User login
Isothiazolinone allergy frequent and underdiagnosed in children
Sensitization to the isothiazolinones MCI (methylchloroisothiazolinone) and MI (methylisothiazolinone), which are used as preservatives in a wide variety of personal and household products, is both frequent and underdiagnosed in U.S. children, according to a report published in Pediatric Dermatology.
These agents are compatible with surfactants and emulsifiers, and because they maintain biocidal activity across a broad range of pH levels they are frequently used as preservatives in products such as wet wipes; shampoos and hair conditioners; soaps, cleansers, and disinfectants; and laundry products. However, they are known to cause contact dermatitis very frequently, and are among the top five contact allergens identified in infants’ patch tests.
A recent survey showed that among 152 pediatric skin care products available at major retail stores, 20% contained MI. These were specifically targeted to infants and children, advertised as being “hypoallergenic,” “natural,” good for “sensitive” skin, and containing “gentle ingredients,” said Alina Goldenberg, MD, of the department of dermatology at the University of California, San Diego, and her associates.
During the past 10 years, only 35 U.S. cases of a positive patch-test reaction to MCI and/or MI have been reported in the literature. To get a more accurate estimate of the true prevalence of pediatric sensitization to MCI and MI, the investigators analyzed information in a database of patch-test results, the Provider Contact Dermatitis Registry. They focused on 1,056 patch tests performed during a 1-year period.
They found 37 positive reactions to combined MCI/MI and another 39 reactions that were negative to combined MCI/MI but positive to MI alone. This shows how important it is to test for sensitization to both formulations separately, Dr. Goldenberg and her associates noted (Pediatr Dermatol. 2017 Mar;34[2]:138-43).
In stark contrast to the reported 35 cases across the entire country during a 10-year period, the investigators found 76 cases (1%) in 1,056 patch tests during a 1-year period.
When test results for MCI/MI and MI alone were compared with those for all other allergens, children sensitized to the isothiazolinones showed marked differences: They were significantly younger, and the location of their dermatitis was more likely to involve the groin and buttocks. This probably is due to the increased use of wet wipes containing MCI and MI being used to clean up urinary and fecal accidents in young children, the researchers said.
The Society for Pediatric Dermatology supported the work. Dr. Goldenberg reported having no relevant financial disclosures; an associate reported serving as a consultant for Johnson & Johnson.
Sensitization to the isothiazolinones MCI (methylchloroisothiazolinone) and MI (methylisothiazolinone), which are used as preservatives in a wide variety of personal and household products, is both frequent and underdiagnosed in U.S. children, according to a report published in Pediatric Dermatology.
These agents are compatible with surfactants and emulsifiers, and because they maintain biocidal activity across a broad range of pH levels they are frequently used as preservatives in products such as wet wipes; shampoos and hair conditioners; soaps, cleansers, and disinfectants; and laundry products. However, they are known to cause contact dermatitis very frequently, and are among the top five contact allergens identified in infants’ patch tests.
A recent survey showed that among 152 pediatric skin care products available at major retail stores, 20% contained MI. These were specifically targeted to infants and children, advertised as being “hypoallergenic,” “natural,” good for “sensitive” skin, and containing “gentle ingredients,” said Alina Goldenberg, MD, of the department of dermatology at the University of California, San Diego, and her associates.
During the past 10 years, only 35 U.S. cases of a positive patch-test reaction to MCI and/or MI have been reported in the literature. To get a more accurate estimate of the true prevalence of pediatric sensitization to MCI and MI, the investigators analyzed information in a database of patch-test results, the Provider Contact Dermatitis Registry. They focused on 1,056 patch tests performed during a 1-year period.
They found 37 positive reactions to combined MCI/MI and another 39 reactions that were negative to combined MCI/MI but positive to MI alone. This shows how important it is to test for sensitization to both formulations separately, Dr. Goldenberg and her associates noted (Pediatr Dermatol. 2017 Mar;34[2]:138-43).
In stark contrast to the reported 35 cases across the entire country during a 10-year period, the investigators found 76 cases (1%) in 1,056 patch tests during a 1-year period.
When test results for MCI/MI and MI alone were compared with those for all other allergens, children sensitized to the isothiazolinones showed marked differences: They were significantly younger, and the location of their dermatitis was more likely to involve the groin and buttocks. This probably is due to the increased use of wet wipes containing MCI and MI being used to clean up urinary and fecal accidents in young children, the researchers said.
The Society for Pediatric Dermatology supported the work. Dr. Goldenberg reported having no relevant financial disclosures; an associate reported serving as a consultant for Johnson & Johnson.
Sensitization to the isothiazolinones MCI (methylchloroisothiazolinone) and MI (methylisothiazolinone), which are used as preservatives in a wide variety of personal and household products, is both frequent and underdiagnosed in U.S. children, according to a report published in Pediatric Dermatology.
These agents are compatible with surfactants and emulsifiers, and because they maintain biocidal activity across a broad range of pH levels they are frequently used as preservatives in products such as wet wipes; shampoos and hair conditioners; soaps, cleansers, and disinfectants; and laundry products. However, they are known to cause contact dermatitis very frequently, and are among the top five contact allergens identified in infants’ patch tests.
A recent survey showed that among 152 pediatric skin care products available at major retail stores, 20% contained MI. These were specifically targeted to infants and children, advertised as being “hypoallergenic,” “natural,” good for “sensitive” skin, and containing “gentle ingredients,” said Alina Goldenberg, MD, of the department of dermatology at the University of California, San Diego, and her associates.
During the past 10 years, only 35 U.S. cases of a positive patch-test reaction to MCI and/or MI have been reported in the literature. To get a more accurate estimate of the true prevalence of pediatric sensitization to MCI and MI, the investigators analyzed information in a database of patch-test results, the Provider Contact Dermatitis Registry. They focused on 1,056 patch tests performed during a 1-year period.
They found 37 positive reactions to combined MCI/MI and another 39 reactions that were negative to combined MCI/MI but positive to MI alone. This shows how important it is to test for sensitization to both formulations separately, Dr. Goldenberg and her associates noted (Pediatr Dermatol. 2017 Mar;34[2]:138-43).
In stark contrast to the reported 35 cases across the entire country during a 10-year period, the investigators found 76 cases (1%) in 1,056 patch tests during a 1-year period.
When test results for MCI/MI and MI alone were compared with those for all other allergens, children sensitized to the isothiazolinones showed marked differences: They were significantly younger, and the location of their dermatitis was more likely to involve the groin and buttocks. This probably is due to the increased use of wet wipes containing MCI and MI being used to clean up urinary and fecal accidents in young children, the researchers said.
The Society for Pediatric Dermatology supported the work. Dr. Goldenberg reported having no relevant financial disclosures; an associate reported serving as a consultant for Johnson & Johnson.
FROM PEDIATRIC DERMATOLOGY
Key clinical point:
Major finding: There were 37 positive patch-test reactions to combined MCI/MI and another 39 reactions that were negative to combined MCI/MI but positive to MI alone.
Data source: An analysis of 1,056 patch-test results recorded in a database by clinicians during a 1-year period.
Disclosures: The Society for Pediatric Dermatology supported the work. Dr. Goldenberg reported having no relevant financial disclosures; an associate reported serving as a consultant for Johnson & Johnson.
Black Linear Streaks on the Face With Pruritic Plaques on the Trunk and Arms
The Diagnosis: Toxicodendron Dermatitis
Toxicodendron dermatitis is an allergic contact dermatitis that can occur after exposure to a plant from the Toxicodendron genus including poison ivy (Toxicodendron radicans), poison oak (Toxicodendron diversilobum), and poison sumac (Toxicodendron vernix). These plants produce urushiol in their oleoresinous sap, which causes intense pruritus, streaks of erythema, and edematous papules followed by vesicles and bullae. Previously sensitized individuals develop symptoms as quickly as 24 to 48 hours after exposure, with a range of 5 hours to 15 days.1-3 Rarely, black spots also can be found on the skin, most prominently after 72 hours of exposure.4
The color change of urushiol-containing sap from pale to black was first documented by Peter Kalm, a Swedish botanist who traveled to North America in the 1700s.5 The black-spot test can be used to identify Toxicodendron species because the sap will turn black when expressed on white paper after a few minutes.6 Manifestation of black lacquer streaks on the skin is rare because concentrated sap is necessary, which typically requires an unusually prolonged exposure with Toxicodendron plants.7
Without treatment, typical Toxicodendron dermatitis resolves in approximately 3 weeks, though it may take up to 6 weeks to clear.2 Early intervention is critical, as urushiol will fully absorb after 30 minutes.2 After contact, complete removal of the oleoresin by washing with mild soap and water within 10 minutes can prevent dermatitis. Early topical corticosteroid application can reduce erythema and pruritus. Extensive or severe involvement, which includes Toxicodendron dermatitis with black spots, is treated with systemic corticosteroids such as prednisone that is tapered over 2 to 3 weeks.1
Our patient had classic findings of Toxicodendron dermatitis; however, initially there was concern for levamisole toxicity by the emergency department, as well-demarcated purpuric or dark skin lesions can be due to morbid conditions such as leukocytoclastic vasculitis or skin necrosis from drug toxicities or infectious etiologies. Dermatology was consulted and these concerns were alleviated on closer skin examination and further questioning. The patient reported that he spent several hours cutting brush that was known to be T vernix (poison sumac) 3 days prior to presentation. Interestingly, the patient did not have similar black streaks on the left side of the face, as he held the weed-trimming saw in his right hand and in effect protected the left side of the face from debris. Furthermore, he had pruritic erythematous plaques on both forearms. The facial black lacquer-like streaks were the result of urushiol oxidation in the setting of prolonged exposure to the poison sumac oleoresin sap during weed trimming. After dermatologic evaluation, the patient was discharged from the emergency department on a 15-day taper of oral prednisone, and he was instructed to wash involved areas and exposed clothing with soap and water, which led to complete resolution.
- Lee NP, Arriola ER. Poison ivy, oak, and sumac dermatitis. West J Med. 1999;171:354-355.
- Gladman AC. Toxicodendron dermatitis: poison ivy, oak, and sumac. Wilderness Environ Med. 2006;17:120-128.
- Gross M, Baer H, Fales H. Urushiols of poisonous anacardiaceae. Phytochemistry. 1975;14:2263-2266.
- Mallory SB, Miller OF 3dU, Tyler WB. Toxicodendron radicans dermatitis with black lacquer deposit on the skin. J Am Acad Dermatol. 1982;6:363-368.
- Benson AB. Peter Kalm's Travels in North America: The English Version of 1770. New York, NY: Dover Publications; 1937.
- Guin JD. The black spot test for recognizing poison ivy and related species. J Am Acad Dermatol. 1980;2:332-333.
- Kurlan JG, Lucky AW. Black spot poison ivy: a report of 5 cases and a review of the literature. J Am Acad Dermatol. 2001;45:246-249.
The Diagnosis: Toxicodendron Dermatitis
Toxicodendron dermatitis is an allergic contact dermatitis that can occur after exposure to a plant from the Toxicodendron genus including poison ivy (Toxicodendron radicans), poison oak (Toxicodendron diversilobum), and poison sumac (Toxicodendron vernix). These plants produce urushiol in their oleoresinous sap, which causes intense pruritus, streaks of erythema, and edematous papules followed by vesicles and bullae. Previously sensitized individuals develop symptoms as quickly as 24 to 48 hours after exposure, with a range of 5 hours to 15 days.1-3 Rarely, black spots also can be found on the skin, most prominently after 72 hours of exposure.4
The color change of urushiol-containing sap from pale to black was first documented by Peter Kalm, a Swedish botanist who traveled to North America in the 1700s.5 The black-spot test can be used to identify Toxicodendron species because the sap will turn black when expressed on white paper after a few minutes.6 Manifestation of black lacquer streaks on the skin is rare because concentrated sap is necessary, which typically requires an unusually prolonged exposure with Toxicodendron plants.7
Without treatment, typical Toxicodendron dermatitis resolves in approximately 3 weeks, though it may take up to 6 weeks to clear.2 Early intervention is critical, as urushiol will fully absorb after 30 minutes.2 After contact, complete removal of the oleoresin by washing with mild soap and water within 10 minutes can prevent dermatitis. Early topical corticosteroid application can reduce erythema and pruritus. Extensive or severe involvement, which includes Toxicodendron dermatitis with black spots, is treated with systemic corticosteroids such as prednisone that is tapered over 2 to 3 weeks.1
Our patient had classic findings of Toxicodendron dermatitis; however, initially there was concern for levamisole toxicity by the emergency department, as well-demarcated purpuric or dark skin lesions can be due to morbid conditions such as leukocytoclastic vasculitis or skin necrosis from drug toxicities or infectious etiologies. Dermatology was consulted and these concerns were alleviated on closer skin examination and further questioning. The patient reported that he spent several hours cutting brush that was known to be T vernix (poison sumac) 3 days prior to presentation. Interestingly, the patient did not have similar black streaks on the left side of the face, as he held the weed-trimming saw in his right hand and in effect protected the left side of the face from debris. Furthermore, he had pruritic erythematous plaques on both forearms. The facial black lacquer-like streaks were the result of urushiol oxidation in the setting of prolonged exposure to the poison sumac oleoresin sap during weed trimming. After dermatologic evaluation, the patient was discharged from the emergency department on a 15-day taper of oral prednisone, and he was instructed to wash involved areas and exposed clothing with soap and water, which led to complete resolution.
The Diagnosis: Toxicodendron Dermatitis
Toxicodendron dermatitis is an allergic contact dermatitis that can occur after exposure to a plant from the Toxicodendron genus including poison ivy (Toxicodendron radicans), poison oak (Toxicodendron diversilobum), and poison sumac (Toxicodendron vernix). These plants produce urushiol in their oleoresinous sap, which causes intense pruritus, streaks of erythema, and edematous papules followed by vesicles and bullae. Previously sensitized individuals develop symptoms as quickly as 24 to 48 hours after exposure, with a range of 5 hours to 15 days.1-3 Rarely, black spots also can be found on the skin, most prominently after 72 hours of exposure.4
The color change of urushiol-containing sap from pale to black was first documented by Peter Kalm, a Swedish botanist who traveled to North America in the 1700s.5 The black-spot test can be used to identify Toxicodendron species because the sap will turn black when expressed on white paper after a few minutes.6 Manifestation of black lacquer streaks on the skin is rare because concentrated sap is necessary, which typically requires an unusually prolonged exposure with Toxicodendron plants.7
Without treatment, typical Toxicodendron dermatitis resolves in approximately 3 weeks, though it may take up to 6 weeks to clear.2 Early intervention is critical, as urushiol will fully absorb after 30 minutes.2 After contact, complete removal of the oleoresin by washing with mild soap and water within 10 minutes can prevent dermatitis. Early topical corticosteroid application can reduce erythema and pruritus. Extensive or severe involvement, which includes Toxicodendron dermatitis with black spots, is treated with systemic corticosteroids such as prednisone that is tapered over 2 to 3 weeks.1
Our patient had classic findings of Toxicodendron dermatitis; however, initially there was concern for levamisole toxicity by the emergency department, as well-demarcated purpuric or dark skin lesions can be due to morbid conditions such as leukocytoclastic vasculitis or skin necrosis from drug toxicities or infectious etiologies. Dermatology was consulted and these concerns were alleviated on closer skin examination and further questioning. The patient reported that he spent several hours cutting brush that was known to be T vernix (poison sumac) 3 days prior to presentation. Interestingly, the patient did not have similar black streaks on the left side of the face, as he held the weed-trimming saw in his right hand and in effect protected the left side of the face from debris. Furthermore, he had pruritic erythematous plaques on both forearms. The facial black lacquer-like streaks were the result of urushiol oxidation in the setting of prolonged exposure to the poison sumac oleoresin sap during weed trimming. After dermatologic evaluation, the patient was discharged from the emergency department on a 15-day taper of oral prednisone, and he was instructed to wash involved areas and exposed clothing with soap and water, which led to complete resolution.
- Lee NP, Arriola ER. Poison ivy, oak, and sumac dermatitis. West J Med. 1999;171:354-355.
- Gladman AC. Toxicodendron dermatitis: poison ivy, oak, and sumac. Wilderness Environ Med. 2006;17:120-128.
- Gross M, Baer H, Fales H. Urushiols of poisonous anacardiaceae. Phytochemistry. 1975;14:2263-2266.
- Mallory SB, Miller OF 3dU, Tyler WB. Toxicodendron radicans dermatitis with black lacquer deposit on the skin. J Am Acad Dermatol. 1982;6:363-368.
- Benson AB. Peter Kalm's Travels in North America: The English Version of 1770. New York, NY: Dover Publications; 1937.
- Guin JD. The black spot test for recognizing poison ivy and related species. J Am Acad Dermatol. 1980;2:332-333.
- Kurlan JG, Lucky AW. Black spot poison ivy: a report of 5 cases and a review of the literature. J Am Acad Dermatol. 2001;45:246-249.
- Lee NP, Arriola ER. Poison ivy, oak, and sumac dermatitis. West J Med. 1999;171:354-355.
- Gladman AC. Toxicodendron dermatitis: poison ivy, oak, and sumac. Wilderness Environ Med. 2006;17:120-128.
- Gross M, Baer H, Fales H. Urushiols of poisonous anacardiaceae. Phytochemistry. 1975;14:2263-2266.
- Mallory SB, Miller OF 3dU, Tyler WB. Toxicodendron radicans dermatitis with black lacquer deposit on the skin. J Am Acad Dermatol. 1982;6:363-368.
- Benson AB. Peter Kalm's Travels in North America: The English Version of 1770. New York, NY: Dover Publications; 1937.
- Guin JD. The black spot test for recognizing poison ivy and related species. J Am Acad Dermatol. 1980;2:332-333.
- Kurlan JG, Lucky AW. Black spot poison ivy: a report of 5 cases and a review of the literature. J Am Acad Dermatol. 2001;45:246-249.

A 68-year-old man presented to the emergency department with pruritic, edematous, pink plaques on the trunk and arms, as well as black linear streaks on the face, prompting dermatology consultation for possible tissue necrosis. The patient reported working outdoors in his garden 3 days prior to presentation.

Allergic Reaction to Vanadium Causes a Diffuse Eczematous Eruption and Titanium Alloy Orthopedic Implant Failure
Metal allergy in patients with orthopedic implants can cause serious problems including dermatitis and implant failure.1 As life expectancy increases, the general population ages, and more metallic orthopedic implants are placed,2 allergy to these implants is expected to be a problem of greater significance. Uncertainty remains regarding best practice for patients with suspected metal implant allergy.1 The major questions are: Who should be tested? When should they be tested? What are the optimal tests to diagnose metal allergy?3-8
We report the case of a patient with vanadium allergy who developed a diffuse eczematous dermatitis and implant failure after receiving a vanadium-containing titanium alloy orthopedic implant in the left foot. This case is remarkable because hypersensitivity reactions to titanium-based hardware are rare, as they traditionally have not been thought to provoke allergic reactions.9
Case Report
A 62-year-old woman who was otherwise healthy presented with an eruption of more than 80 pruritic, nummular, eczematous plaques on the arms, legs, back, and buttocks of 3 weeks’ duration (Figure 1). She had a history of allergy to metal used in costume jewelry. Six weeks prior, the patient underwent implantation of a titanium alloy plate in the left foot for surgical repair of painful deforming osteoarthritis. A radiograph of the foot showed appropriate placement. According to the manufacturer, the plate was composed of the compound Ti6Al4V, which contained 90% titanium, 6% aluminum, and 4% vanadium. The lesions developed on the skin close to but not directly over the surgical site.

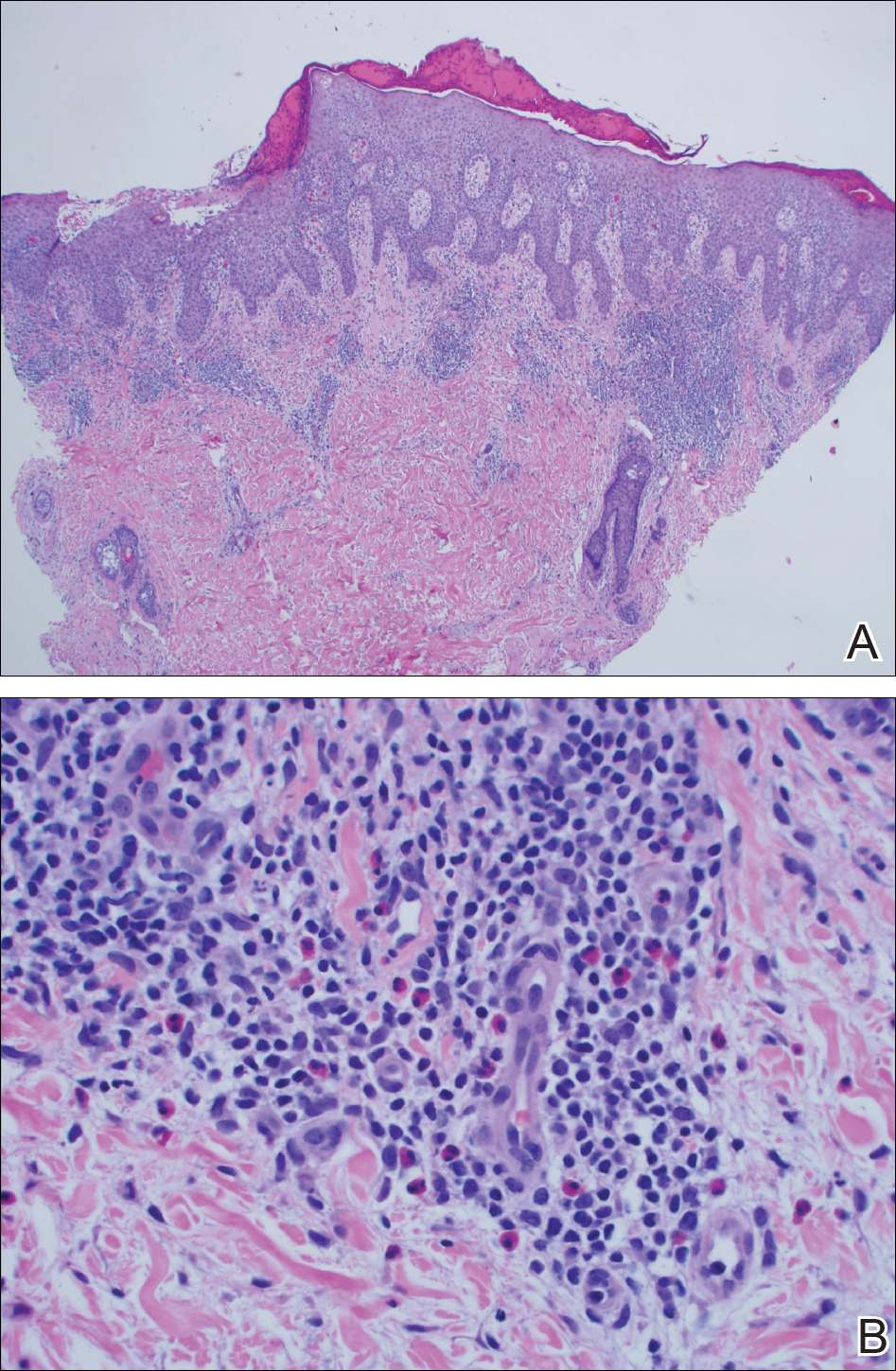
A punch biopsy of one of the lesions on the shoulder showed lymphoeosinophilic spongiosis consistent with a delayed hypersensitivity reaction (Figure 2). There was mild clinical improvement of the eruption with topical steroids. A course of prednisone for systemic effect resulted in clearing of the eruption, but it promptly recurred on cessation of the steroids. The patient was then patch tested using the North American 80 Comprehensive Series, with an additional 59 common textile, shampoo, fragrance, and several metal allergens, all of which were negative.
The patient had persistent pain and swelling at the surgical site, and radiographs taken postoperatively at 6 months showed implant failure (Figure 3). The hardware was surgically removed 8 months after implantation (Figure 4) and the plate and screws were submitted to the Institute for Mineral Resources Geosciences LA-ICP-MS Facility and the Lunar and Planetary Laboratory at the University of Arizona (Tucson, Arizona) for analysis. The skin lesions began to improve days after the hardware was removed and the eruption cleared over the following 3 weeks with no additional treatment.


After the hardware was removed, it was analyzed to determine the elemental composition of the plate and screws, and the patient was then patch tested with the major metal components of the implant: aluminum chloride hexahydrate 2.0% pet, elemental titanium 10.0% pet, titanium dioxide 10.0% pet, titanium (III) nitride 5.0% pet, titanium (III) oxalate decahydrate 5.0% pet, elemental vanadium 5.0% pet, and vanadium (III) chloride 1.0% pet. She demonstrated a 1+ reaction (erythema and induration) to vanadium trichloride at 72 and 96 hours.
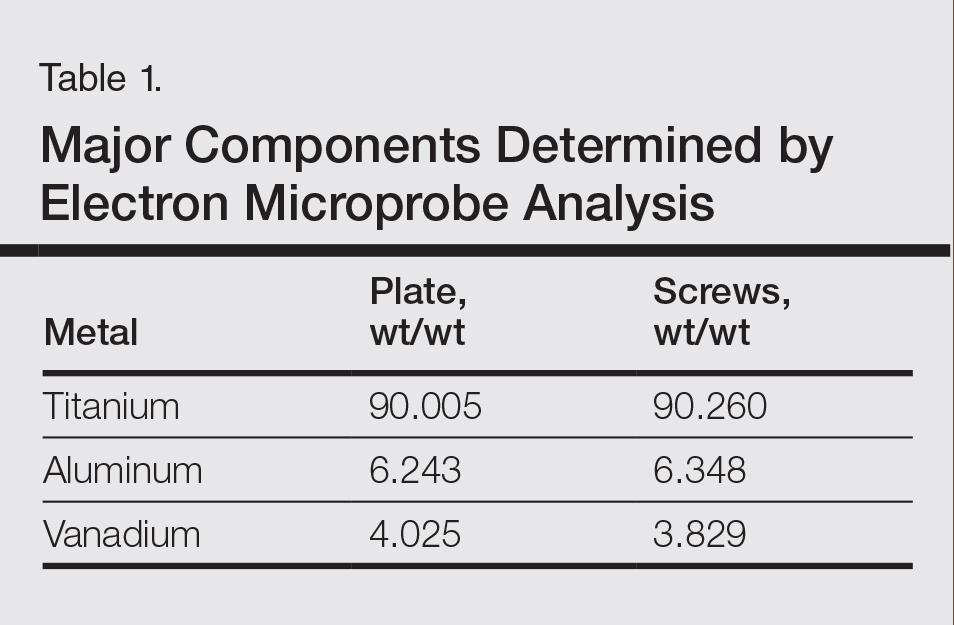
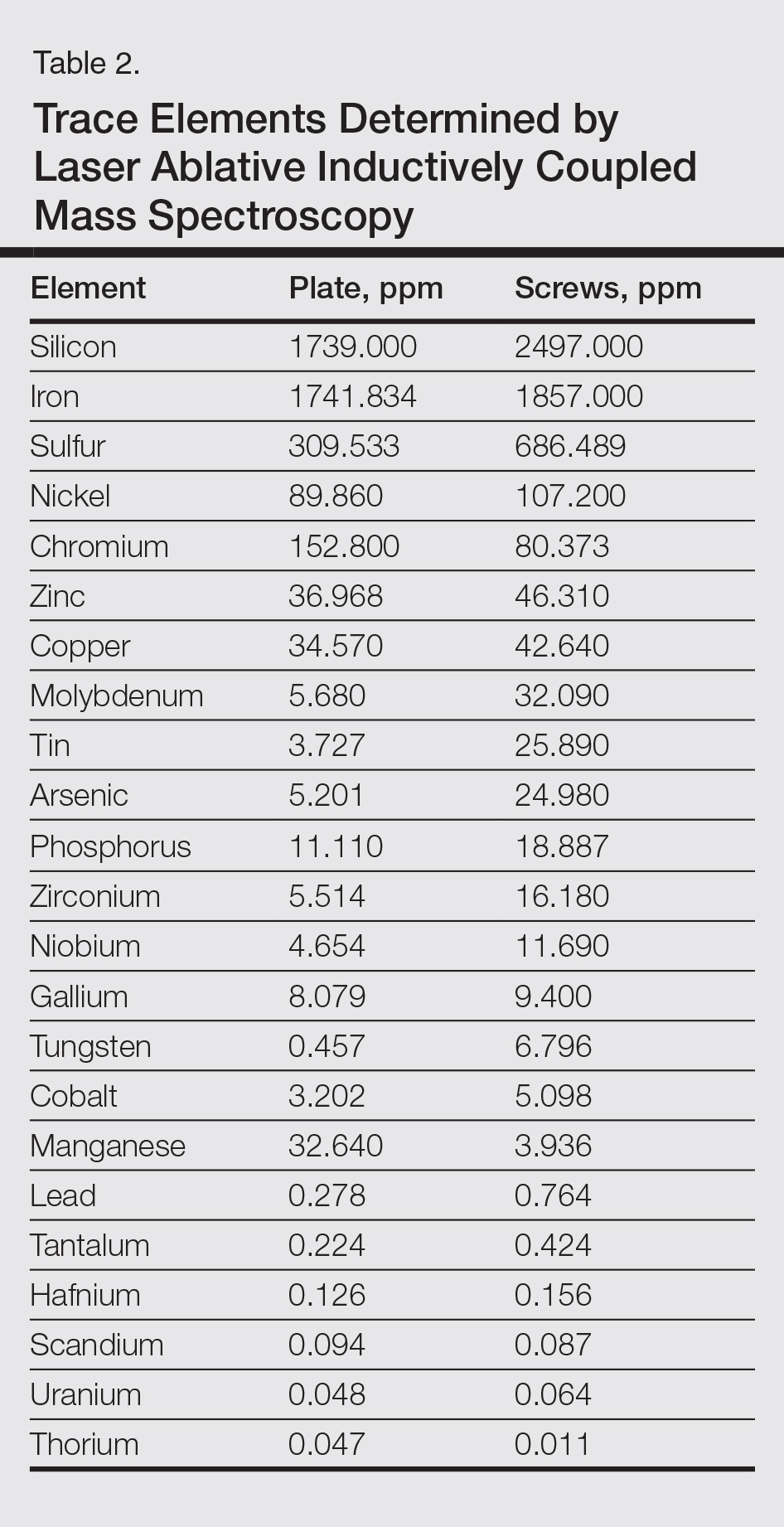
The plate and screws removed from the patient were sterilized and submitted for analysis. Electron microprobe analysis confirmed that the major elemental composition of the plate and screws essentially matched the manufacturer’s listing (Table 1). The trace elements were determined using laser ablative inductively coupled mass spectroscopy, which demonstrated that the screws were of different metal composition from the plate (Table 2). Electron microprobe analysis also was used to determine the microstructure of the plate and screws. The plate had 2 distinct phases consisting of a titanium-aluminum phase and a vanadium phase, whereas the screw was much more homogeneous. Basic electrochemical studies were performed in a salt solution replicating the tissue of the foot. These studies showed that galvanic corrosion could have occurred between the plate and screws due to the differences of composition.
Comment
Titanium is an attractive metal to use in orthopedic implants. It has a high strength-to-weight ratio, a low modulus of elasticity, and good resistance to corrosion. Titanium can be categorized as either commercially pure titanium (cp-Ti) or a titanium alloy. Colloquially, both cp-Ti and titanium alloys are often referred to simply as titanium, but the distinction is important when it comes to medical implants and devices. Commercially pure titanium is more than 99% pure titanium, but up to 1% of its volume can be comprised of impurities.10 In titanium alloys, the alloy elements are intentionally added to create a material with optimal properties. The 2 most common types of titanium that are used for orthopedic implants are cp-Ti and Ti6Al4V, a titanium alloy containing approximately 90% titanium, 6% aluminum, and 4% vanadium. Similar to cp-Ti, titanium alloys also can contain impurities such as aluminum, beryllium, cobalt, chromium, iron, nickel, and palladium, among many others. Although these impurities often are considered negligible from a metallurgy perspective, as they do not change the properties of the material, these trace elements may be present in large enough quantities to cause hypersensitivity reactions.11
Several weeks after implantation of a titanium alloy metal plate in the left foot, a widespread eczematous eruption developed in our patient who had no prior skin disease. The eruption was steroid responsive but did not clear until the plate was removed. Detailed metallurgy analysis confirmed that vanadium was present and was not homogeneously distributed in the plate. The plate also was different in composition from the screws. Additional studies showed that galvanic corrosion between the plate and the chemically different screws might have contributed to the release of vanadium in the tissue.
Vanadium is known to be allergenic, especially in the presence of implant failure.12,13 In our patient, patch testing with more than 100 allergens was negative, except for vanadium trichloride 1%. Our patient’s presentation strongly suggested that she developed a vanadium allergy manifesting as systemic allergic contact dermatitis. She demonstrated no history of skin disease, a widespread eczematous eruption after exposure, histology consistent with systemic contact allergy, a positive patch test to vanadium, and clearance of the eruption on removal of the antigen, which have been proposed as objective criteria that support a diagnosis of metal implant allergy.14 She refused our suggestion to reimplant a portion of the remaining plate under the skin without screws and monitor for recurrence of the eruption. She did not have a lesion overlying the surgical site, but she did develop lesions near the surgical scar. The literature indicates that cutaneous manifestations of allergy to metallic implants can be both localized and generalized.14
Although reports are rare, other researchers have found vanadium allergy in patients with metal orthopedic implants.5,12,13,15 The scarcity of literature on vanadium allergy seems to suggest that it is a rare entity, but we believe that it may be more common. Vanadium allergy may be underdiagnosed because it is not a standard patch test allergen. Furthermore, many of those who do choose to test for it use what we believe to be ineffective formulas of vanadium when patch testing patients. Our patient demonstrated a positive patch test reaction only to vanadium trichloride and not to pure vanadium, which is consistent with the small number of other studies that investigated vanadium allergy.5,12,13,15 We believe that vanadium trichloride is more water soluble than elemental vanadium,16 and thus more likely to identify true vanadium allergy than other test materials.
Although reports of vanadium allergy in patients with metal implants are rare in the medical literature, the material science literature clearly states that vanadium is toxic and that vanadium-containing implants are problematic.17-20 It has been shown that although Ti6Al4V implants are considered highly resistant to corrosion, they will slowly and continuously corrode in a physiologic environment and release titanium, aluminum, and vanadium ions, both systemically and into the peri-implant space.11 To address these problems with vanadium, vanadium-free titanium alloys such as Ti6Al7Nb have specifically been developed for medical use to address the problems caused by vanadium. Ti6Al7Nb contains 7% niobium rather than vanadium and appears to have some improved qualities in surgical implants.17
There is still a great deal of uncertainty around metal implant allergy. Allergy to metal implants can be difficult to diagnose for several reasons. Some metals are not conducive to patch testing because of their low bioavailability. Additionally, we lack validated and standardized patch test formulas for metals that can be diagnosed by patch testing. Furthermore, there is uncertainty about what to do after allergy to a metal implant is diagnosed; in some cases (eg, with more extensive procedures such as total joint replacements), removal or replacement of the implant may be associated with increased risk of further complications.6,21
Conclusion
We suggest that manufacturers consider vanadium-free alloys such as Ti7Al6Nb, which contains niobium instead of vanadium, in their surgical implants,22 and if surgeons have a choice, they should consider using titanium implants with niobium rather than vanadium.10 We suggest that clinicians consider vanadium allergy in patients with Ti6Al4V surgical implants and signs of a hypersensitivity reaction, and include vanadium trichloride 1% when patch testing.
Acknowledgment
The authors would like to thank Nicholas R. Krasnow, PhD (Tucson, Arizona), for his invaluable help coordinating, performing, and interpreting the metal analyses.
- Basko-Plluska JL, Thyssen JP, Schalock PC. Cutaneous and systemic hypersensitivity reactions to metallic implants. Dermatitis. 2011;22:65-79.
- Kurtz S, Ong K, Lau E, et al. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89:780-785.
- Thyssen JP, Johansen JD, Menné T, et al. Hypersensitivity reactions from metallic implants: a future challenge that needs to be addressed. Br J Dermatol. 2010;162:235-236.
- Aquino M, Mucci T. Systemic contact dermatitis and allergy to biomedical devices. Curr Allergy Asthma Rep. 2013;13:518-527.
- Krecisz B, Kiec-Swierczynska M, Chomiczewska-Skora D. Allergy to orthopedic metal implants—a prospective study. Int J Occup Med Environ Health. 2012;25:463-469.
- Atanaskova Mesinkovska N, Tellez A, Molina L, et al. The effect of patch testing on surgical practices and outcomes in orthopedic patients with metal implants. Arch Dermatol. 2012;148:687-693.
- Frigerio E, Pigatto PD, Guzzi G, et al. Metal sensitivity in patients with orthopaedic implants: a prospective study. Contact Dermatitis. 2011;64:273-279.
- Amini M, Mayes WH, Tzeng TH, et al. Evaluation and management of metal hypersensitivity in total joint arthroplasty: a systematic review. J Long Term Eff Med Implants. 2014;24:25-36.
- Thomas P, Bandl WD, Maier S, et al. Hypersensitivity to titanium osteosynthesis with impaired fracture healing, eczema, and T-cell hyperresponsiveness in vitro: case report and review of the literature. Contact Dermatitis. 2006;55:199-202.
- Wood MM, Warshaw EM. Hypersensitivity reactions to titanium: diagnosis and management. Dermatitis. 2015;26:7-25.
- Cadosch D, Chan E, Gautschi OP, et al. Metal is not inert: role of metal ions released by biocorrosion in aseptic loosening—current concepts. J Biomed Mater Res A. 2009;91:1252-1262.
- Granchi D, Cenni E, Trisolino G, et al. Sensitivity to implant materials in patients undergoing total hip replacement. J Biomed Mater Res B Appl Biomater. 2006;77:257-264.
- Granchi D, Cenni E, Tigani D, et al. Sensitivity to implant materials in patients with total knee arthroplasties. Biomaterials. 2008;29:1494-1500.
- Thyssen JP, Menné T, Schalock PC, et al. Pragmatic approach to the clinical work-up of patients with putative allergic disease to metallic orthopaedic implants before and after surgery. Br J Dermatol. 2011;164:473-478.
- Kręcisz B, Kieć-Świerczyńska M, Bąkowicz-Mitura K. Allergy to metals as a cause of orthopedic implant failure. Int J Occup Med Environ Health. 2006;19:178-180.
- Costigan M, Cary R, Dobson S. Vanadium Pentoxide and Other Inorganic Vanadium Compounds. Geneva, Switzerland: World Health Organization; 2001.
- Challa VS, Mali S, Misra RD. Reduced toxicity and superior cellular response of preosteoblasts to Ti-6Al-7Nb alloy and comparison with Ti-6Al-4V. J Biomed Mater Res A. 2013;101:2083-2089.
- Okazaki Y, Rao S, Ito Y, et al. Corrosion resistance, mechanical properties, corrosion fatigue strength and cytocompatibility of new Ti alloys without Al and V. Biomaterials. 1998;19:1197-1215.
- Paszenda Z, Walke W, Jadacka S. Electrochemical investigations of Ti6Al4V and Ti6Al7Nb alloys used on implants in bone surgery. J Achievements Materials Manufacturing Eng. 2010;38:24-32.
- Wang K. The use of titanium for medical applications in the USA. Materials Sci Eng A. 1996:134-137.
- Haseeb M, Butt MF, Altaf T, et al. Indications of implant removal: a study of 83 cases. Int J Health Sci (Qassim). 2017;11:1-7.
- Geetha M, Singh AK, Asokamani R, et al. Ti based biomaterials, the ultimate choice for orthopaedic implants—a review. Progress Materials Sci. 2009;54:397-425.
Metal allergy in patients with orthopedic implants can cause serious problems including dermatitis and implant failure.1 As life expectancy increases, the general population ages, and more metallic orthopedic implants are placed,2 allergy to these implants is expected to be a problem of greater significance. Uncertainty remains regarding best practice for patients with suspected metal implant allergy.1 The major questions are: Who should be tested? When should they be tested? What are the optimal tests to diagnose metal allergy?3-8
We report the case of a patient with vanadium allergy who developed a diffuse eczematous dermatitis and implant failure after receiving a vanadium-containing titanium alloy orthopedic implant in the left foot. This case is remarkable because hypersensitivity reactions to titanium-based hardware are rare, as they traditionally have not been thought to provoke allergic reactions.9
Case Report
A 62-year-old woman who was otherwise healthy presented with an eruption of more than 80 pruritic, nummular, eczematous plaques on the arms, legs, back, and buttocks of 3 weeks’ duration (Figure 1). She had a history of allergy to metal used in costume jewelry. Six weeks prior, the patient underwent implantation of a titanium alloy plate in the left foot for surgical repair of painful deforming osteoarthritis. A radiograph of the foot showed appropriate placement. According to the manufacturer, the plate was composed of the compound Ti6Al4V, which contained 90% titanium, 6% aluminum, and 4% vanadium. The lesions developed on the skin close to but not directly over the surgical site.
A punch biopsy of one of the lesions on the shoulder showed lymphoeosinophilic spongiosis consistent with a delayed hypersensitivity reaction (Figure 2). There was mild clinical improvement of the eruption with topical steroids. A course of prednisone for systemic effect resulted in clearing of the eruption, but it promptly recurred on cessation of the steroids. The patient was then patch tested using the North American 80 Comprehensive Series, with an additional 59 common textile, shampoo, fragrance, and several metal allergens, all of which were negative.
The patient had persistent pain and swelling at the surgical site, and radiographs taken postoperatively at 6 months showed implant failure (Figure 3). The hardware was surgically removed 8 months after implantation (Figure 4) and the plate and screws were submitted to the Institute for Mineral Resources Geosciences LA-ICP-MS Facility and the Lunar and Planetary Laboratory at the University of Arizona (Tucson, Arizona) for analysis. The skin lesions began to improve days after the hardware was removed and the eruption cleared over the following 3 weeks with no additional treatment.
After the hardware was removed, it was analyzed to determine the elemental composition of the plate and screws, and the patient was then patch tested with the major metal components of the implant: aluminum chloride hexahydrate 2.0% pet, elemental titanium 10.0% pet, titanium dioxide 10.0% pet, titanium (III) nitride 5.0% pet, titanium (III) oxalate decahydrate 5.0% pet, elemental vanadium 5.0% pet, and vanadium (III) chloride 1.0% pet. She demonstrated a 1+ reaction (erythema and induration) to vanadium trichloride at 72 and 96 hours.
The plate and screws removed from the patient were sterilized and submitted for analysis. Electron microprobe analysis confirmed that the major elemental composition of the plate and screws essentially matched the manufacturer’s listing (Table 1). The trace elements were determined using laser ablative inductively coupled mass spectroscopy, which demonstrated that the screws were of different metal composition from the plate (Table 2). Electron microprobe analysis also was used to determine the microstructure of the plate and screws. The plate had 2 distinct phases consisting of a titanium-aluminum phase and a vanadium phase, whereas the screw was much more homogeneous. Basic electrochemical studies were performed in a salt solution replicating the tissue of the foot. These studies showed that galvanic corrosion could have occurred between the plate and screws due to the differences of composition.
Comment
Titanium is an attractive metal to use in orthopedic implants. It has a high strength-to-weight ratio, a low modulus of elasticity, and good resistance to corrosion. Titanium can be categorized as either commercially pure titanium (cp-Ti) or a titanium alloy. Colloquially, both cp-Ti and titanium alloys are often referred to simply as titanium, but the distinction is important when it comes to medical implants and devices. Commercially pure titanium is more than 99% pure titanium, but up to 1% of its volume can be comprised of impurities.10 In titanium alloys, the alloy elements are intentionally added to create a material with optimal properties. The 2 most common types of titanium that are used for orthopedic implants are cp-Ti and Ti6Al4V, a titanium alloy containing approximately 90% titanium, 6% aluminum, and 4% vanadium. Similar to cp-Ti, titanium alloys also can contain impurities such as aluminum, beryllium, cobalt, chromium, iron, nickel, and palladium, among many others. Although these impurities often are considered negligible from a metallurgy perspective, as they do not change the properties of the material, these trace elements may be present in large enough quantities to cause hypersensitivity reactions.11
Several weeks after implantation of a titanium alloy metal plate in the left foot, a widespread eczematous eruption developed in our patient who had no prior skin disease. The eruption was steroid responsive but did not clear until the plate was removed. Detailed metallurgy analysis confirmed that vanadium was present and was not homogeneously distributed in the plate. The plate also was different in composition from the screws. Additional studies showed that galvanic corrosion between the plate and the chemically different screws might have contributed to the release of vanadium in the tissue.
Vanadium is known to be allergenic, especially in the presence of implant failure.12,13 In our patient, patch testing with more than 100 allergens was negative, except for vanadium trichloride 1%. Our patient’s presentation strongly suggested that she developed a vanadium allergy manifesting as systemic allergic contact dermatitis. She demonstrated no history of skin disease, a widespread eczematous eruption after exposure, histology consistent with systemic contact allergy, a positive patch test to vanadium, and clearance of the eruption on removal of the antigen, which have been proposed as objective criteria that support a diagnosis of metal implant allergy.14 She refused our suggestion to reimplant a portion of the remaining plate under the skin without screws and monitor for recurrence of the eruption. She did not have a lesion overlying the surgical site, but she did develop lesions near the surgical scar. The literature indicates that cutaneous manifestations of allergy to metallic implants can be both localized and generalized.14
Although reports are rare, other researchers have found vanadium allergy in patients with metal orthopedic implants.5,12,13,15 The scarcity of literature on vanadium allergy seems to suggest that it is a rare entity, but we believe that it may be more common. Vanadium allergy may be underdiagnosed because it is not a standard patch test allergen. Furthermore, many of those who do choose to test for it use what we believe to be ineffective formulas of vanadium when patch testing patients. Our patient demonstrated a positive patch test reaction only to vanadium trichloride and not to pure vanadium, which is consistent with the small number of other studies that investigated vanadium allergy.5,12,13,15 We believe that vanadium trichloride is more water soluble than elemental vanadium,16 and thus more likely to identify true vanadium allergy than other test materials.
Although reports of vanadium allergy in patients with metal implants are rare in the medical literature, the material science literature clearly states that vanadium is toxic and that vanadium-containing implants are problematic.17-20 It has been shown that although Ti6Al4V implants are considered highly resistant to corrosion, they will slowly and continuously corrode in a physiologic environment and release titanium, aluminum, and vanadium ions, both systemically and into the peri-implant space.11 To address these problems with vanadium, vanadium-free titanium alloys such as Ti6Al7Nb have specifically been developed for medical use to address the problems caused by vanadium. Ti6Al7Nb contains 7% niobium rather than vanadium and appears to have some improved qualities in surgical implants.17
There is still a great deal of uncertainty around metal implant allergy. Allergy to metal implants can be difficult to diagnose for several reasons. Some metals are not conducive to patch testing because of their low bioavailability. Additionally, we lack validated and standardized patch test formulas for metals that can be diagnosed by patch testing. Furthermore, there is uncertainty about what to do after allergy to a metal implant is diagnosed; in some cases (eg, with more extensive procedures such as total joint replacements), removal or replacement of the implant may be associated with increased risk of further complications.6,21
Conclusion
We suggest that manufacturers consider vanadium-free alloys such as Ti7Al6Nb, which contains niobium instead of vanadium, in their surgical implants,22 and if surgeons have a choice, they should consider using titanium implants with niobium rather than vanadium.10 We suggest that clinicians consider vanadium allergy in patients with Ti6Al4V surgical implants and signs of a hypersensitivity reaction, and include vanadium trichloride 1% when patch testing.
Acknowledgment
The authors would like to thank Nicholas R. Krasnow, PhD (Tucson, Arizona), for his invaluable help coordinating, performing, and interpreting the metal analyses.
Metal allergy in patients with orthopedic implants can cause serious problems including dermatitis and implant failure.1 As life expectancy increases, the general population ages, and more metallic orthopedic implants are placed,2 allergy to these implants is expected to be a problem of greater significance. Uncertainty remains regarding best practice for patients with suspected metal implant allergy.1 The major questions are: Who should be tested? When should they be tested? What are the optimal tests to diagnose metal allergy?3-8
We report the case of a patient with vanadium allergy who developed a diffuse eczematous dermatitis and implant failure after receiving a vanadium-containing titanium alloy orthopedic implant in the left foot. This case is remarkable because hypersensitivity reactions to titanium-based hardware are rare, as they traditionally have not been thought to provoke allergic reactions.9
Case Report
A 62-year-old woman who was otherwise healthy presented with an eruption of more than 80 pruritic, nummular, eczematous plaques on the arms, legs, back, and buttocks of 3 weeks’ duration (Figure 1). She had a history of allergy to metal used in costume jewelry. Six weeks prior, the patient underwent implantation of a titanium alloy plate in the left foot for surgical repair of painful deforming osteoarthritis. A radiograph of the foot showed appropriate placement. According to the manufacturer, the plate was composed of the compound Ti6Al4V, which contained 90% titanium, 6% aluminum, and 4% vanadium. The lesions developed on the skin close to but not directly over the surgical site.
A punch biopsy of one of the lesions on the shoulder showed lymphoeosinophilic spongiosis consistent with a delayed hypersensitivity reaction (Figure 2). There was mild clinical improvement of the eruption with topical steroids. A course of prednisone for systemic effect resulted in clearing of the eruption, but it promptly recurred on cessation of the steroids. The patient was then patch tested using the North American 80 Comprehensive Series, with an additional 59 common textile, shampoo, fragrance, and several metal allergens, all of which were negative.
The patient had persistent pain and swelling at the surgical site, and radiographs taken postoperatively at 6 months showed implant failure (Figure 3). The hardware was surgically removed 8 months after implantation (Figure 4) and the plate and screws were submitted to the Institute for Mineral Resources Geosciences LA-ICP-MS Facility and the Lunar and Planetary Laboratory at the University of Arizona (Tucson, Arizona) for analysis. The skin lesions began to improve days after the hardware was removed and the eruption cleared over the following 3 weeks with no additional treatment.
After the hardware was removed, it was analyzed to determine the elemental composition of the plate and screws, and the patient was then patch tested with the major metal components of the implant: aluminum chloride hexahydrate 2.0% pet, elemental titanium 10.0% pet, titanium dioxide 10.0% pet, titanium (III) nitride 5.0% pet, titanium (III) oxalate decahydrate 5.0% pet, elemental vanadium 5.0% pet, and vanadium (III) chloride 1.0% pet. She demonstrated a 1+ reaction (erythema and induration) to vanadium trichloride at 72 and 96 hours.
The plate and screws removed from the patient were sterilized and submitted for analysis. Electron microprobe analysis confirmed that the major elemental composition of the plate and screws essentially matched the manufacturer’s listing (Table 1). The trace elements were determined using laser ablative inductively coupled mass spectroscopy, which demonstrated that the screws were of different metal composition from the plate (Table 2). Electron microprobe analysis also was used to determine the microstructure of the plate and screws. The plate had 2 distinct phases consisting of a titanium-aluminum phase and a vanadium phase, whereas the screw was much more homogeneous. Basic electrochemical studies were performed in a salt solution replicating the tissue of the foot. These studies showed that galvanic corrosion could have occurred between the plate and screws due to the differences of composition.
Comment
Titanium is an attractive metal to use in orthopedic implants. It has a high strength-to-weight ratio, a low modulus of elasticity, and good resistance to corrosion. Titanium can be categorized as either commercially pure titanium (cp-Ti) or a titanium alloy. Colloquially, both cp-Ti and titanium alloys are often referred to simply as titanium, but the distinction is important when it comes to medical implants and devices. Commercially pure titanium is more than 99% pure titanium, but up to 1% of its volume can be comprised of impurities.10 In titanium alloys, the alloy elements are intentionally added to create a material with optimal properties. The 2 most common types of titanium that are used for orthopedic implants are cp-Ti and Ti6Al4V, a titanium alloy containing approximately 90% titanium, 6% aluminum, and 4% vanadium. Similar to cp-Ti, titanium alloys also can contain impurities such as aluminum, beryllium, cobalt, chromium, iron, nickel, and palladium, among many others. Although these impurities often are considered negligible from a metallurgy perspective, as they do not change the properties of the material, these trace elements may be present in large enough quantities to cause hypersensitivity reactions.11
Several weeks after implantation of a titanium alloy metal plate in the left foot, a widespread eczematous eruption developed in our patient who had no prior skin disease. The eruption was steroid responsive but did not clear until the plate was removed. Detailed metallurgy analysis confirmed that vanadium was present and was not homogeneously distributed in the plate. The plate also was different in composition from the screws. Additional studies showed that galvanic corrosion between the plate and the chemically different screws might have contributed to the release of vanadium in the tissue.
Vanadium is known to be allergenic, especially in the presence of implant failure.12,13 In our patient, patch testing with more than 100 allergens was negative, except for vanadium trichloride 1%. Our patient’s presentation strongly suggested that she developed a vanadium allergy manifesting as systemic allergic contact dermatitis. She demonstrated no history of skin disease, a widespread eczematous eruption after exposure, histology consistent with systemic contact allergy, a positive patch test to vanadium, and clearance of the eruption on removal of the antigen, which have been proposed as objective criteria that support a diagnosis of metal implant allergy.14 She refused our suggestion to reimplant a portion of the remaining plate under the skin without screws and monitor for recurrence of the eruption. She did not have a lesion overlying the surgical site, but she did develop lesions near the surgical scar. The literature indicates that cutaneous manifestations of allergy to metallic implants can be both localized and generalized.14
Although reports are rare, other researchers have found vanadium allergy in patients with metal orthopedic implants.5,12,13,15 The scarcity of literature on vanadium allergy seems to suggest that it is a rare entity, but we believe that it may be more common. Vanadium allergy may be underdiagnosed because it is not a standard patch test allergen. Furthermore, many of those who do choose to test for it use what we believe to be ineffective formulas of vanadium when patch testing patients. Our patient demonstrated a positive patch test reaction only to vanadium trichloride and not to pure vanadium, which is consistent with the small number of other studies that investigated vanadium allergy.5,12,13,15 We believe that vanadium trichloride is more water soluble than elemental vanadium,16 and thus more likely to identify true vanadium allergy than other test materials.
Although reports of vanadium allergy in patients with metal implants are rare in the medical literature, the material science literature clearly states that vanadium is toxic and that vanadium-containing implants are problematic.17-20 It has been shown that although Ti6Al4V implants are considered highly resistant to corrosion, they will slowly and continuously corrode in a physiologic environment and release titanium, aluminum, and vanadium ions, both systemically and into the peri-implant space.11 To address these problems with vanadium, vanadium-free titanium alloys such as Ti6Al7Nb have specifically been developed for medical use to address the problems caused by vanadium. Ti6Al7Nb contains 7% niobium rather than vanadium and appears to have some improved qualities in surgical implants.17
There is still a great deal of uncertainty around metal implant allergy. Allergy to metal implants can be difficult to diagnose for several reasons. Some metals are not conducive to patch testing because of their low bioavailability. Additionally, we lack validated and standardized patch test formulas for metals that can be diagnosed by patch testing. Furthermore, there is uncertainty about what to do after allergy to a metal implant is diagnosed; in some cases (eg, with more extensive procedures such as total joint replacements), removal or replacement of the implant may be associated with increased risk of further complications.6,21
Conclusion
We suggest that manufacturers consider vanadium-free alloys such as Ti7Al6Nb, which contains niobium instead of vanadium, in their surgical implants,22 and if surgeons have a choice, they should consider using titanium implants with niobium rather than vanadium.10 We suggest that clinicians consider vanadium allergy in patients with Ti6Al4V surgical implants and signs of a hypersensitivity reaction, and include vanadium trichloride 1% when patch testing.
Acknowledgment
The authors would like to thank Nicholas R. Krasnow, PhD (Tucson, Arizona), for his invaluable help coordinating, performing, and interpreting the metal analyses.
- Basko-Plluska JL, Thyssen JP, Schalock PC. Cutaneous and systemic hypersensitivity reactions to metallic implants. Dermatitis. 2011;22:65-79.
- Kurtz S, Ong K, Lau E, et al. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89:780-785.
- Thyssen JP, Johansen JD, Menné T, et al. Hypersensitivity reactions from metallic implants: a future challenge that needs to be addressed. Br J Dermatol. 2010;162:235-236.
- Aquino M, Mucci T. Systemic contact dermatitis and allergy to biomedical devices. Curr Allergy Asthma Rep. 2013;13:518-527.
- Krecisz B, Kiec-Swierczynska M, Chomiczewska-Skora D. Allergy to orthopedic metal implants—a prospective study. Int J Occup Med Environ Health. 2012;25:463-469.
- Atanaskova Mesinkovska N, Tellez A, Molina L, et al. The effect of patch testing on surgical practices and outcomes in orthopedic patients with metal implants. Arch Dermatol. 2012;148:687-693.
- Frigerio E, Pigatto PD, Guzzi G, et al. Metal sensitivity in patients with orthopaedic implants: a prospective study. Contact Dermatitis. 2011;64:273-279.
- Amini M, Mayes WH, Tzeng TH, et al. Evaluation and management of metal hypersensitivity in total joint arthroplasty: a systematic review. J Long Term Eff Med Implants. 2014;24:25-36.
- Thomas P, Bandl WD, Maier S, et al. Hypersensitivity to titanium osteosynthesis with impaired fracture healing, eczema, and T-cell hyperresponsiveness in vitro: case report and review of the literature. Contact Dermatitis. 2006;55:199-202.
- Wood MM, Warshaw EM. Hypersensitivity reactions to titanium: diagnosis and management. Dermatitis. 2015;26:7-25.
- Cadosch D, Chan E, Gautschi OP, et al. Metal is not inert: role of metal ions released by biocorrosion in aseptic loosening—current concepts. J Biomed Mater Res A. 2009;91:1252-1262.
- Granchi D, Cenni E, Trisolino G, et al. Sensitivity to implant materials in patients undergoing total hip replacement. J Biomed Mater Res B Appl Biomater. 2006;77:257-264.
- Granchi D, Cenni E, Tigani D, et al. Sensitivity to implant materials in patients with total knee arthroplasties. Biomaterials. 2008;29:1494-1500.
- Thyssen JP, Menné T, Schalock PC, et al. Pragmatic approach to the clinical work-up of patients with putative allergic disease to metallic orthopaedic implants before and after surgery. Br J Dermatol. 2011;164:473-478.
- Kręcisz B, Kieć-Świerczyńska M, Bąkowicz-Mitura K. Allergy to metals as a cause of orthopedic implant failure. Int J Occup Med Environ Health. 2006;19:178-180.
- Costigan M, Cary R, Dobson S. Vanadium Pentoxide and Other Inorganic Vanadium Compounds. Geneva, Switzerland: World Health Organization; 2001.
- Challa VS, Mali S, Misra RD. Reduced toxicity and superior cellular response of preosteoblasts to Ti-6Al-7Nb alloy and comparison with Ti-6Al-4V. J Biomed Mater Res A. 2013;101:2083-2089.
- Okazaki Y, Rao S, Ito Y, et al. Corrosion resistance, mechanical properties, corrosion fatigue strength and cytocompatibility of new Ti alloys without Al and V. Biomaterials. 1998;19:1197-1215.
- Paszenda Z, Walke W, Jadacka S. Electrochemical investigations of Ti6Al4V and Ti6Al7Nb alloys used on implants in bone surgery. J Achievements Materials Manufacturing Eng. 2010;38:24-32.
- Wang K. The use of titanium for medical applications in the USA. Materials Sci Eng A. 1996:134-137.
- Haseeb M, Butt MF, Altaf T, et al. Indications of implant removal: a study of 83 cases. Int J Health Sci (Qassim). 2017;11:1-7.
- Geetha M, Singh AK, Asokamani R, et al. Ti based biomaterials, the ultimate choice for orthopaedic implants—a review. Progress Materials Sci. 2009;54:397-425.
- Basko-Plluska JL, Thyssen JP, Schalock PC. Cutaneous and systemic hypersensitivity reactions to metallic implants. Dermatitis. 2011;22:65-79.
- Kurtz S, Ong K, Lau E, et al. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89:780-785.
- Thyssen JP, Johansen JD, Menné T, et al. Hypersensitivity reactions from metallic implants: a future challenge that needs to be addressed. Br J Dermatol. 2010;162:235-236.
- Aquino M, Mucci T. Systemic contact dermatitis and allergy to biomedical devices. Curr Allergy Asthma Rep. 2013;13:518-527.
- Krecisz B, Kiec-Swierczynska M, Chomiczewska-Skora D. Allergy to orthopedic metal implants—a prospective study. Int J Occup Med Environ Health. 2012;25:463-469.
- Atanaskova Mesinkovska N, Tellez A, Molina L, et al. The effect of patch testing on surgical practices and outcomes in orthopedic patients with metal implants. Arch Dermatol. 2012;148:687-693.
- Frigerio E, Pigatto PD, Guzzi G, et al. Metal sensitivity in patients with orthopaedic implants: a prospective study. Contact Dermatitis. 2011;64:273-279.
- Amini M, Mayes WH, Tzeng TH, et al. Evaluation and management of metal hypersensitivity in total joint arthroplasty: a systematic review. J Long Term Eff Med Implants. 2014;24:25-36.
- Thomas P, Bandl WD, Maier S, et al. Hypersensitivity to titanium osteosynthesis with impaired fracture healing, eczema, and T-cell hyperresponsiveness in vitro: case report and review of the literature. Contact Dermatitis. 2006;55:199-202.
- Wood MM, Warshaw EM. Hypersensitivity reactions to titanium: diagnosis and management. Dermatitis. 2015;26:7-25.
- Cadosch D, Chan E, Gautschi OP, et al. Metal is not inert: role of metal ions released by biocorrosion in aseptic loosening—current concepts. J Biomed Mater Res A. 2009;91:1252-1262.
- Granchi D, Cenni E, Trisolino G, et al. Sensitivity to implant materials in patients undergoing total hip replacement. J Biomed Mater Res B Appl Biomater. 2006;77:257-264.
- Granchi D, Cenni E, Tigani D, et al. Sensitivity to implant materials in patients with total knee arthroplasties. Biomaterials. 2008;29:1494-1500.
- Thyssen JP, Menné T, Schalock PC, et al. Pragmatic approach to the clinical work-up of patients with putative allergic disease to metallic orthopaedic implants before and after surgery. Br J Dermatol. 2011;164:473-478.
- Kręcisz B, Kieć-Świerczyńska M, Bąkowicz-Mitura K. Allergy to metals as a cause of orthopedic implant failure. Int J Occup Med Environ Health. 2006;19:178-180.
- Costigan M, Cary R, Dobson S. Vanadium Pentoxide and Other Inorganic Vanadium Compounds. Geneva, Switzerland: World Health Organization; 2001.
- Challa VS, Mali S, Misra RD. Reduced toxicity and superior cellular response of preosteoblasts to Ti-6Al-7Nb alloy and comparison with Ti-6Al-4V. J Biomed Mater Res A. 2013;101:2083-2089.
- Okazaki Y, Rao S, Ito Y, et al. Corrosion resistance, mechanical properties, corrosion fatigue strength and cytocompatibility of new Ti alloys without Al and V. Biomaterials. 1998;19:1197-1215.
- Paszenda Z, Walke W, Jadacka S. Electrochemical investigations of Ti6Al4V and Ti6Al7Nb alloys used on implants in bone surgery. J Achievements Materials Manufacturing Eng. 2010;38:24-32.
- Wang K. The use of titanium for medical applications in the USA. Materials Sci Eng A. 1996:134-137.
- Haseeb M, Butt MF, Altaf T, et al. Indications of implant removal: a study of 83 cases. Int J Health Sci (Qassim). 2017;11:1-7.
- Geetha M, Singh AK, Asokamani R, et al. Ti based biomaterials, the ultimate choice for orthopaedic implants—a review. Progress Materials Sci. 2009;54:397-425.
Practice Points
- Vanadium may be an underrecognized allergen in patients with metal implants.
- Consider vanadium allergy in those with surgical implants and signs of hypersensitivity reaction.
- Test for allergy with vanadium trichloride.
- Niobium is an alternative for implants in vanadium-allergic patients.

When atopic dermatitis is really contact dermatitis
ATLANTA – When patients present with atopic dermatitis that worsens, changes distribution, fails to improve, or immediately rebounds, think contact dermatitis, Luz Fonacier, MD, advised at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Clinical signs of contact dermatitis include lesions with an atypical distribution/pattern, such as head, eyelid, or cheilitis/perioral predominance, or lesions on the hand or foot. Also elevate your suspicion in patients with therapy-resistant hand eczema, adult- or childhood-onset atopic dermatitis without childhood eczema, as well as in cases of severe or widespread dermatitis prior to initiating a systemic immunosuppressant. The list of potential allergens to consider includes metal (especially nickel, cobalt, and potassium dichromate), fragrances such as formaldehyde and balsam of Peru, preservatives, as well as topical emollients, corticosteroids, antibiotics, and antiseptics.

Dr. Fonacier, professor of medicine at the State University of New York at Stony Brook and section head of allergy at Winthrop University Hospital, Mineola, N.Y., recommends loading acrylates, fragrances, and allergens in an aqueous vehicle immediately before application. She noted that delayed patch test readings are common to metals, topical antibiotics, and topical corticosteroids, and that positive reactions to gold are often not clinically relevant. “The patch test positivity of gold can be as high as 30% in adults and a little bit less in children, but results from two large studies show clinical relevance in only 10%-15% of cases,” she said. A trial of gold avoidance may be warranted in patients with suspected jewelry allergy, facial or eyelid dermatitis, or exposure through gold dental restorations.
She went on to share tips for reading skin patch tests. The first reading should be done after 48 hours, while the second should be done 3, 4, or 7 days after application. “The second reading helps distinguish irritant from allergic responses,” she said. “Thirty percent of negative tests at 48 hours may be positive on delayed readings.” Most true allergic reactions occur between 72 and 96 hours. Allergens that may peak early include thiuram mix, carba mix, and balsam of Peru. Those that disappear after 5 days include balsam of Peru, benzoic acid, disperse blue #124, fragrance mix, mercury, methyldibromo glutaronitrile, phenoxyethanol, and octyl gallate. Delayed patch test reactions after five days include metals (gold potassium dichromate, nickel, and cobalt), topical antibiotics (neomycin and bacitracin) as well as topic corticosteroids.
Resources she recommended to attendees include the American Contact Dermatitis Society and the Contact Dermatitis Institute. Health and safety information about household products can be found here.
Dr. Fonacier disclosed that she has received research and educational grants from Baxter and Genentech. She is also a consultant to Church and Dwight and Regeneron.
ATLANTA – When patients present with atopic dermatitis that worsens, changes distribution, fails to improve, or immediately rebounds, think contact dermatitis, Luz Fonacier, MD, advised at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Clinical signs of contact dermatitis include lesions with an atypical distribution/pattern, such as head, eyelid, or cheilitis/perioral predominance, or lesions on the hand or foot. Also elevate your suspicion in patients with therapy-resistant hand eczema, adult- or childhood-onset atopic dermatitis without childhood eczema, as well as in cases of severe or widespread dermatitis prior to initiating a systemic immunosuppressant. The list of potential allergens to consider includes metal (especially nickel, cobalt, and potassium dichromate), fragrances such as formaldehyde and balsam of Peru, preservatives, as well as topical emollients, corticosteroids, antibiotics, and antiseptics.
Dr. Fonacier, professor of medicine at the State University of New York at Stony Brook and section head of allergy at Winthrop University Hospital, Mineola, N.Y., recommends loading acrylates, fragrances, and allergens in an aqueous vehicle immediately before application. She noted that delayed patch test readings are common to metals, topical antibiotics, and topical corticosteroids, and that positive reactions to gold are often not clinically relevant. “The patch test positivity of gold can be as high as 30% in adults and a little bit less in children, but results from two large studies show clinical relevance in only 10%-15% of cases,” she said. A trial of gold avoidance may be warranted in patients with suspected jewelry allergy, facial or eyelid dermatitis, or exposure through gold dental restorations.
She went on to share tips for reading skin patch tests. The first reading should be done after 48 hours, while the second should be done 3, 4, or 7 days after application. “The second reading helps distinguish irritant from allergic responses,” she said. “Thirty percent of negative tests at 48 hours may be positive on delayed readings.” Most true allergic reactions occur between 72 and 96 hours. Allergens that may peak early include thiuram mix, carba mix, and balsam of Peru. Those that disappear after 5 days include balsam of Peru, benzoic acid, disperse blue #124, fragrance mix, mercury, methyldibromo glutaronitrile, phenoxyethanol, and octyl gallate. Delayed patch test reactions after five days include metals (gold potassium dichromate, nickel, and cobalt), topical antibiotics (neomycin and bacitracin) as well as topic corticosteroids.
Resources she recommended to attendees include the American Contact Dermatitis Society and the Contact Dermatitis Institute. Health and safety information about household products can be found here.
Dr. Fonacier disclosed that she has received research and educational grants from Baxter and Genentech. She is also a consultant to Church and Dwight and Regeneron.
ATLANTA – When patients present with atopic dermatitis that worsens, changes distribution, fails to improve, or immediately rebounds, think contact dermatitis, Luz Fonacier, MD, advised at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Clinical signs of contact dermatitis include lesions with an atypical distribution/pattern, such as head, eyelid, or cheilitis/perioral predominance, or lesions on the hand or foot. Also elevate your suspicion in patients with therapy-resistant hand eczema, adult- or childhood-onset atopic dermatitis without childhood eczema, as well as in cases of severe or widespread dermatitis prior to initiating a systemic immunosuppressant. The list of potential allergens to consider includes metal (especially nickel, cobalt, and potassium dichromate), fragrances such as formaldehyde and balsam of Peru, preservatives, as well as topical emollients, corticosteroids, antibiotics, and antiseptics.
Dr. Fonacier, professor of medicine at the State University of New York at Stony Brook and section head of allergy at Winthrop University Hospital, Mineola, N.Y., recommends loading acrylates, fragrances, and allergens in an aqueous vehicle immediately before application. She noted that delayed patch test readings are common to metals, topical antibiotics, and topical corticosteroids, and that positive reactions to gold are often not clinically relevant. “The patch test positivity of gold can be as high as 30% in adults and a little bit less in children, but results from two large studies show clinical relevance in only 10%-15% of cases,” she said. A trial of gold avoidance may be warranted in patients with suspected jewelry allergy, facial or eyelid dermatitis, or exposure through gold dental restorations.
She went on to share tips for reading skin patch tests. The first reading should be done after 48 hours, while the second should be done 3, 4, or 7 days after application. “The second reading helps distinguish irritant from allergic responses,” she said. “Thirty percent of negative tests at 48 hours may be positive on delayed readings.” Most true allergic reactions occur between 72 and 96 hours. Allergens that may peak early include thiuram mix, carba mix, and balsam of Peru. Those that disappear after 5 days include balsam of Peru, benzoic acid, disperse blue #124, fragrance mix, mercury, methyldibromo glutaronitrile, phenoxyethanol, and octyl gallate. Delayed patch test reactions after five days include metals (gold potassium dichromate, nickel, and cobalt), topical antibiotics (neomycin and bacitracin) as well as topic corticosteroids.
Resources she recommended to attendees include the American Contact Dermatitis Society and the Contact Dermatitis Institute. Health and safety information about household products can be found here.
Dr. Fonacier disclosed that she has received research and educational grants from Baxter and Genentech. She is also a consultant to Church and Dwight and Regeneron.
EXPERT ANALYSIS AT THE 2017 AAAAI ANNUAL MEETING
Long-term peanut sublingual immunotherapy found safe
ATLANTA – Peanut sublingual immunotherapy induces clinically significant desensitization in the majority of subjects and can induce sustained unresponsiveness in a subset of children treated for 36-60 months, results from a small study suggest.
“Sublingual immunotherapy [SLIT] is an easy-to-administer treatment that appears to be safe, and with extended treatment, may provide a clinically significant amount of protection with the potential for a lasting effect,” one of the study authors, Edwin H. Kim, MD, said in an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology.

To find out, the researchers treated 37 patients with 2 mg of peanut SLIT for 36-60 months and then assessed a 5,000-mg peanut oral food challenge to further assess desensitization. Those who passed the challenge discontinued SLIT for 2-4 weeks and were then re-challenged with 5,000 mg of peanut protein to assess for sustained unresponsiveness.
“Existing data suggested that about 50% of patients on oral immunotherapy develop sustained unresponsiveness, which was defined by being able to tolerate the same full amount of peanut 1 month after stopping therapy,” Dr. Kim said. “As the assumption was that SLIT would have a more modest effect, it was unclear if any patients at all on SLIT would develop sustained unresponsiveness.”
Of the 37 subjects who completed the study, 32 (86%) safely ingested more than 300 mg of peanut and 12 (32%) passed the oral food challenge at the end of SLIT therapy. The median amount of peanut tolerated was 1,750 mg (compared with 1,710 mg in the original 12-month paper). The 12 subjects who passed the oral food challenge were re-challenged with 5,000 mg of peanut 2-4 weeks after discontinuing SLIT. Of these, 10 (27%) demonstrated sustained unresponsiveness. Dr. Kim characterized the results as “better than we would have expected.”
He acknowledged certain limitations to the study, including the lack of an entry food challenge to determine a baseline reaction threshold and the lack of a placebo arm for the study’s extended maintenance phase.
Dr. Kim reported having no financial disclosures.
[email protected]
ATLANTA – Peanut sublingual immunotherapy induces clinically significant desensitization in the majority of subjects and can induce sustained unresponsiveness in a subset of children treated for 36-60 months, results from a small study suggest.
“Sublingual immunotherapy [SLIT] is an easy-to-administer treatment that appears to be safe, and with extended treatment, may provide a clinically significant amount of protection with the potential for a lasting effect,” one of the study authors, Edwin H. Kim, MD, said in an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
To find out, the researchers treated 37 patients with 2 mg of peanut SLIT for 36-60 months and then assessed a 5,000-mg peanut oral food challenge to further assess desensitization. Those who passed the challenge discontinued SLIT for 2-4 weeks and were then re-challenged with 5,000 mg of peanut protein to assess for sustained unresponsiveness.
“Existing data suggested that about 50% of patients on oral immunotherapy develop sustained unresponsiveness, which was defined by being able to tolerate the same full amount of peanut 1 month after stopping therapy,” Dr. Kim said. “As the assumption was that SLIT would have a more modest effect, it was unclear if any patients at all on SLIT would develop sustained unresponsiveness.”
Of the 37 subjects who completed the study, 32 (86%) safely ingested more than 300 mg of peanut and 12 (32%) passed the oral food challenge at the end of SLIT therapy. The median amount of peanut tolerated was 1,750 mg (compared with 1,710 mg in the original 12-month paper). The 12 subjects who passed the oral food challenge were re-challenged with 5,000 mg of peanut 2-4 weeks after discontinuing SLIT. Of these, 10 (27%) demonstrated sustained unresponsiveness. Dr. Kim characterized the results as “better than we would have expected.”
He acknowledged certain limitations to the study, including the lack of an entry food challenge to determine a baseline reaction threshold and the lack of a placebo arm for the study’s extended maintenance phase.
Dr. Kim reported having no financial disclosures.
[email protected]
ATLANTA – Peanut sublingual immunotherapy induces clinically significant desensitization in the majority of subjects and can induce sustained unresponsiveness in a subset of children treated for 36-60 months, results from a small study suggest.
“Sublingual immunotherapy [SLIT] is an easy-to-administer treatment that appears to be safe, and with extended treatment, may provide a clinically significant amount of protection with the potential for a lasting effect,” one of the study authors, Edwin H. Kim, MD, said in an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
To find out, the researchers treated 37 patients with 2 mg of peanut SLIT for 36-60 months and then assessed a 5,000-mg peanut oral food challenge to further assess desensitization. Those who passed the challenge discontinued SLIT for 2-4 weeks and were then re-challenged with 5,000 mg of peanut protein to assess for sustained unresponsiveness.
“Existing data suggested that about 50% of patients on oral immunotherapy develop sustained unresponsiveness, which was defined by being able to tolerate the same full amount of peanut 1 month after stopping therapy,” Dr. Kim said. “As the assumption was that SLIT would have a more modest effect, it was unclear if any patients at all on SLIT would develop sustained unresponsiveness.”
Of the 37 subjects who completed the study, 32 (86%) safely ingested more than 300 mg of peanut and 12 (32%) passed the oral food challenge at the end of SLIT therapy. The median amount of peanut tolerated was 1,750 mg (compared with 1,710 mg in the original 12-month paper). The 12 subjects who passed the oral food challenge were re-challenged with 5,000 mg of peanut 2-4 weeks after discontinuing SLIT. Of these, 10 (27%) demonstrated sustained unresponsiveness. Dr. Kim characterized the results as “better than we would have expected.”
He acknowledged certain limitations to the study, including the lack of an entry food challenge to determine a baseline reaction threshold and the lack of a placebo arm for the study’s extended maintenance phase.
Dr. Kim reported having no financial disclosures.
[email protected]
AT THE 2017 AAAAI ANNUAL MEETING
Key clinical point:
Major finding: Of the children who completed the study, 86% safely ingested more than 300 mg of peanut and 32% passed the oral food challenge at the end of SLIT therapy.
Data source: A study of 37 patients who were treated with 2 mg of peanut SLIT for 36-60 months.
Disclosures: Dr. Kim reported having no financial disclosures.
Teledermatology shows potential for grading patch test results
ORLANDO – Store-and-forward teledermatology may be useful for grading patch test results.
Erin Warshaw, MD, and Sara Hylwa, MD, both of the University of Minnesota, Minneapolis, sought to compare readings of patch test results both in person and via store-and-forward teledermatology. They patch tested patients at the Hennepin County (Minn.) Medical Center with the North American Contact Dermatitis Group screening series; photos were obtained at the 48-hour reading and the final reading (96-160 hours).

Almost all (101 of 107) of patients eligible for the trial were enrolled. Patients were overwhelmingly female (72%) with an average age of 50 years in this single-site study. Most screening panels were applied to the back.
Teledermatology assessment was categorized as successful if it matched the in-person assessment and as a failure if it did not; investigators labeled assessed pairs that did not fully match as indeterminate. Successful matches indicated there was no clinically significant difference between teledermatology and in-person assessment, indeterminate matches indicated that there was possible clinically significant difference, and failure to match indicated definite clinically significant difference.
All readings that were negative both in person and via teledermatology were excluded from the analysis.
At 48 hours, 47.2% of 705 reading pairs were labeled successful and 51.3% were labeled indeterminate. Failure, or complete disagreement, occurred in 1.6%, or 11 individual antigen pairs.
More successes – and failures – were seen at the final reading, with 53.8% of 420 final readings labeled successful, 39.8% labeled indeterminate, and 6.4%, or 27 individual antigen pairs, labeled as failures.
In general, teledermatology was more likely to miss or downplay the severity of reactions in the indeterminate pairs, Dr. Warshaw said. “This makes intuitive sense because when you are with a patient live, often the lighting catches an irritant wrinkle reaction or you can feel the lesion and be much more likely to call it irritant or a mild reaction than you would be from a flat photo.”
In the failure group, teledermatology generally overstated reactions, she added.
Dr. Warshaw said that logistical changes would be needed to make teledermatology more effective for reading patch test reactions in her practice. Their method of marking the patch test grid is to use a surgical marker on the corners, but a highlighter to mark the grid between the antigens. The highlighter simply did not show up well in photographs, she noted.
While not perfect, teledermatology does have promise for reading patch test reactions, she added. “I would love to save patients from having to come for their 48-hour reading... In Minnesota we have these horrible snowstorms. Last week there was a blizzard that was predicted. A third of our patients live 2 hours away from the clinic. If they could have taken photographs instead of trying to come through a blizzard for their final reading, that would be helpful.”
Dr. Warshaw noted that their study assessed only the 70 antigens of the North American Contact Dermatitis Research Group series and that it could have been strengthened by using additional series or the patients’ own products.
[email protected]
On Twitter @denisefulton
ORLANDO – Store-and-forward teledermatology may be useful for grading patch test results.
Erin Warshaw, MD, and Sara Hylwa, MD, both of the University of Minnesota, Minneapolis, sought to compare readings of patch test results both in person and via store-and-forward teledermatology. They patch tested patients at the Hennepin County (Minn.) Medical Center with the North American Contact Dermatitis Group screening series; photos were obtained at the 48-hour reading and the final reading (96-160 hours).
Almost all (101 of 107) of patients eligible for the trial were enrolled. Patients were overwhelmingly female (72%) with an average age of 50 years in this single-site study. Most screening panels were applied to the back.
Teledermatology assessment was categorized as successful if it matched the in-person assessment and as a failure if it did not; investigators labeled assessed pairs that did not fully match as indeterminate. Successful matches indicated there was no clinically significant difference between teledermatology and in-person assessment, indeterminate matches indicated that there was possible clinically significant difference, and failure to match indicated definite clinically significant difference.
All readings that were negative both in person and via teledermatology were excluded from the analysis.
At 48 hours, 47.2% of 705 reading pairs were labeled successful and 51.3% were labeled indeterminate. Failure, or complete disagreement, occurred in 1.6%, or 11 individual antigen pairs.
More successes – and failures – were seen at the final reading, with 53.8% of 420 final readings labeled successful, 39.8% labeled indeterminate, and 6.4%, or 27 individual antigen pairs, labeled as failures.
In general, teledermatology was more likely to miss or downplay the severity of reactions in the indeterminate pairs, Dr. Warshaw said. “This makes intuitive sense because when you are with a patient live, often the lighting catches an irritant wrinkle reaction or you can feel the lesion and be much more likely to call it irritant or a mild reaction than you would be from a flat photo.”
In the failure group, teledermatology generally overstated reactions, she added.
Dr. Warshaw said that logistical changes would be needed to make teledermatology more effective for reading patch test reactions in her practice. Their method of marking the patch test grid is to use a surgical marker on the corners, but a highlighter to mark the grid between the antigens. The highlighter simply did not show up well in photographs, she noted.
While not perfect, teledermatology does have promise for reading patch test reactions, she added. “I would love to save patients from having to come for their 48-hour reading... In Minnesota we have these horrible snowstorms. Last week there was a blizzard that was predicted. A third of our patients live 2 hours away from the clinic. If they could have taken photographs instead of trying to come through a blizzard for their final reading, that would be helpful.”
Dr. Warshaw noted that their study assessed only the 70 antigens of the North American Contact Dermatitis Research Group series and that it could have been strengthened by using additional series or the patients’ own products.
[email protected]
On Twitter @denisefulton
ORLANDO – Store-and-forward teledermatology may be useful for grading patch test results.
Erin Warshaw, MD, and Sara Hylwa, MD, both of the University of Minnesota, Minneapolis, sought to compare readings of patch test results both in person and via store-and-forward teledermatology. They patch tested patients at the Hennepin County (Minn.) Medical Center with the North American Contact Dermatitis Group screening series; photos were obtained at the 48-hour reading and the final reading (96-160 hours).
Almost all (101 of 107) of patients eligible for the trial were enrolled. Patients were overwhelmingly female (72%) with an average age of 50 years in this single-site study. Most screening panels were applied to the back.
Teledermatology assessment was categorized as successful if it matched the in-person assessment and as a failure if it did not; investigators labeled assessed pairs that did not fully match as indeterminate. Successful matches indicated there was no clinically significant difference between teledermatology and in-person assessment, indeterminate matches indicated that there was possible clinically significant difference, and failure to match indicated definite clinically significant difference.
All readings that were negative both in person and via teledermatology were excluded from the analysis.
At 48 hours, 47.2% of 705 reading pairs were labeled successful and 51.3% were labeled indeterminate. Failure, or complete disagreement, occurred in 1.6%, or 11 individual antigen pairs.
More successes – and failures – were seen at the final reading, with 53.8% of 420 final readings labeled successful, 39.8% labeled indeterminate, and 6.4%, or 27 individual antigen pairs, labeled as failures.
In general, teledermatology was more likely to miss or downplay the severity of reactions in the indeterminate pairs, Dr. Warshaw said. “This makes intuitive sense because when you are with a patient live, often the lighting catches an irritant wrinkle reaction or you can feel the lesion and be much more likely to call it irritant or a mild reaction than you would be from a flat photo.”
In the failure group, teledermatology generally overstated reactions, she added.
Dr. Warshaw said that logistical changes would be needed to make teledermatology more effective for reading patch test reactions in her practice. Their method of marking the patch test grid is to use a surgical marker on the corners, but a highlighter to mark the grid between the antigens. The highlighter simply did not show up well in photographs, she noted.
While not perfect, teledermatology does have promise for reading patch test reactions, she added. “I would love to save patients from having to come for their 48-hour reading... In Minnesota we have these horrible snowstorms. Last week there was a blizzard that was predicted. A third of our patients live 2 hours away from the clinic. If they could have taken photographs instead of trying to come through a blizzard for their final reading, that would be helpful.”
Dr. Warshaw noted that their study assessed only the 70 antigens of the North American Contact Dermatitis Research Group series and that it could have been strengthened by using additional series or the patients’ own products.
[email protected]
On Twitter @denisefulton
Key clinical point:
Major finding: Teledermatology readings failed to match in-person final readings 6% of the time.
Data source: Single-site study of 101 patients patch tested with the North American Contact Dermatitis Group series.
Disclosures: Dr. Warshaw declared no relevant conflicts of interest.
Ecofriendly surfactant is allergen of the year
ORLANDO – Alkyl glucosides, mild surfactants derived from natural, sustainable sources, have been named allergen of the year by the American Contact Dermatitis Society.
The ecofriendly nature of these compounds has led to their inclusion in more personal care products in the last decade and a half. Alkyl glucosides are derived from coconut, palm, or rapeseed oil with glucose supplied by corn, wheat starch, or potatoes. They can be found in rinse-off products such as shampoos, shower gels, and liquid cleansers but also in leave-on products such as deodorants, sunscreens, and moisturizers, investigators said at the annual meeting of the American Contact Dermatitis Society, held just prior to the start of the American Academy of Dermatology’s annual meeting.
Camille Loranger, MD, of the department of dermatology, McGill University Health Center, Montreal, presented her institution’s experience with allergic contact dermatitis caused by alkyl glucosides. A total of 3,095 patients were patch tested at the clinic between January 2009 and June 2016. Researchers used the North American Contact Dermatitis Group 65-allergen series, which includes decyl glucoside (5% in petrolatum). Slightly more than half of patients (1,628) also were tested for reactions to lauryl glucoside (3% in petrolatum) as part of an additional cosmetic series. Twenty patients in the larger series reacted to decyl glucoside, while 15 of those who tested for lauryl glucoside reacted. Of those 15 patients, 6 were found to be allergic to decyl glucoside as well (Dermatitis. 2017 Jan/Feb;28[1]:5-13).
Allergy to alkyl glucosides became more common over time in the McGill series. The rate of positivity was low in the early years of the series, but increased from 1.37% of 437 patients in 2014 to 2.2% of 227 patients tested in the first half of 2016, Dr. Loranger said.
“Most of our patients were women with an average age of 48 years,” she added. “Body sites most commonly affected were the head and the hands. Only one case could be attributed to occupational exposure.”
Most patients – 86% – also were atopic (asthma, eczema, and rhinitis).
Products identified as most commonly causing a positive reaction were leave-on moisturizers and hand creams.
Donald V. Belsito, MD, professor of dermatology at Columbia University, N.Y., introduced the allergen of the year, pointing out that the compounds selected are not necessarily “bad actors.”
“The allergen of the year is really chosen to educate dermatologists about allergens that may be of low prevalence but a high relevance,” Dr. Belsito said. The allergens selected “are difficult to test for because they are tested for at irritant concentrations. It doesn’t mean they are these horrible substances that are damaging the world necessarily.”
The ACDS has been naming an allergen of the year since 2004.
[email protected]
On Twitter @denisefulton
ORLANDO – Alkyl glucosides, mild surfactants derived from natural, sustainable sources, have been named allergen of the year by the American Contact Dermatitis Society.
The ecofriendly nature of these compounds has led to their inclusion in more personal care products in the last decade and a half. Alkyl glucosides are derived from coconut, palm, or rapeseed oil with glucose supplied by corn, wheat starch, or potatoes. They can be found in rinse-off products such as shampoos, shower gels, and liquid cleansers but also in leave-on products such as deodorants, sunscreens, and moisturizers, investigators said at the annual meeting of the American Contact Dermatitis Society, held just prior to the start of the American Academy of Dermatology’s annual meeting.
Camille Loranger, MD, of the department of dermatology, McGill University Health Center, Montreal, presented her institution’s experience with allergic contact dermatitis caused by alkyl glucosides. A total of 3,095 patients were patch tested at the clinic between January 2009 and June 2016. Researchers used the North American Contact Dermatitis Group 65-allergen series, which includes decyl glucoside (5% in petrolatum). Slightly more than half of patients (1,628) also were tested for reactions to lauryl glucoside (3% in petrolatum) as part of an additional cosmetic series. Twenty patients in the larger series reacted to decyl glucoside, while 15 of those who tested for lauryl glucoside reacted. Of those 15 patients, 6 were found to be allergic to decyl glucoside as well (Dermatitis. 2017 Jan/Feb;28[1]:5-13).
Allergy to alkyl glucosides became more common over time in the McGill series. The rate of positivity was low in the early years of the series, but increased from 1.37% of 437 patients in 2014 to 2.2% of 227 patients tested in the first half of 2016, Dr. Loranger said.
“Most of our patients were women with an average age of 48 years,” she added. “Body sites most commonly affected were the head and the hands. Only one case could be attributed to occupational exposure.”
Most patients – 86% – also were atopic (asthma, eczema, and rhinitis).
Products identified as most commonly causing a positive reaction were leave-on moisturizers and hand creams.
Donald V. Belsito, MD, professor of dermatology at Columbia University, N.Y., introduced the allergen of the year, pointing out that the compounds selected are not necessarily “bad actors.”
“The allergen of the year is really chosen to educate dermatologists about allergens that may be of low prevalence but a high relevance,” Dr. Belsito said. The allergens selected “are difficult to test for because they are tested for at irritant concentrations. It doesn’t mean they are these horrible substances that are damaging the world necessarily.”
The ACDS has been naming an allergen of the year since 2004.
[email protected]
On Twitter @denisefulton
ORLANDO – Alkyl glucosides, mild surfactants derived from natural, sustainable sources, have been named allergen of the year by the American Contact Dermatitis Society.
The ecofriendly nature of these compounds has led to their inclusion in more personal care products in the last decade and a half. Alkyl glucosides are derived from coconut, palm, or rapeseed oil with glucose supplied by corn, wheat starch, or potatoes. They can be found in rinse-off products such as shampoos, shower gels, and liquid cleansers but also in leave-on products such as deodorants, sunscreens, and moisturizers, investigators said at the annual meeting of the American Contact Dermatitis Society, held just prior to the start of the American Academy of Dermatology’s annual meeting.
Camille Loranger, MD, of the department of dermatology, McGill University Health Center, Montreal, presented her institution’s experience with allergic contact dermatitis caused by alkyl glucosides. A total of 3,095 patients were patch tested at the clinic between January 2009 and June 2016. Researchers used the North American Contact Dermatitis Group 65-allergen series, which includes decyl glucoside (5% in petrolatum). Slightly more than half of patients (1,628) also were tested for reactions to lauryl glucoside (3% in petrolatum) as part of an additional cosmetic series. Twenty patients in the larger series reacted to decyl glucoside, while 15 of those who tested for lauryl glucoside reacted. Of those 15 patients, 6 were found to be allergic to decyl glucoside as well (Dermatitis. 2017 Jan/Feb;28[1]:5-13).
Allergy to alkyl glucosides became more common over time in the McGill series. The rate of positivity was low in the early years of the series, but increased from 1.37% of 437 patients in 2014 to 2.2% of 227 patients tested in the first half of 2016, Dr. Loranger said.
“Most of our patients were women with an average age of 48 years,” she added. “Body sites most commonly affected were the head and the hands. Only one case could be attributed to occupational exposure.”
Most patients – 86% – also were atopic (asthma, eczema, and rhinitis).
Products identified as most commonly causing a positive reaction were leave-on moisturizers and hand creams.
Donald V. Belsito, MD, professor of dermatology at Columbia University, N.Y., introduced the allergen of the year, pointing out that the compounds selected are not necessarily “bad actors.”
“The allergen of the year is really chosen to educate dermatologists about allergens that may be of low prevalence but a high relevance,” Dr. Belsito said. The allergens selected “are difficult to test for because they are tested for at irritant concentrations. It doesn’t mean they are these horrible substances that are damaging the world necessarily.”
The ACDS has been naming an allergen of the year since 2004.
[email protected]
On Twitter @denisefulton
Using Patch Testing to Identify Culprit Agents in Suspected Drug Eruptions


VIDEO: Consider PPIs as a cause of cutaneous reactions
WAILEA, HAWAII – Any proton pump inhibitor (PPI) has the potential to cause skin reactions, so it is important to ask patients about their use, according to J. Mark Jackson, MD, of the University of Louisville (Ky.).
If patients are going to react to a PPI, they usually will do so within 3 or 4 months of starting treatment, rather than in the first week or so of treatment, Dr. Jackson said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Skin reactions to PPIs are often maculopapular, with a flat and a raised component that can be nonspecific, Dr. Jackson noted.
Interestingly, he added, many times patients can switch to a different PPI and not get a skin reaction. However, there are some patients who develop a lupuslike reaction on the skin, and in these cases, there tends to be cross reactivity, “so they couldn’t switch to a different PPI and be risk-free” of the same reaction, he noted.
Dr. Jackson disclosed financial relationships with companies including AbbVie, Amgen, Celgene, Dermira, Galderma, Genentech, Janssen, Lilly, Medimetriks, Merck, Novartis, Pfizer, Promius, and Top MD.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – Any proton pump inhibitor (PPI) has the potential to cause skin reactions, so it is important to ask patients about their use, according to J. Mark Jackson, MD, of the University of Louisville (Ky.).
If patients are going to react to a PPI, they usually will do so within 3 or 4 months of starting treatment, rather than in the first week or so of treatment, Dr. Jackson said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Skin reactions to PPIs are often maculopapular, with a flat and a raised component that can be nonspecific, Dr. Jackson noted.
Interestingly, he added, many times patients can switch to a different PPI and not get a skin reaction. However, there are some patients who develop a lupuslike reaction on the skin, and in these cases, there tends to be cross reactivity, “so they couldn’t switch to a different PPI and be risk-free” of the same reaction, he noted.
Dr. Jackson disclosed financial relationships with companies including AbbVie, Amgen, Celgene, Dermira, Galderma, Genentech, Janssen, Lilly, Medimetriks, Merck, Novartis, Pfizer, Promius, and Top MD.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – Any proton pump inhibitor (PPI) has the potential to cause skin reactions, so it is important to ask patients about their use, according to J. Mark Jackson, MD, of the University of Louisville (Ky.).
If patients are going to react to a PPI, they usually will do so within 3 or 4 months of starting treatment, rather than in the first week or so of treatment, Dr. Jackson said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Skin reactions to PPIs are often maculopapular, with a flat and a raised component that can be nonspecific, Dr. Jackson noted.
Interestingly, he added, many times patients can switch to a different PPI and not get a skin reaction. However, there are some patients who develop a lupuslike reaction on the skin, and in these cases, there tends to be cross reactivity, “so they couldn’t switch to a different PPI and be risk-free” of the same reaction, he noted.
Dr. Jackson disclosed financial relationships with companies including AbbVie, Amgen, Celgene, Dermira, Galderma, Genentech, Janssen, Lilly, Medimetriks, Merck, Novartis, Pfizer, Promius, and Top MD.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT SDEF HAWAII DERMATOLOGY SEMINAR

Contact dermatitis gets personal
Parabens have been eliminated from many personal care products because of health concerns, but from a contact dermatitis standpoint, they have “very low rates of irritancy and allergenicity” and are considered safe and well tolerated, according to Jonathan I. Silverberg, MD, of Northwestern University, Chicago.
“I almost never see a positive reaction to parabens,” Dr. Silverberg said in a presentation on contact dermatitis at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
However, the confirmation of estrogenic activity associated with parabens has led to their replacement in many products – especially personal care products – with other

“MCI/MI is now a common cause of contact dermatitis and can cause severe reactions,” said Dr. Silverberg, director of the Northwestern Medicine Multidisciplinary Eczema Center in Chicago.
An alternative to MCI/MI – methyldibromoglutaronitrile/phenoxyethanol (Euxyl K 400) – also appears in personal care products, such as soaps and shampoos, as well as industrial products such as paints, glues, wood preservatives, and metal-working fluids, Dr. Silverberg noted. This preservative is relatively uncommon in the United States, and in Europe it has been banned from leave-on products since 2005 and from rinse-off products since 2007, he said.
Another paraben alternative, iodopropynyl butylcarbamate, is a relatively uncommon preservative, but it frequently occurs as a positive patch test reaction, Dr. Silverberg said.
Lanolin, a natural ingredient used in topical skin emollients and cosmetics, also has been associated with skin reactions, he added. In addition to personal care products, the increasing range of personal technology products can be sources of contact dermatitis, Dr. Silverberg pointed out. Consider nickel exposure not only from jewelry, but from items such as iPads, iPhones, laptops, and Xbox controllers, when evaluating contact dermatitis in adults and children, he said.
Dr. Silverberg disclosed relationships with companies including AbbVie, Anacor, Celgene, Chugai, Galderma, GlaxoSmithKline, Lilly, Puricore, Medimmune-AstraZeneca, Pfizer, Proctor & Gamble, Puricore, Hoffmann-La Roche, and Regeneron-Sanofi.
SDEF and this news organization are owned by the same parent company.
Parabens have been eliminated from many personal care products because of health concerns, but from a contact dermatitis standpoint, they have “very low rates of irritancy and allergenicity” and are considered safe and well tolerated, according to Jonathan I. Silverberg, MD, of Northwestern University, Chicago.
“I almost never see a positive reaction to parabens,” Dr. Silverberg said in a presentation on contact dermatitis at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
However, the confirmation of estrogenic activity associated with parabens has led to their replacement in many products – especially personal care products – with other
“MCI/MI is now a common cause of contact dermatitis and can cause severe reactions,” said Dr. Silverberg, director of the Northwestern Medicine Multidisciplinary Eczema Center in Chicago.
An alternative to MCI/MI – methyldibromoglutaronitrile/phenoxyethanol (Euxyl K 400) – also appears in personal care products, such as soaps and shampoos, as well as industrial products such as paints, glues, wood preservatives, and metal-working fluids, Dr. Silverberg noted. This preservative is relatively uncommon in the United States, and in Europe it has been banned from leave-on products since 2005 and from rinse-off products since 2007, he said.
Another paraben alternative, iodopropynyl butylcarbamate, is a relatively uncommon preservative, but it frequently occurs as a positive patch test reaction, Dr. Silverberg said.
Lanolin, a natural ingredient used in topical skin emollients and cosmetics, also has been associated with skin reactions, he added. In addition to personal care products, the increasing range of personal technology products can be sources of contact dermatitis, Dr. Silverberg pointed out. Consider nickel exposure not only from jewelry, but from items such as iPads, iPhones, laptops, and Xbox controllers, when evaluating contact dermatitis in adults and children, he said.
Dr. Silverberg disclosed relationships with companies including AbbVie, Anacor, Celgene, Chugai, Galderma, GlaxoSmithKline, Lilly, Puricore, Medimmune-AstraZeneca, Pfizer, Proctor & Gamble, Puricore, Hoffmann-La Roche, and Regeneron-Sanofi.
SDEF and this news organization are owned by the same parent company.
Parabens have been eliminated from many personal care products because of health concerns, but from a contact dermatitis standpoint, they have “very low rates of irritancy and allergenicity” and are considered safe and well tolerated, according to Jonathan I. Silverberg, MD, of Northwestern University, Chicago.
“I almost never see a positive reaction to parabens,” Dr. Silverberg said in a presentation on contact dermatitis at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
However, the confirmation of estrogenic activity associated with parabens has led to their replacement in many products – especially personal care products – with other
“MCI/MI is now a common cause of contact dermatitis and can cause severe reactions,” said Dr. Silverberg, director of the Northwestern Medicine Multidisciplinary Eczema Center in Chicago.
An alternative to MCI/MI – methyldibromoglutaronitrile/phenoxyethanol (Euxyl K 400) – also appears in personal care products, such as soaps and shampoos, as well as industrial products such as paints, glues, wood preservatives, and metal-working fluids, Dr. Silverberg noted. This preservative is relatively uncommon in the United States, and in Europe it has been banned from leave-on products since 2005 and from rinse-off products since 2007, he said.
Another paraben alternative, iodopropynyl butylcarbamate, is a relatively uncommon preservative, but it frequently occurs as a positive patch test reaction, Dr. Silverberg said.
Lanolin, a natural ingredient used in topical skin emollients and cosmetics, also has been associated with skin reactions, he added. In addition to personal care products, the increasing range of personal technology products can be sources of contact dermatitis, Dr. Silverberg pointed out. Consider nickel exposure not only from jewelry, but from items such as iPads, iPhones, laptops, and Xbox controllers, when evaluating contact dermatitis in adults and children, he said.
Dr. Silverberg disclosed relationships with companies including AbbVie, Anacor, Celgene, Chugai, Galderma, GlaxoSmithKline, Lilly, Puricore, Medimmune-AstraZeneca, Pfizer, Proctor & Gamble, Puricore, Hoffmann-La Roche, and Regeneron-Sanofi.
SDEF and this news organization are owned by the same parent company.
FROM SDEF HAWAII DERMATOLOGY SEMINAR