User login
FDA approves plasma product

The FDA has approved a pooled plasma blood product (Octaplas) that can be used to replace coagulation factors in patients with certain medical conditions.
The product is a sterile, frozen solution of human plasma from several donors that has been treated with a solvent detergent process to minimize the risk of serious virus transmission.
The plasma used to manufacture Octaplas is collected from US donors who have been screened and tested for diseases transmitted by blood.
“For patients suffering with clotting disorders, this product provides a viable alternative to single-donor fresh-frozen plasma [FFP] and provides a reduced risk of certain viral transmissions,” said Karen Midthun, MD, director of the FDA’s Center for Biologics Evaluation and Research.
Indications and administration
Octaplas is indicated for the replacement of multiple coagulation factors in patients with acquired deficiencies due to liver disease or undergoing cardiac surgery or liver transplant. Octaplas can also be
used for plasma exchange in patients with thrombotic thrombocytopenic purpura (TTP).
Like FFP, Octaplas should be matched to the recipient’s blood group to help avoid transfusion reactions. Each lot of Octaplas is tested for composition of key clotting factors and is only released if the levels are within acceptable ranges.
The product is administered by intravenous infusion after thawing, using an infusion set with a filter. An aseptic technique must be used throughout the infusion.
The dosage depends upon the clinical situation and the underlying disorder. But 12-15 mL/kg of body weight is a generally accepted starting dose, and it should increase the patient’s plasma coagulation factor levels by about 25%.
It is important to monitor patient response, both clinically and with measurement of prothrombin time, partial thromboplastin time, and/or specific coagulation factor assays.
Prior experience with Octaplas
The FDA’s approval of Octaplas was primarily based on studies conducted in patients with liver disease, liver transplant, heart surgery, and TTP. The most common adverse reactions observed in these trials were shortness of breath, dizziness, chest discomfort, pruritis/rash, headache, and paresthesia.
Additional data supporting the safe use of Octaplas for the US market came from prior use of the product in Europe and other approved markets, where it has been used extensively.
A previous generation of Octaplas was first marketed in 1992, and the current version has been marketed since 2006. In total, more than 2 million patients outside the US have been treated with more than 7 million doses of Octaplas.
The product is manufactured by Octapharma, located in Vienna, Austria. For more information on Octaplas, visit the Octapharma website. ![]()
The FDA has approved a pooled plasma blood product (Octaplas) that can be used to replace coagulation factors in patients with certain medical conditions.
The product is a sterile, frozen solution of human plasma from several donors that has been treated with a solvent detergent process to minimize the risk of serious virus transmission.
The plasma used to manufacture Octaplas is collected from US donors who have been screened and tested for diseases transmitted by blood.
“For patients suffering with clotting disorders, this product provides a viable alternative to single-donor fresh-frozen plasma [FFP] and provides a reduced risk of certain viral transmissions,” said Karen Midthun, MD, director of the FDA’s Center for Biologics Evaluation and Research.
Indications and administration
Octaplas is indicated for the replacement of multiple coagulation factors in patients with acquired deficiencies due to liver disease or undergoing cardiac surgery or liver transplant. Octaplas can also be
used for plasma exchange in patients with thrombotic thrombocytopenic purpura (TTP).
Like FFP, Octaplas should be matched to the recipient’s blood group to help avoid transfusion reactions. Each lot of Octaplas is tested for composition of key clotting factors and is only released if the levels are within acceptable ranges.
The product is administered by intravenous infusion after thawing, using an infusion set with a filter. An aseptic technique must be used throughout the infusion.
The dosage depends upon the clinical situation and the underlying disorder. But 12-15 mL/kg of body weight is a generally accepted starting dose, and it should increase the patient’s plasma coagulation factor levels by about 25%.
It is important to monitor patient response, both clinically and with measurement of prothrombin time, partial thromboplastin time, and/or specific coagulation factor assays.
Prior experience with Octaplas
The FDA’s approval of Octaplas was primarily based on studies conducted in patients with liver disease, liver transplant, heart surgery, and TTP. The most common adverse reactions observed in these trials were shortness of breath, dizziness, chest discomfort, pruritis/rash, headache, and paresthesia.
Additional data supporting the safe use of Octaplas for the US market came from prior use of the product in Europe and other approved markets, where it has been used extensively.
A previous generation of Octaplas was first marketed in 1992, and the current version has been marketed since 2006. In total, more than 2 million patients outside the US have been treated with more than 7 million doses of Octaplas.
The product is manufactured by Octapharma, located in Vienna, Austria. For more information on Octaplas, visit the Octapharma website. ![]()
The FDA has approved a pooled plasma blood product (Octaplas) that can be used to replace coagulation factors in patients with certain medical conditions.
The product is a sterile, frozen solution of human plasma from several donors that has been treated with a solvent detergent process to minimize the risk of serious virus transmission.
The plasma used to manufacture Octaplas is collected from US donors who have been screened and tested for diseases transmitted by blood.
“For patients suffering with clotting disorders, this product provides a viable alternative to single-donor fresh-frozen plasma [FFP] and provides a reduced risk of certain viral transmissions,” said Karen Midthun, MD, director of the FDA’s Center for Biologics Evaluation and Research.
Indications and administration
Octaplas is indicated for the replacement of multiple coagulation factors in patients with acquired deficiencies due to liver disease or undergoing cardiac surgery or liver transplant. Octaplas can also be
used for plasma exchange in patients with thrombotic thrombocytopenic purpura (TTP).
Like FFP, Octaplas should be matched to the recipient’s blood group to help avoid transfusion reactions. Each lot of Octaplas is tested for composition of key clotting factors and is only released if the levels are within acceptable ranges.
The product is administered by intravenous infusion after thawing, using an infusion set with a filter. An aseptic technique must be used throughout the infusion.
The dosage depends upon the clinical situation and the underlying disorder. But 12-15 mL/kg of body weight is a generally accepted starting dose, and it should increase the patient’s plasma coagulation factor levels by about 25%.
It is important to monitor patient response, both clinically and with measurement of prothrombin time, partial thromboplastin time, and/or specific coagulation factor assays.
Prior experience with Octaplas
The FDA’s approval of Octaplas was primarily based on studies conducted in patients with liver disease, liver transplant, heart surgery, and TTP. The most common adverse reactions observed in these trials were shortness of breath, dizziness, chest discomfort, pruritis/rash, headache, and paresthesia.
Additional data supporting the safe use of Octaplas for the US market came from prior use of the product in Europe and other approved markets, where it has been used extensively.
A previous generation of Octaplas was first marketed in 1992, and the current version has been marketed since 2006. In total, more than 2 million patients outside the US have been treated with more than 7 million doses of Octaplas.
The product is manufactured by Octapharma, located in Vienna, Austria. For more information on Octaplas, visit the Octapharma website. ![]()
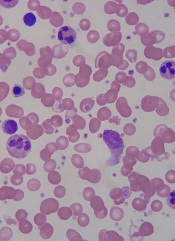
Despite efficacy, most patients discontinued therapy

In a multicenter trial, deferasirox reduced serum ferritin and labile plasma iron (LPI) in transfusion-dependent patients with myelodysplastic syndrome (MDS). A subset of patients also experienced improvements in hematologic parameters.
In spite of these results, nearly 80% of patients discontinued therapy. But researchers said only about 40% of the discontinuations were drug-related; ie, a result of adverse events, abnormal lab values, or drug inefficacy.
Alan F. List, MD, of the Moffitt Cancer Center in Tampa, Florida, and his colleagues reported these results in the Journal of Clinical Oncology. The team’s research was supported by Novartis Pharmaceuticals, the maker of deferasirox.
The researchers analyzed the effects of the drug in 173 patients with low- or intermediate-1-risk MDS. The median patient age was 71 years (range, 21 to 90 years).
Patients had serum ferritin of at least 1000 μg/L, had received at least 20 units of red blood cells, and had ongoing transfusion requirements. The starting dose of deferasirox was 20 mg/kg per day, with dose escalation up to 40 mg/kg per day.
Patients who completed 1 year of therapy (n=91) experienced a median decrease in serum ferritin of 23%. Serum ferritin decreased by 36.7% in patients who completed 2 years of therapy (n=49) and 36.5% in patients who completed 3 years of therapy (n=33).
The investigators measured LPI quarterly during the first year of the study. Nearly 40% of patients (n=68) had elevated LPI at baseline. But, by week 13, LPI levels had normalized in all of the patients.
Twenty-eight percent of patients (n=51) experienced hematologic improvements according to International Working Group 2006 criteria. However, 7 of these patients had received growth factors or MDS therapy.
By the end of the study period, 79.8% of patients (n=138) had discontinued therapy. The reasons included adverse events in 24.8% (n=43), death in 16.1% (n=28), administrative problems in 15.4% (n=27), and abnormal lab values in 13.2% (n=23).
In addition, 6.9% of patients (n=12) chose not to enroll in the extension phase of the study, and 1.7% of patients (n=3) reported an unsatisfactory therapeutic effect. In 1.1% of cases (n=2), the patient no longer required the drug.
The most common drug-related adverse events were gastrointestinal disturbances and increased serum creatinine. Of the 28 patient deaths, none were linked to deferasirox.
“Overall, this study demonstrated improvements in iron parameters in a group of heavily transfused, lower-risk patients with MDS,” Dr List said. “A randomized trial is warranted to better ascertain the clinical impact of deferasirox therapy in lower-risk patients with MDS.” ![]()
In a multicenter trial, deferasirox reduced serum ferritin and labile plasma iron (LPI) in transfusion-dependent patients with myelodysplastic syndrome (MDS). A subset of patients also experienced improvements in hematologic parameters.
In spite of these results, nearly 80% of patients discontinued therapy. But researchers said only about 40% of the discontinuations were drug-related; ie, a result of adverse events, abnormal lab values, or drug inefficacy.
Alan F. List, MD, of the Moffitt Cancer Center in Tampa, Florida, and his colleagues reported these results in the Journal of Clinical Oncology. The team’s research was supported by Novartis Pharmaceuticals, the maker of deferasirox.
The researchers analyzed the effects of the drug in 173 patients with low- or intermediate-1-risk MDS. The median patient age was 71 years (range, 21 to 90 years).
Patients had serum ferritin of at least 1000 μg/L, had received at least 20 units of red blood cells, and had ongoing transfusion requirements. The starting dose of deferasirox was 20 mg/kg per day, with dose escalation up to 40 mg/kg per day.
Patients who completed 1 year of therapy (n=91) experienced a median decrease in serum ferritin of 23%. Serum ferritin decreased by 36.7% in patients who completed 2 years of therapy (n=49) and 36.5% in patients who completed 3 years of therapy (n=33).
The investigators measured LPI quarterly during the first year of the study. Nearly 40% of patients (n=68) had elevated LPI at baseline. But, by week 13, LPI levels had normalized in all of the patients.
Twenty-eight percent of patients (n=51) experienced hematologic improvements according to International Working Group 2006 criteria. However, 7 of these patients had received growth factors or MDS therapy.
By the end of the study period, 79.8% of patients (n=138) had discontinued therapy. The reasons included adverse events in 24.8% (n=43), death in 16.1% (n=28), administrative problems in 15.4% (n=27), and abnormal lab values in 13.2% (n=23).
In addition, 6.9% of patients (n=12) chose not to enroll in the extension phase of the study, and 1.7% of patients (n=3) reported an unsatisfactory therapeutic effect. In 1.1% of cases (n=2), the patient no longer required the drug.
The most common drug-related adverse events were gastrointestinal disturbances and increased serum creatinine. Of the 28 patient deaths, none were linked to deferasirox.
“Overall, this study demonstrated improvements in iron parameters in a group of heavily transfused, lower-risk patients with MDS,” Dr List said. “A randomized trial is warranted to better ascertain the clinical impact of deferasirox therapy in lower-risk patients with MDS.” ![]()
In a multicenter trial, deferasirox reduced serum ferritin and labile plasma iron (LPI) in transfusion-dependent patients with myelodysplastic syndrome (MDS). A subset of patients also experienced improvements in hematologic parameters.
In spite of these results, nearly 80% of patients discontinued therapy. But researchers said only about 40% of the discontinuations were drug-related; ie, a result of adverse events, abnormal lab values, or drug inefficacy.
Alan F. List, MD, of the Moffitt Cancer Center in Tampa, Florida, and his colleagues reported these results in the Journal of Clinical Oncology. The team’s research was supported by Novartis Pharmaceuticals, the maker of deferasirox.
The researchers analyzed the effects of the drug in 173 patients with low- or intermediate-1-risk MDS. The median patient age was 71 years (range, 21 to 90 years).
Patients had serum ferritin of at least 1000 μg/L, had received at least 20 units of red blood cells, and had ongoing transfusion requirements. The starting dose of deferasirox was 20 mg/kg per day, with dose escalation up to 40 mg/kg per day.
Patients who completed 1 year of therapy (n=91) experienced a median decrease in serum ferritin of 23%. Serum ferritin decreased by 36.7% in patients who completed 2 years of therapy (n=49) and 36.5% in patients who completed 3 years of therapy (n=33).
The investigators measured LPI quarterly during the first year of the study. Nearly 40% of patients (n=68) had elevated LPI at baseline. But, by week 13, LPI levels had normalized in all of the patients.
Twenty-eight percent of patients (n=51) experienced hematologic improvements according to International Working Group 2006 criteria. However, 7 of these patients had received growth factors or MDS therapy.
By the end of the study period, 79.8% of patients (n=138) had discontinued therapy. The reasons included adverse events in 24.8% (n=43), death in 16.1% (n=28), administrative problems in 15.4% (n=27), and abnormal lab values in 13.2% (n=23).
In addition, 6.9% of patients (n=12) chose not to enroll in the extension phase of the study, and 1.7% of patients (n=3) reported an unsatisfactory therapeutic effect. In 1.1% of cases (n=2), the patient no longer required the drug.
The most common drug-related adverse events were gastrointestinal disturbances and increased serum creatinine. Of the 28 patient deaths, none were linked to deferasirox.
“Overall, this study demonstrated improvements in iron parameters in a group of heavily transfused, lower-risk patients with MDS,” Dr List said. “A randomized trial is warranted to better ascertain the clinical impact of deferasirox therapy in lower-risk patients with MDS.” ![]()
Drug for aHUS effective but expensive

Congress of the EHA
Photo courtesy of EHA
AMSTERDAM—Eculizumab elicits “phenomenal” results in atypical hemolytic uremic syndrome (aHUS), according to two presentations given at the 17th Annual Congress of the European Hematology Association.
But, as one speaker pointed out, the drug may prove too expensive for a lot of patients.
“It’s the most expensive drug I’ve ever come across in my entire life,” said Adrian Newland, MD, of Barts and The London School of Medicine and Dentistry in the UK.
He noted that the drug costs about £400,000 per year in the UK. And reports have listed the US cost at around $400,000 per year.
Expense aside, the drug elicits “dramatic” improvements in aHUS patients, according to Dr Newland. And he presented data to support that statement during an EHA-JSH joint symposium on platelet disorders.
Ramon Vilalta, MD, of Hospital Vall d’Hebron in Barcelona, Spain, also presented favorable results with eculizumab at the meeting, as abstract 1155.
Dr Vilalta began his presentation by pointing out that aHUS is a life-threatening disease that results in multi-organ damage caused by thrombotic microangiopathy (TMA). And plasma exchange/plasma infusion (PE/PI) therapy does little to alter the poor prognosis in this patient population.
“Our patients—pediatric patients mainly—develop end-stage renal failure and even die, despite treatment [with PE/PI],” he said. “[E]culizumab is an anti-C5 terminal complement blocker that could give some hope in the treatment of these patients.”
In an attempt to prove this theory, Dr Vilalta and his colleagues retrospectively analyzed 19 patients with aHUS. Patients—who ranged in age from 2 months to 17 years—received eculizumab for a median of 6 months (range, less than 1 month to 16 months).
All 19 patients had renal complications prior to receiving eculizumab, and 10 had renal and extra-renal complications. Eight patients had baseline platelet counts less than 150 x 109/L. Eight patients were on dialysis at the start of therapy, and 6 patients had undergone kidney transplant.
The first thing the researchers noticed was that eculizumab increased patients’ platelet counts within a week of administration. And this effect was maintained throughout the study period.
Seven of the 8 patients (88%) with abnormal platelet counts at baseline achieved normalized platelet counts. And 89% of all the patients (17/19) had platelet counts of 150 x 109/L or greater at the data cutoff point.
Eculizumab also reduced the burden of disease, Dr Vilalta said. He and his colleagues observed a significant reduction in the TMA intervention rate, which included the number of PE/PIs and new dialysis events. There were a median of 2 interventions per patient per week before treatment initiation, and a median of 0 interventions during treatment (P<0.0001).
None of the patients required new dialysis, and eculizumab eliminated the need for dialysis in 50% of patients (4/8).
Dr Vilalta also pointed out that eculizumab demonstrated similar efficacy regardless of patients’ mutation status or age. He added that the drug appeared to be well-tolerated, although the retrospective nature of the study did not allow for the full collection of drug-specific adverse events.
Of the side effects the researchers did observe, most were mild or moderate. Nine patients experienced pyrexia, 6 had diarrhea, 6 developed an upper respiratory tract infection, 5 developed a cough, 4 experienced vomiting, 4 had nasal congestion, 4 had tachycardia, and 1 patient developed a meningococcal infection during follow-up.
Dr Newland presented similar results from another study of eculizumab in aHUS. He discussed the results during an EHA-JSH joint symposium on platelet disorders, but the study was also presented at ASH last year as abstract 193.
The study included 17 aHUS patients who received eculizumab for a mean of 58 weeks. All of the patients achieved event-free status, which was defined as 12 weeks or more of stable platelet count, no PE/PI, and no new dialysis. Additionally, 4 of 5 patients were able to discontinue dialysis as a result of treatment with eculizumab.
As in Dr Vilalta’s study, treatment was similarly effective in patients with or without complement regulatory factor mutations. And the drug was generally well-tolerated. Twelve patients experienced adverse events, 1 of which was severe.
“[Eculizumab] showed phenomenal results here,” Dr Newland said. “Patients, particularly those treated earlier in their disease, were able to normalize their renal function.”
He said such an improvement is “dramatic” for this patient population, as 25% of aHUS patients die with the first attack, and 50% go into end-stage renal disease. Therefore, eculizumab can be considered the standard of care for aHUS patients—“if [they] can afford it.” ![]()
Congress of the EHA
Photo courtesy of EHA
AMSTERDAM—Eculizumab elicits “phenomenal” results in atypical hemolytic uremic syndrome (aHUS), according to two presentations given at the 17th Annual Congress of the European Hematology Association.
But, as one speaker pointed out, the drug may prove too expensive for a lot of patients.
“It’s the most expensive drug I’ve ever come across in my entire life,” said Adrian Newland, MD, of Barts and The London School of Medicine and Dentistry in the UK.
He noted that the drug costs about £400,000 per year in the UK. And reports have listed the US cost at around $400,000 per year.
Expense aside, the drug elicits “dramatic” improvements in aHUS patients, according to Dr Newland. And he presented data to support that statement during an EHA-JSH joint symposium on platelet disorders.
Ramon Vilalta, MD, of Hospital Vall d’Hebron in Barcelona, Spain, also presented favorable results with eculizumab at the meeting, as abstract 1155.
Dr Vilalta began his presentation by pointing out that aHUS is a life-threatening disease that results in multi-organ damage caused by thrombotic microangiopathy (TMA). And plasma exchange/plasma infusion (PE/PI) therapy does little to alter the poor prognosis in this patient population.
“Our patients—pediatric patients mainly—develop end-stage renal failure and even die, despite treatment [with PE/PI],” he said. “[E]culizumab is an anti-C5 terminal complement blocker that could give some hope in the treatment of these patients.”
In an attempt to prove this theory, Dr Vilalta and his colleagues retrospectively analyzed 19 patients with aHUS. Patients—who ranged in age from 2 months to 17 years—received eculizumab for a median of 6 months (range, less than 1 month to 16 months).
All 19 patients had renal complications prior to receiving eculizumab, and 10 had renal and extra-renal complications. Eight patients had baseline platelet counts less than 150 x 109/L. Eight patients were on dialysis at the start of therapy, and 6 patients had undergone kidney transplant.
The first thing the researchers noticed was that eculizumab increased patients’ platelet counts within a week of administration. And this effect was maintained throughout the study period.
Seven of the 8 patients (88%) with abnormal platelet counts at baseline achieved normalized platelet counts. And 89% of all the patients (17/19) had platelet counts of 150 x 109/L or greater at the data cutoff point.
Eculizumab also reduced the burden of disease, Dr Vilalta said. He and his colleagues observed a significant reduction in the TMA intervention rate, which included the number of PE/PIs and new dialysis events. There were a median of 2 interventions per patient per week before treatment initiation, and a median of 0 interventions during treatment (P<0.0001).
None of the patients required new dialysis, and eculizumab eliminated the need for dialysis in 50% of patients (4/8).
Dr Vilalta also pointed out that eculizumab demonstrated similar efficacy regardless of patients’ mutation status or age. He added that the drug appeared to be well-tolerated, although the retrospective nature of the study did not allow for the full collection of drug-specific adverse events.
Of the side effects the researchers did observe, most were mild or moderate. Nine patients experienced pyrexia, 6 had diarrhea, 6 developed an upper respiratory tract infection, 5 developed a cough, 4 experienced vomiting, 4 had nasal congestion, 4 had tachycardia, and 1 patient developed a meningococcal infection during follow-up.
Dr Newland presented similar results from another study of eculizumab in aHUS. He discussed the results during an EHA-JSH joint symposium on platelet disorders, but the study was also presented at ASH last year as abstract 193.
The study included 17 aHUS patients who received eculizumab for a mean of 58 weeks. All of the patients achieved event-free status, which was defined as 12 weeks or more of stable platelet count, no PE/PI, and no new dialysis. Additionally, 4 of 5 patients were able to discontinue dialysis as a result of treatment with eculizumab.
As in Dr Vilalta’s study, treatment was similarly effective in patients with or without complement regulatory factor mutations. And the drug was generally well-tolerated. Twelve patients experienced adverse events, 1 of which was severe.
“[Eculizumab] showed phenomenal results here,” Dr Newland said. “Patients, particularly those treated earlier in their disease, were able to normalize their renal function.”
He said such an improvement is “dramatic” for this patient population, as 25% of aHUS patients die with the first attack, and 50% go into end-stage renal disease. Therefore, eculizumab can be considered the standard of care for aHUS patients—“if [they] can afford it.” ![]()
Congress of the EHA
Photo courtesy of EHA
AMSTERDAM—Eculizumab elicits “phenomenal” results in atypical hemolytic uremic syndrome (aHUS), according to two presentations given at the 17th Annual Congress of the European Hematology Association.
But, as one speaker pointed out, the drug may prove too expensive for a lot of patients.
“It’s the most expensive drug I’ve ever come across in my entire life,” said Adrian Newland, MD, of Barts and The London School of Medicine and Dentistry in the UK.
He noted that the drug costs about £400,000 per year in the UK. And reports have listed the US cost at around $400,000 per year.
Expense aside, the drug elicits “dramatic” improvements in aHUS patients, according to Dr Newland. And he presented data to support that statement during an EHA-JSH joint symposium on platelet disorders.
Ramon Vilalta, MD, of Hospital Vall d’Hebron in Barcelona, Spain, also presented favorable results with eculizumab at the meeting, as abstract 1155.
Dr Vilalta began his presentation by pointing out that aHUS is a life-threatening disease that results in multi-organ damage caused by thrombotic microangiopathy (TMA). And plasma exchange/plasma infusion (PE/PI) therapy does little to alter the poor prognosis in this patient population.
“Our patients—pediatric patients mainly—develop end-stage renal failure and even die, despite treatment [with PE/PI],” he said. “[E]culizumab is an anti-C5 terminal complement blocker that could give some hope in the treatment of these patients.”
In an attempt to prove this theory, Dr Vilalta and his colleagues retrospectively analyzed 19 patients with aHUS. Patients—who ranged in age from 2 months to 17 years—received eculizumab for a median of 6 months (range, less than 1 month to 16 months).
All 19 patients had renal complications prior to receiving eculizumab, and 10 had renal and extra-renal complications. Eight patients had baseline platelet counts less than 150 x 109/L. Eight patients were on dialysis at the start of therapy, and 6 patients had undergone kidney transplant.
The first thing the researchers noticed was that eculizumab increased patients’ platelet counts within a week of administration. And this effect was maintained throughout the study period.
Seven of the 8 patients (88%) with abnormal platelet counts at baseline achieved normalized platelet counts. And 89% of all the patients (17/19) had platelet counts of 150 x 109/L or greater at the data cutoff point.
Eculizumab also reduced the burden of disease, Dr Vilalta said. He and his colleagues observed a significant reduction in the TMA intervention rate, which included the number of PE/PIs and new dialysis events. There were a median of 2 interventions per patient per week before treatment initiation, and a median of 0 interventions during treatment (P<0.0001).
None of the patients required new dialysis, and eculizumab eliminated the need for dialysis in 50% of patients (4/8).
Dr Vilalta also pointed out that eculizumab demonstrated similar efficacy regardless of patients’ mutation status or age. He added that the drug appeared to be well-tolerated, although the retrospective nature of the study did not allow for the full collection of drug-specific adverse events.
Of the side effects the researchers did observe, most were mild or moderate. Nine patients experienced pyrexia, 6 had diarrhea, 6 developed an upper respiratory tract infection, 5 developed a cough, 4 experienced vomiting, 4 had nasal congestion, 4 had tachycardia, and 1 patient developed a meningococcal infection during follow-up.
Dr Newland presented similar results from another study of eculizumab in aHUS. He discussed the results during an EHA-JSH joint symposium on platelet disorders, but the study was also presented at ASH last year as abstract 193.
The study included 17 aHUS patients who received eculizumab for a mean of 58 weeks. All of the patients achieved event-free status, which was defined as 12 weeks or more of stable platelet count, no PE/PI, and no new dialysis. Additionally, 4 of 5 patients were able to discontinue dialysis as a result of treatment with eculizumab.
As in Dr Vilalta’s study, treatment was similarly effective in patients with or without complement regulatory factor mutations. And the drug was generally well-tolerated. Twelve patients experienced adverse events, 1 of which was severe.
“[Eculizumab] showed phenomenal results here,” Dr Newland said. “Patients, particularly those treated earlier in their disease, were able to normalize their renal function.”
He said such an improvement is “dramatic” for this patient population, as 25% of aHUS patients die with the first attack, and 50% go into end-stage renal disease. Therefore, eculizumab can be considered the standard of care for aHUS patients—“if [they] can afford it.” ![]()
Hematologists, Hospitalists Differ in Care of Sickle Cell Patients
SAN DIEGO – When caring for patients with sickle cell disease who were hospitalized for vaso-occlusive crisis, hospitalists more often used demand-only patient-controlled analgesia, compared with hematologists.
In addition, symptoms of acute chest syndrome were reported more often among patients cared for by hospitalists than by those cared for by hematologists.
The findings, reported during a poster session at the annual meeting of the American Society of Hematology, underscore the need for improved collaboration between hematologists and hospitalists in the care of patients with sickle cell disease.

These patients have been "increasingly managed by hospitalists rather than adult hematology specialists," the researchers, led by Dr. Nirmish Shah, wrote in their abstract. "Hospitalists provide efficient inpatient management; however, many possess knowledge gaps and carry biases into their relationship with patients with sickle cell disease."
In an effort to better understand the differences between hematologists and hospitalists in the care practices of this patient population, Dr. Shah and his associates reviewed the records of 298 patients with sickle cell disease who were hospitalized for vaso-occlusive crisis at Duke University Medical Center, Durham, N.C., between Sept. 1, 2008, and Jan. 31, 2011. In November of 2009, all inpatient care for patients with sickle cell disease was moved from the hematologists to the hospitalist service, said Dr. Shah, who directs the medical center’s sickle cell transition program.
Of the 298 patients, 120 were cared for by hematologists over 13 months while 178 were cared for by hospitalists over 13 months. The mean age of patients was 32 years.
There were no significant differences between hematologists and hospitalists in standard ordering practices including incentive spirometry, a bowel regimen, an anti-itching medication, and DVT prophylaxis. However, patients cared for by a hematologist had a higher total number of hours on a patient-controlled analgesia device (212 vs. 171 hours).
Dr. Shah also reported that, compared with hospitalists, hematologists were significantly less likely to use demand-only patient-controlled analgesia (23% vs. 42%) and significantly more likely to use both continuous and demand patient-controlled analgesia (67% vs. 54%).
Transfusions were similarly used by clinicians in both specialties. However, the number of units transfused was higher for hematologists, compared with hospitalists (a mean of 2.6 units vs. 1.9 units).
Erythrocytapheresis was used more often by hematologists than by hospitalists, but this difference did not reach statistical significance (6.7% vs. 2.2%).
No patients cared for by hematologists were diagnosed with acute chest syndrome, but 5.6% of those cared for by hospitalists were. In addition, patients cared for by hematologists had a significantly longer hospitalization, compared with those cared for by hospitalists (a mean of 10 days vs. 8.4 days, respectively) and a nonsignificantly lower 7-day readmission rate (6.7% vs. 7.2%) and 30-day readmission rate (35% vs. 40%).
"There often is a knowledge gap in hospitalist care of sickle cell patients," Dr. Shah said in an interview. "Because they may have a gap, it is our job as hematologists to be available as consultants. In addition, we should decide on the right method for controlling pain in this population of patients. I’m not trying to say that [hospitalists are] doing something in a wrong fashion. I think it brings up the idea that we need to collaborate more. At our hospital we’re assigning a nurse practitioner to round independently and help assist hospitalists now, in an attempt to improve our care for patients with sickle cell disease."
Dr. Shah said that he had no relevant financial disclosures.
(**Corrected: An earlier version of this story referred to "anesthesia" rather than "analgesia.")
SAN DIEGO – When caring for patients with sickle cell disease who were hospitalized for vaso-occlusive crisis, hospitalists more often used demand-only patient-controlled analgesia, compared with hematologists.
In addition, symptoms of acute chest syndrome were reported more often among patients cared for by hospitalists than by those cared for by hematologists.
The findings, reported during a poster session at the annual meeting of the American Society of Hematology, underscore the need for improved collaboration between hematologists and hospitalists in the care of patients with sickle cell disease.
These patients have been "increasingly managed by hospitalists rather than adult hematology specialists," the researchers, led by Dr. Nirmish Shah, wrote in their abstract. "Hospitalists provide efficient inpatient management; however, many possess knowledge gaps and carry biases into their relationship with patients with sickle cell disease."
In an effort to better understand the differences between hematologists and hospitalists in the care practices of this patient population, Dr. Shah and his associates reviewed the records of 298 patients with sickle cell disease who were hospitalized for vaso-occlusive crisis at Duke University Medical Center, Durham, N.C., between Sept. 1, 2008, and Jan. 31, 2011. In November of 2009, all inpatient care for patients with sickle cell disease was moved from the hematologists to the hospitalist service, said Dr. Shah, who directs the medical center’s sickle cell transition program.
Of the 298 patients, 120 were cared for by hematologists over 13 months while 178 were cared for by hospitalists over 13 months. The mean age of patients was 32 years.
There were no significant differences between hematologists and hospitalists in standard ordering practices including incentive spirometry, a bowel regimen, an anti-itching medication, and DVT prophylaxis. However, patients cared for by a hematologist had a higher total number of hours on a patient-controlled analgesia device (212 vs. 171 hours).
Dr. Shah also reported that, compared with hospitalists, hematologists were significantly less likely to use demand-only patient-controlled analgesia (23% vs. 42%) and significantly more likely to use both continuous and demand patient-controlled analgesia (67% vs. 54%).
Transfusions were similarly used by clinicians in both specialties. However, the number of units transfused was higher for hematologists, compared with hospitalists (a mean of 2.6 units vs. 1.9 units).
Erythrocytapheresis was used more often by hematologists than by hospitalists, but this difference did not reach statistical significance (6.7% vs. 2.2%).
No patients cared for by hematologists were diagnosed with acute chest syndrome, but 5.6% of those cared for by hospitalists were. In addition, patients cared for by hematologists had a significantly longer hospitalization, compared with those cared for by hospitalists (a mean of 10 days vs. 8.4 days, respectively) and a nonsignificantly lower 7-day readmission rate (6.7% vs. 7.2%) and 30-day readmission rate (35% vs. 40%).
"There often is a knowledge gap in hospitalist care of sickle cell patients," Dr. Shah said in an interview. "Because they may have a gap, it is our job as hematologists to be available as consultants. In addition, we should decide on the right method for controlling pain in this population of patients. I’m not trying to say that [hospitalists are] doing something in a wrong fashion. I think it brings up the idea that we need to collaborate more. At our hospital we’re assigning a nurse practitioner to round independently and help assist hospitalists now, in an attempt to improve our care for patients with sickle cell disease."
Dr. Shah said that he had no relevant financial disclosures.
(**Corrected: An earlier version of this story referred to "anesthesia" rather than "analgesia.")
SAN DIEGO – When caring for patients with sickle cell disease who were hospitalized for vaso-occlusive crisis, hospitalists more often used demand-only patient-controlled analgesia, compared with hematologists.
In addition, symptoms of acute chest syndrome were reported more often among patients cared for by hospitalists than by those cared for by hematologists.
The findings, reported during a poster session at the annual meeting of the American Society of Hematology, underscore the need for improved collaboration between hematologists and hospitalists in the care of patients with sickle cell disease.
These patients have been "increasingly managed by hospitalists rather than adult hematology specialists," the researchers, led by Dr. Nirmish Shah, wrote in their abstract. "Hospitalists provide efficient inpatient management; however, many possess knowledge gaps and carry biases into their relationship with patients with sickle cell disease."
In an effort to better understand the differences between hematologists and hospitalists in the care practices of this patient population, Dr. Shah and his associates reviewed the records of 298 patients with sickle cell disease who were hospitalized for vaso-occlusive crisis at Duke University Medical Center, Durham, N.C., between Sept. 1, 2008, and Jan. 31, 2011. In November of 2009, all inpatient care for patients with sickle cell disease was moved from the hematologists to the hospitalist service, said Dr. Shah, who directs the medical center’s sickle cell transition program.
Of the 298 patients, 120 were cared for by hematologists over 13 months while 178 were cared for by hospitalists over 13 months. The mean age of patients was 32 years.
There were no significant differences between hematologists and hospitalists in standard ordering practices including incentive spirometry, a bowel regimen, an anti-itching medication, and DVT prophylaxis. However, patients cared for by a hematologist had a higher total number of hours on a patient-controlled analgesia device (212 vs. 171 hours).
Dr. Shah also reported that, compared with hospitalists, hematologists were significantly less likely to use demand-only patient-controlled analgesia (23% vs. 42%) and significantly more likely to use both continuous and demand patient-controlled analgesia (67% vs. 54%).
Transfusions were similarly used by clinicians in both specialties. However, the number of units transfused was higher for hematologists, compared with hospitalists (a mean of 2.6 units vs. 1.9 units).
Erythrocytapheresis was used more often by hematologists than by hospitalists, but this difference did not reach statistical significance (6.7% vs. 2.2%).
No patients cared for by hematologists were diagnosed with acute chest syndrome, but 5.6% of those cared for by hospitalists were. In addition, patients cared for by hematologists had a significantly longer hospitalization, compared with those cared for by hospitalists (a mean of 10 days vs. 8.4 days, respectively) and a nonsignificantly lower 7-day readmission rate (6.7% vs. 7.2%) and 30-day readmission rate (35% vs. 40%).
"There often is a knowledge gap in hospitalist care of sickle cell patients," Dr. Shah said in an interview. "Because they may have a gap, it is our job as hematologists to be available as consultants. In addition, we should decide on the right method for controlling pain in this population of patients. I’m not trying to say that [hospitalists are] doing something in a wrong fashion. I think it brings up the idea that we need to collaborate more. At our hospital we’re assigning a nurse practitioner to round independently and help assist hospitalists now, in an attempt to improve our care for patients with sickle cell disease."
Dr. Shah said that he had no relevant financial disclosures.
(**Corrected: An earlier version of this story referred to "anesthesia" rather than "analgesia.")
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF HEMATOLOGY
Major Finding: Compared with sickle cell patients cared for by a hospitalist, those cared for by a hematologist had more hours on a patient-controlled analgesia device (212 vs. 171 hours). In addition, hematologists were significantly less likely than were hospitalists to use demand-only patient-controlled analgesia (23% vs. 42%) and more likely to use both continuous and demand patient-controlled analgesia (67% vs. 54%).
Data Source: A study of 298 patients with sickle cell disease who were hospitalized for vaso-occlusive crisis at Duke University Medical Center between Sept. 1, 2008, and Jan. 31, 2011.
Disclosures: Dr. Shah said that he had no relevant financial disclosures.
New Data Support Continuing Hydroxyurea for Pediatric Sickle Cell
SAN DIEGO – Mounting data from a federally funded follow-up to the BABY HUG study continue to demonstrate that hydroxyurea is a safe and effective treatment for young children with sickle cell anemia.
The results confirm findings published earlier this year from the Pediatric Hydroxyurea Phase III Clinical Trial (BABY HUG), a randomized, placebo-controlled study sponsored by the National Institutes of Health and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
BABY HUG showed that hydroxyurea administered to 9- to 18-month-old children with sickle cell anemia provides significant clinical benefits, including a decrease in pain crises, acute chest syndrome events, and need for transfusion and hospital admission (Lancet 2011; 377:1663-72).
Hydroxyurea is approved to prevent sickle cell complications in adults with sickle cell anemia, but it is not currently indicated for use in children. Dr. Zora R. Rogers discussed the new data during a press briefing prior to a presentation at the annual meeting of the American Society of Hematology.
"We need to complete the data analysis and to critically examine the growth and development of this population with respect to hydroxyurea use," lead author Dr. Rogers said of the follow-up study, which terminates on Dec. 31, 2011. "But on a macroscopic level there [do] not appear to be any differences observed."
In 2008 Dr. Rogers, professor of pediatrics at the University of Texas Southwestern Medical Center, Dallas, and her associates at 14 centers launched the BABY HUG Follow-Up Study I to assess the safety and efficacy of continued treatment with hydroxyurea in infants with sickle cell anemia. The population consisted of 163 children aged 28-44 months who had participated in the original BABY HUG trial and who had completed at least 18 months of randomized treatment of either hydroxyurea or placebo. The researchers collected clinical and laboratory data every 6 months from patient medical records, including use and dosage of hydroxyurea, blood counts, clinical imaging, and frequency of sickle cell-related complications.
Of the 163 families that enrolled children in the follow-up study, 133 (82%) chose open-label hydroxyurea at the beginning of follow-up and every 6 months 65%-75% of the families reported that their children continued to take the drug. No patient developed intolerance or stopped permanently because of toxicity.
Dr. Rogers, clinical director of the bone marrow failure and general hematology program at Children’s Medical Center, Dallas, presented preliminary analyses as of Oct. 18, 2011, that amounted to 497 patient-years of follow-up. Compared with children who are not taking hydroxyurea, those who continue to take hydroxyurea have statistically lower rates of pain crises requiring emergency department visits (a rate of 29 vs. 54 per 100 patient-years, respectively), episodic transfusions (18 vs. 34 per 100 patient-years), and hospital admissions for any reason (73 vs. 132 per 100 patient-years), including acute chest syndrome or febrile illness.
In their abstract, the researchers pointed out that the decrease in acute chest syndrome episodes "is similar to the effect demonstrated with hydroxyurea use in the randomized BABY HUG trial in younger infants and consistent with published trials detailing the benefit of hydroxyurea therapy in older children and adults. The decrease in the rate of admission for febrile events in hydroxyurea-treated patients is also comparable to that in the randomized trial, but the reason for this benefit is uncertain."
There were no differences between the two groups in hospitalization rates for painful events, including dactylitis. Two patients in the non-hydroxyurea group each had a stroke. There were also no differences between the two groups in the frequency of a palpable spleen or rate of acute splenic sequestration crises. Through 36 months of follow up, children taking hydroxyurea had persistently higher hemoglobin and mean corpuscular volume and lower white blood cell count and absolute neutrophil count, compared with those not taking the drug.
Dr. Susan B. Shurin, acting director of the National Heart, Lung, and Blood Institute (NHLBI), characterized the findings as important in efforts to get an early handle on the burden of disease associated with sickle cell anemia.
"The internists who inherit the patients who have gone through pediatric practitioners have a powerful sense that they reach adolescence doing pretty well, and then things kind of fall apart," Dr. Shurin said. "The clear evidence that prevention of organ damage and prevention of complications of sickle cell anemia would be much preferable to trying to manage once they develop has been the motivation" for this work.
The BABY HUG investigators "believe that ongoing follow-up of this cohort is essential to continue to define the potential benefits as the children grow and to observe for late toxicity," Dr. Rogers said. "We are in final discussions with the NHLBI for an additional contract in support of 5 more years of follow-up."
The researchers intend to use the current findings "in support of an FDA application potentially to allow an indication for the use of hydroxyurea in very young children," Dr. Rogers said. "We are also hoping that there will be an interest for the use of this medication in a liquid format, because it’s very hard to get a 1-year-old to take a capsule."
The follow-up study is funded by the National Heart, Lung, and Blood Institute and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
SAN DIEGO – Mounting data from a federally funded follow-up to the BABY HUG study continue to demonstrate that hydroxyurea is a safe and effective treatment for young children with sickle cell anemia.
The results confirm findings published earlier this year from the Pediatric Hydroxyurea Phase III Clinical Trial (BABY HUG), a randomized, placebo-controlled study sponsored by the National Institutes of Health and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
BABY HUG showed that hydroxyurea administered to 9- to 18-month-old children with sickle cell anemia provides significant clinical benefits, including a decrease in pain crises, acute chest syndrome events, and need for transfusion and hospital admission (Lancet 2011; 377:1663-72).
Hydroxyurea is approved to prevent sickle cell complications in adults with sickle cell anemia, but it is not currently indicated for use in children. Dr. Zora R. Rogers discussed the new data during a press briefing prior to a presentation at the annual meeting of the American Society of Hematology.
"We need to complete the data analysis and to critically examine the growth and development of this population with respect to hydroxyurea use," lead author Dr. Rogers said of the follow-up study, which terminates on Dec. 31, 2011. "But on a macroscopic level there [do] not appear to be any differences observed."
In 2008 Dr. Rogers, professor of pediatrics at the University of Texas Southwestern Medical Center, Dallas, and her associates at 14 centers launched the BABY HUG Follow-Up Study I to assess the safety and efficacy of continued treatment with hydroxyurea in infants with sickle cell anemia. The population consisted of 163 children aged 28-44 months who had participated in the original BABY HUG trial and who had completed at least 18 months of randomized treatment of either hydroxyurea or placebo. The researchers collected clinical and laboratory data every 6 months from patient medical records, including use and dosage of hydroxyurea, blood counts, clinical imaging, and frequency of sickle cell-related complications.
Of the 163 families that enrolled children in the follow-up study, 133 (82%) chose open-label hydroxyurea at the beginning of follow-up and every 6 months 65%-75% of the families reported that their children continued to take the drug. No patient developed intolerance or stopped permanently because of toxicity.
Dr. Rogers, clinical director of the bone marrow failure and general hematology program at Children’s Medical Center, Dallas, presented preliminary analyses as of Oct. 18, 2011, that amounted to 497 patient-years of follow-up. Compared with children who are not taking hydroxyurea, those who continue to take hydroxyurea have statistically lower rates of pain crises requiring emergency department visits (a rate of 29 vs. 54 per 100 patient-years, respectively), episodic transfusions (18 vs. 34 per 100 patient-years), and hospital admissions for any reason (73 vs. 132 per 100 patient-years), including acute chest syndrome or febrile illness.
In their abstract, the researchers pointed out that the decrease in acute chest syndrome episodes "is similar to the effect demonstrated with hydroxyurea use in the randomized BABY HUG trial in younger infants and consistent with published trials detailing the benefit of hydroxyurea therapy in older children and adults. The decrease in the rate of admission for febrile events in hydroxyurea-treated patients is also comparable to that in the randomized trial, but the reason for this benefit is uncertain."
There were no differences between the two groups in hospitalization rates for painful events, including dactylitis. Two patients in the non-hydroxyurea group each had a stroke. There were also no differences between the two groups in the frequency of a palpable spleen or rate of acute splenic sequestration crises. Through 36 months of follow up, children taking hydroxyurea had persistently higher hemoglobin and mean corpuscular volume and lower white blood cell count and absolute neutrophil count, compared with those not taking the drug.
Dr. Susan B. Shurin, acting director of the National Heart, Lung, and Blood Institute (NHLBI), characterized the findings as important in efforts to get an early handle on the burden of disease associated with sickle cell anemia.
"The internists who inherit the patients who have gone through pediatric practitioners have a powerful sense that they reach adolescence doing pretty well, and then things kind of fall apart," Dr. Shurin said. "The clear evidence that prevention of organ damage and prevention of complications of sickle cell anemia would be much preferable to trying to manage once they develop has been the motivation" for this work.
The BABY HUG investigators "believe that ongoing follow-up of this cohort is essential to continue to define the potential benefits as the children grow and to observe for late toxicity," Dr. Rogers said. "We are in final discussions with the NHLBI for an additional contract in support of 5 more years of follow-up."
The researchers intend to use the current findings "in support of an FDA application potentially to allow an indication for the use of hydroxyurea in very young children," Dr. Rogers said. "We are also hoping that there will be an interest for the use of this medication in a liquid format, because it’s very hard to get a 1-year-old to take a capsule."
The follow-up study is funded by the National Heart, Lung, and Blood Institute and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
SAN DIEGO – Mounting data from a federally funded follow-up to the BABY HUG study continue to demonstrate that hydroxyurea is a safe and effective treatment for young children with sickle cell anemia.
The results confirm findings published earlier this year from the Pediatric Hydroxyurea Phase III Clinical Trial (BABY HUG), a randomized, placebo-controlled study sponsored by the National Institutes of Health and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
BABY HUG showed that hydroxyurea administered to 9- to 18-month-old children with sickle cell anemia provides significant clinical benefits, including a decrease in pain crises, acute chest syndrome events, and need for transfusion and hospital admission (Lancet 2011; 377:1663-72).
Hydroxyurea is approved to prevent sickle cell complications in adults with sickle cell anemia, but it is not currently indicated for use in children. Dr. Zora R. Rogers discussed the new data during a press briefing prior to a presentation at the annual meeting of the American Society of Hematology.
"We need to complete the data analysis and to critically examine the growth and development of this population with respect to hydroxyurea use," lead author Dr. Rogers said of the follow-up study, which terminates on Dec. 31, 2011. "But on a macroscopic level there [do] not appear to be any differences observed."
In 2008 Dr. Rogers, professor of pediatrics at the University of Texas Southwestern Medical Center, Dallas, and her associates at 14 centers launched the BABY HUG Follow-Up Study I to assess the safety and efficacy of continued treatment with hydroxyurea in infants with sickle cell anemia. The population consisted of 163 children aged 28-44 months who had participated in the original BABY HUG trial and who had completed at least 18 months of randomized treatment of either hydroxyurea or placebo. The researchers collected clinical and laboratory data every 6 months from patient medical records, including use and dosage of hydroxyurea, blood counts, clinical imaging, and frequency of sickle cell-related complications.
Of the 163 families that enrolled children in the follow-up study, 133 (82%) chose open-label hydroxyurea at the beginning of follow-up and every 6 months 65%-75% of the families reported that their children continued to take the drug. No patient developed intolerance or stopped permanently because of toxicity.
Dr. Rogers, clinical director of the bone marrow failure and general hematology program at Children’s Medical Center, Dallas, presented preliminary analyses as of Oct. 18, 2011, that amounted to 497 patient-years of follow-up. Compared with children who are not taking hydroxyurea, those who continue to take hydroxyurea have statistically lower rates of pain crises requiring emergency department visits (a rate of 29 vs. 54 per 100 patient-years, respectively), episodic transfusions (18 vs. 34 per 100 patient-years), and hospital admissions for any reason (73 vs. 132 per 100 patient-years), including acute chest syndrome or febrile illness.
In their abstract, the researchers pointed out that the decrease in acute chest syndrome episodes "is similar to the effect demonstrated with hydroxyurea use in the randomized BABY HUG trial in younger infants and consistent with published trials detailing the benefit of hydroxyurea therapy in older children and adults. The decrease in the rate of admission for febrile events in hydroxyurea-treated patients is also comparable to that in the randomized trial, but the reason for this benefit is uncertain."
There were no differences between the two groups in hospitalization rates for painful events, including dactylitis. Two patients in the non-hydroxyurea group each had a stroke. There were also no differences between the two groups in the frequency of a palpable spleen or rate of acute splenic sequestration crises. Through 36 months of follow up, children taking hydroxyurea had persistently higher hemoglobin and mean corpuscular volume and lower white blood cell count and absolute neutrophil count, compared with those not taking the drug.
Dr. Susan B. Shurin, acting director of the National Heart, Lung, and Blood Institute (NHLBI), characterized the findings as important in efforts to get an early handle on the burden of disease associated with sickle cell anemia.
"The internists who inherit the patients who have gone through pediatric practitioners have a powerful sense that they reach adolescence doing pretty well, and then things kind of fall apart," Dr. Shurin said. "The clear evidence that prevention of organ damage and prevention of complications of sickle cell anemia would be much preferable to trying to manage once they develop has been the motivation" for this work.
The BABY HUG investigators "believe that ongoing follow-up of this cohort is essential to continue to define the potential benefits as the children grow and to observe for late toxicity," Dr. Rogers said. "We are in final discussions with the NHLBI for an additional contract in support of 5 more years of follow-up."
The researchers intend to use the current findings "in support of an FDA application potentially to allow an indication for the use of hydroxyurea in very young children," Dr. Rogers said. "We are also hoping that there will be an interest for the use of this medication in a liquid format, because it’s very hard to get a 1-year-old to take a capsule."
The follow-up study is funded by the National Heart, Lung, and Blood Institute and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF HEMATOLOGY
Major Finding: Compared with children not taking hydroxyurea, those who continue to take hydroxyurea have statistically lower rates of pain crises requiring emergency department visits (rate of 29 vs. 54 per 100 patient-years, respectively), episodic transfusions (18 vs. 34 per 100 patient-years), and hospital admissions for any reason (73 vs. 132 per 100 patient-years), including acute chest syndrome or febrile illness.
Data Source: A study of 163 children aged 28-44 months who had participated in the original Pediatric Hydroxyurea Phase III Clinical Trial (BABY HUG) and who had completed at least 18 months of randomized treatment of either hydroxyurea or placebo.
Disclosures: The study is funded by the National Heart, Lung, and Blood Institute and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
FDA approves deferiprone to treat iron overload
thalassemia
The FDA has approved deferiprone (Ferriprox) to treat iron overload in thalassemia patients who had an inadequate response to prior chelation therapy.
Deferiprone is the first treatment for transfusional iron overload to be approved since 2005, said Richard Pazdur, MD, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research.
The drug’s approval is based on a review of data from 12 clinical studies in 236 patients. Patients participating in the studies did not respond to prior iron chelation therapy.
Deferiprone was considered a success if patients experienced at least a 20% decrease in serum ferritin. And half of the patients included in the review experienced at least a 20% decrease in ferritin levels.
The most common side effects of the drug were nausea, vomiting, abdominal and joint pain, chromaturia, neutropenia, and an increase in the level of a liver enzyme that may be indicative of tissue or liver damage at unsafe amounts. The most serious side effect, seen in about 2% of patients, was the development of agranulocytosis.
Deferiprone has been approved under the FDA’s accelerated approval program, which was designed to provide patients with earlier access to promising new drugs, followed by further studies to confirm the drug’s clinical benefit.
ApoPharma, the company that manufactures deferiprone, has agreed to several post-marketing requirements and commitments. One commitment includes further study of the use of deferiprone in patients with sickle cell disease who have transfusional iron overload. ![]()
thalassemia
The FDA has approved deferiprone (Ferriprox) to treat iron overload in thalassemia patients who had an inadequate response to prior chelation therapy.
Deferiprone is the first treatment for transfusional iron overload to be approved since 2005, said Richard Pazdur, MD, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research.
The drug’s approval is based on a review of data from 12 clinical studies in 236 patients. Patients participating in the studies did not respond to prior iron chelation therapy.
Deferiprone was considered a success if patients experienced at least a 20% decrease in serum ferritin. And half of the patients included in the review experienced at least a 20% decrease in ferritin levels.
The most common side effects of the drug were nausea, vomiting, abdominal and joint pain, chromaturia, neutropenia, and an increase in the level of a liver enzyme that may be indicative of tissue or liver damage at unsafe amounts. The most serious side effect, seen in about 2% of patients, was the development of agranulocytosis.
Deferiprone has been approved under the FDA’s accelerated approval program, which was designed to provide patients with earlier access to promising new drugs, followed by further studies to confirm the drug’s clinical benefit.
ApoPharma, the company that manufactures deferiprone, has agreed to several post-marketing requirements and commitments. One commitment includes further study of the use of deferiprone in patients with sickle cell disease who have transfusional iron overload. ![]()
thalassemia
The FDA has approved deferiprone (Ferriprox) to treat iron overload in thalassemia patients who had an inadequate response to prior chelation therapy.
Deferiprone is the first treatment for transfusional iron overload to be approved since 2005, said Richard Pazdur, MD, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research.
The drug’s approval is based on a review of data from 12 clinical studies in 236 patients. Patients participating in the studies did not respond to prior iron chelation therapy.
Deferiprone was considered a success if patients experienced at least a 20% decrease in serum ferritin. And half of the patients included in the review experienced at least a 20% decrease in ferritin levels.
The most common side effects of the drug were nausea, vomiting, abdominal and joint pain, chromaturia, neutropenia, and an increase in the level of a liver enzyme that may be indicative of tissue or liver damage at unsafe amounts. The most serious side effect, seen in about 2% of patients, was the development of agranulocytosis.
Deferiprone has been approved under the FDA’s accelerated approval program, which was designed to provide patients with earlier access to promising new drugs, followed by further studies to confirm the drug’s clinical benefit.
ApoPharma, the company that manufactures deferiprone, has agreed to several post-marketing requirements and commitments. One commitment includes further study of the use of deferiprone in patients with sickle cell disease who have transfusional iron overload. ![]()
FDA Approves Deferiprone for Transfusional Iron Overload
Deferiprone is approved as a second-line treatment for transfusional iron overload when the condition has not been resolved by chelation therapy in patients with thalassemia, the Food and Drug Administration announced Oct. 14.
The new agent will be marketed as Ferriprox by ApoPharma. The FDA said the Toronto-based company has agreed to several postmarketing requirements and commitments, including further study in patients who have transfusional iron overload after treatment for sickle cell disease.
The FDA’s Oncologic Drugs Advisory Committee recently voted 10-2 that treatment with deferiprone had a favorable benefit-risk profile for treatment of patients with transfusional iron overload when current chelation therapy is inadequate.
As the decision date approached, however, the consumer advocacy group Public Citizen announced that it had sent the FDA a letter opposing approval. Public Citizen contended that APO Pharma had failed to demonstrate the drug is safe and effective in its intended population. The group noted that the FDA had refused to approve deferiprone in 2009 without an additional prospective, randomized, controlled study, but that no such study had been conducted.
"Ferriprox represents the first new FDA-approved treatment for this disorder since 2005."
The FDA announcement said its decision on safety and effectiveness was based on 12 clinical studies in which participating patients had not responded to prior iron chelation therapy.
"Ferriprox was considered a successful treatment for patients who experienced at least a 20% decrease in serum ferritin, a protein that stores iron in the body for later use. Half of the patients in the study experienced at least a 20% decrease in ferritin levels," the agency said.
Thalassemia is a genetic blood disorder that causes anemia. It is treated with frequent blood transfusions, but these can lead to excess iron in the body, a serious, potentially fatal condition. Chelation therapy, a process in which chemical agents remove heavy metals from the body, is the standard of care for transfusional iron overload.
"Ferriprox represents the first new FDA-approved treatment for this disorder since 2005," Dr. Richard Pazdur, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research, said in the FDA announcement.
Deferoxamine (Desferal), an iron chelator administered via a subcutaneous infusion pump (usually 6 nights a week), was approved in 1968, and deferasirox (Exjade), an oral chelator, in 2005. The new agent was approved in Europe in 1999, but had not been able to secure a U.S. go-ahead until the current "accelerated approval."
Ferriprox’s most common side effects have included nausea, vomiting, abdominal and joint pain, chromaturia, neutropenia, and "an increase in the level of a liver enzyme that may be indicative of tissue or liver damage at unsafe amounts," according to the FDA.
The agency said the most serious side effect was the development of agranulocytosis in about 2% of patients treated with Ferriprox.
Deferiprone is approved as a second-line treatment for transfusional iron overload when the condition has not been resolved by chelation therapy in patients with thalassemia, the Food and Drug Administration announced Oct. 14.
The new agent will be marketed as Ferriprox by ApoPharma. The FDA said the Toronto-based company has agreed to several postmarketing requirements and commitments, including further study in patients who have transfusional iron overload after treatment for sickle cell disease.
The FDA’s Oncologic Drugs Advisory Committee recently voted 10-2 that treatment with deferiprone had a favorable benefit-risk profile for treatment of patients with transfusional iron overload when current chelation therapy is inadequate.
As the decision date approached, however, the consumer advocacy group Public Citizen announced that it had sent the FDA a letter opposing approval. Public Citizen contended that APO Pharma had failed to demonstrate the drug is safe and effective in its intended population. The group noted that the FDA had refused to approve deferiprone in 2009 without an additional prospective, randomized, controlled study, but that no such study had been conducted.
"Ferriprox represents the first new FDA-approved treatment for this disorder since 2005."
The FDA announcement said its decision on safety and effectiveness was based on 12 clinical studies in which participating patients had not responded to prior iron chelation therapy.
"Ferriprox was considered a successful treatment for patients who experienced at least a 20% decrease in serum ferritin, a protein that stores iron in the body for later use. Half of the patients in the study experienced at least a 20% decrease in ferritin levels," the agency said.
Thalassemia is a genetic blood disorder that causes anemia. It is treated with frequent blood transfusions, but these can lead to excess iron in the body, a serious, potentially fatal condition. Chelation therapy, a process in which chemical agents remove heavy metals from the body, is the standard of care for transfusional iron overload.
"Ferriprox represents the first new FDA-approved treatment for this disorder since 2005," Dr. Richard Pazdur, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research, said in the FDA announcement.
Deferoxamine (Desferal), an iron chelator administered via a subcutaneous infusion pump (usually 6 nights a week), was approved in 1968, and deferasirox (Exjade), an oral chelator, in 2005. The new agent was approved in Europe in 1999, but had not been able to secure a U.S. go-ahead until the current "accelerated approval."
Ferriprox’s most common side effects have included nausea, vomiting, abdominal and joint pain, chromaturia, neutropenia, and "an increase in the level of a liver enzyme that may be indicative of tissue or liver damage at unsafe amounts," according to the FDA.
The agency said the most serious side effect was the development of agranulocytosis in about 2% of patients treated with Ferriprox.
Deferiprone is approved as a second-line treatment for transfusional iron overload when the condition has not been resolved by chelation therapy in patients with thalassemia, the Food and Drug Administration announced Oct. 14.
The new agent will be marketed as Ferriprox by ApoPharma. The FDA said the Toronto-based company has agreed to several postmarketing requirements and commitments, including further study in patients who have transfusional iron overload after treatment for sickle cell disease.
The FDA’s Oncologic Drugs Advisory Committee recently voted 10-2 that treatment with deferiprone had a favorable benefit-risk profile for treatment of patients with transfusional iron overload when current chelation therapy is inadequate.
As the decision date approached, however, the consumer advocacy group Public Citizen announced that it had sent the FDA a letter opposing approval. Public Citizen contended that APO Pharma had failed to demonstrate the drug is safe and effective in its intended population. The group noted that the FDA had refused to approve deferiprone in 2009 without an additional prospective, randomized, controlled study, but that no such study had been conducted.
"Ferriprox represents the first new FDA-approved treatment for this disorder since 2005."
The FDA announcement said its decision on safety and effectiveness was based on 12 clinical studies in which participating patients had not responded to prior iron chelation therapy.
"Ferriprox was considered a successful treatment for patients who experienced at least a 20% decrease in serum ferritin, a protein that stores iron in the body for later use. Half of the patients in the study experienced at least a 20% decrease in ferritin levels," the agency said.
Thalassemia is a genetic blood disorder that causes anemia. It is treated with frequent blood transfusions, but these can lead to excess iron in the body, a serious, potentially fatal condition. Chelation therapy, a process in which chemical agents remove heavy metals from the body, is the standard of care for transfusional iron overload.
"Ferriprox represents the first new FDA-approved treatment for this disorder since 2005," Dr. Richard Pazdur, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research, said in the FDA announcement.
Deferoxamine (Desferal), an iron chelator administered via a subcutaneous infusion pump (usually 6 nights a week), was approved in 1968, and deferasirox (Exjade), an oral chelator, in 2005. The new agent was approved in Europe in 1999, but had not been able to secure a U.S. go-ahead until the current "accelerated approval."
Ferriprox’s most common side effects have included nausea, vomiting, abdominal and joint pain, chromaturia, neutropenia, and "an increase in the level of a liver enzyme that may be indicative of tissue or liver damage at unsafe amounts," according to the FDA.
The agency said the most serious side effect was the development of agranulocytosis in about 2% of patients treated with Ferriprox.
Team corrects SCD mutation with iPS cells

Credit: James Thomson
Using induced pluripotent stem (iPS) cells, researchers have corrected the genetic alteration that causes sickle cell disease (SCD).
The corrected stem cells were coaxed in vitro into immature red blood cells that then turned on a normal version of the gene.
The researchers caution that the work is years away from clinical use in patients, but it should provide tools for developing gene therapies for SCD and a variety of other hematologic disorders.
“We’re now one step closer to developing a combination cell and gene therapy method that will allow us to use patients’ own cells to treat them,” said lead study author Linzhao Cheng, PhD, of The Johns Hopkins School of Medicine.
Using an adult patient at The Johns Hopkins Hospital as their first case, the researchers isolated the patient’s bone marrow cells. After generating iPS cells from the bone marrow, the team put a normal copy of the hemoglobin gene in place of the defective one using genetic engineering techniques.
The researchers sequenced the DNA from 300 different samples of iPS cells to identify those that contained correct copies of the hemoglobin gene and found 4. Three of these iPS cell lines didn’t pass muster in subsequent tests.
“The beauty of iPS cells is that we can grow a lot of them and then coax them into becoming cells of any kind, including red blood cells,” Dr Cheng said.
In their process, his team converted the corrected iPS cells into immature red blood cells by giving them growth factors. Further testing showed that the normal hemoglobin gene was turned on properly in these cells, although at less than half of normal levels.
“We think these immature red blood cells still behave like embryonic cells and, as a result, are unable to turn on high enough levels of the adult hemoglobin gene,” Dr Cheng said. “We next have to learn how to properly convert these cells into mature red blood cells.”
This research was recently published online in Blood. ![]()
Credit: James Thomson
Using induced pluripotent stem (iPS) cells, researchers have corrected the genetic alteration that causes sickle cell disease (SCD).
The corrected stem cells were coaxed in vitro into immature red blood cells that then turned on a normal version of the gene.
The researchers caution that the work is years away from clinical use in patients, but it should provide tools for developing gene therapies for SCD and a variety of other hematologic disorders.
“We’re now one step closer to developing a combination cell and gene therapy method that will allow us to use patients’ own cells to treat them,” said lead study author Linzhao Cheng, PhD, of The Johns Hopkins School of Medicine.
Using an adult patient at The Johns Hopkins Hospital as their first case, the researchers isolated the patient’s bone marrow cells. After generating iPS cells from the bone marrow, the team put a normal copy of the hemoglobin gene in place of the defective one using genetic engineering techniques.
The researchers sequenced the DNA from 300 different samples of iPS cells to identify those that contained correct copies of the hemoglobin gene and found 4. Three of these iPS cell lines didn’t pass muster in subsequent tests.
“The beauty of iPS cells is that we can grow a lot of them and then coax them into becoming cells of any kind, including red blood cells,” Dr Cheng said.
In their process, his team converted the corrected iPS cells into immature red blood cells by giving them growth factors. Further testing showed that the normal hemoglobin gene was turned on properly in these cells, although at less than half of normal levels.
“We think these immature red blood cells still behave like embryonic cells and, as a result, are unable to turn on high enough levels of the adult hemoglobin gene,” Dr Cheng said. “We next have to learn how to properly convert these cells into mature red blood cells.”
This research was recently published online in Blood. ![]()
Credit: James Thomson
Using induced pluripotent stem (iPS) cells, researchers have corrected the genetic alteration that causes sickle cell disease (SCD).
The corrected stem cells were coaxed in vitro into immature red blood cells that then turned on a normal version of the gene.
The researchers caution that the work is years away from clinical use in patients, but it should provide tools for developing gene therapies for SCD and a variety of other hematologic disorders.
“We’re now one step closer to developing a combination cell and gene therapy method that will allow us to use patients’ own cells to treat them,” said lead study author Linzhao Cheng, PhD, of The Johns Hopkins School of Medicine.
Using an adult patient at The Johns Hopkins Hospital as their first case, the researchers isolated the patient’s bone marrow cells. After generating iPS cells from the bone marrow, the team put a normal copy of the hemoglobin gene in place of the defective one using genetic engineering techniques.
The researchers sequenced the DNA from 300 different samples of iPS cells to identify those that contained correct copies of the hemoglobin gene and found 4. Three of these iPS cell lines didn’t pass muster in subsequent tests.
“The beauty of iPS cells is that we can grow a lot of them and then coax them into becoming cells of any kind, including red blood cells,” Dr Cheng said.
In their process, his team converted the corrected iPS cells into immature red blood cells by giving them growth factors. Further testing showed that the normal hemoglobin gene was turned on properly in these cells, although at less than half of normal levels.
“We think these immature red blood cells still behave like embryonic cells and, as a result, are unable to turn on high enough levels of the adult hemoglobin gene,” Dr Cheng said. “We next have to learn how to properly convert these cells into mature red blood cells.”
This research was recently published online in Blood. ![]()
Eculizumab gets accelerated approval for aHUS
The US Food and Drug Administration (FDA) has granted accelerated approval for eculizumab (Soliris) to treat patients with atypical hemolytic uremic syndrome (aHUS).
This rare and chronic disease can lead to renal failure and is associated with an increased risk of death and stroke. It accounts for 5% to 10% of all cases of hemolytic uremic syndrome and disproportionately affects children.
Eculizumab is a targeted therapy that works by inhibiting proteins that play a role in aHUS. The FDA granted accelerated approval for eculizumab based on data suggesting the drug likely confers a clinical benefit for patients with aHUS.
The FDA’s Accelerated Approval Program allows for earlier approval of drugs that treat serious conditions and fill an unmet medical need based on a surrogate endpoint that is thought to predict clinical benefit. The makers of eculizumab, Alexion Pharmaceuticals, are still required to conduct research to confirm the anticipated clinical benefit.
If this research indicates that eculizumab does provide a clinical benefit, the FDA will grant traditional approval for the drug. If research suggests eculizumab does not provide a clinical benefit, the FDA has regulatory procedures in place that could lead to removing the drug from the market.
There are no other FDA-approved treatments for aHUS. The safety and efficacy of the current standard treatment, plasma therapy (plasma exchange or fresh frozen plasma infusion), have not been studied in well-controlled trials.
Researchers have examined the safety and efficacy of eculizumab in 2 single-arm trials of 37 adult and adolescent patients with aHUS and 1 retrospective study of 19 pediatric and 11 adult patients with aHUS.
Patients treated with eculizumab in these studies experienced a favorable improvement in kidney function, including elimination of the requirement for dialysis in several patients who did not respond to plasma therapy.
Patients treated with eculizumab also exhibited improvement in platelet counts and other blood parameters that correlate with aHUS disease activity.
The most common side effects included hypertension, diarrhea, headache, anemia, vomiting, nausea, upper respiratory and urinary tract infections, and leukopenia.
Eculizumab will continue to be available only through a restricted program. Prescribers must enroll in a registration program and provide a medication guide to patients who receive the drug.
Eculizumab is marketed as Soliris by Alexion Pharmaceuticals, located in Cheshire, Connecticut. ![]()
The US Food and Drug Administration (FDA) has granted accelerated approval for eculizumab (Soliris) to treat patients with atypical hemolytic uremic syndrome (aHUS).
This rare and chronic disease can lead to renal failure and is associated with an increased risk of death and stroke. It accounts for 5% to 10% of all cases of hemolytic uremic syndrome and disproportionately affects children.
Eculizumab is a targeted therapy that works by inhibiting proteins that play a role in aHUS. The FDA granted accelerated approval for eculizumab based on data suggesting the drug likely confers a clinical benefit for patients with aHUS.
The FDA’s Accelerated Approval Program allows for earlier approval of drugs that treat serious conditions and fill an unmet medical need based on a surrogate endpoint that is thought to predict clinical benefit. The makers of eculizumab, Alexion Pharmaceuticals, are still required to conduct research to confirm the anticipated clinical benefit.
If this research indicates that eculizumab does provide a clinical benefit, the FDA will grant traditional approval for the drug. If research suggests eculizumab does not provide a clinical benefit, the FDA has regulatory procedures in place that could lead to removing the drug from the market.
There are no other FDA-approved treatments for aHUS. The safety and efficacy of the current standard treatment, plasma therapy (plasma exchange or fresh frozen plasma infusion), have not been studied in well-controlled trials.
Researchers have examined the safety and efficacy of eculizumab in 2 single-arm trials of 37 adult and adolescent patients with aHUS and 1 retrospective study of 19 pediatric and 11 adult patients with aHUS.
Patients treated with eculizumab in these studies experienced a favorable improvement in kidney function, including elimination of the requirement for dialysis in several patients who did not respond to plasma therapy.
Patients treated with eculizumab also exhibited improvement in platelet counts and other blood parameters that correlate with aHUS disease activity.
The most common side effects included hypertension, diarrhea, headache, anemia, vomiting, nausea, upper respiratory and urinary tract infections, and leukopenia.
Eculizumab will continue to be available only through a restricted program. Prescribers must enroll in a registration program and provide a medication guide to patients who receive the drug.
Eculizumab is marketed as Soliris by Alexion Pharmaceuticals, located in Cheshire, Connecticut. ![]()
The US Food and Drug Administration (FDA) has granted accelerated approval for eculizumab (Soliris) to treat patients with atypical hemolytic uremic syndrome (aHUS).
This rare and chronic disease can lead to renal failure and is associated with an increased risk of death and stroke. It accounts for 5% to 10% of all cases of hemolytic uremic syndrome and disproportionately affects children.
Eculizumab is a targeted therapy that works by inhibiting proteins that play a role in aHUS. The FDA granted accelerated approval for eculizumab based on data suggesting the drug likely confers a clinical benefit for patients with aHUS.
The FDA’s Accelerated Approval Program allows for earlier approval of drugs that treat serious conditions and fill an unmet medical need based on a surrogate endpoint that is thought to predict clinical benefit. The makers of eculizumab, Alexion Pharmaceuticals, are still required to conduct research to confirm the anticipated clinical benefit.
If this research indicates that eculizumab does provide a clinical benefit, the FDA will grant traditional approval for the drug. If research suggests eculizumab does not provide a clinical benefit, the FDA has regulatory procedures in place that could lead to removing the drug from the market.
There are no other FDA-approved treatments for aHUS. The safety and efficacy of the current standard treatment, plasma therapy (plasma exchange or fresh frozen plasma infusion), have not been studied in well-controlled trials.
Researchers have examined the safety and efficacy of eculizumab in 2 single-arm trials of 37 adult and adolescent patients with aHUS and 1 retrospective study of 19 pediatric and 11 adult patients with aHUS.
Patients treated with eculizumab in these studies experienced a favorable improvement in kidney function, including elimination of the requirement for dialysis in several patients who did not respond to plasma therapy.
Patients treated with eculizumab also exhibited improvement in platelet counts and other blood parameters that correlate with aHUS disease activity.
The most common side effects included hypertension, diarrhea, headache, anemia, vomiting, nausea, upper respiratory and urinary tract infections, and leukopenia.
Eculizumab will continue to be available only through a restricted program. Prescribers must enroll in a registration program and provide a medication guide to patients who receive the drug.
Eculizumab is marketed as Soliris by Alexion Pharmaceuticals, located in Cheshire, Connecticut. ![]()
Newly identified NHP2 biallelic mutation can cause dyskeratosis congenita

Copenhagen— Researchers have identified a new biallelic mutation in the telomerase component NHP2, which can cause the premature aging syndrome dyskeratosis congenita.
Thomas J. Vulliamy, PhD, MRCPath, from Barts and the London School of Medicine and Dentistry, presented this finding at the 13th Congress of the European Hematology Association.
Dyskeratosis congenita is a genetically heterogeneous, multisystem disorder. The unifying feature of dyskeratosis congenita is that all mutations identified thus far affect molecules involved in telomere maintenance. Defective telomerase leads to premature aging, bone marrow failure, and a predisposition to 32 cancers.
Investigators analyzed the proteins NHP2 and GAR1 using high performance liquid chromatography screening followed by direct DNA sequencing. NHP2 and GAR1 are key components of telomerase, along with dyskerin and NOP10, and small nucleolar ribonucleoprotein (snoRNP) complexes.
Investigators measured telomere lengths by Southern blot analysis and assessed TERC levels and the effects of siRNA knockdown of gene transcripts using quantitative real-time PCR.
Dr Vulliamy and colleagues found that mutations in NHP2 can cause autosomal recessive dyskeratosis congenita. Patients with NHP2, dyskerin, and NOP10 mutations have short telomeres and low TERC levels.
Investigators concluded that this provided direct evidence of their role in telomere maintenance in humans. They did not find any GAR1 mutations, suggesting that GAR1 has a different impact on the accumulation of TERC.
This abstract was chosen as one of the 5 best of the Congress. ![]()
Copenhagen— Researchers have identified a new biallelic mutation in the telomerase component NHP2, which can cause the premature aging syndrome dyskeratosis congenita.
Thomas J. Vulliamy, PhD, MRCPath, from Barts and the London School of Medicine and Dentistry, presented this finding at the 13th Congress of the European Hematology Association.
Dyskeratosis congenita is a genetically heterogeneous, multisystem disorder. The unifying feature of dyskeratosis congenita is that all mutations identified thus far affect molecules involved in telomere maintenance. Defective telomerase leads to premature aging, bone marrow failure, and a predisposition to 32 cancers.
Investigators analyzed the proteins NHP2 and GAR1 using high performance liquid chromatography screening followed by direct DNA sequencing. NHP2 and GAR1 are key components of telomerase, along with dyskerin and NOP10, and small nucleolar ribonucleoprotein (snoRNP) complexes.
Investigators measured telomere lengths by Southern blot analysis and assessed TERC levels and the effects of siRNA knockdown of gene transcripts using quantitative real-time PCR.
Dr Vulliamy and colleagues found that mutations in NHP2 can cause autosomal recessive dyskeratosis congenita. Patients with NHP2, dyskerin, and NOP10 mutations have short telomeres and low TERC levels.
Investigators concluded that this provided direct evidence of their role in telomere maintenance in humans. They did not find any GAR1 mutations, suggesting that GAR1 has a different impact on the accumulation of TERC.
This abstract was chosen as one of the 5 best of the Congress. ![]()
Copenhagen— Researchers have identified a new biallelic mutation in the telomerase component NHP2, which can cause the premature aging syndrome dyskeratosis congenita.
Thomas J. Vulliamy, PhD, MRCPath, from Barts and the London School of Medicine and Dentistry, presented this finding at the 13th Congress of the European Hematology Association.
Dyskeratosis congenita is a genetically heterogeneous, multisystem disorder. The unifying feature of dyskeratosis congenita is that all mutations identified thus far affect molecules involved in telomere maintenance. Defective telomerase leads to premature aging, bone marrow failure, and a predisposition to 32 cancers.
Investigators analyzed the proteins NHP2 and GAR1 using high performance liquid chromatography screening followed by direct DNA sequencing. NHP2 and GAR1 are key components of telomerase, along with dyskerin and NOP10, and small nucleolar ribonucleoprotein (snoRNP) complexes.
Investigators measured telomere lengths by Southern blot analysis and assessed TERC levels and the effects of siRNA knockdown of gene transcripts using quantitative real-time PCR.
Dr Vulliamy and colleagues found that mutations in NHP2 can cause autosomal recessive dyskeratosis congenita. Patients with NHP2, dyskerin, and NOP10 mutations have short telomeres and low TERC levels.
Investigators concluded that this provided direct evidence of their role in telomere maintenance in humans. They did not find any GAR1 mutations, suggesting that GAR1 has a different impact on the accumulation of TERC.
This abstract was chosen as one of the 5 best of the Congress. ![]()