User login
‘Hill Trip’ Connects Legislators to Hospitalists, Health Care Issues

A veritable perfect storm of relationships brought hospitalist Jairy Hunter, MD, MBA, SFHM, to “Hospitalists on the Hill 2013,” a daylong advocacy affair that preceded HM13 last month.
First, Dr. Hunter was born and bred—and now lives—in South Carolina, a close-knit state where leaders across industries tend to run in the same circles, or at least have relatives who do. Second, Dr. Hunter’s father, Jairy Hunter Jr., is the longtime president of Charleston Southern University, where Sen. Tim Scott (R-S.C.) earned his undergraduate degree when it was still called Baptist College at Charleston. And three, Dr. Hunter is associate executive medical director of one of the state’s flagship health-care institutions, Medical University of South Carolina in Charleston.
So it was that SHM set Dr. Hunter up in meetings with the offices of Scott, Sen. Lindsey Graham (R-S.C.), and Rep. Jim Clyburn (D-S.C.), and—for the day at least—made Dr. Hunter the voice of hospital medicine.
“It was a little bit demystifying of an experience to be able to know there’s actually people you can talk to and you can develop a relationship with,” says Dr. Hunter, who also serves on Team Hospitalist. “I thought that was very rewarding.”
The connections made by Dr. Hunter are the point of the annual trek made by SHM leaders and members to lobby legislators and federal staffers “on the way policies affect your practice and your patients,” SHM says on its website (www.hospitalmedicine.org/advocacy). This year’s volunteer effort was by far the largest ever, says Public Policy Committee chair Ron Greeno, MD, FCCP, MHM. More than 150 hospitalists participated in training, 113 hospitalists visited Capitol Hill, and scores more had to be turned away. All told, hospitalists held 409 individual meetings with legislators and staff members.
“Quite frankly, if we’d have had the budget, we could have had another 100 to 150 people come,” Dr. Greeno says. “That’s how many people wanted to go.”
Dr. Greeno attributes the interest to two factors. One, having the annual meeting at the Gaylord National Resort & Convention Center, just outside Washington, D.C, makes the Hill trip a natural extension. Two, the current landscape of health-care reform has motivated many physicians to become more involved than they might otherwise be. One challenge of having so many first-timers making this year’s trip was making sure they were properly prepared. To hone the message, SHM gave the group a few hours of education by former legislative staffer Stephanie Vance of Advocacy Associates, a communications firm that helps organizations, such as medical societies, tailor their message to policymakers. Vance told hospitalists a personal visit with a constituent often becomes the most influential type of advocacy.
“That’s why it was easy to make an initial connection, because these staffers are from where I’m from, friends with people that I’m friends with,” Dr. Hunter says.

Unique Approach
SHM CEO Larry Wellikson, MD, SFHM, says the society tries to differentiate itself from other organizations through its grassroots approach to advocacy. More important, the society refrains from giving a long list of legislative requests that are self-serving.
“We’re someone they want to talk to because we’re not coming there to just say, ‘Here’s a power play for hospitalists,’” Dr. Wellikson says. “We come and try to provide solutions.”
To that end, this year’s lobbying effort was targeted to topics important both to HM and the health-care system:
- Repealing the sustainable growth rate (SGR) formula for Medicare payments, specifically via the proposed Medicare Physician Payment Innovation Act of 2013 (H.R. 574);
- Solving the quagmire of observation status time not counting toward the required three consecutive overnights as an inpatient needed to qualify for Medicare benefits at a skilled nursing facility, by supporting the Improving Access to Medicare Coverage Act of 2013 (H.R. 1179, S. 569); and
- Getting the federal government to commit to providing $434 million in funding for the Agency for Healthcare Research and Quality (AHRQ) in fiscal 2014.
“The message that we’re sending resonated with the people we met with on both sides of the aisle,” Dr. Greeno says. “The SGR, for instance, they know there needs to be a fix. We want to serve as a resource for them as they start to figure out the answer to the question: What are we going to replace it with?
“What we want to do is make everybody on the Hill understand that we can be relied upon as a resource when they’re looking for solutions,” he says.
Focused on Follow-Up
And that’s where rank-and-filers, such as Dr. Hunter, have to take charge. So for his Hill Day visits, he tried to stand out. Everyone he met with got a lapel pin in the shape of a South Carolina state flag, which has become a popular fashion statement in recent years. And Scott also got a pin from Charleston Southern University, his alma mater. The gestures were small, but they served as icebreakers and reminders that Dr. Hunter and the people he met are bound by service to the residents of the Palmetto State.
Dr. Hunter also hopes the small token will be that little extra that makes him memorable enough that the next time a Congressional staffer has an SGR question, they’ll ask him and not a doctor from another specialty.
“I’m interested to see how much feedback I get back from them,” he says. “I can feed them all day long, but I don’t want to be that crazy guy bugging them. If they respond back to me, I can hopefully make more inroads.”
He certainly would if Dr. Greeno gets his way. Moving forward, SHM hopes to be able to rely more on local advocates pushing for reform than just a once-a-year major event and formal positions drafted by SHM’s staffers or the Public Policy Committee. Dr. Greeno says the physicians who participated in this year’s Hill trip are likely to find they will be asked to be the first cohort of a grassroots initiative meant to deliver the society’s message more routinely.
“These are not easy things to change because there are not easy solutions,” Dr. Greeno adds. “If you have just one meeting on the Hill, you’ll have no impact at all. You have to follow up. You have to do it consistently. And you have to have a consistent message. And we will.”
Richard Quinn is a freelance writer in New Jersey.
A veritable perfect storm of relationships brought hospitalist Jairy Hunter, MD, MBA, SFHM, to “Hospitalists on the Hill 2013,” a daylong advocacy affair that preceded HM13 last month.
First, Dr. Hunter was born and bred—and now lives—in South Carolina, a close-knit state where leaders across industries tend to run in the same circles, or at least have relatives who do. Second, Dr. Hunter’s father, Jairy Hunter Jr., is the longtime president of Charleston Southern University, where Sen. Tim Scott (R-S.C.) earned his undergraduate degree when it was still called Baptist College at Charleston. And three, Dr. Hunter is associate executive medical director of one of the state’s flagship health-care institutions, Medical University of South Carolina in Charleston.
So it was that SHM set Dr. Hunter up in meetings with the offices of Scott, Sen. Lindsey Graham (R-S.C.), and Rep. Jim Clyburn (D-S.C.), and—for the day at least—made Dr. Hunter the voice of hospital medicine.
“It was a little bit demystifying of an experience to be able to know there’s actually people you can talk to and you can develop a relationship with,” says Dr. Hunter, who also serves on Team Hospitalist. “I thought that was very rewarding.”
The connections made by Dr. Hunter are the point of the annual trek made by SHM leaders and members to lobby legislators and federal staffers “on the way policies affect your practice and your patients,” SHM says on its website (www.hospitalmedicine.org/advocacy). This year’s volunteer effort was by far the largest ever, says Public Policy Committee chair Ron Greeno, MD, FCCP, MHM. More than 150 hospitalists participated in training, 113 hospitalists visited Capitol Hill, and scores more had to be turned away. All told, hospitalists held 409 individual meetings with legislators and staff members.
“Quite frankly, if we’d have had the budget, we could have had another 100 to 150 people come,” Dr. Greeno says. “That’s how many people wanted to go.”
Dr. Greeno attributes the interest to two factors. One, having the annual meeting at the Gaylord National Resort & Convention Center, just outside Washington, D.C, makes the Hill trip a natural extension. Two, the current landscape of health-care reform has motivated many physicians to become more involved than they might otherwise be. One challenge of having so many first-timers making this year’s trip was making sure they were properly prepared. To hone the message, SHM gave the group a few hours of education by former legislative staffer Stephanie Vance of Advocacy Associates, a communications firm that helps organizations, such as medical societies, tailor their message to policymakers. Vance told hospitalists a personal visit with a constituent often becomes the most influential type of advocacy.
“That’s why it was easy to make an initial connection, because these staffers are from where I’m from, friends with people that I’m friends with,” Dr. Hunter says.
Unique Approach
SHM CEO Larry Wellikson, MD, SFHM, says the society tries to differentiate itself from other organizations through its grassroots approach to advocacy. More important, the society refrains from giving a long list of legislative requests that are self-serving.
“We’re someone they want to talk to because we’re not coming there to just say, ‘Here’s a power play for hospitalists,’” Dr. Wellikson says. “We come and try to provide solutions.”
To that end, this year’s lobbying effort was targeted to topics important both to HM and the health-care system:
- Repealing the sustainable growth rate (SGR) formula for Medicare payments, specifically via the proposed Medicare Physician Payment Innovation Act of 2013 (H.R. 574);
- Solving the quagmire of observation status time not counting toward the required three consecutive overnights as an inpatient needed to qualify for Medicare benefits at a skilled nursing facility, by supporting the Improving Access to Medicare Coverage Act of 2013 (H.R. 1179, S. 569); and
- Getting the federal government to commit to providing $434 million in funding for the Agency for Healthcare Research and Quality (AHRQ) in fiscal 2014.
“The message that we’re sending resonated with the people we met with on both sides of the aisle,” Dr. Greeno says. “The SGR, for instance, they know there needs to be a fix. We want to serve as a resource for them as they start to figure out the answer to the question: What are we going to replace it with?
“What we want to do is make everybody on the Hill understand that we can be relied upon as a resource when they’re looking for solutions,” he says.
Focused on Follow-Up
And that’s where rank-and-filers, such as Dr. Hunter, have to take charge. So for his Hill Day visits, he tried to stand out. Everyone he met with got a lapel pin in the shape of a South Carolina state flag, which has become a popular fashion statement in recent years. And Scott also got a pin from Charleston Southern University, his alma mater. The gestures were small, but they served as icebreakers and reminders that Dr. Hunter and the people he met are bound by service to the residents of the Palmetto State.
Dr. Hunter also hopes the small token will be that little extra that makes him memorable enough that the next time a Congressional staffer has an SGR question, they’ll ask him and not a doctor from another specialty.
“I’m interested to see how much feedback I get back from them,” he says. “I can feed them all day long, but I don’t want to be that crazy guy bugging them. If they respond back to me, I can hopefully make more inroads.”
He certainly would if Dr. Greeno gets his way. Moving forward, SHM hopes to be able to rely more on local advocates pushing for reform than just a once-a-year major event and formal positions drafted by SHM’s staffers or the Public Policy Committee. Dr. Greeno says the physicians who participated in this year’s Hill trip are likely to find they will be asked to be the first cohort of a grassroots initiative meant to deliver the society’s message more routinely.
“These are not easy things to change because there are not easy solutions,” Dr. Greeno adds. “If you have just one meeting on the Hill, you’ll have no impact at all. You have to follow up. You have to do it consistently. And you have to have a consistent message. And we will.”
Richard Quinn is a freelance writer in New Jersey.
A veritable perfect storm of relationships brought hospitalist Jairy Hunter, MD, MBA, SFHM, to “Hospitalists on the Hill 2013,” a daylong advocacy affair that preceded HM13 last month.
First, Dr. Hunter was born and bred—and now lives—in South Carolina, a close-knit state where leaders across industries tend to run in the same circles, or at least have relatives who do. Second, Dr. Hunter’s father, Jairy Hunter Jr., is the longtime president of Charleston Southern University, where Sen. Tim Scott (R-S.C.) earned his undergraduate degree when it was still called Baptist College at Charleston. And three, Dr. Hunter is associate executive medical director of one of the state’s flagship health-care institutions, Medical University of South Carolina in Charleston.
So it was that SHM set Dr. Hunter up in meetings with the offices of Scott, Sen. Lindsey Graham (R-S.C.), and Rep. Jim Clyburn (D-S.C.), and—for the day at least—made Dr. Hunter the voice of hospital medicine.
“It was a little bit demystifying of an experience to be able to know there’s actually people you can talk to and you can develop a relationship with,” says Dr. Hunter, who also serves on Team Hospitalist. “I thought that was very rewarding.”
The connections made by Dr. Hunter are the point of the annual trek made by SHM leaders and members to lobby legislators and federal staffers “on the way policies affect your practice and your patients,” SHM says on its website (www.hospitalmedicine.org/advocacy). This year’s volunteer effort was by far the largest ever, says Public Policy Committee chair Ron Greeno, MD, FCCP, MHM. More than 150 hospitalists participated in training, 113 hospitalists visited Capitol Hill, and scores more had to be turned away. All told, hospitalists held 409 individual meetings with legislators and staff members.
“Quite frankly, if we’d have had the budget, we could have had another 100 to 150 people come,” Dr. Greeno says. “That’s how many people wanted to go.”
Dr. Greeno attributes the interest to two factors. One, having the annual meeting at the Gaylord National Resort & Convention Center, just outside Washington, D.C, makes the Hill trip a natural extension. Two, the current landscape of health-care reform has motivated many physicians to become more involved than they might otherwise be. One challenge of having so many first-timers making this year’s trip was making sure they were properly prepared. To hone the message, SHM gave the group a few hours of education by former legislative staffer Stephanie Vance of Advocacy Associates, a communications firm that helps organizations, such as medical societies, tailor their message to policymakers. Vance told hospitalists a personal visit with a constituent often becomes the most influential type of advocacy.
“That’s why it was easy to make an initial connection, because these staffers are from where I’m from, friends with people that I’m friends with,” Dr. Hunter says.
Unique Approach
SHM CEO Larry Wellikson, MD, SFHM, says the society tries to differentiate itself from other organizations through its grassroots approach to advocacy. More important, the society refrains from giving a long list of legislative requests that are self-serving.
“We’re someone they want to talk to because we’re not coming there to just say, ‘Here’s a power play for hospitalists,’” Dr. Wellikson says. “We come and try to provide solutions.”
To that end, this year’s lobbying effort was targeted to topics important both to HM and the health-care system:
- Repealing the sustainable growth rate (SGR) formula for Medicare payments, specifically via the proposed Medicare Physician Payment Innovation Act of 2013 (H.R. 574);
- Solving the quagmire of observation status time not counting toward the required three consecutive overnights as an inpatient needed to qualify for Medicare benefits at a skilled nursing facility, by supporting the Improving Access to Medicare Coverage Act of 2013 (H.R. 1179, S. 569); and
- Getting the federal government to commit to providing $434 million in funding for the Agency for Healthcare Research and Quality (AHRQ) in fiscal 2014.
“The message that we’re sending resonated with the people we met with on both sides of the aisle,” Dr. Greeno says. “The SGR, for instance, they know there needs to be a fix. We want to serve as a resource for them as they start to figure out the answer to the question: What are we going to replace it with?
“What we want to do is make everybody on the Hill understand that we can be relied upon as a resource when they’re looking for solutions,” he says.
Focused on Follow-Up
And that’s where rank-and-filers, such as Dr. Hunter, have to take charge. So for his Hill Day visits, he tried to stand out. Everyone he met with got a lapel pin in the shape of a South Carolina state flag, which has become a popular fashion statement in recent years. And Scott also got a pin from Charleston Southern University, his alma mater. The gestures were small, but they served as icebreakers and reminders that Dr. Hunter and the people he met are bound by service to the residents of the Palmetto State.
Dr. Hunter also hopes the small token will be that little extra that makes him memorable enough that the next time a Congressional staffer has an SGR question, they’ll ask him and not a doctor from another specialty.
“I’m interested to see how much feedback I get back from them,” he says. “I can feed them all day long, but I don’t want to be that crazy guy bugging them. If they respond back to me, I can hopefully make more inroads.”
He certainly would if Dr. Greeno gets his way. Moving forward, SHM hopes to be able to rely more on local advocates pushing for reform than just a once-a-year major event and formal positions drafted by SHM’s staffers or the Public Policy Committee. Dr. Greeno says the physicians who participated in this year’s Hill trip are likely to find they will be asked to be the first cohort of a grassroots initiative meant to deliver the society’s message more routinely.
“These are not easy things to change because there are not easy solutions,” Dr. Greeno adds. “If you have just one meeting on the Hill, you’ll have no impact at all. You have to follow up. You have to do it consistently. And you have to have a consistent message. And we will.”
Richard Quinn is a freelance writer in New Jersey.
Hospitalists Can Address Causes of Skyrocketing Health Care Costs


Alarms about our nation’s health-care costs have been sounding for well over a decade. According to the Centers for Medicare & Medicaid Services (CMS), spending on U.S. health care doubled between 1999 and 2011, climbing to $2.7 trillion from $1.3 trillion, and now represents 17.9% of the United States’ GDP.1
“The medical care system is bankrupting the country,” Paul B. Ginsburg, PhD, president of the Center for Studying Health System Change (HSC), based in Washington, D.C., says bluntly. A four-decade-long upward spending trend is “unsustainable,” he wrote in the New England Journal of Medicine with Chapin White, PhD, a senior health researcher at HSC.2
Recent reports suggest that rising premiums and out-of-pocket costs are rendering the price of health care untenable for the average consumer. A 2011 RAND Corp. study found that, for the average American family, the rate of increased costs for health care had outpaced growth in earnings from 1999 to 2009.3 And last year, for the first time, the cost of health care for a typical American family of four surpassed $20,000, the annual Milliman Medical Index reported.4
Should hospitalists be concerned, professionally and personally, about these trends? Absolutely, say hospitalist leaders who spoke with The Hospitalist. HM clinicians have much to contribute at both the macro level (addressing systemic causes of overutilization through quality improvement and other initiatives) and at the micro level, by understanding their personal contributions and by engaging patients and their families in shared decision-making.
But getting at and addressing the root causes of rising health-care costs, according to health-care policy analysts and veteran hospitalists, will require major shifts in thinking and processes.
Contributors to Rising Costs
It’s difficult to pinpoint the root causes of the recent surge in health-care costs. Victor Fuchs, emeritus professor of economics and health research and policy at Stanford University, points to the U.S.’ high administrative costs and complicated billing systems.5 A fragmented, nontransparent system for negotiating fees between insurers and providers also plays a role, as demonstrated in a Consumer Reports investigation into geographic variations in costs for common tests and procedures. A complete blood count might be as low as $15 or as high as $105; a colonoscopy ranges from $800 to $3,160.6
Bradley Flansbaum, DO, MPH, SFHM, an SHM Public Policy Committee member and AMA delegate, says rising costs are a provider-specific issue. He challenges colleagues to take an honest look at their own practice patterns to assess whether they’re contributing to overuse of resources (see “A Lesson in Change,”).
“The culture of practice has developed so that this is not going to change overnight,” says Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City. That’s because many physicians fail to view their own decisions as a problem. For example, says Dr. Flansbaum, “an oncologist may not identify a third round of chemotherapy as an embodiment of the problem, or a gastroenterologist might not embody the colonoscopy at Year Four instead of Year Five as the problem. We must come to grips with the usual mindset, look in the mirror, and admit, ‘Maybe we are part of the problem.’”

—Bradley Flansbaum, DO, MPH, SFHM
Potential Solutions
Hospitalists, intensivists, and ED clinicians are tasked with finding a balance between being prudent stewards of resources and staying within a comfort zone that promotes patient safety. SHM supports the goals of the ABIM Foundation’s Choosing Wisely campaign, which aims to reduce waste by curtailing duplicative and unnecessary care (see “Better Choices, Better Care,” March 2013). Also included in the campaign (www.ChoosingWisely.org) are the American College of Physicians’ recommendations against low-value testing (e.g. obtaining imaging studies in patients with nonspecific low back pain).
“Those recommendations are not going to solve our health spending problem,” says White, “but they are part of a broader move to give permission to clinicians, based on evidence, to follow more conservative practice patterns.”
Still, counters David I. Auerbach, PhD, a health economist at RAND in Boston and author of the RAND study, “there’s another value to these tests that the cost-effectiveness equations do not always consider, which is, they can bring peace of mind. We’re trying to nudge patients down the pathway that we think is best for them without rationing care. That’s a delicate balance.”
Dr. Flansbaum says SHM’s Public Policy Committee has discussed a variety of issues related to rising costs, although the group has not directly tackled advice in the form of a white paper. He suggests some ways that hospitalists can address cost savings:
- Involve patients in shared decision-making, and discuss the evidence against unnecessary testing;
- Utilize generic medications on discharge, when available, especially if patients are uninsured or have limited drug coverage with their insurance plans;
- Use palliative care whenever appropriate; and
- Adhere to transitional-care standards.
On the macro level, HM has “always been the specialty invited to champion the important discussion relating to resource utilization, and the evidence-based medicine driving that resource utilization,” says Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America (HCA) in Nashville, Tenn. He points to SHM’s leadership with Project BOOST (www.hospitalmedicine.org/boost) as one example of addressing the utilization of resources in caring for older adults (see “Resources for Improving Transitions in Care,”).
What else can hospitalists do? Going forward, says Dan Fuller, president and co-founder of IN Compass Health in Alpharetta, Ga., it might be a good idea for the SHM Practice Analysis Committee, of which he’s a member, to look at its possible role in the issue.

—Dr. Frederickson
Embrace Reality
Whatever the downstream developments around the Affordable Care Act, Dr. Ginsburg is “confident” that Medicare policies will continue in a direction of reduced reimbursements. Thomas Frederickson, MD, FACP, FHM, MBA, medical director of the hospital medicine service at Alegent Health in Omaha, Neb., agrees with such an assessment. He also believes that hospitalists are in a prime position to improve care delivery at less cost. To do so, though, requires deliberate partnership-building with outpatient providers to better bridge the transitions of care.
At his institution, Dr. Frederickson says, hospitalists invite themselves to primary-care physicians’ (PCP) meetings. This facilitates rapport so that calls to PCPs at discharge not only communicate essential clinical information, but also build confidence in the hospitalists’ care of their patients. As hospitalists demonstrate value, they must intentionally put metrics in place so that administrators appreciate the need to keep the census at a certain level, Dr. Frederickson says.
“We need the time to make these calls, to sit down with families,” he says. “This adds value to our health system and to society at large.”
SHM does a good job, says Dr. Frost, of being part of the conversation as the hospital C-suite focuses more on episodes of care.
“The intensity of that discussion is getting dialed up and will be driven more by government and the payors,” he adds. The challenge going forward will be to bridge those arenas just outside the acute episode of care, where hospitalists have ownership of processes, to those where they do not have as much control. If payors apply broader definitions to the episode of care, Dr. Frost says, hospitalists might be “invited to play an increasing role, that of ‘transitionist.’”
And in that context, he says, hospitalists need to look at length of stay with a new lens.
Partnership-building will become more important as the definition of “episode of care” expands beyond the hospital stay to the post-acute setting.
“Including post-acute care in the episode of care is a core aspect of the whole” value-based purchasing approach, Dr. Ginsburg says. “Hospitals [and hospitalists] will be wise to opt for the model with the greatest potential to reduce costs, particularly costs incurred by other providers.”
Gretchen Henkel is a freelance writer in California.
References
- Centers for Medicare & Medicaid Services. National health expenditures 2011 highlights. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/highlights.pdf. Accessed May 6, 2013. costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm. Accessed Aug. 2, 2012.
- White C, Ginsburg PB. Slower growth in Medicare spending—is this the new normal? N Engl J Med. 2012;366(12):1073-1075.
- Auerbach DI, Kellermann AL. A decade of health care cost growth has wiped out real income gains for an average US family. Health Aff (Millwood). 2011;30(9):1630-1636.
- Milliman Inc. 2012 Milliman Medical Index. Milliman Inc. website. Available at: http://publications.milliman.com/periodicals/mmi/pdfs/milliman-medical-index-2012.pdf. Accessed Aug. 1, 2012.
- Kolata G. Knotty challenges in health care costs. The New York Times website. Available at: http://www.nytimes.com/2012/03/06/health/policy/an-interview-with-victor-fuchs-on-health-care-costs.html. Accessed March 8, 2012.
- Consumer Reports. That CT scan costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm.
Alarms about our nation’s health-care costs have been sounding for well over a decade. According to the Centers for Medicare & Medicaid Services (CMS), spending on U.S. health care doubled between 1999 and 2011, climbing to $2.7 trillion from $1.3 trillion, and now represents 17.9% of the United States’ GDP.1
“The medical care system is bankrupting the country,” Paul B. Ginsburg, PhD, president of the Center for Studying Health System Change (HSC), based in Washington, D.C., says bluntly. A four-decade-long upward spending trend is “unsustainable,” he wrote in the New England Journal of Medicine with Chapin White, PhD, a senior health researcher at HSC.2
Recent reports suggest that rising premiums and out-of-pocket costs are rendering the price of health care untenable for the average consumer. A 2011 RAND Corp. study found that, for the average American family, the rate of increased costs for health care had outpaced growth in earnings from 1999 to 2009.3 And last year, for the first time, the cost of health care for a typical American family of four surpassed $20,000, the annual Milliman Medical Index reported.4
Should hospitalists be concerned, professionally and personally, about these trends? Absolutely, say hospitalist leaders who spoke with The Hospitalist. HM clinicians have much to contribute at both the macro level (addressing systemic causes of overutilization through quality improvement and other initiatives) and at the micro level, by understanding their personal contributions and by engaging patients and their families in shared decision-making.
But getting at and addressing the root causes of rising health-care costs, according to health-care policy analysts and veteran hospitalists, will require major shifts in thinking and processes.
Contributors to Rising Costs
It’s difficult to pinpoint the root causes of the recent surge in health-care costs. Victor Fuchs, emeritus professor of economics and health research and policy at Stanford University, points to the U.S.’ high administrative costs and complicated billing systems.5 A fragmented, nontransparent system for negotiating fees between insurers and providers also plays a role, as demonstrated in a Consumer Reports investigation into geographic variations in costs for common tests and procedures. A complete blood count might be as low as $15 or as high as $105; a colonoscopy ranges from $800 to $3,160.6
Bradley Flansbaum, DO, MPH, SFHM, an SHM Public Policy Committee member and AMA delegate, says rising costs are a provider-specific issue. He challenges colleagues to take an honest look at their own practice patterns to assess whether they’re contributing to overuse of resources (see “A Lesson in Change,”).
“The culture of practice has developed so that this is not going to change overnight,” says Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City. That’s because many physicians fail to view their own decisions as a problem. For example, says Dr. Flansbaum, “an oncologist may not identify a third round of chemotherapy as an embodiment of the problem, or a gastroenterologist might not embody the colonoscopy at Year Four instead of Year Five as the problem. We must come to grips with the usual mindset, look in the mirror, and admit, ‘Maybe we are part of the problem.’”
—Bradley Flansbaum, DO, MPH, SFHM
Potential Solutions
Hospitalists, intensivists, and ED clinicians are tasked with finding a balance between being prudent stewards of resources and staying within a comfort zone that promotes patient safety. SHM supports the goals of the ABIM Foundation’s Choosing Wisely campaign, which aims to reduce waste by curtailing duplicative and unnecessary care (see “Better Choices, Better Care,” March 2013). Also included in the campaign (www.ChoosingWisely.org) are the American College of Physicians’ recommendations against low-value testing (e.g. obtaining imaging studies in patients with nonspecific low back pain).
“Those recommendations are not going to solve our health spending problem,” says White, “but they are part of a broader move to give permission to clinicians, based on evidence, to follow more conservative practice patterns.”
Still, counters David I. Auerbach, PhD, a health economist at RAND in Boston and author of the RAND study, “there’s another value to these tests that the cost-effectiveness equations do not always consider, which is, they can bring peace of mind. We’re trying to nudge patients down the pathway that we think is best for them without rationing care. That’s a delicate balance.”
Dr. Flansbaum says SHM’s Public Policy Committee has discussed a variety of issues related to rising costs, although the group has not directly tackled advice in the form of a white paper. He suggests some ways that hospitalists can address cost savings:
- Involve patients in shared decision-making, and discuss the evidence against unnecessary testing;
- Utilize generic medications on discharge, when available, especially if patients are uninsured or have limited drug coverage with their insurance plans;
- Use palliative care whenever appropriate; and
- Adhere to transitional-care standards.
On the macro level, HM has “always been the specialty invited to champion the important discussion relating to resource utilization, and the evidence-based medicine driving that resource utilization,” says Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America (HCA) in Nashville, Tenn. He points to SHM’s leadership with Project BOOST (www.hospitalmedicine.org/boost) as one example of addressing the utilization of resources in caring for older adults (see “Resources for Improving Transitions in Care,”).
What else can hospitalists do? Going forward, says Dan Fuller, president and co-founder of IN Compass Health in Alpharetta, Ga., it might be a good idea for the SHM Practice Analysis Committee, of which he’s a member, to look at its possible role in the issue.
—Dr. Frederickson
Embrace Reality
Whatever the downstream developments around the Affordable Care Act, Dr. Ginsburg is “confident” that Medicare policies will continue in a direction of reduced reimbursements. Thomas Frederickson, MD, FACP, FHM, MBA, medical director of the hospital medicine service at Alegent Health in Omaha, Neb., agrees with such an assessment. He also believes that hospitalists are in a prime position to improve care delivery at less cost. To do so, though, requires deliberate partnership-building with outpatient providers to better bridge the transitions of care.
At his institution, Dr. Frederickson says, hospitalists invite themselves to primary-care physicians’ (PCP) meetings. This facilitates rapport so that calls to PCPs at discharge not only communicate essential clinical information, but also build confidence in the hospitalists’ care of their patients. As hospitalists demonstrate value, they must intentionally put metrics in place so that administrators appreciate the need to keep the census at a certain level, Dr. Frederickson says.
“We need the time to make these calls, to sit down with families,” he says. “This adds value to our health system and to society at large.”
SHM does a good job, says Dr. Frost, of being part of the conversation as the hospital C-suite focuses more on episodes of care.
“The intensity of that discussion is getting dialed up and will be driven more by government and the payors,” he adds. The challenge going forward will be to bridge those arenas just outside the acute episode of care, where hospitalists have ownership of processes, to those where they do not have as much control. If payors apply broader definitions to the episode of care, Dr. Frost says, hospitalists might be “invited to play an increasing role, that of ‘transitionist.’”
And in that context, he says, hospitalists need to look at length of stay with a new lens.
Partnership-building will become more important as the definition of “episode of care” expands beyond the hospital stay to the post-acute setting.
“Including post-acute care in the episode of care is a core aspect of the whole” value-based purchasing approach, Dr. Ginsburg says. “Hospitals [and hospitalists] will be wise to opt for the model with the greatest potential to reduce costs, particularly costs incurred by other providers.”
Gretchen Henkel is a freelance writer in California.
References
- Centers for Medicare & Medicaid Services. National health expenditures 2011 highlights. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/highlights.pdf. Accessed May 6, 2013. costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm. Accessed Aug. 2, 2012.
- White C, Ginsburg PB. Slower growth in Medicare spending—is this the new normal? N Engl J Med. 2012;366(12):1073-1075.
- Auerbach DI, Kellermann AL. A decade of health care cost growth has wiped out real income gains for an average US family. Health Aff (Millwood). 2011;30(9):1630-1636.
- Milliman Inc. 2012 Milliman Medical Index. Milliman Inc. website. Available at: http://publications.milliman.com/periodicals/mmi/pdfs/milliman-medical-index-2012.pdf. Accessed Aug. 1, 2012.
- Kolata G. Knotty challenges in health care costs. The New York Times website. Available at: http://www.nytimes.com/2012/03/06/health/policy/an-interview-with-victor-fuchs-on-health-care-costs.html. Accessed March 8, 2012.
- Consumer Reports. That CT scan costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm.
Alarms about our nation’s health-care costs have been sounding for well over a decade. According to the Centers for Medicare & Medicaid Services (CMS), spending on U.S. health care doubled between 1999 and 2011, climbing to $2.7 trillion from $1.3 trillion, and now represents 17.9% of the United States’ GDP.1
“The medical care system is bankrupting the country,” Paul B. Ginsburg, PhD, president of the Center for Studying Health System Change (HSC), based in Washington, D.C., says bluntly. A four-decade-long upward spending trend is “unsustainable,” he wrote in the New England Journal of Medicine with Chapin White, PhD, a senior health researcher at HSC.2
Recent reports suggest that rising premiums and out-of-pocket costs are rendering the price of health care untenable for the average consumer. A 2011 RAND Corp. study found that, for the average American family, the rate of increased costs for health care had outpaced growth in earnings from 1999 to 2009.3 And last year, for the first time, the cost of health care for a typical American family of four surpassed $20,000, the annual Milliman Medical Index reported.4
Should hospitalists be concerned, professionally and personally, about these trends? Absolutely, say hospitalist leaders who spoke with The Hospitalist. HM clinicians have much to contribute at both the macro level (addressing systemic causes of overutilization through quality improvement and other initiatives) and at the micro level, by understanding their personal contributions and by engaging patients and their families in shared decision-making.
But getting at and addressing the root causes of rising health-care costs, according to health-care policy analysts and veteran hospitalists, will require major shifts in thinking and processes.
Contributors to Rising Costs
It’s difficult to pinpoint the root causes of the recent surge in health-care costs. Victor Fuchs, emeritus professor of economics and health research and policy at Stanford University, points to the U.S.’ high administrative costs and complicated billing systems.5 A fragmented, nontransparent system for negotiating fees between insurers and providers also plays a role, as demonstrated in a Consumer Reports investigation into geographic variations in costs for common tests and procedures. A complete blood count might be as low as $15 or as high as $105; a colonoscopy ranges from $800 to $3,160.6
Bradley Flansbaum, DO, MPH, SFHM, an SHM Public Policy Committee member and AMA delegate, says rising costs are a provider-specific issue. He challenges colleagues to take an honest look at their own practice patterns to assess whether they’re contributing to overuse of resources (see “A Lesson in Change,”).
“The culture of practice has developed so that this is not going to change overnight,” says Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City. That’s because many physicians fail to view their own decisions as a problem. For example, says Dr. Flansbaum, “an oncologist may not identify a third round of chemotherapy as an embodiment of the problem, or a gastroenterologist might not embody the colonoscopy at Year Four instead of Year Five as the problem. We must come to grips with the usual mindset, look in the mirror, and admit, ‘Maybe we are part of the problem.’”
—Bradley Flansbaum, DO, MPH, SFHM
Potential Solutions
Hospitalists, intensivists, and ED clinicians are tasked with finding a balance between being prudent stewards of resources and staying within a comfort zone that promotes patient safety. SHM supports the goals of the ABIM Foundation’s Choosing Wisely campaign, which aims to reduce waste by curtailing duplicative and unnecessary care (see “Better Choices, Better Care,” March 2013). Also included in the campaign (www.ChoosingWisely.org) are the American College of Physicians’ recommendations against low-value testing (e.g. obtaining imaging studies in patients with nonspecific low back pain).
“Those recommendations are not going to solve our health spending problem,” says White, “but they are part of a broader move to give permission to clinicians, based on evidence, to follow more conservative practice patterns.”
Still, counters David I. Auerbach, PhD, a health economist at RAND in Boston and author of the RAND study, “there’s another value to these tests that the cost-effectiveness equations do not always consider, which is, they can bring peace of mind. We’re trying to nudge patients down the pathway that we think is best for them without rationing care. That’s a delicate balance.”
Dr. Flansbaum says SHM’s Public Policy Committee has discussed a variety of issues related to rising costs, although the group has not directly tackled advice in the form of a white paper. He suggests some ways that hospitalists can address cost savings:
- Involve patients in shared decision-making, and discuss the evidence against unnecessary testing;
- Utilize generic medications on discharge, when available, especially if patients are uninsured or have limited drug coverage with their insurance plans;
- Use palliative care whenever appropriate; and
- Adhere to transitional-care standards.
On the macro level, HM has “always been the specialty invited to champion the important discussion relating to resource utilization, and the evidence-based medicine driving that resource utilization,” says Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America (HCA) in Nashville, Tenn. He points to SHM’s leadership with Project BOOST (www.hospitalmedicine.org/boost) as one example of addressing the utilization of resources in caring for older adults (see “Resources for Improving Transitions in Care,”).
What else can hospitalists do? Going forward, says Dan Fuller, president and co-founder of IN Compass Health in Alpharetta, Ga., it might be a good idea for the SHM Practice Analysis Committee, of which he’s a member, to look at its possible role in the issue.
—Dr. Frederickson
Embrace Reality
Whatever the downstream developments around the Affordable Care Act, Dr. Ginsburg is “confident” that Medicare policies will continue in a direction of reduced reimbursements. Thomas Frederickson, MD, FACP, FHM, MBA, medical director of the hospital medicine service at Alegent Health in Omaha, Neb., agrees with such an assessment. He also believes that hospitalists are in a prime position to improve care delivery at less cost. To do so, though, requires deliberate partnership-building with outpatient providers to better bridge the transitions of care.
At his institution, Dr. Frederickson says, hospitalists invite themselves to primary-care physicians’ (PCP) meetings. This facilitates rapport so that calls to PCPs at discharge not only communicate essential clinical information, but also build confidence in the hospitalists’ care of their patients. As hospitalists demonstrate value, they must intentionally put metrics in place so that administrators appreciate the need to keep the census at a certain level, Dr. Frederickson says.
“We need the time to make these calls, to sit down with families,” he says. “This adds value to our health system and to society at large.”
SHM does a good job, says Dr. Frost, of being part of the conversation as the hospital C-suite focuses more on episodes of care.
“The intensity of that discussion is getting dialed up and will be driven more by government and the payors,” he adds. The challenge going forward will be to bridge those arenas just outside the acute episode of care, where hospitalists have ownership of processes, to those where they do not have as much control. If payors apply broader definitions to the episode of care, Dr. Frost says, hospitalists might be “invited to play an increasing role, that of ‘transitionist.’”
And in that context, he says, hospitalists need to look at length of stay with a new lens.
Partnership-building will become more important as the definition of “episode of care” expands beyond the hospital stay to the post-acute setting.
“Including post-acute care in the episode of care is a core aspect of the whole” value-based purchasing approach, Dr. Ginsburg says. “Hospitals [and hospitalists] will be wise to opt for the model with the greatest potential to reduce costs, particularly costs incurred by other providers.”
Gretchen Henkel is a freelance writer in California.
References
- Centers for Medicare & Medicaid Services. National health expenditures 2011 highlights. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/highlights.pdf. Accessed May 6, 2013. costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm. Accessed Aug. 2, 2012.
- White C, Ginsburg PB. Slower growth in Medicare spending—is this the new normal? N Engl J Med. 2012;366(12):1073-1075.
- Auerbach DI, Kellermann AL. A decade of health care cost growth has wiped out real income gains for an average US family. Health Aff (Millwood). 2011;30(9):1630-1636.
- Milliman Inc. 2012 Milliman Medical Index. Milliman Inc. website. Available at: http://publications.milliman.com/periodicals/mmi/pdfs/milliman-medical-index-2012.pdf. Accessed Aug. 1, 2012.
- Kolata G. Knotty challenges in health care costs. The New York Times website. Available at: http://www.nytimes.com/2012/03/06/health/policy/an-interview-with-victor-fuchs-on-health-care-costs.html. Accessed March 8, 2012.
- Consumer Reports. That CT scan costs how much? Consumer Reports website. Available at: http://www.consumerreports.org/cro/magazine/ 2012/07/that-ct-scan-costs-how-much/index.htm.
Letters: Medicare Official Says 'Physician Compare' Website Does Not Provide Performance Data on Individual Doctors
I read the article “Call for Transparency in Health-Care Performance Results to Impact Hospitalists” (January 2013, p. 47) by Shaun Frost, MD, SFHM, president of the Society of Hospital Medicine, with interest. I’d like to clarify a key point about Physician Compare. In the article, the statement that the Physician Compare website (www.medicare.gov/find-a-doctor) provides performance information on individual doctors is inaccurate.
The Affordable Care Act (ACA) states that the Centers for Medicare & Medicaid Services (CMS) must have a plan in place by Jan. 1, 2013, to include quality-of-care information on the site. To meet that requirement, CMS has established a plan that initiates a phased approach to public reporting. The 2012 Physician Fee Schedule (PFS) Final Rule was the first step in that phased approach. This rule established that the first measures to be reported on the site would be group-level measures for data collected no sooner than program year 2012. A second critical step is the 2013 PFS Proposed Rule, which outlines a longer-term public reporting plan. According to this plan, we expect the first set of group-level quality measure data to be included on the site in calendar year 2014. We are targeting publishing individual-level quality measures no sooner than 2015 reflecting data collected in program year 2014, if technically feasible.
As you may be aware, Physician Compare is undergoing a redesign to significantly improve the underlying database and thus the information on Physician Compare, as well as the ease of use and functionality of the site. We’ll be unveiling the redesigned site soon. We welcome your feedback and look forward to maintaining a dialogue with you as Physician Compare continues to evolve.
Rashaan Byers, MPH, social science research analyst, Centers forMedicare & Medicaid Services, Center for Clinical Standards & Quality, Quality Measurement & Health Assessment Group
Dr. Frost responds:
I thank Mr. Byers for his clarification regarding the current content on the CMS Physician Compare website, and agree that at the present time the website does not report individual physician clinical performance data.
Physician Compare, however, does currently report if an individual physician participated in the CMS Physician Quality Reporting System (PQRS) by stating “this professional chose to take part in Medicare’s PQRS, and reported quality information satisfactorily for the year 2010.” For those physicians who did not participate in PQRS, their personal website pages do not make reference to the PQRS program.
As the intent of transparency is to educate consumers to make informed choices about where to seek health care, care providers should know that their participation in PQRS is currently publically reported. It is, therefore, possible that patient decisions about whom to seek care from may be influenced by this.
As acknowledged in my January 2013 column in The Hospitalist, Physician Compare currently reports very little information. We should expect this to change, however, as Medicare moves forward with developing a plan to publically report valid and reliable individual physician performance metrics. CMS’ clarification of the timeline by which we can expect to see more detailed information is thus greatly appreciated.
The take-home message for hospitalists is that public reporting of care provider performance will become increasingly comprehensive and transparent in the future. As pointed out, CMS’ present plan targets the publication of individual, physician-level quality measures as soon as 2015, which will reflect actual performance during program year 2014. The measurement period is thus less than one year away, so it behooves us all to focus ever more intently on delivering high-value healthcare.
Shaun Frost, MD, SFHM, past president, SHM
I read the article “Call for Transparency in Health-Care Performance Results to Impact Hospitalists” (January 2013, p. 47) by Shaun Frost, MD, SFHM, president of the Society of Hospital Medicine, with interest. I’d like to clarify a key point about Physician Compare. In the article, the statement that the Physician Compare website (www.medicare.gov/find-a-doctor) provides performance information on individual doctors is inaccurate.
The Affordable Care Act (ACA) states that the Centers for Medicare & Medicaid Services (CMS) must have a plan in place by Jan. 1, 2013, to include quality-of-care information on the site. To meet that requirement, CMS has established a plan that initiates a phased approach to public reporting. The 2012 Physician Fee Schedule (PFS) Final Rule was the first step in that phased approach. This rule established that the first measures to be reported on the site would be group-level measures for data collected no sooner than program year 2012. A second critical step is the 2013 PFS Proposed Rule, which outlines a longer-term public reporting plan. According to this plan, we expect the first set of group-level quality measure data to be included on the site in calendar year 2014. We are targeting publishing individual-level quality measures no sooner than 2015 reflecting data collected in program year 2014, if technically feasible.
As you may be aware, Physician Compare is undergoing a redesign to significantly improve the underlying database and thus the information on Physician Compare, as well as the ease of use and functionality of the site. We’ll be unveiling the redesigned site soon. We welcome your feedback and look forward to maintaining a dialogue with you as Physician Compare continues to evolve.
Rashaan Byers, MPH, social science research analyst, Centers forMedicare & Medicaid Services, Center for Clinical Standards & Quality, Quality Measurement & Health Assessment Group
Dr. Frost responds:
I thank Mr. Byers for his clarification regarding the current content on the CMS Physician Compare website, and agree that at the present time the website does not report individual physician clinical performance data.
Physician Compare, however, does currently report if an individual physician participated in the CMS Physician Quality Reporting System (PQRS) by stating “this professional chose to take part in Medicare’s PQRS, and reported quality information satisfactorily for the year 2010.” For those physicians who did not participate in PQRS, their personal website pages do not make reference to the PQRS program.
As the intent of transparency is to educate consumers to make informed choices about where to seek health care, care providers should know that their participation in PQRS is currently publically reported. It is, therefore, possible that patient decisions about whom to seek care from may be influenced by this.
As acknowledged in my January 2013 column in The Hospitalist, Physician Compare currently reports very little information. We should expect this to change, however, as Medicare moves forward with developing a plan to publically report valid and reliable individual physician performance metrics. CMS’ clarification of the timeline by which we can expect to see more detailed information is thus greatly appreciated.
The take-home message for hospitalists is that public reporting of care provider performance will become increasingly comprehensive and transparent in the future. As pointed out, CMS’ present plan targets the publication of individual, physician-level quality measures as soon as 2015, which will reflect actual performance during program year 2014. The measurement period is thus less than one year away, so it behooves us all to focus ever more intently on delivering high-value healthcare.
Shaun Frost, MD, SFHM, past president, SHM
I read the article “Call for Transparency in Health-Care Performance Results to Impact Hospitalists” (January 2013, p. 47) by Shaun Frost, MD, SFHM, president of the Society of Hospital Medicine, with interest. I’d like to clarify a key point about Physician Compare. In the article, the statement that the Physician Compare website (www.medicare.gov/find-a-doctor) provides performance information on individual doctors is inaccurate.
The Affordable Care Act (ACA) states that the Centers for Medicare & Medicaid Services (CMS) must have a plan in place by Jan. 1, 2013, to include quality-of-care information on the site. To meet that requirement, CMS has established a plan that initiates a phased approach to public reporting. The 2012 Physician Fee Schedule (PFS) Final Rule was the first step in that phased approach. This rule established that the first measures to be reported on the site would be group-level measures for data collected no sooner than program year 2012. A second critical step is the 2013 PFS Proposed Rule, which outlines a longer-term public reporting plan. According to this plan, we expect the first set of group-level quality measure data to be included on the site in calendar year 2014. We are targeting publishing individual-level quality measures no sooner than 2015 reflecting data collected in program year 2014, if technically feasible.
As you may be aware, Physician Compare is undergoing a redesign to significantly improve the underlying database and thus the information on Physician Compare, as well as the ease of use and functionality of the site. We’ll be unveiling the redesigned site soon. We welcome your feedback and look forward to maintaining a dialogue with you as Physician Compare continues to evolve.
Rashaan Byers, MPH, social science research analyst, Centers forMedicare & Medicaid Services, Center for Clinical Standards & Quality, Quality Measurement & Health Assessment Group
Dr. Frost responds:
I thank Mr. Byers for his clarification regarding the current content on the CMS Physician Compare website, and agree that at the present time the website does not report individual physician clinical performance data.
Physician Compare, however, does currently report if an individual physician participated in the CMS Physician Quality Reporting System (PQRS) by stating “this professional chose to take part in Medicare’s PQRS, and reported quality information satisfactorily for the year 2010.” For those physicians who did not participate in PQRS, their personal website pages do not make reference to the PQRS program.
As the intent of transparency is to educate consumers to make informed choices about where to seek health care, care providers should know that their participation in PQRS is currently publically reported. It is, therefore, possible that patient decisions about whom to seek care from may be influenced by this.
As acknowledged in my January 2013 column in The Hospitalist, Physician Compare currently reports very little information. We should expect this to change, however, as Medicare moves forward with developing a plan to publically report valid and reliable individual physician performance metrics. CMS’ clarification of the timeline by which we can expect to see more detailed information is thus greatly appreciated.
The take-home message for hospitalists is that public reporting of care provider performance will become increasingly comprehensive and transparent in the future. As pointed out, CMS’ present plan targets the publication of individual, physician-level quality measures as soon as 2015, which will reflect actual performance during program year 2014. The measurement period is thus less than one year away, so it behooves us all to focus ever more intently on delivering high-value healthcare.
Shaun Frost, MD, SFHM, past president, SHM
Behavioral Economics Can Accelerate Adoption of Choosing Wisely Campaign

SHM has gotten behind the Choosing Wisely campaign in a big way. Earlier this year, SHM announced lists of suggested practices for adult and pediatric hospital medicine (see Table 1). To keep it on the front burner, hospitalists John Bulger and Ian Jenkins held a pre-course at HM13 devoted entirely to quality-improvement (QI) approaches to implementing and sustaining the practices outlined in the campaign. During the main meeting, they did an encore presentation, with Doug Carlson and Ricardo Quinonez presenting the elements of Choosing Wisely for pediatric hospital medicine.
The widely publicized campaign arose from an American Board of Internal Medicine (ABIM) Foundation grant program to “facilitate the development of innovative, emerging strategies to advance appropriate health-care decision-making and stewardship of health-care resources.” (For more information, visit www.abimfoundation.org.)
Adoption of many of the suggested Choosing Wisely practices will require a change in deeply ingrained, habitual behaviors. We assert that rational, reflective, cognitive processes might not be enough to overturn these behaviors, and that we must look to other mental systems to achieve the consistent adoption of the campaign’s suggested practices. An analogy exists in economics, where theories behind classical economics are challenged by behavioral economics.
What is behavioral economics? Classical economics asserts the individual as “homo economicus”: a person making rational, predictable decisions to advance their interests. However, due to social or professional influence, behavior often does not comport to expected ends. We succumb, sympathize, or follow the pack, diverging from the rulebook. Behavioral economics attempts to understand and compensate for these deviations.
In medicine, we often yield to cognitive biases. To simplify decision-making, we generalize our observations to arrive at decisions quickly. Daniel Kahneman, winner of the Nobel Memorial Prize in Economic Sciences, describes Type I thinking as fast and automatic, and Type II thinking as slow and effortful. Using Kahneman’s framework, we attempt to understand where reasoning may stray and, in turn, introduce environmental changes to achieve better outcomes.
How does this relate to Choosing Wisely? Embracing and embedding the practices of the Choosing Wisely campaign in day-to-day practice will require change in how we approach the clinical decisions we make each day. How can we create the conditions so as not to yield to the status quo?
The MINDSPACE framework
King et al in a recent Health Affairs article describe the MINDSPACE framework (see Table 2), which captures nine effects on behavior—messenger, incentives, norms, defaults, salience, priming, affect, commitments, and ego—that mostly involve automatic systems (Kahneman’s Type I), and how we can leverage them to minimize ineffective health care.1 Below, we describe Choosing Wisely’s HM components and how MINDSPACE can help promote better practice.
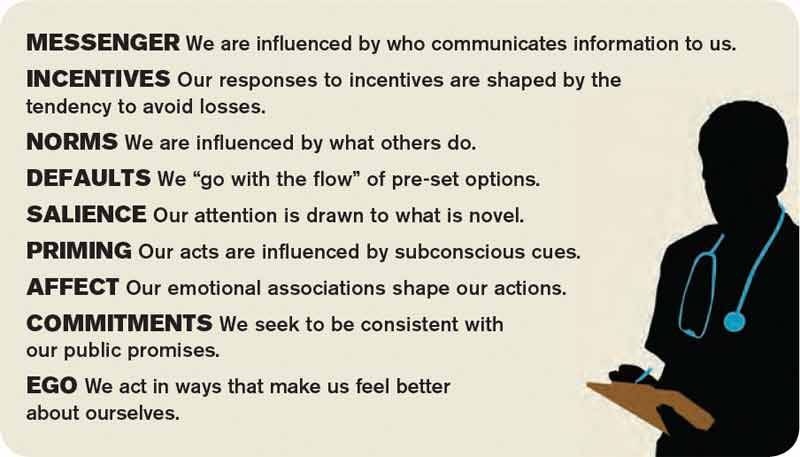
Messenger refers to the importance we place on the source of information conveyed to us. In the campaign, the ABIM Foundation engaged professional societies to come up with a list of specialty-specific practices. We know physicians pay more attention to messages from professional societies than, for example, insurance companies. Having the chair of medicine, the chief of hospital medicine, or the vice president of quality officially sanction the campaign’s practices at your organization leverages messengers.
Incentives, while widely used in health care, have had mixed results in terms of their utility in improving outcomes. People are loss-averse, and behavioral economics leverages that finding, which means incentives structured as penalties seem to have more powerful effects than bonuses. While the familiar pay-for-performance programs might not yield desired results, the evidence base continues to grow, and we have lots to learn. Does a 2% bonus change culture? What would really facilitate modifications in your test ordering patterns?
Norms, or what we perceive as the views of the majority, shape our behavior. How do we establish new ones? We all know the axiom “culture eats strategy for breakfast,” and, like patterned antibiotic administration, redirecting behavior requires examination of why we order items. Often, we order not because the drug combination conforms to standards, but because our training programs imbue us with less-than-ideal habits. These habits become standards, and their root causes require layered examination.
Defaults suggest that we are more likely to embrace a certain behavior if we otherwise need to “opt out” to avoid the behavior. We know that, for example, automatic enrollment in retirement savings plans has dramatically increased participation in such programs. For the Choosing Wisely campaign, the suggested practices should be set up as the default option. Examples include appropriate auto-stop orders for urinary catheters, telemetry, oximetry, or the requirement for added clicks to order daily CBCs. Think about ED orders and how they become substitute defaults once patients arrive on the wards. How do you disrupt the inertia?
Salience is when an individual makes a decision based on what is novel or what their attention is drawn to. Anticipating what subspecialists might expect, what your CMO demands, or what trainees envisage in their supervising attendings all may subconsciously override best judgment and deter best practice.
Priming describes how simple cues—often detected by our subconscious—influence decisions we make. When a physician, perhaps out of concern but often due to poorly reasoned or cavalier messaging, scribes “consider test X,” we involuntarily complete the act. We assume, because of the prime, that we need to act accordingly.
Affect is when we rely on gut feelings to make decisions. Emotions guide our ordering a urinary catheter for incontinence or transfusing to a HGB of 10, even when evidence contradicts what we might know as correct. Countering these actions requires credible stops to convert our emotions to reason (think clinical decision support with teeth).
Commitments are made in advance of an undertaking, behavioral economics suggests, as a way to combat the moment when willpower fails and desired behaviors go by the wayside. By publically signing a contract, in front of your group, chair, or medical director, and going on record as having pledged something, chances of success increase.
Ego, which underpins the need for a positive self-image, can drive the kind of automatic behavior that enables one to compare favorably to others. This effect has driven much of the motivation to perform well on public reporting of hospital quality measures. But ideal reporting of results must be valid; otherwise, attribution of subpar outcomes justifies the usual refrains of “not my responsibility” or the “system needs fixing, not me.”
Conclusions
Choosing Wisely is an ambitious undertaking made up of more than 90 suggested best practices put forth by 25 medical societies. In their book “Nudge,” authors Richard Thaler and Cass Sunstein describe how automatic behaviors arise from the environment or context in which choices to engage in such behaviors are presented.2 For the Choosing Wisely campaign to have staying power, we submit that institutional leaders and front-line clinicians will need to create a context where the safest, most cost-effective choices are the automatic, or nearly automatic, ones.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected]. Dr. Flansbaum is director of hospitalist services at Lenox Hill Hospital in New York City and an SHM Public Policy Committee member.
References
- King D, Greaves F, Vlaev I, Darzi A. Approaches based on behavioral economics could help nudge patients and providers toward lower health spending growth. Health Aff (Millwood). 2013;32(4):661-668.
- Thaler RH, Sunstein CR. Nudge: improving decisions about health, wealth and happiness. New Haven, Conn: Yale University Press; 2008.
SHM has gotten behind the Choosing Wisely campaign in a big way. Earlier this year, SHM announced lists of suggested practices for adult and pediatric hospital medicine (see Table 1). To keep it on the front burner, hospitalists John Bulger and Ian Jenkins held a pre-course at HM13 devoted entirely to quality-improvement (QI) approaches to implementing and sustaining the practices outlined in the campaign. During the main meeting, they did an encore presentation, with Doug Carlson and Ricardo Quinonez presenting the elements of Choosing Wisely for pediatric hospital medicine.
The widely publicized campaign arose from an American Board of Internal Medicine (ABIM) Foundation grant program to “facilitate the development of innovative, emerging strategies to advance appropriate health-care decision-making and stewardship of health-care resources.” (For more information, visit www.abimfoundation.org.)
Adoption of many of the suggested Choosing Wisely practices will require a change in deeply ingrained, habitual behaviors. We assert that rational, reflective, cognitive processes might not be enough to overturn these behaviors, and that we must look to other mental systems to achieve the consistent adoption of the campaign’s suggested practices. An analogy exists in economics, where theories behind classical economics are challenged by behavioral economics.
What is behavioral economics? Classical economics asserts the individual as “homo economicus”: a person making rational, predictable decisions to advance their interests. However, due to social or professional influence, behavior often does not comport to expected ends. We succumb, sympathize, or follow the pack, diverging from the rulebook. Behavioral economics attempts to understand and compensate for these deviations.
In medicine, we often yield to cognitive biases. To simplify decision-making, we generalize our observations to arrive at decisions quickly. Daniel Kahneman, winner of the Nobel Memorial Prize in Economic Sciences, describes Type I thinking as fast and automatic, and Type II thinking as slow and effortful. Using Kahneman’s framework, we attempt to understand where reasoning may stray and, in turn, introduce environmental changes to achieve better outcomes.
How does this relate to Choosing Wisely? Embracing and embedding the practices of the Choosing Wisely campaign in day-to-day practice will require change in how we approach the clinical decisions we make each day. How can we create the conditions so as not to yield to the status quo?
The MINDSPACE framework
King et al in a recent Health Affairs article describe the MINDSPACE framework (see Table 2), which captures nine effects on behavior—messenger, incentives, norms, defaults, salience, priming, affect, commitments, and ego—that mostly involve automatic systems (Kahneman’s Type I), and how we can leverage them to minimize ineffective health care.1 Below, we describe Choosing Wisely’s HM components and how MINDSPACE can help promote better practice.
Messenger refers to the importance we place on the source of information conveyed to us. In the campaign, the ABIM Foundation engaged professional societies to come up with a list of specialty-specific practices. We know physicians pay more attention to messages from professional societies than, for example, insurance companies. Having the chair of medicine, the chief of hospital medicine, or the vice president of quality officially sanction the campaign’s practices at your organization leverages messengers.
Incentives, while widely used in health care, have had mixed results in terms of their utility in improving outcomes. People are loss-averse, and behavioral economics leverages that finding, which means incentives structured as penalties seem to have more powerful effects than bonuses. While the familiar pay-for-performance programs might not yield desired results, the evidence base continues to grow, and we have lots to learn. Does a 2% bonus change culture? What would really facilitate modifications in your test ordering patterns?
Norms, or what we perceive as the views of the majority, shape our behavior. How do we establish new ones? We all know the axiom “culture eats strategy for breakfast,” and, like patterned antibiotic administration, redirecting behavior requires examination of why we order items. Often, we order not because the drug combination conforms to standards, but because our training programs imbue us with less-than-ideal habits. These habits become standards, and their root causes require layered examination.
Defaults suggest that we are more likely to embrace a certain behavior if we otherwise need to “opt out” to avoid the behavior. We know that, for example, automatic enrollment in retirement savings plans has dramatically increased participation in such programs. For the Choosing Wisely campaign, the suggested practices should be set up as the default option. Examples include appropriate auto-stop orders for urinary catheters, telemetry, oximetry, or the requirement for added clicks to order daily CBCs. Think about ED orders and how they become substitute defaults once patients arrive on the wards. How do you disrupt the inertia?
Salience is when an individual makes a decision based on what is novel or what their attention is drawn to. Anticipating what subspecialists might expect, what your CMO demands, or what trainees envisage in their supervising attendings all may subconsciously override best judgment and deter best practice.
Priming describes how simple cues—often detected by our subconscious—influence decisions we make. When a physician, perhaps out of concern but often due to poorly reasoned or cavalier messaging, scribes “consider test X,” we involuntarily complete the act. We assume, because of the prime, that we need to act accordingly.
Affect is when we rely on gut feelings to make decisions. Emotions guide our ordering a urinary catheter for incontinence or transfusing to a HGB of 10, even when evidence contradicts what we might know as correct. Countering these actions requires credible stops to convert our emotions to reason (think clinical decision support with teeth).
Commitments are made in advance of an undertaking, behavioral economics suggests, as a way to combat the moment when willpower fails and desired behaviors go by the wayside. By publically signing a contract, in front of your group, chair, or medical director, and going on record as having pledged something, chances of success increase.
Ego, which underpins the need for a positive self-image, can drive the kind of automatic behavior that enables one to compare favorably to others. This effect has driven much of the motivation to perform well on public reporting of hospital quality measures. But ideal reporting of results must be valid; otherwise, attribution of subpar outcomes justifies the usual refrains of “not my responsibility” or the “system needs fixing, not me.”
Conclusions
Choosing Wisely is an ambitious undertaking made up of more than 90 suggested best practices put forth by 25 medical societies. In their book “Nudge,” authors Richard Thaler and Cass Sunstein describe how automatic behaviors arise from the environment or context in which choices to engage in such behaviors are presented.2 For the Choosing Wisely campaign to have staying power, we submit that institutional leaders and front-line clinicians will need to create a context where the safest, most cost-effective choices are the automatic, or nearly automatic, ones.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected]. Dr. Flansbaum is director of hospitalist services at Lenox Hill Hospital in New York City and an SHM Public Policy Committee member.
References
- King D, Greaves F, Vlaev I, Darzi A. Approaches based on behavioral economics could help nudge patients and providers toward lower health spending growth. Health Aff (Millwood). 2013;32(4):661-668.
- Thaler RH, Sunstein CR. Nudge: improving decisions about health, wealth and happiness. New Haven, Conn: Yale University Press; 2008.
SHM has gotten behind the Choosing Wisely campaign in a big way. Earlier this year, SHM announced lists of suggested practices for adult and pediatric hospital medicine (see Table 1). To keep it on the front burner, hospitalists John Bulger and Ian Jenkins held a pre-course at HM13 devoted entirely to quality-improvement (QI) approaches to implementing and sustaining the practices outlined in the campaign. During the main meeting, they did an encore presentation, with Doug Carlson and Ricardo Quinonez presenting the elements of Choosing Wisely for pediatric hospital medicine.
The widely publicized campaign arose from an American Board of Internal Medicine (ABIM) Foundation grant program to “facilitate the development of innovative, emerging strategies to advance appropriate health-care decision-making and stewardship of health-care resources.” (For more information, visit www.abimfoundation.org.)
Adoption of many of the suggested Choosing Wisely practices will require a change in deeply ingrained, habitual behaviors. We assert that rational, reflective, cognitive processes might not be enough to overturn these behaviors, and that we must look to other mental systems to achieve the consistent adoption of the campaign’s suggested practices. An analogy exists in economics, where theories behind classical economics are challenged by behavioral economics.
What is behavioral economics? Classical economics asserts the individual as “homo economicus”: a person making rational, predictable decisions to advance their interests. However, due to social or professional influence, behavior often does not comport to expected ends. We succumb, sympathize, or follow the pack, diverging from the rulebook. Behavioral economics attempts to understand and compensate for these deviations.
In medicine, we often yield to cognitive biases. To simplify decision-making, we generalize our observations to arrive at decisions quickly. Daniel Kahneman, winner of the Nobel Memorial Prize in Economic Sciences, describes Type I thinking as fast and automatic, and Type II thinking as slow and effortful. Using Kahneman’s framework, we attempt to understand where reasoning may stray and, in turn, introduce environmental changes to achieve better outcomes.
How does this relate to Choosing Wisely? Embracing and embedding the practices of the Choosing Wisely campaign in day-to-day practice will require change in how we approach the clinical decisions we make each day. How can we create the conditions so as not to yield to the status quo?
The MINDSPACE framework
King et al in a recent Health Affairs article describe the MINDSPACE framework (see Table 2), which captures nine effects on behavior—messenger, incentives, norms, defaults, salience, priming, affect, commitments, and ego—that mostly involve automatic systems (Kahneman’s Type I), and how we can leverage them to minimize ineffective health care.1 Below, we describe Choosing Wisely’s HM components and how MINDSPACE can help promote better practice.
Messenger refers to the importance we place on the source of information conveyed to us. In the campaign, the ABIM Foundation engaged professional societies to come up with a list of specialty-specific practices. We know physicians pay more attention to messages from professional societies than, for example, insurance companies. Having the chair of medicine, the chief of hospital medicine, or the vice president of quality officially sanction the campaign’s practices at your organization leverages messengers.
Incentives, while widely used in health care, have had mixed results in terms of their utility in improving outcomes. People are loss-averse, and behavioral economics leverages that finding, which means incentives structured as penalties seem to have more powerful effects than bonuses. While the familiar pay-for-performance programs might not yield desired results, the evidence base continues to grow, and we have lots to learn. Does a 2% bonus change culture? What would really facilitate modifications in your test ordering patterns?
Norms, or what we perceive as the views of the majority, shape our behavior. How do we establish new ones? We all know the axiom “culture eats strategy for breakfast,” and, like patterned antibiotic administration, redirecting behavior requires examination of why we order items. Often, we order not because the drug combination conforms to standards, but because our training programs imbue us with less-than-ideal habits. These habits become standards, and their root causes require layered examination.
Defaults suggest that we are more likely to embrace a certain behavior if we otherwise need to “opt out” to avoid the behavior. We know that, for example, automatic enrollment in retirement savings plans has dramatically increased participation in such programs. For the Choosing Wisely campaign, the suggested practices should be set up as the default option. Examples include appropriate auto-stop orders for urinary catheters, telemetry, oximetry, or the requirement for added clicks to order daily CBCs. Think about ED orders and how they become substitute defaults once patients arrive on the wards. How do you disrupt the inertia?
Salience is when an individual makes a decision based on what is novel or what their attention is drawn to. Anticipating what subspecialists might expect, what your CMO demands, or what trainees envisage in their supervising attendings all may subconsciously override best judgment and deter best practice.
Priming describes how simple cues—often detected by our subconscious—influence decisions we make. When a physician, perhaps out of concern but often due to poorly reasoned or cavalier messaging, scribes “consider test X,” we involuntarily complete the act. We assume, because of the prime, that we need to act accordingly.
Affect is when we rely on gut feelings to make decisions. Emotions guide our ordering a urinary catheter for incontinence or transfusing to a HGB of 10, even when evidence contradicts what we might know as correct. Countering these actions requires credible stops to convert our emotions to reason (think clinical decision support with teeth).
Commitments are made in advance of an undertaking, behavioral economics suggests, as a way to combat the moment when willpower fails and desired behaviors go by the wayside. By publically signing a contract, in front of your group, chair, or medical director, and going on record as having pledged something, chances of success increase.
Ego, which underpins the need for a positive self-image, can drive the kind of automatic behavior that enables one to compare favorably to others. This effect has driven much of the motivation to perform well on public reporting of hospital quality measures. But ideal reporting of results must be valid; otherwise, attribution of subpar outcomes justifies the usual refrains of “not my responsibility” or the “system needs fixing, not me.”
Conclusions
Choosing Wisely is an ambitious undertaking made up of more than 90 suggested best practices put forth by 25 medical societies. In their book “Nudge,” authors Richard Thaler and Cass Sunstein describe how automatic behaviors arise from the environment or context in which choices to engage in such behaviors are presented.2 For the Choosing Wisely campaign to have staying power, we submit that institutional leaders and front-line clinicians will need to create a context where the safest, most cost-effective choices are the automatic, or nearly automatic, ones.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected]. Dr. Flansbaum is director of hospitalist services at Lenox Hill Hospital in New York City and an SHM Public Policy Committee member.
References
- King D, Greaves F, Vlaev I, Darzi A. Approaches based on behavioral economics could help nudge patients and providers toward lower health spending growth. Health Aff (Millwood). 2013;32(4):661-668.
- Thaler RH, Sunstein CR. Nudge: improving decisions about health, wealth and happiness. New Haven, Conn: Yale University Press; 2008.
Nonurgent Pediatric Admissions on Weekends Bump Up Hospital Costs

Clinical question: Do weekend admissions for failure to thrive (FTT) result in higher costs and length of stay (LOS)?
Background: FTT accounts for up to 5% of all admissions for children younger than 2 years of age. The optimal approach to inpatient or outpatient care is not well defined. Hospitalizations sometimes are used to facilitate costly and intense workups for organic disease. Given the nonurgent nature of this condition and expected barriers to efficient workup on weekends, it is likely that weekend admissions for FTT might not add much value.
Study design: Retrospective cohort study.
Setting: Forty-two tertiary-care pediatric hospitals.
Synopsis: A total of 23,332 children younger than 2 were studied over an eight-year period. Saturday and Sunday admissions resulted in an average increase in LOS by 1.93 days and an increase in cost by $2,785 when compared with weekday admissions. Patients admitted on weekends were more likely to have imaging studies and lab tests performed, but were less likely to have a discharge diagnosis of FTT. The authors estimate that if one-half of the weekend admissions from 2010 with a consistent FTT diagnosis at admission and discharge were converted to a Monday admission, $534,145 in savings to the health-care system would result.
One notable limitation of the authors’ conclusions is that patients admitted on weekends appeared to have more organic diagnoses documented and might in fact have been more acutely ill, requiring more workup and intervention. Researchers were not able to further explore this using the administrative data. Nonetheless, a subset of weekend admissions with a consistent FTT diagnosis appeared to represent no value added to the system, and potentially could have resulted in a $3.5 million cost savings had they simply been admitted instead on a weekday.
Bottom line: Nonurgent weekend admissions for FTT are inefficient.
Citation: Thompson RT, Bennett WE, Finnell SME, Downs SM. Increased length of stay and costs associated with weekend admissions for failure to thrive. Pediatrics. 2012;131:e805-e810.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: Do weekend admissions for failure to thrive (FTT) result in higher costs and length of stay (LOS)?
Background: FTT accounts for up to 5% of all admissions for children younger than 2 years of age. The optimal approach to inpatient or outpatient care is not well defined. Hospitalizations sometimes are used to facilitate costly and intense workups for organic disease. Given the nonurgent nature of this condition and expected barriers to efficient workup on weekends, it is likely that weekend admissions for FTT might not add much value.
Study design: Retrospective cohort study.
Setting: Forty-two tertiary-care pediatric hospitals.
Synopsis: A total of 23,332 children younger than 2 were studied over an eight-year period. Saturday and Sunday admissions resulted in an average increase in LOS by 1.93 days and an increase in cost by $2,785 when compared with weekday admissions. Patients admitted on weekends were more likely to have imaging studies and lab tests performed, but were less likely to have a discharge diagnosis of FTT. The authors estimate that if one-half of the weekend admissions from 2010 with a consistent FTT diagnosis at admission and discharge were converted to a Monday admission, $534,145 in savings to the health-care system would result.
One notable limitation of the authors’ conclusions is that patients admitted on weekends appeared to have more organic diagnoses documented and might in fact have been more acutely ill, requiring more workup and intervention. Researchers were not able to further explore this using the administrative data. Nonetheless, a subset of weekend admissions with a consistent FTT diagnosis appeared to represent no value added to the system, and potentially could have resulted in a $3.5 million cost savings had they simply been admitted instead on a weekday.
Bottom line: Nonurgent weekend admissions for FTT are inefficient.
Citation: Thompson RT, Bennett WE, Finnell SME, Downs SM. Increased length of stay and costs associated with weekend admissions for failure to thrive. Pediatrics. 2012;131:e805-e810.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: Do weekend admissions for failure to thrive (FTT) result in higher costs and length of stay (LOS)?
Background: FTT accounts for up to 5% of all admissions for children younger than 2 years of age. The optimal approach to inpatient or outpatient care is not well defined. Hospitalizations sometimes are used to facilitate costly and intense workups for organic disease. Given the nonurgent nature of this condition and expected barriers to efficient workup on weekends, it is likely that weekend admissions for FTT might not add much value.
Study design: Retrospective cohort study.
Setting: Forty-two tertiary-care pediatric hospitals.
Synopsis: A total of 23,332 children younger than 2 were studied over an eight-year period. Saturday and Sunday admissions resulted in an average increase in LOS by 1.93 days and an increase in cost by $2,785 when compared with weekday admissions. Patients admitted on weekends were more likely to have imaging studies and lab tests performed, but were less likely to have a discharge diagnosis of FTT. The authors estimate that if one-half of the weekend admissions from 2010 with a consistent FTT diagnosis at admission and discharge were converted to a Monday admission, $534,145 in savings to the health-care system would result.
One notable limitation of the authors’ conclusions is that patients admitted on weekends appeared to have more organic diagnoses documented and might in fact have been more acutely ill, requiring more workup and intervention. Researchers were not able to further explore this using the administrative data. Nonetheless, a subset of weekend admissions with a consistent FTT diagnosis appeared to represent no value added to the system, and potentially could have resulted in a $3.5 million cost savings had they simply been admitted instead on a weekday.
Bottom line: Nonurgent weekend admissions for FTT are inefficient.
Citation: Thompson RT, Bennett WE, Finnell SME, Downs SM. Increased length of stay and costs associated with weekend admissions for failure to thrive. Pediatrics. 2012;131:e805-e810.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
SHM Supports Clarification to Observational Status Loophole for Medicare Patients
Medicare requires beneficiaries to have at least three consecutive days as a hospital inpatient to qualify for Medicare-covered skilled nursing facility (SNF) care. As the use and duration of observation status continues to rise throughout the nation, patients have been getting caught more frequently within a policy trap: Even though they are physically within the hospital and generally receive care that is indistinguishable from the care received by other inpatients, Medicare is not covering their subsequent SNF stays.
Why? Observation status is considered “outpatient” by both the hospital and Medicare and, therefore, is not counted toward Medicare’s three-day rule.
This leaves seniors on the hook for their skilled nursing care costs, which often exceed their ability to pay. Further, this shortsighted policy might actually result in a net greater cost to Medicare and the health-care system. Faced with mounting costs, many seniors truncate or opt out of SNF care altogether, leaving them vulnerable to added health issues (e.g. dehydration, falls). With new conditions that were not present at the time of the original hospital stay, many of these seniors are at risk to return to the hospital and become another readmission statistic.
As key players in hospitals and, increasingly, in skilled nursing facilities, hospitalists are caught squarely in the middle of this policy. Transitions of care both in and out of these institutions should be guided by sound medical decision-making, not whether Medicare will cover the costs incurred. Although the three-day rule—and, indeed, observation status itself—was originally cast as a cost-containment policy, such policies should incorporate broader care process and delivery reforms that do not add burden to patients when they are at their most vulnerable.
SHM affirms that it is sensible for Medicare to provide coverage for skilled nursing care if a clinician recommends it as part of a treatment plan. Coverage determination should not be beholden to a patient status subject to other systemic pressures, but should reflect the best interest of the patient and the care ordered by providers.
The Improving Access to Medicare Coverage Act, sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio), would clarify the law to indicate that Medicare beneficiaries in observation status are deemed inpatients in the hospital for the purposes of the three-day requirement for SNF coverage. This simple adjustment would ensure that patients are able to access the skilled nursing care they need and that providers do not have to worry about this systemic barrier to patient care.
SHM is actively supporting this legislation. A letter of support was sent to Courtney and Brown earlier this year, and membership was mobilized to take action through our Legislative Action Center (www.hospitalmedicine.org/advocacy). Hospitalists also plan to voice their support for the legislation during Hospitalists on the Hill, to be held this month in conjunction with HM13.
As one of only a few specialty medical societies that are active on this issue, SHM stands out as a leader on health-care-system reforms that improve access to care for patients and reduce administrative barriers to medically appropriate care.
Joshua Lapps is SHM’s government relations specialist.
Medicare requires beneficiaries to have at least three consecutive days as a hospital inpatient to qualify for Medicare-covered skilled nursing facility (SNF) care. As the use and duration of observation status continues to rise throughout the nation, patients have been getting caught more frequently within a policy trap: Even though they are physically within the hospital and generally receive care that is indistinguishable from the care received by other inpatients, Medicare is not covering their subsequent SNF stays.
Why? Observation status is considered “outpatient” by both the hospital and Medicare and, therefore, is not counted toward Medicare’s three-day rule.
This leaves seniors on the hook for their skilled nursing care costs, which often exceed their ability to pay. Further, this shortsighted policy might actually result in a net greater cost to Medicare and the health-care system. Faced with mounting costs, many seniors truncate or opt out of SNF care altogether, leaving them vulnerable to added health issues (e.g. dehydration, falls). With new conditions that were not present at the time of the original hospital stay, many of these seniors are at risk to return to the hospital and become another readmission statistic.
As key players in hospitals and, increasingly, in skilled nursing facilities, hospitalists are caught squarely in the middle of this policy. Transitions of care both in and out of these institutions should be guided by sound medical decision-making, not whether Medicare will cover the costs incurred. Although the three-day rule—and, indeed, observation status itself—was originally cast as a cost-containment policy, such policies should incorporate broader care process and delivery reforms that do not add burden to patients when they are at their most vulnerable.
SHM affirms that it is sensible for Medicare to provide coverage for skilled nursing care if a clinician recommends it as part of a treatment plan. Coverage determination should not be beholden to a patient status subject to other systemic pressures, but should reflect the best interest of the patient and the care ordered by providers.
The Improving Access to Medicare Coverage Act, sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio), would clarify the law to indicate that Medicare beneficiaries in observation status are deemed inpatients in the hospital for the purposes of the three-day requirement for SNF coverage. This simple adjustment would ensure that patients are able to access the skilled nursing care they need and that providers do not have to worry about this systemic barrier to patient care.
SHM is actively supporting this legislation. A letter of support was sent to Courtney and Brown earlier this year, and membership was mobilized to take action through our Legislative Action Center (www.hospitalmedicine.org/advocacy). Hospitalists also plan to voice their support for the legislation during Hospitalists on the Hill, to be held this month in conjunction with HM13.
As one of only a few specialty medical societies that are active on this issue, SHM stands out as a leader on health-care-system reforms that improve access to care for patients and reduce administrative barriers to medically appropriate care.
Joshua Lapps is SHM’s government relations specialist.
Medicare requires beneficiaries to have at least three consecutive days as a hospital inpatient to qualify for Medicare-covered skilled nursing facility (SNF) care. As the use and duration of observation status continues to rise throughout the nation, patients have been getting caught more frequently within a policy trap: Even though they are physically within the hospital and generally receive care that is indistinguishable from the care received by other inpatients, Medicare is not covering their subsequent SNF stays.
Why? Observation status is considered “outpatient” by both the hospital and Medicare and, therefore, is not counted toward Medicare’s three-day rule.
This leaves seniors on the hook for their skilled nursing care costs, which often exceed their ability to pay. Further, this shortsighted policy might actually result in a net greater cost to Medicare and the health-care system. Faced with mounting costs, many seniors truncate or opt out of SNF care altogether, leaving them vulnerable to added health issues (e.g. dehydration, falls). With new conditions that were not present at the time of the original hospital stay, many of these seniors are at risk to return to the hospital and become another readmission statistic.
As key players in hospitals and, increasingly, in skilled nursing facilities, hospitalists are caught squarely in the middle of this policy. Transitions of care both in and out of these institutions should be guided by sound medical decision-making, not whether Medicare will cover the costs incurred. Although the three-day rule—and, indeed, observation status itself—was originally cast as a cost-containment policy, such policies should incorporate broader care process and delivery reforms that do not add burden to patients when they are at their most vulnerable.
SHM affirms that it is sensible for Medicare to provide coverage for skilled nursing care if a clinician recommends it as part of a treatment plan. Coverage determination should not be beholden to a patient status subject to other systemic pressures, but should reflect the best interest of the patient and the care ordered by providers.
The Improving Access to Medicare Coverage Act, sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio), would clarify the law to indicate that Medicare beneficiaries in observation status are deemed inpatients in the hospital for the purposes of the three-day requirement for SNF coverage. This simple adjustment would ensure that patients are able to access the skilled nursing care they need and that providers do not have to worry about this systemic barrier to patient care.
SHM is actively supporting this legislation. A letter of support was sent to Courtney and Brown earlier this year, and membership was mobilized to take action through our Legislative Action Center (www.hospitalmedicine.org/advocacy). Hospitalists also plan to voice their support for the legislation during Hospitalists on the Hill, to be held this month in conjunction with HM13.
As one of only a few specialty medical societies that are active on this issue, SHM stands out as a leader on health-care-system reforms that improve access to care for patients and reduce administrative barriers to medically appropriate care.
Joshua Lapps is SHM’s government relations specialist.
Hospitalists Poised to Advance Health Care Through Teamwork


The problems that ail the American health-care system are numerous, complex, and interrelated. In writing about how to fix our chronically dysfunctional system, Hoffman and Emanuel recently cautioned that single solutions will not be effective.1 In their estimation, “individually implemented changes are divisive rather than unifying,” and “the cure … to this complex problem … will require a multimodal approach with a focus on re-engineering the entire care delivery process.”
If single solutions are insufficient (or even counterproductive and divisive), health care’s key stakeholders must figure out how to work more effectively together. In a nutshell, effective collaboration is critical. Those who collaborate well will thrive in the future, while those who are unable to break down silos to innovatively engage their patients, colleagues, and communities will fail.
Our Tradition of Teamwork
Hospitalists understand the importance of collaboration, as teamwork has been a fundamental value of our specialty since its inception. We have a rich tradition of creating novel, collaborative working relationships with a diverse group of key stakeholders that includes primary-care providers (PCPs), nurses, subspecialists, surgeons, case managers, social workers, nursing homes, transitional-care units, home health agencies, hospice programs, and hospital administrators. We have created innovative, collaborative strategies to effectively and safely comanage patients with other physicians, navigate care transitions, and integrate the input of the many people required to manage day-to-day hospital care.
These experiences will serve us well in a future in which collaboration is essential. We should plan to share our expertise in creating effective teams by assuming leadership roles within our institutions as they implement collaborative initiatives on a larger scale through such concepts as the accountable-care organization (ACO).
We should furthermore plan to seek out new, collaborative opportunities by identifying novel agendas to champion. Two critically important, novel agendas for hospitalists to advance are:
- Enhanced physician-patient collaboration; and
- Collaboration to share and propagate new innovation among hospitalists and HM programs across the country.
True Collaboration with Patients
In my last column, I wrote about how enhancing the patient experience of care will have far-reaching, positive effects on health-care reform.2 Attending to the patient experience has been proven to enhance patient satisfaction, care quality, and care affordability. Initiatives to enhance care experience thus hold promise as global, Triple Aim (better health and better care at lower cost) effectors.
The key to improving patient experience is patient engagement, and the key to patient engagement is incorporating patient expectations into the care planning process. The question thus becomes, “How do physicians identify and appropriately act on patient expectations?” The answer is by collaborating with patients to arrive at care decisions that respect their interests. Care providers must work together with patients to create care plans that respect patient preferences, values, and goals. This will require shared decision-making characterized by collaborative discussions that help patients decide between multiple acceptable health-care choices in accordance with their expectations.
SHM is commissioning a Patient Experience Advisory Board to identify how the society can support its members to effectively collaborate with patients and their loved ones. Expect in the near future to learn more from SHM about how to truly engage your patients to enhance the value of the care you deliver.
The Commodification of Health-Care Quality and Affordability
I recently learned of a subspecialty group that had created a new clinical protocol that promised to deliver higher-quality, more affordable care to their patients. When asked if they would share this with physicians outside of their own group, they flat-out refused. What would motivate a physician group to refuse to collaborate with their community to propagate a new innovation that promises to enhance the value of health care? The answer may lie with an economic concept known as commodification.
Commodification is the process by which an item that possesses no economic interest is assigned monetary worth, and hence how economic values can replace social values that previously governed how the item was treated. Commodification describes a transformation of relationships formerly untainted by commerce into commercial relationships that are influenced by monetary interests.
As payors move away from reimbursing providers simply for performing services (volume-based purchasing) to paying them for the value they deliver (value-based purchasing), we must acknowledge that we are “commodifying” health-care quality and affordability. By doing so, the economic viability of medical practices and health-care institutions will depend on delivering value, and to the extent that this determines a competitive advantage in the marketplace, providers might be reluctant to share innovations in quality and affordability.
We must not let this happen to health care. Competing on the ability to effectively deploy and manage new innovations to enhance quality and affordability is acceptable. Competing, however, on the access to these innovations is ethically unacceptable for an industry that is indispensable to the health and well-being of its consumers.
Coke and Pepsi do not provide indispensable products to society. It is thus fine for soft-drink makers to keep their recipes top secret and fight vigorously to prevent others from gaining access to their innovations. Health-care providers, however, cannot morally defend refusing to share new products and processes that decrease costs, improve patient experience, decrease morbidity, prolong life, or otherwise enhance quality.
We must, therefore, strive to continuously collaborate with our hospitalist colleagues and HM programs across the country to propagate new innovation. When someone builds a better mouse trap, it should be shared freely so that all patients have the opportunity to benefit. We must not let the pursuit of economic competitive advantage prevent us from collaborating and sharing ideas on how to make our health-care system better.
Conclusion
Fixing health care is complicated, and employing collaboration in order to do so will be required. Hospitalists have vast experience in working effectively with others, and should leverage this experience to lead the charge on efforts to enhance physician-patient collaboration. Hospitalists should strive to continuously collaborate with their colleagues to ensure open access to new discoveries that improve health-care quality and affordability. Those interested in learning more about how to be successful collaborators might find it helpful to seek out additional resources on the subject. Collaboration, by Morten T. Hansen, is a good source on how to turn this concept into action.3
References
- Hoffman A, Emanuel E. Reengineering US health care. JAMA. 2013;309(7):661-662.
- Frost, S. A matter of perspective: deconstructing satisfaction measurements by focusing on patient goals. The Hospitalist. 2013:17(3):59.
- Hansen M. Collaboration: how leaders avoid the traps, create unity, and reap big results. Boston: Harvard Business Press; 2009.
The problems that ail the American health-care system are numerous, complex, and interrelated. In writing about how to fix our chronically dysfunctional system, Hoffman and Emanuel recently cautioned that single solutions will not be effective.1 In their estimation, “individually implemented changes are divisive rather than unifying,” and “the cure … to this complex problem … will require a multimodal approach with a focus on re-engineering the entire care delivery process.”
If single solutions are insufficient (or even counterproductive and divisive), health care’s key stakeholders must figure out how to work more effectively together. In a nutshell, effective collaboration is critical. Those who collaborate well will thrive in the future, while those who are unable to break down silos to innovatively engage their patients, colleagues, and communities will fail.
Our Tradition of Teamwork
Hospitalists understand the importance of collaboration, as teamwork has been a fundamental value of our specialty since its inception. We have a rich tradition of creating novel, collaborative working relationships with a diverse group of key stakeholders that includes primary-care providers (PCPs), nurses, subspecialists, surgeons, case managers, social workers, nursing homes, transitional-care units, home health agencies, hospice programs, and hospital administrators. We have created innovative, collaborative strategies to effectively and safely comanage patients with other physicians, navigate care transitions, and integrate the input of the many people required to manage day-to-day hospital care.
These experiences will serve us well in a future in which collaboration is essential. We should plan to share our expertise in creating effective teams by assuming leadership roles within our institutions as they implement collaborative initiatives on a larger scale through such concepts as the accountable-care organization (ACO).
We should furthermore plan to seek out new, collaborative opportunities by identifying novel agendas to champion. Two critically important, novel agendas for hospitalists to advance are:
- Enhanced physician-patient collaboration; and
- Collaboration to share and propagate new innovation among hospitalists and HM programs across the country.
True Collaboration with Patients
In my last column, I wrote about how enhancing the patient experience of care will have far-reaching, positive effects on health-care reform.2 Attending to the patient experience has been proven to enhance patient satisfaction, care quality, and care affordability. Initiatives to enhance care experience thus hold promise as global, Triple Aim (better health and better care at lower cost) effectors.
The key to improving patient experience is patient engagement, and the key to patient engagement is incorporating patient expectations into the care planning process. The question thus becomes, “How do physicians identify and appropriately act on patient expectations?” The answer is by collaborating with patients to arrive at care decisions that respect their interests. Care providers must work together with patients to create care plans that respect patient preferences, values, and goals. This will require shared decision-making characterized by collaborative discussions that help patients decide between multiple acceptable health-care choices in accordance with their expectations.
SHM is commissioning a Patient Experience Advisory Board to identify how the society can support its members to effectively collaborate with patients and their loved ones. Expect in the near future to learn more from SHM about how to truly engage your patients to enhance the value of the care you deliver.
The Commodification of Health-Care Quality and Affordability
I recently learned of a subspecialty group that had created a new clinical protocol that promised to deliver higher-quality, more affordable care to their patients. When asked if they would share this with physicians outside of their own group, they flat-out refused. What would motivate a physician group to refuse to collaborate with their community to propagate a new innovation that promises to enhance the value of health care? The answer may lie with an economic concept known as commodification.
Commodification is the process by which an item that possesses no economic interest is assigned monetary worth, and hence how economic values can replace social values that previously governed how the item was treated. Commodification describes a transformation of relationships formerly untainted by commerce into commercial relationships that are influenced by monetary interests.
As payors move away from reimbursing providers simply for performing services (volume-based purchasing) to paying them for the value they deliver (value-based purchasing), we must acknowledge that we are “commodifying” health-care quality and affordability. By doing so, the economic viability of medical practices and health-care institutions will depend on delivering value, and to the extent that this determines a competitive advantage in the marketplace, providers might be reluctant to share innovations in quality and affordability.
We must not let this happen to health care. Competing on the ability to effectively deploy and manage new innovations to enhance quality and affordability is acceptable. Competing, however, on the access to these innovations is ethically unacceptable for an industry that is indispensable to the health and well-being of its consumers.
Coke and Pepsi do not provide indispensable products to society. It is thus fine for soft-drink makers to keep their recipes top secret and fight vigorously to prevent others from gaining access to their innovations. Health-care providers, however, cannot morally defend refusing to share new products and processes that decrease costs, improve patient experience, decrease morbidity, prolong life, or otherwise enhance quality.
We must, therefore, strive to continuously collaborate with our hospitalist colleagues and HM programs across the country to propagate new innovation. When someone builds a better mouse trap, it should be shared freely so that all patients have the opportunity to benefit. We must not let the pursuit of economic competitive advantage prevent us from collaborating and sharing ideas on how to make our health-care system better.
Conclusion
Fixing health care is complicated, and employing collaboration in order to do so will be required. Hospitalists have vast experience in working effectively with others, and should leverage this experience to lead the charge on efforts to enhance physician-patient collaboration. Hospitalists should strive to continuously collaborate with their colleagues to ensure open access to new discoveries that improve health-care quality and affordability. Those interested in learning more about how to be successful collaborators might find it helpful to seek out additional resources on the subject. Collaboration, by Morten T. Hansen, is a good source on how to turn this concept into action.3
References
- Hoffman A, Emanuel E. Reengineering US health care. JAMA. 2013;309(7):661-662.
- Frost, S. A matter of perspective: deconstructing satisfaction measurements by focusing on patient goals. The Hospitalist. 2013:17(3):59.
- Hansen M. Collaboration: how leaders avoid the traps, create unity, and reap big results. Boston: Harvard Business Press; 2009.
The problems that ail the American health-care system are numerous, complex, and interrelated. In writing about how to fix our chronically dysfunctional system, Hoffman and Emanuel recently cautioned that single solutions will not be effective.1 In their estimation, “individually implemented changes are divisive rather than unifying,” and “the cure … to this complex problem … will require a multimodal approach with a focus on re-engineering the entire care delivery process.”
If single solutions are insufficient (or even counterproductive and divisive), health care’s key stakeholders must figure out how to work more effectively together. In a nutshell, effective collaboration is critical. Those who collaborate well will thrive in the future, while those who are unable to break down silos to innovatively engage their patients, colleagues, and communities will fail.
Our Tradition of Teamwork
Hospitalists understand the importance of collaboration, as teamwork has been a fundamental value of our specialty since its inception. We have a rich tradition of creating novel, collaborative working relationships with a diverse group of key stakeholders that includes primary-care providers (PCPs), nurses, subspecialists, surgeons, case managers, social workers, nursing homes, transitional-care units, home health agencies, hospice programs, and hospital administrators. We have created innovative, collaborative strategies to effectively and safely comanage patients with other physicians, navigate care transitions, and integrate the input of the many people required to manage day-to-day hospital care.
These experiences will serve us well in a future in which collaboration is essential. We should plan to share our expertise in creating effective teams by assuming leadership roles within our institutions as they implement collaborative initiatives on a larger scale through such concepts as the accountable-care organization (ACO).
We should furthermore plan to seek out new, collaborative opportunities by identifying novel agendas to champion. Two critically important, novel agendas for hospitalists to advance are:
- Enhanced physician-patient collaboration; and
- Collaboration to share and propagate new innovation among hospitalists and HM programs across the country.
True Collaboration with Patients
In my last column, I wrote about how enhancing the patient experience of care will have far-reaching, positive effects on health-care reform.2 Attending to the patient experience has been proven to enhance patient satisfaction, care quality, and care affordability. Initiatives to enhance care experience thus hold promise as global, Triple Aim (better health and better care at lower cost) effectors.
The key to improving patient experience is patient engagement, and the key to patient engagement is incorporating patient expectations into the care planning process. The question thus becomes, “How do physicians identify and appropriately act on patient expectations?” The answer is by collaborating with patients to arrive at care decisions that respect their interests. Care providers must work together with patients to create care plans that respect patient preferences, values, and goals. This will require shared decision-making characterized by collaborative discussions that help patients decide between multiple acceptable health-care choices in accordance with their expectations.
SHM is commissioning a Patient Experience Advisory Board to identify how the society can support its members to effectively collaborate with patients and their loved ones. Expect in the near future to learn more from SHM about how to truly engage your patients to enhance the value of the care you deliver.
The Commodification of Health-Care Quality and Affordability
I recently learned of a subspecialty group that had created a new clinical protocol that promised to deliver higher-quality, more affordable care to their patients. When asked if they would share this with physicians outside of their own group, they flat-out refused. What would motivate a physician group to refuse to collaborate with their community to propagate a new innovation that promises to enhance the value of health care? The answer may lie with an economic concept known as commodification.
Commodification is the process by which an item that possesses no economic interest is assigned monetary worth, and hence how economic values can replace social values that previously governed how the item was treated. Commodification describes a transformation of relationships formerly untainted by commerce into commercial relationships that are influenced by monetary interests.
As payors move away from reimbursing providers simply for performing services (volume-based purchasing) to paying them for the value they deliver (value-based purchasing), we must acknowledge that we are “commodifying” health-care quality and affordability. By doing so, the economic viability of medical practices and health-care institutions will depend on delivering value, and to the extent that this determines a competitive advantage in the marketplace, providers might be reluctant to share innovations in quality and affordability.
We must not let this happen to health care. Competing on the ability to effectively deploy and manage new innovations to enhance quality and affordability is acceptable. Competing, however, on the access to these innovations is ethically unacceptable for an industry that is indispensable to the health and well-being of its consumers.
Coke and Pepsi do not provide indispensable products to society. It is thus fine for soft-drink makers to keep their recipes top secret and fight vigorously to prevent others from gaining access to their innovations. Health-care providers, however, cannot morally defend refusing to share new products and processes that decrease costs, improve patient experience, decrease morbidity, prolong life, or otherwise enhance quality.
We must, therefore, strive to continuously collaborate with our hospitalist colleagues and HM programs across the country to propagate new innovation. When someone builds a better mouse trap, it should be shared freely so that all patients have the opportunity to benefit. We must not let the pursuit of economic competitive advantage prevent us from collaborating and sharing ideas on how to make our health-care system better.
Conclusion
Fixing health care is complicated, and employing collaboration in order to do so will be required. Hospitalists have vast experience in working effectively with others, and should leverage this experience to lead the charge on efforts to enhance physician-patient collaboration. Hospitalists should strive to continuously collaborate with their colleagues to ensure open access to new discoveries that improve health-care quality and affordability. Those interested in learning more about how to be successful collaborators might find it helpful to seek out additional resources on the subject. Collaboration, by Morten T. Hansen, is a good source on how to turn this concept into action.3
References
- Hoffman A, Emanuel E. Reengineering US health care. JAMA. 2013;309(7):661-662.
- Frost, S. A matter of perspective: deconstructing satisfaction measurements by focusing on patient goals. The Hospitalist. 2013:17(3):59.
- Hansen M. Collaboration: how leaders avoid the traps, create unity, and reap big results. Boston: Harvard Business Press; 2009.
A Tracheostomy Collar Facilitates Quicker Transition


Each day a patient spends on a ventilator increases pneumonia risk by about 1% (Am J Respir Crit Care Med. 2002;165[7]:867-903). Being unable to move or talk also might induce a sense of helplessness. As a result, many clinicians wean off a ventilator sooner rather than later.
A recent study (JAMA. 2013;309[7]:671-677) has found that unassisted breathing via a tracheostomy collar facilitates a quicker transition than breathing with pressure support after prolonged mechanical ventilation (>21 days). Investigators reported their findings at the Society of Critical Care Medicine’s 42nd Congress in January in San Juan, Puerto Rico.
On average, patients were able to successfully wean four days earlier with unassisted breathing versus pressure support—a significant difference, says lead investigator Amal Jubran, MD, section chief of pulmonary and critical-care medicine at the Edward Hines Jr. VA Hospital in Chicago. No major differences were reported in survival between the two groups at six-month and 12-month intervals after enrollment in the study.
“The faster pace of weaning in the tracheostomy collar group may be related to its effect on clinical decision-making,” says Dr. Jubran, a professor at Loyola University Chicago’s Stritch School of Medicine. “Observing a patient breathing through a tracheostomy collar provides the clinician with a clear view of the patient’s respiratory capabilities.”
In contrast, with pressure support, a clinician’s perception of weanability “is clouded because the patient is receiving ventilator assistance,” she says. “It is extremely difficult to distinguish between how much work the patient is doing and how much work the ventilator is doing.”
Amid this uncertainty, Dr. Jubran adds, clinicians are more likely to accelerate the weaning process in patients who unexpectedly respond well during a tracheostomy collar challenge than in those receiving a low level of pressure support.
In the study, less than 10% of 312 patients—most of whom were elderly—required reconnection to a ventilator after being weaned successfully. Weaning efforts should be restarted only after cardiopulmonary stability has been reached, she says.
Factoring into the equation are the measurements for blood pressure and respiratory rate and the amounts of oxygenation and sedation in patients on ventilators, says Paul Odenbach, MD, SHM, a hospitalist at Abbott Northwestern Hospital in Minneapolis.
“I look at them clinically overall,” he says. “The most important piece is eyeballing them from where they are in their disease trajectory.”
“Are they awake enough to be protecting their airway once they are extubated?” he adds. He has found that a stable airway is more easily achieved with a tracheostomy collar.
Managing heart failure, treating infections, and optimizing nutrition are crucial before weaning off ventilation, says geriatrician Joel Sender, MD, section chief of pulmonary medicine at St. Barnabas Hospital in Bronx, N.Y., and medical director of its Rehabilitation & Continuing Care Center.
“It is important to identify the best candidates for weaning and then apply the best methods,” says Dr. Sender. “Sadly, many patients are not good candidates, and only a portion are successfully weaned.” That’s why “there’s a great need to have a frank discussion with the family to answer their questions and to promote a realistic set of treatment goals.”
Susan Kreimer is a freelance writer based in New York.
Each day a patient spends on a ventilator increases pneumonia risk by about 1% (Am J Respir Crit Care Med. 2002;165[7]:867-903). Being unable to move or talk also might induce a sense of helplessness. As a result, many clinicians wean off a ventilator sooner rather than later.
A recent study (JAMA. 2013;309[7]:671-677) has found that unassisted breathing via a tracheostomy collar facilitates a quicker transition than breathing with pressure support after prolonged mechanical ventilation (>21 days). Investigators reported their findings at the Society of Critical Care Medicine’s 42nd Congress in January in San Juan, Puerto Rico.
On average, patients were able to successfully wean four days earlier with unassisted breathing versus pressure support—a significant difference, says lead investigator Amal Jubran, MD, section chief of pulmonary and critical-care medicine at the Edward Hines Jr. VA Hospital in Chicago. No major differences were reported in survival between the two groups at six-month and 12-month intervals after enrollment in the study.
“The faster pace of weaning in the tracheostomy collar group may be related to its effect on clinical decision-making,” says Dr. Jubran, a professor at Loyola University Chicago’s Stritch School of Medicine. “Observing a patient breathing through a tracheostomy collar provides the clinician with a clear view of the patient’s respiratory capabilities.”
In contrast, with pressure support, a clinician’s perception of weanability “is clouded because the patient is receiving ventilator assistance,” she says. “It is extremely difficult to distinguish between how much work the patient is doing and how much work the ventilator is doing.”
Amid this uncertainty, Dr. Jubran adds, clinicians are more likely to accelerate the weaning process in patients who unexpectedly respond well during a tracheostomy collar challenge than in those receiving a low level of pressure support.
In the study, less than 10% of 312 patients—most of whom were elderly—required reconnection to a ventilator after being weaned successfully. Weaning efforts should be restarted only after cardiopulmonary stability has been reached, she says.
Factoring into the equation are the measurements for blood pressure and respiratory rate and the amounts of oxygenation and sedation in patients on ventilators, says Paul Odenbach, MD, SHM, a hospitalist at Abbott Northwestern Hospital in Minneapolis.
“I look at them clinically overall,” he says. “The most important piece is eyeballing them from where they are in their disease trajectory.”
“Are they awake enough to be protecting their airway once they are extubated?” he adds. He has found that a stable airway is more easily achieved with a tracheostomy collar.
Managing heart failure, treating infections, and optimizing nutrition are crucial before weaning off ventilation, says geriatrician Joel Sender, MD, section chief of pulmonary medicine at St. Barnabas Hospital in Bronx, N.Y., and medical director of its Rehabilitation & Continuing Care Center.
“It is important to identify the best candidates for weaning and then apply the best methods,” says Dr. Sender. “Sadly, many patients are not good candidates, and only a portion are successfully weaned.” That’s why “there’s a great need to have a frank discussion with the family to answer their questions and to promote a realistic set of treatment goals.”
Susan Kreimer is a freelance writer based in New York.
Each day a patient spends on a ventilator increases pneumonia risk by about 1% (Am J Respir Crit Care Med. 2002;165[7]:867-903). Being unable to move or talk also might induce a sense of helplessness. As a result, many clinicians wean off a ventilator sooner rather than later.
A recent study (JAMA. 2013;309[7]:671-677) has found that unassisted breathing via a tracheostomy collar facilitates a quicker transition than breathing with pressure support after prolonged mechanical ventilation (>21 days). Investigators reported their findings at the Society of Critical Care Medicine’s 42nd Congress in January in San Juan, Puerto Rico.
On average, patients were able to successfully wean four days earlier with unassisted breathing versus pressure support—a significant difference, says lead investigator Amal Jubran, MD, section chief of pulmonary and critical-care medicine at the Edward Hines Jr. VA Hospital in Chicago. No major differences were reported in survival between the two groups at six-month and 12-month intervals after enrollment in the study.
“The faster pace of weaning in the tracheostomy collar group may be related to its effect on clinical decision-making,” says Dr. Jubran, a professor at Loyola University Chicago’s Stritch School of Medicine. “Observing a patient breathing through a tracheostomy collar provides the clinician with a clear view of the patient’s respiratory capabilities.”
In contrast, with pressure support, a clinician’s perception of weanability “is clouded because the patient is receiving ventilator assistance,” she says. “It is extremely difficult to distinguish between how much work the patient is doing and how much work the ventilator is doing.”
Amid this uncertainty, Dr. Jubran adds, clinicians are more likely to accelerate the weaning process in patients who unexpectedly respond well during a tracheostomy collar challenge than in those receiving a low level of pressure support.
In the study, less than 10% of 312 patients—most of whom were elderly—required reconnection to a ventilator after being weaned successfully. Weaning efforts should be restarted only after cardiopulmonary stability has been reached, she says.
Factoring into the equation are the measurements for blood pressure and respiratory rate and the amounts of oxygenation and sedation in patients on ventilators, says Paul Odenbach, MD, SHM, a hospitalist at Abbott Northwestern Hospital in Minneapolis.
“I look at them clinically overall,” he says. “The most important piece is eyeballing them from where they are in their disease trajectory.”
“Are they awake enough to be protecting their airway once they are extubated?” he adds. He has found that a stable airway is more easily achieved with a tracheostomy collar.
Managing heart failure, treating infections, and optimizing nutrition are crucial before weaning off ventilation, says geriatrician Joel Sender, MD, section chief of pulmonary medicine at St. Barnabas Hospital in Bronx, N.Y., and medical director of its Rehabilitation & Continuing Care Center.
“It is important to identify the best candidates for weaning and then apply the best methods,” says Dr. Sender. “Sadly, many patients are not good candidates, and only a portion are successfully weaned.” That’s why “there’s a great need to have a frank discussion with the family to answer their questions and to promote a realistic set of treatment goals.”
Susan Kreimer is a freelance writer based in New York.
Hospitalists Can’t Ignore Rise in CRE Infections
Neil Fishman, MD, associate chief medical officer at the University of Pennsylvania Health System in Philadelphia, sounds like a football coach when he says the best way to fight carbapenem-resistant Enterobacteriaceae (CRE) infections is with a good defense. Hospitalists and others should focus on contact precautions, hand hygiene, removing gowns and gloves before entering new rooms, and even suggest better room cleanings when trying to prevent the spread of CRE, he says. In fact, he has worked with SHM leadership for years to engage hospitalists about the “critical necessity of antimicrobial stewardship.”
“They’re all critical to prevent transmission,” says Dr. Fishman, who chairs the CDC’s Health Infection Control Practices Advisory Committee. “That’s part of the things that can be done in the here and now to try to prevent people from getting infected with these organisms. It’s what the CDC calls ‘detect and prevent.’”
Dr. Fishman’s suggestions echo findings in a new CDC report that shows a threefold increase in the proportion of Enterobacteriaceae bugs that proved resistant to carbapenem in the past decade. The data, in the CDC’s Morbidity and Mortality Weekly Report, showed the proportion of reported Enterobacteriacae that were CRE infections jumped to 4.2% in 2011 from 1.2% in 2001, according to data from the National Nosocomial Infection Surveillance system.
“It is a very serious public health threat,” says co-author Alex Kallen, MD, MPH, a medical epidemiologist and outbreak response coordinator in the CDC’s Division of Healthcare Quality Promotion. “Maybe it’s not that common now, but with no action, it has the potential to become much more common—like a lot of the other MDROs [multidrug-resistant organisms] that hospitalists see regularly. [Hospitalists] have a lot of control over some of the things that could potentially lead to increased transmission.”
Part of the problem, Dr. Fishman says, is a lack of antibiotic options. Polymyxins briefly showed success against the bacteria, but performance is waning.
Dr. Fishman estimates it will be up to eight years before a new antibiotic to combat the infection is in widespread use.
Both he and Dr. Kallen say hospitalists can help reduce the spread of CRE through antibiotic stewardship, review of detailed patient histories to ferret out risk factors, and dedication to contact precautions and hand hygiene.
Dr. Kallen notes hospitalists also can play a leadership role in coordinating efforts for patients transferring between hospitals and other institutions (i.e. skilled nursing or assisted-living facilities). Part of being that leader is refusing to dismiss possible CRE cases.
“If you’re a place that doesn’t see this very often, and you see one, that’s a big deal,” Dr. Kallen says. “It needs to be acted on aggressively. Being proactive is much more effective than waiting until it’s common and then trying to intervene.”
Richard Quinn is a freelance writer in New Jersey.
Neil Fishman, MD, associate chief medical officer at the University of Pennsylvania Health System in Philadelphia, sounds like a football coach when he says the best way to fight carbapenem-resistant Enterobacteriaceae (CRE) infections is with a good defense. Hospitalists and others should focus on contact precautions, hand hygiene, removing gowns and gloves before entering new rooms, and even suggest better room cleanings when trying to prevent the spread of CRE, he says. In fact, he has worked with SHM leadership for years to engage hospitalists about the “critical necessity of antimicrobial stewardship.”
“They’re all critical to prevent transmission,” says Dr. Fishman, who chairs the CDC’s Health Infection Control Practices Advisory Committee. “That’s part of the things that can be done in the here and now to try to prevent people from getting infected with these organisms. It’s what the CDC calls ‘detect and prevent.’”
Dr. Fishman’s suggestions echo findings in a new CDC report that shows a threefold increase in the proportion of Enterobacteriaceae bugs that proved resistant to carbapenem in the past decade. The data, in the CDC’s Morbidity and Mortality Weekly Report, showed the proportion of reported Enterobacteriacae that were CRE infections jumped to 4.2% in 2011 from 1.2% in 2001, according to data from the National Nosocomial Infection Surveillance system.
“It is a very serious public health threat,” says co-author Alex Kallen, MD, MPH, a medical epidemiologist and outbreak response coordinator in the CDC’s Division of Healthcare Quality Promotion. “Maybe it’s not that common now, but with no action, it has the potential to become much more common—like a lot of the other MDROs [multidrug-resistant organisms] that hospitalists see regularly. [Hospitalists] have a lot of control over some of the things that could potentially lead to increased transmission.”
Part of the problem, Dr. Fishman says, is a lack of antibiotic options. Polymyxins briefly showed success against the bacteria, but performance is waning.
Dr. Fishman estimates it will be up to eight years before a new antibiotic to combat the infection is in widespread use.
Both he and Dr. Kallen say hospitalists can help reduce the spread of CRE through antibiotic stewardship, review of detailed patient histories to ferret out risk factors, and dedication to contact precautions and hand hygiene.
Dr. Kallen notes hospitalists also can play a leadership role in coordinating efforts for patients transferring between hospitals and other institutions (i.e. skilled nursing or assisted-living facilities). Part of being that leader is refusing to dismiss possible CRE cases.
“If you’re a place that doesn’t see this very often, and you see one, that’s a big deal,” Dr. Kallen says. “It needs to be acted on aggressively. Being proactive is much more effective than waiting until it’s common and then trying to intervene.”
Richard Quinn is a freelance writer in New Jersey.
Neil Fishman, MD, associate chief medical officer at the University of Pennsylvania Health System in Philadelphia, sounds like a football coach when he says the best way to fight carbapenem-resistant Enterobacteriaceae (CRE) infections is with a good defense. Hospitalists and others should focus on contact precautions, hand hygiene, removing gowns and gloves before entering new rooms, and even suggest better room cleanings when trying to prevent the spread of CRE, he says. In fact, he has worked with SHM leadership for years to engage hospitalists about the “critical necessity of antimicrobial stewardship.”
“They’re all critical to prevent transmission,” says Dr. Fishman, who chairs the CDC’s Health Infection Control Practices Advisory Committee. “That’s part of the things that can be done in the here and now to try to prevent people from getting infected with these organisms. It’s what the CDC calls ‘detect and prevent.’”
Dr. Fishman’s suggestions echo findings in a new CDC report that shows a threefold increase in the proportion of Enterobacteriaceae bugs that proved resistant to carbapenem in the past decade. The data, in the CDC’s Morbidity and Mortality Weekly Report, showed the proportion of reported Enterobacteriacae that were CRE infections jumped to 4.2% in 2011 from 1.2% in 2001, according to data from the National Nosocomial Infection Surveillance system.
“It is a very serious public health threat,” says co-author Alex Kallen, MD, MPH, a medical epidemiologist and outbreak response coordinator in the CDC’s Division of Healthcare Quality Promotion. “Maybe it’s not that common now, but with no action, it has the potential to become much more common—like a lot of the other MDROs [multidrug-resistant organisms] that hospitalists see regularly. [Hospitalists] have a lot of control over some of the things that could potentially lead to increased transmission.”
Part of the problem, Dr. Fishman says, is a lack of antibiotic options. Polymyxins briefly showed success against the bacteria, but performance is waning.
Dr. Fishman estimates it will be up to eight years before a new antibiotic to combat the infection is in widespread use.
Both he and Dr. Kallen say hospitalists can help reduce the spread of CRE through antibiotic stewardship, review of detailed patient histories to ferret out risk factors, and dedication to contact precautions and hand hygiene.
Dr. Kallen notes hospitalists also can play a leadership role in coordinating efforts for patients transferring between hospitals and other institutions (i.e. skilled nursing or assisted-living facilities). Part of being that leader is refusing to dismiss possible CRE cases.
“If you’re a place that doesn’t see this very often, and you see one, that’s a big deal,” Dr. Kallen says. “It needs to be acted on aggressively. Being proactive is much more effective than waiting until it’s common and then trying to intervene.”
Richard Quinn is a freelance writer in New Jersey.
Addressing The Joint Commission's Concern About Opioid-Induced Respiratory Depression
The recent article by Susan Kreimer, “Serious Complications from Opioid Overuse in Hospitalized Patients Prompts Nationwide Alert” (February 2013, p. 34) highlights a very important patient safety issue—opioid-induced respiratory depression.
Post-operative patients often manage their pain with patient-controlled analgesia (PCA) pumps. An estimated 14 million patients use PCA annually.1 As the article points out, PCA “offers built-in safety features—if patients become too sedated, they can’t push a button for extra doses—but that isn’t always the case.”
As Dr. Jason McKeown says, “While PCA may be the safest mode of opioid delivery, it is true that regardless of the route of administration, respiratory depression may still occur. To help prevent such incidents from happening, it should be remembered that some of the most significant strides in medicine and surgery are directly attributable to anesthesiology’s advances in patient monitoring.”
With the goal of helping to reduce adverse events and deaths with PCA pumps, the Physician-Patient Alliance for Health & Safety (PPAHS) recently released a safety checklist that reminds caregivers of the essential steps needed to be taken to initiate PCA with a patient, and to continue to assess that patient’s use of PCA. This checklist was developed after consultation with a group of 19 renowned health experts and is a free download at www.ppahs.org.
The checklist provides five recommended steps to have been completed when initiating PCA:
- Risk factors that increase risk of respiratory depression have been considered.
- Pre-procedural cognitive assessment has determined patient is capable of participating in pain management.
However, it should be noted that these first two steps are not an attempt at risk stratification. In reviewing current approaches to address failure-to-rescue, Dr. Andreas Taenzer and his colleagues showed that these current approaches are not able to predict which patients are at risk and at which point the crisis can be detected.
- Patient has been provided with information on proper patient use of PCA pump (other recipients of information—family/visitors) and purpose of monitoring.
The Institute for Safe Medical Practice (www.ismp.org) cautions against PCA proxy and stresses the importance of patient education. The safe use of PCA includes making sure the patient controlling the device actually knows how to use it and the importance of the monitoring used to continuously assess their status.
- Two health-care providers have independently double-checked: patient ID; allergies; drug selection and concentration; dosage adjustments; pump settings; and line attachment to patient and tubing insertion.
Error prevention is critical. The Pennsylvania Patient Safety Authority recently released its analysis of medication errors and adverse drug reactions involving intravenous fentanyl that were reported to them. Researchers found 2,319 events between June 2004 to March 2012; that’s almost 25 events per month. Although one error a day may seem high, their analysis is confined to reports that were made to the authority and only include fentanyl, a potent, synthetic narcotic analgesic with a rapid onset and short duration of action.
- Patient is electronically monitored with both pulse oximetry and capnography.
As Dr. Robert Stoelting, president of the Anesthesia Patient Safety Foundation, recently stated: “The conclusions and recommendations of APSF are that intermittent ‘spot checks’ of [pulse oximetry] and ventilation are not adequate for reliably recognizing clinically significant, evolving, drug-induced, respiratory depression in the postoperative period....APSF recommends that monitoring be continuous and not intermittent, and that continuous electronic monitoring with both pulse oximetry for oxygenation and capnography for the adequacy of ventilation be considered for all patients.”
Frank Federico, a member of the Patient Safety Advisory Group at The Joint Commission and executive director at the Institute for Healthcare Improvement, concurs: “Although nurse spot checks on patients are advisable, pulse oximetry and capnography are essential risk prevention tools in any pain management plan.”
PPAHS encourages all hospitals and health-care facilities to download and utilize the PCA Safety Checklist.
The recent article by Susan Kreimer, “Serious Complications from Opioid Overuse in Hospitalized Patients Prompts Nationwide Alert” (February 2013, p. 34) highlights a very important patient safety issue—opioid-induced respiratory depression.
Post-operative patients often manage their pain with patient-controlled analgesia (PCA) pumps. An estimated 14 million patients use PCA annually.1 As the article points out, PCA “offers built-in safety features—if patients become too sedated, they can’t push a button for extra doses—but that isn’t always the case.”
As Dr. Jason McKeown says, “While PCA may be the safest mode of opioid delivery, it is true that regardless of the route of administration, respiratory depression may still occur. To help prevent such incidents from happening, it should be remembered that some of the most significant strides in medicine and surgery are directly attributable to anesthesiology’s advances in patient monitoring.”
With the goal of helping to reduce adverse events and deaths with PCA pumps, the Physician-Patient Alliance for Health & Safety (PPAHS) recently released a safety checklist that reminds caregivers of the essential steps needed to be taken to initiate PCA with a patient, and to continue to assess that patient’s use of PCA. This checklist was developed after consultation with a group of 19 renowned health experts and is a free download at www.ppahs.org.
The checklist provides five recommended steps to have been completed when initiating PCA:
- Risk factors that increase risk of respiratory depression have been considered.
- Pre-procedural cognitive assessment has determined patient is capable of participating in pain management.
However, it should be noted that these first two steps are not an attempt at risk stratification. In reviewing current approaches to address failure-to-rescue, Dr. Andreas Taenzer and his colleagues showed that these current approaches are not able to predict which patients are at risk and at which point the crisis can be detected.
- Patient has been provided with information on proper patient use of PCA pump (other recipients of information—family/visitors) and purpose of monitoring.
The Institute for Safe Medical Practice (www.ismp.org) cautions against PCA proxy and stresses the importance of patient education. The safe use of PCA includes making sure the patient controlling the device actually knows how to use it and the importance of the monitoring used to continuously assess their status.
- Two health-care providers have independently double-checked: patient ID; allergies; drug selection and concentration; dosage adjustments; pump settings; and line attachment to patient and tubing insertion.
Error prevention is critical. The Pennsylvania Patient Safety Authority recently released its analysis of medication errors and adverse drug reactions involving intravenous fentanyl that were reported to them. Researchers found 2,319 events between June 2004 to March 2012; that’s almost 25 events per month. Although one error a day may seem high, their analysis is confined to reports that were made to the authority and only include fentanyl, a potent, synthetic narcotic analgesic with a rapid onset and short duration of action.
- Patient is electronically monitored with both pulse oximetry and capnography.
As Dr. Robert Stoelting, president of the Anesthesia Patient Safety Foundation, recently stated: “The conclusions and recommendations of APSF are that intermittent ‘spot checks’ of [pulse oximetry] and ventilation are not adequate for reliably recognizing clinically significant, evolving, drug-induced, respiratory depression in the postoperative period....APSF recommends that monitoring be continuous and not intermittent, and that continuous electronic monitoring with both pulse oximetry for oxygenation and capnography for the adequacy of ventilation be considered for all patients.”
Frank Federico, a member of the Patient Safety Advisory Group at The Joint Commission and executive director at the Institute for Healthcare Improvement, concurs: “Although nurse spot checks on patients are advisable, pulse oximetry and capnography are essential risk prevention tools in any pain management plan.”
PPAHS encourages all hospitals and health-care facilities to download and utilize the PCA Safety Checklist.
The recent article by Susan Kreimer, “Serious Complications from Opioid Overuse in Hospitalized Patients Prompts Nationwide Alert” (February 2013, p. 34) highlights a very important patient safety issue—opioid-induced respiratory depression.
Post-operative patients often manage their pain with patient-controlled analgesia (PCA) pumps. An estimated 14 million patients use PCA annually.1 As the article points out, PCA “offers built-in safety features—if patients become too sedated, they can’t push a button for extra doses—but that isn’t always the case.”
As Dr. Jason McKeown says, “While PCA may be the safest mode of opioid delivery, it is true that regardless of the route of administration, respiratory depression may still occur. To help prevent such incidents from happening, it should be remembered that some of the most significant strides in medicine and surgery are directly attributable to anesthesiology’s advances in patient monitoring.”
With the goal of helping to reduce adverse events and deaths with PCA pumps, the Physician-Patient Alliance for Health & Safety (PPAHS) recently released a safety checklist that reminds caregivers of the essential steps needed to be taken to initiate PCA with a patient, and to continue to assess that patient’s use of PCA. This checklist was developed after consultation with a group of 19 renowned health experts and is a free download at www.ppahs.org.
The checklist provides five recommended steps to have been completed when initiating PCA:
- Risk factors that increase risk of respiratory depression have been considered.
- Pre-procedural cognitive assessment has determined patient is capable of participating in pain management.
However, it should be noted that these first two steps are not an attempt at risk stratification. In reviewing current approaches to address failure-to-rescue, Dr. Andreas Taenzer and his colleagues showed that these current approaches are not able to predict which patients are at risk and at which point the crisis can be detected.
- Patient has been provided with information on proper patient use of PCA pump (other recipients of information—family/visitors) and purpose of monitoring.
The Institute for Safe Medical Practice (www.ismp.org) cautions against PCA proxy and stresses the importance of patient education. The safe use of PCA includes making sure the patient controlling the device actually knows how to use it and the importance of the monitoring used to continuously assess their status.
- Two health-care providers have independently double-checked: patient ID; allergies; drug selection and concentration; dosage adjustments; pump settings; and line attachment to patient and tubing insertion.
Error prevention is critical. The Pennsylvania Patient Safety Authority recently released its analysis of medication errors and adverse drug reactions involving intravenous fentanyl that were reported to them. Researchers found 2,319 events between June 2004 to March 2012; that’s almost 25 events per month. Although one error a day may seem high, their analysis is confined to reports that were made to the authority and only include fentanyl, a potent, synthetic narcotic analgesic with a rapid onset and short duration of action.
- Patient is electronically monitored with both pulse oximetry and capnography.
As Dr. Robert Stoelting, president of the Anesthesia Patient Safety Foundation, recently stated: “The conclusions and recommendations of APSF are that intermittent ‘spot checks’ of [pulse oximetry] and ventilation are not adequate for reliably recognizing clinically significant, evolving, drug-induced, respiratory depression in the postoperative period....APSF recommends that monitoring be continuous and not intermittent, and that continuous electronic monitoring with both pulse oximetry for oxygenation and capnography for the adequacy of ventilation be considered for all patients.”
Frank Federico, a member of the Patient Safety Advisory Group at The Joint Commission and executive director at the Institute for Healthcare Improvement, concurs: “Although nurse spot checks on patients are advisable, pulse oximetry and capnography are essential risk prevention tools in any pain management plan.”
PPAHS encourages all hospitals and health-care facilities to download and utilize the PCA Safety Checklist.