User login
Documentation, CMS-Approved Language Key to Getting Paid for Hospitalist Teaching Services

When hospitalists work in academic centers, medical and surgical services are furnished, in part, by a resident within the scope of the hospitalists’ training program. A resident is “an individual who participates in an approved graduate medical education (GME) program or a physician who is not in an approved GME program but who is authorized to practice only in a hospital setting.”1 Resident services are covered by Centers for Medicare & Medicaid Services (CMS) and paid by the Fiscal Intermediary through direct GME and Indirect Medical Education (IME) payments. These services are not billed or paid using the Medicare Physician Fee Schedule. The teaching physician is responsible for supervising the resident’s health-care delivery but is not paid for the resident’s work. The teaching physician is paid for their personal and medically necessary service in providing patient care. The teaching physician has the option to perform the entire service, or perform the self-determined critical or key portion(s) of the service.
Comprehensive Service
Teaching physicians independently see the patient and perform all required elements to support the visit level (e.g. 99233: subsequent hospital care, per day, which requires at least two of the following three key components: a detailed interval history, a detailed examination, or high-complexity medical decision-making).2 The teaching physician writes a note independent of a resident encounter with the patient or documentation. The teaching physician note “stands alone” and does not rely on the resident’s documentation. If the resident saw the patient and documented the encounter, the teaching physician might choose to “link to” the resident note in lieu of personally documenting the entire service. The linking statement must demonstrate teaching physician involvement in the patient encounter and participation in patient management. Use of CMS-approved statements is best to meet these requirements. Statement examples include:3
- “I performed a history and physical examination of the patient and discussed his management with the resident. I reviewed the resident’s note and agree with the documented findings and plan of care.”
- “I saw and evaluated the patient. I agree with the findings and the plan of care as documented in the resident’s note.”
- “I saw and examined the patient. I agree with the resident’s note, except the heart murmur is louder, so I will obtain an echo to evaluate.”
Each of these statements meets the minimum requirements for billing. However, teaching physicians should offer more information in support of other clinical, quality, and regulatory initiatives and mandates, better exemplified in the last example. The reported visit level will be supported by the combined documentation (teaching physician and resident).
The teaching physician submits a claim in their name and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99223-GC). This alerts the Medicare contractor that services were provided under teaching physician rules. Requests for documentation should include a response with medical record entries from the teaching physician and resident.
Critical/Key Portion
“Supervised” service: The resident and teaching physician can round together; they can see the patient at the same time. The teaching physician observes the resident’s performance during the patient encounter, or personally performs self-determined elements of patient care. The resident documents their patient care. The attending must still note their presence in the medical record, performance of the critical or key portions of the service, and involvement in patient management. CMS-accepted statements include:3
- “I was present with the resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident’s note.”
- “I saw the patient with the resident and agree with the resident’s findings and plan.”
Although these statements demonstrate acceptable billing language, they lack patient-specific details that support the teaching physician’s personal contribution to patient care and the quality of their expertise. The teaching physician selects the visit level that represents the combined documentation and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99232-GC).
“Shared” service: The resident sees the patient unaccompanied and documents the corresponding care provided. The teaching physician sees the patient at a different time but performs only the critical or key portions of the service. The case is subsequently discussed with the resident. The teaching physician must document their presence and performance of the critical or key portions of the service, along with any patient management. Using CMS-quoted statements ensures regulatory compliance:3
- “I saw and evaluated the patient. I reviewed the resident’s note and agree, except that the picture is more consistent with pericarditis than myocardial ischemia. Will begin NSAIDs.”
- “I saw and evaluated the patient. Discussed with resident and agree with resident’s findings and plan as documented in the resident’s note.”
- “See resident’s note for details. I saw and evaluated the patient and agree with the resident’s finding and plans as written.”
- “I saw and evaluated the patient. Agree with resident’s note, but lower extremities are weaker, now 3/5; MRI of L/S spine today.”
Once again, the teaching physician selects the visit level that represents the combined documentation and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99233-GC).
EHR Considerations
When seeing patients independent of one another, the timing of the teaching physician and resident encounters does not impact billing. However, the time that the resident encounter is documented in the medical record can significantly impact the payment when reviewed by external auditors. When the resident note is dated and timed later than the teaching physician’s entry, the teaching physician cannot consider the resident’s note for visit-level selection. The teaching physician should not “link to” a resident note that is viewed as “not having been written” prior to the teaching physician note. This would not fulfill the requirements represented in the CMS-approved language “I reviewed the resident’s note and agree.”
Electronic health record (EHR) systems sometimes hinder compliance. If the resident completes the note but does not “finalize” or “close” the encounter until after the teaching physician documents their own note, it can falsely appear that the resident note did not exist at the time the teaching physician created their entry. Because an auditor can only view the finalized entries, the timing of each entry might be erroneously represented. Proper training and closing of encounters can diminish these issues.
Additionally, scribing the attestation is not permitted. Residents cannot document the teaching physician attestation on behalf of the physician under any circumstance. CMS rules require the teaching physician to document their presence, participation, and management of the patient. In an EHR, the teaching physician must document this entry under his/her own log-in and password, which is not to be shared with anyone.
Students
CMS defines student as “an individual who participates in an accredited educational program [e.g. a medical school] that is not an approved GME program.”1 A student is not regarded as a “physician in training,” and the service is not eligible for reimbursement consideration under the teaching physician rules.
Per CMS guidelines, students can document services in the medical record, but the teaching physician may only refer to the student’s systems review and past/family/social history entries. The teaching physician must verify and redocument the history of present illness. A student’s physical exam findings or medical decision-making are not suitable for tethering, and the teaching physician must personally perform and redocument the physical exam and medical decision-making. The visit level reflects only the teaching physician’s personally performed and documented service.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. Guidelines for Teaching Physicians, Interns, Residents. CMS website. Available at: http://www.cms.gov/MLNProducts/downloads/gdelinesteachgresfctsht.pdf. Accessed Jan. 8, 2013.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 100. CMS website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2013.
- Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 30.2. CMS website. Available at: http://www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf. Accessed Jan. 8, 2013.
When hospitalists work in academic centers, medical and surgical services are furnished, in part, by a resident within the scope of the hospitalists’ training program. A resident is “an individual who participates in an approved graduate medical education (GME) program or a physician who is not in an approved GME program but who is authorized to practice only in a hospital setting.”1 Resident services are covered by Centers for Medicare & Medicaid Services (CMS) and paid by the Fiscal Intermediary through direct GME and Indirect Medical Education (IME) payments. These services are not billed or paid using the Medicare Physician Fee Schedule. The teaching physician is responsible for supervising the resident’s health-care delivery but is not paid for the resident’s work. The teaching physician is paid for their personal and medically necessary service in providing patient care. The teaching physician has the option to perform the entire service, or perform the self-determined critical or key portion(s) of the service.
Comprehensive Service
Teaching physicians independently see the patient and perform all required elements to support the visit level (e.g. 99233: subsequent hospital care, per day, which requires at least two of the following three key components: a detailed interval history, a detailed examination, or high-complexity medical decision-making).2 The teaching physician writes a note independent of a resident encounter with the patient or documentation. The teaching physician note “stands alone” and does not rely on the resident’s documentation. If the resident saw the patient and documented the encounter, the teaching physician might choose to “link to” the resident note in lieu of personally documenting the entire service. The linking statement must demonstrate teaching physician involvement in the patient encounter and participation in patient management. Use of CMS-approved statements is best to meet these requirements. Statement examples include:3
- “I performed a history and physical examination of the patient and discussed his management with the resident. I reviewed the resident’s note and agree with the documented findings and plan of care.”
- “I saw and evaluated the patient. I agree with the findings and the plan of care as documented in the resident’s note.”
- “I saw and examined the patient. I agree with the resident’s note, except the heart murmur is louder, so I will obtain an echo to evaluate.”
Each of these statements meets the minimum requirements for billing. However, teaching physicians should offer more information in support of other clinical, quality, and regulatory initiatives and mandates, better exemplified in the last example. The reported visit level will be supported by the combined documentation (teaching physician and resident).
The teaching physician submits a claim in their name and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99223-GC). This alerts the Medicare contractor that services were provided under teaching physician rules. Requests for documentation should include a response with medical record entries from the teaching physician and resident.
Critical/Key Portion
“Supervised” service: The resident and teaching physician can round together; they can see the patient at the same time. The teaching physician observes the resident’s performance during the patient encounter, or personally performs self-determined elements of patient care. The resident documents their patient care. The attending must still note their presence in the medical record, performance of the critical or key portions of the service, and involvement in patient management. CMS-accepted statements include:3
- “I was present with the resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident’s note.”
- “I saw the patient with the resident and agree with the resident’s findings and plan.”
Although these statements demonstrate acceptable billing language, they lack patient-specific details that support the teaching physician’s personal contribution to patient care and the quality of their expertise. The teaching physician selects the visit level that represents the combined documentation and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99232-GC).
“Shared” service: The resident sees the patient unaccompanied and documents the corresponding care provided. The teaching physician sees the patient at a different time but performs only the critical or key portions of the service. The case is subsequently discussed with the resident. The teaching physician must document their presence and performance of the critical or key portions of the service, along with any patient management. Using CMS-quoted statements ensures regulatory compliance:3
- “I saw and evaluated the patient. I reviewed the resident’s note and agree, except that the picture is more consistent with pericarditis than myocardial ischemia. Will begin NSAIDs.”
- “I saw and evaluated the patient. Discussed with resident and agree with resident’s findings and plan as documented in the resident’s note.”
- “See resident’s note for details. I saw and evaluated the patient and agree with the resident’s finding and plans as written.”
- “I saw and evaluated the patient. Agree with resident’s note, but lower extremities are weaker, now 3/5; MRI of L/S spine today.”
Once again, the teaching physician selects the visit level that represents the combined documentation and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99233-GC).
EHR Considerations
When seeing patients independent of one another, the timing of the teaching physician and resident encounters does not impact billing. However, the time that the resident encounter is documented in the medical record can significantly impact the payment when reviewed by external auditors. When the resident note is dated and timed later than the teaching physician’s entry, the teaching physician cannot consider the resident’s note for visit-level selection. The teaching physician should not “link to” a resident note that is viewed as “not having been written” prior to the teaching physician note. This would not fulfill the requirements represented in the CMS-approved language “I reviewed the resident’s note and agree.”
Electronic health record (EHR) systems sometimes hinder compliance. If the resident completes the note but does not “finalize” or “close” the encounter until after the teaching physician documents their own note, it can falsely appear that the resident note did not exist at the time the teaching physician created their entry. Because an auditor can only view the finalized entries, the timing of each entry might be erroneously represented. Proper training and closing of encounters can diminish these issues.
Additionally, scribing the attestation is not permitted. Residents cannot document the teaching physician attestation on behalf of the physician under any circumstance. CMS rules require the teaching physician to document their presence, participation, and management of the patient. In an EHR, the teaching physician must document this entry under his/her own log-in and password, which is not to be shared with anyone.
Students
CMS defines student as “an individual who participates in an accredited educational program [e.g. a medical school] that is not an approved GME program.”1 A student is not regarded as a “physician in training,” and the service is not eligible for reimbursement consideration under the teaching physician rules.
Per CMS guidelines, students can document services in the medical record, but the teaching physician may only refer to the student’s systems review and past/family/social history entries. The teaching physician must verify and redocument the history of present illness. A student’s physical exam findings or medical decision-making are not suitable for tethering, and the teaching physician must personally perform and redocument the physical exam and medical decision-making. The visit level reflects only the teaching physician’s personally performed and documented service.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. Guidelines for Teaching Physicians, Interns, Residents. CMS website. Available at: http://www.cms.gov/MLNProducts/downloads/gdelinesteachgresfctsht.pdf. Accessed Jan. 8, 2013.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 100. CMS website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2013.
- Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 30.2. CMS website. Available at: http://www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf. Accessed Jan. 8, 2013.
When hospitalists work in academic centers, medical and surgical services are furnished, in part, by a resident within the scope of the hospitalists’ training program. A resident is “an individual who participates in an approved graduate medical education (GME) program or a physician who is not in an approved GME program but who is authorized to practice only in a hospital setting.”1 Resident services are covered by Centers for Medicare & Medicaid Services (CMS) and paid by the Fiscal Intermediary through direct GME and Indirect Medical Education (IME) payments. These services are not billed or paid using the Medicare Physician Fee Schedule. The teaching physician is responsible for supervising the resident’s health-care delivery but is not paid for the resident’s work. The teaching physician is paid for their personal and medically necessary service in providing patient care. The teaching physician has the option to perform the entire service, or perform the self-determined critical or key portion(s) of the service.
Comprehensive Service
Teaching physicians independently see the patient and perform all required elements to support the visit level (e.g. 99233: subsequent hospital care, per day, which requires at least two of the following three key components: a detailed interval history, a detailed examination, or high-complexity medical decision-making).2 The teaching physician writes a note independent of a resident encounter with the patient or documentation. The teaching physician note “stands alone” and does not rely on the resident’s documentation. If the resident saw the patient and documented the encounter, the teaching physician might choose to “link to” the resident note in lieu of personally documenting the entire service. The linking statement must demonstrate teaching physician involvement in the patient encounter and participation in patient management. Use of CMS-approved statements is best to meet these requirements. Statement examples include:3
- “I performed a history and physical examination of the patient and discussed his management with the resident. I reviewed the resident’s note and agree with the documented findings and plan of care.”
- “I saw and evaluated the patient. I agree with the findings and the plan of care as documented in the resident’s note.”
- “I saw and examined the patient. I agree with the resident’s note, except the heart murmur is louder, so I will obtain an echo to evaluate.”
Each of these statements meets the minimum requirements for billing. However, teaching physicians should offer more information in support of other clinical, quality, and regulatory initiatives and mandates, better exemplified in the last example. The reported visit level will be supported by the combined documentation (teaching physician and resident).
The teaching physician submits a claim in their name and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99223-GC). This alerts the Medicare contractor that services were provided under teaching physician rules. Requests for documentation should include a response with medical record entries from the teaching physician and resident.
Critical/Key Portion
“Supervised” service: The resident and teaching physician can round together; they can see the patient at the same time. The teaching physician observes the resident’s performance during the patient encounter, or personally performs self-determined elements of patient care. The resident documents their patient care. The attending must still note their presence in the medical record, performance of the critical or key portions of the service, and involvement in patient management. CMS-accepted statements include:3
- “I was present with the resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident’s note.”
- “I saw the patient with the resident and agree with the resident’s findings and plan.”
Although these statements demonstrate acceptable billing language, they lack patient-specific details that support the teaching physician’s personal contribution to patient care and the quality of their expertise. The teaching physician selects the visit level that represents the combined documentation and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99232-GC).
“Shared” service: The resident sees the patient unaccompanied and documents the corresponding care provided. The teaching physician sees the patient at a different time but performs only the critical or key portions of the service. The case is subsequently discussed with the resident. The teaching physician must document their presence and performance of the critical or key portions of the service, along with any patient management. Using CMS-quoted statements ensures regulatory compliance:3
- “I saw and evaluated the patient. I reviewed the resident’s note and agree, except that the picture is more consistent with pericarditis than myocardial ischemia. Will begin NSAIDs.”
- “I saw and evaluated the patient. Discussed with resident and agree with resident’s findings and plan as documented in the resident’s note.”
- “See resident’s note for details. I saw and evaluated the patient and agree with the resident’s finding and plans as written.”
- “I saw and evaluated the patient. Agree with resident’s note, but lower extremities are weaker, now 3/5; MRI of L/S spine today.”
Once again, the teaching physician selects the visit level that represents the combined documentation and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99233-GC).
EHR Considerations
When seeing patients independent of one another, the timing of the teaching physician and resident encounters does not impact billing. However, the time that the resident encounter is documented in the medical record can significantly impact the payment when reviewed by external auditors. When the resident note is dated and timed later than the teaching physician’s entry, the teaching physician cannot consider the resident’s note for visit-level selection. The teaching physician should not “link to” a resident note that is viewed as “not having been written” prior to the teaching physician note. This would not fulfill the requirements represented in the CMS-approved language “I reviewed the resident’s note and agree.”
Electronic health record (EHR) systems sometimes hinder compliance. If the resident completes the note but does not “finalize” or “close” the encounter until after the teaching physician documents their own note, it can falsely appear that the resident note did not exist at the time the teaching physician created their entry. Because an auditor can only view the finalized entries, the timing of each entry might be erroneously represented. Proper training and closing of encounters can diminish these issues.
Additionally, scribing the attestation is not permitted. Residents cannot document the teaching physician attestation on behalf of the physician under any circumstance. CMS rules require the teaching physician to document their presence, participation, and management of the patient. In an EHR, the teaching physician must document this entry under his/her own log-in and password, which is not to be shared with anyone.
Students
CMS defines student as “an individual who participates in an accredited educational program [e.g. a medical school] that is not an approved GME program.”1 A student is not regarded as a “physician in training,” and the service is not eligible for reimbursement consideration under the teaching physician rules.
Per CMS guidelines, students can document services in the medical record, but the teaching physician may only refer to the student’s systems review and past/family/social history entries. The teaching physician must verify and redocument the history of present illness. A student’s physical exam findings or medical decision-making are not suitable for tethering, and the teaching physician must personally perform and redocument the physical exam and medical decision-making. The visit level reflects only the teaching physician’s personally performed and documented service.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. Guidelines for Teaching Physicians, Interns, Residents. CMS website. Available at: http://www.cms.gov/MLNProducts/downloads/gdelinesteachgresfctsht.pdf. Accessed Jan. 8, 2013.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 100. CMS website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2013.
- Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 30.2. CMS website. Available at: http://www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf. Accessed Jan. 8, 2013.
Bill Seeks to Enhance Patient Access to Post-Hospital Benefit
New national legislation proposed in March would change Medicare billing rules to allow patients to more easily access Medicare’s institutional skilled nursing care benefit following a hospital discharge. Currently, patients can get the benefit only after a qualifying three-day hospital stay. If they don’t qualify, they often have to pay out of pocket for the subsequent skilled nursing facility placement.
The Improving Access to Medicare Coverage Act, introduced by Reps. Joe Courtney (D-Conn.) and Tom Latham (R-Iowa) and Sen. Sherrod Brown (D-Ohio), would allow the time patients spend inside the hospital on “observation status” to count toward their required three-day hospital stay. It also would establish a 90-day appeal period for those who have been denied this benefit.
SHM is one of a dozen endorsing organizations, joining the American Medical Association, American Medical Directors Association, and AARP. For more information, check out this month’s “Policy Corner”.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
New national legislation proposed in March would change Medicare billing rules to allow patients to more easily access Medicare’s institutional skilled nursing care benefit following a hospital discharge. Currently, patients can get the benefit only after a qualifying three-day hospital stay. If they don’t qualify, they often have to pay out of pocket for the subsequent skilled nursing facility placement.
The Improving Access to Medicare Coverage Act, introduced by Reps. Joe Courtney (D-Conn.) and Tom Latham (R-Iowa) and Sen. Sherrod Brown (D-Ohio), would allow the time patients spend inside the hospital on “observation status” to count toward their required three-day hospital stay. It also would establish a 90-day appeal period for those who have been denied this benefit.
SHM is one of a dozen endorsing organizations, joining the American Medical Association, American Medical Directors Association, and AARP. For more information, check out this month’s “Policy Corner”.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
New national legislation proposed in March would change Medicare billing rules to allow patients to more easily access Medicare’s institutional skilled nursing care benefit following a hospital discharge. Currently, patients can get the benefit only after a qualifying three-day hospital stay. If they don’t qualify, they often have to pay out of pocket for the subsequent skilled nursing facility placement.
The Improving Access to Medicare Coverage Act, introduced by Reps. Joe Courtney (D-Conn.) and Tom Latham (R-Iowa) and Sen. Sherrod Brown (D-Ohio), would allow the time patients spend inside the hospital on “observation status” to count toward their required three-day hospital stay. It also would establish a 90-day appeal period for those who have been denied this benefit.
SHM is one of a dozen endorsing organizations, joining the American Medical Association, American Medical Directors Association, and AARP. For more information, check out this month’s “Policy Corner”.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
Telehealth Technology Connects Specialists with First Responders in the Field

The VA Ann Arbor Healthcare System in Michigan is mobilizing telehealth technology for a disaster-relief initiative that aims to connect first responders in the field with medical specialists at the Ann Arbor Medical Center. As reported in Healthcare IT News, the Disaster Relief Telehealth System of Orion, Mich.-based JEMS Technology (www.jemstech.com) enables secure, live-streaming video to be sent to specialists, who can review the video and respond with medical advice.5
The Office of Emergency Management at the Ann Arbor VA supports emergency operations from four treatment sites serving 21 counties in Michigan and Ohio, as well as regional disaster preparedness.
In other technology news, the U.S. Army in March awarded a $2.5 million contract to brain-monitoring-device company NeuroWave Systems of Cleveland Heights, Ohio (www.neurowavesystems.com), to develop a wearable, miniaturized brain monitor to assess via electroencephalogram data for traumatic brain injury (TBI) in the field, directly at the point of suspected injury, such as on battlefronts. The device, called SeizTBI, is “small, lightweight, and designed for rapid deployment in austere environments,” explains NeuroWave principal investigator Stephan Bibian, MD. TBI accounted for 22% of U.S. troop casualties in the Iraq and Afghanistan conflicts, but fewer than half were identified in the field.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
The VA Ann Arbor Healthcare System in Michigan is mobilizing telehealth technology for a disaster-relief initiative that aims to connect first responders in the field with medical specialists at the Ann Arbor Medical Center. As reported in Healthcare IT News, the Disaster Relief Telehealth System of Orion, Mich.-based JEMS Technology (www.jemstech.com) enables secure, live-streaming video to be sent to specialists, who can review the video and respond with medical advice.5
The Office of Emergency Management at the Ann Arbor VA supports emergency operations from four treatment sites serving 21 counties in Michigan and Ohio, as well as regional disaster preparedness.
In other technology news, the U.S. Army in March awarded a $2.5 million contract to brain-monitoring-device company NeuroWave Systems of Cleveland Heights, Ohio (www.neurowavesystems.com), to develop a wearable, miniaturized brain monitor to assess via electroencephalogram data for traumatic brain injury (TBI) in the field, directly at the point of suspected injury, such as on battlefronts. The device, called SeizTBI, is “small, lightweight, and designed for rapid deployment in austere environments,” explains NeuroWave principal investigator Stephan Bibian, MD. TBI accounted for 22% of U.S. troop casualties in the Iraq and Afghanistan conflicts, but fewer than half were identified in the field.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
The VA Ann Arbor Healthcare System in Michigan is mobilizing telehealth technology for a disaster-relief initiative that aims to connect first responders in the field with medical specialists at the Ann Arbor Medical Center. As reported in Healthcare IT News, the Disaster Relief Telehealth System of Orion, Mich.-based JEMS Technology (www.jemstech.com) enables secure, live-streaming video to be sent to specialists, who can review the video and respond with medical advice.5
The Office of Emergency Management at the Ann Arbor VA supports emergency operations from four treatment sites serving 21 counties in Michigan and Ohio, as well as regional disaster preparedness.
In other technology news, the U.S. Army in March awarded a $2.5 million contract to brain-monitoring-device company NeuroWave Systems of Cleveland Heights, Ohio (www.neurowavesystems.com), to develop a wearable, miniaturized brain monitor to assess via electroencephalogram data for traumatic brain injury (TBI) in the field, directly at the point of suspected injury, such as on battlefronts. The device, called SeizTBI, is “small, lightweight, and designed for rapid deployment in austere environments,” explains NeuroWave principal investigator Stephan Bibian, MD. TBI accounted for 22% of U.S. troop casualties in the Iraq and Afghanistan conflicts, but fewer than half were identified in the field.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
AMA Report Offers Nine Steps to Help PCPs Prevent Readmissions
The American Medical Association recently released a report developed by a 21-member expert panel proposing a nine-step plan for primary-care-physician (PCP) practices to play an integral role in improving care transitions and preventing avoidable rehospitalizations.2 The report recommends focusing on more than just the hospital-admitting diagnosis, conducting a thorough patient health assessment, clarifying the patient’s short- and long-term goals, and coordinating care with other care settings.
With simultaneous research in JAMA concluding that the vast majority of readmissions are for reasons unrelated to the previous hospital stay, coordination between the inpatient and outpatient teams is crucial to successful transitions of care.3 Moreover, a recent survey showed that nearly 30% of PCPs say they miss alerts about patients’ test results from an electronic health record (EHR) notification system.4 According to the survey by Hardeep Singh, MD, MPH, and colleagues from the Michael E. DeBakey VA Medical Center in Houston, the doctors received on average 63 such alerts per day. Seventy percent reported that they cannot effectively manage the alerts, and more than half said that the current EHR notification system makes it possible to miss test results.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
The American Medical Association recently released a report developed by a 21-member expert panel proposing a nine-step plan for primary-care-physician (PCP) practices to play an integral role in improving care transitions and preventing avoidable rehospitalizations.2 The report recommends focusing on more than just the hospital-admitting diagnosis, conducting a thorough patient health assessment, clarifying the patient’s short- and long-term goals, and coordinating care with other care settings.
With simultaneous research in JAMA concluding that the vast majority of readmissions are for reasons unrelated to the previous hospital stay, coordination between the inpatient and outpatient teams is crucial to successful transitions of care.3 Moreover, a recent survey showed that nearly 30% of PCPs say they miss alerts about patients’ test results from an electronic health record (EHR) notification system.4 According to the survey by Hardeep Singh, MD, MPH, and colleagues from the Michael E. DeBakey VA Medical Center in Houston, the doctors received on average 63 such alerts per day. Seventy percent reported that they cannot effectively manage the alerts, and more than half said that the current EHR notification system makes it possible to miss test results.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
The American Medical Association recently released a report developed by a 21-member expert panel proposing a nine-step plan for primary-care-physician (PCP) practices to play an integral role in improving care transitions and preventing avoidable rehospitalizations.2 The report recommends focusing on more than just the hospital-admitting diagnosis, conducting a thorough patient health assessment, clarifying the patient’s short- and long-term goals, and coordinating care with other care settings.
With simultaneous research in JAMA concluding that the vast majority of readmissions are for reasons unrelated to the previous hospital stay, coordination between the inpatient and outpatient teams is crucial to successful transitions of care.3 Moreover, a recent survey showed that nearly 30% of PCPs say they miss alerts about patients’ test results from an electronic health record (EHR) notification system.4 According to the survey by Hardeep Singh, MD, MPH, and colleagues from the Michael E. DeBakey VA Medical Center in Houston, the doctors received on average 63 such alerts per day. Seventy percent reported that they cannot effectively manage the alerts, and more than half said that the current EHR notification system makes it possible to miss test results.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
UCSF Engages Hospitalists to Improve Patient Communication

In a poster presented at HM12, Kathryn Quinn, MPH, CPPS, FACHE, described how her quality team at the University of California at San Francisco (UCSF) developed a checklist to improve physician communication with patients, then taught it to the attending hospitalist faculty.1 The project began with a list of 29 best practices for patient-physician interaction, as identified in medical literature. Hospitalists then voted for the elements they felt were most important to their practice, as well as those best able to be measured, and a top-10 list was created.
Quinn, the program manager for quality and safety in the division of hospital medicine at UCSF, says the communication best practices were “chosen by the people whose practices we are trying to change.”
The quality team presented the best practices in one-hour training sessions that included small-group role plays, explains co-investigator and UCSF hospitalist Diane Sliwka, MD. The training extended to outpatient physicians, medical specialists, and chief residents. Participants also were provided a laminated pocket card listing the interventions. They also received feedback from structured observations with patients on service.
Quinn says UCSF hospitalists have improved at knocking and asking permission to enter patient rooms, introducing themselves by name and role, and encouraging questions at the end of the interaction. They have been less successful at inquiring about the patient’s concerns early in the interview and at discussing duration of treatment and next steps.
“We learned that it takes more than just talk,” Quinn says. “Just telling physicians how to improve communication doesn’t mean it’s easy to do.”
Still to be determined is the project’s impact on patient satisfaction scores, although the hospitalists reported that they found the training and feedback helpful.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
In a poster presented at HM12, Kathryn Quinn, MPH, CPPS, FACHE, described how her quality team at the University of California at San Francisco (UCSF) developed a checklist to improve physician communication with patients, then taught it to the attending hospitalist faculty.1 The project began with a list of 29 best practices for patient-physician interaction, as identified in medical literature. Hospitalists then voted for the elements they felt were most important to their practice, as well as those best able to be measured, and a top-10 list was created.
Quinn, the program manager for quality and safety in the division of hospital medicine at UCSF, says the communication best practices were “chosen by the people whose practices we are trying to change.”
The quality team presented the best practices in one-hour training sessions that included small-group role plays, explains co-investigator and UCSF hospitalist Diane Sliwka, MD. The training extended to outpatient physicians, medical specialists, and chief residents. Participants also were provided a laminated pocket card listing the interventions. They also received feedback from structured observations with patients on service.
Quinn says UCSF hospitalists have improved at knocking and asking permission to enter patient rooms, introducing themselves by name and role, and encouraging questions at the end of the interaction. They have been less successful at inquiring about the patient’s concerns early in the interview and at discussing duration of treatment and next steps.
“We learned that it takes more than just talk,” Quinn says. “Just telling physicians how to improve communication doesn’t mean it’s easy to do.”
Still to be determined is the project’s impact on patient satisfaction scores, although the hospitalists reported that they found the training and feedback helpful.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
In a poster presented at HM12, Kathryn Quinn, MPH, CPPS, FACHE, described how her quality team at the University of California at San Francisco (UCSF) developed a checklist to improve physician communication with patients, then taught it to the attending hospitalist faculty.1 The project began with a list of 29 best practices for patient-physician interaction, as identified in medical literature. Hospitalists then voted for the elements they felt were most important to their practice, as well as those best able to be measured, and a top-10 list was created.
Quinn, the program manager for quality and safety in the division of hospital medicine at UCSF, says the communication best practices were “chosen by the people whose practices we are trying to change.”
The quality team presented the best practices in one-hour training sessions that included small-group role plays, explains co-investigator and UCSF hospitalist Diane Sliwka, MD. The training extended to outpatient physicians, medical specialists, and chief residents. Participants also were provided a laminated pocket card listing the interventions. They also received feedback from structured observations with patients on service.
Quinn says UCSF hospitalists have improved at knocking and asking permission to enter patient rooms, introducing themselves by name and role, and encouraging questions at the end of the interaction. They have been less successful at inquiring about the patient’s concerns early in the interview and at discussing duration of treatment and next steps.
“We learned that it takes more than just talk,” Quinn says. “Just telling physicians how to improve communication doesn’t mean it’s easy to do.”
Still to be determined is the project’s impact on patient satisfaction scores, although the hospitalists reported that they found the training and feedback helpful.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
Hospitalists Can Get Ahead Through Quality and Patient Safety Initiatives
Are you a hospitalist who, on daily rounds, often thinks, “There’s got to be a better way to do this”? You might be just the type of person who can carve a niche for yourself in hospital quality and patient safety—and advance your career in the process.
Successful navigation of the quality-improvement (QI) and patient-safety domains, according to three veteran hospitalists, requires an initial passion and an incremental approach. Now is an especially good time, they agree, for young hospitalists to engage in these types of initiatives.
Why Do It?
In her capacity as president of the Mid-Atlantic Business Unit for Brentwood, Tenn.-based CogentHMG, Julia Wright, MD, SFHM, FACP, often encourages young recruits to consider participation in QI and patient-safety initiatives. She admits that the transition from residency to a busy HM practice, with its higher patient volumes and a faster pace, can be daunting at first. Still, she tries to cultivate interest in initiatives and establish a realistic timeframe for involvement.
There are many reasons to consider this as a career step. Dr. Wright says that quality and patient safety dovetail with hospitalists’ initial reasons for choosing medicine: to improve patients’ lives.
Janet Nagamine, RN, MD, SFHM, former patient safety officer and assistant chief of quality at Kaiser Permanente in Santa Clara, Calif., describes the fit this way: “I might be a good doctor, but as a hospitalist, I rely on many others within the system to deliver, so my patients can’t get good care until the entire system is running well,” she says. “There are all kinds of opportunities to fix our [hospital] system, and I really believe that hospitalists cannot separate themselves from that engagement.”
Elizabeth Gundersen, MD, FHM, of Fort Lauderdale, Fla., agrees that it’s a natural step to think about the ways to make a difference on a larger level. At her former institution, the University of Massachusetts (UMass) Medical School in Worcester, she parlayed her interest in QI to work her way up from ground-level hospitalist to associate chief of her division and quality officer for the hospital. “Physicians get a lot of satisfaction from helping individual patients,” she says. “One thing I really liked about getting involved with quality improvement was being able to make a difference for patients on a systems level.”
An Incremental Path
The path to her current position began with a very specific issue for Dr. Nagamine, an SHM board member who also serves as a Project BOOST co-investigator. “Although I have been doing patient safety since before they had a name for it, I didn’t start out saying that I wanted a career in quality and safety,” she says. “I was trying to take better care of my patients with diabetes, but controlling their glucose was extremely challenging because all the related variables—timing and amount of their insulin dosage, when and how much they had eaten—were charted in different places. This made it hard to adjust their insulin appropriately.”
It quickly became clear to Dr. Nagamine that the solution had to be systemic. She realized that something as basic as taking care of her patients with diabetes required multiple departments (i.e. dietary, nursing, and pharmacy) to furnish information in an integrated manner. So she joined the diabetes committee and went to work on the issue. She helped devise a flow chart that could be used by all relevant departments. A further evolution on the path emanated from one of her patients receiving the wrong medication. She joined the medication safety committee, became chair, “and the next thing you know, I’m in charge of patient safety, and an assistant chief of quality.”
Training Is Necessary
QI and patient-safety methodologies have become sophisticated disciplines in the past two decades, Dr. Wright says. Access to training in QI basics now is readily available to early-career hospitalists. For example, CogentHMG offers program support for QI so that anyone interested “doesn’t have to start from scratch anymore; we can help show them the way and support them in doing it.”
This month, HM13 (www.hospital medicine2013.org)—just outside Washington, D.C.—will offer multiple sessions on quality, as well as the “Initiating Quality Improvement Projects with Built-In Sustainment” workshop, led by Center for Comprehensive Access and Delivery Research and Evaluation (CADRE) core investigator Peter Kaboli, MD, MS, who will address sustainability.
Beyond methodological tools, success in quality and patient safety requires the ability to motivate people, often across multiple disciplines, Dr. Nagamine says. “If you want things to work better, you must invite the right people to the table. For example, we often forget to include key nonclinical stakeholders,” she adds.
When working with hospitals across the country to implement rapid-response tTeams, Dr. Nagamine often reminds them to invite the operators, or “key people,” in the process.
“If you put patient safety at the core of your initiative and create the context for that, most people will agree that it’s the right thing to do and will get on board, even if it’s an extra step for them,” she says. “Know your audience, listen to their perspective, and learn what matters to them. And to most people, it matters that they give good patient care.”
Gretchen Henkel is a freelance writer in California.
Branch Out: QI and Patient-Safety Initiatives

Pick a passion. It’s best to choose an issue that’s important to you. “It has to be a
passion because much of the time it’s an uphill battle,” says Dr. Gundersen. She started with the issue of reducing readmissions, and with two colleagues pitched the idea of involving the UMass HM group in SHM’s Project BOOST. After that, she set out to become an expert on reducing readmissions, applying what she had learned to other successful initiatives.
Learn the lingo. Dr. Wright advises learning some of the most basic principles, such as Shewhart’s PDCA (Plan-Do-Check-Act) or Deming’s adaptation PDSA (Plan-Do-Study-Act) cycles; the quality tripod; and accessing resources made available from SHM. A member of SHM’s Hospital Quality and Patient Safety Committee, Dr. Wright says a subcommittee for leadership engagement has been created and furnishes tools and training for advancing quality initiatives. The Institute for Healthcare Improvement (www.ihi.org) also offers a wealth of measures, speaker series, and white papers on improvement in health care.
Start small. You can test your ability to work with interdisciplinary departments, often a prerequisite of many quality initiatives, by first joining a committee, Dr. Nagamine advises. “See how effective or persuasive you are in pitching an idea and seeing it through with other departments,” she says.
Brace for a marathon. “Most people,” Dr. Gundersen says, “do not hand you 100% of their cooperation and a budget you can work with.” It takes time to get buy-in, especially if you’re doing interdisciplinary initiatives. If possible, break your projects into achievable units. “Start with some quick wins. Small payoffs here and there can re-energize your team and eventually yield a larger payoff,” she says.
Limit sweat equity. It’s important to put in time at the start of a project to demonstrate your value, but if you’re constantly staying up late working on a project, consider pitching a compensated role to your boss. “Being a good citizen and volunteering for committees is one thing,” Dr. Nagamine cautions, “but taking on leadership roles in too many projects, without dedicated time, is not sustainable and can jeopardize the success of your projects.”
—Gretchen Henkel
Are you a hospitalist who, on daily rounds, often thinks, “There’s got to be a better way to do this”? You might be just the type of person who can carve a niche for yourself in hospital quality and patient safety—and advance your career in the process.
Successful navigation of the quality-improvement (QI) and patient-safety domains, according to three veteran hospitalists, requires an initial passion and an incremental approach. Now is an especially good time, they agree, for young hospitalists to engage in these types of initiatives.
Why Do It?
In her capacity as president of the Mid-Atlantic Business Unit for Brentwood, Tenn.-based CogentHMG, Julia Wright, MD, SFHM, FACP, often encourages young recruits to consider participation in QI and patient-safety initiatives. She admits that the transition from residency to a busy HM practice, with its higher patient volumes and a faster pace, can be daunting at first. Still, she tries to cultivate interest in initiatives and establish a realistic timeframe for involvement.
There are many reasons to consider this as a career step. Dr. Wright says that quality and patient safety dovetail with hospitalists’ initial reasons for choosing medicine: to improve patients’ lives.
Janet Nagamine, RN, MD, SFHM, former patient safety officer and assistant chief of quality at Kaiser Permanente in Santa Clara, Calif., describes the fit this way: “I might be a good doctor, but as a hospitalist, I rely on many others within the system to deliver, so my patients can’t get good care until the entire system is running well,” she says. “There are all kinds of opportunities to fix our [hospital] system, and I really believe that hospitalists cannot separate themselves from that engagement.”
Elizabeth Gundersen, MD, FHM, of Fort Lauderdale, Fla., agrees that it’s a natural step to think about the ways to make a difference on a larger level. At her former institution, the University of Massachusetts (UMass) Medical School in Worcester, she parlayed her interest in QI to work her way up from ground-level hospitalist to associate chief of her division and quality officer for the hospital. “Physicians get a lot of satisfaction from helping individual patients,” she says. “One thing I really liked about getting involved with quality improvement was being able to make a difference for patients on a systems level.”
An Incremental Path
The path to her current position began with a very specific issue for Dr. Nagamine, an SHM board member who also serves as a Project BOOST co-investigator. “Although I have been doing patient safety since before they had a name for it, I didn’t start out saying that I wanted a career in quality and safety,” she says. “I was trying to take better care of my patients with diabetes, but controlling their glucose was extremely challenging because all the related variables—timing and amount of their insulin dosage, when and how much they had eaten—were charted in different places. This made it hard to adjust their insulin appropriately.”
It quickly became clear to Dr. Nagamine that the solution had to be systemic. She realized that something as basic as taking care of her patients with diabetes required multiple departments (i.e. dietary, nursing, and pharmacy) to furnish information in an integrated manner. So she joined the diabetes committee and went to work on the issue. She helped devise a flow chart that could be used by all relevant departments. A further evolution on the path emanated from one of her patients receiving the wrong medication. She joined the medication safety committee, became chair, “and the next thing you know, I’m in charge of patient safety, and an assistant chief of quality.”
Training Is Necessary
QI and patient-safety methodologies have become sophisticated disciplines in the past two decades, Dr. Wright says. Access to training in QI basics now is readily available to early-career hospitalists. For example, CogentHMG offers program support for QI so that anyone interested “doesn’t have to start from scratch anymore; we can help show them the way and support them in doing it.”
This month, HM13 (www.hospital medicine2013.org)—just outside Washington, D.C.—will offer multiple sessions on quality, as well as the “Initiating Quality Improvement Projects with Built-In Sustainment” workshop, led by Center for Comprehensive Access and Delivery Research and Evaluation (CADRE) core investigator Peter Kaboli, MD, MS, who will address sustainability.
Beyond methodological tools, success in quality and patient safety requires the ability to motivate people, often across multiple disciplines, Dr. Nagamine says. “If you want things to work better, you must invite the right people to the table. For example, we often forget to include key nonclinical stakeholders,” she adds.
When working with hospitals across the country to implement rapid-response tTeams, Dr. Nagamine often reminds them to invite the operators, or “key people,” in the process.
“If you put patient safety at the core of your initiative and create the context for that, most people will agree that it’s the right thing to do and will get on board, even if it’s an extra step for them,” she says. “Know your audience, listen to their perspective, and learn what matters to them. And to most people, it matters that they give good patient care.”
Gretchen Henkel is a freelance writer in California.
Branch Out: QI and Patient-Safety Initiatives
Pick a passion. It’s best to choose an issue that’s important to you. “It has to be a
passion because much of the time it’s an uphill battle,” says Dr. Gundersen. She started with the issue of reducing readmissions, and with two colleagues pitched the idea of involving the UMass HM group in SHM’s Project BOOST. After that, she set out to become an expert on reducing readmissions, applying what she had learned to other successful initiatives.
Learn the lingo. Dr. Wright advises learning some of the most basic principles, such as Shewhart’s PDCA (Plan-Do-Check-Act) or Deming’s adaptation PDSA (Plan-Do-Study-Act) cycles; the quality tripod; and accessing resources made available from SHM. A member of SHM’s Hospital Quality and Patient Safety Committee, Dr. Wright says a subcommittee for leadership engagement has been created and furnishes tools and training for advancing quality initiatives. The Institute for Healthcare Improvement (www.ihi.org) also offers a wealth of measures, speaker series, and white papers on improvement in health care.
Start small. You can test your ability to work with interdisciplinary departments, often a prerequisite of many quality initiatives, by first joining a committee, Dr. Nagamine advises. “See how effective or persuasive you are in pitching an idea and seeing it through with other departments,” she says.
Brace for a marathon. “Most people,” Dr. Gundersen says, “do not hand you 100% of their cooperation and a budget you can work with.” It takes time to get buy-in, especially if you’re doing interdisciplinary initiatives. If possible, break your projects into achievable units. “Start with some quick wins. Small payoffs here and there can re-energize your team and eventually yield a larger payoff,” she says.
Limit sweat equity. It’s important to put in time at the start of a project to demonstrate your value, but if you’re constantly staying up late working on a project, consider pitching a compensated role to your boss. “Being a good citizen and volunteering for committees is one thing,” Dr. Nagamine cautions, “but taking on leadership roles in too many projects, without dedicated time, is not sustainable and can jeopardize the success of your projects.”
—Gretchen Henkel
Are you a hospitalist who, on daily rounds, often thinks, “There’s got to be a better way to do this”? You might be just the type of person who can carve a niche for yourself in hospital quality and patient safety—and advance your career in the process.
Successful navigation of the quality-improvement (QI) and patient-safety domains, according to three veteran hospitalists, requires an initial passion and an incremental approach. Now is an especially good time, they agree, for young hospitalists to engage in these types of initiatives.
Why Do It?
In her capacity as president of the Mid-Atlantic Business Unit for Brentwood, Tenn.-based CogentHMG, Julia Wright, MD, SFHM, FACP, often encourages young recruits to consider participation in QI and patient-safety initiatives. She admits that the transition from residency to a busy HM practice, with its higher patient volumes and a faster pace, can be daunting at first. Still, she tries to cultivate interest in initiatives and establish a realistic timeframe for involvement.
There are many reasons to consider this as a career step. Dr. Wright says that quality and patient safety dovetail with hospitalists’ initial reasons for choosing medicine: to improve patients’ lives.
Janet Nagamine, RN, MD, SFHM, former patient safety officer and assistant chief of quality at Kaiser Permanente in Santa Clara, Calif., describes the fit this way: “I might be a good doctor, but as a hospitalist, I rely on many others within the system to deliver, so my patients can’t get good care until the entire system is running well,” she says. “There are all kinds of opportunities to fix our [hospital] system, and I really believe that hospitalists cannot separate themselves from that engagement.”
Elizabeth Gundersen, MD, FHM, of Fort Lauderdale, Fla., agrees that it’s a natural step to think about the ways to make a difference on a larger level. At her former institution, the University of Massachusetts (UMass) Medical School in Worcester, she parlayed her interest in QI to work her way up from ground-level hospitalist to associate chief of her division and quality officer for the hospital. “Physicians get a lot of satisfaction from helping individual patients,” she says. “One thing I really liked about getting involved with quality improvement was being able to make a difference for patients on a systems level.”
An Incremental Path
The path to her current position began with a very specific issue for Dr. Nagamine, an SHM board member who also serves as a Project BOOST co-investigator. “Although I have been doing patient safety since before they had a name for it, I didn’t start out saying that I wanted a career in quality and safety,” she says. “I was trying to take better care of my patients with diabetes, but controlling their glucose was extremely challenging because all the related variables—timing and amount of their insulin dosage, when and how much they had eaten—were charted in different places. This made it hard to adjust their insulin appropriately.”
It quickly became clear to Dr. Nagamine that the solution had to be systemic. She realized that something as basic as taking care of her patients with diabetes required multiple departments (i.e. dietary, nursing, and pharmacy) to furnish information in an integrated manner. So she joined the diabetes committee and went to work on the issue. She helped devise a flow chart that could be used by all relevant departments. A further evolution on the path emanated from one of her patients receiving the wrong medication. She joined the medication safety committee, became chair, “and the next thing you know, I’m in charge of patient safety, and an assistant chief of quality.”
Training Is Necessary
QI and patient-safety methodologies have become sophisticated disciplines in the past two decades, Dr. Wright says. Access to training in QI basics now is readily available to early-career hospitalists. For example, CogentHMG offers program support for QI so that anyone interested “doesn’t have to start from scratch anymore; we can help show them the way and support them in doing it.”
This month, HM13 (www.hospital medicine2013.org)—just outside Washington, D.C.—will offer multiple sessions on quality, as well as the “Initiating Quality Improvement Projects with Built-In Sustainment” workshop, led by Center for Comprehensive Access and Delivery Research and Evaluation (CADRE) core investigator Peter Kaboli, MD, MS, who will address sustainability.
Beyond methodological tools, success in quality and patient safety requires the ability to motivate people, often across multiple disciplines, Dr. Nagamine says. “If you want things to work better, you must invite the right people to the table. For example, we often forget to include key nonclinical stakeholders,” she adds.
When working with hospitals across the country to implement rapid-response tTeams, Dr. Nagamine often reminds them to invite the operators, or “key people,” in the process.
“If you put patient safety at the core of your initiative and create the context for that, most people will agree that it’s the right thing to do and will get on board, even if it’s an extra step for them,” she says. “Know your audience, listen to their perspective, and learn what matters to them. And to most people, it matters that they give good patient care.”
Gretchen Henkel is a freelance writer in California.
Branch Out: QI and Patient-Safety Initiatives
Pick a passion. It’s best to choose an issue that’s important to you. “It has to be a
passion because much of the time it’s an uphill battle,” says Dr. Gundersen. She started with the issue of reducing readmissions, and with two colleagues pitched the idea of involving the UMass HM group in SHM’s Project BOOST. After that, she set out to become an expert on reducing readmissions, applying what she had learned to other successful initiatives.
Learn the lingo. Dr. Wright advises learning some of the most basic principles, such as Shewhart’s PDCA (Plan-Do-Check-Act) or Deming’s adaptation PDSA (Plan-Do-Study-Act) cycles; the quality tripod; and accessing resources made available from SHM. A member of SHM’s Hospital Quality and Patient Safety Committee, Dr. Wright says a subcommittee for leadership engagement has been created and furnishes tools and training for advancing quality initiatives. The Institute for Healthcare Improvement (www.ihi.org) also offers a wealth of measures, speaker series, and white papers on improvement in health care.
Start small. You can test your ability to work with interdisciplinary departments, often a prerequisite of many quality initiatives, by first joining a committee, Dr. Nagamine advises. “See how effective or persuasive you are in pitching an idea and seeing it through with other departments,” she says.
Brace for a marathon. “Most people,” Dr. Gundersen says, “do not hand you 100% of their cooperation and a budget you can work with.” It takes time to get buy-in, especially if you’re doing interdisciplinary initiatives. If possible, break your projects into achievable units. “Start with some quick wins. Small payoffs here and there can re-energize your team and eventually yield a larger payoff,” she says.
Limit sweat equity. It’s important to put in time at the start of a project to demonstrate your value, but if you’re constantly staying up late working on a project, consider pitching a compensated role to your boss. “Being a good citizen and volunteering for committees is one thing,” Dr. Nagamine cautions, “but taking on leadership roles in too many projects, without dedicated time, is not sustainable and can jeopardize the success of your projects.”
—Gretchen Henkel
Drive Change in an ACO

From informal polls I’ve recently conducted of hospitalists, many are not even aware they are part of an accountable-care organization (ACO). And if they are aware, they might not be engaging in meaningful dialogue with ACO leaders about their role in these organizations. But, in the long term, ACOs will need to bring hospitalists to the table in order to be successful.
Are You Part of an ACO?
David Muhlestein, who blogs for Health Affairs, tracks the growth of ACOs around the country. He states that, as of Jan. 31, there were 428 ACOs in the U.S. (see Figure 1).1 In terms of numbers, Florida, Texas, and California lead the nation with 42, 33, and 46 ACOs, respectively. So it is likely that you are part of an ACO. If you are unsure, ask your chief medical officer or president of the medical staff.
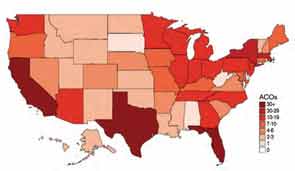
How ACOs Work
All ACOs seek to manage a group, or population, of patients as efficiently as possible while maintaining or improving quality of care. For Medicare ACOs, the goal is to bring together hospitals and physicians in order to share savings derived from efficiencies in care. But before any savings can be shared, the Medicare ACO must demonstrate that it achieved high-quality care across four domains, totaling 33 individual quality measures. (see Table 1)
Main Flavors of ACOs
There are two types of ACOs: private ACOs and Medicare ACOs. Prior to Medicare ACOs, which were launched in January 2012, there were 150 private-sector ACOs, and this number continues to grow. Private ACOs represent a heterogeneous group in terms of reimbursement model. Some operate under shared savings programs; others use full or partial capitation, bundled payments, and/or other types of arrangements. But nearly all ACOs operate under the premise that the incentives used to make care more efficient and less costly can only be applied if measurable quality is maintained or improved. ACOs do not pay doctors or hospitals more unless high quality is demonstrated.
ACO Quality Measures and Hospitalists
Most of the 33 quality measures required by Medicare ACOs are based in ambulatory practice. These include measures related to blood pressure, immunizations, cancer, and fall-risk screening, and measures for diabetics, such as lipids and hemoglobin A1C. However, there are a few measures for which hospitalists should share in accountability, including:
- All-cause hospital readmission rate—risk-standardized;
- Ambulatory sensitive condition hospital admission rates (CHF, COPD); and
- Medication reconciliation after discharge from an inpatient facility.
Four Key Actions for Hospitalists
Hospitalists make a significant contribution to the quality and the financial performance of ACOs. In addition to the quality metrics cited above, hospitalists impact the inpatient portion of the overall population’s cost of care. Furthermore, hospitalists are vital partners in the care coordination required for an ACO to be successful.
Here are four actions I suggest taking in order for your hospitalist group to be effective as participants in an ACO:
- Have a representative from your group participate in ACO committees that address hospital utilization and related matters, such as care coordination impacting pre- and post-hospital care.
- Learn how to work with ACO case managers on care transitions, including post-discharge follow-up and information transfer.
- Understand an ACO’s approach to engagement of and coordination with post-acute-care facilities. The ability of a post-acute facility, such a skilled nursing facility, to accept patients who have complex care needs, to manage changes in condition in the facility when appropriate, and to send complete information upon transfer to the hospital are important strategies for an ACO’s success.
- Understand how an ACO reports quality and cost performance and how savings will be shared among participants.
Mindset Change
If hospitalists are part of the chain of ACO physicians and providers held accountable for the health of a population of patients, we must work more closely with the medical home/neighborhood, post-acute-care facilities, and home-care providers. The change in mindset will occur only if we have a set of tools to get the job done, such as case managers and information technology, and the appropriate incentives to support better care coordination. I encourage my fellow hospitalists to make things happen, instead of taking a passive role in this monumental transformation.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
From informal polls I’ve recently conducted of hospitalists, many are not even aware they are part of an accountable-care organization (ACO). And if they are aware, they might not be engaging in meaningful dialogue with ACO leaders about their role in these organizations. But, in the long term, ACOs will need to bring hospitalists to the table in order to be successful.
Are You Part of an ACO?
David Muhlestein, who blogs for Health Affairs, tracks the growth of ACOs around the country. He states that, as of Jan. 31, there were 428 ACOs in the U.S. (see Figure 1).1 In terms of numbers, Florida, Texas, and California lead the nation with 42, 33, and 46 ACOs, respectively. So it is likely that you are part of an ACO. If you are unsure, ask your chief medical officer or president of the medical staff.
How ACOs Work
All ACOs seek to manage a group, or population, of patients as efficiently as possible while maintaining or improving quality of care. For Medicare ACOs, the goal is to bring together hospitals and physicians in order to share savings derived from efficiencies in care. But before any savings can be shared, the Medicare ACO must demonstrate that it achieved high-quality care across four domains, totaling 33 individual quality measures. (see Table 1)
Main Flavors of ACOs
There are two types of ACOs: private ACOs and Medicare ACOs. Prior to Medicare ACOs, which were launched in January 2012, there were 150 private-sector ACOs, and this number continues to grow. Private ACOs represent a heterogeneous group in terms of reimbursement model. Some operate under shared savings programs; others use full or partial capitation, bundled payments, and/or other types of arrangements. But nearly all ACOs operate under the premise that the incentives used to make care more efficient and less costly can only be applied if measurable quality is maintained or improved. ACOs do not pay doctors or hospitals more unless high quality is demonstrated.
ACO Quality Measures and Hospitalists
Most of the 33 quality measures required by Medicare ACOs are based in ambulatory practice. These include measures related to blood pressure, immunizations, cancer, and fall-risk screening, and measures for diabetics, such as lipids and hemoglobin A1C. However, there are a few measures for which hospitalists should share in accountability, including:
- All-cause hospital readmission rate—risk-standardized;
- Ambulatory sensitive condition hospital admission rates (CHF, COPD); and
- Medication reconciliation after discharge from an inpatient facility.
Four Key Actions for Hospitalists
Hospitalists make a significant contribution to the quality and the financial performance of ACOs. In addition to the quality metrics cited above, hospitalists impact the inpatient portion of the overall population’s cost of care. Furthermore, hospitalists are vital partners in the care coordination required for an ACO to be successful.
Here are four actions I suggest taking in order for your hospitalist group to be effective as participants in an ACO:
- Have a representative from your group participate in ACO committees that address hospital utilization and related matters, such as care coordination impacting pre- and post-hospital care.
- Learn how to work with ACO case managers on care transitions, including post-discharge follow-up and information transfer.
- Understand an ACO’s approach to engagement of and coordination with post-acute-care facilities. The ability of a post-acute facility, such a skilled nursing facility, to accept patients who have complex care needs, to manage changes in condition in the facility when appropriate, and to send complete information upon transfer to the hospital are important strategies for an ACO’s success.
- Understand how an ACO reports quality and cost performance and how savings will be shared among participants.
Mindset Change
If hospitalists are part of the chain of ACO physicians and providers held accountable for the health of a population of patients, we must work more closely with the medical home/neighborhood, post-acute-care facilities, and home-care providers. The change in mindset will occur only if we have a set of tools to get the job done, such as case managers and information technology, and the appropriate incentives to support better care coordination. I encourage my fellow hospitalists to make things happen, instead of taking a passive role in this monumental transformation.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
From informal polls I’ve recently conducted of hospitalists, many are not even aware they are part of an accountable-care organization (ACO). And if they are aware, they might not be engaging in meaningful dialogue with ACO leaders about their role in these organizations. But, in the long term, ACOs will need to bring hospitalists to the table in order to be successful.
Are You Part of an ACO?
David Muhlestein, who blogs for Health Affairs, tracks the growth of ACOs around the country. He states that, as of Jan. 31, there were 428 ACOs in the U.S. (see Figure 1).1 In terms of numbers, Florida, Texas, and California lead the nation with 42, 33, and 46 ACOs, respectively. So it is likely that you are part of an ACO. If you are unsure, ask your chief medical officer or president of the medical staff.
How ACOs Work
All ACOs seek to manage a group, or population, of patients as efficiently as possible while maintaining or improving quality of care. For Medicare ACOs, the goal is to bring together hospitals and physicians in order to share savings derived from efficiencies in care. But before any savings can be shared, the Medicare ACO must demonstrate that it achieved high-quality care across four domains, totaling 33 individual quality measures. (see Table 1)
Main Flavors of ACOs
There are two types of ACOs: private ACOs and Medicare ACOs. Prior to Medicare ACOs, which were launched in January 2012, there were 150 private-sector ACOs, and this number continues to grow. Private ACOs represent a heterogeneous group in terms of reimbursement model. Some operate under shared savings programs; others use full or partial capitation, bundled payments, and/or other types of arrangements. But nearly all ACOs operate under the premise that the incentives used to make care more efficient and less costly can only be applied if measurable quality is maintained or improved. ACOs do not pay doctors or hospitals more unless high quality is demonstrated.
ACO Quality Measures and Hospitalists
Most of the 33 quality measures required by Medicare ACOs are based in ambulatory practice. These include measures related to blood pressure, immunizations, cancer, and fall-risk screening, and measures for diabetics, such as lipids and hemoglobin A1C. However, there are a few measures for which hospitalists should share in accountability, including:
- All-cause hospital readmission rate—risk-standardized;
- Ambulatory sensitive condition hospital admission rates (CHF, COPD); and
- Medication reconciliation after discharge from an inpatient facility.
Four Key Actions for Hospitalists
Hospitalists make a significant contribution to the quality and the financial performance of ACOs. In addition to the quality metrics cited above, hospitalists impact the inpatient portion of the overall population’s cost of care. Furthermore, hospitalists are vital partners in the care coordination required for an ACO to be successful.
Here are four actions I suggest taking in order for your hospitalist group to be effective as participants in an ACO:
- Have a representative from your group participate in ACO committees that address hospital utilization and related matters, such as care coordination impacting pre- and post-hospital care.
- Learn how to work with ACO case managers on care transitions, including post-discharge follow-up and information transfer.
- Understand an ACO’s approach to engagement of and coordination with post-acute-care facilities. The ability of a post-acute facility, such a skilled nursing facility, to accept patients who have complex care needs, to manage changes in condition in the facility when appropriate, and to send complete information upon transfer to the hospital are important strategies for an ACO’s success.
- Understand how an ACO reports quality and cost performance and how savings will be shared among participants.
Mindset Change
If hospitalists are part of the chain of ACO physicians and providers held accountable for the health of a population of patients, we must work more closely with the medical home/neighborhood, post-acute-care facilities, and home-care providers. The change in mindset will occur only if we have a set of tools to get the job done, such as case managers and information technology, and the appropriate incentives to support better care coordination. I encourage my fellow hospitalists to make things happen, instead of taking a passive role in this monumental transformation.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
Win Whitcomb: Front-Line Hospitalists Fight Against Health Care-Associated Infections (HAIs)

2013 marks a turning point in the way hospitals are held accountable for the prevention of healthcare-associated infections (HAIs). It has been known for some time that HAIs are a serious cause of morbidity, with 1 in 20 hospital patients in the U.S. acquiring one. That represents 1.7 million Americans and accounts for about 100,000 lives lost each year. On a personal note, my father died of an HAI after surgery in 2000.
Now, with the Affordable Care Act coming into full swing, hospitals must get serious about preventing HAIs. This presents a major opportunity for hospitalists. There are three ways that hospitals will be affected:
- Since 2008, hospitals have not been reimbursed at a higher rate for vascular catheter-associated infections, catheter-associated urinary tract infections (UTIs), or surgical-site infections when acquired in the hospital.
- Over the next few years, Medicare’s Hospital Value-Based Purchasing (HVBP) program will begin to pay hospitals more or less, depending on how they perform, on six HAIs.
- Beginning in October 2014, in a roll-up measure for hospital-acquired conditions (which include infections), the worst-performing quartile of U.S. hospitals will be penalized 1% of their Medicare inpatient payments (see Table 1, below).
There are six HAIs that will be increasingly tied to hospital reimbursement. Each can be partially or completely prevented based on sets of practices, or care bundles, that require teamwork both in the planning stages and at the bedside. And, of course, the single most important way to reduce the spread of HAIs is to clean your hands before and after each patient encounter.
Clostridium-Difficile-Associated Disease (CDAD)
It is likely that your hospital has some type of CDAD prevention program. Here are a few things to keep in mind for CDAD prevention:
- Avoid alcohol-based hand rubs, because they do not kill C. diff spores. Vigorous hand washing with soap and water is the best approach.
- Use clindamycin, fluoroquinolones, and third-generation cephalosporins judiciously, as their restriction has been associated with reduced rates of CDAD.
- Place patients with suspected or proven C. diff infection on contact precautions, including gloves and gowns.
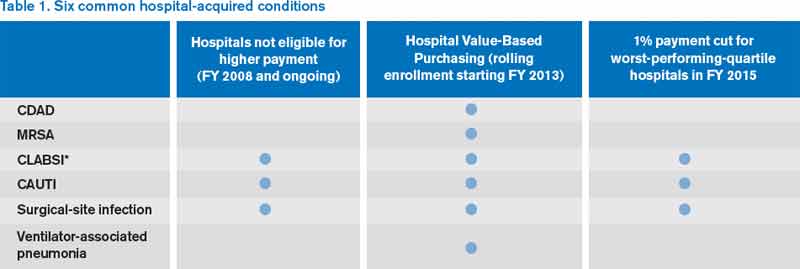
Methicillin-Resistant Staphylococcus Aureus (MRSA)
This includes hospital-acquired MRSA bacteremia. This topic will be discussed in future columns. Approaches to prevention include hand hygiene, cohorting patients, effective environmental cleaning, and antibiotic stewardship.
Central-Line-Associated Bloodstream Infection (CLABSI)
Adherence to the central-line insertion bundle has been conclusively shown to prevent CLABSI. It will become a process measure for HVBP in the near future. Prevention measures include hand hygiene, maximal barrier precautions during insertion, skin antisepsis with chlorhexidine, avoidance of the femoral vein, and daily assessment for readiness to discontinue the central line (which should involve every hospitalist).
Catheter-Associated Urinary Tract Infection (CAUTI)
CAUTI has been mentioned frequently in this column, and for good reason: It is the most common HAI. Although the evidence supporting practices that prevent CAUTI is not as strong as for CLABSI, every institution should have a bundle of practices embedded in nurses’ and doctors’ workflow to prevent CAUTI (see “Quality Meets Finance,” January 2013, p. 31).
Surgical-Site Infection (SSI)
For the most part, SSI can be left to the surgeons and other operating room professionals. However, with increasing involvement of hospitalists in surgical cases, we must have an understanding of how SSIs are prevented. The World Health Organization surgical checklist (www.who.int/patientsafety/safesurgery) is a great starting point for any organization.
Ventilator-Associated Pneumonia (VAP)
For hospitalists who provide critical care, adherence to a VAP prevention bundle includes:
- Elevation of the head of the bed;
- Daily “sedation vacation” and readiness to extubate;
- Oral care with chlorhexidine; and
- Peptic ulcer disease and venous thromboembolism prophylaxis.
In 2009, the U.S. Department of Health and Human Services (HHS) launched an action plan to prevent HAIs. As part of this effort, the Agency for Health Research and Quality (AHRQ) created a comprehensive unit-based safety program (CUSP) aimed at preventing CLABSI and CAUTI. The effort also focuses on safety culture and teamwork. For those interested in participating, visit www.onthecuspstophai.org.
Another way to get involved is to work Partnership for Patients, a public-private partnership led by HHS (http://partnershipforpatients.cms.gov), if a team at your hospital is participating. The Partnership for Patients seeks to reduce harm, including HAIs, by 40% by the end of 2013 compared with a 2010 baseline.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
The View from The Center
As many of you know, SHM recently submitted five recommendations to the American Board of Internal Medicine Foundation’s Choosing Wisely campaign. This campaign encourages physicians and patients to have crucial conversations about appropriate utilization of tests and treatments. Seventeen specialty societies released lists in the second phase of the campaign. Many of the lists, including SHM’s, include recommendations that can help reduce hospital-acquired infections.
For example, one of SHM’s recommendations suggests not placing, or leaving in place, urinary catheters for any reason other than those indicated by the guidelines (e.g. bladder outlet obstruction, acute urinary retention, patient requires prolonged immobilization, to improve comfort for end of life, selected perioperative conditions). As Dr. Whitcomb indicates above, CAUTIs are low-hanging fruit when it comes to improving this condition—the guidelines are clear-cut, and relatively simple protocols can be put into place to prevent CAUTI.
Among the American Academy of Family Physicians and other society recommendations is avoidance of routine prescriptions of antibiotics for acute sinusitis or upper respiratory infections. Good antimicrobial stewardship policies are another approach to reduce or eliminate harmful antibiotic-resistant infections.
SHM will be offering multiple opportunities in the coming months to support your institution in Choosing Wisely. A daylong pre-course and two breakout sessions will be offered at HM13 (www.hospitalmedicine2013.org) addressing how you can implement the various recommendations. Additionally, publications are in the works describing the evidence base for SHM’s “avoid lists.” For resources, more information about SHM’s recommendations, and the latest Choosing Wisely developments, visit www.hospitalmedicine.org/choosingwisely.
2013 marks a turning point in the way hospitals are held accountable for the prevention of healthcare-associated infections (HAIs). It has been known for some time that HAIs are a serious cause of morbidity, with 1 in 20 hospital patients in the U.S. acquiring one. That represents 1.7 million Americans and accounts for about 100,000 lives lost each year. On a personal note, my father died of an HAI after surgery in 2000.
Now, with the Affordable Care Act coming into full swing, hospitals must get serious about preventing HAIs. This presents a major opportunity for hospitalists. There are three ways that hospitals will be affected:
- Since 2008, hospitals have not been reimbursed at a higher rate for vascular catheter-associated infections, catheter-associated urinary tract infections (UTIs), or surgical-site infections when acquired in the hospital.
- Over the next few years, Medicare’s Hospital Value-Based Purchasing (HVBP) program will begin to pay hospitals more or less, depending on how they perform, on six HAIs.
- Beginning in October 2014, in a roll-up measure for hospital-acquired conditions (which include infections), the worst-performing quartile of U.S. hospitals will be penalized 1% of their Medicare inpatient payments (see Table 1, below).
There are six HAIs that will be increasingly tied to hospital reimbursement. Each can be partially or completely prevented based on sets of practices, or care bundles, that require teamwork both in the planning stages and at the bedside. And, of course, the single most important way to reduce the spread of HAIs is to clean your hands before and after each patient encounter.
Clostridium-Difficile-Associated Disease (CDAD)
It is likely that your hospital has some type of CDAD prevention program. Here are a few things to keep in mind for CDAD prevention:
- Avoid alcohol-based hand rubs, because they do not kill C. diff spores. Vigorous hand washing with soap and water is the best approach.
- Use clindamycin, fluoroquinolones, and third-generation cephalosporins judiciously, as their restriction has been associated with reduced rates of CDAD.
- Place patients with suspected or proven C. diff infection on contact precautions, including gloves and gowns.
Methicillin-Resistant Staphylococcus Aureus (MRSA)
This includes hospital-acquired MRSA bacteremia. This topic will be discussed in future columns. Approaches to prevention include hand hygiene, cohorting patients, effective environmental cleaning, and antibiotic stewardship.
Central-Line-Associated Bloodstream Infection (CLABSI)
Adherence to the central-line insertion bundle has been conclusively shown to prevent CLABSI. It will become a process measure for HVBP in the near future. Prevention measures include hand hygiene, maximal barrier precautions during insertion, skin antisepsis with chlorhexidine, avoidance of the femoral vein, and daily assessment for readiness to discontinue the central line (which should involve every hospitalist).
Catheter-Associated Urinary Tract Infection (CAUTI)
CAUTI has been mentioned frequently in this column, and for good reason: It is the most common HAI. Although the evidence supporting practices that prevent CAUTI is not as strong as for CLABSI, every institution should have a bundle of practices embedded in nurses’ and doctors’ workflow to prevent CAUTI (see “Quality Meets Finance,” January 2013, p. 31).
Surgical-Site Infection (SSI)
For the most part, SSI can be left to the surgeons and other operating room professionals. However, with increasing involvement of hospitalists in surgical cases, we must have an understanding of how SSIs are prevented. The World Health Organization surgical checklist (www.who.int/patientsafety/safesurgery) is a great starting point for any organization.
Ventilator-Associated Pneumonia (VAP)
For hospitalists who provide critical care, adherence to a VAP prevention bundle includes:
- Elevation of the head of the bed;
- Daily “sedation vacation” and readiness to extubate;
- Oral care with chlorhexidine; and
- Peptic ulcer disease and venous thromboembolism prophylaxis.
In 2009, the U.S. Department of Health and Human Services (HHS) launched an action plan to prevent HAIs. As part of this effort, the Agency for Health Research and Quality (AHRQ) created a comprehensive unit-based safety program (CUSP) aimed at preventing CLABSI and CAUTI. The effort also focuses on safety culture and teamwork. For those interested in participating, visit www.onthecuspstophai.org.
Another way to get involved is to work Partnership for Patients, a public-private partnership led by HHS (http://partnershipforpatients.cms.gov), if a team at your hospital is participating. The Partnership for Patients seeks to reduce harm, including HAIs, by 40% by the end of 2013 compared with a 2010 baseline.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
The View from The Center
As many of you know, SHM recently submitted five recommendations to the American Board of Internal Medicine Foundation’s Choosing Wisely campaign. This campaign encourages physicians and patients to have crucial conversations about appropriate utilization of tests and treatments. Seventeen specialty societies released lists in the second phase of the campaign. Many of the lists, including SHM’s, include recommendations that can help reduce hospital-acquired infections.
For example, one of SHM’s recommendations suggests not placing, or leaving in place, urinary catheters for any reason other than those indicated by the guidelines (e.g. bladder outlet obstruction, acute urinary retention, patient requires prolonged immobilization, to improve comfort for end of life, selected perioperative conditions). As Dr. Whitcomb indicates above, CAUTIs are low-hanging fruit when it comes to improving this condition—the guidelines are clear-cut, and relatively simple protocols can be put into place to prevent CAUTI.
Among the American Academy of Family Physicians and other society recommendations is avoidance of routine prescriptions of antibiotics for acute sinusitis or upper respiratory infections. Good antimicrobial stewardship policies are another approach to reduce or eliminate harmful antibiotic-resistant infections.
SHM will be offering multiple opportunities in the coming months to support your institution in Choosing Wisely. A daylong pre-course and two breakout sessions will be offered at HM13 (www.hospitalmedicine2013.org) addressing how you can implement the various recommendations. Additionally, publications are in the works describing the evidence base for SHM’s “avoid lists.” For resources, more information about SHM’s recommendations, and the latest Choosing Wisely developments, visit www.hospitalmedicine.org/choosingwisely.
2013 marks a turning point in the way hospitals are held accountable for the prevention of healthcare-associated infections (HAIs). It has been known for some time that HAIs are a serious cause of morbidity, with 1 in 20 hospital patients in the U.S. acquiring one. That represents 1.7 million Americans and accounts for about 100,000 lives lost each year. On a personal note, my father died of an HAI after surgery in 2000.
Now, with the Affordable Care Act coming into full swing, hospitals must get serious about preventing HAIs. This presents a major opportunity for hospitalists. There are three ways that hospitals will be affected:
- Since 2008, hospitals have not been reimbursed at a higher rate for vascular catheter-associated infections, catheter-associated urinary tract infections (UTIs), or surgical-site infections when acquired in the hospital.
- Over the next few years, Medicare’s Hospital Value-Based Purchasing (HVBP) program will begin to pay hospitals more or less, depending on how they perform, on six HAIs.
- Beginning in October 2014, in a roll-up measure for hospital-acquired conditions (which include infections), the worst-performing quartile of U.S. hospitals will be penalized 1% of their Medicare inpatient payments (see Table 1, below).
There are six HAIs that will be increasingly tied to hospital reimbursement. Each can be partially or completely prevented based on sets of practices, or care bundles, that require teamwork both in the planning stages and at the bedside. And, of course, the single most important way to reduce the spread of HAIs is to clean your hands before and after each patient encounter.
Clostridium-Difficile-Associated Disease (CDAD)
It is likely that your hospital has some type of CDAD prevention program. Here are a few things to keep in mind for CDAD prevention:
- Avoid alcohol-based hand rubs, because they do not kill C. diff spores. Vigorous hand washing with soap and water is the best approach.
- Use clindamycin, fluoroquinolones, and third-generation cephalosporins judiciously, as their restriction has been associated with reduced rates of CDAD.
- Place patients with suspected or proven C. diff infection on contact precautions, including gloves and gowns.
Methicillin-Resistant Staphylococcus Aureus (MRSA)
This includes hospital-acquired MRSA bacteremia. This topic will be discussed in future columns. Approaches to prevention include hand hygiene, cohorting patients, effective environmental cleaning, and antibiotic stewardship.
Central-Line-Associated Bloodstream Infection (CLABSI)
Adherence to the central-line insertion bundle has been conclusively shown to prevent CLABSI. It will become a process measure for HVBP in the near future. Prevention measures include hand hygiene, maximal barrier precautions during insertion, skin antisepsis with chlorhexidine, avoidance of the femoral vein, and daily assessment for readiness to discontinue the central line (which should involve every hospitalist).
Catheter-Associated Urinary Tract Infection (CAUTI)
CAUTI has been mentioned frequently in this column, and for good reason: It is the most common HAI. Although the evidence supporting practices that prevent CAUTI is not as strong as for CLABSI, every institution should have a bundle of practices embedded in nurses’ and doctors’ workflow to prevent CAUTI (see “Quality Meets Finance,” January 2013, p. 31).
Surgical-Site Infection (SSI)
For the most part, SSI can be left to the surgeons and other operating room professionals. However, with increasing involvement of hospitalists in surgical cases, we must have an understanding of how SSIs are prevented. The World Health Organization surgical checklist (www.who.int/patientsafety/safesurgery) is a great starting point for any organization.
Ventilator-Associated Pneumonia (VAP)
For hospitalists who provide critical care, adherence to a VAP prevention bundle includes:
- Elevation of the head of the bed;
- Daily “sedation vacation” and readiness to extubate;
- Oral care with chlorhexidine; and
- Peptic ulcer disease and venous thromboembolism prophylaxis.
In 2009, the U.S. Department of Health and Human Services (HHS) launched an action plan to prevent HAIs. As part of this effort, the Agency for Health Research and Quality (AHRQ) created a comprehensive unit-based safety program (CUSP) aimed at preventing CLABSI and CAUTI. The effort also focuses on safety culture and teamwork. For those interested in participating, visit www.onthecuspstophai.org.
Another way to get involved is to work Partnership for Patients, a public-private partnership led by HHS (http://partnershipforpatients.cms.gov), if a team at your hospital is participating. The Partnership for Patients seeks to reduce harm, including HAIs, by 40% by the end of 2013 compared with a 2010 baseline.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
The View from The Center
As many of you know, SHM recently submitted five recommendations to the American Board of Internal Medicine Foundation’s Choosing Wisely campaign. This campaign encourages physicians and patients to have crucial conversations about appropriate utilization of tests and treatments. Seventeen specialty societies released lists in the second phase of the campaign. Many of the lists, including SHM’s, include recommendations that can help reduce hospital-acquired infections.
For example, one of SHM’s recommendations suggests not placing, or leaving in place, urinary catheters for any reason other than those indicated by the guidelines (e.g. bladder outlet obstruction, acute urinary retention, patient requires prolonged immobilization, to improve comfort for end of life, selected perioperative conditions). As Dr. Whitcomb indicates above, CAUTIs are low-hanging fruit when it comes to improving this condition—the guidelines are clear-cut, and relatively simple protocols can be put into place to prevent CAUTI.
Among the American Academy of Family Physicians and other society recommendations is avoidance of routine prescriptions of antibiotics for acute sinusitis or upper respiratory infections. Good antimicrobial stewardship policies are another approach to reduce or eliminate harmful antibiotic-resistant infections.
SHM will be offering multiple opportunities in the coming months to support your institution in Choosing Wisely. A daylong pre-course and two breakout sessions will be offered at HM13 (www.hospitalmedicine2013.org) addressing how you can implement the various recommendations. Additionally, publications are in the works describing the evidence base for SHM’s “avoid lists.” For resources, more information about SHM’s recommendations, and the latest Choosing Wisely developments, visit www.hospitalmedicine.org/choosingwisely.
John Nelson: Excessive Workload a Concern for Many Hospitalists

“Forty percent of physicians reported that their typical inpatient census exceeded safe levels at least monthly.”1
This quote is taken from an article by Henry Michtalik and colleagues that appeared at the end of January this year in JAMA Internal Medicine. In 2010 the authors conducted an on-line survey asking hospitalists their perceptions of their workload. Respondents indicated that with concerning frequency a high workload prevented them from adequately discussing with patients treatment options or answering questions, delay admitting or discharging patients until the next day or shift, or in some other way risk patient safety or the overall quality of their work.
This alarming finding matches my anecdotal experience working with many different hospitalist groups around the country. I think few hospitalists were surprised by the survey’s findings. Excess hospitalist workloads are indeed a problem in some settings, and those who bear them are typically not shy about speaking out.
The demand for hospitalists has exceeded the supply of doctors available to do the work throughout the history of the field. Under the weight of stunningly rapid growth in referral volume, from about 1995 to 2002, it was reasonably common for the original doctors in a hospitalist practice to become overwhelmed and leave for other work after a year or two, sometimes resulting in the collapse of the practice. Most practices are no longer in such a rapid-growth phase, but for many of them, staffing has not yet caught up with workload. The result can be chronic excess work, and even if daily patient volume is not seen as being unsafe, the number of days or shifts worked might be excessive and lead to fatigue and poor performance.
Other Workload Data
The respondents to the Michtalik survey reported that regardless of any assistance, “they could safely see 15 patients per shift, if their effort was 100% clinical.” What we don’t know is how long their shifts were, whether they included things like ICU coverage, and how many shifts they work consecutively or in a year.
SHM’s 2012 State of Hospital Medicine report, which is based on 2011 data, provides additional context. It shows that hospitalists serving adult patients report a median 2,092 billed encounters annually (mean 2,245, standard deviation 1,161). They spread this work over a median 185 shifts (“work periods”) annually (mean 192). While there are lots of methodological problems in manipulating those numbers further, 2,092 encounters divided by 185 shifts yields 11.3 encounters per shift. These numbers exclude academicians who typically spend significant time in activities other than direct patient care, and I’m intentionally ignoring such issues as the night-shift doctor, who typically has low productivity, bringing down the average per full-time doctor in a practice.
The numbers from both surveys are sort of fuzzy because they aren’t audited or verified, but the 2012 State of Hospital Medicine data suggest that typical workloads aren’t too high in most practices, yet 40% of respondents in the Michtalik survey said they were high enough—unreasonably high—to risk quality and safety at least once a month.
One way to reconcile these findings is to take into account the standard deviation in daily volume in a single practice of about 30% to 40% on above or below the mean. If a hospitalist averages 14 encounters each day shift, then he should expect that the daily number might vary between about eight and 20. The Michtalik survey responses were likely reflecting the shifts on the high end.
Perspective
I wonder what a survey of physician workload opinions in other specialties would show, or what a survey of workers across all segments of the U.S. workforce in and out of healthcare would show. Of course, many or most jobs outside of healthcare don’t risk another’s health or well-being as significantly as ours do, but it would still be instructive to know how people in general think about the work they do.
I suspect a significant number of people across many different jobs feel like too much work is expected of them, and they can point to the ways their performance suffers as a result. It is difficult to know what portion of those who report too much work is just complaining versus a thoughtful self-reflection of the determinants of their performance. Lots of hospitalists do face worrisome high workloads, but some would probably still complain even with a much lower workload.
What Can Be Done?
For those practices facing remarkably high patient volumes, the solution is to make sure you’re recruiting additional doctors, and/or NPs/PAs, as fast as you can. But a portion of these practices must first convince their employers that more staff is needed. Some practices face a real uphill battle in getting the required additional funding, and the place to start is with a careful analysis of your current workload—based on hard numbers from your practice, not just anecdotes and estimates.
Don’t forget that some hospitalists put themselves in the position of having to manage high daily patient volumes by choosing a schedule of relatively few worked days annually. For example, a group working a seven-on/seven-off schedule that also has 14 shifts of time off means that each doctor will work only 168.5 shifts annually. Compressing a year’s worth of work into only 168 shifts means that each shift will be busy, and many will involve patient volumes that exceed what is seen as safe.
It could make more sense to titrate that same work volume over more annual shifts so that the average shift is less busy. I would love to see the Michtalik data segregated by those who work many shifts annually versus those who work few shifts. It is possible that those working more shifts have reported excessive workloads less often.
SHM has a role in influencing hospitalist workloads and promotes dissemination of data and opinions about it. At HM13 next month in Washington, D.C., I am leading a session titled “Hospitalist Workload: Is 15 the Right Number?” Although it won’t provide the “right” workload for all hospitalists, it will offer worthwhile data and food for thought.
It is much more difficult to do studies of how workload influences performance than something like effects of sleep deprivation on performance, so we may never get clear answers. You could take some consolation in the fact that successive surveys have shown little change or even modest decreases in annual patient encounters. But then again, maybe that hasn’t helped with excess work since providing hospital care gets harder and more complex every year.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at [email protected].
Reference
“Forty percent of physicians reported that their typical inpatient census exceeded safe levels at least monthly.”1
This quote is taken from an article by Henry Michtalik and colleagues that appeared at the end of January this year in JAMA Internal Medicine. In 2010 the authors conducted an on-line survey asking hospitalists their perceptions of their workload. Respondents indicated that with concerning frequency a high workload prevented them from adequately discussing with patients treatment options or answering questions, delay admitting or discharging patients until the next day or shift, or in some other way risk patient safety or the overall quality of their work.
This alarming finding matches my anecdotal experience working with many different hospitalist groups around the country. I think few hospitalists were surprised by the survey’s findings. Excess hospitalist workloads are indeed a problem in some settings, and those who bear them are typically not shy about speaking out.
The demand for hospitalists has exceeded the supply of doctors available to do the work throughout the history of the field. Under the weight of stunningly rapid growth in referral volume, from about 1995 to 2002, it was reasonably common for the original doctors in a hospitalist practice to become overwhelmed and leave for other work after a year or two, sometimes resulting in the collapse of the practice. Most practices are no longer in such a rapid-growth phase, but for many of them, staffing has not yet caught up with workload. The result can be chronic excess work, and even if daily patient volume is not seen as being unsafe, the number of days or shifts worked might be excessive and lead to fatigue and poor performance.
Other Workload Data
The respondents to the Michtalik survey reported that regardless of any assistance, “they could safely see 15 patients per shift, if their effort was 100% clinical.” What we don’t know is how long their shifts were, whether they included things like ICU coverage, and how many shifts they work consecutively or in a year.
SHM’s 2012 State of Hospital Medicine report, which is based on 2011 data, provides additional context. It shows that hospitalists serving adult patients report a median 2,092 billed encounters annually (mean 2,245, standard deviation 1,161). They spread this work over a median 185 shifts (“work periods”) annually (mean 192). While there are lots of methodological problems in manipulating those numbers further, 2,092 encounters divided by 185 shifts yields 11.3 encounters per shift. These numbers exclude academicians who typically spend significant time in activities other than direct patient care, and I’m intentionally ignoring such issues as the night-shift doctor, who typically has low productivity, bringing down the average per full-time doctor in a practice.
The numbers from both surveys are sort of fuzzy because they aren’t audited or verified, but the 2012 State of Hospital Medicine data suggest that typical workloads aren’t too high in most practices, yet 40% of respondents in the Michtalik survey said they were high enough—unreasonably high—to risk quality and safety at least once a month.
One way to reconcile these findings is to take into account the standard deviation in daily volume in a single practice of about 30% to 40% on above or below the mean. If a hospitalist averages 14 encounters each day shift, then he should expect that the daily number might vary between about eight and 20. The Michtalik survey responses were likely reflecting the shifts on the high end.
Perspective
I wonder what a survey of physician workload opinions in other specialties would show, or what a survey of workers across all segments of the U.S. workforce in and out of healthcare would show. Of course, many or most jobs outside of healthcare don’t risk another’s health or well-being as significantly as ours do, but it would still be instructive to know how people in general think about the work they do.
I suspect a significant number of people across many different jobs feel like too much work is expected of them, and they can point to the ways their performance suffers as a result. It is difficult to know what portion of those who report too much work is just complaining versus a thoughtful self-reflection of the determinants of their performance. Lots of hospitalists do face worrisome high workloads, but some would probably still complain even with a much lower workload.
What Can Be Done?
For those practices facing remarkably high patient volumes, the solution is to make sure you’re recruiting additional doctors, and/or NPs/PAs, as fast as you can. But a portion of these practices must first convince their employers that more staff is needed. Some practices face a real uphill battle in getting the required additional funding, and the place to start is with a careful analysis of your current workload—based on hard numbers from your practice, not just anecdotes and estimates.
Don’t forget that some hospitalists put themselves in the position of having to manage high daily patient volumes by choosing a schedule of relatively few worked days annually. For example, a group working a seven-on/seven-off schedule that also has 14 shifts of time off means that each doctor will work only 168.5 shifts annually. Compressing a year’s worth of work into only 168 shifts means that each shift will be busy, and many will involve patient volumes that exceed what is seen as safe.
It could make more sense to titrate that same work volume over more annual shifts so that the average shift is less busy. I would love to see the Michtalik data segregated by those who work many shifts annually versus those who work few shifts. It is possible that those working more shifts have reported excessive workloads less often.
SHM has a role in influencing hospitalist workloads and promotes dissemination of data and opinions about it. At HM13 next month in Washington, D.C., I am leading a session titled “Hospitalist Workload: Is 15 the Right Number?” Although it won’t provide the “right” workload for all hospitalists, it will offer worthwhile data and food for thought.
It is much more difficult to do studies of how workload influences performance than something like effects of sleep deprivation on performance, so we may never get clear answers. You could take some consolation in the fact that successive surveys have shown little change or even modest decreases in annual patient encounters. But then again, maybe that hasn’t helped with excess work since providing hospital care gets harder and more complex every year.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at [email protected].
Reference
“Forty percent of physicians reported that their typical inpatient census exceeded safe levels at least monthly.”1
This quote is taken from an article by Henry Michtalik and colleagues that appeared at the end of January this year in JAMA Internal Medicine. In 2010 the authors conducted an on-line survey asking hospitalists their perceptions of their workload. Respondents indicated that with concerning frequency a high workload prevented them from adequately discussing with patients treatment options or answering questions, delay admitting or discharging patients until the next day or shift, or in some other way risk patient safety or the overall quality of their work.
This alarming finding matches my anecdotal experience working with many different hospitalist groups around the country. I think few hospitalists were surprised by the survey’s findings. Excess hospitalist workloads are indeed a problem in some settings, and those who bear them are typically not shy about speaking out.
The demand for hospitalists has exceeded the supply of doctors available to do the work throughout the history of the field. Under the weight of stunningly rapid growth in referral volume, from about 1995 to 2002, it was reasonably common for the original doctors in a hospitalist practice to become overwhelmed and leave for other work after a year or two, sometimes resulting in the collapse of the practice. Most practices are no longer in such a rapid-growth phase, but for many of them, staffing has not yet caught up with workload. The result can be chronic excess work, and even if daily patient volume is not seen as being unsafe, the number of days or shifts worked might be excessive and lead to fatigue and poor performance.
Other Workload Data
The respondents to the Michtalik survey reported that regardless of any assistance, “they could safely see 15 patients per shift, if their effort was 100% clinical.” What we don’t know is how long their shifts were, whether they included things like ICU coverage, and how many shifts they work consecutively or in a year.
SHM’s 2012 State of Hospital Medicine report, which is based on 2011 data, provides additional context. It shows that hospitalists serving adult patients report a median 2,092 billed encounters annually (mean 2,245, standard deviation 1,161). They spread this work over a median 185 shifts (“work periods”) annually (mean 192). While there are lots of methodological problems in manipulating those numbers further, 2,092 encounters divided by 185 shifts yields 11.3 encounters per shift. These numbers exclude academicians who typically spend significant time in activities other than direct patient care, and I’m intentionally ignoring such issues as the night-shift doctor, who typically has low productivity, bringing down the average per full-time doctor in a practice.
The numbers from both surveys are sort of fuzzy because they aren’t audited or verified, but the 2012 State of Hospital Medicine data suggest that typical workloads aren’t too high in most practices, yet 40% of respondents in the Michtalik survey said they were high enough—unreasonably high—to risk quality and safety at least once a month.
One way to reconcile these findings is to take into account the standard deviation in daily volume in a single practice of about 30% to 40% on above or below the mean. If a hospitalist averages 14 encounters each day shift, then he should expect that the daily number might vary between about eight and 20. The Michtalik survey responses were likely reflecting the shifts on the high end.
Perspective
I wonder what a survey of physician workload opinions in other specialties would show, or what a survey of workers across all segments of the U.S. workforce in and out of healthcare would show. Of course, many or most jobs outside of healthcare don’t risk another’s health or well-being as significantly as ours do, but it would still be instructive to know how people in general think about the work they do.
I suspect a significant number of people across many different jobs feel like too much work is expected of them, and they can point to the ways their performance suffers as a result. It is difficult to know what portion of those who report too much work is just complaining versus a thoughtful self-reflection of the determinants of their performance. Lots of hospitalists do face worrisome high workloads, but some would probably still complain even with a much lower workload.
What Can Be Done?
For those practices facing remarkably high patient volumes, the solution is to make sure you’re recruiting additional doctors, and/or NPs/PAs, as fast as you can. But a portion of these practices must first convince their employers that more staff is needed. Some practices face a real uphill battle in getting the required additional funding, and the place to start is with a careful analysis of your current workload—based on hard numbers from your practice, not just anecdotes and estimates.
Don’t forget that some hospitalists put themselves in the position of having to manage high daily patient volumes by choosing a schedule of relatively few worked days annually. For example, a group working a seven-on/seven-off schedule that also has 14 shifts of time off means that each doctor will work only 168.5 shifts annually. Compressing a year’s worth of work into only 168 shifts means that each shift will be busy, and many will involve patient volumes that exceed what is seen as safe.
It could make more sense to titrate that same work volume over more annual shifts so that the average shift is less busy. I would love to see the Michtalik data segregated by those who work many shifts annually versus those who work few shifts. It is possible that those working more shifts have reported excessive workloads less often.
SHM has a role in influencing hospitalist workloads and promotes dissemination of data and opinions about it. At HM13 next month in Washington, D.C., I am leading a session titled “Hospitalist Workload: Is 15 the Right Number?” Although it won’t provide the “right” workload for all hospitalists, it will offer worthwhile data and food for thought.
It is much more difficult to do studies of how workload influences performance than something like effects of sleep deprivation on performance, so we may never get clear answers. You could take some consolation in the fact that successive surveys have shown little change or even modest decreases in annual patient encounters. But then again, maybe that hasn’t helped with excess work since providing hospital care gets harder and more complex every year.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at [email protected].
Reference
Bob Wachter Puts Forward Spin on Patient Safety, Quality of Care at HM13

Most hospitalists have heard the adage “If you’ve seen one hospitalist group, you’ve seen one hospitalist group.” Another HM truism is “If you’ve seen one SHM annual meeting, then you’ve seen Bob Wachter, MD, MHM.”
Dr. Wachter, professor, chief of the division of hospital medicine, and chief of the medical service at the University of California at San Francisco Medical Center, is to HM conventions as warfarin is to anticoagulation. His keynote address is the finale to the yearly confab, and HM13’s version is scheduled for noon May 19 at the Gaylord National Harbor Resort & Convention Center in National Harbor, Md.
This year’s address is titled “Quality, Safety, and IT: A Decade of Successes, Failures, Surprises, and Epiphanies.” Dr. Wachter spoke recently with The Hospitalist about his annual tradition.
Question: With your interest in the intersection between healthcare and politics, to be back in D.C. has to be something enjoyable for you to write and talk about.
Answer: It’s a very interesting time in the life of healthcare, in that now that everybody knows that the [Affordable Care Act] is real and not going away, and we’re actually beginning to implement parts of it, you can kind of see what the future is going to look like, and everybody’s responding. And there are parts of that that are very exciting, because they’re forcing us to think about value in new ways. [And] there are parts of it that are somewhat frustrating.
Q: Does that give the hospitalist community the chance to ride herd on more global issues?
A: I think that’s the most optimistic interpretation—that we stick to our knitting, that we continue to be the leaders in improvement, and eventually all of the deals will be done, lawyers will be dismissed, and people will turn back to focusing on performance and say to us, “Thank goodness you’ve been doing this work, because now we realize that it’s not just about contracts; it’s about how we deliver care, and you’re the ones that have been leading the way.”
Q: What’s the most realistic interpretation?
A: This work gets less attention and less support than it needs. … I think we’re going to go through three to five years where we’re continuing to do the work. It’s really important—in many ways, it’s as important as growing—but as its importance is growing, the importance of other things that require more tending-to by the senior leadership is growing even faster. The risk is that there will be a disconnect.
Q: When you see the literature that suggests just how difficult the nuts and bolts implementation of reform is, what message do you want to get across to the people who are going to be listening, in terms of actually implementing all of this?
A: The message I don’t want to get across is “frustration, burnout, and it’s not worth it.” The endgame is worth it. The endgame is not even elective. We have to get to a place where we’re delivering higher-quality, safer, more satisfying care to patients at a lower cost. We’re in a unique position to deliver on that promise. … This is really tough stuff, and it takes time and it takes learning.
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Richard Quinn is a freelance writer in New Jersey.
Most hospitalists have heard the adage “If you’ve seen one hospitalist group, you’ve seen one hospitalist group.” Another HM truism is “If you’ve seen one SHM annual meeting, then you’ve seen Bob Wachter, MD, MHM.”
Dr. Wachter, professor, chief of the division of hospital medicine, and chief of the medical service at the University of California at San Francisco Medical Center, is to HM conventions as warfarin is to anticoagulation. His keynote address is the finale to the yearly confab, and HM13’s version is scheduled for noon May 19 at the Gaylord National Harbor Resort & Convention Center in National Harbor, Md.
This year’s address is titled “Quality, Safety, and IT: A Decade of Successes, Failures, Surprises, and Epiphanies.” Dr. Wachter spoke recently with The Hospitalist about his annual tradition.
Question: With your interest in the intersection between healthcare and politics, to be back in D.C. has to be something enjoyable for you to write and talk about.
Answer: It’s a very interesting time in the life of healthcare, in that now that everybody knows that the [Affordable Care Act] is real and not going away, and we’re actually beginning to implement parts of it, you can kind of see what the future is going to look like, and everybody’s responding. And there are parts of that that are very exciting, because they’re forcing us to think about value in new ways. [And] there are parts of it that are somewhat frustrating.
Q: Does that give the hospitalist community the chance to ride herd on more global issues?
A: I think that’s the most optimistic interpretation—that we stick to our knitting, that we continue to be the leaders in improvement, and eventually all of the deals will be done, lawyers will be dismissed, and people will turn back to focusing on performance and say to us, “Thank goodness you’ve been doing this work, because now we realize that it’s not just about contracts; it’s about how we deliver care, and you’re the ones that have been leading the way.”
Q: What’s the most realistic interpretation?
A: This work gets less attention and less support than it needs. … I think we’re going to go through three to five years where we’re continuing to do the work. It’s really important—in many ways, it’s as important as growing—but as its importance is growing, the importance of other things that require more tending-to by the senior leadership is growing even faster. The risk is that there will be a disconnect.
Q: When you see the literature that suggests just how difficult the nuts and bolts implementation of reform is, what message do you want to get across to the people who are going to be listening, in terms of actually implementing all of this?
A: The message I don’t want to get across is “frustration, burnout, and it’s not worth it.” The endgame is worth it. The endgame is not even elective. We have to get to a place where we’re delivering higher-quality, safer, more satisfying care to patients at a lower cost. We’re in a unique position to deliver on that promise. … This is really tough stuff, and it takes time and it takes learning.
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Richard Quinn is a freelance writer in New Jersey.
Most hospitalists have heard the adage “If you’ve seen one hospitalist group, you’ve seen one hospitalist group.” Another HM truism is “If you’ve seen one SHM annual meeting, then you’ve seen Bob Wachter, MD, MHM.”
Dr. Wachter, professor, chief of the division of hospital medicine, and chief of the medical service at the University of California at San Francisco Medical Center, is to HM conventions as warfarin is to anticoagulation. His keynote address is the finale to the yearly confab, and HM13’s version is scheduled for noon May 19 at the Gaylord National Harbor Resort & Convention Center in National Harbor, Md.
This year’s address is titled “Quality, Safety, and IT: A Decade of Successes, Failures, Surprises, and Epiphanies.” Dr. Wachter spoke recently with The Hospitalist about his annual tradition.
Question: With your interest in the intersection between healthcare and politics, to be back in D.C. has to be something enjoyable for you to write and talk about.
Answer: It’s a very interesting time in the life of healthcare, in that now that everybody knows that the [Affordable Care Act] is real and not going away, and we’re actually beginning to implement parts of it, you can kind of see what the future is going to look like, and everybody’s responding. And there are parts of that that are very exciting, because they’re forcing us to think about value in new ways. [And] there are parts of it that are somewhat frustrating.
Q: Does that give the hospitalist community the chance to ride herd on more global issues?
A: I think that’s the most optimistic interpretation—that we stick to our knitting, that we continue to be the leaders in improvement, and eventually all of the deals will be done, lawyers will be dismissed, and people will turn back to focusing on performance and say to us, “Thank goodness you’ve been doing this work, because now we realize that it’s not just about contracts; it’s about how we deliver care, and you’re the ones that have been leading the way.”
Q: What’s the most realistic interpretation?
A: This work gets less attention and less support than it needs. … I think we’re going to go through three to five years where we’re continuing to do the work. It’s really important—in many ways, it’s as important as growing—but as its importance is growing, the importance of other things that require more tending-to by the senior leadership is growing even faster. The risk is that there will be a disconnect.
Q: When you see the literature that suggests just how difficult the nuts and bolts implementation of reform is, what message do you want to get across to the people who are going to be listening, in terms of actually implementing all of this?
A: The message I don’t want to get across is “frustration, burnout, and it’s not worth it.” The endgame is worth it. The endgame is not even elective. We have to get to a place where we’re delivering higher-quality, safer, more satisfying care to patients at a lower cost. We’re in a unique position to deliver on that promise. … This is really tough stuff, and it takes time and it takes learning.
Check out our 6-minute feature video: "Five Reasons You Should Attend HM13"
Richard Quinn is a freelance writer in New Jersey.