User login
Factors Influencing Outcomes of a Telehealth-Based Physical Activity Program in Older Veterans Postdischarge
Factors Influencing Outcomes of a Telehealth-Based Physical Activity Program in Older Veterans Postdischarge
Deconditioning among hospitalized older adults contributes to significant decline in posthospitalization functional ability, physical performance, and physical activity.1-10 Previous hospital-to-home interventions have targeted improving function and physical activity, including recent programs leveraging home telehealth as a feasible and potentially effective mode of delivering in-home exercise and rehabilitation.11-14 However, pilot interventions have shown mixed effectiveness.11,12,14 This study expands on a previously published intervention describing a pilot home telehealth program for veterans posthospital discharge that demonstrated significant 6-month improvement in physical activity as well as trends in physical function improvement, including among those with cognitive impairment.15 Factors that contribute to improved outcomes are the focus of the present study.
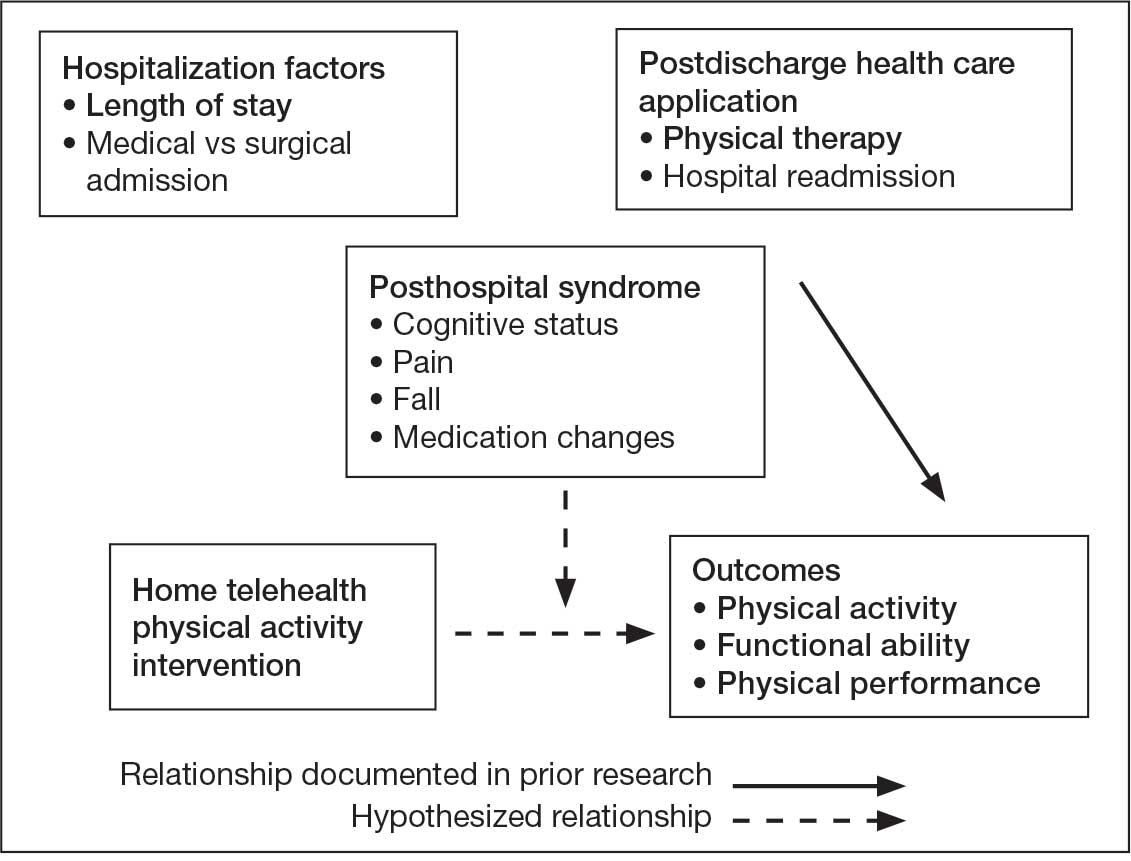
Key factors underlying the complexity of hospital-to-home transitions include hospitalization elements (ie, reason for admission and length of stay), associated posthospital syndromes (ie, postdischarge falls, medication changes, cognitive impairment, and pain), and postdischarge health care application (ie, physical therapy and hospital readmission).16-18 These factors may be associated with postdischarge functional ability, physical performance, and physical activity, but their direct influence on intervention outcomes is unclear (Figure 1).5,7,9,16-20 The objective of this study was to examine the influence of hospitalization, posthospital syndrome, and postdischarge health care application factors on outcomes of a US Department of Veterans Affairs (VA) Video Connect (VVC) intervention to enhance function and physical activity in older adults posthospital discharge.
health care application factors on physical activity, functional ability, and
physical performance intervention outcomes.
Methods
The previous analysis reported on patient characteristics, program feasibility, and preliminary outcomes.13,15 The current study reports on relationships between hospitalization, posthospital syndrome, and postdischarge health care application factors and change in key outcomes, namely postdischarge self-reported functional ability, physical performance, and physical activity from baseline to endpoint.
Participants provided written informed consent. The protocol and consent forms were approved by the VA Ann Arbor Healthcare System (VAAAHS) Research and Development Committee, and the project was registered on clinicaltrials.gov (NCT04045054).
Intervention
The pilot program targeted older adults following recent hospital discharge from VAAAHS. Participants were eligible if they were aged ≥ 50 years, had been discharged following an inpatient stay in the past 1 to 2 weeks, evaluated by physical therapy during hospitalization with stated rehabilitation goals on discharge, and followed by a VAAAHS primary care physician. Participants were either recruited during hospital admission or shortly after discharge.13
An experienced physical activity trainer (PAT) supported the progression of participants’ rehabilitation goals via a home exercise program and coached the patient and caregiver to optimize functional ability, physical performance, and physical activity. The PAT was a nonlicensed research assistant with extensive experience in applying standard physical activity enhancement protocols (eg, increased walking) to older adults with comorbidities. Participation in the program lasted about 6 months. Initiation of the PAT program was delayed if the patient was already receiving postdischarge home-based or outpatient physical therapy. The PAT contacted the patient weekly via VVC for the first 6 weeks, then monthly for a total of 6 months. Each contact included information on optimal walking form, injury prevention, program progression, and ways to incorporate sit-to-stand transitions, nonsitting behavior, and walking into daily routines. The initial VVC contact lasted about 60 minutes and subsequent sessions lasted about 30 minutes.13
Demographic characteristics were self-reported by participants and included age, sex, race, years of education, and marital status. Clinical characteristics were obtained from each participant’s electronic health record (EHR), including copay status, index hospitalization length of stay, admission diagnosis, and postsurgery status (postsurgery vs nonpostsurgery). Intervention adherence was tracked as the number of PAT sessions attended.
Posthospital Syndrome Factors
Participant falls (categorized as those who reported a fall vs those who did not) and medication changes (number of changes reported, including new medication, discontinued medication, dose changes, medication changes, or changes in medication schedule) were reported by participants or caregivers during each VVC contact. Participants completed the Montreal Cognitive Assessment (MoCA) at baseline, and were dichotomized into 2 groups: no cognitive impairment (MoCA score ≥ 26) and mild to moderate cognitive impairment (MoCA score 10-25).13,21
Participants rated how much pain interfered with their normal daily activities since the previous VVC session on a 5-point Likert scale (1, not at all; to 5, extremely).22 Similar to prior research, participants were placed into 2 groups based on their mean pain interference score (individuals with scores from 1.0 to 2.0 in 1 group, and individuals with > 2.0 in another).23-25 Participants were separated into a no or mild pain interference group and a moderate to severe pain interference group. Hospital readmissions (VA and non-VA) and postdischarge physical therapy outcomes were obtained from the participant’s EHR, including primary care visits.
Outcomes
Outcomes were collected at baseline (posthospital discharge) and 6 months postenrollment.
Self-Reported Functional Ability. This measure is provided by participants or caregivers and measured by the Katz Index of Independence in Activities of Daily Living (ADL), Lawton and Brody Instrumental ADL Scale (IADL), Nagi Disability Model, and Rosow-Breslau Scale. The Katz ADL assesses the ability to complete 6 self-care activities and awards 1 point for independence and 0 if the individual is dependent (total score range, 0-6).26 The Lawton and Brody IADL measures an individual’s independence in 8 instrumental ADLs; it awards 1 point for independence and 0 if the individual is dependent (total score range, 0-8).27 The Nagi Disability Model evaluates an individual’s difficulty performing 5 tasks (total score range, 0-5) and tallies the number of items with a response other than “no difficulty at all” (higher total score indicates greater difficulty). 28 The Rosow-Breslau Scale is a 3-item measure of mobility disability; individual responses are 0 (no help) and 1 (requires help or unable); higher total score (range, 0-3) indicates greater disability.29
Physical Performance. Measured using the Short Physical Performance Battery (SPPB), which evaluates standing balance, sit to stand, and walking performance. Scores range from 0 to 4 on the balance, gait speed, and chair stand tests, for a total composite score between 0 and 12 (higher score indicates better performance).30
Physical Activity. Measured using actigraphy, namely a physical activity monitor adherent to the thigh (activ-PAL3TM, PAL Technologies Ltd., Glasgow, UK).31 Participants were instructed to wear the activPal for ≥ 1 week. Participants with a minimum of 5 days of wear were included in this analysis.
Data Analyses
Analyses were performed using SPSS software version 29.0.32 Continuous variables were summarized using mean (SD) or median and IQR using the weighted average method; categorical variables were summarized using frequencies and percentages. Baseline scores on outcome variables were compared by categorical hospitalization, posthospital syndrome, and postdischarge health care application factor variables using Mann-Whitney U tests. The differences between outcome variables from baseline to endpoint were then calculated to produce change scores. Relationships between the number of PAT sessions attended and baseline outcomes and outcome change scores were estimated using Spearman correlations. Relationships between categorical factors (hospitalization, posthospital syndrome, and postdischarge health care application) and outcome variable change scores (which were normally distributed) were examined using Mann-Whitney U tests. Relationships with continuous hospitalization (length of stay) and posthospital syndrome factors (medication changes) were estimated using Spearman correlations. Effect sizes (ES) were estimated with Cohen d; small (d = 0.2), medium (d = 0.5), or large (d ≥ 0.8). Missing data were handled using pairwise deletion.33 Therefore, sample sizes were reported for each analysis. For all statistical tests, P < .05 was considered significant.
Results
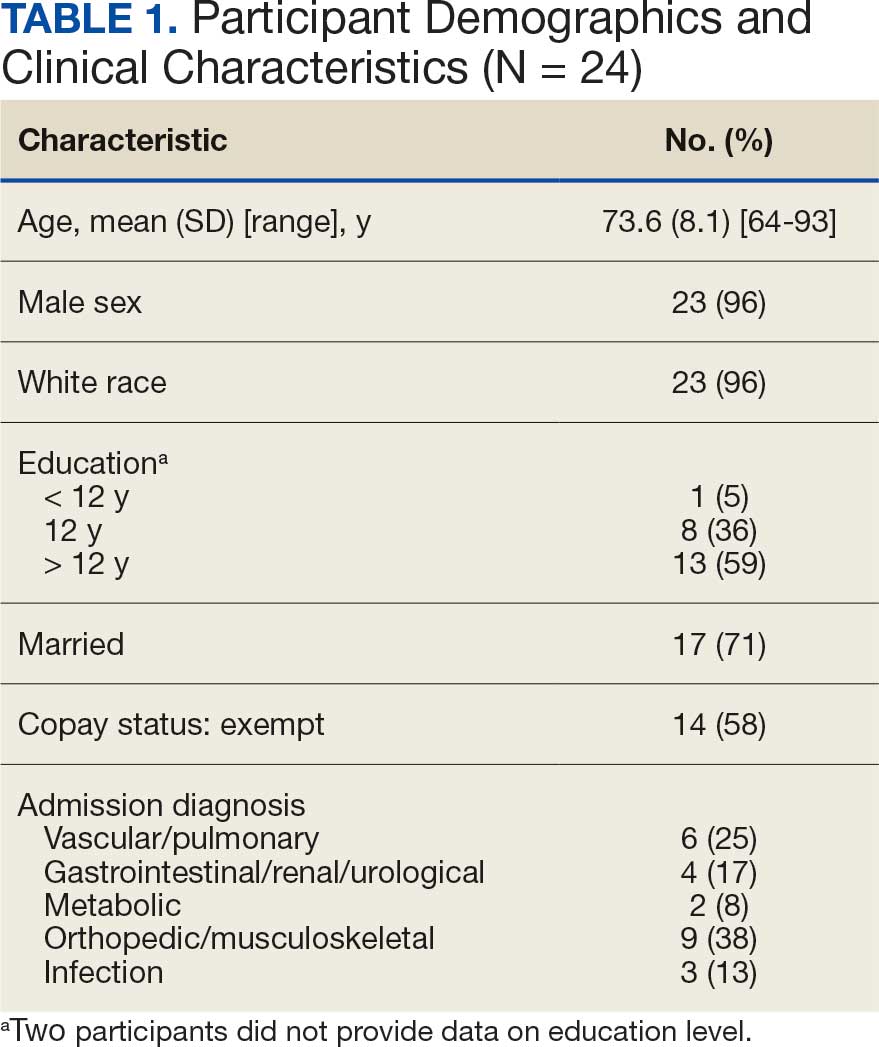
Twenty-four individuals completed the pilot intervention.15 Mean (SD) age was 73.6 (8.1) years (range, 64-93 years) and participants were predominantly White males (Table 1). Eight participants had a high school education only and 13 had more than a high school education. Diagnoses at admission included 9 patients with orthopedic/musculoskeletal conditions (6 were for joint replacement), 6 patients with vascular/pulmonary conditions, and 4 with gastrointestinal/renal/urological conditions. Of the 11 postsurgery participants, 7 were orthopedic, 4 were gastrointestinal, and 1 was peripheral vascular.
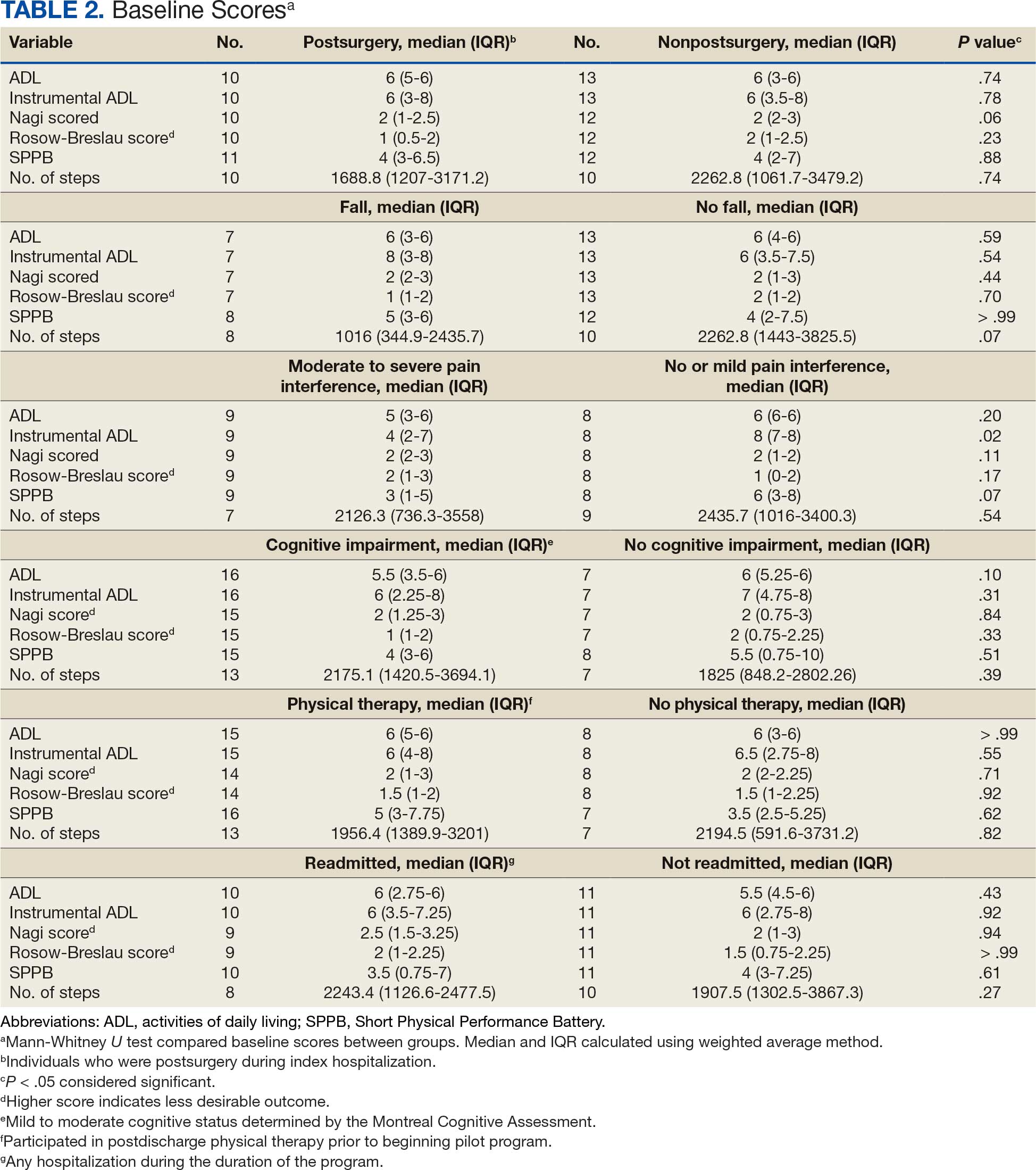
Baseline outcome scores did not differ significantly between groups, except individuals with moderate to severe pain interference reported a significantly lower IADL score (median [IQR] 4 [2-7]) than individuals with mild or moderate pain interference (median [IQR] 8 [7-8]; P = .02) (Table 2). The mean (SD) number of PAT sessions attended was 9.3 (3.7) (range, 3-19). There were no significant relationships between number of sessions attended and any baseline outcome variables or outcome change scores.
Hospitalization Factors
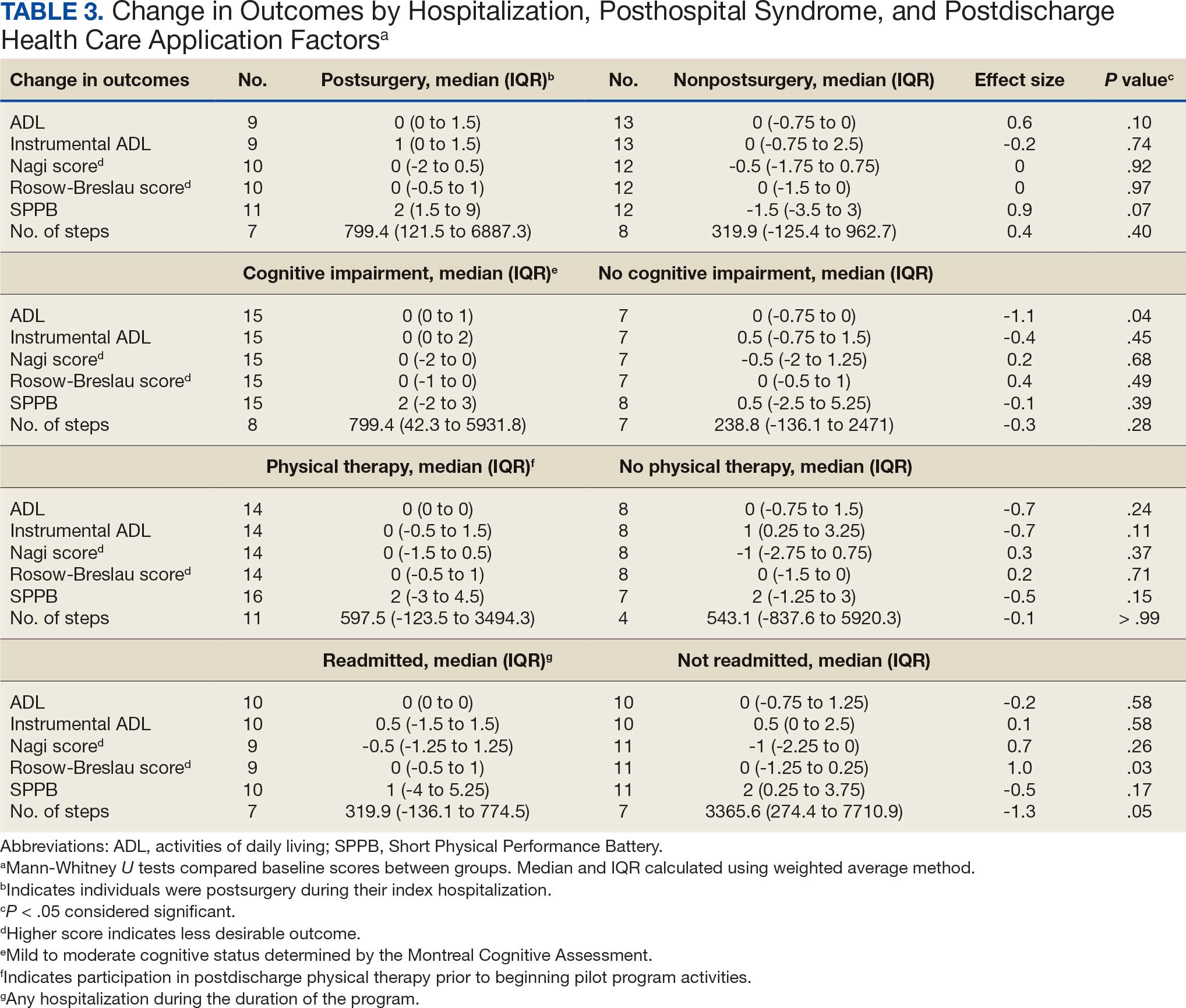
Participants who were postsurgery tended to have greater improvement than individuals who were nonpostsurgery in ADLs (median [IQR] 0 [0-1.5]; ES, 0.6; P = .10) and SPPB (median [IQR] 2 [1.5-9]; ES, 0.9; P = .07), but the improvements were not statistically significant (Table 3). Mean (SD) length of stay of the index hospitalization was 6.7 (6.1) days. Longer length of stay was significantly correlated with an increase in Nagi score (ρ, 0.45; 95% CI, 0.01-0.75). There were no other significant or trending relationships between length of stay and outcome variables.
Posthospital Syndrome Factors
The 16 participants with mild to moderate cognitive impairment had less improvement in ADLs (median [IQR] 0 [0-1]) than the 8 participants with no impairment (median [IQR] 0 [-0.75 to 0]; ES, -1.1; P = .04). Change in outcome variables from baseline to endpoint did not significantly differ between the 8 patients who reported a fall compared with the 13 who did not, nor were any trends observed. Change in outcome variables from baseline to endpoint also did not significantly differ between the 8 participants who reported no or mild pain interference compared with the 10 patients with moderate to severe pain interference, nor were any trends observed. Mean (SD) number of medication changes was 2.5 (1.6). Higher number of medication changes was significantly correlated with a decrease in Rosow-Breslau score (ρ, -0.47; 95% CI, -0.76 to -0.02). There were no other significant or trending relationships between number of medication changes and outcome variables.
Postdischarge Health Care Application Factors
The 16 participants who attended posthospital physical therapy trended towards less improvement in IADLs (median [IQR] 0 [-0.5 to 1.5]; ES, -0.7; P = .11) and SPPB (median [IQR] 2 [-3.0 to 4.5]; ES, -0.5; P = .15) than the 8 patients with no postdischarge physical therapy. Eleven participants were readmitted, while 13 had no readmissions in their medical records between baseline and endpoint. Participants with ≥ 1 readmission experienced a greater increase in Rosow-Breslau score (median [IQR] 0 [-0.5 to 1.0]) than those not readmitted (median [IQR] 0 [-1.25 to 0.25]; ES, 1.0; P = .03). Borderline greater improvement in number of steps was found in those not readmitted (median [IQR] 3365.6 [274.4-7710.9]) compared with those readmitted (median [IQR] 319.9 [-136.1 to 774.5]; ES, -1.3; P = .05). Patients who were readmitted also tended to have lower and not statistically significant improvements in SPPB (median [IQR] 1 [-4.0 to 5.3]) compared with those not readmitted (median [IQR] 2 [0.3-3.8]; ES, -0.5; P = .17) (Table 3).
Discussion
This study examined the association between hospitalization, posthospital syndrome, and postdischarge health care use in patients undergoing a VVC-based intervention following hospital discharge. Participants who had no or mild cognitive impairment, no readmissions, higher medication changes, and a shorter hospital length of stay tended to experience lower disability, including in mobility and ADLs. This suggests individuals who are less clinically complex may be more likely to benefit from this type of virtual rehabilitation program. These findings are consistent with clinical experiences; home-based programs to improve physical activity posthospital discharge can be challenging for those who were medically ill (and did not undergo a specific surgical procedure), cognitively impaired, and become acutely ill and trigger hospital readmission. 15 For example, the sample in this study had higher rates of falls, pain, and readmissions compared to previous research.2,3,34-39
The importance of posthospital syndrome in the context of recovery of function and health at home following hospitalization is well documented.16-18 The potential impact of posthospital syndrome on physical activity-focused interventions is less understood. In our analysis, participants with mild or moderate cognitive impairment tended to become more dependent in their ADLs, while those with no cognitive impairment tended to become more independent in their ADLs. This functional decline over time is perhaps expected in persons with cognitive impairment, but the significant difference with a large ES warrants further consideration on how to tailor interventions to better promote functional recovery in these individuals.40,41 While some cognitive decline may not be preventable, this finding supports the need to promote healthy cognitive aging, identify declines in cognition, and work to mitigate additional decline. Programs specifically designed to promote function and physical activity in older adults with cognitive impairment are needed, especially during care transitions.41-43
While participants reported that falls and pain interference did not have a significant impact on change in outcomes between baseline and endpoint, these areas need further investigation. Falls and pain have been associated with function and physical activity in older adults.42-46 Pain is common, yet underappreciated during older adult hospital-to-home transitions.11,12,45,46 There is a need for more comprehensive assessment of pain (including pain intensity) and qualitative research.
Hospitalization and postdischarge health care application factors may have a significant impact on home-telehealth physical activity intervention success. Individuals who were postsurgery tended to have greater improvements in ADLs and physical performance. Most postsurgery participants had joint replacement surgery. Postsurgery status may not be modifiable, but it is important to note expected differences in recovery between medical and surgical admissions and the need to tailor care based on admission diagnosis. Those with a longer length of hospital stay may be considered at higher risk of suboptimal outcomes postdischarge, which indicates an opportunity for targeting resources and support, in addition to efforts of reducing length of stay where possible.47
Readmissions were significantly related to a change in Rosow-Breslau mobility disability score. This may indicate the detrimental impact a readmission can have on increasing mobility and physical activity postdischarge, or the potential of this pilot program to impact readmissions by increasing mobility and physical activity, contrary to prior physical exercise interventions.5,7,9,48 With 5% to 79% of readmissions considered preventable, continued efforts and program dissemination and implementation to address preventable readmissions are warranted.49 Individuals with postdischarge physical therapy (prior to beginning the pilot program) tended to demonstrate less improvement in disability and physical performance. This relationship needs further investigation; the 2 groups did not appear to have significant differences at baseline, albeit with a small sample size. It is possible they experienced initial improvements with postdischarge physical therapy and plateaued or had little further reserve to improve upon entering the VVC program.
Strengths and Limitations
This pilot program provided evaluative data on the use of VVC to enhance function and physical activity in older adults posthospital discharge. It included individual (eg, fall, pain, cognitive impairment) and health service (eg, readmission, physical therapy) level factors as predictors of function and physical activity posthospitalization.5,7,9,15-19
The results of this pilot project stem from a small sample lacking diversity in terms of race, ethnicity, and sex. There was some variation in baseline and endpoints between participants, and when hospitalization, posthospital syndrome, and postdischarge health care application factors were collected. The majority of participants were recruited within a month postdischarge, and the program lasted about 6 months. Data collection was attempted at regular PAT contacts, but there was some variation in when visits occurred based on participant availability and preference. Some participants had missing data, which was handled using pairwise deletion.33 Larger studies are needed to confirm the findings of this study, particularly the trends that did not reach statistical significance. Home health services other than physical therapy (eg, nursing, occupational therapy) were not fully accounted for and should be considered in future research.
Conclusions
In patients undergoing a 6-month pilot VVC-based physical activity intervention posthospital discharge, improvements in mobility and disability were most likely in those who had no cognitive impairment and were not readmitted. Larger sample and qualitative investigations are necessary to optimize outcomes for patients who meet these clinical profiles.
- Liebzeit D, Bratzke L, Boltz M, Purvis S, King B. Getting back to normal: a grounded theory study of function in post-hospitalized older adults. Gerontologist. 2020;60:704-714. doi:10.1093/geront/gnz057
- Ponzetto M, Zanocchi M, Maero B, et al. Post-hospitalization mortality in the elderly. Arch Gerontol Geriatr. 2003;36:83-91. doi:10.1016/s0167-4943(02)00061-4
- Buurman BM, Hoogerduijn JG, de Haan RJ, et al. Geriatric conditions in acutely hospitalized older patients: prevalence and one-year survival and functional decline. PLoS One. 2011;6:e26951. doi:10.1371/journal.pone.0026951
- Ponzetto M, Maero B, Maina P, et al. Risk factors for early and late mortality in hospitalized older patients: the continuing importance of functional status. J Gerontol A Biol Sci Med Sci. 2003;58:1049-1054. doi:10.1093/gerona/58.11.m1049
- Huang HT, Chang CM, Liu LF, Lin HS, Chen CH. Trajectories and predictors of functional decline of hospitalised older patients. J Clin Nurs. 2013;22:1322-1331. doi:10.1111/jocn.12055
- Boyd CM, Landefeld CS, Counsell SR, et al. Recovery of activities of daily living in older adults after hospitalization for acute medical illness. J Am Geriatr Soc. 2008;56:2171- 2179. doi:10.1111/j.1532-5415.2008.02023.x
- Helvik AS, Selbæk G, Engedal K. Functional decline in older adults one year after hospitalization. Arch Gerontol Geriatr. 2013;57:305-310. doi:10.1016/j.archger.2013.05.008
- Zaslavsky O, Zisberg A, Shadmi E. Impact of functional change before and during hospitalization on functional recovery 1 month following hospitalization. J Gerontol Biol Sci Med Sci. 2015;70:381-386. doi:10.1093/gerona/glu168
- Chen CC, Wang C, Huang GH. Functional trajectory 6 months posthospitalization: a cohort study of older hospitalized patients in Taiwan. Nurs Res. 2008;57:93-100. doi:10.1097/01.NNR.0000313485.18670.e2
- Kleinpell RM, Fletcher K, Jennings BM. Reducing functional decline in hospitalized elderly. In: Hughes RG, ed. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Agency for Healthcare Research and Quality (US); 2008. Accessed September 3, 2025. http://www.ncbi.nlm.nih.gov/books/NBK2629/
- Liebzeit D, Rutkowski R, Arbaje AI, Fields B, Werner NE. A scoping review of interventions for older adults transitioning from hospital to home. J Am Geriatr Soc. 2021;69:2950-2962. doi:10.1111/jgs.17323
- Hladkowicz E, Dumitrascu F, Auais M, et al. Evaluations of postoperative transitions in care for older adults: a scoping review. BMC Geriatr. 2022;22:329. doi:10.1186/s12877-022-02989-6
- Alexander NB, Phillips K, Wagner-Felkey J, et al. Team VA Video Connect (VVC) to optimize mobility and physical activity in post-hospital discharge older veterans: baseline assessment. BMC Geriatr. 2021;21:502. doi:10.1186/s12877-021-02454-w
- Dawson R, Oliveira JS, Kwok WS, et al. Exercise interventions delivered through telehealth to improve physical functioning for older adults with frailty, cognitive, or mobility disability: a systematic review and meta-analysis. Telemed J E Health. 2024;30:940-950. doi:10.1089/tmj.2023.0177
- Liebzeit D, Phillips KK, Hogikyan RV, Cigolle CT, Alexander NB. A pilot home-telehealth program to enhance functional ability, physical performance, and physical activity in older adult veterans post-hospital discharge. Res Gerontol Nurs. 2024;17:271-279. doi:10.3928/19404921-20241105-01
- Krumholz HM. Post-hospital syndrome—an acquired, transient condition of generalized risk. N Engl J Med. 2013;368:100-102. doi:10.1056/NEJMp1212324
- Caraballo C, Dharmarajan K, Krumholz HM. Post hospital syndrome: is the stress of hospitalization causing harm? Rev Esp Cardiol (Engl Ed). 2019;72:896-898. doi:10.1016/j.rec.2019.04.010
- Rawal S, Kwan JL, Razak F, et al. Association of the trauma of hospitalization with 30-day readmission or emergency department visit. JAMA Intern Med. 2019;179:38- 45. doi:10.1001/jamainternmed.2018.5100
- Dutzi I, Schwenk M, Kirchner M, Jooss E, Bauer JM, Hauer K. Influence of cognitive impairment on rehabilitation received and its mediating effect on functional recovery. J Alzheimers Dis. 2021;84:745-756. doi:10.3233/JAD-210620
- Uriz-Otano F, Uriz-Otano JI, Malafarina V. Factors associated with short-term functional recovery in elderly people with a hip fracture. Influence ofcognitiveimpairment. JAmMedDirAssoc. 2015;16:215-220. doi:10.1016/j.jamda.2014.09.009
- Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53:695-699. doi:10.1111/j.1532-5415.2005.53221.x
- Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473-483.
- White RS, Jiang J, Hall CB, et al. Higher perceived stress scale scores are associated with higher pain intensity and pain interference levels in older adults. J Am Geriatr Soc. 2014;62:2350-2356. doi:10.1111/jgs.13135
- Blyth FM, March LM, Brnabic AJ, et al. Chronic pain in Australia: a prevalence study. Pain. 2001;89:127-134. doi:10.1016/s0304-3959(00)00355-9
- Thomas E, Peat G, Harris L, Wilkie R, Croft PR. The prevalence of pain and pain interference in a general population of older adults: cross-sectional findings from the North Staffordshire Osteoarthritis Project (NorStOP). Pain. 2004;110:361-368. doi:10.1016/j.pain.2004.04.017
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914-919. doi:10.1001/jama.1963.03060120024016
- Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179-186.
- Alexander NB, Guire KE, Thelen DG, et al. Self-reported walking ability predicts functional mobility performance in frail older adults. J Am Geriatr Soc. 2000;48:1408-1413. doi:10.1111/j.1532-5415.2000.tb02630.x
- Rosow I, Breslau N. A Guttman health scale for the aged. J Gerontol. 1966;21:556-559. doi:10.1093/geronj/21.4.556
- Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49:M85-M94. doi:10.1093/geronj/49.2.m85
- Chan CS, Slaughter SE, Jones CA, Ickert C, Wagg AS. Measuring activity performance of older adults using the activPAL: a rapid review. Healthcare (Basel). 2017;5:94. doi:10.3390/healthcare5040094
- IBM SPSS software. IBM Corp; 2019. Accessed September 3, 2025. https://www.ibm.com/spss
- Kang H. The prevention and handling of the missing data. Korean J Anesthesiol. 2013;64:402-406. doi:10.4097/kjae.2013.64.5.402
- Epstein AM, Jha AK, Orav EJ. The relationship between hospital admission rates and rehospitalizations. N Engl J Med. 2011;365:2287-2295. doi:10.1056/NEJMsa1101942
- Bogaisky M, Dezieck L. Early hospital readmission of nursing home residents and community-dwelling elderly adults discharged from the geriatrics service of an urban teaching hospital: patterns and risk factors. J Am Geriatr Soc. 2015;63:548-552. doi:10.1111/jgs.13317
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418-1428. doi:10.1056/NEJMsa0803563
- Hoyer EH, Needham DM, Atanelov L, Knox B, Friedman M, Brotman DJ. Association of impaired functional status at hospital discharge and subsequent rehospitalization. J Hosp Med. 2014;9:277-282. doi:10.1002/jhm.2152
- Mahoney J, Sager M, Dunham NC, Johnson J. Risk of falls after hospital discharge. J Am Geriatr Soc. 1994;42:269- 274. doi:10.1111/j.1532-5415.1994.tb01750.x
- Hoffman GJ, Liu H, Alexander NB, Tinetti M, Braun TM, Min LC. Posthospital fall injuries and 30-day readmissions in adults 65 years and older. JAMA Netw Open. 2019;2:e194276. doi:10.1001/jamanetworkopen.2019.4276
- Gill DP, Hubbard RA, Koepsell TD, et al. Differences in rate of functional decline across three dementia types. Alzheimers Dement. 2013;9:S63-S71. doi:10.1016/j.jalz.2012.10.010
- Auyeung TW, Kwok T, Lee J, Leung PC, Leung J, Woo J. Functional decline in cognitive impairment–the relationship between physical and cognitive function. Neuroepidemiology. 2008;31:167-173. doi:10.1159/000154929
- Patti A, Zangla D, Sahin FN, et al. Physical exercise and prevention of falls. Effects of a Pilates training method compared with a general physical activity program. Medicine (Baltimore). 2021;100:e25289. doi:10.1097/MD.0000000000025289
- Nagarkar A, Kulkarni S. Association between daily activities and fall in older adults: an analysis of longitudinal ageing study in India (2017-18). BMC Geriatr. 2022;22:203. doi:10.1186/s12877-022-02879-x
- Ek S, Rizzuto D, Xu W, Calderón-Larrañaga A, Welmer AK. Predictors for functional decline after an injurious fall: a population-based cohort study. Aging Clin Exp Res. 2021;33:2183-2190. doi:10.1007/s40520-020-01747-1
- Dagnino APA, Campos MM. Chronic pain in the elderly: mechanisms and perspectives. Front Hum Neurosci. 2022;16:736688. doi:10.3389/fnhum.2022.736688
- Ritchie CS, Patel K, Boscardin J, et al. Impact of persistent pain on function, cognition, and well-being of older adults. J Am Geriatr Soc. 2023;71:26-35. doi:10.1111/jgs.18125
- Han TS, Murray P, Robin J, et al. Evaluation of the association of length of stay in hospital and outcomes. Int J Qual Health Care. 2022;34:mzab160. doi:10.1093/intqhc/ mzab160
- Lærum-Onsager E, Molin M, Olsen CF, et al. Effect of nutritional and physical exercise intervention on hospital readmission for patients aged 65 or older: a systematic review and meta-analysis of randomized controlled trials. Int J Behav Nutr Phys Act. 2021;18:62. doi:10.1186/s12966-021-01123-w
- Van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: a systematic review. CMAJ. 2011;183:E391-E402. doi:10.1503/cmaj.101860
Deconditioning among hospitalized older adults contributes to significant decline in posthospitalization functional ability, physical performance, and physical activity.1-10 Previous hospital-to-home interventions have targeted improving function and physical activity, including recent programs leveraging home telehealth as a feasible and potentially effective mode of delivering in-home exercise and rehabilitation.11-14 However, pilot interventions have shown mixed effectiveness.11,12,14 This study expands on a previously published intervention describing a pilot home telehealth program for veterans posthospital discharge that demonstrated significant 6-month improvement in physical activity as well as trends in physical function improvement, including among those with cognitive impairment.15 Factors that contribute to improved outcomes are the focus of the present study.
Key factors underlying the complexity of hospital-to-home transitions include hospitalization elements (ie, reason for admission and length of stay), associated posthospital syndromes (ie, postdischarge falls, medication changes, cognitive impairment, and pain), and postdischarge health care application (ie, physical therapy and hospital readmission).16-18 These factors may be associated with postdischarge functional ability, physical performance, and physical activity, but their direct influence on intervention outcomes is unclear (Figure 1).5,7,9,16-20 The objective of this study was to examine the influence of hospitalization, posthospital syndrome, and postdischarge health care application factors on outcomes of a US Department of Veterans Affairs (VA) Video Connect (VVC) intervention to enhance function and physical activity in older adults posthospital discharge.
health care application factors on physical activity, functional ability, and
physical performance intervention outcomes.
Methods
The previous analysis reported on patient characteristics, program feasibility, and preliminary outcomes.13,15 The current study reports on relationships between hospitalization, posthospital syndrome, and postdischarge health care application factors and change in key outcomes, namely postdischarge self-reported functional ability, physical performance, and physical activity from baseline to endpoint.
Participants provided written informed consent. The protocol and consent forms were approved by the VA Ann Arbor Healthcare System (VAAAHS) Research and Development Committee, and the project was registered on clinicaltrials.gov (NCT04045054).
Intervention
The pilot program targeted older adults following recent hospital discharge from VAAAHS. Participants were eligible if they were aged ≥ 50 years, had been discharged following an inpatient stay in the past 1 to 2 weeks, evaluated by physical therapy during hospitalization with stated rehabilitation goals on discharge, and followed by a VAAAHS primary care physician. Participants were either recruited during hospital admission or shortly after discharge.13
An experienced physical activity trainer (PAT) supported the progression of participants’ rehabilitation goals via a home exercise program and coached the patient and caregiver to optimize functional ability, physical performance, and physical activity. The PAT was a nonlicensed research assistant with extensive experience in applying standard physical activity enhancement protocols (eg, increased walking) to older adults with comorbidities. Participation in the program lasted about 6 months. Initiation of the PAT program was delayed if the patient was already receiving postdischarge home-based or outpatient physical therapy. The PAT contacted the patient weekly via VVC for the first 6 weeks, then monthly for a total of 6 months. Each contact included information on optimal walking form, injury prevention, program progression, and ways to incorporate sit-to-stand transitions, nonsitting behavior, and walking into daily routines. The initial VVC contact lasted about 60 minutes and subsequent sessions lasted about 30 minutes.13
Demographic characteristics were self-reported by participants and included age, sex, race, years of education, and marital status. Clinical characteristics were obtained from each participant’s electronic health record (EHR), including copay status, index hospitalization length of stay, admission diagnosis, and postsurgery status (postsurgery vs nonpostsurgery). Intervention adherence was tracked as the number of PAT sessions attended.
Posthospital Syndrome Factors
Participant falls (categorized as those who reported a fall vs those who did not) and medication changes (number of changes reported, including new medication, discontinued medication, dose changes, medication changes, or changes in medication schedule) were reported by participants or caregivers during each VVC contact. Participants completed the Montreal Cognitive Assessment (MoCA) at baseline, and were dichotomized into 2 groups: no cognitive impairment (MoCA score ≥ 26) and mild to moderate cognitive impairment (MoCA score 10-25).13,21
Participants rated how much pain interfered with their normal daily activities since the previous VVC session on a 5-point Likert scale (1, not at all; to 5, extremely).22 Similar to prior research, participants were placed into 2 groups based on their mean pain interference score (individuals with scores from 1.0 to 2.0 in 1 group, and individuals with > 2.0 in another).23-25 Participants were separated into a no or mild pain interference group and a moderate to severe pain interference group. Hospital readmissions (VA and non-VA) and postdischarge physical therapy outcomes were obtained from the participant’s EHR, including primary care visits.
Outcomes
Outcomes were collected at baseline (posthospital discharge) and 6 months postenrollment.
Self-Reported Functional Ability. This measure is provided by participants or caregivers and measured by the Katz Index of Independence in Activities of Daily Living (ADL), Lawton and Brody Instrumental ADL Scale (IADL), Nagi Disability Model, and Rosow-Breslau Scale. The Katz ADL assesses the ability to complete 6 self-care activities and awards 1 point for independence and 0 if the individual is dependent (total score range, 0-6).26 The Lawton and Brody IADL measures an individual’s independence in 8 instrumental ADLs; it awards 1 point for independence and 0 if the individual is dependent (total score range, 0-8).27 The Nagi Disability Model evaluates an individual’s difficulty performing 5 tasks (total score range, 0-5) and tallies the number of items with a response other than “no difficulty at all” (higher total score indicates greater difficulty). 28 The Rosow-Breslau Scale is a 3-item measure of mobility disability; individual responses are 0 (no help) and 1 (requires help or unable); higher total score (range, 0-3) indicates greater disability.29
Physical Performance. Measured using the Short Physical Performance Battery (SPPB), which evaluates standing balance, sit to stand, and walking performance. Scores range from 0 to 4 on the balance, gait speed, and chair stand tests, for a total composite score between 0 and 12 (higher score indicates better performance).30
Physical Activity. Measured using actigraphy, namely a physical activity monitor adherent to the thigh (activ-PAL3TM, PAL Technologies Ltd., Glasgow, UK).31 Participants were instructed to wear the activPal for ≥ 1 week. Participants with a minimum of 5 days of wear were included in this analysis.
Data Analyses
Analyses were performed using SPSS software version 29.0.32 Continuous variables were summarized using mean (SD) or median and IQR using the weighted average method; categorical variables were summarized using frequencies and percentages. Baseline scores on outcome variables were compared by categorical hospitalization, posthospital syndrome, and postdischarge health care application factor variables using Mann-Whitney U tests. The differences between outcome variables from baseline to endpoint were then calculated to produce change scores. Relationships between the number of PAT sessions attended and baseline outcomes and outcome change scores were estimated using Spearman correlations. Relationships between categorical factors (hospitalization, posthospital syndrome, and postdischarge health care application) and outcome variable change scores (which were normally distributed) were examined using Mann-Whitney U tests. Relationships with continuous hospitalization (length of stay) and posthospital syndrome factors (medication changes) were estimated using Spearman correlations. Effect sizes (ES) were estimated with Cohen d; small (d = 0.2), medium (d = 0.5), or large (d ≥ 0.8). Missing data were handled using pairwise deletion.33 Therefore, sample sizes were reported for each analysis. For all statistical tests, P < .05 was considered significant.
Results
Twenty-four individuals completed the pilot intervention.15 Mean (SD) age was 73.6 (8.1) years (range, 64-93 years) and participants were predominantly White males (Table 1). Eight participants had a high school education only and 13 had more than a high school education. Diagnoses at admission included 9 patients with orthopedic/musculoskeletal conditions (6 were for joint replacement), 6 patients with vascular/pulmonary conditions, and 4 with gastrointestinal/renal/urological conditions. Of the 11 postsurgery participants, 7 were orthopedic, 4 were gastrointestinal, and 1 was peripheral vascular.
Baseline outcome scores did not differ significantly between groups, except individuals with moderate to severe pain interference reported a significantly lower IADL score (median [IQR] 4 [2-7]) than individuals with mild or moderate pain interference (median [IQR] 8 [7-8]; P = .02) (Table 2). The mean (SD) number of PAT sessions attended was 9.3 (3.7) (range, 3-19). There were no significant relationships between number of sessions attended and any baseline outcome variables or outcome change scores.
Hospitalization Factors
Participants who were postsurgery tended to have greater improvement than individuals who were nonpostsurgery in ADLs (median [IQR] 0 [0-1.5]; ES, 0.6; P = .10) and SPPB (median [IQR] 2 [1.5-9]; ES, 0.9; P = .07), but the improvements were not statistically significant (Table 3). Mean (SD) length of stay of the index hospitalization was 6.7 (6.1) days. Longer length of stay was significantly correlated with an increase in Nagi score (ρ, 0.45; 95% CI, 0.01-0.75). There were no other significant or trending relationships between length of stay and outcome variables.
Posthospital Syndrome Factors
The 16 participants with mild to moderate cognitive impairment had less improvement in ADLs (median [IQR] 0 [0-1]) than the 8 participants with no impairment (median [IQR] 0 [-0.75 to 0]; ES, -1.1; P = .04). Change in outcome variables from baseline to endpoint did not significantly differ between the 8 patients who reported a fall compared with the 13 who did not, nor were any trends observed. Change in outcome variables from baseline to endpoint also did not significantly differ between the 8 participants who reported no or mild pain interference compared with the 10 patients with moderate to severe pain interference, nor were any trends observed. Mean (SD) number of medication changes was 2.5 (1.6). Higher number of medication changes was significantly correlated with a decrease in Rosow-Breslau score (ρ, -0.47; 95% CI, -0.76 to -0.02). There were no other significant or trending relationships between number of medication changes and outcome variables.
Postdischarge Health Care Application Factors
The 16 participants who attended posthospital physical therapy trended towards less improvement in IADLs (median [IQR] 0 [-0.5 to 1.5]; ES, -0.7; P = .11) and SPPB (median [IQR] 2 [-3.0 to 4.5]; ES, -0.5; P = .15) than the 8 patients with no postdischarge physical therapy. Eleven participants were readmitted, while 13 had no readmissions in their medical records between baseline and endpoint. Participants with ≥ 1 readmission experienced a greater increase in Rosow-Breslau score (median [IQR] 0 [-0.5 to 1.0]) than those not readmitted (median [IQR] 0 [-1.25 to 0.25]; ES, 1.0; P = .03). Borderline greater improvement in number of steps was found in those not readmitted (median [IQR] 3365.6 [274.4-7710.9]) compared with those readmitted (median [IQR] 319.9 [-136.1 to 774.5]; ES, -1.3; P = .05). Patients who were readmitted also tended to have lower and not statistically significant improvements in SPPB (median [IQR] 1 [-4.0 to 5.3]) compared with those not readmitted (median [IQR] 2 [0.3-3.8]; ES, -0.5; P = .17) (Table 3).
Discussion
This study examined the association between hospitalization, posthospital syndrome, and postdischarge health care use in patients undergoing a VVC-based intervention following hospital discharge. Participants who had no or mild cognitive impairment, no readmissions, higher medication changes, and a shorter hospital length of stay tended to experience lower disability, including in mobility and ADLs. This suggests individuals who are less clinically complex may be more likely to benefit from this type of virtual rehabilitation program. These findings are consistent with clinical experiences; home-based programs to improve physical activity posthospital discharge can be challenging for those who were medically ill (and did not undergo a specific surgical procedure), cognitively impaired, and become acutely ill and trigger hospital readmission. 15 For example, the sample in this study had higher rates of falls, pain, and readmissions compared to previous research.2,3,34-39
The importance of posthospital syndrome in the context of recovery of function and health at home following hospitalization is well documented.16-18 The potential impact of posthospital syndrome on physical activity-focused interventions is less understood. In our analysis, participants with mild or moderate cognitive impairment tended to become more dependent in their ADLs, while those with no cognitive impairment tended to become more independent in their ADLs. This functional decline over time is perhaps expected in persons with cognitive impairment, but the significant difference with a large ES warrants further consideration on how to tailor interventions to better promote functional recovery in these individuals.40,41 While some cognitive decline may not be preventable, this finding supports the need to promote healthy cognitive aging, identify declines in cognition, and work to mitigate additional decline. Programs specifically designed to promote function and physical activity in older adults with cognitive impairment are needed, especially during care transitions.41-43
While participants reported that falls and pain interference did not have a significant impact on change in outcomes between baseline and endpoint, these areas need further investigation. Falls and pain have been associated with function and physical activity in older adults.42-46 Pain is common, yet underappreciated during older adult hospital-to-home transitions.11,12,45,46 There is a need for more comprehensive assessment of pain (including pain intensity) and qualitative research.
Hospitalization and postdischarge health care application factors may have a significant impact on home-telehealth physical activity intervention success. Individuals who were postsurgery tended to have greater improvements in ADLs and physical performance. Most postsurgery participants had joint replacement surgery. Postsurgery status may not be modifiable, but it is important to note expected differences in recovery between medical and surgical admissions and the need to tailor care based on admission diagnosis. Those with a longer length of hospital stay may be considered at higher risk of suboptimal outcomes postdischarge, which indicates an opportunity for targeting resources and support, in addition to efforts of reducing length of stay where possible.47
Readmissions were significantly related to a change in Rosow-Breslau mobility disability score. This may indicate the detrimental impact a readmission can have on increasing mobility and physical activity postdischarge, or the potential of this pilot program to impact readmissions by increasing mobility and physical activity, contrary to prior physical exercise interventions.5,7,9,48 With 5% to 79% of readmissions considered preventable, continued efforts and program dissemination and implementation to address preventable readmissions are warranted.49 Individuals with postdischarge physical therapy (prior to beginning the pilot program) tended to demonstrate less improvement in disability and physical performance. This relationship needs further investigation; the 2 groups did not appear to have significant differences at baseline, albeit with a small sample size. It is possible they experienced initial improvements with postdischarge physical therapy and plateaued or had little further reserve to improve upon entering the VVC program.
Strengths and Limitations
This pilot program provided evaluative data on the use of VVC to enhance function and physical activity in older adults posthospital discharge. It included individual (eg, fall, pain, cognitive impairment) and health service (eg, readmission, physical therapy) level factors as predictors of function and physical activity posthospitalization.5,7,9,15-19
The results of this pilot project stem from a small sample lacking diversity in terms of race, ethnicity, and sex. There was some variation in baseline and endpoints between participants, and when hospitalization, posthospital syndrome, and postdischarge health care application factors were collected. The majority of participants were recruited within a month postdischarge, and the program lasted about 6 months. Data collection was attempted at regular PAT contacts, but there was some variation in when visits occurred based on participant availability and preference. Some participants had missing data, which was handled using pairwise deletion.33 Larger studies are needed to confirm the findings of this study, particularly the trends that did not reach statistical significance. Home health services other than physical therapy (eg, nursing, occupational therapy) were not fully accounted for and should be considered in future research.
Conclusions
In patients undergoing a 6-month pilot VVC-based physical activity intervention posthospital discharge, improvements in mobility and disability were most likely in those who had no cognitive impairment and were not readmitted. Larger sample and qualitative investigations are necessary to optimize outcomes for patients who meet these clinical profiles.
Deconditioning among hospitalized older adults contributes to significant decline in posthospitalization functional ability, physical performance, and physical activity.1-10 Previous hospital-to-home interventions have targeted improving function and physical activity, including recent programs leveraging home telehealth as a feasible and potentially effective mode of delivering in-home exercise and rehabilitation.11-14 However, pilot interventions have shown mixed effectiveness.11,12,14 This study expands on a previously published intervention describing a pilot home telehealth program for veterans posthospital discharge that demonstrated significant 6-month improvement in physical activity as well as trends in physical function improvement, including among those with cognitive impairment.15 Factors that contribute to improved outcomes are the focus of the present study.
Key factors underlying the complexity of hospital-to-home transitions include hospitalization elements (ie, reason for admission and length of stay), associated posthospital syndromes (ie, postdischarge falls, medication changes, cognitive impairment, and pain), and postdischarge health care application (ie, physical therapy and hospital readmission).16-18 These factors may be associated with postdischarge functional ability, physical performance, and physical activity, but their direct influence on intervention outcomes is unclear (Figure 1).5,7,9,16-20 The objective of this study was to examine the influence of hospitalization, posthospital syndrome, and postdischarge health care application factors on outcomes of a US Department of Veterans Affairs (VA) Video Connect (VVC) intervention to enhance function and physical activity in older adults posthospital discharge.
health care application factors on physical activity, functional ability, and
physical performance intervention outcomes.
Methods
The previous analysis reported on patient characteristics, program feasibility, and preliminary outcomes.13,15 The current study reports on relationships between hospitalization, posthospital syndrome, and postdischarge health care application factors and change in key outcomes, namely postdischarge self-reported functional ability, physical performance, and physical activity from baseline to endpoint.
Participants provided written informed consent. The protocol and consent forms were approved by the VA Ann Arbor Healthcare System (VAAAHS) Research and Development Committee, and the project was registered on clinicaltrials.gov (NCT04045054).
Intervention
The pilot program targeted older adults following recent hospital discharge from VAAAHS. Participants were eligible if they were aged ≥ 50 years, had been discharged following an inpatient stay in the past 1 to 2 weeks, evaluated by physical therapy during hospitalization with stated rehabilitation goals on discharge, and followed by a VAAAHS primary care physician. Participants were either recruited during hospital admission or shortly after discharge.13
An experienced physical activity trainer (PAT) supported the progression of participants’ rehabilitation goals via a home exercise program and coached the patient and caregiver to optimize functional ability, physical performance, and physical activity. The PAT was a nonlicensed research assistant with extensive experience in applying standard physical activity enhancement protocols (eg, increased walking) to older adults with comorbidities. Participation in the program lasted about 6 months. Initiation of the PAT program was delayed if the patient was already receiving postdischarge home-based or outpatient physical therapy. The PAT contacted the patient weekly via VVC for the first 6 weeks, then monthly for a total of 6 months. Each contact included information on optimal walking form, injury prevention, program progression, and ways to incorporate sit-to-stand transitions, nonsitting behavior, and walking into daily routines. The initial VVC contact lasted about 60 minutes and subsequent sessions lasted about 30 minutes.13
Demographic characteristics were self-reported by participants and included age, sex, race, years of education, and marital status. Clinical characteristics were obtained from each participant’s electronic health record (EHR), including copay status, index hospitalization length of stay, admission diagnosis, and postsurgery status (postsurgery vs nonpostsurgery). Intervention adherence was tracked as the number of PAT sessions attended.
Posthospital Syndrome Factors
Participant falls (categorized as those who reported a fall vs those who did not) and medication changes (number of changes reported, including new medication, discontinued medication, dose changes, medication changes, or changes in medication schedule) were reported by participants or caregivers during each VVC contact. Participants completed the Montreal Cognitive Assessment (MoCA) at baseline, and were dichotomized into 2 groups: no cognitive impairment (MoCA score ≥ 26) and mild to moderate cognitive impairment (MoCA score 10-25).13,21
Participants rated how much pain interfered with their normal daily activities since the previous VVC session on a 5-point Likert scale (1, not at all; to 5, extremely).22 Similar to prior research, participants were placed into 2 groups based on their mean pain interference score (individuals with scores from 1.0 to 2.0 in 1 group, and individuals with > 2.0 in another).23-25 Participants were separated into a no or mild pain interference group and a moderate to severe pain interference group. Hospital readmissions (VA and non-VA) and postdischarge physical therapy outcomes were obtained from the participant’s EHR, including primary care visits.
Outcomes
Outcomes were collected at baseline (posthospital discharge) and 6 months postenrollment.
Self-Reported Functional Ability. This measure is provided by participants or caregivers and measured by the Katz Index of Independence in Activities of Daily Living (ADL), Lawton and Brody Instrumental ADL Scale (IADL), Nagi Disability Model, and Rosow-Breslau Scale. The Katz ADL assesses the ability to complete 6 self-care activities and awards 1 point for independence and 0 if the individual is dependent (total score range, 0-6).26 The Lawton and Brody IADL measures an individual’s independence in 8 instrumental ADLs; it awards 1 point for independence and 0 if the individual is dependent (total score range, 0-8).27 The Nagi Disability Model evaluates an individual’s difficulty performing 5 tasks (total score range, 0-5) and tallies the number of items with a response other than “no difficulty at all” (higher total score indicates greater difficulty). 28 The Rosow-Breslau Scale is a 3-item measure of mobility disability; individual responses are 0 (no help) and 1 (requires help or unable); higher total score (range, 0-3) indicates greater disability.29
Physical Performance. Measured using the Short Physical Performance Battery (SPPB), which evaluates standing balance, sit to stand, and walking performance. Scores range from 0 to 4 on the balance, gait speed, and chair stand tests, for a total composite score between 0 and 12 (higher score indicates better performance).30
Physical Activity. Measured using actigraphy, namely a physical activity monitor adherent to the thigh (activ-PAL3TM, PAL Technologies Ltd., Glasgow, UK).31 Participants were instructed to wear the activPal for ≥ 1 week. Participants with a minimum of 5 days of wear were included in this analysis.
Data Analyses
Analyses were performed using SPSS software version 29.0.32 Continuous variables were summarized using mean (SD) or median and IQR using the weighted average method; categorical variables were summarized using frequencies and percentages. Baseline scores on outcome variables were compared by categorical hospitalization, posthospital syndrome, and postdischarge health care application factor variables using Mann-Whitney U tests. The differences between outcome variables from baseline to endpoint were then calculated to produce change scores. Relationships between the number of PAT sessions attended and baseline outcomes and outcome change scores were estimated using Spearman correlations. Relationships between categorical factors (hospitalization, posthospital syndrome, and postdischarge health care application) and outcome variable change scores (which were normally distributed) were examined using Mann-Whitney U tests. Relationships with continuous hospitalization (length of stay) and posthospital syndrome factors (medication changes) were estimated using Spearman correlations. Effect sizes (ES) were estimated with Cohen d; small (d = 0.2), medium (d = 0.5), or large (d ≥ 0.8). Missing data were handled using pairwise deletion.33 Therefore, sample sizes were reported for each analysis. For all statistical tests, P < .05 was considered significant.
Results
Twenty-four individuals completed the pilot intervention.15 Mean (SD) age was 73.6 (8.1) years (range, 64-93 years) and participants were predominantly White males (Table 1). Eight participants had a high school education only and 13 had more than a high school education. Diagnoses at admission included 9 patients with orthopedic/musculoskeletal conditions (6 were for joint replacement), 6 patients with vascular/pulmonary conditions, and 4 with gastrointestinal/renal/urological conditions. Of the 11 postsurgery participants, 7 were orthopedic, 4 were gastrointestinal, and 1 was peripheral vascular.
Baseline outcome scores did not differ significantly between groups, except individuals with moderate to severe pain interference reported a significantly lower IADL score (median [IQR] 4 [2-7]) than individuals with mild or moderate pain interference (median [IQR] 8 [7-8]; P = .02) (Table 2). The mean (SD) number of PAT sessions attended was 9.3 (3.7) (range, 3-19). There were no significant relationships between number of sessions attended and any baseline outcome variables or outcome change scores.
Hospitalization Factors
Participants who were postsurgery tended to have greater improvement than individuals who were nonpostsurgery in ADLs (median [IQR] 0 [0-1.5]; ES, 0.6; P = .10) and SPPB (median [IQR] 2 [1.5-9]; ES, 0.9; P = .07), but the improvements were not statistically significant (Table 3). Mean (SD) length of stay of the index hospitalization was 6.7 (6.1) days. Longer length of stay was significantly correlated with an increase in Nagi score (ρ, 0.45; 95% CI, 0.01-0.75). There were no other significant or trending relationships between length of stay and outcome variables.
Posthospital Syndrome Factors
The 16 participants with mild to moderate cognitive impairment had less improvement in ADLs (median [IQR] 0 [0-1]) than the 8 participants with no impairment (median [IQR] 0 [-0.75 to 0]; ES, -1.1; P = .04). Change in outcome variables from baseline to endpoint did not significantly differ between the 8 patients who reported a fall compared with the 13 who did not, nor were any trends observed. Change in outcome variables from baseline to endpoint also did not significantly differ between the 8 participants who reported no or mild pain interference compared with the 10 patients with moderate to severe pain interference, nor were any trends observed. Mean (SD) number of medication changes was 2.5 (1.6). Higher number of medication changes was significantly correlated with a decrease in Rosow-Breslau score (ρ, -0.47; 95% CI, -0.76 to -0.02). There were no other significant or trending relationships between number of medication changes and outcome variables.
Postdischarge Health Care Application Factors
The 16 participants who attended posthospital physical therapy trended towards less improvement in IADLs (median [IQR] 0 [-0.5 to 1.5]; ES, -0.7; P = .11) and SPPB (median [IQR] 2 [-3.0 to 4.5]; ES, -0.5; P = .15) than the 8 patients with no postdischarge physical therapy. Eleven participants were readmitted, while 13 had no readmissions in their medical records between baseline and endpoint. Participants with ≥ 1 readmission experienced a greater increase in Rosow-Breslau score (median [IQR] 0 [-0.5 to 1.0]) than those not readmitted (median [IQR] 0 [-1.25 to 0.25]; ES, 1.0; P = .03). Borderline greater improvement in number of steps was found in those not readmitted (median [IQR] 3365.6 [274.4-7710.9]) compared with those readmitted (median [IQR] 319.9 [-136.1 to 774.5]; ES, -1.3; P = .05). Patients who were readmitted also tended to have lower and not statistically significant improvements in SPPB (median [IQR] 1 [-4.0 to 5.3]) compared with those not readmitted (median [IQR] 2 [0.3-3.8]; ES, -0.5; P = .17) (Table 3).
Discussion
This study examined the association between hospitalization, posthospital syndrome, and postdischarge health care use in patients undergoing a VVC-based intervention following hospital discharge. Participants who had no or mild cognitive impairment, no readmissions, higher medication changes, and a shorter hospital length of stay tended to experience lower disability, including in mobility and ADLs. This suggests individuals who are less clinically complex may be more likely to benefit from this type of virtual rehabilitation program. These findings are consistent with clinical experiences; home-based programs to improve physical activity posthospital discharge can be challenging for those who were medically ill (and did not undergo a specific surgical procedure), cognitively impaired, and become acutely ill and trigger hospital readmission. 15 For example, the sample in this study had higher rates of falls, pain, and readmissions compared to previous research.2,3,34-39
The importance of posthospital syndrome in the context of recovery of function and health at home following hospitalization is well documented.16-18 The potential impact of posthospital syndrome on physical activity-focused interventions is less understood. In our analysis, participants with mild or moderate cognitive impairment tended to become more dependent in their ADLs, while those with no cognitive impairment tended to become more independent in their ADLs. This functional decline over time is perhaps expected in persons with cognitive impairment, but the significant difference with a large ES warrants further consideration on how to tailor interventions to better promote functional recovery in these individuals.40,41 While some cognitive decline may not be preventable, this finding supports the need to promote healthy cognitive aging, identify declines in cognition, and work to mitigate additional decline. Programs specifically designed to promote function and physical activity in older adults with cognitive impairment are needed, especially during care transitions.41-43
While participants reported that falls and pain interference did not have a significant impact on change in outcomes between baseline and endpoint, these areas need further investigation. Falls and pain have been associated with function and physical activity in older adults.42-46 Pain is common, yet underappreciated during older adult hospital-to-home transitions.11,12,45,46 There is a need for more comprehensive assessment of pain (including pain intensity) and qualitative research.
Hospitalization and postdischarge health care application factors may have a significant impact on home-telehealth physical activity intervention success. Individuals who were postsurgery tended to have greater improvements in ADLs and physical performance. Most postsurgery participants had joint replacement surgery. Postsurgery status may not be modifiable, but it is important to note expected differences in recovery between medical and surgical admissions and the need to tailor care based on admission diagnosis. Those with a longer length of hospital stay may be considered at higher risk of suboptimal outcomes postdischarge, which indicates an opportunity for targeting resources and support, in addition to efforts of reducing length of stay where possible.47
Readmissions were significantly related to a change in Rosow-Breslau mobility disability score. This may indicate the detrimental impact a readmission can have on increasing mobility and physical activity postdischarge, or the potential of this pilot program to impact readmissions by increasing mobility and physical activity, contrary to prior physical exercise interventions.5,7,9,48 With 5% to 79% of readmissions considered preventable, continued efforts and program dissemination and implementation to address preventable readmissions are warranted.49 Individuals with postdischarge physical therapy (prior to beginning the pilot program) tended to demonstrate less improvement in disability and physical performance. This relationship needs further investigation; the 2 groups did not appear to have significant differences at baseline, albeit with a small sample size. It is possible they experienced initial improvements with postdischarge physical therapy and plateaued or had little further reserve to improve upon entering the VVC program.
Strengths and Limitations
This pilot program provided evaluative data on the use of VVC to enhance function and physical activity in older adults posthospital discharge. It included individual (eg, fall, pain, cognitive impairment) and health service (eg, readmission, physical therapy) level factors as predictors of function and physical activity posthospitalization.5,7,9,15-19
The results of this pilot project stem from a small sample lacking diversity in terms of race, ethnicity, and sex. There was some variation in baseline and endpoints between participants, and when hospitalization, posthospital syndrome, and postdischarge health care application factors were collected. The majority of participants were recruited within a month postdischarge, and the program lasted about 6 months. Data collection was attempted at regular PAT contacts, but there was some variation in when visits occurred based on participant availability and preference. Some participants had missing data, which was handled using pairwise deletion.33 Larger studies are needed to confirm the findings of this study, particularly the trends that did not reach statistical significance. Home health services other than physical therapy (eg, nursing, occupational therapy) were not fully accounted for and should be considered in future research.
Conclusions
In patients undergoing a 6-month pilot VVC-based physical activity intervention posthospital discharge, improvements in mobility and disability were most likely in those who had no cognitive impairment and were not readmitted. Larger sample and qualitative investigations are necessary to optimize outcomes for patients who meet these clinical profiles.
- Liebzeit D, Bratzke L, Boltz M, Purvis S, King B. Getting back to normal: a grounded theory study of function in post-hospitalized older adults. Gerontologist. 2020;60:704-714. doi:10.1093/geront/gnz057
- Ponzetto M, Zanocchi M, Maero B, et al. Post-hospitalization mortality in the elderly. Arch Gerontol Geriatr. 2003;36:83-91. doi:10.1016/s0167-4943(02)00061-4
- Buurman BM, Hoogerduijn JG, de Haan RJ, et al. Geriatric conditions in acutely hospitalized older patients: prevalence and one-year survival and functional decline. PLoS One. 2011;6:e26951. doi:10.1371/journal.pone.0026951
- Ponzetto M, Maero B, Maina P, et al. Risk factors for early and late mortality in hospitalized older patients: the continuing importance of functional status. J Gerontol A Biol Sci Med Sci. 2003;58:1049-1054. doi:10.1093/gerona/58.11.m1049
- Huang HT, Chang CM, Liu LF, Lin HS, Chen CH. Trajectories and predictors of functional decline of hospitalised older patients. J Clin Nurs. 2013;22:1322-1331. doi:10.1111/jocn.12055
- Boyd CM, Landefeld CS, Counsell SR, et al. Recovery of activities of daily living in older adults after hospitalization for acute medical illness. J Am Geriatr Soc. 2008;56:2171- 2179. doi:10.1111/j.1532-5415.2008.02023.x
- Helvik AS, Selbæk G, Engedal K. Functional decline in older adults one year after hospitalization. Arch Gerontol Geriatr. 2013;57:305-310. doi:10.1016/j.archger.2013.05.008
- Zaslavsky O, Zisberg A, Shadmi E. Impact of functional change before and during hospitalization on functional recovery 1 month following hospitalization. J Gerontol Biol Sci Med Sci. 2015;70:381-386. doi:10.1093/gerona/glu168
- Chen CC, Wang C, Huang GH. Functional trajectory 6 months posthospitalization: a cohort study of older hospitalized patients in Taiwan. Nurs Res. 2008;57:93-100. doi:10.1097/01.NNR.0000313485.18670.e2
- Kleinpell RM, Fletcher K, Jennings BM. Reducing functional decline in hospitalized elderly. In: Hughes RG, ed. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Agency for Healthcare Research and Quality (US); 2008. Accessed September 3, 2025. http://www.ncbi.nlm.nih.gov/books/NBK2629/
- Liebzeit D, Rutkowski R, Arbaje AI, Fields B, Werner NE. A scoping review of interventions for older adults transitioning from hospital to home. J Am Geriatr Soc. 2021;69:2950-2962. doi:10.1111/jgs.17323
- Hladkowicz E, Dumitrascu F, Auais M, et al. Evaluations of postoperative transitions in care for older adults: a scoping review. BMC Geriatr. 2022;22:329. doi:10.1186/s12877-022-02989-6
- Alexander NB, Phillips K, Wagner-Felkey J, et al. Team VA Video Connect (VVC) to optimize mobility and physical activity in post-hospital discharge older veterans: baseline assessment. BMC Geriatr. 2021;21:502. doi:10.1186/s12877-021-02454-w
- Dawson R, Oliveira JS, Kwok WS, et al. Exercise interventions delivered through telehealth to improve physical functioning for older adults with frailty, cognitive, or mobility disability: a systematic review and meta-analysis. Telemed J E Health. 2024;30:940-950. doi:10.1089/tmj.2023.0177
- Liebzeit D, Phillips KK, Hogikyan RV, Cigolle CT, Alexander NB. A pilot home-telehealth program to enhance functional ability, physical performance, and physical activity in older adult veterans post-hospital discharge. Res Gerontol Nurs. 2024;17:271-279. doi:10.3928/19404921-20241105-01
- Krumholz HM. Post-hospital syndrome—an acquired, transient condition of generalized risk. N Engl J Med. 2013;368:100-102. doi:10.1056/NEJMp1212324
- Caraballo C, Dharmarajan K, Krumholz HM. Post hospital syndrome: is the stress of hospitalization causing harm? Rev Esp Cardiol (Engl Ed). 2019;72:896-898. doi:10.1016/j.rec.2019.04.010
- Rawal S, Kwan JL, Razak F, et al. Association of the trauma of hospitalization with 30-day readmission or emergency department visit. JAMA Intern Med. 2019;179:38- 45. doi:10.1001/jamainternmed.2018.5100
- Dutzi I, Schwenk M, Kirchner M, Jooss E, Bauer JM, Hauer K. Influence of cognitive impairment on rehabilitation received and its mediating effect on functional recovery. J Alzheimers Dis. 2021;84:745-756. doi:10.3233/JAD-210620
- Uriz-Otano F, Uriz-Otano JI, Malafarina V. Factors associated with short-term functional recovery in elderly people with a hip fracture. Influence ofcognitiveimpairment. JAmMedDirAssoc. 2015;16:215-220. doi:10.1016/j.jamda.2014.09.009
- Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53:695-699. doi:10.1111/j.1532-5415.2005.53221.x
- Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473-483.
- White RS, Jiang J, Hall CB, et al. Higher perceived stress scale scores are associated with higher pain intensity and pain interference levels in older adults. J Am Geriatr Soc. 2014;62:2350-2356. doi:10.1111/jgs.13135
- Blyth FM, March LM, Brnabic AJ, et al. Chronic pain in Australia: a prevalence study. Pain. 2001;89:127-134. doi:10.1016/s0304-3959(00)00355-9
- Thomas E, Peat G, Harris L, Wilkie R, Croft PR. The prevalence of pain and pain interference in a general population of older adults: cross-sectional findings from the North Staffordshire Osteoarthritis Project (NorStOP). Pain. 2004;110:361-368. doi:10.1016/j.pain.2004.04.017
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914-919. doi:10.1001/jama.1963.03060120024016
- Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179-186.
- Alexander NB, Guire KE, Thelen DG, et al. Self-reported walking ability predicts functional mobility performance in frail older adults. J Am Geriatr Soc. 2000;48:1408-1413. doi:10.1111/j.1532-5415.2000.tb02630.x
- Rosow I, Breslau N. A Guttman health scale for the aged. J Gerontol. 1966;21:556-559. doi:10.1093/geronj/21.4.556
- Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49:M85-M94. doi:10.1093/geronj/49.2.m85
- Chan CS, Slaughter SE, Jones CA, Ickert C, Wagg AS. Measuring activity performance of older adults using the activPAL: a rapid review. Healthcare (Basel). 2017;5:94. doi:10.3390/healthcare5040094
- IBM SPSS software. IBM Corp; 2019. Accessed September 3, 2025. https://www.ibm.com/spss
- Kang H. The prevention and handling of the missing data. Korean J Anesthesiol. 2013;64:402-406. doi:10.4097/kjae.2013.64.5.402
- Epstein AM, Jha AK, Orav EJ. The relationship between hospital admission rates and rehospitalizations. N Engl J Med. 2011;365:2287-2295. doi:10.1056/NEJMsa1101942
- Bogaisky M, Dezieck L. Early hospital readmission of nursing home residents and community-dwelling elderly adults discharged from the geriatrics service of an urban teaching hospital: patterns and risk factors. J Am Geriatr Soc. 2015;63:548-552. doi:10.1111/jgs.13317
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418-1428. doi:10.1056/NEJMsa0803563
- Hoyer EH, Needham DM, Atanelov L, Knox B, Friedman M, Brotman DJ. Association of impaired functional status at hospital discharge and subsequent rehospitalization. J Hosp Med. 2014;9:277-282. doi:10.1002/jhm.2152
- Mahoney J, Sager M, Dunham NC, Johnson J. Risk of falls after hospital discharge. J Am Geriatr Soc. 1994;42:269- 274. doi:10.1111/j.1532-5415.1994.tb01750.x
- Hoffman GJ, Liu H, Alexander NB, Tinetti M, Braun TM, Min LC. Posthospital fall injuries and 30-day readmissions in adults 65 years and older. JAMA Netw Open. 2019;2:e194276. doi:10.1001/jamanetworkopen.2019.4276
- Gill DP, Hubbard RA, Koepsell TD, et al. Differences in rate of functional decline across three dementia types. Alzheimers Dement. 2013;9:S63-S71. doi:10.1016/j.jalz.2012.10.010
- Auyeung TW, Kwok T, Lee J, Leung PC, Leung J, Woo J. Functional decline in cognitive impairment–the relationship between physical and cognitive function. Neuroepidemiology. 2008;31:167-173. doi:10.1159/000154929
- Patti A, Zangla D, Sahin FN, et al. Physical exercise and prevention of falls. Effects of a Pilates training method compared with a general physical activity program. Medicine (Baltimore). 2021;100:e25289. doi:10.1097/MD.0000000000025289
- Nagarkar A, Kulkarni S. Association between daily activities and fall in older adults: an analysis of longitudinal ageing study in India (2017-18). BMC Geriatr. 2022;22:203. doi:10.1186/s12877-022-02879-x
- Ek S, Rizzuto D, Xu W, Calderón-Larrañaga A, Welmer AK. Predictors for functional decline after an injurious fall: a population-based cohort study. Aging Clin Exp Res. 2021;33:2183-2190. doi:10.1007/s40520-020-01747-1
- Dagnino APA, Campos MM. Chronic pain in the elderly: mechanisms and perspectives. Front Hum Neurosci. 2022;16:736688. doi:10.3389/fnhum.2022.736688
- Ritchie CS, Patel K, Boscardin J, et al. Impact of persistent pain on function, cognition, and well-being of older adults. J Am Geriatr Soc. 2023;71:26-35. doi:10.1111/jgs.18125
- Han TS, Murray P, Robin J, et al. Evaluation of the association of length of stay in hospital and outcomes. Int J Qual Health Care. 2022;34:mzab160. doi:10.1093/intqhc/ mzab160
- Lærum-Onsager E, Molin M, Olsen CF, et al. Effect of nutritional and physical exercise intervention on hospital readmission for patients aged 65 or older: a systematic review and meta-analysis of randomized controlled trials. Int J Behav Nutr Phys Act. 2021;18:62. doi:10.1186/s12966-021-01123-w
- Van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: a systematic review. CMAJ. 2011;183:E391-E402. doi:10.1503/cmaj.101860
- Liebzeit D, Bratzke L, Boltz M, Purvis S, King B. Getting back to normal: a grounded theory study of function in post-hospitalized older adults. Gerontologist. 2020;60:704-714. doi:10.1093/geront/gnz057
- Ponzetto M, Zanocchi M, Maero B, et al. Post-hospitalization mortality in the elderly. Arch Gerontol Geriatr. 2003;36:83-91. doi:10.1016/s0167-4943(02)00061-4
- Buurman BM, Hoogerduijn JG, de Haan RJ, et al. Geriatric conditions in acutely hospitalized older patients: prevalence and one-year survival and functional decline. PLoS One. 2011;6:e26951. doi:10.1371/journal.pone.0026951
- Ponzetto M, Maero B, Maina P, et al. Risk factors for early and late mortality in hospitalized older patients: the continuing importance of functional status. J Gerontol A Biol Sci Med Sci. 2003;58:1049-1054. doi:10.1093/gerona/58.11.m1049
- Huang HT, Chang CM, Liu LF, Lin HS, Chen CH. Trajectories and predictors of functional decline of hospitalised older patients. J Clin Nurs. 2013;22:1322-1331. doi:10.1111/jocn.12055
- Boyd CM, Landefeld CS, Counsell SR, et al. Recovery of activities of daily living in older adults after hospitalization for acute medical illness. J Am Geriatr Soc. 2008;56:2171- 2179. doi:10.1111/j.1532-5415.2008.02023.x
- Helvik AS, Selbæk G, Engedal K. Functional decline in older adults one year after hospitalization. Arch Gerontol Geriatr. 2013;57:305-310. doi:10.1016/j.archger.2013.05.008
- Zaslavsky O, Zisberg A, Shadmi E. Impact of functional change before and during hospitalization on functional recovery 1 month following hospitalization. J Gerontol Biol Sci Med Sci. 2015;70:381-386. doi:10.1093/gerona/glu168
- Chen CC, Wang C, Huang GH. Functional trajectory 6 months posthospitalization: a cohort study of older hospitalized patients in Taiwan. Nurs Res. 2008;57:93-100. doi:10.1097/01.NNR.0000313485.18670.e2
- Kleinpell RM, Fletcher K, Jennings BM. Reducing functional decline in hospitalized elderly. In: Hughes RG, ed. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Agency for Healthcare Research and Quality (US); 2008. Accessed September 3, 2025. http://www.ncbi.nlm.nih.gov/books/NBK2629/
- Liebzeit D, Rutkowski R, Arbaje AI, Fields B, Werner NE. A scoping review of interventions for older adults transitioning from hospital to home. J Am Geriatr Soc. 2021;69:2950-2962. doi:10.1111/jgs.17323
- Hladkowicz E, Dumitrascu F, Auais M, et al. Evaluations of postoperative transitions in care for older adults: a scoping review. BMC Geriatr. 2022;22:329. doi:10.1186/s12877-022-02989-6
- Alexander NB, Phillips K, Wagner-Felkey J, et al. Team VA Video Connect (VVC) to optimize mobility and physical activity in post-hospital discharge older veterans: baseline assessment. BMC Geriatr. 2021;21:502. doi:10.1186/s12877-021-02454-w
- Dawson R, Oliveira JS, Kwok WS, et al. Exercise interventions delivered through telehealth to improve physical functioning for older adults with frailty, cognitive, or mobility disability: a systematic review and meta-analysis. Telemed J E Health. 2024;30:940-950. doi:10.1089/tmj.2023.0177
- Liebzeit D, Phillips KK, Hogikyan RV, Cigolle CT, Alexander NB. A pilot home-telehealth program to enhance functional ability, physical performance, and physical activity in older adult veterans post-hospital discharge. Res Gerontol Nurs. 2024;17:271-279. doi:10.3928/19404921-20241105-01
- Krumholz HM. Post-hospital syndrome—an acquired, transient condition of generalized risk. N Engl J Med. 2013;368:100-102. doi:10.1056/NEJMp1212324
- Caraballo C, Dharmarajan K, Krumholz HM. Post hospital syndrome: is the stress of hospitalization causing harm? Rev Esp Cardiol (Engl Ed). 2019;72:896-898. doi:10.1016/j.rec.2019.04.010
- Rawal S, Kwan JL, Razak F, et al. Association of the trauma of hospitalization with 30-day readmission or emergency department visit. JAMA Intern Med. 2019;179:38- 45. doi:10.1001/jamainternmed.2018.5100
- Dutzi I, Schwenk M, Kirchner M, Jooss E, Bauer JM, Hauer K. Influence of cognitive impairment on rehabilitation received and its mediating effect on functional recovery. J Alzheimers Dis. 2021;84:745-756. doi:10.3233/JAD-210620
- Uriz-Otano F, Uriz-Otano JI, Malafarina V. Factors associated with short-term functional recovery in elderly people with a hip fracture. Influence ofcognitiveimpairment. JAmMedDirAssoc. 2015;16:215-220. doi:10.1016/j.jamda.2014.09.009
- Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53:695-699. doi:10.1111/j.1532-5415.2005.53221.x
- Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473-483.
- White RS, Jiang J, Hall CB, et al. Higher perceived stress scale scores are associated with higher pain intensity and pain interference levels in older adults. J Am Geriatr Soc. 2014;62:2350-2356. doi:10.1111/jgs.13135
- Blyth FM, March LM, Brnabic AJ, et al. Chronic pain in Australia: a prevalence study. Pain. 2001;89:127-134. doi:10.1016/s0304-3959(00)00355-9
- Thomas E, Peat G, Harris L, Wilkie R, Croft PR. The prevalence of pain and pain interference in a general population of older adults: cross-sectional findings from the North Staffordshire Osteoarthritis Project (NorStOP). Pain. 2004;110:361-368. doi:10.1016/j.pain.2004.04.017
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914-919. doi:10.1001/jama.1963.03060120024016
- Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179-186.
- Alexander NB, Guire KE, Thelen DG, et al. Self-reported walking ability predicts functional mobility performance in frail older adults. J Am Geriatr Soc. 2000;48:1408-1413. doi:10.1111/j.1532-5415.2000.tb02630.x
- Rosow I, Breslau N. A Guttman health scale for the aged. J Gerontol. 1966;21:556-559. doi:10.1093/geronj/21.4.556
- Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49:M85-M94. doi:10.1093/geronj/49.2.m85
- Chan CS, Slaughter SE, Jones CA, Ickert C, Wagg AS. Measuring activity performance of older adults using the activPAL: a rapid review. Healthcare (Basel). 2017;5:94. doi:10.3390/healthcare5040094
- IBM SPSS software. IBM Corp; 2019. Accessed September 3, 2025. https://www.ibm.com/spss
- Kang H. The prevention and handling of the missing data. Korean J Anesthesiol. 2013;64:402-406. doi:10.4097/kjae.2013.64.5.402
- Epstein AM, Jha AK, Orav EJ. The relationship between hospital admission rates and rehospitalizations. N Engl J Med. 2011;365:2287-2295. doi:10.1056/NEJMsa1101942
- Bogaisky M, Dezieck L. Early hospital readmission of nursing home residents and community-dwelling elderly adults discharged from the geriatrics service of an urban teaching hospital: patterns and risk factors. J Am Geriatr Soc. 2015;63:548-552. doi:10.1111/jgs.13317
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418-1428. doi:10.1056/NEJMsa0803563
- Hoyer EH, Needham DM, Atanelov L, Knox B, Friedman M, Brotman DJ. Association of impaired functional status at hospital discharge and subsequent rehospitalization. J Hosp Med. 2014;9:277-282. doi:10.1002/jhm.2152
- Mahoney J, Sager M, Dunham NC, Johnson J. Risk of falls after hospital discharge. J Am Geriatr Soc. 1994;42:269- 274. doi:10.1111/j.1532-5415.1994.tb01750.x
- Hoffman GJ, Liu H, Alexander NB, Tinetti M, Braun TM, Min LC. Posthospital fall injuries and 30-day readmissions in adults 65 years and older. JAMA Netw Open. 2019;2:e194276. doi:10.1001/jamanetworkopen.2019.4276
- Gill DP, Hubbard RA, Koepsell TD, et al. Differences in rate of functional decline across three dementia types. Alzheimers Dement. 2013;9:S63-S71. doi:10.1016/j.jalz.2012.10.010
- Auyeung TW, Kwok T, Lee J, Leung PC, Leung J, Woo J. Functional decline in cognitive impairment–the relationship between physical and cognitive function. Neuroepidemiology. 2008;31:167-173. doi:10.1159/000154929
- Patti A, Zangla D, Sahin FN, et al. Physical exercise and prevention of falls. Effects of a Pilates training method compared with a general physical activity program. Medicine (Baltimore). 2021;100:e25289. doi:10.1097/MD.0000000000025289
- Nagarkar A, Kulkarni S. Association between daily activities and fall in older adults: an analysis of longitudinal ageing study in India (2017-18). BMC Geriatr. 2022;22:203. doi:10.1186/s12877-022-02879-x
- Ek S, Rizzuto D, Xu W, Calderón-Larrañaga A, Welmer AK. Predictors for functional decline after an injurious fall: a population-based cohort study. Aging Clin Exp Res. 2021;33:2183-2190. doi:10.1007/s40520-020-01747-1
- Dagnino APA, Campos MM. Chronic pain in the elderly: mechanisms and perspectives. Front Hum Neurosci. 2022;16:736688. doi:10.3389/fnhum.2022.736688
- Ritchie CS, Patel K, Boscardin J, et al. Impact of persistent pain on function, cognition, and well-being of older adults. J Am Geriatr Soc. 2023;71:26-35. doi:10.1111/jgs.18125
- Han TS, Murray P, Robin J, et al. Evaluation of the association of length of stay in hospital and outcomes. Int J Qual Health Care. 2022;34:mzab160. doi:10.1093/intqhc/ mzab160
- Lærum-Onsager E, Molin M, Olsen CF, et al. Effect of nutritional and physical exercise intervention on hospital readmission for patients aged 65 or older: a systematic review and meta-analysis of randomized controlled trials. Int J Behav Nutr Phys Act. 2021;18:62. doi:10.1186/s12966-021-01123-w
- Van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: a systematic review. CMAJ. 2011;183:E391-E402. doi:10.1503/cmaj.101860
Factors Influencing Outcomes of a Telehealth-Based Physical Activity Program in Older Veterans Postdischarge
Factors Influencing Outcomes of a Telehealth-Based Physical Activity Program in Older Veterans Postdischarge
GLP-1s Increase GERD Risk Over SGLT2 Inhibitors in T2D
in a cohort study of new users.
Risks for GERD were higher overall for each GLP-1 RA type except lixisenatide, and risks for GERD complications were higher in ever-smokers, patients with obesity, and patients with gastric comorbidities.
“The findings were not entirely surprising,” principal author Laurent Azoulay, PhD, of McGill University and Lady Davis Institute for Medical Research, Jewish General Hospital, Montreal, Quebec, Canada, told GI & Hepatology News. “There is a plausible biological mechanism through which GLP-1 RAs could increase the risk of GERD — namely, by delaying gastric emptying, which can lead to symptoms of reflux. Still, it’s always valuable to see whether the clinical data support what we suspect from a physiological standpoint.”
“As with any medication, it’s about balancing benefits and risks — and being proactive when side effects emerge,” he added.
The study was published online in Annals of Internal Medicine.
Duration of Use, Drug Action
Researchers designed an active comparator new-user cohort study emulating a target trial to estimate the effects of GLP-1 RAs compared with SGLT2 inhibitors on the risk for GERD and its complications among patients with T2D.
The study included 24,708 new users of GLP-1 RAs and 89,096 new users of SGLT2 inhibitors. Participants had a mean age of 56 years, and 55% were men. They initiated treatment with the drugs from January 2013 through December 2021, with follow-up through March 2022.
Three-year risk differences (RDs) and risk ratios (RRs) were estimated and weighted using propensity score fine stratification.
Overall, during follow-up, the incidence rate of GERD was 7.9 per 1000 person-years; 138 complications of GERD were observed, with over 90% of them being Barrett’s esophagus.
Over a median follow-up of 3 years, among GLP-1 RA users compared with SGLT2 inhibitor users, the RRs were 1.27 for GERD, with an RD of 0.7 per 100 patients, and 1.55 for complications, with an RD of 0.8 per 1000 patients.
Further analyses found that risks for GERD were higher overall for each GLP-1 RA type except lixisenatide, and risks for GERD complications were higher in ever-smokers, patients with obesity, and those with gastric comorbidities associated with gastric motility. The findings remained robust across sensitivity analyses addressing various types of biases.
The widening incidence curves with duration of use may indicate that mucosal injury and symptom severity correlate with reflux frequency and duration of esophageal acid exposure, the authors suggested.
GERD risk also was higher with long-acting GLP-1 RA use, suggesting that long-acting GLP-1 RAs (liraglutide, exenatide once weekly, dulaglutide, and semaglutide) may have more sustained delaying effects, they noted.
“These potential risks should be weighed against the established clinical benefits of this drug class, particularly in patients at high risk for gastroparesis and GERD,” the authors concluded.
“Given the mechanism through which these drugs may cause GERD, we can reasonably speculate that a similar effect might be observed in individuals without diabetes,” Azoulay added. “That said, a dedicated study would be needed to confirm that.”
Close Monitoring Advised
Caroline Collins, MD, assistant professor at Emory University School of Medicine in Atlanta, agreed with the findings and said the association between GLP-1s and GERD is consistent with what she has observed in her practice.
“I routinely counsel patients about the potential for GERD symptoms as well as other side effects before initiating GLP-1 therapy,” she told GI & Hepatology News. “Several patients on GLP-1s have reported new or worsening reflux symptoms after initiating therapy. Sometimes, we can lower the dose, and the GERD resolves. Other times initiating GERD treatment or discontinuing the medication is appropriate.”
“Patients with T2D are already at increased risk for delayed gastric emptying, which in itself is a contributor to GERD,” said Collins, who was not involved in the study. “Therefore, adding a GLP-1 RA, which further slows gastric motility, may compound this risk. I consider this when assessing which patients are the best candidates for these medications and often monitor more closely in patients with long-standing diabetes and other predisposing factors to GERD.”
Barrett’s esophagus and esophageal cancer generally occur over many years, she noted. “A median follow-up of 3 years may be insufficient to fully assess the long-term risks of serious complications.”
“Chronic cough, a common but often overlooked manifestation of GERD, was not included in the outcome definitions,” she added. Including chronic cough “may have captured a broader picture of reflux-related symptoms.”
The study was funded by a Foundation Scheme grant from the Canadian Institutes of Health Research. Azoulay holds a Distinguished Research Scholar award from the Fonds de recherche du Quebec – Sante and is the recipient of a William Dawson Scholar award from McGill University.
A version of this article appeared on Medscape.com.
in a cohort study of new users.
Risks for GERD were higher overall for each GLP-1 RA type except lixisenatide, and risks for GERD complications were higher in ever-smokers, patients with obesity, and patients with gastric comorbidities.
“The findings were not entirely surprising,” principal author Laurent Azoulay, PhD, of McGill University and Lady Davis Institute for Medical Research, Jewish General Hospital, Montreal, Quebec, Canada, told GI & Hepatology News. “There is a plausible biological mechanism through which GLP-1 RAs could increase the risk of GERD — namely, by delaying gastric emptying, which can lead to symptoms of reflux. Still, it’s always valuable to see whether the clinical data support what we suspect from a physiological standpoint.”
“As with any medication, it’s about balancing benefits and risks — and being proactive when side effects emerge,” he added.
The study was published online in Annals of Internal Medicine.
Duration of Use, Drug Action
Researchers designed an active comparator new-user cohort study emulating a target trial to estimate the effects of GLP-1 RAs compared with SGLT2 inhibitors on the risk for GERD and its complications among patients with T2D.
The study included 24,708 new users of GLP-1 RAs and 89,096 new users of SGLT2 inhibitors. Participants had a mean age of 56 years, and 55% were men. They initiated treatment with the drugs from January 2013 through December 2021, with follow-up through March 2022.
Three-year risk differences (RDs) and risk ratios (RRs) were estimated and weighted using propensity score fine stratification.
Overall, during follow-up, the incidence rate of GERD was 7.9 per 1000 person-years; 138 complications of GERD were observed, with over 90% of them being Barrett’s esophagus.
Over a median follow-up of 3 years, among GLP-1 RA users compared with SGLT2 inhibitor users, the RRs were 1.27 for GERD, with an RD of 0.7 per 100 patients, and 1.55 for complications, with an RD of 0.8 per 1000 patients.
Further analyses found that risks for GERD were higher overall for each GLP-1 RA type except lixisenatide, and risks for GERD complications were higher in ever-smokers, patients with obesity, and those with gastric comorbidities associated with gastric motility. The findings remained robust across sensitivity analyses addressing various types of biases.
The widening incidence curves with duration of use may indicate that mucosal injury and symptom severity correlate with reflux frequency and duration of esophageal acid exposure, the authors suggested.
GERD risk also was higher with long-acting GLP-1 RA use, suggesting that long-acting GLP-1 RAs (liraglutide, exenatide once weekly, dulaglutide, and semaglutide) may have more sustained delaying effects, they noted.
“These potential risks should be weighed against the established clinical benefits of this drug class, particularly in patients at high risk for gastroparesis and GERD,” the authors concluded.
“Given the mechanism through which these drugs may cause GERD, we can reasonably speculate that a similar effect might be observed in individuals without diabetes,” Azoulay added. “That said, a dedicated study would be needed to confirm that.”
Close Monitoring Advised
Caroline Collins, MD, assistant professor at Emory University School of Medicine in Atlanta, agreed with the findings and said the association between GLP-1s and GERD is consistent with what she has observed in her practice.
“I routinely counsel patients about the potential for GERD symptoms as well as other side effects before initiating GLP-1 therapy,” she told GI & Hepatology News. “Several patients on GLP-1s have reported new or worsening reflux symptoms after initiating therapy. Sometimes, we can lower the dose, and the GERD resolves. Other times initiating GERD treatment or discontinuing the medication is appropriate.”
“Patients with T2D are already at increased risk for delayed gastric emptying, which in itself is a contributor to GERD,” said Collins, who was not involved in the study. “Therefore, adding a GLP-1 RA, which further slows gastric motility, may compound this risk. I consider this when assessing which patients are the best candidates for these medications and often monitor more closely in patients with long-standing diabetes and other predisposing factors to GERD.”
Barrett’s esophagus and esophageal cancer generally occur over many years, she noted. “A median follow-up of 3 years may be insufficient to fully assess the long-term risks of serious complications.”
“Chronic cough, a common but often overlooked manifestation of GERD, was not included in the outcome definitions,” she added. Including chronic cough “may have captured a broader picture of reflux-related symptoms.”
The study was funded by a Foundation Scheme grant from the Canadian Institutes of Health Research. Azoulay holds a Distinguished Research Scholar award from the Fonds de recherche du Quebec – Sante and is the recipient of a William Dawson Scholar award from McGill University.
A version of this article appeared on Medscape.com.
in a cohort study of new users.
Risks for GERD were higher overall for each GLP-1 RA type except lixisenatide, and risks for GERD complications were higher in ever-smokers, patients with obesity, and patients with gastric comorbidities.
“The findings were not entirely surprising,” principal author Laurent Azoulay, PhD, of McGill University and Lady Davis Institute for Medical Research, Jewish General Hospital, Montreal, Quebec, Canada, told GI & Hepatology News. “There is a plausible biological mechanism through which GLP-1 RAs could increase the risk of GERD — namely, by delaying gastric emptying, which can lead to symptoms of reflux. Still, it’s always valuable to see whether the clinical data support what we suspect from a physiological standpoint.”
“As with any medication, it’s about balancing benefits and risks — and being proactive when side effects emerge,” he added.
The study was published online in Annals of Internal Medicine.
Duration of Use, Drug Action
Researchers designed an active comparator new-user cohort study emulating a target trial to estimate the effects of GLP-1 RAs compared with SGLT2 inhibitors on the risk for GERD and its complications among patients with T2D.
The study included 24,708 new users of GLP-1 RAs and 89,096 new users of SGLT2 inhibitors. Participants had a mean age of 56 years, and 55% were men. They initiated treatment with the drugs from January 2013 through December 2021, with follow-up through March 2022.
Three-year risk differences (RDs) and risk ratios (RRs) were estimated and weighted using propensity score fine stratification.
Overall, during follow-up, the incidence rate of GERD was 7.9 per 1000 person-years; 138 complications of GERD were observed, with over 90% of them being Barrett’s esophagus.
Over a median follow-up of 3 years, among GLP-1 RA users compared with SGLT2 inhibitor users, the RRs were 1.27 for GERD, with an RD of 0.7 per 100 patients, and 1.55 for complications, with an RD of 0.8 per 1000 patients.
Further analyses found that risks for GERD were higher overall for each GLP-1 RA type except lixisenatide, and risks for GERD complications were higher in ever-smokers, patients with obesity, and those with gastric comorbidities associated with gastric motility. The findings remained robust across sensitivity analyses addressing various types of biases.
The widening incidence curves with duration of use may indicate that mucosal injury and symptom severity correlate with reflux frequency and duration of esophageal acid exposure, the authors suggested.
GERD risk also was higher with long-acting GLP-1 RA use, suggesting that long-acting GLP-1 RAs (liraglutide, exenatide once weekly, dulaglutide, and semaglutide) may have more sustained delaying effects, they noted.
“These potential risks should be weighed against the established clinical benefits of this drug class, particularly in patients at high risk for gastroparesis and GERD,” the authors concluded.
“Given the mechanism through which these drugs may cause GERD, we can reasonably speculate that a similar effect might be observed in individuals without diabetes,” Azoulay added. “That said, a dedicated study would be needed to confirm that.”
Close Monitoring Advised
Caroline Collins, MD, assistant professor at Emory University School of Medicine in Atlanta, agreed with the findings and said the association between GLP-1s and GERD is consistent with what she has observed in her practice.
“I routinely counsel patients about the potential for GERD symptoms as well as other side effects before initiating GLP-1 therapy,” she told GI & Hepatology News. “Several patients on GLP-1s have reported new or worsening reflux symptoms after initiating therapy. Sometimes, we can lower the dose, and the GERD resolves. Other times initiating GERD treatment or discontinuing the medication is appropriate.”
“Patients with T2D are already at increased risk for delayed gastric emptying, which in itself is a contributor to GERD,” said Collins, who was not involved in the study. “Therefore, adding a GLP-1 RA, which further slows gastric motility, may compound this risk. I consider this when assessing which patients are the best candidates for these medications and often monitor more closely in patients with long-standing diabetes and other predisposing factors to GERD.”
Barrett’s esophagus and esophageal cancer generally occur over many years, she noted. “A median follow-up of 3 years may be insufficient to fully assess the long-term risks of serious complications.”
“Chronic cough, a common but often overlooked manifestation of GERD, was not included in the outcome definitions,” she added. Including chronic cough “may have captured a broader picture of reflux-related symptoms.”
The study was funded by a Foundation Scheme grant from the Canadian Institutes of Health Research. Azoulay holds a Distinguished Research Scholar award from the Fonds de recherche du Quebec – Sante and is the recipient of a William Dawson Scholar award from McGill University.
A version of this article appeared on Medscape.com.
Bariatric Surgery May Lower Long-Term CKD Risk
, according to a population-based study in Denmark.
Writing in BMC Nephrology, researchers reported patients with bariatric surgery had an increased 1-year risk for AKI and 10-year risk for nephrolithiasis, alongside a decreased 10-year risk for CKD (stages G3-5) and KFRT, compared with matched patients diagnosed with overweight/obesity who did not undergo surgery.
A Closer Look
Using national registry data, the team identified all adults who underwent Roux-en-Y gastric bypass (RYGB) or sleeve gastrectomy (SG) between January 1, 2006, and December 31, 2018. Each patient was age- and sex-matched (1:5) to patients with hospital-diagnosed overweight/obesity without bariatric surgery. Researchers also compared results against a population cohort matched solely by age and sex. Outcomes included cumulative risks for AKI, nephrolithiasis, CKD (G3-G5), and KFRT.
The cohort comprised 18,827 surgical patients (17,200 RYGB and 1627 SG) and 94,135 matched comparators. Median age was 41 years, 76% were women, and the median follow-up was 8.1 years. At baseline, the median estimated glomerular filtration rate (eGFR) was comparable (103 mL/min/1.73 m2) between both surgery and overweight/obesity control groups, as were A1c levels. There were fewer comorbidities in the population cohort matched only by age and sex than in the overweight/obesity comparison cohort.
Using multivariable Cox regression analyses, the researchers found the 1-year risk for AKI following bariatric surgery was 2.7%. At 10 years, risks were 3.5% for nephrolithiasis, 0.4% for CKD, and 0.2% for KFRT.
Adjusted hazard ratios (HRs) after bariatric surgery vs without bariatric surgery were higher for AKI (HR, 1.63) and nephrolithiasis (HR, 1.73) and lower for CKD (HR, 0.41) and KFRT (HR, 0.63). Results were consistent when compared against the population cohort.
By procedure, the 1-year AKI risk was 2.7% after RYGB and 2.4% after SG vs 2.5% in the overweight/obesity cohort and 1.1% in the population cohort. At 10 years, the risk for incident nephrolithiasis was 3.6% after RYGB and 1.2% after SG vs 2.4% and 1.3% in the overweight/obese and population cohorts, respectively. KFRT risk at 10 years was 0.2% after RYGB and 1.6% after SG vs 0.4% and 0.1% in the overweight/obesity and population cohorts, respectively.
“The increased short-term risk of AKI and nephrolithiasis was expected, given the physiological changes after bariatric surgery, but the long-term reduction in CKD and KFRT was both encouraging and clinically important,” said study investigator Christian Goul Sørensen, MD, Department of Clinical Epidemiology, Department of Clinical Medicine, Aarhus University and Aarhus University Hospital, Aarhus, Denmark. “It was also noteworthy that the results were consistent not only in the obesity-matched comparison cohort but also in the cohort matched solely on age and sex, which further strengthens the validity of our findings.”
RYGB and SG are known to help mitigate obesity-associated complications, such as hypertension, hyperlipidemia, and type 2 diabetes. Studies have suggested that there are improvements in eGFR after bariatric surgery. However, long-term evidence from routine clinical care has not been well studied. Furthermore, RYGB may lead to AKI due to a combination of preoperative, intraoperative, and postoperative factors.
“Obesity is a major driver of kidney disease, often in combination with comorbidities such as diabetes and hypertension,” Sorensen told GI & Hepatology News. “Patients and clinicians face complex decisions about surgery, and understanding both the short-term surgical risks and the long-term kidney benefits is crucial for informed counseling. As bariatric surgery becomes increasingly common worldwide, population-based evidence like this helps guide clinical practice and supports shared decision-making with patients.”
Consistent With Clinical Experience
Panduranga S. Rao, MD, professor of nephrology at the University of Michigan, Ann Arbor, Michigan, who was not involved in the study, called the results consistent with prior clinical experience. He highlighted the strong follow-up and detailed lab and comorbidity data, while noting that the decreasing use of RYGB may limit applicability going forward.
“However, one has to remain vigilant to the risk of nephrolithiasis in the patients who have undergone Roux-en-Y in the past,” he said.
The observation of decreasing risk for CKD with weight loss is particularly relevant, given the growing use of GLP-1s for weight loss, Rao added.
Srinivasan Beddhu, MD, professor of internal medicine and the scientific director of the Cardio-Renal & Metabolism Center at the University of Utah Health in Salt Lake City, said the large national cohort design and outcomes data offer further reassurance about the long-term kidney health effects of bariatric surgery.
“The message that the risks of AKI and nephrolithiasis are outweighed by the long-term kidney protective effects of bariatric surgery is important,” said Beddhu.
Alexander Chang, MD, associate professor and a practicing nephrologist at the Geisinger Health System in Danville, Pennsylvania, noted that the study provided more evidence about RYGB-associated kidney stone risk via fat malabsorption, which raises the levels of fatty acids that bind dietary calcium.
“Calcium normally precipitates with dietary oxalate, and thus, there can be an increase in urinary oxalate,” Chang explained. “There did not appear to be increased risk of nephrolithiasis with sleeve gastrectomy, consistent with other studies.
“This study emphasizes the importance of multidisciplinary care post-bariatric surgery to try to prevent complications such as kidney stones,” Chang added. “This can be tricky but requires trying different strategies to increase fluid intake and calcium citrate supplements with meals.”
The study was partly funded by a grant from the Novo Nordisk Foundation and the Independent Research Fund Denmark. One author reported receiving a speaking fee support from Novo Nordisk for conference attendance. The other authors declared no competing interests. Sørensen, Rao, Beddhu, and Chang had no financial disclosures.
A version of this article appeared on Medscape.com.
, according to a population-based study in Denmark.
Writing in BMC Nephrology, researchers reported patients with bariatric surgery had an increased 1-year risk for AKI and 10-year risk for nephrolithiasis, alongside a decreased 10-year risk for CKD (stages G3-5) and KFRT, compared with matched patients diagnosed with overweight/obesity who did not undergo surgery.
A Closer Look
Using national registry data, the team identified all adults who underwent Roux-en-Y gastric bypass (RYGB) or sleeve gastrectomy (SG) between January 1, 2006, and December 31, 2018. Each patient was age- and sex-matched (1:5) to patients with hospital-diagnosed overweight/obesity without bariatric surgery. Researchers also compared results against a population cohort matched solely by age and sex. Outcomes included cumulative risks for AKI, nephrolithiasis, CKD (G3-G5), and KFRT.
The cohort comprised 18,827 surgical patients (17,200 RYGB and 1627 SG) and 94,135 matched comparators. Median age was 41 years, 76% were women, and the median follow-up was 8.1 years. At baseline, the median estimated glomerular filtration rate (eGFR) was comparable (103 mL/min/1.73 m2) between both surgery and overweight/obesity control groups, as were A1c levels. There were fewer comorbidities in the population cohort matched only by age and sex than in the overweight/obesity comparison cohort.
Using multivariable Cox regression analyses, the researchers found the 1-year risk for AKI following bariatric surgery was 2.7%. At 10 years, risks were 3.5% for nephrolithiasis, 0.4% for CKD, and 0.2% for KFRT.
Adjusted hazard ratios (HRs) after bariatric surgery vs without bariatric surgery were higher for AKI (HR, 1.63) and nephrolithiasis (HR, 1.73) and lower for CKD (HR, 0.41) and KFRT (HR, 0.63). Results were consistent when compared against the population cohort.
By procedure, the 1-year AKI risk was 2.7% after RYGB and 2.4% after SG vs 2.5% in the overweight/obesity cohort and 1.1% in the population cohort. At 10 years, the risk for incident nephrolithiasis was 3.6% after RYGB and 1.2% after SG vs 2.4% and 1.3% in the overweight/obese and population cohorts, respectively. KFRT risk at 10 years was 0.2% after RYGB and 1.6% after SG vs 0.4% and 0.1% in the overweight/obesity and population cohorts, respectively.
“The increased short-term risk of AKI and nephrolithiasis was expected, given the physiological changes after bariatric surgery, but the long-term reduction in CKD and KFRT was both encouraging and clinically important,” said study investigator Christian Goul Sørensen, MD, Department of Clinical Epidemiology, Department of Clinical Medicine, Aarhus University and Aarhus University Hospital, Aarhus, Denmark. “It was also noteworthy that the results were consistent not only in the obesity-matched comparison cohort but also in the cohort matched solely on age and sex, which further strengthens the validity of our findings.”
RYGB and SG are known to help mitigate obesity-associated complications, such as hypertension, hyperlipidemia, and type 2 diabetes. Studies have suggested that there are improvements in eGFR after bariatric surgery. However, long-term evidence from routine clinical care has not been well studied. Furthermore, RYGB may lead to AKI due to a combination of preoperative, intraoperative, and postoperative factors.
“Obesity is a major driver of kidney disease, often in combination with comorbidities such as diabetes and hypertension,” Sorensen told GI & Hepatology News. “Patients and clinicians face complex decisions about surgery, and understanding both the short-term surgical risks and the long-term kidney benefits is crucial for informed counseling. As bariatric surgery becomes increasingly common worldwide, population-based evidence like this helps guide clinical practice and supports shared decision-making with patients.”
Consistent With Clinical Experience
Panduranga S. Rao, MD, professor of nephrology at the University of Michigan, Ann Arbor, Michigan, who was not involved in the study, called the results consistent with prior clinical experience. He highlighted the strong follow-up and detailed lab and comorbidity data, while noting that the decreasing use of RYGB may limit applicability going forward.
“However, one has to remain vigilant to the risk of nephrolithiasis in the patients who have undergone Roux-en-Y in the past,” he said.
The observation of decreasing risk for CKD with weight loss is particularly relevant, given the growing use of GLP-1s for weight loss, Rao added.
Srinivasan Beddhu, MD, professor of internal medicine and the scientific director of the Cardio-Renal & Metabolism Center at the University of Utah Health in Salt Lake City, said the large national cohort design and outcomes data offer further reassurance about the long-term kidney health effects of bariatric surgery.
“The message that the risks of AKI and nephrolithiasis are outweighed by the long-term kidney protective effects of bariatric surgery is important,” said Beddhu.
Alexander Chang, MD, associate professor and a practicing nephrologist at the Geisinger Health System in Danville, Pennsylvania, noted that the study provided more evidence about RYGB-associated kidney stone risk via fat malabsorption, which raises the levels of fatty acids that bind dietary calcium.
“Calcium normally precipitates with dietary oxalate, and thus, there can be an increase in urinary oxalate,” Chang explained. “There did not appear to be increased risk of nephrolithiasis with sleeve gastrectomy, consistent with other studies.
“This study emphasizes the importance of multidisciplinary care post-bariatric surgery to try to prevent complications such as kidney stones,” Chang added. “This can be tricky but requires trying different strategies to increase fluid intake and calcium citrate supplements with meals.”
The study was partly funded by a grant from the Novo Nordisk Foundation and the Independent Research Fund Denmark. One author reported receiving a speaking fee support from Novo Nordisk for conference attendance. The other authors declared no competing interests. Sørensen, Rao, Beddhu, and Chang had no financial disclosures.
A version of this article appeared on Medscape.com.
, according to a population-based study in Denmark.
Writing in BMC Nephrology, researchers reported patients with bariatric surgery had an increased 1-year risk for AKI and 10-year risk for nephrolithiasis, alongside a decreased 10-year risk for CKD (stages G3-5) and KFRT, compared with matched patients diagnosed with overweight/obesity who did not undergo surgery.
A Closer Look
Using national registry data, the team identified all adults who underwent Roux-en-Y gastric bypass (RYGB) or sleeve gastrectomy (SG) between January 1, 2006, and December 31, 2018. Each patient was age- and sex-matched (1:5) to patients with hospital-diagnosed overweight/obesity without bariatric surgery. Researchers also compared results against a population cohort matched solely by age and sex. Outcomes included cumulative risks for AKI, nephrolithiasis, CKD (G3-G5), and KFRT.
The cohort comprised 18,827 surgical patients (17,200 RYGB and 1627 SG) and 94,135 matched comparators. Median age was 41 years, 76% were women, and the median follow-up was 8.1 years. At baseline, the median estimated glomerular filtration rate (eGFR) was comparable (103 mL/min/1.73 m2) between both surgery and overweight/obesity control groups, as were A1c levels. There were fewer comorbidities in the population cohort matched only by age and sex than in the overweight/obesity comparison cohort.
Using multivariable Cox regression analyses, the researchers found the 1-year risk for AKI following bariatric surgery was 2.7%. At 10 years, risks were 3.5% for nephrolithiasis, 0.4% for CKD, and 0.2% for KFRT.
Adjusted hazard ratios (HRs) after bariatric surgery vs without bariatric surgery were higher for AKI (HR, 1.63) and nephrolithiasis (HR, 1.73) and lower for CKD (HR, 0.41) and KFRT (HR, 0.63). Results were consistent when compared against the population cohort.
By procedure, the 1-year AKI risk was 2.7% after RYGB and 2.4% after SG vs 2.5% in the overweight/obesity cohort and 1.1% in the population cohort. At 10 years, the risk for incident nephrolithiasis was 3.6% after RYGB and 1.2% after SG vs 2.4% and 1.3% in the overweight/obese and population cohorts, respectively. KFRT risk at 10 years was 0.2% after RYGB and 1.6% after SG vs 0.4% and 0.1% in the overweight/obesity and population cohorts, respectively.
“The increased short-term risk of AKI and nephrolithiasis was expected, given the physiological changes after bariatric surgery, but the long-term reduction in CKD and KFRT was both encouraging and clinically important,” said study investigator Christian Goul Sørensen, MD, Department of Clinical Epidemiology, Department of Clinical Medicine, Aarhus University and Aarhus University Hospital, Aarhus, Denmark. “It was also noteworthy that the results were consistent not only in the obesity-matched comparison cohort but also in the cohort matched solely on age and sex, which further strengthens the validity of our findings.”
RYGB and SG are known to help mitigate obesity-associated complications, such as hypertension, hyperlipidemia, and type 2 diabetes. Studies have suggested that there are improvements in eGFR after bariatric surgery. However, long-term evidence from routine clinical care has not been well studied. Furthermore, RYGB may lead to AKI due to a combination of preoperative, intraoperative, and postoperative factors.
“Obesity is a major driver of kidney disease, often in combination with comorbidities such as diabetes and hypertension,” Sorensen told GI & Hepatology News. “Patients and clinicians face complex decisions about surgery, and understanding both the short-term surgical risks and the long-term kidney benefits is crucial for informed counseling. As bariatric surgery becomes increasingly common worldwide, population-based evidence like this helps guide clinical practice and supports shared decision-making with patients.”
Consistent With Clinical Experience
Panduranga S. Rao, MD, professor of nephrology at the University of Michigan, Ann Arbor, Michigan, who was not involved in the study, called the results consistent with prior clinical experience. He highlighted the strong follow-up and detailed lab and comorbidity data, while noting that the decreasing use of RYGB may limit applicability going forward.
“However, one has to remain vigilant to the risk of nephrolithiasis in the patients who have undergone Roux-en-Y in the past,” he said.
The observation of decreasing risk for CKD with weight loss is particularly relevant, given the growing use of GLP-1s for weight loss, Rao added.
Srinivasan Beddhu, MD, professor of internal medicine and the scientific director of the Cardio-Renal & Metabolism Center at the University of Utah Health in Salt Lake City, said the large national cohort design and outcomes data offer further reassurance about the long-term kidney health effects of bariatric surgery.
“The message that the risks of AKI and nephrolithiasis are outweighed by the long-term kidney protective effects of bariatric surgery is important,” said Beddhu.
Alexander Chang, MD, associate professor and a practicing nephrologist at the Geisinger Health System in Danville, Pennsylvania, noted that the study provided more evidence about RYGB-associated kidney stone risk via fat malabsorption, which raises the levels of fatty acids that bind dietary calcium.
“Calcium normally precipitates with dietary oxalate, and thus, there can be an increase in urinary oxalate,” Chang explained. “There did not appear to be increased risk of nephrolithiasis with sleeve gastrectomy, consistent with other studies.
“This study emphasizes the importance of multidisciplinary care post-bariatric surgery to try to prevent complications such as kidney stones,” Chang added. “This can be tricky but requires trying different strategies to increase fluid intake and calcium citrate supplements with meals.”
The study was partly funded by a grant from the Novo Nordisk Foundation and the Independent Research Fund Denmark. One author reported receiving a speaking fee support from Novo Nordisk for conference attendance. The other authors declared no competing interests. Sørensen, Rao, Beddhu, and Chang had no financial disclosures.
A version of this article appeared on Medscape.com.
GLP-1 Use After Bariatric Surgery on the Rise
, a large retrospective cohort study showed.
GLP-1 initiation was also more common among women, those who underwent sleeve gastrectomy, and those with lower postoperative weight loss as measured by BMI.
“Some patients do not lose as much weight as expected, or they regain weight after a few years. In such cases, GLP-1 therapies are emerging as an important option for weight management,” said principal investigator Hemalkumar Mehta, PhD, associate professor at Johns Hopkins Bloomberg School of Public Health in Baltimore.
“We also noted many personal stories circulating on social media in which patients shared their experiences using GLP-1 after bariatric surgery,” he told GI & Hepatology News.
But when the researchers reviewed the scientific literature, they found no published evidence on GLP-1 use in this setting and little or no data on outcomes with the newer drugs such as semaglutide and tirzepatide. “This gap motivated us to conduct the current study,” said Mehta. The study was published in JAMA Surgery.
The researchers analyzed data from a national multicenter database of electronic health records of approximately 113 million US adults to characterize the use of and factors associated with GLP-1 initiation after bariatric surgery.
Among 112,858 individuals undergoing bariatric surgery during the study period, the mean age was 45.2 years, and 78.9% were women.
By self-report race, 1.1% were Asian, 22.1% were Black or African American, 64.2% were White individuals, and 12.6% reported belonging to other races (American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, or unknown).
A total of 15,749 individuals (14%) initiated GLP-1s post-surgery, with 3391 (21.5%) beginning within 2 years of surgery and the remainder initiating during postsurgical years 3-4 (32.3%), 5-6 (25.2%), or later (21%).
Notably, the proportion of GLP-1 use increased more in the more recent cohort, from 1.7% in the January 2015-December 2019 cohort to 12.6% from June 2020 to May 2025.
Differences Between Users and Nonusers
Those who initiated GLP-1s differed significantly from those who did not: GLP-1 users vs nonusers were younger (mean age, 44.9 years vs 45.2 years), and use was more common among women vs men (15.1% vs 9.7%), among Black or African American vs White patients (15.8% vs 13.5%), and among those who underwent sleeve gastrectomy vs Roux-en-Y gastric bypass (14.9% vs 12.1%).
Looked at another way, women (adjusted hazard ratio [aHR], 1.61), those undergoing sleeve gastrectomy (aHR, 1.42), and those with type 2 diabetes (aHR, 1.34) were more likely to initiate GLP-1s than their counterparts.
The overall median presurgical BMI was 42. On analyzing obesity classification based on BMI, the researchers found that the chances of GLP-1 use were 1.73 times higher among class 1 obesity patients (BMI, 30.0-34.9), 2.19 times higher among class 2 obesity patients (BMI, 35.0-39.9), and 2.69 times higher among patients with class 3 obesity (BMI ≥ 40) than among overweight patients (BMI, 25.0-29.9).
The median post-surgery BMI for GLP-1 users at drug initiation was 36.7. Each one-unit increase in postsurgical BMI was associated with an 8% increase in the likelihood of GLP-1 initiation (aHR, 1.08).
“Importantly, our study did not specifically evaluate the effectiveness of GLP-1 therapy on weight loss after surgery,” Mehta noted. That issue and others, such as optimal timing for initiating GLP-1s, are currently under investigation.
In a related editorial, Kate Lauer, MD, of the University of Wisconsin-Madison and colleagues noted that the study had several limitations. It relied on data prior to the USFDA approvals of semaglutide and tirzepatide, the two most prescribed GLP-1s currently, potentially limiting its applicability to current practice.
Furthermore, the prescribing data did not capture dose, titration schedules, or adherence, which are “critical for understanding treatment efficacy,” they wrote. “Nonetheless, the findings highlight two important trends: (1) GLP-1s are being increasingly used as an adjunct after bariatric surgery, and (2) there is substantial variability in the timing of their initiation.”
‘Logical’ to Use GLP-1s Post Surgery
Commenting on the study findings for GI & Hepatology News, Louis Aronne, MD, director of the Comprehensive Weight Control Center at Weill Cornell Medicine in New York City, who was not involved in the study, said, “I think it is perfectly logical to use GLP-1s in patients who have had bariatric surgery.”
In this study, weight loss in those who took GLP-1s was about 12% (from a median BMI of 42 pre-surgery to 36.7 when a GLP-1 was initiated), which is significantly less than average, Aronne noted. “The patients still had Class 2 obesity.”
“Obesity is the same as other metabolic diseases,” he added. “We have to use common sense and good medical judgment when treating patients. If surgery isn’t completely effective and weight loss is inadequate, I would recommend medications.”
Of note, his team has found that lower doses of GLP-1s are required in those who have had surgery than in those who have not. “My opinion is that patients who have undergone bariatric surgery seem to be more sensitive to the medications than the average patient, but this hasn’t been carefully studied.”
To prepare patients for the possible use of GLP1s post-surgery, he suggested telling those with very high BMI that “they may need medication in addition to the procedure in order to get the best result.”
Mehta added, “Ultimately, the decision to start GLP-1s after surgery is shared between patients and clinicians. Given the amount of media coverage on GLP-1 therapies, it is not surprising that more patients are initiating these discussions with their doctors.”
Mehta is supported by the US National Institute on Aging and reported receiving grants from the institute for this study; no other funding was reported. Lauer reported receiving grants from the US National Institutes of Health.
A version of this article first appeared on Medscape.com.
, a large retrospective cohort study showed.
GLP-1 initiation was also more common among women, those who underwent sleeve gastrectomy, and those with lower postoperative weight loss as measured by BMI.
“Some patients do not lose as much weight as expected, or they regain weight after a few years. In such cases, GLP-1 therapies are emerging as an important option for weight management,” said principal investigator Hemalkumar Mehta, PhD, associate professor at Johns Hopkins Bloomberg School of Public Health in Baltimore.
“We also noted many personal stories circulating on social media in which patients shared their experiences using GLP-1 after bariatric surgery,” he told GI & Hepatology News.
But when the researchers reviewed the scientific literature, they found no published evidence on GLP-1 use in this setting and little or no data on outcomes with the newer drugs such as semaglutide and tirzepatide. “This gap motivated us to conduct the current study,” said Mehta. The study was published in JAMA Surgery.
The researchers analyzed data from a national multicenter database of electronic health records of approximately 113 million US adults to characterize the use of and factors associated with GLP-1 initiation after bariatric surgery.
Among 112,858 individuals undergoing bariatric surgery during the study period, the mean age was 45.2 years, and 78.9% were women.
By self-report race, 1.1% were Asian, 22.1% were Black or African American, 64.2% were White individuals, and 12.6% reported belonging to other races (American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, or unknown).
A total of 15,749 individuals (14%) initiated GLP-1s post-surgery, with 3391 (21.5%) beginning within 2 years of surgery and the remainder initiating during postsurgical years 3-4 (32.3%), 5-6 (25.2%), or later (21%).
Notably, the proportion of GLP-1 use increased more in the more recent cohort, from 1.7% in the January 2015-December 2019 cohort to 12.6% from June 2020 to May 2025.
Differences Between Users and Nonusers
Those who initiated GLP-1s differed significantly from those who did not: GLP-1 users vs nonusers were younger (mean age, 44.9 years vs 45.2 years), and use was more common among women vs men (15.1% vs 9.7%), among Black or African American vs White patients (15.8% vs 13.5%), and among those who underwent sleeve gastrectomy vs Roux-en-Y gastric bypass (14.9% vs 12.1%).
Looked at another way, women (adjusted hazard ratio [aHR], 1.61), those undergoing sleeve gastrectomy (aHR, 1.42), and those with type 2 diabetes (aHR, 1.34) were more likely to initiate GLP-1s than their counterparts.
The overall median presurgical BMI was 42. On analyzing obesity classification based on BMI, the researchers found that the chances of GLP-1 use were 1.73 times higher among class 1 obesity patients (BMI, 30.0-34.9), 2.19 times higher among class 2 obesity patients (BMI, 35.0-39.9), and 2.69 times higher among patients with class 3 obesity (BMI ≥ 40) than among overweight patients (BMI, 25.0-29.9).
The median post-surgery BMI for GLP-1 users at drug initiation was 36.7. Each one-unit increase in postsurgical BMI was associated with an 8% increase in the likelihood of GLP-1 initiation (aHR, 1.08).
“Importantly, our study did not specifically evaluate the effectiveness of GLP-1 therapy on weight loss after surgery,” Mehta noted. That issue and others, such as optimal timing for initiating GLP-1s, are currently under investigation.
In a related editorial, Kate Lauer, MD, of the University of Wisconsin-Madison and colleagues noted that the study had several limitations. It relied on data prior to the USFDA approvals of semaglutide and tirzepatide, the two most prescribed GLP-1s currently, potentially limiting its applicability to current practice.
Furthermore, the prescribing data did not capture dose, titration schedules, or adherence, which are “critical for understanding treatment efficacy,” they wrote. “Nonetheless, the findings highlight two important trends: (1) GLP-1s are being increasingly used as an adjunct after bariatric surgery, and (2) there is substantial variability in the timing of their initiation.”
‘Logical’ to Use GLP-1s Post Surgery
Commenting on the study findings for GI & Hepatology News, Louis Aronne, MD, director of the Comprehensive Weight Control Center at Weill Cornell Medicine in New York City, who was not involved in the study, said, “I think it is perfectly logical to use GLP-1s in patients who have had bariatric surgery.”
In this study, weight loss in those who took GLP-1s was about 12% (from a median BMI of 42 pre-surgery to 36.7 when a GLP-1 was initiated), which is significantly less than average, Aronne noted. “The patients still had Class 2 obesity.”
“Obesity is the same as other metabolic diseases,” he added. “We have to use common sense and good medical judgment when treating patients. If surgery isn’t completely effective and weight loss is inadequate, I would recommend medications.”
Of note, his team has found that lower doses of GLP-1s are required in those who have had surgery than in those who have not. “My opinion is that patients who have undergone bariatric surgery seem to be more sensitive to the medications than the average patient, but this hasn’t been carefully studied.”
To prepare patients for the possible use of GLP1s post-surgery, he suggested telling those with very high BMI that “they may need medication in addition to the procedure in order to get the best result.”
Mehta added, “Ultimately, the decision to start GLP-1s after surgery is shared between patients and clinicians. Given the amount of media coverage on GLP-1 therapies, it is not surprising that more patients are initiating these discussions with their doctors.”
Mehta is supported by the US National Institute on Aging and reported receiving grants from the institute for this study; no other funding was reported. Lauer reported receiving grants from the US National Institutes of Health.
A version of this article first appeared on Medscape.com.
, a large retrospective cohort study showed.
GLP-1 initiation was also more common among women, those who underwent sleeve gastrectomy, and those with lower postoperative weight loss as measured by BMI.
“Some patients do not lose as much weight as expected, or they regain weight after a few years. In such cases, GLP-1 therapies are emerging as an important option for weight management,” said principal investigator Hemalkumar Mehta, PhD, associate professor at Johns Hopkins Bloomberg School of Public Health in Baltimore.
“We also noted many personal stories circulating on social media in which patients shared their experiences using GLP-1 after bariatric surgery,” he told GI & Hepatology News.
But when the researchers reviewed the scientific literature, they found no published evidence on GLP-1 use in this setting and little or no data on outcomes with the newer drugs such as semaglutide and tirzepatide. “This gap motivated us to conduct the current study,” said Mehta. The study was published in JAMA Surgery.
The researchers analyzed data from a national multicenter database of electronic health records of approximately 113 million US adults to characterize the use of and factors associated with GLP-1 initiation after bariatric surgery.
Among 112,858 individuals undergoing bariatric surgery during the study period, the mean age was 45.2 years, and 78.9% were women.
By self-report race, 1.1% were Asian, 22.1% were Black or African American, 64.2% were White individuals, and 12.6% reported belonging to other races (American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, or unknown).
A total of 15,749 individuals (14%) initiated GLP-1s post-surgery, with 3391 (21.5%) beginning within 2 years of surgery and the remainder initiating during postsurgical years 3-4 (32.3%), 5-6 (25.2%), or later (21%).
Notably, the proportion of GLP-1 use increased more in the more recent cohort, from 1.7% in the January 2015-December 2019 cohort to 12.6% from June 2020 to May 2025.
Differences Between Users and Nonusers
Those who initiated GLP-1s differed significantly from those who did not: GLP-1 users vs nonusers were younger (mean age, 44.9 years vs 45.2 years), and use was more common among women vs men (15.1% vs 9.7%), among Black or African American vs White patients (15.8% vs 13.5%), and among those who underwent sleeve gastrectomy vs Roux-en-Y gastric bypass (14.9% vs 12.1%).
Looked at another way, women (adjusted hazard ratio [aHR], 1.61), those undergoing sleeve gastrectomy (aHR, 1.42), and those with type 2 diabetes (aHR, 1.34) were more likely to initiate GLP-1s than their counterparts.
The overall median presurgical BMI was 42. On analyzing obesity classification based on BMI, the researchers found that the chances of GLP-1 use were 1.73 times higher among class 1 obesity patients (BMI, 30.0-34.9), 2.19 times higher among class 2 obesity patients (BMI, 35.0-39.9), and 2.69 times higher among patients with class 3 obesity (BMI ≥ 40) than among overweight patients (BMI, 25.0-29.9).
The median post-surgery BMI for GLP-1 users at drug initiation was 36.7. Each one-unit increase in postsurgical BMI was associated with an 8% increase in the likelihood of GLP-1 initiation (aHR, 1.08).
“Importantly, our study did not specifically evaluate the effectiveness of GLP-1 therapy on weight loss after surgery,” Mehta noted. That issue and others, such as optimal timing for initiating GLP-1s, are currently under investigation.
In a related editorial, Kate Lauer, MD, of the University of Wisconsin-Madison and colleagues noted that the study had several limitations. It relied on data prior to the USFDA approvals of semaglutide and tirzepatide, the two most prescribed GLP-1s currently, potentially limiting its applicability to current practice.
Furthermore, the prescribing data did not capture dose, titration schedules, or adherence, which are “critical for understanding treatment efficacy,” they wrote. “Nonetheless, the findings highlight two important trends: (1) GLP-1s are being increasingly used as an adjunct after bariatric surgery, and (2) there is substantial variability in the timing of their initiation.”
‘Logical’ to Use GLP-1s Post Surgery
Commenting on the study findings for GI & Hepatology News, Louis Aronne, MD, director of the Comprehensive Weight Control Center at Weill Cornell Medicine in New York City, who was not involved in the study, said, “I think it is perfectly logical to use GLP-1s in patients who have had bariatric surgery.”
In this study, weight loss in those who took GLP-1s was about 12% (from a median BMI of 42 pre-surgery to 36.7 when a GLP-1 was initiated), which is significantly less than average, Aronne noted. “The patients still had Class 2 obesity.”
“Obesity is the same as other metabolic diseases,” he added. “We have to use common sense and good medical judgment when treating patients. If surgery isn’t completely effective and weight loss is inadequate, I would recommend medications.”
Of note, his team has found that lower doses of GLP-1s are required in those who have had surgery than in those who have not. “My opinion is that patients who have undergone bariatric surgery seem to be more sensitive to the medications than the average patient, but this hasn’t been carefully studied.”
To prepare patients for the possible use of GLP1s post-surgery, he suggested telling those with very high BMI that “they may need medication in addition to the procedure in order to get the best result.”
Mehta added, “Ultimately, the decision to start GLP-1s after surgery is shared between patients and clinicians. Given the amount of media coverage on GLP-1 therapies, it is not surprising that more patients are initiating these discussions with their doctors.”
Mehta is supported by the US National Institute on Aging and reported receiving grants from the institute for this study; no other funding was reported. Lauer reported receiving grants from the US National Institutes of Health.
A version of this article first appeared on Medscape.com.
Wegovy Approved for MASH With Fibrosis, No Cirrhosis
The once-weekly 2.4 mg semaglutide subcutaneous injection is given in conjunction with a reduced calorie diet and increased physical activity.
Among people living with overweight or obesity globally, 1 in 3 also have MASH.
The accelerated approval was based on part-one results from the ongoing two-part, phase-3 ESSENCE trial, in which Wegovy demonstrated a significant improvement in liver fibrosis with no worsening of steatohepatitis, as well as resolution of steatohepatitis with no worsening of liver fibrosis, compared with placebo at week 72. Those results were published online in April in The New England Journal of Medicine.
For the trial, 800 participants were randomly assigned to either Wegovy (534 participants) or placebo (266 participants) in addition to lifestyle changes. The mean age was 56 years and the mean BMI was 34. Most patients were white individuals (67.5%) and women (57.1%), and 55.9% of the patients had type 2 diabetes; 250 patients (31.3%) had stage II fibrosis and 550 (68.8%) had stage III fibrosis. Participants were on stable doses of lipid-lowering, glucose-management, and weight-loss medications.
At week 72, the first primary endpoint showed 63% of the 534 people treated with Wegovy achieved resolution of steatohepatitis and no worsening of liver fibrosis compared with 34% of 266 individuals treated with placebo — a statistically significant difference.
The second primary endpoint showed 37% of people treated with Wegovy achieved improvement in liver fibrosis and no worsening of steatohepatitis compared with 22% of those treated with placebo, also a significant difference.
A confirmatory secondary endpoint at week 72 showed 33% of patients treated with Wegovy achieved both resolution of steatohepatitis and improvement in liver fibrosis compared with 16% of those treated with placebo — a statistically significant difference in response rate of 17%.
In addition, 83.5% of the patients in the semaglutide group maintained the target dose of 2.4 mg until week 72.
Wegovy is also indicated, along with diet and physical activity, to reduce the risk for major cardiovascular events in adults with known heart disease and with either obesity or overweight. It is also indicated for adults and children aged 12 years or older with obesity, and some adults with overweight who also have weight-related medical problems, to help them lose excess body weight and keep the weight off.
What’s Next for Wegovy?
In February 2025, Novo Nordisk filed for regulatory approval in the EU, followed by regulatory submission in Japan in May 2025. Also in May, the FDA accepted a filing application for oral semaglutide 25 mg.
Furthermore, “There’s an expected readout of part 2 of ESSENCE in 2029, which aims to demonstrate treatment with Wegovy lowers the risk of liver-related clinical events, compared to placebo, in patients with MASH and F2 or F3 fibrosis at week 240,” a Novo Nordisk spokesperson told GI & Hepatology News.
Although the company has the technology to produce semaglutide as a pill or tablet, she said, “the US launch of oral semaglutide for obesity will be contingent on portfolio prioritization and manufacturing capacity.” The company has not yet submitted the 50 mg oral semaglutide to regulatory authorities.
“The oral form requires more active pharmaceutical ingredient (API),” she noted. “Given that we have a fixed amount of API, the injectable form enables us to treat more patients. We are currently expanding our oral and injectable production capacities globally with the aim of serving as many patients as possible. It requires time to build, install, validate, and ramp-up these production processes.”
A version of this article appeared on Medscape.com.
The once-weekly 2.4 mg semaglutide subcutaneous injection is given in conjunction with a reduced calorie diet and increased physical activity.
Among people living with overweight or obesity globally, 1 in 3 also have MASH.
The accelerated approval was based on part-one results from the ongoing two-part, phase-3 ESSENCE trial, in which Wegovy demonstrated a significant improvement in liver fibrosis with no worsening of steatohepatitis, as well as resolution of steatohepatitis with no worsening of liver fibrosis, compared with placebo at week 72. Those results were published online in April in The New England Journal of Medicine.
For the trial, 800 participants were randomly assigned to either Wegovy (534 participants) or placebo (266 participants) in addition to lifestyle changes. The mean age was 56 years and the mean BMI was 34. Most patients were white individuals (67.5%) and women (57.1%), and 55.9% of the patients had type 2 diabetes; 250 patients (31.3%) had stage II fibrosis and 550 (68.8%) had stage III fibrosis. Participants were on stable doses of lipid-lowering, glucose-management, and weight-loss medications.
At week 72, the first primary endpoint showed 63% of the 534 people treated with Wegovy achieved resolution of steatohepatitis and no worsening of liver fibrosis compared with 34% of 266 individuals treated with placebo — a statistically significant difference.
The second primary endpoint showed 37% of people treated with Wegovy achieved improvement in liver fibrosis and no worsening of steatohepatitis compared with 22% of those treated with placebo, also a significant difference.
A confirmatory secondary endpoint at week 72 showed 33% of patients treated with Wegovy achieved both resolution of steatohepatitis and improvement in liver fibrosis compared with 16% of those treated with placebo — a statistically significant difference in response rate of 17%.
In addition, 83.5% of the patients in the semaglutide group maintained the target dose of 2.4 mg until week 72.
Wegovy is also indicated, along with diet and physical activity, to reduce the risk for major cardiovascular events in adults with known heart disease and with either obesity or overweight. It is also indicated for adults and children aged 12 years or older with obesity, and some adults with overweight who also have weight-related medical problems, to help them lose excess body weight and keep the weight off.
What’s Next for Wegovy?
In February 2025, Novo Nordisk filed for regulatory approval in the EU, followed by regulatory submission in Japan in May 2025. Also in May, the FDA accepted a filing application for oral semaglutide 25 mg.
Furthermore, “There’s an expected readout of part 2 of ESSENCE in 2029, which aims to demonstrate treatment with Wegovy lowers the risk of liver-related clinical events, compared to placebo, in patients with MASH and F2 or F3 fibrosis at week 240,” a Novo Nordisk spokesperson told GI & Hepatology News.
Although the company has the technology to produce semaglutide as a pill or tablet, she said, “the US launch of oral semaglutide for obesity will be contingent on portfolio prioritization and manufacturing capacity.” The company has not yet submitted the 50 mg oral semaglutide to regulatory authorities.
“The oral form requires more active pharmaceutical ingredient (API),” she noted. “Given that we have a fixed amount of API, the injectable form enables us to treat more patients. We are currently expanding our oral and injectable production capacities globally with the aim of serving as many patients as possible. It requires time to build, install, validate, and ramp-up these production processes.”
A version of this article appeared on Medscape.com.
The once-weekly 2.4 mg semaglutide subcutaneous injection is given in conjunction with a reduced calorie diet and increased physical activity.
Among people living with overweight or obesity globally, 1 in 3 also have MASH.
The accelerated approval was based on part-one results from the ongoing two-part, phase-3 ESSENCE trial, in which Wegovy demonstrated a significant improvement in liver fibrosis with no worsening of steatohepatitis, as well as resolution of steatohepatitis with no worsening of liver fibrosis, compared with placebo at week 72. Those results were published online in April in The New England Journal of Medicine.
For the trial, 800 participants were randomly assigned to either Wegovy (534 participants) or placebo (266 participants) in addition to lifestyle changes. The mean age was 56 years and the mean BMI was 34. Most patients were white individuals (67.5%) and women (57.1%), and 55.9% of the patients had type 2 diabetes; 250 patients (31.3%) had stage II fibrosis and 550 (68.8%) had stage III fibrosis. Participants were on stable doses of lipid-lowering, glucose-management, and weight-loss medications.
At week 72, the first primary endpoint showed 63% of the 534 people treated with Wegovy achieved resolution of steatohepatitis and no worsening of liver fibrosis compared with 34% of 266 individuals treated with placebo — a statistically significant difference.
The second primary endpoint showed 37% of people treated with Wegovy achieved improvement in liver fibrosis and no worsening of steatohepatitis compared with 22% of those treated with placebo, also a significant difference.
A confirmatory secondary endpoint at week 72 showed 33% of patients treated with Wegovy achieved both resolution of steatohepatitis and improvement in liver fibrosis compared with 16% of those treated with placebo — a statistically significant difference in response rate of 17%.
In addition, 83.5% of the patients in the semaglutide group maintained the target dose of 2.4 mg until week 72.
Wegovy is also indicated, along with diet and physical activity, to reduce the risk for major cardiovascular events in adults with known heart disease and with either obesity or overweight. It is also indicated for adults and children aged 12 years or older with obesity, and some adults with overweight who also have weight-related medical problems, to help them lose excess body weight and keep the weight off.
What’s Next for Wegovy?
In February 2025, Novo Nordisk filed for regulatory approval in the EU, followed by regulatory submission in Japan in May 2025. Also in May, the FDA accepted a filing application for oral semaglutide 25 mg.
Furthermore, “There’s an expected readout of part 2 of ESSENCE in 2029, which aims to demonstrate treatment with Wegovy lowers the risk of liver-related clinical events, compared to placebo, in patients with MASH and F2 or F3 fibrosis at week 240,” a Novo Nordisk spokesperson told GI & Hepatology News.
Although the company has the technology to produce semaglutide as a pill or tablet, she said, “the US launch of oral semaglutide for obesity will be contingent on portfolio prioritization and manufacturing capacity.” The company has not yet submitted the 50 mg oral semaglutide to regulatory authorities.
“The oral form requires more active pharmaceutical ingredient (API),” she noted. “Given that we have a fixed amount of API, the injectable form enables us to treat more patients. We are currently expanding our oral and injectable production capacities globally with the aim of serving as many patients as possible. It requires time to build, install, validate, and ramp-up these production processes.”
A version of this article appeared on Medscape.com.
Journal Highlights: May-July 2025
Esophagus/Motility
Nguyen AD, et al. AGA Clinical Practice Update on Incorporating Functional Lumen Imaging Probe Into Esophageal Clinical Practice: Expert Review. Gastroenterology. 2025 Jul. doi: 10.1053/j.gastro.2025.05.011.
Hartnett DA, et al. Distribution of Esophageal Eosinophilia as a Predictor of Proton Pump Inhibitor Response in Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.06.032.
Gyawali CP, et al. pH Impedance Monitoring on Proton Pump Inhibitor Therapy Impacts Management Decisions in Proven GERD but not in Unproven GERD. Clin Gastroenterol Hepatol. 2025 May. doi: 10.1016/j.cgh.2025.02.032.
Stomach
Wiklund AK, et al. Risk of Gastric Adenocarcinoma After Eradication of Helicobacter pylori. Gastroenterology. 2025 Feb. doi: 10.1053/j.gastro.2025.01.239.
Sonaiya S, et al. Over-the-Scope Clip versus Standard Endoscopic Therapy as First-Line Intervention for Nonvariceal Upper Gastrointestinal Bleeding: A Cost-Effectiveness Analysis. Tech Innov Gastrointest. 2025 Jun. doi: 10.1016/j.tige.2025.250935.
Colon
Hassan C, et al. Colon Cancer Screening, Surveillance, and Treatment: Novel Artificial Intelligence Driving Strategies in the Management of Colon Lesions. Gastroenterology. 2025 Mar. doi: 10.1053/j.gastro.2025.02.021.

Pancreas
Wilcox CM, et al; US Pancreatic Disease Study Group. Management of the Disconnected Pancreatic Duct in Pancreatic Necrosis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.05.024.
Ghimire C, et al. The effect of advances in pancreatic cancer treatment in population mortality: A SEER-based study. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100739.
Hepatology
Canivet CM, et al. Validation of the AASLD/EASL Multi-Step Screening Strategies for MASLD. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100747.
Miscellaneous
Chang L, et al. Gut Feelings: The Critical Role of Interoception in Obesity and Disorders of Gut-Brain Interaction. Gastroenterology. 2025 Aug. doi: 10.1053/j.gastro.2025.04.002.
Bashiri K, et al. Advancing Hemostatic Powder Technologies for Management of Gastrointestinal Bleeding: Challenges and Solutions. Tech Innov Gastrointest. 2025 Jul. doi: 10.1016/j.tige.2025.250940.
Dr. Trieu is assistant professor of medicine, interventional endoscopy, in the Division of Gastroenterology at Washington University in St. Louis School of Medicine, Missouri.
Esophagus/Motility
Nguyen AD, et al. AGA Clinical Practice Update on Incorporating Functional Lumen Imaging Probe Into Esophageal Clinical Practice: Expert Review. Gastroenterology. 2025 Jul. doi: 10.1053/j.gastro.2025.05.011.
Hartnett DA, et al. Distribution of Esophageal Eosinophilia as a Predictor of Proton Pump Inhibitor Response in Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.06.032.
Gyawali CP, et al. pH Impedance Monitoring on Proton Pump Inhibitor Therapy Impacts Management Decisions in Proven GERD but not in Unproven GERD. Clin Gastroenterol Hepatol. 2025 May. doi: 10.1016/j.cgh.2025.02.032.
Stomach
Wiklund AK, et al. Risk of Gastric Adenocarcinoma After Eradication of Helicobacter pylori. Gastroenterology. 2025 Feb. doi: 10.1053/j.gastro.2025.01.239.
Sonaiya S, et al. Over-the-Scope Clip versus Standard Endoscopic Therapy as First-Line Intervention for Nonvariceal Upper Gastrointestinal Bleeding: A Cost-Effectiveness Analysis. Tech Innov Gastrointest. 2025 Jun. doi: 10.1016/j.tige.2025.250935.
Colon
Hassan C, et al. Colon Cancer Screening, Surveillance, and Treatment: Novel Artificial Intelligence Driving Strategies in the Management of Colon Lesions. Gastroenterology. 2025 Mar. doi: 10.1053/j.gastro.2025.02.021.
Pancreas
Wilcox CM, et al; US Pancreatic Disease Study Group. Management of the Disconnected Pancreatic Duct in Pancreatic Necrosis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.05.024.
Ghimire C, et al. The effect of advances in pancreatic cancer treatment in population mortality: A SEER-based study. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100739.
Hepatology
Canivet CM, et al. Validation of the AASLD/EASL Multi-Step Screening Strategies for MASLD. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100747.
Miscellaneous
Chang L, et al. Gut Feelings: The Critical Role of Interoception in Obesity and Disorders of Gut-Brain Interaction. Gastroenterology. 2025 Aug. doi: 10.1053/j.gastro.2025.04.002.
Bashiri K, et al. Advancing Hemostatic Powder Technologies for Management of Gastrointestinal Bleeding: Challenges and Solutions. Tech Innov Gastrointest. 2025 Jul. doi: 10.1016/j.tige.2025.250940.
Dr. Trieu is assistant professor of medicine, interventional endoscopy, in the Division of Gastroenterology at Washington University in St. Louis School of Medicine, Missouri.
Esophagus/Motility
Nguyen AD, et al. AGA Clinical Practice Update on Incorporating Functional Lumen Imaging Probe Into Esophageal Clinical Practice: Expert Review. Gastroenterology. 2025 Jul. doi: 10.1053/j.gastro.2025.05.011.
Hartnett DA, et al. Distribution of Esophageal Eosinophilia as a Predictor of Proton Pump Inhibitor Response in Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.06.032.
Gyawali CP, et al. pH Impedance Monitoring on Proton Pump Inhibitor Therapy Impacts Management Decisions in Proven GERD but not in Unproven GERD. Clin Gastroenterol Hepatol. 2025 May. doi: 10.1016/j.cgh.2025.02.032.
Stomach
Wiklund AK, et al. Risk of Gastric Adenocarcinoma After Eradication of Helicobacter pylori. Gastroenterology. 2025 Feb. doi: 10.1053/j.gastro.2025.01.239.
Sonaiya S, et al. Over-the-Scope Clip versus Standard Endoscopic Therapy as First-Line Intervention for Nonvariceal Upper Gastrointestinal Bleeding: A Cost-Effectiveness Analysis. Tech Innov Gastrointest. 2025 Jun. doi: 10.1016/j.tige.2025.250935.
Colon
Hassan C, et al. Colon Cancer Screening, Surveillance, and Treatment: Novel Artificial Intelligence Driving Strategies in the Management of Colon Lesions. Gastroenterology. 2025 Mar. doi: 10.1053/j.gastro.2025.02.021.
Pancreas
Wilcox CM, et al; US Pancreatic Disease Study Group. Management of the Disconnected Pancreatic Duct in Pancreatic Necrosis. Clin Gastroenterol Hepatol. 2025 Jul. doi: 10.1016/j.cgh.2025.05.024.
Ghimire C, et al. The effect of advances in pancreatic cancer treatment in population mortality: A SEER-based study. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100739.
Hepatology
Canivet CM, et al. Validation of the AASLD/EASL Multi-Step Screening Strategies for MASLD. Gastro Hep Adv. 2025 Jul. doi: 10.1016/j.gastha.2025.100747.
Miscellaneous
Chang L, et al. Gut Feelings: The Critical Role of Interoception in Obesity and Disorders of Gut-Brain Interaction. Gastroenterology. 2025 Aug. doi: 10.1053/j.gastro.2025.04.002.
Bashiri K, et al. Advancing Hemostatic Powder Technologies for Management of Gastrointestinal Bleeding: Challenges and Solutions. Tech Innov Gastrointest. 2025 Jul. doi: 10.1016/j.tige.2025.250940.
Dr. Trieu is assistant professor of medicine, interventional endoscopy, in the Division of Gastroenterology at Washington University in St. Louis School of Medicine, Missouri.
Data Trends 2025: Obesity
Obesity
Click here to view more from Federal Health Care Data Trends 2025.
1. GBD 2021 US Obesity Forecasting Collaborators. National-level and state-level prevalence of overweight and obesity among children, adolescents, and adults in the USA, 1990-2021, and forecasts up to 2050. Lancet. 2024;404(10469):2278-2298. doi:10.1016/S0140-6736(24)01548-4
2. Breland JY, et al. J Gen Intern Med. 2017;32(Suppl 1):11-17. doi:10.1007/s11606-016-3962-1
3. American Security Project. Costs and consequences: obesity’s compounding impact on the Military Health System. September 2024. Accessed April 21, 2025. https://www.americansecurityproject.org/wp-content/uploads/2024/09/Ref-0295-Costs-and-Consequences-Obesitys-Compounding-Impact-on-the-Military-Health-System.pdf
4. Baser O, et al. Healthcare (Basel). 2023;11(11):1529. doi:10.3390/healthcare11111529
5. Maclin-Akinyemi C, et al. Mil Med. 2017;182(9):e1816-e1823. doi:10.7205/MILMED-D-16-00380.
6. Yang D, et al. Mil Med. 2022;187(7-8):e948-e954. doi:10.1093/milmed/usab292
7. American Security Project. Ready the Reserve: obesity’s impacts on National Guard and Reserve readiness. April 2025. Accessed April 21, 2025. https://www.americansecurityproject.org/white-paper-ready-the-reserve-obesitys-impacts-onnational-guard-and-reserve-readiness/
8. Betancourt JA, et al. Healthcare (Basel). 2020;8(3):191. doi:10.3390/healthcare8030191
9. Breland JY, et al. Psychiatr Serv. 2020;1;71(5):506-509. doi:10.1176/appi.ps.201900078
Click here to view more from Federal Health Care Data Trends 2025.
Click here to view more from Federal Health Care Data Trends 2025.
1. GBD 2021 US Obesity Forecasting Collaborators. National-level and state-level prevalence of overweight and obesity among children, adolescents, and adults in the USA, 1990-2021, and forecasts up to 2050. Lancet. 2024;404(10469):2278-2298. doi:10.1016/S0140-6736(24)01548-4
2. Breland JY, et al. J Gen Intern Med. 2017;32(Suppl 1):11-17. doi:10.1007/s11606-016-3962-1
3. American Security Project. Costs and consequences: obesity’s compounding impact on the Military Health System. September 2024. Accessed April 21, 2025. https://www.americansecurityproject.org/wp-content/uploads/2024/09/Ref-0295-Costs-and-Consequences-Obesitys-Compounding-Impact-on-the-Military-Health-System.pdf
4. Baser O, et al. Healthcare (Basel). 2023;11(11):1529. doi:10.3390/healthcare11111529
5. Maclin-Akinyemi C, et al. Mil Med. 2017;182(9):e1816-e1823. doi:10.7205/MILMED-D-16-00380.
6. Yang D, et al. Mil Med. 2022;187(7-8):e948-e954. doi:10.1093/milmed/usab292
7. American Security Project. Ready the Reserve: obesity’s impacts on National Guard and Reserve readiness. April 2025. Accessed April 21, 2025. https://www.americansecurityproject.org/white-paper-ready-the-reserve-obesitys-impacts-onnational-guard-and-reserve-readiness/
8. Betancourt JA, et al. Healthcare (Basel). 2020;8(3):191. doi:10.3390/healthcare8030191
9. Breland JY, et al. Psychiatr Serv. 2020;1;71(5):506-509. doi:10.1176/appi.ps.201900078
1. GBD 2021 US Obesity Forecasting Collaborators. National-level and state-level prevalence of overweight and obesity among children, adolescents, and adults in the USA, 1990-2021, and forecasts up to 2050. Lancet. 2024;404(10469):2278-2298. doi:10.1016/S0140-6736(24)01548-4
2. Breland JY, et al. J Gen Intern Med. 2017;32(Suppl 1):11-17. doi:10.1007/s11606-016-3962-1
3. American Security Project. Costs and consequences: obesity’s compounding impact on the Military Health System. September 2024. Accessed April 21, 2025. https://www.americansecurityproject.org/wp-content/uploads/2024/09/Ref-0295-Costs-and-Consequences-Obesitys-Compounding-Impact-on-the-Military-Health-System.pdf
4. Baser O, et al. Healthcare (Basel). 2023;11(11):1529. doi:10.3390/healthcare11111529
5. Maclin-Akinyemi C, et al. Mil Med. 2017;182(9):e1816-e1823. doi:10.7205/MILMED-D-16-00380.
6. Yang D, et al. Mil Med. 2022;187(7-8):e948-e954. doi:10.1093/milmed/usab292
7. American Security Project. Ready the Reserve: obesity’s impacts on National Guard and Reserve readiness. April 2025. Accessed April 21, 2025. https://www.americansecurityproject.org/white-paper-ready-the-reserve-obesitys-impacts-onnational-guard-and-reserve-readiness/
8. Betancourt JA, et al. Healthcare (Basel). 2020;8(3):191. doi:10.3390/healthcare8030191
9. Breland JY, et al. Psychiatr Serv. 2020;1;71(5):506-509. doi:10.1176/appi.ps.201900078
Obesity
Obesity
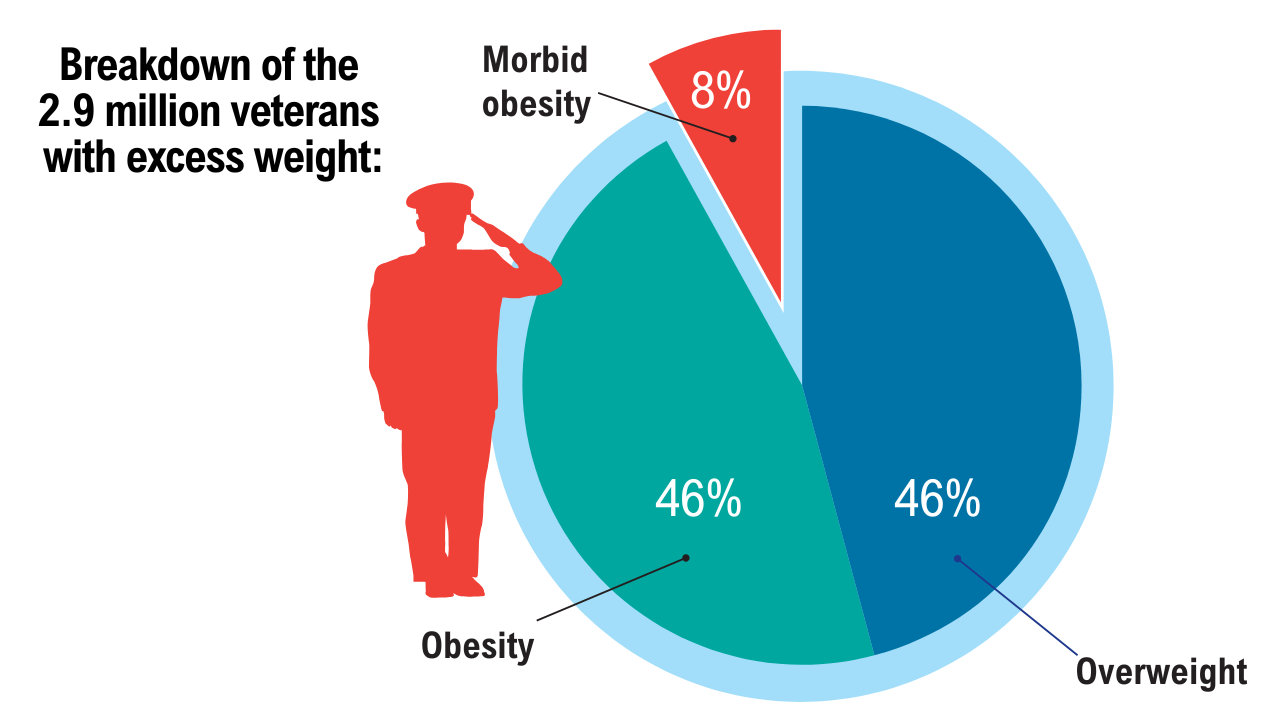
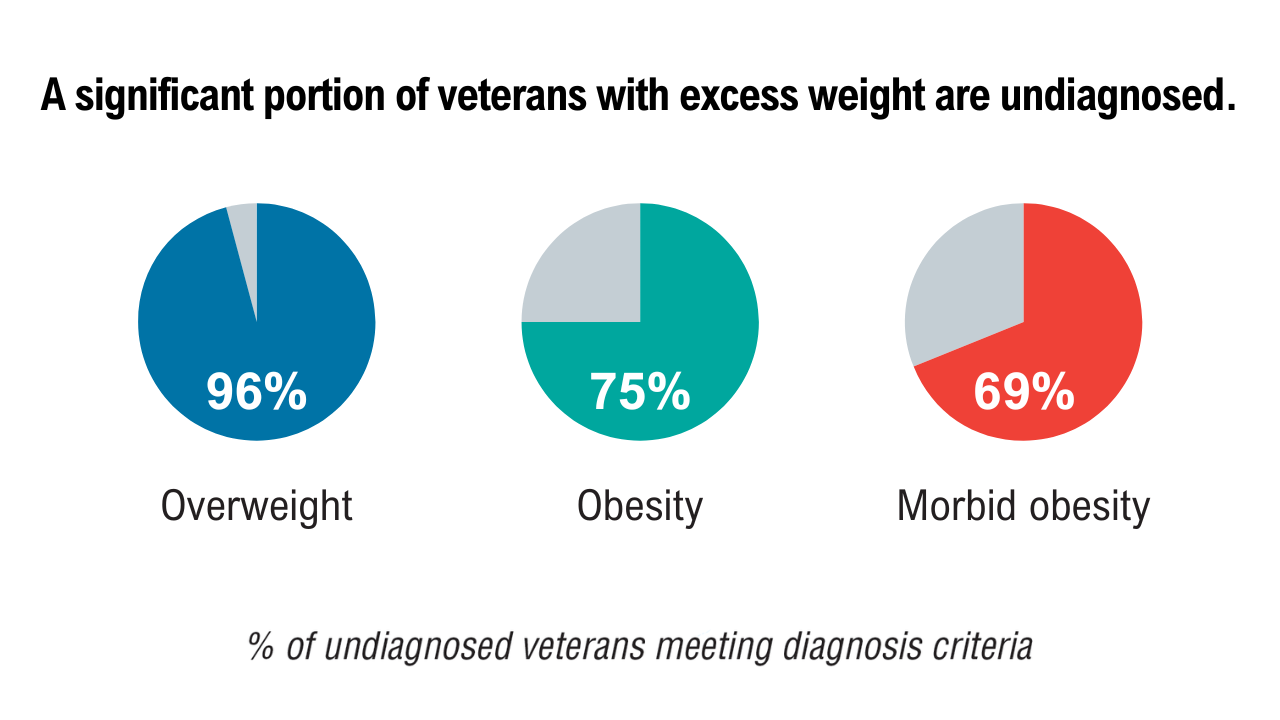
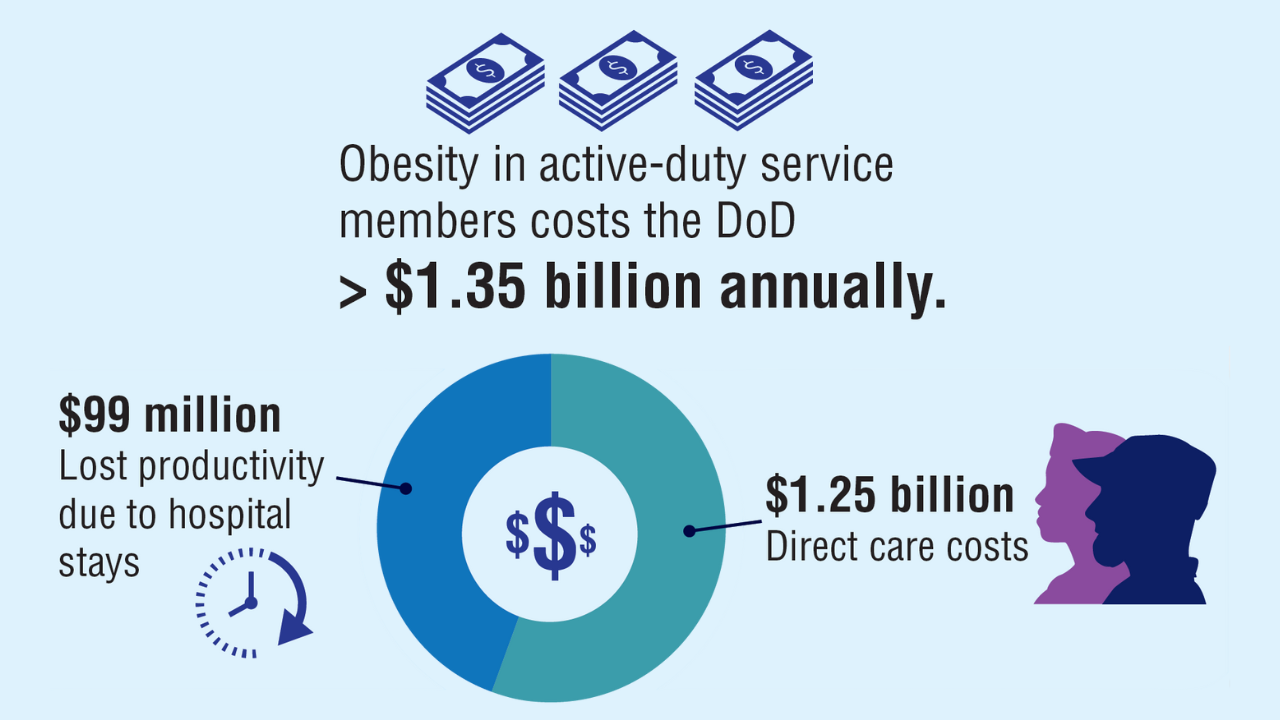
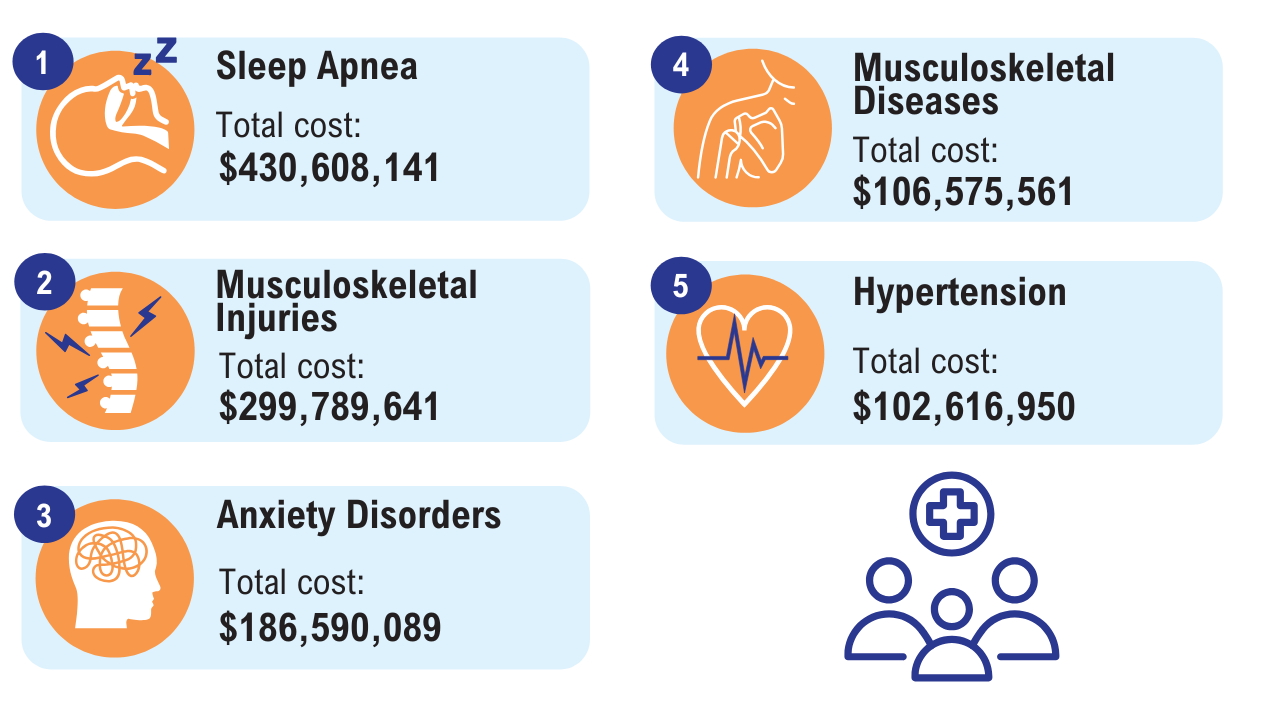
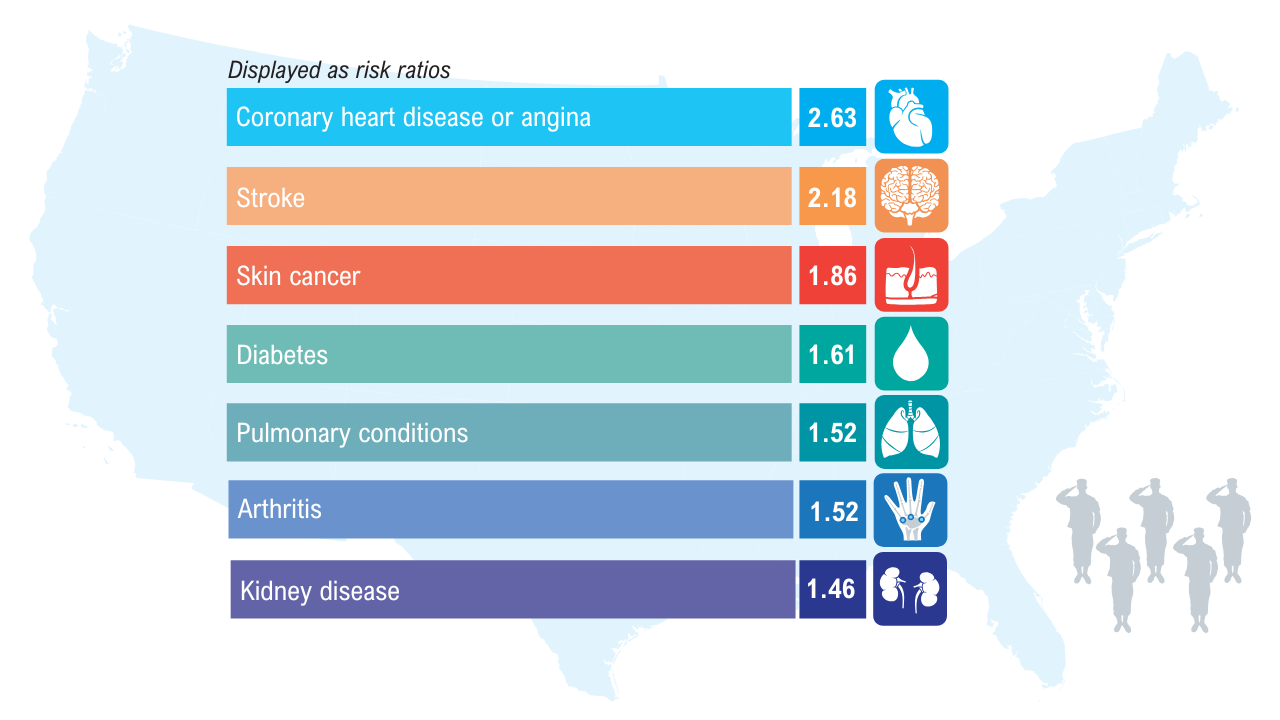
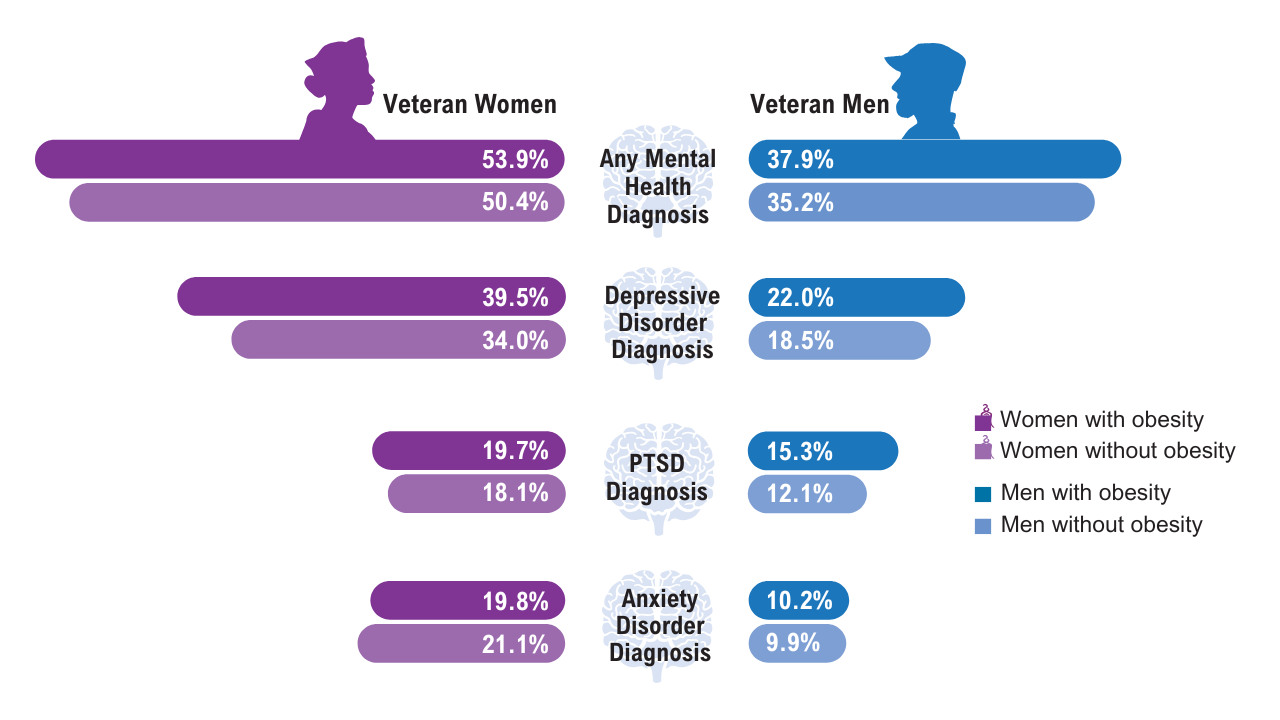
Can Nonresponders to Antiobesity Medicines Be Predicted?
, enabling clinicians to better tailor antiobesity medication (AOM) to the patient.
Currently, patient response to AOMs varies widely, with some patients responding robustly to AOMs and others responding weakly or not at all.
For example, trials of the GLP-1 semaglutide found that 32%-39.6% of people are “super responders,” achieving weight loss in excess of 20%, and a subgroup of 10.2%-16.7% of individuals are nonresponders. Similar variability was found with other AOMs, including the GLP-1 liraglutide and tirzepatide, a dual GLP-1/glucose-dependent insulinotropic polypeptide receptor agonist.
Studies of semaglutide suggest that people with obesity and type 2 diabetes (T2D) lose less weight on the drug than those without T2D, and men tend to lose less weight than women.
However, little else is known about predictors of response rates for various AOMs, and medication selection is typically based on patient or physician preference, comorbidities, medication interactions, and insurance coverage.
Although definitions of a “nonresponder” vary, the Endocrine Society’s latest guideline, which many clinicians follow, states that an AOM is considered effective if patients lose more than 5% of their body weight within 3 months.
Can nonresponders and lower responders be identified and helped? Yes, but it’s complicated.
“Treating obesity effectively means recognizing that not all patients respond the same way to the same treatment, and that’s not a failure; it’s a signal,” said Andres Acosta, MD, PhD, an obesity expert at Mayo Clinic, Rochester, Minnesota, and a cofounder of Phenomix Sciences, a biotech company in Menlo Park, California.

“Obesity is not a single disease. It’s a complex, multifactorial condition driven by diverse biological pathways,” he told GI & Hepatology News. “Semaglutide and other GLP-1s primarily act by reducing appetite and slowing gastric emptying, but not all patients have obesity that is primarily driven by appetite dysregulation.”
Phenotype-Based Profiling
Figuring out what drives an individual’s obesity is where a phenotype-based profiling test could possibly help.
Acosta and colleagues previously used a variety of validated studies and questionnaires to identify four phenotypes that represent distinct biologic drivers of obesity: hungry brain (abnormal satiation), emotional hunger (hedonic eating), hungry gut (abnormal satiety), and slow burn (decreased metabolic rate). In their pragmatic clinical trial, phenotype-guided AOM selection was associated with 1.75-fold greater weight loss after 12 months than the standard approach to drug selection, with mean weight loss of 15.9% and 9%, respectively.
“If a patient’s obesity isn’t primarily rooted in the mechanisms targeted by a particular drug, their response will naturally be limited,” Acosta said. “It’s not that they’re failing the medication; the medication simply isn’t the right match for their biology.”
For their new study, published online in Cell Metabolism, Acosta and colleagues built on their previous research by analyzing the genetic and nongenetic factors that influenced calories needed to reach satiation (Calories to Satiation [CTS]) in adults with obesity. They then used machine learning techniques to develop a CTS gene risk score (CTS-GRS) that could be measured by a DNA saliva test.
The study included 717 adults with obesity (mean age, 41; 75% women) with marked variability in satiation, ranging from 140 to 2166 kcals to reach satiation.
CTS was assessed through an ad libitum meal, combined with physiological and behavioral evaluations, including calorimetry, imaging, blood sampling, and gastric emptying tests. The largest contributors to CTS variability were sex and genetic factors, while other anthropometric measurements played lesser roles.
Various analyses and assessments of participants’ CTS-GRS scores showed that individuals with a high CTS-GRS, or hungry brain phenotype, experienced significantly greater weight loss when treated with phentermine/topiramate than those with a low CTS-GRS, or hungry gut, phenotype. After 52 weeks of treatment, individuals with the hungry brain phenotype lost an average of 17.4% of their body weight compared with 11.2% in those with the hungry gut phenotype.
An analysis of a separate 16-week study showed that patients with the hungry gut phenotype responded better to the GLP-1 liraglutide, losing 6.4% total body weight, compared to 3.3% for those with the hungry brain phenotype.
Overall, the CTS-GRS test predicted drug response with up to 84% accuracy (area under the curve, 0.76 in men and 0.84 in women). The authors acknowledged that these results need to be replicated prospectively and in more diverse populations to validate the test’s predictive ability.
“This kind of phenotype-based profiling allows us to predict which patients are more likely to respond and who might need a different intervention,” Acosta said. “It’s a critical step toward eliminating trial-and-error in obesity treatment.”
The test (MyPhenome test) is used at more than 80 healthcare clinics in the United States, according to Phenomix Sciences, which manufactures it. A company spokesperson said the test does not require FDA approval because it is used to predict obesity phenotypes to help inform treatment, but not to identify specific medications or other interventions. “If it were to do the latter,” the spokesperson said, “it would be considered a ‘companion diagnostic’ and subject to the FDA clearance process.”
What to Do if an AOM Isn’t Working?
It’s one thing to predict whether an individual might do better on one drug vs another, but what should clinicians do meanwhile to optimize weight loss for their patients who may be struggling on a particular drug?
“Efforts to predict the response to GLP-1 therapy have been a hot topic,” noted Sriram Machineni, MD, associate professor at Montefiore Medical Center, Bronx, New York, and founding director of the Fleischer Institute Medical Weight Center at Montefiore Einstein. Although the current study showed that genetic testing could predict responders, like Acosta, he agreed that the results need to be replicated in a prospective manner.
“In the absence of a validated tool for predicting response to specific medications, we use a prioritization process for trialing medications,” Machineni told GI & Hepatology News. “The prioritization is based on the suitability of the side-effect profile to the specific patient, including contraindications; benefits independent of weight loss, such as cardiovascular protection for semaglutide; average efficacy; and financial accessibility for patients.”
Predicting responders isn’t straightforward, said Robert Kushner, MD, professor of medicine and medical education at the Feinberg School of Medicine at Northwestern University and medical director of the Wellness Institute at Northwestern Memorial Hospital in Chicago.
“Despite looking at baseline demographic data such as race, ethnicity, age, weight, and BMI, we are unable to predict who will lose more or less weight,” he told GI & Hepatology News. The one exception is that women generally lose more weight than men. “However, even among females, we cannot discern which females will lose more weight than other females,” he said.
If an individual is not showing sufficient weight loss on a particular medication, “we first explore potential reasons that can be addressed, such as the patient is not taking the medication or is skipping doses,” Kushner said. If need be, they discuss changing to a different drug to improve compliance. He also stresses the importance of making lifestyle changes in diet and physical activity for patients taking AOMs.
Often patients who do not lose at least 5% of their weight within 3 months are not likely to respond well to that medication even if they remain on it. “So, early response rates determine longer-term success,” Kushner said.
Acosta said that if a patient isn’t responding to one class of medication, he pivots to a treatment better aligned with their phenotype. “That could mean switching from a GLP-1 to a medication like [naltrexone/bupropion] or trying a new method altogether,” he said. “The key is that the treatment decision is rooted in the patient’s biology, not just a reaction to short-term results. We also emphasize the importance of long-term follow-up and support.”
The goal isn’t just weight loss but also improved health and quality of life, Acosta said. “Whether through medication, surgery, or behavior change, what matters most is tailoring the care plan to each individual’s unique biology and needs.”
The new study received support from the Mayo Clinic Clinical Research Trials Unit, Vivus Inc., and Phenomix Sciences. Acosta is supported by a National Institutes of Health grant.
Acosta is a co-founder and inventor of intellectual property licensed to Phenomix Sciences Inc.; has served as a consultant for Rhythm Pharmaceuticals, Gila Therapeutics, Amgen, General Mills, Boehringer Ingelheim, Currax Pharmaceuticals, Nestlé, Bausch Health, and Rare Diseases; and has received research support or had contracts with Vivus Inc., Satiogen Pharmaceuticals, Boehringer Ingelheim, and Rhythm Pharmaceuticals. Machineni has been involved in semaglutide and tirzepatide clinical trials and has been a consultant to Novo Nordisk, Eli Lilly and Company, and Rhythm Pharmaceuticals. Kushner is on the scientific advisory board for Novo Nordisk.
A version of this article appeared on Medscape.com.
, enabling clinicians to better tailor antiobesity medication (AOM) to the patient.
Currently, patient response to AOMs varies widely, with some patients responding robustly to AOMs and others responding weakly or not at all.
For example, trials of the GLP-1 semaglutide found that 32%-39.6% of people are “super responders,” achieving weight loss in excess of 20%, and a subgroup of 10.2%-16.7% of individuals are nonresponders. Similar variability was found with other AOMs, including the GLP-1 liraglutide and tirzepatide, a dual GLP-1/glucose-dependent insulinotropic polypeptide receptor agonist.
Studies of semaglutide suggest that people with obesity and type 2 diabetes (T2D) lose less weight on the drug than those without T2D, and men tend to lose less weight than women.
However, little else is known about predictors of response rates for various AOMs, and medication selection is typically based on patient or physician preference, comorbidities, medication interactions, and insurance coverage.
Although definitions of a “nonresponder” vary, the Endocrine Society’s latest guideline, which many clinicians follow, states that an AOM is considered effective if patients lose more than 5% of their body weight within 3 months.
Can nonresponders and lower responders be identified and helped? Yes, but it’s complicated.
“Treating obesity effectively means recognizing that not all patients respond the same way to the same treatment, and that’s not a failure; it’s a signal,” said Andres Acosta, MD, PhD, an obesity expert at Mayo Clinic, Rochester, Minnesota, and a cofounder of Phenomix Sciences, a biotech company in Menlo Park, California.
“Obesity is not a single disease. It’s a complex, multifactorial condition driven by diverse biological pathways,” he told GI & Hepatology News. “Semaglutide and other GLP-1s primarily act by reducing appetite and slowing gastric emptying, but not all patients have obesity that is primarily driven by appetite dysregulation.”
Phenotype-Based Profiling
Figuring out what drives an individual’s obesity is where a phenotype-based profiling test could possibly help.
Acosta and colleagues previously used a variety of validated studies and questionnaires to identify four phenotypes that represent distinct biologic drivers of obesity: hungry brain (abnormal satiation), emotional hunger (hedonic eating), hungry gut (abnormal satiety), and slow burn (decreased metabolic rate). In their pragmatic clinical trial, phenotype-guided AOM selection was associated with 1.75-fold greater weight loss after 12 months than the standard approach to drug selection, with mean weight loss of 15.9% and 9%, respectively.
“If a patient’s obesity isn’t primarily rooted in the mechanisms targeted by a particular drug, their response will naturally be limited,” Acosta said. “It’s not that they’re failing the medication; the medication simply isn’t the right match for their biology.”
For their new study, published online in Cell Metabolism, Acosta and colleagues built on their previous research by analyzing the genetic and nongenetic factors that influenced calories needed to reach satiation (Calories to Satiation [CTS]) in adults with obesity. They then used machine learning techniques to develop a CTS gene risk score (CTS-GRS) that could be measured by a DNA saliva test.
The study included 717 adults with obesity (mean age, 41; 75% women) with marked variability in satiation, ranging from 140 to 2166 kcals to reach satiation.
CTS was assessed through an ad libitum meal, combined with physiological and behavioral evaluations, including calorimetry, imaging, blood sampling, and gastric emptying tests. The largest contributors to CTS variability were sex and genetic factors, while other anthropometric measurements played lesser roles.
Various analyses and assessments of participants’ CTS-GRS scores showed that individuals with a high CTS-GRS, or hungry brain phenotype, experienced significantly greater weight loss when treated with phentermine/topiramate than those with a low CTS-GRS, or hungry gut, phenotype. After 52 weeks of treatment, individuals with the hungry brain phenotype lost an average of 17.4% of their body weight compared with 11.2% in those with the hungry gut phenotype.
An analysis of a separate 16-week study showed that patients with the hungry gut phenotype responded better to the GLP-1 liraglutide, losing 6.4% total body weight, compared to 3.3% for those with the hungry brain phenotype.
Overall, the CTS-GRS test predicted drug response with up to 84% accuracy (area under the curve, 0.76 in men and 0.84 in women). The authors acknowledged that these results need to be replicated prospectively and in more diverse populations to validate the test’s predictive ability.
“This kind of phenotype-based profiling allows us to predict which patients are more likely to respond and who might need a different intervention,” Acosta said. “It’s a critical step toward eliminating trial-and-error in obesity treatment.”
The test (MyPhenome test) is used at more than 80 healthcare clinics in the United States, according to Phenomix Sciences, which manufactures it. A company spokesperson said the test does not require FDA approval because it is used to predict obesity phenotypes to help inform treatment, but not to identify specific medications or other interventions. “If it were to do the latter,” the spokesperson said, “it would be considered a ‘companion diagnostic’ and subject to the FDA clearance process.”
What to Do if an AOM Isn’t Working?
It’s one thing to predict whether an individual might do better on one drug vs another, but what should clinicians do meanwhile to optimize weight loss for their patients who may be struggling on a particular drug?
“Efforts to predict the response to GLP-1 therapy have been a hot topic,” noted Sriram Machineni, MD, associate professor at Montefiore Medical Center, Bronx, New York, and founding director of the Fleischer Institute Medical Weight Center at Montefiore Einstein. Although the current study showed that genetic testing could predict responders, like Acosta, he agreed that the results need to be replicated in a prospective manner.
“In the absence of a validated tool for predicting response to specific medications, we use a prioritization process for trialing medications,” Machineni told GI & Hepatology News. “The prioritization is based on the suitability of the side-effect profile to the specific patient, including contraindications; benefits independent of weight loss, such as cardiovascular protection for semaglutide; average efficacy; and financial accessibility for patients.”
Predicting responders isn’t straightforward, said Robert Kushner, MD, professor of medicine and medical education at the Feinberg School of Medicine at Northwestern University and medical director of the Wellness Institute at Northwestern Memorial Hospital in Chicago.
“Despite looking at baseline demographic data such as race, ethnicity, age, weight, and BMI, we are unable to predict who will lose more or less weight,” he told GI & Hepatology News. The one exception is that women generally lose more weight than men. “However, even among females, we cannot discern which females will lose more weight than other females,” he said.
If an individual is not showing sufficient weight loss on a particular medication, “we first explore potential reasons that can be addressed, such as the patient is not taking the medication or is skipping doses,” Kushner said. If need be, they discuss changing to a different drug to improve compliance. He also stresses the importance of making lifestyle changes in diet and physical activity for patients taking AOMs.
Often patients who do not lose at least 5% of their weight within 3 months are not likely to respond well to that medication even if they remain on it. “So, early response rates determine longer-term success,” Kushner said.
Acosta said that if a patient isn’t responding to one class of medication, he pivots to a treatment better aligned with their phenotype. “That could mean switching from a GLP-1 to a medication like [naltrexone/bupropion] or trying a new method altogether,” he said. “The key is that the treatment decision is rooted in the patient’s biology, not just a reaction to short-term results. We also emphasize the importance of long-term follow-up and support.”
The goal isn’t just weight loss but also improved health and quality of life, Acosta said. “Whether through medication, surgery, or behavior change, what matters most is tailoring the care plan to each individual’s unique biology and needs.”
The new study received support from the Mayo Clinic Clinical Research Trials Unit, Vivus Inc., and Phenomix Sciences. Acosta is supported by a National Institutes of Health grant.
Acosta is a co-founder and inventor of intellectual property licensed to Phenomix Sciences Inc.; has served as a consultant for Rhythm Pharmaceuticals, Gila Therapeutics, Amgen, General Mills, Boehringer Ingelheim, Currax Pharmaceuticals, Nestlé, Bausch Health, and Rare Diseases; and has received research support or had contracts with Vivus Inc., Satiogen Pharmaceuticals, Boehringer Ingelheim, and Rhythm Pharmaceuticals. Machineni has been involved in semaglutide and tirzepatide clinical trials and has been a consultant to Novo Nordisk, Eli Lilly and Company, and Rhythm Pharmaceuticals. Kushner is on the scientific advisory board for Novo Nordisk.
A version of this article appeared on Medscape.com.
, enabling clinicians to better tailor antiobesity medication (AOM) to the patient.
Currently, patient response to AOMs varies widely, with some patients responding robustly to AOMs and others responding weakly or not at all.
For example, trials of the GLP-1 semaglutide found that 32%-39.6% of people are “super responders,” achieving weight loss in excess of 20%, and a subgroup of 10.2%-16.7% of individuals are nonresponders. Similar variability was found with other AOMs, including the GLP-1 liraglutide and tirzepatide, a dual GLP-1/glucose-dependent insulinotropic polypeptide receptor agonist.
Studies of semaglutide suggest that people with obesity and type 2 diabetes (T2D) lose less weight on the drug than those without T2D, and men tend to lose less weight than women.
However, little else is known about predictors of response rates for various AOMs, and medication selection is typically based on patient or physician preference, comorbidities, medication interactions, and insurance coverage.
Although definitions of a “nonresponder” vary, the Endocrine Society’s latest guideline, which many clinicians follow, states that an AOM is considered effective if patients lose more than 5% of their body weight within 3 months.
Can nonresponders and lower responders be identified and helped? Yes, but it’s complicated.
“Treating obesity effectively means recognizing that not all patients respond the same way to the same treatment, and that’s not a failure; it’s a signal,” said Andres Acosta, MD, PhD, an obesity expert at Mayo Clinic, Rochester, Minnesota, and a cofounder of Phenomix Sciences, a biotech company in Menlo Park, California.
“Obesity is not a single disease. It’s a complex, multifactorial condition driven by diverse biological pathways,” he told GI & Hepatology News. “Semaglutide and other GLP-1s primarily act by reducing appetite and slowing gastric emptying, but not all patients have obesity that is primarily driven by appetite dysregulation.”
Phenotype-Based Profiling
Figuring out what drives an individual’s obesity is where a phenotype-based profiling test could possibly help.
Acosta and colleagues previously used a variety of validated studies and questionnaires to identify four phenotypes that represent distinct biologic drivers of obesity: hungry brain (abnormal satiation), emotional hunger (hedonic eating), hungry gut (abnormal satiety), and slow burn (decreased metabolic rate). In their pragmatic clinical trial, phenotype-guided AOM selection was associated with 1.75-fold greater weight loss after 12 months than the standard approach to drug selection, with mean weight loss of 15.9% and 9%, respectively.
“If a patient’s obesity isn’t primarily rooted in the mechanisms targeted by a particular drug, their response will naturally be limited,” Acosta said. “It’s not that they’re failing the medication; the medication simply isn’t the right match for their biology.”
For their new study, published online in Cell Metabolism, Acosta and colleagues built on their previous research by analyzing the genetic and nongenetic factors that influenced calories needed to reach satiation (Calories to Satiation [CTS]) in adults with obesity. They then used machine learning techniques to develop a CTS gene risk score (CTS-GRS) that could be measured by a DNA saliva test.
The study included 717 adults with obesity (mean age, 41; 75% women) with marked variability in satiation, ranging from 140 to 2166 kcals to reach satiation.
CTS was assessed through an ad libitum meal, combined with physiological and behavioral evaluations, including calorimetry, imaging, blood sampling, and gastric emptying tests. The largest contributors to CTS variability were sex and genetic factors, while other anthropometric measurements played lesser roles.
Various analyses and assessments of participants’ CTS-GRS scores showed that individuals with a high CTS-GRS, or hungry brain phenotype, experienced significantly greater weight loss when treated with phentermine/topiramate than those with a low CTS-GRS, or hungry gut, phenotype. After 52 weeks of treatment, individuals with the hungry brain phenotype lost an average of 17.4% of their body weight compared with 11.2% in those with the hungry gut phenotype.
An analysis of a separate 16-week study showed that patients with the hungry gut phenotype responded better to the GLP-1 liraglutide, losing 6.4% total body weight, compared to 3.3% for those with the hungry brain phenotype.
Overall, the CTS-GRS test predicted drug response with up to 84% accuracy (area under the curve, 0.76 in men and 0.84 in women). The authors acknowledged that these results need to be replicated prospectively and in more diverse populations to validate the test’s predictive ability.
“This kind of phenotype-based profiling allows us to predict which patients are more likely to respond and who might need a different intervention,” Acosta said. “It’s a critical step toward eliminating trial-and-error in obesity treatment.”
The test (MyPhenome test) is used at more than 80 healthcare clinics in the United States, according to Phenomix Sciences, which manufactures it. A company spokesperson said the test does not require FDA approval because it is used to predict obesity phenotypes to help inform treatment, but not to identify specific medications or other interventions. “If it were to do the latter,” the spokesperson said, “it would be considered a ‘companion diagnostic’ and subject to the FDA clearance process.”
What to Do if an AOM Isn’t Working?
It’s one thing to predict whether an individual might do better on one drug vs another, but what should clinicians do meanwhile to optimize weight loss for their patients who may be struggling on a particular drug?
“Efforts to predict the response to GLP-1 therapy have been a hot topic,” noted Sriram Machineni, MD, associate professor at Montefiore Medical Center, Bronx, New York, and founding director of the Fleischer Institute Medical Weight Center at Montefiore Einstein. Although the current study showed that genetic testing could predict responders, like Acosta, he agreed that the results need to be replicated in a prospective manner.
“In the absence of a validated tool for predicting response to specific medications, we use a prioritization process for trialing medications,” Machineni told GI & Hepatology News. “The prioritization is based on the suitability of the side-effect profile to the specific patient, including contraindications; benefits independent of weight loss, such as cardiovascular protection for semaglutide; average efficacy; and financial accessibility for patients.”
Predicting responders isn’t straightforward, said Robert Kushner, MD, professor of medicine and medical education at the Feinberg School of Medicine at Northwestern University and medical director of the Wellness Institute at Northwestern Memorial Hospital in Chicago.
“Despite looking at baseline demographic data such as race, ethnicity, age, weight, and BMI, we are unable to predict who will lose more or less weight,” he told GI & Hepatology News. The one exception is that women generally lose more weight than men. “However, even among females, we cannot discern which females will lose more weight than other females,” he said.
If an individual is not showing sufficient weight loss on a particular medication, “we first explore potential reasons that can be addressed, such as the patient is not taking the medication or is skipping doses,” Kushner said. If need be, they discuss changing to a different drug to improve compliance. He also stresses the importance of making lifestyle changes in diet and physical activity for patients taking AOMs.
Often patients who do not lose at least 5% of their weight within 3 months are not likely to respond well to that medication even if they remain on it. “So, early response rates determine longer-term success,” Kushner said.
Acosta said that if a patient isn’t responding to one class of medication, he pivots to a treatment better aligned with their phenotype. “That could mean switching from a GLP-1 to a medication like [naltrexone/bupropion] or trying a new method altogether,” he said. “The key is that the treatment decision is rooted in the patient’s biology, not just a reaction to short-term results. We also emphasize the importance of long-term follow-up and support.”
The goal isn’t just weight loss but also improved health and quality of life, Acosta said. “Whether through medication, surgery, or behavior change, what matters most is tailoring the care plan to each individual’s unique biology and needs.”
The new study received support from the Mayo Clinic Clinical Research Trials Unit, Vivus Inc., and Phenomix Sciences. Acosta is supported by a National Institutes of Health grant.
Acosta is a co-founder and inventor of intellectual property licensed to Phenomix Sciences Inc.; has served as a consultant for Rhythm Pharmaceuticals, Gila Therapeutics, Amgen, General Mills, Boehringer Ingelheim, Currax Pharmaceuticals, Nestlé, Bausch Health, and Rare Diseases; and has received research support or had contracts with Vivus Inc., Satiogen Pharmaceuticals, Boehringer Ingelheim, and Rhythm Pharmaceuticals. Machineni has been involved in semaglutide and tirzepatide clinical trials and has been a consultant to Novo Nordisk, Eli Lilly and Company, and Rhythm Pharmaceuticals. Kushner is on the scientific advisory board for Novo Nordisk.
A version of this article appeared on Medscape.com.
You Are When You Eat: Microbiome Rhythm and Metabolic Health
Similar to circadian rhythms that help regulate when we naturally fall asleep and wake up, microbial rhythms in our gut are naturally active at certain times of the day to help regulate our digestion.
Investigators from the University of California, San Diego sought out to track these microbial rhythms to determine whether aligning the times we eat to when our gut microbes are most active – time-restricted feeding (TRF) – can bolster our metabolic health. Their research was published recently in Cell Host & Microbe.
“Microbial rhythms are daily fluctuations in the composition and function of microbes living in our gut. Much like how our bodies follow an internal clock (circadian rhythm), gut microbes also have their own rhythms, adjusting their activities based on the time of day and when we eat,” said Amir Zarrinpar, MD, PhD, a gastroenterologist at UC San Diego School of Medicine, and senior author of the study.
Zarrinpar and his team were particularly interested in observing whether adopting the TRF approach counteracted the harmful metabolic effects often associated with consuming a high-fat diet.
The study is also notable for the team’s use of technology able to observe real-time microbial changes in the gut — something not previously attainable with existing metagenomics.
How the Study Evolved With New Tech
Researchers separated three groups of mice to analyze their microbiome activity: one on a high-fat diet with unrestricted access, another on the same high-fat diet within a TRF window of 8 hours per day, and a control group on a normal chow diet with unrestricted access.
“In mice, [their] microbial rhythms are well-aligned with their nocturnal lifestyle. For example, during their active (nighttime) period, certain beneficial microbial activities increase, helping digest food, absorb nutrients, and regulate metabolism,” said Zarrinpar. As a result, the team made sure the mice’s TRF window was at night or when they would normally be awake.
“We chose an 8-hour feeding window based on earlier research showing this time period allows mice to consume the same total calories as those with unlimited food access,” said Zarrinpar. “By controlling [the] calories in this way, we ensure any metabolic or microbial benefits we observe are specifically due to the timing of eating, rather than differences in total food intake.”
But before any observations could be made, the team first needed a way to see real-time changes in the animals’ gut microbiomes.
Zarrinpar and his team were able to uncover this, thanks to metatranscriptomics, a technique used to capture real-time microbial activity by profiling RNA transcripts. Compared with the more traditional technique of metagenomics, which could only be used to identify which genes were present, metatranscriptomics provided more in-depth temporal and activity-related context, allowing the team to observe dynamic microbial changes.
“[Metatranscriptomics] helps us understand not just which microbes are present, but specifically what they are doing at any given moment,” said Zarrinpar. “In contrast, metagenomics looks only at microbial DNA, which provides information about what microbes are potentially capable of doing, but doesn’t tell us if those genes are actively expressed. By comparing microbial gene expression (using metatranscriptomics) and microbial gene abundance (using metagenomics) across different diet and feeding conditions in [light and dark] phases, we aimed to identify how feeding timing might influence microbial activity.”
Because metagenomics focuses on stable genetic material, this technique cannot capture the real-time microbial responses to dietary timing presented in rapidly changing, short-lived RNA. At the same time, the instability of the RNA makes it difficult to test hypotheses experimentally and explains why researchers haven’t more widely relied on metatranscriptomics.
To overcome this difficulty, Zarrinpar and his team had to wait to take advantage of improved bioinformatics tools to simplify their analysis of complex datasets. “It took several years for us to analyze this dataset because robust computational tools for metatranscriptomic analysis were not widely available when we initially collected our samples. Additionally, sequencing costs were very high. To clearly identify microbial activity, we needed deep sequencing coverage to distinguish species-level differences in gene expression, especially for genes that are common across multiple types of microbes,” said Zarrinpar.
What They Found
After monitoring these groups of mice for 8 weeks, the results were revealed.
As predicted, “When mice have free access to a high-fat diet, their normal eating behavior changes significantly. Instead of limiting their activity and feeding to their active nighttime period, these mice begin to stay awake and eat during the day, which is their typical rest phase,” Zarrinpar explained.
“This unusual daytime activity interferes with important physiological processes. Consequently, the animals experience circadian misalignment, a condition similar to what human shift workers experience when their sleep-wake and eating cycles don’t match their internal biological clocks,” he continued. “This misalignment can negatively affect metabolism, immunity, and overall health, potentially leading to metabolic diseases.”
For the mice that consumed a high-fat diet within a TRF window, metabolic phenotyping demonstrated that their specific diet regimen had protected them from harmful high-fat induced effects including adiposity, inflammation, and insulin resistance.
Even more promising, the mice not only were protected from metabolic disruption but also experienced physiological improvements including glucose homeostasis and the partial restoration of the daily microbial rhythms absent in the mice with unrestricted access to a high-fat diet.
While the TRF approach did not fully restore the normal, healthy rhythmicity seen in the control mice, the researchers noted distinct shifts in microbial patterns that indicated time-dependent enrichment in genes attributed to lipid and carbohydrate metabolism.
Better Metabolic Health — and Better Tools for Researching It
Thankfully, the latest advancements in sequencing technology, including long-read sequencing methods, are making metatranscriptomics easier for research. “These newer platforms offer greater resolution at a lower cost, making metatranscriptomics increasingly accessible,” said Zarrinpar. With these emerging technologies, he believes metatranscriptomics will become a more standard, widely used method for researchers to better understand the influence of microbial activity on our health.
These tools, for example, enabled Zarrinpar and the team to delve deeper and focus on the transcription of a particular enzyme they identified as a pivotal influence in observable metabolic improvements: bile salt hydrolase (BSH), known to regulate lipid and glucose metabolism. The TRF approach notably enhanced the expression of the BSH gene during the daytime in the gut microbe Dubosiella newyorkensis, which has a functional human equivalent.
To determine why this happened, the team leveraged genetic engineering to insert several active BSH gene variants into a benign strain of gut bacteria to administer to the mice. The only variant to produce metabolic improvements was the one derived from Dubosiella newyorkensis; the mice who were given this BSH-expressing engineered native bacteria (ENB) had increased lean muscle mass, less body fat, lower insulin levels, enhanced insulin sensitivity, and better blood glucose regulation.
“It is still early to know the full clinical potential of this new BSH-expressing engineered native bacterium,” said Zarrinpar. “However, our long-term goal is to develop a therapeutic that can be administered as a single dose, stably colonize the gut, and provide long-lasting metabolic benefits.” Testing the engineered bacteria in obese and diabetic mice on a high-fat diet would be a next step to determine whether its potential indeed holds up. If proven successful, it could then be used to develop future targeted therapies and interventions to treat common metabolic disorders.
With this engineered bacteria, Zarrinpar and his team are hopeful that it alone can replicate the microbial benefits associated with following a TRF dietary schedule. “In our study, the engineered bacterium continuously expressed the enzyme DnBSH1, independently of dietary or environmental factors. As a result, the bacterium provided metabolic benefits similar to those seen with TRF, even without requiring the mice to strictly adhere to a TRF schedule,” said Zarrinpar.
“This suggests the exciting possibility that this engineered microbe might serve either as a replacement for TRF or as a way to enhance its beneficial effects,” he continued. “Further studies will help determine whether combining this ENB with TRF could provide additional or synergistic improvements in metabolic health.”
Looking Ahead
“As the pioneer of the single anastomosis duodenal switch which separates bile from food until halfway down the GI tract, I agree that bile is very important in controlling metabolism and glucose,” said Mitchell Roslin, MD, chief director of bariatric and metabolic surgery at Lenox Hill Hospital, and the Donald and Barbara Zucker School of Medicine, Hempstead, New York, who was not involved in the study. “Using enzymes or medications that work in the GI tract without absorption into the body is very interesting and has great potential. It is an early but exciting prospect.”
However, Roslin expressed some reservations. “I think we are still trying to understand whether the difference in microbiomes is the cause or effect/association. Is the microbiome the difference or is a different microbiome representative of a diet that has more fiber and less processed foods? Thus, while I find this academically fascinating, I think that there are very basic questions that need better answers, before we look at the transcription of bacteria.”
Furthermore, translating the metabolic results observed in mice to humans might not be as straightforward. “Small animal research is mandatory, but how the findings convert to humans is highly speculative,” said Roslin. “Mice that are studied are usually bred for medical research, with reduced genetic variation. Many animal models are more sensitive to time-restricted eating and caloric restriction than humans.”
While it requires further research and validation, this UC San Diego study nevertheless contributes to our overall understanding of host-microbe interactions. “We demonstrate that host circadian rhythms significantly influence microbial function, and conversely, these microbial functions can directly impact host metabolism,” said Zarrinpar. “Importantly, we now have a method to test how specific microbial activities affect host physiology by engineering native gut bacteria.”
Roslin similarly emphasized the importance of continued investment in exploring the microbial ecosystem inside us all. “There is wider evidence that bacteria and microbes are not just passengers using us for a ride but perhaps manipulating every action we take.”
A version of this article appeared on Medscape.com.
Similar to circadian rhythms that help regulate when we naturally fall asleep and wake up, microbial rhythms in our gut are naturally active at certain times of the day to help regulate our digestion.
Investigators from the University of California, San Diego sought out to track these microbial rhythms to determine whether aligning the times we eat to when our gut microbes are most active – time-restricted feeding (TRF) – can bolster our metabolic health. Their research was published recently in Cell Host & Microbe.
“Microbial rhythms are daily fluctuations in the composition and function of microbes living in our gut. Much like how our bodies follow an internal clock (circadian rhythm), gut microbes also have their own rhythms, adjusting their activities based on the time of day and when we eat,” said Amir Zarrinpar, MD, PhD, a gastroenterologist at UC San Diego School of Medicine, and senior author of the study.
Zarrinpar and his team were particularly interested in observing whether adopting the TRF approach counteracted the harmful metabolic effects often associated with consuming a high-fat diet.
The study is also notable for the team’s use of technology able to observe real-time microbial changes in the gut — something not previously attainable with existing metagenomics.
How the Study Evolved With New Tech
Researchers separated three groups of mice to analyze their microbiome activity: one on a high-fat diet with unrestricted access, another on the same high-fat diet within a TRF window of 8 hours per day, and a control group on a normal chow diet with unrestricted access.
“In mice, [their] microbial rhythms are well-aligned with their nocturnal lifestyle. For example, during their active (nighttime) period, certain beneficial microbial activities increase, helping digest food, absorb nutrients, and regulate metabolism,” said Zarrinpar. As a result, the team made sure the mice’s TRF window was at night or when they would normally be awake.
“We chose an 8-hour feeding window based on earlier research showing this time period allows mice to consume the same total calories as those with unlimited food access,” said Zarrinpar. “By controlling [the] calories in this way, we ensure any metabolic or microbial benefits we observe are specifically due to the timing of eating, rather than differences in total food intake.”
But before any observations could be made, the team first needed a way to see real-time changes in the animals’ gut microbiomes.
Zarrinpar and his team were able to uncover this, thanks to metatranscriptomics, a technique used to capture real-time microbial activity by profiling RNA transcripts. Compared with the more traditional technique of metagenomics, which could only be used to identify which genes were present, metatranscriptomics provided more in-depth temporal and activity-related context, allowing the team to observe dynamic microbial changes.
“[Metatranscriptomics] helps us understand not just which microbes are present, but specifically what they are doing at any given moment,” said Zarrinpar. “In contrast, metagenomics looks only at microbial DNA, which provides information about what microbes are potentially capable of doing, but doesn’t tell us if those genes are actively expressed. By comparing microbial gene expression (using metatranscriptomics) and microbial gene abundance (using metagenomics) across different diet and feeding conditions in [light and dark] phases, we aimed to identify how feeding timing might influence microbial activity.”
Because metagenomics focuses on stable genetic material, this technique cannot capture the real-time microbial responses to dietary timing presented in rapidly changing, short-lived RNA. At the same time, the instability of the RNA makes it difficult to test hypotheses experimentally and explains why researchers haven’t more widely relied on metatranscriptomics.
To overcome this difficulty, Zarrinpar and his team had to wait to take advantage of improved bioinformatics tools to simplify their analysis of complex datasets. “It took several years for us to analyze this dataset because robust computational tools for metatranscriptomic analysis were not widely available when we initially collected our samples. Additionally, sequencing costs were very high. To clearly identify microbial activity, we needed deep sequencing coverage to distinguish species-level differences in gene expression, especially for genes that are common across multiple types of microbes,” said Zarrinpar.
What They Found
After monitoring these groups of mice for 8 weeks, the results were revealed.
As predicted, “When mice have free access to a high-fat diet, their normal eating behavior changes significantly. Instead of limiting their activity and feeding to their active nighttime period, these mice begin to stay awake and eat during the day, which is their typical rest phase,” Zarrinpar explained.
“This unusual daytime activity interferes with important physiological processes. Consequently, the animals experience circadian misalignment, a condition similar to what human shift workers experience when their sleep-wake and eating cycles don’t match their internal biological clocks,” he continued. “This misalignment can negatively affect metabolism, immunity, and overall health, potentially leading to metabolic diseases.”
For the mice that consumed a high-fat diet within a TRF window, metabolic phenotyping demonstrated that their specific diet regimen had protected them from harmful high-fat induced effects including adiposity, inflammation, and insulin resistance.
Even more promising, the mice not only were protected from metabolic disruption but also experienced physiological improvements including glucose homeostasis and the partial restoration of the daily microbial rhythms absent in the mice with unrestricted access to a high-fat diet.
While the TRF approach did not fully restore the normal, healthy rhythmicity seen in the control mice, the researchers noted distinct shifts in microbial patterns that indicated time-dependent enrichment in genes attributed to lipid and carbohydrate metabolism.
Better Metabolic Health — and Better Tools for Researching It
Thankfully, the latest advancements in sequencing technology, including long-read sequencing methods, are making metatranscriptomics easier for research. “These newer platforms offer greater resolution at a lower cost, making metatranscriptomics increasingly accessible,” said Zarrinpar. With these emerging technologies, he believes metatranscriptomics will become a more standard, widely used method for researchers to better understand the influence of microbial activity on our health.
These tools, for example, enabled Zarrinpar and the team to delve deeper and focus on the transcription of a particular enzyme they identified as a pivotal influence in observable metabolic improvements: bile salt hydrolase (BSH), known to regulate lipid and glucose metabolism. The TRF approach notably enhanced the expression of the BSH gene during the daytime in the gut microbe Dubosiella newyorkensis, which has a functional human equivalent.
To determine why this happened, the team leveraged genetic engineering to insert several active BSH gene variants into a benign strain of gut bacteria to administer to the mice. The only variant to produce metabolic improvements was the one derived from Dubosiella newyorkensis; the mice who were given this BSH-expressing engineered native bacteria (ENB) had increased lean muscle mass, less body fat, lower insulin levels, enhanced insulin sensitivity, and better blood glucose regulation.
“It is still early to know the full clinical potential of this new BSH-expressing engineered native bacterium,” said Zarrinpar. “However, our long-term goal is to develop a therapeutic that can be administered as a single dose, stably colonize the gut, and provide long-lasting metabolic benefits.” Testing the engineered bacteria in obese and diabetic mice on a high-fat diet would be a next step to determine whether its potential indeed holds up. If proven successful, it could then be used to develop future targeted therapies and interventions to treat common metabolic disorders.
With this engineered bacteria, Zarrinpar and his team are hopeful that it alone can replicate the microbial benefits associated with following a TRF dietary schedule. “In our study, the engineered bacterium continuously expressed the enzyme DnBSH1, independently of dietary or environmental factors. As a result, the bacterium provided metabolic benefits similar to those seen with TRF, even without requiring the mice to strictly adhere to a TRF schedule,” said Zarrinpar.
“This suggests the exciting possibility that this engineered microbe might serve either as a replacement for TRF or as a way to enhance its beneficial effects,” he continued. “Further studies will help determine whether combining this ENB with TRF could provide additional or synergistic improvements in metabolic health.”
Looking Ahead
“As the pioneer of the single anastomosis duodenal switch which separates bile from food until halfway down the GI tract, I agree that bile is very important in controlling metabolism and glucose,” said Mitchell Roslin, MD, chief director of bariatric and metabolic surgery at Lenox Hill Hospital, and the Donald and Barbara Zucker School of Medicine, Hempstead, New York, who was not involved in the study. “Using enzymes or medications that work in the GI tract without absorption into the body is very interesting and has great potential. It is an early but exciting prospect.”
However, Roslin expressed some reservations. “I think we are still trying to understand whether the difference in microbiomes is the cause or effect/association. Is the microbiome the difference or is a different microbiome representative of a diet that has more fiber and less processed foods? Thus, while I find this academically fascinating, I think that there are very basic questions that need better answers, before we look at the transcription of bacteria.”
Furthermore, translating the metabolic results observed in mice to humans might not be as straightforward. “Small animal research is mandatory, but how the findings convert to humans is highly speculative,” said Roslin. “Mice that are studied are usually bred for medical research, with reduced genetic variation. Many animal models are more sensitive to time-restricted eating and caloric restriction than humans.”
While it requires further research and validation, this UC San Diego study nevertheless contributes to our overall understanding of host-microbe interactions. “We demonstrate that host circadian rhythms significantly influence microbial function, and conversely, these microbial functions can directly impact host metabolism,” said Zarrinpar. “Importantly, we now have a method to test how specific microbial activities affect host physiology by engineering native gut bacteria.”
Roslin similarly emphasized the importance of continued investment in exploring the microbial ecosystem inside us all. “There is wider evidence that bacteria and microbes are not just passengers using us for a ride but perhaps manipulating every action we take.”
A version of this article appeared on Medscape.com.
Similar to circadian rhythms that help regulate when we naturally fall asleep and wake up, microbial rhythms in our gut are naturally active at certain times of the day to help regulate our digestion.
Investigators from the University of California, San Diego sought out to track these microbial rhythms to determine whether aligning the times we eat to when our gut microbes are most active – time-restricted feeding (TRF) – can bolster our metabolic health. Their research was published recently in Cell Host & Microbe.
“Microbial rhythms are daily fluctuations in the composition and function of microbes living in our gut. Much like how our bodies follow an internal clock (circadian rhythm), gut microbes also have their own rhythms, adjusting their activities based on the time of day and when we eat,” said Amir Zarrinpar, MD, PhD, a gastroenterologist at UC San Diego School of Medicine, and senior author of the study.
Zarrinpar and his team were particularly interested in observing whether adopting the TRF approach counteracted the harmful metabolic effects often associated with consuming a high-fat diet.
The study is also notable for the team’s use of technology able to observe real-time microbial changes in the gut — something not previously attainable with existing metagenomics.
How the Study Evolved With New Tech
Researchers separated three groups of mice to analyze their microbiome activity: one on a high-fat diet with unrestricted access, another on the same high-fat diet within a TRF window of 8 hours per day, and a control group on a normal chow diet with unrestricted access.
“In mice, [their] microbial rhythms are well-aligned with their nocturnal lifestyle. For example, during their active (nighttime) period, certain beneficial microbial activities increase, helping digest food, absorb nutrients, and regulate metabolism,” said Zarrinpar. As a result, the team made sure the mice’s TRF window was at night or when they would normally be awake.
“We chose an 8-hour feeding window based on earlier research showing this time period allows mice to consume the same total calories as those with unlimited food access,” said Zarrinpar. “By controlling [the] calories in this way, we ensure any metabolic or microbial benefits we observe are specifically due to the timing of eating, rather than differences in total food intake.”
But before any observations could be made, the team first needed a way to see real-time changes in the animals’ gut microbiomes.
Zarrinpar and his team were able to uncover this, thanks to metatranscriptomics, a technique used to capture real-time microbial activity by profiling RNA transcripts. Compared with the more traditional technique of metagenomics, which could only be used to identify which genes were present, metatranscriptomics provided more in-depth temporal and activity-related context, allowing the team to observe dynamic microbial changes.
“[Metatranscriptomics] helps us understand not just which microbes are present, but specifically what they are doing at any given moment,” said Zarrinpar. “In contrast, metagenomics looks only at microbial DNA, which provides information about what microbes are potentially capable of doing, but doesn’t tell us if those genes are actively expressed. By comparing microbial gene expression (using metatranscriptomics) and microbial gene abundance (using metagenomics) across different diet and feeding conditions in [light and dark] phases, we aimed to identify how feeding timing might influence microbial activity.”
Because metagenomics focuses on stable genetic material, this technique cannot capture the real-time microbial responses to dietary timing presented in rapidly changing, short-lived RNA. At the same time, the instability of the RNA makes it difficult to test hypotheses experimentally and explains why researchers haven’t more widely relied on metatranscriptomics.
To overcome this difficulty, Zarrinpar and his team had to wait to take advantage of improved bioinformatics tools to simplify their analysis of complex datasets. “It took several years for us to analyze this dataset because robust computational tools for metatranscriptomic analysis were not widely available when we initially collected our samples. Additionally, sequencing costs were very high. To clearly identify microbial activity, we needed deep sequencing coverage to distinguish species-level differences in gene expression, especially for genes that are common across multiple types of microbes,” said Zarrinpar.
What They Found
After monitoring these groups of mice for 8 weeks, the results were revealed.
As predicted, “When mice have free access to a high-fat diet, their normal eating behavior changes significantly. Instead of limiting their activity and feeding to their active nighttime period, these mice begin to stay awake and eat during the day, which is their typical rest phase,” Zarrinpar explained.
“This unusual daytime activity interferes with important physiological processes. Consequently, the animals experience circadian misalignment, a condition similar to what human shift workers experience when their sleep-wake and eating cycles don’t match their internal biological clocks,” he continued. “This misalignment can negatively affect metabolism, immunity, and overall health, potentially leading to metabolic diseases.”
For the mice that consumed a high-fat diet within a TRF window, metabolic phenotyping demonstrated that their specific diet regimen had protected them from harmful high-fat induced effects including adiposity, inflammation, and insulin resistance.
Even more promising, the mice not only were protected from metabolic disruption but also experienced physiological improvements including glucose homeostasis and the partial restoration of the daily microbial rhythms absent in the mice with unrestricted access to a high-fat diet.
While the TRF approach did not fully restore the normal, healthy rhythmicity seen in the control mice, the researchers noted distinct shifts in microbial patterns that indicated time-dependent enrichment in genes attributed to lipid and carbohydrate metabolism.
Better Metabolic Health — and Better Tools for Researching It
Thankfully, the latest advancements in sequencing technology, including long-read sequencing methods, are making metatranscriptomics easier for research. “These newer platforms offer greater resolution at a lower cost, making metatranscriptomics increasingly accessible,” said Zarrinpar. With these emerging technologies, he believes metatranscriptomics will become a more standard, widely used method for researchers to better understand the influence of microbial activity on our health.
These tools, for example, enabled Zarrinpar and the team to delve deeper and focus on the transcription of a particular enzyme they identified as a pivotal influence in observable metabolic improvements: bile salt hydrolase (BSH), known to regulate lipid and glucose metabolism. The TRF approach notably enhanced the expression of the BSH gene during the daytime in the gut microbe Dubosiella newyorkensis, which has a functional human equivalent.
To determine why this happened, the team leveraged genetic engineering to insert several active BSH gene variants into a benign strain of gut bacteria to administer to the mice. The only variant to produce metabolic improvements was the one derived from Dubosiella newyorkensis; the mice who were given this BSH-expressing engineered native bacteria (ENB) had increased lean muscle mass, less body fat, lower insulin levels, enhanced insulin sensitivity, and better blood glucose regulation.
“It is still early to know the full clinical potential of this new BSH-expressing engineered native bacterium,” said Zarrinpar. “However, our long-term goal is to develop a therapeutic that can be administered as a single dose, stably colonize the gut, and provide long-lasting metabolic benefits.” Testing the engineered bacteria in obese and diabetic mice on a high-fat diet would be a next step to determine whether its potential indeed holds up. If proven successful, it could then be used to develop future targeted therapies and interventions to treat common metabolic disorders.
With this engineered bacteria, Zarrinpar and his team are hopeful that it alone can replicate the microbial benefits associated with following a TRF dietary schedule. “In our study, the engineered bacterium continuously expressed the enzyme DnBSH1, independently of dietary or environmental factors. As a result, the bacterium provided metabolic benefits similar to those seen with TRF, even without requiring the mice to strictly adhere to a TRF schedule,” said Zarrinpar.
“This suggests the exciting possibility that this engineered microbe might serve either as a replacement for TRF or as a way to enhance its beneficial effects,” he continued. “Further studies will help determine whether combining this ENB with TRF could provide additional or synergistic improvements in metabolic health.”
Looking Ahead
“As the pioneer of the single anastomosis duodenal switch which separates bile from food until halfway down the GI tract, I agree that bile is very important in controlling metabolism and glucose,” said Mitchell Roslin, MD, chief director of bariatric and metabolic surgery at Lenox Hill Hospital, and the Donald and Barbara Zucker School of Medicine, Hempstead, New York, who was not involved in the study. “Using enzymes or medications that work in the GI tract without absorption into the body is very interesting and has great potential. It is an early but exciting prospect.”
However, Roslin expressed some reservations. “I think we are still trying to understand whether the difference in microbiomes is the cause or effect/association. Is the microbiome the difference or is a different microbiome representative of a diet that has more fiber and less processed foods? Thus, while I find this academically fascinating, I think that there are very basic questions that need better answers, before we look at the transcription of bacteria.”
Furthermore, translating the metabolic results observed in mice to humans might not be as straightforward. “Small animal research is mandatory, but how the findings convert to humans is highly speculative,” said Roslin. “Mice that are studied are usually bred for medical research, with reduced genetic variation. Many animal models are more sensitive to time-restricted eating and caloric restriction than humans.”
While it requires further research and validation, this UC San Diego study nevertheless contributes to our overall understanding of host-microbe interactions. “We demonstrate that host circadian rhythms significantly influence microbial function, and conversely, these microbial functions can directly impact host metabolism,” said Zarrinpar. “Importantly, we now have a method to test how specific microbial activities affect host physiology by engineering native gut bacteria.”
Roslin similarly emphasized the importance of continued investment in exploring the microbial ecosystem inside us all. “There is wider evidence that bacteria and microbes are not just passengers using us for a ride but perhaps manipulating every action we take.”
A version of this article appeared on Medscape.com.
Novel Gene Risk Score Predicts Outcomes After RYGB Surgery
SAN DIEGO –
The findings suggested that the MyPhenome test (Phenomix Sciences) can help clinicians identify the patients most likely to benefit from bariatric procedures and at a greater risk for long-term weight regain after surgery.
“Patients with both a high genetic risk score and rare mutations in the leptin-melanocortin pathway (LMP) had significantly worse outcomes, maintaining only 4.9% total body weight loss [TBWL] over 15 years compared to up to 24.8% in other genetic groups,” Phenomix Sciences Co-founder Andres Acosta, MD, PhD, told GI & Hepatology News.
The study included details on the score’s development and predictive capability. It was presented at Digestive Disease Week® (DDW) 2025
‘More Precise Bariatric Care’
The researchers recently developed a machine learning-assisted gene risk score for calories to satiation (CTSGRS), which mainly involves genes in the LMP. To assess the role of the score with or without LMP gene variants on weight loss and weight recurrence after RYGB, they identified 707 patients with a history of bariatric procedures from the Mayo Clinic Biobank. Patients with duodenal switch, revisional procedures, or who used antiobesity medications or became pregnant during follow-up were excluded.
To make predictions for 442 of the patients, the team first collected anthropometric data up to 15 years after RYGB. Then they used a two-step approach: Assessing for monogenic variants in the LMP and defining participants as carriers (LMP+) or noncarriers (LMP-). Then they defined the gene risk score (CTSGRS+ or CTSGRS-).
The result was four groups: LMP+/CTSGRS+, LMP+/CTSGRS-, LMP-/CTSGRS+, and LMP-/CTSGRS-. Multiple regression analysis was used to analyze TBWL percentage (TBWL%) between the groups at different timepoints, adjusting for baseline weight, age, and gender.
At the 10-year follow-up, the LMP+/CTSGRS+ group demonstrated a significantly higher weight recurrence (regain) of TBW% compared to the other groups.
At 15 years post-RYGB, the mean TBWL% for LMP+/CTSGRS+ was -4.9 vs -20.3 for LMP+/CTSGRS-, -18.0 for LMP-/CTSGRS+, and -24.8 for LMP-/CTSGRS-.
Further analyses showed that the LMP+/CTSGRS+ group had significantly less weight loss than LMP+/CTSGRS- and LMP-/CTSGRS- groups.
Based on the findings, the authors wrote, “Genotyping patients could improve the implementation of individualized weight-loss interventions, enhance weight-loss outcomes, and/or may explain one of the etiological factors associated with weight recurrence after RYGB.”
Acosta noted, “We’re actively expanding our research to include more diverse populations by age, sex, and race. This includes ongoing analysis to understand whether certain demographic or physiological characteristics affect how the test performs, particularly in the context of bariatric surgery.”
The team also is investigating the benefits of phenotyping for obesity comorbidities such as heart disease and diabetes, he said, and exploring whether early interventions in high-risk patients can prevent long-term weight regain and improve outcomes.
In addition, Acosta said, the team recently launched “the first prospective, placebo-controlled clinical trial using the MyPhenome test to predict response to semaglutide.” That study is based on earlier findings showing that patients identified with a Hungry Gut phenotype lost nearly twice as much weight on semaglutide compared with those who tested negative.
Overall, he concluded, “These findings open the door to more precise bariatric care. When we understand a patient’s biological drivers of obesity, we can make better decisions about the right procedure, follow-up, and long-term support. This moves us away from a one-size-fits-all model to care rooted in each patient’s unique biology.”
Potentially Paradigm-Shifting
Onur Kutlu, MD, associate professor of surgery and director of the Metabolic Surgery and Metabolic Health Program at the Miller School of Medicine, University of Miami, in Miami, Florida, commented on the study for GI & Hepatology News. “By integrating polygenic risk scores into predictive models, the authors offer an innovative method for identifying patients at elevated risk for weight regain following RYGB.”
“Their findings support the hypothesis that genetic predisposition — particularly involving energy homeostasis pathways — may underlie differential postoperative trajectories,” he said. “This approach has the potential to shift the paradigm from reactive to proactive management of weight recurrence.”
Because current options for treat weight regain are “suboptimal,” he said, “prevention becomes paramount. Preoperative identification of high-risk individuals could inform surgical decision-making, enable earlier interventions, and facilitate personalized postoperative monitoring and support.”
“If validated in larger, prospective cohorts, genetic risk stratification could enhance the precision of bariatric care and improve long-term outcomes,” he added. “Future studies should aim to validate these genetic models across diverse populations and explore how integration of behavioral, psychological, and genetic data may further refine patient selection and care pathways.”
The study was funded by Mayo Clinic and Phenomix Sciences. Gila Therapeutics and Phenomix Sciences licensed Acosta’s research technologies from the University of Florida and Mayo Clinic. Acosta declared receiving consultant fees in the past 5 years from Rhythm Pharmaceuticals, Gila Therapeutics, Amgen, General Mills, BI, Currax, Nestle, Phenomix Sciences, Bausch Health, and RareDiseases, as well as funding support from the National Institutes of Health, Vivus Pharmaceuticals, Novo Nordisk, Apollo Endosurgery, Satiogen Pharmaceuticals, Spatz Medical, and Rhythm Pharmaceuticals. Kutlu declared having no conflicts of interest.
A version of this article appeared on Medscape.com.
SAN DIEGO –
The findings suggested that the MyPhenome test (Phenomix Sciences) can help clinicians identify the patients most likely to benefit from bariatric procedures and at a greater risk for long-term weight regain after surgery.
“Patients with both a high genetic risk score and rare mutations in the leptin-melanocortin pathway (LMP) had significantly worse outcomes, maintaining only 4.9% total body weight loss [TBWL] over 15 years compared to up to 24.8% in other genetic groups,” Phenomix Sciences Co-founder Andres Acosta, MD, PhD, told GI & Hepatology News.
The study included details on the score’s development and predictive capability. It was presented at Digestive Disease Week® (DDW) 2025
‘More Precise Bariatric Care’
The researchers recently developed a machine learning-assisted gene risk score for calories to satiation (CTSGRS), which mainly involves genes in the LMP. To assess the role of the score with or without LMP gene variants on weight loss and weight recurrence after RYGB, they identified 707 patients with a history of bariatric procedures from the Mayo Clinic Biobank. Patients with duodenal switch, revisional procedures, or who used antiobesity medications or became pregnant during follow-up were excluded.
To make predictions for 442 of the patients, the team first collected anthropometric data up to 15 years after RYGB. Then they used a two-step approach: Assessing for monogenic variants in the LMP and defining participants as carriers (LMP+) or noncarriers (LMP-). Then they defined the gene risk score (CTSGRS+ or CTSGRS-).
The result was four groups: LMP+/CTSGRS+, LMP+/CTSGRS-, LMP-/CTSGRS+, and LMP-/CTSGRS-. Multiple regression analysis was used to analyze TBWL percentage (TBWL%) between the groups at different timepoints, adjusting for baseline weight, age, and gender.
At the 10-year follow-up, the LMP+/CTSGRS+ group demonstrated a significantly higher weight recurrence (regain) of TBW% compared to the other groups.
At 15 years post-RYGB, the mean TBWL% for LMP+/CTSGRS+ was -4.9 vs -20.3 for LMP+/CTSGRS-, -18.0 for LMP-/CTSGRS+, and -24.8 for LMP-/CTSGRS-.
Further analyses showed that the LMP+/CTSGRS+ group had significantly less weight loss than LMP+/CTSGRS- and LMP-/CTSGRS- groups.
Based on the findings, the authors wrote, “Genotyping patients could improve the implementation of individualized weight-loss interventions, enhance weight-loss outcomes, and/or may explain one of the etiological factors associated with weight recurrence after RYGB.”
Acosta noted, “We’re actively expanding our research to include more diverse populations by age, sex, and race. This includes ongoing analysis to understand whether certain demographic or physiological characteristics affect how the test performs, particularly in the context of bariatric surgery.”
The team also is investigating the benefits of phenotyping for obesity comorbidities such as heart disease and diabetes, he said, and exploring whether early interventions in high-risk patients can prevent long-term weight regain and improve outcomes.
In addition, Acosta said, the team recently launched “the first prospective, placebo-controlled clinical trial using the MyPhenome test to predict response to semaglutide.” That study is based on earlier findings showing that patients identified with a Hungry Gut phenotype lost nearly twice as much weight on semaglutide compared with those who tested negative.
Overall, he concluded, “These findings open the door to more precise bariatric care. When we understand a patient’s biological drivers of obesity, we can make better decisions about the right procedure, follow-up, and long-term support. This moves us away from a one-size-fits-all model to care rooted in each patient’s unique biology.”
Potentially Paradigm-Shifting
Onur Kutlu, MD, associate professor of surgery and director of the Metabolic Surgery and Metabolic Health Program at the Miller School of Medicine, University of Miami, in Miami, Florida, commented on the study for GI & Hepatology News. “By integrating polygenic risk scores into predictive models, the authors offer an innovative method for identifying patients at elevated risk for weight regain following RYGB.”
“Their findings support the hypothesis that genetic predisposition — particularly involving energy homeostasis pathways — may underlie differential postoperative trajectories,” he said. “This approach has the potential to shift the paradigm from reactive to proactive management of weight recurrence.”
Because current options for treat weight regain are “suboptimal,” he said, “prevention becomes paramount. Preoperative identification of high-risk individuals could inform surgical decision-making, enable earlier interventions, and facilitate personalized postoperative monitoring and support.”
“If validated in larger, prospective cohorts, genetic risk stratification could enhance the precision of bariatric care and improve long-term outcomes,” he added. “Future studies should aim to validate these genetic models across diverse populations and explore how integration of behavioral, psychological, and genetic data may further refine patient selection and care pathways.”
The study was funded by Mayo Clinic and Phenomix Sciences. Gila Therapeutics and Phenomix Sciences licensed Acosta’s research technologies from the University of Florida and Mayo Clinic. Acosta declared receiving consultant fees in the past 5 years from Rhythm Pharmaceuticals, Gila Therapeutics, Amgen, General Mills, BI, Currax, Nestle, Phenomix Sciences, Bausch Health, and RareDiseases, as well as funding support from the National Institutes of Health, Vivus Pharmaceuticals, Novo Nordisk, Apollo Endosurgery, Satiogen Pharmaceuticals, Spatz Medical, and Rhythm Pharmaceuticals. Kutlu declared having no conflicts of interest.
A version of this article appeared on Medscape.com.
SAN DIEGO –
The findings suggested that the MyPhenome test (Phenomix Sciences) can help clinicians identify the patients most likely to benefit from bariatric procedures and at a greater risk for long-term weight regain after surgery.
“Patients with both a high genetic risk score and rare mutations in the leptin-melanocortin pathway (LMP) had significantly worse outcomes, maintaining only 4.9% total body weight loss [TBWL] over 15 years compared to up to 24.8% in other genetic groups,” Phenomix Sciences Co-founder Andres Acosta, MD, PhD, told GI & Hepatology News.
The study included details on the score’s development and predictive capability. It was presented at Digestive Disease Week® (DDW) 2025
‘More Precise Bariatric Care’
The researchers recently developed a machine learning-assisted gene risk score for calories to satiation (CTSGRS), which mainly involves genes in the LMP. To assess the role of the score with or without LMP gene variants on weight loss and weight recurrence after RYGB, they identified 707 patients with a history of bariatric procedures from the Mayo Clinic Biobank. Patients with duodenal switch, revisional procedures, or who used antiobesity medications or became pregnant during follow-up were excluded.
To make predictions for 442 of the patients, the team first collected anthropometric data up to 15 years after RYGB. Then they used a two-step approach: Assessing for monogenic variants in the LMP and defining participants as carriers (LMP+) or noncarriers (LMP-). Then they defined the gene risk score (CTSGRS+ or CTSGRS-).
The result was four groups: LMP+/CTSGRS+, LMP+/CTSGRS-, LMP-/CTSGRS+, and LMP-/CTSGRS-. Multiple regression analysis was used to analyze TBWL percentage (TBWL%) between the groups at different timepoints, adjusting for baseline weight, age, and gender.
At the 10-year follow-up, the LMP+/CTSGRS+ group demonstrated a significantly higher weight recurrence (regain) of TBW% compared to the other groups.
At 15 years post-RYGB, the mean TBWL% for LMP+/CTSGRS+ was -4.9 vs -20.3 for LMP+/CTSGRS-, -18.0 for LMP-/CTSGRS+, and -24.8 for LMP-/CTSGRS-.
Further analyses showed that the LMP+/CTSGRS+ group had significantly less weight loss than LMP+/CTSGRS- and LMP-/CTSGRS- groups.
Based on the findings, the authors wrote, “Genotyping patients could improve the implementation of individualized weight-loss interventions, enhance weight-loss outcomes, and/or may explain one of the etiological factors associated with weight recurrence after RYGB.”
Acosta noted, “We’re actively expanding our research to include more diverse populations by age, sex, and race. This includes ongoing analysis to understand whether certain demographic or physiological characteristics affect how the test performs, particularly in the context of bariatric surgery.”
The team also is investigating the benefits of phenotyping for obesity comorbidities such as heart disease and diabetes, he said, and exploring whether early interventions in high-risk patients can prevent long-term weight regain and improve outcomes.
In addition, Acosta said, the team recently launched “the first prospective, placebo-controlled clinical trial using the MyPhenome test to predict response to semaglutide.” That study is based on earlier findings showing that patients identified with a Hungry Gut phenotype lost nearly twice as much weight on semaglutide compared with those who tested negative.
Overall, he concluded, “These findings open the door to more precise bariatric care. When we understand a patient’s biological drivers of obesity, we can make better decisions about the right procedure, follow-up, and long-term support. This moves us away from a one-size-fits-all model to care rooted in each patient’s unique biology.”
Potentially Paradigm-Shifting
Onur Kutlu, MD, associate professor of surgery and director of the Metabolic Surgery and Metabolic Health Program at the Miller School of Medicine, University of Miami, in Miami, Florida, commented on the study for GI & Hepatology News. “By integrating polygenic risk scores into predictive models, the authors offer an innovative method for identifying patients at elevated risk for weight regain following RYGB.”
“Their findings support the hypothesis that genetic predisposition — particularly involving energy homeostasis pathways — may underlie differential postoperative trajectories,” he said. “This approach has the potential to shift the paradigm from reactive to proactive management of weight recurrence.”
Because current options for treat weight regain are “suboptimal,” he said, “prevention becomes paramount. Preoperative identification of high-risk individuals could inform surgical decision-making, enable earlier interventions, and facilitate personalized postoperative monitoring and support.”
“If validated in larger, prospective cohorts, genetic risk stratification could enhance the precision of bariatric care and improve long-term outcomes,” he added. “Future studies should aim to validate these genetic models across diverse populations and explore how integration of behavioral, psychological, and genetic data may further refine patient selection and care pathways.”
The study was funded by Mayo Clinic and Phenomix Sciences. Gila Therapeutics and Phenomix Sciences licensed Acosta’s research technologies from the University of Florida and Mayo Clinic. Acosta declared receiving consultant fees in the past 5 years from Rhythm Pharmaceuticals, Gila Therapeutics, Amgen, General Mills, BI, Currax, Nestle, Phenomix Sciences, Bausch Health, and RareDiseases, as well as funding support from the National Institutes of Health, Vivus Pharmaceuticals, Novo Nordisk, Apollo Endosurgery, Satiogen Pharmaceuticals, Spatz Medical, and Rhythm Pharmaceuticals. Kutlu declared having no conflicts of interest.
A version of this article appeared on Medscape.com.
FROM DDW 2025