User login
AGA Data Trends 2025: IBD
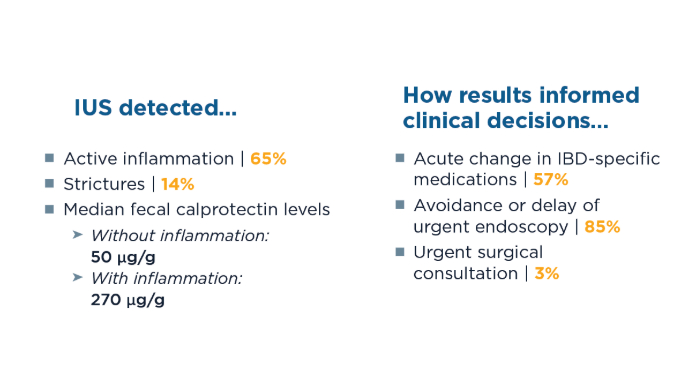
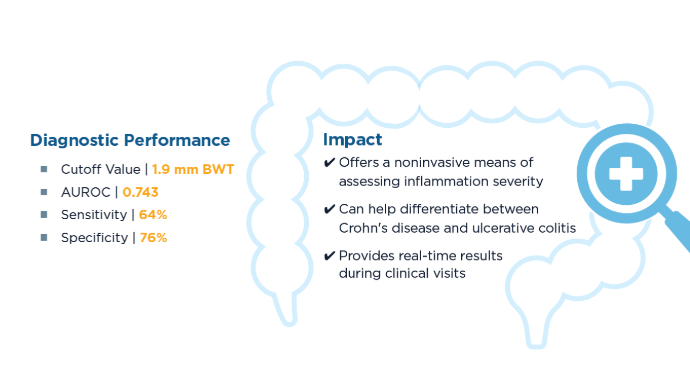
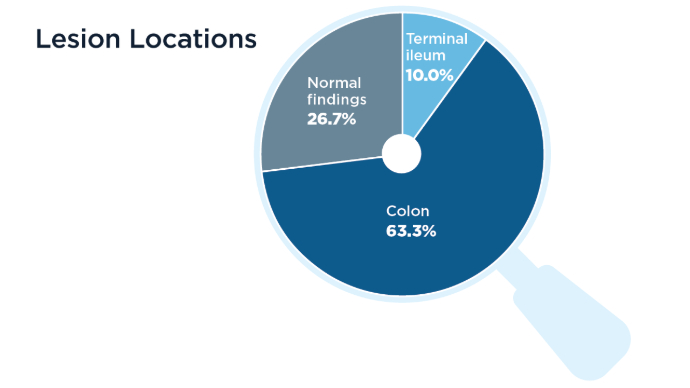
The Role of Bedside Intestinal Ultrasound in IBD Management
- Chavannes M, Dolinger MT, Cohen-Mekelburg S, Abraham B. AGA Clinical Practice update on the Role of Intestinal Ultrasound in Inflammatory Bowel Disease: Commentary. Clin Gastroenterol Hepatol. 2024;22(9):1790-1795.e1. doi:10.1016/j.cgh.2024.04.039
- El-Nakeep S. The intestinal ultrasound role in inflammatory bowel disease in clinical practice and a critical appraisal of the current guidelines (mini-review). Egypt J Intern Med. 2024;36:51. doi:10.1186/s43162-024-00316-6
- Chavannes M, Hart L, Hayati Rezvan P, Dillman JR, Polk DB. Bedside Intestinal Ultrasound Predicts Disease Severity and the Disease Distribution of Pediatric Patients With Inflammatory Bowel Disease: A Pilot Cross-sectional Study. Inflamm Bowel Dis. 2024;30(3):402-409. doi:10.1093/ibd/izad083
- St-Pierre J, Delisle M, Kheirkhahrahimabadi H, et al; International Bowel Ultrasound Group. Bedside Intestinal Ultrasound Performed in an Inflammatory Bowel Disease Urgent Assessment Clinic Improves Clinical Decision-making and Resource Utilization. Crohns Colitis 360. 2023;5(4):otad050. doi:10.1093/crocol/otad050
- Jevdokimova N, Jevdokimov D, Teterina I, Pokrotnieks J, Puķītis A, Mokricka V. Correlation of Intestinal Ultrasound Data With Laboratory Markers of Inflammation for Patients With Inflammatory Bowel Disease. Proc Latv
- Chavannes M, Dolinger MT, Cohen-Mekelburg S, Abraham B. AGA Clinical Practice update on the Role of Intestinal Ultrasound in Inflammatory Bowel Disease: Commentary. Clin Gastroenterol Hepatol. 2024;22(9):1790-1795.e1. doi:10.1016/j.cgh.2024.04.039
- El-Nakeep S. The intestinal ultrasound role in inflammatory bowel disease in clinical practice and a critical appraisal of the current guidelines (mini-review). Egypt J Intern Med. 2024;36:51. doi:10.1186/s43162-024-00316-6
- Chavannes M, Hart L, Hayati Rezvan P, Dillman JR, Polk DB. Bedside Intestinal Ultrasound Predicts Disease Severity and the Disease Distribution of Pediatric Patients With Inflammatory Bowel Disease: A Pilot Cross-sectional Study. Inflamm Bowel Dis. 2024;30(3):402-409. doi:10.1093/ibd/izad083
- St-Pierre J, Delisle M, Kheirkhahrahimabadi H, et al; International Bowel Ultrasound Group. Bedside Intestinal Ultrasound Performed in an Inflammatory Bowel Disease Urgent Assessment Clinic Improves Clinical Decision-making and Resource Utilization. Crohns Colitis 360. 2023;5(4):otad050. doi:10.1093/crocol/otad050
- Jevdokimova N, Jevdokimov D, Teterina I, Pokrotnieks J, Puķītis A, Mokricka V. Correlation of Intestinal Ultrasound Data With Laboratory Markers of Inflammation for Patients With Inflammatory Bowel Disease. Proc Latv
- Chavannes M, Dolinger MT, Cohen-Mekelburg S, Abraham B. AGA Clinical Practice update on the Role of Intestinal Ultrasound in Inflammatory Bowel Disease: Commentary. Clin Gastroenterol Hepatol. 2024;22(9):1790-1795.e1. doi:10.1016/j.cgh.2024.04.039
- El-Nakeep S. The intestinal ultrasound role in inflammatory bowel disease in clinical practice and a critical appraisal of the current guidelines (mini-review). Egypt J Intern Med. 2024;36:51. doi:10.1186/s43162-024-00316-6
- Chavannes M, Hart L, Hayati Rezvan P, Dillman JR, Polk DB. Bedside Intestinal Ultrasound Predicts Disease Severity and the Disease Distribution of Pediatric Patients With Inflammatory Bowel Disease: A Pilot Cross-sectional Study. Inflamm Bowel Dis. 2024;30(3):402-409. doi:10.1093/ibd/izad083
- St-Pierre J, Delisle M, Kheirkhahrahimabadi H, et al; International Bowel Ultrasound Group. Bedside Intestinal Ultrasound Performed in an Inflammatory Bowel Disease Urgent Assessment Clinic Improves Clinical Decision-making and Resource Utilization. Crohns Colitis 360. 2023;5(4):otad050. doi:10.1093/crocol/otad050
- Jevdokimova N, Jevdokimov D, Teterina I, Pokrotnieks J, Puķītis A, Mokricka V. Correlation of Intestinal Ultrasound Data With Laboratory Markers of Inflammation for Patients With Inflammatory Bowel Disease. Proc Latv
The Role of Bedside Intestinal Ultrasound in IBD Management
The Role of Bedside Intestinal Ultrasound in IBD Management
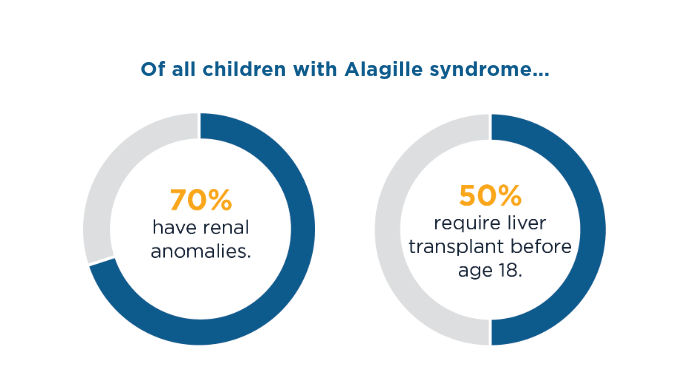
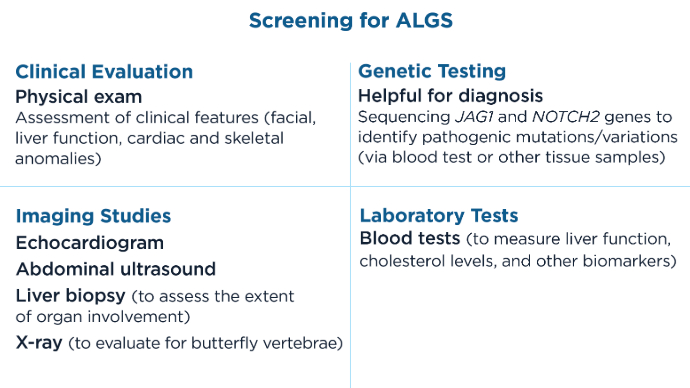
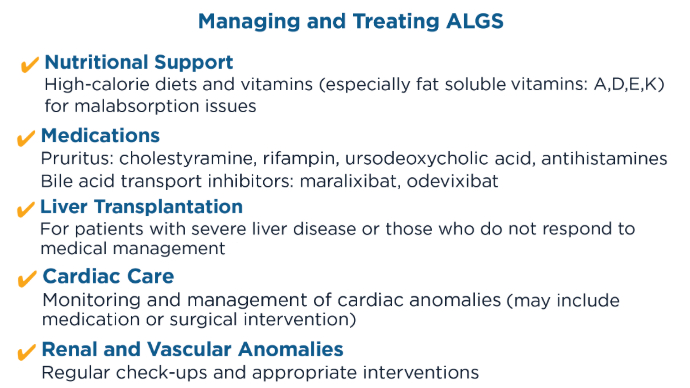
Alagille Syndrome: Epidemiology and Management of a Rare Genetic Disease
Alagille Syndrome: Epidemiology and Management of a Rare Genetic Disease
Yan J, Huang Y, Cao L, et al. Clinical, pathological and genetic characteristics of 17 unrelated children with Alagille Syndrome. BMC Pediatr. 2024;24(1):532. doi:10.1186/s12887-024-04973-y
Cheng K, Rosenthal P. Diagnosis and management of Alagille and progressive familial intrahepatic cholestasis. Hepatol Commun. 2023 Dec 7;7(12):e0314. doi:10.1097/HC9.0000000000000314
Global Allagile Alliance, GALA, website. The GALA Study. Published 2022. Accessed January 27, 2025. https://www.galastudy.com/
Karim F, Hiremath G, Samayoa JC, Said SM. Complex Pulmonary Artery Rehabilitation in Children with Alagille Syndrome: An Early Single-Center Experience of a Successful Collaborative Work. J Cardiovasc Dev Dis. 2024;11(8):232. doi:10.3390/jcdd11080232
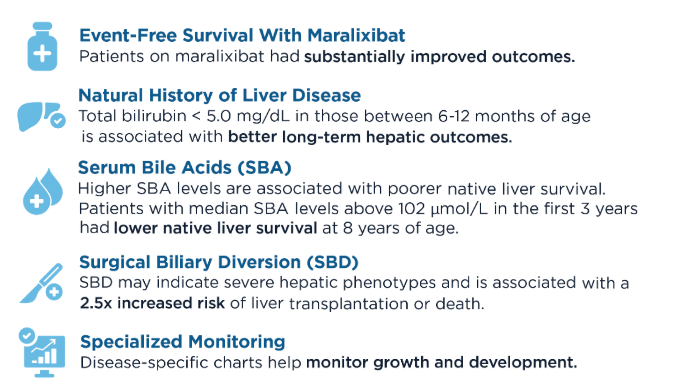
Vandriel SM, Loomes K, Sokal E, et al. Surgical biliary diversion is associated with an increased risk of liver transplantation or death in Alagille syndrome. AASLD Liver Meeting (Boston, USA. 09/11/2023 to 13/11/2023).
Hansen BE, Vandriel SM, Vig P, et al; the Global ALagille Alliance (GALA) Study Group. Event-free survival of maralixibat-treated patients with Alagille syndrome compared to a real-world cohort from GALA. Hepatology. 2024;79(6):1279-1292. doi:10.1097/HEP.0000000000000727
Vandriel SM, Li L-T, She H, et al; the Global ALagille Alliance (GALA) Study Group. Natural history of liver disease in a large international cohort of children with Alagille syndrome: Results from the GALA study. Hepatology. 2023;77(2):512-529. doi:10.1002/hep.32761
Murillo Perez CF, Vandriel SM, Sokal E, et al. Serum bile acids are associated with native liver survival in patients with Alagille syndrome: Results from the GALA Study Group. AASLD Liver Meeting (Boston, USA, 09/11/2023 to 13/11/2023).
Yan J, Huang Y, Cao L, et al. Clinical, pathological and genetic characteristics of 17 unrelated children with Alagille Syndrome. BMC Pediatr. 2024;24(1):532. doi:10.1186/s12887-024-04973-y
Cheng K, Rosenthal P. Diagnosis and management of Alagille and progressive familial intrahepatic cholestasis. Hepatol Commun. 2023 Dec 7;7(12):e0314. doi:10.1097/HC9.0000000000000314
Global Allagile Alliance, GALA, website. The GALA Study. Published 2022. Accessed January 27, 2025. https://www.galastudy.com/
Karim F, Hiremath G, Samayoa JC, Said SM. Complex Pulmonary Artery Rehabilitation in Children with Alagille Syndrome: An Early Single-Center Experience of a Successful Collaborative Work. J Cardiovasc Dev Dis. 2024;11(8):232. doi:10.3390/jcdd11080232
Vandriel SM, Loomes K, Sokal E, et al. Surgical biliary diversion is associated with an increased risk of liver transplantation or death in Alagille syndrome. AASLD Liver Meeting (Boston, USA. 09/11/2023 to 13/11/2023).
Hansen BE, Vandriel SM, Vig P, et al; the Global ALagille Alliance (GALA) Study Group. Event-free survival of maralixibat-treated patients with Alagille syndrome compared to a real-world cohort from GALA. Hepatology. 2024;79(6):1279-1292. doi:10.1097/HEP.0000000000000727
Vandriel SM, Li L-T, She H, et al; the Global ALagille Alliance (GALA) Study Group. Natural history of liver disease in a large international cohort of children with Alagille syndrome: Results from the GALA study. Hepatology. 2023;77(2):512-529. doi:10.1002/hep.32761
Murillo Perez CF, Vandriel SM, Sokal E, et al. Serum bile acids are associated with native liver survival in patients with Alagille syndrome: Results from the GALA Study Group. AASLD Liver Meeting (Boston, USA, 09/11/2023 to 13/11/2023).
Yan J, Huang Y, Cao L, et al. Clinical, pathological and genetic characteristics of 17 unrelated children with Alagille Syndrome. BMC Pediatr. 2024;24(1):532. doi:10.1186/s12887-024-04973-y
Cheng K, Rosenthal P. Diagnosis and management of Alagille and progressive familial intrahepatic cholestasis. Hepatol Commun. 2023 Dec 7;7(12):e0314. doi:10.1097/HC9.0000000000000314
Global Allagile Alliance, GALA, website. The GALA Study. Published 2022. Accessed January 27, 2025. https://www.galastudy.com/
Karim F, Hiremath G, Samayoa JC, Said SM. Complex Pulmonary Artery Rehabilitation in Children with Alagille Syndrome: An Early Single-Center Experience of a Successful Collaborative Work. J Cardiovasc Dev Dis. 2024;11(8):232. doi:10.3390/jcdd11080232
Vandriel SM, Loomes K, Sokal E, et al. Surgical biliary diversion is associated with an increased risk of liver transplantation or death in Alagille syndrome. AASLD Liver Meeting (Boston, USA. 09/11/2023 to 13/11/2023).
Hansen BE, Vandriel SM, Vig P, et al; the Global ALagille Alliance (GALA) Study Group. Event-free survival of maralixibat-treated patients with Alagille syndrome compared to a real-world cohort from GALA. Hepatology. 2024;79(6):1279-1292. doi:10.1097/HEP.0000000000000727
Vandriel SM, Li L-T, She H, et al; the Global ALagille Alliance (GALA) Study Group. Natural history of liver disease in a large international cohort of children with Alagille syndrome: Results from the GALA study. Hepatology. 2023;77(2):512-529. doi:10.1002/hep.32761
Murillo Perez CF, Vandriel SM, Sokal E, et al. Serum bile acids are associated with native liver survival in patients with Alagille syndrome: Results from the GALA Study Group. AASLD Liver Meeting (Boston, USA, 09/11/2023 to 13/11/2023).
Alagille Syndrome: Epidemiology and Management of a Rare Genetic Disease
Alagille Syndrome: Epidemiology and Management of a Rare Genetic Disease
Gastroenterology Data Trends 2025
Gastroenterology Data Trends 2025

GI & Hepatology News and the American Gastroenterological Association (AGA) present Gastroenterology Data Trends 2025, a special report on hot topics in GI told through original infographics and visual storytelling.
In this issue:
The Role of Bedside Intestinal Ultrasound in IBD Management
Bincy Abraham, MD, MS
Obesity Management in the Era of GLP-1: The Role of GLP-1 RAs
Michael Camilleri, MD, MPhil, DSc
Ergonomics in Endoscopy
Amandeep K. Shergill, MD, MS
Optimizing the Delivery of GI Care in Transgender and Gender-Diverse Communities
Kira Newman, MD, PhD
New Therapeutic Frontiers in the Treatment of Eosinophilic Esophagitis
Evan S. Dellon, MD, MPH
New and Emerging Treatments for MASLD/MASH
Naim Alkhouri, MD
Advances in Screening for Barrett’s Esophagus and Esophageal Adenocarcinoma
Joel Rubenstein, MD, MS
Alagille Syndrome: Epidemiology and Management of a Rare Genetic Disease
Alisha Mavis, MD
IBS: Mental Health Factors and Comorbidities
Lin Chang, MD, and Laurie A. Keefer, PhD
GI & Hepatology News and the American Gastroenterological Association (AGA) present Gastroenterology Data Trends 2025, a special report on hot topics in GI told through original infographics and visual storytelling.
In this issue:
The Role of Bedside Intestinal Ultrasound in IBD Management
Bincy Abraham, MD, MS
Obesity Management in the Era of GLP-1: The Role of GLP-1 RAs
Michael Camilleri, MD, MPhil, DSc
Ergonomics in Endoscopy
Amandeep K. Shergill, MD, MS
Optimizing the Delivery of GI Care in Transgender and Gender-Diverse Communities
Kira Newman, MD, PhD
New Therapeutic Frontiers in the Treatment of Eosinophilic Esophagitis
Evan S. Dellon, MD, MPH
New and Emerging Treatments for MASLD/MASH
Naim Alkhouri, MD
Advances in Screening for Barrett’s Esophagus and Esophageal Adenocarcinoma
Joel Rubenstein, MD, MS
Alagille Syndrome: Epidemiology and Management of a Rare Genetic Disease
Alisha Mavis, MD
IBS: Mental Health Factors and Comorbidities
Lin Chang, MD, and Laurie A. Keefer, PhD
GI & Hepatology News and the American Gastroenterological Association (AGA) present Gastroenterology Data Trends 2025, a special report on hot topics in GI told through original infographics and visual storytelling.
In this issue:
The Role of Bedside Intestinal Ultrasound in IBD Management
Bincy Abraham, MD, MS
Obesity Management in the Era of GLP-1: The Role of GLP-1 RAs
Michael Camilleri, MD, MPhil, DSc
Ergonomics in Endoscopy
Amandeep K. Shergill, MD, MS
Optimizing the Delivery of GI Care in Transgender and Gender-Diverse Communities
Kira Newman, MD, PhD
New Therapeutic Frontiers in the Treatment of Eosinophilic Esophagitis
Evan S. Dellon, MD, MPH
New and Emerging Treatments for MASLD/MASH
Naim Alkhouri, MD
Advances in Screening for Barrett’s Esophagus and Esophageal Adenocarcinoma
Joel Rubenstein, MD, MS
Alagille Syndrome: Epidemiology and Management of a Rare Genetic Disease
Alisha Mavis, MD
IBS: Mental Health Factors and Comorbidities
Lin Chang, MD, and Laurie A. Keefer, PhD
Gastroenterology Data Trends 2025
Gastroenterology Data Trends 2025
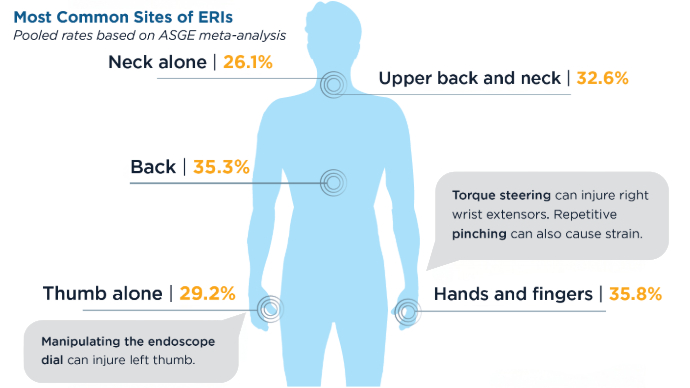
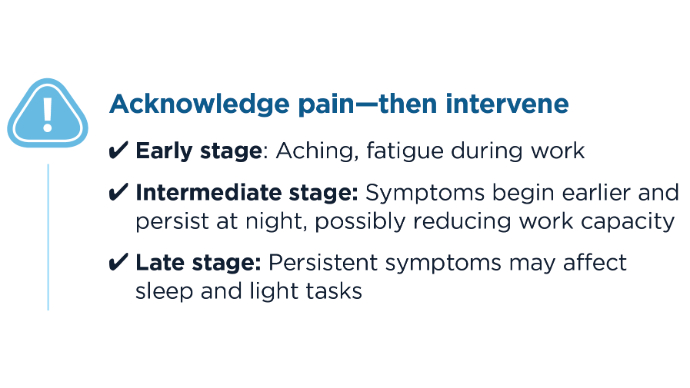
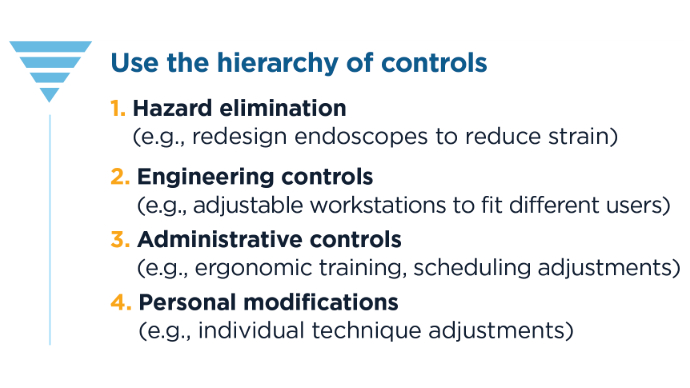
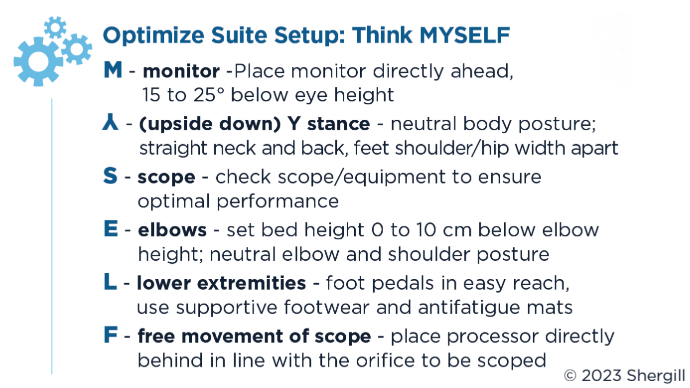
Ergonomics in Endoscopy
Ergonomics in Endoscopy
Click to view more from Gastroenterology Data Trends 2025.
- Ridtitid W, Cote GA, Leung W, et al. Prevalence and risk factors for musculoskeletal injuries related to endoscopy. Gastrointest Endosc. 2015;81(2):294-302 e294.
- Mohan N, Singla M, Pawa S, et al. Gastroenterologists’ goals for ergonomic colonoscopes: results of a national survey. Gastrointest Endosc. 2025;s0016-5107(25)00051-3. doi:10.1016/j.gie.2025.01.027
- Pawa S, Kwon RS, Fishman DS, et al. American Society for Gastrointestinal Endoscopy guideline on the role of ergonomics for prevention of endoscopy-related injury: summary and recommendations. Gastrointest Endosc. 2023;98(4):482-491. Accessed: February 1, 2025. https://www.asge.org/docs/default-source/guidelines/asge-guideline-on-the-role-of-ergonomics-summary.pdf
- Austin K, Schoenberger H, Sesto M, Gaumnitz E, Teo Broman A, Saha S. Musculoskeletal injuries are commonly reported among gastroenterology trainees: Results of a national survey. Dig Dis Sci. 2019;64(6):1439-1447.
- Shergill AK, Rempel D, Barr A, et al. Biomechanical risk factors associated with distal upper extremity musculoskeletal disorders in endoscopists performing colonoscopy. Gastrointest Endosc. 2021;93(3):704–711.e3. doi:10.1016/j.gie.2020.11.001
- Lipowska A, Shergill A. Coping with burnout and repetitive injuries -The hazards of endoscopy: Ergonomics guide the way. GI & Hepatology News. September 1, 2023. Accessed: February 1, 2025. https://www.mdedge.com/gihepnews/article/264737/practice-management/coping-burnout-and-repetitive-injuries/page/0/2
- Taking Care of You: Ergonomic Essentials for Your Practice (DV074). American Society for Gastrointestinal Endoscopy. May 2017. Accessed: February 1, 2025. https://learn.asge.org/Listing/Taking-Care-of-You-Ergonomic-Essentials-for-Your-Practice-DV074-231
- Shergill A, Shin E, Woods K, et al. “MYSELF” - A novel and easy-to-implement pre-procedure ergonomic time-out that reduces endoscopists’ risk of musculoskeletal injury. Gastrointest Endosc. 2024;99(6) Supplement AB154. Accessed: February 1, 2025. https://www.giejournal.org/article/S0016-5107(24)01207-0/abstract
Click to view more from Gastroenterology Data Trends 2025.
Click to view more from Gastroenterology Data Trends 2025.
- Ridtitid W, Cote GA, Leung W, et al. Prevalence and risk factors for musculoskeletal injuries related to endoscopy. Gastrointest Endosc. 2015;81(2):294-302 e294.
- Mohan N, Singla M, Pawa S, et al. Gastroenterologists’ goals for ergonomic colonoscopes: results of a national survey. Gastrointest Endosc. 2025;s0016-5107(25)00051-3. doi:10.1016/j.gie.2025.01.027
- Pawa S, Kwon RS, Fishman DS, et al. American Society for Gastrointestinal Endoscopy guideline on the role of ergonomics for prevention of endoscopy-related injury: summary and recommendations. Gastrointest Endosc. 2023;98(4):482-491. Accessed: February 1, 2025. https://www.asge.org/docs/default-source/guidelines/asge-guideline-on-the-role-of-ergonomics-summary.pdf
- Austin K, Schoenberger H, Sesto M, Gaumnitz E, Teo Broman A, Saha S. Musculoskeletal injuries are commonly reported among gastroenterology trainees: Results of a national survey. Dig Dis Sci. 2019;64(6):1439-1447.
- Shergill AK, Rempel D, Barr A, et al. Biomechanical risk factors associated with distal upper extremity musculoskeletal disorders in endoscopists performing colonoscopy. Gastrointest Endosc. 2021;93(3):704–711.e3. doi:10.1016/j.gie.2020.11.001
- Lipowska A, Shergill A. Coping with burnout and repetitive injuries -The hazards of endoscopy: Ergonomics guide the way. GI & Hepatology News. September 1, 2023. Accessed: February 1, 2025. https://www.mdedge.com/gihepnews/article/264737/practice-management/coping-burnout-and-repetitive-injuries/page/0/2
- Taking Care of You: Ergonomic Essentials for Your Practice (DV074). American Society for Gastrointestinal Endoscopy. May 2017. Accessed: February 1, 2025. https://learn.asge.org/Listing/Taking-Care-of-You-Ergonomic-Essentials-for-Your-Practice-DV074-231
- Shergill A, Shin E, Woods K, et al. “MYSELF” - A novel and easy-to-implement pre-procedure ergonomic time-out that reduces endoscopists’ risk of musculoskeletal injury. Gastrointest Endosc. 2024;99(6) Supplement AB154. Accessed: February 1, 2025. https://www.giejournal.org/article/S0016-5107(24)01207-0/abstract
- Ridtitid W, Cote GA, Leung W, et al. Prevalence and risk factors for musculoskeletal injuries related to endoscopy. Gastrointest Endosc. 2015;81(2):294-302 e294.
- Mohan N, Singla M, Pawa S, et al. Gastroenterologists’ goals for ergonomic colonoscopes: results of a national survey. Gastrointest Endosc. 2025;s0016-5107(25)00051-3. doi:10.1016/j.gie.2025.01.027
- Pawa S, Kwon RS, Fishman DS, et al. American Society for Gastrointestinal Endoscopy guideline on the role of ergonomics for prevention of endoscopy-related injury: summary and recommendations. Gastrointest Endosc. 2023;98(4):482-491. Accessed: February 1, 2025. https://www.asge.org/docs/default-source/guidelines/asge-guideline-on-the-role-of-ergonomics-summary.pdf
- Austin K, Schoenberger H, Sesto M, Gaumnitz E, Teo Broman A, Saha S. Musculoskeletal injuries are commonly reported among gastroenterology trainees: Results of a national survey. Dig Dis Sci. 2019;64(6):1439-1447.
- Shergill AK, Rempel D, Barr A, et al. Biomechanical risk factors associated with distal upper extremity musculoskeletal disorders in endoscopists performing colonoscopy. Gastrointest Endosc. 2021;93(3):704–711.e3. doi:10.1016/j.gie.2020.11.001
- Lipowska A, Shergill A. Coping with burnout and repetitive injuries -The hazards of endoscopy: Ergonomics guide the way. GI & Hepatology News. September 1, 2023. Accessed: February 1, 2025. https://www.mdedge.com/gihepnews/article/264737/practice-management/coping-burnout-and-repetitive-injuries/page/0/2
- Taking Care of You: Ergonomic Essentials for Your Practice (DV074). American Society for Gastrointestinal Endoscopy. May 2017. Accessed: February 1, 2025. https://learn.asge.org/Listing/Taking-Care-of-You-Ergonomic-Essentials-for-Your-Practice-DV074-231
- Shergill A, Shin E, Woods K, et al. “MYSELF” - A novel and easy-to-implement pre-procedure ergonomic time-out that reduces endoscopists’ risk of musculoskeletal injury. Gastrointest Endosc. 2024;99(6) Supplement AB154. Accessed: February 1, 2025. https://www.giejournal.org/article/S0016-5107(24)01207-0/abstract
Ergonomics in Endoscopy
Ergonomics in Endoscopy
Autoimmune Pancreatitis: What’s Really Behind Those Symptoms
“Defined about 30 years ago, autoimmune pancreatitis [AIP] remains a diagnostic challenge,” said Vinciane Rebours, MD, PhD, professor and head of the Pancreatology and Digestive Oncology Department, Beaujon Hospital in Clichy, France. She spoke at the Francophone Days of Hepatology, Gastroenterology, and Digestive Oncology 2025, held in Paris. The challenge lies in the fact that AIP includes two distinct clinical entities, neither of which is truly autoimmune. However, much remains unknown, including its natural history, cancer risk, and optimal treatment strategies. However, some aspects are now better understood.
Autoimmune Pancreatitis
These forms differ in their histological characteristics. Type 1 exhibits lymphoplasmacytic infiltration, extensive fibrosis, and IgG4-positive plasma cells. Type 2 presents with granulocytic lesions similar to those in Crohn’s disease.
Type 1 AIP typically affects men aged 50 years or older and is often associated with jaundice, pseudotumor formation, diabetes, and exocrine pancreatic insufficiency. “It is a systemic disease where lymphoplasmacytic infiltration can affect multiple organs, with the pancreas and lymph nodes most commonly involved,” said Rebours.
A definitive diagnosis of type 1 AIP requires three criteria: Organ involvement, serum IgG4 levels more than twice the normal level, and histological abnormalities on biopsy. If one of these criteria is missing, the diagnosis is considered probable or possible.
Diagnosing type 1 AIP is challenging because it can affect multiple organs, often with few symptoms, leading to significant clinical variability. Type 2 AIP, in contrast, generally affects younger individuals, with no gender preference. It is pathophysiologically distinct and is linked to IBD in 87% of cases. Diagnosis relies on clinical criteria, imaging abnormalities (parenchymal or ductal changes identifiable on scans), response to corticosteroids in symptomatic patients, and the presence of IBD. The absence of IgG4 can also aid in the diagnosis. However, gathering all these elements can be difficult.
Evolving Treatment
Symptomatic patients and those at risk for organ failure, particularly lung and kidney failure, are eligible for induction treatment. This involves the administration of full-dose corticosteroids for 4 weeks, followed by a tapering regimen. Remission was achieved in 99% of type 1 and 92% of type 2 cases. Corticosteroids can also be used as a “trial treatment” to assess corticosteroid sensitivity in patients with type 2 AIP.
The risk for recurrence (in case of nonresponse or recurrence before 12 months posttreatment) is higher in type 1 (one third of cases) than in type 2 (15%). In such cases, immunomodulators, primarily rituximab, are recommended for type 1 AIP. Rituximab can also be used as an induction treatment, either alone or in combination, or as maintenance therapy. Alternatives include mycophenolate mofetil or inebilizumab, which showed an 87% reduction in relapse risk according to data published in 2024.
Maintenance treatment for type 2 AIP is not yet fully standardized. The disease is often managed in a manner similar to that of IBD treatment. Rebours cautioned, “Management cannot stop at the pancreas; it is essential to detect all other paucisymptomatic manifestations through comprehensive annual imaging and biannual biological and functional screenings.”
Monitoring IgG4
Monitoring IgG4 levels is important for therapeutic follow-up but is not the “holy grail” for diagnosis, Rebours acknowledged. For instance, 20% of IgG4-RD cases have normal IgG4 levels, 20% of pancreatic cancers show elevated IgG4 levels, and some patients achieve clinical remission despite persistently abnormal IgG4 levels. Without strong suspicion of type 1 AIP, measuring IgG4 levels is “zero cost-effective.”
This disease, which is associated with the risk for underlying cancer, requires extensive imaging (CT, MRI, and endoscopic ultrasound) to differentiate between AIP and cancer. This step is essential to avoid unnecessary surgery on organs affected by IgG4-RD or for treating cancer with corticosteroids.
A version of this article appeared on Medscape.com.
“Defined about 30 years ago, autoimmune pancreatitis [AIP] remains a diagnostic challenge,” said Vinciane Rebours, MD, PhD, professor and head of the Pancreatology and Digestive Oncology Department, Beaujon Hospital in Clichy, France. She spoke at the Francophone Days of Hepatology, Gastroenterology, and Digestive Oncology 2025, held in Paris. The challenge lies in the fact that AIP includes two distinct clinical entities, neither of which is truly autoimmune. However, much remains unknown, including its natural history, cancer risk, and optimal treatment strategies. However, some aspects are now better understood.
Autoimmune Pancreatitis
These forms differ in their histological characteristics. Type 1 exhibits lymphoplasmacytic infiltration, extensive fibrosis, and IgG4-positive plasma cells. Type 2 presents with granulocytic lesions similar to those in Crohn’s disease.
Type 1 AIP typically affects men aged 50 years or older and is often associated with jaundice, pseudotumor formation, diabetes, and exocrine pancreatic insufficiency. “It is a systemic disease where lymphoplasmacytic infiltration can affect multiple organs, with the pancreas and lymph nodes most commonly involved,” said Rebours.
A definitive diagnosis of type 1 AIP requires three criteria: Organ involvement, serum IgG4 levels more than twice the normal level, and histological abnormalities on biopsy. If one of these criteria is missing, the diagnosis is considered probable or possible.
Diagnosing type 1 AIP is challenging because it can affect multiple organs, often with few symptoms, leading to significant clinical variability. Type 2 AIP, in contrast, generally affects younger individuals, with no gender preference. It is pathophysiologically distinct and is linked to IBD in 87% of cases. Diagnosis relies on clinical criteria, imaging abnormalities (parenchymal or ductal changes identifiable on scans), response to corticosteroids in symptomatic patients, and the presence of IBD. The absence of IgG4 can also aid in the diagnosis. However, gathering all these elements can be difficult.
Evolving Treatment
Symptomatic patients and those at risk for organ failure, particularly lung and kidney failure, are eligible for induction treatment. This involves the administration of full-dose corticosteroids for 4 weeks, followed by a tapering regimen. Remission was achieved in 99% of type 1 and 92% of type 2 cases. Corticosteroids can also be used as a “trial treatment” to assess corticosteroid sensitivity in patients with type 2 AIP.
The risk for recurrence (in case of nonresponse or recurrence before 12 months posttreatment) is higher in type 1 (one third of cases) than in type 2 (15%). In such cases, immunomodulators, primarily rituximab, are recommended for type 1 AIP. Rituximab can also be used as an induction treatment, either alone or in combination, or as maintenance therapy. Alternatives include mycophenolate mofetil or inebilizumab, which showed an 87% reduction in relapse risk according to data published in 2024.
Maintenance treatment for type 2 AIP is not yet fully standardized. The disease is often managed in a manner similar to that of IBD treatment. Rebours cautioned, “Management cannot stop at the pancreas; it is essential to detect all other paucisymptomatic manifestations through comprehensive annual imaging and biannual biological and functional screenings.”
Monitoring IgG4
Monitoring IgG4 levels is important for therapeutic follow-up but is not the “holy grail” for diagnosis, Rebours acknowledged. For instance, 20% of IgG4-RD cases have normal IgG4 levels, 20% of pancreatic cancers show elevated IgG4 levels, and some patients achieve clinical remission despite persistently abnormal IgG4 levels. Without strong suspicion of type 1 AIP, measuring IgG4 levels is “zero cost-effective.”
This disease, which is associated with the risk for underlying cancer, requires extensive imaging (CT, MRI, and endoscopic ultrasound) to differentiate between AIP and cancer. This step is essential to avoid unnecessary surgery on organs affected by IgG4-RD or for treating cancer with corticosteroids.
A version of this article appeared on Medscape.com.
“Defined about 30 years ago, autoimmune pancreatitis [AIP] remains a diagnostic challenge,” said Vinciane Rebours, MD, PhD, professor and head of the Pancreatology and Digestive Oncology Department, Beaujon Hospital in Clichy, France. She spoke at the Francophone Days of Hepatology, Gastroenterology, and Digestive Oncology 2025, held in Paris. The challenge lies in the fact that AIP includes two distinct clinical entities, neither of which is truly autoimmune. However, much remains unknown, including its natural history, cancer risk, and optimal treatment strategies. However, some aspects are now better understood.
Autoimmune Pancreatitis
These forms differ in their histological characteristics. Type 1 exhibits lymphoplasmacytic infiltration, extensive fibrosis, and IgG4-positive plasma cells. Type 2 presents with granulocytic lesions similar to those in Crohn’s disease.
Type 1 AIP typically affects men aged 50 years or older and is often associated with jaundice, pseudotumor formation, diabetes, and exocrine pancreatic insufficiency. “It is a systemic disease where lymphoplasmacytic infiltration can affect multiple organs, with the pancreas and lymph nodes most commonly involved,” said Rebours.
A definitive diagnosis of type 1 AIP requires three criteria: Organ involvement, serum IgG4 levels more than twice the normal level, and histological abnormalities on biopsy. If one of these criteria is missing, the diagnosis is considered probable or possible.
Diagnosing type 1 AIP is challenging because it can affect multiple organs, often with few symptoms, leading to significant clinical variability. Type 2 AIP, in contrast, generally affects younger individuals, with no gender preference. It is pathophysiologically distinct and is linked to IBD in 87% of cases. Diagnosis relies on clinical criteria, imaging abnormalities (parenchymal or ductal changes identifiable on scans), response to corticosteroids in symptomatic patients, and the presence of IBD. The absence of IgG4 can also aid in the diagnosis. However, gathering all these elements can be difficult.
Evolving Treatment
Symptomatic patients and those at risk for organ failure, particularly lung and kidney failure, are eligible for induction treatment. This involves the administration of full-dose corticosteroids for 4 weeks, followed by a tapering regimen. Remission was achieved in 99% of type 1 and 92% of type 2 cases. Corticosteroids can also be used as a “trial treatment” to assess corticosteroid sensitivity in patients with type 2 AIP.
The risk for recurrence (in case of nonresponse or recurrence before 12 months posttreatment) is higher in type 1 (one third of cases) than in type 2 (15%). In such cases, immunomodulators, primarily rituximab, are recommended for type 1 AIP. Rituximab can also be used as an induction treatment, either alone or in combination, or as maintenance therapy. Alternatives include mycophenolate mofetil or inebilizumab, which showed an 87% reduction in relapse risk according to data published in 2024.
Maintenance treatment for type 2 AIP is not yet fully standardized. The disease is often managed in a manner similar to that of IBD treatment. Rebours cautioned, “Management cannot stop at the pancreas; it is essential to detect all other paucisymptomatic manifestations through comprehensive annual imaging and biannual biological and functional screenings.”
Monitoring IgG4
Monitoring IgG4 levels is important for therapeutic follow-up but is not the “holy grail” for diagnosis, Rebours acknowledged. For instance, 20% of IgG4-RD cases have normal IgG4 levels, 20% of pancreatic cancers show elevated IgG4 levels, and some patients achieve clinical remission despite persistently abnormal IgG4 levels. Without strong suspicion of type 1 AIP, measuring IgG4 levels is “zero cost-effective.”
This disease, which is associated with the risk for underlying cancer, requires extensive imaging (CT, MRI, and endoscopic ultrasound) to differentiate between AIP and cancer. This step is essential to avoid unnecessary surgery on organs affected by IgG4-RD or for treating cancer with corticosteroids.
A version of this article appeared on Medscape.com.
New Fecal Product Expected to Enhance Microbiome Research

According to AGA’s Center for Gut Microbiome Research & Education, this critical resource will help advance the utility and reproducibility of microbiome-based diagnostics — “which still remain relatively meaningless clinically, although patients continue to buy direct-to-consumer tests, and a standard reference material will mean there’s a better way to ensure quality control and accuracy.”
Though not a therapeutic, Human Fecal Material RM is expected to speed up gastrointestinal (GI) therapeutics since many microbiome-based drugs are inspired by fecal transplants with human stool as the developmental starting point. A standardized reference material will be an important resource as industry develops and tests new drugs. It can be purchased online at the NIST Store (shop.nist.gov).
The product consists of eight frozen vials of exhaustively studied human feces suspended in aqueous solution. Available are more than 25 pages of data identifying the key microbes and biomolecules in the material. Scientists, including those working at biopharmaceutical and biotech companies, can use this material to further their research and develop new drugs that target the microbiome, including treatments that contain living bacteria.
Development
According to NIST, the stool material is “the most precisely measured, scientifically analyzed, and richly characterized human fecal standard ever produced.
“The project ran for about 6 years from start to finish, the last 2 for manufacturing, characterization, and writing,” said NIST molecular geneticist Scott A. Jackson, PhD, who helped develop the product. “We hope our reference material will lay the foundation for gut microbiome research to thrive and reach its full potential.”
As founder of NIST’s Complex Microbial Systems Group, Jackson is leading international efforts to improve microbiome and metagenomic measurements by organizing inter-lab studies and refining reference materials and methods.
The project collected stool from two cohorts of donors, ie, vegetarians and omnivores, with each cohort comprising four to six donors. Material from each cohort was pooled and homogenized before being aliquoted into 5000 vials per cohort. About 300 tubes from each cohort were picked, and aliquots then underwent multiomic analyses.
Offering his perspective on the new product, Sudhir K. Dutta, MBBS, associate professor in the Division of Gastroenterology and Hepatology at Johns Hopkins University School of Medicine, Baltimore, said, “This tool will be 100% useful for microbiome research.”
And according to Lori Holtz, MD, MSPH, professor of pediatric gastroenterology, hepatology, and nutrition at Washington University School of Medicine in St. Louis, Missouri, the material will aid microbiome research by allowing interpretability and repeatability across studies. “Microbiome research is a relatively new field, and protocols differ from group to group and lab to lab, so it’s been difficult to compare results across studies,” she told GI & Hepatology News. “A standard stool product will allow for greater comparability in preclinical studies and later clinical trials testing interventions to alter the microbiome.”
The NIST developers are looking forward to reaction from the GI research community. “Over the last several years, we’ve released smaller pilot batches of material to smaller groups of stakeholders,” said Jackson. “We’ve used the feedback on these earlier batches to inform the manufacturing and characterization of the final batch that was released in March, but we don’t yet have any feedback yet on the current material.”

Jackson, Dutta, and Holtz disclosed having no relevant competing interests.
A version of this article appeared on Medscape.com.
According to AGA’s Center for Gut Microbiome Research & Education, this critical resource will help advance the utility and reproducibility of microbiome-based diagnostics — “which still remain relatively meaningless clinically, although patients continue to buy direct-to-consumer tests, and a standard reference material will mean there’s a better way to ensure quality control and accuracy.”
Though not a therapeutic, Human Fecal Material RM is expected to speed up gastrointestinal (GI) therapeutics since many microbiome-based drugs are inspired by fecal transplants with human stool as the developmental starting point. A standardized reference material will be an important resource as industry develops and tests new drugs. It can be purchased online at the NIST Store (shop.nist.gov).
The product consists of eight frozen vials of exhaustively studied human feces suspended in aqueous solution. Available are more than 25 pages of data identifying the key microbes and biomolecules in the material. Scientists, including those working at biopharmaceutical and biotech companies, can use this material to further their research and develop new drugs that target the microbiome, including treatments that contain living bacteria.
Development
According to NIST, the stool material is “the most precisely measured, scientifically analyzed, and richly characterized human fecal standard ever produced.
“The project ran for about 6 years from start to finish, the last 2 for manufacturing, characterization, and writing,” said NIST molecular geneticist Scott A. Jackson, PhD, who helped develop the product. “We hope our reference material will lay the foundation for gut microbiome research to thrive and reach its full potential.”
As founder of NIST’s Complex Microbial Systems Group, Jackson is leading international efforts to improve microbiome and metagenomic measurements by organizing inter-lab studies and refining reference materials and methods.
The project collected stool from two cohorts of donors, ie, vegetarians and omnivores, with each cohort comprising four to six donors. Material from each cohort was pooled and homogenized before being aliquoted into 5000 vials per cohort. About 300 tubes from each cohort were picked, and aliquots then underwent multiomic analyses.
Offering his perspective on the new product, Sudhir K. Dutta, MBBS, associate professor in the Division of Gastroenterology and Hepatology at Johns Hopkins University School of Medicine, Baltimore, said, “This tool will be 100% useful for microbiome research.”
And according to Lori Holtz, MD, MSPH, professor of pediatric gastroenterology, hepatology, and nutrition at Washington University School of Medicine in St. Louis, Missouri, the material will aid microbiome research by allowing interpretability and repeatability across studies. “Microbiome research is a relatively new field, and protocols differ from group to group and lab to lab, so it’s been difficult to compare results across studies,” she told GI & Hepatology News. “A standard stool product will allow for greater comparability in preclinical studies and later clinical trials testing interventions to alter the microbiome.”
The NIST developers are looking forward to reaction from the GI research community. “Over the last several years, we’ve released smaller pilot batches of material to smaller groups of stakeholders,” said Jackson. “We’ve used the feedback on these earlier batches to inform the manufacturing and characterization of the final batch that was released in March, but we don’t yet have any feedback yet on the current material.”
Jackson, Dutta, and Holtz disclosed having no relevant competing interests.
A version of this article appeared on Medscape.com.
According to AGA’s Center for Gut Microbiome Research & Education, this critical resource will help advance the utility and reproducibility of microbiome-based diagnostics — “which still remain relatively meaningless clinically, although patients continue to buy direct-to-consumer tests, and a standard reference material will mean there’s a better way to ensure quality control and accuracy.”
Though not a therapeutic, Human Fecal Material RM is expected to speed up gastrointestinal (GI) therapeutics since many microbiome-based drugs are inspired by fecal transplants with human stool as the developmental starting point. A standardized reference material will be an important resource as industry develops and tests new drugs. It can be purchased online at the NIST Store (shop.nist.gov).
The product consists of eight frozen vials of exhaustively studied human feces suspended in aqueous solution. Available are more than 25 pages of data identifying the key microbes and biomolecules in the material. Scientists, including those working at biopharmaceutical and biotech companies, can use this material to further their research and develop new drugs that target the microbiome, including treatments that contain living bacteria.
Development
According to NIST, the stool material is “the most precisely measured, scientifically analyzed, and richly characterized human fecal standard ever produced.
“The project ran for about 6 years from start to finish, the last 2 for manufacturing, characterization, and writing,” said NIST molecular geneticist Scott A. Jackson, PhD, who helped develop the product. “We hope our reference material will lay the foundation for gut microbiome research to thrive and reach its full potential.”
As founder of NIST’s Complex Microbial Systems Group, Jackson is leading international efforts to improve microbiome and metagenomic measurements by organizing inter-lab studies and refining reference materials and methods.
The project collected stool from two cohorts of donors, ie, vegetarians and omnivores, with each cohort comprising four to six donors. Material from each cohort was pooled and homogenized before being aliquoted into 5000 vials per cohort. About 300 tubes from each cohort were picked, and aliquots then underwent multiomic analyses.
Offering his perspective on the new product, Sudhir K. Dutta, MBBS, associate professor in the Division of Gastroenterology and Hepatology at Johns Hopkins University School of Medicine, Baltimore, said, “This tool will be 100% useful for microbiome research.”
And according to Lori Holtz, MD, MSPH, professor of pediatric gastroenterology, hepatology, and nutrition at Washington University School of Medicine in St. Louis, Missouri, the material will aid microbiome research by allowing interpretability and repeatability across studies. “Microbiome research is a relatively new field, and protocols differ from group to group and lab to lab, so it’s been difficult to compare results across studies,” she told GI & Hepatology News. “A standard stool product will allow for greater comparability in preclinical studies and later clinical trials testing interventions to alter the microbiome.”
The NIST developers are looking forward to reaction from the GI research community. “Over the last several years, we’ve released smaller pilot batches of material to smaller groups of stakeholders,” said Jackson. “We’ve used the feedback on these earlier batches to inform the manufacturing and characterization of the final batch that was released in March, but we don’t yet have any feedback yet on the current material.”
Jackson, Dutta, and Holtz disclosed having no relevant competing interests.
A version of this article appeared on Medscape.com.
Experts Recommend Medication for Pediatric MASLD Management
, according to a new joint perspective paper.
Pediatric MASLD is the number-one cause of chronic liver disease in children and the number-one reason for liver transplant listing in young adults aged 18-40 years, said corresponding author Jennifer A. Panganiban, MD, Children’s Hospital of Philadelphia, Philadelphia.
The paper, published in Obesity Pillars, represents “a call to action that has been long overdue,” Panganiban told GI & Hepatology News.
The goal of the authors was to bring global awareness to the recent changes in the pediatric MASLD landscape — especially in medication use — and to empower clinicians treating the disease, she explained.
The recommendations are based on a combination of the latest published evidence and clinical expertise from eight hepatologists/gastroenterologists and two physicians from the Obesity Medicine Association, Centennial, Colorado.
One of the major barriers to MASLD management in children is suboptimal screening resulting in underdiagnosis, said Panganiban. “Unfortunately, only up to 30% of children are being screened in their pediatrician’s office.”
The new guideline outlines the patient care process from screening, referral to a subspecialist, and workup; however, the primary focus is on treatment with medication options that were previously not available or underutilized, she said.
Successful and Sustainable Weight Loss
Adiposity and weight gain make MASLD worse, but weight reduction has been shown to improve the condition, the authors noted. Previous strategies for curbing MASLD in children with obesity have focused mainly on lifestyle changes, but with limited success.
Nevertheless, the authors recommend continuing physical activity and nutrition as treatments for MASLD in children, with a plan tailored specifically to the patient.
In addition, however, they suggest that anti-obesity medications started early in the disease may help reduce costs and improve future outcomes.
Although glucagon-like peptide 1 receptor agonists (GLP-1 RAs) have not yet been studied specifically for pediatric MASLD, data from studies of pediatric obesity, diabetes, and other retrospective studies are encouraging, the authors wrote.
The GLP-1 RAs liraglutide and semaglutide are both approved by the US Food and Drug Administration (FDA) for managing obesity in children and adolescents aged 12 years or older, they noted. And a recent phase 3a randomized trial showed that liraglutide, not yet approved for children younger than 12 years, led to a mean change in body mass index of 5.8% from baseline to 56 weeks in children aged 6-11 years with obesity.
GLP-1 RAs not only are effective for weight management but also improve other metabolic dysfunction indicators including cholesterol and blood pressure, which makes these medications an even more beneficial option for individuals with obesity and MASLD, Panganiban and colleagues wrote.
For example, a recent single-center study of 111 children with MASLD (mean age, 15 years) showed a significant improvement in alanine aminotransferase levels with the use of GLP-1 RAs, although body mass index and weight were unchanged.
Regaining weight after discontinuing GLP-1 RAs is the main barrier to their use for MASLD, the authors noted. In addition, GLP-1 RAs are contraindicated in some situations, such as in those with a history of serious hypersensitivity, and in patients with a personal or family history of either medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 based on animal studies showing an association with the medications and thyroid C–cell tumors.
Other FDA-approved medication options for obesity in children include metformin, topiramate, and phentermine, as well as bupropion, lisdexamfetamine, and setmelanotide, the authors said.
Resmetirom, a thyroid hormone receptor-beta agonist, which is another significant breakthrough in MASLD for adults, has not yet been tested or approved for pediatric use.
In addition to medications, metabolic bariatric surgery has shown effectiveness in children with obesity and/or MASLD by reducing liver fat and reversing fibrosis, as shown in the Teen-LABS study, the authors wrote. However, long-term data on fibrosis reversal are limited, and cost and access remain barriers.
More Research Needed
The joint expert review is intended as an educational tool that may require updates and should not be interpreted as rules for individual patient care, the authors cautioned. And physical activity and nutrition remain the primary treatment of MASLD and should be continued in conjunction with other treatment modalities, they emphasized.
Looking ahead, research is needed to develop accurate and reliable noninvasive biomarkers to diagnose and assess obesity treatment efficacy, Panganiban told GI & Hepatology News.
Also needed are multicenter randomized control trials in children with obesity involving different medications that have been successful in the treatment of metabolic dysfunction–associated steatohepatitis/fibrosis in adults, such as GLP-1 RAs or resmetirom, she added.
Educating Clinicians on Early Identification
When obesity occurs in childhood, it starts a process of additional complications that arise in earlier ages in adults, said Saul J. Karpen, MD, chief scientific officer at the Stravitz-Sanyal Institute for Liver Disease and Metabolic Health, Virginia Commonwealth University, Richmond, Virginia, in an interview.“Given the epidemic of obesity, altered diets, and reduced physical activities during younger ages, it is not easy to identify which children are at greater risk of MASLD,” said Karpen.
“It requires insight from the care providers and often imaging, a blood test, or a referral to a pediatric hepatologist, and not every region has easy access to such expertise,” Karpen said.
The new review is important because it highlights the fact that obesity and its consequences are not limited to adulthood, and that educated clinicians are in a position to get an early start on treatment in children, Karpen noted.
The guideline received no outside funding. Panganiban and Karpen had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
, according to a new joint perspective paper.
Pediatric MASLD is the number-one cause of chronic liver disease in children and the number-one reason for liver transplant listing in young adults aged 18-40 years, said corresponding author Jennifer A. Panganiban, MD, Children’s Hospital of Philadelphia, Philadelphia.
The paper, published in Obesity Pillars, represents “a call to action that has been long overdue,” Panganiban told GI & Hepatology News.
The goal of the authors was to bring global awareness to the recent changes in the pediatric MASLD landscape — especially in medication use — and to empower clinicians treating the disease, she explained.
The recommendations are based on a combination of the latest published evidence and clinical expertise from eight hepatologists/gastroenterologists and two physicians from the Obesity Medicine Association, Centennial, Colorado.
One of the major barriers to MASLD management in children is suboptimal screening resulting in underdiagnosis, said Panganiban. “Unfortunately, only up to 30% of children are being screened in their pediatrician’s office.”
The new guideline outlines the patient care process from screening, referral to a subspecialist, and workup; however, the primary focus is on treatment with medication options that were previously not available or underutilized, she said.
Successful and Sustainable Weight Loss
Adiposity and weight gain make MASLD worse, but weight reduction has been shown to improve the condition, the authors noted. Previous strategies for curbing MASLD in children with obesity have focused mainly on lifestyle changes, but with limited success.
Nevertheless, the authors recommend continuing physical activity and nutrition as treatments for MASLD in children, with a plan tailored specifically to the patient.
In addition, however, they suggest that anti-obesity medications started early in the disease may help reduce costs and improve future outcomes.
Although glucagon-like peptide 1 receptor agonists (GLP-1 RAs) have not yet been studied specifically for pediatric MASLD, data from studies of pediatric obesity, diabetes, and other retrospective studies are encouraging, the authors wrote.
The GLP-1 RAs liraglutide and semaglutide are both approved by the US Food and Drug Administration (FDA) for managing obesity in children and adolescents aged 12 years or older, they noted. And a recent phase 3a randomized trial showed that liraglutide, not yet approved for children younger than 12 years, led to a mean change in body mass index of 5.8% from baseline to 56 weeks in children aged 6-11 years with obesity.
GLP-1 RAs not only are effective for weight management but also improve other metabolic dysfunction indicators including cholesterol and blood pressure, which makes these medications an even more beneficial option for individuals with obesity and MASLD, Panganiban and colleagues wrote.
For example, a recent single-center study of 111 children with MASLD (mean age, 15 years) showed a significant improvement in alanine aminotransferase levels with the use of GLP-1 RAs, although body mass index and weight were unchanged.
Regaining weight after discontinuing GLP-1 RAs is the main barrier to their use for MASLD, the authors noted. In addition, GLP-1 RAs are contraindicated in some situations, such as in those with a history of serious hypersensitivity, and in patients with a personal or family history of either medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 based on animal studies showing an association with the medications and thyroid C–cell tumors.
Other FDA-approved medication options for obesity in children include metformin, topiramate, and phentermine, as well as bupropion, lisdexamfetamine, and setmelanotide, the authors said.
Resmetirom, a thyroid hormone receptor-beta agonist, which is another significant breakthrough in MASLD for adults, has not yet been tested or approved for pediatric use.
In addition to medications, metabolic bariatric surgery has shown effectiveness in children with obesity and/or MASLD by reducing liver fat and reversing fibrosis, as shown in the Teen-LABS study, the authors wrote. However, long-term data on fibrosis reversal are limited, and cost and access remain barriers.
More Research Needed
The joint expert review is intended as an educational tool that may require updates and should not be interpreted as rules for individual patient care, the authors cautioned. And physical activity and nutrition remain the primary treatment of MASLD and should be continued in conjunction with other treatment modalities, they emphasized.
Looking ahead, research is needed to develop accurate and reliable noninvasive biomarkers to diagnose and assess obesity treatment efficacy, Panganiban told GI & Hepatology News.
Also needed are multicenter randomized control trials in children with obesity involving different medications that have been successful in the treatment of metabolic dysfunction–associated steatohepatitis/fibrosis in adults, such as GLP-1 RAs or resmetirom, she added.
Educating Clinicians on Early Identification
When obesity occurs in childhood, it starts a process of additional complications that arise in earlier ages in adults, said Saul J. Karpen, MD, chief scientific officer at the Stravitz-Sanyal Institute for Liver Disease and Metabolic Health, Virginia Commonwealth University, Richmond, Virginia, in an interview.“Given the epidemic of obesity, altered diets, and reduced physical activities during younger ages, it is not easy to identify which children are at greater risk of MASLD,” said Karpen.
“It requires insight from the care providers and often imaging, a blood test, or a referral to a pediatric hepatologist, and not every region has easy access to such expertise,” Karpen said.
The new review is important because it highlights the fact that obesity and its consequences are not limited to adulthood, and that educated clinicians are in a position to get an early start on treatment in children, Karpen noted.
The guideline received no outside funding. Panganiban and Karpen had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
, according to a new joint perspective paper.
Pediatric MASLD is the number-one cause of chronic liver disease in children and the number-one reason for liver transplant listing in young adults aged 18-40 years, said corresponding author Jennifer A. Panganiban, MD, Children’s Hospital of Philadelphia, Philadelphia.
The paper, published in Obesity Pillars, represents “a call to action that has been long overdue,” Panganiban told GI & Hepatology News.
The goal of the authors was to bring global awareness to the recent changes in the pediatric MASLD landscape — especially in medication use — and to empower clinicians treating the disease, she explained.
The recommendations are based on a combination of the latest published evidence and clinical expertise from eight hepatologists/gastroenterologists and two physicians from the Obesity Medicine Association, Centennial, Colorado.
One of the major barriers to MASLD management in children is suboptimal screening resulting in underdiagnosis, said Panganiban. “Unfortunately, only up to 30% of children are being screened in their pediatrician’s office.”
The new guideline outlines the patient care process from screening, referral to a subspecialist, and workup; however, the primary focus is on treatment with medication options that were previously not available or underutilized, she said.
Successful and Sustainable Weight Loss
Adiposity and weight gain make MASLD worse, but weight reduction has been shown to improve the condition, the authors noted. Previous strategies for curbing MASLD in children with obesity have focused mainly on lifestyle changes, but with limited success.
Nevertheless, the authors recommend continuing physical activity and nutrition as treatments for MASLD in children, with a plan tailored specifically to the patient.
In addition, however, they suggest that anti-obesity medications started early in the disease may help reduce costs and improve future outcomes.
Although glucagon-like peptide 1 receptor agonists (GLP-1 RAs) have not yet been studied specifically for pediatric MASLD, data from studies of pediatric obesity, diabetes, and other retrospective studies are encouraging, the authors wrote.
The GLP-1 RAs liraglutide and semaglutide are both approved by the US Food and Drug Administration (FDA) for managing obesity in children and adolescents aged 12 years or older, they noted. And a recent phase 3a randomized trial showed that liraglutide, not yet approved for children younger than 12 years, led to a mean change in body mass index of 5.8% from baseline to 56 weeks in children aged 6-11 years with obesity.
GLP-1 RAs not only are effective for weight management but also improve other metabolic dysfunction indicators including cholesterol and blood pressure, which makes these medications an even more beneficial option for individuals with obesity and MASLD, Panganiban and colleagues wrote.
For example, a recent single-center study of 111 children with MASLD (mean age, 15 years) showed a significant improvement in alanine aminotransferase levels with the use of GLP-1 RAs, although body mass index and weight were unchanged.
Regaining weight after discontinuing GLP-1 RAs is the main barrier to their use for MASLD, the authors noted. In addition, GLP-1 RAs are contraindicated in some situations, such as in those with a history of serious hypersensitivity, and in patients with a personal or family history of either medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 based on animal studies showing an association with the medications and thyroid C–cell tumors.
Other FDA-approved medication options for obesity in children include metformin, topiramate, and phentermine, as well as bupropion, lisdexamfetamine, and setmelanotide, the authors said.
Resmetirom, a thyroid hormone receptor-beta agonist, which is another significant breakthrough in MASLD for adults, has not yet been tested or approved for pediatric use.
In addition to medications, metabolic bariatric surgery has shown effectiveness in children with obesity and/or MASLD by reducing liver fat and reversing fibrosis, as shown in the Teen-LABS study, the authors wrote. However, long-term data on fibrosis reversal are limited, and cost and access remain barriers.
More Research Needed
The joint expert review is intended as an educational tool that may require updates and should not be interpreted as rules for individual patient care, the authors cautioned. And physical activity and nutrition remain the primary treatment of MASLD and should be continued in conjunction with other treatment modalities, they emphasized.
Looking ahead, research is needed to develop accurate and reliable noninvasive biomarkers to diagnose and assess obesity treatment efficacy, Panganiban told GI & Hepatology News.
Also needed are multicenter randomized control trials in children with obesity involving different medications that have been successful in the treatment of metabolic dysfunction–associated steatohepatitis/fibrosis in adults, such as GLP-1 RAs or resmetirom, she added.
Educating Clinicians on Early Identification
When obesity occurs in childhood, it starts a process of additional complications that arise in earlier ages in adults, said Saul J. Karpen, MD, chief scientific officer at the Stravitz-Sanyal Institute for Liver Disease and Metabolic Health, Virginia Commonwealth University, Richmond, Virginia, in an interview.“Given the epidemic of obesity, altered diets, and reduced physical activities during younger ages, it is not easy to identify which children are at greater risk of MASLD,” said Karpen.
“It requires insight from the care providers and often imaging, a blood test, or a referral to a pediatric hepatologist, and not every region has easy access to such expertise,” Karpen said.
The new review is important because it highlights the fact that obesity and its consequences are not limited to adulthood, and that educated clinicians are in a position to get an early start on treatment in children, Karpen noted.
The guideline received no outside funding. Panganiban and Karpen had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Key Blood Proteins Predict MASLD Up to 16 Years in Advance
SAN DIEGO –
“This represents the first high-performance, ultra-early (16 years) predictive model for MASLD,” said first author Shiyi Yu, MD, resident physician in the department of gastroenterology, Guangdong Provincial People’s Hospital in China.
“The findings could be a game-changer for how we screen for and intervene in liver disease,” Yu said at a press briefing for Digestive Disease Week® (DDW) 2025.
“Instead of waiting for symptoms or irreversible damage, we can [identify] high-risk individuals early and take steps to prevent MASLD from developing, which is particularly important because MASLD often progresses silently until advanced stages,” she added.
MASLD is the most common liver disorder in the world and carries a high risk of morbidity and mortality, with a mortality rate that is doubled compared with those without MASLD.
To identify any long-term predictive markers that could be used in simple predictive models, Yu and colleagues evaluated data on 52,952 participants enrolled in the UK Biobank between 2006 and 2010 who did not have MASLD at baseline and were followed up for up to 16.6 years.
Overall, 782 participants were diagnosed with MASLD over the course of the study.
A total of 2,737 blood proteins were analyzed, and among them, the five that emerged as being robust predictive biomarkers for development of MASLD within 5 years included CDHR2 (area under the curve [AUC] = 0.825), FUOM (AUC = 0.815), KRT18 (AUC = 0.810), ACY1 (AUC = 0.803), and GGT1 (AUC = 0.797).
Deviations of the proteins in plasma concentrations were observed up to 16 years prior to MASLD onset, with higher levels of the proteins at baseline associated with up to a nearly 10-times higher risk of MASLD (hazard ratios, 7.05-9.81).
A combination of the five proteins was predictive of incident MASLD at all time frames, including at 5-years (AUC = 0.857), 10-years (AUC = 0.775), and at all time points (AUC = 0.758).
The combined proteins gained even stronger predictive performance when added to key clinical biomarkers such as BMI and daily exercise, with an accuracy of 90.4% at 5 years and 82.2% at 16 years, “surpassing all existing short-term prediction models,” Yu reported.
Similar results were observed with the predictive model in a separate, smaller cohort of 100 participants in China, “further supporting the robustness of the model and showing it can be effective across diverse populations,” she noted in the press briefing.
Potential for Interventions ‘Years Before’ Damage Begins
Yu underscored the potential benefits of informing patients of their risk of MASLD.
“Too often, people do not find out they are at risk for liver disease before they are diagnosed and coping with symptoms,” she said.
A protein-based risk score could “profoundly transform early intervention strategies, triggering personalized lifestyle interventions for high-risk individuals” she said.
With obesity, type 2 diabetes, and high cholesterol levels among key risk factors for MASLD, such personalized interventions could include “counseling on diet, physical activity, and other factors years before liver damage begins, potentially averting disease progression altogether,” Yu noted.
Instead of waiting for abnormal liver function tests or imaging findings, patients could receive more frequent monitoring with annual elastography or ultrasound, for example, she explained.
In addition, “knowing one’s individualized protein-based risk may be more effective than abstract measures such as BMI or liver enzymes in motivating patients, facilitating better patient engagement and adherence,” Yu said.While noting that more work is needed to understand the biology behind the biomarkers, Yu underscored that “this is a big step toward personalized prevention.”
“By finding at-risk patients early, we hope to help stop MASLD before it starts,” she concluded.
Predictive Performance Impressive
Commenting on the study at the press briefing, Loren A. Laine, MD, AGAF, professor of medicine and chief of the Section of Digestive Diseases at the Yale School of Medicine, New Haven, Conn., and council chair of DDW 2025, noted that — as far as AUCs go — even a ranking in the 80% range is considered good. “So, for this to have an accuracy up to the 90s indicates a really excellent [predictive] performance,” he explained.
Laine agreed that the study findings have “the potential value to identify individuals at increased risk,” allowing for early monitoring and interventions.
The interventions “could be either general, such as things like diet and lifestyle, or more specific,” based on the function of these proteins, he added.
Rotonya Carr, MD, the division head of gastroenterology at the University of Washington, Seattle, further highlighted the pressing need for better predictive tools in MASLD.
“The predictions are that if we don’t do anything, as many as 122 million people will be impacted by MASLD” in the US by 2050, she told GI & Hepatology News.
“So, I am very excited about this work because we really don’t have anything right now that predicts who is going to get MASLD,” she said. “We are going to need tools like this, where people have information about their future health in order to make decisions.”
MASLD is known to be a significant risk factor for cardiovascular disease (CVD), and Carr speculated that the findings could lead to the types of predictive tools already available for CVD.
“I see this as being akin to what cardiology has had for quite some time, where they have cardiovascular risk disease calculators in which patients or their physicians can enter data and then estimate their risk of developing cardiovascular disease over, for instance, 10 years,” she said.
Laine’s disclosures include consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept, Merck, and Pfizer. Carr’s disclosures include relationships with Intercept and Novo Nordisk and research funding from Merck.
A version of this article appeared on Medscape.com.
SAN DIEGO –
“This represents the first high-performance, ultra-early (16 years) predictive model for MASLD,” said first author Shiyi Yu, MD, resident physician in the department of gastroenterology, Guangdong Provincial People’s Hospital in China.
“The findings could be a game-changer for how we screen for and intervene in liver disease,” Yu said at a press briefing for Digestive Disease Week® (DDW) 2025.
“Instead of waiting for symptoms or irreversible damage, we can [identify] high-risk individuals early and take steps to prevent MASLD from developing, which is particularly important because MASLD often progresses silently until advanced stages,” she added.
MASLD is the most common liver disorder in the world and carries a high risk of morbidity and mortality, with a mortality rate that is doubled compared with those without MASLD.
To identify any long-term predictive markers that could be used in simple predictive models, Yu and colleagues evaluated data on 52,952 participants enrolled in the UK Biobank between 2006 and 2010 who did not have MASLD at baseline and were followed up for up to 16.6 years.
Overall, 782 participants were diagnosed with MASLD over the course of the study.
A total of 2,737 blood proteins were analyzed, and among them, the five that emerged as being robust predictive biomarkers for development of MASLD within 5 years included CDHR2 (area under the curve [AUC] = 0.825), FUOM (AUC = 0.815), KRT18 (AUC = 0.810), ACY1 (AUC = 0.803), and GGT1 (AUC = 0.797).
Deviations of the proteins in plasma concentrations were observed up to 16 years prior to MASLD onset, with higher levels of the proteins at baseline associated with up to a nearly 10-times higher risk of MASLD (hazard ratios, 7.05-9.81).
A combination of the five proteins was predictive of incident MASLD at all time frames, including at 5-years (AUC = 0.857), 10-years (AUC = 0.775), and at all time points (AUC = 0.758).
The combined proteins gained even stronger predictive performance when added to key clinical biomarkers such as BMI and daily exercise, with an accuracy of 90.4% at 5 years and 82.2% at 16 years, “surpassing all existing short-term prediction models,” Yu reported.
Similar results were observed with the predictive model in a separate, smaller cohort of 100 participants in China, “further supporting the robustness of the model and showing it can be effective across diverse populations,” she noted in the press briefing.
Potential for Interventions ‘Years Before’ Damage Begins
Yu underscored the potential benefits of informing patients of their risk of MASLD.
“Too often, people do not find out they are at risk for liver disease before they are diagnosed and coping with symptoms,” she said.
A protein-based risk score could “profoundly transform early intervention strategies, triggering personalized lifestyle interventions for high-risk individuals” she said.
With obesity, type 2 diabetes, and high cholesterol levels among key risk factors for MASLD, such personalized interventions could include “counseling on diet, physical activity, and other factors years before liver damage begins, potentially averting disease progression altogether,” Yu noted.
Instead of waiting for abnormal liver function tests or imaging findings, patients could receive more frequent monitoring with annual elastography or ultrasound, for example, she explained.
In addition, “knowing one’s individualized protein-based risk may be more effective than abstract measures such as BMI or liver enzymes in motivating patients, facilitating better patient engagement and adherence,” Yu said.While noting that more work is needed to understand the biology behind the biomarkers, Yu underscored that “this is a big step toward personalized prevention.”
“By finding at-risk patients early, we hope to help stop MASLD before it starts,” she concluded.
Predictive Performance Impressive
Commenting on the study at the press briefing, Loren A. Laine, MD, AGAF, professor of medicine and chief of the Section of Digestive Diseases at the Yale School of Medicine, New Haven, Conn., and council chair of DDW 2025, noted that — as far as AUCs go — even a ranking in the 80% range is considered good. “So, for this to have an accuracy up to the 90s indicates a really excellent [predictive] performance,” he explained.
Laine agreed that the study findings have “the potential value to identify individuals at increased risk,” allowing for early monitoring and interventions.
The interventions “could be either general, such as things like diet and lifestyle, or more specific,” based on the function of these proteins, he added.
Rotonya Carr, MD, the division head of gastroenterology at the University of Washington, Seattle, further highlighted the pressing need for better predictive tools in MASLD.
“The predictions are that if we don’t do anything, as many as 122 million people will be impacted by MASLD” in the US by 2050, she told GI & Hepatology News.
“So, I am very excited about this work because we really don’t have anything right now that predicts who is going to get MASLD,” she said. “We are going to need tools like this, where people have information about their future health in order to make decisions.”
MASLD is known to be a significant risk factor for cardiovascular disease (CVD), and Carr speculated that the findings could lead to the types of predictive tools already available for CVD.
“I see this as being akin to what cardiology has had for quite some time, where they have cardiovascular risk disease calculators in which patients or their physicians can enter data and then estimate their risk of developing cardiovascular disease over, for instance, 10 years,” she said.
Laine’s disclosures include consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept, Merck, and Pfizer. Carr’s disclosures include relationships with Intercept and Novo Nordisk and research funding from Merck.
A version of this article appeared on Medscape.com.
SAN DIEGO –
“This represents the first high-performance, ultra-early (16 years) predictive model for MASLD,” said first author Shiyi Yu, MD, resident physician in the department of gastroenterology, Guangdong Provincial People’s Hospital in China.
“The findings could be a game-changer for how we screen for and intervene in liver disease,” Yu said at a press briefing for Digestive Disease Week® (DDW) 2025.
“Instead of waiting for symptoms or irreversible damage, we can [identify] high-risk individuals early and take steps to prevent MASLD from developing, which is particularly important because MASLD often progresses silently until advanced stages,” she added.
MASLD is the most common liver disorder in the world and carries a high risk of morbidity and mortality, with a mortality rate that is doubled compared with those without MASLD.
To identify any long-term predictive markers that could be used in simple predictive models, Yu and colleagues evaluated data on 52,952 participants enrolled in the UK Biobank between 2006 and 2010 who did not have MASLD at baseline and were followed up for up to 16.6 years.
Overall, 782 participants were diagnosed with MASLD over the course of the study.
A total of 2,737 blood proteins were analyzed, and among them, the five that emerged as being robust predictive biomarkers for development of MASLD within 5 years included CDHR2 (area under the curve [AUC] = 0.825), FUOM (AUC = 0.815), KRT18 (AUC = 0.810), ACY1 (AUC = 0.803), and GGT1 (AUC = 0.797).
Deviations of the proteins in plasma concentrations were observed up to 16 years prior to MASLD onset, with higher levels of the proteins at baseline associated with up to a nearly 10-times higher risk of MASLD (hazard ratios, 7.05-9.81).
A combination of the five proteins was predictive of incident MASLD at all time frames, including at 5-years (AUC = 0.857), 10-years (AUC = 0.775), and at all time points (AUC = 0.758).
The combined proteins gained even stronger predictive performance when added to key clinical biomarkers such as BMI and daily exercise, with an accuracy of 90.4% at 5 years and 82.2% at 16 years, “surpassing all existing short-term prediction models,” Yu reported.
Similar results were observed with the predictive model in a separate, smaller cohort of 100 participants in China, “further supporting the robustness of the model and showing it can be effective across diverse populations,” she noted in the press briefing.
Potential for Interventions ‘Years Before’ Damage Begins
Yu underscored the potential benefits of informing patients of their risk of MASLD.
“Too often, people do not find out they are at risk for liver disease before they are diagnosed and coping with symptoms,” she said.
A protein-based risk score could “profoundly transform early intervention strategies, triggering personalized lifestyle interventions for high-risk individuals” she said.
With obesity, type 2 diabetes, and high cholesterol levels among key risk factors for MASLD, such personalized interventions could include “counseling on diet, physical activity, and other factors years before liver damage begins, potentially averting disease progression altogether,” Yu noted.
Instead of waiting for abnormal liver function tests or imaging findings, patients could receive more frequent monitoring with annual elastography or ultrasound, for example, she explained.
In addition, “knowing one’s individualized protein-based risk may be more effective than abstract measures such as BMI or liver enzymes in motivating patients, facilitating better patient engagement and adherence,” Yu said.While noting that more work is needed to understand the biology behind the biomarkers, Yu underscored that “this is a big step toward personalized prevention.”
“By finding at-risk patients early, we hope to help stop MASLD before it starts,” she concluded.
Predictive Performance Impressive
Commenting on the study at the press briefing, Loren A. Laine, MD, AGAF, professor of medicine and chief of the Section of Digestive Diseases at the Yale School of Medicine, New Haven, Conn., and council chair of DDW 2025, noted that — as far as AUCs go — even a ranking in the 80% range is considered good. “So, for this to have an accuracy up to the 90s indicates a really excellent [predictive] performance,” he explained.
Laine agreed that the study findings have “the potential value to identify individuals at increased risk,” allowing for early monitoring and interventions.
The interventions “could be either general, such as things like diet and lifestyle, or more specific,” based on the function of these proteins, he added.
Rotonya Carr, MD, the division head of gastroenterology at the University of Washington, Seattle, further highlighted the pressing need for better predictive tools in MASLD.
“The predictions are that if we don’t do anything, as many as 122 million people will be impacted by MASLD” in the US by 2050, she told GI & Hepatology News.
“So, I am very excited about this work because we really don’t have anything right now that predicts who is going to get MASLD,” she said. “We are going to need tools like this, where people have information about their future health in order to make decisions.”
MASLD is known to be a significant risk factor for cardiovascular disease (CVD), and Carr speculated that the findings could lead to the types of predictive tools already available for CVD.
“I see this as being akin to what cardiology has had for quite some time, where they have cardiovascular risk disease calculators in which patients or their physicians can enter data and then estimate their risk of developing cardiovascular disease over, for instance, 10 years,” she said.
Laine’s disclosures include consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept, Merck, and Pfizer. Carr’s disclosures include relationships with Intercept and Novo Nordisk and research funding from Merck.
A version of this article appeared on Medscape.com.
FROM DDW 2025
Four Key Genes Linked to Worse Gastric Cancer Outcomes
SAN DIEGO – that potentially paves the way for precision oncology and improved targeting of therapies.
“About a third of patients with gastric cancer in our study had somatic mutations or variants of uncertain significance in [one of] four key genes,” lead author Ulysses Ribeiro, MD, PhD, a professor of digestive system surgery at the University of São Paulo School of Medicine in São Paulo, Brazil, said in a press briefing for the study, presented at Digestive Disease Week® (DDW) 2025.
“These patients were more likely to have their cancer come back or to die from the disease, even after surgery and the best chemotherapy and immunotherapy regimens,” said Ribeiro. While treatment strategies in gastric cancer have improved in recent years, resistance to multiple drugs continues, and the 5-year overall survival rate remains low — about 36% — underscoring the critical need for targeted therapies.
In an effort to identify genetic alterations that could have prognostic value, Ribeiro and his colleagues used next-generation DNA sequencing to analyze 21 genes in the tumor samples of 87 patients with gastric cancer who had undergone curative surgery and chemotherapy at the Sao Paulo Cancer Institute, São Paulo, Brazil.
Using Cox regression analysis, they found pathogenic variants or variants of uncertain significance in the following four genes: BRCA2, CDH1, RHOA, and TP53. “We found that 33% of patients carried at least one of these four genes,” Ribeiro told GI & Hepatology News.
Individually, each of the four genes with pathogenic variants or variants of uncertain significance had significantly or near-significantly higher risks in a survival analysis vs wild-type or benign variants, including BRCA2 (hazard ratio [HR], 4.33; P = .030); CDH1 (HR, 7.54; P = .004); RHOA (HR, 29.24; P < .001); and TP53 (HR, 2.82; P = .07).
A further multivariate analysis adjusting for key confounders showed that, when combined, carriers of the genes had lower disease-free survival (P = .005) and worse overall survival (P = .009) than those with none of the mutations.
“Individually, all four genes were related to prognosis in our gastric cancer patients, and when combined, the genes had even a higher difference in prognosis, varying from 2 to 28 times higher,” Ribeiro said.
Overall, factors such as having a more advanced tumor, node, metastasis stage, pathological stage, and the presence of a pathogenic mutation or a variant of uncertain significance in the four genes in the model were independently associated with worse disease-free survival.
Familiar Genes
Some of these genes are highly familiar. BRCA2 is well-known for its role in increasing the risk for breast and ovarian cancers, and CDH1 is known to be associated with hereditary diffuse gastric cancer, which is the most common hereditary cancer syndrome linked to gastric cancer.
TP53, also known as the “guardian of the genome,” is the most commonly altered gene in human cancers, while RHOA is known to be involved in encoding the GTPase protein RhoA, which is key in the regulation of cell shape, motility, and other essential cellular processes.
“This is the first time that these four genes have been shown to strongly relate to these gastric cancer outcomes,” said Ribeiro. This suggests that there’s more than one pathway by which stomach cancer forms and that some stomach cancers are much more aggressive than others.
He noted that “patients without these high-risk mutations” could be given “less aggressive treatment, in some cases sparing them from unnecessary side effects.”
Speaking during the press briefing, Loren A. Laine, MD, AGAF, who is a professor of medicine and chief of the Section of Digestive Diseases at the Yale School of Medicine in New Haven, Connecticut, and council chair of DDW 2025, agreed that “certainly, if these genetic factors, along with other factors, predict risk, this also has implications in practice with respect to the level of monitoring during the follow-up and determining the need for therapy.”
In addition, “it will be interesting to see how much this adds to other known risk factors, such as pathologic stage,” said Laine.
A strength of this study, “which I think is unique, is that it looks at a Western population,” whereas data on gastric as well as esophageal cancer is heavily biased to Eastern regions like China and East Asia, where the rates are much higher than in the West, Alia Qureshi, MD, an associate professor of esophageal and gastric cancer surgery at Oregon Health & Science University in Portland, Oregon, told GI & Hepatology News.
While noting the limitation of the relatively small sample size, Qureshi said the study is nevertheless “exciting and moving the direction we want to go, specifically towards precision medicine [and] precision oncology.”
The study “builds on existing understanding, especially with regard to TP53 and CDH1, and it points to the opportunity to use this data in a way to direct patient care or possibly therapeutic intervention,” she said.
Laine’s disclosures include consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept Pharmaceuticals, Merck, and Pfizer. Qureshi had no disclosures to report.
A version of this article appeared on Medscape.com.
SAN DIEGO – that potentially paves the way for precision oncology and improved targeting of therapies.
“About a third of patients with gastric cancer in our study had somatic mutations or variants of uncertain significance in [one of] four key genes,” lead author Ulysses Ribeiro, MD, PhD, a professor of digestive system surgery at the University of São Paulo School of Medicine in São Paulo, Brazil, said in a press briefing for the study, presented at Digestive Disease Week® (DDW) 2025.
“These patients were more likely to have their cancer come back or to die from the disease, even after surgery and the best chemotherapy and immunotherapy regimens,” said Ribeiro. While treatment strategies in gastric cancer have improved in recent years, resistance to multiple drugs continues, and the 5-year overall survival rate remains low — about 36% — underscoring the critical need for targeted therapies.
In an effort to identify genetic alterations that could have prognostic value, Ribeiro and his colleagues used next-generation DNA sequencing to analyze 21 genes in the tumor samples of 87 patients with gastric cancer who had undergone curative surgery and chemotherapy at the Sao Paulo Cancer Institute, São Paulo, Brazil.
Using Cox regression analysis, they found pathogenic variants or variants of uncertain significance in the following four genes: BRCA2, CDH1, RHOA, and TP53. “We found that 33% of patients carried at least one of these four genes,” Ribeiro told GI & Hepatology News.
Individually, each of the four genes with pathogenic variants or variants of uncertain significance had significantly or near-significantly higher risks in a survival analysis vs wild-type or benign variants, including BRCA2 (hazard ratio [HR], 4.33; P = .030); CDH1 (HR, 7.54; P = .004); RHOA (HR, 29.24; P < .001); and TP53 (HR, 2.82; P = .07).
A further multivariate analysis adjusting for key confounders showed that, when combined, carriers of the genes had lower disease-free survival (P = .005) and worse overall survival (P = .009) than those with none of the mutations.
“Individually, all four genes were related to prognosis in our gastric cancer patients, and when combined, the genes had even a higher difference in prognosis, varying from 2 to 28 times higher,” Ribeiro said.
Overall, factors such as having a more advanced tumor, node, metastasis stage, pathological stage, and the presence of a pathogenic mutation or a variant of uncertain significance in the four genes in the model were independently associated with worse disease-free survival.
Familiar Genes
Some of these genes are highly familiar. BRCA2 is well-known for its role in increasing the risk for breast and ovarian cancers, and CDH1 is known to be associated with hereditary diffuse gastric cancer, which is the most common hereditary cancer syndrome linked to gastric cancer.
TP53, also known as the “guardian of the genome,” is the most commonly altered gene in human cancers, while RHOA is known to be involved in encoding the GTPase protein RhoA, which is key in the regulation of cell shape, motility, and other essential cellular processes.
“This is the first time that these four genes have been shown to strongly relate to these gastric cancer outcomes,” said Ribeiro. This suggests that there’s more than one pathway by which stomach cancer forms and that some stomach cancers are much more aggressive than others.
He noted that “patients without these high-risk mutations” could be given “less aggressive treatment, in some cases sparing them from unnecessary side effects.”
Speaking during the press briefing, Loren A. Laine, MD, AGAF, who is a professor of medicine and chief of the Section of Digestive Diseases at the Yale School of Medicine in New Haven, Connecticut, and council chair of DDW 2025, agreed that “certainly, if these genetic factors, along with other factors, predict risk, this also has implications in practice with respect to the level of monitoring during the follow-up and determining the need for therapy.”
In addition, “it will be interesting to see how much this adds to other known risk factors, such as pathologic stage,” said Laine.
A strength of this study, “which I think is unique, is that it looks at a Western population,” whereas data on gastric as well as esophageal cancer is heavily biased to Eastern regions like China and East Asia, where the rates are much higher than in the West, Alia Qureshi, MD, an associate professor of esophageal and gastric cancer surgery at Oregon Health & Science University in Portland, Oregon, told GI & Hepatology News.
While noting the limitation of the relatively small sample size, Qureshi said the study is nevertheless “exciting and moving the direction we want to go, specifically towards precision medicine [and] precision oncology.”
The study “builds on existing understanding, especially with regard to TP53 and CDH1, and it points to the opportunity to use this data in a way to direct patient care or possibly therapeutic intervention,” she said.
Laine’s disclosures include consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept Pharmaceuticals, Merck, and Pfizer. Qureshi had no disclosures to report.
A version of this article appeared on Medscape.com.
SAN DIEGO – that potentially paves the way for precision oncology and improved targeting of therapies.
“About a third of patients with gastric cancer in our study had somatic mutations or variants of uncertain significance in [one of] four key genes,” lead author Ulysses Ribeiro, MD, PhD, a professor of digestive system surgery at the University of São Paulo School of Medicine in São Paulo, Brazil, said in a press briefing for the study, presented at Digestive Disease Week® (DDW) 2025.
“These patients were more likely to have their cancer come back or to die from the disease, even after surgery and the best chemotherapy and immunotherapy regimens,” said Ribeiro. While treatment strategies in gastric cancer have improved in recent years, resistance to multiple drugs continues, and the 5-year overall survival rate remains low — about 36% — underscoring the critical need for targeted therapies.
In an effort to identify genetic alterations that could have prognostic value, Ribeiro and his colleagues used next-generation DNA sequencing to analyze 21 genes in the tumor samples of 87 patients with gastric cancer who had undergone curative surgery and chemotherapy at the Sao Paulo Cancer Institute, São Paulo, Brazil.
Using Cox regression analysis, they found pathogenic variants or variants of uncertain significance in the following four genes: BRCA2, CDH1, RHOA, and TP53. “We found that 33% of patients carried at least one of these four genes,” Ribeiro told GI & Hepatology News.
Individually, each of the four genes with pathogenic variants or variants of uncertain significance had significantly or near-significantly higher risks in a survival analysis vs wild-type or benign variants, including BRCA2 (hazard ratio [HR], 4.33; P = .030); CDH1 (HR, 7.54; P = .004); RHOA (HR, 29.24; P < .001); and TP53 (HR, 2.82; P = .07).
A further multivariate analysis adjusting for key confounders showed that, when combined, carriers of the genes had lower disease-free survival (P = .005) and worse overall survival (P = .009) than those with none of the mutations.
“Individually, all four genes were related to prognosis in our gastric cancer patients, and when combined, the genes had even a higher difference in prognosis, varying from 2 to 28 times higher,” Ribeiro said.
Overall, factors such as having a more advanced tumor, node, metastasis stage, pathological stage, and the presence of a pathogenic mutation or a variant of uncertain significance in the four genes in the model were independently associated with worse disease-free survival.
Familiar Genes
Some of these genes are highly familiar. BRCA2 is well-known for its role in increasing the risk for breast and ovarian cancers, and CDH1 is known to be associated with hereditary diffuse gastric cancer, which is the most common hereditary cancer syndrome linked to gastric cancer.
TP53, also known as the “guardian of the genome,” is the most commonly altered gene in human cancers, while RHOA is known to be involved in encoding the GTPase protein RhoA, which is key in the regulation of cell shape, motility, and other essential cellular processes.
“This is the first time that these four genes have been shown to strongly relate to these gastric cancer outcomes,” said Ribeiro. This suggests that there’s more than one pathway by which stomach cancer forms and that some stomach cancers are much more aggressive than others.
He noted that “patients without these high-risk mutations” could be given “less aggressive treatment, in some cases sparing them from unnecessary side effects.”
Speaking during the press briefing, Loren A. Laine, MD, AGAF, who is a professor of medicine and chief of the Section of Digestive Diseases at the Yale School of Medicine in New Haven, Connecticut, and council chair of DDW 2025, agreed that “certainly, if these genetic factors, along with other factors, predict risk, this also has implications in practice with respect to the level of monitoring during the follow-up and determining the need for therapy.”
In addition, “it will be interesting to see how much this adds to other known risk factors, such as pathologic stage,” said Laine.
A strength of this study, “which I think is unique, is that it looks at a Western population,” whereas data on gastric as well as esophageal cancer is heavily biased to Eastern regions like China and East Asia, where the rates are much higher than in the West, Alia Qureshi, MD, an associate professor of esophageal and gastric cancer surgery at Oregon Health & Science University in Portland, Oregon, told GI & Hepatology News.
While noting the limitation of the relatively small sample size, Qureshi said the study is nevertheless “exciting and moving the direction we want to go, specifically towards precision medicine [and] precision oncology.”
The study “builds on existing understanding, especially with regard to TP53 and CDH1, and it points to the opportunity to use this data in a way to direct patient care or possibly therapeutic intervention,” she said.
Laine’s disclosures include consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept Pharmaceuticals, Merck, and Pfizer. Qureshi had no disclosures to report.
A version of this article appeared on Medscape.com.
FROM DDW 2025
Targeted CRC Outreach Doubles Screening Rates, Cuts Deaths by Half
SAN DIEGO — A 20-year initiative by Kaiser Permanente Northern California that assessed colorectal cancer (CRC) screening status and offered flexible options for screening has made a huge difference in CRC incidence, deaths, and racial disparities, an analysis showed.
“The program promptly doubled the proportion of people up to date with screening,” reported lead investigator Douglas A. Corley, MD, PhD, AGAF, a research scientist with Kaiser’s Division of Research, at a press briefing held on April 24, ahead of a presentation at the Digestive Disease Week® (DDW) 2025.

Additionally, , he said.
“Ten years ago, there were big gaps in cancer risk and death, especially among our Black patients. Now, those differences are nearly gone,” Corley said.
Closing the Gap
A systematic CRC screening program was implemented across Kaiser Permanente Northern California. The program included proactive outreach to members who were overdue for screening and mailing them fecal immunochemical test (FIT) kits for at-home use.
Corley and colleagues tracked screening status and CRC incidence and mortality annually from 2000 to 2019 among about 1.1 million members aged 50-75 years across 22 medical centers of the integrated healthcare system. The cohort included American Indian or Alaska Native, Asian, Black, Hispanic, Native Hawaiian or Pacific Islander, and White members.
Screening rates via FIT, colonoscopy, or sigmoidoscopy more than doubled after starting the program, from about 37% in the early years to about 80% within a few years, and it stayed that high through 2019, Corley reported.
“Importantly, these large increases occurred across the whole population with only small differences,” he said.
For example, about 76% of Hispanic members, 77% of Black members, 82% of White members, and 83% of Asian members were up to date in the later years and through 2019.
“This shows that systematic, comparable outreach can provide a level playing field for completion of preventive care,” Corley said.
After an expected early uptick in CRC incidence due to early detection, incidence later declined and by 2019 had dropped approximately 30% across the groups.
Long-Standing Disparities Erased
CRC deaths also fell by about 50% across all groups, with the largest decline among Black members, Corley noted.
Racial and ethnic disparities in both CRC incidence and mortality have long existed, with Black patients in particular experiencing higher risks and worse outcomes, likely from a mixture of risk factors and healthcare utilization, Corley said.
Offering outreach and equal access to screening in the Kaiser program erased those long-standing disparities.
“It’s remarkable that some of these large differences in mortality by race and ethnicity that we saw two decades ago, and which are found throughout the United States, are now similar to small chance variation in the population,” Corley said.
Flexibility was key to getting more people screened, he noted. “It’s about reaching people at their homes and offering a choice to patients. It’s an astonishingly simple concept.”
It’s important to note that these findings stem from a large, integrated healthcare system, which may differ from other settings, although similar outreach strategies have succeeded in safety net clinics and smaller practices, Corley added.
By boosting screening rates to 80%, the health system reached the level that’s essentially been defined in the past as our goal of screening programs, said Loren Laine, MD, AGAF, professor of medicine (digestive diseases) at Yale School of Medicine, New Haven, Connecticut, and chair of this year’s DDW.

“It shows that if health systems institute programmatic screening for all their covered individuals, they could markedly increase screening, said Laine, who also served as moderator of the press briefing.
“Most importantly, of course, [screening] was associated with a reduction in colorectal cancer incidence and deaths,” he said.
The study had no commercial funding. Corley reported having no relevant conflicts of interest.
Laine’s disclosures included consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept, Merck, and Pfizer.
A version of this article appeared on Medscape.com.
SAN DIEGO — A 20-year initiative by Kaiser Permanente Northern California that assessed colorectal cancer (CRC) screening status and offered flexible options for screening has made a huge difference in CRC incidence, deaths, and racial disparities, an analysis showed.
“The program promptly doubled the proportion of people up to date with screening,” reported lead investigator Douglas A. Corley, MD, PhD, AGAF, a research scientist with Kaiser’s Division of Research, at a press briefing held on April 24, ahead of a presentation at the Digestive Disease Week® (DDW) 2025.
Additionally, , he said.
“Ten years ago, there were big gaps in cancer risk and death, especially among our Black patients. Now, those differences are nearly gone,” Corley said.
Closing the Gap
A systematic CRC screening program was implemented across Kaiser Permanente Northern California. The program included proactive outreach to members who were overdue for screening and mailing them fecal immunochemical test (FIT) kits for at-home use.
Corley and colleagues tracked screening status and CRC incidence and mortality annually from 2000 to 2019 among about 1.1 million members aged 50-75 years across 22 medical centers of the integrated healthcare system. The cohort included American Indian or Alaska Native, Asian, Black, Hispanic, Native Hawaiian or Pacific Islander, and White members.
Screening rates via FIT, colonoscopy, or sigmoidoscopy more than doubled after starting the program, from about 37% in the early years to about 80% within a few years, and it stayed that high through 2019, Corley reported.
“Importantly, these large increases occurred across the whole population with only small differences,” he said.
For example, about 76% of Hispanic members, 77% of Black members, 82% of White members, and 83% of Asian members were up to date in the later years and through 2019.
“This shows that systematic, comparable outreach can provide a level playing field for completion of preventive care,” Corley said.
After an expected early uptick in CRC incidence due to early detection, incidence later declined and by 2019 had dropped approximately 30% across the groups.
Long-Standing Disparities Erased
CRC deaths also fell by about 50% across all groups, with the largest decline among Black members, Corley noted.
Racial and ethnic disparities in both CRC incidence and mortality have long existed, with Black patients in particular experiencing higher risks and worse outcomes, likely from a mixture of risk factors and healthcare utilization, Corley said.
Offering outreach and equal access to screening in the Kaiser program erased those long-standing disparities.
“It’s remarkable that some of these large differences in mortality by race and ethnicity that we saw two decades ago, and which are found throughout the United States, are now similar to small chance variation in the population,” Corley said.
Flexibility was key to getting more people screened, he noted. “It’s about reaching people at their homes and offering a choice to patients. It’s an astonishingly simple concept.”
It’s important to note that these findings stem from a large, integrated healthcare system, which may differ from other settings, although similar outreach strategies have succeeded in safety net clinics and smaller practices, Corley added.
By boosting screening rates to 80%, the health system reached the level that’s essentially been defined in the past as our goal of screening programs, said Loren Laine, MD, AGAF, professor of medicine (digestive diseases) at Yale School of Medicine, New Haven, Connecticut, and chair of this year’s DDW.
“It shows that if health systems institute programmatic screening for all their covered individuals, they could markedly increase screening, said Laine, who also served as moderator of the press briefing.
“Most importantly, of course, [screening] was associated with a reduction in colorectal cancer incidence and deaths,” he said.
The study had no commercial funding. Corley reported having no relevant conflicts of interest.
Laine’s disclosures included consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept, Merck, and Pfizer.
A version of this article appeared on Medscape.com.
SAN DIEGO — A 20-year initiative by Kaiser Permanente Northern California that assessed colorectal cancer (CRC) screening status and offered flexible options for screening has made a huge difference in CRC incidence, deaths, and racial disparities, an analysis showed.
“The program promptly doubled the proportion of people up to date with screening,” reported lead investigator Douglas A. Corley, MD, PhD, AGAF, a research scientist with Kaiser’s Division of Research, at a press briefing held on April 24, ahead of a presentation at the Digestive Disease Week® (DDW) 2025.
Additionally, , he said.
“Ten years ago, there were big gaps in cancer risk and death, especially among our Black patients. Now, those differences are nearly gone,” Corley said.
Closing the Gap
A systematic CRC screening program was implemented across Kaiser Permanente Northern California. The program included proactive outreach to members who were overdue for screening and mailing them fecal immunochemical test (FIT) kits for at-home use.
Corley and colleagues tracked screening status and CRC incidence and mortality annually from 2000 to 2019 among about 1.1 million members aged 50-75 years across 22 medical centers of the integrated healthcare system. The cohort included American Indian or Alaska Native, Asian, Black, Hispanic, Native Hawaiian or Pacific Islander, and White members.
Screening rates via FIT, colonoscopy, or sigmoidoscopy more than doubled after starting the program, from about 37% in the early years to about 80% within a few years, and it stayed that high through 2019, Corley reported.
“Importantly, these large increases occurred across the whole population with only small differences,” he said.
For example, about 76% of Hispanic members, 77% of Black members, 82% of White members, and 83% of Asian members were up to date in the later years and through 2019.
“This shows that systematic, comparable outreach can provide a level playing field for completion of preventive care,” Corley said.
After an expected early uptick in CRC incidence due to early detection, incidence later declined and by 2019 had dropped approximately 30% across the groups.
Long-Standing Disparities Erased
CRC deaths also fell by about 50% across all groups, with the largest decline among Black members, Corley noted.
Racial and ethnic disparities in both CRC incidence and mortality have long existed, with Black patients in particular experiencing higher risks and worse outcomes, likely from a mixture of risk factors and healthcare utilization, Corley said.
Offering outreach and equal access to screening in the Kaiser program erased those long-standing disparities.
“It’s remarkable that some of these large differences in mortality by race and ethnicity that we saw two decades ago, and which are found throughout the United States, are now similar to small chance variation in the population,” Corley said.
Flexibility was key to getting more people screened, he noted. “It’s about reaching people at their homes and offering a choice to patients. It’s an astonishingly simple concept.”
It’s important to note that these findings stem from a large, integrated healthcare system, which may differ from other settings, although similar outreach strategies have succeeded in safety net clinics and smaller practices, Corley added.
By boosting screening rates to 80%, the health system reached the level that’s essentially been defined in the past as our goal of screening programs, said Loren Laine, MD, AGAF, professor of medicine (digestive diseases) at Yale School of Medicine, New Haven, Connecticut, and chair of this year’s DDW.
“It shows that if health systems institute programmatic screening for all their covered individuals, they could markedly increase screening, said Laine, who also served as moderator of the press briefing.
“Most importantly, of course, [screening] was associated with a reduction in colorectal cancer incidence and deaths,” he said.
The study had no commercial funding. Corley reported having no relevant conflicts of interest.
Laine’s disclosures included consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept, Merck, and Pfizer.
A version of this article appeared on Medscape.com.
FROM DDW 2025