evaluate the patient because the most likely diagnosis is perforated appendicitis with abscess formation.
When the periappendiceal abscess was drained percutaneously, 190 mL of purulent fluid was removed. The cultures were positive for Klebsiella pneumonia, Enterococcus faecalis,and Streptococcus milleri. The patient was given 6 weeks of intravenous antibiotics with improvement in his clinical symptoms. During the interval the findings on his chest radiograph resolved completely. A laproscopic appendectomy 3 months later revealed significant right lower quadrant adhesions. The pathology specimen identified a distorted appendix with regeneration consistent with prior appendicitis. The patient was contacted 4 months after his surgery, and he reported that he was doing well, with no cardiopulmonary or gastrointestinal symptoms.
COMMENTARY
Community‐acquired pneumonia (CAP) is a common cause of acute illness and accounts for nearly 1 million admissions per year in the United States.1 The diagnosis of CAP is made when symptoms including dyspnea, fever, cough, or leukocytosis are present, with confirmation provided by a chest radiograph. Often the diagnosis is clear; however, there is no pathognomonic constellation of signs or symptoms that establish the diagnosis with certainty.2 Many physicians learn that pneumoniaespecially lower‐lobe pneumoniacan lead to abdominal findings such as upper quadrant pain, vomiting, and tenderness to palpation. Conversely, the patient discussed above illustrates that a primary abdominal process can also result in a symptom complex that mimics pneumonia.
The prevalence of CAP coupled with the inherent uncertainty of a clinical diagnosis of CAP leads to an important question: How long is too long before questioning the diagnosis? An analysis of the pneumonia Patient Outcomes Research Trial (PORT) limited to inpatients with CAP examined time to clinical stability. For the majority of patients, abnormal vital signs resolved within 23 days.3 In this study, 29% of patients had severe disease, and not surprisingly, these patients took longer to improve. Using the pneumonia severity index score, which accounts for age, comorbidity, abnormal vital signs, and laboratory data, the patient described in this article would be considered at high risk for death and complication with an estimated mortality of 9%.4 Using a combination of defervescence, resolution of tachycardia, tachypnea, and hypoxemia as markers of clinical stability, a patient like ours should respond within 4 days (with a range of 27 days). On the basis of these dataand the discrepancy between the patient's severe illness and relatively minor pulmonary infiltratesit seems reasonable to have considered this patient as failing CAP therapy as early as the fourth day of hospitalization.
In approximately 10% of hospitalized patients with CAP, the clinical course is protracted.5 When patients do not improve as quickly as expected, the reasons that could explain this should be investigated. In a cohort of 49 patients with CAP who failed therapy the most common reasons for failure to improve were severity of the pneumonia and drug resistance.6 A multicenter study found that the incidence of resistance to penicillin by Streptococcus pneumoniae, the most common bacterial pathogen in CAP, was 30%, with a 4% in vitro resistance rate to ceftriaxone.7 How well in vitro resistance predicts clinical response, however, is unclear. Risk factors for antibiotic resistance include close exposure to children, recent antibiotic use, and recent hospitalization. Immunosuppressive conditions should also be considered in patients who fail to improve. Suppurative complications of pneumoniasuch as empyema, parapneumonic effusion, and lung abscessalso delay recovery.
Another consideration in a patient with what appears to be a nonresolving pneumonia with pleural effusion is that the initial diagnosis is incorrect and the cause is extrathoracic. Pulmonary and cardiac diseases account for more than 90% of effusions, whereas less than 5% of pleural effusions result from intraabdominal causes.8 When should intraabdominal diseases be sought in patients with an effusion, fever, dyspnea, and cough? Light suggests that intraabdominal pathology should be investigated in patients who have pleural effusions without significant parenchymal disease.8 This point is underscored by the experience of our patient, whose chest radiographs showed, despite clinical decline, minimal airspace disease.
Several abdominal entities cause pleural effusion. Pancreatitis, either acute or chronic, with pseudocyst formation is the most common abdominal cause of exudative pleural effusions. Approximately 10% of patients with pancreatic disease will develop effusions, usually left‐sided.9 These left‐sided effusions are also seen in splenic abscesses, usually as a result of endocarditis. Intrahepatic abscess is associated with effusions in 20% of patients.10 A subphrenic abscess, as seen in our patient, is an uncommon cause of exudative pleural effusions. Historically, subphrenic abscesses resulted from a perforated viscus, with ruptured appendicitis the most common cause,11 followed by perforated peptic ulcers and biliary tract disease. With the advent of antibiotics, the causes of subphrenic abscess changed considerably, with the majority of current cases resulting from postsurgical complications.12 The findings of a chest radiograph are abnormal in 80% of patients with subphrenic abscess;1214 an elevated hemidiaphragm and pleural effusion are found in the majority of cases. The symptoms of a subphrenic abscess are nonspecific, and patient's complaints are equally split between predominantly thoracic and predomninantly abdominal complaints.15
Appendicitis, a common disease predominantly of the young, may lead to atypical presentations in older individuals. In a retrospective analysis of 113 patients older than 60 years with appendicitis, 70% presented in an atypical fashion.16 Typical symptoms include right lower quadrant pain, fever, anorexia and a white blood cell count greater than 10,000/mL. Fever was the most frequently absent symptom, seen in only 37% of older patients. In this cohort, approximately one third of older patients waited more than 48 hours prior to presentation. The time between symptom onset and clinical presentation is a strong predictor of perforation risk.17 As in this case, roughly 2% of patients with acute appendicitis will present with perforation and abscess formation.18 In such patients the management is initially conservative. Percutaneous drainage and broad spectrum antibiotics are the treatment of choice, followed by an interval appendectomy in 612 weeks.19 The rationale for delayed surgery is that earlier surgery may disseminate a localized inflammatory process.20
Community‐acquired pneumonia is a more frequent cause of hospital admission than is intraabdominal abscess. Physicians often face the dilemma of when to pursue alternative diagnoses after a patient who is thought to have an atypical presentation of a common disease (ie, CAP) fails to respond to conventional therapy. Although clinicians learn that right upper quadrant pain may be a symptom of pneumonia, our patient revealed that abdominal causes may mimic pneumonia and produce a pleural effusion. Determining whether the primary disease originates above or below the diaphragm is critical to guiding therapy. When patients fail to respond adequately to therapy, clinicians should set a low threshold for deciding to image the abdomen in a patient with modest pulmonary infiltrates, pleural effusion, and abdominal pain.
- ,,, et al.The cost of treating community‐acquired pneumonia.Clin Ther.1998;20:820–827.
- ,,.Does this patient have community‐acquired pneumonia? Diagnosing pneumonia by history and physical examination.JAMA.1997;278:1440–1445.
- ,,, et al.Time to clinical stability in patients hospitalized with community acquired pneumonia. Implications for practice guidelines.JAMA.1998;279:1452–1457.
- ,,, et al.A prediction rule to identify low‐risk patients with community‐acquired pneumonia.N Engl J Med.1997;336:243–250.
- ,,, et al.Utility of fiberoptic bronchoscopy in non resolving pneumonia.Chest.1990;98:1322–1326.
- ,,, et al.Antimicrobial treatment failures in patients with community acquired pneumonia. Causes and prognostic implications.Am J Respir Crit Care Med.2000;162:154–160.
- ,,, et al.Antimicrobial resistance with Streptococcus pneumoniae in the United States, 1997–98.Emerg Infect Dis.1999;5:757–765.
- ,.Pleural effusion. In:Murray JF,Nadel JA, eds.Textbook of respiratory medicine. 3rd ed.Philadelphia:WB Saunders,2000:2013–2041.
- ,,.Significance of pleural effusion in patients with acute pancreatitis.Am J Gastroenterol.1992;87:871–874.
- .Exudative pleural effusions secondary to gastrointestinal diseases.Clin Chest Med.1985;6(1):103–111.
- .Subphrenic abscess.Ann Surg.1963;158:240–248.
- ,,,.Upper abdominal abscess: a continuing and deadly problem.Am J Roentgenol.1980;134:759–765.
- .Subphrenic abscess. A clinical study of 101 cases.Acta Chir Scand.1959;117:388–408.
- ,,.Subphrenic abscess a continuing hazard.Am J Surg.1969:117–122.
- ,.Subphrenic abscess: a thoracoabdominal clinical complex. The changing picture with antibiotics.Am J Surg.1964;108:165–172.
- ,.What have we learned over the past 20 years about appendicitis in the elderly.Am J Surg.2003;185:198–201.
- ,,, et al.Appendicitis: why so complicated? Analysis of 5755 consecutive appendectomies.Am Surg.2000;66:548–554.
- ,,.Appendicitis with a palpable mass.Ann Surg.1981;193:227–229.
- ,,, et al.Nonoperative management of perforated appendicitis without periappendiceal mass.Am J Surg.2000;179:177–181.
- ,,.Appendix. In:Townsend CM, ed.Sabiston textbook of surgery. The biologic basis of modern surgical practice. 16th ed.Philadelphia:W. B. Saunders,2001:917–928.
A 49‐year‐old man presented with 2 days of chills, fever, anorexia, and increased cough and dyspnea. The patient had a history of chronic obstructive pulmonary disease (COPD) and noted that his cough and dyspnea had increased above normal for several days. He was now dyspneic with minimal activity and had slept at a 45‐degree incline the night prior to evaluation due to dyspnea. He noted less improvement than usual with the use of his metered dose inhaler. His cough was occasionally productive of small amounts of white phlegm. He had vomited once. During a coughing episode the patient experienced a sudden onset of sharp right upper quadrant abdominal pain that worsened with coughing and sudden position changes. The patient denied a prior history of abdominal pain or surgery. The patient's last bowel movement was 2 days prior to admission. He denied melena or bright red blood per rectum.
My initial differential diagnosis for this patient's dyspnea and cough is pneumonia, acute exacerbation of COPD, or congestive heart failure. The presence of fever and anorexia increases the likelihood of infectious etiologies, whereas the presence of orthopnea points toward congestive heart failure. Noncardiac processessuch as a large pleural effusion or apical lung diseasecould also cause orthopnea. His abdominal pain could be a result of pneumonia alone (perhaps in the right lower lobe with diaphragmatic irritation), but I am also considering complications of pneumonia such as empyema. Although his abdominal pain, dyspnea, and cough could also be a result of hepatobiliary disease, a perforated viscus, or pancreatitis, we currently have little reason to suspect a direct abdominal etiology. My top diagnosis is community‐acquired pneumonia, perhaps accompanied by pleural effusion.
His medical history was significant for dilated cardiomyopathy and heavy alcohol use. His medications included various meter‐dosed inhalers, bupropion, digoxin, spironolactone, lisinopril, and metoprolol. He had never received corticosteroid therapy and had not previously been hospitalized for COPD‐related problems. He had smoked one pack of cigarettes daily for 40 years.
Heavy alcohol use is associated with an increased risk of several pulmonary infections such as gram‐negative necrotizing pneumonia (classically, Klebsiella pneumoniae), pneumococcal pneumonia, aspiration pneumonia, anaerobic lung abscesses, and tuberculosis. Given his right upper quadrant pain, acute alcoholic hepatitis and alcohol‐related pancreatitis enter the differential. His history of cardiomyopathy makes me consider congestive heart failure as more likely than before, and perhaps his abdominal pain is a result of hepatic congestion from right heart failure. His fever, however, cannot be attributed to cardiac failure. Less likely diagnoses include ischemic conditions related to his cardiomyopathy such as mesenteric ischemia from low perfusion or embolism from a cardiac thrombus. A pulmonary infection remains the most likely diagnosis.
He was an ill‐appearing man in moderate respiratory distress, looking older than his stated age. His temperature was 38.4C, heart rate 129 beats/minute, blood pressure 85/56 mm Hg, respiratory rate 24 breaths/minute, and oxygen saturation 92% on room air. A cardiovascular exam revealed no murmur, gallop, or rub. The jugular venous pulse was not elevated. His lungs were clear to auscultation. Abdominal exam revealed right‐sided abdominal tenderness that appeared to localize to the rectus sheath. Otherwise, the abdomen was soft, with normal bowel sounds and no organomegaly. Rectal examination revealed guaiac negative stool and no focal tenderness. His extremities were normal.
His vital signs are worrisome for impending cardiovascular collapse and shock, possibly due to sepsis. The relatively nonfocal cardiopulmonary exam is surprising given his initial symptoms and makes me wonder if his dyspnea is primarily related to an abdominal process leading to diaphragmatic irritation rather than to a thoracic process. Congestive heart failure seems unlikely given the lack of supportive physical examination findings. His abdominal exam findings are puzzling. Although his abdominal wall tenderness could be benignperhaps from muscular strain or a tear from coughingit could represent a more worrisome process such as infection or a hematoma in the abdominal wall muscles. Mesenteric ischemia is still possible, as the exam is often unimpressive. A hepatic abscess or subphrenic abscess should be considered, as physical exam findings in these conditions can be subtle.
My differential remains relatively unchanged, but I have now put consideration of a hepatic or subphrenic abscess higher on my list. Early empiric broad‐spectrum antibiotics seem necessary.
He had a white blood cell count of 26,700/mL with 92% neutrophils, a hemoglobin of 14.6 g/dL, and a platelet count of 312,000/mL. Sodium was 134 mmol/L, potassium was 4.3 mmol/L, chloride was 94 mmol/L, bicarbonate was 23 mmol/L, blood urea nitrogen was 23 mg/dL, and creatinine was 2.1 mg/dL. The results of the calcium, protein, albumin, and liver function tests were normal. Urinalysis was negative for protein and red blood cells. An electrocardiogram revealed sinus tachycardia. A chest radiograph at admission revealed mild opacities in both lower lobes and the right middle lobe consistent with either atelectasis or pneumonia (Fig. 1). A very small left effusion was also identified.
The additional data reinforce my clinical impression that this process is likely to be infectious. The chest radiograph is consistent with community‐acquired pneumonia, possibly from an atypical pathogen. Given his elevated creatinine, I am also considering a pulmonary‐renal syndrome such as vasculitis, though hematuria was not present. A subphrenic abscess, mesenteric ischemia, or an abdominal wall process (because his abdominal tenderness on exam still needs an explanation) remain possibilities; my suspicion would increase if he does not respond appropriately to therapy for community‐acquired pneumonia.
The clinical team's working diagnosis also was community‐acquired pneumonia. Blood and sputum cultures were obtained, and the patient was treated with intravenous ceftriaxone, azithromycin, and intravenous fluid. By the second day, his creatinine had normalized; however, his hypoxemia had worsened, and he now required supplemental oxygen. His temperature was 39.3C, and his heart rate was 150 beats/minute. The findings of an abdominal ultrasound of the kidneys, spleen, and right upper quadrant were normal.
It is too early to say the patient has failed therapy because a patient can get worse before getting better during the course of antibiotic therapy for community‐acquired pneumonia. Fever, for example, may take up to 7 days to resolve, depending on host factors and the pathogen. Though I typically wait about 72 hours before assuming a patient is not appropriately responding to therapy, the additional information has made me concerned. The degree of tachycardia is significant and warrants an EKG to exclude an arrthymia. I would also repeat the chest radiograph to evaluate for worsening infiltrates or increased pleural effusion.
On the third hospital day, the patient's abdominal pain had decreased with analgesia, but his fever, cough, and dyspnea remained largely unchanged. Antibiotics were changed to intravenous levofloxacin. A repeat chest radiograph revealed elevation of the right hemidiaphragm and bilateral effusions (Fig. 2). An electrocardiogram revealed sinus tachycardia. Blood cultures revealed no growth, and sputum cultures grew oral flora.
A significantly elevated right hemidiaphragm makes me reconsider the diagnosis of simple community‐acquired pneumonia. The differential diagnosis for an elevated hemidiaphragm is best considered by location in relation to the diaphragm. Causes above the diaphragm include rib fracture, atelectasis, pleural thickening, and volume loss of the lung for another reason (e.g., surgery, bronchial obstruction due to tumor or mucus plugging), as well as mimics such as a densely consolidated pneumonia, pulmonary infarction, or a subpulmonary effusion. Diaphragmatic causes include eventration, rupture, phrenic nerve weakness, and intrinsic weakness because of neuromuscular disease (usually bilateral). Causes below the diaphragm that must be considered are subphrenic or liver abscess, liver (and other abdominal) malignancy, pancreatic pseudocyst, and distended bowel. Given the clinical picture, I am focusing below the diaphragmespecially on a possible hepatic or subphrenic abscess (which could be missed on ultrasound) and mimics of it such as dense consolidation or a subpulmonary effusion. Given the lack of response to antibiotics, I need to consider an infection that is not being treated, either because of location (abscess, effusion) or microbiology (tuberculosis, a parasite, a fungus, resistant bacteria). After confirming that the patient has a substantive pleural effusion, he needs a thoracentesis.
On the fourth hospital day, his temperature was 38.8C, and his white blood cell count was 21,000/mL. A right‐sided thoracentesis was performed; approximately 250 cc of fluid was obtained. Pleural fluid analysis revealed bloody fluid, with a white blood cell count of 16,750/mL with 94% neutrophils, 40,000 red blood cells/mL, lactate dehydrogenase of 278 U/L (normal serum value 80200 U/L), protein of 3.7 g/dL, and glucose of 81 mg/dL. A pleural fluid pH was not obtained. A gram stain revealed many white blood cells with no organisms noted. Serum protein was 7.4 g/dL. These results were thought to represent an exudative parapneumonic effusion; levofloxacin and supplemental oxygen were continued.
The pleural fluid appears exudative, but I am not sure this man has a parapneumonic effusion because, despite clinical deterioration, an obvious infiltrate is not seen on interval chest radiography. We must look closely at the fluid because this is a bloody effusion and somewhat atypical for a parapneumonic effusion. Also, the effusion does not appear large enough to explain why he has not improved on the current antibiotics. We should thus reconsider our diagnosis and management. I would obtain additional imaging (such as an abdominal and chest computed tomography [CT]) and perhaps obtain a consultation from the pulmonary team regarding the postulated initial diagnosis of pneumonia with effusion.
On the fifth day of hospitalization, the patient's dyspnea and cough persisted but were improved. His abdominal pain was minimal and felt improved with flatus. Fever continued to 38.8C, and the white blood cell count was 20,000/mL. On examination the patient had decreased breath sounds at the right base and bibasilar crackles. His abdomen was soft, with tenderness in his right upper quadrant only with deep palpation; bowel sounds remained. An ultrasound of the chest was performed to look for a loculated effusion; however, no fluid was identified. The pulmonary consultant thought it likely that the patient had a subpulmonic effusion and recommended CT of the abdomen and chest.
His right upper quadrant tenderness is still unexplained. I would agree with the CT, primarily to evaluate other causes of his elevated diaphragm such as subphrenic or hepatic abscess. For now, I would make no change in antibiotic therapy.
On the sixth hospital day, the patient had an episode of bilious emesis. Chest and abdominal CT revealed collapse of the right middle and lower lobes with a small adjacent effusion, and a 6 6 16 cm abscess intimately opposed to the right lobe of the liver. Extending from the inferior extent of the abscess was a tubular thick‐walled structure connecting to the cecum that was suspicious of a thickened inflamed appendix. There was periappendiceal stranding suggesting inflammation. The small bowel was diffusely dilated up to 4.5 cm, suggesting a small bowel obstruction.
I suspect that his abscess is related to a perforated appendix and that the dilated small bowel is most likely a result of localized irritation of the bowel by the abscess and appendicitis. The collapsed lung is most likely due to local inflammation from the subdiaphragmatic abscess. Treatment should now be changed substantially. I would ask a surgeon to evaluate the patient because the most likely diagnosis is perforated appendicitis with abscess formation.
When the periappendiceal abscess was drained percutaneously, 190 mL of purulent fluid was removed. The cultures were positive for Klebsiella pneumonia, Enterococcus faecalis,and Streptococcus milleri. The patient was given 6 weeks of intravenous antibiotics with improvement in his clinical symptoms. During the interval the findings on his chest radiograph resolved completely. A laproscopic appendectomy 3 months later revealed significant right lower quadrant adhesions. The pathology specimen identified a distorted appendix with regeneration consistent with prior appendicitis. The patient was contacted 4 months after his surgery, and he reported that he was doing well, with no cardiopulmonary or gastrointestinal symptoms.
COMMENTARY
Community‐acquired pneumonia (CAP) is a common cause of acute illness and accounts for nearly 1 million admissions per year in the United States.1 The diagnosis of CAP is made when symptoms including dyspnea, fever, cough, or leukocytosis are present, with confirmation provided by a chest radiograph. Often the diagnosis is clear; however, there is no pathognomonic constellation of signs or symptoms that establish the diagnosis with certainty.2 Many physicians learn that pneumoniaespecially lower‐lobe pneumoniacan lead to abdominal findings such as upper quadrant pain, vomiting, and tenderness to palpation. Conversely, the patient discussed above illustrates that a primary abdominal process can also result in a symptom complex that mimics pneumonia.
The prevalence of CAP coupled with the inherent uncertainty of a clinical diagnosis of CAP leads to an important question: How long is too long before questioning the diagnosis? An analysis of the pneumonia Patient Outcomes Research Trial (PORT) limited to inpatients with CAP examined time to clinical stability. For the majority of patients, abnormal vital signs resolved within 23 days.3 In this study, 29% of patients had severe disease, and not surprisingly, these patients took longer to improve. Using the pneumonia severity index score, which accounts for age, comorbidity, abnormal vital signs, and laboratory data, the patient described in this article would be considered at high risk for death and complication with an estimated mortality of 9%.4 Using a combination of defervescence, resolution of tachycardia, tachypnea, and hypoxemia as markers of clinical stability, a patient like ours should respond within 4 days (with a range of 27 days). On the basis of these dataand the discrepancy between the patient's severe illness and relatively minor pulmonary infiltratesit seems reasonable to have considered this patient as failing CAP therapy as early as the fourth day of hospitalization.
In approximately 10% of hospitalized patients with CAP, the clinical course is protracted.5 When patients do not improve as quickly as expected, the reasons that could explain this should be investigated. In a cohort of 49 patients with CAP who failed therapy the most common reasons for failure to improve were severity of the pneumonia and drug resistance.6 A multicenter study found that the incidence of resistance to penicillin by Streptococcus pneumoniae, the most common bacterial pathogen in CAP, was 30%, with a 4% in vitro resistance rate to ceftriaxone.7 How well in vitro resistance predicts clinical response, however, is unclear. Risk factors for antibiotic resistance include close exposure to children, recent antibiotic use, and recent hospitalization. Immunosuppressive conditions should also be considered in patients who fail to improve. Suppurative complications of pneumoniasuch as empyema, parapneumonic effusion, and lung abscessalso delay recovery.
Another consideration in a patient with what appears to be a nonresolving pneumonia with pleural effusion is that the initial diagnosis is incorrect and the cause is extrathoracic. Pulmonary and cardiac diseases account for more than 90% of effusions, whereas less than 5% of pleural effusions result from intraabdominal causes.8 When should intraabdominal diseases be sought in patients with an effusion, fever, dyspnea, and cough? Light suggests that intraabdominal pathology should be investigated in patients who have pleural effusions without significant parenchymal disease.8 This point is underscored by the experience of our patient, whose chest radiographs showed, despite clinical decline, minimal airspace disease.
Several abdominal entities cause pleural effusion. Pancreatitis, either acute or chronic, with pseudocyst formation is the most common abdominal cause of exudative pleural effusions. Approximately 10% of patients with pancreatic disease will develop effusions, usually left‐sided.9 These left‐sided effusions are also seen in splenic abscesses, usually as a result of endocarditis. Intrahepatic abscess is associated with effusions in 20% of patients.10 A subphrenic abscess, as seen in our patient, is an uncommon cause of exudative pleural effusions. Historically, subphrenic abscesses resulted from a perforated viscus, with ruptured appendicitis the most common cause,11 followed by perforated peptic ulcers and biliary tract disease. With the advent of antibiotics, the causes of subphrenic abscess changed considerably, with the majority of current cases resulting from postsurgical complications.12 The findings of a chest radiograph are abnormal in 80% of patients with subphrenic abscess;1214 an elevated hemidiaphragm and pleural effusion are found in the majority of cases. The symptoms of a subphrenic abscess are nonspecific, and patient's complaints are equally split between predominantly thoracic and predomninantly abdominal complaints.15
Appendicitis, a common disease predominantly of the young, may lead to atypical presentations in older individuals. In a retrospective analysis of 113 patients older than 60 years with appendicitis, 70% presented in an atypical fashion.16 Typical symptoms include right lower quadrant pain, fever, anorexia and a white blood cell count greater than 10,000/mL. Fever was the most frequently absent symptom, seen in only 37% of older patients. In this cohort, approximately one third of older patients waited more than 48 hours prior to presentation. The time between symptom onset and clinical presentation is a strong predictor of perforation risk.17 As in this case, roughly 2% of patients with acute appendicitis will present with perforation and abscess formation.18 In such patients the management is initially conservative. Percutaneous drainage and broad spectrum antibiotics are the treatment of choice, followed by an interval appendectomy in 612 weeks.19 The rationale for delayed surgery is that earlier surgery may disseminate a localized inflammatory process.20
Community‐acquired pneumonia is a more frequent cause of hospital admission than is intraabdominal abscess. Physicians often face the dilemma of when to pursue alternative diagnoses after a patient who is thought to have an atypical presentation of a common disease (ie, CAP) fails to respond to conventional therapy. Although clinicians learn that right upper quadrant pain may be a symptom of pneumonia, our patient revealed that abdominal causes may mimic pneumonia and produce a pleural effusion. Determining whether the primary disease originates above or below the diaphragm is critical to guiding therapy. When patients fail to respond adequately to therapy, clinicians should set a low threshold for deciding to image the abdomen in a patient with modest pulmonary infiltrates, pleural effusion, and abdominal pain.
A 49‐year‐old man presented with 2 days of chills, fever, anorexia, and increased cough and dyspnea. The patient had a history of chronic obstructive pulmonary disease (COPD) and noted that his cough and dyspnea had increased above normal for several days. He was now dyspneic with minimal activity and had slept at a 45‐degree incline the night prior to evaluation due to dyspnea. He noted less improvement than usual with the use of his metered dose inhaler. His cough was occasionally productive of small amounts of white phlegm. He had vomited once. During a coughing episode the patient experienced a sudden onset of sharp right upper quadrant abdominal pain that worsened with coughing and sudden position changes. The patient denied a prior history of abdominal pain or surgery. The patient's last bowel movement was 2 days prior to admission. He denied melena or bright red blood per rectum.
My initial differential diagnosis for this patient's dyspnea and cough is pneumonia, acute exacerbation of COPD, or congestive heart failure. The presence of fever and anorexia increases the likelihood of infectious etiologies, whereas the presence of orthopnea points toward congestive heart failure. Noncardiac processessuch as a large pleural effusion or apical lung diseasecould also cause orthopnea. His abdominal pain could be a result of pneumonia alone (perhaps in the right lower lobe with diaphragmatic irritation), but I am also considering complications of pneumonia such as empyema. Although his abdominal pain, dyspnea, and cough could also be a result of hepatobiliary disease, a perforated viscus, or pancreatitis, we currently have little reason to suspect a direct abdominal etiology. My top diagnosis is community‐acquired pneumonia, perhaps accompanied by pleural effusion.
His medical history was significant for dilated cardiomyopathy and heavy alcohol use. His medications included various meter‐dosed inhalers, bupropion, digoxin, spironolactone, lisinopril, and metoprolol. He had never received corticosteroid therapy and had not previously been hospitalized for COPD‐related problems. He had smoked one pack of cigarettes daily for 40 years.
Heavy alcohol use is associated with an increased risk of several pulmonary infections such as gram‐negative necrotizing pneumonia (classically, Klebsiella pneumoniae), pneumococcal pneumonia, aspiration pneumonia, anaerobic lung abscesses, and tuberculosis. Given his right upper quadrant pain, acute alcoholic hepatitis and alcohol‐related pancreatitis enter the differential. His history of cardiomyopathy makes me consider congestive heart failure as more likely than before, and perhaps his abdominal pain is a result of hepatic congestion from right heart failure. His fever, however, cannot be attributed to cardiac failure. Less likely diagnoses include ischemic conditions related to his cardiomyopathy such as mesenteric ischemia from low perfusion or embolism from a cardiac thrombus. A pulmonary infection remains the most likely diagnosis.
He was an ill‐appearing man in moderate respiratory distress, looking older than his stated age. His temperature was 38.4C, heart rate 129 beats/minute, blood pressure 85/56 mm Hg, respiratory rate 24 breaths/minute, and oxygen saturation 92% on room air. A cardiovascular exam revealed no murmur, gallop, or rub. The jugular venous pulse was not elevated. His lungs were clear to auscultation. Abdominal exam revealed right‐sided abdominal tenderness that appeared to localize to the rectus sheath. Otherwise, the abdomen was soft, with normal bowel sounds and no organomegaly. Rectal examination revealed guaiac negative stool and no focal tenderness. His extremities were normal.
His vital signs are worrisome for impending cardiovascular collapse and shock, possibly due to sepsis. The relatively nonfocal cardiopulmonary exam is surprising given his initial symptoms and makes me wonder if his dyspnea is primarily related to an abdominal process leading to diaphragmatic irritation rather than to a thoracic process. Congestive heart failure seems unlikely given the lack of supportive physical examination findings. His abdominal exam findings are puzzling. Although his abdominal wall tenderness could be benignperhaps from muscular strain or a tear from coughingit could represent a more worrisome process such as infection or a hematoma in the abdominal wall muscles. Mesenteric ischemia is still possible, as the exam is often unimpressive. A hepatic abscess or subphrenic abscess should be considered, as physical exam findings in these conditions can be subtle.
My differential remains relatively unchanged, but I have now put consideration of a hepatic or subphrenic abscess higher on my list. Early empiric broad‐spectrum antibiotics seem necessary.
He had a white blood cell count of 26,700/mL with 92% neutrophils, a hemoglobin of 14.6 g/dL, and a platelet count of 312,000/mL. Sodium was 134 mmol/L, potassium was 4.3 mmol/L, chloride was 94 mmol/L, bicarbonate was 23 mmol/L, blood urea nitrogen was 23 mg/dL, and creatinine was 2.1 mg/dL. The results of the calcium, protein, albumin, and liver function tests were normal. Urinalysis was negative for protein and red blood cells. An electrocardiogram revealed sinus tachycardia. A chest radiograph at admission revealed mild opacities in both lower lobes and the right middle lobe consistent with either atelectasis or pneumonia (Fig. 1). A very small left effusion was also identified.
The additional data reinforce my clinical impression that this process is likely to be infectious. The chest radiograph is consistent with community‐acquired pneumonia, possibly from an atypical pathogen. Given his elevated creatinine, I am also considering a pulmonary‐renal syndrome such as vasculitis, though hematuria was not present. A subphrenic abscess, mesenteric ischemia, or an abdominal wall process (because his abdominal tenderness on exam still needs an explanation) remain possibilities; my suspicion would increase if he does not respond appropriately to therapy for community‐acquired pneumonia.
The clinical team's working diagnosis also was community‐acquired pneumonia. Blood and sputum cultures were obtained, and the patient was treated with intravenous ceftriaxone, azithromycin, and intravenous fluid. By the second day, his creatinine had normalized; however, his hypoxemia had worsened, and he now required supplemental oxygen. His temperature was 39.3C, and his heart rate was 150 beats/minute. The findings of an abdominal ultrasound of the kidneys, spleen, and right upper quadrant were normal.
It is too early to say the patient has failed therapy because a patient can get worse before getting better during the course of antibiotic therapy for community‐acquired pneumonia. Fever, for example, may take up to 7 days to resolve, depending on host factors and the pathogen. Though I typically wait about 72 hours before assuming a patient is not appropriately responding to therapy, the additional information has made me concerned. The degree of tachycardia is significant and warrants an EKG to exclude an arrthymia. I would also repeat the chest radiograph to evaluate for worsening infiltrates or increased pleural effusion.
On the third hospital day, the patient's abdominal pain had decreased with analgesia, but his fever, cough, and dyspnea remained largely unchanged. Antibiotics were changed to intravenous levofloxacin. A repeat chest radiograph revealed elevation of the right hemidiaphragm and bilateral effusions (Fig. 2). An electrocardiogram revealed sinus tachycardia. Blood cultures revealed no growth, and sputum cultures grew oral flora.
A significantly elevated right hemidiaphragm makes me reconsider the diagnosis of simple community‐acquired pneumonia. The differential diagnosis for an elevated hemidiaphragm is best considered by location in relation to the diaphragm. Causes above the diaphragm include rib fracture, atelectasis, pleural thickening, and volume loss of the lung for another reason (e.g., surgery, bronchial obstruction due to tumor or mucus plugging), as well as mimics such as a densely consolidated pneumonia, pulmonary infarction, or a subpulmonary effusion. Diaphragmatic causes include eventration, rupture, phrenic nerve weakness, and intrinsic weakness because of neuromuscular disease (usually bilateral). Causes below the diaphragm that must be considered are subphrenic or liver abscess, liver (and other abdominal) malignancy, pancreatic pseudocyst, and distended bowel. Given the clinical picture, I am focusing below the diaphragmespecially on a possible hepatic or subphrenic abscess (which could be missed on ultrasound) and mimics of it such as dense consolidation or a subpulmonary effusion. Given the lack of response to antibiotics, I need to consider an infection that is not being treated, either because of location (abscess, effusion) or microbiology (tuberculosis, a parasite, a fungus, resistant bacteria). After confirming that the patient has a substantive pleural effusion, he needs a thoracentesis.
On the fourth hospital day, his temperature was 38.8C, and his white blood cell count was 21,000/mL. A right‐sided thoracentesis was performed; approximately 250 cc of fluid was obtained. Pleural fluid analysis revealed bloody fluid, with a white blood cell count of 16,750/mL with 94% neutrophils, 40,000 red blood cells/mL, lactate dehydrogenase of 278 U/L (normal serum value 80200 U/L), protein of 3.7 g/dL, and glucose of 81 mg/dL. A pleural fluid pH was not obtained. A gram stain revealed many white blood cells with no organisms noted. Serum protein was 7.4 g/dL. These results were thought to represent an exudative parapneumonic effusion; levofloxacin and supplemental oxygen were continued.
The pleural fluid appears exudative, but I am not sure this man has a parapneumonic effusion because, despite clinical deterioration, an obvious infiltrate is not seen on interval chest radiography. We must look closely at the fluid because this is a bloody effusion and somewhat atypical for a parapneumonic effusion. Also, the effusion does not appear large enough to explain why he has not improved on the current antibiotics. We should thus reconsider our diagnosis and management. I would obtain additional imaging (such as an abdominal and chest computed tomography [CT]) and perhaps obtain a consultation from the pulmonary team regarding the postulated initial diagnosis of pneumonia with effusion.
On the fifth day of hospitalization, the patient's dyspnea and cough persisted but were improved. His abdominal pain was minimal and felt improved with flatus. Fever continued to 38.8C, and the white blood cell count was 20,000/mL. On examination the patient had decreased breath sounds at the right base and bibasilar crackles. His abdomen was soft, with tenderness in his right upper quadrant only with deep palpation; bowel sounds remained. An ultrasound of the chest was performed to look for a loculated effusion; however, no fluid was identified. The pulmonary consultant thought it likely that the patient had a subpulmonic effusion and recommended CT of the abdomen and chest.
His right upper quadrant tenderness is still unexplained. I would agree with the CT, primarily to evaluate other causes of his elevated diaphragm such as subphrenic or hepatic abscess. For now, I would make no change in antibiotic therapy.
On the sixth hospital day, the patient had an episode of bilious emesis. Chest and abdominal CT revealed collapse of the right middle and lower lobes with a small adjacent effusion, and a 6 6 16 cm abscess intimately opposed to the right lobe of the liver. Extending from the inferior extent of the abscess was a tubular thick‐walled structure connecting to the cecum that was suspicious of a thickened inflamed appendix. There was periappendiceal stranding suggesting inflammation. The small bowel was diffusely dilated up to 4.5 cm, suggesting a small bowel obstruction.
I suspect that his abscess is related to a perforated appendix and that the dilated small bowel is most likely a result of localized irritation of the bowel by the abscess and appendicitis. The collapsed lung is most likely due to local inflammation from the subdiaphragmatic abscess. Treatment should now be changed substantially. I would ask a surgeon to evaluate the patient because the most likely diagnosis is perforated appendicitis with abscess formation.
When the periappendiceal abscess was drained percutaneously, 190 mL of purulent fluid was removed. The cultures were positive for Klebsiella pneumonia, Enterococcus faecalis,and Streptococcus milleri. The patient was given 6 weeks of intravenous antibiotics with improvement in his clinical symptoms. During the interval the findings on his chest radiograph resolved completely. A laproscopic appendectomy 3 months later revealed significant right lower quadrant adhesions. The pathology specimen identified a distorted appendix with regeneration consistent with prior appendicitis. The patient was contacted 4 months after his surgery, and he reported that he was doing well, with no cardiopulmonary or gastrointestinal symptoms.
COMMENTARY
Community‐acquired pneumonia (CAP) is a common cause of acute illness and accounts for nearly 1 million admissions per year in the United States.1 The diagnosis of CAP is made when symptoms including dyspnea, fever, cough, or leukocytosis are present, with confirmation provided by a chest radiograph. Often the diagnosis is clear; however, there is no pathognomonic constellation of signs or symptoms that establish the diagnosis with certainty.2 Many physicians learn that pneumoniaespecially lower‐lobe pneumoniacan lead to abdominal findings such as upper quadrant pain, vomiting, and tenderness to palpation. Conversely, the patient discussed above illustrates that a primary abdominal process can also result in a symptom complex that mimics pneumonia.
The prevalence of CAP coupled with the inherent uncertainty of a clinical diagnosis of CAP leads to an important question: How long is too long before questioning the diagnosis? An analysis of the pneumonia Patient Outcomes Research Trial (PORT) limited to inpatients with CAP examined time to clinical stability. For the majority of patients, abnormal vital signs resolved within 23 days.3 In this study, 29% of patients had severe disease, and not surprisingly, these patients took longer to improve. Using the pneumonia severity index score, which accounts for age, comorbidity, abnormal vital signs, and laboratory data, the patient described in this article would be considered at high risk for death and complication with an estimated mortality of 9%.4 Using a combination of defervescence, resolution of tachycardia, tachypnea, and hypoxemia as markers of clinical stability, a patient like ours should respond within 4 days (with a range of 27 days). On the basis of these dataand the discrepancy between the patient's severe illness and relatively minor pulmonary infiltratesit seems reasonable to have considered this patient as failing CAP therapy as early as the fourth day of hospitalization.
In approximately 10% of hospitalized patients with CAP, the clinical course is protracted.5 When patients do not improve as quickly as expected, the reasons that could explain this should be investigated. In a cohort of 49 patients with CAP who failed therapy the most common reasons for failure to improve were severity of the pneumonia and drug resistance.6 A multicenter study found that the incidence of resistance to penicillin by Streptococcus pneumoniae, the most common bacterial pathogen in CAP, was 30%, with a 4% in vitro resistance rate to ceftriaxone.7 How well in vitro resistance predicts clinical response, however, is unclear. Risk factors for antibiotic resistance include close exposure to children, recent antibiotic use, and recent hospitalization. Immunosuppressive conditions should also be considered in patients who fail to improve. Suppurative complications of pneumoniasuch as empyema, parapneumonic effusion, and lung abscessalso delay recovery.
Another consideration in a patient with what appears to be a nonresolving pneumonia with pleural effusion is that the initial diagnosis is incorrect and the cause is extrathoracic. Pulmonary and cardiac diseases account for more than 90% of effusions, whereas less than 5% of pleural effusions result from intraabdominal causes.8 When should intraabdominal diseases be sought in patients with an effusion, fever, dyspnea, and cough? Light suggests that intraabdominal pathology should be investigated in patients who have pleural effusions without significant parenchymal disease.8 This point is underscored by the experience of our patient, whose chest radiographs showed, despite clinical decline, minimal airspace disease.
Several abdominal entities cause pleural effusion. Pancreatitis, either acute or chronic, with pseudocyst formation is the most common abdominal cause of exudative pleural effusions. Approximately 10% of patients with pancreatic disease will develop effusions, usually left‐sided.9 These left‐sided effusions are also seen in splenic abscesses, usually as a result of endocarditis. Intrahepatic abscess is associated with effusions in 20% of patients.10 A subphrenic abscess, as seen in our patient, is an uncommon cause of exudative pleural effusions. Historically, subphrenic abscesses resulted from a perforated viscus, with ruptured appendicitis the most common cause,11 followed by perforated peptic ulcers and biliary tract disease. With the advent of antibiotics, the causes of subphrenic abscess changed considerably, with the majority of current cases resulting from postsurgical complications.12 The findings of a chest radiograph are abnormal in 80% of patients with subphrenic abscess;1214 an elevated hemidiaphragm and pleural effusion are found in the majority of cases. The symptoms of a subphrenic abscess are nonspecific, and patient's complaints are equally split between predominantly thoracic and predomninantly abdominal complaints.15
Appendicitis, a common disease predominantly of the young, may lead to atypical presentations in older individuals. In a retrospective analysis of 113 patients older than 60 years with appendicitis, 70% presented in an atypical fashion.16 Typical symptoms include right lower quadrant pain, fever, anorexia and a white blood cell count greater than 10,000/mL. Fever was the most frequently absent symptom, seen in only 37% of older patients. In this cohort, approximately one third of older patients waited more than 48 hours prior to presentation. The time between symptom onset and clinical presentation is a strong predictor of perforation risk.17 As in this case, roughly 2% of patients with acute appendicitis will present with perforation and abscess formation.18 In such patients the management is initially conservative. Percutaneous drainage and broad spectrum antibiotics are the treatment of choice, followed by an interval appendectomy in 612 weeks.19 The rationale for delayed surgery is that earlier surgery may disseminate a localized inflammatory process.20
Community‐acquired pneumonia is a more frequent cause of hospital admission than is intraabdominal abscess. Physicians often face the dilemma of when to pursue alternative diagnoses after a patient who is thought to have an atypical presentation of a common disease (ie, CAP) fails to respond to conventional therapy. Although clinicians learn that right upper quadrant pain may be a symptom of pneumonia, our patient revealed that abdominal causes may mimic pneumonia and produce a pleural effusion. Determining whether the primary disease originates above or below the diaphragm is critical to guiding therapy. When patients fail to respond adequately to therapy, clinicians should set a low threshold for deciding to image the abdomen in a patient with modest pulmonary infiltrates, pleural effusion, and abdominal pain.
- ,,, et al.The cost of treating community‐acquired pneumonia.Clin Ther.1998;20:820–827.
- ,,.Does this patient have community‐acquired pneumonia? Diagnosing pneumonia by history and physical examination.JAMA.1997;278:1440–1445.
- ,,, et al.Time to clinical stability in patients hospitalized with community acquired pneumonia. Implications for practice guidelines.JAMA.1998;279:1452–1457.
- ,,, et al.A prediction rule to identify low‐risk patients with community‐acquired pneumonia.N Engl J Med.1997;336:243–250.
- ,,, et al.Utility of fiberoptic bronchoscopy in non resolving pneumonia.Chest.1990;98:1322–1326.
- ,,, et al.Antimicrobial treatment failures in patients with community acquired pneumonia. Causes and prognostic implications.Am J Respir Crit Care Med.2000;162:154–160.
- ,,, et al.Antimicrobial resistance with Streptococcus pneumoniae in the United States, 1997–98.Emerg Infect Dis.1999;5:757–765.
- ,.Pleural effusion. In:Murray JF,Nadel JA, eds.Textbook of respiratory medicine. 3rd ed.Philadelphia:WB Saunders,2000:2013–2041.
- ,,.Significance of pleural effusion in patients with acute pancreatitis.Am J Gastroenterol.1992;87:871–874.
- .Exudative pleural effusions secondary to gastrointestinal diseases.Clin Chest Med.1985;6(1):103–111.
- .Subphrenic abscess.Ann Surg.1963;158:240–248.
- ,,,.Upper abdominal abscess: a continuing and deadly problem.Am J Roentgenol.1980;134:759–765.
- .Subphrenic abscess. A clinical study of 101 cases.Acta Chir Scand.1959;117:388–408.
- ,,.Subphrenic abscess a continuing hazard.Am J Surg.1969:117–122.
- ,.Subphrenic abscess: a thoracoabdominal clinical complex. The changing picture with antibiotics.Am J Surg.1964;108:165–172.
- ,.What have we learned over the past 20 years about appendicitis in the elderly.Am J Surg.2003;185:198–201.
- ,,, et al.Appendicitis: why so complicated? Analysis of 5755 consecutive appendectomies.Am Surg.2000;66:548–554.
- ,,.Appendicitis with a palpable mass.Ann Surg.1981;193:227–229.
- ,,, et al.Nonoperative management of perforated appendicitis without periappendiceal mass.Am J Surg.2000;179:177–181.
- ,,.Appendix. In:Townsend CM, ed.Sabiston textbook of surgery. The biologic basis of modern surgical practice. 16th ed.Philadelphia:W. B. Saunders,2001:917–928.
- ,,, et al.The cost of treating community‐acquired pneumonia.Clin Ther.1998;20:820–827.
- ,,.Does this patient have community‐acquired pneumonia? Diagnosing pneumonia by history and physical examination.JAMA.1997;278:1440–1445.
- ,,, et al.Time to clinical stability in patients hospitalized with community acquired pneumonia. Implications for practice guidelines.JAMA.1998;279:1452–1457.
- ,,, et al.A prediction rule to identify low‐risk patients with community‐acquired pneumonia.N Engl J Med.1997;336:243–250.
- ,,, et al.Utility of fiberoptic bronchoscopy in non resolving pneumonia.Chest.1990;98:1322–1326.
- ,,, et al.Antimicrobial treatment failures in patients with community acquired pneumonia. Causes and prognostic implications.Am J Respir Crit Care Med.2000;162:154–160.
- ,,, et al.Antimicrobial resistance with Streptococcus pneumoniae in the United States, 1997–98.Emerg Infect Dis.1999;5:757–765.
- ,.Pleural effusion. In:Murray JF,Nadel JA, eds.Textbook of respiratory medicine. 3rd ed.Philadelphia:WB Saunders,2000:2013–2041.
- ,,.Significance of pleural effusion in patients with acute pancreatitis.Am J Gastroenterol.1992;87:871–874.
- .Exudative pleural effusions secondary to gastrointestinal diseases.Clin Chest Med.1985;6(1):103–111.
- .Subphrenic abscess.Ann Surg.1963;158:240–248.
- ,,,.Upper abdominal abscess: a continuing and deadly problem.Am J Roentgenol.1980;134:759–765.
- .Subphrenic abscess. A clinical study of 101 cases.Acta Chir Scand.1959;117:388–408.
- ,,.Subphrenic abscess a continuing hazard.Am J Surg.1969:117–122.
- ,.Subphrenic abscess: a thoracoabdominal clinical complex. The changing picture with antibiotics.Am J Surg.1964;108:165–172.
- ,.What have we learned over the past 20 years about appendicitis in the elderly.Am J Surg.2003;185:198–201.
- ,,, et al.Appendicitis: why so complicated? Analysis of 5755 consecutive appendectomies.Am Surg.2000;66:548–554.
- ,,.Appendicitis with a palpable mass.Ann Surg.1981;193:227–229.
- ,,, et al.Nonoperative management of perforated appendicitis without periappendiceal mass.Am J Surg.2000;179:177–181.
- ,,.Appendix. In:Townsend CM, ed.Sabiston textbook of surgery. The biologic basis of modern surgical practice. 16th ed.Philadelphia:W. B. Saunders,2001:917–928.
Hospital‐Acquired Gastrointestinal Bleeding
Gastrointestinal bleeding occurring in hospitalized patients admitted for nongastrointestinal disorders has been extensively studied in intensive care unit patients. However, a systematic study in noncritically ill medical patients has not yet been done. In critically ill patients the incidence of hospital‐acquired gastrointestinal bleeding (GIB) varies from 0.17% to 5%, depending on its definition.16 These bleeding events significantly increase the morbidity and duration of hospitalization.1, 5, 79
Risk factors for bleeding in the intensive care unit include mechanical ventilation, coagulopathy, burns, chronic renal failure, and neurological insults.15 Several studies have found that stress ulcer prophylaxis with histamine‐2 (H2) receptor antagonists, sucralfate, or proton pump inhibitors (PPIs) decreases bleeding in this group of patients, with a relative risk reduction of 29%61%.10, 11 However, use of these drugs outside this high‐risk group has been questioned because of the low overall risk of bleeding.1, 11, 12 Despite their being an unproven benefit in the noncritically ill population, prophylactic H2 antagonists or PPIs are prescribed in an indiscriminant fashion to up to 30%50% of patients admitted to the hospital,13, 14 suggesting that physician preference dictates this practice. To shed light on this issue in noncritically ill patients, we conducted a retrospective casecontrol study in order to identify risk factors that predict hospital‐acquired gastrointestinal bleeding in this group of patients and to assess whether treatment with prophylactic acid suppression was associated with fewer bleeding events. We also sought to characterize the endoscopic lesions in these patients.
MATERIALS AND METHODS
Study Patients
The institutional review board of the Cleveland Clinic Foundation (Cleveland, OH) approved this study. All patients admitted to the General Internal Medicine service between January 1, 1999, and December 31, 2002, were eligible for inclusion. Two types of cases were included: 1) patients admitted for nongastrointestinal illnesses who developed bleeding at least 24 hours after admission and required esophagogastroduodenoscopy (EGD) during hospitalization (designated in‐hospital bleeding), and 2) patients admitted with gastrointestinal bleeding (requiring EGD) who had been hospitalized on the General Medical service during the preceding 4 weeks for a nongastrointestinal illness (designated out‐of‐hospital bleeding). This second group was included to identify risk factors for delayed bleeding that might not be obvious during hospitalization.
Medical records of all General Medicine patients who underwent EGD were reviewed in a standardized fashion (Fig. 1). We excluded patients with documented gastrointestinal complaints (including bleeding) at the time of the index admission or within 24 hours of admission, bleeding in the intensive care unit (ICU) or in another hospital prior to transfer to the General Medicine service, or a history of gastrointestinal bleeding during the month prior to admission. ICU stay prior to General Medicine admission, if not associated with GI bleeding, was not an exclusion criterion for our study.
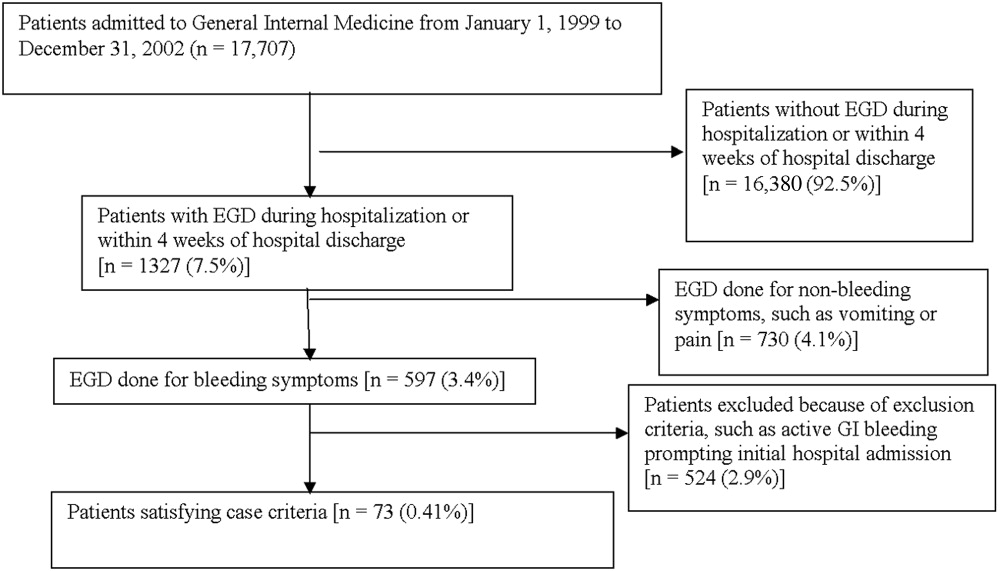
Controls, also without any acute gastrointestinal symptoms at admission, were randomly matched to cases in a 1:1 ratio by date of admission. We used this liberal matching strategy because any factors matched for would no longer be eligible to be risk factors for bleeding. If more than one control was admitted on the same day as a case, then a random number was used to select the control.
Definition of Prophylactic Acid Suppression
We defined prophylactic acid suppression as in‐hospital de novo treatment with histamine‐2 receptor antagonists and/or proton pump inhibitors received prior to the onset of any symptoms that would suggest GI bleeding (for cases) or any time during hospitalization (for controls). Patients taking these drugs prior to admission were deemed ineligible for in‐hospital prophylactic acid blockade and were excluded from the related analyses.
Data Collection
We extracted demographic information, medical history, medication usage, and laboratory data by chart review. For those patients readmitted for gastrointestinal bleeding following discharge, data from the initial (nongastrointestinal illnessassociated) hospitalization were recorded. Bleeding symptoms triggering endoscopy were grouped into four categories: 1) melena or hematochezia; 2) hematemesis (frank blood in vomitus or coffee‐grounds emesis); 3) melena or hematochezia plus hematemesis (both 1 and 2); 4) stool positivity for occult blood or unexplained drop in hemoglobin in the absence of overt bleeding. Endoscopic findings were categorized by the nature of the visualized lesions, and if multiple lesions were noted, the endoscopist's impression of the most likely bleeding site was used to define the source of bleeding. We recorded colonoscopy findings for patients undergoing this evaluation.
Statistical Analysis
We analyzed data utilizing JMP 5.1 (SAS Institute, Cary, NC). Random controls were chosen using computer‐generated random numbers. The proportions of patients with various categorical characteristics were compared using the chi‐square test or Fisher's exact test as appropriate. We used the Student t test or Wilcoxon's test to compare continuous variables. Odds ratios and adjusted odds ratios were calculated by logistic regression. Two‐tailed P values less than .05 were considered statistically significant.
RESULTS: Identification of Cases and Controls
Of 17,707 patients admitted to the General Medicine service, 1327 (7.5%) underwent EGD during hospitalization or within 1 month of discharge. Only 73 (0.41%) of the total number of patients met the case definition (Fig. 1). Of these cases, 62 (84.9%) had developed gastrointestinal bleeding during the index hospitalization, whereas 11 (15.1%) were readmitted for bleeding within 4 weeks of hospital discharge. The remaining 1254 patients who underwent EGD were excluded based on exclusion criteria, including an absence of documented bleeding prompting the EGD.
Clinical Risk Factors for Bleeding
In univariate analysis, as shown in Table 1, predictors of GIB included: 1) age (P = .02); 2) admission diagnosis (P = .01); 3) preexisting coronary artery disease (P = .004); 4) treatment with blood‐thinning medications, including warfarin (P = .0004), intravenous heparin (P = .0003), and clopidogrel (P = .02); and 5) treatment with PPIs (P = .02). After adjusting for the use of full‐dose anticoagulation and/or clopidogrel, the only of these risk factors that remained significantly associated with GIB was treatment with PPIs prior to hospitalization (adjusted OR = 2.1; 95% CI 1.17.0; P = .04), suggesting that PPI treatment in the outpatient setting may be a marker for GI vulnerability.
| Characteristic | Cases n = 73 | Controls n = 73 | Unadjusted | Adjusted for treatment with full‐dose anticoagulants or clopidogrel | ||
|---|---|---|---|---|---|---|
| Odds ratio (95% CI) | P value (2‐tailed) | Odds ratio (95% CI) | P value (2‐tailed) | |||
| ||||||
| Demographics | ||||||
| Women | 36 (49.3%) | 29 (39.7%) | 1.5 (0.82.9) | .24 | 1.6 (0.83.3) | .19 |
| Age (years), mean (SD) | 71.6 (13.7) | 65.7 (17.2) | 1.5 (1.12.1)c | .02 | 1.3 (0.91.8) | .19 |
| Caucasian | 42 (58.3%) | 32 (44.4%) | 1.7 (0.93.4) | .09 | 1.3 (0.62.6) | .50 |
| Nursing home residents | 5 (6.9%) | 5 (6.9%) | 1.0 (0.33.7) | >.99 | 0.5 (0.12.2) | .35 |
| Admission diagnosisa | .01d | .30d | ||||
| Cardiovascular (non‐thrombotic) | 15 (20.5%) | 6 (8.2%) | 2.9 (1.18.5) | .04 | 2.1 (0.76.5) | .19 |
| Arterial or venous thrombosis | 13 (17.8%) | 2 (2.7%) | 7.9 (2.050.4) | .009 | 3.3 (0.822.1) | .15 |
| Infection | 21 (28.8%) | 24 (32.9%) | 0.8 (0.41.7) | .59 | 1.1 (0.52.3) | .86 |
| Pulmonary (noninfectious) | 4 (5.5%) | 10 (13.7%) | 0.4 (0.11.2) | .10 | 0.5 (0.11.7) | .31 |
| Altered level of consciousness | 7 (9.6%) | 10 (13.7%) | 0.7 (0.21.8) | .44 | 0.7 (0.22.2) | .59 |
| Other | 13 (17.8%) | 21 (28.8%) | 0.5 (0.21.2) | .12 | 0.6 (0.31.5) | .29 |
| Baseline medical conditions | ||||||
| Diabetes mellitus | 28 (38.4%) | 25 (34.3%) | 1.2 (0.62.4) | .61 | 1.3 (0.62.7) | .48 |
| Hypertension | 50 (68.5%) | 48 (65.8%) | 1.1 (0.62.3) | .72 | 1.2 (0.52.5) | .71 |
| Coronary artery disease | 36 (49.3%) | 19 (26.0%) | 2.8 (1.45.6) | .004 | 2.0 (1.04.3) | .06 |
| Atrial fibrillation | 18 (24.7%) | 10 (13.7%) | 2.1 (0.95.0) | .09 | 1.4 (0.53.6) | .49 |
| Congestive heart failure | 25 (34.3%) | 16 (21.9%) | 1.9 (0.93.9) | .10 | 1.5 (0.73.3) | .35 |
| Renal insufficiency (creatinine > 2) | 18 (24.7%) | 11 (15.1%) | 1.8 (0.84.4) | .14 | 1.9 (0.84.7) | .33 |
| Chronic obstructive pulmonary disease | 21 (28.8%) | 20 (27.4%) | 1.1 (0.52.2) | .85 | 1.5 (0.73.4) | .29 |
| Stroke | 13 (17.8%) | 16 (21.9%) | 0.8 (0.31.7) | .53 | 0.7 (0.31.6) | .39 |
| Active malignancy | 6 (8.2%) | 8 (11.0%) | 0.7 (0.32.2) | .57 | 1.0 (0.33.5) | .80 |
| Gastroesophageal reflux (GERD) | 10 (13.7%) | 10 (13.7%) | 1.0 (0.42.6) | >.99 | 1.0 (0.32.7) | .92 |
| Liver disease | 7 (9.6%) | 6 (8.2%) | 1.2 (0.43.9) | .77 | 1.4 (0.44.9) | .59 |
| Peptic ulcer disease | 13 (17.8%) | 5 (6.9%) | 2.9 (1.09.6) | .04 | 2.7 (0.99.4) | .09 |
| Colonic disease (diverticulosis, polyp, or AVM) | 7 (9.6%) | 4 (5.5%) | 1.8 (0.57.3) | .34 | 1.2 (0.35.2) | .79 |
| Prior gastrointestinal hemorrhage | 15 (20.1%) | 7 (9.6%) | 2.4 (1.06.8) | .06 | 2.0 (0.75.8) | .20 |
| Tobacco abuse (current smoking) | 9 (12.3%) | 18 (24.7%) | 0.4 (0.21.0) | .05 | 0.6 (0.21.5) | .26 |
| Heavy drinking (>8 drinks/day) | 2 (2.7%) | 2 (2.7%) | 1.0 (0.18.5) | >.99 | 1.3 (0.111.7) | .83 |
| Medication exposure prior to bleeding (excluding acid blockade)b | ||||||
| Aspirin (with or without NSAID) | 34 (46.6%) | 32 (43.8%) | 1.1 (0.62.1) | .74 | 0.7 (0.31.5) | .42 |
| Nonselective NSAID (without aspirin) | 3 (4.1%) | 5 (6.9%) | 0.6 (0.12.5) | .72 | 0.6 (0.12.6) | .44 |
| COX‐2 inhibitors | 3 (4.1%) | 7 (9.6%) | 0.4 (0.11.5) | .18 | 0.3 (0.11.4) | .15 |
| Glucocorticoids | 17 (23.3%) | 20 (27.4%) | 0.8 (0.41.7) | .57 | 0.9 (0.42.1) | .89 |
| Warfarin | 24 (32.9%) | 7 (9.6%) | 4.6 (1.912.4) | .004 | N/A | N/A |
| Unfractionated heparin, UFH (full‐dose intravenous | 23 (31.5%) | 6 (20.7%) | 5.1 (2.114.8) | .0003 | N/A | N/A |
| Full‐dose low‐molecular‐weight heparin (LMWH) | 2 (2.7%) | 0 (0%) | infinity | .50 | N/A | N/A |
| Clopidogrel | 9 (12.3%) | 2 (2.7%) | 5.0 (1.233.5) | .02 | N/A | N/A |
| Prophylactic LMWH or UFH (among 103 patients not on full‐dose anticoagulants) | 19 (47.5%) | 32 (50.8%) | 0.9 (0.41.9) | .74 | N/A | N/A |
| Any treatment with warfarin, full‐dose UFH, full‐ dose LMWH, and/or clopidogrel | 41 (56.2%) | 14 (19.2%) | 5.4 (2.611.7) | <.0001 | N/A | N/A |
| Gastric acid suppression (prior to any gastrointestinal hemorrhage) | ||||||
| H2‐receptor antagonists (H2RA) (total) | 11 (15.1%) | 19 (26.0%) | 0.5 (0.21.1) | .10 | 0.6 (0.31.5) | .31 |
| Taken prior to admission | 6 (8.2%) | 9 (12.3%) | 0.6 (0.21.9) | .41 | 0.6 (0.22.1) | .47 |
| Started de novo at admission | 5 (6.9%) | 10 (13.7%) | 0.5 (0.11.4) | .17 | 0.7 (0.22.2) | .53 |
| Proton‐pump inhibitor (PPI) (total) | 28 (38.6%) | 16 (21.9%) | 2.2 (1.14.7) | .03 | 2.1 (1.04.6) | .07 |
| Taken prior to admission | 20 (27.4%) | 9 (12.3%) | 2.2 (1.14.7) | .02 | 2.7 (1.17.0) | .04 |
| Started de novo at admission | 8 (11.0%) | 7 (9.6%) | 1.2 (0.43.5) | .79 | 1.0 (0.33.2) | .99 |
| Any treatment with PPI or H2RA prior to hemorrhage (total) | 39 (53.4%) | 33 (45.2%) | 1.4 (0.72.7) | .32 | 1.5 (0.73.0) | .28 |
| Taken prior to admission | 26 (35.6%) | 18 (24.7%) | 1.7 (0.83.5) | .15 | 1.7 (0.83.7) | .18 |
| Started de novo at admission (among the 102 patients not taking prior to admission) | 13 (27.7%) | 15 (27.3%) | 1.0 (0.42.4) | .97 | 1.1 (0.42.9) | .80 |
Among patients on warfarin, the peak international normalized ratio (median [IQR]) was 3.0 (1.25.0) for cases and 1.9 (1.64.8) for controls (P = .52). For those on heparin (23 cases and 6 controls), the median peak activated partial thromboplastin time (aPTT) was 67 (5082) and 128 (67180) seconds for cases and controls, respectively (P = .03), a surprising finding that was likely a result of type III error and small sample size.
Outcomes
We found no evidence of major complications from bleeding, as shown in Table 2. As expected, cases were more likely to receive blood transfusions than were controls, but clinically serious outcomes were uncommon in both groups.
| Characteristic | Cases n = 73 | Controls n = 73 | P value |
|---|---|---|---|
| |||
| Pulmonary complicationsa | 4 ( 5.5%) | 2 (2.7%) | .68 |
| Cardiac complicationsb | 4 ( 5.5%) | 3 (4.1%) | >.99 |
| Acute renal failure requiring dialysis | 0 ( 0.0%) | 1 (1.4%) | >.99 |
| Stroke or transient cerebral ischemia | 1 ( 1.4%) | 1 (1.4%) | >.99 |
| Transfer to intensive care unit | 9 (12.3%) | 4 (5.5%) | .14 |
| Blood transfusion required | 46 (63.0%) | 3 (4.1%) | <.0001 |
| All‐cause mortality | 3 ( 4.1%) | 2 (2.7%) | >.99 |
Gastrointestinal Symptoms and Endoscopic Findings
Bleeding symptoms prompting EGD and associated endoscopic findings are shown in Table 3. Findings on colonoscopy (performed in 34 patients) are included. Overall, 54 (74%) patients had a detected abnormality on EGD and/or colonoscopy that was believed to be a likely source of bleeding by the endoscopist, and 19 (26%) had no apparent culprit lesions. Melena and stool positivity for occult blood were the most common manifestations of gastrointestinal bleeding (77%) and also accounted for all the normal endoscopic evaluations. Of the 21 ulcers, 18 (85.7%) had a clean base, 1 (4.8%) had a red spot, and 2 (9.5%) had an adherent clot. None had a bleeding vessel. Endoscopic treatment was performed in one patient and angiography in one patient. A possible gastric stromal tumor (not the source of bleeding) was seen in one patient, but no mucosal malignant lesions were identified. Of the 73 cases, 41 (56.2% of cases and 0.2% of the total cohort of 17,707 patients) had culprit lesions that might have been preventable with gastric acid suppression (including peptic ulcers, esophagitis, and duodenitis).
| Most likely primary source of bleeding based on EGD with or without colonoscopya | Hematemesis only n = 10 (13.7% of cases) | Melena or hematochezia n = 33 (45.2% of cases) | Hematemesis plus either melena or hematochezia n = 4 (5.5% of cases) | Occult blood (+) and/or drop in hemoglobin (without overt bleeding) n = 26 (35.6% of cases) |
|---|---|---|---|---|
| ||||
| Normal (no lesions identified n = 19 (26.0% of cases) | 0 | 12 | 0 | 7 |
| Peptic ulcer n = 21 (28.8% of cases) | 4 | 10 | 0 | 7 |
| Esophagitis n = 8 (11.0% of cases) | 2 | 2 | 2 | 2 |
| Gastritis or duodenitis n = 12 (16.4% of cases) | 1 | 6 | 1 | 4 |
| Lower GI source only n = 1 (1.4% of cases) | 0 | 0 | 0 | 1 |
| Miscellaneous upper GI sourceb n = 12 (16.4% of cases) | 3 | 3 | 1 | 5 |
Prophylactic Gastric Acid Suppression
One hundred and two patients were not taking any acid‐suppressive prophylaxis on admission to the hospital. Of these patients, on admission 28 (27.5%) were prescribed either histamine‐2 receptor antagonists or proton pump inhibitors. We identified no clinical features associated with the prescriptions for these medications (Table 4), suggesting that physician preference, rather than perceived risk factors for bleeding, determined which patients received prophylactic acid blockade. There was no association between this prophylaxis and GI bleeding, but because of the small size of our sample, the confidence interval was wide (OR = 1.0; 95% CI 0.42.4; P = .97). In the analysis of the subgroup of patients receiving anticoagulation or clopidogrel, prophylaxis showed a nonsignificant trend toward benefit (OR = 0.71; 95% CI 0.23.9; P = .67). There was no significant interaction between the presence of anticoagulation or clopidogrel and prophylaxis (P = .61). Similarly, when we excluded those without prior GI bleeding from analysis, there was still no apparent protective effect of acid‐suppressive prophylaxis (OR = 1.0; 95% CI 0.42.5; P = .97). Finally, there was no significant association between the use of prophylaxis and lesions (theoretically) preventable by acid blockade (OR = 0.9; 95% CI 0.32.3; P = .84).
| Characteristic | Prophylaxis | |||
|---|---|---|---|---|
| Initiated n = 28 (27.5%) | Withheld n = 74 (72.5%) | Odds ratio (95% CI) | P value | |
| ||||
| Cases | ||||
| All lesions | 13 (46.4%) | 34 (46.0%) | 1.0 (0.42.4) | .97 |
| Lesions preventable with acid blockadeb | 8 (28.6%) | 20 (27.0%) | 1.1 (0.42.8) | .88 |
| Demographics | ||||
| Age, in years (SD) | 70.3 (18.6) | 66.9 (15.7) | 1.2 (0.81.9) | .40 |
| Female | 10 (35.7%) | 36 (48.7%) | 0.6 (0.21.4) | .24 |
| Medical history | ||||
| Prior gastrointestinal bleeding | 4 (14.3%) | 7 ( 9.5%) | 1.6 (0.45.8) | .49 |
| History of GERD | 1 ( 3.6%) | 4 ( 5.4%) | 0.6 (0.04.6) | >.99 |
| History of peptic ulcer disease | 3 (10.7%) | 5 ( 6.8%) | 1.7 (0.37.3) | .68 |
| Hospitalization variables | ||||
| Transferred from ICU | 2 ( 7.1%) | 4 ( 5.4%) | 1.3 (0.27.3) | .67 |
| Cardiovascular admission diagnosis | 7 (25.0%) | 21 (28.4%) | 0.8 (0.32.2) | .73 |
| Medication exposure | ||||
| Aspirin (with or without NSAID) | 13 (46.4%) | 30 (40.5%) | 1.3 (0.53.1) | .59 |
| NSAID alone (nonselective) | 2 ( 7.1%) | 4 ( 5.4%) | 1.3 (0.27.3) | .67 |
| Glucocorticoids | 6 (21.4%) | 19 (25.7%) | 0.8 (0.32.2) | .65 |
| Warfarin, clopidogrel, or IV heparin | 9 (32.1%) | 28 (37.8%) | 0.8 (0.31.9) | .59 |
DISCUSSION
Our data suggest that the incidence of hospital‐acquired gastrointestinal bleeding in noncritically ill medical patients is low (approximately 0.4%) and that treatment with anticoagulants or clopidogrel predisposes to this complication. Anticoagulation is a well‐known risk factor for gastrointestinal bleeding, with an estimated odds ratio of 2416; our study confirmed this risk.
Although some studies have questioned the utility of prophylactic acid blockade in the intensive care unit,15 the weight of current evidence supports prophylaxis in selected critically ill patients. In a randomized double‐blind study of 1200 mechanically ventilated patients, the relative risk of gastrointestinal bleeding in patients treated with ranitidine was 0.44 (95% CI 0.210.92 P = .02).11 Many experts discourage indiscriminant use of prophylaxes, even by patients in intensive care units, recommending that it be used only in patients with established risk factors for bleeding.1, 12
Despite the absence of evidence of any benefit of the use of prophylactic acid blockade outside the intensive care unit, this practice is common. In our study, 27.5% of patients who were not on outpatient acid suppression medications (PPIs or H2 antagonists) were started on them on admission to the hospital, presumably as prophylaxes, as we excluded patients admitted for acute gastrointestinal complaints. Other studies have reported prophylaxis rates of 30%50%.13, 14 Many patients started on this prophylaxis during hospitalization go on to take these drugs following discharge, creating an unnecessary economic burden.13, 14 In our study, GI prophylaxis did not appear to prevent hospital‐acquired gastrointestinal bleeding. However, the odds ratio associating the use of prophylactic acid suppression with gastrointestinal bleeding (1.0) was associated with a wide 95% confidence interval (0.42.4), so we cannot exclude the possibility that these medications might provide a relative risk reduction that we were unable to detect. Finally, although gastrointestinal bleeding in the intensive care unit is associated with significant morbidity and mortality,8, 9 we found no evidence to suggest that gastrointestinal bleeding in our patients was associated with poor outcomes.
In interpreting the data from this study, it is important to note that the definition of hospital‐acquired gastrointestinal bleeding in the literature has been inconsistent. Some studies have required that bleeding be hemodynamically significant1, 2, 5, 11a stringent criterion that may be present in only 10%15% of patients with bleeding16whereas other studies defined gastrointestinal bleeding on the basis of occult‐blood‐positive nasogastric aspirates or positive endoscopic findings.7, 15 Because the definition used in the present study required a hard clinical event (EGD), it excluded bleeding events that were considered clinically insignificant by treating physicians. We justified this definition on our belief that any bleeding that warrants invasive evaluation is clinically relevant because it is expensive and puts the patient at some physical risk. Even though some of our patients were diagnosed with GIB without obvious melena or hematemesis (ie, based on stool positivity for occult blood), many of these patients had significant drops in hemoglobin during hospitalization, which, accompanied by occult blood positivity, justified inpatient EGD. We do not believe our definition of GI bleeding was too restrictive, at least for our institution, as physicians at the Cleveland Clinic generally pursue inpatient EGD with clinically apparent gastrointestinal bleeding; we maintain that bleeding that is minor enough not to change management is of limited clinical relevance. Nevertheless, the threshold for EGD at a given institution could affect the rate of EGD for soft indications and the overall prevalence of nosocomial GI bleeding based on our definition.
It also is worth noting that our definition of nosocomial bleeding encompassed some patients with recent hospitalization on the medical service who bled following discharge (15% of cases in this study). This inclusion criterion was chosen because of our concern that the stress of hospitalization might lead to complications even after discharge. We chose an arbitrary postdischarge cutoff of 4 weeks. When we excluded these patients from analysis, the results were similar (data not shown). Although it is possible that we missed some patient who presented to other institutions with GI bleeding following discharge from the Cleveland Clinic, we suspect that the number of such patients was very small based on current referral patterns.
We do not have complete information to determine exactly why patients were on acid‐suppressive therapy prior to admission, but the available data suggest that many had gastroesophageal reflux disease (GERD), PUD, or prior GI bleeding. For this reason, we focused the investigation of the potential efficacy of prophylactic initiation of acid blockade among patients who at presentation were not taking these medications, as prior GERD (or undocumented GIB) leading to chronic use of acid blockade may predispose to subsequent GIB. Although we analyzed only those patients who had newly started taking acid‐suppressive medications, we acknowledge that a few of them may have been started on these medications for other reasons, like chest pain or GERD. However, the evidence suggests that an overwhelming number are started on these medications for the sole purpose of GI prophylaxis.13, 14
Our study was limited by its retrospective casecontrol design. However, because of the low prevalence of hospital‐acquired gastrointestinal bleeding outside the critical care unit, a prospective study would have to enroll thousands of patients in order to generate statistically meaningful results.
In summary, hospital‐acquired gastrointestinal bleeding outside the intensive care unit is uncommon, with an incidence of about 0.4% according to our definition of bleeding. We found no evidence that these bleeding episodes are associated with increased mortality or with occult malignancy. Furthermore, we found no evidence that prophylactic gastric acid suppression prevents these events, and only 41 patients (0.2% of the total cohort) had lesions that might be preventable with gastric acid blockade. We discourage the indiscriminant use of prophylactic acid suppressants in general medical patients.
Acknowledgements
The authors thank Donna M. Richey and Betty Lou Harrison for clerical support.
- ,,, et al.Risk factors for gastrointestinal bleeding in critically ill patients. Canadian Critical Care Trials Group.N Engl J Med.1994;330:377–381.
- ,,, et al.Risk factors for clinically important upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group.Crit Care Med.1999;27:2812–2817.
- ,,,,.Prospective evaluation of the risk of upper gastrointestinal bleeding after admission to a medical intensive care unit.Am J Med.1984;76:623–630.
- ,,, et al.Risk factors for hospitalized gastrointestinal bleeding among older persons. Cardiovascular Health Study Investigators.J Am Geriatr Soc.2001;49:126–133.
- ,.Gastrointestinal bleeding in the hospitalized patient: a case–control study to assess risk factors, causes, and outcome.Am J Med.1998;104:349–354.
- ,,.Characterization of gastrointestinal bleeding in severely ill hospitalized patients.Crit Care Med.2000;28:46–50.
- ,,,,.Clinically significant gastrointestinal bleeding in critically ill patients in an era of prophylaxis.Am J Gastroenterol.2000;95:2801–2806.
- ,,, et al.The attributable mortality and length of intensive care unit stay of clinically important gastrointestinal bleeding in critically ill patients.Crit Care.2001;5:368–375.
- ,,,.Risks for developing critical illness with GI hemorrhage.Chest.2000;118:473–478.
- .Stress ulcer prophylaxis: gastrointestinal bleeding and nosocomial pneumonia. Best evidence synthesis.Scand J GastroenterolSuppl.1995;210:48–52.
- ,,, et al.A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group.N Engl J Med.1998;338:791–797.
- ,.Stress ulcer: is routine prophylaxis necessary?Am J Gastroenterol.1995;90:708–712.
- ,,, et al.Hospital use of acid‐suppressive medications and its fall‐out on prescribing in general practice: a 1‐month survey.Aliment Pharmacol Ther.2003;17:1503–1506.
- ,,.Overuse of acid‐suppressive therapy in hospitalized patients.Am J Gastroenterol.2000;95:3118–122.
- ,,, et al.Prophylaxis for stress‐related gastric hemorrhage in the medical intensive care unit. A randomized, controlled, single‐blind study.Ann Intern Med.1994;121:568–575.
- .Low incidence of hemodynamic instability in patients with gastrointestinal hemorrhage.South Med J.1996;89:386–390.
Gastrointestinal bleeding occurring in hospitalized patients admitted for nongastrointestinal disorders has been extensively studied in intensive care unit patients. However, a systematic study in noncritically ill medical patients has not yet been done. In critically ill patients the incidence of hospital‐acquired gastrointestinal bleeding (GIB) varies from 0.17% to 5%, depending on its definition.16 These bleeding events significantly increase the morbidity and duration of hospitalization.1, 5, 79
Risk factors for bleeding in the intensive care unit include mechanical ventilation, coagulopathy, burns, chronic renal failure, and neurological insults.15 Several studies have found that stress ulcer prophylaxis with histamine‐2 (H2) receptor antagonists, sucralfate, or proton pump inhibitors (PPIs) decreases bleeding in this group of patients, with a relative risk reduction of 29%61%.10, 11 However, use of these drugs outside this high‐risk group has been questioned because of the low overall risk of bleeding.1, 11, 12 Despite their being an unproven benefit in the noncritically ill population, prophylactic H2 antagonists or PPIs are prescribed in an indiscriminant fashion to up to 30%50% of patients admitted to the hospital,13, 14 suggesting that physician preference dictates this practice. To shed light on this issue in noncritically ill patients, we conducted a retrospective casecontrol study in order to identify risk factors that predict hospital‐acquired gastrointestinal bleeding in this group of patients and to assess whether treatment with prophylactic acid suppression was associated with fewer bleeding events. We also sought to characterize the endoscopic lesions in these patients.
MATERIALS AND METHODS
Study Patients
The institutional review board of the Cleveland Clinic Foundation (Cleveland, OH) approved this study. All patients admitted to the General Internal Medicine service between January 1, 1999, and December 31, 2002, were eligible for inclusion. Two types of cases were included: 1) patients admitted for nongastrointestinal illnesses who developed bleeding at least 24 hours after admission and required esophagogastroduodenoscopy (EGD) during hospitalization (designated in‐hospital bleeding), and 2) patients admitted with gastrointestinal bleeding (requiring EGD) who had been hospitalized on the General Medical service during the preceding 4 weeks for a nongastrointestinal illness (designated out‐of‐hospital bleeding). This second group was included to identify risk factors for delayed bleeding that might not be obvious during hospitalization.
Medical records of all General Medicine patients who underwent EGD were reviewed in a standardized fashion (Fig. 1). We excluded patients with documented gastrointestinal complaints (including bleeding) at the time of the index admission or within 24 hours of admission, bleeding in the intensive care unit (ICU) or in another hospital prior to transfer to the General Medicine service, or a history of gastrointestinal bleeding during the month prior to admission. ICU stay prior to General Medicine admission, if not associated with GI bleeding, was not an exclusion criterion for our study.
Controls, also without any acute gastrointestinal symptoms at admission, were randomly matched to cases in a 1:1 ratio by date of admission. We used this liberal matching strategy because any factors matched for would no longer be eligible to be risk factors for bleeding. If more than one control was admitted on the same day as a case, then a random number was used to select the control.
Definition of Prophylactic Acid Suppression
We defined prophylactic acid suppression as in‐hospital de novo treatment with histamine‐2 receptor antagonists and/or proton pump inhibitors received prior to the onset of any symptoms that would suggest GI bleeding (for cases) or any time during hospitalization (for controls). Patients taking these drugs prior to admission were deemed ineligible for in‐hospital prophylactic acid blockade and were excluded from the related analyses.
Data Collection
We extracted demographic information, medical history, medication usage, and laboratory data by chart review. For those patients readmitted for gastrointestinal bleeding following discharge, data from the initial (nongastrointestinal illnessassociated) hospitalization were recorded. Bleeding symptoms triggering endoscopy were grouped into four categories: 1) melena or hematochezia; 2) hematemesis (frank blood in vomitus or coffee‐grounds emesis); 3) melena or hematochezia plus hematemesis (both 1 and 2); 4) stool positivity for occult blood or unexplained drop in hemoglobin in the absence of overt bleeding. Endoscopic findings were categorized by the nature of the visualized lesions, and if multiple lesions were noted, the endoscopist's impression of the most likely bleeding site was used to define the source of bleeding. We recorded colonoscopy findings for patients undergoing this evaluation.
Statistical Analysis
We analyzed data utilizing JMP 5.1 (SAS Institute, Cary, NC). Random controls were chosen using computer‐generated random numbers. The proportions of patients with various categorical characteristics were compared using the chi‐square test or Fisher's exact test as appropriate. We used the Student t test or Wilcoxon's test to compare continuous variables. Odds ratios and adjusted odds ratios were calculated by logistic regression. Two‐tailed P values less than .05 were considered statistically significant.
RESULTS: Identification of Cases and Controls
Of 17,707 patients admitted to the General Medicine service, 1327 (7.5%) underwent EGD during hospitalization or within 1 month of discharge. Only 73 (0.41%) of the total number of patients met the case definition (Fig. 1). Of these cases, 62 (84.9%) had developed gastrointestinal bleeding during the index hospitalization, whereas 11 (15.1%) were readmitted for bleeding within 4 weeks of hospital discharge. The remaining 1254 patients who underwent EGD were excluded based on exclusion criteria, including an absence of documented bleeding prompting the EGD.
Clinical Risk Factors for Bleeding
In univariate analysis, as shown in Table 1, predictors of GIB included: 1) age (P = .02); 2) admission diagnosis (P = .01); 3) preexisting coronary artery disease (P = .004); 4) treatment with blood‐thinning medications, including warfarin (P = .0004), intravenous heparin (P = .0003), and clopidogrel (P = .02); and 5) treatment with PPIs (P = .02). After adjusting for the use of full‐dose anticoagulation and/or clopidogrel, the only of these risk factors that remained significantly associated with GIB was treatment with PPIs prior to hospitalization (adjusted OR = 2.1; 95% CI 1.17.0; P = .04), suggesting that PPI treatment in the outpatient setting may be a marker for GI vulnerability.
| Characteristic | Cases n = 73 | Controls n = 73 | Unadjusted | Adjusted for treatment with full‐dose anticoagulants or clopidogrel | ||
|---|---|---|---|---|---|---|
| Odds ratio (95% CI) | P value (2‐tailed) | Odds ratio (95% CI) | P value (2‐tailed) | |||
| ||||||
| Demographics | ||||||
| Women | 36 (49.3%) | 29 (39.7%) | 1.5 (0.82.9) | .24 | 1.6 (0.83.3) | .19 |
| Age (years), mean (SD) | 71.6 (13.7) | 65.7 (17.2) | 1.5 (1.12.1)c | .02 | 1.3 (0.91.8) | .19 |
| Caucasian | 42 (58.3%) | 32 (44.4%) | 1.7 (0.93.4) | .09 | 1.3 (0.62.6) | .50 |
| Nursing home residents | 5 (6.9%) | 5 (6.9%) | 1.0 (0.33.7) | >.99 | 0.5 (0.12.2) | .35 |
| Admission diagnosisa | .01d | .30d | ||||
| Cardiovascular (non‐thrombotic) | 15 (20.5%) | 6 (8.2%) | 2.9 (1.18.5) | .04 | 2.1 (0.76.5) | .19 |
| Arterial or venous thrombosis | 13 (17.8%) | 2 (2.7%) | 7.9 (2.050.4) | .009 | 3.3 (0.822.1) | .15 |
| Infection | 21 (28.8%) | 24 (32.9%) | 0.8 (0.41.7) | .59 | 1.1 (0.52.3) | .86 |
| Pulmonary (noninfectious) | 4 (5.5%) | 10 (13.7%) | 0.4 (0.11.2) | .10 | 0.5 (0.11.7) | .31 |
| Altered level of consciousness | 7 (9.6%) | 10 (13.7%) | 0.7 (0.21.8) | .44 | 0.7 (0.22.2) | .59 |
| Other | 13 (17.8%) | 21 (28.8%) | 0.5 (0.21.2) | .12 | 0.6 (0.31.5) | .29 |
| Baseline medical conditions | ||||||
| Diabetes mellitus | 28 (38.4%) | 25 (34.3%) | 1.2 (0.62.4) | .61 | 1.3 (0.62.7) | .48 |
| Hypertension | 50 (68.5%) | 48 (65.8%) | 1.1 (0.62.3) | .72 | 1.2 (0.52.5) | .71 |
| Coronary artery disease | 36 (49.3%) | 19 (26.0%) | 2.8 (1.45.6) | .004 | 2.0 (1.04.3) | .06 |
| Atrial fibrillation | 18 (24.7%) | 10 (13.7%) | 2.1 (0.95.0) | .09 | 1.4 (0.53.6) | .49 |
| Congestive heart failure | 25 (34.3%) | 16 (21.9%) | 1.9 (0.93.9) | .10 | 1.5 (0.73.3) | .35 |
| Renal insufficiency (creatinine > 2) | 18 (24.7%) | 11 (15.1%) | 1.8 (0.84.4) | .14 | 1.9 (0.84.7) | .33 |
| Chronic obstructive pulmonary disease | 21 (28.8%) | 20 (27.4%) | 1.1 (0.52.2) | .85 | 1.5 (0.73.4) | .29 |
| Stroke | 13 (17.8%) | 16 (21.9%) | 0.8 (0.31.7) | .53 | 0.7 (0.31.6) | .39 |
| Active malignancy | 6 (8.2%) | 8 (11.0%) | 0.7 (0.32.2) | .57 | 1.0 (0.33.5) | .80 |
| Gastroesophageal reflux (GERD) | 10 (13.7%) | 10 (13.7%) | 1.0 (0.42.6) | >.99 | 1.0 (0.32.7) | .92 |
| Liver disease | 7 (9.6%) | 6 (8.2%) | 1.2 (0.43.9) | .77 | 1.4 (0.44.9) | .59 |
| Peptic ulcer disease | 13 (17.8%) | 5 (6.9%) | 2.9 (1.09.6) | .04 | 2.7 (0.99.4) | .09 |
| Colonic disease (diverticulosis, polyp, or AVM) | 7 (9.6%) | 4 (5.5%) | 1.8 (0.57.3) | .34 | 1.2 (0.35.2) | .79 |
| Prior gastrointestinal hemorrhage | 15 (20.1%) | 7 (9.6%) | 2.4 (1.06.8) | .06 | 2.0 (0.75.8) | .20 |
| Tobacco abuse (current smoking) | 9 (12.3%) | 18 (24.7%) | 0.4 (0.21.0) | .05 | 0.6 (0.21.5) | .26 |
| Heavy drinking (>8 drinks/day) | 2 (2.7%) | 2 (2.7%) | 1.0 (0.18.5) | >.99 | 1.3 (0.111.7) | .83 |
| Medication exposure prior to bleeding (excluding acid blockade)b | ||||||
| Aspirin (with or without NSAID) | 34 (46.6%) | 32 (43.8%) | 1.1 (0.62.1) | .74 | 0.7 (0.31.5) | .42 |
| Nonselective NSAID (without aspirin) | 3 (4.1%) | 5 (6.9%) | 0.6 (0.12.5) | .72 | 0.6 (0.12.6) | .44 |
| COX‐2 inhibitors | 3 (4.1%) | 7 (9.6%) | 0.4 (0.11.5) | .18 | 0.3 (0.11.4) | .15 |
| Glucocorticoids | 17 (23.3%) | 20 (27.4%) | 0.8 (0.41.7) | .57 | 0.9 (0.42.1) | .89 |
| Warfarin | 24 (32.9%) | 7 (9.6%) | 4.6 (1.912.4) | .004 | N/A | N/A |
| Unfractionated heparin, UFH (full‐dose intravenous | 23 (31.5%) | 6 (20.7%) | 5.1 (2.114.8) | .0003 | N/A | N/A |
| Full‐dose low‐molecular‐weight heparin (LMWH) | 2 (2.7%) | 0 (0%) | infinity | .50 | N/A | N/A |
| Clopidogrel | 9 (12.3%) | 2 (2.7%) | 5.0 (1.233.5) | .02 | N/A | N/A |
| Prophylactic LMWH or UFH (among 103 patients not on full‐dose anticoagulants) | 19 (47.5%) | 32 (50.8%) | 0.9 (0.41.9) | .74 | N/A | N/A |
| Any treatment with warfarin, full‐dose UFH, full‐ dose LMWH, and/or clopidogrel | 41 (56.2%) | 14 (19.2%) | 5.4 (2.611.7) | <.0001 | N/A | N/A |
| Gastric acid suppression (prior to any gastrointestinal hemorrhage) | ||||||
| H2‐receptor antagonists (H2RA) (total) | 11 (15.1%) | 19 (26.0%) | 0.5 (0.21.1) | .10 | 0.6 (0.31.5) | .31 |
| Taken prior to admission | 6 (8.2%) | 9 (12.3%) | 0.6 (0.21.9) | .41 | 0.6 (0.22.1) | .47 |
| Started de novo at admission | 5 (6.9%) | 10 (13.7%) | 0.5 (0.11.4) | .17 | 0.7 (0.22.2) | .53 |
| Proton‐pump inhibitor (PPI) (total) | 28 (38.6%) | 16 (21.9%) | 2.2 (1.14.7) | .03 | 2.1 (1.04.6) | .07 |
| Taken prior to admission | 20 (27.4%) | 9 (12.3%) | 2.2 (1.14.7) | .02 | 2.7 (1.17.0) | .04 |
| Started de novo at admission | 8 (11.0%) | 7 (9.6%) | 1.2 (0.43.5) | .79 | 1.0 (0.33.2) | .99 |
| Any treatment with PPI or H2RA prior to hemorrhage (total) | 39 (53.4%) | 33 (45.2%) | 1.4 (0.72.7) | .32 | 1.5 (0.73.0) | .28 |
| Taken prior to admission | 26 (35.6%) | 18 (24.7%) | 1.7 (0.83.5) | .15 | 1.7 (0.83.7) | .18 |
| Started de novo at admission (among the 102 patients not taking prior to admission) | 13 (27.7%) | 15 (27.3%) | 1.0 (0.42.4) | .97 | 1.1 (0.42.9) | .80 |
Among patients on warfarin, the peak international normalized ratio (median [IQR]) was 3.0 (1.25.0) for cases and 1.9 (1.64.8) for controls (P = .52). For those on heparin (23 cases and 6 controls), the median peak activated partial thromboplastin time (aPTT) was 67 (5082) and 128 (67180) seconds for cases and controls, respectively (P = .03), a surprising finding that was likely a result of type III error and small sample size.
Outcomes
We found no evidence of major complications from bleeding, as shown in Table 2. As expected, cases were more likely to receive blood transfusions than were controls, but clinically serious outcomes were uncommon in both groups.
| Characteristic | Cases n = 73 | Controls n = 73 | P value |
|---|---|---|---|
| |||
| Pulmonary complicationsa | 4 ( 5.5%) | 2 (2.7%) | .68 |
| Cardiac complicationsb | 4 ( 5.5%) | 3 (4.1%) | >.99 |
| Acute renal failure requiring dialysis | 0 ( 0.0%) | 1 (1.4%) | >.99 |
| Stroke or transient cerebral ischemia | 1 ( 1.4%) | 1 (1.4%) | >.99 |
| Transfer to intensive care unit | 9 (12.3%) | 4 (5.5%) | .14 |
| Blood transfusion required | 46 (63.0%) | 3 (4.1%) | <.0001 |
| All‐cause mortality | 3 ( 4.1%) | 2 (2.7%) | >.99 |
Gastrointestinal Symptoms and Endoscopic Findings
Bleeding symptoms prompting EGD and associated endoscopic findings are shown in Table 3. Findings on colonoscopy (performed in 34 patients) are included. Overall, 54 (74%) patients had a detected abnormality on EGD and/or colonoscopy that was believed to be a likely source of bleeding by the endoscopist, and 19 (26%) had no apparent culprit lesions. Melena and stool positivity for occult blood were the most common manifestations of gastrointestinal bleeding (77%) and also accounted for all the normal endoscopic evaluations. Of the 21 ulcers, 18 (85.7%) had a clean base, 1 (4.8%) had a red spot, and 2 (9.5%) had an adherent clot. None had a bleeding vessel. Endoscopic treatment was performed in one patient and angiography in one patient. A possible gastric stromal tumor (not the source of bleeding) was seen in one patient, but no mucosal malignant lesions were identified. Of the 73 cases, 41 (56.2% of cases and 0.2% of the total cohort of 17,707 patients) had culprit lesions that might have been preventable with gastric acid suppression (including peptic ulcers, esophagitis, and duodenitis).
| Most likely primary source of bleeding based on EGD with or without colonoscopya | Hematemesis only n = 10 (13.7% of cases) | Melena or hematochezia n = 33 (45.2% of cases) | Hematemesis plus either melena or hematochezia n = 4 (5.5% of cases) | Occult blood (+) and/or drop in hemoglobin (without overt bleeding) n = 26 (35.6% of cases) |
|---|---|---|---|---|
| ||||
| Normal (no lesions identified n = 19 (26.0% of cases) | 0 | 12 | 0 | 7 |
| Peptic ulcer n = 21 (28.8% of cases) | 4 | 10 | 0 | 7 |
| Esophagitis n = 8 (11.0% of cases) | 2 | 2 | 2 | 2 |
| Gastritis or duodenitis n = 12 (16.4% of cases) | 1 | 6 | 1 | 4 |
| Lower GI source only n = 1 (1.4% of cases) | 0 | 0 | 0 | 1 |
| Miscellaneous upper GI sourceb n = 12 (16.4% of cases) | 3 | 3 | 1 | 5 |
Prophylactic Gastric Acid Suppression
One hundred and two patients were not taking any acid‐suppressive prophylaxis on admission to the hospital. Of these patients, on admission 28 (27.5%) were prescribed either histamine‐2 receptor antagonists or proton pump inhibitors. We identified no clinical features associated with the prescriptions for these medications (Table 4), suggesting that physician preference, rather than perceived risk factors for bleeding, determined which patients received prophylactic acid blockade. There was no association between this prophylaxis and GI bleeding, but because of the small size of our sample, the confidence interval was wide (OR = 1.0; 95% CI 0.42.4; P = .97). In the analysis of the subgroup of patients receiving anticoagulation or clopidogrel, prophylaxis showed a nonsignificant trend toward benefit (OR = 0.71; 95% CI 0.23.9; P = .67). There was no significant interaction between the presence of anticoagulation or clopidogrel and prophylaxis (P = .61). Similarly, when we excluded those without prior GI bleeding from analysis, there was still no apparent protective effect of acid‐suppressive prophylaxis (OR = 1.0; 95% CI 0.42.5; P = .97). Finally, there was no significant association between the use of prophylaxis and lesions (theoretically) preventable by acid blockade (OR = 0.9; 95% CI 0.32.3; P = .84).
| Characteristic | Prophylaxis | |||
|---|---|---|---|---|
| Initiated n = 28 (27.5%) | Withheld n = 74 (72.5%) | Odds ratio (95% CI) | P value | |
| ||||
| Cases | ||||
| All lesions | 13 (46.4%) | 34 (46.0%) | 1.0 (0.42.4) | .97 |
| Lesions preventable with acid blockadeb | 8 (28.6%) | 20 (27.0%) | 1.1 (0.42.8) | .88 |
| Demographics | ||||
| Age, in years (SD) | 70.3 (18.6) | 66.9 (15.7) | 1.2 (0.81.9) | .40 |
| Female | 10 (35.7%) | 36 (48.7%) | 0.6 (0.21.4) | .24 |
| Medical history | ||||
| Prior gastrointestinal bleeding | 4 (14.3%) | 7 ( 9.5%) | 1.6 (0.45.8) | .49 |
| History of GERD | 1 ( 3.6%) | 4 ( 5.4%) | 0.6 (0.04.6) | >.99 |
| History of peptic ulcer disease | 3 (10.7%) | 5 ( 6.8%) | 1.7 (0.37.3) | .68 |
| Hospitalization variables | ||||
| Transferred from ICU | 2 ( 7.1%) | 4 ( 5.4%) | 1.3 (0.27.3) | .67 |
| Cardiovascular admission diagnosis | 7 (25.0%) | 21 (28.4%) | 0.8 (0.32.2) | .73 |
| Medication exposure | ||||
| Aspirin (with or without NSAID) | 13 (46.4%) | 30 (40.5%) | 1.3 (0.53.1) | .59 |
| NSAID alone (nonselective) | 2 ( 7.1%) | 4 ( 5.4%) | 1.3 (0.27.3) | .67 |
| Glucocorticoids | 6 (21.4%) | 19 (25.7%) | 0.8 (0.32.2) | .65 |
| Warfarin, clopidogrel, or IV heparin | 9 (32.1%) | 28 (37.8%) | 0.8 (0.31.9) | .59 |
DISCUSSION
Our data suggest that the incidence of hospital‐acquired gastrointestinal bleeding in noncritically ill medical patients is low (approximately 0.4%) and that treatment with anticoagulants or clopidogrel predisposes to this complication. Anticoagulation is a well‐known risk factor for gastrointestinal bleeding, with an estimated odds ratio of 2416; our study confirmed this risk.
Although some studies have questioned the utility of prophylactic acid blockade in the intensive care unit,15 the weight of current evidence supports prophylaxis in selected critically ill patients. In a randomized double‐blind study of 1200 mechanically ventilated patients, the relative risk of gastrointestinal bleeding in patients treated with ranitidine was 0.44 (95% CI 0.210.92 P = .02).11 Many experts discourage indiscriminant use of prophylaxes, even by patients in intensive care units, recommending that it be used only in patients with established risk factors for bleeding.1, 12
Despite the absence of evidence of any benefit of the use of prophylactic acid blockade outside the intensive care unit, this practice is common. In our study, 27.5% of patients who were not on outpatient acid suppression medications (PPIs or H2 antagonists) were started on them on admission to the hospital, presumably as prophylaxes, as we excluded patients admitted for acute gastrointestinal complaints. Other studies have reported prophylaxis rates of 30%50%.13, 14 Many patients started on this prophylaxis during hospitalization go on to take these drugs following discharge, creating an unnecessary economic burden.13, 14 In our study, GI prophylaxis did not appear to prevent hospital‐acquired gastrointestinal bleeding. However, the odds ratio associating the use of prophylactic acid suppression with gastrointestinal bleeding (1.0) was associated with a wide 95% confidence interval (0.42.4), so we cannot exclude the possibility that these medications might provide a relative risk reduction that we were unable to detect. Finally, although gastrointestinal bleeding in the intensive care unit is associated with significant morbidity and mortality,8, 9 we found no evidence to suggest that gastrointestinal bleeding in our patients was associated with poor outcomes.
In interpreting the data from this study, it is important to note that the definition of hospital‐acquired gastrointestinal bleeding in the literature has been inconsistent. Some studies have required that bleeding be hemodynamically significant1, 2, 5, 11a stringent criterion that may be present in only 10%15% of patients with bleeding16whereas other studies defined gastrointestinal bleeding on the basis of occult‐blood‐positive nasogastric aspirates or positive endoscopic findings.7, 15 Because the definition used in the present study required a hard clinical event (EGD), it excluded bleeding events that were considered clinically insignificant by treating physicians. We justified this definition on our belief that any bleeding that warrants invasive evaluation is clinically relevant because it is expensive and puts the patient at some physical risk. Even though some of our patients were diagnosed with GIB without obvious melena or hematemesis (ie, based on stool positivity for occult blood), many of these patients had significant drops in hemoglobin during hospitalization, which, accompanied by occult blood positivity, justified inpatient EGD. We do not believe our definition of GI bleeding was too restrictive, at least for our institution, as physicians at the Cleveland Clinic generally pursue inpatient EGD with clinically apparent gastrointestinal bleeding; we maintain that bleeding that is minor enough not to change management is of limited clinical relevance. Nevertheless, the threshold for EGD at a given institution could affect the rate of EGD for soft indications and the overall prevalence of nosocomial GI bleeding based on our definition.
It also is worth noting that our definition of nosocomial bleeding encompassed some patients with recent hospitalization on the medical service who bled following discharge (15% of cases in this study). This inclusion criterion was chosen because of our concern that the stress of hospitalization might lead to complications even after discharge. We chose an arbitrary postdischarge cutoff of 4 weeks. When we excluded these patients from analysis, the results were similar (data not shown). Although it is possible that we missed some patient who presented to other institutions with GI bleeding following discharge from the Cleveland Clinic, we suspect that the number of such patients was very small based on current referral patterns.
We do not have complete information to determine exactly why patients were on acid‐suppressive therapy prior to admission, but the available data suggest that many had gastroesophageal reflux disease (GERD), PUD, or prior GI bleeding. For this reason, we focused the investigation of the potential efficacy of prophylactic initiation of acid blockade among patients who at presentation were not taking these medications, as prior GERD (or undocumented GIB) leading to chronic use of acid blockade may predispose to subsequent GIB. Although we analyzed only those patients who had newly started taking acid‐suppressive medications, we acknowledge that a few of them may have been started on these medications for other reasons, like chest pain or GERD. However, the evidence suggests that an overwhelming number are started on these medications for the sole purpose of GI prophylaxis.13, 14
Our study was limited by its retrospective casecontrol design. However, because of the low prevalence of hospital‐acquired gastrointestinal bleeding outside the critical care unit, a prospective study would have to enroll thousands of patients in order to generate statistically meaningful results.
In summary, hospital‐acquired gastrointestinal bleeding outside the intensive care unit is uncommon, with an incidence of about 0.4% according to our definition of bleeding. We found no evidence that these bleeding episodes are associated with increased mortality or with occult malignancy. Furthermore, we found no evidence that prophylactic gastric acid suppression prevents these events, and only 41 patients (0.2% of the total cohort) had lesions that might be preventable with gastric acid blockade. We discourage the indiscriminant use of prophylactic acid suppressants in general medical patients.
Acknowledgements
The authors thank Donna M. Richey and Betty Lou Harrison for clerical support.
Gastrointestinal bleeding occurring in hospitalized patients admitted for nongastrointestinal disorders has been extensively studied in intensive care unit patients. However, a systematic study in noncritically ill medical patients has not yet been done. In critically ill patients the incidence of hospital‐acquired gastrointestinal bleeding (GIB) varies from 0.17% to 5%, depending on its definition.16 These bleeding events significantly increase the morbidity and duration of hospitalization.1, 5, 79
Risk factors for bleeding in the intensive care unit include mechanical ventilation, coagulopathy, burns, chronic renal failure, and neurological insults.15 Several studies have found that stress ulcer prophylaxis with histamine‐2 (H2) receptor antagonists, sucralfate, or proton pump inhibitors (PPIs) decreases bleeding in this group of patients, with a relative risk reduction of 29%61%.10, 11 However, use of these drugs outside this high‐risk group has been questioned because of the low overall risk of bleeding.1, 11, 12 Despite their being an unproven benefit in the noncritically ill population, prophylactic H2 antagonists or PPIs are prescribed in an indiscriminant fashion to up to 30%50% of patients admitted to the hospital,13, 14 suggesting that physician preference dictates this practice. To shed light on this issue in noncritically ill patients, we conducted a retrospective casecontrol study in order to identify risk factors that predict hospital‐acquired gastrointestinal bleeding in this group of patients and to assess whether treatment with prophylactic acid suppression was associated with fewer bleeding events. We also sought to characterize the endoscopic lesions in these patients.
MATERIALS AND METHODS
Study Patients
The institutional review board of the Cleveland Clinic Foundation (Cleveland, OH) approved this study. All patients admitted to the General Internal Medicine service between January 1, 1999, and December 31, 2002, were eligible for inclusion. Two types of cases were included: 1) patients admitted for nongastrointestinal illnesses who developed bleeding at least 24 hours after admission and required esophagogastroduodenoscopy (EGD) during hospitalization (designated in‐hospital bleeding), and 2) patients admitted with gastrointestinal bleeding (requiring EGD) who had been hospitalized on the General Medical service during the preceding 4 weeks for a nongastrointestinal illness (designated out‐of‐hospital bleeding). This second group was included to identify risk factors for delayed bleeding that might not be obvious during hospitalization.
Medical records of all General Medicine patients who underwent EGD were reviewed in a standardized fashion (Fig. 1). We excluded patients with documented gastrointestinal complaints (including bleeding) at the time of the index admission or within 24 hours of admission, bleeding in the intensive care unit (ICU) or in another hospital prior to transfer to the General Medicine service, or a history of gastrointestinal bleeding during the month prior to admission. ICU stay prior to General Medicine admission, if not associated with GI bleeding, was not an exclusion criterion for our study.
Controls, also without any acute gastrointestinal symptoms at admission, were randomly matched to cases in a 1:1 ratio by date of admission. We used this liberal matching strategy because any factors matched for would no longer be eligible to be risk factors for bleeding. If more than one control was admitted on the same day as a case, then a random number was used to select the control.
Definition of Prophylactic Acid Suppression
We defined prophylactic acid suppression as in‐hospital de novo treatment with histamine‐2 receptor antagonists and/or proton pump inhibitors received prior to the onset of any symptoms that would suggest GI bleeding (for cases) or any time during hospitalization (for controls). Patients taking these drugs prior to admission were deemed ineligible for in‐hospital prophylactic acid blockade and were excluded from the related analyses.
Data Collection
We extracted demographic information, medical history, medication usage, and laboratory data by chart review. For those patients readmitted for gastrointestinal bleeding following discharge, data from the initial (nongastrointestinal illnessassociated) hospitalization were recorded. Bleeding symptoms triggering endoscopy were grouped into four categories: 1) melena or hematochezia; 2) hematemesis (frank blood in vomitus or coffee‐grounds emesis); 3) melena or hematochezia plus hematemesis (both 1 and 2); 4) stool positivity for occult blood or unexplained drop in hemoglobin in the absence of overt bleeding. Endoscopic findings were categorized by the nature of the visualized lesions, and if multiple lesions were noted, the endoscopist's impression of the most likely bleeding site was used to define the source of bleeding. We recorded colonoscopy findings for patients undergoing this evaluation.
Statistical Analysis
We analyzed data utilizing JMP 5.1 (SAS Institute, Cary, NC). Random controls were chosen using computer‐generated random numbers. The proportions of patients with various categorical characteristics were compared using the chi‐square test or Fisher's exact test as appropriate. We used the Student t test or Wilcoxon's test to compare continuous variables. Odds ratios and adjusted odds ratios were calculated by logistic regression. Two‐tailed P values less than .05 were considered statistically significant.
RESULTS: Identification of Cases and Controls
Of 17,707 patients admitted to the General Medicine service, 1327 (7.5%) underwent EGD during hospitalization or within 1 month of discharge. Only 73 (0.41%) of the total number of patients met the case definition (Fig. 1). Of these cases, 62 (84.9%) had developed gastrointestinal bleeding during the index hospitalization, whereas 11 (15.1%) were readmitted for bleeding within 4 weeks of hospital discharge. The remaining 1254 patients who underwent EGD were excluded based on exclusion criteria, including an absence of documented bleeding prompting the EGD.
Clinical Risk Factors for Bleeding
In univariate analysis, as shown in Table 1, predictors of GIB included: 1) age (P = .02); 2) admission diagnosis (P = .01); 3) preexisting coronary artery disease (P = .004); 4) treatment with blood‐thinning medications, including warfarin (P = .0004), intravenous heparin (P = .0003), and clopidogrel (P = .02); and 5) treatment with PPIs (P = .02). After adjusting for the use of full‐dose anticoagulation and/or clopidogrel, the only of these risk factors that remained significantly associated with GIB was treatment with PPIs prior to hospitalization (adjusted OR = 2.1; 95% CI 1.17.0; P = .04), suggesting that PPI treatment in the outpatient setting may be a marker for GI vulnerability.
| Characteristic | Cases n = 73 | Controls n = 73 | Unadjusted | Adjusted for treatment with full‐dose anticoagulants or clopidogrel | ||
|---|---|---|---|---|---|---|
| Odds ratio (95% CI) | P value (2‐tailed) | Odds ratio (95% CI) | P value (2‐tailed) | |||
| ||||||
| Demographics | ||||||
| Women | 36 (49.3%) | 29 (39.7%) | 1.5 (0.82.9) | .24 | 1.6 (0.83.3) | .19 |
| Age (years), mean (SD) | 71.6 (13.7) | 65.7 (17.2) | 1.5 (1.12.1)c | .02 | 1.3 (0.91.8) | .19 |
| Caucasian | 42 (58.3%) | 32 (44.4%) | 1.7 (0.93.4) | .09 | 1.3 (0.62.6) | .50 |
| Nursing home residents | 5 (6.9%) | 5 (6.9%) | 1.0 (0.33.7) | >.99 | 0.5 (0.12.2) | .35 |
| Admission diagnosisa | .01d | .30d | ||||
| Cardiovascular (non‐thrombotic) | 15 (20.5%) | 6 (8.2%) | 2.9 (1.18.5) | .04 | 2.1 (0.76.5) | .19 |
| Arterial or venous thrombosis | 13 (17.8%) | 2 (2.7%) | 7.9 (2.050.4) | .009 | 3.3 (0.822.1) | .15 |
| Infection | 21 (28.8%) | 24 (32.9%) | 0.8 (0.41.7) | .59 | 1.1 (0.52.3) | .86 |
| Pulmonary (noninfectious) | 4 (5.5%) | 10 (13.7%) | 0.4 (0.11.2) | .10 | 0.5 (0.11.7) | .31 |
| Altered level of consciousness | 7 (9.6%) | 10 (13.7%) | 0.7 (0.21.8) | .44 | 0.7 (0.22.2) | .59 |
| Other | 13 (17.8%) | 21 (28.8%) | 0.5 (0.21.2) | .12 | 0.6 (0.31.5) | .29 |
| Baseline medical conditions | ||||||
| Diabetes mellitus | 28 (38.4%) | 25 (34.3%) | 1.2 (0.62.4) | .61 | 1.3 (0.62.7) | .48 |
| Hypertension | 50 (68.5%) | 48 (65.8%) | 1.1 (0.62.3) | .72 | 1.2 (0.52.5) | .71 |
| Coronary artery disease | 36 (49.3%) | 19 (26.0%) | 2.8 (1.45.6) | .004 | 2.0 (1.04.3) | .06 |
| Atrial fibrillation | 18 (24.7%) | 10 (13.7%) | 2.1 (0.95.0) | .09 | 1.4 (0.53.6) | .49 |
| Congestive heart failure | 25 (34.3%) | 16 (21.9%) | 1.9 (0.93.9) | .10 | 1.5 (0.73.3) | .35 |
| Renal insufficiency (creatinine > 2) | 18 (24.7%) | 11 (15.1%) | 1.8 (0.84.4) | .14 | 1.9 (0.84.7) | .33 |
| Chronic obstructive pulmonary disease | 21 (28.8%) | 20 (27.4%) | 1.1 (0.52.2) | .85 | 1.5 (0.73.4) | .29 |
| Stroke | 13 (17.8%) | 16 (21.9%) | 0.8 (0.31.7) | .53 | 0.7 (0.31.6) | .39 |
| Active malignancy | 6 (8.2%) | 8 (11.0%) | 0.7 (0.32.2) | .57 | 1.0 (0.33.5) | .80 |
| Gastroesophageal reflux (GERD) | 10 (13.7%) | 10 (13.7%) | 1.0 (0.42.6) | >.99 | 1.0 (0.32.7) | .92 |
| Liver disease | 7 (9.6%) | 6 (8.2%) | 1.2 (0.43.9) | .77 | 1.4 (0.44.9) | .59 |
| Peptic ulcer disease | 13 (17.8%) | 5 (6.9%) | 2.9 (1.09.6) | .04 | 2.7 (0.99.4) | .09 |
| Colonic disease (diverticulosis, polyp, or AVM) | 7 (9.6%) | 4 (5.5%) | 1.8 (0.57.3) | .34 | 1.2 (0.35.2) | .79 |
| Prior gastrointestinal hemorrhage | 15 (20.1%) | 7 (9.6%) | 2.4 (1.06.8) | .06 | 2.0 (0.75.8) | .20 |
| Tobacco abuse (current smoking) | 9 (12.3%) | 18 (24.7%) | 0.4 (0.21.0) | .05 | 0.6 (0.21.5) | .26 |
| Heavy drinking (>8 drinks/day) | 2 (2.7%) | 2 (2.7%) | 1.0 (0.18.5) | >.99 | 1.3 (0.111.7) | .83 |
| Medication exposure prior to bleeding (excluding acid blockade)b | ||||||
| Aspirin (with or without NSAID) | 34 (46.6%) | 32 (43.8%) | 1.1 (0.62.1) | .74 | 0.7 (0.31.5) | .42 |
| Nonselective NSAID (without aspirin) | 3 (4.1%) | 5 (6.9%) | 0.6 (0.12.5) | .72 | 0.6 (0.12.6) | .44 |
| COX‐2 inhibitors | 3 (4.1%) | 7 (9.6%) | 0.4 (0.11.5) | .18 | 0.3 (0.11.4) | .15 |
| Glucocorticoids | 17 (23.3%) | 20 (27.4%) | 0.8 (0.41.7) | .57 | 0.9 (0.42.1) | .89 |
| Warfarin | 24 (32.9%) | 7 (9.6%) | 4.6 (1.912.4) | .004 | N/A | N/A |
| Unfractionated heparin, UFH (full‐dose intravenous | 23 (31.5%) | 6 (20.7%) | 5.1 (2.114.8) | .0003 | N/A | N/A |
| Full‐dose low‐molecular‐weight heparin (LMWH) | 2 (2.7%) | 0 (0%) | infinity | .50 | N/A | N/A |
| Clopidogrel | 9 (12.3%) | 2 (2.7%) | 5.0 (1.233.5) | .02 | N/A | N/A |
| Prophylactic LMWH or UFH (among 103 patients not on full‐dose anticoagulants) | 19 (47.5%) | 32 (50.8%) | 0.9 (0.41.9) | .74 | N/A | N/A |
| Any treatment with warfarin, full‐dose UFH, full‐ dose LMWH, and/or clopidogrel | 41 (56.2%) | 14 (19.2%) | 5.4 (2.611.7) | <.0001 | N/A | N/A |
| Gastric acid suppression (prior to any gastrointestinal hemorrhage) | ||||||
| H2‐receptor antagonists (H2RA) (total) | 11 (15.1%) | 19 (26.0%) | 0.5 (0.21.1) | .10 | 0.6 (0.31.5) | .31 |
| Taken prior to admission | 6 (8.2%) | 9 (12.3%) | 0.6 (0.21.9) | .41 | 0.6 (0.22.1) | .47 |
| Started de novo at admission | 5 (6.9%) | 10 (13.7%) | 0.5 (0.11.4) | .17 | 0.7 (0.22.2) | .53 |
| Proton‐pump inhibitor (PPI) (total) | 28 (38.6%) | 16 (21.9%) | 2.2 (1.14.7) | .03 | 2.1 (1.04.6) | .07 |
| Taken prior to admission | 20 (27.4%) | 9 (12.3%) | 2.2 (1.14.7) | .02 | 2.7 (1.17.0) | .04 |
| Started de novo at admission | 8 (11.0%) | 7 (9.6%) | 1.2 (0.43.5) | .79 | 1.0 (0.33.2) | .99 |
| Any treatment with PPI or H2RA prior to hemorrhage (total) | 39 (53.4%) | 33 (45.2%) | 1.4 (0.72.7) | .32 | 1.5 (0.73.0) | .28 |
| Taken prior to admission | 26 (35.6%) | 18 (24.7%) | 1.7 (0.83.5) | .15 | 1.7 (0.83.7) | .18 |
| Started de novo at admission (among the 102 patients not taking prior to admission) | 13 (27.7%) | 15 (27.3%) | 1.0 (0.42.4) | .97 | 1.1 (0.42.9) | .80 |
Among patients on warfarin, the peak international normalized ratio (median [IQR]) was 3.0 (1.25.0) for cases and 1.9 (1.64.8) for controls (P = .52). For those on heparin (23 cases and 6 controls), the median peak activated partial thromboplastin time (aPTT) was 67 (5082) and 128 (67180) seconds for cases and controls, respectively (P = .03), a surprising finding that was likely a result of type III error and small sample size.
Outcomes
We found no evidence of major complications from bleeding, as shown in Table 2. As expected, cases were more likely to receive blood transfusions than were controls, but clinically serious outcomes were uncommon in both groups.
| Characteristic | Cases n = 73 | Controls n = 73 | P value |
|---|---|---|---|
| |||
| Pulmonary complicationsa | 4 ( 5.5%) | 2 (2.7%) | .68 |
| Cardiac complicationsb | 4 ( 5.5%) | 3 (4.1%) | >.99 |
| Acute renal failure requiring dialysis | 0 ( 0.0%) | 1 (1.4%) | >.99 |
| Stroke or transient cerebral ischemia | 1 ( 1.4%) | 1 (1.4%) | >.99 |
| Transfer to intensive care unit | 9 (12.3%) | 4 (5.5%) | .14 |
| Blood transfusion required | 46 (63.0%) | 3 (4.1%) | <.0001 |
| All‐cause mortality | 3 ( 4.1%) | 2 (2.7%) | >.99 |
Gastrointestinal Symptoms and Endoscopic Findings
Bleeding symptoms prompting EGD and associated endoscopic findings are shown in Table 3. Findings on colonoscopy (performed in 34 patients) are included. Overall, 54 (74%) patients had a detected abnormality on EGD and/or colonoscopy that was believed to be a likely source of bleeding by the endoscopist, and 19 (26%) had no apparent culprit lesions. Melena and stool positivity for occult blood were the most common manifestations of gastrointestinal bleeding (77%) and also accounted for all the normal endoscopic evaluations. Of the 21 ulcers, 18 (85.7%) had a clean base, 1 (4.8%) had a red spot, and 2 (9.5%) had an adherent clot. None had a bleeding vessel. Endoscopic treatment was performed in one patient and angiography in one patient. A possible gastric stromal tumor (not the source of bleeding) was seen in one patient, but no mucosal malignant lesions were identified. Of the 73 cases, 41 (56.2% of cases and 0.2% of the total cohort of 17,707 patients) had culprit lesions that might have been preventable with gastric acid suppression (including peptic ulcers, esophagitis, and duodenitis).
| Most likely primary source of bleeding based on EGD with or without colonoscopya | Hematemesis only n = 10 (13.7% of cases) | Melena or hematochezia n = 33 (45.2% of cases) | Hematemesis plus either melena or hematochezia n = 4 (5.5% of cases) | Occult blood (+) and/or drop in hemoglobin (without overt bleeding) n = 26 (35.6% of cases) |
|---|---|---|---|---|
| ||||
| Normal (no lesions identified n = 19 (26.0% of cases) | 0 | 12 | 0 | 7 |
| Peptic ulcer n = 21 (28.8% of cases) | 4 | 10 | 0 | 7 |
| Esophagitis n = 8 (11.0% of cases) | 2 | 2 | 2 | 2 |
| Gastritis or duodenitis n = 12 (16.4% of cases) | 1 | 6 | 1 | 4 |
| Lower GI source only n = 1 (1.4% of cases) | 0 | 0 | 0 | 1 |
| Miscellaneous upper GI sourceb n = 12 (16.4% of cases) | 3 | 3 | 1 | 5 |
Prophylactic Gastric Acid Suppression
One hundred and two patients were not taking any acid‐suppressive prophylaxis on admission to the hospital. Of these patients, on admission 28 (27.5%) were prescribed either histamine‐2 receptor antagonists or proton pump inhibitors. We identified no clinical features associated with the prescriptions for these medications (Table 4), suggesting that physician preference, rather than perceived risk factors for bleeding, determined which patients received prophylactic acid blockade. There was no association between this prophylaxis and GI bleeding, but because of the small size of our sample, the confidence interval was wide (OR = 1.0; 95% CI 0.42.4; P = .97). In the analysis of the subgroup of patients receiving anticoagulation or clopidogrel, prophylaxis showed a nonsignificant trend toward benefit (OR = 0.71; 95% CI 0.23.9; P = .67). There was no significant interaction between the presence of anticoagulation or clopidogrel and prophylaxis (P = .61). Similarly, when we excluded those without prior GI bleeding from analysis, there was still no apparent protective effect of acid‐suppressive prophylaxis (OR = 1.0; 95% CI 0.42.5; P = .97). Finally, there was no significant association between the use of prophylaxis and lesions (theoretically) preventable by acid blockade (OR = 0.9; 95% CI 0.32.3; P = .84).
| Characteristic | Prophylaxis | |||
|---|---|---|---|---|
| Initiated n = 28 (27.5%) | Withheld n = 74 (72.5%) | Odds ratio (95% CI) | P value | |
| ||||
| Cases | ||||
| All lesions | 13 (46.4%) | 34 (46.0%) | 1.0 (0.42.4) | .97 |
| Lesions preventable with acid blockadeb | 8 (28.6%) | 20 (27.0%) | 1.1 (0.42.8) | .88 |
| Demographics | ||||
| Age, in years (SD) | 70.3 (18.6) | 66.9 (15.7) | 1.2 (0.81.9) | .40 |
| Female | 10 (35.7%) | 36 (48.7%) | 0.6 (0.21.4) | .24 |
| Medical history | ||||
| Prior gastrointestinal bleeding | 4 (14.3%) | 7 ( 9.5%) | 1.6 (0.45.8) | .49 |
| History of GERD | 1 ( 3.6%) | 4 ( 5.4%) | 0.6 (0.04.6) | >.99 |
| History of peptic ulcer disease | 3 (10.7%) | 5 ( 6.8%) | 1.7 (0.37.3) | .68 |
| Hospitalization variables | ||||
| Transferred from ICU | 2 ( 7.1%) | 4 ( 5.4%) | 1.3 (0.27.3) | .67 |
| Cardiovascular admission diagnosis | 7 (25.0%) | 21 (28.4%) | 0.8 (0.32.2) | .73 |
| Medication exposure | ||||
| Aspirin (with or without NSAID) | 13 (46.4%) | 30 (40.5%) | 1.3 (0.53.1) | .59 |
| NSAID alone (nonselective) | 2 ( 7.1%) | 4 ( 5.4%) | 1.3 (0.27.3) | .67 |
| Glucocorticoids | 6 (21.4%) | 19 (25.7%) | 0.8 (0.32.2) | .65 |
| Warfarin, clopidogrel, or IV heparin | 9 (32.1%) | 28 (37.8%) | 0.8 (0.31.9) | .59 |
DISCUSSION
Our data suggest that the incidence of hospital‐acquired gastrointestinal bleeding in noncritically ill medical patients is low (approximately 0.4%) and that treatment with anticoagulants or clopidogrel predisposes to this complication. Anticoagulation is a well‐known risk factor for gastrointestinal bleeding, with an estimated odds ratio of 2416; our study confirmed this risk.
Although some studies have questioned the utility of prophylactic acid blockade in the intensive care unit,15 the weight of current evidence supports prophylaxis in selected critically ill patients. In a randomized double‐blind study of 1200 mechanically ventilated patients, the relative risk of gastrointestinal bleeding in patients treated with ranitidine was 0.44 (95% CI 0.210.92 P = .02).11 Many experts discourage indiscriminant use of prophylaxes, even by patients in intensive care units, recommending that it be used only in patients with established risk factors for bleeding.1, 12
Despite the absence of evidence of any benefit of the use of prophylactic acid blockade outside the intensive care unit, this practice is common. In our study, 27.5% of patients who were not on outpatient acid suppression medications (PPIs or H2 antagonists) were started on them on admission to the hospital, presumably as prophylaxes, as we excluded patients admitted for acute gastrointestinal complaints. Other studies have reported prophylaxis rates of 30%50%.13, 14 Many patients started on this prophylaxis during hospitalization go on to take these drugs following discharge, creating an unnecessary economic burden.13, 14 In our study, GI prophylaxis did not appear to prevent hospital‐acquired gastrointestinal bleeding. However, the odds ratio associating the use of prophylactic acid suppression with gastrointestinal bleeding (1.0) was associated with a wide 95% confidence interval (0.42.4), so we cannot exclude the possibility that these medications might provide a relative risk reduction that we were unable to detect. Finally, although gastrointestinal bleeding in the intensive care unit is associated with significant morbidity and mortality,8, 9 we found no evidence to suggest that gastrointestinal bleeding in our patients was associated with poor outcomes.
In interpreting the data from this study, it is important to note that the definition of hospital‐acquired gastrointestinal bleeding in the literature has been inconsistent. Some studies have required that bleeding be hemodynamically significant1, 2, 5, 11a stringent criterion that may be present in only 10%15% of patients with bleeding16whereas other studies defined gastrointestinal bleeding on the basis of occult‐blood‐positive nasogastric aspirates or positive endoscopic findings.7, 15 Because the definition used in the present study required a hard clinical event (EGD), it excluded bleeding events that were considered clinically insignificant by treating physicians. We justified this definition on our belief that any bleeding that warrants invasive evaluation is clinically relevant because it is expensive and puts the patient at some physical risk. Even though some of our patients were diagnosed with GIB without obvious melena or hematemesis (ie, based on stool positivity for occult blood), many of these patients had significant drops in hemoglobin during hospitalization, which, accompanied by occult blood positivity, justified inpatient EGD. We do not believe our definition of GI bleeding was too restrictive, at least for our institution, as physicians at the Cleveland Clinic generally pursue inpatient EGD with clinically apparent gastrointestinal bleeding; we maintain that bleeding that is minor enough not to change management is of limited clinical relevance. Nevertheless, the threshold for EGD at a given institution could affect the rate of EGD for soft indications and the overall prevalence of nosocomial GI bleeding based on our definition.
It also is worth noting that our definition of nosocomial bleeding encompassed some patients with recent hospitalization on the medical service who bled following discharge (15% of cases in this study). This inclusion criterion was chosen because of our concern that the stress of hospitalization might lead to complications even after discharge. We chose an arbitrary postdischarge cutoff of 4 weeks. When we excluded these patients from analysis, the results were similar (data not shown). Although it is possible that we missed some patient who presented to other institutions with GI bleeding following discharge from the Cleveland Clinic, we suspect that the number of such patients was very small based on current referral patterns.
We do not have complete information to determine exactly why patients were on acid‐suppressive therapy prior to admission, but the available data suggest that many had gastroesophageal reflux disease (GERD), PUD, or prior GI bleeding. For this reason, we focused the investigation of the potential efficacy of prophylactic initiation of acid blockade among patients who at presentation were not taking these medications, as prior GERD (or undocumented GIB) leading to chronic use of acid blockade may predispose to subsequent GIB. Although we analyzed only those patients who had newly started taking acid‐suppressive medications, we acknowledge that a few of them may have been started on these medications for other reasons, like chest pain or GERD. However, the evidence suggests that an overwhelming number are started on these medications for the sole purpose of GI prophylaxis.13, 14
Our study was limited by its retrospective casecontrol design. However, because of the low prevalence of hospital‐acquired gastrointestinal bleeding outside the critical care unit, a prospective study would have to enroll thousands of patients in order to generate statistically meaningful results.
In summary, hospital‐acquired gastrointestinal bleeding outside the intensive care unit is uncommon, with an incidence of about 0.4% according to our definition of bleeding. We found no evidence that these bleeding episodes are associated with increased mortality or with occult malignancy. Furthermore, we found no evidence that prophylactic gastric acid suppression prevents these events, and only 41 patients (0.2% of the total cohort) had lesions that might be preventable with gastric acid blockade. We discourage the indiscriminant use of prophylactic acid suppressants in general medical patients.
Acknowledgements
The authors thank Donna M. Richey and Betty Lou Harrison for clerical support.
- ,,, et al.Risk factors for gastrointestinal bleeding in critically ill patients. Canadian Critical Care Trials Group.N Engl J Med.1994;330:377–381.
- ,,, et al.Risk factors for clinically important upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group.Crit Care Med.1999;27:2812–2817.
- ,,,,.Prospective evaluation of the risk of upper gastrointestinal bleeding after admission to a medical intensive care unit.Am J Med.1984;76:623–630.
- ,,, et al.Risk factors for hospitalized gastrointestinal bleeding among older persons. Cardiovascular Health Study Investigators.J Am Geriatr Soc.2001;49:126–133.
- ,.Gastrointestinal bleeding in the hospitalized patient: a case–control study to assess risk factors, causes, and outcome.Am J Med.1998;104:349–354.
- ,,.Characterization of gastrointestinal bleeding in severely ill hospitalized patients.Crit Care Med.2000;28:46–50.
- ,,,,.Clinically significant gastrointestinal bleeding in critically ill patients in an era of prophylaxis.Am J Gastroenterol.2000;95:2801–2806.
- ,,, et al.The attributable mortality and length of intensive care unit stay of clinically important gastrointestinal bleeding in critically ill patients.Crit Care.2001;5:368–375.
- ,,,.Risks for developing critical illness with GI hemorrhage.Chest.2000;118:473–478.
- .Stress ulcer prophylaxis: gastrointestinal bleeding and nosocomial pneumonia. Best evidence synthesis.Scand J GastroenterolSuppl.1995;210:48–52.
- ,,, et al.A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group.N Engl J Med.1998;338:791–797.
- ,.Stress ulcer: is routine prophylaxis necessary?Am J Gastroenterol.1995;90:708–712.
- ,,, et al.Hospital use of acid‐suppressive medications and its fall‐out on prescribing in general practice: a 1‐month survey.Aliment Pharmacol Ther.2003;17:1503–1506.
- ,,.Overuse of acid‐suppressive therapy in hospitalized patients.Am J Gastroenterol.2000;95:3118–122.
- ,,, et al.Prophylaxis for stress‐related gastric hemorrhage in the medical intensive care unit. A randomized, controlled, single‐blind study.Ann Intern Med.1994;121:568–575.
- .Low incidence of hemodynamic instability in patients with gastrointestinal hemorrhage.South Med J.1996;89:386–390.
- ,,, et al.Risk factors for gastrointestinal bleeding in critically ill patients. Canadian Critical Care Trials Group.N Engl J Med.1994;330:377–381.
- ,,, et al.Risk factors for clinically important upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group.Crit Care Med.1999;27:2812–2817.
- ,,,,.Prospective evaluation of the risk of upper gastrointestinal bleeding after admission to a medical intensive care unit.Am J Med.1984;76:623–630.
- ,,, et al.Risk factors for hospitalized gastrointestinal bleeding among older persons. Cardiovascular Health Study Investigators.J Am Geriatr Soc.2001;49:126–133.
- ,.Gastrointestinal bleeding in the hospitalized patient: a case–control study to assess risk factors, causes, and outcome.Am J Med.1998;104:349–354.
- ,,.Characterization of gastrointestinal bleeding in severely ill hospitalized patients.Crit Care Med.2000;28:46–50.
- ,,,,.Clinically significant gastrointestinal bleeding in critically ill patients in an era of prophylaxis.Am J Gastroenterol.2000;95:2801–2806.
- ,,, et al.The attributable mortality and length of intensive care unit stay of clinically important gastrointestinal bleeding in critically ill patients.Crit Care.2001;5:368–375.
- ,,,.Risks for developing critical illness with GI hemorrhage.Chest.2000;118:473–478.
- .Stress ulcer prophylaxis: gastrointestinal bleeding and nosocomial pneumonia. Best evidence synthesis.Scand J GastroenterolSuppl.1995;210:48–52.
- ,,, et al.A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group.N Engl J Med.1998;338:791–797.
- ,.Stress ulcer: is routine prophylaxis necessary?Am J Gastroenterol.1995;90:708–712.
- ,,, et al.Hospital use of acid‐suppressive medications and its fall‐out on prescribing in general practice: a 1‐month survey.Aliment Pharmacol Ther.2003;17:1503–1506.
- ,,.Overuse of acid‐suppressive therapy in hospitalized patients.Am J Gastroenterol.2000;95:3118–122.
- ,,, et al.Prophylaxis for stress‐related gastric hemorrhage in the medical intensive care unit. A randomized, controlled, single‐blind study.Ann Intern Med.1994;121:568–575.
- .Low incidence of hemodynamic instability in patients with gastrointestinal hemorrhage.South Med J.1996;89:386–390.
Copyright © 2006 Society of Hospital Medicine
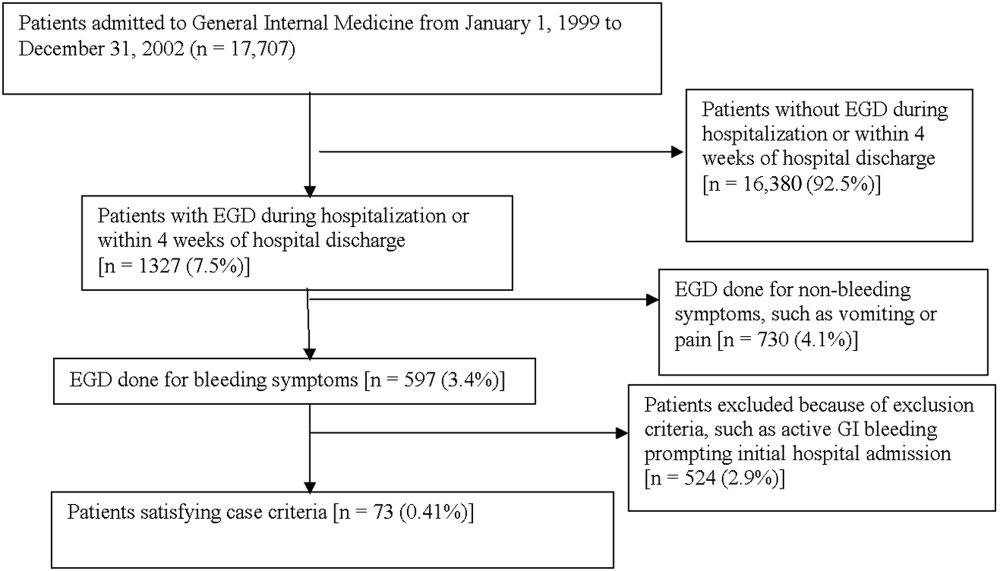
Editorial
It is right and fitting that an article focused on palliative care appears in the inaugural issue of the Journal of Hospital Medicine (JHM).1 Both hospital medicine and palliative care are rapidly growing fields expanding in response to quality and economic imperatives. Both fields recognize the need to develop systems to care for seriously ill patients and to work within interdisciplinary teams. In fact, a natural and mutually beneficial relationship should exist between these two fields. For palliative care, hospital medicine and hospitalists offer the physicians and systems approach to care that could guarantee access to high‐quality palliative care for all hospitalized patients. In addition, hospitalists offer the promise of increasing the number of hospital‐based palliative care programs as the presence of a hospitalist program is strongly associated with having or starting such a program.2, 3 For hospital medicine and hospitalists, palliative care offers a compassionate and high‐quality response to the challenge of caring for seriously and terminally ill patients and their families. By each embracing the other, both fields could find willing and eager partners in the quest to provide the highest possible quality of care for hospitalized patients.
In this first issue of JHM, Dr. Meier offers hospitalists an intriguing and attractive picture of palliative care. She describes how the growth of palliative care is driven by the needs of an ever‐larger group of patients living with chronic and life‐threatening illness and evidence of high quality and satisfaction for these patients who have many physical, emotional, psychological, and spiritual concerns. Dr. Meier also demonstrates how hospital‐based palliative care can coordinate with hospices to provide the continuity of care for terminally ill patients that is often elusive at hospital discharge. Finally, Dr. Meier provides a practical list of resources for clinicians seeking further training in the field. No doubt hospitalists will appreciate this list as the core competencies in hospital medicine, published as a supplement to this issue of JHM, include palliative care, pain management, communication, and discharge planning.
As Dr. Meier states in her article Palliative Care in Hospitals, many types of clinicians can provide palliative care in hospitals, including general internists, nurses, geriatricians, oncologists, hospitalists, and others, yet hospitalists are likely to emerge as the predominant providers of palliative care to hospitalized patients.4 That 75% of Americans die in institutionalized settings, where hospitalists are becoming the dominant providers of care, will drive this prediction.5 In addition, hospitalists are increasingly leading efforts in quality improvement, patient satisfaction, and patient safety.6 Of necessity these initiatives will involve the sickest hospitalized patients and will look to palliative care as a proven response for improving quality and increasing satisfaction.
Hospital medicine and palliative care have other aspects in common that make a melding of the two fields beneficial. Both fields recognize and emphasize the need for interdisciplinary care; good communication between members of the health care team and between health care providers and patients; and timely, effective, and responsible discharge planning. Finally, both fields often rely on multiple sources of funding including professional fee billing and support from the hospital for the added value that programs provide. Sharing so many issues in common should help hospital medicine and palliative care form strong links.
For these links to take hold and for the benefits of this partnership to bear fruit, members of both fields, and especially those with a foot in each, need to reach out. For hospitalists this means getting educated in palliative care, an area for which hospitalists recognize they are underprepared.7 Each hospitalist must be able to provide primary, basic palliative care to each patient.8 Some hospitalists will discover the rewards of palliative care and seek further training and even board certification. These hospitalists can start or join palliative care teams in their institutions. Finally, some hospitalists will become experts in palliative care and join or lead palliative care programs at tertiary care centers. In turn, palliative care providers must reach out to hospitalists. Palliative care clinicians should seek out hospitalists at their institutions and hospices should contact hospitalists at their local hospitals. These programs need to invite hospitalists to participate in the palliative care team and suggest how their services can help the patients of hospitalists. This natural alliance can come about only if both sides reach out.
A partnership between palliative care and hospital medicine will be good for patients and their families as well as for each field, as hospitalists enable realization of the goal of providing palliative care to every patient in the United States. In addition, this partnership will be good for hospitalists who embrace this work. Palliative care can connect us to the humanism and compassion that brought so many of us to medicine and can serve as an antidote to burnout. Furthermore, by caring for patients with life‐threatening illnesses we remember that our time is limited and that each day is a gift. We recognize the importance of making the most of our time regardless of how long we have and of choosing carefully how and with whom we spend our time.
In this first issue of JHM, Dr. Meier makes a strong argument for the need and continued growth of palliative care in hospitals, lays out a strategy for achieving this growth through education and program development, and in doing so, opens the door to hope for the future. Through palliative care we can offer patients hope for healing when cure is not possible, for comfort in the face of suffering, and for what can still be despite all that cannot. The possibility that hospitalists could provide all patients access to palliative care is cause enough for hope. The knowledge that hospitalists will play a major role in making this possibility a reality and may become the predominant providers of palliative care can make that hope a reality.
- .Palliative care in hospitals.J Hosp Med.2006;1:21–28.
- ,.Prevalence and structure of palliative care services in California hospitals.Arch Intern Med.2003;163:1084–1088.
- ,,,,,.Evaluation of the California Hospital Initiative in Palliative Services (CHIPS).Arch Intern Med. In press.
- ,.Palliative care and the hospitalist: an opportunity for cross‐fertilization.Am J Med.2001;111:10S–14S.
- Field MJ,Cassell CK, Eds.Approaching death: improving care at the end of life.Washington, DC:National Academy Press,1997.
- ,.The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- ,,,.Hospitalists' perceptions of their residency training needs: results of a national survey.Am J Med.2001;111:247–254.
- .Secondary and tertiary palliative care in US hospitals.JAMA.2002;287:875–881.
It is right and fitting that an article focused on palliative care appears in the inaugural issue of the Journal of Hospital Medicine (JHM).1 Both hospital medicine and palliative care are rapidly growing fields expanding in response to quality and economic imperatives. Both fields recognize the need to develop systems to care for seriously ill patients and to work within interdisciplinary teams. In fact, a natural and mutually beneficial relationship should exist between these two fields. For palliative care, hospital medicine and hospitalists offer the physicians and systems approach to care that could guarantee access to high‐quality palliative care for all hospitalized patients. In addition, hospitalists offer the promise of increasing the number of hospital‐based palliative care programs as the presence of a hospitalist program is strongly associated with having or starting such a program.2, 3 For hospital medicine and hospitalists, palliative care offers a compassionate and high‐quality response to the challenge of caring for seriously and terminally ill patients and their families. By each embracing the other, both fields could find willing and eager partners in the quest to provide the highest possible quality of care for hospitalized patients.
In this first issue of JHM, Dr. Meier offers hospitalists an intriguing and attractive picture of palliative care. She describes how the growth of palliative care is driven by the needs of an ever‐larger group of patients living with chronic and life‐threatening illness and evidence of high quality and satisfaction for these patients who have many physical, emotional, psychological, and spiritual concerns. Dr. Meier also demonstrates how hospital‐based palliative care can coordinate with hospices to provide the continuity of care for terminally ill patients that is often elusive at hospital discharge. Finally, Dr. Meier provides a practical list of resources for clinicians seeking further training in the field. No doubt hospitalists will appreciate this list as the core competencies in hospital medicine, published as a supplement to this issue of JHM, include palliative care, pain management, communication, and discharge planning.
As Dr. Meier states in her article Palliative Care in Hospitals, many types of clinicians can provide palliative care in hospitals, including general internists, nurses, geriatricians, oncologists, hospitalists, and others, yet hospitalists are likely to emerge as the predominant providers of palliative care to hospitalized patients.4 That 75% of Americans die in institutionalized settings, where hospitalists are becoming the dominant providers of care, will drive this prediction.5 In addition, hospitalists are increasingly leading efforts in quality improvement, patient satisfaction, and patient safety.6 Of necessity these initiatives will involve the sickest hospitalized patients and will look to palliative care as a proven response for improving quality and increasing satisfaction.
Hospital medicine and palliative care have other aspects in common that make a melding of the two fields beneficial. Both fields recognize and emphasize the need for interdisciplinary care; good communication between members of the health care team and between health care providers and patients; and timely, effective, and responsible discharge planning. Finally, both fields often rely on multiple sources of funding including professional fee billing and support from the hospital for the added value that programs provide. Sharing so many issues in common should help hospital medicine and palliative care form strong links.
For these links to take hold and for the benefits of this partnership to bear fruit, members of both fields, and especially those with a foot in each, need to reach out. For hospitalists this means getting educated in palliative care, an area for which hospitalists recognize they are underprepared.7 Each hospitalist must be able to provide primary, basic palliative care to each patient.8 Some hospitalists will discover the rewards of palliative care and seek further training and even board certification. These hospitalists can start or join palliative care teams in their institutions. Finally, some hospitalists will become experts in palliative care and join or lead palliative care programs at tertiary care centers. In turn, palliative care providers must reach out to hospitalists. Palliative care clinicians should seek out hospitalists at their institutions and hospices should contact hospitalists at their local hospitals. These programs need to invite hospitalists to participate in the palliative care team and suggest how their services can help the patients of hospitalists. This natural alliance can come about only if both sides reach out.
A partnership between palliative care and hospital medicine will be good for patients and their families as well as for each field, as hospitalists enable realization of the goal of providing palliative care to every patient in the United States. In addition, this partnership will be good for hospitalists who embrace this work. Palliative care can connect us to the humanism and compassion that brought so many of us to medicine and can serve as an antidote to burnout. Furthermore, by caring for patients with life‐threatening illnesses we remember that our time is limited and that each day is a gift. We recognize the importance of making the most of our time regardless of how long we have and of choosing carefully how and with whom we spend our time.
In this first issue of JHM, Dr. Meier makes a strong argument for the need and continued growth of palliative care in hospitals, lays out a strategy for achieving this growth through education and program development, and in doing so, opens the door to hope for the future. Through palliative care we can offer patients hope for healing when cure is not possible, for comfort in the face of suffering, and for what can still be despite all that cannot. The possibility that hospitalists could provide all patients access to palliative care is cause enough for hope. The knowledge that hospitalists will play a major role in making this possibility a reality and may become the predominant providers of palliative care can make that hope a reality.
It is right and fitting that an article focused on palliative care appears in the inaugural issue of the Journal of Hospital Medicine (JHM).1 Both hospital medicine and palliative care are rapidly growing fields expanding in response to quality and economic imperatives. Both fields recognize the need to develop systems to care for seriously ill patients and to work within interdisciplinary teams. In fact, a natural and mutually beneficial relationship should exist between these two fields. For palliative care, hospital medicine and hospitalists offer the physicians and systems approach to care that could guarantee access to high‐quality palliative care for all hospitalized patients. In addition, hospitalists offer the promise of increasing the number of hospital‐based palliative care programs as the presence of a hospitalist program is strongly associated with having or starting such a program.2, 3 For hospital medicine and hospitalists, palliative care offers a compassionate and high‐quality response to the challenge of caring for seriously and terminally ill patients and their families. By each embracing the other, both fields could find willing and eager partners in the quest to provide the highest possible quality of care for hospitalized patients.
In this first issue of JHM, Dr. Meier offers hospitalists an intriguing and attractive picture of palliative care. She describes how the growth of palliative care is driven by the needs of an ever‐larger group of patients living with chronic and life‐threatening illness and evidence of high quality and satisfaction for these patients who have many physical, emotional, psychological, and spiritual concerns. Dr. Meier also demonstrates how hospital‐based palliative care can coordinate with hospices to provide the continuity of care for terminally ill patients that is often elusive at hospital discharge. Finally, Dr. Meier provides a practical list of resources for clinicians seeking further training in the field. No doubt hospitalists will appreciate this list as the core competencies in hospital medicine, published as a supplement to this issue of JHM, include palliative care, pain management, communication, and discharge planning.
As Dr. Meier states in her article Palliative Care in Hospitals, many types of clinicians can provide palliative care in hospitals, including general internists, nurses, geriatricians, oncologists, hospitalists, and others, yet hospitalists are likely to emerge as the predominant providers of palliative care to hospitalized patients.4 That 75% of Americans die in institutionalized settings, where hospitalists are becoming the dominant providers of care, will drive this prediction.5 In addition, hospitalists are increasingly leading efforts in quality improvement, patient satisfaction, and patient safety.6 Of necessity these initiatives will involve the sickest hospitalized patients and will look to palliative care as a proven response for improving quality and increasing satisfaction.
Hospital medicine and palliative care have other aspects in common that make a melding of the two fields beneficial. Both fields recognize and emphasize the need for interdisciplinary care; good communication between members of the health care team and between health care providers and patients; and timely, effective, and responsible discharge planning. Finally, both fields often rely on multiple sources of funding including professional fee billing and support from the hospital for the added value that programs provide. Sharing so many issues in common should help hospital medicine and palliative care form strong links.
For these links to take hold and for the benefits of this partnership to bear fruit, members of both fields, and especially those with a foot in each, need to reach out. For hospitalists this means getting educated in palliative care, an area for which hospitalists recognize they are underprepared.7 Each hospitalist must be able to provide primary, basic palliative care to each patient.8 Some hospitalists will discover the rewards of palliative care and seek further training and even board certification. These hospitalists can start or join palliative care teams in their institutions. Finally, some hospitalists will become experts in palliative care and join or lead palliative care programs at tertiary care centers. In turn, palliative care providers must reach out to hospitalists. Palliative care clinicians should seek out hospitalists at their institutions and hospices should contact hospitalists at their local hospitals. These programs need to invite hospitalists to participate in the palliative care team and suggest how their services can help the patients of hospitalists. This natural alliance can come about only if both sides reach out.
A partnership between palliative care and hospital medicine will be good for patients and their families as well as for each field, as hospitalists enable realization of the goal of providing palliative care to every patient in the United States. In addition, this partnership will be good for hospitalists who embrace this work. Palliative care can connect us to the humanism and compassion that brought so many of us to medicine and can serve as an antidote to burnout. Furthermore, by caring for patients with life‐threatening illnesses we remember that our time is limited and that each day is a gift. We recognize the importance of making the most of our time regardless of how long we have and of choosing carefully how and with whom we spend our time.
In this first issue of JHM, Dr. Meier makes a strong argument for the need and continued growth of palliative care in hospitals, lays out a strategy for achieving this growth through education and program development, and in doing so, opens the door to hope for the future. Through palliative care we can offer patients hope for healing when cure is not possible, for comfort in the face of suffering, and for what can still be despite all that cannot. The possibility that hospitalists could provide all patients access to palliative care is cause enough for hope. The knowledge that hospitalists will play a major role in making this possibility a reality and may become the predominant providers of palliative care can make that hope a reality.
- .Palliative care in hospitals.J Hosp Med.2006;1:21–28.
- ,.Prevalence and structure of palliative care services in California hospitals.Arch Intern Med.2003;163:1084–1088.
- ,,,,,.Evaluation of the California Hospital Initiative in Palliative Services (CHIPS).Arch Intern Med. In press.
- ,.Palliative care and the hospitalist: an opportunity for cross‐fertilization.Am J Med.2001;111:10S–14S.
- Field MJ,Cassell CK, Eds.Approaching death: improving care at the end of life.Washington, DC:National Academy Press,1997.
- ,.The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- ,,,.Hospitalists' perceptions of their residency training needs: results of a national survey.Am J Med.2001;111:247–254.
- .Secondary and tertiary palliative care in US hospitals.JAMA.2002;287:875–881.
- .Palliative care in hospitals.J Hosp Med.2006;1:21–28.
- ,.Prevalence and structure of palliative care services in California hospitals.Arch Intern Med.2003;163:1084–1088.
- ,,,,,.Evaluation of the California Hospital Initiative in Palliative Services (CHIPS).Arch Intern Med. In press.
- ,.Palliative care and the hospitalist: an opportunity for cross‐fertilization.Am J Med.2001;111:10S–14S.
- Field MJ,Cassell CK, Eds.Approaching death: improving care at the end of life.Washington, DC:National Academy Press,1997.
- ,.The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- ,,,.Hospitalists' perceptions of their residency training needs: results of a national survey.Am J Med.2001;111:247–254.
- .Secondary and tertiary palliative care in US hospitals.JAMA.2002;287:875–881.